User login
How to cut the CRT nonresponder rate
SNOWMASS, COLO. – The 12-lead Holter monitor is an invaluable and underutilized tool for turning cardiac resynchronization therapy nonresponders into responders, according to Dr. N.A. Mark Estes III.
“The Achilles heel of CRT right now is the failure to respond that occurs in one-quarter to one-third of patients who receive the device. And I think it’s less and less due to a problem of poor patient selection or technical failure, but instead due to common mistakes made in patients who’ve been properly selected and in whom a CRT device has been placed appropriately. I think there’s a lot of room for improvement here,” said Dr. Estes, director of the cardiac arrhythmia center and professor of medicine at Tufts University in Boston.
One common mistake is to accept at face value the CRT device counter when it shows a high percentage of ventricular pacing that’s supposed to be indicative of adequate biventricular pacing in patients. That’s not reliable in patients with coexisting heart failure and atrial fibrillation. In fact, the device pacing counter can markedly overestimate the degree of effective biventricular pacing in patients with permanent atrial fibrillation undergoing CRT. That’s because it may incorrectly count fusion and pseudofusion beats as paced events, even though ventricular capture and atrioventricular resynchronization fail to occur during such beats. The 12-lead Holter monitor will tell the real story regarding ventricular rate control and the percentage of fully paced beats, Dr. Estes said at the Annual Cardiovascular Conference at Snowmass.
“In patients with atrial fibrillation, you can’t just do an EKG, and you can’t just do an interrogation of the device and see that they have 90% or 95% biventricular pacing, which is the sweet spot you need to be North of to make sure they’re having benefit. You really need to do the 24-hour Holter monitor,” the cardiologist emphasized.
“It happens all the time,” he continued. “It happens in my own institution, where we have people come in with heart failure who are being evaluated for an LVAD [left ventricular assist device] because when their CRT device is interrogated, it shows 95% pacing. Everyone’s getting ready to put in the LVAD, and we put them on a Holter monitor and guess what? They’re 60% paced. And sometimes you can have dramatic – really dramatic – improvements by just slowing the ventricular response.”
Increasingly, however, he and his fellow electrophysiologists are alternatively turning to atrioventricular junction ablation in suitable candidates for the catheter-based procedure in order to improve their clinical response to CRT.
Dr. Estes cited a study by Columbia University cardiologists as being highly influential in shaping the new understanding of how to use 12-lead Holter monitoring to identify patients with atrial fibrillation who aren’t responding to CRT. They studied 19 patients with permanent atrial fibrillation who were on CRT, all of whom were on beta-blockers, amiodarone, and digoxin for rate control. Although device interrogation showed all 19 patients had in excess of 90% biventricular pacing 12 months after CRT implantation, only 9 patients were actually clinical responders to CRT as defined by at least a 1-grade improvement in New York Heart Association functional class.
Upon wearing an ambulatory 12-lead Holter monitor for 24 hours, only the nine patients with clinical improvement in response to CRT actually had effective pacing; 94% of their heart beats over the course of 24 hours were fully paced, with a mere 2% fusion beats and less than 4% pseudofusion beats. The other 10 patients had an average of only 60% fully paced beats, along with 16% fusion and 24% pseudofusion beats.
The CRT clinical responders also showed evidence of reverse remodeling, with significantly greater improvements in left ventricular ejection fraction, end-systolic dimension, end-diastolic diameter, and end-systolic and end-diastolic volume, compared with nonresponders.
The lesson, according to the investigators, is that the percentage of biventricular pacing, as obtained from CRT device interrogation, is an unreliable indicator of effective pacing in patients with permanent atrial fibrillation. The goal of CRT programming in this population is to try to achieve 100% biventricular capture on the 12-lead Holter monitor (J. Am. Coll. Cardiol. 2009;53:1050-5).
A series of landmark randomized trials has established that in suitable candidates for CRT with NYHA class I through ambulatory class IV heart failure with reduced ejection fraction, the device therapy provides on average about a 17% reduction in all-cause mortality and a 29% decrease in hospitalizations for heart failure above and beyond the benefits obtained through guideline-directed medical therapy. However, the improvements seen in patients with NYHA class I symptoms are less impressive than in those with NYHA class II-IV disease. And it’s possible that the randomized controlled trials overestimate the true benefit from CRT.
“This is a group of extremely experienced investigators who know the literature well. They’re typically quite savvy with patient selection, and they’re vested in getting the right patients into these trials. Unfortunately, there’s not a registry of all eligible patients, so we can’t tell exactly how those patients were selected. It would have been helpful,” Dr. Estes said.
It’s clear from the randomized trials that the ideal patient for CRT is a woman under age 65 with nonischemic cardiomyopathy with a left bundle branch block, normal sinus rhythm, and a QRS duration of 150 milliseconds or more. That’s who’s most likely to obtain clinical benefit from the therapy. The flip side of that is that an older male patient with ischemia, atrial fibrillation, a QRS of 120-150 milliseconds, and non–left bundle branch block is less likely to respond.
“We’ve figured this out. I think we’ve gotten pretty good at giving patients an honest estimate of their probability of responding independent of our ability to get a lead into a good spot in the coronary sinus,” Dr. Estes said. “More than 95% of patients can be adequately resynchronized currently with the tools we have, so it’s not the barrier that it once represented. We have many different techniques available.”
Despite intensive efforts by investigators using sophisticated nuclear studies, echocardiography, and MRI, however, nothing to date has been able to predict who’s going to respond to CRT as well as a simple electrical parameter: the QRS duration.
“It remains really the gold standard. It’s an electrical marker for what is a mechanical event,” Dr. Estes said.
He reported serving as a consultant to Medtronic, St. Jude Medical, and Boston Scientific and receiving research support from Boston Scientific and St. Jude Medical.
SNOWMASS, COLO. – The 12-lead Holter monitor is an invaluable and underutilized tool for turning cardiac resynchronization therapy nonresponders into responders, according to Dr. N.A. Mark Estes III.
“The Achilles heel of CRT right now is the failure to respond that occurs in one-quarter to one-third of patients who receive the device. And I think it’s less and less due to a problem of poor patient selection or technical failure, but instead due to common mistakes made in patients who’ve been properly selected and in whom a CRT device has been placed appropriately. I think there’s a lot of room for improvement here,” said Dr. Estes, director of the cardiac arrhythmia center and professor of medicine at Tufts University in Boston.
One common mistake is to accept at face value the CRT device counter when it shows a high percentage of ventricular pacing that’s supposed to be indicative of adequate biventricular pacing in patients. That’s not reliable in patients with coexisting heart failure and atrial fibrillation. In fact, the device pacing counter can markedly overestimate the degree of effective biventricular pacing in patients with permanent atrial fibrillation undergoing CRT. That’s because it may incorrectly count fusion and pseudofusion beats as paced events, even though ventricular capture and atrioventricular resynchronization fail to occur during such beats. The 12-lead Holter monitor will tell the real story regarding ventricular rate control and the percentage of fully paced beats, Dr. Estes said at the Annual Cardiovascular Conference at Snowmass.
“In patients with atrial fibrillation, you can’t just do an EKG, and you can’t just do an interrogation of the device and see that they have 90% or 95% biventricular pacing, which is the sweet spot you need to be North of to make sure they’re having benefit. You really need to do the 24-hour Holter monitor,” the cardiologist emphasized.
“It happens all the time,” he continued. “It happens in my own institution, where we have people come in with heart failure who are being evaluated for an LVAD [left ventricular assist device] because when their CRT device is interrogated, it shows 95% pacing. Everyone’s getting ready to put in the LVAD, and we put them on a Holter monitor and guess what? They’re 60% paced. And sometimes you can have dramatic – really dramatic – improvements by just slowing the ventricular response.”
Increasingly, however, he and his fellow electrophysiologists are alternatively turning to atrioventricular junction ablation in suitable candidates for the catheter-based procedure in order to improve their clinical response to CRT.
Dr. Estes cited a study by Columbia University cardiologists as being highly influential in shaping the new understanding of how to use 12-lead Holter monitoring to identify patients with atrial fibrillation who aren’t responding to CRT. They studied 19 patients with permanent atrial fibrillation who were on CRT, all of whom were on beta-blockers, amiodarone, and digoxin for rate control. Although device interrogation showed all 19 patients had in excess of 90% biventricular pacing 12 months after CRT implantation, only 9 patients were actually clinical responders to CRT as defined by at least a 1-grade improvement in New York Heart Association functional class.
Upon wearing an ambulatory 12-lead Holter monitor for 24 hours, only the nine patients with clinical improvement in response to CRT actually had effective pacing; 94% of their heart beats over the course of 24 hours were fully paced, with a mere 2% fusion beats and less than 4% pseudofusion beats. The other 10 patients had an average of only 60% fully paced beats, along with 16% fusion and 24% pseudofusion beats.
The CRT clinical responders also showed evidence of reverse remodeling, with significantly greater improvements in left ventricular ejection fraction, end-systolic dimension, end-diastolic diameter, and end-systolic and end-diastolic volume, compared with nonresponders.
The lesson, according to the investigators, is that the percentage of biventricular pacing, as obtained from CRT device interrogation, is an unreliable indicator of effective pacing in patients with permanent atrial fibrillation. The goal of CRT programming in this population is to try to achieve 100% biventricular capture on the 12-lead Holter monitor (J. Am. Coll. Cardiol. 2009;53:1050-5).
A series of landmark randomized trials has established that in suitable candidates for CRT with NYHA class I through ambulatory class IV heart failure with reduced ejection fraction, the device therapy provides on average about a 17% reduction in all-cause mortality and a 29% decrease in hospitalizations for heart failure above and beyond the benefits obtained through guideline-directed medical therapy. However, the improvements seen in patients with NYHA class I symptoms are less impressive than in those with NYHA class II-IV disease. And it’s possible that the randomized controlled trials overestimate the true benefit from CRT.
“This is a group of extremely experienced investigators who know the literature well. They’re typically quite savvy with patient selection, and they’re vested in getting the right patients into these trials. Unfortunately, there’s not a registry of all eligible patients, so we can’t tell exactly how those patients were selected. It would have been helpful,” Dr. Estes said.
It’s clear from the randomized trials that the ideal patient for CRT is a woman under age 65 with nonischemic cardiomyopathy with a left bundle branch block, normal sinus rhythm, and a QRS duration of 150 milliseconds or more. That’s who’s most likely to obtain clinical benefit from the therapy. The flip side of that is that an older male patient with ischemia, atrial fibrillation, a QRS of 120-150 milliseconds, and non–left bundle branch block is less likely to respond.
“We’ve figured this out. I think we’ve gotten pretty good at giving patients an honest estimate of their probability of responding independent of our ability to get a lead into a good spot in the coronary sinus,” Dr. Estes said. “More than 95% of patients can be adequately resynchronized currently with the tools we have, so it’s not the barrier that it once represented. We have many different techniques available.”
Despite intensive efforts by investigators using sophisticated nuclear studies, echocardiography, and MRI, however, nothing to date has been able to predict who’s going to respond to CRT as well as a simple electrical parameter: the QRS duration.
“It remains really the gold standard. It’s an electrical marker for what is a mechanical event,” Dr. Estes said.
He reported serving as a consultant to Medtronic, St. Jude Medical, and Boston Scientific and receiving research support from Boston Scientific and St. Jude Medical.
SNOWMASS, COLO. – The 12-lead Holter monitor is an invaluable and underutilized tool for turning cardiac resynchronization therapy nonresponders into responders, according to Dr. N.A. Mark Estes III.
“The Achilles heel of CRT right now is the failure to respond that occurs in one-quarter to one-third of patients who receive the device. And I think it’s less and less due to a problem of poor patient selection or technical failure, but instead due to common mistakes made in patients who’ve been properly selected and in whom a CRT device has been placed appropriately. I think there’s a lot of room for improvement here,” said Dr. Estes, director of the cardiac arrhythmia center and professor of medicine at Tufts University in Boston.
One common mistake is to accept at face value the CRT device counter when it shows a high percentage of ventricular pacing that’s supposed to be indicative of adequate biventricular pacing in patients. That’s not reliable in patients with coexisting heart failure and atrial fibrillation. In fact, the device pacing counter can markedly overestimate the degree of effective biventricular pacing in patients with permanent atrial fibrillation undergoing CRT. That’s because it may incorrectly count fusion and pseudofusion beats as paced events, even though ventricular capture and atrioventricular resynchronization fail to occur during such beats. The 12-lead Holter monitor will tell the real story regarding ventricular rate control and the percentage of fully paced beats, Dr. Estes said at the Annual Cardiovascular Conference at Snowmass.
“In patients with atrial fibrillation, you can’t just do an EKG, and you can’t just do an interrogation of the device and see that they have 90% or 95% biventricular pacing, which is the sweet spot you need to be North of to make sure they’re having benefit. You really need to do the 24-hour Holter monitor,” the cardiologist emphasized.
“It happens all the time,” he continued. “It happens in my own institution, where we have people come in with heart failure who are being evaluated for an LVAD [left ventricular assist device] because when their CRT device is interrogated, it shows 95% pacing. Everyone’s getting ready to put in the LVAD, and we put them on a Holter monitor and guess what? They’re 60% paced. And sometimes you can have dramatic – really dramatic – improvements by just slowing the ventricular response.”
Increasingly, however, he and his fellow electrophysiologists are alternatively turning to atrioventricular junction ablation in suitable candidates for the catheter-based procedure in order to improve their clinical response to CRT.
Dr. Estes cited a study by Columbia University cardiologists as being highly influential in shaping the new understanding of how to use 12-lead Holter monitoring to identify patients with atrial fibrillation who aren’t responding to CRT. They studied 19 patients with permanent atrial fibrillation who were on CRT, all of whom were on beta-blockers, amiodarone, and digoxin for rate control. Although device interrogation showed all 19 patients had in excess of 90% biventricular pacing 12 months after CRT implantation, only 9 patients were actually clinical responders to CRT as defined by at least a 1-grade improvement in New York Heart Association functional class.
Upon wearing an ambulatory 12-lead Holter monitor for 24 hours, only the nine patients with clinical improvement in response to CRT actually had effective pacing; 94% of their heart beats over the course of 24 hours were fully paced, with a mere 2% fusion beats and less than 4% pseudofusion beats. The other 10 patients had an average of only 60% fully paced beats, along with 16% fusion and 24% pseudofusion beats.
The CRT clinical responders also showed evidence of reverse remodeling, with significantly greater improvements in left ventricular ejection fraction, end-systolic dimension, end-diastolic diameter, and end-systolic and end-diastolic volume, compared with nonresponders.
The lesson, according to the investigators, is that the percentage of biventricular pacing, as obtained from CRT device interrogation, is an unreliable indicator of effective pacing in patients with permanent atrial fibrillation. The goal of CRT programming in this population is to try to achieve 100% biventricular capture on the 12-lead Holter monitor (J. Am. Coll. Cardiol. 2009;53:1050-5).
A series of landmark randomized trials has established that in suitable candidates for CRT with NYHA class I through ambulatory class IV heart failure with reduced ejection fraction, the device therapy provides on average about a 17% reduction in all-cause mortality and a 29% decrease in hospitalizations for heart failure above and beyond the benefits obtained through guideline-directed medical therapy. However, the improvements seen in patients with NYHA class I symptoms are less impressive than in those with NYHA class II-IV disease. And it’s possible that the randomized controlled trials overestimate the true benefit from CRT.
“This is a group of extremely experienced investigators who know the literature well. They’re typically quite savvy with patient selection, and they’re vested in getting the right patients into these trials. Unfortunately, there’s not a registry of all eligible patients, so we can’t tell exactly how those patients were selected. It would have been helpful,” Dr. Estes said.
It’s clear from the randomized trials that the ideal patient for CRT is a woman under age 65 with nonischemic cardiomyopathy with a left bundle branch block, normal sinus rhythm, and a QRS duration of 150 milliseconds or more. That’s who’s most likely to obtain clinical benefit from the therapy. The flip side of that is that an older male patient with ischemia, atrial fibrillation, a QRS of 120-150 milliseconds, and non–left bundle branch block is less likely to respond.
“We’ve figured this out. I think we’ve gotten pretty good at giving patients an honest estimate of their probability of responding independent of our ability to get a lead into a good spot in the coronary sinus,” Dr. Estes said. “More than 95% of patients can be adequately resynchronized currently with the tools we have, so it’s not the barrier that it once represented. We have many different techniques available.”
Despite intensive efforts by investigators using sophisticated nuclear studies, echocardiography, and MRI, however, nothing to date has been able to predict who’s going to respond to CRT as well as a simple electrical parameter: the QRS duration.
“It remains really the gold standard. It’s an electrical marker for what is a mechanical event,” Dr. Estes said.
He reported serving as a consultant to Medtronic, St. Jude Medical, and Boston Scientific and receiving research support from Boston Scientific and St. Jude Medical.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
New concerns rise over iatrogenic hydroxychloroquine retinopathy
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
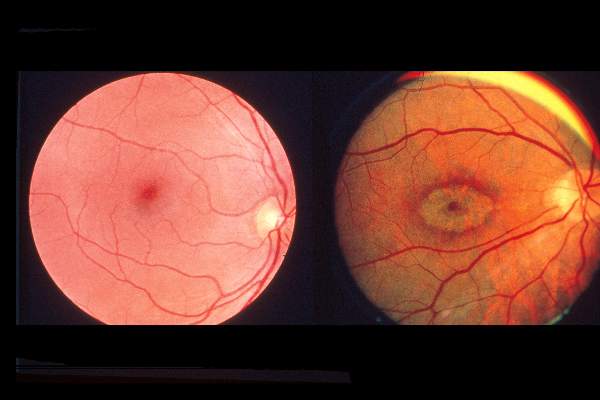
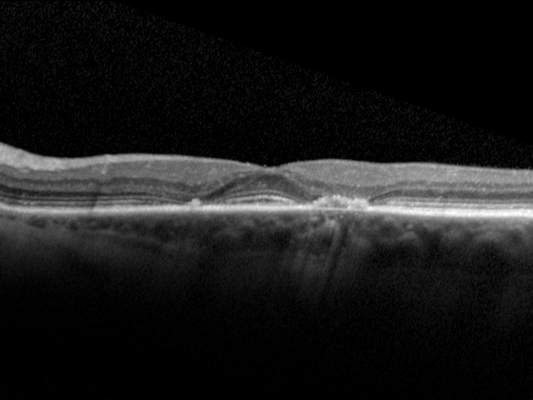
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
SNOWMASS, COLO. – The risk of irreversible hydroxychloroquine toxic retinopathy is much greater than previously appreciated, Dr. James T. Rosenbaum cautioned at the Winter Rheumatology Symposium sponsored by the American College of Rheumatology.
“I remember when I was a fellow a paper was published saying Plaquenil [hydroxychloroquine] is safer than aspirin, it lowers lipids, and everyone should be taking it,” recalled Dr. Rosenbaum, professor of inflammatory diseases and chief of the division of arthritis and rheumatic diseases at Oregon Health and Science University, and chief of ophthalmology at the Devers Eye Institute in Portland, Ore.
He doesn’t feel that way anymore.
Dr. Rosenbaum highlighted a major recent study from Kaiser Permanente of Northern California which underscored the retinal hazards of long-term hydroxychloroquine. The retrospective, case-control study included 2,361 Kaiser Permanente patients who used the drug continuously for at least 5 years.
Evaluation by visual field testing and/or spectral domain optical coherence tomography (OCT) showed the overall prevalence of retinal thinning and photoreceptor damage or visual field loss was 7.5%. The risk climbed with greater daily dosage and duration of therapy, reaching a prevalence of nearly 20% after 20 years on hydroxychloroquine (JAMA Ophthalmol. 2014;132:1453-60).
“This really shakes my belief,” Dr. Rosenbaum confessed. “I really thought that anyone could take hydroxychloroquine with great impunity, but it turns out we really have to be careful with the dosage and the duration of therapy. I think we probably should routinely be reducing the dosage after 5 years of use, and in females who are under 5’6” we might need to be adjusting the dosage.
“Look, I think hydroxychloroquine is the greatest drug. I think everyone with rheumatoid arthritis and lupus should be on hydroxychloroquine. But I do think that after 5 years you want to monitor, and you should start thinking about having the patient take the drug 12 times per week instead of 14 times per week,” he added.
Dr. Rosenbaum called OCT “an absolutely invaluable diagnostic technique.” It provides objective findings enabling physicians to catch hydroxychloroquine retinopathy early, well before development of the classic hydroxychloroquine-induced severe bullseye maculopathy.
With no risk to the patient, the OCT laser reflects off the eye, permitting close inspection of the nine layers of the retina. Toxicity due to hydroxychloroquine or other antimalarials is manifest in what ophthalmologists call the flying saucer sign or sombrero sign because of its distinctive appearance, the result of fovial thinning and loss of the inner segment/outer segment junction.
Dr. Rosenbaum credited Dr. Michael F. Marmor, professor of ophthalmology at Stanford (Calif.) University, as the driving force behind the new appreciation of the full scope of hydroxychloroquine toxic retinopathy. Dr. Marmor was coauthor of the recent Kaiser Permanente study and has also collaborated with rheumatologist Dr. Fred Wolfe of the National Databank for Rheumatic Diseases in a large study (Arthritis Care Res. 2010;62:775-84). In addition, Dr. Marmor chaired the American Academy of Ophthalmology committee that drew up revised guidelines for screening for hydroxychloroquine retinopathy (Ophthalmology 2011;118:415-22).
Those guidelines call for screening when a patient first goes on hydroxychloroquine and then not again until the 5-year mark, since toxicity is rare within the first 5 years of treatment. After 5 years of use, annual screening is recommended. The screening should include a visual field exam as well as one of the advanced objective technologies: spectral domain OCT, autofluorescence, or multifocal electroretinography. Use of the outmoded Amsler grid is discouraged.
Dr. Rosenbaum advised his colleagues to send their patients to a practitioner who utilizes spectral domain OCT.
“Multifocal ERG is painful, time consuming, and you wouldn’t want to undergo it. Autofluorescence is equally as good as OCT but not as many centers do it; optometrists now often have OCT in their office,” he observed.
The Kaiser Permanente study identified several key risk factors for hydroxychloroquine retinopathy. The investigators were unable to identify a safe dosage of hydroxychloroquine, but they noted that for daily consumption of 4.0-5.0 mg/kg of real body weight, the prevalence was low – less than 2% – for the first 10 years of use. However, the prevalence climbed sharply thereafter. The researchers determined that real body weight predicted risk better than did ideal weight and should be used by clinicians in their dosing calculations. Patients on more than 5.0 mg/kg of real body weight daily had a 5.7-fold greater prevalence of hydroxychloroquine retinopathy.
Chronic kidney disease, defined as an estimated glomerular filtration rate below 60 mL/min, was associated with a twofold increased risk. Concurrent use of tamoxifen – a drug that appears to be toxic to the retina in its own right – was associated with a 4.6-fold increased risk of hydroxychloroquine retinopathy.
Audience members at the symposium asked how worried they and their patients really need to be, and just how often these subtle early abnormalities translate to functional visual impairment.
“When you can see the structural damage and see the damage functionally on the field exam, and you know that it’s going to increase over time, I think you need an awfully good lawyer to continue with the use of therapy,” Dr. Rosenbaum replied. “This is early change, and many patients may not even be aware of it. But I would much rather find it early than persist with treatment. And I’m thankful that now we have a mechanism to prevent it from progressing.”
Does the retinopathy reverse upon drug discontinuation? “Maybe a smidgen, but it’s neurologic damage. I think for the most part, if you catch it early and it stabilizes, that’s the best we can do,” according to Dr. Rosenbaum.
And remember: Eighty percent of people who have taken hydroxychloroquine for 20 years do not have retinal toxicity, he added.
Dr. Rosenbaum reported receiving consulting fees from a dozen pharmaceutical companies and research grants from AbbVie, Eyegate, Genentech, and pSivida.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
How to tell constrictive pericarditis from mimickers
SNOWMASS, COLO. – Differentiating constrictive pericarditis from restrictive cardiomyopathy in patients with right heart failure with a normal ejection fraction is “one of the most difficult diagnostic challenges in cardiology today,” but reliable results can be achieved using a careful step-by-step approach, Dr. Rick A. Nishimura said at the Annual Cardiovascular Conference at Snowmass.
Under current terminology for heart failure, cardiologists speak of HFrEF, or heart failure with reduced ejection fraction, and HFpEF, or heart failure with preserved ejection fraction. But there is a third group of patients who are often mistakenly thought to have HFpEF: those with severe right heart failure and a normal ejection fraction, classically caused by constrictive pericarditis or restrictive cardiomyopathy.
Unlike patients with HFpEF, these people are not hypertensive and they don’t have pulmonary congestion. Instead, they present predominantly with ascites, peripheral edema, fatigue, and marked elevation in jugular venous pressure, noted Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn.
Before elaborating on his own tried-and-true, step-by-step approach, he highlighted several diagnostic procedures he considers less than reliable. One is advanced imaging with CT or MRI looking for the pericardial thickening that is widely viewed as an anatomic hallmark of constrictive pericarditis.
“Remember, 22% of patients with proven constrictive pericarditis actually have a normal pericardium on CT or MRI, because it’s their fibrotic epicardium that’s causing the constrictive pericarditis. And roughly 70% of patients are going to have some thickened pericardium after radiation therapy or coronary artery bypass graft surgery without having constrictive pericarditis. So CT and MRI are helpful, but they’re not going to be diagnostic,” according to the cardiologist.
Similarly, while it’s often been said that constrictive pericarditis can be diagnosed based upon a classic trio of hemodynamic findings obtained through heart catheterization – namely, early rapid filling with a left ventricular end-diastolic pressure equal to the right ventricular end-diastolic pressure, a right ventricular end-diastolic pressure greater than one-third of the right ventricular systolic pressure, and a pulmonary artery pressure below 50 mm Hg – these criteria didn’t reliably separate the last 100 patients who came to the catheterization lab at the Mayo Clinic with either constrictive pericarditis or restrictive cardiomyopathy, he continued.
Dr. Nishimura’s approach to the work-up of patients with unexplained right heart failure and a normal ejection begins with the history and physical examination. The history in a patient with constrictive pericarditis is classically one of radiation therapy years earlier for a malignancy, or prior CABG surgery. And the physical exam has to reveal the presence of high neck veins.
“If you don’t see high neck veins due to elevated jugular venous pressure with rapid x and y descents, the patient doesn’t have constrictive pericarditis, no matter what the echocardiogram shows,” Dr. Nishimura asserted.
If those findings are present, however, then on 2-D echocardiography he’s looking for three things that point to constrictive pericarditis: a brisk septal shudder due to rapid filling in early diastole with every heart beat; an early diastolic posterior motion of the intraventricular septum, known as the septal bounce, that occurs as a consequence of the less compliant ventricular walls; and dilation of the inferior vena cava indicative of increased right atrial pressure.
When all three findings are present on 2-D echo, he turns to Doppler echo for hemodynamic information. If Doppler shows a reduction in transmitral driving pressure from the lungs to the heart during inspiration, as the intrathoracic pressure drops but the left ventricular pressure does not, the work-up is done. That patient has constrictive pericarditis and needs to be referred to surgery for pericardiectomy, which will bring rapid improvement.
In roughly one-quarter of patients with constrictive pericarditis, however, that full constellation of 2-D and Doppler echocardiographic findings isn’t present. It then becomes necessary to move on to cardiac catheterization. The first two things to look for in the cath lab are elevated end-equalization of diastolic pressures and low cardiac output.
“If they’re in the cath lab and they’ve got normal filling pressures and a normal cardiac output, they do not have clinically significant constrictive pericarditis, no matter what the echo shows. So those two things are necessary to see, but of course they’re not diagnostic. So we go further,” Dr. Nishimura said.
A patient with constrictive pericarditis will have enhanced ventricular interaction arising from the restraint imposed by a rigid, diseased pericardium. That’s crucial. This increased ventricular interaction is manifest as an increase in the size of the right ventricle during inspiration while the area of the left ventricle is getting smaller.
In contrast, during inspiration and expiration in a patient with restrictive cardiomyopathy, as the right ventricle gets smaller, so does the left ventricle.
“The ratio of the right ventricle to left ventricle area under the curve during inspiration versus expiration gives a very nice distinction between constrictive pericarditis and restrictive cardiomyopathy. Enhanced ventricular interaction is the most sensitive and specific finding for constrictive pericarditis,” according to Dr. Nishimura.
He added that, in addition to constrictive pericarditis and restrictive cardiomyopathy, there is a third and underappreciated cause of right heart failure with a normal ejection fraction: severe tricuspid regurgitation. This abnormality may not be readily apparent upon echocardiography in a patient with a pacemaker lead or automatic implantable cardioverter-defibrillator lead, which can cause acoustic shadowing that results in underestimation of the severity of tricuspid regurgitation. The clue here is the observation of hepatic vein systolic flow reversal, which can only be caused by severe tricuspid regurgitation.
“Think tricuspid regurgitation in patients who have a pacemaker lead or AICD, and also in older women with longstanding atrial fibrillation who dilate their tricuspid annulus and develop more and more tricuspid regurgitation. Take those patients to the cath lab and do a right ventriculogram, which will show tricuspid regurgitation,” Dr. Nishimura advised.
He reported having no financial conflicts.
SNOWMASS, COLO. – Differentiating constrictive pericarditis from restrictive cardiomyopathy in patients with right heart failure with a normal ejection fraction is “one of the most difficult diagnostic challenges in cardiology today,” but reliable results can be achieved using a careful step-by-step approach, Dr. Rick A. Nishimura said at the Annual Cardiovascular Conference at Snowmass.
Under current terminology for heart failure, cardiologists speak of HFrEF, or heart failure with reduced ejection fraction, and HFpEF, or heart failure with preserved ejection fraction. But there is a third group of patients who are often mistakenly thought to have HFpEF: those with severe right heart failure and a normal ejection fraction, classically caused by constrictive pericarditis or restrictive cardiomyopathy.
Unlike patients with HFpEF, these people are not hypertensive and they don’t have pulmonary congestion. Instead, they present predominantly with ascites, peripheral edema, fatigue, and marked elevation in jugular venous pressure, noted Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn.
Before elaborating on his own tried-and-true, step-by-step approach, he highlighted several diagnostic procedures he considers less than reliable. One is advanced imaging with CT or MRI looking for the pericardial thickening that is widely viewed as an anatomic hallmark of constrictive pericarditis.
“Remember, 22% of patients with proven constrictive pericarditis actually have a normal pericardium on CT or MRI, because it’s their fibrotic epicardium that’s causing the constrictive pericarditis. And roughly 70% of patients are going to have some thickened pericardium after radiation therapy or coronary artery bypass graft surgery without having constrictive pericarditis. So CT and MRI are helpful, but they’re not going to be diagnostic,” according to the cardiologist.
Similarly, while it’s often been said that constrictive pericarditis can be diagnosed based upon a classic trio of hemodynamic findings obtained through heart catheterization – namely, early rapid filling with a left ventricular end-diastolic pressure equal to the right ventricular end-diastolic pressure, a right ventricular end-diastolic pressure greater than one-third of the right ventricular systolic pressure, and a pulmonary artery pressure below 50 mm Hg – these criteria didn’t reliably separate the last 100 patients who came to the catheterization lab at the Mayo Clinic with either constrictive pericarditis or restrictive cardiomyopathy, he continued.
Dr. Nishimura’s approach to the work-up of patients with unexplained right heart failure and a normal ejection begins with the history and physical examination. The history in a patient with constrictive pericarditis is classically one of radiation therapy years earlier for a malignancy, or prior CABG surgery. And the physical exam has to reveal the presence of high neck veins.
“If you don’t see high neck veins due to elevated jugular venous pressure with rapid x and y descents, the patient doesn’t have constrictive pericarditis, no matter what the echocardiogram shows,” Dr. Nishimura asserted.
If those findings are present, however, then on 2-D echocardiography he’s looking for three things that point to constrictive pericarditis: a brisk septal shudder due to rapid filling in early diastole with every heart beat; an early diastolic posterior motion of the intraventricular septum, known as the septal bounce, that occurs as a consequence of the less compliant ventricular walls; and dilation of the inferior vena cava indicative of increased right atrial pressure.
When all three findings are present on 2-D echo, he turns to Doppler echo for hemodynamic information. If Doppler shows a reduction in transmitral driving pressure from the lungs to the heart during inspiration, as the intrathoracic pressure drops but the left ventricular pressure does not, the work-up is done. That patient has constrictive pericarditis and needs to be referred to surgery for pericardiectomy, which will bring rapid improvement.
In roughly one-quarter of patients with constrictive pericarditis, however, that full constellation of 2-D and Doppler echocardiographic findings isn’t present. It then becomes necessary to move on to cardiac catheterization. The first two things to look for in the cath lab are elevated end-equalization of diastolic pressures and low cardiac output.
“If they’re in the cath lab and they’ve got normal filling pressures and a normal cardiac output, they do not have clinically significant constrictive pericarditis, no matter what the echo shows. So those two things are necessary to see, but of course they’re not diagnostic. So we go further,” Dr. Nishimura said.
A patient with constrictive pericarditis will have enhanced ventricular interaction arising from the restraint imposed by a rigid, diseased pericardium. That’s crucial. This increased ventricular interaction is manifest as an increase in the size of the right ventricle during inspiration while the area of the left ventricle is getting smaller.
In contrast, during inspiration and expiration in a patient with restrictive cardiomyopathy, as the right ventricle gets smaller, so does the left ventricle.
“The ratio of the right ventricle to left ventricle area under the curve during inspiration versus expiration gives a very nice distinction between constrictive pericarditis and restrictive cardiomyopathy. Enhanced ventricular interaction is the most sensitive and specific finding for constrictive pericarditis,” according to Dr. Nishimura.
He added that, in addition to constrictive pericarditis and restrictive cardiomyopathy, there is a third and underappreciated cause of right heart failure with a normal ejection fraction: severe tricuspid regurgitation. This abnormality may not be readily apparent upon echocardiography in a patient with a pacemaker lead or automatic implantable cardioverter-defibrillator lead, which can cause acoustic shadowing that results in underestimation of the severity of tricuspid regurgitation. The clue here is the observation of hepatic vein systolic flow reversal, which can only be caused by severe tricuspid regurgitation.
“Think tricuspid regurgitation in patients who have a pacemaker lead or AICD, and also in older women with longstanding atrial fibrillation who dilate their tricuspid annulus and develop more and more tricuspid regurgitation. Take those patients to the cath lab and do a right ventriculogram, which will show tricuspid regurgitation,” Dr. Nishimura advised.
He reported having no financial conflicts.
SNOWMASS, COLO. – Differentiating constrictive pericarditis from restrictive cardiomyopathy in patients with right heart failure with a normal ejection fraction is “one of the most difficult diagnostic challenges in cardiology today,” but reliable results can be achieved using a careful step-by-step approach, Dr. Rick A. Nishimura said at the Annual Cardiovascular Conference at Snowmass.
Under current terminology for heart failure, cardiologists speak of HFrEF, or heart failure with reduced ejection fraction, and HFpEF, or heart failure with preserved ejection fraction. But there is a third group of patients who are often mistakenly thought to have HFpEF: those with severe right heart failure and a normal ejection fraction, classically caused by constrictive pericarditis or restrictive cardiomyopathy.
Unlike patients with HFpEF, these people are not hypertensive and they don’t have pulmonary congestion. Instead, they present predominantly with ascites, peripheral edema, fatigue, and marked elevation in jugular venous pressure, noted Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn.
Before elaborating on his own tried-and-true, step-by-step approach, he highlighted several diagnostic procedures he considers less than reliable. One is advanced imaging with CT or MRI looking for the pericardial thickening that is widely viewed as an anatomic hallmark of constrictive pericarditis.
“Remember, 22% of patients with proven constrictive pericarditis actually have a normal pericardium on CT or MRI, because it’s their fibrotic epicardium that’s causing the constrictive pericarditis. And roughly 70% of patients are going to have some thickened pericardium after radiation therapy or coronary artery bypass graft surgery without having constrictive pericarditis. So CT and MRI are helpful, but they’re not going to be diagnostic,” according to the cardiologist.
Similarly, while it’s often been said that constrictive pericarditis can be diagnosed based upon a classic trio of hemodynamic findings obtained through heart catheterization – namely, early rapid filling with a left ventricular end-diastolic pressure equal to the right ventricular end-diastolic pressure, a right ventricular end-diastolic pressure greater than one-third of the right ventricular systolic pressure, and a pulmonary artery pressure below 50 mm Hg – these criteria didn’t reliably separate the last 100 patients who came to the catheterization lab at the Mayo Clinic with either constrictive pericarditis or restrictive cardiomyopathy, he continued.
Dr. Nishimura’s approach to the work-up of patients with unexplained right heart failure and a normal ejection begins with the history and physical examination. The history in a patient with constrictive pericarditis is classically one of radiation therapy years earlier for a malignancy, or prior CABG surgery. And the physical exam has to reveal the presence of high neck veins.
“If you don’t see high neck veins due to elevated jugular venous pressure with rapid x and y descents, the patient doesn’t have constrictive pericarditis, no matter what the echocardiogram shows,” Dr. Nishimura asserted.
If those findings are present, however, then on 2-D echocardiography he’s looking for three things that point to constrictive pericarditis: a brisk septal shudder due to rapid filling in early diastole with every heart beat; an early diastolic posterior motion of the intraventricular septum, known as the septal bounce, that occurs as a consequence of the less compliant ventricular walls; and dilation of the inferior vena cava indicative of increased right atrial pressure.
When all three findings are present on 2-D echo, he turns to Doppler echo for hemodynamic information. If Doppler shows a reduction in transmitral driving pressure from the lungs to the heart during inspiration, as the intrathoracic pressure drops but the left ventricular pressure does not, the work-up is done. That patient has constrictive pericarditis and needs to be referred to surgery for pericardiectomy, which will bring rapid improvement.
In roughly one-quarter of patients with constrictive pericarditis, however, that full constellation of 2-D and Doppler echocardiographic findings isn’t present. It then becomes necessary to move on to cardiac catheterization. The first two things to look for in the cath lab are elevated end-equalization of diastolic pressures and low cardiac output.
“If they’re in the cath lab and they’ve got normal filling pressures and a normal cardiac output, they do not have clinically significant constrictive pericarditis, no matter what the echo shows. So those two things are necessary to see, but of course they’re not diagnostic. So we go further,” Dr. Nishimura said.
A patient with constrictive pericarditis will have enhanced ventricular interaction arising from the restraint imposed by a rigid, diseased pericardium. That’s crucial. This increased ventricular interaction is manifest as an increase in the size of the right ventricle during inspiration while the area of the left ventricle is getting smaller.
In contrast, during inspiration and expiration in a patient with restrictive cardiomyopathy, as the right ventricle gets smaller, so does the left ventricle.
“The ratio of the right ventricle to left ventricle area under the curve during inspiration versus expiration gives a very nice distinction between constrictive pericarditis and restrictive cardiomyopathy. Enhanced ventricular interaction is the most sensitive and specific finding for constrictive pericarditis,” according to Dr. Nishimura.
He added that, in addition to constrictive pericarditis and restrictive cardiomyopathy, there is a third and underappreciated cause of right heart failure with a normal ejection fraction: severe tricuspid regurgitation. This abnormality may not be readily apparent upon echocardiography in a patient with a pacemaker lead or automatic implantable cardioverter-defibrillator lead, which can cause acoustic shadowing that results in underestimation of the severity of tricuspid regurgitation. The clue here is the observation of hepatic vein systolic flow reversal, which can only be caused by severe tricuspid regurgitation.
“Think tricuspid regurgitation in patients who have a pacemaker lead or AICD, and also in older women with longstanding atrial fibrillation who dilate their tricuspid annulus and develop more and more tricuspid regurgitation. Take those patients to the cath lab and do a right ventriculogram, which will show tricuspid regurgitation,” Dr. Nishimura advised.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Stage trumps biology for most small triple-negative breast cancers
SAN ANTONIO – Patients with stage T1a or T1b triple-negative breast cancer have an excellent prognosis even without chemotherapy, according to Dr. Eric P. Winer.
“There’s a perception on the part of many patients and physicians that all triple-negative breast cancer is bad, and that it’s destined to threaten and ultimately take a woman’s life. But even in an era where biology is king, stage still matters,” he observed at the San Antonio Breast Cancer Symposium.

He was a coinvestigator in a recent prospective cohort study which included 4,113 women with stage T1a or 1b breast cancer – that is, a tumor size no greater than 10 mm in its greatest dimension – without regional lymph node metastases or evidence of distant metastases. The patients, drawn from the National Comprehensive Cancer Network database, were treated in accord with institutional practice and followed for a median of 5.5 years.
Slightly over half of those in the subset with triple-negative breast cancer (TNBC) got chemotherapy. Those who received chemotherapy for T1a TNBC as defined by a tumor size not greater than 5 mm had a 5-year distant relapse-free survival (DRFS) of 100%, but the rate was still close to 95% in those not treated with chemotherapy. Outcomes were also quite favorable for patients with T1b TNBC who didn’t receive chemotherapy (J. Clin. Oncol. 2014;32:2142-50), said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
He noted that the findings in this study echo those of an earlier study by investigators at University of Texas M.D. Anderson Cancer Center, Houston, who reported a 5-year DRFS rate of 96% in 125 patients with T1a or 1b, lymph node-negative TNBC untreated with chemotherapy (J. Clin. Oncol. 2009;27:5700-6).
Dr. Winer said that while the consensus among most experts is that standard adjuvant chemotherapy regimens for patients with stage 2 or 3 TNBC include both anthracyclines and taxanes, his own view is that for patients with stage 1 TNBC “if you’re going to pursue chemotherapy, then treatment with a somewhat less toxic, shorter regimen would seem to be more appropriate.”
SAN ANTONIO – Patients with stage T1a or T1b triple-negative breast cancer have an excellent prognosis even without chemotherapy, according to Dr. Eric P. Winer.
“There’s a perception on the part of many patients and physicians that all triple-negative breast cancer is bad, and that it’s destined to threaten and ultimately take a woman’s life. But even in an era where biology is king, stage still matters,” he observed at the San Antonio Breast Cancer Symposium.
He was a coinvestigator in a recent prospective cohort study which included 4,113 women with stage T1a or 1b breast cancer – that is, a tumor size no greater than 10 mm in its greatest dimension – without regional lymph node metastases or evidence of distant metastases. The patients, drawn from the National Comprehensive Cancer Network database, were treated in accord with institutional practice and followed for a median of 5.5 years.
Slightly over half of those in the subset with triple-negative breast cancer (TNBC) got chemotherapy. Those who received chemotherapy for T1a TNBC as defined by a tumor size not greater than 5 mm had a 5-year distant relapse-free survival (DRFS) of 100%, but the rate was still close to 95% in those not treated with chemotherapy. Outcomes were also quite favorable for patients with T1b TNBC who didn’t receive chemotherapy (J. Clin. Oncol. 2014;32:2142-50), said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
He noted that the findings in this study echo those of an earlier study by investigators at University of Texas M.D. Anderson Cancer Center, Houston, who reported a 5-year DRFS rate of 96% in 125 patients with T1a or 1b, lymph node-negative TNBC untreated with chemotherapy (J. Clin. Oncol. 2009;27:5700-6).
Dr. Winer said that while the consensus among most experts is that standard adjuvant chemotherapy regimens for patients with stage 2 or 3 TNBC include both anthracyclines and taxanes, his own view is that for patients with stage 1 TNBC “if you’re going to pursue chemotherapy, then treatment with a somewhat less toxic, shorter regimen would seem to be more appropriate.”
SAN ANTONIO – Patients with stage T1a or T1b triple-negative breast cancer have an excellent prognosis even without chemotherapy, according to Dr. Eric P. Winer.
“There’s a perception on the part of many patients and physicians that all triple-negative breast cancer is bad, and that it’s destined to threaten and ultimately take a woman’s life. But even in an era where biology is king, stage still matters,” he observed at the San Antonio Breast Cancer Symposium.
He was a coinvestigator in a recent prospective cohort study which included 4,113 women with stage T1a or 1b breast cancer – that is, a tumor size no greater than 10 mm in its greatest dimension – without regional lymph node metastases or evidence of distant metastases. The patients, drawn from the National Comprehensive Cancer Network database, were treated in accord with institutional practice and followed for a median of 5.5 years.
Slightly over half of those in the subset with triple-negative breast cancer (TNBC) got chemotherapy. Those who received chemotherapy for T1a TNBC as defined by a tumor size not greater than 5 mm had a 5-year distant relapse-free survival (DRFS) of 100%, but the rate was still close to 95% in those not treated with chemotherapy. Outcomes were also quite favorable for patients with T1b TNBC who didn’t receive chemotherapy (J. Clin. Oncol. 2014;32:2142-50), said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
He noted that the findings in this study echo those of an earlier study by investigators at University of Texas M.D. Anderson Cancer Center, Houston, who reported a 5-year DRFS rate of 96% in 125 patients with T1a or 1b, lymph node-negative TNBC untreated with chemotherapy (J. Clin. Oncol. 2009;27:5700-6).
Dr. Winer said that while the consensus among most experts is that standard adjuvant chemotherapy regimens for patients with stage 2 or 3 TNBC include both anthracyclines and taxanes, his own view is that for patients with stage 1 TNBC “if you’re going to pursue chemotherapy, then treatment with a somewhat less toxic, shorter regimen would seem to be more appropriate.”
EXPERT ANALYSIS FROM SABCS 2014

HFpEF: Time for a new approach
SNOWMASS, COLO. – The plethora of comorbidities typically present in patients with heart failure with preserved ejection fraction is increasingly thought to be a key driver of the cardiac structural remodeling and poor clinical outcomes characteristic of this increasingly common condition.
“The new message is that even though HFpHF [heart failure with preserved ejection fraction] is a problem of the heart involving diastolic filling and structural remodeling of the ventricle, it’s also a problem of factors outside the heart. Outcomes are driven not just by the cardiac abnormalities, but by the comorbidities that are so common in this elderly population,” Dr. Akshay S. Desai said at the annual Cardiovascular Conference at Snowmass.
“The evolving theoretical model is one that emphasizes the role these comorbidities play, not just in remodeling of the heart, but also in microvascular inflammation, with its consequences for inflammatory cell migration, transforming growth factor–beta activation, myocardial fibrosis, oxidative stress, endothelial inflammation, and downstream impairment of cyclic guanosine monophosphate signaling,” explained Dr. Desai of Brigham and Women’s Hospital, Boston.
He credited Dr. Walter J. Paulus of the Institute for Cardiovascular Research at VU University Medical Center, Amsterdam, as being the primary developer of the new paradigm, which veers away from the traditional emphasis upon excessive afterload as the primary driver of diastolic dysfunction.
As elaborated in detail by Dr. Paulus, the noncardiac comorbidities that are so highly prevalent in HFpEF – especially obesity, diabetes, chronic obstructive pulmonary disease, hypertension, chronic kidney disease, and anemia – induce a systemic inflammatory state which promotes diastolic left ventricular stiffness, cardiac hypertrophy, and the development of heart failure. Dr. Paulus has buttressed his theoretical framework with endomyocardial biopsy studies that document abnormal myocyte structure and function (J. Am. Coll. Cardiol. 2013;62:263-71).
Dr. Desai said the fresh perspective provided by Dr. Paulus is most welcome because it is easily tested, and also because it points to new pathways for treatment. New therapeutic targets are needed desperately because of the striking lack of progress to date in treatment of HFpEF. No drug has been convincingly shown effective in reducing the morbidity and mortality of HFpEF, although a secondary analysis of the flawed TOPCAT trial did strongly suggest spironolactone may reduce the risks of mortality and heart failure hospitalizations (Circulation 2015;131:34-42).
Clinical trials that are now planned or underway as a consequence of the new HFpEF paradigm are investigating novel treatment strategies targeting low myocardial nitric oxide bioavailability and endothelial dysfunction. Agents under study include statins, interleukin-1 receptor antagonists, oral nitrates aimed at boosting cellular levels of nitric oxide, the oral soluble guanylate cyclase stimulator riociguat (Adempas), and the phosphodiesterase-5 inhibitor sildenafil.
Also, all eyes are on the 4,300 patient, 37-country, phase III, randomized PARAGON HF study which began last summer. PARAGON is evaluating LCZ696, the combined angiotensin receptor neprilysin inhibitor that scored a smashing success in heart failure with reduced ejection fraction in the landmark PARADIGM-HF study (N. Engl. J. Med. 2014;371:993-1004).
The rising prevalence of diabetes, obesity, and other proinflammatory chronic conditions could help explain the increasing proportion of patients with heart failure who have HFpEF.
“Depending on where you draw the cut point for preserved ejection fraction, you could say half or as many as 60% of patients hospitalized for decompensated heart failure do so in the setting of preserved ejection fraction,” Dr. Desai observed.
It’s noteworthy that the trajectory of decline following hospitalization for heart failure is similar in HFpEF and heart failure with reduced ejection fraction.
While awaiting the outcome of clinical trials of novel treatments, and with so little evidence-based therapy available at this point, physicians should redouble their efforts to aggressively manage hypertension and other comorbidities in an effort to prevent HFpEF or slow its progression. The favorable TOPCAT results in the Western Hemisphere are also worthy of consideration, the cardiologist argued.
Dr. Desai reported serving as a consultant to 5AM Ventures, AtCor Medical, Novartis, and St. Jude Medical.
SNOWMASS, COLO. – The plethora of comorbidities typically present in patients with heart failure with preserved ejection fraction is increasingly thought to be a key driver of the cardiac structural remodeling and poor clinical outcomes characteristic of this increasingly common condition.
“The new message is that even though HFpHF [heart failure with preserved ejection fraction] is a problem of the heart involving diastolic filling and structural remodeling of the ventricle, it’s also a problem of factors outside the heart. Outcomes are driven not just by the cardiac abnormalities, but by the comorbidities that are so common in this elderly population,” Dr. Akshay S. Desai said at the annual Cardiovascular Conference at Snowmass.
“The evolving theoretical model is one that emphasizes the role these comorbidities play, not just in remodeling of the heart, but also in microvascular inflammation, with its consequences for inflammatory cell migration, transforming growth factor–beta activation, myocardial fibrosis, oxidative stress, endothelial inflammation, and downstream impairment of cyclic guanosine monophosphate signaling,” explained Dr. Desai of Brigham and Women’s Hospital, Boston.
He credited Dr. Walter J. Paulus of the Institute for Cardiovascular Research at VU University Medical Center, Amsterdam, as being the primary developer of the new paradigm, which veers away from the traditional emphasis upon excessive afterload as the primary driver of diastolic dysfunction.
As elaborated in detail by Dr. Paulus, the noncardiac comorbidities that are so highly prevalent in HFpEF – especially obesity, diabetes, chronic obstructive pulmonary disease, hypertension, chronic kidney disease, and anemia – induce a systemic inflammatory state which promotes diastolic left ventricular stiffness, cardiac hypertrophy, and the development of heart failure. Dr. Paulus has buttressed his theoretical framework with endomyocardial biopsy studies that document abnormal myocyte structure and function (J. Am. Coll. Cardiol. 2013;62:263-71).
Dr. Desai said the fresh perspective provided by Dr. Paulus is most welcome because it is easily tested, and also because it points to new pathways for treatment. New therapeutic targets are needed desperately because of the striking lack of progress to date in treatment of HFpEF. No drug has been convincingly shown effective in reducing the morbidity and mortality of HFpEF, although a secondary analysis of the flawed TOPCAT trial did strongly suggest spironolactone may reduce the risks of mortality and heart failure hospitalizations (Circulation 2015;131:34-42).
Clinical trials that are now planned or underway as a consequence of the new HFpEF paradigm are investigating novel treatment strategies targeting low myocardial nitric oxide bioavailability and endothelial dysfunction. Agents under study include statins, interleukin-1 receptor antagonists, oral nitrates aimed at boosting cellular levels of nitric oxide, the oral soluble guanylate cyclase stimulator riociguat (Adempas), and the phosphodiesterase-5 inhibitor sildenafil.
Also, all eyes are on the 4,300 patient, 37-country, phase III, randomized PARAGON HF study which began last summer. PARAGON is evaluating LCZ696, the combined angiotensin receptor neprilysin inhibitor that scored a smashing success in heart failure with reduced ejection fraction in the landmark PARADIGM-HF study (N. Engl. J. Med. 2014;371:993-1004).
The rising prevalence of diabetes, obesity, and other proinflammatory chronic conditions could help explain the increasing proportion of patients with heart failure who have HFpEF.
“Depending on where you draw the cut point for preserved ejection fraction, you could say half or as many as 60% of patients hospitalized for decompensated heart failure do so in the setting of preserved ejection fraction,” Dr. Desai observed.
It’s noteworthy that the trajectory of decline following hospitalization for heart failure is similar in HFpEF and heart failure with reduced ejection fraction.
While awaiting the outcome of clinical trials of novel treatments, and with so little evidence-based therapy available at this point, physicians should redouble their efforts to aggressively manage hypertension and other comorbidities in an effort to prevent HFpEF or slow its progression. The favorable TOPCAT results in the Western Hemisphere are also worthy of consideration, the cardiologist argued.
Dr. Desai reported serving as a consultant to 5AM Ventures, AtCor Medical, Novartis, and St. Jude Medical.
SNOWMASS, COLO. – The plethora of comorbidities typically present in patients with heart failure with preserved ejection fraction is increasingly thought to be a key driver of the cardiac structural remodeling and poor clinical outcomes characteristic of this increasingly common condition.
“The new message is that even though HFpHF [heart failure with preserved ejection fraction] is a problem of the heart involving diastolic filling and structural remodeling of the ventricle, it’s also a problem of factors outside the heart. Outcomes are driven not just by the cardiac abnormalities, but by the comorbidities that are so common in this elderly population,” Dr. Akshay S. Desai said at the annual Cardiovascular Conference at Snowmass.
“The evolving theoretical model is one that emphasizes the role these comorbidities play, not just in remodeling of the heart, but also in microvascular inflammation, with its consequences for inflammatory cell migration, transforming growth factor–beta activation, myocardial fibrosis, oxidative stress, endothelial inflammation, and downstream impairment of cyclic guanosine monophosphate signaling,” explained Dr. Desai of Brigham and Women’s Hospital, Boston.
He credited Dr. Walter J. Paulus of the Institute for Cardiovascular Research at VU University Medical Center, Amsterdam, as being the primary developer of the new paradigm, which veers away from the traditional emphasis upon excessive afterload as the primary driver of diastolic dysfunction.
As elaborated in detail by Dr. Paulus, the noncardiac comorbidities that are so highly prevalent in HFpEF – especially obesity, diabetes, chronic obstructive pulmonary disease, hypertension, chronic kidney disease, and anemia – induce a systemic inflammatory state which promotes diastolic left ventricular stiffness, cardiac hypertrophy, and the development of heart failure. Dr. Paulus has buttressed his theoretical framework with endomyocardial biopsy studies that document abnormal myocyte structure and function (J. Am. Coll. Cardiol. 2013;62:263-71).
Dr. Desai said the fresh perspective provided by Dr. Paulus is most welcome because it is easily tested, and also because it points to new pathways for treatment. New therapeutic targets are needed desperately because of the striking lack of progress to date in treatment of HFpEF. No drug has been convincingly shown effective in reducing the morbidity and mortality of HFpEF, although a secondary analysis of the flawed TOPCAT trial did strongly suggest spironolactone may reduce the risks of mortality and heart failure hospitalizations (Circulation 2015;131:34-42).
Clinical trials that are now planned or underway as a consequence of the new HFpEF paradigm are investigating novel treatment strategies targeting low myocardial nitric oxide bioavailability and endothelial dysfunction. Agents under study include statins, interleukin-1 receptor antagonists, oral nitrates aimed at boosting cellular levels of nitric oxide, the oral soluble guanylate cyclase stimulator riociguat (Adempas), and the phosphodiesterase-5 inhibitor sildenafil.
Also, all eyes are on the 4,300 patient, 37-country, phase III, randomized PARAGON HF study which began last summer. PARAGON is evaluating LCZ696, the combined angiotensin receptor neprilysin inhibitor that scored a smashing success in heart failure with reduced ejection fraction in the landmark PARADIGM-HF study (N. Engl. J. Med. 2014;371:993-1004).
The rising prevalence of diabetes, obesity, and other proinflammatory chronic conditions could help explain the increasing proportion of patients with heart failure who have HFpEF.
“Depending on where you draw the cut point for preserved ejection fraction, you could say half or as many as 60% of patients hospitalized for decompensated heart failure do so in the setting of preserved ejection fraction,” Dr. Desai observed.
It’s noteworthy that the trajectory of decline following hospitalization for heart failure is similar in HFpEF and heart failure with reduced ejection fraction.
While awaiting the outcome of clinical trials of novel treatments, and with so little evidence-based therapy available at this point, physicians should redouble their efforts to aggressively manage hypertension and other comorbidities in an effort to prevent HFpEF or slow its progression. The favorable TOPCAT results in the Western Hemisphere are also worthy of consideration, the cardiologist argued.
Dr. Desai reported serving as a consultant to 5AM Ventures, AtCor Medical, Novartis, and St. Jude Medical.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Controversy continues over platinum for TNBC patients
SAN ANTONIO – Oncologists are split over the use of platinum compounds as adjuvant or neoadjuvant therapy for triple-negative breast cancer patients, a rift likely to continue until definitive outcome data become available several years from now.
“In the U.S., I would say that about half of all medical oncologists are now in a fairly routine manner giving carboplatin in this setting,” Dr. Eric P. Winer estimated at the San Antonio Breast Cancer Symposium.
He’s not among them.

“Is carboplatin ready for prime time use in the adjuvant or neoadjuvant setting in triple-negative breast cancer? I personally feel we first need a definitive study showing improvement in disease-free survival and/or overall survival, or something close to that,” said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
Proponents of platinum salts cite two positive phase II randomized trials – GeparSixto and CALGB 40603 – which demonstrated significantly higher pathologic complete response (pCR) rates in patients with stage II or III triple-negative breast cancer (TNBC) with the addition of carboplatin to neoadjuvant chemotherapy.
The pro-platinum camp points to evidence suggesting a pCR in women with TNBC appears to be a good surrogate endpoint for event-free survival and overall survival, as shown in a recent meta-analysis by Dr. Patricia Cortazar of the Food and Drug Administration and her coworkers. The investigators concluded that pCR in response to neoadjuvant therapy with various regimens was associated with a 76% improvement in event-free survival and an 84% improvement in overall survival in 557 women with TNBC (Lancet 2014;384:164-72).
“The two phase II studies are going in the same direction,” observed Dr. Gunter von Minckwitz of the German Breast Group and principal investigator in the GeparSixto trial. “We have surveyed our group of investigators, and they are all using platinum in triple-negative breast cancer. The German guidelines say you can, but you don’t have to.”
But Dr. Winer, and by his estimate roughly half of all American medical oncologists, remain unconvinced.
“I think we should all keep in mind that pCR is a marker of better outcome, it’s not necessarily a required step in the process,” he said.
He’s leery of relying upon pCR as a surrogate endpoint in light of the deeply disappointing BEATRICE experience. The phase III BEATRICE trial included nearly 2,600 women with TNBC who were randomized to adjuvant chemotherapy alone or in combination with bevacizumab. The bevacizumab group had a higher pCR, but no improvement in disease-free survival or overall survival (Lancet Oncol. 2013;14:933-42).
“I would hate to see us all indiscriminately adding platinum to standard regimens, increasing toxicity, particularly if it is not associated with long-term benefit,” Dr. Winer said. “And even if it is associated with long-term benefit, I want to tease out who really benefits and which triple-negative patients are most sensitive to these agents.”
Progress is occurring in this area, he added. In GeparSixto, the addition of neoadjuvant carboplatin to paclitaxel and nonpegylated liposomal doxorubicin was associated with a 66.7% pCR rate in the subgroup of TNBC patients with a BRCA 1 or 2 germline mutation and a 43.5% rate in those without such mutations (Lancet Oncol. 2014;15:747-56).

Moreover, in the phase III Triple Negative Breast Cancer Trial (TNT) presented at this year’s San Antonio symposium, Dr. Andrew N.J. Tutt reported that in a prespecified analysis of the small subgroup comprising 43 BRCA mutation-positive patients, the objective response rate was 68% in those randomized to carboplatin, compared with 33% in those assigned to docetaxel. Moreover, mean progression-free survival was 6.8 months with carboplatin, significantly better than the 4.8 months with docetaxel or the 3.1 months in carboplatin-treated patients without a BRCA 1/2 mutation.
The TNT trial included 376 patients with metastatic or recurrent locally advanced TNBC randomized to single agent therapy. While the study provides no evidence of a superior response to carboplatin, compared with docetaxel in unselected patients with metastatic TNBC, it does support BRCA 1/2 mutation genotyping as part of decision making regarding therapy in metastatic TNBC and familial breast cancer, according to Dr. Tutt, professor of breast oncology at the Institute of Cancer Research, London.
The trial also tested the utility of Myriad Genetics’ novel Homologous Recombination Deficiency (HRD) score as a predictor of platinum-responsiveness of TNBC and concluded it was without benefit.
Dr. Winer noted that TNBC accounts for only about 15% of breast cancers. Still, that’s roughly 35,000 new cases per year in the United States alone – and TNBC is responsible for a disproportionate degree of breast cancer mortality.
“Perhaps in patients with BRCA 1 or 2 mutations, we’re getting close to thinking that platinum may be a standard, but even here I would await the completion of ongoing trials before we embrace that concept,” he said.
Among these studies is the 12-258 INFORM trial, a multicenter study in which 166 newly diagnosed breast cancer patients with BRCA1 or 2 mutations are being randomized to preoperative cisplatin or doxorubicin/cyclophosphamide.
Dr. William M. Sikov, principal investigator for the CALGB 40603 trial (J. Clin. Oncol. 2015;33:13-21), predicted there will be little crossover between the platinum-user and nonuser camps until definitive trials report whether the therapy improves relapse-free or overall survival.
“One group will say, ‘There’s an absolute increase in pathologic complete response with carboplatin in these two studies, and I’m convinced it’s a beneficial drug in these patients.’ It’s inexpensive, it’s available, although not approved for triple negative breast cancer, and it has some hematologic toxicities. But we have no long-term outcomes yet. I don’t think the TNT results will change anyone’s mind,” according to Dr. Sikov of Women and Infants Hospital in Providence, R.I.
Dr. Winer reported receiving research funding from Genentech. Dr. Sikov serves as a consultant to AbbVie and Celgene. Dr. Tutt reported having no financial conflicts.
SAN ANTONIO – Oncologists are split over the use of platinum compounds as adjuvant or neoadjuvant therapy for triple-negative breast cancer patients, a rift likely to continue until definitive outcome data become available several years from now.
“In the U.S., I would say that about half of all medical oncologists are now in a fairly routine manner giving carboplatin in this setting,” Dr. Eric P. Winer estimated at the San Antonio Breast Cancer Symposium.
He’s not among them.
“Is carboplatin ready for prime time use in the adjuvant or neoadjuvant setting in triple-negative breast cancer? I personally feel we first need a definitive study showing improvement in disease-free survival and/or overall survival, or something close to that,” said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
Proponents of platinum salts cite two positive phase II randomized trials – GeparSixto and CALGB 40603 – which demonstrated significantly higher pathologic complete response (pCR) rates in patients with stage II or III triple-negative breast cancer (TNBC) with the addition of carboplatin to neoadjuvant chemotherapy.
The pro-platinum camp points to evidence suggesting a pCR in women with TNBC appears to be a good surrogate endpoint for event-free survival and overall survival, as shown in a recent meta-analysis by Dr. Patricia Cortazar of the Food and Drug Administration and her coworkers. The investigators concluded that pCR in response to neoadjuvant therapy with various regimens was associated with a 76% improvement in event-free survival and an 84% improvement in overall survival in 557 women with TNBC (Lancet 2014;384:164-72).
“The two phase II studies are going in the same direction,” observed Dr. Gunter von Minckwitz of the German Breast Group and principal investigator in the GeparSixto trial. “We have surveyed our group of investigators, and they are all using platinum in triple-negative breast cancer. The German guidelines say you can, but you don’t have to.”
But Dr. Winer, and by his estimate roughly half of all American medical oncologists, remain unconvinced.
“I think we should all keep in mind that pCR is a marker of better outcome, it’s not necessarily a required step in the process,” he said.
He’s leery of relying upon pCR as a surrogate endpoint in light of the deeply disappointing BEATRICE experience. The phase III BEATRICE trial included nearly 2,600 women with TNBC who were randomized to adjuvant chemotherapy alone or in combination with bevacizumab. The bevacizumab group had a higher pCR, but no improvement in disease-free survival or overall survival (Lancet Oncol. 2013;14:933-42).
“I would hate to see us all indiscriminately adding platinum to standard regimens, increasing toxicity, particularly if it is not associated with long-term benefit,” Dr. Winer said. “And even if it is associated with long-term benefit, I want to tease out who really benefits and which triple-negative patients are most sensitive to these agents.”
Progress is occurring in this area, he added. In GeparSixto, the addition of neoadjuvant carboplatin to paclitaxel and nonpegylated liposomal doxorubicin was associated with a 66.7% pCR rate in the subgroup of TNBC patients with a BRCA 1 or 2 germline mutation and a 43.5% rate in those without such mutations (Lancet Oncol. 2014;15:747-56).
Moreover, in the phase III Triple Negative Breast Cancer Trial (TNT) presented at this year’s San Antonio symposium, Dr. Andrew N.J. Tutt reported that in a prespecified analysis of the small subgroup comprising 43 BRCA mutation-positive patients, the objective response rate was 68% in those randomized to carboplatin, compared with 33% in those assigned to docetaxel. Moreover, mean progression-free survival was 6.8 months with carboplatin, significantly better than the 4.8 months with docetaxel or the 3.1 months in carboplatin-treated patients without a BRCA 1/2 mutation.
The TNT trial included 376 patients with metastatic or recurrent locally advanced TNBC randomized to single agent therapy. While the study provides no evidence of a superior response to carboplatin, compared with docetaxel in unselected patients with metastatic TNBC, it does support BRCA 1/2 mutation genotyping as part of decision making regarding therapy in metastatic TNBC and familial breast cancer, according to Dr. Tutt, professor of breast oncology at the Institute of Cancer Research, London.
The trial also tested the utility of Myriad Genetics’ novel Homologous Recombination Deficiency (HRD) score as a predictor of platinum-responsiveness of TNBC and concluded it was without benefit.
Dr. Winer noted that TNBC accounts for only about 15% of breast cancers. Still, that’s roughly 35,000 new cases per year in the United States alone – and TNBC is responsible for a disproportionate degree of breast cancer mortality.
“Perhaps in patients with BRCA 1 or 2 mutations, we’re getting close to thinking that platinum may be a standard, but even here I would await the completion of ongoing trials before we embrace that concept,” he said.
Among these studies is the 12-258 INFORM trial, a multicenter study in which 166 newly diagnosed breast cancer patients with BRCA1 or 2 mutations are being randomized to preoperative cisplatin or doxorubicin/cyclophosphamide.
Dr. William M. Sikov, principal investigator for the CALGB 40603 trial (J. Clin. Oncol. 2015;33:13-21), predicted there will be little crossover between the platinum-user and nonuser camps until definitive trials report whether the therapy improves relapse-free or overall survival.
“One group will say, ‘There’s an absolute increase in pathologic complete response with carboplatin in these two studies, and I’m convinced it’s a beneficial drug in these patients.’ It’s inexpensive, it’s available, although not approved for triple negative breast cancer, and it has some hematologic toxicities. But we have no long-term outcomes yet. I don’t think the TNT results will change anyone’s mind,” according to Dr. Sikov of Women and Infants Hospital in Providence, R.I.
Dr. Winer reported receiving research funding from Genentech. Dr. Sikov serves as a consultant to AbbVie and Celgene. Dr. Tutt reported having no financial conflicts.
SAN ANTONIO – Oncologists are split over the use of platinum compounds as adjuvant or neoadjuvant therapy for triple-negative breast cancer patients, a rift likely to continue until definitive outcome data become available several years from now.
“In the U.S., I would say that about half of all medical oncologists are now in a fairly routine manner giving carboplatin in this setting,” Dr. Eric P. Winer estimated at the San Antonio Breast Cancer Symposium.
He’s not among them.
“Is carboplatin ready for prime time use in the adjuvant or neoadjuvant setting in triple-negative breast cancer? I personally feel we first need a definitive study showing improvement in disease-free survival and/or overall survival, or something close to that,” said Dr. Winer, chief of the division of women’s cancers at the Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston.
Proponents of platinum salts cite two positive phase II randomized trials – GeparSixto and CALGB 40603 – which demonstrated significantly higher pathologic complete response (pCR) rates in patients with stage II or III triple-negative breast cancer (TNBC) with the addition of carboplatin to neoadjuvant chemotherapy.
The pro-platinum camp points to evidence suggesting a pCR in women with TNBC appears to be a good surrogate endpoint for event-free survival and overall survival, as shown in a recent meta-analysis by Dr. Patricia Cortazar of the Food and Drug Administration and her coworkers. The investigators concluded that pCR in response to neoadjuvant therapy with various regimens was associated with a 76% improvement in event-free survival and an 84% improvement in overall survival in 557 women with TNBC (Lancet 2014;384:164-72).
“The two phase II studies are going in the same direction,” observed Dr. Gunter von Minckwitz of the German Breast Group and principal investigator in the GeparSixto trial. “We have surveyed our group of investigators, and they are all using platinum in triple-negative breast cancer. The German guidelines say you can, but you don’t have to.”
But Dr. Winer, and by his estimate roughly half of all American medical oncologists, remain unconvinced.
“I think we should all keep in mind that pCR is a marker of better outcome, it’s not necessarily a required step in the process,” he said.
He’s leery of relying upon pCR as a surrogate endpoint in light of the deeply disappointing BEATRICE experience. The phase III BEATRICE trial included nearly 2,600 women with TNBC who were randomized to adjuvant chemotherapy alone or in combination with bevacizumab. The bevacizumab group had a higher pCR, but no improvement in disease-free survival or overall survival (Lancet Oncol. 2013;14:933-42).
“I would hate to see us all indiscriminately adding platinum to standard regimens, increasing toxicity, particularly if it is not associated with long-term benefit,” Dr. Winer said. “And even if it is associated with long-term benefit, I want to tease out who really benefits and which triple-negative patients are most sensitive to these agents.”
Progress is occurring in this area, he added. In GeparSixto, the addition of neoadjuvant carboplatin to paclitaxel and nonpegylated liposomal doxorubicin was associated with a 66.7% pCR rate in the subgroup of TNBC patients with a BRCA 1 or 2 germline mutation and a 43.5% rate in those without such mutations (Lancet Oncol. 2014;15:747-56).
Moreover, in the phase III Triple Negative Breast Cancer Trial (TNT) presented at this year’s San Antonio symposium, Dr. Andrew N.J. Tutt reported that in a prespecified analysis of the small subgroup comprising 43 BRCA mutation-positive patients, the objective response rate was 68% in those randomized to carboplatin, compared with 33% in those assigned to docetaxel. Moreover, mean progression-free survival was 6.8 months with carboplatin, significantly better than the 4.8 months with docetaxel or the 3.1 months in carboplatin-treated patients without a BRCA 1/2 mutation.
The TNT trial included 376 patients with metastatic or recurrent locally advanced TNBC randomized to single agent therapy. While the study provides no evidence of a superior response to carboplatin, compared with docetaxel in unselected patients with metastatic TNBC, it does support BRCA 1/2 mutation genotyping as part of decision making regarding therapy in metastatic TNBC and familial breast cancer, according to Dr. Tutt, professor of breast oncology at the Institute of Cancer Research, London.
The trial also tested the utility of Myriad Genetics’ novel Homologous Recombination Deficiency (HRD) score as a predictor of platinum-responsiveness of TNBC and concluded it was without benefit.
Dr. Winer noted that TNBC accounts for only about 15% of breast cancers. Still, that’s roughly 35,000 new cases per year in the United States alone – and TNBC is responsible for a disproportionate degree of breast cancer mortality.
“Perhaps in patients with BRCA 1 or 2 mutations, we’re getting close to thinking that platinum may be a standard, but even here I would await the completion of ongoing trials before we embrace that concept,” he said.
Among these studies is the 12-258 INFORM trial, a multicenter study in which 166 newly diagnosed breast cancer patients with BRCA1 or 2 mutations are being randomized to preoperative cisplatin or doxorubicin/cyclophosphamide.
Dr. William M. Sikov, principal investigator for the CALGB 40603 trial (J. Clin. Oncol. 2015;33:13-21), predicted there will be little crossover between the platinum-user and nonuser camps until definitive trials report whether the therapy improves relapse-free or overall survival.
“One group will say, ‘There’s an absolute increase in pathologic complete response with carboplatin in these two studies, and I’m convinced it’s a beneficial drug in these patients.’ It’s inexpensive, it’s available, although not approved for triple negative breast cancer, and it has some hematologic toxicities. But we have no long-term outcomes yet. I don’t think the TNT results will change anyone’s mind,” according to Dr. Sikov of Women and Infants Hospital in Providence, R.I.
Dr. Winer reported receiving research funding from Genentech. Dr. Sikov serves as a consultant to AbbVie and Celgene. Dr. Tutt reported having no financial conflicts.
EXPERT ANALYSIS FROM SABCS 2014

Breast Cancer Patients Show Poor Adherence to Cardiovascular, Diabetes Medications
SAN ANTONIO – Hypertension, dyslipidemia, and type 2 diabetes are common among breast cancer survivors – and so is nonadherence to medications prescribed for these major comorbid conditions.
That was the central finding from COMBO (Commonly Used Medications and Breast Cancer Outcomes), a retrospective cohort study of 4,216 breast cancer survivors belonging to Group Health Cooperative, Gregory S. Calip, Pharm.D., reported at the San Antonio Breast Cancer Symposium.
“This is the first study to investigate breast cancer characteristics and treatments in relation to nonadherence to chronic medications for hypertension, diabetes, and dyslipidemia,” said Dr. Calip of the University of Illinois, Chicago. “Our results suggest that some breast cancer treatments may be associated with nonadherence to antihypertensive agents and oral diabetes medications, but not statins. These findings highlight possible opportunities to improve comorbid condition care in the growing population of breast cancer survivors.”
The irony is that while experiencing breast cancer understandably renders survivors deeply concerned about the prospect of cancer-related death, by not taking their medications for these common comorbid conditions these women increase their overall mortality risk, and particularly their risk of death due to cardiovascular disease and stroke.
The women in the COMBO study had been diagnosed with stage I or II breast cancer during 1990-2008 and did not experience recurrence or a second primary breast cancer during their second year after breast cancer diagnosis. Their medication adherence during that second year was measured via automated health plan pharmacy dispensing records. Patients were classified as nonadherent if their medication possession ratio, or MPR, was less than 0.8.
Antihypertensive agents were prescribed for 1,929 of the subjects, statins for 1,072, and oral diabetes drugs for 449.
During days 366-730 post breast cancer diagnosis, 37% of the women were nonadherent to antihypertensive medications, 39% to prescribed statins, and 75% to their oral diabetes medications.
Common forms of breast cancer therapy were independently associated with increased likelihood of nonadherence in multivariate logistic regression analysis. For example, chemotherapy was associated with a 67% increased likelihood of nonadherence to diabetes medications during year 2 after breast cancer diagnosis. Patients who received radiation therapy or hormonal therapy were, respectively, 21% and 25% more likely to be nonadherent to antihypertensive therapy.
Continue for risk factors >>
One factor associated with increased likelihood of adherence to medications for comorbid conditions was greater contact with a primary care physician. Breast cancer survivors who saw their primary care physicians two or more times during year 2 post diagnosis were 70% less likely to be nonadherent to antihypertensive therapy than were those who visited their primary care physicians less frequently.
Greater body mass index was associated with significantly less likelihood of nonadherence to antihypertensive agents but not statins or diabetes medications. When researchers used a BMI below 25 kg/m2 for reference, patients with a BMI of 25-29.9 were 39% less likely to be nonadherent to antihypertensive therapy, those with a BMI of 30-34.9 kg/m2 were 46% less likely, and women with a BMI of 35 kg/m2 or greater were 63% less likely to be nonadherent to their antihypertensive therapy.
A higher Charlson comorbidity score of 2 or more during the first year following breast cancer diagnosis was associated with a 51% reduction in likelihood of nonadherence to diabetes medications during year 2 and a 46% lower nonadherence rate for statins than in patients with a Charlson score below 2.
As reported in previous studies of non-cancer patients, younger age was associated with increased nonadherence. This was true across the board for all three medication classes, although the age effect was most dramatic with respect to nonadherence to statins and oral diabetes medications. Fifty- to 54-year-olds were 3.4- and 1.8-fold more likely than were women age 65 or older to be nonadherent to diabetes drugs and statins, respectively, while breast cancer survivors under age 50 were 7.1- and 2.8-fold more likely to be nonadherent to those types of medications.
Discussant Dawn L. Hershman called the COMBO study medication nonadherence rates “pretty awful.” And if breast cancer survivors aren’t taking their medications for chronic comorbid conditions, it’s not much of a leap to think they may not be adherent to their breast cancer–related medications, she said. She urged her fellow breast cancer specialists to think beyond their specialty focus, consider the patient as a whole, and do what they can to promote adherence to medications targeting these potentially serious comorbidities.
“So, what can we do? We can try to engage technology,” said Dr. Hershman, a medical oncologist at Columbia University, New York.
She cited a randomized, controlled trial by other investigators which showed that automated phone calls reminding patients to take their cardiovascular medications had a salutary effect. In addition, she was an investigator in a large study of text messaging as an effective tool for improving adherence to hormonal therapy.
The COMBO study was supported by the National Cancer Institute and the University of Washington, Seattle. Dr. Calip reported having no financial conflicts.
SAN ANTONIO – Hypertension, dyslipidemia, and type 2 diabetes are common among breast cancer survivors – and so is nonadherence to medications prescribed for these major comorbid conditions.
That was the central finding from COMBO (Commonly Used Medications and Breast Cancer Outcomes), a retrospective cohort study of 4,216 breast cancer survivors belonging to Group Health Cooperative, Gregory S. Calip, Pharm.D., reported at the San Antonio Breast Cancer Symposium.
“This is the first study to investigate breast cancer characteristics and treatments in relation to nonadherence to chronic medications for hypertension, diabetes, and dyslipidemia,” said Dr. Calip of the University of Illinois, Chicago. “Our results suggest that some breast cancer treatments may be associated with nonadherence to antihypertensive agents and oral diabetes medications, but not statins. These findings highlight possible opportunities to improve comorbid condition care in the growing population of breast cancer survivors.”
The irony is that while experiencing breast cancer understandably renders survivors deeply concerned about the prospect of cancer-related death, by not taking their medications for these common comorbid conditions these women increase their overall mortality risk, and particularly their risk of death due to cardiovascular disease and stroke.
The women in the COMBO study had been diagnosed with stage I or II breast cancer during 1990-2008 and did not experience recurrence or a second primary breast cancer during their second year after breast cancer diagnosis. Their medication adherence during that second year was measured via automated health plan pharmacy dispensing records. Patients were classified as nonadherent if their medication possession ratio, or MPR, was less than 0.8.
Antihypertensive agents were prescribed for 1,929 of the subjects, statins for 1,072, and oral diabetes drugs for 449.
During days 366-730 post breast cancer diagnosis, 37% of the women were nonadherent to antihypertensive medications, 39% to prescribed statins, and 75% to their oral diabetes medications.
Common forms of breast cancer therapy were independently associated with increased likelihood of nonadherence in multivariate logistic regression analysis. For example, chemotherapy was associated with a 67% increased likelihood of nonadherence to diabetes medications during year 2 after breast cancer diagnosis. Patients who received radiation therapy or hormonal therapy were, respectively, 21% and 25% more likely to be nonadherent to antihypertensive therapy.
Continue for risk factors >>
One factor associated with increased likelihood of adherence to medications for comorbid conditions was greater contact with a primary care physician. Breast cancer survivors who saw their primary care physicians two or more times during year 2 post diagnosis were 70% less likely to be nonadherent to antihypertensive therapy than were those who visited their primary care physicians less frequently.
Greater body mass index was associated with significantly less likelihood of nonadherence to antihypertensive agents but not statins or diabetes medications. When researchers used a BMI below 25 kg/m2 for reference, patients with a BMI of 25-29.9 were 39% less likely to be nonadherent to antihypertensive therapy, those with a BMI of 30-34.9 kg/m2 were 46% less likely, and women with a BMI of 35 kg/m2 or greater were 63% less likely to be nonadherent to their antihypertensive therapy.
A higher Charlson comorbidity score of 2 or more during the first year following breast cancer diagnosis was associated with a 51% reduction in likelihood of nonadherence to diabetes medications during year 2 and a 46% lower nonadherence rate for statins than in patients with a Charlson score below 2.
As reported in previous studies of non-cancer patients, younger age was associated with increased nonadherence. This was true across the board for all three medication classes, although the age effect was most dramatic with respect to nonadherence to statins and oral diabetes medications. Fifty- to 54-year-olds were 3.4- and 1.8-fold more likely than were women age 65 or older to be nonadherent to diabetes drugs and statins, respectively, while breast cancer survivors under age 50 were 7.1- and 2.8-fold more likely to be nonadherent to those types of medications.
Discussant Dawn L. Hershman called the COMBO study medication nonadherence rates “pretty awful.” And if breast cancer survivors aren’t taking their medications for chronic comorbid conditions, it’s not much of a leap to think they may not be adherent to their breast cancer–related medications, she said. She urged her fellow breast cancer specialists to think beyond their specialty focus, consider the patient as a whole, and do what they can to promote adherence to medications targeting these potentially serious comorbidities.
“So, what can we do? We can try to engage technology,” said Dr. Hershman, a medical oncologist at Columbia University, New York.
She cited a randomized, controlled trial by other investigators which showed that automated phone calls reminding patients to take their cardiovascular medications had a salutary effect. In addition, she was an investigator in a large study of text messaging as an effective tool for improving adherence to hormonal therapy.
The COMBO study was supported by the National Cancer Institute and the University of Washington, Seattle. Dr. Calip reported having no financial conflicts.
SAN ANTONIO – Hypertension, dyslipidemia, and type 2 diabetes are common among breast cancer survivors – and so is nonadherence to medications prescribed for these major comorbid conditions.
That was the central finding from COMBO (Commonly Used Medications and Breast Cancer Outcomes), a retrospective cohort study of 4,216 breast cancer survivors belonging to Group Health Cooperative, Gregory S. Calip, Pharm.D., reported at the San Antonio Breast Cancer Symposium.
“This is the first study to investigate breast cancer characteristics and treatments in relation to nonadherence to chronic medications for hypertension, diabetes, and dyslipidemia,” said Dr. Calip of the University of Illinois, Chicago. “Our results suggest that some breast cancer treatments may be associated with nonadherence to antihypertensive agents and oral diabetes medications, but not statins. These findings highlight possible opportunities to improve comorbid condition care in the growing population of breast cancer survivors.”
The irony is that while experiencing breast cancer understandably renders survivors deeply concerned about the prospect of cancer-related death, by not taking their medications for these common comorbid conditions these women increase their overall mortality risk, and particularly their risk of death due to cardiovascular disease and stroke.
The women in the COMBO study had been diagnosed with stage I or II breast cancer during 1990-2008 and did not experience recurrence or a second primary breast cancer during their second year after breast cancer diagnosis. Their medication adherence during that second year was measured via automated health plan pharmacy dispensing records. Patients were classified as nonadherent if their medication possession ratio, or MPR, was less than 0.8.
Antihypertensive agents were prescribed for 1,929 of the subjects, statins for 1,072, and oral diabetes drugs for 449.
During days 366-730 post breast cancer diagnosis, 37% of the women were nonadherent to antihypertensive medications, 39% to prescribed statins, and 75% to their oral diabetes medications.
Common forms of breast cancer therapy were independently associated with increased likelihood of nonadherence in multivariate logistic regression analysis. For example, chemotherapy was associated with a 67% increased likelihood of nonadherence to diabetes medications during year 2 after breast cancer diagnosis. Patients who received radiation therapy or hormonal therapy were, respectively, 21% and 25% more likely to be nonadherent to antihypertensive therapy.
Continue for risk factors >>
One factor associated with increased likelihood of adherence to medications for comorbid conditions was greater contact with a primary care physician. Breast cancer survivors who saw their primary care physicians two or more times during year 2 post diagnosis were 70% less likely to be nonadherent to antihypertensive therapy than were those who visited their primary care physicians less frequently.
Greater body mass index was associated with significantly less likelihood of nonadherence to antihypertensive agents but not statins or diabetes medications. When researchers used a BMI below 25 kg/m2 for reference, patients with a BMI of 25-29.9 were 39% less likely to be nonadherent to antihypertensive therapy, those with a BMI of 30-34.9 kg/m2 were 46% less likely, and women with a BMI of 35 kg/m2 or greater were 63% less likely to be nonadherent to their antihypertensive therapy.
A higher Charlson comorbidity score of 2 or more during the first year following breast cancer diagnosis was associated with a 51% reduction in likelihood of nonadherence to diabetes medications during year 2 and a 46% lower nonadherence rate for statins than in patients with a Charlson score below 2.
As reported in previous studies of non-cancer patients, younger age was associated with increased nonadherence. This was true across the board for all three medication classes, although the age effect was most dramatic with respect to nonadherence to statins and oral diabetes medications. Fifty- to 54-year-olds were 3.4- and 1.8-fold more likely than were women age 65 or older to be nonadherent to diabetes drugs and statins, respectively, while breast cancer survivors under age 50 were 7.1- and 2.8-fold more likely to be nonadherent to those types of medications.
Discussant Dawn L. Hershman called the COMBO study medication nonadherence rates “pretty awful.” And if breast cancer survivors aren’t taking their medications for chronic comorbid conditions, it’s not much of a leap to think they may not be adherent to their breast cancer–related medications, she said. She urged her fellow breast cancer specialists to think beyond their specialty focus, consider the patient as a whole, and do what they can to promote adherence to medications targeting these potentially serious comorbidities.
“So, what can we do? We can try to engage technology,” said Dr. Hershman, a medical oncologist at Columbia University, New York.
She cited a randomized, controlled trial by other investigators which showed that automated phone calls reminding patients to take their cardiovascular medications had a salutary effect. In addition, she was an investigator in a large study of text messaging as an effective tool for improving adherence to hormonal therapy.
The COMBO study was supported by the National Cancer Institute and the University of Washington, Seattle. Dr. Calip reported having no financial conflicts.
Breast cancer patients show poor adherence to cardiovascular, diabetes medications
SAN ANTONIO – Hypertension, dyslipidemia, and type 2 diabetes are common among breast cancer survivors – and so is nonadherence to medications prescribed for these major comorbid conditions.
That was the central finding from COMBO (Commonly Used Medications and Breast Cancer Outcomes), a retrospective cohort study of 4,216 breast cancer survivors belonging to Group Health Cooperative, Gregory S. Calip, Pharm.D., reported at the San Antonio Breast Cancer Symposium.

“This is the first study to investigate breast cancer characteristics and treatments in relation to nonadherence to chronic medications for hypertension, diabetes, and dyslipidemia,” said Dr. Calip of the University of Illinois, Chicago. “Our results suggest that some breast cancer treatments may be associated with nonadherence to antihypertensive agents and oral diabetes medications, but not statins. These findings highlight possible opportunities to improve comorbid condition care in the growing population of breast cancer survivors.”
The irony is that while experiencing breast cancer understandably renders survivors deeply concerned about the prospect of cancer-related death, by not taking their medications for these common comorbid conditions these women increase their overall mortality risk, and particularly their risk of death due to cardiovascular disease and stroke.
The women in the COMBO study had been diagnosed with stage I or II breast cancer during 1990-2008 and did not experience recurrence or a second primary breast cancer during their second year after breast cancer diagnosis. Their medication adherence during that second year was measured via automated health plan pharmacy dispensing records. Patients were classified as nonadherent if their medication possession ratio, or MPR, was less than 0.8.
Antihypertensive agents were prescribed for 1,929 of the subjects, statins for 1,072, and oral diabetes drugs for 449.
During days 366-730 post breast cancer diagnosis, 37% of the women were nonadherent to antihypertensive medications, 39% to prescribed statins, and 75% to their oral diabetes medications.
Common forms of breast cancer therapy were independently associated with increased likelihood of nonadherence in multivariate logistic regression analysis. For example, chemotherapy was associated with a 67% increased likelihood of nonadherence to diabetes medications during year 2 after breast cancer diagnosis. Patients who received radiation therapy or hormonal therapy were, respectively, 21% and 25% more likely to be nonadherent to antihypertensive therapy.
One factor associated with increased likelihood of adherence to medications for comorbid conditions was greater contact with a primary care physician. Breast cancer survivors who saw their primary care physicians two or more times during year 2 post diagnosis were 70% less likely to be nonadherent to antihypertensive therapy than were those who visited their primary care physicians less frequently.
Greater body mass index was associated with significantly less likelihood of nonadherence to antihypertensive agents but not statins or diabetes medications. When researchers used a BMI below 25 kg/m2 for reference, patients with a BMI of 25-29.9 were 39% less likely to be nonadherent to antihypertensive therapy, those with a BMI of 30-34.9 kg/m2 were 46% less likely, and women with a BMI of 35 kg/m2 or greater were 63% less likely to be nonadherent to their antihypertensive therapy.
A higher Charlson comorbidity score of 2 or more during the first year following breast cancer diagnosis was associated with a 51% reduction in likelihood of nonadherence to diabetes medications during year 2 and a 46% lower nonadherence rate for statins than in patients with a Charlson score below 2.
As reported in previous studies of non-cancer patients, younger age was associated with increased nonadherence. This was true across the board for all three medication classes, although the age effect was most dramatic with respect to nonadherence to statins and oral diabetes medications. Fifty- to 54-year-olds were 3.4- and 1.8-fold more likely than were women age 65 or older to be nonadherent to diabetes drugs and statins, respectively, while breast cancer survivors under age 50 were 7.1- and 2.8-fold more likely to be nonadherent to those types of medications.

Discussant Dawn L. Hershman called the COMBO study medication nonadherence rates “pretty awful.” And if breast cancer survivors aren’t taking their medications for chronic comorbid conditions, it’s not much of a leap to think they may not be adherent to their breast cancer–related medications, she said. She urged her fellow breast cancer specialists to think beyond their specialty focus, consider the patient as a whole, and do what they can to promote adherence to medications targeting these potentially serious comorbidities.
“So, what can we do? We can try to engage technology,” said Dr. Hershman, a medical oncologist at Columbia University, New York.
She cited a randomized, controlled trial by other investigators which showed that automated phone calls reminding patients to take their cardiovascular medications had a salutary effect. In addition, she was an investigator in a large study of text messaging as an effective tool for improving adherence to hormonal therapy.
The COMBO study was supported by the National Cancer Institute and the University of Washington, Seattle. Dr. Calip reported having no financial conflicts.
SAN ANTONIO – Hypertension, dyslipidemia, and type 2 diabetes are common among breast cancer survivors – and so is nonadherence to medications prescribed for these major comorbid conditions.
That was the central finding from COMBO (Commonly Used Medications and Breast Cancer Outcomes), a retrospective cohort study of 4,216 breast cancer survivors belonging to Group Health Cooperative, Gregory S. Calip, Pharm.D., reported at the San Antonio Breast Cancer Symposium.
“This is the first study to investigate breast cancer characteristics and treatments in relation to nonadherence to chronic medications for hypertension, diabetes, and dyslipidemia,” said Dr. Calip of the University of Illinois, Chicago. “Our results suggest that some breast cancer treatments may be associated with nonadherence to antihypertensive agents and oral diabetes medications, but not statins. These findings highlight possible opportunities to improve comorbid condition care in the growing population of breast cancer survivors.”
The irony is that while experiencing breast cancer understandably renders survivors deeply concerned about the prospect of cancer-related death, by not taking their medications for these common comorbid conditions these women increase their overall mortality risk, and particularly their risk of death due to cardiovascular disease and stroke.
The women in the COMBO study had been diagnosed with stage I or II breast cancer during 1990-2008 and did not experience recurrence or a second primary breast cancer during their second year after breast cancer diagnosis. Their medication adherence during that second year was measured via automated health plan pharmacy dispensing records. Patients were classified as nonadherent if their medication possession ratio, or MPR, was less than 0.8.
Antihypertensive agents were prescribed for 1,929 of the subjects, statins for 1,072, and oral diabetes drugs for 449.
During days 366-730 post breast cancer diagnosis, 37% of the women were nonadherent to antihypertensive medications, 39% to prescribed statins, and 75% to their oral diabetes medications.
Common forms of breast cancer therapy were independently associated with increased likelihood of nonadherence in multivariate logistic regression analysis. For example, chemotherapy was associated with a 67% increased likelihood of nonadherence to diabetes medications during year 2 after breast cancer diagnosis. Patients who received radiation therapy or hormonal therapy were, respectively, 21% and 25% more likely to be nonadherent to antihypertensive therapy.
One factor associated with increased likelihood of adherence to medications for comorbid conditions was greater contact with a primary care physician. Breast cancer survivors who saw their primary care physicians two or more times during year 2 post diagnosis were 70% less likely to be nonadherent to antihypertensive therapy than were those who visited their primary care physicians less frequently.
Greater body mass index was associated with significantly less likelihood of nonadherence to antihypertensive agents but not statins or diabetes medications. When researchers used a BMI below 25 kg/m2 for reference, patients with a BMI of 25-29.9 were 39% less likely to be nonadherent to antihypertensive therapy, those with a BMI of 30-34.9 kg/m2 were 46% less likely, and women with a BMI of 35 kg/m2 or greater were 63% less likely to be nonadherent to their antihypertensive therapy.
A higher Charlson comorbidity score of 2 or more during the first year following breast cancer diagnosis was associated with a 51% reduction in likelihood of nonadherence to diabetes medications during year 2 and a 46% lower nonadherence rate for statins than in patients with a Charlson score below 2.
As reported in previous studies of non-cancer patients, younger age was associated with increased nonadherence. This was true across the board for all three medication classes, although the age effect was most dramatic with respect to nonadherence to statins and oral diabetes medications. Fifty- to 54-year-olds were 3.4- and 1.8-fold more likely than were women age 65 or older to be nonadherent to diabetes drugs and statins, respectively, while breast cancer survivors under age 50 were 7.1- and 2.8-fold more likely to be nonadherent to those types of medications.
Discussant Dawn L. Hershman called the COMBO study medication nonadherence rates “pretty awful.” And if breast cancer survivors aren’t taking their medications for chronic comorbid conditions, it’s not much of a leap to think they may not be adherent to their breast cancer–related medications, she said. She urged her fellow breast cancer specialists to think beyond their specialty focus, consider the patient as a whole, and do what they can to promote adherence to medications targeting these potentially serious comorbidities.
“So, what can we do? We can try to engage technology,” said Dr. Hershman, a medical oncologist at Columbia University, New York.
She cited a randomized, controlled trial by other investigators which showed that automated phone calls reminding patients to take their cardiovascular medications had a salutary effect. In addition, she was an investigator in a large study of text messaging as an effective tool for improving adherence to hormonal therapy.
The COMBO study was supported by the National Cancer Institute and the University of Washington, Seattle. Dr. Calip reported having no financial conflicts.
SAN ANTONIO – Hypertension, dyslipidemia, and type 2 diabetes are common among breast cancer survivors – and so is nonadherence to medications prescribed for these major comorbid conditions.
That was the central finding from COMBO (Commonly Used Medications and Breast Cancer Outcomes), a retrospective cohort study of 4,216 breast cancer survivors belonging to Group Health Cooperative, Gregory S. Calip, Pharm.D., reported at the San Antonio Breast Cancer Symposium.
“This is the first study to investigate breast cancer characteristics and treatments in relation to nonadherence to chronic medications for hypertension, diabetes, and dyslipidemia,” said Dr. Calip of the University of Illinois, Chicago. “Our results suggest that some breast cancer treatments may be associated with nonadherence to antihypertensive agents and oral diabetes medications, but not statins. These findings highlight possible opportunities to improve comorbid condition care in the growing population of breast cancer survivors.”
The irony is that while experiencing breast cancer understandably renders survivors deeply concerned about the prospect of cancer-related death, by not taking their medications for these common comorbid conditions these women increase their overall mortality risk, and particularly their risk of death due to cardiovascular disease and stroke.
The women in the COMBO study had been diagnosed with stage I or II breast cancer during 1990-2008 and did not experience recurrence or a second primary breast cancer during their second year after breast cancer diagnosis. Their medication adherence during that second year was measured via automated health plan pharmacy dispensing records. Patients were classified as nonadherent if their medication possession ratio, or MPR, was less than 0.8.
Antihypertensive agents were prescribed for 1,929 of the subjects, statins for 1,072, and oral diabetes drugs for 449.
During days 366-730 post breast cancer diagnosis, 37% of the women were nonadherent to antihypertensive medications, 39% to prescribed statins, and 75% to their oral diabetes medications.
Common forms of breast cancer therapy were independently associated with increased likelihood of nonadherence in multivariate logistic regression analysis. For example, chemotherapy was associated with a 67% increased likelihood of nonadherence to diabetes medications during year 2 after breast cancer diagnosis. Patients who received radiation therapy or hormonal therapy were, respectively, 21% and 25% more likely to be nonadherent to antihypertensive therapy.
One factor associated with increased likelihood of adherence to medications for comorbid conditions was greater contact with a primary care physician. Breast cancer survivors who saw their primary care physicians two or more times during year 2 post diagnosis were 70% less likely to be nonadherent to antihypertensive therapy than were those who visited their primary care physicians less frequently.
Greater body mass index was associated with significantly less likelihood of nonadherence to antihypertensive agents but not statins or diabetes medications. When researchers used a BMI below 25 kg/m2 for reference, patients with a BMI of 25-29.9 were 39% less likely to be nonadherent to antihypertensive therapy, those with a BMI of 30-34.9 kg/m2 were 46% less likely, and women with a BMI of 35 kg/m2 or greater were 63% less likely to be nonadherent to their antihypertensive therapy.
A higher Charlson comorbidity score of 2 or more during the first year following breast cancer diagnosis was associated with a 51% reduction in likelihood of nonadherence to diabetes medications during year 2 and a 46% lower nonadherence rate for statins than in patients with a Charlson score below 2.
As reported in previous studies of non-cancer patients, younger age was associated with increased nonadherence. This was true across the board for all three medication classes, although the age effect was most dramatic with respect to nonadherence to statins and oral diabetes medications. Fifty- to 54-year-olds were 3.4- and 1.8-fold more likely than were women age 65 or older to be nonadherent to diabetes drugs and statins, respectively, while breast cancer survivors under age 50 were 7.1- and 2.8-fold more likely to be nonadherent to those types of medications.
Discussant Dawn L. Hershman called the COMBO study medication nonadherence rates “pretty awful.” And if breast cancer survivors aren’t taking their medications for chronic comorbid conditions, it’s not much of a leap to think they may not be adherent to their breast cancer–related medications, she said. She urged her fellow breast cancer specialists to think beyond their specialty focus, consider the patient as a whole, and do what they can to promote adherence to medications targeting these potentially serious comorbidities.
“So, what can we do? We can try to engage technology,” said Dr. Hershman, a medical oncologist at Columbia University, New York.
She cited a randomized, controlled trial by other investigators which showed that automated phone calls reminding patients to take their cardiovascular medications had a salutary effect. In addition, she was an investigator in a large study of text messaging as an effective tool for improving adherence to hormonal therapy.
The COMBO study was supported by the National Cancer Institute and the University of Washington, Seattle. Dr. Calip reported having no financial conflicts.
AT SABCS 2014
Key clinical point: Breast cancer survivors’ adherence rates to medications prescribed for comorbid hypertension, dyslipidemia, and type 2 diabetes were characterized as “pretty awful.”
Major finding: During the second year after breast cancer diagnosis, the rates of nonadherence to antihypertensive agents, statins, and oral diabetes medications were 37%, 75%, and 39%, respectively.
Data source: COMBO, a retrospective cohort study involving 4,216 breast cancer survivors without a disease recurrence or second primary breast cancer during the first 2 years post diagnosis.
Disclosures: The National Cancer Institute and the University of Washington supported the study. Dr. Calip reported having no financial conflicts.

Laser improves oral mucositis in breast cancer patients
SAN ANTONIO – Low-level laser therapy proved highly effective in managing chemotherapy-induced oral mucositis in a retrospective study.
Although this was the first study of low-level laser therapy in breast cancer patients, this form of therapy is already widely used to prevent and treat oral mucositis in hematopoietic stem cell transplant recipients as well as in patients with head and neck cancer. These preliminary findings in a breast cancer population warrant confirmation in a randomized controlled trial, Sandrine Censabella, Ph.D., said at the San Antonio Breast Cancer Symposium.
Roughly 40% of patients develop oral mucositis as a consequence of standard-dose chemotherapy. Oral mucositis is the most debilitating, severe, and costly nonhematologic complication of oncologic therapy. It compromises both quality of life and treatment outcomes, said Dr. Censabella of Jessa Hospital in Hasselt, Belgium.
She reported on 93 patients with stage 0-IV breast cancer and chemotherapy-induced oral mucositis who received low-level laser therapy using a gallium arsenide laser at 665-nm wavelength and 100 mW of output power combined with a continuous-emission infrared laser with an output power of 500 mW. The laser energy, 4 J per application point, was delivered via a 600-mcm optical fiber.
The treatment schedule was two sessions per week until lesion healing occurred. Depending on the extent of the oral mucositis, up to seven oral sites could be treated: lips, tongue, palate, inside of the two cheeks, tonsils, and mouth floor.
Outcomes were assessed in a standardized fashion by trained nurses using the World Health Organization 0-4 grading scale, where 0 means unaffected, 1 represents soreness and erythema, 2 means erythema and ulcers but with an ability to eat solid foods, 3 is for patients with ulcers who require a liquid diet only, and 4 is for patients incapable of oral nutritional intake. In addition, investigators calculated an oral mucositis score for every patient by adding up the WHO grades at all affected sites.
Laser therapy began a mean of 49 days after the start of chemotherapy, which was anthracycline based in two-thirds of cases. The mean age of the women was 54.8 years.
Subjects received a mean of 5.7 laser treatment sessions, during which they showed a significant reduction in oral mucositis severity. At baseline, 60% of patients had WHO grade 2 lesions, a rate that dropped to 30% at the end of treatment several weeks later. While only 12% of patients were WHO grade 1 at baseline, 65% were at the conclusion of the laser treatment program. Twenty-eight percent of women were WHO grade 3 at entry, compared with just 5.4% after laser treatment.
The mean baseline combined oral mucositis score averaged 6.6, improving to 2.78 at treatment’s end.
Self-reported pain scores improved from 5.14 at baseline on a 10-point scale to 1.64 at the conclusion of laser therapy.
At the end of laser therapy, only 2% had a worse WHO grade than at baseline, 8.6% had a worse composite oral mucositis score, and no one reported more pain than at entry.
“These findings are the first to document a beneficial effect of low-level laser therapy in a large group of breast cancer patients and suggest that low-level laser therapy might become a standard management for oral mucositis in all cancer patients,” Dr. Censabella said.
She reported having no financial conflicts regarding this study.
SAN ANTONIO – Low-level laser therapy proved highly effective in managing chemotherapy-induced oral mucositis in a retrospective study.
Although this was the first study of low-level laser therapy in breast cancer patients, this form of therapy is already widely used to prevent and treat oral mucositis in hematopoietic stem cell transplant recipients as well as in patients with head and neck cancer. These preliminary findings in a breast cancer population warrant confirmation in a randomized controlled trial, Sandrine Censabella, Ph.D., said at the San Antonio Breast Cancer Symposium.
Roughly 40% of patients develop oral mucositis as a consequence of standard-dose chemotherapy. Oral mucositis is the most debilitating, severe, and costly nonhematologic complication of oncologic therapy. It compromises both quality of life and treatment outcomes, said Dr. Censabella of Jessa Hospital in Hasselt, Belgium.
She reported on 93 patients with stage 0-IV breast cancer and chemotherapy-induced oral mucositis who received low-level laser therapy using a gallium arsenide laser at 665-nm wavelength and 100 mW of output power combined with a continuous-emission infrared laser with an output power of 500 mW. The laser energy, 4 J per application point, was delivered via a 600-mcm optical fiber.
The treatment schedule was two sessions per week until lesion healing occurred. Depending on the extent of the oral mucositis, up to seven oral sites could be treated: lips, tongue, palate, inside of the two cheeks, tonsils, and mouth floor.
Outcomes were assessed in a standardized fashion by trained nurses using the World Health Organization 0-4 grading scale, where 0 means unaffected, 1 represents soreness and erythema, 2 means erythema and ulcers but with an ability to eat solid foods, 3 is for patients with ulcers who require a liquid diet only, and 4 is for patients incapable of oral nutritional intake. In addition, investigators calculated an oral mucositis score for every patient by adding up the WHO grades at all affected sites.
Laser therapy began a mean of 49 days after the start of chemotherapy, which was anthracycline based in two-thirds of cases. The mean age of the women was 54.8 years.
Subjects received a mean of 5.7 laser treatment sessions, during which they showed a significant reduction in oral mucositis severity. At baseline, 60% of patients had WHO grade 2 lesions, a rate that dropped to 30% at the end of treatment several weeks later. While only 12% of patients were WHO grade 1 at baseline, 65% were at the conclusion of the laser treatment program. Twenty-eight percent of women were WHO grade 3 at entry, compared with just 5.4% after laser treatment.
The mean baseline combined oral mucositis score averaged 6.6, improving to 2.78 at treatment’s end.
Self-reported pain scores improved from 5.14 at baseline on a 10-point scale to 1.64 at the conclusion of laser therapy.
At the end of laser therapy, only 2% had a worse WHO grade than at baseline, 8.6% had a worse composite oral mucositis score, and no one reported more pain than at entry.
“These findings are the first to document a beneficial effect of low-level laser therapy in a large group of breast cancer patients and suggest that low-level laser therapy might become a standard management for oral mucositis in all cancer patients,” Dr. Censabella said.
She reported having no financial conflicts regarding this study.
SAN ANTONIO – Low-level laser therapy proved highly effective in managing chemotherapy-induced oral mucositis in a retrospective study.
Although this was the first study of low-level laser therapy in breast cancer patients, this form of therapy is already widely used to prevent and treat oral mucositis in hematopoietic stem cell transplant recipients as well as in patients with head and neck cancer. These preliminary findings in a breast cancer population warrant confirmation in a randomized controlled trial, Sandrine Censabella, Ph.D., said at the San Antonio Breast Cancer Symposium.
Roughly 40% of patients develop oral mucositis as a consequence of standard-dose chemotherapy. Oral mucositis is the most debilitating, severe, and costly nonhematologic complication of oncologic therapy. It compromises both quality of life and treatment outcomes, said Dr. Censabella of Jessa Hospital in Hasselt, Belgium.
She reported on 93 patients with stage 0-IV breast cancer and chemotherapy-induced oral mucositis who received low-level laser therapy using a gallium arsenide laser at 665-nm wavelength and 100 mW of output power combined with a continuous-emission infrared laser with an output power of 500 mW. The laser energy, 4 J per application point, was delivered via a 600-mcm optical fiber.
The treatment schedule was two sessions per week until lesion healing occurred. Depending on the extent of the oral mucositis, up to seven oral sites could be treated: lips, tongue, palate, inside of the two cheeks, tonsils, and mouth floor.
Outcomes were assessed in a standardized fashion by trained nurses using the World Health Organization 0-4 grading scale, where 0 means unaffected, 1 represents soreness and erythema, 2 means erythema and ulcers but with an ability to eat solid foods, 3 is for patients with ulcers who require a liquid diet only, and 4 is for patients incapable of oral nutritional intake. In addition, investigators calculated an oral mucositis score for every patient by adding up the WHO grades at all affected sites.
Laser therapy began a mean of 49 days after the start of chemotherapy, which was anthracycline based in two-thirds of cases. The mean age of the women was 54.8 years.
Subjects received a mean of 5.7 laser treatment sessions, during which they showed a significant reduction in oral mucositis severity. At baseline, 60% of patients had WHO grade 2 lesions, a rate that dropped to 30% at the end of treatment several weeks later. While only 12% of patients were WHO grade 1 at baseline, 65% were at the conclusion of the laser treatment program. Twenty-eight percent of women were WHO grade 3 at entry, compared with just 5.4% after laser treatment.
The mean baseline combined oral mucositis score averaged 6.6, improving to 2.78 at treatment’s end.
Self-reported pain scores improved from 5.14 at baseline on a 10-point scale to 1.64 at the conclusion of laser therapy.
At the end of laser therapy, only 2% had a worse WHO grade than at baseline, 8.6% had a worse composite oral mucositis score, and no one reported more pain than at entry.
“These findings are the first to document a beneficial effect of low-level laser therapy in a large group of breast cancer patients and suggest that low-level laser therapy might become a standard management for oral mucositis in all cancer patients,” Dr. Censabella said.
She reported having no financial conflicts regarding this study.
AT SABCS 2014
Key clinical point: Breast cancer patients with oral mucositis caused by chemotherapy can experience relief with low-level laser therapy.
Major finding: The mean oral mucositis severity score was more than halved after fewer than six laser therapy sessions, from 6.6 at baseline to 2.78.
Data source: A retrospective study of 93 breast cancer patients whose oral mucositis was treated with twice-weekly laser sessions using a gallium arsenide laser in combination with a continuous-emission infrared laser.
Disclosures: The presenter reported having no financial conflicts regarding this study, which was conducted free of commercial support.
Transcatheter mitral valve replacement poised for takeoff
SNOWMASS, COLO. – Early feasibility trials of transcatheter mitral valve replacement in patients with significant functional mitral regurgitation have received Food and Drug Administration approval and are about to commence in the United States.
“This is deja vu all over again. This is TAVR [transcatheter aortic valve replacement] 10 years ago. And we’re about to see the same level of investment and enthusiasm in the mitral space that we saw in TAVR 10 years ago,” Dr. Michael J. Mack predicted at the Annual Cardiovascular Conference at Snowmass.

As a pioneer of TAVR in the United States, he knows very well what that looks like. While serving as president of the Society of Thoracic Surgeons, he forged an epic cross-specialty collaboration with then–ACC President Dr. David R. Holmes Jr. that led to creation of an unprecedented joint STS/ACC TAVR Registry and fostered the concept of the heart team approach.
Dr. Mack said that at present, there are five “very promising” devices for transcatheter mitral valve replacement (TMVR), four with human experience. Three of the five – the Edwards Fortis, Neovasc Tiara, and the Tendyne device – have received FDA approval for early human feasibility trials, to begin imminently.
“Eighteen of these procedures have been done worldwide, all in Europe or Paraguay. This is a new day at the FDA, and the FDA – with a worldwide experience of only 18 – is allowing three early feasibility trials of 15 patients each at three U.S. centers, starting immediately. By the end of the year there will be experience with 45 transcatheter mitral valve replacements in the United States,” observed Dr. Mack, medical director of Baylor Health Care System in Plano, Tex.
All three devices under evaluation will be placed via a transapical approach using a mini-thoracotomy. This has proved to be a much simpler delivery route than the transfemoral approach. The TMVR procedure relies heavily upon 3-D echocardiography and fluoroscopy.
“There’s now a very robust field of mitral valve imaging, just like we’ve seen over the last 10 years for the aortic valve,” Dr. Mack said. “We’re learning a lot about mitral valve anatomy and papillary muscle positioning that we didn’t know before. What we’ve learned from TAVR is all coming over to the mitral space.”
The rationale for TMVR is that the open surgical experience has shown recurrent mitral regurgitation is vastly more common after mitral valve repair than replacement.
Nevertheless, transcatheter mitral valve repair is already here, and its role may grow substantially. The MitraClip device received FDA approval in Fall 2013 for percutaneous repair of severely symptomatic primary degenerative mitral regurgitation in patients who have a reasonable life expectancy but prohibitive surgical risk due to comorbidities. The device is designed to clip the valve leaflets together without surgical suturing. Roughly 1,500 MitraClip procedures have been done to date in the United States, and the initial commercial experience will be presented as a late-breaker at the annual ACC meeting in San Diego in March.
Together with cardiologist Dr. Gregg W. Stone, Dr. Mack is co–principal investigator of the COAPT trial, in which the MitraClip is being studied as a treatment for significant functional or secondary mitral regurgitation, as opposed to the primary degenerative mitral regurgitation for which it’s already indicated. If this major clinical trial yields positive results, the role of the MitraClip will greatly expand.
The COAPT trial is sponsored by Abbott Vascular. Dr. Mack reported receiving research grants from Abbott and Edwards Lifesciences.
SNOWMASS, COLO. – Early feasibility trials of transcatheter mitral valve replacement in patients with significant functional mitral regurgitation have received Food and Drug Administration approval and are about to commence in the United States.
“This is deja vu all over again. This is TAVR [transcatheter aortic valve replacement] 10 years ago. And we’re about to see the same level of investment and enthusiasm in the mitral space that we saw in TAVR 10 years ago,” Dr. Michael J. Mack predicted at the Annual Cardiovascular Conference at Snowmass.
As a pioneer of TAVR in the United States, he knows very well what that looks like. While serving as president of the Society of Thoracic Surgeons, he forged an epic cross-specialty collaboration with then–ACC President Dr. David R. Holmes Jr. that led to creation of an unprecedented joint STS/ACC TAVR Registry and fostered the concept of the heart team approach.
Dr. Mack said that at present, there are five “very promising” devices for transcatheter mitral valve replacement (TMVR), four with human experience. Three of the five – the Edwards Fortis, Neovasc Tiara, and the Tendyne device – have received FDA approval for early human feasibility trials, to begin imminently.
“Eighteen of these procedures have been done worldwide, all in Europe or Paraguay. This is a new day at the FDA, and the FDA – with a worldwide experience of only 18 – is allowing three early feasibility trials of 15 patients each at three U.S. centers, starting immediately. By the end of the year there will be experience with 45 transcatheter mitral valve replacements in the United States,” observed Dr. Mack, medical director of Baylor Health Care System in Plano, Tex.
All three devices under evaluation will be placed via a transapical approach using a mini-thoracotomy. This has proved to be a much simpler delivery route than the transfemoral approach. The TMVR procedure relies heavily upon 3-D echocardiography and fluoroscopy.
“There’s now a very robust field of mitral valve imaging, just like we’ve seen over the last 10 years for the aortic valve,” Dr. Mack said. “We’re learning a lot about mitral valve anatomy and papillary muscle positioning that we didn’t know before. What we’ve learned from TAVR is all coming over to the mitral space.”
The rationale for TMVR is that the open surgical experience has shown recurrent mitral regurgitation is vastly more common after mitral valve repair than replacement.
Nevertheless, transcatheter mitral valve repair is already here, and its role may grow substantially. The MitraClip device received FDA approval in Fall 2013 for percutaneous repair of severely symptomatic primary degenerative mitral regurgitation in patients who have a reasonable life expectancy but prohibitive surgical risk due to comorbidities. The device is designed to clip the valve leaflets together without surgical suturing. Roughly 1,500 MitraClip procedures have been done to date in the United States, and the initial commercial experience will be presented as a late-breaker at the annual ACC meeting in San Diego in March.
Together with cardiologist Dr. Gregg W. Stone, Dr. Mack is co–principal investigator of the COAPT trial, in which the MitraClip is being studied as a treatment for significant functional or secondary mitral regurgitation, as opposed to the primary degenerative mitral regurgitation for which it’s already indicated. If this major clinical trial yields positive results, the role of the MitraClip will greatly expand.
The COAPT trial is sponsored by Abbott Vascular. Dr. Mack reported receiving research grants from Abbott and Edwards Lifesciences.
SNOWMASS, COLO. – Early feasibility trials of transcatheter mitral valve replacement in patients with significant functional mitral regurgitation have received Food and Drug Administration approval and are about to commence in the United States.
“This is deja vu all over again. This is TAVR [transcatheter aortic valve replacement] 10 years ago. And we’re about to see the same level of investment and enthusiasm in the mitral space that we saw in TAVR 10 years ago,” Dr. Michael J. Mack predicted at the Annual Cardiovascular Conference at Snowmass.
As a pioneer of TAVR in the United States, he knows very well what that looks like. While serving as president of the Society of Thoracic Surgeons, he forged an epic cross-specialty collaboration with then–ACC President Dr. David R. Holmes Jr. that led to creation of an unprecedented joint STS/ACC TAVR Registry and fostered the concept of the heart team approach.
Dr. Mack said that at present, there are five “very promising” devices for transcatheter mitral valve replacement (TMVR), four with human experience. Three of the five – the Edwards Fortis, Neovasc Tiara, and the Tendyne device – have received FDA approval for early human feasibility trials, to begin imminently.
“Eighteen of these procedures have been done worldwide, all in Europe or Paraguay. This is a new day at the FDA, and the FDA – with a worldwide experience of only 18 – is allowing three early feasibility trials of 15 patients each at three U.S. centers, starting immediately. By the end of the year there will be experience with 45 transcatheter mitral valve replacements in the United States,” observed Dr. Mack, medical director of Baylor Health Care System in Plano, Tex.
All three devices under evaluation will be placed via a transapical approach using a mini-thoracotomy. This has proved to be a much simpler delivery route than the transfemoral approach. The TMVR procedure relies heavily upon 3-D echocardiography and fluoroscopy.
“There’s now a very robust field of mitral valve imaging, just like we’ve seen over the last 10 years for the aortic valve,” Dr. Mack said. “We’re learning a lot about mitral valve anatomy and papillary muscle positioning that we didn’t know before. What we’ve learned from TAVR is all coming over to the mitral space.”
The rationale for TMVR is that the open surgical experience has shown recurrent mitral regurgitation is vastly more common after mitral valve repair than replacement.
Nevertheless, transcatheter mitral valve repair is already here, and its role may grow substantially. The MitraClip device received FDA approval in Fall 2013 for percutaneous repair of severely symptomatic primary degenerative mitral regurgitation in patients who have a reasonable life expectancy but prohibitive surgical risk due to comorbidities. The device is designed to clip the valve leaflets together without surgical suturing. Roughly 1,500 MitraClip procedures have been done to date in the United States, and the initial commercial experience will be presented as a late-breaker at the annual ACC meeting in San Diego in March.
Together with cardiologist Dr. Gregg W. Stone, Dr. Mack is co–principal investigator of the COAPT trial, in which the MitraClip is being studied as a treatment for significant functional or secondary mitral regurgitation, as opposed to the primary degenerative mitral regurgitation for which it’s already indicated. If this major clinical trial yields positive results, the role of the MitraClip will greatly expand.
The COAPT trial is sponsored by Abbott Vascular. Dr. Mack reported receiving research grants from Abbott and Edwards Lifesciences.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
