User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
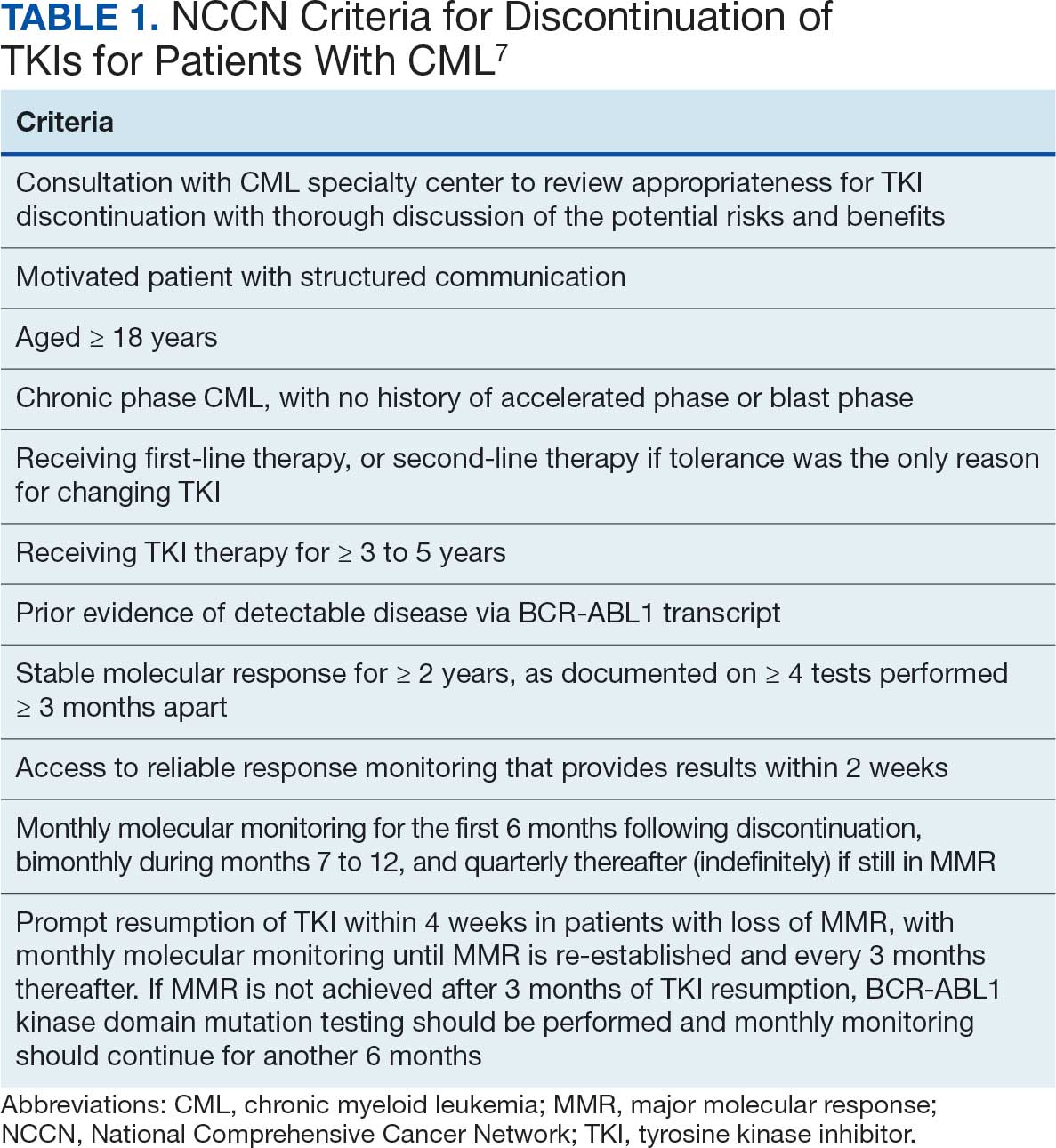
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
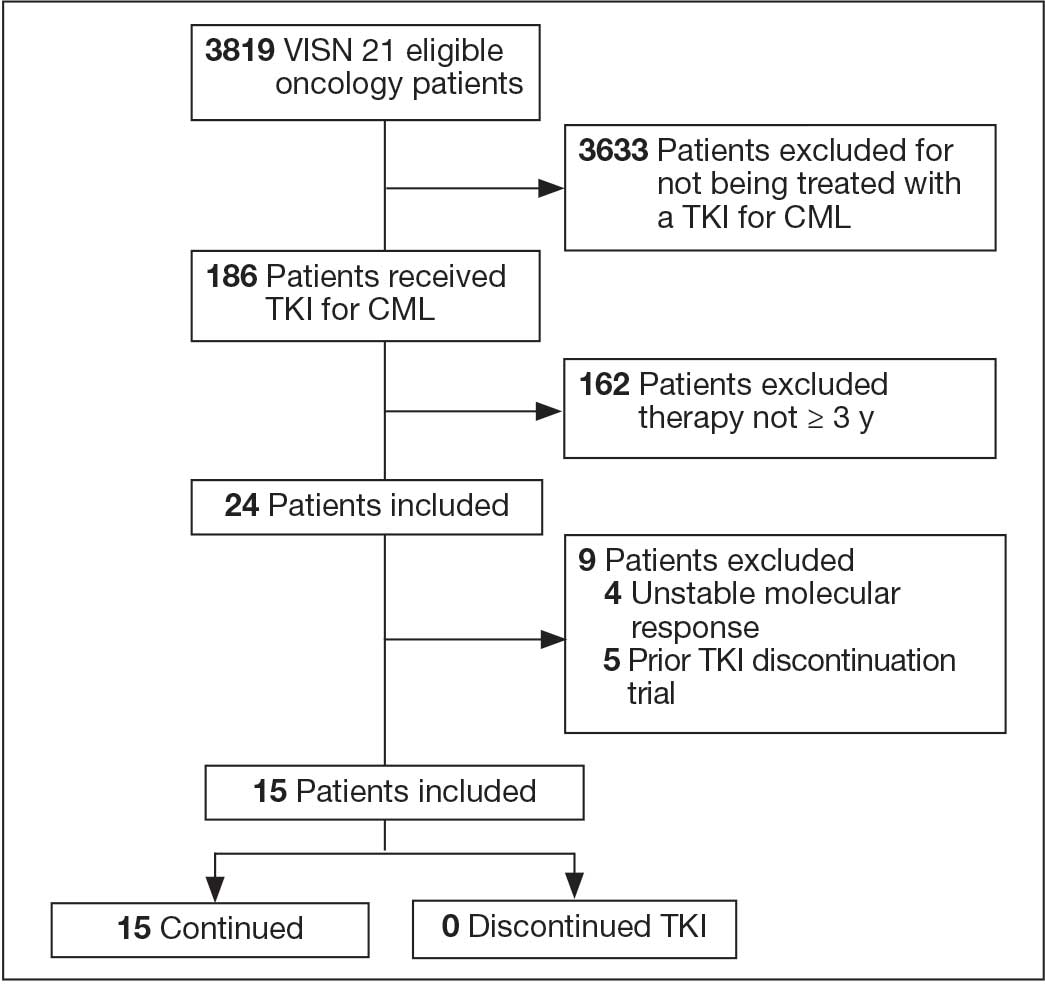
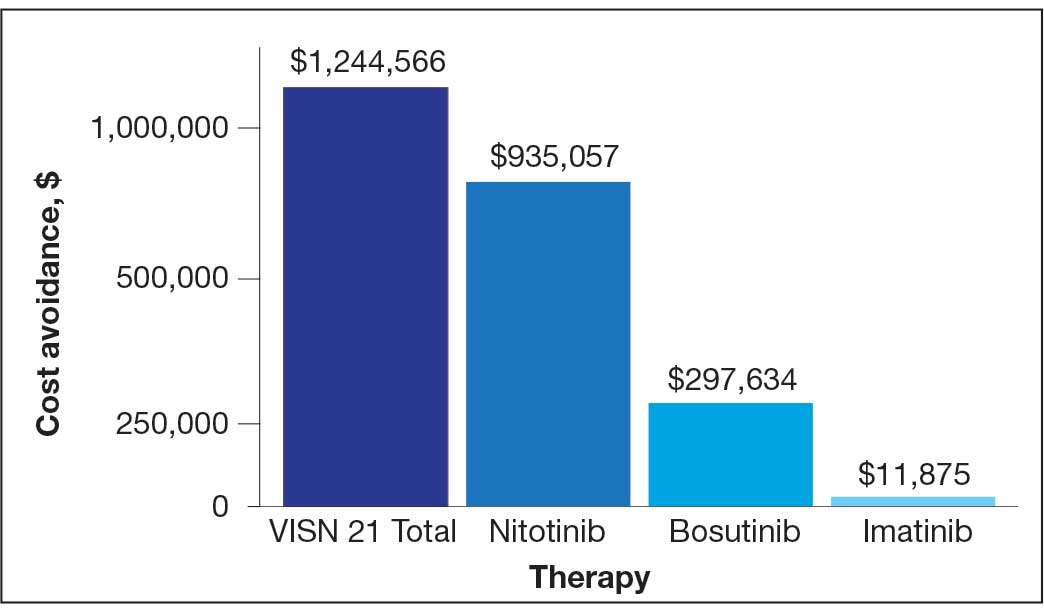
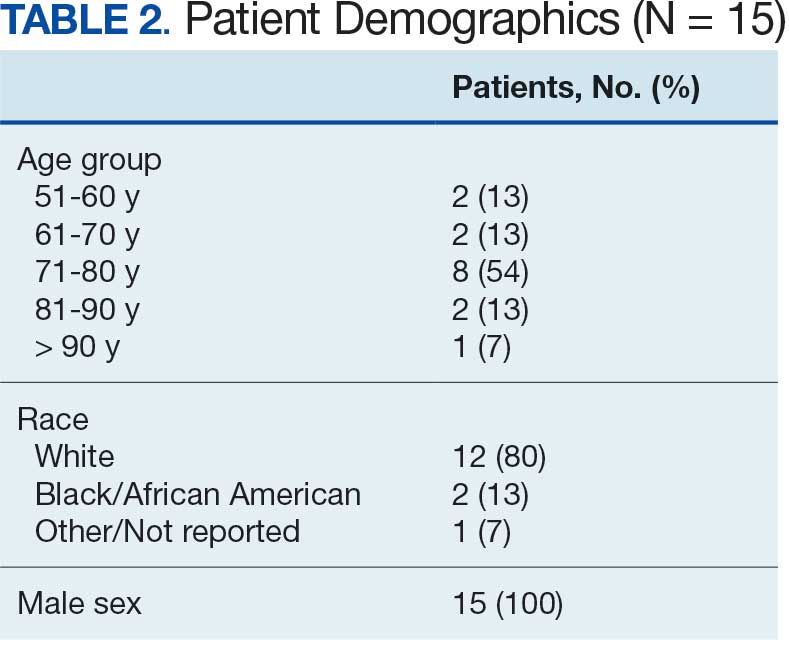
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Cervical Cancer Screening Gaps Persist After 65 Years of Age
Cervical Cancer Screening Gaps Persist After 65 Years of Age
TOPLINE:
Among women aged > 65 years who were at a high risk for cervical cancer and required screening, only 5.2% received appropriate screening. Women with a history of high-grade cervical dysplasia had a greater likelihood of appropriate screening.
METHODOLOGY:
- Researchers conducted a retrospective study to assess the rates of appropriate cervical cancer screening among 1787 women aged 66 years or older (median, 76 years; 96.3% White) who had a Medicare wellness visit or an annual gynecologic visit in a healthcare system in 2022.
- Data on age at the last cervical cancer screening, history of hysterectomy, human papillomavirus (HPV) status, and history of a diagnosis of cervical cancer or cervical dysplasia, high-grade dysplasia, and immune deficiency status were assessed.
- Participants were categorized into 2 groups: those at high risk for cervical cancer (prior high-grade cervical dysplasia or cancer, an immunocompromised status, or lack of two normal cytology results in the past 10 years; n = 250) and those at average risk (having no high-risk features and adequate prior screening or having a prior hysterectomy with no history of high-grade cervical dysplasia; n = 1537).
- The screening cessation criteria were based on adequate prior screening, defined as two prior negative cervical cancer screenings in the past 10 years, the absence of high-grade cervical dysplasia or cervical cancer, and no immune deficiency.
TAKEAWAY:
- Overall, 4.9% of patients had a history of inadequate prior screening; among women at high risk, 5.2% were appropriately screened.
- The odds of continued screening were greater for women with a history of a positive HPV test results (adjusted odds ratio [aOR], 3.4; P = .016), a history of high-grade cervical dysplasia (aOR, 3.8; P = .009), and those without prior hysterectomy (aOR, 2.2; P = .005).
- Among women at high risk for cervical cancer, those with a history of high-grade cervical dysplasia had increased odds of appropriate screening (aOR, 6.7; P = .002), whereas the odds decreased with every 5-year increase in age (aOR, 0.5; P = .031). Women with prior hysterectomy were less likely to be over-screened (aOR, 0.3; P < .001) than those without.
- Among the 79 women who underwent screening, 97.5% had normal cytology results; the remaining women had abnormal cytology results (atypical squamous cells of undetermined significance or atypical squamous cells); all patients with abnormal cytology results met high-risk criteria and were screened appropriately.
IN PRACTICE:
“[The study] findings suggest that most clinicians and patients are aware of recommendations to stop cervical cancer screening after age 65 years. However, there may be a lack of awareness regarding continued screening in high-risk patients or those with inadequate prior screening. The lack of prior screening history and results in the medical record suggests that providers may not understand the importance of these factors to inform cervical cancer screening in older patients,” the authors of the study wrote.
SOURCE:
The study was led by Daniel Rodriguez, BS, Kolschowsky Research and Education Institute, Sarasota Memorial Health Care System, Sarasota, Florida. It was published online on April 23, 2026, in the Journal of Lower Genital Tract Disease.
LIMITATIONS:
Screening history in electronic medical records may be incomplete.
DISCLOSURES:
The Sarasota Memorial Healthcare Foundation provided financial support for this research. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among women aged > 65 years who were at a high risk for cervical cancer and required screening, only 5.2% received appropriate screening. Women with a history of high-grade cervical dysplasia had a greater likelihood of appropriate screening.
METHODOLOGY:
- Researchers conducted a retrospective study to assess the rates of appropriate cervical cancer screening among 1787 women aged 66 years or older (median, 76 years; 96.3% White) who had a Medicare wellness visit or an annual gynecologic visit in a healthcare system in 2022.
- Data on age at the last cervical cancer screening, history of hysterectomy, human papillomavirus (HPV) status, and history of a diagnosis of cervical cancer or cervical dysplasia, high-grade dysplasia, and immune deficiency status were assessed.
- Participants were categorized into 2 groups: those at high risk for cervical cancer (prior high-grade cervical dysplasia or cancer, an immunocompromised status, or lack of two normal cytology results in the past 10 years; n = 250) and those at average risk (having no high-risk features and adequate prior screening or having a prior hysterectomy with no history of high-grade cervical dysplasia; n = 1537).
- The screening cessation criteria were based on adequate prior screening, defined as two prior negative cervical cancer screenings in the past 10 years, the absence of high-grade cervical dysplasia or cervical cancer, and no immune deficiency.
TAKEAWAY:
- Overall, 4.9% of patients had a history of inadequate prior screening; among women at high risk, 5.2% were appropriately screened.
- The odds of continued screening were greater for women with a history of a positive HPV test results (adjusted odds ratio [aOR], 3.4; P = .016), a history of high-grade cervical dysplasia (aOR, 3.8; P = .009), and those without prior hysterectomy (aOR, 2.2; P = .005).
- Among women at high risk for cervical cancer, those with a history of high-grade cervical dysplasia had increased odds of appropriate screening (aOR, 6.7; P = .002), whereas the odds decreased with every 5-year increase in age (aOR, 0.5; P = .031). Women with prior hysterectomy were less likely to be over-screened (aOR, 0.3; P < .001) than those without.
- Among the 79 women who underwent screening, 97.5% had normal cytology results; the remaining women had abnormal cytology results (atypical squamous cells of undetermined significance or atypical squamous cells); all patients with abnormal cytology results met high-risk criteria and were screened appropriately.
IN PRACTICE:
“[The study] findings suggest that most clinicians and patients are aware of recommendations to stop cervical cancer screening after age 65 years. However, there may be a lack of awareness regarding continued screening in high-risk patients or those with inadequate prior screening. The lack of prior screening history and results in the medical record suggests that providers may not understand the importance of these factors to inform cervical cancer screening in older patients,” the authors of the study wrote.
SOURCE:
The study was led by Daniel Rodriguez, BS, Kolschowsky Research and Education Institute, Sarasota Memorial Health Care System, Sarasota, Florida. It was published online on April 23, 2026, in the Journal of Lower Genital Tract Disease.
LIMITATIONS:
Screening history in electronic medical records may be incomplete.
DISCLOSURES:
The Sarasota Memorial Healthcare Foundation provided financial support for this research. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among women aged > 65 years who were at a high risk for cervical cancer and required screening, only 5.2% received appropriate screening. Women with a history of high-grade cervical dysplasia had a greater likelihood of appropriate screening.
METHODOLOGY:
- Researchers conducted a retrospective study to assess the rates of appropriate cervical cancer screening among 1787 women aged 66 years or older (median, 76 years; 96.3% White) who had a Medicare wellness visit or an annual gynecologic visit in a healthcare system in 2022.
- Data on age at the last cervical cancer screening, history of hysterectomy, human papillomavirus (HPV) status, and history of a diagnosis of cervical cancer or cervical dysplasia, high-grade dysplasia, and immune deficiency status were assessed.
- Participants were categorized into 2 groups: those at high risk for cervical cancer (prior high-grade cervical dysplasia or cancer, an immunocompromised status, or lack of two normal cytology results in the past 10 years; n = 250) and those at average risk (having no high-risk features and adequate prior screening or having a prior hysterectomy with no history of high-grade cervical dysplasia; n = 1537).
- The screening cessation criteria were based on adequate prior screening, defined as two prior negative cervical cancer screenings in the past 10 years, the absence of high-grade cervical dysplasia or cervical cancer, and no immune deficiency.
TAKEAWAY:
- Overall, 4.9% of patients had a history of inadequate prior screening; among women at high risk, 5.2% were appropriately screened.
- The odds of continued screening were greater for women with a history of a positive HPV test results (adjusted odds ratio [aOR], 3.4; P = .016), a history of high-grade cervical dysplasia (aOR, 3.8; P = .009), and those without prior hysterectomy (aOR, 2.2; P = .005).
- Among women at high risk for cervical cancer, those with a history of high-grade cervical dysplasia had increased odds of appropriate screening (aOR, 6.7; P = .002), whereas the odds decreased with every 5-year increase in age (aOR, 0.5; P = .031). Women with prior hysterectomy were less likely to be over-screened (aOR, 0.3; P < .001) than those without.
- Among the 79 women who underwent screening, 97.5% had normal cytology results; the remaining women had abnormal cytology results (atypical squamous cells of undetermined significance or atypical squamous cells); all patients with abnormal cytology results met high-risk criteria and were screened appropriately.
IN PRACTICE:
“[The study] findings suggest that most clinicians and patients are aware of recommendations to stop cervical cancer screening after age 65 years. However, there may be a lack of awareness regarding continued screening in high-risk patients or those with inadequate prior screening. The lack of prior screening history and results in the medical record suggests that providers may not understand the importance of these factors to inform cervical cancer screening in older patients,” the authors of the study wrote.
SOURCE:
The study was led by Daniel Rodriguez, BS, Kolschowsky Research and Education Institute, Sarasota Memorial Health Care System, Sarasota, Florida. It was published online on April 23, 2026, in the Journal of Lower Genital Tract Disease.
LIMITATIONS:
Screening history in electronic medical records may be incomplete.
DISCLOSURES:
The Sarasota Memorial Healthcare Foundation provided financial support for this research. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Cervical Cancer Screening Gaps Persist After 65 Years of Age
Cervical Cancer Screening Gaps Persist After 65 Years of Age
Pumping Iron May Aid Recovery After Breast Cancer Surgery
Pumping Iron May Aid Recovery After Breast Cancer Surgery
Women who undergo surgery for breast cancer often hear that they should take it easy with exercise during recovery. But new research looking at intense strength training puts that advice into question.
The study, of nearly 200 women who’d undergone lumpectomy or mastectomy, found that a 3-month weight-training program helped patients make substantial gains in strength, mobility, balance, and body composition.
And while previous studies have examined resistance exercise during breast cancer surgery recovery, this program pumped up the intensity: Most women progressed to deadlifting 100 to 200 pounds, even though few had ever performed strength training before.
“Most of these patients can do a lot more than we think,” said principal investigator Colin Champ, MD, director of the Exercise Oncology and Resiliency Center at Allegheny Health Network in Pittsburgh.
The findings were presented at The American Society of Breast Surgeons (ASBrS) Annual Meeting, held in Seattle from April 29 to May 3.
Pumping Up the Intensity
For the analysis, Champ and his colleagues pooled the results of 3 small prospective studies of their strength conditioning program, including one that previously reported no worsening in patients’ lymphedema, and instead, showed signs of improvement.
The researchers evaluated program participants’ physical and functional gains and whether any of those parameters differed by the extent of their breast cancer surgery.
In total, there were 197 participants, including 85 who’d undergone mastectomies and 112 who’d had lumpectomies; 26 patients also had axillary lymph node dissection.
All of the women attended the same 3-month supervised strength-training program, starting at various points in their recovery process. Nearly half started at 3 months postdiagnosis.
According to Champ, the program addresses a full range of motion, with the exercise intensity building over a short period — similar to what professional athletes do in early training. The specific exercises include split squats, dumbbell presses, and dumbbell rows, done 3 days per week, for about 45-60 minutes.
Most participants, Champ said, start with deadlifting around 70 pounds (lifting weight from the floor to hip level). “If you can carry groceries, you can deadlift 60 or 70 pounds,” he noted.
Each month, the weight and sets increase, while the repetitions decrease.
“We just had a woman in her 70s who deadlifted about 200 pounds” as the program progressed, Champ said.
Benefits Regardless of Surgery Type
Women in the current analysis underwent baseline and post-program testing of body composition and functional parameters, including strength, mobility, and balance. Mastectomy patients (median age, 51 years) were younger than lumpectomy patients (median age, 59 years). They were also more likely to have had chemotherapy (45% vs 27%).
Overall, Champ’s team found that both surgery groups showed statistically significant improvements in muscle and body fat percentages over the course of the program, with muscle mass increasing by 1 percentage point on average and body fat declining by 1.5 percentage points.
Similarly, functional movement scores, grip strength, loads lifted, and balance skills also improved, with comparable benefits regardless of surgery type or whether lymph node dissection was performed.
By the end of the program’s third week, Champ said, most women could deadlift 100-pound weights. And by the 3-month mark, many were able to lift 200-pound loads.
Champ called the results empowering, and he hopes they help reframe the traditional mindset that intense strength training is too heavy a lift after breast cancer surgery.
A surgical oncologist who was not involved in the study agreed.
“This gives us something concrete to say to patients,” said Tina Hieken, MD, of the Mayo Clinic in Rochester, Minnesota. “We have more data to say it’s safe for you to exercise.’’
Hieken, who chaired the meeting’s scientific program committee, also noted that the findings pertain to women of all baseline fitness levels.
For her part, Hieken already encourages patients to walk for exercise and spend time outdoors — in part for the mental well-being benefits.
With patients facing so much uncertainty after a cancer diagnosis, she said, “this is something an individual can take control of.”
Champ and Hieken had no disclosures.
A version of this article first appeared on Medscape.com.
Women who undergo surgery for breast cancer often hear that they should take it easy with exercise during recovery. But new research looking at intense strength training puts that advice into question.
The study, of nearly 200 women who’d undergone lumpectomy or mastectomy, found that a 3-month weight-training program helped patients make substantial gains in strength, mobility, balance, and body composition.
And while previous studies have examined resistance exercise during breast cancer surgery recovery, this program pumped up the intensity: Most women progressed to deadlifting 100 to 200 pounds, even though few had ever performed strength training before.
“Most of these patients can do a lot more than we think,” said principal investigator Colin Champ, MD, director of the Exercise Oncology and Resiliency Center at Allegheny Health Network in Pittsburgh.
The findings were presented at The American Society of Breast Surgeons (ASBrS) Annual Meeting, held in Seattle from April 29 to May 3.
Pumping Up the Intensity
For the analysis, Champ and his colleagues pooled the results of 3 small prospective studies of their strength conditioning program, including one that previously reported no worsening in patients’ lymphedema, and instead, showed signs of improvement.
The researchers evaluated program participants’ physical and functional gains and whether any of those parameters differed by the extent of their breast cancer surgery.
In total, there were 197 participants, including 85 who’d undergone mastectomies and 112 who’d had lumpectomies; 26 patients also had axillary lymph node dissection.
All of the women attended the same 3-month supervised strength-training program, starting at various points in their recovery process. Nearly half started at 3 months postdiagnosis.
According to Champ, the program addresses a full range of motion, with the exercise intensity building over a short period — similar to what professional athletes do in early training. The specific exercises include split squats, dumbbell presses, and dumbbell rows, done 3 days per week, for about 45-60 minutes.
Most participants, Champ said, start with deadlifting around 70 pounds (lifting weight from the floor to hip level). “If you can carry groceries, you can deadlift 60 or 70 pounds,” he noted.
Each month, the weight and sets increase, while the repetitions decrease.
“We just had a woman in her 70s who deadlifted about 200 pounds” as the program progressed, Champ said.
Benefits Regardless of Surgery Type
Women in the current analysis underwent baseline and post-program testing of body composition and functional parameters, including strength, mobility, and balance. Mastectomy patients (median age, 51 years) were younger than lumpectomy patients (median age, 59 years). They were also more likely to have had chemotherapy (45% vs 27%).
Overall, Champ’s team found that both surgery groups showed statistically significant improvements in muscle and body fat percentages over the course of the program, with muscle mass increasing by 1 percentage point on average and body fat declining by 1.5 percentage points.
Similarly, functional movement scores, grip strength, loads lifted, and balance skills also improved, with comparable benefits regardless of surgery type or whether lymph node dissection was performed.
By the end of the program’s third week, Champ said, most women could deadlift 100-pound weights. And by the 3-month mark, many were able to lift 200-pound loads.
Champ called the results empowering, and he hopes they help reframe the traditional mindset that intense strength training is too heavy a lift after breast cancer surgery.
A surgical oncologist who was not involved in the study agreed.
“This gives us something concrete to say to patients,” said Tina Hieken, MD, of the Mayo Clinic in Rochester, Minnesota. “We have more data to say it’s safe for you to exercise.’’
Hieken, who chaired the meeting’s scientific program committee, also noted that the findings pertain to women of all baseline fitness levels.
For her part, Hieken already encourages patients to walk for exercise and spend time outdoors — in part for the mental well-being benefits.
With patients facing so much uncertainty after a cancer diagnosis, she said, “this is something an individual can take control of.”
Champ and Hieken had no disclosures.
A version of this article first appeared on Medscape.com.
Women who undergo surgery for breast cancer often hear that they should take it easy with exercise during recovery. But new research looking at intense strength training puts that advice into question.
The study, of nearly 200 women who’d undergone lumpectomy or mastectomy, found that a 3-month weight-training program helped patients make substantial gains in strength, mobility, balance, and body composition.
And while previous studies have examined resistance exercise during breast cancer surgery recovery, this program pumped up the intensity: Most women progressed to deadlifting 100 to 200 pounds, even though few had ever performed strength training before.
“Most of these patients can do a lot more than we think,” said principal investigator Colin Champ, MD, director of the Exercise Oncology and Resiliency Center at Allegheny Health Network in Pittsburgh.
The findings were presented at The American Society of Breast Surgeons (ASBrS) Annual Meeting, held in Seattle from April 29 to May 3.
Pumping Up the Intensity
For the analysis, Champ and his colleagues pooled the results of 3 small prospective studies of their strength conditioning program, including one that previously reported no worsening in patients’ lymphedema, and instead, showed signs of improvement.
The researchers evaluated program participants’ physical and functional gains and whether any of those parameters differed by the extent of their breast cancer surgery.
In total, there were 197 participants, including 85 who’d undergone mastectomies and 112 who’d had lumpectomies; 26 patients also had axillary lymph node dissection.
All of the women attended the same 3-month supervised strength-training program, starting at various points in their recovery process. Nearly half started at 3 months postdiagnosis.
According to Champ, the program addresses a full range of motion, with the exercise intensity building over a short period — similar to what professional athletes do in early training. The specific exercises include split squats, dumbbell presses, and dumbbell rows, done 3 days per week, for about 45-60 minutes.
Most participants, Champ said, start with deadlifting around 70 pounds (lifting weight from the floor to hip level). “If you can carry groceries, you can deadlift 60 or 70 pounds,” he noted.
Each month, the weight and sets increase, while the repetitions decrease.
“We just had a woman in her 70s who deadlifted about 200 pounds” as the program progressed, Champ said.
Benefits Regardless of Surgery Type
Women in the current analysis underwent baseline and post-program testing of body composition and functional parameters, including strength, mobility, and balance. Mastectomy patients (median age, 51 years) were younger than lumpectomy patients (median age, 59 years). They were also more likely to have had chemotherapy (45% vs 27%).
Overall, Champ’s team found that both surgery groups showed statistically significant improvements in muscle and body fat percentages over the course of the program, with muscle mass increasing by 1 percentage point on average and body fat declining by 1.5 percentage points.
Similarly, functional movement scores, grip strength, loads lifted, and balance skills also improved, with comparable benefits regardless of surgery type or whether lymph node dissection was performed.
By the end of the program’s third week, Champ said, most women could deadlift 100-pound weights. And by the 3-month mark, many were able to lift 200-pound loads.
Champ called the results empowering, and he hopes they help reframe the traditional mindset that intense strength training is too heavy a lift after breast cancer surgery.
A surgical oncologist who was not involved in the study agreed.
“This gives us something concrete to say to patients,” said Tina Hieken, MD, of the Mayo Clinic in Rochester, Minnesota. “We have more data to say it’s safe for you to exercise.’’
Hieken, who chaired the meeting’s scientific program committee, also noted that the findings pertain to women of all baseline fitness levels.
For her part, Hieken already encourages patients to walk for exercise and spend time outdoors — in part for the mental well-being benefits.
With patients facing so much uncertainty after a cancer diagnosis, she said, “this is something an individual can take control of.”
Champ and Hieken had no disclosures.
A version of this article first appeared on Medscape.com.
Pumping Iron May Aid Recovery After Breast Cancer Surgery
Pumping Iron May Aid Recovery After Breast Cancer Surgery
Can Dual Immunotherapy Replace Surgery in Gastric Cancer?
Can Dual Immunotherapy Replace Surgery in Gastric Cancer?
Dual checkpoint blockade allowed 70.6% of patients with microsatellite instability-high (MSI-H) resectable gastric or gastroesophageal junction adenocarcinoma (G/GEJAC) to avoid surgery in a small cohort of the INFINITY study.
MSI-H tumors account for roughly 10% of early G/GEJACs. They respond well to immunotherapy, with high rates of pathologic complete responses. The Italian INFINITY trial set out to test whether some patients with these tumors might not need gastrectomy.
The trial treated MSI-H patients with durvalumab 1500 mg once a month for 3 months along with 1 300-mg dose of the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blocker tremelimumab on day 1. The 18 patients in cohort 1 proceeded to surgery, with a 60% pathologic complete response rate. An additional 18 patients in cohort 2 were the subject of a presentation at the American Association for Cancer Research (AACR) Annual Meeting 2026. These patients were assessed for clinical complete response; if present, they went on to surveillance; if not, they had surgery.
To qualify for a clinical complete response and surveillance, patients were required to have negative findings on CT and PET scans; tumor-informed circulating tumor DNA (ctDNA); and upper endoscopy with ultrasound, including bite-on-bite biopsies and nodal sampling. Surveillance afterward included CT, endoscopy with biopsies, and ctDNA every 12 weeks for up to 2 years.
Among 17 evaluable patients, 1 withdrew consent during immunotherapy, 13 (76%) had a clinical complete response and started surveillance, and the other 4 went to surgery. One patient in the surveillance group had a local regrowth after 4 months, underwent salvage surgery, and remained disease-free. At a median follow-up of 27.1 months, there were no additional progression events.
Overall, 12 of the 17 patients (70.6%) were gastrectomy-free at 2 years without additional treatment. Progression-free survival was 94.1%, and all patients were alive.
“The results are very encouraging,” lead investigator Alberto Leone, MD, said while presenting the results at the AACR annual meeting.
“Nonoperative management could be a safe and effective strategy for patients achieving a clinical complete response after only 3 months of dual immunotherapy,” said Leone, who is a gastrointestinal medical oncologist at the Istituto Nazionale dei Tumori, Milan, Italy. “However, the optimal strategy needs to be established in larger randomized trials.”
Study discussant Yelena Janjagian, MD, gastrointestinal medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, said the findings were important, particularly given that 70.6% of patients avoided a potentially life-altering gastrectomy.
In addition to surgery, the study also calls into question the need for chemotherapy, long the backbone of management alongside surgery, she said. To replace it, however, “it appears that dual checkpoint blockade will be required for a chemotherapy-free approach to achieve organ preservation.”
“Anti-PD-1 alone is not sufficient; we need CTLA-4 to expand and reactivate tumor-specific immunity,” Janjagian continued.
Ultimately, she expects immunotherapy to shift management of MSI-H cancers away from surgery, although some patients will still likely need an operation.
In addition to being MSI-H, patients in the study were mismatch repair deficient and Epstein-Barr virus-negative with T2/T3 tumors; T4 tumors were excluded.
Tumor-agnostic plasma ctDNA was positive at baseline in 13 patients and cleared in 11 after treatment. Higher baseline plasma ctDNA trended toward a lower likelihood of reaching a clinical complete response. Specificity was 100%, so when positive, the test was “very highly informative,” Leone said.
Three patients had grade 3 adverse events (hyperthyroidism, increased gamma-glutamyl transferase, and colitis) that resolved with steroids. There were no grade 4 events, treatment discontinuation, or deaths.
The work was funded by the GONO Foundation and AstraZeneca, the maker of durvalumab and tremelimumab. Leone reported having no disclosures. Janjagian reported having extensive industry ties, including travel funding, consulting fees, and research support from AstraZeneca.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net
A version of this article first appeared on Medscape.com.
Dual checkpoint blockade allowed 70.6% of patients with microsatellite instability-high (MSI-H) resectable gastric or gastroesophageal junction adenocarcinoma (G/GEJAC) to avoid surgery in a small cohort of the INFINITY study.
MSI-H tumors account for roughly 10% of early G/GEJACs. They respond well to immunotherapy, with high rates of pathologic complete responses. The Italian INFINITY trial set out to test whether some patients with these tumors might not need gastrectomy.
The trial treated MSI-H patients with durvalumab 1500 mg once a month for 3 months along with 1 300-mg dose of the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blocker tremelimumab on day 1. The 18 patients in cohort 1 proceeded to surgery, with a 60% pathologic complete response rate. An additional 18 patients in cohort 2 were the subject of a presentation at the American Association for Cancer Research (AACR) Annual Meeting 2026. These patients were assessed for clinical complete response; if present, they went on to surveillance; if not, they had surgery.
To qualify for a clinical complete response and surveillance, patients were required to have negative findings on CT and PET scans; tumor-informed circulating tumor DNA (ctDNA); and upper endoscopy with ultrasound, including bite-on-bite biopsies and nodal sampling. Surveillance afterward included CT, endoscopy with biopsies, and ctDNA every 12 weeks for up to 2 years.
Among 17 evaluable patients, 1 withdrew consent during immunotherapy, 13 (76%) had a clinical complete response and started surveillance, and the other 4 went to surgery. One patient in the surveillance group had a local regrowth after 4 months, underwent salvage surgery, and remained disease-free. At a median follow-up of 27.1 months, there were no additional progression events.
Overall, 12 of the 17 patients (70.6%) were gastrectomy-free at 2 years without additional treatment. Progression-free survival was 94.1%, and all patients were alive.
“The results are very encouraging,” lead investigator Alberto Leone, MD, said while presenting the results at the AACR annual meeting.
“Nonoperative management could be a safe and effective strategy for patients achieving a clinical complete response after only 3 months of dual immunotherapy,” said Leone, who is a gastrointestinal medical oncologist at the Istituto Nazionale dei Tumori, Milan, Italy. “However, the optimal strategy needs to be established in larger randomized trials.”
Study discussant Yelena Janjagian, MD, gastrointestinal medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, said the findings were important, particularly given that 70.6% of patients avoided a potentially life-altering gastrectomy.
In addition to surgery, the study also calls into question the need for chemotherapy, long the backbone of management alongside surgery, she said. To replace it, however, “it appears that dual checkpoint blockade will be required for a chemotherapy-free approach to achieve organ preservation.”
“Anti-PD-1 alone is not sufficient; we need CTLA-4 to expand and reactivate tumor-specific immunity,” Janjagian continued.
Ultimately, she expects immunotherapy to shift management of MSI-H cancers away from surgery, although some patients will still likely need an operation.
In addition to being MSI-H, patients in the study were mismatch repair deficient and Epstein-Barr virus-negative with T2/T3 tumors; T4 tumors were excluded.
Tumor-agnostic plasma ctDNA was positive at baseline in 13 patients and cleared in 11 after treatment. Higher baseline plasma ctDNA trended toward a lower likelihood of reaching a clinical complete response. Specificity was 100%, so when positive, the test was “very highly informative,” Leone said.
Three patients had grade 3 adverse events (hyperthyroidism, increased gamma-glutamyl transferase, and colitis) that resolved with steroids. There were no grade 4 events, treatment discontinuation, or deaths.
The work was funded by the GONO Foundation and AstraZeneca, the maker of durvalumab and tremelimumab. Leone reported having no disclosures. Janjagian reported having extensive industry ties, including travel funding, consulting fees, and research support from AstraZeneca.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net
A version of this article first appeared on Medscape.com.
Dual checkpoint blockade allowed 70.6% of patients with microsatellite instability-high (MSI-H) resectable gastric or gastroesophageal junction adenocarcinoma (G/GEJAC) to avoid surgery in a small cohort of the INFINITY study.
MSI-H tumors account for roughly 10% of early G/GEJACs. They respond well to immunotherapy, with high rates of pathologic complete responses. The Italian INFINITY trial set out to test whether some patients with these tumors might not need gastrectomy.
The trial treated MSI-H patients with durvalumab 1500 mg once a month for 3 months along with 1 300-mg dose of the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blocker tremelimumab on day 1. The 18 patients in cohort 1 proceeded to surgery, with a 60% pathologic complete response rate. An additional 18 patients in cohort 2 were the subject of a presentation at the American Association for Cancer Research (AACR) Annual Meeting 2026. These patients were assessed for clinical complete response; if present, they went on to surveillance; if not, they had surgery.
To qualify for a clinical complete response and surveillance, patients were required to have negative findings on CT and PET scans; tumor-informed circulating tumor DNA (ctDNA); and upper endoscopy with ultrasound, including bite-on-bite biopsies and nodal sampling. Surveillance afterward included CT, endoscopy with biopsies, and ctDNA every 12 weeks for up to 2 years.
Among 17 evaluable patients, 1 withdrew consent during immunotherapy, 13 (76%) had a clinical complete response and started surveillance, and the other 4 went to surgery. One patient in the surveillance group had a local regrowth after 4 months, underwent salvage surgery, and remained disease-free. At a median follow-up of 27.1 months, there were no additional progression events.
Overall, 12 of the 17 patients (70.6%) were gastrectomy-free at 2 years without additional treatment. Progression-free survival was 94.1%, and all patients were alive.
“The results are very encouraging,” lead investigator Alberto Leone, MD, said while presenting the results at the AACR annual meeting.
“Nonoperative management could be a safe and effective strategy for patients achieving a clinical complete response after only 3 months of dual immunotherapy,” said Leone, who is a gastrointestinal medical oncologist at the Istituto Nazionale dei Tumori, Milan, Italy. “However, the optimal strategy needs to be established in larger randomized trials.”
Study discussant Yelena Janjagian, MD, gastrointestinal medical oncologist at Memorial Sloan Kettering Cancer Center in New York City, said the findings were important, particularly given that 70.6% of patients avoided a potentially life-altering gastrectomy.
In addition to surgery, the study also calls into question the need for chemotherapy, long the backbone of management alongside surgery, she said. To replace it, however, “it appears that dual checkpoint blockade will be required for a chemotherapy-free approach to achieve organ preservation.”
“Anti-PD-1 alone is not sufficient; we need CTLA-4 to expand and reactivate tumor-specific immunity,” Janjagian continued.
Ultimately, she expects immunotherapy to shift management of MSI-H cancers away from surgery, although some patients will still likely need an operation.
In addition to being MSI-H, patients in the study were mismatch repair deficient and Epstein-Barr virus-negative with T2/T3 tumors; T4 tumors were excluded.
Tumor-agnostic plasma ctDNA was positive at baseline in 13 patients and cleared in 11 after treatment. Higher baseline plasma ctDNA trended toward a lower likelihood of reaching a clinical complete response. Specificity was 100%, so when positive, the test was “very highly informative,” Leone said.
Three patients had grade 3 adverse events (hyperthyroidism, increased gamma-glutamyl transferase, and colitis) that resolved with steroids. There were no grade 4 events, treatment discontinuation, or deaths.
The work was funded by the GONO Foundation and AstraZeneca, the maker of durvalumab and tremelimumab. Leone reported having no disclosures. Janjagian reported having extensive industry ties, including travel funding, consulting fees, and research support from AstraZeneca.
M. Alexander Otto is a physician assistant with a master’s degree in medical science and a journalism degree from Newhouse. He is an award-winning medical journalist who worked for several major news outlets before joining Medscape. Alex is also an MIT Knight Science Journalism fellow. Email: aotto@medscape.net
A version of this article first appeared on Medscape.com.
Can Dual Immunotherapy Replace Surgery in Gastric Cancer?
Can Dual Immunotherapy Replace Surgery in Gastric Cancer?
Pancreatic Cancer Vaccine Still Shows Promise 6 Years Out
Pancreatic Cancer Vaccine Still Shows Promise 6 Years Out
A personalized messenger RNA (mRNA) vaccine for pancreatic cancer continues to show promise for improving patient survival, according to 6-year follow-up results of a phase 1 clinical study.
Among the 8 out of 16 patients in the study who initially experienced an immune response to the vaccine, seven (87.5%) were still alive at follow-up, lead investigator Vinod P. Balachandran, MD, reported at the American Association for Cancer Research (AACR) Annual Meeting 2026.
Of the eight patients who did not respond, two (25%) were still alive, with a median survival time of 3.4 years. “This suggests that personalized vaccines can stimulate the immune system in some pancreatic cancer patients, and that these patients continue to do well for several years after vaccination,” said Balachandran, director of the Olayan Center for Cancer Vaccines at Memorial Sloan Kettering Cancer Center in New York City.
The findings suggest that this vaccine has the potential to improve outcomes in patients with pancreatic cancer, which is one of the deadliest cancers, he said.
The 5-year survival rate for pancreatic cancer is currently 13%, according to the American Cancer Society’s Cancer Statistics 2026 report.
Initial results of the trial evaluating the individualized neoantigen vaccine — autogene cevumeran, which is being developed by BioNTech and Genentech — were published in Nature in February 2025.
After pancreatic cancer surgery and chemo-immunotherapy, patients with pancreatic ductal adenocarcinoma (PDAC) received a vaccine personalized to each patient based on unique changes in their tumor DNA.
The eight patients with vaccine-induced T cells had prolonged recurrence-free survival (RFS; median not reached), whereas nonresponders had a median RFS of 13.4 months, the authors had reported in the Nature paper.
This correlation was not confounded by other factors, including those associated with the patient, tumor, treatment, and host immune fitness, Balachandran noted.
In the responders, the T-cell clones had “high magnitude and exceptional longevity,” with an average estimated lifespan of 7.7 years, he said.
A fundamental challenge in developing cancer vaccines has been generating durable functional T cells specific for tumor antigens, and these findings suggest that mRNA-lipoplex vaccines against somatic mutation-derived neoantigens like autogene cevumeran may help overcome this challenge in pancreatic cancer, he and his colleagues concluded in the Nature paper.
The latest findings presented at the AACR annual meeting further underscore the potential of this approach.
At the 6-year follow-up, median RFS was “still not reached” in the vaccine responders vs 1.1 year in the nonresponders, he noted.
“This translates to a difference in overall survival,” he said. “Seven of eight [responders to the vaccine] are still alive 4.5-6 years after surgery.”
And of the 2 of 8 nonresponders still alive, one appears to be mounting a subclinical vaccine-induced T-cell response, he added, noting that this “suggests that inducible vaccine immunity may also impact survival in PDAC.”
“The implication here, we believe, is that even if a cancer has very mutational by-products [like PDAC], these mutational by-products can empower potent and composite immunity,” he said. “This is important because it could potentially expand vaccine eligibility to many cancers.”
Currently, there are about 50 neoantigen vaccine trials in solid tumors ongoing worldwide, he noted.
Memorial Sloan Kettering reports that Genentech and BioNTech are now testing autogene cevumeran in a larger patient population at numerous sites worldwide.
Balachandran reported receiving research support from Genentech, Merck Sharp & Dohme, and AbbVie.
Sharon Worcester, MA, is an award-winning medical journalist based in Birmingham, Alabama, writing for Medscape, MDedge, and other affiliate sites. She currently covers oncology, but she has also written on a variety of other medical specialties and healthcare topics. She can be reached at sworcester@mdedge.com or on X: @SW_MedReporter.
A version of this article first appeared on Medscape.com.
A personalized messenger RNA (mRNA) vaccine for pancreatic cancer continues to show promise for improving patient survival, according to 6-year follow-up results of a phase 1 clinical study.
Among the 8 out of 16 patients in the study who initially experienced an immune response to the vaccine, seven (87.5%) were still alive at follow-up, lead investigator Vinod P. Balachandran, MD, reported at the American Association for Cancer Research (AACR) Annual Meeting 2026.
Of the eight patients who did not respond, two (25%) were still alive, with a median survival time of 3.4 years. “This suggests that personalized vaccines can stimulate the immune system in some pancreatic cancer patients, and that these patients continue to do well for several years after vaccination,” said Balachandran, director of the Olayan Center for Cancer Vaccines at Memorial Sloan Kettering Cancer Center in New York City.
The findings suggest that this vaccine has the potential to improve outcomes in patients with pancreatic cancer, which is one of the deadliest cancers, he said.
The 5-year survival rate for pancreatic cancer is currently 13%, according to the American Cancer Society’s Cancer Statistics 2026 report.
Initial results of the trial evaluating the individualized neoantigen vaccine — autogene cevumeran, which is being developed by BioNTech and Genentech — were published in Nature in February 2025.
After pancreatic cancer surgery and chemo-immunotherapy, patients with pancreatic ductal adenocarcinoma (PDAC) received a vaccine personalized to each patient based on unique changes in their tumor DNA.
The eight patients with vaccine-induced T cells had prolonged recurrence-free survival (RFS; median not reached), whereas nonresponders had a median RFS of 13.4 months, the authors had reported in the Nature paper.
This correlation was not confounded by other factors, including those associated with the patient, tumor, treatment, and host immune fitness, Balachandran noted.
In the responders, the T-cell clones had “high magnitude and exceptional longevity,” with an average estimated lifespan of 7.7 years, he said.
A fundamental challenge in developing cancer vaccines has been generating durable functional T cells specific for tumor antigens, and these findings suggest that mRNA-lipoplex vaccines against somatic mutation-derived neoantigens like autogene cevumeran may help overcome this challenge in pancreatic cancer, he and his colleagues concluded in the Nature paper.
The latest findings presented at the AACR annual meeting further underscore the potential of this approach.
At the 6-year follow-up, median RFS was “still not reached” in the vaccine responders vs 1.1 year in the nonresponders, he noted.
“This translates to a difference in overall survival,” he said. “Seven of eight [responders to the vaccine] are still alive 4.5-6 years after surgery.”
And of the 2 of 8 nonresponders still alive, one appears to be mounting a subclinical vaccine-induced T-cell response, he added, noting that this “suggests that inducible vaccine immunity may also impact survival in PDAC.”
“The implication here, we believe, is that even if a cancer has very mutational by-products [like PDAC], these mutational by-products can empower potent and composite immunity,” he said. “This is important because it could potentially expand vaccine eligibility to many cancers.”
Currently, there are about 50 neoantigen vaccine trials in solid tumors ongoing worldwide, he noted.
Memorial Sloan Kettering reports that Genentech and BioNTech are now testing autogene cevumeran in a larger patient population at numerous sites worldwide.
Balachandran reported receiving research support from Genentech, Merck Sharp & Dohme, and AbbVie.
Sharon Worcester, MA, is an award-winning medical journalist based in Birmingham, Alabama, writing for Medscape, MDedge, and other affiliate sites. She currently covers oncology, but she has also written on a variety of other medical specialties and healthcare topics. She can be reached at sworcester@mdedge.com or on X: @SW_MedReporter.
A version of this article first appeared on Medscape.com.
A personalized messenger RNA (mRNA) vaccine for pancreatic cancer continues to show promise for improving patient survival, according to 6-year follow-up results of a phase 1 clinical study.
Among the 8 out of 16 patients in the study who initially experienced an immune response to the vaccine, seven (87.5%) were still alive at follow-up, lead investigator Vinod P. Balachandran, MD, reported at the American Association for Cancer Research (AACR) Annual Meeting 2026.
Of the eight patients who did not respond, two (25%) were still alive, with a median survival time of 3.4 years. “This suggests that personalized vaccines can stimulate the immune system in some pancreatic cancer patients, and that these patients continue to do well for several years after vaccination,” said Balachandran, director of the Olayan Center for Cancer Vaccines at Memorial Sloan Kettering Cancer Center in New York City.
The findings suggest that this vaccine has the potential to improve outcomes in patients with pancreatic cancer, which is one of the deadliest cancers, he said.
The 5-year survival rate for pancreatic cancer is currently 13%, according to the American Cancer Society’s Cancer Statistics 2026 report.
Initial results of the trial evaluating the individualized neoantigen vaccine — autogene cevumeran, which is being developed by BioNTech and Genentech — were published in Nature in February 2025.
After pancreatic cancer surgery and chemo-immunotherapy, patients with pancreatic ductal adenocarcinoma (PDAC) received a vaccine personalized to each patient based on unique changes in their tumor DNA.
The eight patients with vaccine-induced T cells had prolonged recurrence-free survival (RFS; median not reached), whereas nonresponders had a median RFS of 13.4 months, the authors had reported in the Nature paper.
This correlation was not confounded by other factors, including those associated with the patient, tumor, treatment, and host immune fitness, Balachandran noted.
In the responders, the T-cell clones had “high magnitude and exceptional longevity,” with an average estimated lifespan of 7.7 years, he said.
A fundamental challenge in developing cancer vaccines has been generating durable functional T cells specific for tumor antigens, and these findings suggest that mRNA-lipoplex vaccines against somatic mutation-derived neoantigens like autogene cevumeran may help overcome this challenge in pancreatic cancer, he and his colleagues concluded in the Nature paper.
The latest findings presented at the AACR annual meeting further underscore the potential of this approach.
At the 6-year follow-up, median RFS was “still not reached” in the vaccine responders vs 1.1 year in the nonresponders, he noted.
“This translates to a difference in overall survival,” he said. “Seven of eight [responders to the vaccine] are still alive 4.5-6 years after surgery.”
And of the 2 of 8 nonresponders still alive, one appears to be mounting a subclinical vaccine-induced T-cell response, he added, noting that this “suggests that inducible vaccine immunity may also impact survival in PDAC.”
“The implication here, we believe, is that even if a cancer has very mutational by-products [like PDAC], these mutational by-products can empower potent and composite immunity,” he said. “This is important because it could potentially expand vaccine eligibility to many cancers.”
Currently, there are about 50 neoantigen vaccine trials in solid tumors ongoing worldwide, he noted.
Memorial Sloan Kettering reports that Genentech and BioNTech are now testing autogene cevumeran in a larger patient population at numerous sites worldwide.
Balachandran reported receiving research support from Genentech, Merck Sharp & Dohme, and AbbVie.
Sharon Worcester, MA, is an award-winning medical journalist based in Birmingham, Alabama, writing for Medscape, MDedge, and other affiliate sites. She currently covers oncology, but she has also written on a variety of other medical specialties and healthcare topics. She can be reached at sworcester@mdedge.com or on X: @SW_MedReporter.
A version of this article first appeared on Medscape.com.
Pancreatic Cancer Vaccine Still Shows Promise 6 Years Out
Pancreatic Cancer Vaccine Still Shows Promise 6 Years Out
Military Women Survive Ovarian Cancer at Higher Rates
Military Women Survive Ovarian Cancer at Higher Rates
Women with epithelial ovarian cancer treated in the US Department of Defense (DoD) universal health care system demonstrate better 5-year survival compared with similar patients from the national population. The survival advantage persists across multiple age groups and disease stages, with particularly notable improvements in patients aged 35-49 years and those with stage III disease.
METHODOLOGY:
- Researchers compared 1504 patients with invasive stage I-IV epithelial ovarian carcinoma from the Automated Center Tumor Registry (ACTUR) for the DoD with 6016 matched patients from the 18-region Surveillance, Epidemiology, and End Results (SEER) program between 1987 and 2013.
- Patients from ACTUR were matched in a 1:4 ratio with SEER patients stratified for age, race, year of diagnosis, and histology, including serous carcinoma, clear cell carcinoma, mucinous carcinoma, and endometrioid carcinoma with adenocarcinoma subtypes.
- Five-year overall survival was evaluated using the Kaplan-Meier method and compared using log-rank test, with median follow-up time of 46 months in ACTUR and 44 months in SEER.
- Adjusted hazard ratio (AHR) and 95% CI for all-cause mortality were estimated from multivariable Cox proportional regression modeling controlling for age, race, year of diagnosis, region of diagnosis, stage, histology, and grade.
TAKEAWAY:
- Overall survival differs between registries: 5-year survival of 53.2% in ACTUR vs 47.7% in matched SEER cohort (log-rank P = .001).
- In the primary adjusted model, ACTUR is associated with a lower risk for all-cause mortality vs SEER (AHR, 0.83; 95% CI, 0.76-0.91; P < .0001).
- Subset results retain lower adjusted risk for death for ACTUR vs SEER among ages 35-49 years (AHR, 0.66; 95% CI, 0.52-0.83; P = .0005), ages ≥ 65 years (AHR, 0.82; 95% CI, 0.70-0.96; P = .016), and stage III cancer (AHR, 0.79; 95% CI, 0.69-0.91; P = .0015).
- Histology-stratified findings show lower adjusted risk for death in ACTUR vs SEER for clear cell carcinoma (AHR, 0.63; 95% CI, 0.43-0.93; P =.02) and for endometrioid and other adenocarcinomas (AHR, 0.68; 95% CI, 0.56-0.81; P < .0001).
IN PRACTICE:
"This study is envisioned to be a stepping stone to further investigations of survival and other cancer health outcomes starting with patients diagnosed between 2014 and 2024 with epithelial carcinoma of the ovary, fallopian tube, or primary peritoneum in the DoD Healthcare System versus the national population or other Healthcare Systems,” wrote the authors of the study. “Dedicated funding and support in the [Military Health System] are needed to invest in infrastructure, technology, security, education, and research.”
SOURCE:
The study was led by Kathleen M. Darcy, PhD, and Christopher M. Tarney, MD, from the Gynecologic Cancer Center of Excellence, Department of Gynecologic Surgery & Obstetrics, Uniformed Services University, Walter Reed National Military Medical Center in Bethesda, Maryland. It was published online in Military Medicine.
LIMITATIONS:
The retrospective cohort study design limits causal inference. Although groups were balanced by age, race, year, and region of diagnosis, other demographic factors and socioeconomic variables such as patient comorbidities, educational attainment, household income, and health insurance status were not available and may have affected results. The databases fundamentally differ in how data are acquired, with ACTUR following hospital-based Facility Oncology Registry Data Standards and SEER being a national population-based registry, potentially affecting data quality, consistency, and reliability of survival outcome comparisons. The inclusion of patients diagnosed only through 2013 represents a limitation as it does not allow for contemporary evaluation of survival outcomes, particularly given advances over the past decade including maximal cytoreductive effort to no residual disease, increased adoption of neoadjuvant chemotherapy, and introduction of targeted maintenance agents. The study could not incorporate details regarding residual disease status or control for specifics regarding surgical and medical management, including primary vs interval debulking surgery or the type and timing of agents utilized in first-line, maintenance, and recurrent disease settings. Data regarding circulating biomarkers including CA125, molecular subtypes or alterations, and stratification by homologous recombination deficiency vs proficiency status were not available. Epithelial carcinomas of the fallopian tube and primary peritoneum were excluded from this study, which now are commonly incorporated with ovarian carcinomas. Results may not be generalizable to other populations given the unique characteristics of the Military Health System beneficiary population.
DISCLOSURES:
This research received funding from the Uniformed Services University from the Defense Health Program to the Henry M. Jackson Foundation for the Advancement of Military Medicine Inc., including award HU0001-18-2-0032 to the Murtha Cancer Center Research Program and awards HU0001-19-2-0031 and HU0001-24-2-0047 to the Gynecologic Cancer Center of Excellence Program. All coauthors disclosed no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Women with epithelial ovarian cancer treated in the US Department of Defense (DoD) universal health care system demonstrate better 5-year survival compared with similar patients from the national population. The survival advantage persists across multiple age groups and disease stages, with particularly notable improvements in patients aged 35-49 years and those with stage III disease.
METHODOLOGY:
- Researchers compared 1504 patients with invasive stage I-IV epithelial ovarian carcinoma from the Automated Center Tumor Registry (ACTUR) for the DoD with 6016 matched patients from the 18-region Surveillance, Epidemiology, and End Results (SEER) program between 1987 and 2013.
- Patients from ACTUR were matched in a 1:4 ratio with SEER patients stratified for age, race, year of diagnosis, and histology, including serous carcinoma, clear cell carcinoma, mucinous carcinoma, and endometrioid carcinoma with adenocarcinoma subtypes.
- Five-year overall survival was evaluated using the Kaplan-Meier method and compared using log-rank test, with median follow-up time of 46 months in ACTUR and 44 months in SEER.
- Adjusted hazard ratio (AHR) and 95% CI for all-cause mortality were estimated from multivariable Cox proportional regression modeling controlling for age, race, year of diagnosis, region of diagnosis, stage, histology, and grade.
TAKEAWAY:
- Overall survival differs between registries: 5-year survival of 53.2% in ACTUR vs 47.7% in matched SEER cohort (log-rank P = .001).
- In the primary adjusted model, ACTUR is associated with a lower risk for all-cause mortality vs SEER (AHR, 0.83; 95% CI, 0.76-0.91; P < .0001).
- Subset results retain lower adjusted risk for death for ACTUR vs SEER among ages 35-49 years (AHR, 0.66; 95% CI, 0.52-0.83; P = .0005), ages ≥ 65 years (AHR, 0.82; 95% CI, 0.70-0.96; P = .016), and stage III cancer (AHR, 0.79; 95% CI, 0.69-0.91; P = .0015).
- Histology-stratified findings show lower adjusted risk for death in ACTUR vs SEER for clear cell carcinoma (AHR, 0.63; 95% CI, 0.43-0.93; P =.02) and for endometrioid and other adenocarcinomas (AHR, 0.68; 95% CI, 0.56-0.81; P < .0001).
IN PRACTICE:
"This study is envisioned to be a stepping stone to further investigations of survival and other cancer health outcomes starting with patients diagnosed between 2014 and 2024 with epithelial carcinoma of the ovary, fallopian tube, or primary peritoneum in the DoD Healthcare System versus the national population or other Healthcare Systems,” wrote the authors of the study. “Dedicated funding and support in the [Military Health System] are needed to invest in infrastructure, technology, security, education, and research.”
SOURCE:
The study was led by Kathleen M. Darcy, PhD, and Christopher M. Tarney, MD, from the Gynecologic Cancer Center of Excellence, Department of Gynecologic Surgery & Obstetrics, Uniformed Services University, Walter Reed National Military Medical Center in Bethesda, Maryland. It was published online in Military Medicine.
LIMITATIONS:
The retrospective cohort study design limits causal inference. Although groups were balanced by age, race, year, and region of diagnosis, other demographic factors and socioeconomic variables such as patient comorbidities, educational attainment, household income, and health insurance status were not available and may have affected results. The databases fundamentally differ in how data are acquired, with ACTUR following hospital-based Facility Oncology Registry Data Standards and SEER being a national population-based registry, potentially affecting data quality, consistency, and reliability of survival outcome comparisons. The inclusion of patients diagnosed only through 2013 represents a limitation as it does not allow for contemporary evaluation of survival outcomes, particularly given advances over the past decade including maximal cytoreductive effort to no residual disease, increased adoption of neoadjuvant chemotherapy, and introduction of targeted maintenance agents. The study could not incorporate details regarding residual disease status or control for specifics regarding surgical and medical management, including primary vs interval debulking surgery or the type and timing of agents utilized in first-line, maintenance, and recurrent disease settings. Data regarding circulating biomarkers including CA125, molecular subtypes or alterations, and stratification by homologous recombination deficiency vs proficiency status were not available. Epithelial carcinomas of the fallopian tube and primary peritoneum were excluded from this study, which now are commonly incorporated with ovarian carcinomas. Results may not be generalizable to other populations given the unique characteristics of the Military Health System beneficiary population.
DISCLOSURES:
This research received funding from the Uniformed Services University from the Defense Health Program to the Henry M. Jackson Foundation for the Advancement of Military Medicine Inc., including award HU0001-18-2-0032 to the Murtha Cancer Center Research Program and awards HU0001-19-2-0031 and HU0001-24-2-0047 to the Gynecologic Cancer Center of Excellence Program. All coauthors disclosed no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Women with epithelial ovarian cancer treated in the US Department of Defense (DoD) universal health care system demonstrate better 5-year survival compared with similar patients from the national population. The survival advantage persists across multiple age groups and disease stages, with particularly notable improvements in patients aged 35-49 years and those with stage III disease.
METHODOLOGY:
- Researchers compared 1504 patients with invasive stage I-IV epithelial ovarian carcinoma from the Automated Center Tumor Registry (ACTUR) for the DoD with 6016 matched patients from the 18-region Surveillance, Epidemiology, and End Results (SEER) program between 1987 and 2013.
- Patients from ACTUR were matched in a 1:4 ratio with SEER patients stratified for age, race, year of diagnosis, and histology, including serous carcinoma, clear cell carcinoma, mucinous carcinoma, and endometrioid carcinoma with adenocarcinoma subtypes.
- Five-year overall survival was evaluated using the Kaplan-Meier method and compared using log-rank test, with median follow-up time of 46 months in ACTUR and 44 months in SEER.
- Adjusted hazard ratio (AHR) and 95% CI for all-cause mortality were estimated from multivariable Cox proportional regression modeling controlling for age, race, year of diagnosis, region of diagnosis, stage, histology, and grade.
TAKEAWAY:
- Overall survival differs between registries: 5-year survival of 53.2% in ACTUR vs 47.7% in matched SEER cohort (log-rank P = .001).
- In the primary adjusted model, ACTUR is associated with a lower risk for all-cause mortality vs SEER (AHR, 0.83; 95% CI, 0.76-0.91; P < .0001).
- Subset results retain lower adjusted risk for death for ACTUR vs SEER among ages 35-49 years (AHR, 0.66; 95% CI, 0.52-0.83; P = .0005), ages ≥ 65 years (AHR, 0.82; 95% CI, 0.70-0.96; P = .016), and stage III cancer (AHR, 0.79; 95% CI, 0.69-0.91; P = .0015).
- Histology-stratified findings show lower adjusted risk for death in ACTUR vs SEER for clear cell carcinoma (AHR, 0.63; 95% CI, 0.43-0.93; P =.02) and for endometrioid and other adenocarcinomas (AHR, 0.68; 95% CI, 0.56-0.81; P < .0001).
IN PRACTICE:
"This study is envisioned to be a stepping stone to further investigations of survival and other cancer health outcomes starting with patients diagnosed between 2014 and 2024 with epithelial carcinoma of the ovary, fallopian tube, or primary peritoneum in the DoD Healthcare System versus the national population or other Healthcare Systems,” wrote the authors of the study. “Dedicated funding and support in the [Military Health System] are needed to invest in infrastructure, technology, security, education, and research.”
SOURCE:
The study was led by Kathleen M. Darcy, PhD, and Christopher M. Tarney, MD, from the Gynecologic Cancer Center of Excellence, Department of Gynecologic Surgery & Obstetrics, Uniformed Services University, Walter Reed National Military Medical Center in Bethesda, Maryland. It was published online in Military Medicine.
LIMITATIONS:
The retrospective cohort study design limits causal inference. Although groups were balanced by age, race, year, and region of diagnosis, other demographic factors and socioeconomic variables such as patient comorbidities, educational attainment, household income, and health insurance status were not available and may have affected results. The databases fundamentally differ in how data are acquired, with ACTUR following hospital-based Facility Oncology Registry Data Standards and SEER being a national population-based registry, potentially affecting data quality, consistency, and reliability of survival outcome comparisons. The inclusion of patients diagnosed only through 2013 represents a limitation as it does not allow for contemporary evaluation of survival outcomes, particularly given advances over the past decade including maximal cytoreductive effort to no residual disease, increased adoption of neoadjuvant chemotherapy, and introduction of targeted maintenance agents. The study could not incorporate details regarding residual disease status or control for specifics regarding surgical and medical management, including primary vs interval debulking surgery or the type and timing of agents utilized in first-line, maintenance, and recurrent disease settings. Data regarding circulating biomarkers including CA125, molecular subtypes or alterations, and stratification by homologous recombination deficiency vs proficiency status were not available. Epithelial carcinomas of the fallopian tube and primary peritoneum were excluded from this study, which now are commonly incorporated with ovarian carcinomas. Results may not be generalizable to other populations given the unique characteristics of the Military Health System beneficiary population.
DISCLOSURES:
This research received funding from the Uniformed Services University from the Defense Health Program to the Henry M. Jackson Foundation for the Advancement of Military Medicine Inc., including award HU0001-18-2-0032 to the Murtha Cancer Center Research Program and awards HU0001-19-2-0031 and HU0001-24-2-0047 to the Gynecologic Cancer Center of Excellence Program. All coauthors disclosed no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Military Women Survive Ovarian Cancer at Higher Rates
Military Women Survive Ovarian Cancer at Higher Rates
No Survival Gain With Adjuvant Therapy in Stage III Melanoma
Offering adjuvant therapy to patients with stage III melanoma offers no melanoma-specific or overall survival benefit, reveals extended follow-up from the first population-based national study to estimate the impact of the treatment.
Hildur Helgadottir, MD, PhD, presented the new findings at the 22nd European Association of Dermato-Oncology (EADO) Congress 2026 on April 24 and described the lead-up to the latest update on the study.
To investigate the impact of adjuvant treatment in patients with stage III melanoma, researchers initially conducted a study in which they used the Swedish Melanoma Registry (SweMR) to identify a precohort of those treated before the introduction of adjuvant therapy in 2018 and a postcohort of those treated subsequently, following both groups out to 2023, she explained.
The analysis revealed no significant difference in melanoma-specific survival between the two groups, at a hazard ratio of 0.92, nor in overall survival, at a hazard ratio of 0.93 (P = .60 for both). However, median follow-up differed between the groups, at 69 months vs 39 months for the precohort vs the postcohort.
Helgadottir, who is a senior research specialist at the Karolinska Comprehensive Cancer Center in Stockholm, Sweden, said that when the earlier results were presented at the European Society for Medical Oncology 2024, there was some criticism that the follow-up was not long enough and that there was no information on the actual adjuvant treatment received in the postcohort patients.
The researchers therefore extended their study out to 2024 to increase the median follow-up to 60 months vs 92 months in the postcohort group vs the precohort group.
They also focused patient selection on patients aged less than 75 years because exposure to adjuvant therapy in older patients was low and restricted the analysis to sentinel lymph node-positive stage IIIB-D cutaneous melanoma diagnosed between 2016 and 2020. This was because adjuvant exposure in stage IIIA disease was low, and patients with clinically detected stage III melanoma started to receive neoadjuvant therapy from 2022 onward.
The current analysis, which was recently published in the European Journal of Cancer, involved 287 patients in the precohort and 349 in the postcohort, who had a median age of 60.0 years and 61.0 years, respectively, and of whom 62.0% and 60.5%, respectively, were male. The groups were well balanced in terms of baseline disease characteristics.
Helgadottir explained that 73% of patients in the postcohort received some form of adjuvant treatment, with the majority treated with PD-1 inhibitors, and a smaller proportion given B-Raf serine-threonine kinase inhibitors. The main reasons for not giving adjuvant therapy were favorable tumor characteristics and the presence of comorbidities.
Five-year melanoma-specific survival rates in the precohorts and postcohorts were 71.4% vs 73.2%, at a hazard ratio adjusted for age, sex, and American Joint Committee on Cancer stage of 1.01 (P = .931). Five-year overall survival rates were 67.3% vs 70.1%, at an adjusted hazard ratio of 0.96 (P = .791).
Helgadottir showed that there were also no significant survival differences in any of the prespecified subgroups for neither melanoma-specific nor overall survival.
There were, again, no significant differences in survival outcomes between the two patient groups, she reported.
The latest results are similar to those from another study conducted in Netherlands and a Danish analysis, Helgadottir said.
Taken together, and “considering the side effects and the costs, it is possible that we will go back to closely following up our patients and treating only at relapse,” she said, “and optimally, of course, that will be already in the neoadjuvant setting.”
“And of course we will need biomarkers because there could be some patients that really need adjuvant treatment, but we need to identify these patients,” continued Helgadottir. Overall survival results from KEYNOTE-054, which compares pembrolizumab with placebo after resection of high-risk stage III melanoma, are awaited, she continued.
Helgadottir explained that adjuvant treatment for stage III melanoma was approved in Sweden in 2018, with treatments freely available to all Swedish residents.
The SweMR is a population-based national register that has near-complete and detailed data on primary cutaneous melanomas, including nodal status and satellite and in-transit disease, and is linked to the national Cause of Death Registry. Helgadottir noted, however, that the SweMR does not contain any information on relapses or the nature of the oncologic treatment received by patients with melanoma.
Following her presentation, she was challenged by an audience member as to whether, on the basis of her findings, she would go back to following up with patients and treating at relapses.
“Maybe we should do that and believe in our own data, and we do. But still, the gold standard must always be the randomized clinical trial,” Helgadottir responded. “So I think, although that we believe in this data, we also want to see the results of the randomized studies.”
The audience member commented that she can see in the data from her own institution that they treat fewer and fewer patients with melanoma with adjuvant therapy by discussing it more thoroughly and being stricter on who should receive it.
Helgadottir agreed, adding that “based on this experience, we did not introduce it to stage II patients because it’s always harder to go back” once a group of patients has started to receive a treatment.
The research was supported by Regional Cancer Centres in Sweden and with grants from the Swedish Cancer Society, Region Stockholm, and the Cancer Research Funds of Radiumhemmet. Helgadottir declared having relationships with Bristol Myers Squibb, Merck Sharp & Dohme, Pierre Fabre, and Novartis.
The trial was supported by SkinVision. The researchers declared having no relevant financial relationships.
This article was previously published by Medscape.
Offering adjuvant therapy to patients with stage III melanoma offers no melanoma-specific or overall survival benefit, reveals extended follow-up from the first population-based national study to estimate the impact of the treatment.
Hildur Helgadottir, MD, PhD, presented the new findings at the 22nd European Association of Dermato-Oncology (EADO) Congress 2026 on April 24 and described the lead-up to the latest update on the study.
To investigate the impact of adjuvant treatment in patients with stage III melanoma, researchers initially conducted a study in which they used the Swedish Melanoma Registry (SweMR) to identify a precohort of those treated before the introduction of adjuvant therapy in 2018 and a postcohort of those treated subsequently, following both groups out to 2023, she explained.
The analysis revealed no significant difference in melanoma-specific survival between the two groups, at a hazard ratio of 0.92, nor in overall survival, at a hazard ratio of 0.93 (P = .60 for both). However, median follow-up differed between the groups, at 69 months vs 39 months for the precohort vs the postcohort.
Helgadottir, who is a senior research specialist at the Karolinska Comprehensive Cancer Center in Stockholm, Sweden, said that when the earlier results were presented at the European Society for Medical Oncology 2024, there was some criticism that the follow-up was not long enough and that there was no information on the actual adjuvant treatment received in the postcohort patients.
The researchers therefore extended their study out to 2024 to increase the median follow-up to 60 months vs 92 months in the postcohort group vs the precohort group.
They also focused patient selection on patients aged less than 75 years because exposure to adjuvant therapy in older patients was low and restricted the analysis to sentinel lymph node-positive stage IIIB-D cutaneous melanoma diagnosed between 2016 and 2020. This was because adjuvant exposure in stage IIIA disease was low, and patients with clinically detected stage III melanoma started to receive neoadjuvant therapy from 2022 onward.
The current analysis, which was recently published in the European Journal of Cancer, involved 287 patients in the precohort and 349 in the postcohort, who had a median age of 60.0 years and 61.0 years, respectively, and of whom 62.0% and 60.5%, respectively, were male. The groups were well balanced in terms of baseline disease characteristics.
Helgadottir explained that 73% of patients in the postcohort received some form of adjuvant treatment, with the majority treated with PD-1 inhibitors, and a smaller proportion given B-Raf serine-threonine kinase inhibitors. The main reasons for not giving adjuvant therapy were favorable tumor characteristics and the presence of comorbidities.
Five-year melanoma-specific survival rates in the precohorts and postcohorts were 71.4% vs 73.2%, at a hazard ratio adjusted for age, sex, and American Joint Committee on Cancer stage of 1.01 (P = .931). Five-year overall survival rates were 67.3% vs 70.1%, at an adjusted hazard ratio of 0.96 (P = .791).
Helgadottir showed that there were also no significant survival differences in any of the prespecified subgroups for neither melanoma-specific nor overall survival.
There were, again, no significant differences in survival outcomes between the two patient groups, she reported.
The latest results are similar to those from another study conducted in Netherlands and a Danish analysis, Helgadottir said.
Taken together, and “considering the side effects and the costs, it is possible that we will go back to closely following up our patients and treating only at relapse,” she said, “and optimally, of course, that will be already in the neoadjuvant setting.”
“And of course we will need biomarkers because there could be some patients that really need adjuvant treatment, but we need to identify these patients,” continued Helgadottir. Overall survival results from KEYNOTE-054, which compares pembrolizumab with placebo after resection of high-risk stage III melanoma, are awaited, she continued.
Helgadottir explained that adjuvant treatment for stage III melanoma was approved in Sweden in 2018, with treatments freely available to all Swedish residents.
The SweMR is a population-based national register that has near-complete and detailed data on primary cutaneous melanomas, including nodal status and satellite and in-transit disease, and is linked to the national Cause of Death Registry. Helgadottir noted, however, that the SweMR does not contain any information on relapses or the nature of the oncologic treatment received by patients with melanoma.
Following her presentation, she was challenged by an audience member as to whether, on the basis of her findings, she would go back to following up with patients and treating at relapses.
“Maybe we should do that and believe in our own data, and we do. But still, the gold standard must always be the randomized clinical trial,” Helgadottir responded. “So I think, although that we believe in this data, we also want to see the results of the randomized studies.”
The audience member commented that she can see in the data from her own institution that they treat fewer and fewer patients with melanoma with adjuvant therapy by discussing it more thoroughly and being stricter on who should receive it.
Helgadottir agreed, adding that “based on this experience, we did not introduce it to stage II patients because it’s always harder to go back” once a group of patients has started to receive a treatment.
The research was supported by Regional Cancer Centres in Sweden and with grants from the Swedish Cancer Society, Region Stockholm, and the Cancer Research Funds of Radiumhemmet. Helgadottir declared having relationships with Bristol Myers Squibb, Merck Sharp & Dohme, Pierre Fabre, and Novartis.
The trial was supported by SkinVision. The researchers declared having no relevant financial relationships.
This article was previously published by Medscape.
Offering adjuvant therapy to patients with stage III melanoma offers no melanoma-specific or overall survival benefit, reveals extended follow-up from the first population-based national study to estimate the impact of the treatment.
Hildur Helgadottir, MD, PhD, presented the new findings at the 22nd European Association of Dermato-Oncology (EADO) Congress 2026 on April 24 and described the lead-up to the latest update on the study.
To investigate the impact of adjuvant treatment in patients with stage III melanoma, researchers initially conducted a study in which they used the Swedish Melanoma Registry (SweMR) to identify a precohort of those treated before the introduction of adjuvant therapy in 2018 and a postcohort of those treated subsequently, following both groups out to 2023, she explained.
The analysis revealed no significant difference in melanoma-specific survival between the two groups, at a hazard ratio of 0.92, nor in overall survival, at a hazard ratio of 0.93 (P = .60 for both). However, median follow-up differed between the groups, at 69 months vs 39 months for the precohort vs the postcohort.
Helgadottir, who is a senior research specialist at the Karolinska Comprehensive Cancer Center in Stockholm, Sweden, said that when the earlier results were presented at the European Society for Medical Oncology 2024, there was some criticism that the follow-up was not long enough and that there was no information on the actual adjuvant treatment received in the postcohort patients.
The researchers therefore extended their study out to 2024 to increase the median follow-up to 60 months vs 92 months in the postcohort group vs the precohort group.
They also focused patient selection on patients aged less than 75 years because exposure to adjuvant therapy in older patients was low and restricted the analysis to sentinel lymph node-positive stage IIIB-D cutaneous melanoma diagnosed between 2016 and 2020. This was because adjuvant exposure in stage IIIA disease was low, and patients with clinically detected stage III melanoma started to receive neoadjuvant therapy from 2022 onward.
The current analysis, which was recently published in the European Journal of Cancer, involved 287 patients in the precohort and 349 in the postcohort, who had a median age of 60.0 years and 61.0 years, respectively, and of whom 62.0% and 60.5%, respectively, were male. The groups were well balanced in terms of baseline disease characteristics.
Helgadottir explained that 73% of patients in the postcohort received some form of adjuvant treatment, with the majority treated with PD-1 inhibitors, and a smaller proportion given B-Raf serine-threonine kinase inhibitors. The main reasons for not giving adjuvant therapy were favorable tumor characteristics and the presence of comorbidities.
Five-year melanoma-specific survival rates in the precohorts and postcohorts were 71.4% vs 73.2%, at a hazard ratio adjusted for age, sex, and American Joint Committee on Cancer stage of 1.01 (P = .931). Five-year overall survival rates were 67.3% vs 70.1%, at an adjusted hazard ratio of 0.96 (P = .791).
Helgadottir showed that there were also no significant survival differences in any of the prespecified subgroups for neither melanoma-specific nor overall survival.
There were, again, no significant differences in survival outcomes between the two patient groups, she reported.
The latest results are similar to those from another study conducted in Netherlands and a Danish analysis, Helgadottir said.
Taken together, and “considering the side effects and the costs, it is possible that we will go back to closely following up our patients and treating only at relapse,” she said, “and optimally, of course, that will be already in the neoadjuvant setting.”
“And of course we will need biomarkers because there could be some patients that really need adjuvant treatment, but we need to identify these patients,” continued Helgadottir. Overall survival results from KEYNOTE-054, which compares pembrolizumab with placebo after resection of high-risk stage III melanoma, are awaited, she continued.
Helgadottir explained that adjuvant treatment for stage III melanoma was approved in Sweden in 2018, with treatments freely available to all Swedish residents.
The SweMR is a population-based national register that has near-complete and detailed data on primary cutaneous melanomas, including nodal status and satellite and in-transit disease, and is linked to the national Cause of Death Registry. Helgadottir noted, however, that the SweMR does not contain any information on relapses or the nature of the oncologic treatment received by patients with melanoma.
Following her presentation, she was challenged by an audience member as to whether, on the basis of her findings, she would go back to following up with patients and treating at relapses.
“Maybe we should do that and believe in our own data, and we do. But still, the gold standard must always be the randomized clinical trial,” Helgadottir responded. “So I think, although that we believe in this data, we also want to see the results of the randomized studies.”
The audience member commented that she can see in the data from her own institution that they treat fewer and fewer patients with melanoma with adjuvant therapy by discussing it more thoroughly and being stricter on who should receive it.
Helgadottir agreed, adding that “based on this experience, we did not introduce it to stage II patients because it’s always harder to go back” once a group of patients has started to receive a treatment.
The research was supported by Regional Cancer Centres in Sweden and with grants from the Swedish Cancer Society, Region Stockholm, and the Cancer Research Funds of Radiumhemmet. Helgadottir declared having relationships with Bristol Myers Squibb, Merck Sharp & Dohme, Pierre Fabre, and Novartis.
The trial was supported by SkinVision. The researchers declared having no relevant financial relationships.
This article was previously published by Medscape.
AI Skin Cancer Apps: Do They Work?
An AI-based skin assessment app may drive up healthcare visits for benign lesions, with unclear benefits for skin cancer detection, a Dutch clinical trial has found.
The trial, of nearly 20,000 patients in one health insurance plan, found that those given free access to the app were no more likely to be diagnosed with skin cancer over 1 year than participants assigned to a control group with no app access. They were, however, more likely to make healthcare visits for benign skin lesions.
The results came as a surprise, lead researcher Marlies Wakkee, MD, PhD, said during a presentation at the European Association of Dermato-Oncology (EADO) Congress 2026, held in Prague, Czech Republic.
“We were a bit flabbergasted,” said Wakkee, of Erasmus MC in Rotterdam, Netherlands. “We were, of course, expecting that those who would use this intervention app would have more skin cancer diagnoses than those who did not.”
She did, however, point to a potential reason for the lack of benefit: A deeper look at the data suggested that participants in the control group might have been particularly motivated to see their doctor for suspicious skin growths.
Can AI Apps Fill a Gap?
Wakkee pointed out that routine skin cancer screening via clinical skin examination is considered infeasible in many countries. Current guidance from the US Preventive Services Task Force says there is insufficient evidence to assess the balance of benefits and harms from widespread screening.
A plethora of AI-based skin assessment apps have entered the market in recent years, Wakkee said, and in theory, they have the potential to aid in earlier skin cancer diagnosis. But, she added, the technology also comes with potential harms, ranging from spurring healthcare visits for benign lesions to missing true cancers.
The current trial focused on the SkinVision app. It relies on a convolutional neural network to analyze images of skin lesions captured by the user’s smartphone and provides risk assessments of low, medium or high; a tele-dermatology team is available for support.
The app has been reimbursed in Netherlands via health insurance companies since 2019, and by 2021, it was available to 2.2 million insurees, with an uptake of about 1%, according to Wakkee.
In a previous study, the researchers used insurance claims data to study 18,960 app users and compare them with 56,880 nonusers. They found that app use was associated with an increased likelihood of being diagnosed with cutaneous malignancies and premalignancies but also benign tumors and nevi.
“So there’s a group in there that just is very worried about their skin,” Wakkee said.
To investigate further, her team conducted the SPOT-study, a randomized controlled trial in which roughly 226,000 adults covered by a Dutch nonprofit health insurance provider were invited to take part.
Of those, just over 19,000 agreed and were randomly assigned to either an intervention group that had free access to the skin app for 12 months or a control group that had no access. They were told that if they had any skin lesions they were worried about, they should visit their general practitioner.
During that period, the study found there was no significant difference in rates of histologically verified melanoma between the intervention and control groups, at 0.26% vs 0.31% — a risk difference of -0.05% (P = .68).
Similarly, the groups showed no difference in rates of any type of skin cancer, including squamous cell and basal cell carcinomas, at 2.66% in the intervention group vs 2.27% in the control group (P = .10). Rates of premalignant lesions were also comparable (6.9% vs 6.3%; P = .23).
The researchers then examined participants’ claims data to look at healthcare visits for benign skin lesions. There, app users did have a significantly higher rate, at 3.9% vs 2.6% (P < .001).
A Case of Inherent Bias?
The lack of benefit for skin cancer detection prompted the researchers to view the data from a different angle. They compared their trial participants with over 200,000 nonresponders from the health insurance plan. And that’s when a difference emerged.
Overall, trial participants were nearly three times more likely to have a skin premalignancy or malignancy diagnosed during that period, at 6.7% vs 2.4% (P < .001).
Wakkee said that because trial participants were told that the study aimed to gauge “the potential impact of this technology” in assessing skin lesions, that might have created an inherent bias. Participants assigned to the control group may have been motivated to have any worrisome skin growth checked out by their general practitioners.
In addition, Wakkee cautioned that the 12-month results are based on a small number of cancer cases, making it difficult to draw firm conclusions about the app’s performance. The trial has a second phase, where both groups were given free access to the app for 12 months, then followed for an additional 24 months.
Longer-term data are needed, Wakkee noted, in part to see whether people’s app usage changes over time.
Future Questions
Audience members at the presentation raised questions about how AI-based apps could be best deployed for skin cancer detection — including whether they might work better in the hands of clinicians rather than patients.
Wakkee said that clinicians would need a more advanced technology than that included in the app used in this trial. But future studies, she said, will look at whether the app can be used in a more targeted way, specifically, as a triage tool for people who are already concerned about something on their skin, to help them decide if they need to visit their doctor.
One presentation attendee wondered whether people given a low-risk result by the app were likely to be reassured or still make an appointment.
Wakkee said her team has begun to dig into that question. In a pilot study, 50 patients who wanted to see their general practitioner for a skin lesion were asked: If you received a low-risk rating on the skin app, would you still visit your doctor?
“Half of them said they would stay at home,” Wakkee said. She added, however, that her team is conducting a follow-up study to see what people actually do.
The trial was supported by SkinVision. The researchers declared having no relevant financial relationships.
This article was previously published by Medscape.
An AI-based skin assessment app may drive up healthcare visits for benign lesions, with unclear benefits for skin cancer detection, a Dutch clinical trial has found.
The trial, of nearly 20,000 patients in one health insurance plan, found that those given free access to the app were no more likely to be diagnosed with skin cancer over 1 year than participants assigned to a control group with no app access. They were, however, more likely to make healthcare visits for benign skin lesions.
The results came as a surprise, lead researcher Marlies Wakkee, MD, PhD, said during a presentation at the European Association of Dermato-Oncology (EADO) Congress 2026, held in Prague, Czech Republic.
“We were a bit flabbergasted,” said Wakkee, of Erasmus MC in Rotterdam, Netherlands. “We were, of course, expecting that those who would use this intervention app would have more skin cancer diagnoses than those who did not.”
She did, however, point to a potential reason for the lack of benefit: A deeper look at the data suggested that participants in the control group might have been particularly motivated to see their doctor for suspicious skin growths.
Can AI Apps Fill a Gap?
Wakkee pointed out that routine skin cancer screening via clinical skin examination is considered infeasible in many countries. Current guidance from the US Preventive Services Task Force says there is insufficient evidence to assess the balance of benefits and harms from widespread screening.
A plethora of AI-based skin assessment apps have entered the market in recent years, Wakkee said, and in theory, they have the potential to aid in earlier skin cancer diagnosis. But, she added, the technology also comes with potential harms, ranging from spurring healthcare visits for benign lesions to missing true cancers.
The current trial focused on the SkinVision app. It relies on a convolutional neural network to analyze images of skin lesions captured by the user’s smartphone and provides risk assessments of low, medium or high; a tele-dermatology team is available for support.
The app has been reimbursed in Netherlands via health insurance companies since 2019, and by 2021, it was available to 2.2 million insurees, with an uptake of about 1%, according to Wakkee.
In a previous study, the researchers used insurance claims data to study 18,960 app users and compare them with 56,880 nonusers. They found that app use was associated with an increased likelihood of being diagnosed with cutaneous malignancies and premalignancies but also benign tumors and nevi.
“So there’s a group in there that just is very worried about their skin,” Wakkee said.
To investigate further, her team conducted the SPOT-study, a randomized controlled trial in which roughly 226,000 adults covered by a Dutch nonprofit health insurance provider were invited to take part.
Of those, just over 19,000 agreed and were randomly assigned to either an intervention group that had free access to the skin app for 12 months or a control group that had no access. They were told that if they had any skin lesions they were worried about, they should visit their general practitioner.
During that period, the study found there was no significant difference in rates of histologically verified melanoma between the intervention and control groups, at 0.26% vs 0.31% — a risk difference of -0.05% (P = .68).
Similarly, the groups showed no difference in rates of any type of skin cancer, including squamous cell and basal cell carcinomas, at 2.66% in the intervention group vs 2.27% in the control group (P = .10). Rates of premalignant lesions were also comparable (6.9% vs 6.3%; P = .23).
The researchers then examined participants’ claims data to look at healthcare visits for benign skin lesions. There, app users did have a significantly higher rate, at 3.9% vs 2.6% (P < .001).
A Case of Inherent Bias?
The lack of benefit for skin cancer detection prompted the researchers to view the data from a different angle. They compared their trial participants with over 200,000 nonresponders from the health insurance plan. And that’s when a difference emerged.
Overall, trial participants were nearly three times more likely to have a skin premalignancy or malignancy diagnosed during that period, at 6.7% vs 2.4% (P < .001).
Wakkee said that because trial participants were told that the study aimed to gauge “the potential impact of this technology” in assessing skin lesions, that might have created an inherent bias. Participants assigned to the control group may have been motivated to have any worrisome skin growth checked out by their general practitioners.
In addition, Wakkee cautioned that the 12-month results are based on a small number of cancer cases, making it difficult to draw firm conclusions about the app’s performance. The trial has a second phase, where both groups were given free access to the app for 12 months, then followed for an additional 24 months.
Longer-term data are needed, Wakkee noted, in part to see whether people’s app usage changes over time.
Future Questions
Audience members at the presentation raised questions about how AI-based apps could be best deployed for skin cancer detection — including whether they might work better in the hands of clinicians rather than patients.
Wakkee said that clinicians would need a more advanced technology than that included in the app used in this trial. But future studies, she said, will look at whether the app can be used in a more targeted way, specifically, as a triage tool for people who are already concerned about something on their skin, to help them decide if they need to visit their doctor.
One presentation attendee wondered whether people given a low-risk result by the app were likely to be reassured or still make an appointment.
Wakkee said her team has begun to dig into that question. In a pilot study, 50 patients who wanted to see their general practitioner for a skin lesion were asked: If you received a low-risk rating on the skin app, would you still visit your doctor?
“Half of them said they would stay at home,” Wakkee said. She added, however, that her team is conducting a follow-up study to see what people actually do.
The trial was supported by SkinVision. The researchers declared having no relevant financial relationships.
This article was previously published by Medscape.
An AI-based skin assessment app may drive up healthcare visits for benign lesions, with unclear benefits for skin cancer detection, a Dutch clinical trial has found.
The trial, of nearly 20,000 patients in one health insurance plan, found that those given free access to the app were no more likely to be diagnosed with skin cancer over 1 year than participants assigned to a control group with no app access. They were, however, more likely to make healthcare visits for benign skin lesions.
The results came as a surprise, lead researcher Marlies Wakkee, MD, PhD, said during a presentation at the European Association of Dermato-Oncology (EADO) Congress 2026, held in Prague, Czech Republic.
“We were a bit flabbergasted,” said Wakkee, of Erasmus MC in Rotterdam, Netherlands. “We were, of course, expecting that those who would use this intervention app would have more skin cancer diagnoses than those who did not.”
She did, however, point to a potential reason for the lack of benefit: A deeper look at the data suggested that participants in the control group might have been particularly motivated to see their doctor for suspicious skin growths.
Can AI Apps Fill a Gap?
Wakkee pointed out that routine skin cancer screening via clinical skin examination is considered infeasible in many countries. Current guidance from the US Preventive Services Task Force says there is insufficient evidence to assess the balance of benefits and harms from widespread screening.
A plethora of AI-based skin assessment apps have entered the market in recent years, Wakkee said, and in theory, they have the potential to aid in earlier skin cancer diagnosis. But, she added, the technology also comes with potential harms, ranging from spurring healthcare visits for benign lesions to missing true cancers.
The current trial focused on the SkinVision app. It relies on a convolutional neural network to analyze images of skin lesions captured by the user’s smartphone and provides risk assessments of low, medium or high; a tele-dermatology team is available for support.
The app has been reimbursed in Netherlands via health insurance companies since 2019, and by 2021, it was available to 2.2 million insurees, with an uptake of about 1%, according to Wakkee.
In a previous study, the researchers used insurance claims data to study 18,960 app users and compare them with 56,880 nonusers. They found that app use was associated with an increased likelihood of being diagnosed with cutaneous malignancies and premalignancies but also benign tumors and nevi.
“So there’s a group in there that just is very worried about their skin,” Wakkee said.
To investigate further, her team conducted the SPOT-study, a randomized controlled trial in which roughly 226,000 adults covered by a Dutch nonprofit health insurance provider were invited to take part.
Of those, just over 19,000 agreed and were randomly assigned to either an intervention group that had free access to the skin app for 12 months or a control group that had no access. They were told that if they had any skin lesions they were worried about, they should visit their general practitioner.
During that period, the study found there was no significant difference in rates of histologically verified melanoma between the intervention and control groups, at 0.26% vs 0.31% — a risk difference of -0.05% (P = .68).
Similarly, the groups showed no difference in rates of any type of skin cancer, including squamous cell and basal cell carcinomas, at 2.66% in the intervention group vs 2.27% in the control group (P = .10). Rates of premalignant lesions were also comparable (6.9% vs 6.3%; P = .23).
The researchers then examined participants’ claims data to look at healthcare visits for benign skin lesions. There, app users did have a significantly higher rate, at 3.9% vs 2.6% (P < .001).
A Case of Inherent Bias?
The lack of benefit for skin cancer detection prompted the researchers to view the data from a different angle. They compared their trial participants with over 200,000 nonresponders from the health insurance plan. And that’s when a difference emerged.
Overall, trial participants were nearly three times more likely to have a skin premalignancy or malignancy diagnosed during that period, at 6.7% vs 2.4% (P < .001).
Wakkee said that because trial participants were told that the study aimed to gauge “the potential impact of this technology” in assessing skin lesions, that might have created an inherent bias. Participants assigned to the control group may have been motivated to have any worrisome skin growth checked out by their general practitioners.
In addition, Wakkee cautioned that the 12-month results are based on a small number of cancer cases, making it difficult to draw firm conclusions about the app’s performance. The trial has a second phase, where both groups were given free access to the app for 12 months, then followed for an additional 24 months.
Longer-term data are needed, Wakkee noted, in part to see whether people’s app usage changes over time.
Future Questions
Audience members at the presentation raised questions about how AI-based apps could be best deployed for skin cancer detection — including whether they might work better in the hands of clinicians rather than patients.
Wakkee said that clinicians would need a more advanced technology than that included in the app used in this trial. But future studies, she said, will look at whether the app can be used in a more targeted way, specifically, as a triage tool for people who are already concerned about something on their skin, to help them decide if they need to visit their doctor.
One presentation attendee wondered whether people given a low-risk result by the app were likely to be reassured or still make an appointment.
Wakkee said her team has begun to dig into that question. In a pilot study, 50 patients who wanted to see their general practitioner for a skin lesion were asked: If you received a low-risk rating on the skin app, would you still visit your doctor?
“Half of them said they would stay at home,” Wakkee said. She added, however, that her team is conducting a follow-up study to see what people actually do.
The trial was supported by SkinVision. The researchers declared having no relevant financial relationships.
This article was previously published by Medscape.
Wildfire Smoke Linked to Potential Risks for Some Cancers
Wildfire smoke exposure may be associated with increased risks for multiple types of cancer, suggests an analysis of prospective cohort data from over 90,000 individuals.
To determine how this widespread pollution might be affecting cancer risk, senior author Shuguang Leng, MBBS, PhD, and colleagues analyzed data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. That prospective national study enrolled approximately 154,000 participants between 1993 and 2001 and tracked cancer incidence through 2018. Of these, 91,460 participants had wildfire smoke exposure data and were included in the analysis.
During the 2006-2018 exposure period, the investigators identified incident cases of 242 ovarian, 800 colorectal, 896 bladder, 1696 hematopoietic, 1739 breast, and 1758 lung cancers, as well as 1127 melanoma cases. The median 36-month moving average for wildfire smoke PM2.5 (fine particulate matter) across the cohort was 0.37 µg/m3.
Wildfire smoke exposure was significantly associated with increased risks for lung, colorectal, breast, bladder, and hematopoietic cancer, according to the results of the study presented by Leng at American Association for Cancer Research (AACR) Annual Meeting 2026.
Each 1 µg/m3 increase in the 36-month moving average of wildfire smoke PM2.5 was associated with a 63% higher risk for hematopoietic cancer (HR, 1.63; 95% CI, 1.02-2.60), a nearly twofold higher risk for lung cancer (hazard ratio [HR], 1.92; 95% CI, 1.18-3.15), more than twofold higher risks for breast cancer (HR, 2.09; 95% CI, 1.34-3.26) and colorectal cancer (HR, 2.31; 95% CI, 1.11-4.81), and a more than threefold higher risk for bladder cancer (HR, 3.49; 95% CI, 1.66-7.34). No significant associations were observed for ovarian cancer or melanoma.
The investigators quantified wildfire smoke exposure at each participant’s residence on a monthly basis using three measures: near-ground wildfire smoke PM2.5, wildfire smoke black carbon, and satellite-derived wildfire smoke plume-day counts, with measurements available from 2006 until first cancer diagnosis or last contact.
Given evidence that 3 years of air pollution exposure can influence the development of epidermal growth factor receptor-positive lung adenocarcinoma, the team modeled exposure as a time-varying variable using 36-month moving averages preceding each month. HRs were estimated using Cox proportional hazards models stratified by study center, with restricted cubic splines applied to evaluate dose-response relationships. Models were adjusted for age, sex, race and ethnicity, education, smoking history, BMI, and trial arm.
All five cancer types linked with wildfire smoke exposure showed linear dose-response relationships, Leng noted, “which means the higher the exposure, the higher the cancer risk.”
Results based on wildfire smoke plume-day counts were generally consistent with those for PM2.5, while associations for black carbon exposure were observed only for breast and bladder cancers.
With wildfires on the rise, these findings suggest that the resulting smoke may become a “major driver for cancer burden in the US in the coming decades,” said Leng, of the University of New Mexico Comprehensive Cancer Center, Albuquerque, New Mexico.
“Wildfire smoke has become a major source of air pollution in the United States,” he continued. Large fires in the US are three times more common than they were 50 years ago, and the “tons of toxicants and particles” released by these fires “can travel hundreds of miles to affect communities far away.”
The investigators also conducted histology-specific analyses, finding that adenocarcinoma showed the strongest association with wildfire smoke among lung cancer subtypes. Among colorectal cancers, proximal tumors appeared more sensitive to wildfire smoke exposure, while among bladder cancers, the association was strongest for muscle-invasive disease.
Wildfire Smoke Exposure Expected to Rise
Under even the most conservative climate projections, wildfire smoke exposure in the US is expected to rise over the next 20-30 years, Leng said.
Annual average wildfire smoke PM2.5 levels, currently estimated at around 0.5 µg/m3, could rise to 1 µg/m3. Based on the study’s dose-response data, this would correspond to substantially greater cancer risk.
There will be “a much larger area” of the US exposed “at a much higher dose,” Leng predicted.
Mitigating the Risks of Wildfire Smoke
This is a “strong hypothesis-generating study,” Jun Wu, PhD, professor of environmental and occupational health at the UC Irvine Program in Public Health, Irvine, California, told Medscape Medical News.
“This is one of the first large, prospective US cohort studies to examine wildfire smoke specifically in relation to cancer risk, especially cancer sites beyond the lung,” Wu said. “A major strength is that the PLCO platform has around 91,000 participants with longitudinal follow-up and detailed covariate data, including smoking history, which is often a weak point in previous air pollution-cancer studies.”
According to Wu, who was not involved in the analysis but recently published data linking wildfire smoke exposure to preterm birth, the reported risks for colorectal, breast, bladder, and hematopoietic cancers represent novel contributions to the literature. However, she cautioned against viewing the specific HRs as a precise estimates of risk due to wide confidence intervals.
The findings should encourage individuals, public health officials, and clinicians to mitigate the risks of wildfire smoke, Wu said.
Specifically, she suggested that public health assessments expand beyond acute outcomes like emergency department visits to include long-term endpoints such as cancer, while community clean-air shelters need to be made more widely available.
She advised clinicians to incorporate wildfire exposure into routine patient histories and to provide vulnerable patients — such as those with asthma, chronic obstructive pulmonary disease, heart failure, or pregnancy — with smoke-season action plans.
Risk mitigation begins with awareness, according to Wu, who advised individuals check their local air quality index on AirNow.gov or PurpleAir.
On smoky days, she suggested prioritizing indoor air quality by keeping windows closed and running air purifiers. If going outside on such days is necessary, she suggested an N95 or KN95 mask, as these offer “meaningful protection,” while cloth and surgical masks do not.
These preventive steps may have once been out of the ordinary, Wu said, but the risk for wildfire smoke exposure is becoming a part of everyday life.
“The common thread is a shift in framing,” Wu said. “Wildfire smoke has traditionally been treated as an acute event, but the emerging evidence points to a chronic environmental exposure. Both our clinical and public health systems have room to grow into that reality.”
The analysis was funded by the National Institutes of Health. The investigators and Wu reported having no conflicts of interest.
This article was previously published on Medscape.
Wildfire smoke exposure may be associated with increased risks for multiple types of cancer, suggests an analysis of prospective cohort data from over 90,000 individuals.
To determine how this widespread pollution might be affecting cancer risk, senior author Shuguang Leng, MBBS, PhD, and colleagues analyzed data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. That prospective national study enrolled approximately 154,000 participants between 1993 and 2001 and tracked cancer incidence through 2018. Of these, 91,460 participants had wildfire smoke exposure data and were included in the analysis.
During the 2006-2018 exposure period, the investigators identified incident cases of 242 ovarian, 800 colorectal, 896 bladder, 1696 hematopoietic, 1739 breast, and 1758 lung cancers, as well as 1127 melanoma cases. The median 36-month moving average for wildfire smoke PM2.5 (fine particulate matter) across the cohort was 0.37 µg/m3.
Wildfire smoke exposure was significantly associated with increased risks for lung, colorectal, breast, bladder, and hematopoietic cancer, according to the results of the study presented by Leng at American Association for Cancer Research (AACR) Annual Meeting 2026.
Each 1 µg/m3 increase in the 36-month moving average of wildfire smoke PM2.5 was associated with a 63% higher risk for hematopoietic cancer (HR, 1.63; 95% CI, 1.02-2.60), a nearly twofold higher risk for lung cancer (hazard ratio [HR], 1.92; 95% CI, 1.18-3.15), more than twofold higher risks for breast cancer (HR, 2.09; 95% CI, 1.34-3.26) and colorectal cancer (HR, 2.31; 95% CI, 1.11-4.81), and a more than threefold higher risk for bladder cancer (HR, 3.49; 95% CI, 1.66-7.34). No significant associations were observed for ovarian cancer or melanoma.
The investigators quantified wildfire smoke exposure at each participant’s residence on a monthly basis using three measures: near-ground wildfire smoke PM2.5, wildfire smoke black carbon, and satellite-derived wildfire smoke plume-day counts, with measurements available from 2006 until first cancer diagnosis or last contact.
Given evidence that 3 years of air pollution exposure can influence the development of epidermal growth factor receptor-positive lung adenocarcinoma, the team modeled exposure as a time-varying variable using 36-month moving averages preceding each month. HRs were estimated using Cox proportional hazards models stratified by study center, with restricted cubic splines applied to evaluate dose-response relationships. Models were adjusted for age, sex, race and ethnicity, education, smoking history, BMI, and trial arm.
All five cancer types linked with wildfire smoke exposure showed linear dose-response relationships, Leng noted, “which means the higher the exposure, the higher the cancer risk.”
Results based on wildfire smoke plume-day counts were generally consistent with those for PM2.5, while associations for black carbon exposure were observed only for breast and bladder cancers.
With wildfires on the rise, these findings suggest that the resulting smoke may become a “major driver for cancer burden in the US in the coming decades,” said Leng, of the University of New Mexico Comprehensive Cancer Center, Albuquerque, New Mexico.
“Wildfire smoke has become a major source of air pollution in the United States,” he continued. Large fires in the US are three times more common than they were 50 years ago, and the “tons of toxicants and particles” released by these fires “can travel hundreds of miles to affect communities far away.”
The investigators also conducted histology-specific analyses, finding that adenocarcinoma showed the strongest association with wildfire smoke among lung cancer subtypes. Among colorectal cancers, proximal tumors appeared more sensitive to wildfire smoke exposure, while among bladder cancers, the association was strongest for muscle-invasive disease.
Wildfire Smoke Exposure Expected to Rise
Under even the most conservative climate projections, wildfire smoke exposure in the US is expected to rise over the next 20-30 years, Leng said.
Annual average wildfire smoke PM2.5 levels, currently estimated at around 0.5 µg/m3, could rise to 1 µg/m3. Based on the study’s dose-response data, this would correspond to substantially greater cancer risk.
There will be “a much larger area” of the US exposed “at a much higher dose,” Leng predicted.
Mitigating the Risks of Wildfire Smoke
This is a “strong hypothesis-generating study,” Jun Wu, PhD, professor of environmental and occupational health at the UC Irvine Program in Public Health, Irvine, California, told Medscape Medical News.
“This is one of the first large, prospective US cohort studies to examine wildfire smoke specifically in relation to cancer risk, especially cancer sites beyond the lung,” Wu said. “A major strength is that the PLCO platform has around 91,000 participants with longitudinal follow-up and detailed covariate data, including smoking history, which is often a weak point in previous air pollution-cancer studies.”
According to Wu, who was not involved in the analysis but recently published data linking wildfire smoke exposure to preterm birth, the reported risks for colorectal, breast, bladder, and hematopoietic cancers represent novel contributions to the literature. However, she cautioned against viewing the specific HRs as a precise estimates of risk due to wide confidence intervals.
The findings should encourage individuals, public health officials, and clinicians to mitigate the risks of wildfire smoke, Wu said.
Specifically, she suggested that public health assessments expand beyond acute outcomes like emergency department visits to include long-term endpoints such as cancer, while community clean-air shelters need to be made more widely available.
She advised clinicians to incorporate wildfire exposure into routine patient histories and to provide vulnerable patients — such as those with asthma, chronic obstructive pulmonary disease, heart failure, or pregnancy — with smoke-season action plans.
Risk mitigation begins with awareness, according to Wu, who advised individuals check their local air quality index on AirNow.gov or PurpleAir.
On smoky days, she suggested prioritizing indoor air quality by keeping windows closed and running air purifiers. If going outside on such days is necessary, she suggested an N95 or KN95 mask, as these offer “meaningful protection,” while cloth and surgical masks do not.
These preventive steps may have once been out of the ordinary, Wu said, but the risk for wildfire smoke exposure is becoming a part of everyday life.
“The common thread is a shift in framing,” Wu said. “Wildfire smoke has traditionally been treated as an acute event, but the emerging evidence points to a chronic environmental exposure. Both our clinical and public health systems have room to grow into that reality.”
The analysis was funded by the National Institutes of Health. The investigators and Wu reported having no conflicts of interest.
This article was previously published on Medscape.
Wildfire smoke exposure may be associated with increased risks for multiple types of cancer, suggests an analysis of prospective cohort data from over 90,000 individuals.
To determine how this widespread pollution might be affecting cancer risk, senior author Shuguang Leng, MBBS, PhD, and colleagues analyzed data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. That prospective national study enrolled approximately 154,000 participants between 1993 and 2001 and tracked cancer incidence through 2018. Of these, 91,460 participants had wildfire smoke exposure data and were included in the analysis.
During the 2006-2018 exposure period, the investigators identified incident cases of 242 ovarian, 800 colorectal, 896 bladder, 1696 hematopoietic, 1739 breast, and 1758 lung cancers, as well as 1127 melanoma cases. The median 36-month moving average for wildfire smoke PM2.5 (fine particulate matter) across the cohort was 0.37 µg/m3.
Wildfire smoke exposure was significantly associated with increased risks for lung, colorectal, breast, bladder, and hematopoietic cancer, according to the results of the study presented by Leng at American Association for Cancer Research (AACR) Annual Meeting 2026.
Each 1 µg/m3 increase in the 36-month moving average of wildfire smoke PM2.5 was associated with a 63% higher risk for hematopoietic cancer (HR, 1.63; 95% CI, 1.02-2.60), a nearly twofold higher risk for lung cancer (hazard ratio [HR], 1.92; 95% CI, 1.18-3.15), more than twofold higher risks for breast cancer (HR, 2.09; 95% CI, 1.34-3.26) and colorectal cancer (HR, 2.31; 95% CI, 1.11-4.81), and a more than threefold higher risk for bladder cancer (HR, 3.49; 95% CI, 1.66-7.34). No significant associations were observed for ovarian cancer or melanoma.
The investigators quantified wildfire smoke exposure at each participant’s residence on a monthly basis using three measures: near-ground wildfire smoke PM2.5, wildfire smoke black carbon, and satellite-derived wildfire smoke plume-day counts, with measurements available from 2006 until first cancer diagnosis or last contact.
Given evidence that 3 years of air pollution exposure can influence the development of epidermal growth factor receptor-positive lung adenocarcinoma, the team modeled exposure as a time-varying variable using 36-month moving averages preceding each month. HRs were estimated using Cox proportional hazards models stratified by study center, with restricted cubic splines applied to evaluate dose-response relationships. Models were adjusted for age, sex, race and ethnicity, education, smoking history, BMI, and trial arm.
All five cancer types linked with wildfire smoke exposure showed linear dose-response relationships, Leng noted, “which means the higher the exposure, the higher the cancer risk.”
Results based on wildfire smoke plume-day counts were generally consistent with those for PM2.5, while associations for black carbon exposure were observed only for breast and bladder cancers.
With wildfires on the rise, these findings suggest that the resulting smoke may become a “major driver for cancer burden in the US in the coming decades,” said Leng, of the University of New Mexico Comprehensive Cancer Center, Albuquerque, New Mexico.
“Wildfire smoke has become a major source of air pollution in the United States,” he continued. Large fires in the US are three times more common than they were 50 years ago, and the “tons of toxicants and particles” released by these fires “can travel hundreds of miles to affect communities far away.”
The investigators also conducted histology-specific analyses, finding that adenocarcinoma showed the strongest association with wildfire smoke among lung cancer subtypes. Among colorectal cancers, proximal tumors appeared more sensitive to wildfire smoke exposure, while among bladder cancers, the association was strongest for muscle-invasive disease.
Wildfire Smoke Exposure Expected to Rise
Under even the most conservative climate projections, wildfire smoke exposure in the US is expected to rise over the next 20-30 years, Leng said.
Annual average wildfire smoke PM2.5 levels, currently estimated at around 0.5 µg/m3, could rise to 1 µg/m3. Based on the study’s dose-response data, this would correspond to substantially greater cancer risk.
There will be “a much larger area” of the US exposed “at a much higher dose,” Leng predicted.
Mitigating the Risks of Wildfire Smoke
This is a “strong hypothesis-generating study,” Jun Wu, PhD, professor of environmental and occupational health at the UC Irvine Program in Public Health, Irvine, California, told Medscape Medical News.
“This is one of the first large, prospective US cohort studies to examine wildfire smoke specifically in relation to cancer risk, especially cancer sites beyond the lung,” Wu said. “A major strength is that the PLCO platform has around 91,000 participants with longitudinal follow-up and detailed covariate data, including smoking history, which is often a weak point in previous air pollution-cancer studies.”
According to Wu, who was not involved in the analysis but recently published data linking wildfire smoke exposure to preterm birth, the reported risks for colorectal, breast, bladder, and hematopoietic cancers represent novel contributions to the literature. However, she cautioned against viewing the specific HRs as a precise estimates of risk due to wide confidence intervals.
The findings should encourage individuals, public health officials, and clinicians to mitigate the risks of wildfire smoke, Wu said.
Specifically, she suggested that public health assessments expand beyond acute outcomes like emergency department visits to include long-term endpoints such as cancer, while community clean-air shelters need to be made more widely available.
She advised clinicians to incorporate wildfire exposure into routine patient histories and to provide vulnerable patients — such as those with asthma, chronic obstructive pulmonary disease, heart failure, or pregnancy — with smoke-season action plans.
Risk mitigation begins with awareness, according to Wu, who advised individuals check their local air quality index on AirNow.gov or PurpleAir.
On smoky days, she suggested prioritizing indoor air quality by keeping windows closed and running air purifiers. If going outside on such days is necessary, she suggested an N95 or KN95 mask, as these offer “meaningful protection,” while cloth and surgical masks do not.
These preventive steps may have once been out of the ordinary, Wu said, but the risk for wildfire smoke exposure is becoming a part of everyday life.
“The common thread is a shift in framing,” Wu said. “Wildfire smoke has traditionally been treated as an acute event, but the emerging evidence points to a chronic environmental exposure. Both our clinical and public health systems have room to grow into that reality.”
The analysis was funded by the National Institutes of Health. The investigators and Wu reported having no conflicts of interest.
This article was previously published on Medscape.
Many Veterans With H&N Cancer Face Access, Equity Barriers
TOPLINE: In 75,453 veterans with head and neck squamous cell carcinoma (HNSCC), 36.4% live in rural or highly rural areas and 32.0% have a national area deprivation index (ADI) ≥ 75. The average drive time to the nearest tertiary or complex US Department of Veterans Affairs (VA) facility is 94 minutes, highlighting potential access and equity barriers related to rurality, deprivation, and distance.
METHODOLOGY:
A retrospective descriptive study using nationwide VA data from fiscal years 2012 to 2022 identified 75,453 veterans with head and neck squamous cell carcinoma (HNSCC) by International Classification of Diseases, Ninth Revision and International Classification of Diseases, Tenth Revision codes.
Patients were grouped into 5 primary tumor subsites: oral cavity, oropharynx, hypopharynx, larynx, and nasopharynx.
Rurality was classified using Rural-Urban Commuting Area-derived urban, rural, and highly rural scores; socioeconomic disadvantage was measured with national ADI scores.
Travel burden was assessed using time and distance to the nearest primary, secondary, and tertiary VA facilities.
TAKEAWAY:
Oropharyngeal cancer (OPC) cases among veterans increased from 26.3% in 2012 to 46.0% in 2022, while laryngeal cancers decreased from 41.2% to 29.3%.
HNSCCs locations included 35.6% in the larynx, 34.4% in the oropharynx, 22.6% in the oral cavity 3.7% in the hypopharynx, and 3.7% in the nasopharynx.
Veterans with OPC were younger than non-OPC patients and more likely to be White; > 70% were current or former smokers.
IN PRACTICE: “Understanding the geographic and socioeconomic landscape of veterans with HNSCC will allow us to tease out the factors associated with poor outcomes and ultimately design interventions that target high-risk veteran populations to improve overall health outcomes,” the authors argued.
SOURCE: The study was led by researchers at the Veterans Affairs Pittsburgh Healthcare System. It was published online in Head & Neck.
LIMITATIONS: The inability to extract accurate data from a large dataset, challenges in obtaining tumor stage information due to varying documentation practices across physicians and treatment courses, and the inability to assess HPV or p16 data for the cohort represents significant limitations that may have impacted interpretation of results. Clinical outcome measures and cause of death assessment were limited in this national database, affecting the ability to draw conclusions regarding the impact of rurality, area deprivation, and travel time on outcomes.
DISCLOSURES: Chad Brenner reported holding several patents related to the development and use of circulating tumor DNA tests in patients with HNSCC. Jose P. Zevallos disclosed being the founder, equity shareholder, and board member of Droplet Biosciences and Echogenesis Therapeutics, serving as chief scientific advisor and shareholder of Vine Medical, and acting as a consultant for Merck and Johnson & Johnson. Matthew E. Spector reported serving as a consultant for Hologic. Kristen L. Zayan, Jennifer L. McCoy, Monique Y. Boudreaux-Kelly, Zachary Hahn, John Hotchkiss, and Jessica H. Maxwell declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: In 75,453 veterans with head and neck squamous cell carcinoma (HNSCC), 36.4% live in rural or highly rural areas and 32.0% have a national area deprivation index (ADI) ≥ 75. The average drive time to the nearest tertiary or complex US Department of Veterans Affairs (VA) facility is 94 minutes, highlighting potential access and equity barriers related to rurality, deprivation, and distance.
METHODOLOGY:
A retrospective descriptive study using nationwide VA data from fiscal years 2012 to 2022 identified 75,453 veterans with head and neck squamous cell carcinoma (HNSCC) by International Classification of Diseases, Ninth Revision and International Classification of Diseases, Tenth Revision codes.
Patients were grouped into 5 primary tumor subsites: oral cavity, oropharynx, hypopharynx, larynx, and nasopharynx.
Rurality was classified using Rural-Urban Commuting Area-derived urban, rural, and highly rural scores; socioeconomic disadvantage was measured with national ADI scores.
Travel burden was assessed using time and distance to the nearest primary, secondary, and tertiary VA facilities.
TAKEAWAY:
Oropharyngeal cancer (OPC) cases among veterans increased from 26.3% in 2012 to 46.0% in 2022, while laryngeal cancers decreased from 41.2% to 29.3%.
HNSCCs locations included 35.6% in the larynx, 34.4% in the oropharynx, 22.6% in the oral cavity 3.7% in the hypopharynx, and 3.7% in the nasopharynx.
Veterans with OPC were younger than non-OPC patients and more likely to be White; > 70% were current or former smokers.
IN PRACTICE: “Understanding the geographic and socioeconomic landscape of veterans with HNSCC will allow us to tease out the factors associated with poor outcomes and ultimately design interventions that target high-risk veteran populations to improve overall health outcomes,” the authors argued.
SOURCE: The study was led by researchers at the Veterans Affairs Pittsburgh Healthcare System. It was published online in Head & Neck.
LIMITATIONS: The inability to extract accurate data from a large dataset, challenges in obtaining tumor stage information due to varying documentation practices across physicians and treatment courses, and the inability to assess HPV or p16 data for the cohort represents significant limitations that may have impacted interpretation of results. Clinical outcome measures and cause of death assessment were limited in this national database, affecting the ability to draw conclusions regarding the impact of rurality, area deprivation, and travel time on outcomes.
DISCLOSURES: Chad Brenner reported holding several patents related to the development and use of circulating tumor DNA tests in patients with HNSCC. Jose P. Zevallos disclosed being the founder, equity shareholder, and board member of Droplet Biosciences and Echogenesis Therapeutics, serving as chief scientific advisor and shareholder of Vine Medical, and acting as a consultant for Merck and Johnson & Johnson. Matthew E. Spector reported serving as a consultant for Hologic. Kristen L. Zayan, Jennifer L. McCoy, Monique Y. Boudreaux-Kelly, Zachary Hahn, John Hotchkiss, and Jessica H. Maxwell declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: In 75,453 veterans with head and neck squamous cell carcinoma (HNSCC), 36.4% live in rural or highly rural areas and 32.0% have a national area deprivation index (ADI) ≥ 75. The average drive time to the nearest tertiary or complex US Department of Veterans Affairs (VA) facility is 94 minutes, highlighting potential access and equity barriers related to rurality, deprivation, and distance.
METHODOLOGY:
A retrospective descriptive study using nationwide VA data from fiscal years 2012 to 2022 identified 75,453 veterans with head and neck squamous cell carcinoma (HNSCC) by International Classification of Diseases, Ninth Revision and International Classification of Diseases, Tenth Revision codes.
Patients were grouped into 5 primary tumor subsites: oral cavity, oropharynx, hypopharynx, larynx, and nasopharynx.
Rurality was classified using Rural-Urban Commuting Area-derived urban, rural, and highly rural scores; socioeconomic disadvantage was measured with national ADI scores.
Travel burden was assessed using time and distance to the nearest primary, secondary, and tertiary VA facilities.
TAKEAWAY:
Oropharyngeal cancer (OPC) cases among veterans increased from 26.3% in 2012 to 46.0% in 2022, while laryngeal cancers decreased from 41.2% to 29.3%.
HNSCCs locations included 35.6% in the larynx, 34.4% in the oropharynx, 22.6% in the oral cavity 3.7% in the hypopharynx, and 3.7% in the nasopharynx.
Veterans with OPC were younger than non-OPC patients and more likely to be White; > 70% were current or former smokers.
IN PRACTICE: “Understanding the geographic and socioeconomic landscape of veterans with HNSCC will allow us to tease out the factors associated with poor outcomes and ultimately design interventions that target high-risk veteran populations to improve overall health outcomes,” the authors argued.
SOURCE: The study was led by researchers at the Veterans Affairs Pittsburgh Healthcare System. It was published online in Head & Neck.
LIMITATIONS: The inability to extract accurate data from a large dataset, challenges in obtaining tumor stage information due to varying documentation practices across physicians and treatment courses, and the inability to assess HPV or p16 data for the cohort represents significant limitations that may have impacted interpretation of results. Clinical outcome measures and cause of death assessment were limited in this national database, affecting the ability to draw conclusions regarding the impact of rurality, area deprivation, and travel time on outcomes.
DISCLOSURES: Chad Brenner reported holding several patents related to the development and use of circulating tumor DNA tests in patients with HNSCC. Jose P. Zevallos disclosed being the founder, equity shareholder, and board member of Droplet Biosciences and Echogenesis Therapeutics, serving as chief scientific advisor and shareholder of Vine Medical, and acting as a consultant for Merck and Johnson & Johnson. Matthew E. Spector reported serving as a consultant for Hologic. Kristen L. Zayan, Jennifer L. McCoy, Monique Y. Boudreaux-Kelly, Zachary Hahn, John Hotchkiss, and Jessica H. Maxwell declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.