User login
Medicaid Payments for Some Primary-Care Services Reach Parity with Medicare Levels
On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulation implementing increased Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
Covered Medicaid services include evaluation and management codes between 99201 and 99499 when used by physicians with a specialty designation of family medicine, general internal medicine, or pediatric medicine. CMS also finalized a policy to qualify services provided by subspecialists related to the designated primary-care specialists board-certified by the American Board of Medical Specialties, American Osteopathic Association, and the American Board of Physician Specialties. Advanced-practice clinicians also qualify for the increased payment when services are furnished under a physician’s personal supervision.
In commenting on the proposed rule, SHM stated that hospitalists should qualify for purposes of the increased payment because they are an important part of the “team” of clinicians required to treat many common conditions within the Medicaid population, and that hospitalists often provide the first contact and facilitate an entry point into the comprehensive care network.
CMS agreed.
The codes included in the pay increase will be limited to traditional primary care but also will include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services.
Hospitalists will qualify for the enhanced payment, but it remains somewhat unclear how individual states will handle the increase. State Medicaid agencies could pay physicians based on their self-attestation alone or in conjunction with any other provider enrollment requirements that currently exist in the state. Further, inclusion of a code does not require a state to pay for the service if it is not already covered under the state’s Medicaid program. All other state coverage and payment policy rules related to the services also remain in effect.
Timing of the pay increase also remains unclear. The statute requires that states make higher payments for services provided on or after Jan. 1, 2013, but for many physicians, the higher payment might be longer in coming despite being retroactive to the January deadline. States must submit a State Plan Amendment (SPA) to reflect the fee schedule rate increases by March 31, 2013, and CMS may then take up to 90 days to review and approve the SPA. Therefore, it could be six months or longer before eligible physicians and practitioners receive any of the payment increase.
States will receive an estimated $5.8 billion in 2013 and $6.1 billion in 2014 in federal funds to meet this two-year requirement, unless Congress acts to extend or fund the provision permanently. In response to an SHM suggestion on the potential to extend the increase, CMS will be collecting relevant data on the impact of the pay increase on Medicaid patients.
Even with the remaining uncertainty and timing issues, this is a change in payment policy that presents an important shift in the valuation of primary-care services, including some services provided by hospitalists. Medicaid services are notoriously undervalued, and this increase to providers will certainly have a positive impact on the accessibility of care for patients.
Josh Boswell is SHM’s interim senior manager of government relations.
On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulation implementing increased Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
Covered Medicaid services include evaluation and management codes between 99201 and 99499 when used by physicians with a specialty designation of family medicine, general internal medicine, or pediatric medicine. CMS also finalized a policy to qualify services provided by subspecialists related to the designated primary-care specialists board-certified by the American Board of Medical Specialties, American Osteopathic Association, and the American Board of Physician Specialties. Advanced-practice clinicians also qualify for the increased payment when services are furnished under a physician’s personal supervision.
In commenting on the proposed rule, SHM stated that hospitalists should qualify for purposes of the increased payment because they are an important part of the “team” of clinicians required to treat many common conditions within the Medicaid population, and that hospitalists often provide the first contact and facilitate an entry point into the comprehensive care network.
CMS agreed.
The codes included in the pay increase will be limited to traditional primary care but also will include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services.
Hospitalists will qualify for the enhanced payment, but it remains somewhat unclear how individual states will handle the increase. State Medicaid agencies could pay physicians based on their self-attestation alone or in conjunction with any other provider enrollment requirements that currently exist in the state. Further, inclusion of a code does not require a state to pay for the service if it is not already covered under the state’s Medicaid program. All other state coverage and payment policy rules related to the services also remain in effect.
Timing of the pay increase also remains unclear. The statute requires that states make higher payments for services provided on or after Jan. 1, 2013, but for many physicians, the higher payment might be longer in coming despite being retroactive to the January deadline. States must submit a State Plan Amendment (SPA) to reflect the fee schedule rate increases by March 31, 2013, and CMS may then take up to 90 days to review and approve the SPA. Therefore, it could be six months or longer before eligible physicians and practitioners receive any of the payment increase.
States will receive an estimated $5.8 billion in 2013 and $6.1 billion in 2014 in federal funds to meet this two-year requirement, unless Congress acts to extend or fund the provision permanently. In response to an SHM suggestion on the potential to extend the increase, CMS will be collecting relevant data on the impact of the pay increase on Medicaid patients.
Even with the remaining uncertainty and timing issues, this is a change in payment policy that presents an important shift in the valuation of primary-care services, including some services provided by hospitalists. Medicaid services are notoriously undervalued, and this increase to providers will certainly have a positive impact on the accessibility of care for patients.
Josh Boswell is SHM’s interim senior manager of government relations.
On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulation implementing increased Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
Covered Medicaid services include evaluation and management codes between 99201 and 99499 when used by physicians with a specialty designation of family medicine, general internal medicine, or pediatric medicine. CMS also finalized a policy to qualify services provided by subspecialists related to the designated primary-care specialists board-certified by the American Board of Medical Specialties, American Osteopathic Association, and the American Board of Physician Specialties. Advanced-practice clinicians also qualify for the increased payment when services are furnished under a physician’s personal supervision.
In commenting on the proposed rule, SHM stated that hospitalists should qualify for purposes of the increased payment because they are an important part of the “team” of clinicians required to treat many common conditions within the Medicaid population, and that hospitalists often provide the first contact and facilitate an entry point into the comprehensive care network.
CMS agreed.
The codes included in the pay increase will be limited to traditional primary care but also will include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services.
Hospitalists will qualify for the enhanced payment, but it remains somewhat unclear how individual states will handle the increase. State Medicaid agencies could pay physicians based on their self-attestation alone or in conjunction with any other provider enrollment requirements that currently exist in the state. Further, inclusion of a code does not require a state to pay for the service if it is not already covered under the state’s Medicaid program. All other state coverage and payment policy rules related to the services also remain in effect.
Timing of the pay increase also remains unclear. The statute requires that states make higher payments for services provided on or after Jan. 1, 2013, but for many physicians, the higher payment might be longer in coming despite being retroactive to the January deadline. States must submit a State Plan Amendment (SPA) to reflect the fee schedule rate increases by March 31, 2013, and CMS may then take up to 90 days to review and approve the SPA. Therefore, it could be six months or longer before eligible physicians and practitioners receive any of the payment increase.
States will receive an estimated $5.8 billion in 2013 and $6.1 billion in 2014 in federal funds to meet this two-year requirement, unless Congress acts to extend or fund the provision permanently. In response to an SHM suggestion on the potential to extend the increase, CMS will be collecting relevant data on the impact of the pay increase on Medicaid patients.
Even with the remaining uncertainty and timing issues, this is a change in payment policy that presents an important shift in the valuation of primary-care services, including some services provided by hospitalists. Medicaid services are notoriously undervalued, and this increase to providers will certainly have a positive impact on the accessibility of care for patients.
Josh Boswell is SHM’s interim senior manager of government relations.

Medicare Imaging Payments Fell 21% Since 2006
CHICAGO – After a meteoric rise that peaked in 2006, Medicare reimbursements for noninvasive diagnostic imaging fell by 21% in 2010, a new analysis shows.
But Medicare’s total payments in 2010 were still 60% greater than what it paid a decade earlier.
"I think we in radiology can hope that this big cut in payments will convince the feds and payers that enough has been taken out of imaging and hopefully no more cuts will occur in the future year," Dr. David C. Levin said at the annual meeting of the Radiological Society of North America. "Unfortunately, I don’t think we can hang our hats on that hope."

Even without the so-called "fiscal cliff" around the corner, federal policy makers began cutting reimbursement for imaging services starting with the Deficit Reduction Act in 2006. Imaging has been identified in recent years as the most rapidly growing of all physician services, and it is well known that radiologists are highly compensated, he said.
As a result, efforts have been made by the Centers for Medicare and Medicaid Services to rein in reimbursements for imaging. This trend continues in the recently released final rules for the Hospital Outpatient Prospective Payment System (HOPPS).
To track these trends, the investigators used the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2000-2010. These files provide data on volume and allowed reimbursements for every procedure code. All noninvasive diagnostic imaging codes, covering all specialties and all places of service, were selected and aggregated.
From 2000 to 2006, Medicare Part B payments to physicians for noninvasive diagnostic imaging rose from $5.9 billion to $11.9 billion – a 101% increase over those years.
There was a sharp reversal in 2007 when the Deficit Reduction Act first took effect, followed by a slight rise in 2008 and progressive declines to $9.45 billion in 2010, representing a 21% decrease from 2006, said Dr. David Levin, founder of the Center for Research on Utilization of Imaging Services (CRUISE) at Thomas Jefferson University Hospital in Philadelphia.
"That’s obviously a huge hit," he said.
When looked at by specialty, radiologists’ payments from Medicare rose 81% from $2.93 billion in 2000 to $5.3 billion in 2006, before dropping 11% to $4.7 billion in 2010.
Cardiologists, the second-largest group of imaging providers, suffered more than radiologists, Dr. Levin said. Their payments fell 33% to $1.9 billion in 2010, after rising 126% from $1.3 billion in 2000 to $2.9 billion in 2006.
Medicare spent $2.3 billion on imaging services to all other physicians in 2006, a 115% increase from $1.1 billion in 2000, before throttling back 17% to $1.9 billion in 2010.
Medicare payments to independent testing facilities increased 124% from 2000 to 2006, before declining 37% from 2006 to 2010.
The Deficit Reduction Act was the biggest reason for the drop in Part B payments for noninvasive diagnostic imaging – but other factors played a role, particularly in the progressive declines seen after 2007, Dr. Levin said.
Those factors include the Multiple Payment Procedure Reduction, the Centers for Medicare and Medicaid Services’ practice expense revaluation that cut the hourly rate for noninvasive diagnostic imaging from $204 to $135, an increase in the assumed equipment utilization rate from 50% to 75%, and a decrease in the volume of advanced imaging.
Finally, there was the bundling of codes for transthoracic echocardiogram, radionuclide myocardial infusion imaging, abdominal and pelvic computed tomography, and coronary CT angiography. "These had tremendous impacts," he added.
Dr. Levin reported serving as a consultant for HealthHelp and as a director for Outpatient Imaging Affiliates. CRUISE is funded in part by the American College of Radiology.
CHICAGO – After a meteoric rise that peaked in 2006, Medicare reimbursements for noninvasive diagnostic imaging fell by 21% in 2010, a new analysis shows.
But Medicare’s total payments in 2010 were still 60% greater than what it paid a decade earlier.
"I think we in radiology can hope that this big cut in payments will convince the feds and payers that enough has been taken out of imaging and hopefully no more cuts will occur in the future year," Dr. David C. Levin said at the annual meeting of the Radiological Society of North America. "Unfortunately, I don’t think we can hang our hats on that hope."
Even without the so-called "fiscal cliff" around the corner, federal policy makers began cutting reimbursement for imaging services starting with the Deficit Reduction Act in 2006. Imaging has been identified in recent years as the most rapidly growing of all physician services, and it is well known that radiologists are highly compensated, he said.
As a result, efforts have been made by the Centers for Medicare and Medicaid Services to rein in reimbursements for imaging. This trend continues in the recently released final rules for the Hospital Outpatient Prospective Payment System (HOPPS).
To track these trends, the investigators used the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2000-2010. These files provide data on volume and allowed reimbursements for every procedure code. All noninvasive diagnostic imaging codes, covering all specialties and all places of service, were selected and aggregated.
From 2000 to 2006, Medicare Part B payments to physicians for noninvasive diagnostic imaging rose from $5.9 billion to $11.9 billion – a 101% increase over those years.
There was a sharp reversal in 2007 when the Deficit Reduction Act first took effect, followed by a slight rise in 2008 and progressive declines to $9.45 billion in 2010, representing a 21% decrease from 2006, said Dr. David Levin, founder of the Center for Research on Utilization of Imaging Services (CRUISE) at Thomas Jefferson University Hospital in Philadelphia.
"That’s obviously a huge hit," he said.
When looked at by specialty, radiologists’ payments from Medicare rose 81% from $2.93 billion in 2000 to $5.3 billion in 2006, before dropping 11% to $4.7 billion in 2010.
Cardiologists, the second-largest group of imaging providers, suffered more than radiologists, Dr. Levin said. Their payments fell 33% to $1.9 billion in 2010, after rising 126% from $1.3 billion in 2000 to $2.9 billion in 2006.
Medicare spent $2.3 billion on imaging services to all other physicians in 2006, a 115% increase from $1.1 billion in 2000, before throttling back 17% to $1.9 billion in 2010.
Medicare payments to independent testing facilities increased 124% from 2000 to 2006, before declining 37% from 2006 to 2010.
The Deficit Reduction Act was the biggest reason for the drop in Part B payments for noninvasive diagnostic imaging – but other factors played a role, particularly in the progressive declines seen after 2007, Dr. Levin said.
Those factors include the Multiple Payment Procedure Reduction, the Centers for Medicare and Medicaid Services’ practice expense revaluation that cut the hourly rate for noninvasive diagnostic imaging from $204 to $135, an increase in the assumed equipment utilization rate from 50% to 75%, and a decrease in the volume of advanced imaging.
Finally, there was the bundling of codes for transthoracic echocardiogram, radionuclide myocardial infusion imaging, abdominal and pelvic computed tomography, and coronary CT angiography. "These had tremendous impacts," he added.
Dr. Levin reported serving as a consultant for HealthHelp and as a director for Outpatient Imaging Affiliates. CRUISE is funded in part by the American College of Radiology.
CHICAGO – After a meteoric rise that peaked in 2006, Medicare reimbursements for noninvasive diagnostic imaging fell by 21% in 2010, a new analysis shows.
But Medicare’s total payments in 2010 were still 60% greater than what it paid a decade earlier.
"I think we in radiology can hope that this big cut in payments will convince the feds and payers that enough has been taken out of imaging and hopefully no more cuts will occur in the future year," Dr. David C. Levin said at the annual meeting of the Radiological Society of North America. "Unfortunately, I don’t think we can hang our hats on that hope."
Even without the so-called "fiscal cliff" around the corner, federal policy makers began cutting reimbursement for imaging services starting with the Deficit Reduction Act in 2006. Imaging has been identified in recent years as the most rapidly growing of all physician services, and it is well known that radiologists are highly compensated, he said.
As a result, efforts have been made by the Centers for Medicare and Medicaid Services to rein in reimbursements for imaging. This trend continues in the recently released final rules for the Hospital Outpatient Prospective Payment System (HOPPS).
To track these trends, the investigators used the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2000-2010. These files provide data on volume and allowed reimbursements for every procedure code. All noninvasive diagnostic imaging codes, covering all specialties and all places of service, were selected and aggregated.
From 2000 to 2006, Medicare Part B payments to physicians for noninvasive diagnostic imaging rose from $5.9 billion to $11.9 billion – a 101% increase over those years.
There was a sharp reversal in 2007 when the Deficit Reduction Act first took effect, followed by a slight rise in 2008 and progressive declines to $9.45 billion in 2010, representing a 21% decrease from 2006, said Dr. David Levin, founder of the Center for Research on Utilization of Imaging Services (CRUISE) at Thomas Jefferson University Hospital in Philadelphia.
"That’s obviously a huge hit," he said.
When looked at by specialty, radiologists’ payments from Medicare rose 81% from $2.93 billion in 2000 to $5.3 billion in 2006, before dropping 11% to $4.7 billion in 2010.
Cardiologists, the second-largest group of imaging providers, suffered more than radiologists, Dr. Levin said. Their payments fell 33% to $1.9 billion in 2010, after rising 126% from $1.3 billion in 2000 to $2.9 billion in 2006.
Medicare spent $2.3 billion on imaging services to all other physicians in 2006, a 115% increase from $1.1 billion in 2000, before throttling back 17% to $1.9 billion in 2010.
Medicare payments to independent testing facilities increased 124% from 2000 to 2006, before declining 37% from 2006 to 2010.
The Deficit Reduction Act was the biggest reason for the drop in Part B payments for noninvasive diagnostic imaging – but other factors played a role, particularly in the progressive declines seen after 2007, Dr. Levin said.
Those factors include the Multiple Payment Procedure Reduction, the Centers for Medicare and Medicaid Services’ practice expense revaluation that cut the hourly rate for noninvasive diagnostic imaging from $204 to $135, an increase in the assumed equipment utilization rate from 50% to 75%, and a decrease in the volume of advanced imaging.
Finally, there was the bundling of codes for transthoracic echocardiogram, radionuclide myocardial infusion imaging, abdominal and pelvic computed tomography, and coronary CT angiography. "These had tremendous impacts," he added.
Dr. Levin reported serving as a consultant for HealthHelp and as a director for Outpatient Imaging Affiliates. CRUISE is funded in part by the American College of Radiology.
AT THE ANNUAL MEETING OF THE RADIOLOGICAL SOCIETY OF NORTH AMERICA
Major Finding: Medicare Part B payments for noninvasive diagnostic imaging rose 101% from $5.9 million in 2000 to $11.9 billion in 2006, before falling 21% to $9.45 billion in 2010.
Data Source: Analysis of the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2000-2010.
Disclosures: Dr. Levin reported serving as a consultant for HealthHelp and as a director for Outpatient Imaging Affiliates. CRUISE is funded in part by the American College of Radiology.
Performance Disconnect: Measures Don’t Improve Hospitals’ Readmissions Experience
Two recent studies have reached the same surprising conclusion: Adherence to national quality and performance guidelines does not translate into reduced readmissions rates.
Sula Mazimba, MD, MPH, and colleagues at Kettering Medical Center in Kettering, Ohio, focused on congestive heart failure (CHF) patients, documenting compliance with four core CHF performance measures at discharge and subsequent 30-day readmissions. Only one measure-assessment of left ventricular function-had a significant association with readmissions.
A second study published the same month looked at a wider range of diagnoses in a Medicare population at more than 2,000 hospitals nationwide. That study reached similar conclusions about the disconnect between hospitals that followed Hospital Compare process quality measures and their readmission rates.
Dr. Mazimba says hospitalists and other physicians involved in quality improvement (QI) should be more involved in defining quality measures that reflect quality of care for their patients.
“We should be looking for parameters that have a higher yield for outcomes, such as preventing readmissions,” he says, encouraging better symptom management before the CHF patient is hospitalized and enhanced coordination of care after discharge.
Alpesh Amin, MD, MBA, SFHM, professor and chair of the department of medicine and executive director of the hospitalist program at the University of California at Irvine, says the findings are important, but he adds that the core quality measures studied were never designed to address readmissions.
“The challenge is to find a way to connect the dots between the core measures and readmissions,” he says.
Learn more about the four "core" heart failure quality measures for hospitals by visiting the Resource Rooms on the SHM website, or check out this 80-page implementation guide, “Improving Heart Failure Care for Hospitalized Patients [PDF],” also available on SHM’s website.
Read The Hospitalist columnist Win Whitcomb’s take on readmissions penalty programs.
Two recent studies have reached the same surprising conclusion: Adherence to national quality and performance guidelines does not translate into reduced readmissions rates.
Sula Mazimba, MD, MPH, and colleagues at Kettering Medical Center in Kettering, Ohio, focused on congestive heart failure (CHF) patients, documenting compliance with four core CHF performance measures at discharge and subsequent 30-day readmissions. Only one measure-assessment of left ventricular function-had a significant association with readmissions.
A second study published the same month looked at a wider range of diagnoses in a Medicare population at more than 2,000 hospitals nationwide. That study reached similar conclusions about the disconnect between hospitals that followed Hospital Compare process quality measures and their readmission rates.
Dr. Mazimba says hospitalists and other physicians involved in quality improvement (QI) should be more involved in defining quality measures that reflect quality of care for their patients.
“We should be looking for parameters that have a higher yield for outcomes, such as preventing readmissions,” he says, encouraging better symptom management before the CHF patient is hospitalized and enhanced coordination of care after discharge.
Alpesh Amin, MD, MBA, SFHM, professor and chair of the department of medicine and executive director of the hospitalist program at the University of California at Irvine, says the findings are important, but he adds that the core quality measures studied were never designed to address readmissions.
“The challenge is to find a way to connect the dots between the core measures and readmissions,” he says.
Learn more about the four "core" heart failure quality measures for hospitals by visiting the Resource Rooms on the SHM website, or check out this 80-page implementation guide, “Improving Heart Failure Care for Hospitalized Patients [PDF],” also available on SHM’s website.
Read The Hospitalist columnist Win Whitcomb’s take on readmissions penalty programs.
Two recent studies have reached the same surprising conclusion: Adherence to national quality and performance guidelines does not translate into reduced readmissions rates.
Sula Mazimba, MD, MPH, and colleagues at Kettering Medical Center in Kettering, Ohio, focused on congestive heart failure (CHF) patients, documenting compliance with four core CHF performance measures at discharge and subsequent 30-day readmissions. Only one measure-assessment of left ventricular function-had a significant association with readmissions.
A second study published the same month looked at a wider range of diagnoses in a Medicare population at more than 2,000 hospitals nationwide. That study reached similar conclusions about the disconnect between hospitals that followed Hospital Compare process quality measures and their readmission rates.
Dr. Mazimba says hospitalists and other physicians involved in quality improvement (QI) should be more involved in defining quality measures that reflect quality of care for their patients.
“We should be looking for parameters that have a higher yield for outcomes, such as preventing readmissions,” he says, encouraging better symptom management before the CHF patient is hospitalized and enhanced coordination of care after discharge.
Alpesh Amin, MD, MBA, SFHM, professor and chair of the department of medicine and executive director of the hospitalist program at the University of California at Irvine, says the findings are important, but he adds that the core quality measures studied were never designed to address readmissions.
“The challenge is to find a way to connect the dots between the core measures and readmissions,” he says.
Learn more about the four "core" heart failure quality measures for hospitals by visiting the Resource Rooms on the SHM website, or check out this 80-page implementation guide, “Improving Heart Failure Care for Hospitalized Patients [PDF],” also available on SHM’s website.
Read The Hospitalist columnist Win Whitcomb’s take on readmissions penalty programs.
Medical Researchers Need Access to The Social Security Death Master File
The Social Security Public Death Master File (DMF) has served as a valuable source of data for medical researchers, providing information critical for long-term survival and epidemiological studies. The DMF includes death records received by the Social Security Administration (SSA) from families, hospitals, funeral homes and financial institutions dating from 1936 to the present. Since 2002, the DMF has also included death records supplied by state governments, which constitute approximately 35% of the newest death records located in the DMF. However, as of November 1, 2011, the SSA no longer discloses state-supplied death records in the public version of the DMF. Because state records constitute such a large portion of the most current and relevant data in the DMF, the loss of this affordable database of death records has substantial negative implications for medical researchers and other groups who rely on the data for financial and research purposes. The American Association for Thoracic Surgery (AATS) has been working with other specialty societies to advocate for restored access to the full DMF for medical researchers.

Importance of the DMF to Medical Research
The DMF is a popular research tool because it is updated weekly and the full DMF file plus weekly updates can cost as little as $8,500 annually. The Center for Disease Control and Prevention (CDC) keeps a more complete record of deaths, but the CDC database is only updated annually and can cost much more than the DMF to use for larger studies because the cost of use increases with the number of individuals searched. Therefore, the DMF is an important and affordable, though incomplete, source of data for medical researchers and practitioners, as well as members of the financial services industry and individuals performing genealogical research.
Medical researchers use the DMF to track the mortality rates of organ transplant recipients, monitor the survival rates of participants in long-term research studies, and evaluate the safety and effectiveness of various procedures and medical devices by comparing survival outcomes. The DMF is particularly useful in helping researchers track subjects who have moved and cannot be located or who have continued treatment in different institutions. Additionally, because the DMF includes the age, location, and other demographic data of decedents, researchers can study the effect of these variables on mortality outcomes. Without such information, these subjects would not be included in research results, affecting the comprehensiveness and accuracy of the studies.
According to the National Technical Information Service (NTIS), the government agency responsible for managing access to the DMF, insurance companies, fraud prevention companies, and financial institutions use the DMF to ensure the accuracy and legitimacy of various transactions. For example, insurance companies regularly check the DMF to confirm that insurance or annuity beneficiaries are still living. Recently, the New York Department of Financial Services ordered life insurance companies to search the DMF for names of policyholders to help ensure that beneficiaries unaware of the policy would be paid.
Additionally, according to the NTIS, the DMF is used to prevent identity fraud by financial services providers, government entities and fraud prevention services. By comparing the personal information supplied by an applicant against the information provided in the DMF, these institutions can ensure that applicants for government services or credit cards, for example, are not fraudulently using the personal information of a deceased individual.
Finally, professional and amateur genealogists use data from the DMF to create family trees and study family health histories. According to the Records Preservation and Access Committee, a coalition of various genealogical societies, genealogists must have access to the Social Security numbers of decedents to make certain that they have identified the correct decedent in their research. Particularly when genealogical research involves locating information about a decedent with a common name, accessing death records connected to a Social Security number is necessary for accurate research.
Improper Uses of the DMF: Identity Theft and Incorrect Death Reporting
Because the DMF includes a decedent’s full Social Security number, its role in facilitating identity theft has become an issue of increasing concern to the SSA, Congress, and consumer advocacy groups. Witnesses in a Congressional hearing on the DMF held in February reported that identity thieves are using the personal information of deceased children listed in the DMF to file false tax returns by listing the child as a dependent.
CNN Money reports that identity thieves use the personal information of over two million deceased Americans per year for purposes of opening bank and credit card accounts. Although the number of these identity thefts resulting from the use of DMF data specifically has not yet been studied, the potential for abuse by users of the DMF has contributed to the current and proposed restrictions to DMF data accessibility.
In addition to concerns regarding the publication of personal information of deceased individuals, members of Congress and consumer protection groups are also concerned about the publication of personal information of living people mistakenly placed on the DMF. According to the SSA, the names and personal information of over 14,000 living people per year are accidently placed in the DMF. In addition to the risks associated with having such personal information publically available, being listed in the DMF can have severe financial implications.
Because fraud prevention services use the DMF to cross-check accounts and applications to ensure that a criminal is not fraudulently using a deceased person’s identity, individuals listed may not be able to apply for a loan or open bank accounts, or may have their accounts closed, resulting in months of inconvenience until the SSA corrects the mistake. Due to the increasing rate of identity theft and the relative ease of finding information from the DMF on the Internet, consumer protection advocates concerned with the amount of personal information listed have argued that the risks of the public availability of such information justify eliminating public access to the DMF entirely.
Changes in Access to the DMF
In 1980, a court-mandated settlement required the SSA to disclose information from all of the death records it received, including the Social Security numbers, names, birthdays, and dates of death of the decedents. In 1983, however, Congress amended the statutes governing the SSA to exempt state death records from the public disclosure requirement, while continuing to allow the SSA to share the data with other governmental agencies. Despite the 1983 legislation exempting such records from required public disclosure, the SSA publicly reported information received from state death records beginning in 2002. However, due to controversy surrounding incorrect death reports in the DMF and identity thefts arising from personal information allegedly gathered from the DMF, the SSA concluded last year that it could no longer disclose death records obtained from state governments. According to a recent New York Times article, as a result of this decision four million entries were removed from the DMF and the number of new entries per year is expected to drop by approximately 35% compared to the amount of 2010 records.
Since 2011, several bills have been introduced in Congress to further restrict access to the DMF. Last year, Representative Samuel Johnson (R-TX) proposed new legislation, the Keeping IDs Safe Act of 2011 (H.R. 3475), that would limit the use of all DMF data to law enforcement, tax administration, and federal and state agency research purposes only. Senator Bill Nelson (D-FL) included a provision in his proposed Identity Theft and Tax Fraud Prevention Act (S. 3432) that would forbid the SSA from disclosing any information in the DMF regarding a recently deceased individual in order to combat tax fraud.
Potential Solutions to Provide Medical Researchers Access to the DMF
By refusing to disclose state death records to appropriate users of the DMF, the SSA has failed to balance the valid concerns of protecting personal information with the need for researchers and other legitimate users to have access to information needed to efficiently track deceased individuals. As previously discussed, Representative Johnson’s proposed legislation goes even further than the recent SSA policy change, eliminating almost all public access to the DMF. According to Toby McIntosh from Bloomberg BNA, this past summer the SSA and various financial entities began discussions that would allow these groups to continue to access the DMF provided that they undertake various security measures to ensure the privacy of the data received. This form of "limited access" and imposition of security requirements on users could easily be extended to medical researchers. Likewise, the DMF limitations found in Senator Nelson’s proposed Identity Theft and Tax Fraud Prevention Act include an exception for "certified" users, defined as those users who need access to the DMF for the detection and prevention of fraud. AATS and other medical societies have urged Congress to recognize the importance of the full DMF data for medical research and include medical researchers in the groups permitted to access the full DMF. Both of these pieces of legislation can be amended to ensure that DMF data stays out of the hands of criminals while continuing to allow medical researchers access to this valuable database.
Please contact your local representative and senator to encourage them to support a medical research exception to any legislation that would restrict public access to the DMF. Legislation that imposes restrictions on public access to the DMF while including tailored exceptions for carefully screened and monitored users would address the potential for abusive use of the DMF, while permitting complete and timely access to those who rely on it for legitimate purposes.
Ms. Halpern is counsel at Hogan Lovells in Washington, D.C. and writes on medico-legal issues for the American Association for Thoracic Surgery.
The Social Security Public Death Master File (DMF) has served as a valuable source of data for medical researchers, providing information critical for long-term survival and epidemiological studies. The DMF includes death records received by the Social Security Administration (SSA) from families, hospitals, funeral homes and financial institutions dating from 1936 to the present. Since 2002, the DMF has also included death records supplied by state governments, which constitute approximately 35% of the newest death records located in the DMF. However, as of November 1, 2011, the SSA no longer discloses state-supplied death records in the public version of the DMF. Because state records constitute such a large portion of the most current and relevant data in the DMF, the loss of this affordable database of death records has substantial negative implications for medical researchers and other groups who rely on the data for financial and research purposes. The American Association for Thoracic Surgery (AATS) has been working with other specialty societies to advocate for restored access to the full DMF for medical researchers.
Importance of the DMF to Medical Research
The DMF is a popular research tool because it is updated weekly and the full DMF file plus weekly updates can cost as little as $8,500 annually. The Center for Disease Control and Prevention (CDC) keeps a more complete record of deaths, but the CDC database is only updated annually and can cost much more than the DMF to use for larger studies because the cost of use increases with the number of individuals searched. Therefore, the DMF is an important and affordable, though incomplete, source of data for medical researchers and practitioners, as well as members of the financial services industry and individuals performing genealogical research.
Medical researchers use the DMF to track the mortality rates of organ transplant recipients, monitor the survival rates of participants in long-term research studies, and evaluate the safety and effectiveness of various procedures and medical devices by comparing survival outcomes. The DMF is particularly useful in helping researchers track subjects who have moved and cannot be located or who have continued treatment in different institutions. Additionally, because the DMF includes the age, location, and other demographic data of decedents, researchers can study the effect of these variables on mortality outcomes. Without such information, these subjects would not be included in research results, affecting the comprehensiveness and accuracy of the studies.
According to the National Technical Information Service (NTIS), the government agency responsible for managing access to the DMF, insurance companies, fraud prevention companies, and financial institutions use the DMF to ensure the accuracy and legitimacy of various transactions. For example, insurance companies regularly check the DMF to confirm that insurance or annuity beneficiaries are still living. Recently, the New York Department of Financial Services ordered life insurance companies to search the DMF for names of policyholders to help ensure that beneficiaries unaware of the policy would be paid.
Additionally, according to the NTIS, the DMF is used to prevent identity fraud by financial services providers, government entities and fraud prevention services. By comparing the personal information supplied by an applicant against the information provided in the DMF, these institutions can ensure that applicants for government services or credit cards, for example, are not fraudulently using the personal information of a deceased individual.
Finally, professional and amateur genealogists use data from the DMF to create family trees and study family health histories. According to the Records Preservation and Access Committee, a coalition of various genealogical societies, genealogists must have access to the Social Security numbers of decedents to make certain that they have identified the correct decedent in their research. Particularly when genealogical research involves locating information about a decedent with a common name, accessing death records connected to a Social Security number is necessary for accurate research.
Improper Uses of the DMF: Identity Theft and Incorrect Death Reporting
Because the DMF includes a decedent’s full Social Security number, its role in facilitating identity theft has become an issue of increasing concern to the SSA, Congress, and consumer advocacy groups. Witnesses in a Congressional hearing on the DMF held in February reported that identity thieves are using the personal information of deceased children listed in the DMF to file false tax returns by listing the child as a dependent.
CNN Money reports that identity thieves use the personal information of over two million deceased Americans per year for purposes of opening bank and credit card accounts. Although the number of these identity thefts resulting from the use of DMF data specifically has not yet been studied, the potential for abuse by users of the DMF has contributed to the current and proposed restrictions to DMF data accessibility.
In addition to concerns regarding the publication of personal information of deceased individuals, members of Congress and consumer protection groups are also concerned about the publication of personal information of living people mistakenly placed on the DMF. According to the SSA, the names and personal information of over 14,000 living people per year are accidently placed in the DMF. In addition to the risks associated with having such personal information publically available, being listed in the DMF can have severe financial implications.
Because fraud prevention services use the DMF to cross-check accounts and applications to ensure that a criminal is not fraudulently using a deceased person’s identity, individuals listed may not be able to apply for a loan or open bank accounts, or may have their accounts closed, resulting in months of inconvenience until the SSA corrects the mistake. Due to the increasing rate of identity theft and the relative ease of finding information from the DMF on the Internet, consumer protection advocates concerned with the amount of personal information listed have argued that the risks of the public availability of such information justify eliminating public access to the DMF entirely.
Changes in Access to the DMF
In 1980, a court-mandated settlement required the SSA to disclose information from all of the death records it received, including the Social Security numbers, names, birthdays, and dates of death of the decedents. In 1983, however, Congress amended the statutes governing the SSA to exempt state death records from the public disclosure requirement, while continuing to allow the SSA to share the data with other governmental agencies. Despite the 1983 legislation exempting such records from required public disclosure, the SSA publicly reported information received from state death records beginning in 2002. However, due to controversy surrounding incorrect death reports in the DMF and identity thefts arising from personal information allegedly gathered from the DMF, the SSA concluded last year that it could no longer disclose death records obtained from state governments. According to a recent New York Times article, as a result of this decision four million entries were removed from the DMF and the number of new entries per year is expected to drop by approximately 35% compared to the amount of 2010 records.
Since 2011, several bills have been introduced in Congress to further restrict access to the DMF. Last year, Representative Samuel Johnson (R-TX) proposed new legislation, the Keeping IDs Safe Act of 2011 (H.R. 3475), that would limit the use of all DMF data to law enforcement, tax administration, and federal and state agency research purposes only. Senator Bill Nelson (D-FL) included a provision in his proposed Identity Theft and Tax Fraud Prevention Act (S. 3432) that would forbid the SSA from disclosing any information in the DMF regarding a recently deceased individual in order to combat tax fraud.
Potential Solutions to Provide Medical Researchers Access to the DMF
By refusing to disclose state death records to appropriate users of the DMF, the SSA has failed to balance the valid concerns of protecting personal information with the need for researchers and other legitimate users to have access to information needed to efficiently track deceased individuals. As previously discussed, Representative Johnson’s proposed legislation goes even further than the recent SSA policy change, eliminating almost all public access to the DMF. According to Toby McIntosh from Bloomberg BNA, this past summer the SSA and various financial entities began discussions that would allow these groups to continue to access the DMF provided that they undertake various security measures to ensure the privacy of the data received. This form of "limited access" and imposition of security requirements on users could easily be extended to medical researchers. Likewise, the DMF limitations found in Senator Nelson’s proposed Identity Theft and Tax Fraud Prevention Act include an exception for "certified" users, defined as those users who need access to the DMF for the detection and prevention of fraud. AATS and other medical societies have urged Congress to recognize the importance of the full DMF data for medical research and include medical researchers in the groups permitted to access the full DMF. Both of these pieces of legislation can be amended to ensure that DMF data stays out of the hands of criminals while continuing to allow medical researchers access to this valuable database.
Please contact your local representative and senator to encourage them to support a medical research exception to any legislation that would restrict public access to the DMF. Legislation that imposes restrictions on public access to the DMF while including tailored exceptions for carefully screened and monitored users would address the potential for abusive use of the DMF, while permitting complete and timely access to those who rely on it for legitimate purposes.
Ms. Halpern is counsel at Hogan Lovells in Washington, D.C. and writes on medico-legal issues for the American Association for Thoracic Surgery.
The Social Security Public Death Master File (DMF) has served as a valuable source of data for medical researchers, providing information critical for long-term survival and epidemiological studies. The DMF includes death records received by the Social Security Administration (SSA) from families, hospitals, funeral homes and financial institutions dating from 1936 to the present. Since 2002, the DMF has also included death records supplied by state governments, which constitute approximately 35% of the newest death records located in the DMF. However, as of November 1, 2011, the SSA no longer discloses state-supplied death records in the public version of the DMF. Because state records constitute such a large portion of the most current and relevant data in the DMF, the loss of this affordable database of death records has substantial negative implications for medical researchers and other groups who rely on the data for financial and research purposes. The American Association for Thoracic Surgery (AATS) has been working with other specialty societies to advocate for restored access to the full DMF for medical researchers.
Importance of the DMF to Medical Research
The DMF is a popular research tool because it is updated weekly and the full DMF file plus weekly updates can cost as little as $8,500 annually. The Center for Disease Control and Prevention (CDC) keeps a more complete record of deaths, but the CDC database is only updated annually and can cost much more than the DMF to use for larger studies because the cost of use increases with the number of individuals searched. Therefore, the DMF is an important and affordable, though incomplete, source of data for medical researchers and practitioners, as well as members of the financial services industry and individuals performing genealogical research.
Medical researchers use the DMF to track the mortality rates of organ transplant recipients, monitor the survival rates of participants in long-term research studies, and evaluate the safety and effectiveness of various procedures and medical devices by comparing survival outcomes. The DMF is particularly useful in helping researchers track subjects who have moved and cannot be located or who have continued treatment in different institutions. Additionally, because the DMF includes the age, location, and other demographic data of decedents, researchers can study the effect of these variables on mortality outcomes. Without such information, these subjects would not be included in research results, affecting the comprehensiveness and accuracy of the studies.
According to the National Technical Information Service (NTIS), the government agency responsible for managing access to the DMF, insurance companies, fraud prevention companies, and financial institutions use the DMF to ensure the accuracy and legitimacy of various transactions. For example, insurance companies regularly check the DMF to confirm that insurance or annuity beneficiaries are still living. Recently, the New York Department of Financial Services ordered life insurance companies to search the DMF for names of policyholders to help ensure that beneficiaries unaware of the policy would be paid.
Additionally, according to the NTIS, the DMF is used to prevent identity fraud by financial services providers, government entities and fraud prevention services. By comparing the personal information supplied by an applicant against the information provided in the DMF, these institutions can ensure that applicants for government services or credit cards, for example, are not fraudulently using the personal information of a deceased individual.
Finally, professional and amateur genealogists use data from the DMF to create family trees and study family health histories. According to the Records Preservation and Access Committee, a coalition of various genealogical societies, genealogists must have access to the Social Security numbers of decedents to make certain that they have identified the correct decedent in their research. Particularly when genealogical research involves locating information about a decedent with a common name, accessing death records connected to a Social Security number is necessary for accurate research.
Improper Uses of the DMF: Identity Theft and Incorrect Death Reporting
Because the DMF includes a decedent’s full Social Security number, its role in facilitating identity theft has become an issue of increasing concern to the SSA, Congress, and consumer advocacy groups. Witnesses in a Congressional hearing on the DMF held in February reported that identity thieves are using the personal information of deceased children listed in the DMF to file false tax returns by listing the child as a dependent.
CNN Money reports that identity thieves use the personal information of over two million deceased Americans per year for purposes of opening bank and credit card accounts. Although the number of these identity thefts resulting from the use of DMF data specifically has not yet been studied, the potential for abuse by users of the DMF has contributed to the current and proposed restrictions to DMF data accessibility.
In addition to concerns regarding the publication of personal information of deceased individuals, members of Congress and consumer protection groups are also concerned about the publication of personal information of living people mistakenly placed on the DMF. According to the SSA, the names and personal information of over 14,000 living people per year are accidently placed in the DMF. In addition to the risks associated with having such personal information publically available, being listed in the DMF can have severe financial implications.
Because fraud prevention services use the DMF to cross-check accounts and applications to ensure that a criminal is not fraudulently using a deceased person’s identity, individuals listed may not be able to apply for a loan or open bank accounts, or may have their accounts closed, resulting in months of inconvenience until the SSA corrects the mistake. Due to the increasing rate of identity theft and the relative ease of finding information from the DMF on the Internet, consumer protection advocates concerned with the amount of personal information listed have argued that the risks of the public availability of such information justify eliminating public access to the DMF entirely.
Changes in Access to the DMF
In 1980, a court-mandated settlement required the SSA to disclose information from all of the death records it received, including the Social Security numbers, names, birthdays, and dates of death of the decedents. In 1983, however, Congress amended the statutes governing the SSA to exempt state death records from the public disclosure requirement, while continuing to allow the SSA to share the data with other governmental agencies. Despite the 1983 legislation exempting such records from required public disclosure, the SSA publicly reported information received from state death records beginning in 2002. However, due to controversy surrounding incorrect death reports in the DMF and identity thefts arising from personal information allegedly gathered from the DMF, the SSA concluded last year that it could no longer disclose death records obtained from state governments. According to a recent New York Times article, as a result of this decision four million entries were removed from the DMF and the number of new entries per year is expected to drop by approximately 35% compared to the amount of 2010 records.
Since 2011, several bills have been introduced in Congress to further restrict access to the DMF. Last year, Representative Samuel Johnson (R-TX) proposed new legislation, the Keeping IDs Safe Act of 2011 (H.R. 3475), that would limit the use of all DMF data to law enforcement, tax administration, and federal and state agency research purposes only. Senator Bill Nelson (D-FL) included a provision in his proposed Identity Theft and Tax Fraud Prevention Act (S. 3432) that would forbid the SSA from disclosing any information in the DMF regarding a recently deceased individual in order to combat tax fraud.
Potential Solutions to Provide Medical Researchers Access to the DMF
By refusing to disclose state death records to appropriate users of the DMF, the SSA has failed to balance the valid concerns of protecting personal information with the need for researchers and other legitimate users to have access to information needed to efficiently track deceased individuals. As previously discussed, Representative Johnson’s proposed legislation goes even further than the recent SSA policy change, eliminating almost all public access to the DMF. According to Toby McIntosh from Bloomberg BNA, this past summer the SSA and various financial entities began discussions that would allow these groups to continue to access the DMF provided that they undertake various security measures to ensure the privacy of the data received. This form of "limited access" and imposition of security requirements on users could easily be extended to medical researchers. Likewise, the DMF limitations found in Senator Nelson’s proposed Identity Theft and Tax Fraud Prevention Act include an exception for "certified" users, defined as those users who need access to the DMF for the detection and prevention of fraud. AATS and other medical societies have urged Congress to recognize the importance of the full DMF data for medical research and include medical researchers in the groups permitted to access the full DMF. Both of these pieces of legislation can be amended to ensure that DMF data stays out of the hands of criminals while continuing to allow medical researchers access to this valuable database.
Please contact your local representative and senator to encourage them to support a medical research exception to any legislation that would restrict public access to the DMF. Legislation that imposes restrictions on public access to the DMF while including tailored exceptions for carefully screened and monitored users would address the potential for abusive use of the DMF, while permitting complete and timely access to those who rely on it for legitimate purposes.
Ms. Halpern is counsel at Hogan Lovells in Washington, D.C. and writes on medico-legal issues for the American Association for Thoracic Surgery.

Soaring Healthcare Expenses Draw Attention to Price Transparency As Cost Control
As efforts intensify to rein in the soaring cost of healthcare, greater attention is being paid to the cost-control potential of price transparency. Initially envisioned as a consumer-driven dynamic, price transparency beckons physicians to consider much more seriously the cost impacts of their diagnostic and treatment decisions.
Consumer-Driven Approach
The U.S. Department of Health and Human Services (HHS) regards price transparency as an important weapon in its armamentarium of “value-driven” approaches to drive down the cost of healthcare. By unleashing the energy of the savvy shopper and empowering consumers with the ability to compare the price and quality of healthcare services, they can make informed choices of their doctors and hospitals. In turn, HHS hopes to motivate the entire system to provide better care for less money.
That “empowered consumerism” principle is the guiding impetus for the Affordable Care Act’s state-regulated health insurance exchange apparatus, which, beginning in 2014, will present a side-by-side comparison of health plan choices, premium costs, and out-of-pocket copays in a way that is designed to help consumers shop for better-value health plans.
Some health plans are using price transparency to nudge consumers to choose lower-cost healthcare service options. Anthem BlueCross BlueShield, for example, has launched the Compass SmartShopper program (www.compasssmartshopper.com), which gives members in New Hampshire, Connecticut, and Indiana $50 to $200 if they get a diagnostic test or surgical procedure at a less expensive facility. Anthem notes that the cost for the same service can vary greatly. For example, hernia repairs range in price from $4,026 to $7,498, and colonoscopies range from $1,450 to $2,973.
New price transparency tools also are available (HealthCareBlueBook.com and FairHealthConsumer.org, for example) to help consumers who face high deductibles or out-of-pocket costs to find “fair prices” for surgeries, hospital stays, doctor visits, and medical tests—and shop accordingly.
Despite these developments, however, there is limited evidence that the “empowered consumerism” approach to price transparency will spur consumers to choose lower-cost providers. Some experts note that many consumers equate higher-cost providers with higher quality, and caution that healthcare cost-profiling initiatives might even have the perverse effect of deterring them from seeking these providers.1 Cost measures, they argue, must be tied to quality information in order to neutralize the typical association of high costs with higher quality.1
Provider-Driven Approach
There are healthcare price transparency initiatives that address the supply side of the healthcare cost equation. These initiatives seek to educate physicians about the ways in which their clinical decisions drive cost and affect what patients pay for care. Some believe that this approach has the potential to make a much bigger dent in cost containment than the empowered-consumerism approach.
“Ninety percent of healthcare cost comes from a physician’s pen, but a lot of that spending doesn’t help patients get better,” says Neel Shah, MD, a Harvard-affiliated OBGYN and executive director of Costs of Care (www.costsofcare.org), a nonprofit aimed at empowering both patients and their caregivers to deflate medical bills. The challenge, he adds, is making physicians aware of how their decisions can inflate costs unnecessarily, and giving them the training and tools they need to take appropriate action.
“Just as the patient-safety movement helped caregivers think about how to prevent unintended harm, a new movement is needed to educate doctors, nurses, and other caregivers about the cost and value of their decisions, so they can avoid waste and protect patients from unintended financial harms as well,” Dr. Shah says.
Costs of Care recently launched its Teaching Value Project, which employs Web-based video education modules to help medical students and residents learn to optimize both quality and cost in clinical decision-making.
“We’re also developing an iPhone app to put cost and quality information at physicians’ fingertips at the critical moment when medical decisions are made,” Dr. Shah adds. “Just being able to see the price variation—an ultrasound versus a CT scan, a generic versus a brand-name medication, or the cost of a marginally valuable test—can help drive physician ordering behavior.”
Hospitalist Impacts
Robert A. Bessler, MD, CEO of Tacoma, Wash.-based hospitalist management firm Sound Physicians, says his hospitalists spend about $2 million a year “with their pen or computerized physician order entry.” A quarter of the cost is pharmacy-related, and the “majority of the rest is from bed-days.”

“The most expensive thing we do is make the decision to admit,” Dr. Bessler notes. “With hospitals switching from revenue centers to cost centers in a population health/ACO [accountable-care organization] environment, an increasingly important part of the hospitalist’s job will be asking
questions, such as, ‘Could this patient go to a nursing home tonight from the ER?’ and ‘Can my colleague in the post-acute environment take care of this patient, with the same effective outcome, if we provide more intense services in the nursing home, going forward?’”
Because most diagnostic testing is done on the front end of an inpatient’s stay, the hospitalist’s main contribution to cost control is to get that diagnosis right and use consults to answer specific questions, Dr. Bessler explains. “There is a direct correlation between the number of consults and the volume of procedures which lead to higher inpatient costs,” he adds.
As hospitals convert to value-based care models, and pressure increases on hospitalists to ramp up their analysis and sharing of cost data and resource utilization, not all physicians will find that conversion easy.

—Neel Shah, MD, executive director, Costs of Care
“We are trained to take good care of our patients, not to be financial stewards of the healthcare system,” says SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, SFHM. “Now, physicians are being asked to do both—to watch our resource use without looking like we’re selling out to payors. You’re putting physicians in a difficult position. Will they say to patients, ‘You can’t have this service’? When does being pragmatic stewards of resources become rationing?” he cautions.
Dr. Shah concedes that there is a perceived tension between “what’s best” for my patient and “what’s best” for society. “We, as a profession, haven’t given serious attention to how to navigate those tensions,” he says.
Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York City, says it’s time to start down the transparency road.
“Otherwise, we will have a centralized body making these decisions for us,” he says.
Christopher Guadagnino is a freelance medical writer in Philadelphia.
Reference
As efforts intensify to rein in the soaring cost of healthcare, greater attention is being paid to the cost-control potential of price transparency. Initially envisioned as a consumer-driven dynamic, price transparency beckons physicians to consider much more seriously the cost impacts of their diagnostic and treatment decisions.
Consumer-Driven Approach
The U.S. Department of Health and Human Services (HHS) regards price transparency as an important weapon in its armamentarium of “value-driven” approaches to drive down the cost of healthcare. By unleashing the energy of the savvy shopper and empowering consumers with the ability to compare the price and quality of healthcare services, they can make informed choices of their doctors and hospitals. In turn, HHS hopes to motivate the entire system to provide better care for less money.
That “empowered consumerism” principle is the guiding impetus for the Affordable Care Act’s state-regulated health insurance exchange apparatus, which, beginning in 2014, will present a side-by-side comparison of health plan choices, premium costs, and out-of-pocket copays in a way that is designed to help consumers shop for better-value health plans.
Some health plans are using price transparency to nudge consumers to choose lower-cost healthcare service options. Anthem BlueCross BlueShield, for example, has launched the Compass SmartShopper program (www.compasssmartshopper.com), which gives members in New Hampshire, Connecticut, and Indiana $50 to $200 if they get a diagnostic test or surgical procedure at a less expensive facility. Anthem notes that the cost for the same service can vary greatly. For example, hernia repairs range in price from $4,026 to $7,498, and colonoscopies range from $1,450 to $2,973.
New price transparency tools also are available (HealthCareBlueBook.com and FairHealthConsumer.org, for example) to help consumers who face high deductibles or out-of-pocket costs to find “fair prices” for surgeries, hospital stays, doctor visits, and medical tests—and shop accordingly.
Despite these developments, however, there is limited evidence that the “empowered consumerism” approach to price transparency will spur consumers to choose lower-cost providers. Some experts note that many consumers equate higher-cost providers with higher quality, and caution that healthcare cost-profiling initiatives might even have the perverse effect of deterring them from seeking these providers.1 Cost measures, they argue, must be tied to quality information in order to neutralize the typical association of high costs with higher quality.1
Provider-Driven Approach
There are healthcare price transparency initiatives that address the supply side of the healthcare cost equation. These initiatives seek to educate physicians about the ways in which their clinical decisions drive cost and affect what patients pay for care. Some believe that this approach has the potential to make a much bigger dent in cost containment than the empowered-consumerism approach.
“Ninety percent of healthcare cost comes from a physician’s pen, but a lot of that spending doesn’t help patients get better,” says Neel Shah, MD, a Harvard-affiliated OBGYN and executive director of Costs of Care (www.costsofcare.org), a nonprofit aimed at empowering both patients and their caregivers to deflate medical bills. The challenge, he adds, is making physicians aware of how their decisions can inflate costs unnecessarily, and giving them the training and tools they need to take appropriate action.
“Just as the patient-safety movement helped caregivers think about how to prevent unintended harm, a new movement is needed to educate doctors, nurses, and other caregivers about the cost and value of their decisions, so they can avoid waste and protect patients from unintended financial harms as well,” Dr. Shah says.
Costs of Care recently launched its Teaching Value Project, which employs Web-based video education modules to help medical students and residents learn to optimize both quality and cost in clinical decision-making.
“We’re also developing an iPhone app to put cost and quality information at physicians’ fingertips at the critical moment when medical decisions are made,” Dr. Shah adds. “Just being able to see the price variation—an ultrasound versus a CT scan, a generic versus a brand-name medication, or the cost of a marginally valuable test—can help drive physician ordering behavior.”
Hospitalist Impacts
Robert A. Bessler, MD, CEO of Tacoma, Wash.-based hospitalist management firm Sound Physicians, says his hospitalists spend about $2 million a year “with their pen or computerized physician order entry.” A quarter of the cost is pharmacy-related, and the “majority of the rest is from bed-days.”
“The most expensive thing we do is make the decision to admit,” Dr. Bessler notes. “With hospitals switching from revenue centers to cost centers in a population health/ACO [accountable-care organization] environment, an increasingly important part of the hospitalist’s job will be asking
questions, such as, ‘Could this patient go to a nursing home tonight from the ER?’ and ‘Can my colleague in the post-acute environment take care of this patient, with the same effective outcome, if we provide more intense services in the nursing home, going forward?’”
Because most diagnostic testing is done on the front end of an inpatient’s stay, the hospitalist’s main contribution to cost control is to get that diagnosis right and use consults to answer specific questions, Dr. Bessler explains. “There is a direct correlation between the number of consults and the volume of procedures which lead to higher inpatient costs,” he adds.
As hospitals convert to value-based care models, and pressure increases on hospitalists to ramp up their analysis and sharing of cost data and resource utilization, not all physicians will find that conversion easy.
—Neel Shah, MD, executive director, Costs of Care
“We are trained to take good care of our patients, not to be financial stewards of the healthcare system,” says SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, SFHM. “Now, physicians are being asked to do both—to watch our resource use without looking like we’re selling out to payors. You’re putting physicians in a difficult position. Will they say to patients, ‘You can’t have this service’? When does being pragmatic stewards of resources become rationing?” he cautions.
Dr. Shah concedes that there is a perceived tension between “what’s best” for my patient and “what’s best” for society. “We, as a profession, haven’t given serious attention to how to navigate those tensions,” he says.
Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York City, says it’s time to start down the transparency road.
“Otherwise, we will have a centralized body making these decisions for us,” he says.
Christopher Guadagnino is a freelance medical writer in Philadelphia.
Reference
As efforts intensify to rein in the soaring cost of healthcare, greater attention is being paid to the cost-control potential of price transparency. Initially envisioned as a consumer-driven dynamic, price transparency beckons physicians to consider much more seriously the cost impacts of their diagnostic and treatment decisions.
Consumer-Driven Approach
The U.S. Department of Health and Human Services (HHS) regards price transparency as an important weapon in its armamentarium of “value-driven” approaches to drive down the cost of healthcare. By unleashing the energy of the savvy shopper and empowering consumers with the ability to compare the price and quality of healthcare services, they can make informed choices of their doctors and hospitals. In turn, HHS hopes to motivate the entire system to provide better care for less money.
That “empowered consumerism” principle is the guiding impetus for the Affordable Care Act’s state-regulated health insurance exchange apparatus, which, beginning in 2014, will present a side-by-side comparison of health plan choices, premium costs, and out-of-pocket copays in a way that is designed to help consumers shop for better-value health plans.
Some health plans are using price transparency to nudge consumers to choose lower-cost healthcare service options. Anthem BlueCross BlueShield, for example, has launched the Compass SmartShopper program (www.compasssmartshopper.com), which gives members in New Hampshire, Connecticut, and Indiana $50 to $200 if they get a diagnostic test or surgical procedure at a less expensive facility. Anthem notes that the cost for the same service can vary greatly. For example, hernia repairs range in price from $4,026 to $7,498, and colonoscopies range from $1,450 to $2,973.
New price transparency tools also are available (HealthCareBlueBook.com and FairHealthConsumer.org, for example) to help consumers who face high deductibles or out-of-pocket costs to find “fair prices” for surgeries, hospital stays, doctor visits, and medical tests—and shop accordingly.
Despite these developments, however, there is limited evidence that the “empowered consumerism” approach to price transparency will spur consumers to choose lower-cost providers. Some experts note that many consumers equate higher-cost providers with higher quality, and caution that healthcare cost-profiling initiatives might even have the perverse effect of deterring them from seeking these providers.1 Cost measures, they argue, must be tied to quality information in order to neutralize the typical association of high costs with higher quality.1
Provider-Driven Approach
There are healthcare price transparency initiatives that address the supply side of the healthcare cost equation. These initiatives seek to educate physicians about the ways in which their clinical decisions drive cost and affect what patients pay for care. Some believe that this approach has the potential to make a much bigger dent in cost containment than the empowered-consumerism approach.
“Ninety percent of healthcare cost comes from a physician’s pen, but a lot of that spending doesn’t help patients get better,” says Neel Shah, MD, a Harvard-affiliated OBGYN and executive director of Costs of Care (www.costsofcare.org), a nonprofit aimed at empowering both patients and their caregivers to deflate medical bills. The challenge, he adds, is making physicians aware of how their decisions can inflate costs unnecessarily, and giving them the training and tools they need to take appropriate action.
“Just as the patient-safety movement helped caregivers think about how to prevent unintended harm, a new movement is needed to educate doctors, nurses, and other caregivers about the cost and value of their decisions, so they can avoid waste and protect patients from unintended financial harms as well,” Dr. Shah says.
Costs of Care recently launched its Teaching Value Project, which employs Web-based video education modules to help medical students and residents learn to optimize both quality and cost in clinical decision-making.
“We’re also developing an iPhone app to put cost and quality information at physicians’ fingertips at the critical moment when medical decisions are made,” Dr. Shah adds. “Just being able to see the price variation—an ultrasound versus a CT scan, a generic versus a brand-name medication, or the cost of a marginally valuable test—can help drive physician ordering behavior.”
Hospitalist Impacts
Robert A. Bessler, MD, CEO of Tacoma, Wash.-based hospitalist management firm Sound Physicians, says his hospitalists spend about $2 million a year “with their pen or computerized physician order entry.” A quarter of the cost is pharmacy-related, and the “majority of the rest is from bed-days.”
“The most expensive thing we do is make the decision to admit,” Dr. Bessler notes. “With hospitals switching from revenue centers to cost centers in a population health/ACO [accountable-care organization] environment, an increasingly important part of the hospitalist’s job will be asking
questions, such as, ‘Could this patient go to a nursing home tonight from the ER?’ and ‘Can my colleague in the post-acute environment take care of this patient, with the same effective outcome, if we provide more intense services in the nursing home, going forward?’”
Because most diagnostic testing is done on the front end of an inpatient’s stay, the hospitalist’s main contribution to cost control is to get that diagnosis right and use consults to answer specific questions, Dr. Bessler explains. “There is a direct correlation between the number of consults and the volume of procedures which lead to higher inpatient costs,” he adds.
As hospitals convert to value-based care models, and pressure increases on hospitalists to ramp up their analysis and sharing of cost data and resource utilization, not all physicians will find that conversion easy.
—Neel Shah, MD, executive director, Costs of Care
“We are trained to take good care of our patients, not to be financial stewards of the healthcare system,” says SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, SFHM. “Now, physicians are being asked to do both—to watch our resource use without looking like we’re selling out to payors. You’re putting physicians in a difficult position. Will they say to patients, ‘You can’t have this service’? When does being pragmatic stewards of resources become rationing?” he cautions.
Dr. Shah concedes that there is a perceived tension between “what’s best” for my patient and “what’s best” for society. “We, as a profession, haven’t given serious attention to how to navigate those tensions,” he says.
Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York City, says it’s time to start down the transparency road.
“Otherwise, we will have a centralized body making these decisions for us,” he says.
Christopher Guadagnino is a freelance medical writer in Philadelphia.
Reference
iPad Rollout at UC-Irvine Medical Center Prompts Security Measures
The University of California’s Irvine Medical Center has been issuing iPads to its incoming class of 100 medical students and to all 18 resident physicians in its department of emergency medicine.1 The entire medical curriculum is on the iPad and employs document sharing via the SharePoint collaborative software platform, says Adam Gold, the medical center’s director of emerging technologies.
But the use of these new technologies and subsequent clamoring by students, professors, physicians, and other staff to connect their own mobile devices to the network have led to the establishment of security and management guidelines for monitoring technology use, now spelled out in the new “Bring Your Own Device” policy, Gold explains.
Reference
The University of California’s Irvine Medical Center has been issuing iPads to its incoming class of 100 medical students and to all 18 resident physicians in its department of emergency medicine.1 The entire medical curriculum is on the iPad and employs document sharing via the SharePoint collaborative software platform, says Adam Gold, the medical center’s director of emerging technologies.
But the use of these new technologies and subsequent clamoring by students, professors, physicians, and other staff to connect their own mobile devices to the network have led to the establishment of security and management guidelines for monitoring technology use, now spelled out in the new “Bring Your Own Device” policy, Gold explains.
Reference
The University of California’s Irvine Medical Center has been issuing iPads to its incoming class of 100 medical students and to all 18 resident physicians in its department of emergency medicine.1 The entire medical curriculum is on the iPad and employs document sharing via the SharePoint collaborative software platform, says Adam Gold, the medical center’s director of emerging technologies.
But the use of these new technologies and subsequent clamoring by students, professors, physicians, and other staff to connect their own mobile devices to the network have led to the establishment of security and management guidelines for monitoring technology use, now spelled out in the new “Bring Your Own Device” policy, Gold explains.
Reference
Guidelines Help Hospitalists Manage Acute Coronary Syndrome Patients

Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
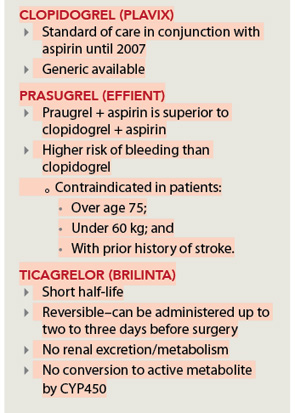
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
The Numerators: Treating Noncompliant, Medically Complicated Hospital Patients

We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
Reference
We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
Reference
We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
Reference
Recommendations for Antithrombotic and Thrombolytic Therapy
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.