User login
Resident Education, Feedback, Incentives Improve Patient Satisfaction
Editor’s note: This article first appeared on SHM’s “The Hospital Leader” blog.
Patient satisfaction survey performance is becoming increasingly important for hospitals, because the ratings are being used by payers in pay-for-performance programs more and more (including the CMS Hospital Value-Based Purchasing program). CMS also recently released its “Five-Star Quality Rating System” for hospitals, which publicly grades hospitals, using one to five stars, based on their patient satisfaction scores.
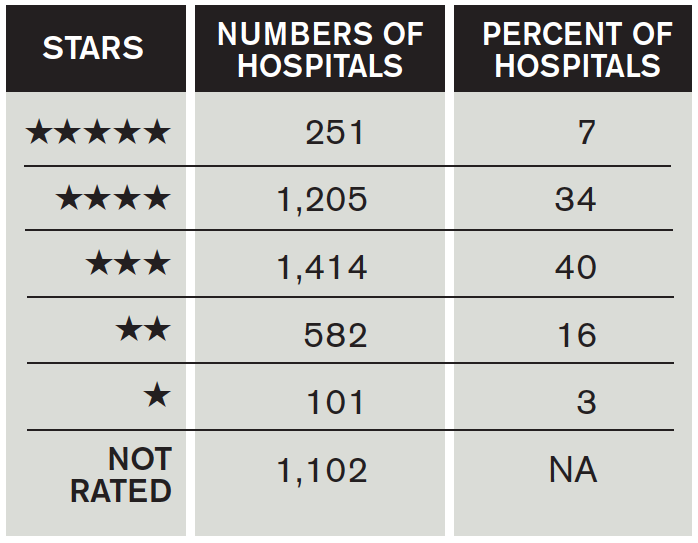
How Did Hospitals Do in Medicare’s Patient Quality Ratings?
Unfortunately, there is little literature to guide physicians on exactly HOW to improve patient satisfaction scores for themselves or their groups. A recent publication in the Journal of Hospital Medicine found a feasible and effective intervention to improve patient satisfaction scores among trainees, the methodology of which could easily be applied to hospitalists.
Gaurav Banka, MD, a former internal medicine resident (and current cardiology fellow) at UCLA Hospital, was interviewed about his team’s recent publication in the Journal of Hospital Medicine. In the interview, he opined about “improving patient satisfaction through resident education, feedback, and incentives.” The study he published found that this combination of interventions among internal medicine residents improved relevant HCAHPS scores by approximately 8%.
The following are excerpts from a Q&A session I had with Dr. Banka:
Question: Can you briefly summarize the intervention(s)?
Answer: There were three total interventions put in place simultaneously: an educational conference on best practices in patient communication, a recognition-reward program (recognition within the department and a movie package for high performers), and real-time feedback to the residents from their patients via a survey. The last component was the most impactful to the residents. Patients were randomly surveyed on how their residents were communicating with them, and the results were sent to the resident for review and self-reflection within weeks.
Q: How did you become interested in resident interventions to improve HCAHPS?
A: I noticed as an intern [that] there was almost no emphasis placed on patient communication skills, and there was almost no feedback given to residents on how they were performing. I felt that this was a very important piece of feedback that residents were lacking and was very interested in creating a program that would help them learn new communication skills and get feedback on how they were doing.
Q: How should hospitalists use this study information to change their practice?
A: Hospital medicine programs should have some way to measure and give feedback to individual hospitalists on what the patient is experiencing with respect to communication. The intervention from this study should be easily scalable to any practice. There was almost no cost associated with the patient survey distribution, and it gave incredibly valuable individualized feedback about communication skills directly from the patients themselves. It should be feasible to implement this type of audit and feedback within any size hospital medicine program.
Q: Were there any unexpected findings in your study?
A: We were surprised at how much of an impact it had on HCAHPS scores. Not only did it impact physician communication ratings, but [it] also had an impressive impact on overall hospital ratings.
Q: Where does this take us with respect to future research efforts?
A: Our team is now working on expanding this program to other residency programs, as well as expanding it to attending physicians, within and outside the department of medicine.
In summary, Dr. Banka’s team found this relatively simple intervention was able to sizably improve the HCAHPS scores of recipient providers. Such interventions should be seriously considered by hospital medicine programs looking to improve their publicly reported patient satisfaction scores.
Editor’s note: This article first appeared on SHM’s “The Hospital Leader” blog.
Patient satisfaction survey performance is becoming increasingly important for hospitals, because the ratings are being used by payers in pay-for-performance programs more and more (including the CMS Hospital Value-Based Purchasing program). CMS also recently released its “Five-Star Quality Rating System” for hospitals, which publicly grades hospitals, using one to five stars, based on their patient satisfaction scores.
How Did Hospitals Do in Medicare’s Patient Quality Ratings?
Unfortunately, there is little literature to guide physicians on exactly HOW to improve patient satisfaction scores for themselves or their groups. A recent publication in the Journal of Hospital Medicine found a feasible and effective intervention to improve patient satisfaction scores among trainees, the methodology of which could easily be applied to hospitalists.
Gaurav Banka, MD, a former internal medicine resident (and current cardiology fellow) at UCLA Hospital, was interviewed about his team’s recent publication in the Journal of Hospital Medicine. In the interview, he opined about “improving patient satisfaction through resident education, feedback, and incentives.” The study he published found that this combination of interventions among internal medicine residents improved relevant HCAHPS scores by approximately 8%.
The following are excerpts from a Q&A session I had with Dr. Banka:
Question: Can you briefly summarize the intervention(s)?
Answer: There were three total interventions put in place simultaneously: an educational conference on best practices in patient communication, a recognition-reward program (recognition within the department and a movie package for high performers), and real-time feedback to the residents from their patients via a survey. The last component was the most impactful to the residents. Patients were randomly surveyed on how their residents were communicating with them, and the results were sent to the resident for review and self-reflection within weeks.
Q: How did you become interested in resident interventions to improve HCAHPS?
A: I noticed as an intern [that] there was almost no emphasis placed on patient communication skills, and there was almost no feedback given to residents on how they were performing. I felt that this was a very important piece of feedback that residents were lacking and was very interested in creating a program that would help them learn new communication skills and get feedback on how they were doing.
Q: How should hospitalists use this study information to change their practice?
A: Hospital medicine programs should have some way to measure and give feedback to individual hospitalists on what the patient is experiencing with respect to communication. The intervention from this study should be easily scalable to any practice. There was almost no cost associated with the patient survey distribution, and it gave incredibly valuable individualized feedback about communication skills directly from the patients themselves. It should be feasible to implement this type of audit and feedback within any size hospital medicine program.
Q: Were there any unexpected findings in your study?
A: We were surprised at how much of an impact it had on HCAHPS scores. Not only did it impact physician communication ratings, but [it] also had an impressive impact on overall hospital ratings.
Q: Where does this take us with respect to future research efforts?
A: Our team is now working on expanding this program to other residency programs, as well as expanding it to attending physicians, within and outside the department of medicine.
In summary, Dr. Banka’s team found this relatively simple intervention was able to sizably improve the HCAHPS scores of recipient providers. Such interventions should be seriously considered by hospital medicine programs looking to improve their publicly reported patient satisfaction scores.
Editor’s note: This article first appeared on SHM’s “The Hospital Leader” blog.
Patient satisfaction survey performance is becoming increasingly important for hospitals, because the ratings are being used by payers in pay-for-performance programs more and more (including the CMS Hospital Value-Based Purchasing program). CMS also recently released its “Five-Star Quality Rating System” for hospitals, which publicly grades hospitals, using one to five stars, based on their patient satisfaction scores.
How Did Hospitals Do in Medicare’s Patient Quality Ratings?
Unfortunately, there is little literature to guide physicians on exactly HOW to improve patient satisfaction scores for themselves or their groups. A recent publication in the Journal of Hospital Medicine found a feasible and effective intervention to improve patient satisfaction scores among trainees, the methodology of which could easily be applied to hospitalists.
Gaurav Banka, MD, a former internal medicine resident (and current cardiology fellow) at UCLA Hospital, was interviewed about his team’s recent publication in the Journal of Hospital Medicine. In the interview, he opined about “improving patient satisfaction through resident education, feedback, and incentives.” The study he published found that this combination of interventions among internal medicine residents improved relevant HCAHPS scores by approximately 8%.
The following are excerpts from a Q&A session I had with Dr. Banka:
Question: Can you briefly summarize the intervention(s)?
Answer: There were three total interventions put in place simultaneously: an educational conference on best practices in patient communication, a recognition-reward program (recognition within the department and a movie package for high performers), and real-time feedback to the residents from their patients via a survey. The last component was the most impactful to the residents. Patients were randomly surveyed on how their residents were communicating with them, and the results were sent to the resident for review and self-reflection within weeks.
Q: How did you become interested in resident interventions to improve HCAHPS?
A: I noticed as an intern [that] there was almost no emphasis placed on patient communication skills, and there was almost no feedback given to residents on how they were performing. I felt that this was a very important piece of feedback that residents were lacking and was very interested in creating a program that would help them learn new communication skills and get feedback on how they were doing.
Q: How should hospitalists use this study information to change their practice?
A: Hospital medicine programs should have some way to measure and give feedback to individual hospitalists on what the patient is experiencing with respect to communication. The intervention from this study should be easily scalable to any practice. There was almost no cost associated with the patient survey distribution, and it gave incredibly valuable individualized feedback about communication skills directly from the patients themselves. It should be feasible to implement this type of audit and feedback within any size hospital medicine program.
Q: Were there any unexpected findings in your study?
A: We were surprised at how much of an impact it had on HCAHPS scores. Not only did it impact physician communication ratings, but [it] also had an impressive impact on overall hospital ratings.
Q: Where does this take us with respect to future research efforts?
A: Our team is now working on expanding this program to other residency programs, as well as expanding it to attending physicians, within and outside the department of medicine.
In summary, Dr. Banka’s team found this relatively simple intervention was able to sizably improve the HCAHPS scores of recipient providers. Such interventions should be seriously considered by hospital medicine programs looking to improve their publicly reported patient satisfaction scores.
Hospitalists' Role in Improving Patient Experience: A Baldridge Winner's Perspective
Understanding and improving the patient care experience has become a vital component of delivering high quality care. According to a new survey of American Society for Quality (ASQ) healthcare quality experts, more than 80% of respondents said improving communications between caregivers and patients and easing access to treatment across the entire continuum of care should be top priorities for improving patient experience. For Hill Country Memorial (HCM) in Fredericksburg, Texas, winner of the Malcolm Baldrige National Quality Award, accomplishing this kind of top-level patient experience performance involved engaging physicians—particularly hospitalists—using voice of the customer (VOC) input.
HCM did not achieve overnight success, however; instead, the facility achieved year-over-year improvement in finance and growth, patient experience, quality of care, and workforce environment and engagement (see Figure 1).

HCM developed a systematic VOC input-to-action process in which listening and learning methods during annual planning led them to institute a hospitalist program. Results included:
- Improved access to primary care, achieved by increasing the physicians’ hours of availability in their clinics, and improved work-life balance, enhancing engagement and alignment of the medical staff and HCM;
- Reductions in delays in admissions, discharges, and length of stay; and
- Real-time review and management of clinical data, not just during the daily rounding as had been done previously.
One of the major hurdles in the way of achieving patient satisfaction, according to the ASQ patient experience survey, is care that is fragmented and uncoordinated because of communication issues. HCM has overcome those hurdles using strategies such as a daily afternoon huddle in which hospitalists meet with a multidisciplinary team so that everyone understands patient action plans and current concerns. The process of discharge planning begins in these huddles so that more complex issues are initiated on day one of the hospital stay.
A new rounding communication process, called GIFT for greet, inform, find out, and time, has dramatically improved patient satisfaction and engagement. GIFT enables hospitalists to greet a patient with a personal introduction and an explanation of their position and responsibilities. Hospitalists always sit while engaging the patient, and they make it a point to acknowledge not only the patient but everyone present in the room. Personalized “baseball cards” featuring the hospitalist’s background, including personal interests and hobbies, are handed out to patients or family members. Hospitalists take time to inform the patient and appropriate family members and caregivers of all diagnostic test results and the clinical response of treatment to date. Treatment plans and further diagnostic tests or procedures are discussed. A report of all consultants who have joined or will be joining in the care, along with their roles in the treatment planned, is fully vetted.
One key to a successful patient experience is discovering the concerns of the patient, family members, friends, and caregivers. Emotional issues become as important as the physical needs of the patient; these are openly addressed. Ask not “What’s the matter?” but instead “What matters to you?”
Timing the hospitalist’s return to see the patient and the anticipated date of transition of care is the last item in the rounding interaction. The date should be as accurate as possible to reduce patient anxiety and help the patient understand that the hospitalist really cares.
The hospitalist program has also strengthened the relationship between nurses and physicians. Nurses know the hospitalists’ practice patterns well, which allows them to help manage patient interactions and minimize patient anxiety and frustration. The physician-patient relationship is reinforced when nurse leaders include hospitalist satisfaction questions during daily rounding to identify concerns that can be clarified or resolved in real time.
The systematic VOC approach has enabled HCM to design, manage, and improve its key work process at multiple levels of the organization. These processes are reviewed and refined periodically to respond to the changing healthcare environment and stay focused on creating value for customers.
Chip Caldwell is chairman of Caldwell Butler, a firm specializing in coaching organizations to achieve world class performance in margin improvement, patient experience, physician/clinical enterprise, and capacity optimization. Jayne Pope, MBA, RN, is CEO of Hill Country Memorial Hospital in Fredericksburg, Texas. James Partin, MD, is CMO at Hill Country Memorial.
Understanding and improving the patient care experience has become a vital component of delivering high quality care. According to a new survey of American Society for Quality (ASQ) healthcare quality experts, more than 80% of respondents said improving communications between caregivers and patients and easing access to treatment across the entire continuum of care should be top priorities for improving patient experience. For Hill Country Memorial (HCM) in Fredericksburg, Texas, winner of the Malcolm Baldrige National Quality Award, accomplishing this kind of top-level patient experience performance involved engaging physicians—particularly hospitalists—using voice of the customer (VOC) input.
HCM did not achieve overnight success, however; instead, the facility achieved year-over-year improvement in finance and growth, patient experience, quality of care, and workforce environment and engagement (see Figure 1).
HCM developed a systematic VOC input-to-action process in which listening and learning methods during annual planning led them to institute a hospitalist program. Results included:
- Improved access to primary care, achieved by increasing the physicians’ hours of availability in their clinics, and improved work-life balance, enhancing engagement and alignment of the medical staff and HCM;
- Reductions in delays in admissions, discharges, and length of stay; and
- Real-time review and management of clinical data, not just during the daily rounding as had been done previously.
One of the major hurdles in the way of achieving patient satisfaction, according to the ASQ patient experience survey, is care that is fragmented and uncoordinated because of communication issues. HCM has overcome those hurdles using strategies such as a daily afternoon huddle in which hospitalists meet with a multidisciplinary team so that everyone understands patient action plans and current concerns. The process of discharge planning begins in these huddles so that more complex issues are initiated on day one of the hospital stay.
A new rounding communication process, called GIFT for greet, inform, find out, and time, has dramatically improved patient satisfaction and engagement. GIFT enables hospitalists to greet a patient with a personal introduction and an explanation of their position and responsibilities. Hospitalists always sit while engaging the patient, and they make it a point to acknowledge not only the patient but everyone present in the room. Personalized “baseball cards” featuring the hospitalist’s background, including personal interests and hobbies, are handed out to patients or family members. Hospitalists take time to inform the patient and appropriate family members and caregivers of all diagnostic test results and the clinical response of treatment to date. Treatment plans and further diagnostic tests or procedures are discussed. A report of all consultants who have joined or will be joining in the care, along with their roles in the treatment planned, is fully vetted.
One key to a successful patient experience is discovering the concerns of the patient, family members, friends, and caregivers. Emotional issues become as important as the physical needs of the patient; these are openly addressed. Ask not “What’s the matter?” but instead “What matters to you?”
Timing the hospitalist’s return to see the patient and the anticipated date of transition of care is the last item in the rounding interaction. The date should be as accurate as possible to reduce patient anxiety and help the patient understand that the hospitalist really cares.
The hospitalist program has also strengthened the relationship between nurses and physicians. Nurses know the hospitalists’ practice patterns well, which allows them to help manage patient interactions and minimize patient anxiety and frustration. The physician-patient relationship is reinforced when nurse leaders include hospitalist satisfaction questions during daily rounding to identify concerns that can be clarified or resolved in real time.
The systematic VOC approach has enabled HCM to design, manage, and improve its key work process at multiple levels of the organization. These processes are reviewed and refined periodically to respond to the changing healthcare environment and stay focused on creating value for customers.
Chip Caldwell is chairman of Caldwell Butler, a firm specializing in coaching organizations to achieve world class performance in margin improvement, patient experience, physician/clinical enterprise, and capacity optimization. Jayne Pope, MBA, RN, is CEO of Hill Country Memorial Hospital in Fredericksburg, Texas. James Partin, MD, is CMO at Hill Country Memorial.
Understanding and improving the patient care experience has become a vital component of delivering high quality care. According to a new survey of American Society for Quality (ASQ) healthcare quality experts, more than 80% of respondents said improving communications between caregivers and patients and easing access to treatment across the entire continuum of care should be top priorities for improving patient experience. For Hill Country Memorial (HCM) in Fredericksburg, Texas, winner of the Malcolm Baldrige National Quality Award, accomplishing this kind of top-level patient experience performance involved engaging physicians—particularly hospitalists—using voice of the customer (VOC) input.
HCM did not achieve overnight success, however; instead, the facility achieved year-over-year improvement in finance and growth, patient experience, quality of care, and workforce environment and engagement (see Figure 1).
HCM developed a systematic VOC input-to-action process in which listening and learning methods during annual planning led them to institute a hospitalist program. Results included:
- Improved access to primary care, achieved by increasing the physicians’ hours of availability in their clinics, and improved work-life balance, enhancing engagement and alignment of the medical staff and HCM;
- Reductions in delays in admissions, discharges, and length of stay; and
- Real-time review and management of clinical data, not just during the daily rounding as had been done previously.
One of the major hurdles in the way of achieving patient satisfaction, according to the ASQ patient experience survey, is care that is fragmented and uncoordinated because of communication issues. HCM has overcome those hurdles using strategies such as a daily afternoon huddle in which hospitalists meet with a multidisciplinary team so that everyone understands patient action plans and current concerns. The process of discharge planning begins in these huddles so that more complex issues are initiated on day one of the hospital stay.
A new rounding communication process, called GIFT for greet, inform, find out, and time, has dramatically improved patient satisfaction and engagement. GIFT enables hospitalists to greet a patient with a personal introduction and an explanation of their position and responsibilities. Hospitalists always sit while engaging the patient, and they make it a point to acknowledge not only the patient but everyone present in the room. Personalized “baseball cards” featuring the hospitalist’s background, including personal interests and hobbies, are handed out to patients or family members. Hospitalists take time to inform the patient and appropriate family members and caregivers of all diagnostic test results and the clinical response of treatment to date. Treatment plans and further diagnostic tests or procedures are discussed. A report of all consultants who have joined or will be joining in the care, along with their roles in the treatment planned, is fully vetted.
One key to a successful patient experience is discovering the concerns of the patient, family members, friends, and caregivers. Emotional issues become as important as the physical needs of the patient; these are openly addressed. Ask not “What’s the matter?” but instead “What matters to you?”
Timing the hospitalist’s return to see the patient and the anticipated date of transition of care is the last item in the rounding interaction. The date should be as accurate as possible to reduce patient anxiety and help the patient understand that the hospitalist really cares.
The hospitalist program has also strengthened the relationship between nurses and physicians. Nurses know the hospitalists’ practice patterns well, which allows them to help manage patient interactions and minimize patient anxiety and frustration. The physician-patient relationship is reinforced when nurse leaders include hospitalist satisfaction questions during daily rounding to identify concerns that can be clarified or resolved in real time.
The systematic VOC approach has enabled HCM to design, manage, and improve its key work process at multiple levels of the organization. These processes are reviewed and refined periodically to respond to the changing healthcare environment and stay focused on creating value for customers.
Chip Caldwell is chairman of Caldwell Butler, a firm specializing in coaching organizations to achieve world class performance in margin improvement, patient experience, physician/clinical enterprise, and capacity optimization. Jayne Pope, MBA, RN, is CEO of Hill Country Memorial Hospital in Fredericksburg, Texas. James Partin, MD, is CMO at Hill Country Memorial.
Post-Procedural Bridging Therapy for Secondary Prevention of VTE Increases Rate of Bleeding
Clinical question: Is post-procedural bridging therapy necessary for secondary prevention of VTE?
Background: Bridging therapy has been studied to stratify peri-procedural risk for patients with atrial fibrillation and mechanical heart valves. Data examining the necessity of post-procedural bridging for secondary prevention of VTE are lacking.
Study design: Retrospective, cohort study.
Setting: Single-state, integrated, healthcare delivery system.
Synopsis: A retrospective analysis of patients treated with warfarin for VTE prior to undergoing an invasive procedure was conducted from January 2006 through March 2012 to evaluate the occurrence of post-procedural bleeding secondary to bridging therapy, as well as the occurrence of VTE if bridging therapy was withheld.
Nearly 19,000 procedures were evaluated, of which 1,812 were included in the study. Of note, 11,710 procedures were excluded because the indication for anticoagulation was not VTE. The primary outcome was post-procedure bleeding events at 30 days, while secondary outcomes included severe bleeding events, recurrent VTE, and 30-day mortality. Patient risk of recurrent VTE was stratified into low-, medium-, and high-risk categories based on AT9 current guidelines.
Clinically relevant bleeding events occurred in 2.7% (15/555) of bridged patients and in 0.2% (2/1257) of non-bridged patients (hazard ratio of 17.2). With respect to VTE recurrence, there were three events in the non-bridged group and zero in the bridged group, which was not statistically significant (P=0.56). No VTE events were seen in the high-risk group, and there was no mortality at 30 days across any group.
Bottom line: Peri-procedural bridging therapy for VTE is associated with higher risk of bleeding, but there is not a significant risk of recurrent VTE if bridging therapy is withheld.
Citation: Clark NP, Witt DM, Davies LE, et al. Bleeding, recurrent venous thromboembolism, and mortality risks during warfarin interruption for invasive procedures. JAMA Intern Med. 2015;175(7):1163-1168. doi:10.1001/jamainternmed.2015.1843.
Clinical question: Is post-procedural bridging therapy necessary for secondary prevention of VTE?
Background: Bridging therapy has been studied to stratify peri-procedural risk for patients with atrial fibrillation and mechanical heart valves. Data examining the necessity of post-procedural bridging for secondary prevention of VTE are lacking.
Study design: Retrospective, cohort study.
Setting: Single-state, integrated, healthcare delivery system.
Synopsis: A retrospective analysis of patients treated with warfarin for VTE prior to undergoing an invasive procedure was conducted from January 2006 through March 2012 to evaluate the occurrence of post-procedural bleeding secondary to bridging therapy, as well as the occurrence of VTE if bridging therapy was withheld.
Nearly 19,000 procedures were evaluated, of which 1,812 were included in the study. Of note, 11,710 procedures were excluded because the indication for anticoagulation was not VTE. The primary outcome was post-procedure bleeding events at 30 days, while secondary outcomes included severe bleeding events, recurrent VTE, and 30-day mortality. Patient risk of recurrent VTE was stratified into low-, medium-, and high-risk categories based on AT9 current guidelines.
Clinically relevant bleeding events occurred in 2.7% (15/555) of bridged patients and in 0.2% (2/1257) of non-bridged patients (hazard ratio of 17.2). With respect to VTE recurrence, there were three events in the non-bridged group and zero in the bridged group, which was not statistically significant (P=0.56). No VTE events were seen in the high-risk group, and there was no mortality at 30 days across any group.
Bottom line: Peri-procedural bridging therapy for VTE is associated with higher risk of bleeding, but there is not a significant risk of recurrent VTE if bridging therapy is withheld.
Citation: Clark NP, Witt DM, Davies LE, et al. Bleeding, recurrent venous thromboembolism, and mortality risks during warfarin interruption for invasive procedures. JAMA Intern Med. 2015;175(7):1163-1168. doi:10.1001/jamainternmed.2015.1843.
Clinical question: Is post-procedural bridging therapy necessary for secondary prevention of VTE?
Background: Bridging therapy has been studied to stratify peri-procedural risk for patients with atrial fibrillation and mechanical heart valves. Data examining the necessity of post-procedural bridging for secondary prevention of VTE are lacking.
Study design: Retrospective, cohort study.
Setting: Single-state, integrated, healthcare delivery system.
Synopsis: A retrospective analysis of patients treated with warfarin for VTE prior to undergoing an invasive procedure was conducted from January 2006 through March 2012 to evaluate the occurrence of post-procedural bleeding secondary to bridging therapy, as well as the occurrence of VTE if bridging therapy was withheld.
Nearly 19,000 procedures were evaluated, of which 1,812 were included in the study. Of note, 11,710 procedures were excluded because the indication for anticoagulation was not VTE. The primary outcome was post-procedure bleeding events at 30 days, while secondary outcomes included severe bleeding events, recurrent VTE, and 30-day mortality. Patient risk of recurrent VTE was stratified into low-, medium-, and high-risk categories based on AT9 current guidelines.
Clinically relevant bleeding events occurred in 2.7% (15/555) of bridged patients and in 0.2% (2/1257) of non-bridged patients (hazard ratio of 17.2). With respect to VTE recurrence, there were three events in the non-bridged group and zero in the bridged group, which was not statistically significant (P=0.56). No VTE events were seen in the high-risk group, and there was no mortality at 30 days across any group.
Bottom line: Peri-procedural bridging therapy for VTE is associated with higher risk of bleeding, but there is not a significant risk of recurrent VTE if bridging therapy is withheld.
Citation: Clark NP, Witt DM, Davies LE, et al. Bleeding, recurrent venous thromboembolism, and mortality risks during warfarin interruption for invasive procedures. JAMA Intern Med. 2015;175(7):1163-1168. doi:10.1001/jamainternmed.2015.1843.
Listen Now: Highlights of the September 2015 Issue of The Hospitalist
In this month's issue, our special report on the patient experience includes Dr. Jairy Hunter talking about things that impact the patient experience on the ward; Dr. Nasim Afsar discusses on how her love of science was sparked; and we feature the latest in HM clinical literature.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/09/September-2015-Hospitalist-Highlights.mp3"][/audio]
In this month's issue, our special report on the patient experience includes Dr. Jairy Hunter talking about things that impact the patient experience on the ward; Dr. Nasim Afsar discusses on how her love of science was sparked; and we feature the latest in HM clinical literature.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/09/September-2015-Hospitalist-Highlights.mp3"][/audio]
In this month's issue, our special report on the patient experience includes Dr. Jairy Hunter talking about things that impact the patient experience on the ward; Dr. Nasim Afsar discusses on how her love of science was sparked; and we feature the latest in HM clinical literature.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/09/September-2015-Hospitalist-Highlights.mp3"][/audio]
Short-Course Antimicrobial Therapy Outcomes for Intraabdominal Infection
Clinical question: Does a short, fixed duration of antibiotic therapy for complicated intraabdominal infections lead to equivalent outcomes and less antibiotic exposure than the traditional approach?
Background: Published guidelines recommend appropriate antimicrobial agents for intraabdominal infections, but the optimal duration of therapy remains unclear. Most practitioners continue to treat for 10-14 days and until all physiologic evidence of the systemic inflammatory response syndrome (SIRS) has resolved. More recently, small studies have suggested that a shorter course may lead to equivalent outcomes with decreased antibiotic exposure.
Study design: Open-label, multicenter, randomized control trial.
Setting: Twenty-three sites throughout the U.S. and Canada.
Synopsis: In the short-course group, 257 patients were randomized to receive antimicrobial therapy for four full days after their index source-control procedure; 260 patients in the control group received antimicrobial therapy until two days after resolution of the physiological abnormalities related to SIRS. The median duration of therapy was 4.0 days (interquartile range [IQR], 4.0-5.0) for the experimental group and 8.0 days (IQR 5.0-10.0) in the control group (95% CI, -4.7 to -3.3; P<0.001).
There was no significant difference in surgical site infection, recurrent intraabdominal infection, or death between the experimental and control groups (21.8% vs. 22.3%, 95% CI -7.0 to 8.0; P=0.92). In the experimental group, 47 patients did not adhere to the protocol, all of whom received a longer antimicrobial treatment course than specified in the protocol.
This trial excluded patients without adequate source control and included a small number of immunocompromised hosts. The rate of nonadherence to the protocol was high, at 18% of patients in the experimental group. The calculated sample size to assert equivalence between groups was not achieved, although the results are suggestive of equivalence.
Bottom line: A shorter course of antimicrobial therapy for complicated intraabdominal infections might lead to equivalent outcomes with less antibiotic exposure compared with current practice; however, it is challenging for providers to stop antimicrobial therapy while patients continue to show physiologic evidence of SIRS.
Citation: Sawyer RG, Claridge JA, Nathens AB, et al. Trial of short-course antimicrobial therapy for intraabdominal infection. NEJM. 2015;372(21):1996-2005.
Clinical question: Does a short, fixed duration of antibiotic therapy for complicated intraabdominal infections lead to equivalent outcomes and less antibiotic exposure than the traditional approach?
Background: Published guidelines recommend appropriate antimicrobial agents for intraabdominal infections, but the optimal duration of therapy remains unclear. Most practitioners continue to treat for 10-14 days and until all physiologic evidence of the systemic inflammatory response syndrome (SIRS) has resolved. More recently, small studies have suggested that a shorter course may lead to equivalent outcomes with decreased antibiotic exposure.
Study design: Open-label, multicenter, randomized control trial.
Setting: Twenty-three sites throughout the U.S. and Canada.
Synopsis: In the short-course group, 257 patients were randomized to receive antimicrobial therapy for four full days after their index source-control procedure; 260 patients in the control group received antimicrobial therapy until two days after resolution of the physiological abnormalities related to SIRS. The median duration of therapy was 4.0 days (interquartile range [IQR], 4.0-5.0) for the experimental group and 8.0 days (IQR 5.0-10.0) in the control group (95% CI, -4.7 to -3.3; P<0.001).
There was no significant difference in surgical site infection, recurrent intraabdominal infection, or death between the experimental and control groups (21.8% vs. 22.3%, 95% CI -7.0 to 8.0; P=0.92). In the experimental group, 47 patients did not adhere to the protocol, all of whom received a longer antimicrobial treatment course than specified in the protocol.
This trial excluded patients without adequate source control and included a small number of immunocompromised hosts. The rate of nonadherence to the protocol was high, at 18% of patients in the experimental group. The calculated sample size to assert equivalence between groups was not achieved, although the results are suggestive of equivalence.
Bottom line: A shorter course of antimicrobial therapy for complicated intraabdominal infections might lead to equivalent outcomes with less antibiotic exposure compared with current practice; however, it is challenging for providers to stop antimicrobial therapy while patients continue to show physiologic evidence of SIRS.
Citation: Sawyer RG, Claridge JA, Nathens AB, et al. Trial of short-course antimicrobial therapy for intraabdominal infection. NEJM. 2015;372(21):1996-2005.
Clinical question: Does a short, fixed duration of antibiotic therapy for complicated intraabdominal infections lead to equivalent outcomes and less antibiotic exposure than the traditional approach?
Background: Published guidelines recommend appropriate antimicrobial agents for intraabdominal infections, but the optimal duration of therapy remains unclear. Most practitioners continue to treat for 10-14 days and until all physiologic evidence of the systemic inflammatory response syndrome (SIRS) has resolved. More recently, small studies have suggested that a shorter course may lead to equivalent outcomes with decreased antibiotic exposure.
Study design: Open-label, multicenter, randomized control trial.
Setting: Twenty-three sites throughout the U.S. and Canada.
Synopsis: In the short-course group, 257 patients were randomized to receive antimicrobial therapy for four full days after their index source-control procedure; 260 patients in the control group received antimicrobial therapy until two days after resolution of the physiological abnormalities related to SIRS. The median duration of therapy was 4.0 days (interquartile range [IQR], 4.0-5.0) for the experimental group and 8.0 days (IQR 5.0-10.0) in the control group (95% CI, -4.7 to -3.3; P<0.001).
There was no significant difference in surgical site infection, recurrent intraabdominal infection, or death between the experimental and control groups (21.8% vs. 22.3%, 95% CI -7.0 to 8.0; P=0.92). In the experimental group, 47 patients did not adhere to the protocol, all of whom received a longer antimicrobial treatment course than specified in the protocol.
This trial excluded patients without adequate source control and included a small number of immunocompromised hosts. The rate of nonadherence to the protocol was high, at 18% of patients in the experimental group. The calculated sample size to assert equivalence between groups was not achieved, although the results are suggestive of equivalence.
Bottom line: A shorter course of antimicrobial therapy for complicated intraabdominal infections might lead to equivalent outcomes with less antibiotic exposure compared with current practice; however, it is challenging for providers to stop antimicrobial therapy while patients continue to show physiologic evidence of SIRS.
Citation: Sawyer RG, Claridge JA, Nathens AB, et al. Trial of short-course antimicrobial therapy for intraabdominal infection. NEJM. 2015;372(21):1996-2005.
Clinical Care Conundrums Provide Learning Potential for Hospitalists

At A Glance
Series: Hospital Medicine: Current Concepts
Title: Clinical Care Conundrums: Challenging Diagnoses in Hospital Medicine
Edited by: James C. Pile, Thomas E. Baudendistel, Brian Harte
Series Editors: Scott Flanders, Sanjay Saint
Pages: 208
Clinical Care Conundrums is written in 22 chapters, each discussing a clinical case presentation in a format similar to the series by the same name, published frequently in the Journal of Hospital Medicine.
An expert clinician’s approach to the “clinical conundrums” is disclosed using the presentation of an actual patient case in a prototypical “morning report” style. As in a patient care situation, sequential pieces of information are provided to the expert clinician, who is unfamiliar with the case. The focus of each case is the thought processes of both the clinical team caring for the patient and the commentator.
Excerpt
“Clinicians rely heavily on diagnostic test information, yet diagnostic tests are also susceptible to error. About 18% of critical laboratory results are judged nonrepresentative of the patient’s clinical condition after a chart review. …CT scans have 1.7% misinterpretation rate. Pathologic discrepancies occur in 11%-19% of cancer biopsy specimens. These data should remind clinicians to question…”
Each case provides great learning potential, not only in the unusual presentation of common diseases or more typical presentations of unusual diseases, but also in discussions of the possibilities in differential diagnoses. The range of information is wide. Readers are taken through discussions of conditions infrequently encountered but potentially fatal in the event of missed or delayed diagnosis, such as strongyloides hyperinfection, a condition that we are reminded is not always accompanied by eosinophilia. Some discussions of the more common conditions include:
- Evaluation of confusion;
- Etiologies of cirrhosis;
- Malignancies associated with hypercalcemia; and
- Work-up for new-onset seizures.
My interest remained high throughout the book, because I never knew what to expect. For example, a patient presenting with acute chest pain caused by esophageal perforation resulting in delayed diagnosis might follow the index case presentation of Whipple’s disease. We are also reminded that, despite the insistence of Gregory House, MD, (Dr. House is the titular character from the television series “House”) that “it’s never lupus,” it sometimes is actually lupus. A couple of interesting lupus cases are presented in a realistically perplexing manner, followed by beneficial discussion.
Analysis
The real value in this book lies in continued reminders of how and why clinicians make diagnostic errors. In fact, an early chapter in the book deals explicitly with improving diagnostic safety.
Robert Wachter, MD, MHM, reminds us in the introductory chapter that diagnostic errors comprise nearly one in five preventable adverse events. Until recently, diagnostic errors have been given relatively little attention, most likely because they are difficult to measure and harder to fix.
As hospital-based providers, the more awareness we have about the “anatomy and physiology” of both good and faulty decision making, the more likely we are to make better decisions. This book can be a crucial resource for any hospital-based care provider.
Dr. Lindsey is medical director of hospital-based physician services at Hospital Corporation of America (HCA).
At A Glance
Series: Hospital Medicine: Current Concepts
Title: Clinical Care Conundrums: Challenging Diagnoses in Hospital Medicine
Edited by: James C. Pile, Thomas E. Baudendistel, Brian Harte
Series Editors: Scott Flanders, Sanjay Saint
Pages: 208
Clinical Care Conundrums is written in 22 chapters, each discussing a clinical case presentation in a format similar to the series by the same name, published frequently in the Journal of Hospital Medicine.
An expert clinician’s approach to the “clinical conundrums” is disclosed using the presentation of an actual patient case in a prototypical “morning report” style. As in a patient care situation, sequential pieces of information are provided to the expert clinician, who is unfamiliar with the case. The focus of each case is the thought processes of both the clinical team caring for the patient and the commentator.
Excerpt
“Clinicians rely heavily on diagnostic test information, yet diagnostic tests are also susceptible to error. About 18% of critical laboratory results are judged nonrepresentative of the patient’s clinical condition after a chart review. …CT scans have 1.7% misinterpretation rate. Pathologic discrepancies occur in 11%-19% of cancer biopsy specimens. These data should remind clinicians to question…”
Each case provides great learning potential, not only in the unusual presentation of common diseases or more typical presentations of unusual diseases, but also in discussions of the possibilities in differential diagnoses. The range of information is wide. Readers are taken through discussions of conditions infrequently encountered but potentially fatal in the event of missed or delayed diagnosis, such as strongyloides hyperinfection, a condition that we are reminded is not always accompanied by eosinophilia. Some discussions of the more common conditions include:
- Evaluation of confusion;
- Etiologies of cirrhosis;
- Malignancies associated with hypercalcemia; and
- Work-up for new-onset seizures.
My interest remained high throughout the book, because I never knew what to expect. For example, a patient presenting with acute chest pain caused by esophageal perforation resulting in delayed diagnosis might follow the index case presentation of Whipple’s disease. We are also reminded that, despite the insistence of Gregory House, MD, (Dr. House is the titular character from the television series “House”) that “it’s never lupus,” it sometimes is actually lupus. A couple of interesting lupus cases are presented in a realistically perplexing manner, followed by beneficial discussion.
Analysis
The real value in this book lies in continued reminders of how and why clinicians make diagnostic errors. In fact, an early chapter in the book deals explicitly with improving diagnostic safety.
Robert Wachter, MD, MHM, reminds us in the introductory chapter that diagnostic errors comprise nearly one in five preventable adverse events. Until recently, diagnostic errors have been given relatively little attention, most likely because they are difficult to measure and harder to fix.
As hospital-based providers, the more awareness we have about the “anatomy and physiology” of both good and faulty decision making, the more likely we are to make better decisions. This book can be a crucial resource for any hospital-based care provider.
Dr. Lindsey is medical director of hospital-based physician services at Hospital Corporation of America (HCA).
At A Glance
Series: Hospital Medicine: Current Concepts
Title: Clinical Care Conundrums: Challenging Diagnoses in Hospital Medicine
Edited by: James C. Pile, Thomas E. Baudendistel, Brian Harte
Series Editors: Scott Flanders, Sanjay Saint
Pages: 208
Clinical Care Conundrums is written in 22 chapters, each discussing a clinical case presentation in a format similar to the series by the same name, published frequently in the Journal of Hospital Medicine.
An expert clinician’s approach to the “clinical conundrums” is disclosed using the presentation of an actual patient case in a prototypical “morning report” style. As in a patient care situation, sequential pieces of information are provided to the expert clinician, who is unfamiliar with the case. The focus of each case is the thought processes of both the clinical team caring for the patient and the commentator.
Excerpt
“Clinicians rely heavily on diagnostic test information, yet diagnostic tests are also susceptible to error. About 18% of critical laboratory results are judged nonrepresentative of the patient’s clinical condition after a chart review. …CT scans have 1.7% misinterpretation rate. Pathologic discrepancies occur in 11%-19% of cancer biopsy specimens. These data should remind clinicians to question…”
Each case provides great learning potential, not only in the unusual presentation of common diseases or more typical presentations of unusual diseases, but also in discussions of the possibilities in differential diagnoses. The range of information is wide. Readers are taken through discussions of conditions infrequently encountered but potentially fatal in the event of missed or delayed diagnosis, such as strongyloides hyperinfection, a condition that we are reminded is not always accompanied by eosinophilia. Some discussions of the more common conditions include:
- Evaluation of confusion;
- Etiologies of cirrhosis;
- Malignancies associated with hypercalcemia; and
- Work-up for new-onset seizures.
My interest remained high throughout the book, because I never knew what to expect. For example, a patient presenting with acute chest pain caused by esophageal perforation resulting in delayed diagnosis might follow the index case presentation of Whipple’s disease. We are also reminded that, despite the insistence of Gregory House, MD, (Dr. House is the titular character from the television series “House”) that “it’s never lupus,” it sometimes is actually lupus. A couple of interesting lupus cases are presented in a realistically perplexing manner, followed by beneficial discussion.
Analysis
The real value in this book lies in continued reminders of how and why clinicians make diagnostic errors. In fact, an early chapter in the book deals explicitly with improving diagnostic safety.
Robert Wachter, MD, MHM, reminds us in the introductory chapter that diagnostic errors comprise nearly one in five preventable adverse events. Until recently, diagnostic errors have been given relatively little attention, most likely because they are difficult to measure and harder to fix.
As hospital-based providers, the more awareness we have about the “anatomy and physiology” of both good and faulty decision making, the more likely we are to make better decisions. This book can be a crucial resource for any hospital-based care provider.
Dr. Lindsey is medical director of hospital-based physician services at Hospital Corporation of America (HCA).
{kind=link}
Hospitalist Elizabeth Cook, MD, Pursues Lifetime of Learning

Physicians are lifelong learners by definition. But Elizabeth Cook, MD, is still an actual student.
Dr. Cook, medical director of the hospitalist division of Medical Associates of Central Virginia in Lynchburg, Va., is working toward her master’s degree in public health (MPH) leadership at the University of North Carolina in Chapel Hill, N.C. She is on target to graduate in 2016.
“I am interested in health policy and how the big decisions made at high levels are translated into day-to-day operations,” she says. “Oftentimes the unintended consequences are substantial for some of these decisions. I think it is important for those who do the daily provider work to be a part of the process to help inform the decisions.”
That day-to-day work for Dr. Cook now includes serving as one of seven new members of Team Hospitalist, the volunteer editorial advisory board of The Hospitalist.
Question: Why did you choose a career in medicine?
Answer: A long series of events. My undergrad degree was in television/film/radio production. I was working in the field but was exposed to the field of medicine for the first time after I tore an ACL [anterior cruciate ligament] and had knee surgery. Some friends worked in medicine and, between their encouragement and my fascination with medicine and the way the body works, I decided to change directions and pursued a medical degree.

Q: How/when did you decide to become a hospitalist?
A: I hated inpatient medicine when I was in medical school and as a family practice resident. I intended to open a private practice (family practice) office, but a mentor convinced me to take a job as hospitalist as an interim step while working on putting together the office. I did open the office with intention to transition to just that long term. After doing both for a while, I started to really enjoy the collegiality and pace of hospitalist work and decided to close the office and do hospitalist work full time. That was 14 years ago, and I’ve never second-guessed my decision.
Q: Was there a specific person who steered you to hospital medicine?
A: A part-time faculty member at the residency where I trained really encouraged me to try hospitalist work. He felt like I would enjoy the pace and the ability to interact with specialists and colleagues, and he was absolutely right. I still thank him and sometimes rib him about it when things are really crazy.
Q: What do you like most about working as a hospitalist?
A: I love the pace and the constant interaction with specialists, nursing staff, and other providers. I also have a great group of fellow hospitalists. We have been a very stable group, and some of us have been together for a long time doing this. Almost feels like family. I also like the constant learning that takes place in the interactions with specialists. They keep us on the cutting edge of medicine, and the patients always provide a new and interesting challenge to learn from.
Q: What do you dislike most?
A: We have a very flexible schedule, but it does require lots of weekends and evenings. It makes it hard to have a social life and do things with people outside of medicine who maintain the usual (Monday to Friday) life.
Q: What’s the best advice you ever received?
A: Have fun with whatever you are doing.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The patients are much sicker and more complicated than when I first started. We have become really good at managing a lot of things as outpatients, so what is left is a lot of really challenging, time-consuming patients. It’s intellectually rewarding but can be exhausting when you are seeing 16 to 20 patients a day like that.
Q: What’s the biggest change you would like to see in HM?
A: I think we need better coordination with care and more connection to the outpatient setting. I often feel like I am sending my patients out into a black hole, and I just hope they end up with all the things I have ordered and recommended.
Q: For group leaders, why is it important for you to continue seeing patients?
A: Seeing patients is critical. It keeps me in touch with the issues and challenges that my providers deal with. It also creates a sense of teamwork and puts us on equal footing rather than my being perceived as a distant administrator.
Q: As a hospitalist, seeing most of your patients for the very first time, what aspect of patient care is most challenging?
A: Being in the hospital, by its very nature, places patients and families in circumstances that are often scary and out of their control. It creates a lot of emotions that can charge interactions. After so many years, the management and diagnosis can lose their sense of impact for providers, as it is daily routine. It is important to remember the patients’ perspective and learn ways to reassure and inform to defuse some of the high emotions.
Q: What aspect of patient care is most rewarding?
A: When a patient comes in very sick and I am able to identify and treat the problem and watch them make a good recovery. It feels like I am doing something meaningful and important in life.
Q: What is your biggest professional challenge?
A: Interacting with hospital administration, as there are often competing demands and desires that require politics, collaboration, and people skills to get everyone pulling in the same direction.
Q: What’s next professionally?
A: I am not sure. I am eager to see what doors the MPH opens for me. I would be interested in consulting work, helping smaller programs look at opportunities for growth and ways to collaborate and align interests with their hospital administrators. Also, working in health policy interests me.
Q: If you weren’t a doctor, what would you be doing right now?
A: I have written a book and a screenplay and really enjoy that. In my dream world, I would be able to work full time as an author.
Richard Quinn is a freelance journalist in New Jersey.
Physicians are lifelong learners by definition. But Elizabeth Cook, MD, is still an actual student.
Dr. Cook, medical director of the hospitalist division of Medical Associates of Central Virginia in Lynchburg, Va., is working toward her master’s degree in public health (MPH) leadership at the University of North Carolina in Chapel Hill, N.C. She is on target to graduate in 2016.
“I am interested in health policy and how the big decisions made at high levels are translated into day-to-day operations,” she says. “Oftentimes the unintended consequences are substantial for some of these decisions. I think it is important for those who do the daily provider work to be a part of the process to help inform the decisions.”
That day-to-day work for Dr. Cook now includes serving as one of seven new members of Team Hospitalist, the volunteer editorial advisory board of The Hospitalist.
Question: Why did you choose a career in medicine?
Answer: A long series of events. My undergrad degree was in television/film/radio production. I was working in the field but was exposed to the field of medicine for the first time after I tore an ACL [anterior cruciate ligament] and had knee surgery. Some friends worked in medicine and, between their encouragement and my fascination with medicine and the way the body works, I decided to change directions and pursued a medical degree.
Q: How/when did you decide to become a hospitalist?
A: I hated inpatient medicine when I was in medical school and as a family practice resident. I intended to open a private practice (family practice) office, but a mentor convinced me to take a job as hospitalist as an interim step while working on putting together the office. I did open the office with intention to transition to just that long term. After doing both for a while, I started to really enjoy the collegiality and pace of hospitalist work and decided to close the office and do hospitalist work full time. That was 14 years ago, and I’ve never second-guessed my decision.
Q: Was there a specific person who steered you to hospital medicine?
A: A part-time faculty member at the residency where I trained really encouraged me to try hospitalist work. He felt like I would enjoy the pace and the ability to interact with specialists and colleagues, and he was absolutely right. I still thank him and sometimes rib him about it when things are really crazy.
Q: What do you like most about working as a hospitalist?
A: I love the pace and the constant interaction with specialists, nursing staff, and other providers. I also have a great group of fellow hospitalists. We have been a very stable group, and some of us have been together for a long time doing this. Almost feels like family. I also like the constant learning that takes place in the interactions with specialists. They keep us on the cutting edge of medicine, and the patients always provide a new and interesting challenge to learn from.
Q: What do you dislike most?
A: We have a very flexible schedule, but it does require lots of weekends and evenings. It makes it hard to have a social life and do things with people outside of medicine who maintain the usual (Monday to Friday) life.
Q: What’s the best advice you ever received?
A: Have fun with whatever you are doing.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The patients are much sicker and more complicated than when I first started. We have become really good at managing a lot of things as outpatients, so what is left is a lot of really challenging, time-consuming patients. It’s intellectually rewarding but can be exhausting when you are seeing 16 to 20 patients a day like that.
Q: What’s the biggest change you would like to see in HM?
A: I think we need better coordination with care and more connection to the outpatient setting. I often feel like I am sending my patients out into a black hole, and I just hope they end up with all the things I have ordered and recommended.
Q: For group leaders, why is it important for you to continue seeing patients?
A: Seeing patients is critical. It keeps me in touch with the issues and challenges that my providers deal with. It also creates a sense of teamwork and puts us on equal footing rather than my being perceived as a distant administrator.
Q: As a hospitalist, seeing most of your patients for the very first time, what aspect of patient care is most challenging?
A: Being in the hospital, by its very nature, places patients and families in circumstances that are often scary and out of their control. It creates a lot of emotions that can charge interactions. After so many years, the management and diagnosis can lose their sense of impact for providers, as it is daily routine. It is important to remember the patients’ perspective and learn ways to reassure and inform to defuse some of the high emotions.
Q: What aspect of patient care is most rewarding?
A: When a patient comes in very sick and I am able to identify and treat the problem and watch them make a good recovery. It feels like I am doing something meaningful and important in life.
Q: What is your biggest professional challenge?
A: Interacting with hospital administration, as there are often competing demands and desires that require politics, collaboration, and people skills to get everyone pulling in the same direction.
Q: What’s next professionally?
A: I am not sure. I am eager to see what doors the MPH opens for me. I would be interested in consulting work, helping smaller programs look at opportunities for growth and ways to collaborate and align interests with their hospital administrators. Also, working in health policy interests me.
Q: If you weren’t a doctor, what would you be doing right now?
A: I have written a book and a screenplay and really enjoy that. In my dream world, I would be able to work full time as an author.
Richard Quinn is a freelance journalist in New Jersey.
Physicians are lifelong learners by definition. But Elizabeth Cook, MD, is still an actual student.
Dr. Cook, medical director of the hospitalist division of Medical Associates of Central Virginia in Lynchburg, Va., is working toward her master’s degree in public health (MPH) leadership at the University of North Carolina in Chapel Hill, N.C. She is on target to graduate in 2016.
“I am interested in health policy and how the big decisions made at high levels are translated into day-to-day operations,” she says. “Oftentimes the unintended consequences are substantial for some of these decisions. I think it is important for those who do the daily provider work to be a part of the process to help inform the decisions.”
That day-to-day work for Dr. Cook now includes serving as one of seven new members of Team Hospitalist, the volunteer editorial advisory board of The Hospitalist.
Question: Why did you choose a career in medicine?
Answer: A long series of events. My undergrad degree was in television/film/radio production. I was working in the field but was exposed to the field of medicine for the first time after I tore an ACL [anterior cruciate ligament] and had knee surgery. Some friends worked in medicine and, between their encouragement and my fascination with medicine and the way the body works, I decided to change directions and pursued a medical degree.
Q: How/when did you decide to become a hospitalist?
A: I hated inpatient medicine when I was in medical school and as a family practice resident. I intended to open a private practice (family practice) office, but a mentor convinced me to take a job as hospitalist as an interim step while working on putting together the office. I did open the office with intention to transition to just that long term. After doing both for a while, I started to really enjoy the collegiality and pace of hospitalist work and decided to close the office and do hospitalist work full time. That was 14 years ago, and I’ve never second-guessed my decision.
Q: Was there a specific person who steered you to hospital medicine?
A: A part-time faculty member at the residency where I trained really encouraged me to try hospitalist work. He felt like I would enjoy the pace and the ability to interact with specialists and colleagues, and he was absolutely right. I still thank him and sometimes rib him about it when things are really crazy.
Q: What do you like most about working as a hospitalist?
A: I love the pace and the constant interaction with specialists, nursing staff, and other providers. I also have a great group of fellow hospitalists. We have been a very stable group, and some of us have been together for a long time doing this. Almost feels like family. I also like the constant learning that takes place in the interactions with specialists. They keep us on the cutting edge of medicine, and the patients always provide a new and interesting challenge to learn from.
Q: What do you dislike most?
A: We have a very flexible schedule, but it does require lots of weekends and evenings. It makes it hard to have a social life and do things with people outside of medicine who maintain the usual (Monday to Friday) life.
Q: What’s the best advice you ever received?
A: Have fun with whatever you are doing.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The patients are much sicker and more complicated than when I first started. We have become really good at managing a lot of things as outpatients, so what is left is a lot of really challenging, time-consuming patients. It’s intellectually rewarding but can be exhausting when you are seeing 16 to 20 patients a day like that.
Q: What’s the biggest change you would like to see in HM?
A: I think we need better coordination with care and more connection to the outpatient setting. I often feel like I am sending my patients out into a black hole, and I just hope they end up with all the things I have ordered and recommended.
Q: For group leaders, why is it important for you to continue seeing patients?
A: Seeing patients is critical. It keeps me in touch with the issues and challenges that my providers deal with. It also creates a sense of teamwork and puts us on equal footing rather than my being perceived as a distant administrator.
Q: As a hospitalist, seeing most of your patients for the very first time, what aspect of patient care is most challenging?
A: Being in the hospital, by its very nature, places patients and families in circumstances that are often scary and out of their control. It creates a lot of emotions that can charge interactions. After so many years, the management and diagnosis can lose their sense of impact for providers, as it is daily routine. It is important to remember the patients’ perspective and learn ways to reassure and inform to defuse some of the high emotions.
Q: What aspect of patient care is most rewarding?
A: When a patient comes in very sick and I am able to identify and treat the problem and watch them make a good recovery. It feels like I am doing something meaningful and important in life.
Q: What is your biggest professional challenge?
A: Interacting with hospital administration, as there are often competing demands and desires that require politics, collaboration, and people skills to get everyone pulling in the same direction.
Q: What’s next professionally?
A: I am not sure. I am eager to see what doors the MPH opens for me. I would be interested in consulting work, helping smaller programs look at opportunities for growth and ways to collaborate and align interests with their hospital administrators. Also, working in health policy interests me.
Q: If you weren’t a doctor, what would you be doing right now?
A: I have written a book and a screenplay and really enjoy that. In my dream world, I would be able to work full time as an author.
Richard Quinn is a freelance journalist in New Jersey.
Hospitalist-Led Quality Initiatives Plentiful at Community Hospitals
Community hospitals offer multiple opportunities for hospitalists to become involved in both quality assurance and quality improvement. To help steer the right approach and avoid possible missteps, it’s important to acknowledge the differences between the community and academic settings, according to two medical directors with whom we spoke.
For example, in the rural, 47-bed Riverside Tappahannock Hospital where Randy Ferrance, DC, MD, SFHM, is medical director for hospital-based quality, cost effectiveness is king.
“We live on a thin margin, and being sure we provide cost-effective care is the difference between having adequate nursing and not,” he says. It’s a critical difference from academic institutions, he notes, where “there is protected time to do QI, research, and administrative tasks.”
Dr. Ferrance advises those interested in tackling quality projects to “make sure that the project is tied to quality measures and that you’re being cognizant of the cost impact.”
Although much of the work around quality assurance and quality improvement in the community hospital setting is being tackled by nonphysician administrative partners, “those people are usually more than happy to develop a physician partner,” says Colleen A. McCoy, MD, PhD, medical director for hospital medicine at Williamsport (Pa.) Regional Medical Center, a part of the Susquehanna Health System.
“The idea is to look for quality projects where there is a quantifiable financial payoff to the hospital,” she says. That could be a Centers for Medicare and Medicaid Services (CMS) core measure or helping to rewrite an order set for new inpatient guidelines on stroke, as Dr. McCoy did at her hospital.
First Order of Business
Dr. McCoy has been actively engaged in quality initiatives since she joined Williams-port in 2012. She cautions new hospitalists to spend the first six months at their new job developing a reputation for clinical excellence and attention to detail.
“Having a reputation that is respected clinically opens many doors,” she says. As generalists, hospitalists interact with a wider variety of staff than specialists. This leads to broad early exposure to a diverse group of decision makers in your institution. “As a hospitalist, you can get a lot of credibility in your organization much sooner than, for example, a young cardiologist or a young gastroenterologist,” she notes.
It is also important for new hospitalists to be mindful of their position in the organization and to watch how their institutions work and operate, so that when they propose a project they are not doing so from a critical standpoint.
“Unrequested input is often seen as criticism,” she says.
Dr. Ferrance agrees. “It’s always a good idea to make sure we focus on processes and not on people in the process.”
Meeting the Mark
“If you want to leapfrog into doing things quickly, you have to be very savvy about the cost impact of your quality improvement,” continues Dr. McCoy. She and Dr. Ferrance advise those just getting started to consider tackling core measures that are reported to CMS or to identify other quality improvement projects that can be financially quantified.
Early on at Riverside Tappahannock Hospital, Dr. Ferrance participated in root cause analyses and developed (at that time) paper-based standard order sets with quality measures attached to them.

Because of her attention to detail during her orientation at Williamsport, Dr. McCoy, who had been a clinical instructor at Emory University and worked for Kaiser Permanente, quickly spotted some necessary omissions regarding DVT prophylaxis. She helped rewrite the ICU admission order sets, inserting a query for DVT prophylaxis. That one intervention helped to increase compliance on a CMS core measure.
Assess Advancement Ops
Is your community hospital open to QI projects? Dr. McCoy says candidates should ask direct questions during job interviews to assess a prospective employer’s approach to quality. She suggests two fair questions:
- Is it possible, within my first two years here as a junior staff member, to participate in a QI project?
- If I were successful in that venture, is this organization open and able to give me more opportunities in that field?
It is key for the medical director to know who in the administrative organization of the hospital would really appreciate a physician partner or physician champion for new projects. If young hospitalists are interested in such projects, they should make that known to their medical directors.
“Having the senior person in your group make a connection with your [administrative] partner is how things get done in the community medical center,” Dr. McCoy says.
Dr. Ferrance’s HM group comprises four physicians and one nurse practitioner, so “there are plenty of QI projects to go around.”
“I would be more than happy to give them [junior staff hospitalists] any QI project they are interested in taking on,” he adds. “With medicine evolving as it does, we need to revisit processes every two to three years.” For example, drug shortages and cost increases often necessitate formulary cutbacks and the need for a change in administration protocols.
When selecting a QI project, it pays to stay ahead of the game, Dr. McCoy says. She encourages hospitalists to be aware of the next core measures and volunteer to help develop guidelines. She helped create a new protocol for inpatient tissue plasminogen activator (tPa) evaluation for acute stroke, which was a recent recommendation for stroke center certification. This approach was key in helping Williamsport retain its accreditation as a stroke center. The hospital has garnered multiple accolades from the Joint Commission, U.S. News and World Report, and other reporting agencies.
“The community setting is a much smaller world than academia,” she says. But smaller can be good for one’s career advancement. “If you hit a project out of the park and it makes your hospital look better, you can very quickly get a promotion or an increase in other opportunities. These types of projects may lead to the hospital asking, ‘Have you thought about being director of the hospital medicine group or taking a leadership role in hospital operations?’”
Gretchen Henkel is a freelance writer in California.
Community hospitals offer multiple opportunities for hospitalists to become involved in both quality assurance and quality improvement. To help steer the right approach and avoid possible missteps, it’s important to acknowledge the differences between the community and academic settings, according to two medical directors with whom we spoke.
For example, in the rural, 47-bed Riverside Tappahannock Hospital where Randy Ferrance, DC, MD, SFHM, is medical director for hospital-based quality, cost effectiveness is king.
“We live on a thin margin, and being sure we provide cost-effective care is the difference between having adequate nursing and not,” he says. It’s a critical difference from academic institutions, he notes, where “there is protected time to do QI, research, and administrative tasks.”
Dr. Ferrance advises those interested in tackling quality projects to “make sure that the project is tied to quality measures and that you’re being cognizant of the cost impact.”
Although much of the work around quality assurance and quality improvement in the community hospital setting is being tackled by nonphysician administrative partners, “those people are usually more than happy to develop a physician partner,” says Colleen A. McCoy, MD, PhD, medical director for hospital medicine at Williamsport (Pa.) Regional Medical Center, a part of the Susquehanna Health System.
“The idea is to look for quality projects where there is a quantifiable financial payoff to the hospital,” she says. That could be a Centers for Medicare and Medicaid Services (CMS) core measure or helping to rewrite an order set for new inpatient guidelines on stroke, as Dr. McCoy did at her hospital.
First Order of Business
Dr. McCoy has been actively engaged in quality initiatives since she joined Williams-port in 2012. She cautions new hospitalists to spend the first six months at their new job developing a reputation for clinical excellence and attention to detail.
“Having a reputation that is respected clinically opens many doors,” she says. As generalists, hospitalists interact with a wider variety of staff than specialists. This leads to broad early exposure to a diverse group of decision makers in your institution. “As a hospitalist, you can get a lot of credibility in your organization much sooner than, for example, a young cardiologist or a young gastroenterologist,” she notes.
It is also important for new hospitalists to be mindful of their position in the organization and to watch how their institutions work and operate, so that when they propose a project they are not doing so from a critical standpoint.
“Unrequested input is often seen as criticism,” she says.
Dr. Ferrance agrees. “It’s always a good idea to make sure we focus on processes and not on people in the process.”
Meeting the Mark
“If you want to leapfrog into doing things quickly, you have to be very savvy about the cost impact of your quality improvement,” continues Dr. McCoy. She and Dr. Ferrance advise those just getting started to consider tackling core measures that are reported to CMS or to identify other quality improvement projects that can be financially quantified.
Early on at Riverside Tappahannock Hospital, Dr. Ferrance participated in root cause analyses and developed (at that time) paper-based standard order sets with quality measures attached to them.
Because of her attention to detail during her orientation at Williamsport, Dr. McCoy, who had been a clinical instructor at Emory University and worked for Kaiser Permanente, quickly spotted some necessary omissions regarding DVT prophylaxis. She helped rewrite the ICU admission order sets, inserting a query for DVT prophylaxis. That one intervention helped to increase compliance on a CMS core measure.
Assess Advancement Ops
Is your community hospital open to QI projects? Dr. McCoy says candidates should ask direct questions during job interviews to assess a prospective employer’s approach to quality. She suggests two fair questions:
- Is it possible, within my first two years here as a junior staff member, to participate in a QI project?
- If I were successful in that venture, is this organization open and able to give me more opportunities in that field?
It is key for the medical director to know who in the administrative organization of the hospital would really appreciate a physician partner or physician champion for new projects. If young hospitalists are interested in such projects, they should make that known to their medical directors.
“Having the senior person in your group make a connection with your [administrative] partner is how things get done in the community medical center,” Dr. McCoy says.
Dr. Ferrance’s HM group comprises four physicians and one nurse practitioner, so “there are plenty of QI projects to go around.”
“I would be more than happy to give them [junior staff hospitalists] any QI project they are interested in taking on,” he adds. “With medicine evolving as it does, we need to revisit processes every two to three years.” For example, drug shortages and cost increases often necessitate formulary cutbacks and the need for a change in administration protocols.
When selecting a QI project, it pays to stay ahead of the game, Dr. McCoy says. She encourages hospitalists to be aware of the next core measures and volunteer to help develop guidelines. She helped create a new protocol for inpatient tissue plasminogen activator (tPa) evaluation for acute stroke, which was a recent recommendation for stroke center certification. This approach was key in helping Williamsport retain its accreditation as a stroke center. The hospital has garnered multiple accolades from the Joint Commission, U.S. News and World Report, and other reporting agencies.
“The community setting is a much smaller world than academia,” she says. But smaller can be good for one’s career advancement. “If you hit a project out of the park and it makes your hospital look better, you can very quickly get a promotion or an increase in other opportunities. These types of projects may lead to the hospital asking, ‘Have you thought about being director of the hospital medicine group or taking a leadership role in hospital operations?’”
Gretchen Henkel is a freelance writer in California.
Community hospitals offer multiple opportunities for hospitalists to become involved in both quality assurance and quality improvement. To help steer the right approach and avoid possible missteps, it’s important to acknowledge the differences between the community and academic settings, according to two medical directors with whom we spoke.
For example, in the rural, 47-bed Riverside Tappahannock Hospital where Randy Ferrance, DC, MD, SFHM, is medical director for hospital-based quality, cost effectiveness is king.
“We live on a thin margin, and being sure we provide cost-effective care is the difference between having adequate nursing and not,” he says. It’s a critical difference from academic institutions, he notes, where “there is protected time to do QI, research, and administrative tasks.”
Dr. Ferrance advises those interested in tackling quality projects to “make sure that the project is tied to quality measures and that you’re being cognizant of the cost impact.”
Although much of the work around quality assurance and quality improvement in the community hospital setting is being tackled by nonphysician administrative partners, “those people are usually more than happy to develop a physician partner,” says Colleen A. McCoy, MD, PhD, medical director for hospital medicine at Williamsport (Pa.) Regional Medical Center, a part of the Susquehanna Health System.
“The idea is to look for quality projects where there is a quantifiable financial payoff to the hospital,” she says. That could be a Centers for Medicare and Medicaid Services (CMS) core measure or helping to rewrite an order set for new inpatient guidelines on stroke, as Dr. McCoy did at her hospital.
First Order of Business
Dr. McCoy has been actively engaged in quality initiatives since she joined Williams-port in 2012. She cautions new hospitalists to spend the first six months at their new job developing a reputation for clinical excellence and attention to detail.
“Having a reputation that is respected clinically opens many doors,” she says. As generalists, hospitalists interact with a wider variety of staff than specialists. This leads to broad early exposure to a diverse group of decision makers in your institution. “As a hospitalist, you can get a lot of credibility in your organization much sooner than, for example, a young cardiologist or a young gastroenterologist,” she notes.
It is also important for new hospitalists to be mindful of their position in the organization and to watch how their institutions work and operate, so that when they propose a project they are not doing so from a critical standpoint.
“Unrequested input is often seen as criticism,” she says.
Dr. Ferrance agrees. “It’s always a good idea to make sure we focus on processes and not on people in the process.”
Meeting the Mark
“If you want to leapfrog into doing things quickly, you have to be very savvy about the cost impact of your quality improvement,” continues Dr. McCoy. She and Dr. Ferrance advise those just getting started to consider tackling core measures that are reported to CMS or to identify other quality improvement projects that can be financially quantified.
Early on at Riverside Tappahannock Hospital, Dr. Ferrance participated in root cause analyses and developed (at that time) paper-based standard order sets with quality measures attached to them.
Because of her attention to detail during her orientation at Williamsport, Dr. McCoy, who had been a clinical instructor at Emory University and worked for Kaiser Permanente, quickly spotted some necessary omissions regarding DVT prophylaxis. She helped rewrite the ICU admission order sets, inserting a query for DVT prophylaxis. That one intervention helped to increase compliance on a CMS core measure.
Assess Advancement Ops
Is your community hospital open to QI projects? Dr. McCoy says candidates should ask direct questions during job interviews to assess a prospective employer’s approach to quality. She suggests two fair questions:
- Is it possible, within my first two years here as a junior staff member, to participate in a QI project?
- If I were successful in that venture, is this organization open and able to give me more opportunities in that field?
It is key for the medical director to know who in the administrative organization of the hospital would really appreciate a physician partner or physician champion for new projects. If young hospitalists are interested in such projects, they should make that known to their medical directors.
“Having the senior person in your group make a connection with your [administrative] partner is how things get done in the community medical center,” Dr. McCoy says.
Dr. Ferrance’s HM group comprises four physicians and one nurse practitioner, so “there are plenty of QI projects to go around.”
“I would be more than happy to give them [junior staff hospitalists] any QI project they are interested in taking on,” he adds. “With medicine evolving as it does, we need to revisit processes every two to three years.” For example, drug shortages and cost increases often necessitate formulary cutbacks and the need for a change in administration protocols.
When selecting a QI project, it pays to stay ahead of the game, Dr. McCoy says. She encourages hospitalists to be aware of the next core measures and volunteer to help develop guidelines. She helped create a new protocol for inpatient tissue plasminogen activator (tPa) evaluation for acute stroke, which was a recent recommendation for stroke center certification. This approach was key in helping Williamsport retain its accreditation as a stroke center. The hospital has garnered multiple accolades from the Joint Commission, U.S. News and World Report, and other reporting agencies.
“The community setting is a much smaller world than academia,” she says. But smaller can be good for one’s career advancement. “If you hit a project out of the park and it makes your hospital look better, you can very quickly get a promotion or an increase in other opportunities. These types of projects may lead to the hospital asking, ‘Have you thought about being director of the hospital medicine group or taking a leadership role in hospital operations?’”
Gretchen Henkel is a freelance writer in California.
Physicians Critical of Proposed Changes to Medicare's Two-Midnight Rule

In the wake of proposed changes to the Centers for Medicare and Medicaid Services’ two-midnight rule, physicians say new flexibilities and changes to the policy’s auditing mechanism add more uncertainty and ambiguity.
The 2016 Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System proposed rule was published on July 1, 2015, and included changes in response to concerns about portions of the original two-midnight rule.1 By classifying an inpatient stay as any hospitalization lasting more than two midnights, the rule, which attempted to clarify which services warranted billing under Part B and which qualified for Part A, initially was intended to limit the long observation stays negatively impacting Medicare beneficiaries. However, aggressive reviews by recovery auditors (RAs) and the notion that physician judgment was taking a backseat to arbitrary CMS policy caused a backlash.
In 2014, CMS solicited feedback on the two-midnight rule. SHM suggested a two-tiered approach to address immediate and long-term patient care needs.
“SHM suggests CMS pursue broader solutions to observation status instead of making minor adjustments to the two-midnight rule,” wrote then-SHM President Burke Kealey, MD, SFHM, in a public comment letter to CMS in June 2014. “However, SHM does recognize that in the interim, the two-midnight policy needs to be refined in order to reflect the realities of patient care. Some situations may not be appropriate for classification as outpatient, regardless of the length of stay.”
The proposed changes were supposed to be a solution, but some are saying that CMS has missed the mark. In trying to give physicians more flexibility to determine patient status at the time of admissions, the rule instead may leave physician judgment open to additional scrutiny. Also, the nature of short inpatient stay reviews by Quality Improvement Organizations (QIOs), rather than RAs, remains unclear, and an additional point of concern involves the question of how RAs will factor in.
“My personal opinion is that it will only muddy the waters, in terms of payment for [and] documentation and reviews of short stays for Medicare beneficiaries,” says Jeannine Engel, MD, FACP, in a statement she wrote and shared by email. Dr. Engel is an internist and physician advisor for billing compliance at University of Utah Health Care in Salt Lake City. “No matter who reviews medical documentation, when subjective criteria are used, there is room for interpretation.”
CMS has not defined what constitutes adequate documentation to justify short inpatient stays, nor has it indicated the threshold for “high rates of denials” that would kick reviews over to RAs.
“Details are lacking, and then what makes it even more confusing is what they’ve done with the tweak in policy is further muddied the definition of inpatient,” says Charles Locke, MD, internist and senior physician advisor at Johns Hopkins University School of Medicine in Baltimore. “Whether you agree or disagree with the two-midnight rule, it actually made more clear what inpatient should be.”
According to CMS, the two-midnight rule has reduced observation stays lasting longer than two midnights by 11%, and inpatient admissions are anticipated to increase. But, physicians say, it’s a billing distinction rather than one that impacts patient care.
“The reality is when you take someone in the hospital as outpatient, they can receive every service and care identical to inpatient,” Dr. Locke says. “CMS seems hung up on the idea that in the hospital there are two levels of care.”
In fact, with the changes, “CMS had all but abandoned the term ‘inpatient hospital care’ in favor of simply ‘hospital care.’ Now it is back,” says Dr. Engel, who is also a professor of medicine at Huntsman Cancer Institute. “The two-midnight rule was a payment policy, not a ‘care policy.’ Now we may be back to debating what constitutes ‘inpatient care’ versus what could have been ‘safely delivered in a different/lower status such as observation.’”
Dr. Engel and Dr. Locke recently published a study of RAs and the two-midnight rule in the Journal of Hospital Medicine, with University of Wisconsin-Madison School of Medicine and Public Health hospitalist Ann Sheehy, MD.2
The AHA-CMS Quarrel
In addition to SHM, other organizations are heartened by CMS’s responsiveness. Priya Bathija, senior associate director of policy at the American Hospital Association, called them a “step in the right direction,” but also highlighted some of the group’s lingering concerns.
“We think it’s a good thing they’re using QIOs as first-line medical review as opposed to RAs, but we still want to make sure RAs will not make inappropriate denials of claims,” Bathija says.
The AHA is fighting a legal battle against the U.S. Department of Health and Human Services over a 0.2% reduction in inpatient payments through the two-midnight rule, maintained in the proposed changes, which CMS says are warranted based on a projected increase in inpatient service claims.3 The AHA disputes these actuarial values, Bathija says.
The AHA is calling upon CMS to make changes to short stay payments and submitted a letter to CMS outlining six models.4 The agency accepted comment on the proposed changes through August 30.
The fundamental issue, however, is that the Medicare payment system is vastly out of date, Dr. Locke says. “What I have advocated is to get rid of Part A and Part B distinction, just like private insurance,” he says, “so when you’re hospitalized, you’re hospitalized, and there is no distinction except inpatient extended, recovery outpatient, or extended outpatient observation.”
If the proposed rule changes are finalized, hospitals are going to have to learn to live with them, despite ambiguous guidance, and adjust their workflow, Dr. Locke says.
“It costs a lot of money and time, and hospitals don’t want to do something thinking they’re doing it in good faith but then the Inspector General says you owe $10 million,” he says. “In general, I and others don’t see this fixing any fundamental problems.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- U.S. Department of Health and Human Services. Medicare program: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center payment systems and quality reporting programs; short inpatient hospital stays; transition for certain Medicare-dependent, small rural hospitals under the Hospital Inpatient Prospective Payment System. July 1, 2015. Accessed July 29, 2015.
- Sheehy AM, Locke C, Engel JZ, et al. Recovery audit contractor audits and appeals at three academic medical centers. J Hosp Med. 2015;10(4):212-219. doi: 10.1002/jhm.2332.
- American Hospital Association. Associations, hospitals challenge two-midnight rule in federal court. April 14, 2014. Accessed July 29, 2015.
- Fishman LE. RE: Two-midnight policy and potential short stay payment solutions [letter]. American Hospital Association. February 13, 2015. Accessed July 29, 2015.
In the wake of proposed changes to the Centers for Medicare and Medicaid Services’ two-midnight rule, physicians say new flexibilities and changes to the policy’s auditing mechanism add more uncertainty and ambiguity.
The 2016 Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System proposed rule was published on July 1, 2015, and included changes in response to concerns about portions of the original two-midnight rule.1 By classifying an inpatient stay as any hospitalization lasting more than two midnights, the rule, which attempted to clarify which services warranted billing under Part B and which qualified for Part A, initially was intended to limit the long observation stays negatively impacting Medicare beneficiaries. However, aggressive reviews by recovery auditors (RAs) and the notion that physician judgment was taking a backseat to arbitrary CMS policy caused a backlash.
In 2014, CMS solicited feedback on the two-midnight rule. SHM suggested a two-tiered approach to address immediate and long-term patient care needs.
“SHM suggests CMS pursue broader solutions to observation status instead of making minor adjustments to the two-midnight rule,” wrote then-SHM President Burke Kealey, MD, SFHM, in a public comment letter to CMS in June 2014. “However, SHM does recognize that in the interim, the two-midnight policy needs to be refined in order to reflect the realities of patient care. Some situations may not be appropriate for classification as outpatient, regardless of the length of stay.”
The proposed changes were supposed to be a solution, but some are saying that CMS has missed the mark. In trying to give physicians more flexibility to determine patient status at the time of admissions, the rule instead may leave physician judgment open to additional scrutiny. Also, the nature of short inpatient stay reviews by Quality Improvement Organizations (QIOs), rather than RAs, remains unclear, and an additional point of concern involves the question of how RAs will factor in.
“My personal opinion is that it will only muddy the waters, in terms of payment for [and] documentation and reviews of short stays for Medicare beneficiaries,” says Jeannine Engel, MD, FACP, in a statement she wrote and shared by email. Dr. Engel is an internist and physician advisor for billing compliance at University of Utah Health Care in Salt Lake City. “No matter who reviews medical documentation, when subjective criteria are used, there is room for interpretation.”
CMS has not defined what constitutes adequate documentation to justify short inpatient stays, nor has it indicated the threshold for “high rates of denials” that would kick reviews over to RAs.
“Details are lacking, and then what makes it even more confusing is what they’ve done with the tweak in policy is further muddied the definition of inpatient,” says Charles Locke, MD, internist and senior physician advisor at Johns Hopkins University School of Medicine in Baltimore. “Whether you agree or disagree with the two-midnight rule, it actually made more clear what inpatient should be.”
According to CMS, the two-midnight rule has reduced observation stays lasting longer than two midnights by 11%, and inpatient admissions are anticipated to increase. But, physicians say, it’s a billing distinction rather than one that impacts patient care.
“The reality is when you take someone in the hospital as outpatient, they can receive every service and care identical to inpatient,” Dr. Locke says. “CMS seems hung up on the idea that in the hospital there are two levels of care.”
In fact, with the changes, “CMS had all but abandoned the term ‘inpatient hospital care’ in favor of simply ‘hospital care.’ Now it is back,” says Dr. Engel, who is also a professor of medicine at Huntsman Cancer Institute. “The two-midnight rule was a payment policy, not a ‘care policy.’ Now we may be back to debating what constitutes ‘inpatient care’ versus what could have been ‘safely delivered in a different/lower status such as observation.’”
Dr. Engel and Dr. Locke recently published a study of RAs and the two-midnight rule in the Journal of Hospital Medicine, with University of Wisconsin-Madison School of Medicine and Public Health hospitalist Ann Sheehy, MD.2
The AHA-CMS Quarrel
In addition to SHM, other organizations are heartened by CMS’s responsiveness. Priya Bathija, senior associate director of policy at the American Hospital Association, called them a “step in the right direction,” but also highlighted some of the group’s lingering concerns.
“We think it’s a good thing they’re using QIOs as first-line medical review as opposed to RAs, but we still want to make sure RAs will not make inappropriate denials of claims,” Bathija says.
The AHA is fighting a legal battle against the U.S. Department of Health and Human Services over a 0.2% reduction in inpatient payments through the two-midnight rule, maintained in the proposed changes, which CMS says are warranted based on a projected increase in inpatient service claims.3 The AHA disputes these actuarial values, Bathija says.
The AHA is calling upon CMS to make changes to short stay payments and submitted a letter to CMS outlining six models.4 The agency accepted comment on the proposed changes through August 30.
The fundamental issue, however, is that the Medicare payment system is vastly out of date, Dr. Locke says. “What I have advocated is to get rid of Part A and Part B distinction, just like private insurance,” he says, “so when you’re hospitalized, you’re hospitalized, and there is no distinction except inpatient extended, recovery outpatient, or extended outpatient observation.”
If the proposed rule changes are finalized, hospitals are going to have to learn to live with them, despite ambiguous guidance, and adjust their workflow, Dr. Locke says.
“It costs a lot of money and time, and hospitals don’t want to do something thinking they’re doing it in good faith but then the Inspector General says you owe $10 million,” he says. “In general, I and others don’t see this fixing any fundamental problems.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- U.S. Department of Health and Human Services. Medicare program: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center payment systems and quality reporting programs; short inpatient hospital stays; transition for certain Medicare-dependent, small rural hospitals under the Hospital Inpatient Prospective Payment System. July 1, 2015. Accessed July 29, 2015.
- Sheehy AM, Locke C, Engel JZ, et al. Recovery audit contractor audits and appeals at three academic medical centers. J Hosp Med. 2015;10(4):212-219. doi: 10.1002/jhm.2332.
- American Hospital Association. Associations, hospitals challenge two-midnight rule in federal court. April 14, 2014. Accessed July 29, 2015.
- Fishman LE. RE: Two-midnight policy and potential short stay payment solutions [letter]. American Hospital Association. February 13, 2015. Accessed July 29, 2015.
In the wake of proposed changes to the Centers for Medicare and Medicaid Services’ two-midnight rule, physicians say new flexibilities and changes to the policy’s auditing mechanism add more uncertainty and ambiguity.
The 2016 Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System proposed rule was published on July 1, 2015, and included changes in response to concerns about portions of the original two-midnight rule.1 By classifying an inpatient stay as any hospitalization lasting more than two midnights, the rule, which attempted to clarify which services warranted billing under Part B and which qualified for Part A, initially was intended to limit the long observation stays negatively impacting Medicare beneficiaries. However, aggressive reviews by recovery auditors (RAs) and the notion that physician judgment was taking a backseat to arbitrary CMS policy caused a backlash.
In 2014, CMS solicited feedback on the two-midnight rule. SHM suggested a two-tiered approach to address immediate and long-term patient care needs.
“SHM suggests CMS pursue broader solutions to observation status instead of making minor adjustments to the two-midnight rule,” wrote then-SHM President Burke Kealey, MD, SFHM, in a public comment letter to CMS in June 2014. “However, SHM does recognize that in the interim, the two-midnight policy needs to be refined in order to reflect the realities of patient care. Some situations may not be appropriate for classification as outpatient, regardless of the length of stay.”
The proposed changes were supposed to be a solution, but some are saying that CMS has missed the mark. In trying to give physicians more flexibility to determine patient status at the time of admissions, the rule instead may leave physician judgment open to additional scrutiny. Also, the nature of short inpatient stay reviews by Quality Improvement Organizations (QIOs), rather than RAs, remains unclear, and an additional point of concern involves the question of how RAs will factor in.
“My personal opinion is that it will only muddy the waters, in terms of payment for [and] documentation and reviews of short stays for Medicare beneficiaries,” says Jeannine Engel, MD, FACP, in a statement she wrote and shared by email. Dr. Engel is an internist and physician advisor for billing compliance at University of Utah Health Care in Salt Lake City. “No matter who reviews medical documentation, when subjective criteria are used, there is room for interpretation.”
CMS has not defined what constitutes adequate documentation to justify short inpatient stays, nor has it indicated the threshold for “high rates of denials” that would kick reviews over to RAs.
“Details are lacking, and then what makes it even more confusing is what they’ve done with the tweak in policy is further muddied the definition of inpatient,” says Charles Locke, MD, internist and senior physician advisor at Johns Hopkins University School of Medicine in Baltimore. “Whether you agree or disagree with the two-midnight rule, it actually made more clear what inpatient should be.”
According to CMS, the two-midnight rule has reduced observation stays lasting longer than two midnights by 11%, and inpatient admissions are anticipated to increase. But, physicians say, it’s a billing distinction rather than one that impacts patient care.
“The reality is when you take someone in the hospital as outpatient, they can receive every service and care identical to inpatient,” Dr. Locke says. “CMS seems hung up on the idea that in the hospital there are two levels of care.”
In fact, with the changes, “CMS had all but abandoned the term ‘inpatient hospital care’ in favor of simply ‘hospital care.’ Now it is back,” says Dr. Engel, who is also a professor of medicine at Huntsman Cancer Institute. “The two-midnight rule was a payment policy, not a ‘care policy.’ Now we may be back to debating what constitutes ‘inpatient care’ versus what could have been ‘safely delivered in a different/lower status such as observation.’”
Dr. Engel and Dr. Locke recently published a study of RAs and the two-midnight rule in the Journal of Hospital Medicine, with University of Wisconsin-Madison School of Medicine and Public Health hospitalist Ann Sheehy, MD.2
The AHA-CMS Quarrel
In addition to SHM, other organizations are heartened by CMS’s responsiveness. Priya Bathija, senior associate director of policy at the American Hospital Association, called them a “step in the right direction,” but also highlighted some of the group’s lingering concerns.
“We think it’s a good thing they’re using QIOs as first-line medical review as opposed to RAs, but we still want to make sure RAs will not make inappropriate denials of claims,” Bathija says.
The AHA is fighting a legal battle against the U.S. Department of Health and Human Services over a 0.2% reduction in inpatient payments through the two-midnight rule, maintained in the proposed changes, which CMS says are warranted based on a projected increase in inpatient service claims.3 The AHA disputes these actuarial values, Bathija says.
The AHA is calling upon CMS to make changes to short stay payments and submitted a letter to CMS outlining six models.4 The agency accepted comment on the proposed changes through August 30.
The fundamental issue, however, is that the Medicare payment system is vastly out of date, Dr. Locke says. “What I have advocated is to get rid of Part A and Part B distinction, just like private insurance,” he says, “so when you’re hospitalized, you’re hospitalized, and there is no distinction except inpatient extended, recovery outpatient, or extended outpatient observation.”
If the proposed rule changes are finalized, hospitals are going to have to learn to live with them, despite ambiguous guidance, and adjust their workflow, Dr. Locke says.
“It costs a lot of money and time, and hospitals don’t want to do something thinking they’re doing it in good faith but then the Inspector General says you owe $10 million,” he says. “In general, I and others don’t see this fixing any fundamental problems.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- U.S. Department of Health and Human Services. Medicare program: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center payment systems and quality reporting programs; short inpatient hospital stays; transition for certain Medicare-dependent, small rural hospitals under the Hospital Inpatient Prospective Payment System. July 1, 2015. Accessed July 29, 2015.
- Sheehy AM, Locke C, Engel JZ, et al. Recovery audit contractor audits and appeals at three academic medical centers. J Hosp Med. 2015;10(4):212-219. doi: 10.1002/jhm.2332.
- American Hospital Association. Associations, hospitals challenge two-midnight rule in federal court. April 14, 2014. Accessed July 29, 2015.
- Fishman LE. RE: Two-midnight policy and potential short stay payment solutions [letter]. American Hospital Association. February 13, 2015. Accessed July 29, 2015.
Effects of Peri-Operative Beta-Blockade in Noncardiac Surgery Vary Based on Cardiac Risk Factors
Clinical question: In patients undergoing noncardiac surgery, are peri-operative beta blockers beneficial in those at high risk and harmful in those at low risk?
Background: Despite multiple RCTs, the exact utility of peri-operative beta-blockade remains unclear, especially in those patients considered low cardiac risk. While initial research prompted guidelines that encouraged the liberal use of peri-operative beta blockers, more recent studies have drawn attention to their potential adverse effects, prompting further investigation.
Study design: Retrospective, observational, cohort study.
Setting: One hundred nineteen Veterans Administration medical centers.
Synopsis: Through the modeling of data from 326,489 patients who underwent noncardiac surgery between 2008 and 2013, this study assessed the effects of beta blocker usage and cardiac risk factors on 30-day surgical mortality.
Analysis demonstrated a significant difference in the effect of beta blocker use on mortality based on the number of cardiac risk factors. For patients with no cardiac risk factors, those receiving beta blockers were at increased risk of death (odds ratio 1.19, 95% confidence interval 1.06-1.35). Among patients with three to four cardiac risk factors, however, those on beta blockers had a decreased risk of death (odds ratio 0.63, 95% confidence interval 0.43-0.93).
Bottom line: In noncardiac surgery, use of beta blockers may be beneficial for those at high cardiac risk and detrimental to those without cardiac risk factors.
Citation: Friedell ML, Van Way CW 3rd, Freyberg RW, Almenoff PL. Beta-blockade and operative mortality in noncardiac surgery: harmful or helpful? JAMA Surgery. 2015;150(7):658-664. doi:10.1001/jamasurg.2015.86.
Clinical question: In patients undergoing noncardiac surgery, are peri-operative beta blockers beneficial in those at high risk and harmful in those at low risk?
Background: Despite multiple RCTs, the exact utility of peri-operative beta-blockade remains unclear, especially in those patients considered low cardiac risk. While initial research prompted guidelines that encouraged the liberal use of peri-operative beta blockers, more recent studies have drawn attention to their potential adverse effects, prompting further investigation.
Study design: Retrospective, observational, cohort study.
Setting: One hundred nineteen Veterans Administration medical centers.
Synopsis: Through the modeling of data from 326,489 patients who underwent noncardiac surgery between 2008 and 2013, this study assessed the effects of beta blocker usage and cardiac risk factors on 30-day surgical mortality.
Analysis demonstrated a significant difference in the effect of beta blocker use on mortality based on the number of cardiac risk factors. For patients with no cardiac risk factors, those receiving beta blockers were at increased risk of death (odds ratio 1.19, 95% confidence interval 1.06-1.35). Among patients with three to four cardiac risk factors, however, those on beta blockers had a decreased risk of death (odds ratio 0.63, 95% confidence interval 0.43-0.93).
Bottom line: In noncardiac surgery, use of beta blockers may be beneficial for those at high cardiac risk and detrimental to those without cardiac risk factors.
Citation: Friedell ML, Van Way CW 3rd, Freyberg RW, Almenoff PL. Beta-blockade and operative mortality in noncardiac surgery: harmful or helpful? JAMA Surgery. 2015;150(7):658-664. doi:10.1001/jamasurg.2015.86.
Clinical question: In patients undergoing noncardiac surgery, are peri-operative beta blockers beneficial in those at high risk and harmful in those at low risk?
Background: Despite multiple RCTs, the exact utility of peri-operative beta-blockade remains unclear, especially in those patients considered low cardiac risk. While initial research prompted guidelines that encouraged the liberal use of peri-operative beta blockers, more recent studies have drawn attention to their potential adverse effects, prompting further investigation.
Study design: Retrospective, observational, cohort study.
Setting: One hundred nineteen Veterans Administration medical centers.
Synopsis: Through the modeling of data from 326,489 patients who underwent noncardiac surgery between 2008 and 2013, this study assessed the effects of beta blocker usage and cardiac risk factors on 30-day surgical mortality.
Analysis demonstrated a significant difference in the effect of beta blocker use on mortality based on the number of cardiac risk factors. For patients with no cardiac risk factors, those receiving beta blockers were at increased risk of death (odds ratio 1.19, 95% confidence interval 1.06-1.35). Among patients with three to four cardiac risk factors, however, those on beta blockers had a decreased risk of death (odds ratio 0.63, 95% confidence interval 0.43-0.93).
Bottom line: In noncardiac surgery, use of beta blockers may be beneficial for those at high cardiac risk and detrimental to those without cardiac risk factors.
Citation: Friedell ML, Van Way CW 3rd, Freyberg RW, Almenoff PL. Beta-blockade and operative mortality in noncardiac surgery: harmful or helpful? JAMA Surgery. 2015;150(7):658-664. doi:10.1001/jamasurg.2015.86.