User login
Community Service Helps Hospitalists Build Connections, Earn Credibility


Hospitalist Brian Bossard, MD, FACP, FHM, founder and medical director of Inpatient Physician Associates, which serves Bryan Health Medical Center in Lincoln, Neb., as well as Columbus (Neb.) Community Hospital and Great Plains Regional Medical Center in North Platte, recalls a time when the suggestion of community involvement was a non-starter for physicians. Twenty years ago, he says, “the idea was that physicians work so many hours that there wasn’t time for community involvement.” In the ensuing years, the advent of shift-based work has created an opportunity for hospitalists to connect to community.
Learning the ropes takes the majority of a physician’s time in the first year or two on a new assignment right after residency, Dr. Bossard says. But after initial orientation, young hospitalists in their group are encouraged to become “joiners.”
“We identify activities that the physicians can participate in—many of them medically related, such as sitting on the board of a local blood bank,” he says. “Feeling a part of something bigger, and participating in areas outside of your direct control, can add to satisfaction.”
And that, in turn, can lead to engaged, satisfied, happy, and retained physicians.
Closing the Credibility Gap
David Grace, MD, FHM, SFHM area medical officer for The Schumacher Group’s Hospital Medicine Division in Lafayette, La., agrees that community involvement can lead to improved engagement, as well as a better sense of belonging and job satisfaction. He also encourages younger hospitalists to become engaged in their local communities. Participating in volunteer activities can lead to:
- Better public understanding of what hospitalists do;
- Better relationships with key hospital and community stakeholders; and
- Better use of down time for long-distance hospitalist commuters.
Regarding his first point, Dr. Grace finds that despite the growth of the hospitalist movement, many consumers still do not understand the role hospitalists play in patient care. Encountering hospitalists in the community helps patients put a public and familiar face on the concept. Community involvement can function as “direct-to-consumer advertising,” he says, when patients express a preference for hospitals based on their interface with hospitalists in the community. He notes that “the smaller the town, the more likely there will be a dividing line between the community and ‘outsiders.’ The chance to go from being an outsider to an insider can have a profound effect on your success, your future, and your happiness.”
Because the business of healthcare is based on relationships, interacting with hospital stakeholders at youth sporting events and other gatherings gives hospitalists a chance to build relationships away from the pressures of the work environment. At the core of community involvement, Dr. Grace says, is the reality that “we are social creatures. There’s something about developing a bond away from the hospital that provides a unique strength, compared to a bond formed solely in the hospital environment.”
Manikandan Nagendran, MD, medical director of the hospital medicine program at Dauterive Hospital in New Iberia, La., has strengthened his professional relationships through community participation. After completing his residency, he joined the Schumacher hospitalist program at Dauterive Hospital. Burt Bujard, MD, who had begun the HM program just two years prior, took Dr. Nagendran under his wing. Not only did he introduce Dr. Nagendran to community primary care providers and specialists, he also fostered his involvement with some of the hospital’s traditions, such as the Gumbo Cook-Off and annual Berry Ball. Organized by all the physicians and their spouses, “the Berry Ball is a great social event to meet lots of nurses, doctors, and administrative people,” Dr. Nagendran says.
During last year’s cook-off, he volunteered to help his group’s nurse practitioner and her husband, both New Iberia residents, set up their booth and serve gumbo to the public.
“When you encounter another physician or hospital administrator at an event, you always get to know something different about that person,” he says. “When you meet people on a different level at a social event, and exchange phone numbers, your relationship changes in many ways.”
Since he maintains his home in Lafayette, a 30-minute commute away, he wanted to invest time in New Iberia community activities. “One of the reasons I go to these events,” he says, “is so they understand that I’m part of their community here.
“When you meet these people in the hospital after an event, you are seen as more approachable. Especially for hospitalists, we need to build relationships.”
Six years ago, the Dauterive hospital medicine program had 15 contracts with community PCPs. That number is now up to 58.
And when Dr. Bujard retired in 2011, Dr. Nagendran became medical director.
Dr. Grace notes that community involvement can also serve to keep one’s life in balance. Referring to the “systolic/diastolic lifestyle” of hospitalist shifts, he says that “introducing a little bit of community and enjoyment into your down time can also increase job satisfaction during your work time.”
Gretchen Henkel is a freelance writer in San Luis Obispo, Calif.
Hospitalist Brian Bossard, MD, FACP, FHM, founder and medical director of Inpatient Physician Associates, which serves Bryan Health Medical Center in Lincoln, Neb., as well as Columbus (Neb.) Community Hospital and Great Plains Regional Medical Center in North Platte, recalls a time when the suggestion of community involvement was a non-starter for physicians. Twenty years ago, he says, “the idea was that physicians work so many hours that there wasn’t time for community involvement.” In the ensuing years, the advent of shift-based work has created an opportunity for hospitalists to connect to community.
Learning the ropes takes the majority of a physician’s time in the first year or two on a new assignment right after residency, Dr. Bossard says. But after initial orientation, young hospitalists in their group are encouraged to become “joiners.”
“We identify activities that the physicians can participate in—many of them medically related, such as sitting on the board of a local blood bank,” he says. “Feeling a part of something bigger, and participating in areas outside of your direct control, can add to satisfaction.”
And that, in turn, can lead to engaged, satisfied, happy, and retained physicians.
Closing the Credibility Gap
David Grace, MD, FHM, SFHM area medical officer for The Schumacher Group’s Hospital Medicine Division in Lafayette, La., agrees that community involvement can lead to improved engagement, as well as a better sense of belonging and job satisfaction. He also encourages younger hospitalists to become engaged in their local communities. Participating in volunteer activities can lead to:
- Better public understanding of what hospitalists do;
- Better relationships with key hospital and community stakeholders; and
- Better use of down time for long-distance hospitalist commuters.
Regarding his first point, Dr. Grace finds that despite the growth of the hospitalist movement, many consumers still do not understand the role hospitalists play in patient care. Encountering hospitalists in the community helps patients put a public and familiar face on the concept. Community involvement can function as “direct-to-consumer advertising,” he says, when patients express a preference for hospitals based on their interface with hospitalists in the community. He notes that “the smaller the town, the more likely there will be a dividing line between the community and ‘outsiders.’ The chance to go from being an outsider to an insider can have a profound effect on your success, your future, and your happiness.”
Because the business of healthcare is based on relationships, interacting with hospital stakeholders at youth sporting events and other gatherings gives hospitalists a chance to build relationships away from the pressures of the work environment. At the core of community involvement, Dr. Grace says, is the reality that “we are social creatures. There’s something about developing a bond away from the hospital that provides a unique strength, compared to a bond formed solely in the hospital environment.”
Manikandan Nagendran, MD, medical director of the hospital medicine program at Dauterive Hospital in New Iberia, La., has strengthened his professional relationships through community participation. After completing his residency, he joined the Schumacher hospitalist program at Dauterive Hospital. Burt Bujard, MD, who had begun the HM program just two years prior, took Dr. Nagendran under his wing. Not only did he introduce Dr. Nagendran to community primary care providers and specialists, he also fostered his involvement with some of the hospital’s traditions, such as the Gumbo Cook-Off and annual Berry Ball. Organized by all the physicians and their spouses, “the Berry Ball is a great social event to meet lots of nurses, doctors, and administrative people,” Dr. Nagendran says.
During last year’s cook-off, he volunteered to help his group’s nurse practitioner and her husband, both New Iberia residents, set up their booth and serve gumbo to the public.
“When you encounter another physician or hospital administrator at an event, you always get to know something different about that person,” he says. “When you meet people on a different level at a social event, and exchange phone numbers, your relationship changes in many ways.”
Since he maintains his home in Lafayette, a 30-minute commute away, he wanted to invest time in New Iberia community activities. “One of the reasons I go to these events,” he says, “is so they understand that I’m part of their community here.
“When you meet these people in the hospital after an event, you are seen as more approachable. Especially for hospitalists, we need to build relationships.”
Six years ago, the Dauterive hospital medicine program had 15 contracts with community PCPs. That number is now up to 58.
And when Dr. Bujard retired in 2011, Dr. Nagendran became medical director.
Dr. Grace notes that community involvement can also serve to keep one’s life in balance. Referring to the “systolic/diastolic lifestyle” of hospitalist shifts, he says that “introducing a little bit of community and enjoyment into your down time can also increase job satisfaction during your work time.”
Gretchen Henkel is a freelance writer in San Luis Obispo, Calif.
Hospitalist Brian Bossard, MD, FACP, FHM, founder and medical director of Inpatient Physician Associates, which serves Bryan Health Medical Center in Lincoln, Neb., as well as Columbus (Neb.) Community Hospital and Great Plains Regional Medical Center in North Platte, recalls a time when the suggestion of community involvement was a non-starter for physicians. Twenty years ago, he says, “the idea was that physicians work so many hours that there wasn’t time for community involvement.” In the ensuing years, the advent of shift-based work has created an opportunity for hospitalists to connect to community.
Learning the ropes takes the majority of a physician’s time in the first year or two on a new assignment right after residency, Dr. Bossard says. But after initial orientation, young hospitalists in their group are encouraged to become “joiners.”
“We identify activities that the physicians can participate in—many of them medically related, such as sitting on the board of a local blood bank,” he says. “Feeling a part of something bigger, and participating in areas outside of your direct control, can add to satisfaction.”
And that, in turn, can lead to engaged, satisfied, happy, and retained physicians.
Closing the Credibility Gap
David Grace, MD, FHM, SFHM area medical officer for The Schumacher Group’s Hospital Medicine Division in Lafayette, La., agrees that community involvement can lead to improved engagement, as well as a better sense of belonging and job satisfaction. He also encourages younger hospitalists to become engaged in their local communities. Participating in volunteer activities can lead to:
- Better public understanding of what hospitalists do;
- Better relationships with key hospital and community stakeholders; and
- Better use of down time for long-distance hospitalist commuters.
Regarding his first point, Dr. Grace finds that despite the growth of the hospitalist movement, many consumers still do not understand the role hospitalists play in patient care. Encountering hospitalists in the community helps patients put a public and familiar face on the concept. Community involvement can function as “direct-to-consumer advertising,” he says, when patients express a preference for hospitals based on their interface with hospitalists in the community. He notes that “the smaller the town, the more likely there will be a dividing line between the community and ‘outsiders.’ The chance to go from being an outsider to an insider can have a profound effect on your success, your future, and your happiness.”
Because the business of healthcare is based on relationships, interacting with hospital stakeholders at youth sporting events and other gatherings gives hospitalists a chance to build relationships away from the pressures of the work environment. At the core of community involvement, Dr. Grace says, is the reality that “we are social creatures. There’s something about developing a bond away from the hospital that provides a unique strength, compared to a bond formed solely in the hospital environment.”
Manikandan Nagendran, MD, medical director of the hospital medicine program at Dauterive Hospital in New Iberia, La., has strengthened his professional relationships through community participation. After completing his residency, he joined the Schumacher hospitalist program at Dauterive Hospital. Burt Bujard, MD, who had begun the HM program just two years prior, took Dr. Nagendran under his wing. Not only did he introduce Dr. Nagendran to community primary care providers and specialists, he also fostered his involvement with some of the hospital’s traditions, such as the Gumbo Cook-Off and annual Berry Ball. Organized by all the physicians and their spouses, “the Berry Ball is a great social event to meet lots of nurses, doctors, and administrative people,” Dr. Nagendran says.
During last year’s cook-off, he volunteered to help his group’s nurse practitioner and her husband, both New Iberia residents, set up their booth and serve gumbo to the public.
“When you encounter another physician or hospital administrator at an event, you always get to know something different about that person,” he says. “When you meet people on a different level at a social event, and exchange phone numbers, your relationship changes in many ways.”
Since he maintains his home in Lafayette, a 30-minute commute away, he wanted to invest time in New Iberia community activities. “One of the reasons I go to these events,” he says, “is so they understand that I’m part of their community here.
“When you meet these people in the hospital after an event, you are seen as more approachable. Especially for hospitalists, we need to build relationships.”
Six years ago, the Dauterive hospital medicine program had 15 contracts with community PCPs. That number is now up to 58.
And when Dr. Bujard retired in 2011, Dr. Nagendran became medical director.
Dr. Grace notes that community involvement can also serve to keep one’s life in balance. Referring to the “systolic/diastolic lifestyle” of hospitalist shifts, he says that “introducing a little bit of community and enjoyment into your down time can also increase job satisfaction during your work time.”
Gretchen Henkel is a freelance writer in San Luis Obispo, Calif.
Delay in ICD-10 Implementation to Impact Hospitalists, Physicians, Payers
On April 1, President Obama signed into law a bill that again delays a permanent fix of the sustainable growth rate formula, or SGR, the so-called “doc fix.” The bill also contained a surprise provision added by Congress to delay implementation of the switch from ICD-9 to ICD-10. The mandated conversion was supposed to take place by October 1 of this year; its delay will have a range of impacts on everyone from physicians to payers.
Hospitalists and others must weigh their options going forward, as many health systems and groups are already well on their way toward compliance with the 2014 deadline.
At this point, prevailing wisdom is that Congress added the delay as an appeasement to physician groups that would be unhappy about its failure to pass an SGR replacement, says Jeffrey Smith, senior director of federal affairs for CHIME, the College of Healthcare Information Management Executives.
“The appeasement, if in fact that was the motivation, was too little too late,” Smith says, adding Congress “caused a lot of unnecessary chaos.”
For instance, according to Modern Healthcare, executives at Catholic Health Initiatives had already invested millions of dollars updating software programs to handle the coding switch ahead of a new electronic health record system roll-out in 89 of its hospitals, which would not have been ready by the ICD-10 deadline.
“Anyone in the process has to circle the wagons again and reconsider their timelines,” Smith says. “The legislation has punished people trying to do the right thing.”
The transition to ICD-10 is a massive update to the 30-year-old ICD-9 codes, which no longer adequately reflect medical diagnoses, procedures, technology, and knowledge. There are five times more diagnosis codes and 21 times more procedural codes in ICD-10. It’s been on the table for at least a decade, and this was not the first delay.
In 2012, when fewer groups were on their way to compliance, CMS estimated that a one-year push-back of ICD-10 conversion could cost up to $306 million. With the latest delay, the American Health Information Management Association says CMS now estimates those costs between $1 billion and $6.6 billion.
However, according to the American Medical Association, which has actively lobbied to stop ICD-10 altogether, the costs of implementing ICD-10 range from $57,000 for small physician practices to as high as $8 million for large practices.
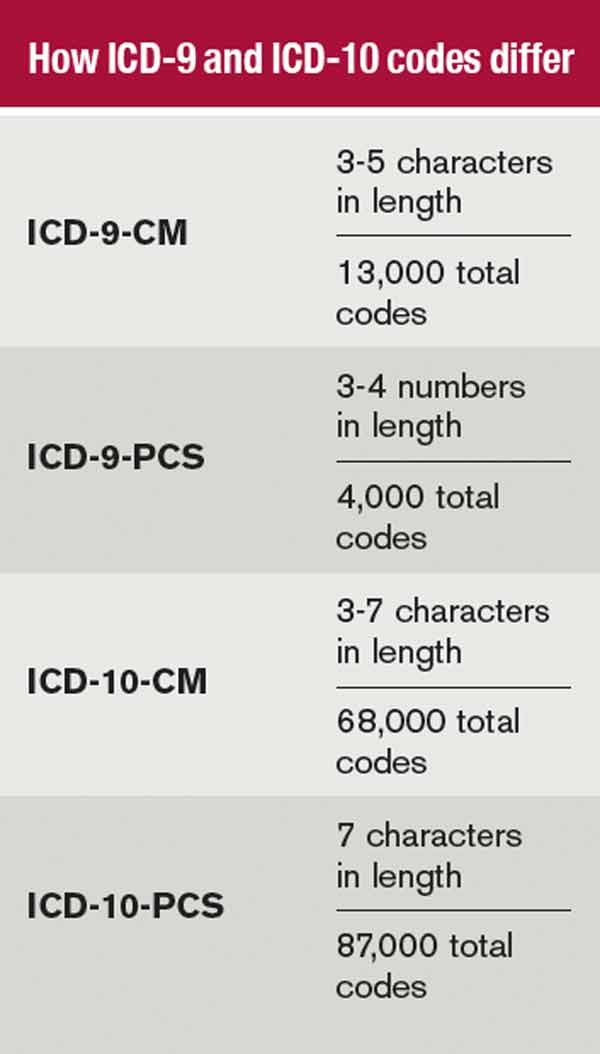
The increased number of codes, the increased number of characters per code, and the increased specificity require significant planning, training, software updates, and financial investments.
The Medical Group Management Association (MGMA) also pushed for ICD-10 delay, concerned that many groups would not be ready by Oct. 1. MGMA surveys showed as much, says Robert Tennant, senior policy advisor for MGMA.“We were concerned that if everyone has to flip the switch at the same time, there will be huge problems, as there were for healthcare.gov,” Tennant explains.
What MGMA would like to see is more thorough end-to-end testing and staggered roll-outs. Hospitals and health plans should be permitted to start using ICD-10 coding when they're ready, even if ahead of the next deadline, Tennant said. MGMA would also like to see a period of dual coding built in.
The ball is now in CMS' court.
“I think that CMS has within its power … the ability to embolden the industry to be more confident,” Smith says. “Even if it’s not going to require ICD-10 codes [by October 2014], hopefully they are still doing testing, still doing benchmarking, and by the time the deadline rolls around, it will touch every sector of the healthcare economy.”
Hospitalists, Smith says, should be more involved in the conversation going forward, to help maintain the momentum and preserve the investments made by their groups and institutions. Those not ready should push for compliance, rather than finding themselves in the same position a year from now.
Many of the hospital CIOs (chief information officers) he has talked to say that while they are stopping the car, they are keeping the engine running. Some will push for dual coding, even if only internally, because it’s proving to be a valuable tool in understanding their patient populations.
“It’s a frustrating time any time you have to kind of stop something with so much momentum, with hundreds of millions, if not billions, spent in advance of the conversion,” Smith says. “It does nothing to help care in this country to stay on ICD-9. Everybody understands those codes are completely exhausted, and the data we are getting out of it, while workable, is certainly not going to get us where we need to be in terms of transforming healthcare.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
On April 1, President Obama signed into law a bill that again delays a permanent fix of the sustainable growth rate formula, or SGR, the so-called “doc fix.” The bill also contained a surprise provision added by Congress to delay implementation of the switch from ICD-9 to ICD-10. The mandated conversion was supposed to take place by October 1 of this year; its delay will have a range of impacts on everyone from physicians to payers.
Hospitalists and others must weigh their options going forward, as many health systems and groups are already well on their way toward compliance with the 2014 deadline.
At this point, prevailing wisdom is that Congress added the delay as an appeasement to physician groups that would be unhappy about its failure to pass an SGR replacement, says Jeffrey Smith, senior director of federal affairs for CHIME, the College of Healthcare Information Management Executives.
“The appeasement, if in fact that was the motivation, was too little too late,” Smith says, adding Congress “caused a lot of unnecessary chaos.”
For instance, according to Modern Healthcare, executives at Catholic Health Initiatives had already invested millions of dollars updating software programs to handle the coding switch ahead of a new electronic health record system roll-out in 89 of its hospitals, which would not have been ready by the ICD-10 deadline.
“Anyone in the process has to circle the wagons again and reconsider their timelines,” Smith says. “The legislation has punished people trying to do the right thing.”
The transition to ICD-10 is a massive update to the 30-year-old ICD-9 codes, which no longer adequately reflect medical diagnoses, procedures, technology, and knowledge. There are five times more diagnosis codes and 21 times more procedural codes in ICD-10. It’s been on the table for at least a decade, and this was not the first delay.
In 2012, when fewer groups were on their way to compliance, CMS estimated that a one-year push-back of ICD-10 conversion could cost up to $306 million. With the latest delay, the American Health Information Management Association says CMS now estimates those costs between $1 billion and $6.6 billion.
However, according to the American Medical Association, which has actively lobbied to stop ICD-10 altogether, the costs of implementing ICD-10 range from $57,000 for small physician practices to as high as $8 million for large practices.
The increased number of codes, the increased number of characters per code, and the increased specificity require significant planning, training, software updates, and financial investments.
The Medical Group Management Association (MGMA) also pushed for ICD-10 delay, concerned that many groups would not be ready by Oct. 1. MGMA surveys showed as much, says Robert Tennant, senior policy advisor for MGMA.“We were concerned that if everyone has to flip the switch at the same time, there will be huge problems, as there were for healthcare.gov,” Tennant explains.
What MGMA would like to see is more thorough end-to-end testing and staggered roll-outs. Hospitals and health plans should be permitted to start using ICD-10 coding when they're ready, even if ahead of the next deadline, Tennant said. MGMA would also like to see a period of dual coding built in.
The ball is now in CMS' court.
“I think that CMS has within its power … the ability to embolden the industry to be more confident,” Smith says. “Even if it’s not going to require ICD-10 codes [by October 2014], hopefully they are still doing testing, still doing benchmarking, and by the time the deadline rolls around, it will touch every sector of the healthcare economy.”
Hospitalists, Smith says, should be more involved in the conversation going forward, to help maintain the momentum and preserve the investments made by their groups and institutions. Those not ready should push for compliance, rather than finding themselves in the same position a year from now.
Many of the hospital CIOs (chief information officers) he has talked to say that while they are stopping the car, they are keeping the engine running. Some will push for dual coding, even if only internally, because it’s proving to be a valuable tool in understanding their patient populations.
“It’s a frustrating time any time you have to kind of stop something with so much momentum, with hundreds of millions, if not billions, spent in advance of the conversion,” Smith says. “It does nothing to help care in this country to stay on ICD-9. Everybody understands those codes are completely exhausted, and the data we are getting out of it, while workable, is certainly not going to get us where we need to be in terms of transforming healthcare.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
On April 1, President Obama signed into law a bill that again delays a permanent fix of the sustainable growth rate formula, or SGR, the so-called “doc fix.” The bill also contained a surprise provision added by Congress to delay implementation of the switch from ICD-9 to ICD-10. The mandated conversion was supposed to take place by October 1 of this year; its delay will have a range of impacts on everyone from physicians to payers.
Hospitalists and others must weigh their options going forward, as many health systems and groups are already well on their way toward compliance with the 2014 deadline.
At this point, prevailing wisdom is that Congress added the delay as an appeasement to physician groups that would be unhappy about its failure to pass an SGR replacement, says Jeffrey Smith, senior director of federal affairs for CHIME, the College of Healthcare Information Management Executives.
“The appeasement, if in fact that was the motivation, was too little too late,” Smith says, adding Congress “caused a lot of unnecessary chaos.”
For instance, according to Modern Healthcare, executives at Catholic Health Initiatives had already invested millions of dollars updating software programs to handle the coding switch ahead of a new electronic health record system roll-out in 89 of its hospitals, which would not have been ready by the ICD-10 deadline.
“Anyone in the process has to circle the wagons again and reconsider their timelines,” Smith says. “The legislation has punished people trying to do the right thing.”
The transition to ICD-10 is a massive update to the 30-year-old ICD-9 codes, which no longer adequately reflect medical diagnoses, procedures, technology, and knowledge. There are five times more diagnosis codes and 21 times more procedural codes in ICD-10. It’s been on the table for at least a decade, and this was not the first delay.
In 2012, when fewer groups were on their way to compliance, CMS estimated that a one-year push-back of ICD-10 conversion could cost up to $306 million. With the latest delay, the American Health Information Management Association says CMS now estimates those costs between $1 billion and $6.6 billion.
However, according to the American Medical Association, which has actively lobbied to stop ICD-10 altogether, the costs of implementing ICD-10 range from $57,000 for small physician practices to as high as $8 million for large practices.
The increased number of codes, the increased number of characters per code, and the increased specificity require significant planning, training, software updates, and financial investments.
The Medical Group Management Association (MGMA) also pushed for ICD-10 delay, concerned that many groups would not be ready by Oct. 1. MGMA surveys showed as much, says Robert Tennant, senior policy advisor for MGMA.“We were concerned that if everyone has to flip the switch at the same time, there will be huge problems, as there were for healthcare.gov,” Tennant explains.
What MGMA would like to see is more thorough end-to-end testing and staggered roll-outs. Hospitals and health plans should be permitted to start using ICD-10 coding when they're ready, even if ahead of the next deadline, Tennant said. MGMA would also like to see a period of dual coding built in.
The ball is now in CMS' court.
“I think that CMS has within its power … the ability to embolden the industry to be more confident,” Smith says. “Even if it’s not going to require ICD-10 codes [by October 2014], hopefully they are still doing testing, still doing benchmarking, and by the time the deadline rolls around, it will touch every sector of the healthcare economy.”
Hospitalists, Smith says, should be more involved in the conversation going forward, to help maintain the momentum and preserve the investments made by their groups and institutions. Those not ready should push for compliance, rather than finding themselves in the same position a year from now.
Many of the hospital CIOs (chief information officers) he has talked to say that while they are stopping the car, they are keeping the engine running. Some will push for dual coding, even if only internally, because it’s proving to be a valuable tool in understanding their patient populations.
“It’s a frustrating time any time you have to kind of stop something with so much momentum, with hundreds of millions, if not billions, spent in advance of the conversion,” Smith says. “It does nothing to help care in this country to stay on ICD-9. Everybody understands those codes are completely exhausted, and the data we are getting out of it, while workable, is certainly not going to get us where we need to be in terms of transforming healthcare.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
Hospitals Lose $45.9 Billion in Uncompensated Care in 2012
Dollar value of uncompensated care provided by U.S. hospitals in 2012, expressed in terms of actual costs, according to data from the American Hospital Association’s Annual Survey of Hospitals.6 This figure represents 6.1% of total costs, an increase of 11.7% from 2011. The total includes both bad debt and charity care provided to patients unable to pay for their care, AHA says, but does not include underpayments by Medicare and Medicaid.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Dollar value of uncompensated care provided by U.S. hospitals in 2012, expressed in terms of actual costs, according to data from the American Hospital Association’s Annual Survey of Hospitals.6 This figure represents 6.1% of total costs, an increase of 11.7% from 2011. The total includes both bad debt and charity care provided to patients unable to pay for their care, AHA says, but does not include underpayments by Medicare and Medicaid.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Dollar value of uncompensated care provided by U.S. hospitals in 2012, expressed in terms of actual costs, according to data from the American Hospital Association’s Annual Survey of Hospitals.6 This figure represents 6.1% of total costs, an increase of 11.7% from 2011. The total includes both bad debt and charity care provided to patients unable to pay for their care, AHA says, but does not include underpayments by Medicare and Medicaid.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Health Information Technology Could Improve Hospital Discharge Planning

An RIV poster presented at SHM’s annual meeting describes the application of health information technology to improve the quality of hospital discharge summaries.4 Lead author Kristen Lewis, MD, in the clinical division of hospital medicine at The Ohio State University (OSU) Wexner Medical Center in Columbus, described how SHM’s 2009 “Transitions of Care Consensus Policy Statement” was adopted as the medical center’s standard of care—although at baseline this standard was being fully met at the hospital only 4% of the time.5 Discharge summaries frequently lacked important information, including tests pending at discharge, and were not made available to those clinicians who needed them following discharge.
“We developed, piloted, and implemented an innovative electronic discharge summary template that incorporated prompts and automatically populated core components of a quality discharge summary,” Dr. Lewis says, adding that the process also offered opportunities for customization and free-text entries. Initial experience following a series of multidisciplinary educational initiatives to help physicians and case managers understand these mechanisms found full compliance rising to 75%.
Next steps for the project include improving the availability of discharge data for primary care providers, specialist physicians, and extended care facilities not affiliated with OSU; inclusion of the discharge summary in the “After Visit Summary” given to patients; and assessment of outpatient providers’ satisfaction with the process.
For more information about the electronic discharge template, contact Dr. Lewis at kristen.lewis@osumc.edu.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
An RIV poster presented at SHM’s annual meeting describes the application of health information technology to improve the quality of hospital discharge summaries.4 Lead author Kristen Lewis, MD, in the clinical division of hospital medicine at The Ohio State University (OSU) Wexner Medical Center in Columbus, described how SHM’s 2009 “Transitions of Care Consensus Policy Statement” was adopted as the medical center’s standard of care—although at baseline this standard was being fully met at the hospital only 4% of the time.5 Discharge summaries frequently lacked important information, including tests pending at discharge, and were not made available to those clinicians who needed them following discharge.
“We developed, piloted, and implemented an innovative electronic discharge summary template that incorporated prompts and automatically populated core components of a quality discharge summary,” Dr. Lewis says, adding that the process also offered opportunities for customization and free-text entries. Initial experience following a series of multidisciplinary educational initiatives to help physicians and case managers understand these mechanisms found full compliance rising to 75%.
Next steps for the project include improving the availability of discharge data for primary care providers, specialist physicians, and extended care facilities not affiliated with OSU; inclusion of the discharge summary in the “After Visit Summary” given to patients; and assessment of outpatient providers’ satisfaction with the process.
For more information about the electronic discharge template, contact Dr. Lewis at kristen.lewis@osumc.edu.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
An RIV poster presented at SHM’s annual meeting describes the application of health information technology to improve the quality of hospital discharge summaries.4 Lead author Kristen Lewis, MD, in the clinical division of hospital medicine at The Ohio State University (OSU) Wexner Medical Center in Columbus, described how SHM’s 2009 “Transitions of Care Consensus Policy Statement” was adopted as the medical center’s standard of care—although at baseline this standard was being fully met at the hospital only 4% of the time.5 Discharge summaries frequently lacked important information, including tests pending at discharge, and were not made available to those clinicians who needed them following discharge.
“We developed, piloted, and implemented an innovative electronic discharge summary template that incorporated prompts and automatically populated core components of a quality discharge summary,” Dr. Lewis says, adding that the process also offered opportunities for customization and free-text entries. Initial experience following a series of multidisciplinary educational initiatives to help physicians and case managers understand these mechanisms found full compliance rising to 75%.
Next steps for the project include improving the availability of discharge data for primary care providers, specialist physicians, and extended care facilities not affiliated with OSU; inclusion of the discharge summary in the “After Visit Summary” given to patients; and assessment of outpatient providers’ satisfaction with the process.
For more information about the electronic discharge template, contact Dr. Lewis at kristen.lewis@osumc.edu.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Yogurt May Reduce Clostridium Difficile Infection Rate

The Philadelphia Inquirer recently reported that Holy Redeemer Hospital in Meadowbrook, Pa., cut its incidence of Clostridium difficile by two-thirds after its nutritionists began encouraging hospitalized patients with orders for antibiotics for more than one day to eat a widely available brand of yogurt.2 Seventy-five C. diff cases were reported in the hospital during 2011 and only 23 in 2012. The facility won an innovation award for the program from the Hospital and Healthsystem Association of Pennsylvania.
Other hospitals dispense probiotic dietary supplements, shown to have benefits against C. diff, in granular form. Medical experts have expressed skepticism that dispensing yogurt made the difference in cutting C. diff infections, arguing that there has not been enough research yet to support its widespread implementation in hospital settings.
Nationally, 337,000 cases of C. diff are reported in hospitals each year. A recent study reports that its spores are still commonly carried on the hands of healthcare workers who rubbed alcohol on their hands shortly after providing routine care to patients.3 Risk factors independently associated with hand contamination among healthcare workers in the exposed group included high-risk contacts and at least one contact without the use of gloves.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
The Philadelphia Inquirer recently reported that Holy Redeemer Hospital in Meadowbrook, Pa., cut its incidence of Clostridium difficile by two-thirds after its nutritionists began encouraging hospitalized patients with orders for antibiotics for more than one day to eat a widely available brand of yogurt.2 Seventy-five C. diff cases were reported in the hospital during 2011 and only 23 in 2012. The facility won an innovation award for the program from the Hospital and Healthsystem Association of Pennsylvania.
Other hospitals dispense probiotic dietary supplements, shown to have benefits against C. diff, in granular form. Medical experts have expressed skepticism that dispensing yogurt made the difference in cutting C. diff infections, arguing that there has not been enough research yet to support its widespread implementation in hospital settings.
Nationally, 337,000 cases of C. diff are reported in hospitals each year. A recent study reports that its spores are still commonly carried on the hands of healthcare workers who rubbed alcohol on their hands shortly after providing routine care to patients.3 Risk factors independently associated with hand contamination among healthcare workers in the exposed group included high-risk contacts and at least one contact without the use of gloves.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
The Philadelphia Inquirer recently reported that Holy Redeemer Hospital in Meadowbrook, Pa., cut its incidence of Clostridium difficile by two-thirds after its nutritionists began encouraging hospitalized patients with orders for antibiotics for more than one day to eat a widely available brand of yogurt.2 Seventy-five C. diff cases were reported in the hospital during 2011 and only 23 in 2012. The facility won an innovation award for the program from the Hospital and Healthsystem Association of Pennsylvania.
Other hospitals dispense probiotic dietary supplements, shown to have benefits against C. diff, in granular form. Medical experts have expressed skepticism that dispensing yogurt made the difference in cutting C. diff infections, arguing that there has not been enough research yet to support its widespread implementation in hospital settings.
Nationally, 337,000 cases of C. diff are reported in hospitals each year. A recent study reports that its spores are still commonly carried on the hands of healthcare workers who rubbed alcohol on their hands shortly after providing routine care to patients.3 Risk factors independently associated with hand contamination among healthcare workers in the exposed group included high-risk contacts and at least one contact without the use of gloves.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Home Hospice Providers Offer Best Practices for End-of-Life Care

New research from the Birmingham, Ala., Veterans Affairs Medical Center and the University of Alabama-Birmingham, published in the Journal of General Internal Medicine, finds that clinical techniques and care processes imported from home-based hospice professionals improved outcomes for hospitalized patients approaching the end of their lives.1
The project, conducted in six VA medical centers, employed a multi-modal strategy for improving end-of-life care processes, with staff training for all hospital providers in how to identify actively dying patients and then communicate this information to their families. Best clinical practices, supported by electronic order sets and paper-based educational materials, were implemented. Patients also were encouraged to eat what—and when—they wanted, to sit up in bed, and to receive family visitors at all hours.
“I started the project years ago, when I noticed that patients on hospice care at home often seemed more comfortable, while if I brought them into the hospital, they sometimes got worse,” says lead author F. Amos Bailey, MD. “We went out to the home to observe what the hospice nurses were doing and then came back to the hospital to write order sets to reflect that practice.”
Key quality endpoints included:
- Rates of orders for opioid pain medications;
- Anti-psychotic medications and scopolamine for death rattle;
- Completion of advance directives; and
- Consultations for palliative care and pastoral care.
Patients were more likely to have their pain relieved and symptoms addressed, according to chart reviews of 6,066 patients who died before or after the intervention was launched.
“All of the processes we measured moved in the direction of increased comfort,” Dr. Bailey says.
This is the first study to show that palliative care techniques developed in the home setting can have an impact on end-of-life care. That’s important, he adds, because most patients die in hospitals or nursing homes.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
New research from the Birmingham, Ala., Veterans Affairs Medical Center and the University of Alabama-Birmingham, published in the Journal of General Internal Medicine, finds that clinical techniques and care processes imported from home-based hospice professionals improved outcomes for hospitalized patients approaching the end of their lives.1
The project, conducted in six VA medical centers, employed a multi-modal strategy for improving end-of-life care processes, with staff training for all hospital providers in how to identify actively dying patients and then communicate this information to their families. Best clinical practices, supported by electronic order sets and paper-based educational materials, were implemented. Patients also were encouraged to eat what—and when—they wanted, to sit up in bed, and to receive family visitors at all hours.
“I started the project years ago, when I noticed that patients on hospice care at home often seemed more comfortable, while if I brought them into the hospital, they sometimes got worse,” says lead author F. Amos Bailey, MD. “We went out to the home to observe what the hospice nurses were doing and then came back to the hospital to write order sets to reflect that practice.”
Key quality endpoints included:
- Rates of orders for opioid pain medications;
- Anti-psychotic medications and scopolamine for death rattle;
- Completion of advance directives; and
- Consultations for palliative care and pastoral care.
Patients were more likely to have their pain relieved and symptoms addressed, according to chart reviews of 6,066 patients who died before or after the intervention was launched.
“All of the processes we measured moved in the direction of increased comfort,” Dr. Bailey says.
This is the first study to show that palliative care techniques developed in the home setting can have an impact on end-of-life care. That’s important, he adds, because most patients die in hospitals or nursing homes.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
New research from the Birmingham, Ala., Veterans Affairs Medical Center and the University of Alabama-Birmingham, published in the Journal of General Internal Medicine, finds that clinical techniques and care processes imported from home-based hospice professionals improved outcomes for hospitalized patients approaching the end of their lives.1
The project, conducted in six VA medical centers, employed a multi-modal strategy for improving end-of-life care processes, with staff training for all hospital providers in how to identify actively dying patients and then communicate this information to their families. Best clinical practices, supported by electronic order sets and paper-based educational materials, were implemented. Patients also were encouraged to eat what—and when—they wanted, to sit up in bed, and to receive family visitors at all hours.
“I started the project years ago, when I noticed that patients on hospice care at home often seemed more comfortable, while if I brought them into the hospital, they sometimes got worse,” says lead author F. Amos Bailey, MD. “We went out to the home to observe what the hospice nurses were doing and then came back to the hospital to write order sets to reflect that practice.”
Key quality endpoints included:
- Rates of orders for opioid pain medications;
- Anti-psychotic medications and scopolamine for death rattle;
- Completion of advance directives; and
- Consultations for palliative care and pastoral care.
Patients were more likely to have their pain relieved and symptoms addressed, according to chart reviews of 6,066 patients who died before or after the intervention was launched.
“All of the processes we measured moved in the direction of increased comfort,” Dr. Bailey says.
This is the first study to show that palliative care techniques developed in the home setting can have an impact on end-of-life care. That’s important, he adds, because most patients die in hospitals or nursing homes.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Klaus Suehler, MD, FHM, Is Rooted in Hospital Medicine
Klaus Suehler, MD, FHM, grew up in Germany and studied in Munich but dreamed of one day becoming the next Marcus Welby, MD. So he trained in Minnesota and has now worked for the same physician group for nearly two decades.
“Like many of us, I had some romantic ideas of being a doctor, running around with my black bag, figuring out a patient’s diagnosis that everyone else had missed,” says Dr. Suehler, one of the newest members of Team Hospitalist, the volunteer editorial advisory group for The Hospitalist. “As I was more seriously contemplating medicine, hospital medicine [presented] an intellectual challenge, the opportunity of applying science outside of a lab, and to be of service and to develop relationships with one’s patients.”
Dr. Suehler says internal medicine appealed to him because it was, and still is, “somewhat of an art” and affords him professional freedom. In 1994, straight out of residency, he joined Midwest Internal Medicine in Coon Rapids, Minn., an internal medicine group that, at the time, was breaking ground by dedicating physicians to hospital-based positions.
“The time was right. … Being at the hospital was kind of a continuation of residency anyhow. Some of my friends at my teaching hospital were starting a hospitalist service as well, and the whole concept appealed to me,” he says. “After juggling outpatient clinic and my weeks at the hospital for about five to six years, I finally became a full-time hospitalist.”
Since 2000, he has worked only as a hospitalist with Midwest Internal Medicine, serving as the hospitalist group’s leader for eight of those years.
Question: What do you like most about working as a hospitalist?
Answer: I like the challenging cases and the opportunity to collaborate with other specialists and the staff on the wards. We always learn from each other within our hospitalist group, as we are taking care of each other’s patients. There is ample opportunity to informally discuss complex patients and their treatment.
Q: What do you dislike most?
A: Overly busy call nights. I must say, though, at least at our hospital we have the opportunity to close our service for admissions, if we feel the workload would no longer be safe.
Q: What’s the best advice you ever received?
A: There was no single advice that I can recall related to my HM practice. What really helped very much was the ongoing input and advice that I received through formal leadership training, which I received during the time as the leader of our group. It helped me to be more grounded, resilient, and effective, both as a professional and a person.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The field has essentially become its own specialty. There is an increased focus on the operational part of taking care of patients in the hospital, as well as the transitions, which goes beyond the medical aspects of patient care for, let’s say, patients presenting with congestive heart failure.
Q: Why is it important for group leaders to continue seeing patients?
A: It adds credibility to their leadership. There is nothing like shouldering new responsibilities or high workloads together with your partners.
Q: Outside of patient care, what about your job interests you the most?
A: Quality and patient safety are of great interest for me. Our hospitalist group consists of about 25 hospitalists, but there are about 200 hospitalists within our health system. I participate in a steering committee within the larger system to improve medication reconciliation.
I also continue to be interested in leadership. Especially in the years to come, with all the upcoming changes in the delivery of care, performance measures, and modes of reimbursement, there will be an increased need for physician leaders.
Q: What is your biggest professional challenge?
A: It is a good sign that I have to think for a while to come up with an answer. It probably is taking care of patients with narcotic addictions or difficult personalities. Every given week there are probably one or two such patients on the service. It is challenging to do these patients justice and to provide the appropriate medical care.
Q: What is your biggest professional reward?
A: The respect of my physician colleagues, the nursing staff, and the gratitude of my patients and their families. One of my most moving experiences was when a former patient of mine walked over to my table in a Chinese restaurant and said: “Thank you for saving my life!”
Q: You were one of the first hospitalists designated Fellow in Hospital Medicine. What does that mean to you?
A: It gave me some formal recognition for the years of service I have put into HM, both in patient care and leadership, as well as for my level of experience.
Q: When you aren’t working, what is important to you?
A: The relationships with the people around me (marriage, family, friendship). In terms of what I do, it is traveling, exercising, reading, and being appreciative of the moment.
Q: Where do you see yourself in 10 years?
A: I want to continue to work as a hospitalist. I am looking into leadership opportunities. I can see shifting my focus more toward leadership or consulting roles again within the next 10 years.
Q: If you weren’t a doctor, what would you be doing right now?
A: I think I would be a lawyer. I know there is a perceived friction between these professions, but there are some common themes, such as providing expert advice or professional help in times of need.
Q: What’s the best book you’ve read recently?
A: The Angel’s Game by Carlos Ruiz Zafon. It is an incredibly captivating story, with a marvelous imagery of old Barcelona before the Spanish Civil War.
Q: How many Apple products do you interface with in a given week?
A: Two: iPhone and iPad.
Richard Quinn is a freelance writer in New Jersey.
Klaus Suehler, MD, FHM, grew up in Germany and studied in Munich but dreamed of one day becoming the next Marcus Welby, MD. So he trained in Minnesota and has now worked for the same physician group for nearly two decades.
“Like many of us, I had some romantic ideas of being a doctor, running around with my black bag, figuring out a patient’s diagnosis that everyone else had missed,” says Dr. Suehler, one of the newest members of Team Hospitalist, the volunteer editorial advisory group for The Hospitalist. “As I was more seriously contemplating medicine, hospital medicine [presented] an intellectual challenge, the opportunity of applying science outside of a lab, and to be of service and to develop relationships with one’s patients.”
Dr. Suehler says internal medicine appealed to him because it was, and still is, “somewhat of an art” and affords him professional freedom. In 1994, straight out of residency, he joined Midwest Internal Medicine in Coon Rapids, Minn., an internal medicine group that, at the time, was breaking ground by dedicating physicians to hospital-based positions.
“The time was right. … Being at the hospital was kind of a continuation of residency anyhow. Some of my friends at my teaching hospital were starting a hospitalist service as well, and the whole concept appealed to me,” he says. “After juggling outpatient clinic and my weeks at the hospital for about five to six years, I finally became a full-time hospitalist.”
Since 2000, he has worked only as a hospitalist with Midwest Internal Medicine, serving as the hospitalist group’s leader for eight of those years.
Question: What do you like most about working as a hospitalist?
Answer: I like the challenging cases and the opportunity to collaborate with other specialists and the staff on the wards. We always learn from each other within our hospitalist group, as we are taking care of each other’s patients. There is ample opportunity to informally discuss complex patients and their treatment.
Q: What do you dislike most?
A: Overly busy call nights. I must say, though, at least at our hospital we have the opportunity to close our service for admissions, if we feel the workload would no longer be safe.
Q: What’s the best advice you ever received?
A: There was no single advice that I can recall related to my HM practice. What really helped very much was the ongoing input and advice that I received through formal leadership training, which I received during the time as the leader of our group. It helped me to be more grounded, resilient, and effective, both as a professional and a person.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The field has essentially become its own specialty. There is an increased focus on the operational part of taking care of patients in the hospital, as well as the transitions, which goes beyond the medical aspects of patient care for, let’s say, patients presenting with congestive heart failure.
Q: Why is it important for group leaders to continue seeing patients?
A: It adds credibility to their leadership. There is nothing like shouldering new responsibilities or high workloads together with your partners.
Q: Outside of patient care, what about your job interests you the most?
A: Quality and patient safety are of great interest for me. Our hospitalist group consists of about 25 hospitalists, but there are about 200 hospitalists within our health system. I participate in a steering committee within the larger system to improve medication reconciliation.
I also continue to be interested in leadership. Especially in the years to come, with all the upcoming changes in the delivery of care, performance measures, and modes of reimbursement, there will be an increased need for physician leaders.
Q: What is your biggest professional challenge?
A: It is a good sign that I have to think for a while to come up with an answer. It probably is taking care of patients with narcotic addictions or difficult personalities. Every given week there are probably one or two such patients on the service. It is challenging to do these patients justice and to provide the appropriate medical care.
Q: What is your biggest professional reward?
A: The respect of my physician colleagues, the nursing staff, and the gratitude of my patients and their families. One of my most moving experiences was when a former patient of mine walked over to my table in a Chinese restaurant and said: “Thank you for saving my life!”
Q: You were one of the first hospitalists designated Fellow in Hospital Medicine. What does that mean to you?
A: It gave me some formal recognition for the years of service I have put into HM, both in patient care and leadership, as well as for my level of experience.
Q: When you aren’t working, what is important to you?
A: The relationships with the people around me (marriage, family, friendship). In terms of what I do, it is traveling, exercising, reading, and being appreciative of the moment.
Q: Where do you see yourself in 10 years?
A: I want to continue to work as a hospitalist. I am looking into leadership opportunities. I can see shifting my focus more toward leadership or consulting roles again within the next 10 years.
Q: If you weren’t a doctor, what would you be doing right now?
A: I think I would be a lawyer. I know there is a perceived friction between these professions, but there are some common themes, such as providing expert advice or professional help in times of need.
Q: What’s the best book you’ve read recently?
A: The Angel’s Game by Carlos Ruiz Zafon. It is an incredibly captivating story, with a marvelous imagery of old Barcelona before the Spanish Civil War.
Q: How many Apple products do you interface with in a given week?
A: Two: iPhone and iPad.
Richard Quinn is a freelance writer in New Jersey.
Klaus Suehler, MD, FHM, grew up in Germany and studied in Munich but dreamed of one day becoming the next Marcus Welby, MD. So he trained in Minnesota and has now worked for the same physician group for nearly two decades.
“Like many of us, I had some romantic ideas of being a doctor, running around with my black bag, figuring out a patient’s diagnosis that everyone else had missed,” says Dr. Suehler, one of the newest members of Team Hospitalist, the volunteer editorial advisory group for The Hospitalist. “As I was more seriously contemplating medicine, hospital medicine [presented] an intellectual challenge, the opportunity of applying science outside of a lab, and to be of service and to develop relationships with one’s patients.”
Dr. Suehler says internal medicine appealed to him because it was, and still is, “somewhat of an art” and affords him professional freedom. In 1994, straight out of residency, he joined Midwest Internal Medicine in Coon Rapids, Minn., an internal medicine group that, at the time, was breaking ground by dedicating physicians to hospital-based positions.
“The time was right. … Being at the hospital was kind of a continuation of residency anyhow. Some of my friends at my teaching hospital were starting a hospitalist service as well, and the whole concept appealed to me,” he says. “After juggling outpatient clinic and my weeks at the hospital for about five to six years, I finally became a full-time hospitalist.”
Since 2000, he has worked only as a hospitalist with Midwest Internal Medicine, serving as the hospitalist group’s leader for eight of those years.
Question: What do you like most about working as a hospitalist?
Answer: I like the challenging cases and the opportunity to collaborate with other specialists and the staff on the wards. We always learn from each other within our hospitalist group, as we are taking care of each other’s patients. There is ample opportunity to informally discuss complex patients and their treatment.
Q: What do you dislike most?
A: Overly busy call nights. I must say, though, at least at our hospital we have the opportunity to close our service for admissions, if we feel the workload would no longer be safe.
Q: What’s the best advice you ever received?
A: There was no single advice that I can recall related to my HM practice. What really helped very much was the ongoing input and advice that I received through formal leadership training, which I received during the time as the leader of our group. It helped me to be more grounded, resilient, and effective, both as a professional and a person.
Q: What’s the biggest change you’ve seen in HM in your career?
A: The field has essentially become its own specialty. There is an increased focus on the operational part of taking care of patients in the hospital, as well as the transitions, which goes beyond the medical aspects of patient care for, let’s say, patients presenting with congestive heart failure.
Q: Why is it important for group leaders to continue seeing patients?
A: It adds credibility to their leadership. There is nothing like shouldering new responsibilities or high workloads together with your partners.
Q: Outside of patient care, what about your job interests you the most?
A: Quality and patient safety are of great interest for me. Our hospitalist group consists of about 25 hospitalists, but there are about 200 hospitalists within our health system. I participate in a steering committee within the larger system to improve medication reconciliation.
I also continue to be interested in leadership. Especially in the years to come, with all the upcoming changes in the delivery of care, performance measures, and modes of reimbursement, there will be an increased need for physician leaders.
Q: What is your biggest professional challenge?
A: It is a good sign that I have to think for a while to come up with an answer. It probably is taking care of patients with narcotic addictions or difficult personalities. Every given week there are probably one or two such patients on the service. It is challenging to do these patients justice and to provide the appropriate medical care.
Q: What is your biggest professional reward?
A: The respect of my physician colleagues, the nursing staff, and the gratitude of my patients and their families. One of my most moving experiences was when a former patient of mine walked over to my table in a Chinese restaurant and said: “Thank you for saving my life!”
Q: You were one of the first hospitalists designated Fellow in Hospital Medicine. What does that mean to you?
A: It gave me some formal recognition for the years of service I have put into HM, both in patient care and leadership, as well as for my level of experience.
Q: When you aren’t working, what is important to you?
A: The relationships with the people around me (marriage, family, friendship). In terms of what I do, it is traveling, exercising, reading, and being appreciative of the moment.
Q: Where do you see yourself in 10 years?
A: I want to continue to work as a hospitalist. I am looking into leadership opportunities. I can see shifting my focus more toward leadership or consulting roles again within the next 10 years.
Q: If you weren’t a doctor, what would you be doing right now?
A: I think I would be a lawyer. I know there is a perceived friction between these professions, but there are some common themes, such as providing expert advice or professional help in times of need.
Q: What’s the best book you’ve read recently?
A: The Angel’s Game by Carlos Ruiz Zafon. It is an incredibly captivating story, with a marvelous imagery of old Barcelona before the Spanish Civil War.
Q: How many Apple products do you interface with in a given week?
A: Two: iPhone and iPad.
Richard Quinn is a freelance writer in New Jersey.
When Should You Suspect Kawasaki Disease as the Cause of Fever in an Infant?
Case
A seven-week-old Hispanic female with a history of prematurity (born at 35 weeks by C-section) presents to the ED with four days of fever as high as 102°F and new-onset cyanotic spells. Cultures of blood, urine, and cerebrospinal fluid obtained 48 hours prior to admission were negative, but she continued to have intermittent fevers and developed a macular, non-pruritic rash on her hands and feet, with associated non-bilious emesis. One day prior to admission, she began to have episodes of apnea, with color change and cyanosis of her lips and eyelids. In the ED, her vital signs include a rectal temperature of 38.4°C, heart rate of 178/min, respiratory rate of 27/min, and blood pressure of 79/66. Examination reveals a non-toxic-appearing infant, with no conjunctival or oropharyngeal abnormalities, unremarkable heart and lung exam, and a blanching, erythematous macular rash on her hands, lower legs, and feet.
When should you suspect Kawasaki disease (KD) as the cause of fever in an infant?
Background
KD is an acute systemic vasculitis of unknown etiology that occurs in children. Affecting the small- and medium-sized arteries, with a striking predilection for coronary arteries, it is the leading cause of acquired pediatric heart disease in Japan and the U.S.1 Occurring predominantly in children younger than five years, KD has been diagnosed in infants and in young adults.2 The incidence of KD is lowest among white children and highest among Asians and Pacific Islanders, with the highest incidence in children of Japanese descent.
A recent epidemiologic study performed in Taiwan showed an incidence of 69 cases per 100,000 per year among children younger than five years, with a male/female ratio of 1.62:1.3 The peak of mortality occurs 15-45 days after onset of fever, although sudden cardiac death may occur many years later. Recurrence rate is approximately 3%. In the U.S., the estimated incidence ranges from nine to 18 per 100,000 children younger than five years per year.4
Review of Data
Because there is no specific diagnostic test or pathognomonic clinical feature, clinical diagnostic criteria have been established to guide physicians. KD diagnosis traditionally requires fever for at least five days and the presence of at least four of the following five principal features:
- bilateral conjunctival injection;
- changes in the mucous membranes of the upper respiratory tract (injected pharynx, infected, fissured lips, strawberry tongue);
- polymorphous rash;
- changes of the extremities (peripheral edema, erythema, periungual desquamation); and
- cervical lymphadenopathy.5
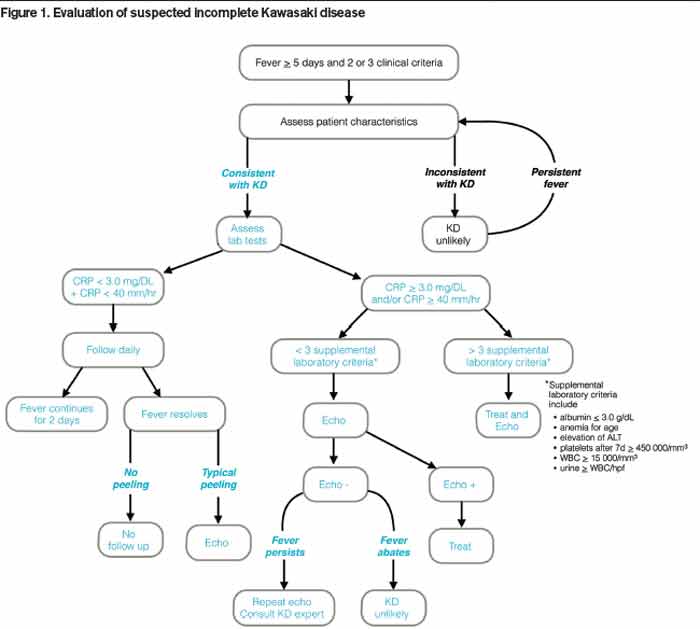
The fever, which is remittent, typically peaks at 39ºC to 40ºC. The mean duration of untreated fever is 11 days; with prompt treatment, fever typically subsides in two days. Bilateral painless non-exudative conjunctival injection begins shortly after onset of fever, involves typically bulbar conjunctiva, and is not associated with edema.
Erythematous rash usually appears within five days of onset of fever and is often a diffuse, nonspecific maculopapular eruption that is commonly pronounced in the perineal region. The appearance might be urticarial, micropustular, or erythema multiforme-like. Changes in extremities include erythema of palms and soles and tender induration of the hands and feet. Subsequently, desquamation begins in the periungual area within two to three weeks after the onset of fever. Typically, peeling begins around the nail folds of fingers, followed by the toes. The least common of the principal clinical features is tender unilateral anterior cervical lymphadenopathy (1.5 cm or greater in diameter).
When a patient presents with a history, examination, and laboratory findings consistent with KD without meeting the typical diagnostic standard, incomplete KD should be considered. The term “incomplete” is favored over “atypical” for this pre-sentation, because these patients are otherwise similar to other patients with KD. Patients with fever for five or fewer days and fewer than four principal features can be diagnosed as having KD when coronary artery disease is detected by two-dimensional echocardiography or coronary angiography (see Figure 1, p. 10). In the presence of four or more principal criteria, KD can be diagnosed before day four of the illness by an experienced clinician.6 Features less consistent with KD include the presence of exudative conjunctivitis, exudative pharyngitis, discrete intraoral lesions, bullous or vesicular rash, or generalized adenopathy.
If clinical features are consistent with KD, further risk stratification with erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) will determine whether patients are followed daily (if low) or if supplementary laboratory tests should be done (see Figure 1, p. 10). If three or more of supplementary laboratory criteria are present (albumin ≤3.0 g/dL, anemia for age, elevation of alanine aminotransferase (ALT), platelet count after seven days is 450 000/mm3 or greater, white blood cell count is 15,000/mm3 or greater, and urinary sediment containing 10 white blood cells/high-power field or more), echocardiogram should be performed and treatment initiated if abnormal.6
Young infants are more likely to manifest an incomplete presentation of KD, with a polymorphous rash being the most common symptom other than fever in this age group.7 Acute phase symptoms were also more likely to progress rapidly in this age group, with a higher risk of developing cardiac sequelae.8 As a result, any infant under the age of six months with fever for more than seven days and no other clear etiology should be evaluated for KD even in the absence of other diagnostic criteria.9
Other clinical manifestations of KD may include:
- Irritability: more notable in KD than in other febrile illnesses;
- Arthralgia and arthritis: may occur in the first week;
- Gastrointestinal complaints and findings: hepatomegaly, jaundice; and
- Abnormal chest X-ray findings: may be present in as many as 15% of patients.

Cardiovascular manifestations can be prominent in the acute phase of KD and are the leading cause of long-term morbidity and mortality. Coronary artery aneurysms occur in 20% of affected children with KD. Other cardiovascular complications include myocardial ischemia and ensuing depressed contractility and arrhythmias, as well as vascular obstruction in peripheral arteries.
A subset of KD patients develops hemodynamic instability requiring management in a critical care setting. This phenomenon has been named Kawasaki disease shock syndrome, where hemodynamic instability is not related to administration of intravenous immunoglobulin (IVIG). Patients are more likely to be female, to have laboratory findings consistent with greater inflammation, and to have impaired systolic and diastolic function. They also exhibit resistance to IVIG more often and have higher rates of coronary artery dilation and aneurysm formation.10
Differential diagnoses for KD may include viral infections, scarlet fever, staphylococcal scalded skin syndrome, toxic shock syndrome, Rocky Mountain spotted fever, cervical lymphadenitis, drug hypersensitivity, Stevens-Johnson syndrome, systemic idiopathic arthritis, leptospirosis, and mercury hypersensitivity reaction.11
Work-Up
Laboratory evaluation of a patient with suspected KD should include:
- Complete blood count (CBC) with differential: leukocytosis, anemia, thrombocytosis that peaks in the third week is characteristic. A manual differential may reveal an increase in band forms.
- Acute phase reactants: If C-reactive protein (CRP) is 3 mg/dL or greater and erythrocyte sedimentation rate (ESR) is 40 mm/hr or greater, supplementary laboratory work-up should be done. Make sure not to cloud classic with incomplete KD; the stepwise lab evaluation only pertains to the latter.
- Liver panel: Elevated ALT and gamma-glutamyl transferase (GGT), mild hyperbilirubinemia, or hypoalbuminemia may be present.
- Urinalysis: Sterile pyuria may be present; if present, it may be of urethral origin, and catheterized samples could miss this finding.12
Lack of elevated inflammatory markers (CRP is less than 3 mg/dl and ESR is less than 40 mm/hr) and the presence of two or three principal clinical features warrant ongoing daily monitoring of ESR, CRP, and fever until day seven of illness. If the fever resolves but is followed by peeling of extremities, an echocardiogram should be done. Lumbar puncture might help differentiate from CNS infectious etiologies, but about 50% of KD patients have a cerebrospinal fluid pleocytosis.
Echocardiography is the preferred imaging modality for the initial cardiovascular evaluation and follow-up.1 It has a sensitivity of 100% and specificity of 96% for the detection of proximal coronary aneurysms.13 Coronary aneurysms are clinically silent in most cases and can manifest with delayed complications, such as myocardial infarction or sudden death. Imaging plays an important role in the early diagnosis of these aneurysms and in estimating their number, size, and location, important elements in making a therapeutic decision.14
Although the echocardiography should be done as soon as KD is suspected, definitive treatment must not be delayed. Evaluation of all coronary artery segments, as well as cardiac contractility and presence of effusion, should be noted on echocardiography. In the absence of complications, echocardiography is performed at the time of diagnosis and at two weeks and six to eight weeks after disease onset.11
Treatment
Treatment goals for Kawasaki disease in the acute phase are reduction of systemic and coronary arterial inflammation and prevention of coronary thrombosis. The long-term therapy in individuals who develop coronary aneurysms is aimed at preventing myocardial ischemia or infarction.6 The current standard of care for the treatment of children in the U.S. is anti-inflammatory therapy with:
- immunoglobulin (IVIG) in a single 2 g/kg/dose infused over 10–12 hours, accompanied by;
- high-dose aspirin (80–100 mg/kg/day orally in four divided doses).6,15
IVIG administration within 10 days of the onset of fever results in more favorable outcomes. Live virus vaccines should be delayed to 11 months after administration of IVIG. Both aspirin and IVIG have anti-inflammatory effects. This regimen applies to patients without abnormalities on initial echocardiography. High-dose aspirin typically is continued for 48-72 hours after the child becomes afebrile. Thereafter, low-dose aspirin (3-5 mg/kg/day) is prescribed until patient shows no evidence of coronary changes, typically by six to eight weeks after onset of illness. Children with coronary abnormalities should continue aspirin indefinitely.
Approximately 10% of patients are IVIG-resistant and have persistent or recurrent fever for at least 36 hours after completion of the infusion. The current recommendation is to re-treat with IVIG at the same dose. If the patient has fever 36 hours after the second dose of IVIG, this is considered true treatment failure.
Other possible treatments for KD refractory to IVIG include IV methylprednisolone (30 mg/kg over two to three hours daily for three days) or infliximab.16 Even with prompt treatment, 5% of children who have KD develop coronary artery dilation, and 1% develop giant aneurysms.
Back to the Case
Initial laboratory evaluation revealed white blood cell count of 19.0×103 cells/mm3, hemoglobin of 8.9 gm/dL, CRP of 17.9 mg/dL, and ESR of 73 mm/hr. Because of persistent fevers for 48 hours after admission in the absence of another cause to explain the illness, the KD service was consulted. Echocardiography revealed dilatation of the left main (z-score 4.23) and proximal right (z-score 2.59), confirming the diagnosis of KD. Ejection fraction was read as qualitatively normal.
The infant received infliximab and IVIG, as well as high-dose aspirin, clopidogrel, and propranolol. This treatment regimen was directed by a KD expert and was more aggressive than typical therapy due to the severity of presentation. She received blood transfusions for worsening symptomatic anemia (hemoglobin 7.0 gm/dL) with hypoxia.
Following her IVIG infusion, she remained afebrile with progressive reduction in her CRP. She was discharged on hospital day seven on aspirin until her next follow-up, with propranolol for three days to limit potential tachycardia. At her three-week follow-up visit, her ESR had improved to 8 mm/hr. Her echocardiogram revealed a normal ejection fraction. Echocardiography revealed resolution of all abnormalities except for a borderline prominence of the right coronary artery (z-score 2.11). At this time it was recommended that her aspirin be discontinued.
She continues to be followed by the KD service as an outpatient and has done well without cardiovascular symptoms four months after her diagnosis.
Bottom Line
KD can manifest an incomplete presentation, especially in infants under the age of six months. Clinicians should maintain a high level of suspicion for KD in young infants with unexplained fevers lasting more than seven days.
Dr. Gurevich-Panigrahi is a fellow in pediatric hospital medicine at Cleveland Clinic Children’s Hospital. Dr. Kanegaye is a clinical professor of pediatrics at the University of California San Diego (UCSD) School of Medicine and attending physician in the emergency care center at Rady Children’s Hospital San Diego. Dr. Chang is associate clinical professor of pediatrics and medicine at UCSD School of Medicine, a pediatric hospitalist at Rady Children’s, and pediatric editor of The Hospitalist.
References
- Hendaoui L, Stanson AW, Habib Bouhaouala M, Joffre F, eds. Systemic Vasculitis: Imaging Features. New York: Springer; 2012.
- Manlhiot C, Yeung RS, Clarizia NA, Chahal N, McCrindle BW. Kawasaki disease at the extremes of the age spectrum. Pediatrics. 2009;124(3):e410-e415.
- Huang WC, Huang LM, Chang IS, et al. Epidemiologic features of Kawasaki disease in Taiwan, 2003-2006. Pediatrics. 2009;123(3):e401-405.
- Holman RC, Belay ED, Christensen KY, Folkema AM, Steiner CA, Schonberger LB. Hospitalizations for Kawasaki syndrome among children in the United States, 1997-2007. Pediatr Infect Dis J. 2010;29(6):483-438.
- Council on Cardiovascular Disease in the Young, Committee on Rheumatic Fever Endocarditis, Kawasaki Disease, American Heart Association. Diagnostic guidelines for Kawasaki disease. Circulation. 2001;103:335-336.
- Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110(17):2747-2771.
- Shiozawa Y, Inuzuka R, Harita Y, Kagawa J. Age-related differences in the course of the acute phase symptoms of Kawasaki disease. Pediatr Infect Dis J. 2013;32(9):e365-369.
- Genizi J, Miron D, Spiegel R, Fink D, Horowitz Y. Kawasaki disease in very young infants: high prevalence of atypical presentation and coronary arteritis. Clin Pediatr (Phila.). 2003;42(3):263-267.
- Sundel R. Incomplete (atypical) Kawasaki disease. UpToDate. Available at: http://www.uptodate.com/contents/incomplete-atypical-kawasaki-disease. Accessed June 9, 2014.
- Kanegaye JT, Wilder MS, Molkara D, et al. Recognition of a Kawasaki disease shock syndrome. Pediatrics. 2009;123(5):e783-e789.
- Fimbres AM, Shulman ST. Kawasaki disease. Pediatr Rev. 2008;29(9):308-315.
- Shike H, Kanegaye JT, Best BM, Pancheri J, Burns JC. Pyuria associated with acute Kawasaki disease and fever from other causes. Pediatr Infect Dis J. 2009;28(5):440-443.
- Capannari TE, Daniels SR, Meyer RA, Schwartz DC, Kaplan S. Sensitivity, specificity and predictive value of two-dimensional echocardiography in detecting coronary artery aneurysms in patients with Kawasaki disease. J Am Coll Cardiol. 1986;7(2):355-360.
- Mavrogeni S, Papadopoulos G, Karanasios E, Cokkinos DV. How to image Kawasaki disease: a validation of different imaging techniques. Int J Cardiol. 2008;124(1):27-31.
- Burns JC, Glodé MP. Kawasaki syndrome. Lancet. 2004;364(9433):533-544.
- Ghelani SJ, Pastor W, Parikh K. Demographic and treatment variability of refractory Kawasaki Disease: a multicenter analysis from 2005 to 2009. Hosp Pediatr. 2012;2(2):71-76.
Case
A seven-week-old Hispanic female with a history of prematurity (born at 35 weeks by C-section) presents to the ED with four days of fever as high as 102°F and new-onset cyanotic spells. Cultures of blood, urine, and cerebrospinal fluid obtained 48 hours prior to admission were negative, but she continued to have intermittent fevers and developed a macular, non-pruritic rash on her hands and feet, with associated non-bilious emesis. One day prior to admission, she began to have episodes of apnea, with color change and cyanosis of her lips and eyelids. In the ED, her vital signs include a rectal temperature of 38.4°C, heart rate of 178/min, respiratory rate of 27/min, and blood pressure of 79/66. Examination reveals a non-toxic-appearing infant, with no conjunctival or oropharyngeal abnormalities, unremarkable heart and lung exam, and a blanching, erythematous macular rash on her hands, lower legs, and feet.
When should you suspect Kawasaki disease (KD) as the cause of fever in an infant?
Background
KD is an acute systemic vasculitis of unknown etiology that occurs in children. Affecting the small- and medium-sized arteries, with a striking predilection for coronary arteries, it is the leading cause of acquired pediatric heart disease in Japan and the U.S.1 Occurring predominantly in children younger than five years, KD has been diagnosed in infants and in young adults.2 The incidence of KD is lowest among white children and highest among Asians and Pacific Islanders, with the highest incidence in children of Japanese descent.
A recent epidemiologic study performed in Taiwan showed an incidence of 69 cases per 100,000 per year among children younger than five years, with a male/female ratio of 1.62:1.3 The peak of mortality occurs 15-45 days after onset of fever, although sudden cardiac death may occur many years later. Recurrence rate is approximately 3%. In the U.S., the estimated incidence ranges from nine to 18 per 100,000 children younger than five years per year.4
Review of Data
Because there is no specific diagnostic test or pathognomonic clinical feature, clinical diagnostic criteria have been established to guide physicians. KD diagnosis traditionally requires fever for at least five days and the presence of at least four of the following five principal features:
- bilateral conjunctival injection;
- changes in the mucous membranes of the upper respiratory tract (injected pharynx, infected, fissured lips, strawberry tongue);
- polymorphous rash;
- changes of the extremities (peripheral edema, erythema, periungual desquamation); and
- cervical lymphadenopathy.5
The fever, which is remittent, typically peaks at 39ºC to 40ºC. The mean duration of untreated fever is 11 days; with prompt treatment, fever typically subsides in two days. Bilateral painless non-exudative conjunctival injection begins shortly after onset of fever, involves typically bulbar conjunctiva, and is not associated with edema.
Erythematous rash usually appears within five days of onset of fever and is often a diffuse, nonspecific maculopapular eruption that is commonly pronounced in the perineal region. The appearance might be urticarial, micropustular, or erythema multiforme-like. Changes in extremities include erythema of palms and soles and tender induration of the hands and feet. Subsequently, desquamation begins in the periungual area within two to three weeks after the onset of fever. Typically, peeling begins around the nail folds of fingers, followed by the toes. The least common of the principal clinical features is tender unilateral anterior cervical lymphadenopathy (1.5 cm or greater in diameter).
When a patient presents with a history, examination, and laboratory findings consistent with KD without meeting the typical diagnostic standard, incomplete KD should be considered. The term “incomplete” is favored over “atypical” for this pre-sentation, because these patients are otherwise similar to other patients with KD. Patients with fever for five or fewer days and fewer than four principal features can be diagnosed as having KD when coronary artery disease is detected by two-dimensional echocardiography or coronary angiography (see Figure 1, p. 10). In the presence of four or more principal criteria, KD can be diagnosed before day four of the illness by an experienced clinician.6 Features less consistent with KD include the presence of exudative conjunctivitis, exudative pharyngitis, discrete intraoral lesions, bullous or vesicular rash, or generalized adenopathy.
If clinical features are consistent with KD, further risk stratification with erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) will determine whether patients are followed daily (if low) or if supplementary laboratory tests should be done (see Figure 1, p. 10). If three or more of supplementary laboratory criteria are present (albumin ≤3.0 g/dL, anemia for age, elevation of alanine aminotransferase (ALT), platelet count after seven days is 450 000/mm3 or greater, white blood cell count is 15,000/mm3 or greater, and urinary sediment containing 10 white blood cells/high-power field or more), echocardiogram should be performed and treatment initiated if abnormal.6
Young infants are more likely to manifest an incomplete presentation of KD, with a polymorphous rash being the most common symptom other than fever in this age group.7 Acute phase symptoms were also more likely to progress rapidly in this age group, with a higher risk of developing cardiac sequelae.8 As a result, any infant under the age of six months with fever for more than seven days and no other clear etiology should be evaluated for KD even in the absence of other diagnostic criteria.9
Other clinical manifestations of KD may include:
- Irritability: more notable in KD than in other febrile illnesses;
- Arthralgia and arthritis: may occur in the first week;
- Gastrointestinal complaints and findings: hepatomegaly, jaundice; and
- Abnormal chest X-ray findings: may be present in as many as 15% of patients.
Cardiovascular manifestations can be prominent in the acute phase of KD and are the leading cause of long-term morbidity and mortality. Coronary artery aneurysms occur in 20% of affected children with KD. Other cardiovascular complications include myocardial ischemia and ensuing depressed contractility and arrhythmias, as well as vascular obstruction in peripheral arteries.
A subset of KD patients develops hemodynamic instability requiring management in a critical care setting. This phenomenon has been named Kawasaki disease shock syndrome, where hemodynamic instability is not related to administration of intravenous immunoglobulin (IVIG). Patients are more likely to be female, to have laboratory findings consistent with greater inflammation, and to have impaired systolic and diastolic function. They also exhibit resistance to IVIG more often and have higher rates of coronary artery dilation and aneurysm formation.10
Differential diagnoses for KD may include viral infections, scarlet fever, staphylococcal scalded skin syndrome, toxic shock syndrome, Rocky Mountain spotted fever, cervical lymphadenitis, drug hypersensitivity, Stevens-Johnson syndrome, systemic idiopathic arthritis, leptospirosis, and mercury hypersensitivity reaction.11
Work-Up
Laboratory evaluation of a patient with suspected KD should include:
- Complete blood count (CBC) with differential: leukocytosis, anemia, thrombocytosis that peaks in the third week is characteristic. A manual differential may reveal an increase in band forms.
- Acute phase reactants: If C-reactive protein (CRP) is 3 mg/dL or greater and erythrocyte sedimentation rate (ESR) is 40 mm/hr or greater, supplementary laboratory work-up should be done. Make sure not to cloud classic with incomplete KD; the stepwise lab evaluation only pertains to the latter.
- Liver panel: Elevated ALT and gamma-glutamyl transferase (GGT), mild hyperbilirubinemia, or hypoalbuminemia may be present.
- Urinalysis: Sterile pyuria may be present; if present, it may be of urethral origin, and catheterized samples could miss this finding.12
Lack of elevated inflammatory markers (CRP is less than 3 mg/dl and ESR is less than 40 mm/hr) and the presence of two or three principal clinical features warrant ongoing daily monitoring of ESR, CRP, and fever until day seven of illness. If the fever resolves but is followed by peeling of extremities, an echocardiogram should be done. Lumbar puncture might help differentiate from CNS infectious etiologies, but about 50% of KD patients have a cerebrospinal fluid pleocytosis.
Echocardiography is the preferred imaging modality for the initial cardiovascular evaluation and follow-up.1 It has a sensitivity of 100% and specificity of 96% for the detection of proximal coronary aneurysms.13 Coronary aneurysms are clinically silent in most cases and can manifest with delayed complications, such as myocardial infarction or sudden death. Imaging plays an important role in the early diagnosis of these aneurysms and in estimating their number, size, and location, important elements in making a therapeutic decision.14
Although the echocardiography should be done as soon as KD is suspected, definitive treatment must not be delayed. Evaluation of all coronary artery segments, as well as cardiac contractility and presence of effusion, should be noted on echocardiography. In the absence of complications, echocardiography is performed at the time of diagnosis and at two weeks and six to eight weeks after disease onset.11
Treatment
Treatment goals for Kawasaki disease in the acute phase are reduction of systemic and coronary arterial inflammation and prevention of coronary thrombosis. The long-term therapy in individuals who develop coronary aneurysms is aimed at preventing myocardial ischemia or infarction.6 The current standard of care for the treatment of children in the U.S. is anti-inflammatory therapy with:
- immunoglobulin (IVIG) in a single 2 g/kg/dose infused over 10–12 hours, accompanied by;
- high-dose aspirin (80–100 mg/kg/day orally in four divided doses).6,15
IVIG administration within 10 days of the onset of fever results in more favorable outcomes. Live virus vaccines should be delayed to 11 months after administration of IVIG. Both aspirin and IVIG have anti-inflammatory effects. This regimen applies to patients without abnormalities on initial echocardiography. High-dose aspirin typically is continued for 48-72 hours after the child becomes afebrile. Thereafter, low-dose aspirin (3-5 mg/kg/day) is prescribed until patient shows no evidence of coronary changes, typically by six to eight weeks after onset of illness. Children with coronary abnormalities should continue aspirin indefinitely.
Approximately 10% of patients are IVIG-resistant and have persistent or recurrent fever for at least 36 hours after completion of the infusion. The current recommendation is to re-treat with IVIG at the same dose. If the patient has fever 36 hours after the second dose of IVIG, this is considered true treatment failure.
Other possible treatments for KD refractory to IVIG include IV methylprednisolone (30 mg/kg over two to three hours daily for three days) or infliximab.16 Even with prompt treatment, 5% of children who have KD develop coronary artery dilation, and 1% develop giant aneurysms.
Back to the Case
Initial laboratory evaluation revealed white blood cell count of 19.0×103 cells/mm3, hemoglobin of 8.9 gm/dL, CRP of 17.9 mg/dL, and ESR of 73 mm/hr. Because of persistent fevers for 48 hours after admission in the absence of another cause to explain the illness, the KD service was consulted. Echocardiography revealed dilatation of the left main (z-score 4.23) and proximal right (z-score 2.59), confirming the diagnosis of KD. Ejection fraction was read as qualitatively normal.
The infant received infliximab and IVIG, as well as high-dose aspirin, clopidogrel, and propranolol. This treatment regimen was directed by a KD expert and was more aggressive than typical therapy due to the severity of presentation. She received blood transfusions for worsening symptomatic anemia (hemoglobin 7.0 gm/dL) with hypoxia.
Following her IVIG infusion, she remained afebrile with progressive reduction in her CRP. She was discharged on hospital day seven on aspirin until her next follow-up, with propranolol for three days to limit potential tachycardia. At her three-week follow-up visit, her ESR had improved to 8 mm/hr. Her echocardiogram revealed a normal ejection fraction. Echocardiography revealed resolution of all abnormalities except for a borderline prominence of the right coronary artery (z-score 2.11). At this time it was recommended that her aspirin be discontinued.
She continues to be followed by the KD service as an outpatient and has done well without cardiovascular symptoms four months after her diagnosis.
Bottom Line
KD can manifest an incomplete presentation, especially in infants under the age of six months. Clinicians should maintain a high level of suspicion for KD in young infants with unexplained fevers lasting more than seven days.
Dr. Gurevich-Panigrahi is a fellow in pediatric hospital medicine at Cleveland Clinic Children’s Hospital. Dr. Kanegaye is a clinical professor of pediatrics at the University of California San Diego (UCSD) School of Medicine and attending physician in the emergency care center at Rady Children’s Hospital San Diego. Dr. Chang is associate clinical professor of pediatrics and medicine at UCSD School of Medicine, a pediatric hospitalist at Rady Children’s, and pediatric editor of The Hospitalist.
References
- Hendaoui L, Stanson AW, Habib Bouhaouala M, Joffre F, eds. Systemic Vasculitis: Imaging Features. New York: Springer; 2012.
- Manlhiot C, Yeung RS, Clarizia NA, Chahal N, McCrindle BW. Kawasaki disease at the extremes of the age spectrum. Pediatrics. 2009;124(3):e410-e415.
- Huang WC, Huang LM, Chang IS, et al. Epidemiologic features of Kawasaki disease in Taiwan, 2003-2006. Pediatrics. 2009;123(3):e401-405.
- Holman RC, Belay ED, Christensen KY, Folkema AM, Steiner CA, Schonberger LB. Hospitalizations for Kawasaki syndrome among children in the United States, 1997-2007. Pediatr Infect Dis J. 2010;29(6):483-438.
- Council on Cardiovascular Disease in the Young, Committee on Rheumatic Fever Endocarditis, Kawasaki Disease, American Heart Association. Diagnostic guidelines for Kawasaki disease. Circulation. 2001;103:335-336.
- Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110(17):2747-2771.
- Shiozawa Y, Inuzuka R, Harita Y, Kagawa J. Age-related differences in the course of the acute phase symptoms of Kawasaki disease. Pediatr Infect Dis J. 2013;32(9):e365-369.
- Genizi J, Miron D, Spiegel R, Fink D, Horowitz Y. Kawasaki disease in very young infants: high prevalence of atypical presentation and coronary arteritis. Clin Pediatr (Phila.). 2003;42(3):263-267.
- Sundel R. Incomplete (atypical) Kawasaki disease. UpToDate. Available at: http://www.uptodate.com/contents/incomplete-atypical-kawasaki-disease. Accessed June 9, 2014.
- Kanegaye JT, Wilder MS, Molkara D, et al. Recognition of a Kawasaki disease shock syndrome. Pediatrics. 2009;123(5):e783-e789.
- Fimbres AM, Shulman ST. Kawasaki disease. Pediatr Rev. 2008;29(9):308-315.
- Shike H, Kanegaye JT, Best BM, Pancheri J, Burns JC. Pyuria associated with acute Kawasaki disease and fever from other causes. Pediatr Infect Dis J. 2009;28(5):440-443.
- Capannari TE, Daniels SR, Meyer RA, Schwartz DC, Kaplan S. Sensitivity, specificity and predictive value of two-dimensional echocardiography in detecting coronary artery aneurysms in patients with Kawasaki disease. J Am Coll Cardiol. 1986;7(2):355-360.
- Mavrogeni S, Papadopoulos G, Karanasios E, Cokkinos DV. How to image Kawasaki disease: a validation of different imaging techniques. Int J Cardiol. 2008;124(1):27-31.
- Burns JC, Glodé MP. Kawasaki syndrome. Lancet. 2004;364(9433):533-544.
- Ghelani SJ, Pastor W, Parikh K. Demographic and treatment variability of refractory Kawasaki Disease: a multicenter analysis from 2005 to 2009. Hosp Pediatr. 2012;2(2):71-76.
Case
A seven-week-old Hispanic female with a history of prematurity (born at 35 weeks by C-section) presents to the ED with four days of fever as high as 102°F and new-onset cyanotic spells. Cultures of blood, urine, and cerebrospinal fluid obtained 48 hours prior to admission were negative, but she continued to have intermittent fevers and developed a macular, non-pruritic rash on her hands and feet, with associated non-bilious emesis. One day prior to admission, she began to have episodes of apnea, with color change and cyanosis of her lips and eyelids. In the ED, her vital signs include a rectal temperature of 38.4°C, heart rate of 178/min, respiratory rate of 27/min, and blood pressure of 79/66. Examination reveals a non-toxic-appearing infant, with no conjunctival or oropharyngeal abnormalities, unremarkable heart and lung exam, and a blanching, erythematous macular rash on her hands, lower legs, and feet.
When should you suspect Kawasaki disease (KD) as the cause of fever in an infant?
Background
KD is an acute systemic vasculitis of unknown etiology that occurs in children. Affecting the small- and medium-sized arteries, with a striking predilection for coronary arteries, it is the leading cause of acquired pediatric heart disease in Japan and the U.S.1 Occurring predominantly in children younger than five years, KD has been diagnosed in infants and in young adults.2 The incidence of KD is lowest among white children and highest among Asians and Pacific Islanders, with the highest incidence in children of Japanese descent.
A recent epidemiologic study performed in Taiwan showed an incidence of 69 cases per 100,000 per year among children younger than five years, with a male/female ratio of 1.62:1.3 The peak of mortality occurs 15-45 days after onset of fever, although sudden cardiac death may occur many years later. Recurrence rate is approximately 3%. In the U.S., the estimated incidence ranges from nine to 18 per 100,000 children younger than five years per year.4
Review of Data
Because there is no specific diagnostic test or pathognomonic clinical feature, clinical diagnostic criteria have been established to guide physicians. KD diagnosis traditionally requires fever for at least five days and the presence of at least four of the following five principal features:
- bilateral conjunctival injection;
- changes in the mucous membranes of the upper respiratory tract (injected pharynx, infected, fissured lips, strawberry tongue);
- polymorphous rash;
- changes of the extremities (peripheral edema, erythema, periungual desquamation); and
- cervical lymphadenopathy.5
The fever, which is remittent, typically peaks at 39ºC to 40ºC. The mean duration of untreated fever is 11 days; with prompt treatment, fever typically subsides in two days. Bilateral painless non-exudative conjunctival injection begins shortly after onset of fever, involves typically bulbar conjunctiva, and is not associated with edema.
Erythematous rash usually appears within five days of onset of fever and is often a diffuse, nonspecific maculopapular eruption that is commonly pronounced in the perineal region. The appearance might be urticarial, micropustular, or erythema multiforme-like. Changes in extremities include erythema of palms and soles and tender induration of the hands and feet. Subsequently, desquamation begins in the periungual area within two to three weeks after the onset of fever. Typically, peeling begins around the nail folds of fingers, followed by the toes. The least common of the principal clinical features is tender unilateral anterior cervical lymphadenopathy (1.5 cm or greater in diameter).
When a patient presents with a history, examination, and laboratory findings consistent with KD without meeting the typical diagnostic standard, incomplete KD should be considered. The term “incomplete” is favored over “atypical” for this pre-sentation, because these patients are otherwise similar to other patients with KD. Patients with fever for five or fewer days and fewer than four principal features can be diagnosed as having KD when coronary artery disease is detected by two-dimensional echocardiography or coronary angiography (see Figure 1, p. 10). In the presence of four or more principal criteria, KD can be diagnosed before day four of the illness by an experienced clinician.6 Features less consistent with KD include the presence of exudative conjunctivitis, exudative pharyngitis, discrete intraoral lesions, bullous or vesicular rash, or generalized adenopathy.
If clinical features are consistent with KD, further risk stratification with erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) will determine whether patients are followed daily (if low) or if supplementary laboratory tests should be done (see Figure 1, p. 10). If three or more of supplementary laboratory criteria are present (albumin ≤3.0 g/dL, anemia for age, elevation of alanine aminotransferase (ALT), platelet count after seven days is 450 000/mm3 or greater, white blood cell count is 15,000/mm3 or greater, and urinary sediment containing 10 white blood cells/high-power field or more), echocardiogram should be performed and treatment initiated if abnormal.6
Young infants are more likely to manifest an incomplete presentation of KD, with a polymorphous rash being the most common symptom other than fever in this age group.7 Acute phase symptoms were also more likely to progress rapidly in this age group, with a higher risk of developing cardiac sequelae.8 As a result, any infant under the age of six months with fever for more than seven days and no other clear etiology should be evaluated for KD even in the absence of other diagnostic criteria.9
Other clinical manifestations of KD may include:
- Irritability: more notable in KD than in other febrile illnesses;
- Arthralgia and arthritis: may occur in the first week;
- Gastrointestinal complaints and findings: hepatomegaly, jaundice; and
- Abnormal chest X-ray findings: may be present in as many as 15% of patients.
Cardiovascular manifestations can be prominent in the acute phase of KD and are the leading cause of long-term morbidity and mortality. Coronary artery aneurysms occur in 20% of affected children with KD. Other cardiovascular complications include myocardial ischemia and ensuing depressed contractility and arrhythmias, as well as vascular obstruction in peripheral arteries.
A subset of KD patients develops hemodynamic instability requiring management in a critical care setting. This phenomenon has been named Kawasaki disease shock syndrome, where hemodynamic instability is not related to administration of intravenous immunoglobulin (IVIG). Patients are more likely to be female, to have laboratory findings consistent with greater inflammation, and to have impaired systolic and diastolic function. They also exhibit resistance to IVIG more often and have higher rates of coronary artery dilation and aneurysm formation.10
Differential diagnoses for KD may include viral infections, scarlet fever, staphylococcal scalded skin syndrome, toxic shock syndrome, Rocky Mountain spotted fever, cervical lymphadenitis, drug hypersensitivity, Stevens-Johnson syndrome, systemic idiopathic arthritis, leptospirosis, and mercury hypersensitivity reaction.11
Work-Up
Laboratory evaluation of a patient with suspected KD should include:
- Complete blood count (CBC) with differential: leukocytosis, anemia, thrombocytosis that peaks in the third week is characteristic. A manual differential may reveal an increase in band forms.
- Acute phase reactants: If C-reactive protein (CRP) is 3 mg/dL or greater and erythrocyte sedimentation rate (ESR) is 40 mm/hr or greater, supplementary laboratory work-up should be done. Make sure not to cloud classic with incomplete KD; the stepwise lab evaluation only pertains to the latter.
- Liver panel: Elevated ALT and gamma-glutamyl transferase (GGT), mild hyperbilirubinemia, or hypoalbuminemia may be present.
- Urinalysis: Sterile pyuria may be present; if present, it may be of urethral origin, and catheterized samples could miss this finding.12
Lack of elevated inflammatory markers (CRP is less than 3 mg/dl and ESR is less than 40 mm/hr) and the presence of two or three principal clinical features warrant ongoing daily monitoring of ESR, CRP, and fever until day seven of illness. If the fever resolves but is followed by peeling of extremities, an echocardiogram should be done. Lumbar puncture might help differentiate from CNS infectious etiologies, but about 50% of KD patients have a cerebrospinal fluid pleocytosis.
Echocardiography is the preferred imaging modality for the initial cardiovascular evaluation and follow-up.1 It has a sensitivity of 100% and specificity of 96% for the detection of proximal coronary aneurysms.13 Coronary aneurysms are clinically silent in most cases and can manifest with delayed complications, such as myocardial infarction or sudden death. Imaging plays an important role in the early diagnosis of these aneurysms and in estimating their number, size, and location, important elements in making a therapeutic decision.14
Although the echocardiography should be done as soon as KD is suspected, definitive treatment must not be delayed. Evaluation of all coronary artery segments, as well as cardiac contractility and presence of effusion, should be noted on echocardiography. In the absence of complications, echocardiography is performed at the time of diagnosis and at two weeks and six to eight weeks after disease onset.11
Treatment
Treatment goals for Kawasaki disease in the acute phase are reduction of systemic and coronary arterial inflammation and prevention of coronary thrombosis. The long-term therapy in individuals who develop coronary aneurysms is aimed at preventing myocardial ischemia or infarction.6 The current standard of care for the treatment of children in the U.S. is anti-inflammatory therapy with:
- immunoglobulin (IVIG) in a single 2 g/kg/dose infused over 10–12 hours, accompanied by;
- high-dose aspirin (80–100 mg/kg/day orally in four divided doses).6,15
IVIG administration within 10 days of the onset of fever results in more favorable outcomes. Live virus vaccines should be delayed to 11 months after administration of IVIG. Both aspirin and IVIG have anti-inflammatory effects. This regimen applies to patients without abnormalities on initial echocardiography. High-dose aspirin typically is continued for 48-72 hours after the child becomes afebrile. Thereafter, low-dose aspirin (3-5 mg/kg/day) is prescribed until patient shows no evidence of coronary changes, typically by six to eight weeks after onset of illness. Children with coronary abnormalities should continue aspirin indefinitely.
Approximately 10% of patients are IVIG-resistant and have persistent or recurrent fever for at least 36 hours after completion of the infusion. The current recommendation is to re-treat with IVIG at the same dose. If the patient has fever 36 hours after the second dose of IVIG, this is considered true treatment failure.
Other possible treatments for KD refractory to IVIG include IV methylprednisolone (30 mg/kg over two to three hours daily for three days) or infliximab.16 Even with prompt treatment, 5% of children who have KD develop coronary artery dilation, and 1% develop giant aneurysms.
Back to the Case
Initial laboratory evaluation revealed white blood cell count of 19.0×103 cells/mm3, hemoglobin of 8.9 gm/dL, CRP of 17.9 mg/dL, and ESR of 73 mm/hr. Because of persistent fevers for 48 hours after admission in the absence of another cause to explain the illness, the KD service was consulted. Echocardiography revealed dilatation of the left main (z-score 4.23) and proximal right (z-score 2.59), confirming the diagnosis of KD. Ejection fraction was read as qualitatively normal.
The infant received infliximab and IVIG, as well as high-dose aspirin, clopidogrel, and propranolol. This treatment regimen was directed by a KD expert and was more aggressive than typical therapy due to the severity of presentation. She received blood transfusions for worsening symptomatic anemia (hemoglobin 7.0 gm/dL) with hypoxia.
Following her IVIG infusion, she remained afebrile with progressive reduction in her CRP. She was discharged on hospital day seven on aspirin until her next follow-up, with propranolol for three days to limit potential tachycardia. At her three-week follow-up visit, her ESR had improved to 8 mm/hr. Her echocardiogram revealed a normal ejection fraction. Echocardiography revealed resolution of all abnormalities except for a borderline prominence of the right coronary artery (z-score 2.11). At this time it was recommended that her aspirin be discontinued.
She continues to be followed by the KD service as an outpatient and has done well without cardiovascular symptoms four months after her diagnosis.
Bottom Line
KD can manifest an incomplete presentation, especially in infants under the age of six months. Clinicians should maintain a high level of suspicion for KD in young infants with unexplained fevers lasting more than seven days.
Dr. Gurevich-Panigrahi is a fellow in pediatric hospital medicine at Cleveland Clinic Children’s Hospital. Dr. Kanegaye is a clinical professor of pediatrics at the University of California San Diego (UCSD) School of Medicine and attending physician in the emergency care center at Rady Children’s Hospital San Diego. Dr. Chang is associate clinical professor of pediatrics and medicine at UCSD School of Medicine, a pediatric hospitalist at Rady Children’s, and pediatric editor of The Hospitalist.
References
- Hendaoui L, Stanson AW, Habib Bouhaouala M, Joffre F, eds. Systemic Vasculitis: Imaging Features. New York: Springer; 2012.
- Manlhiot C, Yeung RS, Clarizia NA, Chahal N, McCrindle BW. Kawasaki disease at the extremes of the age spectrum. Pediatrics. 2009;124(3):e410-e415.
- Huang WC, Huang LM, Chang IS, et al. Epidemiologic features of Kawasaki disease in Taiwan, 2003-2006. Pediatrics. 2009;123(3):e401-405.
- Holman RC, Belay ED, Christensen KY, Folkema AM, Steiner CA, Schonberger LB. Hospitalizations for Kawasaki syndrome among children in the United States, 1997-2007. Pediatr Infect Dis J. 2010;29(6):483-438.
- Council on Cardiovascular Disease in the Young, Committee on Rheumatic Fever Endocarditis, Kawasaki Disease, American Heart Association. Diagnostic guidelines for Kawasaki disease. Circulation. 2001;103:335-336.
- Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110(17):2747-2771.
- Shiozawa Y, Inuzuka R, Harita Y, Kagawa J. Age-related differences in the course of the acute phase symptoms of Kawasaki disease. Pediatr Infect Dis J. 2013;32(9):e365-369.
- Genizi J, Miron D, Spiegel R, Fink D, Horowitz Y. Kawasaki disease in very young infants: high prevalence of atypical presentation and coronary arteritis. Clin Pediatr (Phila.). 2003;42(3):263-267.
- Sundel R. Incomplete (atypical) Kawasaki disease. UpToDate. Available at: http://www.uptodate.com/contents/incomplete-atypical-kawasaki-disease. Accessed June 9, 2014.
- Kanegaye JT, Wilder MS, Molkara D, et al. Recognition of a Kawasaki disease shock syndrome. Pediatrics. 2009;123(5):e783-e789.
- Fimbres AM, Shulman ST. Kawasaki disease. Pediatr Rev. 2008;29(9):308-315.
- Shike H, Kanegaye JT, Best BM, Pancheri J, Burns JC. Pyuria associated with acute Kawasaki disease and fever from other causes. Pediatr Infect Dis J. 2009;28(5):440-443.
- Capannari TE, Daniels SR, Meyer RA, Schwartz DC, Kaplan S. Sensitivity, specificity and predictive value of two-dimensional echocardiography in detecting coronary artery aneurysms in patients with Kawasaki disease. J Am Coll Cardiol. 1986;7(2):355-360.
- Mavrogeni S, Papadopoulos G, Karanasios E, Cokkinos DV. How to image Kawasaki disease: a validation of different imaging techniques. Int J Cardiol. 2008;124(1):27-31.
- Burns JC, Glodé MP. Kawasaki syndrome. Lancet. 2004;364(9433):533-544.
- Ghelani SJ, Pastor W, Parikh K. Demographic and treatment variability of refractory Kawasaki Disease: a multicenter analysis from 2005 to 2009. Hosp Pediatr. 2012;2(2):71-76.
Movers and Shakers in Hospital Medicine

Michael Campbell, MD, has been named one of the 2013 Physicians of the Year at Lake Health community health system in Lake County, Ohio. Dr. Campbell is a hospitalist who is board certified in family practice. He has been with Lake Health since 2011.
Nitish Kosaraju, MD, and Jocelyn Hendricks, DO, both received the 2013 Hospitalist of the Year award for an acute care practice from IPC The Hospitalist Company, based in North Hollywood, Calif. Dr. Kosaraju is a practice group leader for IPC in Houston and has been an IPC hospitalist since 2010. Dr. Hendricks is a practice group leader in Tucson, Ariz., and has been part of IPC since 2004.
Pedram Taher, MD, received IPC’s 2013 Hospitalist of the Year award for a post-acute care practice. Dr. Taher has worked for IPC since 2009 and is a practice group leader in the San Francisco Bay area.
Tammy Hilliard, FNP-C, earned IPC’s 2013 Hospitalist of the Year award for a non-physician provider. Hilliard has been with IPC since 2009 and now serves as a nurse practitioner and practice group representative in Phoenix, Ariz.
Jeffrey Harris, MD, received IPC’s 2013 Newcomer Clinician of the Year award. Dr. Harris is a neuro-hospitalist in San Antonio, Texas, and joined IPC in January 2013.
Corbi Milligan, MD, was featured in Murfreesboro Magazine for her exemplary leadership as the EmCare hospitalist site medical director for TriStar StoneCrest Medical Center in Smyrna, Tenn. Dr. Milligan oversees 10 hospitalists in her role and has been with TriStar StoneCrest since 2004.

Business Moves
St. Anthony’s Memorial Hospital in Effingham, Ill., has announced a brand new hospitalist program. The 146-bed acute care center will staff two full-time hospitalists.
Laurens County Memorial Hospital (LCMH) in Clinton, S.C., has partnered with the hospitalist program at Greenville Health System (GHS) in Greenville, S.C., to provide 24-hour hospitalist services. GHS’s lead hospitalist, Kevin Gilroy, MD, will oversee the new program at LCMH. GHS is a public, nonprofit healthcare system comprising seven regional medical centers, including LCMH, as well as numerous post-acute care facilities and offices.
The hospitalist program at Erlanger Health System in Chattanooga, Tenn., will now be managed by MDP Management, a Chattanooga-based physician management company. Erlanger’s hospitalist program has 18 full-time physicians at the nonprofit, level-one trauma center.
IPC The Hospitalist Company has acquired the post-acute hospitalist practice CAP Medical Group, PLLC, in New Hartford, N.Y. CAP Medical Group has served the Oneida County area of upstate New York since 2007. IPC oversees hospitalist services in over 400 hospitals and 1,100 post-acute care practices across the country.
Michael Campbell, MD, has been named one of the 2013 Physicians of the Year at Lake Health community health system in Lake County, Ohio. Dr. Campbell is a hospitalist who is board certified in family practice. He has been with Lake Health since 2011.
Nitish Kosaraju, MD, and Jocelyn Hendricks, DO, both received the 2013 Hospitalist of the Year award for an acute care practice from IPC The Hospitalist Company, based in North Hollywood, Calif. Dr. Kosaraju is a practice group leader for IPC in Houston and has been an IPC hospitalist since 2010. Dr. Hendricks is a practice group leader in Tucson, Ariz., and has been part of IPC since 2004.
Pedram Taher, MD, received IPC’s 2013 Hospitalist of the Year award for a post-acute care practice. Dr. Taher has worked for IPC since 2009 and is a practice group leader in the San Francisco Bay area.
Tammy Hilliard, FNP-C, earned IPC’s 2013 Hospitalist of the Year award for a non-physician provider. Hilliard has been with IPC since 2009 and now serves as a nurse practitioner and practice group representative in Phoenix, Ariz.
Jeffrey Harris, MD, received IPC’s 2013 Newcomer Clinician of the Year award. Dr. Harris is a neuro-hospitalist in San Antonio, Texas, and joined IPC in January 2013.
Corbi Milligan, MD, was featured in Murfreesboro Magazine for her exemplary leadership as the EmCare hospitalist site medical director for TriStar StoneCrest Medical Center in Smyrna, Tenn. Dr. Milligan oversees 10 hospitalists in her role and has been with TriStar StoneCrest since 2004.
Business Moves
St. Anthony’s Memorial Hospital in Effingham, Ill., has announced a brand new hospitalist program. The 146-bed acute care center will staff two full-time hospitalists.
Laurens County Memorial Hospital (LCMH) in Clinton, S.C., has partnered with the hospitalist program at Greenville Health System (GHS) in Greenville, S.C., to provide 24-hour hospitalist services. GHS’s lead hospitalist, Kevin Gilroy, MD, will oversee the new program at LCMH. GHS is a public, nonprofit healthcare system comprising seven regional medical centers, including LCMH, as well as numerous post-acute care facilities and offices.
The hospitalist program at Erlanger Health System in Chattanooga, Tenn., will now be managed by MDP Management, a Chattanooga-based physician management company. Erlanger’s hospitalist program has 18 full-time physicians at the nonprofit, level-one trauma center.
IPC The Hospitalist Company has acquired the post-acute hospitalist practice CAP Medical Group, PLLC, in New Hartford, N.Y. CAP Medical Group has served the Oneida County area of upstate New York since 2007. IPC oversees hospitalist services in over 400 hospitals and 1,100 post-acute care practices across the country.
Michael Campbell, MD, has been named one of the 2013 Physicians of the Year at Lake Health community health system in Lake County, Ohio. Dr. Campbell is a hospitalist who is board certified in family practice. He has been with Lake Health since 2011.
Nitish Kosaraju, MD, and Jocelyn Hendricks, DO, both received the 2013 Hospitalist of the Year award for an acute care practice from IPC The Hospitalist Company, based in North Hollywood, Calif. Dr. Kosaraju is a practice group leader for IPC in Houston and has been an IPC hospitalist since 2010. Dr. Hendricks is a practice group leader in Tucson, Ariz., and has been part of IPC since 2004.
Pedram Taher, MD, received IPC’s 2013 Hospitalist of the Year award for a post-acute care practice. Dr. Taher has worked for IPC since 2009 and is a practice group leader in the San Francisco Bay area.
Tammy Hilliard, FNP-C, earned IPC’s 2013 Hospitalist of the Year award for a non-physician provider. Hilliard has been with IPC since 2009 and now serves as a nurse practitioner and practice group representative in Phoenix, Ariz.
Jeffrey Harris, MD, received IPC’s 2013 Newcomer Clinician of the Year award. Dr. Harris is a neuro-hospitalist in San Antonio, Texas, and joined IPC in January 2013.
Corbi Milligan, MD, was featured in Murfreesboro Magazine for her exemplary leadership as the EmCare hospitalist site medical director for TriStar StoneCrest Medical Center in Smyrna, Tenn. Dr. Milligan oversees 10 hospitalists in her role and has been with TriStar StoneCrest since 2004.
Business Moves
St. Anthony’s Memorial Hospital in Effingham, Ill., has announced a brand new hospitalist program. The 146-bed acute care center will staff two full-time hospitalists.
Laurens County Memorial Hospital (LCMH) in Clinton, S.C., has partnered with the hospitalist program at Greenville Health System (GHS) in Greenville, S.C., to provide 24-hour hospitalist services. GHS’s lead hospitalist, Kevin Gilroy, MD, will oversee the new program at LCMH. GHS is a public, nonprofit healthcare system comprising seven regional medical centers, including LCMH, as well as numerous post-acute care facilities and offices.
The hospitalist program at Erlanger Health System in Chattanooga, Tenn., will now be managed by MDP Management, a Chattanooga-based physician management company. Erlanger’s hospitalist program has 18 full-time physicians at the nonprofit, level-one trauma center.
IPC The Hospitalist Company has acquired the post-acute hospitalist practice CAP Medical Group, PLLC, in New Hartford, N.Y. CAP Medical Group has served the Oneida County area of upstate New York since 2007. IPC oversees hospitalist services in over 400 hospitals and 1,100 post-acute care practices across the country.
Society of Hospital Medicine Improves Online Career Center
Looking to recruit new hospitalists? Or are you a hospitalist looking for a change? Visit the new SHM Career Center (www.shmcareercenter.org) to recruit and look for new jobs. The new site enables visitors to highlight their favorite opportunities, get alerts via e-mail, and search through hospitalist jobs across the country. Recruiters will find easy-to-use instructions for posting jobs and searching through resumes.
Looking to recruit new hospitalists? Or are you a hospitalist looking for a change? Visit the new SHM Career Center (www.shmcareercenter.org) to recruit and look for new jobs. The new site enables visitors to highlight their favorite opportunities, get alerts via e-mail, and search through hospitalist jobs across the country. Recruiters will find easy-to-use instructions for posting jobs and searching through resumes.
Looking to recruit new hospitalists? Or are you a hospitalist looking for a change? Visit the new SHM Career Center (www.shmcareercenter.org) to recruit and look for new jobs. The new site enables visitors to highlight their favorite opportunities, get alerts via e-mail, and search through hospitalist jobs across the country. Recruiters will find easy-to-use instructions for posting jobs and searching through resumes.