User login
How to control weight gain when prescribing antidepressants
The prevalence of undesired weight gain in the United States has reached an all-time high, with 68.5% of adults identified as overweight (body mass index [BMI] ≥25) or obese (BMI ≥30), 34.5% considered obese, and 6.4% considered extremely obese (BMI ≥40).1 Reasons for weight gain include various physical and nutritional factors in a patient’s life, but sometimes weight gain is iatrogenic. Many medications we prescribe are associated with weight gain, including most antidepressants and atypical antipsychotics. Clinicians might minimize or overlook the risk of weight gain when prescribing antidepressants.
Patients with major depression often have associated weight loss. Regaining weight can be seen as sign of successful treatment of depressive symptoms. If weight gain after treatment exceeds the amount of weight loss attributed to depression, however, medication could have caused the excessive gain. This is considered a side effect, or iatrogenic weight gain, and should not be considered normal or clinically acceptable.
Patients who are overweight or obese when beginning antidepressant treatment might be at greater medical risk when placed on a medication that can cause additional weight gain. The time to onset of weight gain during treatment can predict weight gain patterns; those affected in the first month are most at risk of future excessive weight gain.2
In this article, we discuss:
- considerations when prescribing antidepressants
- ways to approach weight gain
- medications available to assist in weight loss.
Our general recommendations
Screen. The United States Preventive Services Task Force maintains a Class-B recommendation for screening all patients for obesity. This means that the Task Force’s review panel determined that such screening is at least moderately or substantially beneficial.3 Screening is important in a setting of potential weight gain in patients taking an antidepressant.
Educate and treat. Provide at least some education and encouragement about eating a healthy diet and exercising, or refer the patient to a nutritionist or dietician. Next, initiate psychotherapy (motivational interviewing, cognitive-behavioral therapy [CBT]) as needed. Reserve anti-obesity medications for those who do not respond to weight loss efforts or who might be taking an antidepressant for the long term.
The need for medical management of weight gain has given rise to specialists who treat this complicated, multifactorial condition. Whether psychiatrists should be seen as a substitution for their specialty is not the purpose of this review; rather, how we might more effectively (1) work on our patients’ behalf to mitigate potential weight gain from the treatments that we prescribe and (2) participate in consultations that we’ve provided on their behalf.
BMI is not an absolute marker of healthBMI likely should not be viewed as a marker with absolute prognostic certainty of overall health of an overweight or obese person: An overweight person considered healthy from a cardiovascular and metabolic perspective could still benefit from preventing further weight gain.
Tomiyama et al4 concluded that BMI itself was insufficient to stratify health in a meaningful way—and that such a focus would lead to overweight and obese people in otherwise good health being penalized unfairly through higher health insurance premiums, and would divert focus on those with less optimal health but a normal BMI. The researchers’ goal was to use blood pressure, lipid levels, and glycemic markers as surrogate markers of health, and then statistically compare results with patients’ corresponding BMI. Their findings showed that approximately one-half of people who are overweight and 29% of obese people can be considered healthy.4
Potential causes of weight gainThere may be more than one reason for weight gain during depression treatment, so a multifactorial management approach might be necessary, depending on the patient’s medication regimen. Appetite might be influenced by physical (chemical, metabolic) and psychological (cultural, familial) factors. The following sections focus on specific antidepressant classes and their proclivity for weight gain.
Serotonergic antidepressantsMany patients with depression are treated with medications that alter serotonin levels in the body, such as selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs). This neurotransmitter often is affected through depression treatment, and therefore might be a factor contributing to unintended weight gain. In mice bred to lack serotonin 5-HT2c receptors in proopiomelanocortin (POMC) neurons, the expected anorectic reaction to serotonergic agents often is reversed, causing a robust increase in hyperphagia and obesity.5 This effect indicates that 5-HT2c receptor stimulation might control appetite and feeding.
After SSRI or SNRI treatment, accumulation of serotonin over time in the synaptic cleft is thought to result in down-regulation of 5-HT2c receptors. This may cause a relative absence of 5-HT2c receptors, similar to what is seen in mice who lack them biologically. The loss of these receptors or their activity often will result in excessive weight gain. Some sedating antidepressants (mirtazapine) and some second-generation antipsychotics (SGAs) (olanzapine, quetiapine) directly block 5-HT2c receptors and might cause more rapid weight gain. Lorcaserin, a selective 5-HT2c receptor agonist, theoretically could reverse this proposed weight gain mechanism and suppress appetite by activating the POMC pathway in the hypothalamus.
Continue to: Among SSRIs and SNRIs
Among SSRIs and SNRIs, paroxetine might be one of the worst for provoking long-term weight gain; a study showed an average increase of 2.73 kg over a 4-month period.6
Theoretically, SNRIs have the ability to increase noradrenergic tone. This might be associated with nausea and a decline in appetite or it might generally curb appetite. These agents likely will cause less future weight gain. SNRIs typically induce more noradrenergic tone at increasingly higher dosages. There may be a dose-response curve in this manner. Levomilnacipran likely is the most noradrenergic of the SNRIs; recent regulatory studies suggest no statistically significant weight gain over the long term.7
Sedating antidepressants
Mirtazapine has receptor-blocking effects on noradrenergic α-2 and serotonergic 5-HT2a and 5-HT2c receptors. Additionally, histamine blocking of H1 receptors can contribute to additional weight gain, similar to what is seen with some SGAs. H1 antagonism dampens satiety response, resulting in increased caloric intake. In that case, or when specific SGAs are used for managing depression, appetite increases (H1 antagonism) and metabolism slows (possibly 5-HT2c antagonism, muscarinic receptor antagonism, etc.), thus allowing for greater adipose tissue growth and leptin insensitivity.
In a meta-analysis, mean weight increased by 1.74 kg (P < .0001) in the first 4 to 12 weeks of mirtazapine treatment, with greater variability in periods >4 months.6 Among the more novel antidepressants released since the era of tricyclic antidepressants (TCAs) or monoamine oxidase inhibitor, mirtazapine might have the greatest weight gain potential.
Trazodone and nefazodone block 5-HT2a and 5-HT2c receptors, as well as serotonin reuptake transporters. Compared with trazodone, nefazodone has a more potent effect on 5-HT2a receptor antagonism and a less potent effect on 5-HT2c receptors, and also mildly inhibits uptake of norepinephrine—meaning that this drug might have less weight gain potential. These medications are not used frequently for treating depression, but trazodone is used as an adjunctive agent for insomnia. Used even at off-label low dosages, trazodone exerts H1-histaminic and α-1 adrenergic antagonistic properties, decreasing the level of consciousness and allowing sedation and somnolence. Because of its fast onset and relatively short duration of action, it can improve depression symptoms by promoting restful sleep as well as by facilitating monoamine neurotransmission. It also might add to weight gain because of its pharmacodynamic receptor profile.
Tricyclic antidepressants
Amitriptyline can be associated with release of tumor necrosis factor-alpha, which is implicated in causing weight gain. Many TCAs block H1 (amitriptyline, imipramine, clomipramine), likely causing weight gain. Most TCAs antagonize muscarinic receptors as well. The more noradrenergic TCAs could curb appetite (nortriptyline, desipramine, protriptyline) similar to SNRIs, therefore countering some of the weight gain drive.
As an example, in a meta-analysis examining weight gain with antidepressants, amitriptyline was associated with weight gain of 1.52 kg above baseline in the acute period (4 to 12 weeks) and 2.24 kg above baseline at 4 to 7 months.6 These results of the acute phase should be viewed cautiously because the authors reported high heterogeneity among these studies, and the possibility of publication bias (Egger test, P < .0001). In the same meta-analysis, the even the more noradrenergic nortriptyline was associated with an increase of 2.0 kg on average over baseline during acute treatment, with that number dropping to 1.24 kg over baseline at ≥4 months.6
Newer antidepressants
Vilazodone is a weak SSRI that aggressively partially agonizes pre-synaptic and post-synaptic 5-HT1a receptors in the CNS. This dual site 5-HT1a action is somewhat unique among antidepressants. This type of agent sometimes is called multimodal,8 or could be considered an “SSRI +” antidepressant. These drugs are SSRIs at the core but have additional 5-HT receptor modulating capabilities. Vilazodone has a favorable weight gain profile, as suggested in a 52-week trial reporting 1.7 kg gain over 52 weeks, compared with an average of 6.8 to 10 kg for long-term SSRI therapy.9
Vortioxetine is a stronger SSRI that also partially agonizes presynaptic 5-HT1a receptors. In addition, it antagonizes 5-HT1d, 5-HT3, and 5-HT7 receptors, giving it a unique pharmacodynamic profile.10 Vortioxetine also had minimal impact on drug-induced weight gain in 52-week studies, with data from 2 trials indicating either minimal weight gain in 6.1% of patients (mean increase of 0.41 kg over 52 weeks)11 or gain that was not statistically significant.12
Levomilnacipran is unique in that it has the most aggressive norepinephrine reuptake inhibition of all SNRIs.13 Again, increased noradrenergic tone might curb appetite and caloric intake. Many SNRIs cause low-grade nausea, which could account for decreased appetite. Long-term, 52-week data for this drug also shows minimal proclivity for weight gain, with the trial participants reporting a slight decrease of 4.34 kg on average from baseline.14
Continue to: Addressing weight gain
Addressing weight gain
Lifestyle modification. Eating smaller portions, combined with restricting foods high in calories and fat, should be the first step. A simple suggestion to a patient to eat the same foods, but remove 20% of the portion, is a simple intervention akin to that of suggesting sleep hygiene practices for insomnia management. Under medical supervision or with referral to a dietician or nutritionist, more rigid caloric restrictions could be employed.
Commercial weight-loss programs, such as Weight Watchers or Curves, can be helpful; some insurers will only cover medications for weight loss if one of these programs have been tried or is used in combination with medication. Some patients might ask about extreme weight-loss measures, such as low-calorie diets combined with intense exercise programs that have been popularized in the media. Although the motivation to initiate and maintain meaningful weight loss should be encouraged, doing so in a more gradual manner should be the goal.
Addressing portion size is a good approach in the early stages of managing obesity. Restaurants often serve portions that have more calories than should be consumed in one meal. Visual cues can influence this trend; using smaller plates can help reduce caloric intake.15
Exercise, sustained for at least 45 minutes, can have long-lasting effects, with a small study showing an increase in metabolic rate of 190 ± 71.4 kcal (P < .001) above baseline for 14 hours after exercise.16 Endurance exercise training is associated with a significant decrease in total cholesterol, triglycerides, and low-density lipoprotein cholesterol, as well as an increase in the high-density lipoprotein level over a 24-week period.17
Encouraging an exercise regimen that is appropriate for your patient can help maintain weight loss. In small trials,18,19 high-intensity exercise was shown to help suppress appetite and decrease 24-hour caloric consumption by 6% to 11%.18
Psychotherapy can become an important intervention for initiating and maintaining weight loss. CBT can help patients recognize and modify lifestyle components, and reinforce behaviors that promote weight loss. This can come from setting realistic weight loss goals; preventing triggering factors that lead to overeating; encouraging portion control during meals; and promoting exercise habits.
In a small, randomized controlled trial (RCT) examining weight loss in obese women, those who underwent CBT and psychoeducation for 2 hours a week for 10 weeks in addition to dietary changes and exercise showed an average weight loss of 10.4 kg at 18-month follow-up, compared with weight gain of 2.3 kg in the control group.20 The short duration of treatment in this study might be desirable to reduce cost and utilization of services. Group formats also could be employed.
Motivational interviewing is a useful tool in addiction psychiatry and shows promise for treating obesity and overeating as well. The approach may differ slightly because weight-loss therapy involves behavior modification rather than behavior cessation. In a meta-analysis of data from RCTs exploring motivational interviewing and its use as an intervention for weight loss, those in the intervention groups experienced significant weight loss as indicated by BMI decreasing a standardized mean difference of −0.51, compared with control groups.21
Medical management considerations
Diagnostics. Recognition and early intervention are instrumental in successfully treating medication-associated weight gain. It is important to obtain any family history of obesity, diabetes, hypertension, and hyperlipidemia. This will likely indicate a patient’s risk for weight gain before initiating medication.
Obtain vital signs at every visit, including blood pressure. Monitoring weight at every clinical visit can be used to calculate and monitor BMI, while also asking the patient to maintain a log of weight measurements obtained at home. Measuring abdominal girth is important to watch for metabolic syndrome, although often this is the least measured variable.
Laboratory testing is helpful. Obtaining a baseline lipid panel and a fasting glucose level (consider measuring hemoglobin A1c in patients with diabetes) is warranted. Including thyroid markers, such as thyroid-stimulating hormone and thyroxine (free T4), might be important considerations, because inadequate management of hypothyroidism can complicate the clinical picture.
Follow-up testing should be ordered every 3 to 12 months to monitor progress if your patient is showing signs of rapid weight gain, or if BMI nears ≥30 kg/m². These guidelines generally are assigned for prescribing of SGAs, but can be applied when using any psychotropic with weight gain potential.
Medications to considerWhen considering the medication regimen as an intervention point, consider changing the antidepressant to one that is not associated with significant weight gain. Although not specifically indicated as a monotherapy for weight loss, switching to or augmenting therapy with bupropion could aid weight loss through appetite suppression.20 Some newer antidepressants, such as vilazodone, vortioxetine, and levomilnacipran, might have less propensity to cause weight gain. In patients with severe depression, augmenting with medications containing amphetamine or methylphenidate could cause some weight loss, but greater care should be taken because of cardiovascular effects and dependency issues.
Continue to: Discussing with your patient...
Discussing with your patient the possibility of changing or worsening depressive symptoms when adding or switching medications allows them to be aware and engaged in the process and can encourage them to notice and report changes. Developing a sensible schedule to taper an existing medication slowly over several weeks and allowing a new one to build up gradually to a therapeutic level can help minimize adverse effects or a discontinuation syndrome.
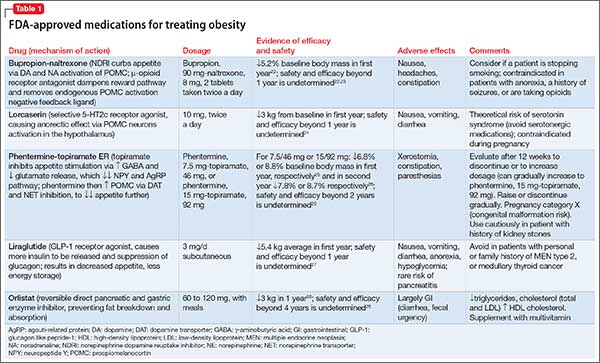
If switching antidepressants is not possible, or is ineffective, an anti-obesity medication (Table 122-29) can be considered. These medications should not be considered first-line in weight loss management, but reserved for more difficult or refractory weight loss challenges and in patients who are not able to participate in weight loss or dieting programs because of cognitive disorders, a history of nonadherance, financial or travel limitations, or in those with poor social support systems such as homelessness.
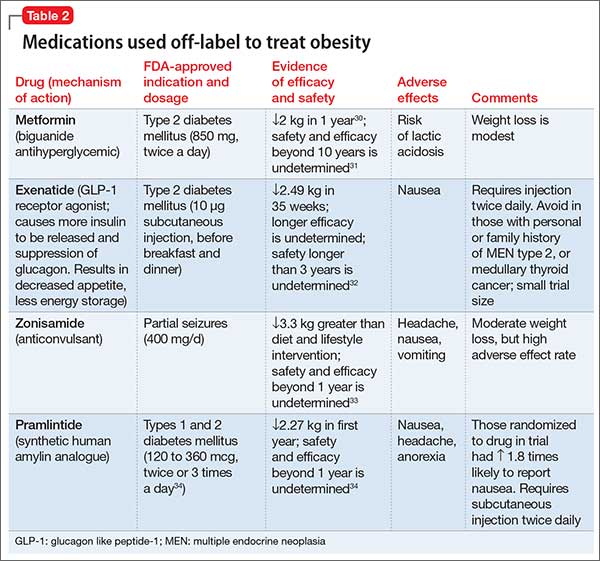
Some of these medications are not reimbursed by insurance companies; therefore, consider the financial burden to the patient and their capacity for adherence to therapy, and discuss this challenge before initiating treatment. There is some evidence for using medications off-label to treat obesity (Table 2,30-34).
Anti-obesity medications typically are considered for patients with a BMI >30 or in any overweight patient with diabetes, hyperlipidemia, or cardiovascular disease. As always, discuss with patients and their primary care provider the potential benefits and risks of adding any of these or other medications to an existing treatment regimen.
If weight loss goals are not met, consider discontinuing anti-obesity therapy. Patients and physicians should be cognizant of the need to continue long-term maintenance on these medications after successful treatment—perhaps indefinitely, because patients frequently regain weight after medication is discontinued.
Bottom Line
Many antidepressants are known to increase the risk of excessive weight gain, although risk of weigh gain varies among antidepressant classes. First, advise changes in diet and exercise; next, initiate psychotherapy as indicated, and then consider referral to a nutritionist. Consider switching to an antidepressant with less potential for causing weight gain or adding bupropion, which could lead to weight loss, if your patient can tolerate it. If these strategies are unsuccessful, consider an anti-obesity medication.
Related Resource
1. Ogden CL, Carroll MD, Kit BK, et al. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806-814.
2. Vandenberghe F, Gholam-Rezaee M, Saigí-Morgui N, et al. Importance of early weight changes to predict long-term weight gain during psychotropic drug treatment. J Clin Psychiatry. 2015;76(11):e1417-e1423.
3. Grade Definitions. Electronic Preventive Services Selector (ePSS). http://epss.ahrq.gov/ePSS/gradedef.jsp. Accessed May 2, 2016.
4. Tomiyama AJ, Hunger JM, Nguyen-Cuu J, et al. Misclassification of cardiometabolic health when using body mass index categories in NHANES 2005-2012 [published online February 4, 2016]. Int J Obes (Lond). doi: 10.1038/ijo.2016.17.
5. Berglund ED, Liu C, Sohn J, et al. Serotonin 2C receptors in pro-opiomelanocortin neurons regulate energy and glucose homeostasis. J Clin Invest. 2013;123(12):5061-5070.
6. Serretti A, Mandelli L. Antidepressants and body weight: a comprehensive review and meta-anaylsis. J Clin Psychiatry. 2010;71(10):1259-1272.
7. Mago R, Forero G, Greenberg WM, et al. Safety and tolerability of levomilnacipran ER in major depressive disorder: results from an open-label, 48-week extension study. Clin Drug Investig. 2013;33(10):761-771.
8. Schwartz TL, Siddiqui UA, Stahl SM. Vilazodone: a brief pharmacological and clinical review of the novel serotonin partial agonist and reuptake inhibitor. Ther Adv Psychopharmacol. 2011;1(3):81-87.
9. Robinson DS, Kajdasz DK, Gallipoli S, et al. A 1-year, open-label study assessing the safety and tolerability of vilazodone in patients with major depressive disorder. J Clin Psychopharmacol. 2011;31(5):643-646.
10. Stahl SM. Modes and nodes explain the mechanism of action of vortioxetine, a multimodal agent (MMA): actions at serotonin receptors may enhance downstream release of four pro-cognitive neurotransmitters. CNS Spectr. 2015;20(6):515-519.
11. Jacobsen PL, Harper L, Chrones L, et al. Safety and tolerability of vortioxetine (15 and 20 mg) in patients with major depressive disorder: results of an open-label, flexible-dose, 52-week extension study. Int Clin Psychopharmacol. 2015;30(5):255-264.
12. Boulenger JP, Loft H, Olsen CK. Efficacy and safety of vortioxetine (Lu AA21004), 15 and 20 mg/day: a randomized, double-blind, placebo-controlled, duloxetine-referenced study in the acute treatment of adult patients with major depressive disorder. Int Clin Psychopharmacol. 2014;29(3):138-149.
13. Grady MM, Stahl SM. Novel agents in development for the treatment of depression. CNS Spectr. 2013;18(suppl 1):37-40; quiz 41.
14. Mago R, Forero G, Greenberg WM, et al. Safety and tolerability of levomilnacipran ER in major depressive disorder: results from an open-label, 48-week extension study. Clin Drug Investig. 2013;33(10):761-771.
15. Hollands GJ, Shemilt I, Marteau TM, et al. Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco. Cochrane Database Syst Rev. 2015;9:CD011045.
16. Knab AM, Shanely RA, Corbin KD, et al. A 45-minute vigorous exercise bout increases metabolic rate for 14 hours. Med Sci Sports Exerc. 2011;43(9):1643-1648.
17. Halverstadt A, Phares DA, Wilund KR, et al. Endurance exercise training raises high-density lipoprotein cholesterol and lowers small low-density lipoprotein and very low-density lipoprotein independent of body fat phenotypes in older men and women. Metabolism. 2007;56(4):444-450.
18. Thivel D, Isacco L, Montaurier C, et al. The 24-h energy intake of obese adolescents is spontaneously reduced after intensive exercise: a randomized controlled trial in calorimetric chambers [published online January 17, 2012]. PLoS One. 2012;7(1):e29840. doi: 10.1371/journal.pone.0029840.
19. Sim AY, Wallman KE, Fairchild TJ, et al. High-intensity intermittent exercise attenuates ad-libitum energy intake. Int J Obes (Lond). 2014;38(3):417-422.
20. Stahre L, Tärnell B, Håkanson CE, et al. A randomized controlled trial of two weight-reducing short-term group treatment programs for obesity with an 18-month follow-up. Int J Behav Med. 2007;14(1):48-55.
21. Armstrong MJ, Mottershead TA, Ronksley PE, et al. Motivational interviewing to improve weight loss in overweight and/or obese patients: a systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2011;12(9):709-723.
22. Apovian CM, Aronne L, Rubino D, et al. A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity (Silver Springs). 2013;21(5):935-943.
23. Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595-605.
24. Fidler MC, Sanchez M, Raether B, et al; BLOSSOM Clinical Trial Group. A one-year randomized trial of lorcaserin for weight loss in obese and overweight adults: the BLOSSOM trial. J Clin Endocrinol Metab. 2011;96(10):3067-3077.
25. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial [Erratum in Lancet. 2011;377(9776):1494]. Lancet. 2011;377(9774):1341-1352.
26. Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297-308.
27. Pi-Sunyer X, Astrup A, Fujioka K, et al; SCALE Obesity and Prediabetes NN8022-1839 Study Group. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11-22.
28. Leblanc ES, O’Connor E, Whitlock EP, et al. Effectiveness of primary care-relevant treatments for obesity in adults: a systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2011;155(7):434-447.
29. Torgerson JS, Hauptman J, Boldrin MN, et al. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155-161.
30. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393-403.
31. McDonagh MS, Selph S, Ozpinar A, et al. Systematic review of the benefits and risks of metformin in treating obesity in children aged 18 years and younger. JAMA Pediatr. 2014;168(2):178-184.
32. Dushay J, Gao C, Gopalakrishnan GS, et al. Short-term exenatide treatment leads to significant weight loss in a subset of obese women without diabetes. Diabetes Care. 2012;35(1):4-11.
33. Gadde KM, Kopping MF, Wagner HR 2nd, et al. Zonisamide for weight reduction in obese adults: a 1-year randomized controlled trial. Arch Intern Med. 2012;172(20):1557-1564.
34. Singh-Franco D, Perez A, Harrington C. The effect of pramlintide acetate on glycemic control and weight in patients with type 2 diabetes mellitus and in obese patients without diabetes: a systematic review and meta-analysis. Diabetes Obes Metab. 2011;13(2):169-180.
The prevalence of undesired weight gain in the United States has reached an all-time high, with 68.5% of adults identified as overweight (body mass index [BMI] ≥25) or obese (BMI ≥30), 34.5% considered obese, and 6.4% considered extremely obese (BMI ≥40).1 Reasons for weight gain include various physical and nutritional factors in a patient’s life, but sometimes weight gain is iatrogenic. Many medications we prescribe are associated with weight gain, including most antidepressants and atypical antipsychotics. Clinicians might minimize or overlook the risk of weight gain when prescribing antidepressants.
Patients with major depression often have associated weight loss. Regaining weight can be seen as sign of successful treatment of depressive symptoms. If weight gain after treatment exceeds the amount of weight loss attributed to depression, however, medication could have caused the excessive gain. This is considered a side effect, or iatrogenic weight gain, and should not be considered normal or clinically acceptable.
Patients who are overweight or obese when beginning antidepressant treatment might be at greater medical risk when placed on a medication that can cause additional weight gain. The time to onset of weight gain during treatment can predict weight gain patterns; those affected in the first month are most at risk of future excessive weight gain.2
In this article, we discuss:
- considerations when prescribing antidepressants
- ways to approach weight gain
- medications available to assist in weight loss.
Our general recommendations
Screen. The United States Preventive Services Task Force maintains a Class-B recommendation for screening all patients for obesity. This means that the Task Force’s review panel determined that such screening is at least moderately or substantially beneficial.3 Screening is important in a setting of potential weight gain in patients taking an antidepressant.
Educate and treat. Provide at least some education and encouragement about eating a healthy diet and exercising, or refer the patient to a nutritionist or dietician. Next, initiate psychotherapy (motivational interviewing, cognitive-behavioral therapy [CBT]) as needed. Reserve anti-obesity medications for those who do not respond to weight loss efforts or who might be taking an antidepressant for the long term.
The need for medical management of weight gain has given rise to specialists who treat this complicated, multifactorial condition. Whether psychiatrists should be seen as a substitution for their specialty is not the purpose of this review; rather, how we might more effectively (1) work on our patients’ behalf to mitigate potential weight gain from the treatments that we prescribe and (2) participate in consultations that we’ve provided on their behalf.
BMI is not an absolute marker of healthBMI likely should not be viewed as a marker with absolute prognostic certainty of overall health of an overweight or obese person: An overweight person considered healthy from a cardiovascular and metabolic perspective could still benefit from preventing further weight gain.
Tomiyama et al4 concluded that BMI itself was insufficient to stratify health in a meaningful way—and that such a focus would lead to overweight and obese people in otherwise good health being penalized unfairly through higher health insurance premiums, and would divert focus on those with less optimal health but a normal BMI. The researchers’ goal was to use blood pressure, lipid levels, and glycemic markers as surrogate markers of health, and then statistically compare results with patients’ corresponding BMI. Their findings showed that approximately one-half of people who are overweight and 29% of obese people can be considered healthy.4
Potential causes of weight gainThere may be more than one reason for weight gain during depression treatment, so a multifactorial management approach might be necessary, depending on the patient’s medication regimen. Appetite might be influenced by physical (chemical, metabolic) and psychological (cultural, familial) factors. The following sections focus on specific antidepressant classes and their proclivity for weight gain.
Serotonergic antidepressantsMany patients with depression are treated with medications that alter serotonin levels in the body, such as selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs). This neurotransmitter often is affected through depression treatment, and therefore might be a factor contributing to unintended weight gain. In mice bred to lack serotonin 5-HT2c receptors in proopiomelanocortin (POMC) neurons, the expected anorectic reaction to serotonergic agents often is reversed, causing a robust increase in hyperphagia and obesity.5 This effect indicates that 5-HT2c receptor stimulation might control appetite and feeding.
After SSRI or SNRI treatment, accumulation of serotonin over time in the synaptic cleft is thought to result in down-regulation of 5-HT2c receptors. This may cause a relative absence of 5-HT2c receptors, similar to what is seen in mice who lack them biologically. The loss of these receptors or their activity often will result in excessive weight gain. Some sedating antidepressants (mirtazapine) and some second-generation antipsychotics (SGAs) (olanzapine, quetiapine) directly block 5-HT2c receptors and might cause more rapid weight gain. Lorcaserin, a selective 5-HT2c receptor agonist, theoretically could reverse this proposed weight gain mechanism and suppress appetite by activating the POMC pathway in the hypothalamus.
Continue to: Among SSRIs and SNRIs
Among SSRIs and SNRIs, paroxetine might be one of the worst for provoking long-term weight gain; a study showed an average increase of 2.73 kg over a 4-month period.6
Theoretically, SNRIs have the ability to increase noradrenergic tone. This might be associated with nausea and a decline in appetite or it might generally curb appetite. These agents likely will cause less future weight gain. SNRIs typically induce more noradrenergic tone at increasingly higher dosages. There may be a dose-response curve in this manner. Levomilnacipran likely is the most noradrenergic of the SNRIs; recent regulatory studies suggest no statistically significant weight gain over the long term.7
Sedating antidepressants
Mirtazapine has receptor-blocking effects on noradrenergic α-2 and serotonergic 5-HT2a and 5-HT2c receptors. Additionally, histamine blocking of H1 receptors can contribute to additional weight gain, similar to what is seen with some SGAs. H1 antagonism dampens satiety response, resulting in increased caloric intake. In that case, or when specific SGAs are used for managing depression, appetite increases (H1 antagonism) and metabolism slows (possibly 5-HT2c antagonism, muscarinic receptor antagonism, etc.), thus allowing for greater adipose tissue growth and leptin insensitivity.
In a meta-analysis, mean weight increased by 1.74 kg (P < .0001) in the first 4 to 12 weeks of mirtazapine treatment, with greater variability in periods >4 months.6 Among the more novel antidepressants released since the era of tricyclic antidepressants (TCAs) or monoamine oxidase inhibitor, mirtazapine might have the greatest weight gain potential.
Trazodone and nefazodone block 5-HT2a and 5-HT2c receptors, as well as serotonin reuptake transporters. Compared with trazodone, nefazodone has a more potent effect on 5-HT2a receptor antagonism and a less potent effect on 5-HT2c receptors, and also mildly inhibits uptake of norepinephrine—meaning that this drug might have less weight gain potential. These medications are not used frequently for treating depression, but trazodone is used as an adjunctive agent for insomnia. Used even at off-label low dosages, trazodone exerts H1-histaminic and α-1 adrenergic antagonistic properties, decreasing the level of consciousness and allowing sedation and somnolence. Because of its fast onset and relatively short duration of action, it can improve depression symptoms by promoting restful sleep as well as by facilitating monoamine neurotransmission. It also might add to weight gain because of its pharmacodynamic receptor profile.
Tricyclic antidepressants
Amitriptyline can be associated with release of tumor necrosis factor-alpha, which is implicated in causing weight gain. Many TCAs block H1 (amitriptyline, imipramine, clomipramine), likely causing weight gain. Most TCAs antagonize muscarinic receptors as well. The more noradrenergic TCAs could curb appetite (nortriptyline, desipramine, protriptyline) similar to SNRIs, therefore countering some of the weight gain drive.
As an example, in a meta-analysis examining weight gain with antidepressants, amitriptyline was associated with weight gain of 1.52 kg above baseline in the acute period (4 to 12 weeks) and 2.24 kg above baseline at 4 to 7 months.6 These results of the acute phase should be viewed cautiously because the authors reported high heterogeneity among these studies, and the possibility of publication bias (Egger test, P < .0001). In the same meta-analysis, the even the more noradrenergic nortriptyline was associated with an increase of 2.0 kg on average over baseline during acute treatment, with that number dropping to 1.24 kg over baseline at ≥4 months.6
Newer antidepressants
Vilazodone is a weak SSRI that aggressively partially agonizes pre-synaptic and post-synaptic 5-HT1a receptors in the CNS. This dual site 5-HT1a action is somewhat unique among antidepressants. This type of agent sometimes is called multimodal,8 or could be considered an “SSRI +” antidepressant. These drugs are SSRIs at the core but have additional 5-HT receptor modulating capabilities. Vilazodone has a favorable weight gain profile, as suggested in a 52-week trial reporting 1.7 kg gain over 52 weeks, compared with an average of 6.8 to 10 kg for long-term SSRI therapy.9
Vortioxetine is a stronger SSRI that also partially agonizes presynaptic 5-HT1a receptors. In addition, it antagonizes 5-HT1d, 5-HT3, and 5-HT7 receptors, giving it a unique pharmacodynamic profile.10 Vortioxetine also had minimal impact on drug-induced weight gain in 52-week studies, with data from 2 trials indicating either minimal weight gain in 6.1% of patients (mean increase of 0.41 kg over 52 weeks)11 or gain that was not statistically significant.12
Levomilnacipran is unique in that it has the most aggressive norepinephrine reuptake inhibition of all SNRIs.13 Again, increased noradrenergic tone might curb appetite and caloric intake. Many SNRIs cause low-grade nausea, which could account for decreased appetite. Long-term, 52-week data for this drug also shows minimal proclivity for weight gain, with the trial participants reporting a slight decrease of 4.34 kg on average from baseline.14
Continue to: Addressing weight gain
Addressing weight gain
Lifestyle modification. Eating smaller portions, combined with restricting foods high in calories and fat, should be the first step. A simple suggestion to a patient to eat the same foods, but remove 20% of the portion, is a simple intervention akin to that of suggesting sleep hygiene practices for insomnia management. Under medical supervision or with referral to a dietician or nutritionist, more rigid caloric restrictions could be employed.
Commercial weight-loss programs, such as Weight Watchers or Curves, can be helpful; some insurers will only cover medications for weight loss if one of these programs have been tried or is used in combination with medication. Some patients might ask about extreme weight-loss measures, such as low-calorie diets combined with intense exercise programs that have been popularized in the media. Although the motivation to initiate and maintain meaningful weight loss should be encouraged, doing so in a more gradual manner should be the goal.
Addressing portion size is a good approach in the early stages of managing obesity. Restaurants often serve portions that have more calories than should be consumed in one meal. Visual cues can influence this trend; using smaller plates can help reduce caloric intake.15
Exercise, sustained for at least 45 minutes, can have long-lasting effects, with a small study showing an increase in metabolic rate of 190 ± 71.4 kcal (P < .001) above baseline for 14 hours after exercise.16 Endurance exercise training is associated with a significant decrease in total cholesterol, triglycerides, and low-density lipoprotein cholesterol, as well as an increase in the high-density lipoprotein level over a 24-week period.17
Encouraging an exercise regimen that is appropriate for your patient can help maintain weight loss. In small trials,18,19 high-intensity exercise was shown to help suppress appetite and decrease 24-hour caloric consumption by 6% to 11%.18
Psychotherapy can become an important intervention for initiating and maintaining weight loss. CBT can help patients recognize and modify lifestyle components, and reinforce behaviors that promote weight loss. This can come from setting realistic weight loss goals; preventing triggering factors that lead to overeating; encouraging portion control during meals; and promoting exercise habits.
In a small, randomized controlled trial (RCT) examining weight loss in obese women, those who underwent CBT and psychoeducation for 2 hours a week for 10 weeks in addition to dietary changes and exercise showed an average weight loss of 10.4 kg at 18-month follow-up, compared with weight gain of 2.3 kg in the control group.20 The short duration of treatment in this study might be desirable to reduce cost and utilization of services. Group formats also could be employed.
Motivational interviewing is a useful tool in addiction psychiatry and shows promise for treating obesity and overeating as well. The approach may differ slightly because weight-loss therapy involves behavior modification rather than behavior cessation. In a meta-analysis of data from RCTs exploring motivational interviewing and its use as an intervention for weight loss, those in the intervention groups experienced significant weight loss as indicated by BMI decreasing a standardized mean difference of −0.51, compared with control groups.21
Medical management considerations
Diagnostics. Recognition and early intervention are instrumental in successfully treating medication-associated weight gain. It is important to obtain any family history of obesity, diabetes, hypertension, and hyperlipidemia. This will likely indicate a patient’s risk for weight gain before initiating medication.
Obtain vital signs at every visit, including blood pressure. Monitoring weight at every clinical visit can be used to calculate and monitor BMI, while also asking the patient to maintain a log of weight measurements obtained at home. Measuring abdominal girth is important to watch for metabolic syndrome, although often this is the least measured variable.
Laboratory testing is helpful. Obtaining a baseline lipid panel and a fasting glucose level (consider measuring hemoglobin A1c in patients with diabetes) is warranted. Including thyroid markers, such as thyroid-stimulating hormone and thyroxine (free T4), might be important considerations, because inadequate management of hypothyroidism can complicate the clinical picture.
Follow-up testing should be ordered every 3 to 12 months to monitor progress if your patient is showing signs of rapid weight gain, or if BMI nears ≥30 kg/m². These guidelines generally are assigned for prescribing of SGAs, but can be applied when using any psychotropic with weight gain potential.
Medications to considerWhen considering the medication regimen as an intervention point, consider changing the antidepressant to one that is not associated with significant weight gain. Although not specifically indicated as a monotherapy for weight loss, switching to or augmenting therapy with bupropion could aid weight loss through appetite suppression.20 Some newer antidepressants, such as vilazodone, vortioxetine, and levomilnacipran, might have less propensity to cause weight gain. In patients with severe depression, augmenting with medications containing amphetamine or methylphenidate could cause some weight loss, but greater care should be taken because of cardiovascular effects and dependency issues.
Continue to: Discussing with your patient...
Discussing with your patient the possibility of changing or worsening depressive symptoms when adding or switching medications allows them to be aware and engaged in the process and can encourage them to notice and report changes. Developing a sensible schedule to taper an existing medication slowly over several weeks and allowing a new one to build up gradually to a therapeutic level can help minimize adverse effects or a discontinuation syndrome.
If switching antidepressants is not possible, or is ineffective, an anti-obesity medication (Table 122-29) can be considered. These medications should not be considered first-line in weight loss management, but reserved for more difficult or refractory weight loss challenges and in patients who are not able to participate in weight loss or dieting programs because of cognitive disorders, a history of nonadherance, financial or travel limitations, or in those with poor social support systems such as homelessness.
Some of these medications are not reimbursed by insurance companies; therefore, consider the financial burden to the patient and their capacity for adherence to therapy, and discuss this challenge before initiating treatment. There is some evidence for using medications off-label to treat obesity (Table 2,30-34).
Anti-obesity medications typically are considered for patients with a BMI >30 or in any overweight patient with diabetes, hyperlipidemia, or cardiovascular disease. As always, discuss with patients and their primary care provider the potential benefits and risks of adding any of these or other medications to an existing treatment regimen.
If weight loss goals are not met, consider discontinuing anti-obesity therapy. Patients and physicians should be cognizant of the need to continue long-term maintenance on these medications after successful treatment—perhaps indefinitely, because patients frequently regain weight after medication is discontinued.
Bottom Line
Many antidepressants are known to increase the risk of excessive weight gain, although risk of weigh gain varies among antidepressant classes. First, advise changes in diet and exercise; next, initiate psychotherapy as indicated, and then consider referral to a nutritionist. Consider switching to an antidepressant with less potential for causing weight gain or adding bupropion, which could lead to weight loss, if your patient can tolerate it. If these strategies are unsuccessful, consider an anti-obesity medication.
Related Resource
The prevalence of undesired weight gain in the United States has reached an all-time high, with 68.5% of adults identified as overweight (body mass index [BMI] ≥25) or obese (BMI ≥30), 34.5% considered obese, and 6.4% considered extremely obese (BMI ≥40).1 Reasons for weight gain include various physical and nutritional factors in a patient’s life, but sometimes weight gain is iatrogenic. Many medications we prescribe are associated with weight gain, including most antidepressants and atypical antipsychotics. Clinicians might minimize or overlook the risk of weight gain when prescribing antidepressants.
Patients with major depression often have associated weight loss. Regaining weight can be seen as sign of successful treatment of depressive symptoms. If weight gain after treatment exceeds the amount of weight loss attributed to depression, however, medication could have caused the excessive gain. This is considered a side effect, or iatrogenic weight gain, and should not be considered normal or clinically acceptable.
Patients who are overweight or obese when beginning antidepressant treatment might be at greater medical risk when placed on a medication that can cause additional weight gain. The time to onset of weight gain during treatment can predict weight gain patterns; those affected in the first month are most at risk of future excessive weight gain.2
In this article, we discuss:
- considerations when prescribing antidepressants
- ways to approach weight gain
- medications available to assist in weight loss.
Our general recommendations
Screen. The United States Preventive Services Task Force maintains a Class-B recommendation for screening all patients for obesity. This means that the Task Force’s review panel determined that such screening is at least moderately or substantially beneficial.3 Screening is important in a setting of potential weight gain in patients taking an antidepressant.
Educate and treat. Provide at least some education and encouragement about eating a healthy diet and exercising, or refer the patient to a nutritionist or dietician. Next, initiate psychotherapy (motivational interviewing, cognitive-behavioral therapy [CBT]) as needed. Reserve anti-obesity medications for those who do not respond to weight loss efforts or who might be taking an antidepressant for the long term.
The need for medical management of weight gain has given rise to specialists who treat this complicated, multifactorial condition. Whether psychiatrists should be seen as a substitution for their specialty is not the purpose of this review; rather, how we might more effectively (1) work on our patients’ behalf to mitigate potential weight gain from the treatments that we prescribe and (2) participate in consultations that we’ve provided on their behalf.
BMI is not an absolute marker of healthBMI likely should not be viewed as a marker with absolute prognostic certainty of overall health of an overweight or obese person: An overweight person considered healthy from a cardiovascular and metabolic perspective could still benefit from preventing further weight gain.
Tomiyama et al4 concluded that BMI itself was insufficient to stratify health in a meaningful way—and that such a focus would lead to overweight and obese people in otherwise good health being penalized unfairly through higher health insurance premiums, and would divert focus on those with less optimal health but a normal BMI. The researchers’ goal was to use blood pressure, lipid levels, and glycemic markers as surrogate markers of health, and then statistically compare results with patients’ corresponding BMI. Their findings showed that approximately one-half of people who are overweight and 29% of obese people can be considered healthy.4
Potential causes of weight gainThere may be more than one reason for weight gain during depression treatment, so a multifactorial management approach might be necessary, depending on the patient’s medication regimen. Appetite might be influenced by physical (chemical, metabolic) and psychological (cultural, familial) factors. The following sections focus on specific antidepressant classes and their proclivity for weight gain.
Serotonergic antidepressantsMany patients with depression are treated with medications that alter serotonin levels in the body, such as selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs). This neurotransmitter often is affected through depression treatment, and therefore might be a factor contributing to unintended weight gain. In mice bred to lack serotonin 5-HT2c receptors in proopiomelanocortin (POMC) neurons, the expected anorectic reaction to serotonergic agents often is reversed, causing a robust increase in hyperphagia and obesity.5 This effect indicates that 5-HT2c receptor stimulation might control appetite and feeding.
After SSRI or SNRI treatment, accumulation of serotonin over time in the synaptic cleft is thought to result in down-regulation of 5-HT2c receptors. This may cause a relative absence of 5-HT2c receptors, similar to what is seen in mice who lack them biologically. The loss of these receptors or their activity often will result in excessive weight gain. Some sedating antidepressants (mirtazapine) and some second-generation antipsychotics (SGAs) (olanzapine, quetiapine) directly block 5-HT2c receptors and might cause more rapid weight gain. Lorcaserin, a selective 5-HT2c receptor agonist, theoretically could reverse this proposed weight gain mechanism and suppress appetite by activating the POMC pathway in the hypothalamus.
Continue to: Among SSRIs and SNRIs
Among SSRIs and SNRIs, paroxetine might be one of the worst for provoking long-term weight gain; a study showed an average increase of 2.73 kg over a 4-month period.6
Theoretically, SNRIs have the ability to increase noradrenergic tone. This might be associated with nausea and a decline in appetite or it might generally curb appetite. These agents likely will cause less future weight gain. SNRIs typically induce more noradrenergic tone at increasingly higher dosages. There may be a dose-response curve in this manner. Levomilnacipran likely is the most noradrenergic of the SNRIs; recent regulatory studies suggest no statistically significant weight gain over the long term.7
Sedating antidepressants
Mirtazapine has receptor-blocking effects on noradrenergic α-2 and serotonergic 5-HT2a and 5-HT2c receptors. Additionally, histamine blocking of H1 receptors can contribute to additional weight gain, similar to what is seen with some SGAs. H1 antagonism dampens satiety response, resulting in increased caloric intake. In that case, or when specific SGAs are used for managing depression, appetite increases (H1 antagonism) and metabolism slows (possibly 5-HT2c antagonism, muscarinic receptor antagonism, etc.), thus allowing for greater adipose tissue growth and leptin insensitivity.
In a meta-analysis, mean weight increased by 1.74 kg (P < .0001) in the first 4 to 12 weeks of mirtazapine treatment, with greater variability in periods >4 months.6 Among the more novel antidepressants released since the era of tricyclic antidepressants (TCAs) or monoamine oxidase inhibitor, mirtazapine might have the greatest weight gain potential.
Trazodone and nefazodone block 5-HT2a and 5-HT2c receptors, as well as serotonin reuptake transporters. Compared with trazodone, nefazodone has a more potent effect on 5-HT2a receptor antagonism and a less potent effect on 5-HT2c receptors, and also mildly inhibits uptake of norepinephrine—meaning that this drug might have less weight gain potential. These medications are not used frequently for treating depression, but trazodone is used as an adjunctive agent for insomnia. Used even at off-label low dosages, trazodone exerts H1-histaminic and α-1 adrenergic antagonistic properties, decreasing the level of consciousness and allowing sedation and somnolence. Because of its fast onset and relatively short duration of action, it can improve depression symptoms by promoting restful sleep as well as by facilitating monoamine neurotransmission. It also might add to weight gain because of its pharmacodynamic receptor profile.
Tricyclic antidepressants
Amitriptyline can be associated with release of tumor necrosis factor-alpha, which is implicated in causing weight gain. Many TCAs block H1 (amitriptyline, imipramine, clomipramine), likely causing weight gain. Most TCAs antagonize muscarinic receptors as well. The more noradrenergic TCAs could curb appetite (nortriptyline, desipramine, protriptyline) similar to SNRIs, therefore countering some of the weight gain drive.
As an example, in a meta-analysis examining weight gain with antidepressants, amitriptyline was associated with weight gain of 1.52 kg above baseline in the acute period (4 to 12 weeks) and 2.24 kg above baseline at 4 to 7 months.6 These results of the acute phase should be viewed cautiously because the authors reported high heterogeneity among these studies, and the possibility of publication bias (Egger test, P < .0001). In the same meta-analysis, the even the more noradrenergic nortriptyline was associated with an increase of 2.0 kg on average over baseline during acute treatment, with that number dropping to 1.24 kg over baseline at ≥4 months.6
Newer antidepressants
Vilazodone is a weak SSRI that aggressively partially agonizes pre-synaptic and post-synaptic 5-HT1a receptors in the CNS. This dual site 5-HT1a action is somewhat unique among antidepressants. This type of agent sometimes is called multimodal,8 or could be considered an “SSRI +” antidepressant. These drugs are SSRIs at the core but have additional 5-HT receptor modulating capabilities. Vilazodone has a favorable weight gain profile, as suggested in a 52-week trial reporting 1.7 kg gain over 52 weeks, compared with an average of 6.8 to 10 kg for long-term SSRI therapy.9
Vortioxetine is a stronger SSRI that also partially agonizes presynaptic 5-HT1a receptors. In addition, it antagonizes 5-HT1d, 5-HT3, and 5-HT7 receptors, giving it a unique pharmacodynamic profile.10 Vortioxetine also had minimal impact on drug-induced weight gain in 52-week studies, with data from 2 trials indicating either minimal weight gain in 6.1% of patients (mean increase of 0.41 kg over 52 weeks)11 or gain that was not statistically significant.12
Levomilnacipran is unique in that it has the most aggressive norepinephrine reuptake inhibition of all SNRIs.13 Again, increased noradrenergic tone might curb appetite and caloric intake. Many SNRIs cause low-grade nausea, which could account for decreased appetite. Long-term, 52-week data for this drug also shows minimal proclivity for weight gain, with the trial participants reporting a slight decrease of 4.34 kg on average from baseline.14
Continue to: Addressing weight gain
Addressing weight gain
Lifestyle modification. Eating smaller portions, combined with restricting foods high in calories and fat, should be the first step. A simple suggestion to a patient to eat the same foods, but remove 20% of the portion, is a simple intervention akin to that of suggesting sleep hygiene practices for insomnia management. Under medical supervision or with referral to a dietician or nutritionist, more rigid caloric restrictions could be employed.
Commercial weight-loss programs, such as Weight Watchers or Curves, can be helpful; some insurers will only cover medications for weight loss if one of these programs have been tried or is used in combination with medication. Some patients might ask about extreme weight-loss measures, such as low-calorie diets combined with intense exercise programs that have been popularized in the media. Although the motivation to initiate and maintain meaningful weight loss should be encouraged, doing so in a more gradual manner should be the goal.
Addressing portion size is a good approach in the early stages of managing obesity. Restaurants often serve portions that have more calories than should be consumed in one meal. Visual cues can influence this trend; using smaller plates can help reduce caloric intake.15
Exercise, sustained for at least 45 minutes, can have long-lasting effects, with a small study showing an increase in metabolic rate of 190 ± 71.4 kcal (P < .001) above baseline for 14 hours after exercise.16 Endurance exercise training is associated with a significant decrease in total cholesterol, triglycerides, and low-density lipoprotein cholesterol, as well as an increase in the high-density lipoprotein level over a 24-week period.17
Encouraging an exercise regimen that is appropriate for your patient can help maintain weight loss. In small trials,18,19 high-intensity exercise was shown to help suppress appetite and decrease 24-hour caloric consumption by 6% to 11%.18
Psychotherapy can become an important intervention for initiating and maintaining weight loss. CBT can help patients recognize and modify lifestyle components, and reinforce behaviors that promote weight loss. This can come from setting realistic weight loss goals; preventing triggering factors that lead to overeating; encouraging portion control during meals; and promoting exercise habits.
In a small, randomized controlled trial (RCT) examining weight loss in obese women, those who underwent CBT and psychoeducation for 2 hours a week for 10 weeks in addition to dietary changes and exercise showed an average weight loss of 10.4 kg at 18-month follow-up, compared with weight gain of 2.3 kg in the control group.20 The short duration of treatment in this study might be desirable to reduce cost and utilization of services. Group formats also could be employed.
Motivational interviewing is a useful tool in addiction psychiatry and shows promise for treating obesity and overeating as well. The approach may differ slightly because weight-loss therapy involves behavior modification rather than behavior cessation. In a meta-analysis of data from RCTs exploring motivational interviewing and its use as an intervention for weight loss, those in the intervention groups experienced significant weight loss as indicated by BMI decreasing a standardized mean difference of −0.51, compared with control groups.21
Medical management considerations
Diagnostics. Recognition and early intervention are instrumental in successfully treating medication-associated weight gain. It is important to obtain any family history of obesity, diabetes, hypertension, and hyperlipidemia. This will likely indicate a patient’s risk for weight gain before initiating medication.
Obtain vital signs at every visit, including blood pressure. Monitoring weight at every clinical visit can be used to calculate and monitor BMI, while also asking the patient to maintain a log of weight measurements obtained at home. Measuring abdominal girth is important to watch for metabolic syndrome, although often this is the least measured variable.
Laboratory testing is helpful. Obtaining a baseline lipid panel and a fasting glucose level (consider measuring hemoglobin A1c in patients with diabetes) is warranted. Including thyroid markers, such as thyroid-stimulating hormone and thyroxine (free T4), might be important considerations, because inadequate management of hypothyroidism can complicate the clinical picture.
Follow-up testing should be ordered every 3 to 12 months to monitor progress if your patient is showing signs of rapid weight gain, or if BMI nears ≥30 kg/m². These guidelines generally are assigned for prescribing of SGAs, but can be applied when using any psychotropic with weight gain potential.
Medications to considerWhen considering the medication regimen as an intervention point, consider changing the antidepressant to one that is not associated with significant weight gain. Although not specifically indicated as a monotherapy for weight loss, switching to or augmenting therapy with bupropion could aid weight loss through appetite suppression.20 Some newer antidepressants, such as vilazodone, vortioxetine, and levomilnacipran, might have less propensity to cause weight gain. In patients with severe depression, augmenting with medications containing amphetamine or methylphenidate could cause some weight loss, but greater care should be taken because of cardiovascular effects and dependency issues.
Continue to: Discussing with your patient...
Discussing with your patient the possibility of changing or worsening depressive symptoms when adding or switching medications allows them to be aware and engaged in the process and can encourage them to notice and report changes. Developing a sensible schedule to taper an existing medication slowly over several weeks and allowing a new one to build up gradually to a therapeutic level can help minimize adverse effects or a discontinuation syndrome.
If switching antidepressants is not possible, or is ineffective, an anti-obesity medication (Table 122-29) can be considered. These medications should not be considered first-line in weight loss management, but reserved for more difficult or refractory weight loss challenges and in patients who are not able to participate in weight loss or dieting programs because of cognitive disorders, a history of nonadherance, financial or travel limitations, or in those with poor social support systems such as homelessness.
Some of these medications are not reimbursed by insurance companies; therefore, consider the financial burden to the patient and their capacity for adherence to therapy, and discuss this challenge before initiating treatment. There is some evidence for using medications off-label to treat obesity (Table 2,30-34).
Anti-obesity medications typically are considered for patients with a BMI >30 or in any overweight patient with diabetes, hyperlipidemia, or cardiovascular disease. As always, discuss with patients and their primary care provider the potential benefits and risks of adding any of these or other medications to an existing treatment regimen.
If weight loss goals are not met, consider discontinuing anti-obesity therapy. Patients and physicians should be cognizant of the need to continue long-term maintenance on these medications after successful treatment—perhaps indefinitely, because patients frequently regain weight after medication is discontinued.
Bottom Line
Many antidepressants are known to increase the risk of excessive weight gain, although risk of weigh gain varies among antidepressant classes. First, advise changes in diet and exercise; next, initiate psychotherapy as indicated, and then consider referral to a nutritionist. Consider switching to an antidepressant with less potential for causing weight gain or adding bupropion, which could lead to weight loss, if your patient can tolerate it. If these strategies are unsuccessful, consider an anti-obesity medication.
Related Resource
1. Ogden CL, Carroll MD, Kit BK, et al. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806-814.
2. Vandenberghe F, Gholam-Rezaee M, Saigí-Morgui N, et al. Importance of early weight changes to predict long-term weight gain during psychotropic drug treatment. J Clin Psychiatry. 2015;76(11):e1417-e1423.
3. Grade Definitions. Electronic Preventive Services Selector (ePSS). http://epss.ahrq.gov/ePSS/gradedef.jsp. Accessed May 2, 2016.
4. Tomiyama AJ, Hunger JM, Nguyen-Cuu J, et al. Misclassification of cardiometabolic health when using body mass index categories in NHANES 2005-2012 [published online February 4, 2016]. Int J Obes (Lond). doi: 10.1038/ijo.2016.17.
5. Berglund ED, Liu C, Sohn J, et al. Serotonin 2C receptors in pro-opiomelanocortin neurons regulate energy and glucose homeostasis. J Clin Invest. 2013;123(12):5061-5070.
6. Serretti A, Mandelli L. Antidepressants and body weight: a comprehensive review and meta-anaylsis. J Clin Psychiatry. 2010;71(10):1259-1272.
7. Mago R, Forero G, Greenberg WM, et al. Safety and tolerability of levomilnacipran ER in major depressive disorder: results from an open-label, 48-week extension study. Clin Drug Investig. 2013;33(10):761-771.
8. Schwartz TL, Siddiqui UA, Stahl SM. Vilazodone: a brief pharmacological and clinical review of the novel serotonin partial agonist and reuptake inhibitor. Ther Adv Psychopharmacol. 2011;1(3):81-87.
9. Robinson DS, Kajdasz DK, Gallipoli S, et al. A 1-year, open-label study assessing the safety and tolerability of vilazodone in patients with major depressive disorder. J Clin Psychopharmacol. 2011;31(5):643-646.
10. Stahl SM. Modes and nodes explain the mechanism of action of vortioxetine, a multimodal agent (MMA): actions at serotonin receptors may enhance downstream release of four pro-cognitive neurotransmitters. CNS Spectr. 2015;20(6):515-519.
11. Jacobsen PL, Harper L, Chrones L, et al. Safety and tolerability of vortioxetine (15 and 20 mg) in patients with major depressive disorder: results of an open-label, flexible-dose, 52-week extension study. Int Clin Psychopharmacol. 2015;30(5):255-264.
12. Boulenger JP, Loft H, Olsen CK. Efficacy and safety of vortioxetine (Lu AA21004), 15 and 20 mg/day: a randomized, double-blind, placebo-controlled, duloxetine-referenced study in the acute treatment of adult patients with major depressive disorder. Int Clin Psychopharmacol. 2014;29(3):138-149.
13. Grady MM, Stahl SM. Novel agents in development for the treatment of depression. CNS Spectr. 2013;18(suppl 1):37-40; quiz 41.
14. Mago R, Forero G, Greenberg WM, et al. Safety and tolerability of levomilnacipran ER in major depressive disorder: results from an open-label, 48-week extension study. Clin Drug Investig. 2013;33(10):761-771.
15. Hollands GJ, Shemilt I, Marteau TM, et al. Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco. Cochrane Database Syst Rev. 2015;9:CD011045.
16. Knab AM, Shanely RA, Corbin KD, et al. A 45-minute vigorous exercise bout increases metabolic rate for 14 hours. Med Sci Sports Exerc. 2011;43(9):1643-1648.
17. Halverstadt A, Phares DA, Wilund KR, et al. Endurance exercise training raises high-density lipoprotein cholesterol and lowers small low-density lipoprotein and very low-density lipoprotein independent of body fat phenotypes in older men and women. Metabolism. 2007;56(4):444-450.
18. Thivel D, Isacco L, Montaurier C, et al. The 24-h energy intake of obese adolescents is spontaneously reduced after intensive exercise: a randomized controlled trial in calorimetric chambers [published online January 17, 2012]. PLoS One. 2012;7(1):e29840. doi: 10.1371/journal.pone.0029840.
19. Sim AY, Wallman KE, Fairchild TJ, et al. High-intensity intermittent exercise attenuates ad-libitum energy intake. Int J Obes (Lond). 2014;38(3):417-422.
20. Stahre L, Tärnell B, Håkanson CE, et al. A randomized controlled trial of two weight-reducing short-term group treatment programs for obesity with an 18-month follow-up. Int J Behav Med. 2007;14(1):48-55.
21. Armstrong MJ, Mottershead TA, Ronksley PE, et al. Motivational interviewing to improve weight loss in overweight and/or obese patients: a systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2011;12(9):709-723.
22. Apovian CM, Aronne L, Rubino D, et al. A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity (Silver Springs). 2013;21(5):935-943.
23. Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595-605.
24. Fidler MC, Sanchez M, Raether B, et al; BLOSSOM Clinical Trial Group. A one-year randomized trial of lorcaserin for weight loss in obese and overweight adults: the BLOSSOM trial. J Clin Endocrinol Metab. 2011;96(10):3067-3077.
25. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial [Erratum in Lancet. 2011;377(9776):1494]. Lancet. 2011;377(9774):1341-1352.
26. Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297-308.
27. Pi-Sunyer X, Astrup A, Fujioka K, et al; SCALE Obesity and Prediabetes NN8022-1839 Study Group. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11-22.
28. Leblanc ES, O’Connor E, Whitlock EP, et al. Effectiveness of primary care-relevant treatments for obesity in adults: a systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2011;155(7):434-447.
29. Torgerson JS, Hauptman J, Boldrin MN, et al. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155-161.
30. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393-403.
31. McDonagh MS, Selph S, Ozpinar A, et al. Systematic review of the benefits and risks of metformin in treating obesity in children aged 18 years and younger. JAMA Pediatr. 2014;168(2):178-184.
32. Dushay J, Gao C, Gopalakrishnan GS, et al. Short-term exenatide treatment leads to significant weight loss in a subset of obese women without diabetes. Diabetes Care. 2012;35(1):4-11.
33. Gadde KM, Kopping MF, Wagner HR 2nd, et al. Zonisamide for weight reduction in obese adults: a 1-year randomized controlled trial. Arch Intern Med. 2012;172(20):1557-1564.
34. Singh-Franco D, Perez A, Harrington C. The effect of pramlintide acetate on glycemic control and weight in patients with type 2 diabetes mellitus and in obese patients without diabetes: a systematic review and meta-analysis. Diabetes Obes Metab. 2011;13(2):169-180.
1. Ogden CL, Carroll MD, Kit BK, et al. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806-814.
2. Vandenberghe F, Gholam-Rezaee M, Saigí-Morgui N, et al. Importance of early weight changes to predict long-term weight gain during psychotropic drug treatment. J Clin Psychiatry. 2015;76(11):e1417-e1423.
3. Grade Definitions. Electronic Preventive Services Selector (ePSS). http://epss.ahrq.gov/ePSS/gradedef.jsp. Accessed May 2, 2016.
4. Tomiyama AJ, Hunger JM, Nguyen-Cuu J, et al. Misclassification of cardiometabolic health when using body mass index categories in NHANES 2005-2012 [published online February 4, 2016]. Int J Obes (Lond). doi: 10.1038/ijo.2016.17.
5. Berglund ED, Liu C, Sohn J, et al. Serotonin 2C receptors in pro-opiomelanocortin neurons regulate energy and glucose homeostasis. J Clin Invest. 2013;123(12):5061-5070.
6. Serretti A, Mandelli L. Antidepressants and body weight: a comprehensive review and meta-anaylsis. J Clin Psychiatry. 2010;71(10):1259-1272.
7. Mago R, Forero G, Greenberg WM, et al. Safety and tolerability of levomilnacipran ER in major depressive disorder: results from an open-label, 48-week extension study. Clin Drug Investig. 2013;33(10):761-771.
8. Schwartz TL, Siddiqui UA, Stahl SM. Vilazodone: a brief pharmacological and clinical review of the novel serotonin partial agonist and reuptake inhibitor. Ther Adv Psychopharmacol. 2011;1(3):81-87.
9. Robinson DS, Kajdasz DK, Gallipoli S, et al. A 1-year, open-label study assessing the safety and tolerability of vilazodone in patients with major depressive disorder. J Clin Psychopharmacol. 2011;31(5):643-646.
10. Stahl SM. Modes and nodes explain the mechanism of action of vortioxetine, a multimodal agent (MMA): actions at serotonin receptors may enhance downstream release of four pro-cognitive neurotransmitters. CNS Spectr. 2015;20(6):515-519.
11. Jacobsen PL, Harper L, Chrones L, et al. Safety and tolerability of vortioxetine (15 and 20 mg) in patients with major depressive disorder: results of an open-label, flexible-dose, 52-week extension study. Int Clin Psychopharmacol. 2015;30(5):255-264.
12. Boulenger JP, Loft H, Olsen CK. Efficacy and safety of vortioxetine (Lu AA21004), 15 and 20 mg/day: a randomized, double-blind, placebo-controlled, duloxetine-referenced study in the acute treatment of adult patients with major depressive disorder. Int Clin Psychopharmacol. 2014;29(3):138-149.
13. Grady MM, Stahl SM. Novel agents in development for the treatment of depression. CNS Spectr. 2013;18(suppl 1):37-40; quiz 41.
14. Mago R, Forero G, Greenberg WM, et al. Safety and tolerability of levomilnacipran ER in major depressive disorder: results from an open-label, 48-week extension study. Clin Drug Investig. 2013;33(10):761-771.
15. Hollands GJ, Shemilt I, Marteau TM, et al. Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco. Cochrane Database Syst Rev. 2015;9:CD011045.
16. Knab AM, Shanely RA, Corbin KD, et al. A 45-minute vigorous exercise bout increases metabolic rate for 14 hours. Med Sci Sports Exerc. 2011;43(9):1643-1648.
17. Halverstadt A, Phares DA, Wilund KR, et al. Endurance exercise training raises high-density lipoprotein cholesterol and lowers small low-density lipoprotein and very low-density lipoprotein independent of body fat phenotypes in older men and women. Metabolism. 2007;56(4):444-450.
18. Thivel D, Isacco L, Montaurier C, et al. The 24-h energy intake of obese adolescents is spontaneously reduced after intensive exercise: a randomized controlled trial in calorimetric chambers [published online January 17, 2012]. PLoS One. 2012;7(1):e29840. doi: 10.1371/journal.pone.0029840.
19. Sim AY, Wallman KE, Fairchild TJ, et al. High-intensity intermittent exercise attenuates ad-libitum energy intake. Int J Obes (Lond). 2014;38(3):417-422.
20. Stahre L, Tärnell B, Håkanson CE, et al. A randomized controlled trial of two weight-reducing short-term group treatment programs for obesity with an 18-month follow-up. Int J Behav Med. 2007;14(1):48-55.
21. Armstrong MJ, Mottershead TA, Ronksley PE, et al. Motivational interviewing to improve weight loss in overweight and/or obese patients: a systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2011;12(9):709-723.
22. Apovian CM, Aronne L, Rubino D, et al. A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity (Silver Springs). 2013;21(5):935-943.
23. Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595-605.
24. Fidler MC, Sanchez M, Raether B, et al; BLOSSOM Clinical Trial Group. A one-year randomized trial of lorcaserin for weight loss in obese and overweight adults: the BLOSSOM trial. J Clin Endocrinol Metab. 2011;96(10):3067-3077.
25. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial [Erratum in Lancet. 2011;377(9776):1494]. Lancet. 2011;377(9774):1341-1352.
26. Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297-308.
27. Pi-Sunyer X, Astrup A, Fujioka K, et al; SCALE Obesity and Prediabetes NN8022-1839 Study Group. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med. 2015;373(1):11-22.
28. Leblanc ES, O’Connor E, Whitlock EP, et al. Effectiveness of primary care-relevant treatments for obesity in adults: a systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2011;155(7):434-447.
29. Torgerson JS, Hauptman J, Boldrin MN, et al. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care. 2004;27(1):155-161.
30. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393-403.
31. McDonagh MS, Selph S, Ozpinar A, et al. Systematic review of the benefits and risks of metformin in treating obesity in children aged 18 years and younger. JAMA Pediatr. 2014;168(2):178-184.
32. Dushay J, Gao C, Gopalakrishnan GS, et al. Short-term exenatide treatment leads to significant weight loss in a subset of obese women without diabetes. Diabetes Care. 2012;35(1):4-11.
33. Gadde KM, Kopping MF, Wagner HR 2nd, et al. Zonisamide for weight reduction in obese adults: a 1-year randomized controlled trial. Arch Intern Med. 2012;172(20):1557-1564.
34. Singh-Franco D, Perez A, Harrington C. The effect of pramlintide acetate on glycemic control and weight in patients with type 2 diabetes mellitus and in obese patients without diabetes: a systematic review and meta-analysis. Diabetes Obes Metab. 2011;13(2):169-180.

Benzodiazepines might succeed as monotherapy for cannabinoid-induced catatonia
We found the case report “Unresponsive and mute after he smoked ‘Spice’” (Cases That Test Your Skills, Current Psychiatry. March 2016 p. 65-70) intriguing because we recently published an article that discusses 3 similar cases of DSM-5 unspecified catatonia.1 The diagnosis of unspecified catatonia applies to catatonia that does not fully meet criteria for either catatonic disorder associated with another mental disorder or catatonic disorder associated with another medical disorder.
In Case 3 of our article, we described a patient who presented with unspecified catatonia after smoking a synthetic cannabinoid. The patient had been diagnosed with schizophrenia 4 years prior, but had not been adherent to treatment with an antipsychotic regimen since his diagnosis. His companion reported he had been smoking “K2” before he presented to the hospital. He was admitted to acute psychiatry, treated with oral lorazepam, 1 mg, 3 times a day, and improved within 3 days. He did not require electroconvulsive therapy (ECT). We have followed this patient through electronic medical records for 2.5 years after this hospitalization. He has not presented with re-emergent signs or symptoms of catatonia.
We also have conducted a literature review of synthetic cannabinoids and catatonia. As synthetic cannabinoids are a relatively recent phenomena, we recognize that reviews on catatonia might not include such substances.2 Our literature review shows there are no other published cases of patients who returned to baseline functioning after treat<hl name="3"/>ment with benzodiazepine (ie, lorazepam) monotherapy.
It appears that, in similar cases of Cannabis-induced or synthetic cannabinoid-induced catatonia, return to baseline level of functioning before hospitalization required ECT in addition to benzodiazepines. Therefore, we feel it is important to note that in some cases, such as with our patient, Cannabis-induced catatonia might resolve with benzodiazepine monotherapy.
Shannon M. O’Connell, DO
PGY-3 Psychiatry Resident
Brendan T. Carroll, MD
Clinical Assistant Professor
Ohio University Heritage College of Osteopathic Medicine
Athens, Ohio
Chillicothe Veterans Affairs Medical Center
Chillicothe, Ohio
1. Bottoms J, Carroll BT. Unspecified catatonia: 3 cases. In Carroll BT, Spiegel DR, eds. Catatonia on the consultation liaison service and other clinical settings. New York, NY: Nova Science Publishers; 2015.
2. The Guidelines and Evidence-Based Medicine Subcommittee of the Academy of Psycho-somatic Medicine (APM); The European Association of Psychosomatic Medicine (EAPM). Catatonia in medically ill patients: evidence-based medicine (EBM) monograph for psychosomatic medicine practice. http://www.apm.org/library/monographs/catatonia/Catatonia_APM-EAPM_2015-04-17.pdf. Published April 17, 2015. Accessed May 3, 2016.
We found the case report “Unresponsive and mute after he smoked ‘Spice’” (Cases That Test Your Skills, Current Psychiatry. March 2016 p. 65-70) intriguing because we recently published an article that discusses 3 similar cases of DSM-5 unspecified catatonia.1 The diagnosis of unspecified catatonia applies to catatonia that does not fully meet criteria for either catatonic disorder associated with another mental disorder or catatonic disorder associated with another medical disorder.
In Case 3 of our article, we described a patient who presented with unspecified catatonia after smoking a synthetic cannabinoid. The patient had been diagnosed with schizophrenia 4 years prior, but had not been adherent to treatment with an antipsychotic regimen since his diagnosis. His companion reported he had been smoking “K2” before he presented to the hospital. He was admitted to acute psychiatry, treated with oral lorazepam, 1 mg, 3 times a day, and improved within 3 days. He did not require electroconvulsive therapy (ECT). We have followed this patient through electronic medical records for 2.5 years after this hospitalization. He has not presented with re-emergent signs or symptoms of catatonia.
We also have conducted a literature review of synthetic cannabinoids and catatonia. As synthetic cannabinoids are a relatively recent phenomena, we recognize that reviews on catatonia might not include such substances.2 Our literature review shows there are no other published cases of patients who returned to baseline functioning after treat<hl name="3"/>ment with benzodiazepine (ie, lorazepam) monotherapy.
It appears that, in similar cases of Cannabis-induced or synthetic cannabinoid-induced catatonia, return to baseline level of functioning before hospitalization required ECT in addition to benzodiazepines. Therefore, we feel it is important to note that in some cases, such as with our patient, Cannabis-induced catatonia might resolve with benzodiazepine monotherapy.
Shannon M. O’Connell, DO
PGY-3 Psychiatry Resident
Brendan T. Carroll, MD
Clinical Assistant Professor
Ohio University Heritage College of Osteopathic Medicine
Athens, Ohio
Chillicothe Veterans Affairs Medical Center
Chillicothe, Ohio
We found the case report “Unresponsive and mute after he smoked ‘Spice’” (Cases That Test Your Skills, Current Psychiatry. March 2016 p. 65-70) intriguing because we recently published an article that discusses 3 similar cases of DSM-5 unspecified catatonia.1 The diagnosis of unspecified catatonia applies to catatonia that does not fully meet criteria for either catatonic disorder associated with another mental disorder or catatonic disorder associated with another medical disorder.
In Case 3 of our article, we described a patient who presented with unspecified catatonia after smoking a synthetic cannabinoid. The patient had been diagnosed with schizophrenia 4 years prior, but had not been adherent to treatment with an antipsychotic regimen since his diagnosis. His companion reported he had been smoking “K2” before he presented to the hospital. He was admitted to acute psychiatry, treated with oral lorazepam, 1 mg, 3 times a day, and improved within 3 days. He did not require electroconvulsive therapy (ECT). We have followed this patient through electronic medical records for 2.5 years after this hospitalization. He has not presented with re-emergent signs or symptoms of catatonia.
We also have conducted a literature review of synthetic cannabinoids and catatonia. As synthetic cannabinoids are a relatively recent phenomena, we recognize that reviews on catatonia might not include such substances.2 Our literature review shows there are no other published cases of patients who returned to baseline functioning after treat<hl name="3"/>ment with benzodiazepine (ie, lorazepam) monotherapy.
It appears that, in similar cases of Cannabis-induced or synthetic cannabinoid-induced catatonia, return to baseline level of functioning before hospitalization required ECT in addition to benzodiazepines. Therefore, we feel it is important to note that in some cases, such as with our patient, Cannabis-induced catatonia might resolve with benzodiazepine monotherapy.
Shannon M. O’Connell, DO
PGY-3 Psychiatry Resident
Brendan T. Carroll, MD
Clinical Assistant Professor
Ohio University Heritage College of Osteopathic Medicine
Athens, Ohio
Chillicothe Veterans Affairs Medical Center
Chillicothe, Ohio
1. Bottoms J, Carroll BT. Unspecified catatonia: 3 cases. In Carroll BT, Spiegel DR, eds. Catatonia on the consultation liaison service and other clinical settings. New York, NY: Nova Science Publishers; 2015.
2. The Guidelines and Evidence-Based Medicine Subcommittee of the Academy of Psycho-somatic Medicine (APM); The European Association of Psychosomatic Medicine (EAPM). Catatonia in medically ill patients: evidence-based medicine (EBM) monograph for psychosomatic medicine practice. http://www.apm.org/library/monographs/catatonia/Catatonia_APM-EAPM_2015-04-17.pdf. Published April 17, 2015. Accessed May 3, 2016.
1. Bottoms J, Carroll BT. Unspecified catatonia: 3 cases. In Carroll BT, Spiegel DR, eds. Catatonia on the consultation liaison service and other clinical settings. New York, NY: Nova Science Publishers; 2015.
2. The Guidelines and Evidence-Based Medicine Subcommittee of the Academy of Psycho-somatic Medicine (APM); The European Association of Psychosomatic Medicine (EAPM). Catatonia in medically ill patients: evidence-based medicine (EBM) monograph for psychosomatic medicine practice. http://www.apm.org/library/monographs/catatonia/Catatonia_APM-EAPM_2015-04-17.pdf. Published April 17, 2015. Accessed May 3, 2016.

Does Natalizumab Benefit Patients With Secondary Progressive MS?
VANCOUVER—Among patients with secondary progressive multiple sclerosis (MS), natalizumab does not delay progression of ambulatory disability, according to phase III trial results presented at the 68th Annual Meeting of the American Academy of Neurology. The drug may slow progression of upper-extremity disability, however, researchers said.
Natalizumab, a recombinant humanized monoclonal antibody against alpha-4 beta-1 integrin, reduces inflammation by inhibiting the transmigration of leukocytes into the brain. It is FDA-approved to treat relapsing-remitting MS, and data have suggested that the drug also may benefit patients with progressive forms of MS.
To investigate whether natalizumab slows disability progression unrelated to relapses in patients with secondary progressive MS, Deborah Steiner, MD, Medical Director at Biogen, and colleagues conducted ASCEND, a multicenter, double-blind, placebo-controlled, randomized trial.

The primary end point was the proportion of participants with confirmed disability progression on the EDSS, Nine-Hole Peg Test, or Timed 25-Foot Walk at six months and at the end of the trial. On the EDSS, progression was defined as an increase of at least 1.0 from a baseline EDSS score of 5.5 or less, or an increase of at least 0.5 from a baseline EDSS score of 6 or more. On the Timed 25-Foot Walk, progression was defined as an increase of 20% or more from baseline. On the Nine-Hole Peg Test, progression was defined as an increase of 20% or more on either hand.
ASCEND did not meet its primary end point. The proportion of progressors was higher in the placebo-treated group (48%) than in the natalizumab-treated group (44%), but the difference was not statistically significant.
Natalizumab treatment was, however, associated with a statistically significant reduction of upper-extremity disability progression, as measured by the Nine-Hole Peg Test. Fifteen percent of participants who received natalizumab had confirmed disability progression on the Nine-Hole Peg Test, compared with 23% of participants who received placebo (odds ratio, 0.56). Dr. Steiner noted that ABILHAND, a patient-reported upper-extremity outcome, clearly differentiated Nine-Hole Peg Test progressors from nonprogressors. This finding “confirms the meaningfulness” of the treatment’s effect on upper extremity disability, the researchers said.
On the Nine-Hole Peg Test, estimated probabilities of confirmed progression over two years showed increased separation over time between the natalizumab and placebo arms. “In contrast, no significant separation over time was observed between natalizumab- and placebo-treated patients on the Timed 25-Foot Walk (38.3% vs 39.2%) or EDSS (17.4% vs 16.7%) components of the primary end point,” the researchers said.
“There’s a striking contrast between the lack of effect on ambulatory function … and the effect on upper-extremity function,” Dr. Steiner said.
Natalizumab was generally well tolerated, with adverse events consistent with its known safety profile.
The study was supported by Biogen in Cambridge, Massachusetts.
—Jake Remaly
Suggested Reading
Sellebjerg F, Cadavid D, Steiner D, et al. Exploring potential mechanisms of action of natalizumab in secondary progressive multiple sclerosis. Ther Adv Neurol Disord. 2016;9(1):31-43.
VANCOUVER—Among patients with secondary progressive multiple sclerosis (MS), natalizumab does not delay progression of ambulatory disability, according to phase III trial results presented at the 68th Annual Meeting of the American Academy of Neurology. The drug may slow progression of upper-extremity disability, however, researchers said.
Natalizumab, a recombinant humanized monoclonal antibody against alpha-4 beta-1 integrin, reduces inflammation by inhibiting the transmigration of leukocytes into the brain. It is FDA-approved to treat relapsing-remitting MS, and data have suggested that the drug also may benefit patients with progressive forms of MS.
To investigate whether natalizumab slows disability progression unrelated to relapses in patients with secondary progressive MS, Deborah Steiner, MD, Medical Director at Biogen, and colleagues conducted ASCEND, a multicenter, double-blind, placebo-controlled, randomized trial.
The primary end point was the proportion of participants with confirmed disability progression on the EDSS, Nine-Hole Peg Test, or Timed 25-Foot Walk at six months and at the end of the trial. On the EDSS, progression was defined as an increase of at least 1.0 from a baseline EDSS score of 5.5 or less, or an increase of at least 0.5 from a baseline EDSS score of 6 or more. On the Timed 25-Foot Walk, progression was defined as an increase of 20% or more from baseline. On the Nine-Hole Peg Test, progression was defined as an increase of 20% or more on either hand.
ASCEND did not meet its primary end point. The proportion of progressors was higher in the placebo-treated group (48%) than in the natalizumab-treated group (44%), but the difference was not statistically significant.
Natalizumab treatment was, however, associated with a statistically significant reduction of upper-extremity disability progression, as measured by the Nine-Hole Peg Test. Fifteen percent of participants who received natalizumab had confirmed disability progression on the Nine-Hole Peg Test, compared with 23% of participants who received placebo (odds ratio, 0.56). Dr. Steiner noted that ABILHAND, a patient-reported upper-extremity outcome, clearly differentiated Nine-Hole Peg Test progressors from nonprogressors. This finding “confirms the meaningfulness” of the treatment’s effect on upper extremity disability, the researchers said.
On the Nine-Hole Peg Test, estimated probabilities of confirmed progression over two years showed increased separation over time between the natalizumab and placebo arms. “In contrast, no significant separation over time was observed between natalizumab- and placebo-treated patients on the Timed 25-Foot Walk (38.3% vs 39.2%) or EDSS (17.4% vs 16.7%) components of the primary end point,” the researchers said.
“There’s a striking contrast between the lack of effect on ambulatory function … and the effect on upper-extremity function,” Dr. Steiner said.
Natalizumab was generally well tolerated, with adverse events consistent with its known safety profile.
The study was supported by Biogen in Cambridge, Massachusetts.
—Jake Remaly
VANCOUVER—Among patients with secondary progressive multiple sclerosis (MS), natalizumab does not delay progression of ambulatory disability, according to phase III trial results presented at the 68th Annual Meeting of the American Academy of Neurology. The drug may slow progression of upper-extremity disability, however, researchers said.
Natalizumab, a recombinant humanized monoclonal antibody against alpha-4 beta-1 integrin, reduces inflammation by inhibiting the transmigration of leukocytes into the brain. It is FDA-approved to treat relapsing-remitting MS, and data have suggested that the drug also may benefit patients with progressive forms of MS.
To investigate whether natalizumab slows disability progression unrelated to relapses in patients with secondary progressive MS, Deborah Steiner, MD, Medical Director at Biogen, and colleagues conducted ASCEND, a multicenter, double-blind, placebo-controlled, randomized trial.
The primary end point was the proportion of participants with confirmed disability progression on the EDSS, Nine-Hole Peg Test, or Timed 25-Foot Walk at six months and at the end of the trial. On the EDSS, progression was defined as an increase of at least 1.0 from a baseline EDSS score of 5.5 or less, or an increase of at least 0.5 from a baseline EDSS score of 6 or more. On the Timed 25-Foot Walk, progression was defined as an increase of 20% or more from baseline. On the Nine-Hole Peg Test, progression was defined as an increase of 20% or more on either hand.
ASCEND did not meet its primary end point. The proportion of progressors was higher in the placebo-treated group (48%) than in the natalizumab-treated group (44%), but the difference was not statistically significant.
Natalizumab treatment was, however, associated with a statistically significant reduction of upper-extremity disability progression, as measured by the Nine-Hole Peg Test. Fifteen percent of participants who received natalizumab had confirmed disability progression on the Nine-Hole Peg Test, compared with 23% of participants who received placebo (odds ratio, 0.56). Dr. Steiner noted that ABILHAND, a patient-reported upper-extremity outcome, clearly differentiated Nine-Hole Peg Test progressors from nonprogressors. This finding “confirms the meaningfulness” of the treatment’s effect on upper extremity disability, the researchers said.
On the Nine-Hole Peg Test, estimated probabilities of confirmed progression over two years showed increased separation over time between the natalizumab and placebo arms. “In contrast, no significant separation over time was observed between natalizumab- and placebo-treated patients on the Timed 25-Foot Walk (38.3% vs 39.2%) or EDSS (17.4% vs 16.7%) components of the primary end point,” the researchers said.
“There’s a striking contrast between the lack of effect on ambulatory function … and the effect on upper-extremity function,” Dr. Steiner said.
Natalizumab was generally well tolerated, with adverse events consistent with its known safety profile.
The study was supported by Biogen in Cambridge, Massachusetts.
—Jake Remaly
Suggested Reading
Sellebjerg F, Cadavid D, Steiner D, et al. Exploring potential mechanisms of action of natalizumab in secondary progressive multiple sclerosis. Ther Adv Neurol Disord. 2016;9(1):31-43.
Suggested Reading
Sellebjerg F, Cadavid D, Steiner D, et al. Exploring potential mechanisms of action of natalizumab in secondary progressive multiple sclerosis. Ther Adv Neurol Disord. 2016;9(1):31-43.

The scourge of societal anosognosia about the mentally ill
What if this increase had occurred in cardiovascular disease or cancer (both on the decline, in fact, thanks to the intense attention they receive)? I think there would have been a public outcry, followed by demands by Congress that the National Institutes of Health and the CDC address this catastrophic rise immediately. And billions of dollars would then be earmarked to prevent these 2 diseases.
How sad that society has “forgotten” that mental illness has deadly consequences, often leading to suicide (42,773 deaths in 2014 alone2—the second most common cause among people age 15 to 253)! Hundreds of thousands of people attempt suicide every year, and those who do not lose their life often end up injured or maimed. Millions who suffer depression, bipolar disorder, schizophrenia, anxiety, posttraumatic stress disorder, or a substance use disorder are at high risk of suicide, and many never receive the timely intervention that might save their life.
Our national blind spot
It is poignant that the CDC report was released in spring: The rate of suicide is highest in April and May, when the light-dark cycle is reversed. This springtime peak runs contrary to the common belief that the rate of suicide is highest during winter months. The Annual Meeting of the American Psychiatric Association convenes in May, such that, ironically, thousands of psychiatrists are away from their office exactly when their patients might need them most
Lack of attention to the high risk of suicide among all ages and both sexes is emblematic of society’s inexplicable neglect of the needs of the mentally ill. That neglect is fueled, and exacerbated, by the destructive stigma attached to brain disorders that display psychiatric symptoms. As a neuropsychiatrist, I label this neglect societal anosognosia—the same as the lack of insight seen in patients with acute schizophrenia, who are unaware of how impaired they are and insist that they are not sick. (Anosognosia also occurs in stroke patients who deny that their limb is paralyzed and insist that all is well.)
Loss of insight can have serious consequences for patients who lose the ability to monitor and evaluate their physical and mental health. Just as patients with anosognosia think they do not need help, a society that fails to attend to the mental illness of its citizens endangers their overall health and welfare.
From neglect of mental illness many hazards arise
Tens of millions of Americans suffer from mental illness, according to the National Institute of Mental Health-sponsored Epidemiologic Catchment Area Study.4 The last thing these people can afford is societal anosognosia, which deprives them of necessary and timely access to psychiatric care.
Societal anosognosia is associated with numerous hazards for persons with mental illness, including:
- Lack of compassion, which is readily available for people with a medical ailment (broken bones, cardiovascular disease, cancer).
- Lack of adequate, affordable health insurance and financial support, compared with what is available for non-psychiatric disorders.
- Shortage of publicly funded programs and mental health practitioners to provide prevention and intervention for those who consider ending their life during an episode of depression, psychosis, stress, or a panic attack.
- Allowing the stigma to continue unabated. Why are there strict laws about hate crimes, but not about stigma? Why does society continue to portray depression and anxiety as a personal weakness or failure, while patients with Parkinson’s disease or multiple sclerosis who have motor weakness are not stigmatized for their physical deficits?
- Transforming the seriously mentally ill into felons by arresting and jailing them because of erratic behavior—instead of hospitalizing them for the medical care they need. The transinstitutionalization of the mentally ill—from state hospitals to prisons—is one of the most shameful consequences of societal anosognosia, burdening our patients with the dual stigma of being a criminal and mentally ill.
- Turning a blind eye to abuses by insurance companies. More appalling is the perpetuation of restricted health coverage despite the passage of parity laws! Why are sensory and motor disorders of brain lesions covered fully, while the thought, emotional, and behavior disorders of the brain covered only partially?
- Consent laws that restrict psychiatrists from medicating acutely psychotic or depressed patients unless they consent—but no laws that restrict a cardiologist from immediately treating an unconscious heart attack patient who cannot consent, or an obtunded stroke patient who cannot communicate? The duration of untreated psychosis or depression has been shown repeatedly to have deleterious effects on brain tissue and functional outcomes, yet treatment of an acutely ill psychiatric patient is often delayed until a court order is obtained. When was the last time a court order was needed to treat an acute myocardial infarction?
- Failure to recognize that premature mortality (by approximately 25 years) is a devastating consequence of mental illness, whether from suicide or cardiometabolic risk factors due to smoking, substance use (often used to self-medicate because proper treatment is lacking), poor diet, and sedentary living.
- Failure to provide basic primary care to people with severe mental illness, and the much lower use of life-saving diagnostic and treatment procedures offered to these patients, compared with non-psychiatric patients.
- Inadequate funding for research on psychiatric disorders, compared with other medical disorders—even though direct and indirect costs of mental illness to society (hundreds of billions of dollars a year) far exceed costs of most medical disorders.
- Severe shortage of rehabilitation programs for the mentally ill, compared with many other medical disorders. Why does paralysis of the mind receive far less support than paralysis of the legs or arms?
The rising suicide rate reflects poorly on us
Societal anosognosia is a global scourge, affecting many underdeveloped countries. Why do developed nations, like ours, have the same blind spot for mental illness? Might ignorance and discrimination be universal?
The tragic rise in the rate of death by suicide in men and women, among all age groups, year after year, is stunningly incongruent when juxtaposed against the elimination of smallpox and other communicable diseases through a concerted societal effort to support scientific advances in vaccine development. Societal anosognosia appears to be selective: We have comprehensive insight about diseases of the body but not diseases of the mind.
The essence and soul of a society are the collective minds of its citizens, not their bodies. Societal anosognosia is a serious dysfunction of its mind, and a rising suicide rate is a symptom of that pathological dysfunction.
1. Curtin SC, Warner M, Hedegaard H, et al. Increase in suicide in the United States, 1999-2014. National Center for Health Statistics Data Brief No. 241. Atlanta, GA: National Center for Health Statistics, U.S. Department of Health and Human Services; 2016.
2. Ten leading causes of death by age group, United States – 2014. Centers for Disease Control and Prevention. http://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_age_group_2014_1050w760h.gif. Accessed May 20, 2016.
3. Morris M. Stemming the rising tide of suicide. Clinical Psychiatry News. http://www.clinicalpsychiatrynews.com/specialty-focus/depression/single-article-page/stemming-the-rising-tide-of-suicide/01cd45cabfc693bedb0e30bb6cb0b89e.html. Published April 26, 2016. Accessed May 13, 2016.
4. Robins LN, Regier DA, eds. Psychiatric disorders in America: the Epidemiologic Catchment Area Study. New York, NY: Free Press; 1990.
What if this increase had occurred in cardiovascular disease or cancer (both on the decline, in fact, thanks to the intense attention they receive)? I think there would have been a public outcry, followed by demands by Congress that the National Institutes of Health and the CDC address this catastrophic rise immediately. And billions of dollars would then be earmarked to prevent these 2 diseases.
How sad that society has “forgotten” that mental illness has deadly consequences, often leading to suicide (42,773 deaths in 2014 alone2—the second most common cause among people age 15 to 253)! Hundreds of thousands of people attempt suicide every year, and those who do not lose their life often end up injured or maimed. Millions who suffer depression, bipolar disorder, schizophrenia, anxiety, posttraumatic stress disorder, or a substance use disorder are at high risk of suicide, and many never receive the timely intervention that might save their life.
Our national blind spot
It is poignant that the CDC report was released in spring: The rate of suicide is highest in April and May, when the light-dark cycle is reversed. This springtime peak runs contrary to the common belief that the rate of suicide is highest during winter months. The Annual Meeting of the American Psychiatric Association convenes in May, such that, ironically, thousands of psychiatrists are away from their office exactly when their patients might need them most
Lack of attention to the high risk of suicide among all ages and both sexes is emblematic of society’s inexplicable neglect of the needs of the mentally ill. That neglect is fueled, and exacerbated, by the destructive stigma attached to brain disorders that display psychiatric symptoms. As a neuropsychiatrist, I label this neglect societal anosognosia—the same as the lack of insight seen in patients with acute schizophrenia, who are unaware of how impaired they are and insist that they are not sick. (Anosognosia also occurs in stroke patients who deny that their limb is paralyzed and insist that all is well.)
Loss of insight can have serious consequences for patients who lose the ability to monitor and evaluate their physical and mental health. Just as patients with anosognosia think they do not need help, a society that fails to attend to the mental illness of its citizens endangers their overall health and welfare.
From neglect of mental illness many hazards arise
Tens of millions of Americans suffer from mental illness, according to the National Institute of Mental Health-sponsored Epidemiologic Catchment Area Study.4 The last thing these people can afford is societal anosognosia, which deprives them of necessary and timely access to psychiatric care.
Societal anosognosia is associated with numerous hazards for persons with mental illness, including:
- Lack of compassion, which is readily available for people with a medical ailment (broken bones, cardiovascular disease, cancer).
- Lack of adequate, affordable health insurance and financial support, compared with what is available for non-psychiatric disorders.
- Shortage of publicly funded programs and mental health practitioners to provide prevention and intervention for those who consider ending their life during an episode of depression, psychosis, stress, or a panic attack.
- Allowing the stigma to continue unabated. Why are there strict laws about hate crimes, but not about stigma? Why does society continue to portray depression and anxiety as a personal weakness or failure, while patients with Parkinson’s disease or multiple sclerosis who have motor weakness are not stigmatized for their physical deficits?
- Transforming the seriously mentally ill into felons by arresting and jailing them because of erratic behavior—instead of hospitalizing them for the medical care they need. The transinstitutionalization of the mentally ill—from state hospitals to prisons—is one of the most shameful consequences of societal anosognosia, burdening our patients with the dual stigma of being a criminal and mentally ill.
- Turning a blind eye to abuses by insurance companies. More appalling is the perpetuation of restricted health coverage despite the passage of parity laws! Why are sensory and motor disorders of brain lesions covered fully, while the thought, emotional, and behavior disorders of the brain covered only partially?
- Consent laws that restrict psychiatrists from medicating acutely psychotic or depressed patients unless they consent—but no laws that restrict a cardiologist from immediately treating an unconscious heart attack patient who cannot consent, or an obtunded stroke patient who cannot communicate? The duration of untreated psychosis or depression has been shown repeatedly to have deleterious effects on brain tissue and functional outcomes, yet treatment of an acutely ill psychiatric patient is often delayed until a court order is obtained. When was the last time a court order was needed to treat an acute myocardial infarction?
- Failure to recognize that premature mortality (by approximately 25 years) is a devastating consequence of mental illness, whether from suicide or cardiometabolic risk factors due to smoking, substance use (often used to self-medicate because proper treatment is lacking), poor diet, and sedentary living.
- Failure to provide basic primary care to people with severe mental illness, and the much lower use of life-saving diagnostic and treatment procedures offered to these patients, compared with non-psychiatric patients.
- Inadequate funding for research on psychiatric disorders, compared with other medical disorders—even though direct and indirect costs of mental illness to society (hundreds of billions of dollars a year) far exceed costs of most medical disorders.
- Severe shortage of rehabilitation programs for the mentally ill, compared with many other medical disorders. Why does paralysis of the mind receive far less support than paralysis of the legs or arms?
The rising suicide rate reflects poorly on us
Societal anosognosia is a global scourge, affecting many underdeveloped countries. Why do developed nations, like ours, have the same blind spot for mental illness? Might ignorance and discrimination be universal?
The tragic rise in the rate of death by suicide in men and women, among all age groups, year after year, is stunningly incongruent when juxtaposed against the elimination of smallpox and other communicable diseases through a concerted societal effort to support scientific advances in vaccine development. Societal anosognosia appears to be selective: We have comprehensive insight about diseases of the body but not diseases of the mind.
The essence and soul of a society are the collective minds of its citizens, not their bodies. Societal anosognosia is a serious dysfunction of its mind, and a rising suicide rate is a symptom of that pathological dysfunction.
What if this increase had occurred in cardiovascular disease or cancer (both on the decline, in fact, thanks to the intense attention they receive)? I think there would have been a public outcry, followed by demands by Congress that the National Institutes of Health and the CDC address this catastrophic rise immediately. And billions of dollars would then be earmarked to prevent these 2 diseases.
How sad that society has “forgotten” that mental illness has deadly consequences, often leading to suicide (42,773 deaths in 2014 alone2—the second most common cause among people age 15 to 253)! Hundreds of thousands of people attempt suicide every year, and those who do not lose their life often end up injured or maimed. Millions who suffer depression, bipolar disorder, schizophrenia, anxiety, posttraumatic stress disorder, or a substance use disorder are at high risk of suicide, and many never receive the timely intervention that might save their life.
Our national blind spot
It is poignant that the CDC report was released in spring: The rate of suicide is highest in April and May, when the light-dark cycle is reversed. This springtime peak runs contrary to the common belief that the rate of suicide is highest during winter months. The Annual Meeting of the American Psychiatric Association convenes in May, such that, ironically, thousands of psychiatrists are away from their office exactly when their patients might need them most
Lack of attention to the high risk of suicide among all ages and both sexes is emblematic of society’s inexplicable neglect of the needs of the mentally ill. That neglect is fueled, and exacerbated, by the destructive stigma attached to brain disorders that display psychiatric symptoms. As a neuropsychiatrist, I label this neglect societal anosognosia—the same as the lack of insight seen in patients with acute schizophrenia, who are unaware of how impaired they are and insist that they are not sick. (Anosognosia also occurs in stroke patients who deny that their limb is paralyzed and insist that all is well.)
Loss of insight can have serious consequences for patients who lose the ability to monitor and evaluate their physical and mental health. Just as patients with anosognosia think they do not need help, a society that fails to attend to the mental illness of its citizens endangers their overall health and welfare.
From neglect of mental illness many hazards arise
Tens of millions of Americans suffer from mental illness, according to the National Institute of Mental Health-sponsored Epidemiologic Catchment Area Study.4 The last thing these people can afford is societal anosognosia, which deprives them of necessary and timely access to psychiatric care.
Societal anosognosia is associated with numerous hazards for persons with mental illness, including:
- Lack of compassion, which is readily available for people with a medical ailment (broken bones, cardiovascular disease, cancer).
- Lack of adequate, affordable health insurance and financial support, compared with what is available for non-psychiatric disorders.
- Shortage of publicly funded programs and mental health practitioners to provide prevention and intervention for those who consider ending their life during an episode of depression, psychosis, stress, or a panic attack.
- Allowing the stigma to continue unabated. Why are there strict laws about hate crimes, but not about stigma? Why does society continue to portray depression and anxiety as a personal weakness or failure, while patients with Parkinson’s disease or multiple sclerosis who have motor weakness are not stigmatized for their physical deficits?
- Transforming the seriously mentally ill into felons by arresting and jailing them because of erratic behavior—instead of hospitalizing them for the medical care they need. The transinstitutionalization of the mentally ill—from state hospitals to prisons—is one of the most shameful consequences of societal anosognosia, burdening our patients with the dual stigma of being a criminal and mentally ill.
- Turning a blind eye to abuses by insurance companies. More appalling is the perpetuation of restricted health coverage despite the passage of parity laws! Why are sensory and motor disorders of brain lesions covered fully, while the thought, emotional, and behavior disorders of the brain covered only partially?
- Consent laws that restrict psychiatrists from medicating acutely psychotic or depressed patients unless they consent—but no laws that restrict a cardiologist from immediately treating an unconscious heart attack patient who cannot consent, or an obtunded stroke patient who cannot communicate? The duration of untreated psychosis or depression has been shown repeatedly to have deleterious effects on brain tissue and functional outcomes, yet treatment of an acutely ill psychiatric patient is often delayed until a court order is obtained. When was the last time a court order was needed to treat an acute myocardial infarction?
- Failure to recognize that premature mortality (by approximately 25 years) is a devastating consequence of mental illness, whether from suicide or cardiometabolic risk factors due to smoking, substance use (often used to self-medicate because proper treatment is lacking), poor diet, and sedentary living.
- Failure to provide basic primary care to people with severe mental illness, and the much lower use of life-saving diagnostic and treatment procedures offered to these patients, compared with non-psychiatric patients.
- Inadequate funding for research on psychiatric disorders, compared with other medical disorders—even though direct and indirect costs of mental illness to society (hundreds of billions of dollars a year) far exceed costs of most medical disorders.
- Severe shortage of rehabilitation programs for the mentally ill, compared with many other medical disorders. Why does paralysis of the mind receive far less support than paralysis of the legs or arms?
The rising suicide rate reflects poorly on us
Societal anosognosia is a global scourge, affecting many underdeveloped countries. Why do developed nations, like ours, have the same blind spot for mental illness? Might ignorance and discrimination be universal?
The tragic rise in the rate of death by suicide in men and women, among all age groups, year after year, is stunningly incongruent when juxtaposed against the elimination of smallpox and other communicable diseases through a concerted societal effort to support scientific advances in vaccine development. Societal anosognosia appears to be selective: We have comprehensive insight about diseases of the body but not diseases of the mind.
The essence and soul of a society are the collective minds of its citizens, not their bodies. Societal anosognosia is a serious dysfunction of its mind, and a rising suicide rate is a symptom of that pathological dysfunction.
1. Curtin SC, Warner M, Hedegaard H, et al. Increase in suicide in the United States, 1999-2014. National Center for Health Statistics Data Brief No. 241. Atlanta, GA: National Center for Health Statistics, U.S. Department of Health and Human Services; 2016.
2. Ten leading causes of death by age group, United States – 2014. Centers for Disease Control and Prevention. http://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_age_group_2014_1050w760h.gif. Accessed May 20, 2016.
3. Morris M. Stemming the rising tide of suicide. Clinical Psychiatry News. http://www.clinicalpsychiatrynews.com/specialty-focus/depression/single-article-page/stemming-the-rising-tide-of-suicide/01cd45cabfc693bedb0e30bb6cb0b89e.html. Published April 26, 2016. Accessed May 13, 2016.
4. Robins LN, Regier DA, eds. Psychiatric disorders in America: the Epidemiologic Catchment Area Study. New York, NY: Free Press; 1990.
1. Curtin SC, Warner M, Hedegaard H, et al. Increase in suicide in the United States, 1999-2014. National Center for Health Statistics Data Brief No. 241. Atlanta, GA: National Center for Health Statistics, U.S. Department of Health and Human Services; 2016.
2. Ten leading causes of death by age group, United States – 2014. Centers for Disease Control and Prevention. http://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_age_group_2014_1050w760h.gif. Accessed May 20, 2016.
3. Morris M. Stemming the rising tide of suicide. Clinical Psychiatry News. http://www.clinicalpsychiatrynews.com/specialty-focus/depression/single-article-page/stemming-the-rising-tide-of-suicide/01cd45cabfc693bedb0e30bb6cb0b89e.html. Published April 26, 2016. Accessed May 13, 2016.
4. Robins LN, Regier DA, eds. Psychiatric disorders in America: the Epidemiologic Catchment Area Study. New York, NY: Free Press; 1990.
Sudden Unexpected Death in Epilepsy: An Update
Pooja Patel, MD
Selim Benbadis, MD
Dr. Patel is a fourth year neurology resident at the University of South Florida and will begin an epilepsy fellowship at the University of South Florida in July.
Dr. Benbadis is Professor and Director of the Comprehensive Epilepsy Program at the University of South Florida and Tampa General Hospital in Tampa, Florida.
Sudden unexpected death in epilepsy (SUDEP) is the most common cause of death in patients with intractable epilepsy. SUDEP accounts for 7.5% to 17% of all deaths related to epilepsy and has an annual incidence of 3 to 9 per 1000 in the general epilepsy population. Even with such a high prevalence, epilepsy patients, their families, and even many physicians are unaware of the mortality and risk of SUDEP. SUDEP has recently received significant attention in the scientific literature due to its high prevalence and lack of well-defined mechanisms. Understanding the modifiable risk factors and pathophysiology of SUDEP is critically important to help delineate preventive strategies.
Several mechanisms have been proposed to play a role in the pathophysiology of SUDEP. Recent literature have included new insights derived from combined data from older and newer studies where clues were obtained from witnessed SUDEP cases, Epilepsy Monitoring Unit observation of SUDEP cases, physiological data obtained from nonfatal seizures, and animal models. Based on many cohort studies, the initial mechanism is thought to be due to hypoventilation or apnea resulting from the seizure itself. The prone position is thought to contribute to prolonged oxygen desaturation by causing loss of arousal and inability to sense increased carbon dioxide levels. This in turn can cause secondary cardiac arrhythmias that are fatal. The other proposed mechanism is primary cardiac arrhythmia resulting from autonomic dysfunction before, during, or after a seizure. Additionally, serotonergic neurons might contribute as well by causing combination of hypoventilation and seizure. Experts also have suggested that genetic mutations cause primary dysfunction leading to fatal seizures; however, this requires further research.
Based on recent findings about the pathophysiology of SUDEP, several preventive measures have been suggested. The critical preventive measure is still believed to be good control of seizures, as uncontrolled generalized tonic-clonic seizures continue to be the biggest risk factor of SUDEP. Good control of seizures can be difficult in chronic refractory epilepsy and early referral should be made to an epilepsy center. Several studies evaluating patients after epilepsy surgery have discovered that surgery reduces patients’ likelihood of SUDEP. A study done in 2000 evaluated vagus nerve stimulation (VNS) implantation and SUDEP risk, and concluded that during the first 2 years the risk of SUDEP was higher than isolated use of some of the antiepileptics. However, after a 2-year follow-up, the risk of SUDEP was remarkably lower. The initial higher rate was likely due to the fact that VNS was implanted in refractory patients who had failed antiepileptics and were candidates for surgery. Experts believe that VNS is likely protective toward SUDEP as it reduces the amount of generalized tonic-clonic seizures.
Sleep is considered to be high risk for SUDEP because of the higher number of seizures occurring in sleep and hormonal and autonomic changes occurring at nighttime, which increase SUDEP risk. Use of a bed where the head can be adjusted to be higher than the feet, a supine sleep position, a special pillow to prevent suffocation, and even supervision at night has been recommended to reduce the risk of SUDEP. Supervision at night, which includes a supervising person sharing the same bedroom, special precautions such as regular checks throughout the night, or use of a monitoring device, was associated with a decreased risk of SUDEP in a recent study. Medications such as alpha-blockers and beta-blockers might be considered as they can reduce sympathetic discharge and prevent cardiac arrhythmias. Selective serotonin reuptake inhibitors can also reduce ictal hypoxemia and can help prevent a potential mechanism leading to SUDEP.
SUDEP is a significant burden in the field of epilepsy because of its mortality, but it is a subject that is not known well among patients, family, and providers. A recent Australian study reported that only a minority of adult patients with epilepsy had heard about SUDEP from their neurologists. Due to limited experience and knowledge of SUDEP, some neurologists may be unable to provide the appropriate education to patients and their families. The first qualitative study to explore opinions of bereaved relatives on whether to discuss SUDEP with patients was recently performed in the United States. The study showed that 91% of parents of epilepsy patients and 89.5% of adults with epilepsy would have preferred to have information about SUDEP. These respondents would have liked their neurologists in particular to discuss SUDEP so that they could have focused on preventive techniques. Study results suggest a lack of knowledge and the need for more awareness of SUDEP among the epilepsy population. It should be the neurologists’ responsibility to discuss and inform patients and their families about SUDEP at an appropriate time based on their diagnosis.
Resources such as the SUDEP-7 inventory can be used to help physicians identify patients with refractory epilepsy at risk for SUDEP. In 2011, the first SUDEP-7 inventory was found to be associated to two biomarkers: vagus-mediated heart rate variability and post-ictal generalized electroencephalogram suppression. In 2015, this inventory was modified to the revised SUDEP-7 inventory, which re-evaluated the association with heart rate. Results indicated that older age, longer duration of epilepsy, and presence of developmental disability had direct influence on vagus-mediated heart rate variability and thus increased SUDEP risk. The higher the SUDEP-7 inventory score, the higher the risk of SUDEP. SUDEP-7 inventory and other similar inventories can be a valuable tool for risk stratification and in turn can be used when deciding whether or not to have discussion of SUDEP with patients and families.
In conclusion, SUDEP continues to be a growing concern of mortality in the epilepsy population. Recent research has shed light on its pathophysiologic mechanism, which will in turn help us determine preventive techniques for vulnerable patients. Hopefully, increased SUDEP awareness will help physicians be more knowledgeable and comfortable in leading the discussion of SUDEP. Further research is still needed to uncover the role of genetics using animal and human models.
Sources
Annegers JF, Coan SP, Hauser WA, Leestma J. Epilepsy, vagal nerve stimulation by the NCP system, all-cause mortality and sudden, unexpected, unexplained death. Epilepsia. 2000;41(5):549-553.
Dlouhy BJ, Gehlbach BK, Richerson GB. Sudden unexpected death in epilepsy: basic mechanisms and clinical implications for prevention. J Neurol Neurosurg Psychiatry. 2016;87(4):402-413.
Morse AM, Kothare SV. Pediatric sudden unexpected death in epilepsy. Pediatr Neurol. 2016;57:7-16.
Novak JL, Miller PR, Markovic D, Meymandi SK, DeGiorgio CM. Risk assessment for sudden death in epilepsy: the SUDEP-7 inventory. Front Neurol. 2015;6:252.
Pansani AP, Colugnati DB, Scorza CA, de Almeida AC, Cavalheiro EA, Scorza FA. Furthering our understanding of SUDEP: the role of animal models. Expert Rev Neurother. 2016;16(5):561-572.
RamachandranNair R, Jack SM, Strohm S. SUDEP: to discuss or not? recommendations from bereaved relatives. Epilepsy Behav. 2016;56:20-25.
Pooja Patel, MD
Selim Benbadis, MD
Dr. Patel is a fourth year neurology resident at the University of South Florida and will begin an epilepsy fellowship at the University of South Florida in July.
Dr. Benbadis is Professor and Director of the Comprehensive Epilepsy Program at the University of South Florida and Tampa General Hospital in Tampa, Florida.
Sudden unexpected death in epilepsy (SUDEP) is the most common cause of death in patients with intractable epilepsy. SUDEP accounts for 7.5% to 17% of all deaths related to epilepsy and has an annual incidence of 3 to 9 per 1000 in the general epilepsy population. Even with such a high prevalence, epilepsy patients, their families, and even many physicians are unaware of the mortality and risk of SUDEP. SUDEP has recently received significant attention in the scientific literature due to its high prevalence and lack of well-defined mechanisms. Understanding the modifiable risk factors and pathophysiology of SUDEP is critically important to help delineate preventive strategies.
Several mechanisms have been proposed to play a role in the pathophysiology of SUDEP. Recent literature have included new insights derived from combined data from older and newer studies where clues were obtained from witnessed SUDEP cases, Epilepsy Monitoring Unit observation of SUDEP cases, physiological data obtained from nonfatal seizures, and animal models. Based on many cohort studies, the initial mechanism is thought to be due to hypoventilation or apnea resulting from the seizure itself. The prone position is thought to contribute to prolonged oxygen desaturation by causing loss of arousal and inability to sense increased carbon dioxide levels. This in turn can cause secondary cardiac arrhythmias that are fatal. The other proposed mechanism is primary cardiac arrhythmia resulting from autonomic dysfunction before, during, or after a seizure. Additionally, serotonergic neurons might contribute as well by causing combination of hypoventilation and seizure. Experts also have suggested that genetic mutations cause primary dysfunction leading to fatal seizures; however, this requires further research.
Based on recent findings about the pathophysiology of SUDEP, several preventive measures have been suggested. The critical preventive measure is still believed to be good control of seizures, as uncontrolled generalized tonic-clonic seizures continue to be the biggest risk factor of SUDEP. Good control of seizures can be difficult in chronic refractory epilepsy and early referral should be made to an epilepsy center. Several studies evaluating patients after epilepsy surgery have discovered that surgery reduces patients’ likelihood of SUDEP. A study done in 2000 evaluated vagus nerve stimulation (VNS) implantation and SUDEP risk, and concluded that during the first 2 years the risk of SUDEP was higher than isolated use of some of the antiepileptics. However, after a 2-year follow-up, the risk of SUDEP was remarkably lower. The initial higher rate was likely due to the fact that VNS was implanted in refractory patients who had failed antiepileptics and were candidates for surgery. Experts believe that VNS is likely protective toward SUDEP as it reduces the amount of generalized tonic-clonic seizures.
Sleep is considered to be high risk for SUDEP because of the higher number of seizures occurring in sleep and hormonal and autonomic changes occurring at nighttime, which increase SUDEP risk. Use of a bed where the head can be adjusted to be higher than the feet, a supine sleep position, a special pillow to prevent suffocation, and even supervision at night has been recommended to reduce the risk of SUDEP. Supervision at night, which includes a supervising person sharing the same bedroom, special precautions such as regular checks throughout the night, or use of a monitoring device, was associated with a decreased risk of SUDEP in a recent study. Medications such as alpha-blockers and beta-blockers might be considered as they can reduce sympathetic discharge and prevent cardiac arrhythmias. Selective serotonin reuptake inhibitors can also reduce ictal hypoxemia and can help prevent a potential mechanism leading to SUDEP.
SUDEP is a significant burden in the field of epilepsy because of its mortality, but it is a subject that is not known well among patients, family, and providers. A recent Australian study reported that only a minority of adult patients with epilepsy had heard about SUDEP from their neurologists. Due to limited experience and knowledge of SUDEP, some neurologists may be unable to provide the appropriate education to patients and their families. The first qualitative study to explore opinions of bereaved relatives on whether to discuss SUDEP with patients was recently performed in the United States. The study showed that 91% of parents of epilepsy patients and 89.5% of adults with epilepsy would have preferred to have information about SUDEP. These respondents would have liked their neurologists in particular to discuss SUDEP so that they could have focused on preventive techniques. Study results suggest a lack of knowledge and the need for more awareness of SUDEP among the epilepsy population. It should be the neurologists’ responsibility to discuss and inform patients and their families about SUDEP at an appropriate time based on their diagnosis.
Resources such as the SUDEP-7 inventory can be used to help physicians identify patients with refractory epilepsy at risk for SUDEP. In 2011, the first SUDEP-7 inventory was found to be associated to two biomarkers: vagus-mediated heart rate variability and post-ictal generalized electroencephalogram suppression. In 2015, this inventory was modified to the revised SUDEP-7 inventory, which re-evaluated the association with heart rate. Results indicated that older age, longer duration of epilepsy, and presence of developmental disability had direct influence on vagus-mediated heart rate variability and thus increased SUDEP risk. The higher the SUDEP-7 inventory score, the higher the risk of SUDEP. SUDEP-7 inventory and other similar inventories can be a valuable tool for risk stratification and in turn can be used when deciding whether or not to have discussion of SUDEP with patients and families.
In conclusion, SUDEP continues to be a growing concern of mortality in the epilepsy population. Recent research has shed light on its pathophysiologic mechanism, which will in turn help us determine preventive techniques for vulnerable patients. Hopefully, increased SUDEP awareness will help physicians be more knowledgeable and comfortable in leading the discussion of SUDEP. Further research is still needed to uncover the role of genetics using animal and human models.
Sources
Annegers JF, Coan SP, Hauser WA, Leestma J. Epilepsy, vagal nerve stimulation by the NCP system, all-cause mortality and sudden, unexpected, unexplained death. Epilepsia. 2000;41(5):549-553.
Dlouhy BJ, Gehlbach BK, Richerson GB. Sudden unexpected death in epilepsy: basic mechanisms and clinical implications for prevention. J Neurol Neurosurg Psychiatry. 2016;87(4):402-413.
Morse AM, Kothare SV. Pediatric sudden unexpected death in epilepsy. Pediatr Neurol. 2016;57:7-16.
Novak JL, Miller PR, Markovic D, Meymandi SK, DeGiorgio CM. Risk assessment for sudden death in epilepsy: the SUDEP-7 inventory. Front Neurol. 2015;6:252.
Pansani AP, Colugnati DB, Scorza CA, de Almeida AC, Cavalheiro EA, Scorza FA. Furthering our understanding of SUDEP: the role of animal models. Expert Rev Neurother. 2016;16(5):561-572.
RamachandranNair R, Jack SM, Strohm S. SUDEP: to discuss or not? recommendations from bereaved relatives. Epilepsy Behav. 2016;56:20-25.
Pooja Patel, MD
Selim Benbadis, MD
Dr. Patel is a fourth year neurology resident at the University of South Florida and will begin an epilepsy fellowship at the University of South Florida in July.
Dr. Benbadis is Professor and Director of the Comprehensive Epilepsy Program at the University of South Florida and Tampa General Hospital in Tampa, Florida.
Sudden unexpected death in epilepsy (SUDEP) is the most common cause of death in patients with intractable epilepsy. SUDEP accounts for 7.5% to 17% of all deaths related to epilepsy and has an annual incidence of 3 to 9 per 1000 in the general epilepsy population. Even with such a high prevalence, epilepsy patients, their families, and even many physicians are unaware of the mortality and risk of SUDEP. SUDEP has recently received significant attention in the scientific literature due to its high prevalence and lack of well-defined mechanisms. Understanding the modifiable risk factors and pathophysiology of SUDEP is critically important to help delineate preventive strategies.
Several mechanisms have been proposed to play a role in the pathophysiology of SUDEP. Recent literature have included new insights derived from combined data from older and newer studies where clues were obtained from witnessed SUDEP cases, Epilepsy Monitoring Unit observation of SUDEP cases, physiological data obtained from nonfatal seizures, and animal models. Based on many cohort studies, the initial mechanism is thought to be due to hypoventilation or apnea resulting from the seizure itself. The prone position is thought to contribute to prolonged oxygen desaturation by causing loss of arousal and inability to sense increased carbon dioxide levels. This in turn can cause secondary cardiac arrhythmias that are fatal. The other proposed mechanism is primary cardiac arrhythmia resulting from autonomic dysfunction before, during, or after a seizure. Additionally, serotonergic neurons might contribute as well by causing combination of hypoventilation and seizure. Experts also have suggested that genetic mutations cause primary dysfunction leading to fatal seizures; however, this requires further research.
Based on recent findings about the pathophysiology of SUDEP, several preventive measures have been suggested. The critical preventive measure is still believed to be good control of seizures, as uncontrolled generalized tonic-clonic seizures continue to be the biggest risk factor of SUDEP. Good control of seizures can be difficult in chronic refractory epilepsy and early referral should be made to an epilepsy center. Several studies evaluating patients after epilepsy surgery have discovered that surgery reduces patients’ likelihood of SUDEP. A study done in 2000 evaluated vagus nerve stimulation (VNS) implantation and SUDEP risk, and concluded that during the first 2 years the risk of SUDEP was higher than isolated use of some of the antiepileptics. However, after a 2-year follow-up, the risk of SUDEP was remarkably lower. The initial higher rate was likely due to the fact that VNS was implanted in refractory patients who had failed antiepileptics and were candidates for surgery. Experts believe that VNS is likely protective toward SUDEP as it reduces the amount of generalized tonic-clonic seizures.
Sleep is considered to be high risk for SUDEP because of the higher number of seizures occurring in sleep and hormonal and autonomic changes occurring at nighttime, which increase SUDEP risk. Use of a bed where the head can be adjusted to be higher than the feet, a supine sleep position, a special pillow to prevent suffocation, and even supervision at night has been recommended to reduce the risk of SUDEP. Supervision at night, which includes a supervising person sharing the same bedroom, special precautions such as regular checks throughout the night, or use of a monitoring device, was associated with a decreased risk of SUDEP in a recent study. Medications such as alpha-blockers and beta-blockers might be considered as they can reduce sympathetic discharge and prevent cardiac arrhythmias. Selective serotonin reuptake inhibitors can also reduce ictal hypoxemia and can help prevent a potential mechanism leading to SUDEP.
SUDEP is a significant burden in the field of epilepsy because of its mortality, but it is a subject that is not known well among patients, family, and providers. A recent Australian study reported that only a minority of adult patients with epilepsy had heard about SUDEP from their neurologists. Due to limited experience and knowledge of SUDEP, some neurologists may be unable to provide the appropriate education to patients and their families. The first qualitative study to explore opinions of bereaved relatives on whether to discuss SUDEP with patients was recently performed in the United States. The study showed that 91% of parents of epilepsy patients and 89.5% of adults with epilepsy would have preferred to have information about SUDEP. These respondents would have liked their neurologists in particular to discuss SUDEP so that they could have focused on preventive techniques. Study results suggest a lack of knowledge and the need for more awareness of SUDEP among the epilepsy population. It should be the neurologists’ responsibility to discuss and inform patients and their families about SUDEP at an appropriate time based on their diagnosis.
Resources such as the SUDEP-7 inventory can be used to help physicians identify patients with refractory epilepsy at risk for SUDEP. In 2011, the first SUDEP-7 inventory was found to be associated to two biomarkers: vagus-mediated heart rate variability and post-ictal generalized electroencephalogram suppression. In 2015, this inventory was modified to the revised SUDEP-7 inventory, which re-evaluated the association with heart rate. Results indicated that older age, longer duration of epilepsy, and presence of developmental disability had direct influence on vagus-mediated heart rate variability and thus increased SUDEP risk. The higher the SUDEP-7 inventory score, the higher the risk of SUDEP. SUDEP-7 inventory and other similar inventories can be a valuable tool for risk stratification and in turn can be used when deciding whether or not to have discussion of SUDEP with patients and families.
In conclusion, SUDEP continues to be a growing concern of mortality in the epilepsy population. Recent research has shed light on its pathophysiologic mechanism, which will in turn help us determine preventive techniques for vulnerable patients. Hopefully, increased SUDEP awareness will help physicians be more knowledgeable and comfortable in leading the discussion of SUDEP. Further research is still needed to uncover the role of genetics using animal and human models.
Sources
Annegers JF, Coan SP, Hauser WA, Leestma J. Epilepsy, vagal nerve stimulation by the NCP system, all-cause mortality and sudden, unexpected, unexplained death. Epilepsia. 2000;41(5):549-553.
Dlouhy BJ, Gehlbach BK, Richerson GB. Sudden unexpected death in epilepsy: basic mechanisms and clinical implications for prevention. J Neurol Neurosurg Psychiatry. 2016;87(4):402-413.
Morse AM, Kothare SV. Pediatric sudden unexpected death in epilepsy. Pediatr Neurol. 2016;57:7-16.
Novak JL, Miller PR, Markovic D, Meymandi SK, DeGiorgio CM. Risk assessment for sudden death in epilepsy: the SUDEP-7 inventory. Front Neurol. 2015;6:252.
Pansani AP, Colugnati DB, Scorza CA, de Almeida AC, Cavalheiro EA, Scorza FA. Furthering our understanding of SUDEP: the role of animal models. Expert Rev Neurother. 2016;16(5):561-572.
RamachandranNair R, Jack SM, Strohm S. SUDEP: to discuss or not? recommendations from bereaved relatives. Epilepsy Behav. 2016;56:20-25.
Blood Pressure Trajectories May Affect Risk of Stroke and Mortality
Trajectories of blood pressure in mid to late life are associated with incident stroke and mortality, according to research published online ahead of print May 9 in Hypertension.
Most associations between blood pressure—a major modifiable risk factor for stroke—and incident stroke have been based on blood pressure measurements taken at a single time point.
Although long-term trajectories of blood pressure can vary considerably in the elderly, studies have not looked at the long-term blood pressure trajectories in mid to late life or at whether such trajectories relate to stroke, said M. Arfan Ikram, MD, PhD, senior study author and Associate Professor of Neuroepidemiology at Erasmus University Medical Center in Rotterdam, the Netherlands.

M. Arfan Ikram, MD, PhD
To identify long-term trajectories of blood pressure in a population-based study and examine the risk of stroke within those trajectories, Dr. Ikram and colleagues evaluated the course of systolic blood pressure in 6,745 participants within the Rotterdam Study.
Participants resided in Ommoord, a suburb of Rotterdam, and received baseline examinations starting in 1990. The investigators used data from five follow-up visits, which occurred every three to four years from 1990 to 2011. During each follow-up visit, blood pressure was measured twice in the right arm, in sitting position, after a resting period of five minutes. Researchers used the average of the two measurements. The investigators focused on systolic blood pressure because it is the best predictor of cardiovascular events.
Participants’ ages ranged from 55 to 106, and 60% were women. Participants had a mean follow-up of 13.5 years.
Four Trajectories
The investigators jointly modeled participants’ risk of stroke and competing causes of death using joint latent class mixed modeling. When assessing blood pressure trajectories, the researchers found that the joint latent class model with four trajectory classes had the best fit.
Class 1, the largest class, included 4,938 participants. It was characterized by a gradually increasing blood pressure, starting at an average of 120 mm Hg at age 55 and increasing to an average of 160 mm Hg at age 95. Class 2, with 822 participants, was characterized by a similar blood pressure at age 55, but a much steeper increase in blood pressure, to an average of 200 mm Hg. The two other classes were characterized by a relatively higher baseline blood pressure. In class 3 (870 participants), the average baseline blood pressure of 140 mm Hg had modest variation over time. In class 4 (115 patients), the average baseline blood pressure of 160 mm Hg decreased after age 65.
People in class 4 were more frequently men. Use of blood pressure-lowering medication was similar between classes at baseline. At the end of follow-up, classes 3 and 4 had higher proportions of blood pressure-lowering medication users. Frequency of current smokers varied between classes, with particularly higher frequencies in classes 2 and 4.
Groups’ Risk Varied
During the study period, 1,053 participants had a stroke. Researchers also studied the number of deaths that occurred from nonstroke health events. They adjusted for sex and baseline blood-pressure lowering medication.
Classes 2, 3, and 4 had a significantly and substantially higher risk of stroke, compared with class 1 (ie, 4.7% to 13.6% vs 0.7%). Classes 2 and 4 had the highest risk of dying of other causes. The risk of dying of other causes in class 3 was similar to that of class 1. The risk of stroke in class 3, however, continued to increase until older age and was highest overall.
In all, 2,546 people (51.5%) in class 1, 575 (70.0%) people in class 2, 288 (33.1%) people in class 3, and 87 (75.7%) people in class 4 died due to a nonstroke-related cause. Between 25% and 38% of nonstroke deaths were due to cardiovascular events.
In multivariable-adjusted models that controlled for cholesterol, lipid-lowering medication, BMI, smoking, alcohol use, diabetes mellitus type 2, and antithrombotic medication, the results were relatively similar, the researchers said. The risk of stroke in classes 2 and 4 was attenuated by data adjustment, whereas the risk increased in class 3.
“Assessing trajectories of blood pressure provides a more nuanced understanding of the associations between blood pressure, stroke, and mortality,” the authors said.
The researchers noted that people in class 2 with steep increases in blood pressure might not receive effective treatment in time under current guidelines, and future studies could determine whether this class can be a target for prevention.
Effect of Slope
Prior studies that examined blood pressure trajectories in young to middle-aged people identified several parallel trajectories and found that long-term higher blood pressure related to more cardiovascular pathology.
“In our older population, we also observed that the class with a high mid-life blood pressure had the highest risk of stroke and death, compared to the class with the lowest blood pressure,” Dr. Ikram and colleagues said. “However, a novel finding of our study is that the slope of increase was associated with an increasing risk of stroke and competing causes of death. Namely, we identified two classes characterized by equally low baseline blood pressure and increasing trajectories, but only the class characterized by steep increases had a high risk of stroke and death. Of note, the risks in that class were even similar to the class with a high mid-life blood pressure.”
The large study population, the use of repeated measures of blood pressure over a long follow-up, and thorough collection of stroke assessments were among the study’s strengths. The study was not large enough to examine stroke subtypes, the authors said. In addition, the study’s population was geographically limited and mostly white, although the findings likely apply to people from other communities, Dr. Ikram said.
“Blood pressure should be measured regularly because it can change markedly over the course of a couple years and put you at high risk for an adverse event,” said Dr. Ikram. “Since the risks of stroke and death differ across these trajectory paths, they are potentially important for preventive strategies.”
—Jake Remaly
Suggested Reading
Portegies ML, Mirza SS, Verlinden VJ, et al. Mid- to late-life trajectories of blood pressure and the risk of stroke: the Rotterdam Study. Hypertension. 2016 May 9 [Epub ahead of print].
Trajectories of blood pressure in mid to late life are associated with incident stroke and mortality, according to research published online ahead of print May 9 in Hypertension.
Most associations between blood pressure—a major modifiable risk factor for stroke—and incident stroke have been based on blood pressure measurements taken at a single time point.
Although long-term trajectories of blood pressure can vary considerably in the elderly, studies have not looked at the long-term blood pressure trajectories in mid to late life or at whether such trajectories relate to stroke, said M. Arfan Ikram, MD, PhD, senior study author and Associate Professor of Neuroepidemiology at Erasmus University Medical Center in Rotterdam, the Netherlands.
M. Arfan Ikram, MD, PhD
To identify long-term trajectories of blood pressure in a population-based study and examine the risk of stroke within those trajectories, Dr. Ikram and colleagues evaluated the course of systolic blood pressure in 6,745 participants within the Rotterdam Study.
Participants resided in Ommoord, a suburb of Rotterdam, and received baseline examinations starting in 1990. The investigators used data from five follow-up visits, which occurred every three to four years from 1990 to 2011. During each follow-up visit, blood pressure was measured twice in the right arm, in sitting position, after a resting period of five minutes. Researchers used the average of the two measurements. The investigators focused on systolic blood pressure because it is the best predictor of cardiovascular events.
Participants’ ages ranged from 55 to 106, and 60% were women. Participants had a mean follow-up of 13.5 years.
Four Trajectories
The investigators jointly modeled participants’ risk of stroke and competing causes of death using joint latent class mixed modeling. When assessing blood pressure trajectories, the researchers found that the joint latent class model with four trajectory classes had the best fit.
Class 1, the largest class, included 4,938 participants. It was characterized by a gradually increasing blood pressure, starting at an average of 120 mm Hg at age 55 and increasing to an average of 160 mm Hg at age 95. Class 2, with 822 participants, was characterized by a similar blood pressure at age 55, but a much steeper increase in blood pressure, to an average of 200 mm Hg. The two other classes were characterized by a relatively higher baseline blood pressure. In class 3 (870 participants), the average baseline blood pressure of 140 mm Hg had modest variation over time. In class 4 (115 patients), the average baseline blood pressure of 160 mm Hg decreased after age 65.
People in class 4 were more frequently men. Use of blood pressure-lowering medication was similar between classes at baseline. At the end of follow-up, classes 3 and 4 had higher proportions of blood pressure-lowering medication users. Frequency of current smokers varied between classes, with particularly higher frequencies in classes 2 and 4.
Groups’ Risk Varied
During the study period, 1,053 participants had a stroke. Researchers also studied the number of deaths that occurred from nonstroke health events. They adjusted for sex and baseline blood-pressure lowering medication.
Classes 2, 3, and 4 had a significantly and substantially higher risk of stroke, compared with class 1 (ie, 4.7% to 13.6% vs 0.7%). Classes 2 and 4 had the highest risk of dying of other causes. The risk of dying of other causes in class 3 was similar to that of class 1. The risk of stroke in class 3, however, continued to increase until older age and was highest overall.
In all, 2,546 people (51.5%) in class 1, 575 (70.0%) people in class 2, 288 (33.1%) people in class 3, and 87 (75.7%) people in class 4 died due to a nonstroke-related cause. Between 25% and 38% of nonstroke deaths were due to cardiovascular events.
In multivariable-adjusted models that controlled for cholesterol, lipid-lowering medication, BMI, smoking, alcohol use, diabetes mellitus type 2, and antithrombotic medication, the results were relatively similar, the researchers said. The risk of stroke in classes 2 and 4 was attenuated by data adjustment, whereas the risk increased in class 3.
“Assessing trajectories of blood pressure provides a more nuanced understanding of the associations between blood pressure, stroke, and mortality,” the authors said.
The researchers noted that people in class 2 with steep increases in blood pressure might not receive effective treatment in time under current guidelines, and future studies could determine whether this class can be a target for prevention.
Effect of Slope
Prior studies that examined blood pressure trajectories in young to middle-aged people identified several parallel trajectories and found that long-term higher blood pressure related to more cardiovascular pathology.
“In our older population, we also observed that the class with a high mid-life blood pressure had the highest risk of stroke and death, compared to the class with the lowest blood pressure,” Dr. Ikram and colleagues said. “However, a novel finding of our study is that the slope of increase was associated with an increasing risk of stroke and competing causes of death. Namely, we identified two classes characterized by equally low baseline blood pressure and increasing trajectories, but only the class characterized by steep increases had a high risk of stroke and death. Of note, the risks in that class were even similar to the class with a high mid-life blood pressure.”
The large study population, the use of repeated measures of blood pressure over a long follow-up, and thorough collection of stroke assessments were among the study’s strengths. The study was not large enough to examine stroke subtypes, the authors said. In addition, the study’s population was geographically limited and mostly white, although the findings likely apply to people from other communities, Dr. Ikram said.
“Blood pressure should be measured regularly because it can change markedly over the course of a couple years and put you at high risk for an adverse event,” said Dr. Ikram. “Since the risks of stroke and death differ across these trajectory paths, they are potentially important for preventive strategies.”
—Jake Remaly
Trajectories of blood pressure in mid to late life are associated with incident stroke and mortality, according to research published online ahead of print May 9 in Hypertension.
Most associations between blood pressure—a major modifiable risk factor for stroke—and incident stroke have been based on blood pressure measurements taken at a single time point.
Although long-term trajectories of blood pressure can vary considerably in the elderly, studies have not looked at the long-term blood pressure trajectories in mid to late life or at whether such trajectories relate to stroke, said M. Arfan Ikram, MD, PhD, senior study author and Associate Professor of Neuroepidemiology at Erasmus University Medical Center in Rotterdam, the Netherlands.
M. Arfan Ikram, MD, PhD
To identify long-term trajectories of blood pressure in a population-based study and examine the risk of stroke within those trajectories, Dr. Ikram and colleagues evaluated the course of systolic blood pressure in 6,745 participants within the Rotterdam Study.
Participants resided in Ommoord, a suburb of Rotterdam, and received baseline examinations starting in 1990. The investigators used data from five follow-up visits, which occurred every three to four years from 1990 to 2011. During each follow-up visit, blood pressure was measured twice in the right arm, in sitting position, after a resting period of five minutes. Researchers used the average of the two measurements. The investigators focused on systolic blood pressure because it is the best predictor of cardiovascular events.
Participants’ ages ranged from 55 to 106, and 60% were women. Participants had a mean follow-up of 13.5 years.
Four Trajectories
The investigators jointly modeled participants’ risk of stroke and competing causes of death using joint latent class mixed modeling. When assessing blood pressure trajectories, the researchers found that the joint latent class model with four trajectory classes had the best fit.
Class 1, the largest class, included 4,938 participants. It was characterized by a gradually increasing blood pressure, starting at an average of 120 mm Hg at age 55 and increasing to an average of 160 mm Hg at age 95. Class 2, with 822 participants, was characterized by a similar blood pressure at age 55, but a much steeper increase in blood pressure, to an average of 200 mm Hg. The two other classes were characterized by a relatively higher baseline blood pressure. In class 3 (870 participants), the average baseline blood pressure of 140 mm Hg had modest variation over time. In class 4 (115 patients), the average baseline blood pressure of 160 mm Hg decreased after age 65.
People in class 4 were more frequently men. Use of blood pressure-lowering medication was similar between classes at baseline. At the end of follow-up, classes 3 and 4 had higher proportions of blood pressure-lowering medication users. Frequency of current smokers varied between classes, with particularly higher frequencies in classes 2 and 4.
Groups’ Risk Varied
During the study period, 1,053 participants had a stroke. Researchers also studied the number of deaths that occurred from nonstroke health events. They adjusted for sex and baseline blood-pressure lowering medication.
Classes 2, 3, and 4 had a significantly and substantially higher risk of stroke, compared with class 1 (ie, 4.7% to 13.6% vs 0.7%). Classes 2 and 4 had the highest risk of dying of other causes. The risk of dying of other causes in class 3 was similar to that of class 1. The risk of stroke in class 3, however, continued to increase until older age and was highest overall.
In all, 2,546 people (51.5%) in class 1, 575 (70.0%) people in class 2, 288 (33.1%) people in class 3, and 87 (75.7%) people in class 4 died due to a nonstroke-related cause. Between 25% and 38% of nonstroke deaths were due to cardiovascular events.
In multivariable-adjusted models that controlled for cholesterol, lipid-lowering medication, BMI, smoking, alcohol use, diabetes mellitus type 2, and antithrombotic medication, the results were relatively similar, the researchers said. The risk of stroke in classes 2 and 4 was attenuated by data adjustment, whereas the risk increased in class 3.
“Assessing trajectories of blood pressure provides a more nuanced understanding of the associations between blood pressure, stroke, and mortality,” the authors said.
The researchers noted that people in class 2 with steep increases in blood pressure might not receive effective treatment in time under current guidelines, and future studies could determine whether this class can be a target for prevention.
Effect of Slope
Prior studies that examined blood pressure trajectories in young to middle-aged people identified several parallel trajectories and found that long-term higher blood pressure related to more cardiovascular pathology.
“In our older population, we also observed that the class with a high mid-life blood pressure had the highest risk of stroke and death, compared to the class with the lowest blood pressure,” Dr. Ikram and colleagues said. “However, a novel finding of our study is that the slope of increase was associated with an increasing risk of stroke and competing causes of death. Namely, we identified two classes characterized by equally low baseline blood pressure and increasing trajectories, but only the class characterized by steep increases had a high risk of stroke and death. Of note, the risks in that class were even similar to the class with a high mid-life blood pressure.”
The large study population, the use of repeated measures of blood pressure over a long follow-up, and thorough collection of stroke assessments were among the study’s strengths. The study was not large enough to examine stroke subtypes, the authors said. In addition, the study’s population was geographically limited and mostly white, although the findings likely apply to people from other communities, Dr. Ikram said.
“Blood pressure should be measured regularly because it can change markedly over the course of a couple years and put you at high risk for an adverse event,” said Dr. Ikram. “Since the risks of stroke and death differ across these trajectory paths, they are potentially important for preventive strategies.”
—Jake Remaly
Suggested Reading
Portegies ML, Mirza SS, Verlinden VJ, et al. Mid- to late-life trajectories of blood pressure and the risk of stroke: the Rotterdam Study. Hypertension. 2016 May 9 [Epub ahead of print].
Suggested Reading
Portegies ML, Mirza SS, Verlinden VJ, et al. Mid- to late-life trajectories of blood pressure and the risk of stroke: the Rotterdam Study. Hypertension. 2016 May 9 [Epub ahead of print].

Age, lower baseline ALC increase dimethyl fumarate lymphopenia risk
VANCOUVER – The risk of dimethyl fumarate lymphopenia – and perhaps progressive multifocal leukoencephalopathy – is greatest in patients 60 years or older and those with baseline absolute lymphocyte counts below 2 x 109/L, according to a review of 206 patients with relapsing-remitting or progressive multiple sclerosis from the University of Rochester (N.Y.).
A total of 87 patients (42%), all of whom were on dimethyl fumarate (DMF; Tecfidera) for at least 3 months, developed lymphopenia with an absolute lymphocyte count (ALC) below 0.91 x 109/L. That’s not a surprise; lymphopenia is a well-known side effect of the drug, and the rates in Rochester were similar to what was reported in clinical trials. The greatest concern with DMF lymphopenia is subsequent progressive multifocal leukoencephalopathy (PML); a handful of cases have been reported in lymphopenic patients, none in the University of Rochester review.
What was surprising was that in the 34 patients aged 60 years or older, 24 (71%) developed lymphopenia, versus 62 (36%) of the 172 under 60 years old (P = .0005). Meanwhile, of 93 patients with baseline ALCs below 2 x 109/L, 49 (53%) became lymphopenic, versus 34 of 104 patients (33%) who started DMF with higher lymphocyte counts (P = .0006). A total of nine patients in the study did not have a baseline ALC available.

“If I had a patient who was 70 years old with a low baseline lymphocyte count, [these findings] would weigh into my decisions about choosing” this medication. “Age and baseline ALC may guide future selection of patients for DMF therapy,” neurologist and investigator Dr. Jessica Robb said at the annual meeting of the American Academy of Neurology.
Also, because higher grade lymphopenia didn’t resolve in most cases until the drug was stopped, “if I had a patient who developed more severe grade 3 or 4 lymphopenia, I would probably have a lower threshold for” discontinuation. “I would probably think about changing medication more quickly rather than leaving them on [DMF] and hoping that their lymphopenia resolves,” Dr. Robb said.
The Rochester findings are in line with a 2015 report from Washington University, St. Louis, that also indicated a higher risk of moderate to severe lymphopenia in older patients and those with lower baseline ALCs, as well as recent natalizumab (Tysabri) users. Grade 2 or worse lymphopenia “is unlikely to resolve while on the drug,” the St. Louis investigators concluded (Mult Scler J Exp Transl Clin. 2015 Jan-Dec;1:2055217315596994).
Taken together, the two studies are important because there’s otherwise not much else in the medical literature identifying DMF lymphopenia risk factors. Lymphopenia and PML are also concerns with other multiple sclerosis (MS) agents.
“The increased prevalence of lymphopenia in older patients and in patients with a lower baseline ALC suggests a failure of lymphopoiesis triggered by DMF therapy. Indeed, lymphopoiesis declines with age due to thymic involution and decreased production of naive lymphocytes. ... Whether these consequences of normal aging could be amplified by DMF is an avenue for future study,” the St. Louis team said.
“The significance of increased risk for lymphopenia in patients recently exposed to natalizumab is not immediately obvious. ... Natalizumab is known to expand circulating leukocytes, including progenitor cells. If in turn, DMF causes lymphocyte apoptosis or arrest of differentiation, then patients sequentially exposed to natalizumab and DMF might have a larger number of circulating lymphocytes vulnerable to DMF effects than other patients,” they said.
Food and Drug Administration labeling for DMF recommends lymphocyte counts at baseline, 6 months, and every 6-12 months thereafter. However, European regulators recently recommended lymphocyte counts at baseline and every 3 months to catch problems early, as well as baseline MRIs as references for possible PML.
Standard, 240-mg twice-daily dosing was used at the University of Rochester, and the mean age in the study was 49 years. The majority of patients were women, and the mean duration of MS was 11 years. Almost three-quarters of the patients were new to immunosuppression, and none of the patients developed serious infections.
The University of Rochester team noted a higher rate of grade 1 lymphopenia than reported in clinical trials (18% vs. 10%). Twelve patients (6%) discontinued DMF because of lymphopenia.
Dr. Robb and the other investigators had no relevant disclosures.
VANCOUVER – The risk of dimethyl fumarate lymphopenia – and perhaps progressive multifocal leukoencephalopathy – is greatest in patients 60 years or older and those with baseline absolute lymphocyte counts below 2 x 109/L, according to a review of 206 patients with relapsing-remitting or progressive multiple sclerosis from the University of Rochester (N.Y.).
A total of 87 patients (42%), all of whom were on dimethyl fumarate (DMF; Tecfidera) for at least 3 months, developed lymphopenia with an absolute lymphocyte count (ALC) below 0.91 x 109/L. That’s not a surprise; lymphopenia is a well-known side effect of the drug, and the rates in Rochester were similar to what was reported in clinical trials. The greatest concern with DMF lymphopenia is subsequent progressive multifocal leukoencephalopathy (PML); a handful of cases have been reported in lymphopenic patients, none in the University of Rochester review.
What was surprising was that in the 34 patients aged 60 years or older, 24 (71%) developed lymphopenia, versus 62 (36%) of the 172 under 60 years old (P = .0005). Meanwhile, of 93 patients with baseline ALCs below 2 x 109/L, 49 (53%) became lymphopenic, versus 34 of 104 patients (33%) who started DMF with higher lymphocyte counts (P = .0006). A total of nine patients in the study did not have a baseline ALC available.
“If I had a patient who was 70 years old with a low baseline lymphocyte count, [these findings] would weigh into my decisions about choosing” this medication. “Age and baseline ALC may guide future selection of patients for DMF therapy,” neurologist and investigator Dr. Jessica Robb said at the annual meeting of the American Academy of Neurology.
Also, because higher grade lymphopenia didn’t resolve in most cases until the drug was stopped, “if I had a patient who developed more severe grade 3 or 4 lymphopenia, I would probably have a lower threshold for” discontinuation. “I would probably think about changing medication more quickly rather than leaving them on [DMF] and hoping that their lymphopenia resolves,” Dr. Robb said.
The Rochester findings are in line with a 2015 report from Washington University, St. Louis, that also indicated a higher risk of moderate to severe lymphopenia in older patients and those with lower baseline ALCs, as well as recent natalizumab (Tysabri) users. Grade 2 or worse lymphopenia “is unlikely to resolve while on the drug,” the St. Louis investigators concluded (Mult Scler J Exp Transl Clin. 2015 Jan-Dec;1:2055217315596994).
Taken together, the two studies are important because there’s otherwise not much else in the medical literature identifying DMF lymphopenia risk factors. Lymphopenia and PML are also concerns with other multiple sclerosis (MS) agents.
“The increased prevalence of lymphopenia in older patients and in patients with a lower baseline ALC suggests a failure of lymphopoiesis triggered by DMF therapy. Indeed, lymphopoiesis declines with age due to thymic involution and decreased production of naive lymphocytes. ... Whether these consequences of normal aging could be amplified by DMF is an avenue for future study,” the St. Louis team said.
“The significance of increased risk for lymphopenia in patients recently exposed to natalizumab is not immediately obvious. ... Natalizumab is known to expand circulating leukocytes, including progenitor cells. If in turn, DMF causes lymphocyte apoptosis or arrest of differentiation, then patients sequentially exposed to natalizumab and DMF might have a larger number of circulating lymphocytes vulnerable to DMF effects than other patients,” they said.
Food and Drug Administration labeling for DMF recommends lymphocyte counts at baseline, 6 months, and every 6-12 months thereafter. However, European regulators recently recommended lymphocyte counts at baseline and every 3 months to catch problems early, as well as baseline MRIs as references for possible PML.
Standard, 240-mg twice-daily dosing was used at the University of Rochester, and the mean age in the study was 49 years. The majority of patients were women, and the mean duration of MS was 11 years. Almost three-quarters of the patients were new to immunosuppression, and none of the patients developed serious infections.
The University of Rochester team noted a higher rate of grade 1 lymphopenia than reported in clinical trials (18% vs. 10%). Twelve patients (6%) discontinued DMF because of lymphopenia.
Dr. Robb and the other investigators had no relevant disclosures.
VANCOUVER – The risk of dimethyl fumarate lymphopenia – and perhaps progressive multifocal leukoencephalopathy – is greatest in patients 60 years or older and those with baseline absolute lymphocyte counts below 2 x 109/L, according to a review of 206 patients with relapsing-remitting or progressive multiple sclerosis from the University of Rochester (N.Y.).
A total of 87 patients (42%), all of whom were on dimethyl fumarate (DMF; Tecfidera) for at least 3 months, developed lymphopenia with an absolute lymphocyte count (ALC) below 0.91 x 109/L. That’s not a surprise; lymphopenia is a well-known side effect of the drug, and the rates in Rochester were similar to what was reported in clinical trials. The greatest concern with DMF lymphopenia is subsequent progressive multifocal leukoencephalopathy (PML); a handful of cases have been reported in lymphopenic patients, none in the University of Rochester review.
What was surprising was that in the 34 patients aged 60 years or older, 24 (71%) developed lymphopenia, versus 62 (36%) of the 172 under 60 years old (P = .0005). Meanwhile, of 93 patients with baseline ALCs below 2 x 109/L, 49 (53%) became lymphopenic, versus 34 of 104 patients (33%) who started DMF with higher lymphocyte counts (P = .0006). A total of nine patients in the study did not have a baseline ALC available.
“If I had a patient who was 70 years old with a low baseline lymphocyte count, [these findings] would weigh into my decisions about choosing” this medication. “Age and baseline ALC may guide future selection of patients for DMF therapy,” neurologist and investigator Dr. Jessica Robb said at the annual meeting of the American Academy of Neurology.
Also, because higher grade lymphopenia didn’t resolve in most cases until the drug was stopped, “if I had a patient who developed more severe grade 3 or 4 lymphopenia, I would probably have a lower threshold for” discontinuation. “I would probably think about changing medication more quickly rather than leaving them on [DMF] and hoping that their lymphopenia resolves,” Dr. Robb said.
The Rochester findings are in line with a 2015 report from Washington University, St. Louis, that also indicated a higher risk of moderate to severe lymphopenia in older patients and those with lower baseline ALCs, as well as recent natalizumab (Tysabri) users. Grade 2 or worse lymphopenia “is unlikely to resolve while on the drug,” the St. Louis investigators concluded (Mult Scler J Exp Transl Clin. 2015 Jan-Dec;1:2055217315596994).
Taken together, the two studies are important because there’s otherwise not much else in the medical literature identifying DMF lymphopenia risk factors. Lymphopenia and PML are also concerns with other multiple sclerosis (MS) agents.
“The increased prevalence of lymphopenia in older patients and in patients with a lower baseline ALC suggests a failure of lymphopoiesis triggered by DMF therapy. Indeed, lymphopoiesis declines with age due to thymic involution and decreased production of naive lymphocytes. ... Whether these consequences of normal aging could be amplified by DMF is an avenue for future study,” the St. Louis team said.
“The significance of increased risk for lymphopenia in patients recently exposed to natalizumab is not immediately obvious. ... Natalizumab is known to expand circulating leukocytes, including progenitor cells. If in turn, DMF causes lymphocyte apoptosis or arrest of differentiation, then patients sequentially exposed to natalizumab and DMF might have a larger number of circulating lymphocytes vulnerable to DMF effects than other patients,” they said.
Food and Drug Administration labeling for DMF recommends lymphocyte counts at baseline, 6 months, and every 6-12 months thereafter. However, European regulators recently recommended lymphocyte counts at baseline and every 3 months to catch problems early, as well as baseline MRIs as references for possible PML.
Standard, 240-mg twice-daily dosing was used at the University of Rochester, and the mean age in the study was 49 years. The majority of patients were women, and the mean duration of MS was 11 years. Almost three-quarters of the patients were new to immunosuppression, and none of the patients developed serious infections.
The University of Rochester team noted a higher rate of grade 1 lymphopenia than reported in clinical trials (18% vs. 10%). Twelve patients (6%) discontinued DMF because of lymphopenia.
Dr. Robb and the other investigators had no relevant disclosures.
AT THE AAN 2016 ANNUAL MEETING
Key clinical point: Dimethyl fumarate is probably not the best option for older patients with lower baseline lymphocyte counts.
Major finding: Among 34 patients aged 60 years or older, 24 (71%) developed lymphopenia, versus 62 (36%) of the 172 under 60 years old (P = .0005). Meanwhile, of 93 patients with baseline ALCs below 2 x 109/L, 49 (53%) became lymphopenic, versus 34 of 104 patients (33%) who started DMF with higher lymphocyte counts (P = .0006).
Data source: Review of 206 patients with relapsing-remitting or progressive multiple sclerosis
Disclosures: The investigators had no disclosures.

Keys to Success on the Focused Practice in Hospital Medicine Exam

- Enroll in the Focused Practice in Hospital Medicine MOC program by August 1 at www.abim.org.
- Schedule a seat for the exam before August 15 at www.abim.org.
- Order SHM SPARK, the missing piece of the MOC exam-prep puzzle.
SHM recently developed the only MOC exam-preparation tool by hospitalists for hospitalists, SHM SPARK. It complements tools already on the market and will help hospitalists succeed on the upcoming exam. SHM SPARK delivers 175 vignette-style multiple-choice questions that bridge the primary knowledge gaps found within existing MOC exam-preparation products and provides in-depth review on:
- Palliative care, ethics, and decision making
- Patient safety
- Perioperative care and consultative co-management
- Quality, cost, and clinical reasoning
SHM SPARK offers detailed learning objectives and discussion points and allows users to define individual areas of strengths and weaknesses. Users can claim 58 ABIM MOC Medical Knowledge points upon completion of all four modules with a minimum passing score of 80%. After successful completion of all four modules, participants may claim up to 10.5 AMA PRA Category 1 credits.
- Enroll in the Focused Practice in Hospital Medicine MOC program by August 1 at www.abim.org.
- Schedule a seat for the exam before August 15 at www.abim.org.
- Order SHM SPARK, the missing piece of the MOC exam-prep puzzle.
SHM recently developed the only MOC exam-preparation tool by hospitalists for hospitalists, SHM SPARK. It complements tools already on the market and will help hospitalists succeed on the upcoming exam. SHM SPARK delivers 175 vignette-style multiple-choice questions that bridge the primary knowledge gaps found within existing MOC exam-preparation products and provides in-depth review on:
- Palliative care, ethics, and decision making
- Patient safety
- Perioperative care and consultative co-management
- Quality, cost, and clinical reasoning
SHM SPARK offers detailed learning objectives and discussion points and allows users to define individual areas of strengths and weaknesses. Users can claim 58 ABIM MOC Medical Knowledge points upon completion of all four modules with a minimum passing score of 80%. After successful completion of all four modules, participants may claim up to 10.5 AMA PRA Category 1 credits.
- Enroll in the Focused Practice in Hospital Medicine MOC program by August 1 at www.abim.org.
- Schedule a seat for the exam before August 15 at www.abim.org.
- Order SHM SPARK, the missing piece of the MOC exam-prep puzzle.
SHM recently developed the only MOC exam-preparation tool by hospitalists for hospitalists, SHM SPARK. It complements tools already on the market and will help hospitalists succeed on the upcoming exam. SHM SPARK delivers 175 vignette-style multiple-choice questions that bridge the primary knowledge gaps found within existing MOC exam-preparation products and provides in-depth review on:
- Palliative care, ethics, and decision making
- Patient safety
- Perioperative care and consultative co-management
- Quality, cost, and clinical reasoning
SHM SPARK offers detailed learning objectives and discussion points and allows users to define individual areas of strengths and weaknesses. Users can claim 58 ABIM MOC Medical Knowledge points upon completion of all four modules with a minimum passing score of 80%. After successful completion of all four modules, participants may claim up to 10.5 AMA PRA Category 1 credits.

Update on the Interstate Medical Licensure Compact
In 2014, the Society of Hospital Medicine endorsed the Interstate Medical Licensure Compact as a way to address divergent physician licensing requirements among states. The thrust of SHM’s reasoning was that differing licensing policies across state lines not only hinder the ability of hospitalists to quickly adjust staffing to meet the needs of hospitals and patients but also create extensive, costly, and often redundant administrative hurdles for individual hospitalists and hospital medicine groups. For hospitalists looking to relocate to another state, practice in multiple states, provide telemedicine services, or even take on some per diem work, the Interstate Medical Licensure Compact should be of great help.
To briefly summarize, states participating in the compact agree to share information with one another and work together in streamlining the licensing process. For example, the compact aims to reduce redundant licensing requirements by creating one place where physicians submit basic information such as their education credentials. The compact does not establish a national license; a license to practice medicine will still be issued by individual state medical boards. Physicians will still need to be licensed in the state where the patient is located, but the difference is that the process of obtaining a license will be streamlined significantly.
To join the Interstate Medical Licensure Compact, state legislatures must enact the compact into state law. Two years in, the compact is now being implemented in 12 states: Alabama, Idaho, Illinois, Iowa, Minnesota, Montana, Nevada, South Dakota, Utah, West Virginia, Wisconsin, and Wyoming. States where it has been introduced but not yet adopted include Alaska, Arizona, Colorado, Kansas, Maryland, Michigan, Mississippi, Nebraska, New Hampshire, Oklahoma, Pennsylvania, Rhode Island, Vermont, and Washington.
Licenses via the compact process are not currently being issued, but representatives from the 12 participating states have begun to formally meet and are working out the administrative procedures needed to begin expedited licensure processes. With a core group of states adopting and implementing the compact, it will be important for state officials to hear why adoption of the compact is important to physicians.
This presents an opportunity for hospitalists residing in holdout states to participate in some advocacy work at the state level—on their own, as a group, or even within one of SHM’s many state chapters. To find your local chapter and get involved, visit www.hospitalmedicine.org/chapters.
To assist, detailed information on the Interstate Medical Licensure Compact can be found at www.licenseportability.org, and SHM advocacy staff is available to address questions members may have about getting started. You can reach them via email at advocacy@hospitalmedicine.org. TH
Josh Boswell is SHM’s director of government affairs.
In 2014, the Society of Hospital Medicine endorsed the Interstate Medical Licensure Compact as a way to address divergent physician licensing requirements among states. The thrust of SHM’s reasoning was that differing licensing policies across state lines not only hinder the ability of hospitalists to quickly adjust staffing to meet the needs of hospitals and patients but also create extensive, costly, and often redundant administrative hurdles for individual hospitalists and hospital medicine groups. For hospitalists looking to relocate to another state, practice in multiple states, provide telemedicine services, or even take on some per diem work, the Interstate Medical Licensure Compact should be of great help.
To briefly summarize, states participating in the compact agree to share information with one another and work together in streamlining the licensing process. For example, the compact aims to reduce redundant licensing requirements by creating one place where physicians submit basic information such as their education credentials. The compact does not establish a national license; a license to practice medicine will still be issued by individual state medical boards. Physicians will still need to be licensed in the state where the patient is located, but the difference is that the process of obtaining a license will be streamlined significantly.
To join the Interstate Medical Licensure Compact, state legislatures must enact the compact into state law. Two years in, the compact is now being implemented in 12 states: Alabama, Idaho, Illinois, Iowa, Minnesota, Montana, Nevada, South Dakota, Utah, West Virginia, Wisconsin, and Wyoming. States where it has been introduced but not yet adopted include Alaska, Arizona, Colorado, Kansas, Maryland, Michigan, Mississippi, Nebraska, New Hampshire, Oklahoma, Pennsylvania, Rhode Island, Vermont, and Washington.
Licenses via the compact process are not currently being issued, but representatives from the 12 participating states have begun to formally meet and are working out the administrative procedures needed to begin expedited licensure processes. With a core group of states adopting and implementing the compact, it will be important for state officials to hear why adoption of the compact is important to physicians.
This presents an opportunity for hospitalists residing in holdout states to participate in some advocacy work at the state level—on their own, as a group, or even within one of SHM’s many state chapters. To find your local chapter and get involved, visit www.hospitalmedicine.org/chapters.
To assist, detailed information on the Interstate Medical Licensure Compact can be found at www.licenseportability.org, and SHM advocacy staff is available to address questions members may have about getting started. You can reach them via email at advocacy@hospitalmedicine.org. TH
Josh Boswell is SHM’s director of government affairs.
In 2014, the Society of Hospital Medicine endorsed the Interstate Medical Licensure Compact as a way to address divergent physician licensing requirements among states. The thrust of SHM’s reasoning was that differing licensing policies across state lines not only hinder the ability of hospitalists to quickly adjust staffing to meet the needs of hospitals and patients but also create extensive, costly, and often redundant administrative hurdles for individual hospitalists and hospital medicine groups. For hospitalists looking to relocate to another state, practice in multiple states, provide telemedicine services, or even take on some per diem work, the Interstate Medical Licensure Compact should be of great help.
To briefly summarize, states participating in the compact agree to share information with one another and work together in streamlining the licensing process. For example, the compact aims to reduce redundant licensing requirements by creating one place where physicians submit basic information such as their education credentials. The compact does not establish a national license; a license to practice medicine will still be issued by individual state medical boards. Physicians will still need to be licensed in the state where the patient is located, but the difference is that the process of obtaining a license will be streamlined significantly.
To join the Interstate Medical Licensure Compact, state legislatures must enact the compact into state law. Two years in, the compact is now being implemented in 12 states: Alabama, Idaho, Illinois, Iowa, Minnesota, Montana, Nevada, South Dakota, Utah, West Virginia, Wisconsin, and Wyoming. States where it has been introduced but not yet adopted include Alaska, Arizona, Colorado, Kansas, Maryland, Michigan, Mississippi, Nebraska, New Hampshire, Oklahoma, Pennsylvania, Rhode Island, Vermont, and Washington.
Licenses via the compact process are not currently being issued, but representatives from the 12 participating states have begun to formally meet and are working out the administrative procedures needed to begin expedited licensure processes. With a core group of states adopting and implementing the compact, it will be important for state officials to hear why adoption of the compact is important to physicians.
This presents an opportunity for hospitalists residing in holdout states to participate in some advocacy work at the state level—on their own, as a group, or even within one of SHM’s many state chapters. To find your local chapter and get involved, visit www.hospitalmedicine.org/chapters.
To assist, detailed information on the Interstate Medical Licensure Compact can be found at www.licenseportability.org, and SHM advocacy staff is available to address questions members may have about getting started. You can reach them via email at advocacy@hospitalmedicine.org. TH
Josh Boswell is SHM’s director of government affairs.
FDA approves CMV test for use in HSCT recipients
The US Food and Drug Administration (FDA) has approved the first cytomegalovirus (CMV) test for use in hematopoietic stem cell transplant (HSCT) recipients.
With this approval, the COBAS® AmpliPrep/COBAS® TaqMan® CMV Test is available for monitoring CMV treatment in all types of transplant patients in the US.
The test, which was developed by Roche, is an in vitro nucleic acid amplification test that quantitates CMV DNA in human plasma.
It is intended to aid the management of HSCT recipients and solid-organ transplant recipients who are undergoing anti-CMV therapy.
In this population, serial DNA measurements can be used to assess virological response to antiviral treatment. The results from the test must be interpreted within the context of all relevant clinical and laboratory findings.
The COBAS® AmpliPrep/COBAS® TaqMan® CMV Test is not intended for use as a screening test for the presence of CMV DNA in blood or blood products.
The test is designed for use on the automated COBAS® AmpliPrep/COBAS® TaqMan® System, an established platform for viral load monitoring of multiple infectious diseases.
The system combines the COBAS® AmpliPrep Instrument for automated sample preparation and the COBAS® TaqMan® Analyzer or the smaller COBAS® TaqMan® 48 Analyzer for automated real-time PCR amplification and detection.
The COBAS® AmpliPrep/COBAS® TaqMan® System has parallel processing with other molecular diagnostics assays targeting other diseases. Roche’s AmpErase enzyme is also included in each test and is designed to prevent cross-contamination of samples and labs. ![]()
The US Food and Drug Administration (FDA) has approved the first cytomegalovirus (CMV) test for use in hematopoietic stem cell transplant (HSCT) recipients.
With this approval, the COBAS® AmpliPrep/COBAS® TaqMan® CMV Test is available for monitoring CMV treatment in all types of transplant patients in the US.
The test, which was developed by Roche, is an in vitro nucleic acid amplification test that quantitates CMV DNA in human plasma.
It is intended to aid the management of HSCT recipients and solid-organ transplant recipients who are undergoing anti-CMV therapy.
In this population, serial DNA measurements can be used to assess virological response to antiviral treatment. The results from the test must be interpreted within the context of all relevant clinical and laboratory findings.
The COBAS® AmpliPrep/COBAS® TaqMan® CMV Test is not intended for use as a screening test for the presence of CMV DNA in blood or blood products.
The test is designed for use on the automated COBAS® AmpliPrep/COBAS® TaqMan® System, an established platform for viral load monitoring of multiple infectious diseases.
The system combines the COBAS® AmpliPrep Instrument for automated sample preparation and the COBAS® TaqMan® Analyzer or the smaller COBAS® TaqMan® 48 Analyzer for automated real-time PCR amplification and detection.
The COBAS® AmpliPrep/COBAS® TaqMan® System has parallel processing with other molecular diagnostics assays targeting other diseases. Roche’s AmpErase enzyme is also included in each test and is designed to prevent cross-contamination of samples and labs. ![]()
The US Food and Drug Administration (FDA) has approved the first cytomegalovirus (CMV) test for use in hematopoietic stem cell transplant (HSCT) recipients.
With this approval, the COBAS® AmpliPrep/COBAS® TaqMan® CMV Test is available for monitoring CMV treatment in all types of transplant patients in the US.
The test, which was developed by Roche, is an in vitro nucleic acid amplification test that quantitates CMV DNA in human plasma.
It is intended to aid the management of HSCT recipients and solid-organ transplant recipients who are undergoing anti-CMV therapy.
In this population, serial DNA measurements can be used to assess virological response to antiviral treatment. The results from the test must be interpreted within the context of all relevant clinical and laboratory findings.
The COBAS® AmpliPrep/COBAS® TaqMan® CMV Test is not intended for use as a screening test for the presence of CMV DNA in blood or blood products.
The test is designed for use on the automated COBAS® AmpliPrep/COBAS® TaqMan® System, an established platform for viral load monitoring of multiple infectious diseases.
The system combines the COBAS® AmpliPrep Instrument for automated sample preparation and the COBAS® TaqMan® Analyzer or the smaller COBAS® TaqMan® 48 Analyzer for automated real-time PCR amplification and detection.
The COBAS® AmpliPrep/COBAS® TaqMan® System has parallel processing with other molecular diagnostics assays targeting other diseases. Roche’s AmpErase enzyme is also included in each test and is designed to prevent cross-contamination of samples and labs. ![]()