User login
GRAPPA initiatives continue to chart the way for psoriasis, psoriatic arthritis
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) meeting was held in Stockholm this year on July 7 and 8. This year’s meeting was packed with updates regarding numerous projects, including, but not limited to, educational initiatives, research work streams, inclusion of patients in the research process in psoriasis and psoriatic arthritis (PsA), and updating of the core set of outcome measures to be included in both psoriasis and PsA clinical trials through Outcome Measures in Rheumatology (OMERACT) and International Dermatology Outcome Measures (IDEOM) initiatives.
Among the most exciting initiatives was the review of the 2015 GRAPPA PsA Treatment Recommendations. The new treatment recommendations began 2 years ago and have included extensive literature reviews, small group discussions, and large group surveys. The final manuscript includes overarching principles and specific recommendations broken down by disease manifestations (for example, peripheral arthritis, axial disease, enthesitis, dactylitis, skin psoriasis, and nail disease). Changes from the 2009 GRAPPA Treatment Recommendations (Ann. Rheum. Dis. 2009;68:1387-94) include addition of new therapies (for example, phosphodiesterase-4 inhibitors, interleukin (IL) 12/23 inhibitors, IL-17 inhibitors) and recommendations for screening for comorbidities, as well as a table noting the influence of comorbidities on therapy selection. Each recommendation is supported as “weak” or “strong” depending on the level of evidence. Patient research partners were involved in all steps of the process. The final manuscript has been submitted for publication.

In addition to treating the disease, better defining the disease is also of critical importance. In particular, defining a “flare” of rheumatoid arthritis or PsA has been quite difficult, and there has been great interest in building an assessment tool to measure the occurrence of flare. During the meeting, Dr. Anna Moverley and Dr. Philip Helliwell, both from the NIHR Musculoskeletal Biomedical Research Unit, Leeds (England) Institute of Rheumatic & Musculoskeletal Medicine, presented their work to date on defining PsA flares. They began their work by conducting a qualitative analysis of 18 patient interviews to identify themes related to having a PsA flare. Domains (or themes) identified included physical, psychological, social withdrawal, fatigue, and loss of function. In addition, patients described flare triggers, timing of flares, preflare management, and flare management. The results of this study were recently published in a paper titled, “It’s not just the joints, it’s the whole thing: qualitative analysis of patients’ experience of flare in psoriatic arthritis” (Rheumatology 2015;54:1448-54). The team then used these themes to create a Delphi survey, which was sent to both patients and physicians. Working groups at GRAPPA were used to determine the next steps, in particular whether a physician or patient tool (or both) should be developed.
Care of the patient with PsA from a multispecialty perspective was discussed in the “combined clinics” presentation. Several academic centers across North America have developed combined dermatology-rheumatology clinics. The functioning of these clinics varies widely from monthly dual clinics in which the dermatologist and rheumatologist see the patient together for virtual combined clinics in which time is set aside for discussion of shared patients. The advantages of these dual clinics include rich educational opportunities for medical students, residents, and fellows; the ideal clinical care model for patients; enhanced patient satisfaction with their care; improved patient care and quicker transition to a disease-modifying agent when indicated; and physician satisfaction and learning opportunities through collaborative work. Institutions using these collaborative models have combined to form the Psoriasis and Psoriatic Arthritis Clinics Multicenter Advancement Network (PPACMAN). The group has had two meetings and has developed research initiatives that are moving forward. Another goal of the group is to assist others centers interested in creating similar collaborative clinics.
The GRAPPA PsA BioDam (Psoriatic Arthritis Biomarkers for Joint Damage) initiative was also discussed at the meeting. The goal of this initiative is to examine soluble biomarkers as predictors of structural damage in PsA. Blood samples are taken at enrollment and then patients are followed prospectively. At 24 months of follow-up, repeat radiographs are obtained to monitor the development of new erosions. In addition to plain film radiographs, three sites are now also including MRI to assess for erosions. The study team, led by Dr. Oliver FitzGerald, hopes to begin analyzing some of the results from the study in the next 1-2 years.
Dr. Ogdie-Beatty is director of the Penn Psoriatic Arthritis Clinic at the University of Pennsylvania, Philadelphia, and is a member of the GRAPPA Steering Committee.
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) meeting was held in Stockholm this year on July 7 and 8. This year’s meeting was packed with updates regarding numerous projects, including, but not limited to, educational initiatives, research work streams, inclusion of patients in the research process in psoriasis and psoriatic arthritis (PsA), and updating of the core set of outcome measures to be included in both psoriasis and PsA clinical trials through Outcome Measures in Rheumatology (OMERACT) and International Dermatology Outcome Measures (IDEOM) initiatives.
Among the most exciting initiatives was the review of the 2015 GRAPPA PsA Treatment Recommendations. The new treatment recommendations began 2 years ago and have included extensive literature reviews, small group discussions, and large group surveys. The final manuscript includes overarching principles and specific recommendations broken down by disease manifestations (for example, peripheral arthritis, axial disease, enthesitis, dactylitis, skin psoriasis, and nail disease). Changes from the 2009 GRAPPA Treatment Recommendations (Ann. Rheum. Dis. 2009;68:1387-94) include addition of new therapies (for example, phosphodiesterase-4 inhibitors, interleukin (IL) 12/23 inhibitors, IL-17 inhibitors) and recommendations for screening for comorbidities, as well as a table noting the influence of comorbidities on therapy selection. Each recommendation is supported as “weak” or “strong” depending on the level of evidence. Patient research partners were involved in all steps of the process. The final manuscript has been submitted for publication.
In addition to treating the disease, better defining the disease is also of critical importance. In particular, defining a “flare” of rheumatoid arthritis or PsA has been quite difficult, and there has been great interest in building an assessment tool to measure the occurrence of flare. During the meeting, Dr. Anna Moverley and Dr. Philip Helliwell, both from the NIHR Musculoskeletal Biomedical Research Unit, Leeds (England) Institute of Rheumatic & Musculoskeletal Medicine, presented their work to date on defining PsA flares. They began their work by conducting a qualitative analysis of 18 patient interviews to identify themes related to having a PsA flare. Domains (or themes) identified included physical, psychological, social withdrawal, fatigue, and loss of function. In addition, patients described flare triggers, timing of flares, preflare management, and flare management. The results of this study were recently published in a paper titled, “It’s not just the joints, it’s the whole thing: qualitative analysis of patients’ experience of flare in psoriatic arthritis” (Rheumatology 2015;54:1448-54). The team then used these themes to create a Delphi survey, which was sent to both patients and physicians. Working groups at GRAPPA were used to determine the next steps, in particular whether a physician or patient tool (or both) should be developed.
Care of the patient with PsA from a multispecialty perspective was discussed in the “combined clinics” presentation. Several academic centers across North America have developed combined dermatology-rheumatology clinics. The functioning of these clinics varies widely from monthly dual clinics in which the dermatologist and rheumatologist see the patient together for virtual combined clinics in which time is set aside for discussion of shared patients. The advantages of these dual clinics include rich educational opportunities for medical students, residents, and fellows; the ideal clinical care model for patients; enhanced patient satisfaction with their care; improved patient care and quicker transition to a disease-modifying agent when indicated; and physician satisfaction and learning opportunities through collaborative work. Institutions using these collaborative models have combined to form the Psoriasis and Psoriatic Arthritis Clinics Multicenter Advancement Network (PPACMAN). The group has had two meetings and has developed research initiatives that are moving forward. Another goal of the group is to assist others centers interested in creating similar collaborative clinics.
The GRAPPA PsA BioDam (Psoriatic Arthritis Biomarkers for Joint Damage) initiative was also discussed at the meeting. The goal of this initiative is to examine soluble biomarkers as predictors of structural damage in PsA. Blood samples are taken at enrollment and then patients are followed prospectively. At 24 months of follow-up, repeat radiographs are obtained to monitor the development of new erosions. In addition to plain film radiographs, three sites are now also including MRI to assess for erosions. The study team, led by Dr. Oliver FitzGerald, hopes to begin analyzing some of the results from the study in the next 1-2 years.
Dr. Ogdie-Beatty is director of the Penn Psoriatic Arthritis Clinic at the University of Pennsylvania, Philadelphia, and is a member of the GRAPPA Steering Committee.
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) meeting was held in Stockholm this year on July 7 and 8. This year’s meeting was packed with updates regarding numerous projects, including, but not limited to, educational initiatives, research work streams, inclusion of patients in the research process in psoriasis and psoriatic arthritis (PsA), and updating of the core set of outcome measures to be included in both psoriasis and PsA clinical trials through Outcome Measures in Rheumatology (OMERACT) and International Dermatology Outcome Measures (IDEOM) initiatives.
Among the most exciting initiatives was the review of the 2015 GRAPPA PsA Treatment Recommendations. The new treatment recommendations began 2 years ago and have included extensive literature reviews, small group discussions, and large group surveys. The final manuscript includes overarching principles and specific recommendations broken down by disease manifestations (for example, peripheral arthritis, axial disease, enthesitis, dactylitis, skin psoriasis, and nail disease). Changes from the 2009 GRAPPA Treatment Recommendations (Ann. Rheum. Dis. 2009;68:1387-94) include addition of new therapies (for example, phosphodiesterase-4 inhibitors, interleukin (IL) 12/23 inhibitors, IL-17 inhibitors) and recommendations for screening for comorbidities, as well as a table noting the influence of comorbidities on therapy selection. Each recommendation is supported as “weak” or “strong” depending on the level of evidence. Patient research partners were involved in all steps of the process. The final manuscript has been submitted for publication.
In addition to treating the disease, better defining the disease is also of critical importance. In particular, defining a “flare” of rheumatoid arthritis or PsA has been quite difficult, and there has been great interest in building an assessment tool to measure the occurrence of flare. During the meeting, Dr. Anna Moverley and Dr. Philip Helliwell, both from the NIHR Musculoskeletal Biomedical Research Unit, Leeds (England) Institute of Rheumatic & Musculoskeletal Medicine, presented their work to date on defining PsA flares. They began their work by conducting a qualitative analysis of 18 patient interviews to identify themes related to having a PsA flare. Domains (or themes) identified included physical, psychological, social withdrawal, fatigue, and loss of function. In addition, patients described flare triggers, timing of flares, preflare management, and flare management. The results of this study were recently published in a paper titled, “It’s not just the joints, it’s the whole thing: qualitative analysis of patients’ experience of flare in psoriatic arthritis” (Rheumatology 2015;54:1448-54). The team then used these themes to create a Delphi survey, which was sent to both patients and physicians. Working groups at GRAPPA were used to determine the next steps, in particular whether a physician or patient tool (or both) should be developed.
Care of the patient with PsA from a multispecialty perspective was discussed in the “combined clinics” presentation. Several academic centers across North America have developed combined dermatology-rheumatology clinics. The functioning of these clinics varies widely from monthly dual clinics in which the dermatologist and rheumatologist see the patient together for virtual combined clinics in which time is set aside for discussion of shared patients. The advantages of these dual clinics include rich educational opportunities for medical students, residents, and fellows; the ideal clinical care model for patients; enhanced patient satisfaction with their care; improved patient care and quicker transition to a disease-modifying agent when indicated; and physician satisfaction and learning opportunities through collaborative work. Institutions using these collaborative models have combined to form the Psoriasis and Psoriatic Arthritis Clinics Multicenter Advancement Network (PPACMAN). The group has had two meetings and has developed research initiatives that are moving forward. Another goal of the group is to assist others centers interested in creating similar collaborative clinics.
The GRAPPA PsA BioDam (Psoriatic Arthritis Biomarkers for Joint Damage) initiative was also discussed at the meeting. The goal of this initiative is to examine soluble biomarkers as predictors of structural damage in PsA. Blood samples are taken at enrollment and then patients are followed prospectively. At 24 months of follow-up, repeat radiographs are obtained to monitor the development of new erosions. In addition to plain film radiographs, three sites are now also including MRI to assess for erosions. The study team, led by Dr. Oliver FitzGerald, hopes to begin analyzing some of the results from the study in the next 1-2 years.
Dr. Ogdie-Beatty is director of the Penn Psoriatic Arthritis Clinic at the University of Pennsylvania, Philadelphia, and is a member of the GRAPPA Steering Committee.

A call to action on metabolic syndrome and pediatric psoriasis
VANCOUVER – Dermatologists and primary care physicians working collaboratively have a golden opportunity to improve the long-term health of pediatric psoriasis patients by addressing their predisposition to components of the metabolic syndrome, Dr. Amy S. Paller declared at the World Congress of Dermatology.
“I think we as dermatologists should be in touch with the primary care doctors of every one of our children with psoriasis. Together, we should be thinking about whether the child has metabolic issues and working jointly to most effectively counsel and evaluate these children for their potential risk for these metabolic disorders,” said Dr. Paller, professor and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Pediatric psoriasis is commonly associated with other comorbid conditions in addition to metabolic disorders. But the metabolic syndrome has recently become the focus of increasing attention given that cardiovascular disease is the No. 1 cause of death in the United States, and it appears that children with psoriasis may be getting a jump start on the atherosclerotic process.

By now, it’s well established that plaque psoriasis in adults is strongly associated with increased risks of diabetes, obesity, dyslipidemia, the metabolic syndrome, and cardiovascular disease. Mounting evidence indicates children and adolescents with psoriasis face the same risks.
Everyone knows how difficult it can be to make the long-term lifestyle changes that reverse obesity and its related metabolic disorders. But dermatologists, pediatricians, and family physicians have some leverage when it comes to pediatric psoriasis.
“Think about the fact that 30% of children with psoriasis have a first-degree relative with psoriasis, usually a parent. I think we need to think about counseling young adults with psoriasis early on, especially if that adult is overweight or obese, about the need for adopting a healthy lifestyle. If they do that, it’s not just for themselves but for their children, and we just might prevent pediatric psoriasis in that family or temper its severity through that healthy lifestyle intervention,” Dr. Paller continued.
The hope is that effectively addressing the metabolic comorbidities of pediatric psoriasis will modulate and improve the skin disease; in other words, that weight loss could improve psoriasis. As yet, however, that’s just a hope, as there is no persuasive supporting evidence.
“We’re looking towards ongoing adult trials to give us some clues about whether that’s the case,” she said.
Evidence for comorbidities
Some of the key evidence regarding the metabolic comorbidities of pediatric psoriasis comes from a landmark German epidemiologic study involving 33,981 pediatric psoriasis patients. The prevalence of psoriasis in German youth rose linearly from 0.12% at age 1 year to 1.2% at age 18. Pediatric psoriasis patients had significantly higher rates of diabetes, hyperlipidemia, obesity, and hypertension than did nonpsoriatic controls (Br. J. Dermatol. 2010;162:633-6).
A Kaiser Permanente study of nearly 711,000 youths aged 2-19 years showed that those who were overweight were 2.8-fold more likely than normal-weight youth to have severe or widespread psoriasis, while those who were moderately obese were at 2.9-fold increased risk and extremely obese youth were at 4.2-fold increased risk. Among adolescents, having psoriasis was associated with significantly higher mean total and LDL cholesterol, triglycerides, and alanine aminotransferase levels (J. Pediatr. 2011;159:577-83).
Recent evidence suggests that even before increased levels of LDL cholesterol and triglycerides are apparent in children with psoriasis, abnormalities in lipid function are present and may potentially serve as a novel marker for early cardiovascular risk. Dr. Paller cited a study presented by Dr. Wynnis L. Tom of Rady Children’s Hospital, San Diego, at the 2015 annual meeting of the Society for Investigative Dermatology. The case-control study included 50 children with psoriasis and 50 matched controls with a mean age of 13 years.
Like other investigators, Dr. Tom found that the psoriatic children had higher waist/hip ratios and more insulin resistance. While fasting lipid levels didn’t differ between the two groups, the psoriasis patients had significantly higher levels of atherogenic apolipoprotein B, fewer of the particularly cardioprotective large-size HDL particles, and reduced HDL efflux capacity. Stay tuned regarding these potential early markers, Dr. Paller advised.
She was lead author of a 409-patient international study that showed the risks of obesity and a high waist circumference rise with greater severity of pediatric psoriasis. Children with severe psoriasis were at 4.92-fold increased risk of obesity, compared with controls, while even those with mild psoriasis were at 3.6-fold increased risk (JAMA Dermatol. 2013;149:166-76).
Which comes first?
The question arises: Which comes first in children, the excess adiposity or the psoriasis? Dr. Paller said that although the final word isn’t in, she and her coworkers found in a pilot study of 27 overweight or obese children with psoriasis that excess adiposity typically came first. Moreover, among the roughly one-half of children with a family history of obesity, onset of psoriasis occurred a full 3 years earlier than in those without a positive family history (JAMA Dermatol. 2014;150:573-4).
In another small study, this by investigators at Tufts University, Boston, 6 of 20 children with psoriasis (30%) met criteria for the metabolic syndrome, compared with just 1 of 20 matched nonpsoriatic controls (Pediatr. Dermatol. 2013;30:700-5).
Dr. Paller said that if dermatologists and primary care physicians are to successfully collaborate in tackling the comorbid metabolic disorders associated with pediatric psoriasis, a prerequisite is that dermatologists are going to have to do a better job of educating their primary care colleagues about the skin disease as manifest in children.
“I think it’s very important that pediatricians are aware that psoriasis is a risk factor for metabolic syndrome. But pediatric psoriasis is often misdiagnosed by primary care physicians who mistake it for eczema or tinea infection or contact dermatitis,” according to the pediatric dermatologist.
In one eye-catching Australian study, she noted, a mere 9% of patients with pediatric psoriasis were correctly diagnosed before referral to a dermatologist (Australas. J. Dermatol. 2012;53:98-105).
Pediatric psoriasis: not just skin deep
In addition to the increased risk of metabolic disorders faced by pediatric psoriasis patients, other common comorbidities include depression, anxiety disorders, impaired self-esteem and quality of life, arthritis, and Crohn’s disease, Dr. Paller observed.
• Quality of life. “The quality of life impact of psoriasis is profound. It’s a highly visible disorder, which affects the development of self-esteem and social relationships,” Dr. Paller said.
Investigators at Texas A&M University applied the Pediatric Quality of Life Inventory Version 4.0 to 208 patients aged 2-17 years with moderate to severe psoriasis and compared the results to published data on children with arthritis, asthma, diabetes, and psychiatric disorders. Health-related quality of life turned out to be more impaired in the psoriasis patients than in those with diabetes. The quality-of-life impairment associated with pediatric psoriasis was comparable to that of having asthma or arthritis, albeit not as severe as for pediatric psychiatric disorders (Eur. J. Pediatr. 2012;171:485-92).
• Psychiatric disorders. A study of more than 7,400 pediatric psoriasis patients concluded they had an adjusted 25% increased risk of developing depression, compared with psoriasis-free controls, as well as a 32% increased risk of anxiety disorders and a 55% greater risk of bipolar disorder (J. Am. Acad. Dermatol. 2012;67:651-7.e2).
• Psoriatic arthritis. An estimated 1 in 10 U.S. children with psoriasis report having arthritis, often classified as juvenile idiopathic arthritis (JAMA Dermatol. 2013;149:1180-5).
• Crohn’s disease. A large German epidemiologic study concluded that psoriasis was associated with a 3.69-fold increased risk of Crohn’s disease. There was no increased risk of ulcerative colitis (Br. J. Dermatol. 2010;162:633-6).
Dr. Paller reported receiving research grants from Amgen and Leo and serving as a consultant to AbbVie.
VANCOUVER – Dermatologists and primary care physicians working collaboratively have a golden opportunity to improve the long-term health of pediatric psoriasis patients by addressing their predisposition to components of the metabolic syndrome, Dr. Amy S. Paller declared at the World Congress of Dermatology.
“I think we as dermatologists should be in touch with the primary care doctors of every one of our children with psoriasis. Together, we should be thinking about whether the child has metabolic issues and working jointly to most effectively counsel and evaluate these children for their potential risk for these metabolic disorders,” said Dr. Paller, professor and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Pediatric psoriasis is commonly associated with other comorbid conditions in addition to metabolic disorders. But the metabolic syndrome has recently become the focus of increasing attention given that cardiovascular disease is the No. 1 cause of death in the United States, and it appears that children with psoriasis may be getting a jump start on the atherosclerotic process.
By now, it’s well established that plaque psoriasis in adults is strongly associated with increased risks of diabetes, obesity, dyslipidemia, the metabolic syndrome, and cardiovascular disease. Mounting evidence indicates children and adolescents with psoriasis face the same risks.
Everyone knows how difficult it can be to make the long-term lifestyle changes that reverse obesity and its related metabolic disorders. But dermatologists, pediatricians, and family physicians have some leverage when it comes to pediatric psoriasis.
“Think about the fact that 30% of children with psoriasis have a first-degree relative with psoriasis, usually a parent. I think we need to think about counseling young adults with psoriasis early on, especially if that adult is overweight or obese, about the need for adopting a healthy lifestyle. If they do that, it’s not just for themselves but for their children, and we just might prevent pediatric psoriasis in that family or temper its severity through that healthy lifestyle intervention,” Dr. Paller continued.
The hope is that effectively addressing the metabolic comorbidities of pediatric psoriasis will modulate and improve the skin disease; in other words, that weight loss could improve psoriasis. As yet, however, that’s just a hope, as there is no persuasive supporting evidence.
“We’re looking towards ongoing adult trials to give us some clues about whether that’s the case,” she said.
Evidence for comorbidities
Some of the key evidence regarding the metabolic comorbidities of pediatric psoriasis comes from a landmark German epidemiologic study involving 33,981 pediatric psoriasis patients. The prevalence of psoriasis in German youth rose linearly from 0.12% at age 1 year to 1.2% at age 18. Pediatric psoriasis patients had significantly higher rates of diabetes, hyperlipidemia, obesity, and hypertension than did nonpsoriatic controls (Br. J. Dermatol. 2010;162:633-6).
A Kaiser Permanente study of nearly 711,000 youths aged 2-19 years showed that those who were overweight were 2.8-fold more likely than normal-weight youth to have severe or widespread psoriasis, while those who were moderately obese were at 2.9-fold increased risk and extremely obese youth were at 4.2-fold increased risk. Among adolescents, having psoriasis was associated with significantly higher mean total and LDL cholesterol, triglycerides, and alanine aminotransferase levels (J. Pediatr. 2011;159:577-83).
Recent evidence suggests that even before increased levels of LDL cholesterol and triglycerides are apparent in children with psoriasis, abnormalities in lipid function are present and may potentially serve as a novel marker for early cardiovascular risk. Dr. Paller cited a study presented by Dr. Wynnis L. Tom of Rady Children’s Hospital, San Diego, at the 2015 annual meeting of the Society for Investigative Dermatology. The case-control study included 50 children with psoriasis and 50 matched controls with a mean age of 13 years.
Like other investigators, Dr. Tom found that the psoriatic children had higher waist/hip ratios and more insulin resistance. While fasting lipid levels didn’t differ between the two groups, the psoriasis patients had significantly higher levels of atherogenic apolipoprotein B, fewer of the particularly cardioprotective large-size HDL particles, and reduced HDL efflux capacity. Stay tuned regarding these potential early markers, Dr. Paller advised.
She was lead author of a 409-patient international study that showed the risks of obesity and a high waist circumference rise with greater severity of pediatric psoriasis. Children with severe psoriasis were at 4.92-fold increased risk of obesity, compared with controls, while even those with mild psoriasis were at 3.6-fold increased risk (JAMA Dermatol. 2013;149:166-76).
Which comes first?
The question arises: Which comes first in children, the excess adiposity or the psoriasis? Dr. Paller said that although the final word isn’t in, she and her coworkers found in a pilot study of 27 overweight or obese children with psoriasis that excess adiposity typically came first. Moreover, among the roughly one-half of children with a family history of obesity, onset of psoriasis occurred a full 3 years earlier than in those without a positive family history (JAMA Dermatol. 2014;150:573-4).
In another small study, this by investigators at Tufts University, Boston, 6 of 20 children with psoriasis (30%) met criteria for the metabolic syndrome, compared with just 1 of 20 matched nonpsoriatic controls (Pediatr. Dermatol. 2013;30:700-5).
Dr. Paller said that if dermatologists and primary care physicians are to successfully collaborate in tackling the comorbid metabolic disorders associated with pediatric psoriasis, a prerequisite is that dermatologists are going to have to do a better job of educating their primary care colleagues about the skin disease as manifest in children.
“I think it’s very important that pediatricians are aware that psoriasis is a risk factor for metabolic syndrome. But pediatric psoriasis is often misdiagnosed by primary care physicians who mistake it for eczema or tinea infection or contact dermatitis,” according to the pediatric dermatologist.
In one eye-catching Australian study, she noted, a mere 9% of patients with pediatric psoriasis were correctly diagnosed before referral to a dermatologist (Australas. J. Dermatol. 2012;53:98-105).
Pediatric psoriasis: not just skin deep
In addition to the increased risk of metabolic disorders faced by pediatric psoriasis patients, other common comorbidities include depression, anxiety disorders, impaired self-esteem and quality of life, arthritis, and Crohn’s disease, Dr. Paller observed.
• Quality of life. “The quality of life impact of psoriasis is profound. It’s a highly visible disorder, which affects the development of self-esteem and social relationships,” Dr. Paller said.
Investigators at Texas A&M University applied the Pediatric Quality of Life Inventory Version 4.0 to 208 patients aged 2-17 years with moderate to severe psoriasis and compared the results to published data on children with arthritis, asthma, diabetes, and psychiatric disorders. Health-related quality of life turned out to be more impaired in the psoriasis patients than in those with diabetes. The quality-of-life impairment associated with pediatric psoriasis was comparable to that of having asthma or arthritis, albeit not as severe as for pediatric psychiatric disorders (Eur. J. Pediatr. 2012;171:485-92).
• Psychiatric disorders. A study of more than 7,400 pediatric psoriasis patients concluded they had an adjusted 25% increased risk of developing depression, compared with psoriasis-free controls, as well as a 32% increased risk of anxiety disorders and a 55% greater risk of bipolar disorder (J. Am. Acad. Dermatol. 2012;67:651-7.e2).
• Psoriatic arthritis. An estimated 1 in 10 U.S. children with psoriasis report having arthritis, often classified as juvenile idiopathic arthritis (JAMA Dermatol. 2013;149:1180-5).
• Crohn’s disease. A large German epidemiologic study concluded that psoriasis was associated with a 3.69-fold increased risk of Crohn’s disease. There was no increased risk of ulcerative colitis (Br. J. Dermatol. 2010;162:633-6).
Dr. Paller reported receiving research grants from Amgen and Leo and serving as a consultant to AbbVie.
VANCOUVER – Dermatologists and primary care physicians working collaboratively have a golden opportunity to improve the long-term health of pediatric psoriasis patients by addressing their predisposition to components of the metabolic syndrome, Dr. Amy S. Paller declared at the World Congress of Dermatology.
“I think we as dermatologists should be in touch with the primary care doctors of every one of our children with psoriasis. Together, we should be thinking about whether the child has metabolic issues and working jointly to most effectively counsel and evaluate these children for their potential risk for these metabolic disorders,” said Dr. Paller, professor and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Pediatric psoriasis is commonly associated with other comorbid conditions in addition to metabolic disorders. But the metabolic syndrome has recently become the focus of increasing attention given that cardiovascular disease is the No. 1 cause of death in the United States, and it appears that children with psoriasis may be getting a jump start on the atherosclerotic process.
By now, it’s well established that plaque psoriasis in adults is strongly associated with increased risks of diabetes, obesity, dyslipidemia, the metabolic syndrome, and cardiovascular disease. Mounting evidence indicates children and adolescents with psoriasis face the same risks.
Everyone knows how difficult it can be to make the long-term lifestyle changes that reverse obesity and its related metabolic disorders. But dermatologists, pediatricians, and family physicians have some leverage when it comes to pediatric psoriasis.
“Think about the fact that 30% of children with psoriasis have a first-degree relative with psoriasis, usually a parent. I think we need to think about counseling young adults with psoriasis early on, especially if that adult is overweight or obese, about the need for adopting a healthy lifestyle. If they do that, it’s not just for themselves but for their children, and we just might prevent pediatric psoriasis in that family or temper its severity through that healthy lifestyle intervention,” Dr. Paller continued.
The hope is that effectively addressing the metabolic comorbidities of pediatric psoriasis will modulate and improve the skin disease; in other words, that weight loss could improve psoriasis. As yet, however, that’s just a hope, as there is no persuasive supporting evidence.
“We’re looking towards ongoing adult trials to give us some clues about whether that’s the case,” she said.
Evidence for comorbidities
Some of the key evidence regarding the metabolic comorbidities of pediatric psoriasis comes from a landmark German epidemiologic study involving 33,981 pediatric psoriasis patients. The prevalence of psoriasis in German youth rose linearly from 0.12% at age 1 year to 1.2% at age 18. Pediatric psoriasis patients had significantly higher rates of diabetes, hyperlipidemia, obesity, and hypertension than did nonpsoriatic controls (Br. J. Dermatol. 2010;162:633-6).
A Kaiser Permanente study of nearly 711,000 youths aged 2-19 years showed that those who were overweight were 2.8-fold more likely than normal-weight youth to have severe or widespread psoriasis, while those who were moderately obese were at 2.9-fold increased risk and extremely obese youth were at 4.2-fold increased risk. Among adolescents, having psoriasis was associated with significantly higher mean total and LDL cholesterol, triglycerides, and alanine aminotransferase levels (J. Pediatr. 2011;159:577-83).
Recent evidence suggests that even before increased levels of LDL cholesterol and triglycerides are apparent in children with psoriasis, abnormalities in lipid function are present and may potentially serve as a novel marker for early cardiovascular risk. Dr. Paller cited a study presented by Dr. Wynnis L. Tom of Rady Children’s Hospital, San Diego, at the 2015 annual meeting of the Society for Investigative Dermatology. The case-control study included 50 children with psoriasis and 50 matched controls with a mean age of 13 years.
Like other investigators, Dr. Tom found that the psoriatic children had higher waist/hip ratios and more insulin resistance. While fasting lipid levels didn’t differ between the two groups, the psoriasis patients had significantly higher levels of atherogenic apolipoprotein B, fewer of the particularly cardioprotective large-size HDL particles, and reduced HDL efflux capacity. Stay tuned regarding these potential early markers, Dr. Paller advised.
She was lead author of a 409-patient international study that showed the risks of obesity and a high waist circumference rise with greater severity of pediatric psoriasis. Children with severe psoriasis were at 4.92-fold increased risk of obesity, compared with controls, while even those with mild psoriasis were at 3.6-fold increased risk (JAMA Dermatol. 2013;149:166-76).
Which comes first?
The question arises: Which comes first in children, the excess adiposity or the psoriasis? Dr. Paller said that although the final word isn’t in, she and her coworkers found in a pilot study of 27 overweight or obese children with psoriasis that excess adiposity typically came first. Moreover, among the roughly one-half of children with a family history of obesity, onset of psoriasis occurred a full 3 years earlier than in those without a positive family history (JAMA Dermatol. 2014;150:573-4).
In another small study, this by investigators at Tufts University, Boston, 6 of 20 children with psoriasis (30%) met criteria for the metabolic syndrome, compared with just 1 of 20 matched nonpsoriatic controls (Pediatr. Dermatol. 2013;30:700-5).
Dr. Paller said that if dermatologists and primary care physicians are to successfully collaborate in tackling the comorbid metabolic disorders associated with pediatric psoriasis, a prerequisite is that dermatologists are going to have to do a better job of educating their primary care colleagues about the skin disease as manifest in children.
“I think it’s very important that pediatricians are aware that psoriasis is a risk factor for metabolic syndrome. But pediatric psoriasis is often misdiagnosed by primary care physicians who mistake it for eczema or tinea infection or contact dermatitis,” according to the pediatric dermatologist.
In one eye-catching Australian study, she noted, a mere 9% of patients with pediatric psoriasis were correctly diagnosed before referral to a dermatologist (Australas. J. Dermatol. 2012;53:98-105).
Pediatric psoriasis: not just skin deep
In addition to the increased risk of metabolic disorders faced by pediatric psoriasis patients, other common comorbidities include depression, anxiety disorders, impaired self-esteem and quality of life, arthritis, and Crohn’s disease, Dr. Paller observed.
• Quality of life. “The quality of life impact of psoriasis is profound. It’s a highly visible disorder, which affects the development of self-esteem and social relationships,” Dr. Paller said.
Investigators at Texas A&M University applied the Pediatric Quality of Life Inventory Version 4.0 to 208 patients aged 2-17 years with moderate to severe psoriasis and compared the results to published data on children with arthritis, asthma, diabetes, and psychiatric disorders. Health-related quality of life turned out to be more impaired in the psoriasis patients than in those with diabetes. The quality-of-life impairment associated with pediatric psoriasis was comparable to that of having asthma or arthritis, albeit not as severe as for pediatric psychiatric disorders (Eur. J. Pediatr. 2012;171:485-92).
• Psychiatric disorders. A study of more than 7,400 pediatric psoriasis patients concluded they had an adjusted 25% increased risk of developing depression, compared with psoriasis-free controls, as well as a 32% increased risk of anxiety disorders and a 55% greater risk of bipolar disorder (J. Am. Acad. Dermatol. 2012;67:651-7.e2).
• Psoriatic arthritis. An estimated 1 in 10 U.S. children with psoriasis report having arthritis, often classified as juvenile idiopathic arthritis (JAMA Dermatol. 2013;149:1180-5).
• Crohn’s disease. A large German epidemiologic study concluded that psoriasis was associated with a 3.69-fold increased risk of Crohn’s disease. There was no increased risk of ulcerative colitis (Br. J. Dermatol. 2010;162:633-6).
Dr. Paller reported receiving research grants from Amgen and Leo and serving as a consultant to AbbVie.
EXPERT ANALYSIS FROM WCD 2015

Secukinumab proves successful against psoriatic arthritis in FUTURE 2 trial
Treatment of psoriatic arthritis over 24 weeks with the human anti-interleukin-17A monoclonal antibody secukinumab allowed a significantly higher percentage of patients who received 150-mg and 300-mg doses to achieve at least 20% improvement in the American College of Rheumatology response criteria than did placebo.
The results of the multicenter, double-blind, randomized, placebo-controlled FUTURE 2 trial hinted at the effectiveness of the 300-mg dosing regimen in treating patients who previously had not responded to treatment with tumor necrosis factor (TNF) inhibitors and did not show differences in effectiveness when used together with methotrexate. The drug did not have any particularly worrisome treatment-related adverse events, Dr. Iain McInnes of the University of Glasgow (Scotland) and his colleagues reported (Lancet 2015 June 28 [doi:10.1016/S0140-6736(15)61134-5]).
At week 24, ACR20 responses occurred in 54 of 100 patients who received secukinumab 300 mg, 51 of 100 who took the 150-mg dosing regimen, 29 of 99 on the 75-mg dosing regimen, and 15 of 98 on placebo. The odds for achieving ACR20 at 24 weeks were nearly sevenfold higher for the 300-mg dose (odds ratio, 6.81; 95% confidence interval, 3.42-13.56; P < .0001) and 150-mg doses (OR, 6.52; 95% CI, 3.25-13.08; P < .0001) than with placebo.
In an editorial accompanying the report, Dr. Philip Helliwell and Dr. Laura Coates of the University of Leeds (England) said that it is important to note that responses at week 24 were similar to those observed at weeks 12 and 16 so that patients and physicians can “get an idea of response (or non-response) at an early timepoint” (Lancet 2015 June 28 [doi:10.1016/S0140-6736(15)61170-9]).
Although radiographic progression wasn’t assessed in the FUTURE 2 trial, Dr. Helliwell and Dr. Coates noted that secukinumab inhibited radiographic damage in the unpublished FUTURE-1 trial, so “in view of its position in the cytokine hierarchy, interleukin-17 inhibition might prevent both of these features, and future studies with this class of drug should investigate this issue in detail.”
The lower response that seemed to have occurred in the secukinumab-treated patients who had previously used TNF inhibitors vs. those who had not “is in keeping with data for other treatments such as ustekinumab,” they wrote. The fact that there appeared to be a dose-response effect between the patients who received 150 mg secukinumab vs. 300 mg and had previously used TNF inhibitors suggests that the 300-mg dose might be more appropriate for patients who did not respond to TNF inhibitors and/or have moderate to severe psoriasis, for whom the 300-mg dose is already approved and recommended.
Read our meeting coverage of the FUTURE 2 trial at ACR 2014 here.
Treatment of psoriatic arthritis over 24 weeks with the human anti-interleukin-17A monoclonal antibody secukinumab allowed a significantly higher percentage of patients who received 150-mg and 300-mg doses to achieve at least 20% improvement in the American College of Rheumatology response criteria than did placebo.
The results of the multicenter, double-blind, randomized, placebo-controlled FUTURE 2 trial hinted at the effectiveness of the 300-mg dosing regimen in treating patients who previously had not responded to treatment with tumor necrosis factor (TNF) inhibitors and did not show differences in effectiveness when used together with methotrexate. The drug did not have any particularly worrisome treatment-related adverse events, Dr. Iain McInnes of the University of Glasgow (Scotland) and his colleagues reported (Lancet 2015 June 28 [doi:10.1016/S0140-6736(15)61134-5]).
At week 24, ACR20 responses occurred in 54 of 100 patients who received secukinumab 300 mg, 51 of 100 who took the 150-mg dosing regimen, 29 of 99 on the 75-mg dosing regimen, and 15 of 98 on placebo. The odds for achieving ACR20 at 24 weeks were nearly sevenfold higher for the 300-mg dose (odds ratio, 6.81; 95% confidence interval, 3.42-13.56; P < .0001) and 150-mg doses (OR, 6.52; 95% CI, 3.25-13.08; P < .0001) than with placebo.
In an editorial accompanying the report, Dr. Philip Helliwell and Dr. Laura Coates of the University of Leeds (England) said that it is important to note that responses at week 24 were similar to those observed at weeks 12 and 16 so that patients and physicians can “get an idea of response (or non-response) at an early timepoint” (Lancet 2015 June 28 [doi:10.1016/S0140-6736(15)61170-9]).
Although radiographic progression wasn’t assessed in the FUTURE 2 trial, Dr. Helliwell and Dr. Coates noted that secukinumab inhibited radiographic damage in the unpublished FUTURE-1 trial, so “in view of its position in the cytokine hierarchy, interleukin-17 inhibition might prevent both of these features, and future studies with this class of drug should investigate this issue in detail.”
The lower response that seemed to have occurred in the secukinumab-treated patients who had previously used TNF inhibitors vs. those who had not “is in keeping with data for other treatments such as ustekinumab,” they wrote. The fact that there appeared to be a dose-response effect between the patients who received 150 mg secukinumab vs. 300 mg and had previously used TNF inhibitors suggests that the 300-mg dose might be more appropriate for patients who did not respond to TNF inhibitors and/or have moderate to severe psoriasis, for whom the 300-mg dose is already approved and recommended.
Read our meeting coverage of the FUTURE 2 trial at ACR 2014 here.
Treatment of psoriatic arthritis over 24 weeks with the human anti-interleukin-17A monoclonal antibody secukinumab allowed a significantly higher percentage of patients who received 150-mg and 300-mg doses to achieve at least 20% improvement in the American College of Rheumatology response criteria than did placebo.
The results of the multicenter, double-blind, randomized, placebo-controlled FUTURE 2 trial hinted at the effectiveness of the 300-mg dosing regimen in treating patients who previously had not responded to treatment with tumor necrosis factor (TNF) inhibitors and did not show differences in effectiveness when used together with methotrexate. The drug did not have any particularly worrisome treatment-related adverse events, Dr. Iain McInnes of the University of Glasgow (Scotland) and his colleagues reported (Lancet 2015 June 28 [doi:10.1016/S0140-6736(15)61134-5]).
At week 24, ACR20 responses occurred in 54 of 100 patients who received secukinumab 300 mg, 51 of 100 who took the 150-mg dosing regimen, 29 of 99 on the 75-mg dosing regimen, and 15 of 98 on placebo. The odds for achieving ACR20 at 24 weeks were nearly sevenfold higher for the 300-mg dose (odds ratio, 6.81; 95% confidence interval, 3.42-13.56; P < .0001) and 150-mg doses (OR, 6.52; 95% CI, 3.25-13.08; P < .0001) than with placebo.
In an editorial accompanying the report, Dr. Philip Helliwell and Dr. Laura Coates of the University of Leeds (England) said that it is important to note that responses at week 24 were similar to those observed at weeks 12 and 16 so that patients and physicians can “get an idea of response (or non-response) at an early timepoint” (Lancet 2015 June 28 [doi:10.1016/S0140-6736(15)61170-9]).
Although radiographic progression wasn’t assessed in the FUTURE 2 trial, Dr. Helliwell and Dr. Coates noted that secukinumab inhibited radiographic damage in the unpublished FUTURE-1 trial, so “in view of its position in the cytokine hierarchy, interleukin-17 inhibition might prevent both of these features, and future studies with this class of drug should investigate this issue in detail.”
The lower response that seemed to have occurred in the secukinumab-treated patients who had previously used TNF inhibitors vs. those who had not “is in keeping with data for other treatments such as ustekinumab,” they wrote. The fact that there appeared to be a dose-response effect between the patients who received 150 mg secukinumab vs. 300 mg and had previously used TNF inhibitors suggests that the 300-mg dose might be more appropriate for patients who did not respond to TNF inhibitors and/or have moderate to severe psoriasis, for whom the 300-mg dose is already approved and recommended.
Read our meeting coverage of the FUTURE 2 trial at ACR 2014 here.
Undiagnosed Psoriatic Arthritis
Of all the comorbidities associated with psoriasis, psoriatic arthritis (PsA) is the most common and one of the most problematic. Early recognition, diagnosis, and treatment of PsA can help prevent or limit extensive joint damage that occurs in later stages of the disease. Because cutaneous psoriasis precedes the onset of PsA in 84% of patients with psoriasis, it is incumbent upon dermatologists to be the first line of defense in the screening for joint problems. However, the efficacy of PsA screening remains unknown.
In a recent article published online on June 5 in the Journal of the American Academy of Dermatology, Villani et al performed an analysis to determine the point prevalence of undiagnosed PsA in patients with psoriasis, utilizing a systematic search of the literature and meta-analysis. Searching PubMed, Cochrane, and Embase databases, the authors identified 394 studies for review. None of the studies sought to determine the prevalence of undiagnosed PsA in patients with psoriasis.
The investigators made the assumption that the prevalence of newly diagnosed PsA in patients with psoriasis at the time they sought medical care could be a reasonable estimate of this value. Seven epidemiological studies and 5 studies on PsA screening questionnaires were selected for review and were used to clearly identify patients with newly diagnosed PsA.
The authors found that the prevalence of undiagnosed PsA was 15.5% when all studies were analyzed and 10.1% when only epidemiological studies were included. The high prevalence of undiagnosed PsA in patients with psoriasis reinforces the recommendation that dermatologists need to screen all patients with psoriasis for PsA.
What’s the issue?
The findings of this study are not surprising. Therefore, it is important that we double our efforts to screen patients for PsA to address this comorbidity as early as possible. Improved algorithms for screening of patients for PsA would be a welcome advancement. How will you improve your screening methods for PsA?
Of all the comorbidities associated with psoriasis, psoriatic arthritis (PsA) is the most common and one of the most problematic. Early recognition, diagnosis, and treatment of PsA can help prevent or limit extensive joint damage that occurs in later stages of the disease. Because cutaneous psoriasis precedes the onset of PsA in 84% of patients with psoriasis, it is incumbent upon dermatologists to be the first line of defense in the screening for joint problems. However, the efficacy of PsA screening remains unknown.
In a recent article published online on June 5 in the Journal of the American Academy of Dermatology, Villani et al performed an analysis to determine the point prevalence of undiagnosed PsA in patients with psoriasis, utilizing a systematic search of the literature and meta-analysis. Searching PubMed, Cochrane, and Embase databases, the authors identified 394 studies for review. None of the studies sought to determine the prevalence of undiagnosed PsA in patients with psoriasis.
The investigators made the assumption that the prevalence of newly diagnosed PsA in patients with psoriasis at the time they sought medical care could be a reasonable estimate of this value. Seven epidemiological studies and 5 studies on PsA screening questionnaires were selected for review and were used to clearly identify patients with newly diagnosed PsA.
The authors found that the prevalence of undiagnosed PsA was 15.5% when all studies were analyzed and 10.1% when only epidemiological studies were included. The high prevalence of undiagnosed PsA in patients with psoriasis reinforces the recommendation that dermatologists need to screen all patients with psoriasis for PsA.
What’s the issue?
The findings of this study are not surprising. Therefore, it is important that we double our efforts to screen patients for PsA to address this comorbidity as early as possible. Improved algorithms for screening of patients for PsA would be a welcome advancement. How will you improve your screening methods for PsA?
Of all the comorbidities associated with psoriasis, psoriatic arthritis (PsA) is the most common and one of the most problematic. Early recognition, diagnosis, and treatment of PsA can help prevent or limit extensive joint damage that occurs in later stages of the disease. Because cutaneous psoriasis precedes the onset of PsA in 84% of patients with psoriasis, it is incumbent upon dermatologists to be the first line of defense in the screening for joint problems. However, the efficacy of PsA screening remains unknown.
In a recent article published online on June 5 in the Journal of the American Academy of Dermatology, Villani et al performed an analysis to determine the point prevalence of undiagnosed PsA in patients with psoriasis, utilizing a systematic search of the literature and meta-analysis. Searching PubMed, Cochrane, and Embase databases, the authors identified 394 studies for review. None of the studies sought to determine the prevalence of undiagnosed PsA in patients with psoriasis.
The investigators made the assumption that the prevalence of newly diagnosed PsA in patients with psoriasis at the time they sought medical care could be a reasonable estimate of this value. Seven epidemiological studies and 5 studies on PsA screening questionnaires were selected for review and were used to clearly identify patients with newly diagnosed PsA.
The authors found that the prevalence of undiagnosed PsA was 15.5% when all studies were analyzed and 10.1% when only epidemiological studies were included. The high prevalence of undiagnosed PsA in patients with psoriasis reinforces the recommendation that dermatologists need to screen all patients with psoriasis for PsA.
What’s the issue?
The findings of this study are not surprising. Therefore, it is important that we double our efforts to screen patients for PsA to address this comorbidity as early as possible. Improved algorithms for screening of patients for PsA would be a welcome advancement. How will you improve your screening methods for PsA?

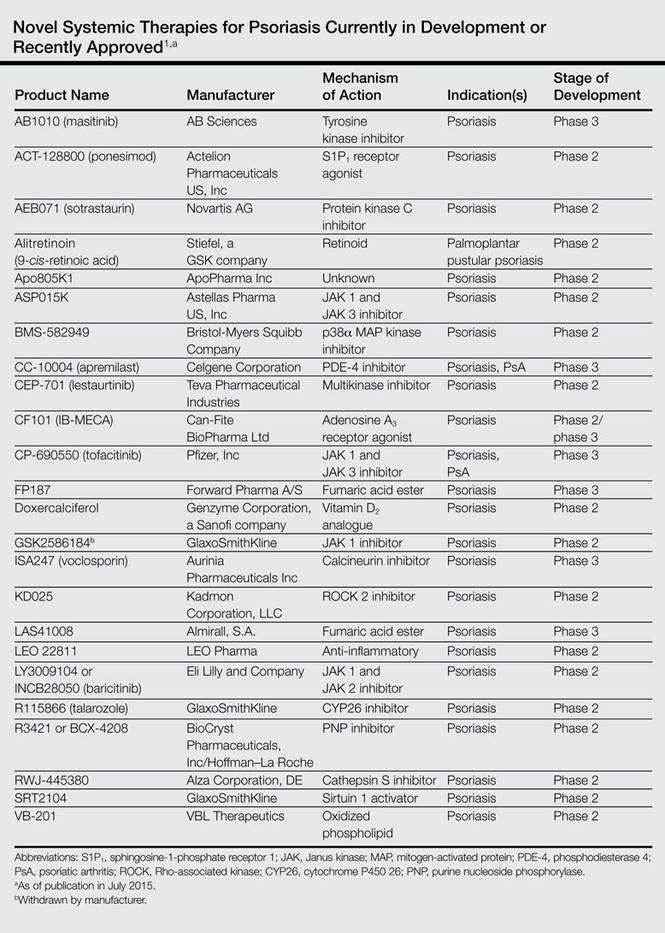
Novel Psoriasis Therapies and Patient Outcomes, Part 3: Systemic Medications
Evolving knowledge of the underlying pathogenesis of psoriasis has afforded the development of a broad spectrum of nonbiologic systemic medications with therapeutic potential in moderate to severe psoriasis and psoriatic arthritis (PsA). The targets for these medications are antagonists of proinflammatory mediators such as tyrosine kinase, protein kinase, Janus kinase (JAK), p38α mitogen-activated protein (MAP) kinase, phosphodiesterase 4 (PDE-4), calcineurin, Rho-associated kinase (ROCK) 2, cytochrome P450 26 (CYP26), and purine nucleoside phosphorylase (PNP); agonists of anti-inflammatory mediators such as sphingosine-1-phosphate receptor 1 (S1P1) and adeno-sine A3 receptor; and myriad other mechanisms. A brief introduction to some of these therapies presently in phase 2 and phase 3 clinical trials are presented (Table).1
Masitinib (Tyrosine Kinase Inhibitor)
Masitinib (formerly known as AB1010)(AB Sciences) is a tyrosine kinase inhibitor that is purported to decrease inflammation by inhibiting stem cell factor receptor (c-kit) and consequently limiting mast cell degranulation.2 A randomized, placebo-controlled, double-blind phase 3 study evaluating its efficacy as an oral formulation was completed, but the results were not available at the time of publication (registered at www.clinicaltrials.gov with the identifier NCT01045577).
Ponesimod (S1P1 Receptor Agonist)
Ponesimod (formerly known as ACT-128800)(Actelion Pharmaceuticals US, Inc) is an orally formulated S1P1 receptor agonist. Sphingosine-1-phosphate receptor 1 is necessary for lymphoid chemotaxis.3 A randomized, placebo-controlled, double-blind phase 2 trial of 326 patients demonstrated 75% improvement in psoriasis area and severity index (PASI) score at week 16 in 13.4%, 46.0%, and 48.1% of participants receiving placebo, ponesimod 20 mg, and ponesimod 40 mg, respectively.4 At week 28, PASI 75 scores for participants transitioned from ponesimod 40 mg to placebo or ponesimod 20 mg to placebo and those maintained on ponesimod 20 mg and 40 mg were 40.4%, 42.2%, 77.4%, and 71.4%, respectively. This study demonstrated benefit of treatment with ponesimod versus placebo with increased efficacy using maintenance therapy.4
Sotrastaurin (Protein Kinase C Inhibitor)
Sotrastaurin (formerly known as AEB071)(Novartis AG) is an oral medication that inhibitsprotein kinase C, thereby limiting CD28-induced activation of T cells. Furthermore, it increases forkhead box P3 expression, which is important, as proinflammatory IL-17 production is stimulated in regulatory T cells with lost forkhead box P3 expression.5 In a study of 32 patients who received placebo or sotrastaurin 25, 100, 200, or 300 mg twice daily for 2 weeks, the mean PASI score was reduced by 69% for the 300-mg group versus 5.3% for placebo.6 A randomized, placebo-controlled, double-blind phase 2 study was completed for patients with moderate to severe psoriasis, but the results were not available at the time of publication (NCT00885196).
Alitretinoin (Retinoid)
Alitretinoin (9-cis-retinoic acid; Stiefel, a GSK company) is an oral retinoid with purported promise for patients with palmoplantar pustular psoriasis recalcitrant to conventional therapies. In one study, 7 participants with palmoplantar psoriasis received alitretinoin 30 mg daily for 12 weeks with 60% to 90% clinical improvement noted using the visual analog scale and palmoplantar pustular PASI to assess response.7 A randomized, placebo-controlled, double-blind phase 2 trial of alitretinoin assessing the success of alitretinoin in patients with palmoplantar psoriasis recalcitrant to topical treatments was completed, but the results were not available at the time of publication (NCT01245140).
Apo805K1 (Unknown Mechanism of Action)
Apo805K1 (ApoPharma Inc) is an oral agent whose mechanism of action has not been disclosed. A randomized, placebo-controlled, double-blind phase 2 trial in patients with moderate to severe psoriasis with a treatment duration of 14 days has been completed. For 12 weeks there was a daily dosing regimen of Apo805K1 10, 30, 60, or 100 mg or placebo, with 12 patients in each treatment group. The proportion of patients achieving PASI 75 was 16.7%, 0%, 0%, 8.3%, and 16.7%, respectively (P=.1975). The number of participants with adverse events reported ranged between 4 to 7, with the greatest number of adverse events reported in the 30-mg subset.8 It may be of interest to repeat the study with a larger sample size.
ASP015K (JAK 1 and JAK 3 Inhibitor)
ASP015K (Astellas Pharma US, Inc) is the first of the JAK inhibitors that will be discussed in this section. Janus kinase inhibitors represent a group of tyrosine kinases that regulate cytokine-mediated signaling pathways through the activation of signal transducer and activator of transcription proteins via phosphorylation in the cytoplasm, which in turn control the transcription of genes that generate inflammation. ASP015K and tofacitinib (formerly known as CP-690550)(Pfizer, Inc) inhibit JAK 1 and JAK 3, whereas GSK2586184 (GlaxoSmithKline) inhibits JAK 1 and baricitinib (formerly known as LY3009104 or INCB28050)(Eli Lilly and Company) inhibits JAK 1 and JAK 2.9 In a 6-week, dose-escalation phase 2 trial in patients with moderate to severe psoriasis, ASP015K showed a dose-dependent decline in PASI, psoriasis static global assessment, and body surface area.10
BMS-582949 (p38α MAP Kinase Inhibitor)
BMS-582949 (Bristol-Myers Squibb Company) is an oral p38α MAP kinase inhibitor.11 Along with c-Jun N-terminal kinase and extracellular signal-regulated protein kinases 1 and 2, MAP kinase plays a role in the pathogenesis of psoriasis.12 A randomized, placebo-controlled, double-blind, 12-week phase 2a study of placebo versus BMS-582949 dosed at 10, 30, and 100 mg has been completed, but the results were not available at the time of publication (NCT00399906).
Apremilast (PDE-4 Inhibitor)
Apremilast (formerly known as CC-10004)(Celgene Corporation) is an oral PDE-4 inhibitor that acts to inhibit the degradation of cyclic adenosine monophosphate. It is approved by the US Food and Drug Administration for moderate to severe plaque psoriasis13 and is a particularly good treatment for patients with recalcitrant disease.14 Several studies on apremilast have been published, including a phase 2 trial of 204 participants receiving placebo or apremilast 20 mg or 40 mg twice daily with American College of Rheumatology (ACR) 20% improvement response of 11.8%, 35.8%, and 43.5%, respectively.15 The phase 3 PALACE 1, 2, 3, and 4 trials also demonstrated therapeutic efficacy.16 In PALACE 1, 504 patients receiving placebo or apremilast 20 mg and 30 mg twice daily had an ACR20 of 19%, 31%, and 40%, respectively. In the PALACE 4 study, ACR20 was achieved by 58% of participants at week 52, but the ACR50 and ACR70 rates were less impressive.16
Lestaurtinib (Multikinase Inhibitor)
Lestaurtinib (formerly known as CEP-701)(Teva Pharmaceutical Industries) is an oral multikinase inhibitor for which a 12-week, nonrandomized, dose-escalation phase 2 study was completed, but the results were not available at the time of publication (NCT00236119).
CF101 (Adenosine A3 Receptor Agonist)
CF101 (IB-MECA; Can-Fite BioPharma Ltd) is an oral adenosine A3 receptor agonist. Adenosine A3 is a G protein–coupled receptor that has an anti-inflammatory role, which lends itself to the treatment of inflammatory conditions such as rheumatoid arthritis.17 In a randomized, placebo-controlled, double-blind phase 2 trial of 75 patients who received placebo or CF101 1, 2, or 4 mg twice daily for 12 weeks, PASI 50 or greater was reported in 35.3% of participants in the 2-mg group, which was statistically significant at weeks 8 (P=.047) and 12 (P=.031).18 A randomized, placebo-controlled, double-blind, 16-week phase 2/phase 3 trial in patients with moderate to severe psoriasis treated with CF101 2 mg twice daily versus placebo is ongoing but not recruiting participants (NCT01265667).
Tofacitinib (JAK 1 and JAK 3 Inhibitor)
Tofacitinib is a JAK 1 and JAK 3 inhibitor that is available in both topical and oral formulations. Many studies have been published on tofacitinib, including a dose-ranging phase 2b trial of 197 patients randomized to placebo or tofacitinib 2, 5, or 15 mg daily in which 2.0%, 25.0% (P<.001), 40.8% (P<.0001), and 66.7% (P<.0001) of participants in each treatment group, respectively, achieved PASI 75 at week 12.19 Another 12-week phase 2b trial in patients with moderate to severe psoriasis explored the effectiveness of oral formulations of tofacitinib based on body location, namely the head and neck, arms, trunk, and legs.20 Designed with twice-daily placebo and tofacitinib 2-, 5-, and 15-mg treatment arms, the target plaque severity score demonstrated a statistically significant dose-responsive improvement in each of the 4 anatomic regions (P<.01).
Two randomized, double-blinded, placebo-controlled phase 3 trials of tofacitinib have been completed. One trial compared the safety and effectiveness of tofacitinib and etanercept in patients with moderate to severe psoriasis.21 The 329 participants were randomized to treatment with oral tofacitinib 5 mg or 10 mg twice daily with placebo subcutaneous (SQ) injections twice weekly; oral placebo twice daily with etanercept 50-mg SQ injections twice weekly; or oral placebo twice daily with placebo SQ injection twice weekly. At week 12, PASI 75 was achieved in 39.51%, 63.64%, 58.81%, and 5.61% of participants in each treatment group, respectively. Thus, tofacitinib 10 mg and etanercept 50 mg were the first and second best performers in this study design.21
In the other phase 3 trial, the efficacy and safety of treatment, treatment withdrawal, and subsequent resumption of treatment with tofacitinib was examined in 290 patients who received either tofacitinib 5 mg or 10 mg or placebo twice daily for 24 weeks.22 In the withdrawal period, the percentage of patients who maintained a PASI 75 response in the tofacitinib 5-mg group was 56.2% versus 23.3% in the placebo group at week 16 (P<.0008). In the 10-mg group, 62.3% of participants maintained PASI 75 at week 16 versus 26.1% in the placebo group (P<.0001). During the re-treatment period for those who showed a greater than 50% reduction in week 24 PASI during treatment withdrawal (N=102), 50.0% of the tofacitinib 5-mg group showed PASI 75 versus 31.58% of the placebo group at week 16. In the tofacitinib 10-mg group, PASI 75 was seen in 0% versus 50.85% in the placebo group. Of note, only 5 participants who demonstrated a greater than 50% reduction in week 24 PASI response following withdrawal of therapy were in the tofacitinib 5- or 10-mg groups, as the rest were in the placebo group.22
FP187 (Fumaric Acid Ester)
FP187 (Forward Pharma A/S) is an oral fumaric acid ester whose underlying mechanism is thought to be elevation of glutathione levels that decreases the amount of inflammatory cytokines by blocking the translocation of nuclear factor κB. Other fumaric acid esters such as monoethyl fumarate and dimethyl fumarate have been used in Europe for the management of psoriasis.23 A phase 2 study of the safety and effectiveness of FP187 for moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01230138). A phase 3 trial examining the efficacy of FP187 in managing moderate to severe psoriasis was not yet open for participant recruitment at the time of publication (NCT01815723).
Doxercalciferol (Vitamin D2 Analogue)
Doxercalciferol (1α-hydroxyvitamin D2; Genzyme Corporation, a Sanofi company) is an oral prodrug of vitamin D.24 Topical preparations of vitamin D analogues approved by the US Food and Drug Administration such as calcipotriene are mainstays in psoriasis management. Doxercalciferol has been used for other therapeutic applications such as decreasing elevated parathyroid hormone levels.25 Research has demonstrated that CYP24A1 can extrahepatically regulate the activation of vitamin D prodrugs in cutaneous tissues.26 In a phase 2 study examining the efficacy and safety of doxercalciferol in patients with moderate to severe psoriasis, 111 patients were randomized to placebo or doxercalciferol 2.5, 5, or 7.5 mg daily for 24 weeks (NCT00601107). At week 12, PASI 50 was similar regardless of the treatment administered, reported at 20.0%, 20.0%, 17.9%, and 20.0%, respectively (P=1.000).27
GSK2586184 (JAK 1 Inhibitor)
GSK2586184 is an oral JAK 1 inhibitor. A placebo-controlled, double-blind, dose-dependent phase 2 study of GSK2586184 in patients with chronic plaque psoriasis who were randomized to placebo or GSK2586184 100, 200, and 400 mg twice daily for 84 days has been completed, but the results were not available at the time of publication (NCT01782664). Of note, despite clinical promise, due to potential adverse effects of the medication that included a possible interaction with statin medication, the manufacturer decided against pursuing GSK2586184 as a treatment in the management of psoriasis.28
Voclosporin (Calcineurin Inhibitor)
Voclosporin (formerly known as ISA247)(Aurinia Pharmaceuticals Inc) is an oral calcineurin inhibitor that is purported to be as effective as cyclospor-ine A with less associated toxicity. A 12-week randomized, placebo-controlled, double-blind phase 2 trial demonstrated PASI 75 in 0%, 18.2%, and 66.7% of 201 participants receiving placebo, voclospo-rin 0.5 mg/kg, and voclosporin 1.5 mg/kg twice daily, respectively (P<.0001). Elevated serum creatinine levels within the high range of normal were noted in the 1.5-mg/kg group.29 A 12-week phase 3 study of 451 patients randomized to placebo or voclospo-rin 0.2-, 0.3-, or 0.4-mg/kg treatment groups similarly demonstrated a dose-responsive PASI 75 of 4%, 16%, 25%, and 47%, respectively, that was maintained at week 24. Mild to moderate decreases in glomerular filtration rates were noted in 8 patients in the 0.3- and 0.4-mg/kg subsets.30 Another phase 2 study of voclosporin in patients with moderate to severe psoriasis showed improvements according to the psoriasis disability index and dermatology life quality index.31
Three randomized, placebo-controlled, double-blind phase 3 trials have been completed for voclosporin, but the results were not available at the time of publication. The phase 3 ESSENCE trial compared voclosporin to placebo and ciclosporin controls (NCT00408187). Two phase 3 trials known as the SPIRIT trials—one a 12-week study (NCT00244842) and the other a 36-week extension trial (NCT00258713)—compared the efficacy of placebo to voclosporin administered at 0.2-, 0.3-, and 0.4-mg/kg doses.
KD025 (ROCK 2 Inhibitor)
KD025 (Kadmon Corporation, LLC) is an oral ROCK 2 inhibitor. The inhibition of ROCK in the ras homolog gene family, member A/ROCK pathway has been targeted therapeutically for pulmonary arterial hypertension,32 glaucoma,33 and many other uses. A phase 2a study assessing the tolerability and safety profile of KD025 in patients with moderate to severe psoriasis was completed, but the results were not available at the time of publication (NCT02106195).
LAS41008 (Fumaric Acid Ester)
LAS41008 (Almirall, S.A.) is purported to be an oral dimethyl fumarate that inhibits endothelial cell proliferation, migration, and differentiation.34 A phase 3 trial comparing the safety and effectiveness of LAS41008, LASW1835 (an active comparator), and placebo in patients with moderate to severe psoriasis is ongoing but not recruiting participants (NCT01726933).
LEO 22811 (Anti-inflammatory)
LEO 22811 (LEO Pharma) is an oral anti-inflammatory agent for the treatment of psoriasis. Two clinical trials have been completed, the results of which have not yet been published. A phase 1 trial assessing the tolerability and safety profile of LEO 22811 (NCT00833872) and a phase 2 proof-of-concept study assessing dose response of LEO 22811 versus placebo (NCT01116895) were completed, but the results were not available at the time of publication.
Baricitinib (JAK 1 and JAK 2 Inhibitor)
As noted above, baricitinib (LY3009104 or INCB28050) is a JAK 1 and JAK 2 inhibitor. A phase 2b trial examining dose response for LY3009104 or baricitinib administration in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01490632).
Talarozole (CYP26 Inhibitor)
Talarozole (formerly known as R115866)(GlaxoSmithKline) is a selective oral CYP26 inhibitor that could serve to regulate the degradation of all-trans retinoic acid in the management of conditions such as acne and psoriasis. One phase 2 nonrandomized, open-label study (NCT00725348) and another phase 2 randomized, placebo-controlled, double-blind, dose-dependent trial examining the effectiveness and safety profile of 12-week talarozole treatment in patients with severe plaque psoriasis have been completed, but the results were not available at the time of publication (NCT00716144).
R3421 or BCX-4208 (PNP Inhibitor)
R3421 or BCX-4208 (BioCryst Pharmaceuticals, Inc/Hoffman–La Roche) is an oral PNP inhibitor that may help regulate apoptosis of T cells and B cells.35 A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT00504270).
RWJ-445380 (Cathepsin S Inhibitor)
RWJ-445380 (Alza Corporation, DE) is an oral cathepsin S inhibitor. Cathepsin S is produced by antigen-presenting cells and activates CD4+ T cells via presentation of antigen by class II major histocompatibility complex.36 A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial evaluating the tolerability, safety, pharmacodynamics, and pharmacokinetics of RWJ-445380 in patients with plaque psoriasis has been completed, but the results were not available at the time of publication (NCT00396422).
SRT2104 (Sirtuin 1 Activator)
SRT2104 (GlaxoSmithKline) is a selective oral NAD+-dependent deacetylase sirtuin 1 activator. Sirtuins help regulate apoptosis, inflammation, and other important cellular mechanisms.37 A randomized, open-label phase 1 trial examining drug bioavailability (NCT01702493) and a randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial studying the efficacy, tolerability, and safety of SRT2104 in patients with moderate to severe psoriasis have been completed (NCT01154101), but the results were not available at the time of publication.
VB-201 (Oxidized Phospholipid)
VB-201 (VBL Therapeutics) is an orally administered oxidized phospholipid analogue with anti-inflammatory effects.38 Oxidized phospholipids are another element in the intricate spectrum of inflammatory mediators. A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial of VB-201 20 mg or 80 mg daily in patients with moderate to severe psoriasis was completed, but the results were not available at the time of publication (NCT01001468). Another randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial of VB-201 80 mg and 160 mg twice daily in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01837420).
Conclusion
We are living in an exciting time in the treatment of psoriasis and PsA, with promising novel therapies afforded by the discovery of new therapeutic targets. In this 3-part series, we have reviewed topical, systemic, and biologic therapies that currently are in phase 2 through phase 4 clinical trials or have recently been approved by the US Food and Drug Administration for the management of psoriasis and PsA. These treatments offer patients and their caregivers the prospect of more targeted therapeutic regimens that offer enhanced clinical outcomes with more favorable side-effect profiles. As clinicians and researchers build upon this knowledge in the years to come, we can offer psoriasis patients an increasingly diverse and powerful therapeutic armamentarium.
1. Lu PD, Mazza JM. Research pipeline III: biologic therapies. In: Weinberg JM, Lebwohl M, eds. Advances in Psoriasis. New York, NY: Springer; 2014:227-242.
2. Humbert M, de Blay F, Garcia G, et al. Masitinib, a c-kit/PDGF receptor tyrosine kinase inhibitor, improves disease control in severe corticosteroid-dependent asthmatics. Allergy. 2009;64:1194-1201.
3. Krause A, Brossard P, D’Ambrosio D, et al. Population pharmacokinetics and pharmacodynamics of ponesimod, a selective S1P1 receptor modulator. J Pharmacokinet Pharmacodyn. 2014;41:261-278.
4. Vaclavkova A, Chimenti S, Arenberger P, et al. Oral ponesimod in patients with chronic plaque psoriasis: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet. 2014;384:2036-2045.
5. He X, Koenen HJ, Smeets RL, et al. Targeting PKC in human T cells using sotrastaurin (AEB071) preserves regulatory T cells and prevents IL-17 production. J Invest Dermatol. 2014;134:975-983.
6. Skvara H, Dawid M, Kleyn E, et al. The PKC inhibitor AEB071 may be a therapeutic option for psoriasis. J Clin Invest. 2008;118:3151-3159.
7. Irla N, Navarini AA, Yawalkar N. Alitretinoin abrogates innate inflammation in palmoplantar pustular psoriasis. Br J Dermatol. 2012;167:1170-1174.
8. Study to evaluate Apo805K1 in subjects with moderate to severe chronic plaque psoriasis (NCT01483924). https://clinicaltrials.gov/ct2/results?term=NCT01483924&Search=Search. Updated February 9, 2015. Accessed June 23, 2015.
9. Kofoed K, Skov L, Zachariae C. New drugs and treatment targets in psoriasis. Acta Derm Venereol. 2015;95:133-139.
10. Gooderham M. Small molecules: an overview of emerging therapeutic options in the treatment of psoriasis. Skin Therapy Lett. 2013;18:1-4.
11. Liu C, Lin J, Wrobleski ST, et al. Discovery of 4-(5-(cyclopropylcarbamoyl)-2-methylphenylamino)-5-methyl-N-propylpyrrolo[1,2-f][1,2,4]triazine-6-carboxamide (BMS-582949), a clinical p38a MAP kinase inhibitor for the treatment of inflammatory diseases. J Med Chem. 2010;53:6629-6639.
12. Mavropoulos A, Rigopoulou EI, Liaskos C, et al. The role of p38 MAPK in the aetiopathogenesis of psoriasis and psoriatic arthritis. Clin Dev Immunol. 2013;2013:569751.
13. Oral OTEZLA® (apremilast) approved by the U.S. Food and Drug Administration for the treatment of patients with moderate to severe plaque psoriasis [news release]. Summit, NJ: Celegene Corporation; September 23, 2014. http://ir.celgene.com/releasedetail.cfm?releaseid=872240. Accessed June 23, 2015.
14. Gottlieb AB, Matheson RT, Menter A, et al. Efficacy, tolerability, and pharmacodynamics of apremilast in recalcitrant plaque psoriasis: a phase II open-label study. J Drugs Dermatol. 2013;12:888-897.
15. Moustafa F, Feldman SR. A review of phosphodiesterase-inhibition and the potential role for phosphodiesterase 4-inhibitors in clinical dermatology. Dermatol Online J. 2014;20:22608.
16. Huynh D, Kavanaugh A. Psoriatic arthritis: current therapy and future approaches. Rheumatology (Oxford). 2015;54:20-28.
17. Fishman P, Bar-Yehuda S, Liang BT, et al. Pharmacological and therapeutic effects of A3 adenosine receptor agonists. Drug Discov Today. 2012;17:359-366.
18. David M, Akerman L, Ziv M, et al. Treatment of plaque-type psoriasis with oral CF101: data from an exploratory randomized phase 2 clinical trial. J Eur Acad Dermatol Venereol. 2012;26:361-367.
19. Papp KA, Menter A, Strober B, et al. Efficacy and safety of tofacitinib, an oral Janus kinase inhibitor, in the treatment of psoriasis: a phase 2b randomized placebo-controlled dose-ranging study. Br J Dermatol. 2012;167:668-677.
20. Menter A, Papp KA, Tan H, et al. Efficacy of tofacitinib, an oral Janus kinase inhibitor, on clinical signs of moderate-to-severe plaque psoriasis in different body regions. J Drugs Dermatol. 2014;13:252-256.
21. A phase 3, multi site, randomized, double blind, placebo controlled study of the efficacy and safety comparing CP-690,550 and etanercept in subjects with moderate to severe chronic plaque psoriasis (NCT01241591). https://clinicaltrials.gov/ct2/show/NCT01241591?term=01241591&rank=1. Updated May 8, 2014. Accessed June 16, 2015.
22. A study to evaluate the effects and safety of treatment, treatment withdrawal, followed by re-treatment with CP-690,550 in subjects with moderate to severe chronic plaque psoriasis (NCT01186744). https://clinicaltrials.gov/ct2/show/NCT01186744?term=01186744&rank=1. Updated May 14, 2014. Accessed June 16, 2015.
23. Rostami Yazdi M, Mrowietz U. Fumaric acid esters. Clin Dermatol. 2008;26:522-526.
24. Kubodera N. A new look at the most successful prodrugs for active vitamin D (D hormone): alfacalcidol and doxercalciferol. Molecules. 2009;14:3869-3880.
25. Brown AJ. Therapeutic uses of vitamin D analogues. Am J Kidney Dis. 2001;38(5 suppl 5):S3-S19.
26. Masuda S, Strugnell SA, Knutson JC, et al. Evidence for the activation of 1alpha-hydroxyvitamin D2 by 25-hydroxyvitamin D-24-hydroxylase: delineation of pathways involving 1alpha,24-dihydroxyvitamin D2 and 1alpha,25-dihydroxyvitamin D2. Biochim Biophys Acta. 2006;1761:221-234.
27. A study to evaluate the safety and effectiveness of doxercalciferol capsules in participants with moderate to severe psoriasis (NCT00601107). https://clinicaltrials.gov/ct2/show/NCT00601107?term=00601107&rank=1. Updated April 2, 2014. Accessed June 16, 2015.
28. GSK discloses good efficacy in psoriasis with GSK2856184 [news release]. Mechelen, Belgium: Galapagos NV; November 6, 2014. http://www.globenewswire.com/news-release/2014/11/06/680358/10106744/en/GSK-discloses-good-efficacy-in-psoriasis-with-GSK2856184.html. Accessed June 24, 2015.
29. Bissonnette R, Papp K, Poulin Y, et al. A randomized, multicenter, double-blind, placebo-controlled phase 2 trial of ISA247 in patients with chronic plaque psoriasis. J Am Acad Dermatol. 2006;54:472-478.
30. Papp K, Bissonnette R, Rosoph L, et al. Efficacy of ISA247 in plaque psoriasis: a randomised, multicentre, double-blind, placebo-controlled phase III study. Lancet. 2008;371:1337-1342.
31. Gupta AK, Langley RG, Lynde C, et al. ISA247: quality of life results from a phase II, randomized, placebo-controlled study. J Cutan Med Surg. 2008;12:268-275.
32. Antoniu SA. Targeting RhoA/ROCK pathway in pulmonary arterial hypertension. Expert Opin Ther Targets. 2012;16:355-363.
33. Challa P, Arnold JJ. Rho-kinase inhibitors offer a new approach in the treatment of glaucoma. Expert Opin Investig Drugs. 2014;23:81-95.
34. National Institute for Health Research Horizon Scanning Centre. Dimethyl fumarate for plaque psoriasis. http://www.hsc.nihr.ac.uk/files/downloads/2228/2526.163fbff8.Dimethylfumarate_Nov13.pdf. Published November 2013. Accessed June 15, 2015.
35. Bantia S, Parker C, Upshaw R, et al. Potent orally bioavailable purine nucleoside phosphorylase inhibitor BCX-4208 induces apoptosis in B- and T-lymphocytes—a novel treatment approach for autoimmune diseases, organ transplantation and hematologic malignancies. Int Immunopharmacol. 2010;10:784-790.
36. García-Pérez ME, Stevanovic T, Poubelle PE. New therapies under development for psoriasis treatment. Curr Opin Pediatr. 2013;25:480-487.
37. Villalba JM, Alcaín FJ. Sirtuin activators and inhibitors. Biofactors. 2012;38:349-359.
38. Feige E, Mendel I, George J, et al. Modified phospholipids as anti-inflammatory compounds. Curr Opin Lipidol. 2010;21:525-529.
Evolving knowledge of the underlying pathogenesis of psoriasis has afforded the development of a broad spectrum of nonbiologic systemic medications with therapeutic potential in moderate to severe psoriasis and psoriatic arthritis (PsA). The targets for these medications are antagonists of proinflammatory mediators such as tyrosine kinase, protein kinase, Janus kinase (JAK), p38α mitogen-activated protein (MAP) kinase, phosphodiesterase 4 (PDE-4), calcineurin, Rho-associated kinase (ROCK) 2, cytochrome P450 26 (CYP26), and purine nucleoside phosphorylase (PNP); agonists of anti-inflammatory mediators such as sphingosine-1-phosphate receptor 1 (S1P1) and adeno-sine A3 receptor; and myriad other mechanisms. A brief introduction to some of these therapies presently in phase 2 and phase 3 clinical trials are presented (Table).1
Masitinib (Tyrosine Kinase Inhibitor)
Masitinib (formerly known as AB1010)(AB Sciences) is a tyrosine kinase inhibitor that is purported to decrease inflammation by inhibiting stem cell factor receptor (c-kit) and consequently limiting mast cell degranulation.2 A randomized, placebo-controlled, double-blind phase 3 study evaluating its efficacy as an oral formulation was completed, but the results were not available at the time of publication (registered at www.clinicaltrials.gov with the identifier NCT01045577).
Ponesimod (S1P1 Receptor Agonist)
Ponesimod (formerly known as ACT-128800)(Actelion Pharmaceuticals US, Inc) is an orally formulated S1P1 receptor agonist. Sphingosine-1-phosphate receptor 1 is necessary for lymphoid chemotaxis.3 A randomized, placebo-controlled, double-blind phase 2 trial of 326 patients demonstrated 75% improvement in psoriasis area and severity index (PASI) score at week 16 in 13.4%, 46.0%, and 48.1% of participants receiving placebo, ponesimod 20 mg, and ponesimod 40 mg, respectively.4 At week 28, PASI 75 scores for participants transitioned from ponesimod 40 mg to placebo or ponesimod 20 mg to placebo and those maintained on ponesimod 20 mg and 40 mg were 40.4%, 42.2%, 77.4%, and 71.4%, respectively. This study demonstrated benefit of treatment with ponesimod versus placebo with increased efficacy using maintenance therapy.4
Sotrastaurin (Protein Kinase C Inhibitor)
Sotrastaurin (formerly known as AEB071)(Novartis AG) is an oral medication that inhibitsprotein kinase C, thereby limiting CD28-induced activation of T cells. Furthermore, it increases forkhead box P3 expression, which is important, as proinflammatory IL-17 production is stimulated in regulatory T cells with lost forkhead box P3 expression.5 In a study of 32 patients who received placebo or sotrastaurin 25, 100, 200, or 300 mg twice daily for 2 weeks, the mean PASI score was reduced by 69% for the 300-mg group versus 5.3% for placebo.6 A randomized, placebo-controlled, double-blind phase 2 study was completed for patients with moderate to severe psoriasis, but the results were not available at the time of publication (NCT00885196).
Alitretinoin (Retinoid)
Alitretinoin (9-cis-retinoic acid; Stiefel, a GSK company) is an oral retinoid with purported promise for patients with palmoplantar pustular psoriasis recalcitrant to conventional therapies. In one study, 7 participants with palmoplantar psoriasis received alitretinoin 30 mg daily for 12 weeks with 60% to 90% clinical improvement noted using the visual analog scale and palmoplantar pustular PASI to assess response.7 A randomized, placebo-controlled, double-blind phase 2 trial of alitretinoin assessing the success of alitretinoin in patients with palmoplantar psoriasis recalcitrant to topical treatments was completed, but the results were not available at the time of publication (NCT01245140).
Apo805K1 (Unknown Mechanism of Action)
Apo805K1 (ApoPharma Inc) is an oral agent whose mechanism of action has not been disclosed. A randomized, placebo-controlled, double-blind phase 2 trial in patients with moderate to severe psoriasis with a treatment duration of 14 days has been completed. For 12 weeks there was a daily dosing regimen of Apo805K1 10, 30, 60, or 100 mg or placebo, with 12 patients in each treatment group. The proportion of patients achieving PASI 75 was 16.7%, 0%, 0%, 8.3%, and 16.7%, respectively (P=.1975). The number of participants with adverse events reported ranged between 4 to 7, with the greatest number of adverse events reported in the 30-mg subset.8 It may be of interest to repeat the study with a larger sample size.
ASP015K (JAK 1 and JAK 3 Inhibitor)
ASP015K (Astellas Pharma US, Inc) is the first of the JAK inhibitors that will be discussed in this section. Janus kinase inhibitors represent a group of tyrosine kinases that regulate cytokine-mediated signaling pathways through the activation of signal transducer and activator of transcription proteins via phosphorylation in the cytoplasm, which in turn control the transcription of genes that generate inflammation. ASP015K and tofacitinib (formerly known as CP-690550)(Pfizer, Inc) inhibit JAK 1 and JAK 3, whereas GSK2586184 (GlaxoSmithKline) inhibits JAK 1 and baricitinib (formerly known as LY3009104 or INCB28050)(Eli Lilly and Company) inhibits JAK 1 and JAK 2.9 In a 6-week, dose-escalation phase 2 trial in patients with moderate to severe psoriasis, ASP015K showed a dose-dependent decline in PASI, psoriasis static global assessment, and body surface area.10
BMS-582949 (p38α MAP Kinase Inhibitor)
BMS-582949 (Bristol-Myers Squibb Company) is an oral p38α MAP kinase inhibitor.11 Along with c-Jun N-terminal kinase and extracellular signal-regulated protein kinases 1 and 2, MAP kinase plays a role in the pathogenesis of psoriasis.12 A randomized, placebo-controlled, double-blind, 12-week phase 2a study of placebo versus BMS-582949 dosed at 10, 30, and 100 mg has been completed, but the results were not available at the time of publication (NCT00399906).
Apremilast (PDE-4 Inhibitor)
Apremilast (formerly known as CC-10004)(Celgene Corporation) is an oral PDE-4 inhibitor that acts to inhibit the degradation of cyclic adenosine monophosphate. It is approved by the US Food and Drug Administration for moderate to severe plaque psoriasis13 and is a particularly good treatment for patients with recalcitrant disease.14 Several studies on apremilast have been published, including a phase 2 trial of 204 participants receiving placebo or apremilast 20 mg or 40 mg twice daily with American College of Rheumatology (ACR) 20% improvement response of 11.8%, 35.8%, and 43.5%, respectively.15 The phase 3 PALACE 1, 2, 3, and 4 trials also demonstrated therapeutic efficacy.16 In PALACE 1, 504 patients receiving placebo or apremilast 20 mg and 30 mg twice daily had an ACR20 of 19%, 31%, and 40%, respectively. In the PALACE 4 study, ACR20 was achieved by 58% of participants at week 52, but the ACR50 and ACR70 rates were less impressive.16
Lestaurtinib (Multikinase Inhibitor)
Lestaurtinib (formerly known as CEP-701)(Teva Pharmaceutical Industries) is an oral multikinase inhibitor for which a 12-week, nonrandomized, dose-escalation phase 2 study was completed, but the results were not available at the time of publication (NCT00236119).
CF101 (Adenosine A3 Receptor Agonist)
CF101 (IB-MECA; Can-Fite BioPharma Ltd) is an oral adenosine A3 receptor agonist. Adenosine A3 is a G protein–coupled receptor that has an anti-inflammatory role, which lends itself to the treatment of inflammatory conditions such as rheumatoid arthritis.17 In a randomized, placebo-controlled, double-blind phase 2 trial of 75 patients who received placebo or CF101 1, 2, or 4 mg twice daily for 12 weeks, PASI 50 or greater was reported in 35.3% of participants in the 2-mg group, which was statistically significant at weeks 8 (P=.047) and 12 (P=.031).18 A randomized, placebo-controlled, double-blind, 16-week phase 2/phase 3 trial in patients with moderate to severe psoriasis treated with CF101 2 mg twice daily versus placebo is ongoing but not recruiting participants (NCT01265667).
Tofacitinib (JAK 1 and JAK 3 Inhibitor)
Tofacitinib is a JAK 1 and JAK 3 inhibitor that is available in both topical and oral formulations. Many studies have been published on tofacitinib, including a dose-ranging phase 2b trial of 197 patients randomized to placebo or tofacitinib 2, 5, or 15 mg daily in which 2.0%, 25.0% (P<.001), 40.8% (P<.0001), and 66.7% (P<.0001) of participants in each treatment group, respectively, achieved PASI 75 at week 12.19 Another 12-week phase 2b trial in patients with moderate to severe psoriasis explored the effectiveness of oral formulations of tofacitinib based on body location, namely the head and neck, arms, trunk, and legs.20 Designed with twice-daily placebo and tofacitinib 2-, 5-, and 15-mg treatment arms, the target plaque severity score demonstrated a statistically significant dose-responsive improvement in each of the 4 anatomic regions (P<.01).
Two randomized, double-blinded, placebo-controlled phase 3 trials of tofacitinib have been completed. One trial compared the safety and effectiveness of tofacitinib and etanercept in patients with moderate to severe psoriasis.21 The 329 participants were randomized to treatment with oral tofacitinib 5 mg or 10 mg twice daily with placebo subcutaneous (SQ) injections twice weekly; oral placebo twice daily with etanercept 50-mg SQ injections twice weekly; or oral placebo twice daily with placebo SQ injection twice weekly. At week 12, PASI 75 was achieved in 39.51%, 63.64%, 58.81%, and 5.61% of participants in each treatment group, respectively. Thus, tofacitinib 10 mg and etanercept 50 mg were the first and second best performers in this study design.21
In the other phase 3 trial, the efficacy and safety of treatment, treatment withdrawal, and subsequent resumption of treatment with tofacitinib was examined in 290 patients who received either tofacitinib 5 mg or 10 mg or placebo twice daily for 24 weeks.22 In the withdrawal period, the percentage of patients who maintained a PASI 75 response in the tofacitinib 5-mg group was 56.2% versus 23.3% in the placebo group at week 16 (P<.0008). In the 10-mg group, 62.3% of participants maintained PASI 75 at week 16 versus 26.1% in the placebo group (P<.0001). During the re-treatment period for those who showed a greater than 50% reduction in week 24 PASI during treatment withdrawal (N=102), 50.0% of the tofacitinib 5-mg group showed PASI 75 versus 31.58% of the placebo group at week 16. In the tofacitinib 10-mg group, PASI 75 was seen in 0% versus 50.85% in the placebo group. Of note, only 5 participants who demonstrated a greater than 50% reduction in week 24 PASI response following withdrawal of therapy were in the tofacitinib 5- or 10-mg groups, as the rest were in the placebo group.22
FP187 (Fumaric Acid Ester)
FP187 (Forward Pharma A/S) is an oral fumaric acid ester whose underlying mechanism is thought to be elevation of glutathione levels that decreases the amount of inflammatory cytokines by blocking the translocation of nuclear factor κB. Other fumaric acid esters such as monoethyl fumarate and dimethyl fumarate have been used in Europe for the management of psoriasis.23 A phase 2 study of the safety and effectiveness of FP187 for moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01230138). A phase 3 trial examining the efficacy of FP187 in managing moderate to severe psoriasis was not yet open for participant recruitment at the time of publication (NCT01815723).
Doxercalciferol (Vitamin D2 Analogue)
Doxercalciferol (1α-hydroxyvitamin D2; Genzyme Corporation, a Sanofi company) is an oral prodrug of vitamin D.24 Topical preparations of vitamin D analogues approved by the US Food and Drug Administration such as calcipotriene are mainstays in psoriasis management. Doxercalciferol has been used for other therapeutic applications such as decreasing elevated parathyroid hormone levels.25 Research has demonstrated that CYP24A1 can extrahepatically regulate the activation of vitamin D prodrugs in cutaneous tissues.26 In a phase 2 study examining the efficacy and safety of doxercalciferol in patients with moderate to severe psoriasis, 111 patients were randomized to placebo or doxercalciferol 2.5, 5, or 7.5 mg daily for 24 weeks (NCT00601107). At week 12, PASI 50 was similar regardless of the treatment administered, reported at 20.0%, 20.0%, 17.9%, and 20.0%, respectively (P=1.000).27
GSK2586184 (JAK 1 Inhibitor)
GSK2586184 is an oral JAK 1 inhibitor. A placebo-controlled, double-blind, dose-dependent phase 2 study of GSK2586184 in patients with chronic plaque psoriasis who were randomized to placebo or GSK2586184 100, 200, and 400 mg twice daily for 84 days has been completed, but the results were not available at the time of publication (NCT01782664). Of note, despite clinical promise, due to potential adverse effects of the medication that included a possible interaction with statin medication, the manufacturer decided against pursuing GSK2586184 as a treatment in the management of psoriasis.28
Voclosporin (Calcineurin Inhibitor)
Voclosporin (formerly known as ISA247)(Aurinia Pharmaceuticals Inc) is an oral calcineurin inhibitor that is purported to be as effective as cyclospor-ine A with less associated toxicity. A 12-week randomized, placebo-controlled, double-blind phase 2 trial demonstrated PASI 75 in 0%, 18.2%, and 66.7% of 201 participants receiving placebo, voclospo-rin 0.5 mg/kg, and voclosporin 1.5 mg/kg twice daily, respectively (P<.0001). Elevated serum creatinine levels within the high range of normal were noted in the 1.5-mg/kg group.29 A 12-week phase 3 study of 451 patients randomized to placebo or voclospo-rin 0.2-, 0.3-, or 0.4-mg/kg treatment groups similarly demonstrated a dose-responsive PASI 75 of 4%, 16%, 25%, and 47%, respectively, that was maintained at week 24. Mild to moderate decreases in glomerular filtration rates were noted in 8 patients in the 0.3- and 0.4-mg/kg subsets.30 Another phase 2 study of voclosporin in patients with moderate to severe psoriasis showed improvements according to the psoriasis disability index and dermatology life quality index.31
Three randomized, placebo-controlled, double-blind phase 3 trials have been completed for voclosporin, but the results were not available at the time of publication. The phase 3 ESSENCE trial compared voclosporin to placebo and ciclosporin controls (NCT00408187). Two phase 3 trials known as the SPIRIT trials—one a 12-week study (NCT00244842) and the other a 36-week extension trial (NCT00258713)—compared the efficacy of placebo to voclosporin administered at 0.2-, 0.3-, and 0.4-mg/kg doses.
KD025 (ROCK 2 Inhibitor)
KD025 (Kadmon Corporation, LLC) is an oral ROCK 2 inhibitor. The inhibition of ROCK in the ras homolog gene family, member A/ROCK pathway has been targeted therapeutically for pulmonary arterial hypertension,32 glaucoma,33 and many other uses. A phase 2a study assessing the tolerability and safety profile of KD025 in patients with moderate to severe psoriasis was completed, but the results were not available at the time of publication (NCT02106195).
LAS41008 (Fumaric Acid Ester)
LAS41008 (Almirall, S.A.) is purported to be an oral dimethyl fumarate that inhibits endothelial cell proliferation, migration, and differentiation.34 A phase 3 trial comparing the safety and effectiveness of LAS41008, LASW1835 (an active comparator), and placebo in patients with moderate to severe psoriasis is ongoing but not recruiting participants (NCT01726933).
LEO 22811 (Anti-inflammatory)
LEO 22811 (LEO Pharma) is an oral anti-inflammatory agent for the treatment of psoriasis. Two clinical trials have been completed, the results of which have not yet been published. A phase 1 trial assessing the tolerability and safety profile of LEO 22811 (NCT00833872) and a phase 2 proof-of-concept study assessing dose response of LEO 22811 versus placebo (NCT01116895) were completed, but the results were not available at the time of publication.
Baricitinib (JAK 1 and JAK 2 Inhibitor)
As noted above, baricitinib (LY3009104 or INCB28050) is a JAK 1 and JAK 2 inhibitor. A phase 2b trial examining dose response for LY3009104 or baricitinib administration in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01490632).
Talarozole (CYP26 Inhibitor)
Talarozole (formerly known as R115866)(GlaxoSmithKline) is a selective oral CYP26 inhibitor that could serve to regulate the degradation of all-trans retinoic acid in the management of conditions such as acne and psoriasis. One phase 2 nonrandomized, open-label study (NCT00725348) and another phase 2 randomized, placebo-controlled, double-blind, dose-dependent trial examining the effectiveness and safety profile of 12-week talarozole treatment in patients with severe plaque psoriasis have been completed, but the results were not available at the time of publication (NCT00716144).
R3421 or BCX-4208 (PNP Inhibitor)
R3421 or BCX-4208 (BioCryst Pharmaceuticals, Inc/Hoffman–La Roche) is an oral PNP inhibitor that may help regulate apoptosis of T cells and B cells.35 A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT00504270).
RWJ-445380 (Cathepsin S Inhibitor)
RWJ-445380 (Alza Corporation, DE) is an oral cathepsin S inhibitor. Cathepsin S is produced by antigen-presenting cells and activates CD4+ T cells via presentation of antigen by class II major histocompatibility complex.36 A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial evaluating the tolerability, safety, pharmacodynamics, and pharmacokinetics of RWJ-445380 in patients with plaque psoriasis has been completed, but the results were not available at the time of publication (NCT00396422).
SRT2104 (Sirtuin 1 Activator)
SRT2104 (GlaxoSmithKline) is a selective oral NAD+-dependent deacetylase sirtuin 1 activator. Sirtuins help regulate apoptosis, inflammation, and other important cellular mechanisms.37 A randomized, open-label phase 1 trial examining drug bioavailability (NCT01702493) and a randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial studying the efficacy, tolerability, and safety of SRT2104 in patients with moderate to severe psoriasis have been completed (NCT01154101), but the results were not available at the time of publication.
VB-201 (Oxidized Phospholipid)
VB-201 (VBL Therapeutics) is an orally administered oxidized phospholipid analogue with anti-inflammatory effects.38 Oxidized phospholipids are another element in the intricate spectrum of inflammatory mediators. A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial of VB-201 20 mg or 80 mg daily in patients with moderate to severe psoriasis was completed, but the results were not available at the time of publication (NCT01001468). Another randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial of VB-201 80 mg and 160 mg twice daily in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01837420).
Conclusion
We are living in an exciting time in the treatment of psoriasis and PsA, with promising novel therapies afforded by the discovery of new therapeutic targets. In this 3-part series, we have reviewed topical, systemic, and biologic therapies that currently are in phase 2 through phase 4 clinical trials or have recently been approved by the US Food and Drug Administration for the management of psoriasis and PsA. These treatments offer patients and their caregivers the prospect of more targeted therapeutic regimens that offer enhanced clinical outcomes with more favorable side-effect profiles. As clinicians and researchers build upon this knowledge in the years to come, we can offer psoriasis patients an increasingly diverse and powerful therapeutic armamentarium.
Evolving knowledge of the underlying pathogenesis of psoriasis has afforded the development of a broad spectrum of nonbiologic systemic medications with therapeutic potential in moderate to severe psoriasis and psoriatic arthritis (PsA). The targets for these medications are antagonists of proinflammatory mediators such as tyrosine kinase, protein kinase, Janus kinase (JAK), p38α mitogen-activated protein (MAP) kinase, phosphodiesterase 4 (PDE-4), calcineurin, Rho-associated kinase (ROCK) 2, cytochrome P450 26 (CYP26), and purine nucleoside phosphorylase (PNP); agonists of anti-inflammatory mediators such as sphingosine-1-phosphate receptor 1 (S1P1) and adeno-sine A3 receptor; and myriad other mechanisms. A brief introduction to some of these therapies presently in phase 2 and phase 3 clinical trials are presented (Table).1
Masitinib (Tyrosine Kinase Inhibitor)
Masitinib (formerly known as AB1010)(AB Sciences) is a tyrosine kinase inhibitor that is purported to decrease inflammation by inhibiting stem cell factor receptor (c-kit) and consequently limiting mast cell degranulation.2 A randomized, placebo-controlled, double-blind phase 3 study evaluating its efficacy as an oral formulation was completed, but the results were not available at the time of publication (registered at www.clinicaltrials.gov with the identifier NCT01045577).
Ponesimod (S1P1 Receptor Agonist)
Ponesimod (formerly known as ACT-128800)(Actelion Pharmaceuticals US, Inc) is an orally formulated S1P1 receptor agonist. Sphingosine-1-phosphate receptor 1 is necessary for lymphoid chemotaxis.3 A randomized, placebo-controlled, double-blind phase 2 trial of 326 patients demonstrated 75% improvement in psoriasis area and severity index (PASI) score at week 16 in 13.4%, 46.0%, and 48.1% of participants receiving placebo, ponesimod 20 mg, and ponesimod 40 mg, respectively.4 At week 28, PASI 75 scores for participants transitioned from ponesimod 40 mg to placebo or ponesimod 20 mg to placebo and those maintained on ponesimod 20 mg and 40 mg were 40.4%, 42.2%, 77.4%, and 71.4%, respectively. This study demonstrated benefit of treatment with ponesimod versus placebo with increased efficacy using maintenance therapy.4
Sotrastaurin (Protein Kinase C Inhibitor)
Sotrastaurin (formerly known as AEB071)(Novartis AG) is an oral medication that inhibitsprotein kinase C, thereby limiting CD28-induced activation of T cells. Furthermore, it increases forkhead box P3 expression, which is important, as proinflammatory IL-17 production is stimulated in regulatory T cells with lost forkhead box P3 expression.5 In a study of 32 patients who received placebo or sotrastaurin 25, 100, 200, or 300 mg twice daily for 2 weeks, the mean PASI score was reduced by 69% for the 300-mg group versus 5.3% for placebo.6 A randomized, placebo-controlled, double-blind phase 2 study was completed for patients with moderate to severe psoriasis, but the results were not available at the time of publication (NCT00885196).
Alitretinoin (Retinoid)
Alitretinoin (9-cis-retinoic acid; Stiefel, a GSK company) is an oral retinoid with purported promise for patients with palmoplantar pustular psoriasis recalcitrant to conventional therapies. In one study, 7 participants with palmoplantar psoriasis received alitretinoin 30 mg daily for 12 weeks with 60% to 90% clinical improvement noted using the visual analog scale and palmoplantar pustular PASI to assess response.7 A randomized, placebo-controlled, double-blind phase 2 trial of alitretinoin assessing the success of alitretinoin in patients with palmoplantar psoriasis recalcitrant to topical treatments was completed, but the results were not available at the time of publication (NCT01245140).
Apo805K1 (Unknown Mechanism of Action)
Apo805K1 (ApoPharma Inc) is an oral agent whose mechanism of action has not been disclosed. A randomized, placebo-controlled, double-blind phase 2 trial in patients with moderate to severe psoriasis with a treatment duration of 14 days has been completed. For 12 weeks there was a daily dosing regimen of Apo805K1 10, 30, 60, or 100 mg or placebo, with 12 patients in each treatment group. The proportion of patients achieving PASI 75 was 16.7%, 0%, 0%, 8.3%, and 16.7%, respectively (P=.1975). The number of participants with adverse events reported ranged between 4 to 7, with the greatest number of adverse events reported in the 30-mg subset.8 It may be of interest to repeat the study with a larger sample size.
ASP015K (JAK 1 and JAK 3 Inhibitor)
ASP015K (Astellas Pharma US, Inc) is the first of the JAK inhibitors that will be discussed in this section. Janus kinase inhibitors represent a group of tyrosine kinases that regulate cytokine-mediated signaling pathways through the activation of signal transducer and activator of transcription proteins via phosphorylation in the cytoplasm, which in turn control the transcription of genes that generate inflammation. ASP015K and tofacitinib (formerly known as CP-690550)(Pfizer, Inc) inhibit JAK 1 and JAK 3, whereas GSK2586184 (GlaxoSmithKline) inhibits JAK 1 and baricitinib (formerly known as LY3009104 or INCB28050)(Eli Lilly and Company) inhibits JAK 1 and JAK 2.9 In a 6-week, dose-escalation phase 2 trial in patients with moderate to severe psoriasis, ASP015K showed a dose-dependent decline in PASI, psoriasis static global assessment, and body surface area.10
BMS-582949 (p38α MAP Kinase Inhibitor)
BMS-582949 (Bristol-Myers Squibb Company) is an oral p38α MAP kinase inhibitor.11 Along with c-Jun N-terminal kinase and extracellular signal-regulated protein kinases 1 and 2, MAP kinase plays a role in the pathogenesis of psoriasis.12 A randomized, placebo-controlled, double-blind, 12-week phase 2a study of placebo versus BMS-582949 dosed at 10, 30, and 100 mg has been completed, but the results were not available at the time of publication (NCT00399906).
Apremilast (PDE-4 Inhibitor)
Apremilast (formerly known as CC-10004)(Celgene Corporation) is an oral PDE-4 inhibitor that acts to inhibit the degradation of cyclic adenosine monophosphate. It is approved by the US Food and Drug Administration for moderate to severe plaque psoriasis13 and is a particularly good treatment for patients with recalcitrant disease.14 Several studies on apremilast have been published, including a phase 2 trial of 204 participants receiving placebo or apremilast 20 mg or 40 mg twice daily with American College of Rheumatology (ACR) 20% improvement response of 11.8%, 35.8%, and 43.5%, respectively.15 The phase 3 PALACE 1, 2, 3, and 4 trials also demonstrated therapeutic efficacy.16 In PALACE 1, 504 patients receiving placebo or apremilast 20 mg and 30 mg twice daily had an ACR20 of 19%, 31%, and 40%, respectively. In the PALACE 4 study, ACR20 was achieved by 58% of participants at week 52, but the ACR50 and ACR70 rates were less impressive.16
Lestaurtinib (Multikinase Inhibitor)
Lestaurtinib (formerly known as CEP-701)(Teva Pharmaceutical Industries) is an oral multikinase inhibitor for which a 12-week, nonrandomized, dose-escalation phase 2 study was completed, but the results were not available at the time of publication (NCT00236119).
CF101 (Adenosine A3 Receptor Agonist)
CF101 (IB-MECA; Can-Fite BioPharma Ltd) is an oral adenosine A3 receptor agonist. Adenosine A3 is a G protein–coupled receptor that has an anti-inflammatory role, which lends itself to the treatment of inflammatory conditions such as rheumatoid arthritis.17 In a randomized, placebo-controlled, double-blind phase 2 trial of 75 patients who received placebo or CF101 1, 2, or 4 mg twice daily for 12 weeks, PASI 50 or greater was reported in 35.3% of participants in the 2-mg group, which was statistically significant at weeks 8 (P=.047) and 12 (P=.031).18 A randomized, placebo-controlled, double-blind, 16-week phase 2/phase 3 trial in patients with moderate to severe psoriasis treated with CF101 2 mg twice daily versus placebo is ongoing but not recruiting participants (NCT01265667).
Tofacitinib (JAK 1 and JAK 3 Inhibitor)
Tofacitinib is a JAK 1 and JAK 3 inhibitor that is available in both topical and oral formulations. Many studies have been published on tofacitinib, including a dose-ranging phase 2b trial of 197 patients randomized to placebo or tofacitinib 2, 5, or 15 mg daily in which 2.0%, 25.0% (P<.001), 40.8% (P<.0001), and 66.7% (P<.0001) of participants in each treatment group, respectively, achieved PASI 75 at week 12.19 Another 12-week phase 2b trial in patients with moderate to severe psoriasis explored the effectiveness of oral formulations of tofacitinib based on body location, namely the head and neck, arms, trunk, and legs.20 Designed with twice-daily placebo and tofacitinib 2-, 5-, and 15-mg treatment arms, the target plaque severity score demonstrated a statistically significant dose-responsive improvement in each of the 4 anatomic regions (P<.01).
Two randomized, double-blinded, placebo-controlled phase 3 trials of tofacitinib have been completed. One trial compared the safety and effectiveness of tofacitinib and etanercept in patients with moderate to severe psoriasis.21 The 329 participants were randomized to treatment with oral tofacitinib 5 mg or 10 mg twice daily with placebo subcutaneous (SQ) injections twice weekly; oral placebo twice daily with etanercept 50-mg SQ injections twice weekly; or oral placebo twice daily with placebo SQ injection twice weekly. At week 12, PASI 75 was achieved in 39.51%, 63.64%, 58.81%, and 5.61% of participants in each treatment group, respectively. Thus, tofacitinib 10 mg and etanercept 50 mg were the first and second best performers in this study design.21
In the other phase 3 trial, the efficacy and safety of treatment, treatment withdrawal, and subsequent resumption of treatment with tofacitinib was examined in 290 patients who received either tofacitinib 5 mg or 10 mg or placebo twice daily for 24 weeks.22 In the withdrawal period, the percentage of patients who maintained a PASI 75 response in the tofacitinib 5-mg group was 56.2% versus 23.3% in the placebo group at week 16 (P<.0008). In the 10-mg group, 62.3% of participants maintained PASI 75 at week 16 versus 26.1% in the placebo group (P<.0001). During the re-treatment period for those who showed a greater than 50% reduction in week 24 PASI during treatment withdrawal (N=102), 50.0% of the tofacitinib 5-mg group showed PASI 75 versus 31.58% of the placebo group at week 16. In the tofacitinib 10-mg group, PASI 75 was seen in 0% versus 50.85% in the placebo group. Of note, only 5 participants who demonstrated a greater than 50% reduction in week 24 PASI response following withdrawal of therapy were in the tofacitinib 5- or 10-mg groups, as the rest were in the placebo group.22
FP187 (Fumaric Acid Ester)
FP187 (Forward Pharma A/S) is an oral fumaric acid ester whose underlying mechanism is thought to be elevation of glutathione levels that decreases the amount of inflammatory cytokines by blocking the translocation of nuclear factor κB. Other fumaric acid esters such as monoethyl fumarate and dimethyl fumarate have been used in Europe for the management of psoriasis.23 A phase 2 study of the safety and effectiveness of FP187 for moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01230138). A phase 3 trial examining the efficacy of FP187 in managing moderate to severe psoriasis was not yet open for participant recruitment at the time of publication (NCT01815723).
Doxercalciferol (Vitamin D2 Analogue)
Doxercalciferol (1α-hydroxyvitamin D2; Genzyme Corporation, a Sanofi company) is an oral prodrug of vitamin D.24 Topical preparations of vitamin D analogues approved by the US Food and Drug Administration such as calcipotriene are mainstays in psoriasis management. Doxercalciferol has been used for other therapeutic applications such as decreasing elevated parathyroid hormone levels.25 Research has demonstrated that CYP24A1 can extrahepatically regulate the activation of vitamin D prodrugs in cutaneous tissues.26 In a phase 2 study examining the efficacy and safety of doxercalciferol in patients with moderate to severe psoriasis, 111 patients were randomized to placebo or doxercalciferol 2.5, 5, or 7.5 mg daily for 24 weeks (NCT00601107). At week 12, PASI 50 was similar regardless of the treatment administered, reported at 20.0%, 20.0%, 17.9%, and 20.0%, respectively (P=1.000).27
GSK2586184 (JAK 1 Inhibitor)
GSK2586184 is an oral JAK 1 inhibitor. A placebo-controlled, double-blind, dose-dependent phase 2 study of GSK2586184 in patients with chronic plaque psoriasis who were randomized to placebo or GSK2586184 100, 200, and 400 mg twice daily for 84 days has been completed, but the results were not available at the time of publication (NCT01782664). Of note, despite clinical promise, due to potential adverse effects of the medication that included a possible interaction with statin medication, the manufacturer decided against pursuing GSK2586184 as a treatment in the management of psoriasis.28
Voclosporin (Calcineurin Inhibitor)
Voclosporin (formerly known as ISA247)(Aurinia Pharmaceuticals Inc) is an oral calcineurin inhibitor that is purported to be as effective as cyclospor-ine A with less associated toxicity. A 12-week randomized, placebo-controlled, double-blind phase 2 trial demonstrated PASI 75 in 0%, 18.2%, and 66.7% of 201 participants receiving placebo, voclospo-rin 0.5 mg/kg, and voclosporin 1.5 mg/kg twice daily, respectively (P<.0001). Elevated serum creatinine levels within the high range of normal were noted in the 1.5-mg/kg group.29 A 12-week phase 3 study of 451 patients randomized to placebo or voclospo-rin 0.2-, 0.3-, or 0.4-mg/kg treatment groups similarly demonstrated a dose-responsive PASI 75 of 4%, 16%, 25%, and 47%, respectively, that was maintained at week 24. Mild to moderate decreases in glomerular filtration rates were noted in 8 patients in the 0.3- and 0.4-mg/kg subsets.30 Another phase 2 study of voclosporin in patients with moderate to severe psoriasis showed improvements according to the psoriasis disability index and dermatology life quality index.31
Three randomized, placebo-controlled, double-blind phase 3 trials have been completed for voclosporin, but the results were not available at the time of publication. The phase 3 ESSENCE trial compared voclosporin to placebo and ciclosporin controls (NCT00408187). Two phase 3 trials known as the SPIRIT trials—one a 12-week study (NCT00244842) and the other a 36-week extension trial (NCT00258713)—compared the efficacy of placebo to voclosporin administered at 0.2-, 0.3-, and 0.4-mg/kg doses.
KD025 (ROCK 2 Inhibitor)
KD025 (Kadmon Corporation, LLC) is an oral ROCK 2 inhibitor. The inhibition of ROCK in the ras homolog gene family, member A/ROCK pathway has been targeted therapeutically for pulmonary arterial hypertension,32 glaucoma,33 and many other uses. A phase 2a study assessing the tolerability and safety profile of KD025 in patients with moderate to severe psoriasis was completed, but the results were not available at the time of publication (NCT02106195).
LAS41008 (Fumaric Acid Ester)
LAS41008 (Almirall, S.A.) is purported to be an oral dimethyl fumarate that inhibits endothelial cell proliferation, migration, and differentiation.34 A phase 3 trial comparing the safety and effectiveness of LAS41008, LASW1835 (an active comparator), and placebo in patients with moderate to severe psoriasis is ongoing but not recruiting participants (NCT01726933).
LEO 22811 (Anti-inflammatory)
LEO 22811 (LEO Pharma) is an oral anti-inflammatory agent for the treatment of psoriasis. Two clinical trials have been completed, the results of which have not yet been published. A phase 1 trial assessing the tolerability and safety profile of LEO 22811 (NCT00833872) and a phase 2 proof-of-concept study assessing dose response of LEO 22811 versus placebo (NCT01116895) were completed, but the results were not available at the time of publication.
Baricitinib (JAK 1 and JAK 2 Inhibitor)
As noted above, baricitinib (LY3009104 or INCB28050) is a JAK 1 and JAK 2 inhibitor. A phase 2b trial examining dose response for LY3009104 or baricitinib administration in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01490632).
Talarozole (CYP26 Inhibitor)
Talarozole (formerly known as R115866)(GlaxoSmithKline) is a selective oral CYP26 inhibitor that could serve to regulate the degradation of all-trans retinoic acid in the management of conditions such as acne and psoriasis. One phase 2 nonrandomized, open-label study (NCT00725348) and another phase 2 randomized, placebo-controlled, double-blind, dose-dependent trial examining the effectiveness and safety profile of 12-week talarozole treatment in patients with severe plaque psoriasis have been completed, but the results were not available at the time of publication (NCT00716144).
R3421 or BCX-4208 (PNP Inhibitor)
R3421 or BCX-4208 (BioCryst Pharmaceuticals, Inc/Hoffman–La Roche) is an oral PNP inhibitor that may help regulate apoptosis of T cells and B cells.35 A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT00504270).
RWJ-445380 (Cathepsin S Inhibitor)
RWJ-445380 (Alza Corporation, DE) is an oral cathepsin S inhibitor. Cathepsin S is produced by antigen-presenting cells and activates CD4+ T cells via presentation of antigen by class II major histocompatibility complex.36 A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial evaluating the tolerability, safety, pharmacodynamics, and pharmacokinetics of RWJ-445380 in patients with plaque psoriasis has been completed, but the results were not available at the time of publication (NCT00396422).
SRT2104 (Sirtuin 1 Activator)
SRT2104 (GlaxoSmithKline) is a selective oral NAD+-dependent deacetylase sirtuin 1 activator. Sirtuins help regulate apoptosis, inflammation, and other important cellular mechanisms.37 A randomized, open-label phase 1 trial examining drug bioavailability (NCT01702493) and a randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial studying the efficacy, tolerability, and safety of SRT2104 in patients with moderate to severe psoriasis have been completed (NCT01154101), but the results were not available at the time of publication.
VB-201 (Oxidized Phospholipid)
VB-201 (VBL Therapeutics) is an orally administered oxidized phospholipid analogue with anti-inflammatory effects.38 Oxidized phospholipids are another element in the intricate spectrum of inflammatory mediators. A randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial of VB-201 20 mg or 80 mg daily in patients with moderate to severe psoriasis was completed, but the results were not available at the time of publication (NCT01001468). Another randomized, placebo-controlled, double-blind, dose-dependent phase 2 trial of VB-201 80 mg and 160 mg twice daily in patients with moderate to severe psoriasis has been completed, but the results were not available at the time of publication (NCT01837420).
Conclusion
We are living in an exciting time in the treatment of psoriasis and PsA, with promising novel therapies afforded by the discovery of new therapeutic targets. In this 3-part series, we have reviewed topical, systemic, and biologic therapies that currently are in phase 2 through phase 4 clinical trials or have recently been approved by the US Food and Drug Administration for the management of psoriasis and PsA. These treatments offer patients and their caregivers the prospect of more targeted therapeutic regimens that offer enhanced clinical outcomes with more favorable side-effect profiles. As clinicians and researchers build upon this knowledge in the years to come, we can offer psoriasis patients an increasingly diverse and powerful therapeutic armamentarium.
1. Lu PD, Mazza JM. Research pipeline III: biologic therapies. In: Weinberg JM, Lebwohl M, eds. Advances in Psoriasis. New York, NY: Springer; 2014:227-242.
2. Humbert M, de Blay F, Garcia G, et al. Masitinib, a c-kit/PDGF receptor tyrosine kinase inhibitor, improves disease control in severe corticosteroid-dependent asthmatics. Allergy. 2009;64:1194-1201.
3. Krause A, Brossard P, D’Ambrosio D, et al. Population pharmacokinetics and pharmacodynamics of ponesimod, a selective S1P1 receptor modulator. J Pharmacokinet Pharmacodyn. 2014;41:261-278.
4. Vaclavkova A, Chimenti S, Arenberger P, et al. Oral ponesimod in patients with chronic plaque psoriasis: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet. 2014;384:2036-2045.
5. He X, Koenen HJ, Smeets RL, et al. Targeting PKC in human T cells using sotrastaurin (AEB071) preserves regulatory T cells and prevents IL-17 production. J Invest Dermatol. 2014;134:975-983.
6. Skvara H, Dawid M, Kleyn E, et al. The PKC inhibitor AEB071 may be a therapeutic option for psoriasis. J Clin Invest. 2008;118:3151-3159.
7. Irla N, Navarini AA, Yawalkar N. Alitretinoin abrogates innate inflammation in palmoplantar pustular psoriasis. Br J Dermatol. 2012;167:1170-1174.
8. Study to evaluate Apo805K1 in subjects with moderate to severe chronic plaque psoriasis (NCT01483924). https://clinicaltrials.gov/ct2/results?term=NCT01483924&Search=Search. Updated February 9, 2015. Accessed June 23, 2015.
9. Kofoed K, Skov L, Zachariae C. New drugs and treatment targets in psoriasis. Acta Derm Venereol. 2015;95:133-139.
10. Gooderham M. Small molecules: an overview of emerging therapeutic options in the treatment of psoriasis. Skin Therapy Lett. 2013;18:1-4.
11. Liu C, Lin J, Wrobleski ST, et al. Discovery of 4-(5-(cyclopropylcarbamoyl)-2-methylphenylamino)-5-methyl-N-propylpyrrolo[1,2-f][1,2,4]triazine-6-carboxamide (BMS-582949), a clinical p38a MAP kinase inhibitor for the treatment of inflammatory diseases. J Med Chem. 2010;53:6629-6639.
12. Mavropoulos A, Rigopoulou EI, Liaskos C, et al. The role of p38 MAPK in the aetiopathogenesis of psoriasis and psoriatic arthritis. Clin Dev Immunol. 2013;2013:569751.
13. Oral OTEZLA® (apremilast) approved by the U.S. Food and Drug Administration for the treatment of patients with moderate to severe plaque psoriasis [news release]. Summit, NJ: Celegene Corporation; September 23, 2014. http://ir.celgene.com/releasedetail.cfm?releaseid=872240. Accessed June 23, 2015.
14. Gottlieb AB, Matheson RT, Menter A, et al. Efficacy, tolerability, and pharmacodynamics of apremilast in recalcitrant plaque psoriasis: a phase II open-label study. J Drugs Dermatol. 2013;12:888-897.
15. Moustafa F, Feldman SR. A review of phosphodiesterase-inhibition and the potential role for phosphodiesterase 4-inhibitors in clinical dermatology. Dermatol Online J. 2014;20:22608.
16. Huynh D, Kavanaugh A. Psoriatic arthritis: current therapy and future approaches. Rheumatology (Oxford). 2015;54:20-28.
17. Fishman P, Bar-Yehuda S, Liang BT, et al. Pharmacological and therapeutic effects of A3 adenosine receptor agonists. Drug Discov Today. 2012;17:359-366.
18. David M, Akerman L, Ziv M, et al. Treatment of plaque-type psoriasis with oral CF101: data from an exploratory randomized phase 2 clinical trial. J Eur Acad Dermatol Venereol. 2012;26:361-367.
19. Papp KA, Menter A, Strober B, et al. Efficacy and safety of tofacitinib, an oral Janus kinase inhibitor, in the treatment of psoriasis: a phase 2b randomized placebo-controlled dose-ranging study. Br J Dermatol. 2012;167:668-677.
20. Menter A, Papp KA, Tan H, et al. Efficacy of tofacitinib, an oral Janus kinase inhibitor, on clinical signs of moderate-to-severe plaque psoriasis in different body regions. J Drugs Dermatol. 2014;13:252-256.
21. A phase 3, multi site, randomized, double blind, placebo controlled study of the efficacy and safety comparing CP-690,550 and etanercept in subjects with moderate to severe chronic plaque psoriasis (NCT01241591). https://clinicaltrials.gov/ct2/show/NCT01241591?term=01241591&rank=1. Updated May 8, 2014. Accessed June 16, 2015.
22. A study to evaluate the effects and safety of treatment, treatment withdrawal, followed by re-treatment with CP-690,550 in subjects with moderate to severe chronic plaque psoriasis (NCT01186744). https://clinicaltrials.gov/ct2/show/NCT01186744?term=01186744&rank=1. Updated May 14, 2014. Accessed June 16, 2015.
23. Rostami Yazdi M, Mrowietz U. Fumaric acid esters. Clin Dermatol. 2008;26:522-526.
24. Kubodera N. A new look at the most successful prodrugs for active vitamin D (D hormone): alfacalcidol and doxercalciferol. Molecules. 2009;14:3869-3880.
25. Brown AJ. Therapeutic uses of vitamin D analogues. Am J Kidney Dis. 2001;38(5 suppl 5):S3-S19.
26. Masuda S, Strugnell SA, Knutson JC, et al. Evidence for the activation of 1alpha-hydroxyvitamin D2 by 25-hydroxyvitamin D-24-hydroxylase: delineation of pathways involving 1alpha,24-dihydroxyvitamin D2 and 1alpha,25-dihydroxyvitamin D2. Biochim Biophys Acta. 2006;1761:221-234.
27. A study to evaluate the safety and effectiveness of doxercalciferol capsules in participants with moderate to severe psoriasis (NCT00601107). https://clinicaltrials.gov/ct2/show/NCT00601107?term=00601107&rank=1. Updated April 2, 2014. Accessed June 16, 2015.
28. GSK discloses good efficacy in psoriasis with GSK2856184 [news release]. Mechelen, Belgium: Galapagos NV; November 6, 2014. http://www.globenewswire.com/news-release/2014/11/06/680358/10106744/en/GSK-discloses-good-efficacy-in-psoriasis-with-GSK2856184.html. Accessed June 24, 2015.
29. Bissonnette R, Papp K, Poulin Y, et al. A randomized, multicenter, double-blind, placebo-controlled phase 2 trial of ISA247 in patients with chronic plaque psoriasis. J Am Acad Dermatol. 2006;54:472-478.
30. Papp K, Bissonnette R, Rosoph L, et al. Efficacy of ISA247 in plaque psoriasis: a randomised, multicentre, double-blind, placebo-controlled phase III study. Lancet. 2008;371:1337-1342.
31. Gupta AK, Langley RG, Lynde C, et al. ISA247: quality of life results from a phase II, randomized, placebo-controlled study. J Cutan Med Surg. 2008;12:268-275.
32. Antoniu SA. Targeting RhoA/ROCK pathway in pulmonary arterial hypertension. Expert Opin Ther Targets. 2012;16:355-363.
33. Challa P, Arnold JJ. Rho-kinase inhibitors offer a new approach in the treatment of glaucoma. Expert Opin Investig Drugs. 2014;23:81-95.
34. National Institute for Health Research Horizon Scanning Centre. Dimethyl fumarate for plaque psoriasis. http://www.hsc.nihr.ac.uk/files/downloads/2228/2526.163fbff8.Dimethylfumarate_Nov13.pdf. Published November 2013. Accessed June 15, 2015.
35. Bantia S, Parker C, Upshaw R, et al. Potent orally bioavailable purine nucleoside phosphorylase inhibitor BCX-4208 induces apoptosis in B- and T-lymphocytes—a novel treatment approach for autoimmune diseases, organ transplantation and hematologic malignancies. Int Immunopharmacol. 2010;10:784-790.
36. García-Pérez ME, Stevanovic T, Poubelle PE. New therapies under development for psoriasis treatment. Curr Opin Pediatr. 2013;25:480-487.
37. Villalba JM, Alcaín FJ. Sirtuin activators and inhibitors. Biofactors. 2012;38:349-359.
38. Feige E, Mendel I, George J, et al. Modified phospholipids as anti-inflammatory compounds. Curr Opin Lipidol. 2010;21:525-529.
1. Lu PD, Mazza JM. Research pipeline III: biologic therapies. In: Weinberg JM, Lebwohl M, eds. Advances in Psoriasis. New York, NY: Springer; 2014:227-242.
2. Humbert M, de Blay F, Garcia G, et al. Masitinib, a c-kit/PDGF receptor tyrosine kinase inhibitor, improves disease control in severe corticosteroid-dependent asthmatics. Allergy. 2009;64:1194-1201.
3. Krause A, Brossard P, D’Ambrosio D, et al. Population pharmacokinetics and pharmacodynamics of ponesimod, a selective S1P1 receptor modulator. J Pharmacokinet Pharmacodyn. 2014;41:261-278.
4. Vaclavkova A, Chimenti S, Arenberger P, et al. Oral ponesimod in patients with chronic plaque psoriasis: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet. 2014;384:2036-2045.
5. He X, Koenen HJ, Smeets RL, et al. Targeting PKC in human T cells using sotrastaurin (AEB071) preserves regulatory T cells and prevents IL-17 production. J Invest Dermatol. 2014;134:975-983.
6. Skvara H, Dawid M, Kleyn E, et al. The PKC inhibitor AEB071 may be a therapeutic option for psoriasis. J Clin Invest. 2008;118:3151-3159.
7. Irla N, Navarini AA, Yawalkar N. Alitretinoin abrogates innate inflammation in palmoplantar pustular psoriasis. Br J Dermatol. 2012;167:1170-1174.
8. Study to evaluate Apo805K1 in subjects with moderate to severe chronic plaque psoriasis (NCT01483924). https://clinicaltrials.gov/ct2/results?term=NCT01483924&Search=Search. Updated February 9, 2015. Accessed June 23, 2015.
9. Kofoed K, Skov L, Zachariae C. New drugs and treatment targets in psoriasis. Acta Derm Venereol. 2015;95:133-139.
10. Gooderham M. Small molecules: an overview of emerging therapeutic options in the treatment of psoriasis. Skin Therapy Lett. 2013;18:1-4.
11. Liu C, Lin J, Wrobleski ST, et al. Discovery of 4-(5-(cyclopropylcarbamoyl)-2-methylphenylamino)-5-methyl-N-propylpyrrolo[1,2-f][1,2,4]triazine-6-carboxamide (BMS-582949), a clinical p38a MAP kinase inhibitor for the treatment of inflammatory diseases. J Med Chem. 2010;53:6629-6639.
12. Mavropoulos A, Rigopoulou EI, Liaskos C, et al. The role of p38 MAPK in the aetiopathogenesis of psoriasis and psoriatic arthritis. Clin Dev Immunol. 2013;2013:569751.
13. Oral OTEZLA® (apremilast) approved by the U.S. Food and Drug Administration for the treatment of patients with moderate to severe plaque psoriasis [news release]. Summit, NJ: Celegene Corporation; September 23, 2014. http://ir.celgene.com/releasedetail.cfm?releaseid=872240. Accessed June 23, 2015.
14. Gottlieb AB, Matheson RT, Menter A, et al. Efficacy, tolerability, and pharmacodynamics of apremilast in recalcitrant plaque psoriasis: a phase II open-label study. J Drugs Dermatol. 2013;12:888-897.
15. Moustafa F, Feldman SR. A review of phosphodiesterase-inhibition and the potential role for phosphodiesterase 4-inhibitors in clinical dermatology. Dermatol Online J. 2014;20:22608.
16. Huynh D, Kavanaugh A. Psoriatic arthritis: current therapy and future approaches. Rheumatology (Oxford). 2015;54:20-28.
17. Fishman P, Bar-Yehuda S, Liang BT, et al. Pharmacological and therapeutic effects of A3 adenosine receptor agonists. Drug Discov Today. 2012;17:359-366.
18. David M, Akerman L, Ziv M, et al. Treatment of plaque-type psoriasis with oral CF101: data from an exploratory randomized phase 2 clinical trial. J Eur Acad Dermatol Venereol. 2012;26:361-367.
19. Papp KA, Menter A, Strober B, et al. Efficacy and safety of tofacitinib, an oral Janus kinase inhibitor, in the treatment of psoriasis: a phase 2b randomized placebo-controlled dose-ranging study. Br J Dermatol. 2012;167:668-677.
20. Menter A, Papp KA, Tan H, et al. Efficacy of tofacitinib, an oral Janus kinase inhibitor, on clinical signs of moderate-to-severe plaque psoriasis in different body regions. J Drugs Dermatol. 2014;13:252-256.
21. A phase 3, multi site, randomized, double blind, placebo controlled study of the efficacy and safety comparing CP-690,550 and etanercept in subjects with moderate to severe chronic plaque psoriasis (NCT01241591). https://clinicaltrials.gov/ct2/show/NCT01241591?term=01241591&rank=1. Updated May 8, 2014. Accessed June 16, 2015.
22. A study to evaluate the effects and safety of treatment, treatment withdrawal, followed by re-treatment with CP-690,550 in subjects with moderate to severe chronic plaque psoriasis (NCT01186744). https://clinicaltrials.gov/ct2/show/NCT01186744?term=01186744&rank=1. Updated May 14, 2014. Accessed June 16, 2015.
23. Rostami Yazdi M, Mrowietz U. Fumaric acid esters. Clin Dermatol. 2008;26:522-526.
24. Kubodera N. A new look at the most successful prodrugs for active vitamin D (D hormone): alfacalcidol and doxercalciferol. Molecules. 2009;14:3869-3880.
25. Brown AJ. Therapeutic uses of vitamin D analogues. Am J Kidney Dis. 2001;38(5 suppl 5):S3-S19.
26. Masuda S, Strugnell SA, Knutson JC, et al. Evidence for the activation of 1alpha-hydroxyvitamin D2 by 25-hydroxyvitamin D-24-hydroxylase: delineation of pathways involving 1alpha,24-dihydroxyvitamin D2 and 1alpha,25-dihydroxyvitamin D2. Biochim Biophys Acta. 2006;1761:221-234.
27. A study to evaluate the safety and effectiveness of doxercalciferol capsules in participants with moderate to severe psoriasis (NCT00601107). https://clinicaltrials.gov/ct2/show/NCT00601107?term=00601107&rank=1. Updated April 2, 2014. Accessed June 16, 2015.
28. GSK discloses good efficacy in psoriasis with GSK2856184 [news release]. Mechelen, Belgium: Galapagos NV; November 6, 2014. http://www.globenewswire.com/news-release/2014/11/06/680358/10106744/en/GSK-discloses-good-efficacy-in-psoriasis-with-GSK2856184.html. Accessed June 24, 2015.
29. Bissonnette R, Papp K, Poulin Y, et al. A randomized, multicenter, double-blind, placebo-controlled phase 2 trial of ISA247 in patients with chronic plaque psoriasis. J Am Acad Dermatol. 2006;54:472-478.
30. Papp K, Bissonnette R, Rosoph L, et al. Efficacy of ISA247 in plaque psoriasis: a randomised, multicentre, double-blind, placebo-controlled phase III study. Lancet. 2008;371:1337-1342.
31. Gupta AK, Langley RG, Lynde C, et al. ISA247: quality of life results from a phase II, randomized, placebo-controlled study. J Cutan Med Surg. 2008;12:268-275.
32. Antoniu SA. Targeting RhoA/ROCK pathway in pulmonary arterial hypertension. Expert Opin Ther Targets. 2012;16:355-363.
33. Challa P, Arnold JJ. Rho-kinase inhibitors offer a new approach in the treatment of glaucoma. Expert Opin Investig Drugs. 2014;23:81-95.
34. National Institute for Health Research Horizon Scanning Centre. Dimethyl fumarate for plaque psoriasis. http://www.hsc.nihr.ac.uk/files/downloads/2228/2526.163fbff8.Dimethylfumarate_Nov13.pdf. Published November 2013. Accessed June 15, 2015.
35. Bantia S, Parker C, Upshaw R, et al. Potent orally bioavailable purine nucleoside phosphorylase inhibitor BCX-4208 induces apoptosis in B- and T-lymphocytes—a novel treatment approach for autoimmune diseases, organ transplantation and hematologic malignancies. Int Immunopharmacol. 2010;10:784-790.
36. García-Pérez ME, Stevanovic T, Poubelle PE. New therapies under development for psoriasis treatment. Curr Opin Pediatr. 2013;25:480-487.
37. Villalba JM, Alcaín FJ. Sirtuin activators and inhibitors. Biofactors. 2012;38:349-359.
38. Feige E, Mendel I, George J, et al. Modified phospholipids as anti-inflammatory compounds. Curr Opin Lipidol. 2010;21:525-529.
Practice Points
- A wide spectrum of promising nonbiologic systemic medications presently are in development or were recently approved for the management of moderate to severe psoriasis and psoriatic arthritis (PsA).
- Systemic medications broaden the therapeutic armamentarium for patients with psoriasis and PsA, offering targeted therapeutic regimens that afford enhanced clinical outcomes with favorable side-effect profiles.

WCD: Touch avoidance is a new dimension of psoriatic impairment
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.

“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.
“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.
“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
AT WCD 2015
Key clinical point: Touch avoidance among psoriasis patients is an important new patient-reported outcome having a major negative quality-of-life impact.
Major finding: A total of 48 of a large group of psoriasis patients reported having avoided touching others, or having others touching them, within the prior 2 weeks because of how their skin looks or feels.
Data source: This was an online survey of 1,109 psoriasis patients.
Disclosures: The study was supported by the National Psoriasis Foundation. Dr. April Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.

Screening for Psoriatic Arthritis in Psoriasis Patients
Delayed diagnosis of psoriatic arthritis (PsA) can have profound effects, such as irreversible joint damage, poor quality of life, and decreased response to treatment; however, many cases of PsA are not diagnosed until up to 2 years after onset of symptoms. Dr. Saakshi Khattri discusses screening questions for PsA that dermatologists should address when treating patients with psoriasis and emphasizes that collaboration between dermatologists and rheumatologists is essential to early diagnosis and treatment of PsA.
The psoriasis audiocast series is created in collaboration with Cutis® and the National Psoriasis Foundation®.
Suggested Reading
Armstrong AW, Robertson AD, Wu J, et al. Undertreatment, treatment trends, and treatment dissatisfaction among patients with psoriasis and psoriatic arthritis in the United States: findings from the National Psoriasis Foundation surveys, 2003-2011. JAMA Dermatol. 2013;149:1180-1185.
Delayed diagnosis of psoriatic arthritis (PsA) can have profound effects, such as irreversible joint damage, poor quality of life, and decreased response to treatment; however, many cases of PsA are not diagnosed until up to 2 years after onset of symptoms. Dr. Saakshi Khattri discusses screening questions for PsA that dermatologists should address when treating patients with psoriasis and emphasizes that collaboration between dermatologists and rheumatologists is essential to early diagnosis and treatment of PsA.
The psoriasis audiocast series is created in collaboration with Cutis® and the National Psoriasis Foundation®.
Delayed diagnosis of psoriatic arthritis (PsA) can have profound effects, such as irreversible joint damage, poor quality of life, and decreased response to treatment; however, many cases of PsA are not diagnosed until up to 2 years after onset of symptoms. Dr. Saakshi Khattri discusses screening questions for PsA that dermatologists should address when treating patients with psoriasis and emphasizes that collaboration between dermatologists and rheumatologists is essential to early diagnosis and treatment of PsA.
The psoriasis audiocast series is created in collaboration with Cutis® and the National Psoriasis Foundation®.
Suggested Reading
Armstrong AW, Robertson AD, Wu J, et al. Undertreatment, treatment trends, and treatment dissatisfaction among patients with psoriasis and psoriatic arthritis in the United States: findings from the National Psoriasis Foundation surveys, 2003-2011. JAMA Dermatol. 2013;149:1180-1185.
Suggested Reading
Armstrong AW, Robertson AD, Wu J, et al. Undertreatment, treatment trends, and treatment dissatisfaction among patients with psoriasis and psoriatic arthritis in the United States: findings from the National Psoriasis Foundation surveys, 2003-2011. JAMA Dermatol. 2013;149:1180-1185.
Guselkumab prevails in phase II psoriasis trial
Guselkumab, a monoclonal antibody that specifically inhibits interleukin-23 signaling, was safe and more effective than placebo or adalimumab against plaque psoriasis in a phase II clinical trial, according to a report published online July 9 in the New England Journal of Medicine.
The 1-year randomized double-blind study, funded and administered by the maker of guselkumab, involved 293 adult patients treated at 31 sites in North America and 12 in Europe. The median duration of disease was 19 years. Study participants were randomly assigned to receive one of five subcutaneous doses of the agent (5 mg, 15 mg, 50 mg, 100 mg, or 200 mg) at two different dosing intervals (208 patients), matching placebo (42 patients), or adalimumab (43 patients) for 40 weeks and were followed for an additional 12 weeks. At 16 weeks, patients in the placebo group crossed over to receive 100 mg of guselkumab every 8 weeks, said Dr. Kenneth B. Gordon of Northwestern University, Chicago, and his associates.

The primary efficacy endpoint – the proportion of patients at week 16 with a Physician’s Global Assessment score of 0 or 1 – was significantly higher in every guselkumab dosing group (34%, 61%, 79%, 86%, and 83%, respectively) than in the placebo group (7%). In addition, the proportion of patients showing a 75%, 90%, or 100% improvement in Psoriasis Area and Severity Index score was significantly higher in each guselkumab group than in the placebo group. Scores on the Dermatology Life Quality Index also showed significantly greater improvement from baseline to week 16 in the guselkumab groups.
The findings were similar when patients taking the higher doses of guselkumab were compared with those taking adalimumab. At week 16, the proportion of patients with a PGA score of 0 or 1 was 58% with adalimumab, compared with 79%, 86%, and 83% at the highest doses of guselkumab (50 mg, 100 mg, or 200 mg). And at week 40, the proportion of patients with a PGA score of 0 or 1 was significantly higher in those taking 50 mg (71%), 100 mg (77%), or 200 mg (81%) guselkumab than in patients taking adalimumab (49%). The response to guselkumab was noted at the earliest patient assessment at week 4, peaked at week 20, and was maintained through week 40, Dr. Gordon and his associates said (N. Engl. J. Med. 2015 July 9 [doi:10.1056/NEJMoa1501646]).
The rates of adverse events, serious adverse events, and infections were similar across all the treatment groups. At week 16, infections were reported in 20% of patients taking guselkumab, 14% of those taking placebo, and 12% of those taking adalimumab. At final follow-up, infections were reported in 30% of patients taking guselkumab and 35% taking adalimumab. This study had a limited ability to assess uncommon adverse events; three patients taking guselkumab had major cardiovascular events during treatment, but “it is difficult to interpret the significance” of such events, the investigators said.
They added that larger and longer-term phase III trials are now underway to further assess the efficacy and safety of guselkumab for this indication. Moreover, their study results “validate the use of interleukin-23 as a therapeutic target by showing that therapy involving selective antagonism of this single cytokine in patients with moderate to severe plaque psoriasis is highly efficacious, as compared with adalimumab therapy,” Dr. Gordon and his associates said.
Guselkumab, a monoclonal antibody that specifically inhibits interleukin-23 signaling, was safe and more effective than placebo or adalimumab against plaque psoriasis in a phase II clinical trial, according to a report published online July 9 in the New England Journal of Medicine.
The 1-year randomized double-blind study, funded and administered by the maker of guselkumab, involved 293 adult patients treated at 31 sites in North America and 12 in Europe. The median duration of disease was 19 years. Study participants were randomly assigned to receive one of five subcutaneous doses of the agent (5 mg, 15 mg, 50 mg, 100 mg, or 200 mg) at two different dosing intervals (208 patients), matching placebo (42 patients), or adalimumab (43 patients) for 40 weeks and were followed for an additional 12 weeks. At 16 weeks, patients in the placebo group crossed over to receive 100 mg of guselkumab every 8 weeks, said Dr. Kenneth B. Gordon of Northwestern University, Chicago, and his associates.
The primary efficacy endpoint – the proportion of patients at week 16 with a Physician’s Global Assessment score of 0 or 1 – was significantly higher in every guselkumab dosing group (34%, 61%, 79%, 86%, and 83%, respectively) than in the placebo group (7%). In addition, the proportion of patients showing a 75%, 90%, or 100% improvement in Psoriasis Area and Severity Index score was significantly higher in each guselkumab group than in the placebo group. Scores on the Dermatology Life Quality Index also showed significantly greater improvement from baseline to week 16 in the guselkumab groups.
The findings were similar when patients taking the higher doses of guselkumab were compared with those taking adalimumab. At week 16, the proportion of patients with a PGA score of 0 or 1 was 58% with adalimumab, compared with 79%, 86%, and 83% at the highest doses of guselkumab (50 mg, 100 mg, or 200 mg). And at week 40, the proportion of patients with a PGA score of 0 or 1 was significantly higher in those taking 50 mg (71%), 100 mg (77%), or 200 mg (81%) guselkumab than in patients taking adalimumab (49%). The response to guselkumab was noted at the earliest patient assessment at week 4, peaked at week 20, and was maintained through week 40, Dr. Gordon and his associates said (N. Engl. J. Med. 2015 July 9 [doi:10.1056/NEJMoa1501646]).
The rates of adverse events, serious adverse events, and infections were similar across all the treatment groups. At week 16, infections were reported in 20% of patients taking guselkumab, 14% of those taking placebo, and 12% of those taking adalimumab. At final follow-up, infections were reported in 30% of patients taking guselkumab and 35% taking adalimumab. This study had a limited ability to assess uncommon adverse events; three patients taking guselkumab had major cardiovascular events during treatment, but “it is difficult to interpret the significance” of such events, the investigators said.
They added that larger and longer-term phase III trials are now underway to further assess the efficacy and safety of guselkumab for this indication. Moreover, their study results “validate the use of interleukin-23 as a therapeutic target by showing that therapy involving selective antagonism of this single cytokine in patients with moderate to severe plaque psoriasis is highly efficacious, as compared with adalimumab therapy,” Dr. Gordon and his associates said.
Guselkumab, a monoclonal antibody that specifically inhibits interleukin-23 signaling, was safe and more effective than placebo or adalimumab against plaque psoriasis in a phase II clinical trial, according to a report published online July 9 in the New England Journal of Medicine.
The 1-year randomized double-blind study, funded and administered by the maker of guselkumab, involved 293 adult patients treated at 31 sites in North America and 12 in Europe. The median duration of disease was 19 years. Study participants were randomly assigned to receive one of five subcutaneous doses of the agent (5 mg, 15 mg, 50 mg, 100 mg, or 200 mg) at two different dosing intervals (208 patients), matching placebo (42 patients), or adalimumab (43 patients) for 40 weeks and were followed for an additional 12 weeks. At 16 weeks, patients in the placebo group crossed over to receive 100 mg of guselkumab every 8 weeks, said Dr. Kenneth B. Gordon of Northwestern University, Chicago, and his associates.
The primary efficacy endpoint – the proportion of patients at week 16 with a Physician’s Global Assessment score of 0 or 1 – was significantly higher in every guselkumab dosing group (34%, 61%, 79%, 86%, and 83%, respectively) than in the placebo group (7%). In addition, the proportion of patients showing a 75%, 90%, or 100% improvement in Psoriasis Area and Severity Index score was significantly higher in each guselkumab group than in the placebo group. Scores on the Dermatology Life Quality Index also showed significantly greater improvement from baseline to week 16 in the guselkumab groups.
The findings were similar when patients taking the higher doses of guselkumab were compared with those taking adalimumab. At week 16, the proportion of patients with a PGA score of 0 or 1 was 58% with adalimumab, compared with 79%, 86%, and 83% at the highest doses of guselkumab (50 mg, 100 mg, or 200 mg). And at week 40, the proportion of patients with a PGA score of 0 or 1 was significantly higher in those taking 50 mg (71%), 100 mg (77%), or 200 mg (81%) guselkumab than in patients taking adalimumab (49%). The response to guselkumab was noted at the earliest patient assessment at week 4, peaked at week 20, and was maintained through week 40, Dr. Gordon and his associates said (N. Engl. J. Med. 2015 July 9 [doi:10.1056/NEJMoa1501646]).
The rates of adverse events, serious adverse events, and infections were similar across all the treatment groups. At week 16, infections were reported in 20% of patients taking guselkumab, 14% of those taking placebo, and 12% of those taking adalimumab. At final follow-up, infections were reported in 30% of patients taking guselkumab and 35% taking adalimumab. This study had a limited ability to assess uncommon adverse events; three patients taking guselkumab had major cardiovascular events during treatment, but “it is difficult to interpret the significance” of such events, the investigators said.
They added that larger and longer-term phase III trials are now underway to further assess the efficacy and safety of guselkumab for this indication. Moreover, their study results “validate the use of interleukin-23 as a therapeutic target by showing that therapy involving selective antagonism of this single cytokine in patients with moderate to severe plaque psoriasis is highly efficacious, as compared with adalimumab therapy,” Dr. Gordon and his associates said.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Guselkumab was safe and more effective than placebo and adalimumab against plaque psoriasis in a phase II industry-sponsored trial.
Major finding: The primary efficacy endpoint – the proportion of patients at week 16 with a Physician’s Global Assessment score of 0 or 1 – was significantly higher in every guselkumab group (34%, 61%, 79%, 86%, and 83%, respectively) than in the placebo group (7%).
Data source: A 1-year double-blind randomized phase II trial involving 293 adults at 43 sites in North America and Europe.
Disclosures: The trial was sponsored by Janssen, maker of guselkumab. Janssen supplied the study drugs, collected and analyzed the data, and helped write the report. Dr. Gordon reported receiving grants and personal fees from Janssen, AbbVie, Amgen, Celgene, Eli Lilly, Novartis, Pfizer, and Medac; his associates reported ties to numerous industry sources.

Clinical Trial Update: Topical Therapy for Plaque Psoriasis
Comparison of 122-0551 Foam Versus Vehicle for Plaque Psoriasis
Product: 122-0551 foam
Sponsor: Therapeutics, Inc
Stage of development: Phase 3
ClinicalTrials.gov Identifier: NCT02368210
Study start: January 2015
Study completion: October 2015 (August 2015 final collection date for primary outcome measure)
This phase 3 study will compare the efficacy and safety of 122-0551 foam (a glucocorticoid receptor agonist) and vehicle foam applied twice daily for 2 weeks in participants (aged ≥18 years) with plaque psoriasis.
The primary outcome measure will include the proportion of participants rated a “treatment success” based on the investigator global assessment.
Secondary outcome measures will include the proportion of participants rated a “treatment success” for each of the clinical signs of psoriasis: scaling, erythema, and plaque elevation.
HPA Axis Suppression Following Treatment With Desoximetasone Topical Spray 0.25% in Pediatric Patients With Plaque Psoriasis
Product: Topicort® (desoximetasone) topical spray 0.25%
Sponsor: Taro Pharmaceuticals USA
Stage of development: Phase 4
ClinicalTrials.gov Identifier: NCT02340169
Study start: December 2014
Study completion: April 2016
This open-label, postmarketing safety study will evaluate the potential of Topicort (desoximetasone) topical spray 0.25% to suppress hypothalamic-pituitary-adrenal (HPA) axis function following twice daily dosing for 28 days in pediatric patients aged 2 to 17 years with moderate to severe plaque psoriasis. Participants will be serially enrolled into 3 cohorts.
The primary outcome measure will include HPA axis function suppression as measured by cortisol response test.
Secondary outcome measures will include evaluation of efficacy parameters, pharmacokinetics, and adverse events.
Long-term Safety and Efficacy of Calcitriol 3 µg/g Ointment in Pediatric Participants With Plaque Psoriasis
Product: Calcitriol 3 µg/g ointment
Sponsor: Galderma
Stage of development: Phase 4
ClinicalTrials.gov Identifier: NCT02125279
Study start: May 2014
Study completion: October 2016
This multicenter study will evaluate the safety and efficacy of calcitriol 3 µg/g ointment applied twice daily (without occlusion) to treat pediatric participants aged 2 to 17 years with mild to moderate plaque psoriasis for up to 26 weeks.
The primary outcome measure will include laboratory parameters related to calcium metabolism after 26 weeks of topical treatment with calcitriol 3 µg/g.
Evaluation of Calcipotriene Foam 0.005% Versus Vehicle Foam in Pediatric Patients With Plaque Psoriasis
Product: STF 115469 foam (calcipotriene foam 0.005%)
Sponsor: GlaxoSmithKline
Stage of development: Phase 3
ClinicalTrials.gov Identifier: NCT01582932
Study start: April 2013
Study completion: April 2019
This multicenter study will compare calcipotriene foam 0.005% with vehicle foam in pediatric participants aged 2 to 11 years (inclusive) with mild to moderate plaque psoriasis. Study participants or a primary caregiver will apply calcipotriene foam 0.005% as a thin layer twice daily (morning and evening) on the body and scalp (excluding the face) for up to 8 weeks.
The primary outcome measure will include treatment success.
Secondary outcome measures will include erythema, scaling, and plaque thickness.
Comparison of 122-0551 Foam Versus Vehicle for Plaque Psoriasis
Product: 122-0551 foam
Sponsor: Therapeutics, Inc
Stage of development: Phase 3
ClinicalTrials.gov Identifier: NCT02368210
Study start: January 2015
Study completion: October 2015 (August 2015 final collection date for primary outcome measure)
This phase 3 study will compare the efficacy and safety of 122-0551 foam (a glucocorticoid receptor agonist) and vehicle foam applied twice daily for 2 weeks in participants (aged ≥18 years) with plaque psoriasis.
The primary outcome measure will include the proportion of participants rated a “treatment success” based on the investigator global assessment.
Secondary outcome measures will include the proportion of participants rated a “treatment success” for each of the clinical signs of psoriasis: scaling, erythema, and plaque elevation.
HPA Axis Suppression Following Treatment With Desoximetasone Topical Spray 0.25% in Pediatric Patients With Plaque Psoriasis
Product: Topicort® (desoximetasone) topical spray 0.25%
Sponsor: Taro Pharmaceuticals USA
Stage of development: Phase 4
ClinicalTrials.gov Identifier: NCT02340169
Study start: December 2014
Study completion: April 2016
This open-label, postmarketing safety study will evaluate the potential of Topicort (desoximetasone) topical spray 0.25% to suppress hypothalamic-pituitary-adrenal (HPA) axis function following twice daily dosing for 28 days in pediatric patients aged 2 to 17 years with moderate to severe plaque psoriasis. Participants will be serially enrolled into 3 cohorts.
The primary outcome measure will include HPA axis function suppression as measured by cortisol response test.
Secondary outcome measures will include evaluation of efficacy parameters, pharmacokinetics, and adverse events.
Long-term Safety and Efficacy of Calcitriol 3 µg/g Ointment in Pediatric Participants With Plaque Psoriasis
Product: Calcitriol 3 µg/g ointment
Sponsor: Galderma
Stage of development: Phase 4
ClinicalTrials.gov Identifier: NCT02125279
Study start: May 2014
Study completion: October 2016
This multicenter study will evaluate the safety and efficacy of calcitriol 3 µg/g ointment applied twice daily (without occlusion) to treat pediatric participants aged 2 to 17 years with mild to moderate plaque psoriasis for up to 26 weeks.
The primary outcome measure will include laboratory parameters related to calcium metabolism after 26 weeks of topical treatment with calcitriol 3 µg/g.
Evaluation of Calcipotriene Foam 0.005% Versus Vehicle Foam in Pediatric Patients With Plaque Psoriasis
Product: STF 115469 foam (calcipotriene foam 0.005%)
Sponsor: GlaxoSmithKline
Stage of development: Phase 3
ClinicalTrials.gov Identifier: NCT01582932
Study start: April 2013
Study completion: April 2019
This multicenter study will compare calcipotriene foam 0.005% with vehicle foam in pediatric participants aged 2 to 11 years (inclusive) with mild to moderate plaque psoriasis. Study participants or a primary caregiver will apply calcipotriene foam 0.005% as a thin layer twice daily (morning and evening) on the body and scalp (excluding the face) for up to 8 weeks.
The primary outcome measure will include treatment success.
Secondary outcome measures will include erythema, scaling, and plaque thickness.
Comparison of 122-0551 Foam Versus Vehicle for Plaque Psoriasis
Product: 122-0551 foam
Sponsor: Therapeutics, Inc
Stage of development: Phase 3
ClinicalTrials.gov Identifier: NCT02368210
Study start: January 2015
Study completion: October 2015 (August 2015 final collection date for primary outcome measure)
This phase 3 study will compare the efficacy and safety of 122-0551 foam (a glucocorticoid receptor agonist) and vehicle foam applied twice daily for 2 weeks in participants (aged ≥18 years) with plaque psoriasis.
The primary outcome measure will include the proportion of participants rated a “treatment success” based on the investigator global assessment.
Secondary outcome measures will include the proportion of participants rated a “treatment success” for each of the clinical signs of psoriasis: scaling, erythema, and plaque elevation.
HPA Axis Suppression Following Treatment With Desoximetasone Topical Spray 0.25% in Pediatric Patients With Plaque Psoriasis
Product: Topicort® (desoximetasone) topical spray 0.25%
Sponsor: Taro Pharmaceuticals USA
Stage of development: Phase 4
ClinicalTrials.gov Identifier: NCT02340169
Study start: December 2014
Study completion: April 2016
This open-label, postmarketing safety study will evaluate the potential of Topicort (desoximetasone) topical spray 0.25% to suppress hypothalamic-pituitary-adrenal (HPA) axis function following twice daily dosing for 28 days in pediatric patients aged 2 to 17 years with moderate to severe plaque psoriasis. Participants will be serially enrolled into 3 cohorts.
The primary outcome measure will include HPA axis function suppression as measured by cortisol response test.
Secondary outcome measures will include evaluation of efficacy parameters, pharmacokinetics, and adverse events.
Long-term Safety and Efficacy of Calcitriol 3 µg/g Ointment in Pediatric Participants With Plaque Psoriasis
Product: Calcitriol 3 µg/g ointment
Sponsor: Galderma
Stage of development: Phase 4
ClinicalTrials.gov Identifier: NCT02125279
Study start: May 2014
Study completion: October 2016
This multicenter study will evaluate the safety and efficacy of calcitriol 3 µg/g ointment applied twice daily (without occlusion) to treat pediatric participants aged 2 to 17 years with mild to moderate plaque psoriasis for up to 26 weeks.
The primary outcome measure will include laboratory parameters related to calcium metabolism after 26 weeks of topical treatment with calcitriol 3 µg/g.
Evaluation of Calcipotriene Foam 0.005% Versus Vehicle Foam in Pediatric Patients With Plaque Psoriasis
Product: STF 115469 foam (calcipotriene foam 0.005%)
Sponsor: GlaxoSmithKline
Stage of development: Phase 3
ClinicalTrials.gov Identifier: NCT01582932
Study start: April 2013
Study completion: April 2019
This multicenter study will compare calcipotriene foam 0.005% with vehicle foam in pediatric participants aged 2 to 11 years (inclusive) with mild to moderate plaque psoriasis. Study participants or a primary caregiver will apply calcipotriene foam 0.005% as a thin layer twice daily (morning and evening) on the body and scalp (excluding the face) for up to 8 weeks.
The primary outcome measure will include treatment success.
Secondary outcome measures will include erythema, scaling, and plaque thickness.
EULAR’s psoriatic arthritis recommendations gain new drugs
ROME – Tumor necrosis factor inhibitors remain the mainstay of treatment for patients with psoriatic arthritis who don’t fully respond to treatment with a nonsteroidal anti-inflammatory drug and at least one conventional synthetic disease-modifying antirheumatic drug in newly updated treatment recommendations written by a task force of the European League Against Rheumatism.
The revised recommendations for psoriatic arthritis (PsA) replace what EULAR had last released in 2011 and published in 2012 (Ann. Rheum. Dis. 2012;71:4-12) and also add three new drug options not mentioned in the 2011 version that the panel now endorsed as alternatives to a tumor necrosis factor (TNF) inhibitor when a TNF inhibitor is not appropriate. The three additions are ustekinumab (Stelara), which acts by inhibiting interleukin- (IL-)12 and IL-23, secukinumab (Cosentyx), which acts by inhibiting IL-17, and apremilast (Otezla), which inhibits phosphodiesterase-4. Ustekinumab and secukinumab are considered biological disease-modifying antirheumatic drugs (bDMARDs), like the TNF inhibitors, while apremilast occupies a new classification niche as a targeted synthetic DMARD, said Dr. Laure Gossec, convener of the PsA treatment task force, at the European Congress of Rheumatology.

Although ustekinumab, secukinumab, and apremilast all have a role to play in managing selected PsA patients, they all remain second line to TNF inhibitors, stressed Dr. Gossec, professor of rheumatology at Pierre and Marie Curie University in Paris. A TNF inhibitor is the first agent to turn to when treatment with an NSAID and a conventional synthetic DMARD fails to bring about remission or minimal disease activity essentially because of its much longer track record of safety and efficacy, she said. Specifically, TNF inhibitors have been studied long term and have demonstrated their safety in registries, they have not been surpassed for efficacy by any other agent using indirect comparisons, and now that biosimilar TNF inhibitors have entered the market they also could potentially offer a price advantage, compared with newer agents.
But for some patients, TNF inhibitors are not appropriate, such as a patient with certain comorbidities or a history of infections that would make a TNF inhibitor contraindicated, she said. For these patients, one of the other types of biologic DMARDS now available would be the top alternative. In other patients, a comorbidity profile or a history of infections might make any biologic DMARD contraindicated, in which case the targeted synthetic DMARD apremilast is an appropriate alternative, she said.
The revised recommendations contain several other new items:
• For patients with active enthesitis, dactylitis, or both and an insufficient response to an NSAID or local glucocorticoid injections, then a TNF inhibitor or alternatively an IL-12 and IL-23 inhibitor (currently ustekinumab) or an IL-17 inhibitor (currently secukinumab) may be considered. Conventional synthetic DMARDS are ineffective for these patients, while in contrast all of the biologic DMARDs are effective, but the TNF inhibitors have an edge because of greater experience with the class in this setting.
• For patients with predominantly axial disease that is active and insufficiently responsive to NSAID treatment, a biologic DMARD should be considered, specifically a TNF inhibitor. Conventional synthetic DMARDs also have no efficacy for these patients, and few data exist regarding the efficacy of IL-12 and IL-23 inhibitors or IL-17 inhibitors.
• When patients fail to respond adequately to one biologic DMARD, switching to another biologic DMARD should be considered. This could involve switching from one TNF inhibitor to another, as some evidence exists that this could be effective. Alternatively, it could involve switching to a IL-12 and IL-23 inhibitor, an IL-17 inhibitor, or possibly a targeted synthetic DMARD (currently apremilast). The task force did not endorse any particular order of these drugs when switching occurs.
Dr. Gossec has been a consultant to AbbVie, Bristol-Myers Squibb, Celgene, Chugai, Janssen, Novartis, Pfizer, Roche, and UCB.
On Twitter @mitchelzoler
ROME – Tumor necrosis factor inhibitors remain the mainstay of treatment for patients with psoriatic arthritis who don’t fully respond to treatment with a nonsteroidal anti-inflammatory drug and at least one conventional synthetic disease-modifying antirheumatic drug in newly updated treatment recommendations written by a task force of the European League Against Rheumatism.
The revised recommendations for psoriatic arthritis (PsA) replace what EULAR had last released in 2011 and published in 2012 (Ann. Rheum. Dis. 2012;71:4-12) and also add three new drug options not mentioned in the 2011 version that the panel now endorsed as alternatives to a tumor necrosis factor (TNF) inhibitor when a TNF inhibitor is not appropriate. The three additions are ustekinumab (Stelara), which acts by inhibiting interleukin- (IL-)12 and IL-23, secukinumab (Cosentyx), which acts by inhibiting IL-17, and apremilast (Otezla), which inhibits phosphodiesterase-4. Ustekinumab and secukinumab are considered biological disease-modifying antirheumatic drugs (bDMARDs), like the TNF inhibitors, while apremilast occupies a new classification niche as a targeted synthetic DMARD, said Dr. Laure Gossec, convener of the PsA treatment task force, at the European Congress of Rheumatology.
Although ustekinumab, secukinumab, and apremilast all have a role to play in managing selected PsA patients, they all remain second line to TNF inhibitors, stressed Dr. Gossec, professor of rheumatology at Pierre and Marie Curie University in Paris. A TNF inhibitor is the first agent to turn to when treatment with an NSAID and a conventional synthetic DMARD fails to bring about remission or minimal disease activity essentially because of its much longer track record of safety and efficacy, she said. Specifically, TNF inhibitors have been studied long term and have demonstrated their safety in registries, they have not been surpassed for efficacy by any other agent using indirect comparisons, and now that biosimilar TNF inhibitors have entered the market they also could potentially offer a price advantage, compared with newer agents.
But for some patients, TNF inhibitors are not appropriate, such as a patient with certain comorbidities or a history of infections that would make a TNF inhibitor contraindicated, she said. For these patients, one of the other types of biologic DMARDS now available would be the top alternative. In other patients, a comorbidity profile or a history of infections might make any biologic DMARD contraindicated, in which case the targeted synthetic DMARD apremilast is an appropriate alternative, she said.
The revised recommendations contain several other new items:
• For patients with active enthesitis, dactylitis, or both and an insufficient response to an NSAID or local glucocorticoid injections, then a TNF inhibitor or alternatively an IL-12 and IL-23 inhibitor (currently ustekinumab) or an IL-17 inhibitor (currently secukinumab) may be considered. Conventional synthetic DMARDS are ineffective for these patients, while in contrast all of the biologic DMARDs are effective, but the TNF inhibitors have an edge because of greater experience with the class in this setting.
• For patients with predominantly axial disease that is active and insufficiently responsive to NSAID treatment, a biologic DMARD should be considered, specifically a TNF inhibitor. Conventional synthetic DMARDs also have no efficacy for these patients, and few data exist regarding the efficacy of IL-12 and IL-23 inhibitors or IL-17 inhibitors.
• When patients fail to respond adequately to one biologic DMARD, switching to another biologic DMARD should be considered. This could involve switching from one TNF inhibitor to another, as some evidence exists that this could be effective. Alternatively, it could involve switching to a IL-12 and IL-23 inhibitor, an IL-17 inhibitor, or possibly a targeted synthetic DMARD (currently apremilast). The task force did not endorse any particular order of these drugs when switching occurs.
Dr. Gossec has been a consultant to AbbVie, Bristol-Myers Squibb, Celgene, Chugai, Janssen, Novartis, Pfizer, Roche, and UCB.
On Twitter @mitchelzoler
ROME – Tumor necrosis factor inhibitors remain the mainstay of treatment for patients with psoriatic arthritis who don’t fully respond to treatment with a nonsteroidal anti-inflammatory drug and at least one conventional synthetic disease-modifying antirheumatic drug in newly updated treatment recommendations written by a task force of the European League Against Rheumatism.
The revised recommendations for psoriatic arthritis (PsA) replace what EULAR had last released in 2011 and published in 2012 (Ann. Rheum. Dis. 2012;71:4-12) and also add three new drug options not mentioned in the 2011 version that the panel now endorsed as alternatives to a tumor necrosis factor (TNF) inhibitor when a TNF inhibitor is not appropriate. The three additions are ustekinumab (Stelara), which acts by inhibiting interleukin- (IL-)12 and IL-23, secukinumab (Cosentyx), which acts by inhibiting IL-17, and apremilast (Otezla), which inhibits phosphodiesterase-4. Ustekinumab and secukinumab are considered biological disease-modifying antirheumatic drugs (bDMARDs), like the TNF inhibitors, while apremilast occupies a new classification niche as a targeted synthetic DMARD, said Dr. Laure Gossec, convener of the PsA treatment task force, at the European Congress of Rheumatology.
Although ustekinumab, secukinumab, and apremilast all have a role to play in managing selected PsA patients, they all remain second line to TNF inhibitors, stressed Dr. Gossec, professor of rheumatology at Pierre and Marie Curie University in Paris. A TNF inhibitor is the first agent to turn to when treatment with an NSAID and a conventional synthetic DMARD fails to bring about remission or minimal disease activity essentially because of its much longer track record of safety and efficacy, she said. Specifically, TNF inhibitors have been studied long term and have demonstrated their safety in registries, they have not been surpassed for efficacy by any other agent using indirect comparisons, and now that biosimilar TNF inhibitors have entered the market they also could potentially offer a price advantage, compared with newer agents.
But for some patients, TNF inhibitors are not appropriate, such as a patient with certain comorbidities or a history of infections that would make a TNF inhibitor contraindicated, she said. For these patients, one of the other types of biologic DMARDS now available would be the top alternative. In other patients, a comorbidity profile or a history of infections might make any biologic DMARD contraindicated, in which case the targeted synthetic DMARD apremilast is an appropriate alternative, she said.
The revised recommendations contain several other new items:
• For patients with active enthesitis, dactylitis, or both and an insufficient response to an NSAID or local glucocorticoid injections, then a TNF inhibitor or alternatively an IL-12 and IL-23 inhibitor (currently ustekinumab) or an IL-17 inhibitor (currently secukinumab) may be considered. Conventional synthetic DMARDS are ineffective for these patients, while in contrast all of the biologic DMARDs are effective, but the TNF inhibitors have an edge because of greater experience with the class in this setting.
• For patients with predominantly axial disease that is active and insufficiently responsive to NSAID treatment, a biologic DMARD should be considered, specifically a TNF inhibitor. Conventional synthetic DMARDs also have no efficacy for these patients, and few data exist regarding the efficacy of IL-12 and IL-23 inhibitors or IL-17 inhibitors.
• When patients fail to respond adequately to one biologic DMARD, switching to another biologic DMARD should be considered. This could involve switching from one TNF inhibitor to another, as some evidence exists that this could be effective. Alternatively, it could involve switching to a IL-12 and IL-23 inhibitor, an IL-17 inhibitor, or possibly a targeted synthetic DMARD (currently apremilast). The task force did not endorse any particular order of these drugs when switching occurs.
Dr. Gossec has been a consultant to AbbVie, Bristol-Myers Squibb, Celgene, Chugai, Janssen, Novartis, Pfizer, Roche, and UCB.
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE EULAR 2015 CONGRESS