User login
New Thinking, Higher Expectations Needed to Solve Hospital Readmission Problem


As we enter a new era of health-care and payment reform, we are all keenly aware of the need to limit unnecessary readmissions. We have been given tools and tips on how to most efficiently and effectively transition patients from the hospital setting to the outpatient world in order to limit the chances that they will “bounce back” to us, resulting in penalties to our hospital or health-care system. Tools such as Project BOOST and others help us to educate patients, transfer information effectively, follow up on patients post-discharge, and reconcile medications safely across the continuum of care. But without a competent and committed provider of care to “catch” the patient on the other side, we might just be dropping the ball yet again.
It is imperative as we look to safely transition patients into the next level of care that we, as hospitalists, get outside the box and begin to engage the community of care providers outside our walls, and yes, even outside of our control. We have been down this road before with other quality initiatives, which at first glance appeared to be outside our sphere of influence—such projects as post-operative antibiotic use and hospitalwide DVT prophylaxis. Given the right hospitalist leader, with the right set of leadership tools, these quality-improvement (QI) projects have been widely successful in many environments.
I would suggest that the issue of safe transitions for our patients is no different, and maybe more important, to the health and safety of our patients.
Solving the readmission problem on a local level requires an analytical approach, much like a “root-cause analysis.” We need to begin to examine the sources of our readmitted patients, as well as the routes of our discharged patients, and we need to ask ourselves if we are continuing to feed patients into the vicious circle that results in readmissions. Are there post-acute-care facilities in your area that are responsible for more than their fair share of patients returning to your service? If so, why do we continue to discharge patients to their care? Is it because we are pressured to lower length of stay, and any bed at the next level of care is better than another day in the acute-care hospital? At some point, this reasoning fails, and given the penalties coming soon, it may be better to begin to more discriminately discharge patients to facilities that provide higher-quality care and assist us in our goals to reduce unnecessary readmissions. Leading the charge in this endeavor also necessitates that we begin to engage those providers on the other side, making them aware of the quality data related to their facility and providing education and resources to assist them in improving their performance.
Realities of the Care Continuum
Several options pertaining to hospitalist groups are available. The first, already a large movement in our current marketplace, is to extend the current hospitalist group across the chasm and begin to deliver care in those post-acute facilities. Long-term acute care (LTAC) and skilled nursing facilities (SNF) are prime examples of this movement; the obvious advantage lies in the effective control of quality and efficient transfer of information that a single group can achieve when it extends to these facilities. Obviously, manpower issues and financial support are drawbacks in a model such as this.
More realistically, a group might consider taking a less aggressive approach to this problem. Educating care providers and assisting these facilities with QI projects would require fewer resources and might provide a higher return on investment (ROI) for your group and hospital. Engaging these physicians, nonphysician providers, and facility administrators is key to our ability to impact this problem. Demanding quality care for our discharged patients in terms of timeliness of follow-up, adherence to care paths, and responsiveness to changes in condition should be non-negotiable and factored into our development of referral patterns.
As our population of patients continues to be more acutely ill, and the level of care provided at post-acute care facilities continues to rise, our current reality is that a majority of these patients, at any given time, meet hospital admissions criteria. Preventing readmissions requires that post-acute care providers have mechanisms in place to stop the “knee-jerk” transfer to the emergency department, rather than attempt to evaluate and treat the patient in the facility. Interact II (http://interact2.net/index.aspx) is a resource that provides tools for post-acute-care facilities to use in monitoring their own internal data around acute-care transfers. It also provides tracking tools, communication strategies, advanced-care-planning tools, and clinical pathways for limiting the number of acute-care transfers. The reality is, once these patients end up in the emergency department, they are likely to be referred to us for consideration of readmission. The best way to stop this is to stop the transfer before it happens.
Demand Better
We, as hospitalists, need to begin to leverage our own “buying power” as it relates to the care of our patients post-discharge. We can start by educating and assisting care providers on a local level to improve compliance with well-known standards of care that prevent unnecessary readmissions. We need to be prepared to wield our collective weight as a specialty to demand from our post-acute care colleagues what has been demanded of us over the last several years: quality and value. Make no mistake—hospitalists have to get outside the box.
Dr. Harrington is an SHM board member and chief medical officer of Locum Leaders in Alpharetta, Ga.
As we enter a new era of health-care and payment reform, we are all keenly aware of the need to limit unnecessary readmissions. We have been given tools and tips on how to most efficiently and effectively transition patients from the hospital setting to the outpatient world in order to limit the chances that they will “bounce back” to us, resulting in penalties to our hospital or health-care system. Tools such as Project BOOST and others help us to educate patients, transfer information effectively, follow up on patients post-discharge, and reconcile medications safely across the continuum of care. But without a competent and committed provider of care to “catch” the patient on the other side, we might just be dropping the ball yet again.
It is imperative as we look to safely transition patients into the next level of care that we, as hospitalists, get outside the box and begin to engage the community of care providers outside our walls, and yes, even outside of our control. We have been down this road before with other quality initiatives, which at first glance appeared to be outside our sphere of influence—such projects as post-operative antibiotic use and hospitalwide DVT prophylaxis. Given the right hospitalist leader, with the right set of leadership tools, these quality-improvement (QI) projects have been widely successful in many environments.
I would suggest that the issue of safe transitions for our patients is no different, and maybe more important, to the health and safety of our patients.
Solving the readmission problem on a local level requires an analytical approach, much like a “root-cause analysis.” We need to begin to examine the sources of our readmitted patients, as well as the routes of our discharged patients, and we need to ask ourselves if we are continuing to feed patients into the vicious circle that results in readmissions. Are there post-acute-care facilities in your area that are responsible for more than their fair share of patients returning to your service? If so, why do we continue to discharge patients to their care? Is it because we are pressured to lower length of stay, and any bed at the next level of care is better than another day in the acute-care hospital? At some point, this reasoning fails, and given the penalties coming soon, it may be better to begin to more discriminately discharge patients to facilities that provide higher-quality care and assist us in our goals to reduce unnecessary readmissions. Leading the charge in this endeavor also necessitates that we begin to engage those providers on the other side, making them aware of the quality data related to their facility and providing education and resources to assist them in improving their performance.
Realities of the Care Continuum
Several options pertaining to hospitalist groups are available. The first, already a large movement in our current marketplace, is to extend the current hospitalist group across the chasm and begin to deliver care in those post-acute facilities. Long-term acute care (LTAC) and skilled nursing facilities (SNF) are prime examples of this movement; the obvious advantage lies in the effective control of quality and efficient transfer of information that a single group can achieve when it extends to these facilities. Obviously, manpower issues and financial support are drawbacks in a model such as this.
More realistically, a group might consider taking a less aggressive approach to this problem. Educating care providers and assisting these facilities with QI projects would require fewer resources and might provide a higher return on investment (ROI) for your group and hospital. Engaging these physicians, nonphysician providers, and facility administrators is key to our ability to impact this problem. Demanding quality care for our discharged patients in terms of timeliness of follow-up, adherence to care paths, and responsiveness to changes in condition should be non-negotiable and factored into our development of referral patterns.
As our population of patients continues to be more acutely ill, and the level of care provided at post-acute care facilities continues to rise, our current reality is that a majority of these patients, at any given time, meet hospital admissions criteria. Preventing readmissions requires that post-acute care providers have mechanisms in place to stop the “knee-jerk” transfer to the emergency department, rather than attempt to evaluate and treat the patient in the facility. Interact II (http://interact2.net/index.aspx) is a resource that provides tools for post-acute-care facilities to use in monitoring their own internal data around acute-care transfers. It also provides tracking tools, communication strategies, advanced-care-planning tools, and clinical pathways for limiting the number of acute-care transfers. The reality is, once these patients end up in the emergency department, they are likely to be referred to us for consideration of readmission. The best way to stop this is to stop the transfer before it happens.
Demand Better
We, as hospitalists, need to begin to leverage our own “buying power” as it relates to the care of our patients post-discharge. We can start by educating and assisting care providers on a local level to improve compliance with well-known standards of care that prevent unnecessary readmissions. We need to be prepared to wield our collective weight as a specialty to demand from our post-acute care colleagues what has been demanded of us over the last several years: quality and value. Make no mistake—hospitalists have to get outside the box.
Dr. Harrington is an SHM board member and chief medical officer of Locum Leaders in Alpharetta, Ga.
As we enter a new era of health-care and payment reform, we are all keenly aware of the need to limit unnecessary readmissions. We have been given tools and tips on how to most efficiently and effectively transition patients from the hospital setting to the outpatient world in order to limit the chances that they will “bounce back” to us, resulting in penalties to our hospital or health-care system. Tools such as Project BOOST and others help us to educate patients, transfer information effectively, follow up on patients post-discharge, and reconcile medications safely across the continuum of care. But without a competent and committed provider of care to “catch” the patient on the other side, we might just be dropping the ball yet again.
It is imperative as we look to safely transition patients into the next level of care that we, as hospitalists, get outside the box and begin to engage the community of care providers outside our walls, and yes, even outside of our control. We have been down this road before with other quality initiatives, which at first glance appeared to be outside our sphere of influence—such projects as post-operative antibiotic use and hospitalwide DVT prophylaxis. Given the right hospitalist leader, with the right set of leadership tools, these quality-improvement (QI) projects have been widely successful in many environments.
I would suggest that the issue of safe transitions for our patients is no different, and maybe more important, to the health and safety of our patients.
Solving the readmission problem on a local level requires an analytical approach, much like a “root-cause analysis.” We need to begin to examine the sources of our readmitted patients, as well as the routes of our discharged patients, and we need to ask ourselves if we are continuing to feed patients into the vicious circle that results in readmissions. Are there post-acute-care facilities in your area that are responsible for more than their fair share of patients returning to your service? If so, why do we continue to discharge patients to their care? Is it because we are pressured to lower length of stay, and any bed at the next level of care is better than another day in the acute-care hospital? At some point, this reasoning fails, and given the penalties coming soon, it may be better to begin to more discriminately discharge patients to facilities that provide higher-quality care and assist us in our goals to reduce unnecessary readmissions. Leading the charge in this endeavor also necessitates that we begin to engage those providers on the other side, making them aware of the quality data related to their facility and providing education and resources to assist them in improving their performance.
Realities of the Care Continuum
Several options pertaining to hospitalist groups are available. The first, already a large movement in our current marketplace, is to extend the current hospitalist group across the chasm and begin to deliver care in those post-acute facilities. Long-term acute care (LTAC) and skilled nursing facilities (SNF) are prime examples of this movement; the obvious advantage lies in the effective control of quality and efficient transfer of information that a single group can achieve when it extends to these facilities. Obviously, manpower issues and financial support are drawbacks in a model such as this.
More realistically, a group might consider taking a less aggressive approach to this problem. Educating care providers and assisting these facilities with QI projects would require fewer resources and might provide a higher return on investment (ROI) for your group and hospital. Engaging these physicians, nonphysician providers, and facility administrators is key to our ability to impact this problem. Demanding quality care for our discharged patients in terms of timeliness of follow-up, adherence to care paths, and responsiveness to changes in condition should be non-negotiable and factored into our development of referral patterns.
As our population of patients continues to be more acutely ill, and the level of care provided at post-acute care facilities continues to rise, our current reality is that a majority of these patients, at any given time, meet hospital admissions criteria. Preventing readmissions requires that post-acute care providers have mechanisms in place to stop the “knee-jerk” transfer to the emergency department, rather than attempt to evaluate and treat the patient in the facility. Interact II (http://interact2.net/index.aspx) is a resource that provides tools for post-acute-care facilities to use in monitoring their own internal data around acute-care transfers. It also provides tracking tools, communication strategies, advanced-care-planning tools, and clinical pathways for limiting the number of acute-care transfers. The reality is, once these patients end up in the emergency department, they are likely to be referred to us for consideration of readmission. The best way to stop this is to stop the transfer before it happens.
Demand Better
We, as hospitalists, need to begin to leverage our own “buying power” as it relates to the care of our patients post-discharge. We can start by educating and assisting care providers on a local level to improve compliance with well-known standards of care that prevent unnecessary readmissions. We need to be prepared to wield our collective weight as a specialty to demand from our post-acute care colleagues what has been demanded of us over the last several years: quality and value. Make no mistake—hospitalists have to get outside the box.
Dr. Harrington is an SHM board member and chief medical officer of Locum Leaders in Alpharetta, Ga.
Project BOOST Study Documents Modest Impact on 30-Day Hospital Readmissions

Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Wasteful Practices in Hospital Cardiac Services Identified
A recent article in the American Journal of Medical Quality reviewed 366 cardiac-related medical studies and 21 practice guidelines to identify eight measures of potential waste in hospital cardiac services.4 The wasteful measures included excess use of higher-cost implantable cardioverter-defibrillators and similar cardiac devices, the use of dual-chamber defibrillators rather than single-chamber devices, and excess lengths of stay in the hospital. The eight measures were validated with data from 261 hospitals.
The authors emphasize that their set of measures is not designed to determine clinical appropriateness but to highlight areas of potential overutilization that can be benchmarked with other hospitals.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
A recent article in the American Journal of Medical Quality reviewed 366 cardiac-related medical studies and 21 practice guidelines to identify eight measures of potential waste in hospital cardiac services.4 The wasteful measures included excess use of higher-cost implantable cardioverter-defibrillators and similar cardiac devices, the use of dual-chamber defibrillators rather than single-chamber devices, and excess lengths of stay in the hospital. The eight measures were validated with data from 261 hospitals.
The authors emphasize that their set of measures is not designed to determine clinical appropriateness but to highlight areas of potential overutilization that can be benchmarked with other hospitals.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
A recent article in the American Journal of Medical Quality reviewed 366 cardiac-related medical studies and 21 practice guidelines to identify eight measures of potential waste in hospital cardiac services.4 The wasteful measures included excess use of higher-cost implantable cardioverter-defibrillators and similar cardiac devices, the use of dual-chamber defibrillators rather than single-chamber devices, and excess lengths of stay in the hospital. The eight measures were validated with data from 261 hospitals.
The authors emphasize that their set of measures is not designed to determine clinical appropriateness but to highlight areas of potential overutilization that can be benchmarked with other hospitals.
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
Applied Psychology Improves Hand Hygiene in Hospitals
According to a recent New York Times report, hand-hygiene compliance in hospitals can be as low as 30%, with serious implications regarding hospital-acquired infections.1 While many initiatives have employed secret observers, vibrating badges, or hand-washing coaches, a Research, Innovations, and Clinical Vignettes (RIV) poster at HM13 outlined how a multidisciplinary committee at University of Colorado Hospital in Aurora applied principles of psychology to the challenge of compliance.2
The initiative focused on behavioral changes: surreptitiously auditing staff behaviors, real-time feedback, and immediate public corrections for observed nonadherence on the test unit from an infection-control champion. The study randomly assigned daily auditing responsibilities across all members of the nursing staff, including aides. Taking a page from soccer referees, auditors handed out red tickets to hygiene violators—and individually wrapped Life Savers to reinforce adherence.
When unprofessional behavior is the response to a verbal correction, leadership has to be prepared to act, explains hospitalist and lead author Ethan Cumbler, MD, FACP.
“We need to stop thinking about hospital staff and physicians as rational actors when it comes to hand hygiene, but as social animals who will respond to positive and negative reinforcements and group culture,” he says.
Noncompliant hand hygiene is largely unconscious behavior that needs to be brought to conscious attention but is amenable to change, Dr. Cumbler says, adding that “unit leadership steps in for repeated nonadherence or an unprofessional response to correction. We have never needed to intervene more than once with the same person.”
Hand-hygiene adherence reached 97% on the pilot unit in the second quarter of 2012 and has remained at that level, Dr. Cumbler says. Additionally, iatrogenic infections dropped to zero from 4.8 per 1,000 urinary catheter days, with bloodstream infections falling at a similar rate.
Similar results with hand-hygiene compliance have been reported at St. Mary’s Health Center in St. Louis, which has been testing a system that reminds nurses to wash their hands at various checkpoints in the hospital, tracking their compliance with a badge that turns green when registering the presence of hand sanitizer, thereby informing patients that the nurse’s hands are clean.
The system, developed by Biovigil Hygiene Technologies of Ann Arbor, Mich., started on two pilot units last year, where compliance has grown to 97% and 99%, respectively. System set-up can cost about $2,000 per patient room, plus monthly subscriptions per employee, but more hospitals in the system could sign on next year, reports the St. Louis Post-Dispatch.3
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
According to a recent New York Times report, hand-hygiene compliance in hospitals can be as low as 30%, with serious implications regarding hospital-acquired infections.1 While many initiatives have employed secret observers, vibrating badges, or hand-washing coaches, a Research, Innovations, and Clinical Vignettes (RIV) poster at HM13 outlined how a multidisciplinary committee at University of Colorado Hospital in Aurora applied principles of psychology to the challenge of compliance.2
The initiative focused on behavioral changes: surreptitiously auditing staff behaviors, real-time feedback, and immediate public corrections for observed nonadherence on the test unit from an infection-control champion. The study randomly assigned daily auditing responsibilities across all members of the nursing staff, including aides. Taking a page from soccer referees, auditors handed out red tickets to hygiene violators—and individually wrapped Life Savers to reinforce adherence.
When unprofessional behavior is the response to a verbal correction, leadership has to be prepared to act, explains hospitalist and lead author Ethan Cumbler, MD, FACP.
“We need to stop thinking about hospital staff and physicians as rational actors when it comes to hand hygiene, but as social animals who will respond to positive and negative reinforcements and group culture,” he says.
Noncompliant hand hygiene is largely unconscious behavior that needs to be brought to conscious attention but is amenable to change, Dr. Cumbler says, adding that “unit leadership steps in for repeated nonadherence or an unprofessional response to correction. We have never needed to intervene more than once with the same person.”
Hand-hygiene adherence reached 97% on the pilot unit in the second quarter of 2012 and has remained at that level, Dr. Cumbler says. Additionally, iatrogenic infections dropped to zero from 4.8 per 1,000 urinary catheter days, with bloodstream infections falling at a similar rate.
Similar results with hand-hygiene compliance have been reported at St. Mary’s Health Center in St. Louis, which has been testing a system that reminds nurses to wash their hands at various checkpoints in the hospital, tracking their compliance with a badge that turns green when registering the presence of hand sanitizer, thereby informing patients that the nurse’s hands are clean.
The system, developed by Biovigil Hygiene Technologies of Ann Arbor, Mich., started on two pilot units last year, where compliance has grown to 97% and 99%, respectively. System set-up can cost about $2,000 per patient room, plus monthly subscriptions per employee, but more hospitals in the system could sign on next year, reports the St. Louis Post-Dispatch.3
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
According to a recent New York Times report, hand-hygiene compliance in hospitals can be as low as 30%, with serious implications regarding hospital-acquired infections.1 While many initiatives have employed secret observers, vibrating badges, or hand-washing coaches, a Research, Innovations, and Clinical Vignettes (RIV) poster at HM13 outlined how a multidisciplinary committee at University of Colorado Hospital in Aurora applied principles of psychology to the challenge of compliance.2
The initiative focused on behavioral changes: surreptitiously auditing staff behaviors, real-time feedback, and immediate public corrections for observed nonadherence on the test unit from an infection-control champion. The study randomly assigned daily auditing responsibilities across all members of the nursing staff, including aides. Taking a page from soccer referees, auditors handed out red tickets to hygiene violators—and individually wrapped Life Savers to reinforce adherence.
When unprofessional behavior is the response to a verbal correction, leadership has to be prepared to act, explains hospitalist and lead author Ethan Cumbler, MD, FACP.
“We need to stop thinking about hospital staff and physicians as rational actors when it comes to hand hygiene, but as social animals who will respond to positive and negative reinforcements and group culture,” he says.
Noncompliant hand hygiene is largely unconscious behavior that needs to be brought to conscious attention but is amenable to change, Dr. Cumbler says, adding that “unit leadership steps in for repeated nonadherence or an unprofessional response to correction. We have never needed to intervene more than once with the same person.”
Hand-hygiene adherence reached 97% on the pilot unit in the second quarter of 2012 and has remained at that level, Dr. Cumbler says. Additionally, iatrogenic infections dropped to zero from 4.8 per 1,000 urinary catheter days, with bloodstream infections falling at a similar rate.
Similar results with hand-hygiene compliance have been reported at St. Mary’s Health Center in St. Louis, which has been testing a system that reminds nurses to wash their hands at various checkpoints in the hospital, tracking their compliance with a badge that turns green when registering the presence of hand sanitizer, thereby informing patients that the nurse’s hands are clean.
The system, developed by Biovigil Hygiene Technologies of Ann Arbor, Mich., started on two pilot units last year, where compliance has grown to 97% and 99%, respectively. System set-up can cost about $2,000 per patient room, plus monthly subscriptions per employee, but more hospitals in the system could sign on next year, reports the St. Louis Post-Dispatch.3
Larry Beresford is a freelance writer in San Francisco.
References
- Hartocollis A. With money at risk, hospitals push staff to wash hands. The New York Times website. Available at: http://www.nytimes.com/2013/05/29/nyregion/hospitals-struggle-to-get-workers-to-wash-their-hands.html?pagewanted=all&_r=0. Accessed May 28, 2013.
- Cumbler E, Castillo L, Satorie L, et al. Culture change in infection control: applying psychological principles to improve hand hygiene. J Nurs Care Qual. 2013 May 10 [Epub ahead of print].
- Bernhard B. High tech hand washing comes to St. Louis hospital. St. Louis Post-Dispatch website. Available at: http://www.stltoday.com/lifestyles/health-med-fit/health/high-tech-hand-washing-comes-to-st-louis-hospital/article_9379065d-85ff-5643-bae2-899254cb22fa.html. Accessed June 27, 2013.
- Lowe TJ, Partovian C, Kroch E, Martin J, Bankowitz R. Measuring cardiac waste: the Premier cardiac waste measures. Am J Med Qual. 2013 May 29 [Epub ahead of print].
- Elixhauser A, Steiner C. Readmissions to U.S. hospitals by diagnosis, 2010. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb153.pdf. Accessed July 15, 2013.
- Jackson Healthcare. Filling the void: 2013 physician outlook & practice trends. Jackson Healthcare website. Available at: http://www.jacksonhealthcare.com/media/193525/jc-2013physiciantrends-void_ebk0513.pdf. Accessed July 15, 2013.
Patient Satisfaction Surveys Not Accurate Measure of Hospitalists’ Performance

Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
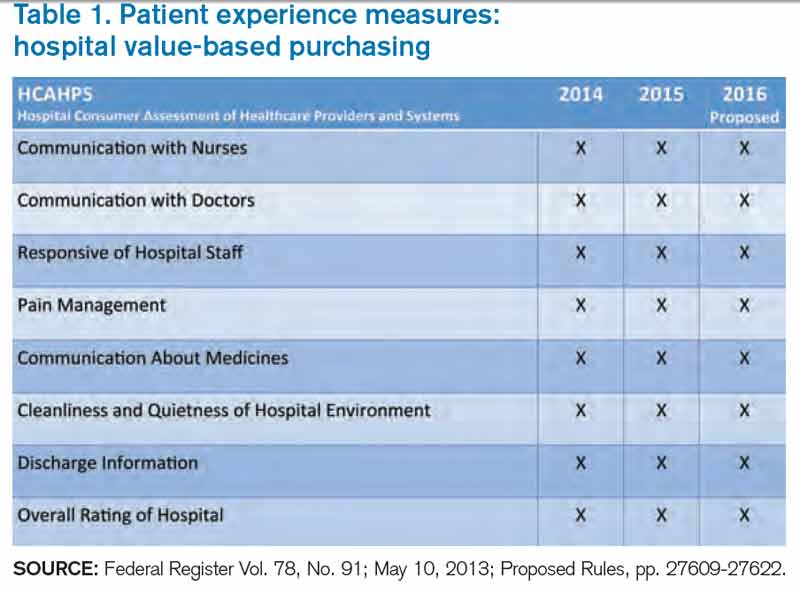
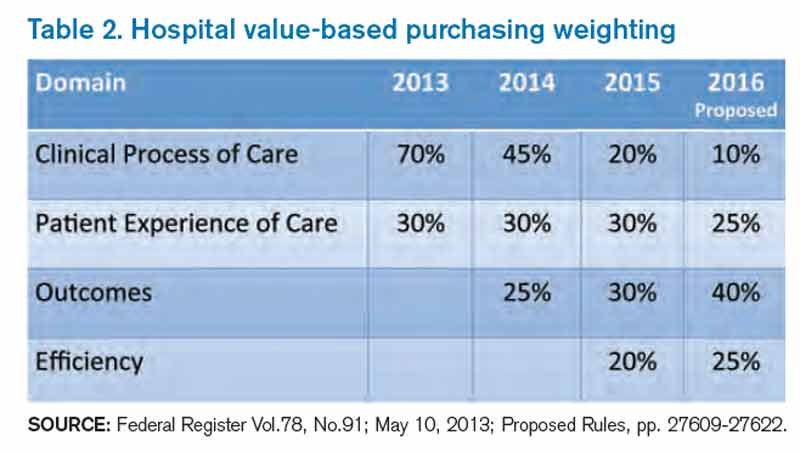
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Feeling frustrated with your group’s patient-satisfaction performance? Wondering why your chief (fill in the blank) officer glazes over when you try to explain why your hospitalist group’s Hospital Consumer Assessment of Healthcare Providers and System (HCAHPS) scores for doctor communication are in a percentile rivaling the numeric age of your children?
It is likely that the C-suite administrator overseeing your hospitalist group has a portion of their pay based on HCAHPS or other patient-satisfaction (also called patient experience) scores. And for good reason: The Centers for Medicare & Medicaid Services (CMS) Hospital Value-Based Purchasing (HVBP) program that started Oct. 1, 2012, has placed your hospital’s Medicare reimbursement at risk based on its HCAHPS scores.
HVBP and Patient Satisfaction
Patient satisfaction will remain an important part of HVBP in the coming years. Table 1 (below) shows the domains that will be included in fiscal years 2014 (which starts Oct. 1, 2013), 2015, and 2016. Table 2 (below) depicts the percent weighting the patient-satisfaction domain will receive through 2016. You may recall that HVBP is a program in which all hospitals place 1% to 2% (2013 through 2017, starting at 1% and increasing each year by 0.25% so that by 2017%, it is 2%) of their CMS inpatient payments in a withhold pool and, based on performance, can make back some, all, or an amount in excess of the amount placed in the withhold pool.
Source: Federal Register Vol. 78, No. 91; May 10, 2013; Proposed Rules, pp. 27609-27622.
Source: Federal Register Vol.78, No.91; May 10, 2013; Proposed Rules, pp. 27609-27622.
End In Itself
A colleague of mine recently asked, “Is an increase in patient satisfaction associated with higher quality of care and better patient safety?” The point here: It doesn’t matter. Patient satisfaction is an end in itself, and we should strive to maximize it, or at least put ourselves in the place of the patient and design care accordingly.
For Hospitalists: A Starting Point
There is a conundrum for hospitalists vis-à-vis patient satisfaction. Follow this chain of logic: The hospitals at which we work are incented to perform well on the HCAHPS domains. Hospitals pay a lot for hospitalists. Hospitalists can impact many of the HCAHPS domains. So shouldn’t hospitalists be judged according to HCAHPS scores?
Yes and no.
HCAHPS as a survey is intended to measure a patient’s overall experience of receiving care in the hospital. For example, from the “Doctor Communication” domain, we have questions like “how often did doctors treat you with courtesy and respect?” And “how often did doctors explain things in a way you could understand?”
These questions, like all in HCAHPS, are not designed to get at individual doctor performance, or even performance of a group of doctors, such as hospitalists. Instead, they are designed to measure a patient’s overall experience with the hospitalization, and “Doctor Communication” questions are designed to assess satisfaction with “doctors” collectively.
The Need for Hospitalist-Specific Satisfaction Surveys
So while HCAHPS is not designed to measure hospitalist performance with regard to patient satisfaction, it is a reasonable interim step for hospitals to judge hospitalists according to HCAHPS. However, this should be a bridge to a strategy that adopts hospitalist-specific patient-satisfaction questionnaires in the future and not an end in itself.
Why? Perhaps the biggest reason is that HCAHPS scores are neither specific nor timely enough to form the basis of improvement efforts for hospitalists. If a hospitalist receives a low score on the “Doctor Communication” domain, the scores are likely to be three to nine months old. How can we legitimately assign (and then modify) behaviors based on those scores?
Further, because the survey is not built to measure patient satisfaction specifically with hospitalists, the results are unlikely to engender meaningful and sustained behavior change. Hospitalists I talk to are generally bewildered and confused by HCAHPS scores attributed to them or their groups. Even if they understand the scores, I almost never see true quality improvement (plan-do-study-act) based on specific HCAHPS results. Instead, I see hospitalists trying to adhere to “best practices,” with no adjustments made along the way based on performance.
Nearly all the prominent patient satisfaction vendors have developed a survey instrument specifically designed for hospitalists. Each has an approach to appropriately attribute performance to the hospitalist in question, and each has a battery of questions that is designed to capture patient satisfaction with the hospitalist. Although use of these surveys involves an added financial commitment, I submit that because hospitalists have an unparalleled proximity to hospitalized patients, such an investment is worthy of consideration and has an accompanying business case, thanks to HVBP. The results of these surveys may form the basis of legitimate, targeted feedback to hospitalists, who may then adjust their approach to patient interactions. Such performance improvement should result in improved HCAHPS scores.
In sum, hospitalists should pay close attention to patient satisfaction and embrace HCAHPS. However, we should be looking beyond HCAHPS to survey instruments that fairly and accurately measure our performance. Such surveys will be more widely accepted by the hospitalists they are measuring, and will allow hospitalists to perform meaningful quality improvement based on the results. Although hospitalist-specific surveys will require an investment, the increased patient satisfaction that results should be the basis of a favorable return on that investment.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Career Boost a Benefit of Winning SHM’s Research, Innovations, and Clinical Vignettes Poster Competition
Back to the Furture Past RIV winners talk about what the recognition meant for their careers By Larry Beresford

After winning SHM’s annual Research, Innovations, and Clinical Vignettes (RIV) scientific abstract and poster competition for an abstract illustrating a program that promoted flu vaccinations for families of neonatal patients, Shetal Shah, MD, FAAP, became a leading advocate for two laws mandating that New York hospitals offer vaccinations to families.
A poster that described a VTE prevention program led Gregory Maynard, MD, MSc, SFHM, to join SHM’s VTE Prevention Collaborative and, eventually, to become senior vice president of the society’s Center for Hospital Innovation and Improvement.
A prize-winning innovations poster for improving team communication by Vineet Chopra, MD, MS, FACP, FHM, and colleagues later took off as a new technology company.
Leonard Feldman, MD, FAAP, SFHM, won for a poster that explained online CME curriculum for hospitalists as consultants; the curriculum now resides on SHM’s website.
The evidence is clear: RIV abstracts are a vital part of hospital medicine.
Nearly 800 abstracts were submitted for HM13.
Awards are given in three categories:
- Research posters report clinical or basic science data, systematically review a clinical problem, or address efficiency, cost, or method of health-care delivery or medical decision-making;
- Innovations posters describe an existing innovative program in hospital medicine, often with preliminary data; and
- Clinical vignettes, either adult or pediatric, report on one or more cases illustrating a new disease entity, a prominent or unusual feature of an established disease, or an area of clinical controversy.
The Hospitalist asked 11 past RIV winners what the poster contest meant to their careers. Some added more data and analysis and went on to be published in such medical journals as the Journal of Hospital Medicine. Some used the recognition to launch or boost research-oriented careers; others saw their careers go in different directions.
“Winning a national poster competition gives you the confidence to continue to pursue your interest and take it to a higher level, like successfully competing for funding and publishing your line of inquiry,” says hospitalist and researcher Vineet Arora, MD, MPP, FHM, of the University of Chicago, who won the 2006 RIV research competition. “Sometimes, presenting posters can be lonely, but at SHM, you get a lot of traffic. You get a chance to practice your spiel, communicating science and research in a very concise way, which is an important skill to have.”
David Metzger, MD, PhD, also from the University of Chicago, who won the RIV research award in 2005, says recognition is a big deal, but “one of the biggest values of the RIV competition is just getting information out to colleagues, with the opportunity to talk with your peers. That’s the real prize.
“I’ve been involved in presenting posters at SHM every year that the society has been in existence,” he says. “I’ve met so many people and talked about what they’re doing. That’s what a medical society should do—bring people together like this.”

Title: Administrator, academic consult service; teaching staff physician
Institution: Saint Joseph Mercy Hospital, Ypsilanti, Mich.
Year: 2008
RIV: “A Case of Salty Voluminous Urine” (clinical vignette)
Dr. Tassava was honored two years in a row for topics drawn from her experience as a hospitalist working in the surgical ICU. Her HM08 entry won top poster, and her HM09 poster, “Permissive Hypernatremia: Co-Management of Intracranial Pressure in a Patient with Diabetes Insipidus,” was selected for an oral presentation.
The HM09 vignette described how the hypernatremia that occurs with diabetes insipidus could be used in a novel way to control intracranial pressure in a 17-year-old patient who had a traumatic brain injury from an auto accident.
“She had a beautiful outcome,” Dr. Tassava says. “She started college and she came back to our unit for a visit after her recovery.”
Dr. Tassava enjoyed the opportunity to explain to her peers how diabetes insipidus presented and how she managed the case. “I was a little surprised at how much discussion was generated by my case,” she says, “even though I knew this was an important and novel approach.”
When her hospital added intensivists, her work and research in the ICU ended and her career moved more toward hospitalist administration. She now runs the academic consult service at St. Joseph, serves as lead physician for the orthopedic surgery floor, instructs and mentors medical residents, and chairs the hospital’s Coagulation Collaborative Practice Team (Coagulation CPT). She credits the RIV honors with helping her to gain recognition as an academic hospitalist who was nominated for leadership roles. She has moved out of research for now but plans to pursue anticoagulation research in the future.
“I really appreciated the recognition for my curiosity and scientific approach, which was acknowledged by my surgical colleagues,” Dr. Tassava says. “I absolutely love the CPT. I am the hospital’s principal educator with regard to anticoagulation. Over the past year, I have given medicine and cardiology grand rounds, and have presented on the newest anticoagulants.”
Dr. Tassava still collaborates with her residents on abstracts, several of which have been submitted to SHM, the American College of Physicians, and other medical societies.
“I still love research,” she says. “I have a million ideas.”

Title: Chief of the division of hospital medicine; senior vice president, SHM’s Center for Innovation and Improvement
Institution: University of California at San Diego (UCSD)
Year: 2008
RIV: “Prevention of Hospital-Acquired Venous Thromboembolism: Prospective Validation of a VTE Risk Assessment Model and Protocol” (research)
Citations: Maynard G, Stein J. Designing and implementing effective VTE prevention protocols: lessons from collaboratives. J Thromb Thrombolysis. 2010;29(2):159-166. Maynard G, Morris T, Jenkins I, et al. Optimizing prevention of hospital acquired venous thromboembolism: prospective validation of a VTE risk assessment model. J Hosp Med. 2010;5(1):10-18.
Dr. Maynard’s abstract described a project funded by the federal Agency for Healthcare Research and Quality to design and implement an organized, comprehensive protocol for VTE prevention within the hospital setting. The project also included a toolkit to help other hospitals do the same thing. The same group received SHM’s Award of Excellence for Teamwork.
This work, combined with similar efforts by Jason Stein, MD, and colleagues at Emory University in Atlanta and others, provided the foundation for SHM’s VTE resource room and the mentored implementation program of SHM’s VTE Prevention Collaborative, which had been launched in 2007 as one of the society’s first large-scale quality-improvement (QI) initiatives.
“SHM wanted to do something about VTE prevention, and when we got our AHRQ grant, I was interested in doing the same,” Dr. Maynard says. “We published our implementation guides on the AHRQ and SHM websites, along with a lot of valuable supporting materials.”
Dr. Maynard later took on leadership roles with SHM’s quality initiatives on glycemic control and care transitions, which made him the logical choice to become senior vice president of SHM’s Center for Hospital Innovation and Improvement.
He says the RIV honor lifted his profile not only within SHM, but also throughout the field, and it was instrumental in obtaining continued funding to advance the VTE initiative. “We did this tremendous work—with great results,” he says. “But I don’t think our local administrators appreciated it quite as much until we started to get external, national recognition.”
Dr. Maynard earned his master’s degree in biostatistics and clinical research design from the University of Michigan—skills he later brought to the academic setting at UCSD.
“It was a nice way for a hospitalist, who’s really a medical generalist, to become an expert in something,” he says. “I could never be more of an expert in cardiology than a cardiologist, or more of an expert in DVT than a hematologist or critical-care specialist. But I could help both of them do what they couldn’t do as effectively, which was to implement protocols reliably using a QI framework.”

Title: Assistant professor of general internal medicine, hospital medicine, and public health
Institution: Vanderbilt University, Nashville, Tenn.
Year: 2009
RIV: “Predictors of Early Post-Discharge Mortality in Critically Ill Patients: Lessons for Quality Performance and Quality Assessment” (research)
Citation: Vasilevskis EE, Kuzniewicz MW, Cason BA, et al. Predictors of early post-discharge mortality in critically ill patients: a retrospective cohort study from the California Intensive Care Outcomes project. J Crit Care. 2011;26(1):65-75.
Dr. Vasilevskis has submitted abstracts to the RIV competition almost every year since 2007, when he was completing a fellowship at the University of California at San Francisco’s Institute for Health Policy Studies. He was honored in 2009 for a project based on the California Intensive Care Outcomes Project, which drew data from 35 hospitals to demonstrate that shortening ICU length of stay was predictive of early post-discharge mortality in the most severely ill patients.
He has continued to research quality and safety in the ICU, and he has published dozens of journal articles.
“My initial focus was on traditional mortality and length-of-stay outcomes,” he says. “I am now pursuing additional outcomes, most notably delirium in the ICU patient. I work with an amazing group of researchers that are trying to better measure, define, and treat delirium in the ICU—an outcome associated with a number of poor patient outcomes.”
Dr. Vasilevskis also is researching the causes of hospital readmissions and the development of novel ways to improve care transitions for elderly patients. He is pursuing a master’s of public health at Vanderbilt, and is co-principal investigator of an investigation of the Hospital Medicine Reengineering Network to improve transitions of care, supported by the Association of American Medical Colleges.
In addition to his 2009 win, he captured the HM10 and HM12 research categories. His HM12 poster, “Veterans Administration Acute Care 30-Day Mortality Model: Development, Validation and Performance Variation,” was singled out by the judging committee for its impressive sample size (1,114,327 patients in a retrospective cohort study of 131 VA hospitals), as well as for how it combined administrative and clinical risk models.
Dr. Vasilevskis says the opportunity to present his research at SHM and the recognition he received encouraged him to continue as a hospitalist engaged in medical research. He has been a member of SHM’s Research Committee since 2009, an RIV judge at HM11, and chaired the HM13 RIV competition subcommittee.

Title: Assistant professor of medicine
Institution: University of Michigan Health System, Ann Arbor
Year: 2009
RIV: “MComm: Redefining Medical Communications in the 21st Century” (innovations)
Early in his career, Dr. Chopra was curious about how to improve the way patient care is delivered in the hospital setting. He was particularly interested in the inordinate amount of time hospitalists spend every day on communication.
“I saw one-way paging systems as a problem for communication between members of the medical team,” he says. “Doctors get paged and break off from what they’re doing to return the page—to someone who often isn’t there to take the call back. Sometimes the system gives us the wrong number or a cryptic message that makes no sense.”
A technological solution to this problem, which he and hospitalist Prasanth Gogineni, MD, conceived, designed, and created, then tested at the University of Michigan, is called MComm. Dr. Chopra describes it as a novel, uniform way of messaging for the entire medical team using wireless servers, PUSH technology, and iPhones. MComm was built around existing hospital workflow and patient-specific task lists, assigning priority to each message and documenting that it was delivered. The junior faculty members submitted an abstract about their innovative application, not really expecting it to get accepted. But when it won the poster competition and was selected for a plenary presentation, things got busy in a hurry. Specifically, the university hospital’s Office of Technology Transfer took a keen interest.
“We met with a number of people who had business experience in the health-care-technology space and found a CEO for the company we formed to develop MComm,” Dr. Chopra says. “I found myself getting pulled into it very quickly, with a lot of conversations about commercialization, revenue-sharing models, intellectual property, and the like.”
But running a company was not something Dr. Chopra wanted to do. Two years ago, that company, Synaptin, went one way and he went another—he stayed at Michigan as a medical researcher. He remains deeply interested in how care is delivered to hospitalized patients, but with a focus on such patient-safety questions as how to prevent negative outcomes from indwelling venous catheters.
“Winning the poster competition opened doors for me—there’s no doubt in my mind,” he says. “We demonstrated the ability to deliver a project of significance, from concept to prototype, without formal training in this area. If we didn’t have that recognition, I’m not sure I would have been ready to step into a research career as quickly. It helped me realize that medical research was what I wanted to do.”
Title: Associate program director, internal-medicine residency; assistant dean of scholarship and discovery
Institution: Pritzker School of Medicine, University of Chicago
Year: 2006
RIV: “Measuring Quality of Hospital Care for Vulnerable Elders: Use of ACOVE Quality Indicators” (research)
Citation: Arora VM, Fish M, Basu A, et al. Relationship between quality of care of hospitalized vulnerable elders and postdischarge mortality. J Am Geriatrics. 2010;58:1642-1648.

Title: Associate professor, department of medicine; associate faculty member, Harris School and the Department of Economics
Institution: University of Chicago
Year: 2005
RIV: “Effects of Hospitalists on Outcomes and Costs in a Multicenter Trial of Academic Hospitalists” (research)
Dr. Meltzer was the lead author, with 11 other prominent hospitalists, of an abstract based on a multisite study of the cost and outcome implications of the hospitalist model—still a relatively new concept in 2001, when the research began. Although the study did not uncover large cost savings realized from the hospitalist model of care, as some advocates had hoped, important findings and implications for the emerging field were teased out of the data.
At the time, only a few randomly controlled, multisite studies of costs and outcomes for the hospitalist model had been performed. The study, Dr. Meltzer says, required a complicated analysis to discover that hospitalists, in fact, saved their facilities money, with their most important impact realized post-hospitalization, such as on nursing-home costs. It was important to control for spillover effect and the fact that hospitalists do a better job of teaching house staff, while a physician’s years of experience was another important variable, he says.
Dr. Meltzer was a medical researcher interested in medical specialization when the term “hospitalist” was first coined in 1996. “I thought, here was a chance to study a medical specialty in its formative stages,” he says.
He still works as a hospitalist, although with limited clinical time. In addition to his administrative work as division chief, he directs the Center for Health and the Social Sciences at the University of Chicago. His research interests include cost-effectiveness, technology assessment, and information research.
In 2010, his poster “Effects of Hospitalists on 1-Year Post-Discharge Resource Utilization by Medicare Beneficiaries” took the top prize in the HM10 research competition. In 2011, he was appointed to the methodology committee of the federal Patient-Centered Outcomes Research Institute (PCORI), which was created by the Affordable Care Act to advise the government on clinical-effectiveness research. He also sits on the Advisory Council to the National Institute of General Medical Sciences at the Institute of Medicine, and on the Congressional Budget Office’s panel of health advisors.
In a career full of recognition, Dr. Meltzer says it’s hard to pinpoint the impact of winning the poster contest. But he has continued to submit abstracts to SHM every year and appreciates the opportunities for interaction with peers at the poster exhibits.

Title: Director of perioperative and consultative medicine
Institution: University of Michigan, Ann Arbor
Year: 2006
RIV: “Disseminated Histoplasmosis Presenting As Painful Oral Ulcers” (clinical vignettes)
Dr. Grant’s winning vignette presented a patient with a complex medical history, including heart disease and four months of painful oral ulcers, for which prior evaluations had been inconclusive, despite conducting biopsies. Following administration of high-dose corticosteroids, the patient’s condition worsened on multiple fronts. The vignette showed how the medical team was able to diagnose an unusual presentation of a fungal infection called histoplasmosis, which is prevalent in parts of the Midwest surrounding the Ohio and Mississippi river valleys.
“We see a lot of cases in the hospital where there are different angles you could take to turn it into a clinical vignette or a nice poster with good teaching points,” Dr. Grant says. “In this case, just digging deeper into the actual diagnosis was important because the empiric use of steroids can be fatal for some patients. Steroids are given for a lot of good reasons, but in this patient they caused immune suppression, allowing a smoldering infection to become very active.”
Dr. Grant did not submit the vignette for publication. “That was probably a mistake on my part,” he says, acknowledging the common complaint of too little time and too many competing priorities. But his interest in research has continued.
“I became involved at a national level with issues of perioperative medicine and last August published a textbook on the subject,” he reports.1 “VTE is another area of interest I have developed since my hospital medicine fellowship.”
He serves as the VTE resource expert on the Michigan Hospital Medicine Safety Consortium, a quality collaborative of more than 40 hospitals with Blue Cross/Blue Shield of Michigan. “It’s exciting to be able to look at the risk factors, what kinds of patients get VTEs, and whether they were appropriately prophylaxed in the hospital,” he says.
VTE is a national quality priority, and Dr. Grant expects abstracts to emerge from the consortium’s work.
He says he appreciates the opportunities that arise from participating in poster sessions at SHM, where medical students, residents, and working hospitalists talk to the presenters of interesting cases.
“It gives you a real back-and-forth, which is good for the person asking the question and for the presenter,” he says, noting hospitalists from other parts of the country were not as familiar with histoplasmosis.
He says winning the HM06 poster contest helped him “get his feet wet” and feel more prepared for a career in academic hospital medicine. “I’m sure the award solidified my employers’ satisfaction in hiring me—and in giving me more desirable academic roles and responsibilities,” he adds.

Title: Assistant professor of medicine pediatrics; director of the general internal-medicine comprehensive consultation service
Institution: Johns Hopkins Hospital, Baltimore
Year: 2009
RIV: “An Internet-Based Consult Curriculum for Hospitalists” (innovations)
Dr. Feldman’s poster described an online CME curriculum for hospitalists acting as medical consultants. The concept grew out of a perceived deficiency in his own medical education when, in 2004, he was asked to lead the consultation service at Johns Hopkins—just six months after finishing his residency.
“I had no idea what I was doing as a general-internal-medicine consultant,” he says. “I maybe received two weeks of experience as a consultant during my residency. I was willing to take it on, learning on the job and asking for help. But it occurred to me that I’m probably not alone in feeling unprepared.”
In his quest for self-education, Dr. Feldman wondered whether he should write a textbook on the subject. “But the information changes so quickly, I thought I’d have a better chance to reach people online,” he notes.
After talking to publishers and CME companies, he came up with the concept of learning modules on perioperative and consultative medicine topics, which could be taken online while earning CME credits. Johns Hopkins served as the CME certifier, and medical-education company Advanced Studies in Medicine joined as a partner. Once the project got off the ground, a medical advisory committee was convened.
“Winning the SHM poster competition is a great honor to have on a CV. It really helps to legitimize your name in the world of hospital medicine,” Dr. Feldman says. “It also provided confirmation that we were on the right track with the curriculum project. People valued what we were doing.”
Dr. Feldman and SHM have since become affiliated, and the “Consultative and Perioperative Medicine Essentials for Hospitalists” modules are available on SHM’s website (www.shmconsults.com). The site has 12,000 registered members completing 500 CME modules every month.
“I do a lot of the editing still,” Dr. Feldman says. “We update the modules every two years and are still creating new ones.”
Dr. Feldman also pursues a number of clinical-research interests, including resident education and costs of care.

Title: Assistant professor of medicine
Institution: Medical University of South Carolina, Charleston
Year: 2009
RIV: “Intensivists versus Hospitalists in the ICU: A Prospective Cohort Study Comparing Mortality and Length of Stay Between Two Staffing Models” (research) Citation: Wise KR, Akopov VA, Williams BR, Ido MS, Leeper KV, Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective and observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189.
Dr. Wise was recognized for research that began while she worked at Emory University in Atlanta, comparing hospitalists and intensivists in such outcomes as length of stay and mortality rates for patients in the ICU. The study was one of the first statistically rigorous examinations of this critical quality question. With an eye toward improving patient safety, national quality advocates such as the Leapfrog Group have called for hospitals to employ intensivists (critical-care specialists) to manage the care of ICU patients. In reality, Dr. Wise says, there aren’t enough intensivists to meet the need.
“Hospitalists are in the ICU anyway,” she says. “We just don’t have enough data to answer how well they do [in comparison to intensivists].”
Through a prospective cohort study of more than 1,000 patients, Dr. Wise’s group found that there was essentially no statistical difference in mortality rates between patients treated by intensivist teams or hospitalist ICU teams.
“We were also able to look at some of the intermediate-acuity patients—fairly complicated but not requiring ventilators,” she explains. “Our study wasn’t sufficiently powered for this subgroup, but it was an interesting piece of data to raise the question: Where should we deploy this scarce resource of intensivists? Which pockets of patients?”
Presenting her abstract at SHM’s annual meeting was a “good experience.”
“I’d done public speaking before, but never with an audience of about 500 people,” she says. “To go out there and field their questions was a real professional growing experience. Several people interested in the topic sought me out at the conference, introduced themselves, and we have subsequently stayed in touch.”
The manuscript published in JHM has been cited four times, including in a position paper from SHM and the Society of Critical Care Medicine.3 Another outgrowth of the research was being asked to contribute a chapter on hospitalists’ role in the ICU to a textbook on hospital medicine. Based on her still-fresh HM presentation, Dr. Wise was one of the few publicly identified experts on the subject. The chapter, co-authored by fellow Emory hospitalist Michael Heisler, MD, MPH, “The Role of the Hospitalist in Critical Care” was included in Principles and Practices of Hospital Medicine.4

Title: Neonatal intensivist
Institution: Stony Brook University Hospital, Great Neck, N.Y.
Year: 2006
RIV: “Administration of Inactivated Trivalent Influenza Vaccine (TIV) to Parents of Infants in the Neonatal Intensive Care Unit (NICU): A Novel Strategy to Increase Vaccination Rates” (innovations)
Citation: Shah SI, Caprio M, Hendricks-Munoz K. Administration of inactivated trivalent influenza vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2007;120;e617-e621.
Dr. Shah was in his final year of a fellowship in neonatology at New York University when he took on the challenge of improving immunization access to protect premature, highly vulnerable patients in the NICU from influenza infections. Because these children are too young to be vaccinated directly, the concept of cocooning them from infection involves extending protection to everyone around them.
“We came up with the idea of offering flu vaccinations 24/7 in the NICU to the children’s parents,” he says. “It worked well for us as a way to define an indicated therapy for a defined population, even if it was a little outside the box. By the end of the flu season, 95% of the parents were vaccinated.”
SHM recognized the project as the top RIV innovations poster at HM06, but that was just the beginning.
“When I moved to SUNY Stony Brook, I continued to study and advocate for these vaccinations,” Dr. Shah says. “We were giving 500 to 700 vaccinations a year. Then I wrote a national resolution for the American Academy of Pediatrics, which was significant because it meant AAP was behind the project.”
Dr. Shah later became chair of AAP’s Long Island Chapter Legislative Committee and joined a statewide pediatric advocacy group. In 2009, the New York legislature enacted the Neonatal Influenza Protection Act, which required hospitals in the state to offer parents the vaccine, with Dr. Shah’s research and advocacy providing an essential basis for its passage. He’s even been recognized for his research in congressional citations.
Based on that success with influenza vaccinations, Dr. Shah and his colleagues looked at other diseases, starting with pertussis, and then tetanus, diphtheria, and whooping cough.5 All the while, they continued tracking immunization rates. A second state law, passed in 2011, added pertussis to the vaccinations. Next on his advocacy agenda is a project to promote smoking-cessation interventions in the NICU.6
“These parents come to see us every day,” he says. “What can we do, through the parents, to promote the health and well-being of their high-risk newborns?”

Title: Assistant professor of medicine; medical director of inpatient palliative-care consultation
Institution: University of Texas Health Sciences Center, San Antonio
Year: 2009
RIV: “When to Depend on the Kinins of Strangers: An Unusual Case of Abdominal Pain” (clinical vignettes)
Publication: An article on the ethics of determining code status for patients with advanced cancer and a book chapter on the “last hours of life” for a forthcoming book on palliative care and hospital medicine.
As a medical resident, Dr. Morrow met a 27-year-old woman who had chronic abdominal pain and had made multiple visits to the ED for this complaint. The patient had a history of substance abuse and requested dilaudid for her pain—making it easy for staff to consign her to the stereotype of the difficult patient.
“I met her after an interesting finding,” he says. “It turns out that on the previous emergency room visit, she received a CAT scan, which showed duodenal and small-bowel thickening consistent with hereditary angioedema, although with an unusual presentation. As it happened, we had onsite a world expert in angioedema.”
The expert was able to confirm the diagnosis, Dr. Morrow says.
“By giving her this ‘legitimate,’ organic diagnosis, it just changed the whole dynamic of her relationship with her doctors,” he says. “She knew that they knew something was really wrong. The residents were empowered to have something to hang their hats on. And we were able to get better control of her pain.”
Dr. Morrow says he came on the scene late in the discovery process, but he helped to solve the puzzle, and then put together the abstract and poster that told the story of making the diagnosis.
“In my previous job, I was hired as a hospitalist but helped to build the palliative-care program within the hospital-medicine service,” he says. “In my current job, I was brought in to build the inpatient palliative-care-consultation service, although I still moonlight as a hospitalist to stay sharp.”
Dr. Morrow says he enjoys sharing stories of difficult cases and submitting case studies about them to medical conferences, often with clever titles incorporating puns (e.g. the 2009 SHM poster citing kinins, polypeptides in the blood that cause inflammation). Another example is “The Angina Monologues,” a story of an 82-year-old patient with chronic angina pectoris and complex pain syndromes that were difficult to bring under control. Palliative care also emphasizes patients’ stories, he says, in order to understand the person behind the diagnosis.
Larry Beresford is a freelance writer in San Francisco. References available at www.the-hospitalist.org.
References
2. Yoder J. Association between hospital noise levels and inpatient sleep among middle-aged and older adults: Far from a quiet night. Abstract, Society of Hospital Medicine, 2011.
3. McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS. Principles and Practice of Hospital Medicine. McGraw-Hill Medical; New York City: 2012.
4. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. J Hosp Med. 2012;7:359-364.
5. Dylag A, Shah SI. Administration of tetanus, diphtheria, and acellular pertussis vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2008;122:e550-e555.
6. Shah S. Smoking cessation counseling and PPSV 23-valent pneumococcal polysaccharide vaccine administration parents of neonatal intensive care unit (NICU)-admitted infants: A life-changing opportunity. J Neonatal-Perinatal Med. 2011;4:263-267.
Back to the Furture Past RIV winners talk about what the recognition meant for their careers By Larry Beresford
After winning SHM’s annual Research, Innovations, and Clinical Vignettes (RIV) scientific abstract and poster competition for an abstract illustrating a program that promoted flu vaccinations for families of neonatal patients, Shetal Shah, MD, FAAP, became a leading advocate for two laws mandating that New York hospitals offer vaccinations to families.
A poster that described a VTE prevention program led Gregory Maynard, MD, MSc, SFHM, to join SHM’s VTE Prevention Collaborative and, eventually, to become senior vice president of the society’s Center for Hospital Innovation and Improvement.
A prize-winning innovations poster for improving team communication by Vineet Chopra, MD, MS, FACP, FHM, and colleagues later took off as a new technology company.
Leonard Feldman, MD, FAAP, SFHM, won for a poster that explained online CME curriculum for hospitalists as consultants; the curriculum now resides on SHM’s website.
The evidence is clear: RIV abstracts are a vital part of hospital medicine.
Nearly 800 abstracts were submitted for HM13.
Awards are given in three categories:
- Research posters report clinical or basic science data, systematically review a clinical problem, or address efficiency, cost, or method of health-care delivery or medical decision-making;
- Innovations posters describe an existing innovative program in hospital medicine, often with preliminary data; and
- Clinical vignettes, either adult or pediatric, report on one or more cases illustrating a new disease entity, a prominent or unusual feature of an established disease, or an area of clinical controversy.
The Hospitalist asked 11 past RIV winners what the poster contest meant to their careers. Some added more data and analysis and went on to be published in such medical journals as the Journal of Hospital Medicine. Some used the recognition to launch or boost research-oriented careers; others saw their careers go in different directions.
“Winning a national poster competition gives you the confidence to continue to pursue your interest and take it to a higher level, like successfully competing for funding and publishing your line of inquiry,” says hospitalist and researcher Vineet Arora, MD, MPP, FHM, of the University of Chicago, who won the 2006 RIV research competition. “Sometimes, presenting posters can be lonely, but at SHM, you get a lot of traffic. You get a chance to practice your spiel, communicating science and research in a very concise way, which is an important skill to have.”
David Metzger, MD, PhD, also from the University of Chicago, who won the RIV research award in 2005, says recognition is a big deal, but “one of the biggest values of the RIV competition is just getting information out to colleagues, with the opportunity to talk with your peers. That’s the real prize.
“I’ve been involved in presenting posters at SHM every year that the society has been in existence,” he says. “I’ve met so many people and talked about what they’re doing. That’s what a medical society should do—bring people together like this.”
Title: Administrator, academic consult service; teaching staff physician
Institution: Saint Joseph Mercy Hospital, Ypsilanti, Mich.
Year: 2008
RIV: “A Case of Salty Voluminous Urine” (clinical vignette)
Dr. Tassava was honored two years in a row for topics drawn from her experience as a hospitalist working in the surgical ICU. Her HM08 entry won top poster, and her HM09 poster, “Permissive Hypernatremia: Co-Management of Intracranial Pressure in a Patient with Diabetes Insipidus,” was selected for an oral presentation.
The HM09 vignette described how the hypernatremia that occurs with diabetes insipidus could be used in a novel way to control intracranial pressure in a 17-year-old patient who had a traumatic brain injury from an auto accident.
“She had a beautiful outcome,” Dr. Tassava says. “She started college and she came back to our unit for a visit after her recovery.”
Dr. Tassava enjoyed the opportunity to explain to her peers how diabetes insipidus presented and how she managed the case. “I was a little surprised at how much discussion was generated by my case,” she says, “even though I knew this was an important and novel approach.”
When her hospital added intensivists, her work and research in the ICU ended and her career moved more toward hospitalist administration. She now runs the academic consult service at St. Joseph, serves as lead physician for the orthopedic surgery floor, instructs and mentors medical residents, and chairs the hospital’s Coagulation Collaborative Practice Team (Coagulation CPT). She credits the RIV honors with helping her to gain recognition as an academic hospitalist who was nominated for leadership roles. She has moved out of research for now but plans to pursue anticoagulation research in the future.
“I really appreciated the recognition for my curiosity and scientific approach, which was acknowledged by my surgical colleagues,” Dr. Tassava says. “I absolutely love the CPT. I am the hospital’s principal educator with regard to anticoagulation. Over the past year, I have given medicine and cardiology grand rounds, and have presented on the newest anticoagulants.”
Dr. Tassava still collaborates with her residents on abstracts, several of which have been submitted to SHM, the American College of Physicians, and other medical societies.
“I still love research,” she says. “I have a million ideas.”
Title: Chief of the division of hospital medicine; senior vice president, SHM’s Center for Innovation and Improvement
Institution: University of California at San Diego (UCSD)
Year: 2008
RIV: “Prevention of Hospital-Acquired Venous Thromboembolism: Prospective Validation of a VTE Risk Assessment Model and Protocol” (research)
Citations: Maynard G, Stein J. Designing and implementing effective VTE prevention protocols: lessons from collaboratives. J Thromb Thrombolysis. 2010;29(2):159-166. Maynard G, Morris T, Jenkins I, et al. Optimizing prevention of hospital acquired venous thromboembolism: prospective validation of a VTE risk assessment model. J Hosp Med. 2010;5(1):10-18.
Dr. Maynard’s abstract described a project funded by the federal Agency for Healthcare Research and Quality to design and implement an organized, comprehensive protocol for VTE prevention within the hospital setting. The project also included a toolkit to help other hospitals do the same thing. The same group received SHM’s Award of Excellence for Teamwork.
This work, combined with similar efforts by Jason Stein, MD, and colleagues at Emory University in Atlanta and others, provided the foundation for SHM’s VTE resource room and the mentored implementation program of SHM’s VTE Prevention Collaborative, which had been launched in 2007 as one of the society’s first large-scale quality-improvement (QI) initiatives.
“SHM wanted to do something about VTE prevention, and when we got our AHRQ grant, I was interested in doing the same,” Dr. Maynard says. “We published our implementation guides on the AHRQ and SHM websites, along with a lot of valuable supporting materials.”
Dr. Maynard later took on leadership roles with SHM’s quality initiatives on glycemic control and care transitions, which made him the logical choice to become senior vice president of SHM’s Center for Hospital Innovation and Improvement.
He says the RIV honor lifted his profile not only within SHM, but also throughout the field, and it was instrumental in obtaining continued funding to advance the VTE initiative. “We did this tremendous work—with great results,” he says. “But I don’t think our local administrators appreciated it quite as much until we started to get external, national recognition.”
Dr. Maynard earned his master’s degree in biostatistics and clinical research design from the University of Michigan—skills he later brought to the academic setting at UCSD.
“It was a nice way for a hospitalist, who’s really a medical generalist, to become an expert in something,” he says. “I could never be more of an expert in cardiology than a cardiologist, or more of an expert in DVT than a hematologist or critical-care specialist. But I could help both of them do what they couldn’t do as effectively, which was to implement protocols reliably using a QI framework.”
Title: Assistant professor of general internal medicine, hospital medicine, and public health
Institution: Vanderbilt University, Nashville, Tenn.
Year: 2009
RIV: “Predictors of Early Post-Discharge Mortality in Critically Ill Patients: Lessons for Quality Performance and Quality Assessment” (research)
Citation: Vasilevskis EE, Kuzniewicz MW, Cason BA, et al. Predictors of early post-discharge mortality in critically ill patients: a retrospective cohort study from the California Intensive Care Outcomes project. J Crit Care. 2011;26(1):65-75.
Dr. Vasilevskis has submitted abstracts to the RIV competition almost every year since 2007, when he was completing a fellowship at the University of California at San Francisco’s Institute for Health Policy Studies. He was honored in 2009 for a project based on the California Intensive Care Outcomes Project, which drew data from 35 hospitals to demonstrate that shortening ICU length of stay was predictive of early post-discharge mortality in the most severely ill patients.
He has continued to research quality and safety in the ICU, and he has published dozens of journal articles.
“My initial focus was on traditional mortality and length-of-stay outcomes,” he says. “I am now pursuing additional outcomes, most notably delirium in the ICU patient. I work with an amazing group of researchers that are trying to better measure, define, and treat delirium in the ICU—an outcome associated with a number of poor patient outcomes.”
Dr. Vasilevskis also is researching the causes of hospital readmissions and the development of novel ways to improve care transitions for elderly patients. He is pursuing a master’s of public health at Vanderbilt, and is co-principal investigator of an investigation of the Hospital Medicine Reengineering Network to improve transitions of care, supported by the Association of American Medical Colleges.
In addition to his 2009 win, he captured the HM10 and HM12 research categories. His HM12 poster, “Veterans Administration Acute Care 30-Day Mortality Model: Development, Validation and Performance Variation,” was singled out by the judging committee for its impressive sample size (1,114,327 patients in a retrospective cohort study of 131 VA hospitals), as well as for how it combined administrative and clinical risk models.
Dr. Vasilevskis says the opportunity to present his research at SHM and the recognition he received encouraged him to continue as a hospitalist engaged in medical research. He has been a member of SHM’s Research Committee since 2009, an RIV judge at HM11, and chaired the HM13 RIV competition subcommittee.
Title: Assistant professor of medicine
Institution: University of Michigan Health System, Ann Arbor
Year: 2009
RIV: “MComm: Redefining Medical Communications in the 21st Century” (innovations)
Early in his career, Dr. Chopra was curious about how to improve the way patient care is delivered in the hospital setting. He was particularly interested in the inordinate amount of time hospitalists spend every day on communication.
“I saw one-way paging systems as a problem for communication between members of the medical team,” he says. “Doctors get paged and break off from what they’re doing to return the page—to someone who often isn’t there to take the call back. Sometimes the system gives us the wrong number or a cryptic message that makes no sense.”
A technological solution to this problem, which he and hospitalist Prasanth Gogineni, MD, conceived, designed, and created, then tested at the University of Michigan, is called MComm. Dr. Chopra describes it as a novel, uniform way of messaging for the entire medical team using wireless servers, PUSH technology, and iPhones. MComm was built around existing hospital workflow and patient-specific task lists, assigning priority to each message and documenting that it was delivered. The junior faculty members submitted an abstract about their innovative application, not really expecting it to get accepted. But when it won the poster competition and was selected for a plenary presentation, things got busy in a hurry. Specifically, the university hospital’s Office of Technology Transfer took a keen interest.
“We met with a number of people who had business experience in the health-care-technology space and found a CEO for the company we formed to develop MComm,” Dr. Chopra says. “I found myself getting pulled into it very quickly, with a lot of conversations about commercialization, revenue-sharing models, intellectual property, and the like.”
But running a company was not something Dr. Chopra wanted to do. Two years ago, that company, Synaptin, went one way and he went another—he stayed at Michigan as a medical researcher. He remains deeply interested in how care is delivered to hospitalized patients, but with a focus on such patient-safety questions as how to prevent negative outcomes from indwelling venous catheters.
“Winning the poster competition opened doors for me—there’s no doubt in my mind,” he says. “We demonstrated the ability to deliver a project of significance, from concept to prototype, without formal training in this area. If we didn’t have that recognition, I’m not sure I would have been ready to step into a research career as quickly. It helped me realize that medical research was what I wanted to do.”
Title: Associate program director, internal-medicine residency; assistant dean of scholarship and discovery
Institution: Pritzker School of Medicine, University of Chicago
Year: 2006
RIV: “Measuring Quality of Hospital Care for Vulnerable Elders: Use of ACOVE Quality Indicators” (research)
Citation: Arora VM, Fish M, Basu A, et al. Relationship between quality of care of hospitalized vulnerable elders and postdischarge mortality. J Am Geriatrics. 2010;58:1642-1648.
Title: Associate professor, department of medicine; associate faculty member, Harris School and the Department of Economics
Institution: University of Chicago
Year: 2005
RIV: “Effects of Hospitalists on Outcomes and Costs in a Multicenter Trial of Academic Hospitalists” (research)
Dr. Meltzer was the lead author, with 11 other prominent hospitalists, of an abstract based on a multisite study of the cost and outcome implications of the hospitalist model—still a relatively new concept in 2001, when the research began. Although the study did not uncover large cost savings realized from the hospitalist model of care, as some advocates had hoped, important findings and implications for the emerging field were teased out of the data.
At the time, only a few randomly controlled, multisite studies of costs and outcomes for the hospitalist model had been performed. The study, Dr. Meltzer says, required a complicated analysis to discover that hospitalists, in fact, saved their facilities money, with their most important impact realized post-hospitalization, such as on nursing-home costs. It was important to control for spillover effect and the fact that hospitalists do a better job of teaching house staff, while a physician’s years of experience was another important variable, he says.
Dr. Meltzer was a medical researcher interested in medical specialization when the term “hospitalist” was first coined in 1996. “I thought, here was a chance to study a medical specialty in its formative stages,” he says.
He still works as a hospitalist, although with limited clinical time. In addition to his administrative work as division chief, he directs the Center for Health and the Social Sciences at the University of Chicago. His research interests include cost-effectiveness, technology assessment, and information research.
In 2010, his poster “Effects of Hospitalists on 1-Year Post-Discharge Resource Utilization by Medicare Beneficiaries” took the top prize in the HM10 research competition. In 2011, he was appointed to the methodology committee of the federal Patient-Centered Outcomes Research Institute (PCORI), which was created by the Affordable Care Act to advise the government on clinical-effectiveness research. He also sits on the Advisory Council to the National Institute of General Medical Sciences at the Institute of Medicine, and on the Congressional Budget Office’s panel of health advisors.
In a career full of recognition, Dr. Meltzer says it’s hard to pinpoint the impact of winning the poster contest. But he has continued to submit abstracts to SHM every year and appreciates the opportunities for interaction with peers at the poster exhibits.
Title: Director of perioperative and consultative medicine
Institution: University of Michigan, Ann Arbor
Year: 2006
RIV: “Disseminated Histoplasmosis Presenting As Painful Oral Ulcers” (clinical vignettes)
Dr. Grant’s winning vignette presented a patient with a complex medical history, including heart disease and four months of painful oral ulcers, for which prior evaluations had been inconclusive, despite conducting biopsies. Following administration of high-dose corticosteroids, the patient’s condition worsened on multiple fronts. The vignette showed how the medical team was able to diagnose an unusual presentation of a fungal infection called histoplasmosis, which is prevalent in parts of the Midwest surrounding the Ohio and Mississippi river valleys.
“We see a lot of cases in the hospital where there are different angles you could take to turn it into a clinical vignette or a nice poster with good teaching points,” Dr. Grant says. “In this case, just digging deeper into the actual diagnosis was important because the empiric use of steroids can be fatal for some patients. Steroids are given for a lot of good reasons, but in this patient they caused immune suppression, allowing a smoldering infection to become very active.”
Dr. Grant did not submit the vignette for publication. “That was probably a mistake on my part,” he says, acknowledging the common complaint of too little time and too many competing priorities. But his interest in research has continued.
“I became involved at a national level with issues of perioperative medicine and last August published a textbook on the subject,” he reports.1 “VTE is another area of interest I have developed since my hospital medicine fellowship.”
He serves as the VTE resource expert on the Michigan Hospital Medicine Safety Consortium, a quality collaborative of more than 40 hospitals with Blue Cross/Blue Shield of Michigan. “It’s exciting to be able to look at the risk factors, what kinds of patients get VTEs, and whether they were appropriately prophylaxed in the hospital,” he says.
VTE is a national quality priority, and Dr. Grant expects abstracts to emerge from the consortium’s work.
He says he appreciates the opportunities that arise from participating in poster sessions at SHM, where medical students, residents, and working hospitalists talk to the presenters of interesting cases.
“It gives you a real back-and-forth, which is good for the person asking the question and for the presenter,” he says, noting hospitalists from other parts of the country were not as familiar with histoplasmosis.
He says winning the HM06 poster contest helped him “get his feet wet” and feel more prepared for a career in academic hospital medicine. “I’m sure the award solidified my employers’ satisfaction in hiring me—and in giving me more desirable academic roles and responsibilities,” he adds.
Title: Assistant professor of medicine pediatrics; director of the general internal-medicine comprehensive consultation service
Institution: Johns Hopkins Hospital, Baltimore
Year: 2009
RIV: “An Internet-Based Consult Curriculum for Hospitalists” (innovations)
Dr. Feldman’s poster described an online CME curriculum for hospitalists acting as medical consultants. The concept grew out of a perceived deficiency in his own medical education when, in 2004, he was asked to lead the consultation service at Johns Hopkins—just six months after finishing his residency.
“I had no idea what I was doing as a general-internal-medicine consultant,” he says. “I maybe received two weeks of experience as a consultant during my residency. I was willing to take it on, learning on the job and asking for help. But it occurred to me that I’m probably not alone in feeling unprepared.”
In his quest for self-education, Dr. Feldman wondered whether he should write a textbook on the subject. “But the information changes so quickly, I thought I’d have a better chance to reach people online,” he notes.
After talking to publishers and CME companies, he came up with the concept of learning modules on perioperative and consultative medicine topics, which could be taken online while earning CME credits. Johns Hopkins served as the CME certifier, and medical-education company Advanced Studies in Medicine joined as a partner. Once the project got off the ground, a medical advisory committee was convened.
“Winning the SHM poster competition is a great honor to have on a CV. It really helps to legitimize your name in the world of hospital medicine,” Dr. Feldman says. “It also provided confirmation that we were on the right track with the curriculum project. People valued what we were doing.”
Dr. Feldman and SHM have since become affiliated, and the “Consultative and Perioperative Medicine Essentials for Hospitalists” modules are available on SHM’s website (www.shmconsults.com). The site has 12,000 registered members completing 500 CME modules every month.
“I do a lot of the editing still,” Dr. Feldman says. “We update the modules every two years and are still creating new ones.”
Dr. Feldman also pursues a number of clinical-research interests, including resident education and costs of care.
Title: Assistant professor of medicine
Institution: Medical University of South Carolina, Charleston
Year: 2009
RIV: “Intensivists versus Hospitalists in the ICU: A Prospective Cohort Study Comparing Mortality and Length of Stay Between Two Staffing Models” (research) Citation: Wise KR, Akopov VA, Williams BR, Ido MS, Leeper KV, Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective and observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189.
Dr. Wise was recognized for research that began while she worked at Emory University in Atlanta, comparing hospitalists and intensivists in such outcomes as length of stay and mortality rates for patients in the ICU. The study was one of the first statistically rigorous examinations of this critical quality question. With an eye toward improving patient safety, national quality advocates such as the Leapfrog Group have called for hospitals to employ intensivists (critical-care specialists) to manage the care of ICU patients. In reality, Dr. Wise says, there aren’t enough intensivists to meet the need.
“Hospitalists are in the ICU anyway,” she says. “We just don’t have enough data to answer how well they do [in comparison to intensivists].”
Through a prospective cohort study of more than 1,000 patients, Dr. Wise’s group found that there was essentially no statistical difference in mortality rates between patients treated by intensivist teams or hospitalist ICU teams.
“We were also able to look at some of the intermediate-acuity patients—fairly complicated but not requiring ventilators,” she explains. “Our study wasn’t sufficiently powered for this subgroup, but it was an interesting piece of data to raise the question: Where should we deploy this scarce resource of intensivists? Which pockets of patients?”
Presenting her abstract at SHM’s annual meeting was a “good experience.”
“I’d done public speaking before, but never with an audience of about 500 people,” she says. “To go out there and field their questions was a real professional growing experience. Several people interested in the topic sought me out at the conference, introduced themselves, and we have subsequently stayed in touch.”
The manuscript published in JHM has been cited four times, including in a position paper from SHM and the Society of Critical Care Medicine.3 Another outgrowth of the research was being asked to contribute a chapter on hospitalists’ role in the ICU to a textbook on hospital medicine. Based on her still-fresh HM presentation, Dr. Wise was one of the few publicly identified experts on the subject. The chapter, co-authored by fellow Emory hospitalist Michael Heisler, MD, MPH, “The Role of the Hospitalist in Critical Care” was included in Principles and Practices of Hospital Medicine.4
Title: Neonatal intensivist
Institution: Stony Brook University Hospital, Great Neck, N.Y.
Year: 2006
RIV: “Administration of Inactivated Trivalent Influenza Vaccine (TIV) to Parents of Infants in the Neonatal Intensive Care Unit (NICU): A Novel Strategy to Increase Vaccination Rates” (innovations)
Citation: Shah SI, Caprio M, Hendricks-Munoz K. Administration of inactivated trivalent influenza vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2007;120;e617-e621.
Dr. Shah was in his final year of a fellowship in neonatology at New York University when he took on the challenge of improving immunization access to protect premature, highly vulnerable patients in the NICU from influenza infections. Because these children are too young to be vaccinated directly, the concept of cocooning them from infection involves extending protection to everyone around them.
“We came up with the idea of offering flu vaccinations 24/7 in the NICU to the children’s parents,” he says. “It worked well for us as a way to define an indicated therapy for a defined population, even if it was a little outside the box. By the end of the flu season, 95% of the parents were vaccinated.”
SHM recognized the project as the top RIV innovations poster at HM06, but that was just the beginning.
“When I moved to SUNY Stony Brook, I continued to study and advocate for these vaccinations,” Dr. Shah says. “We were giving 500 to 700 vaccinations a year. Then I wrote a national resolution for the American Academy of Pediatrics, which was significant because it meant AAP was behind the project.”
Dr. Shah later became chair of AAP’s Long Island Chapter Legislative Committee and joined a statewide pediatric advocacy group. In 2009, the New York legislature enacted the Neonatal Influenza Protection Act, which required hospitals in the state to offer parents the vaccine, with Dr. Shah’s research and advocacy providing an essential basis for its passage. He’s even been recognized for his research in congressional citations.
Based on that success with influenza vaccinations, Dr. Shah and his colleagues looked at other diseases, starting with pertussis, and then tetanus, diphtheria, and whooping cough.5 All the while, they continued tracking immunization rates. A second state law, passed in 2011, added pertussis to the vaccinations. Next on his advocacy agenda is a project to promote smoking-cessation interventions in the NICU.6
“These parents come to see us every day,” he says. “What can we do, through the parents, to promote the health and well-being of their high-risk newborns?”
Title: Assistant professor of medicine; medical director of inpatient palliative-care consultation
Institution: University of Texas Health Sciences Center, San Antonio
Year: 2009
RIV: “When to Depend on the Kinins of Strangers: An Unusual Case of Abdominal Pain” (clinical vignettes)
Publication: An article on the ethics of determining code status for patients with advanced cancer and a book chapter on the “last hours of life” for a forthcoming book on palliative care and hospital medicine.
As a medical resident, Dr. Morrow met a 27-year-old woman who had chronic abdominal pain and had made multiple visits to the ED for this complaint. The patient had a history of substance abuse and requested dilaudid for her pain—making it easy for staff to consign her to the stereotype of the difficult patient.
“I met her after an interesting finding,” he says. “It turns out that on the previous emergency room visit, she received a CAT scan, which showed duodenal and small-bowel thickening consistent with hereditary angioedema, although with an unusual presentation. As it happened, we had onsite a world expert in angioedema.”
The expert was able to confirm the diagnosis, Dr. Morrow says.
“By giving her this ‘legitimate,’ organic diagnosis, it just changed the whole dynamic of her relationship with her doctors,” he says. “She knew that they knew something was really wrong. The residents were empowered to have something to hang their hats on. And we were able to get better control of her pain.”
Dr. Morrow says he came on the scene late in the discovery process, but he helped to solve the puzzle, and then put together the abstract and poster that told the story of making the diagnosis.
“In my previous job, I was hired as a hospitalist but helped to build the palliative-care program within the hospital-medicine service,” he says. “In my current job, I was brought in to build the inpatient palliative-care-consultation service, although I still moonlight as a hospitalist to stay sharp.”
Dr. Morrow says he enjoys sharing stories of difficult cases and submitting case studies about them to medical conferences, often with clever titles incorporating puns (e.g. the 2009 SHM poster citing kinins, polypeptides in the blood that cause inflammation). Another example is “The Angina Monologues,” a story of an 82-year-old patient with chronic angina pectoris and complex pain syndromes that were difficult to bring under control. Palliative care also emphasizes patients’ stories, he says, in order to understand the person behind the diagnosis.
Larry Beresford is a freelance writer in San Francisco. References available at www.the-hospitalist.org.
References
2. Yoder J. Association between hospital noise levels and inpatient sleep among middle-aged and older adults: Far from a quiet night. Abstract, Society of Hospital Medicine, 2011.
3. McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS. Principles and Practice of Hospital Medicine. McGraw-Hill Medical; New York City: 2012.
4. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. J Hosp Med. 2012;7:359-364.
5. Dylag A, Shah SI. Administration of tetanus, diphtheria, and acellular pertussis vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2008;122:e550-e555.
6. Shah S. Smoking cessation counseling and PPSV 23-valent pneumococcal polysaccharide vaccine administration parents of neonatal intensive care unit (NICU)-admitted infants: A life-changing opportunity. J Neonatal-Perinatal Med. 2011;4:263-267.
Back to the Furture Past RIV winners talk about what the recognition meant for their careers By Larry Beresford
After winning SHM’s annual Research, Innovations, and Clinical Vignettes (RIV) scientific abstract and poster competition for an abstract illustrating a program that promoted flu vaccinations for families of neonatal patients, Shetal Shah, MD, FAAP, became a leading advocate for two laws mandating that New York hospitals offer vaccinations to families.
A poster that described a VTE prevention program led Gregory Maynard, MD, MSc, SFHM, to join SHM’s VTE Prevention Collaborative and, eventually, to become senior vice president of the society’s Center for Hospital Innovation and Improvement.
A prize-winning innovations poster for improving team communication by Vineet Chopra, MD, MS, FACP, FHM, and colleagues later took off as a new technology company.
Leonard Feldman, MD, FAAP, SFHM, won for a poster that explained online CME curriculum for hospitalists as consultants; the curriculum now resides on SHM’s website.
The evidence is clear: RIV abstracts are a vital part of hospital medicine.
Nearly 800 abstracts were submitted for HM13.
Awards are given in three categories:
- Research posters report clinical or basic science data, systematically review a clinical problem, or address efficiency, cost, or method of health-care delivery or medical decision-making;
- Innovations posters describe an existing innovative program in hospital medicine, often with preliminary data; and
- Clinical vignettes, either adult or pediatric, report on one or more cases illustrating a new disease entity, a prominent or unusual feature of an established disease, or an area of clinical controversy.
The Hospitalist asked 11 past RIV winners what the poster contest meant to their careers. Some added more data and analysis and went on to be published in such medical journals as the Journal of Hospital Medicine. Some used the recognition to launch or boost research-oriented careers; others saw their careers go in different directions.
“Winning a national poster competition gives you the confidence to continue to pursue your interest and take it to a higher level, like successfully competing for funding and publishing your line of inquiry,” says hospitalist and researcher Vineet Arora, MD, MPP, FHM, of the University of Chicago, who won the 2006 RIV research competition. “Sometimes, presenting posters can be lonely, but at SHM, you get a lot of traffic. You get a chance to practice your spiel, communicating science and research in a very concise way, which is an important skill to have.”
David Metzger, MD, PhD, also from the University of Chicago, who won the RIV research award in 2005, says recognition is a big deal, but “one of the biggest values of the RIV competition is just getting information out to colleagues, with the opportunity to talk with your peers. That’s the real prize.
“I’ve been involved in presenting posters at SHM every year that the society has been in existence,” he says. “I’ve met so many people and talked about what they’re doing. That’s what a medical society should do—bring people together like this.”
Title: Administrator, academic consult service; teaching staff physician
Institution: Saint Joseph Mercy Hospital, Ypsilanti, Mich.
Year: 2008
RIV: “A Case of Salty Voluminous Urine” (clinical vignette)
Dr. Tassava was honored two years in a row for topics drawn from her experience as a hospitalist working in the surgical ICU. Her HM08 entry won top poster, and her HM09 poster, “Permissive Hypernatremia: Co-Management of Intracranial Pressure in a Patient with Diabetes Insipidus,” was selected for an oral presentation.
The HM09 vignette described how the hypernatremia that occurs with diabetes insipidus could be used in a novel way to control intracranial pressure in a 17-year-old patient who had a traumatic brain injury from an auto accident.
“She had a beautiful outcome,” Dr. Tassava says. “She started college and she came back to our unit for a visit after her recovery.”
Dr. Tassava enjoyed the opportunity to explain to her peers how diabetes insipidus presented and how she managed the case. “I was a little surprised at how much discussion was generated by my case,” she says, “even though I knew this was an important and novel approach.”
When her hospital added intensivists, her work and research in the ICU ended and her career moved more toward hospitalist administration. She now runs the academic consult service at St. Joseph, serves as lead physician for the orthopedic surgery floor, instructs and mentors medical residents, and chairs the hospital’s Coagulation Collaborative Practice Team (Coagulation CPT). She credits the RIV honors with helping her to gain recognition as an academic hospitalist who was nominated for leadership roles. She has moved out of research for now but plans to pursue anticoagulation research in the future.
“I really appreciated the recognition for my curiosity and scientific approach, which was acknowledged by my surgical colleagues,” Dr. Tassava says. “I absolutely love the CPT. I am the hospital’s principal educator with regard to anticoagulation. Over the past year, I have given medicine and cardiology grand rounds, and have presented on the newest anticoagulants.”
Dr. Tassava still collaborates with her residents on abstracts, several of which have been submitted to SHM, the American College of Physicians, and other medical societies.
“I still love research,” she says. “I have a million ideas.”
Title: Chief of the division of hospital medicine; senior vice president, SHM’s Center for Innovation and Improvement
Institution: University of California at San Diego (UCSD)
Year: 2008
RIV: “Prevention of Hospital-Acquired Venous Thromboembolism: Prospective Validation of a VTE Risk Assessment Model and Protocol” (research)
Citations: Maynard G, Stein J. Designing and implementing effective VTE prevention protocols: lessons from collaboratives. J Thromb Thrombolysis. 2010;29(2):159-166. Maynard G, Morris T, Jenkins I, et al. Optimizing prevention of hospital acquired venous thromboembolism: prospective validation of a VTE risk assessment model. J Hosp Med. 2010;5(1):10-18.
Dr. Maynard’s abstract described a project funded by the federal Agency for Healthcare Research and Quality to design and implement an organized, comprehensive protocol for VTE prevention within the hospital setting. The project also included a toolkit to help other hospitals do the same thing. The same group received SHM’s Award of Excellence for Teamwork.
This work, combined with similar efforts by Jason Stein, MD, and colleagues at Emory University in Atlanta and others, provided the foundation for SHM’s VTE resource room and the mentored implementation program of SHM’s VTE Prevention Collaborative, which had been launched in 2007 as one of the society’s first large-scale quality-improvement (QI) initiatives.
“SHM wanted to do something about VTE prevention, and when we got our AHRQ grant, I was interested in doing the same,” Dr. Maynard says. “We published our implementation guides on the AHRQ and SHM websites, along with a lot of valuable supporting materials.”
Dr. Maynard later took on leadership roles with SHM’s quality initiatives on glycemic control and care transitions, which made him the logical choice to become senior vice president of SHM’s Center for Hospital Innovation and Improvement.
He says the RIV honor lifted his profile not only within SHM, but also throughout the field, and it was instrumental in obtaining continued funding to advance the VTE initiative. “We did this tremendous work—with great results,” he says. “But I don’t think our local administrators appreciated it quite as much until we started to get external, national recognition.”
Dr. Maynard earned his master’s degree in biostatistics and clinical research design from the University of Michigan—skills he later brought to the academic setting at UCSD.
“It was a nice way for a hospitalist, who’s really a medical generalist, to become an expert in something,” he says. “I could never be more of an expert in cardiology than a cardiologist, or more of an expert in DVT than a hematologist or critical-care specialist. But I could help both of them do what they couldn’t do as effectively, which was to implement protocols reliably using a QI framework.”
Title: Assistant professor of general internal medicine, hospital medicine, and public health
Institution: Vanderbilt University, Nashville, Tenn.
Year: 2009
RIV: “Predictors of Early Post-Discharge Mortality in Critically Ill Patients: Lessons for Quality Performance and Quality Assessment” (research)
Citation: Vasilevskis EE, Kuzniewicz MW, Cason BA, et al. Predictors of early post-discharge mortality in critically ill patients: a retrospective cohort study from the California Intensive Care Outcomes project. J Crit Care. 2011;26(1):65-75.
Dr. Vasilevskis has submitted abstracts to the RIV competition almost every year since 2007, when he was completing a fellowship at the University of California at San Francisco’s Institute for Health Policy Studies. He was honored in 2009 for a project based on the California Intensive Care Outcomes Project, which drew data from 35 hospitals to demonstrate that shortening ICU length of stay was predictive of early post-discharge mortality in the most severely ill patients.
He has continued to research quality and safety in the ICU, and he has published dozens of journal articles.
“My initial focus was on traditional mortality and length-of-stay outcomes,” he says. “I am now pursuing additional outcomes, most notably delirium in the ICU patient. I work with an amazing group of researchers that are trying to better measure, define, and treat delirium in the ICU—an outcome associated with a number of poor patient outcomes.”
Dr. Vasilevskis also is researching the causes of hospital readmissions and the development of novel ways to improve care transitions for elderly patients. He is pursuing a master’s of public health at Vanderbilt, and is co-principal investigator of an investigation of the Hospital Medicine Reengineering Network to improve transitions of care, supported by the Association of American Medical Colleges.
In addition to his 2009 win, he captured the HM10 and HM12 research categories. His HM12 poster, “Veterans Administration Acute Care 30-Day Mortality Model: Development, Validation and Performance Variation,” was singled out by the judging committee for its impressive sample size (1,114,327 patients in a retrospective cohort study of 131 VA hospitals), as well as for how it combined administrative and clinical risk models.
Dr. Vasilevskis says the opportunity to present his research at SHM and the recognition he received encouraged him to continue as a hospitalist engaged in medical research. He has been a member of SHM’s Research Committee since 2009, an RIV judge at HM11, and chaired the HM13 RIV competition subcommittee.
Title: Assistant professor of medicine
Institution: University of Michigan Health System, Ann Arbor
Year: 2009
RIV: “MComm: Redefining Medical Communications in the 21st Century” (innovations)
Early in his career, Dr. Chopra was curious about how to improve the way patient care is delivered in the hospital setting. He was particularly interested in the inordinate amount of time hospitalists spend every day on communication.
“I saw one-way paging systems as a problem for communication between members of the medical team,” he says. “Doctors get paged and break off from what they’re doing to return the page—to someone who often isn’t there to take the call back. Sometimes the system gives us the wrong number or a cryptic message that makes no sense.”
A technological solution to this problem, which he and hospitalist Prasanth Gogineni, MD, conceived, designed, and created, then tested at the University of Michigan, is called MComm. Dr. Chopra describes it as a novel, uniform way of messaging for the entire medical team using wireless servers, PUSH technology, and iPhones. MComm was built around existing hospital workflow and patient-specific task lists, assigning priority to each message and documenting that it was delivered. The junior faculty members submitted an abstract about their innovative application, not really expecting it to get accepted. But when it won the poster competition and was selected for a plenary presentation, things got busy in a hurry. Specifically, the university hospital’s Office of Technology Transfer took a keen interest.
“We met with a number of people who had business experience in the health-care-technology space and found a CEO for the company we formed to develop MComm,” Dr. Chopra says. “I found myself getting pulled into it very quickly, with a lot of conversations about commercialization, revenue-sharing models, intellectual property, and the like.”
But running a company was not something Dr. Chopra wanted to do. Two years ago, that company, Synaptin, went one way and he went another—he stayed at Michigan as a medical researcher. He remains deeply interested in how care is delivered to hospitalized patients, but with a focus on such patient-safety questions as how to prevent negative outcomes from indwelling venous catheters.
“Winning the poster competition opened doors for me—there’s no doubt in my mind,” he says. “We demonstrated the ability to deliver a project of significance, from concept to prototype, without formal training in this area. If we didn’t have that recognition, I’m not sure I would have been ready to step into a research career as quickly. It helped me realize that medical research was what I wanted to do.”
Title: Associate program director, internal-medicine residency; assistant dean of scholarship and discovery
Institution: Pritzker School of Medicine, University of Chicago
Year: 2006
RIV: “Measuring Quality of Hospital Care for Vulnerable Elders: Use of ACOVE Quality Indicators” (research)
Citation: Arora VM, Fish M, Basu A, et al. Relationship between quality of care of hospitalized vulnerable elders and postdischarge mortality. J Am Geriatrics. 2010;58:1642-1648.
Title: Associate professor, department of medicine; associate faculty member, Harris School and the Department of Economics
Institution: University of Chicago
Year: 2005
RIV: “Effects of Hospitalists on Outcomes and Costs in a Multicenter Trial of Academic Hospitalists” (research)
Dr. Meltzer was the lead author, with 11 other prominent hospitalists, of an abstract based on a multisite study of the cost and outcome implications of the hospitalist model—still a relatively new concept in 2001, when the research began. Although the study did not uncover large cost savings realized from the hospitalist model of care, as some advocates had hoped, important findings and implications for the emerging field were teased out of the data.
At the time, only a few randomly controlled, multisite studies of costs and outcomes for the hospitalist model had been performed. The study, Dr. Meltzer says, required a complicated analysis to discover that hospitalists, in fact, saved their facilities money, with their most important impact realized post-hospitalization, such as on nursing-home costs. It was important to control for spillover effect and the fact that hospitalists do a better job of teaching house staff, while a physician’s years of experience was another important variable, he says.
Dr. Meltzer was a medical researcher interested in medical specialization when the term “hospitalist” was first coined in 1996. “I thought, here was a chance to study a medical specialty in its formative stages,” he says.
He still works as a hospitalist, although with limited clinical time. In addition to his administrative work as division chief, he directs the Center for Health and the Social Sciences at the University of Chicago. His research interests include cost-effectiveness, technology assessment, and information research.
In 2010, his poster “Effects of Hospitalists on 1-Year Post-Discharge Resource Utilization by Medicare Beneficiaries” took the top prize in the HM10 research competition. In 2011, he was appointed to the methodology committee of the federal Patient-Centered Outcomes Research Institute (PCORI), which was created by the Affordable Care Act to advise the government on clinical-effectiveness research. He also sits on the Advisory Council to the National Institute of General Medical Sciences at the Institute of Medicine, and on the Congressional Budget Office’s panel of health advisors.
In a career full of recognition, Dr. Meltzer says it’s hard to pinpoint the impact of winning the poster contest. But he has continued to submit abstracts to SHM every year and appreciates the opportunities for interaction with peers at the poster exhibits.
Title: Director of perioperative and consultative medicine
Institution: University of Michigan, Ann Arbor
Year: 2006
RIV: “Disseminated Histoplasmosis Presenting As Painful Oral Ulcers” (clinical vignettes)
Dr. Grant’s winning vignette presented a patient with a complex medical history, including heart disease and four months of painful oral ulcers, for which prior evaluations had been inconclusive, despite conducting biopsies. Following administration of high-dose corticosteroids, the patient’s condition worsened on multiple fronts. The vignette showed how the medical team was able to diagnose an unusual presentation of a fungal infection called histoplasmosis, which is prevalent in parts of the Midwest surrounding the Ohio and Mississippi river valleys.
“We see a lot of cases in the hospital where there are different angles you could take to turn it into a clinical vignette or a nice poster with good teaching points,” Dr. Grant says. “In this case, just digging deeper into the actual diagnosis was important because the empiric use of steroids can be fatal for some patients. Steroids are given for a lot of good reasons, but in this patient they caused immune suppression, allowing a smoldering infection to become very active.”
Dr. Grant did not submit the vignette for publication. “That was probably a mistake on my part,” he says, acknowledging the common complaint of too little time and too many competing priorities. But his interest in research has continued.
“I became involved at a national level with issues of perioperative medicine and last August published a textbook on the subject,” he reports.1 “VTE is another area of interest I have developed since my hospital medicine fellowship.”
He serves as the VTE resource expert on the Michigan Hospital Medicine Safety Consortium, a quality collaborative of more than 40 hospitals with Blue Cross/Blue Shield of Michigan. “It’s exciting to be able to look at the risk factors, what kinds of patients get VTEs, and whether they were appropriately prophylaxed in the hospital,” he says.
VTE is a national quality priority, and Dr. Grant expects abstracts to emerge from the consortium’s work.
He says he appreciates the opportunities that arise from participating in poster sessions at SHM, where medical students, residents, and working hospitalists talk to the presenters of interesting cases.
“It gives you a real back-and-forth, which is good for the person asking the question and for the presenter,” he says, noting hospitalists from other parts of the country were not as familiar with histoplasmosis.
He says winning the HM06 poster contest helped him “get his feet wet” and feel more prepared for a career in academic hospital medicine. “I’m sure the award solidified my employers’ satisfaction in hiring me—and in giving me more desirable academic roles and responsibilities,” he adds.
Title: Assistant professor of medicine pediatrics; director of the general internal-medicine comprehensive consultation service
Institution: Johns Hopkins Hospital, Baltimore
Year: 2009
RIV: “An Internet-Based Consult Curriculum for Hospitalists” (innovations)
Dr. Feldman’s poster described an online CME curriculum for hospitalists acting as medical consultants. The concept grew out of a perceived deficiency in his own medical education when, in 2004, he was asked to lead the consultation service at Johns Hopkins—just six months after finishing his residency.
“I had no idea what I was doing as a general-internal-medicine consultant,” he says. “I maybe received two weeks of experience as a consultant during my residency. I was willing to take it on, learning on the job and asking for help. But it occurred to me that I’m probably not alone in feeling unprepared.”
In his quest for self-education, Dr. Feldman wondered whether he should write a textbook on the subject. “But the information changes so quickly, I thought I’d have a better chance to reach people online,” he notes.
After talking to publishers and CME companies, he came up with the concept of learning modules on perioperative and consultative medicine topics, which could be taken online while earning CME credits. Johns Hopkins served as the CME certifier, and medical-education company Advanced Studies in Medicine joined as a partner. Once the project got off the ground, a medical advisory committee was convened.
“Winning the SHM poster competition is a great honor to have on a CV. It really helps to legitimize your name in the world of hospital medicine,” Dr. Feldman says. “It also provided confirmation that we were on the right track with the curriculum project. People valued what we were doing.”
Dr. Feldman and SHM have since become affiliated, and the “Consultative and Perioperative Medicine Essentials for Hospitalists” modules are available on SHM’s website (www.shmconsults.com). The site has 12,000 registered members completing 500 CME modules every month.
“I do a lot of the editing still,” Dr. Feldman says. “We update the modules every two years and are still creating new ones.”
Dr. Feldman also pursues a number of clinical-research interests, including resident education and costs of care.
Title: Assistant professor of medicine
Institution: Medical University of South Carolina, Charleston
Year: 2009
RIV: “Intensivists versus Hospitalists in the ICU: A Prospective Cohort Study Comparing Mortality and Length of Stay Between Two Staffing Models” (research) Citation: Wise KR, Akopov VA, Williams BR, Ido MS, Leeper KV, Dressler DD. Hospitalists and intensivists in the medical ICU: a prospective and observational study comparing mortality and length of stay between two staffing models. J Hosp Med. 2012;7(3):183-189.
Dr. Wise was recognized for research that began while she worked at Emory University in Atlanta, comparing hospitalists and intensivists in such outcomes as length of stay and mortality rates for patients in the ICU. The study was one of the first statistically rigorous examinations of this critical quality question. With an eye toward improving patient safety, national quality advocates such as the Leapfrog Group have called for hospitals to employ intensivists (critical-care specialists) to manage the care of ICU patients. In reality, Dr. Wise says, there aren’t enough intensivists to meet the need.
“Hospitalists are in the ICU anyway,” she says. “We just don’t have enough data to answer how well they do [in comparison to intensivists].”
Through a prospective cohort study of more than 1,000 patients, Dr. Wise’s group found that there was essentially no statistical difference in mortality rates between patients treated by intensivist teams or hospitalist ICU teams.
“We were also able to look at some of the intermediate-acuity patients—fairly complicated but not requiring ventilators,” she explains. “Our study wasn’t sufficiently powered for this subgroup, but it was an interesting piece of data to raise the question: Where should we deploy this scarce resource of intensivists? Which pockets of patients?”
Presenting her abstract at SHM’s annual meeting was a “good experience.”
“I’d done public speaking before, but never with an audience of about 500 people,” she says. “To go out there and field their questions was a real professional growing experience. Several people interested in the topic sought me out at the conference, introduced themselves, and we have subsequently stayed in touch.”
The manuscript published in JHM has been cited four times, including in a position paper from SHM and the Society of Critical Care Medicine.3 Another outgrowth of the research was being asked to contribute a chapter on hospitalists’ role in the ICU to a textbook on hospital medicine. Based on her still-fresh HM presentation, Dr. Wise was one of the few publicly identified experts on the subject. The chapter, co-authored by fellow Emory hospitalist Michael Heisler, MD, MPH, “The Role of the Hospitalist in Critical Care” was included in Principles and Practices of Hospital Medicine.4
Title: Neonatal intensivist
Institution: Stony Brook University Hospital, Great Neck, N.Y.
Year: 2006
RIV: “Administration of Inactivated Trivalent Influenza Vaccine (TIV) to Parents of Infants in the Neonatal Intensive Care Unit (NICU): A Novel Strategy to Increase Vaccination Rates” (innovations)
Citation: Shah SI, Caprio M, Hendricks-Munoz K. Administration of inactivated trivalent influenza vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2007;120;e617-e621.
Dr. Shah was in his final year of a fellowship in neonatology at New York University when he took on the challenge of improving immunization access to protect premature, highly vulnerable patients in the NICU from influenza infections. Because these children are too young to be vaccinated directly, the concept of cocooning them from infection involves extending protection to everyone around them.
“We came up with the idea of offering flu vaccinations 24/7 in the NICU to the children’s parents,” he says. “It worked well for us as a way to define an indicated therapy for a defined population, even if it was a little outside the box. By the end of the flu season, 95% of the parents were vaccinated.”
SHM recognized the project as the top RIV innovations poster at HM06, but that was just the beginning.
“When I moved to SUNY Stony Brook, I continued to study and advocate for these vaccinations,” Dr. Shah says. “We were giving 500 to 700 vaccinations a year. Then I wrote a national resolution for the American Academy of Pediatrics, which was significant because it meant AAP was behind the project.”
Dr. Shah later became chair of AAP’s Long Island Chapter Legislative Committee and joined a statewide pediatric advocacy group. In 2009, the New York legislature enacted the Neonatal Influenza Protection Act, which required hospitals in the state to offer parents the vaccine, with Dr. Shah’s research and advocacy providing an essential basis for its passage. He’s even been recognized for his research in congressional citations.
Based on that success with influenza vaccinations, Dr. Shah and his colleagues looked at other diseases, starting with pertussis, and then tetanus, diphtheria, and whooping cough.5 All the while, they continued tracking immunization rates. A second state law, passed in 2011, added pertussis to the vaccinations. Next on his advocacy agenda is a project to promote smoking-cessation interventions in the NICU.6
“These parents come to see us every day,” he says. “What can we do, through the parents, to promote the health and well-being of their high-risk newborns?”
Title: Assistant professor of medicine; medical director of inpatient palliative-care consultation
Institution: University of Texas Health Sciences Center, San Antonio
Year: 2009
RIV: “When to Depend on the Kinins of Strangers: An Unusual Case of Abdominal Pain” (clinical vignettes)
Publication: An article on the ethics of determining code status for patients with advanced cancer and a book chapter on the “last hours of life” for a forthcoming book on palliative care and hospital medicine.
As a medical resident, Dr. Morrow met a 27-year-old woman who had chronic abdominal pain and had made multiple visits to the ED for this complaint. The patient had a history of substance abuse and requested dilaudid for her pain—making it easy for staff to consign her to the stereotype of the difficult patient.
“I met her after an interesting finding,” he says. “It turns out that on the previous emergency room visit, she received a CAT scan, which showed duodenal and small-bowel thickening consistent with hereditary angioedema, although with an unusual presentation. As it happened, we had onsite a world expert in angioedema.”
The expert was able to confirm the diagnosis, Dr. Morrow says.
“By giving her this ‘legitimate,’ organic diagnosis, it just changed the whole dynamic of her relationship with her doctors,” he says. “She knew that they knew something was really wrong. The residents were empowered to have something to hang their hats on. And we were able to get better control of her pain.”
Dr. Morrow says he came on the scene late in the discovery process, but he helped to solve the puzzle, and then put together the abstract and poster that told the story of making the diagnosis.
“In my previous job, I was hired as a hospitalist but helped to build the palliative-care program within the hospital-medicine service,” he says. “In my current job, I was brought in to build the inpatient palliative-care-consultation service, although I still moonlight as a hospitalist to stay sharp.”
Dr. Morrow says he enjoys sharing stories of difficult cases and submitting case studies about them to medical conferences, often with clever titles incorporating puns (e.g. the 2009 SHM poster citing kinins, polypeptides in the blood that cause inflammation). Another example is “The Angina Monologues,” a story of an 82-year-old patient with chronic angina pectoris and complex pain syndromes that were difficult to bring under control. Palliative care also emphasizes patients’ stories, he says, in order to understand the person behind the diagnosis.
Larry Beresford is a freelance writer in San Francisco. References available at www.the-hospitalist.org.
References
2. Yoder J. Association between hospital noise levels and inpatient sleep among middle-aged and older adults: Far from a quiet night. Abstract, Society of Hospital Medicine, 2011.
3. McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS. Principles and Practice of Hospital Medicine. McGraw-Hill Medical; New York City: 2012.
4. Siegal EM, Dressler DD, Dichter JR, Gorman MJ, Lipsett PA. Training a hospitalist workforce to address the intensivist shortage in American hospitals: a position paper from the Society of Hospital Medicine and the Society of Critical Care Medicine. J Hosp Med. 2012;7:359-364.
5. Dylag A, Shah SI. Administration of tetanus, diphtheria, and acellular pertussis vaccine to parents of high-risk infants in the neonatal intensive care unit. Pediatrics. 2008;122:e550-e555.
6. Shah S. Smoking cessation counseling and PPSV 23-valent pneumococcal polysaccharide vaccine administration parents of neonatal intensive care unit (NICU)-admitted infants: A life-changing opportunity. J Neonatal-Perinatal Med. 2011;4:263-267.
Medicare Penalties Make Hospital-Acquired-Infection Solutions a Priority
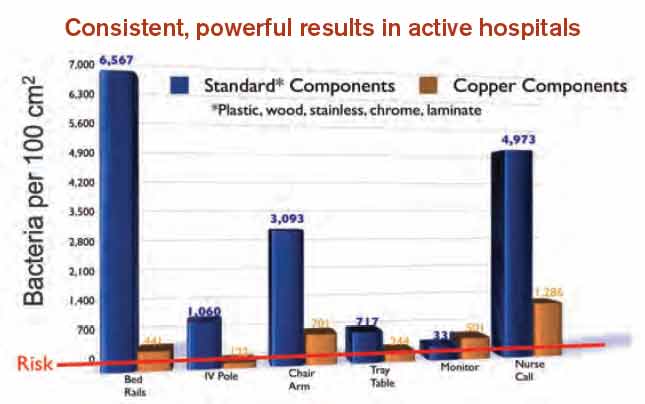
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
How Copper Could Solve Problem of Hospital-Acquired Infections

—James Pile, MD, FACP, SFHM, vice chair, department of hospital medicine, Cleveland Clinic
Hospital-acquired infections (HAIs) are on the rise despite efforts to decrease them. HAIs cause an estimated 100,000 deaths annually and account for up to $45 billion in health-care costs. Adding fuel to the fire, bacteria increasingly are becoming resistant to last-resort drugs. Despite this gloomy outlook, a recent study in Infection Control and Hospital Epidemiology shows that a material known for its antimicrobial properties for more than 4,000 years—copper—might be a light at the end of this darkening tunnel.1
Ancient Indians stored water in copper pots to prevent illness, says lead study author Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, and medical director for infection prevention at the Medical University of South Carolina (MUSC) in Charleston. But copper rarely is used in that manner today because molded plastics and stainless steel are less expensive and easier to mass-produce.
Dr. Salgado explains that the antimicrobial effect of copper-alloy surfaces is a result of the metal stealing electrons from the bacteria when they come into contact with each other. “Once the bacteria donate the electrons to the copper metal, this places the organism into a state of electrical-charge deficit,” she says. “As a consequence, free radicals are generated inside the cell, which ultimately leads to the cell’s death.”
Copper-alloy surfaces kill 99.9% of bacteria in less than two hours, says Harold T. Michels, PhD, PE, senior vice president of technology and technical services for Copper Development Association Inc. in New York, who was a study author. On other surfaces, bacteria may live for multiple days or even months.
Unlike current methods used to decrease HAIs (i.e. hand-washing and sanitizing surfaces), copper components don’t require human intervention or compliance to be effective.
“It supplements what these other things can do; it’s in the background and it’s always working,” Michels says.

—Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, medical director for infection prevention, Medical University of South Carolina, Charleston
Study Specifics
To conduct the study, copper prototypes of items touched most frequently by patients, health-care providers, and visitors were made and placed in patient rooms located within ICUs. “We placed the copper around the patient [much like a defensive perimeter] to reduce the likelihood that the health-care worker or visitor would introduce the infectious agent to the patient,” says the study’s lead investigator, Michael Schmidt, PhD, a professor and vice chair of MUSC’s department of microbiology and immunology.
Then, bacterial loads were measured on each object. For every study room, there was a control room without copper objects. Researchers were most interested in methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE). For a period of time, bacterial burdens were measured in both copper rooms and control rooms.
Results exceeded the researchers’ expectations. Although only 7% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases. The rate of HAI and/or MRSA or VRE colonization in ICU rooms with copper-alloy surfaces was significantly lower than that in standard ICU rooms (0.071 versus 0.123). For HAIs only, the rate was reduced to 0.034 from 0.081.3
“We were pleasantly surprised with the reductions,” Dr. Salgado says. “We consistently saw a more than 50% reduction in HAIs in all study sites.”
Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association, is an advocate for making the health-care system simpler and safer for consumers. She says copper is a “game-changer.”
“It’s a brand-new way of thinking about decreasing the number of HAIs,” she says.
Green Light?
In light of the study’s encouraging findings, hospitalist and infectious-disease specialist James Pile, MD, FACP, SFHM, vice chair of the Department of Hospital Medicine at Cleveland Clinic, says that although study results appear valid, “it didn’t provide any final answers.”

“It would be premature for a hospital to install copper based on this study,” he says, adding he didn’t find the study results surprising, because copper is known to have antimicrobial properties.
But, Dr. Pile says, the study did provide proof of concept and opens the door for larger, more definitive studies that will show if installing copper in hospital rooms is worthwhile.
“If future studies confirm earlier results, then hospitals should seriously consider copper installations,” he says.
Barriers to Implementation
Despite the promising outlook for copper in dramatically reducing HAIs, implantation of copper components is off to a slow start.
Negotiations with the Environmental Protection Agency, the federal agency with jurisdiction over public-health claims for antimicrobial surfaces, started in 2004. Testing started in 2005. Although federal registration was completed in February 2008, it wasn’t until late 2011 that all regulatory issues were resolved for manufacturers.
“The regulatory process created delays in educating hospitals and the public about copper’s effectiveness in killing certain bacteria,” Dr. Georgiou explains. “As a result, American manufacturers with the ability to make copper components weren’t developing products because they couldn’t sell them.”
Now that the regulatory issues have been resolved, U.S. manufacturers are beginning to make copper components. The first wave of commercial products came on the market in late 2011. Meanwhile, European countries have not been delayed and are well ahead of U.S. hospitals in implementing copper components.
Presently, nine U.S. hospitals have installed some form of copper components, including door hardware, cabinet pulls, sinks, stretchers, and IV poles, Michels reports.
Despite these advances, hospitals may be slow to incorporate copper components due to a variety of reasons:
Cost. Dr. Pile believes that cost will be the major barrier. “Installing copper surfaces won’t be cheap,” he says. “But, then again, HAIs are very costly. I think it will be more difficult to justify their existence if they can be prevented. If copper is effective in preventing HAIs, it would prove to be cost-effective over time.”
Dr. Salgado concurs. “A study needs to be done on the cost-effectiveness of copper surfaces,” she says. “Health economists estimate that if copper surfaces were incorporated into ICUs, after three to six months, those surfaces would pay for themselves. That is not a long time period. Hospitals need to understand that there will be upfront costs but that they will realize benefits downstream.”
The Center for Medicare & Medicaid Services (CMS) has reported that one infection adds $43,000 in patient costs.4 A typical U.S. hospital room contains $100,000 worth of goods and equipment.
“When you do the math using the amount of copper in our study, the cost would be between $1 and $10 per patient,” Dr. Schmidt says. “It’s also important to note that an infection adds 19 days to a patient’s hospital stay.”
Aesthetics. For some, appearance may be a concern. “Copper is actually an appealing material that is offered in an array of colors and surface finishes,” Dr. Michels says. Because a copper-and-brass combination is more prone to tarnishing, a copper-nickel alloy may be more desirable.
Availability. Copper components are not produced and marketed to U.S. hospitals; however, they are available. “We are hoping with our study and future studies that some medical-device companies, as well as hospital-furniture manufacturers, will jump on board to look at ways to mass-produce items,” Dr. Salgado says.
Acceptance. The study published in Infection Control and Hospital Epidemiology validated the effectiveness of copper in decreasing HAIs. This pilot study, however, was not blinded.3
“It was pretty apparent to providers where copper surfaces were located, which tends to result in some bias. Future studies will, hopefully, try to answer questions regarding healthcare providers’ behaviors with different surfaces,” says Dr. Salgado, noting researchers in California and Chile also are studying the effects of copper surfaces in hospitals.
Possible loss of efficacy. Even if a surface is effective initially, Dr. Pile points out that it’s possible for that to change. “I have a theoretical concern that, over time, bacterial pathogens may develop a tolerance to copper,” he says. “Bacterial adversaries have been able to overcome any type of treatment that we have devised for them thus far. But this remains to be seen.”
This has been an issue with other surfaces; once microbes establish a foothold, it is hard to eliminate them. But Dr. Schmidt says because bacteria are killed so quickly on copper surfaces and cleaning is only required once daily, the ability to establish a foothold is greatly reduced, if not completely eliminated.

—Harold T. Michels, PhD, PE, senior vice president of technology and technical services, Copper Development Association Inc.
Champion Proven Strategies
Dr. Pile sees antimicrobial stewardship as a great opportunity for hospitalists as a specialty. In fact, the Centers for Disease Control and Prevention is partnering with HM groups on piloting multiple antimicrobial stewardship initiatives at several sites.
Dr. Pile suggests that leaders spearhead formal quality-improvement efforts, be involved with patient-safety efforts, and serve as physician champions.
“No one is better positioned to do this than hospitalists, because we own the hospital environment,” he says. “We have an incredible stake in making sure that our inpatient environment provides safe and high-value care.”
As a result of the published study, Dr. Salgado says discussions are underway with hospital leaders at MUSC to determine if copper surfaces will be used in its ICUs and, if so, how changes will be implemented.
Karen Appold is a freelance writer in Pennsylvania.
References
- Klevens RM, Edwards JR, Richards CL, et al. Estimating healthcare-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160-166.
- Scott RD. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Atlanta: Centers for Disease Control and Prevention, 2009.
- Salgado CD, Sepkowitz KA, John JF, et al. Copper Surfaces Reduce the Rate of Healthcare-Acquired Infections in the Intensive Care Unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
- Healthcare Cost and Utilization Project. Statistical Brief No. 94. Agency for Healthcare Research and Quality. Aug. 2010. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb94.pdf. Accessed Aug. 6, 2013.
—James Pile, MD, FACP, SFHM, vice chair, department of hospital medicine, Cleveland Clinic
Hospital-acquired infections (HAIs) are on the rise despite efforts to decrease them. HAIs cause an estimated 100,000 deaths annually and account for up to $45 billion in health-care costs. Adding fuel to the fire, bacteria increasingly are becoming resistant to last-resort drugs. Despite this gloomy outlook, a recent study in Infection Control and Hospital Epidemiology shows that a material known for its antimicrobial properties for more than 4,000 years—copper—might be a light at the end of this darkening tunnel.1
Ancient Indians stored water in copper pots to prevent illness, says lead study author Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, and medical director for infection prevention at the Medical University of South Carolina (MUSC) in Charleston. But copper rarely is used in that manner today because molded plastics and stainless steel are less expensive and easier to mass-produce.
Dr. Salgado explains that the antimicrobial effect of copper-alloy surfaces is a result of the metal stealing electrons from the bacteria when they come into contact with each other. “Once the bacteria donate the electrons to the copper metal, this places the organism into a state of electrical-charge deficit,” she says. “As a consequence, free radicals are generated inside the cell, which ultimately leads to the cell’s death.”
Copper-alloy surfaces kill 99.9% of bacteria in less than two hours, says Harold T. Michels, PhD, PE, senior vice president of technology and technical services for Copper Development Association Inc. in New York, who was a study author. On other surfaces, bacteria may live for multiple days or even months.
Unlike current methods used to decrease HAIs (i.e. hand-washing and sanitizing surfaces), copper components don’t require human intervention or compliance to be effective.
“It supplements what these other things can do; it’s in the background and it’s always working,” Michels says.
—Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, medical director for infection prevention, Medical University of South Carolina, Charleston
Study Specifics
To conduct the study, copper prototypes of items touched most frequently by patients, health-care providers, and visitors were made and placed in patient rooms located within ICUs. “We placed the copper around the patient [much like a defensive perimeter] to reduce the likelihood that the health-care worker or visitor would introduce the infectious agent to the patient,” says the study’s lead investigator, Michael Schmidt, PhD, a professor and vice chair of MUSC’s department of microbiology and immunology.
Then, bacterial loads were measured on each object. For every study room, there was a control room without copper objects. Researchers were most interested in methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE). For a period of time, bacterial burdens were measured in both copper rooms and control rooms.
Results exceeded the researchers’ expectations. Although only 7% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases. The rate of HAI and/or MRSA or VRE colonization in ICU rooms with copper-alloy surfaces was significantly lower than that in standard ICU rooms (0.071 versus 0.123). For HAIs only, the rate was reduced to 0.034 from 0.081.3
“We were pleasantly surprised with the reductions,” Dr. Salgado says. “We consistently saw a more than 50% reduction in HAIs in all study sites.”
Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association, is an advocate for making the health-care system simpler and safer for consumers. She says copper is a “game-changer.”
“It’s a brand-new way of thinking about decreasing the number of HAIs,” she says.
Green Light?
In light of the study’s encouraging findings, hospitalist and infectious-disease specialist James Pile, MD, FACP, SFHM, vice chair of the Department of Hospital Medicine at Cleveland Clinic, says that although study results appear valid, “it didn’t provide any final answers.”
“It would be premature for a hospital to install copper based on this study,” he says, adding he didn’t find the study results surprising, because copper is known to have antimicrobial properties.
But, Dr. Pile says, the study did provide proof of concept and opens the door for larger, more definitive studies that will show if installing copper in hospital rooms is worthwhile.
“If future studies confirm earlier results, then hospitals should seriously consider copper installations,” he says.
Barriers to Implementation
Despite the promising outlook for copper in dramatically reducing HAIs, implantation of copper components is off to a slow start.
Negotiations with the Environmental Protection Agency, the federal agency with jurisdiction over public-health claims for antimicrobial surfaces, started in 2004. Testing started in 2005. Although federal registration was completed in February 2008, it wasn’t until late 2011 that all regulatory issues were resolved for manufacturers.
“The regulatory process created delays in educating hospitals and the public about copper’s effectiveness in killing certain bacteria,” Dr. Georgiou explains. “As a result, American manufacturers with the ability to make copper components weren’t developing products because they couldn’t sell them.”
Now that the regulatory issues have been resolved, U.S. manufacturers are beginning to make copper components. The first wave of commercial products came on the market in late 2011. Meanwhile, European countries have not been delayed and are well ahead of U.S. hospitals in implementing copper components.
Presently, nine U.S. hospitals have installed some form of copper components, including door hardware, cabinet pulls, sinks, stretchers, and IV poles, Michels reports.
Despite these advances, hospitals may be slow to incorporate copper components due to a variety of reasons:
Cost. Dr. Pile believes that cost will be the major barrier. “Installing copper surfaces won’t be cheap,” he says. “But, then again, HAIs are very costly. I think it will be more difficult to justify their existence if they can be prevented. If copper is effective in preventing HAIs, it would prove to be cost-effective over time.”
Dr. Salgado concurs. “A study needs to be done on the cost-effectiveness of copper surfaces,” she says. “Health economists estimate that if copper surfaces were incorporated into ICUs, after three to six months, those surfaces would pay for themselves. That is not a long time period. Hospitals need to understand that there will be upfront costs but that they will realize benefits downstream.”
The Center for Medicare & Medicaid Services (CMS) has reported that one infection adds $43,000 in patient costs.4 A typical U.S. hospital room contains $100,000 worth of goods and equipment.
“When you do the math using the amount of copper in our study, the cost would be between $1 and $10 per patient,” Dr. Schmidt says. “It’s also important to note that an infection adds 19 days to a patient’s hospital stay.”
Aesthetics. For some, appearance may be a concern. “Copper is actually an appealing material that is offered in an array of colors and surface finishes,” Dr. Michels says. Because a copper-and-brass combination is more prone to tarnishing, a copper-nickel alloy may be more desirable.
Availability. Copper components are not produced and marketed to U.S. hospitals; however, they are available. “We are hoping with our study and future studies that some medical-device companies, as well as hospital-furniture manufacturers, will jump on board to look at ways to mass-produce items,” Dr. Salgado says.
Acceptance. The study published in Infection Control and Hospital Epidemiology validated the effectiveness of copper in decreasing HAIs. This pilot study, however, was not blinded.3
“It was pretty apparent to providers where copper surfaces were located, which tends to result in some bias. Future studies will, hopefully, try to answer questions regarding healthcare providers’ behaviors with different surfaces,” says Dr. Salgado, noting researchers in California and Chile also are studying the effects of copper surfaces in hospitals.
Possible loss of efficacy. Even if a surface is effective initially, Dr. Pile points out that it’s possible for that to change. “I have a theoretical concern that, over time, bacterial pathogens may develop a tolerance to copper,” he says. “Bacterial adversaries have been able to overcome any type of treatment that we have devised for them thus far. But this remains to be seen.”
This has been an issue with other surfaces; once microbes establish a foothold, it is hard to eliminate them. But Dr. Schmidt says because bacteria are killed so quickly on copper surfaces and cleaning is only required once daily, the ability to establish a foothold is greatly reduced, if not completely eliminated.
—Harold T. Michels, PhD, PE, senior vice president of technology and technical services, Copper Development Association Inc.
Champion Proven Strategies
Dr. Pile sees antimicrobial stewardship as a great opportunity for hospitalists as a specialty. In fact, the Centers for Disease Control and Prevention is partnering with HM groups on piloting multiple antimicrobial stewardship initiatives at several sites.
Dr. Pile suggests that leaders spearhead formal quality-improvement efforts, be involved with patient-safety efforts, and serve as physician champions.
“No one is better positioned to do this than hospitalists, because we own the hospital environment,” he says. “We have an incredible stake in making sure that our inpatient environment provides safe and high-value care.”
As a result of the published study, Dr. Salgado says discussions are underway with hospital leaders at MUSC to determine if copper surfaces will be used in its ICUs and, if so, how changes will be implemented.
Karen Appold is a freelance writer in Pennsylvania.
References
- Klevens RM, Edwards JR, Richards CL, et al. Estimating healthcare-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160-166.
- Scott RD. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Atlanta: Centers for Disease Control and Prevention, 2009.
- Salgado CD, Sepkowitz KA, John JF, et al. Copper Surfaces Reduce the Rate of Healthcare-Acquired Infections in the Intensive Care Unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
- Healthcare Cost and Utilization Project. Statistical Brief No. 94. Agency for Healthcare Research and Quality. Aug. 2010. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb94.pdf. Accessed Aug. 6, 2013.
—James Pile, MD, FACP, SFHM, vice chair, department of hospital medicine, Cleveland Clinic
Hospital-acquired infections (HAIs) are on the rise despite efforts to decrease them. HAIs cause an estimated 100,000 deaths annually and account for up to $45 billion in health-care costs. Adding fuel to the fire, bacteria increasingly are becoming resistant to last-resort drugs. Despite this gloomy outlook, a recent study in Infection Control and Hospital Epidemiology shows that a material known for its antimicrobial properties for more than 4,000 years—copper—might be a light at the end of this darkening tunnel.1
Ancient Indians stored water in copper pots to prevent illness, says lead study author Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, and medical director for infection prevention at the Medical University of South Carolina (MUSC) in Charleston. But copper rarely is used in that manner today because molded plastics and stainless steel are less expensive and easier to mass-produce.
Dr. Salgado explains that the antimicrobial effect of copper-alloy surfaces is a result of the metal stealing electrons from the bacteria when they come into contact with each other. “Once the bacteria donate the electrons to the copper metal, this places the organism into a state of electrical-charge deficit,” she says. “As a consequence, free radicals are generated inside the cell, which ultimately leads to the cell’s death.”
Copper-alloy surfaces kill 99.9% of bacteria in less than two hours, says Harold T. Michels, PhD, PE, senior vice president of technology and technical services for Copper Development Association Inc. in New York, who was a study author. On other surfaces, bacteria may live for multiple days or even months.
Unlike current methods used to decrease HAIs (i.e. hand-washing and sanitizing surfaces), copper components don’t require human intervention or compliance to be effective.
“It supplements what these other things can do; it’s in the background and it’s always working,” Michels says.
—Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, medical director for infection prevention, Medical University of South Carolina, Charleston
Study Specifics
To conduct the study, copper prototypes of items touched most frequently by patients, health-care providers, and visitors were made and placed in patient rooms located within ICUs. “We placed the copper around the patient [much like a defensive perimeter] to reduce the likelihood that the health-care worker or visitor would introduce the infectious agent to the patient,” says the study’s lead investigator, Michael Schmidt, PhD, a professor and vice chair of MUSC’s department of microbiology and immunology.
Then, bacterial loads were measured on each object. For every study room, there was a control room without copper objects. Researchers were most interested in methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE). For a period of time, bacterial burdens were measured in both copper rooms and control rooms.
Results exceeded the researchers’ expectations. Although only 7% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases. The rate of HAI and/or MRSA or VRE colonization in ICU rooms with copper-alloy surfaces was significantly lower than that in standard ICU rooms (0.071 versus 0.123). For HAIs only, the rate was reduced to 0.034 from 0.081.3
“We were pleasantly surprised with the reductions,” Dr. Salgado says. “We consistently saw a more than 50% reduction in HAIs in all study sites.”
Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association, is an advocate for making the health-care system simpler and safer for consumers. She says copper is a “game-changer.”
“It’s a brand-new way of thinking about decreasing the number of HAIs,” she says.
Green Light?
In light of the study’s encouraging findings, hospitalist and infectious-disease specialist James Pile, MD, FACP, SFHM, vice chair of the Department of Hospital Medicine at Cleveland Clinic, says that although study results appear valid, “it didn’t provide any final answers.”
“It would be premature for a hospital to install copper based on this study,” he says, adding he didn’t find the study results surprising, because copper is known to have antimicrobial properties.
But, Dr. Pile says, the study did provide proof of concept and opens the door for larger, more definitive studies that will show if installing copper in hospital rooms is worthwhile.
“If future studies confirm earlier results, then hospitals should seriously consider copper installations,” he says.
Barriers to Implementation
Despite the promising outlook for copper in dramatically reducing HAIs, implantation of copper components is off to a slow start.
Negotiations with the Environmental Protection Agency, the federal agency with jurisdiction over public-health claims for antimicrobial surfaces, started in 2004. Testing started in 2005. Although federal registration was completed in February 2008, it wasn’t until late 2011 that all regulatory issues were resolved for manufacturers.
“The regulatory process created delays in educating hospitals and the public about copper’s effectiveness in killing certain bacteria,” Dr. Georgiou explains. “As a result, American manufacturers with the ability to make copper components weren’t developing products because they couldn’t sell them.”
Now that the regulatory issues have been resolved, U.S. manufacturers are beginning to make copper components. The first wave of commercial products came on the market in late 2011. Meanwhile, European countries have not been delayed and are well ahead of U.S. hospitals in implementing copper components.
Presently, nine U.S. hospitals have installed some form of copper components, including door hardware, cabinet pulls, sinks, stretchers, and IV poles, Michels reports.
Despite these advances, hospitals may be slow to incorporate copper components due to a variety of reasons:
Cost. Dr. Pile believes that cost will be the major barrier. “Installing copper surfaces won’t be cheap,” he says. “But, then again, HAIs are very costly. I think it will be more difficult to justify their existence if they can be prevented. If copper is effective in preventing HAIs, it would prove to be cost-effective over time.”
Dr. Salgado concurs. “A study needs to be done on the cost-effectiveness of copper surfaces,” she says. “Health economists estimate that if copper surfaces were incorporated into ICUs, after three to six months, those surfaces would pay for themselves. That is not a long time period. Hospitals need to understand that there will be upfront costs but that they will realize benefits downstream.”
The Center for Medicare & Medicaid Services (CMS) has reported that one infection adds $43,000 in patient costs.4 A typical U.S. hospital room contains $100,000 worth of goods and equipment.
“When you do the math using the amount of copper in our study, the cost would be between $1 and $10 per patient,” Dr. Schmidt says. “It’s also important to note that an infection adds 19 days to a patient’s hospital stay.”
Aesthetics. For some, appearance may be a concern. “Copper is actually an appealing material that is offered in an array of colors and surface finishes,” Dr. Michels says. Because a copper-and-brass combination is more prone to tarnishing, a copper-nickel alloy may be more desirable.
Availability. Copper components are not produced and marketed to U.S. hospitals; however, they are available. “We are hoping with our study and future studies that some medical-device companies, as well as hospital-furniture manufacturers, will jump on board to look at ways to mass-produce items,” Dr. Salgado says.
Acceptance. The study published in Infection Control and Hospital Epidemiology validated the effectiveness of copper in decreasing HAIs. This pilot study, however, was not blinded.3
“It was pretty apparent to providers where copper surfaces were located, which tends to result in some bias. Future studies will, hopefully, try to answer questions regarding healthcare providers’ behaviors with different surfaces,” says Dr. Salgado, noting researchers in California and Chile also are studying the effects of copper surfaces in hospitals.
Possible loss of efficacy. Even if a surface is effective initially, Dr. Pile points out that it’s possible for that to change. “I have a theoretical concern that, over time, bacterial pathogens may develop a tolerance to copper,” he says. “Bacterial adversaries have been able to overcome any type of treatment that we have devised for them thus far. But this remains to be seen.”
This has been an issue with other surfaces; once microbes establish a foothold, it is hard to eliminate them. But Dr. Schmidt says because bacteria are killed so quickly on copper surfaces and cleaning is only required once daily, the ability to establish a foothold is greatly reduced, if not completely eliminated.
—Harold T. Michels, PhD, PE, senior vice president of technology and technical services, Copper Development Association Inc.
Champion Proven Strategies
Dr. Pile sees antimicrobial stewardship as a great opportunity for hospitalists as a specialty. In fact, the Centers for Disease Control and Prevention is partnering with HM groups on piloting multiple antimicrobial stewardship initiatives at several sites.
Dr. Pile suggests that leaders spearhead formal quality-improvement efforts, be involved with patient-safety efforts, and serve as physician champions.
“No one is better positioned to do this than hospitalists, because we own the hospital environment,” he says. “We have an incredible stake in making sure that our inpatient environment provides safe and high-value care.”
As a result of the published study, Dr. Salgado says discussions are underway with hospital leaders at MUSC to determine if copper surfaces will be used in its ICUs and, if so, how changes will be implemented.
Karen Appold is a freelance writer in Pennsylvania.
References
- Klevens RM, Edwards JR, Richards CL, et al. Estimating healthcare-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160-166.
- Scott RD. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Atlanta: Centers for Disease Control and Prevention, 2009.
- Salgado CD, Sepkowitz KA, John JF, et al. Copper Surfaces Reduce the Rate of Healthcare-Acquired Infections in the Intensive Care Unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
- Healthcare Cost and Utilization Project. Statistical Brief No. 94. Agency for Healthcare Research and Quality. Aug. 2010. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb94.pdf. Accessed Aug. 6, 2013.
Listen to Project BOOST lead analyst Luke Hansen, MD, MPH, discuss the outcomes study published in JHM
Click here to listen to our interview with Dr. Hansen
Click here to listen to our interview with Dr. Hansen
Click here to listen to our interview with Dr. Hansen
11 Things Neurologists Think Hospitalists Need To Know

11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.

Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.

Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians

The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.