User login
Reconciliation Act

Pharmacist Kristine M. Gleason, RPh, got the chance to personally test her ability to help ED providers with medication reconciliation—known by most in healthcare as “med rec”—when she broke her leg a couple of years ago. No problem, she thought: “I’ve been involved in med-rec efforts for eight-plus years.”
But when asked to provide her current medications, Gleason, who is the clinical quality leader in the department of clinical quality and analytics at Northwestern Memorial Hospital in Chicago, says she was in pain and overwhelmed. “I couldn’t even remember my children’s names, let alone the names and dosages of my aspirin and my thyroid medication,” she says. Moreover, she didn’t carry a list in her wallet because “I’m a pharmacist and I do med rec,” she says.
Gleason’s experience highlights why, six years after The Joint Commission introduced medication reconciliation as National Patient Safety Goal (NPSG) No. 8, hospitals and providers still struggle with the process.1 As a younger patient, Gleason took few medications. But for the majority of elderly inpatients with comorbid conditions, just establishing the patient’s medication list can bring the whole process to a halt; without that foundational list, reconciling other medications becomes problematic.
Although the commission has taken the goals under review and has, since July 1, required compliance with the revised NPSG 03.06.01 (see “Additional Resources,”), hospitalization-associated adverse drug events continue to mount. A recent Canadian study caused a ripple this summer with its findings that patients discharged from acute-care hospitals were at higher risk for unintentional discontinuation of their medications prescribed for chronic diseases than control groups, and those who had an ICU stay are at even higher risk.2
There’s been no shortage of med-rec initiatives in recent years. Medication reconciliation was at the top of the list for ways to prevent errors when the Institute for Healthcare Improvement launched its “5 Million Lives Campaign” in December 2006. SHM weighed in on the issue in 2010 with a consensus statement on key principles and necessary first steps in med rec.3
“This isn’t a new problem,” Gleason says. “Med rec has become more heightened because we have many more medications and complex therapies, more care providers, more specialists—more players, if you will.”
The March launch of the Hospital Readmissions Reduction Program, part of the Centers for Medicaid & Medicare Services’ (CMS) Inpatient Prospective Payment System, will again shine the spotlight on med rec’s role in the prevention of 30-day readmissions. The Hospitalist talked with researchers, pharmacists, and hospitalists about the reasons behind medication discrepancies, and their strategies for addressing mismatches.
Why So Difficult?
The goal of medication reconciliation is to generate and maintain an accurate and coherent record of patients’ medications across all transitions of care, which sounds straightforward enough. But the process involves much more than just checking items off a list, says Jeffrey Schnipper, MD, MPH, FHM, currently the principal investigator for the $1.5 million study funded by the Agency for Healthcare Research and Quality (AHRQ) to research and implement best practices in med rec, dubbed MARQUIS (Multicenter Medication Reconciliation Quality Improvement Study). Those immersed in med rec know that it’s nonlinear, multilayered, and surprisingly complex, requiring partnerships among diverse providers across many domains of care.
“Medication reconciliation gets right at all the weaknesses of our healthcare system,” says Dr. Schnipper, a hospitalist and director of clinical research for the HM service at Brigham and Women’s Hospital (BWH) and assistant professor of medicine at Harvard Medical School, both in Boston. “We have an excellent healthcare system in so many ways, but what we do not do such a good job of is coordination of care across settings, easy transfer of information, and having one person who is responsible for the accuracy of a patient’s health information.”
Dr. Schnipper’s studies attest to the common occurrence of unintentional medical discrepancies, pointing to the need for accurate medication histories, identifying high-risk patients for intensive interventions, and careful med rec at time of discharge.4
Other factors might come into play, says Ted Tsomides, MD, PhD, an attending physician on the HM service at WakeMed Hospital and assistant professor of medicine at the University of North Carolina’s School of Medicine in Raleigh, N.C. For example, he surmises that a “fatigue factor” sets in for some providers. “After five years of working on any initiative, people get worn out and push it to the back burner, unless they are really incentivized to stay on it,” he says.
List Capture
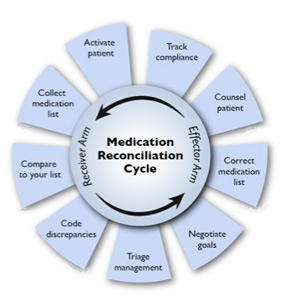
Medication reconciliation is a multifaceted process, and the first step is to gather the history of medications the patient has been taking. Hospitalist Blake J. Lesselroth, MD, MBI, assistant professor of medicine and medical informatics and director of the Portland Patient Safety Center of Inquiry at the Portland VA Medical Center in Oregon, points out that “the initial exposure to the patient is like a pencil sketch. You start to realize that med rec involves iterative loops of communication between you, the patient, and other knowledge resources (see Figure 1). As you start to pull in more information, you begin to complete your narrative. At the end of hospitalization, you’ve got a vibrant portrait with much more nuance to it. So it can’t be a linear process.”
—Kristine M. Gleason, RPh, clinical quality leader, department of clinical quality and analytics, Northwestern Memorial Hospital, Chicago
The list is dynamic, especially in the ICU setting, says Gleason, where it represents only one point in time.
In a closed system, such as the Veterans Administration or Kaiser Permanente, it’s often easier to establish a patient’s ongoing medications. With an integrated electronic health record (EHR), providers can call up the patient’s list of medications during admittance to the hospital. Verifying those medications remains critical: The health record lists patients’ prescriptions, but that doesn’t always mean they have actually filled or are taking those medications.
At the Kaiser Permanente Southern California site in Santa Clarita, Calif., where hospitalist David W. Wong, MD, works, pharmacists review their medications with patients when they are admitted, provide any needed consultation, then repeat the process at discharge. “So far,” Dr. Wong says, “this has resulted in the best medication reconciliation that we’ve seen.”
Pharmacy Is Key
In 2006, Kenneth Boockvar, MD, of the James J. Peters VA Medical Center in Bronx, N.Y., found in a pre- and post-intervention study that using pharmacists to ferret out and communicate prescribing discrepancies to physicians resulted in lower risk of adverse drug events (ADEs) for patients transferred between the hospital and the nursing home.5 Likewise, Dr. Schnipper and his colleagues found that using pharmacists to conduct medication reviews, counsel patients at discharge, and make follow-up telephone calls to patients was associated with a lower rate of preventable ADEs 30 days after hospital discharge.6
At United Hospital System’s (UHS) Kenosha Medical Center campus in Kenosha, Wis., pharmacists play a key role in generating medication lists for incoming patients. Hospitalist Corey Black, MD, regional medical director for Cogent HMG, says many patients do not recall their medications or the dosages, so UHS utilizes a team approach: If patients come in during evenings or weekends, pharmacists start calling local pharmacies to track down patients’ medication lists. “We also try to have family members bring in any medication containers they can find,” he adds. Due to a Wisconsin state law mandating nursing homes to send medication lists along with patients, generating a list is much easier.
Dr. Tsomides is a physician sponsor of a new med-rec initiative at WakeMed. With a steering committee that includes representatives from stakeholder services (medicine, nursing, pharmacy, administration, etc.), the group plans to hire and train pharmacy techs who will take home medication lists in the ED, lifting that responsibility from physicians’ task lists.
Is IT the Answer?
Would many of the barriers to med rec go away with universal EHR? So far, the literature has not borne out the superiority of using EHR to facilitate better med rec.
Peter Kaboli and colleagues found that the computerized medication record reflected what patients were actually taking for only 5.3% of the 493 VA patients enrolled in a study at the Iowa City VA.7 Kenneth Boockvar and colleagues at the Bronx VA found no difference in the overall incidence of ADEs caused by medication discrepancies between VA patients with an EHR and non-VA patients without an EHR.8 A group of researchers with Partners HealthCare in Boston evaluated a secure, Web-based patient portal to produce more accurate medication lists. The patients using this system had just as many discrepancies between medication lists and self-reporting as those who did not.9
Dr. Lesselroth, who has devised a patient kiosk touch-screen tool for reconciling patients’ medication lists and has faced barriers when implementing said technology, says med rec is much more “organic” than strictly mechanical. “It invokes theories of learning from the cognitive sciences,” he says. “We haven’t actually built tools that help people with their problem representation, with understanding not just how medications reconcile with the prior setting of care, but whether they make clinical sense within the new context of care. That requires a quantum leap in thinking.”
Re-Brand the Message
Drs. Schnipper and Tsomides believe that when The Joint Committee first coined the term “medication reconciliation” and advanced it as a mandate, most providers associated it with a regulatory requirement, and understandably so. Dr. Schnipper says med rec could be improved if providers think about it in the context of accurate orders that translate to greater patient safety. “After all,” he says, “hospitalists are ultimately responsible for the medication orders written for their patients.
“This is not about regulatory requirements,” he continues. “This is about medication safety and transitions of care. You can spend an hour on deciding what dose of Lasix you want to send this patient home on, but if the patient then takes the wrong dose of Lasix because they don’t know what they were supposed to be taking, then all that good medical care is undone.”
The med rec conversation has come full circle, then, as being truly an issue of delivering patient-centered care. (For more on this topic, visit the-hospitalist.org to read “Patient Engagement Critical.”) Rather than focusing on the sometimes-befuddling term of medication reconciliation, providers should see med rec as part of an integrated medication management process that aims to take better care of patients through prevention and treatment, Gleason says.
The med rec issue is about effective communication at every transition of care. And that’s why, says Dr. Schnipper, “Hospitalists should own this process. We don’t have to do the process entirely by ourselves—and shouldn’t. But we are responsible for errors that happen during transitions in care and we should own these initiatives.”
He notes that all six hospitals enrolled in the MARQUIS study have hospitalists at the forefront of their quality-improvement (QI) efforts.
“Medication reconciliation is potentially a high-risk process, and there are no silver bullets” for globally addressing the process, says Dorothea Wild, MD, chief hospitalist at Griffin Hospital, a 160-bed acute care hospital in Derby, Conn.
—Jeffrey Schnipper, MD, MPH, FHM, hospitalist and director of clinical research, Brigham and Women’s Hospital Hospitalist Service, assistant professor of medicine, Harvard Medical School, Boston
Dr. Wild draws a parallel between med rec and blood transfusions. Just as with correct transfusing procedures, “we envision a process where at least two people independently verify what patients’ medications are,” she says. The meds list is started in the ED by nursing staff, is verified by the ED attending, verified again by the admitting team, and triple-checked by the admitting attending. Thus, says Dr. Wild, med rec becomes a shared responsibility.
Dr. Lesselroth wholeheartedly agrees with the approach.
“This is everybody’s job,” he says. “In a larger world view, med rec is all about trying to find a medication regimen that harmonizes with what the patient can do, that improves their probability of adherence, and that also helps us gather information when the patient returns and we re-embrace them in the care model. Theoretically, then, everybody [interfacing with a patient] becomes a clutch player.”
Gretchen Henkel is a freelance writer in California.
Target High-Risk Patients

Pharmacist Kristine M. Gleason, RPh, was the lead author of Northwestern Memorial Hospital’s MATCH (Medications at Transitions and Clinical Handoffs) study, which formed the basis for the recommendations contained in a toolkit generated by the research team (see “Additional Resources,” p. 20).10 Comparing pharmacist and hospitalist medication histories with medication orders, the authors uncovered medication errors for one-third of the study’s 651 patients at admission. The majority of errors (85%) originated in patients’ medication histories. As a result of the study, Gleason explains, the authors recommend that admitting physicians focus on older patients with polypharmacy to reduce medication errors.
Roberta Barber, PharmD, MPH, assistant vice president of pharmacy at Virtua Health in Mount Holly, N.J., oversees pharmacy operations for Virtua’s four hospital campuses. She is involved in med rec/readmission initiatives that focus on such disease states as congestive heart failure that are likely to result in discrepancies. “We can’t have dedicated pharmacists for every unit and every patient, so we have to strategically pick where we can have the most impact.”
References
- Joint Commission on Accreditation of Healthcare Organizations. 2005 Hospital Accreditation Standards. JCO website. Available at: http://www.jointcommissioninternational.org/ JCI-Accredited-Organizations/. Accessed Dec. 7, 2011.
- Bell CM, Brener SS, Gunraj N, et al. Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;306:840-847.
- Greenwald JL, Halasyamani L, Green J, et al. Making inpatient medication patient centered, clinically relevant and implementable: a consensus statement on key principles and necessary first steps. J Hosp Med. 2010;5:477-485.
- Pippins JR, Gandhi TK, Hamann C, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23:1414-1422.
- Boockvar KS, Carlson HL, Giambanco V, et al. Medication reconciliation for reducing drug-discrepancy adverse events. Am J Geriatr Pharmacother. 2006;4:236-243.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166:565-571.
- Kaboli PJ, McClimon JB, Hoth AB, et al. Assessing the accuracy of computerized medication histories. Am J Manag Care. 2004;10(11 Pt 2):872-877.
- Boockvar KS, Livote EE, Goldstein N, et al. Electronic health records and adverse drug events after patient transfer. Qual Saf Health Care. 2010;5:Epub(Aug 19).
- Staroselsky M, Volk LA, Tsurikova R, et al. An effort to improve electronic health record medication list accuracy between visits: patients’ and physicians’ responses. Int J Med Inform. 2008;77:153-160.
- Gleason KM, McDaniel MR, Feinglass J, et al. Results of the Medications at Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25:441-447.
Pharmacist Kristine M. Gleason, RPh, got the chance to personally test her ability to help ED providers with medication reconciliation—known by most in healthcare as “med rec”—when she broke her leg a couple of years ago. No problem, she thought: “I’ve been involved in med-rec efforts for eight-plus years.”
But when asked to provide her current medications, Gleason, who is the clinical quality leader in the department of clinical quality and analytics at Northwestern Memorial Hospital in Chicago, says she was in pain and overwhelmed. “I couldn’t even remember my children’s names, let alone the names and dosages of my aspirin and my thyroid medication,” she says. Moreover, she didn’t carry a list in her wallet because “I’m a pharmacist and I do med rec,” she says.
Gleason’s experience highlights why, six years after The Joint Commission introduced medication reconciliation as National Patient Safety Goal (NPSG) No. 8, hospitals and providers still struggle with the process.1 As a younger patient, Gleason took few medications. But for the majority of elderly inpatients with comorbid conditions, just establishing the patient’s medication list can bring the whole process to a halt; without that foundational list, reconciling other medications becomes problematic.
Although the commission has taken the goals under review and has, since July 1, required compliance with the revised NPSG 03.06.01 (see “Additional Resources,”), hospitalization-associated adverse drug events continue to mount. A recent Canadian study caused a ripple this summer with its findings that patients discharged from acute-care hospitals were at higher risk for unintentional discontinuation of their medications prescribed for chronic diseases than control groups, and those who had an ICU stay are at even higher risk.2
There’s been no shortage of med-rec initiatives in recent years. Medication reconciliation was at the top of the list for ways to prevent errors when the Institute for Healthcare Improvement launched its “5 Million Lives Campaign” in December 2006. SHM weighed in on the issue in 2010 with a consensus statement on key principles and necessary first steps in med rec.3
“This isn’t a new problem,” Gleason says. “Med rec has become more heightened because we have many more medications and complex therapies, more care providers, more specialists—more players, if you will.”
The March launch of the Hospital Readmissions Reduction Program, part of the Centers for Medicaid & Medicare Services’ (CMS) Inpatient Prospective Payment System, will again shine the spotlight on med rec’s role in the prevention of 30-day readmissions. The Hospitalist talked with researchers, pharmacists, and hospitalists about the reasons behind medication discrepancies, and their strategies for addressing mismatches.
Why So Difficult?
The goal of medication reconciliation is to generate and maintain an accurate and coherent record of patients’ medications across all transitions of care, which sounds straightforward enough. But the process involves much more than just checking items off a list, says Jeffrey Schnipper, MD, MPH, FHM, currently the principal investigator for the $1.5 million study funded by the Agency for Healthcare Research and Quality (AHRQ) to research and implement best practices in med rec, dubbed MARQUIS (Multicenter Medication Reconciliation Quality Improvement Study). Those immersed in med rec know that it’s nonlinear, multilayered, and surprisingly complex, requiring partnerships among diverse providers across many domains of care.
“Medication reconciliation gets right at all the weaknesses of our healthcare system,” says Dr. Schnipper, a hospitalist and director of clinical research for the HM service at Brigham and Women’s Hospital (BWH) and assistant professor of medicine at Harvard Medical School, both in Boston. “We have an excellent healthcare system in so many ways, but what we do not do such a good job of is coordination of care across settings, easy transfer of information, and having one person who is responsible for the accuracy of a patient’s health information.”
Dr. Schnipper’s studies attest to the common occurrence of unintentional medical discrepancies, pointing to the need for accurate medication histories, identifying high-risk patients for intensive interventions, and careful med rec at time of discharge.4
Other factors might come into play, says Ted Tsomides, MD, PhD, an attending physician on the HM service at WakeMed Hospital and assistant professor of medicine at the University of North Carolina’s School of Medicine in Raleigh, N.C. For example, he surmises that a “fatigue factor” sets in for some providers. “After five years of working on any initiative, people get worn out and push it to the back burner, unless they are really incentivized to stay on it,” he says.
List Capture
Medication reconciliation is a multifaceted process, and the first step is to gather the history of medications the patient has been taking. Hospitalist Blake J. Lesselroth, MD, MBI, assistant professor of medicine and medical informatics and director of the Portland Patient Safety Center of Inquiry at the Portland VA Medical Center in Oregon, points out that “the initial exposure to the patient is like a pencil sketch. You start to realize that med rec involves iterative loops of communication between you, the patient, and other knowledge resources (see Figure 1). As you start to pull in more information, you begin to complete your narrative. At the end of hospitalization, you’ve got a vibrant portrait with much more nuance to it. So it can’t be a linear process.”
—Kristine M. Gleason, RPh, clinical quality leader, department of clinical quality and analytics, Northwestern Memorial Hospital, Chicago
The list is dynamic, especially in the ICU setting, says Gleason, where it represents only one point in time.
In a closed system, such as the Veterans Administration or Kaiser Permanente, it’s often easier to establish a patient’s ongoing medications. With an integrated electronic health record (EHR), providers can call up the patient’s list of medications during admittance to the hospital. Verifying those medications remains critical: The health record lists patients’ prescriptions, but that doesn’t always mean they have actually filled or are taking those medications.
At the Kaiser Permanente Southern California site in Santa Clarita, Calif., where hospitalist David W. Wong, MD, works, pharmacists review their medications with patients when they are admitted, provide any needed consultation, then repeat the process at discharge. “So far,” Dr. Wong says, “this has resulted in the best medication reconciliation that we’ve seen.”
Pharmacy Is Key
In 2006, Kenneth Boockvar, MD, of the James J. Peters VA Medical Center in Bronx, N.Y., found in a pre- and post-intervention study that using pharmacists to ferret out and communicate prescribing discrepancies to physicians resulted in lower risk of adverse drug events (ADEs) for patients transferred between the hospital and the nursing home.5 Likewise, Dr. Schnipper and his colleagues found that using pharmacists to conduct medication reviews, counsel patients at discharge, and make follow-up telephone calls to patients was associated with a lower rate of preventable ADEs 30 days after hospital discharge.6
At United Hospital System’s (UHS) Kenosha Medical Center campus in Kenosha, Wis., pharmacists play a key role in generating medication lists for incoming patients. Hospitalist Corey Black, MD, regional medical director for Cogent HMG, says many patients do not recall their medications or the dosages, so UHS utilizes a team approach: If patients come in during evenings or weekends, pharmacists start calling local pharmacies to track down patients’ medication lists. “We also try to have family members bring in any medication containers they can find,” he adds. Due to a Wisconsin state law mandating nursing homes to send medication lists along with patients, generating a list is much easier.
Dr. Tsomides is a physician sponsor of a new med-rec initiative at WakeMed. With a steering committee that includes representatives from stakeholder services (medicine, nursing, pharmacy, administration, etc.), the group plans to hire and train pharmacy techs who will take home medication lists in the ED, lifting that responsibility from physicians’ task lists.
Is IT the Answer?
Would many of the barriers to med rec go away with universal EHR? So far, the literature has not borne out the superiority of using EHR to facilitate better med rec.
Peter Kaboli and colleagues found that the computerized medication record reflected what patients were actually taking for only 5.3% of the 493 VA patients enrolled in a study at the Iowa City VA.7 Kenneth Boockvar and colleagues at the Bronx VA found no difference in the overall incidence of ADEs caused by medication discrepancies between VA patients with an EHR and non-VA patients without an EHR.8 A group of researchers with Partners HealthCare in Boston evaluated a secure, Web-based patient portal to produce more accurate medication lists. The patients using this system had just as many discrepancies between medication lists and self-reporting as those who did not.9
Dr. Lesselroth, who has devised a patient kiosk touch-screen tool for reconciling patients’ medication lists and has faced barriers when implementing said technology, says med rec is much more “organic” than strictly mechanical. “It invokes theories of learning from the cognitive sciences,” he says. “We haven’t actually built tools that help people with their problem representation, with understanding not just how medications reconcile with the prior setting of care, but whether they make clinical sense within the new context of care. That requires a quantum leap in thinking.”
Re-Brand the Message
Drs. Schnipper and Tsomides believe that when The Joint Committee first coined the term “medication reconciliation” and advanced it as a mandate, most providers associated it with a regulatory requirement, and understandably so. Dr. Schnipper says med rec could be improved if providers think about it in the context of accurate orders that translate to greater patient safety. “After all,” he says, “hospitalists are ultimately responsible for the medication orders written for their patients.
“This is not about regulatory requirements,” he continues. “This is about medication safety and transitions of care. You can spend an hour on deciding what dose of Lasix you want to send this patient home on, but if the patient then takes the wrong dose of Lasix because they don’t know what they were supposed to be taking, then all that good medical care is undone.”
The med rec conversation has come full circle, then, as being truly an issue of delivering patient-centered care. (For more on this topic, visit the-hospitalist.org to read “Patient Engagement Critical.”) Rather than focusing on the sometimes-befuddling term of medication reconciliation, providers should see med rec as part of an integrated medication management process that aims to take better care of patients through prevention and treatment, Gleason says.
The med rec issue is about effective communication at every transition of care. And that’s why, says Dr. Schnipper, “Hospitalists should own this process. We don’t have to do the process entirely by ourselves—and shouldn’t. But we are responsible for errors that happen during transitions in care and we should own these initiatives.”
He notes that all six hospitals enrolled in the MARQUIS study have hospitalists at the forefront of their quality-improvement (QI) efforts.
“Medication reconciliation is potentially a high-risk process, and there are no silver bullets” for globally addressing the process, says Dorothea Wild, MD, chief hospitalist at Griffin Hospital, a 160-bed acute care hospital in Derby, Conn.
—Jeffrey Schnipper, MD, MPH, FHM, hospitalist and director of clinical research, Brigham and Women’s Hospital Hospitalist Service, assistant professor of medicine, Harvard Medical School, Boston
Dr. Wild draws a parallel between med rec and blood transfusions. Just as with correct transfusing procedures, “we envision a process where at least two people independently verify what patients’ medications are,” she says. The meds list is started in the ED by nursing staff, is verified by the ED attending, verified again by the admitting team, and triple-checked by the admitting attending. Thus, says Dr. Wild, med rec becomes a shared responsibility.
Dr. Lesselroth wholeheartedly agrees with the approach.
“This is everybody’s job,” he says. “In a larger world view, med rec is all about trying to find a medication regimen that harmonizes with what the patient can do, that improves their probability of adherence, and that also helps us gather information when the patient returns and we re-embrace them in the care model. Theoretically, then, everybody [interfacing with a patient] becomes a clutch player.”
Gretchen Henkel is a freelance writer in California.
Target High-Risk Patients
Pharmacist Kristine M. Gleason, RPh, was the lead author of Northwestern Memorial Hospital’s MATCH (Medications at Transitions and Clinical Handoffs) study, which formed the basis for the recommendations contained in a toolkit generated by the research team (see “Additional Resources,” p. 20).10 Comparing pharmacist and hospitalist medication histories with medication orders, the authors uncovered medication errors for one-third of the study’s 651 patients at admission. The majority of errors (85%) originated in patients’ medication histories. As a result of the study, Gleason explains, the authors recommend that admitting physicians focus on older patients with polypharmacy to reduce medication errors.
Roberta Barber, PharmD, MPH, assistant vice president of pharmacy at Virtua Health in Mount Holly, N.J., oversees pharmacy operations for Virtua’s four hospital campuses. She is involved in med rec/readmission initiatives that focus on such disease states as congestive heart failure that are likely to result in discrepancies. “We can’t have dedicated pharmacists for every unit and every patient, so we have to strategically pick where we can have the most impact.”
References
- Joint Commission on Accreditation of Healthcare Organizations. 2005 Hospital Accreditation Standards. JCO website. Available at: http://www.jointcommissioninternational.org/ JCI-Accredited-Organizations/. Accessed Dec. 7, 2011.
- Bell CM, Brener SS, Gunraj N, et al. Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;306:840-847.
- Greenwald JL, Halasyamani L, Green J, et al. Making inpatient medication patient centered, clinically relevant and implementable: a consensus statement on key principles and necessary first steps. J Hosp Med. 2010;5:477-485.
- Pippins JR, Gandhi TK, Hamann C, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23:1414-1422.
- Boockvar KS, Carlson HL, Giambanco V, et al. Medication reconciliation for reducing drug-discrepancy adverse events. Am J Geriatr Pharmacother. 2006;4:236-243.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166:565-571.
- Kaboli PJ, McClimon JB, Hoth AB, et al. Assessing the accuracy of computerized medication histories. Am J Manag Care. 2004;10(11 Pt 2):872-877.
- Boockvar KS, Livote EE, Goldstein N, et al. Electronic health records and adverse drug events after patient transfer. Qual Saf Health Care. 2010;5:Epub(Aug 19).
- Staroselsky M, Volk LA, Tsurikova R, et al. An effort to improve electronic health record medication list accuracy between visits: patients’ and physicians’ responses. Int J Med Inform. 2008;77:153-160.
- Gleason KM, McDaniel MR, Feinglass J, et al. Results of the Medications at Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25:441-447.
Pharmacist Kristine M. Gleason, RPh, got the chance to personally test her ability to help ED providers with medication reconciliation—known by most in healthcare as “med rec”—when she broke her leg a couple of years ago. No problem, she thought: “I’ve been involved in med-rec efforts for eight-plus years.”
But when asked to provide her current medications, Gleason, who is the clinical quality leader in the department of clinical quality and analytics at Northwestern Memorial Hospital in Chicago, says she was in pain and overwhelmed. “I couldn’t even remember my children’s names, let alone the names and dosages of my aspirin and my thyroid medication,” she says. Moreover, she didn’t carry a list in her wallet because “I’m a pharmacist and I do med rec,” she says.
Gleason’s experience highlights why, six years after The Joint Commission introduced medication reconciliation as National Patient Safety Goal (NPSG) No. 8, hospitals and providers still struggle with the process.1 As a younger patient, Gleason took few medications. But for the majority of elderly inpatients with comorbid conditions, just establishing the patient’s medication list can bring the whole process to a halt; without that foundational list, reconciling other medications becomes problematic.
Although the commission has taken the goals under review and has, since July 1, required compliance with the revised NPSG 03.06.01 (see “Additional Resources,”), hospitalization-associated adverse drug events continue to mount. A recent Canadian study caused a ripple this summer with its findings that patients discharged from acute-care hospitals were at higher risk for unintentional discontinuation of their medications prescribed for chronic diseases than control groups, and those who had an ICU stay are at even higher risk.2
There’s been no shortage of med-rec initiatives in recent years. Medication reconciliation was at the top of the list for ways to prevent errors when the Institute for Healthcare Improvement launched its “5 Million Lives Campaign” in December 2006. SHM weighed in on the issue in 2010 with a consensus statement on key principles and necessary first steps in med rec.3
“This isn’t a new problem,” Gleason says. “Med rec has become more heightened because we have many more medications and complex therapies, more care providers, more specialists—more players, if you will.”
The March launch of the Hospital Readmissions Reduction Program, part of the Centers for Medicaid & Medicare Services’ (CMS) Inpatient Prospective Payment System, will again shine the spotlight on med rec’s role in the prevention of 30-day readmissions. The Hospitalist talked with researchers, pharmacists, and hospitalists about the reasons behind medication discrepancies, and their strategies for addressing mismatches.
Why So Difficult?
The goal of medication reconciliation is to generate and maintain an accurate and coherent record of patients’ medications across all transitions of care, which sounds straightforward enough. But the process involves much more than just checking items off a list, says Jeffrey Schnipper, MD, MPH, FHM, currently the principal investigator for the $1.5 million study funded by the Agency for Healthcare Research and Quality (AHRQ) to research and implement best practices in med rec, dubbed MARQUIS (Multicenter Medication Reconciliation Quality Improvement Study). Those immersed in med rec know that it’s nonlinear, multilayered, and surprisingly complex, requiring partnerships among diverse providers across many domains of care.
“Medication reconciliation gets right at all the weaknesses of our healthcare system,” says Dr. Schnipper, a hospitalist and director of clinical research for the HM service at Brigham and Women’s Hospital (BWH) and assistant professor of medicine at Harvard Medical School, both in Boston. “We have an excellent healthcare system in so many ways, but what we do not do such a good job of is coordination of care across settings, easy transfer of information, and having one person who is responsible for the accuracy of a patient’s health information.”
Dr. Schnipper’s studies attest to the common occurrence of unintentional medical discrepancies, pointing to the need for accurate medication histories, identifying high-risk patients for intensive interventions, and careful med rec at time of discharge.4
Other factors might come into play, says Ted Tsomides, MD, PhD, an attending physician on the HM service at WakeMed Hospital and assistant professor of medicine at the University of North Carolina’s School of Medicine in Raleigh, N.C. For example, he surmises that a “fatigue factor” sets in for some providers. “After five years of working on any initiative, people get worn out and push it to the back burner, unless they are really incentivized to stay on it,” he says.
List Capture
Medication reconciliation is a multifaceted process, and the first step is to gather the history of medications the patient has been taking. Hospitalist Blake J. Lesselroth, MD, MBI, assistant professor of medicine and medical informatics and director of the Portland Patient Safety Center of Inquiry at the Portland VA Medical Center in Oregon, points out that “the initial exposure to the patient is like a pencil sketch. You start to realize that med rec involves iterative loops of communication between you, the patient, and other knowledge resources (see Figure 1). As you start to pull in more information, you begin to complete your narrative. At the end of hospitalization, you’ve got a vibrant portrait with much more nuance to it. So it can’t be a linear process.”
—Kristine M. Gleason, RPh, clinical quality leader, department of clinical quality and analytics, Northwestern Memorial Hospital, Chicago
The list is dynamic, especially in the ICU setting, says Gleason, where it represents only one point in time.
In a closed system, such as the Veterans Administration or Kaiser Permanente, it’s often easier to establish a patient’s ongoing medications. With an integrated electronic health record (EHR), providers can call up the patient’s list of medications during admittance to the hospital. Verifying those medications remains critical: The health record lists patients’ prescriptions, but that doesn’t always mean they have actually filled or are taking those medications.
At the Kaiser Permanente Southern California site in Santa Clarita, Calif., where hospitalist David W. Wong, MD, works, pharmacists review their medications with patients when they are admitted, provide any needed consultation, then repeat the process at discharge. “So far,” Dr. Wong says, “this has resulted in the best medication reconciliation that we’ve seen.”
Pharmacy Is Key
In 2006, Kenneth Boockvar, MD, of the James J. Peters VA Medical Center in Bronx, N.Y., found in a pre- and post-intervention study that using pharmacists to ferret out and communicate prescribing discrepancies to physicians resulted in lower risk of adverse drug events (ADEs) for patients transferred between the hospital and the nursing home.5 Likewise, Dr. Schnipper and his colleagues found that using pharmacists to conduct medication reviews, counsel patients at discharge, and make follow-up telephone calls to patients was associated with a lower rate of preventable ADEs 30 days after hospital discharge.6
At United Hospital System’s (UHS) Kenosha Medical Center campus in Kenosha, Wis., pharmacists play a key role in generating medication lists for incoming patients. Hospitalist Corey Black, MD, regional medical director for Cogent HMG, says many patients do not recall their medications or the dosages, so UHS utilizes a team approach: If patients come in during evenings or weekends, pharmacists start calling local pharmacies to track down patients’ medication lists. “We also try to have family members bring in any medication containers they can find,” he adds. Due to a Wisconsin state law mandating nursing homes to send medication lists along with patients, generating a list is much easier.
Dr. Tsomides is a physician sponsor of a new med-rec initiative at WakeMed. With a steering committee that includes representatives from stakeholder services (medicine, nursing, pharmacy, administration, etc.), the group plans to hire and train pharmacy techs who will take home medication lists in the ED, lifting that responsibility from physicians’ task lists.
Is IT the Answer?
Would many of the barriers to med rec go away with universal EHR? So far, the literature has not borne out the superiority of using EHR to facilitate better med rec.
Peter Kaboli and colleagues found that the computerized medication record reflected what patients were actually taking for only 5.3% of the 493 VA patients enrolled in a study at the Iowa City VA.7 Kenneth Boockvar and colleagues at the Bronx VA found no difference in the overall incidence of ADEs caused by medication discrepancies between VA patients with an EHR and non-VA patients without an EHR.8 A group of researchers with Partners HealthCare in Boston evaluated a secure, Web-based patient portal to produce more accurate medication lists. The patients using this system had just as many discrepancies between medication lists and self-reporting as those who did not.9
Dr. Lesselroth, who has devised a patient kiosk touch-screen tool for reconciling patients’ medication lists and has faced barriers when implementing said technology, says med rec is much more “organic” than strictly mechanical. “It invokes theories of learning from the cognitive sciences,” he says. “We haven’t actually built tools that help people with their problem representation, with understanding not just how medications reconcile with the prior setting of care, but whether they make clinical sense within the new context of care. That requires a quantum leap in thinking.”
Re-Brand the Message
Drs. Schnipper and Tsomides believe that when The Joint Committee first coined the term “medication reconciliation” and advanced it as a mandate, most providers associated it with a regulatory requirement, and understandably so. Dr. Schnipper says med rec could be improved if providers think about it in the context of accurate orders that translate to greater patient safety. “After all,” he says, “hospitalists are ultimately responsible for the medication orders written for their patients.
“This is not about regulatory requirements,” he continues. “This is about medication safety and transitions of care. You can spend an hour on deciding what dose of Lasix you want to send this patient home on, but if the patient then takes the wrong dose of Lasix because they don’t know what they were supposed to be taking, then all that good medical care is undone.”
The med rec conversation has come full circle, then, as being truly an issue of delivering patient-centered care. (For more on this topic, visit the-hospitalist.org to read “Patient Engagement Critical.”) Rather than focusing on the sometimes-befuddling term of medication reconciliation, providers should see med rec as part of an integrated medication management process that aims to take better care of patients through prevention and treatment, Gleason says.
The med rec issue is about effective communication at every transition of care. And that’s why, says Dr. Schnipper, “Hospitalists should own this process. We don’t have to do the process entirely by ourselves—and shouldn’t. But we are responsible for errors that happen during transitions in care and we should own these initiatives.”
He notes that all six hospitals enrolled in the MARQUIS study have hospitalists at the forefront of their quality-improvement (QI) efforts.
“Medication reconciliation is potentially a high-risk process, and there are no silver bullets” for globally addressing the process, says Dorothea Wild, MD, chief hospitalist at Griffin Hospital, a 160-bed acute care hospital in Derby, Conn.
—Jeffrey Schnipper, MD, MPH, FHM, hospitalist and director of clinical research, Brigham and Women’s Hospital Hospitalist Service, assistant professor of medicine, Harvard Medical School, Boston
Dr. Wild draws a parallel between med rec and blood transfusions. Just as with correct transfusing procedures, “we envision a process where at least two people independently verify what patients’ medications are,” she says. The meds list is started in the ED by nursing staff, is verified by the ED attending, verified again by the admitting team, and triple-checked by the admitting attending. Thus, says Dr. Wild, med rec becomes a shared responsibility.
Dr. Lesselroth wholeheartedly agrees with the approach.
“This is everybody’s job,” he says. “In a larger world view, med rec is all about trying to find a medication regimen that harmonizes with what the patient can do, that improves their probability of adherence, and that also helps us gather information when the patient returns and we re-embrace them in the care model. Theoretically, then, everybody [interfacing with a patient] becomes a clutch player.”
Gretchen Henkel is a freelance writer in California.
Target High-Risk Patients
Pharmacist Kristine M. Gleason, RPh, was the lead author of Northwestern Memorial Hospital’s MATCH (Medications at Transitions and Clinical Handoffs) study, which formed the basis for the recommendations contained in a toolkit generated by the research team (see “Additional Resources,” p. 20).10 Comparing pharmacist and hospitalist medication histories with medication orders, the authors uncovered medication errors for one-third of the study’s 651 patients at admission. The majority of errors (85%) originated in patients’ medication histories. As a result of the study, Gleason explains, the authors recommend that admitting physicians focus on older patients with polypharmacy to reduce medication errors.
Roberta Barber, PharmD, MPH, assistant vice president of pharmacy at Virtua Health in Mount Holly, N.J., oversees pharmacy operations for Virtua’s four hospital campuses. She is involved in med rec/readmission initiatives that focus on such disease states as congestive heart failure that are likely to result in discrepancies. “We can’t have dedicated pharmacists for every unit and every patient, so we have to strategically pick where we can have the most impact.”
References
- Joint Commission on Accreditation of Healthcare Organizations. 2005 Hospital Accreditation Standards. JCO website. Available at: http://www.jointcommissioninternational.org/ JCI-Accredited-Organizations/. Accessed Dec. 7, 2011.
- Bell CM, Brener SS, Gunraj N, et al. Association of ICU or hospital admission with unintentional discontinuation of medications for chronic diseases. JAMA. 2011;306:840-847.
- Greenwald JL, Halasyamani L, Green J, et al. Making inpatient medication patient centered, clinically relevant and implementable: a consensus statement on key principles and necessary first steps. J Hosp Med. 2010;5:477-485.
- Pippins JR, Gandhi TK, Hamann C, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23:1414-1422.
- Boockvar KS, Carlson HL, Giambanco V, et al. Medication reconciliation for reducing drug-discrepancy adverse events. Am J Geriatr Pharmacother. 2006;4:236-243.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166:565-571.
- Kaboli PJ, McClimon JB, Hoth AB, et al. Assessing the accuracy of computerized medication histories. Am J Manag Care. 2004;10(11 Pt 2):872-877.
- Boockvar KS, Livote EE, Goldstein N, et al. Electronic health records and adverse drug events after patient transfer. Qual Saf Health Care. 2010;5:Epub(Aug 19).
- Staroselsky M, Volk LA, Tsurikova R, et al. An effort to improve electronic health record medication list accuracy between visits: patients’ and physicians’ responses. Int J Med Inform. 2008;77:153-160.
- Gleason KM, McDaniel MR, Feinglass J, et al. Results of the Medications at Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25:441-447.
Policy Corner: An Inside Look at the Most Pressing Policy Issues
In early November, the Institute of Medicine (IOM) released a report on the current status of health information technology (HIT). Although the report was developed at the request of the Office of the National Coordinator (ONC), the arm within the Department of Health and Human Services (HHS) responsible for promoting the use of HIT, not everything in the report was positive—and could leave the impression that HIT is not quite as successful as some think.
The report recommends that the ONC should work with the private and public sectors to make comparative user experiences across vendors publicly available.
Many hospitalists have developed significant expertise with HIT, played significant roles in its effective implementation and use, and are acutely aware of implementation pitfalls. This practical experience could be very helpful in working with the ONC to develop solutions. It is for this reason that hospitalists should reach out to the ONC and offer their expertise instead of waiting for the ONC to act.
The report, “Patient Safety and Health IT: Building Safer Systems for Better Care,” did praise HIT’s potential for eventual cost savings and increased patient safety but stopped short of being a ringing endorsement of the pace HM is taking toward implementation initiatives, such as meaningful use. An overall theme of the report is that greater oversight of HIT is needed to protect patients from potential medical errors associated with its use.
A few of the recommendations given by the IOM to achieve a greater level of safety range from the establishment of a mechanism for vendors and users to report health IT-related deaths, injuries, or unsafe conditions to possible FDA regulation of the systems themselves.
Information-sharing and reporting in a nonpunitive environment, as recommended by the IOM, would go a long way when it comes to remedying or avoiding IT-related problems, and hospitalists probably have some ideas about how this could be done.
Unfortunately, IT vendor contracts often prevent the open sharing of information, so working toward doing away with such contract terms might be a worthy step before making a push toward overall FDA regulation and the unintended consequences that may come with it.
At first glance, FDA regulation seems like the easiest solution because the FDA can theoretically control every aspect of what might go wrong with HIT, but at what cost would such regulation come? FDA approval can be long, complicated and expensive. The whole process could result in cutting-edge technology becoming outdated by the time approval is granted or innovations being overlooked entirely because of a negative cost-benefit analysis. Furthermore, the expense associated with FDA approval could in turn increase the cost of already costly electronic health records (EHR).
Despite the myriad problems that can arise if implementation moves too fast, HIT holds promise and has shown success when done well.
SHM is currently working to position hospitalists as a resource for the ONC, so hospitalists with expertise in this area should not hesitate to come forward with ideas on how to make HIT work better and more safely. HIT is not going to go away, so the best option is to help make it better.
In early November, the Institute of Medicine (IOM) released a report on the current status of health information technology (HIT). Although the report was developed at the request of the Office of the National Coordinator (ONC), the arm within the Department of Health and Human Services (HHS) responsible for promoting the use of HIT, not everything in the report was positive—and could leave the impression that HIT is not quite as successful as some think.
The report recommends that the ONC should work with the private and public sectors to make comparative user experiences across vendors publicly available.
Many hospitalists have developed significant expertise with HIT, played significant roles in its effective implementation and use, and are acutely aware of implementation pitfalls. This practical experience could be very helpful in working with the ONC to develop solutions. It is for this reason that hospitalists should reach out to the ONC and offer their expertise instead of waiting for the ONC to act.
The report, “Patient Safety and Health IT: Building Safer Systems for Better Care,” did praise HIT’s potential for eventual cost savings and increased patient safety but stopped short of being a ringing endorsement of the pace HM is taking toward implementation initiatives, such as meaningful use. An overall theme of the report is that greater oversight of HIT is needed to protect patients from potential medical errors associated with its use.
A few of the recommendations given by the IOM to achieve a greater level of safety range from the establishment of a mechanism for vendors and users to report health IT-related deaths, injuries, or unsafe conditions to possible FDA regulation of the systems themselves.
Information-sharing and reporting in a nonpunitive environment, as recommended by the IOM, would go a long way when it comes to remedying or avoiding IT-related problems, and hospitalists probably have some ideas about how this could be done.
Unfortunately, IT vendor contracts often prevent the open sharing of information, so working toward doing away with such contract terms might be a worthy step before making a push toward overall FDA regulation and the unintended consequences that may come with it.
At first glance, FDA regulation seems like the easiest solution because the FDA can theoretically control every aspect of what might go wrong with HIT, but at what cost would such regulation come? FDA approval can be long, complicated and expensive. The whole process could result in cutting-edge technology becoming outdated by the time approval is granted or innovations being overlooked entirely because of a negative cost-benefit analysis. Furthermore, the expense associated with FDA approval could in turn increase the cost of already costly electronic health records (EHR).
Despite the myriad problems that can arise if implementation moves too fast, HIT holds promise and has shown success when done well.
SHM is currently working to position hospitalists as a resource for the ONC, so hospitalists with expertise in this area should not hesitate to come forward with ideas on how to make HIT work better and more safely. HIT is not going to go away, so the best option is to help make it better.
In early November, the Institute of Medicine (IOM) released a report on the current status of health information technology (HIT). Although the report was developed at the request of the Office of the National Coordinator (ONC), the arm within the Department of Health and Human Services (HHS) responsible for promoting the use of HIT, not everything in the report was positive—and could leave the impression that HIT is not quite as successful as some think.
The report recommends that the ONC should work with the private and public sectors to make comparative user experiences across vendors publicly available.
Many hospitalists have developed significant expertise with HIT, played significant roles in its effective implementation and use, and are acutely aware of implementation pitfalls. This practical experience could be very helpful in working with the ONC to develop solutions. It is for this reason that hospitalists should reach out to the ONC and offer their expertise instead of waiting for the ONC to act.
The report, “Patient Safety and Health IT: Building Safer Systems for Better Care,” did praise HIT’s potential for eventual cost savings and increased patient safety but stopped short of being a ringing endorsement of the pace HM is taking toward implementation initiatives, such as meaningful use. An overall theme of the report is that greater oversight of HIT is needed to protect patients from potential medical errors associated with its use.
A few of the recommendations given by the IOM to achieve a greater level of safety range from the establishment of a mechanism for vendors and users to report health IT-related deaths, injuries, or unsafe conditions to possible FDA regulation of the systems themselves.
Information-sharing and reporting in a nonpunitive environment, as recommended by the IOM, would go a long way when it comes to remedying or avoiding IT-related problems, and hospitalists probably have some ideas about how this could be done.
Unfortunately, IT vendor contracts often prevent the open sharing of information, so working toward doing away with such contract terms might be a worthy step before making a push toward overall FDA regulation and the unintended consequences that may come with it.
At first glance, FDA regulation seems like the easiest solution because the FDA can theoretically control every aspect of what might go wrong with HIT, but at what cost would such regulation come? FDA approval can be long, complicated and expensive. The whole process could result in cutting-edge technology becoming outdated by the time approval is granted or innovations being overlooked entirely because of a negative cost-benefit analysis. Furthermore, the expense associated with FDA approval could in turn increase the cost of already costly electronic health records (EHR).
Despite the myriad problems that can arise if implementation moves too fast, HIT holds promise and has shown success when done well.
SHM is currently working to position hospitalists as a resource for the ONC, so hospitalists with expertise in this area should not hesitate to come forward with ideas on how to make HIT work better and more safely. HIT is not going to go away, so the best option is to help make it better.
IOM Report Outlines Health IT Concerns
The Institute of Medicine in November issued a new report, “Patient Safety and Health IT (HIT): Building Safer Systems for Better Care,” which identifies potential harm that could stem from a digital healthcare system and proposes 10 recommendations. Many of the suggestions are directed at the U.S. Secretary of Health and Human Services, urging the office to work with the private sector and research groups on patient safety, ensure the free exchange of information on healthcare information technology (HIT) issues, and create a process for reporting HIT-related deaths and injuries.
“Concerns about potential harm are emerging as providers increasingly rely on electronic medical records, secure patient portals, and other technologies to deliver care,” the report states, but there is a lack of published research quantifying the risks. For more on the HIT report, check out the Policy Corner.
The Institute of Medicine in November issued a new report, “Patient Safety and Health IT (HIT): Building Safer Systems for Better Care,” which identifies potential harm that could stem from a digital healthcare system and proposes 10 recommendations. Many of the suggestions are directed at the U.S. Secretary of Health and Human Services, urging the office to work with the private sector and research groups on patient safety, ensure the free exchange of information on healthcare information technology (HIT) issues, and create a process for reporting HIT-related deaths and injuries.
“Concerns about potential harm are emerging as providers increasingly rely on electronic medical records, secure patient portals, and other technologies to deliver care,” the report states, but there is a lack of published research quantifying the risks. For more on the HIT report, check out the Policy Corner.
The Institute of Medicine in November issued a new report, “Patient Safety and Health IT (HIT): Building Safer Systems for Better Care,” which identifies potential harm that could stem from a digital healthcare system and proposes 10 recommendations. Many of the suggestions are directed at the U.S. Secretary of Health and Human Services, urging the office to work with the private sector and research groups on patient safety, ensure the free exchange of information on healthcare information technology (HIT) issues, and create a process for reporting HIT-related deaths and injuries.
“Concerns about potential harm are emerging as providers increasingly rely on electronic medical records, secure patient portals, and other technologies to deliver care,” the report states, but there is a lack of published research quantifying the risks. For more on the HIT report, check out the Policy Corner.
Six Ways You Can Help Reduce HAIs in Your Hospital
- Encourage good hand hygiene. This should be obvious, but hospitals are struggling to achieve compliance rates of even 50%. One study has found significant improvement by appealing to medical providers’ altruistic sense: “Hand hygiene prevents patients from catching diseases.”1
- Embrace checklists. If they work for airline pilots, they can work for you. Study after study has supported their effectiveness, particularly in preventing CLABSIs and CAUTIs when well-integrated into a multifaceted approach.
- Bundle up. A bundled approach that emphasized proper hand hygiene, disinfection, catheter avoidance, and timely removal cut CLABSI rates by morethan half, on average, in Veterans Administration ICUs throughout the U.S.2
- Team up. For a C. diff-reduction effort at Kaiser Permanente Medical Center in Santa Clara, Calif., success meant getting doctors, nurses, specialists, and administrators on board, both to brainstorm and to sustain momentum.
- Be a role model. Consistently following HAI-prevention protocols, such as contact precautions, can make adherence contagious—in a very good way.
- Be an innovator. By virtue of being ubiquitous in inpatient wards, hospitalists know what works and what doesn’t; your insight can be particularly valuable for a team-based, HAI-reduction effort.
References
- Grant AM, Hofmann DA. It’s not all about me: Motivating hospital hand hygiene by focusing on patients. Psychol Sci. 2011;22:1494-1499.
- Render ML, Hasselbeck R, Freyberg RW, Hofer TP, et al. Reduction of central line infections in Veterans Administration intensive care units: an observational cohort using a central infrastructure to support learning and improvement. BMJ Qual Saf. 2011;20(8):725-732.
- Encourage good hand hygiene. This should be obvious, but hospitals are struggling to achieve compliance rates of even 50%. One study has found significant improvement by appealing to medical providers’ altruistic sense: “Hand hygiene prevents patients from catching diseases.”1
- Embrace checklists. If they work for airline pilots, they can work for you. Study after study has supported their effectiveness, particularly in preventing CLABSIs and CAUTIs when well-integrated into a multifaceted approach.
- Bundle up. A bundled approach that emphasized proper hand hygiene, disinfection, catheter avoidance, and timely removal cut CLABSI rates by morethan half, on average, in Veterans Administration ICUs throughout the U.S.2
- Team up. For a C. diff-reduction effort at Kaiser Permanente Medical Center in Santa Clara, Calif., success meant getting doctors, nurses, specialists, and administrators on board, both to brainstorm and to sustain momentum.
- Be a role model. Consistently following HAI-prevention protocols, such as contact precautions, can make adherence contagious—in a very good way.
- Be an innovator. By virtue of being ubiquitous in inpatient wards, hospitalists know what works and what doesn’t; your insight can be particularly valuable for a team-based, HAI-reduction effort.
References
- Grant AM, Hofmann DA. It’s not all about me: Motivating hospital hand hygiene by focusing on patients. Psychol Sci. 2011;22:1494-1499.
- Render ML, Hasselbeck R, Freyberg RW, Hofer TP, et al. Reduction of central line infections in Veterans Administration intensive care units: an observational cohort using a central infrastructure to support learning and improvement. BMJ Qual Saf. 2011;20(8):725-732.
- Encourage good hand hygiene. This should be obvious, but hospitals are struggling to achieve compliance rates of even 50%. One study has found significant improvement by appealing to medical providers’ altruistic sense: “Hand hygiene prevents patients from catching diseases.”1
- Embrace checklists. If they work for airline pilots, they can work for you. Study after study has supported their effectiveness, particularly in preventing CLABSIs and CAUTIs when well-integrated into a multifaceted approach.
- Bundle up. A bundled approach that emphasized proper hand hygiene, disinfection, catheter avoidance, and timely removal cut CLABSI rates by morethan half, on average, in Veterans Administration ICUs throughout the U.S.2
- Team up. For a C. diff-reduction effort at Kaiser Permanente Medical Center in Santa Clara, Calif., success meant getting doctors, nurses, specialists, and administrators on board, both to brainstorm and to sustain momentum.
- Be a role model. Consistently following HAI-prevention protocols, such as contact precautions, can make adherence contagious—in a very good way.
- Be an innovator. By virtue of being ubiquitous in inpatient wards, hospitalists know what works and what doesn’t; your insight can be particularly valuable for a team-based, HAI-reduction effort.
References
- Grant AM, Hofmann DA. It’s not all about me: Motivating hospital hand hygiene by focusing on patients. Psychol Sci. 2011;22:1494-1499.
- Render ML, Hasselbeck R, Freyberg RW, Hofer TP, et al. Reduction of central line infections in Veterans Administration intensive care units: an observational cohort using a central infrastructure to support learning and improvement. BMJ Qual Saf. 2011;20(8):725-732.
Gut Reaction
At 480-bed Emory University Hospital Midtown in Atlanta, the physicians and staff seemingly are doing all the right things to foil one of hospital’s archenemies: Clostridium difficile. The bacteria, better known as C. diff, is responsible for a sharp rise in hospital-acquired infections over the past decade, rivaling even MRSA.
In 2010, Emory Midtown launched a campaign to boost awareness of the importance of hand washing before and after treating patients infected with C. diff and those likely to be infected. They also began using the polymerase-chain-reaction-based assay to detect the bacteria, a test with much higher sensitivity that helps to more efficiently identify those infected so control measures can be more prompt and targeted. They use a hypochlorite mixture to clean the rooms of those infected, which is considered a must. And a committee monitors the use of antibiotics to prevent overuse—often the scapegoat for the rise of the hard-to-kill bacteria.
Still, at Emory, the rate of C. diff is about the same as the national average, says hospitalist Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine and a member of the antimicrobial stewardship and infectious disease control committees at Midtown. While Dr. Kobaidze says her institution is doing a good job of trying to keep C. diff under control, she thinks hospitalists can do more.
“My feeling is that we are not as involved as we’re supposed to be,” she says. “I think we need to be a little bit more proactive, be involved in committees and research activities across the hospital.”
—Kevin Kavanagh, MD, founder, Health Watch USA
You Are Not Alone
The experience at Emory Midtown is far from unusual—healthcare facilities, and hospitalists, across the country have seen healthcare-related C. diff cases more than double since 2001 to between 400,000 and 500,000 a year, says Carolyn Gould, MD, a medical epidemiologist in the division of healthcare quality promotion at the Centers for Disease Control and Prevention (CDC) in Atlanta.
Hospitalists, whether they realize it or not, are intimately involved in how well the C. diff outbreak is controlled. Infectious-disease (ID) specialists say hospitalists are perfectly situated to make an impact in efforts to help curb the outbreak.
“Hospitalists are critical to this effort,” Dr. Gould says. “They’re in the hospital day in and day out, and they’re constantly interacting with the patients, staff, and administration. They’re often the first on the scene to see a patient who might have suddenly developed diarrhea; they’re the first to react. I think they’re in a prime position to play a leadership role to prevent C. diff infections.”
They’re also situated well to work with infection-control experts on antimicrobial stewardship programs, she says.
“I look at hospitalists just like I would have looked at internists managing their own patients 15 years ago,” says Stuart Cohen, MD, an ID expert with the University of California at Davis and a fellow with the Infectious Diseases Society of America who was lead author of the latest published IDSA guidelines on C. diff treatment. “And so they’re the first-line people.”
continued below...
Mayo Shows How a Simple Step Can Make Big Difference in C. Diff

Sometimes even when it comes to a huge problem like widespread bacterial infections, simplicity is best.
The Mayo Clinic, in a project to cut the rate of C. diff infections, asked its workers to do one extra thing: Wipe down high-touch areas with bleach wipes. The effort worked; infections were all but eradicated in units that had been having five to seven infections per month.
The results of the project, recently published in Infectious Control and Hospital Epidemiology, show the importance of simple steps as long as they’re carried out regularly and thoroughly.1
The project began when Robert Orenstein, DO, associate professor of medicine in infectious diseases who then worked in Rochester, Minn., established a surveillance network for C. diff infections at Mayo Clinic at the time when such infections were being noted more widely throughout the U.S. and Canada. The network began tracking the cases and found that one inpatient medical unit primarily composed of patients with gastrointestinal diseases had a C. diff rate 10 times higher than the rest of the hospital. Surveillance also showed that universally gloved hematology and oncology units had substantially lower rates of C. diff infection despite high-risk patients.
Dr. Orenstein knew he had to make a change in the GI unit, but it wasn’t feasible to institute universal gloving, so he turned to bleach wipes.

Twice a day, housekeeping staff wiped down all “high-touch” areas (light switches, toilet handles, bed rails) in all of the rooms. The wipes contain 0.55% sodium hypochlorite. Within six months, the number of C. diff cases fell to almost zero.
“We were just in shock,” Dr. Orenstein says. He attributed the improvement to a reduction in the “colonization pressure”—if a high concentration of patients with C. diff can cause abundant transmissions quickly, the opposite is also true.
The greatly improved figures were shared with housekeeping, which initially complained about the smell but were encouraged to keep doors open and rooms ventilated. The bleach wipes, which Dr. Orenstein acknowledges mean an additional expense, leave a white residue when dry, so the surfaces are wiped down with water after the recommended contact time.
Dr. Orenstein notes that the results came even without a change in hand hygiene, which he had deemed not feasible because of the hospital’s lack of sinks. He isn’t diminishing the importance of hand washing, but the project does show how effective a single step can be.
The key, Dr. Orenstein adds, might be that it was just one change involving just one group of staff. “Why we think it was so effective is it was really one group that had to change their behavior and we worked with them, educated them,” he says.
He emphasizes that the wipes don’t come at the expense of other measures, like thorough cleaning of all rooms and antibiotic stewardship programs.
“You do all of those and do them well,” he says, “then you get the reduction of C. diff in the hospital.”
A Tough Bug
Believed to be aided largely by the use of broad-spectrum antibiotics that knock out the colon’s natural flora, C. diff in the hospital—as well as nursing homes and acute-care facilities—has raged for much of the past decade. Its rise is tied to the emergence of a new hypervirulent strain known as BI/NAP1/027, or NAP1 for short. The strain is highly resistant to fluoroquinolones, such as ciprofloxacin and levofloxacin, which are used often in healthcare settings.
“A fluoroquinolone will wipe out a lot of your normal flora in your gut,” Dr. Gould says. “But it won’t wipe out C. diff, in particular this hypervirulent strain. And so this strain can flourish in the presence of fluoroquinolones.” The strain produces up to 15 to 20 times more toxins than other C. diff strains, according to some data, she adds.
Vancomycin (Vanconin) and metronidazole (Flagyl) are the most common antibiotics used to treat patients infected with C. diff. Mortality rates are higher among the elderly, largely because of their weaker immune system, Dr. Gould says. Studies have generally shown mortality rates of 10% or a bit lower.1
More recent studies have shown that the number of hospital-related C. diff cases might have begun to level off in 2008 and 2009. Dr. Gould says she thinks the leveling off is for real, but there is debate over what the immediate future holds.
“There’s a lot of work and initiatives, especially state-based initiatives, that are being done in hospitals. And there’s reason to believe they’re effective,” she says, adding it’s harder to get a good picture of the problem in long-term care facilities and in the community.
Dr. Cohen with the IDSA says it’s too soon to say whether the problem is hitting a plateau. “CDC data are always a couple of years behind,” he says. “Until you see another data point, you can’t tell whether that’s just a transient flattening and whether it’s going to keep going up or not.”
Kevin Kavanagh, MD, founder of the patient advocacy group Health Watch USA and a retired otolaryngologist in Kentucky who has taken a keen interest in the C. diff problem, says he doesn’t think the end of the tunnel is within view yet.
“I think C. diff is going to get worse before it gets better,” Dr. Kavanagh says. “And that’s not necessarily because the healthcare profession isn’t doing due diligence. This is a tough organism.—it can be tough to treat and can be very tough to kill.”
The Best Defense?
Because C. diff lives within protective spores, sound hand hygiene practices and room-cleaning practices are essential for keeping infections to a minimum. Alcohol-based hand sanitizers, effective against other organisms including MRSA, do not kill C. diff. The bacteria must be mechanically removed through hand washing.
And even hand washing might not be totally effective at getting rid of the spores, which means it’s important for healthcare workers to gown and glove in high-risk rooms.
Sodium hypochlorite solutions, or bleach mixtures, have to be used to clean rooms occupied by patients with C. diff, and the prevailing thought is to clean the rooms of patients suspected of having C. diff, even if those cases might not be confirmed.
Equally important to cleaning and hand washing is systemwide emphasis on antibiotic stewardship. A 2011 study at the State University of New York Buffalo found that the risk of a C. diff infection rose with the number of antibiotics taken.2

—Carolyn Gould, MD, medical epidemiologist, division of healthcare quality promotion, Centers of Disease Control and Prevention, Atlanta
While a broad-spectrum antibiotic might be necessary at first, once the results of cultures are received, the treatment should be finely tailored to kill only the problem bacteria so that the body’s natural defenses aren’t broken down, Dr. Gould explains.
“If someone is very sick and you’re not sure what is going on, it’s very reasonable to treat them empirically with broad-spectrum antibiotics,” she says. “The important thing is that you send the appropriate cultures before so that you know what you’re treating and you can optimize those antibiotics with daily assessments.”

It’s clear why an overreliance on broad-spectrum drugs prevails in U.S. health settings, Dr. Cohen acknowledges. Recent literature suggests treating critically ill patients with wide-ranging antimicrobials as the mortality rate can be twice as high with narrower options. “I think people have gotten very quick to give broad-spectrum therapy,” he says.
continued below...
Knocking Out Clostridium Difficile

Here are the guidelines on treatment of C. diff infections (CDI) as recommended by the Infectious Diseases Society of America:
First steps:
- Discontinue therapy with the inciting antimicrobial agent(s) as soon as possible as this may influence the risk of CDI recurrence.
- When severe or complicated CDI is suspected, initiate empirical treatment as soon as the diagnosis is suspected.
- If the stool toxin assay result is negative, the decision to initiate, stop, or continue treatment must be individualized.
- If possible, avoid use of antiperistaltic agents as they may obscure symptoms and precipitate toxic megacolon.
Treatment of initial episode:
- Metronidazole is the drug of choice for the initial episode of mild to moderate CDI. The dosage is 500 mg orally three times per day for 10 to 14 days.
- Vancomycin is the drug of choice for an initial episode of severe CDI. The dosage is 125 mg orally four times per day for 10 to 14 days.
- Vancomycin administered orally (and per rectum if ileus is present) with or without intravenously administered metronidazole is the regimen of choice for the treatment of severe complicated CDI. The vancomycin dosage is 500 mg orally four times per day and 500 mg in approximately 100 mL normal saline per rectum every six hours as a retention enema, and the metronidazole dosage is 500 mg intravenously every eight hours.
Severely ill patients:
Consider colectomy for severely ill patients. Monitoring the serum lactate level and the peripheral blood white blood cell count may be helpful in prompting a decision to operate because a serum lactate level rising to 5 mmol/L and a white blood cell count rising to 50,000 cells per mL have been associated with greatly increased perioperative mortality. If surgical management is necessary, perform subtotal colectomy with preservation of the rectum.
Treatment of recurrences:
- Treatment of the first recurrence of CDI is usually with the same regimen as for the initial episode but should be stratified by disease severity (mild-to-moderate, severe, or severe complicated) as is recommended for treatment of the initial CDI episode.
- Do not use metronidazole beyond the first recurrence of CDI or for long-term chronic therapy because of potential for cumulative neurotoxicity.
- Treatment of the second or later recurrence of CDI with vancomycin therapy using a tapered and/or pulse regimen is the preferred next strategy.
Probiotics:
Administration of currently available probiotics is not recommended to prevent primary CDI as there are limited data to support this approach and there is a potential risk of bloodstream infection.
Source: Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infection Control and Hospital Epidemiology. 2010;31(5):431–455.
National Response, Localized Attention
Dr. Kavanagh of Health Watch USA says that more information about C. diff is needed, particularly publicly available numbers of infections at hospitals. Some states require those figures to be reported, but most don’t. And there is no current federal mandate on reporting of C. diff cases, although acute-care hospitals will be required to report C. diff infection rates starting in 2013.
“We really have scant data,” he says. “There is not a lot of reporting if you look at the nation on a whole. And I think that underscores one of the reasons why you need to have data for action. You need to have reporting of these organisms to the National Healthcare Safety Network so that the CDC can monitor and can make plans and can do effective interventions.
“You want to know where the areas of highest infection are,” he adds. “You want to know what interventions work and don’t work. If you don’t have a national coordinated reporting system, it really makes it difficult to address the problem. C. diff is going to be much harder to control than MRSA or other bacteria because it changes into a hard-to-kill dormant spore stage and then re-occurs at some point.”
The Centers for Medicare & Medicaid Services (CMS) has proposed adding C. diff infections to the list of hospital-acquired conditions that will not be reimbursable. It is widely hoped that such a measure will go a long way toward stamping out the problem.
Dr. Kobaidze of Emory notes that C. diff is a dynamic problem, always adapting and posing new challenges. And hospitalists should be more involved in answering these questions through research. One recent question, she points out, is whether proton pump inhibitor use is related to the rise of C. diff.
Ultimately, though, controlling C. diff in hospitals might come down to what is done day to day inside the hospital. And hospitalists can play a big role.
Danielle Scheurer, MD, MSCR, SFHM, a hospitalist and medical director of quality at the Medical University of South Carolina in Charleston, says that a full-time pharmacist on the hospital’s antimicrobial stewardship committee is always reviewing antibiotic prescriptions and is prepared to flag cases in which a broad-spectrum is used when one with a more narrow scope might be more appropriate.
The hospital has done its best, as part of its “renovation cycle,” to standardize the layouts of rooms “so that the second you open the door you know exactly where the alcohol gel is and where the soap and the sink is going to be.” The idea is to make compliance as “mindless” as possible. Such efforts can be hampered by structural limitations though, she says.
HM group leaders, she suggests, can play an important part simply by being good role models—gowning and gloving without complaint before entering high-risk rooms and reinforcing the message that such efforts have real effects on patient safety.
But she also acknowledges that “it always sounds easy....There has to be some level of redundancy built into the hospital system. This is more of a system thing than the individual hospitalist.”
One level of redundancy at MUSC that has been particularly effective, she says, are “secret shoppers” who keep an eye out for medical teams that might not be washing their hands as they go in and out of high-risk rooms. Each unit is responsible for their hand hygiene numbers—which include both self-reported figures and those obtained by the secret onlookers—and those numbers are made available to the hospital.
Those units with the best numbers are sometimes given a reward, such as a pizza party, but it’s colleagues’ knowledge of the numbers that matters most, she says.
“That, in and of itself, is a powerful motivator,” Dr. Scheurer says. “We bring it to all of our quality operations meetings, all the administrators, the CEO, the CMO. It’s very motivating for every unit. They don’t want to be the trailing unit.”
Tom Collins is a freelance medical writer based in Miami.
References
- Orenstein R, Aronhalt KC, McManus JE Jr., Fedraw LA. A targeted strategy to wipe out Clostridium difficile. Infect Control Hosp Epidemiol. 2011;32(11):1137-1139.
- Stevens V, Dumyati G, Fine LS, Fisher SG, van Wijngaarden E. Cumulative antibiotic exposures over time and the risk of Clostridium difficile infection. Clin Infect Dis. 2011;53(1):42-48.
What Hospitalists Can Do

Here are suggestions, as provided by ID experts and hospitalist leaders, on what hospitalists can do to battle C. diff infections:
Short-term steps:
- Wash hands before entering and upon leaving rooms occupied by patients with C. diff infections and those strongly suspected of having C. diff infections.
- Continue using alcohol-based hand sanitizers in addition to hand washing to prevent other types of outbreaks.
- Ensure that infected patients, and those suspected of being infected, are isolated, possibly even for 48 hours after diarrhea resolves, as research shows the patients can still transmit the spores.
- In units with high C. diff rates, consider universal gloving, not just for patients with known infection.
- Use more highly sensitive tests, such as polymerase chain reaction, or PCR, rather than enzyme immunoassays to more efficiently identify affected patients.
- Avoid testing patients with formed stools.
- Ensure that rooms of infected patients and patients strongly suspected of being infected are cleaned with a hypochlorite solution.
- Taper the use of broad-spectrum antibiotics in non-C. diff patients after test results are obtained.
- Encourage patients to question their healthcare practitioners about hand hygiene and use of antibiotics.
Long-term steps:
- Be involved with your hospital’s antimicrobial stewardship program.
- Conduct research into C. diff to explore its causes and treatments.
- Be a good role model for the rest of your group, emphasizing good practices and a strong patient-safety message.
At 480-bed Emory University Hospital Midtown in Atlanta, the physicians and staff seemingly are doing all the right things to foil one of hospital’s archenemies: Clostridium difficile. The bacteria, better known as C. diff, is responsible for a sharp rise in hospital-acquired infections over the past decade, rivaling even MRSA.
In 2010, Emory Midtown launched a campaign to boost awareness of the importance of hand washing before and after treating patients infected with C. diff and those likely to be infected. They also began using the polymerase-chain-reaction-based assay to detect the bacteria, a test with much higher sensitivity that helps to more efficiently identify those infected so control measures can be more prompt and targeted. They use a hypochlorite mixture to clean the rooms of those infected, which is considered a must. And a committee monitors the use of antibiotics to prevent overuse—often the scapegoat for the rise of the hard-to-kill bacteria.
Still, at Emory, the rate of C. diff is about the same as the national average, says hospitalist Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine and a member of the antimicrobial stewardship and infectious disease control committees at Midtown. While Dr. Kobaidze says her institution is doing a good job of trying to keep C. diff under control, she thinks hospitalists can do more.
“My feeling is that we are not as involved as we’re supposed to be,” she says. “I think we need to be a little bit more proactive, be involved in committees and research activities across the hospital.”
—Kevin Kavanagh, MD, founder, Health Watch USA
You Are Not Alone
The experience at Emory Midtown is far from unusual—healthcare facilities, and hospitalists, across the country have seen healthcare-related C. diff cases more than double since 2001 to between 400,000 and 500,000 a year, says Carolyn Gould, MD, a medical epidemiologist in the division of healthcare quality promotion at the Centers for Disease Control and Prevention (CDC) in Atlanta.
Hospitalists, whether they realize it or not, are intimately involved in how well the C. diff outbreak is controlled. Infectious-disease (ID) specialists say hospitalists are perfectly situated to make an impact in efforts to help curb the outbreak.
“Hospitalists are critical to this effort,” Dr. Gould says. “They’re in the hospital day in and day out, and they’re constantly interacting with the patients, staff, and administration. They’re often the first on the scene to see a patient who might have suddenly developed diarrhea; they’re the first to react. I think they’re in a prime position to play a leadership role to prevent C. diff infections.”
They’re also situated well to work with infection-control experts on antimicrobial stewardship programs, she says.
“I look at hospitalists just like I would have looked at internists managing their own patients 15 years ago,” says Stuart Cohen, MD, an ID expert with the University of California at Davis and a fellow with the Infectious Diseases Society of America who was lead author of the latest published IDSA guidelines on C. diff treatment. “And so they’re the first-line people.”
continued below...
Mayo Shows How a Simple Step Can Make Big Difference in C. Diff
Sometimes even when it comes to a huge problem like widespread bacterial infections, simplicity is best.
The Mayo Clinic, in a project to cut the rate of C. diff infections, asked its workers to do one extra thing: Wipe down high-touch areas with bleach wipes. The effort worked; infections were all but eradicated in units that had been having five to seven infections per month.
The results of the project, recently published in Infectious Control and Hospital Epidemiology, show the importance of simple steps as long as they’re carried out regularly and thoroughly.1
The project began when Robert Orenstein, DO, associate professor of medicine in infectious diseases who then worked in Rochester, Minn., established a surveillance network for C. diff infections at Mayo Clinic at the time when such infections were being noted more widely throughout the U.S. and Canada. The network began tracking the cases and found that one inpatient medical unit primarily composed of patients with gastrointestinal diseases had a C. diff rate 10 times higher than the rest of the hospital. Surveillance also showed that universally gloved hematology and oncology units had substantially lower rates of C. diff infection despite high-risk patients.
Dr. Orenstein knew he had to make a change in the GI unit, but it wasn’t feasible to institute universal gloving, so he turned to bleach wipes.
Twice a day, housekeeping staff wiped down all “high-touch” areas (light switches, toilet handles, bed rails) in all of the rooms. The wipes contain 0.55% sodium hypochlorite. Within six months, the number of C. diff cases fell to almost zero.
“We were just in shock,” Dr. Orenstein says. He attributed the improvement to a reduction in the “colonization pressure”—if a high concentration of patients with C. diff can cause abundant transmissions quickly, the opposite is also true.
The greatly improved figures were shared with housekeeping, which initially complained about the smell but were encouraged to keep doors open and rooms ventilated. The bleach wipes, which Dr. Orenstein acknowledges mean an additional expense, leave a white residue when dry, so the surfaces are wiped down with water after the recommended contact time.
Dr. Orenstein notes that the results came even without a change in hand hygiene, which he had deemed not feasible because of the hospital’s lack of sinks. He isn’t diminishing the importance of hand washing, but the project does show how effective a single step can be.
The key, Dr. Orenstein adds, might be that it was just one change involving just one group of staff. “Why we think it was so effective is it was really one group that had to change their behavior and we worked with them, educated them,” he says.
He emphasizes that the wipes don’t come at the expense of other measures, like thorough cleaning of all rooms and antibiotic stewardship programs.
“You do all of those and do them well,” he says, “then you get the reduction of C. diff in the hospital.”
A Tough Bug
Believed to be aided largely by the use of broad-spectrum antibiotics that knock out the colon’s natural flora, C. diff in the hospital—as well as nursing homes and acute-care facilities—has raged for much of the past decade. Its rise is tied to the emergence of a new hypervirulent strain known as BI/NAP1/027, or NAP1 for short. The strain is highly resistant to fluoroquinolones, such as ciprofloxacin and levofloxacin, which are used often in healthcare settings.
“A fluoroquinolone will wipe out a lot of your normal flora in your gut,” Dr. Gould says. “But it won’t wipe out C. diff, in particular this hypervirulent strain. And so this strain can flourish in the presence of fluoroquinolones.” The strain produces up to 15 to 20 times more toxins than other C. diff strains, according to some data, she adds.
Vancomycin (Vanconin) and metronidazole (Flagyl) are the most common antibiotics used to treat patients infected with C. diff. Mortality rates are higher among the elderly, largely because of their weaker immune system, Dr. Gould says. Studies have generally shown mortality rates of 10% or a bit lower.1
More recent studies have shown that the number of hospital-related C. diff cases might have begun to level off in 2008 and 2009. Dr. Gould says she thinks the leveling off is for real, but there is debate over what the immediate future holds.
“There’s a lot of work and initiatives, especially state-based initiatives, that are being done in hospitals. And there’s reason to believe they’re effective,” she says, adding it’s harder to get a good picture of the problem in long-term care facilities and in the community.
Dr. Cohen with the IDSA says it’s too soon to say whether the problem is hitting a plateau. “CDC data are always a couple of years behind,” he says. “Until you see another data point, you can’t tell whether that’s just a transient flattening and whether it’s going to keep going up or not.”
Kevin Kavanagh, MD, founder of the patient advocacy group Health Watch USA and a retired otolaryngologist in Kentucky who has taken a keen interest in the C. diff problem, says he doesn’t think the end of the tunnel is within view yet.
“I think C. diff is going to get worse before it gets better,” Dr. Kavanagh says. “And that’s not necessarily because the healthcare profession isn’t doing due diligence. This is a tough organism.—it can be tough to treat and can be very tough to kill.”
The Best Defense?
Because C. diff lives within protective spores, sound hand hygiene practices and room-cleaning practices are essential for keeping infections to a minimum. Alcohol-based hand sanitizers, effective against other organisms including MRSA, do not kill C. diff. The bacteria must be mechanically removed through hand washing.
And even hand washing might not be totally effective at getting rid of the spores, which means it’s important for healthcare workers to gown and glove in high-risk rooms.
Sodium hypochlorite solutions, or bleach mixtures, have to be used to clean rooms occupied by patients with C. diff, and the prevailing thought is to clean the rooms of patients suspected of having C. diff, even if those cases might not be confirmed.
Equally important to cleaning and hand washing is systemwide emphasis on antibiotic stewardship. A 2011 study at the State University of New York Buffalo found that the risk of a C. diff infection rose with the number of antibiotics taken.2
—Carolyn Gould, MD, medical epidemiologist, division of healthcare quality promotion, Centers of Disease Control and Prevention, Atlanta
While a broad-spectrum antibiotic might be necessary at first, once the results of cultures are received, the treatment should be finely tailored to kill only the problem bacteria so that the body’s natural defenses aren’t broken down, Dr. Gould explains.
“If someone is very sick and you’re not sure what is going on, it’s very reasonable to treat them empirically with broad-spectrum antibiotics,” she says. “The important thing is that you send the appropriate cultures before so that you know what you’re treating and you can optimize those antibiotics with daily assessments.”
It’s clear why an overreliance on broad-spectrum drugs prevails in U.S. health settings, Dr. Cohen acknowledges. Recent literature suggests treating critically ill patients with wide-ranging antimicrobials as the mortality rate can be twice as high with narrower options. “I think people have gotten very quick to give broad-spectrum therapy,” he says.
continued below...
Knocking Out Clostridium Difficile
Here are the guidelines on treatment of C. diff infections (CDI) as recommended by the Infectious Diseases Society of America:
First steps:
- Discontinue therapy with the inciting antimicrobial agent(s) as soon as possible as this may influence the risk of CDI recurrence.
- When severe or complicated CDI is suspected, initiate empirical treatment as soon as the diagnosis is suspected.
- If the stool toxin assay result is negative, the decision to initiate, stop, or continue treatment must be individualized.
- If possible, avoid use of antiperistaltic agents as they may obscure symptoms and precipitate toxic megacolon.
Treatment of initial episode:
- Metronidazole is the drug of choice for the initial episode of mild to moderate CDI. The dosage is 500 mg orally three times per day for 10 to 14 days.
- Vancomycin is the drug of choice for an initial episode of severe CDI. The dosage is 125 mg orally four times per day for 10 to 14 days.
- Vancomycin administered orally (and per rectum if ileus is present) with or without intravenously administered metronidazole is the regimen of choice for the treatment of severe complicated CDI. The vancomycin dosage is 500 mg orally four times per day and 500 mg in approximately 100 mL normal saline per rectum every six hours as a retention enema, and the metronidazole dosage is 500 mg intravenously every eight hours.
Severely ill patients:
Consider colectomy for severely ill patients. Monitoring the serum lactate level and the peripheral blood white blood cell count may be helpful in prompting a decision to operate because a serum lactate level rising to 5 mmol/L and a white blood cell count rising to 50,000 cells per mL have been associated with greatly increased perioperative mortality. If surgical management is necessary, perform subtotal colectomy with preservation of the rectum.
Treatment of recurrences:
- Treatment of the first recurrence of CDI is usually with the same regimen as for the initial episode but should be stratified by disease severity (mild-to-moderate, severe, or severe complicated) as is recommended for treatment of the initial CDI episode.
- Do not use metronidazole beyond the first recurrence of CDI or for long-term chronic therapy because of potential for cumulative neurotoxicity.
- Treatment of the second or later recurrence of CDI with vancomycin therapy using a tapered and/or pulse regimen is the preferred next strategy.
Probiotics:
Administration of currently available probiotics is not recommended to prevent primary CDI as there are limited data to support this approach and there is a potential risk of bloodstream infection.
Source: Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infection Control and Hospital Epidemiology. 2010;31(5):431–455.
National Response, Localized Attention
Dr. Kavanagh of Health Watch USA says that more information about C. diff is needed, particularly publicly available numbers of infections at hospitals. Some states require those figures to be reported, but most don’t. And there is no current federal mandate on reporting of C. diff cases, although acute-care hospitals will be required to report C. diff infection rates starting in 2013.
“We really have scant data,” he says. “There is not a lot of reporting if you look at the nation on a whole. And I think that underscores one of the reasons why you need to have data for action. You need to have reporting of these organisms to the National Healthcare Safety Network so that the CDC can monitor and can make plans and can do effective interventions.
“You want to know where the areas of highest infection are,” he adds. “You want to know what interventions work and don’t work. If you don’t have a national coordinated reporting system, it really makes it difficult to address the problem. C. diff is going to be much harder to control than MRSA or other bacteria because it changes into a hard-to-kill dormant spore stage and then re-occurs at some point.”
The Centers for Medicare & Medicaid Services (CMS) has proposed adding C. diff infections to the list of hospital-acquired conditions that will not be reimbursable. It is widely hoped that such a measure will go a long way toward stamping out the problem.
Dr. Kobaidze of Emory notes that C. diff is a dynamic problem, always adapting and posing new challenges. And hospitalists should be more involved in answering these questions through research. One recent question, she points out, is whether proton pump inhibitor use is related to the rise of C. diff.
Ultimately, though, controlling C. diff in hospitals might come down to what is done day to day inside the hospital. And hospitalists can play a big role.
Danielle Scheurer, MD, MSCR, SFHM, a hospitalist and medical director of quality at the Medical University of South Carolina in Charleston, says that a full-time pharmacist on the hospital’s antimicrobial stewardship committee is always reviewing antibiotic prescriptions and is prepared to flag cases in which a broad-spectrum is used when one with a more narrow scope might be more appropriate.
The hospital has done its best, as part of its “renovation cycle,” to standardize the layouts of rooms “so that the second you open the door you know exactly where the alcohol gel is and where the soap and the sink is going to be.” The idea is to make compliance as “mindless” as possible. Such efforts can be hampered by structural limitations though, she says.
HM group leaders, she suggests, can play an important part simply by being good role models—gowning and gloving without complaint before entering high-risk rooms and reinforcing the message that such efforts have real effects on patient safety.
But she also acknowledges that “it always sounds easy....There has to be some level of redundancy built into the hospital system. This is more of a system thing than the individual hospitalist.”
One level of redundancy at MUSC that has been particularly effective, she says, are “secret shoppers” who keep an eye out for medical teams that might not be washing their hands as they go in and out of high-risk rooms. Each unit is responsible for their hand hygiene numbers—which include both self-reported figures and those obtained by the secret onlookers—and those numbers are made available to the hospital.
Those units with the best numbers are sometimes given a reward, such as a pizza party, but it’s colleagues’ knowledge of the numbers that matters most, she says.
“That, in and of itself, is a powerful motivator,” Dr. Scheurer says. “We bring it to all of our quality operations meetings, all the administrators, the CEO, the CMO. It’s very motivating for every unit. They don’t want to be the trailing unit.”
Tom Collins is a freelance medical writer based in Miami.
References
- Orenstein R, Aronhalt KC, McManus JE Jr., Fedraw LA. A targeted strategy to wipe out Clostridium difficile. Infect Control Hosp Epidemiol. 2011;32(11):1137-1139.
- Stevens V, Dumyati G, Fine LS, Fisher SG, van Wijngaarden E. Cumulative antibiotic exposures over time and the risk of Clostridium difficile infection. Clin Infect Dis. 2011;53(1):42-48.
What Hospitalists Can Do
Here are suggestions, as provided by ID experts and hospitalist leaders, on what hospitalists can do to battle C. diff infections:
Short-term steps:
- Wash hands before entering and upon leaving rooms occupied by patients with C. diff infections and those strongly suspected of having C. diff infections.
- Continue using alcohol-based hand sanitizers in addition to hand washing to prevent other types of outbreaks.
- Ensure that infected patients, and those suspected of being infected, are isolated, possibly even for 48 hours after diarrhea resolves, as research shows the patients can still transmit the spores.
- In units with high C. diff rates, consider universal gloving, not just for patients with known infection.
- Use more highly sensitive tests, such as polymerase chain reaction, or PCR, rather than enzyme immunoassays to more efficiently identify affected patients.
- Avoid testing patients with formed stools.
- Ensure that rooms of infected patients and patients strongly suspected of being infected are cleaned with a hypochlorite solution.
- Taper the use of broad-spectrum antibiotics in non-C. diff patients after test results are obtained.
- Encourage patients to question their healthcare practitioners about hand hygiene and use of antibiotics.
Long-term steps:
- Be involved with your hospital’s antimicrobial stewardship program.
- Conduct research into C. diff to explore its causes and treatments.
- Be a good role model for the rest of your group, emphasizing good practices and a strong patient-safety message.
At 480-bed Emory University Hospital Midtown in Atlanta, the physicians and staff seemingly are doing all the right things to foil one of hospital’s archenemies: Clostridium difficile. The bacteria, better known as C. diff, is responsible for a sharp rise in hospital-acquired infections over the past decade, rivaling even MRSA.
In 2010, Emory Midtown launched a campaign to boost awareness of the importance of hand washing before and after treating patients infected with C. diff and those likely to be infected. They also began using the polymerase-chain-reaction-based assay to detect the bacteria, a test with much higher sensitivity that helps to more efficiently identify those infected so control measures can be more prompt and targeted. They use a hypochlorite mixture to clean the rooms of those infected, which is considered a must. And a committee monitors the use of antibiotics to prevent overuse—often the scapegoat for the rise of the hard-to-kill bacteria.
Still, at Emory, the rate of C. diff is about the same as the national average, says hospitalist Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine and a member of the antimicrobial stewardship and infectious disease control committees at Midtown. While Dr. Kobaidze says her institution is doing a good job of trying to keep C. diff under control, she thinks hospitalists can do more.
“My feeling is that we are not as involved as we’re supposed to be,” she says. “I think we need to be a little bit more proactive, be involved in committees and research activities across the hospital.”
—Kevin Kavanagh, MD, founder, Health Watch USA
You Are Not Alone
The experience at Emory Midtown is far from unusual—healthcare facilities, and hospitalists, across the country have seen healthcare-related C. diff cases more than double since 2001 to between 400,000 and 500,000 a year, says Carolyn Gould, MD, a medical epidemiologist in the division of healthcare quality promotion at the Centers for Disease Control and Prevention (CDC) in Atlanta.
Hospitalists, whether they realize it or not, are intimately involved in how well the C. diff outbreak is controlled. Infectious-disease (ID) specialists say hospitalists are perfectly situated to make an impact in efforts to help curb the outbreak.
“Hospitalists are critical to this effort,” Dr. Gould says. “They’re in the hospital day in and day out, and they’re constantly interacting with the patients, staff, and administration. They’re often the first on the scene to see a patient who might have suddenly developed diarrhea; they’re the first to react. I think they’re in a prime position to play a leadership role to prevent C. diff infections.”
They’re also situated well to work with infection-control experts on antimicrobial stewardship programs, she says.
“I look at hospitalists just like I would have looked at internists managing their own patients 15 years ago,” says Stuart Cohen, MD, an ID expert with the University of California at Davis and a fellow with the Infectious Diseases Society of America who was lead author of the latest published IDSA guidelines on C. diff treatment. “And so they’re the first-line people.”
continued below...
Mayo Shows How a Simple Step Can Make Big Difference in C. Diff
Sometimes even when it comes to a huge problem like widespread bacterial infections, simplicity is best.
The Mayo Clinic, in a project to cut the rate of C. diff infections, asked its workers to do one extra thing: Wipe down high-touch areas with bleach wipes. The effort worked; infections were all but eradicated in units that had been having five to seven infections per month.
The results of the project, recently published in Infectious Control and Hospital Epidemiology, show the importance of simple steps as long as they’re carried out regularly and thoroughly.1
The project began when Robert Orenstein, DO, associate professor of medicine in infectious diseases who then worked in Rochester, Minn., established a surveillance network for C. diff infections at Mayo Clinic at the time when such infections were being noted more widely throughout the U.S. and Canada. The network began tracking the cases and found that one inpatient medical unit primarily composed of patients with gastrointestinal diseases had a C. diff rate 10 times higher than the rest of the hospital. Surveillance also showed that universally gloved hematology and oncology units had substantially lower rates of C. diff infection despite high-risk patients.
Dr. Orenstein knew he had to make a change in the GI unit, but it wasn’t feasible to institute universal gloving, so he turned to bleach wipes.
Twice a day, housekeeping staff wiped down all “high-touch” areas (light switches, toilet handles, bed rails) in all of the rooms. The wipes contain 0.55% sodium hypochlorite. Within six months, the number of C. diff cases fell to almost zero.
“We were just in shock,” Dr. Orenstein says. He attributed the improvement to a reduction in the “colonization pressure”—if a high concentration of patients with C. diff can cause abundant transmissions quickly, the opposite is also true.
The greatly improved figures were shared with housekeeping, which initially complained about the smell but were encouraged to keep doors open and rooms ventilated. The bleach wipes, which Dr. Orenstein acknowledges mean an additional expense, leave a white residue when dry, so the surfaces are wiped down with water after the recommended contact time.
Dr. Orenstein notes that the results came even without a change in hand hygiene, which he had deemed not feasible because of the hospital’s lack of sinks. He isn’t diminishing the importance of hand washing, but the project does show how effective a single step can be.
The key, Dr. Orenstein adds, might be that it was just one change involving just one group of staff. “Why we think it was so effective is it was really one group that had to change their behavior and we worked with them, educated them,” he says.
He emphasizes that the wipes don’t come at the expense of other measures, like thorough cleaning of all rooms and antibiotic stewardship programs.
“You do all of those and do them well,” he says, “then you get the reduction of C. diff in the hospital.”
A Tough Bug
Believed to be aided largely by the use of broad-spectrum antibiotics that knock out the colon’s natural flora, C. diff in the hospital—as well as nursing homes and acute-care facilities—has raged for much of the past decade. Its rise is tied to the emergence of a new hypervirulent strain known as BI/NAP1/027, or NAP1 for short. The strain is highly resistant to fluoroquinolones, such as ciprofloxacin and levofloxacin, which are used often in healthcare settings.
“A fluoroquinolone will wipe out a lot of your normal flora in your gut,” Dr. Gould says. “But it won’t wipe out C. diff, in particular this hypervirulent strain. And so this strain can flourish in the presence of fluoroquinolones.” The strain produces up to 15 to 20 times more toxins than other C. diff strains, according to some data, she adds.
Vancomycin (Vanconin) and metronidazole (Flagyl) are the most common antibiotics used to treat patients infected with C. diff. Mortality rates are higher among the elderly, largely because of their weaker immune system, Dr. Gould says. Studies have generally shown mortality rates of 10% or a bit lower.1
More recent studies have shown that the number of hospital-related C. diff cases might have begun to level off in 2008 and 2009. Dr. Gould says she thinks the leveling off is for real, but there is debate over what the immediate future holds.
“There’s a lot of work and initiatives, especially state-based initiatives, that are being done in hospitals. And there’s reason to believe they’re effective,” she says, adding it’s harder to get a good picture of the problem in long-term care facilities and in the community.
Dr. Cohen with the IDSA says it’s too soon to say whether the problem is hitting a plateau. “CDC data are always a couple of years behind,” he says. “Until you see another data point, you can’t tell whether that’s just a transient flattening and whether it’s going to keep going up or not.”
Kevin Kavanagh, MD, founder of the patient advocacy group Health Watch USA and a retired otolaryngologist in Kentucky who has taken a keen interest in the C. diff problem, says he doesn’t think the end of the tunnel is within view yet.
“I think C. diff is going to get worse before it gets better,” Dr. Kavanagh says. “And that’s not necessarily because the healthcare profession isn’t doing due diligence. This is a tough organism.—it can be tough to treat and can be very tough to kill.”
The Best Defense?
Because C. diff lives within protective spores, sound hand hygiene practices and room-cleaning practices are essential for keeping infections to a minimum. Alcohol-based hand sanitizers, effective against other organisms including MRSA, do not kill C. diff. The bacteria must be mechanically removed through hand washing.
And even hand washing might not be totally effective at getting rid of the spores, which means it’s important for healthcare workers to gown and glove in high-risk rooms.
Sodium hypochlorite solutions, or bleach mixtures, have to be used to clean rooms occupied by patients with C. diff, and the prevailing thought is to clean the rooms of patients suspected of having C. diff, even if those cases might not be confirmed.
Equally important to cleaning and hand washing is systemwide emphasis on antibiotic stewardship. A 2011 study at the State University of New York Buffalo found that the risk of a C. diff infection rose with the number of antibiotics taken.2
—Carolyn Gould, MD, medical epidemiologist, division of healthcare quality promotion, Centers of Disease Control and Prevention, Atlanta
While a broad-spectrum antibiotic might be necessary at first, once the results of cultures are received, the treatment should be finely tailored to kill only the problem bacteria so that the body’s natural defenses aren’t broken down, Dr. Gould explains.
“If someone is very sick and you’re not sure what is going on, it’s very reasonable to treat them empirically with broad-spectrum antibiotics,” she says. “The important thing is that you send the appropriate cultures before so that you know what you’re treating and you can optimize those antibiotics with daily assessments.”
It’s clear why an overreliance on broad-spectrum drugs prevails in U.S. health settings, Dr. Cohen acknowledges. Recent literature suggests treating critically ill patients with wide-ranging antimicrobials as the mortality rate can be twice as high with narrower options. “I think people have gotten very quick to give broad-spectrum therapy,” he says.
continued below...
Knocking Out Clostridium Difficile
Here are the guidelines on treatment of C. diff infections (CDI) as recommended by the Infectious Diseases Society of America:
First steps:
- Discontinue therapy with the inciting antimicrobial agent(s) as soon as possible as this may influence the risk of CDI recurrence.
- When severe or complicated CDI is suspected, initiate empirical treatment as soon as the diagnosis is suspected.
- If the stool toxin assay result is negative, the decision to initiate, stop, or continue treatment must be individualized.
- If possible, avoid use of antiperistaltic agents as they may obscure symptoms and precipitate toxic megacolon.
Treatment of initial episode:
- Metronidazole is the drug of choice for the initial episode of mild to moderate CDI. The dosage is 500 mg orally three times per day for 10 to 14 days.
- Vancomycin is the drug of choice for an initial episode of severe CDI. The dosage is 125 mg orally four times per day for 10 to 14 days.
- Vancomycin administered orally (and per rectum if ileus is present) with or without intravenously administered metronidazole is the regimen of choice for the treatment of severe complicated CDI. The vancomycin dosage is 500 mg orally four times per day and 500 mg in approximately 100 mL normal saline per rectum every six hours as a retention enema, and the metronidazole dosage is 500 mg intravenously every eight hours.
Severely ill patients:
Consider colectomy for severely ill patients. Monitoring the serum lactate level and the peripheral blood white blood cell count may be helpful in prompting a decision to operate because a serum lactate level rising to 5 mmol/L and a white blood cell count rising to 50,000 cells per mL have been associated with greatly increased perioperative mortality. If surgical management is necessary, perform subtotal colectomy with preservation of the rectum.
Treatment of recurrences:
- Treatment of the first recurrence of CDI is usually with the same regimen as for the initial episode but should be stratified by disease severity (mild-to-moderate, severe, or severe complicated) as is recommended for treatment of the initial CDI episode.
- Do not use metronidazole beyond the first recurrence of CDI or for long-term chronic therapy because of potential for cumulative neurotoxicity.
- Treatment of the second or later recurrence of CDI with vancomycin therapy using a tapered and/or pulse regimen is the preferred next strategy.
Probiotics:
Administration of currently available probiotics is not recommended to prevent primary CDI as there are limited data to support this approach and there is a potential risk of bloodstream infection.
Source: Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infection Control and Hospital Epidemiology. 2010;31(5):431–455.
National Response, Localized Attention
Dr. Kavanagh of Health Watch USA says that more information about C. diff is needed, particularly publicly available numbers of infections at hospitals. Some states require those figures to be reported, but most don’t. And there is no current federal mandate on reporting of C. diff cases, although acute-care hospitals will be required to report C. diff infection rates starting in 2013.
“We really have scant data,” he says. “There is not a lot of reporting if you look at the nation on a whole. And I think that underscores one of the reasons why you need to have data for action. You need to have reporting of these organisms to the National Healthcare Safety Network so that the CDC can monitor and can make plans and can do effective interventions.
“You want to know where the areas of highest infection are,” he adds. “You want to know what interventions work and don’t work. If you don’t have a national coordinated reporting system, it really makes it difficult to address the problem. C. diff is going to be much harder to control than MRSA or other bacteria because it changes into a hard-to-kill dormant spore stage and then re-occurs at some point.”
The Centers for Medicare & Medicaid Services (CMS) has proposed adding C. diff infections to the list of hospital-acquired conditions that will not be reimbursable. It is widely hoped that such a measure will go a long way toward stamping out the problem.
Dr. Kobaidze of Emory notes that C. diff is a dynamic problem, always adapting and posing new challenges. And hospitalists should be more involved in answering these questions through research. One recent question, she points out, is whether proton pump inhibitor use is related to the rise of C. diff.
Ultimately, though, controlling C. diff in hospitals might come down to what is done day to day inside the hospital. And hospitalists can play a big role.
Danielle Scheurer, MD, MSCR, SFHM, a hospitalist and medical director of quality at the Medical University of South Carolina in Charleston, says that a full-time pharmacist on the hospital’s antimicrobial stewardship committee is always reviewing antibiotic prescriptions and is prepared to flag cases in which a broad-spectrum is used when one with a more narrow scope might be more appropriate.
The hospital has done its best, as part of its “renovation cycle,” to standardize the layouts of rooms “so that the second you open the door you know exactly where the alcohol gel is and where the soap and the sink is going to be.” The idea is to make compliance as “mindless” as possible. Such efforts can be hampered by structural limitations though, she says.
HM group leaders, she suggests, can play an important part simply by being good role models—gowning and gloving without complaint before entering high-risk rooms and reinforcing the message that such efforts have real effects on patient safety.
But she also acknowledges that “it always sounds easy....There has to be some level of redundancy built into the hospital system. This is more of a system thing than the individual hospitalist.”
One level of redundancy at MUSC that has been particularly effective, she says, are “secret shoppers” who keep an eye out for medical teams that might not be washing their hands as they go in and out of high-risk rooms. Each unit is responsible for their hand hygiene numbers—which include both self-reported figures and those obtained by the secret onlookers—and those numbers are made available to the hospital.
Those units with the best numbers are sometimes given a reward, such as a pizza party, but it’s colleagues’ knowledge of the numbers that matters most, she says.
“That, in and of itself, is a powerful motivator,” Dr. Scheurer says. “We bring it to all of our quality operations meetings, all the administrators, the CEO, the CMO. It’s very motivating for every unit. They don’t want to be the trailing unit.”
Tom Collins is a freelance medical writer based in Miami.
References
- Orenstein R, Aronhalt KC, McManus JE Jr., Fedraw LA. A targeted strategy to wipe out Clostridium difficile. Infect Control Hosp Epidemiol. 2011;32(11):1137-1139.
- Stevens V, Dumyati G, Fine LS, Fisher SG, van Wijngaarden E. Cumulative antibiotic exposures over time and the risk of Clostridium difficile infection. Clin Infect Dis. 2011;53(1):42-48.
What Hospitalists Can Do
Here are suggestions, as provided by ID experts and hospitalist leaders, on what hospitalists can do to battle C. diff infections:
Short-term steps:
- Wash hands before entering and upon leaving rooms occupied by patients with C. diff infections and those strongly suspected of having C. diff infections.
- Continue using alcohol-based hand sanitizers in addition to hand washing to prevent other types of outbreaks.
- Ensure that infected patients, and those suspected of being infected, are isolated, possibly even for 48 hours after diarrhea resolves, as research shows the patients can still transmit the spores.
- In units with high C. diff rates, consider universal gloving, not just for patients with known infection.
- Use more highly sensitive tests, such as polymerase chain reaction, or PCR, rather than enzyme immunoassays to more efficiently identify affected patients.
- Avoid testing patients with formed stools.
- Ensure that rooms of infected patients and patients strongly suspected of being infected are cleaned with a hypochlorite solution.
- Taper the use of broad-spectrum antibiotics in non-C. diff patients after test results are obtained.
- Encourage patients to question their healthcare practitioners about hand hygiene and use of antibiotics.
Long-term steps:
- Be involved with your hospital’s antimicrobial stewardship program.
- Conduct research into C. diff to explore its causes and treatments.
- Be a good role model for the rest of your group, emphasizing good practices and a strong patient-safety message.
Simple Interventions Save Lives
A new Health Affairs study tested three relatively simple and inexpensive interventions on a hospital unit to prevent the kinds of hospital-acquired infections that cause the deaths of an estimated 99,000 patients each year. Principal investigator Bradford Harris, MD, and colleagues conducted the research on a pediatric ICU at the University of North Carolina at Chapel Hill School of Medicine, finding that patients admitted after these interventions were implemented left the hospital on average two days earlier, at lower cost, and with a 2.3% lower death rate. Study authors projected annual savings of $12 million for a single PICU.1
The simple measures include strict enforcement of standard hand hygiene policies; guideline-recommended measures for ventilator patients, such as elevating the head of the hospital bed; and compliance with guidelines for maintaining central line catheters, along with educational posters and the use of oral care kits.
A recent article in the “Cleveland Plain Dealer” describes efforts in that city’s hospitals to enforce proper hand hygiene.2 MetroHealth Medical Center hired four employees it calls “infection prevention observers,” whose entire job is to make sure that every caregiver who comes near a patient washes his or her hands. They openly appear on the units carrying clipboards and filling out sheets tracking non-compliance.
The hospital’s hand hygiene compliance rate has reached 98% on all medical units (nationwide, the rate is around 50%), while bloodstream infections have dropped to one-third of what they were in 2010. Cleveland Clinic and University Hospitals achieved similar compliance by employing secret observers of staff hand-washing.
CDC epidemiologist and hand hygiene expert Kate Ellingson, MD, told the newspaper that while awareness of the importance of hand hygiene has long been understood, it is difficult for healthcare workers to follow. But hospitals that use employee monitors, post data, and implement other hand hygiene initiatives tend to show strong compliance.
References
- Harris BD, Hanson H, Christy C, et al. Strict hand hygiene and other practices shortened stays and cut costs and mortality in a pediatric intensive care unit. Health Affairs. 2011;30(9):1751-1761.
- Tribble SJ. Cleveland MetroHealth Medical Center increases hand washing, reduces infections. “Cleveland Plain Dealer” website. Available at: http://www.cleveland.com/healthfit/index.ssf/2011/09/metrohealth_increases_hand_was.html. Accessed Oct. 15, 2011.
A new Health Affairs study tested three relatively simple and inexpensive interventions on a hospital unit to prevent the kinds of hospital-acquired infections that cause the deaths of an estimated 99,000 patients each year. Principal investigator Bradford Harris, MD, and colleagues conducted the research on a pediatric ICU at the University of North Carolina at Chapel Hill School of Medicine, finding that patients admitted after these interventions were implemented left the hospital on average two days earlier, at lower cost, and with a 2.3% lower death rate. Study authors projected annual savings of $12 million for a single PICU.1
The simple measures include strict enforcement of standard hand hygiene policies; guideline-recommended measures for ventilator patients, such as elevating the head of the hospital bed; and compliance with guidelines for maintaining central line catheters, along with educational posters and the use of oral care kits.
A recent article in the “Cleveland Plain Dealer” describes efforts in that city’s hospitals to enforce proper hand hygiene.2 MetroHealth Medical Center hired four employees it calls “infection prevention observers,” whose entire job is to make sure that every caregiver who comes near a patient washes his or her hands. They openly appear on the units carrying clipboards and filling out sheets tracking non-compliance.
The hospital’s hand hygiene compliance rate has reached 98% on all medical units (nationwide, the rate is around 50%), while bloodstream infections have dropped to one-third of what they were in 2010. Cleveland Clinic and University Hospitals achieved similar compliance by employing secret observers of staff hand-washing.
CDC epidemiologist and hand hygiene expert Kate Ellingson, MD, told the newspaper that while awareness of the importance of hand hygiene has long been understood, it is difficult for healthcare workers to follow. But hospitals that use employee monitors, post data, and implement other hand hygiene initiatives tend to show strong compliance.
References
- Harris BD, Hanson H, Christy C, et al. Strict hand hygiene and other practices shortened stays and cut costs and mortality in a pediatric intensive care unit. Health Affairs. 2011;30(9):1751-1761.
- Tribble SJ. Cleveland MetroHealth Medical Center increases hand washing, reduces infections. “Cleveland Plain Dealer” website. Available at: http://www.cleveland.com/healthfit/index.ssf/2011/09/metrohealth_increases_hand_was.html. Accessed Oct. 15, 2011.
A new Health Affairs study tested three relatively simple and inexpensive interventions on a hospital unit to prevent the kinds of hospital-acquired infections that cause the deaths of an estimated 99,000 patients each year. Principal investigator Bradford Harris, MD, and colleagues conducted the research on a pediatric ICU at the University of North Carolina at Chapel Hill School of Medicine, finding that patients admitted after these interventions were implemented left the hospital on average two days earlier, at lower cost, and with a 2.3% lower death rate. Study authors projected annual savings of $12 million for a single PICU.1
The simple measures include strict enforcement of standard hand hygiene policies; guideline-recommended measures for ventilator patients, such as elevating the head of the hospital bed; and compliance with guidelines for maintaining central line catheters, along with educational posters and the use of oral care kits.
A recent article in the “Cleveland Plain Dealer” describes efforts in that city’s hospitals to enforce proper hand hygiene.2 MetroHealth Medical Center hired four employees it calls “infection prevention observers,” whose entire job is to make sure that every caregiver who comes near a patient washes his or her hands. They openly appear on the units carrying clipboards and filling out sheets tracking non-compliance.
The hospital’s hand hygiene compliance rate has reached 98% on all medical units (nationwide, the rate is around 50%), while bloodstream infections have dropped to one-third of what they were in 2010. Cleveland Clinic and University Hospitals achieved similar compliance by employing secret observers of staff hand-washing.
CDC epidemiologist and hand hygiene expert Kate Ellingson, MD, told the newspaper that while awareness of the importance of hand hygiene has long been understood, it is difficult for healthcare workers to follow. But hospitals that use employee monitors, post data, and implement other hand hygiene initiatives tend to show strong compliance.
References
- Harris BD, Hanson H, Christy C, et al. Strict hand hygiene and other practices shortened stays and cut costs and mortality in a pediatric intensive care unit. Health Affairs. 2011;30(9):1751-1761.
- Tribble SJ. Cleveland MetroHealth Medical Center increases hand washing, reduces infections. “Cleveland Plain Dealer” website. Available at: http://www.cleveland.com/healthfit/index.ssf/2011/09/metrohealth_increases_hand_was.html. Accessed Oct. 15, 2011.
Dartmouth Atlas: Little Progress Reducing Readmissions
The newest Dartmouth Atlas report, released Sept. 28, documents striking variation in 30-day hospital readmission rates for Medicare patients across 308 hospital-referral regions.1 The authors found little progress in decreasing 30-day readmissions from 2004 to 2009, while for some conditions and many regions, rates actually went up.
National readmission rates following surgery were 12.7% in both 2004 and 2009; readmissions for medical conditions rose slightly, from 15.9% to 16.1%, over the same period. Only 42% of hospitalized Medicare patients discharged to home had a PCP contact within 14 days of discharge, according to the report.
The Dartmouth Atlas Project (www.dartmouthatlas.org) documents geographic variation in healthcare utilization unrelated to outcome. It offers an extensive database for comparison by state, county, region and facility.
The new report is the first to identify an association nationally between readmissions rates and “the overall intensity of inpatient care provided to patients within a region or hospital,” with patterns of relatively high hospital utilization often corresponding with areas of higher readmissions. “Other patients are readmitted simply because they live in a locale where the hospital is used more frequently as a site of care,” the authors note.
Without continuous, high-quality care coordination across sites, the authors write, discharged patients can repeatedly bounce back to emergency rooms and hospitals.
Reference
The newest Dartmouth Atlas report, released Sept. 28, documents striking variation in 30-day hospital readmission rates for Medicare patients across 308 hospital-referral regions.1 The authors found little progress in decreasing 30-day readmissions from 2004 to 2009, while for some conditions and many regions, rates actually went up.
National readmission rates following surgery were 12.7% in both 2004 and 2009; readmissions for medical conditions rose slightly, from 15.9% to 16.1%, over the same period. Only 42% of hospitalized Medicare patients discharged to home had a PCP contact within 14 days of discharge, according to the report.
The Dartmouth Atlas Project (www.dartmouthatlas.org) documents geographic variation in healthcare utilization unrelated to outcome. It offers an extensive database for comparison by state, county, region and facility.
The new report is the first to identify an association nationally between readmissions rates and “the overall intensity of inpatient care provided to patients within a region or hospital,” with patterns of relatively high hospital utilization often corresponding with areas of higher readmissions. “Other patients are readmitted simply because they live in a locale where the hospital is used more frequently as a site of care,” the authors note.
Without continuous, high-quality care coordination across sites, the authors write, discharged patients can repeatedly bounce back to emergency rooms and hospitals.
Reference
The newest Dartmouth Atlas report, released Sept. 28, documents striking variation in 30-day hospital readmission rates for Medicare patients across 308 hospital-referral regions.1 The authors found little progress in decreasing 30-day readmissions from 2004 to 2009, while for some conditions and many regions, rates actually went up.
National readmission rates following surgery were 12.7% in both 2004 and 2009; readmissions for medical conditions rose slightly, from 15.9% to 16.1%, over the same period. Only 42% of hospitalized Medicare patients discharged to home had a PCP contact within 14 days of discharge, according to the report.
The Dartmouth Atlas Project (www.dartmouthatlas.org) documents geographic variation in healthcare utilization unrelated to outcome. It offers an extensive database for comparison by state, county, region and facility.
The new report is the first to identify an association nationally between readmissions rates and “the overall intensity of inpatient care provided to patients within a region or hospital,” with patterns of relatively high hospital utilization often corresponding with areas of higher readmissions. “Other patients are readmitted simply because they live in a locale where the hospital is used more frequently as a site of care,” the authors note.
Without continuous, high-quality care coordination across sites, the authors write, discharged patients can repeatedly bounce back to emergency rooms and hospitals.
Reference
By the Numbers: 209,000
Projected total number of adult in-hospital cardiac arrests that are treated with a resuscitation response each year in U.S. hospitals.1 Raina Merchant, MD, and colleagues from the University of Pennsylvania Health System derived several estimates from the American Heart Association’s Get with the Guidelines-Resuscitation registry for 2003 to 2007, weighted for total U.S. hospital bed days. Survival rate for in-hospital cardiac arrests is 21%, compared with 10% for arrests in other settings. But the authors note that arrests might be rising, which is “important for understanding the burden of in-hospital cardiac arrest and developing strategies to improve care for hospitalized patients,” Dr. Merchant says.
Reference
Projected total number of adult in-hospital cardiac arrests that are treated with a resuscitation response each year in U.S. hospitals.1 Raina Merchant, MD, and colleagues from the University of Pennsylvania Health System derived several estimates from the American Heart Association’s Get with the Guidelines-Resuscitation registry for 2003 to 2007, weighted for total U.S. hospital bed days. Survival rate for in-hospital cardiac arrests is 21%, compared with 10% for arrests in other settings. But the authors note that arrests might be rising, which is “important for understanding the burden of in-hospital cardiac arrest and developing strategies to improve care for hospitalized patients,” Dr. Merchant says.
Reference
Projected total number of adult in-hospital cardiac arrests that are treated with a resuscitation response each year in U.S. hospitals.1 Raina Merchant, MD, and colleagues from the University of Pennsylvania Health System derived several estimates from the American Heart Association’s Get with the Guidelines-Resuscitation registry for 2003 to 2007, weighted for total U.S. hospital bed days. Survival rate for in-hospital cardiac arrests is 21%, compared with 10% for arrests in other settings. But the authors note that arrests might be rising, which is “important for understanding the burden of in-hospital cardiac arrest and developing strategies to improve care for hospitalized patients,” Dr. Merchant says.
Reference
Lost in Transition

It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at JosephLi@hospitalmedicine.org.
Dr. Li is president of SHM.
It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at JosephLi@hospitalmedicine.org.
Dr. Li is president of SHM.
It’s been nearly two decades since I graduated from medical school. I think back and I honestly do not remember any lectures about transitions of care.
During residency, I remember some attending physicians would insist that when I discharged patients from the hospital, the patients had to leave with post-discharge appointments in hand. Like any diligent intern, I did as I was told. I telephoned the administrative assistants in clinic and booked follow-up appointments for my patients. I always asked for the first available appointment. Why? Because that was what my senior resident told me to do. I suspect he learned that from his resident as well.
Sometimes the appointment was scheduled for the week following discharge; other times it was six months later. I honestly didn’t give it much thought. There was a blank on the discharge paperwork and I filled it in with a date and time. I was doing my job—or so I thought.
Can you imagine if someone just gave you a slip of paper today telling you when to show up to get your teeth cleaned without consulting your schedule? How about scheduling the oil change for your car at a garage 100 miles away? Seems pretty silly, doesn’t it? Nothing about it seems customer-centric or cost-efficient.
With such a system in place, why are we surprised when patients do not show up for their follow-up appointments? When the patient presents to the ED later and is readmitted to the hospital, we label them as “non-compliant” because they failed to show up for their follow-up appointment.
Inefficient, Ineffective, Inappropriate
There are multiple problems with the above situation. The first problem: Why are doctors calling to schedule follow-up appointments in the first place? Do we ask airline pilots to serve refreshments? I suppose they could, but I’d rather they concentrate on flying the plane. It also seems like an awful waste of money and resources when we could accomplish the same feat with less-expensive airline attendants who are better trained to interact with passengers.
At most teaching hospitals across the country, I suspect we still rely on trainees to book follow-up appointments for patients. At hospitals without trainees, I suspect some of this responsibility falls on nurses and unit coordinators. Again, I wonder how often these people are actually in a position to schedule an appointment that the patient is likely to keep—or whether they are filling in a box on a checklist like I used to do.
Common Problem?
How do other industries address this issue? Well, many utilize customer service representatives to help consumers book their appointments. Some industries have advanced software, which allows consumers to book their own appointment online. I have to tell you that I am chuckling as I write this. I’m chuckling not because this is funny—I am just amazed that something that is so common sense is not utilized consistently across the hospital industry. When was the last time you actually called a hotel to book a room? Most of us find it so much more convenient to book airline tickets or hotel rooms online.
If we were to create a system with the consumer’s satisfaction and cost in mind, would you rely on trainees, nurses, or unit coordinators to book follow-up appointments? I suppose Hypothetical System 2.0 would include consumer representatives speaking with patients to book appointments. Hypothetical System 3.0 would allow patients and/or a family member to book the appointment online.
I can tell you that folks at Beth Israel Deaconess Medical Center in Boston, where I work, have given this some thought. We are nowhere near a 3.0 version, but we do rely on professional appointment-makers to work with our hospitalized patients to book follow-up appointments. Inpatient providers put in the order online requesting follow-up appointments for their hospitalized patients. The online application asks the provider to specify the requests. Does the patient need follow-up with specialists, as well as their primary outpatient provider? The inpatient provider can specify the window of time in which they recommend follow-up for the patient. If I want my patient to follow up with their primary-care physician (PCP) within one week and with their cardiologist within two weeks, the appointment-maker will work with the patient and the respective doctors’ offices to make this happen. I am contacted only if any issues arise.
All of this information is provided to the patient with their other discharge paperwork. Some of you might be asking: How can the hospital afford to pay for this software and for the cadre of professional appointment-makers? I am wondering how hospitals can afford not to. It’s like worrying about the cost of a college degree until you realize how difficult it is trying to get a job without one.
Part of the PCP “access” problem we have in this country is due to the fact that not every patient shows up for scheduled appointments. Our appointment-makers minimize the “no show” rate because, by speaking with patients about their schedules, they are providing appointments to patients with knowledge that they are likely to make the appointment. One of the things we learned at Beth Israel was that our trainees were sometimes requesting appointments for patients within one week of discharge when I knew darn well that the patient was unlikely to make that appointment because the patient most likely would still be at rehab.
Prior to this system, we also had the occasional PCP who was upset because we booked their patient’s follow-up with a specialist who was outside that PCP’s “inner circle” of specialists. How in the world are any of us supposed to remember this information?
Well, our professional appointment-makers utilize this information as part of the algorithm they follow when booking appointments for patients. As our nation moves towards a value-based purchasing system for healthcare, we don’t need to recreate the wheel; we can adopt proven practices from other cost-effective industries—and we can improve customer satisfaction.
I am interested in hearing how appointments are arranged for your hospitalized patients. Send me your thoughts at JosephLi@hospitalmedicine.org.
Dr. Li is president of SHM.
Quality, Defined

Pornography. There can be few better hooks for readers than that. Just typing the word is a bit uncomfortable. As is, I imagine, reading it. But it’s effective, and likely why you’ve made it to word 37 of my column—34 words further than you usually get, I imagine.
“What about pornography?” you ask with bated breath. “What could pornography possibly have to do with hospital medicine?” your mind wonders. “Is this the column that (finally) gets Glasheen fired?” the ambulance chaser in you titillates.
By now, you’ve no doubt heard the famous Potter Stewart definition of pornography: “I know it when I see it.” That’s how the former U.S. Supreme Court justice described his threshold for recognizing pornography. It was made famous in a 1960s decision about whether a particular movie scene was protected by the 1st Amendment right to free speech or, indeed, a pornographic obscenity to be censured. Stewart, who clearly recognized the need to “define” pornography, also recognized the inherent challenges in doing so. The I-know-it-when-I-see-it benchmark is, of course, flawed, but I defy you to come up with a better definition.
Quality Is, of Course…
I was thinking about pornography (another discomforting phrase to type) recently—and Potter Stewart’s challenge in defining it, specifically—when I was asked about quality in healthcare. The query, which occurred during a several-hour, mind-numbing meeting (is there another type of several-hour meeting?), was “What is quality?” The question, laced with hostility and dripping with antagonism, was posed by a senior physician and directed pointedly at me. Indignantly, I cleared my throat, mentally stepping onto my pedestal to ceremoniously topple this academic egghead with my erudite response.
“Well, quality is, of course,” I confidently retorted, the “of course” added to demonstrate my moral superiority, “the ability to … uhhh, you see … ummmm, you know.” At which point I again cleared my throat not once, not twice, but a socially awkward three times before employing the timed-honored, full-body shock-twitch that signifies that you’ve just received an urgent vibrate page (faked, of course) and excused myself from the meeting, never to return.
The reality is that I struggle to define quality. Like Chief Justice Stewart, I think I know quality when I see it, but more precise definitions can be elusive.
And distracting.
It’s Not My Job
Just this morning, I read a news release from a respected physician group trumpeting the fact that their advocacy resulted in the federal government reducing the number of quality data-point requirements in their final rule for accountable-care organizations (ACOs) from 66 to 33. Trumpeting? Is this a good thing? Should we be supporting fewer quality measures? The article quoted a physician leader saying that the original reporting requirements were too burdensome. Too burdensome to whom? My guess is the recipients of our care, often referred to as our patients, wouldn’t categorize quality assurance as “too burdensome.”
I was at another meeting recently in which a respected colleague related her take on the physician role in improving quality. “I don’t think that’s a physician’s job. That’s what we have a quality department for,” she noted. “It’s just too expensive, time-consuming, and boring for physicians to do that kind of work.”
Too burdensome? Not a physician’s job to ensure the delivery of quality care? While I understand the sentiment (the need to have support staff collecting data, recognition of the huge infrastructure requirements, etc.), I can’t help but think that these types of responses are a large part of the struggle we are having with improving quality.
Then again, I would hazard that 0.0 percent of physicians would argue with the premise that we are obliged by the Hippocratic Oath, our moral compass, and our sense of professionalism to provide the best possible care to our patients. If we accept that we aren’t doing that—and we aren’t—then what is the disconnect? Why aren’t we seeking more quality data points? Why isn’t this “our job”?
Definitional Disconnect
Well, the truth is, it is our job. And we know it. The problem is that quality isn’t universally defined and the process of trying to define it often distracts us from the true task at hand—improving patient care.
Few of us would argue that a wrong-site surgery or anaphylaxis from administration of a medication known to have caused an allergy represents a suboptimal level of care. But more often than not, we see quality being measured and defined in less concrete, more obscure ways—ways that my eyes may not view as low-quality. These definitions are inherently flawed and breed contempt among providers who are told they aren’t passing muster in metrics they don’t see as “quality.”
So the real disconnect is definitional. Is quality defined by the Institute of Medicine characteristics of safe, effective, patient-centered, timely, efficient, and equitable care? Or is it the rates of underuse, overuse, and misuse of medical treatments and procedures? Or is it defined by individual quality metrics such as those captured by the Centers for Medicare & Medicaid Services (CMS)—you know, things like hospital fall rates, perioperative antibiotic usage, beta-blockers after MI, or whether a patient reported their bathroom as being clean?
Is 30% of the quality of care that we deliver referable to the patient experience (as measured by HCAHPS), as the new value-based purchasing program would have us believe? Is it hospital accreditation through the Joint Commission? Or physician certification through our parent boards? Is quality measured by a physician’s cognitive or technical skills, or where they went to school? Is it experience, medical knowledge, guideline usage?
We use such a mystifying array of metrics to define quality that it confuses the issue such that physicians who personally believe they are doing a good job can become disenfranchised. To a physician who provides clinically appropriate care around a surgical procedure or treatment of pneumonia, it can be demeaning and demoralizing to suggest that his or her patient did not receive “high quality” care because the bathroom wasn’t clean or the patient didn’t get a flu shot. Yet, this is the message we often send—a message that alienates many physicians, making them cynical about quality and disengaged in quality improvement. The result is that they seek fewer quality data points and defer the job of improving quality to someone else.
Make no mistake: Quality measures have an important role in our healthcare landscape. But to the degree that defining quality confuses, alienates, or disenfranchises providers, we should stop trying to define it. Quality is not a thing, a metric, or an outcome. It is not an elusive, unquantifiable creature that is achievable only by the elite. Quality is simply providing the best possible care. And quality improvement is simply closing the gap between the best possible care and actual care.
In this regard, we can learn a lot from Potter Stewart. We know quality when we see it. And we know what an absence of quality looks like.
Let’s close that gap by putting less energy into defining quality, and putting more energy into the tenacious pursuit of quality.
Dr. Glasheen is physician editor of The Hospitalist.
Pornography. There can be few better hooks for readers than that. Just typing the word is a bit uncomfortable. As is, I imagine, reading it. But it’s effective, and likely why you’ve made it to word 37 of my column—34 words further than you usually get, I imagine.
“What about pornography?” you ask with bated breath. “What could pornography possibly have to do with hospital medicine?” your mind wonders. “Is this the column that (finally) gets Glasheen fired?” the ambulance chaser in you titillates.
By now, you’ve no doubt heard the famous Potter Stewart definition of pornography: “I know it when I see it.” That’s how the former U.S. Supreme Court justice described his threshold for recognizing pornography. It was made famous in a 1960s decision about whether a particular movie scene was protected by the 1st Amendment right to free speech or, indeed, a pornographic obscenity to be censured. Stewart, who clearly recognized the need to “define” pornography, also recognized the inherent challenges in doing so. The I-know-it-when-I-see-it benchmark is, of course, flawed, but I defy you to come up with a better definition.
Quality Is, of Course…
I was thinking about pornography (another discomforting phrase to type) recently—and Potter Stewart’s challenge in defining it, specifically—when I was asked about quality in healthcare. The query, which occurred during a several-hour, mind-numbing meeting (is there another type of several-hour meeting?), was “What is quality?” The question, laced with hostility and dripping with antagonism, was posed by a senior physician and directed pointedly at me. Indignantly, I cleared my throat, mentally stepping onto my pedestal to ceremoniously topple this academic egghead with my erudite response.
“Well, quality is, of course,” I confidently retorted, the “of course” added to demonstrate my moral superiority, “the ability to … uhhh, you see … ummmm, you know.” At which point I again cleared my throat not once, not twice, but a socially awkward three times before employing the timed-honored, full-body shock-twitch that signifies that you’ve just received an urgent vibrate page (faked, of course) and excused myself from the meeting, never to return.
The reality is that I struggle to define quality. Like Chief Justice Stewart, I think I know quality when I see it, but more precise definitions can be elusive.
And distracting.
It’s Not My Job
Just this morning, I read a news release from a respected physician group trumpeting the fact that their advocacy resulted in the federal government reducing the number of quality data-point requirements in their final rule for accountable-care organizations (ACOs) from 66 to 33. Trumpeting? Is this a good thing? Should we be supporting fewer quality measures? The article quoted a physician leader saying that the original reporting requirements were too burdensome. Too burdensome to whom? My guess is the recipients of our care, often referred to as our patients, wouldn’t categorize quality assurance as “too burdensome.”
I was at another meeting recently in which a respected colleague related her take on the physician role in improving quality. “I don’t think that’s a physician’s job. That’s what we have a quality department for,” she noted. “It’s just too expensive, time-consuming, and boring for physicians to do that kind of work.”
Too burdensome? Not a physician’s job to ensure the delivery of quality care? While I understand the sentiment (the need to have support staff collecting data, recognition of the huge infrastructure requirements, etc.), I can’t help but think that these types of responses are a large part of the struggle we are having with improving quality.
Then again, I would hazard that 0.0 percent of physicians would argue with the premise that we are obliged by the Hippocratic Oath, our moral compass, and our sense of professionalism to provide the best possible care to our patients. If we accept that we aren’t doing that—and we aren’t—then what is the disconnect? Why aren’t we seeking more quality data points? Why isn’t this “our job”?
Definitional Disconnect
Well, the truth is, it is our job. And we know it. The problem is that quality isn’t universally defined and the process of trying to define it often distracts us from the true task at hand—improving patient care.
Few of us would argue that a wrong-site surgery or anaphylaxis from administration of a medication known to have caused an allergy represents a suboptimal level of care. But more often than not, we see quality being measured and defined in less concrete, more obscure ways—ways that my eyes may not view as low-quality. These definitions are inherently flawed and breed contempt among providers who are told they aren’t passing muster in metrics they don’t see as “quality.”
So the real disconnect is definitional. Is quality defined by the Institute of Medicine characteristics of safe, effective, patient-centered, timely, efficient, and equitable care? Or is it the rates of underuse, overuse, and misuse of medical treatments and procedures? Or is it defined by individual quality metrics such as those captured by the Centers for Medicare & Medicaid Services (CMS)—you know, things like hospital fall rates, perioperative antibiotic usage, beta-blockers after MI, or whether a patient reported their bathroom as being clean?
Is 30% of the quality of care that we deliver referable to the patient experience (as measured by HCAHPS), as the new value-based purchasing program would have us believe? Is it hospital accreditation through the Joint Commission? Or physician certification through our parent boards? Is quality measured by a physician’s cognitive or technical skills, or where they went to school? Is it experience, medical knowledge, guideline usage?
We use such a mystifying array of metrics to define quality that it confuses the issue such that physicians who personally believe they are doing a good job can become disenfranchised. To a physician who provides clinically appropriate care around a surgical procedure or treatment of pneumonia, it can be demeaning and demoralizing to suggest that his or her patient did not receive “high quality” care because the bathroom wasn’t clean or the patient didn’t get a flu shot. Yet, this is the message we often send—a message that alienates many physicians, making them cynical about quality and disengaged in quality improvement. The result is that they seek fewer quality data points and defer the job of improving quality to someone else.
Make no mistake: Quality measures have an important role in our healthcare landscape. But to the degree that defining quality confuses, alienates, or disenfranchises providers, we should stop trying to define it. Quality is not a thing, a metric, or an outcome. It is not an elusive, unquantifiable creature that is achievable only by the elite. Quality is simply providing the best possible care. And quality improvement is simply closing the gap between the best possible care and actual care.
In this regard, we can learn a lot from Potter Stewart. We know quality when we see it. And we know what an absence of quality looks like.
Let’s close that gap by putting less energy into defining quality, and putting more energy into the tenacious pursuit of quality.
Dr. Glasheen is physician editor of The Hospitalist.
Pornography. There can be few better hooks for readers than that. Just typing the word is a bit uncomfortable. As is, I imagine, reading it. But it’s effective, and likely why you’ve made it to word 37 of my column—34 words further than you usually get, I imagine.
“What about pornography?” you ask with bated breath. “What could pornography possibly have to do with hospital medicine?” your mind wonders. “Is this the column that (finally) gets Glasheen fired?” the ambulance chaser in you titillates.
By now, you’ve no doubt heard the famous Potter Stewart definition of pornography: “I know it when I see it.” That’s how the former U.S. Supreme Court justice described his threshold for recognizing pornography. It was made famous in a 1960s decision about whether a particular movie scene was protected by the 1st Amendment right to free speech or, indeed, a pornographic obscenity to be censured. Stewart, who clearly recognized the need to “define” pornography, also recognized the inherent challenges in doing so. The I-know-it-when-I-see-it benchmark is, of course, flawed, but I defy you to come up with a better definition.
Quality Is, of Course…
I was thinking about pornography (another discomforting phrase to type) recently—and Potter Stewart’s challenge in defining it, specifically—when I was asked about quality in healthcare. The query, which occurred during a several-hour, mind-numbing meeting (is there another type of several-hour meeting?), was “What is quality?” The question, laced with hostility and dripping with antagonism, was posed by a senior physician and directed pointedly at me. Indignantly, I cleared my throat, mentally stepping onto my pedestal to ceremoniously topple this academic egghead with my erudite response.
“Well, quality is, of course,” I confidently retorted, the “of course” added to demonstrate my moral superiority, “the ability to … uhhh, you see … ummmm, you know.” At which point I again cleared my throat not once, not twice, but a socially awkward three times before employing the timed-honored, full-body shock-twitch that signifies that you’ve just received an urgent vibrate page (faked, of course) and excused myself from the meeting, never to return.
The reality is that I struggle to define quality. Like Chief Justice Stewart, I think I know quality when I see it, but more precise definitions can be elusive.
And distracting.
It’s Not My Job
Just this morning, I read a news release from a respected physician group trumpeting the fact that their advocacy resulted in the federal government reducing the number of quality data-point requirements in their final rule for accountable-care organizations (ACOs) from 66 to 33. Trumpeting? Is this a good thing? Should we be supporting fewer quality measures? The article quoted a physician leader saying that the original reporting requirements were too burdensome. Too burdensome to whom? My guess is the recipients of our care, often referred to as our patients, wouldn’t categorize quality assurance as “too burdensome.”
I was at another meeting recently in which a respected colleague related her take on the physician role in improving quality. “I don’t think that’s a physician’s job. That’s what we have a quality department for,” she noted. “It’s just too expensive, time-consuming, and boring for physicians to do that kind of work.”
Too burdensome? Not a physician’s job to ensure the delivery of quality care? While I understand the sentiment (the need to have support staff collecting data, recognition of the huge infrastructure requirements, etc.), I can’t help but think that these types of responses are a large part of the struggle we are having with improving quality.
Then again, I would hazard that 0.0 percent of physicians would argue with the premise that we are obliged by the Hippocratic Oath, our moral compass, and our sense of professionalism to provide the best possible care to our patients. If we accept that we aren’t doing that—and we aren’t—then what is the disconnect? Why aren’t we seeking more quality data points? Why isn’t this “our job”?
Definitional Disconnect
Well, the truth is, it is our job. And we know it. The problem is that quality isn’t universally defined and the process of trying to define it often distracts us from the true task at hand—improving patient care.
Few of us would argue that a wrong-site surgery or anaphylaxis from administration of a medication known to have caused an allergy represents a suboptimal level of care. But more often than not, we see quality being measured and defined in less concrete, more obscure ways—ways that my eyes may not view as low-quality. These definitions are inherently flawed and breed contempt among providers who are told they aren’t passing muster in metrics they don’t see as “quality.”
So the real disconnect is definitional. Is quality defined by the Institute of Medicine characteristics of safe, effective, patient-centered, timely, efficient, and equitable care? Or is it the rates of underuse, overuse, and misuse of medical treatments and procedures? Or is it defined by individual quality metrics such as those captured by the Centers for Medicare & Medicaid Services (CMS)—you know, things like hospital fall rates, perioperative antibiotic usage, beta-blockers after MI, or whether a patient reported their bathroom as being clean?
Is 30% of the quality of care that we deliver referable to the patient experience (as measured by HCAHPS), as the new value-based purchasing program would have us believe? Is it hospital accreditation through the Joint Commission? Or physician certification through our parent boards? Is quality measured by a physician’s cognitive or technical skills, or where they went to school? Is it experience, medical knowledge, guideline usage?
We use such a mystifying array of metrics to define quality that it confuses the issue such that physicians who personally believe they are doing a good job can become disenfranchised. To a physician who provides clinically appropriate care around a surgical procedure or treatment of pneumonia, it can be demeaning and demoralizing to suggest that his or her patient did not receive “high quality” care because the bathroom wasn’t clean or the patient didn’t get a flu shot. Yet, this is the message we often send—a message that alienates many physicians, making them cynical about quality and disengaged in quality improvement. The result is that they seek fewer quality data points and defer the job of improving quality to someone else.
Make no mistake: Quality measures have an important role in our healthcare landscape. But to the degree that defining quality confuses, alienates, or disenfranchises providers, we should stop trying to define it. Quality is not a thing, a metric, or an outcome. It is not an elusive, unquantifiable creature that is achievable only by the elite. Quality is simply providing the best possible care. And quality improvement is simply closing the gap between the best possible care and actual care.
In this regard, we can learn a lot from Potter Stewart. We know quality when we see it. And we know what an absence of quality looks like.
Let’s close that gap by putting less energy into defining quality, and putting more energy into the tenacious pursuit of quality.
Dr. Glasheen is physician editor of The Hospitalist.