User login
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
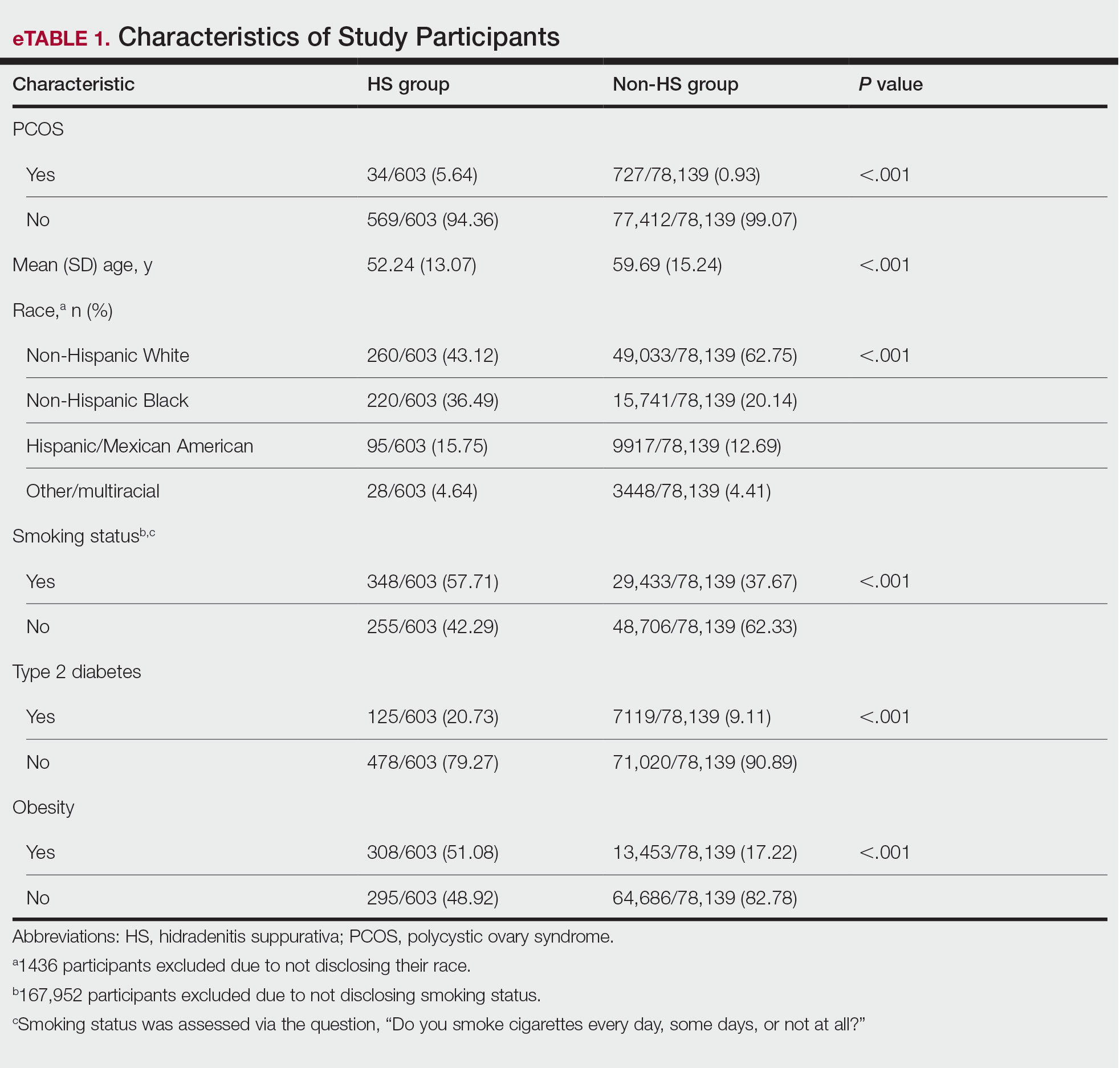
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
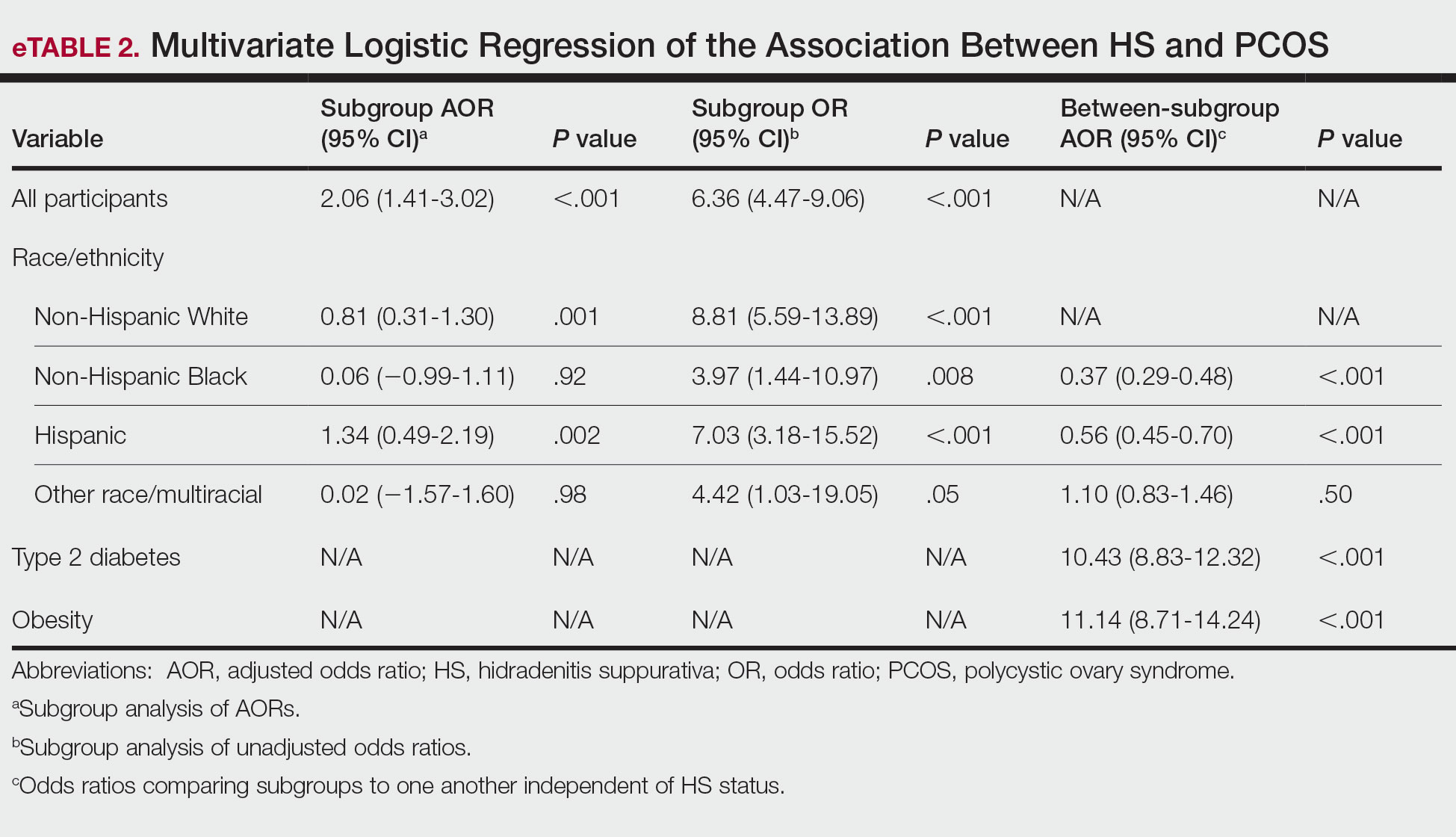
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
PRACTICE POINTS
- Patients with hidradenitis suppurativa were 2.06 times more likely to have polycystic ovary syndrome (PCOS) than patients without HS after controlling for age, race/ ethnicity, tobacco use, type 2 diabetes, and obesity.
- Non-Hispanic Black and Hispanic patients were less likely than White patients to have a diagnosis of PCOS, potentially reflecting underdiagnosis in these populations.
- Individuals with type 2 diabetes and obesity were 10.43 and 11.14 times more likely, respectively, to have PCOS.
