User login
Using apps in clinical practice: 8 studies
COVID-19’s increased demand on the mental health care delivery system led to expanded utilization of technology-based solutions, including digital tools to deliver care.1 Technology-based solutions include both synchronous telehealth (eg, real-time interactive audio/video visits) and asynchronous tools such as smartphone applications (apps). Both real-time telehealth and apps continue to gain popularity. More than 10,000 mental health–related apps are available, and that number continues to rise.2 Numerous web- or mobile-based apps are available to aid in the treatment of various psychiatric conditions, including generalized anxiety disorder (GAD), major depressive disorder, insomnia, and posttraumatic stress disorder (PTSD).
Clinicians may find it challenging to choose the best psychiatry-related apps to recommend to patients. This dilemma calls for an approach to help clinicians select apps that are safe and effective.2 The American Psychiatric Association provides information to help mental health professionals navigate these issues and identify which aspects to consider when selecting an app for clinical use.3 The M-Health Index and Navigation Database also provides a set of objective evaluative criteria and offers guidance on choosing apps.4
In this article, we review 8 randomized controlled trials (RCTs) of mental health–related apps. We took several steps to ensure the RCTs we included were impactful and meaningful. First, we conducted a general search using mainstream search engines to assess which psychiatric apps were most popular for use in clinical practice. Using this list, we conducted a scholarly search engine query of RCTs using the name of the apps as a search parameter along with the following keywords: “mobile,” “web,” “applications,” and “psychiatry.” This search yielded approximately 50 results, which were narrowed down based on content and interest to a list of 8 articles (Table5-12). These articles were then graded using the limitations of each study as the primary substrate for evaluation.

1. Linardon J, Shatte A, Rosato J, et al. Efficacy of a transdiagnostic cognitive-behavioral intervention for eating disorder psychopathology delivered through a smartphone app: a randomized controlled trial. Psychol Med. 2022;52(9):1679-1690. doi:10.1017/S0033291720003426
Many patients with eating disorders are unable to receive effective treatment due to problems with accessing health care. Smartphone apps may help bridge the treatment gap for patients in this position. Linardon et al5 developed an app that uses the principles of cognitive-behavioral therapy (CBT) for treating eating disorders and conducted this study to evaluate its effectiveness.
Study design
- This RCT assigned individuals who reported episodes of binge eating to a group that used a mobile app (n = 197) or to a waiting list (n = 195). At baseline, 42% of participants exhibited diagnostic-level symptoms of bulimia nervosa and 31% had symptoms of binge-eating disorder.
- Assessments took place at baseline, Week 4, and Week 8.
- The primary outcome was global levels of eating disorder psychopathology.
- Secondary outcomes were other eating disorder symptoms, impairment, and distress.
Outcomes
- Compared to the control group, participants who used the mobile app reported greater reductions in global eating disorder psychopathology (d = -0.80).
- Significant effects were also observed for secondary outcomes except compensatory behavior frequency.
- Overall, participants reported they were satisfied with the app.
Continue to: Conclusions/limitations
Conclusions/limitations
- Findings show this app could potentially be a cost-effective and easily accessible option for patients who cannot receive standard treatment for eating disorders.
- Limitations: The overall posttest attrition rate was 35%.
2. Christoforou M, Sáez Fonseca JA, Tsakanikos E. Two novel cognitive behavioral therapy–based mobile apps for agoraphobia: randomized controlled trial. J Med Internet Res. 2017;19(11):e398. doi:10.2196/jmir.7747
CBT is generally the most accepted first-line treatment for agoraphobia. However, numerous barriers to obtaining CBT can prevent successful treatment. Limited research has evaluated the efficacy of apps for treating agoraphobia. Christoforou et al6 conducted an RCT to determine the effectiveness of a self-guided smartphone app for improving agoraphobic symptoms, compared to a mobile app used to treat anxiety.
Study design
- Participants (N = 170) who self-identified as having agoraphobia were randomly assigned to use a smartphone app designed to target agoraphobia (Agoraphobia Free) or a smartphone app designed to help with symptoms of anxiety (Stress Free) for 12 weeks. Both apps were based on established cognitive behavioral principles.
- Assessment occurred at baseline, midpoint, and end point.
- The primary outcome was symptom severity as measured by the Panic and Agoraphobia Scale (PAS).
Outcomes
- Both groups experienced statistically significant improvements in symptom severity over time. The differences in PAS score were -5.97 (95% CI, -8.49 to -3.44, P < .001) for Agoraphobia Free and -6.35 (95% CI, -8.82 to -3.87, P < .001) for Stress Free.
- There were no significant between-group differences in symptom severity.
Continue to: Conclusions/limitations
Conclusions/limitations
- This study is the first RCT to show that patients with agoraphobia could benefit from mobile-based interventions.
- Limitations: There was no waitlist control group. Limited information was collected about participant characteristics; there were no data on comorbid disorders, other psychological or physiological treatments, or other demographic characteristics such as ethnicity or computer literacy.
3. Everitt N, Broadbent J, Richardson B, et al. Exploring the features of an app-based just-in-time intervention for depression. J Affect Disord. 2021;291:279-287. doi:10.1016/j.jad.2021.05.021
The apps MoodTracker, ImproveYourMood, and ImproveYourMood+ deliver content “just in time” (in response to acute negative symptoms) to help patients with depression. In an RCT, Everitt et al7 evaluated delivering acute care for depressive mood states via a smartphone app. They sought to delineate whether symptom improvement was due to microintervention content, mood augmentation, or just-in-time prompts to use content.
Study design
- Participants (N = 235) from the general population who said they wanted to improve their mood were randomly assigned to a waitlist control group (n = 55) or 1 of 3 intervention groups: MoodTracker (monitoring-only; n = 58), ImproveYourMood (monitoring and content; n = 62), or ImproveYourMood+ (monitoring, content, and prompts; n = 60).
- The microintervention content provided by these apps consisted of 4 audio files of brief (2- to 3-minute) mindfulness and relaxation exercises. Participants used the assigned app for 3 weeks.
- Depressive symptoms, anxiety symptoms, and negative automatic thoughts were assessed at baseline, immediately following the intervention, and 1 month after the intervention using the 9-item Patient Health Questionnaire (PHQ-9), 7-item GAD scale (GAD-7), and 8-item Automatic Thoughts Questionnaire, respectively.
Outcomes
- Compared to the waitlist control group, participants in the ImproveYourMood group showed greater declines in depressive symptoms and anxiety symptoms (at follow-up only), and negative automatic thoughts (at both postintervention and follow-up).
- Those in the ImproveYourMood+ group only showed significantly greater improvements for automatic negative thoughts (at postintervention).
- MoodTracker participants did not differ from waitlist controls for any variables at any timepoints.
Continue to: Conclusions/limitations
Conclusions/limitations
- This study suggests that using microinterventions in acute settings can effectively reduce depressive symptoms both as they occur, and 1 to 2 months later.
- Limitations: The study featured a naturalistic design, where participants self-selected whether they wanted to use the program. Participants did not complete eligibility assessments or receive compensation, and the study had high dropout rates, ranging from 20% for the waitlist control group to 67% for the ImproveYourMood+ group.
4. McLean C, Davis CA, Miller M, et al. The effects of an exposure-based mobile app on symptoms of posttraumatic stress disorder in veterans: pilot randomized controlled trial. JMIR Mhealth Uhealth. 2022;10(11):e38951. doi:10.2196/38951
Veterans with PTSD face barriers when receiving trauma-focused treatments such as exposure therapy or CBT. Smartphone apps may help veterans self-treat and self-manage their PTSD symptoms. McLean et al8 studied the efficacy of Renew, a smartphone app that uses exposure therapy and social support to treat PTSD.
Study design
- In this pilot RCT, 93 veterans with clinically significant PTSD symptoms were randomly assigned to use the Renew app with and without support from a research staff member (active use group) or to a waitlist (delayed use group) for 6 weeks.
- The PTSD Checklist for DSM-5 (PCL-5) was used to measure PTSD symptoms at preintervention, postintervention, and 6-week follow-up.
- Most participants (69%) were women, and the mean age was 49.
Outcomes
- Compared to the delayed use group, participants in the active use group experienced a larger decrease in PCL-5 score (-6.14 vs -1.84). However, this difference was not statistically significant (P = .29), and the effect size was small (d = -0.39).
- There was no difference in engagement with the app between participants who received support from a research staff member and those who did not receive such support.
Continue to: Conclusions/limitations
Conclusions/limitations
- Renew may show promise as a tool to reduce PTSD symptoms in veterans.
- Educating family and friends on how to best support a patient using a mobile mental health app may help improve the efficacy of Renew and increase app engagement.
- Limitations: Because the study was conducted in veterans, the results may not be generalizable to other populations. Because most data collection occurred during the first wave of the COVID-19 pandemic in the United States, COVID-19–related stress may have impacted PTSD symptoms, app engagement, or outcomes.
5. Graham AK, Greene CJ, Kwasny MJ, et al. Coached mobile app platform for the treatment of depression and anxiety among primary care patients: a randomized clinical trial. JAMA Psychiatry. 2020;77(9):906-914. doi:10.1001/jamapsychiatry.2020.1011
Many cases of depression and anxiety are initially treated in primary care settings. However, these settings may have limited resources and inadequate training, and mobile interventions might be helpful to augment patient care. Graham et al9 studied the mobile platform IntelliCare to determine its efficacy as a tool to be used in primary care settings to treat depression and anxiety.
Study design
- This RCT randomly assigned adult primary care patients (N = 146) who screened positive for depression on the PHQ-9 (score ≥10) or anxiety on the GAD-7 (score ≥8) to the coach-supported IntelliCare platform, which consisted of 5 clinically focused apps, or to a waitlist control group. Interventions were delivered over 8 weeks.
- Overall, 122 (83.6%) patients were diagnosed with depression and 131 (89.7%) were diagnosed with anxiety.
- The primary outcomes were changes in depression (as measured by change in PHQ-9 score) and anxiety (change in GAD-7 score) during the intervention period.
Outcomes
- Participants who used the IntelliCare platform had a greater reduction in depression and anxiety symptoms compared to waitlist controls, and changes were sustained over 2-month follow-up.
- The least square means (LSM) difference in depression scores at Week 4 was 2.91 (SE = 0.83; d = 0.43) and at Week 8 was 4.37 (SE = 0.83; d = 0.64). The LSM difference in anxiety scores at Week 4 was 2.51 (SE = 0.78; d = 0.41) and at Week 8 was 3.33 (SE = 0.76; d = 0.55).
- A median number of 93 and 98 sessions among participants with depression and anxiety were recorded, respectively, indicating high use of the IntelliCare platform.
Continue to: Conclusions/limitations
Conclusions/limitations
- The IntelliCare platform was shown to be effective in reducing depression and anxiety among primary care patients. Simple apps can be bundled together and used by patients in conjunction to treat their individual needs.
- Limitations: The study had a limited follow-up period and did not record participants’ use of other apps. Slightly more than one-half (56%) of participants were taking an antidepressant.
6. Wilhelm S, Weingarden H, Greenberg JL, et al. Efficacy of app-based cognitive behavioral therapy for body dysmorphic disorder with coach support: initial randomized controlled clinical trial. Psychother Psychosom. 2022;91(4):277-285. doi:10.1159/000524628
Body dysmorphic disorder (BDD) is a severe yet undertreated disorder. Apps can improve access to treatment for patients experiencing BDD. Wilhelm et al10 studied the usability and efficacy of a coach-supported app called Perspectives that was specifically designed for treating BDD. Perspectives provide CBT in 7 modules: psychoeducation, cognitive restructuring, exposure, response prevention, mindfulness, attention retraining, and relapse prevention.
Study design
- Adults (N = 80) with primary BDD were assigned to use the Perspectives app for 12 weeks or to a waitlist control group. Participants were predominately female (84%) and White (71%), with a mean age of 27.
- Coaches promoted engagement and answered questions via in-app messaging and phone calls.
- Blinded independent evaluators used the Yale-Brown Obsessive Compulsive Scale Modified for BDD (BDD-YBOCS) to measure BDD severity at baseline, midtreatment (Week 6), and end of treatment (Week 12).
- Secondary outcomes included BDD-related insight, depression, quality of life, and functioning. Various scales were used to measure these outcomes.
Outcomes
- In intent-to-treat analyses, patients who received CBT via the Perspectives app had significantly lower BDD severity at the end of treatment compared to the waitlist control group, with a mean (SD) BDD-YBOCS score of 16.8 (7.5) vs 26.7 (6.2), with P < .001 and d = 1.44.
- Slightly more than one-half (52%) of those who used Perspectives achieved full or partial remission, compared to 8% in the waitlist control group.
Continue to: Conclusions/limitations
Conclusions/limitations
- CBT delivered via the Perspectives app and a coach proved to be effective treatment for adults with BDD.
- Adoption of the application was relatively high; 86% of Perspectives users were very or mostly satisfied.
- Limitations: Because the participants in this study were predominantly female and White, the findings might not be generalizable to other populations.
7. Kuhn E, Miller KE, Puran D, et al. A pilot randomized controlled trial of the Insomnia Coach mobile app to assess its feasibility, acceptability, and potential efficacy. Behav Ther. 2022;53(3):440-457. doi:10.1016/j.beth.2021.11.003
Insomnia remains a substantial problem among military veterans. First-line treatments for the disorder are sleep hygiene modification and CBT. Access to CBT is limited, especially for veterans. Kuhn et al11 studied the effectiveness of using Insomnia Coach, a CBT for insomnia–based app, to improve insomnia symptoms.
Study design
- Fifty US veterans who were mostly male (58%) with a mean age of 44.5 and moderate insomnia symptoms were randomized to use Insomnia Coach (n = 25) or to a waitlist control group (n = 25) for 6 weeks.
- All participants completed self-report measures and sleep diaries at baseline, posttreatment, and follow-up (12 weeks). Those who used the app (n = 15) completed a qualitative interview at posttreatment.
Outcomes
- At posttreatment, 28% of participants who used Insomnia Coach achieved clinically significant improvement, vs 4% of waitlist control participants. There was also a significant treatment effect on daytime sleep-related impairment (P = .044, d = -0.6).
- Additional treatment effects emerged at follow-up for insomnia severity, sleep onset latency, global sleep quality, and depression symptoms.
- Based on self-reports and qualitative interview responses, participants’ perceptions of Insomnia Coach were favorable. Three-fourths of participants used the app through 6 weeks and engaged with active elements.
Continue to: Conclusions/limitations
Conclusions/limitations
- Insomnia Coach may provide an accessible and convenient public health intervention for patients who aren’t receiving adequate care or CBT.
- Limitations: Because this study evaluated only veterans, the findings might not be generalizable to other populations.
8. Dahne J, Lejuez CW, Diaz VA, et al. Pilot randomized trial of a self-help behavioral activation mobile app for utilization in primary care. Behav Ther. 2019;50(4):817-827. doi:10.1016/j.beth.2018.12.003
Previous mobile technologies have shown the ability to treat depression in primary care settings. Moodivate is a self-help mobile app based on the Brief Behavioral Activation Treatment for Depression, which is an evidence-based treatment. This app is designed to help the user reengage in positive, nondepressed activities by identifying, scheduling, and completing activities. Dahne et al12 investigated the feasibility and efficacy of Moodivate for depressive symptoms in primary care patients.
Study design
- Participants (N = 52) were recruited from primary care practices and randomized 2:2:1 to receive Moodivate, a CBT-based mobile app called MoodKit, or treatment as usual (no app). All participants had an initial PHQ-8 score >10.
- Participants completed assessments of depressive symptoms (PHQ-8) weekly for 8 weeks.
- App analytics data were captured to examine if the use of Moodivate was feasible. (Analytics were not available for MoodKit).
Outcomes
- Participants who used Moodivate had a mean (SD) of 46.76 (30.10) sessions throughout the trial, spent 3.50 (2.76) minutes using the app per session, and spent 120.76 (101.02) minutes using the app in total.
- Nearly 70% of Moodivate participants continued to use the app 1 month after trial enrollment and 50% at the end of the 8-week follow-up period.
- Compared to the treatment as usual group, participants who used Moodivate and those who used MoodKit experienced significant decreases in depressive symptoms over time.
Conclusions/limitations
- The results show that for primary care patients with depression, the use of Moodivate is feasible and may reduce depressive symptoms.
- Limitations: For the first 3 months of enrollment, patients who met diagnostic criteria for a current major depressive episode were excluded. This study did not assess duration of medication use (ie, whether a study participant was stabilized on medication or recently started taking a new medication) and therefore could not ascertain whether treatment gains were a result of the use of the app or of possible new medication use.
1. Torous J, Jän Myrick K, Rauseo-Ricupero N, et al. Digital mental health and COVID-19: using technology today to accelerate the curve on access and quality tomorrow. JMIR Ment Health. 2020;7(3):e18848. doi:10.2196/18848
2. Camacho E, Cohen A, Torous J. Assessment of mental health services available through smartphone apps. JAMA Netw Open. 2022;5(12):e2248784. doi:10.1001/jamanetworkopen.2022.48784
3. American Psychiatric Association. APP Advisor: An American Psychiatric Association Initiative. Accessed April 28, 2023. https://www.psychiatry.org/psychiatrists/practice/mental-health-apps
4. Lagan S, Aquino P, Emerson MR, et al. Actionable health app evaluation: translating expert frameworks into objective metrics. NPJ Digit Med. 2020;3:100. doi:10.1038/s41746-020-00312-4
5. Linardon J, Shatte A, Rosato J, et al. Efficacy of a transdiagnostic cognitive-behavioral intervention for eating disorder psychopathology delivered through a smartphone app: a randomized controlled trial. Psychol Med. 2022;52(9):1679-1690. doi:10.1017/S0033291720003426
6. Christoforou M, Sáez Fonseca JA, Tsakanikos E. Two novel cognitive behavioral therapy–based mobile apps for agoraphobia: randomized controlled trial. J Med Internet Res. 2017;19(11):e398. doi:10.2196/jmir.7747
7. Everitt N, Broadbent J, Richardson B, et al. Exploring the features of an app-based just-in-time intervention for depression. J Affect Disord. 2021;291:279-287. doi:10.1016/j.jad.2021.05.021
8. McLean C, Davis CA, Miller M, et al. The effects of an exposure-based mobile app on symptoms of posttraumatic stress disorder in veterans: pilot randomized controlled trial. JMIR Mhealth Uhealth. 2022;10(11):e38951. doi:10.2196/38951
9. Graham AK, Greene CJ, Kwasny MJ, et al. Coached mobile app platform for the treatment of depression and anxiety among primary care patients: a randomized clinical trial. JAMA Psychiatry. 2020;77(9):906-914. doi:10.1001/jamapsychiatry.2020.1011
10. Wilhelm S, Weingarden H, Greenberg JL, et al. Efficacy of app-based cognitive behavioral therapy for body dysmorphic disorder with coach support: initial randomized controlled clinical trial. Psychother Psychosom. 2022;91(4):277-285. doi:10.1159/000524628
11. Kuhn E, Miller KE, Puran D, et al. A pilot randomized controlled trial of the Insomnia Coach mobile app to assess its feasibility, acceptability, and potential efficacy. Behav Ther. 2022;53(3):440-457. doi:10.1016/j.beth.2021.11.003
12. Dahne J, Lejuez CW, Diaz VA, et al. Pilot randomized trial of a self-help behavioral activation mobile app for utilization in primary care. Behav Ther. 2019;50(4):817-827. doi:10.1016/j.beth.2018.12.003
COVID-19’s increased demand on the mental health care delivery system led to expanded utilization of technology-based solutions, including digital tools to deliver care.1 Technology-based solutions include both synchronous telehealth (eg, real-time interactive audio/video visits) and asynchronous tools such as smartphone applications (apps). Both real-time telehealth and apps continue to gain popularity. More than 10,000 mental health–related apps are available, and that number continues to rise.2 Numerous web- or mobile-based apps are available to aid in the treatment of various psychiatric conditions, including generalized anxiety disorder (GAD), major depressive disorder, insomnia, and posttraumatic stress disorder (PTSD).
Clinicians may find it challenging to choose the best psychiatry-related apps to recommend to patients. This dilemma calls for an approach to help clinicians select apps that are safe and effective.2 The American Psychiatric Association provides information to help mental health professionals navigate these issues and identify which aspects to consider when selecting an app for clinical use.3 The M-Health Index and Navigation Database also provides a set of objective evaluative criteria and offers guidance on choosing apps.4
In this article, we review 8 randomized controlled trials (RCTs) of mental health–related apps. We took several steps to ensure the RCTs we included were impactful and meaningful. First, we conducted a general search using mainstream search engines to assess which psychiatric apps were most popular for use in clinical practice. Using this list, we conducted a scholarly search engine query of RCTs using the name of the apps as a search parameter along with the following keywords: “mobile,” “web,” “applications,” and “psychiatry.” This search yielded approximately 50 results, which were narrowed down based on content and interest to a list of 8 articles (Table5-12). These articles were then graded using the limitations of each study as the primary substrate for evaluation.
1. Linardon J, Shatte A, Rosato J, et al. Efficacy of a transdiagnostic cognitive-behavioral intervention for eating disorder psychopathology delivered through a smartphone app: a randomized controlled trial. Psychol Med. 2022;52(9):1679-1690. doi:10.1017/S0033291720003426
Many patients with eating disorders are unable to receive effective treatment due to problems with accessing health care. Smartphone apps may help bridge the treatment gap for patients in this position. Linardon et al5 developed an app that uses the principles of cognitive-behavioral therapy (CBT) for treating eating disorders and conducted this study to evaluate its effectiveness.
Study design
- This RCT assigned individuals who reported episodes of binge eating to a group that used a mobile app (n = 197) or to a waiting list (n = 195). At baseline, 42% of participants exhibited diagnostic-level symptoms of bulimia nervosa and 31% had symptoms of binge-eating disorder.
- Assessments took place at baseline, Week 4, and Week 8.
- The primary outcome was global levels of eating disorder psychopathology.
- Secondary outcomes were other eating disorder symptoms, impairment, and distress.
Outcomes
- Compared to the control group, participants who used the mobile app reported greater reductions in global eating disorder psychopathology (d = -0.80).
- Significant effects were also observed for secondary outcomes except compensatory behavior frequency.
- Overall, participants reported they were satisfied with the app.
Continue to: Conclusions/limitations
Conclusions/limitations
- Findings show this app could potentially be a cost-effective and easily accessible option for patients who cannot receive standard treatment for eating disorders.
- Limitations: The overall posttest attrition rate was 35%.
2. Christoforou M, Sáez Fonseca JA, Tsakanikos E. Two novel cognitive behavioral therapy–based mobile apps for agoraphobia: randomized controlled trial. J Med Internet Res. 2017;19(11):e398. doi:10.2196/jmir.7747
CBT is generally the most accepted first-line treatment for agoraphobia. However, numerous barriers to obtaining CBT can prevent successful treatment. Limited research has evaluated the efficacy of apps for treating agoraphobia. Christoforou et al6 conducted an RCT to determine the effectiveness of a self-guided smartphone app for improving agoraphobic symptoms, compared to a mobile app used to treat anxiety.
Study design
- Participants (N = 170) who self-identified as having agoraphobia were randomly assigned to use a smartphone app designed to target agoraphobia (Agoraphobia Free) or a smartphone app designed to help with symptoms of anxiety (Stress Free) for 12 weeks. Both apps were based on established cognitive behavioral principles.
- Assessment occurred at baseline, midpoint, and end point.
- The primary outcome was symptom severity as measured by the Panic and Agoraphobia Scale (PAS).
Outcomes
- Both groups experienced statistically significant improvements in symptom severity over time. The differences in PAS score were -5.97 (95% CI, -8.49 to -3.44, P < .001) for Agoraphobia Free and -6.35 (95% CI, -8.82 to -3.87, P < .001) for Stress Free.
- There were no significant between-group differences in symptom severity.
Continue to: Conclusions/limitations
Conclusions/limitations
- This study is the first RCT to show that patients with agoraphobia could benefit from mobile-based interventions.
- Limitations: There was no waitlist control group. Limited information was collected about participant characteristics; there were no data on comorbid disorders, other psychological or physiological treatments, or other demographic characteristics such as ethnicity or computer literacy.
3. Everitt N, Broadbent J, Richardson B, et al. Exploring the features of an app-based just-in-time intervention for depression. J Affect Disord. 2021;291:279-287. doi:10.1016/j.jad.2021.05.021
The apps MoodTracker, ImproveYourMood, and ImproveYourMood+ deliver content “just in time” (in response to acute negative symptoms) to help patients with depression. In an RCT, Everitt et al7 evaluated delivering acute care for depressive mood states via a smartphone app. They sought to delineate whether symptom improvement was due to microintervention content, mood augmentation, or just-in-time prompts to use content.
Study design
- Participants (N = 235) from the general population who said they wanted to improve their mood were randomly assigned to a waitlist control group (n = 55) or 1 of 3 intervention groups: MoodTracker (monitoring-only; n = 58), ImproveYourMood (monitoring and content; n = 62), or ImproveYourMood+ (monitoring, content, and prompts; n = 60).
- The microintervention content provided by these apps consisted of 4 audio files of brief (2- to 3-minute) mindfulness and relaxation exercises. Participants used the assigned app for 3 weeks.
- Depressive symptoms, anxiety symptoms, and negative automatic thoughts were assessed at baseline, immediately following the intervention, and 1 month after the intervention using the 9-item Patient Health Questionnaire (PHQ-9), 7-item GAD scale (GAD-7), and 8-item Automatic Thoughts Questionnaire, respectively.
Outcomes
- Compared to the waitlist control group, participants in the ImproveYourMood group showed greater declines in depressive symptoms and anxiety symptoms (at follow-up only), and negative automatic thoughts (at both postintervention and follow-up).
- Those in the ImproveYourMood+ group only showed significantly greater improvements for automatic negative thoughts (at postintervention).
- MoodTracker participants did not differ from waitlist controls for any variables at any timepoints.
Continue to: Conclusions/limitations
Conclusions/limitations
- This study suggests that using microinterventions in acute settings can effectively reduce depressive symptoms both as they occur, and 1 to 2 months later.
- Limitations: The study featured a naturalistic design, where participants self-selected whether they wanted to use the program. Participants did not complete eligibility assessments or receive compensation, and the study had high dropout rates, ranging from 20% for the waitlist control group to 67% for the ImproveYourMood+ group.
4. McLean C, Davis CA, Miller M, et al. The effects of an exposure-based mobile app on symptoms of posttraumatic stress disorder in veterans: pilot randomized controlled trial. JMIR Mhealth Uhealth. 2022;10(11):e38951. doi:10.2196/38951
Veterans with PTSD face barriers when receiving trauma-focused treatments such as exposure therapy or CBT. Smartphone apps may help veterans self-treat and self-manage their PTSD symptoms. McLean et al8 studied the efficacy of Renew, a smartphone app that uses exposure therapy and social support to treat PTSD.
Study design
- In this pilot RCT, 93 veterans with clinically significant PTSD symptoms were randomly assigned to use the Renew app with and without support from a research staff member (active use group) or to a waitlist (delayed use group) for 6 weeks.
- The PTSD Checklist for DSM-5 (PCL-5) was used to measure PTSD symptoms at preintervention, postintervention, and 6-week follow-up.
- Most participants (69%) were women, and the mean age was 49.
Outcomes
- Compared to the delayed use group, participants in the active use group experienced a larger decrease in PCL-5 score (-6.14 vs -1.84). However, this difference was not statistically significant (P = .29), and the effect size was small (d = -0.39).
- There was no difference in engagement with the app between participants who received support from a research staff member and those who did not receive such support.
Continue to: Conclusions/limitations
Conclusions/limitations
- Renew may show promise as a tool to reduce PTSD symptoms in veterans.
- Educating family and friends on how to best support a patient using a mobile mental health app may help improve the efficacy of Renew and increase app engagement.
- Limitations: Because the study was conducted in veterans, the results may not be generalizable to other populations. Because most data collection occurred during the first wave of the COVID-19 pandemic in the United States, COVID-19–related stress may have impacted PTSD symptoms, app engagement, or outcomes.
5. Graham AK, Greene CJ, Kwasny MJ, et al. Coached mobile app platform for the treatment of depression and anxiety among primary care patients: a randomized clinical trial. JAMA Psychiatry. 2020;77(9):906-914. doi:10.1001/jamapsychiatry.2020.1011
Many cases of depression and anxiety are initially treated in primary care settings. However, these settings may have limited resources and inadequate training, and mobile interventions might be helpful to augment patient care. Graham et al9 studied the mobile platform IntelliCare to determine its efficacy as a tool to be used in primary care settings to treat depression and anxiety.
Study design
- This RCT randomly assigned adult primary care patients (N = 146) who screened positive for depression on the PHQ-9 (score ≥10) or anxiety on the GAD-7 (score ≥8) to the coach-supported IntelliCare platform, which consisted of 5 clinically focused apps, or to a waitlist control group. Interventions were delivered over 8 weeks.
- Overall, 122 (83.6%) patients were diagnosed with depression and 131 (89.7%) were diagnosed with anxiety.
- The primary outcomes were changes in depression (as measured by change in PHQ-9 score) and anxiety (change in GAD-7 score) during the intervention period.
Outcomes
- Participants who used the IntelliCare platform had a greater reduction in depression and anxiety symptoms compared to waitlist controls, and changes were sustained over 2-month follow-up.
- The least square means (LSM) difference in depression scores at Week 4 was 2.91 (SE = 0.83; d = 0.43) and at Week 8 was 4.37 (SE = 0.83; d = 0.64). The LSM difference in anxiety scores at Week 4 was 2.51 (SE = 0.78; d = 0.41) and at Week 8 was 3.33 (SE = 0.76; d = 0.55).
- A median number of 93 and 98 sessions among participants with depression and anxiety were recorded, respectively, indicating high use of the IntelliCare platform.
Continue to: Conclusions/limitations
Conclusions/limitations
- The IntelliCare platform was shown to be effective in reducing depression and anxiety among primary care patients. Simple apps can be bundled together and used by patients in conjunction to treat their individual needs.
- Limitations: The study had a limited follow-up period and did not record participants’ use of other apps. Slightly more than one-half (56%) of participants were taking an antidepressant.
6. Wilhelm S, Weingarden H, Greenberg JL, et al. Efficacy of app-based cognitive behavioral therapy for body dysmorphic disorder with coach support: initial randomized controlled clinical trial. Psychother Psychosom. 2022;91(4):277-285. doi:10.1159/000524628
Body dysmorphic disorder (BDD) is a severe yet undertreated disorder. Apps can improve access to treatment for patients experiencing BDD. Wilhelm et al10 studied the usability and efficacy of a coach-supported app called Perspectives that was specifically designed for treating BDD. Perspectives provide CBT in 7 modules: psychoeducation, cognitive restructuring, exposure, response prevention, mindfulness, attention retraining, and relapse prevention.
Study design
- Adults (N = 80) with primary BDD were assigned to use the Perspectives app for 12 weeks or to a waitlist control group. Participants were predominately female (84%) and White (71%), with a mean age of 27.
- Coaches promoted engagement and answered questions via in-app messaging and phone calls.
- Blinded independent evaluators used the Yale-Brown Obsessive Compulsive Scale Modified for BDD (BDD-YBOCS) to measure BDD severity at baseline, midtreatment (Week 6), and end of treatment (Week 12).
- Secondary outcomes included BDD-related insight, depression, quality of life, and functioning. Various scales were used to measure these outcomes.
Outcomes
- In intent-to-treat analyses, patients who received CBT via the Perspectives app had significantly lower BDD severity at the end of treatment compared to the waitlist control group, with a mean (SD) BDD-YBOCS score of 16.8 (7.5) vs 26.7 (6.2), with P < .001 and d = 1.44.
- Slightly more than one-half (52%) of those who used Perspectives achieved full or partial remission, compared to 8% in the waitlist control group.
Continue to: Conclusions/limitations
Conclusions/limitations
- CBT delivered via the Perspectives app and a coach proved to be effective treatment for adults with BDD.
- Adoption of the application was relatively high; 86% of Perspectives users were very or mostly satisfied.
- Limitations: Because the participants in this study were predominantly female and White, the findings might not be generalizable to other populations.
7. Kuhn E, Miller KE, Puran D, et al. A pilot randomized controlled trial of the Insomnia Coach mobile app to assess its feasibility, acceptability, and potential efficacy. Behav Ther. 2022;53(3):440-457. doi:10.1016/j.beth.2021.11.003
Insomnia remains a substantial problem among military veterans. First-line treatments for the disorder are sleep hygiene modification and CBT. Access to CBT is limited, especially for veterans. Kuhn et al11 studied the effectiveness of using Insomnia Coach, a CBT for insomnia–based app, to improve insomnia symptoms.
Study design
- Fifty US veterans who were mostly male (58%) with a mean age of 44.5 and moderate insomnia symptoms were randomized to use Insomnia Coach (n = 25) or to a waitlist control group (n = 25) for 6 weeks.
- All participants completed self-report measures and sleep diaries at baseline, posttreatment, and follow-up (12 weeks). Those who used the app (n = 15) completed a qualitative interview at posttreatment.
Outcomes
- At posttreatment, 28% of participants who used Insomnia Coach achieved clinically significant improvement, vs 4% of waitlist control participants. There was also a significant treatment effect on daytime sleep-related impairment (P = .044, d = -0.6).
- Additional treatment effects emerged at follow-up for insomnia severity, sleep onset latency, global sleep quality, and depression symptoms.
- Based on self-reports and qualitative interview responses, participants’ perceptions of Insomnia Coach were favorable. Three-fourths of participants used the app through 6 weeks and engaged with active elements.
Continue to: Conclusions/limitations
Conclusions/limitations
- Insomnia Coach may provide an accessible and convenient public health intervention for patients who aren’t receiving adequate care or CBT.
- Limitations: Because this study evaluated only veterans, the findings might not be generalizable to other populations.
8. Dahne J, Lejuez CW, Diaz VA, et al. Pilot randomized trial of a self-help behavioral activation mobile app for utilization in primary care. Behav Ther. 2019;50(4):817-827. doi:10.1016/j.beth.2018.12.003
Previous mobile technologies have shown the ability to treat depression in primary care settings. Moodivate is a self-help mobile app based on the Brief Behavioral Activation Treatment for Depression, which is an evidence-based treatment. This app is designed to help the user reengage in positive, nondepressed activities by identifying, scheduling, and completing activities. Dahne et al12 investigated the feasibility and efficacy of Moodivate for depressive symptoms in primary care patients.
Study design
- Participants (N = 52) were recruited from primary care practices and randomized 2:2:1 to receive Moodivate, a CBT-based mobile app called MoodKit, or treatment as usual (no app). All participants had an initial PHQ-8 score >10.
- Participants completed assessments of depressive symptoms (PHQ-8) weekly for 8 weeks.
- App analytics data were captured to examine if the use of Moodivate was feasible. (Analytics were not available for MoodKit).
Outcomes
- Participants who used Moodivate had a mean (SD) of 46.76 (30.10) sessions throughout the trial, spent 3.50 (2.76) minutes using the app per session, and spent 120.76 (101.02) minutes using the app in total.
- Nearly 70% of Moodivate participants continued to use the app 1 month after trial enrollment and 50% at the end of the 8-week follow-up period.
- Compared to the treatment as usual group, participants who used Moodivate and those who used MoodKit experienced significant decreases in depressive symptoms over time.
Conclusions/limitations
- The results show that for primary care patients with depression, the use of Moodivate is feasible and may reduce depressive symptoms.
- Limitations: For the first 3 months of enrollment, patients who met diagnostic criteria for a current major depressive episode were excluded. This study did not assess duration of medication use (ie, whether a study participant was stabilized on medication or recently started taking a new medication) and therefore could not ascertain whether treatment gains were a result of the use of the app or of possible new medication use.
COVID-19’s increased demand on the mental health care delivery system led to expanded utilization of technology-based solutions, including digital tools to deliver care.1 Technology-based solutions include both synchronous telehealth (eg, real-time interactive audio/video visits) and asynchronous tools such as smartphone applications (apps). Both real-time telehealth and apps continue to gain popularity. More than 10,000 mental health–related apps are available, and that number continues to rise.2 Numerous web- or mobile-based apps are available to aid in the treatment of various psychiatric conditions, including generalized anxiety disorder (GAD), major depressive disorder, insomnia, and posttraumatic stress disorder (PTSD).
Clinicians may find it challenging to choose the best psychiatry-related apps to recommend to patients. This dilemma calls for an approach to help clinicians select apps that are safe and effective.2 The American Psychiatric Association provides information to help mental health professionals navigate these issues and identify which aspects to consider when selecting an app for clinical use.3 The M-Health Index and Navigation Database also provides a set of objective evaluative criteria and offers guidance on choosing apps.4
In this article, we review 8 randomized controlled trials (RCTs) of mental health–related apps. We took several steps to ensure the RCTs we included were impactful and meaningful. First, we conducted a general search using mainstream search engines to assess which psychiatric apps were most popular for use in clinical practice. Using this list, we conducted a scholarly search engine query of RCTs using the name of the apps as a search parameter along with the following keywords: “mobile,” “web,” “applications,” and “psychiatry.” This search yielded approximately 50 results, which were narrowed down based on content and interest to a list of 8 articles (Table5-12). These articles were then graded using the limitations of each study as the primary substrate for evaluation.
1. Linardon J, Shatte A, Rosato J, et al. Efficacy of a transdiagnostic cognitive-behavioral intervention for eating disorder psychopathology delivered through a smartphone app: a randomized controlled trial. Psychol Med. 2022;52(9):1679-1690. doi:10.1017/S0033291720003426
Many patients with eating disorders are unable to receive effective treatment due to problems with accessing health care. Smartphone apps may help bridge the treatment gap for patients in this position. Linardon et al5 developed an app that uses the principles of cognitive-behavioral therapy (CBT) for treating eating disorders and conducted this study to evaluate its effectiveness.
Study design
- This RCT assigned individuals who reported episodes of binge eating to a group that used a mobile app (n = 197) or to a waiting list (n = 195). At baseline, 42% of participants exhibited diagnostic-level symptoms of bulimia nervosa and 31% had symptoms of binge-eating disorder.
- Assessments took place at baseline, Week 4, and Week 8.
- The primary outcome was global levels of eating disorder psychopathology.
- Secondary outcomes were other eating disorder symptoms, impairment, and distress.
Outcomes
- Compared to the control group, participants who used the mobile app reported greater reductions in global eating disorder psychopathology (d = -0.80).
- Significant effects were also observed for secondary outcomes except compensatory behavior frequency.
- Overall, participants reported they were satisfied with the app.
Continue to: Conclusions/limitations
Conclusions/limitations
- Findings show this app could potentially be a cost-effective and easily accessible option for patients who cannot receive standard treatment for eating disorders.
- Limitations: The overall posttest attrition rate was 35%.
2. Christoforou M, Sáez Fonseca JA, Tsakanikos E. Two novel cognitive behavioral therapy–based mobile apps for agoraphobia: randomized controlled trial. J Med Internet Res. 2017;19(11):e398. doi:10.2196/jmir.7747
CBT is generally the most accepted first-line treatment for agoraphobia. However, numerous barriers to obtaining CBT can prevent successful treatment. Limited research has evaluated the efficacy of apps for treating agoraphobia. Christoforou et al6 conducted an RCT to determine the effectiveness of a self-guided smartphone app for improving agoraphobic symptoms, compared to a mobile app used to treat anxiety.
Study design
- Participants (N = 170) who self-identified as having agoraphobia were randomly assigned to use a smartphone app designed to target agoraphobia (Agoraphobia Free) or a smartphone app designed to help with symptoms of anxiety (Stress Free) for 12 weeks. Both apps were based on established cognitive behavioral principles.
- Assessment occurred at baseline, midpoint, and end point.
- The primary outcome was symptom severity as measured by the Panic and Agoraphobia Scale (PAS).
Outcomes
- Both groups experienced statistically significant improvements in symptom severity over time. The differences in PAS score were -5.97 (95% CI, -8.49 to -3.44, P < .001) for Agoraphobia Free and -6.35 (95% CI, -8.82 to -3.87, P < .001) for Stress Free.
- There were no significant between-group differences in symptom severity.
Continue to: Conclusions/limitations
Conclusions/limitations
- This study is the first RCT to show that patients with agoraphobia could benefit from mobile-based interventions.
- Limitations: There was no waitlist control group. Limited information was collected about participant characteristics; there were no data on comorbid disorders, other psychological or physiological treatments, or other demographic characteristics such as ethnicity or computer literacy.
3. Everitt N, Broadbent J, Richardson B, et al. Exploring the features of an app-based just-in-time intervention for depression. J Affect Disord. 2021;291:279-287. doi:10.1016/j.jad.2021.05.021
The apps MoodTracker, ImproveYourMood, and ImproveYourMood+ deliver content “just in time” (in response to acute negative symptoms) to help patients with depression. In an RCT, Everitt et al7 evaluated delivering acute care for depressive mood states via a smartphone app. They sought to delineate whether symptom improvement was due to microintervention content, mood augmentation, or just-in-time prompts to use content.
Study design
- Participants (N = 235) from the general population who said they wanted to improve their mood were randomly assigned to a waitlist control group (n = 55) or 1 of 3 intervention groups: MoodTracker (monitoring-only; n = 58), ImproveYourMood (monitoring and content; n = 62), or ImproveYourMood+ (monitoring, content, and prompts; n = 60).
- The microintervention content provided by these apps consisted of 4 audio files of brief (2- to 3-minute) mindfulness and relaxation exercises. Participants used the assigned app for 3 weeks.
- Depressive symptoms, anxiety symptoms, and negative automatic thoughts were assessed at baseline, immediately following the intervention, and 1 month after the intervention using the 9-item Patient Health Questionnaire (PHQ-9), 7-item GAD scale (GAD-7), and 8-item Automatic Thoughts Questionnaire, respectively.
Outcomes
- Compared to the waitlist control group, participants in the ImproveYourMood group showed greater declines in depressive symptoms and anxiety symptoms (at follow-up only), and negative automatic thoughts (at both postintervention and follow-up).
- Those in the ImproveYourMood+ group only showed significantly greater improvements for automatic negative thoughts (at postintervention).
- MoodTracker participants did not differ from waitlist controls for any variables at any timepoints.
Continue to: Conclusions/limitations
Conclusions/limitations
- This study suggests that using microinterventions in acute settings can effectively reduce depressive symptoms both as they occur, and 1 to 2 months later.
- Limitations: The study featured a naturalistic design, where participants self-selected whether they wanted to use the program. Participants did not complete eligibility assessments or receive compensation, and the study had high dropout rates, ranging from 20% for the waitlist control group to 67% for the ImproveYourMood+ group.
4. McLean C, Davis CA, Miller M, et al. The effects of an exposure-based mobile app on symptoms of posttraumatic stress disorder in veterans: pilot randomized controlled trial. JMIR Mhealth Uhealth. 2022;10(11):e38951. doi:10.2196/38951
Veterans with PTSD face barriers when receiving trauma-focused treatments such as exposure therapy or CBT. Smartphone apps may help veterans self-treat and self-manage their PTSD symptoms. McLean et al8 studied the efficacy of Renew, a smartphone app that uses exposure therapy and social support to treat PTSD.
Study design
- In this pilot RCT, 93 veterans with clinically significant PTSD symptoms were randomly assigned to use the Renew app with and without support from a research staff member (active use group) or to a waitlist (delayed use group) for 6 weeks.
- The PTSD Checklist for DSM-5 (PCL-5) was used to measure PTSD symptoms at preintervention, postintervention, and 6-week follow-up.
- Most participants (69%) were women, and the mean age was 49.
Outcomes
- Compared to the delayed use group, participants in the active use group experienced a larger decrease in PCL-5 score (-6.14 vs -1.84). However, this difference was not statistically significant (P = .29), and the effect size was small (d = -0.39).
- There was no difference in engagement with the app between participants who received support from a research staff member and those who did not receive such support.
Continue to: Conclusions/limitations
Conclusions/limitations
- Renew may show promise as a tool to reduce PTSD symptoms in veterans.
- Educating family and friends on how to best support a patient using a mobile mental health app may help improve the efficacy of Renew and increase app engagement.
- Limitations: Because the study was conducted in veterans, the results may not be generalizable to other populations. Because most data collection occurred during the first wave of the COVID-19 pandemic in the United States, COVID-19–related stress may have impacted PTSD symptoms, app engagement, or outcomes.
5. Graham AK, Greene CJ, Kwasny MJ, et al. Coached mobile app platform for the treatment of depression and anxiety among primary care patients: a randomized clinical trial. JAMA Psychiatry. 2020;77(9):906-914. doi:10.1001/jamapsychiatry.2020.1011
Many cases of depression and anxiety are initially treated in primary care settings. However, these settings may have limited resources and inadequate training, and mobile interventions might be helpful to augment patient care. Graham et al9 studied the mobile platform IntelliCare to determine its efficacy as a tool to be used in primary care settings to treat depression and anxiety.
Study design
- This RCT randomly assigned adult primary care patients (N = 146) who screened positive for depression on the PHQ-9 (score ≥10) or anxiety on the GAD-7 (score ≥8) to the coach-supported IntelliCare platform, which consisted of 5 clinically focused apps, or to a waitlist control group. Interventions were delivered over 8 weeks.
- Overall, 122 (83.6%) patients were diagnosed with depression and 131 (89.7%) were diagnosed with anxiety.
- The primary outcomes were changes in depression (as measured by change in PHQ-9 score) and anxiety (change in GAD-7 score) during the intervention period.
Outcomes
- Participants who used the IntelliCare platform had a greater reduction in depression and anxiety symptoms compared to waitlist controls, and changes were sustained over 2-month follow-up.
- The least square means (LSM) difference in depression scores at Week 4 was 2.91 (SE = 0.83; d = 0.43) and at Week 8 was 4.37 (SE = 0.83; d = 0.64). The LSM difference in anxiety scores at Week 4 was 2.51 (SE = 0.78; d = 0.41) and at Week 8 was 3.33 (SE = 0.76; d = 0.55).
- A median number of 93 and 98 sessions among participants with depression and anxiety were recorded, respectively, indicating high use of the IntelliCare platform.
Continue to: Conclusions/limitations
Conclusions/limitations
- The IntelliCare platform was shown to be effective in reducing depression and anxiety among primary care patients. Simple apps can be bundled together and used by patients in conjunction to treat their individual needs.
- Limitations: The study had a limited follow-up period and did not record participants’ use of other apps. Slightly more than one-half (56%) of participants were taking an antidepressant.
6. Wilhelm S, Weingarden H, Greenberg JL, et al. Efficacy of app-based cognitive behavioral therapy for body dysmorphic disorder with coach support: initial randomized controlled clinical trial. Psychother Psychosom. 2022;91(4):277-285. doi:10.1159/000524628
Body dysmorphic disorder (BDD) is a severe yet undertreated disorder. Apps can improve access to treatment for patients experiencing BDD. Wilhelm et al10 studied the usability and efficacy of a coach-supported app called Perspectives that was specifically designed for treating BDD. Perspectives provide CBT in 7 modules: psychoeducation, cognitive restructuring, exposure, response prevention, mindfulness, attention retraining, and relapse prevention.
Study design
- Adults (N = 80) with primary BDD were assigned to use the Perspectives app for 12 weeks or to a waitlist control group. Participants were predominately female (84%) and White (71%), with a mean age of 27.
- Coaches promoted engagement and answered questions via in-app messaging and phone calls.
- Blinded independent evaluators used the Yale-Brown Obsessive Compulsive Scale Modified for BDD (BDD-YBOCS) to measure BDD severity at baseline, midtreatment (Week 6), and end of treatment (Week 12).
- Secondary outcomes included BDD-related insight, depression, quality of life, and functioning. Various scales were used to measure these outcomes.
Outcomes
- In intent-to-treat analyses, patients who received CBT via the Perspectives app had significantly lower BDD severity at the end of treatment compared to the waitlist control group, with a mean (SD) BDD-YBOCS score of 16.8 (7.5) vs 26.7 (6.2), with P < .001 and d = 1.44.
- Slightly more than one-half (52%) of those who used Perspectives achieved full or partial remission, compared to 8% in the waitlist control group.
Continue to: Conclusions/limitations
Conclusions/limitations
- CBT delivered via the Perspectives app and a coach proved to be effective treatment for adults with BDD.
- Adoption of the application was relatively high; 86% of Perspectives users were very or mostly satisfied.
- Limitations: Because the participants in this study were predominantly female and White, the findings might not be generalizable to other populations.
7. Kuhn E, Miller KE, Puran D, et al. A pilot randomized controlled trial of the Insomnia Coach mobile app to assess its feasibility, acceptability, and potential efficacy. Behav Ther. 2022;53(3):440-457. doi:10.1016/j.beth.2021.11.003
Insomnia remains a substantial problem among military veterans. First-line treatments for the disorder are sleep hygiene modification and CBT. Access to CBT is limited, especially for veterans. Kuhn et al11 studied the effectiveness of using Insomnia Coach, a CBT for insomnia–based app, to improve insomnia symptoms.
Study design
- Fifty US veterans who were mostly male (58%) with a mean age of 44.5 and moderate insomnia symptoms were randomized to use Insomnia Coach (n = 25) or to a waitlist control group (n = 25) for 6 weeks.
- All participants completed self-report measures and sleep diaries at baseline, posttreatment, and follow-up (12 weeks). Those who used the app (n = 15) completed a qualitative interview at posttreatment.
Outcomes
- At posttreatment, 28% of participants who used Insomnia Coach achieved clinically significant improvement, vs 4% of waitlist control participants. There was also a significant treatment effect on daytime sleep-related impairment (P = .044, d = -0.6).
- Additional treatment effects emerged at follow-up for insomnia severity, sleep onset latency, global sleep quality, and depression symptoms.
- Based on self-reports and qualitative interview responses, participants’ perceptions of Insomnia Coach were favorable. Three-fourths of participants used the app through 6 weeks and engaged with active elements.
Continue to: Conclusions/limitations
Conclusions/limitations
- Insomnia Coach may provide an accessible and convenient public health intervention for patients who aren’t receiving adequate care or CBT.
- Limitations: Because this study evaluated only veterans, the findings might not be generalizable to other populations.
8. Dahne J, Lejuez CW, Diaz VA, et al. Pilot randomized trial of a self-help behavioral activation mobile app for utilization in primary care. Behav Ther. 2019;50(4):817-827. doi:10.1016/j.beth.2018.12.003
Previous mobile technologies have shown the ability to treat depression in primary care settings. Moodivate is a self-help mobile app based on the Brief Behavioral Activation Treatment for Depression, which is an evidence-based treatment. This app is designed to help the user reengage in positive, nondepressed activities by identifying, scheduling, and completing activities. Dahne et al12 investigated the feasibility and efficacy of Moodivate for depressive symptoms in primary care patients.
Study design
- Participants (N = 52) were recruited from primary care practices and randomized 2:2:1 to receive Moodivate, a CBT-based mobile app called MoodKit, or treatment as usual (no app). All participants had an initial PHQ-8 score >10.
- Participants completed assessments of depressive symptoms (PHQ-8) weekly for 8 weeks.
- App analytics data were captured to examine if the use of Moodivate was feasible. (Analytics were not available for MoodKit).
Outcomes
- Participants who used Moodivate had a mean (SD) of 46.76 (30.10) sessions throughout the trial, spent 3.50 (2.76) minutes using the app per session, and spent 120.76 (101.02) minutes using the app in total.
- Nearly 70% of Moodivate participants continued to use the app 1 month after trial enrollment and 50% at the end of the 8-week follow-up period.
- Compared to the treatment as usual group, participants who used Moodivate and those who used MoodKit experienced significant decreases in depressive symptoms over time.
Conclusions/limitations
- The results show that for primary care patients with depression, the use of Moodivate is feasible and may reduce depressive symptoms.
- Limitations: For the first 3 months of enrollment, patients who met diagnostic criteria for a current major depressive episode were excluded. This study did not assess duration of medication use (ie, whether a study participant was stabilized on medication or recently started taking a new medication) and therefore could not ascertain whether treatment gains were a result of the use of the app or of possible new medication use.
1. Torous J, Jän Myrick K, Rauseo-Ricupero N, et al. Digital mental health and COVID-19: using technology today to accelerate the curve on access and quality tomorrow. JMIR Ment Health. 2020;7(3):e18848. doi:10.2196/18848
2. Camacho E, Cohen A, Torous J. Assessment of mental health services available through smartphone apps. JAMA Netw Open. 2022;5(12):e2248784. doi:10.1001/jamanetworkopen.2022.48784
3. American Psychiatric Association. APP Advisor: An American Psychiatric Association Initiative. Accessed April 28, 2023. https://www.psychiatry.org/psychiatrists/practice/mental-health-apps
4. Lagan S, Aquino P, Emerson MR, et al. Actionable health app evaluation: translating expert frameworks into objective metrics. NPJ Digit Med. 2020;3:100. doi:10.1038/s41746-020-00312-4
5. Linardon J, Shatte A, Rosato J, et al. Efficacy of a transdiagnostic cognitive-behavioral intervention for eating disorder psychopathology delivered through a smartphone app: a randomized controlled trial. Psychol Med. 2022;52(9):1679-1690. doi:10.1017/S0033291720003426
6. Christoforou M, Sáez Fonseca JA, Tsakanikos E. Two novel cognitive behavioral therapy–based mobile apps for agoraphobia: randomized controlled trial. J Med Internet Res. 2017;19(11):e398. doi:10.2196/jmir.7747
7. Everitt N, Broadbent J, Richardson B, et al. Exploring the features of an app-based just-in-time intervention for depression. J Affect Disord. 2021;291:279-287. doi:10.1016/j.jad.2021.05.021
8. McLean C, Davis CA, Miller M, et al. The effects of an exposure-based mobile app on symptoms of posttraumatic stress disorder in veterans: pilot randomized controlled trial. JMIR Mhealth Uhealth. 2022;10(11):e38951. doi:10.2196/38951
9. Graham AK, Greene CJ, Kwasny MJ, et al. Coached mobile app platform for the treatment of depression and anxiety among primary care patients: a randomized clinical trial. JAMA Psychiatry. 2020;77(9):906-914. doi:10.1001/jamapsychiatry.2020.1011
10. Wilhelm S, Weingarden H, Greenberg JL, et al. Efficacy of app-based cognitive behavioral therapy for body dysmorphic disorder with coach support: initial randomized controlled clinical trial. Psychother Psychosom. 2022;91(4):277-285. doi:10.1159/000524628
11. Kuhn E, Miller KE, Puran D, et al. A pilot randomized controlled trial of the Insomnia Coach mobile app to assess its feasibility, acceptability, and potential efficacy. Behav Ther. 2022;53(3):440-457. doi:10.1016/j.beth.2021.11.003
12. Dahne J, Lejuez CW, Diaz VA, et al. Pilot randomized trial of a self-help behavioral activation mobile app for utilization in primary care. Behav Ther. 2019;50(4):817-827. doi:10.1016/j.beth.2018.12.003
1. Torous J, Jän Myrick K, Rauseo-Ricupero N, et al. Digital mental health and COVID-19: using technology today to accelerate the curve on access and quality tomorrow. JMIR Ment Health. 2020;7(3):e18848. doi:10.2196/18848
2. Camacho E, Cohen A, Torous J. Assessment of mental health services available through smartphone apps. JAMA Netw Open. 2022;5(12):e2248784. doi:10.1001/jamanetworkopen.2022.48784
3. American Psychiatric Association. APP Advisor: An American Psychiatric Association Initiative. Accessed April 28, 2023. https://www.psychiatry.org/psychiatrists/practice/mental-health-apps
4. Lagan S, Aquino P, Emerson MR, et al. Actionable health app evaluation: translating expert frameworks into objective metrics. NPJ Digit Med. 2020;3:100. doi:10.1038/s41746-020-00312-4
5. Linardon J, Shatte A, Rosato J, et al. Efficacy of a transdiagnostic cognitive-behavioral intervention for eating disorder psychopathology delivered through a smartphone app: a randomized controlled trial. Psychol Med. 2022;52(9):1679-1690. doi:10.1017/S0033291720003426
6. Christoforou M, Sáez Fonseca JA, Tsakanikos E. Two novel cognitive behavioral therapy–based mobile apps for agoraphobia: randomized controlled trial. J Med Internet Res. 2017;19(11):e398. doi:10.2196/jmir.7747
7. Everitt N, Broadbent J, Richardson B, et al. Exploring the features of an app-based just-in-time intervention for depression. J Affect Disord. 2021;291:279-287. doi:10.1016/j.jad.2021.05.021
8. McLean C, Davis CA, Miller M, et al. The effects of an exposure-based mobile app on symptoms of posttraumatic stress disorder in veterans: pilot randomized controlled trial. JMIR Mhealth Uhealth. 2022;10(11):e38951. doi:10.2196/38951
9. Graham AK, Greene CJ, Kwasny MJ, et al. Coached mobile app platform for the treatment of depression and anxiety among primary care patients: a randomized clinical trial. JAMA Psychiatry. 2020;77(9):906-914. doi:10.1001/jamapsychiatry.2020.1011
10. Wilhelm S, Weingarden H, Greenberg JL, et al. Efficacy of app-based cognitive behavioral therapy for body dysmorphic disorder with coach support: initial randomized controlled clinical trial. Psychother Psychosom. 2022;91(4):277-285. doi:10.1159/000524628
11. Kuhn E, Miller KE, Puran D, et al. A pilot randomized controlled trial of the Insomnia Coach mobile app to assess its feasibility, acceptability, and potential efficacy. Behav Ther. 2022;53(3):440-457. doi:10.1016/j.beth.2021.11.003
12. Dahne J, Lejuez CW, Diaz VA, et al. Pilot randomized trial of a self-help behavioral activation mobile app for utilization in primary care. Behav Ther. 2019;50(4):817-827. doi:10.1016/j.beth.2018.12.003

Father’s influence impacts whether their infant is breastfed, follows safe sleeping practices
Infants of fathers who want their child to breastfeed are more likely to be part of a family unit that starts and continues breastfeeding, and fathers informed of safe sleep practices are more likely to follow those sleeping recommendations for their infant, according to the results of a recent survey published in Pediatrics.
The results suggest that the researchers said.
“Our findings underscore that new fathers are a critical audience to promote breastfeeding and safe infant sleep,” John James Parker, MD, instructor of pediatrics at Northwestern University, Chicago, stated in a press release. “Many families do not gain the health benefits from breastfeeding because they are not provided the support to breastfeed successfully. Fathers need to be directly engaged in breastfeeding discussions, and providers need to describe the important role fathers play in breastfeeding success.”
Population-based survey results
Dr. Parker and colleagues used the Pregnancy Risk Assessment Monitoring System (PRAMS) for Dads population-based survey to evaluate the rate of adherence to breastfeeding and infant sleep practices recommended by the American Academy of Pediatrics. In total, 250 fathers in Georgia were surveyed between October 2018 and July 2019 about whether their infants were breastfeeding and if they were breastfeeding at 8 weeks. The fathers were also asked how often the infant slept in a back sleeping position, on an approved sleep surface, and sleeping with no soft objects or soft bedding.
In addition to surveying fathers on their attitudes on breastfeeding and whether they followed safe infant sleep practices, the researchers collected information on paternal sociodemographic characteristics such as age, race and ethnicity, education, health insurance status, and marital status. Overall, a majority fathers who responded to the survey were between 25 years and 34 years old (56.5%), non-Hispanic White (44.7%), had a high school diploma or less (43.7%) or completed college (37.1%), and were married (65.2%).
Dr. Parker and colleagues found fathers surveyed said 86.1% of infants were ever breastfed, which decreased to 63.4% at 8 weeks. Compared with fathers who did not want their infant to breastfeed or expressed no opinion, fathers who wanted to have the infant’s mother breastfeed had a higher likelihood of reporting breastfeeding initiation (adjusted prevalence ratio, 1.39; 95% confidence interval, 1.15-1.68) and breastfeeding at 8 weeks (aPR, 2.33; 95% CI, 1.59-3.42). Having a college degree was also associated with the infant breastfeeding (93.6% vs. 75.1%; aPR, 1.25; 95% CI, 1.06-1.46) and breastfeeding at 8 weeks (74.7% vs. 52.0%; aPR, 1.44; 95% CI, 1.08-1.91), compared with fathers who graduated from high school or less.
Regarding safe infant sleeping practices, 81.18% of fathers said they placed their infants on their back to sleep, but 44.1% said they did not use soft bedding, and 31.9% said they used an approved sleep surface. In total, 99.4% of fathers put their infant to sleep, and 68.4% said they received information on all three infant safe sleeping practices, while 15.7% said they followed all three sleeping recommendations. A health care provider was the most common person giving advice to the father on placing the infant to sleep on their back (84.7%); to use a safe sleep surface such as a crib, bassinet, or pack-and-play (78.7%); and receiving information about what not to place in the infant’s bed (79.1%).
The survey found non-Hispanic Black fathers reported they were less likely to put the infant to sleep on their back (62.5% vs. 89.5%; aPR, 0.70; 95% CI, 0.54-0.90) and not use soft bedding (28.1% vs. 54.1%; aPR, 0.52; 95% CI, 0.30-0.89), compared with non-Hispanic White fathers. College graduates were more likely to not use soft bedding (61.4% vs. 31.9%; aPR, 1.92; 95% CI, 1.25-2.95), more likely to get advice on placing the infant on their back for sleep (94.3% vs. 73.6%; aPR, 1.28; 95% CI, 1.09-1.51), and more likely to receive advice on what not to place in the infant’s bed (88.1% vs. 68.5%; aPR, 1.29; 95% CI, 1.06-1.57), compared with fathers with a high school diploma or less.
“Fathers need to receive counseling on all the safe sleep practices for their infants,” Dr. Parker said. “To reduce racial disparities in sudden unexpected infant death, we need tailored strategies to increase safe infant sleep practices in the Black community, including public campaigns to increase awareness and home visiting programs. These interventions must involve both parents to be most effective.”
Educational efforts should recognize father’s contributions
In an interview, Deborah E. Campbell, MD, chief of neonatology at the Children’s Hospital at Montefiore, New York, said the survey “adds further important information on the role of fathers both in the care of their infants and young children, but also in terms of supporting the birth parent and a number of the parenting decisions, whether it’s breastfeeding as well as safe sleep practices for the infant.”

The benefits of breastfeeding are important for the infant but also for the health of the family and the community, Dr. Campbell explained, noting that breastfeeding can aid in preventing chronic disease and cancer. Promoting safe sleep practices for infants, on the other hand, helps reduce factors such as infant mortality and sudden unexpected infant death.
While PRAMS has existed for decades, PRAMS for Dads is relatively new and localized as a pilot program in Georgia, Dr. Campbell noted. The pilot program “really shows that you can get helpful information, and it would be wonderful to see that model expanded to begin to look at the father’s role in other states as well.”
To improve adherence to breastfeeding and infant safe sleeping practices, creating broadly educational efforts that include and recognize the contributions of the father are important, especially as fathers today are generally more involved and engaged than in past generations, Dr. Campbell said. For instance, pediatric or family practice offices could be structured in a way that welcomes fathers and appreciates them, rather than focusing solely on the birth mother or the baby.
“I think certainly as we have greater diversity among our families, greater diversity within our communities, just more varied family constellations, recognizing and valuing each member of the family becomes important and then providing them with the information and the tools,” she said.
While health literacy is important, structural inequalities in care provision in health care settings mean that “it’s honestly much more likely that an educated parent is going to have an opportunity to hear more of those messages,” Dr. Campbell said. “They are much more likely to be able to go to childbirth classes, go to the pediatrician visits, take off from work, have leaves so that they can spend time in the hospital during the infant’s stay and the birth parent’s initial recoveries so that they have greater opportunity to get those messages.”
Fathers with lower educational attainment may have good health literacy, but may be unable to be around for these conversations. “Education is really a proxy for a lot of other structural issues,” she said.
Educational messages around safe sleeping practices for the infant should acknowledge that many families might not have the space to have a dedicated room with a crib for an infant, and offer assurances that other safe sleeping options exist, such as a pack-and-play or Moses basket. The most important message to get across to parents is that the baby is “sleeping alone” in a firm, noninclined surface and does not have bedding or other objects around them.
It is not just the infant’s bed that should follow the AAP recommendations: the family bed should also be a firm surface free of soft objects and bedding for breastfeeding, Dr. Campbell noted. If a parent falls asleep while breastfeeding in bed, the AAP’s most recent guidance notes the parent should move the infant to a separate sleep space as soon as they wake up, but the Academy also acknowledges how that can be challenging in early months with sleep deprivation.
“I think it’s dealing with the realities of having a new baby and trying to create the safest environment for that baby, one that supports and promotes breastfeeding as well as safe sleep,” she said.
In families where there are “strong cultural beliefs and traditions” about the baby sleeping with the parents, it is important to “convey the messages in a way that, that honors and values, family traditions and customs, but also assures the safety of the infant,” Dr. Campbell said.
This study was supported by the Centers for Disease Control and Prevention and CDC Innovation Fund. The authors reported no relevant conflicts of interest. Dr. Campbell reported no relevant conflicts of interest.
Infants of fathers who want their child to breastfeed are more likely to be part of a family unit that starts and continues breastfeeding, and fathers informed of safe sleep practices are more likely to follow those sleeping recommendations for their infant, according to the results of a recent survey published in Pediatrics.
The results suggest that the researchers said.
“Our findings underscore that new fathers are a critical audience to promote breastfeeding and safe infant sleep,” John James Parker, MD, instructor of pediatrics at Northwestern University, Chicago, stated in a press release. “Many families do not gain the health benefits from breastfeeding because they are not provided the support to breastfeed successfully. Fathers need to be directly engaged in breastfeeding discussions, and providers need to describe the important role fathers play in breastfeeding success.”
Population-based survey results
Dr. Parker and colleagues used the Pregnancy Risk Assessment Monitoring System (PRAMS) for Dads population-based survey to evaluate the rate of adherence to breastfeeding and infant sleep practices recommended by the American Academy of Pediatrics. In total, 250 fathers in Georgia were surveyed between October 2018 and July 2019 about whether their infants were breastfeeding and if they were breastfeeding at 8 weeks. The fathers were also asked how often the infant slept in a back sleeping position, on an approved sleep surface, and sleeping with no soft objects or soft bedding.
In addition to surveying fathers on their attitudes on breastfeeding and whether they followed safe infant sleep practices, the researchers collected information on paternal sociodemographic characteristics such as age, race and ethnicity, education, health insurance status, and marital status. Overall, a majority fathers who responded to the survey were between 25 years and 34 years old (56.5%), non-Hispanic White (44.7%), had a high school diploma or less (43.7%) or completed college (37.1%), and were married (65.2%).
Dr. Parker and colleagues found fathers surveyed said 86.1% of infants were ever breastfed, which decreased to 63.4% at 8 weeks. Compared with fathers who did not want their infant to breastfeed or expressed no opinion, fathers who wanted to have the infant’s mother breastfeed had a higher likelihood of reporting breastfeeding initiation (adjusted prevalence ratio, 1.39; 95% confidence interval, 1.15-1.68) and breastfeeding at 8 weeks (aPR, 2.33; 95% CI, 1.59-3.42). Having a college degree was also associated with the infant breastfeeding (93.6% vs. 75.1%; aPR, 1.25; 95% CI, 1.06-1.46) and breastfeeding at 8 weeks (74.7% vs. 52.0%; aPR, 1.44; 95% CI, 1.08-1.91), compared with fathers who graduated from high school or less.
Regarding safe infant sleeping practices, 81.18% of fathers said they placed their infants on their back to sleep, but 44.1% said they did not use soft bedding, and 31.9% said they used an approved sleep surface. In total, 99.4% of fathers put their infant to sleep, and 68.4% said they received information on all three infant safe sleeping practices, while 15.7% said they followed all three sleeping recommendations. A health care provider was the most common person giving advice to the father on placing the infant to sleep on their back (84.7%); to use a safe sleep surface such as a crib, bassinet, or pack-and-play (78.7%); and receiving information about what not to place in the infant’s bed (79.1%).
The survey found non-Hispanic Black fathers reported they were less likely to put the infant to sleep on their back (62.5% vs. 89.5%; aPR, 0.70; 95% CI, 0.54-0.90) and not use soft bedding (28.1% vs. 54.1%; aPR, 0.52; 95% CI, 0.30-0.89), compared with non-Hispanic White fathers. College graduates were more likely to not use soft bedding (61.4% vs. 31.9%; aPR, 1.92; 95% CI, 1.25-2.95), more likely to get advice on placing the infant on their back for sleep (94.3% vs. 73.6%; aPR, 1.28; 95% CI, 1.09-1.51), and more likely to receive advice on what not to place in the infant’s bed (88.1% vs. 68.5%; aPR, 1.29; 95% CI, 1.06-1.57), compared with fathers with a high school diploma or less.
“Fathers need to receive counseling on all the safe sleep practices for their infants,” Dr. Parker said. “To reduce racial disparities in sudden unexpected infant death, we need tailored strategies to increase safe infant sleep practices in the Black community, including public campaigns to increase awareness and home visiting programs. These interventions must involve both parents to be most effective.”
Educational efforts should recognize father’s contributions
In an interview, Deborah E. Campbell, MD, chief of neonatology at the Children’s Hospital at Montefiore, New York, said the survey “adds further important information on the role of fathers both in the care of their infants and young children, but also in terms of supporting the birth parent and a number of the parenting decisions, whether it’s breastfeeding as well as safe sleep practices for the infant.”
The benefits of breastfeeding are important for the infant but also for the health of the family and the community, Dr. Campbell explained, noting that breastfeeding can aid in preventing chronic disease and cancer. Promoting safe sleep practices for infants, on the other hand, helps reduce factors such as infant mortality and sudden unexpected infant death.
While PRAMS has existed for decades, PRAMS for Dads is relatively new and localized as a pilot program in Georgia, Dr. Campbell noted. The pilot program “really shows that you can get helpful information, and it would be wonderful to see that model expanded to begin to look at the father’s role in other states as well.”
To improve adherence to breastfeeding and infant safe sleeping practices, creating broadly educational efforts that include and recognize the contributions of the father are important, especially as fathers today are generally more involved and engaged than in past generations, Dr. Campbell said. For instance, pediatric or family practice offices could be structured in a way that welcomes fathers and appreciates them, rather than focusing solely on the birth mother or the baby.
“I think certainly as we have greater diversity among our families, greater diversity within our communities, just more varied family constellations, recognizing and valuing each member of the family becomes important and then providing them with the information and the tools,” she said.
While health literacy is important, structural inequalities in care provision in health care settings mean that “it’s honestly much more likely that an educated parent is going to have an opportunity to hear more of those messages,” Dr. Campbell said. “They are much more likely to be able to go to childbirth classes, go to the pediatrician visits, take off from work, have leaves so that they can spend time in the hospital during the infant’s stay and the birth parent’s initial recoveries so that they have greater opportunity to get those messages.”
Fathers with lower educational attainment may have good health literacy, but may be unable to be around for these conversations. “Education is really a proxy for a lot of other structural issues,” she said.
Educational messages around safe sleeping practices for the infant should acknowledge that many families might not have the space to have a dedicated room with a crib for an infant, and offer assurances that other safe sleeping options exist, such as a pack-and-play or Moses basket. The most important message to get across to parents is that the baby is “sleeping alone” in a firm, noninclined surface and does not have bedding or other objects around them.
It is not just the infant’s bed that should follow the AAP recommendations: the family bed should also be a firm surface free of soft objects and bedding for breastfeeding, Dr. Campbell noted. If a parent falls asleep while breastfeeding in bed, the AAP’s most recent guidance notes the parent should move the infant to a separate sleep space as soon as they wake up, but the Academy also acknowledges how that can be challenging in early months with sleep deprivation.
“I think it’s dealing with the realities of having a new baby and trying to create the safest environment for that baby, one that supports and promotes breastfeeding as well as safe sleep,” she said.
In families where there are “strong cultural beliefs and traditions” about the baby sleeping with the parents, it is important to “convey the messages in a way that, that honors and values, family traditions and customs, but also assures the safety of the infant,” Dr. Campbell said.
This study was supported by the Centers for Disease Control and Prevention and CDC Innovation Fund. The authors reported no relevant conflicts of interest. Dr. Campbell reported no relevant conflicts of interest.
Infants of fathers who want their child to breastfeed are more likely to be part of a family unit that starts and continues breastfeeding, and fathers informed of safe sleep practices are more likely to follow those sleeping recommendations for their infant, according to the results of a recent survey published in Pediatrics.
The results suggest that the researchers said.
“Our findings underscore that new fathers are a critical audience to promote breastfeeding and safe infant sleep,” John James Parker, MD, instructor of pediatrics at Northwestern University, Chicago, stated in a press release. “Many families do not gain the health benefits from breastfeeding because they are not provided the support to breastfeed successfully. Fathers need to be directly engaged in breastfeeding discussions, and providers need to describe the important role fathers play in breastfeeding success.”
Population-based survey results
Dr. Parker and colleagues used the Pregnancy Risk Assessment Monitoring System (PRAMS) for Dads population-based survey to evaluate the rate of adherence to breastfeeding and infant sleep practices recommended by the American Academy of Pediatrics. In total, 250 fathers in Georgia were surveyed between October 2018 and July 2019 about whether their infants were breastfeeding and if they were breastfeeding at 8 weeks. The fathers were also asked how often the infant slept in a back sleeping position, on an approved sleep surface, and sleeping with no soft objects or soft bedding.
In addition to surveying fathers on their attitudes on breastfeeding and whether they followed safe infant sleep practices, the researchers collected information on paternal sociodemographic characteristics such as age, race and ethnicity, education, health insurance status, and marital status. Overall, a majority fathers who responded to the survey were between 25 years and 34 years old (56.5%), non-Hispanic White (44.7%), had a high school diploma or less (43.7%) or completed college (37.1%), and were married (65.2%).
Dr. Parker and colleagues found fathers surveyed said 86.1% of infants were ever breastfed, which decreased to 63.4% at 8 weeks. Compared with fathers who did not want their infant to breastfeed or expressed no opinion, fathers who wanted to have the infant’s mother breastfeed had a higher likelihood of reporting breastfeeding initiation (adjusted prevalence ratio, 1.39; 95% confidence interval, 1.15-1.68) and breastfeeding at 8 weeks (aPR, 2.33; 95% CI, 1.59-3.42). Having a college degree was also associated with the infant breastfeeding (93.6% vs. 75.1%; aPR, 1.25; 95% CI, 1.06-1.46) and breastfeeding at 8 weeks (74.7% vs. 52.0%; aPR, 1.44; 95% CI, 1.08-1.91), compared with fathers who graduated from high school or less.
Regarding safe infant sleeping practices, 81.18% of fathers said they placed their infants on their back to sleep, but 44.1% said they did not use soft bedding, and 31.9% said they used an approved sleep surface. In total, 99.4% of fathers put their infant to sleep, and 68.4% said they received information on all three infant safe sleeping practices, while 15.7% said they followed all three sleeping recommendations. A health care provider was the most common person giving advice to the father on placing the infant to sleep on their back (84.7%); to use a safe sleep surface such as a crib, bassinet, or pack-and-play (78.7%); and receiving information about what not to place in the infant’s bed (79.1%).
The survey found non-Hispanic Black fathers reported they were less likely to put the infant to sleep on their back (62.5% vs. 89.5%; aPR, 0.70; 95% CI, 0.54-0.90) and not use soft bedding (28.1% vs. 54.1%; aPR, 0.52; 95% CI, 0.30-0.89), compared with non-Hispanic White fathers. College graduates were more likely to not use soft bedding (61.4% vs. 31.9%; aPR, 1.92; 95% CI, 1.25-2.95), more likely to get advice on placing the infant on their back for sleep (94.3% vs. 73.6%; aPR, 1.28; 95% CI, 1.09-1.51), and more likely to receive advice on what not to place in the infant’s bed (88.1% vs. 68.5%; aPR, 1.29; 95% CI, 1.06-1.57), compared with fathers with a high school diploma or less.
“Fathers need to receive counseling on all the safe sleep practices for their infants,” Dr. Parker said. “To reduce racial disparities in sudden unexpected infant death, we need tailored strategies to increase safe infant sleep practices in the Black community, including public campaigns to increase awareness and home visiting programs. These interventions must involve both parents to be most effective.”
Educational efforts should recognize father’s contributions
In an interview, Deborah E. Campbell, MD, chief of neonatology at the Children’s Hospital at Montefiore, New York, said the survey “adds further important information on the role of fathers both in the care of their infants and young children, but also in terms of supporting the birth parent and a number of the parenting decisions, whether it’s breastfeeding as well as safe sleep practices for the infant.”
The benefits of breastfeeding are important for the infant but also for the health of the family and the community, Dr. Campbell explained, noting that breastfeeding can aid in preventing chronic disease and cancer. Promoting safe sleep practices for infants, on the other hand, helps reduce factors such as infant mortality and sudden unexpected infant death.
While PRAMS has existed for decades, PRAMS for Dads is relatively new and localized as a pilot program in Georgia, Dr. Campbell noted. The pilot program “really shows that you can get helpful information, and it would be wonderful to see that model expanded to begin to look at the father’s role in other states as well.”
To improve adherence to breastfeeding and infant safe sleeping practices, creating broadly educational efforts that include and recognize the contributions of the father are important, especially as fathers today are generally more involved and engaged than in past generations, Dr. Campbell said. For instance, pediatric or family practice offices could be structured in a way that welcomes fathers and appreciates them, rather than focusing solely on the birth mother or the baby.
“I think certainly as we have greater diversity among our families, greater diversity within our communities, just more varied family constellations, recognizing and valuing each member of the family becomes important and then providing them with the information and the tools,” she said.
While health literacy is important, structural inequalities in care provision in health care settings mean that “it’s honestly much more likely that an educated parent is going to have an opportunity to hear more of those messages,” Dr. Campbell said. “They are much more likely to be able to go to childbirth classes, go to the pediatrician visits, take off from work, have leaves so that they can spend time in the hospital during the infant’s stay and the birth parent’s initial recoveries so that they have greater opportunity to get those messages.”
Fathers with lower educational attainment may have good health literacy, but may be unable to be around for these conversations. “Education is really a proxy for a lot of other structural issues,” she said.
Educational messages around safe sleeping practices for the infant should acknowledge that many families might not have the space to have a dedicated room with a crib for an infant, and offer assurances that other safe sleeping options exist, such as a pack-and-play or Moses basket. The most important message to get across to parents is that the baby is “sleeping alone” in a firm, noninclined surface and does not have bedding or other objects around them.
It is not just the infant’s bed that should follow the AAP recommendations: the family bed should also be a firm surface free of soft objects and bedding for breastfeeding, Dr. Campbell noted. If a parent falls asleep while breastfeeding in bed, the AAP’s most recent guidance notes the parent should move the infant to a separate sleep space as soon as they wake up, but the Academy also acknowledges how that can be challenging in early months with sleep deprivation.
“I think it’s dealing with the realities of having a new baby and trying to create the safest environment for that baby, one that supports and promotes breastfeeding as well as safe sleep,” she said.
In families where there are “strong cultural beliefs and traditions” about the baby sleeping with the parents, it is important to “convey the messages in a way that, that honors and values, family traditions and customs, but also assures the safety of the infant,” Dr. Campbell said.
This study was supported by the Centers for Disease Control and Prevention and CDC Innovation Fund. The authors reported no relevant conflicts of interest. Dr. Campbell reported no relevant conflicts of interest.
FROM PEDIATRICS
Poor sleep tied to increased injury from falls, motor vehicle accidents
Confirming the importance of sleep health, new research shows that short and disrupted sleep increases the risk of fall-related and motor vehicle–related injury among U.S. adults.
Among the study’s key findings – adults who get 4 hours or less nightly and those who have trouble staying asleep are significantly more likely to be injured than peers who sleep the recommended 7-8 hours and those who never have trouble staying asleep.
The findings were presented at SLEEP 2023: 37th Annual Meeting of the Associated Professional Sleep Societies.
‘Stark differences’
In 2020, 55.4 million (roughly 1 in 6) Americans sought medical attention for nonfatal, preventable injuries.
“Poor sleep has been identified as a risk factor for preventable injuries,” study investigator Clarence Locklear, MA, who is a PhD student with the Center for Translational Sleep and Circadian Sciences, University of Miami Miller School of Medicine, told this news organization.
For the study, the researchers examined associations between different types of sleep problems and different types of injuries utilizing data on 31,568 adults who participated in the 2020 National Health Interview Survey.
They investigated three types of injuries (fall-related, sports-related, and motor vehicle–related) and four domains of past-month sleep health: (1) sleep quantity: very short (≤ 4 hours), short (5-6 hours), healthy (7-8 hours), or long (≥ 9 hours); (2) sleep quality: trouble falling asleep and trouble staying asleep; (3) feeling well rested upon waking up; and (4) sleep medications.
Overall, 9% of adults suffered an injury in the prior 3 months. Among injured adults, 47% had a fall-related injury, 29% had a sports-related injury, and 6% had a motor vehicle–related injury.
Adults with very short sleep, those with short sleep, and those with long sleep were 37%, 15%, and 22% more likely to be injured, respectively, than adults with healthy sleep (P < .05), the researchers found.
Those who had trouble staying asleep were 36% more likely to be injured than peers who never had trouble staying asleep (P < .01).
Adults who never woke up feeling rested and those who woke up feeling rested only on some days were 49% and 36% more likely to be injured (P < .01), respectively, than peers who always felt rested on waking.
Individuals who on some days took medication for sleep were 24% (P < .05) more likely to suffer an injury and those who took sleep medication every day were 36% (P < .001) more likely to get injured than those who never took sleep medication.
“These are pretty stark differences,” said Mr. Locklear.
Regarding injury type, those who had trouble staying asleep some days were 22% (P < .05) more likely to have a fall-related injury and were 3.5 times (P < .01) more likely to experience a motor vehicle–related injury than peers who didn’t have trouble staying asleep.
People who took sleep medication most days were 2.4 times more likely to suffer a fall than those who never took sleep medication. In addition, adults who reported long sleep (9+ hours nightly) were 43% less likely to have sports-related injuries (P < .05) than healthy sleepers (7-8 hours).
Quantity and quality matter
Michael Breus, PhD, clinical psychologist and founder of TheSleepDoctor.com, said the results are “not particularly surprising but are consistent with other data.”
Dr. Breus said, “Many people don’t realize it’s not just sleep deprivation, in terms of minutes, that’s a problem. Our quality of sleep also matters. You can get 8 hours of crappy sleep and still injure yourself playing sports or get into a car accident due to poor reaction time.”
As previously reported by this news organization, the American Heart Association recently added healthy sleep as an essential component of heart health. “It’s nice to see them recognize that sleep is a big deal, and we’ve got the data to back it up,” said Dr. Breus.
He noted that people often ask him what’s the one thing they can do to improve sleep.
“The answer is always, wake up at the same time every single day, including the weekend, because your circadian system realigns every single morning.
“I solve maybe 50%-60% of people’s problems by just telling them to just wake up at the same time 7 days a week. I personally have been doing it for a very long time,” said Dr. Breus.
The study was supported by the National Heart Lung and Blood Institute. Mr. Locklear and Dr. Breus have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Confirming the importance of sleep health, new research shows that short and disrupted sleep increases the risk of fall-related and motor vehicle–related injury among U.S. adults.
Among the study’s key findings – adults who get 4 hours or less nightly and those who have trouble staying asleep are significantly more likely to be injured than peers who sleep the recommended 7-8 hours and those who never have trouble staying asleep.
The findings were presented at SLEEP 2023: 37th Annual Meeting of the Associated Professional Sleep Societies.
‘Stark differences’
In 2020, 55.4 million (roughly 1 in 6) Americans sought medical attention for nonfatal, preventable injuries.
“Poor sleep has been identified as a risk factor for preventable injuries,” study investigator Clarence Locklear, MA, who is a PhD student with the Center for Translational Sleep and Circadian Sciences, University of Miami Miller School of Medicine, told this news organization.
For the study, the researchers examined associations between different types of sleep problems and different types of injuries utilizing data on 31,568 adults who participated in the 2020 National Health Interview Survey.
They investigated three types of injuries (fall-related, sports-related, and motor vehicle–related) and four domains of past-month sleep health: (1) sleep quantity: very short (≤ 4 hours), short (5-6 hours), healthy (7-8 hours), or long (≥ 9 hours); (2) sleep quality: trouble falling asleep and trouble staying asleep; (3) feeling well rested upon waking up; and (4) sleep medications.
Overall, 9% of adults suffered an injury in the prior 3 months. Among injured adults, 47% had a fall-related injury, 29% had a sports-related injury, and 6% had a motor vehicle–related injury.
Adults with very short sleep, those with short sleep, and those with long sleep were 37%, 15%, and 22% more likely to be injured, respectively, than adults with healthy sleep (P < .05), the researchers found.
Those who had trouble staying asleep were 36% more likely to be injured than peers who never had trouble staying asleep (P < .01).
Adults who never woke up feeling rested and those who woke up feeling rested only on some days were 49% and 36% more likely to be injured (P < .01), respectively, than peers who always felt rested on waking.
Individuals who on some days took medication for sleep were 24% (P < .05) more likely to suffer an injury and those who took sleep medication every day were 36% (P < .001) more likely to get injured than those who never took sleep medication.
“These are pretty stark differences,” said Mr. Locklear.
Regarding injury type, those who had trouble staying asleep some days were 22% (P < .05) more likely to have a fall-related injury and were 3.5 times (P < .01) more likely to experience a motor vehicle–related injury than peers who didn’t have trouble staying asleep.
People who took sleep medication most days were 2.4 times more likely to suffer a fall than those who never took sleep medication. In addition, adults who reported long sleep (9+ hours nightly) were 43% less likely to have sports-related injuries (P < .05) than healthy sleepers (7-8 hours).
Quantity and quality matter
Michael Breus, PhD, clinical psychologist and founder of TheSleepDoctor.com, said the results are “not particularly surprising but are consistent with other data.”
Dr. Breus said, “Many people don’t realize it’s not just sleep deprivation, in terms of minutes, that’s a problem. Our quality of sleep also matters. You can get 8 hours of crappy sleep and still injure yourself playing sports or get into a car accident due to poor reaction time.”
As previously reported by this news organization, the American Heart Association recently added healthy sleep as an essential component of heart health. “It’s nice to see them recognize that sleep is a big deal, and we’ve got the data to back it up,” said Dr. Breus.
He noted that people often ask him what’s the one thing they can do to improve sleep.
“The answer is always, wake up at the same time every single day, including the weekend, because your circadian system realigns every single morning.
“I solve maybe 50%-60% of people’s problems by just telling them to just wake up at the same time 7 days a week. I personally have been doing it for a very long time,” said Dr. Breus.
The study was supported by the National Heart Lung and Blood Institute. Mr. Locklear and Dr. Breus have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Confirming the importance of sleep health, new research shows that short and disrupted sleep increases the risk of fall-related and motor vehicle–related injury among U.S. adults.
Among the study’s key findings – adults who get 4 hours or less nightly and those who have trouble staying asleep are significantly more likely to be injured than peers who sleep the recommended 7-8 hours and those who never have trouble staying asleep.
The findings were presented at SLEEP 2023: 37th Annual Meeting of the Associated Professional Sleep Societies.
‘Stark differences’
In 2020, 55.4 million (roughly 1 in 6) Americans sought medical attention for nonfatal, preventable injuries.
“Poor sleep has been identified as a risk factor for preventable injuries,” study investigator Clarence Locklear, MA, who is a PhD student with the Center for Translational Sleep and Circadian Sciences, University of Miami Miller School of Medicine, told this news organization.
For the study, the researchers examined associations between different types of sleep problems and different types of injuries utilizing data on 31,568 adults who participated in the 2020 National Health Interview Survey.
They investigated three types of injuries (fall-related, sports-related, and motor vehicle–related) and four domains of past-month sleep health: (1) sleep quantity: very short (≤ 4 hours), short (5-6 hours), healthy (7-8 hours), or long (≥ 9 hours); (2) sleep quality: trouble falling asleep and trouble staying asleep; (3) feeling well rested upon waking up; and (4) sleep medications.
Overall, 9% of adults suffered an injury in the prior 3 months. Among injured adults, 47% had a fall-related injury, 29% had a sports-related injury, and 6% had a motor vehicle–related injury.
Adults with very short sleep, those with short sleep, and those with long sleep were 37%, 15%, and 22% more likely to be injured, respectively, than adults with healthy sleep (P < .05), the researchers found.
Those who had trouble staying asleep were 36% more likely to be injured than peers who never had trouble staying asleep (P < .01).
Adults who never woke up feeling rested and those who woke up feeling rested only on some days were 49% and 36% more likely to be injured (P < .01), respectively, than peers who always felt rested on waking.
Individuals who on some days took medication for sleep were 24% (P < .05) more likely to suffer an injury and those who took sleep medication every day were 36% (P < .001) more likely to get injured than those who never took sleep medication.
“These are pretty stark differences,” said Mr. Locklear.
Regarding injury type, those who had trouble staying asleep some days were 22% (P < .05) more likely to have a fall-related injury and were 3.5 times (P < .01) more likely to experience a motor vehicle–related injury than peers who didn’t have trouble staying asleep.
People who took sleep medication most days were 2.4 times more likely to suffer a fall than those who never took sleep medication. In addition, adults who reported long sleep (9+ hours nightly) were 43% less likely to have sports-related injuries (P < .05) than healthy sleepers (7-8 hours).
Quantity and quality matter
Michael Breus, PhD, clinical psychologist and founder of TheSleepDoctor.com, said the results are “not particularly surprising but are consistent with other data.”
Dr. Breus said, “Many people don’t realize it’s not just sleep deprivation, in terms of minutes, that’s a problem. Our quality of sleep also matters. You can get 8 hours of crappy sleep and still injure yourself playing sports or get into a car accident due to poor reaction time.”
As previously reported by this news organization, the American Heart Association recently added healthy sleep as an essential component of heart health. “It’s nice to see them recognize that sleep is a big deal, and we’ve got the data to back it up,” said Dr. Breus.
He noted that people often ask him what’s the one thing they can do to improve sleep.
“The answer is always, wake up at the same time every single day, including the weekend, because your circadian system realigns every single morning.
“I solve maybe 50%-60% of people’s problems by just telling them to just wake up at the same time 7 days a week. I personally have been doing it for a very long time,” said Dr. Breus.
The study was supported by the National Heart Lung and Blood Institute. Mr. Locklear and Dr. Breus have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Smart-bed technology reveals insomnia, flu risk link
The study of smart-bed sleepers found that there was a statistically significant correlation between a higher number of episodes of influenza-like illnesses (ILI) per year with longer duration compared to people without insomnia.
However, more research is needed to determine causality and whether insomnia may predispose to ILI or whether ILI affects long-term sleep behavior, the researchers noted.
“Several lines of evidence make me think that it’s more likely that insomnia makes one more vulnerable to influenza through pathways that involve decreased immune function,” study investigator Gary Garcia-Molina, PhD, with Sleep Number Labs, San Jose, Calif., said in an interview.
Sleep disorders, including insomnia, can dampen immune function and an individual’s ability to fight off illness, he noted.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Smart, connected devices
Pathophysiological responses to respiratory viral infection affect sleep duration and quality in addition to breathing function. “Smart” and “connected” devices that monitor biosignals over time have shown promise for monitoring infectious disease.
In an earlier study presented at SLEEP 2021, Dr. Garcia-Molina and colleagues found that real-world biometric data obtained from a smart bed can help predict and track symptoms of COVID-19 and other respiratory infections. They showed that worsening of COVID-19 symptoms correlated with an increase in sleep duration, breathing rate, and heart rate and a decrease in sleep quality.
In the new study, the researchers evaluated vulnerability to ILI in people with insomnia.
They quantified insomnia over time using the insomnia severity index (ISI). They quantified ILI vulnerability using an established artificial intelligence model they developed that estimates the daily probability of ILI symptoms from a Sleep Number smart bed using ballistocardiograph sensors.
Smart bed data – including daily and restful sleep duration, sleep latency, sleep quality, heart rate, breathing rate and motion level – were queried from 2019 (pre-COVID) and 2021.
A total of 1,680 smart sleepers had nearly constant ISI scores over the study period, with 249 having insomnia and 1,431 not having insomnia.
Data from both 2019 and 2021 show that smart sleepers with insomnia had significantly more and longer ILI episodes per year, compared with peers without insomnia.
For 2019, individuals without insomnia had 1.2 ILI episodes on average, which was significantly less (P < .01) than individuals with insomnia, at 1.5 episodes. The average ILI episode duration for those without insomnia was 4.3 days, which was significantly lower (P < .01) in those with insomnia group, at 6.1 days.
The data for 2021 show similar results, with the no-insomnia group having significantly fewer (P < .01) ILI episodes (about 1.2), compared with the insomnia group (about 1.5).
The average ILI episode duration for the no-insomnia group was 5 days, which was significantly less (P < .01) than the insomnia group, at 6.1 days.
The researchers said their study adds to other data on the relationship between sleep and overall health and well-being. It also highlights the potential health risk of insomnia and the importance of identifying and treating sleep disorders.
“Sleep has such a profound influence on health and wellness and the ability to capture these data unobtrusively in such an easy way and with such a large number of participants paves the way to investigate different aspects of health and disease,” Dr. Garcia-Molina said.
Rich data source
In a comment, Adam C. Powell, PhD, president of Payer+Provider Syndicate, a management advisory and operational consulting firm, said “smart beds provide a new data source for passively monitoring the health of individuals.”
“Unlike active monitoring methods requiring self-report, passive monitoring enables data to be captured without an individual taking any action. This data can be potentially integrated with data from other sources, such as pedometers, smart scales, and smart blood pressure cuffs, to gain a more holistic understanding of how an individual’s activities and behaviors impact their well-being,” said Dr. Powell, who wasn’t involved in the study.
There are some methodological limitations to the study, he noted.
“While the dependent variables examined were the duration and presence of episodes of influenza-like illness, they did not directly measure these episodes. Instead, they calculated the daily probability of influenza-like illness symptoms using a model that received input from the ballistocardiograph sensors in the smart beds,” Dr. Powell noted.
“The model used to calculate daily probability of influenza-like illness was created by examining associations between individuals’ smart-bed sensor data and population-level trends in influenza-like illness reported by the Centers for Disease Control and Prevention,” he explained.
Nonetheless, the findings are “consistent with the literature. It has been established by other researchers that impaired sleep is associated with greater risk of influenza, as well as other illnesses,” Dr. Powell said.
Funding for the study was provided by Sleep Number. Dr. Garcia-Molina and five coauthors are employed by Sleep Number. Dr. Powell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study of smart-bed sleepers found that there was a statistically significant correlation between a higher number of episodes of influenza-like illnesses (ILI) per year with longer duration compared to people without insomnia.
However, more research is needed to determine causality and whether insomnia may predispose to ILI or whether ILI affects long-term sleep behavior, the researchers noted.
“Several lines of evidence make me think that it’s more likely that insomnia makes one more vulnerable to influenza through pathways that involve decreased immune function,” study investigator Gary Garcia-Molina, PhD, with Sleep Number Labs, San Jose, Calif., said in an interview.
Sleep disorders, including insomnia, can dampen immune function and an individual’s ability to fight off illness, he noted.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Smart, connected devices
Pathophysiological responses to respiratory viral infection affect sleep duration and quality in addition to breathing function. “Smart” and “connected” devices that monitor biosignals over time have shown promise for monitoring infectious disease.
In an earlier study presented at SLEEP 2021, Dr. Garcia-Molina and colleagues found that real-world biometric data obtained from a smart bed can help predict and track symptoms of COVID-19 and other respiratory infections. They showed that worsening of COVID-19 symptoms correlated with an increase in sleep duration, breathing rate, and heart rate and a decrease in sleep quality.
In the new study, the researchers evaluated vulnerability to ILI in people with insomnia.
They quantified insomnia over time using the insomnia severity index (ISI). They quantified ILI vulnerability using an established artificial intelligence model they developed that estimates the daily probability of ILI symptoms from a Sleep Number smart bed using ballistocardiograph sensors.
Smart bed data – including daily and restful sleep duration, sleep latency, sleep quality, heart rate, breathing rate and motion level – were queried from 2019 (pre-COVID) and 2021.
A total of 1,680 smart sleepers had nearly constant ISI scores over the study period, with 249 having insomnia and 1,431 not having insomnia.
Data from both 2019 and 2021 show that smart sleepers with insomnia had significantly more and longer ILI episodes per year, compared with peers without insomnia.
For 2019, individuals without insomnia had 1.2 ILI episodes on average, which was significantly less (P < .01) than individuals with insomnia, at 1.5 episodes. The average ILI episode duration for those without insomnia was 4.3 days, which was significantly lower (P < .01) in those with insomnia group, at 6.1 days.
The data for 2021 show similar results, with the no-insomnia group having significantly fewer (P < .01) ILI episodes (about 1.2), compared with the insomnia group (about 1.5).
The average ILI episode duration for the no-insomnia group was 5 days, which was significantly less (P < .01) than the insomnia group, at 6.1 days.
The researchers said their study adds to other data on the relationship between sleep and overall health and well-being. It also highlights the potential health risk of insomnia and the importance of identifying and treating sleep disorders.
“Sleep has such a profound influence on health and wellness and the ability to capture these data unobtrusively in such an easy way and with such a large number of participants paves the way to investigate different aspects of health and disease,” Dr. Garcia-Molina said.
Rich data source
In a comment, Adam C. Powell, PhD, president of Payer+Provider Syndicate, a management advisory and operational consulting firm, said “smart beds provide a new data source for passively monitoring the health of individuals.”
“Unlike active monitoring methods requiring self-report, passive monitoring enables data to be captured without an individual taking any action. This data can be potentially integrated with data from other sources, such as pedometers, smart scales, and smart blood pressure cuffs, to gain a more holistic understanding of how an individual’s activities and behaviors impact their well-being,” said Dr. Powell, who wasn’t involved in the study.
There are some methodological limitations to the study, he noted.
“While the dependent variables examined were the duration and presence of episodes of influenza-like illness, they did not directly measure these episodes. Instead, they calculated the daily probability of influenza-like illness symptoms using a model that received input from the ballistocardiograph sensors in the smart beds,” Dr. Powell noted.
“The model used to calculate daily probability of influenza-like illness was created by examining associations between individuals’ smart-bed sensor data and population-level trends in influenza-like illness reported by the Centers for Disease Control and Prevention,” he explained.
Nonetheless, the findings are “consistent with the literature. It has been established by other researchers that impaired sleep is associated with greater risk of influenza, as well as other illnesses,” Dr. Powell said.
Funding for the study was provided by Sleep Number. Dr. Garcia-Molina and five coauthors are employed by Sleep Number. Dr. Powell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study of smart-bed sleepers found that there was a statistically significant correlation between a higher number of episodes of influenza-like illnesses (ILI) per year with longer duration compared to people without insomnia.
However, more research is needed to determine causality and whether insomnia may predispose to ILI or whether ILI affects long-term sleep behavior, the researchers noted.
“Several lines of evidence make me think that it’s more likely that insomnia makes one more vulnerable to influenza through pathways that involve decreased immune function,” study investigator Gary Garcia-Molina, PhD, with Sleep Number Labs, San Jose, Calif., said in an interview.
Sleep disorders, including insomnia, can dampen immune function and an individual’s ability to fight off illness, he noted.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Smart, connected devices
Pathophysiological responses to respiratory viral infection affect sleep duration and quality in addition to breathing function. “Smart” and “connected” devices that monitor biosignals over time have shown promise for monitoring infectious disease.
In an earlier study presented at SLEEP 2021, Dr. Garcia-Molina and colleagues found that real-world biometric data obtained from a smart bed can help predict and track symptoms of COVID-19 and other respiratory infections. They showed that worsening of COVID-19 symptoms correlated with an increase in sleep duration, breathing rate, and heart rate and a decrease in sleep quality.
In the new study, the researchers evaluated vulnerability to ILI in people with insomnia.
They quantified insomnia over time using the insomnia severity index (ISI). They quantified ILI vulnerability using an established artificial intelligence model they developed that estimates the daily probability of ILI symptoms from a Sleep Number smart bed using ballistocardiograph sensors.
Smart bed data – including daily and restful sleep duration, sleep latency, sleep quality, heart rate, breathing rate and motion level – were queried from 2019 (pre-COVID) and 2021.
A total of 1,680 smart sleepers had nearly constant ISI scores over the study period, with 249 having insomnia and 1,431 not having insomnia.
Data from both 2019 and 2021 show that smart sleepers with insomnia had significantly more and longer ILI episodes per year, compared with peers without insomnia.
For 2019, individuals without insomnia had 1.2 ILI episodes on average, which was significantly less (P < .01) than individuals with insomnia, at 1.5 episodes. The average ILI episode duration for those without insomnia was 4.3 days, which was significantly lower (P < .01) in those with insomnia group, at 6.1 days.
The data for 2021 show similar results, with the no-insomnia group having significantly fewer (P < .01) ILI episodes (about 1.2), compared with the insomnia group (about 1.5).
The average ILI episode duration for the no-insomnia group was 5 days, which was significantly less (P < .01) than the insomnia group, at 6.1 days.
The researchers said their study adds to other data on the relationship between sleep and overall health and well-being. It also highlights the potential health risk of insomnia and the importance of identifying and treating sleep disorders.
“Sleep has such a profound influence on health and wellness and the ability to capture these data unobtrusively in such an easy way and with such a large number of participants paves the way to investigate different aspects of health and disease,” Dr. Garcia-Molina said.
Rich data source
In a comment, Adam C. Powell, PhD, president of Payer+Provider Syndicate, a management advisory and operational consulting firm, said “smart beds provide a new data source for passively monitoring the health of individuals.”
“Unlike active monitoring methods requiring self-report, passive monitoring enables data to be captured without an individual taking any action. This data can be potentially integrated with data from other sources, such as pedometers, smart scales, and smart blood pressure cuffs, to gain a more holistic understanding of how an individual’s activities and behaviors impact their well-being,” said Dr. Powell, who wasn’t involved in the study.
There are some methodological limitations to the study, he noted.
“While the dependent variables examined were the duration and presence of episodes of influenza-like illness, they did not directly measure these episodes. Instead, they calculated the daily probability of influenza-like illness symptoms using a model that received input from the ballistocardiograph sensors in the smart beds,” Dr. Powell noted.
“The model used to calculate daily probability of influenza-like illness was created by examining associations between individuals’ smart-bed sensor data and population-level trends in influenza-like illness reported by the Centers for Disease Control and Prevention,” he explained.
Nonetheless, the findings are “consistent with the literature. It has been established by other researchers that impaired sleep is associated with greater risk of influenza, as well as other illnesses,” Dr. Powell said.
Funding for the study was provided by Sleep Number. Dr. Garcia-Molina and five coauthors are employed by Sleep Number. Dr. Powell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2023
Poor outcomes in fibrotic ILD attributed to nocturnal hypoxemia
In patients with fibrotic interstitial lung disease, nocturnal hypoxemia is associated with poor clinical outcomes, according to results of a prospective observational cohort study.
While both obstructive sleep apnea (OSA) and nocturnal hypoxemia (NH) are known to be common in patients with fibrotic interstitial lung disease (F-ILD), how they affect disease outcomes has remained unclear, Katherine J. Myall, MBChB, and colleagues reported in their published study. They noted that deposition of extracellular matrix within the lung parenchyma found in F-ILD is associated with restrictive lung disease and impaired gas exchange leading to progressive breathlessness and exercise intolerance and ultimately respiratory failure.
Prior research has suggested that sleep architecture is disrupted in F-ILD, with nocturnal desaturations from relative hypoventilation during rapid-eye movement sleep and higher incidence of OSA. While disrupted sleep architecture has been associated with poorer outcomes including worse survival, the relationship between sleep and F-ILD is not well understood, especially whether either total time spent in sleep with hypoxemia or repeated desaturations and arousals seen in OSA might promote disease progression, the researchers wrote.
They conducted a prospective observational cohort study among 102 idiopathic pulmonary fibrosis patients without daytime hypoxemia (74.5% male; age 73.0 years), among whom 91.1% and 31.4% had nocturnal hypoxemia (NH) and obstructive sleep apnea (OSA), respectively. There were no significant differences between those with and without NH or OSA at baseline. The study’s primary outcome measure was change in King’s Brief Interstitial Lung Disease questionnaire (KBILD) at 12 months from baseline. The secondary outcome measures were annualized change in forced vital capacity (FVC), transfer factor for carbon monoxide (TLCO), and mortality at 12 months.
Mortality association?
The analysis showed NH was associated with a more rapid decline in both quality of life (KBILD change –11.3 in the NH group vs. –6.7 in those without NH, P = .005) and higher all-cause mortality at 1 year (hazard ratio [HR], 8.21; 95% confidence interval [CI], 2.40-28.1, P < .001). There was no increased risk of death in patients with OSA compared with those without (HR, 2.78; 95% CI 0.85-9.12, P = .19), and OSA in the absence of NH was not associated with worsening of KBILD scores (P = .30). Analysis of findings did not reveal any relationship between disease severity and sleep characteristics.
“This suggests that the excess mortality demonstrated in earlier studies of patients with OSA may be related to prolonged hypoxemia rather than sleep disruption or the other deleterious physiological effects of OSA, such as sympathetic excitation,” noted Dr. Myall and colleagues. Underscoring that the current study is the first to elucidate the contribution of prolonged NH to disease progression and death in this population, they added that since the central process in the development of idiopathic pulmonary fibrosis is thought to be one of repeated or sustained lung injury, one hypothesis is that prolonged hypoxia of the alveolar epithelium due to prolonged nocturnal hypoxemia may be the source of this insult.
“These data provide support for screening for nocturnal hypoxemia, as well as obstructive sleep apnea in patients with F-ILD to allow early identification of these potentially modifiable conditions. Trials of CPAP and nocturnal oxygen therapy would offer a potential intervention to correct prolonged nocturnal hypoxemia, offering the potential to improve quality of life and survival for patients who otherwise have limited treatment options,” the researchers concluded.
A possible limitations of the study was the fact that patients were offered referral for CPAP therapy, and were used in the analysis only if they elected not to commence therapy. This may have introduced a bias, although there was no statistically significant difference between patients who opted to be referred and those who did not, according to the authors.
Dr. Myall reported having no conflicts of interest to declare.
In patients with fibrotic interstitial lung disease, nocturnal hypoxemia is associated with poor clinical outcomes, according to results of a prospective observational cohort study.
While both obstructive sleep apnea (OSA) and nocturnal hypoxemia (NH) are known to be common in patients with fibrotic interstitial lung disease (F-ILD), how they affect disease outcomes has remained unclear, Katherine J. Myall, MBChB, and colleagues reported in their published study. They noted that deposition of extracellular matrix within the lung parenchyma found in F-ILD is associated with restrictive lung disease and impaired gas exchange leading to progressive breathlessness and exercise intolerance and ultimately respiratory failure.
Prior research has suggested that sleep architecture is disrupted in F-ILD, with nocturnal desaturations from relative hypoventilation during rapid-eye movement sleep and higher incidence of OSA. While disrupted sleep architecture has been associated with poorer outcomes including worse survival, the relationship between sleep and F-ILD is not well understood, especially whether either total time spent in sleep with hypoxemia or repeated desaturations and arousals seen in OSA might promote disease progression, the researchers wrote.
They conducted a prospective observational cohort study among 102 idiopathic pulmonary fibrosis patients without daytime hypoxemia (74.5% male; age 73.0 years), among whom 91.1% and 31.4% had nocturnal hypoxemia (NH) and obstructive sleep apnea (OSA), respectively. There were no significant differences between those with and without NH or OSA at baseline. The study’s primary outcome measure was change in King’s Brief Interstitial Lung Disease questionnaire (KBILD) at 12 months from baseline. The secondary outcome measures were annualized change in forced vital capacity (FVC), transfer factor for carbon monoxide (TLCO), and mortality at 12 months.
Mortality association?
The analysis showed NH was associated with a more rapid decline in both quality of life (KBILD change –11.3 in the NH group vs. –6.7 in those without NH, P = .005) and higher all-cause mortality at 1 year (hazard ratio [HR], 8.21; 95% confidence interval [CI], 2.40-28.1, P < .001). There was no increased risk of death in patients with OSA compared with those without (HR, 2.78; 95% CI 0.85-9.12, P = .19), and OSA in the absence of NH was not associated with worsening of KBILD scores (P = .30). Analysis of findings did not reveal any relationship between disease severity and sleep characteristics.
“This suggests that the excess mortality demonstrated in earlier studies of patients with OSA may be related to prolonged hypoxemia rather than sleep disruption or the other deleterious physiological effects of OSA, such as sympathetic excitation,” noted Dr. Myall and colleagues. Underscoring that the current study is the first to elucidate the contribution of prolonged NH to disease progression and death in this population, they added that since the central process in the development of idiopathic pulmonary fibrosis is thought to be one of repeated or sustained lung injury, one hypothesis is that prolonged hypoxia of the alveolar epithelium due to prolonged nocturnal hypoxemia may be the source of this insult.
“These data provide support for screening for nocturnal hypoxemia, as well as obstructive sleep apnea in patients with F-ILD to allow early identification of these potentially modifiable conditions. Trials of CPAP and nocturnal oxygen therapy would offer a potential intervention to correct prolonged nocturnal hypoxemia, offering the potential to improve quality of life and survival for patients who otherwise have limited treatment options,” the researchers concluded.
A possible limitations of the study was the fact that patients were offered referral for CPAP therapy, and were used in the analysis only if they elected not to commence therapy. This may have introduced a bias, although there was no statistically significant difference between patients who opted to be referred and those who did not, according to the authors.
Dr. Myall reported having no conflicts of interest to declare.
In patients with fibrotic interstitial lung disease, nocturnal hypoxemia is associated with poor clinical outcomes, according to results of a prospective observational cohort study.
While both obstructive sleep apnea (OSA) and nocturnal hypoxemia (NH) are known to be common in patients with fibrotic interstitial lung disease (F-ILD), how they affect disease outcomes has remained unclear, Katherine J. Myall, MBChB, and colleagues reported in their published study. They noted that deposition of extracellular matrix within the lung parenchyma found in F-ILD is associated with restrictive lung disease and impaired gas exchange leading to progressive breathlessness and exercise intolerance and ultimately respiratory failure.
Prior research has suggested that sleep architecture is disrupted in F-ILD, with nocturnal desaturations from relative hypoventilation during rapid-eye movement sleep and higher incidence of OSA. While disrupted sleep architecture has been associated with poorer outcomes including worse survival, the relationship between sleep and F-ILD is not well understood, especially whether either total time spent in sleep with hypoxemia or repeated desaturations and arousals seen in OSA might promote disease progression, the researchers wrote.
They conducted a prospective observational cohort study among 102 idiopathic pulmonary fibrosis patients without daytime hypoxemia (74.5% male; age 73.0 years), among whom 91.1% and 31.4% had nocturnal hypoxemia (NH) and obstructive sleep apnea (OSA), respectively. There were no significant differences between those with and without NH or OSA at baseline. The study’s primary outcome measure was change in King’s Brief Interstitial Lung Disease questionnaire (KBILD) at 12 months from baseline. The secondary outcome measures were annualized change in forced vital capacity (FVC), transfer factor for carbon monoxide (TLCO), and mortality at 12 months.
Mortality association?
The analysis showed NH was associated with a more rapid decline in both quality of life (KBILD change –11.3 in the NH group vs. –6.7 in those without NH, P = .005) and higher all-cause mortality at 1 year (hazard ratio [HR], 8.21; 95% confidence interval [CI], 2.40-28.1, P < .001). There was no increased risk of death in patients with OSA compared with those without (HR, 2.78; 95% CI 0.85-9.12, P = .19), and OSA in the absence of NH was not associated with worsening of KBILD scores (P = .30). Analysis of findings did not reveal any relationship between disease severity and sleep characteristics.
“This suggests that the excess mortality demonstrated in earlier studies of patients with OSA may be related to prolonged hypoxemia rather than sleep disruption or the other deleterious physiological effects of OSA, such as sympathetic excitation,” noted Dr. Myall and colleagues. Underscoring that the current study is the first to elucidate the contribution of prolonged NH to disease progression and death in this population, they added that since the central process in the development of idiopathic pulmonary fibrosis is thought to be one of repeated or sustained lung injury, one hypothesis is that prolonged hypoxia of the alveolar epithelium due to prolonged nocturnal hypoxemia may be the source of this insult.
“These data provide support for screening for nocturnal hypoxemia, as well as obstructive sleep apnea in patients with F-ILD to allow early identification of these potentially modifiable conditions. Trials of CPAP and nocturnal oxygen therapy would offer a potential intervention to correct prolonged nocturnal hypoxemia, offering the potential to improve quality of life and survival for patients who otherwise have limited treatment options,” the researchers concluded.
A possible limitations of the study was the fact that patients were offered referral for CPAP therapy, and were used in the analysis only if they elected not to commence therapy. This may have introduced a bias, although there was no statistically significant difference between patients who opted to be referred and those who did not, according to the authors.
Dr. Myall reported having no conflicts of interest to declare.
FROM THE JOURNAL CHEST
Regular, optimal sleep tied to lower mortality risk
INDIANAPOLIS –
In a diverse group of older adults, those with regular and optimal sleep had about a 40% lower risk of dying of any cause during follow-up compared with peers who had irregular and insufficient sleep.
“If sleep were an 8-hour pill, it would be beneficial to take the full dose at regular times consistently,” lead researcher Joon Chung, PhD, of Harvard Medical School and Brigham and Women’s Hospital, Boston, said in a news release.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Broad adverse health effects
“Evidence is mounting that irregular sleep is associated with pretty broad adverse health outcomes, most prominently cardiometabolic disease, obesity, and cardiovascular disease,” Dr. Chungsaid in an interview.

In the current study, the researchers estimated the association of regular sleep of optimal sleep duration with all-cause mortality using data from 1,759 adults the Multi-Ethnic Study of Atherosclerosis Sleep Study.
Sleep regularity and duration were classified using 7 days of data gathered by wrist actigraphy. Adults were categorized as “regular-optimal” sleepers (n = 1,015) or “irregular-insufficient” sleepers (n = 744).
During 7 years of follow-up, 176 people died. In the fully adjusted model, the regular-optimal group had a 39% lower mortality risk compared with the irregular-insufficient sleep group (hazard ratio, 0.61;95% confidence interval [CI], 0.45-0.83). The findings were robust in sensitivity analyses.
The regular and optimal duration sleep pattern maps behaviorally to regular bed and wake times, suggesting potential health benefits of adherence to recommended sleep practices, the researchers noted.
“Results suggest benefits of expanding the public conversation on getting ‘a good night’s sleep’ and broadening this goal to getting many good nights of sleep, in a row, on weekdays and weekends,” Dr. Chung said in the release.
He further said that “getting adequate, regular sleep seems to be something that is good for all. I don’t know of anyone who wouldn’t benefit.”
Fariha Abassi-Feinberg, MD, spokesperson for the American Academy of Sleep Medicine and sleep specialist with the Millennium Physician Group, Fort Myers, Fla., agreed.
“We know our bodies have an internal clock, known as the circadian rhythm, which regulates various biological processes, including sleep-wake cycles. Sticking to a consistent sleep schedule allows your body to align its natural rhythm with the external day-night cycle. This synchronization promotes better sleep quality and therefore better health,” said Dr. Abassi-Feinberg, who wasn’t involved in the study.
“The AASM recommends adults try to aim for at least 7 hours of sleep and I often tell my patients that keeping a regular routine is best for your sleep and health,” she said in an interview.
Funding for the study was provided by the American Academy of Sleep Medicine Foundation and the National Institutes of Health. Dr. Chung and Dr. Abassi-Feinberg report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
INDIANAPOLIS –
In a diverse group of older adults, those with regular and optimal sleep had about a 40% lower risk of dying of any cause during follow-up compared with peers who had irregular and insufficient sleep.
“If sleep were an 8-hour pill, it would be beneficial to take the full dose at regular times consistently,” lead researcher Joon Chung, PhD, of Harvard Medical School and Brigham and Women’s Hospital, Boston, said in a news release.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Broad adverse health effects
“Evidence is mounting that irregular sleep is associated with pretty broad adverse health outcomes, most prominently cardiometabolic disease, obesity, and cardiovascular disease,” Dr. Chungsaid in an interview.
In the current study, the researchers estimated the association of regular sleep of optimal sleep duration with all-cause mortality using data from 1,759 adults the Multi-Ethnic Study of Atherosclerosis Sleep Study.
Sleep regularity and duration were classified using 7 days of data gathered by wrist actigraphy. Adults were categorized as “regular-optimal” sleepers (n = 1,015) or “irregular-insufficient” sleepers (n = 744).
During 7 years of follow-up, 176 people died. In the fully adjusted model, the regular-optimal group had a 39% lower mortality risk compared with the irregular-insufficient sleep group (hazard ratio, 0.61;95% confidence interval [CI], 0.45-0.83). The findings were robust in sensitivity analyses.
The regular and optimal duration sleep pattern maps behaviorally to regular bed and wake times, suggesting potential health benefits of adherence to recommended sleep practices, the researchers noted.
“Results suggest benefits of expanding the public conversation on getting ‘a good night’s sleep’ and broadening this goal to getting many good nights of sleep, in a row, on weekdays and weekends,” Dr. Chung said in the release.
He further said that “getting adequate, regular sleep seems to be something that is good for all. I don’t know of anyone who wouldn’t benefit.”
Fariha Abassi-Feinberg, MD, spokesperson for the American Academy of Sleep Medicine and sleep specialist with the Millennium Physician Group, Fort Myers, Fla., agreed.
“We know our bodies have an internal clock, known as the circadian rhythm, which regulates various biological processes, including sleep-wake cycles. Sticking to a consistent sleep schedule allows your body to align its natural rhythm with the external day-night cycle. This synchronization promotes better sleep quality and therefore better health,” said Dr. Abassi-Feinberg, who wasn’t involved in the study.
“The AASM recommends adults try to aim for at least 7 hours of sleep and I often tell my patients that keeping a regular routine is best for your sleep and health,” she said in an interview.
Funding for the study was provided by the American Academy of Sleep Medicine Foundation and the National Institutes of Health. Dr. Chung and Dr. Abassi-Feinberg report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
INDIANAPOLIS –
In a diverse group of older adults, those with regular and optimal sleep had about a 40% lower risk of dying of any cause during follow-up compared with peers who had irregular and insufficient sleep.
“If sleep were an 8-hour pill, it would be beneficial to take the full dose at regular times consistently,” lead researcher Joon Chung, PhD, of Harvard Medical School and Brigham and Women’s Hospital, Boston, said in a news release.
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Broad adverse health effects
“Evidence is mounting that irregular sleep is associated with pretty broad adverse health outcomes, most prominently cardiometabolic disease, obesity, and cardiovascular disease,” Dr. Chungsaid in an interview.
In the current study, the researchers estimated the association of regular sleep of optimal sleep duration with all-cause mortality using data from 1,759 adults the Multi-Ethnic Study of Atherosclerosis Sleep Study.
Sleep regularity and duration were classified using 7 days of data gathered by wrist actigraphy. Adults were categorized as “regular-optimal” sleepers (n = 1,015) or “irregular-insufficient” sleepers (n = 744).
During 7 years of follow-up, 176 people died. In the fully adjusted model, the regular-optimal group had a 39% lower mortality risk compared with the irregular-insufficient sleep group (hazard ratio, 0.61;95% confidence interval [CI], 0.45-0.83). The findings were robust in sensitivity analyses.
The regular and optimal duration sleep pattern maps behaviorally to regular bed and wake times, suggesting potential health benefits of adherence to recommended sleep practices, the researchers noted.
“Results suggest benefits of expanding the public conversation on getting ‘a good night’s sleep’ and broadening this goal to getting many good nights of sleep, in a row, on weekdays and weekends,” Dr. Chung said in the release.
He further said that “getting adequate, regular sleep seems to be something that is good for all. I don’t know of anyone who wouldn’t benefit.”
Fariha Abassi-Feinberg, MD, spokesperson for the American Academy of Sleep Medicine and sleep specialist with the Millennium Physician Group, Fort Myers, Fla., agreed.
“We know our bodies have an internal clock, known as the circadian rhythm, which regulates various biological processes, including sleep-wake cycles. Sticking to a consistent sleep schedule allows your body to align its natural rhythm with the external day-night cycle. This synchronization promotes better sleep quality and therefore better health,” said Dr. Abassi-Feinberg, who wasn’t involved in the study.
“The AASM recommends adults try to aim for at least 7 hours of sleep and I often tell my patients that keeping a regular routine is best for your sleep and health,” she said in an interview.
Funding for the study was provided by the American Academy of Sleep Medicine Foundation and the National Institutes of Health. Dr. Chung and Dr. Abassi-Feinberg report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
AT SLEEP 2023
Don’t screen, just listen
A recent study published in the journal Academic Pediatrics suggests that during health maintenance visits clinicians are giving too little attention to their patients’ sleep problems. Using a questionnaire, researchers surveyed patients’ caregivers’ concerns and observations regarding a variety of sleep problems. The investigators then reviewed the clinicians’ documentation of what transpired at the visit and found that while over 90% of the caregivers reported their child had at least one sleep related problem, only 20% of the clinicians documented the problem. And, only 12% documented a management plan regarding the sleep concerns.
I am always bit skeptical about studies that rely on clinicians’ “documentation” because clinicians are busy people and don’t always remember to record things they’ve discussed. You and I know that the lawyers’ dictum “if it wasn’t documented it didn’t happen” is rubbish. However, I still find the basic finding of this study concerning. If we are failing to ask about or even listen to caregivers’ concerns about something as important as sleep, we are missing the boat ... a very large boat.

How could this be happening? First, sleep may have fallen victim to the bloated list of topics that well-intentioned single-issue preventive health advocates have tacked on to the health maintenance visit. It’s a burden that few of us can manage without cutting corners.
However, it is more troubling to me that so many clinicians have chosen sleep as one of those corners to cut. This oversight suggests to me that too many of us have failed to realize from our own observations that sleep is incredibly important to the health of our patients ... and to ourselves.
I will admit that I am extremely sensitive to the importance of sleep. Some might say my sensitivity borders on an obsession. But, the literature is clear and becoming more voluminous every year that sleep is important to the mental health of our patients and their caregivers to things like obesity, to symptoms that suggest an attention-deficit/hyperactivity disorder, to school success, and to migraine ... to name just a few.
It may be that most of us realize the importance of sleep but feel our society has allowed itself to become so sleep deprived that there is little chance we can turn the ship around by spending just a few minutes trying help a family undo their deeply ingrained sleep unfriendly habits.
I am tempted to join those of you who see sleep depravation as a “why bother” issue. But, I’m not ready to throw in the towel. Even simply sharing your observations about the importance of sleep in the whole wellness picture may have an effect.
One of the benefits of retiring in the same community in which I practiced for over 40 years is that at least every month or two I encounter a parent who thanks me for sharing my views on the importance of sleep. They may not recall the little tip or two I gave them, but it seems that urging them to put sleep near the top of their lifestyle priority list has made the difference for them.
If I have failed in getting you to join me in my crusade against sleep deprivation, at least take to heart the most basic message of this study. That is that the investigators found only 20% of clinicians were addressing a concern that 90% of the caregivers shared. It happened to be sleep, but it could have been anything.
The authors of the study suggest that we need to be more assiduous in our screening for sleep problems. On the contrary. You and I know we don’t need more screening. We just need to be better listeners.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
A recent study published in the journal Academic Pediatrics suggests that during health maintenance visits clinicians are giving too little attention to their patients’ sleep problems. Using a questionnaire, researchers surveyed patients’ caregivers’ concerns and observations regarding a variety of sleep problems. The investigators then reviewed the clinicians’ documentation of what transpired at the visit and found that while over 90% of the caregivers reported their child had at least one sleep related problem, only 20% of the clinicians documented the problem. And, only 12% documented a management plan regarding the sleep concerns.
I am always bit skeptical about studies that rely on clinicians’ “documentation” because clinicians are busy people and don’t always remember to record things they’ve discussed. You and I know that the lawyers’ dictum “if it wasn’t documented it didn’t happen” is rubbish. However, I still find the basic finding of this study concerning. If we are failing to ask about or even listen to caregivers’ concerns about something as important as sleep, we are missing the boat ... a very large boat.
How could this be happening? First, sleep may have fallen victim to the bloated list of topics that well-intentioned single-issue preventive health advocates have tacked on to the health maintenance visit. It’s a burden that few of us can manage without cutting corners.
However, it is more troubling to me that so many clinicians have chosen sleep as one of those corners to cut. This oversight suggests to me that too many of us have failed to realize from our own observations that sleep is incredibly important to the health of our patients ... and to ourselves.
I will admit that I am extremely sensitive to the importance of sleep. Some might say my sensitivity borders on an obsession. But, the literature is clear and becoming more voluminous every year that sleep is important to the mental health of our patients and their caregivers to things like obesity, to symptoms that suggest an attention-deficit/hyperactivity disorder, to school success, and to migraine ... to name just a few.
It may be that most of us realize the importance of sleep but feel our society has allowed itself to become so sleep deprived that there is little chance we can turn the ship around by spending just a few minutes trying help a family undo their deeply ingrained sleep unfriendly habits.
I am tempted to join those of you who see sleep depravation as a “why bother” issue. But, I’m not ready to throw in the towel. Even simply sharing your observations about the importance of sleep in the whole wellness picture may have an effect.
One of the benefits of retiring in the same community in which I practiced for over 40 years is that at least every month or two I encounter a parent who thanks me for sharing my views on the importance of sleep. They may not recall the little tip or two I gave them, but it seems that urging them to put sleep near the top of their lifestyle priority list has made the difference for them.
If I have failed in getting you to join me in my crusade against sleep deprivation, at least take to heart the most basic message of this study. That is that the investigators found only 20% of clinicians were addressing a concern that 90% of the caregivers shared. It happened to be sleep, but it could have been anything.
The authors of the study suggest that we need to be more assiduous in our screening for sleep problems. On the contrary. You and I know we don’t need more screening. We just need to be better listeners.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
A recent study published in the journal Academic Pediatrics suggests that during health maintenance visits clinicians are giving too little attention to their patients’ sleep problems. Using a questionnaire, researchers surveyed patients’ caregivers’ concerns and observations regarding a variety of sleep problems. The investigators then reviewed the clinicians’ documentation of what transpired at the visit and found that while over 90% of the caregivers reported their child had at least one sleep related problem, only 20% of the clinicians documented the problem. And, only 12% documented a management plan regarding the sleep concerns.
I am always bit skeptical about studies that rely on clinicians’ “documentation” because clinicians are busy people and don’t always remember to record things they’ve discussed. You and I know that the lawyers’ dictum “if it wasn’t documented it didn’t happen” is rubbish. However, I still find the basic finding of this study concerning. If we are failing to ask about or even listen to caregivers’ concerns about something as important as sleep, we are missing the boat ... a very large boat.
How could this be happening? First, sleep may have fallen victim to the bloated list of topics that well-intentioned single-issue preventive health advocates have tacked on to the health maintenance visit. It’s a burden that few of us can manage without cutting corners.
However, it is more troubling to me that so many clinicians have chosen sleep as one of those corners to cut. This oversight suggests to me that too many of us have failed to realize from our own observations that sleep is incredibly important to the health of our patients ... and to ourselves.
I will admit that I am extremely sensitive to the importance of sleep. Some might say my sensitivity borders on an obsession. But, the literature is clear and becoming more voluminous every year that sleep is important to the mental health of our patients and their caregivers to things like obesity, to symptoms that suggest an attention-deficit/hyperactivity disorder, to school success, and to migraine ... to name just a few.
It may be that most of us realize the importance of sleep but feel our society has allowed itself to become so sleep deprived that there is little chance we can turn the ship around by spending just a few minutes trying help a family undo their deeply ingrained sleep unfriendly habits.
I am tempted to join those of you who see sleep depravation as a “why bother” issue. But, I’m not ready to throw in the towel. Even simply sharing your observations about the importance of sleep in the whole wellness picture may have an effect.
One of the benefits of retiring in the same community in which I practiced for over 40 years is that at least every month or two I encounter a parent who thanks me for sharing my views on the importance of sleep. They may not recall the little tip or two I gave them, but it seems that urging them to put sleep near the top of their lifestyle priority list has made the difference for them.
If I have failed in getting you to join me in my crusade against sleep deprivation, at least take to heart the most basic message of this study. That is that the investigators found only 20% of clinicians were addressing a concern that 90% of the caregivers shared. It happened to be sleep, but it could have been anything.
The authors of the study suggest that we need to be more assiduous in our screening for sleep problems. On the contrary. You and I know we don’t need more screening. We just need to be better listeners.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Suicidality risk in youth at highest at night
Investigators found that suicidal ideation and attempts were lowest in the mornings and highest in the evenings, particularly among youth with higher levels of self-critical rumination.
“These are preliminary findings, and there is a need for more data, but they signal potentially that there’s a need for support, particularly at nighttime, and that there might be a potential of targeting self-critical rumination in daily lives of youth,” said lead researcher Anastacia Kudinova, PhD, with the department of psychiatry and human behavior, Alpert Medical School of Brown University, Providence, R.I.
The findings were presented at the late-breaker session at the annual meeting of the Associated Professional Sleep Societies.
Urgent need
Suicidal ideation (SI) is a “robust” predictor of suicidal behavior and, “alarmingly,” both suicidal ideation and suicidal behavior have been increasing, Dr. Kudinova said.
“There is an urgent need to describe proximal time-period risk factors for suicide so that we can identify who is at a greater suicide risk on the time scale of weeks, days, or even hours,” she told attendees.
The researchers asked 165 psychiatrically hospitalized youth aged 11-18 (72% female) about the time of day of their most recent suicide attempt.
More than half (58%) said it occurred in the evenings and nights, followed by daytime (35%) and mornings (7%).
They also assessed the timing of suicidal ideation at home in 61 youth aged 12-15 (61% female) who were discharged after a partial hospitalization program.
They did this using ecological momentary assessments (EMAs) three times a day over 2 weeks. EMAs study people’s thoughts and behavior in their daily lives by repeatedly collecting data in an individual’s normal environment at or close to the time they carry out that behavior.
As in the other sample, youth in this sample also experienced significantly more frequent suicidal ideation later in the day (P < .01).
There was also a significant moderating effect of self-criticism (P < .01), such that more self-critical youth evidenced the highest levels of suicidal ideation later in the day.
True variation or mechanics?
Reached for comment, Paul Nestadt, MD, with Johns Hopkins Bloomberg School of Public Health, Baltimore, noted that EMA is becoming “an interesting way to track high-resolution temporal variation in suicidal ideation and other psych symptoms.”
Dr. Nestadt, who was not involved in the study, said that “it’s not surprising” that the majority of youth attempted suicide in evenings and nights, “as adolescents are generally being supervised in a school setting during daytime hours. It may not be the fluctuation in suicidality that impacts attempt timing so much as the mechanics – it is very hard to attempt suicide in math class.”
The same may be true for the youth in the second sample who were in the partial hospital program. “During the day, they were in therapy groups where feelings of suicidal ideation would have been solicited and addressed in real time,” Dr. Nestadt noted.
“Again, suicidal ideation later in the day may be a practical effect of how they are occupied in the partial hospital program, as opposed to some inherent suicidal ideation increase linked to something endogenous, such as circadian rhythm or cortisol level rises. That said, we do often see more attempts in the evenings in adults as well,” he added.
A vulnerable time
Also weighing in, Casey O’Brien, PsyD, a psychologist in the department of psychiatry at Columbia University Irving Medical Center, New York, said the findings in this study “track” with what she sees in the clinic.
Teens often report in session that the “unstructured time of night – especially the time when they usually should be getting to bed but are kind of staying up – tends to be a very vulnerable time for them,” Dr. O’Brien said in an interview.
“It’s really nice to have research confirm a lot of what we see reported anecdotally from the teens we work with,” said Dr. O’Brien.
Dr. O’Brien heads the intensive adolescent dialectical behavior therapy (DBT) program at Columbia for young people struggling with mental health issues.
“Within the DBT framework, we try to really focus on accepting that this is a vulnerable time and then planning ahead for what the strategies are that they can use to help them transition to bed quickly and smoothly,” Dr. O’Brien said.
These strategies may include spending time with their parents before bed, reading, or building into their bedtime routines things that they find soothing and comforting, like taking a longer shower or having comfortable pajamas to change into, she explained.
“We also work a lot on sleep hygiene strategies to help develop a regular bedtime and have a consistent sleep-wake cycle. We also will plan ahead for using distress tolerance skills during times of emotional vulnerability,” Dr. O’Brien said.
The Columbia DBT program also offers phone coaching “so teens can reach out to a therapist for help using skills outside of a therapeutic hour, and we do find that we get more coaching calls closer to around bedtime,” Dr. O’Brien said.
Support for the study was provided by the National Institute of Mental Health and Bradley Hospital COBRE Center. Dr. Kudinova, Dr. Nestadt, and Dr. O’Brien have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators found that suicidal ideation and attempts were lowest in the mornings and highest in the evenings, particularly among youth with higher levels of self-critical rumination.
“These are preliminary findings, and there is a need for more data, but they signal potentially that there’s a need for support, particularly at nighttime, and that there might be a potential of targeting self-critical rumination in daily lives of youth,” said lead researcher Anastacia Kudinova, PhD, with the department of psychiatry and human behavior, Alpert Medical School of Brown University, Providence, R.I.
The findings were presented at the late-breaker session at the annual meeting of the Associated Professional Sleep Societies.
Urgent need
Suicidal ideation (SI) is a “robust” predictor of suicidal behavior and, “alarmingly,” both suicidal ideation and suicidal behavior have been increasing, Dr. Kudinova said.
“There is an urgent need to describe proximal time-period risk factors for suicide so that we can identify who is at a greater suicide risk on the time scale of weeks, days, or even hours,” she told attendees.
The researchers asked 165 psychiatrically hospitalized youth aged 11-18 (72% female) about the time of day of their most recent suicide attempt.
More than half (58%) said it occurred in the evenings and nights, followed by daytime (35%) and mornings (7%).
They also assessed the timing of suicidal ideation at home in 61 youth aged 12-15 (61% female) who were discharged after a partial hospitalization program.
They did this using ecological momentary assessments (EMAs) three times a day over 2 weeks. EMAs study people’s thoughts and behavior in their daily lives by repeatedly collecting data in an individual’s normal environment at or close to the time they carry out that behavior.
As in the other sample, youth in this sample also experienced significantly more frequent suicidal ideation later in the day (P < .01).
There was also a significant moderating effect of self-criticism (P < .01), such that more self-critical youth evidenced the highest levels of suicidal ideation later in the day.
True variation or mechanics?
Reached for comment, Paul Nestadt, MD, with Johns Hopkins Bloomberg School of Public Health, Baltimore, noted that EMA is becoming “an interesting way to track high-resolution temporal variation in suicidal ideation and other psych symptoms.”
Dr. Nestadt, who was not involved in the study, said that “it’s not surprising” that the majority of youth attempted suicide in evenings and nights, “as adolescents are generally being supervised in a school setting during daytime hours. It may not be the fluctuation in suicidality that impacts attempt timing so much as the mechanics – it is very hard to attempt suicide in math class.”
The same may be true for the youth in the second sample who were in the partial hospital program. “During the day, they were in therapy groups where feelings of suicidal ideation would have been solicited and addressed in real time,” Dr. Nestadt noted.
“Again, suicidal ideation later in the day may be a practical effect of how they are occupied in the partial hospital program, as opposed to some inherent suicidal ideation increase linked to something endogenous, such as circadian rhythm or cortisol level rises. That said, we do often see more attempts in the evenings in adults as well,” he added.
A vulnerable time
Also weighing in, Casey O’Brien, PsyD, a psychologist in the department of psychiatry at Columbia University Irving Medical Center, New York, said the findings in this study “track” with what she sees in the clinic.
Teens often report in session that the “unstructured time of night – especially the time when they usually should be getting to bed but are kind of staying up – tends to be a very vulnerable time for them,” Dr. O’Brien said in an interview.
“It’s really nice to have research confirm a lot of what we see reported anecdotally from the teens we work with,” said Dr. O’Brien.
Dr. O’Brien heads the intensive adolescent dialectical behavior therapy (DBT) program at Columbia for young people struggling with mental health issues.
“Within the DBT framework, we try to really focus on accepting that this is a vulnerable time and then planning ahead for what the strategies are that they can use to help them transition to bed quickly and smoothly,” Dr. O’Brien said.
These strategies may include spending time with their parents before bed, reading, or building into their bedtime routines things that they find soothing and comforting, like taking a longer shower or having comfortable pajamas to change into, she explained.
“We also work a lot on sleep hygiene strategies to help develop a regular bedtime and have a consistent sleep-wake cycle. We also will plan ahead for using distress tolerance skills during times of emotional vulnerability,” Dr. O’Brien said.
The Columbia DBT program also offers phone coaching “so teens can reach out to a therapist for help using skills outside of a therapeutic hour, and we do find that we get more coaching calls closer to around bedtime,” Dr. O’Brien said.
Support for the study was provided by the National Institute of Mental Health and Bradley Hospital COBRE Center. Dr. Kudinova, Dr. Nestadt, and Dr. O’Brien have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators found that suicidal ideation and attempts were lowest in the mornings and highest in the evenings, particularly among youth with higher levels of self-critical rumination.
“These are preliminary findings, and there is a need for more data, but they signal potentially that there’s a need for support, particularly at nighttime, and that there might be a potential of targeting self-critical rumination in daily lives of youth,” said lead researcher Anastacia Kudinova, PhD, with the department of psychiatry and human behavior, Alpert Medical School of Brown University, Providence, R.I.
The findings were presented at the late-breaker session at the annual meeting of the Associated Professional Sleep Societies.
Urgent need
Suicidal ideation (SI) is a “robust” predictor of suicidal behavior and, “alarmingly,” both suicidal ideation and suicidal behavior have been increasing, Dr. Kudinova said.
“There is an urgent need to describe proximal time-period risk factors for suicide so that we can identify who is at a greater suicide risk on the time scale of weeks, days, or even hours,” she told attendees.
The researchers asked 165 psychiatrically hospitalized youth aged 11-18 (72% female) about the time of day of their most recent suicide attempt.
More than half (58%) said it occurred in the evenings and nights, followed by daytime (35%) and mornings (7%).
They also assessed the timing of suicidal ideation at home in 61 youth aged 12-15 (61% female) who were discharged after a partial hospitalization program.
They did this using ecological momentary assessments (EMAs) three times a day over 2 weeks. EMAs study people’s thoughts and behavior in their daily lives by repeatedly collecting data in an individual’s normal environment at or close to the time they carry out that behavior.
As in the other sample, youth in this sample also experienced significantly more frequent suicidal ideation later in the day (P < .01).
There was also a significant moderating effect of self-criticism (P < .01), such that more self-critical youth evidenced the highest levels of suicidal ideation later in the day.
True variation or mechanics?
Reached for comment, Paul Nestadt, MD, with Johns Hopkins Bloomberg School of Public Health, Baltimore, noted that EMA is becoming “an interesting way to track high-resolution temporal variation in suicidal ideation and other psych symptoms.”
Dr. Nestadt, who was not involved in the study, said that “it’s not surprising” that the majority of youth attempted suicide in evenings and nights, “as adolescents are generally being supervised in a school setting during daytime hours. It may not be the fluctuation in suicidality that impacts attempt timing so much as the mechanics – it is very hard to attempt suicide in math class.”
The same may be true for the youth in the second sample who were in the partial hospital program. “During the day, they were in therapy groups where feelings of suicidal ideation would have been solicited and addressed in real time,” Dr. Nestadt noted.
“Again, suicidal ideation later in the day may be a practical effect of how they are occupied in the partial hospital program, as opposed to some inherent suicidal ideation increase linked to something endogenous, such as circadian rhythm or cortisol level rises. That said, we do often see more attempts in the evenings in adults as well,” he added.
A vulnerable time
Also weighing in, Casey O’Brien, PsyD, a psychologist in the department of psychiatry at Columbia University Irving Medical Center, New York, said the findings in this study “track” with what she sees in the clinic.
Teens often report in session that the “unstructured time of night – especially the time when they usually should be getting to bed but are kind of staying up – tends to be a very vulnerable time for them,” Dr. O’Brien said in an interview.
“It’s really nice to have research confirm a lot of what we see reported anecdotally from the teens we work with,” said Dr. O’Brien.
Dr. O’Brien heads the intensive adolescent dialectical behavior therapy (DBT) program at Columbia for young people struggling with mental health issues.
“Within the DBT framework, we try to really focus on accepting that this is a vulnerable time and then planning ahead for what the strategies are that they can use to help them transition to bed quickly and smoothly,” Dr. O’Brien said.
These strategies may include spending time with their parents before bed, reading, or building into their bedtime routines things that they find soothing and comforting, like taking a longer shower or having comfortable pajamas to change into, she explained.
“We also work a lot on sleep hygiene strategies to help develop a regular bedtime and have a consistent sleep-wake cycle. We also will plan ahead for using distress tolerance skills during times of emotional vulnerability,” Dr. O’Brien said.
The Columbia DBT program also offers phone coaching “so teens can reach out to a therapist for help using skills outside of a therapeutic hour, and we do find that we get more coaching calls closer to around bedtime,” Dr. O’Brien said.
Support for the study was provided by the National Institute of Mental Health and Bradley Hospital COBRE Center. Dr. Kudinova, Dr. Nestadt, and Dr. O’Brien have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2023
Unlocking the riddle of REM sleep
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.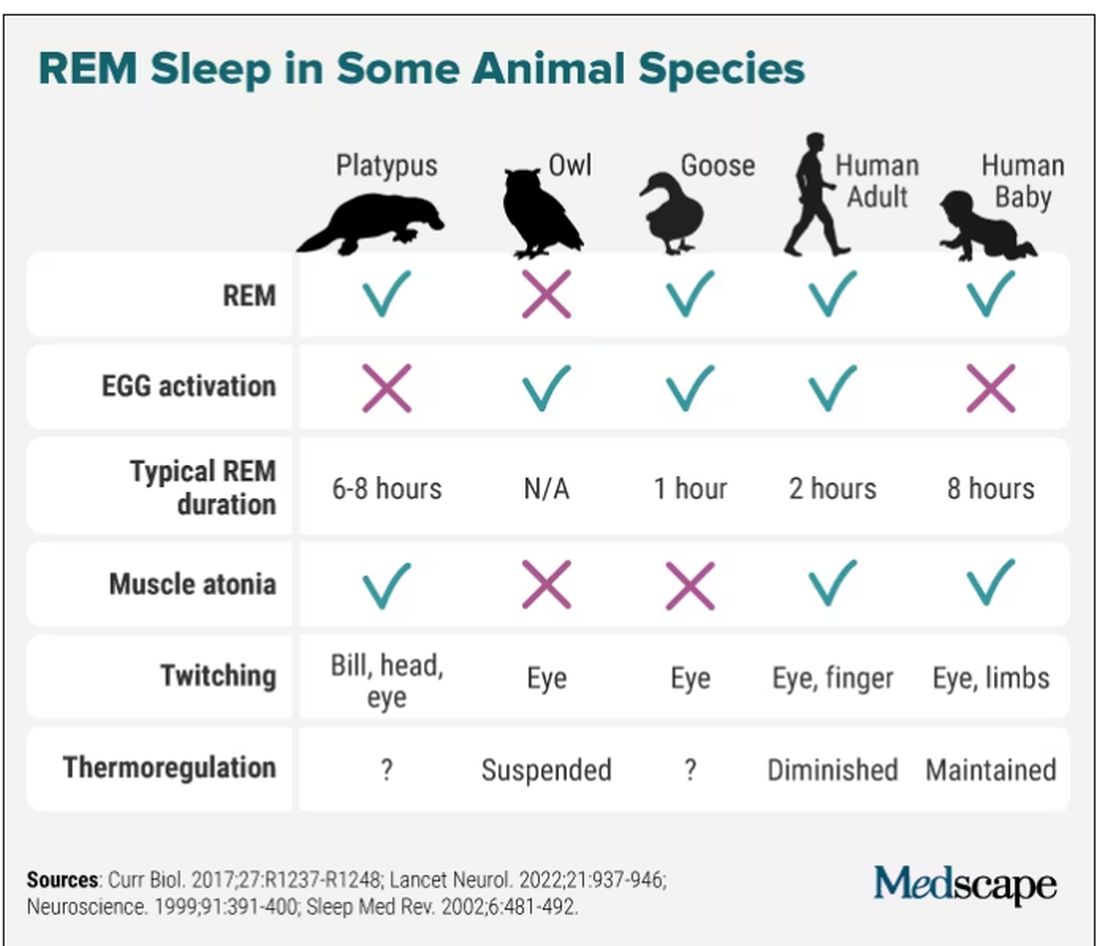
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Prenatal sleep problems, depression linked to poorer outcomes
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
AT ACOG 2023