User login
Whither the percutaneous MitraClip for mitral regurgitation?
SNOWMASS, COLO. – The ongoing COAPT trial will not only determine the future of the MitraClip device for transcatheter mitral valve repair, it will also answer a key broader question: Does fixing functional mitral regurgitation even provide meaningful clinical benefit?
“This is an extremely important study because we don’t know whether correcting secondary [mitral regurgitation (MR)] does anything to change the prognosis or survival in the disease. The [Food and Drug Administration] gets kudos for insisting on this study. This will be a major trial in which we learn whether interrupting functional MR adds anything to guideline-directed medical therapy or not,” Dr. Michael J. Mack predicted at the Annual Cardiovascular Conference at Snowmass.

The distinction between primary degenerative MR and secondary functional MR is key. In primary MR, the problem is that the valve itself has worn out. Secondary MR is a disease of the left ventricle, not the mitral valve. The source of the valve problem in secondary MR lies in a dilated left ventricle, which causes stretching of the valve annulus and displacement of the papillary muscles. This left ventricular dilation can be caused by either ischemic or nonischemic dilated cardiomyopathy. Regardless, functional MR is a disorder of left ventricular remodeling in which anatomically normal valve leaflets don’t coapt sufficiently.
The MitraClip device is designed for percutaneous repair of MR in patients deemed at unacceptable risk for surgery. The device clips the valve leaflets together without surgical suturing. The MitraClip won FDA approval in fall 2013 for repair of severely symptomatic primary degenerative mitral regurgitation in patients who have a reasonable life expectancy but prohibitive surgical risk due to comorbidities. Roughly 1,500 MitraClip procedures have been done to date in the United States, and the initial commercial experience will be presented as a late-breaker at the annual meeting of the American College of Cardiology in San Diego in March.
Functional MR is a whole different story. The FDA decided that for the MitraClip to gain an additional indication for functional or secondary MR, a randomized controlled trial would be required. Moreover, after considerable debate among valve experts, the FDA decreed that the control group should consist of patients on guideline-directed medical therapy since – much to the surprise of many physicians and surgeons – to date there is actually no persuasive evidence that surgical repair or replacement is effective therapy for functional MR, explained Dr. Mack, former president of the Society of Thoracic Surgeons and medical director at Baylor Health Care System in Plano, Tex.
Dr. Mack and Columbia University cardiologist Dr. Gregg W. Stone serve as co–principal investigators of COAPT, scheduled to include about 420 high-surgical-risk patients with severely symptomatic secondary MR at 75 U.S. sites. Patients will be followed clinically and by transthoracic echocardiography for 5 years, with the primary endpoint being the 2-year rates of survival and freedom from repeat hospitalization for heart failure.
Patients with both ischemic and nonischemic cardiomyopathies are being enrolled. However, their outcomes will be analyzed separately because investigators believe these disorders may not respond in the same way to any interventional therapy.
“I think that nonischemic cardiomyopathy is an idiopathic disease of unknown etiology, and probably multiple etiologies. It’s reasonable to think that in ischemic MR there’s something we can treat and in that way prevent a progressive process from ongoing, and even cause some reverse remodeling. I don’t think we have any clue in nonischemic cardiomyopathies as to what the disease causes are and whether correcting the secondary MR will cause reverse remodeling. So if I were to bet one way or another on which one’s going to respond better to MitraClip therapy, I would say ischemic cardiomyopathy,” the surgeon said.
As to who’s at prohibitive surgical risk and therefore potentially eligible for percutaneous repair, the criteria established for use of the MitraClip for its approved indication also apply to candidates for the COAPT trial. These criteria include an STS mortality score of 8%-10% or more, a porcelain aorta, severe COPD, advanced liver disease, frailty, severe mitral annular calcification, what surgeons call a “hostile chest” due to prior sternectomy or other causes, and/or severe pulmonary hypertension. The determination is to be made jointly by a cardiologist and surgeon functioning within a local heart team.
Enrollment in the COAPT study has been “extremely difficult” because of widespread, albeit misplaced, pro-surgery bias, but the roster should be filled by the end of the year, Dr. Mack said.
He observed that a major disadvantage of the MitraClip is that it does only one thing: clip the leaflets together.
“In surgery, at least for primary MR, we never do one thing. We’ll resect, we’ll put cords in, we’ll do an annuloplasty,” he explained.
In the future – post COAPT – a likely scenario is that the MitraClip will routinely be employed together with a complementary percutaneous posterior mitral annuloplasty procedure, he said. The top candidate, in his view, is the Valtech Cardioband device.
“That’s the one with the most experience and success for transcatheter mitral annuloplasty. It’s done under 3-D transesophageal echocardiographic guidance. Thirty patients have been enrolled in a European feasibility trial, with a device success rate of 88%. Eighty-five percent of those 30 patients are none-to-trace MR at 6 months’ follow-up,” said Dr. Mack.
Dr. Bernard J. Gersh said that he totally agrees with Dr. Mack’s prediction of divergent outcomes in COAPT depending upon whether patients have ischemic or nonischemic dilated cardiomyopathy.
“As you look at the history of surgical procedures, those that are directed to a mechanism are successful, and those that are directed to the consequences of something are not. Idiopathic dilated cardiomyopathy is a totally different disease – it’s dysfunctional cells, we don’t really know why, and there’s very little fibrosis or scar. It’s a completely different mechanism. So I agree: If I had to bet, it’d be that it’s in ischemic MR that the MitraClip is relevant,” said Dr. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.
The COAPT trial is sponsored by Abbott Vascular. Dr. Mack reported receiving research grants from Abbott and Edwards Lifesciences.
SNOWMASS, COLO. – The ongoing COAPT trial will not only determine the future of the MitraClip device for transcatheter mitral valve repair, it will also answer a key broader question: Does fixing functional mitral regurgitation even provide meaningful clinical benefit?
“This is an extremely important study because we don’t know whether correcting secondary [mitral regurgitation (MR)] does anything to change the prognosis or survival in the disease. The [Food and Drug Administration] gets kudos for insisting on this study. This will be a major trial in which we learn whether interrupting functional MR adds anything to guideline-directed medical therapy or not,” Dr. Michael J. Mack predicted at the Annual Cardiovascular Conference at Snowmass.
The distinction between primary degenerative MR and secondary functional MR is key. In primary MR, the problem is that the valve itself has worn out. Secondary MR is a disease of the left ventricle, not the mitral valve. The source of the valve problem in secondary MR lies in a dilated left ventricle, which causes stretching of the valve annulus and displacement of the papillary muscles. This left ventricular dilation can be caused by either ischemic or nonischemic dilated cardiomyopathy. Regardless, functional MR is a disorder of left ventricular remodeling in which anatomically normal valve leaflets don’t coapt sufficiently.
The MitraClip device is designed for percutaneous repair of MR in patients deemed at unacceptable risk for surgery. The device clips the valve leaflets together without surgical suturing. The MitraClip won FDA approval in fall 2013 for repair of severely symptomatic primary degenerative mitral regurgitation in patients who have a reasonable life expectancy but prohibitive surgical risk due to comorbidities. Roughly 1,500 MitraClip procedures have been done to date in the United States, and the initial commercial experience will be presented as a late-breaker at the annual meeting of the American College of Cardiology in San Diego in March.
Functional MR is a whole different story. The FDA decided that for the MitraClip to gain an additional indication for functional or secondary MR, a randomized controlled trial would be required. Moreover, after considerable debate among valve experts, the FDA decreed that the control group should consist of patients on guideline-directed medical therapy since – much to the surprise of many physicians and surgeons – to date there is actually no persuasive evidence that surgical repair or replacement is effective therapy for functional MR, explained Dr. Mack, former president of the Society of Thoracic Surgeons and medical director at Baylor Health Care System in Plano, Tex.
Dr. Mack and Columbia University cardiologist Dr. Gregg W. Stone serve as co–principal investigators of COAPT, scheduled to include about 420 high-surgical-risk patients with severely symptomatic secondary MR at 75 U.S. sites. Patients will be followed clinically and by transthoracic echocardiography for 5 years, with the primary endpoint being the 2-year rates of survival and freedom from repeat hospitalization for heart failure.
Patients with both ischemic and nonischemic cardiomyopathies are being enrolled. However, their outcomes will be analyzed separately because investigators believe these disorders may not respond in the same way to any interventional therapy.
“I think that nonischemic cardiomyopathy is an idiopathic disease of unknown etiology, and probably multiple etiologies. It’s reasonable to think that in ischemic MR there’s something we can treat and in that way prevent a progressive process from ongoing, and even cause some reverse remodeling. I don’t think we have any clue in nonischemic cardiomyopathies as to what the disease causes are and whether correcting the secondary MR will cause reverse remodeling. So if I were to bet one way or another on which one’s going to respond better to MitraClip therapy, I would say ischemic cardiomyopathy,” the surgeon said.
As to who’s at prohibitive surgical risk and therefore potentially eligible for percutaneous repair, the criteria established for use of the MitraClip for its approved indication also apply to candidates for the COAPT trial. These criteria include an STS mortality score of 8%-10% or more, a porcelain aorta, severe COPD, advanced liver disease, frailty, severe mitral annular calcification, what surgeons call a “hostile chest” due to prior sternectomy or other causes, and/or severe pulmonary hypertension. The determination is to be made jointly by a cardiologist and surgeon functioning within a local heart team.
Enrollment in the COAPT study has been “extremely difficult” because of widespread, albeit misplaced, pro-surgery bias, but the roster should be filled by the end of the year, Dr. Mack said.
He observed that a major disadvantage of the MitraClip is that it does only one thing: clip the leaflets together.
“In surgery, at least for primary MR, we never do one thing. We’ll resect, we’ll put cords in, we’ll do an annuloplasty,” he explained.
In the future – post COAPT – a likely scenario is that the MitraClip will routinely be employed together with a complementary percutaneous posterior mitral annuloplasty procedure, he said. The top candidate, in his view, is the Valtech Cardioband device.
“That’s the one with the most experience and success for transcatheter mitral annuloplasty. It’s done under 3-D transesophageal echocardiographic guidance. Thirty patients have been enrolled in a European feasibility trial, with a device success rate of 88%. Eighty-five percent of those 30 patients are none-to-trace MR at 6 months’ follow-up,” said Dr. Mack.
Dr. Bernard J. Gersh said that he totally agrees with Dr. Mack’s prediction of divergent outcomes in COAPT depending upon whether patients have ischemic or nonischemic dilated cardiomyopathy.
“As you look at the history of surgical procedures, those that are directed to a mechanism are successful, and those that are directed to the consequences of something are not. Idiopathic dilated cardiomyopathy is a totally different disease – it’s dysfunctional cells, we don’t really know why, and there’s very little fibrosis or scar. It’s a completely different mechanism. So I agree: If I had to bet, it’d be that it’s in ischemic MR that the MitraClip is relevant,” said Dr. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.
The COAPT trial is sponsored by Abbott Vascular. Dr. Mack reported receiving research grants from Abbott and Edwards Lifesciences.
SNOWMASS, COLO. – The ongoing COAPT trial will not only determine the future of the MitraClip device for transcatheter mitral valve repair, it will also answer a key broader question: Does fixing functional mitral regurgitation even provide meaningful clinical benefit?
“This is an extremely important study because we don’t know whether correcting secondary [mitral regurgitation (MR)] does anything to change the prognosis or survival in the disease. The [Food and Drug Administration] gets kudos for insisting on this study. This will be a major trial in which we learn whether interrupting functional MR adds anything to guideline-directed medical therapy or not,” Dr. Michael J. Mack predicted at the Annual Cardiovascular Conference at Snowmass.
The distinction between primary degenerative MR and secondary functional MR is key. In primary MR, the problem is that the valve itself has worn out. Secondary MR is a disease of the left ventricle, not the mitral valve. The source of the valve problem in secondary MR lies in a dilated left ventricle, which causes stretching of the valve annulus and displacement of the papillary muscles. This left ventricular dilation can be caused by either ischemic or nonischemic dilated cardiomyopathy. Regardless, functional MR is a disorder of left ventricular remodeling in which anatomically normal valve leaflets don’t coapt sufficiently.
The MitraClip device is designed for percutaneous repair of MR in patients deemed at unacceptable risk for surgery. The device clips the valve leaflets together without surgical suturing. The MitraClip won FDA approval in fall 2013 for repair of severely symptomatic primary degenerative mitral regurgitation in patients who have a reasonable life expectancy but prohibitive surgical risk due to comorbidities. Roughly 1,500 MitraClip procedures have been done to date in the United States, and the initial commercial experience will be presented as a late-breaker at the annual meeting of the American College of Cardiology in San Diego in March.
Functional MR is a whole different story. The FDA decided that for the MitraClip to gain an additional indication for functional or secondary MR, a randomized controlled trial would be required. Moreover, after considerable debate among valve experts, the FDA decreed that the control group should consist of patients on guideline-directed medical therapy since – much to the surprise of many physicians and surgeons – to date there is actually no persuasive evidence that surgical repair or replacement is effective therapy for functional MR, explained Dr. Mack, former president of the Society of Thoracic Surgeons and medical director at Baylor Health Care System in Plano, Tex.
Dr. Mack and Columbia University cardiologist Dr. Gregg W. Stone serve as co–principal investigators of COAPT, scheduled to include about 420 high-surgical-risk patients with severely symptomatic secondary MR at 75 U.S. sites. Patients will be followed clinically and by transthoracic echocardiography for 5 years, with the primary endpoint being the 2-year rates of survival and freedom from repeat hospitalization for heart failure.
Patients with both ischemic and nonischemic cardiomyopathies are being enrolled. However, their outcomes will be analyzed separately because investigators believe these disorders may not respond in the same way to any interventional therapy.
“I think that nonischemic cardiomyopathy is an idiopathic disease of unknown etiology, and probably multiple etiologies. It’s reasonable to think that in ischemic MR there’s something we can treat and in that way prevent a progressive process from ongoing, and even cause some reverse remodeling. I don’t think we have any clue in nonischemic cardiomyopathies as to what the disease causes are and whether correcting the secondary MR will cause reverse remodeling. So if I were to bet one way or another on which one’s going to respond better to MitraClip therapy, I would say ischemic cardiomyopathy,” the surgeon said.
As to who’s at prohibitive surgical risk and therefore potentially eligible for percutaneous repair, the criteria established for use of the MitraClip for its approved indication also apply to candidates for the COAPT trial. These criteria include an STS mortality score of 8%-10% or more, a porcelain aorta, severe COPD, advanced liver disease, frailty, severe mitral annular calcification, what surgeons call a “hostile chest” due to prior sternectomy or other causes, and/or severe pulmonary hypertension. The determination is to be made jointly by a cardiologist and surgeon functioning within a local heart team.
Enrollment in the COAPT study has been “extremely difficult” because of widespread, albeit misplaced, pro-surgery bias, but the roster should be filled by the end of the year, Dr. Mack said.
He observed that a major disadvantage of the MitraClip is that it does only one thing: clip the leaflets together.
“In surgery, at least for primary MR, we never do one thing. We’ll resect, we’ll put cords in, we’ll do an annuloplasty,” he explained.
In the future – post COAPT – a likely scenario is that the MitraClip will routinely be employed together with a complementary percutaneous posterior mitral annuloplasty procedure, he said. The top candidate, in his view, is the Valtech Cardioband device.
“That’s the one with the most experience and success for transcatheter mitral annuloplasty. It’s done under 3-D transesophageal echocardiographic guidance. Thirty patients have been enrolled in a European feasibility trial, with a device success rate of 88%. Eighty-five percent of those 30 patients are none-to-trace MR at 6 months’ follow-up,” said Dr. Mack.
Dr. Bernard J. Gersh said that he totally agrees with Dr. Mack’s prediction of divergent outcomes in COAPT depending upon whether patients have ischemic or nonischemic dilated cardiomyopathy.
“As you look at the history of surgical procedures, those that are directed to a mechanism are successful, and those that are directed to the consequences of something are not. Idiopathic dilated cardiomyopathy is a totally different disease – it’s dysfunctional cells, we don’t really know why, and there’s very little fibrosis or scar. It’s a completely different mechanism. So I agree: If I had to bet, it’d be that it’s in ischemic MR that the MitraClip is relevant,” said Dr. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.
The COAPT trial is sponsored by Abbott Vascular. Dr. Mack reported receiving research grants from Abbott and Edwards Lifesciences.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Most cardiologists misstep on aspirin in ACS
SNOWMASS, COLO. – U.S. cardiologists are glaringly out of touch with the guidelines on maintenance aspirin dosing in patients with acute coronary syndrome, American College of Cardiology President Dr. Patrick T. O’Gara said at the Annual Cardiovascular Conference at Snowmass.
The latest AHA/ACC guidelines state that maintenance aspirin therapy at 81 mg/day to be continued indefinitely is preferred over 325 mg/day in patients with ACS, regardless of whether they have received a coronary stent or noninvasive medical management (Circulation 2014 Dec 23;130(25):e344-426).
“This statement has been out there in the guidelines for several years now. Yet the last time we interrogated the NCDR [National Cardiovascular Data Registry], 70% of patients with ACS were discharged on 325 mg/day of aspirin in the U.S.,” said Dr. O’Gara, professor of medicine at Harvard Medical School and director of clinical cardiology at Brigham and Women’s Hospital, Boston.
The recommendation in the guidelines is based on several solid studies, including OASIS 7, which in more than 25,000 randomized patients showed no difference in outcomes when aspirin at 75-100 mg/day was compared with 300-325 mg/day, but an increased incidence of bleeding at the higher dose (N. Engl. J. Med. 2010;363:930-42).
“Aspirin at 81 mg/day is not inferior with respect to clinical efficacy and it’s superior with respect to its safety outcome. But here in the United States we are still very much wedded to using 325 mg of aspirin. I’m not exactly sure of the reasons for that. Maybe it’s a catch up phenomenon,” Dr. O’Gara commented.
In the setting of percutaneous coronary intervention with a bare metal or drug-eluting stent for patients with either non–ST-elevation ACS or ST-elevation MI, the AHA/ACC guidelines give a class I recommendation for at least 12 months of dual-antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor. Either ticagrelor (Brilinta) at 90 mg twice daily or prasugrel (Effient) once daily at 10 mg is recommended over clopidogrel at 75 mg/day in patients who can take those medications safely; this guidance is based on ticagrelor’s superior efficacy compared with clopidogrel as shown in TRITON TIMI-38 (N. Engl. J. Med. 2007;357:2001-15) and prasugrel’s superiority in the PLATO trial (N. Engl. J. Med. 2009;361:1045-57).
The AHA/ACC guidelines give a relatively tepid level IIb recommendation that continuation of DAPT beyond 12 months may be considered in stent recipients. Many observers expect a stronger endorsement in the next iteration of the guidelines on the strength of the recent DAPT study, which showed that 30 months of DAPT was better than 12 in terms of major adverse cardiac and cerebrovascular events (N. Engl. J. Med. 2014;371:2155-66).
“Interestingly enough, the mechanism of benefit had less to do with prevention of stent thrombosis than it did with prevention of recurrent MI and stroke. This renders into much sharper focus the question of whether we’re treating the patient or we’re treating the stent. This result would imply that we’re treating the patient,” Dr. O’Gara observed.
The guidelines also include a bail-out option which states that if the risk of bleeding outweighs the anticipated benefit, it’s reasonable to discontinue DAPT before 12 months.
“I don’t know a single practitioner who’s not had to withdraw one or both elements of DAPT because of bleeding or because of the need for unanticipated noncardiac surgery. It’s a fact of life, and sometimes you have to just hope for the best,” the cardiologist said.
He reported having no financial conflicts of interest.
SNOWMASS, COLO. – U.S. cardiologists are glaringly out of touch with the guidelines on maintenance aspirin dosing in patients with acute coronary syndrome, American College of Cardiology President Dr. Patrick T. O’Gara said at the Annual Cardiovascular Conference at Snowmass.
The latest AHA/ACC guidelines state that maintenance aspirin therapy at 81 mg/day to be continued indefinitely is preferred over 325 mg/day in patients with ACS, regardless of whether they have received a coronary stent or noninvasive medical management (Circulation 2014 Dec 23;130(25):e344-426).
“This statement has been out there in the guidelines for several years now. Yet the last time we interrogated the NCDR [National Cardiovascular Data Registry], 70% of patients with ACS were discharged on 325 mg/day of aspirin in the U.S.,” said Dr. O’Gara, professor of medicine at Harvard Medical School and director of clinical cardiology at Brigham and Women’s Hospital, Boston.
The recommendation in the guidelines is based on several solid studies, including OASIS 7, which in more than 25,000 randomized patients showed no difference in outcomes when aspirin at 75-100 mg/day was compared with 300-325 mg/day, but an increased incidence of bleeding at the higher dose (N. Engl. J. Med. 2010;363:930-42).
“Aspirin at 81 mg/day is not inferior with respect to clinical efficacy and it’s superior with respect to its safety outcome. But here in the United States we are still very much wedded to using 325 mg of aspirin. I’m not exactly sure of the reasons for that. Maybe it’s a catch up phenomenon,” Dr. O’Gara commented.
In the setting of percutaneous coronary intervention with a bare metal or drug-eluting stent for patients with either non–ST-elevation ACS or ST-elevation MI, the AHA/ACC guidelines give a class I recommendation for at least 12 months of dual-antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor. Either ticagrelor (Brilinta) at 90 mg twice daily or prasugrel (Effient) once daily at 10 mg is recommended over clopidogrel at 75 mg/day in patients who can take those medications safely; this guidance is based on ticagrelor’s superior efficacy compared with clopidogrel as shown in TRITON TIMI-38 (N. Engl. J. Med. 2007;357:2001-15) and prasugrel’s superiority in the PLATO trial (N. Engl. J. Med. 2009;361:1045-57).
The AHA/ACC guidelines give a relatively tepid level IIb recommendation that continuation of DAPT beyond 12 months may be considered in stent recipients. Many observers expect a stronger endorsement in the next iteration of the guidelines on the strength of the recent DAPT study, which showed that 30 months of DAPT was better than 12 in terms of major adverse cardiac and cerebrovascular events (N. Engl. J. Med. 2014;371:2155-66).
“Interestingly enough, the mechanism of benefit had less to do with prevention of stent thrombosis than it did with prevention of recurrent MI and stroke. This renders into much sharper focus the question of whether we’re treating the patient or we’re treating the stent. This result would imply that we’re treating the patient,” Dr. O’Gara observed.
The guidelines also include a bail-out option which states that if the risk of bleeding outweighs the anticipated benefit, it’s reasonable to discontinue DAPT before 12 months.
“I don’t know a single practitioner who’s not had to withdraw one or both elements of DAPT because of bleeding or because of the need for unanticipated noncardiac surgery. It’s a fact of life, and sometimes you have to just hope for the best,” the cardiologist said.
He reported having no financial conflicts of interest.
SNOWMASS, COLO. – U.S. cardiologists are glaringly out of touch with the guidelines on maintenance aspirin dosing in patients with acute coronary syndrome, American College of Cardiology President Dr. Patrick T. O’Gara said at the Annual Cardiovascular Conference at Snowmass.
The latest AHA/ACC guidelines state that maintenance aspirin therapy at 81 mg/day to be continued indefinitely is preferred over 325 mg/day in patients with ACS, regardless of whether they have received a coronary stent or noninvasive medical management (Circulation 2014 Dec 23;130(25):e344-426).
“This statement has been out there in the guidelines for several years now. Yet the last time we interrogated the NCDR [National Cardiovascular Data Registry], 70% of patients with ACS were discharged on 325 mg/day of aspirin in the U.S.,” said Dr. O’Gara, professor of medicine at Harvard Medical School and director of clinical cardiology at Brigham and Women’s Hospital, Boston.
The recommendation in the guidelines is based on several solid studies, including OASIS 7, which in more than 25,000 randomized patients showed no difference in outcomes when aspirin at 75-100 mg/day was compared with 300-325 mg/day, but an increased incidence of bleeding at the higher dose (N. Engl. J. Med. 2010;363:930-42).
“Aspirin at 81 mg/day is not inferior with respect to clinical efficacy and it’s superior with respect to its safety outcome. But here in the United States we are still very much wedded to using 325 mg of aspirin. I’m not exactly sure of the reasons for that. Maybe it’s a catch up phenomenon,” Dr. O’Gara commented.
In the setting of percutaneous coronary intervention with a bare metal or drug-eluting stent for patients with either non–ST-elevation ACS or ST-elevation MI, the AHA/ACC guidelines give a class I recommendation for at least 12 months of dual-antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor. Either ticagrelor (Brilinta) at 90 mg twice daily or prasugrel (Effient) once daily at 10 mg is recommended over clopidogrel at 75 mg/day in patients who can take those medications safely; this guidance is based on ticagrelor’s superior efficacy compared with clopidogrel as shown in TRITON TIMI-38 (N. Engl. J. Med. 2007;357:2001-15) and prasugrel’s superiority in the PLATO trial (N. Engl. J. Med. 2009;361:1045-57).
The AHA/ACC guidelines give a relatively tepid level IIb recommendation that continuation of DAPT beyond 12 months may be considered in stent recipients. Many observers expect a stronger endorsement in the next iteration of the guidelines on the strength of the recent DAPT study, which showed that 30 months of DAPT was better than 12 in terms of major adverse cardiac and cerebrovascular events (N. Engl. J. Med. 2014;371:2155-66).
“Interestingly enough, the mechanism of benefit had less to do with prevention of stent thrombosis than it did with prevention of recurrent MI and stroke. This renders into much sharper focus the question of whether we’re treating the patient or we’re treating the stent. This result would imply that we’re treating the patient,” Dr. O’Gara observed.
The guidelines also include a bail-out option which states that if the risk of bleeding outweighs the anticipated benefit, it’s reasonable to discontinue DAPT before 12 months.
“I don’t know a single practitioner who’s not had to withdraw one or both elements of DAPT because of bleeding or because of the need for unanticipated noncardiac surgery. It’s a fact of life, and sometimes you have to just hope for the best,” the cardiologist said.
He reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Renal denervation therapy: What’s next
SNOWMASS, COLO. – Reports of the demise of catheter-based renal denervation therapy for resistant hypertension in light of the disappointing SYMPLICITY HTN-3 trial results are greatly exaggerated, according to Dr. Bernard J. Gersh.
“I think what we can say about renal denervation is that the initial enthusiasm has been tempered and the number of unanswered questions is not decreasing. But the concept, I assure you, still maintains its promise,” the cardiologist said at the annual Cardiovascular Conference at Snowmass.

Expectations for SYMPLICITY HTN-3 were sky high in the cardiology and business worlds on the basis of the prior unblinded SYMPLICITY HTN-1 and -2 studies showing renal denervation (RDN) achieved spectacular reductions in systolic blood pressure of 25-30 mm Hg in patients with multidrug-resistant hypertension. As the chair of the SYMPLICITY HTN-3 data safety monitoring board, he knew the outcome prior to release of the results, and he was struck that during that period the talk at cardiology conferences was only of next-generation RDN catheters and expanded indications, such as heart failure and even metabolic syndrome. Absolutely no one seemed to entertain the possibility that the results wouldn’t be positive.
So the general reaction to the SYMPLICITY HTN-3 results was profound, crushing disappointment. The trial, which was the first blinded, controlled study of RDN, showed significant reduction in blood pressure at 6 months in the RDN recipients, but a similar reduction in medically managed controls who underwent a sham RDN procedure, making for a neutral study outcome (N. Engl. J. Med. 2014;370:1393-59).
Yet the physiologic basis remains strong for RDN as a treatment for hypertension, heart failure, and perhaps other cardiovascular disorders in which sympathetic nervous system activation plays a crucial role, according to Dr. Gersh, who chaired the data safety monitoring board for SYMPLICITY HTN-3 and is a professor of medicine at the Mayo Clinic in Rochester, Minn.
He cited a recommended review written by a pioneer in the field, Dr. Murray Esler of Australia, who observed that increased renal sympathetic nervous system activity increases the secretion rate of renin, reduces renal blood flow, and boosts renal tubular sodium reabsorption while reducing urinary sodium excretion, all actions that contribute to hypertension (Exp. Physiol. 2011;96:611-22).
Dr. Gersh ticked off many potential explanations for the neutral outcome in SYMPLICITY HTN-3, including the placebo effect; regression to the mean; operator inexperience; limitations of the current technology; and the likelihood that a fair number of study participants didn’t have true treatment-resistant hypertension, but were merely resistant to taking their medication until they entered a structured, supervised randomized trial setting. The power of a placebo procedure is not to be underestimated, the cardiologist emphasized. He cited a striking illustration from another field of medicine, in which a recent meta-analysis of 137 controlled studies in more than 33,000 patients with knee osteoarthritis showed that intra-articular placebo injections outperformed oral naproxen, celecoxib, and placebo in terms of pain relief (Ann. Intern. Med. 2015;162:46-54).
Regression to the mean definitely occurred in SYMPLICITY HTN-3, as evidenced by the fact that reductions in office systolic blood pressure (SBP) averaged 25.7 and 19.7 mm Hg, respectively, in RDN recipients and controls with a baseline greater than 184 mm Hg, compared with 13.8 and 9.8 mm Hg in those with a lower baseline SBP, of 170-184 mm Hg, Dr. Gersh continued.
Operator inexperience was likely a factor in the study outcomes: Nearly one-third of the operators dad done just one procedure. And while the study protocol called for four to six ablations per side, a recent secondary analysis of SYMPLICITY HTN-3 showed that the greater the number of ablations, the greater the drop in SBP. Patients who received at least seven ablations per side averaged a nearly threefold larger blood pressure reduction at 6 months, compared with those who got five or six per side (Eur. Heart J. 2015;36:219-27).
Some 39% of study participants had a medication change because of side effects during the 6-month trial. This confounds attempts to assess the true impact of RDN. To answer this question, the Food and Drug Administration recently granted Boston Scientific approval to test RDN in a sham-controlled trial in patients with mild to moderate hypertension after a 4-week medication washout period. The 6-month trial is due to start shortly. This is an important study because it will demonstrate whether RDN in its present form actually works.
“Clearly, what we’ve learned in SYMPLICITY HTN-3 is ‘resistant’ hypertension is amenable to expert pharmacologic control. This raises an interesting question: If renal nerve denervation works, could we offer it as an alternative to taking two or three drugs for the next 10 or 20 years? That might be, in certain patient populations, a very attractive option. That’s why we’ve got to show whether this procedure works well,” according to Dr. Gersh.
Now that SYMPLICITY HTN-3 has provided a reality check, the necessary next steps include improving the technology. Current levels of achieved RDN using only proximal ablation are suboptimal. What’s needed are higher-energy, multipolar electrodes that deliver energy both proximally and distally; such equipment is well along in development.
A thornier limitation involves the lack of a method for immediate testing of the completeness of an RDN procedure in a given patient. Unlike in coronary stent placement, where an interventional cardiologist can immediately see angiographically whether the device is properly seated, RDN operators have no way to tell intraprocedurally whether effective RDN has been achieved. Two methods now under investigation are intra-arterial adenosine and urinary biomarkers of nerve degradation.
The pathophysiology of hypertension is variable, so efforts are underway to identify patient subsets in which sympathetic nervous system overactivity is a primary underlying mechanism and RDN should have its greatest impact.
“I think renal denervation is still worthy of investigation, particularly in patients with resistant hypertension and perhaps other disease states characterized by sympathetic overactivity, such as heart failure,” Dr. Gersh concluded. “How do I think it’s going to all turn out? I just don’t know. We’ll see. We need the trials. I don’t think we should close the book on this very exciting technique. I simply don’t know what the trials are going to show.”
SYMPLICITY HTN-3 was funded by Medtronic. Dr. Gersh reported serving as a consultant to Merck and Ortho-McNeil-Janssen and on data safety monitoring boards for trials sponsored by Baxter, Medtronic, and Teva Pharmaceuticals.
SNOWMASS, COLO. – Reports of the demise of catheter-based renal denervation therapy for resistant hypertension in light of the disappointing SYMPLICITY HTN-3 trial results are greatly exaggerated, according to Dr. Bernard J. Gersh.
“I think what we can say about renal denervation is that the initial enthusiasm has been tempered and the number of unanswered questions is not decreasing. But the concept, I assure you, still maintains its promise,” the cardiologist said at the annual Cardiovascular Conference at Snowmass.
Expectations for SYMPLICITY HTN-3 were sky high in the cardiology and business worlds on the basis of the prior unblinded SYMPLICITY HTN-1 and -2 studies showing renal denervation (RDN) achieved spectacular reductions in systolic blood pressure of 25-30 mm Hg in patients with multidrug-resistant hypertension. As the chair of the SYMPLICITY HTN-3 data safety monitoring board, he knew the outcome prior to release of the results, and he was struck that during that period the talk at cardiology conferences was only of next-generation RDN catheters and expanded indications, such as heart failure and even metabolic syndrome. Absolutely no one seemed to entertain the possibility that the results wouldn’t be positive.
So the general reaction to the SYMPLICITY HTN-3 results was profound, crushing disappointment. The trial, which was the first blinded, controlled study of RDN, showed significant reduction in blood pressure at 6 months in the RDN recipients, but a similar reduction in medically managed controls who underwent a sham RDN procedure, making for a neutral study outcome (N. Engl. J. Med. 2014;370:1393-59).
Yet the physiologic basis remains strong for RDN as a treatment for hypertension, heart failure, and perhaps other cardiovascular disorders in which sympathetic nervous system activation plays a crucial role, according to Dr. Gersh, who chaired the data safety monitoring board for SYMPLICITY HTN-3 and is a professor of medicine at the Mayo Clinic in Rochester, Minn.
He cited a recommended review written by a pioneer in the field, Dr. Murray Esler of Australia, who observed that increased renal sympathetic nervous system activity increases the secretion rate of renin, reduces renal blood flow, and boosts renal tubular sodium reabsorption while reducing urinary sodium excretion, all actions that contribute to hypertension (Exp. Physiol. 2011;96:611-22).
Dr. Gersh ticked off many potential explanations for the neutral outcome in SYMPLICITY HTN-3, including the placebo effect; regression to the mean; operator inexperience; limitations of the current technology; and the likelihood that a fair number of study participants didn’t have true treatment-resistant hypertension, but were merely resistant to taking their medication until they entered a structured, supervised randomized trial setting. The power of a placebo procedure is not to be underestimated, the cardiologist emphasized. He cited a striking illustration from another field of medicine, in which a recent meta-analysis of 137 controlled studies in more than 33,000 patients with knee osteoarthritis showed that intra-articular placebo injections outperformed oral naproxen, celecoxib, and placebo in terms of pain relief (Ann. Intern. Med. 2015;162:46-54).
Regression to the mean definitely occurred in SYMPLICITY HTN-3, as evidenced by the fact that reductions in office systolic blood pressure (SBP) averaged 25.7 and 19.7 mm Hg, respectively, in RDN recipients and controls with a baseline greater than 184 mm Hg, compared with 13.8 and 9.8 mm Hg in those with a lower baseline SBP, of 170-184 mm Hg, Dr. Gersh continued.
Operator inexperience was likely a factor in the study outcomes: Nearly one-third of the operators dad done just one procedure. And while the study protocol called for four to six ablations per side, a recent secondary analysis of SYMPLICITY HTN-3 showed that the greater the number of ablations, the greater the drop in SBP. Patients who received at least seven ablations per side averaged a nearly threefold larger blood pressure reduction at 6 months, compared with those who got five or six per side (Eur. Heart J. 2015;36:219-27).
Some 39% of study participants had a medication change because of side effects during the 6-month trial. This confounds attempts to assess the true impact of RDN. To answer this question, the Food and Drug Administration recently granted Boston Scientific approval to test RDN in a sham-controlled trial in patients with mild to moderate hypertension after a 4-week medication washout period. The 6-month trial is due to start shortly. This is an important study because it will demonstrate whether RDN in its present form actually works.
“Clearly, what we’ve learned in SYMPLICITY HTN-3 is ‘resistant’ hypertension is amenable to expert pharmacologic control. This raises an interesting question: If renal nerve denervation works, could we offer it as an alternative to taking two or three drugs for the next 10 or 20 years? That might be, in certain patient populations, a very attractive option. That’s why we’ve got to show whether this procedure works well,” according to Dr. Gersh.
Now that SYMPLICITY HTN-3 has provided a reality check, the necessary next steps include improving the technology. Current levels of achieved RDN using only proximal ablation are suboptimal. What’s needed are higher-energy, multipolar electrodes that deliver energy both proximally and distally; such equipment is well along in development.
A thornier limitation involves the lack of a method for immediate testing of the completeness of an RDN procedure in a given patient. Unlike in coronary stent placement, where an interventional cardiologist can immediately see angiographically whether the device is properly seated, RDN operators have no way to tell intraprocedurally whether effective RDN has been achieved. Two methods now under investigation are intra-arterial adenosine and urinary biomarkers of nerve degradation.
The pathophysiology of hypertension is variable, so efforts are underway to identify patient subsets in which sympathetic nervous system overactivity is a primary underlying mechanism and RDN should have its greatest impact.
“I think renal denervation is still worthy of investigation, particularly in patients with resistant hypertension and perhaps other disease states characterized by sympathetic overactivity, such as heart failure,” Dr. Gersh concluded. “How do I think it’s going to all turn out? I just don’t know. We’ll see. We need the trials. I don’t think we should close the book on this very exciting technique. I simply don’t know what the trials are going to show.”
SYMPLICITY HTN-3 was funded by Medtronic. Dr. Gersh reported serving as a consultant to Merck and Ortho-McNeil-Janssen and on data safety monitoring boards for trials sponsored by Baxter, Medtronic, and Teva Pharmaceuticals.
SNOWMASS, COLO. – Reports of the demise of catheter-based renal denervation therapy for resistant hypertension in light of the disappointing SYMPLICITY HTN-3 trial results are greatly exaggerated, according to Dr. Bernard J. Gersh.
“I think what we can say about renal denervation is that the initial enthusiasm has been tempered and the number of unanswered questions is not decreasing. But the concept, I assure you, still maintains its promise,” the cardiologist said at the annual Cardiovascular Conference at Snowmass.
Expectations for SYMPLICITY HTN-3 were sky high in the cardiology and business worlds on the basis of the prior unblinded SYMPLICITY HTN-1 and -2 studies showing renal denervation (RDN) achieved spectacular reductions in systolic blood pressure of 25-30 mm Hg in patients with multidrug-resistant hypertension. As the chair of the SYMPLICITY HTN-3 data safety monitoring board, he knew the outcome prior to release of the results, and he was struck that during that period the talk at cardiology conferences was only of next-generation RDN catheters and expanded indications, such as heart failure and even metabolic syndrome. Absolutely no one seemed to entertain the possibility that the results wouldn’t be positive.
So the general reaction to the SYMPLICITY HTN-3 results was profound, crushing disappointment. The trial, which was the first blinded, controlled study of RDN, showed significant reduction in blood pressure at 6 months in the RDN recipients, but a similar reduction in medically managed controls who underwent a sham RDN procedure, making for a neutral study outcome (N. Engl. J. Med. 2014;370:1393-59).
Yet the physiologic basis remains strong for RDN as a treatment for hypertension, heart failure, and perhaps other cardiovascular disorders in which sympathetic nervous system activation plays a crucial role, according to Dr. Gersh, who chaired the data safety monitoring board for SYMPLICITY HTN-3 and is a professor of medicine at the Mayo Clinic in Rochester, Minn.
He cited a recommended review written by a pioneer in the field, Dr. Murray Esler of Australia, who observed that increased renal sympathetic nervous system activity increases the secretion rate of renin, reduces renal blood flow, and boosts renal tubular sodium reabsorption while reducing urinary sodium excretion, all actions that contribute to hypertension (Exp. Physiol. 2011;96:611-22).
Dr. Gersh ticked off many potential explanations for the neutral outcome in SYMPLICITY HTN-3, including the placebo effect; regression to the mean; operator inexperience; limitations of the current technology; and the likelihood that a fair number of study participants didn’t have true treatment-resistant hypertension, but were merely resistant to taking their medication until they entered a structured, supervised randomized trial setting. The power of a placebo procedure is not to be underestimated, the cardiologist emphasized. He cited a striking illustration from another field of medicine, in which a recent meta-analysis of 137 controlled studies in more than 33,000 patients with knee osteoarthritis showed that intra-articular placebo injections outperformed oral naproxen, celecoxib, and placebo in terms of pain relief (Ann. Intern. Med. 2015;162:46-54).
Regression to the mean definitely occurred in SYMPLICITY HTN-3, as evidenced by the fact that reductions in office systolic blood pressure (SBP) averaged 25.7 and 19.7 mm Hg, respectively, in RDN recipients and controls with a baseline greater than 184 mm Hg, compared with 13.8 and 9.8 mm Hg in those with a lower baseline SBP, of 170-184 mm Hg, Dr. Gersh continued.
Operator inexperience was likely a factor in the study outcomes: Nearly one-third of the operators dad done just one procedure. And while the study protocol called for four to six ablations per side, a recent secondary analysis of SYMPLICITY HTN-3 showed that the greater the number of ablations, the greater the drop in SBP. Patients who received at least seven ablations per side averaged a nearly threefold larger blood pressure reduction at 6 months, compared with those who got five or six per side (Eur. Heart J. 2015;36:219-27).
Some 39% of study participants had a medication change because of side effects during the 6-month trial. This confounds attempts to assess the true impact of RDN. To answer this question, the Food and Drug Administration recently granted Boston Scientific approval to test RDN in a sham-controlled trial in patients with mild to moderate hypertension after a 4-week medication washout period. The 6-month trial is due to start shortly. This is an important study because it will demonstrate whether RDN in its present form actually works.
“Clearly, what we’ve learned in SYMPLICITY HTN-3 is ‘resistant’ hypertension is amenable to expert pharmacologic control. This raises an interesting question: If renal nerve denervation works, could we offer it as an alternative to taking two or three drugs for the next 10 or 20 years? That might be, in certain patient populations, a very attractive option. That’s why we’ve got to show whether this procedure works well,” according to Dr. Gersh.
Now that SYMPLICITY HTN-3 has provided a reality check, the necessary next steps include improving the technology. Current levels of achieved RDN using only proximal ablation are suboptimal. What’s needed are higher-energy, multipolar electrodes that deliver energy both proximally and distally; such equipment is well along in development.
A thornier limitation involves the lack of a method for immediate testing of the completeness of an RDN procedure in a given patient. Unlike in coronary stent placement, where an interventional cardiologist can immediately see angiographically whether the device is properly seated, RDN operators have no way to tell intraprocedurally whether effective RDN has been achieved. Two methods now under investigation are intra-arterial adenosine and urinary biomarkers of nerve degradation.
The pathophysiology of hypertension is variable, so efforts are underway to identify patient subsets in which sympathetic nervous system overactivity is a primary underlying mechanism and RDN should have its greatest impact.
“I think renal denervation is still worthy of investigation, particularly in patients with resistant hypertension and perhaps other disease states characterized by sympathetic overactivity, such as heart failure,” Dr. Gersh concluded. “How do I think it’s going to all turn out? I just don’t know. We’ll see. We need the trials. I don’t think we should close the book on this very exciting technique. I simply don’t know what the trials are going to show.”
SYMPLICITY HTN-3 was funded by Medtronic. Dr. Gersh reported serving as a consultant to Merck and Ortho-McNeil-Janssen and on data safety monitoring boards for trials sponsored by Baxter, Medtronic, and Teva Pharmaceuticals.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Commonly cited lymphedema risk factors ‘myth-busted’
SAN ANTONIO – Breast cancer patients are often advised that in order to avoid developing lymphedema they should shun blood pressure cuffs, injections, and blood draws on their at-risk arm as well as airplane travel unless wearing a compression sleeve.
All these recommendations are anecdotally based. None withstood formal evaluation in a prospective study of 710 breast cancer patients with 860 treated and thus potentially at-risk breasts, Chantal M. Ferguson reported at the San Antonio Breast Cancer Symposium.
“Our findings don’t support current guidelines regarding these activities and suggest that further studies are needed to determine if these guidelines are appropriate,” said Ms. Ferguson of Massachusetts General Hospital, Boston.

Standard practice for newly diagnosed breast cancer patients at Mass. General is to enter into a prospective screening program for lymphedema, a chronic, painful swelling caused by damage to the lymphatic system secondary to breast cancer therapy.
Breast cancer patients routinely have bilateral arm volume measurements taken using a perometer preoperatively, postoperatively, after finishing chemotherapy and radiotherapy, and at 3- to 7-month intervals thereafter following completion of treatment. At each measurement, data are collected on exposures to airplane flights, blood pressure readings, and the other often-cited putative risk factors.
The incidence of lymphedema among the 710 patients in the study at 24 months was 7.05%. The diagnosis required at least a 10% increase in arm volume, compared with the untreated side. For women who underwent bilateral breast surgery, a weight-adjusted volume change formula was employed.
Consistent with the medical literature, axial lymph node dissection and a higher preoperative body mass index were significantly associated with the development of lymphedema. So was self-reported trauma to the at-risk arm, although the reported trauma ranged in severity from bruises to fractures in motor vehicle accidents.
Session cochair Dr. Michelle E. Melisko observed that few medical oncologists are well informed about lymphedema or the numerous and highly complex functions of the lymphatic system, so she was favorably impressed that physicians at Mass. General have incorporated structured screening for the disorder as part of the institutional standard of care.
She cautioned, however, that rates of the risk factor events under study were relatively low. For example, only 17% of the breast cancer patients had one or more blood pressure measurements taken on their at-risk arm during 2 years of prospective follow-up, 9% had one or more blood draws, and 15% of patients flew for a total of 12 hours or more.
“I’m not sure that we can take these data to say we can let patients go hog wild and get their blood pressure measured all the time on that arm. This is a large prospective trial featuring a broad range of patient ages and BMIs, and both lumpectomy and mastectomy patients, and the trial adds a lot to the literature, but it does need to be interpreted with caution,” said Dr. Melisko of the University of California, San Francisco.
The study was funded by the National Cancer Institute and the Adele McKinnon Research Fund for Breast Cancer–related Lymphedema. Ms. Ferguson reported having no financial conflicts.
SAN ANTONIO – Breast cancer patients are often advised that in order to avoid developing lymphedema they should shun blood pressure cuffs, injections, and blood draws on their at-risk arm as well as airplane travel unless wearing a compression sleeve.
All these recommendations are anecdotally based. None withstood formal evaluation in a prospective study of 710 breast cancer patients with 860 treated and thus potentially at-risk breasts, Chantal M. Ferguson reported at the San Antonio Breast Cancer Symposium.
“Our findings don’t support current guidelines regarding these activities and suggest that further studies are needed to determine if these guidelines are appropriate,” said Ms. Ferguson of Massachusetts General Hospital, Boston.
Standard practice for newly diagnosed breast cancer patients at Mass. General is to enter into a prospective screening program for lymphedema, a chronic, painful swelling caused by damage to the lymphatic system secondary to breast cancer therapy.
Breast cancer patients routinely have bilateral arm volume measurements taken using a perometer preoperatively, postoperatively, after finishing chemotherapy and radiotherapy, and at 3- to 7-month intervals thereafter following completion of treatment. At each measurement, data are collected on exposures to airplane flights, blood pressure readings, and the other often-cited putative risk factors.
The incidence of lymphedema among the 710 patients in the study at 24 months was 7.05%. The diagnosis required at least a 10% increase in arm volume, compared with the untreated side. For women who underwent bilateral breast surgery, a weight-adjusted volume change formula was employed.
Consistent with the medical literature, axial lymph node dissection and a higher preoperative body mass index were significantly associated with the development of lymphedema. So was self-reported trauma to the at-risk arm, although the reported trauma ranged in severity from bruises to fractures in motor vehicle accidents.
Session cochair Dr. Michelle E. Melisko observed that few medical oncologists are well informed about lymphedema or the numerous and highly complex functions of the lymphatic system, so she was favorably impressed that physicians at Mass. General have incorporated structured screening for the disorder as part of the institutional standard of care.
She cautioned, however, that rates of the risk factor events under study were relatively low. For example, only 17% of the breast cancer patients had one or more blood pressure measurements taken on their at-risk arm during 2 years of prospective follow-up, 9% had one or more blood draws, and 15% of patients flew for a total of 12 hours or more.
“I’m not sure that we can take these data to say we can let patients go hog wild and get their blood pressure measured all the time on that arm. This is a large prospective trial featuring a broad range of patient ages and BMIs, and both lumpectomy and mastectomy patients, and the trial adds a lot to the literature, but it does need to be interpreted with caution,” said Dr. Melisko of the University of California, San Francisco.
The study was funded by the National Cancer Institute and the Adele McKinnon Research Fund for Breast Cancer–related Lymphedema. Ms. Ferguson reported having no financial conflicts.
SAN ANTONIO – Breast cancer patients are often advised that in order to avoid developing lymphedema they should shun blood pressure cuffs, injections, and blood draws on their at-risk arm as well as airplane travel unless wearing a compression sleeve.
All these recommendations are anecdotally based. None withstood formal evaluation in a prospective study of 710 breast cancer patients with 860 treated and thus potentially at-risk breasts, Chantal M. Ferguson reported at the San Antonio Breast Cancer Symposium.
“Our findings don’t support current guidelines regarding these activities and suggest that further studies are needed to determine if these guidelines are appropriate,” said Ms. Ferguson of Massachusetts General Hospital, Boston.
Standard practice for newly diagnosed breast cancer patients at Mass. General is to enter into a prospective screening program for lymphedema, a chronic, painful swelling caused by damage to the lymphatic system secondary to breast cancer therapy.
Breast cancer patients routinely have bilateral arm volume measurements taken using a perometer preoperatively, postoperatively, after finishing chemotherapy and radiotherapy, and at 3- to 7-month intervals thereafter following completion of treatment. At each measurement, data are collected on exposures to airplane flights, blood pressure readings, and the other often-cited putative risk factors.
The incidence of lymphedema among the 710 patients in the study at 24 months was 7.05%. The diagnosis required at least a 10% increase in arm volume, compared with the untreated side. For women who underwent bilateral breast surgery, a weight-adjusted volume change formula was employed.
Consistent with the medical literature, axial lymph node dissection and a higher preoperative body mass index were significantly associated with the development of lymphedema. So was self-reported trauma to the at-risk arm, although the reported trauma ranged in severity from bruises to fractures in motor vehicle accidents.
Session cochair Dr. Michelle E. Melisko observed that few medical oncologists are well informed about lymphedema or the numerous and highly complex functions of the lymphatic system, so she was favorably impressed that physicians at Mass. General have incorporated structured screening for the disorder as part of the institutional standard of care.
She cautioned, however, that rates of the risk factor events under study were relatively low. For example, only 17% of the breast cancer patients had one or more blood pressure measurements taken on their at-risk arm during 2 years of prospective follow-up, 9% had one or more blood draws, and 15% of patients flew for a total of 12 hours or more.
“I’m not sure that we can take these data to say we can let patients go hog wild and get their blood pressure measured all the time on that arm. This is a large prospective trial featuring a broad range of patient ages and BMIs, and both lumpectomy and mastectomy patients, and the trial adds a lot to the literature, but it does need to be interpreted with caution,” said Dr. Melisko of the University of California, San Francisco.
The study was funded by the National Cancer Institute and the Adele McKinnon Research Fund for Breast Cancer–related Lymphedema. Ms. Ferguson reported having no financial conflicts.
AT SABCS 2014
Key clinical point: In order to reduce their risk of lymphedema, breast cancer patients are often advised to avoid certain activities which turned out not to be associated with the chronic disorder in a prospective study.
Major finding: Blood draws, injections, and blood pressure measurements on the at-risk arm did not prove to be risk factors for lymphedema. Neither was airplane travel without a compression sleeve.
Data source: This was a prospective study of 710 breast cancer patients with 860 treated breasts, 7.05% of whom developed lymphedema during 24 months of follow-up.
Disclosures: The study was funded by the National Cancer Institute and the Adele McKinnon Research Fund for Breast Cancer-Related Lymphedema. Ms. Ferguson reported having no financial conflicts.

Shifting surgical strategies in ischemic mitral regurgitation
SNOWMASS, COLO. – In a major reversal of longstanding opinion, thought leaders in cardiothoracic surgery now increasingly favor mitral valve replacement over repair in patients with severe ischemic mitral regurgitation.
The overwhelming preference among both surgeons and cardiologists has been for mitral valve repair, but recent randomized trial evidence shows that mitral valve replacement provides a more durable correction with no increase in adverse events. That’s persuaded many surgical leaders to move towards replacement until improved repair strategies can be developed, Dr. Vinod H. Thourani said at the Annual Cardiovascular Conference at Snowmass.

“When I do a replacement in a patient, the cardiologist will call me and ask why. He’ll say, ‘I was hoping you were going to do a repair.’ Now we have to completely change our mentality about this,” said Dr. Thourani, professor of surgery and codirector of the Structural Heart and Valve Center at Emory University in Atlanta.
That need for a mind-shift goes for cardiothoracic surgeons as well as cardiologists, he added, pointing to an analysis of the Society of Thoracic Surgeons adult cardiac surgery database for 2008-2012 showing roughly a 65%-35% preference for repair over replacement.
The evidence favoring mitral valve replacement is so new it didn’t make it into the deliberations that generated the freshly minted 2014 ACC/AHA guidelines on valvular heart disease management (J. Am. Coll. Cardiol. 2014;63:e57-185), which state that “there is no conclusive evidence for superiority of repair or replacement” in severe ischemic mitral regurgitation (MR). That statement is no longer true, in Dr. Thourani’s view.
He highlighted a multicenter randomized trial conducted by the Cardiothoracic Surgical Trials Network (CSTN) in which 251 patients with severe ischemic mitral regurgitation were randomized to repair or replacement. The primary endpoint – change in left ventricular end-systolic volume index indicative of reversal of ventricular remodeling – improved similarly in both groups. Nor did the two treatment groups differ significantly in 30-day and 12-month mortality or rates of stroke, heart failure, bleeding, infection, and other major adverse events. The eye opener was that 32.6% of patients in the repair group had moderate or severe mitral regurgitation at 12 months, compared with just 2.3% in the replacement group (N. Engl. J. Med. 2014;370:23-32).
“This study was done at a group of high-functioning academic centers where surgeons are supposed to know how to do repair and do replacement, yet one-third of our patients have come back with moderate to severe MR after repair. This has opened up a lot of discussion among surgeons as to what we should be doing,” noted Dr. Thourani, who participated in the trial.
One-year mortality was 14.2% in the repair group and a statistically similar 17.6% in the valve-replacement group, but Dr. Thourani anticipates a steeper mortality rise ahead for the repair group. “It’ll be interesting to see where these patients living with recurrent MR will be at the 2- and 5-year marks,” he said.
In a subsequent analysis, the CSTN investigators examined whether baseline clinical and echocardiographic characteristics in patients randomized to repair could identify a subgroup at high risk for recurrent moderate-to-severe mitral regurgitation or death within 2 years post surgery. They identified a predictive model that shows promise, with a favorable area under the receiver operating characteristic curve of 0.82.
The model is based on 10 factors: age; gender; race; body mass index; New York Heart Association class; effective regurgitant orifice area; basal aneurysm/dyskinesia; and history of coronary artery bypass grafting, percutaneous coronary intervention, or ventricular arrhythmias (J. Thorac. Cardiovasc. Surg. 2014 Nov 6. pii: S0022-5223(14)01772-3).
Of these 10 variables, the standout predictor was basal aneurysm/dyskinesia. “If you repair those patients, they have a really high likelihood of having worse outcomes,” according to Dr. Thourani.
This analysis of the CSTN repair subgroup shed new light on the MR-recurrence phenomenon. Roughly 30% of patients had recurrent moderate or severe MR at 1 month after surgery. By 24 months, that figure had climbed to 46%. There was little progression from moderate to severe MR over time, but MR recurrence was a dynamic phenomenon: Roughly 10% of affected patients experienced reversal of recurrent MR at various time points.
The randomized CSTN findings showing better results with mitral valve replacement were supported by the results of the Italian Study on the Treatment of Ischemic Mitral Regurgitation (ISTIMIR). This was a multicenter observational study of 1,006 patients with ischemic MR, 30% of whom underwent valve replacement while 70% had a repair. In a propensity-matched multivariate logistic regression analysis, mitral valve repair was associated with a 2.84-fold increased risk of reoperation within 8 years (J. Thorac. Cardiovasc. Surg. 2013;145:128-39).
Although mitral annuloplasty remains the current standard of care for repair of severe ischemic MR in 2015, “we’re realizing this isn’t necessarily the right thing to do” because of that high recurrent MR rate, Dr. Thourani said. There is a growing understanding that a subannular component is required to achieve a truly successful repair. A variety of promising subannular approaches are being developed. He is particularly enthusiastic about his own group’s work involving creation of a papillary muscle sling to achieve papillary approximation – the results have been encouraging in roughly 40 treated sheep and pigs. Human studies are coming.
Ischemic MR develops secondary to an acute MI, which imposes volume overload on the left ventricle, with increasing wall stress, left ventricular remodeling and heart failure, papillary muscle disarray, annular dilation, and MR. The incidence of heart failure within 5 years is threefold higher if an MI occurs with ischemic MR than without it, the surgeon observed.
The CSTN studies were sponsored by the National Institutes of Health and the Canadian Institutes of Health. Dr. Thourani reported serving as a consultant to Edwards Lifesciences and St. Jude Medical and receiving research grants from Abbott, Boston Scientific, Medtronic, and Sorin.
SNOWMASS, COLO. – In a major reversal of longstanding opinion, thought leaders in cardiothoracic surgery now increasingly favor mitral valve replacement over repair in patients with severe ischemic mitral regurgitation.
The overwhelming preference among both surgeons and cardiologists has been for mitral valve repair, but recent randomized trial evidence shows that mitral valve replacement provides a more durable correction with no increase in adverse events. That’s persuaded many surgical leaders to move towards replacement until improved repair strategies can be developed, Dr. Vinod H. Thourani said at the Annual Cardiovascular Conference at Snowmass.
“When I do a replacement in a patient, the cardiologist will call me and ask why. He’ll say, ‘I was hoping you were going to do a repair.’ Now we have to completely change our mentality about this,” said Dr. Thourani, professor of surgery and codirector of the Structural Heart and Valve Center at Emory University in Atlanta.
That need for a mind-shift goes for cardiothoracic surgeons as well as cardiologists, he added, pointing to an analysis of the Society of Thoracic Surgeons adult cardiac surgery database for 2008-2012 showing roughly a 65%-35% preference for repair over replacement.
The evidence favoring mitral valve replacement is so new it didn’t make it into the deliberations that generated the freshly minted 2014 ACC/AHA guidelines on valvular heart disease management (J. Am. Coll. Cardiol. 2014;63:e57-185), which state that “there is no conclusive evidence for superiority of repair or replacement” in severe ischemic mitral regurgitation (MR). That statement is no longer true, in Dr. Thourani’s view.
He highlighted a multicenter randomized trial conducted by the Cardiothoracic Surgical Trials Network (CSTN) in which 251 patients with severe ischemic mitral regurgitation were randomized to repair or replacement. The primary endpoint – change in left ventricular end-systolic volume index indicative of reversal of ventricular remodeling – improved similarly in both groups. Nor did the two treatment groups differ significantly in 30-day and 12-month mortality or rates of stroke, heart failure, bleeding, infection, and other major adverse events. The eye opener was that 32.6% of patients in the repair group had moderate or severe mitral regurgitation at 12 months, compared with just 2.3% in the replacement group (N. Engl. J. Med. 2014;370:23-32).
“This study was done at a group of high-functioning academic centers where surgeons are supposed to know how to do repair and do replacement, yet one-third of our patients have come back with moderate to severe MR after repair. This has opened up a lot of discussion among surgeons as to what we should be doing,” noted Dr. Thourani, who participated in the trial.
One-year mortality was 14.2% in the repair group and a statistically similar 17.6% in the valve-replacement group, but Dr. Thourani anticipates a steeper mortality rise ahead for the repair group. “It’ll be interesting to see where these patients living with recurrent MR will be at the 2- and 5-year marks,” he said.
In a subsequent analysis, the CSTN investigators examined whether baseline clinical and echocardiographic characteristics in patients randomized to repair could identify a subgroup at high risk for recurrent moderate-to-severe mitral regurgitation or death within 2 years post surgery. They identified a predictive model that shows promise, with a favorable area under the receiver operating characteristic curve of 0.82.
The model is based on 10 factors: age; gender; race; body mass index; New York Heart Association class; effective regurgitant orifice area; basal aneurysm/dyskinesia; and history of coronary artery bypass grafting, percutaneous coronary intervention, or ventricular arrhythmias (J. Thorac. Cardiovasc. Surg. 2014 Nov 6. pii: S0022-5223(14)01772-3).
Of these 10 variables, the standout predictor was basal aneurysm/dyskinesia. “If you repair those patients, they have a really high likelihood of having worse outcomes,” according to Dr. Thourani.
This analysis of the CSTN repair subgroup shed new light on the MR-recurrence phenomenon. Roughly 30% of patients had recurrent moderate or severe MR at 1 month after surgery. By 24 months, that figure had climbed to 46%. There was little progression from moderate to severe MR over time, but MR recurrence was a dynamic phenomenon: Roughly 10% of affected patients experienced reversal of recurrent MR at various time points.
The randomized CSTN findings showing better results with mitral valve replacement were supported by the results of the Italian Study on the Treatment of Ischemic Mitral Regurgitation (ISTIMIR). This was a multicenter observational study of 1,006 patients with ischemic MR, 30% of whom underwent valve replacement while 70% had a repair. In a propensity-matched multivariate logistic regression analysis, mitral valve repair was associated with a 2.84-fold increased risk of reoperation within 8 years (J. Thorac. Cardiovasc. Surg. 2013;145:128-39).
Although mitral annuloplasty remains the current standard of care for repair of severe ischemic MR in 2015, “we’re realizing this isn’t necessarily the right thing to do” because of that high recurrent MR rate, Dr. Thourani said. There is a growing understanding that a subannular component is required to achieve a truly successful repair. A variety of promising subannular approaches are being developed. He is particularly enthusiastic about his own group’s work involving creation of a papillary muscle sling to achieve papillary approximation – the results have been encouraging in roughly 40 treated sheep and pigs. Human studies are coming.
Ischemic MR develops secondary to an acute MI, which imposes volume overload on the left ventricle, with increasing wall stress, left ventricular remodeling and heart failure, papillary muscle disarray, annular dilation, and MR. The incidence of heart failure within 5 years is threefold higher if an MI occurs with ischemic MR than without it, the surgeon observed.
The CSTN studies were sponsored by the National Institutes of Health and the Canadian Institutes of Health. Dr. Thourani reported serving as a consultant to Edwards Lifesciences and St. Jude Medical and receiving research grants from Abbott, Boston Scientific, Medtronic, and Sorin.
SNOWMASS, COLO. – In a major reversal of longstanding opinion, thought leaders in cardiothoracic surgery now increasingly favor mitral valve replacement over repair in patients with severe ischemic mitral regurgitation.
The overwhelming preference among both surgeons and cardiologists has been for mitral valve repair, but recent randomized trial evidence shows that mitral valve replacement provides a more durable correction with no increase in adverse events. That’s persuaded many surgical leaders to move towards replacement until improved repair strategies can be developed, Dr. Vinod H. Thourani said at the Annual Cardiovascular Conference at Snowmass.
“When I do a replacement in a patient, the cardiologist will call me and ask why. He’ll say, ‘I was hoping you were going to do a repair.’ Now we have to completely change our mentality about this,” said Dr. Thourani, professor of surgery and codirector of the Structural Heart and Valve Center at Emory University in Atlanta.
That need for a mind-shift goes for cardiothoracic surgeons as well as cardiologists, he added, pointing to an analysis of the Society of Thoracic Surgeons adult cardiac surgery database for 2008-2012 showing roughly a 65%-35% preference for repair over replacement.
The evidence favoring mitral valve replacement is so new it didn’t make it into the deliberations that generated the freshly minted 2014 ACC/AHA guidelines on valvular heart disease management (J. Am. Coll. Cardiol. 2014;63:e57-185), which state that “there is no conclusive evidence for superiority of repair or replacement” in severe ischemic mitral regurgitation (MR). That statement is no longer true, in Dr. Thourani’s view.
He highlighted a multicenter randomized trial conducted by the Cardiothoracic Surgical Trials Network (CSTN) in which 251 patients with severe ischemic mitral regurgitation were randomized to repair or replacement. The primary endpoint – change in left ventricular end-systolic volume index indicative of reversal of ventricular remodeling – improved similarly in both groups. Nor did the two treatment groups differ significantly in 30-day and 12-month mortality or rates of stroke, heart failure, bleeding, infection, and other major adverse events. The eye opener was that 32.6% of patients in the repair group had moderate or severe mitral regurgitation at 12 months, compared with just 2.3% in the replacement group (N. Engl. J. Med. 2014;370:23-32).
“This study was done at a group of high-functioning academic centers where surgeons are supposed to know how to do repair and do replacement, yet one-third of our patients have come back with moderate to severe MR after repair. This has opened up a lot of discussion among surgeons as to what we should be doing,” noted Dr. Thourani, who participated in the trial.
One-year mortality was 14.2% in the repair group and a statistically similar 17.6% in the valve-replacement group, but Dr. Thourani anticipates a steeper mortality rise ahead for the repair group. “It’ll be interesting to see where these patients living with recurrent MR will be at the 2- and 5-year marks,” he said.
In a subsequent analysis, the CSTN investigators examined whether baseline clinical and echocardiographic characteristics in patients randomized to repair could identify a subgroup at high risk for recurrent moderate-to-severe mitral regurgitation or death within 2 years post surgery. They identified a predictive model that shows promise, with a favorable area under the receiver operating characteristic curve of 0.82.
The model is based on 10 factors: age; gender; race; body mass index; New York Heart Association class; effective regurgitant orifice area; basal aneurysm/dyskinesia; and history of coronary artery bypass grafting, percutaneous coronary intervention, or ventricular arrhythmias (J. Thorac. Cardiovasc. Surg. 2014 Nov 6. pii: S0022-5223(14)01772-3).
Of these 10 variables, the standout predictor was basal aneurysm/dyskinesia. “If you repair those patients, they have a really high likelihood of having worse outcomes,” according to Dr. Thourani.
This analysis of the CSTN repair subgroup shed new light on the MR-recurrence phenomenon. Roughly 30% of patients had recurrent moderate or severe MR at 1 month after surgery. By 24 months, that figure had climbed to 46%. There was little progression from moderate to severe MR over time, but MR recurrence was a dynamic phenomenon: Roughly 10% of affected patients experienced reversal of recurrent MR at various time points.
The randomized CSTN findings showing better results with mitral valve replacement were supported by the results of the Italian Study on the Treatment of Ischemic Mitral Regurgitation (ISTIMIR). This was a multicenter observational study of 1,006 patients with ischemic MR, 30% of whom underwent valve replacement while 70% had a repair. In a propensity-matched multivariate logistic regression analysis, mitral valve repair was associated with a 2.84-fold increased risk of reoperation within 8 years (J. Thorac. Cardiovasc. Surg. 2013;145:128-39).
Although mitral annuloplasty remains the current standard of care for repair of severe ischemic MR in 2015, “we’re realizing this isn’t necessarily the right thing to do” because of that high recurrent MR rate, Dr. Thourani said. There is a growing understanding that a subannular component is required to achieve a truly successful repair. A variety of promising subannular approaches are being developed. He is particularly enthusiastic about his own group’s work involving creation of a papillary muscle sling to achieve papillary approximation – the results have been encouraging in roughly 40 treated sheep and pigs. Human studies are coming.
Ischemic MR develops secondary to an acute MI, which imposes volume overload on the left ventricle, with increasing wall stress, left ventricular remodeling and heart failure, papillary muscle disarray, annular dilation, and MR. The incidence of heart failure within 5 years is threefold higher if an MI occurs with ischemic MR than without it, the surgeon observed.
The CSTN studies were sponsored by the National Institutes of Health and the Canadian Institutes of Health. Dr. Thourani reported serving as a consultant to Edwards Lifesciences and St. Jude Medical and receiving research grants from Abbott, Boston Scientific, Medtronic, and Sorin.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Aromatase inhibitors linked to cardiovascular disease
SAN ANTONIO – Adjuvant aromatase inhibitor therapy in postmenopausal breast cancer survivors was associated with an increased risk of incident nonischemic cardiovascular disease, compared with tamoxifen users in a large prospective study conducted at Kaiser Permanente.
The elevation in risk was comparable in women on aromatase inhibitors (AIs) only and in those who used sequential tamoxifen followed by an AI, Reina Haque, Ph.D., reported at the San Antonio Breast Cancer Symposium.
She presented a prospective cohort study of 13,273 postmenopausal women free of known cardiovascular disease at the time of their breast cancer diagnosis during 1991-2010. Thirty-two percent of them used adjuvant tamoxifen only, 29% used an aromatase inhibitor (AI) only, 20% switched from adjuvant tamoxifen to an AI, and the rest used neither endocrine therapy.

During a mean of 5.5 and maximum 22 years of prospective follow-up, 3,711 women experienced their first cardiovascular disease event. Neither rates of ischemic heart disease nor stroke differed significantly among the groups on tamoxifen, AIs, both in sequence, or neither. However, those on adjuvant AI therapy had an adjusted 26% greater risk of ‘other’ cardiovascular disease, compared with women on tamoxifen only.
The category of ‘other’ cardiovascular disease was comprised of heart failure, arrhythmia, cardiomyopathy, pericarditis, and valvular dysfunction, explained Dr. Haque, a research scientist at Kaiser Permanente of Southern California, Pasadena.
Similarly, women who switched from tamoxifen to an AI were at 28% greater risk of developing ‘other’ cardiovascular disease, compared with those on tamoxifen alone in a multivariate Cox analysis adjusted for age, demographics, comorbid conditions, cancer treatment, tumor characteristics, and use of antihypertensive agents and other cardiovascular medications.
In the subset of 7,982 patients who underwent breast irradiation, those on an adjuvant AI who received left-sided breast radiation therapy were at an adjusted 21% increased risk of all forms of cardiovascular disease – ischemic as well as other – compared with those who got left-sided breast irradiation and took tamoxifen.
As this was an observational study, the results warrant cautious interpretation, Dr. Haque said. Nevertheless, this is a study based upon 72,886 women-years of prospective follow-up and a large number of cardiovascular events, she noted.
The study was funded by the California Breast Cancer Research Program and the National Cancer Institute. Dr. Haque reported having no financial conflicts.
SAN ANTONIO – Adjuvant aromatase inhibitor therapy in postmenopausal breast cancer survivors was associated with an increased risk of incident nonischemic cardiovascular disease, compared with tamoxifen users in a large prospective study conducted at Kaiser Permanente.
The elevation in risk was comparable in women on aromatase inhibitors (AIs) only and in those who used sequential tamoxifen followed by an AI, Reina Haque, Ph.D., reported at the San Antonio Breast Cancer Symposium.
She presented a prospective cohort study of 13,273 postmenopausal women free of known cardiovascular disease at the time of their breast cancer diagnosis during 1991-2010. Thirty-two percent of them used adjuvant tamoxifen only, 29% used an aromatase inhibitor (AI) only, 20% switched from adjuvant tamoxifen to an AI, and the rest used neither endocrine therapy.
During a mean of 5.5 and maximum 22 years of prospective follow-up, 3,711 women experienced their first cardiovascular disease event. Neither rates of ischemic heart disease nor stroke differed significantly among the groups on tamoxifen, AIs, both in sequence, or neither. However, those on adjuvant AI therapy had an adjusted 26% greater risk of ‘other’ cardiovascular disease, compared with women on tamoxifen only.
The category of ‘other’ cardiovascular disease was comprised of heart failure, arrhythmia, cardiomyopathy, pericarditis, and valvular dysfunction, explained Dr. Haque, a research scientist at Kaiser Permanente of Southern California, Pasadena.
Similarly, women who switched from tamoxifen to an AI were at 28% greater risk of developing ‘other’ cardiovascular disease, compared with those on tamoxifen alone in a multivariate Cox analysis adjusted for age, demographics, comorbid conditions, cancer treatment, tumor characteristics, and use of antihypertensive agents and other cardiovascular medications.
In the subset of 7,982 patients who underwent breast irradiation, those on an adjuvant AI who received left-sided breast radiation therapy were at an adjusted 21% increased risk of all forms of cardiovascular disease – ischemic as well as other – compared with those who got left-sided breast irradiation and took tamoxifen.
As this was an observational study, the results warrant cautious interpretation, Dr. Haque said. Nevertheless, this is a study based upon 72,886 women-years of prospective follow-up and a large number of cardiovascular events, she noted.
The study was funded by the California Breast Cancer Research Program and the National Cancer Institute. Dr. Haque reported having no financial conflicts.
SAN ANTONIO – Adjuvant aromatase inhibitor therapy in postmenopausal breast cancer survivors was associated with an increased risk of incident nonischemic cardiovascular disease, compared with tamoxifen users in a large prospective study conducted at Kaiser Permanente.
The elevation in risk was comparable in women on aromatase inhibitors (AIs) only and in those who used sequential tamoxifen followed by an AI, Reina Haque, Ph.D., reported at the San Antonio Breast Cancer Symposium.
She presented a prospective cohort study of 13,273 postmenopausal women free of known cardiovascular disease at the time of their breast cancer diagnosis during 1991-2010. Thirty-two percent of them used adjuvant tamoxifen only, 29% used an aromatase inhibitor (AI) only, 20% switched from adjuvant tamoxifen to an AI, and the rest used neither endocrine therapy.
During a mean of 5.5 and maximum 22 years of prospective follow-up, 3,711 women experienced their first cardiovascular disease event. Neither rates of ischemic heart disease nor stroke differed significantly among the groups on tamoxifen, AIs, both in sequence, or neither. However, those on adjuvant AI therapy had an adjusted 26% greater risk of ‘other’ cardiovascular disease, compared with women on tamoxifen only.
The category of ‘other’ cardiovascular disease was comprised of heart failure, arrhythmia, cardiomyopathy, pericarditis, and valvular dysfunction, explained Dr. Haque, a research scientist at Kaiser Permanente of Southern California, Pasadena.
Similarly, women who switched from tamoxifen to an AI were at 28% greater risk of developing ‘other’ cardiovascular disease, compared with those on tamoxifen alone in a multivariate Cox analysis adjusted for age, demographics, comorbid conditions, cancer treatment, tumor characteristics, and use of antihypertensive agents and other cardiovascular medications.
In the subset of 7,982 patients who underwent breast irradiation, those on an adjuvant AI who received left-sided breast radiation therapy were at an adjusted 21% increased risk of all forms of cardiovascular disease – ischemic as well as other – compared with those who got left-sided breast irradiation and took tamoxifen.
As this was an observational study, the results warrant cautious interpretation, Dr. Haque said. Nevertheless, this is a study based upon 72,886 women-years of prospective follow-up and a large number of cardiovascular events, she noted.
The study was funded by the California Breast Cancer Research Program and the National Cancer Institute. Dr. Haque reported having no financial conflicts.
AT SABCS 2014
Key clinical point: Breast cancer patients who take an adjuvant aromatase inhibitor have a higher risk of new-onset nonischemic cardiovascular disease than those on tamoxifen.
Major finding: Patients on an adjuvant aromatase inhibitor only or on sequential tamoxifen followed by an aromatase inhibitor had an adjusted 26%-28% greater risk of nonischemic cardiovascular disease events than those on tamoxifen only.
Data source: This was a prospective cohort study of 13,273 breast cancer patients with 72,886 woman-years of follow-up.
Disclosures: The study was funded by the California Breast Cancer Research Program and the National Cancer Institute. Dr. Haque reported having no financial conflicts.

Data scarce on risk modifiers for second primary cancers
SAN ANTONIO – Though breast cancer survivors have a two- to sixfold higher risk of developing a second primary cancer compared with women in the general population, only a handful of studies have investigated potential ways for women to mitigate this risk, Dr. Christopher I. Li said at the San Antonio Breast Cancer Symposium.
The best established modifiable risk factors for a second primary contralateral breast cancer are obesity, smoking, and excessive alcohol consumption, while chemotherapy, adjuvant aromatase inhibitors, and tamoxifen are protective, he said
In addition, one study has found bisphosphonates have a protective effect against contralateral breast cancer (CBC), and another has identified diabetes mellitus as a significant risk factor. However, these two studies – both conducted by Dr. Li and coworkers – are the only ones to date that have looked at these potential risk modifiers. Confirmatory studies are warranted, emphasized Dr. Li, professor of epidemiology at the University of Washington and head of the translational research program at the Fred Hutchinson Cancer Research Center, Seattle.

An estimated 10% of breast cancer survivors will develop a second, distinct primary cancer. The most common site is the contralateral breast. Indeed, 35% of all second primary cancers in breast cancer survivors occur there. Lung cancer is next most common, accounting for 18%, followed by endometrial cancer at 10%, and colorectal cancer, which comprises 8% of all secondary primary cancers in breast cancer survivors.
Despite the high incidence of CBC, only three studies with 200 or more cases have looked at modifiable risk factors.
One was a population-based nested case-control study by Dr. Li and coworkers. It included 367 CBC cases and a control group of 734 matched breast cancer survivors without a second primary cancer. The investigators identified three modifiable risk factors for CBC: a body mass index of 30 kg/m2 or greater, associated with an adjusted 1.5-fold increased risk; consumption of at least seven alcoholic drinks per week after the first breast cancer diagnosis, with a 1.9-fold risk; and current smoking, which conferred a 2.2-fold increased risk.
Upon further analysis, however, an important interaction was noted between alcohol consumption and current smoking such that neither behavior alone was associated with significantly increased risk of CBC. But current smokers who also drank at least seven alcoholic beverages per week were at a highly significant 7.2-fold increased risk (J. Clin. Oncol. 2009;27:5312-8).
Today, bisphosphonates are widely prescribed to prevent and treat bone metastases in breast cancer patients. Dr. Li and coinvestigators conducted a nested case-control study looking at the use of bisphosphonates for another indication: the prevention of osteoporosis-related events. The study comparison involved 351 patients with CBC and 662 controls who were breast cancer survivors without CBC. They found that patients who had ever used a bisphosphonate for 6 months or longer were 47% less likely to develop a CBC.
Moreover, the protective effect increased with duration of therapy. Among current bisphosphonate users who had been taking the medication for at least 6 months, there was an adjusted 59% reduction in the risk of CBC. For current users of at least 12 months, there was a 69% reduction in relative risk compared to nonusers. And among current users of a bisphosphonate for 24 months or longer, the relative risk reduction climbed to 79%, (J. Natl. Cancer Inst. 2011;103:1752-60).
The diabetes study included 332 patients who developed a second primary CBC and 616 matched controls with only a first breast cancer. Women diagnosed with diabetes prior to age 54 had a 6.2-fold increased risk of CBC after Dr. Li and coworkers controlled for obesity and other potential confounders in a conditional logistic regression analysis, while those diagnosed with diabetes at age 55 or older had a twofold increased risk (Breast Cancer Res. Treat. 2011;125:545-51). If these findings are confirmed in another study, more frequent surveillance for CBC will be warranted in diabetic breast cancer survivors, Dr. Li said.
One risk factor for CBC that patients can’t modify involves their breast cancer subtype. In another population-based nested case-control study, this one involving 482 women with a first breast cancer followed by a CBC and 1,506 controls with only a first breast cancer, Dr. Li and colleagues showed that women with HER2-overexpressing primary disease – estrogen receptor-negative/HER2-positive tumors – had a twofold greater likelihood of CBC compared with women who were ER-positive/HER2 positive.
Women with triple-negative breast cancer had an increased risk of CBC that did not become significant until at least 4 years had gone by since diagnosis of the first breast cancer. At that point they had a 2.2-fold greater risk of CBC and patients with HER2-overexpressing disease had a 2.7-fold greater risk compared with ER-positive/HER2-positive patients.
Patients with these more aggressive breast cancer subtypes – the HER2-overexpressing and triple-negative forms of the disease – were also at particularly high risk for more advanced stage CBC. Their CBCs were greater than three times more likely to be at a regional or distant stage at diagnosis than those occurring in patients with ER-positive/HER2-positive primary breast cancer (Breast Cancer Res. Treat. 2012;135:849-55).
Dr. Li closed by noting that the growing problem of CBC is finally receiving extra attention from funding agencies. A new Consortium of CBC has been created, enabling investigators from 28 different CBC studies to interact more closely. The consortium is led by physicians at Memorial Sloan Kettering Cancer Center in New York, and at Fred Hutchinson.
The National Cancer Institute recently approved funding for a new population-based case-control study focusing on second primary cancers. It will include 700 controls with only a single breast cancer diagnosis along with 600 women with a second primary cancer of the lung, 600 with CBC, 350 with a second primary colorectal cancer, and another 350 with a second primary in the endometrium. The study will look in-depth at risk factors, treatments, and clinical and molecular characteristics and their impact on second primary cancers in breast cancer patients.
“We really hope through this study to move the field forward,” Dr. Li said.
His studies have been funded by the National Institutes of Health. He reported having no financial conflicts.
SAN ANTONIO – Though breast cancer survivors have a two- to sixfold higher risk of developing a second primary cancer compared with women in the general population, only a handful of studies have investigated potential ways for women to mitigate this risk, Dr. Christopher I. Li said at the San Antonio Breast Cancer Symposium.
The best established modifiable risk factors for a second primary contralateral breast cancer are obesity, smoking, and excessive alcohol consumption, while chemotherapy, adjuvant aromatase inhibitors, and tamoxifen are protective, he said
In addition, one study has found bisphosphonates have a protective effect against contralateral breast cancer (CBC), and another has identified diabetes mellitus as a significant risk factor. However, these two studies – both conducted by Dr. Li and coworkers – are the only ones to date that have looked at these potential risk modifiers. Confirmatory studies are warranted, emphasized Dr. Li, professor of epidemiology at the University of Washington and head of the translational research program at the Fred Hutchinson Cancer Research Center, Seattle.
An estimated 10% of breast cancer survivors will develop a second, distinct primary cancer. The most common site is the contralateral breast. Indeed, 35% of all second primary cancers in breast cancer survivors occur there. Lung cancer is next most common, accounting for 18%, followed by endometrial cancer at 10%, and colorectal cancer, which comprises 8% of all secondary primary cancers in breast cancer survivors.
Despite the high incidence of CBC, only three studies with 200 or more cases have looked at modifiable risk factors.
One was a population-based nested case-control study by Dr. Li and coworkers. It included 367 CBC cases and a control group of 734 matched breast cancer survivors without a second primary cancer. The investigators identified three modifiable risk factors for CBC: a body mass index of 30 kg/m2 or greater, associated with an adjusted 1.5-fold increased risk; consumption of at least seven alcoholic drinks per week after the first breast cancer diagnosis, with a 1.9-fold risk; and current smoking, which conferred a 2.2-fold increased risk.
Upon further analysis, however, an important interaction was noted between alcohol consumption and current smoking such that neither behavior alone was associated with significantly increased risk of CBC. But current smokers who also drank at least seven alcoholic beverages per week were at a highly significant 7.2-fold increased risk (J. Clin. Oncol. 2009;27:5312-8).
Today, bisphosphonates are widely prescribed to prevent and treat bone metastases in breast cancer patients. Dr. Li and coinvestigators conducted a nested case-control study looking at the use of bisphosphonates for another indication: the prevention of osteoporosis-related events. The study comparison involved 351 patients with CBC and 662 controls who were breast cancer survivors without CBC. They found that patients who had ever used a bisphosphonate for 6 months or longer were 47% less likely to develop a CBC.
Moreover, the protective effect increased with duration of therapy. Among current bisphosphonate users who had been taking the medication for at least 6 months, there was an adjusted 59% reduction in the risk of CBC. For current users of at least 12 months, there was a 69% reduction in relative risk compared to nonusers. And among current users of a bisphosphonate for 24 months or longer, the relative risk reduction climbed to 79%, (J. Natl. Cancer Inst. 2011;103:1752-60).
The diabetes study included 332 patients who developed a second primary CBC and 616 matched controls with only a first breast cancer. Women diagnosed with diabetes prior to age 54 had a 6.2-fold increased risk of CBC after Dr. Li and coworkers controlled for obesity and other potential confounders in a conditional logistic regression analysis, while those diagnosed with diabetes at age 55 or older had a twofold increased risk (Breast Cancer Res. Treat. 2011;125:545-51). If these findings are confirmed in another study, more frequent surveillance for CBC will be warranted in diabetic breast cancer survivors, Dr. Li said.
One risk factor for CBC that patients can’t modify involves their breast cancer subtype. In another population-based nested case-control study, this one involving 482 women with a first breast cancer followed by a CBC and 1,506 controls with only a first breast cancer, Dr. Li and colleagues showed that women with HER2-overexpressing primary disease – estrogen receptor-negative/HER2-positive tumors – had a twofold greater likelihood of CBC compared with women who were ER-positive/HER2 positive.
Women with triple-negative breast cancer had an increased risk of CBC that did not become significant until at least 4 years had gone by since diagnosis of the first breast cancer. At that point they had a 2.2-fold greater risk of CBC and patients with HER2-overexpressing disease had a 2.7-fold greater risk compared with ER-positive/HER2-positive patients.
Patients with these more aggressive breast cancer subtypes – the HER2-overexpressing and triple-negative forms of the disease – were also at particularly high risk for more advanced stage CBC. Their CBCs were greater than three times more likely to be at a regional or distant stage at diagnosis than those occurring in patients with ER-positive/HER2-positive primary breast cancer (Breast Cancer Res. Treat. 2012;135:849-55).
Dr. Li closed by noting that the growing problem of CBC is finally receiving extra attention from funding agencies. A new Consortium of CBC has been created, enabling investigators from 28 different CBC studies to interact more closely. The consortium is led by physicians at Memorial Sloan Kettering Cancer Center in New York, and at Fred Hutchinson.
The National Cancer Institute recently approved funding for a new population-based case-control study focusing on second primary cancers. It will include 700 controls with only a single breast cancer diagnosis along with 600 women with a second primary cancer of the lung, 600 with CBC, 350 with a second primary colorectal cancer, and another 350 with a second primary in the endometrium. The study will look in-depth at risk factors, treatments, and clinical and molecular characteristics and their impact on second primary cancers in breast cancer patients.
“We really hope through this study to move the field forward,” Dr. Li said.
His studies have been funded by the National Institutes of Health. He reported having no financial conflicts.
SAN ANTONIO – Though breast cancer survivors have a two- to sixfold higher risk of developing a second primary cancer compared with women in the general population, only a handful of studies have investigated potential ways for women to mitigate this risk, Dr. Christopher I. Li said at the San Antonio Breast Cancer Symposium.
The best established modifiable risk factors for a second primary contralateral breast cancer are obesity, smoking, and excessive alcohol consumption, while chemotherapy, adjuvant aromatase inhibitors, and tamoxifen are protective, he said
In addition, one study has found bisphosphonates have a protective effect against contralateral breast cancer (CBC), and another has identified diabetes mellitus as a significant risk factor. However, these two studies – both conducted by Dr. Li and coworkers – are the only ones to date that have looked at these potential risk modifiers. Confirmatory studies are warranted, emphasized Dr. Li, professor of epidemiology at the University of Washington and head of the translational research program at the Fred Hutchinson Cancer Research Center, Seattle.
An estimated 10% of breast cancer survivors will develop a second, distinct primary cancer. The most common site is the contralateral breast. Indeed, 35% of all second primary cancers in breast cancer survivors occur there. Lung cancer is next most common, accounting for 18%, followed by endometrial cancer at 10%, and colorectal cancer, which comprises 8% of all secondary primary cancers in breast cancer survivors.
Despite the high incidence of CBC, only three studies with 200 or more cases have looked at modifiable risk factors.
One was a population-based nested case-control study by Dr. Li and coworkers. It included 367 CBC cases and a control group of 734 matched breast cancer survivors without a second primary cancer. The investigators identified three modifiable risk factors for CBC: a body mass index of 30 kg/m2 or greater, associated with an adjusted 1.5-fold increased risk; consumption of at least seven alcoholic drinks per week after the first breast cancer diagnosis, with a 1.9-fold risk; and current smoking, which conferred a 2.2-fold increased risk.
Upon further analysis, however, an important interaction was noted between alcohol consumption and current smoking such that neither behavior alone was associated with significantly increased risk of CBC. But current smokers who also drank at least seven alcoholic beverages per week were at a highly significant 7.2-fold increased risk (J. Clin. Oncol. 2009;27:5312-8).
Today, bisphosphonates are widely prescribed to prevent and treat bone metastases in breast cancer patients. Dr. Li and coinvestigators conducted a nested case-control study looking at the use of bisphosphonates for another indication: the prevention of osteoporosis-related events. The study comparison involved 351 patients with CBC and 662 controls who were breast cancer survivors without CBC. They found that patients who had ever used a bisphosphonate for 6 months or longer were 47% less likely to develop a CBC.
Moreover, the protective effect increased with duration of therapy. Among current bisphosphonate users who had been taking the medication for at least 6 months, there was an adjusted 59% reduction in the risk of CBC. For current users of at least 12 months, there was a 69% reduction in relative risk compared to nonusers. And among current users of a bisphosphonate for 24 months or longer, the relative risk reduction climbed to 79%, (J. Natl. Cancer Inst. 2011;103:1752-60).
The diabetes study included 332 patients who developed a second primary CBC and 616 matched controls with only a first breast cancer. Women diagnosed with diabetes prior to age 54 had a 6.2-fold increased risk of CBC after Dr. Li and coworkers controlled for obesity and other potential confounders in a conditional logistic regression analysis, while those diagnosed with diabetes at age 55 or older had a twofold increased risk (Breast Cancer Res. Treat. 2011;125:545-51). If these findings are confirmed in another study, more frequent surveillance for CBC will be warranted in diabetic breast cancer survivors, Dr. Li said.
One risk factor for CBC that patients can’t modify involves their breast cancer subtype. In another population-based nested case-control study, this one involving 482 women with a first breast cancer followed by a CBC and 1,506 controls with only a first breast cancer, Dr. Li and colleagues showed that women with HER2-overexpressing primary disease – estrogen receptor-negative/HER2-positive tumors – had a twofold greater likelihood of CBC compared with women who were ER-positive/HER2 positive.
Women with triple-negative breast cancer had an increased risk of CBC that did not become significant until at least 4 years had gone by since diagnosis of the first breast cancer. At that point they had a 2.2-fold greater risk of CBC and patients with HER2-overexpressing disease had a 2.7-fold greater risk compared with ER-positive/HER2-positive patients.
Patients with these more aggressive breast cancer subtypes – the HER2-overexpressing and triple-negative forms of the disease – were also at particularly high risk for more advanced stage CBC. Their CBCs were greater than three times more likely to be at a regional or distant stage at diagnosis than those occurring in patients with ER-positive/HER2-positive primary breast cancer (Breast Cancer Res. Treat. 2012;135:849-55).
Dr. Li closed by noting that the growing problem of CBC is finally receiving extra attention from funding agencies. A new Consortium of CBC has been created, enabling investigators from 28 different CBC studies to interact more closely. The consortium is led by physicians at Memorial Sloan Kettering Cancer Center in New York, and at Fred Hutchinson.
The National Cancer Institute recently approved funding for a new population-based case-control study focusing on second primary cancers. It will include 700 controls with only a single breast cancer diagnosis along with 600 women with a second primary cancer of the lung, 600 with CBC, 350 with a second primary colorectal cancer, and another 350 with a second primary in the endometrium. The study will look in-depth at risk factors, treatments, and clinical and molecular characteristics and their impact on second primary cancers in breast cancer patients.
“We really hope through this study to move the field forward,” Dr. Li said.
His studies have been funded by the National Institutes of Health. He reported having no financial conflicts.
EXPERT ANALYSIS FROM SABCS 2014
Residual SYNTAX score a boon to interventional cardiology
SNOWMASS, COLO. – The residual SYNTAX score is a powerful indicator of 5-year all-cause mortality after percutaneous coronary intervention for triple-vessel or unprotected left main coronary artery disease, Dr. David R. Holmes Jr. said at the Annual Cardiovascular Conference at Snowmass.
Cardiologists will find the residual SYNTAX score enormously valuable in shared decision making as to whether an individual with complex coronary artery disease is a reasonable candidate for PCI or better off with coronary artery bypass graft (CABG), predicted Dr. Holmes, professor of medicine at the Mayo Clinic in Rochester, Minn.
“I think the residual SYNTAX score is incredibly important. We need to be cognizant of it in our patient selection. I think we’ll see more and more use of it going forward,” the cardiologist said.
The SYNTAX score, as well as the residual SYNTAX score, grew out of the SYNTAX trial (Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery), a multicenter, prospective, randomized study of PCI versus CABG in 1,800 all-comers with triple-vessel or unprotected left main coronary artery disease (CAD) who were deemed eligible for both revascularization strategies. The trial was led by a who’s who of prominent American and European interventional cardiologists and heart surgeons, including Dr. Holmes (N. Engl. J. Med. 2009;360:961-72)
“SYNTAX is probably the most pivotally important trial in cardiovascular revascularization strategies in the past 10 years or so. An important thing to remember from this study is that the SYNTAX score should be used in all patients with multivessel disease,” he said.
The SYNTAX score (www.syntaxscore.com) is an objective, quantitative measure of CAD complexity that takes into account factors including total occlusions, lesion tortuosity and length, calcifications, and bifurcations. It was calculated preprocedurally in all study participants.
Five years of follow-up established the baseline SYNTAX score to be a useful guide as to whether surgery or PCI is the better strategy in a given individual. Patients in the top tertile for SYNTAX score, with a score of 33 or greater, had a significantly lower 5-year mortality if randomized to CABG: 11.4%, compared with 19.2% for PCI. Mortality didn’t differ between surgically and percutaneously revascularized patients with an intermediate-range SYNTAX score of 23-32, although the composite major adverse cardiac and cerebrovascular event (MACCE) rate was significantly lower in the CABG arm at 25.8%, compared with 36% for PCI. In contrast, among patients with a SYNTAX score of 22 or less, MACCE rates were similar regardless of treatment strategy.
Based on the 5-year MACCE rates, SYNTAX investigators estimated that 71% of all patients with triple-vessel or unprotected left main coronary artery disease are best treated with CABG, adding that, for the remaining 29%, PCI is “a very reasonable alternative” (Lancet 2013;381:629-38).
The mean baseline SYNTAX score in the trial was 28.4. The mean residual score was 4.5. The residual SYNTAX score measures the extent of remaining obstructive coronary disease after revascularization. SYNTAX investigators validated the residual SYNTAX score as a potent predictor of 5-year mortality and other adverse outcomes in a separate analysis of 5-year outcomes in the 903 subjects randomized to PCI.
This analysis was done to validate the concept of “reasonable incomplete revascularization,” which the SYNTAX investigators concluded was a residual SYNTAX score of 8 or less. That’s because 5-year all-cause mortality in patients with a residual SYNTAX score of greater than 0-8 wasn’t significantly different than the 8.5% rate in the 43% of PCI recipients with a residual SYNTAX score of 0, which is indicative of complete revascularization. In contrast, the 17% of patients with a residual score above 8 had a 35% mortality rate (Circulation 2013;128:141-51).
Dr. Holmes recommended that cardiologists who are considering whether to recommend PCI or CABG for patients with multivessel CAD make a baseline estimate of the likely residual SYNTAX Score based upon what they can reasonably expect to achieve with PCI. For example, if a patient has multiple total occlusions and the cardiologist isn’t comfortable tackling such lesions, the estimated residual SYNTAX score is likely to be sufficiently high to point to CABG as the better option.
“If you don’t think you can provide pretty complete revascularization to viable myocardium, then much more consideration should be given to surgery,” he said.
Dr. Holmes reported serving as a consultant to Boston Scientific, which funded the SYNTAX trial.
SNOWMASS, COLO. – The residual SYNTAX score is a powerful indicator of 5-year all-cause mortality after percutaneous coronary intervention for triple-vessel or unprotected left main coronary artery disease, Dr. David R. Holmes Jr. said at the Annual Cardiovascular Conference at Snowmass.
Cardiologists will find the residual SYNTAX score enormously valuable in shared decision making as to whether an individual with complex coronary artery disease is a reasonable candidate for PCI or better off with coronary artery bypass graft (CABG), predicted Dr. Holmes, professor of medicine at the Mayo Clinic in Rochester, Minn.
“I think the residual SYNTAX score is incredibly important. We need to be cognizant of it in our patient selection. I think we’ll see more and more use of it going forward,” the cardiologist said.
The SYNTAX score, as well as the residual SYNTAX score, grew out of the SYNTAX trial (Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery), a multicenter, prospective, randomized study of PCI versus CABG in 1,800 all-comers with triple-vessel or unprotected left main coronary artery disease (CAD) who were deemed eligible for both revascularization strategies. The trial was led by a who’s who of prominent American and European interventional cardiologists and heart surgeons, including Dr. Holmes (N. Engl. J. Med. 2009;360:961-72)
“SYNTAX is probably the most pivotally important trial in cardiovascular revascularization strategies in the past 10 years or so. An important thing to remember from this study is that the SYNTAX score should be used in all patients with multivessel disease,” he said.
The SYNTAX score (www.syntaxscore.com) is an objective, quantitative measure of CAD complexity that takes into account factors including total occlusions, lesion tortuosity and length, calcifications, and bifurcations. It was calculated preprocedurally in all study participants.
Five years of follow-up established the baseline SYNTAX score to be a useful guide as to whether surgery or PCI is the better strategy in a given individual. Patients in the top tertile for SYNTAX score, with a score of 33 or greater, had a significantly lower 5-year mortality if randomized to CABG: 11.4%, compared with 19.2% for PCI. Mortality didn’t differ between surgically and percutaneously revascularized patients with an intermediate-range SYNTAX score of 23-32, although the composite major adverse cardiac and cerebrovascular event (MACCE) rate was significantly lower in the CABG arm at 25.8%, compared with 36% for PCI. In contrast, among patients with a SYNTAX score of 22 or less, MACCE rates were similar regardless of treatment strategy.
Based on the 5-year MACCE rates, SYNTAX investigators estimated that 71% of all patients with triple-vessel or unprotected left main coronary artery disease are best treated with CABG, adding that, for the remaining 29%, PCI is “a very reasonable alternative” (Lancet 2013;381:629-38).
The mean baseline SYNTAX score in the trial was 28.4. The mean residual score was 4.5. The residual SYNTAX score measures the extent of remaining obstructive coronary disease after revascularization. SYNTAX investigators validated the residual SYNTAX score as a potent predictor of 5-year mortality and other adverse outcomes in a separate analysis of 5-year outcomes in the 903 subjects randomized to PCI.
This analysis was done to validate the concept of “reasonable incomplete revascularization,” which the SYNTAX investigators concluded was a residual SYNTAX score of 8 or less. That’s because 5-year all-cause mortality in patients with a residual SYNTAX score of greater than 0-8 wasn’t significantly different than the 8.5% rate in the 43% of PCI recipients with a residual SYNTAX score of 0, which is indicative of complete revascularization. In contrast, the 17% of patients with a residual score above 8 had a 35% mortality rate (Circulation 2013;128:141-51).
Dr. Holmes recommended that cardiologists who are considering whether to recommend PCI or CABG for patients with multivessel CAD make a baseline estimate of the likely residual SYNTAX Score based upon what they can reasonably expect to achieve with PCI. For example, if a patient has multiple total occlusions and the cardiologist isn’t comfortable tackling such lesions, the estimated residual SYNTAX score is likely to be sufficiently high to point to CABG as the better option.
“If you don’t think you can provide pretty complete revascularization to viable myocardium, then much more consideration should be given to surgery,” he said.
Dr. Holmes reported serving as a consultant to Boston Scientific, which funded the SYNTAX trial.
SNOWMASS, COLO. – The residual SYNTAX score is a powerful indicator of 5-year all-cause mortality after percutaneous coronary intervention for triple-vessel or unprotected left main coronary artery disease, Dr. David R. Holmes Jr. said at the Annual Cardiovascular Conference at Snowmass.
Cardiologists will find the residual SYNTAX score enormously valuable in shared decision making as to whether an individual with complex coronary artery disease is a reasonable candidate for PCI or better off with coronary artery bypass graft (CABG), predicted Dr. Holmes, professor of medicine at the Mayo Clinic in Rochester, Minn.
“I think the residual SYNTAX score is incredibly important. We need to be cognizant of it in our patient selection. I think we’ll see more and more use of it going forward,” the cardiologist said.
The SYNTAX score, as well as the residual SYNTAX score, grew out of the SYNTAX trial (Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery), a multicenter, prospective, randomized study of PCI versus CABG in 1,800 all-comers with triple-vessel or unprotected left main coronary artery disease (CAD) who were deemed eligible for both revascularization strategies. The trial was led by a who’s who of prominent American and European interventional cardiologists and heart surgeons, including Dr. Holmes (N. Engl. J. Med. 2009;360:961-72)
“SYNTAX is probably the most pivotally important trial in cardiovascular revascularization strategies in the past 10 years or so. An important thing to remember from this study is that the SYNTAX score should be used in all patients with multivessel disease,” he said.
The SYNTAX score (www.syntaxscore.com) is an objective, quantitative measure of CAD complexity that takes into account factors including total occlusions, lesion tortuosity and length, calcifications, and bifurcations. It was calculated preprocedurally in all study participants.
Five years of follow-up established the baseline SYNTAX score to be a useful guide as to whether surgery or PCI is the better strategy in a given individual. Patients in the top tertile for SYNTAX score, with a score of 33 or greater, had a significantly lower 5-year mortality if randomized to CABG: 11.4%, compared with 19.2% for PCI. Mortality didn’t differ between surgically and percutaneously revascularized patients with an intermediate-range SYNTAX score of 23-32, although the composite major adverse cardiac and cerebrovascular event (MACCE) rate was significantly lower in the CABG arm at 25.8%, compared with 36% for PCI. In contrast, among patients with a SYNTAX score of 22 or less, MACCE rates were similar regardless of treatment strategy.
Based on the 5-year MACCE rates, SYNTAX investigators estimated that 71% of all patients with triple-vessel or unprotected left main coronary artery disease are best treated with CABG, adding that, for the remaining 29%, PCI is “a very reasonable alternative” (Lancet 2013;381:629-38).
The mean baseline SYNTAX score in the trial was 28.4. The mean residual score was 4.5. The residual SYNTAX score measures the extent of remaining obstructive coronary disease after revascularization. SYNTAX investigators validated the residual SYNTAX score as a potent predictor of 5-year mortality and other adverse outcomes in a separate analysis of 5-year outcomes in the 903 subjects randomized to PCI.
This analysis was done to validate the concept of “reasonable incomplete revascularization,” which the SYNTAX investigators concluded was a residual SYNTAX score of 8 or less. That’s because 5-year all-cause mortality in patients with a residual SYNTAX score of greater than 0-8 wasn’t significantly different than the 8.5% rate in the 43% of PCI recipients with a residual SYNTAX score of 0, which is indicative of complete revascularization. In contrast, the 17% of patients with a residual score above 8 had a 35% mortality rate (Circulation 2013;128:141-51).
Dr. Holmes recommended that cardiologists who are considering whether to recommend PCI or CABG for patients with multivessel CAD make a baseline estimate of the likely residual SYNTAX Score based upon what they can reasonably expect to achieve with PCI. For example, if a patient has multiple total occlusions and the cardiologist isn’t comfortable tackling such lesions, the estimated residual SYNTAX score is likely to be sufficiently high to point to CABG as the better option.
“If you don’t think you can provide pretty complete revascularization to viable myocardium, then much more consideration should be given to surgery,” he said.
Dr. Holmes reported serving as a consultant to Boston Scientific, which funded the SYNTAX trial.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
The high cost of treatment-resistant hypertension
CHICAGO– Prepare for sticker shock: Researchers have put a price tag on direct medical expenditures for treatment-resistant hypertension, and it’s a big one.
Indeed, apparent treatment-resistant hypertension (aTRH) is associated with an estimated $11.3-$17.9 billion per year in direct medical expenditures above and beyond expenditures for nonresistant hypertension in the United States, Steven M. Smith, Pharm.D., reported at the American Heart Association scientific sessions.
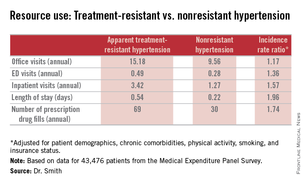
This is a conservative estimate based on an assumed 5% prevalence of aTRH among U.S. adults with hypertension, which may be a low figure, according to Dr. Smith of the University of Florida, Gainesville.
He presented an analysis of data on direct medical expenditures and health care utilization for 43,476 patients with hypertension in the nationally representative U.S. Medical Expenditure Panel Survey, of whom 1,924 met the criteria for aTRH as defined by a requirement for drugs from at least four antihypertensive medications classes in order to achieve blood pressure control.
While aTRH is known to be associated with higher rates of major adverse cardiovascular events and increased mortality relative to nonresistant hypertension, the financial costs associated with this condition haven’t previously been carefully examined.
Mean annual health care expenditures for individuals with aTRH were $20,018, more than twice the $9,814 figure for patients with nonresistant hypertension. But patients with aTRH were older, heavier, less likely to have a high income, and differed in additional ways from the much larger group with nonresistant hypertension. In a multivariate analysis adjusted for these potential confounders, aTRH was associated with $2,413 in excess annual medical expenditures and $1,253 in excess total prescription expenditures, for a total of $3,647 excess total annual health care expenditures per person, compared with subjects with nonresistant hypertension.
New preventive strategies are clearly in order, Dr. Smith concluded.
He reported having no financial conflicts regarding this study, which was conducted without industry funding.
CHICAGO– Prepare for sticker shock: Researchers have put a price tag on direct medical expenditures for treatment-resistant hypertension, and it’s a big one.
Indeed, apparent treatment-resistant hypertension (aTRH) is associated with an estimated $11.3-$17.9 billion per year in direct medical expenditures above and beyond expenditures for nonresistant hypertension in the United States, Steven M. Smith, Pharm.D., reported at the American Heart Association scientific sessions.
This is a conservative estimate based on an assumed 5% prevalence of aTRH among U.S. adults with hypertension, which may be a low figure, according to Dr. Smith of the University of Florida, Gainesville.
He presented an analysis of data on direct medical expenditures and health care utilization for 43,476 patients with hypertension in the nationally representative U.S. Medical Expenditure Panel Survey, of whom 1,924 met the criteria for aTRH as defined by a requirement for drugs from at least four antihypertensive medications classes in order to achieve blood pressure control.
While aTRH is known to be associated with higher rates of major adverse cardiovascular events and increased mortality relative to nonresistant hypertension, the financial costs associated with this condition haven’t previously been carefully examined.
Mean annual health care expenditures for individuals with aTRH were $20,018, more than twice the $9,814 figure for patients with nonresistant hypertension. But patients with aTRH were older, heavier, less likely to have a high income, and differed in additional ways from the much larger group with nonresistant hypertension. In a multivariate analysis adjusted for these potential confounders, aTRH was associated with $2,413 in excess annual medical expenditures and $1,253 in excess total prescription expenditures, for a total of $3,647 excess total annual health care expenditures per person, compared with subjects with nonresistant hypertension.
New preventive strategies are clearly in order, Dr. Smith concluded.
He reported having no financial conflicts regarding this study, which was conducted without industry funding.
CHICAGO– Prepare for sticker shock: Researchers have put a price tag on direct medical expenditures for treatment-resistant hypertension, and it’s a big one.
Indeed, apparent treatment-resistant hypertension (aTRH) is associated with an estimated $11.3-$17.9 billion per year in direct medical expenditures above and beyond expenditures for nonresistant hypertension in the United States, Steven M. Smith, Pharm.D., reported at the American Heart Association scientific sessions.
This is a conservative estimate based on an assumed 5% prevalence of aTRH among U.S. adults with hypertension, which may be a low figure, according to Dr. Smith of the University of Florida, Gainesville.
He presented an analysis of data on direct medical expenditures and health care utilization for 43,476 patients with hypertension in the nationally representative U.S. Medical Expenditure Panel Survey, of whom 1,924 met the criteria for aTRH as defined by a requirement for drugs from at least four antihypertensive medications classes in order to achieve blood pressure control.
While aTRH is known to be associated with higher rates of major adverse cardiovascular events and increased mortality relative to nonresistant hypertension, the financial costs associated with this condition haven’t previously been carefully examined.
Mean annual health care expenditures for individuals with aTRH were $20,018, more than twice the $9,814 figure for patients with nonresistant hypertension. But patients with aTRH were older, heavier, less likely to have a high income, and differed in additional ways from the much larger group with nonresistant hypertension. In a multivariate analysis adjusted for these potential confounders, aTRH was associated with $2,413 in excess annual medical expenditures and $1,253 in excess total prescription expenditures, for a total of $3,647 excess total annual health care expenditures per person, compared with subjects with nonresistant hypertension.
New preventive strategies are clearly in order, Dr. Smith concluded.
He reported having no financial conflicts regarding this study, which was conducted without industry funding.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Direct medical expenditures for apparent treatment-resistant hypertension amount to up to an additional $17.9 billion annually beyond the cost associated with nonresistant hypertension.
Major finding: Patients with apparent treatment-resistant hypertension averaged twice as many office visits and nearly three times as many inpatient stays annually, compared with individuals with nonresistant hypertension. Moreover, their average hospital stay was twice as long.
Data source: A retrospective analysis of prospectively collected data on 43,476 persons with hypertension included in the U.S. Medical Expenditure Panel Survey.
Disclosures: The presenter reported having no financial conflicts regarding this study, which was conducted free of commercial funding.
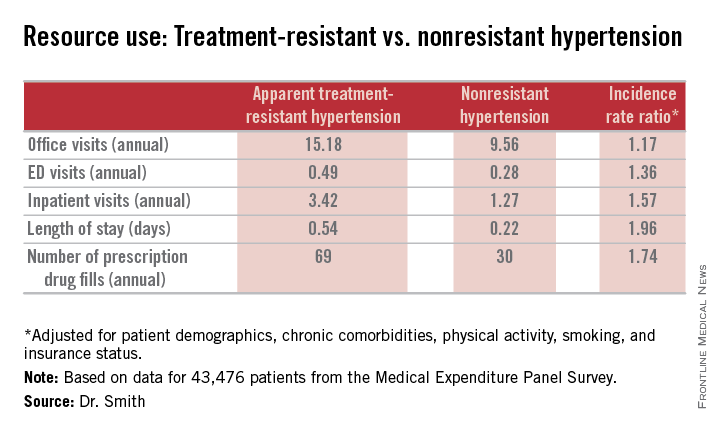
Promising new therapy for critical limb ischemia
CHICAGO – A single set of intramuscular injections of stromal cell–derived factor-1 in patients with critical limb ischemia showed safety as well as evidence of efficacy through 12 months of follow-up in the STOP-CLI trial.
“Patients treated with JVS-100 demonstrated dose-dependent improvement across multiple patient-centered outcomes, including pain, quality of life, and wound healing, with less change in macrovascular objective measures in this small study,” Dr. Melina R. Kibbe reported at the American Heart Association scientific sessions. JVS-100 is a nonviral plasmid encoding human stromal cell–derived factor-1 (SDF-1), a natural chemokine protein that promotes angiogenesis by recruiting endothelial progenitor cells from the bone marrow to ischemic sites, explained Dr. Kibbe, professor and vice chair of surgical research and deputy director of the Simpson Querrey Institute for BioNanotechnology at Northwestern University, Chicago.

STOP-CLI was an exploratory, phase IIa, double-blind, first-in-humans study involving 48 patients with Rutherford classification 4 or 5 critical climb ischemia (CLI). All had an ankle-brachial index of 0.4 or lower, an ankle systolic blood pressure of 70 mm Hg or less or a toe systolic blood pressure of 50 or less, and were poor candidates for surgical revascularization. None had Buerger’s disease.
Participants were randomized to one of four study arms, and within each study arm further randomized 3:1 to stromal cell–derived factor-1 (SDF-1) or placebo injections. The patients received either 8 or 16 injections, each containing either 0.5 or 1.0 mg of SDF-1 or placebo. The injections, given in a single session, were placed at least 0.5 cm apart throughout the ischemic area of the affected limb.
By chance, most patients randomized to the placebo group were Rutherford 4, a category of CLI defined by rest pain, while the majority in the active treatment arms were Rutherford 5, a more severe disease manifestation characterized by ulcers. As a consequence, the SDF-1 recipients also had far larger nonhealing wounds, with an average area of 6.4 cm2, compared with 1.5 cm2, in controls.
The SDF-1 injections proved safe and were well tolerated, with no treatment-related serious adverse events and no safety signals evident in the laboratory results.
Turning to efficacy endpoints, Dr. Kibbe said self-rated visual analog scale pain scores showed clear, dose-dependent improvement over time in the SDF-1 treatment cohorts and no change in controls.
Similarly, the active treatment groups showed improved quality of life scores on all domains of the Short Form-36: physical functioning, bodily pain, general health, social functioning, energy/fatigue, emotional well-being, and overall physical and mental health, the surgeon continued.
Wound area decreased significantly in the SDF-1-treated groups, with the biggest reduction – more than 8 cm2 – being noted in the three patients who received eight 1-mg injections. That was also the group with the largest wounds at baseline, with an average area of 11.4 cm2.
Of note, the major limb amputation rate was “remarkably low” for patients with such severe CLI, according to Dr. Kibbe. The rate was less than 10% over the course of 12 months, with one patient in each of the four active treatment arms having a major amputation at time intervals of 58-112 days post injection. No major limb amputations occurred in the control group.
There was a hint of improvement with SDF-1 therapy over placebo in ankle-brachial index and transcutaneous oxygen pressure, but the between-group differences were too narrow in this study to allow for any conclusions. That must await planned much larger phase III trials, according to Dr. Kibbe.
Audience members, citing the numerous failures of once-promising stem cell therapies for CLI at phase III testing over the last 10-15 years, wondered why Dr. Kibbe thinks SDF-1 will fare any better.
“This is much debated and discussed among all the people involved in these kinds of trials,” she replied. “I’d say, briefly, that a lot of it has to do with patient selection. I think when you have a mixed bag of patients in a trial, including patients with Buerger’s disease, treated in multiple different countries, using different definitions of when to amputate, all those things come into play and could account for why those phase III trials were not successful.”
“Having been involved in lots of the different gene- and cell-based therapy trials, I think one of the unique benefits of this therapy is that it kind of bridges between the two. SDF-1 basically homes your endothelial progenitor cells to the site of ischemic injury for enhanced vasculogenesis. But SDF-1 also has direct effects on endothelial cells, including stimulating proliferation and preventing apoptosis,” she added.
JVS-100 has also successfully completed a phase II clinical trial for the treatment of heart failure. In addition, the agent is being developed as a treatment for acute MI, chronic angina, and for muscle regeneration.
The STOP-CLI study was sponsored by Juventas Therapeutics. Dr. Kibbe reported serving as a consultant to Johnson & Johnson/Cordis and Pluristem.
CHICAGO – A single set of intramuscular injections of stromal cell–derived factor-1 in patients with critical limb ischemia showed safety as well as evidence of efficacy through 12 months of follow-up in the STOP-CLI trial.
“Patients treated with JVS-100 demonstrated dose-dependent improvement across multiple patient-centered outcomes, including pain, quality of life, and wound healing, with less change in macrovascular objective measures in this small study,” Dr. Melina R. Kibbe reported at the American Heart Association scientific sessions. JVS-100 is a nonviral plasmid encoding human stromal cell–derived factor-1 (SDF-1), a natural chemokine protein that promotes angiogenesis by recruiting endothelial progenitor cells from the bone marrow to ischemic sites, explained Dr. Kibbe, professor and vice chair of surgical research and deputy director of the Simpson Querrey Institute for BioNanotechnology at Northwestern University, Chicago.
STOP-CLI was an exploratory, phase IIa, double-blind, first-in-humans study involving 48 patients with Rutherford classification 4 or 5 critical climb ischemia (CLI). All had an ankle-brachial index of 0.4 or lower, an ankle systolic blood pressure of 70 mm Hg or less or a toe systolic blood pressure of 50 or less, and were poor candidates for surgical revascularization. None had Buerger’s disease.
Participants were randomized to one of four study arms, and within each study arm further randomized 3:1 to stromal cell–derived factor-1 (SDF-1) or placebo injections. The patients received either 8 or 16 injections, each containing either 0.5 or 1.0 mg of SDF-1 or placebo. The injections, given in a single session, were placed at least 0.5 cm apart throughout the ischemic area of the affected limb.
By chance, most patients randomized to the placebo group were Rutherford 4, a category of CLI defined by rest pain, while the majority in the active treatment arms were Rutherford 5, a more severe disease manifestation characterized by ulcers. As a consequence, the SDF-1 recipients also had far larger nonhealing wounds, with an average area of 6.4 cm2, compared with 1.5 cm2, in controls.
The SDF-1 injections proved safe and were well tolerated, with no treatment-related serious adverse events and no safety signals evident in the laboratory results.
Turning to efficacy endpoints, Dr. Kibbe said self-rated visual analog scale pain scores showed clear, dose-dependent improvement over time in the SDF-1 treatment cohorts and no change in controls.
Similarly, the active treatment groups showed improved quality of life scores on all domains of the Short Form-36: physical functioning, bodily pain, general health, social functioning, energy/fatigue, emotional well-being, and overall physical and mental health, the surgeon continued.
Wound area decreased significantly in the SDF-1-treated groups, with the biggest reduction – more than 8 cm2 – being noted in the three patients who received eight 1-mg injections. That was also the group with the largest wounds at baseline, with an average area of 11.4 cm2.
Of note, the major limb amputation rate was “remarkably low” for patients with such severe CLI, according to Dr. Kibbe. The rate was less than 10% over the course of 12 months, with one patient in each of the four active treatment arms having a major amputation at time intervals of 58-112 days post injection. No major limb amputations occurred in the control group.
There was a hint of improvement with SDF-1 therapy over placebo in ankle-brachial index and transcutaneous oxygen pressure, but the between-group differences were too narrow in this study to allow for any conclusions. That must await planned much larger phase III trials, according to Dr. Kibbe.
Audience members, citing the numerous failures of once-promising stem cell therapies for CLI at phase III testing over the last 10-15 years, wondered why Dr. Kibbe thinks SDF-1 will fare any better.
“This is much debated and discussed among all the people involved in these kinds of trials,” she replied. “I’d say, briefly, that a lot of it has to do with patient selection. I think when you have a mixed bag of patients in a trial, including patients with Buerger’s disease, treated in multiple different countries, using different definitions of when to amputate, all those things come into play and could account for why those phase III trials were not successful.”
“Having been involved in lots of the different gene- and cell-based therapy trials, I think one of the unique benefits of this therapy is that it kind of bridges between the two. SDF-1 basically homes your endothelial progenitor cells to the site of ischemic injury for enhanced vasculogenesis. But SDF-1 also has direct effects on endothelial cells, including stimulating proliferation and preventing apoptosis,” she added.
JVS-100 has also successfully completed a phase II clinical trial for the treatment of heart failure. In addition, the agent is being developed as a treatment for acute MI, chronic angina, and for muscle regeneration.
The STOP-CLI study was sponsored by Juventas Therapeutics. Dr. Kibbe reported serving as a consultant to Johnson & Johnson/Cordis and Pluristem.
CHICAGO – A single set of intramuscular injections of stromal cell–derived factor-1 in patients with critical limb ischemia showed safety as well as evidence of efficacy through 12 months of follow-up in the STOP-CLI trial.
“Patients treated with JVS-100 demonstrated dose-dependent improvement across multiple patient-centered outcomes, including pain, quality of life, and wound healing, with less change in macrovascular objective measures in this small study,” Dr. Melina R. Kibbe reported at the American Heart Association scientific sessions. JVS-100 is a nonviral plasmid encoding human stromal cell–derived factor-1 (SDF-1), a natural chemokine protein that promotes angiogenesis by recruiting endothelial progenitor cells from the bone marrow to ischemic sites, explained Dr. Kibbe, professor and vice chair of surgical research and deputy director of the Simpson Querrey Institute for BioNanotechnology at Northwestern University, Chicago.
STOP-CLI was an exploratory, phase IIa, double-blind, first-in-humans study involving 48 patients with Rutherford classification 4 or 5 critical climb ischemia (CLI). All had an ankle-brachial index of 0.4 or lower, an ankle systolic blood pressure of 70 mm Hg or less or a toe systolic blood pressure of 50 or less, and were poor candidates for surgical revascularization. None had Buerger’s disease.
Participants were randomized to one of four study arms, and within each study arm further randomized 3:1 to stromal cell–derived factor-1 (SDF-1) or placebo injections. The patients received either 8 or 16 injections, each containing either 0.5 or 1.0 mg of SDF-1 or placebo. The injections, given in a single session, were placed at least 0.5 cm apart throughout the ischemic area of the affected limb.
By chance, most patients randomized to the placebo group were Rutherford 4, a category of CLI defined by rest pain, while the majority in the active treatment arms were Rutherford 5, a more severe disease manifestation characterized by ulcers. As a consequence, the SDF-1 recipients also had far larger nonhealing wounds, with an average area of 6.4 cm2, compared with 1.5 cm2, in controls.
The SDF-1 injections proved safe and were well tolerated, with no treatment-related serious adverse events and no safety signals evident in the laboratory results.
Turning to efficacy endpoints, Dr. Kibbe said self-rated visual analog scale pain scores showed clear, dose-dependent improvement over time in the SDF-1 treatment cohorts and no change in controls.
Similarly, the active treatment groups showed improved quality of life scores on all domains of the Short Form-36: physical functioning, bodily pain, general health, social functioning, energy/fatigue, emotional well-being, and overall physical and mental health, the surgeon continued.
Wound area decreased significantly in the SDF-1-treated groups, with the biggest reduction – more than 8 cm2 – being noted in the three patients who received eight 1-mg injections. That was also the group with the largest wounds at baseline, with an average area of 11.4 cm2.
Of note, the major limb amputation rate was “remarkably low” for patients with such severe CLI, according to Dr. Kibbe. The rate was less than 10% over the course of 12 months, with one patient in each of the four active treatment arms having a major amputation at time intervals of 58-112 days post injection. No major limb amputations occurred in the control group.
There was a hint of improvement with SDF-1 therapy over placebo in ankle-brachial index and transcutaneous oxygen pressure, but the between-group differences were too narrow in this study to allow for any conclusions. That must await planned much larger phase III trials, according to Dr. Kibbe.
Audience members, citing the numerous failures of once-promising stem cell therapies for CLI at phase III testing over the last 10-15 years, wondered why Dr. Kibbe thinks SDF-1 will fare any better.
“This is much debated and discussed among all the people involved in these kinds of trials,” she replied. “I’d say, briefly, that a lot of it has to do with patient selection. I think when you have a mixed bag of patients in a trial, including patients with Buerger’s disease, treated in multiple different countries, using different definitions of when to amputate, all those things come into play and could account for why those phase III trials were not successful.”
“Having been involved in lots of the different gene- and cell-based therapy trials, I think one of the unique benefits of this therapy is that it kind of bridges between the two. SDF-1 basically homes your endothelial progenitor cells to the site of ischemic injury for enhanced vasculogenesis. But SDF-1 also has direct effects on endothelial cells, including stimulating proliferation and preventing apoptosis,” she added.
JVS-100 has also successfully completed a phase II clinical trial for the treatment of heart failure. In addition, the agent is being developed as a treatment for acute MI, chronic angina, and for muscle regeneration.
The STOP-CLI study was sponsored by Juventas Therapeutics. Dr. Kibbe reported serving as a consultant to Johnson & Johnson/Cordis and Pluristem.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Intramuscular injections of stromal cell–derived factor-1 in patients with critical limb ischemia demonstrated safety and efficacy; the therapy is moving forward to phase III testing.
Major finding: The major limb amputation rate was less than 10% during 12 months of follow-up after a single dose of the novel therapy.
Data source: The STOP-CLI trial was a phase IIa, 12-month, randomized, double-blind, placebo-controlled, six-center trial including 48 patients with critical limb ischemia.
Disclosures: The STOP-CLI trial was sponsored by Juventas Therapeutics. The presenter reported serving as a consultant to Johnson & Johnson/Cordis and Pluristem.
