User login
Lipoprotein(a) and Cardiovascular Disease
Cardiovascular disease (CVD) is the leading cause of death in the United States. CVD-related diseases affect 83.6 million people in the US and are responsible for almost 800,000 deaths annually.1 The myriad underlying causes for these disorders range from inadequate lifestyle management to genetic abnormalities. One genetically determined abnormality is lipoprotein(a), or Lp(a).2-4
It is estimated that 25% of the US population has elevated Lp(a) levels (> 30 mg/dL) that are clinically significant.5 Lp(a) is recognized as an independent risk factor for CVD, stroke, retinal artery occlusions, and restenosis of vein grafts.2-5
Regardless of practice type, clinicians at some point in their career will see a “vasculopath.” Many of these patients have undiagnosed familial hypercholesterolemia, which affects 1 in 200 to 300 patients in the US and manifests with LDL cholesterol (LDL-C) levels ≥ 190 mg/dL.6-8 Other patients may have CVD with relatively “normal” traditional lipids, more aggressive premature disease, and/or progressive disease despite “usual therapy.”
As clinical lipid specialists working both in cardiology and endocrinology, the authors find the lack of evaluation for additional abnormalities in high-risk patients to be quite disturbing. The patient most commonly seen with the Lp(a) abnormality is one with CVD onset approximately one decade earlier than expected, along with a family history of premature CVD or closure of recently placed stents. Unfortunately, this may result in disease in the second or third decade for men and third or fourth decade for women.
Of course, CVD can leave patients with less productive lives and increase the burden to the health care system and to society. A positive outcome of identification of this apolipoprotein abnormality is that it may prompt evaluation of other family members prior to the inception of vascular disease. When it is identified in the asymptomatic, disease-free patient, aggressive risk reduction—in the form of lifestyle management and medication—may delay or prevent disease onset.
Continue for identification of the problem >>
Identification of the problem
Office visits seldom include a thorough and complete patient history. A “good” family history should include first-degree relatives. Time-constrained practitioners may take a rudimentary family history of immediate relatives when a pedigree of the patient would be more appropriate.
Pedigree assessment offers a more specific picture of disease in families and identifies prevalence and incidence. Busy clinicians could have patients use an online resource to generate their own family pedigree. Or, as in most practices, a medical assistant or other appropriate office staff could initiate the process in the chart.
Patients with premature or advanced disease and significant family history need further investigation. A suspect history would include multiple family members with disease earlier in life than expected and perhaps early cardiovascular death. The personal history of the patient may include multiple cardiovascular incidents despite therapeutic intervention; despite taking lipid-lowering and/or antiplatelet therapy, the patient will present with progressive disease. Often, disease manifests in multiple areas of the vasculature or as restenosis of previous interventions.
Genetics
Lp(a) results from a genetic variation of the apolipoprotein(a) (LPA) locus on chromosome 6q27. Lp(a) is comprised of an apolipoprotein(b) (apoB)–containing LDL molecule that is bonded to LPA. LPA is structurally similar to plasminogen, the precursor for plasmin that degrades fibrin in blood clots. Due to this similarity, LPA can competitively inhibit plasmin activity and thereby increase risk for thrombosis.4,9
Continue for physical examination >>
Physical Examination
Patients with very elevated LDL-C levels in whom Lp(a) is also high may present with other outward stigmata of dyslipidemia. Visualization of the eye may reveal evidence of severe dyslipidemia with arcus cornea. This arcus can present as unilateral, bilateral, inferior, superior, or mixed and is representative of the buildup of cholesterol that cannot be removed from the body by normal means. Further examination may reveal tendon xanthomas, which are also representative of a genetic cholesterol disorder—in most cases, familial hypercholesterolemia.7
Laboratory Workup
In patients who are known or suspected to be at high risk for CVD, the laboratory workup should include a fasting lipid panel, with Lp(a) and apoB; a comprehensive metabolic profile to establish renal and liver function (as therapeutic interventions utilize these organs for metabolism); and a fasting glucose measurement to rule out occult diabetes, which enhances risk factors. Thyroid function is also assessed, secondary to its deleterious effects on lipid metabolism.
Lp(a) results must be interpreted in the context of ethnicity; significance will vary. For example, both the African-American and Asian populations have been found to have high levels of Lp(a), but these are generally felt to be less atherogenic in African Americans. No major differences have been identified for other populations. It is, however, important to note that those patients with nephropathies and elevated Lp(a) carry a higher risk for coronary artery disease.
Lp(a) levels will remain relatively steady throughout life, negating the need for routine monitoring once a patient’s levels have been established. The exception is postmenopausal women, in whom Lp(a) levels may increase due to changes in estrogen. It is prudent to assess Lp(a) in women both pre- and postmenopause, based on data from the Women’s Health Study.10
Continue for diagnosis and treatment >>
Diagnosis and Treatment
Elevated Lp(a), which is found in 25% to 35% of the population, is diagnosed at a level > 30 mg/dL, regardless of sex.4,9 In conjunction with known disease, elevated Lp(a) is sufficient to warrant consideration of very aggressive treatment. In these circumstances, the provider may consider a target LDL-C level ≤ 70 mg/dL.6,7,11 In primary prevention, clinicians should consider lowering this threshold. Levels that may have been considered appropriate in a low- or moderate-risk patient (≤ 160 mg/dL and ≤ 130 mg/dL, respectively) may be reduced to ≤ 130 mg/dL and ≤ 100 mg/dL, respectively.6,11
There is no peer-reviewed evidence with regard to lifestyle management (exercise and diet) for reduction of Lp(a). However, it is reasonable to recommend that high-risk patients adopt healthier regimens.
Management of elevated Lp(a) includes consideration of pharmacologic intervention. Since Lp(a) is prothrombotic, all patients without contraindications should at least be taking low-dose (81-mg) aspirin. Those with evidence of thrombotic events may need lifetime antiplatelet therapy.12 Statin therapy has mixed and minimal effects on Lp(a), although it remains the mainstay of treatment due to its effects on LDL-C and other lipoproteins.13 Although long-term data are lacking, there is some anecdotal evidence of improvement with fibrate therapy. However, it is not recommended for treatment of elevated Lp(a).14
Nicotinic acid has had the longest and most robust history for reduction of Lp(a).9,12 However, recent studies examining combination therapy with statins and nicotinic acid have yielded discouraging results—and in some cases have suggested negative outcomes with this combination.15,16 High doses (4-5 g for immediate release and 2-3 g for sustained release) of nicotinic acid are necessary to produce beneficial results on Lp(a) or other lipid abnormalities (eg, elevated triglycerides, low HDL cholesterol).17 Use of OTC nicotinic acid is not recommended, since these products are considered dietary supplements and regulated as such, raising the potential for untoward adverse effects and/or the possibility that little to no active ingredient is present.18-20
Results from the Women’s Health Study and the Heart and Estrogen/progestin Replacement Study suggested that estrogen might be an effective therapy. In one analysis, women with elevated Lp(a) derived greater potential cardioprotective effects from hormone replacement therapy (HRT) than those with lower Lp(a), and the researchers noted a “significant interaction” between baseline Lp(a), HRT treatment, and CVD risk. However, use of HRT is not approved for treatment of vascular risk today, due to the potential for adverse effects.10,21
A novel therapy, in the form of PCSK9 inhibition, has been shown to reduce LDL-C significantly; reduction in Lp(a) was also observed. The FDA recently approved two PCSK9 inhibitors (alirocumab and evolocumab) for use, although the primary indication is for further reduction in LDL-C on top of the maximally tolerated dose of statin therapy, not for reduction of Lp(a).22,23
Apheresis has been shown to have positive effects in reducing ongoing vascular events in select patient populations. It is approved by the FDA for treatment of refractory LDL-C, mostly in patients with familial hypercholesterolemia, but it is not indicated for treatment of elevated Lp(a). However, since Lp(a) tracks with LDL-C, it is also removed during the process; about a 50% reduction in Lp(a) levels has been noted, although levels rebound posttreatment. To date, reimbursement issues remain in the absence of an FDA indication and due to the paucity of treatment centers in the US.24,25
Follow-up. The therapies mentioned require routine evaluation to assess tolerability and safety, as recommended in the prescribing information. Patients with known CVD should undergo an appropriate cardiac workup annually to evaluate for occult progression of disease. Patients require further evaluation of related cardiovascular risk factors and adherence with medication regimens. For primary prevention patients, annual follow-up is also recommended to assess for any changes in health status, lifestyle, or medication adherence.
Continue for conclusion >>
Conclusion
The average health care provider frequently performs the standard evaluation of a patient at risk for, or with, CVD. However, a subset of this population may be at increased cardiovascular risk due to Lp(a), a common genetic risk factor that can be responsible for premature or progressive CVD. Because of the aggressive nature of this disorder and the young age at which it influences the development of vascular disease, health care providers must be more vigilant about looking beyond the obvious in patients with familial hypercholesterolemia or family history of premature CVD.
Patients with progressive disease must be more thoroughly evaluated; there are already more than 63 million persons with elevated Lp(a) in the US—and many more undiagnosed—who may benefit from aggressive care. Underdiagnosis has been associated with decreased quality and productivity in the work environment, decreased quality of life, increased use of health dollars, and possibly early loss of life.
While the test for Lp(a) is readily available, the cost may not be covered by insurance and therefore may be passed on to the patient. It would behoove health care professionals to lobby for coverage as a means to reduce the prevalence of CVD, the number one cause of mortality in the US.
References
1. Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive Summary: heart disease and stroke statistics—2014 Update: a report from the American Heart Association. Circulation. 2014;129:399-410.
2. Bennet A, Di Angelantonio E, Erqou S, et al. Lipoprotein(a) levels and risk of future coronary heart disease: large-scale prospective data [published corrections appear in Arch Intern Med. 2008;168(10):1089 and Arch Intern Med. 2008;168(10):1096]. Arch Intern Med. 2008;168(6):598-608.
3. Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301(22):2331-2339.
4. Suk DJ, Rifai N, Buring JE, Ridker PM. Lipoprotein(a), hormone replacement therapy, and risk of future cardiovascular events. J Am Coll Cardiol. 2008;52(2):124-131.
5. Scanu AM. Lipoprotein(a). A genetic risk factor for premature coronary heart disease. JAMA. 1992;267(24):3326-3329.
6. Goldberg AC, Hopkins PN, Toth PP; National Lipid Association Expert Panel on Familial Hypercholesterolemia. Familial hypercholesterolemia: screening, diagnosis and management of pediatric and adult patients: clinical guidance from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J Clin Lipid. 2011;5(3 suppl):S1-S8.
7. Ito M, McGowan MP, Moriarty PM; National Lipid Association Expert Panel on Familial Hypercholesterolemia. Management of familial hypercholesterolemias in adult patients: recommendations from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J Clin Lipid. 2011;5(3 suppl):S38-S45.
8. Sjouke B, Kusters DM, Kindt I, et al. Homozygous autosomal dominant hypercholesterolaemia in the Netherlands: prevalence, genotype-phenotype relationship, and clinical outcome. Eur Heart J. 2014 Feb 28. [Epub ahead of print]
9. Nordestgaard BG, Chapman MJ, Ray K, et al; European Atherosclerosis Society Consensus Panel. Lipoprotein (a) as a cardiovascular risk factor: current status. Eur Heart J. 2010; 31(23):2844-2853.
10. Suk DJ, Rifai N, Buring JE, Ridker PM. Lipoprotein(a), measured with an assay independent of apolipoprotein(a) isoform size, and risk of future cardiovascular events among initially healthy women. JAMA. 2006;296 (11):1363-1370.
11. Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. 2004;110(2):227-239.
12. Jacobson TA. Lipoprotein (a), cardiovascular disease, and contemporary management. Mayo Clin Proc. 2013;88(11):1294-1311.
13. Hunninghake DB, Stein EA, Mellies MJ. Effects of one year of treatment with pravastatin, an HMG-CoA reductase inhibitor, on lipoprotein a. J Clin Pharmacol. 1993;33 (6):574-580.
14. Jones PH, Pownall HJ, Patsch W, et al. Effect of gemfibrozil on levels of lipoprotein[a] in type 2 hyperlipoproteinemic subjects. J Lipid Res. 1996;37(6):1298-1308.
15. Boden WE, Probstfield JL, Anderson T, et al; AIM-HIGH investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011; 365(24):2255-2267.
16. Landray MJ, Haynes R, Hopewell JC, et al; HPS2-THRIVE Collaborative Group. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371 (3):203-212.
17. Morgan JM, Capuzzi DM, Guyton JR. A new extended-release niacin (Niaspan): efficacy, tolerability, and safety in hypercholesterolemic patients. Am J Cardiol. 1998;82 (12A): 29U-34U.
18. Piepho RW. The pharmacokinetics and pharmacodynamics of agents proven to raise high-density lipoprotein cholesterol. Am J Cardiol. 2000;86(12A):35L-40L.
19. Guyton JR, Bays HE. Safety considerations with niacin therapy. Am J Cardiol. 2007; 99(6A):22C-31C.
20. McKenney JM, Proctor JD, Harris S, Chinchili VM. A comparison of the efficacy and toxic effects of sustained- vs immediate-release niacin in hypercholesterolemic patients. JAMA. 1994;271(9):672-677.
21. Shlipak MG, Simon JA, Vittinghoff E, et al. Estrogen and progestin, lipoprotein(a), and the risk of recurrent coronary heart disease events after menopause. JAMA. 2000;283 (14):1845-1852.
22. Marbach JA, McKeon JL, Ross JL, Duffy D. Novel treatments for familial hypercholesterolemia: pharmacogenetics at work. Pharmacotherapy. 2014;34(9):961-972.
23. Stein EA, Mellis S, Yancopoulos GD, et al. Effect of a monoclonal antibody to PCSK9 on LDL cholesterol. N Engl J Med. 2012;366(12): 1108-1118.
24. Sachais BS, Katz J, Ross J, Rader DJ. Long-term effects of LDL apheresis in patients with severe hypercholesterolemia. J Clin Apher. 2005;20:252-255.
25. Waldmann E, Parhofer K. Lipoprotein apheresis to treat elevated lipoprotein(a). J Lipid Res. 2016 Feb 17. [Epub ahead of print]
Clinician Reviews in partnership with![]()
John H. Sink practices at The Jones Center for Diabetes and Endocrine Wellness in Macon, Georgia. Joyce L. Ross is President of the National Lipid Association and Past President of the Preventive Cardiovascular Nurses Association. Mr. Sink has no disclosures relevant to the content of this article. Ms. Ross is on the Speakers’ Bureau for Sanofi/Regeneron, AstraZeneca, Abbott/AbbVie, Amarin, and Amgen; she is also a consultant for Amarin.
Clinician Reviews in partnership with![]()
John H. Sink practices at The Jones Center for Diabetes and Endocrine Wellness in Macon, Georgia. Joyce L. Ross is President of the National Lipid Association and Past President of the Preventive Cardiovascular Nurses Association. Mr. Sink has no disclosures relevant to the content of this article. Ms. Ross is on the Speakers’ Bureau for Sanofi/Regeneron, AstraZeneca, Abbott/AbbVie, Amarin, and Amgen; she is also a consultant for Amarin.
Clinician Reviews in partnership with![]()
John H. Sink practices at The Jones Center for Diabetes and Endocrine Wellness in Macon, Georgia. Joyce L. Ross is President of the National Lipid Association and Past President of the Preventive Cardiovascular Nurses Association. Mr. Sink has no disclosures relevant to the content of this article. Ms. Ross is on the Speakers’ Bureau for Sanofi/Regeneron, AstraZeneca, Abbott/AbbVie, Amarin, and Amgen; she is also a consultant for Amarin.
Cardiovascular disease (CVD) is the leading cause of death in the United States. CVD-related diseases affect 83.6 million people in the US and are responsible for almost 800,000 deaths annually.1 The myriad underlying causes for these disorders range from inadequate lifestyle management to genetic abnormalities. One genetically determined abnormality is lipoprotein(a), or Lp(a).2-4
It is estimated that 25% of the US population has elevated Lp(a) levels (> 30 mg/dL) that are clinically significant.5 Lp(a) is recognized as an independent risk factor for CVD, stroke, retinal artery occlusions, and restenosis of vein grafts.2-5
Regardless of practice type, clinicians at some point in their career will see a “vasculopath.” Many of these patients have undiagnosed familial hypercholesterolemia, which affects 1 in 200 to 300 patients in the US and manifests with LDL cholesterol (LDL-C) levels ≥ 190 mg/dL.6-8 Other patients may have CVD with relatively “normal” traditional lipids, more aggressive premature disease, and/or progressive disease despite “usual therapy.”
As clinical lipid specialists working both in cardiology and endocrinology, the authors find the lack of evaluation for additional abnormalities in high-risk patients to be quite disturbing. The patient most commonly seen with the Lp(a) abnormality is one with CVD onset approximately one decade earlier than expected, along with a family history of premature CVD or closure of recently placed stents. Unfortunately, this may result in disease in the second or third decade for men and third or fourth decade for women.
Of course, CVD can leave patients with less productive lives and increase the burden to the health care system and to society. A positive outcome of identification of this apolipoprotein abnormality is that it may prompt evaluation of other family members prior to the inception of vascular disease. When it is identified in the asymptomatic, disease-free patient, aggressive risk reduction—in the form of lifestyle management and medication—may delay or prevent disease onset.
Continue for identification of the problem >>
Identification of the problem
Office visits seldom include a thorough and complete patient history. A “good” family history should include first-degree relatives. Time-constrained practitioners may take a rudimentary family history of immediate relatives when a pedigree of the patient would be more appropriate.
Pedigree assessment offers a more specific picture of disease in families and identifies prevalence and incidence. Busy clinicians could have patients use an online resource to generate their own family pedigree. Or, as in most practices, a medical assistant or other appropriate office staff could initiate the process in the chart.
Patients with premature or advanced disease and significant family history need further investigation. A suspect history would include multiple family members with disease earlier in life than expected and perhaps early cardiovascular death. The personal history of the patient may include multiple cardiovascular incidents despite therapeutic intervention; despite taking lipid-lowering and/or antiplatelet therapy, the patient will present with progressive disease. Often, disease manifests in multiple areas of the vasculature or as restenosis of previous interventions.
Genetics
Lp(a) results from a genetic variation of the apolipoprotein(a) (LPA) locus on chromosome 6q27. Lp(a) is comprised of an apolipoprotein(b) (apoB)–containing LDL molecule that is bonded to LPA. LPA is structurally similar to plasminogen, the precursor for plasmin that degrades fibrin in blood clots. Due to this similarity, LPA can competitively inhibit plasmin activity and thereby increase risk for thrombosis.4,9
Continue for physical examination >>
Physical Examination
Patients with very elevated LDL-C levels in whom Lp(a) is also high may present with other outward stigmata of dyslipidemia. Visualization of the eye may reveal evidence of severe dyslipidemia with arcus cornea. This arcus can present as unilateral, bilateral, inferior, superior, or mixed and is representative of the buildup of cholesterol that cannot be removed from the body by normal means. Further examination may reveal tendon xanthomas, which are also representative of a genetic cholesterol disorder—in most cases, familial hypercholesterolemia.7
Laboratory Workup
In patients who are known or suspected to be at high risk for CVD, the laboratory workup should include a fasting lipid panel, with Lp(a) and apoB; a comprehensive metabolic profile to establish renal and liver function (as therapeutic interventions utilize these organs for metabolism); and a fasting glucose measurement to rule out occult diabetes, which enhances risk factors. Thyroid function is also assessed, secondary to its deleterious effects on lipid metabolism.
Lp(a) results must be interpreted in the context of ethnicity; significance will vary. For example, both the African-American and Asian populations have been found to have high levels of Lp(a), but these are generally felt to be less atherogenic in African Americans. No major differences have been identified for other populations. It is, however, important to note that those patients with nephropathies and elevated Lp(a) carry a higher risk for coronary artery disease.
Lp(a) levels will remain relatively steady throughout life, negating the need for routine monitoring once a patient’s levels have been established. The exception is postmenopausal women, in whom Lp(a) levels may increase due to changes in estrogen. It is prudent to assess Lp(a) in women both pre- and postmenopause, based on data from the Women’s Health Study.10
Continue for diagnosis and treatment >>
Diagnosis and Treatment
Elevated Lp(a), which is found in 25% to 35% of the population, is diagnosed at a level > 30 mg/dL, regardless of sex.4,9 In conjunction with known disease, elevated Lp(a) is sufficient to warrant consideration of very aggressive treatment. In these circumstances, the provider may consider a target LDL-C level ≤ 70 mg/dL.6,7,11 In primary prevention, clinicians should consider lowering this threshold. Levels that may have been considered appropriate in a low- or moderate-risk patient (≤ 160 mg/dL and ≤ 130 mg/dL, respectively) may be reduced to ≤ 130 mg/dL and ≤ 100 mg/dL, respectively.6,11
There is no peer-reviewed evidence with regard to lifestyle management (exercise and diet) for reduction of Lp(a). However, it is reasonable to recommend that high-risk patients adopt healthier regimens.
Management of elevated Lp(a) includes consideration of pharmacologic intervention. Since Lp(a) is prothrombotic, all patients without contraindications should at least be taking low-dose (81-mg) aspirin. Those with evidence of thrombotic events may need lifetime antiplatelet therapy.12 Statin therapy has mixed and minimal effects on Lp(a), although it remains the mainstay of treatment due to its effects on LDL-C and other lipoproteins.13 Although long-term data are lacking, there is some anecdotal evidence of improvement with fibrate therapy. However, it is not recommended for treatment of elevated Lp(a).14
Nicotinic acid has had the longest and most robust history for reduction of Lp(a).9,12 However, recent studies examining combination therapy with statins and nicotinic acid have yielded discouraging results—and in some cases have suggested negative outcomes with this combination.15,16 High doses (4-5 g for immediate release and 2-3 g for sustained release) of nicotinic acid are necessary to produce beneficial results on Lp(a) or other lipid abnormalities (eg, elevated triglycerides, low HDL cholesterol).17 Use of OTC nicotinic acid is not recommended, since these products are considered dietary supplements and regulated as such, raising the potential for untoward adverse effects and/or the possibility that little to no active ingredient is present.18-20
Results from the Women’s Health Study and the Heart and Estrogen/progestin Replacement Study suggested that estrogen might be an effective therapy. In one analysis, women with elevated Lp(a) derived greater potential cardioprotective effects from hormone replacement therapy (HRT) than those with lower Lp(a), and the researchers noted a “significant interaction” between baseline Lp(a), HRT treatment, and CVD risk. However, use of HRT is not approved for treatment of vascular risk today, due to the potential for adverse effects.10,21
A novel therapy, in the form of PCSK9 inhibition, has been shown to reduce LDL-C significantly; reduction in Lp(a) was also observed. The FDA recently approved two PCSK9 inhibitors (alirocumab and evolocumab) for use, although the primary indication is for further reduction in LDL-C on top of the maximally tolerated dose of statin therapy, not for reduction of Lp(a).22,23
Apheresis has been shown to have positive effects in reducing ongoing vascular events in select patient populations. It is approved by the FDA for treatment of refractory LDL-C, mostly in patients with familial hypercholesterolemia, but it is not indicated for treatment of elevated Lp(a). However, since Lp(a) tracks with LDL-C, it is also removed during the process; about a 50% reduction in Lp(a) levels has been noted, although levels rebound posttreatment. To date, reimbursement issues remain in the absence of an FDA indication and due to the paucity of treatment centers in the US.24,25
Follow-up. The therapies mentioned require routine evaluation to assess tolerability and safety, as recommended in the prescribing information. Patients with known CVD should undergo an appropriate cardiac workup annually to evaluate for occult progression of disease. Patients require further evaluation of related cardiovascular risk factors and adherence with medication regimens. For primary prevention patients, annual follow-up is also recommended to assess for any changes in health status, lifestyle, or medication adherence.
Continue for conclusion >>
Conclusion
The average health care provider frequently performs the standard evaluation of a patient at risk for, or with, CVD. However, a subset of this population may be at increased cardiovascular risk due to Lp(a), a common genetic risk factor that can be responsible for premature or progressive CVD. Because of the aggressive nature of this disorder and the young age at which it influences the development of vascular disease, health care providers must be more vigilant about looking beyond the obvious in patients with familial hypercholesterolemia or family history of premature CVD.
Patients with progressive disease must be more thoroughly evaluated; there are already more than 63 million persons with elevated Lp(a) in the US—and many more undiagnosed—who may benefit from aggressive care. Underdiagnosis has been associated with decreased quality and productivity in the work environment, decreased quality of life, increased use of health dollars, and possibly early loss of life.
While the test for Lp(a) is readily available, the cost may not be covered by insurance and therefore may be passed on to the patient. It would behoove health care professionals to lobby for coverage as a means to reduce the prevalence of CVD, the number one cause of mortality in the US.
References
1. Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive Summary: heart disease and stroke statistics—2014 Update: a report from the American Heart Association. Circulation. 2014;129:399-410.
2. Bennet A, Di Angelantonio E, Erqou S, et al. Lipoprotein(a) levels and risk of future coronary heart disease: large-scale prospective data [published corrections appear in Arch Intern Med. 2008;168(10):1089 and Arch Intern Med. 2008;168(10):1096]. Arch Intern Med. 2008;168(6):598-608.
3. Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301(22):2331-2339.
4. Suk DJ, Rifai N, Buring JE, Ridker PM. Lipoprotein(a), hormone replacement therapy, and risk of future cardiovascular events. J Am Coll Cardiol. 2008;52(2):124-131.
5. Scanu AM. Lipoprotein(a). A genetic risk factor for premature coronary heart disease. JAMA. 1992;267(24):3326-3329.
6. Goldberg AC, Hopkins PN, Toth PP; National Lipid Association Expert Panel on Familial Hypercholesterolemia. Familial hypercholesterolemia: screening, diagnosis and management of pediatric and adult patients: clinical guidance from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J Clin Lipid. 2011;5(3 suppl):S1-S8.
7. Ito M, McGowan MP, Moriarty PM; National Lipid Association Expert Panel on Familial Hypercholesterolemia. Management of familial hypercholesterolemias in adult patients: recommendations from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J Clin Lipid. 2011;5(3 suppl):S38-S45.
8. Sjouke B, Kusters DM, Kindt I, et al. Homozygous autosomal dominant hypercholesterolaemia in the Netherlands: prevalence, genotype-phenotype relationship, and clinical outcome. Eur Heart J. 2014 Feb 28. [Epub ahead of print]
9. Nordestgaard BG, Chapman MJ, Ray K, et al; European Atherosclerosis Society Consensus Panel. Lipoprotein (a) as a cardiovascular risk factor: current status. Eur Heart J. 2010; 31(23):2844-2853.
10. Suk DJ, Rifai N, Buring JE, Ridker PM. Lipoprotein(a), measured with an assay independent of apolipoprotein(a) isoform size, and risk of future cardiovascular events among initially healthy women. JAMA. 2006;296 (11):1363-1370.
11. Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. 2004;110(2):227-239.
12. Jacobson TA. Lipoprotein (a), cardiovascular disease, and contemporary management. Mayo Clin Proc. 2013;88(11):1294-1311.
13. Hunninghake DB, Stein EA, Mellies MJ. Effects of one year of treatment with pravastatin, an HMG-CoA reductase inhibitor, on lipoprotein a. J Clin Pharmacol. 1993;33 (6):574-580.
14. Jones PH, Pownall HJ, Patsch W, et al. Effect of gemfibrozil on levels of lipoprotein[a] in type 2 hyperlipoproteinemic subjects. J Lipid Res. 1996;37(6):1298-1308.
15. Boden WE, Probstfield JL, Anderson T, et al; AIM-HIGH investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011; 365(24):2255-2267.
16. Landray MJ, Haynes R, Hopewell JC, et al; HPS2-THRIVE Collaborative Group. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371 (3):203-212.
17. Morgan JM, Capuzzi DM, Guyton JR. A new extended-release niacin (Niaspan): efficacy, tolerability, and safety in hypercholesterolemic patients. Am J Cardiol. 1998;82 (12A): 29U-34U.
18. Piepho RW. The pharmacokinetics and pharmacodynamics of agents proven to raise high-density lipoprotein cholesterol. Am J Cardiol. 2000;86(12A):35L-40L.
19. Guyton JR, Bays HE. Safety considerations with niacin therapy. Am J Cardiol. 2007; 99(6A):22C-31C.
20. McKenney JM, Proctor JD, Harris S, Chinchili VM. A comparison of the efficacy and toxic effects of sustained- vs immediate-release niacin in hypercholesterolemic patients. JAMA. 1994;271(9):672-677.
21. Shlipak MG, Simon JA, Vittinghoff E, et al. Estrogen and progestin, lipoprotein(a), and the risk of recurrent coronary heart disease events after menopause. JAMA. 2000;283 (14):1845-1852.
22. Marbach JA, McKeon JL, Ross JL, Duffy D. Novel treatments for familial hypercholesterolemia: pharmacogenetics at work. Pharmacotherapy. 2014;34(9):961-972.
23. Stein EA, Mellis S, Yancopoulos GD, et al. Effect of a monoclonal antibody to PCSK9 on LDL cholesterol. N Engl J Med. 2012;366(12): 1108-1118.
24. Sachais BS, Katz J, Ross J, Rader DJ. Long-term effects of LDL apheresis in patients with severe hypercholesterolemia. J Clin Apher. 2005;20:252-255.
25. Waldmann E, Parhofer K. Lipoprotein apheresis to treat elevated lipoprotein(a). J Lipid Res. 2016 Feb 17. [Epub ahead of print]
Cardiovascular disease (CVD) is the leading cause of death in the United States. CVD-related diseases affect 83.6 million people in the US and are responsible for almost 800,000 deaths annually.1 The myriad underlying causes for these disorders range from inadequate lifestyle management to genetic abnormalities. One genetically determined abnormality is lipoprotein(a), or Lp(a).2-4
It is estimated that 25% of the US population has elevated Lp(a) levels (> 30 mg/dL) that are clinically significant.5 Lp(a) is recognized as an independent risk factor for CVD, stroke, retinal artery occlusions, and restenosis of vein grafts.2-5
Regardless of practice type, clinicians at some point in their career will see a “vasculopath.” Many of these patients have undiagnosed familial hypercholesterolemia, which affects 1 in 200 to 300 patients in the US and manifests with LDL cholesterol (LDL-C) levels ≥ 190 mg/dL.6-8 Other patients may have CVD with relatively “normal” traditional lipids, more aggressive premature disease, and/or progressive disease despite “usual therapy.”
As clinical lipid specialists working both in cardiology and endocrinology, the authors find the lack of evaluation for additional abnormalities in high-risk patients to be quite disturbing. The patient most commonly seen with the Lp(a) abnormality is one with CVD onset approximately one decade earlier than expected, along with a family history of premature CVD or closure of recently placed stents. Unfortunately, this may result in disease in the second or third decade for men and third or fourth decade for women.
Of course, CVD can leave patients with less productive lives and increase the burden to the health care system and to society. A positive outcome of identification of this apolipoprotein abnormality is that it may prompt evaluation of other family members prior to the inception of vascular disease. When it is identified in the asymptomatic, disease-free patient, aggressive risk reduction—in the form of lifestyle management and medication—may delay or prevent disease onset.
Continue for identification of the problem >>
Identification of the problem
Office visits seldom include a thorough and complete patient history. A “good” family history should include first-degree relatives. Time-constrained practitioners may take a rudimentary family history of immediate relatives when a pedigree of the patient would be more appropriate.
Pedigree assessment offers a more specific picture of disease in families and identifies prevalence and incidence. Busy clinicians could have patients use an online resource to generate their own family pedigree. Or, as in most practices, a medical assistant or other appropriate office staff could initiate the process in the chart.
Patients with premature or advanced disease and significant family history need further investigation. A suspect history would include multiple family members with disease earlier in life than expected and perhaps early cardiovascular death. The personal history of the patient may include multiple cardiovascular incidents despite therapeutic intervention; despite taking lipid-lowering and/or antiplatelet therapy, the patient will present with progressive disease. Often, disease manifests in multiple areas of the vasculature or as restenosis of previous interventions.
Genetics
Lp(a) results from a genetic variation of the apolipoprotein(a) (LPA) locus on chromosome 6q27. Lp(a) is comprised of an apolipoprotein(b) (apoB)–containing LDL molecule that is bonded to LPA. LPA is structurally similar to plasminogen, the precursor for plasmin that degrades fibrin in blood clots. Due to this similarity, LPA can competitively inhibit plasmin activity and thereby increase risk for thrombosis.4,9
Continue for physical examination >>
Physical Examination
Patients with very elevated LDL-C levels in whom Lp(a) is also high may present with other outward stigmata of dyslipidemia. Visualization of the eye may reveal evidence of severe dyslipidemia with arcus cornea. This arcus can present as unilateral, bilateral, inferior, superior, or mixed and is representative of the buildup of cholesterol that cannot be removed from the body by normal means. Further examination may reveal tendon xanthomas, which are also representative of a genetic cholesterol disorder—in most cases, familial hypercholesterolemia.7
Laboratory Workup
In patients who are known or suspected to be at high risk for CVD, the laboratory workup should include a fasting lipid panel, with Lp(a) and apoB; a comprehensive metabolic profile to establish renal and liver function (as therapeutic interventions utilize these organs for metabolism); and a fasting glucose measurement to rule out occult diabetes, which enhances risk factors. Thyroid function is also assessed, secondary to its deleterious effects on lipid metabolism.
Lp(a) results must be interpreted in the context of ethnicity; significance will vary. For example, both the African-American and Asian populations have been found to have high levels of Lp(a), but these are generally felt to be less atherogenic in African Americans. No major differences have been identified for other populations. It is, however, important to note that those patients with nephropathies and elevated Lp(a) carry a higher risk for coronary artery disease.
Lp(a) levels will remain relatively steady throughout life, negating the need for routine monitoring once a patient’s levels have been established. The exception is postmenopausal women, in whom Lp(a) levels may increase due to changes in estrogen. It is prudent to assess Lp(a) in women both pre- and postmenopause, based on data from the Women’s Health Study.10
Continue for diagnosis and treatment >>
Diagnosis and Treatment
Elevated Lp(a), which is found in 25% to 35% of the population, is diagnosed at a level > 30 mg/dL, regardless of sex.4,9 In conjunction with known disease, elevated Lp(a) is sufficient to warrant consideration of very aggressive treatment. In these circumstances, the provider may consider a target LDL-C level ≤ 70 mg/dL.6,7,11 In primary prevention, clinicians should consider lowering this threshold. Levels that may have been considered appropriate in a low- or moderate-risk patient (≤ 160 mg/dL and ≤ 130 mg/dL, respectively) may be reduced to ≤ 130 mg/dL and ≤ 100 mg/dL, respectively.6,11
There is no peer-reviewed evidence with regard to lifestyle management (exercise and diet) for reduction of Lp(a). However, it is reasonable to recommend that high-risk patients adopt healthier regimens.
Management of elevated Lp(a) includes consideration of pharmacologic intervention. Since Lp(a) is prothrombotic, all patients without contraindications should at least be taking low-dose (81-mg) aspirin. Those with evidence of thrombotic events may need lifetime antiplatelet therapy.12 Statin therapy has mixed and minimal effects on Lp(a), although it remains the mainstay of treatment due to its effects on LDL-C and other lipoproteins.13 Although long-term data are lacking, there is some anecdotal evidence of improvement with fibrate therapy. However, it is not recommended for treatment of elevated Lp(a).14
Nicotinic acid has had the longest and most robust history for reduction of Lp(a).9,12 However, recent studies examining combination therapy with statins and nicotinic acid have yielded discouraging results—and in some cases have suggested negative outcomes with this combination.15,16 High doses (4-5 g for immediate release and 2-3 g for sustained release) of nicotinic acid are necessary to produce beneficial results on Lp(a) or other lipid abnormalities (eg, elevated triglycerides, low HDL cholesterol).17 Use of OTC nicotinic acid is not recommended, since these products are considered dietary supplements and regulated as such, raising the potential for untoward adverse effects and/or the possibility that little to no active ingredient is present.18-20
Results from the Women’s Health Study and the Heart and Estrogen/progestin Replacement Study suggested that estrogen might be an effective therapy. In one analysis, women with elevated Lp(a) derived greater potential cardioprotective effects from hormone replacement therapy (HRT) than those with lower Lp(a), and the researchers noted a “significant interaction” between baseline Lp(a), HRT treatment, and CVD risk. However, use of HRT is not approved for treatment of vascular risk today, due to the potential for adverse effects.10,21
A novel therapy, in the form of PCSK9 inhibition, has been shown to reduce LDL-C significantly; reduction in Lp(a) was also observed. The FDA recently approved two PCSK9 inhibitors (alirocumab and evolocumab) for use, although the primary indication is for further reduction in LDL-C on top of the maximally tolerated dose of statin therapy, not for reduction of Lp(a).22,23
Apheresis has been shown to have positive effects in reducing ongoing vascular events in select patient populations. It is approved by the FDA for treatment of refractory LDL-C, mostly in patients with familial hypercholesterolemia, but it is not indicated for treatment of elevated Lp(a). However, since Lp(a) tracks with LDL-C, it is also removed during the process; about a 50% reduction in Lp(a) levels has been noted, although levels rebound posttreatment. To date, reimbursement issues remain in the absence of an FDA indication and due to the paucity of treatment centers in the US.24,25
Follow-up. The therapies mentioned require routine evaluation to assess tolerability and safety, as recommended in the prescribing information. Patients with known CVD should undergo an appropriate cardiac workup annually to evaluate for occult progression of disease. Patients require further evaluation of related cardiovascular risk factors and adherence with medication regimens. For primary prevention patients, annual follow-up is also recommended to assess for any changes in health status, lifestyle, or medication adherence.
Continue for conclusion >>
Conclusion
The average health care provider frequently performs the standard evaluation of a patient at risk for, or with, CVD. However, a subset of this population may be at increased cardiovascular risk due to Lp(a), a common genetic risk factor that can be responsible for premature or progressive CVD. Because of the aggressive nature of this disorder and the young age at which it influences the development of vascular disease, health care providers must be more vigilant about looking beyond the obvious in patients with familial hypercholesterolemia or family history of premature CVD.
Patients with progressive disease must be more thoroughly evaluated; there are already more than 63 million persons with elevated Lp(a) in the US—and many more undiagnosed—who may benefit from aggressive care. Underdiagnosis has been associated with decreased quality and productivity in the work environment, decreased quality of life, increased use of health dollars, and possibly early loss of life.
While the test for Lp(a) is readily available, the cost may not be covered by insurance and therefore may be passed on to the patient. It would behoove health care professionals to lobby for coverage as a means to reduce the prevalence of CVD, the number one cause of mortality in the US.
References
1. Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive Summary: heart disease and stroke statistics—2014 Update: a report from the American Heart Association. Circulation. 2014;129:399-410.
2. Bennet A, Di Angelantonio E, Erqou S, et al. Lipoprotein(a) levels and risk of future coronary heart disease: large-scale prospective data [published corrections appear in Arch Intern Med. 2008;168(10):1089 and Arch Intern Med. 2008;168(10):1096]. Arch Intern Med. 2008;168(6):598-608.
3. Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301(22):2331-2339.
4. Suk DJ, Rifai N, Buring JE, Ridker PM. Lipoprotein(a), hormone replacement therapy, and risk of future cardiovascular events. J Am Coll Cardiol. 2008;52(2):124-131.
5. Scanu AM. Lipoprotein(a). A genetic risk factor for premature coronary heart disease. JAMA. 1992;267(24):3326-3329.
6. Goldberg AC, Hopkins PN, Toth PP; National Lipid Association Expert Panel on Familial Hypercholesterolemia. Familial hypercholesterolemia: screening, diagnosis and management of pediatric and adult patients: clinical guidance from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J Clin Lipid. 2011;5(3 suppl):S1-S8.
7. Ito M, McGowan MP, Moriarty PM; National Lipid Association Expert Panel on Familial Hypercholesterolemia. Management of familial hypercholesterolemias in adult patients: recommendations from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J Clin Lipid. 2011;5(3 suppl):S38-S45.
8. Sjouke B, Kusters DM, Kindt I, et al. Homozygous autosomal dominant hypercholesterolaemia in the Netherlands: prevalence, genotype-phenotype relationship, and clinical outcome. Eur Heart J. 2014 Feb 28. [Epub ahead of print]
9. Nordestgaard BG, Chapman MJ, Ray K, et al; European Atherosclerosis Society Consensus Panel. Lipoprotein (a) as a cardiovascular risk factor: current status. Eur Heart J. 2010; 31(23):2844-2853.
10. Suk DJ, Rifai N, Buring JE, Ridker PM. Lipoprotein(a), measured with an assay independent of apolipoprotein(a) isoform size, and risk of future cardiovascular events among initially healthy women. JAMA. 2006;296 (11):1363-1370.
11. Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. 2004;110(2):227-239.
12. Jacobson TA. Lipoprotein (a), cardiovascular disease, and contemporary management. Mayo Clin Proc. 2013;88(11):1294-1311.
13. Hunninghake DB, Stein EA, Mellies MJ. Effects of one year of treatment with pravastatin, an HMG-CoA reductase inhibitor, on lipoprotein a. J Clin Pharmacol. 1993;33 (6):574-580.
14. Jones PH, Pownall HJ, Patsch W, et al. Effect of gemfibrozil on levels of lipoprotein[a] in type 2 hyperlipoproteinemic subjects. J Lipid Res. 1996;37(6):1298-1308.
15. Boden WE, Probstfield JL, Anderson T, et al; AIM-HIGH investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011; 365(24):2255-2267.
16. Landray MJ, Haynes R, Hopewell JC, et al; HPS2-THRIVE Collaborative Group. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371 (3):203-212.
17. Morgan JM, Capuzzi DM, Guyton JR. A new extended-release niacin (Niaspan): efficacy, tolerability, and safety in hypercholesterolemic patients. Am J Cardiol. 1998;82 (12A): 29U-34U.
18. Piepho RW. The pharmacokinetics and pharmacodynamics of agents proven to raise high-density lipoprotein cholesterol. Am J Cardiol. 2000;86(12A):35L-40L.
19. Guyton JR, Bays HE. Safety considerations with niacin therapy. Am J Cardiol. 2007; 99(6A):22C-31C.
20. McKenney JM, Proctor JD, Harris S, Chinchili VM. A comparison of the efficacy and toxic effects of sustained- vs immediate-release niacin in hypercholesterolemic patients. JAMA. 1994;271(9):672-677.
21. Shlipak MG, Simon JA, Vittinghoff E, et al. Estrogen and progestin, lipoprotein(a), and the risk of recurrent coronary heart disease events after menopause. JAMA. 2000;283 (14):1845-1852.
22. Marbach JA, McKeon JL, Ross JL, Duffy D. Novel treatments for familial hypercholesterolemia: pharmacogenetics at work. Pharmacotherapy. 2014;34(9):961-972.
23. Stein EA, Mellis S, Yancopoulos GD, et al. Effect of a monoclonal antibody to PCSK9 on LDL cholesterol. N Engl J Med. 2012;366(12): 1108-1118.
24. Sachais BS, Katz J, Ross J, Rader DJ. Long-term effects of LDL apheresis in patients with severe hypercholesterolemia. J Clin Apher. 2005;20:252-255.
25. Waldmann E, Parhofer K. Lipoprotein apheresis to treat elevated lipoprotein(a). J Lipid Res. 2016 Feb 17. [Epub ahead of print]
In hemophilia A, emicizumab cuts bleeding; plasma-derived factor VIII less likely to trigger antibodies
Patients with severe hemophilia A treated with plasma-derived factor VIII, as compared with recombinant factor VIII, had a lower risk of developing neutralizing antibodies, based on a recent report from the randomized SIPPET trial published in the New England Journal of Medicine.
In a second study, also published in the journal, prophylactic treatment with the bispecific antibody emicizumab decreased bleeding in patients with or without neutralizing antibodies.

Of 125 patients with severe hemophilia A who were treated with plasma-derived factor VIII with von Willebrand factor, 29 (23.2%) developed inhibitors, compared with 47 of 126 patients (37.3%) treated with recombinant factor VIII. In the plasma-derived group, 20 (16.0%) had high-titer inhibitors compared with 30 (23.8%) in the recombinant group. Cox regression models showed an 87% higher rate of inhibitor development with recombinant factor VIII (hazard ratio, 1.87; 95% confidence interval, 1.17-2.96). For development of high-titer inhibitors, the HR was 1.69 (95% CI, 0.96-2.98).
Previous observational studies have suggested greater immunogenicity of recombinant vs. plasm-derived factor VIII, but the results remained inconclusive. Meta-analyses of studies have been hindered by differences in design, enrollment criteria, definition of hemophilia A, sample size, method of inhibitor detection, and intervals of follow-up testing, according to Dr. Flora Peyvandi of the IRCCS Maggiore Hospital, University of Milan and colleagues. “Our trial was specifically designed to compare the immunogenicity of factor VIII products. As a result of randomization, the main risk factors for inhibitor development were evenly distributed between the two factor VIII classes,” they wrote, adding, “The finding that native factor VIII products from human plasma are less immunogenic than those engineered by recombinant DNA technology in animal cell lines has the potential to affect treatment strategies and open new investigations to better understand the mechanisms of the immunogenicity of various factor VIII preparations.” (N Engl J Med. 2016 May 25. doi: 10.1200/JCO.2015.64.0730).
The Survey of Inhibitors in Plasma-Product Exposed Toddlers (SIPPET) clinical trial randomized 251 patients with severe hemophilia A who received infusions of plasma-derived or recombinant factor VIII. The investigators found no association between risk of inhibitor development and race, intensity of treatment, or age at first treatment.
The second study, a 12-week dose-escalation trial of emicizumab, included 18 patients with severe hemophilia A, aged 12-59 years. Patients were assigned to one of three cohorts and received a once-weekly subcutaneous dose of 0.3, 1, or 3 mg per kilogram of body weight. During prophylactic emicizumab treatment, median annualized bleeding rates decreased from 32.5 (range, 8.1-77.1) to 4.4 (0.0-59.5) in cohort 1, from 18.3 (range, 10.1-38.6) to 0.0 (range, 0.0-4.3) in cohort 2, and from 15.2 (range, 0.0-32.5) to 0.0 (range, 0.0-4.2) in cohort 3. The annualized bleeding rate decreased regardless of factor VIII inhibitor status. Of 11 patients with factor VIII inhibitors, 8 (73%) had no bleeding episodes; 5 of 7 patients without factor VIII inhibitors (71%) had no bleeding episodes.
“This study showed that once-weekly subcutaneous administration of emicizumab as prophylaxis is safe and has the potential to reduce or prevent bleeding episodes in patients who have severe hemophilia A with or without factor VIII inhibitors,” wrote Dr. Midori Shima of Nara Medical University, Kashihara, Japan, and colleagues (N. Engl J Med. 2016 May 25. doi: 10.1056/NEJMoa1511769).
Emicizumab had an acceptable safety profile. In total, 43 adverse events were reported in 15 of 18 patients. All were mild, except two moderate events – an upper respiratory tract infection and a headache. Events thought to be treatment related included malaise, injection-site erythema, injection-site rash, diarrhea, increased C-reactive protein level, and increased blood creatine kinase level.
Dr. Peyvandi and coauthors disclosed consulting, advising, research funding and other relationships with several industry sources, including Grifols, Kedrion, and LFB. Dr. Shima and coauthors disclosed consulting, advising, research funding and other relationships with several industry sources, including Chugai Pharmaceuticals, which supported the study.
The studies by Peyvandi et al. and Shima et al. bring exciting news to patients with hemophilia. Peyvandi et al. report the influence of factor VIII product source on the cumulative incidence of inhibitors in children with severe hemophilia. Exclusive use of recombinant factor VIII through the highest-risk period increased the cumulative incidence of all inhibitors, compared with plasma-derived factor VIII. Factor VIII protein glycosylation and von Willebrand factor association play a role in endocytosis, clearance, and antigen presentation and are altered by recombinant technology, which lends plausibility to the implication of product source affecting inhibitor generation. The results may lead to valuable mechanistic insight into factor VIII immunogenicity.
In the second study, Shima et al. evaluate once-weekly administration of emicizumab in patients with severe hemophilia. The bifunctional antibody functions as a conformation replica of factor VIII, forming a thrombin-generating complex with factors IX and X. Emicizumab would likely not induce or be inhibited by factor VIII–neutralizing antibodies, and its subcutaneous bioavailability permits a once-weekly treatment regimen instead of intravenous infusion. The study reports impressive short-term decreases in annualized bleeding rates in both inhibitor-positive and inhibitor-negative patients. The next steps in testing more substantial and sustained thrombin generation required for the treatment of acute hemorrhage will be important for emicizumab.
If proven feasible as a therapeutic agent, emicizumab may play a role in mediating factor VIII immunogenicity. Early sustained treatment with emicizumab in children could ultimately affect the epidemiology of neutralizing antibodies.
The clinical and scientific ramifications of these two studies will take time to be fully realized but offer exciting potential as therapeutic options where new approaches to bypassing the factor VIII requirement have so far fallen short (N Engl J Med. 2016 May 25. doi: 10.1056/NEJMe1603419).
Dr. Donna DiMichele is the deputy director of the Division of Blood Diseases and Resources at the National Heart, Lung, and Blood Institute, part of the National Institutes of Health. These remarks were part of an editorial accompanying two reports in the New England Journal of Medicine. Dr. DiMichele reports personal fees from Chugai Pharmaceuticals outside the submitted work. She was an early founding member of the SIPPET study Steering Committee but resigned when she came to NIH in 2010.
The studies by Peyvandi et al. and Shima et al. bring exciting news to patients with hemophilia. Peyvandi et al. report the influence of factor VIII product source on the cumulative incidence of inhibitors in children with severe hemophilia. Exclusive use of recombinant factor VIII through the highest-risk period increased the cumulative incidence of all inhibitors, compared with plasma-derived factor VIII. Factor VIII protein glycosylation and von Willebrand factor association play a role in endocytosis, clearance, and antigen presentation and are altered by recombinant technology, which lends plausibility to the implication of product source affecting inhibitor generation. The results may lead to valuable mechanistic insight into factor VIII immunogenicity.
In the second study, Shima et al. evaluate once-weekly administration of emicizumab in patients with severe hemophilia. The bifunctional antibody functions as a conformation replica of factor VIII, forming a thrombin-generating complex with factors IX and X. Emicizumab would likely not induce or be inhibited by factor VIII–neutralizing antibodies, and its subcutaneous bioavailability permits a once-weekly treatment regimen instead of intravenous infusion. The study reports impressive short-term decreases in annualized bleeding rates in both inhibitor-positive and inhibitor-negative patients. The next steps in testing more substantial and sustained thrombin generation required for the treatment of acute hemorrhage will be important for emicizumab.
If proven feasible as a therapeutic agent, emicizumab may play a role in mediating factor VIII immunogenicity. Early sustained treatment with emicizumab in children could ultimately affect the epidemiology of neutralizing antibodies.
The clinical and scientific ramifications of these two studies will take time to be fully realized but offer exciting potential as therapeutic options where new approaches to bypassing the factor VIII requirement have so far fallen short (N Engl J Med. 2016 May 25. doi: 10.1056/NEJMe1603419).
Dr. Donna DiMichele is the deputy director of the Division of Blood Diseases and Resources at the National Heart, Lung, and Blood Institute, part of the National Institutes of Health. These remarks were part of an editorial accompanying two reports in the New England Journal of Medicine. Dr. DiMichele reports personal fees from Chugai Pharmaceuticals outside the submitted work. She was an early founding member of the SIPPET study Steering Committee but resigned when she came to NIH in 2010.
The studies by Peyvandi et al. and Shima et al. bring exciting news to patients with hemophilia. Peyvandi et al. report the influence of factor VIII product source on the cumulative incidence of inhibitors in children with severe hemophilia. Exclusive use of recombinant factor VIII through the highest-risk period increased the cumulative incidence of all inhibitors, compared with plasma-derived factor VIII. Factor VIII protein glycosylation and von Willebrand factor association play a role in endocytosis, clearance, and antigen presentation and are altered by recombinant technology, which lends plausibility to the implication of product source affecting inhibitor generation. The results may lead to valuable mechanistic insight into factor VIII immunogenicity.
In the second study, Shima et al. evaluate once-weekly administration of emicizumab in patients with severe hemophilia. The bifunctional antibody functions as a conformation replica of factor VIII, forming a thrombin-generating complex with factors IX and X. Emicizumab would likely not induce or be inhibited by factor VIII–neutralizing antibodies, and its subcutaneous bioavailability permits a once-weekly treatment regimen instead of intravenous infusion. The study reports impressive short-term decreases in annualized bleeding rates in both inhibitor-positive and inhibitor-negative patients. The next steps in testing more substantial and sustained thrombin generation required for the treatment of acute hemorrhage will be important for emicizumab.
If proven feasible as a therapeutic agent, emicizumab may play a role in mediating factor VIII immunogenicity. Early sustained treatment with emicizumab in children could ultimately affect the epidemiology of neutralizing antibodies.
The clinical and scientific ramifications of these two studies will take time to be fully realized but offer exciting potential as therapeutic options where new approaches to bypassing the factor VIII requirement have so far fallen short (N Engl J Med. 2016 May 25. doi: 10.1056/NEJMe1603419).
Dr. Donna DiMichele is the deputy director of the Division of Blood Diseases and Resources at the National Heart, Lung, and Blood Institute, part of the National Institutes of Health. These remarks were part of an editorial accompanying two reports in the New England Journal of Medicine. Dr. DiMichele reports personal fees from Chugai Pharmaceuticals outside the submitted work. She was an early founding member of the SIPPET study Steering Committee but resigned when she came to NIH in 2010.
Patients with severe hemophilia A treated with plasma-derived factor VIII, as compared with recombinant factor VIII, had a lower risk of developing neutralizing antibodies, based on a recent report from the randomized SIPPET trial published in the New England Journal of Medicine.
In a second study, also published in the journal, prophylactic treatment with the bispecific antibody emicizumab decreased bleeding in patients with or without neutralizing antibodies.
Of 125 patients with severe hemophilia A who were treated with plasma-derived factor VIII with von Willebrand factor, 29 (23.2%) developed inhibitors, compared with 47 of 126 patients (37.3%) treated with recombinant factor VIII. In the plasma-derived group, 20 (16.0%) had high-titer inhibitors compared with 30 (23.8%) in the recombinant group. Cox regression models showed an 87% higher rate of inhibitor development with recombinant factor VIII (hazard ratio, 1.87; 95% confidence interval, 1.17-2.96). For development of high-titer inhibitors, the HR was 1.69 (95% CI, 0.96-2.98).
Previous observational studies have suggested greater immunogenicity of recombinant vs. plasm-derived factor VIII, but the results remained inconclusive. Meta-analyses of studies have been hindered by differences in design, enrollment criteria, definition of hemophilia A, sample size, method of inhibitor detection, and intervals of follow-up testing, according to Dr. Flora Peyvandi of the IRCCS Maggiore Hospital, University of Milan and colleagues. “Our trial was specifically designed to compare the immunogenicity of factor VIII products. As a result of randomization, the main risk factors for inhibitor development were evenly distributed between the two factor VIII classes,” they wrote, adding, “The finding that native factor VIII products from human plasma are less immunogenic than those engineered by recombinant DNA technology in animal cell lines has the potential to affect treatment strategies and open new investigations to better understand the mechanisms of the immunogenicity of various factor VIII preparations.” (N Engl J Med. 2016 May 25. doi: 10.1200/JCO.2015.64.0730).
The Survey of Inhibitors in Plasma-Product Exposed Toddlers (SIPPET) clinical trial randomized 251 patients with severe hemophilia A who received infusions of plasma-derived or recombinant factor VIII. The investigators found no association between risk of inhibitor development and race, intensity of treatment, or age at first treatment.
The second study, a 12-week dose-escalation trial of emicizumab, included 18 patients with severe hemophilia A, aged 12-59 years. Patients were assigned to one of three cohorts and received a once-weekly subcutaneous dose of 0.3, 1, or 3 mg per kilogram of body weight. During prophylactic emicizumab treatment, median annualized bleeding rates decreased from 32.5 (range, 8.1-77.1) to 4.4 (0.0-59.5) in cohort 1, from 18.3 (range, 10.1-38.6) to 0.0 (range, 0.0-4.3) in cohort 2, and from 15.2 (range, 0.0-32.5) to 0.0 (range, 0.0-4.2) in cohort 3. The annualized bleeding rate decreased regardless of factor VIII inhibitor status. Of 11 patients with factor VIII inhibitors, 8 (73%) had no bleeding episodes; 5 of 7 patients without factor VIII inhibitors (71%) had no bleeding episodes.
“This study showed that once-weekly subcutaneous administration of emicizumab as prophylaxis is safe and has the potential to reduce or prevent bleeding episodes in patients who have severe hemophilia A with or without factor VIII inhibitors,” wrote Dr. Midori Shima of Nara Medical University, Kashihara, Japan, and colleagues (N. Engl J Med. 2016 May 25. doi: 10.1056/NEJMoa1511769).
Emicizumab had an acceptable safety profile. In total, 43 adverse events were reported in 15 of 18 patients. All were mild, except two moderate events – an upper respiratory tract infection and a headache. Events thought to be treatment related included malaise, injection-site erythema, injection-site rash, diarrhea, increased C-reactive protein level, and increased blood creatine kinase level.
Dr. Peyvandi and coauthors disclosed consulting, advising, research funding and other relationships with several industry sources, including Grifols, Kedrion, and LFB. Dr. Shima and coauthors disclosed consulting, advising, research funding and other relationships with several industry sources, including Chugai Pharmaceuticals, which supported the study.
Patients with severe hemophilia A treated with plasma-derived factor VIII, as compared with recombinant factor VIII, had a lower risk of developing neutralizing antibodies, based on a recent report from the randomized SIPPET trial published in the New England Journal of Medicine.
In a second study, also published in the journal, prophylactic treatment with the bispecific antibody emicizumab decreased bleeding in patients with or without neutralizing antibodies.
Of 125 patients with severe hemophilia A who were treated with plasma-derived factor VIII with von Willebrand factor, 29 (23.2%) developed inhibitors, compared with 47 of 126 patients (37.3%) treated with recombinant factor VIII. In the plasma-derived group, 20 (16.0%) had high-titer inhibitors compared with 30 (23.8%) in the recombinant group. Cox regression models showed an 87% higher rate of inhibitor development with recombinant factor VIII (hazard ratio, 1.87; 95% confidence interval, 1.17-2.96). For development of high-titer inhibitors, the HR was 1.69 (95% CI, 0.96-2.98).
Previous observational studies have suggested greater immunogenicity of recombinant vs. plasm-derived factor VIII, but the results remained inconclusive. Meta-analyses of studies have been hindered by differences in design, enrollment criteria, definition of hemophilia A, sample size, method of inhibitor detection, and intervals of follow-up testing, according to Dr. Flora Peyvandi of the IRCCS Maggiore Hospital, University of Milan and colleagues. “Our trial was specifically designed to compare the immunogenicity of factor VIII products. As a result of randomization, the main risk factors for inhibitor development were evenly distributed between the two factor VIII classes,” they wrote, adding, “The finding that native factor VIII products from human plasma are less immunogenic than those engineered by recombinant DNA technology in animal cell lines has the potential to affect treatment strategies and open new investigations to better understand the mechanisms of the immunogenicity of various factor VIII preparations.” (N Engl J Med. 2016 May 25. doi: 10.1200/JCO.2015.64.0730).
The Survey of Inhibitors in Plasma-Product Exposed Toddlers (SIPPET) clinical trial randomized 251 patients with severe hemophilia A who received infusions of plasma-derived or recombinant factor VIII. The investigators found no association between risk of inhibitor development and race, intensity of treatment, or age at first treatment.
The second study, a 12-week dose-escalation trial of emicizumab, included 18 patients with severe hemophilia A, aged 12-59 years. Patients were assigned to one of three cohorts and received a once-weekly subcutaneous dose of 0.3, 1, or 3 mg per kilogram of body weight. During prophylactic emicizumab treatment, median annualized bleeding rates decreased from 32.5 (range, 8.1-77.1) to 4.4 (0.0-59.5) in cohort 1, from 18.3 (range, 10.1-38.6) to 0.0 (range, 0.0-4.3) in cohort 2, and from 15.2 (range, 0.0-32.5) to 0.0 (range, 0.0-4.2) in cohort 3. The annualized bleeding rate decreased regardless of factor VIII inhibitor status. Of 11 patients with factor VIII inhibitors, 8 (73%) had no bleeding episodes; 5 of 7 patients without factor VIII inhibitors (71%) had no bleeding episodes.
“This study showed that once-weekly subcutaneous administration of emicizumab as prophylaxis is safe and has the potential to reduce or prevent bleeding episodes in patients who have severe hemophilia A with or without factor VIII inhibitors,” wrote Dr. Midori Shima of Nara Medical University, Kashihara, Japan, and colleagues (N. Engl J Med. 2016 May 25. doi: 10.1056/NEJMoa1511769).
Emicizumab had an acceptable safety profile. In total, 43 adverse events were reported in 15 of 18 patients. All were mild, except two moderate events – an upper respiratory tract infection and a headache. Events thought to be treatment related included malaise, injection-site erythema, injection-site rash, diarrhea, increased C-reactive protein level, and increased blood creatine kinase level.
Dr. Peyvandi and coauthors disclosed consulting, advising, research funding and other relationships with several industry sources, including Grifols, Kedrion, and LFB. Dr. Shima and coauthors disclosed consulting, advising, research funding and other relationships with several industry sources, including Chugai Pharmaceuticals, which supported the study.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical points: Plasma-derived factor VIII carries lower risk of developing neutralizing antibodies than recombinant factor VIII; once-weekly emicizumab decreased bleeding in hemophilia A patients with or without neutralizing antibodies.
Major findings: Inhibitors developed in 23% of patients treated with plasma-derived factor VIII (16% high titer), compared with 37% treated with recombinant factor VIII (24% high titer); during prophylactic treatment with emicizumab, bleeding rates were markedly reduced, and more than 70% of patients had no bleeding episodes.
Data sources: The Survey of Inhibitors in Plasma-Product Exposed Toddlers (SIPPET) randomized trial evaluated 251 patients with severe hemophilia A who received plasma-derived or recombinant factor VIII; emicizumab was evaluated in a 12-week, open-label, nonrandomized dose-escalation study of 18 patients.
Disclosures: Dr. Peyvandi and coauthors disclosed consulting, advising, research funding and other relationships with several industry sources, including Grifols, Kedrion, and LFB. Dr. Shima and coauthors disclosed consulting, advising, research funding and other relationships with several industry sources, including Chugai Pharmaceuticals, which supported the study.

Ocrelizumab bests interferon for relapsing MS at 2 years
VANCOUVER – Ocrelizumab, a B-cell depleting humanized monoclonal antibody being developed by Hoffman–La Roche, consistently outperformed interferon beta-1a (Rebif) for relapsing multiple sclerosis in two phase III trials reported at the annual meeting of the American Academy of Neurology.
The identical trials, dubbed OPERA I and OPERA II, each had about 800 patients. Subjects were randomized one-to-one to intravenous ocrelizumab 600 mg every 24 weeks or to subcutaneous interferon beta-1a 44 micrograms three times weekly over 96 weeks. Patients had early disease; a significant portion were naive to multiple sclerosis (MS) treatments.
At 96 weeks, 47.9% and 47.5% of ocrelizumab patients versus 29.2% and 25.1% of interferon patients had no evidence of disease activity (NEDA) in the two studies. NEDA is a composite score defined as no relapses, no confirmed disability progression, and no new or enlarging T2 or gadolinium-enhancing T1 lesions.
Across both studies, relapses occurred in about 20% of ocrelizumab patients versus about 35% of interferon patients. About 10% of ocrelizumab, but about 15% of interferon patients, had clinical disease progression. Similarly, about 10% of ocrelizumab patients developed new gadolinium-enhancing lesions, compared with about 35% in the interferon groups. New or enlarging T2 lesions were found in about 40% in the ocrelizumab groups but in more than 60% in the interferon arms.
After week 24, 96% percent of ocrelizumab patients, compared with 60%-70% on interferon, were free of new or enlarging T2 lesions.
In short, ocrelizumab “resulted in greater achievement of NEDA versus [interferon] over 96 weeks, with elimination of new/enlarging T2 lesions in nearly all patients after week 24,” the researchers concluded.

“These are very impressive numbers,” especially because ocrelizumab was compared with a standard treatment. “There was a wonderful constancy of results” across the trials; “a very highly effective treatment is emerging for multiple sclerosis,” said investigator and presenter Dr. Anthony Traboulsee, a neurologist at the University of British Columbia, Vancouver, who also noted that in many cases, patients opted to stay on ocrelizumab at the end of the trials.
Dr. Traboulsee did not present safety data. A previous report of 24-week results found that infusion reactions were significantly more common with ocrelizumab than with interferon beta-1a (34% vs. 9.7%). Otherwise, there were similar rates of serious adverse events, including serious infections, and there were no cases of progressive multifocal leukoencephalopathy (PML). The PML and infection findings are especially important; Roche shelved earlier attempts to develop the biologic for lupus and rheumatoid arthritis due to serious and opportunistic infections, some of which were fatal.
Roche plans to submit its approval package to the Food and Drug Administration in the first half of 2016; the tentative brand name is Ocrevus. FDA granted the biologic breakthrough, fast-track status for primary progressive MS based on the strength of an earlier phase III trial. At present, there are no MS agents indicated for primary progressive disease.
Patients in OPERA were 37 years old, on average, and two-thirds were women. The mean baseline score on the Extended Disability Status Scale was 2.77, and the mean time since diagnosis was about 4 years. Patients had about 1.5 relapses in the first and second year before entering the studies.
The positive results – and the increasing buzz about ocrelizumab in the MS community – raise the question of how it will fit into the MS armamentarium if it’s approved, which seems likely. A review in Therapeutic Advances in Neurological Disorders tackled the issue in January, before the OPERA results were made public (2016 Jan; 9[1]:44-52).
It’s unclear if ocrelizumab will become the go-to option when patients progress on first-line agents such as interferon and glatiramer acetate. Phase II data suggest ocrelizumab’s “effect on clinical disease activity [seems] to be of the same magnitude compared with that of fingolimod and natalizumab,” and will likely be an alternative to natalizumab and alemtuzumab. “Ocrelizumab seems to have a more favourable risk–benefit profile compared with natalizumab in JC [John Cunningham] virus antibody–positive patients, whereas natalizumab in JC virus antibody–negative patients appears safer. Hence, ocrelizumab could be an attractive option among second-line therapies in patients who are JC virus antibody positive, whereas natalizumab or alternatively oral fingolimod would be the first choice among second-line therapies in JC virus antibody–negative patients,” said authors Dr. Per Soelberg Sorensen and Dr. Morten Blinkenberg, both MS neurologists at the University of Copenhagen.
“It needs to be emphasized that long-term data on the safety of ocrelizumab in the treatment of MS is warranted, and therefore post-marketing safety programs will be needed.” The risk of PML with long-term use is unknown. “Another unsolved question is whether ocrelizumab therapy should be applied at fixed intervals, e.g. every 6 months [as in OPERA], or if re-treatment should be guided by the recovery of CD19-positive B cells,” they said.
In any case, infusion reactions with ocrelizumab should be less than with rituximab (Rituxan), another B-cell depleter used off-label for MS, because ocrelizumab is a more humanized antibody.
OPERA 1 and 2 were funded by Hoffmann–La Roche. Dr. Traboulsee is a paid speaker, consultant, and researcher for the company. Other investigators also reported various ties to Roche; several are employees. The review authors had no disclosures.
VANCOUVER – Ocrelizumab, a B-cell depleting humanized monoclonal antibody being developed by Hoffman–La Roche, consistently outperformed interferon beta-1a (Rebif) for relapsing multiple sclerosis in two phase III trials reported at the annual meeting of the American Academy of Neurology.
The identical trials, dubbed OPERA I and OPERA II, each had about 800 patients. Subjects were randomized one-to-one to intravenous ocrelizumab 600 mg every 24 weeks or to subcutaneous interferon beta-1a 44 micrograms three times weekly over 96 weeks. Patients had early disease; a significant portion were naive to multiple sclerosis (MS) treatments.
At 96 weeks, 47.9% and 47.5% of ocrelizumab patients versus 29.2% and 25.1% of interferon patients had no evidence of disease activity (NEDA) in the two studies. NEDA is a composite score defined as no relapses, no confirmed disability progression, and no new or enlarging T2 or gadolinium-enhancing T1 lesions.
Across both studies, relapses occurred in about 20% of ocrelizumab patients versus about 35% of interferon patients. About 10% of ocrelizumab, but about 15% of interferon patients, had clinical disease progression. Similarly, about 10% of ocrelizumab patients developed new gadolinium-enhancing lesions, compared with about 35% in the interferon groups. New or enlarging T2 lesions were found in about 40% in the ocrelizumab groups but in more than 60% in the interferon arms.
After week 24, 96% percent of ocrelizumab patients, compared with 60%-70% on interferon, were free of new or enlarging T2 lesions.
In short, ocrelizumab “resulted in greater achievement of NEDA versus [interferon] over 96 weeks, with elimination of new/enlarging T2 lesions in nearly all patients after week 24,” the researchers concluded.
“These are very impressive numbers,” especially because ocrelizumab was compared with a standard treatment. “There was a wonderful constancy of results” across the trials; “a very highly effective treatment is emerging for multiple sclerosis,” said investigator and presenter Dr. Anthony Traboulsee, a neurologist at the University of British Columbia, Vancouver, who also noted that in many cases, patients opted to stay on ocrelizumab at the end of the trials.
Dr. Traboulsee did not present safety data. A previous report of 24-week results found that infusion reactions were significantly more common with ocrelizumab than with interferon beta-1a (34% vs. 9.7%). Otherwise, there were similar rates of serious adverse events, including serious infections, and there were no cases of progressive multifocal leukoencephalopathy (PML). The PML and infection findings are especially important; Roche shelved earlier attempts to develop the biologic for lupus and rheumatoid arthritis due to serious and opportunistic infections, some of which were fatal.
Roche plans to submit its approval package to the Food and Drug Administration in the first half of 2016; the tentative brand name is Ocrevus. FDA granted the biologic breakthrough, fast-track status for primary progressive MS based on the strength of an earlier phase III trial. At present, there are no MS agents indicated for primary progressive disease.
Patients in OPERA were 37 years old, on average, and two-thirds were women. The mean baseline score on the Extended Disability Status Scale was 2.77, and the mean time since diagnosis was about 4 years. Patients had about 1.5 relapses in the first and second year before entering the studies.
The positive results – and the increasing buzz about ocrelizumab in the MS community – raise the question of how it will fit into the MS armamentarium if it’s approved, which seems likely. A review in Therapeutic Advances in Neurological Disorders tackled the issue in January, before the OPERA results were made public (2016 Jan; 9[1]:44-52).
It’s unclear if ocrelizumab will become the go-to option when patients progress on first-line agents such as interferon and glatiramer acetate. Phase II data suggest ocrelizumab’s “effect on clinical disease activity [seems] to be of the same magnitude compared with that of fingolimod and natalizumab,” and will likely be an alternative to natalizumab and alemtuzumab. “Ocrelizumab seems to have a more favourable risk–benefit profile compared with natalizumab in JC [John Cunningham] virus antibody–positive patients, whereas natalizumab in JC virus antibody–negative patients appears safer. Hence, ocrelizumab could be an attractive option among second-line therapies in patients who are JC virus antibody positive, whereas natalizumab or alternatively oral fingolimod would be the first choice among second-line therapies in JC virus antibody–negative patients,” said authors Dr. Per Soelberg Sorensen and Dr. Morten Blinkenberg, both MS neurologists at the University of Copenhagen.
“It needs to be emphasized that long-term data on the safety of ocrelizumab in the treatment of MS is warranted, and therefore post-marketing safety programs will be needed.” The risk of PML with long-term use is unknown. “Another unsolved question is whether ocrelizumab therapy should be applied at fixed intervals, e.g. every 6 months [as in OPERA], or if re-treatment should be guided by the recovery of CD19-positive B cells,” they said.
In any case, infusion reactions with ocrelizumab should be less than with rituximab (Rituxan), another B-cell depleter used off-label for MS, because ocrelizumab is a more humanized antibody.
OPERA 1 and 2 were funded by Hoffmann–La Roche. Dr. Traboulsee is a paid speaker, consultant, and researcher for the company. Other investigators also reported various ties to Roche; several are employees. The review authors had no disclosures.
VANCOUVER – Ocrelizumab, a B-cell depleting humanized monoclonal antibody being developed by Hoffman–La Roche, consistently outperformed interferon beta-1a (Rebif) for relapsing multiple sclerosis in two phase III trials reported at the annual meeting of the American Academy of Neurology.
The identical trials, dubbed OPERA I and OPERA II, each had about 800 patients. Subjects were randomized one-to-one to intravenous ocrelizumab 600 mg every 24 weeks or to subcutaneous interferon beta-1a 44 micrograms three times weekly over 96 weeks. Patients had early disease; a significant portion were naive to multiple sclerosis (MS) treatments.
At 96 weeks, 47.9% and 47.5% of ocrelizumab patients versus 29.2% and 25.1% of interferon patients had no evidence of disease activity (NEDA) in the two studies. NEDA is a composite score defined as no relapses, no confirmed disability progression, and no new or enlarging T2 or gadolinium-enhancing T1 lesions.
Across both studies, relapses occurred in about 20% of ocrelizumab patients versus about 35% of interferon patients. About 10% of ocrelizumab, but about 15% of interferon patients, had clinical disease progression. Similarly, about 10% of ocrelizumab patients developed new gadolinium-enhancing lesions, compared with about 35% in the interferon groups. New or enlarging T2 lesions were found in about 40% in the ocrelizumab groups but in more than 60% in the interferon arms.
After week 24, 96% percent of ocrelizumab patients, compared with 60%-70% on interferon, were free of new or enlarging T2 lesions.
In short, ocrelizumab “resulted in greater achievement of NEDA versus [interferon] over 96 weeks, with elimination of new/enlarging T2 lesions in nearly all patients after week 24,” the researchers concluded.
“These are very impressive numbers,” especially because ocrelizumab was compared with a standard treatment. “There was a wonderful constancy of results” across the trials; “a very highly effective treatment is emerging for multiple sclerosis,” said investigator and presenter Dr. Anthony Traboulsee, a neurologist at the University of British Columbia, Vancouver, who also noted that in many cases, patients opted to stay on ocrelizumab at the end of the trials.
Dr. Traboulsee did not present safety data. A previous report of 24-week results found that infusion reactions were significantly more common with ocrelizumab than with interferon beta-1a (34% vs. 9.7%). Otherwise, there were similar rates of serious adverse events, including serious infections, and there were no cases of progressive multifocal leukoencephalopathy (PML). The PML and infection findings are especially important; Roche shelved earlier attempts to develop the biologic for lupus and rheumatoid arthritis due to serious and opportunistic infections, some of which were fatal.
Roche plans to submit its approval package to the Food and Drug Administration in the first half of 2016; the tentative brand name is Ocrevus. FDA granted the biologic breakthrough, fast-track status for primary progressive MS based on the strength of an earlier phase III trial. At present, there are no MS agents indicated for primary progressive disease.
Patients in OPERA were 37 years old, on average, and two-thirds were women. The mean baseline score on the Extended Disability Status Scale was 2.77, and the mean time since diagnosis was about 4 years. Patients had about 1.5 relapses in the first and second year before entering the studies.
The positive results – and the increasing buzz about ocrelizumab in the MS community – raise the question of how it will fit into the MS armamentarium if it’s approved, which seems likely. A review in Therapeutic Advances in Neurological Disorders tackled the issue in January, before the OPERA results were made public (2016 Jan; 9[1]:44-52).
It’s unclear if ocrelizumab will become the go-to option when patients progress on first-line agents such as interferon and glatiramer acetate. Phase II data suggest ocrelizumab’s “effect on clinical disease activity [seems] to be of the same magnitude compared with that of fingolimod and natalizumab,” and will likely be an alternative to natalizumab and alemtuzumab. “Ocrelizumab seems to have a more favourable risk–benefit profile compared with natalizumab in JC [John Cunningham] virus antibody–positive patients, whereas natalizumab in JC virus antibody–negative patients appears safer. Hence, ocrelizumab could be an attractive option among second-line therapies in patients who are JC virus antibody positive, whereas natalizumab or alternatively oral fingolimod would be the first choice among second-line therapies in JC virus antibody–negative patients,” said authors Dr. Per Soelberg Sorensen and Dr. Morten Blinkenberg, both MS neurologists at the University of Copenhagen.
“It needs to be emphasized that long-term data on the safety of ocrelizumab in the treatment of MS is warranted, and therefore post-marketing safety programs will be needed.” The risk of PML with long-term use is unknown. “Another unsolved question is whether ocrelizumab therapy should be applied at fixed intervals, e.g. every 6 months [as in OPERA], or if re-treatment should be guided by the recovery of CD19-positive B cells,” they said.
In any case, infusion reactions with ocrelizumab should be less than with rituximab (Rituxan), another B-cell depleter used off-label for MS, because ocrelizumab is a more humanized antibody.
OPERA 1 and 2 were funded by Hoffmann–La Roche. Dr. Traboulsee is a paid speaker, consultant, and researcher for the company. Other investigators also reported various ties to Roche; several are employees. The review authors had no disclosures.
AT THE AAN 2016 ANNUAL MEETING
Key clinical point: Ocrelizumab, a B-cell depleting humanized monoclonal antibody being developed by Hoffman–La Roche, consistently outperformed interferon beta-1a (Rebif) for relapsing multiple sclerosis in two phase III trials reported at the American Academy of Neurology annual meeting.
Major finding: At 96 weeks, 47.9% and 47.5% of ocrelizumab patients versus 29.2% and 25.1% of interferon patients had no evidence of disease activity in the two studies.
Data source: Two phase III trials with about 1,600 relapsing MS patients.
Disclosures: OPERA 1 and 2 were funded by Hoffmann–La Roche. The presenter is a paid speaker, consultant, and researcher for the company. Other investigators also reported various ties to Roche; several are employees.

Watchman registry provides reassuring answers on device safety
PARIS – Results of the real-world EWOLUTION registry of recipients of the Watchman device for stroke prevention provide reassuring answers to several key questions which have slowed physician uptake of the left atrial appendage closure device, Dr. Martin W. Bergmann said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“EWOLUTION, with more than 1,000 patients, is I think the study that we’ve needed to make this intervention happen in routine practice as a procedure for stroke prevention in atrial fibrillation,” declared Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.

EWOLUTION is a prospective, single-arm, multicenter registry including 1,025 recipients of the first-generation version of the Watchman, a transcatheter device for left atrial appendage closure as a means of stroke prevention in patients with atrial fibrillation (AF). These were high-risk patients: 50% of them had a CHA2DS2-VASc score of 5 or higher, and 72% of participants were deemed unsuitable for warfarin. EWOLUTION was conducted at 47 sites in Europe, the Middle East, and Russia. Dr. Bergmann presented the 3-month outcomes, a key period for device-related complications because protective epithelialization of the device isn’t yet complete. Follow-up will continue at the 1- and 2-year marks.
Among the key findings in the domain of procedural success: The rate of successful device implantation was 98.5%. A complete seal or an echocardiographic color jet of 5 mm or less at the time of implantation was achieved in 99.7% of cases, and this remained the case in 98.9% at 3 months.
With regard to safety, the stroke rate was 0.4%, device embolization occurred in 0.4%, and the pericardial effusion/tamponade rate was 0.7%, all of which are lower rates than in earlier clinical trials.
Just over 4% of patients experienced device-related adverse events with full recovery at the 3-month follow-up. These were mostly bleeding events at the groin access site. More importantly, only 0.5% of patients had device-related serious adverse events that weren’t resolved at 3 months.
“This 0.5% is a major step forward,” Dr. Bergmann said. “This includes all pericardial effusions, all device embolizations, all periprocedural strokes – everything involving the procedure that puts a patient at risk. In fact, that 0.5% risk for left atrial appendage closure with the Watchman is pretty much the same risk as if you refer your patient with AF to an electrophysiologist for pulmonary vein isolation.”
One key question answered by EWOLUTION is, do you need to be an expert in the procedure in order to get excellent results? The answer, Dr. Bergmann said, is emphatically “no.” Interventionalists at the 47 participating sites varied widely in their experience with left atrial appendage occlusion, so investigators divided the sites into quartiles based upon experience and patient volumes contributed to the registry. While cardiologists in the most experienced centers had a significantly higher rate of successful device release on the first try, the most- and least-experienced centers did equally well on the endpoint that really counts: a complete or near-complete seal of the left atrial appendage at follow-up. Complication rates didn’t differ by site experience, either.
Another important practical question that’s been holding up wider adoption of the Watchman concerns how best to handle postimplantation antithrombotic therapy. Here the EWOLUTION registry provides a partial answer: 607 patients were on dual antiplatelet therapy, 113 were on a novel anticoagulant (NOAC), 159 were on warfarin, 67 were on nothing at all, and the rest were on a single antiplatelet agent. And there was no significant difference between any of these groups in the 3-month rates of thrombus on the device, bleeding events, stroke, or other adverse events.
“The main message is there is no difference in serious adverse events between any of the drug regimens. So if you’re in a situation where you can’t give any medication to reduce stroke risk because the bleeding risk is so high, you can go for left atrial appendage closure technology and give them nothing post implant,” according to Dr. Bergmann.
He added that he’d personally try to avoid that strategy: “You want to have some coverage.”

Also noteworthy is that 113 Watchman recipients did well with 3 months of NOAC monotherapy. The appeal of that approach is the short half-life of those agents in the event of a bleeding problem.
Discussant Dr. Farrel Hellig commented that EWOLUTION demonstrates that the Watchman procedure is predictable and safe, with an impressively low complication rate even in inexperienced centers. For that, he added, kudos goes to Boston Scientific, which markets the Watchman, for rolling out an effective physician training program.
“The most important topic to discuss is bleeding, because a bleeding rate of 4.1% at 3 months is certainly not insignificant,” he continued. “It appears, firstly, from EWOLUTION that it’s safe to omit warfarin. I think the most important thing we’d like to know now is could a postprocedure NOAC be the best option, and can aspirin be eliminated in the long term?”
“Is it too early to recommend a NOAC-only for a period of time post procedure? Perhaps. But I think this would be an important next clinical trial: a NOAC-only for a period post procedure with no aspirin to follow. This is the next piece of information we need to complete the puzzle and for left atrial appendage closure to reach its full potential,” according to Dr. Hellig of the University of Cape Town (South Africa).
The EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann reported serving as a consultant to Boston Scientific and Biosense Webster and receiving honoraria from more than a half-dozen pharmaceutical and device companies.
PARIS – Results of the real-world EWOLUTION registry of recipients of the Watchman device for stroke prevention provide reassuring answers to several key questions which have slowed physician uptake of the left atrial appendage closure device, Dr. Martin W. Bergmann said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“EWOLUTION, with more than 1,000 patients, is I think the study that we’ve needed to make this intervention happen in routine practice as a procedure for stroke prevention in atrial fibrillation,” declared Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.
EWOLUTION is a prospective, single-arm, multicenter registry including 1,025 recipients of the first-generation version of the Watchman, a transcatheter device for left atrial appendage closure as a means of stroke prevention in patients with atrial fibrillation (AF). These were high-risk patients: 50% of them had a CHA2DS2-VASc score of 5 or higher, and 72% of participants were deemed unsuitable for warfarin. EWOLUTION was conducted at 47 sites in Europe, the Middle East, and Russia. Dr. Bergmann presented the 3-month outcomes, a key period for device-related complications because protective epithelialization of the device isn’t yet complete. Follow-up will continue at the 1- and 2-year marks.
Among the key findings in the domain of procedural success: The rate of successful device implantation was 98.5%. A complete seal or an echocardiographic color jet of 5 mm or less at the time of implantation was achieved in 99.7% of cases, and this remained the case in 98.9% at 3 months.
With regard to safety, the stroke rate was 0.4%, device embolization occurred in 0.4%, and the pericardial effusion/tamponade rate was 0.7%, all of which are lower rates than in earlier clinical trials.
Just over 4% of patients experienced device-related adverse events with full recovery at the 3-month follow-up. These were mostly bleeding events at the groin access site. More importantly, only 0.5% of patients had device-related serious adverse events that weren’t resolved at 3 months.
“This 0.5% is a major step forward,” Dr. Bergmann said. “This includes all pericardial effusions, all device embolizations, all periprocedural strokes – everything involving the procedure that puts a patient at risk. In fact, that 0.5% risk for left atrial appendage closure with the Watchman is pretty much the same risk as if you refer your patient with AF to an electrophysiologist for pulmonary vein isolation.”
One key question answered by EWOLUTION is, do you need to be an expert in the procedure in order to get excellent results? The answer, Dr. Bergmann said, is emphatically “no.” Interventionalists at the 47 participating sites varied widely in their experience with left atrial appendage occlusion, so investigators divided the sites into quartiles based upon experience and patient volumes contributed to the registry. While cardiologists in the most experienced centers had a significantly higher rate of successful device release on the first try, the most- and least-experienced centers did equally well on the endpoint that really counts: a complete or near-complete seal of the left atrial appendage at follow-up. Complication rates didn’t differ by site experience, either.
Another important practical question that’s been holding up wider adoption of the Watchman concerns how best to handle postimplantation antithrombotic therapy. Here the EWOLUTION registry provides a partial answer: 607 patients were on dual antiplatelet therapy, 113 were on a novel anticoagulant (NOAC), 159 were on warfarin, 67 were on nothing at all, and the rest were on a single antiplatelet agent. And there was no significant difference between any of these groups in the 3-month rates of thrombus on the device, bleeding events, stroke, or other adverse events.
“The main message is there is no difference in serious adverse events between any of the drug regimens. So if you’re in a situation where you can’t give any medication to reduce stroke risk because the bleeding risk is so high, you can go for left atrial appendage closure technology and give them nothing post implant,” according to Dr. Bergmann.
He added that he’d personally try to avoid that strategy: “You want to have some coverage.”
Also noteworthy is that 113 Watchman recipients did well with 3 months of NOAC monotherapy. The appeal of that approach is the short half-life of those agents in the event of a bleeding problem.
Discussant Dr. Farrel Hellig commented that EWOLUTION demonstrates that the Watchman procedure is predictable and safe, with an impressively low complication rate even in inexperienced centers. For that, he added, kudos goes to Boston Scientific, which markets the Watchman, for rolling out an effective physician training program.
“The most important topic to discuss is bleeding, because a bleeding rate of 4.1% at 3 months is certainly not insignificant,” he continued. “It appears, firstly, from EWOLUTION that it’s safe to omit warfarin. I think the most important thing we’d like to know now is could a postprocedure NOAC be the best option, and can aspirin be eliminated in the long term?”
“Is it too early to recommend a NOAC-only for a period of time post procedure? Perhaps. But I think this would be an important next clinical trial: a NOAC-only for a period post procedure with no aspirin to follow. This is the next piece of information we need to complete the puzzle and for left atrial appendage closure to reach its full potential,” according to Dr. Hellig of the University of Cape Town (South Africa).
The EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann reported serving as a consultant to Boston Scientific and Biosense Webster and receiving honoraria from more than a half-dozen pharmaceutical and device companies.
PARIS – Results of the real-world EWOLUTION registry of recipients of the Watchman device for stroke prevention provide reassuring answers to several key questions which have slowed physician uptake of the left atrial appendage closure device, Dr. Martin W. Bergmann said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“EWOLUTION, with more than 1,000 patients, is I think the study that we’ve needed to make this intervention happen in routine practice as a procedure for stroke prevention in atrial fibrillation,” declared Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.
EWOLUTION is a prospective, single-arm, multicenter registry including 1,025 recipients of the first-generation version of the Watchman, a transcatheter device for left atrial appendage closure as a means of stroke prevention in patients with atrial fibrillation (AF). These were high-risk patients: 50% of them had a CHA2DS2-VASc score of 5 or higher, and 72% of participants were deemed unsuitable for warfarin. EWOLUTION was conducted at 47 sites in Europe, the Middle East, and Russia. Dr. Bergmann presented the 3-month outcomes, a key period for device-related complications because protective epithelialization of the device isn’t yet complete. Follow-up will continue at the 1- and 2-year marks.
Among the key findings in the domain of procedural success: The rate of successful device implantation was 98.5%. A complete seal or an echocardiographic color jet of 5 mm or less at the time of implantation was achieved in 99.7% of cases, and this remained the case in 98.9% at 3 months.
With regard to safety, the stroke rate was 0.4%, device embolization occurred in 0.4%, and the pericardial effusion/tamponade rate was 0.7%, all of which are lower rates than in earlier clinical trials.
Just over 4% of patients experienced device-related adverse events with full recovery at the 3-month follow-up. These were mostly bleeding events at the groin access site. More importantly, only 0.5% of patients had device-related serious adverse events that weren’t resolved at 3 months.
“This 0.5% is a major step forward,” Dr. Bergmann said. “This includes all pericardial effusions, all device embolizations, all periprocedural strokes – everything involving the procedure that puts a patient at risk. In fact, that 0.5% risk for left atrial appendage closure with the Watchman is pretty much the same risk as if you refer your patient with AF to an electrophysiologist for pulmonary vein isolation.”
One key question answered by EWOLUTION is, do you need to be an expert in the procedure in order to get excellent results? The answer, Dr. Bergmann said, is emphatically “no.” Interventionalists at the 47 participating sites varied widely in their experience with left atrial appendage occlusion, so investigators divided the sites into quartiles based upon experience and patient volumes contributed to the registry. While cardiologists in the most experienced centers had a significantly higher rate of successful device release on the first try, the most- and least-experienced centers did equally well on the endpoint that really counts: a complete or near-complete seal of the left atrial appendage at follow-up. Complication rates didn’t differ by site experience, either.
Another important practical question that’s been holding up wider adoption of the Watchman concerns how best to handle postimplantation antithrombotic therapy. Here the EWOLUTION registry provides a partial answer: 607 patients were on dual antiplatelet therapy, 113 were on a novel anticoagulant (NOAC), 159 were on warfarin, 67 were on nothing at all, and the rest were on a single antiplatelet agent. And there was no significant difference between any of these groups in the 3-month rates of thrombus on the device, bleeding events, stroke, or other adverse events.
“The main message is there is no difference in serious adverse events between any of the drug regimens. So if you’re in a situation where you can’t give any medication to reduce stroke risk because the bleeding risk is so high, you can go for left atrial appendage closure technology and give them nothing post implant,” according to Dr. Bergmann.
He added that he’d personally try to avoid that strategy: “You want to have some coverage.”
Also noteworthy is that 113 Watchman recipients did well with 3 months of NOAC monotherapy. The appeal of that approach is the short half-life of those agents in the event of a bleeding problem.
Discussant Dr. Farrel Hellig commented that EWOLUTION demonstrates that the Watchman procedure is predictable and safe, with an impressively low complication rate even in inexperienced centers. For that, he added, kudos goes to Boston Scientific, which markets the Watchman, for rolling out an effective physician training program.
“The most important topic to discuss is bleeding, because a bleeding rate of 4.1% at 3 months is certainly not insignificant,” he continued. “It appears, firstly, from EWOLUTION that it’s safe to omit warfarin. I think the most important thing we’d like to know now is could a postprocedure NOAC be the best option, and can aspirin be eliminated in the long term?”
“Is it too early to recommend a NOAC-only for a period of time post procedure? Perhaps. But I think this would be an important next clinical trial: a NOAC-only for a period post procedure with no aspirin to follow. This is the next piece of information we need to complete the puzzle and for left atrial appendage closure to reach its full potential,” according to Dr. Hellig of the University of Cape Town (South Africa).
The EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann reported serving as a consultant to Boston Scientific and Biosense Webster and receiving honoraria from more than a half-dozen pharmaceutical and device companies.
AT EUROPCR 2016
Key clinical point: You don’t have to be an expert at implanting the Watchman left atrial appendage closure device to achieve the same sort of sky-high procedural success and low complication rates the experts do.
Major finding: The Watchman device successfully sealed off the left atrial appendage in 98.9% of cases at 3 months follow-up, with rates closely similar at the least- and most-experienced centers.
Data source: EWOLUTION is a prospective, multicenter, real-world registry of 1,025 recipients of the Watchman left atrial appendage closure device at 47 sites in Europe, the Middle East, and Russia.
Disclosures: The EWOLUTION registry is sponsored by Boston Scientific. The presenter reported serving as a consultant to Boston Scientific and Biosense Webster and receiving honoraria from more than a half-dozen pharmaceutical and device companies.

ASCT still a player for multiple myeloma
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
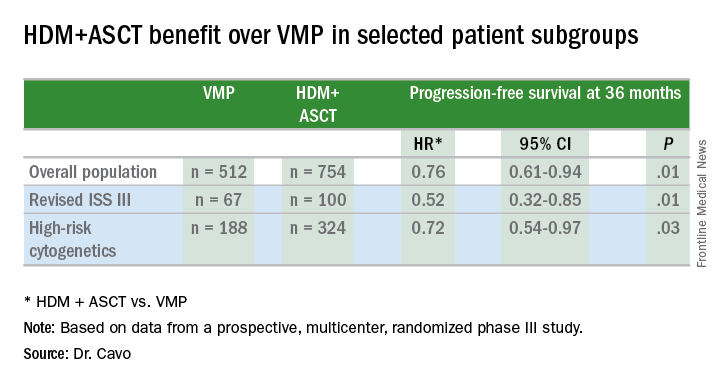
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
Even in this era of novel therapies for multiple myeloma, for patients with newly diagnosed disease, autologous stem cell transplant (ASCT) after chemotherapy provides benefits in terms of disease progression and extent of response, compared with chemotherapy alone. The benefit of ASCT was especially pronounced among certain groups of high-risk patients.
Novel proteasome inhibitors and immunomodulators “have dramatically increased the complete response rate and significantly extended progression-free survival and overall survival in previously untreated multiple myeloma patients,” Dr. Michele Cavo, head of the Seragnoli Institute of Hematology at the University of Bologna School of Medicine in Italy, said at a presscast in advance of the annual meeting of the American Society of Clinical Oncology.
But questions remain about how these newer agents perform, compared with high-dose melphalan (HDM) followed by ASCT, traditionally seen as the standard of care for younger and fit patients with newly diagnosed disease.
EMN02/HO95 is a large, prospective, multicenter, intergroup, randomized phase III study that addresses this question, as well as single vs. double ASCT and the use of consolidation therapy or not. The study includes patients 65 years old or younger, and the trial protocol involves induction therapy with bortezomib (Velcade)–cyclophosphamide-dexamethasone (VCD) and subsequent collection of peripheral blood stem cells.
Patients were then randomly assigned to receive bortezomib-melphalan-prednisone (VMP) or HDM as intensification therapy in centers that had a single ASCT policy. For those centers doing double (tandem) ASCT procedures, the randomization was to VMP vs. HDM + single ASCT vs. HDM + double ASCT.
Patients in each treatment arm then underwent another randomization to consolidation therapy with bortezomib-lenalidomide (Revlimid)–dexamethasone or no consolidation. All patients received lenalidomide maintenance until disease progression or toxicity. At the time of a preliminary analysis of trial data in January 2016, results from the second randomization to consolidation or no consolidation therapy were not yet complete. This first prespecified interim analysis was performed after at least 33% of the required events had occurred.
Early results show ASCT benefit
Early results on 1,266 patients (VMP, n = 512; HDM, n = 754) show that a median progression-free survival (PFS) was not yet reached after a median follow-up of 23.9 months from the first randomization (to VMP vs. HDM+ASCT), the primary endpoint of the trial.
In the overall patient population, patients achieved a significant 24% benefit in PFS when given HDM+ASCT up front (hazard ratio, 0.76 vs. VMP), and this benefit extended to certain patient subgroups, as well.
“PFS benefit with bortezomib-based ASCT was of relevance for patients at high risk of early relapse, in particular for those with revised ISS [International Staging System] stage III and high-risk cytogenetic profiles, who had a relative reduction in the risk of progression or death of 48% and 28%, respectively,” Dr. Cavo said.
Other predictors of longer PFS were ISS stage I (HR, 0.44; 95% confidence interval, 0.28-067; P less than .0001), standard risk cytogenetics (HR, 0.57; 95% CI, 0.41-0.78; P less than .0001), randomization to the HDM+ASCT arm (HR, 0.61; 95% CI, 0.45-0.82; P = .001), and less than 60% bone marrow plasma cells (HR, 0.67; 95% CI, 0.48-0.99; P = .014).
More patients receiving ASCT up front had a significantly greater reduction in tumor volume of at least 90%, as indicated by the composite of very good partial remission, complete response, and stringent complete response, which was achieved in 74.0% in the VMP arm and in 84.4% of the HDM+ASCT arm (P less than .0001).
For patients at low risk of relapse, Dr. Cavo said longer follow up will be needed to compare the different arms of the study, and future analyses will delineate the effects of consolidation or no consolidation therapy and the use of the VMP regimen, compared with single or double ASCT.
ASCO president Dr. Julie Vose said that even with effective novel agents available, older, proven approaches still retain their value. “This study demonstrated that combining the best of both worlds – initial therapy with a novel agent followed by stem cell transplant – resulted in the best patient outcomes,” she said.
FROM THE 2016 ASCO ANNUAL MEETING
Key clinical point: ASCT bested bortezomib for newly diagnosed younger multiple myeloma patients.
Major finding: Multiple myeloma patients showed 24% PFS prolongation with up front HDM+ASCT.
Data source: EMN02/HO95, a prospective, multicenter, intergroup, randomized phase III study of 1,266 patients.
Disclosures: The study was funded by HOVON, the Hemato Oncology Foundation for Adults in the Netherlands. Dr. Cavo disclosed relationships with Janssen, Takeda, Amgen, Bristol-Myers Squibb, and Celgene. Dr. Vose disclosed relationships with Sanofi Aventis, Seattle Genetics, Acerta, Bristol-Myers Squibb, Celgene, Genentech, GlaxoSmithKline, Incyte, Janssen Biotech, Kite Pharma, Pharmacyclics, and Spectrum Pharmaceuticals.
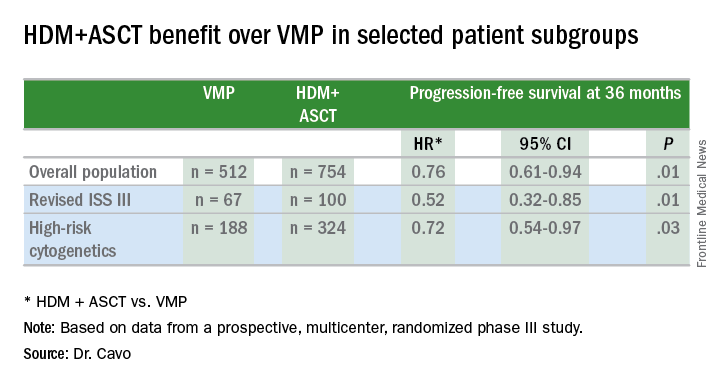
SIMPle smartphone app shows promise for bipolar disorder psychoeducation
ATLANTA – A new smartphone application aimed at providing psychoeducation to patients with bipolar disorder was well received and showed promise for improving outcomes in a feasibility study, according to Dr. Eduard Vieta.
Early results of the study showed that adherence was quite high, with retention at 76% among 49 patients with bipolar disorder who tested the SIMPle app (Self Monitoring and Psychoeducation in Bipolar Patients with a Smartphone Application), Dr. Vieta said at the annual meeting of the American Psychiatric Association.

The app, currently available for free for Android and iPhones, is an interactive educational program that includes weekly and daily tests, with alerts for patients to take medications or see their doctor.
The patients in the study were representative of generally stable bipolar disorder patients in a real-world setting, as the app ideally would be used by those who are “in near remission or at least not acutely ill,” said Dr. Vieta of the University of Barcelona.
“People like the app and did follow the daily and weekly tests, which is a good sign,” he said, noting that satisfaction was high, and good correlation between test scores and mood changes suggested that the app is reliable for monitoring mood changes.
There were 10 suicide alerts during the study that were quickly addressed because messages were received immediately, he said.
The latest version of the app includes simpler navigation, rewards for fulfilling the daily and weekly testing, and medication reminders.
Dr. Vieta and his colleagues at the University of Barcelona previously have demonstrated the value of psychoeducation among patients with bipolar disorder. They developed a successful psychoeducation program in the late 1990s, which led to a trial published in 2003 and development of a training manual in 2006 that has been translated into numerous languages.
The program and trial showed that adding psychoeducation to medication in patients with bipolar disorder improves outcomes in terms of relapse and hospitalizations: the rate of relapses in the study was reduced by nearly 80%, Dr. Vieta said.
Providing such education, however, which has become a standard of care, is limited by the need for personnel training and by staffing and financial resource constraints.
“We wanted something nonstigmatizing but also linked to the clinical care team. … Clearly, we would like to make this intervention more widely available without compromising quality,” Dr. Vieta said, describing the impetus for the SIMPle app.
A phase II, randomized controlled study of the app is now underway, he said, adding that “this is really quite exciting. … There is huge potential for things we can do with this app.”
Dr. Vieta is a consultant or adviser for several pharmaceutical companies. He also has received research grants, honoraria, or consulting fees from numerous entities.
ATLANTA – A new smartphone application aimed at providing psychoeducation to patients with bipolar disorder was well received and showed promise for improving outcomes in a feasibility study, according to Dr. Eduard Vieta.
Early results of the study showed that adherence was quite high, with retention at 76% among 49 patients with bipolar disorder who tested the SIMPle app (Self Monitoring and Psychoeducation in Bipolar Patients with a Smartphone Application), Dr. Vieta said at the annual meeting of the American Psychiatric Association.
The app, currently available for free for Android and iPhones, is an interactive educational program that includes weekly and daily tests, with alerts for patients to take medications or see their doctor.
The patients in the study were representative of generally stable bipolar disorder patients in a real-world setting, as the app ideally would be used by those who are “in near remission or at least not acutely ill,” said Dr. Vieta of the University of Barcelona.
“People like the app and did follow the daily and weekly tests, which is a good sign,” he said, noting that satisfaction was high, and good correlation between test scores and mood changes suggested that the app is reliable for monitoring mood changes.
There were 10 suicide alerts during the study that were quickly addressed because messages were received immediately, he said.
The latest version of the app includes simpler navigation, rewards for fulfilling the daily and weekly testing, and medication reminders.
Dr. Vieta and his colleagues at the University of Barcelona previously have demonstrated the value of psychoeducation among patients with bipolar disorder. They developed a successful psychoeducation program in the late 1990s, which led to a trial published in 2003 and development of a training manual in 2006 that has been translated into numerous languages.
The program and trial showed that adding psychoeducation to medication in patients with bipolar disorder improves outcomes in terms of relapse and hospitalizations: the rate of relapses in the study was reduced by nearly 80%, Dr. Vieta said.
Providing such education, however, which has become a standard of care, is limited by the need for personnel training and by staffing and financial resource constraints.
“We wanted something nonstigmatizing but also linked to the clinical care team. … Clearly, we would like to make this intervention more widely available without compromising quality,” Dr. Vieta said, describing the impetus for the SIMPle app.
A phase II, randomized controlled study of the app is now underway, he said, adding that “this is really quite exciting. … There is huge potential for things we can do with this app.”
Dr. Vieta is a consultant or adviser for several pharmaceutical companies. He also has received research grants, honoraria, or consulting fees from numerous entities.
ATLANTA – A new smartphone application aimed at providing psychoeducation to patients with bipolar disorder was well received and showed promise for improving outcomes in a feasibility study, according to Dr. Eduard Vieta.
Early results of the study showed that adherence was quite high, with retention at 76% among 49 patients with bipolar disorder who tested the SIMPle app (Self Monitoring and Psychoeducation in Bipolar Patients with a Smartphone Application), Dr. Vieta said at the annual meeting of the American Psychiatric Association.
The app, currently available for free for Android and iPhones, is an interactive educational program that includes weekly and daily tests, with alerts for patients to take medications or see their doctor.
The patients in the study were representative of generally stable bipolar disorder patients in a real-world setting, as the app ideally would be used by those who are “in near remission or at least not acutely ill,” said Dr. Vieta of the University of Barcelona.
“People like the app and did follow the daily and weekly tests, which is a good sign,” he said, noting that satisfaction was high, and good correlation between test scores and mood changes suggested that the app is reliable for monitoring mood changes.
There were 10 suicide alerts during the study that were quickly addressed because messages were received immediately, he said.
The latest version of the app includes simpler navigation, rewards for fulfilling the daily and weekly testing, and medication reminders.
Dr. Vieta and his colleagues at the University of Barcelona previously have demonstrated the value of psychoeducation among patients with bipolar disorder. They developed a successful psychoeducation program in the late 1990s, which led to a trial published in 2003 and development of a training manual in 2006 that has been translated into numerous languages.
The program and trial showed that adding psychoeducation to medication in patients with bipolar disorder improves outcomes in terms of relapse and hospitalizations: the rate of relapses in the study was reduced by nearly 80%, Dr. Vieta said.
Providing such education, however, which has become a standard of care, is limited by the need for personnel training and by staffing and financial resource constraints.
“We wanted something nonstigmatizing but also linked to the clinical care team. … Clearly, we would like to make this intervention more widely available without compromising quality,” Dr. Vieta said, describing the impetus for the SIMPle app.
A phase II, randomized controlled study of the app is now underway, he said, adding that “this is really quite exciting. … There is huge potential for things we can do with this app.”
Dr. Vieta is a consultant or adviser for several pharmaceutical companies. He also has received research grants, honoraria, or consulting fees from numerous entities.
AT THE APA ANNUAL MEETING
Key clinical point: A new smartphone application aimed at providing psychoeducation to patients with bipolar disorder was well received and showed promise for improving outcomes in a feasibility study.
Major finding: Adherence was good and retention was high at 76%.
Data source: A feasibility study involving 49 patients.
Disclosures: Dr. Vieta is a consultant or advisor for several pharmaceutical companies. He also has received research grants, honoraria, or consulting fees from numerous entities.

Statins, but not aspirin, linked to lower pancreatic cancer risk
SAN DIEGO – Statin use, but not aspirin use, showed a protective effect against pancreatic ductal adenocarcinoma in a large prospective case-control study.
“There also appears to be no chemoenhancing effect from combining the two drugs,” Dr. Livia Archibugi of Hospital Sant’Andrea in Rome, Italy, said at the annual Digestive Disease Week. The study also confirmed known risk factors for pancreatic cancer, “supporting the genuineness of our population,” she and her associates said.

This is the first epidemiologic study to look at both aspirin and statins in relationship to pancreatic cancer. Both types of drugs have shown anticarcinogenic effects in laboratory and epidemiologic studies, Dr. Archibugi noted. For example, aspirin blocks mTOR, NF-kappa B and Wnt signaling, which inhibits carcinogenesis and angiogenesis and promotes apoptosis and DNA mismatch repair. A recent meta-analysis, found a 23% lower risk of pancreatic cancer among aspirin users than nonusers, but the study did not assess concurrent statin use.
Statins, for their part, are both immunomodulatory and anti-inflammatory, and inhibit angiogenesis at low doses, said Dr. Archibugi. However, studies have yielded mixed results about whether they reduce the risk of pancreatic cancer, she noted.
Therefore, between 2005 and 2016, she and her colleagues used questionnaires to study environmental exposures and the family and individual health histories of 408 consecutive patients with pancreatic ductal adenocarcinoma and 816 age- and sex-matched controls. The controls were gastroenterology patients at the same hospital and did not have chronic obstructive pulmonary disease, cirrhosis, chronic kidney failure, acute bleeding, inflammatory bowel disease, or a history of cancer in the past 5 years. The study was large enough to have an 80% power to detect an odds ratio of 0.65 for the relationship between incident pancreatic cancer and either aspirin or statin exposure, and an odds ratio of 0.5 for dual exposure, Dr. Archibugi noted.
Reported statin use was significantly more common among controls (24%) than cases (18%; P = .03), and controls were more likely than cases to report taking either low-dose (less than 20 mg) or high-dose (greater than 20 mg) statins, the investigators found. Proportionally more controls also reported at least a 5-year history of statin use. After controlling for age, sex, and known risk factors, only statin use was significantly associated with incident pancreatic cancer in the multivariate analysis (OR, 0.59; 95% confidence interval, 0.42-0.85; P = .004). The protective effect of statins held up in subgroups stratified by gender, age, and statin type, Dr. Archibugi said.
In contrast, statistically similar proportions of cases (19%) and controls (23%) reported using aspirin, and although aspirin use was inversely linked to incident pancreatic cancer in the univariate analysis, the effect lost significance in the multivariable analysis (OR, 0.78; 95% CI, 0.54-1.11). Moreover, patients who took both aspirin and statins were no less likely to develop pancreatic cancer than those who took only statins.
Like all case-control studies, recall bias could have affected the associations, she noted. However, the same analyses correlated pancreatic cancer with several known risk factors, including smoking (OR, 1.8), heavy drinking (OR, 1.7), diabetes (OR, 1.8), chronic pancreatitis (OR, 14.3), and first-degree family history of pancreatic cancer (OR, 3.1).
Dr. Archibugi and her associates had no disclosures.
SAN DIEGO – Statin use, but not aspirin use, showed a protective effect against pancreatic ductal adenocarcinoma in a large prospective case-control study.
“There also appears to be no chemoenhancing effect from combining the two drugs,” Dr. Livia Archibugi of Hospital Sant’Andrea in Rome, Italy, said at the annual Digestive Disease Week. The study also confirmed known risk factors for pancreatic cancer, “supporting the genuineness of our population,” she and her associates said.
This is the first epidemiologic study to look at both aspirin and statins in relationship to pancreatic cancer. Both types of drugs have shown anticarcinogenic effects in laboratory and epidemiologic studies, Dr. Archibugi noted. For example, aspirin blocks mTOR, NF-kappa B and Wnt signaling, which inhibits carcinogenesis and angiogenesis and promotes apoptosis and DNA mismatch repair. A recent meta-analysis, found a 23% lower risk of pancreatic cancer among aspirin users than nonusers, but the study did not assess concurrent statin use.
Statins, for their part, are both immunomodulatory and anti-inflammatory, and inhibit angiogenesis at low doses, said Dr. Archibugi. However, studies have yielded mixed results about whether they reduce the risk of pancreatic cancer, she noted.
Therefore, between 2005 and 2016, she and her colleagues used questionnaires to study environmental exposures and the family and individual health histories of 408 consecutive patients with pancreatic ductal adenocarcinoma and 816 age- and sex-matched controls. The controls were gastroenterology patients at the same hospital and did not have chronic obstructive pulmonary disease, cirrhosis, chronic kidney failure, acute bleeding, inflammatory bowel disease, or a history of cancer in the past 5 years. The study was large enough to have an 80% power to detect an odds ratio of 0.65 for the relationship between incident pancreatic cancer and either aspirin or statin exposure, and an odds ratio of 0.5 for dual exposure, Dr. Archibugi noted.
Reported statin use was significantly more common among controls (24%) than cases (18%; P = .03), and controls were more likely than cases to report taking either low-dose (less than 20 mg) or high-dose (greater than 20 mg) statins, the investigators found. Proportionally more controls also reported at least a 5-year history of statin use. After controlling for age, sex, and known risk factors, only statin use was significantly associated with incident pancreatic cancer in the multivariate analysis (OR, 0.59; 95% confidence interval, 0.42-0.85; P = .004). The protective effect of statins held up in subgroups stratified by gender, age, and statin type, Dr. Archibugi said.
In contrast, statistically similar proportions of cases (19%) and controls (23%) reported using aspirin, and although aspirin use was inversely linked to incident pancreatic cancer in the univariate analysis, the effect lost significance in the multivariable analysis (OR, 0.78; 95% CI, 0.54-1.11). Moreover, patients who took both aspirin and statins were no less likely to develop pancreatic cancer than those who took only statins.
Like all case-control studies, recall bias could have affected the associations, she noted. However, the same analyses correlated pancreatic cancer with several known risk factors, including smoking (OR, 1.8), heavy drinking (OR, 1.7), diabetes (OR, 1.8), chronic pancreatitis (OR, 14.3), and first-degree family history of pancreatic cancer (OR, 3.1).
Dr. Archibugi and her associates had no disclosures.
SAN DIEGO – Statin use, but not aspirin use, showed a protective effect against pancreatic ductal adenocarcinoma in a large prospective case-control study.
“There also appears to be no chemoenhancing effect from combining the two drugs,” Dr. Livia Archibugi of Hospital Sant’Andrea in Rome, Italy, said at the annual Digestive Disease Week. The study also confirmed known risk factors for pancreatic cancer, “supporting the genuineness of our population,” she and her associates said.
This is the first epidemiologic study to look at both aspirin and statins in relationship to pancreatic cancer. Both types of drugs have shown anticarcinogenic effects in laboratory and epidemiologic studies, Dr. Archibugi noted. For example, aspirin blocks mTOR, NF-kappa B and Wnt signaling, which inhibits carcinogenesis and angiogenesis and promotes apoptosis and DNA mismatch repair. A recent meta-analysis, found a 23% lower risk of pancreatic cancer among aspirin users than nonusers, but the study did not assess concurrent statin use.
Statins, for their part, are both immunomodulatory and anti-inflammatory, and inhibit angiogenesis at low doses, said Dr. Archibugi. However, studies have yielded mixed results about whether they reduce the risk of pancreatic cancer, she noted.
Therefore, between 2005 and 2016, she and her colleagues used questionnaires to study environmental exposures and the family and individual health histories of 408 consecutive patients with pancreatic ductal adenocarcinoma and 816 age- and sex-matched controls. The controls were gastroenterology patients at the same hospital and did not have chronic obstructive pulmonary disease, cirrhosis, chronic kidney failure, acute bleeding, inflammatory bowel disease, or a history of cancer in the past 5 years. The study was large enough to have an 80% power to detect an odds ratio of 0.65 for the relationship between incident pancreatic cancer and either aspirin or statin exposure, and an odds ratio of 0.5 for dual exposure, Dr. Archibugi noted.
Reported statin use was significantly more common among controls (24%) than cases (18%; P = .03), and controls were more likely than cases to report taking either low-dose (less than 20 mg) or high-dose (greater than 20 mg) statins, the investigators found. Proportionally more controls also reported at least a 5-year history of statin use. After controlling for age, sex, and known risk factors, only statin use was significantly associated with incident pancreatic cancer in the multivariate analysis (OR, 0.59; 95% confidence interval, 0.42-0.85; P = .004). The protective effect of statins held up in subgroups stratified by gender, age, and statin type, Dr. Archibugi said.
In contrast, statistically similar proportions of cases (19%) and controls (23%) reported using aspirin, and although aspirin use was inversely linked to incident pancreatic cancer in the univariate analysis, the effect lost significance in the multivariable analysis (OR, 0.78; 95% CI, 0.54-1.11). Moreover, patients who took both aspirin and statins were no less likely to develop pancreatic cancer than those who took only statins.
Like all case-control studies, recall bias could have affected the associations, she noted. However, the same analyses correlated pancreatic cancer with several known risk factors, including smoking (OR, 1.8), heavy drinking (OR, 1.7), diabetes (OR, 1.8), chronic pancreatitis (OR, 14.3), and first-degree family history of pancreatic cancer (OR, 3.1).
Dr. Archibugi and her associates had no disclosures.
AT DDW® 2016
Key clinical point: Statin use was linked to lower odds of pancreatic ductal adenocarcinoma, while aspirin use was not.
Major finding: Statin use was the only statistically significant protective factor in the multivariate analysis, with an adjusted OR of 0.59 (P = .004).
Data source: A prospective case-control study of 408 patients with pancreatic cancer and 816 age- and sex-matched hospital controls.
Disclosures: Dr. Archibugi and her associates had no disclosures.

Pediatric Dermatology: 2016

- New options for acne treatment
- Expert critiques isotretinoin controversies
- Busting atopic dermatitis therapy myths
- Promising new topicals for treating eczema
- Cut simple carbs to clear acne
- Two conditions raise suspicion for pediatric psoriasis
- Ask teens with acne about whey protein
Faculty
Lawrence F. Eichenfield, M.D.
Chief of pediatric and adolescent dermatology
Rady Children’s Hospital—San Diego
Professor of medicine and pediatrics
University of California, San Diego
Director, Rady Children’s Hospital/UCSD’s Eczema and Inflammatory Skin Disease Center
Andrew Krakowski, M.D.
Board-certified dermatologist and pediatric dermatologist with a clinical research focus on acne, eczema, and the application of lasers/photomedicine in children
Chief medical officer for DermOne, LLC
West Conshohocken, Pa.
Disclosures: Dr. Eichenfield has served as an investigator and/or consultant for Anacor Pharmaceuticals, Otsuka Pharmaceuticals, and Regeneron Pharmaceuticals. Dr. Krakowski said he had no relevant financial disclosures.
©Copyright 2016, by Frontline Medical Communications Inc. All rights reserved.
- New options for acne treatment
- Expert critiques isotretinoin controversies
- Busting atopic dermatitis therapy myths
- Promising new topicals for treating eczema
- Cut simple carbs to clear acne
- Two conditions raise suspicion for pediatric psoriasis
- Ask teens with acne about whey protein
Faculty
Lawrence F. Eichenfield, M.D.
Chief of pediatric and adolescent dermatology
Rady Children’s Hospital—San Diego
Professor of medicine and pediatrics
University of California, San Diego
Director, Rady Children’s Hospital/UCSD’s Eczema and Inflammatory Skin Disease Center
Andrew Krakowski, M.D.
Board-certified dermatologist and pediatric dermatologist with a clinical research focus on acne, eczema, and the application of lasers/photomedicine in children
Chief medical officer for DermOne, LLC
West Conshohocken, Pa.
Disclosures: Dr. Eichenfield has served as an investigator and/or consultant for Anacor Pharmaceuticals, Otsuka Pharmaceuticals, and Regeneron Pharmaceuticals. Dr. Krakowski said he had no relevant financial disclosures.
©Copyright 2016, by Frontline Medical Communications Inc. All rights reserved.
- New options for acne treatment
- Expert critiques isotretinoin controversies
- Busting atopic dermatitis therapy myths
- Promising new topicals for treating eczema
- Cut simple carbs to clear acne
- Two conditions raise suspicion for pediatric psoriasis
- Ask teens with acne about whey protein
Faculty
Lawrence F. Eichenfield, M.D.
Chief of pediatric and adolescent dermatology
Rady Children’s Hospital—San Diego
Professor of medicine and pediatrics
University of California, San Diego
Director, Rady Children’s Hospital/UCSD’s Eczema and Inflammatory Skin Disease Center
Andrew Krakowski, M.D.
Board-certified dermatologist and pediatric dermatologist with a clinical research focus on acne, eczema, and the application of lasers/photomedicine in children
Chief medical officer for DermOne, LLC
West Conshohocken, Pa.
Disclosures: Dr. Eichenfield has served as an investigator and/or consultant for Anacor Pharmaceuticals, Otsuka Pharmaceuticals, and Regeneron Pharmaceuticals. Dr. Krakowski said he had no relevant financial disclosures.
©Copyright 2016, by Frontline Medical Communications Inc. All rights reserved.
Don’t Miss the 2016 Heart Valve Summit: Medical, Surgical & Interventional Decision Making
October 20-22, 2016
Radisson Blu Aqua Hotel
Chicago, IL
Course Directors
David H. Adams
Steven F. Bolling
Robert O. Bonow
Howard C. Herrmann
Nurse Planner
Michele Mistovich
Course Overview
The American College of Cardiology and the American Association for Thoracic Surgery are again partnering to bring together cardiologists and surgeons in a cooperative, case-based course to address the rapid advances in the treatment of valvular heart disease (VHD).
Focusing on interactivity and practical decision-making, this unique conference will engage participants in discussions, debates and potential controversies using real-world cases. Its renowned faculty will include experts on the cutting edge of clinically relevant VHD data.
The interdisciplinary course emphasizes clinical decision-making with medical, surgical and interventional options for patient care, taking into account that constantly changing management tools can impact the surgical team. There will be breakout sessions for cardiologists, cardiac surgeons, nurses and physician assistants designed to help specialists manage their unique challenges from a team perspective.
Target Audience
Cardiologists, interventional cardiologists, cardiothoracic surgeons, internists, nurses, physician assistants and health care professionals involved in VHD evaluation, diagnosis and/or management.
October 20-22, 2016
Radisson Blu Aqua Hotel
Chicago, IL
Course Directors
David H. Adams
Steven F. Bolling
Robert O. Bonow
Howard C. Herrmann
Nurse Planner
Michele Mistovich
Course Overview
The American College of Cardiology and the American Association for Thoracic Surgery are again partnering to bring together cardiologists and surgeons in a cooperative, case-based course to address the rapid advances in the treatment of valvular heart disease (VHD).
Focusing on interactivity and practical decision-making, this unique conference will engage participants in discussions, debates and potential controversies using real-world cases. Its renowned faculty will include experts on the cutting edge of clinically relevant VHD data.
The interdisciplinary course emphasizes clinical decision-making with medical, surgical and interventional options for patient care, taking into account that constantly changing management tools can impact the surgical team. There will be breakout sessions for cardiologists, cardiac surgeons, nurses and physician assistants designed to help specialists manage their unique challenges from a team perspective.
Target Audience
Cardiologists, interventional cardiologists, cardiothoracic surgeons, internists, nurses, physician assistants and health care professionals involved in VHD evaluation, diagnosis and/or management.
October 20-22, 2016
Radisson Blu Aqua Hotel
Chicago, IL
Course Directors
David H. Adams
Steven F. Bolling
Robert O. Bonow
Howard C. Herrmann
Nurse Planner
Michele Mistovich
Course Overview
The American College of Cardiology and the American Association for Thoracic Surgery are again partnering to bring together cardiologists and surgeons in a cooperative, case-based course to address the rapid advances in the treatment of valvular heart disease (VHD).
Focusing on interactivity and practical decision-making, this unique conference will engage participants in discussions, debates and potential controversies using real-world cases. Its renowned faculty will include experts on the cutting edge of clinically relevant VHD data.
The interdisciplinary course emphasizes clinical decision-making with medical, surgical and interventional options for patient care, taking into account that constantly changing management tools can impact the surgical team. There will be breakout sessions for cardiologists, cardiac surgeons, nurses and physician assistants designed to help specialists manage their unique challenges from a team perspective.
Target Audience
Cardiologists, interventional cardiologists, cardiothoracic surgeons, internists, nurses, physician assistants and health care professionals involved in VHD evaluation, diagnosis and/or management.

Answers to Clinical Questions in Primary Care Management of People with Obesity

