User login
IBD: Patients struggle with presenteeism, mental health
Anxiety and depression are common among individuals with inflammatory bowel disease (IBD) who are in remission, and the conditions are linked to unemployment and presenteeism, according to a prospective study.
Previous studies have found a heightened risk of anxiety and depression in IBD, as well as an association with poor treatment compliance and greater morbidity. Presenteeism, defined as reduced productivity due to a physical or mental condition, is increasingly recognized as an indirect economic cost of chronic conditions that may exact a higher cost than absenteeism.

More than one-third of patients with IBD experienced presenteeism in one study. Other studies have examined exercise in chronic diseases, and most find an association between more exercise and lower rates of anxiety and depression. To date, few studies have examined a combination of physical activity, mental health, and presenteeism in the context of IBD.
The new study, published in the Journal of Crohn’s and Colitis, “is very important, as presenteeism is not commonly discussed in any formal, measurable way in the IBD space,” said Laurie Keefer, PhD, professor of medicine and a gastropsychologist at Icahn School of Medicine, who was asked to comment on the research. “While conducted in Europe and Israel, the study also has relevance in the U.S. since, here, employers typically pay for health care – so absenteeism, presenteeism, and health care cost are all intertwined.”

“The study confirmed high rates of depression and anxiety after a diagnosis of IBD. One high-quality aspect of this study was that the diagnosis of depression and anxiety was confirmed by a medical practitioner,” said Dr. Keefer.
The results suggest that current efforts to screen IBD patients for depression and anxiety may not be enough, according to Stephen Lupe, PsyD, who was also asked to comment on the study. He noted that almost half of the patients had symptoms of anxiety or depression as measured by the Hospital Anxiety and Depression Score (HADS). “We’re missing all kinds of people,” said Dr. Lupe, who is director of behavioral medicine for the department of gastroenterology, hepatology, and nutrition at the Cleveland Clinic. He cited other data that show that, if someone develops depression, they are more likely to have a surgical outcome, and they are more likely to have problems with medication adherence. They likely will have more flares and less time in remission. “We need to be screening for it as part of care,” he said.
The researchers prospectively studied 585 IBD patients who were in clinical remission at 8 centers in Europe and Israel between September 2020 and March 2021. Participants filled out the HADS and The Stanford Presenteeism scale (SPS-6). A total of 62.2% of the participants had CD; 53.0% were male. Participants’ mean age was 39 years. Among the group, 10.8% had a pre existing diagnosis of anxiety or depression at the time of IBD diagnosis, and an additional 14.2% were later diagnosed with anxiety or depression.
Less than half, 46.1%, of IBD patients had a score 8 or higher in the HADS-anxiety (HADS-A) or HADS-depression (HADS-D) subscale, a cutoff that suggests evidence of clinical depression or anxiety. A total of 27.4% had a score of 11 or higher, indicating a mood disorder. High HADS-A score was associated with female gender (odds ratio, 1.91; P < 0.05), long duration of disease (OR, 1.04; P < 0.01), and perianal disease (P < 0.023). The authors speculate that the latter result may be due to a higher burden of symptoms. Three-quarters, 74.5%, of patients were employed; 34.0% experienced presenteeism as defined by SPS-6 score less than or equal to 18.
The researchers found that 23.0% of the patients were sedentary, and this was more common among individuals with HADS-A or HADS-D scores greater than or equal to 8. Among those experiencing presenteeism, 50% were sedentary, 29.4% were active, and 20.6% were moderately active (P < 0.01). Individuals with higher HADS-A or HADS-D scores had a greater likelihood of being sedentary (P < 0.05).
One limitation of the study was that the questionnaires were translated into the respective languages and scores were taken at only one time point.
“Rather than relying on the patient to come forward and seek help,” physicians should familiarize themselves with these validated screening tools “in order to increase the diagnostic rate of such pathologies and enable a better holistic care for the IBD patients,” the authors concluded. “Active involvement of a psychologist and/or a psychiatrist, as part of the IBD team, should be pursued to further improve the patients’ quality of life, which has emerged as one of the top priority outcomes in IBD.”
Dr. Lupe said that the findings regarding presenteeism are consistent with his experience. He pointed out that IBD patients must be more aware of their body and vigilant in managing symptoms, and he speculated that that could detract from concentration at work. He said that the study shows the need for a holistic approach to treatment. “When someone is coping with a chronic disease, like ulcerative colitis or Crohn’s disease, it affects the whole person,” including psychologically, professionally, and personally. “These are bidirectional relationships, so that if someone’s social life starts falling down, it’s more contributory to the development of something like depression and anxiety, and maybe that’s contributory to complications that come up in a disease state like Crohn’s disease or ulcerative colitis.”
The study did not receive funding, but two authors disclosed relations with AbbVie, Janssen, Pfizer, and other companies. Dr. Keefer is a cofounder and has equity ownership In Trellus Health. Dr. Lupe has no relevant financial disclosures.
Anxiety and depression are common among individuals with inflammatory bowel disease (IBD) who are in remission, and the conditions are linked to unemployment and presenteeism, according to a prospective study.
Previous studies have found a heightened risk of anxiety and depression in IBD, as well as an association with poor treatment compliance and greater morbidity. Presenteeism, defined as reduced productivity due to a physical or mental condition, is increasingly recognized as an indirect economic cost of chronic conditions that may exact a higher cost than absenteeism.
More than one-third of patients with IBD experienced presenteeism in one study. Other studies have examined exercise in chronic diseases, and most find an association between more exercise and lower rates of anxiety and depression. To date, few studies have examined a combination of physical activity, mental health, and presenteeism in the context of IBD.
The new study, published in the Journal of Crohn’s and Colitis, “is very important, as presenteeism is not commonly discussed in any formal, measurable way in the IBD space,” said Laurie Keefer, PhD, professor of medicine and a gastropsychologist at Icahn School of Medicine, who was asked to comment on the research. “While conducted in Europe and Israel, the study also has relevance in the U.S. since, here, employers typically pay for health care – so absenteeism, presenteeism, and health care cost are all intertwined.”
“The study confirmed high rates of depression and anxiety after a diagnosis of IBD. One high-quality aspect of this study was that the diagnosis of depression and anxiety was confirmed by a medical practitioner,” said Dr. Keefer.
The results suggest that current efforts to screen IBD patients for depression and anxiety may not be enough, according to Stephen Lupe, PsyD, who was also asked to comment on the study. He noted that almost half of the patients had symptoms of anxiety or depression as measured by the Hospital Anxiety and Depression Score (HADS). “We’re missing all kinds of people,” said Dr. Lupe, who is director of behavioral medicine for the department of gastroenterology, hepatology, and nutrition at the Cleveland Clinic. He cited other data that show that, if someone develops depression, they are more likely to have a surgical outcome, and they are more likely to have problems with medication adherence. They likely will have more flares and less time in remission. “We need to be screening for it as part of care,” he said.
The researchers prospectively studied 585 IBD patients who were in clinical remission at 8 centers in Europe and Israel between September 2020 and March 2021. Participants filled out the HADS and The Stanford Presenteeism scale (SPS-6). A total of 62.2% of the participants had CD; 53.0% were male. Participants’ mean age was 39 years. Among the group, 10.8% had a pre existing diagnosis of anxiety or depression at the time of IBD diagnosis, and an additional 14.2% were later diagnosed with anxiety or depression.
Less than half, 46.1%, of IBD patients had a score 8 or higher in the HADS-anxiety (HADS-A) or HADS-depression (HADS-D) subscale, a cutoff that suggests evidence of clinical depression or anxiety. A total of 27.4% had a score of 11 or higher, indicating a mood disorder. High HADS-A score was associated with female gender (odds ratio, 1.91; P < 0.05), long duration of disease (OR, 1.04; P < 0.01), and perianal disease (P < 0.023). The authors speculate that the latter result may be due to a higher burden of symptoms. Three-quarters, 74.5%, of patients were employed; 34.0% experienced presenteeism as defined by SPS-6 score less than or equal to 18.
The researchers found that 23.0% of the patients were sedentary, and this was more common among individuals with HADS-A or HADS-D scores greater than or equal to 8. Among those experiencing presenteeism, 50% were sedentary, 29.4% were active, and 20.6% were moderately active (P < 0.01). Individuals with higher HADS-A or HADS-D scores had a greater likelihood of being sedentary (P < 0.05).
One limitation of the study was that the questionnaires were translated into the respective languages and scores were taken at only one time point.
“Rather than relying on the patient to come forward and seek help,” physicians should familiarize themselves with these validated screening tools “in order to increase the diagnostic rate of such pathologies and enable a better holistic care for the IBD patients,” the authors concluded. “Active involvement of a psychologist and/or a psychiatrist, as part of the IBD team, should be pursued to further improve the patients’ quality of life, which has emerged as one of the top priority outcomes in IBD.”
Dr. Lupe said that the findings regarding presenteeism are consistent with his experience. He pointed out that IBD patients must be more aware of their body and vigilant in managing symptoms, and he speculated that that could detract from concentration at work. He said that the study shows the need for a holistic approach to treatment. “When someone is coping with a chronic disease, like ulcerative colitis or Crohn’s disease, it affects the whole person,” including psychologically, professionally, and personally. “These are bidirectional relationships, so that if someone’s social life starts falling down, it’s more contributory to the development of something like depression and anxiety, and maybe that’s contributory to complications that come up in a disease state like Crohn’s disease or ulcerative colitis.”
The study did not receive funding, but two authors disclosed relations with AbbVie, Janssen, Pfizer, and other companies. Dr. Keefer is a cofounder and has equity ownership In Trellus Health. Dr. Lupe has no relevant financial disclosures.
Anxiety and depression are common among individuals with inflammatory bowel disease (IBD) who are in remission, and the conditions are linked to unemployment and presenteeism, according to a prospective study.
Previous studies have found a heightened risk of anxiety and depression in IBD, as well as an association with poor treatment compliance and greater morbidity. Presenteeism, defined as reduced productivity due to a physical or mental condition, is increasingly recognized as an indirect economic cost of chronic conditions that may exact a higher cost than absenteeism.
More than one-third of patients with IBD experienced presenteeism in one study. Other studies have examined exercise in chronic diseases, and most find an association between more exercise and lower rates of anxiety and depression. To date, few studies have examined a combination of physical activity, mental health, and presenteeism in the context of IBD.
The new study, published in the Journal of Crohn’s and Colitis, “is very important, as presenteeism is not commonly discussed in any formal, measurable way in the IBD space,” said Laurie Keefer, PhD, professor of medicine and a gastropsychologist at Icahn School of Medicine, who was asked to comment on the research. “While conducted in Europe and Israel, the study also has relevance in the U.S. since, here, employers typically pay for health care – so absenteeism, presenteeism, and health care cost are all intertwined.”
“The study confirmed high rates of depression and anxiety after a diagnosis of IBD. One high-quality aspect of this study was that the diagnosis of depression and anxiety was confirmed by a medical practitioner,” said Dr. Keefer.
The results suggest that current efforts to screen IBD patients for depression and anxiety may not be enough, according to Stephen Lupe, PsyD, who was also asked to comment on the study. He noted that almost half of the patients had symptoms of anxiety or depression as measured by the Hospital Anxiety and Depression Score (HADS). “We’re missing all kinds of people,” said Dr. Lupe, who is director of behavioral medicine for the department of gastroenterology, hepatology, and nutrition at the Cleveland Clinic. He cited other data that show that, if someone develops depression, they are more likely to have a surgical outcome, and they are more likely to have problems with medication adherence. They likely will have more flares and less time in remission. “We need to be screening for it as part of care,” he said.
The researchers prospectively studied 585 IBD patients who were in clinical remission at 8 centers in Europe and Israel between September 2020 and March 2021. Participants filled out the HADS and The Stanford Presenteeism scale (SPS-6). A total of 62.2% of the participants had CD; 53.0% were male. Participants’ mean age was 39 years. Among the group, 10.8% had a pre existing diagnosis of anxiety or depression at the time of IBD diagnosis, and an additional 14.2% were later diagnosed with anxiety or depression.
Less than half, 46.1%, of IBD patients had a score 8 or higher in the HADS-anxiety (HADS-A) or HADS-depression (HADS-D) subscale, a cutoff that suggests evidence of clinical depression or anxiety. A total of 27.4% had a score of 11 or higher, indicating a mood disorder. High HADS-A score was associated with female gender (odds ratio, 1.91; P < 0.05), long duration of disease (OR, 1.04; P < 0.01), and perianal disease (P < 0.023). The authors speculate that the latter result may be due to a higher burden of symptoms. Three-quarters, 74.5%, of patients were employed; 34.0% experienced presenteeism as defined by SPS-6 score less than or equal to 18.
The researchers found that 23.0% of the patients were sedentary, and this was more common among individuals with HADS-A or HADS-D scores greater than or equal to 8. Among those experiencing presenteeism, 50% were sedentary, 29.4% were active, and 20.6% were moderately active (P < 0.01). Individuals with higher HADS-A or HADS-D scores had a greater likelihood of being sedentary (P < 0.05).
One limitation of the study was that the questionnaires were translated into the respective languages and scores were taken at only one time point.
“Rather than relying on the patient to come forward and seek help,” physicians should familiarize themselves with these validated screening tools “in order to increase the diagnostic rate of such pathologies and enable a better holistic care for the IBD patients,” the authors concluded. “Active involvement of a psychologist and/or a psychiatrist, as part of the IBD team, should be pursued to further improve the patients’ quality of life, which has emerged as one of the top priority outcomes in IBD.”
Dr. Lupe said that the findings regarding presenteeism are consistent with his experience. He pointed out that IBD patients must be more aware of their body and vigilant in managing symptoms, and he speculated that that could detract from concentration at work. He said that the study shows the need for a holistic approach to treatment. “When someone is coping with a chronic disease, like ulcerative colitis or Crohn’s disease, it affects the whole person,” including psychologically, professionally, and personally. “These are bidirectional relationships, so that if someone’s social life starts falling down, it’s more contributory to the development of something like depression and anxiety, and maybe that’s contributory to complications that come up in a disease state like Crohn’s disease or ulcerative colitis.”
The study did not receive funding, but two authors disclosed relations with AbbVie, Janssen, Pfizer, and other companies. Dr. Keefer is a cofounder and has equity ownership In Trellus Health. Dr. Lupe has no relevant financial disclosures.
REPORTING FROM JOURNAL OF CROHN'S AND COLITIS
Atypical anxiety offers intervention target in Parkinson’s disease
Anxiety is common in Parkinson’s disease (PD) and has been shown to increase functional disability and decrease quality of life, but atypical presentations of anxiety are underrecognized and often undertreated in PD patients, wrote Nadeeka N. Dissanayaka, PhD, of the University of Queensland, Brisbane, Australia, and colleagues.
In a study published in the American Journal of Geriatric Psychiatry , the researchers conducted a systematic review of 60 studies to better characterize atypical PD-related anxiety. Fourteen studies involved Anxiety Not Otherwise Specified (NOS), 31 included fluctuating anxiety symptoms, and 22 included Fear of Falling (FOF).
Overall, the average prevalence rate for anxiety disorders in the PD population was 31%.
Anxiety NOS, fluctuating anxiety, and FOF accounted for a weighted mean prevalence of 14.9%, 34.19%, and 51.5%, respectively.
The symptomatology of anxiety NOS included psychological distress about the PD diagnosis, insecurity about the future, fear of losing control of motor and bodily functions, and social embarrassment. Clinically, anxiety NOS was associated with a range of factors including minor depression, on-off motor symptoms, muscle cramps, poor quality of life, and gait impairment.
The symptomatology of fluctuating anxiety was assessed in 9 studies of the “on” motor state and 16 studies of both “on” and “off.” Symptoms associated with the off state included panic attacks, feeling anxious or sad, and avoiding situations, as well as palpitations, dizziness, chills, and hot flashes.
Clinically, studies showed that anxiety was more severe in the off-medication state, and symptoms were reduced in the on state. Data from some studies showed that fluctuating anxiety was more common in PD patients who were female, and who had a younger age of PD onset and longer disease duration.
The symptomatology of FOF included associations between FOF and difficulty with walking and gait: Using a walker or other device, more frequent freezing in place, hesitation when turning, and slower speed while walking. Clinically, characteristics associated with FOF included older age, needing assistance for activities of daily living, a history of falls, and reduced quality of life.
The results of the review were limited by several factors including the varying assessment techniques, and the lack of data on treatment for atypical anxiety in PD, the researchers noted. “To our knowledge there are no treatment trials focused on Anxiety NOS,” and studies on the treatment of fluctuating anxiety and FOF are preliminary, they said.
However, the results support the need for early identification and classification of PD-related anxiety to improve treatment strategies and long-term outcomes, the researchers concluded. In the absence of evidence-based treatment strategies, “Given the heterogeneity of anxiety presentations in PD, the importance of tailoring interventions to meet the specific needs and unique symptom profiles of each individual cannot be overstated,” and routine screening of PD patients for anxiety every 6-12 months is recommended, they emphasized.
Dr. Dissanayaka disclosed support from the National Health and Medical Research Boosting Dementia Research Leadership Fellowship.
Anxiety is common in Parkinson’s disease (PD) and has been shown to increase functional disability and decrease quality of life, but atypical presentations of anxiety are underrecognized and often undertreated in PD patients, wrote Nadeeka N. Dissanayaka, PhD, of the University of Queensland, Brisbane, Australia, and colleagues.
In a study published in the American Journal of Geriatric Psychiatry , the researchers conducted a systematic review of 60 studies to better characterize atypical PD-related anxiety. Fourteen studies involved Anxiety Not Otherwise Specified (NOS), 31 included fluctuating anxiety symptoms, and 22 included Fear of Falling (FOF).
Overall, the average prevalence rate for anxiety disorders in the PD population was 31%.
Anxiety NOS, fluctuating anxiety, and FOF accounted for a weighted mean prevalence of 14.9%, 34.19%, and 51.5%, respectively.
The symptomatology of anxiety NOS included psychological distress about the PD diagnosis, insecurity about the future, fear of losing control of motor and bodily functions, and social embarrassment. Clinically, anxiety NOS was associated with a range of factors including minor depression, on-off motor symptoms, muscle cramps, poor quality of life, and gait impairment.
The symptomatology of fluctuating anxiety was assessed in 9 studies of the “on” motor state and 16 studies of both “on” and “off.” Symptoms associated with the off state included panic attacks, feeling anxious or sad, and avoiding situations, as well as palpitations, dizziness, chills, and hot flashes.
Clinically, studies showed that anxiety was more severe in the off-medication state, and symptoms were reduced in the on state. Data from some studies showed that fluctuating anxiety was more common in PD patients who were female, and who had a younger age of PD onset and longer disease duration.
The symptomatology of FOF included associations between FOF and difficulty with walking and gait: Using a walker or other device, more frequent freezing in place, hesitation when turning, and slower speed while walking. Clinically, characteristics associated with FOF included older age, needing assistance for activities of daily living, a history of falls, and reduced quality of life.
The results of the review were limited by several factors including the varying assessment techniques, and the lack of data on treatment for atypical anxiety in PD, the researchers noted. “To our knowledge there are no treatment trials focused on Anxiety NOS,” and studies on the treatment of fluctuating anxiety and FOF are preliminary, they said.
However, the results support the need for early identification and classification of PD-related anxiety to improve treatment strategies and long-term outcomes, the researchers concluded. In the absence of evidence-based treatment strategies, “Given the heterogeneity of anxiety presentations in PD, the importance of tailoring interventions to meet the specific needs and unique symptom profiles of each individual cannot be overstated,” and routine screening of PD patients for anxiety every 6-12 months is recommended, they emphasized.
Dr. Dissanayaka disclosed support from the National Health and Medical Research Boosting Dementia Research Leadership Fellowship.
Anxiety is common in Parkinson’s disease (PD) and has been shown to increase functional disability and decrease quality of life, but atypical presentations of anxiety are underrecognized and often undertreated in PD patients, wrote Nadeeka N. Dissanayaka, PhD, of the University of Queensland, Brisbane, Australia, and colleagues.
In a study published in the American Journal of Geriatric Psychiatry , the researchers conducted a systematic review of 60 studies to better characterize atypical PD-related anxiety. Fourteen studies involved Anxiety Not Otherwise Specified (NOS), 31 included fluctuating anxiety symptoms, and 22 included Fear of Falling (FOF).
Overall, the average prevalence rate for anxiety disorders in the PD population was 31%.
Anxiety NOS, fluctuating anxiety, and FOF accounted for a weighted mean prevalence of 14.9%, 34.19%, and 51.5%, respectively.
The symptomatology of anxiety NOS included psychological distress about the PD diagnosis, insecurity about the future, fear of losing control of motor and bodily functions, and social embarrassment. Clinically, anxiety NOS was associated with a range of factors including minor depression, on-off motor symptoms, muscle cramps, poor quality of life, and gait impairment.
The symptomatology of fluctuating anxiety was assessed in 9 studies of the “on” motor state and 16 studies of both “on” and “off.” Symptoms associated with the off state included panic attacks, feeling anxious or sad, and avoiding situations, as well as palpitations, dizziness, chills, and hot flashes.
Clinically, studies showed that anxiety was more severe in the off-medication state, and symptoms were reduced in the on state. Data from some studies showed that fluctuating anxiety was more common in PD patients who were female, and who had a younger age of PD onset and longer disease duration.
The symptomatology of FOF included associations between FOF and difficulty with walking and gait: Using a walker or other device, more frequent freezing in place, hesitation when turning, and slower speed while walking. Clinically, characteristics associated with FOF included older age, needing assistance for activities of daily living, a history of falls, and reduced quality of life.
The results of the review were limited by several factors including the varying assessment techniques, and the lack of data on treatment for atypical anxiety in PD, the researchers noted. “To our knowledge there are no treatment trials focused on Anxiety NOS,” and studies on the treatment of fluctuating anxiety and FOF are preliminary, they said.
However, the results support the need for early identification and classification of PD-related anxiety to improve treatment strategies and long-term outcomes, the researchers concluded. In the absence of evidence-based treatment strategies, “Given the heterogeneity of anxiety presentations in PD, the importance of tailoring interventions to meet the specific needs and unique symptom profiles of each individual cannot be overstated,” and routine screening of PD patients for anxiety every 6-12 months is recommended, they emphasized.
Dr. Dissanayaka disclosed support from the National Health and Medical Research Boosting Dementia Research Leadership Fellowship.
FROM THE AMERICAN JOURNAL OF GERIATRIC PSYCHIATRY
Study finds social media use negatively affects male and female adolescents at different ages
A cross-sectional study in the United Kingdom has revealed an association between social media use and lower life satisfaction among children and adolescents aged 10-21 years.
“[Our] study provides evidence for age- and sex-specific windows of sensitivity to social media use in adolescence,” lead author Amy Orben, PhD, of the University of Cambridge (England), and colleagues wrote. The findings were published in Nature Communications.
The researchers analyzed cross-sectional and longitudinal data from the Understanding Society dataset and the Millennium Cohort Study. The cross-sectional data was used to investigate the existence of developmental windows of sensitivity to social media, while the longitudinal data was used to evaluate whether sex-specific windows of sensitivity to social media were present during the adolescence period.
These two datasets comprised 84,011 participants aged 10-80 years old. After applying the modeling framework, 17,409 participants aged 10-21 years were included in the analysis.
Longitudinal analyses revealed different developmental windows of sensitivity to social media during adolescence, with higher estimated social media use predicting lower life satisfaction scores 1 year later (regression coefficient [beta], −0.02; 95% confidence interval, −0.03 to −0.01; P = .004).
Among females, the researchers observed a window of sensitivity to social media between the ages of 11 and 13, with higher estimated social media use predicting lower life satisfaction ratings 1 year later (age 11: beta, −0.11; 95% CI, −0.21 to −0.02; P = .020; age 12: beta, −0.14; 95% CI, −0.22 to −0.07; P < .001; age 13: beta, −0.08; 95% CI, −0.15 to −0.01; P = .019).
Among males, a similar window was observed between the ages of 14 and 15 (age 14: beta, −0.10; 95% CI, −0.17 to −0.03; P = .005; age 15: beta, –0.18; 95% CI, −0.29 to −0.08; P = .001).
Furthermore, they showed that a later increase in sensitivity to social media, which was present at age 19 for both females and males, suggested a different underlying process was present in late adolescence (females: beta, −0.16; 95% CI, −0.25 to −0.07; P < .001; males: beta, −0.16; 95% CI, −0.26 to −0.07; P = .001).
“Speculatively, this might be related to changes in the social environment such as a move away from home and subsequent disruptions in social networks,” the researchers wrote.
Importantly, Dr. Orben and colleagues noted that these results should be interpreted with caution. Owing to the cross-sectional nature of the data, causality cannot be inferred from these findings.
“The findings reported here may enable investigation of potential mechanisms of interest, for example, in datasets with pubertal or additional social measurements,” they wrote. “One could also carry out more targeted investigations, for example, by examining the mental health measures only completed by select age ranges in the datasets.”
Digital literacy is important, expert says
“Digital literacy and education about social media use is warranted for all ages, starting young,” Yalda T. Uhls, MBA, PhD, of the department of psychology at the University of California, Los Angeles, said in an interview. “Attending to underlying issues for vulnerable ages, such as anxiety, as well as parental support is critical.”
“I would urge social media platforms to pay attention to what kinds of content they are making available to ensure the highest possible quality, and to embed things like suggestions for pauses and other ways to check in on someone who may be experiencing distress when on socials,” Dr. Uhls said. “We also need to increase access to mental health resources for young people and social media could help provide information for those experiencing issues.”
This study was supported by the University of Cambridge and the UK Medical Research Council. The authors reported no relevant disclosures. Dr. Uhls had no relevant disclosures.
A cross-sectional study in the United Kingdom has revealed an association between social media use and lower life satisfaction among children and adolescents aged 10-21 years.
“[Our] study provides evidence for age- and sex-specific windows of sensitivity to social media use in adolescence,” lead author Amy Orben, PhD, of the University of Cambridge (England), and colleagues wrote. The findings were published in Nature Communications.
The researchers analyzed cross-sectional and longitudinal data from the Understanding Society dataset and the Millennium Cohort Study. The cross-sectional data was used to investigate the existence of developmental windows of sensitivity to social media, while the longitudinal data was used to evaluate whether sex-specific windows of sensitivity to social media were present during the adolescence period.
These two datasets comprised 84,011 participants aged 10-80 years old. After applying the modeling framework, 17,409 participants aged 10-21 years were included in the analysis.
Longitudinal analyses revealed different developmental windows of sensitivity to social media during adolescence, with higher estimated social media use predicting lower life satisfaction scores 1 year later (regression coefficient [beta], −0.02; 95% confidence interval, −0.03 to −0.01; P = .004).
Among females, the researchers observed a window of sensitivity to social media between the ages of 11 and 13, with higher estimated social media use predicting lower life satisfaction ratings 1 year later (age 11: beta, −0.11; 95% CI, −0.21 to −0.02; P = .020; age 12: beta, −0.14; 95% CI, −0.22 to −0.07; P < .001; age 13: beta, −0.08; 95% CI, −0.15 to −0.01; P = .019).
Among males, a similar window was observed between the ages of 14 and 15 (age 14: beta, −0.10; 95% CI, −0.17 to −0.03; P = .005; age 15: beta, –0.18; 95% CI, −0.29 to −0.08; P = .001).
Furthermore, they showed that a later increase in sensitivity to social media, which was present at age 19 for both females and males, suggested a different underlying process was present in late adolescence (females: beta, −0.16; 95% CI, −0.25 to −0.07; P < .001; males: beta, −0.16; 95% CI, −0.26 to −0.07; P = .001).
“Speculatively, this might be related to changes in the social environment such as a move away from home and subsequent disruptions in social networks,” the researchers wrote.
Importantly, Dr. Orben and colleagues noted that these results should be interpreted with caution. Owing to the cross-sectional nature of the data, causality cannot be inferred from these findings.
“The findings reported here may enable investigation of potential mechanisms of interest, for example, in datasets with pubertal or additional social measurements,” they wrote. “One could also carry out more targeted investigations, for example, by examining the mental health measures only completed by select age ranges in the datasets.”
Digital literacy is important, expert says
“Digital literacy and education about social media use is warranted for all ages, starting young,” Yalda T. Uhls, MBA, PhD, of the department of psychology at the University of California, Los Angeles, said in an interview. “Attending to underlying issues for vulnerable ages, such as anxiety, as well as parental support is critical.”
“I would urge social media platforms to pay attention to what kinds of content they are making available to ensure the highest possible quality, and to embed things like suggestions for pauses and other ways to check in on someone who may be experiencing distress when on socials,” Dr. Uhls said. “We also need to increase access to mental health resources for young people and social media could help provide information for those experiencing issues.”
This study was supported by the University of Cambridge and the UK Medical Research Council. The authors reported no relevant disclosures. Dr. Uhls had no relevant disclosures.
A cross-sectional study in the United Kingdom has revealed an association between social media use and lower life satisfaction among children and adolescents aged 10-21 years.
“[Our] study provides evidence for age- and sex-specific windows of sensitivity to social media use in adolescence,” lead author Amy Orben, PhD, of the University of Cambridge (England), and colleagues wrote. The findings were published in Nature Communications.
The researchers analyzed cross-sectional and longitudinal data from the Understanding Society dataset and the Millennium Cohort Study. The cross-sectional data was used to investigate the existence of developmental windows of sensitivity to social media, while the longitudinal data was used to evaluate whether sex-specific windows of sensitivity to social media were present during the adolescence period.
These two datasets comprised 84,011 participants aged 10-80 years old. After applying the modeling framework, 17,409 participants aged 10-21 years were included in the analysis.
Longitudinal analyses revealed different developmental windows of sensitivity to social media during adolescence, with higher estimated social media use predicting lower life satisfaction scores 1 year later (regression coefficient [beta], −0.02; 95% confidence interval, −0.03 to −0.01; P = .004).
Among females, the researchers observed a window of sensitivity to social media between the ages of 11 and 13, with higher estimated social media use predicting lower life satisfaction ratings 1 year later (age 11: beta, −0.11; 95% CI, −0.21 to −0.02; P = .020; age 12: beta, −0.14; 95% CI, −0.22 to −0.07; P < .001; age 13: beta, −0.08; 95% CI, −0.15 to −0.01; P = .019).
Among males, a similar window was observed between the ages of 14 and 15 (age 14: beta, −0.10; 95% CI, −0.17 to −0.03; P = .005; age 15: beta, –0.18; 95% CI, −0.29 to −0.08; P = .001).
Furthermore, they showed that a later increase in sensitivity to social media, which was present at age 19 for both females and males, suggested a different underlying process was present in late adolescence (females: beta, −0.16; 95% CI, −0.25 to −0.07; P < .001; males: beta, −0.16; 95% CI, −0.26 to −0.07; P = .001).
“Speculatively, this might be related to changes in the social environment such as a move away from home and subsequent disruptions in social networks,” the researchers wrote.
Importantly, Dr. Orben and colleagues noted that these results should be interpreted with caution. Owing to the cross-sectional nature of the data, causality cannot be inferred from these findings.
“The findings reported here may enable investigation of potential mechanisms of interest, for example, in datasets with pubertal or additional social measurements,” they wrote. “One could also carry out more targeted investigations, for example, by examining the mental health measures only completed by select age ranges in the datasets.”
Digital literacy is important, expert says
“Digital literacy and education about social media use is warranted for all ages, starting young,” Yalda T. Uhls, MBA, PhD, of the department of psychology at the University of California, Los Angeles, said in an interview. “Attending to underlying issues for vulnerable ages, such as anxiety, as well as parental support is critical.”
“I would urge social media platforms to pay attention to what kinds of content they are making available to ensure the highest possible quality, and to embed things like suggestions for pauses and other ways to check in on someone who may be experiencing distress when on socials,” Dr. Uhls said. “We also need to increase access to mental health resources for young people and social media could help provide information for those experiencing issues.”
This study was supported by the University of Cambridge and the UK Medical Research Council. The authors reported no relevant disclosures. Dr. Uhls had no relevant disclosures.
FROM NATURE COMMUNICATIONS
Microdosing psychedelics: Untapped potential in psychiatry?
In her month-long memoir, A Really Good Day: How Microdosing Made a Mega Difference in My Mood, My Marriage, and My Life (Knopf, 2017), author Ayelet Waldman turns herself into a one-woman experiment.
Over a single month she takes one-tenth of a recreational dose of LSD every third day. She plots her emotions, her productivity, and her pain along the way. Ms. Waldman obtains the LSD in a single vial, enough for 10 doses, from a researcher, who is retiring. What she’s looking for, she tells the reader, is a really good day – something that has been elusive in her turbulent life.

Although psychedelics remain illegal for both recreational and therapeutic use, they are increasingly being studied at academic centers, and there is hope that they will offer something that our traditional medications might not. However, these are not “micro” doses, but full doses of psychedelic agents that induce clinically-monitored “trips” in order to treat conditions such as depression, anorexia nervosa, or for smoking cessation, to name just a few.
Yet
Because these drugs are illegal under most circumstances, many of the studies involve surveys of users in their natural environments who are already microdosing in an uncontrolled manner. In a 2019 study published in PLOS One, Vince Polito and Richard Stevenson, from Macquarie University, Sydney, gave daily surveys of psychological functioning to 98 microdosers over 6 weeks. Several participants were excluded for using doses that were too high or for concurrent use of other illicit substances.
Whereas the authors found that many people claimed to have positive experiences, there was an increase in neuroticism in some of the subjects. There was no control group and no uniformity to what the subject claimed to be ingesting with regard to dose, frequency, substance, or verification of the chemical content.
University of Chicago neuroscientist Harriet De Wit, PhD, leads one of the few laboratories that conducts controlled, double-blind studies looking at microdosing LSD.
“With microdosing there are expectations, and we don’t know if it’s the expectation or the agent that is making a difference,” she explained. And when asked who in her experience is experimenting with microdosing psychedelics, she expounded “Everybody under the sun!”
Dr. De Wit notes that people microdose to increase their creativity, productivity, focus, and energy, to heighten their spiritual awareness, improve empathy and social relational skills, and to improve their mood – all purported benefits of low-dose psychedelics.
Her group published a study in Addiction Biology, in which 39 subjects were administered low doses of LSD four times over 2 weeks. To address the issues of expectation, the subjects were not told they were participating in a study of hallucinogens specifically but were instead given a list of pharmaceuticals in different classes that they might be given. Microdoses of LSD did not improve either mood or performance, but they did appear to be safe, and they produced no adverse effects.
To date, studies on microdosing have looked at their effects on healthy populations, and the practice has been associated with “Silicon Valley techies” looking for performance enhancement. Ms. Waldman, however, is different.
She is open about her diagnosis of bipolar disorder, and her long history with therapy and medications. As she describes herself in the beginning of her book, she is emotionally uncomfortable, and both irritable and reactive to the point that her life is propelled by interpersonal chaos. In her uncontrolled ‘study,’ she is an N of 1, and she is pleased with the results. Microdosing, she believes, helped her become less irritable, more resilient, and in fact, have some very good days.
By the end of her memoir, she was looking for a way to continue microdosing but was unsure how to safely obtain more LSD and be certain of its purity. Her experience does raise the possibility that microdoses may have therapeutic benefits in people with certain psychiatric conditions, but this has yet to be studied.
J. Raymond DePaulo Jr., MD, is the chair of the National Network of Depression Centers and a distinguished service professor at Johns Hopkins Hospital, Baltimore. “Microdosing of psychedelics is very problematic for two equally serious reasons,” he cautioned. “There is no control over what it is that people are actually taking, it is completely unstudied scientifically, and there is no agreement on what a ‘micro’ dose is.”
He noted that one of his patients thought he was taking psilocybin. A chemical analysis was done that revealed the agent to contain a combination of THC, a stimulant, morphine, and fluoxetine. There wasn’t a trace of psilocybin. “Mislabeling is the rule, not the exception,” Dr. DePaulo has concluded.
He also believes the placebo effect has a powerful role with microdosing. “It’s not working because of what is in the pill, more likely it is working because of what is advertised to be in it.”
Ms. De Wit noted that when she started her study, she tried to find people who were elevated on measures of depression or anxiety, but she was not looking for a specific clinical population of patients with these clinical diagnoses. “We found a handful of people, and they improved, but so did those in the placebo group; they all got better.”
Psychedelic agents interact with antidepressants, so subjects in controlled studies need to go off their medications before enrolling – this is a limiting factor in studies of both macro- and microdosing. Ms. De Wit also notes that there are logistical and practical obstacles – it is difficult to get approval to use these agents, and the patients have to remain in the lab and be observed for several hours after they are administered, just as with standard doses.
As might be expected, data collection and anecdotal microdosing experiences are rampant on the internet. The social media forum Reddit alone boasts 192,000 members in its microdosing group, while Imperial College London invites microdosers to take part in surveys intended to add to the body of knowledge. But despite its popularity, there is little in the way of prospective, agent-verified, placebo-controlled research exploring whether or not microdosing is truly beneficial beyond just anecdotal evidence.
Perhaps microdosing is a fad, or perhaps it offers some benefits to some people. Given the current interest in the therapeutic uses of psychedelics, it would be useful to have controlled studies of lower doses that don’t carry the risk of “bad trips.”
Certainly, psychiatry could use more agents to address mental health issues, and society might benefit from the use of agents that are proven to be evidence-based options for improving creativity and productivity. Anything that has potential to reduce psychiatric suffering seems worthy of further study to delineate which populations could be helped or harmed.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins in Baltimore. Dr. Miller has no conflicts of interest.
A version of this article first appeared on Medscape.com.
In her month-long memoir, A Really Good Day: How Microdosing Made a Mega Difference in My Mood, My Marriage, and My Life (Knopf, 2017), author Ayelet Waldman turns herself into a one-woman experiment.
Over a single month she takes one-tenth of a recreational dose of LSD every third day. She plots her emotions, her productivity, and her pain along the way. Ms. Waldman obtains the LSD in a single vial, enough for 10 doses, from a researcher, who is retiring. What she’s looking for, she tells the reader, is a really good day – something that has been elusive in her turbulent life.
Although psychedelics remain illegal for both recreational and therapeutic use, they are increasingly being studied at academic centers, and there is hope that they will offer something that our traditional medications might not. However, these are not “micro” doses, but full doses of psychedelic agents that induce clinically-monitored “trips” in order to treat conditions such as depression, anorexia nervosa, or for smoking cessation, to name just a few.
Yet
Because these drugs are illegal under most circumstances, many of the studies involve surveys of users in their natural environments who are already microdosing in an uncontrolled manner. In a 2019 study published in PLOS One, Vince Polito and Richard Stevenson, from Macquarie University, Sydney, gave daily surveys of psychological functioning to 98 microdosers over 6 weeks. Several participants were excluded for using doses that were too high or for concurrent use of other illicit substances.
Whereas the authors found that many people claimed to have positive experiences, there was an increase in neuroticism in some of the subjects. There was no control group and no uniformity to what the subject claimed to be ingesting with regard to dose, frequency, substance, or verification of the chemical content.
University of Chicago neuroscientist Harriet De Wit, PhD, leads one of the few laboratories that conducts controlled, double-blind studies looking at microdosing LSD.
“With microdosing there are expectations, and we don’t know if it’s the expectation or the agent that is making a difference,” she explained. And when asked who in her experience is experimenting with microdosing psychedelics, she expounded “Everybody under the sun!”
Dr. De Wit notes that people microdose to increase their creativity, productivity, focus, and energy, to heighten their spiritual awareness, improve empathy and social relational skills, and to improve their mood – all purported benefits of low-dose psychedelics.
Her group published a study in Addiction Biology, in which 39 subjects were administered low doses of LSD four times over 2 weeks. To address the issues of expectation, the subjects were not told they were participating in a study of hallucinogens specifically but were instead given a list of pharmaceuticals in different classes that they might be given. Microdoses of LSD did not improve either mood or performance, but they did appear to be safe, and they produced no adverse effects.
To date, studies on microdosing have looked at their effects on healthy populations, and the practice has been associated with “Silicon Valley techies” looking for performance enhancement. Ms. Waldman, however, is different.
She is open about her diagnosis of bipolar disorder, and her long history with therapy and medications. As she describes herself in the beginning of her book, she is emotionally uncomfortable, and both irritable and reactive to the point that her life is propelled by interpersonal chaos. In her uncontrolled ‘study,’ she is an N of 1, and she is pleased with the results. Microdosing, she believes, helped her become less irritable, more resilient, and in fact, have some very good days.
By the end of her memoir, she was looking for a way to continue microdosing but was unsure how to safely obtain more LSD and be certain of its purity. Her experience does raise the possibility that microdoses may have therapeutic benefits in people with certain psychiatric conditions, but this has yet to be studied.
J. Raymond DePaulo Jr., MD, is the chair of the National Network of Depression Centers and a distinguished service professor at Johns Hopkins Hospital, Baltimore. “Microdosing of psychedelics is very problematic for two equally serious reasons,” he cautioned. “There is no control over what it is that people are actually taking, it is completely unstudied scientifically, and there is no agreement on what a ‘micro’ dose is.”
He noted that one of his patients thought he was taking psilocybin. A chemical analysis was done that revealed the agent to contain a combination of THC, a stimulant, morphine, and fluoxetine. There wasn’t a trace of psilocybin. “Mislabeling is the rule, not the exception,” Dr. DePaulo has concluded.
He also believes the placebo effect has a powerful role with microdosing. “It’s not working because of what is in the pill, more likely it is working because of what is advertised to be in it.”
Ms. De Wit noted that when she started her study, she tried to find people who were elevated on measures of depression or anxiety, but she was not looking for a specific clinical population of patients with these clinical diagnoses. “We found a handful of people, and they improved, but so did those in the placebo group; they all got better.”
Psychedelic agents interact with antidepressants, so subjects in controlled studies need to go off their medications before enrolling – this is a limiting factor in studies of both macro- and microdosing. Ms. De Wit also notes that there are logistical and practical obstacles – it is difficult to get approval to use these agents, and the patients have to remain in the lab and be observed for several hours after they are administered, just as with standard doses.
As might be expected, data collection and anecdotal microdosing experiences are rampant on the internet. The social media forum Reddit alone boasts 192,000 members in its microdosing group, while Imperial College London invites microdosers to take part in surveys intended to add to the body of knowledge. But despite its popularity, there is little in the way of prospective, agent-verified, placebo-controlled research exploring whether or not microdosing is truly beneficial beyond just anecdotal evidence.
Perhaps microdosing is a fad, or perhaps it offers some benefits to some people. Given the current interest in the therapeutic uses of psychedelics, it would be useful to have controlled studies of lower doses that don’t carry the risk of “bad trips.”
Certainly, psychiatry could use more agents to address mental health issues, and society might benefit from the use of agents that are proven to be evidence-based options for improving creativity and productivity. Anything that has potential to reduce psychiatric suffering seems worthy of further study to delineate which populations could be helped or harmed.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins in Baltimore. Dr. Miller has no conflicts of interest.
A version of this article first appeared on Medscape.com.
In her month-long memoir, A Really Good Day: How Microdosing Made a Mega Difference in My Mood, My Marriage, and My Life (Knopf, 2017), author Ayelet Waldman turns herself into a one-woman experiment.
Over a single month she takes one-tenth of a recreational dose of LSD every third day. She plots her emotions, her productivity, and her pain along the way. Ms. Waldman obtains the LSD in a single vial, enough for 10 doses, from a researcher, who is retiring. What she’s looking for, she tells the reader, is a really good day – something that has been elusive in her turbulent life.
Although psychedelics remain illegal for both recreational and therapeutic use, they are increasingly being studied at academic centers, and there is hope that they will offer something that our traditional medications might not. However, these are not “micro” doses, but full doses of psychedelic agents that induce clinically-monitored “trips” in order to treat conditions such as depression, anorexia nervosa, or for smoking cessation, to name just a few.
Yet
Because these drugs are illegal under most circumstances, many of the studies involve surveys of users in their natural environments who are already microdosing in an uncontrolled manner. In a 2019 study published in PLOS One, Vince Polito and Richard Stevenson, from Macquarie University, Sydney, gave daily surveys of psychological functioning to 98 microdosers over 6 weeks. Several participants were excluded for using doses that were too high or for concurrent use of other illicit substances.
Whereas the authors found that many people claimed to have positive experiences, there was an increase in neuroticism in some of the subjects. There was no control group and no uniformity to what the subject claimed to be ingesting with regard to dose, frequency, substance, or verification of the chemical content.
University of Chicago neuroscientist Harriet De Wit, PhD, leads one of the few laboratories that conducts controlled, double-blind studies looking at microdosing LSD.
“With microdosing there are expectations, and we don’t know if it’s the expectation or the agent that is making a difference,” she explained. And when asked who in her experience is experimenting with microdosing psychedelics, she expounded “Everybody under the sun!”
Dr. De Wit notes that people microdose to increase their creativity, productivity, focus, and energy, to heighten their spiritual awareness, improve empathy and social relational skills, and to improve their mood – all purported benefits of low-dose psychedelics.
Her group published a study in Addiction Biology, in which 39 subjects were administered low doses of LSD four times over 2 weeks. To address the issues of expectation, the subjects were not told they were participating in a study of hallucinogens specifically but were instead given a list of pharmaceuticals in different classes that they might be given. Microdoses of LSD did not improve either mood or performance, but they did appear to be safe, and they produced no adverse effects.
To date, studies on microdosing have looked at their effects on healthy populations, and the practice has been associated with “Silicon Valley techies” looking for performance enhancement. Ms. Waldman, however, is different.
She is open about her diagnosis of bipolar disorder, and her long history with therapy and medications. As she describes herself in the beginning of her book, she is emotionally uncomfortable, and both irritable and reactive to the point that her life is propelled by interpersonal chaos. In her uncontrolled ‘study,’ she is an N of 1, and she is pleased with the results. Microdosing, she believes, helped her become less irritable, more resilient, and in fact, have some very good days.
By the end of her memoir, she was looking for a way to continue microdosing but was unsure how to safely obtain more LSD and be certain of its purity. Her experience does raise the possibility that microdoses may have therapeutic benefits in people with certain psychiatric conditions, but this has yet to be studied.
J. Raymond DePaulo Jr., MD, is the chair of the National Network of Depression Centers and a distinguished service professor at Johns Hopkins Hospital, Baltimore. “Microdosing of psychedelics is very problematic for two equally serious reasons,” he cautioned. “There is no control over what it is that people are actually taking, it is completely unstudied scientifically, and there is no agreement on what a ‘micro’ dose is.”
He noted that one of his patients thought he was taking psilocybin. A chemical analysis was done that revealed the agent to contain a combination of THC, a stimulant, morphine, and fluoxetine. There wasn’t a trace of psilocybin. “Mislabeling is the rule, not the exception,” Dr. DePaulo has concluded.
He also believes the placebo effect has a powerful role with microdosing. “It’s not working because of what is in the pill, more likely it is working because of what is advertised to be in it.”
Ms. De Wit noted that when she started her study, she tried to find people who were elevated on measures of depression or anxiety, but she was not looking for a specific clinical population of patients with these clinical diagnoses. “We found a handful of people, and they improved, but so did those in the placebo group; they all got better.”
Psychedelic agents interact with antidepressants, so subjects in controlled studies need to go off their medications before enrolling – this is a limiting factor in studies of both macro- and microdosing. Ms. De Wit also notes that there are logistical and practical obstacles – it is difficult to get approval to use these agents, and the patients have to remain in the lab and be observed for several hours after they are administered, just as with standard doses.
As might be expected, data collection and anecdotal microdosing experiences are rampant on the internet. The social media forum Reddit alone boasts 192,000 members in its microdosing group, while Imperial College London invites microdosers to take part in surveys intended to add to the body of knowledge. But despite its popularity, there is little in the way of prospective, agent-verified, placebo-controlled research exploring whether or not microdosing is truly beneficial beyond just anecdotal evidence.
Perhaps microdosing is a fad, or perhaps it offers some benefits to some people. Given the current interest in the therapeutic uses of psychedelics, it would be useful to have controlled studies of lower doses that don’t carry the risk of “bad trips.”
Certainly, psychiatry could use more agents to address mental health issues, and society might benefit from the use of agents that are proven to be evidence-based options for improving creativity and productivity. Anything that has potential to reduce psychiatric suffering seems worthy of further study to delineate which populations could be helped or harmed.
Dr. Miller is a coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins in Baltimore. Dr. Miller has no conflicts of interest.
A version of this article first appeared on Medscape.com.
High-intensity exercise helps patients with anxiety quit smoking
DENVER –
Results from a randomized study of 150 participants reporting symptoms of anxiety showed that among daily smokers who received a personalized, high-intensity aerobic intervention, rates of smoking abstinence were nearly twice as great as for those who received a lower-intensity exercise intervention.

“We are encouraged in the sense that we feel we have a targeted [smoking cessation] intervention to tailor to people with high anxiety sensitivity,” lead author Jasper A. Smits, PhD, professor at the Institute for Mental Health Research and the department of psychology, the University of Texas at Austin, told attendees during a presentation of the findings at the Anxiety and Depression Association of America (ADAA) 2022. The findings were recently published in Addiction.
Effective as CBT
Previous research shows that relatively short periods of exercise, lasting as little as 2 weeks, were associated with reductions in anxiety equivalent to 12 weeks of cognitive-behavioral therapy (CBT).
In light of these earlier findings, Dr. Smits and colleagues investigated the effect of an exercise intervention for smoking cessation based on the knowledge that individuals with anxiety disorders are more likely to smoke and less likely to succeed in quitting.
The initial study, which was published in 2016, included 136 smokers with high “anxiety sensitivity,” a heightened sensitivity to normal sensations associated with anxiety, potentially leading to panic attacks or other disorders.
Results showed that participation in the researchers’ Smoking Treatment Enhancement Program (STEP) was associated with significant improvements in prolonged smoking abstinence among those with high anxiety sensitivity but not those with low anxiety.
Building on these results, the new study evaluated the exercise program at a community level at four YMCA centers. This time all participants had high anxiety sensitivity, defined as a score of 23 or higher on the Anxiety Sensitivity Index–3.
The study included 150 adult participants who had high anxiety, were daily smokers, were motivated to quit smoking, and who reported that they did not currently participate in regular moderate exercise.
All participants (67.3% women; mean age, 38.6 years) took part in STEP, which included a 15-week exercise intervention with a personal trainer. Of the participants, 77 individuals were randomly assigned to receive high-intensity aerobic training that targeted 60%-85% of their heart rate reserve (HRR), while the other 73 were assigned to a lower-intensity control group in which training was only targeted to 20%-40% of their HRR.
All participants also received standard behavioral support with phone- or text-based CBT and nicotine replacement therapy (NRT).
The centers’ fitness instructors served as case managers who oversaw the smoking cessation exercise regimens of high-intensity versus low-intensity exercise. A broad array of aerobic exercise options were permitted, with the instructors working with participants to personalize their regimens.
“It’s important to take into consideration patients’ preferences [and] to work with the fitness instructors to find the right activity,” Dr. Smits said. He noted that options may include intense yoga or swimming. “So I think we just need to be creative in thinking about exercise as being more than just running,” he noted.
Abstinence rate doubled
The study’s primary endpoint was abstinence, defined as biologically verified 7-day point prevalence abstinence.
Results at 6-month follow-up showed that the primary endpoint was achieved by 27.6% of the higher-intensity intervention group, compared with just 14.8% of the lower-intensity group (odds ratio, 2.2; P = .005).
“It was encouraging to see we roughly doubled the abstinence rate at the 6-month follow-up,” Dr. Smits said. “Those receiving the high-intensity exercise intervention had greater abstinence rates spanning the entire study period versus the standard treatment.”
Of note, declines in anxiety sensitivity, as measured on the Reiss-Epstein-Gursky Anxiety Sensitivity Index, were observed in both groups. However, there was no significant difference in changes between the two groups.
Dr. Smits noted the investigators initially speculated that exercise would improve cessation success in individuals with anxiety sensitivity by providing exposure to the types of sensations that may trigger their anxiety, such as sweating and an accelerated heart rate, providing an opportunity for “extinction training” by desensitizing them to these experiences.
In addition, high-intensity exercise may also mitigate other anxiety symptoms, including panic disorder, pain, depression, overeating, and posttraumatic stress disorder, Dr. Smits said.
Real-world evidence
Commenting on the findings, Sahib S. Khalsa, MD, PhD, director of clinical operations at the Laureate Institute for Brain Research and associate professor at the University of Tulsa, Oklahoma, noted that the real-world nature of the study suggests its results are widely applicable.

It is also important to note that both the current and previous studies conducted by the investigators included NRT, “and thus the effects are more likely to be reflective of a grouping of therapies, something that is more reflective of current practice,” said Dr. Khalsa, who was not involved in the research.
He noted that initiating as well as maintaining exercise motivation over longer periods is challenging.
“The study likely addressed this challenge by using fitness instructors, which may be an important criterion for successful deployment of the intervention. We also don’t know whether maintaining an active exercise regimen is critical to maintaining smoking cessation,” Dr. Khalsa added.
Dr. Smits is a consultant for Big Health. Dr. Khalsa has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
DENVER –
Results from a randomized study of 150 participants reporting symptoms of anxiety showed that among daily smokers who received a personalized, high-intensity aerobic intervention, rates of smoking abstinence were nearly twice as great as for those who received a lower-intensity exercise intervention.
“We are encouraged in the sense that we feel we have a targeted [smoking cessation] intervention to tailor to people with high anxiety sensitivity,” lead author Jasper A. Smits, PhD, professor at the Institute for Mental Health Research and the department of psychology, the University of Texas at Austin, told attendees during a presentation of the findings at the Anxiety and Depression Association of America (ADAA) 2022. The findings were recently published in Addiction.
Effective as CBT
Previous research shows that relatively short periods of exercise, lasting as little as 2 weeks, were associated with reductions in anxiety equivalent to 12 weeks of cognitive-behavioral therapy (CBT).
In light of these earlier findings, Dr. Smits and colleagues investigated the effect of an exercise intervention for smoking cessation based on the knowledge that individuals with anxiety disorders are more likely to smoke and less likely to succeed in quitting.
The initial study, which was published in 2016, included 136 smokers with high “anxiety sensitivity,” a heightened sensitivity to normal sensations associated with anxiety, potentially leading to panic attacks or other disorders.
Results showed that participation in the researchers’ Smoking Treatment Enhancement Program (STEP) was associated with significant improvements in prolonged smoking abstinence among those with high anxiety sensitivity but not those with low anxiety.
Building on these results, the new study evaluated the exercise program at a community level at four YMCA centers. This time all participants had high anxiety sensitivity, defined as a score of 23 or higher on the Anxiety Sensitivity Index–3.
The study included 150 adult participants who had high anxiety, were daily smokers, were motivated to quit smoking, and who reported that they did not currently participate in regular moderate exercise.
All participants (67.3% women; mean age, 38.6 years) took part in STEP, which included a 15-week exercise intervention with a personal trainer. Of the participants, 77 individuals were randomly assigned to receive high-intensity aerobic training that targeted 60%-85% of their heart rate reserve (HRR), while the other 73 were assigned to a lower-intensity control group in which training was only targeted to 20%-40% of their HRR.
All participants also received standard behavioral support with phone- or text-based CBT and nicotine replacement therapy (NRT).
The centers’ fitness instructors served as case managers who oversaw the smoking cessation exercise regimens of high-intensity versus low-intensity exercise. A broad array of aerobic exercise options were permitted, with the instructors working with participants to personalize their regimens.
“It’s important to take into consideration patients’ preferences [and] to work with the fitness instructors to find the right activity,” Dr. Smits said. He noted that options may include intense yoga or swimming. “So I think we just need to be creative in thinking about exercise as being more than just running,” he noted.
Abstinence rate doubled
The study’s primary endpoint was abstinence, defined as biologically verified 7-day point prevalence abstinence.
Results at 6-month follow-up showed that the primary endpoint was achieved by 27.6% of the higher-intensity intervention group, compared with just 14.8% of the lower-intensity group (odds ratio, 2.2; P = .005).
“It was encouraging to see we roughly doubled the abstinence rate at the 6-month follow-up,” Dr. Smits said. “Those receiving the high-intensity exercise intervention had greater abstinence rates spanning the entire study period versus the standard treatment.”
Of note, declines in anxiety sensitivity, as measured on the Reiss-Epstein-Gursky Anxiety Sensitivity Index, were observed in both groups. However, there was no significant difference in changes between the two groups.
Dr. Smits noted the investigators initially speculated that exercise would improve cessation success in individuals with anxiety sensitivity by providing exposure to the types of sensations that may trigger their anxiety, such as sweating and an accelerated heart rate, providing an opportunity for “extinction training” by desensitizing them to these experiences.
In addition, high-intensity exercise may also mitigate other anxiety symptoms, including panic disorder, pain, depression, overeating, and posttraumatic stress disorder, Dr. Smits said.
Real-world evidence
Commenting on the findings, Sahib S. Khalsa, MD, PhD, director of clinical operations at the Laureate Institute for Brain Research and associate professor at the University of Tulsa, Oklahoma, noted that the real-world nature of the study suggests its results are widely applicable.
It is also important to note that both the current and previous studies conducted by the investigators included NRT, “and thus the effects are more likely to be reflective of a grouping of therapies, something that is more reflective of current practice,” said Dr. Khalsa, who was not involved in the research.
He noted that initiating as well as maintaining exercise motivation over longer periods is challenging.
“The study likely addressed this challenge by using fitness instructors, which may be an important criterion for successful deployment of the intervention. We also don’t know whether maintaining an active exercise regimen is critical to maintaining smoking cessation,” Dr. Khalsa added.
Dr. Smits is a consultant for Big Health. Dr. Khalsa has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
DENVER –
Results from a randomized study of 150 participants reporting symptoms of anxiety showed that among daily smokers who received a personalized, high-intensity aerobic intervention, rates of smoking abstinence were nearly twice as great as for those who received a lower-intensity exercise intervention.
“We are encouraged in the sense that we feel we have a targeted [smoking cessation] intervention to tailor to people with high anxiety sensitivity,” lead author Jasper A. Smits, PhD, professor at the Institute for Mental Health Research and the department of psychology, the University of Texas at Austin, told attendees during a presentation of the findings at the Anxiety and Depression Association of America (ADAA) 2022. The findings were recently published in Addiction.
Effective as CBT
Previous research shows that relatively short periods of exercise, lasting as little as 2 weeks, were associated with reductions in anxiety equivalent to 12 weeks of cognitive-behavioral therapy (CBT).
In light of these earlier findings, Dr. Smits and colleagues investigated the effect of an exercise intervention for smoking cessation based on the knowledge that individuals with anxiety disorders are more likely to smoke and less likely to succeed in quitting.
The initial study, which was published in 2016, included 136 smokers with high “anxiety sensitivity,” a heightened sensitivity to normal sensations associated with anxiety, potentially leading to panic attacks or other disorders.
Results showed that participation in the researchers’ Smoking Treatment Enhancement Program (STEP) was associated with significant improvements in prolonged smoking abstinence among those with high anxiety sensitivity but not those with low anxiety.
Building on these results, the new study evaluated the exercise program at a community level at four YMCA centers. This time all participants had high anxiety sensitivity, defined as a score of 23 or higher on the Anxiety Sensitivity Index–3.
The study included 150 adult participants who had high anxiety, were daily smokers, were motivated to quit smoking, and who reported that they did not currently participate in regular moderate exercise.
All participants (67.3% women; mean age, 38.6 years) took part in STEP, which included a 15-week exercise intervention with a personal trainer. Of the participants, 77 individuals were randomly assigned to receive high-intensity aerobic training that targeted 60%-85% of their heart rate reserve (HRR), while the other 73 were assigned to a lower-intensity control group in which training was only targeted to 20%-40% of their HRR.
All participants also received standard behavioral support with phone- or text-based CBT and nicotine replacement therapy (NRT).
The centers’ fitness instructors served as case managers who oversaw the smoking cessation exercise regimens of high-intensity versus low-intensity exercise. A broad array of aerobic exercise options were permitted, with the instructors working with participants to personalize their regimens.
“It’s important to take into consideration patients’ preferences [and] to work with the fitness instructors to find the right activity,” Dr. Smits said. He noted that options may include intense yoga or swimming. “So I think we just need to be creative in thinking about exercise as being more than just running,” he noted.
Abstinence rate doubled
The study’s primary endpoint was abstinence, defined as biologically verified 7-day point prevalence abstinence.
Results at 6-month follow-up showed that the primary endpoint was achieved by 27.6% of the higher-intensity intervention group, compared with just 14.8% of the lower-intensity group (odds ratio, 2.2; P = .005).
“It was encouraging to see we roughly doubled the abstinence rate at the 6-month follow-up,” Dr. Smits said. “Those receiving the high-intensity exercise intervention had greater abstinence rates spanning the entire study period versus the standard treatment.”
Of note, declines in anxiety sensitivity, as measured on the Reiss-Epstein-Gursky Anxiety Sensitivity Index, were observed in both groups. However, there was no significant difference in changes between the two groups.
Dr. Smits noted the investigators initially speculated that exercise would improve cessation success in individuals with anxiety sensitivity by providing exposure to the types of sensations that may trigger their anxiety, such as sweating and an accelerated heart rate, providing an opportunity for “extinction training” by desensitizing them to these experiences.
In addition, high-intensity exercise may also mitigate other anxiety symptoms, including panic disorder, pain, depression, overeating, and posttraumatic stress disorder, Dr. Smits said.
Real-world evidence
Commenting on the findings, Sahib S. Khalsa, MD, PhD, director of clinical operations at the Laureate Institute for Brain Research and associate professor at the University of Tulsa, Oklahoma, noted that the real-world nature of the study suggests its results are widely applicable.
It is also important to note that both the current and previous studies conducted by the investigators included NRT, “and thus the effects are more likely to be reflective of a grouping of therapies, something that is more reflective of current practice,” said Dr. Khalsa, who was not involved in the research.
He noted that initiating as well as maintaining exercise motivation over longer periods is challenging.
“The study likely addressed this challenge by using fitness instructors, which may be an important criterion for successful deployment of the intervention. We also don’t know whether maintaining an active exercise regimen is critical to maintaining smoking cessation,” Dr. Khalsa added.
Dr. Smits is a consultant for Big Health. Dr. Khalsa has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ADAA 2022
Common eye disorder in children tied to mental illness
Misaligned eyes in children are associated with an increased prevalence of mental illness, results of a large study suggest.
“Psychiatrists who have a patient with depression or anxiety and notice that patient also has strabismus might think about the link between those two conditions and refer that patient,” study investigator Stacy L. Pineles, MD, professor, department of ophthalmology, University of California, Los Angeles, told this news organization.

The study was published online March 10 in JAMA Ophthalmology.
A common condition
Strabismus, a condition in which the eyes don’t line up or are “crossed,” is one of the most common eye diseases in children, with some estimates suggesting it affects more than 1.5 million American youth.
Patients with strabismus have problems making eye contact and are affected socially and functionally, said Dr. Pineles. They’re often met with a negative bias, as shown by children’s responses to pictures of faces with and without strabismus, she said.
There is a signal from previous research suggesting that strabismus is linked to a higher risk of mental illness. However, most of these studies were small and had relatively homogenous populations, said Dr. Pineles.
The new study includes over 12 million children (mean age, 8.0 years) from a private health insurance claims database that represents diverse races and ethnicities as well as geographic regions across the United States.
The sample included 352,636 children with strabismus and 11,652,553 children with no diagnosed eye disease who served as controls. Most participants were White (51.6%), came from a family with an annual household income of $40,000 or more (51.0%), had point-of-service insurance (68.7%), and had at least one comorbid condition (64.5%).
The study evaluated five mental illness diagnoses. These included anxiety disorder, depressive disorder, substance use or addictive disorder, bipolar disorder, and schizophrenia.
Overall, children with strabismus had a higher prevalence of all these illnesses, with the exception of substance use disorder.
After adjusting for age, sex, race and ethnicity, census region, education level of caregiver, family net worth, and presence of at least one comorbid condition, the odds ratios among those with versus without strabismus were: 2.01 (95% confidence interval, 1.99-2.04; P < .001) for anxiety disorder, 1.83 (95% CI, 1.76-1.90; P < .001) for schizophrenia, 1.64 (95% CI, 1.59-1.70; P < .001) for bipolar disorder, and 1.61 (95% CI, 1.59-1.63; P < .001) for depressive disorder.
Substance use disorder had a negative unadjusted association with strabismus, but after adjustment for confounders, the association was not significant (OR, 0.99; 95% CI, 0.97-1.02; P = .48).
Dr. Pineles noted that the study participants, who were all under age 19, may be too young to have substance use disorders.
The results for substance use disorders provided something of an “internal control” and reaffirmed results for the other four conditions, said Dr. Pineles.
“When you do research on such a large database, you’re very likely to find significant associations; the dataset is so large that even very small differences become statistically significant. It was interesting that not everything gave us a positive association.”
Researchers divided the strabismus group into those with esotropia, where the eyes turn inward (52.2%), exotropia, where they turn outward (46.3%), and hypertropia, where one eye wanders upward (12.5%). Investigators found that all three conditions were associated with increased risk of anxiety disorder, depressive disorder, bipolar disorders, and schizophrenia.
Investigators note that rates in the current study were lower than in previous studies, which showed that children with congenital esotropia were 2.6 times more likely to receive a mental health diagnosis, and children with intermittent exotropia were 2.7 times more likely to receive a mental health diagnosis.
“It is probable that our study found a lower risk than these studies, because our study was cross-sectional and claims based, whereas these studies observed the children to early adulthood and were based on medical records,” the investigators note.
It’s impossible to determine from this study how strabismus is connected to mental illness. However, Dr. Pineles believes depression and anxiety might be tied to strabismus via teasing, which affects self-esteem, although genetics could also play a role. For conditions such as schizophrenia, a shared genetic link with strabismus might be more likely, she added.
“Schizophrenia is a pretty severe diagnosis, so just being teased or having poor self-esteem is probably not enough” to develop schizophrenia.
Based on her clinical experience, Dr. Pineles said that realigning the eyes of patients with milder forms of depression or anxiety “definitely anecdotally helps these patients a lot.”
Dr. Pineles and colleagues have another paper in press that examines mental illnesses and other serious eye disorders in children and shows similar findings, she said.
Implications for insurance coverage?
In an accompanying editorial, experts, led by S. Grace Prakalapakorn, MD, department of ophthalmology and pediatrics, Duke University Medical Center, Durham, N.C., noted the exclusion of children covered under government insurance or without insurance is an important study limitation, largely because socioeconomic status is a risk factor for poor mental health.
The editorialists point to studies showing that surgical correction of ocular misalignments may be associated with reduced anxiety and depression. However, health insurance coverage for such surgical correction “may not be available owing to a misconception that these conditions are ‘cosmetic’.”
Evidence of the broader association of strabismus with physical and mental health “may play an important role in shifting policy to promote insurance coverage for timely strabismus care,” they write.
As many mental health disorders begin in childhood or adolescence, “it is paramount to identify, address, and, if possible, prevent mental health disorders at a young age, because failure to intervene in a timely fashion can have lifelong health consequences,” say Dr. Prakalapakorn and colleagues.
With mental health conditions and disorders increasing worldwide, compounded by the stressors of the COVID-19 pandemic, additional studies are needed to explore the causal relationships between ocular and psychiatric phenomena, their treatment, and outcomes, they add.
The study was supported by a grant from the National Eye Institute and an unrestricted grant from Research to Prevent Blindness. Dr. Pineles has reported no relevant conflicts of interest. Commentary author Manpreet K. Singh, MD, has reported receiving research support from Stanford’s Maternal Child Health Research Institute and Stanford’s Department of Psychiatry and Behavioral Sciences, the National Institute of Mental Health, the National Institute on Aging, the Patient-Centered Outcomes Research Institute, Johnson & Johnson, Allergan, and the Brain and Behavior Research Foundation; serving on the advisory board for Sunovion and Skyland Trail; serving as a consultant for Johnson & Johnson; previously serving as a consultant for X, the moonshot factory, Alphabet, and Limbix Health; receiving honoraria from the American Academy of Child and Adolescent Psychiatry; and receiving royalties from American Psychiatric Association Publishing and Thrive Global. Commentary author Nathan Congdon, MD, has reported receiving personal fees from Belkin Vision outside the submitted work.
A version of this article first appeared on Medscape.com.
Misaligned eyes in children are associated with an increased prevalence of mental illness, results of a large study suggest.
“Psychiatrists who have a patient with depression or anxiety and notice that patient also has strabismus might think about the link between those two conditions and refer that patient,” study investigator Stacy L. Pineles, MD, professor, department of ophthalmology, University of California, Los Angeles, told this news organization.
The study was published online March 10 in JAMA Ophthalmology.
A common condition
Strabismus, a condition in which the eyes don’t line up or are “crossed,” is one of the most common eye diseases in children, with some estimates suggesting it affects more than 1.5 million American youth.
Patients with strabismus have problems making eye contact and are affected socially and functionally, said Dr. Pineles. They’re often met with a negative bias, as shown by children’s responses to pictures of faces with and without strabismus, she said.
There is a signal from previous research suggesting that strabismus is linked to a higher risk of mental illness. However, most of these studies were small and had relatively homogenous populations, said Dr. Pineles.
The new study includes over 12 million children (mean age, 8.0 years) from a private health insurance claims database that represents diverse races and ethnicities as well as geographic regions across the United States.
The sample included 352,636 children with strabismus and 11,652,553 children with no diagnosed eye disease who served as controls. Most participants were White (51.6%), came from a family with an annual household income of $40,000 or more (51.0%), had point-of-service insurance (68.7%), and had at least one comorbid condition (64.5%).
The study evaluated five mental illness diagnoses. These included anxiety disorder, depressive disorder, substance use or addictive disorder, bipolar disorder, and schizophrenia.
Overall, children with strabismus had a higher prevalence of all these illnesses, with the exception of substance use disorder.
After adjusting for age, sex, race and ethnicity, census region, education level of caregiver, family net worth, and presence of at least one comorbid condition, the odds ratios among those with versus without strabismus were: 2.01 (95% confidence interval, 1.99-2.04; P < .001) for anxiety disorder, 1.83 (95% CI, 1.76-1.90; P < .001) for schizophrenia, 1.64 (95% CI, 1.59-1.70; P < .001) for bipolar disorder, and 1.61 (95% CI, 1.59-1.63; P < .001) for depressive disorder.
Substance use disorder had a negative unadjusted association with strabismus, but after adjustment for confounders, the association was not significant (OR, 0.99; 95% CI, 0.97-1.02; P = .48).
Dr. Pineles noted that the study participants, who were all under age 19, may be too young to have substance use disorders.
The results for substance use disorders provided something of an “internal control” and reaffirmed results for the other four conditions, said Dr. Pineles.
“When you do research on such a large database, you’re very likely to find significant associations; the dataset is so large that even very small differences become statistically significant. It was interesting that not everything gave us a positive association.”
Researchers divided the strabismus group into those with esotropia, where the eyes turn inward (52.2%), exotropia, where they turn outward (46.3%), and hypertropia, where one eye wanders upward (12.5%). Investigators found that all three conditions were associated with increased risk of anxiety disorder, depressive disorder, bipolar disorders, and schizophrenia.
Investigators note that rates in the current study were lower than in previous studies, which showed that children with congenital esotropia were 2.6 times more likely to receive a mental health diagnosis, and children with intermittent exotropia were 2.7 times more likely to receive a mental health diagnosis.
“It is probable that our study found a lower risk than these studies, because our study was cross-sectional and claims based, whereas these studies observed the children to early adulthood and were based on medical records,” the investigators note.
It’s impossible to determine from this study how strabismus is connected to mental illness. However, Dr. Pineles believes depression and anxiety might be tied to strabismus via teasing, which affects self-esteem, although genetics could also play a role. For conditions such as schizophrenia, a shared genetic link with strabismus might be more likely, she added.
“Schizophrenia is a pretty severe diagnosis, so just being teased or having poor self-esteem is probably not enough” to develop schizophrenia.
Based on her clinical experience, Dr. Pineles said that realigning the eyes of patients with milder forms of depression or anxiety “definitely anecdotally helps these patients a lot.”
Dr. Pineles and colleagues have another paper in press that examines mental illnesses and other serious eye disorders in children and shows similar findings, she said.
Implications for insurance coverage?
In an accompanying editorial, experts, led by S. Grace Prakalapakorn, MD, department of ophthalmology and pediatrics, Duke University Medical Center, Durham, N.C., noted the exclusion of children covered under government insurance or without insurance is an important study limitation, largely because socioeconomic status is a risk factor for poor mental health.
The editorialists point to studies showing that surgical correction of ocular misalignments may be associated with reduced anxiety and depression. However, health insurance coverage for such surgical correction “may not be available owing to a misconception that these conditions are ‘cosmetic’.”
Evidence of the broader association of strabismus with physical and mental health “may play an important role in shifting policy to promote insurance coverage for timely strabismus care,” they write.
As many mental health disorders begin in childhood or adolescence, “it is paramount to identify, address, and, if possible, prevent mental health disorders at a young age, because failure to intervene in a timely fashion can have lifelong health consequences,” say Dr. Prakalapakorn and colleagues.
With mental health conditions and disorders increasing worldwide, compounded by the stressors of the COVID-19 pandemic, additional studies are needed to explore the causal relationships between ocular and psychiatric phenomena, their treatment, and outcomes, they add.
The study was supported by a grant from the National Eye Institute and an unrestricted grant from Research to Prevent Blindness. Dr. Pineles has reported no relevant conflicts of interest. Commentary author Manpreet K. Singh, MD, has reported receiving research support from Stanford’s Maternal Child Health Research Institute and Stanford’s Department of Psychiatry and Behavioral Sciences, the National Institute of Mental Health, the National Institute on Aging, the Patient-Centered Outcomes Research Institute, Johnson & Johnson, Allergan, and the Brain and Behavior Research Foundation; serving on the advisory board for Sunovion and Skyland Trail; serving as a consultant for Johnson & Johnson; previously serving as a consultant for X, the moonshot factory, Alphabet, and Limbix Health; receiving honoraria from the American Academy of Child and Adolescent Psychiatry; and receiving royalties from American Psychiatric Association Publishing and Thrive Global. Commentary author Nathan Congdon, MD, has reported receiving personal fees from Belkin Vision outside the submitted work.
A version of this article first appeared on Medscape.com.
Misaligned eyes in children are associated with an increased prevalence of mental illness, results of a large study suggest.
“Psychiatrists who have a patient with depression or anxiety and notice that patient also has strabismus might think about the link between those two conditions and refer that patient,” study investigator Stacy L. Pineles, MD, professor, department of ophthalmology, University of California, Los Angeles, told this news organization.
The study was published online March 10 in JAMA Ophthalmology.
A common condition
Strabismus, a condition in which the eyes don’t line up or are “crossed,” is one of the most common eye diseases in children, with some estimates suggesting it affects more than 1.5 million American youth.
Patients with strabismus have problems making eye contact and are affected socially and functionally, said Dr. Pineles. They’re often met with a negative bias, as shown by children’s responses to pictures of faces with and without strabismus, she said.
There is a signal from previous research suggesting that strabismus is linked to a higher risk of mental illness. However, most of these studies were small and had relatively homogenous populations, said Dr. Pineles.
The new study includes over 12 million children (mean age, 8.0 years) from a private health insurance claims database that represents diverse races and ethnicities as well as geographic regions across the United States.
The sample included 352,636 children with strabismus and 11,652,553 children with no diagnosed eye disease who served as controls. Most participants were White (51.6%), came from a family with an annual household income of $40,000 or more (51.0%), had point-of-service insurance (68.7%), and had at least one comorbid condition (64.5%).
The study evaluated five mental illness diagnoses. These included anxiety disorder, depressive disorder, substance use or addictive disorder, bipolar disorder, and schizophrenia.
Overall, children with strabismus had a higher prevalence of all these illnesses, with the exception of substance use disorder.
After adjusting for age, sex, race and ethnicity, census region, education level of caregiver, family net worth, and presence of at least one comorbid condition, the odds ratios among those with versus without strabismus were: 2.01 (95% confidence interval, 1.99-2.04; P < .001) for anxiety disorder, 1.83 (95% CI, 1.76-1.90; P < .001) for schizophrenia, 1.64 (95% CI, 1.59-1.70; P < .001) for bipolar disorder, and 1.61 (95% CI, 1.59-1.63; P < .001) for depressive disorder.
Substance use disorder had a negative unadjusted association with strabismus, but after adjustment for confounders, the association was not significant (OR, 0.99; 95% CI, 0.97-1.02; P = .48).
Dr. Pineles noted that the study participants, who were all under age 19, may be too young to have substance use disorders.
The results for substance use disorders provided something of an “internal control” and reaffirmed results for the other four conditions, said Dr. Pineles.
“When you do research on such a large database, you’re very likely to find significant associations; the dataset is so large that even very small differences become statistically significant. It was interesting that not everything gave us a positive association.”
Researchers divided the strabismus group into those with esotropia, where the eyes turn inward (52.2%), exotropia, where they turn outward (46.3%), and hypertropia, where one eye wanders upward (12.5%). Investigators found that all three conditions were associated with increased risk of anxiety disorder, depressive disorder, bipolar disorders, and schizophrenia.
Investigators note that rates in the current study were lower than in previous studies, which showed that children with congenital esotropia were 2.6 times more likely to receive a mental health diagnosis, and children with intermittent exotropia were 2.7 times more likely to receive a mental health diagnosis.
“It is probable that our study found a lower risk than these studies, because our study was cross-sectional and claims based, whereas these studies observed the children to early adulthood and were based on medical records,” the investigators note.
It’s impossible to determine from this study how strabismus is connected to mental illness. However, Dr. Pineles believes depression and anxiety might be tied to strabismus via teasing, which affects self-esteem, although genetics could also play a role. For conditions such as schizophrenia, a shared genetic link with strabismus might be more likely, she added.
“Schizophrenia is a pretty severe diagnosis, so just being teased or having poor self-esteem is probably not enough” to develop schizophrenia.
Based on her clinical experience, Dr. Pineles said that realigning the eyes of patients with milder forms of depression or anxiety “definitely anecdotally helps these patients a lot.”
Dr. Pineles and colleagues have another paper in press that examines mental illnesses and other serious eye disorders in children and shows similar findings, she said.
Implications for insurance coverage?
In an accompanying editorial, experts, led by S. Grace Prakalapakorn, MD, department of ophthalmology and pediatrics, Duke University Medical Center, Durham, N.C., noted the exclusion of children covered under government insurance or without insurance is an important study limitation, largely because socioeconomic status is a risk factor for poor mental health.
The editorialists point to studies showing that surgical correction of ocular misalignments may be associated with reduced anxiety and depression. However, health insurance coverage for such surgical correction “may not be available owing to a misconception that these conditions are ‘cosmetic’.”
Evidence of the broader association of strabismus with physical and mental health “may play an important role in shifting policy to promote insurance coverage for timely strabismus care,” they write.
As many mental health disorders begin in childhood or adolescence, “it is paramount to identify, address, and, if possible, prevent mental health disorders at a young age, because failure to intervene in a timely fashion can have lifelong health consequences,” say Dr. Prakalapakorn and colleagues.
With mental health conditions and disorders increasing worldwide, compounded by the stressors of the COVID-19 pandemic, additional studies are needed to explore the causal relationships between ocular and psychiatric phenomena, their treatment, and outcomes, they add.
The study was supported by a grant from the National Eye Institute and an unrestricted grant from Research to Prevent Blindness. Dr. Pineles has reported no relevant conflicts of interest. Commentary author Manpreet K. Singh, MD, has reported receiving research support from Stanford’s Maternal Child Health Research Institute and Stanford’s Department of Psychiatry and Behavioral Sciences, the National Institute of Mental Health, the National Institute on Aging, the Patient-Centered Outcomes Research Institute, Johnson & Johnson, Allergan, and the Brain and Behavior Research Foundation; serving on the advisory board for Sunovion and Skyland Trail; serving as a consultant for Johnson & Johnson; previously serving as a consultant for X, the moonshot factory, Alphabet, and Limbix Health; receiving honoraria from the American Academy of Child and Adolescent Psychiatry; and receiving royalties from American Psychiatric Association Publishing and Thrive Global. Commentary author Nathan Congdon, MD, has reported receiving personal fees from Belkin Vision outside the submitted work.
A version of this article first appeared on Medscape.com.
‘Alarming’ worldwide decline in mental health
The Mental Health Million project of Sapien Labs issued its second report, published online March 15, encompassing 34 countries and over 220,000 Internet-enabled adults. It found a continued decline in mental health in all age groups and genders, with English-speaking countries having the lowest mental well-being.
The decline was significantly correlated with the stringency of COVID-19 lockdown measures in each country and was directionally correlated to the cases and deaths per million.
The youngest age group (18-24 years) reported the poorest mental well-being, with better mental health scores rising in every successively older age group.
“Some of our findings, especially regarding mental health in young adults, are alarming,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, told this news organization.
“Our data, which are continually updated in real time, are freely available for nonprofit, noncommercial use and research, and we hope that researchers will get involved in an interdisciplinary way that spans sociology, economics, psychiatry, and other fields,” she said.
Pioneering research
Dr. Thiagarajan and her team pioneered the Mental Health Million project, an ongoing research initiative utilizing a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability.”
The MHQ consists of 47 “elements of mental well-being,” with scores ranging from –100 to +200. (Negative scores indicate poorer mental well-being.) The MHQ categorizes respondents as “clinical, at-risk, enduring, managing, succeeding, and thriving” and computes scores on the basis of six broad dimensions of mental health: core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
As reported by this news organization, Sapien Lab’s first Mental Health State of the World report (n = 49,000 adults) was conducted in eight English-speaking countries in 2020. Participants were compared to a smaller sample of people from the same countries polled in 2019.
In this year’s report, “we expanded quite substantially,” Dr. Thiagarajan said. The project added Spanish, French, and Arabic and recruited participants from 34 countries on six continents (n = 223,087) via advertising on Google and Facebook.

Economic prosperity not protective
Across the eight English-speaking countries, there was a decline in mental well-being of 3% from 2020 to 2021, which was smaller than the 8% decline from 2019 to 2020. The percentage of people who were “distressed or struggling” increased from 26% to 30% in 2021.
“Now that a lot of pandemic issue seems to be easing up, I hope we’ll see mental well-being coming back up, but at least it’s a smaller decline than we saw between 2019 and 2020,” said Dr. Thiagarajan.
The decline across countries from 2019 to 2021 was significantly correlated with the stringency of governmental COVID-19-related measures (based on the Oxford COVID-19 Government Response Tracker, 2022; r = .54) and directionally correlated to the cases and deaths per million.
In total, 30% of respondents in English-speaking countries had mental well-being scores in the “distressed” or “struggling” range – higher than the Middle Eastern countries, North Africa, Latin America, and Europe (23%, 23%, 24%, and 18%, respectively).
Only 36% of participants in the English-speaking countries, the Middle East, and North Africa reported “thriving or succeeding,” vs. 45% and 46% in Latin America and Europe, respectively. Venezuela topped the list with an average MHQ of 91, while the United Kingdom and South Africa had the lowest scores, at 46 each.
Mental well-being was slightly higher in males than in females but was dramatically lower in nonbinary/third-gender respondents. In fact, those identifying as nonbinary/third gender had the lowest mental well-being of any group.
Across all countries and languages, higher education was associated with better mental well-being. Employment was also associated with superior mental well-being, compared with being unemployed – particularly in core English-speaking countries.
However, “country indicators of economic prosperity were negatively correlated with mental well-being, particularly for young adults and males, belying the commonly held belief that national economic prosperity translates into greater mental well-being,” said Dr. Thiagarajan.
‘Stark’ contrast
The most dramatic finding was the difference in mental well-being between younger and older adults, which was two- to threefold larger than differences in other dimensions (for example, age, gender, employment). Even the maximum difference between countries overall (15%) was still smaller than the generational gap within any region.
While only 7% (6%- 9%) of participants aged ≥65 years were “distressed and struggling” with their mental well-being to a “clinical” extent, 44% (38%-50%) of those aged 18-24 years reported mental well-being scores in the “distressed or struggling” range – representing a “growing gap between generations that, while present prior to the COVID-19 pandemic, has since been exacerbated,” the authors state.
With every successive decrement in age group, mental well-being “plummeted,” Dr. Thiagarajan said. She noted that research conducted prior to 2010 in several regions of the world showed that young adults typically had the highest well-being. “Our findings stand in stark contrast to these previous patterns.”
The relationship between lockdown stringency and poorer mental health could play a role. “The impact of social isolation may be most strongly felt in younger people,” she said.
Internet a culprit?
“Within almost every region, scores for cognition and drive and motivation were highest while mood and outlook and social self were the lowest,” the authors report.
The aggregate percentage of respondents who reported being “distressed or struggling” in the various MHQ dimensions is shown in the following table.
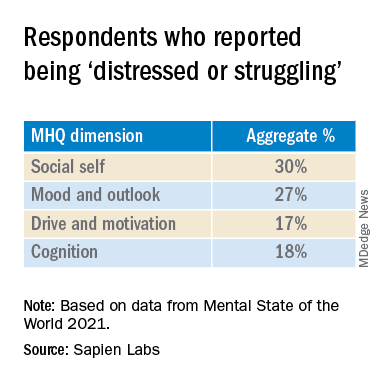
In particular, English-speaking countries scored lowest on the social self scale.
The sense of social self is “how you see yourself with respect to others, how you relate to others and the ability to form strong, stable relationships and maintain them with other people,” said Dr. Thiagarajan.
Internet use might account for the “massive” difference between the youngest and the oldest generations, she suggested. “Following 2010, mobile phone penetration picked up and rose rapidly. ... Mobile phones took over the world.”
Time spent on the Internet – an estimated 7-10 hours per day – “eats into the time people in older generations used in building the social self. Kids who grow up on the Internet are losing thousands of hours in social interactions, which is challenging their ability to form relationships, how they see themselves, and how they fit into the social fabric,” Dr. Thiagarajan added
Sedentary time
Commenting for this news organization, Bernardo Ng, MD, a member of the American Psychiatric Association’s Council on International Psychiatry and Global Health and medical director of Sun Valley Research Center, Imperial, Calif., called the report “interesting, with an impressive sample size” and an “impressive geographic distribution.”

Dr. Ng, who was not involved in the report, said, “I did not think the impact of Internet use on mental health was as dramatic before looking at this report.
“On the other hand, I have personally been interested in the impact of sedentarism in mental health – not only emotionally but also biologically. Sedentarism, which is directly related to screen use time, produces inflammation that worsens brain function.”

Also commenting, Ken Duckworth, MD, chief medical officer of the National Alliance of Mental Illness, called the survey “extremely well timed and creative, although it looked only at Internet-enabled populations, so one cannot make too many overall pronouncements, because a lot of people don’t have access to the Internet.”
The data regarding young people are particularly powerful. “The idea that young people are having a decrease in their experience of mental health across the world is something I haven’t seen before.”
Dr. Duckworth suggested the reason might “have to do with the impact of the COVID lockdown on normal development that young people go through, while older people don’t struggle with these developmental challenges in the same way.”
A version of this article first appeared on Medscape.com.
The Mental Health Million project of Sapien Labs issued its second report, published online March 15, encompassing 34 countries and over 220,000 Internet-enabled adults. It found a continued decline in mental health in all age groups and genders, with English-speaking countries having the lowest mental well-being.
The decline was significantly correlated with the stringency of COVID-19 lockdown measures in each country and was directionally correlated to the cases and deaths per million.
The youngest age group (18-24 years) reported the poorest mental well-being, with better mental health scores rising in every successively older age group.
“Some of our findings, especially regarding mental health in young adults, are alarming,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, told this news organization.
“Our data, which are continually updated in real time, are freely available for nonprofit, noncommercial use and research, and we hope that researchers will get involved in an interdisciplinary way that spans sociology, economics, psychiatry, and other fields,” she said.
Pioneering research
Dr. Thiagarajan and her team pioneered the Mental Health Million project, an ongoing research initiative utilizing a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability.”
The MHQ consists of 47 “elements of mental well-being,” with scores ranging from –100 to +200. (Negative scores indicate poorer mental well-being.) The MHQ categorizes respondents as “clinical, at-risk, enduring, managing, succeeding, and thriving” and computes scores on the basis of six broad dimensions of mental health: core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
As reported by this news organization, Sapien Lab’s first Mental Health State of the World report (n = 49,000 adults) was conducted in eight English-speaking countries in 2020. Participants were compared to a smaller sample of people from the same countries polled in 2019.
In this year’s report, “we expanded quite substantially,” Dr. Thiagarajan said. The project added Spanish, French, and Arabic and recruited participants from 34 countries on six continents (n = 223,087) via advertising on Google and Facebook.
Economic prosperity not protective
Across the eight English-speaking countries, there was a decline in mental well-being of 3% from 2020 to 2021, which was smaller than the 8% decline from 2019 to 2020. The percentage of people who were “distressed or struggling” increased from 26% to 30% in 2021.
“Now that a lot of pandemic issue seems to be easing up, I hope we’ll see mental well-being coming back up, but at least it’s a smaller decline than we saw between 2019 and 2020,” said Dr. Thiagarajan.
The decline across countries from 2019 to 2021 was significantly correlated with the stringency of governmental COVID-19-related measures (based on the Oxford COVID-19 Government Response Tracker, 2022; r = .54) and directionally correlated to the cases and deaths per million.
In total, 30% of respondents in English-speaking countries had mental well-being scores in the “distressed” or “struggling” range – higher than the Middle Eastern countries, North Africa, Latin America, and Europe (23%, 23%, 24%, and 18%, respectively).
Only 36% of participants in the English-speaking countries, the Middle East, and North Africa reported “thriving or succeeding,” vs. 45% and 46% in Latin America and Europe, respectively. Venezuela topped the list with an average MHQ of 91, while the United Kingdom and South Africa had the lowest scores, at 46 each.
Mental well-being was slightly higher in males than in females but was dramatically lower in nonbinary/third-gender respondents. In fact, those identifying as nonbinary/third gender had the lowest mental well-being of any group.
Across all countries and languages, higher education was associated with better mental well-being. Employment was also associated with superior mental well-being, compared with being unemployed – particularly in core English-speaking countries.
However, “country indicators of economic prosperity were negatively correlated with mental well-being, particularly for young adults and males, belying the commonly held belief that national economic prosperity translates into greater mental well-being,” said Dr. Thiagarajan.
‘Stark’ contrast
The most dramatic finding was the difference in mental well-being between younger and older adults, which was two- to threefold larger than differences in other dimensions (for example, age, gender, employment). Even the maximum difference between countries overall (15%) was still smaller than the generational gap within any region.
While only 7% (6%- 9%) of participants aged ≥65 years were “distressed and struggling” with their mental well-being to a “clinical” extent, 44% (38%-50%) of those aged 18-24 years reported mental well-being scores in the “distressed or struggling” range – representing a “growing gap between generations that, while present prior to the COVID-19 pandemic, has since been exacerbated,” the authors state.
With every successive decrement in age group, mental well-being “plummeted,” Dr. Thiagarajan said. She noted that research conducted prior to 2010 in several regions of the world showed that young adults typically had the highest well-being. “Our findings stand in stark contrast to these previous patterns.”
The relationship between lockdown stringency and poorer mental health could play a role. “The impact of social isolation may be most strongly felt in younger people,” she said.
Internet a culprit?
“Within almost every region, scores for cognition and drive and motivation were highest while mood and outlook and social self were the lowest,” the authors report.
The aggregate percentage of respondents who reported being “distressed or struggling” in the various MHQ dimensions is shown in the following table.
In particular, English-speaking countries scored lowest on the social self scale.
The sense of social self is “how you see yourself with respect to others, how you relate to others and the ability to form strong, stable relationships and maintain them with other people,” said Dr. Thiagarajan.
Internet use might account for the “massive” difference between the youngest and the oldest generations, she suggested. “Following 2010, mobile phone penetration picked up and rose rapidly. ... Mobile phones took over the world.”
Time spent on the Internet – an estimated 7-10 hours per day – “eats into the time people in older generations used in building the social self. Kids who grow up on the Internet are losing thousands of hours in social interactions, which is challenging their ability to form relationships, how they see themselves, and how they fit into the social fabric,” Dr. Thiagarajan added
Sedentary time
Commenting for this news organization, Bernardo Ng, MD, a member of the American Psychiatric Association’s Council on International Psychiatry and Global Health and medical director of Sun Valley Research Center, Imperial, Calif., called the report “interesting, with an impressive sample size” and an “impressive geographic distribution.”
Dr. Ng, who was not involved in the report, said, “I did not think the impact of Internet use on mental health was as dramatic before looking at this report.
“On the other hand, I have personally been interested in the impact of sedentarism in mental health – not only emotionally but also biologically. Sedentarism, which is directly related to screen use time, produces inflammation that worsens brain function.”
Also commenting, Ken Duckworth, MD, chief medical officer of the National Alliance of Mental Illness, called the survey “extremely well timed and creative, although it looked only at Internet-enabled populations, so one cannot make too many overall pronouncements, because a lot of people don’t have access to the Internet.”
The data regarding young people are particularly powerful. “The idea that young people are having a decrease in their experience of mental health across the world is something I haven’t seen before.”
Dr. Duckworth suggested the reason might “have to do with the impact of the COVID lockdown on normal development that young people go through, while older people don’t struggle with these developmental challenges in the same way.”
A version of this article first appeared on Medscape.com.
The Mental Health Million project of Sapien Labs issued its second report, published online March 15, encompassing 34 countries and over 220,000 Internet-enabled adults. It found a continued decline in mental health in all age groups and genders, with English-speaking countries having the lowest mental well-being.
The decline was significantly correlated with the stringency of COVID-19 lockdown measures in each country and was directionally correlated to the cases and deaths per million.
The youngest age group (18-24 years) reported the poorest mental well-being, with better mental health scores rising in every successively older age group.
“Some of our findings, especially regarding mental health in young adults, are alarming,” Tara Thiagarajan, PhD, Sapien Labs founder and chief scientist, told this news organization.
“Our data, which are continually updated in real time, are freely available for nonprofit, noncommercial use and research, and we hope that researchers will get involved in an interdisciplinary way that spans sociology, economics, psychiatry, and other fields,” she said.
Pioneering research
Dr. Thiagarajan and her team pioneered the Mental Health Million project, an ongoing research initiative utilizing a “free and anonymous assessment tool,” the Mental Health Quotient (MHQ), which “encompasses a comprehensive view of our emotional, social, and cognitive function and capability.”
The MHQ consists of 47 “elements of mental well-being,” with scores ranging from –100 to +200. (Negative scores indicate poorer mental well-being.) The MHQ categorizes respondents as “clinical, at-risk, enduring, managing, succeeding, and thriving” and computes scores on the basis of six broad dimensions of mental health: core cognition, complex cognition, mood and outlook, drive and motivation, social self, and mind-body connection.
As reported by this news organization, Sapien Lab’s first Mental Health State of the World report (n = 49,000 adults) was conducted in eight English-speaking countries in 2020. Participants were compared to a smaller sample of people from the same countries polled in 2019.
In this year’s report, “we expanded quite substantially,” Dr. Thiagarajan said. The project added Spanish, French, and Arabic and recruited participants from 34 countries on six continents (n = 223,087) via advertising on Google and Facebook.
Economic prosperity not protective
Across the eight English-speaking countries, there was a decline in mental well-being of 3% from 2020 to 2021, which was smaller than the 8% decline from 2019 to 2020. The percentage of people who were “distressed or struggling” increased from 26% to 30% in 2021.
“Now that a lot of pandemic issue seems to be easing up, I hope we’ll see mental well-being coming back up, but at least it’s a smaller decline than we saw between 2019 and 2020,” said Dr. Thiagarajan.
The decline across countries from 2019 to 2021 was significantly correlated with the stringency of governmental COVID-19-related measures (based on the Oxford COVID-19 Government Response Tracker, 2022; r = .54) and directionally correlated to the cases and deaths per million.
In total, 30% of respondents in English-speaking countries had mental well-being scores in the “distressed” or “struggling” range – higher than the Middle Eastern countries, North Africa, Latin America, and Europe (23%, 23%, 24%, and 18%, respectively).
Only 36% of participants in the English-speaking countries, the Middle East, and North Africa reported “thriving or succeeding,” vs. 45% and 46% in Latin America and Europe, respectively. Venezuela topped the list with an average MHQ of 91, while the United Kingdom and South Africa had the lowest scores, at 46 each.
Mental well-being was slightly higher in males than in females but was dramatically lower in nonbinary/third-gender respondents. In fact, those identifying as nonbinary/third gender had the lowest mental well-being of any group.
Across all countries and languages, higher education was associated with better mental well-being. Employment was also associated with superior mental well-being, compared with being unemployed – particularly in core English-speaking countries.
However, “country indicators of economic prosperity were negatively correlated with mental well-being, particularly for young adults and males, belying the commonly held belief that national economic prosperity translates into greater mental well-being,” said Dr. Thiagarajan.
‘Stark’ contrast
The most dramatic finding was the difference in mental well-being between younger and older adults, which was two- to threefold larger than differences in other dimensions (for example, age, gender, employment). Even the maximum difference between countries overall (15%) was still smaller than the generational gap within any region.
While only 7% (6%- 9%) of participants aged ≥65 years were “distressed and struggling” with their mental well-being to a “clinical” extent, 44% (38%-50%) of those aged 18-24 years reported mental well-being scores in the “distressed or struggling” range – representing a “growing gap between generations that, while present prior to the COVID-19 pandemic, has since been exacerbated,” the authors state.
With every successive decrement in age group, mental well-being “plummeted,” Dr. Thiagarajan said. She noted that research conducted prior to 2010 in several regions of the world showed that young adults typically had the highest well-being. “Our findings stand in stark contrast to these previous patterns.”
The relationship between lockdown stringency and poorer mental health could play a role. “The impact of social isolation may be most strongly felt in younger people,” she said.
Internet a culprit?
“Within almost every region, scores for cognition and drive and motivation were highest while mood and outlook and social self were the lowest,” the authors report.
The aggregate percentage of respondents who reported being “distressed or struggling” in the various MHQ dimensions is shown in the following table.
In particular, English-speaking countries scored lowest on the social self scale.
The sense of social self is “how you see yourself with respect to others, how you relate to others and the ability to form strong, stable relationships and maintain them with other people,” said Dr. Thiagarajan.
Internet use might account for the “massive” difference between the youngest and the oldest generations, she suggested. “Following 2010, mobile phone penetration picked up and rose rapidly. ... Mobile phones took over the world.”
Time spent on the Internet – an estimated 7-10 hours per day – “eats into the time people in older generations used in building the social self. Kids who grow up on the Internet are losing thousands of hours in social interactions, which is challenging their ability to form relationships, how they see themselves, and how they fit into the social fabric,” Dr. Thiagarajan added
Sedentary time
Commenting for this news organization, Bernardo Ng, MD, a member of the American Psychiatric Association’s Council on International Psychiatry and Global Health and medical director of Sun Valley Research Center, Imperial, Calif., called the report “interesting, with an impressive sample size” and an “impressive geographic distribution.”
Dr. Ng, who was not involved in the report, said, “I did not think the impact of Internet use on mental health was as dramatic before looking at this report.
“On the other hand, I have personally been interested in the impact of sedentarism in mental health – not only emotionally but also biologically. Sedentarism, which is directly related to screen use time, produces inflammation that worsens brain function.”
Also commenting, Ken Duckworth, MD, chief medical officer of the National Alliance of Mental Illness, called the survey “extremely well timed and creative, although it looked only at Internet-enabled populations, so one cannot make too many overall pronouncements, because a lot of people don’t have access to the Internet.”
The data regarding young people are particularly powerful. “The idea that young people are having a decrease in their experience of mental health across the world is something I haven’t seen before.”
Dr. Duckworth suggested the reason might “have to do with the impact of the COVID lockdown on normal development that young people go through, while older people don’t struggle with these developmental challenges in the same way.”
A version of this article first appeared on Medscape.com.
Navigating patient requests for an emotional support animal
When Serena-Lian Sakheim-Devine’s best friend from childhood died of cancer, she felt sad and lonely while away at college. Wanting something warm to snuggle, she got a guinea pig and named her Basil. Then she got two more and called them Nutmeg and Paprika. The three became her Spice Girls.
“They were of great comfort to me, but also to others at times of need,” said Ms. Sakheim-Devine, 26, who lived with them in a dormitory at Smith College, an all-women’s institution in Northampton, Mass.
Her therapist wrote a letter and sent it to the disability office at Smith, which permitted the guinea pigs as emotional support animals (ESAs). Eventually, though, she wanted a dog to help manage her PTSD, depression, anxiety, and panic attacks. So, she adopted a beagle from a shelter.
Once again, a therapist provided a letter, and Ms. Sakheim-Devine was allowed to keep the beagle, Finnian, then about 13 years old, in her dorm room on the condition that she give up the guinea pigs, which she did.
She and Finnian bonded almost instantly. When she woke up drenched in sweat, unable to move or speak, the dog sensed how tense she was. Finnian licked her hands, got her fingers moving, and helped ground her.
“I didn’t really teach her that. She just knew,” said Ms. Sakheim-Devine, now a safety engineer who lives in New Haven, Conn. “It was incredible how well connected we were, even from the get-go.”
The therapeutic benefits of four-legged friends
Although there is limited scientific literature on the therapeutic use of ESAs, there are well-established benefits of having pets that also apply in these situations. Animals can provide distraction from stress, alleviate loneliness, and instill a sense of responsibility, said Rachel A. Davis, MD, associate professor of psychiatry and neurosurgery at the University of Colorado at Denver, Aurora.
They add structure to a person’s day by needing to be fed at specific times, and they can help the human get exercise. “Patients have reported improved sense of meaning in life and purpose,” Dr. Davis said.
Examples include depression, anxiety, obsessive-compulsive disorder, panic attacks, and PTSD.
ESAs differ from psychiatric service animals, which are trained to perform specific tasks, such as applying deep pressure that calms the owner. By their mere existence, ESAs provide emotional benefits to a person with a mental health disability.
“Social support, even from an animal, can really help people feel less alone, better about themselves, and safer from unpleasantness or even a physical attack,” said David Spiegel, MD, professor and associate chair of psychiatry and behavioral sciences and director of the Center on Stress and Health at Stanford (Calif.) University.
Writing a letter on your patient’s behalf
Writing a letter that serves as proof of a person’s need for an ESA is a request that mental health professionals sometimes receive from patients. The letter can grant access to housing without additional cost regardless of no-pet polices, and some employers may allow an ESA at work as a reasonable accommodation for a psychological disability. Until recently, an ESA could accompany its owner on a plane, but most airlines no longer permit this, partly because some passengers falsely claim their pets as ESAs.
Before crafting a letter for someone with an ESA, Dr. Spiegel asks for the patient’s permission to elaborate on the clinical condition that merits professional help and to explain how the animal relieves associated symptoms.
The Fair Housing Act, a federal law, requires a landlord to grant a reasonable accommodation involving an emotional support or other assistance animal. Such an accommodation honors a request to live on the property despite a no-pets policy. It also waives a pet deposit, fee, or other rules involving animals on the premises.
Landlords are usually supportive of a request to permit an ESA, said Jonathan Betlinski, MD, associate professor and director of the public psychiatry division at Oregon Health and Science University, Portland. None of his patients have experienced any difficulties once they obtained a letter from him.
However, “anytime somebody asks me about a letter for an ESA, that’s the time to have a conversation. It’s not automatic,” Dr. Betlinski said. The discussion involves learning about the type of animal a patient has and how it helps his or her emotional state.
Because of privacy concerns, Dr. Betlinski doesn’t disclose the specific diagnosis in the letter unless the patient signs a release of information. The laws pertaining to ESAs only require his letter to note that an individual has a qualifying diagnosis and that an ESA helps improve symptoms, but it’s not necessary to explain how.
“You can see where writing the letter is a fine balancing act,” he said. But he finds it helpful to mention any training the animal has completed, such as the Canine Good Citizen course sponsored by the American Kennel Club.
Most of the letters Luis Anez, PsyD, a clinical psychologist and associate professor of psychiatry at Yale University, New Haven, Conn., has written for this purpose were in support of ESAs in housing. But he also recalled providing a letter for a patient who was flying to Puerto Rico with an ESA. The letters are generally provided only to established patients with psychiatric diagnoses.
Without a letter, “we’ve seen people say: ‘I’d rather be homeless than part with my dog,’ ”said Dr. Anez, who is also director of Hispanic services at Connecticut Mental Health Center in New Haven, a partnership between Yale and the Connecticut Department of Mental Health and Addiction Services. Before getting an ESA, Dr. Anez recommends that individuals become aware of their landlord’s policies on possible restrictions relating to dog sizes and breeds.
Additional considerations
An ESA doesn’t necessarily have to be a dog. “It certainly could be a cat. It could be a parrot, too,” said Stephen Stern, MD, a psychiatrist in private practice in Mount Kisco, N.Y. But, “if they say that their emotional support animal is an earthworm, that would make you wonder,” he added half-jokingly.
Dr. Stern only writes an ESA letter for a patient with whom he has an ongoing professional relationship. For instance, if he’s treating someone for depression and that patient tells him how the animal helps relieve symptoms, then that is sufficient justification to write a letter.
“Because you know them, you’ve assessed that what they’re saying is plausible,” said Dr. Stern, who is also an adjunct professor of psychiatry at the University of Texas Health Science in San Antonio, where he conducted research on companion dogs for veterans with PTSD and continues to collaborate with colleagues via email and Zoom.
While veterans benefit from ESAs, some live in housing that doesn’t permit animals, said Beth Zimmerman, founder and executive director of Pets for Patriots, a nationally operating nonprofit organization in Long Beach, N.Y., that partners with shelters and animal welfare groups to adopt dogs and cats for companionship and emotional support. She said an ESA can be “a wonderful complement to other forms of therapy that a veteran may undertake.
“Most of the time when the veteran encounters a problem, it’s because the landlord is ill-informed of the law,” Dr. Zimmerman said. “We provide information to the veteran to share with the landlord or building management, and always recommend taking a very amicable approach. In our experience, with very few exceptions, once the landlord understands his or her responsibilities under the law, they will permit the veteran to have that emotional support animal in their dwelling.”
For Kristin Lowe, a chocolate Labrador-Weimaraner mix named Lola provided emotional support from her puppy days until her death at age 12 in May 2021. Ms. Lowe’s psychiatrist provided letters that allowed Lola to live in her apartment and to travel on commercial airline flights.
“She was so connected to me,” said Ms. Lowe, 34, who lives in Denver and works as an administrative office worker in physical therapy. “She was a part of me. She could read every emotion that I had.”
Now, Ms. Lowe relies on Henry, an Australian shepherd puppy, to help her cope with obsessive-compulsive disorder, major depressive disorder, and an eating disorder. She described him as “a very happy little guy and a constant tail wagger – and that lights up something in me.”
More information, which is provided by the U.S. Department of Housing and Urban Development, can be found here.
A version of this article first appeared on Medscape.com.
When Serena-Lian Sakheim-Devine’s best friend from childhood died of cancer, she felt sad and lonely while away at college. Wanting something warm to snuggle, she got a guinea pig and named her Basil. Then she got two more and called them Nutmeg and Paprika. The three became her Spice Girls.
“They were of great comfort to me, but also to others at times of need,” said Ms. Sakheim-Devine, 26, who lived with them in a dormitory at Smith College, an all-women’s institution in Northampton, Mass.
Her therapist wrote a letter and sent it to the disability office at Smith, which permitted the guinea pigs as emotional support animals (ESAs). Eventually, though, she wanted a dog to help manage her PTSD, depression, anxiety, and panic attacks. So, she adopted a beagle from a shelter.
Once again, a therapist provided a letter, and Ms. Sakheim-Devine was allowed to keep the beagle, Finnian, then about 13 years old, in her dorm room on the condition that she give up the guinea pigs, which she did.
She and Finnian bonded almost instantly. When she woke up drenched in sweat, unable to move or speak, the dog sensed how tense she was. Finnian licked her hands, got her fingers moving, and helped ground her.
“I didn’t really teach her that. She just knew,” said Ms. Sakheim-Devine, now a safety engineer who lives in New Haven, Conn. “It was incredible how well connected we were, even from the get-go.”
The therapeutic benefits of four-legged friends
Although there is limited scientific literature on the therapeutic use of ESAs, there are well-established benefits of having pets that also apply in these situations. Animals can provide distraction from stress, alleviate loneliness, and instill a sense of responsibility, said Rachel A. Davis, MD, associate professor of psychiatry and neurosurgery at the University of Colorado at Denver, Aurora.
They add structure to a person’s day by needing to be fed at specific times, and they can help the human get exercise. “Patients have reported improved sense of meaning in life and purpose,” Dr. Davis said.
Examples include depression, anxiety, obsessive-compulsive disorder, panic attacks, and PTSD.
ESAs differ from psychiatric service animals, which are trained to perform specific tasks, such as applying deep pressure that calms the owner. By their mere existence, ESAs provide emotional benefits to a person with a mental health disability.
“Social support, even from an animal, can really help people feel less alone, better about themselves, and safer from unpleasantness or even a physical attack,” said David Spiegel, MD, professor and associate chair of psychiatry and behavioral sciences and director of the Center on Stress and Health at Stanford (Calif.) University.
Writing a letter on your patient’s behalf
Writing a letter that serves as proof of a person’s need for an ESA is a request that mental health professionals sometimes receive from patients. The letter can grant access to housing without additional cost regardless of no-pet polices, and some employers may allow an ESA at work as a reasonable accommodation for a psychological disability. Until recently, an ESA could accompany its owner on a plane, but most airlines no longer permit this, partly because some passengers falsely claim their pets as ESAs.
Before crafting a letter for someone with an ESA, Dr. Spiegel asks for the patient’s permission to elaborate on the clinical condition that merits professional help and to explain how the animal relieves associated symptoms.
The Fair Housing Act, a federal law, requires a landlord to grant a reasonable accommodation involving an emotional support or other assistance animal. Such an accommodation honors a request to live on the property despite a no-pets policy. It also waives a pet deposit, fee, or other rules involving animals on the premises.
Landlords are usually supportive of a request to permit an ESA, said Jonathan Betlinski, MD, associate professor and director of the public psychiatry division at Oregon Health and Science University, Portland. None of his patients have experienced any difficulties once they obtained a letter from him.
However, “anytime somebody asks me about a letter for an ESA, that’s the time to have a conversation. It’s not automatic,” Dr. Betlinski said. The discussion involves learning about the type of animal a patient has and how it helps his or her emotional state.
Because of privacy concerns, Dr. Betlinski doesn’t disclose the specific diagnosis in the letter unless the patient signs a release of information. The laws pertaining to ESAs only require his letter to note that an individual has a qualifying diagnosis and that an ESA helps improve symptoms, but it’s not necessary to explain how.
“You can see where writing the letter is a fine balancing act,” he said. But he finds it helpful to mention any training the animal has completed, such as the Canine Good Citizen course sponsored by the American Kennel Club.
Most of the letters Luis Anez, PsyD, a clinical psychologist and associate professor of psychiatry at Yale University, New Haven, Conn., has written for this purpose were in support of ESAs in housing. But he also recalled providing a letter for a patient who was flying to Puerto Rico with an ESA. The letters are generally provided only to established patients with psychiatric diagnoses.
Without a letter, “we’ve seen people say: ‘I’d rather be homeless than part with my dog,’ ”said Dr. Anez, who is also director of Hispanic services at Connecticut Mental Health Center in New Haven, a partnership between Yale and the Connecticut Department of Mental Health and Addiction Services. Before getting an ESA, Dr. Anez recommends that individuals become aware of their landlord’s policies on possible restrictions relating to dog sizes and breeds.
Additional considerations
An ESA doesn’t necessarily have to be a dog. “It certainly could be a cat. It could be a parrot, too,” said Stephen Stern, MD, a psychiatrist in private practice in Mount Kisco, N.Y. But, “if they say that their emotional support animal is an earthworm, that would make you wonder,” he added half-jokingly.
Dr. Stern only writes an ESA letter for a patient with whom he has an ongoing professional relationship. For instance, if he’s treating someone for depression and that patient tells him how the animal helps relieve symptoms, then that is sufficient justification to write a letter.
“Because you know them, you’ve assessed that what they’re saying is plausible,” said Dr. Stern, who is also an adjunct professor of psychiatry at the University of Texas Health Science in San Antonio, where he conducted research on companion dogs for veterans with PTSD and continues to collaborate with colleagues via email and Zoom.
While veterans benefit from ESAs, some live in housing that doesn’t permit animals, said Beth Zimmerman, founder and executive director of Pets for Patriots, a nationally operating nonprofit organization in Long Beach, N.Y., that partners with shelters and animal welfare groups to adopt dogs and cats for companionship and emotional support. She said an ESA can be “a wonderful complement to other forms of therapy that a veteran may undertake.
“Most of the time when the veteran encounters a problem, it’s because the landlord is ill-informed of the law,” Dr. Zimmerman said. “We provide information to the veteran to share with the landlord or building management, and always recommend taking a very amicable approach. In our experience, with very few exceptions, once the landlord understands his or her responsibilities under the law, they will permit the veteran to have that emotional support animal in their dwelling.”
For Kristin Lowe, a chocolate Labrador-Weimaraner mix named Lola provided emotional support from her puppy days until her death at age 12 in May 2021. Ms. Lowe’s psychiatrist provided letters that allowed Lola to live in her apartment and to travel on commercial airline flights.
“She was so connected to me,” said Ms. Lowe, 34, who lives in Denver and works as an administrative office worker in physical therapy. “She was a part of me. She could read every emotion that I had.”
Now, Ms. Lowe relies on Henry, an Australian shepherd puppy, to help her cope with obsessive-compulsive disorder, major depressive disorder, and an eating disorder. She described him as “a very happy little guy and a constant tail wagger – and that lights up something in me.”
More information, which is provided by the U.S. Department of Housing and Urban Development, can be found here.
A version of this article first appeared on Medscape.com.
When Serena-Lian Sakheim-Devine’s best friend from childhood died of cancer, she felt sad and lonely while away at college. Wanting something warm to snuggle, she got a guinea pig and named her Basil. Then she got two more and called them Nutmeg and Paprika. The three became her Spice Girls.
“They were of great comfort to me, but also to others at times of need,” said Ms. Sakheim-Devine, 26, who lived with them in a dormitory at Smith College, an all-women’s institution in Northampton, Mass.
Her therapist wrote a letter and sent it to the disability office at Smith, which permitted the guinea pigs as emotional support animals (ESAs). Eventually, though, she wanted a dog to help manage her PTSD, depression, anxiety, and panic attacks. So, she adopted a beagle from a shelter.
Once again, a therapist provided a letter, and Ms. Sakheim-Devine was allowed to keep the beagle, Finnian, then about 13 years old, in her dorm room on the condition that she give up the guinea pigs, which she did.
She and Finnian bonded almost instantly. When she woke up drenched in sweat, unable to move or speak, the dog sensed how tense she was. Finnian licked her hands, got her fingers moving, and helped ground her.
“I didn’t really teach her that. She just knew,” said Ms. Sakheim-Devine, now a safety engineer who lives in New Haven, Conn. “It was incredible how well connected we were, even from the get-go.”
The therapeutic benefits of four-legged friends
Although there is limited scientific literature on the therapeutic use of ESAs, there are well-established benefits of having pets that also apply in these situations. Animals can provide distraction from stress, alleviate loneliness, and instill a sense of responsibility, said Rachel A. Davis, MD, associate professor of psychiatry and neurosurgery at the University of Colorado at Denver, Aurora.
They add structure to a person’s day by needing to be fed at specific times, and they can help the human get exercise. “Patients have reported improved sense of meaning in life and purpose,” Dr. Davis said.
Examples include depression, anxiety, obsessive-compulsive disorder, panic attacks, and PTSD.
ESAs differ from psychiatric service animals, which are trained to perform specific tasks, such as applying deep pressure that calms the owner. By their mere existence, ESAs provide emotional benefits to a person with a mental health disability.
“Social support, even from an animal, can really help people feel less alone, better about themselves, and safer from unpleasantness or even a physical attack,” said David Spiegel, MD, professor and associate chair of psychiatry and behavioral sciences and director of the Center on Stress and Health at Stanford (Calif.) University.
Writing a letter on your patient’s behalf
Writing a letter that serves as proof of a person’s need for an ESA is a request that mental health professionals sometimes receive from patients. The letter can grant access to housing without additional cost regardless of no-pet polices, and some employers may allow an ESA at work as a reasonable accommodation for a psychological disability. Until recently, an ESA could accompany its owner on a plane, but most airlines no longer permit this, partly because some passengers falsely claim their pets as ESAs.
Before crafting a letter for someone with an ESA, Dr. Spiegel asks for the patient’s permission to elaborate on the clinical condition that merits professional help and to explain how the animal relieves associated symptoms.
The Fair Housing Act, a federal law, requires a landlord to grant a reasonable accommodation involving an emotional support or other assistance animal. Such an accommodation honors a request to live on the property despite a no-pets policy. It also waives a pet deposit, fee, or other rules involving animals on the premises.
Landlords are usually supportive of a request to permit an ESA, said Jonathan Betlinski, MD, associate professor and director of the public psychiatry division at Oregon Health and Science University, Portland. None of his patients have experienced any difficulties once they obtained a letter from him.
However, “anytime somebody asks me about a letter for an ESA, that’s the time to have a conversation. It’s not automatic,” Dr. Betlinski said. The discussion involves learning about the type of animal a patient has and how it helps his or her emotional state.
Because of privacy concerns, Dr. Betlinski doesn’t disclose the specific diagnosis in the letter unless the patient signs a release of information. The laws pertaining to ESAs only require his letter to note that an individual has a qualifying diagnosis and that an ESA helps improve symptoms, but it’s not necessary to explain how.
“You can see where writing the letter is a fine balancing act,” he said. But he finds it helpful to mention any training the animal has completed, such as the Canine Good Citizen course sponsored by the American Kennel Club.
Most of the letters Luis Anez, PsyD, a clinical psychologist and associate professor of psychiatry at Yale University, New Haven, Conn., has written for this purpose were in support of ESAs in housing. But he also recalled providing a letter for a patient who was flying to Puerto Rico with an ESA. The letters are generally provided only to established patients with psychiatric diagnoses.
Without a letter, “we’ve seen people say: ‘I’d rather be homeless than part with my dog,’ ”said Dr. Anez, who is also director of Hispanic services at Connecticut Mental Health Center in New Haven, a partnership between Yale and the Connecticut Department of Mental Health and Addiction Services. Before getting an ESA, Dr. Anez recommends that individuals become aware of their landlord’s policies on possible restrictions relating to dog sizes and breeds.
Additional considerations
An ESA doesn’t necessarily have to be a dog. “It certainly could be a cat. It could be a parrot, too,” said Stephen Stern, MD, a psychiatrist in private practice in Mount Kisco, N.Y. But, “if they say that their emotional support animal is an earthworm, that would make you wonder,” he added half-jokingly.
Dr. Stern only writes an ESA letter for a patient with whom he has an ongoing professional relationship. For instance, if he’s treating someone for depression and that patient tells him how the animal helps relieve symptoms, then that is sufficient justification to write a letter.
“Because you know them, you’ve assessed that what they’re saying is plausible,” said Dr. Stern, who is also an adjunct professor of psychiatry at the University of Texas Health Science in San Antonio, where he conducted research on companion dogs for veterans with PTSD and continues to collaborate with colleagues via email and Zoom.
While veterans benefit from ESAs, some live in housing that doesn’t permit animals, said Beth Zimmerman, founder and executive director of Pets for Patriots, a nationally operating nonprofit organization in Long Beach, N.Y., that partners with shelters and animal welfare groups to adopt dogs and cats for companionship and emotional support. She said an ESA can be “a wonderful complement to other forms of therapy that a veteran may undertake.
“Most of the time when the veteran encounters a problem, it’s because the landlord is ill-informed of the law,” Dr. Zimmerman said. “We provide information to the veteran to share with the landlord or building management, and always recommend taking a very amicable approach. In our experience, with very few exceptions, once the landlord understands his or her responsibilities under the law, they will permit the veteran to have that emotional support animal in their dwelling.”
For Kristin Lowe, a chocolate Labrador-Weimaraner mix named Lola provided emotional support from her puppy days until her death at age 12 in May 2021. Ms. Lowe’s psychiatrist provided letters that allowed Lola to live in her apartment and to travel on commercial airline flights.
“She was so connected to me,” said Ms. Lowe, 34, who lives in Denver and works as an administrative office worker in physical therapy. “She was a part of me. She could read every emotion that I had.”
Now, Ms. Lowe relies on Henry, an Australian shepherd puppy, to help her cope with obsessive-compulsive disorder, major depressive disorder, and an eating disorder. She described him as “a very happy little guy and a constant tail wagger – and that lights up something in me.”
More information, which is provided by the U.S. Department of Housing and Urban Development, can be found here.
A version of this article first appeared on Medscape.com.

Addiction expert says CBD may help people cut cannabis use
PARIS – Following the suspension of the decree that banned the sale of cannabidiol (CBD) flowers, raw cannabis is again available in France for over-the-counter sales. The “feel-good” plant is praised for its relaxing properties.

The suspension of the ban, which lasted for 3 weeks, is a mixed blessing for businesses that sell CBD-based products in France. Professional organizations in this booming sector filed a petition with France’s highest administrative court, the Council of State. At the end of January, the court suspended the government decree that banned the sale of cannabis-derived CBD flowers and leaves; however, it has yet to hand down a final decision as to the legality of the decree.
In just a few years, numerous shops have opened across France. They no longer have to settle for selling processed CBD products such as chocolate, oils, cookies – even wine. They can resume the sale of CBD hemp, which mainly comes in clusters of flower buds and can be smoked or used as an infusion.
Cannabis-derived CBD must have less than 0.2% tetrahydrocannabinol (THC) to be considered “feel-good hemp,” which is used in various consumer goods (such as food, cosmetics, and e-cigarette liquids) and is praised for its calming effects. But not all hemp is the same. Medical hemp, which is currently in clinical trials, combines varying doses of CBD and THC. And then there is THC-rich psychotropic hemp, which is illegal to sell.
The government’s decree cites health concerns as a justification for the ban. While uncertainties remain, “research studies have shown that CBD acts on dopamine and serotonin receptors in the brain. ... Therefore, using CBD can produce psychoactive, sedative, and sleep-inducing effects.” In addition to a preventive approach, the authorities cite the difficulties in distinguishing cannabis-derived CBD from THC-rich illegal cannabis – difficulties that complicate efforts in the war on drugs.
The government’s position sows confusion among consumers, who are attracted by the arguments in favor of CBD and intrigued by the promise of the substance’s calming effects. This confusion is heightened by the fact that there are not enough scientific data either to declare that CBD poses a real risk or, alternatively, to confirm that it has beneficial effects. While some studies have suggested that CBD has a potential benefit for treating anxiety, pain, and sleep problems, others suggest that it may instead be a placebo effect.
What actual benefit can be expected from CBD-derived products, in particular from using the plant’s raw extracts? We asked Dan Velea, MD, an addiction psychiatrist in Paris, to give us his thoughts.
What do you think of the government’s position of banning the sale of cannabis-derived CBD flowers and leaves?
Dr. Velea: I don’t understand the reasoning behind this ban. Unlike THC, CBD is not an addictive substance. We’ve suspected that CBD had beneficial effects ever since noting that, just like THC, it could bind to the two types of cannabinoid receptors found in our bodies, CB1 and CB2, but without inducing a psychotropic effect or giving rise to dependence.
The CBD-derived products that are available on the market have infinitesimal amounts of THC – the threshold is 0.2% – which pose no risk. These products seem to be a particularly good alternative for certain at-risk users who are looking for a way that will help them cut down on their use of “traditional” cannabis, which has THC. However, due to a lack of research, the benefits of CBD cannot be confirmed.
Now that the decree’s been suspended, we can leave behind the ideological debate that has been built around cannabis in France. It’s time to focus only on discussions based on science. On that note, we also have to encourage people to do more research into cannabis’s therapeutic value.
You believe that CBD can help people cut down on their cannabis use. Is that based on what you see in your practice as an addiction specialist?
Dr. Velea: Of course, they don’t get the same dazzling effect that’s produced by THC, very high concentrations of which are often found in cannabis. But for them, the sensation they get from CBD is still pleasant. They describe it as having a soothing and fun effect; they quite like it. Given that the vast majority of people use cannabis recreationally, we can consider that this effect is no small benefit.
Even those who are highly dependent prefer to alternate, using CBD during the day and having just one THC joint in the evening. This makes them feel a lot better. In addition, it clearly reduces the health risks. In my opinion, CBD can be viewed as an alternative for people whose cannabis use is problematic. If a patient asks me about it, I give them an unequivocal answer: There are fewer risks associated with CBD than with regular cannabis.
Isn’t there still a risk for abuse? A dose of cannabidiol that shouldn’t be exceeded?
Dr. Velea: Honestly, apart from the harmful effects of smoking CBD, I don’t see any health risks associated with its use. I’ve never had a patient present with complaints after using these products. No one has ever told me that they became addicted or experienced psychotropic effects. There are no changes in behavior, even at high doses. It should be mentioned that World Health Organization experts hold that there’s no abuse or dependence potential associated with the use of pure CBD. Furthermore, they say that the product is generally well tolerated.
What other actual benefits does CBD have? People mention its relaxing, even anxiolytic, effects.
Dr. Velea: CBD-derived products are praised for their relaxing properties, which particularly help improve one’s sleep. It’s a question of knowing whether these are actual benefits or whether a placebo effect is involved here – something that would be enhanced in a person who firmly believes that these products bring about a sense of well-being. Even when CBD is used for pain relief, we can’t rule out the placebo effect as playing an important role in the outcome.
Some patients with serious diseases have been able to find comfort by using CBD. However, because there haven’t been any well-designed randomized studies, we’ve never been able to show clearly that the beneficial effect comes from the product itself. It’s also possible that the soothing, muscle-relaxing effect induced by CBD’s stimulation of cannabinoid receptors is actually what’s helping to relieve the pain. But this has yet to be proved.
So, what position can a doctor take toward patients who express their desire to use CBD-derived products?
Dr. Velea: Without reliable studies to back them up, it’s difficult to say. Also, at the moment, there are legal gray areas that don’t allow doctors to take a position. As a result, users are put at a disadvantage and not given the opportunity to make the choice to use CBD-derived products in an informed manner. Even so, I think that as long as we don’t have scientific data, the use of these products must be limited to recreational use with the aim of bringing about relaxation. In the case of a sleep disorder, for example, doctors can’t replace standard therapeutic management aimed at improving the patient’s sleep cycles. For now, the only genuinely interesting aspect of CBD that I can see is that it makes it possible to cut down on the use of THC-containing cannabis.
A version of this article first appeared on Medscape.com.
PARIS – Following the suspension of the decree that banned the sale of cannabidiol (CBD) flowers, raw cannabis is again available in France for over-the-counter sales. The “feel-good” plant is praised for its relaxing properties.
The suspension of the ban, which lasted for 3 weeks, is a mixed blessing for businesses that sell CBD-based products in France. Professional organizations in this booming sector filed a petition with France’s highest administrative court, the Council of State. At the end of January, the court suspended the government decree that banned the sale of cannabis-derived CBD flowers and leaves; however, it has yet to hand down a final decision as to the legality of the decree.
In just a few years, numerous shops have opened across France. They no longer have to settle for selling processed CBD products such as chocolate, oils, cookies – even wine. They can resume the sale of CBD hemp, which mainly comes in clusters of flower buds and can be smoked or used as an infusion.
Cannabis-derived CBD must have less than 0.2% tetrahydrocannabinol (THC) to be considered “feel-good hemp,” which is used in various consumer goods (such as food, cosmetics, and e-cigarette liquids) and is praised for its calming effects. But not all hemp is the same. Medical hemp, which is currently in clinical trials, combines varying doses of CBD and THC. And then there is THC-rich psychotropic hemp, which is illegal to sell.
The government’s decree cites health concerns as a justification for the ban. While uncertainties remain, “research studies have shown that CBD acts on dopamine and serotonin receptors in the brain. ... Therefore, using CBD can produce psychoactive, sedative, and sleep-inducing effects.” In addition to a preventive approach, the authorities cite the difficulties in distinguishing cannabis-derived CBD from THC-rich illegal cannabis – difficulties that complicate efforts in the war on drugs.
The government’s position sows confusion among consumers, who are attracted by the arguments in favor of CBD and intrigued by the promise of the substance’s calming effects. This confusion is heightened by the fact that there are not enough scientific data either to declare that CBD poses a real risk or, alternatively, to confirm that it has beneficial effects. While some studies have suggested that CBD has a potential benefit for treating anxiety, pain, and sleep problems, others suggest that it may instead be a placebo effect.
What actual benefit can be expected from CBD-derived products, in particular from using the plant’s raw extracts? We asked Dan Velea, MD, an addiction psychiatrist in Paris, to give us his thoughts.
What do you think of the government’s position of banning the sale of cannabis-derived CBD flowers and leaves?
Dr. Velea: I don’t understand the reasoning behind this ban. Unlike THC, CBD is not an addictive substance. We’ve suspected that CBD had beneficial effects ever since noting that, just like THC, it could bind to the two types of cannabinoid receptors found in our bodies, CB1 and CB2, but without inducing a psychotropic effect or giving rise to dependence.
The CBD-derived products that are available on the market have infinitesimal amounts of THC – the threshold is 0.2% – which pose no risk. These products seem to be a particularly good alternative for certain at-risk users who are looking for a way that will help them cut down on their use of “traditional” cannabis, which has THC. However, due to a lack of research, the benefits of CBD cannot be confirmed.
Now that the decree’s been suspended, we can leave behind the ideological debate that has been built around cannabis in France. It’s time to focus only on discussions based on science. On that note, we also have to encourage people to do more research into cannabis’s therapeutic value.
You believe that CBD can help people cut down on their cannabis use. Is that based on what you see in your practice as an addiction specialist?
Dr. Velea: Of course, they don’t get the same dazzling effect that’s produced by THC, very high concentrations of which are often found in cannabis. But for them, the sensation they get from CBD is still pleasant. They describe it as having a soothing and fun effect; they quite like it. Given that the vast majority of people use cannabis recreationally, we can consider that this effect is no small benefit.
Even those who are highly dependent prefer to alternate, using CBD during the day and having just one THC joint in the evening. This makes them feel a lot better. In addition, it clearly reduces the health risks. In my opinion, CBD can be viewed as an alternative for people whose cannabis use is problematic. If a patient asks me about it, I give them an unequivocal answer: There are fewer risks associated with CBD than with regular cannabis.
Isn’t there still a risk for abuse? A dose of cannabidiol that shouldn’t be exceeded?
Dr. Velea: Honestly, apart from the harmful effects of smoking CBD, I don’t see any health risks associated with its use. I’ve never had a patient present with complaints after using these products. No one has ever told me that they became addicted or experienced psychotropic effects. There are no changes in behavior, even at high doses. It should be mentioned that World Health Organization experts hold that there’s no abuse or dependence potential associated with the use of pure CBD. Furthermore, they say that the product is generally well tolerated.
What other actual benefits does CBD have? People mention its relaxing, even anxiolytic, effects.
Dr. Velea: CBD-derived products are praised for their relaxing properties, which particularly help improve one’s sleep. It’s a question of knowing whether these are actual benefits or whether a placebo effect is involved here – something that would be enhanced in a person who firmly believes that these products bring about a sense of well-being. Even when CBD is used for pain relief, we can’t rule out the placebo effect as playing an important role in the outcome.
Some patients with serious diseases have been able to find comfort by using CBD. However, because there haven’t been any well-designed randomized studies, we’ve never been able to show clearly that the beneficial effect comes from the product itself. It’s also possible that the soothing, muscle-relaxing effect induced by CBD’s stimulation of cannabinoid receptors is actually what’s helping to relieve the pain. But this has yet to be proved.
So, what position can a doctor take toward patients who express their desire to use CBD-derived products?
Dr. Velea: Without reliable studies to back them up, it’s difficult to say. Also, at the moment, there are legal gray areas that don’t allow doctors to take a position. As a result, users are put at a disadvantage and not given the opportunity to make the choice to use CBD-derived products in an informed manner. Even so, I think that as long as we don’t have scientific data, the use of these products must be limited to recreational use with the aim of bringing about relaxation. In the case of a sleep disorder, for example, doctors can’t replace standard therapeutic management aimed at improving the patient’s sleep cycles. For now, the only genuinely interesting aspect of CBD that I can see is that it makes it possible to cut down on the use of THC-containing cannabis.
A version of this article first appeared on Medscape.com.
PARIS – Following the suspension of the decree that banned the sale of cannabidiol (CBD) flowers, raw cannabis is again available in France for over-the-counter sales. The “feel-good” plant is praised for its relaxing properties.
The suspension of the ban, which lasted for 3 weeks, is a mixed blessing for businesses that sell CBD-based products in France. Professional organizations in this booming sector filed a petition with France’s highest administrative court, the Council of State. At the end of January, the court suspended the government decree that banned the sale of cannabis-derived CBD flowers and leaves; however, it has yet to hand down a final decision as to the legality of the decree.
In just a few years, numerous shops have opened across France. They no longer have to settle for selling processed CBD products such as chocolate, oils, cookies – even wine. They can resume the sale of CBD hemp, which mainly comes in clusters of flower buds and can be smoked or used as an infusion.
Cannabis-derived CBD must have less than 0.2% tetrahydrocannabinol (THC) to be considered “feel-good hemp,” which is used in various consumer goods (such as food, cosmetics, and e-cigarette liquids) and is praised for its calming effects. But not all hemp is the same. Medical hemp, which is currently in clinical trials, combines varying doses of CBD and THC. And then there is THC-rich psychotropic hemp, which is illegal to sell.
The government’s decree cites health concerns as a justification for the ban. While uncertainties remain, “research studies have shown that CBD acts on dopamine and serotonin receptors in the brain. ... Therefore, using CBD can produce psychoactive, sedative, and sleep-inducing effects.” In addition to a preventive approach, the authorities cite the difficulties in distinguishing cannabis-derived CBD from THC-rich illegal cannabis – difficulties that complicate efforts in the war on drugs.
The government’s position sows confusion among consumers, who are attracted by the arguments in favor of CBD and intrigued by the promise of the substance’s calming effects. This confusion is heightened by the fact that there are not enough scientific data either to declare that CBD poses a real risk or, alternatively, to confirm that it has beneficial effects. While some studies have suggested that CBD has a potential benefit for treating anxiety, pain, and sleep problems, others suggest that it may instead be a placebo effect.
What actual benefit can be expected from CBD-derived products, in particular from using the plant’s raw extracts? We asked Dan Velea, MD, an addiction psychiatrist in Paris, to give us his thoughts.
What do you think of the government’s position of banning the sale of cannabis-derived CBD flowers and leaves?
Dr. Velea: I don’t understand the reasoning behind this ban. Unlike THC, CBD is not an addictive substance. We’ve suspected that CBD had beneficial effects ever since noting that, just like THC, it could bind to the two types of cannabinoid receptors found in our bodies, CB1 and CB2, but without inducing a psychotropic effect or giving rise to dependence.
The CBD-derived products that are available on the market have infinitesimal amounts of THC – the threshold is 0.2% – which pose no risk. These products seem to be a particularly good alternative for certain at-risk users who are looking for a way that will help them cut down on their use of “traditional” cannabis, which has THC. However, due to a lack of research, the benefits of CBD cannot be confirmed.
Now that the decree’s been suspended, we can leave behind the ideological debate that has been built around cannabis in France. It’s time to focus only on discussions based on science. On that note, we also have to encourage people to do more research into cannabis’s therapeutic value.
You believe that CBD can help people cut down on their cannabis use. Is that based on what you see in your practice as an addiction specialist?
Dr. Velea: Of course, they don’t get the same dazzling effect that’s produced by THC, very high concentrations of which are often found in cannabis. But for them, the sensation they get from CBD is still pleasant. They describe it as having a soothing and fun effect; they quite like it. Given that the vast majority of people use cannabis recreationally, we can consider that this effect is no small benefit.
Even those who are highly dependent prefer to alternate, using CBD during the day and having just one THC joint in the evening. This makes them feel a lot better. In addition, it clearly reduces the health risks. In my opinion, CBD can be viewed as an alternative for people whose cannabis use is problematic. If a patient asks me about it, I give them an unequivocal answer: There are fewer risks associated with CBD than with regular cannabis.
Isn’t there still a risk for abuse? A dose of cannabidiol that shouldn’t be exceeded?
Dr. Velea: Honestly, apart from the harmful effects of smoking CBD, I don’t see any health risks associated with its use. I’ve never had a patient present with complaints after using these products. No one has ever told me that they became addicted or experienced psychotropic effects. There are no changes in behavior, even at high doses. It should be mentioned that World Health Organization experts hold that there’s no abuse or dependence potential associated with the use of pure CBD. Furthermore, they say that the product is generally well tolerated.
What other actual benefits does CBD have? People mention its relaxing, even anxiolytic, effects.
Dr. Velea: CBD-derived products are praised for their relaxing properties, which particularly help improve one’s sleep. It’s a question of knowing whether these are actual benefits or whether a placebo effect is involved here – something that would be enhanced in a person who firmly believes that these products bring about a sense of well-being. Even when CBD is used for pain relief, we can’t rule out the placebo effect as playing an important role in the outcome.
Some patients with serious diseases have been able to find comfort by using CBD. However, because there haven’t been any well-designed randomized studies, we’ve never been able to show clearly that the beneficial effect comes from the product itself. It’s also possible that the soothing, muscle-relaxing effect induced by CBD’s stimulation of cannabinoid receptors is actually what’s helping to relieve the pain. But this has yet to be proved.
So, what position can a doctor take toward patients who express their desire to use CBD-derived products?
Dr. Velea: Without reliable studies to back them up, it’s difficult to say. Also, at the moment, there are legal gray areas that don’t allow doctors to take a position. As a result, users are put at a disadvantage and not given the opportunity to make the choice to use CBD-derived products in an informed manner. Even so, I think that as long as we don’t have scientific data, the use of these products must be limited to recreational use with the aim of bringing about relaxation. In the case of a sleep disorder, for example, doctors can’t replace standard therapeutic management aimed at improving the patient’s sleep cycles. For now, the only genuinely interesting aspect of CBD that I can see is that it makes it possible to cut down on the use of THC-containing cannabis.
A version of this article first appeared on Medscape.com.
Routine pharmacogenetic testing in psychiatry not indicated
LAS VEGAS –
“It’s misleading to rely on results of genetic tests to drive clinical treatment,” Dr. Nurmi, a child and adolescent psychiatrist in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “There’s a lot of hope and promise there. But currently, we only know the tip of the iceberg about how drugs work and the genetics influencing these effects. Current testing is probably a very poor reflection of the complexity of drug effects.”
According to Dr. Nurmi, there are at least 165 Food and Drug Administration–approved drugs with pharmacogenetic information on 64 different biomarkers – 37% with CYP p450 notations. Of these, 32 psychiatric drugs have pharmacogenetic information, and most of them are dosing recommendations based on whether a patient has the variant. However, there is wide public acceptance of genetic testing in preventing the wrong drug from being used, in selecting the best drug dose, and avoiding side effects (Pharmacogenomics 2012;12[3]:197-204). “Most people have a lot of hope [for genetic testing in psychiatry],” Dr. Nurmi said. “But is the science really there? It doesn’t matter, because these companies are doing it, and you are being shown these reports from patients. Whether or not the science supports it, we’re going to have to interpret these reports and explain them to our patients – even if we don’t order them.”
Currently, she continued, clinicians practice trial and error prescribing where they might try one treatment in a class that they think that will work based on previous literature. If nothing works, they try another one. If that’s intolerable, they try a third treatment, and so on. “When we finally find the right treatment, it can take some time to get the dosing right,” Dr. Nurmi said. “So, it can take many months to get a child on the right medication. Precision treatment, on the other hand, would start off by taking a saliva or blood sample to get a printout that lets physicians know which drugs might be used with caution because they might lack efficacy at standard doses, which ones would likely have adverse effects at standard doses, and which are the best choices and what are the dosing recommendations for those choices. If we could get all the information to guide us, that would be a useful product, but right now, we don’t know enough to be able to make these determinations.”
Current evidence-based genetic testing supports a limited role for CYP2D6 and CYP2C19 genotyping because most psychiatric drugs are metabolized by those two enzymes. Poor metabolizers have two dysfunctional copies of the enzyme-encoding gene. This results in increased drug plasma levels with a potentially increased rate of adverse effects.
“Intermediate and extensive metabolizers usually have a normal phenotype, but you can also have ultrarapid metabolizers who have duplications or other enhancing mutations of the CYP gene,” Dr. Nurmi said. “This can result in lower bioavailability and possibly efficacy. Psychiatrists treat poor metabolizers and ultrarapid metabolizers all the time, because the variants are very common.” An estimated 10% of White people are poor metabolizers at the CYP2D6 gene while about 7% are ultrarapid metabolizers. At the same time, an estimated 20% of Asians, Africans, and Whites are poor metabolizers at the CYP2C19 gene. “So, you’re seeing a lot of this in your practice, and you’re probably changing dosing based on genetic differences in metabolism,” she said.
The only FDA pharmacodynamic treatment guideline is for the risk of Stevens-Johnson syndrome (SJS) with the use of carbamazepine. In a study of 44 patients with SJS, all were positive for the HLA-B*1502 variant, compared with 3% of carbamazepine-tolerant patients (Nature 2004;428[6982]:486). The frequency of carrying this variant is an estimated 1:10,000 among Whites and 1:1,000 among Asians. In 2007, the FDA recommended that patients of Asian ancestry should be screened for HLA-B*1502 prior to starting carbamazepine.
Genetic variation also predicts clinical outcome with atomoxetine use. “Most child psychiatrists I know think atomoxetine doesn’t work as a second-line nonstimulant medication for ADHD,” Dr. Nurmi said. “I’d like to convince you that why you think it doesn’t work is because of the genetics.” In a study published in 2019, Dr. Nurmi and colleagues reviewed medical literature and provided therapeutic recommendations for atomoxetine therapy based on CYP2D6 genotype (Clin Pharmacol Ther 2019 Jul;106[1]:94-102). They observed 10- to 30-fold plasma differences in drug exposure between normal metabolizers and poor metabolizers.
“Poor metabolizers therefore get more benefit, but they are also going to get more side effects,” she said. “FDA recommended doses are inadequate for normal metabolizers, so they had to make guidelines based on poor metabolizers because there would be too much risk for them at higher doses. One-third of individuals require doses above the FDA limit to achieve a therapeutic drug level.”
Dr. Nurmi warned that the existing evidence base for using these genetic tests in children “is really poor. There is no data in adults with any diagnosis other than depression, and even those studies are plagued by concerns. When you’re implementing decision support tools in your practice, the key factors are patient presentation, history and symptoms, your clinical skills, the evidence base, FDA recommendations, and patient autonomy. Appropriate incorporation of genetic data should include avoiding a medication with high toxicity (like SJS), titration planning (dose and titration speed adjustments), and choosing between medications in the same class with an indication or evidence base for the target disorder.” She added that while the benefit of current genetic testing is limited, it may help some patients feel more comfortable tolerating a medication. “For example, being able to tell someone with anxiety that their genetics suggests that they will not have side effects could be very powerful,” she said.
In a 2018 safety communication, the FDA warned the public about its concerns with companies making claims about how to use genetic test results to manage medication treatments that are not supported by recommendations in the FDA-approved drug labeling or other scientific evidence. The American Academy of Child and Adolescent Psychiatry also published a guide for patients and families.
Dr. Nurmi disclosed that she is an unpaid advisory board member for Myriad Genetics and the Tourette Association of America, a paid adviser for Teva Pharmaceuticals, and a recipient of research support from Emalex Pharmaceuticals. She has received research funding from the National Institutes Health, the International OCD Foundation, the Tourette Association of America, and the Brain & Behavior Research Foundation.
LAS VEGAS –
“It’s misleading to rely on results of genetic tests to drive clinical treatment,” Dr. Nurmi, a child and adolescent psychiatrist in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “There’s a lot of hope and promise there. But currently, we only know the tip of the iceberg about how drugs work and the genetics influencing these effects. Current testing is probably a very poor reflection of the complexity of drug effects.”
According to Dr. Nurmi, there are at least 165 Food and Drug Administration–approved drugs with pharmacogenetic information on 64 different biomarkers – 37% with CYP p450 notations. Of these, 32 psychiatric drugs have pharmacogenetic information, and most of them are dosing recommendations based on whether a patient has the variant. However, there is wide public acceptance of genetic testing in preventing the wrong drug from being used, in selecting the best drug dose, and avoiding side effects (Pharmacogenomics 2012;12[3]:197-204). “Most people have a lot of hope [for genetic testing in psychiatry],” Dr. Nurmi said. “But is the science really there? It doesn’t matter, because these companies are doing it, and you are being shown these reports from patients. Whether or not the science supports it, we’re going to have to interpret these reports and explain them to our patients – even if we don’t order them.”
Currently, she continued, clinicians practice trial and error prescribing where they might try one treatment in a class that they think that will work based on previous literature. If nothing works, they try another one. If that’s intolerable, they try a third treatment, and so on. “When we finally find the right treatment, it can take some time to get the dosing right,” Dr. Nurmi said. “So, it can take many months to get a child on the right medication. Precision treatment, on the other hand, would start off by taking a saliva or blood sample to get a printout that lets physicians know which drugs might be used with caution because they might lack efficacy at standard doses, which ones would likely have adverse effects at standard doses, and which are the best choices and what are the dosing recommendations for those choices. If we could get all the information to guide us, that would be a useful product, but right now, we don’t know enough to be able to make these determinations.”
Current evidence-based genetic testing supports a limited role for CYP2D6 and CYP2C19 genotyping because most psychiatric drugs are metabolized by those two enzymes. Poor metabolizers have two dysfunctional copies of the enzyme-encoding gene. This results in increased drug plasma levels with a potentially increased rate of adverse effects.
“Intermediate and extensive metabolizers usually have a normal phenotype, but you can also have ultrarapid metabolizers who have duplications or other enhancing mutations of the CYP gene,” Dr. Nurmi said. “This can result in lower bioavailability and possibly efficacy. Psychiatrists treat poor metabolizers and ultrarapid metabolizers all the time, because the variants are very common.” An estimated 10% of White people are poor metabolizers at the CYP2D6 gene while about 7% are ultrarapid metabolizers. At the same time, an estimated 20% of Asians, Africans, and Whites are poor metabolizers at the CYP2C19 gene. “So, you’re seeing a lot of this in your practice, and you’re probably changing dosing based on genetic differences in metabolism,” she said.
The only FDA pharmacodynamic treatment guideline is for the risk of Stevens-Johnson syndrome (SJS) with the use of carbamazepine. In a study of 44 patients with SJS, all were positive for the HLA-B*1502 variant, compared with 3% of carbamazepine-tolerant patients (Nature 2004;428[6982]:486). The frequency of carrying this variant is an estimated 1:10,000 among Whites and 1:1,000 among Asians. In 2007, the FDA recommended that patients of Asian ancestry should be screened for HLA-B*1502 prior to starting carbamazepine.
Genetic variation also predicts clinical outcome with atomoxetine use. “Most child psychiatrists I know think atomoxetine doesn’t work as a second-line nonstimulant medication for ADHD,” Dr. Nurmi said. “I’d like to convince you that why you think it doesn’t work is because of the genetics.” In a study published in 2019, Dr. Nurmi and colleagues reviewed medical literature and provided therapeutic recommendations for atomoxetine therapy based on CYP2D6 genotype (Clin Pharmacol Ther 2019 Jul;106[1]:94-102). They observed 10- to 30-fold plasma differences in drug exposure between normal metabolizers and poor metabolizers.
“Poor metabolizers therefore get more benefit, but they are also going to get more side effects,” she said. “FDA recommended doses are inadequate for normal metabolizers, so they had to make guidelines based on poor metabolizers because there would be too much risk for them at higher doses. One-third of individuals require doses above the FDA limit to achieve a therapeutic drug level.”
Dr. Nurmi warned that the existing evidence base for using these genetic tests in children “is really poor. There is no data in adults with any diagnosis other than depression, and even those studies are plagued by concerns. When you’re implementing decision support tools in your practice, the key factors are patient presentation, history and symptoms, your clinical skills, the evidence base, FDA recommendations, and patient autonomy. Appropriate incorporation of genetic data should include avoiding a medication with high toxicity (like SJS), titration planning (dose and titration speed adjustments), and choosing between medications in the same class with an indication or evidence base for the target disorder.” She added that while the benefit of current genetic testing is limited, it may help some patients feel more comfortable tolerating a medication. “For example, being able to tell someone with anxiety that their genetics suggests that they will not have side effects could be very powerful,” she said.
In a 2018 safety communication, the FDA warned the public about its concerns with companies making claims about how to use genetic test results to manage medication treatments that are not supported by recommendations in the FDA-approved drug labeling or other scientific evidence. The American Academy of Child and Adolescent Psychiatry also published a guide for patients and families.
Dr. Nurmi disclosed that she is an unpaid advisory board member for Myriad Genetics and the Tourette Association of America, a paid adviser for Teva Pharmaceuticals, and a recipient of research support from Emalex Pharmaceuticals. She has received research funding from the National Institutes Health, the International OCD Foundation, the Tourette Association of America, and the Brain & Behavior Research Foundation.
LAS VEGAS –
“It’s misleading to rely on results of genetic tests to drive clinical treatment,” Dr. Nurmi, a child and adolescent psychiatrist in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles, said during an annual psychopharmacology update held by the Nevada Psychiatric Association. “There’s a lot of hope and promise there. But currently, we only know the tip of the iceberg about how drugs work and the genetics influencing these effects. Current testing is probably a very poor reflection of the complexity of drug effects.”
According to Dr. Nurmi, there are at least 165 Food and Drug Administration–approved drugs with pharmacogenetic information on 64 different biomarkers – 37% with CYP p450 notations. Of these, 32 psychiatric drugs have pharmacogenetic information, and most of them are dosing recommendations based on whether a patient has the variant. However, there is wide public acceptance of genetic testing in preventing the wrong drug from being used, in selecting the best drug dose, and avoiding side effects (Pharmacogenomics 2012;12[3]:197-204). “Most people have a lot of hope [for genetic testing in psychiatry],” Dr. Nurmi said. “But is the science really there? It doesn’t matter, because these companies are doing it, and you are being shown these reports from patients. Whether or not the science supports it, we’re going to have to interpret these reports and explain them to our patients – even if we don’t order them.”
Currently, she continued, clinicians practice trial and error prescribing where they might try one treatment in a class that they think that will work based on previous literature. If nothing works, they try another one. If that’s intolerable, they try a third treatment, and so on. “When we finally find the right treatment, it can take some time to get the dosing right,” Dr. Nurmi said. “So, it can take many months to get a child on the right medication. Precision treatment, on the other hand, would start off by taking a saliva or blood sample to get a printout that lets physicians know which drugs might be used with caution because they might lack efficacy at standard doses, which ones would likely have adverse effects at standard doses, and which are the best choices and what are the dosing recommendations for those choices. If we could get all the information to guide us, that would be a useful product, but right now, we don’t know enough to be able to make these determinations.”
Current evidence-based genetic testing supports a limited role for CYP2D6 and CYP2C19 genotyping because most psychiatric drugs are metabolized by those two enzymes. Poor metabolizers have two dysfunctional copies of the enzyme-encoding gene. This results in increased drug plasma levels with a potentially increased rate of adverse effects.
“Intermediate and extensive metabolizers usually have a normal phenotype, but you can also have ultrarapid metabolizers who have duplications or other enhancing mutations of the CYP gene,” Dr. Nurmi said. “This can result in lower bioavailability and possibly efficacy. Psychiatrists treat poor metabolizers and ultrarapid metabolizers all the time, because the variants are very common.” An estimated 10% of White people are poor metabolizers at the CYP2D6 gene while about 7% are ultrarapid metabolizers. At the same time, an estimated 20% of Asians, Africans, and Whites are poor metabolizers at the CYP2C19 gene. “So, you’re seeing a lot of this in your practice, and you’re probably changing dosing based on genetic differences in metabolism,” she said.
The only FDA pharmacodynamic treatment guideline is for the risk of Stevens-Johnson syndrome (SJS) with the use of carbamazepine. In a study of 44 patients with SJS, all were positive for the HLA-B*1502 variant, compared with 3% of carbamazepine-tolerant patients (Nature 2004;428[6982]:486). The frequency of carrying this variant is an estimated 1:10,000 among Whites and 1:1,000 among Asians. In 2007, the FDA recommended that patients of Asian ancestry should be screened for HLA-B*1502 prior to starting carbamazepine.
Genetic variation also predicts clinical outcome with atomoxetine use. “Most child psychiatrists I know think atomoxetine doesn’t work as a second-line nonstimulant medication for ADHD,” Dr. Nurmi said. “I’d like to convince you that why you think it doesn’t work is because of the genetics.” In a study published in 2019, Dr. Nurmi and colleagues reviewed medical literature and provided therapeutic recommendations for atomoxetine therapy based on CYP2D6 genotype (Clin Pharmacol Ther 2019 Jul;106[1]:94-102). They observed 10- to 30-fold plasma differences in drug exposure between normal metabolizers and poor metabolizers.
“Poor metabolizers therefore get more benefit, but they are also going to get more side effects,” she said. “FDA recommended doses are inadequate for normal metabolizers, so they had to make guidelines based on poor metabolizers because there would be too much risk for them at higher doses. One-third of individuals require doses above the FDA limit to achieve a therapeutic drug level.”
Dr. Nurmi warned that the existing evidence base for using these genetic tests in children “is really poor. There is no data in adults with any diagnosis other than depression, and even those studies are plagued by concerns. When you’re implementing decision support tools in your practice, the key factors are patient presentation, history and symptoms, your clinical skills, the evidence base, FDA recommendations, and patient autonomy. Appropriate incorporation of genetic data should include avoiding a medication with high toxicity (like SJS), titration planning (dose and titration speed adjustments), and choosing between medications in the same class with an indication or evidence base for the target disorder.” She added that while the benefit of current genetic testing is limited, it may help some patients feel more comfortable tolerating a medication. “For example, being able to tell someone with anxiety that their genetics suggests that they will not have side effects could be very powerful,” she said.
In a 2018 safety communication, the FDA warned the public about its concerns with companies making claims about how to use genetic test results to manage medication treatments that are not supported by recommendations in the FDA-approved drug labeling or other scientific evidence. The American Academy of Child and Adolescent Psychiatry also published a guide for patients and families.
Dr. Nurmi disclosed that she is an unpaid advisory board member for Myriad Genetics and the Tourette Association of America, a paid adviser for Teva Pharmaceuticals, and a recipient of research support from Emalex Pharmaceuticals. She has received research funding from the National Institutes Health, the International OCD Foundation, the Tourette Association of America, and the Brain & Behavior Research Foundation.
REPORTING FROM NPA 2022