User login
Early Detection of Melanoma: Harnessing Untapped Resources
WAIKOLOA, HAWAII – Improved early detection of fast-growing, lethal melanomas will require out-of-the-box thinking, such as providing dermatoscopes for patients to use at home and educating hairdressers and other nondermatologists on how to detect melanoma.
"At least three companies are now designing dermatoscopes for patient use. Patients will be able to buy the dermatoscope at a pharmacy and do self-examination or examine their spouse. That, I think, is going to be a reality within the next 5 years," Dr. Ashfaq A. Marghoob predicted at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).

A key feature of these devices will be the capability of hooking into a smart phone for wireless transmission of suspicious images to a skin cancer expert for assessment.
Dr. Marghoob and his coworkers first proposed dermoscopy as a tool with untapped potential for skin self-examination in selected patients in an article last year (Arch. Dermatol. 2011;147:53-8).
But patient empowerment is only part of what’s needed in order to improve early detection of the fast-growing killer subtype of melanoma. Dr. Marghoob and his coworkers are now conducting a prospective study to evaluate the impact of a 20-minute education session for hair care professionals about how they can aid in detecting skin cancers on the scalp, neck, and face.
This study was a direct outgrowth of a survey the investigators conducted at a Houston convention of barbers and hairstylists. Forty-nine percent of respondents indicated they were highly receptive to participating in a skin cancer education program. During the preceding month, 37% of respondents had looked at more than half of their customers’ scalps for suspicious lesions, 29% had looked at more than half of their customers’ necks, and 15% had checked more than half of their customers’ faces (Arch. Dermatol. 2011;147:1159-65).
Melanoma of the scalp and neck accounted for 10% of all melanoma deaths in the United States from 1973 to 2003. Barbers and hairstylists are in a unique position to detect skin cancers in those locations because they typically see their customers on a regular basis, spend a fair amount of time with them at each visit, have good rapport, and often discuss health issues.
The larger goal underlying this project, Dr. Marghoob explained, is to develop a cadre of expertly trained lay community workers to examine areas of the skin that are difficult for people to see for themselves and which often go overlooked by physicians. In addition to hair professionals, other workers ideally suited to serve as lay skin cancer educators and examiners include massage therapists, manicurists, cosmetologists, and electrologists.
Dr. Marghoob has also been involved in efforts to teach dermoscopy to primary care physicians and other nondermatologist physicians, including ob.gyns., pediatricians, and plastic surgeons. Moreover, he recently conducted a study in which second-year medical students were issued dermatoscopes and trained in their use.
"We found they get better at diagnosing skin cancer and are paying more attention to the skin. All we really want them to do is really look at the skin while they’re doing a physical examination," he said.
He has also been encouraging internists and family physicians to take advantage of opportunistic skin screening situations. For example, when they’re listening to the lungs and heart with a stethoscope, he urges primary care physicians to have patients take their shirt off so they can take a close look at the truncal skin rather than simply slip the bell of the scope underneath the shirt.
Another potentially fruitful means of improving upon the gains achieved in early detection of skin cancer would be targeted screening of older men, a high-risk group for fast-growing nodular melanomas, Dr. Marghoob added.
He reported having no financial conflicts. SDEF and this news organization are owned by Elsevier.
WAIKOLOA, HAWAII – Improved early detection of fast-growing, lethal melanomas will require out-of-the-box thinking, such as providing dermatoscopes for patients to use at home and educating hairdressers and other nondermatologists on how to detect melanoma.
"At least three companies are now designing dermatoscopes for patient use. Patients will be able to buy the dermatoscope at a pharmacy and do self-examination or examine their spouse. That, I think, is going to be a reality within the next 5 years," Dr. Ashfaq A. Marghoob predicted at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
A key feature of these devices will be the capability of hooking into a smart phone for wireless transmission of suspicious images to a skin cancer expert for assessment.
Dr. Marghoob and his coworkers first proposed dermoscopy as a tool with untapped potential for skin self-examination in selected patients in an article last year (Arch. Dermatol. 2011;147:53-8).
But patient empowerment is only part of what’s needed in order to improve early detection of the fast-growing killer subtype of melanoma. Dr. Marghoob and his coworkers are now conducting a prospective study to evaluate the impact of a 20-minute education session for hair care professionals about how they can aid in detecting skin cancers on the scalp, neck, and face.
This study was a direct outgrowth of a survey the investigators conducted at a Houston convention of barbers and hairstylists. Forty-nine percent of respondents indicated they were highly receptive to participating in a skin cancer education program. During the preceding month, 37% of respondents had looked at more than half of their customers’ scalps for suspicious lesions, 29% had looked at more than half of their customers’ necks, and 15% had checked more than half of their customers’ faces (Arch. Dermatol. 2011;147:1159-65).
Melanoma of the scalp and neck accounted for 10% of all melanoma deaths in the United States from 1973 to 2003. Barbers and hairstylists are in a unique position to detect skin cancers in those locations because they typically see their customers on a regular basis, spend a fair amount of time with them at each visit, have good rapport, and often discuss health issues.
The larger goal underlying this project, Dr. Marghoob explained, is to develop a cadre of expertly trained lay community workers to examine areas of the skin that are difficult for people to see for themselves and which often go overlooked by physicians. In addition to hair professionals, other workers ideally suited to serve as lay skin cancer educators and examiners include massage therapists, manicurists, cosmetologists, and electrologists.
Dr. Marghoob has also been involved in efforts to teach dermoscopy to primary care physicians and other nondermatologist physicians, including ob.gyns., pediatricians, and plastic surgeons. Moreover, he recently conducted a study in which second-year medical students were issued dermatoscopes and trained in their use.
"We found they get better at diagnosing skin cancer and are paying more attention to the skin. All we really want them to do is really look at the skin while they’re doing a physical examination," he said.
He has also been encouraging internists and family physicians to take advantage of opportunistic skin screening situations. For example, when they’re listening to the lungs and heart with a stethoscope, he urges primary care physicians to have patients take their shirt off so they can take a close look at the truncal skin rather than simply slip the bell of the scope underneath the shirt.
Another potentially fruitful means of improving upon the gains achieved in early detection of skin cancer would be targeted screening of older men, a high-risk group for fast-growing nodular melanomas, Dr. Marghoob added.
He reported having no financial conflicts. SDEF and this news organization are owned by Elsevier.
WAIKOLOA, HAWAII – Improved early detection of fast-growing, lethal melanomas will require out-of-the-box thinking, such as providing dermatoscopes for patients to use at home and educating hairdressers and other nondermatologists on how to detect melanoma.
"At least three companies are now designing dermatoscopes for patient use. Patients will be able to buy the dermatoscope at a pharmacy and do self-examination or examine their spouse. That, I think, is going to be a reality within the next 5 years," Dr. Ashfaq A. Marghoob predicted at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
A key feature of these devices will be the capability of hooking into a smart phone for wireless transmission of suspicious images to a skin cancer expert for assessment.
Dr. Marghoob and his coworkers first proposed dermoscopy as a tool with untapped potential for skin self-examination in selected patients in an article last year (Arch. Dermatol. 2011;147:53-8).
But patient empowerment is only part of what’s needed in order to improve early detection of the fast-growing killer subtype of melanoma. Dr. Marghoob and his coworkers are now conducting a prospective study to evaluate the impact of a 20-minute education session for hair care professionals about how they can aid in detecting skin cancers on the scalp, neck, and face.
This study was a direct outgrowth of a survey the investigators conducted at a Houston convention of barbers and hairstylists. Forty-nine percent of respondents indicated they were highly receptive to participating in a skin cancer education program. During the preceding month, 37% of respondents had looked at more than half of their customers’ scalps for suspicious lesions, 29% had looked at more than half of their customers’ necks, and 15% had checked more than half of their customers’ faces (Arch. Dermatol. 2011;147:1159-65).
Melanoma of the scalp and neck accounted for 10% of all melanoma deaths in the United States from 1973 to 2003. Barbers and hairstylists are in a unique position to detect skin cancers in those locations because they typically see their customers on a regular basis, spend a fair amount of time with them at each visit, have good rapport, and often discuss health issues.
The larger goal underlying this project, Dr. Marghoob explained, is to develop a cadre of expertly trained lay community workers to examine areas of the skin that are difficult for people to see for themselves and which often go overlooked by physicians. In addition to hair professionals, other workers ideally suited to serve as lay skin cancer educators and examiners include massage therapists, manicurists, cosmetologists, and electrologists.
Dr. Marghoob has also been involved in efforts to teach dermoscopy to primary care physicians and other nondermatologist physicians, including ob.gyns., pediatricians, and plastic surgeons. Moreover, he recently conducted a study in which second-year medical students were issued dermatoscopes and trained in their use.
"We found they get better at diagnosing skin cancer and are paying more attention to the skin. All we really want them to do is really look at the skin while they’re doing a physical examination," he said.
He has also been encouraging internists and family physicians to take advantage of opportunistic skin screening situations. For example, when they’re listening to the lungs and heart with a stethoscope, he urges primary care physicians to have patients take their shirt off so they can take a close look at the truncal skin rather than simply slip the bell of the scope underneath the shirt.
Another potentially fruitful means of improving upon the gains achieved in early detection of skin cancer would be targeted screening of older men, a high-risk group for fast-growing nodular melanomas, Dr. Marghoob added.
He reported having no financial conflicts. SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR
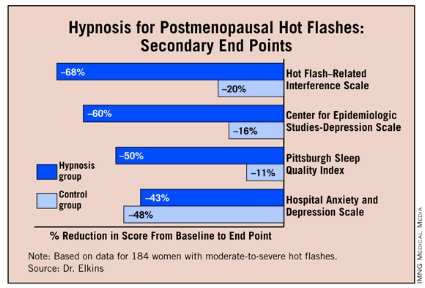
Hypnosis Chills Out Severe Postmenopausal Hot Flashes
NEW ORLEANS – A five-session hypnosis program reduced the frequency and severity of postmenopausal hot flashes by 80%, according to the results of a randomized controlled trial presented at the annual meeting of the Society of Behavioral Medicine.
"It appears that hypnosis, when properly applied, can be a safe and effective treatment for hot flashes. And side benefits appear likely. We had a lot of women comment that they were generally feeling better; improvement in sleep was a big deal," Gary Elkins, Ph.D., said in presenting the results at the meeting. This trial was honored by the society as the outstanding study in the field of complementary and alternative medicine during the past year.
Dr. Elkins and his colleagues randomized 184 postmenopausal women with moderate to severe hot flashes to either five weekly hypnosis sessions or a structured attention control condition of equal duration.
Hot flash frequency and severity scores as recorded in patients’ daily hot flash diaries fell by about 70% at 5 weeks and even further to 80% at 12 weeks of follow-up, 7 weeks after the intervention ended, reported Dr. Elkins, professor of psychology and neuroscience at Baylor University in Waco, Tex.
Another key study end point was change in physiologically measured hot flashes obtained via a 24-hour skin conductance monitor sensitive to sweating; this tool was particularly helpful in getting objective data on nighttime hot flashes. Hot flashes as documented by the monitor, the Biologic HF Recorder with computer linkage, declined by about 50% at 5 weeks and 60% at 12 weeks. In contrast, the control group showed a 10% decrease in hot flashes at 5 weeks and a 15% reduction at 12 weeks.
Secondary end points assessing sleep, depression, and hot flash–related interference with daily life also showed marked improvement in the hypnosis group.
The intervention entailed hypnotic induction with relaxation and direct and indirect suggestions, dissociation, and mental imagery evoking coolness, such as walking down a mountain path on a cool day. The imagery was individualized to incorporate places a patient had been and things she’d experienced. The emphasis was on teaching patients self-hypnosis with the goal of patient empowerment, the psychologist explained.
Results with the hypnosis intervention compare favorably with studies of other proposed treatments for hot flashes. For instance, the nonpharmacologic therapies black cohosh, soy, and vitamin E have been shown "virtually indistinguishable" from placebo, according to Dr. Elkins.
Venlafaxine and SSRIs have achieved roughly a 50% reduction in hot flashes in clinical trials. While that’s a clinically meaningful improvement, it’s a weaker effect than seen in the hypnosis trial. Moreover, Dr. Elkins noted, some women don’t want to take drugs or they experience limiting side effects. Hormone replacement therapy, formerly the standard treatment for hot flashes, has fallen into disfavor since the 16,000-subject Women’s Health Initiative was halted early due to a 26% increase in breast cancer, a 29% increase in coronary heart disease, and a 41% greater risk of stroke than in the placebo arm (JAMA 2004; 29:1701-12).
The critical next step in this hypnosis research project is to disseminate the required therapeutic skills as widely as possible. After all, it’s estimated that more than 25 million American women experience hot flashes, and 4 million of them are severely affected.
"I think we’ve shown this is a very effective therapy, but we need to find a way to make it widely available," the researcher observed.

He and his coinvestigators are pursuing a twofold dissemination strategy. They are developing a treatment manual for interested health care professionals, although "that’s still not going to create an army of practitioners," Dr. Elkins noted. So in addition, the investigators plan to put a guided hypnotic intervention on a CD for self-treatment.
"That could be very widely distributed. Even if it’s not quite as effective, I think that’s going to be the long-term way to go," according to the psychologist.
In an earlier, smaller randomized trial, Dr. Elkins showed that hypnosis also was highly effective in reducing hot flashes in breast cancer survivors on hormone-suppressing therapy (J. Clin. Oncol. 2008;26:5022-6). Unlike the new study in women with postmenopausal hot flashes, however, the study in breast cancer patients relied solely on patient self-reported symptoms without physiologic monitoring.
The trial was funded by the National Institutes of Health’s National Center for Complementary and Alternative Medicine. Dr. Elkins and his colleagues reported having no financial conflict.
Venlafaxine, SSRIs,
NEW ORLEANS – A five-session hypnosis program reduced the frequency and severity of postmenopausal hot flashes by 80%, according to the results of a randomized controlled trial presented at the annual meeting of the Society of Behavioral Medicine.
"It appears that hypnosis, when properly applied, can be a safe and effective treatment for hot flashes. And side benefits appear likely. We had a lot of women comment that they were generally feeling better; improvement in sleep was a big deal," Gary Elkins, Ph.D., said in presenting the results at the meeting. This trial was honored by the society as the outstanding study in the field of complementary and alternative medicine during the past year.
Dr. Elkins and his colleagues randomized 184 postmenopausal women with moderate to severe hot flashes to either five weekly hypnosis sessions or a structured attention control condition of equal duration.
Hot flash frequency and severity scores as recorded in patients’ daily hot flash diaries fell by about 70% at 5 weeks and even further to 80% at 12 weeks of follow-up, 7 weeks after the intervention ended, reported Dr. Elkins, professor of psychology and neuroscience at Baylor University in Waco, Tex.
Another key study end point was change in physiologically measured hot flashes obtained via a 24-hour skin conductance monitor sensitive to sweating; this tool was particularly helpful in getting objective data on nighttime hot flashes. Hot flashes as documented by the monitor, the Biologic HF Recorder with computer linkage, declined by about 50% at 5 weeks and 60% at 12 weeks. In contrast, the control group showed a 10% decrease in hot flashes at 5 weeks and a 15% reduction at 12 weeks.
Secondary end points assessing sleep, depression, and hot flash–related interference with daily life also showed marked improvement in the hypnosis group.
The intervention entailed hypnotic induction with relaxation and direct and indirect suggestions, dissociation, and mental imagery evoking coolness, such as walking down a mountain path on a cool day. The imagery was individualized to incorporate places a patient had been and things she’d experienced. The emphasis was on teaching patients self-hypnosis with the goal of patient empowerment, the psychologist explained.
Results with the hypnosis intervention compare favorably with studies of other proposed treatments for hot flashes. For instance, the nonpharmacologic therapies black cohosh, soy, and vitamin E have been shown "virtually indistinguishable" from placebo, according to Dr. Elkins.
Venlafaxine and SSRIs have achieved roughly a 50% reduction in hot flashes in clinical trials. While that’s a clinically meaningful improvement, it’s a weaker effect than seen in the hypnosis trial. Moreover, Dr. Elkins noted, some women don’t want to take drugs or they experience limiting side effects. Hormone replacement therapy, formerly the standard treatment for hot flashes, has fallen into disfavor since the 16,000-subject Women’s Health Initiative was halted early due to a 26% increase in breast cancer, a 29% increase in coronary heart disease, and a 41% greater risk of stroke than in the placebo arm (JAMA 2004; 29:1701-12).
The critical next step in this hypnosis research project is to disseminate the required therapeutic skills as widely as possible. After all, it’s estimated that more than 25 million American women experience hot flashes, and 4 million of them are severely affected.
"I think we’ve shown this is a very effective therapy, but we need to find a way to make it widely available," the researcher observed.
He and his coinvestigators are pursuing a twofold dissemination strategy. They are developing a treatment manual for interested health care professionals, although "that’s still not going to create an army of practitioners," Dr. Elkins noted. So in addition, the investigators plan to put a guided hypnotic intervention on a CD for self-treatment.
"That could be very widely distributed. Even if it’s not quite as effective, I think that’s going to be the long-term way to go," according to the psychologist.
In an earlier, smaller randomized trial, Dr. Elkins showed that hypnosis also was highly effective in reducing hot flashes in breast cancer survivors on hormone-suppressing therapy (J. Clin. Oncol. 2008;26:5022-6). Unlike the new study in women with postmenopausal hot flashes, however, the study in breast cancer patients relied solely on patient self-reported symptoms without physiologic monitoring.
The trial was funded by the National Institutes of Health’s National Center for Complementary and Alternative Medicine. Dr. Elkins and his colleagues reported having no financial conflict.
NEW ORLEANS – A five-session hypnosis program reduced the frequency and severity of postmenopausal hot flashes by 80%, according to the results of a randomized controlled trial presented at the annual meeting of the Society of Behavioral Medicine.
"It appears that hypnosis, when properly applied, can be a safe and effective treatment for hot flashes. And side benefits appear likely. We had a lot of women comment that they were generally feeling better; improvement in sleep was a big deal," Gary Elkins, Ph.D., said in presenting the results at the meeting. This trial was honored by the society as the outstanding study in the field of complementary and alternative medicine during the past year.
Dr. Elkins and his colleagues randomized 184 postmenopausal women with moderate to severe hot flashes to either five weekly hypnosis sessions or a structured attention control condition of equal duration.
Hot flash frequency and severity scores as recorded in patients’ daily hot flash diaries fell by about 70% at 5 weeks and even further to 80% at 12 weeks of follow-up, 7 weeks after the intervention ended, reported Dr. Elkins, professor of psychology and neuroscience at Baylor University in Waco, Tex.
Another key study end point was change in physiologically measured hot flashes obtained via a 24-hour skin conductance monitor sensitive to sweating; this tool was particularly helpful in getting objective data on nighttime hot flashes. Hot flashes as documented by the monitor, the Biologic HF Recorder with computer linkage, declined by about 50% at 5 weeks and 60% at 12 weeks. In contrast, the control group showed a 10% decrease in hot flashes at 5 weeks and a 15% reduction at 12 weeks.
Secondary end points assessing sleep, depression, and hot flash–related interference with daily life also showed marked improvement in the hypnosis group.
The intervention entailed hypnotic induction with relaxation and direct and indirect suggestions, dissociation, and mental imagery evoking coolness, such as walking down a mountain path on a cool day. The imagery was individualized to incorporate places a patient had been and things she’d experienced. The emphasis was on teaching patients self-hypnosis with the goal of patient empowerment, the psychologist explained.
Results with the hypnosis intervention compare favorably with studies of other proposed treatments for hot flashes. For instance, the nonpharmacologic therapies black cohosh, soy, and vitamin E have been shown "virtually indistinguishable" from placebo, according to Dr. Elkins.
Venlafaxine and SSRIs have achieved roughly a 50% reduction in hot flashes in clinical trials. While that’s a clinically meaningful improvement, it’s a weaker effect than seen in the hypnosis trial. Moreover, Dr. Elkins noted, some women don’t want to take drugs or they experience limiting side effects. Hormone replacement therapy, formerly the standard treatment for hot flashes, has fallen into disfavor since the 16,000-subject Women’s Health Initiative was halted early due to a 26% increase in breast cancer, a 29% increase in coronary heart disease, and a 41% greater risk of stroke than in the placebo arm (JAMA 2004; 29:1701-12).
The critical next step in this hypnosis research project is to disseminate the required therapeutic skills as widely as possible. After all, it’s estimated that more than 25 million American women experience hot flashes, and 4 million of them are severely affected.
"I think we’ve shown this is a very effective therapy, but we need to find a way to make it widely available," the researcher observed.
He and his coinvestigators are pursuing a twofold dissemination strategy. They are developing a treatment manual for interested health care professionals, although "that’s still not going to create an army of practitioners," Dr. Elkins noted. So in addition, the investigators plan to put a guided hypnotic intervention on a CD for self-treatment.
"That could be very widely distributed. Even if it’s not quite as effective, I think that’s going to be the long-term way to go," according to the psychologist.
In an earlier, smaller randomized trial, Dr. Elkins showed that hypnosis also was highly effective in reducing hot flashes in breast cancer survivors on hormone-suppressing therapy (J. Clin. Oncol. 2008;26:5022-6). Unlike the new study in women with postmenopausal hot flashes, however, the study in breast cancer patients relied solely on patient self-reported symptoms without physiologic monitoring.
The trial was funded by the National Institutes of Health’s National Center for Complementary and Alternative Medicine. Dr. Elkins and his colleagues reported having no financial conflict.
Venlafaxine, SSRIs,
Venlafaxine, SSRIs,
FROM THE ANNUAL MEETING OF THE SOCIETY OF BEHAVIORAL MEDICINE
Lowering Cholesterol in Childhood Pays Off Later
CHICAGO – Lowering LDL cholesterol early in life would prevent three times more cardiovascular events per unit of LDL-reduction compared to the current practice of initiating LDL-lowering statin therapy decades later, based on the findings of a novel genomic analysis known as a mendelian randomized controlled trial.
"People who’ve already been exposed to a lifetime of (elevated levels of) LDL have developed a certain underlying atherosclerotic burden. Lowering LDL at that point – even intensively – can merely stabilize the plaque or cause it to regress only slightly. One is still left with an underlying atherosclerotic plaque that can disrupt and cause symptoms or acute events. The alternative would be to start much earlier in life, before the plaque develops. And that’s what we tested," Dr. Brian A. Ference explained at the annual meeting of the American College of Cardiology.

Dr. Ference emphasized that he wasn’t arguing in favor of routinely starting statin therapy in children with high LDL levels. "A reasonable policy may be to promote a greater awareness of LDL cholesterol levels and a new emphasis on diet and lifestyle to keep LDL low, and in those persons in their 20s who can’t maintain ideal levels of cholesterol – somewhere between 50 and 70 mg/dL – it may be reasonable at that time to begin contemplating adding medication to prevent the development of atherosclerotic plaque."
His mendelian randomized controlled trial was not a conventional prospective clinical trial. That would be utterly impractical because it would take half a century or more. Rather, the mendelian randomized controlled trial was essentially a series of nine natural randomized trials conducted using a database comprised of more than 326,000 people whose genetic status was known with regard to nine single nucleotide polymorphisms (SNPs) associated with low LDL levels throughout life.
"We based this study on the concept of in vivo randomization, which suggests that at the time of conception polymorphisms are allocated randomly and that inheriting an allele that is associated with a lower LDL is analogous to being randomized at the time of birth to a medicine that lowers LDL for the whole of one’s lifetime. In contrast, inheriting the other allele is analogous to being allocated to usual care. So if one compares the risk of coronary [heart] disease (CHD) between the two groups, it should be analogous to a long-term trial," according to Dr. Ference, director of the cardiovascular genomic research center at Wayne State University, Detroit.
He and his fellow researchers compared CHD rates in individuals with the low-LDL SNPs to those in the huge database without the SNPs. Next they compared CHD rates in subjects with each of the nine SNPs to rates in statin-treated patients included in a large meta-analysis of statin randomized controlled trials that was carried out by the Cholesterol Treatment Trialists’ Collaboration.
Each of the nine SNPs was consistently associated with a 55% reduction in CHD risk for each 39 mg/dL lower lifetime exposure to LDL. In contrast, to achieve the same 55% reduction in CHD risk by starting statin therapy at age 63 – the average age at enrollment in the statin trials – a 116 mg/dL decrease in LDL would be required.
Dr. Ference noted that the nine SNPs lowered LDL via different mechanisms, suggesting that the associated beneficial decrease in CHD was mediated through LDL lowering per se and that the manner in which the reductions are achieved wasn’t important. Thus, lowering LDL via diet and exercise beginning early in life should be as effective in terms of reducing CHD risk as any other means of doing so, including drug therapy.
Dr. Ference reported having no financial conflicts.
The observation that having a low LDL cholesterol level from birth is associated with a marked decrease in cardiovascular events, much greater than would be seen by starting statin therapy at age 60-65, has profound public health implications.
There is, however, a hitch: naturally occurring low LDL levels and the levels achieved on treatment are not the same thing, and they may be associated with different degrees of risk.
The Framingham Risk Score is illustrative. The Framingham tool grants a certain point score if a patient’s blood pressure is within a desirable range, but the points double if that blood pressure is achieved through antihypertensive drug therapy.
Dr. Noel Bairey Merz is director of the Women’s Heart Center and the Preventive and Rehabilitative Cardiac Center at Cedars-Sinai Medical Center, Los Angeles. She made her remarks as the study discussant at the meeting. She reported no conflicts of interest related to the study.
The observation that having a low LDL cholesterol level from birth is associated with a marked decrease in cardiovascular events, much greater than would be seen by starting statin therapy at age 60-65, has profound public health implications.
There is, however, a hitch: naturally occurring low LDL levels and the levels achieved on treatment are not the same thing, and they may be associated with different degrees of risk.
The Framingham Risk Score is illustrative. The Framingham tool grants a certain point score if a patient’s blood pressure is within a desirable range, but the points double if that blood pressure is achieved through antihypertensive drug therapy.
Dr. Noel Bairey Merz is director of the Women’s Heart Center and the Preventive and Rehabilitative Cardiac Center at Cedars-Sinai Medical Center, Los Angeles. She made her remarks as the study discussant at the meeting. She reported no conflicts of interest related to the study.
The observation that having a low LDL cholesterol level from birth is associated with a marked decrease in cardiovascular events, much greater than would be seen by starting statin therapy at age 60-65, has profound public health implications.
There is, however, a hitch: naturally occurring low LDL levels and the levels achieved on treatment are not the same thing, and they may be associated with different degrees of risk.
The Framingham Risk Score is illustrative. The Framingham tool grants a certain point score if a patient’s blood pressure is within a desirable range, but the points double if that blood pressure is achieved through antihypertensive drug therapy.
Dr. Noel Bairey Merz is director of the Women’s Heart Center and the Preventive and Rehabilitative Cardiac Center at Cedars-Sinai Medical Center, Los Angeles. She made her remarks as the study discussant at the meeting. She reported no conflicts of interest related to the study.
CHICAGO – Lowering LDL cholesterol early in life would prevent three times more cardiovascular events per unit of LDL-reduction compared to the current practice of initiating LDL-lowering statin therapy decades later, based on the findings of a novel genomic analysis known as a mendelian randomized controlled trial.
"People who’ve already been exposed to a lifetime of (elevated levels of) LDL have developed a certain underlying atherosclerotic burden. Lowering LDL at that point – even intensively – can merely stabilize the plaque or cause it to regress only slightly. One is still left with an underlying atherosclerotic plaque that can disrupt and cause symptoms or acute events. The alternative would be to start much earlier in life, before the plaque develops. And that’s what we tested," Dr. Brian A. Ference explained at the annual meeting of the American College of Cardiology.
Dr. Ference emphasized that he wasn’t arguing in favor of routinely starting statin therapy in children with high LDL levels. "A reasonable policy may be to promote a greater awareness of LDL cholesterol levels and a new emphasis on diet and lifestyle to keep LDL low, and in those persons in their 20s who can’t maintain ideal levels of cholesterol – somewhere between 50 and 70 mg/dL – it may be reasonable at that time to begin contemplating adding medication to prevent the development of atherosclerotic plaque."
His mendelian randomized controlled trial was not a conventional prospective clinical trial. That would be utterly impractical because it would take half a century or more. Rather, the mendelian randomized controlled trial was essentially a series of nine natural randomized trials conducted using a database comprised of more than 326,000 people whose genetic status was known with regard to nine single nucleotide polymorphisms (SNPs) associated with low LDL levels throughout life.
"We based this study on the concept of in vivo randomization, which suggests that at the time of conception polymorphisms are allocated randomly and that inheriting an allele that is associated with a lower LDL is analogous to being randomized at the time of birth to a medicine that lowers LDL for the whole of one’s lifetime. In contrast, inheriting the other allele is analogous to being allocated to usual care. So if one compares the risk of coronary [heart] disease (CHD) between the two groups, it should be analogous to a long-term trial," according to Dr. Ference, director of the cardiovascular genomic research center at Wayne State University, Detroit.
He and his fellow researchers compared CHD rates in individuals with the low-LDL SNPs to those in the huge database without the SNPs. Next they compared CHD rates in subjects with each of the nine SNPs to rates in statin-treated patients included in a large meta-analysis of statin randomized controlled trials that was carried out by the Cholesterol Treatment Trialists’ Collaboration.
Each of the nine SNPs was consistently associated with a 55% reduction in CHD risk for each 39 mg/dL lower lifetime exposure to LDL. In contrast, to achieve the same 55% reduction in CHD risk by starting statin therapy at age 63 – the average age at enrollment in the statin trials – a 116 mg/dL decrease in LDL would be required.
Dr. Ference noted that the nine SNPs lowered LDL via different mechanisms, suggesting that the associated beneficial decrease in CHD was mediated through LDL lowering per se and that the manner in which the reductions are achieved wasn’t important. Thus, lowering LDL via diet and exercise beginning early in life should be as effective in terms of reducing CHD risk as any other means of doing so, including drug therapy.
Dr. Ference reported having no financial conflicts.
CHICAGO – Lowering LDL cholesterol early in life would prevent three times more cardiovascular events per unit of LDL-reduction compared to the current practice of initiating LDL-lowering statin therapy decades later, based on the findings of a novel genomic analysis known as a mendelian randomized controlled trial.
"People who’ve already been exposed to a lifetime of (elevated levels of) LDL have developed a certain underlying atherosclerotic burden. Lowering LDL at that point – even intensively – can merely stabilize the plaque or cause it to regress only slightly. One is still left with an underlying atherosclerotic plaque that can disrupt and cause symptoms or acute events. The alternative would be to start much earlier in life, before the plaque develops. And that’s what we tested," Dr. Brian A. Ference explained at the annual meeting of the American College of Cardiology.
Dr. Ference emphasized that he wasn’t arguing in favor of routinely starting statin therapy in children with high LDL levels. "A reasonable policy may be to promote a greater awareness of LDL cholesterol levels and a new emphasis on diet and lifestyle to keep LDL low, and in those persons in their 20s who can’t maintain ideal levels of cholesterol – somewhere between 50 and 70 mg/dL – it may be reasonable at that time to begin contemplating adding medication to prevent the development of atherosclerotic plaque."
His mendelian randomized controlled trial was not a conventional prospective clinical trial. That would be utterly impractical because it would take half a century or more. Rather, the mendelian randomized controlled trial was essentially a series of nine natural randomized trials conducted using a database comprised of more than 326,000 people whose genetic status was known with regard to nine single nucleotide polymorphisms (SNPs) associated with low LDL levels throughout life.
"We based this study on the concept of in vivo randomization, which suggests that at the time of conception polymorphisms are allocated randomly and that inheriting an allele that is associated with a lower LDL is analogous to being randomized at the time of birth to a medicine that lowers LDL for the whole of one’s lifetime. In contrast, inheriting the other allele is analogous to being allocated to usual care. So if one compares the risk of coronary [heart] disease (CHD) between the two groups, it should be analogous to a long-term trial," according to Dr. Ference, director of the cardiovascular genomic research center at Wayne State University, Detroit.
He and his fellow researchers compared CHD rates in individuals with the low-LDL SNPs to those in the huge database without the SNPs. Next they compared CHD rates in subjects with each of the nine SNPs to rates in statin-treated patients included in a large meta-analysis of statin randomized controlled trials that was carried out by the Cholesterol Treatment Trialists’ Collaboration.
Each of the nine SNPs was consistently associated with a 55% reduction in CHD risk for each 39 mg/dL lower lifetime exposure to LDL. In contrast, to achieve the same 55% reduction in CHD risk by starting statin therapy at age 63 – the average age at enrollment in the statin trials – a 116 mg/dL decrease in LDL would be required.
Dr. Ference noted that the nine SNPs lowered LDL via different mechanisms, suggesting that the associated beneficial decrease in CHD was mediated through LDL lowering per se and that the manner in which the reductions are achieved wasn’t important. Thus, lowering LDL via diet and exercise beginning early in life should be as effective in terms of reducing CHD risk as any other means of doing so, including drug therapy.
Dr. Ference reported having no financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Each of the nine SNPs was consistently associated with a 55% reduction in CHD risk for each 39 mg/dL lower lifetime exposure to LDL. To achieve the same 55% reduction in CHD risk by starting statin therapy at age 63, a 116 mg/dL decrease in LDL would be required.
Data Source: The mendelian randomized controlled trial was a series of nine randomized trials conducted using a database of more than 326,000 people whose genetic status was known with regard to nine single nucleotide polymorphisms associated with low LDL levels throughout life.
Disclosures: Dr. Ference reported having no financial conflicts.
Psychostimulants, Ketamine Improve Depression Quickly in Hospice
DENVER – Methylphenidate and oral ketamine show considerable promise as extremely rapid-acting, safe, and cost-effective treatments for depression in the hospice setting.
Moreover, early indications are that ketamine might be even more effective as the treatment of anxiety disorders than as an antidepressant in this population nearing end of life, Dr. Scott A. Irwin said at the conference.

This is off-label therapy. But standard antidepressant medications and guideline-recommended treatment algorithms for depression just don’t cut it in the hospice setting. The reason is quite simple: "We don’t have that kind of time," noted Dr. Irwin, director of psychiatry programs at the Institute for Palliative Medicine at San Diego Hospice.
For example, current American Psychiatric Association guidelines for treatment of moderate to severe depression call for 6-8 weeks of antidepressant medication and psychotherapy before switching agents or adding a second one in the event there hasn’t been at least moderate improvement. Patients are then supposed to be monitored for another 6-8 weeks. Yet, the median time in hospice care in the United States is only about 3 weeks. One-third of patients at San Diego Hospice die within the first week.
In one study of more than 1,000 consecutive patients in a palliative care unit, three-quarters of those who were prescribed an antidepressant got the medication only during their last 2 weeks of life. That’s not enough time to allow relief of symptoms, the psychiatrist said.
The prevalence of major depressive disorder in palliative care patients has been estimated at about 15%. No published randomized controlled trials have examined methylphenidate for treatment of such episodes in palliative care settings. But mechanistically, it is sound, Dr. Irwin said, since the psychostimulant blocks reuptake of dopamine in central adrenergic neurons and inhibits reuptake of serotonin and norepinephrine as well, just like standard antidepressants. There have been encouraging review articles, and Dr. Irwin presented his own highly promising retrospective blinded chart review study.
His study included 64 palliative care patients with psychiatrist-diagnosed depressive disorders treated in various ways, with treatment efficacy and side effects evaluated using the Clinical Global Impressions Scale (CGI).
Twenty of 21 methylphenidate-treated patients (95%) were blindly rated as having a significant clinical response, as were 4 of 9 (44%) treated with selective serotonin reuptake inhibitors (SSRIs), 3 of 13 (23%) who received other antidepressants, and 0 of 21 who received usual care alone. The time to response was 4 days with methylphenidate, 10 days with SSRIs, and about 5 days with other antidepressants. Those response times for standard antidepressants are much shorter than expected and require further study, according to Dr. Irwin.
Methylphenidate was blindly rated as significantly more effective than were the nonstimulant antidepressants. The mean score on the CGI 0-4 efficacy scale, in which lower is better, was 2.33 in methylphenidate-treated patients, compared with 3.06 with nonstimulant antidepressants.
On the other hand, side effects were significantly greater with methylphenidate: a mean score of 1.72, compared with 1.13. However, Dr. Irwin characterized side effects in the 1.0-2.0 range on the CGI as being in the "mild and don’t worry about-it" level.
It’s readily apparent within the first day or two if methylphenidate is going to be effective, he continued.
Somatic symptoms, which are very common in palliative care patients, typically improve markedly in methylphenidate-treated patients as their depression improves. However, anxiety increases in a minority of treated patients as depression wanes, sometimes requiring methylphenidate discontinuation, said Dr. Irwin, who is also a faculty psychiatrist at the University of California, San Diego.
He is now conducting a prospective open-label study of methylphenidate in hospice patients having a current major depressive episode. The study employs a flexible dosing schedule with dosing changes on days 3, 7, and 14, and a maximum dose of 20 mg b.i.d. But he finds it extremely challenging to conduct clinical trials in hospice patients because of their high death rate, its unpredictable timing, and informed consent issues.
Turning to ketamine for depression, Dr. Irwin said exciting preliminary evidence in nonhospice patients suggests that a single intravenous infusion of the anesthetic improves depression literally within minutes and that the effect lasts for weeks.
As it turns out, hospice physicians already have long experience using ketamine, not as an antidepressant but for treatment of pain, including cancer pain. They view ketamine as a familiar and inexpensive analgesic that they’re comfortable giving by the oral, subcutaneous, and transdermal routes.
Dr. Irwin is in the midst of conducting an open label pilot study to evaluate the efficacy and tolerability of oral ketamine for the treatment of major depression in hospice patients. Fourteen of a planned 20 patients have completed the 28-day study. The dosing is 0.5 mg/kg of the intravenous ketamine solution mixed in cherry syrup to hide the universally loathed taste. Treatment is once daily.
The therapeutic efficacy has been impressive, as reflected in a drop in average scores on the Hospital Anxiety and Depression Scale from about 20 to 5.
"Interestingly, several patients had diagnosable severe anxiety disorders that went away completely. We’re finding that anxiety may be even more affected by ketamine than depression," Dr. Irwin said.
The high burden of somatic symptoms present in these patients also lightened significantly, with scores on the Adverse Symptom Checklist falling from about 28 to 5. This doesn’t appear to be a result of the drug’s analgesic effect, because some patients didn’t have significant pain, while in others the somatic symptoms improved while pain scores remained unchanged.
Another 30 or so San Diego Hospice patients have received oral ketamine outside of the pilot study, with similar benefits.
"We’ve gone to nightly dosing. And if you see a decrement in benefit, bump up the dose by 20%," Dr. Irwin advised in response to audience questions.
He called depression near the end of life a major yet widely underappreciated public health problem. The consequences of untreated depression in these patients include longer inpatient hospital stays, worsening medical illness, greater difficulty in treating pain and nausea, and interference with making preparations for death. Untreated depression also impedes interactions with caregivers and, most importantly, with loved ones.
Dr. Irwin recalled one of the first hospice patients for whom he prescribed methylphenidate. After 24 hours on treatment, the man no longer met criteria for major depressive disorder. He lived for another week with newly restored enjoyment of nature and his family. Dr. Irwin learned of his death when he ran into the patient’s daughter in the parking lot.
"She said, ‘I want to thank you for giving me my father back. I will now remember him as the great man he always was, and not the miserable man that he’d become for the last 6 months,’ "
Dr. Irwin said. "So we changed her life for decades.
"If anyone asks you, ‘Why bother treating depression in hospice when you’re only changing the last few days?’ tell them it’s a family experience. It’s not just about the patient."
He reported having no financial conflicts.
DENVER – Methylphenidate and oral ketamine show considerable promise as extremely rapid-acting, safe, and cost-effective treatments for depression in the hospice setting.
Moreover, early indications are that ketamine might be even more effective as the treatment of anxiety disorders than as an antidepressant in this population nearing end of life, Dr. Scott A. Irwin said at the conference.
This is off-label therapy. But standard antidepressant medications and guideline-recommended treatment algorithms for depression just don’t cut it in the hospice setting. The reason is quite simple: "We don’t have that kind of time," noted Dr. Irwin, director of psychiatry programs at the Institute for Palliative Medicine at San Diego Hospice.
For example, current American Psychiatric Association guidelines for treatment of moderate to severe depression call for 6-8 weeks of antidepressant medication and psychotherapy before switching agents or adding a second one in the event there hasn’t been at least moderate improvement. Patients are then supposed to be monitored for another 6-8 weeks. Yet, the median time in hospice care in the United States is only about 3 weeks. One-third of patients at San Diego Hospice die within the first week.
In one study of more than 1,000 consecutive patients in a palliative care unit, three-quarters of those who were prescribed an antidepressant got the medication only during their last 2 weeks of life. That’s not enough time to allow relief of symptoms, the psychiatrist said.
The prevalence of major depressive disorder in palliative care patients has been estimated at about 15%. No published randomized controlled trials have examined methylphenidate for treatment of such episodes in palliative care settings. But mechanistically, it is sound, Dr. Irwin said, since the psychostimulant blocks reuptake of dopamine in central adrenergic neurons and inhibits reuptake of serotonin and norepinephrine as well, just like standard antidepressants. There have been encouraging review articles, and Dr. Irwin presented his own highly promising retrospective blinded chart review study.
His study included 64 palliative care patients with psychiatrist-diagnosed depressive disorders treated in various ways, with treatment efficacy and side effects evaluated using the Clinical Global Impressions Scale (CGI).
Twenty of 21 methylphenidate-treated patients (95%) were blindly rated as having a significant clinical response, as were 4 of 9 (44%) treated with selective serotonin reuptake inhibitors (SSRIs), 3 of 13 (23%) who received other antidepressants, and 0 of 21 who received usual care alone. The time to response was 4 days with methylphenidate, 10 days with SSRIs, and about 5 days with other antidepressants. Those response times for standard antidepressants are much shorter than expected and require further study, according to Dr. Irwin.
Methylphenidate was blindly rated as significantly more effective than were the nonstimulant antidepressants. The mean score on the CGI 0-4 efficacy scale, in which lower is better, was 2.33 in methylphenidate-treated patients, compared with 3.06 with nonstimulant antidepressants.
On the other hand, side effects were significantly greater with methylphenidate: a mean score of 1.72, compared with 1.13. However, Dr. Irwin characterized side effects in the 1.0-2.0 range on the CGI as being in the "mild and don’t worry about-it" level.
It’s readily apparent within the first day or two if methylphenidate is going to be effective, he continued.
Somatic symptoms, which are very common in palliative care patients, typically improve markedly in methylphenidate-treated patients as their depression improves. However, anxiety increases in a minority of treated patients as depression wanes, sometimes requiring methylphenidate discontinuation, said Dr. Irwin, who is also a faculty psychiatrist at the University of California, San Diego.
He is now conducting a prospective open-label study of methylphenidate in hospice patients having a current major depressive episode. The study employs a flexible dosing schedule with dosing changes on days 3, 7, and 14, and a maximum dose of 20 mg b.i.d. But he finds it extremely challenging to conduct clinical trials in hospice patients because of their high death rate, its unpredictable timing, and informed consent issues.
Turning to ketamine for depression, Dr. Irwin said exciting preliminary evidence in nonhospice patients suggests that a single intravenous infusion of the anesthetic improves depression literally within minutes and that the effect lasts for weeks.
As it turns out, hospice physicians already have long experience using ketamine, not as an antidepressant but for treatment of pain, including cancer pain. They view ketamine as a familiar and inexpensive analgesic that they’re comfortable giving by the oral, subcutaneous, and transdermal routes.
Dr. Irwin is in the midst of conducting an open label pilot study to evaluate the efficacy and tolerability of oral ketamine for the treatment of major depression in hospice patients. Fourteen of a planned 20 patients have completed the 28-day study. The dosing is 0.5 mg/kg of the intravenous ketamine solution mixed in cherry syrup to hide the universally loathed taste. Treatment is once daily.
The therapeutic efficacy has been impressive, as reflected in a drop in average scores on the Hospital Anxiety and Depression Scale from about 20 to 5.
"Interestingly, several patients had diagnosable severe anxiety disorders that went away completely. We’re finding that anxiety may be even more affected by ketamine than depression," Dr. Irwin said.
The high burden of somatic symptoms present in these patients also lightened significantly, with scores on the Adverse Symptom Checklist falling from about 28 to 5. This doesn’t appear to be a result of the drug’s analgesic effect, because some patients didn’t have significant pain, while in others the somatic symptoms improved while pain scores remained unchanged.
Another 30 or so San Diego Hospice patients have received oral ketamine outside of the pilot study, with similar benefits.
"We’ve gone to nightly dosing. And if you see a decrement in benefit, bump up the dose by 20%," Dr. Irwin advised in response to audience questions.
He called depression near the end of life a major yet widely underappreciated public health problem. The consequences of untreated depression in these patients include longer inpatient hospital stays, worsening medical illness, greater difficulty in treating pain and nausea, and interference with making preparations for death. Untreated depression also impedes interactions with caregivers and, most importantly, with loved ones.
Dr. Irwin recalled one of the first hospice patients for whom he prescribed methylphenidate. After 24 hours on treatment, the man no longer met criteria for major depressive disorder. He lived for another week with newly restored enjoyment of nature and his family. Dr. Irwin learned of his death when he ran into the patient’s daughter in the parking lot.
"She said, ‘I want to thank you for giving me my father back. I will now remember him as the great man he always was, and not the miserable man that he’d become for the last 6 months,’ "
Dr. Irwin said. "So we changed her life for decades.
"If anyone asks you, ‘Why bother treating depression in hospice when you’re only changing the last few days?’ tell them it’s a family experience. It’s not just about the patient."
He reported having no financial conflicts.
DENVER – Methylphenidate and oral ketamine show considerable promise as extremely rapid-acting, safe, and cost-effective treatments for depression in the hospice setting.
Moreover, early indications are that ketamine might be even more effective as the treatment of anxiety disorders than as an antidepressant in this population nearing end of life, Dr. Scott A. Irwin said at the conference.
This is off-label therapy. But standard antidepressant medications and guideline-recommended treatment algorithms for depression just don’t cut it in the hospice setting. The reason is quite simple: "We don’t have that kind of time," noted Dr. Irwin, director of psychiatry programs at the Institute for Palliative Medicine at San Diego Hospice.
For example, current American Psychiatric Association guidelines for treatment of moderate to severe depression call for 6-8 weeks of antidepressant medication and psychotherapy before switching agents or adding a second one in the event there hasn’t been at least moderate improvement. Patients are then supposed to be monitored for another 6-8 weeks. Yet, the median time in hospice care in the United States is only about 3 weeks. One-third of patients at San Diego Hospice die within the first week.
In one study of more than 1,000 consecutive patients in a palliative care unit, three-quarters of those who were prescribed an antidepressant got the medication only during their last 2 weeks of life. That’s not enough time to allow relief of symptoms, the psychiatrist said.
The prevalence of major depressive disorder in palliative care patients has been estimated at about 15%. No published randomized controlled trials have examined methylphenidate for treatment of such episodes in palliative care settings. But mechanistically, it is sound, Dr. Irwin said, since the psychostimulant blocks reuptake of dopamine in central adrenergic neurons and inhibits reuptake of serotonin and norepinephrine as well, just like standard antidepressants. There have been encouraging review articles, and Dr. Irwin presented his own highly promising retrospective blinded chart review study.
His study included 64 palliative care patients with psychiatrist-diagnosed depressive disorders treated in various ways, with treatment efficacy and side effects evaluated using the Clinical Global Impressions Scale (CGI).
Twenty of 21 methylphenidate-treated patients (95%) were blindly rated as having a significant clinical response, as were 4 of 9 (44%) treated with selective serotonin reuptake inhibitors (SSRIs), 3 of 13 (23%) who received other antidepressants, and 0 of 21 who received usual care alone. The time to response was 4 days with methylphenidate, 10 days with SSRIs, and about 5 days with other antidepressants. Those response times for standard antidepressants are much shorter than expected and require further study, according to Dr. Irwin.
Methylphenidate was blindly rated as significantly more effective than were the nonstimulant antidepressants. The mean score on the CGI 0-4 efficacy scale, in which lower is better, was 2.33 in methylphenidate-treated patients, compared with 3.06 with nonstimulant antidepressants.
On the other hand, side effects were significantly greater with methylphenidate: a mean score of 1.72, compared with 1.13. However, Dr. Irwin characterized side effects in the 1.0-2.0 range on the CGI as being in the "mild and don’t worry about-it" level.
It’s readily apparent within the first day or two if methylphenidate is going to be effective, he continued.
Somatic symptoms, which are very common in palliative care patients, typically improve markedly in methylphenidate-treated patients as their depression improves. However, anxiety increases in a minority of treated patients as depression wanes, sometimes requiring methylphenidate discontinuation, said Dr. Irwin, who is also a faculty psychiatrist at the University of California, San Diego.
He is now conducting a prospective open-label study of methylphenidate in hospice patients having a current major depressive episode. The study employs a flexible dosing schedule with dosing changes on days 3, 7, and 14, and a maximum dose of 20 mg b.i.d. But he finds it extremely challenging to conduct clinical trials in hospice patients because of their high death rate, its unpredictable timing, and informed consent issues.
Turning to ketamine for depression, Dr. Irwin said exciting preliminary evidence in nonhospice patients suggests that a single intravenous infusion of the anesthetic improves depression literally within minutes and that the effect lasts for weeks.
As it turns out, hospice physicians already have long experience using ketamine, not as an antidepressant but for treatment of pain, including cancer pain. They view ketamine as a familiar and inexpensive analgesic that they’re comfortable giving by the oral, subcutaneous, and transdermal routes.
Dr. Irwin is in the midst of conducting an open label pilot study to evaluate the efficacy and tolerability of oral ketamine for the treatment of major depression in hospice patients. Fourteen of a planned 20 patients have completed the 28-day study. The dosing is 0.5 mg/kg of the intravenous ketamine solution mixed in cherry syrup to hide the universally loathed taste. Treatment is once daily.
The therapeutic efficacy has been impressive, as reflected in a drop in average scores on the Hospital Anxiety and Depression Scale from about 20 to 5.
"Interestingly, several patients had diagnosable severe anxiety disorders that went away completely. We’re finding that anxiety may be even more affected by ketamine than depression," Dr. Irwin said.
The high burden of somatic symptoms present in these patients also lightened significantly, with scores on the Adverse Symptom Checklist falling from about 28 to 5. This doesn’t appear to be a result of the drug’s analgesic effect, because some patients didn’t have significant pain, while in others the somatic symptoms improved while pain scores remained unchanged.
Another 30 or so San Diego Hospice patients have received oral ketamine outside of the pilot study, with similar benefits.
"We’ve gone to nightly dosing. And if you see a decrement in benefit, bump up the dose by 20%," Dr. Irwin advised in response to audience questions.
He called depression near the end of life a major yet widely underappreciated public health problem. The consequences of untreated depression in these patients include longer inpatient hospital stays, worsening medical illness, greater difficulty in treating pain and nausea, and interference with making preparations for death. Untreated depression also impedes interactions with caregivers and, most importantly, with loved ones.
Dr. Irwin recalled one of the first hospice patients for whom he prescribed methylphenidate. After 24 hours on treatment, the man no longer met criteria for major depressive disorder. He lived for another week with newly restored enjoyment of nature and his family. Dr. Irwin learned of his death when he ran into the patient’s daughter in the parking lot.
"She said, ‘I want to thank you for giving me my father back. I will now remember him as the great man he always was, and not the miserable man that he’d become for the last 6 months,’ "
Dr. Irwin said. "So we changed her life for decades.
"If anyone asks you, ‘Why bother treating depression in hospice when you’re only changing the last few days?’ tell them it’s a family experience. It’s not just about the patient."
He reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL ASSEMBLY OF THE AMERICAN ACADEMY OF HOSPICE AND PALLIATIVE MEDICINE
Gains in Melanoma Survival Attributed to Patient Awareness
WAIKOLOA, HAWAII – The improvement in melanoma survival over the past 4 decades can be attributed to effective public education campaigns, increased patient awareness, and improved physician skills and diagnostic tools, according to Dr. Ashfaq A. Marghoob.
It has been nothing short of phenomenal, he said, especially considering it can’t be credited to major therapeutic advances because up until a couple years ago there weren’t any.

Survival at 5 years for all-stage melanomas of the skin climbed from less than 60% in 1970 to 91% in 2011, he said at the Hawaii Dermatology Seminar sponsored by the Skin Disease Education Foundation (SDEF). But while this is a triumph deserving of celebration, the statistics are somewhat deceiving, said Dr. Marghoob, a dermatologist at Memorial Sloan-Kettering Cancer Center in New York.
He is among a growing number of experts who believe that many thin melanomas detected through screening efforts are slow-growing, indolent skin cancers that sometimes regress and in any event will never become thick or dangerous – never result in death – within the range of current life expectancy. He noted that there is ample precedence, namely, indolent forms of prostate cancer, lymphoma, and breast cancer.
Dr. Marghoob was part of an international team that demonstrated the existence of a slow-growing subtype of melanoma. In a series of 103 melanomas excised after a median follow-up of 20 months, most of the lesions were still in situ or in an early invasive stage. Only three lesions were 1-mm thick or more. There was no correlation between tumor thickness and follow-up time (Br. J. Dermatol. 2010;162:267-73). Growing support exists among epidemiologists for the concept that there are three distinct, unrelated melanoma subtypes (Br. J. Dermatol. 2007;157:338-43). One subtype consists of thin, slow-growing melanomas – the kind that have been steadily increasing in incidence for decades. These are associated with intermittent sun exposure and often arise on the trunk among numerous background nevi. These melanomas are amenable to detection via screening or periodic surveillance. But they only rarely metastasize.
A second type of slow-growing melanoma often occurs on the head and neck of individuals with continuous sun exposure. The incidence of this subtype of melanoma is slowly increasing.
The third and most concerning melanoma subtype consists of thick, fast-growing lesions occurring in individuals with many nevi, but that are not associated with sun exposure. The incidence of these fast-growing, high-lethality melanomas has remained steady over time because they often escape detection as a result of their accelerated growth rate. Improved early detection is a high priority, and it will require creative new approaches, he said.
But in terms of celebrating rising 5-year melanoma survival rates, a contributory landmark event, in Dr. Marghoob’s view, was the increased awareness about melanoma after introduction of the ABCD mnemonic, devised chiefly for primary care physicians and the general public. This was later enhanced by the "ugly duckling" campaign, which taught physicians and patients that melanomas are generally recognizable as outlier lesions.
Multiple studies have shown that skin cancer specialists using visual examination alone – incorporating the ABCDs and ugly duckling concept – can typically diagnose melanoma with a sensitivity of 70% and specificity of 75%. The number needed to treat (NNT) or benign-to-malignant biopsy ratio is 1:12-15.
With the aid of total body photography for assistance in patient follow-up, the NNT improves to 10.
Dermoscopy has been another important advance. It enables physicians to pick up melanomas not detectable by any other method. Skin cancer specialists who supplement visual examination with dermoscopy typically have 90% sensitivity and 86% specificity for the diagnosis of melanoma. The NNT improves to 4-7, Dr. Marghoob continued.
Recent studies indicate these numbers get even better with the use of confocal microscopy during skin examination.
Using a review of his own practice to illustrate the strong trend for improved diagnosis, Dr. Marghoob noted that in 1998 his NNT was 12.5. He adopted dermoscopy in 1999, and in 2000, when he was using dermoscopy routinely, his NNT improved to 7. During both 2006 and 2007 it was 3, he said.
"We have gotten better at diagnosing melanoma and we will continue to improve," he concluded.
He reported having no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
WAIKOLOA, HAWAII – The improvement in melanoma survival over the past 4 decades can be attributed to effective public education campaigns, increased patient awareness, and improved physician skills and diagnostic tools, according to Dr. Ashfaq A. Marghoob.
It has been nothing short of phenomenal, he said, especially considering it can’t be credited to major therapeutic advances because up until a couple years ago there weren’t any.
Survival at 5 years for all-stage melanomas of the skin climbed from less than 60% in 1970 to 91% in 2011, he said at the Hawaii Dermatology Seminar sponsored by the Skin Disease Education Foundation (SDEF). But while this is a triumph deserving of celebration, the statistics are somewhat deceiving, said Dr. Marghoob, a dermatologist at Memorial Sloan-Kettering Cancer Center in New York.
He is among a growing number of experts who believe that many thin melanomas detected through screening efforts are slow-growing, indolent skin cancers that sometimes regress and in any event will never become thick or dangerous – never result in death – within the range of current life expectancy. He noted that there is ample precedence, namely, indolent forms of prostate cancer, lymphoma, and breast cancer.
Dr. Marghoob was part of an international team that demonstrated the existence of a slow-growing subtype of melanoma. In a series of 103 melanomas excised after a median follow-up of 20 months, most of the lesions were still in situ or in an early invasive stage. Only three lesions were 1-mm thick or more. There was no correlation between tumor thickness and follow-up time (Br. J. Dermatol. 2010;162:267-73). Growing support exists among epidemiologists for the concept that there are three distinct, unrelated melanoma subtypes (Br. J. Dermatol. 2007;157:338-43). One subtype consists of thin, slow-growing melanomas – the kind that have been steadily increasing in incidence for decades. These are associated with intermittent sun exposure and often arise on the trunk among numerous background nevi. These melanomas are amenable to detection via screening or periodic surveillance. But they only rarely metastasize.
A second type of slow-growing melanoma often occurs on the head and neck of individuals with continuous sun exposure. The incidence of this subtype of melanoma is slowly increasing.
The third and most concerning melanoma subtype consists of thick, fast-growing lesions occurring in individuals with many nevi, but that are not associated with sun exposure. The incidence of these fast-growing, high-lethality melanomas has remained steady over time because they often escape detection as a result of their accelerated growth rate. Improved early detection is a high priority, and it will require creative new approaches, he said.
But in terms of celebrating rising 5-year melanoma survival rates, a contributory landmark event, in Dr. Marghoob’s view, was the increased awareness about melanoma after introduction of the ABCD mnemonic, devised chiefly for primary care physicians and the general public. This was later enhanced by the "ugly duckling" campaign, which taught physicians and patients that melanomas are generally recognizable as outlier lesions.
Multiple studies have shown that skin cancer specialists using visual examination alone – incorporating the ABCDs and ugly duckling concept – can typically diagnose melanoma with a sensitivity of 70% and specificity of 75%. The number needed to treat (NNT) or benign-to-malignant biopsy ratio is 1:12-15.
With the aid of total body photography for assistance in patient follow-up, the NNT improves to 10.
Dermoscopy has been another important advance. It enables physicians to pick up melanomas not detectable by any other method. Skin cancer specialists who supplement visual examination with dermoscopy typically have 90% sensitivity and 86% specificity for the diagnosis of melanoma. The NNT improves to 4-7, Dr. Marghoob continued.
Recent studies indicate these numbers get even better with the use of confocal microscopy during skin examination.
Using a review of his own practice to illustrate the strong trend for improved diagnosis, Dr. Marghoob noted that in 1998 his NNT was 12.5. He adopted dermoscopy in 1999, and in 2000, when he was using dermoscopy routinely, his NNT improved to 7. During both 2006 and 2007 it was 3, he said.
"We have gotten better at diagnosing melanoma and we will continue to improve," he concluded.
He reported having no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
WAIKOLOA, HAWAII – The improvement in melanoma survival over the past 4 decades can be attributed to effective public education campaigns, increased patient awareness, and improved physician skills and diagnostic tools, according to Dr. Ashfaq A. Marghoob.
It has been nothing short of phenomenal, he said, especially considering it can’t be credited to major therapeutic advances because up until a couple years ago there weren’t any.
Survival at 5 years for all-stage melanomas of the skin climbed from less than 60% in 1970 to 91% in 2011, he said at the Hawaii Dermatology Seminar sponsored by the Skin Disease Education Foundation (SDEF). But while this is a triumph deserving of celebration, the statistics are somewhat deceiving, said Dr. Marghoob, a dermatologist at Memorial Sloan-Kettering Cancer Center in New York.
He is among a growing number of experts who believe that many thin melanomas detected through screening efforts are slow-growing, indolent skin cancers that sometimes regress and in any event will never become thick or dangerous – never result in death – within the range of current life expectancy. He noted that there is ample precedence, namely, indolent forms of prostate cancer, lymphoma, and breast cancer.
Dr. Marghoob was part of an international team that demonstrated the existence of a slow-growing subtype of melanoma. In a series of 103 melanomas excised after a median follow-up of 20 months, most of the lesions were still in situ or in an early invasive stage. Only three lesions were 1-mm thick or more. There was no correlation between tumor thickness and follow-up time (Br. J. Dermatol. 2010;162:267-73). Growing support exists among epidemiologists for the concept that there are three distinct, unrelated melanoma subtypes (Br. J. Dermatol. 2007;157:338-43). One subtype consists of thin, slow-growing melanomas – the kind that have been steadily increasing in incidence for decades. These are associated with intermittent sun exposure and often arise on the trunk among numerous background nevi. These melanomas are amenable to detection via screening or periodic surveillance. But they only rarely metastasize.
A second type of slow-growing melanoma often occurs on the head and neck of individuals with continuous sun exposure. The incidence of this subtype of melanoma is slowly increasing.
The third and most concerning melanoma subtype consists of thick, fast-growing lesions occurring in individuals with many nevi, but that are not associated with sun exposure. The incidence of these fast-growing, high-lethality melanomas has remained steady over time because they often escape detection as a result of their accelerated growth rate. Improved early detection is a high priority, and it will require creative new approaches, he said.
But in terms of celebrating rising 5-year melanoma survival rates, a contributory landmark event, in Dr. Marghoob’s view, was the increased awareness about melanoma after introduction of the ABCD mnemonic, devised chiefly for primary care physicians and the general public. This was later enhanced by the "ugly duckling" campaign, which taught physicians and patients that melanomas are generally recognizable as outlier lesions.
Multiple studies have shown that skin cancer specialists using visual examination alone – incorporating the ABCDs and ugly duckling concept – can typically diagnose melanoma with a sensitivity of 70% and specificity of 75%. The number needed to treat (NNT) or benign-to-malignant biopsy ratio is 1:12-15.
With the aid of total body photography for assistance in patient follow-up, the NNT improves to 10.
Dermoscopy has been another important advance. It enables physicians to pick up melanomas not detectable by any other method. Skin cancer specialists who supplement visual examination with dermoscopy typically have 90% sensitivity and 86% specificity for the diagnosis of melanoma. The NNT improves to 4-7, Dr. Marghoob continued.
Recent studies indicate these numbers get even better with the use of confocal microscopy during skin examination.
Using a review of his own practice to illustrate the strong trend for improved diagnosis, Dr. Marghoob noted that in 1998 his NNT was 12.5. He adopted dermoscopy in 1999, and in 2000, when he was using dermoscopy routinely, his NNT improved to 7. During both 2006 and 2007 it was 3, he said.
"We have gotten better at diagnosing melanoma and we will continue to improve," he concluded.
He reported having no relevant financial disclosures. SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR
Total Body Exam Reduces Melanoma Mortality
WAIKOLOA, HAWAII – An organized program of population-based total body skin examination screening for skin cancer has been shown to significantly reduce melanoma mortality.
"This is quite astounding. It is very impressive to see that a total body skin exam can reduce mortality. It forces us all to think about whether we should do this in a very, very large population, as we now do in Germany," said Dr. Andreas Blum, professor of dermatology at the University of Tübingen (Germany).

He presented highlights of the SCREEN (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany) project, in which all residents of the state of Schleswig-Holstein were eligible for a standardized total body skin exam during a 1-year study period. This was to date the world’s largest systematic population-based skin cancer screening program, he said.
Nineteen percent of the Schleswig-Holstein adult population – more than 360,000 citizens – participated. A total of 3,103 skin cancers were found, including 585 melanomas, for a rate of 1.6 melanomas per 1,000 persons screened. Basal cell carcinomas were detected at a rate of 5.4 malignancies per 1,000, and squamous cell carcinomas at 1.1 per 1,000 people screened. Five lesion excisions had to be performed to detect one malignancy.
Using the incidence of melanoma in Schleswig-Holstein during the 2 years prior to the SCREEN project as a baseline, the incidence of melanoma during the SCREEN project increased by 16% in men and by 38% in women.
The key study finding was a significant decrease in melanoma mortality documented 5 years after SCREEN ended. The observed melanoma mortality rate in men was 0.79 per 100,000 population, compared with an expected 2.0 per 100,000. Among women, the observed mortality was 0.66 per 100,000, compared with an expected 1.3 per 100,000. Thus, the observed mortality because of earlier detection of melanoma in the screened area was less than 50% of expected, Dr. Blum said at the Hawaii Dermatology Seminar sponsored by the Skin Disease Education Foundation (SDEF).
The screening project had a two-tiered structure. Most participants were first screened by a primary care physician or other nondermatologist. In the event of suspicious findings and/or skin cancer risk factors, the participant was referred to a dermatologist who performed the biopsies. All participating physicians first had to attend an 8-hour training course. Of note, 116 of the 118 dermatologists in Schleswig-Holstein participated in SCREEN, as did nearly two-thirds of eligible nondermatologists (J. Am. Acad. Dermatol. 2012;66:201-11).
Following up on the unprecedented success of the SCREEN project, German dermatologists next proposed a randomized controlled trial in order to provide the highest-level evidence that mass skin cancer screening reduces melanoma mortality. However, government health officials found SCREEN persuasive and nixed the idea of a large and costly randomized trial. Instead, Germany has launched a national skin cancer screening program, according to Dr. Blum. All 45 million Germans aged 35 years and older are now eligible to be screened for skin cancer once every 2 years; whether the health care system can cope with the demand remains to be seen.
Another recent project evaluating the benefits of total body skin examination for skin cancer screening also reported favorable results, he noted.
Investigators in a multicenter study screened more than 14,000 patients with a total body skin exam. Participants were consecutive adults presenting with a localized dermatologic problem, such as a skin infection, that wouldn’t ordinarily result in a total body skin exam. The total body skin exams detected 40 patients (0.3%) with melanoma. Five benign lesions were excised for each melanoma detected. Another 2.1% of patients had at least one nonmelanoma skin cancer detected by total body skin exam. On average, 400 patients had to be examined by total body skin exam in order to find 1 melanoma (J. Am. Acad. Dermatol. 2012;66:212-9).
"I see around 150 new patients per week, so that means every third week I see a new melanoma," Dr. Blum said.
Total body skin examination has long been a controversial issue. The U.S. Preventive Services Task Force found insufficient evidence to recommend screening adults for skin cancer (Ann. Intern. Med. 2009;150:188-93). That stance will now need to be revisited in light of these two large projects, said Dr. Blum.
He predicted that the cost involved in routine total body skin examinations is likely to be a critical source of controversy. Using the National Cancer Institute’s estimate that 12.5% of melanomas are fatal, and assuming the cost of a total body skin exam to be $50, he estimated that routine total body skin exams in the SCREEN project cost $240,000 per melanoma death avoided.
In his own specialized skin cancer clinic, where he sees a more select patient population, Dr. Blum estimated that routine total body skin examination costs about $65,000 per melanoma death avoided. And when he plugged in the numbers provided by his colleague Dr. Ashfaq A. Marghoob, pertaining to the skin cancer clinic at Memorial Sloan-Kettering Cancer Center in New York, Dr. Blum once again came up with a figure of roughly $65,000 per melanoma death avoided.
"The range is quite high. I think the cost debate will continue," Dr. Blum predicted.
He reported having no financial conflicts.
SDEF and this news organization are owned by Elsevier.
WAIKOLOA, HAWAII – An organized program of population-based total body skin examination screening for skin cancer has been shown to significantly reduce melanoma mortality.
"This is quite astounding. It is very impressive to see that a total body skin exam can reduce mortality. It forces us all to think about whether we should do this in a very, very large population, as we now do in Germany," said Dr. Andreas Blum, professor of dermatology at the University of Tübingen (Germany).
He presented highlights of the SCREEN (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany) project, in which all residents of the state of Schleswig-Holstein were eligible for a standardized total body skin exam during a 1-year study period. This was to date the world’s largest systematic population-based skin cancer screening program, he said.
Nineteen percent of the Schleswig-Holstein adult population – more than 360,000 citizens – participated. A total of 3,103 skin cancers were found, including 585 melanomas, for a rate of 1.6 melanomas per 1,000 persons screened. Basal cell carcinomas were detected at a rate of 5.4 malignancies per 1,000, and squamous cell carcinomas at 1.1 per 1,000 people screened. Five lesion excisions had to be performed to detect one malignancy.
Using the incidence of melanoma in Schleswig-Holstein during the 2 years prior to the SCREEN project as a baseline, the incidence of melanoma during the SCREEN project increased by 16% in men and by 38% in women.
The key study finding was a significant decrease in melanoma mortality documented 5 years after SCREEN ended. The observed melanoma mortality rate in men was 0.79 per 100,000 population, compared with an expected 2.0 per 100,000. Among women, the observed mortality was 0.66 per 100,000, compared with an expected 1.3 per 100,000. Thus, the observed mortality because of earlier detection of melanoma in the screened area was less than 50% of expected, Dr. Blum said at the Hawaii Dermatology Seminar sponsored by the Skin Disease Education Foundation (SDEF).
The screening project had a two-tiered structure. Most participants were first screened by a primary care physician or other nondermatologist. In the event of suspicious findings and/or skin cancer risk factors, the participant was referred to a dermatologist who performed the biopsies. All participating physicians first had to attend an 8-hour training course. Of note, 116 of the 118 dermatologists in Schleswig-Holstein participated in SCREEN, as did nearly two-thirds of eligible nondermatologists (J. Am. Acad. Dermatol. 2012;66:201-11).
Following up on the unprecedented success of the SCREEN project, German dermatologists next proposed a randomized controlled trial in order to provide the highest-level evidence that mass skin cancer screening reduces melanoma mortality. However, government health officials found SCREEN persuasive and nixed the idea of a large and costly randomized trial. Instead, Germany has launched a national skin cancer screening program, according to Dr. Blum. All 45 million Germans aged 35 years and older are now eligible to be screened for skin cancer once every 2 years; whether the health care system can cope with the demand remains to be seen.
Another recent project evaluating the benefits of total body skin examination for skin cancer screening also reported favorable results, he noted.
Investigators in a multicenter study screened more than 14,000 patients with a total body skin exam. Participants were consecutive adults presenting with a localized dermatologic problem, such as a skin infection, that wouldn’t ordinarily result in a total body skin exam. The total body skin exams detected 40 patients (0.3%) with melanoma. Five benign lesions were excised for each melanoma detected. Another 2.1% of patients had at least one nonmelanoma skin cancer detected by total body skin exam. On average, 400 patients had to be examined by total body skin exam in order to find 1 melanoma (J. Am. Acad. Dermatol. 2012;66:212-9).
"I see around 150 new patients per week, so that means every third week I see a new melanoma," Dr. Blum said.
Total body skin examination has long been a controversial issue. The U.S. Preventive Services Task Force found insufficient evidence to recommend screening adults for skin cancer (Ann. Intern. Med. 2009;150:188-93). That stance will now need to be revisited in light of these two large projects, said Dr. Blum.
He predicted that the cost involved in routine total body skin examinations is likely to be a critical source of controversy. Using the National Cancer Institute’s estimate that 12.5% of melanomas are fatal, and assuming the cost of a total body skin exam to be $50, he estimated that routine total body skin exams in the SCREEN project cost $240,000 per melanoma death avoided.
In his own specialized skin cancer clinic, where he sees a more select patient population, Dr. Blum estimated that routine total body skin examination costs about $65,000 per melanoma death avoided. And when he plugged in the numbers provided by his colleague Dr. Ashfaq A. Marghoob, pertaining to the skin cancer clinic at Memorial Sloan-Kettering Cancer Center in New York, Dr. Blum once again came up with a figure of roughly $65,000 per melanoma death avoided.
"The range is quite high. I think the cost debate will continue," Dr. Blum predicted.
He reported having no financial conflicts.
SDEF and this news organization are owned by Elsevier.
WAIKOLOA, HAWAII – An organized program of population-based total body skin examination screening for skin cancer has been shown to significantly reduce melanoma mortality.
"This is quite astounding. It is very impressive to see that a total body skin exam can reduce mortality. It forces us all to think about whether we should do this in a very, very large population, as we now do in Germany," said Dr. Andreas Blum, professor of dermatology at the University of Tübingen (Germany).
He presented highlights of the SCREEN (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany) project, in which all residents of the state of Schleswig-Holstein were eligible for a standardized total body skin exam during a 1-year study period. This was to date the world’s largest systematic population-based skin cancer screening program, he said.
Nineteen percent of the Schleswig-Holstein adult population – more than 360,000 citizens – participated. A total of 3,103 skin cancers were found, including 585 melanomas, for a rate of 1.6 melanomas per 1,000 persons screened. Basal cell carcinomas were detected at a rate of 5.4 malignancies per 1,000, and squamous cell carcinomas at 1.1 per 1,000 people screened. Five lesion excisions had to be performed to detect one malignancy.
Using the incidence of melanoma in Schleswig-Holstein during the 2 years prior to the SCREEN project as a baseline, the incidence of melanoma during the SCREEN project increased by 16% in men and by 38% in women.
The key study finding was a significant decrease in melanoma mortality documented 5 years after SCREEN ended. The observed melanoma mortality rate in men was 0.79 per 100,000 population, compared with an expected 2.0 per 100,000. Among women, the observed mortality was 0.66 per 100,000, compared with an expected 1.3 per 100,000. Thus, the observed mortality because of earlier detection of melanoma in the screened area was less than 50% of expected, Dr. Blum said at the Hawaii Dermatology Seminar sponsored by the Skin Disease Education Foundation (SDEF).
The screening project had a two-tiered structure. Most participants were first screened by a primary care physician or other nondermatologist. In the event of suspicious findings and/or skin cancer risk factors, the participant was referred to a dermatologist who performed the biopsies. All participating physicians first had to attend an 8-hour training course. Of note, 116 of the 118 dermatologists in Schleswig-Holstein participated in SCREEN, as did nearly two-thirds of eligible nondermatologists (J. Am. Acad. Dermatol. 2012;66:201-11).
Following up on the unprecedented success of the SCREEN project, German dermatologists next proposed a randomized controlled trial in order to provide the highest-level evidence that mass skin cancer screening reduces melanoma mortality. However, government health officials found SCREEN persuasive and nixed the idea of a large and costly randomized trial. Instead, Germany has launched a national skin cancer screening program, according to Dr. Blum. All 45 million Germans aged 35 years and older are now eligible to be screened for skin cancer once every 2 years; whether the health care system can cope with the demand remains to be seen.
Another recent project evaluating the benefits of total body skin examination for skin cancer screening also reported favorable results, he noted.
Investigators in a multicenter study screened more than 14,000 patients with a total body skin exam. Participants were consecutive adults presenting with a localized dermatologic problem, such as a skin infection, that wouldn’t ordinarily result in a total body skin exam. The total body skin exams detected 40 patients (0.3%) with melanoma. Five benign lesions were excised for each melanoma detected. Another 2.1% of patients had at least one nonmelanoma skin cancer detected by total body skin exam. On average, 400 patients had to be examined by total body skin exam in order to find 1 melanoma (J. Am. Acad. Dermatol. 2012;66:212-9).
"I see around 150 new patients per week, so that means every third week I see a new melanoma," Dr. Blum said.
Total body skin examination has long been a controversial issue. The U.S. Preventive Services Task Force found insufficient evidence to recommend screening adults for skin cancer (Ann. Intern. Med. 2009;150:188-93). That stance will now need to be revisited in light of these two large projects, said Dr. Blum.
He predicted that the cost involved in routine total body skin examinations is likely to be a critical source of controversy. Using the National Cancer Institute’s estimate that 12.5% of melanomas are fatal, and assuming the cost of a total body skin exam to be $50, he estimated that routine total body skin exams in the SCREEN project cost $240,000 per melanoma death avoided.
In his own specialized skin cancer clinic, where he sees a more select patient population, Dr. Blum estimated that routine total body skin examination costs about $65,000 per melanoma death avoided. And when he plugged in the numbers provided by his colleague Dr. Ashfaq A. Marghoob, pertaining to the skin cancer clinic at Memorial Sloan-Kettering Cancer Center in New York, Dr. Blum once again came up with a figure of roughly $65,000 per melanoma death avoided.
"The range is quite high. I think the cost debate will continue," Dr. Blum predicted.
He reported having no financial conflicts.
SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM THE HAWAII DERMATOLOGY SEMINAR
Zotarolimus Stent: Short-Term Dual Antiplatelet Therapy Is Safe
CHICAGO – A 3-month regimen of dual antiplatelet therapy may be a safe and effective alternative to the standard 12 months in selected recipients of the zotarolimus-eluting Endeavor stent.
This was the main finding of the 2,117-patient randomized, prospective RESET (Real Safety and Efficacy of 3-Month Dual Antiplatelet Therapy Following Zotarolimus-Eluting Stent Implantation) trial.

RESET was an open-label, randomized trial conducted at 26 South Korean centers. It was designed as a noninferiority study, meaning it was set up to evaluate the hypothesis that 3 months of dual antiplatelet therapy (DAPT) with clopidogrel and aspirin following implantation of the Endeavor drug-eluting stent doesn’t yield worse clinical outcomes than does the standard 12 months of DAPT.
Dr. Myeong-Ki Hong volunteered that an important study limitation in RESET was the exclusion of high-risk patients from participation. Among those ineligible were patients with a history of peripheral artery disease or cerebrovascular accident, those in cardiogenic shock or with a left ventricular ejection fraction less than 40%, and patients with severe renal or hepatic renal dysfunction. The lessons of RESET may not be applicable to such individuals.
Participants in RESET underwent percutaneous coronary intervention and implantation of a drug-eluting stent for unstable angina, acute MI, or stable angina. Half of RESET participants were randomized to receive the Endeavor stent with 3 months of DAPT before discontinuing clopidogrel and carrying on with aspirin monotherapy; the other half received various other drug-eluting stents accompanied by the standard, guideline-recommended 12 months of DAPT.
The primary study end point was the 12-month composite of cardiovascular death, acute MI, stent thrombosis, ischemia-driven target vessel revascularization, and TIMI (thrombolysis in myocardial infarction) major or minor bleeding. The combined end point occurred in exactly 4.7% of subjects in each study arm, Dr. Hong reported at the annual meeting of the American College of Cardiology.
The secondary end point (comprising all-cause mortality, stent thrombosis, or MI at 12 months of follow-up) occurred in 0.8% of patients assigned to 3 months of DAPT and 1.3% of controls, a nonsignificant difference, noted Dr. Hong, professor of medicine at Yonsei University, Seoul.
A key aim of DAPT, he pointed out, is the prevention of stent thrombosis. Two cases occurred in Endeavor stent recipients, both during their 3 months on DAPT; notably, no cases occurred in this group after discontinuation of clopidogrel. In contrast, three cases of stent thrombosis occurred in the control group on 12 months of DAPT, all during months 3-12.
Downsides of prolonged DAPT include increased risk of bleeding, financial cost, and poor patient adherence. Dr. Hong cited the following situations in which (based upon RESET) the placement of a zotarolimus-eluting stent and 3 months of DAPT might be useful:
• Patients at increased risk for bleeding complications.
• Patients with a high likelihood of noncardiac surgery or other invasive procedures in the coming year.
• Patients at low anatomical risk of stent thrombosis.
• Patients who are likely to be nonadherent to the prolonged DAPT regimen.
An impetus for the RESET trial was an earlier Korean registry that reported favorable long-term outcomes in 661 patients whose clopidogrel was discontinued 3 months after implantation of a zotarolimus-eluting stent (Circ. J. 2010;74:2314-21).
Audience member Dr. Antonio Colombo of Milan, who was honored as a "Legend of Cardiology" at the conference, rose to note that most studies from Korea and Japan report stent thrombosis rates that are half those seen in Europe and North America.
"I believe it’s not easy to translate these RESET conclusions to other populations. I think some genetic or other factors may play a role in these low thrombosis rates," he observed.
The study was sponsored by the South Korean Ministry of Health and Welfare, the Cardiovascular Research Center of Seoul, and Medtronic. Dr. Hong reported having no financial conflicts. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
One of take-away lesson from this study is that in an anatomically low-risk population such as this, with a reference vessel diameter of 3.0 mm and an average of 1.3 treated lesions per patient, we’re getting very good with our drug-eluting stents. The expected 1-year event rate of about 10% was more than double what was actually observed.
Dr. Matthew J. Price |

These low event rates in both study arms underscore how difficult it’s going to be to ever definitively prove that short-duration DAPT is safe. RESET was a noninferiority study, and even with more than 2,100 randomized patients, the statistical noninferiority margins were broad enough that it’s theoretically possible for a safety signal to have gone undetected.
Matthew J. Price, M.D., is director of the cardiac catheterization laboratory at the Scripps Clinic in La Jolla, Calif. He was the study discussant at the meeting. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
One of take-away lesson from this study is that in an anatomically low-risk population such as this, with a reference vessel diameter of 3.0 mm and an average of 1.3 treated lesions per patient, we’re getting very good with our drug-eluting stents. The expected 1-year event rate of about 10% was more than double what was actually observed.
Dr. Matthew J. Price |
These low event rates in both study arms underscore how difficult it’s going to be to ever definitively prove that short-duration DAPT is safe. RESET was a noninferiority study, and even with more than 2,100 randomized patients, the statistical noninferiority margins were broad enough that it’s theoretically possible for a safety signal to have gone undetected.
Matthew J. Price, M.D., is director of the cardiac catheterization laboratory at the Scripps Clinic in La Jolla, Calif. He was the study discussant at the meeting. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
One of take-away lesson from this study is that in an anatomically low-risk population such as this, with a reference vessel diameter of 3.0 mm and an average of 1.3 treated lesions per patient, we’re getting very good with our drug-eluting stents. The expected 1-year event rate of about 10% was more than double what was actually observed.
Dr. Matthew J. Price |
These low event rates in both study arms underscore how difficult it’s going to be to ever definitively prove that short-duration DAPT is safe. RESET was a noninferiority study, and even with more than 2,100 randomized patients, the statistical noninferiority margins were broad enough that it’s theoretically possible for a safety signal to have gone undetected.
Matthew J. Price, M.D., is director of the cardiac catheterization laboratory at the Scripps Clinic in La Jolla, Calif. He was the study discussant at the meeting. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
CHICAGO – A 3-month regimen of dual antiplatelet therapy may be a safe and effective alternative to the standard 12 months in selected recipients of the zotarolimus-eluting Endeavor stent.
This was the main finding of the 2,117-patient randomized, prospective RESET (Real Safety and Efficacy of 3-Month Dual Antiplatelet Therapy Following Zotarolimus-Eluting Stent Implantation) trial.
RESET was an open-label, randomized trial conducted at 26 South Korean centers. It was designed as a noninferiority study, meaning it was set up to evaluate the hypothesis that 3 months of dual antiplatelet therapy (DAPT) with clopidogrel and aspirin following implantation of the Endeavor drug-eluting stent doesn’t yield worse clinical outcomes than does the standard 12 months of DAPT.
Dr. Myeong-Ki Hong volunteered that an important study limitation in RESET was the exclusion of high-risk patients from participation. Among those ineligible were patients with a history of peripheral artery disease or cerebrovascular accident, those in cardiogenic shock or with a left ventricular ejection fraction less than 40%, and patients with severe renal or hepatic renal dysfunction. The lessons of RESET may not be applicable to such individuals.
Participants in RESET underwent percutaneous coronary intervention and implantation of a drug-eluting stent for unstable angina, acute MI, or stable angina. Half of RESET participants were randomized to receive the Endeavor stent with 3 months of DAPT before discontinuing clopidogrel and carrying on with aspirin monotherapy; the other half received various other drug-eluting stents accompanied by the standard, guideline-recommended 12 months of DAPT.
The primary study end point was the 12-month composite of cardiovascular death, acute MI, stent thrombosis, ischemia-driven target vessel revascularization, and TIMI (thrombolysis in myocardial infarction) major or minor bleeding. The combined end point occurred in exactly 4.7% of subjects in each study arm, Dr. Hong reported at the annual meeting of the American College of Cardiology.
The secondary end point (comprising all-cause mortality, stent thrombosis, or MI at 12 months of follow-up) occurred in 0.8% of patients assigned to 3 months of DAPT and 1.3% of controls, a nonsignificant difference, noted Dr. Hong, professor of medicine at Yonsei University, Seoul.
A key aim of DAPT, he pointed out, is the prevention of stent thrombosis. Two cases occurred in Endeavor stent recipients, both during their 3 months on DAPT; notably, no cases occurred in this group after discontinuation of clopidogrel. In contrast, three cases of stent thrombosis occurred in the control group on 12 months of DAPT, all during months 3-12.
Downsides of prolonged DAPT include increased risk of bleeding, financial cost, and poor patient adherence. Dr. Hong cited the following situations in which (based upon RESET) the placement of a zotarolimus-eluting stent and 3 months of DAPT might be useful:
• Patients at increased risk for bleeding complications.
• Patients with a high likelihood of noncardiac surgery or other invasive procedures in the coming year.
• Patients at low anatomical risk of stent thrombosis.
• Patients who are likely to be nonadherent to the prolonged DAPT regimen.
An impetus for the RESET trial was an earlier Korean registry that reported favorable long-term outcomes in 661 patients whose clopidogrel was discontinued 3 months after implantation of a zotarolimus-eluting stent (Circ. J. 2010;74:2314-21).
Audience member Dr. Antonio Colombo of Milan, who was honored as a "Legend of Cardiology" at the conference, rose to note that most studies from Korea and Japan report stent thrombosis rates that are half those seen in Europe and North America.
"I believe it’s not easy to translate these RESET conclusions to other populations. I think some genetic or other factors may play a role in these low thrombosis rates," he observed.
The study was sponsored by the South Korean Ministry of Health and Welfare, the Cardiovascular Research Center of Seoul, and Medtronic. Dr. Hong reported having no financial conflicts. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
CHICAGO – A 3-month regimen of dual antiplatelet therapy may be a safe and effective alternative to the standard 12 months in selected recipients of the zotarolimus-eluting Endeavor stent.
This was the main finding of the 2,117-patient randomized, prospective RESET (Real Safety and Efficacy of 3-Month Dual Antiplatelet Therapy Following Zotarolimus-Eluting Stent Implantation) trial.
RESET was an open-label, randomized trial conducted at 26 South Korean centers. It was designed as a noninferiority study, meaning it was set up to evaluate the hypothesis that 3 months of dual antiplatelet therapy (DAPT) with clopidogrel and aspirin following implantation of the Endeavor drug-eluting stent doesn’t yield worse clinical outcomes than does the standard 12 months of DAPT.
Dr. Myeong-Ki Hong volunteered that an important study limitation in RESET was the exclusion of high-risk patients from participation. Among those ineligible were patients with a history of peripheral artery disease or cerebrovascular accident, those in cardiogenic shock or with a left ventricular ejection fraction less than 40%, and patients with severe renal or hepatic renal dysfunction. The lessons of RESET may not be applicable to such individuals.
Participants in RESET underwent percutaneous coronary intervention and implantation of a drug-eluting stent for unstable angina, acute MI, or stable angina. Half of RESET participants were randomized to receive the Endeavor stent with 3 months of DAPT before discontinuing clopidogrel and carrying on with aspirin monotherapy; the other half received various other drug-eluting stents accompanied by the standard, guideline-recommended 12 months of DAPT.
The primary study end point was the 12-month composite of cardiovascular death, acute MI, stent thrombosis, ischemia-driven target vessel revascularization, and TIMI (thrombolysis in myocardial infarction) major or minor bleeding. The combined end point occurred in exactly 4.7% of subjects in each study arm, Dr. Hong reported at the annual meeting of the American College of Cardiology.
The secondary end point (comprising all-cause mortality, stent thrombosis, or MI at 12 months of follow-up) occurred in 0.8% of patients assigned to 3 months of DAPT and 1.3% of controls, a nonsignificant difference, noted Dr. Hong, professor of medicine at Yonsei University, Seoul.
A key aim of DAPT, he pointed out, is the prevention of stent thrombosis. Two cases occurred in Endeavor stent recipients, both during their 3 months on DAPT; notably, no cases occurred in this group after discontinuation of clopidogrel. In contrast, three cases of stent thrombosis occurred in the control group on 12 months of DAPT, all during months 3-12.
Downsides of prolonged DAPT include increased risk of bleeding, financial cost, and poor patient adherence. Dr. Hong cited the following situations in which (based upon RESET) the placement of a zotarolimus-eluting stent and 3 months of DAPT might be useful:
• Patients at increased risk for bleeding complications.
• Patients with a high likelihood of noncardiac surgery or other invasive procedures in the coming year.
• Patients at low anatomical risk of stent thrombosis.
• Patients who are likely to be nonadherent to the prolonged DAPT regimen.
An impetus for the RESET trial was an earlier Korean registry that reported favorable long-term outcomes in 661 patients whose clopidogrel was discontinued 3 months after implantation of a zotarolimus-eluting stent (Circ. J. 2010;74:2314-21).
Audience member Dr. Antonio Colombo of Milan, who was honored as a "Legend of Cardiology" at the conference, rose to note that most studies from Korea and Japan report stent thrombosis rates that are half those seen in Europe and North America.
"I believe it’s not easy to translate these RESET conclusions to other populations. I think some genetic or other factors may play a role in these low thrombosis rates," he observed.
The study was sponsored by the South Korean Ministry of Health and Welfare, the Cardiovascular Research Center of Seoul, and Medtronic. Dr. Hong reported having no financial conflicts. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Patients assigned to 3 months of dual antiplatelet therapy following implantation of a zotarolimus-eluting stent had a 1-year combined adverse event rate of 4.7%, identical to that in recipients of other drug-eluting stents plus the standard 12 months of dual antiplatelet therapy.
Data Source: An open-label, randomized trial including 2,117 patients who received a zotarolimus-eluting Endeavor stent and 3 months of dual antiplatelet therapy, or a different drug-eluting stent and the standard 12 months of dual antiplatelet therapy.
Disclosures: The study was sponsored by the South Korean Ministry of Health and Welfare, the Cardiovascular Research Center of Seoul, and Medtronic.
Acupuncture Improves Heart Rate Variability in CHD
CHICAGO – Traditional acupuncture improves heart rate variability, and it may prove to reduce the risk of sudden death for patients with established coronary heart disease, a pilot study suggests.
The blinded study with a sham-acupuncture control arm demonstrated that acupuncture accomplishes autonomic remodeling via sympathovagal modulation as reflected in increased heart rate variability (HRV), according to Dr. Puja K. Mehta of the Women's Heart Center at Cedars-Sinai Medical Center, Los Angeles. The clinically meaningful improvements in heart rate variability in this pilot study lay the groundwork for a future large outcome-based clinical trial of traditional acupuncture in patients with known CHD.
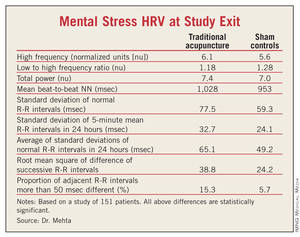
Diminished HRV in patients with CHD is accepted as a predictor of sudden cardiac death risk in clinical trials, Dr. Mehta noted at the annual meeting of the American College of Cardiology.
Sudden cardiac death accounts for roughly 150,000 deaths annually in Americans with established CHD. Traditional cardiovascular risk factors don’t fully account for the sudden cardiac death risk.
She reported on 151 patients with established CHD who were randomized to traditional acupuncture, sham acupuncture, or a wait-list control arm. The acupuncture, performed with stainless steel needles, was done three times per week for 12 weeks. Eight active CHD-specific traditional acupuncture sites were targeted. The sham-treatment group received a previously validated sham procedure at nonacupuncture sites. Patients were blinded as to whether they got real or sham acupuncture.
Heart rate variability was measured at baseline and after 12 weeks using 24-hour time and frequency domain measures and during a 5-minute mental arithmetic stress test and a 5-minute forehead cold pressor test.
Compared with the sham-treated controls, the traditional acupuncture recipients had 17% more high frequency HRV as determined by efferent vagal activity and 31% more heart rate variability on mental arithmetic stress testing at study’s end.
Dr. Mehta said that these results may actually underestimate the true clinical effect size of traditional acupuncture because sham acupuncture has previously been shown to have some mild therapeutic benefit compared with conventional placebos.
At study’s end, there were no differences between the acupuncture and sham control groups in blood pressure, serum lipids, insulin resistance, C-reactive protein, salivary cortisol, paroxysmal atrial tachyarrhythmia, or psychosocial variables, she noted.
The pilot study was supported by grants from the National Institutes of Health-National Center for Complementary and Alternative Medicine, the Barbara Streisand Women’s Cardiovascular Research and Education Program at Cedars-Sinai Medical Center, and foundation grants. Dr. Mehta reported having no financial conflicts.
CHICAGO – Traditional acupuncture improves heart rate variability, and it may prove to reduce the risk of sudden death for patients with established coronary heart disease, a pilot study suggests.
The blinded study with a sham-acupuncture control arm demonstrated that acupuncture accomplishes autonomic remodeling via sympathovagal modulation as reflected in increased heart rate variability (HRV), according to Dr. Puja K. Mehta of the Women's Heart Center at Cedars-Sinai Medical Center, Los Angeles. The clinically meaningful improvements in heart rate variability in this pilot study lay the groundwork for a future large outcome-based clinical trial of traditional acupuncture in patients with known CHD.
Diminished HRV in patients with CHD is accepted as a predictor of sudden cardiac death risk in clinical trials, Dr. Mehta noted at the annual meeting of the American College of Cardiology.
Sudden cardiac death accounts for roughly 150,000 deaths annually in Americans with established CHD. Traditional cardiovascular risk factors don’t fully account for the sudden cardiac death risk.
She reported on 151 patients with established CHD who were randomized to traditional acupuncture, sham acupuncture, or a wait-list control arm. The acupuncture, performed with stainless steel needles, was done three times per week for 12 weeks. Eight active CHD-specific traditional acupuncture sites were targeted. The sham-treatment group received a previously validated sham procedure at nonacupuncture sites. Patients were blinded as to whether they got real or sham acupuncture.
Heart rate variability was measured at baseline and after 12 weeks using 24-hour time and frequency domain measures and during a 5-minute mental arithmetic stress test and a 5-minute forehead cold pressor test.
Compared with the sham-treated controls, the traditional acupuncture recipients had 17% more high frequency HRV as determined by efferent vagal activity and 31% more heart rate variability on mental arithmetic stress testing at study’s end.
Dr. Mehta said that these results may actually underestimate the true clinical effect size of traditional acupuncture because sham acupuncture has previously been shown to have some mild therapeutic benefit compared with conventional placebos.
At study’s end, there were no differences between the acupuncture and sham control groups in blood pressure, serum lipids, insulin resistance, C-reactive protein, salivary cortisol, paroxysmal atrial tachyarrhythmia, or psychosocial variables, she noted.
The pilot study was supported by grants from the National Institutes of Health-National Center for Complementary and Alternative Medicine, the Barbara Streisand Women’s Cardiovascular Research and Education Program at Cedars-Sinai Medical Center, and foundation grants. Dr. Mehta reported having no financial conflicts.
CHICAGO – Traditional acupuncture improves heart rate variability, and it may prove to reduce the risk of sudden death for patients with established coronary heart disease, a pilot study suggests.
The blinded study with a sham-acupuncture control arm demonstrated that acupuncture accomplishes autonomic remodeling via sympathovagal modulation as reflected in increased heart rate variability (HRV), according to Dr. Puja K. Mehta of the Women's Heart Center at Cedars-Sinai Medical Center, Los Angeles. The clinically meaningful improvements in heart rate variability in this pilot study lay the groundwork for a future large outcome-based clinical trial of traditional acupuncture in patients with known CHD.
Diminished HRV in patients with CHD is accepted as a predictor of sudden cardiac death risk in clinical trials, Dr. Mehta noted at the annual meeting of the American College of Cardiology.
Sudden cardiac death accounts for roughly 150,000 deaths annually in Americans with established CHD. Traditional cardiovascular risk factors don’t fully account for the sudden cardiac death risk.
She reported on 151 patients with established CHD who were randomized to traditional acupuncture, sham acupuncture, or a wait-list control arm. The acupuncture, performed with stainless steel needles, was done three times per week for 12 weeks. Eight active CHD-specific traditional acupuncture sites were targeted. The sham-treatment group received a previously validated sham procedure at nonacupuncture sites. Patients were blinded as to whether they got real or sham acupuncture.
Heart rate variability was measured at baseline and after 12 weeks using 24-hour time and frequency domain measures and during a 5-minute mental arithmetic stress test and a 5-minute forehead cold pressor test.
Compared with the sham-treated controls, the traditional acupuncture recipients had 17% more high frequency HRV as determined by efferent vagal activity and 31% more heart rate variability on mental arithmetic stress testing at study’s end.
Dr. Mehta said that these results may actually underestimate the true clinical effect size of traditional acupuncture because sham acupuncture has previously been shown to have some mild therapeutic benefit compared with conventional placebos.
At study’s end, there were no differences between the acupuncture and sham control groups in blood pressure, serum lipids, insulin resistance, C-reactive protein, salivary cortisol, paroxysmal atrial tachyarrhythmia, or psychosocial variables, she noted.
The pilot study was supported by grants from the National Institutes of Health-National Center for Complementary and Alternative Medicine, the Barbara Streisand Women’s Cardiovascular Research and Education Program at Cedars-Sinai Medical Center, and foundation grants. Dr. Mehta reported having no financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Compared with sham-treated controls, traditional acupuncture recipients had 17% more high frequency heart rate variability as determined by efferent vagal activity and 31% more heart rate variability on mental arithmetic stress testing at study’s end.
Data Source: The study included 151 patients with established CHD who were randomized to traditional acupuncture, sham acupuncture, or a wait-list control arm.
Disclosures: The pilot study was supported by grants from the National Institutes of Health-National Center for Complementary and Alternative Medicine, the Barbara Streisand Women’s Cardiovascular Research and Education Program at Cedars-Sinai Medical Center, and foundation grants. Dr. Mehta reported having no financial conflicts.
Ob.Gyn. Offices Ideal for Heart Risk Screening
CHICAGO – Cardiologists and ob.gyns. teamed up for a pilot project of the Women’s Cardiovascular Health Initiative aimed at improving primary cardiovascular prevention in middle-aged women.
An ob.gyn. is often the primary care physician for many middle-aged women, Dr. Jennifer Yu explained at the conference. The goal was to upgrade cardiovascular screening and education in ob.gyn. practices, without distracting ob.gyns. from their focus on reproductive health, and to direct at-risk women to specialized care as needed.
The project, sponsored by the nonprofit Cardiovascular Research Foundation, was implemented at 10 community-based ob.gyn. clinics around the country. Patients completed a one-page questionnaire addressing traditional and gestational cardiovascular risk factors and any current symptoms.
During a recent 2-year period, 2,234 middle-age women visiting these 10 clinics for routine ob.gyn. care completed the one-page survey and had their blood pressure measured. The payoff was substantial: 87% of the women turned out to have cardiovascular risk factors, and 42% had cardiovascular symptoms. In many cases, the women were unaware of their risk factors or the potential significance of their cardiovascular symptoms, according to Dr. Yu of Mount Sinai Medical Center, New York.
The project addresses the misconception that coronary artery disease is mainly a man’s disease, she said. Heart disease also is the No.1 cause of death in women, and cardiovascular mortality among women in the 35- to 44-year-old age group is rising by 1% annually.
The mean age of participants was 53 years; 56% were postmenopausal, and 27% of the postmenopausal women were on hormone replacement therapy.
The most prevalent cardiovascular symptoms included claudication in 10%, palpitations in 14%, exertional chest pain in 8%, resting chest pain in 10%, and shortness of breath in 35%.
Most of the women reported being sedentary; 14% had high blood pressure, 21% were hypercholesterolemic, and 7.5% had diabetes.
A history of gestational diabetes was reported by 8.8%, a history of gestational hypertension by 10%, and preeclampsia by 7.6%.
About 76% of the women had another primary care provider besides their ob.gyn. Those women were more likely to be aware that they had cardiovascular risk factors than were the 6% who indicated they had no primary care provider and the 18% who said their ob.gyn. is their primary care provider.
Among women with elevated blood pressure, 13% with a non–ob.gyn. primary care physician were unaware that they had high blood pressure, compared with 22% of hypertensive women with an ob.gyn. as their primary care physician and 27% of those with no primary care provider.
Similarly, 31% of women with a non–ob.gyn. primary care provider were unaware they were hypercholesterolemic, as were 38% of those whose ob.gyn. was their primary care physician and 51% of women with no primary care provider.
Of diabetic women with a non–ob.gyn. primary care provider, 18% didn’t know they had diabetes or were unaware of the associated cardiovascular risk. This was the case for 19% of diabetic women with an ob.gyn. primary care provider and 26% of women without a primary care provider.
One-quarter of the screened women were subsequently referred to another health care provider, typically a cardiologist, endocrinologist, or primary care physician.
The questionnaire was developed in consultation with leaders from the American College of Cardiology, the American Congress of Obstetricians and Gynecologists, and the Society of Cardiovascular Angiography and Interventions – Women in Innovations. The pilot screening was funded by Abbott Vascular. Dr. Yu reported having no financial conflicts.
CHICAGO – Cardiologists and ob.gyns. teamed up for a pilot project of the Women’s Cardiovascular Health Initiative aimed at improving primary cardiovascular prevention in middle-aged women.
An ob.gyn. is often the primary care physician for many middle-aged women, Dr. Jennifer Yu explained at the conference. The goal was to upgrade cardiovascular screening and education in ob.gyn. practices, without distracting ob.gyns. from their focus on reproductive health, and to direct at-risk women to specialized care as needed.
The project, sponsored by the nonprofit Cardiovascular Research Foundation, was implemented at 10 community-based ob.gyn. clinics around the country. Patients completed a one-page questionnaire addressing traditional and gestational cardiovascular risk factors and any current symptoms.
During a recent 2-year period, 2,234 middle-age women visiting these 10 clinics for routine ob.gyn. care completed the one-page survey and had their blood pressure measured. The payoff was substantial: 87% of the women turned out to have cardiovascular risk factors, and 42% had cardiovascular symptoms. In many cases, the women were unaware of their risk factors or the potential significance of their cardiovascular symptoms, according to Dr. Yu of Mount Sinai Medical Center, New York.
The project addresses the misconception that coronary artery disease is mainly a man’s disease, she said. Heart disease also is the No.1 cause of death in women, and cardiovascular mortality among women in the 35- to 44-year-old age group is rising by 1% annually.
The mean age of participants was 53 years; 56% were postmenopausal, and 27% of the postmenopausal women were on hormone replacement therapy.
The most prevalent cardiovascular symptoms included claudication in 10%, palpitations in 14%, exertional chest pain in 8%, resting chest pain in 10%, and shortness of breath in 35%.
Most of the women reported being sedentary; 14% had high blood pressure, 21% were hypercholesterolemic, and 7.5% had diabetes.
A history of gestational diabetes was reported by 8.8%, a history of gestational hypertension by 10%, and preeclampsia by 7.6%.
About 76% of the women had another primary care provider besides their ob.gyn. Those women were more likely to be aware that they had cardiovascular risk factors than were the 6% who indicated they had no primary care provider and the 18% who said their ob.gyn. is their primary care provider.
Among women with elevated blood pressure, 13% with a non–ob.gyn. primary care physician were unaware that they had high blood pressure, compared with 22% of hypertensive women with an ob.gyn. as their primary care physician and 27% of those with no primary care provider.
Similarly, 31% of women with a non–ob.gyn. primary care provider were unaware they were hypercholesterolemic, as were 38% of those whose ob.gyn. was their primary care physician and 51% of women with no primary care provider.
Of diabetic women with a non–ob.gyn. primary care provider, 18% didn’t know they had diabetes or were unaware of the associated cardiovascular risk. This was the case for 19% of diabetic women with an ob.gyn. primary care provider and 26% of women without a primary care provider.
One-quarter of the screened women were subsequently referred to another health care provider, typically a cardiologist, endocrinologist, or primary care physician.
The questionnaire was developed in consultation with leaders from the American College of Cardiology, the American Congress of Obstetricians and Gynecologists, and the Society of Cardiovascular Angiography and Interventions – Women in Innovations. The pilot screening was funded by Abbott Vascular. Dr. Yu reported having no financial conflicts.
CHICAGO – Cardiologists and ob.gyns. teamed up for a pilot project of the Women’s Cardiovascular Health Initiative aimed at improving primary cardiovascular prevention in middle-aged women.
An ob.gyn. is often the primary care physician for many middle-aged women, Dr. Jennifer Yu explained at the conference. The goal was to upgrade cardiovascular screening and education in ob.gyn. practices, without distracting ob.gyns. from their focus on reproductive health, and to direct at-risk women to specialized care as needed.
The project, sponsored by the nonprofit Cardiovascular Research Foundation, was implemented at 10 community-based ob.gyn. clinics around the country. Patients completed a one-page questionnaire addressing traditional and gestational cardiovascular risk factors and any current symptoms.
During a recent 2-year period, 2,234 middle-age women visiting these 10 clinics for routine ob.gyn. care completed the one-page survey and had their blood pressure measured. The payoff was substantial: 87% of the women turned out to have cardiovascular risk factors, and 42% had cardiovascular symptoms. In many cases, the women were unaware of their risk factors or the potential significance of their cardiovascular symptoms, according to Dr. Yu of Mount Sinai Medical Center, New York.
The project addresses the misconception that coronary artery disease is mainly a man’s disease, she said. Heart disease also is the No.1 cause of death in women, and cardiovascular mortality among women in the 35- to 44-year-old age group is rising by 1% annually.
The mean age of participants was 53 years; 56% were postmenopausal, and 27% of the postmenopausal women were on hormone replacement therapy.
The most prevalent cardiovascular symptoms included claudication in 10%, palpitations in 14%, exertional chest pain in 8%, resting chest pain in 10%, and shortness of breath in 35%.
Most of the women reported being sedentary; 14% had high blood pressure, 21% were hypercholesterolemic, and 7.5% had diabetes.
A history of gestational diabetes was reported by 8.8%, a history of gestational hypertension by 10%, and preeclampsia by 7.6%.
About 76% of the women had another primary care provider besides their ob.gyn. Those women were more likely to be aware that they had cardiovascular risk factors than were the 6% who indicated they had no primary care provider and the 18% who said their ob.gyn. is their primary care provider.
Among women with elevated blood pressure, 13% with a non–ob.gyn. primary care physician were unaware that they had high blood pressure, compared with 22% of hypertensive women with an ob.gyn. as their primary care physician and 27% of those with no primary care provider.
Similarly, 31% of women with a non–ob.gyn. primary care provider were unaware they were hypercholesterolemic, as were 38% of those whose ob.gyn. was their primary care physician and 51% of women with no primary care provider.
Of diabetic women with a non–ob.gyn. primary care provider, 18% didn’t know they had diabetes or were unaware of the associated cardiovascular risk. This was the case for 19% of diabetic women with an ob.gyn. primary care provider and 26% of women without a primary care provider.
One-quarter of the screened women were subsequently referred to another health care provider, typically a cardiologist, endocrinologist, or primary care physician.
The questionnaire was developed in consultation with leaders from the American College of Cardiology, the American Congress of Obstetricians and Gynecologists, and the Society of Cardiovascular Angiography and Interventions – Women in Innovations. The pilot screening was funded by Abbott Vascular. Dr. Yu reported having no financial conflicts.
FROM THE ANNUAL SCIENTIFIC SESSION OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Of those screened, 87% of the women turned out to have cardiovascular risk factors and 42% had cardiovascular symptoms.
Data Source: During a 2-year period, 2,234 middle-age women were screened at 10 ob.gyn. practices and completed a one-page survey and blood pressure screening.
Disclosures: The questionnaire was developed in consultation with leaders from the American College of Cardiology, the American Congress of Obstetricians and Gynecologists, and the Society of Cardiovascular Angiography and Interventions – Women in Innovations. The pilot screening was funded by Abbott Vascular. Dr. Yu reported having no financial conflicts
Promising New Cellulite Therapies Target Fibrous Septae
WAIKOLOA, HAWAII – Cellulite therapy may finally be moving out of the dark ages of overhyped claims made on behalf of interventions of little or no value to an era of treatments that actually work.
And what appears to work, according to Dr. Michael S. Kaminer, are therapies that cut the fibrous septae tethering the dermis to deeper tissues.
"I think it’s likely that the vertical pull of the fibrous septae tends to pull down on the cellulite in the skin and causes the cellulite dimples," he explained at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).

The fibrous septae theory of the etiology of cellulite is relatively new. It has gained substantial credence as a result of encouraging clinical trial data showing long-term effectiveness for two devices targeting cellulite via severing fibrous septae: the Cellulaze 1,440-nm Nd:YAG laser and the Cabochon Aesthetics controlled subcision system for subdermal undermining, according to Dr. Kaminer, who is a managing partner at SkinCare Physicians, Chestnut Hill, Mass.
Cellulaze, developed by Cynosure, recently received Food and Drug Administration marketing approval for the treatment of cellulite. It is also approved across Europe for this indication. The Cabochon device for subcutaneous release of fibrous septae in patients with cellulite is still in clinical trials.
Dr. Kaminer said Americans spend an estimated $3 billion annually on ineffective treatments for cellulite. These therapies, many of which have been the beneficiaries of claims he termed "outrageous," aim to either reduce or redistribute subcutaneous fat or to thicken the skin surface through methods such as suction massage, which creates skin edema that temporarily camouflages the cellulite dimples. Among the myriad of available therapies are skin wraps, various injectables, and focused ultrasound. But the effect sizes are small and the results, if any, last for a matter of weeks.
"Until very recently, there was absolutely no reason to pay attention to cellulite except to counsel patients as to the fact that they shouldn’t waste their money, unless they feel good about wasting their money," Dr. Kaminer said.
The situation has changed dramatically with the emergence of fibrous septae as the prime therapeutic target. Cellulaze can be used for laser lipolysis; however, in addition, the handpiece for the cannula can be turned in such a way that the laser beam can be used like a saw to cut through the fibrous septae, with resultant long-term improvement in cellulite.
In U.S. clinical trials, the average increase in skin thickness following Cellulaze therapy was 23% at 1 month and 27% at 1 year. Skin elasticity improved over baseline by 32.5% at 1 month and 21% at 1 year. Sixty-eight percent of patients demonstrated significant improvement in cellulite based upon analysis of photographs, as did 65% when assessed by Vectra 3D surface imaging.
Patient self-evaluations rated the results as good to excellent at 1 month in 76% of cases. Physicians judged the results as good to excellent in 69% of cases. These results have held up at 1 year of follow-up, noted Dr. Kaminer, who also is with the dermatology departments of Yale University, New Haven, Conn.; Dartmouth College, Hanover, N.H.; and Brown University, Providence, R.I.
The downside of Cellulaze is that it is an invasive therapy that requires tumescent anesthesia. And given that the history of the field of cellulite therapy is one of hype far in excess of reality, Dr. Kaminer indicated that a healthy skepticism is appropriate.
"For me, I’m going to approach this with caution. I think Cellulaze is a great idea, and I think it gets to what many people believe is the root of cellulite. But I’d like to see it around for a little longer before we all jump on the bandwagon," he said.
The Cabochon system draws a small section of skin affected by cellulite into a handpiece so that a percutaneously inserted cutting tool can be utilized to cut the fibrous septae. Dr. Kaminer was an investigator in a two-site, 56-patient clinical trial with a 6- to 12-month follow-up.
In independent blinded physician review of before and after photos, 78% of patients were judged to have improved at least one full grade in severity at 6 months, such that, for example, those whose cellulite was rated severe at baseline were judged to have moderate or mild cellulite at follow-up.
At baseline, the average cellulite severity score was about 4.5 on a 0-6 scale. At 90 days, the average severity score had dropped to 3, and at 180 days to roughly 2.5. Ninety-four percent of patients were rated by independent physicians as having improved by at least 1 point on the 0-6 scale.
Of the 33 U.S. patients followed for 1 year, 87% felt their appearance was improved and 77% were satisfied with their treatment at all time points.
Seroma formation was an issue early on, until investigators realized the problem resulted from treating adjacent sites at the same depth. Seven of 31 patients treated in that manner had a seroma in excess of 2 cc at 1 month’s follow-up. But once operators began utilizing the device’s automated guidance system to vary the cutting depth at adjacent sites – for example, treating one area at a depth of 6 mm and an adjacent area at 10 mm of depth seromas were no longer a problem. None of 25 patients treated in this fashion had a seroma in excess of 2 cc 1 month post treatment, said Dr. Kaminer.
He reported that he serves as a consultant to Cabochon and has received research funding and equipment from Cynosure.
SDEF and this news organization are owned by Elsevier.
WAIKOLOA, HAWAII – Cellulite therapy may finally be moving out of the dark ages of overhyped claims made on behalf of interventions of little or no value to an era of treatments that actually work.
And what appears to work, according to Dr. Michael S. Kaminer, are therapies that cut the fibrous septae tethering the dermis to deeper tissues.
"I think it’s likely that the vertical pull of the fibrous septae tends to pull down on the cellulite in the skin and causes the cellulite dimples," he explained at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
The fibrous septae theory of the etiology of cellulite is relatively new. It has gained substantial credence as a result of encouraging clinical trial data showing long-term effectiveness for two devices targeting cellulite via severing fibrous septae: the Cellulaze 1,440-nm Nd:YAG laser and the Cabochon Aesthetics controlled subcision system for subdermal undermining, according to Dr. Kaminer, who is a managing partner at SkinCare Physicians, Chestnut Hill, Mass.
Cellulaze, developed by Cynosure, recently received Food and Drug Administration marketing approval for the treatment of cellulite. It is also approved across Europe for this indication. The Cabochon device for subcutaneous release of fibrous septae in patients with cellulite is still in clinical trials.
Dr. Kaminer said Americans spend an estimated $3 billion annually on ineffective treatments for cellulite. These therapies, many of which have been the beneficiaries of claims he termed "outrageous," aim to either reduce or redistribute subcutaneous fat or to thicken the skin surface through methods such as suction massage, which creates skin edema that temporarily camouflages the cellulite dimples. Among the myriad of available therapies are skin wraps, various injectables, and focused ultrasound. But the effect sizes are small and the results, if any, last for a matter of weeks.
"Until very recently, there was absolutely no reason to pay attention to cellulite except to counsel patients as to the fact that they shouldn’t waste their money, unless they feel good about wasting their money," Dr. Kaminer said.
The situation has changed dramatically with the emergence of fibrous septae as the prime therapeutic target. Cellulaze can be used for laser lipolysis; however, in addition, the handpiece for the cannula can be turned in such a way that the laser beam can be used like a saw to cut through the fibrous septae, with resultant long-term improvement in cellulite.
In U.S. clinical trials, the average increase in skin thickness following Cellulaze therapy was 23% at 1 month and 27% at 1 year. Skin elasticity improved over baseline by 32.5% at 1 month and 21% at 1 year. Sixty-eight percent of patients demonstrated significant improvement in cellulite based upon analysis of photographs, as did 65% when assessed by Vectra 3D surface imaging.
Patient self-evaluations rated the results as good to excellent at 1 month in 76% of cases. Physicians judged the results as good to excellent in 69% of cases. These results have held up at 1 year of follow-up, noted Dr. Kaminer, who also is with the dermatology departments of Yale University, New Haven, Conn.; Dartmouth College, Hanover, N.H.; and Brown University, Providence, R.I.
The downside of Cellulaze is that it is an invasive therapy that requires tumescent anesthesia. And given that the history of the field of cellulite therapy is one of hype far in excess of reality, Dr. Kaminer indicated that a healthy skepticism is appropriate.
"For me, I’m going to approach this with caution. I think Cellulaze is a great idea, and I think it gets to what many people believe is the root of cellulite. But I’d like to see it around for a little longer before we all jump on the bandwagon," he said.
The Cabochon system draws a small section of skin affected by cellulite into a handpiece so that a percutaneously inserted cutting tool can be utilized to cut the fibrous septae. Dr. Kaminer was an investigator in a two-site, 56-patient clinical trial with a 6- to 12-month follow-up.
In independent blinded physician review of before and after photos, 78% of patients were judged to have improved at least one full grade in severity at 6 months, such that, for example, those whose cellulite was rated severe at baseline were judged to have moderate or mild cellulite at follow-up.
At baseline, the average cellulite severity score was about 4.5 on a 0-6 scale. At 90 days, the average severity score had dropped to 3, and at 180 days to roughly 2.5. Ninety-four percent of patients were rated by independent physicians as having improved by at least 1 point on the 0-6 scale.
Of the 33 U.S. patients followed for 1 year, 87% felt their appearance was improved and 77% were satisfied with their treatment at all time points.
Seroma formation was an issue early on, until investigators realized the problem resulted from treating adjacent sites at the same depth. Seven of 31 patients treated in that manner had a seroma in excess of 2 cc at 1 month’s follow-up. But once operators began utilizing the device’s automated guidance system to vary the cutting depth at adjacent sites – for example, treating one area at a depth of 6 mm and an adjacent area at 10 mm of depth seromas were no longer a problem. None of 25 patients treated in this fashion had a seroma in excess of 2 cc 1 month post treatment, said Dr. Kaminer.
He reported that he serves as a consultant to Cabochon and has received research funding and equipment from Cynosure.
SDEF and this news organization are owned by Elsevier.
WAIKOLOA, HAWAII – Cellulite therapy may finally be moving out of the dark ages of overhyped claims made on behalf of interventions of little or no value to an era of treatments that actually work.
And what appears to work, according to Dr. Michael S. Kaminer, are therapies that cut the fibrous septae tethering the dermis to deeper tissues.
"I think it’s likely that the vertical pull of the fibrous septae tends to pull down on the cellulite in the skin and causes the cellulite dimples," he explained at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
The fibrous septae theory of the etiology of cellulite is relatively new. It has gained substantial credence as a result of encouraging clinical trial data showing long-term effectiveness for two devices targeting cellulite via severing fibrous septae: the Cellulaze 1,440-nm Nd:YAG laser and the Cabochon Aesthetics controlled subcision system for subdermal undermining, according to Dr. Kaminer, who is a managing partner at SkinCare Physicians, Chestnut Hill, Mass.
Cellulaze, developed by Cynosure, recently received Food and Drug Administration marketing approval for the treatment of cellulite. It is also approved across Europe for this indication. The Cabochon device for subcutaneous release of fibrous septae in patients with cellulite is still in clinical trials.
Dr. Kaminer said Americans spend an estimated $3 billion annually on ineffective treatments for cellulite. These therapies, many of which have been the beneficiaries of claims he termed "outrageous," aim to either reduce or redistribute subcutaneous fat or to thicken the skin surface through methods such as suction massage, which creates skin edema that temporarily camouflages the cellulite dimples. Among the myriad of available therapies are skin wraps, various injectables, and focused ultrasound. But the effect sizes are small and the results, if any, last for a matter of weeks.
"Until very recently, there was absolutely no reason to pay attention to cellulite except to counsel patients as to the fact that they shouldn’t waste their money, unless they feel good about wasting their money," Dr. Kaminer said.
The situation has changed dramatically with the emergence of fibrous septae as the prime therapeutic target. Cellulaze can be used for laser lipolysis; however, in addition, the handpiece for the cannula can be turned in such a way that the laser beam can be used like a saw to cut through the fibrous septae, with resultant long-term improvement in cellulite.
In U.S. clinical trials, the average increase in skin thickness following Cellulaze therapy was 23% at 1 month and 27% at 1 year. Skin elasticity improved over baseline by 32.5% at 1 month and 21% at 1 year. Sixty-eight percent of patients demonstrated significant improvement in cellulite based upon analysis of photographs, as did 65% when assessed by Vectra 3D surface imaging.
Patient self-evaluations rated the results as good to excellent at 1 month in 76% of cases. Physicians judged the results as good to excellent in 69% of cases. These results have held up at 1 year of follow-up, noted Dr. Kaminer, who also is with the dermatology departments of Yale University, New Haven, Conn.; Dartmouth College, Hanover, N.H.; and Brown University, Providence, R.I.
The downside of Cellulaze is that it is an invasive therapy that requires tumescent anesthesia. And given that the history of the field of cellulite therapy is one of hype far in excess of reality, Dr. Kaminer indicated that a healthy skepticism is appropriate.
"For me, I’m going to approach this with caution. I think Cellulaze is a great idea, and I think it gets to what many people believe is the root of cellulite. But I’d like to see it around for a little longer before we all jump on the bandwagon," he said.
The Cabochon system draws a small section of skin affected by cellulite into a handpiece so that a percutaneously inserted cutting tool can be utilized to cut the fibrous septae. Dr. Kaminer was an investigator in a two-site, 56-patient clinical trial with a 6- to 12-month follow-up.
In independent blinded physician review of before and after photos, 78% of patients were judged to have improved at least one full grade in severity at 6 months, such that, for example, those whose cellulite was rated severe at baseline were judged to have moderate or mild cellulite at follow-up.
At baseline, the average cellulite severity score was about 4.5 on a 0-6 scale. At 90 days, the average severity score had dropped to 3, and at 180 days to roughly 2.5. Ninety-four percent of patients were rated by independent physicians as having improved by at least 1 point on the 0-6 scale.
Of the 33 U.S. patients followed for 1 year, 87% felt their appearance was improved and 77% were satisfied with their treatment at all time points.
Seroma formation was an issue early on, until investigators realized the problem resulted from treating adjacent sites at the same depth. Seven of 31 patients treated in that manner had a seroma in excess of 2 cc at 1 month’s follow-up. But once operators began utilizing the device’s automated guidance system to vary the cutting depth at adjacent sites – for example, treating one area at a depth of 6 mm and an adjacent area at 10 mm of depth seromas were no longer a problem. None of 25 patients treated in this fashion had a seroma in excess of 2 cc 1 month post treatment, said Dr. Kaminer.
He reported that he serves as a consultant to Cabochon and has received research funding and equipment from Cynosure.
SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR