User login


After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
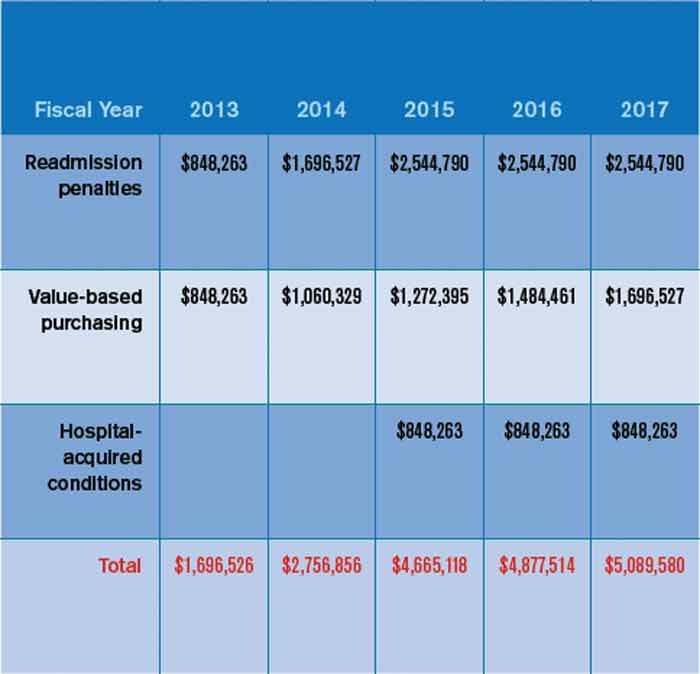
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.