User login
A Primer to Natural Hair Care Practices in Black Patients
The phenomenon of natural (nonchemically treated) hair in individuals of African and Afro-Caribbean descent is sweeping across the United States. The ideals of beauty among this patient population have shifted from a relaxed, straightened, noncurly look to a more natural curly and/or kinky appearance. The discussion on natural hair versus straight hair has been brought to the mainstream by films such as Good Hair (2009). Furthermore, major hair care companies have increased their marketing of natural hair products to address the needs of these patients.
Popular traumatic hair care practices such as chemical relaxation and thermal straightening may lead to hair damage. Although the role of hair care practices in various scalp and hair disorders is ambiguous, traumatic practices commonly are performed by patients who are diagnosed with dermatologic conditions such as scarring alopecia.1 Alopecia is the fourth most common dermatologic diagnosis in black patients.2 Central centrifugal cicatricial alopecia is the most common form of scarring alopecia in this patient population3 and has been associated with traumatic hair care practices. As a result, many patients have switched to natural hairstyles that are less traumatic and damaging, often due to recommendations by dermatologists.
As the US population continues to become more diverse, dermatologists will be faced with many questions regarding hair disease and natural hair care in patients with skin of color. A basic understanding of hair care practices among black individuals is important to aid in the diagnosis and treatment of hair shaft and scalp disorders.4 When patients switch to natural hairstyles, are dermatologists prepared to answer questions that may arise during this process? This article will familiarize dermatologists with basic hair care terminology and general recommendations they can make to black patients who are transitioning to natural hairstyles.
Characteristics of Hair in the Skin of Color Population
A basic understanding of the structural properties of hair is fundamental. Human hair is categorized into 3 groups: Asian, Caucasian, and African.5 African hair typically is curly and, depending on the degree of the curl, is more susceptible to damage due to increased mechanical fragility. It also has a tendency to form knots and fissures along the hair shaft, which causes additional fracturing with simple manipulation. African hair grows more slowly than Asian and Caucasian hair, which can be discouraging to patients. It also has a lower water concentration and does not become coated with sebum as naturally as straightened hair.5 A simplified explanation of these characteristics can help patients understand how to proceed in managing and styling their natural hair.
As physicians, it is important for us to treat any underlying conditions related to the hair and scalp in black patients. Common dermatologic conditions such as seborrheic dermatitis, lupus, folliculitis, and alopecia can affect patients’ hair health. In addition to traumatic hair care practices, inflammation secondary to bacterial infections can contribute to the onset of central centrifugal cicatricial alopecia.6 Therefore, a detailed history and physical examination are needed to evaluate the etiology of associated symptoms. Treatment of these associated symptoms will aid in the overall care of patients.
Transitioning to Natural Hairstyles
Following evaluation and treatment of any hair or scalp conditions, how can dermatologists help black patients transition to natural hairstyles? The term transition refers to the process of switching from a chemically relaxed or thermally straightened hairstyle to a natural hairstyle. Dermatologists must understand the common terminology used to describe natural hair practices in this patient population.
There are several methods patients can use to transition from chemically treated hairstyles to natural hairstyles. Patients may consider the option of the “big chop,” or cutting off all chemically treated hair. This option typically leaves women with very short hairstyles down to the new growth, or hair that has grown since the last chemical relaxer. Other commonly used methods during the transition phase include protective styling (eg, braids, weaves, extensions) or simply growing out the chemically treated hair.
Protective styling methods such as braids, weaves, and extensions allow hair to be easily styled while the chemically treated hair grows out over time.7 Typically, protective styles may be worn for weeks to months, allowing hair growth without hair breakage and shedding. Hair weaving is a practice that incorporates artificial (synthetic) or human hair into one’s natural scalp hair.8 There are various techniques to extend hair including clip-in extensions, hair bonding and fusion with adhesives, sewing hair into braided hair, or the application of single strands of hair into a cap made of nylon mesh known as a lace front. Braided styles, weaves, and hair extensions cannot be washed as often as natural hair, but it is important to remind patients to replenish moisture as often as possible. Moisturizing or greasing the exposed scalp and proximal hair shafts can assist with water retention. It is imperative to inform patients that overuse of tight braids and glues for weaves and extensions may further damage the hair and scalp. Some of the natural ingredients commonly used in moisturizers include olive oil, jojoba oil, coconut oil, castor oil, and glycerin. These products can commonly cause pomade acne, which should be recognized and treated by dermatologists. Furthermore, long weaves and extensions can put excess weight on natural hair causing breakage. To prevent breakage, wearing an updo (a hairstyle in which the hair is pulled upward) can reduce the heavy strain on the hair.
Dermatologists should remind patients who wish to grow out chemically treated hair to frequently moisturize the hair and scalp as well as to avoid trauma to prevent hair breakage. As the natural hair grows out, the patient will experience varying hair textures from the natural curly hair to the previously processed straightened hair; as a result, the hair may tangle and become damaged. Manual detangling and detangling conditioners can help prevent damage. Patients should be advised to detangle the hair in sections first with the fingers, then with a wide-tooth comb working retrograde from the hair end to the roots.
Frequent hair trimming, ranging from every 4 to 6 weeks to every 2 to 4 months, should be recommended to patients who are experiencing breakage or wish to prevent damage. Trimming damaged hair can relieve excess weight on the natural hair and remove split ends, which promotes hair growth. Braiding and other lengthening techniques can prevent the hair from curling upon itself or tangling, causing less kinking and thereby decreasing the need for trimming.7 Wearing bonnets, using satin pillowcases, and wearing protective hairstyles while sleeping also can decrease hair breakage and hair loss. A commonly used hairstyle to protect the hair while sleeping is called “pineappling,” which is used to preserve and protect curls. This technique is described as gathering the hair in a high but loose ponytail at the top of the head. For patients with straightened hair, wrapping the hair underneath a bonnet or satin scarf while sleeping can prevent damage.
Managing Natural Hairstyles
An important factor in the management of natural hairstyles is the retention of hair moisture, as there is less water content in African hair compared to other hair types.5 Overuse of heat and harsh shampoos can strip moisture from the hair. Similar to patients with atopic dermatitis who should restore and maintain the skin barrier to prevent transepidermal water loss, it is important to remind patients with natural hairstyles to avoid using products and styling practices that may further deplete water content in the hair. Moisture is crucial to healthy hair.
A common culprit in shampoos that leads to hair dryness is sodium lauryl sulfate/sodium laureth sulfate, a detergent/surfactant used as a foaming agent. Sodium lauryl sulfate is a potent degreaser that binds dirt and excess product on the hair and scalp. It also dissolves oil in the hair, causing additional dryness and breakage.
Patients with natural hairstyles commonly use sulfate-free shampoos to prevent stripping the hair of its moisture and natural oils. Another method used to prevent hair dryness is co-washing, or washing the hair with a conditioner. Co-washing can effectively cleanse the hair while maintaining moisture. The use of cationic ingredients in conditioners aids in sealing moisture within the hair shaft. Hair consists of the negatively charged protein keratin, which binds to cationic surfactants in conditioners.9 The hydrophobic ends of the surfactant prevent the substance from being rinsed out and act to restore the hair barrier.
Silicone is another important ingredient in hair care products. In patients with natural hair, there are varying views on the use of products containing silicone. Silicones are added to products designed to coat the hair, adding shine, retaining moisture, and providing thermal protection. Silicones are used to provide “slip.” Slip is a term that is commonly used among patients with natural hair to describe how slippery a product is and how easily the product will help comb or detangle the hair. There are 2 basic types of silicones: water insoluble and water soluble. Water-insoluble silicones traditionally build up on the hair and require surfactant-containing shampoos to becompletely removed. Residue buildup on the hair weighs the hair down and causes damage. In contrast, water-soluble silicones do not build up and typically do not cause damage.
Silicones with the prefixes PEG- or PPG- typically are water soluble and will not build up on the hair. Dimethicone copolyol and lauryl methicone copolyol are other water-soluble silicones. In general, water-soluble silicones provide moisturizing properties without leaving residue. Other silicones such as amodimethicone and cyclomethicone are not water soluble but have properties that prevent buildup.
It is common practice for patients with natural hairstyles to avoid using water-insoluble silicones. As dermatologists, we can recommend silicone-free conditioners or conditioners containing water-soluble silicones to prevent hair dehydration and subsequent breakage. It may be advantageous to have patients try various products to determine which ones work best for their hair.
More Resources for Patients
Dermatologists have extensive knowledge of the pathophysiology of skin, hair, and nail diseases; however, despite our vast knowledge, we also need to recognize our limits. In addition to increasing your own knowledge of natural hair care practices to help your patients, it is important to recommend that your patients search for additional resources to aid in their transition to natural hairstyles. Natural hairstylists can be great resources for patients to help with hair management. In the current digital age, there also are thousands of blogs and social media forums dedicated to the topic of natural hair care. Advising patients to consult natural hair care resources can be beneficial, but as hair specialists, it also is important for us to dispel any false information that our patients may receive. As physicians, it is essential not only to manage patients who present to our offices with conditions resulting from damaging hair practices but also to help prevent such conditions from occurring. Although there may not be an overwhelming amount of evidence-based medical research to guide our decisions, we also can learn from the thousands of patients who have articulated their stories and experiences. Through observing and listening to our patients, we can incorporate this new knowledge in the management of our patients.
1. Shah SK, Alexis AF. Central centrifugal cicatricial alopecia: retrospective chart review. J Cutan Med Surg. 2010;14:212-222.
2. Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007;80:387-394.
3. Uhlenhake EE, Mehregan DM. Prospective histologic examinations in patients who practice traumatic hairstyling [published online ahead of print March 3, 2013]. Int J Dermatol. 2013;52:1506-1512.
4. Roseborough IE, McMichael AJ. Hair care practices in African-American patients. Semin Cutan Med Surg. 2009;28:103-108.
5. Kelly AP, Taylor S, eds. Dermatology for Skin of Color. New York: McGraw-Hill; 2009.
6. Kyei A, Bergfeld WF, Piliang M, et al. Medical and environmental risk factors for the development of central centrifugal cicatricial alopecia: a population study [published online ahead of print April 11, 2011]. Arch Dermatol. 2011;147:909-914.
7. Walton N, Carter ET. Better Than Good Hair: The Curly Girl Guide to Healthy, Gorgeous Natural Hair! New York, NY: Amistad; 2013.
8. Quinn CR, Quinn TM, Kelly AP. Hair care practices in African American women. Cutis. 2003;72:280-282, 285-289.
9. Cruz CF, Fernandes MM, Gomes AC, et al. Keratins and lipids in ethnic hair [published online ahead of print January 24, 2013]. Int J Cosmet Sci. 2013;35:244-249.
The phenomenon of natural (nonchemically treated) hair in individuals of African and Afro-Caribbean descent is sweeping across the United States. The ideals of beauty among this patient population have shifted from a relaxed, straightened, noncurly look to a more natural curly and/or kinky appearance. The discussion on natural hair versus straight hair has been brought to the mainstream by films such as Good Hair (2009). Furthermore, major hair care companies have increased their marketing of natural hair products to address the needs of these patients.
Popular traumatic hair care practices such as chemical relaxation and thermal straightening may lead to hair damage. Although the role of hair care practices in various scalp and hair disorders is ambiguous, traumatic practices commonly are performed by patients who are diagnosed with dermatologic conditions such as scarring alopecia.1 Alopecia is the fourth most common dermatologic diagnosis in black patients.2 Central centrifugal cicatricial alopecia is the most common form of scarring alopecia in this patient population3 and has been associated with traumatic hair care practices. As a result, many patients have switched to natural hairstyles that are less traumatic and damaging, often due to recommendations by dermatologists.
As the US population continues to become more diverse, dermatologists will be faced with many questions regarding hair disease and natural hair care in patients with skin of color. A basic understanding of hair care practices among black individuals is important to aid in the diagnosis and treatment of hair shaft and scalp disorders.4 When patients switch to natural hairstyles, are dermatologists prepared to answer questions that may arise during this process? This article will familiarize dermatologists with basic hair care terminology and general recommendations they can make to black patients who are transitioning to natural hairstyles.
Characteristics of Hair in the Skin of Color Population
A basic understanding of the structural properties of hair is fundamental. Human hair is categorized into 3 groups: Asian, Caucasian, and African.5 African hair typically is curly and, depending on the degree of the curl, is more susceptible to damage due to increased mechanical fragility. It also has a tendency to form knots and fissures along the hair shaft, which causes additional fracturing with simple manipulation. African hair grows more slowly than Asian and Caucasian hair, which can be discouraging to patients. It also has a lower water concentration and does not become coated with sebum as naturally as straightened hair.5 A simplified explanation of these characteristics can help patients understand how to proceed in managing and styling their natural hair.
As physicians, it is important for us to treat any underlying conditions related to the hair and scalp in black patients. Common dermatologic conditions such as seborrheic dermatitis, lupus, folliculitis, and alopecia can affect patients’ hair health. In addition to traumatic hair care practices, inflammation secondary to bacterial infections can contribute to the onset of central centrifugal cicatricial alopecia.6 Therefore, a detailed history and physical examination are needed to evaluate the etiology of associated symptoms. Treatment of these associated symptoms will aid in the overall care of patients.
Transitioning to Natural Hairstyles
Following evaluation and treatment of any hair or scalp conditions, how can dermatologists help black patients transition to natural hairstyles? The term transition refers to the process of switching from a chemically relaxed or thermally straightened hairstyle to a natural hairstyle. Dermatologists must understand the common terminology used to describe natural hair practices in this patient population.
There are several methods patients can use to transition from chemically treated hairstyles to natural hairstyles. Patients may consider the option of the “big chop,” or cutting off all chemically treated hair. This option typically leaves women with very short hairstyles down to the new growth, or hair that has grown since the last chemical relaxer. Other commonly used methods during the transition phase include protective styling (eg, braids, weaves, extensions) or simply growing out the chemically treated hair.
Protective styling methods such as braids, weaves, and extensions allow hair to be easily styled while the chemically treated hair grows out over time.7 Typically, protective styles may be worn for weeks to months, allowing hair growth without hair breakage and shedding. Hair weaving is a practice that incorporates artificial (synthetic) or human hair into one’s natural scalp hair.8 There are various techniques to extend hair including clip-in extensions, hair bonding and fusion with adhesives, sewing hair into braided hair, or the application of single strands of hair into a cap made of nylon mesh known as a lace front. Braided styles, weaves, and hair extensions cannot be washed as often as natural hair, but it is important to remind patients to replenish moisture as often as possible. Moisturizing or greasing the exposed scalp and proximal hair shafts can assist with water retention. It is imperative to inform patients that overuse of tight braids and glues for weaves and extensions may further damage the hair and scalp. Some of the natural ingredients commonly used in moisturizers include olive oil, jojoba oil, coconut oil, castor oil, and glycerin. These products can commonly cause pomade acne, which should be recognized and treated by dermatologists. Furthermore, long weaves and extensions can put excess weight on natural hair causing breakage. To prevent breakage, wearing an updo (a hairstyle in which the hair is pulled upward) can reduce the heavy strain on the hair.
Dermatologists should remind patients who wish to grow out chemically treated hair to frequently moisturize the hair and scalp as well as to avoid trauma to prevent hair breakage. As the natural hair grows out, the patient will experience varying hair textures from the natural curly hair to the previously processed straightened hair; as a result, the hair may tangle and become damaged. Manual detangling and detangling conditioners can help prevent damage. Patients should be advised to detangle the hair in sections first with the fingers, then with a wide-tooth comb working retrograde from the hair end to the roots.
Frequent hair trimming, ranging from every 4 to 6 weeks to every 2 to 4 months, should be recommended to patients who are experiencing breakage or wish to prevent damage. Trimming damaged hair can relieve excess weight on the natural hair and remove split ends, which promotes hair growth. Braiding and other lengthening techniques can prevent the hair from curling upon itself or tangling, causing less kinking and thereby decreasing the need for trimming.7 Wearing bonnets, using satin pillowcases, and wearing protective hairstyles while sleeping also can decrease hair breakage and hair loss. A commonly used hairstyle to protect the hair while sleeping is called “pineappling,” which is used to preserve and protect curls. This technique is described as gathering the hair in a high but loose ponytail at the top of the head. For patients with straightened hair, wrapping the hair underneath a bonnet or satin scarf while sleeping can prevent damage.
Managing Natural Hairstyles
An important factor in the management of natural hairstyles is the retention of hair moisture, as there is less water content in African hair compared to other hair types.5 Overuse of heat and harsh shampoos can strip moisture from the hair. Similar to patients with atopic dermatitis who should restore and maintain the skin barrier to prevent transepidermal water loss, it is important to remind patients with natural hairstyles to avoid using products and styling practices that may further deplete water content in the hair. Moisture is crucial to healthy hair.
A common culprit in shampoos that leads to hair dryness is sodium lauryl sulfate/sodium laureth sulfate, a detergent/surfactant used as a foaming agent. Sodium lauryl sulfate is a potent degreaser that binds dirt and excess product on the hair and scalp. It also dissolves oil in the hair, causing additional dryness and breakage.
Patients with natural hairstyles commonly use sulfate-free shampoos to prevent stripping the hair of its moisture and natural oils. Another method used to prevent hair dryness is co-washing, or washing the hair with a conditioner. Co-washing can effectively cleanse the hair while maintaining moisture. The use of cationic ingredients in conditioners aids in sealing moisture within the hair shaft. Hair consists of the negatively charged protein keratin, which binds to cationic surfactants in conditioners.9 The hydrophobic ends of the surfactant prevent the substance from being rinsed out and act to restore the hair barrier.
Silicone is another important ingredient in hair care products. In patients with natural hair, there are varying views on the use of products containing silicone. Silicones are added to products designed to coat the hair, adding shine, retaining moisture, and providing thermal protection. Silicones are used to provide “slip.” Slip is a term that is commonly used among patients with natural hair to describe how slippery a product is and how easily the product will help comb or detangle the hair. There are 2 basic types of silicones: water insoluble and water soluble. Water-insoluble silicones traditionally build up on the hair and require surfactant-containing shampoos to becompletely removed. Residue buildup on the hair weighs the hair down and causes damage. In contrast, water-soluble silicones do not build up and typically do not cause damage.
Silicones with the prefixes PEG- or PPG- typically are water soluble and will not build up on the hair. Dimethicone copolyol and lauryl methicone copolyol are other water-soluble silicones. In general, water-soluble silicones provide moisturizing properties without leaving residue. Other silicones such as amodimethicone and cyclomethicone are not water soluble but have properties that prevent buildup.
It is common practice for patients with natural hairstyles to avoid using water-insoluble silicones. As dermatologists, we can recommend silicone-free conditioners or conditioners containing water-soluble silicones to prevent hair dehydration and subsequent breakage. It may be advantageous to have patients try various products to determine which ones work best for their hair.
More Resources for Patients
Dermatologists have extensive knowledge of the pathophysiology of skin, hair, and nail diseases; however, despite our vast knowledge, we also need to recognize our limits. In addition to increasing your own knowledge of natural hair care practices to help your patients, it is important to recommend that your patients search for additional resources to aid in their transition to natural hairstyles. Natural hairstylists can be great resources for patients to help with hair management. In the current digital age, there also are thousands of blogs and social media forums dedicated to the topic of natural hair care. Advising patients to consult natural hair care resources can be beneficial, but as hair specialists, it also is important for us to dispel any false information that our patients may receive. As physicians, it is essential not only to manage patients who present to our offices with conditions resulting from damaging hair practices but also to help prevent such conditions from occurring. Although there may not be an overwhelming amount of evidence-based medical research to guide our decisions, we also can learn from the thousands of patients who have articulated their stories and experiences. Through observing and listening to our patients, we can incorporate this new knowledge in the management of our patients.
The phenomenon of natural (nonchemically treated) hair in individuals of African and Afro-Caribbean descent is sweeping across the United States. The ideals of beauty among this patient population have shifted from a relaxed, straightened, noncurly look to a more natural curly and/or kinky appearance. The discussion on natural hair versus straight hair has been brought to the mainstream by films such as Good Hair (2009). Furthermore, major hair care companies have increased their marketing of natural hair products to address the needs of these patients.
Popular traumatic hair care practices such as chemical relaxation and thermal straightening may lead to hair damage. Although the role of hair care practices in various scalp and hair disorders is ambiguous, traumatic practices commonly are performed by patients who are diagnosed with dermatologic conditions such as scarring alopecia.1 Alopecia is the fourth most common dermatologic diagnosis in black patients.2 Central centrifugal cicatricial alopecia is the most common form of scarring alopecia in this patient population3 and has been associated with traumatic hair care practices. As a result, many patients have switched to natural hairstyles that are less traumatic and damaging, often due to recommendations by dermatologists.
As the US population continues to become more diverse, dermatologists will be faced with many questions regarding hair disease and natural hair care in patients with skin of color. A basic understanding of hair care practices among black individuals is important to aid in the diagnosis and treatment of hair shaft and scalp disorders.4 When patients switch to natural hairstyles, are dermatologists prepared to answer questions that may arise during this process? This article will familiarize dermatologists with basic hair care terminology and general recommendations they can make to black patients who are transitioning to natural hairstyles.
Characteristics of Hair in the Skin of Color Population
A basic understanding of the structural properties of hair is fundamental. Human hair is categorized into 3 groups: Asian, Caucasian, and African.5 African hair typically is curly and, depending on the degree of the curl, is more susceptible to damage due to increased mechanical fragility. It also has a tendency to form knots and fissures along the hair shaft, which causes additional fracturing with simple manipulation. African hair grows more slowly than Asian and Caucasian hair, which can be discouraging to patients. It also has a lower water concentration and does not become coated with sebum as naturally as straightened hair.5 A simplified explanation of these characteristics can help patients understand how to proceed in managing and styling their natural hair.
As physicians, it is important for us to treat any underlying conditions related to the hair and scalp in black patients. Common dermatologic conditions such as seborrheic dermatitis, lupus, folliculitis, and alopecia can affect patients’ hair health. In addition to traumatic hair care practices, inflammation secondary to bacterial infections can contribute to the onset of central centrifugal cicatricial alopecia.6 Therefore, a detailed history and physical examination are needed to evaluate the etiology of associated symptoms. Treatment of these associated symptoms will aid in the overall care of patients.
Transitioning to Natural Hairstyles
Following evaluation and treatment of any hair or scalp conditions, how can dermatologists help black patients transition to natural hairstyles? The term transition refers to the process of switching from a chemically relaxed or thermally straightened hairstyle to a natural hairstyle. Dermatologists must understand the common terminology used to describe natural hair practices in this patient population.
There are several methods patients can use to transition from chemically treated hairstyles to natural hairstyles. Patients may consider the option of the “big chop,” or cutting off all chemically treated hair. This option typically leaves women with very short hairstyles down to the new growth, or hair that has grown since the last chemical relaxer. Other commonly used methods during the transition phase include protective styling (eg, braids, weaves, extensions) or simply growing out the chemically treated hair.
Protective styling methods such as braids, weaves, and extensions allow hair to be easily styled while the chemically treated hair grows out over time.7 Typically, protective styles may be worn for weeks to months, allowing hair growth without hair breakage and shedding. Hair weaving is a practice that incorporates artificial (synthetic) or human hair into one’s natural scalp hair.8 There are various techniques to extend hair including clip-in extensions, hair bonding and fusion with adhesives, sewing hair into braided hair, or the application of single strands of hair into a cap made of nylon mesh known as a lace front. Braided styles, weaves, and hair extensions cannot be washed as often as natural hair, but it is important to remind patients to replenish moisture as often as possible. Moisturizing or greasing the exposed scalp and proximal hair shafts can assist with water retention. It is imperative to inform patients that overuse of tight braids and glues for weaves and extensions may further damage the hair and scalp. Some of the natural ingredients commonly used in moisturizers include olive oil, jojoba oil, coconut oil, castor oil, and glycerin. These products can commonly cause pomade acne, which should be recognized and treated by dermatologists. Furthermore, long weaves and extensions can put excess weight on natural hair causing breakage. To prevent breakage, wearing an updo (a hairstyle in which the hair is pulled upward) can reduce the heavy strain on the hair.
Dermatologists should remind patients who wish to grow out chemically treated hair to frequently moisturize the hair and scalp as well as to avoid trauma to prevent hair breakage. As the natural hair grows out, the patient will experience varying hair textures from the natural curly hair to the previously processed straightened hair; as a result, the hair may tangle and become damaged. Manual detangling and detangling conditioners can help prevent damage. Patients should be advised to detangle the hair in sections first with the fingers, then with a wide-tooth comb working retrograde from the hair end to the roots.
Frequent hair trimming, ranging from every 4 to 6 weeks to every 2 to 4 months, should be recommended to patients who are experiencing breakage or wish to prevent damage. Trimming damaged hair can relieve excess weight on the natural hair and remove split ends, which promotes hair growth. Braiding and other lengthening techniques can prevent the hair from curling upon itself or tangling, causing less kinking and thereby decreasing the need for trimming.7 Wearing bonnets, using satin pillowcases, and wearing protective hairstyles while sleeping also can decrease hair breakage and hair loss. A commonly used hairstyle to protect the hair while sleeping is called “pineappling,” which is used to preserve and protect curls. This technique is described as gathering the hair in a high but loose ponytail at the top of the head. For patients with straightened hair, wrapping the hair underneath a bonnet or satin scarf while sleeping can prevent damage.
Managing Natural Hairstyles
An important factor in the management of natural hairstyles is the retention of hair moisture, as there is less water content in African hair compared to other hair types.5 Overuse of heat and harsh shampoos can strip moisture from the hair. Similar to patients with atopic dermatitis who should restore and maintain the skin barrier to prevent transepidermal water loss, it is important to remind patients with natural hairstyles to avoid using products and styling practices that may further deplete water content in the hair. Moisture is crucial to healthy hair.
A common culprit in shampoos that leads to hair dryness is sodium lauryl sulfate/sodium laureth sulfate, a detergent/surfactant used as a foaming agent. Sodium lauryl sulfate is a potent degreaser that binds dirt and excess product on the hair and scalp. It also dissolves oil in the hair, causing additional dryness and breakage.
Patients with natural hairstyles commonly use sulfate-free shampoos to prevent stripping the hair of its moisture and natural oils. Another method used to prevent hair dryness is co-washing, or washing the hair with a conditioner. Co-washing can effectively cleanse the hair while maintaining moisture. The use of cationic ingredients in conditioners aids in sealing moisture within the hair shaft. Hair consists of the negatively charged protein keratin, which binds to cationic surfactants in conditioners.9 The hydrophobic ends of the surfactant prevent the substance from being rinsed out and act to restore the hair barrier.
Silicone is another important ingredient in hair care products. In patients with natural hair, there are varying views on the use of products containing silicone. Silicones are added to products designed to coat the hair, adding shine, retaining moisture, and providing thermal protection. Silicones are used to provide “slip.” Slip is a term that is commonly used among patients with natural hair to describe how slippery a product is and how easily the product will help comb or detangle the hair. There are 2 basic types of silicones: water insoluble and water soluble. Water-insoluble silicones traditionally build up on the hair and require surfactant-containing shampoos to becompletely removed. Residue buildup on the hair weighs the hair down and causes damage. In contrast, water-soluble silicones do not build up and typically do not cause damage.
Silicones with the prefixes PEG- or PPG- typically are water soluble and will not build up on the hair. Dimethicone copolyol and lauryl methicone copolyol are other water-soluble silicones. In general, water-soluble silicones provide moisturizing properties without leaving residue. Other silicones such as amodimethicone and cyclomethicone are not water soluble but have properties that prevent buildup.
It is common practice for patients with natural hairstyles to avoid using water-insoluble silicones. As dermatologists, we can recommend silicone-free conditioners or conditioners containing water-soluble silicones to prevent hair dehydration and subsequent breakage. It may be advantageous to have patients try various products to determine which ones work best for their hair.
More Resources for Patients
Dermatologists have extensive knowledge of the pathophysiology of skin, hair, and nail diseases; however, despite our vast knowledge, we also need to recognize our limits. In addition to increasing your own knowledge of natural hair care practices to help your patients, it is important to recommend that your patients search for additional resources to aid in their transition to natural hairstyles. Natural hairstylists can be great resources for patients to help with hair management. In the current digital age, there also are thousands of blogs and social media forums dedicated to the topic of natural hair care. Advising patients to consult natural hair care resources can be beneficial, but as hair specialists, it also is important for us to dispel any false information that our patients may receive. As physicians, it is essential not only to manage patients who present to our offices with conditions resulting from damaging hair practices but also to help prevent such conditions from occurring. Although there may not be an overwhelming amount of evidence-based medical research to guide our decisions, we also can learn from the thousands of patients who have articulated their stories and experiences. Through observing and listening to our patients, we can incorporate this new knowledge in the management of our patients.
1. Shah SK, Alexis AF. Central centrifugal cicatricial alopecia: retrospective chart review. J Cutan Med Surg. 2010;14:212-222.
2. Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007;80:387-394.
3. Uhlenhake EE, Mehregan DM. Prospective histologic examinations in patients who practice traumatic hairstyling [published online ahead of print March 3, 2013]. Int J Dermatol. 2013;52:1506-1512.
4. Roseborough IE, McMichael AJ. Hair care practices in African-American patients. Semin Cutan Med Surg. 2009;28:103-108.
5. Kelly AP, Taylor S, eds. Dermatology for Skin of Color. New York: McGraw-Hill; 2009.
6. Kyei A, Bergfeld WF, Piliang M, et al. Medical and environmental risk factors for the development of central centrifugal cicatricial alopecia: a population study [published online ahead of print April 11, 2011]. Arch Dermatol. 2011;147:909-914.
7. Walton N, Carter ET. Better Than Good Hair: The Curly Girl Guide to Healthy, Gorgeous Natural Hair! New York, NY: Amistad; 2013.
8. Quinn CR, Quinn TM, Kelly AP. Hair care practices in African American women. Cutis. 2003;72:280-282, 285-289.
9. Cruz CF, Fernandes MM, Gomes AC, et al. Keratins and lipids in ethnic hair [published online ahead of print January 24, 2013]. Int J Cosmet Sci. 2013;35:244-249.
1. Shah SK, Alexis AF. Central centrifugal cicatricial alopecia: retrospective chart review. J Cutan Med Surg. 2010;14:212-222.
2. Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007;80:387-394.
3. Uhlenhake EE, Mehregan DM. Prospective histologic examinations in patients who practice traumatic hairstyling [published online ahead of print March 3, 2013]. Int J Dermatol. 2013;52:1506-1512.
4. Roseborough IE, McMichael AJ. Hair care practices in African-American patients. Semin Cutan Med Surg. 2009;28:103-108.
5. Kelly AP, Taylor S, eds. Dermatology for Skin of Color. New York: McGraw-Hill; 2009.
6. Kyei A, Bergfeld WF, Piliang M, et al. Medical and environmental risk factors for the development of central centrifugal cicatricial alopecia: a population study [published online ahead of print April 11, 2011]. Arch Dermatol. 2011;147:909-914.
7. Walton N, Carter ET. Better Than Good Hair: The Curly Girl Guide to Healthy, Gorgeous Natural Hair! New York, NY: Amistad; 2013.
8. Quinn CR, Quinn TM, Kelly AP. Hair care practices in African American women. Cutis. 2003;72:280-282, 285-289.
9. Cruz CF, Fernandes MM, Gomes AC, et al. Keratins and lipids in ethnic hair [published online ahead of print January 24, 2013]. Int J Cosmet Sci. 2013;35:244-249.
Practice Points
- Many scalp and hair diseases in patients of African and Afro-Caribbean descent result from traumatic hairstyling practices and poor management. Proper care of these patients requires an understanding of hair variances and styling techniques across ethnicities.
- The use of protective hairstyles and adequate trimming can aid black patients in the transition to healthier natural hair.
- The use of natural oils for scalp health and the avoidance of products containing chemicals that remove moisture from the hair are helpful in maintaining healthy natural hair.

Aging process is complex in highly active adults
The aging process is highly individualistic and complex, even when many confounding factors are removed, according to Ross D. Pollock, Ph.D., and his associates.
In a cross-sectional study of 125 highly active male and female cyclists aged 55-79 years, some associations were found between age and function, with maximal rate of oxygen consumption showing the closest association. The age of a given individual, however, could not be determined from his or her physiological profiling, even in functions for which some correlation was found, because of high variance.
Further study is needed to find reliable biomarkers of aging as well as the relationship between age and physiological function, the researchers concluded.
Read the full article at the Journal of Physiology (2015;593:657-80 [doi:10.1113/jphysiol.2014.282863]).
The aging process is highly individualistic and complex, even when many confounding factors are removed, according to Ross D. Pollock, Ph.D., and his associates.
In a cross-sectional study of 125 highly active male and female cyclists aged 55-79 years, some associations were found between age and function, with maximal rate of oxygen consumption showing the closest association. The age of a given individual, however, could not be determined from his or her physiological profiling, even in functions for which some correlation was found, because of high variance.
Further study is needed to find reliable biomarkers of aging as well as the relationship between age and physiological function, the researchers concluded.
Read the full article at the Journal of Physiology (2015;593:657-80 [doi:10.1113/jphysiol.2014.282863]).
The aging process is highly individualistic and complex, even when many confounding factors are removed, according to Ross D. Pollock, Ph.D., and his associates.
In a cross-sectional study of 125 highly active male and female cyclists aged 55-79 years, some associations were found between age and function, with maximal rate of oxygen consumption showing the closest association. The age of a given individual, however, could not be determined from his or her physiological profiling, even in functions for which some correlation was found, because of high variance.
Further study is needed to find reliable biomarkers of aging as well as the relationship between age and physiological function, the researchers concluded.
Read the full article at the Journal of Physiology (2015;593:657-80 [doi:10.1113/jphysiol.2014.282863]).
Treatment for dark lower eyelid circles
NEW ORLEANS – Addressing the problem of dark lower eyelid circles may require the use of multiple modalities, but defining the cause is the first step toward effective treatment, Dr. Joel E. Kopelman said at the annual meeting of the American Academy of Cosmetic Surgery.
Lower eyelid dark circles affect patients of all ages and races and often create a fatigued and sad appearance. Loss of volume in the eyelid, midfacial, and orbital areas; superficial and deep pigmentation; thin, translucent skin with a paucity of fat between the skin and orbicularis muscle; and shadowing from herniated or pseudo-herniated protruding fat all might contribute to the appearance of dark lower eyelid circles, he said.

By first identifying the source of the dark circles, practitioners can make informed decisions about the correct course of treatment. “Some are easier to treat than others, but each one presents its own challenge,” said Dr. Kopelman, an ophthalmic plastic surgeon in Ridgewood, N.J.
Correcting the appearance of lower eyelid circles entails the use of one or more modalities, depending upon the etiology of the problem. “Volume restoration alone doesn’t address the entire problem, nor does it maximize the opportunity for improvement,” Dr. Kopelman said. “The issue of pigmentation is one that we often overlook.”
He recommends a primary skin evaluation with the use of a Wood’s lamp, which will assess the depth of pigmentation and intensify superficial pigment. If skin hyperpigmentation is the cause of the dark circles, lightening the skin with topical phenolic or nonphenolic depigmenting agents, and/or laser therapy, might help to significantly reduce lower eyelid skin pigmentation.
Hydroquinone (HQ) and Kojic acid are considered the strongest phenolic bleaching agents, he noted. Topical application of these compounds should start at twice a day for 4-6 weeks, but long-term use of these treatments can lead to irritation, so treatment should be spread out and/or lessened as needed.
Nonphenolic bleaching compounds also can be used to treat pigmentation. “Over time, these compounds can yield nice blanching without the toxicity of HQ, but you have to use them for several months to get the kind of results you want,” he added.
Melanozyme (lignin peroxidase) is another treatment effective at reducing pigment. “This is sometimes used in conjunction with hydroquinone right away, since Melanozyme breaks down existing melanin rather than trying to prevent melanin from forming,” Dr. Kopelman stated. There is no delay in activation with the use of Melanozyme, as opposed to the use of HQ, which usually takes several weeks to have a suppressive effect on pigment generating cells. He recommends an initial therapy regimen of a phenolic bleaching agent with or without the use of Melanozyme, and the substitution of nonphenolic compounds in a long-term therapy regimen.
Fractionated lasers also can be used to apply these drugs, he reported. The protocol involves creating a channel of predetermined depth and density, which allows for immediate application and penetration of topical drugs. Dr. Kopelman recommends applying medication immediately after delivering the fractionated laser treatment to the pigmented area, which will allow the medicine to better penetrate into the deeper layers of skin.
Chemical peels and laser resurfacing can be used as a secondary level of therapy, but “these can induce postinflammatory hyperpigmentation, so I’m very cautious about using anything that delivers heat or strong chemicals, as they can make things worse,” he warned. Laser treatment can be used as a tertiary level of treatment to disrupt melanin production. “But using lasers around the eyelids can be dangerous, so you have to be very cautious,” he added.
Patients must understand that the process of treating dark undereye circles takes time, and realistic expectations are a central part of the process, Dr. Kopelman emphasized. Often, multiple modalities are necessary to achieve an improvement, so patients must commit to long-term treatment, be compliant with applying medication on a daily basis, avoid sun exposure, and wear polarized sunglasses and sunblocks to prevent the sun from stimulating melanin production and achieve improved aesthetic outcomes.
Dr. Kopelman reported no relevant financial disclosures.
NEW ORLEANS – Addressing the problem of dark lower eyelid circles may require the use of multiple modalities, but defining the cause is the first step toward effective treatment, Dr. Joel E. Kopelman said at the annual meeting of the American Academy of Cosmetic Surgery.
Lower eyelid dark circles affect patients of all ages and races and often create a fatigued and sad appearance. Loss of volume in the eyelid, midfacial, and orbital areas; superficial and deep pigmentation; thin, translucent skin with a paucity of fat between the skin and orbicularis muscle; and shadowing from herniated or pseudo-herniated protruding fat all might contribute to the appearance of dark lower eyelid circles, he said.
By first identifying the source of the dark circles, practitioners can make informed decisions about the correct course of treatment. “Some are easier to treat than others, but each one presents its own challenge,” said Dr. Kopelman, an ophthalmic plastic surgeon in Ridgewood, N.J.
Correcting the appearance of lower eyelid circles entails the use of one or more modalities, depending upon the etiology of the problem. “Volume restoration alone doesn’t address the entire problem, nor does it maximize the opportunity for improvement,” Dr. Kopelman said. “The issue of pigmentation is one that we often overlook.”
He recommends a primary skin evaluation with the use of a Wood’s lamp, which will assess the depth of pigmentation and intensify superficial pigment. If skin hyperpigmentation is the cause of the dark circles, lightening the skin with topical phenolic or nonphenolic depigmenting agents, and/or laser therapy, might help to significantly reduce lower eyelid skin pigmentation.
Hydroquinone (HQ) and Kojic acid are considered the strongest phenolic bleaching agents, he noted. Topical application of these compounds should start at twice a day for 4-6 weeks, but long-term use of these treatments can lead to irritation, so treatment should be spread out and/or lessened as needed.
Nonphenolic bleaching compounds also can be used to treat pigmentation. “Over time, these compounds can yield nice blanching without the toxicity of HQ, but you have to use them for several months to get the kind of results you want,” he added.
Melanozyme (lignin peroxidase) is another treatment effective at reducing pigment. “This is sometimes used in conjunction with hydroquinone right away, since Melanozyme breaks down existing melanin rather than trying to prevent melanin from forming,” Dr. Kopelman stated. There is no delay in activation with the use of Melanozyme, as opposed to the use of HQ, which usually takes several weeks to have a suppressive effect on pigment generating cells. He recommends an initial therapy regimen of a phenolic bleaching agent with or without the use of Melanozyme, and the substitution of nonphenolic compounds in a long-term therapy regimen.
Fractionated lasers also can be used to apply these drugs, he reported. The protocol involves creating a channel of predetermined depth and density, which allows for immediate application and penetration of topical drugs. Dr. Kopelman recommends applying medication immediately after delivering the fractionated laser treatment to the pigmented area, which will allow the medicine to better penetrate into the deeper layers of skin.
Chemical peels and laser resurfacing can be used as a secondary level of therapy, but “these can induce postinflammatory hyperpigmentation, so I’m very cautious about using anything that delivers heat or strong chemicals, as they can make things worse,” he warned. Laser treatment can be used as a tertiary level of treatment to disrupt melanin production. “But using lasers around the eyelids can be dangerous, so you have to be very cautious,” he added.
Patients must understand that the process of treating dark undereye circles takes time, and realistic expectations are a central part of the process, Dr. Kopelman emphasized. Often, multiple modalities are necessary to achieve an improvement, so patients must commit to long-term treatment, be compliant with applying medication on a daily basis, avoid sun exposure, and wear polarized sunglasses and sunblocks to prevent the sun from stimulating melanin production and achieve improved aesthetic outcomes.
Dr. Kopelman reported no relevant financial disclosures.
NEW ORLEANS – Addressing the problem of dark lower eyelid circles may require the use of multiple modalities, but defining the cause is the first step toward effective treatment, Dr. Joel E. Kopelman said at the annual meeting of the American Academy of Cosmetic Surgery.
Lower eyelid dark circles affect patients of all ages and races and often create a fatigued and sad appearance. Loss of volume in the eyelid, midfacial, and orbital areas; superficial and deep pigmentation; thin, translucent skin with a paucity of fat between the skin and orbicularis muscle; and shadowing from herniated or pseudo-herniated protruding fat all might contribute to the appearance of dark lower eyelid circles, he said.
By first identifying the source of the dark circles, practitioners can make informed decisions about the correct course of treatment. “Some are easier to treat than others, but each one presents its own challenge,” said Dr. Kopelman, an ophthalmic plastic surgeon in Ridgewood, N.J.
Correcting the appearance of lower eyelid circles entails the use of one or more modalities, depending upon the etiology of the problem. “Volume restoration alone doesn’t address the entire problem, nor does it maximize the opportunity for improvement,” Dr. Kopelman said. “The issue of pigmentation is one that we often overlook.”
He recommends a primary skin evaluation with the use of a Wood’s lamp, which will assess the depth of pigmentation and intensify superficial pigment. If skin hyperpigmentation is the cause of the dark circles, lightening the skin with topical phenolic or nonphenolic depigmenting agents, and/or laser therapy, might help to significantly reduce lower eyelid skin pigmentation.
Hydroquinone (HQ) and Kojic acid are considered the strongest phenolic bleaching agents, he noted. Topical application of these compounds should start at twice a day for 4-6 weeks, but long-term use of these treatments can lead to irritation, so treatment should be spread out and/or lessened as needed.
Nonphenolic bleaching compounds also can be used to treat pigmentation. “Over time, these compounds can yield nice blanching without the toxicity of HQ, but you have to use them for several months to get the kind of results you want,” he added.
Melanozyme (lignin peroxidase) is another treatment effective at reducing pigment. “This is sometimes used in conjunction with hydroquinone right away, since Melanozyme breaks down existing melanin rather than trying to prevent melanin from forming,” Dr. Kopelman stated. There is no delay in activation with the use of Melanozyme, as opposed to the use of HQ, which usually takes several weeks to have a suppressive effect on pigment generating cells. He recommends an initial therapy regimen of a phenolic bleaching agent with or without the use of Melanozyme, and the substitution of nonphenolic compounds in a long-term therapy regimen.
Fractionated lasers also can be used to apply these drugs, he reported. The protocol involves creating a channel of predetermined depth and density, which allows for immediate application and penetration of topical drugs. Dr. Kopelman recommends applying medication immediately after delivering the fractionated laser treatment to the pigmented area, which will allow the medicine to better penetrate into the deeper layers of skin.
Chemical peels and laser resurfacing can be used as a secondary level of therapy, but “these can induce postinflammatory hyperpigmentation, so I’m very cautious about using anything that delivers heat or strong chemicals, as they can make things worse,” he warned. Laser treatment can be used as a tertiary level of treatment to disrupt melanin production. “But using lasers around the eyelids can be dangerous, so you have to be very cautious,” he added.
Patients must understand that the process of treating dark undereye circles takes time, and realistic expectations are a central part of the process, Dr. Kopelman emphasized. Often, multiple modalities are necessary to achieve an improvement, so patients must commit to long-term treatment, be compliant with applying medication on a daily basis, avoid sun exposure, and wear polarized sunglasses and sunblocks to prevent the sun from stimulating melanin production and achieve improved aesthetic outcomes.
Dr. Kopelman reported no relevant financial disclosures.
EXPERT ANALYSIS FROM THE AACS ANNUAL MEETING

Patient preparation maximizes resurfacing results
NEW ORLEANS – Knowledge of skin anatomy and methods of proper pretreatment will enhance and extend the results of skin-resurfacing modalities, according to Dr. Suzan Obagi.
Skin resurfacing procedures continue to grow in popularity, and newer resurfacing modalities with less recovery time are regularly being introduced, Dr. Obagi said at the annual meeting of the American Academy of Cosmetic Surgery.

“Managing the skin properly by appropriately evaluating and treating it before, during, and after a skin resurfacing procedure will allow us to expand the base of patients we can treat safely, improve and maximize their results, and reduce complications,” she added.
The most common patient concerns are acne, wrinkles, pores, rosacea, facial redness, sensitive skin, and discoloration, said Dr. Obagi of the University of Pittsburgh.
“We hear about these issues all the time, so we need to know how to properly address them,” she noted. Discuss a range of procedures and the downtime associated with each modality when advising patients. “What patients do at home is equally – if not more – important than what is done in the office,” she stressed. “This puts some of the responsibility on them [patients]; we can only fix so much, but they have to be partners with us in this process.”
Aesthetic skin concerns can be treated with chemical peels, lasers, fillers, and skin-tightening procedures, but anyone performing surgery without first preparing the patient’s skin is doing the patient a disservice, Dr. Obagi stated.

Topical agents should be considered prior to other treatments, she advised. “A patient with excessive wrinkles will not achieve the desired result through a face-lift alone; I want to fix their skin first, and then do the face-lift if needed,” she noted. Similarly, skin problems such as rosacea and acne must be addressed before considering resurfacing modalities, as resurfacing skin that is actively inflamed will only exacerbate the issue, she said.
To maximize results from a skin-resurfacing modality, skin must be healthy before it is treated. “If you laser away just one brown spot, you’ll have a healthy spot of skin surrounded by a sea of sun damage,” said Dr. Obagi. Healthy skin heals faster and scars are less noticeable when sun damage is primarily addressed. This process serves as a test of patient compliance with instructions, she added.
The importance of topical agents in a preoperative skin care regimen cannot be overstated, she said. A retinoid should always be used to activate and stimulate keratinocytes and fibroblasts, and hydroquinone should be used to stimulate melanocytes. The use of hydroquinone is controversial, but claims regarding its carcinogenic properties have not been supported in the literature, said Dr. Obagi. “If you want to see results, become comfortable speaking to the safety of hydroquinone and using it properly in your patients,” she added. Mineral-based sunblock should take the place of a daily moisturizer, and a product containing zinc or titanium is recommended. “Many of us work under fluorescent light; even the visible spectrum of light interacts with tissue and causes some of the aging we’re seeing, and chemical sunscreens don’t touch that spectrum,” she stated. Finally, supportive topical agents such as AHAs, benzoyl peroxide, and astringents can be added as needed to a topical skin care regimen depending on a patient’s skin concerns.
Pre-resurfacing goals include controlling acne and rosacea, testing compliance, enhancing wound healing, and controlling pigment production. When all of these issues are addressed prior to resurfacing, results are enhanced. “Always do a skin conditioning treatment, as this makes results more dramatic,” said Dr. Obagi. “I usually do a pre-resurfacing regimen for 6 weeks on a lighter-skinned patient; on a patient with darker skin I continue the regimen for about 12 weeks before I feel I can safely treat them,” she said.
Resurfacing treatments must be tailored to differing levels of the skin for different conditions, Dr. Obagi noted. Sun damage resides very superficially in the epidermis, wrinkles and scars can reside superficially or deeper, and acne and rosacea involve deeper layers of the skin. Some treatments will not go deep enough in the skin to address certain problems, so it is crucial to address treatment depths to where the problem actually resides. “Although new lasers are constantly introduced, one thing that has remained stable is skin cells; we know we can only target certain ones,” she added.
Cellular targets for skin health restoration in the keratinocytes involve normalizing turnover and improving atypia; in the melanocytes, the targets involve decreasing pigment production and enhancing melanin distribution. Deeper in the dermis, cellular targets for skin health in the fibroblasts include increasing collagen, elastin and glycosaminoglycans (GAGs). “We want to take these cells and really stimulate and control them at every level, so we can make patients heal the way we want them to post procedurally,” explained Dr. Obagi.
For best results, postresurfacing goals should involve resuming control of acne and rosacea, monitoring for complications such as infections, and enhancing wound healing through such modalities as steroids, antibiotics, or low-level lasers when appropriate. “However, the most crucial postresurfacing goal is controlling pigmentation. Don’t wait for hyperpigmentation to occur; it is much harder to treat than it is to prevent,” Dr. Obagi emphasized.
Establishing a proper skin care regimen prior to a procedure is vital in combating aging, and will in turn produce better and longer-lasting procedure results with fewer complications, said Dr. Obagi. Further, communicating with patients and involving them in their own skin care establishes trust and confidence. These patients will be happier with their surgical results, will report for regular follow-ups, and will serve as sources of referral. “If you deliver results before you even get to the procedure, the patient will trust you implicitly,” Dr. Obagi said.
Dr. Obagi reported serving on the scientific advisory board for Valeant Pharmaceuticals.
NEW ORLEANS – Knowledge of skin anatomy and methods of proper pretreatment will enhance and extend the results of skin-resurfacing modalities, according to Dr. Suzan Obagi.
Skin resurfacing procedures continue to grow in popularity, and newer resurfacing modalities with less recovery time are regularly being introduced, Dr. Obagi said at the annual meeting of the American Academy of Cosmetic Surgery.
“Managing the skin properly by appropriately evaluating and treating it before, during, and after a skin resurfacing procedure will allow us to expand the base of patients we can treat safely, improve and maximize their results, and reduce complications,” she added.
The most common patient concerns are acne, wrinkles, pores, rosacea, facial redness, sensitive skin, and discoloration, said Dr. Obagi of the University of Pittsburgh.
“We hear about these issues all the time, so we need to know how to properly address them,” she noted. Discuss a range of procedures and the downtime associated with each modality when advising patients. “What patients do at home is equally – if not more – important than what is done in the office,” she stressed. “This puts some of the responsibility on them [patients]; we can only fix so much, but they have to be partners with us in this process.”
Aesthetic skin concerns can be treated with chemical peels, lasers, fillers, and skin-tightening procedures, but anyone performing surgery without first preparing the patient’s skin is doing the patient a disservice, Dr. Obagi stated.
Topical agents should be considered prior to other treatments, she advised. “A patient with excessive wrinkles will not achieve the desired result through a face-lift alone; I want to fix their skin first, and then do the face-lift if needed,” she noted. Similarly, skin problems such as rosacea and acne must be addressed before considering resurfacing modalities, as resurfacing skin that is actively inflamed will only exacerbate the issue, she said.
To maximize results from a skin-resurfacing modality, skin must be healthy before it is treated. “If you laser away just one brown spot, you’ll have a healthy spot of skin surrounded by a sea of sun damage,” said Dr. Obagi. Healthy skin heals faster and scars are less noticeable when sun damage is primarily addressed. This process serves as a test of patient compliance with instructions, she added.
The importance of topical agents in a preoperative skin care regimen cannot be overstated, she said. A retinoid should always be used to activate and stimulate keratinocytes and fibroblasts, and hydroquinone should be used to stimulate melanocytes. The use of hydroquinone is controversial, but claims regarding its carcinogenic properties have not been supported in the literature, said Dr. Obagi. “If you want to see results, become comfortable speaking to the safety of hydroquinone and using it properly in your patients,” she added. Mineral-based sunblock should take the place of a daily moisturizer, and a product containing zinc or titanium is recommended. “Many of us work under fluorescent light; even the visible spectrum of light interacts with tissue and causes some of the aging we’re seeing, and chemical sunscreens don’t touch that spectrum,” she stated. Finally, supportive topical agents such as AHAs, benzoyl peroxide, and astringents can be added as needed to a topical skin care regimen depending on a patient’s skin concerns.
Pre-resurfacing goals include controlling acne and rosacea, testing compliance, enhancing wound healing, and controlling pigment production. When all of these issues are addressed prior to resurfacing, results are enhanced. “Always do a skin conditioning treatment, as this makes results more dramatic,” said Dr. Obagi. “I usually do a pre-resurfacing regimen for 6 weeks on a lighter-skinned patient; on a patient with darker skin I continue the regimen for about 12 weeks before I feel I can safely treat them,” she said.
Resurfacing treatments must be tailored to differing levels of the skin for different conditions, Dr. Obagi noted. Sun damage resides very superficially in the epidermis, wrinkles and scars can reside superficially or deeper, and acne and rosacea involve deeper layers of the skin. Some treatments will not go deep enough in the skin to address certain problems, so it is crucial to address treatment depths to where the problem actually resides. “Although new lasers are constantly introduced, one thing that has remained stable is skin cells; we know we can only target certain ones,” she added.
Cellular targets for skin health restoration in the keratinocytes involve normalizing turnover and improving atypia; in the melanocytes, the targets involve decreasing pigment production and enhancing melanin distribution. Deeper in the dermis, cellular targets for skin health in the fibroblasts include increasing collagen, elastin and glycosaminoglycans (GAGs). “We want to take these cells and really stimulate and control them at every level, so we can make patients heal the way we want them to post procedurally,” explained Dr. Obagi.
For best results, postresurfacing goals should involve resuming control of acne and rosacea, monitoring for complications such as infections, and enhancing wound healing through such modalities as steroids, antibiotics, or low-level lasers when appropriate. “However, the most crucial postresurfacing goal is controlling pigmentation. Don’t wait for hyperpigmentation to occur; it is much harder to treat than it is to prevent,” Dr. Obagi emphasized.
Establishing a proper skin care regimen prior to a procedure is vital in combating aging, and will in turn produce better and longer-lasting procedure results with fewer complications, said Dr. Obagi. Further, communicating with patients and involving them in their own skin care establishes trust and confidence. These patients will be happier with their surgical results, will report for regular follow-ups, and will serve as sources of referral. “If you deliver results before you even get to the procedure, the patient will trust you implicitly,” Dr. Obagi said.
Dr. Obagi reported serving on the scientific advisory board for Valeant Pharmaceuticals.
NEW ORLEANS – Knowledge of skin anatomy and methods of proper pretreatment will enhance and extend the results of skin-resurfacing modalities, according to Dr. Suzan Obagi.
Skin resurfacing procedures continue to grow in popularity, and newer resurfacing modalities with less recovery time are regularly being introduced, Dr. Obagi said at the annual meeting of the American Academy of Cosmetic Surgery.
“Managing the skin properly by appropriately evaluating and treating it before, during, and after a skin resurfacing procedure will allow us to expand the base of patients we can treat safely, improve and maximize their results, and reduce complications,” she added.
The most common patient concerns are acne, wrinkles, pores, rosacea, facial redness, sensitive skin, and discoloration, said Dr. Obagi of the University of Pittsburgh.
“We hear about these issues all the time, so we need to know how to properly address them,” she noted. Discuss a range of procedures and the downtime associated with each modality when advising patients. “What patients do at home is equally – if not more – important than what is done in the office,” she stressed. “This puts some of the responsibility on them [patients]; we can only fix so much, but they have to be partners with us in this process.”
Aesthetic skin concerns can be treated with chemical peels, lasers, fillers, and skin-tightening procedures, but anyone performing surgery without first preparing the patient’s skin is doing the patient a disservice, Dr. Obagi stated.
Topical agents should be considered prior to other treatments, she advised. “A patient with excessive wrinkles will not achieve the desired result through a face-lift alone; I want to fix their skin first, and then do the face-lift if needed,” she noted. Similarly, skin problems such as rosacea and acne must be addressed before considering resurfacing modalities, as resurfacing skin that is actively inflamed will only exacerbate the issue, she said.
To maximize results from a skin-resurfacing modality, skin must be healthy before it is treated. “If you laser away just one brown spot, you’ll have a healthy spot of skin surrounded by a sea of sun damage,” said Dr. Obagi. Healthy skin heals faster and scars are less noticeable when sun damage is primarily addressed. This process serves as a test of patient compliance with instructions, she added.
The importance of topical agents in a preoperative skin care regimen cannot be overstated, she said. A retinoid should always be used to activate and stimulate keratinocytes and fibroblasts, and hydroquinone should be used to stimulate melanocytes. The use of hydroquinone is controversial, but claims regarding its carcinogenic properties have not been supported in the literature, said Dr. Obagi. “If you want to see results, become comfortable speaking to the safety of hydroquinone and using it properly in your patients,” she added. Mineral-based sunblock should take the place of a daily moisturizer, and a product containing zinc or titanium is recommended. “Many of us work under fluorescent light; even the visible spectrum of light interacts with tissue and causes some of the aging we’re seeing, and chemical sunscreens don’t touch that spectrum,” she stated. Finally, supportive topical agents such as AHAs, benzoyl peroxide, and astringents can be added as needed to a topical skin care regimen depending on a patient’s skin concerns.
Pre-resurfacing goals include controlling acne and rosacea, testing compliance, enhancing wound healing, and controlling pigment production. When all of these issues are addressed prior to resurfacing, results are enhanced. “Always do a skin conditioning treatment, as this makes results more dramatic,” said Dr. Obagi. “I usually do a pre-resurfacing regimen for 6 weeks on a lighter-skinned patient; on a patient with darker skin I continue the regimen for about 12 weeks before I feel I can safely treat them,” she said.
Resurfacing treatments must be tailored to differing levels of the skin for different conditions, Dr. Obagi noted. Sun damage resides very superficially in the epidermis, wrinkles and scars can reside superficially or deeper, and acne and rosacea involve deeper layers of the skin. Some treatments will not go deep enough in the skin to address certain problems, so it is crucial to address treatment depths to where the problem actually resides. “Although new lasers are constantly introduced, one thing that has remained stable is skin cells; we know we can only target certain ones,” she added.
Cellular targets for skin health restoration in the keratinocytes involve normalizing turnover and improving atypia; in the melanocytes, the targets involve decreasing pigment production and enhancing melanin distribution. Deeper in the dermis, cellular targets for skin health in the fibroblasts include increasing collagen, elastin and glycosaminoglycans (GAGs). “We want to take these cells and really stimulate and control them at every level, so we can make patients heal the way we want them to post procedurally,” explained Dr. Obagi.
For best results, postresurfacing goals should involve resuming control of acne and rosacea, monitoring for complications such as infections, and enhancing wound healing through such modalities as steroids, antibiotics, or low-level lasers when appropriate. “However, the most crucial postresurfacing goal is controlling pigmentation. Don’t wait for hyperpigmentation to occur; it is much harder to treat than it is to prevent,” Dr. Obagi emphasized.
Establishing a proper skin care regimen prior to a procedure is vital in combating aging, and will in turn produce better and longer-lasting procedure results with fewer complications, said Dr. Obagi. Further, communicating with patients and involving them in their own skin care establishes trust and confidence. These patients will be happier with their surgical results, will report for regular follow-ups, and will serve as sources of referral. “If you deliver results before you even get to the procedure, the patient will trust you implicitly,” Dr. Obagi said.
Dr. Obagi reported serving on the scientific advisory board for Valeant Pharmaceuticals.
EXPERT ANALYSIS FROM THE AACS ANNUAL MEETING
Dermatologic Emergencies
Dermatologic emergency may sound like an oxymoron, but there are many emergencies that dermatology residents may encounter in their careers. In some instances the skin is the primary organ that is affected, while in others cutaneous symptoms and life-threatening signs are important diagnostic clues for what may lie beneath the skin.
As residents who are occasionally on call or on consultation services, it is important for us to recognize dermatologic emergencies quickly because some of these conditions can acutely evolve and become lethal if a diagnosis is not made early in the disease course with the appropriate treatment administered. Dermatologic emergencies can range from severe drug reactions, infections, autoimmune exacerbations, and inflammatory conditions (eg, erythroderma) to environmental insults such as burns (Figure 1) and child abuse.1

Critical Infections
Some dermatologic emergencies are infectious in origin, and although these infections are most commonly bacterial (eg, necrotizing fasciitis), they also can range from viral to fungal (eg, mucormycosis) in nature. Some areas with large populations of immunocompromised patients (eg, human immunodeficiency virus–positive patients, organ transplant recipients) may warrant a high index of suspicion for possible zebras (rare conditions) and opportunistic infections that may quickly escalate to life-threatening situations.
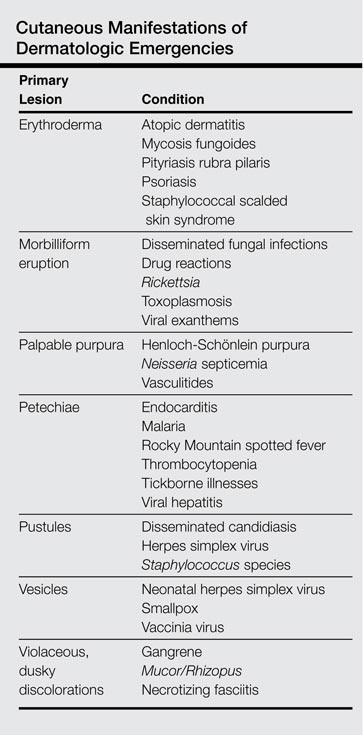
Although few cutaneous manifestations in emergent infections are pathognomonic, they sometimes can be categorized according to the appearance of the primary lesion: erythrodermic (eg, staphylococcal scalded skin syndrome), maculopapular (eg, Lyme disease), purpuric/petechial (eg, Rocky Mountain spotted fever), pustular (eg, disseminated candidiasis), or vesicular (eg, neonatal herpes simplex virus)(Table). On consultations, dermatology residents frequently get called to evaluate hemorrhagic and ischemic lesions in inpatients (Figure 2). Aside from infectious causes, the differential diagnosis may include coagulation abnormalities (eg, concurrent anticoagulant therapies), vasculitides, poisoning, vascular disease, or Stevens-Johnson syndrome and toxic epidermal necrolysis, which can occasionally present with hemorrhagic lesions.1,2

Necrotizing Fasciitis
Dermatology residents may frequently encounter necrotizing fasciitis, either in clinic or on the wards (Figure 3). Recognition of the skin signs in this condition is essential to patient survival. As an intern, I once had an attending teach me that patients with necrotizing fasciitis only have a couple of hours to live. The rapid unfolding of this flesh-eating disease and its high morbidity and mortality has led to recent attention in the press and media.

Although necrotizing fasciitis may be caused by several different bacterial organisms (eg, gram positive, gram negative, polymicrobial), it usually is rapidly progressive, destroying muscle and subcutaneous tissues in a matter of hours.3 Bacteria usually enter through a traumatic or present wound and quickly move along fascial planes, destroying blood vessels and whatever subcutaneous tissues happen to be in the way. Within the first few hours, the involved area that was initially erythematous becomes indurated, woody, extremely painful, and dusky, indicating a lack of circulation to the area. Extensive debridement is required until reaching noninfected tissue that is no longer purulent, necrotic, or woody to the touch. If necrotizing fasciitis is not diagnosed and treated early, patients may lose one or several limbs and death may occur.
Key findings of necrotizing fasciitis include systemic toxicity, localized painful induration, well-defined dusky blue discoloration, and a lack of bleeding or purulent discharge on incision and squeezing of the affected tissue. Crepitation or a crackling sensation can occasionally be felt when palpating the area secondary to gas formation in the tissue, though it is not always present. Patients with necrotizing fasciitis often initially present to dermatology clinics because the first manifestation happens to be in the skin. The role of dermatologists in treating this critical condition may prompt recognition and collaboration with other specialists to reach a viable outcome for the patient.3
Drug Reactions
Cutaneous drug eruptions usually are relatively benign, consisting of a morbilliform eruption often without any other accompanying symptoms. However, sometimes these reactions can present as exfoliative dermatitis or red man syndrome in which patients can develop total body erythema with diffuse scaling and pruritus.4 Aside from drug reactions, other causes of exfoliative dermatitis such as psoriasis, atopic and seborrheic dermatitis, mycosis fungoides, and lymphoma should be ruled out. Other drug eruptions that can be classified as dermatologic emergencies include leukocytoclastic vasculitis, severe urticaria or angioedema, erythema multiforme, or Stevens-Johnson syndrome and toxic epidermal necrolysis.

Severe Acne
If not treated promptly, serious cases of acne can lead to severe scarring and psychologic problems. Acne fulminans is characterized by a rapid eruption of suppurative and large, highly inflamed nodules, plaques, and cysts that result in ragged ulcerations and cicatrization of the chest, back, and occasionally the face. Systemic symptoms of fever, arthralgia, leukocytosis, and myalgia suggest an upregulation of the immune system in affected patients.
Final Comment
In summary, dermatologic emergencies do exist and some may present with characteristic skin findings. In almost all cases, collaboration with other departments such as trauma, burn, internal medicine, rheumatology, and infectious diseases is extremely helpful in diagnosing and treating these medical emergencies. Collaboration can provide insight into how brainstorming through different approaches can lead to a better outcome whether it be solving the cause of a puzzling rash in a patient with multiple comorbidities or surgically removing a bullet from a trauma patient (Figure 4). Recognition of specific cutaneous manifestations and early diagnosis of dermatologic emergencies can be lifesaving.
1. McQueen A, Martin SA, Lio PA. Derm emergencies: detecting early signs of trouble. J Fam Pract. 2012;61:71-78.
2. Bennion S. Dermatologic emergencies. In: Fitzpatrick J, Morelli J, eds. Dermatology Secrets Plus. 4th ed. Philadelphia, PA: Mosby; 2011:442-452.
3. Sarani B, Strong M, Pascual J, et al. Necrotizing fasciitis: current concepts and review of the literature. J Am Coll Surg. 2009;208:279-288.
4. Wolf R, Orion E, Marcos B, et al. Life-threatening acute adverse cutaneous drug reactions. Clin Dermatol. 2005;23:171-181.
Dermatologic emergency may sound like an oxymoron, but there are many emergencies that dermatology residents may encounter in their careers. In some instances the skin is the primary organ that is affected, while in others cutaneous symptoms and life-threatening signs are important diagnostic clues for what may lie beneath the skin.
As residents who are occasionally on call or on consultation services, it is important for us to recognize dermatologic emergencies quickly because some of these conditions can acutely evolve and become lethal if a diagnosis is not made early in the disease course with the appropriate treatment administered. Dermatologic emergencies can range from severe drug reactions, infections, autoimmune exacerbations, and inflammatory conditions (eg, erythroderma) to environmental insults such as burns (Figure 1) and child abuse.1
Critical Infections
Some dermatologic emergencies are infectious in origin, and although these infections are most commonly bacterial (eg, necrotizing fasciitis), they also can range from viral to fungal (eg, mucormycosis) in nature. Some areas with large populations of immunocompromised patients (eg, human immunodeficiency virus–positive patients, organ transplant recipients) may warrant a high index of suspicion for possible zebras (rare conditions) and opportunistic infections that may quickly escalate to life-threatening situations.
Although few cutaneous manifestations in emergent infections are pathognomonic, they sometimes can be categorized according to the appearance of the primary lesion: erythrodermic (eg, staphylococcal scalded skin syndrome), maculopapular (eg, Lyme disease), purpuric/petechial (eg, Rocky Mountain spotted fever), pustular (eg, disseminated candidiasis), or vesicular (eg, neonatal herpes simplex virus)(Table). On consultations, dermatology residents frequently get called to evaluate hemorrhagic and ischemic lesions in inpatients (Figure 2). Aside from infectious causes, the differential diagnosis may include coagulation abnormalities (eg, concurrent anticoagulant therapies), vasculitides, poisoning, vascular disease, or Stevens-Johnson syndrome and toxic epidermal necrolysis, which can occasionally present with hemorrhagic lesions.1,2
Necrotizing Fasciitis
Dermatology residents may frequently encounter necrotizing fasciitis, either in clinic or on the wards (Figure 3). Recognition of the skin signs in this condition is essential to patient survival. As an intern, I once had an attending teach me that patients with necrotizing fasciitis only have a couple of hours to live. The rapid unfolding of this flesh-eating disease and its high morbidity and mortality has led to recent attention in the press and media.
Although necrotizing fasciitis may be caused by several different bacterial organisms (eg, gram positive, gram negative, polymicrobial), it usually is rapidly progressive, destroying muscle and subcutaneous tissues in a matter of hours.3 Bacteria usually enter through a traumatic or present wound and quickly move along fascial planes, destroying blood vessels and whatever subcutaneous tissues happen to be in the way. Within the first few hours, the involved area that was initially erythematous becomes indurated, woody, extremely painful, and dusky, indicating a lack of circulation to the area. Extensive debridement is required until reaching noninfected tissue that is no longer purulent, necrotic, or woody to the touch. If necrotizing fasciitis is not diagnosed and treated early, patients may lose one or several limbs and death may occur.
Key findings of necrotizing fasciitis include systemic toxicity, localized painful induration, well-defined dusky blue discoloration, and a lack of bleeding or purulent discharge on incision and squeezing of the affected tissue. Crepitation or a crackling sensation can occasionally be felt when palpating the area secondary to gas formation in the tissue, though it is not always present. Patients with necrotizing fasciitis often initially present to dermatology clinics because the first manifestation happens to be in the skin. The role of dermatologists in treating this critical condition may prompt recognition and collaboration with other specialists to reach a viable outcome for the patient.3
Drug Reactions
Cutaneous drug eruptions usually are relatively benign, consisting of a morbilliform eruption often without any other accompanying symptoms. However, sometimes these reactions can present as exfoliative dermatitis or red man syndrome in which patients can develop total body erythema with diffuse scaling and pruritus.4 Aside from drug reactions, other causes of exfoliative dermatitis such as psoriasis, atopic and seborrheic dermatitis, mycosis fungoides, and lymphoma should be ruled out. Other drug eruptions that can be classified as dermatologic emergencies include leukocytoclastic vasculitis, severe urticaria or angioedema, erythema multiforme, or Stevens-Johnson syndrome and toxic epidermal necrolysis.
Severe Acne
If not treated promptly, serious cases of acne can lead to severe scarring and psychologic problems. Acne fulminans is characterized by a rapid eruption of suppurative and large, highly inflamed nodules, plaques, and cysts that result in ragged ulcerations and cicatrization of the chest, back, and occasionally the face. Systemic symptoms of fever, arthralgia, leukocytosis, and myalgia suggest an upregulation of the immune system in affected patients.
Final Comment
In summary, dermatologic emergencies do exist and some may present with characteristic skin findings. In almost all cases, collaboration with other departments such as trauma, burn, internal medicine, rheumatology, and infectious diseases is extremely helpful in diagnosing and treating these medical emergencies. Collaboration can provide insight into how brainstorming through different approaches can lead to a better outcome whether it be solving the cause of a puzzling rash in a patient with multiple comorbidities or surgically removing a bullet from a trauma patient (Figure 4). Recognition of specific cutaneous manifestations and early diagnosis of dermatologic emergencies can be lifesaving.
Dermatologic emergency may sound like an oxymoron, but there are many emergencies that dermatology residents may encounter in their careers. In some instances the skin is the primary organ that is affected, while in others cutaneous symptoms and life-threatening signs are important diagnostic clues for what may lie beneath the skin.
As residents who are occasionally on call or on consultation services, it is important for us to recognize dermatologic emergencies quickly because some of these conditions can acutely evolve and become lethal if a diagnosis is not made early in the disease course with the appropriate treatment administered. Dermatologic emergencies can range from severe drug reactions, infections, autoimmune exacerbations, and inflammatory conditions (eg, erythroderma) to environmental insults such as burns (Figure 1) and child abuse.1
Critical Infections
Some dermatologic emergencies are infectious in origin, and although these infections are most commonly bacterial (eg, necrotizing fasciitis), they also can range from viral to fungal (eg, mucormycosis) in nature. Some areas with large populations of immunocompromised patients (eg, human immunodeficiency virus–positive patients, organ transplant recipients) may warrant a high index of suspicion for possible zebras (rare conditions) and opportunistic infections that may quickly escalate to life-threatening situations.
Although few cutaneous manifestations in emergent infections are pathognomonic, they sometimes can be categorized according to the appearance of the primary lesion: erythrodermic (eg, staphylococcal scalded skin syndrome), maculopapular (eg, Lyme disease), purpuric/petechial (eg, Rocky Mountain spotted fever), pustular (eg, disseminated candidiasis), or vesicular (eg, neonatal herpes simplex virus)(Table). On consultations, dermatology residents frequently get called to evaluate hemorrhagic and ischemic lesions in inpatients (Figure 2). Aside from infectious causes, the differential diagnosis may include coagulation abnormalities (eg, concurrent anticoagulant therapies), vasculitides, poisoning, vascular disease, or Stevens-Johnson syndrome and toxic epidermal necrolysis, which can occasionally present with hemorrhagic lesions.1,2
Necrotizing Fasciitis
Dermatology residents may frequently encounter necrotizing fasciitis, either in clinic or on the wards (Figure 3). Recognition of the skin signs in this condition is essential to patient survival. As an intern, I once had an attending teach me that patients with necrotizing fasciitis only have a couple of hours to live. The rapid unfolding of this flesh-eating disease and its high morbidity and mortality has led to recent attention in the press and media.
Although necrotizing fasciitis may be caused by several different bacterial organisms (eg, gram positive, gram negative, polymicrobial), it usually is rapidly progressive, destroying muscle and subcutaneous tissues in a matter of hours.3 Bacteria usually enter through a traumatic or present wound and quickly move along fascial planes, destroying blood vessels and whatever subcutaneous tissues happen to be in the way. Within the first few hours, the involved area that was initially erythematous becomes indurated, woody, extremely painful, and dusky, indicating a lack of circulation to the area. Extensive debridement is required until reaching noninfected tissue that is no longer purulent, necrotic, or woody to the touch. If necrotizing fasciitis is not diagnosed and treated early, patients may lose one or several limbs and death may occur.
Key findings of necrotizing fasciitis include systemic toxicity, localized painful induration, well-defined dusky blue discoloration, and a lack of bleeding or purulent discharge on incision and squeezing of the affected tissue. Crepitation or a crackling sensation can occasionally be felt when palpating the area secondary to gas formation in the tissue, though it is not always present. Patients with necrotizing fasciitis often initially present to dermatology clinics because the first manifestation happens to be in the skin. The role of dermatologists in treating this critical condition may prompt recognition and collaboration with other specialists to reach a viable outcome for the patient.3
Drug Reactions
Cutaneous drug eruptions usually are relatively benign, consisting of a morbilliform eruption often without any other accompanying symptoms. However, sometimes these reactions can present as exfoliative dermatitis or red man syndrome in which patients can develop total body erythema with diffuse scaling and pruritus.4 Aside from drug reactions, other causes of exfoliative dermatitis such as psoriasis, atopic and seborrheic dermatitis, mycosis fungoides, and lymphoma should be ruled out. Other drug eruptions that can be classified as dermatologic emergencies include leukocytoclastic vasculitis, severe urticaria or angioedema, erythema multiforme, or Stevens-Johnson syndrome and toxic epidermal necrolysis.
Severe Acne
If not treated promptly, serious cases of acne can lead to severe scarring and psychologic problems. Acne fulminans is characterized by a rapid eruption of suppurative and large, highly inflamed nodules, plaques, and cysts that result in ragged ulcerations and cicatrization of the chest, back, and occasionally the face. Systemic symptoms of fever, arthralgia, leukocytosis, and myalgia suggest an upregulation of the immune system in affected patients.
Final Comment
In summary, dermatologic emergencies do exist and some may present with characteristic skin findings. In almost all cases, collaboration with other departments such as trauma, burn, internal medicine, rheumatology, and infectious diseases is extremely helpful in diagnosing and treating these medical emergencies. Collaboration can provide insight into how brainstorming through different approaches can lead to a better outcome whether it be solving the cause of a puzzling rash in a patient with multiple comorbidities or surgically removing a bullet from a trauma patient (Figure 4). Recognition of specific cutaneous manifestations and early diagnosis of dermatologic emergencies can be lifesaving.
1. McQueen A, Martin SA, Lio PA. Derm emergencies: detecting early signs of trouble. J Fam Pract. 2012;61:71-78.
2. Bennion S. Dermatologic emergencies. In: Fitzpatrick J, Morelli J, eds. Dermatology Secrets Plus. 4th ed. Philadelphia, PA: Mosby; 2011:442-452.
3. Sarani B, Strong M, Pascual J, et al. Necrotizing fasciitis: current concepts and review of the literature. J Am Coll Surg. 2009;208:279-288.
4. Wolf R, Orion E, Marcos B, et al. Life-threatening acute adverse cutaneous drug reactions. Clin Dermatol. 2005;23:171-181.
1. McQueen A, Martin SA, Lio PA. Derm emergencies: detecting early signs of trouble. J Fam Pract. 2012;61:71-78.
2. Bennion S. Dermatologic emergencies. In: Fitzpatrick J, Morelli J, eds. Dermatology Secrets Plus. 4th ed. Philadelphia, PA: Mosby; 2011:442-452.
3. Sarani B, Strong M, Pascual J, et al. Necrotizing fasciitis: current concepts and review of the literature. J Am Coll Surg. 2009;208:279-288.
4. Wolf R, Orion E, Marcos B, et al. Life-threatening acute adverse cutaneous drug reactions. Clin Dermatol. 2005;23:171-181.

Cosmetic Corner: Dermatologists Weigh in on Aftershaves
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top aftershaves. Consideration must be given to:
- The Art of Shaving Pre-Shave Oil
- CeraVe Facial Moisturizing Lotion AM
- Post Shave Cooling Gel
Cutis invites readers to send us their recommendations. Skin care products for babies, hand sanitizers, and cleansers for rosacea patients will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top aftershaves. Consideration must be given to:
- The Art of Shaving Pre-Shave Oil
- CeraVe Facial Moisturizing Lotion AM
- Post Shave Cooling Gel
Cutis invites readers to send us their recommendations. Skin care products for babies, hand sanitizers, and cleansers for rosacea patients will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top aftershaves. Consideration must be given to:
- The Art of Shaving Pre-Shave Oil
- CeraVe Facial Moisturizing Lotion AM
- Post Shave Cooling Gel
Cutis invites readers to send us their recommendations. Skin care products for babies, hand sanitizers, and cleansers for rosacea patients will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
Consider five factors when selecting laser or peel
NEW ORLEANS – When deciding whether to laser or peel, safety is enhanced and postoperative results are more favorable when five factors are considered, according to Dr. Suzan Obagi of the Cosmetic Surgery and Skin Health Center at University of Pittsburgh Medical Center.
“When I look at a patient and I am deciding on a skin resurfacing modality, I go through a checklist in my head to evaluate their skin color, thickness, and anatomy; the depth of their skin problem; and the number of treatments the patient will be willing to go through,” she noted in a presentation at the annual meeting of the American Academy of Cosmetic Surgery.

Consider every factor and to inform patients of the risks and benefits associated with each skin resurfacing modality, she said.
“Peels and lasers don’t work the same way, and comparing them is like comparing apples and oranges,” she noted.
In general, lighter skin responds well to a wide variety of peels and laser treatments, and fares particularly well when treated with lasers, said Dr. Obagi. However, patients with darker skin present a special challenge because they are more likely to present with a number of skin problems such as melasma, lentigines, ephelides, post-inflammatory hyperpigmentation (PIH), post-inflammatory erythema (PIE), acne scars, and dermatosis papulosa nigra (DPN). These patients often require a combination of modalities to address their concerns.
The depth of the skin problem should be carefully considered, as different modalities to treat specific indications are targeted to various depths, Dr. Obagi noted. Photodamage is a superficial condition that she typically treats with peels, while superficial scars and rhytids, can be treated with a combination of lasers and peels. Deep scars and rhytids that reside deeper in the skin should be treated with lasers.
“You can try to reach some of these deeper problems with peels and superficial laser peels, but you may end up in trouble from pushing a modality deeper than you can control it,” stressed Dr. Obagi. “When I see deep acne scars, I immediately know to use a laser; no chemical peel is going to address that,” she added.
Thin skin is easier to treat with peels, and lasers are safer to use on thick skin, she said. Thicker skin can be treated with peels, but requires the application of more solution. “It’s harder to get results when doing a peel on thick skin, so I prefer to do laser resurfacing,” said Dr. Obagi. “On thin skin, I’d rather do a chemical peel and save the laser for the areas that really need it.”

When evaluating the anatomic area of the skin to be treated, remember that lasers cannot be used on certain parts of the face, noted Dr. Obagi. The areas around the hairline, eyes, ears, and neck pose the most risk when using lasers. “If you laser around the eyebrows, you’ll burn them off; if you laser the neck, you sometimes learn the hard way that the neck isn’t very forgiving,” she said.
Finally, consider the number of treatments needed to achieve the desired result in conjunction with the number of treatments a patient is willing to go through, Dr. Obagi said. Fractionated lasers, by definition, do not treat 100% of the skin in one session; they cover 20%-40% of the skin surface, and multiple treatments are recommended for optimal results. Each treatment requires 5-7 days of recovery time, and pain can be managed with oral and local anesthesia.
“When using lasers, I prefer to treat more aggressively with fewer sessions,” she added.
Conversely, medium-depth peels are suitable for all skin types and anatomic areas and cover 100% of the skin being treated. Optimal results can usually be achieved in one session followed by 7 days of recovery time. Pain is managed with oral sedation, and the whole face can be treated in 20-30 minutes, noted Dr. Obagi.
Additionally, medical conditions such as autoimmune diseases, and social habits such as smoking should be considered when choosing a treatment, as these conditions can affect healing time.
Dr. Obagi reported serving on the scientific advisory board for Valeant Pharmaceuticals.
NEW ORLEANS – When deciding whether to laser or peel, safety is enhanced and postoperative results are more favorable when five factors are considered, according to Dr. Suzan Obagi of the Cosmetic Surgery and Skin Health Center at University of Pittsburgh Medical Center.
“When I look at a patient and I am deciding on a skin resurfacing modality, I go through a checklist in my head to evaluate their skin color, thickness, and anatomy; the depth of their skin problem; and the number of treatments the patient will be willing to go through,” she noted in a presentation at the annual meeting of the American Academy of Cosmetic Surgery.
Consider every factor and to inform patients of the risks and benefits associated with each skin resurfacing modality, she said.
“Peels and lasers don’t work the same way, and comparing them is like comparing apples and oranges,” she noted.
In general, lighter skin responds well to a wide variety of peels and laser treatments, and fares particularly well when treated with lasers, said Dr. Obagi. However, patients with darker skin present a special challenge because they are more likely to present with a number of skin problems such as melasma, lentigines, ephelides, post-inflammatory hyperpigmentation (PIH), post-inflammatory erythema (PIE), acne scars, and dermatosis papulosa nigra (DPN). These patients often require a combination of modalities to address their concerns.
The depth of the skin problem should be carefully considered, as different modalities to treat specific indications are targeted to various depths, Dr. Obagi noted. Photodamage is a superficial condition that she typically treats with peels, while superficial scars and rhytids, can be treated with a combination of lasers and peels. Deep scars and rhytids that reside deeper in the skin should be treated with lasers.
“You can try to reach some of these deeper problems with peels and superficial laser peels, but you may end up in trouble from pushing a modality deeper than you can control it,” stressed Dr. Obagi. “When I see deep acne scars, I immediately know to use a laser; no chemical peel is going to address that,” she added.
Thin skin is easier to treat with peels, and lasers are safer to use on thick skin, she said. Thicker skin can be treated with peels, but requires the application of more solution. “It’s harder to get results when doing a peel on thick skin, so I prefer to do laser resurfacing,” said Dr. Obagi. “On thin skin, I’d rather do a chemical peel and save the laser for the areas that really need it.”
When evaluating the anatomic area of the skin to be treated, remember that lasers cannot be used on certain parts of the face, noted Dr. Obagi. The areas around the hairline, eyes, ears, and neck pose the most risk when using lasers. “If you laser around the eyebrows, you’ll burn them off; if you laser the neck, you sometimes learn the hard way that the neck isn’t very forgiving,” she said.
Finally, consider the number of treatments needed to achieve the desired result in conjunction with the number of treatments a patient is willing to go through, Dr. Obagi said. Fractionated lasers, by definition, do not treat 100% of the skin in one session; they cover 20%-40% of the skin surface, and multiple treatments are recommended for optimal results. Each treatment requires 5-7 days of recovery time, and pain can be managed with oral and local anesthesia.
“When using lasers, I prefer to treat more aggressively with fewer sessions,” she added.
Conversely, medium-depth peels are suitable for all skin types and anatomic areas and cover 100% of the skin being treated. Optimal results can usually be achieved in one session followed by 7 days of recovery time. Pain is managed with oral sedation, and the whole face can be treated in 20-30 minutes, noted Dr. Obagi.
Additionally, medical conditions such as autoimmune diseases, and social habits such as smoking should be considered when choosing a treatment, as these conditions can affect healing time.
Dr. Obagi reported serving on the scientific advisory board for Valeant Pharmaceuticals.
NEW ORLEANS – When deciding whether to laser or peel, safety is enhanced and postoperative results are more favorable when five factors are considered, according to Dr. Suzan Obagi of the Cosmetic Surgery and Skin Health Center at University of Pittsburgh Medical Center.
“When I look at a patient and I am deciding on a skin resurfacing modality, I go through a checklist in my head to evaluate their skin color, thickness, and anatomy; the depth of their skin problem; and the number of treatments the patient will be willing to go through,” she noted in a presentation at the annual meeting of the American Academy of Cosmetic Surgery.
Consider every factor and to inform patients of the risks and benefits associated with each skin resurfacing modality, she said.
“Peels and lasers don’t work the same way, and comparing them is like comparing apples and oranges,” she noted.
In general, lighter skin responds well to a wide variety of peels and laser treatments, and fares particularly well when treated with lasers, said Dr. Obagi. However, patients with darker skin present a special challenge because they are more likely to present with a number of skin problems such as melasma, lentigines, ephelides, post-inflammatory hyperpigmentation (PIH), post-inflammatory erythema (PIE), acne scars, and dermatosis papulosa nigra (DPN). These patients often require a combination of modalities to address their concerns.
The depth of the skin problem should be carefully considered, as different modalities to treat specific indications are targeted to various depths, Dr. Obagi noted. Photodamage is a superficial condition that she typically treats with peels, while superficial scars and rhytids, can be treated with a combination of lasers and peels. Deep scars and rhytids that reside deeper in the skin should be treated with lasers.
“You can try to reach some of these deeper problems with peels and superficial laser peels, but you may end up in trouble from pushing a modality deeper than you can control it,” stressed Dr. Obagi. “When I see deep acne scars, I immediately know to use a laser; no chemical peel is going to address that,” she added.
Thin skin is easier to treat with peels, and lasers are safer to use on thick skin, she said. Thicker skin can be treated with peels, but requires the application of more solution. “It’s harder to get results when doing a peel on thick skin, so I prefer to do laser resurfacing,” said Dr. Obagi. “On thin skin, I’d rather do a chemical peel and save the laser for the areas that really need it.”
When evaluating the anatomic area of the skin to be treated, remember that lasers cannot be used on certain parts of the face, noted Dr. Obagi. The areas around the hairline, eyes, ears, and neck pose the most risk when using lasers. “If you laser around the eyebrows, you’ll burn them off; if you laser the neck, you sometimes learn the hard way that the neck isn’t very forgiving,” she said.
Finally, consider the number of treatments needed to achieve the desired result in conjunction with the number of treatments a patient is willing to go through, Dr. Obagi said. Fractionated lasers, by definition, do not treat 100% of the skin in one session; they cover 20%-40% of the skin surface, and multiple treatments are recommended for optimal results. Each treatment requires 5-7 days of recovery time, and pain can be managed with oral and local anesthesia.
“When using lasers, I prefer to treat more aggressively with fewer sessions,” she added.
Conversely, medium-depth peels are suitable for all skin types and anatomic areas and cover 100% of the skin being treated. Optimal results can usually be achieved in one session followed by 7 days of recovery time. Pain is managed with oral sedation, and the whole face can be treated in 20-30 minutes, noted Dr. Obagi.
Additionally, medical conditions such as autoimmune diseases, and social habits such as smoking should be considered when choosing a treatment, as these conditions can affect healing time.
Dr. Obagi reported serving on the scientific advisory board for Valeant Pharmaceuticals.
AT THE AACS ANNUAL MEETING

Silver sulfadiazine linked to delayed wound healing in mice
Silver sulfadiazine appeared to disrupt cytokine activity, suppress macrophage recruitment, and inhibit collagen deposition and re-epithelialization in mice with full-thickness burns, the researchers reported.
“Our data suggest a mechanism by which [silver sulfadiazine] impairs wound healing … though further investigations are necessary,” said coauthors Jamie Rosen and Angelo Landriscina and their associates at the Albert Einstein College of Medicine, New York.
Silver sulfadiazine (SSD) is a broad-spectrum antimicrobial used widely for treating second- and third-degree burns. Despite its popularity, some past studies have found it inferior to other wound treatments. To explore why, the investigators created two full-thickness thermal burns each on the backs of 102 mice and treated 46 of the mice with 50 mcL of 1% SSD cream per wound/day. The other mice served as untreated controls (J. Invest. Dermatol. 2015 [doi: 10.1038/jid.2015.21])
Photographs and computerized wound measurements showed that by day 3, the SSD group had greater wound expansion than did the control group (49.7%, compared with 23.8%; P < .0002), said the researchers. Furthermore, the SSD group had only 16.3% wound closure by day 10, compared with 42.1% for controls (P < .005). Cytokine assays also showed that the SSD group also had lower expression of IL-1 and IL-1ra, while histologic studies revealed fewer macrophages and less collagen deposition and re-epithelialization.
“We hypothesize that SSD alters gene expression of IL-1 family genes, resulting in impaired downstream cytokine production and ultimately delayed wound healing,” concluded the authors. But because data in mice do not always translate to humans, more studies would be needed to confirm the mechanism.
The investigators reported no funding sources and declared no relevant financial disclosures.
Silver sulfadiazine appeared to disrupt cytokine activity, suppress macrophage recruitment, and inhibit collagen deposition and re-epithelialization in mice with full-thickness burns, the researchers reported.
“Our data suggest a mechanism by which [silver sulfadiazine] impairs wound healing … though further investigations are necessary,” said coauthors Jamie Rosen and Angelo Landriscina and their associates at the Albert Einstein College of Medicine, New York.
Silver sulfadiazine (SSD) is a broad-spectrum antimicrobial used widely for treating second- and third-degree burns. Despite its popularity, some past studies have found it inferior to other wound treatments. To explore why, the investigators created two full-thickness thermal burns each on the backs of 102 mice and treated 46 of the mice with 50 mcL of 1% SSD cream per wound/day. The other mice served as untreated controls (J. Invest. Dermatol. 2015 [doi: 10.1038/jid.2015.21])
Photographs and computerized wound measurements showed that by day 3, the SSD group had greater wound expansion than did the control group (49.7%, compared with 23.8%; P < .0002), said the researchers. Furthermore, the SSD group had only 16.3% wound closure by day 10, compared with 42.1% for controls (P < .005). Cytokine assays also showed that the SSD group also had lower expression of IL-1 and IL-1ra, while histologic studies revealed fewer macrophages and less collagen deposition and re-epithelialization.
“We hypothesize that SSD alters gene expression of IL-1 family genes, resulting in impaired downstream cytokine production and ultimately delayed wound healing,” concluded the authors. But because data in mice do not always translate to humans, more studies would be needed to confirm the mechanism.
The investigators reported no funding sources and declared no relevant financial disclosures.
Silver sulfadiazine appeared to disrupt cytokine activity, suppress macrophage recruitment, and inhibit collagen deposition and re-epithelialization in mice with full-thickness burns, the researchers reported.
“Our data suggest a mechanism by which [silver sulfadiazine] impairs wound healing … though further investigations are necessary,” said coauthors Jamie Rosen and Angelo Landriscina and their associates at the Albert Einstein College of Medicine, New York.
Silver sulfadiazine (SSD) is a broad-spectrum antimicrobial used widely for treating second- and third-degree burns. Despite its popularity, some past studies have found it inferior to other wound treatments. To explore why, the investigators created two full-thickness thermal burns each on the backs of 102 mice and treated 46 of the mice with 50 mcL of 1% SSD cream per wound/day. The other mice served as untreated controls (J. Invest. Dermatol. 2015 [doi: 10.1038/jid.2015.21])
Photographs and computerized wound measurements showed that by day 3, the SSD group had greater wound expansion than did the control group (49.7%, compared with 23.8%; P < .0002), said the researchers. Furthermore, the SSD group had only 16.3% wound closure by day 10, compared with 42.1% for controls (P < .005). Cytokine assays also showed that the SSD group also had lower expression of IL-1 and IL-1ra, while histologic studies revealed fewer macrophages and less collagen deposition and re-epithelialization.
“We hypothesize that SSD alters gene expression of IL-1 family genes, resulting in impaired downstream cytokine production and ultimately delayed wound healing,” concluded the authors. But because data in mice do not always translate to humans, more studies would be needed to confirm the mechanism.
The investigators reported no funding sources and declared no relevant financial disclosures.
Key clinical point: Silver sulfadiazine may impair wound healing.
Major finding: By day 10, mice treated with silver sulfadiazine had only 16.2% wound closure, compared with 42.1% for untreated controls (P < .005).
Data source: Histologic, clinical, and cytokine evaluations of 102 mice with full-thickness burns.
Disclosures: The investigators reported no funding sources and declared no relevant financial disclosures.
Hand rejuvenation
The three most exposed areas of the body that give away a person’s age are the face, neck, and hands. Rejuvenation of the hands is an often simple and nice addition to facial and neck aesthetic rejuvenation.
When examining aging hands, the three most prominent features are decreased volume in the interosseous spaces (leading to increased crepiness of the skin and increased show of extensor tendons), lentigines, and prominent veins. Therefore, the treatment for hands is quite simple: Restore volume, treat the pigmented lesions, and if needed, treat the prominent veins.
The anatomy of the dorsal hand can be divided into three major compartments. First, the skin, which on the dorsal hand is quite pliable. Second, the subcutaneous tissue, which consists of a loose areolar tissue where the lymphatics and veins lie. Third, beneath the subcutaneous tissue is the dorsal fascia of the hand, which is contiguous with extensor tendons and underlying compartments. It is in the subcutaneous layer (or loose areolar tissue) where fillers or fat are placed to treat volume loss.
While several fillers are currently used off label for hand rejuvenation, the Food and Drug Administration is meeting in February to consider officially approving Radiesse for this indication. Currently, hyaluronic acid (HA) fillers, calcium- hydroxylapatite (Radiesse), poly-L-lactic acid, and autologous fat are all utilized. I tend to use HAs in this location because of the reversibility, if needed, and decreased risk of nodule formation. Several techniques exist, including injecting between each tendon space vs. a bolus technique. I tend to use a bolus technique, where one or two boluses are injected while tenting the skin up to ensure injection into the correct plane and to avoid the vessels. Subsequently, the boluses are massaged into place while the patient makes a fist.
Once the interosseous spaces have been treated, the veins often appear less prominent and often don’t require direct treatment. I typically do not treat the dorsal hand veins, but sclerotherapy can be performed. Lentigines may be treated with a variety of devices including intense pulse light, Q-switched lasers, and fractionated nonablative lasers. Chemical peels and topical antipigment agents also may help to a lesser degree or also may be used for maintenance to keep the lentigines away.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.
The three most exposed areas of the body that give away a person’s age are the face, neck, and hands. Rejuvenation of the hands is an often simple and nice addition to facial and neck aesthetic rejuvenation.
When examining aging hands, the three most prominent features are decreased volume in the interosseous spaces (leading to increased crepiness of the skin and increased show of extensor tendons), lentigines, and prominent veins. Therefore, the treatment for hands is quite simple: Restore volume, treat the pigmented lesions, and if needed, treat the prominent veins.
The anatomy of the dorsal hand can be divided into three major compartments. First, the skin, which on the dorsal hand is quite pliable. Second, the subcutaneous tissue, which consists of a loose areolar tissue where the lymphatics and veins lie. Third, beneath the subcutaneous tissue is the dorsal fascia of the hand, which is contiguous with extensor tendons and underlying compartments. It is in the subcutaneous layer (or loose areolar tissue) where fillers or fat are placed to treat volume loss.
While several fillers are currently used off label for hand rejuvenation, the Food and Drug Administration is meeting in February to consider officially approving Radiesse for this indication. Currently, hyaluronic acid (HA) fillers, calcium- hydroxylapatite (Radiesse), poly-L-lactic acid, and autologous fat are all utilized. I tend to use HAs in this location because of the reversibility, if needed, and decreased risk of nodule formation. Several techniques exist, including injecting between each tendon space vs. a bolus technique. I tend to use a bolus technique, where one or two boluses are injected while tenting the skin up to ensure injection into the correct plane and to avoid the vessels. Subsequently, the boluses are massaged into place while the patient makes a fist.
Once the interosseous spaces have been treated, the veins often appear less prominent and often don’t require direct treatment. I typically do not treat the dorsal hand veins, but sclerotherapy can be performed. Lentigines may be treated with a variety of devices including intense pulse light, Q-switched lasers, and fractionated nonablative lasers. Chemical peels and topical antipigment agents also may help to a lesser degree or also may be used for maintenance to keep the lentigines away.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.
The three most exposed areas of the body that give away a person’s age are the face, neck, and hands. Rejuvenation of the hands is an often simple and nice addition to facial and neck aesthetic rejuvenation.
When examining aging hands, the three most prominent features are decreased volume in the interosseous spaces (leading to increased crepiness of the skin and increased show of extensor tendons), lentigines, and prominent veins. Therefore, the treatment for hands is quite simple: Restore volume, treat the pigmented lesions, and if needed, treat the prominent veins.
The anatomy of the dorsal hand can be divided into three major compartments. First, the skin, which on the dorsal hand is quite pliable. Second, the subcutaneous tissue, which consists of a loose areolar tissue where the lymphatics and veins lie. Third, beneath the subcutaneous tissue is the dorsal fascia of the hand, which is contiguous with extensor tendons and underlying compartments. It is in the subcutaneous layer (or loose areolar tissue) where fillers or fat are placed to treat volume loss.
While several fillers are currently used off label for hand rejuvenation, the Food and Drug Administration is meeting in February to consider officially approving Radiesse for this indication. Currently, hyaluronic acid (HA) fillers, calcium- hydroxylapatite (Radiesse), poly-L-lactic acid, and autologous fat are all utilized. I tend to use HAs in this location because of the reversibility, if needed, and decreased risk of nodule formation. Several techniques exist, including injecting between each tendon space vs. a bolus technique. I tend to use a bolus technique, where one or two boluses are injected while tenting the skin up to ensure injection into the correct plane and to avoid the vessels. Subsequently, the boluses are massaged into place while the patient makes a fist.
Once the interosseous spaces have been treated, the veins often appear less prominent and often don’t require direct treatment. I typically do not treat the dorsal hand veins, but sclerotherapy can be performed. Lentigines may be treated with a variety of devices including intense pulse light, Q-switched lasers, and fractionated nonablative lasers. Chemical peels and topical antipigment agents also may help to a lesser degree or also may be used for maintenance to keep the lentigines away.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.

Simple early interventions enhance dermatologic care across the lifespan
ORLANDO – Generational dermatology can be conceptualized by looking at patients now in their 50s, 60s, and 70s and thinking about what aspects of aging could have been targeted 20 years ago had currently available tools been available then, according to Dr. Wendy E. Roberts.
“What interventions would we select for our patients, and what tools do we have that we did not have then?” said Dr. Roberts of Rancho Mirage, Calif.

One area for intervention that stands out is integumentary system collapse, with such features as stress tears, purpura, and photodamage, she said, noting that these aren’t things that happen overnight. Preventive measures, beginning with a focus on the skin barrier, can go a long way toward preventing this type of organ damage.
“Skin barrier has been upgraded to a major feature of a variety of common disease states, so I encourage everyone to start your therapeutic plan by assessing this skin care component – assessing the integrity of the skin,” she said, explaining that entities including xerosis, pruritus, purpura, and rosacea share a common factor: skin barrier abnormalities.
Understanding what is normal, what indicates injury, and what is considered progressive pathology with respect to skin barrier is important.
Consider xerosis, for example.
For a long time, the condition was relegated to “just dry skin.” But xerosis is the No. 1 aging skin issue for both men and women, she noted.
Further, it contributes to other important skin pathology, including pruritus, lichen simplex chronicus, and foot fissures.
“This happens because over the course of our lifetime, we have decreasing epidermal keratinocyte transit time,” she explained.
Of note, foot ulcers are a billion dollar burden on the American health care system, and a major contributing factor – accounting for about 70% of foot ulcers – is hyperkeratosis, she said, adding that “there’s something to be said about foot care and moisturization.”
“I always recommend this in my evolving aging patients. It’s something we really need to think about, and we can’t wait to think about it in the 7th decade,” she said referring to moisturization and good skin care habits.
Moisturization is the key, and it involves the use of protectants that produce an additional barrier to water loss, hydration with moisturizers that decrease transepidermal water loss and restore water to the epidermis, and emollients that intercalate and form a nice skin barrier. Using all three is advisable, as each has a specific function, she said.
Other pearls for xerosis management include a review of all possible contributors: photodamage, menopausal status, hormonal status, comorbidities, thyroid status, and emerging medication issues. Statins and systemic retinoids, in particular, can contribute.
Climate and living environment also should be considered, as cold (and use of heating units), high altitude, and desert areas can increase the risk of xerosis.
Advise patients with xerosis to avoid prolonged contact with hot water and with detergent cleansers (in lieu of moisturizing cleansers), and recommend twice daily application of cream- or oil-based vehicles rather than lotions. Supplements, including omega-3s, vitamin A, vitamin B, and primrose may also provide some benefit, she said.
Among the other tools that Dr. Roberts recommended for use earlier in life to help improve outcomes across the lifespan are imaging technologies and full-body skin exams.
Visual interactive systems that can bring patients awareness regarding the aging process, and imaging of pigmented lesions via dermoscopy that can help track changes over time are examples of imaging modalities that can be used. Programs exist that allow patients to log in to a program from home and view the images of their skin online.
Examples include Touch MD by Alphaeon, MelaFind by MELA Sciences, and Visia by Canfield Scientific which can be useful not only for cosmetic dermatology, but also for medical dermatology, she said.
“These tools aren’t just research tools; these tools really help communicate the attributes of all aspects of aging skin and can be very beneficial,” she said.
Such images can be useful in children as well, as they can show the early effects of photodamage and encourage parents to begin sun protection efforts early.
Full-body skin exams are a must, because the most deadly skin cancers occur most often on typically covered sites. Such exams also can be used as a tool to discuss medical, cosmetic, and oncologic issues that are important throughout the aging process, she said.
Dr. Roberts reported that she is a speaker or consultant for, and/or has received honoraria from Allergan, Colorescience, L’Oreal, La Roche-Posay, NeoStrata, SkinMedica, Theraplex, and Top MD Skincare.
ORLANDO – Generational dermatology can be conceptualized by looking at patients now in their 50s, 60s, and 70s and thinking about what aspects of aging could have been targeted 20 years ago had currently available tools been available then, according to Dr. Wendy E. Roberts.
“What interventions would we select for our patients, and what tools do we have that we did not have then?” said Dr. Roberts of Rancho Mirage, Calif.
One area for intervention that stands out is integumentary system collapse, with such features as stress tears, purpura, and photodamage, she said, noting that these aren’t things that happen overnight. Preventive measures, beginning with a focus on the skin barrier, can go a long way toward preventing this type of organ damage.
“Skin barrier has been upgraded to a major feature of a variety of common disease states, so I encourage everyone to start your therapeutic plan by assessing this skin care component – assessing the integrity of the skin,” she said, explaining that entities including xerosis, pruritus, purpura, and rosacea share a common factor: skin barrier abnormalities.
Understanding what is normal, what indicates injury, and what is considered progressive pathology with respect to skin barrier is important.
Consider xerosis, for example.
For a long time, the condition was relegated to “just dry skin.” But xerosis is the No. 1 aging skin issue for both men and women, she noted.
Further, it contributes to other important skin pathology, including pruritus, lichen simplex chronicus, and foot fissures.
“This happens because over the course of our lifetime, we have decreasing epidermal keratinocyte transit time,” she explained.
Of note, foot ulcers are a billion dollar burden on the American health care system, and a major contributing factor – accounting for about 70% of foot ulcers – is hyperkeratosis, she said, adding that “there’s something to be said about foot care and moisturization.”
“I always recommend this in my evolving aging patients. It’s something we really need to think about, and we can’t wait to think about it in the 7th decade,” she said referring to moisturization and good skin care habits.
Moisturization is the key, and it involves the use of protectants that produce an additional barrier to water loss, hydration with moisturizers that decrease transepidermal water loss and restore water to the epidermis, and emollients that intercalate and form a nice skin barrier. Using all three is advisable, as each has a specific function, she said.
Other pearls for xerosis management include a review of all possible contributors: photodamage, menopausal status, hormonal status, comorbidities, thyroid status, and emerging medication issues. Statins and systemic retinoids, in particular, can contribute.
Climate and living environment also should be considered, as cold (and use of heating units), high altitude, and desert areas can increase the risk of xerosis.
Advise patients with xerosis to avoid prolonged contact with hot water and with detergent cleansers (in lieu of moisturizing cleansers), and recommend twice daily application of cream- or oil-based vehicles rather than lotions. Supplements, including omega-3s, vitamin A, vitamin B, and primrose may also provide some benefit, she said.
Among the other tools that Dr. Roberts recommended for use earlier in life to help improve outcomes across the lifespan are imaging technologies and full-body skin exams.
Visual interactive systems that can bring patients awareness regarding the aging process, and imaging of pigmented lesions via dermoscopy that can help track changes over time are examples of imaging modalities that can be used. Programs exist that allow patients to log in to a program from home and view the images of their skin online.
Examples include Touch MD by Alphaeon, MelaFind by MELA Sciences, and Visia by Canfield Scientific which can be useful not only for cosmetic dermatology, but also for medical dermatology, she said.
“These tools aren’t just research tools; these tools really help communicate the attributes of all aspects of aging skin and can be very beneficial,” she said.
Such images can be useful in children as well, as they can show the early effects of photodamage and encourage parents to begin sun protection efforts early.
Full-body skin exams are a must, because the most deadly skin cancers occur most often on typically covered sites. Such exams also can be used as a tool to discuss medical, cosmetic, and oncologic issues that are important throughout the aging process, she said.
Dr. Roberts reported that she is a speaker or consultant for, and/or has received honoraria from Allergan, Colorescience, L’Oreal, La Roche-Posay, NeoStrata, SkinMedica, Theraplex, and Top MD Skincare.
ORLANDO – Generational dermatology can be conceptualized by looking at patients now in their 50s, 60s, and 70s and thinking about what aspects of aging could have been targeted 20 years ago had currently available tools been available then, according to Dr. Wendy E. Roberts.
“What interventions would we select for our patients, and what tools do we have that we did not have then?” said Dr. Roberts of Rancho Mirage, Calif.
One area for intervention that stands out is integumentary system collapse, with such features as stress tears, purpura, and photodamage, she said, noting that these aren’t things that happen overnight. Preventive measures, beginning with a focus on the skin barrier, can go a long way toward preventing this type of organ damage.
“Skin barrier has been upgraded to a major feature of a variety of common disease states, so I encourage everyone to start your therapeutic plan by assessing this skin care component – assessing the integrity of the skin,” she said, explaining that entities including xerosis, pruritus, purpura, and rosacea share a common factor: skin barrier abnormalities.
Understanding what is normal, what indicates injury, and what is considered progressive pathology with respect to skin barrier is important.
Consider xerosis, for example.
For a long time, the condition was relegated to “just dry skin.” But xerosis is the No. 1 aging skin issue for both men and women, she noted.
Further, it contributes to other important skin pathology, including pruritus, lichen simplex chronicus, and foot fissures.
“This happens because over the course of our lifetime, we have decreasing epidermal keratinocyte transit time,” she explained.
Of note, foot ulcers are a billion dollar burden on the American health care system, and a major contributing factor – accounting for about 70% of foot ulcers – is hyperkeratosis, she said, adding that “there’s something to be said about foot care and moisturization.”
“I always recommend this in my evolving aging patients. It’s something we really need to think about, and we can’t wait to think about it in the 7th decade,” she said referring to moisturization and good skin care habits.
Moisturization is the key, and it involves the use of protectants that produce an additional barrier to water loss, hydration with moisturizers that decrease transepidermal water loss and restore water to the epidermis, and emollients that intercalate and form a nice skin barrier. Using all three is advisable, as each has a specific function, she said.
Other pearls for xerosis management include a review of all possible contributors: photodamage, menopausal status, hormonal status, comorbidities, thyroid status, and emerging medication issues. Statins and systemic retinoids, in particular, can contribute.
Climate and living environment also should be considered, as cold (and use of heating units), high altitude, and desert areas can increase the risk of xerosis.
Advise patients with xerosis to avoid prolonged contact with hot water and with detergent cleansers (in lieu of moisturizing cleansers), and recommend twice daily application of cream- or oil-based vehicles rather than lotions. Supplements, including omega-3s, vitamin A, vitamin B, and primrose may also provide some benefit, she said.
Among the other tools that Dr. Roberts recommended for use earlier in life to help improve outcomes across the lifespan are imaging technologies and full-body skin exams.
Visual interactive systems that can bring patients awareness regarding the aging process, and imaging of pigmented lesions via dermoscopy that can help track changes over time are examples of imaging modalities that can be used. Programs exist that allow patients to log in to a program from home and view the images of their skin online.
Examples include Touch MD by Alphaeon, MelaFind by MELA Sciences, and Visia by Canfield Scientific which can be useful not only for cosmetic dermatology, but also for medical dermatology, she said.
“These tools aren’t just research tools; these tools really help communicate the attributes of all aspects of aging skin and can be very beneficial,” she said.
Such images can be useful in children as well, as they can show the early effects of photodamage and encourage parents to begin sun protection efforts early.
Full-body skin exams are a must, because the most deadly skin cancers occur most often on typically covered sites. Such exams also can be used as a tool to discuss medical, cosmetic, and oncologic issues that are important throughout the aging process, she said.
Dr. Roberts reported that she is a speaker or consultant for, and/or has received honoraria from Allergan, Colorescience, L’Oreal, La Roche-Posay, NeoStrata, SkinMedica, Theraplex, and Top MD Skincare.
EXPERT ANALYSIS FROM THE ODAC CONFERENCE
