User login
Larry Beresford is an Oakland, Calif.-based freelance medical journalist with a breadth of experience writing about the policy, financial, clinical, management and human aspects of hospice, palliative care, end-of-life care, death, and dying. He is a longtime contributor to The Hospitalist, for which he covers re-admissions, pain management, palliative care, physician stress and burnout, quality improvement, waste prevention, practice management, innovation, and technology. He also contributes to Medscape. Learn more about his work at www.larryberesford.com; follow him on Twitter @larryberesford.
The state of hospital medicine in 2018
Productivity, pay, and roles remain center stage
In a national health care environment undergoing unprecedented transformation, the specialty of hospital medicine appears to be an island of relative stability, a conclusion that is supported by the principal findings from SHM’s 2018 State of Hospital Medicine (SoHM) report.

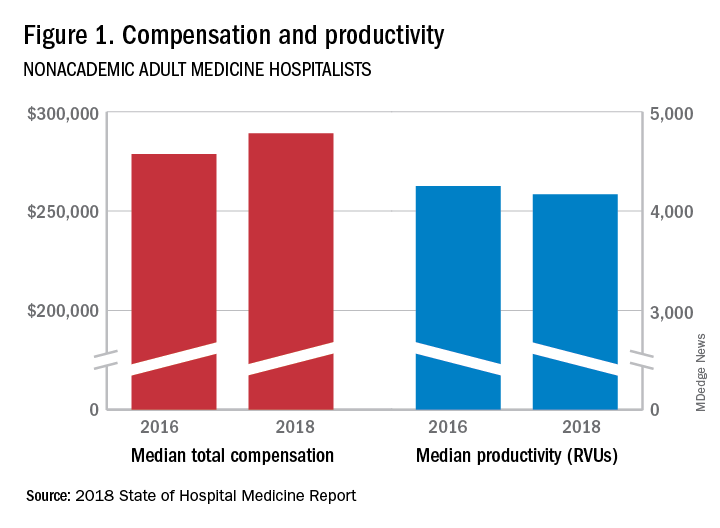
The report of hospitalist group practice characteristics, as well as other key data defining the field’s current status, that the Society of Hospital Medicine puts out every 2 years reveals that overall salaries for hospitalist physicians are up by 3.8% since 2016. Although productivity, as measured by work relative value units (RVUs), remained largely flat over the same period, financial support per full-time equivalent (FTE) physician position to hospitalist groups from their hospitals and health systems is up significantly.
Total support per FTE averaged $176,657 in 2018, 12% higher than in 2016, noted Leslie Flores, MHA, SFHM, of Nelson Flores Hospital Medicine Consultants, and a member of SHM’s Practice Analysis Committee, which oversees the biennial survey. Compensation and productivity data were collected by the Medical Group Management Association and licensed by SHM for inclusion in its report.
These findings – particularly the flat productivity – raise questions about long-term sustainability, Ms. Flores said. “What is going on? Do hospital administrators still recognize the value hospitalists bring to the operations and the quality of their hospitals? Or is paying the subsidy just a cost of doing business – a necessity for most hospitals in a setting where demand for hospitalist positions remains high?”
Andrew White, MD, FACP, SFHM, chair of SHM’s Practice Analysis Committee and director of the hospital medicine service at the University of Washington Medical Center, Seattle, said basic market forces dictate that it is “pretty much inconceivable” to run a modern hospital of any size without hospitalists.

“Clearly, demand outstrips supply, which drives up salaries and support, whether CEOs feel that the hospitalist group is earning that support or not,” Dr. White said. “The unfilled hospitalist positions we identified speak to ongoing projected greater demand than supply. That said, hospitalists and group leaders can’t be complacent and must collaborate effectively with hospitals to provide highly valuable services.” Turnover of hospitalist positions was up slightly, he noted, at 7.4% in 2018, from 6.9% in 2016, reversing a trend of previous years.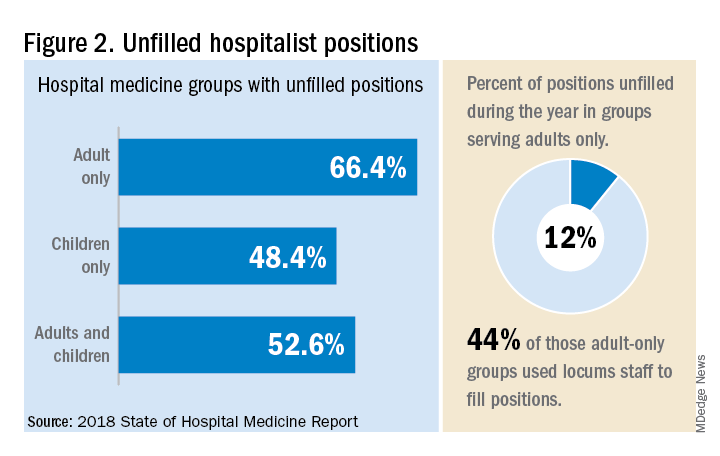
But will these trends continue at a time when hospitals face continued pressure to cut costs, as the hospital medicine subsidy may represent one of their largest cost centers? Because the size of hospitalist groups continues to grow, hospitals’ total subsidy for hospital medicine is going up faster than the percentage increase in support per FTE.
How do hospitalists use the SoHM report?
Dr. White called the 2018 SoHM report the “most representative and balanced sample to date” of hospitalist group practices, with some of the highest quality data, thanks to more robust participation in the survey by pediatric groups and improved distribution among hospitalist management companies and academic programs.
“Not that past reports had major flaws, but this version is more authoritative, reflecting an intentional effort by our Practice Analysis Committee to bring in more participants from key groups,” he said.
The biennial report has been around long enough to achieve brand recognition in the field as the most authoritative source of information regarding hospitalist practice, he added. “We worked hard this year to balance the participants, with more of our responses than in the past coming from multi-hospital groups, whether 4 to 5 sites, or 20 to 30.”
Surveys were conducted online in January and February of 2018 in response to invitations mailed and emailed to targeted hospital medicine group leaders. A total of 569 groups completed the survey, representing 8,889 hospitalist FTEs, approximately 16% of the total hospitalist workforce. Responses were presented in several categories, including by size of program, region and employment model. Groups that care for adults only represented 87.9% of the surveys, while groups that care for children only were 6.7% and groups that care for both adults and children were 5.4%.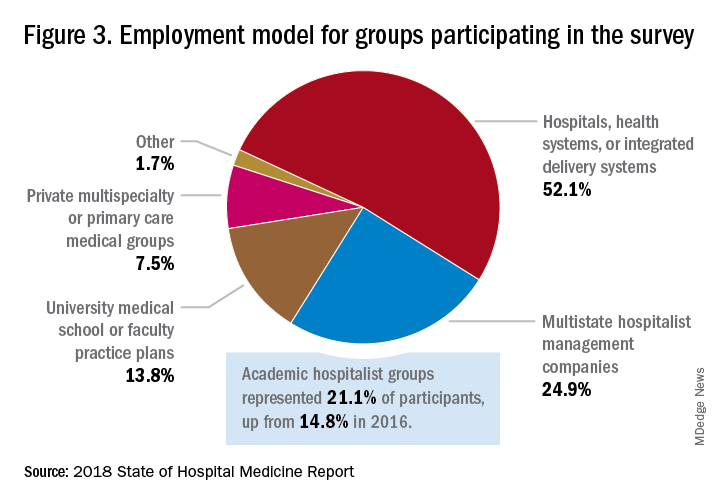
“This survey doesn’t tell us what should be best practice in hospital medicine,” Dr. White said, only what is actual current practice. He uses it in his own health system to not only contextualize and justify his group’s performance metrics for hospital administrators – relative to national and categorical averages – but also to see if the direction his group is following is consistent with what’s going on in the larger field.
“These data offer a very powerful resource regarding the trends in hospital medicine,” said Romil Chadha, MD, MPH, FACP, SFHM, associate division chief for operations in the division of hospital medicine at the University of Kentucky and UK Healthcare, Lexington. “It is my repository of data to go before my administrators for decisions that need to be made or to pilot new programs.” 
Dr. Chadha also uses the data to help answer compensation, scheduling, and support questions from his group’s members.
Thomas McIlraith, MD, immediate past chairman of the hospital medicine department at Mercy Medical Group, Sacramento, Calif., said the report’s value is that it allows comparisons of salaries in different settings, and to see, for example, how night staffing is structured. “A lot of leaders I spoke to at SHM’s 2018 Leadership Academy in Vancouver were saying they didn’t feel up to parity with the national standards. You can use the report to look at the state of hospital medicine nationally and make comparisons,” he said.
Calls for more productivity
Roberta Himebaugh, MBA, SFHM, senior vice president of acute care services for the national hospitalist management company TeamHealth, and cochair of the SHM Practice Administrators Special Interest Group, said her company’s clients have traditionally asked for greater productivity from their hospitalist contracts as a way to decrease overall costs. Some markets are starting to see a change in that approach, she noted.
“Recently there’s been an increased focus on paying hospitalists to focus on quality rather than just productivity. Some of our clients are willing to pay for that, and we are trying to assign value to this non-billable time or adjust our productivity standards appropriately. I think hospitals definitely understand the value of non-billable services from hospitalists, but still will push us on the productivity targets,” Ms. Himebaugh said.

“I don’t believe hospital medicine can be sustainable long term on flat productivity or flat RVUs,” she added. “Yet the costs of burnout associated with pushing higher productivity are not sustainable, either.” So what are the answers? She said many inefficiencies are involved in responding to inquiries on the floor that could have been addressed another way, or waiting for the turnaround of diagnostic tests.
“Maybe we don’t need physicians to be in the hospital 24/7 if we have access to telehealth, or a partnership with the emergency department, or greater use of advanced care practice providers,” Ms. Himebaugh said. “Our hospitals are examining those options, and we have to look at how we can become more efficient and less costly. At TeamHealth, we are trying to staff for value – looking at patient flow patterns and adjusting our schedules accordingly. Is there a bolus of admissions tied to emergency department shift changes, or to certain days of the week? How can we move from the 12-hour shift that begins at 7 a.m. and ends at 7 p.m., and instead provide coverage for when the patients are there?”
Mark Williams, MD, MHM, chief of the division of hospital medicine at the University of Kentucky, Lexington, said he appreciates the volume of data in the report but wishes for even more survey participants, which could make the breakouts for subgroups such as academic hospitalists more robust. Other current sources of hospitalist salary data include the Association of American Medical Colleges (AAMC), which produces compensation reports to help medical schools and teaching hospitals with benchmarking, and the Faculty Practice Solution Center developed jointly by AAMC and Vizient to provide faculty practice plans with analytic tools. The Medical Group Management Association (MGMA) is another valuable source of information, some of which was licensed for inclusion in the SoHM report.
“There is no source of absolute truth that hospitalists can point to,” Dr. Williams said. “I will present my data and my administrators will reply: ‘We have our own data.’ Our institution has consistently ranked first or second nationwide for the sickest patients. We take more Medicaid and dually eligible patients, who have a lot of social issues. They take a lot of time to manage medically and the RVUs don’t reflect that. And yet I’m still judged by my RVUs generated per hospitalist. Hospital administrators understandably want to get the most productivity, and they are looking for their own data for average productivity numbers.”
Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., said that hospital medicine’s flat productivity trends would be difficult to sustain in the business world. But there aren’t easy or obvious ways to increase hospitalists’ productivity. The SoHM report also shows that as productivity increases, total compensation increases but at a lower rate, resulting in a gradual decrease in compensation per RVU.
Pressures to increase productivity can be a double-edged sword, Dr. Williams added. Demanding that doctors make more billable visits faster to generate more RVUs can be a recipe for burnout and turnover, with huge costs associated with recruiting replacements.
“If there was recent turnover of hospitalists at the hospital, with the need to find replacements, there may be institutional memory about that,” he said. “But where are hospitals spending their money? Bottom line, we still need to learn to cut our costs.”
How is hospitalist practice evolving?
In addition to payment and productivity data, the SoHM report provides a current picture of the evolving state of hospitalist group practices. A key thread is how the work hospitalists are doing, and the way they do it, is changing, with new information about comanagement roles, dedicated admitters, night coverage, geographic rounding, and the like.
Making greater use of nurse practitioners and physician assistants (NPs/PAs), may be one way to change the flat productivity trends, Dr. Brown said. With a cost per RVU that’s roughly half that of a doctor’s, NPs/PAs could contribute to the bottom line. But he sees surprisingly large variation in how hospitalist groups are using them. Typically, they are deployed at a ratio of four doctors to one NP/PA, but that ratio could be two to one or even one to one, he said.

Use of NPs/PAs by academic hospitalist groups is up, from 52.1% in 2016 to 75.7% in 2018. For adult-only groups, 76.8% had NPs/PAs, with higher rates in hospitals and health systems and lower rates in the West region. But a lot of groups are using these practitioners for nonproductive work, and some are failing to generate any billing income, Dr. Brown said.
“The rate at which NPs/PAs performed billable services was higher in physician-owned practices, resulting in a lower cost per RVU, suggesting that many practices may be underutilizing their NPs/PAs or not sharing the work.” Not every NP or PA wants to or is able to care for very complex patients, Dr. Brown said, “but you want a system where the NP and PA can work at the highest level permitted by state law.”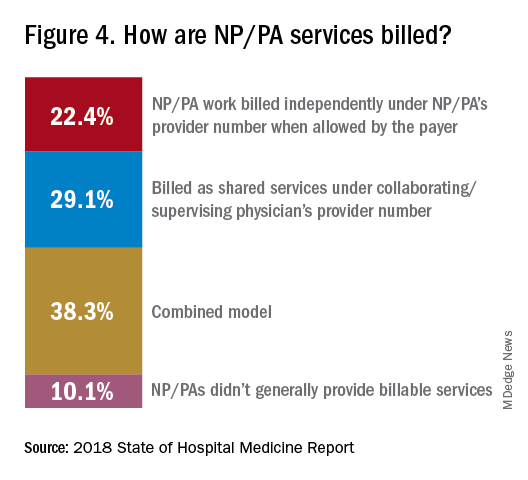
The predominant scheduling model of hospital medicine, 7 days on duty followed by 7 days off, has diminished somewhat in recent years. There appears to be some fluctuation and a gradual move away from 7 on/7 off toward some kind of variable approach, since the former may not be physically sustainable for the doctor over the long haul, Dr. Brown said. Some groups are experimenting with a combined approach.
“I think balancing workload with manpower has always been a challenge for our field. Maybe we should be working shorter shifts or fewer days and making sure our hospitalists aren’t ever sitting around idle,” he said. “And could we come in on nonclinical days to do administrative tasks? I think the solution is out there, but we haven’t created the algorithms to define that yet. If you could somehow use the data for volume, number of beds, nurse staffing, etc., by year and seasonally, you might be able to reliably predict census. This is about applying data hospitals already have in their electronic health records, but utilizing the data in ways that are more helpful.”
Dr. McIlraith added that a big driver of the future of hospital medicine will be the evolution of the EHR and the digitalization of health care, as hospitals learn how to leverage more of what’s in their EHRs. “The impact will grow for hospitalists through the creation and maturation of big data systems – and the learning that can be extracted from what’s contained in the electronic health record.”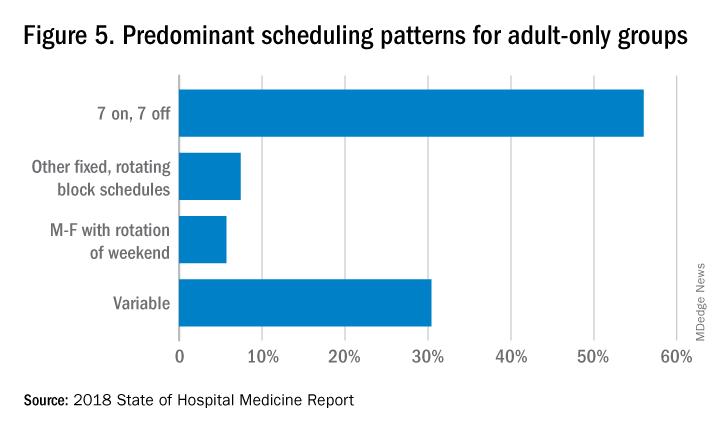
Another important question for hospitalist groups is their model of backup scheduling, to make sure there is a replacement available if a scheduled doctor calls in sick or if demand is unexpectedly high.
“In today’s world, this is how we have traditionally managed unpredictability,” Dr. Brown said. “You don’t know when you will need it, but if you need it, you want it immediately. So how do you pay for it – only when the doctor comes in, or also an amount just for being on call?” Some groups pay for both, he said, others for neither.
“We are a group of 70 hospitalists, and if someone is sick you can’t just shut down the service,” said Dr. Chadha. “We are one of the few to use incentives for both, which could include a 1-week decrease in clinical shifts in exchange for 2 weeks of backup. We have times with 25% usage of backup number 1, and 10% usage of backup number 2,” he noted. “But the goal is for our hospitalists to have assurances that there is a backup system and that it works.”
The presence of nocturnists in hospitals continues to rise, with 76.1% of adults-only groups having nocturnists, 27.6% of children-only groups, and 68.2% of adults and children groups. Geographic or unit-based hospital assignments have grown to 36.4% of adult-only groups.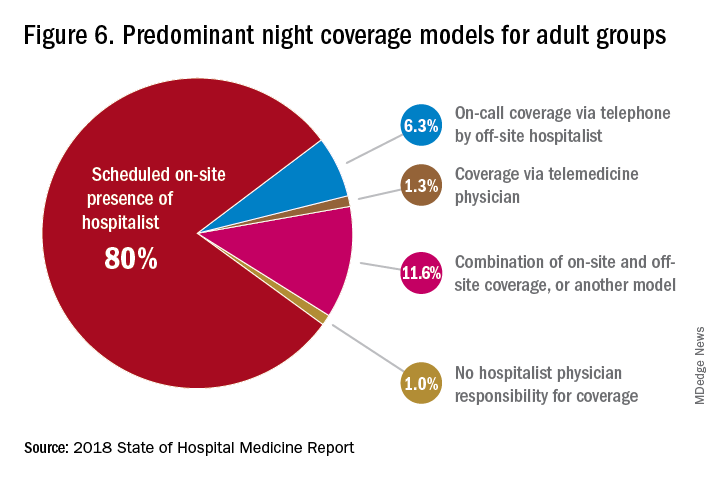
What are hospitalists’ other new roles?
“We have a large group of 50 doctors, with about 40 FTEs, and we are evolving from the traditional generalist role toward more subspecialty comanagement,” said Bryan Huang, MD, physician adviser and associate clinical professor in the division of hospital medicine at the University of California–San Diego. “Our hospitalists are asking what it means to be an academic hospitalist as our teaching roles have shrunk.”

Dr. Huang recently took on a new role as physician adviser for his hospital in such areas as utilization review, patient flow, and length of stay. “I’m spearheading a work group to address quality issues – all of which involve collaboration with other professionals. We also developed an admitting role here for a hospitalist whose sole role for the day is to admit patients.” Nationally up to 51.2% of hospitalist groups utilize a dedicated daytime admitter.
The report found that hospital services for which hospitalists are more likely to be attendings than consultants include GI/liver, 78.4%; palliative care, 77.3%; neurology/stroke, 73.6%; oncology, 67.8%; cardiology, 56.9%; and critical care, 50.7%. Conditions where hospitalists are more likely to consult rather than admit and attend include neurosurgery, orthopedics, general surgery, cardiovascular surgery, and other surgical subspecialties.
Other hospital services routinely provided by adult-only hospitalists include care of patients in an ICU setting (62.7%); primary responsibility for observation units (54.6%); primary clinical responsibility for rapid response teams (48.8%); primary responsibility for code blue or cardiac arrest teams (43.8%); nighttime admissions or tuck-in services (33.9%); and medical procedures (31.5%). For pediatric hospital medicine groups, care of healthy newborns and medical procedures were among the most common services provided, while for hospitalists serving adults and children, rapid response teams, ICUs, and specialty units were most common.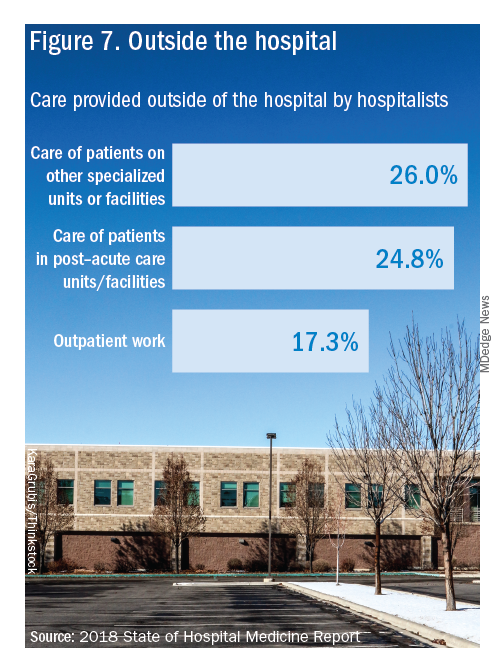
New models of payment for health care
As the larger health care system is being transformed by new payment models and benefit structures, including accountable care organizations (ACOs), value-based purchasing, bundled payments, and other forms of population-based coverage – which is described as a volume-to-value shift in health care – how are these new models affecting hospitalists?
Observers say penetration of these new models varies widely by locality but they haven’t had much direct impact on hospitalists’ practices – at least not yet. However, as hospitals and health systems find themselves needing to learn new ways to invest their resources differently in response to these trends, what matters to the hospital should be of great importance to the hospitalist group.
“I haven’t seen a lot of dramatic changes in how hospitalists engage with value-based purchasing,” Dr. White said. “If we know that someone is part of an ACO, the instinctual – and right – response is to treat them like any other patient. But we still need to be committed to not waste resources.”
Hospitalists are the best people to understand the intricacies of how the health care system works under value-based approaches, Dr. Huang said. “That’s why so many hospitalists have taken leadership positions in their hospitals. I think all of this translates to the practical, day-to-day work of hospitalists, reflected in our focus on readmissions and length of stay.”
Dr. Williams said the health care system still hasn’t turned the corner from fee-for-service to value-based purchasing. “It still represents a tiny fraction of the income of hospitalists. Hospitals still have to focus on the bottom line, as fee-for-service reimbursement for hospitalized patients continues to get squeezed, and ACOs aren’t exactly paying premium rates either. Ask almost any hospital CEO what drives their bottom line today and the answer is volume – along with optimizing productivity. Pretty much every place I look, the future does not look terribly rosy for hospitals.”
Ms. Himebaugh said she is bullish on hospital medicine, in the sense that it’s unlikely to go away anytime soon. “Hospitalists are needed and provide value. But I don’t think we have devised the right model yet. I’m not sure our current model is sustainable. We need to find new models we can afford that don’t require squeezing our providers.”
For more information about the 2018 State of Hospital Medicine Report, contact SHM’s Practice Management Department at: survey@hospitalmedicine.org or call 800-843-3360. See also: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/.
Productivity, pay, and roles remain center stage
Productivity, pay, and roles remain center stage
In a national health care environment undergoing unprecedented transformation, the specialty of hospital medicine appears to be an island of relative stability, a conclusion that is supported by the principal findings from SHM’s 2018 State of Hospital Medicine (SoHM) report.
The report of hospitalist group practice characteristics, as well as other key data defining the field’s current status, that the Society of Hospital Medicine puts out every 2 years reveals that overall salaries for hospitalist physicians are up by 3.8% since 2016. Although productivity, as measured by work relative value units (RVUs), remained largely flat over the same period, financial support per full-time equivalent (FTE) physician position to hospitalist groups from their hospitals and health systems is up significantly.
Total support per FTE averaged $176,657 in 2018, 12% higher than in 2016, noted Leslie Flores, MHA, SFHM, of Nelson Flores Hospital Medicine Consultants, and a member of SHM’s Practice Analysis Committee, which oversees the biennial survey. Compensation and productivity data were collected by the Medical Group Management Association and licensed by SHM for inclusion in its report.
These findings – particularly the flat productivity – raise questions about long-term sustainability, Ms. Flores said. “What is going on? Do hospital administrators still recognize the value hospitalists bring to the operations and the quality of their hospitals? Or is paying the subsidy just a cost of doing business – a necessity for most hospitals in a setting where demand for hospitalist positions remains high?”
Andrew White, MD, FACP, SFHM, chair of SHM’s Practice Analysis Committee and director of the hospital medicine service at the University of Washington Medical Center, Seattle, said basic market forces dictate that it is “pretty much inconceivable” to run a modern hospital of any size without hospitalists.
“Clearly, demand outstrips supply, which drives up salaries and support, whether CEOs feel that the hospitalist group is earning that support or not,” Dr. White said. “The unfilled hospitalist positions we identified speak to ongoing projected greater demand than supply. That said, hospitalists and group leaders can’t be complacent and must collaborate effectively with hospitals to provide highly valuable services.” Turnover of hospitalist positions was up slightly, he noted, at 7.4% in 2018, from 6.9% in 2016, reversing a trend of previous years.
But will these trends continue at a time when hospitals face continued pressure to cut costs, as the hospital medicine subsidy may represent one of their largest cost centers? Because the size of hospitalist groups continues to grow, hospitals’ total subsidy for hospital medicine is going up faster than the percentage increase in support per FTE.
How do hospitalists use the SoHM report?
Dr. White called the 2018 SoHM report the “most representative and balanced sample to date” of hospitalist group practices, with some of the highest quality data, thanks to more robust participation in the survey by pediatric groups and improved distribution among hospitalist management companies and academic programs.
“Not that past reports had major flaws, but this version is more authoritative, reflecting an intentional effort by our Practice Analysis Committee to bring in more participants from key groups,” he said.
The biennial report has been around long enough to achieve brand recognition in the field as the most authoritative source of information regarding hospitalist practice, he added. “We worked hard this year to balance the participants, with more of our responses than in the past coming from multi-hospital groups, whether 4 to 5 sites, or 20 to 30.”
Surveys were conducted online in January and February of 2018 in response to invitations mailed and emailed to targeted hospital medicine group leaders. A total of 569 groups completed the survey, representing 8,889 hospitalist FTEs, approximately 16% of the total hospitalist workforce. Responses were presented in several categories, including by size of program, region and employment model. Groups that care for adults only represented 87.9% of the surveys, while groups that care for children only were 6.7% and groups that care for both adults and children were 5.4%.
“This survey doesn’t tell us what should be best practice in hospital medicine,” Dr. White said, only what is actual current practice. He uses it in his own health system to not only contextualize and justify his group’s performance metrics for hospital administrators – relative to national and categorical averages – but also to see if the direction his group is following is consistent with what’s going on in the larger field.
“These data offer a very powerful resource regarding the trends in hospital medicine,” said Romil Chadha, MD, MPH, FACP, SFHM, associate division chief for operations in the division of hospital medicine at the University of Kentucky and UK Healthcare, Lexington. “It is my repository of data to go before my administrators for decisions that need to be made or to pilot new programs.”
Dr. Chadha also uses the data to help answer compensation, scheduling, and support questions from his group’s members.
Thomas McIlraith, MD, immediate past chairman of the hospital medicine department at Mercy Medical Group, Sacramento, Calif., said the report’s value is that it allows comparisons of salaries in different settings, and to see, for example, how night staffing is structured. “A lot of leaders I spoke to at SHM’s 2018 Leadership Academy in Vancouver were saying they didn’t feel up to parity with the national standards. You can use the report to look at the state of hospital medicine nationally and make comparisons,” he said.
Calls for more productivity
Roberta Himebaugh, MBA, SFHM, senior vice president of acute care services for the national hospitalist management company TeamHealth, and cochair of the SHM Practice Administrators Special Interest Group, said her company’s clients have traditionally asked for greater productivity from their hospitalist contracts as a way to decrease overall costs. Some markets are starting to see a change in that approach, she noted.
“Recently there’s been an increased focus on paying hospitalists to focus on quality rather than just productivity. Some of our clients are willing to pay for that, and we are trying to assign value to this non-billable time or adjust our productivity standards appropriately. I think hospitals definitely understand the value of non-billable services from hospitalists, but still will push us on the productivity targets,” Ms. Himebaugh said.
“I don’t believe hospital medicine can be sustainable long term on flat productivity or flat RVUs,” she added. “Yet the costs of burnout associated with pushing higher productivity are not sustainable, either.” So what are the answers? She said many inefficiencies are involved in responding to inquiries on the floor that could have been addressed another way, or waiting for the turnaround of diagnostic tests.
“Maybe we don’t need physicians to be in the hospital 24/7 if we have access to telehealth, or a partnership with the emergency department, or greater use of advanced care practice providers,” Ms. Himebaugh said. “Our hospitals are examining those options, and we have to look at how we can become more efficient and less costly. At TeamHealth, we are trying to staff for value – looking at patient flow patterns and adjusting our schedules accordingly. Is there a bolus of admissions tied to emergency department shift changes, or to certain days of the week? How can we move from the 12-hour shift that begins at 7 a.m. and ends at 7 p.m., and instead provide coverage for when the patients are there?”
Mark Williams, MD, MHM, chief of the division of hospital medicine at the University of Kentucky, Lexington, said he appreciates the volume of data in the report but wishes for even more survey participants, which could make the breakouts for subgroups such as academic hospitalists more robust. Other current sources of hospitalist salary data include the Association of American Medical Colleges (AAMC), which produces compensation reports to help medical schools and teaching hospitals with benchmarking, and the Faculty Practice Solution Center developed jointly by AAMC and Vizient to provide faculty practice plans with analytic tools. The Medical Group Management Association (MGMA) is another valuable source of information, some of which was licensed for inclusion in the SoHM report.
“There is no source of absolute truth that hospitalists can point to,” Dr. Williams said. “I will present my data and my administrators will reply: ‘We have our own data.’ Our institution has consistently ranked first or second nationwide for the sickest patients. We take more Medicaid and dually eligible patients, who have a lot of social issues. They take a lot of time to manage medically and the RVUs don’t reflect that. And yet I’m still judged by my RVUs generated per hospitalist. Hospital administrators understandably want to get the most productivity, and they are looking for their own data for average productivity numbers.”
Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., said that hospital medicine’s flat productivity trends would be difficult to sustain in the business world. But there aren’t easy or obvious ways to increase hospitalists’ productivity. The SoHM report also shows that as productivity increases, total compensation increases but at a lower rate, resulting in a gradual decrease in compensation per RVU.
Pressures to increase productivity can be a double-edged sword, Dr. Williams added. Demanding that doctors make more billable visits faster to generate more RVUs can be a recipe for burnout and turnover, with huge costs associated with recruiting replacements.
“If there was recent turnover of hospitalists at the hospital, with the need to find replacements, there may be institutional memory about that,” he said. “But where are hospitals spending their money? Bottom line, we still need to learn to cut our costs.”
How is hospitalist practice evolving?
In addition to payment and productivity data, the SoHM report provides a current picture of the evolving state of hospitalist group practices. A key thread is how the work hospitalists are doing, and the way they do it, is changing, with new information about comanagement roles, dedicated admitters, night coverage, geographic rounding, and the like.
Making greater use of nurse practitioners and physician assistants (NPs/PAs), may be one way to change the flat productivity trends, Dr. Brown said. With a cost per RVU that’s roughly half that of a doctor’s, NPs/PAs could contribute to the bottom line. But he sees surprisingly large variation in how hospitalist groups are using them. Typically, they are deployed at a ratio of four doctors to one NP/PA, but that ratio could be two to one or even one to one, he said.
Use of NPs/PAs by academic hospitalist groups is up, from 52.1% in 2016 to 75.7% in 2018. For adult-only groups, 76.8% had NPs/PAs, with higher rates in hospitals and health systems and lower rates in the West region. But a lot of groups are using these practitioners for nonproductive work, and some are failing to generate any billing income, Dr. Brown said.
“The rate at which NPs/PAs performed billable services was higher in physician-owned practices, resulting in a lower cost per RVU, suggesting that many practices may be underutilizing their NPs/PAs or not sharing the work.” Not every NP or PA wants to or is able to care for very complex patients, Dr. Brown said, “but you want a system where the NP and PA can work at the highest level permitted by state law.”
The predominant scheduling model of hospital medicine, 7 days on duty followed by 7 days off, has diminished somewhat in recent years. There appears to be some fluctuation and a gradual move away from 7 on/7 off toward some kind of variable approach, since the former may not be physically sustainable for the doctor over the long haul, Dr. Brown said. Some groups are experimenting with a combined approach.
“I think balancing workload with manpower has always been a challenge for our field. Maybe we should be working shorter shifts or fewer days and making sure our hospitalists aren’t ever sitting around idle,” he said. “And could we come in on nonclinical days to do administrative tasks? I think the solution is out there, but we haven’t created the algorithms to define that yet. If you could somehow use the data for volume, number of beds, nurse staffing, etc., by year and seasonally, you might be able to reliably predict census. This is about applying data hospitals already have in their electronic health records, but utilizing the data in ways that are more helpful.”
Dr. McIlraith added that a big driver of the future of hospital medicine will be the evolution of the EHR and the digitalization of health care, as hospitals learn how to leverage more of what’s in their EHRs. “The impact will grow for hospitalists through the creation and maturation of big data systems – and the learning that can be extracted from what’s contained in the electronic health record.”
Another important question for hospitalist groups is their model of backup scheduling, to make sure there is a replacement available if a scheduled doctor calls in sick or if demand is unexpectedly high.
“In today’s world, this is how we have traditionally managed unpredictability,” Dr. Brown said. “You don’t know when you will need it, but if you need it, you want it immediately. So how do you pay for it – only when the doctor comes in, or also an amount just for being on call?” Some groups pay for both, he said, others for neither.
“We are a group of 70 hospitalists, and if someone is sick you can’t just shut down the service,” said Dr. Chadha. “We are one of the few to use incentives for both, which could include a 1-week decrease in clinical shifts in exchange for 2 weeks of backup. We have times with 25% usage of backup number 1, and 10% usage of backup number 2,” he noted. “But the goal is for our hospitalists to have assurances that there is a backup system and that it works.”
The presence of nocturnists in hospitals continues to rise, with 76.1% of adults-only groups having nocturnists, 27.6% of children-only groups, and 68.2% of adults and children groups. Geographic or unit-based hospital assignments have grown to 36.4% of adult-only groups.
What are hospitalists’ other new roles?
“We have a large group of 50 doctors, with about 40 FTEs, and we are evolving from the traditional generalist role toward more subspecialty comanagement,” said Bryan Huang, MD, physician adviser and associate clinical professor in the division of hospital medicine at the University of California–San Diego. “Our hospitalists are asking what it means to be an academic hospitalist as our teaching roles have shrunk.”
Dr. Huang recently took on a new role as physician adviser for his hospital in such areas as utilization review, patient flow, and length of stay. “I’m spearheading a work group to address quality issues – all of which involve collaboration with other professionals. We also developed an admitting role here for a hospitalist whose sole role for the day is to admit patients.” Nationally up to 51.2% of hospitalist groups utilize a dedicated daytime admitter.
The report found that hospital services for which hospitalists are more likely to be attendings than consultants include GI/liver, 78.4%; palliative care, 77.3%; neurology/stroke, 73.6%; oncology, 67.8%; cardiology, 56.9%; and critical care, 50.7%. Conditions where hospitalists are more likely to consult rather than admit and attend include neurosurgery, orthopedics, general surgery, cardiovascular surgery, and other surgical subspecialties.
Other hospital services routinely provided by adult-only hospitalists include care of patients in an ICU setting (62.7%); primary responsibility for observation units (54.6%); primary clinical responsibility for rapid response teams (48.8%); primary responsibility for code blue or cardiac arrest teams (43.8%); nighttime admissions or tuck-in services (33.9%); and medical procedures (31.5%). For pediatric hospital medicine groups, care of healthy newborns and medical procedures were among the most common services provided, while for hospitalists serving adults and children, rapid response teams, ICUs, and specialty units were most common.
New models of payment for health care
As the larger health care system is being transformed by new payment models and benefit structures, including accountable care organizations (ACOs), value-based purchasing, bundled payments, and other forms of population-based coverage – which is described as a volume-to-value shift in health care – how are these new models affecting hospitalists?
Observers say penetration of these new models varies widely by locality but they haven’t had much direct impact on hospitalists’ practices – at least not yet. However, as hospitals and health systems find themselves needing to learn new ways to invest their resources differently in response to these trends, what matters to the hospital should be of great importance to the hospitalist group.
“I haven’t seen a lot of dramatic changes in how hospitalists engage with value-based purchasing,” Dr. White said. “If we know that someone is part of an ACO, the instinctual – and right – response is to treat them like any other patient. But we still need to be committed to not waste resources.”
Hospitalists are the best people to understand the intricacies of how the health care system works under value-based approaches, Dr. Huang said. “That’s why so many hospitalists have taken leadership positions in their hospitals. I think all of this translates to the practical, day-to-day work of hospitalists, reflected in our focus on readmissions and length of stay.”
Dr. Williams said the health care system still hasn’t turned the corner from fee-for-service to value-based purchasing. “It still represents a tiny fraction of the income of hospitalists. Hospitals still have to focus on the bottom line, as fee-for-service reimbursement for hospitalized patients continues to get squeezed, and ACOs aren’t exactly paying premium rates either. Ask almost any hospital CEO what drives their bottom line today and the answer is volume – along with optimizing productivity. Pretty much every place I look, the future does not look terribly rosy for hospitals.”
Ms. Himebaugh said she is bullish on hospital medicine, in the sense that it’s unlikely to go away anytime soon. “Hospitalists are needed and provide value. But I don’t think we have devised the right model yet. I’m not sure our current model is sustainable. We need to find new models we can afford that don’t require squeezing our providers.”
For more information about the 2018 State of Hospital Medicine Report, contact SHM’s Practice Management Department at: survey@hospitalmedicine.org or call 800-843-3360. See also: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/.
In a national health care environment undergoing unprecedented transformation, the specialty of hospital medicine appears to be an island of relative stability, a conclusion that is supported by the principal findings from SHM’s 2018 State of Hospital Medicine (SoHM) report.
The report of hospitalist group practice characteristics, as well as other key data defining the field’s current status, that the Society of Hospital Medicine puts out every 2 years reveals that overall salaries for hospitalist physicians are up by 3.8% since 2016. Although productivity, as measured by work relative value units (RVUs), remained largely flat over the same period, financial support per full-time equivalent (FTE) physician position to hospitalist groups from their hospitals and health systems is up significantly.
Total support per FTE averaged $176,657 in 2018, 12% higher than in 2016, noted Leslie Flores, MHA, SFHM, of Nelson Flores Hospital Medicine Consultants, and a member of SHM’s Practice Analysis Committee, which oversees the biennial survey. Compensation and productivity data were collected by the Medical Group Management Association and licensed by SHM for inclusion in its report.
These findings – particularly the flat productivity – raise questions about long-term sustainability, Ms. Flores said. “What is going on? Do hospital administrators still recognize the value hospitalists bring to the operations and the quality of their hospitals? Or is paying the subsidy just a cost of doing business – a necessity for most hospitals in a setting where demand for hospitalist positions remains high?”
Andrew White, MD, FACP, SFHM, chair of SHM’s Practice Analysis Committee and director of the hospital medicine service at the University of Washington Medical Center, Seattle, said basic market forces dictate that it is “pretty much inconceivable” to run a modern hospital of any size without hospitalists.
“Clearly, demand outstrips supply, which drives up salaries and support, whether CEOs feel that the hospitalist group is earning that support or not,” Dr. White said. “The unfilled hospitalist positions we identified speak to ongoing projected greater demand than supply. That said, hospitalists and group leaders can’t be complacent and must collaborate effectively with hospitals to provide highly valuable services.” Turnover of hospitalist positions was up slightly, he noted, at 7.4% in 2018, from 6.9% in 2016, reversing a trend of previous years.
But will these trends continue at a time when hospitals face continued pressure to cut costs, as the hospital medicine subsidy may represent one of their largest cost centers? Because the size of hospitalist groups continues to grow, hospitals’ total subsidy for hospital medicine is going up faster than the percentage increase in support per FTE.
How do hospitalists use the SoHM report?
Dr. White called the 2018 SoHM report the “most representative and balanced sample to date” of hospitalist group practices, with some of the highest quality data, thanks to more robust participation in the survey by pediatric groups and improved distribution among hospitalist management companies and academic programs.
“Not that past reports had major flaws, but this version is more authoritative, reflecting an intentional effort by our Practice Analysis Committee to bring in more participants from key groups,” he said.
The biennial report has been around long enough to achieve brand recognition in the field as the most authoritative source of information regarding hospitalist practice, he added. “We worked hard this year to balance the participants, with more of our responses than in the past coming from multi-hospital groups, whether 4 to 5 sites, or 20 to 30.”
Surveys were conducted online in January and February of 2018 in response to invitations mailed and emailed to targeted hospital medicine group leaders. A total of 569 groups completed the survey, representing 8,889 hospitalist FTEs, approximately 16% of the total hospitalist workforce. Responses were presented in several categories, including by size of program, region and employment model. Groups that care for adults only represented 87.9% of the surveys, while groups that care for children only were 6.7% and groups that care for both adults and children were 5.4%.
“This survey doesn’t tell us what should be best practice in hospital medicine,” Dr. White said, only what is actual current practice. He uses it in his own health system to not only contextualize and justify his group’s performance metrics for hospital administrators – relative to national and categorical averages – but also to see if the direction his group is following is consistent with what’s going on in the larger field.
“These data offer a very powerful resource regarding the trends in hospital medicine,” said Romil Chadha, MD, MPH, FACP, SFHM, associate division chief for operations in the division of hospital medicine at the University of Kentucky and UK Healthcare, Lexington. “It is my repository of data to go before my administrators for decisions that need to be made or to pilot new programs.”
Dr. Chadha also uses the data to help answer compensation, scheduling, and support questions from his group’s members.
Thomas McIlraith, MD, immediate past chairman of the hospital medicine department at Mercy Medical Group, Sacramento, Calif., said the report’s value is that it allows comparisons of salaries in different settings, and to see, for example, how night staffing is structured. “A lot of leaders I spoke to at SHM’s 2018 Leadership Academy in Vancouver were saying they didn’t feel up to parity with the national standards. You can use the report to look at the state of hospital medicine nationally and make comparisons,” he said.
Calls for more productivity
Roberta Himebaugh, MBA, SFHM, senior vice president of acute care services for the national hospitalist management company TeamHealth, and cochair of the SHM Practice Administrators Special Interest Group, said her company’s clients have traditionally asked for greater productivity from their hospitalist contracts as a way to decrease overall costs. Some markets are starting to see a change in that approach, she noted.
“Recently there’s been an increased focus on paying hospitalists to focus on quality rather than just productivity. Some of our clients are willing to pay for that, and we are trying to assign value to this non-billable time or adjust our productivity standards appropriately. I think hospitals definitely understand the value of non-billable services from hospitalists, but still will push us on the productivity targets,” Ms. Himebaugh said.
“I don’t believe hospital medicine can be sustainable long term on flat productivity or flat RVUs,” she added. “Yet the costs of burnout associated with pushing higher productivity are not sustainable, either.” So what are the answers? She said many inefficiencies are involved in responding to inquiries on the floor that could have been addressed another way, or waiting for the turnaround of diagnostic tests.
“Maybe we don’t need physicians to be in the hospital 24/7 if we have access to telehealth, or a partnership with the emergency department, or greater use of advanced care practice providers,” Ms. Himebaugh said. “Our hospitals are examining those options, and we have to look at how we can become more efficient and less costly. At TeamHealth, we are trying to staff for value – looking at patient flow patterns and adjusting our schedules accordingly. Is there a bolus of admissions tied to emergency department shift changes, or to certain days of the week? How can we move from the 12-hour shift that begins at 7 a.m. and ends at 7 p.m., and instead provide coverage for when the patients are there?”
Mark Williams, MD, MHM, chief of the division of hospital medicine at the University of Kentucky, Lexington, said he appreciates the volume of data in the report but wishes for even more survey participants, which could make the breakouts for subgroups such as academic hospitalists more robust. Other current sources of hospitalist salary data include the Association of American Medical Colleges (AAMC), which produces compensation reports to help medical schools and teaching hospitals with benchmarking, and the Faculty Practice Solution Center developed jointly by AAMC and Vizient to provide faculty practice plans with analytic tools. The Medical Group Management Association (MGMA) is another valuable source of information, some of which was licensed for inclusion in the SoHM report.
“There is no source of absolute truth that hospitalists can point to,” Dr. Williams said. “I will present my data and my administrators will reply: ‘We have our own data.’ Our institution has consistently ranked first or second nationwide for the sickest patients. We take more Medicaid and dually eligible patients, who have a lot of social issues. They take a lot of time to manage medically and the RVUs don’t reflect that. And yet I’m still judged by my RVUs generated per hospitalist. Hospital administrators understandably want to get the most productivity, and they are looking for their own data for average productivity numbers.”
Ryan Brown, MD, specialty medical director for hospital medicine with Atrium Health in Charlotte, N.C., said that hospital medicine’s flat productivity trends would be difficult to sustain in the business world. But there aren’t easy or obvious ways to increase hospitalists’ productivity. The SoHM report also shows that as productivity increases, total compensation increases but at a lower rate, resulting in a gradual decrease in compensation per RVU.
Pressures to increase productivity can be a double-edged sword, Dr. Williams added. Demanding that doctors make more billable visits faster to generate more RVUs can be a recipe for burnout and turnover, with huge costs associated with recruiting replacements.
“If there was recent turnover of hospitalists at the hospital, with the need to find replacements, there may be institutional memory about that,” he said. “But where are hospitals spending their money? Bottom line, we still need to learn to cut our costs.”
How is hospitalist practice evolving?
In addition to payment and productivity data, the SoHM report provides a current picture of the evolving state of hospitalist group practices. A key thread is how the work hospitalists are doing, and the way they do it, is changing, with new information about comanagement roles, dedicated admitters, night coverage, geographic rounding, and the like.
Making greater use of nurse practitioners and physician assistants (NPs/PAs), may be one way to change the flat productivity trends, Dr. Brown said. With a cost per RVU that’s roughly half that of a doctor’s, NPs/PAs could contribute to the bottom line. But he sees surprisingly large variation in how hospitalist groups are using them. Typically, they are deployed at a ratio of four doctors to one NP/PA, but that ratio could be two to one or even one to one, he said.
Use of NPs/PAs by academic hospitalist groups is up, from 52.1% in 2016 to 75.7% in 2018. For adult-only groups, 76.8% had NPs/PAs, with higher rates in hospitals and health systems and lower rates in the West region. But a lot of groups are using these practitioners for nonproductive work, and some are failing to generate any billing income, Dr. Brown said.
“The rate at which NPs/PAs performed billable services was higher in physician-owned practices, resulting in a lower cost per RVU, suggesting that many practices may be underutilizing their NPs/PAs or not sharing the work.” Not every NP or PA wants to or is able to care for very complex patients, Dr. Brown said, “but you want a system where the NP and PA can work at the highest level permitted by state law.”
The predominant scheduling model of hospital medicine, 7 days on duty followed by 7 days off, has diminished somewhat in recent years. There appears to be some fluctuation and a gradual move away from 7 on/7 off toward some kind of variable approach, since the former may not be physically sustainable for the doctor over the long haul, Dr. Brown said. Some groups are experimenting with a combined approach.
“I think balancing workload with manpower has always been a challenge for our field. Maybe we should be working shorter shifts or fewer days and making sure our hospitalists aren’t ever sitting around idle,” he said. “And could we come in on nonclinical days to do administrative tasks? I think the solution is out there, but we haven’t created the algorithms to define that yet. If you could somehow use the data for volume, number of beds, nurse staffing, etc., by year and seasonally, you might be able to reliably predict census. This is about applying data hospitals already have in their electronic health records, but utilizing the data in ways that are more helpful.”
Dr. McIlraith added that a big driver of the future of hospital medicine will be the evolution of the EHR and the digitalization of health care, as hospitals learn how to leverage more of what’s in their EHRs. “The impact will grow for hospitalists through the creation and maturation of big data systems – and the learning that can be extracted from what’s contained in the electronic health record.”
Another important question for hospitalist groups is their model of backup scheduling, to make sure there is a replacement available if a scheduled doctor calls in sick or if demand is unexpectedly high.
“In today’s world, this is how we have traditionally managed unpredictability,” Dr. Brown said. “You don’t know when you will need it, but if you need it, you want it immediately. So how do you pay for it – only when the doctor comes in, or also an amount just for being on call?” Some groups pay for both, he said, others for neither.
“We are a group of 70 hospitalists, and if someone is sick you can’t just shut down the service,” said Dr. Chadha. “We are one of the few to use incentives for both, which could include a 1-week decrease in clinical shifts in exchange for 2 weeks of backup. We have times with 25% usage of backup number 1, and 10% usage of backup number 2,” he noted. “But the goal is for our hospitalists to have assurances that there is a backup system and that it works.”
The presence of nocturnists in hospitals continues to rise, with 76.1% of adults-only groups having nocturnists, 27.6% of children-only groups, and 68.2% of adults and children groups. Geographic or unit-based hospital assignments have grown to 36.4% of adult-only groups.
What are hospitalists’ other new roles?
“We have a large group of 50 doctors, with about 40 FTEs, and we are evolving from the traditional generalist role toward more subspecialty comanagement,” said Bryan Huang, MD, physician adviser and associate clinical professor in the division of hospital medicine at the University of California–San Diego. “Our hospitalists are asking what it means to be an academic hospitalist as our teaching roles have shrunk.”
Dr. Huang recently took on a new role as physician adviser for his hospital in such areas as utilization review, patient flow, and length of stay. “I’m spearheading a work group to address quality issues – all of which involve collaboration with other professionals. We also developed an admitting role here for a hospitalist whose sole role for the day is to admit patients.” Nationally up to 51.2% of hospitalist groups utilize a dedicated daytime admitter.
The report found that hospital services for which hospitalists are more likely to be attendings than consultants include GI/liver, 78.4%; palliative care, 77.3%; neurology/stroke, 73.6%; oncology, 67.8%; cardiology, 56.9%; and critical care, 50.7%. Conditions where hospitalists are more likely to consult rather than admit and attend include neurosurgery, orthopedics, general surgery, cardiovascular surgery, and other surgical subspecialties.
Other hospital services routinely provided by adult-only hospitalists include care of patients in an ICU setting (62.7%); primary responsibility for observation units (54.6%); primary clinical responsibility for rapid response teams (48.8%); primary responsibility for code blue or cardiac arrest teams (43.8%); nighttime admissions or tuck-in services (33.9%); and medical procedures (31.5%). For pediatric hospital medicine groups, care of healthy newborns and medical procedures were among the most common services provided, while for hospitalists serving adults and children, rapid response teams, ICUs, and specialty units were most common.
New models of payment for health care
As the larger health care system is being transformed by new payment models and benefit structures, including accountable care organizations (ACOs), value-based purchasing, bundled payments, and other forms of population-based coverage – which is described as a volume-to-value shift in health care – how are these new models affecting hospitalists?
Observers say penetration of these new models varies widely by locality but they haven’t had much direct impact on hospitalists’ practices – at least not yet. However, as hospitals and health systems find themselves needing to learn new ways to invest their resources differently in response to these trends, what matters to the hospital should be of great importance to the hospitalist group.
“I haven’t seen a lot of dramatic changes in how hospitalists engage with value-based purchasing,” Dr. White said. “If we know that someone is part of an ACO, the instinctual – and right – response is to treat them like any other patient. But we still need to be committed to not waste resources.”
Hospitalists are the best people to understand the intricacies of how the health care system works under value-based approaches, Dr. Huang said. “That’s why so many hospitalists have taken leadership positions in their hospitals. I think all of this translates to the practical, day-to-day work of hospitalists, reflected in our focus on readmissions and length of stay.”
Dr. Williams said the health care system still hasn’t turned the corner from fee-for-service to value-based purchasing. “It still represents a tiny fraction of the income of hospitalists. Hospitals still have to focus on the bottom line, as fee-for-service reimbursement for hospitalized patients continues to get squeezed, and ACOs aren’t exactly paying premium rates either. Ask almost any hospital CEO what drives their bottom line today and the answer is volume – along with optimizing productivity. Pretty much every place I look, the future does not look terribly rosy for hospitals.”
Ms. Himebaugh said she is bullish on hospital medicine, in the sense that it’s unlikely to go away anytime soon. “Hospitalists are needed and provide value. But I don’t think we have devised the right model yet. I’m not sure our current model is sustainable. We need to find new models we can afford that don’t require squeezing our providers.”
For more information about the 2018 State of Hospital Medicine Report, contact SHM’s Practice Management Department at: survey@hospitalmedicine.org or call 800-843-3360. See also: https://www.hospitalmedicine.org/practice-management/shms-state-of-hospital-medicine/.
A deep commitment to veterans’ medical needs
VA hospitalist Dr. Mel Anderson loves his work
Mel C. Anderson, MD, FACP, section chief of hospital medicine for the Veterans Administration of Eastern Colorado, and his hospitalist colleagues share a mission to care for the men and women who served their country in the armed forces and are now being served by the VA.

“That mission binds us together in a deep and impactful way,” he said. “One of the greatest joys of my life has been to dedicate, with the teams I lead, our hearts and minds to serving this population of veterans.”
Approximately 400 hospitalists work nationwide in the VA, the country’s largest integrated health system, typically in groups of about a dozen. Not every VA medical center employs hospitalists; this depends on local tradition and size of the facility. Dr. Anderson was for several years the lone hospitalist at the VA Medical Center in Denver, starting in 2005, and now he heads a group of 17. The Denver facility employs five inpatient teams plus nocturnists, supported by residents, interns, and medical students in training from the University of Colorado at Denver, Aurora, to deliver all of its inpatient medical care.
“We also have an open ICU here. Hospitalists are able to follow their patients across the hospital, and we can make the decision to move them to the ICU,” Dr. Anderson said. The Denver group also established a hospitalist-staffed postdischarge clinic, where patients can reconnect with their hospital team. “It’s not to supplant primary care but to help promote safe transit as the patient moves back to the community,” he said. “We’ve also developed a surgery consult service for orthopedics and other surgical subspecialties.”
The VA’s integrated electronic medical record facilitates communication between hospitalists and primary care physicians, with instant messaging for updating the PCPs on the patient’s hospital stay.
The Denver VA hospitalists value their collegial culture, Dr. Anderson said. “We are invested in our group and in one another and in life-long learning. I often ask my group for their feedback. It’s one of the singular joys of my career to lead such a wonderful group, which has been built up person by person. I hired every single member. As much as their clinical skills and the achievements on their curriculum vitae were important, I also paid attention to their interpersonal communication skills.”
Members of the Denver hospitalist group also share an academic focus and commitment to scholarship and research. Dr. Anderson’s academic emphasis is on how to promote teaching and faculty development through organized bedside rounding and how to orient students to teaching as a potential career path. He is associate program director for medicine residencies at the University of Colorado and leads its Clinician/Educator Pathway.
The VA hospital’s interdisciplinary bedside rounding initiative involves the medicine team – students, residents, attending – and pharmacist, plus the patient’s bedside nurse and nurse care coordinator. “We have worked on fostering an interdisciplinary culture, and we’re very proud of the rounding model we developed here. We all round together at the bedside, and typically that might include 7 or 8 people,” Dr. Anderson explained.
“In planning this program, we used a Rapid Performance Improvement Project team with a nurse, pharmacist, and physical therapist helping us envision how to redesign rounds to overcome the time constraints,” he said. “We altered nurses’ work flow to permit them to join the rounding for their patients, and we moved morning medication administration to 7 a.m., so it wouldn’t get in the way of the rounding. We now audit rates of physician-to-nurse communication on rounds and how often we successfully achieve the nurse’s participation.”1 This approach has also cut rates of phone pages from nurses to house staff, and substantially increased job satisfaction.
What’s different in the VA?
The work of hospitalists in the VA is mostly similar to other hospital settings, but perhaps with more intensity, Dr. Anderson said. There are comorbidities such as higher rates of PTSD, alcohol use disorder, substance abuse, and mental health issues – all of which have an effect over time on patients. But veterans also have different attitudes about, for example, pain.
“When patients are asked to rate their pain on a scale of 0 to 10, for a veteran of a foreign war, 2 out of 10 is not the same as someone else’s 2 out of 10. How do we compensate for that difference?” he said. “And while awareness of PTSD and efforts to mitigate its impact have made incredible gains over the past 15 years, we still see a lot of these issues and their manifestations in social challenges such as homelessness. We are fortunate to have VA outpatient services and homeless veteran programs to help with these issues.”
There is a different paradigm for care at the VA, Dr. Anderson said. “We are a not-for-profit institution with the welfare of veterans as our primary aim. Beyond their health and wellness, that means supporting them in other ways and reaching out into the community. As doctors and nurses we feel a kinship around that mission, although we also have to be stewards of taxpayer dollars. We recognize that the VA is a large and complicated, somewhat inertia-laden organization in which making changes can be very challenging. But there are also opportunities as a national organization to effect changes on a national scale.”
Dr. Anderson chairs the VA’s Hospitalist Field Advisory Committee (HFAC), a group of about eight hospitalists empaneled to advise the system’s Office of Specialty Care Services on clinical policy and program development. They serve 3-year terms and meet monthly by phone and annually in Washington. The HFAC’s last annual meeting occurred in mid-September 2018 in Washington with a focus on developing a hospital medicine annual survey and needs assessment, revisiting strategic goals, and convening multilateral meetings with the chiefs of medicine and emergency medicine FACs.
“Our biggest emphasis is clinical – this includes clinical pathways, best practices for managing PTSD or acute coronary syndrome, and the like. We also share management issues, such as how to configure medical records or arrange night coverage. This is a national conversation to share what some sites have already experienced and learned,” Dr. Anderson said.
“We also have a VA Academic Hospitalist Subcommittee, working together on multisite research studies and on resident education protocols. Because we’re a large system, we’re able to connect with one another and leverage what we’ve learned. I get emails almost every day about research topics from colleagues across the country,” he said. A collaborative website and email distribution list allows doctors to post questions to their peers nationwide.
A calling for hospital medicine
Before moving to Denver, Dr. Anderson served as a major in the Air Force Medical Corps and was based at the David Grant US Air Force Medical Center on Travis Air Force Base in California – which is where he did his residency. In the course of a “traditionalist” internal medical training, including 4-month stints on hospital wards in addition to outpatient services, he realized he had a calling for hospital medicine.
In a job at the Providence (R.I.) VA Medical Center, he exclusively practiced outpatient care, but he found that he missed key aspects of inpatient work, such as the intensity of the clinical issues and teaching encounters. “I cold-called the hospital’s chief of medicine and volunteered to start mentoring inpatient residents,” Dr. Anderson said. “That was 17 years ago.”
Another abiding interest derived from Dr. Anderson’s military service is travel medicine. While a physician in the Air Force, he was deployed to Haiti in 1995 and to Nicaragua in 2000, where he treated thousands of patients – both U.S. service personnel and local populations.
“In Haiti, our primary mission was for U.S. troops who were still based there following the 1994 Operation Uphold Democracy intervention, but there were a lot fewer of them, so we mostly kept busy providing care to Haitian nationals,” he said. “That work was eye opening, to say the least,” and led to a professional interest in tropical illnesses. “Since then, I’ve been a visiting professor for the University of Colorado posted to the University of Zimbabwe in Harare in 2012 and 2016.”
What gives Dr. Anderson such joy and enthusiasm for his VA work? “I am a curious lifelong learner. Every day, there are 10 new things I need to learn, whether clinically or operationally in a big hospital system or just the day-to-day realities of leading a group of physicians. I never feel like I’m treading water,” he said. He is also energized by teaching – seeing “the light bulb go on” for the students he is instructing – and by serving as a role model for doctors in training.
“As I contemplate all the simultaneous balls I have in the air, including our recent move into a new hospital building, sometimes I think it is kind of crazy to be doing as much as I do,” he said. “But I also take time away, balancing work versus nonwork.” He spends quality time with his wife of 21 years, 17-year-old daughter, other relatives, and friends, as well as on physical activity, reading books about philosophy, and his hobby of rebuilding motorcycles, which he says offers a kind of meditative calm.
“I also feel a deep sense of service – to patients, colleagues, students, and to the mission of the VA,” Dr. Anderson said. “There is truly something special about caring for the veteran. It’s hard to articulate, but it really keeps us coming back for more. I’ve had vets sing to me, tell jokes, do magic tricks, share their war stories. I’ve had patients open up to me in ways that were both profound and humbling.”
References
1. Young E et al. Impact of altered medication administration time on interdisciplinary bedside rounds on academic medical ward. J Nurs Care Qual. 2017 Jul/Sep;32(3):218-225.
VA hospitalist Dr. Mel Anderson loves his work
VA hospitalist Dr. Mel Anderson loves his work
Mel C. Anderson, MD, FACP, section chief of hospital medicine for the Veterans Administration of Eastern Colorado, and his hospitalist colleagues share a mission to care for the men and women who served their country in the armed forces and are now being served by the VA.
“That mission binds us together in a deep and impactful way,” he said. “One of the greatest joys of my life has been to dedicate, with the teams I lead, our hearts and minds to serving this population of veterans.”
Approximately 400 hospitalists work nationwide in the VA, the country’s largest integrated health system, typically in groups of about a dozen. Not every VA medical center employs hospitalists; this depends on local tradition and size of the facility. Dr. Anderson was for several years the lone hospitalist at the VA Medical Center in Denver, starting in 2005, and now he heads a group of 17. The Denver facility employs five inpatient teams plus nocturnists, supported by residents, interns, and medical students in training from the University of Colorado at Denver, Aurora, to deliver all of its inpatient medical care.
“We also have an open ICU here. Hospitalists are able to follow their patients across the hospital, and we can make the decision to move them to the ICU,” Dr. Anderson said. The Denver group also established a hospitalist-staffed postdischarge clinic, where patients can reconnect with their hospital team. “It’s not to supplant primary care but to help promote safe transit as the patient moves back to the community,” he said. “We’ve also developed a surgery consult service for orthopedics and other surgical subspecialties.”
The VA’s integrated electronic medical record facilitates communication between hospitalists and primary care physicians, with instant messaging for updating the PCPs on the patient’s hospital stay.
The Denver VA hospitalists value their collegial culture, Dr. Anderson said. “We are invested in our group and in one another and in life-long learning. I often ask my group for their feedback. It’s one of the singular joys of my career to lead such a wonderful group, which has been built up person by person. I hired every single member. As much as their clinical skills and the achievements on their curriculum vitae were important, I also paid attention to their interpersonal communication skills.”
Members of the Denver hospitalist group also share an academic focus and commitment to scholarship and research. Dr. Anderson’s academic emphasis is on how to promote teaching and faculty development through organized bedside rounding and how to orient students to teaching as a potential career path. He is associate program director for medicine residencies at the University of Colorado and leads its Clinician/Educator Pathway.
The VA hospital’s interdisciplinary bedside rounding initiative involves the medicine team – students, residents, attending – and pharmacist, plus the patient’s bedside nurse and nurse care coordinator. “We have worked on fostering an interdisciplinary culture, and we’re very proud of the rounding model we developed here. We all round together at the bedside, and typically that might include 7 or 8 people,” Dr. Anderson explained.
“In planning this program, we used a Rapid Performance Improvement Project team with a nurse, pharmacist, and physical therapist helping us envision how to redesign rounds to overcome the time constraints,” he said. “We altered nurses’ work flow to permit them to join the rounding for their patients, and we moved morning medication administration to 7 a.m., so it wouldn’t get in the way of the rounding. We now audit rates of physician-to-nurse communication on rounds and how often we successfully achieve the nurse’s participation.”1 This approach has also cut rates of phone pages from nurses to house staff, and substantially increased job satisfaction.
What’s different in the VA?
The work of hospitalists in the VA is mostly similar to other hospital settings, but perhaps with more intensity, Dr. Anderson said. There are comorbidities such as higher rates of PTSD, alcohol use disorder, substance abuse, and mental health issues – all of which have an effect over time on patients. But veterans also have different attitudes about, for example, pain.
“When patients are asked to rate their pain on a scale of 0 to 10, for a veteran of a foreign war, 2 out of 10 is not the same as someone else’s 2 out of 10. How do we compensate for that difference?” he said. “And while awareness of PTSD and efforts to mitigate its impact have made incredible gains over the past 15 years, we still see a lot of these issues and their manifestations in social challenges such as homelessness. We are fortunate to have VA outpatient services and homeless veteran programs to help with these issues.”
There is a different paradigm for care at the VA, Dr. Anderson said. “We are a not-for-profit institution with the welfare of veterans as our primary aim. Beyond their health and wellness, that means supporting them in other ways and reaching out into the community. As doctors and nurses we feel a kinship around that mission, although we also have to be stewards of taxpayer dollars. We recognize that the VA is a large and complicated, somewhat inertia-laden organization in which making changes can be very challenging. But there are also opportunities as a national organization to effect changes on a national scale.”
Dr. Anderson chairs the VA’s Hospitalist Field Advisory Committee (HFAC), a group of about eight hospitalists empaneled to advise the system’s Office of Specialty Care Services on clinical policy and program development. They serve 3-year terms and meet monthly by phone and annually in Washington. The HFAC’s last annual meeting occurred in mid-September 2018 in Washington with a focus on developing a hospital medicine annual survey and needs assessment, revisiting strategic goals, and convening multilateral meetings with the chiefs of medicine and emergency medicine FACs.
“Our biggest emphasis is clinical – this includes clinical pathways, best practices for managing PTSD or acute coronary syndrome, and the like. We also share management issues, such as how to configure medical records or arrange night coverage. This is a national conversation to share what some sites have already experienced and learned,” Dr. Anderson said.
“We also have a VA Academic Hospitalist Subcommittee, working together on multisite research studies and on resident education protocols. Because we’re a large system, we’re able to connect with one another and leverage what we’ve learned. I get emails almost every day about research topics from colleagues across the country,” he said. A collaborative website and email distribution list allows doctors to post questions to their peers nationwide.
A calling for hospital medicine
Before moving to Denver, Dr. Anderson served as a major in the Air Force Medical Corps and was based at the David Grant US Air Force Medical Center on Travis Air Force Base in California – which is where he did his residency. In the course of a “traditionalist” internal medical training, including 4-month stints on hospital wards in addition to outpatient services, he realized he had a calling for hospital medicine.
In a job at the Providence (R.I.) VA Medical Center, he exclusively practiced outpatient care, but he found that he missed key aspects of inpatient work, such as the intensity of the clinical issues and teaching encounters. “I cold-called the hospital’s chief of medicine and volunteered to start mentoring inpatient residents,” Dr. Anderson said. “That was 17 years ago.”
Another abiding interest derived from Dr. Anderson’s military service is travel medicine. While a physician in the Air Force, he was deployed to Haiti in 1995 and to Nicaragua in 2000, where he treated thousands of patients – both U.S. service personnel and local populations.
“In Haiti, our primary mission was for U.S. troops who were still based there following the 1994 Operation Uphold Democracy intervention, but there were a lot fewer of them, so we mostly kept busy providing care to Haitian nationals,” he said. “That work was eye opening, to say the least,” and led to a professional interest in tropical illnesses. “Since then, I’ve been a visiting professor for the University of Colorado posted to the University of Zimbabwe in Harare in 2012 and 2016.”
What gives Dr. Anderson such joy and enthusiasm for his VA work? “I am a curious lifelong learner. Every day, there are 10 new things I need to learn, whether clinically or operationally in a big hospital system or just the day-to-day realities of leading a group of physicians. I never feel like I’m treading water,” he said. He is also energized by teaching – seeing “the light bulb go on” for the students he is instructing – and by serving as a role model for doctors in training.
“As I contemplate all the simultaneous balls I have in the air, including our recent move into a new hospital building, sometimes I think it is kind of crazy to be doing as much as I do,” he said. “But I also take time away, balancing work versus nonwork.” He spends quality time with his wife of 21 years, 17-year-old daughter, other relatives, and friends, as well as on physical activity, reading books about philosophy, and his hobby of rebuilding motorcycles, which he says offers a kind of meditative calm.
“I also feel a deep sense of service – to patients, colleagues, students, and to the mission of the VA,” Dr. Anderson said. “There is truly something special about caring for the veteran. It’s hard to articulate, but it really keeps us coming back for more. I’ve had vets sing to me, tell jokes, do magic tricks, share their war stories. I’ve had patients open up to me in ways that were both profound and humbling.”
References
1. Young E et al. Impact of altered medication administration time on interdisciplinary bedside rounds on academic medical ward. J Nurs Care Qual. 2017 Jul/Sep;32(3):218-225.
Mel C. Anderson, MD, FACP, section chief of hospital medicine for the Veterans Administration of Eastern Colorado, and his hospitalist colleagues share a mission to care for the men and women who served their country in the armed forces and are now being served by the VA.
“That mission binds us together in a deep and impactful way,” he said. “One of the greatest joys of my life has been to dedicate, with the teams I lead, our hearts and minds to serving this population of veterans.”
Approximately 400 hospitalists work nationwide in the VA, the country’s largest integrated health system, typically in groups of about a dozen. Not every VA medical center employs hospitalists; this depends on local tradition and size of the facility. Dr. Anderson was for several years the lone hospitalist at the VA Medical Center in Denver, starting in 2005, and now he heads a group of 17. The Denver facility employs five inpatient teams plus nocturnists, supported by residents, interns, and medical students in training from the University of Colorado at Denver, Aurora, to deliver all of its inpatient medical care.
“We also have an open ICU here. Hospitalists are able to follow their patients across the hospital, and we can make the decision to move them to the ICU,” Dr. Anderson said. The Denver group also established a hospitalist-staffed postdischarge clinic, where patients can reconnect with their hospital team. “It’s not to supplant primary care but to help promote safe transit as the patient moves back to the community,” he said. “We’ve also developed a surgery consult service for orthopedics and other surgical subspecialties.”
The VA’s integrated electronic medical record facilitates communication between hospitalists and primary care physicians, with instant messaging for updating the PCPs on the patient’s hospital stay.
The Denver VA hospitalists value their collegial culture, Dr. Anderson said. “We are invested in our group and in one another and in life-long learning. I often ask my group for their feedback. It’s one of the singular joys of my career to lead such a wonderful group, which has been built up person by person. I hired every single member. As much as their clinical skills and the achievements on their curriculum vitae were important, I also paid attention to their interpersonal communication skills.”
Members of the Denver hospitalist group also share an academic focus and commitment to scholarship and research. Dr. Anderson’s academic emphasis is on how to promote teaching and faculty development through organized bedside rounding and how to orient students to teaching as a potential career path. He is associate program director for medicine residencies at the University of Colorado and leads its Clinician/Educator Pathway.
The VA hospital’s interdisciplinary bedside rounding initiative involves the medicine team – students, residents, attending – and pharmacist, plus the patient’s bedside nurse and nurse care coordinator. “We have worked on fostering an interdisciplinary culture, and we’re very proud of the rounding model we developed here. We all round together at the bedside, and typically that might include 7 or 8 people,” Dr. Anderson explained.
“In planning this program, we used a Rapid Performance Improvement Project team with a nurse, pharmacist, and physical therapist helping us envision how to redesign rounds to overcome the time constraints,” he said. “We altered nurses’ work flow to permit them to join the rounding for their patients, and we moved morning medication administration to 7 a.m., so it wouldn’t get in the way of the rounding. We now audit rates of physician-to-nurse communication on rounds and how often we successfully achieve the nurse’s participation.”1 This approach has also cut rates of phone pages from nurses to house staff, and substantially increased job satisfaction.
What’s different in the VA?
The work of hospitalists in the VA is mostly similar to other hospital settings, but perhaps with more intensity, Dr. Anderson said. There are comorbidities such as higher rates of PTSD, alcohol use disorder, substance abuse, and mental health issues – all of which have an effect over time on patients. But veterans also have different attitudes about, for example, pain.
“When patients are asked to rate their pain on a scale of 0 to 10, for a veteran of a foreign war, 2 out of 10 is not the same as someone else’s 2 out of 10. How do we compensate for that difference?” he said. “And while awareness of PTSD and efforts to mitigate its impact have made incredible gains over the past 15 years, we still see a lot of these issues and their manifestations in social challenges such as homelessness. We are fortunate to have VA outpatient services and homeless veteran programs to help with these issues.”
There is a different paradigm for care at the VA, Dr. Anderson said. “We are a not-for-profit institution with the welfare of veterans as our primary aim. Beyond their health and wellness, that means supporting them in other ways and reaching out into the community. As doctors and nurses we feel a kinship around that mission, although we also have to be stewards of taxpayer dollars. We recognize that the VA is a large and complicated, somewhat inertia-laden organization in which making changes can be very challenging. But there are also opportunities as a national organization to effect changes on a national scale.”
Dr. Anderson chairs the VA’s Hospitalist Field Advisory Committee (HFAC), a group of about eight hospitalists empaneled to advise the system’s Office of Specialty Care Services on clinical policy and program development. They serve 3-year terms and meet monthly by phone and annually in Washington. The HFAC’s last annual meeting occurred in mid-September 2018 in Washington with a focus on developing a hospital medicine annual survey and needs assessment, revisiting strategic goals, and convening multilateral meetings with the chiefs of medicine and emergency medicine FACs.
“Our biggest emphasis is clinical – this includes clinical pathways, best practices for managing PTSD or acute coronary syndrome, and the like. We also share management issues, such as how to configure medical records or arrange night coverage. This is a national conversation to share what some sites have already experienced and learned,” Dr. Anderson said.
“We also have a VA Academic Hospitalist Subcommittee, working together on multisite research studies and on resident education protocols. Because we’re a large system, we’re able to connect with one another and leverage what we’ve learned. I get emails almost every day about research topics from colleagues across the country,” he said. A collaborative website and email distribution list allows doctors to post questions to their peers nationwide.
A calling for hospital medicine
Before moving to Denver, Dr. Anderson served as a major in the Air Force Medical Corps and was based at the David Grant US Air Force Medical Center on Travis Air Force Base in California – which is where he did his residency. In the course of a “traditionalist” internal medical training, including 4-month stints on hospital wards in addition to outpatient services, he realized he had a calling for hospital medicine.
In a job at the Providence (R.I.) VA Medical Center, he exclusively practiced outpatient care, but he found that he missed key aspects of inpatient work, such as the intensity of the clinical issues and teaching encounters. “I cold-called the hospital’s chief of medicine and volunteered to start mentoring inpatient residents,” Dr. Anderson said. “That was 17 years ago.”
Another abiding interest derived from Dr. Anderson’s military service is travel medicine. While a physician in the Air Force, he was deployed to Haiti in 1995 and to Nicaragua in 2000, where he treated thousands of patients – both U.S. service personnel and local populations.
“In Haiti, our primary mission was for U.S. troops who were still based there following the 1994 Operation Uphold Democracy intervention, but there were a lot fewer of them, so we mostly kept busy providing care to Haitian nationals,” he said. “That work was eye opening, to say the least,” and led to a professional interest in tropical illnesses. “Since then, I’ve been a visiting professor for the University of Colorado posted to the University of Zimbabwe in Harare in 2012 and 2016.”
What gives Dr. Anderson such joy and enthusiasm for his VA work? “I am a curious lifelong learner. Every day, there are 10 new things I need to learn, whether clinically or operationally in a big hospital system or just the day-to-day realities of leading a group of physicians. I never feel like I’m treading water,” he said. He is also energized by teaching – seeing “the light bulb go on” for the students he is instructing – and by serving as a role model for doctors in training.
“As I contemplate all the simultaneous balls I have in the air, including our recent move into a new hospital building, sometimes I think it is kind of crazy to be doing as much as I do,” he said. “But I also take time away, balancing work versus nonwork.” He spends quality time with his wife of 21 years, 17-year-old daughter, other relatives, and friends, as well as on physical activity, reading books about philosophy, and his hobby of rebuilding motorcycles, which he says offers a kind of meditative calm.
“I also feel a deep sense of service – to patients, colleagues, students, and to the mission of the VA,” Dr. Anderson said. “There is truly something special about caring for the veteran. It’s hard to articulate, but it really keeps us coming back for more. I’ve had vets sing to me, tell jokes, do magic tricks, share their war stories. I’ve had patients open up to me in ways that were both profound and humbling.”
References
1. Young E et al. Impact of altered medication administration time on interdisciplinary bedside rounds on academic medical ward. J Nurs Care Qual. 2017 Jul/Sep;32(3):218-225.
Hospitalist groups explore use of medical scribes
Can scribes reduce doctors’ job stress?
Physician stress and burnout remain major concerns for the U.S. health care system, with frustrations over the electronic health record (EHR) driving much of the dissatisfaction experienced by hospitalists and other physicians in the hospital.1 Underlying the EHR conundrum is a deeper question: Is entering clinical data on a computer the best use of a doctor’s time and professional skills? Or could a portion of that clerical function be delegated to nonphysicians?
Trained medical scribes, charting specialists who input EHR data for physicians on rounds, have been offered as a solution to potentially affect job stress for physicians and shorten their work days. But while scribes have been used and tested by different hospitalist groups around the country, the concept has not taken off in hospital medicine the way it has in certain other settings, such as emergency departments.
“The demand for scribes doesn’t seem to have materialized in a big way for hospital medicine,” said John Nelson, MD, MHM, a hospitalist and consultant in Bellevue, Wash., and a cofounder of the Society of Hospital Medicine. “I’m not convinced that scribes have had a big impact on hospitalist burnout.” It’s difficult to share scribes between doctors on a shift, and it’s a problem if the scribe and doctor get physically separated in the hospital. There’s also the question of who should pay the scribe’s salary, Dr. Nelson said.
Frustrations with the EHR can be a major factor in the experience of physician burnout, but Dr. Nelson said hospitalists can get proficient more quickly because they’re using the same computer system all day. “The bigger problem is that other doctors like surgeons don’t learn how to use the EHR and dump their routine tasks involving the EHR on the hospitalist, which means more work that is less satisfying.”
Could pairing a scribe with a hospitalist improve efficiency and decrease costs relative to the expense of employing the scribe? Are there specific settings, applications, and caseloads in hospital medicine where it makes more sense to use a scribe to support and assist doctors while they’re meeting with patients, with the doctor reviewing and editing the scribe’s work for accuracy? Could the scribe even help with physician staffing shortages by making doctors more productive?
TeamHealth, a national physician services company based in Knoxville, Tenn., has used scribes in emergency departments for years but had concluded that they made less sense for its hospitalist groups after a failure to document significant net increases in productivity, according to a 2015 report in The Hospitalist.2 Michael Corvini, MD, FACP, FACEP, TeamHealth’s new regional medical director for acute care services, said he brought extensive positive experience with scribes to his new job and is quite excited about their potential for hospital medicine. “When I came to TeamHealth in July, I began to suggest that there was unrealized potential for scribes,” he said.
Dr. Corvini noted that a potential benefit of scribes for patients is that their presence may allow for more face time with the doctor. Providers, relieved of worrying about completing the chart in its entirety would be more able to focus on the patient and critical thinking. There are even benefits for scribes themselves. Often scribes are medical students, and those who are interested in pursuing a future in the health professions gain invaluable experience in the workings of medicine. “They are making a real contribution to patient care. They are a member of the health care team,” he said.
Dr. Corvini sees two primary areas in which scribes can contribute to hospital medicine. The first is shadowing the physician who is admitting patients during a high-volume admissions shift. Regular tasks like capturing the patient’s medication list and populating the History and Physical document lend themselves well to data entry by scribes, in contrast to completing more routine daily progress notes, which does not.
“They can also be helpful when there is a major transition from paper charting to the EHR or from one EHR system to another, when there is a lot of stress on the physician and risk for lost billing revenue,” Dr. Corvini said. “If scribes are trained in a particular EHR, they could help teach the physician how to use it.” TeamHealth is now in the process of running a trial of scribes at one of its sites, and the organization plans to measure productivity, provider satisfaction, and HCAHPS patient satisfaction scores.
A workaround – or a problem solver?
In a 2015 Viewpoint article in JAMA,3 George Gellert, MD, MPH, MPA, former chief medical information officer for the CHRISTUS Santa Rosa health system in San Antonio, Texas, and his coauthors labeled the use of scribes as a “workaround” that could curtail efforts to make EHRs more functionally operational because their use allows physicians to be satisfied with inferior EHR products.
In an interview, Dr. Gellert stated that he hasn’t changed his views about the negative consequences of scribes on EHR improvement. “The work of clinicians in using and advancing EHR technology is presently the only method we have for massively distributing and ensuring the use of evidence-based medicine,” he said. “That in turn is a critical strategy for reducing high rates of medical errors through a variety of decision-support applications.”
For better or worse, EHRs are an essential part of the solution to the epidemic of preventable, medical error–caused patient deaths, Dr. Gellert said. He also believes that substantial progress has already been made in advancing EHR usability, as reflected in the most recent product releases by leading EHR companies. However, considerable evolution is still needed in both usability and optimization of clinical decision support.
“With respect to your readers, my recommendation is to not use medical scribes, or else delimit their use to only where absolutely required. Instead, develop systematic processes to regularly capture specific physician concerns with the EHR being used, and transmit that critical information to their EHR vendor with a clear expectation that the manufacturer will address the issue in the near term, or at least in their next major product iteration or generation,” Dr. Gellert said.
By contrast, at the Management of the Hospitalized Patient conference in San Francisco in October 2015, Christine Sinsky, MD, FACP, vice president for professional satisfaction at the American Medical Association, identified documentation assistance as a helpful intervention for physician stress and burnout.4 In a recent email, Dr. Sinsky called documentation assistance “the most powerful intervention to give patients the time, attention, and care they need from their physicians. The data entry and data retrieval work of health care has grown over the last decade. Sharing this work with nonphysicians allows society to get the most value for its investment in physicians’ training.”
Dr. Sinsky calls documentation assistance – such as that provided by medical scribes – “a logical and strategic delegation of work according to ability for greater value,” not a workaround. She said it makes patient care safer by allowing physicians to focus on medical decision making and relationship building – rather than record keeping.
Experience from the front lines
Eric Edwards, MD, FAAP, FHM, of the division of hospital medicine at the University of North Carolina’s Hillsborough Hospital campus, recently presented a poster on his group’s experience with medical scribes at a meeting of the North Carolina Triangle Chapter of SHM. Their research concluded that scribes can be successfully incorporated into an inpatient hospital medicine practice and thus increase provider satisfaction and decrease the time clinicians spend charting.
“We were able to get the support of the hospital administration to pilot the use of scribes 3 days per week, which we’ve now done for almost a year,” Dr. Edwards said. Scribes are employed through a local company, MedScribes, and they work alongside admitting hospitalists during their 10-hour shifts. The hospitalists have been overwhelmingly positive about their experience, he said. “We established that it saves the physician 15 minutes per patient encounter by helping with documentation.”
It’s important that the scribe gets to know an individual provider’s personal preferences, Dr. Edwards said. Some hospitalists create their own charting templates. There’s also a need to train the clinician in how to use the medical scribe. For example, physicians are instructed to call out physical findings during their exam, which simultaneously informs the patient while allowing the scribe to document the exam.
“We are working on getting more formal data about the scribe experience,” he added. “But we have found that our providers love it, and it improves their efficiency and productivity. The danger is if the physician becomes too reliant on the scribe and fails to exercise due diligence in reviewing the scribe’s notes to ensure that all relevant information is in the chart and irrelevant information is not. We need to make sure we are carefully reviewing and signing off on the scribe’s notes,” he explained.
“I think we’re years away from improving the EHR to the point that would allow us to call it doctor friendly,” Dr. Edwards said. “For now, the scribe is a great way to alleviate some of the physician’s burden. But for hospitalist groups to use scribes successfully, it can’t be done haphazardly. We are lucky to have an experienced local scribe company to partner with. They provide systematic training and orientation. It’s also important that scribes are trained in the specific EHR that they will be using.”
Christine Lum Lung, MD, SFHM, CEO and medical director of Northern Colorado Hospitalists, a hospital medicine group at the University of Colorado’s North Campus hospitals in Fort Collins, has been studying the use of scribes since 2014. “We had a gap in bringing on new doctors fast enough for our group’s needs, so I looked into the return on investment from scribes and pitched it to our group,” she said. “It’s difficult to say what has been the actual impact on caseload, but we all think it has reduced physician workdays by an hour or greater.”
The 32-member hospitalist group, which covers two facilities, has a designated director of scribes who periodically surveys the hospitalists’ satisfaction with the scribes. “Now we all embrace the use of scribes. Satisfaction is high, and quality of life has improved,” Dr. Lum Lung said. “It’s hard to quantify, but we feel like it helps with burnout for us to be able to leave work earlier, and it alleviates some of the other stresses in our workday.”
She said scribes are important to the medical team not just with managing the EHR but also with other burdens such as documenting compliance with code status, VTEs, and other quality requirements, and to help with other regulatory issues. Scribes can look up lab values and radiology reports. When there are downtimes, they can prepare discharge plans.
Typically, there are five scribes on duty for 18 hours a day at each hospital, Dr. Lum Lung said. But only those doctors primarily doing admissions are assured of having a scribe to round with them. “Most doctors in the group would say the greatest efficiency of scribes is with admitting,” she said. The company that provides scribes to the UC hospitals, ScribeAmerica, handles administration, training, and human resource issues, and the scribe team has a designated Lead Scribe and Quality Scribe at their facility.
Studying the benefits
Andrew Friedson, PhD, a health care economist at the University of Colorado in Denver, recently conducted a 9-month randomized experiment in three hospital emergency rooms in the Denver area to determine the effects of scribes on measures of emergency physician productivity.5 He found that scribes reduced patient wait times in the emergency department by about 13 minutes per patient, while greatly decreasing the amount of time physicians spent after a shift completing their charting, which thus lowered overtime costs for ED physicians.

“This is one of the first times medical scribes have been studied with a randomized, controlled trial,” Dr. Friedson said. “I tracked the amount of overtime, patient waiting, and charge capture for each encounter. These were hospitals where the emergency doctors weren’t allowed to go home until their charting was done.” He discovered that there was a large drop in the time between when patients arrived at the ED and when a decision was made regarding whether to admit them. Additionally, charge capture increased significantly, and physicians had more time to perform medical procedures. Dr. Friedson believes that his findings hold implications for other settings and medical groups, including hospital medicine. To the extent that scribes free up hospitalists to perform tasks other than charting, they should provide an efficiency benefit.
So why hasn’t the medical scribe caught on in a bigger way for hospitalists, compared with ED physicians? For Dr. Corvini, the ED is an obvious, high-pressure, high-volume setting where the cost of the scribe can be easily recouped. “That doesn’t exist in such an obvious fashion in hospital medicine, except where high-volume admissions are concentrated in a single physician’s caseload,” he said. Not all hospitalist groups will fit that model. Some may divide admissions between hospitalists on a shift, and others may not be large enough to experience significant caseload pressures.
“EDs are obviously time pressured, and once scribes demonstrate the ability to produce documentation in a high-quality fashion, they are quickly accepted. In hospital medicine, the time pressures are different – not necessarily less, but different,” Dr. Corvini said. There are also differences in physician responsibilities between the ED and hospital medicine, as well as in physicians’ willingness to let go of documentation responsibilities. “My prediction, if the scribe test is rolled out successfully in TeamHealth, with measurable benefits, it will be adopted in other settings where it fits.”
References
1. Shanafelt TD et al. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016 Jul;91(7):836-48.
2. Collins TR. Use of medical scribes spurs debate about costs, difficulties of electronic health records. The Hospitalist; 2015 Oct.
3. Gellert GA et al. The rise of the medical scribe industry: Implications for the advancement of electronic health records. JAMA; 2015;313(13):1315-6.
4. Beresford L. Electronic Health Records Key Driver of Physician Burnout. The Hospitalist; 2015 Dec.
5. Friedson AI. Medical scribes as an input in healthcare production: Evidence from a randomized experiment. Am J Health Econ. 2017 Oct 2. doi: /10.1162/ajhe_a_00103.
Can scribes reduce doctors’ job stress?
Can scribes reduce doctors’ job stress?
Physician stress and burnout remain major concerns for the U.S. health care system, with frustrations over the electronic health record (EHR) driving much of the dissatisfaction experienced by hospitalists and other physicians in the hospital.1 Underlying the EHR conundrum is a deeper question: Is entering clinical data on a computer the best use of a doctor’s time and professional skills? Or could a portion of that clerical function be delegated to nonphysicians?
Trained medical scribes, charting specialists who input EHR data for physicians on rounds, have been offered as a solution to potentially affect job stress for physicians and shorten their work days. But while scribes have been used and tested by different hospitalist groups around the country, the concept has not taken off in hospital medicine the way it has in certain other settings, such as emergency departments.
“The demand for scribes doesn’t seem to have materialized in a big way for hospital medicine,” said John Nelson, MD, MHM, a hospitalist and consultant in Bellevue, Wash., and a cofounder of the Society of Hospital Medicine. “I’m not convinced that scribes have had a big impact on hospitalist burnout.” It’s difficult to share scribes between doctors on a shift, and it’s a problem if the scribe and doctor get physically separated in the hospital. There’s also the question of who should pay the scribe’s salary, Dr. Nelson said.
Frustrations with the EHR can be a major factor in the experience of physician burnout, but Dr. Nelson said hospitalists can get proficient more quickly because they’re using the same computer system all day. “The bigger problem is that other doctors like surgeons don’t learn how to use the EHR and dump their routine tasks involving the EHR on the hospitalist, which means more work that is less satisfying.”
Could pairing a scribe with a hospitalist improve efficiency and decrease costs relative to the expense of employing the scribe? Are there specific settings, applications, and caseloads in hospital medicine where it makes more sense to use a scribe to support and assist doctors while they’re meeting with patients, with the doctor reviewing and editing the scribe’s work for accuracy? Could the scribe even help with physician staffing shortages by making doctors more productive?
TeamHealth, a national physician services company based in Knoxville, Tenn., has used scribes in emergency departments for years but had concluded that they made less sense for its hospitalist groups after a failure to document significant net increases in productivity, according to a 2015 report in The Hospitalist.2 Michael Corvini, MD, FACP, FACEP, TeamHealth’s new regional medical director for acute care services, said he brought extensive positive experience with scribes to his new job and is quite excited about their potential for hospital medicine. “When I came to TeamHealth in July, I began to suggest that there was unrealized potential for scribes,” he said.
Dr. Corvini noted that a potential benefit of scribes for patients is that their presence may allow for more face time with the doctor. Providers, relieved of worrying about completing the chart in its entirety would be more able to focus on the patient and critical thinking. There are even benefits for scribes themselves. Often scribes are medical students, and those who are interested in pursuing a future in the health professions gain invaluable experience in the workings of medicine. “They are making a real contribution to patient care. They are a member of the health care team,” he said.
Dr. Corvini sees two primary areas in which scribes can contribute to hospital medicine. The first is shadowing the physician who is admitting patients during a high-volume admissions shift. Regular tasks like capturing the patient’s medication list and populating the History and Physical document lend themselves well to data entry by scribes, in contrast to completing more routine daily progress notes, which does not.
“They can also be helpful when there is a major transition from paper charting to the EHR or from one EHR system to another, when there is a lot of stress on the physician and risk for lost billing revenue,” Dr. Corvini said. “If scribes are trained in a particular EHR, they could help teach the physician how to use it.” TeamHealth is now in the process of running a trial of scribes at one of its sites, and the organization plans to measure productivity, provider satisfaction, and HCAHPS patient satisfaction scores.
A workaround – or a problem solver?
In a 2015 Viewpoint article in JAMA,3 George Gellert, MD, MPH, MPA, former chief medical information officer for the CHRISTUS Santa Rosa health system in San Antonio, Texas, and his coauthors labeled the use of scribes as a “workaround” that could curtail efforts to make EHRs more functionally operational because their use allows physicians to be satisfied with inferior EHR products.
In an interview, Dr. Gellert stated that he hasn’t changed his views about the negative consequences of scribes on EHR improvement. “The work of clinicians in using and advancing EHR technology is presently the only method we have for massively distributing and ensuring the use of evidence-based medicine,” he said. “That in turn is a critical strategy for reducing high rates of medical errors through a variety of decision-support applications.”
For better or worse, EHRs are an essential part of the solution to the epidemic of preventable, medical error–caused patient deaths, Dr. Gellert said. He also believes that substantial progress has already been made in advancing EHR usability, as reflected in the most recent product releases by leading EHR companies. However, considerable evolution is still needed in both usability and optimization of clinical decision support.
“With respect to your readers, my recommendation is to not use medical scribes, or else delimit their use to only where absolutely required. Instead, develop systematic processes to regularly capture specific physician concerns with the EHR being used, and transmit that critical information to their EHR vendor with a clear expectation that the manufacturer will address the issue in the near term, or at least in their next major product iteration or generation,” Dr. Gellert said.
By contrast, at the Management of the Hospitalized Patient conference in San Francisco in October 2015, Christine Sinsky, MD, FACP, vice president for professional satisfaction at the American Medical Association, identified documentation assistance as a helpful intervention for physician stress and burnout.4 In a recent email, Dr. Sinsky called documentation assistance “the most powerful intervention to give patients the time, attention, and care they need from their physicians. The data entry and data retrieval work of health care has grown over the last decade. Sharing this work with nonphysicians allows society to get the most value for its investment in physicians’ training.”
Dr. Sinsky calls documentation assistance – such as that provided by medical scribes – “a logical and strategic delegation of work according to ability for greater value,” not a workaround. She said it makes patient care safer by allowing physicians to focus on medical decision making and relationship building – rather than record keeping.
Experience from the front lines
Eric Edwards, MD, FAAP, FHM, of the division of hospital medicine at the University of North Carolina’s Hillsborough Hospital campus, recently presented a poster on his group’s experience with medical scribes at a meeting of the North Carolina Triangle Chapter of SHM. Their research concluded that scribes can be successfully incorporated into an inpatient hospital medicine practice and thus increase provider satisfaction and decrease the time clinicians spend charting.
“We were able to get the support of the hospital administration to pilot the use of scribes 3 days per week, which we’ve now done for almost a year,” Dr. Edwards said. Scribes are employed through a local company, MedScribes, and they work alongside admitting hospitalists during their 10-hour shifts. The hospitalists have been overwhelmingly positive about their experience, he said. “We established that it saves the physician 15 minutes per patient encounter by helping with documentation.”
It’s important that the scribe gets to know an individual provider’s personal preferences, Dr. Edwards said. Some hospitalists create their own charting templates. There’s also a need to train the clinician in how to use the medical scribe. For example, physicians are instructed to call out physical findings during their exam, which simultaneously informs the patient while allowing the scribe to document the exam.
“We are working on getting more formal data about the scribe experience,” he added. “But we have found that our providers love it, and it improves their efficiency and productivity. The danger is if the physician becomes too reliant on the scribe and fails to exercise due diligence in reviewing the scribe’s notes to ensure that all relevant information is in the chart and irrelevant information is not. We need to make sure we are carefully reviewing and signing off on the scribe’s notes,” he explained.
“I think we’re years away from improving the EHR to the point that would allow us to call it doctor friendly,” Dr. Edwards said. “For now, the scribe is a great way to alleviate some of the physician’s burden. But for hospitalist groups to use scribes successfully, it can’t be done haphazardly. We are lucky to have an experienced local scribe company to partner with. They provide systematic training and orientation. It’s also important that scribes are trained in the specific EHR that they will be using.”
Christine Lum Lung, MD, SFHM, CEO and medical director of Northern Colorado Hospitalists, a hospital medicine group at the University of Colorado’s North Campus hospitals in Fort Collins, has been studying the use of scribes since 2014. “We had a gap in bringing on new doctors fast enough for our group’s needs, so I looked into the return on investment from scribes and pitched it to our group,” she said. “It’s difficult to say what has been the actual impact on caseload, but we all think it has reduced physician workdays by an hour or greater.”
The 32-member hospitalist group, which covers two facilities, has a designated director of scribes who periodically surveys the hospitalists’ satisfaction with the scribes. “Now we all embrace the use of scribes. Satisfaction is high, and quality of life has improved,” Dr. Lum Lung said. “It’s hard to quantify, but we feel like it helps with burnout for us to be able to leave work earlier, and it alleviates some of the other stresses in our workday.”
She said scribes are important to the medical team not just with managing the EHR but also with other burdens such as documenting compliance with code status, VTEs, and other quality requirements, and to help with other regulatory issues. Scribes can look up lab values and radiology reports. When there are downtimes, they can prepare discharge plans.
Typically, there are five scribes on duty for 18 hours a day at each hospital, Dr. Lum Lung said. But only those doctors primarily doing admissions are assured of having a scribe to round with them. “Most doctors in the group would say the greatest efficiency of scribes is with admitting,” she said. The company that provides scribes to the UC hospitals, ScribeAmerica, handles administration, training, and human resource issues, and the scribe team has a designated Lead Scribe and Quality Scribe at their facility.
Studying the benefits
Andrew Friedson, PhD, a health care economist at the University of Colorado in Denver, recently conducted a 9-month randomized experiment in three hospital emergency rooms in the Denver area to determine the effects of scribes on measures of emergency physician productivity.5 He found that scribes reduced patient wait times in the emergency department by about 13 minutes per patient, while greatly decreasing the amount of time physicians spent after a shift completing their charting, which thus lowered overtime costs for ED physicians.
“This is one of the first times medical scribes have been studied with a randomized, controlled trial,” Dr. Friedson said. “I tracked the amount of overtime, patient waiting, and charge capture for each encounter. These were hospitals where the emergency doctors weren’t allowed to go home until their charting was done.” He discovered that there was a large drop in the time between when patients arrived at the ED and when a decision was made regarding whether to admit them. Additionally, charge capture increased significantly, and physicians had more time to perform medical procedures. Dr. Friedson believes that his findings hold implications for other settings and medical groups, including hospital medicine. To the extent that scribes free up hospitalists to perform tasks other than charting, they should provide an efficiency benefit.
So why hasn’t the medical scribe caught on in a bigger way for hospitalists, compared with ED physicians? For Dr. Corvini, the ED is an obvious, high-pressure, high-volume setting where the cost of the scribe can be easily recouped. “That doesn’t exist in such an obvious fashion in hospital medicine, except where high-volume admissions are concentrated in a single physician’s caseload,” he said. Not all hospitalist groups will fit that model. Some may divide admissions between hospitalists on a shift, and others may not be large enough to experience significant caseload pressures.
“EDs are obviously time pressured, and once scribes demonstrate the ability to produce documentation in a high-quality fashion, they are quickly accepted. In hospital medicine, the time pressures are different – not necessarily less, but different,” Dr. Corvini said. There are also differences in physician responsibilities between the ED and hospital medicine, as well as in physicians’ willingness to let go of documentation responsibilities. “My prediction, if the scribe test is rolled out successfully in TeamHealth, with measurable benefits, it will be adopted in other settings where it fits.”
References
1. Shanafelt TD et al. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016 Jul;91(7):836-48.
2. Collins TR. Use of medical scribes spurs debate about costs, difficulties of electronic health records. The Hospitalist; 2015 Oct.
3. Gellert GA et al. The rise of the medical scribe industry: Implications for the advancement of electronic health records. JAMA; 2015;313(13):1315-6.
4. Beresford L. Electronic Health Records Key Driver of Physician Burnout. The Hospitalist; 2015 Dec.
5. Friedson AI. Medical scribes as an input in healthcare production: Evidence from a randomized experiment. Am J Health Econ. 2017 Oct 2. doi: /10.1162/ajhe_a_00103.
Physician stress and burnout remain major concerns for the U.S. health care system, with frustrations over the electronic health record (EHR) driving much of the dissatisfaction experienced by hospitalists and other physicians in the hospital.1 Underlying the EHR conundrum is a deeper question: Is entering clinical data on a computer the best use of a doctor’s time and professional skills? Or could a portion of that clerical function be delegated to nonphysicians?
Trained medical scribes, charting specialists who input EHR data for physicians on rounds, have been offered as a solution to potentially affect job stress for physicians and shorten their work days. But while scribes have been used and tested by different hospitalist groups around the country, the concept has not taken off in hospital medicine the way it has in certain other settings, such as emergency departments.
“The demand for scribes doesn’t seem to have materialized in a big way for hospital medicine,” said John Nelson, MD, MHM, a hospitalist and consultant in Bellevue, Wash., and a cofounder of the Society of Hospital Medicine. “I’m not convinced that scribes have had a big impact on hospitalist burnout.” It’s difficult to share scribes between doctors on a shift, and it’s a problem if the scribe and doctor get physically separated in the hospital. There’s also the question of who should pay the scribe’s salary, Dr. Nelson said.
Frustrations with the EHR can be a major factor in the experience of physician burnout, but Dr. Nelson said hospitalists can get proficient more quickly because they’re using the same computer system all day. “The bigger problem is that other doctors like surgeons don’t learn how to use the EHR and dump their routine tasks involving the EHR on the hospitalist, which means more work that is less satisfying.”
Could pairing a scribe with a hospitalist improve efficiency and decrease costs relative to the expense of employing the scribe? Are there specific settings, applications, and caseloads in hospital medicine where it makes more sense to use a scribe to support and assist doctors while they’re meeting with patients, with the doctor reviewing and editing the scribe’s work for accuracy? Could the scribe even help with physician staffing shortages by making doctors more productive?
TeamHealth, a national physician services company based in Knoxville, Tenn., has used scribes in emergency departments for years but had concluded that they made less sense for its hospitalist groups after a failure to document significant net increases in productivity, according to a 2015 report in The Hospitalist.2 Michael Corvini, MD, FACP, FACEP, TeamHealth’s new regional medical director for acute care services, said he brought extensive positive experience with scribes to his new job and is quite excited about their potential for hospital medicine. “When I came to TeamHealth in July, I began to suggest that there was unrealized potential for scribes,” he said.
Dr. Corvini noted that a potential benefit of scribes for patients is that their presence may allow for more face time with the doctor. Providers, relieved of worrying about completing the chart in its entirety would be more able to focus on the patient and critical thinking. There are even benefits for scribes themselves. Often scribes are medical students, and those who are interested in pursuing a future in the health professions gain invaluable experience in the workings of medicine. “They are making a real contribution to patient care. They are a member of the health care team,” he said.
Dr. Corvini sees two primary areas in which scribes can contribute to hospital medicine. The first is shadowing the physician who is admitting patients during a high-volume admissions shift. Regular tasks like capturing the patient’s medication list and populating the History and Physical document lend themselves well to data entry by scribes, in contrast to completing more routine daily progress notes, which does not.
“They can also be helpful when there is a major transition from paper charting to the EHR or from one EHR system to another, when there is a lot of stress on the physician and risk for lost billing revenue,” Dr. Corvini said. “If scribes are trained in a particular EHR, they could help teach the physician how to use it.” TeamHealth is now in the process of running a trial of scribes at one of its sites, and the organization plans to measure productivity, provider satisfaction, and HCAHPS patient satisfaction scores.
A workaround – or a problem solver?
In a 2015 Viewpoint article in JAMA,3 George Gellert, MD, MPH, MPA, former chief medical information officer for the CHRISTUS Santa Rosa health system in San Antonio, Texas, and his coauthors labeled the use of scribes as a “workaround” that could curtail efforts to make EHRs more functionally operational because their use allows physicians to be satisfied with inferior EHR products.
In an interview, Dr. Gellert stated that he hasn’t changed his views about the negative consequences of scribes on EHR improvement. “The work of clinicians in using and advancing EHR technology is presently the only method we have for massively distributing and ensuring the use of evidence-based medicine,” he said. “That in turn is a critical strategy for reducing high rates of medical errors through a variety of decision-support applications.”
For better or worse, EHRs are an essential part of the solution to the epidemic of preventable, medical error–caused patient deaths, Dr. Gellert said. He also believes that substantial progress has already been made in advancing EHR usability, as reflected in the most recent product releases by leading EHR companies. However, considerable evolution is still needed in both usability and optimization of clinical decision support.
“With respect to your readers, my recommendation is to not use medical scribes, or else delimit their use to only where absolutely required. Instead, develop systematic processes to regularly capture specific physician concerns with the EHR being used, and transmit that critical information to their EHR vendor with a clear expectation that the manufacturer will address the issue in the near term, or at least in their next major product iteration or generation,” Dr. Gellert said.
By contrast, at the Management of the Hospitalized Patient conference in San Francisco in October 2015, Christine Sinsky, MD, FACP, vice president for professional satisfaction at the American Medical Association, identified documentation assistance as a helpful intervention for physician stress and burnout.4 In a recent email, Dr. Sinsky called documentation assistance “the most powerful intervention to give patients the time, attention, and care they need from their physicians. The data entry and data retrieval work of health care has grown over the last decade. Sharing this work with nonphysicians allows society to get the most value for its investment in physicians’ training.”
Dr. Sinsky calls documentation assistance – such as that provided by medical scribes – “a logical and strategic delegation of work according to ability for greater value,” not a workaround. She said it makes patient care safer by allowing physicians to focus on medical decision making and relationship building – rather than record keeping.
Experience from the front lines
Eric Edwards, MD, FAAP, FHM, of the division of hospital medicine at the University of North Carolina’s Hillsborough Hospital campus, recently presented a poster on his group’s experience with medical scribes at a meeting of the North Carolina Triangle Chapter of SHM. Their research concluded that scribes can be successfully incorporated into an inpatient hospital medicine practice and thus increase provider satisfaction and decrease the time clinicians spend charting.
“We were able to get the support of the hospital administration to pilot the use of scribes 3 days per week, which we’ve now done for almost a year,” Dr. Edwards said. Scribes are employed through a local company, MedScribes, and they work alongside admitting hospitalists during their 10-hour shifts. The hospitalists have been overwhelmingly positive about their experience, he said. “We established that it saves the physician 15 minutes per patient encounter by helping with documentation.”
It’s important that the scribe gets to know an individual provider’s personal preferences, Dr. Edwards said. Some hospitalists create their own charting templates. There’s also a need to train the clinician in how to use the medical scribe. For example, physicians are instructed to call out physical findings during their exam, which simultaneously informs the patient while allowing the scribe to document the exam.
“We are working on getting more formal data about the scribe experience,” he added. “But we have found that our providers love it, and it improves their efficiency and productivity. The danger is if the physician becomes too reliant on the scribe and fails to exercise due diligence in reviewing the scribe’s notes to ensure that all relevant information is in the chart and irrelevant information is not. We need to make sure we are carefully reviewing and signing off on the scribe’s notes,” he explained.
“I think we’re years away from improving the EHR to the point that would allow us to call it doctor friendly,” Dr. Edwards said. “For now, the scribe is a great way to alleviate some of the physician’s burden. But for hospitalist groups to use scribes successfully, it can’t be done haphazardly. We are lucky to have an experienced local scribe company to partner with. They provide systematic training and orientation. It’s also important that scribes are trained in the specific EHR that they will be using.”
Christine Lum Lung, MD, SFHM, CEO and medical director of Northern Colorado Hospitalists, a hospital medicine group at the University of Colorado’s North Campus hospitals in Fort Collins, has been studying the use of scribes since 2014. “We had a gap in bringing on new doctors fast enough for our group’s needs, so I looked into the return on investment from scribes and pitched it to our group,” she said. “It’s difficult to say what has been the actual impact on caseload, but we all think it has reduced physician workdays by an hour or greater.”
The 32-member hospitalist group, which covers two facilities, has a designated director of scribes who periodically surveys the hospitalists’ satisfaction with the scribes. “Now we all embrace the use of scribes. Satisfaction is high, and quality of life has improved,” Dr. Lum Lung said. “It’s hard to quantify, but we feel like it helps with burnout for us to be able to leave work earlier, and it alleviates some of the other stresses in our workday.”
She said scribes are important to the medical team not just with managing the EHR but also with other burdens such as documenting compliance with code status, VTEs, and other quality requirements, and to help with other regulatory issues. Scribes can look up lab values and radiology reports. When there are downtimes, they can prepare discharge plans.
Typically, there are five scribes on duty for 18 hours a day at each hospital, Dr. Lum Lung said. But only those doctors primarily doing admissions are assured of having a scribe to round with them. “Most doctors in the group would say the greatest efficiency of scribes is with admitting,” she said. The company that provides scribes to the UC hospitals, ScribeAmerica, handles administration, training, and human resource issues, and the scribe team has a designated Lead Scribe and Quality Scribe at their facility.
Studying the benefits
Andrew Friedson, PhD, a health care economist at the University of Colorado in Denver, recently conducted a 9-month randomized experiment in three hospital emergency rooms in the Denver area to determine the effects of scribes on measures of emergency physician productivity.5 He found that scribes reduced patient wait times in the emergency department by about 13 minutes per patient, while greatly decreasing the amount of time physicians spent after a shift completing their charting, which thus lowered overtime costs for ED physicians.
“This is one of the first times medical scribes have been studied with a randomized, controlled trial,” Dr. Friedson said. “I tracked the amount of overtime, patient waiting, and charge capture for each encounter. These were hospitals where the emergency doctors weren’t allowed to go home until their charting was done.” He discovered that there was a large drop in the time between when patients arrived at the ED and when a decision was made regarding whether to admit them. Additionally, charge capture increased significantly, and physicians had more time to perform medical procedures. Dr. Friedson believes that his findings hold implications for other settings and medical groups, including hospital medicine. To the extent that scribes free up hospitalists to perform tasks other than charting, they should provide an efficiency benefit.
So why hasn’t the medical scribe caught on in a bigger way for hospitalists, compared with ED physicians? For Dr. Corvini, the ED is an obvious, high-pressure, high-volume setting where the cost of the scribe can be easily recouped. “That doesn’t exist in such an obvious fashion in hospital medicine, except where high-volume admissions are concentrated in a single physician’s caseload,” he said. Not all hospitalist groups will fit that model. Some may divide admissions between hospitalists on a shift, and others may not be large enough to experience significant caseload pressures.
“EDs are obviously time pressured, and once scribes demonstrate the ability to produce documentation in a high-quality fashion, they are quickly accepted. In hospital medicine, the time pressures are different – not necessarily less, but different,” Dr. Corvini said. There are also differences in physician responsibilities between the ED and hospital medicine, as well as in physicians’ willingness to let go of documentation responsibilities. “My prediction, if the scribe test is rolled out successfully in TeamHealth, with measurable benefits, it will be adopted in other settings where it fits.”
References
1. Shanafelt TD et al. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016 Jul;91(7):836-48.
2. Collins TR. Use of medical scribes spurs debate about costs, difficulties of electronic health records. The Hospitalist; 2015 Oct.
3. Gellert GA et al. The rise of the medical scribe industry: Implications for the advancement of electronic health records. JAMA; 2015;313(13):1315-6.
4. Beresford L. Electronic Health Records Key Driver of Physician Burnout. The Hospitalist; 2015 Dec.
5. Friedson AI. Medical scribes as an input in healthcare production: Evidence from a randomized experiment. Am J Health Econ. 2017 Oct 2. doi: /10.1162/ajhe_a_00103.
Hospitalists target inpatient glycemic control
SHM benchmarks provide ‘objective format’ for improving outcomes
Physicians are trained to manage their patients’ diabetes and often do a meticulous job – one on one. But in order to maximize glycemic control outcomes throughout the hospital, you need a kind of diabetic epidemiology team to focus on the data, said Andjela Drincic, MD, an endocrinologist at Nebraska Medicine, the clinical partner of the University of Nebraska Medical Center in Omaha.

As medical director for diabetes stewardship, Dr. Drincic serves as the epidemiologic lead for her hospital, which has worked systematically to improve inpatient glycemic control since 2012 – with help from the Society of Hospital Medicine.
“You need a team and to set up a system that works, with protocols and some way of knowing if the protocols are succeeding,” Dr. Drincic said. “Quality improvement targets are never static.” She credited SHM’s glycemic control eQUIPS (Electronic Quality Improvement Program), an online quality improvement resource and collaborative of 104 participating hospitals, for providing the support and the data needed to drive glycemic QI efforts at Nebraska Medicine. SHM provided reporting metrics, quarterly benchmarking reports, a library of tools and resources, an implementation guide, educational webinars on demand and, for some participants, mentored implementation with the advice of a leading expert in the field.
One big reason for giving more attention to glycemic control in the hospital is patient safety, said Gregory Maynard, MD, MHM, clinical professor and chief quality officer at the University of California–Davis Medical Center and SHM’s project team leader for eQUIPS.
“Hyperglycemia in hospitalized patients is an extraordinarily common and growing problem, affecting up to 40%-50% of patients in the hospital,” he said. In 2012, 7.7 million hospital stays involved patients with diabetes, the seventh leading cause of death in the United States.1
Hyperglycemia is linked to elevated rates of medical complications, infections, wound complications, hospital mortality, length of stay, readmissions, and ICU admissions, along with other outcomes not directly related to diabetes. Hyperglycemia in hospitalized patients who have not been given a diagnosis of diabetes is, if anything, more dangerous. Add the related risk for hypoglycemia, and clinicians are challenged to keep their patients controlled within the zone between the extremes of hyper- and hypoglycemia. The American Diabetes Association recently issued recommendations with more relaxed glucose targets between 140 and 180 mg/dL for most patients in non–intensive care settings.2
“To not have a standardized way of managing hyperglycemia for your hospital seems like an enormous missed opportunity,” Dr. Maynard said. “If someone comes into the hospital with a chronic condition of diabetes that you ignore, just maintaining them in the hospital and sending them back out into the world without addressing the underlying condition is not good care. You have missed an important opportunity to alter the course of a serious chronic condition.”
Dr. Maynard said SHM recognized this opportunity when it established eQUIPS. “Hospitalists are often tasked with taking care of patients with glycemic issues because there may not be an endocrinologist readily accessible in the hospital,” he said. “We have seen through our benchmarking in eQUIPS incredible variability – with 10-fold differences in hyperglycemia and hypoglycemia rates between the best- and worst-performing sites. The biggest variable is whether the hospital systematically manages glycemic control. We have also shown that achieving high levels of glycemic control and low hypoglycemia rates concurrently is very possible.”
Reliable benchmarks
Nebraska Medicine enrolled in eQUIPS in 2012.
“We utilize SHM’s glucometrics (standardized analyses of inpatient glycemic control data).”3 said Dr. Drincic. “I was looking for a reliable glucometric system and some way to make comparisons with other hospitals when I came across the data Dr. Maynard published about SHM via a PubMed search. We needed outcomes that are validated in the literature and comparison groups.”
Nebraska Medicine has also received a certificate of distinction for inpatient diabetes care from the Joint Commission, and Dr. Drincic is active in PRIDE (Planning Research in Inpatient Diabetes), a national consortium of leading investigators in inpatient diabetes care formed to promote collaborative research. The PRIDE group meets yearly at the ADA conference, communicates regularly by email, and publishes articles.
“Once a year I present our glycemic control data to our administration and to the quality and safety committees at the hospital. I have been pleased with the level of support we have received,” Dr. Drincic said. “We needed a mandate to do this, but when I reported the impact on readmissions and other outcomes, I got the full support of administration. This would have been a lot harder without SHM.”
Engagement with hospitalists is another key to the glucose management project’s success, Dr. Drincic said. “We as endocrinologists think we know how to manage diabetes, but hospitalists have the daunting task of dealing with all of the patient’s medical issues. If we don’t have a strong collaboration, how can we change practice hospitalwide?” Rachel Thompson, MD, SFHM, Nebraska Medicine’s chief of hospital medicine, participates in the glucose management project, Dr. Drincic said.
“We occasionally are guests at hospitalist meetings to share new glucose treatment algorithms,” she said. “We’re also looking at collaborating on other quality initiatives, for example, studying how perioperative dexamethasone affects glycemic control. We built this relationship with hospitalists by establishing trust while trying to shed a reputation as ‘sugar police.’ I don’t want hospitalists saying ‘There she goes again’ whenever I come on the unit. We have tried to establish personal relationships and figure out what the hospitalists need, especially relative to EPIC (the hospital’s electronic medical record software).”
Dr. Thompson said her group’s recent growth to nearly 70 clinicians has increased its footprint hospitalwide and given hospitalists a greater opportunity to influence glycemic control. “We see up to a third of the patients in the hospital outside of the ICU. Glycemic control is something you learn as a hospitalist – It’s a very important frontline quality issue. In the patient list on EPIC every morning we have a field highlighting all patients with glycemic control issues,” she said.
“Poor glucose control is associated with poor outcomes for our patients. We need the right systems in place for patient safety. Moreover, if we are ignoring glycemic control when the patient is in the hospital, we’re sending the wrong message and setting a bad example for our patients when they return home.”
Lack of clear metrics
A significant defect in the infrastructure of many glucose management programs is the lack of clear metrics for outcomes, Dr. Maynard said. Nearly one-third of hospitals in the United States have no standardized metric to track the quality of their inpatient glycemic management, a sobering statistic considering that the first step in any QI initiative is to define and measure the problem at hand.
“I believe the main reason that glycemic control has been left off hospitals’ radar screens is that we still have not adopted national, publicly reported quality measures for glycemic control, although those were proposed recently by a government interagency work group,” Dr. Maynard said. “Until that happens, we’ll continue to see uneven response.”
The first step for frontline hospitalists is to learn and understand the basics of glucose control, for example, basal bolus insulin administration, and to stop writing orders for sliding scale insulin as the sole means of controlling hyperglycemia.
“Develop and adopt standards of practice for insulin administration in your hospital,” Dr. Maynard said. “Be part of the solution, not the problem. Once you get into the weeds – patients on steroids or on total parenteral nutrition – it can get tricky. But it’s important to get the basics right and move beyond inertia on this topic.”
The glycemic team at Nebraska Medicine includes, in addition to Dr. Drincic and Dr. Thompson, an endocrinology fellow, diabetes case managers, resource nurses, nurse leadership, pharmacists, inpatient care transitions coordinators, and representatives from pediatrics and critical care, all working to impact the overall quality of glycemic management in the hospital. Jon Knezevich, PharmD is diabetes stewardship pharmacy coordinator, and Shelly Lautenbaugh, RN, CDE, is diabetes lead care manager and diabetes coordinator for the Joint Commission certificate program. Diabetes stewardship also includes online and live training courses and a class in acute glucose management for the diabetes resource nurses, who bring the knowledge back to their units.
The glucose team’s job is to make sure patients are cared for safely, using appropriate policies and procedures, education, and training, Ms. Lautenbaugh said. “We have a mission as a hospital to transform people’s lives. We try to live our values, and everything follows from the focus on patient safety,” she added. “If our patients can receive extraordinary care and leave better informed about their condition than when they came in, and then we don’t see them again, we’ve achieved our ultimate goal.”
Hyperglycemia is most often not the primary reason why patients are hospitalized, Ms. Lautenbaugh said. “But we need to give them appropriate glucose management regardless. We’ve worked with bedside staff, nurse leadership, and teams to develop plans to raise our outcome scores. We have a lot of different outcomes we examine, and it’s always evolving.”
Quality metrics are incorporated into the electronic medical record, but those reports are not timely enough for day-to-day management, Dr. Knezevich said. “So we created a diabetes dashboard, constantly updated in real time to identify patients who are out of glycemic control.” The measures tracked include a mean patient day glucose score, percentage of readings within recommended limits, mean time between measured low readings and next documented reading or resolution of hypoglycemia, readmission rates, and diabetes nutrition assessments.
For hospitals with diabetes certificates, the Joint Commission also requires that every patient with hyperglycemia receives a clinic visit 30 days after discharge to make sure they are receiving appropriate follow-up care. Other facets of the Nebraska glycemic initiative include utilizing the hospital’s voluntary “Meds to Beds” program, which brings prescribed medications to the patient’s room at discharge. “We offer a diabetes discharge kit for patients who are self-pay, with all of the insulin and medical supplies they will need to get to the 30-day follow-up visit,” Dr. Knezevich said. “We can dream up amazing treatment regimens, but if they can’t afford the medications, what have we accomplished?”
SHM’s external benchmarks have provided an objective format for comparing and improving outcomes, Ms. Lautenbaugh said. “We like to see where we are and use the data to make significant improvements, but we’re also focused on internal assessments. If we make changes for a given metric, how does it affect performance in other areas?” One important metric is percentage of glucose readings within target range hospitalwide. “Our overall goal is 75%. It was 72% in April 2018, and we’ve raised it to 74.4%. It’s a small gain but it shows steady progress. Little steps make small but steady improvement,” she said.
“One area where we were not pleased was the occurrence of hypoglycemia,” Ms. Lautenbaugh said. “We did a root cause analysis of every hypoglycemic event, including several reports for patients who didn’t have diabetes at all. We had to weed out some that weren’t pertinent to our quality questions, but for those that are, the diabetes case manager calls the provider to make sure they were aware of the incident. We were able to identify the outliers in noncritical care, which we’re now able to tackle using a systematic approach.”
Get on the bus
Hospitalists are also integrally involved in a hospital glycemic improvement initiative at Orange Regional Medical Center (ORMC) in Middletown, N.Y.

The Glycemic Improvement Team (GIT) was formed in 2012 when a new hospital campus opened and EPIC was implemented as the hospital’s EMR. But glycemic control has taken on greater focus since 2015, when ORMC enrolled in eQUIPS, said Lorraine Porcaro, RN, the hospital’s diabetes clinical manager. The glycemic control team includes representatives from medicine, nursing, case management, laboratory, nutrition, pharmacy, wound care, and quality improvement.
Implementing the new EMR offered the opportunity to track a number of medical values in real time, Ms. Porcaro said. ORMC has focused its glycemic quality improvement efforts on hypoglycemia and hyperglycemia, with a recent emphasis on the need for improvements related to glucose reassessment 15 minutes post hypoglycemia treatment. More than a hundred “Diabetes Champions” have completed 16 hours of advanced training in diabetes and provide in-unit mentorship for other staff.
The ORMC team’s glycemic improvement “bus” is a rolling cart that goes from unit to unit supplying nurse education, reminders, copies of department-specific policies and protocols, and treats for staff. “It’s what we’re known for,” Ms. Porcaro said. Pens with the motto: “Don’t Miss the Bus! Retest in 15!” summarize the GIT’s current focus on post–hypoglycemia treatment retesting.
Hospitalists were part of the glycemic improvement process at ORMC from the beginning and are still involved, said Adrian Paraschiv, MD, FHM, a hospitalist and assistant director of the medical center, as well as the ORMC director of clinical information technology. ORMC initiated hospitalist coverage in 1998 and now has three HM groups, two of them represented on the glycemic improvement team.
“Like any hospital, we feel we should minimize hypoglycemic events,” Dr. Paraschiv explained. “This became important for other hospital departments, and we recognized we needed a major QI initiative to improve our outcomes hospitalwide. In the process, we noticed what other people were saying: Results from improving glycemic control included reduced length of stay, cost, and infections. That provided motivation for the hospital to support our initiative.”
Glucose management isn’t only about blood sugar, but whether the patient ate or not, their other blood work, the level of education for patient and staff, and a variety of other inputs, Dr. Paraschiv said. “All of these things were in the EMR but all over the place. EPIC had an incipient structure for pulling the data together, and we modified it to show everything that’s going on with the patient’s glycemic control on a single screen. We can build order sets and issue different reports.”
Today at ORMC, hypoglycemia is reassessed within 30 minutes more than 50% of the time. “It will never be at 100%, but we wanted to at least be at the national mean for eQUIPS hospitals. Our stretch goal was to be in the top quartile, and by the end of 2017, we realized that goal,” Ms. Porcaro said. Sometimes, because of changes in patients and staff, the GIT needs to repeat the education and review policies. “Since then, it’s been a matter of continuing staff education; sharing glucose data with stakeholders; talking about goals for ICU and non-ICU units; and, when needed, rolling out the bus.”
Participation in eQUIPS has made it possible to gather this information in one place and present it in a way that makes sense to physicians, Dr. Paraschiv said. “Dr. Maynard and SHM showed us how to put the data together to add value. Using these tools, we started looking at our processes, what needed to change, and what we are able to change. Now we’re examining what happens afterward. Can we use the electronic system to automatically alert physicians to make changes to the treatment regimen in real time? We continue to improve using upgrades to our EMR, such as an alert system with best practice advisories for the clinician. We now think we can actually achieve what we set out to achieve,” he said.
“Our idea was that we needed to market this program throughout the hospital – starting from the kitchen, meal delivery staff, IT, laboratory, medical and nursing staff,” Ms. Porcaro said. “The issue is multifactorial – it’s for the entire hospital. My heart is warmed when I see the woman who delivers the meals asking the patient: ‘Have you gotten your insulin shot?’ ”
References
1. Corvino L et al. “Management of diabetes and hyperglycemia in hospitalized patients.” Updated 2017 Oct 1 in De Groot LJ et al. editors. Endotext. South Dartmouth (MA): MDText.com 2000.
2. American Diabetes Association. Glycemic targets. Diabetes Care 2017 Jan;40(Suppl 1):S48-56.
3. Maynard G et al. “Design and implementation of a web-based reporting and benchmarking center for inpatient glucometrics.” J Diabetes Sci Technol. 2014 May 12;8(4):630-40.
SHM benchmarks provide ‘objective format’ for improving outcomes
SHM benchmarks provide ‘objective format’ for improving outcomes
Physicians are trained to manage their patients’ diabetes and often do a meticulous job – one on one. But in order to maximize glycemic control outcomes throughout the hospital, you need a kind of diabetic epidemiology team to focus on the data, said Andjela Drincic, MD, an endocrinologist at Nebraska Medicine, the clinical partner of the University of Nebraska Medical Center in Omaha.
As medical director for diabetes stewardship, Dr. Drincic serves as the epidemiologic lead for her hospital, which has worked systematically to improve inpatient glycemic control since 2012 – with help from the Society of Hospital Medicine.
“You need a team and to set up a system that works, with protocols and some way of knowing if the protocols are succeeding,” Dr. Drincic said. “Quality improvement targets are never static.” She credited SHM’s glycemic control eQUIPS (Electronic Quality Improvement Program), an online quality improvement resource and collaborative of 104 participating hospitals, for providing the support and the data needed to drive glycemic QI efforts at Nebraska Medicine. SHM provided reporting metrics, quarterly benchmarking reports, a library of tools and resources, an implementation guide, educational webinars on demand and, for some participants, mentored implementation with the advice of a leading expert in the field.
One big reason for giving more attention to glycemic control in the hospital is patient safety, said Gregory Maynard, MD, MHM, clinical professor and chief quality officer at the University of California–Davis Medical Center and SHM’s project team leader for eQUIPS.
“Hyperglycemia in hospitalized patients is an extraordinarily common and growing problem, affecting up to 40%-50% of patients in the hospital,” he said. In 2012, 7.7 million hospital stays involved patients with diabetes, the seventh leading cause of death in the United States.1
Hyperglycemia is linked to elevated rates of medical complications, infections, wound complications, hospital mortality, length of stay, readmissions, and ICU admissions, along with other outcomes not directly related to diabetes. Hyperglycemia in hospitalized patients who have not been given a diagnosis of diabetes is, if anything, more dangerous. Add the related risk for hypoglycemia, and clinicians are challenged to keep their patients controlled within the zone between the extremes of hyper- and hypoglycemia. The American Diabetes Association recently issued recommendations with more relaxed glucose targets between 140 and 180 mg/dL for most patients in non–intensive care settings.2
“To not have a standardized way of managing hyperglycemia for your hospital seems like an enormous missed opportunity,” Dr. Maynard said. “If someone comes into the hospital with a chronic condition of diabetes that you ignore, just maintaining them in the hospital and sending them back out into the world without addressing the underlying condition is not good care. You have missed an important opportunity to alter the course of a serious chronic condition.”
Dr. Maynard said SHM recognized this opportunity when it established eQUIPS. “Hospitalists are often tasked with taking care of patients with glycemic issues because there may not be an endocrinologist readily accessible in the hospital,” he said. “We have seen through our benchmarking in eQUIPS incredible variability – with 10-fold differences in hyperglycemia and hypoglycemia rates between the best- and worst-performing sites. The biggest variable is whether the hospital systematically manages glycemic control. We have also shown that achieving high levels of glycemic control and low hypoglycemia rates concurrently is very possible.”
Reliable benchmarks
Nebraska Medicine enrolled in eQUIPS in 2012.
“We utilize SHM’s glucometrics (standardized analyses of inpatient glycemic control data).”3 said Dr. Drincic. “I was looking for a reliable glucometric system and some way to make comparisons with other hospitals when I came across the data Dr. Maynard published about SHM via a PubMed search. We needed outcomes that are validated in the literature and comparison groups.”
Nebraska Medicine has also received a certificate of distinction for inpatient diabetes care from the Joint Commission, and Dr. Drincic is active in PRIDE (Planning Research in Inpatient Diabetes), a national consortium of leading investigators in inpatient diabetes care formed to promote collaborative research. The PRIDE group meets yearly at the ADA conference, communicates regularly by email, and publishes articles.
“Once a year I present our glycemic control data to our administration and to the quality and safety committees at the hospital. I have been pleased with the level of support we have received,” Dr. Drincic said. “We needed a mandate to do this, but when I reported the impact on readmissions and other outcomes, I got the full support of administration. This would have been a lot harder without SHM.”
Engagement with hospitalists is another key to the glucose management project’s success, Dr. Drincic said. “We as endocrinologists think we know how to manage diabetes, but hospitalists have the daunting task of dealing with all of the patient’s medical issues. If we don’t have a strong collaboration, how can we change practice hospitalwide?” Rachel Thompson, MD, SFHM, Nebraska Medicine’s chief of hospital medicine, participates in the glucose management project, Dr. Drincic said.
“We occasionally are guests at hospitalist meetings to share new glucose treatment algorithms,” she said. “We’re also looking at collaborating on other quality initiatives, for example, studying how perioperative dexamethasone affects glycemic control. We built this relationship with hospitalists by establishing trust while trying to shed a reputation as ‘sugar police.’ I don’t want hospitalists saying ‘There she goes again’ whenever I come on the unit. We have tried to establish personal relationships and figure out what the hospitalists need, especially relative to EPIC (the hospital’s electronic medical record software).”
Dr. Thompson said her group’s recent growth to nearly 70 clinicians has increased its footprint hospitalwide and given hospitalists a greater opportunity to influence glycemic control. “We see up to a third of the patients in the hospital outside of the ICU. Glycemic control is something you learn as a hospitalist – It’s a very important frontline quality issue. In the patient list on EPIC every morning we have a field highlighting all patients with glycemic control issues,” she said.
“Poor glucose control is associated with poor outcomes for our patients. We need the right systems in place for patient safety. Moreover, if we are ignoring glycemic control when the patient is in the hospital, we’re sending the wrong message and setting a bad example for our patients when they return home.”
Lack of clear metrics
A significant defect in the infrastructure of many glucose management programs is the lack of clear metrics for outcomes, Dr. Maynard said. Nearly one-third of hospitals in the United States have no standardized metric to track the quality of their inpatient glycemic management, a sobering statistic considering that the first step in any QI initiative is to define and measure the problem at hand.
“I believe the main reason that glycemic control has been left off hospitals’ radar screens is that we still have not adopted national, publicly reported quality measures for glycemic control, although those were proposed recently by a government interagency work group,” Dr. Maynard said. “Until that happens, we’ll continue to see uneven response.”
The first step for frontline hospitalists is to learn and understand the basics of glucose control, for example, basal bolus insulin administration, and to stop writing orders for sliding scale insulin as the sole means of controlling hyperglycemia.
“Develop and adopt standards of practice for insulin administration in your hospital,” Dr. Maynard said. “Be part of the solution, not the problem. Once you get into the weeds – patients on steroids or on total parenteral nutrition – it can get tricky. But it’s important to get the basics right and move beyond inertia on this topic.”
The glycemic team at Nebraska Medicine includes, in addition to Dr. Drincic and Dr. Thompson, an endocrinology fellow, diabetes case managers, resource nurses, nurse leadership, pharmacists, inpatient care transitions coordinators, and representatives from pediatrics and critical care, all working to impact the overall quality of glycemic management in the hospital. Jon Knezevich, PharmD is diabetes stewardship pharmacy coordinator, and Shelly Lautenbaugh, RN, CDE, is diabetes lead care manager and diabetes coordinator for the Joint Commission certificate program. Diabetes stewardship also includes online and live training courses and a class in acute glucose management for the diabetes resource nurses, who bring the knowledge back to their units.
The glucose team’s job is to make sure patients are cared for safely, using appropriate policies and procedures, education, and training, Ms. Lautenbaugh said. “We have a mission as a hospital to transform people’s lives. We try to live our values, and everything follows from the focus on patient safety,” she added. “If our patients can receive extraordinary care and leave better informed about their condition than when they came in, and then we don’t see them again, we’ve achieved our ultimate goal.”
Hyperglycemia is most often not the primary reason why patients are hospitalized, Ms. Lautenbaugh said. “But we need to give them appropriate glucose management regardless. We’ve worked with bedside staff, nurse leadership, and teams to develop plans to raise our outcome scores. We have a lot of different outcomes we examine, and it’s always evolving.”
Quality metrics are incorporated into the electronic medical record, but those reports are not timely enough for day-to-day management, Dr. Knezevich said. “So we created a diabetes dashboard, constantly updated in real time to identify patients who are out of glycemic control.” The measures tracked include a mean patient day glucose score, percentage of readings within recommended limits, mean time between measured low readings and next documented reading or resolution of hypoglycemia, readmission rates, and diabetes nutrition assessments.
For hospitals with diabetes certificates, the Joint Commission also requires that every patient with hyperglycemia receives a clinic visit 30 days after discharge to make sure they are receiving appropriate follow-up care. Other facets of the Nebraska glycemic initiative include utilizing the hospital’s voluntary “Meds to Beds” program, which brings prescribed medications to the patient’s room at discharge. “We offer a diabetes discharge kit for patients who are self-pay, with all of the insulin and medical supplies they will need to get to the 30-day follow-up visit,” Dr. Knezevich said. “We can dream up amazing treatment regimens, but if they can’t afford the medications, what have we accomplished?”
SHM’s external benchmarks have provided an objective format for comparing and improving outcomes, Ms. Lautenbaugh said. “We like to see where we are and use the data to make significant improvements, but we’re also focused on internal assessments. If we make changes for a given metric, how does it affect performance in other areas?” One important metric is percentage of glucose readings within target range hospitalwide. “Our overall goal is 75%. It was 72% in April 2018, and we’ve raised it to 74.4%. It’s a small gain but it shows steady progress. Little steps make small but steady improvement,” she said.
“One area where we were not pleased was the occurrence of hypoglycemia,” Ms. Lautenbaugh said. “We did a root cause analysis of every hypoglycemic event, including several reports for patients who didn’t have diabetes at all. We had to weed out some that weren’t pertinent to our quality questions, but for those that are, the diabetes case manager calls the provider to make sure they were aware of the incident. We were able to identify the outliers in noncritical care, which we’re now able to tackle using a systematic approach.”
Get on the bus
Hospitalists are also integrally involved in a hospital glycemic improvement initiative at Orange Regional Medical Center (ORMC) in Middletown, N.Y.
The Glycemic Improvement Team (GIT) was formed in 2012 when a new hospital campus opened and EPIC was implemented as the hospital’s EMR. But glycemic control has taken on greater focus since 2015, when ORMC enrolled in eQUIPS, said Lorraine Porcaro, RN, the hospital’s diabetes clinical manager. The glycemic control team includes representatives from medicine, nursing, case management, laboratory, nutrition, pharmacy, wound care, and quality improvement.
Implementing the new EMR offered the opportunity to track a number of medical values in real time, Ms. Porcaro said. ORMC has focused its glycemic quality improvement efforts on hypoglycemia and hyperglycemia, with a recent emphasis on the need for improvements related to glucose reassessment 15 minutes post hypoglycemia treatment. More than a hundred “Diabetes Champions” have completed 16 hours of advanced training in diabetes and provide in-unit mentorship for other staff.
The ORMC team’s glycemic improvement “bus” is a rolling cart that goes from unit to unit supplying nurse education, reminders, copies of department-specific policies and protocols, and treats for staff. “It’s what we’re known for,” Ms. Porcaro said. Pens with the motto: “Don’t Miss the Bus! Retest in 15!” summarize the GIT’s current focus on post–hypoglycemia treatment retesting.
Hospitalists were part of the glycemic improvement process at ORMC from the beginning and are still involved, said Adrian Paraschiv, MD, FHM, a hospitalist and assistant director of the medical center, as well as the ORMC director of clinical information technology. ORMC initiated hospitalist coverage in 1998 and now has three HM groups, two of them represented on the glycemic improvement team.
“Like any hospital, we feel we should minimize hypoglycemic events,” Dr. Paraschiv explained. “This became important for other hospital departments, and we recognized we needed a major QI initiative to improve our outcomes hospitalwide. In the process, we noticed what other people were saying: Results from improving glycemic control included reduced length of stay, cost, and infections. That provided motivation for the hospital to support our initiative.”
Glucose management isn’t only about blood sugar, but whether the patient ate or not, their other blood work, the level of education for patient and staff, and a variety of other inputs, Dr. Paraschiv said. “All of these things were in the EMR but all over the place. EPIC had an incipient structure for pulling the data together, and we modified it to show everything that’s going on with the patient’s glycemic control on a single screen. We can build order sets and issue different reports.”
Today at ORMC, hypoglycemia is reassessed within 30 minutes more than 50% of the time. “It will never be at 100%, but we wanted to at least be at the national mean for eQUIPS hospitals. Our stretch goal was to be in the top quartile, and by the end of 2017, we realized that goal,” Ms. Porcaro said. Sometimes, because of changes in patients and staff, the GIT needs to repeat the education and review policies. “Since then, it’s been a matter of continuing staff education; sharing glucose data with stakeholders; talking about goals for ICU and non-ICU units; and, when needed, rolling out the bus.”
Participation in eQUIPS has made it possible to gather this information in one place and present it in a way that makes sense to physicians, Dr. Paraschiv said. “Dr. Maynard and SHM showed us how to put the data together to add value. Using these tools, we started looking at our processes, what needed to change, and what we are able to change. Now we’re examining what happens afterward. Can we use the electronic system to automatically alert physicians to make changes to the treatment regimen in real time? We continue to improve using upgrades to our EMR, such as an alert system with best practice advisories for the clinician. We now think we can actually achieve what we set out to achieve,” he said.
“Our idea was that we needed to market this program throughout the hospital – starting from the kitchen, meal delivery staff, IT, laboratory, medical and nursing staff,” Ms. Porcaro said. “The issue is multifactorial – it’s for the entire hospital. My heart is warmed when I see the woman who delivers the meals asking the patient: ‘Have you gotten your insulin shot?’ ”
References
1. Corvino L et al. “Management of diabetes and hyperglycemia in hospitalized patients.” Updated 2017 Oct 1 in De Groot LJ et al. editors. Endotext. South Dartmouth (MA): MDText.com 2000.
2. American Diabetes Association. Glycemic targets. Diabetes Care 2017 Jan;40(Suppl 1):S48-56.
3. Maynard G et al. “Design and implementation of a web-based reporting and benchmarking center for inpatient glucometrics.” J Diabetes Sci Technol. 2014 May 12;8(4):630-40.
Physicians are trained to manage their patients’ diabetes and often do a meticulous job – one on one. But in order to maximize glycemic control outcomes throughout the hospital, you need a kind of diabetic epidemiology team to focus on the data, said Andjela Drincic, MD, an endocrinologist at Nebraska Medicine, the clinical partner of the University of Nebraska Medical Center in Omaha.
As medical director for diabetes stewardship, Dr. Drincic serves as the epidemiologic lead for her hospital, which has worked systematically to improve inpatient glycemic control since 2012 – with help from the Society of Hospital Medicine.
“You need a team and to set up a system that works, with protocols and some way of knowing if the protocols are succeeding,” Dr. Drincic said. “Quality improvement targets are never static.” She credited SHM’s glycemic control eQUIPS (Electronic Quality Improvement Program), an online quality improvement resource and collaborative of 104 participating hospitals, for providing the support and the data needed to drive glycemic QI efforts at Nebraska Medicine. SHM provided reporting metrics, quarterly benchmarking reports, a library of tools and resources, an implementation guide, educational webinars on demand and, for some participants, mentored implementation with the advice of a leading expert in the field.
One big reason for giving more attention to glycemic control in the hospital is patient safety, said Gregory Maynard, MD, MHM, clinical professor and chief quality officer at the University of California–Davis Medical Center and SHM’s project team leader for eQUIPS.
“Hyperglycemia in hospitalized patients is an extraordinarily common and growing problem, affecting up to 40%-50% of patients in the hospital,” he said. In 2012, 7.7 million hospital stays involved patients with diabetes, the seventh leading cause of death in the United States.1
Hyperglycemia is linked to elevated rates of medical complications, infections, wound complications, hospital mortality, length of stay, readmissions, and ICU admissions, along with other outcomes not directly related to diabetes. Hyperglycemia in hospitalized patients who have not been given a diagnosis of diabetes is, if anything, more dangerous. Add the related risk for hypoglycemia, and clinicians are challenged to keep their patients controlled within the zone between the extremes of hyper- and hypoglycemia. The American Diabetes Association recently issued recommendations with more relaxed glucose targets between 140 and 180 mg/dL for most patients in non–intensive care settings.2
“To not have a standardized way of managing hyperglycemia for your hospital seems like an enormous missed opportunity,” Dr. Maynard said. “If someone comes into the hospital with a chronic condition of diabetes that you ignore, just maintaining them in the hospital and sending them back out into the world without addressing the underlying condition is not good care. You have missed an important opportunity to alter the course of a serious chronic condition.”
Dr. Maynard said SHM recognized this opportunity when it established eQUIPS. “Hospitalists are often tasked with taking care of patients with glycemic issues because there may not be an endocrinologist readily accessible in the hospital,” he said. “We have seen through our benchmarking in eQUIPS incredible variability – with 10-fold differences in hyperglycemia and hypoglycemia rates between the best- and worst-performing sites. The biggest variable is whether the hospital systematically manages glycemic control. We have also shown that achieving high levels of glycemic control and low hypoglycemia rates concurrently is very possible.”
Reliable benchmarks
Nebraska Medicine enrolled in eQUIPS in 2012.
“We utilize SHM’s glucometrics (standardized analyses of inpatient glycemic control data).”3 said Dr. Drincic. “I was looking for a reliable glucometric system and some way to make comparisons with other hospitals when I came across the data Dr. Maynard published about SHM via a PubMed search. We needed outcomes that are validated in the literature and comparison groups.”
Nebraska Medicine has also received a certificate of distinction for inpatient diabetes care from the Joint Commission, and Dr. Drincic is active in PRIDE (Planning Research in Inpatient Diabetes), a national consortium of leading investigators in inpatient diabetes care formed to promote collaborative research. The PRIDE group meets yearly at the ADA conference, communicates regularly by email, and publishes articles.
“Once a year I present our glycemic control data to our administration and to the quality and safety committees at the hospital. I have been pleased with the level of support we have received,” Dr. Drincic said. “We needed a mandate to do this, but when I reported the impact on readmissions and other outcomes, I got the full support of administration. This would have been a lot harder without SHM.”
Engagement with hospitalists is another key to the glucose management project’s success, Dr. Drincic said. “We as endocrinologists think we know how to manage diabetes, but hospitalists have the daunting task of dealing with all of the patient’s medical issues. If we don’t have a strong collaboration, how can we change practice hospitalwide?” Rachel Thompson, MD, SFHM, Nebraska Medicine’s chief of hospital medicine, participates in the glucose management project, Dr. Drincic said.
“We occasionally are guests at hospitalist meetings to share new glucose treatment algorithms,” she said. “We’re also looking at collaborating on other quality initiatives, for example, studying how perioperative dexamethasone affects glycemic control. We built this relationship with hospitalists by establishing trust while trying to shed a reputation as ‘sugar police.’ I don’t want hospitalists saying ‘There she goes again’ whenever I come on the unit. We have tried to establish personal relationships and figure out what the hospitalists need, especially relative to EPIC (the hospital’s electronic medical record software).”
Dr. Thompson said her group’s recent growth to nearly 70 clinicians has increased its footprint hospitalwide and given hospitalists a greater opportunity to influence glycemic control. “We see up to a third of the patients in the hospital outside of the ICU. Glycemic control is something you learn as a hospitalist – It’s a very important frontline quality issue. In the patient list on EPIC every morning we have a field highlighting all patients with glycemic control issues,” she said.
“Poor glucose control is associated with poor outcomes for our patients. We need the right systems in place for patient safety. Moreover, if we are ignoring glycemic control when the patient is in the hospital, we’re sending the wrong message and setting a bad example for our patients when they return home.”
Lack of clear metrics
A significant defect in the infrastructure of many glucose management programs is the lack of clear metrics for outcomes, Dr. Maynard said. Nearly one-third of hospitals in the United States have no standardized metric to track the quality of their inpatient glycemic management, a sobering statistic considering that the first step in any QI initiative is to define and measure the problem at hand.
“I believe the main reason that glycemic control has been left off hospitals’ radar screens is that we still have not adopted national, publicly reported quality measures for glycemic control, although those were proposed recently by a government interagency work group,” Dr. Maynard said. “Until that happens, we’ll continue to see uneven response.”
The first step for frontline hospitalists is to learn and understand the basics of glucose control, for example, basal bolus insulin administration, and to stop writing orders for sliding scale insulin as the sole means of controlling hyperglycemia.
“Develop and adopt standards of practice for insulin administration in your hospital,” Dr. Maynard said. “Be part of the solution, not the problem. Once you get into the weeds – patients on steroids or on total parenteral nutrition – it can get tricky. But it’s important to get the basics right and move beyond inertia on this topic.”
The glycemic team at Nebraska Medicine includes, in addition to Dr. Drincic and Dr. Thompson, an endocrinology fellow, diabetes case managers, resource nurses, nurse leadership, pharmacists, inpatient care transitions coordinators, and representatives from pediatrics and critical care, all working to impact the overall quality of glycemic management in the hospital. Jon Knezevich, PharmD is diabetes stewardship pharmacy coordinator, and Shelly Lautenbaugh, RN, CDE, is diabetes lead care manager and diabetes coordinator for the Joint Commission certificate program. Diabetes stewardship also includes online and live training courses and a class in acute glucose management for the diabetes resource nurses, who bring the knowledge back to their units.
The glucose team’s job is to make sure patients are cared for safely, using appropriate policies and procedures, education, and training, Ms. Lautenbaugh said. “We have a mission as a hospital to transform people’s lives. We try to live our values, and everything follows from the focus on patient safety,” she added. “If our patients can receive extraordinary care and leave better informed about their condition than when they came in, and then we don’t see them again, we’ve achieved our ultimate goal.”
Hyperglycemia is most often not the primary reason why patients are hospitalized, Ms. Lautenbaugh said. “But we need to give them appropriate glucose management regardless. We’ve worked with bedside staff, nurse leadership, and teams to develop plans to raise our outcome scores. We have a lot of different outcomes we examine, and it’s always evolving.”
Quality metrics are incorporated into the electronic medical record, but those reports are not timely enough for day-to-day management, Dr. Knezevich said. “So we created a diabetes dashboard, constantly updated in real time to identify patients who are out of glycemic control.” The measures tracked include a mean patient day glucose score, percentage of readings within recommended limits, mean time between measured low readings and next documented reading or resolution of hypoglycemia, readmission rates, and diabetes nutrition assessments.
For hospitals with diabetes certificates, the Joint Commission also requires that every patient with hyperglycemia receives a clinic visit 30 days after discharge to make sure they are receiving appropriate follow-up care. Other facets of the Nebraska glycemic initiative include utilizing the hospital’s voluntary “Meds to Beds” program, which brings prescribed medications to the patient’s room at discharge. “We offer a diabetes discharge kit for patients who are self-pay, with all of the insulin and medical supplies they will need to get to the 30-day follow-up visit,” Dr. Knezevich said. “We can dream up amazing treatment regimens, but if they can’t afford the medications, what have we accomplished?”
SHM’s external benchmarks have provided an objective format for comparing and improving outcomes, Ms. Lautenbaugh said. “We like to see where we are and use the data to make significant improvements, but we’re also focused on internal assessments. If we make changes for a given metric, how does it affect performance in other areas?” One important metric is percentage of glucose readings within target range hospitalwide. “Our overall goal is 75%. It was 72% in April 2018, and we’ve raised it to 74.4%. It’s a small gain but it shows steady progress. Little steps make small but steady improvement,” she said.
“One area where we were not pleased was the occurrence of hypoglycemia,” Ms. Lautenbaugh said. “We did a root cause analysis of every hypoglycemic event, including several reports for patients who didn’t have diabetes at all. We had to weed out some that weren’t pertinent to our quality questions, but for those that are, the diabetes case manager calls the provider to make sure they were aware of the incident. We were able to identify the outliers in noncritical care, which we’re now able to tackle using a systematic approach.”
Get on the bus
Hospitalists are also integrally involved in a hospital glycemic improvement initiative at Orange Regional Medical Center (ORMC) in Middletown, N.Y.
The Glycemic Improvement Team (GIT) was formed in 2012 when a new hospital campus opened and EPIC was implemented as the hospital’s EMR. But glycemic control has taken on greater focus since 2015, when ORMC enrolled in eQUIPS, said Lorraine Porcaro, RN, the hospital’s diabetes clinical manager. The glycemic control team includes representatives from medicine, nursing, case management, laboratory, nutrition, pharmacy, wound care, and quality improvement.
Implementing the new EMR offered the opportunity to track a number of medical values in real time, Ms. Porcaro said. ORMC has focused its glycemic quality improvement efforts on hypoglycemia and hyperglycemia, with a recent emphasis on the need for improvements related to glucose reassessment 15 minutes post hypoglycemia treatment. More than a hundred “Diabetes Champions” have completed 16 hours of advanced training in diabetes and provide in-unit mentorship for other staff.
The ORMC team’s glycemic improvement “bus” is a rolling cart that goes from unit to unit supplying nurse education, reminders, copies of department-specific policies and protocols, and treats for staff. “It’s what we’re known for,” Ms. Porcaro said. Pens with the motto: “Don’t Miss the Bus! Retest in 15!” summarize the GIT’s current focus on post–hypoglycemia treatment retesting.
Hospitalists were part of the glycemic improvement process at ORMC from the beginning and are still involved, said Adrian Paraschiv, MD, FHM, a hospitalist and assistant director of the medical center, as well as the ORMC director of clinical information technology. ORMC initiated hospitalist coverage in 1998 and now has three HM groups, two of them represented on the glycemic improvement team.
“Like any hospital, we feel we should minimize hypoglycemic events,” Dr. Paraschiv explained. “This became important for other hospital departments, and we recognized we needed a major QI initiative to improve our outcomes hospitalwide. In the process, we noticed what other people were saying: Results from improving glycemic control included reduced length of stay, cost, and infections. That provided motivation for the hospital to support our initiative.”
Glucose management isn’t only about blood sugar, but whether the patient ate or not, their other blood work, the level of education for patient and staff, and a variety of other inputs, Dr. Paraschiv said. “All of these things were in the EMR but all over the place. EPIC had an incipient structure for pulling the data together, and we modified it to show everything that’s going on with the patient’s glycemic control on a single screen. We can build order sets and issue different reports.”
Today at ORMC, hypoglycemia is reassessed within 30 minutes more than 50% of the time. “It will never be at 100%, but we wanted to at least be at the national mean for eQUIPS hospitals. Our stretch goal was to be in the top quartile, and by the end of 2017, we realized that goal,” Ms. Porcaro said. Sometimes, because of changes in patients and staff, the GIT needs to repeat the education and review policies. “Since then, it’s been a matter of continuing staff education; sharing glucose data with stakeholders; talking about goals for ICU and non-ICU units; and, when needed, rolling out the bus.”
Participation in eQUIPS has made it possible to gather this information in one place and present it in a way that makes sense to physicians, Dr. Paraschiv said. “Dr. Maynard and SHM showed us how to put the data together to add value. Using these tools, we started looking at our processes, what needed to change, and what we are able to change. Now we’re examining what happens afterward. Can we use the electronic system to automatically alert physicians to make changes to the treatment regimen in real time? We continue to improve using upgrades to our EMR, such as an alert system with best practice advisories for the clinician. We now think we can actually achieve what we set out to achieve,” he said.
“Our idea was that we needed to market this program throughout the hospital – starting from the kitchen, meal delivery staff, IT, laboratory, medical and nursing staff,” Ms. Porcaro said. “The issue is multifactorial – it’s for the entire hospital. My heart is warmed when I see the woman who delivers the meals asking the patient: ‘Have you gotten your insulin shot?’ ”
References
1. Corvino L et al. “Management of diabetes and hyperglycemia in hospitalized patients.” Updated 2017 Oct 1 in De Groot LJ et al. editors. Endotext. South Dartmouth (MA): MDText.com 2000.
2. American Diabetes Association. Glycemic targets. Diabetes Care 2017 Jan;40(Suppl 1):S48-56.
3. Maynard G et al. “Design and implementation of a web-based reporting and benchmarking center for inpatient glucometrics.” J Diabetes Sci Technol. 2014 May 12;8(4):630-40.
How will SNF readmissions penalties affect hospitalists?
Starting in 2018, skilled nursing facilities (SNFs), like acute care hospitals before them, will be subject to a penalty of up to 2% of their Medicare reimbursement for posting higher-than-average rates of hospital readmissions.
The Protecting Access to Medicare Act of 2014 established a value-based purchasing component for SNFs, including incentives for high-performing facilities and a measure for all-cause, all-condition readmissions to any hospital from the SNF within 30 days following hospital discharge – designed to recognize and reward, or punish, facilities’ performance on preventing unnecessary readmissions. Public reporting of SNF quality data, including readmission rates, started in October 2017. Penalties follow a year later. Some patients’ readmissions could trigger penalties for both the hospital and the SNF.
According to 2010 data, 23.5% of patients discharged from acute care hospitals to SNFs were readmitted to the hospital within 30 days, at a financial cost of $10,362 per readmission or $4.34 billion per year.1 Seventy eight percent of these readmissions were labeled avoidable. More recent evidence suggests that hospitalization rates for dual-eligible patients living in long-term care facilities decreased by 31% between 2010 and 2015.2As increasing numbers of hospitalists spend some or all of their work week in post-acute care settings, how will the SNF readmission penalty affect their relationships with post-acute facilities?
Experts say SNFs – as with hospitals before them – lack the ability to allocate rewards or penalties for readmission rate performance to individual doctors. But increasingly close collaborative relationships between post-acute facilities and the hospitalists who work in post-acute care mean that the hospitalist has an important role in helping the SNF to manage its readmissions exposure.
“Hospitals and hospitalists want to keep good relationships with the SNFs they partner with, for a variety of reasons,” Dr. Frizner said. “We believe that the best way to reduce readmissions and unplanned transfers from the SNF is for the doctor to know the patient. We need dedicated doctors in the facility. We want hospitalists who already know the patient to come to the facility and see the patient there.”
The hospitalist’s role in post-acute care
Hospitalists who work in post-acute care typically make scheduled, billable medical visits to patients in long-term care facilities, and may also take on roles such as facility medical director or contribute to quality improvement. Relationships may be initiated by a facility seeking more medical coverage, by a hospitalist group seeking additional work or an ability to impact on the post-acute care delivered to hospital patients discharged to the facility, or by health systems, health plans, or accountable care organizations seeking to better manage the quality of care transitions for their beneficiaries.

“What I’m seeing is that with opportunities for bundled payments, we all have new incentives for moving patients along and reducing waste,” Dr. Boutwell said. “For hospitalists practicing in SNFs, it’s going to be a much bigger phenomenon. They’ll be called to reevaluate patients and make more visits than they have been accustomed to.” She hopes SNFs are studying what happened with hospitals’ readmission penalties, and will respond more quickly and effectively to their own penalty exposure.
“What we are seeing is an effort to shift folks to lower cost – but still clinically appropriate – levels of care,” he said. “These dynamics will force SNFs to reevaluate and improve their clinical competencies, to accept patients and then treat them in place. It’s no longer acceptable for the medical director to make rounds in person twice a month and do the rest by telephone.”
Instead, someone needs to be on site several times a week, working with nursing staff and developing protocols and pathways to control variability, Dr. Harrington said. “And in many cases that will be a hospitalist. Hospitalists are finding ways to partner and provide that level of care. I believe good hospitalist groups can change the facility for the better, and fairly quickly.”
What happens in post-acute care
Cari Levy, MD, PhD, who does hospital coverage and post-acute care for a number of facilities and home health agencies in the Denver area, calls the changes coming to SNFs a thrilling time for post-acute care.
“Suddenly medical professionals care about what happens in the post-acute world,” she said. “Everyone is now looking at the same measures. If this works the way it should, there would be a lot more mutual respect between providers.”
SNFs that are concerned about their readmissions rates will want to do root cause analysis to figure out what’s going on, Dr. Levy said. “Maybe the doctor didn’t do a good assessment. Maybe it was just a tough case. Once you start talking, you’ll develop systems to help everyone responsible. Hospitalists can be part of that conversation,” she said.
“You can have a good outcome at Shady Oaks and a terrible outcome at Whispering Pines, for all sorts of reasons. The hospital wants to make sure we’re sending patients to facilities that produce good outcomes,” he explained. “But there has to be communication between providers – the SNF medical director, the hospitalists, and the emergency department.”
A TeamHealth doctor in Phoenix has convened a consortium of providers from different care settings to meet and talk about cases and how they could have gone better. “The reality is, these conversations are going on all over,” Dr. Wilborn said. “What’s driving them is the realization of what we all need to do in this new environment.”
Opportunities from reforms
Robert Burke, MD, FHM, assistant chief of Hospital Medicine at the Denver VA Medical Center, is lead author of a study in the Journal of Hospital Medicine highlighting implications and opportunities from reforms in post-acute care.3 Hospitalists may not appreciate that post-acute care is poised to undergo transformative change from the recently legislated reforms, opening opportunities for hospitalists to improve health care value by improving transitions of care, he noted.
“My sense is that payment reform will put pressure on physicians to use home health care more often than institutional care, because of the cost pressures. We know that hospitalists choose long-term care facility placements less often when participating in bundled payment,” Dr. Burke said. “I think few hospitalists really know what happens on a day-to-day basis in SNFs – or in patients’ homes, for that matter.”
According to Dr. Burke, there’s just not enough data currently to guide these decisions. He said that, based on his research, the best thing hospitalists can do is try to understand what’s available in post-acute spaces, and build relationships with post-acute facilities.
“Find ways to get feedback on your discharge decisions,” he said. “Here in Colorado, we met recently with the local chapter of the Society for Post-Acute and Long-Term Care Medicine, also known as AMDA. It’s been revealing for everyone involved.”
He recommends AMDA’s learning modules – which are designed for doctors who are new to long-term care – to any hospitalist who is entering the post-acute world.
References
1. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010 Jan-Feb;29(1):57-64.
2. Brennan N et al. Data Brief: Sharp reduction in avoidable hospitalizations among long-term care facility residents. The CMS Blog, 2017 Jan 17.
3. Burke RE et al. Post-acute care reform: Implications and opportunities for hospitalists. J Hosp Med. 2017 Jan;12(1);46-51.
Starting in 2018, skilled nursing facilities (SNFs), like acute care hospitals before them, will be subject to a penalty of up to 2% of their Medicare reimbursement for posting higher-than-average rates of hospital readmissions.
The Protecting Access to Medicare Act of 2014 established a value-based purchasing component for SNFs, including incentives for high-performing facilities and a measure for all-cause, all-condition readmissions to any hospital from the SNF within 30 days following hospital discharge – designed to recognize and reward, or punish, facilities’ performance on preventing unnecessary readmissions. Public reporting of SNF quality data, including readmission rates, started in October 2017. Penalties follow a year later. Some patients’ readmissions could trigger penalties for both the hospital and the SNF.
According to 2010 data, 23.5% of patients discharged from acute care hospitals to SNFs were readmitted to the hospital within 30 days, at a financial cost of $10,362 per readmission or $4.34 billion per year.1 Seventy eight percent of these readmissions were labeled avoidable. More recent evidence suggests that hospitalization rates for dual-eligible patients living in long-term care facilities decreased by 31% between 2010 and 2015.2As increasing numbers of hospitalists spend some or all of their work week in post-acute care settings, how will the SNF readmission penalty affect their relationships with post-acute facilities?
Experts say SNFs – as with hospitals before them – lack the ability to allocate rewards or penalties for readmission rate performance to individual doctors. But increasingly close collaborative relationships between post-acute facilities and the hospitalists who work in post-acute care mean that the hospitalist has an important role in helping the SNF to manage its readmissions exposure.
“Hospitals and hospitalists want to keep good relationships with the SNFs they partner with, for a variety of reasons,” Dr. Frizner said. “We believe that the best way to reduce readmissions and unplanned transfers from the SNF is for the doctor to know the patient. We need dedicated doctors in the facility. We want hospitalists who already know the patient to come to the facility and see the patient there.”
The hospitalist’s role in post-acute care
Hospitalists who work in post-acute care typically make scheduled, billable medical visits to patients in long-term care facilities, and may also take on roles such as facility medical director or contribute to quality improvement. Relationships may be initiated by a facility seeking more medical coverage, by a hospitalist group seeking additional work or an ability to impact on the post-acute care delivered to hospital patients discharged to the facility, or by health systems, health plans, or accountable care organizations seeking to better manage the quality of care transitions for their beneficiaries.
“What I’m seeing is that with opportunities for bundled payments, we all have new incentives for moving patients along and reducing waste,” Dr. Boutwell said. “For hospitalists practicing in SNFs, it’s going to be a much bigger phenomenon. They’ll be called to reevaluate patients and make more visits than they have been accustomed to.” She hopes SNFs are studying what happened with hospitals’ readmission penalties, and will respond more quickly and effectively to their own penalty exposure.
“What we are seeing is an effort to shift folks to lower cost – but still clinically appropriate – levels of care,” he said. “These dynamics will force SNFs to reevaluate and improve their clinical competencies, to accept patients and then treat them in place. It’s no longer acceptable for the medical director to make rounds in person twice a month and do the rest by telephone.”
Instead, someone needs to be on site several times a week, working with nursing staff and developing protocols and pathways to control variability, Dr. Harrington said. “And in many cases that will be a hospitalist. Hospitalists are finding ways to partner and provide that level of care. I believe good hospitalist groups can change the facility for the better, and fairly quickly.”
What happens in post-acute care
Cari Levy, MD, PhD, who does hospital coverage and post-acute care for a number of facilities and home health agencies in the Denver area, calls the changes coming to SNFs a thrilling time for post-acute care.
“Suddenly medical professionals care about what happens in the post-acute world,” she said. “Everyone is now looking at the same measures. If this works the way it should, there would be a lot more mutual respect between providers.”
SNFs that are concerned about their readmissions rates will want to do root cause analysis to figure out what’s going on, Dr. Levy said. “Maybe the doctor didn’t do a good assessment. Maybe it was just a tough case. Once you start talking, you’ll develop systems to help everyone responsible. Hospitalists can be part of that conversation,” she said.
“You can have a good outcome at Shady Oaks and a terrible outcome at Whispering Pines, for all sorts of reasons. The hospital wants to make sure we’re sending patients to facilities that produce good outcomes,” he explained. “But there has to be communication between providers – the SNF medical director, the hospitalists, and the emergency department.”
A TeamHealth doctor in Phoenix has convened a consortium of providers from different care settings to meet and talk about cases and how they could have gone better. “The reality is, these conversations are going on all over,” Dr. Wilborn said. “What’s driving them is the realization of what we all need to do in this new environment.”
Opportunities from reforms
Robert Burke, MD, FHM, assistant chief of Hospital Medicine at the Denver VA Medical Center, is lead author of a study in the Journal of Hospital Medicine highlighting implications and opportunities from reforms in post-acute care.3 Hospitalists may not appreciate that post-acute care is poised to undergo transformative change from the recently legislated reforms, opening opportunities for hospitalists to improve health care value by improving transitions of care, he noted.
“My sense is that payment reform will put pressure on physicians to use home health care more often than institutional care, because of the cost pressures. We know that hospitalists choose long-term care facility placements less often when participating in bundled payment,” Dr. Burke said. “I think few hospitalists really know what happens on a day-to-day basis in SNFs – or in patients’ homes, for that matter.”
According to Dr. Burke, there’s just not enough data currently to guide these decisions. He said that, based on his research, the best thing hospitalists can do is try to understand what’s available in post-acute spaces, and build relationships with post-acute facilities.
“Find ways to get feedback on your discharge decisions,” he said. “Here in Colorado, we met recently with the local chapter of the Society for Post-Acute and Long-Term Care Medicine, also known as AMDA. It’s been revealing for everyone involved.”
He recommends AMDA’s learning modules – which are designed for doctors who are new to long-term care – to any hospitalist who is entering the post-acute world.
References
1. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010 Jan-Feb;29(1):57-64.
2. Brennan N et al. Data Brief: Sharp reduction in avoidable hospitalizations among long-term care facility residents. The CMS Blog, 2017 Jan 17.
3. Burke RE et al. Post-acute care reform: Implications and opportunities for hospitalists. J Hosp Med. 2017 Jan;12(1);46-51.
Starting in 2018, skilled nursing facilities (SNFs), like acute care hospitals before them, will be subject to a penalty of up to 2% of their Medicare reimbursement for posting higher-than-average rates of hospital readmissions.
The Protecting Access to Medicare Act of 2014 established a value-based purchasing component for SNFs, including incentives for high-performing facilities and a measure for all-cause, all-condition readmissions to any hospital from the SNF within 30 days following hospital discharge – designed to recognize and reward, or punish, facilities’ performance on preventing unnecessary readmissions. Public reporting of SNF quality data, including readmission rates, started in October 2017. Penalties follow a year later. Some patients’ readmissions could trigger penalties for both the hospital and the SNF.
According to 2010 data, 23.5% of patients discharged from acute care hospitals to SNFs were readmitted to the hospital within 30 days, at a financial cost of $10,362 per readmission or $4.34 billion per year.1 Seventy eight percent of these readmissions were labeled avoidable. More recent evidence suggests that hospitalization rates for dual-eligible patients living in long-term care facilities decreased by 31% between 2010 and 2015.2As increasing numbers of hospitalists spend some or all of their work week in post-acute care settings, how will the SNF readmission penalty affect their relationships with post-acute facilities?
Experts say SNFs – as with hospitals before them – lack the ability to allocate rewards or penalties for readmission rate performance to individual doctors. But increasingly close collaborative relationships between post-acute facilities and the hospitalists who work in post-acute care mean that the hospitalist has an important role in helping the SNF to manage its readmissions exposure.
“Hospitals and hospitalists want to keep good relationships with the SNFs they partner with, for a variety of reasons,” Dr. Frizner said. “We believe that the best way to reduce readmissions and unplanned transfers from the SNF is for the doctor to know the patient. We need dedicated doctors in the facility. We want hospitalists who already know the patient to come to the facility and see the patient there.”
The hospitalist’s role in post-acute care
Hospitalists who work in post-acute care typically make scheduled, billable medical visits to patients in long-term care facilities, and may also take on roles such as facility medical director or contribute to quality improvement. Relationships may be initiated by a facility seeking more medical coverage, by a hospitalist group seeking additional work or an ability to impact on the post-acute care delivered to hospital patients discharged to the facility, or by health systems, health plans, or accountable care organizations seeking to better manage the quality of care transitions for their beneficiaries.
“What I’m seeing is that with opportunities for bundled payments, we all have new incentives for moving patients along and reducing waste,” Dr. Boutwell said. “For hospitalists practicing in SNFs, it’s going to be a much bigger phenomenon. They’ll be called to reevaluate patients and make more visits than they have been accustomed to.” She hopes SNFs are studying what happened with hospitals’ readmission penalties, and will respond more quickly and effectively to their own penalty exposure.
“What we are seeing is an effort to shift folks to lower cost – but still clinically appropriate – levels of care,” he said. “These dynamics will force SNFs to reevaluate and improve their clinical competencies, to accept patients and then treat them in place. It’s no longer acceptable for the medical director to make rounds in person twice a month and do the rest by telephone.”
Instead, someone needs to be on site several times a week, working with nursing staff and developing protocols and pathways to control variability, Dr. Harrington said. “And in many cases that will be a hospitalist. Hospitalists are finding ways to partner and provide that level of care. I believe good hospitalist groups can change the facility for the better, and fairly quickly.”
What happens in post-acute care
Cari Levy, MD, PhD, who does hospital coverage and post-acute care for a number of facilities and home health agencies in the Denver area, calls the changes coming to SNFs a thrilling time for post-acute care.
“Suddenly medical professionals care about what happens in the post-acute world,” she said. “Everyone is now looking at the same measures. If this works the way it should, there would be a lot more mutual respect between providers.”
SNFs that are concerned about their readmissions rates will want to do root cause analysis to figure out what’s going on, Dr. Levy said. “Maybe the doctor didn’t do a good assessment. Maybe it was just a tough case. Once you start talking, you’ll develop systems to help everyone responsible. Hospitalists can be part of that conversation,” she said.
“You can have a good outcome at Shady Oaks and a terrible outcome at Whispering Pines, for all sorts of reasons. The hospital wants to make sure we’re sending patients to facilities that produce good outcomes,” he explained. “But there has to be communication between providers – the SNF medical director, the hospitalists, and the emergency department.”
A TeamHealth doctor in Phoenix has convened a consortium of providers from different care settings to meet and talk about cases and how they could have gone better. “The reality is, these conversations are going on all over,” Dr. Wilborn said. “What’s driving them is the realization of what we all need to do in this new environment.”
Opportunities from reforms
Robert Burke, MD, FHM, assistant chief of Hospital Medicine at the Denver VA Medical Center, is lead author of a study in the Journal of Hospital Medicine highlighting implications and opportunities from reforms in post-acute care.3 Hospitalists may not appreciate that post-acute care is poised to undergo transformative change from the recently legislated reforms, opening opportunities for hospitalists to improve health care value by improving transitions of care, he noted.
“My sense is that payment reform will put pressure on physicians to use home health care more often than institutional care, because of the cost pressures. We know that hospitalists choose long-term care facility placements less often when participating in bundled payment,” Dr. Burke said. “I think few hospitalists really know what happens on a day-to-day basis in SNFs – or in patients’ homes, for that matter.”
According to Dr. Burke, there’s just not enough data currently to guide these decisions. He said that, based on his research, the best thing hospitalists can do is try to understand what’s available in post-acute spaces, and build relationships with post-acute facilities.
“Find ways to get feedback on your discharge decisions,” he said. “Here in Colorado, we met recently with the local chapter of the Society for Post-Acute and Long-Term Care Medicine, also known as AMDA. It’s been revealing for everyone involved.”
He recommends AMDA’s learning modules – which are designed for doctors who are new to long-term care – to any hospitalist who is entering the post-acute world.
References
1. Mor V et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff (Millwood). 2010 Jan-Feb;29(1):57-64.
2. Brennan N et al. Data Brief: Sharp reduction in avoidable hospitalizations among long-term care facility residents. The CMS Blog, 2017 Jan 17.
3. Burke RE et al. Post-acute care reform: Implications and opportunities for hospitalists. J Hosp Med. 2017 Jan;12(1);46-51.
Hospital readmissions penalties now in 5th year
With the Hospital Readmissions Reduction Program (HRRP) in its 5th year, what has been the impact on hospitals and on hospitalists?
First of all, a lot of penalties have been paid by hospitals. According to an analysis by Kaiser Health News,1 the Centers for Medicare and Medicaid Services will withhold $528 million from 2,597 hospitals in the current fiscal year, Oct. 1, 2016 to Sept. 30, 2017, for readmissions for six diagnoses that occurred between July 2012 and June 2015. The number of penalized hospitals is down slightly from 2,665 the year before, but the total annual withhold will go up by $108 million.
HRRP exacts Medicare payment penalties from hospitals that have rates of readmissions – within 30 days of discharge – that are higher than expected, based on national rates and the health of their patient population. The maximum penalty is now up to 3% of a hospital’s Medicare reimbursement. Hospitals are being penalized an average of 0.73% of their annual Medicare reimbursement, and cumulative HRRP penalties will reach nearly $1.9 billion by the end of the fiscal year, Kaiser Health News reports.2
“Basically, we chose to introduce the idea of measuring readmissions because we felt it represented an adverse outcome for many people that was being ignored; that risk could be reduced; and improvements would yield benefits for people as well as save money for the health care system,” he told The Hospitalist.
“More than anything, HRRP has sharpened the focus on considering the episode of care from the patient’s perspective – rather than just focusing on venues of care like the hospitalization alone,” Dr. Krumholz said. “The focus on readmission forced many of us in the health professions to consider what the experience was like to leave the acute setting – how information flowed, what kind of concerns people had, the degree to which they understood what had happened to them, the extent to which they were prepared for the next steps.”
Once the patient leaves the hospital, there are myriad factors that will influence their likelihood of returning, notes researcher Karen Joynt, MD, MPH, of the Department of Health Policy and Management at Harvard’s School of Public Health, Boston. “The proportion of patients readmitted to the hospital because of gross error is low, but sometimes we’re too optimistic about our patients’ ability to manage postdischarge,” she said.
“We all know we can do better at providing softer landings, and anyone who’s ever been a hospital patient or a family member of one knows that leaving the hospital is incredibly tumultuous. I experienced that with my own parents, and it’s frightening, even if everything is done right. It’s still a very vulnerable time.”
HRRP has fundamentally changed the conversation about hospital care, Dr. Joynt said. “I think we need to change the conversation even more and talk more about how to prevent admissions in the first place. As a clinician, I think we need to be more innovative, recognizing that the ways we’ll make a real difference probably has more to do with what happens outside of the hospital. My personal hope is that new alternate payment models like accountable care organizations will lead to more creative partnerships with other providers.”
What have we learned about readmissions in 5 years?
A lot of recently published research about readmissions has documented modest decreases in overall readmissions nationally, from over 21% to under 18% between 2007 and 2014, although most of the reduction occurred in the first couple of years after HRRP was announced and it has since largely leveled off.
Other research has tried to explore the relationship between readmissions rates and other outcomes that might matter more to patients or that might be better proxies for the quality of the hospital experience. Is readmission rate a true measure of quality, or just a utilization measure? Research has also tried to document what works: what are the best strategies for preventing avoidable readmissions by improving the discharge process, care transitions, and the coordination of care postdischarge in the community – although no silver bullet has yet been identified.
A recent effort to inject more equity into the penalties program, contained in the wide-ranging 21st Century Cures Act signed into law by President Obama in December 2016, requires Medicare to account for patients’ socio-economic backgrounds when it calculates reductions in its payments to hospitals under HRRP. The law directs the government to change the way pay for performance is applied to safety net hospitals by setting different penalty thresholds for hospitals based on the proportion of their patients who are dually eligible for Medicare and Medicaid.
It remains to be seen how this will be implemented and with what impact. But some critics have continued to question whether hospitals should be held accountable for readmissions, whether 30 days is the correct time frame for that accountability, and whether some hospitals might be simply taking the penalty hit rather than investing in the hard work of care transitions.
Impact on working hospitalists
One expert, Ashish Jha, MD, MPH, director of Harvard’s Global Health Institute, wants to see hospitalists get more engaged in the conversation about how to improve hospital care overall.

Experts say there aren’t metrics available that could allocate penalties to individual hospitalists for their performance in readmissions prevention. But hospitals, clearly, are paying attention, and hospitalist groups may find that part of their negotiation of quality and performance incentives with the hospital includes readmissions.
“There are so many other variables that go into transitions of care, and it would be unreasonable to try to hold the individual doctor responsible for all of them,” he said. But accountability can be passed on to the hospitalist group. “My hospital contracts with a national hospitalist company and our agreement has quality measures that we review with them. We ask them to focus on readmissions.”
Dr. Harte said that when patients are discharged from the hospital, they go from an environment where everything is taken care of for them, to total responsibility for their self-care. Yet we are asking ever more from patients in terms of self-management.
“We need to focus on the human side of the experience. The hospital is a place to be avoided wherever possible,” he said. Yet some readmissions are largely unpreventable. Hospitalists should focus on the patient’s greatest risk of preventable readmission. “Is it health literacy? Is it transportation?”
Readmissions at the front lines
Preetham Talari, MD, FACP, FHM, hospitalist at University of Kentucky HealthCare in Lexington, has an interest in health care safety, quality improvement, and value. He has led the university’s site participation in Project BOOST, the Society of Hospital Medicine’s national mentored quality improvement initiative for care transitions. Dr. Talari also led a quality initiative at the university called the Interprofessional Teamwork Innovation Model to systematize teamwork, first piloted on a 30-bed hospitalist unit where he is medical director.

“Readmissions are not just about doctors, they are more about patient factors, socioeconomic factors, where they live,” Dr. Talari said. “Those are harder to impact, but in my experience, it comes down to thinking about the patient’s needs before discharge – really from the time of admission: What are all the things we can do in the hospital to make sure the patient is safely transitioned home?”
According to Dr. Talari, complex issues like readmissions don’t depend on just one, two, or three factors. “But we do the interventions believing that it will improve processes and outcomes, and then add another intervention and another,” he said. “All of these interventions will add up like a jigsaw puzzle to achieve a final, sustainable outcome. One thing I believe is hospitalists should be leading these efforts.”
Better interventions, better infrastructure
Leora Horwitz, MD, MHS, director of the Center for Healthcare Innovation and Delivery Science at New York University School of Public Health, says the biggest change she has seen resulting from readmissions penalties is that transitions of care are now understood to be both important and the responsibility of front line hospitalists. “That was not true 5 or 10 years ago. We used to spend hours admitting patients to the hospital and then 5 minutes on their discharge.”

“We’ve also learned that the infrastructure can be built better. Historically, hospital discharge summaries have been abysmal. But we can automate the importation of pending labs into the electronic health record. These are things you can change for everybody by changing your template. Sit down in a room together every afternoon to talk about what will happen to the patients when they go home. That’s become standard at our hospital. That was never done before.”
Evidence for improved outcomes is mixed, Dr. Horwitz noted. However, she pointed out, is there any evidence that readmissions penalties have produced adverse outcomes? Did they increase mortality, or length of stay? “So far the evidence suggests that they did not,” she said.
“I think it’s generally likely that the work we have done has resulted in better care. Thousands of people haven’t had to go back to the hospital, and that’s a good thing.”
Recent research on readmissions penalties
A survey by Yale researchers, published in JAMA in December 2016, found that hospitals financially penalized under HRRP reduced their readmissions rates at a higher rate than nonpenalized hospitals, “which implies that penalties can improve quality and readmission performance for hospitals with the most room for improvement,” coauthor Kumar Dharmarajan, MD, MBA, said in a statement.4 The hospitals responded to external pressures – in other words, financial penalties worked. But most of the reduction happened in the 2 years before actual penalties went into effect, which suggests that further improvement will not be easy, the authors note.
A survey of the attitudes of hospital leaders on the HRRP found that it has had a major impact on their efforts to reduce readmissions rates, although the failure to take sociodemographic factors into account was a major complaint for these leaders.5 Most said the penalties were too large, but 42.5% believed HRRP was likely to improve quality.
Some have questioned whether readmissions penalties were just encouraging hospitals to reduce their rates by keeping returning patients in observation units rather than formally readmitting them. Zuckerman et al. in the New England Journal of Medicine found no evidence that changes in observation unit stays accounted for the documented decrease in readmissions.6
But according to Papanicolas et al. in Health Affairs, patient hospital experience has improved only modestly under hospital value-based purchasing for U.S. hospitals, with no evidence that the program has had a beneficial effect on overall patient experience.7 Another study from Harvard by Figueroa et al. found that evidence is lacking that hospital value-based purchasing leads to lower mortality rates.8
“Patients and caregivers tell us: Hey, you people are the experts. You’ve taken care of lots of people with my medical condition before. You should know what my needs are going to be postdischarge and help me anticipate them,” he said.
References
1. Rau J. Medicare’s Readmission Penalties Hit New High. Kaiser Health News. 2016 Aug 2.
2. Boccuti C, Casillas G. Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program. Kaiser Health News, 2016 Sep 30.
3. Keenan PS, Normand SLT, Lin Z, et al. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ Cardiovasc Qual Outcomes. 2008;1:29-37.
4. Desai NR, Ross JS, Kwon JY, et al. Association between hospital penalty status under the Hospital Readmission Reduction Program and readmission rates for target and nontarget conditions. JAMA. 2016 Dec 27;316(24):2647-56.
5. Joynt KE, Figueroa JF, Orav EJ, Jha AK. Opinions on the Hospital Readmissions Reduction Program: Results of a national survey of hospital leaders. Am J Manag Care. 2016 Aug 1;222(8):e287-94.
6. Zuckerman RB, Sheingold SH, Orav EJ, et al. Readmissions, observation, and the Hospital Readmissions Reduction Program. N Engl J Med. 2016 Apr 21;374(16):1543-51.
7. Papanicolas I, Figueroa JF, Orav EJ, Jha AK. Patient hospital experience improved modestly, but no evidence Medicare incentives promoted meaningful gain. Health Aff (Millwood). 2017 Jan;36(1):133-40.
8. Figueroa JF, Tsugawa Y, Zheng J, et al. Association between the value-based purchasing pay for performance program and patient mortality in US hospitals: observational study. BMJ. 2016;353:i2214.
With the Hospital Readmissions Reduction Program (HRRP) in its 5th year, what has been the impact on hospitals and on hospitalists?
First of all, a lot of penalties have been paid by hospitals. According to an analysis by Kaiser Health News,1 the Centers for Medicare and Medicaid Services will withhold $528 million from 2,597 hospitals in the current fiscal year, Oct. 1, 2016 to Sept. 30, 2017, for readmissions for six diagnoses that occurred between July 2012 and June 2015. The number of penalized hospitals is down slightly from 2,665 the year before, but the total annual withhold will go up by $108 million.
HRRP exacts Medicare payment penalties from hospitals that have rates of readmissions – within 30 days of discharge – that are higher than expected, based on national rates and the health of their patient population. The maximum penalty is now up to 3% of a hospital’s Medicare reimbursement. Hospitals are being penalized an average of 0.73% of their annual Medicare reimbursement, and cumulative HRRP penalties will reach nearly $1.9 billion by the end of the fiscal year, Kaiser Health News reports.2
“Basically, we chose to introduce the idea of measuring readmissions because we felt it represented an adverse outcome for many people that was being ignored; that risk could be reduced; and improvements would yield benefits for people as well as save money for the health care system,” he told The Hospitalist.
“More than anything, HRRP has sharpened the focus on considering the episode of care from the patient’s perspective – rather than just focusing on venues of care like the hospitalization alone,” Dr. Krumholz said. “The focus on readmission forced many of us in the health professions to consider what the experience was like to leave the acute setting – how information flowed, what kind of concerns people had, the degree to which they understood what had happened to them, the extent to which they were prepared for the next steps.”
Once the patient leaves the hospital, there are myriad factors that will influence their likelihood of returning, notes researcher Karen Joynt, MD, MPH, of the Department of Health Policy and Management at Harvard’s School of Public Health, Boston. “The proportion of patients readmitted to the hospital because of gross error is low, but sometimes we’re too optimistic about our patients’ ability to manage postdischarge,” she said.
“We all know we can do better at providing softer landings, and anyone who’s ever been a hospital patient or a family member of one knows that leaving the hospital is incredibly tumultuous. I experienced that with my own parents, and it’s frightening, even if everything is done right. It’s still a very vulnerable time.”
HRRP has fundamentally changed the conversation about hospital care, Dr. Joynt said. “I think we need to change the conversation even more and talk more about how to prevent admissions in the first place. As a clinician, I think we need to be more innovative, recognizing that the ways we’ll make a real difference probably has more to do with what happens outside of the hospital. My personal hope is that new alternate payment models like accountable care organizations will lead to more creative partnerships with other providers.”
What have we learned about readmissions in 5 years?
A lot of recently published research about readmissions has documented modest decreases in overall readmissions nationally, from over 21% to under 18% between 2007 and 2014, although most of the reduction occurred in the first couple of years after HRRP was announced and it has since largely leveled off.
Other research has tried to explore the relationship between readmissions rates and other outcomes that might matter more to patients or that might be better proxies for the quality of the hospital experience. Is readmission rate a true measure of quality, or just a utilization measure? Research has also tried to document what works: what are the best strategies for preventing avoidable readmissions by improving the discharge process, care transitions, and the coordination of care postdischarge in the community – although no silver bullet has yet been identified.
A recent effort to inject more equity into the penalties program, contained in the wide-ranging 21st Century Cures Act signed into law by President Obama in December 2016, requires Medicare to account for patients’ socio-economic backgrounds when it calculates reductions in its payments to hospitals under HRRP. The law directs the government to change the way pay for performance is applied to safety net hospitals by setting different penalty thresholds for hospitals based on the proportion of their patients who are dually eligible for Medicare and Medicaid.
It remains to be seen how this will be implemented and with what impact. But some critics have continued to question whether hospitals should be held accountable for readmissions, whether 30 days is the correct time frame for that accountability, and whether some hospitals might be simply taking the penalty hit rather than investing in the hard work of care transitions.
Impact on working hospitalists
One expert, Ashish Jha, MD, MPH, director of Harvard’s Global Health Institute, wants to see hospitalists get more engaged in the conversation about how to improve hospital care overall.
Experts say there aren’t metrics available that could allocate penalties to individual hospitalists for their performance in readmissions prevention. But hospitals, clearly, are paying attention, and hospitalist groups may find that part of their negotiation of quality and performance incentives with the hospital includes readmissions.
“There are so many other variables that go into transitions of care, and it would be unreasonable to try to hold the individual doctor responsible for all of them,” he said. But accountability can be passed on to the hospitalist group. “My hospital contracts with a national hospitalist company and our agreement has quality measures that we review with them. We ask them to focus on readmissions.”
Dr. Harte said that when patients are discharged from the hospital, they go from an environment where everything is taken care of for them, to total responsibility for their self-care. Yet we are asking ever more from patients in terms of self-management.
“We need to focus on the human side of the experience. The hospital is a place to be avoided wherever possible,” he said. Yet some readmissions are largely unpreventable. Hospitalists should focus on the patient’s greatest risk of preventable readmission. “Is it health literacy? Is it transportation?”
Readmissions at the front lines
Preetham Talari, MD, FACP, FHM, hospitalist at University of Kentucky HealthCare in Lexington, has an interest in health care safety, quality improvement, and value. He has led the university’s site participation in Project BOOST, the Society of Hospital Medicine’s national mentored quality improvement initiative for care transitions. Dr. Talari also led a quality initiative at the university called the Interprofessional Teamwork Innovation Model to systematize teamwork, first piloted on a 30-bed hospitalist unit where he is medical director.
“Readmissions are not just about doctors, they are more about patient factors, socioeconomic factors, where they live,” Dr. Talari said. “Those are harder to impact, but in my experience, it comes down to thinking about the patient’s needs before discharge – really from the time of admission: What are all the things we can do in the hospital to make sure the patient is safely transitioned home?”
According to Dr. Talari, complex issues like readmissions don’t depend on just one, two, or three factors. “But we do the interventions believing that it will improve processes and outcomes, and then add another intervention and another,” he said. “All of these interventions will add up like a jigsaw puzzle to achieve a final, sustainable outcome. One thing I believe is hospitalists should be leading these efforts.”
Better interventions, better infrastructure
Leora Horwitz, MD, MHS, director of the Center for Healthcare Innovation and Delivery Science at New York University School of Public Health, says the biggest change she has seen resulting from readmissions penalties is that transitions of care are now understood to be both important and the responsibility of front line hospitalists. “That was not true 5 or 10 years ago. We used to spend hours admitting patients to the hospital and then 5 minutes on their discharge.”
“We’ve also learned that the infrastructure can be built better. Historically, hospital discharge summaries have been abysmal. But we can automate the importation of pending labs into the electronic health record. These are things you can change for everybody by changing your template. Sit down in a room together every afternoon to talk about what will happen to the patients when they go home. That’s become standard at our hospital. That was never done before.”
Evidence for improved outcomes is mixed, Dr. Horwitz noted. However, she pointed out, is there any evidence that readmissions penalties have produced adverse outcomes? Did they increase mortality, or length of stay? “So far the evidence suggests that they did not,” she said.
“I think it’s generally likely that the work we have done has resulted in better care. Thousands of people haven’t had to go back to the hospital, and that’s a good thing.”
Recent research on readmissions penalties
A survey by Yale researchers, published in JAMA in December 2016, found that hospitals financially penalized under HRRP reduced their readmissions rates at a higher rate than nonpenalized hospitals, “which implies that penalties can improve quality and readmission performance for hospitals with the most room for improvement,” coauthor Kumar Dharmarajan, MD, MBA, said in a statement.4 The hospitals responded to external pressures – in other words, financial penalties worked. But most of the reduction happened in the 2 years before actual penalties went into effect, which suggests that further improvement will not be easy, the authors note.
A survey of the attitudes of hospital leaders on the HRRP found that it has had a major impact on their efforts to reduce readmissions rates, although the failure to take sociodemographic factors into account was a major complaint for these leaders.5 Most said the penalties were too large, but 42.5% believed HRRP was likely to improve quality.
Some have questioned whether readmissions penalties were just encouraging hospitals to reduce their rates by keeping returning patients in observation units rather than formally readmitting them. Zuckerman et al. in the New England Journal of Medicine found no evidence that changes in observation unit stays accounted for the documented decrease in readmissions.6
But according to Papanicolas et al. in Health Affairs, patient hospital experience has improved only modestly under hospital value-based purchasing for U.S. hospitals, with no evidence that the program has had a beneficial effect on overall patient experience.7 Another study from Harvard by Figueroa et al. found that evidence is lacking that hospital value-based purchasing leads to lower mortality rates.8
“Patients and caregivers tell us: Hey, you people are the experts. You’ve taken care of lots of people with my medical condition before. You should know what my needs are going to be postdischarge and help me anticipate them,” he said.
References
1. Rau J. Medicare’s Readmission Penalties Hit New High. Kaiser Health News. 2016 Aug 2.
2. Boccuti C, Casillas G. Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program. Kaiser Health News, 2016 Sep 30.
3. Keenan PS, Normand SLT, Lin Z, et al. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ Cardiovasc Qual Outcomes. 2008;1:29-37.
4. Desai NR, Ross JS, Kwon JY, et al. Association between hospital penalty status under the Hospital Readmission Reduction Program and readmission rates for target and nontarget conditions. JAMA. 2016 Dec 27;316(24):2647-56.
5. Joynt KE, Figueroa JF, Orav EJ, Jha AK. Opinions on the Hospital Readmissions Reduction Program: Results of a national survey of hospital leaders. Am J Manag Care. 2016 Aug 1;222(8):e287-94.
6. Zuckerman RB, Sheingold SH, Orav EJ, et al. Readmissions, observation, and the Hospital Readmissions Reduction Program. N Engl J Med. 2016 Apr 21;374(16):1543-51.
7. Papanicolas I, Figueroa JF, Orav EJ, Jha AK. Patient hospital experience improved modestly, but no evidence Medicare incentives promoted meaningful gain. Health Aff (Millwood). 2017 Jan;36(1):133-40.
8. Figueroa JF, Tsugawa Y, Zheng J, et al. Association between the value-based purchasing pay for performance program and patient mortality in US hospitals: observational study. BMJ. 2016;353:i2214.
With the Hospital Readmissions Reduction Program (HRRP) in its 5th year, what has been the impact on hospitals and on hospitalists?
First of all, a lot of penalties have been paid by hospitals. According to an analysis by Kaiser Health News,1 the Centers for Medicare and Medicaid Services will withhold $528 million from 2,597 hospitals in the current fiscal year, Oct. 1, 2016 to Sept. 30, 2017, for readmissions for six diagnoses that occurred between July 2012 and June 2015. The number of penalized hospitals is down slightly from 2,665 the year before, but the total annual withhold will go up by $108 million.
HRRP exacts Medicare payment penalties from hospitals that have rates of readmissions – within 30 days of discharge – that are higher than expected, based on national rates and the health of their patient population. The maximum penalty is now up to 3% of a hospital’s Medicare reimbursement. Hospitals are being penalized an average of 0.73% of their annual Medicare reimbursement, and cumulative HRRP penalties will reach nearly $1.9 billion by the end of the fiscal year, Kaiser Health News reports.2
“Basically, we chose to introduce the idea of measuring readmissions because we felt it represented an adverse outcome for many people that was being ignored; that risk could be reduced; and improvements would yield benefits for people as well as save money for the health care system,” he told The Hospitalist.
“More than anything, HRRP has sharpened the focus on considering the episode of care from the patient’s perspective – rather than just focusing on venues of care like the hospitalization alone,” Dr. Krumholz said. “The focus on readmission forced many of us in the health professions to consider what the experience was like to leave the acute setting – how information flowed, what kind of concerns people had, the degree to which they understood what had happened to them, the extent to which they were prepared for the next steps.”
Once the patient leaves the hospital, there are myriad factors that will influence their likelihood of returning, notes researcher Karen Joynt, MD, MPH, of the Department of Health Policy and Management at Harvard’s School of Public Health, Boston. “The proportion of patients readmitted to the hospital because of gross error is low, but sometimes we’re too optimistic about our patients’ ability to manage postdischarge,” she said.
“We all know we can do better at providing softer landings, and anyone who’s ever been a hospital patient or a family member of one knows that leaving the hospital is incredibly tumultuous. I experienced that with my own parents, and it’s frightening, even if everything is done right. It’s still a very vulnerable time.”
HRRP has fundamentally changed the conversation about hospital care, Dr. Joynt said. “I think we need to change the conversation even more and talk more about how to prevent admissions in the first place. As a clinician, I think we need to be more innovative, recognizing that the ways we’ll make a real difference probably has more to do with what happens outside of the hospital. My personal hope is that new alternate payment models like accountable care organizations will lead to more creative partnerships with other providers.”
What have we learned about readmissions in 5 years?
A lot of recently published research about readmissions has documented modest decreases in overall readmissions nationally, from over 21% to under 18% between 2007 and 2014, although most of the reduction occurred in the first couple of years after HRRP was announced and it has since largely leveled off.
Other research has tried to explore the relationship between readmissions rates and other outcomes that might matter more to patients or that might be better proxies for the quality of the hospital experience. Is readmission rate a true measure of quality, or just a utilization measure? Research has also tried to document what works: what are the best strategies for preventing avoidable readmissions by improving the discharge process, care transitions, and the coordination of care postdischarge in the community – although no silver bullet has yet been identified.
A recent effort to inject more equity into the penalties program, contained in the wide-ranging 21st Century Cures Act signed into law by President Obama in December 2016, requires Medicare to account for patients’ socio-economic backgrounds when it calculates reductions in its payments to hospitals under HRRP. The law directs the government to change the way pay for performance is applied to safety net hospitals by setting different penalty thresholds for hospitals based on the proportion of their patients who are dually eligible for Medicare and Medicaid.
It remains to be seen how this will be implemented and with what impact. But some critics have continued to question whether hospitals should be held accountable for readmissions, whether 30 days is the correct time frame for that accountability, and whether some hospitals might be simply taking the penalty hit rather than investing in the hard work of care transitions.
Impact on working hospitalists
One expert, Ashish Jha, MD, MPH, director of Harvard’s Global Health Institute, wants to see hospitalists get more engaged in the conversation about how to improve hospital care overall.
Experts say there aren’t metrics available that could allocate penalties to individual hospitalists for their performance in readmissions prevention. But hospitals, clearly, are paying attention, and hospitalist groups may find that part of their negotiation of quality and performance incentives with the hospital includes readmissions.
“There are so many other variables that go into transitions of care, and it would be unreasonable to try to hold the individual doctor responsible for all of them,” he said. But accountability can be passed on to the hospitalist group. “My hospital contracts with a national hospitalist company and our agreement has quality measures that we review with them. We ask them to focus on readmissions.”
Dr. Harte said that when patients are discharged from the hospital, they go from an environment where everything is taken care of for them, to total responsibility for their self-care. Yet we are asking ever more from patients in terms of self-management.
“We need to focus on the human side of the experience. The hospital is a place to be avoided wherever possible,” he said. Yet some readmissions are largely unpreventable. Hospitalists should focus on the patient’s greatest risk of preventable readmission. “Is it health literacy? Is it transportation?”
Readmissions at the front lines
Preetham Talari, MD, FACP, FHM, hospitalist at University of Kentucky HealthCare in Lexington, has an interest in health care safety, quality improvement, and value. He has led the university’s site participation in Project BOOST, the Society of Hospital Medicine’s national mentored quality improvement initiative for care transitions. Dr. Talari also led a quality initiative at the university called the Interprofessional Teamwork Innovation Model to systematize teamwork, first piloted on a 30-bed hospitalist unit where he is medical director.
“Readmissions are not just about doctors, they are more about patient factors, socioeconomic factors, where they live,” Dr. Talari said. “Those are harder to impact, but in my experience, it comes down to thinking about the patient’s needs before discharge – really from the time of admission: What are all the things we can do in the hospital to make sure the patient is safely transitioned home?”
According to Dr. Talari, complex issues like readmissions don’t depend on just one, two, or three factors. “But we do the interventions believing that it will improve processes and outcomes, and then add another intervention and another,” he said. “All of these interventions will add up like a jigsaw puzzle to achieve a final, sustainable outcome. One thing I believe is hospitalists should be leading these efforts.”
Better interventions, better infrastructure
Leora Horwitz, MD, MHS, director of the Center for Healthcare Innovation and Delivery Science at New York University School of Public Health, says the biggest change she has seen resulting from readmissions penalties is that transitions of care are now understood to be both important and the responsibility of front line hospitalists. “That was not true 5 or 10 years ago. We used to spend hours admitting patients to the hospital and then 5 minutes on their discharge.”
“We’ve also learned that the infrastructure can be built better. Historically, hospital discharge summaries have been abysmal. But we can automate the importation of pending labs into the electronic health record. These are things you can change for everybody by changing your template. Sit down in a room together every afternoon to talk about what will happen to the patients when they go home. That’s become standard at our hospital. That was never done before.”
Evidence for improved outcomes is mixed, Dr. Horwitz noted. However, she pointed out, is there any evidence that readmissions penalties have produced adverse outcomes? Did they increase mortality, or length of stay? “So far the evidence suggests that they did not,” she said.
“I think it’s generally likely that the work we have done has resulted in better care. Thousands of people haven’t had to go back to the hospital, and that’s a good thing.”
Recent research on readmissions penalties
A survey by Yale researchers, published in JAMA in December 2016, found that hospitals financially penalized under HRRP reduced their readmissions rates at a higher rate than nonpenalized hospitals, “which implies that penalties can improve quality and readmission performance for hospitals with the most room for improvement,” coauthor Kumar Dharmarajan, MD, MBA, said in a statement.4 The hospitals responded to external pressures – in other words, financial penalties worked. But most of the reduction happened in the 2 years before actual penalties went into effect, which suggests that further improvement will not be easy, the authors note.
A survey of the attitudes of hospital leaders on the HRRP found that it has had a major impact on their efforts to reduce readmissions rates, although the failure to take sociodemographic factors into account was a major complaint for these leaders.5 Most said the penalties were too large, but 42.5% believed HRRP was likely to improve quality.
Some have questioned whether readmissions penalties were just encouraging hospitals to reduce their rates by keeping returning patients in observation units rather than formally readmitting them. Zuckerman et al. in the New England Journal of Medicine found no evidence that changes in observation unit stays accounted for the documented decrease in readmissions.6
But according to Papanicolas et al. in Health Affairs, patient hospital experience has improved only modestly under hospital value-based purchasing for U.S. hospitals, with no evidence that the program has had a beneficial effect on overall patient experience.7 Another study from Harvard by Figueroa et al. found that evidence is lacking that hospital value-based purchasing leads to lower mortality rates.8
“Patients and caregivers tell us: Hey, you people are the experts. You’ve taken care of lots of people with my medical condition before. You should know what my needs are going to be postdischarge and help me anticipate them,” he said.
References
1. Rau J. Medicare’s Readmission Penalties Hit New High. Kaiser Health News. 2016 Aug 2.
2. Boccuti C, Casillas G. Aiming for Fewer Hospital U-turns: The Medicare Hospital Readmission Reduction Program. Kaiser Health News, 2016 Sep 30.
3. Keenan PS, Normand SLT, Lin Z, et al. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ Cardiovasc Qual Outcomes. 2008;1:29-37.
4. Desai NR, Ross JS, Kwon JY, et al. Association between hospital penalty status under the Hospital Readmission Reduction Program and readmission rates for target and nontarget conditions. JAMA. 2016 Dec 27;316(24):2647-56.
5. Joynt KE, Figueroa JF, Orav EJ, Jha AK. Opinions on the Hospital Readmissions Reduction Program: Results of a national survey of hospital leaders. Am J Manag Care. 2016 Aug 1;222(8):e287-94.
6. Zuckerman RB, Sheingold SH, Orav EJ, et al. Readmissions, observation, and the Hospital Readmissions Reduction Program. N Engl J Med. 2016 Apr 21;374(16):1543-51.
7. Papanicolas I, Figueroa JF, Orav EJ, Jha AK. Patient hospital experience improved modestly, but no evidence Medicare incentives promoted meaningful gain. Health Aff (Millwood). 2017 Jan;36(1):133-40.
8. Figueroa JF, Tsugawa Y, Zheng J, et al. Association between the value-based purchasing pay for performance program and patient mortality in US hospitals: observational study. BMJ. 2016;353:i2214.
Pediatric hospital medicine marches toward subspecialty recognition
Pediatric hospital medicine is moving quickly toward recognition as a board-certified, fellowship-trained medical subspecialty, joining 14 other pediatric subspecialties now certified by the American Board of Pediatrics (ABP).
It was approved as a subspecialty by the American Board of Medical Specialties (ABMS) at its October 2016 board meeting in Chicago in response to a petition from the ABP. Following years of discussion within the field,1 it will take 2 more years to describe pediatric hospital medicine’s specialized knowledge base and write test questions for biannual board exams that are projected to commence in the fall of 2019.
Eventually, starting in 2025, pediatric hospitalists will need to complete a fellowship of 2 years or more if they wish to sit for the exam and become board-certified in the field. But for the next 7 years, hospitalists in current practice will be able to qualify based on their work experience. Maintenance of certification requirements likely will be similar to those in other subspecialties, and doctors certified in pediatric hospital medicine won’t be required to maintain general pediatric certification, Dr. Rauch said.
Formal eligibility criteria have not been set, but likely will include working half-time overall in pediatric-related activities, and quarter-time in clinical practice in pediatric hospital medicine for 4 years prior to qualifying for the exam. How the hours might break down between clinical and other hospital responsibilities, and between pediatric or adult patients, still needs to be determined, Dr. Rauch said. He added that the experiential pathway is likely to be defined broadly, with latitude for determinations based on percentages of time worked, rather than absolute number of hours worked. Local pediatric institutions will be granted latitude to determine how that “plays out” in real world situations, he said, “and an ABP credentialing committee will be available to hear appeals for people who have complicated life circumstances.”
“I was part of a committee that explored these issues. We were an independent group of hospitalists who decided that board certification was a good way to advance the field,” Dr. Quinonez said. “We’ve seen what subspecialty certification has done, for example, for pediatric emergency medicine and pediatric critical care medicine – advancing them tremendously from a research standpoint and helping to develop a distinct body of knowledge reflecting increased severity of illness in hospitalized children.”
Discrepancy between practicing hospitalists, fellowships
An estimated 4,000 pediatric hospitalists now practice in the United States, and 2,100 of those belong to the American Academy of Pediatrics’ Section on Hospital Medicine. There are 40 pediatric hospital medicine fellowship programs listed on the website of AAP’s Section on Hospital Medicine (http://phmfellows.org/phm-programs/), although formal training assessment criteria will be needed for the American College of Graduate Medical Education to recognize programs that qualify their fellows to sit for the PHM exam. A wide gap is anticipated between the demand for pediatric hospitalists and currently available fellowship training slots to generate new candidates for board certification, although Dr. Rauch projects that fellowship slots will double in coming years.
“My message to the field is that historically, board certification has been the launching point for further development of the field,” Dr. Rauch said. “It leads to standardization of who is a subspecialist. Right now, who is a pediatric hospitalist is subject to wide variation. We need to standardize training and to create for this field the same distinction and stature as other medical subspecialties,” he said, noting that subspecialty status also has ramifications for academic settings, and for career advancement and career satisfaction for the individuals who choose to pursue it.
“I know there has been some hue and cry about this in the field, but in most cases certification will not change a pediatric hospitalist’s ability to obtain a job,” he said. “Already, you can’t become a division leader at a children’s hospital without additional training. This isn’t going to change that reality. But for people who don’t want to follow an academic career path, there will never be enough board-certified or fellowship-trained pediatric hospitalists to fill all of the pediatric positions in all the hospitals in the country. Community hospitals aren’t going to say: We won’t hire you unless you are board certified.”
Is the fellowship good for the field?
The subspecialty development process clearly is moving forward. Those in favor believe it will increase scholarship, research, and recognition for the subspecialty by the public for its specialized body of knowledge. But not everyone in the field agrees. Last fall The Hospitalist published3 an opinion piece questioning the need for fellowship-based board certification in pediatric hospital medicine. The author recommended instead retaining the current voluntary approach to fellowships and establishing a pediatric “focused practice” incorporated into residency training, much as the American Board of Internal Medicine and the American Board of Family Medicine have done for hospitalists in adult medicine.

“Will it lead to uncertainty among those currently in residency programs? If you are a pediatric resident and you want to become a board-certified pediatric hospitalist, you’ll need at least 2 years more of training. Is that going to deter qualified individuals?” Dr. Chang said. “The people this decision will impact the most are med-peds doctors – who complete a combined internal medicine and pediatrics residency – and part-timers. They may find themselves in a difficult position if the number of hours don’t add up for them to sit for the boards. For the most part, we’ll have to wait and see for answers to these questions.”
Brian Alverson, MD, FAAP, current chair of the AAP’s Section on Hospital Medicine and associate professor of pediatrics at Brown University, Providence, R.I., says he can see both sides of the debate.
But at the same time, there is a significant opportunity cost for doing 2 more years of fellowship training, Dr. Alverson said.
“We don’t know how much the board certification test will improve actual care,” he noted. “Does it truly identify higher quality doctors, or just doctors who are good at taking multiple choice exams? There are a number of people in pediatrics who do a lot of different things in their jobs, and it’s important that they not lose their ability to practice in the field. Two-thirds of our work force is in community hospitals, not academic medical centers. They work hard to provide the backbone of hospital care for young patients, and many of them are unlikely to ever do a fellowship.”
Nonetheless, Dr. Alverson believes pediatric hospitalists needn’t worry. “You still have plenty of time to figure out what’s going to happen in your hospital,” he said.
References
1. Section on Hospital Medicine. Guiding principles for pediatric hospital medicine program. Pediatrics; 2013; 132:782-786.
2. Stucky E. The Pediatric Hospital Medicine Core Competencies. Wiley-Blackwell; 2010.
3. Feldman LS, Monash B, Eniasivam A. Why required pediatric hospital medicine fellowships are unnecessary. The Hospitalist Magazine, October 8, 2016.
Pediatric hospital medicine is moving quickly toward recognition as a board-certified, fellowship-trained medical subspecialty, joining 14 other pediatric subspecialties now certified by the American Board of Pediatrics (ABP).
It was approved as a subspecialty by the American Board of Medical Specialties (ABMS) at its October 2016 board meeting in Chicago in response to a petition from the ABP. Following years of discussion within the field,1 it will take 2 more years to describe pediatric hospital medicine’s specialized knowledge base and write test questions for biannual board exams that are projected to commence in the fall of 2019.
Eventually, starting in 2025, pediatric hospitalists will need to complete a fellowship of 2 years or more if they wish to sit for the exam and become board-certified in the field. But for the next 7 years, hospitalists in current practice will be able to qualify based on their work experience. Maintenance of certification requirements likely will be similar to those in other subspecialties, and doctors certified in pediatric hospital medicine won’t be required to maintain general pediatric certification, Dr. Rauch said.
Formal eligibility criteria have not been set, but likely will include working half-time overall in pediatric-related activities, and quarter-time in clinical practice in pediatric hospital medicine for 4 years prior to qualifying for the exam. How the hours might break down between clinical and other hospital responsibilities, and between pediatric or adult patients, still needs to be determined, Dr. Rauch said. He added that the experiential pathway is likely to be defined broadly, with latitude for determinations based on percentages of time worked, rather than absolute number of hours worked. Local pediatric institutions will be granted latitude to determine how that “plays out” in real world situations, he said, “and an ABP credentialing committee will be available to hear appeals for people who have complicated life circumstances.”
“I was part of a committee that explored these issues. We were an independent group of hospitalists who decided that board certification was a good way to advance the field,” Dr. Quinonez said. “We’ve seen what subspecialty certification has done, for example, for pediatric emergency medicine and pediatric critical care medicine – advancing them tremendously from a research standpoint and helping to develop a distinct body of knowledge reflecting increased severity of illness in hospitalized children.”
Discrepancy between practicing hospitalists, fellowships
An estimated 4,000 pediatric hospitalists now practice in the United States, and 2,100 of those belong to the American Academy of Pediatrics’ Section on Hospital Medicine. There are 40 pediatric hospital medicine fellowship programs listed on the website of AAP’s Section on Hospital Medicine (http://phmfellows.org/phm-programs/), although formal training assessment criteria will be needed for the American College of Graduate Medical Education to recognize programs that qualify their fellows to sit for the PHM exam. A wide gap is anticipated between the demand for pediatric hospitalists and currently available fellowship training slots to generate new candidates for board certification, although Dr. Rauch projects that fellowship slots will double in coming years.
“My message to the field is that historically, board certification has been the launching point for further development of the field,” Dr. Rauch said. “It leads to standardization of who is a subspecialist. Right now, who is a pediatric hospitalist is subject to wide variation. We need to standardize training and to create for this field the same distinction and stature as other medical subspecialties,” he said, noting that subspecialty status also has ramifications for academic settings, and for career advancement and career satisfaction for the individuals who choose to pursue it.
“I know there has been some hue and cry about this in the field, but in most cases certification will not change a pediatric hospitalist’s ability to obtain a job,” he said. “Already, you can’t become a division leader at a children’s hospital without additional training. This isn’t going to change that reality. But for people who don’t want to follow an academic career path, there will never be enough board-certified or fellowship-trained pediatric hospitalists to fill all of the pediatric positions in all the hospitals in the country. Community hospitals aren’t going to say: We won’t hire you unless you are board certified.”
Is the fellowship good for the field?
The subspecialty development process clearly is moving forward. Those in favor believe it will increase scholarship, research, and recognition for the subspecialty by the public for its specialized body of knowledge. But not everyone in the field agrees. Last fall The Hospitalist published3 an opinion piece questioning the need for fellowship-based board certification in pediatric hospital medicine. The author recommended instead retaining the current voluntary approach to fellowships and establishing a pediatric “focused practice” incorporated into residency training, much as the American Board of Internal Medicine and the American Board of Family Medicine have done for hospitalists in adult medicine.
“Will it lead to uncertainty among those currently in residency programs? If you are a pediatric resident and you want to become a board-certified pediatric hospitalist, you’ll need at least 2 years more of training. Is that going to deter qualified individuals?” Dr. Chang said. “The people this decision will impact the most are med-peds doctors – who complete a combined internal medicine and pediatrics residency – and part-timers. They may find themselves in a difficult position if the number of hours don’t add up for them to sit for the boards. For the most part, we’ll have to wait and see for answers to these questions.”
Brian Alverson, MD, FAAP, current chair of the AAP’s Section on Hospital Medicine and associate professor of pediatrics at Brown University, Providence, R.I., says he can see both sides of the debate.
But at the same time, there is a significant opportunity cost for doing 2 more years of fellowship training, Dr. Alverson said.
“We don’t know how much the board certification test will improve actual care,” he noted. “Does it truly identify higher quality doctors, or just doctors who are good at taking multiple choice exams? There are a number of people in pediatrics who do a lot of different things in their jobs, and it’s important that they not lose their ability to practice in the field. Two-thirds of our work force is in community hospitals, not academic medical centers. They work hard to provide the backbone of hospital care for young patients, and many of them are unlikely to ever do a fellowship.”
Nonetheless, Dr. Alverson believes pediatric hospitalists needn’t worry. “You still have plenty of time to figure out what’s going to happen in your hospital,” he said.
References
1. Section on Hospital Medicine. Guiding principles for pediatric hospital medicine program. Pediatrics; 2013; 132:782-786.
2. Stucky E. The Pediatric Hospital Medicine Core Competencies. Wiley-Blackwell; 2010.
3. Feldman LS, Monash B, Eniasivam A. Why required pediatric hospital medicine fellowships are unnecessary. The Hospitalist Magazine, October 8, 2016.
Pediatric hospital medicine is moving quickly toward recognition as a board-certified, fellowship-trained medical subspecialty, joining 14 other pediatric subspecialties now certified by the American Board of Pediatrics (ABP).
It was approved as a subspecialty by the American Board of Medical Specialties (ABMS) at its October 2016 board meeting in Chicago in response to a petition from the ABP. Following years of discussion within the field,1 it will take 2 more years to describe pediatric hospital medicine’s specialized knowledge base and write test questions for biannual board exams that are projected to commence in the fall of 2019.
Eventually, starting in 2025, pediatric hospitalists will need to complete a fellowship of 2 years or more if they wish to sit for the exam and become board-certified in the field. But for the next 7 years, hospitalists in current practice will be able to qualify based on their work experience. Maintenance of certification requirements likely will be similar to those in other subspecialties, and doctors certified in pediatric hospital medicine won’t be required to maintain general pediatric certification, Dr. Rauch said.
Formal eligibility criteria have not been set, but likely will include working half-time overall in pediatric-related activities, and quarter-time in clinical practice in pediatric hospital medicine for 4 years prior to qualifying for the exam. How the hours might break down between clinical and other hospital responsibilities, and between pediatric or adult patients, still needs to be determined, Dr. Rauch said. He added that the experiential pathway is likely to be defined broadly, with latitude for determinations based on percentages of time worked, rather than absolute number of hours worked. Local pediatric institutions will be granted latitude to determine how that “plays out” in real world situations, he said, “and an ABP credentialing committee will be available to hear appeals for people who have complicated life circumstances.”
“I was part of a committee that explored these issues. We were an independent group of hospitalists who decided that board certification was a good way to advance the field,” Dr. Quinonez said. “We’ve seen what subspecialty certification has done, for example, for pediatric emergency medicine and pediatric critical care medicine – advancing them tremendously from a research standpoint and helping to develop a distinct body of knowledge reflecting increased severity of illness in hospitalized children.”
Discrepancy between practicing hospitalists, fellowships
An estimated 4,000 pediatric hospitalists now practice in the United States, and 2,100 of those belong to the American Academy of Pediatrics’ Section on Hospital Medicine. There are 40 pediatric hospital medicine fellowship programs listed on the website of AAP’s Section on Hospital Medicine (http://phmfellows.org/phm-programs/), although formal training assessment criteria will be needed for the American College of Graduate Medical Education to recognize programs that qualify their fellows to sit for the PHM exam. A wide gap is anticipated between the demand for pediatric hospitalists and currently available fellowship training slots to generate new candidates for board certification, although Dr. Rauch projects that fellowship slots will double in coming years.
“My message to the field is that historically, board certification has been the launching point for further development of the field,” Dr. Rauch said. “It leads to standardization of who is a subspecialist. Right now, who is a pediatric hospitalist is subject to wide variation. We need to standardize training and to create for this field the same distinction and stature as other medical subspecialties,” he said, noting that subspecialty status also has ramifications for academic settings, and for career advancement and career satisfaction for the individuals who choose to pursue it.
“I know there has been some hue and cry about this in the field, but in most cases certification will not change a pediatric hospitalist’s ability to obtain a job,” he said. “Already, you can’t become a division leader at a children’s hospital without additional training. This isn’t going to change that reality. But for people who don’t want to follow an academic career path, there will never be enough board-certified or fellowship-trained pediatric hospitalists to fill all of the pediatric positions in all the hospitals in the country. Community hospitals aren’t going to say: We won’t hire you unless you are board certified.”
Is the fellowship good for the field?
The subspecialty development process clearly is moving forward. Those in favor believe it will increase scholarship, research, and recognition for the subspecialty by the public for its specialized body of knowledge. But not everyone in the field agrees. Last fall The Hospitalist published3 an opinion piece questioning the need for fellowship-based board certification in pediatric hospital medicine. The author recommended instead retaining the current voluntary approach to fellowships and establishing a pediatric “focused practice” incorporated into residency training, much as the American Board of Internal Medicine and the American Board of Family Medicine have done for hospitalists in adult medicine.
“Will it lead to uncertainty among those currently in residency programs? If you are a pediatric resident and you want to become a board-certified pediatric hospitalist, you’ll need at least 2 years more of training. Is that going to deter qualified individuals?” Dr. Chang said. “The people this decision will impact the most are med-peds doctors – who complete a combined internal medicine and pediatrics residency – and part-timers. They may find themselves in a difficult position if the number of hours don’t add up for them to sit for the boards. For the most part, we’ll have to wait and see for answers to these questions.”
Brian Alverson, MD, FAAP, current chair of the AAP’s Section on Hospital Medicine and associate professor of pediatrics at Brown University, Providence, R.I., says he can see both sides of the debate.
But at the same time, there is a significant opportunity cost for doing 2 more years of fellowship training, Dr. Alverson said.
“We don’t know how much the board certification test will improve actual care,” he noted. “Does it truly identify higher quality doctors, or just doctors who are good at taking multiple choice exams? There are a number of people in pediatrics who do a lot of different things in their jobs, and it’s important that they not lose their ability to practice in the field. Two-thirds of our work force is in community hospitals, not academic medical centers. They work hard to provide the backbone of hospital care for young patients, and many of them are unlikely to ever do a fellowship.”
Nonetheless, Dr. Alverson believes pediatric hospitalists needn’t worry. “You still have plenty of time to figure out what’s going to happen in your hospital,” he said.
References
1. Section on Hospital Medicine. Guiding principles for pediatric hospital medicine program. Pediatrics; 2013; 132:782-786.
2. Stucky E. The Pediatric Hospital Medicine Core Competencies. Wiley-Blackwell; 2010.
3. Feldman LS, Monash B, Eniasivam A. Why required pediatric hospital medicine fellowships are unnecessary. The Hospitalist Magazine, October 8, 2016.
10 Things Hospitalists Need to Know about Palliative Care

In fact, according to the 2015 Palliative Care Report Card from the Center to Advance Palliative Care (CAPC), 67 percent of hospitals with 50 or more beds had a designated palliative care program.1
While core palliative care skills can be performed by frontline clinicians including hospitalists, specialty palliative care consults are the ones who are called in for complicated cases. The Hospitalist asked several palliative care experts for advice on how to clarify definitions, distinctions, and roles. This is what they told us:
Palliative care is not synonymous with end-of-life care.
Palliative care advocates call this the biggest misconception they struggle to overcome, with the potential to inhibit its contributions to patient care in the hospital. Palliative care, they say, is for any patient with a serious illness who is struggling to cope with the fallout from that illness in their lives.
“Our biggest impact can come earlier in the illness,” says Jeanie Youngwerth, MD, director of the University of Colorado Hospital’s Palliative Care Consult Service in Aurora. “We help people do the best they can for as long as they can. If you’re even considering a palliative-care consult, then do it sooner rather than later.”

Palliative care can offer more than just help with difficult conversations, adds Daniel Fischberg, MD, PhD, FAAHPM, medical director of the Pain and Palliative Care Department at The Queen’s Medical Center in Honolulu. For example, the palliative-care team can work with patients to clarify their expectations and goals for care, plan for what comes next, and address troubling symptoms—whether physical or emotional, Dr. Fischberg says.
“We can really help patients and families who are facing unique and challenging needs,” he says.
The experts also say that palliative care is not synonymous with hospice care, which is a comprehensive service that provides specialized terminal care for patients with a prognosis of six months or fewer to live. Both, however, share many of the same principles and techniques of symptom management and psycho-social-spiritual support. But some patients and families may associate a palliative-care referral with hospice care or have other misconceptions and fears about it. Hospitalists are challenged to provide a consistent message clarifying that palliative care can be helpful for seriously ill patients regardless of prognosis or other medical treatments they’re receiving.
“It’s human nature not to want to deal with our mortality, and any word that gets associated with death and dying can turn people off,” says Joseph Rotella, MD, chief medical officer of the American Academy of Hospice and Palliative Medicine (AAHPM). “The best way to prevent this is to define it in terms of patient and family needs: ‘Let’s bring in our comfort specialists.’ Doctors should not apologize when referring to a service that has proven its value. We should be happy to recommend it often and early.”
Patients with serious illness can benefit from palliative care.
CAPC defines palliative care as “specialized medical care for people with serious illnesses.” It focuses on providing patients with relief from the symptoms and stress of a serious illness, regardless of their diagnosis, at any age and at any stage of a serious illness. This service is provided by a specially trained interdisciplinary palliative-care team of doctors, nurses, and other specialists who work together with patients’ other doctors. Their goal is to improve quality of life for both patients and their families with an extra layer of support.
Palliative care is also a medical specialty that involves specialty training, including year-long hospice and palliative medicine (HPM) fellowships now offered at 112 sites accredited by the Accreditation Council for Graduate Medical Education. Subspecialty board certification is also available through 10 collaborating medical specialty boards within the American Board of Medical Specialties as well as by the American Osteopathic Association. Palliative-care programs are now certified by The Joint Commission, with similar recognition under development by the Community Health Accreditation Partner.
Palliative care is intended for patients facing challenges.
Palliative care is intended for patients who might be expected to face stresses and challenges in any area of their lives as a result of serious illness. This may include, for example, patients who experience frequent emergency department visits, hospital readmissions, or prolonged ICU stays, as well as cancer patients who are admitted to the hospital solely to address out-of-control symptoms resulting from their disease and its treatment.
“We can help with the burdens of any challenging symptoms,” Dr. Fischberg says.
Other examples of appropriate palliative-care referrals are when next steps for patients’ treatment are not clear, when there are questions about patients’ real goals of care, and when unmet needs such as unrelieved symptoms have put their families in a state of distress, whether physical, emotional, social, or spiritual. Patients may need guidance about weighing their care options.
Palliative care is also available for children and their families.
The philosophy and organization of palliative care for delivering compassionate care for children with chronic, complex, or life-threatening conditions are much the same as for adults. In 2013, the American Academy of Pediatrics issued a Pediatric Palliative Care and Hospice Care policy statement,2 which outlined core commitments in such areas as respecting and partnering with patients and families and pursuing care that is high-quality, readily accessible, and equitable.
As with adults, a referral for palliative care typically is most helpful for the more complex cases, says Joanne Wolfe, MD, MPH, director of Pediatric Palliative Care at Boston Children’s Hospital. The palliative care team can offer emotional support to the parents of children with complex illnesses and help them understand confusing treatment options. The children, too, need a sounding board.
“If I were teaching a group of hospitalists, I would emphasize foundational principles of palliative care, starting with relationship and understanding patients’ and families’ goals of care,” Dr. Wolfe says. If the family is struggling to cope with the illness and the hospitalist doesn’t have good answers, that’s when to call palliative care, she adds.
Palliative care’s role is not to talk patients and their families out of treatments.
The palliative-care team tries to enter cases without an agenda, Dr. Fischberg says, rather than aiming to get patients to stop treatments or agree to a do-not-resuscitate (DNR) order.
“We’re interested in what the hospitalist thinks about what best care for this patient looks like but also in eliciting the patient’s values and preferences,” he says.
Palliative-care professionals are skilled at delicately communicating bad news and helping patients and families clarify what their goals of care really are, says Robert Crook, MD, FACP, associate medical director of Mount Carmel Hospice and Palliative Care in Columbus, Ohio.
“It’s more about helping to improve communication between the primary-care team and the patient and family—not talking somebody out of something but helping them understand each other better,” Dr. Crook says.
Palliative care can reduce costs of care on average, but it does not achieve this by rationing care or denying treatments.
“We’re not there to cut costs or to get patients discharged sooner or to steer them away from costly treatments,” explains Dr. Rotella. “The last thing a palliative-care team wants is to be viewed as a care rationer. But if the patient understands what’s really going on, they often won’t want treatments that don’t help. So, in that way, we are part of the solution.”
Dr. Rotella calls this cost-effectiveness a side effect of palliative care, when patients are empowered to make decisions about their own care. “That’s where you achieve the triple aim,” he says. “They feel better about it because they are in the driver’s seat. If a patient wants a treatment consistent with their values, we will advocate for it.”
One study found that patients at eight U.S. hospitals who received palliative care incurred significantly lower hospital costs than a matched group receiving usual care, with an average reduction in direct hospital costs of almost $1,700 for patients discharged alive and almost $5,000 per admission for patients who died in the hospital.3 Another study found that early palliative care interventions for cancer patients led to significant improvements in both quality of life and mood compared with patients receiving standard care, with less cost and fewer aggressive treatments at the end of life but longer survival.4
One of the main tools of the palliative care team is the family meeting.
Family meetings are scheduled to allow as many family members as possible to attend, and the primary-care team and relevant specialists typically are also invited. Many palliative-care teams use a standardized format that involves introductions, clarification of each participant’s understanding of the patient’s prognosis, and an effort to reconcile the patient’s hopes and values with medical realities and possibilities, Dr. Fischberg explains.
“That is such a critical component of our care, where we make sure the patient and family are fully informed and foster shared decision making that results in patients being more comfortable with care that better matches what they want,” says Dr. Rotella.
The palliative-care team typically becomes involved via a consultation request from a patient’s attending physician.
“A big part of our job is doing our homework,” Dr. Youngwerth says. “We’ll talk to the team about what’s going on. We want to get as much information as possible about the patient, about prognosis, about the perspectives of people caring for them. Don’t be surprised if the palliative-care team contacts you to get your input on the prognosis and other medical details in order to best inform their discussion with the patient and family.”
Then the palliative-care team will follow consult protocol in reporting back to the primary medical team.
Palliative-care teams can assist busy hospitalists with difficult patient conversations.
“When I’m on the hospitalist service, I’ll pull in the palliative-care team,” Dr. Youngwerth explains. “It’s not that I don’t have the skills; I don’t have the time.”
Conversations aimed at clarifying goals of care can take 90 minutes or more, but the palliative-care team will take as much time as needed to achieve clarification.
It’s important that hospitalists remain involved in these cases, says Christian Sinclair, MD, assistant professor in the division of palliative medicine at the University of Kansas Medical Center in Kansas City and president-elect of AAHPM.
“Just because you have access to palliative-care services, don’t miss the chance to enhance your own communication skills and your ability to address these issues head on,” Dr. Sinclair says.
American Academy of Hospice and Palliative Medicine is a participant in Choosing Wisely.
The Choosing Wisely program, initiated by the American Board of Internal Medicine Foundation, invites medical societies to identify five treatments that should be questioned by physicians and patients based on lack of supporting evidence in the research base. The Society of Hospital Medicine is also a participant in this initiative.
For AAHPM, one of its recommendations was: “Don’t delay palliative care for a patient with serious illness who has a physical, psychological, social, or spiritual distress because they are pursuing disease-directed treatment.” Other Choosing Wisely suggestions include not recommending feeding tubes for patients with advanced dementia, not leaving implantable cardioverter defibrillators (ICDs) activated when these are not consistent with patient/family goals of care, and not recommending more than a single fraction of palliative radiation for an uncomplicated painful bone metastasis.
Different palliative-care programs provide different services.
It is important for hospitalists to learn their local palliative-care programs and what they emphasize and are able to offer—or not, says Dr. Sinclair.
“There are so many different models,” he says. “Spend some time reaching out to them, outside of actual consults, and find out what their comfort level is on various issues. Hospitalists and palliative-care teams should get to know each other better.”
Access to palliative care and the comprehensiveness of the team and services can vary between hospitals, while access to community-based palliative care outside of the hospital is even more variable.
“Palliative-care teams often have a better sense of our partners in the community and access to community-based palliative care,” Dr. Fischberg says.
References
- Morrison RS, Meier DE. America’s Care of Serious Illness: 2015 State-by-State Report Card on Access to Palliative Care in Our Nation’s Hospitals. New York, NY: Center to Advance Palliative Care; 2015.
- American Academy of Pediatrics. Policy statement: pediatric palliative care and hospice care commitments, guidelines, and recommendations. Pediatr. 2013;132(5):966-972.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Temel JS, Greer JA, Muzikansky et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
In fact, according to the 2015 Palliative Care Report Card from the Center to Advance Palliative Care (CAPC), 67 percent of hospitals with 50 or more beds had a designated palliative care program.1
While core palliative care skills can be performed by frontline clinicians including hospitalists, specialty palliative care consults are the ones who are called in for complicated cases. The Hospitalist asked several palliative care experts for advice on how to clarify definitions, distinctions, and roles. This is what they told us:
Palliative care is not synonymous with end-of-life care.
Palliative care advocates call this the biggest misconception they struggle to overcome, with the potential to inhibit its contributions to patient care in the hospital. Palliative care, they say, is for any patient with a serious illness who is struggling to cope with the fallout from that illness in their lives.
“Our biggest impact can come earlier in the illness,” says Jeanie Youngwerth, MD, director of the University of Colorado Hospital’s Palliative Care Consult Service in Aurora. “We help people do the best they can for as long as they can. If you’re even considering a palliative-care consult, then do it sooner rather than later.”
Palliative care can offer more than just help with difficult conversations, adds Daniel Fischberg, MD, PhD, FAAHPM, medical director of the Pain and Palliative Care Department at The Queen’s Medical Center in Honolulu. For example, the palliative-care team can work with patients to clarify their expectations and goals for care, plan for what comes next, and address troubling symptoms—whether physical or emotional, Dr. Fischberg says.
“We can really help patients and families who are facing unique and challenging needs,” he says.
The experts also say that palliative care is not synonymous with hospice care, which is a comprehensive service that provides specialized terminal care for patients with a prognosis of six months or fewer to live. Both, however, share many of the same principles and techniques of symptom management and psycho-social-spiritual support. But some patients and families may associate a palliative-care referral with hospice care or have other misconceptions and fears about it. Hospitalists are challenged to provide a consistent message clarifying that palliative care can be helpful for seriously ill patients regardless of prognosis or other medical treatments they’re receiving.
“It’s human nature not to want to deal with our mortality, and any word that gets associated with death and dying can turn people off,” says Joseph Rotella, MD, chief medical officer of the American Academy of Hospice and Palliative Medicine (AAHPM). “The best way to prevent this is to define it in terms of patient and family needs: ‘Let’s bring in our comfort specialists.’ Doctors should not apologize when referring to a service that has proven its value. We should be happy to recommend it often and early.”
Patients with serious illness can benefit from palliative care.
CAPC defines palliative care as “specialized medical care for people with serious illnesses.” It focuses on providing patients with relief from the symptoms and stress of a serious illness, regardless of their diagnosis, at any age and at any stage of a serious illness. This service is provided by a specially trained interdisciplinary palliative-care team of doctors, nurses, and other specialists who work together with patients’ other doctors. Their goal is to improve quality of life for both patients and their families with an extra layer of support.
Palliative care is also a medical specialty that involves specialty training, including year-long hospice and palliative medicine (HPM) fellowships now offered at 112 sites accredited by the Accreditation Council for Graduate Medical Education. Subspecialty board certification is also available through 10 collaborating medical specialty boards within the American Board of Medical Specialties as well as by the American Osteopathic Association. Palliative-care programs are now certified by The Joint Commission, with similar recognition under development by the Community Health Accreditation Partner.
Palliative care is intended for patients facing challenges.
Palliative care is intended for patients who might be expected to face stresses and challenges in any area of their lives as a result of serious illness. This may include, for example, patients who experience frequent emergency department visits, hospital readmissions, or prolonged ICU stays, as well as cancer patients who are admitted to the hospital solely to address out-of-control symptoms resulting from their disease and its treatment.
“We can help with the burdens of any challenging symptoms,” Dr. Fischberg says.
Other examples of appropriate palliative-care referrals are when next steps for patients’ treatment are not clear, when there are questions about patients’ real goals of care, and when unmet needs such as unrelieved symptoms have put their families in a state of distress, whether physical, emotional, social, or spiritual. Patients may need guidance about weighing their care options.
Palliative care is also available for children and their families.
The philosophy and organization of palliative care for delivering compassionate care for children with chronic, complex, or life-threatening conditions are much the same as for adults. In 2013, the American Academy of Pediatrics issued a Pediatric Palliative Care and Hospice Care policy statement,2 which outlined core commitments in such areas as respecting and partnering with patients and families and pursuing care that is high-quality, readily accessible, and equitable.
As with adults, a referral for palliative care typically is most helpful for the more complex cases, says Joanne Wolfe, MD, MPH, director of Pediatric Palliative Care at Boston Children’s Hospital. The palliative care team can offer emotional support to the parents of children with complex illnesses and help them understand confusing treatment options. The children, too, need a sounding board.
“If I were teaching a group of hospitalists, I would emphasize foundational principles of palliative care, starting with relationship and understanding patients’ and families’ goals of care,” Dr. Wolfe says. If the family is struggling to cope with the illness and the hospitalist doesn’t have good answers, that’s when to call palliative care, she adds.
Palliative care’s role is not to talk patients and their families out of treatments.
The palliative-care team tries to enter cases without an agenda, Dr. Fischberg says, rather than aiming to get patients to stop treatments or agree to a do-not-resuscitate (DNR) order.
“We’re interested in what the hospitalist thinks about what best care for this patient looks like but also in eliciting the patient’s values and preferences,” he says.
Palliative-care professionals are skilled at delicately communicating bad news and helping patients and families clarify what their goals of care really are, says Robert Crook, MD, FACP, associate medical director of Mount Carmel Hospice and Palliative Care in Columbus, Ohio.
“It’s more about helping to improve communication between the primary-care team and the patient and family—not talking somebody out of something but helping them understand each other better,” Dr. Crook says.
Palliative care can reduce costs of care on average, but it does not achieve this by rationing care or denying treatments.
“We’re not there to cut costs or to get patients discharged sooner or to steer them away from costly treatments,” explains Dr. Rotella. “The last thing a palliative-care team wants is to be viewed as a care rationer. But if the patient understands what’s really going on, they often won’t want treatments that don’t help. So, in that way, we are part of the solution.”
Dr. Rotella calls this cost-effectiveness a side effect of palliative care, when patients are empowered to make decisions about their own care. “That’s where you achieve the triple aim,” he says. “They feel better about it because they are in the driver’s seat. If a patient wants a treatment consistent with their values, we will advocate for it.”
One study found that patients at eight U.S. hospitals who received palliative care incurred significantly lower hospital costs than a matched group receiving usual care, with an average reduction in direct hospital costs of almost $1,700 for patients discharged alive and almost $5,000 per admission for patients who died in the hospital.3 Another study found that early palliative care interventions for cancer patients led to significant improvements in both quality of life and mood compared with patients receiving standard care, with less cost and fewer aggressive treatments at the end of life but longer survival.4
One of the main tools of the palliative care team is the family meeting.
Family meetings are scheduled to allow as many family members as possible to attend, and the primary-care team and relevant specialists typically are also invited. Many palliative-care teams use a standardized format that involves introductions, clarification of each participant’s understanding of the patient’s prognosis, and an effort to reconcile the patient’s hopes and values with medical realities and possibilities, Dr. Fischberg explains.
“That is such a critical component of our care, where we make sure the patient and family are fully informed and foster shared decision making that results in patients being more comfortable with care that better matches what they want,” says Dr. Rotella.
The palliative-care team typically becomes involved via a consultation request from a patient’s attending physician.
“A big part of our job is doing our homework,” Dr. Youngwerth says. “We’ll talk to the team about what’s going on. We want to get as much information as possible about the patient, about prognosis, about the perspectives of people caring for them. Don’t be surprised if the palliative-care team contacts you to get your input on the prognosis and other medical details in order to best inform their discussion with the patient and family.”
Then the palliative-care team will follow consult protocol in reporting back to the primary medical team.
Palliative-care teams can assist busy hospitalists with difficult patient conversations.
“When I’m on the hospitalist service, I’ll pull in the palliative-care team,” Dr. Youngwerth explains. “It’s not that I don’t have the skills; I don’t have the time.”
Conversations aimed at clarifying goals of care can take 90 minutes or more, but the palliative-care team will take as much time as needed to achieve clarification.
It’s important that hospitalists remain involved in these cases, says Christian Sinclair, MD, assistant professor in the division of palliative medicine at the University of Kansas Medical Center in Kansas City and president-elect of AAHPM.
“Just because you have access to palliative-care services, don’t miss the chance to enhance your own communication skills and your ability to address these issues head on,” Dr. Sinclair says.
American Academy of Hospice and Palliative Medicine is a participant in Choosing Wisely.
The Choosing Wisely program, initiated by the American Board of Internal Medicine Foundation, invites medical societies to identify five treatments that should be questioned by physicians and patients based on lack of supporting evidence in the research base. The Society of Hospital Medicine is also a participant in this initiative.
For AAHPM, one of its recommendations was: “Don’t delay palliative care for a patient with serious illness who has a physical, psychological, social, or spiritual distress because they are pursuing disease-directed treatment.” Other Choosing Wisely suggestions include not recommending feeding tubes for patients with advanced dementia, not leaving implantable cardioverter defibrillators (ICDs) activated when these are not consistent with patient/family goals of care, and not recommending more than a single fraction of palliative radiation for an uncomplicated painful bone metastasis.
Different palliative-care programs provide different services.
It is important for hospitalists to learn their local palliative-care programs and what they emphasize and are able to offer—or not, says Dr. Sinclair.
“There are so many different models,” he says. “Spend some time reaching out to them, outside of actual consults, and find out what their comfort level is on various issues. Hospitalists and palliative-care teams should get to know each other better.”
Access to palliative care and the comprehensiveness of the team and services can vary between hospitals, while access to community-based palliative care outside of the hospital is even more variable.
“Palliative-care teams often have a better sense of our partners in the community and access to community-based palliative care,” Dr. Fischberg says.
References
- Morrison RS, Meier DE. America’s Care of Serious Illness: 2015 State-by-State Report Card on Access to Palliative Care in Our Nation’s Hospitals. New York, NY: Center to Advance Palliative Care; 2015.
- American Academy of Pediatrics. Policy statement: pediatric palliative care and hospice care commitments, guidelines, and recommendations. Pediatr. 2013;132(5):966-972.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Temel JS, Greer JA, Muzikansky et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
In fact, according to the 2015 Palliative Care Report Card from the Center to Advance Palliative Care (CAPC), 67 percent of hospitals with 50 or more beds had a designated palliative care program.1
While core palliative care skills can be performed by frontline clinicians including hospitalists, specialty palliative care consults are the ones who are called in for complicated cases. The Hospitalist asked several palliative care experts for advice on how to clarify definitions, distinctions, and roles. This is what they told us:
Palliative care is not synonymous with end-of-life care.
Palliative care advocates call this the biggest misconception they struggle to overcome, with the potential to inhibit its contributions to patient care in the hospital. Palliative care, they say, is for any patient with a serious illness who is struggling to cope with the fallout from that illness in their lives.
“Our biggest impact can come earlier in the illness,” says Jeanie Youngwerth, MD, director of the University of Colorado Hospital’s Palliative Care Consult Service in Aurora. “We help people do the best they can for as long as they can. If you’re even considering a palliative-care consult, then do it sooner rather than later.”
Palliative care can offer more than just help with difficult conversations, adds Daniel Fischberg, MD, PhD, FAAHPM, medical director of the Pain and Palliative Care Department at The Queen’s Medical Center in Honolulu. For example, the palliative-care team can work with patients to clarify their expectations and goals for care, plan for what comes next, and address troubling symptoms—whether physical or emotional, Dr. Fischberg says.
“We can really help patients and families who are facing unique and challenging needs,” he says.
The experts also say that palliative care is not synonymous with hospice care, which is a comprehensive service that provides specialized terminal care for patients with a prognosis of six months or fewer to live. Both, however, share many of the same principles and techniques of symptom management and psycho-social-spiritual support. But some patients and families may associate a palliative-care referral with hospice care or have other misconceptions and fears about it. Hospitalists are challenged to provide a consistent message clarifying that palliative care can be helpful for seriously ill patients regardless of prognosis or other medical treatments they’re receiving.
“It’s human nature not to want to deal with our mortality, and any word that gets associated with death and dying can turn people off,” says Joseph Rotella, MD, chief medical officer of the American Academy of Hospice and Palliative Medicine (AAHPM). “The best way to prevent this is to define it in terms of patient and family needs: ‘Let’s bring in our comfort specialists.’ Doctors should not apologize when referring to a service that has proven its value. We should be happy to recommend it often and early.”
Patients with serious illness can benefit from palliative care.
CAPC defines palliative care as “specialized medical care for people with serious illnesses.” It focuses on providing patients with relief from the symptoms and stress of a serious illness, regardless of their diagnosis, at any age and at any stage of a serious illness. This service is provided by a specially trained interdisciplinary palliative-care team of doctors, nurses, and other specialists who work together with patients’ other doctors. Their goal is to improve quality of life for both patients and their families with an extra layer of support.
Palliative care is also a medical specialty that involves specialty training, including year-long hospice and palliative medicine (HPM) fellowships now offered at 112 sites accredited by the Accreditation Council for Graduate Medical Education. Subspecialty board certification is also available through 10 collaborating medical specialty boards within the American Board of Medical Specialties as well as by the American Osteopathic Association. Palliative-care programs are now certified by The Joint Commission, with similar recognition under development by the Community Health Accreditation Partner.
Palliative care is intended for patients facing challenges.
Palliative care is intended for patients who might be expected to face stresses and challenges in any area of their lives as a result of serious illness. This may include, for example, patients who experience frequent emergency department visits, hospital readmissions, or prolonged ICU stays, as well as cancer patients who are admitted to the hospital solely to address out-of-control symptoms resulting from their disease and its treatment.
“We can help with the burdens of any challenging symptoms,” Dr. Fischberg says.
Other examples of appropriate palliative-care referrals are when next steps for patients’ treatment are not clear, when there are questions about patients’ real goals of care, and when unmet needs such as unrelieved symptoms have put their families in a state of distress, whether physical, emotional, social, or spiritual. Patients may need guidance about weighing their care options.
Palliative care is also available for children and their families.
The philosophy and organization of palliative care for delivering compassionate care for children with chronic, complex, or life-threatening conditions are much the same as for adults. In 2013, the American Academy of Pediatrics issued a Pediatric Palliative Care and Hospice Care policy statement,2 which outlined core commitments in such areas as respecting and partnering with patients and families and pursuing care that is high-quality, readily accessible, and equitable.
As with adults, a referral for palliative care typically is most helpful for the more complex cases, says Joanne Wolfe, MD, MPH, director of Pediatric Palliative Care at Boston Children’s Hospital. The palliative care team can offer emotional support to the parents of children with complex illnesses and help them understand confusing treatment options. The children, too, need a sounding board.
“If I were teaching a group of hospitalists, I would emphasize foundational principles of palliative care, starting with relationship and understanding patients’ and families’ goals of care,” Dr. Wolfe says. If the family is struggling to cope with the illness and the hospitalist doesn’t have good answers, that’s when to call palliative care, she adds.
Palliative care’s role is not to talk patients and their families out of treatments.
The palliative-care team tries to enter cases without an agenda, Dr. Fischberg says, rather than aiming to get patients to stop treatments or agree to a do-not-resuscitate (DNR) order.
“We’re interested in what the hospitalist thinks about what best care for this patient looks like but also in eliciting the patient’s values and preferences,” he says.
Palliative-care professionals are skilled at delicately communicating bad news and helping patients and families clarify what their goals of care really are, says Robert Crook, MD, FACP, associate medical director of Mount Carmel Hospice and Palliative Care in Columbus, Ohio.
“It’s more about helping to improve communication between the primary-care team and the patient and family—not talking somebody out of something but helping them understand each other better,” Dr. Crook says.
Palliative care can reduce costs of care on average, but it does not achieve this by rationing care or denying treatments.
“We’re not there to cut costs or to get patients discharged sooner or to steer them away from costly treatments,” explains Dr. Rotella. “The last thing a palliative-care team wants is to be viewed as a care rationer. But if the patient understands what’s really going on, they often won’t want treatments that don’t help. So, in that way, we are part of the solution.”
Dr. Rotella calls this cost-effectiveness a side effect of palliative care, when patients are empowered to make decisions about their own care. “That’s where you achieve the triple aim,” he says. “They feel better about it because they are in the driver’s seat. If a patient wants a treatment consistent with their values, we will advocate for it.”
One study found that patients at eight U.S. hospitals who received palliative care incurred significantly lower hospital costs than a matched group receiving usual care, with an average reduction in direct hospital costs of almost $1,700 for patients discharged alive and almost $5,000 per admission for patients who died in the hospital.3 Another study found that early palliative care interventions for cancer patients led to significant improvements in both quality of life and mood compared with patients receiving standard care, with less cost and fewer aggressive treatments at the end of life but longer survival.4
One of the main tools of the palliative care team is the family meeting.
Family meetings are scheduled to allow as many family members as possible to attend, and the primary-care team and relevant specialists typically are also invited. Many palliative-care teams use a standardized format that involves introductions, clarification of each participant’s understanding of the patient’s prognosis, and an effort to reconcile the patient’s hopes and values with medical realities and possibilities, Dr. Fischberg explains.
“That is such a critical component of our care, where we make sure the patient and family are fully informed and foster shared decision making that results in patients being more comfortable with care that better matches what they want,” says Dr. Rotella.
The palliative-care team typically becomes involved via a consultation request from a patient’s attending physician.
“A big part of our job is doing our homework,” Dr. Youngwerth says. “We’ll talk to the team about what’s going on. We want to get as much information as possible about the patient, about prognosis, about the perspectives of people caring for them. Don’t be surprised if the palliative-care team contacts you to get your input on the prognosis and other medical details in order to best inform their discussion with the patient and family.”
Then the palliative-care team will follow consult protocol in reporting back to the primary medical team.
Palliative-care teams can assist busy hospitalists with difficult patient conversations.
“When I’m on the hospitalist service, I’ll pull in the palliative-care team,” Dr. Youngwerth explains. “It’s not that I don’t have the skills; I don’t have the time.”
Conversations aimed at clarifying goals of care can take 90 minutes or more, but the palliative-care team will take as much time as needed to achieve clarification.
It’s important that hospitalists remain involved in these cases, says Christian Sinclair, MD, assistant professor in the division of palliative medicine at the University of Kansas Medical Center in Kansas City and president-elect of AAHPM.
“Just because you have access to palliative-care services, don’t miss the chance to enhance your own communication skills and your ability to address these issues head on,” Dr. Sinclair says.
American Academy of Hospice and Palliative Medicine is a participant in Choosing Wisely.
The Choosing Wisely program, initiated by the American Board of Internal Medicine Foundation, invites medical societies to identify five treatments that should be questioned by physicians and patients based on lack of supporting evidence in the research base. The Society of Hospital Medicine is also a participant in this initiative.
For AAHPM, one of its recommendations was: “Don’t delay palliative care for a patient with serious illness who has a physical, psychological, social, or spiritual distress because they are pursuing disease-directed treatment.” Other Choosing Wisely suggestions include not recommending feeding tubes for patients with advanced dementia, not leaving implantable cardioverter defibrillators (ICDs) activated when these are not consistent with patient/family goals of care, and not recommending more than a single fraction of palliative radiation for an uncomplicated painful bone metastasis.
Different palliative-care programs provide different services.
It is important for hospitalists to learn their local palliative-care programs and what they emphasize and are able to offer—or not, says Dr. Sinclair.
“There are so many different models,” he says. “Spend some time reaching out to them, outside of actual consults, and find out what their comfort level is on various issues. Hospitalists and palliative-care teams should get to know each other better.”
Access to palliative care and the comprehensiveness of the team and services can vary between hospitals, while access to community-based palliative care outside of the hospital is even more variable.
“Palliative-care teams often have a better sense of our partners in the community and access to community-based palliative care,” Dr. Fischberg says.
References
- Morrison RS, Meier DE. America’s Care of Serious Illness: 2015 State-by-State Report Card on Access to Palliative Care in Our Nation’s Hospitals. New York, NY: Center to Advance Palliative Care; 2015.
- American Academy of Pediatrics. Policy statement: pediatric palliative care and hospice care commitments, guidelines, and recommendations. Pediatr. 2013;132(5):966-972.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
- Temel JS, Greer JA, Muzikansky et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.

PAs, NPs Seizing Key Leadership Roles in HM Groups, Health Systems
Since hospital medicine’s early days, hospitalist physicians have worked alongside physician assistants (PAs) and nurse practitioners (NPs). Some PAs and NPs have ascended to positions of leadership in their HM groups or health systems, in some cases even supervising the physicians.

The Hospitalist connected with six PA and NP leaders in hospital medicine to discuss their career paths as well as the nature and scope of their jobs. They described leadership as a complex, multidimensional concept, with often more of a collaborative model than a clear-cut supervisory relationship with clinicians. Most said they don’t try to be the “boss” of their group and have found ways to impact key decisions.
They also emphasized that PAs and NPs bring special skills and perspectives to team building. Many have supplemented frontline clinical experience with leadership training. And when it comes to decision making, their responsibilities can include hiring, scheduling, training, mentoring, information technology, quality improvement, and other essential functions of the group.
Edwin Lopez, MBA, PA-C

Workplace: St. Elizabeth is a 25-bed critical-access hospital serving a semi-rural bedroom community of 11,000 people an hour southeast of Seattle. It belongs to the nine-hospital CHI Franciscan Health system, and the HM group includes four physicians and four PAs providing 24-hour coverage. The physicians and PAs work in paired teams in the hospital and an 80-bed skilled nursing facility (SNF) across the street. Lopez heads St. Elizabeth’s HM group and is associate medical director of the SNF.
Background: Lopez graduated from the PA program at the University of Washington in 1982 and spent seven years as a PA with a cardiothoracic surgery practice in Tacoma. Then he established his own firm providing PA staffing services for six cardiac surgery programs in western Washington. In 1997, he co-founded an MD/PA hospitalist service covering three hospitals for a Seattle insurance company. That program grew into a larger group that was acquired by CHI Franciscan.
Lopez took time off to earn his MBA in health policy at the University of Washington and Harvard Kennedy School in Boston.
Eight years ago as part of an acquisition, CHI Franciscan asked Lopez to launch an HM program at St. Elizabeth. From the start, he developed the program as a collaborative model. The HM group now covers almost 90% of hospital admissions, manages the ICU, takes calls to admit patients from the ED, and rounds daily on patients in a small hospital that doesn’t have access to a lot of medical specialists.
St. Elizabeth’s has since flourished to become one of the health system’s top performers on quality metrics like HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores. However, Lopez admits readmission rates remain high. He noticed that a big part of the readmission problem was coming from the facility across the street, so he proposed the HM group start providing daily coverage to the SNF. In the group’s first year covering the SNF, the hospital’s readmission rate dropped to 5% from 35%.
Listen: Edwin Lopez, PA-C, discusses post-acute Care in the U.S. health system
Responsibilities: Lopez spends roughly half his time seeing patients, which he considers the most satisfying half. The other half is managing and setting clinical and administrative direction for the group.
“My responsibility is to ensure that there is appropriate physician and PA coverage 24-7 in both facilities,” he says, adding he also handles hiring and personnel issue. “We have an understanding here. I help guide, mentor, and direct the team, with the support of our regional medical director.”
The story: Lopez credits his current position to Joe Wilczek, a visionary CEO who came to the health system 18 years ago and retired in 2015.
“Joe and Franciscan’s chief medical officer and system director of hospital medicine came to me and said, ‘We’d like you to go over there and see what you can do at St. Elizabeth.’ There was a definite mandate, with markers they wanted me to reach. They said, ‘If you succeed, we will build you a new hospital building.’”
The new building opened in 2012.
Lopez says he has spent much of his career in quiet oblivion.
“It took five or six years here before people started noticing that our quality and performance were among the highest in the system,” he says. “For my entire 33-year career in medicine, I was never driven by the money. I grew up believing in service and got into medicine to make a difference, to leave a place better than I found it.”
He occasionally fields questions about his role as a PA group leader, which he tries to overcome by building trust, just as he overcame initial resistance to the hospital medicine program at St. Elizabeth from community physicians.
“I am very clear, we as a team are very clear, that we’re all worker bees here. We build strong relationships. We consider ourselves family,” he says. “When family issues come up, we need to sit down and talk about them, even when it may be uncomfortable.”
Laurie Benton, RN, MPAS, PhD, PA-C, DFAAPA

Workplace: Baylor Scott & White Health is the largest nonprofit health system in Texas, with 46 hospitals and 500 multispecialty clinics. Scott & White Memorial Hospital is a 636-bed specialty care and teaching hospital. Its hospital medicine program includes 40 physicians and 34 NP/PAs caring for an average daily census of 240 patients. They cover an observation service, consult service, and long-term acute-care service.
Background: Benton has a PhD in health administration. She has practiced hospital medicine at Scott & White Memorial Hospital since 2000 and before that at Emanuel Hospital in Portland, Ore. Currently an orthopedic hospitalist PA, she has worked in cardiothoracic surgery, critical care, and nephrology settings.
She became the system director for APPs in September 2013. In that role, she leads and represents 428 APPs, including hospitalist, intensivist, and cardiology PAs, in the system’s 26-hospital Central Region. She sits on the board of directors of the American Academy of Physician Assistants and has been on workforce committees for the National Commission on Certification of Physician Assistants and on the CME committee of the National Kidney Foundation.
Responsibilities: Benton coordinates everything, including PAs, advanced practice nurses, and nurse anesthetists, in settings across the healthcare continuum.
“I was appointed by our hospital medicine board and administration to be the APP leader. I report to the chief medical officer,” she says. “But I still see patients; it’s my passion. I’m not ready to give it up completely.”
Benton’s schedule includes two 10-hour clinical shifts per week. The other three days she works on administrative tasks. She attends board meetings as well as regular meetings with the system’s top executives and officers, including the chair of the board and the senior vice president for medical affairs.
“I have a seat on staff credentialing, benefits, and compensation committees, and I’m part of continuing medical education and disaster planning. Pretty much any of the committees we have here, I’m invited to be on,” she says. “I make sure I’m up-to-date on all of the new regulations and have information on any policies that have to do with APPs.”
The story: Benton says her PA training, including mentorship from Edwin Lopez, placed a strong emphasis on helping students develop leadership skills and interests.
“While I was working in nephrology, my supervising physician mentored me and encouraged me to move forward with my education,” she says. Along the way, she participated in a yearlong executive-education program and taught at the University of Texas McCombs School of Business. “Right off, it was not easy because while people saw me as a very strong, very confident provider, they didn’t see me as an administrator. When I worked with administrators, they were speaking a different language. I’d speak medicine, and they’d speak administration. It took a while to learn how to communicate with them.”
She says non-physician professionals traditionally have reported up through a physician and “never had their own voice. … Now that we have our leadership ladder here, it’s still new to some administrators,” she says. “I want to make sure PAs are part of the solution to high-quality healthcare.
“When I’m at the leadership table, we’re working together. The physicians respect my opinion, giving me the opportunity to interact like anyone else at the table.”
Catherine Boyd, MS, PA-C

Workplace: Essex is a private hospitalist group founded in 2007 by James Tollman, MD, FHM, who remains its CEO. It has 34 clinical members, including 16 physicians, 12 PAs, and six NPs. It began providing hospitalist medical care to several hospitals on Massachusetts’ North Shore under contract, then to a psychiatric hospital and a detox treatment center. In recent years, it has expanded into the post-acute arena, providing coverage to 14 SNFs, which now constitute the majority of its business. It also is active with two accountable-care organization networks.
Background: After three years as a respiratory therapist, Boyd enrolled in a PA program at Massachusetts College of Pharmacy and Health Sciences. After graduating in 2005, she worked as a hospitalist and intensivist, including as team leader for the medical emergency team at Lahey Health & Medical Center in Burlington, Mass., and in the PACE (Program of All-Inclusive Care for the Elderly) Internal Medical Department with Partners HealthCare until mid-2014, when she was invited to join Essex.
Responsibilities: “This job is not one thing; I dabble in everything,” says Boyd, who describes herself as the group’s chief operating officer for professional affairs. “I provide direct supervision to our PAs and NPs but also to our independent contractors, including moonlighting physicians. And I help to supervise the full-time physicians.”
She works on system issues, on-site training and mentorship, and implementation of a new electronic health record (EHR) and charge capture system while trying to improve bed flow and quality and decrease clinicians’ job frustrations. She also monitors developments in Medicare regulations.
“I check in with every one of our full-time providers weekly, and I try to offset some of the minutiae of their workday so that they can focus on their patients,” she explains. “Dr. Tollman and I feel that we bring a healthy work-lifestyle balance to the group. We encourage that in our staff. If they are happy in their jobs, it makes quality of care better.”
Boyd also maintains a clinical practice as a hospitalist, with her clinical duties flexing up and down based on patient demand and management needs.
The story: When Boyd was a respiratory therapist at a small community hospital, she worked one-on-one with a physician assistant who inspired her to change careers.
“I really liked what she did. As a PA, I worked to broaden my skill set on a critical care service for seven years,” she says. “But then my two kids got older and I wanted a more flexible schedule. Dr. Tollman came across my résumé when he was looking for a clinician to run operations for Essex.”
Building on 10 years of clinical experience, Boyd has tried to earn the trust of the other clinicians.
“They know they can come to me with questions. I like to think I practice active listening. When there is a problem, I do a case review and try to get all the facts,” she says. “When you earn their trust, the credentials tend to fall away, especially with the doctors I work with on a daily basis.”
Daniel Ladd, PA-C, DFAAPA

Workplace: Founded in 1993 as Hospitalists of Northern Michigan, iNDIGO Health Partners is one of the country’s largest private hospitalist companies, employing 150 physicians, PAs, and NPs who practice at seven hospitals across the state. The program also provides nighttime hospitalist services via telehealth and pediatric hospital medicine. It recently added 10 post-acute providers to work in SNFs and assisted living facilities.
Background: While working as a nurse’s aide, meeting and being inspired by some of the earliest PAs in Michigan, Ladd pursued PA training at Mercy College in Detroit. After graduating in 1984, he was hired by a cardiology practice at Detroit Medical Center. When he moved upstate to Traverse City in 1997, he landed a position as lead PA at another cardiology practice, acting as its liaison to PAs in the hospital. He joined iNDIGO in 2006.
“Jim Levy, one of the first PA hospitalists in Michigan, was an integral part of founding iNDIGO and now is our vice president of human resources,” Ladd says. “He asked me to join iNDIGO, and I jumped at the chance. Hospital medicine was a new opportunity for me and one with more opportunities for PAs to advance than cardiology.”
In 2009, when the company reorganized, the firm’s leadership recognized the need to establish a liaison group as a buffer between the providers and the company. Ladd became president of its new board of managers.
“From there, my position evolved to what it is today,” he says.
Levy calls Ladd a role model and leader, with great credibility among site program directors, hospital CMOs, and providers.
Responsibilities: Ladd gave up his clinical practice as a hospitalist in 2014 in response to growing management responsibilities.
“I do and I don’t miss it,” he says. “I miss the camaraderie of clinical practice, the foxhole mentality on the front lines. But I feel where I am now that I am able to help our providers give better care.
“Concretely, what I do is to help our practitioners and our medical directors at the clinical sites, some of whom are PAs and NPs, supporting them with leadership and education. I listen to their issues, translating and bringing to bear the resources of our company.”
Those resources include staffing, working conditions, office space, and the application of mobile medical technology for billing and clinical decision support.
“A lot of my communication is via email. I feel I am able to make a point without being inflammatory, by stating my purpose—the rationale for my position—and asking for what I need,” Ladd says. “This role is very accepted at iNDIGO. The corollary is that physician leaders who report to me are also comfortable in our relationship. It’s not about me being a PA and them being physicians but about us being colleagues in medicine.
“I’m in a position where I understand their world and am able to help them.”
The story: Encouraged by what he calls “visionary” leaders, Ladd has taken a number of steps to ascend to his current position as chief clinical officer.
“Even going back to the Boy Scouts, I was always one to step forward and volunteer for leadership,” he says. “I was president of my PA class in college and involved with the state association of PAs, as well as taking leadership training through the American Academy of Physician Assistants. I had the good fortune to be hired by a brilliant cardiologist at Detroit Medical Center. … He was the first to encourage me to be not just an excellent clinician but also a leader. He got me involved in implementing the EHR and in medication reconciliation. He promoted me as a PA to his patients and allowed me to become the face of our clinical practice, running the clinical side of the practice.”
Ladd also credits iNDIGO’s leaders for an approach of hiring the best people regardless of degree.
“If they happen to be PAs, great. The company’s vision is to have people with vision and skills to lead, not just based on credentials,” he says. “They established that as a baseline, and now it’s the culture here. We have PAs who are key drivers of the efficiency of this program.”
It hasn’t eliminated the occasional “I’m the physician, I’m delegating to you, and you have to do what I say,” Ladd admits. But he knows handling those situations is part of his job as a practice leader.
“It requires patience and understanding and the ability to see the issue from multiple perspectives,” he says, “and then synthesize all of that into a reasonable solution for all concerned.”
Arnold Facklam III, MSN, FNP-BC, FHM

Workplace: United Memorial has 100 beds and is part of the four-hospital Rochester Regional Health System. Kaleida Health has four acute-care hospitals in western New York. Based an hour apart, they compete, but both now get hospitalist services from Infinity Health Hospitalists of Western New York, a hospitalist group of 30 to 35 providers privately owned by local hospitalist John Patti, MD.
Background: Facklam has been a nocturnist since 2009, when he completed an NP program at D’Youville College in Buffalo. He worked 15 to 17 night shifts a month, first at Kaleida’s DeGraff Memorial Hospital and then at United Memorial, starting in 2013 as a per diem and vacation fill-in, then full-time since 2015. He now works for Infinity Health Hospitalists.
While working as a hospitalist, Facklam became involved with the MSO of Kaleida Health, starting on its Advanced Practice Provider Committee, which represents more than 600 NPs and PAs. Now chair of the committee, he leads change in the scope of practice for NPs and PAs and acts as liaison between APPs and the hospitals and health system.
Responsibilities: As a full-time nocturnist, Facklam has to squeeze in time for his role as director of advanced practice providers. He offers guidance and oversight, under the direction of the vice president of medical affairs, to all NPs, PAs, nurse midwives, and nurse anesthetists. He also is in charge of its rapid response and code blue team coverage at night, plus provides clinical education to family practice medical students and residents overnight in the hospital. He has worked on hospital quality improvement projects since 2012.
Facklam, who acknowledges type A personality tendencies, also maintains two to three night shifts per month at Kaleida’s Millard Suburban Hospital.
In 2012, he became a member, eventually a voting member, of Kaleida’s system-wide MSO Medical Executive Committee, which is responsible for rule making, disciplinary action, and the provision of medical care within the system.
“The MSO is the mechanism for accountability for professional practice,” he says. He is also active in SHM’s NP/PA Committee and now sits on SHM’s Public Policy Committee.
The story: “Working as a nocturnist has given me the flexibility to look into advanced management training,” he says, including Six Sigma green belt course work and certificate training. While at DeGraff, he heard about a call for membership on the NP/PA committee.
“They quickly realized the benefits of having someone with a background like mine on board,” he said. “As a nocturnist, I started going to more meetings and getting involved when the easier thing to do might have been to drive home and go to bed.”
Along the way, he learned a lot about hospital systems and how they work.
“Having been in healthcare for 23 years, I know the hierarchical approach,” Facklam says. “But the times are changing. As medicine becomes broader and more difficult to manage, it has to become more of a team approach. If you look at the data, there won’t be enough physicians in the near future. PAs and NPs can help fill that need.”
Crystal Therrien, MS, ACNP-BC

Workplace: UMass Medical Center encompasses three campuses in central Massachusetts, including University, Memorial, and Marlborough. The hospital medicine division covers all three campuses with 40 to 45 FTEs of physicians and 20 of APPs. Therrien has been with the department since October 2009—her first job after completing NP training—and assumed her leadership role in June 2012.
Responsibilities: Therrien supervises the UMass hospital medicine division’s Affiliate Practitioner Group. She works with physicians on the executive council, coordinates the medicine service, and coordinates cross-coverage with other services in the hospital, including urology, neurology, surgery, GI, interventional radiology, and bone marrow transplants.
Hospitalist staff work 12-hour shifts, providing 24-hour coverage in the hospital, with one physician and two APPs scheduled at night.
“Because we are available 24-7 in house, I work closely with our scheduler. There is also a lot of coordination with subspecialty services in the hospital and on the observation unit,” she says. “I’m also responsible for interviewing and hiring AP candidates, including credentialing, and with the mentorship program. I chair the rapid response program and host our monthly staff meetings,” which involve both business and didactic presentations. She also serves on the hospital’s NP advisory council.
Before Therrien became the lead NP, her predecessor was assigned at 5% administrative.
“I started out 25% administrative because the program has expanded so quickly,” she says, noting that now she is 50% clinic and 50% administrative. “To be a good leader, I think I need to keep my feet on the ground in patient care.”
The story: Therrien worked as an EMT, a volunteer firefighter, and an ED tech before pursuing a degree in nursing.
“I grew up in a house where my dad was a firefighter and my mom was an EMT,” she says. “We were taught the importance of helping others and being selfless. I always had a leadership mentality.”
Therrien credits her physician colleagues for their commitment and support.
“It can be a little more difficult outside of our department,” she says. “They don’t always understand my role. Some of the attendings have not worked with affiliated providers before, but they have worked with residents. So there’s an interesting dynamic for them to learn how to work with us.”
Kimberly Eisenstock, MD, FHM, the clinical chief of hospital medicine, says that when she was looking for someone new to lead the affiliated practitioners, she wanted “a leader who understood their training and where they could be best utilized. Crystal volunteered. Boy, did she! She was the most experienced and enthusiastic candidate, with the most people-oriented skills.”
Dr. Eisenstock says she doesn’t start new roles or programs for the affiliated practitioners without getting the green light from Therrien.
“Crystal now represents the voice for how the division decides to employ APPs and the strategies we use to fill various roles,” she says. TH
Larry Beresford is a freelance writer in Alameda, Calif.
How NPs, PAs Can Prepare for Greater Leadership Roles
Michael Huckabee, MPAS, PhD, PA-C, is director of the Division of Physician Assistant Education at the University of Nebraska Medical Center in Omaha, where he trains both entry-level students and mid-career practitioners pursuing distance learning.

“When PAs are group leaders, they need to have the ability and orientation to involve all of their physicians in decision making,” Huckabee says. “This is a collaborative model of leadership. A term we use in leadership training is called ‘persuasive mapping’—the ability to influence others through reasoning to do something greater.”
What does Huckabee look for in students who might have a knack for leadership but could use a nudge in that direction?
“It’s a person who is somewhat gregarious and who builds strong relationships with others. They come to him or her for advice and ideas. But also with some level of humility—aware and accepting of personal limitations. These are the folks where we can say, ‘Let’s talk about your leadership skills and where we can strengthen you to be better prepared for the opportunities that can come up,’” he explains.
Huckabee says PAs need to get their names into consideration for opportunities on hospital committees such as pharmacy, credentialing, or ethics.
“You have to be well-versed about where you fit as a professional, relative to other advanced practitioners, and how the system works,” he says. “You have to be at the table, looking for opportunities to move the organization forward.”
Laurie Benton, PhD, MPAS, PA-C, RN, DFAAPA, who is the system director of advanced practice professionals for the Baylor Scott & White Health in Dallas, offers some additional advice for PAs and NPs who would like to rise to positions of leadership in their hospital groups or health systems.
“I recommend taking as many leadership classes as your facility offers,” she says. “Also consider taking outside leadership courses and even getting a second degree in business.”
Benton also says NPs and PAs should get involved in state and national professional and specialty associations. For example, the National Commission on Certification of Physician Assistants now offers a certificate of added qualifications in hospital medicine.
“That is where you will learn a great deal about laws that govern PAs and upcoming legislation that could affect what PAs are allowed to do and how they get paid,” she says, as well as the credentialing and boarding of PAs and NPs, which vary from state to state and from hospital to hospital.
—Larry Beresford
Since hospital medicine’s early days, hospitalist physicians have worked alongside physician assistants (PAs) and nurse practitioners (NPs). Some PAs and NPs have ascended to positions of leadership in their HM groups or health systems, in some cases even supervising the physicians.
The Hospitalist connected with six PA and NP leaders in hospital medicine to discuss their career paths as well as the nature and scope of their jobs. They described leadership as a complex, multidimensional concept, with often more of a collaborative model than a clear-cut supervisory relationship with clinicians. Most said they don’t try to be the “boss” of their group and have found ways to impact key decisions.
They also emphasized that PAs and NPs bring special skills and perspectives to team building. Many have supplemented frontline clinical experience with leadership training. And when it comes to decision making, their responsibilities can include hiring, scheduling, training, mentoring, information technology, quality improvement, and other essential functions of the group.
Edwin Lopez, MBA, PA-C
Workplace: St. Elizabeth is a 25-bed critical-access hospital serving a semi-rural bedroom community of 11,000 people an hour southeast of Seattle. It belongs to the nine-hospital CHI Franciscan Health system, and the HM group includes four physicians and four PAs providing 24-hour coverage. The physicians and PAs work in paired teams in the hospital and an 80-bed skilled nursing facility (SNF) across the street. Lopez heads St. Elizabeth’s HM group and is associate medical director of the SNF.
Background: Lopez graduated from the PA program at the University of Washington in 1982 and spent seven years as a PA with a cardiothoracic surgery practice in Tacoma. Then he established his own firm providing PA staffing services for six cardiac surgery programs in western Washington. In 1997, he co-founded an MD/PA hospitalist service covering three hospitals for a Seattle insurance company. That program grew into a larger group that was acquired by CHI Franciscan.
Lopez took time off to earn his MBA in health policy at the University of Washington and Harvard Kennedy School in Boston.
Eight years ago as part of an acquisition, CHI Franciscan asked Lopez to launch an HM program at St. Elizabeth. From the start, he developed the program as a collaborative model. The HM group now covers almost 90% of hospital admissions, manages the ICU, takes calls to admit patients from the ED, and rounds daily on patients in a small hospital that doesn’t have access to a lot of medical specialists.
St. Elizabeth’s has since flourished to become one of the health system’s top performers on quality metrics like HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores. However, Lopez admits readmission rates remain high. He noticed that a big part of the readmission problem was coming from the facility across the street, so he proposed the HM group start providing daily coverage to the SNF. In the group’s first year covering the SNF, the hospital’s readmission rate dropped to 5% from 35%.
Listen: Edwin Lopez, PA-C, discusses post-acute Care in the U.S. health system
Responsibilities: Lopez spends roughly half his time seeing patients, which he considers the most satisfying half. The other half is managing and setting clinical and administrative direction for the group.
“My responsibility is to ensure that there is appropriate physician and PA coverage 24-7 in both facilities,” he says, adding he also handles hiring and personnel issue. “We have an understanding here. I help guide, mentor, and direct the team, with the support of our regional medical director.”
The story: Lopez credits his current position to Joe Wilczek, a visionary CEO who came to the health system 18 years ago and retired in 2015.
“Joe and Franciscan’s chief medical officer and system director of hospital medicine came to me and said, ‘We’d like you to go over there and see what you can do at St. Elizabeth.’ There was a definite mandate, with markers they wanted me to reach. They said, ‘If you succeed, we will build you a new hospital building.’”
The new building opened in 2012.
Lopez says he has spent much of his career in quiet oblivion.
“It took five or six years here before people started noticing that our quality and performance were among the highest in the system,” he says. “For my entire 33-year career in medicine, I was never driven by the money. I grew up believing in service and got into medicine to make a difference, to leave a place better than I found it.”
He occasionally fields questions about his role as a PA group leader, which he tries to overcome by building trust, just as he overcame initial resistance to the hospital medicine program at St. Elizabeth from community physicians.
“I am very clear, we as a team are very clear, that we’re all worker bees here. We build strong relationships. We consider ourselves family,” he says. “When family issues come up, we need to sit down and talk about them, even when it may be uncomfortable.”
Laurie Benton, RN, MPAS, PhD, PA-C, DFAAPA
Workplace: Baylor Scott & White Health is the largest nonprofit health system in Texas, with 46 hospitals and 500 multispecialty clinics. Scott & White Memorial Hospital is a 636-bed specialty care and teaching hospital. Its hospital medicine program includes 40 physicians and 34 NP/PAs caring for an average daily census of 240 patients. They cover an observation service, consult service, and long-term acute-care service.
Background: Benton has a PhD in health administration. She has practiced hospital medicine at Scott & White Memorial Hospital since 2000 and before that at Emanuel Hospital in Portland, Ore. Currently an orthopedic hospitalist PA, she has worked in cardiothoracic surgery, critical care, and nephrology settings.
She became the system director for APPs in September 2013. In that role, she leads and represents 428 APPs, including hospitalist, intensivist, and cardiology PAs, in the system’s 26-hospital Central Region. She sits on the board of directors of the American Academy of Physician Assistants and has been on workforce committees for the National Commission on Certification of Physician Assistants and on the CME committee of the National Kidney Foundation.
Responsibilities: Benton coordinates everything, including PAs, advanced practice nurses, and nurse anesthetists, in settings across the healthcare continuum.
“I was appointed by our hospital medicine board and administration to be the APP leader. I report to the chief medical officer,” she says. “But I still see patients; it’s my passion. I’m not ready to give it up completely.”
Benton’s schedule includes two 10-hour clinical shifts per week. The other three days she works on administrative tasks. She attends board meetings as well as regular meetings with the system’s top executives and officers, including the chair of the board and the senior vice president for medical affairs.
“I have a seat on staff credentialing, benefits, and compensation committees, and I’m part of continuing medical education and disaster planning. Pretty much any of the committees we have here, I’m invited to be on,” she says. “I make sure I’m up-to-date on all of the new regulations and have information on any policies that have to do with APPs.”
The story: Benton says her PA training, including mentorship from Edwin Lopez, placed a strong emphasis on helping students develop leadership skills and interests.
“While I was working in nephrology, my supervising physician mentored me and encouraged me to move forward with my education,” she says. Along the way, she participated in a yearlong executive-education program and taught at the University of Texas McCombs School of Business. “Right off, it was not easy because while people saw me as a very strong, very confident provider, they didn’t see me as an administrator. When I worked with administrators, they were speaking a different language. I’d speak medicine, and they’d speak administration. It took a while to learn how to communicate with them.”
She says non-physician professionals traditionally have reported up through a physician and “never had their own voice. … Now that we have our leadership ladder here, it’s still new to some administrators,” she says. “I want to make sure PAs are part of the solution to high-quality healthcare.
“When I’m at the leadership table, we’re working together. The physicians respect my opinion, giving me the opportunity to interact like anyone else at the table.”
Catherine Boyd, MS, PA-C
Workplace: Essex is a private hospitalist group founded in 2007 by James Tollman, MD, FHM, who remains its CEO. It has 34 clinical members, including 16 physicians, 12 PAs, and six NPs. It began providing hospitalist medical care to several hospitals on Massachusetts’ North Shore under contract, then to a psychiatric hospital and a detox treatment center. In recent years, it has expanded into the post-acute arena, providing coverage to 14 SNFs, which now constitute the majority of its business. It also is active with two accountable-care organization networks.
Background: After three years as a respiratory therapist, Boyd enrolled in a PA program at Massachusetts College of Pharmacy and Health Sciences. After graduating in 2005, she worked as a hospitalist and intensivist, including as team leader for the medical emergency team at Lahey Health & Medical Center in Burlington, Mass., and in the PACE (Program of All-Inclusive Care for the Elderly) Internal Medical Department with Partners HealthCare until mid-2014, when she was invited to join Essex.
Responsibilities: “This job is not one thing; I dabble in everything,” says Boyd, who describes herself as the group’s chief operating officer for professional affairs. “I provide direct supervision to our PAs and NPs but also to our independent contractors, including moonlighting physicians. And I help to supervise the full-time physicians.”
She works on system issues, on-site training and mentorship, and implementation of a new electronic health record (EHR) and charge capture system while trying to improve bed flow and quality and decrease clinicians’ job frustrations. She also monitors developments in Medicare regulations.
“I check in with every one of our full-time providers weekly, and I try to offset some of the minutiae of their workday so that they can focus on their patients,” she explains. “Dr. Tollman and I feel that we bring a healthy work-lifestyle balance to the group. We encourage that in our staff. If they are happy in their jobs, it makes quality of care better.”
Boyd also maintains a clinical practice as a hospitalist, with her clinical duties flexing up and down based on patient demand and management needs.
The story: When Boyd was a respiratory therapist at a small community hospital, she worked one-on-one with a physician assistant who inspired her to change careers.
“I really liked what she did. As a PA, I worked to broaden my skill set on a critical care service for seven years,” she says. “But then my two kids got older and I wanted a more flexible schedule. Dr. Tollman came across my résumé when he was looking for a clinician to run operations for Essex.”
Building on 10 years of clinical experience, Boyd has tried to earn the trust of the other clinicians.
“They know they can come to me with questions. I like to think I practice active listening. When there is a problem, I do a case review and try to get all the facts,” she says. “When you earn their trust, the credentials tend to fall away, especially with the doctors I work with on a daily basis.”
Daniel Ladd, PA-C, DFAAPA
Workplace: Founded in 1993 as Hospitalists of Northern Michigan, iNDIGO Health Partners is one of the country’s largest private hospitalist companies, employing 150 physicians, PAs, and NPs who practice at seven hospitals across the state. The program also provides nighttime hospitalist services via telehealth and pediatric hospital medicine. It recently added 10 post-acute providers to work in SNFs and assisted living facilities.
Background: While working as a nurse’s aide, meeting and being inspired by some of the earliest PAs in Michigan, Ladd pursued PA training at Mercy College in Detroit. After graduating in 1984, he was hired by a cardiology practice at Detroit Medical Center. When he moved upstate to Traverse City in 1997, he landed a position as lead PA at another cardiology practice, acting as its liaison to PAs in the hospital. He joined iNDIGO in 2006.
“Jim Levy, one of the first PA hospitalists in Michigan, was an integral part of founding iNDIGO and now is our vice president of human resources,” Ladd says. “He asked me to join iNDIGO, and I jumped at the chance. Hospital medicine was a new opportunity for me and one with more opportunities for PAs to advance than cardiology.”
In 2009, when the company reorganized, the firm’s leadership recognized the need to establish a liaison group as a buffer between the providers and the company. Ladd became president of its new board of managers.
“From there, my position evolved to what it is today,” he says.
Levy calls Ladd a role model and leader, with great credibility among site program directors, hospital CMOs, and providers.
Responsibilities: Ladd gave up his clinical practice as a hospitalist in 2014 in response to growing management responsibilities.
“I do and I don’t miss it,” he says. “I miss the camaraderie of clinical practice, the foxhole mentality on the front lines. But I feel where I am now that I am able to help our providers give better care.
“Concretely, what I do is to help our practitioners and our medical directors at the clinical sites, some of whom are PAs and NPs, supporting them with leadership and education. I listen to their issues, translating and bringing to bear the resources of our company.”
Those resources include staffing, working conditions, office space, and the application of mobile medical technology for billing and clinical decision support.
“A lot of my communication is via email. I feel I am able to make a point without being inflammatory, by stating my purpose—the rationale for my position—and asking for what I need,” Ladd says. “This role is very accepted at iNDIGO. The corollary is that physician leaders who report to me are also comfortable in our relationship. It’s not about me being a PA and them being physicians but about us being colleagues in medicine.
“I’m in a position where I understand their world and am able to help them.”
The story: Encouraged by what he calls “visionary” leaders, Ladd has taken a number of steps to ascend to his current position as chief clinical officer.
“Even going back to the Boy Scouts, I was always one to step forward and volunteer for leadership,” he says. “I was president of my PA class in college and involved with the state association of PAs, as well as taking leadership training through the American Academy of Physician Assistants. I had the good fortune to be hired by a brilliant cardiologist at Detroit Medical Center. … He was the first to encourage me to be not just an excellent clinician but also a leader. He got me involved in implementing the EHR and in medication reconciliation. He promoted me as a PA to his patients and allowed me to become the face of our clinical practice, running the clinical side of the practice.”
Ladd also credits iNDIGO’s leaders for an approach of hiring the best people regardless of degree.
“If they happen to be PAs, great. The company’s vision is to have people with vision and skills to lead, not just based on credentials,” he says. “They established that as a baseline, and now it’s the culture here. We have PAs who are key drivers of the efficiency of this program.”
It hasn’t eliminated the occasional “I’m the physician, I’m delegating to you, and you have to do what I say,” Ladd admits. But he knows handling those situations is part of his job as a practice leader.
“It requires patience and understanding and the ability to see the issue from multiple perspectives,” he says, “and then synthesize all of that into a reasonable solution for all concerned.”
Arnold Facklam III, MSN, FNP-BC, FHM
Workplace: United Memorial has 100 beds and is part of the four-hospital Rochester Regional Health System. Kaleida Health has four acute-care hospitals in western New York. Based an hour apart, they compete, but both now get hospitalist services from Infinity Health Hospitalists of Western New York, a hospitalist group of 30 to 35 providers privately owned by local hospitalist John Patti, MD.
Background: Facklam has been a nocturnist since 2009, when he completed an NP program at D’Youville College in Buffalo. He worked 15 to 17 night shifts a month, first at Kaleida’s DeGraff Memorial Hospital and then at United Memorial, starting in 2013 as a per diem and vacation fill-in, then full-time since 2015. He now works for Infinity Health Hospitalists.
While working as a hospitalist, Facklam became involved with the MSO of Kaleida Health, starting on its Advanced Practice Provider Committee, which represents more than 600 NPs and PAs. Now chair of the committee, he leads change in the scope of practice for NPs and PAs and acts as liaison between APPs and the hospitals and health system.
Responsibilities: As a full-time nocturnist, Facklam has to squeeze in time for his role as director of advanced practice providers. He offers guidance and oversight, under the direction of the vice president of medical affairs, to all NPs, PAs, nurse midwives, and nurse anesthetists. He also is in charge of its rapid response and code blue team coverage at night, plus provides clinical education to family practice medical students and residents overnight in the hospital. He has worked on hospital quality improvement projects since 2012.
Facklam, who acknowledges type A personality tendencies, also maintains two to three night shifts per month at Kaleida’s Millard Suburban Hospital.
In 2012, he became a member, eventually a voting member, of Kaleida’s system-wide MSO Medical Executive Committee, which is responsible for rule making, disciplinary action, and the provision of medical care within the system.
“The MSO is the mechanism for accountability for professional practice,” he says. He is also active in SHM’s NP/PA Committee and now sits on SHM’s Public Policy Committee.
The story: “Working as a nocturnist has given me the flexibility to look into advanced management training,” he says, including Six Sigma green belt course work and certificate training. While at DeGraff, he heard about a call for membership on the NP/PA committee.
“They quickly realized the benefits of having someone with a background like mine on board,” he said. “As a nocturnist, I started going to more meetings and getting involved when the easier thing to do might have been to drive home and go to bed.”
Along the way, he learned a lot about hospital systems and how they work.
“Having been in healthcare for 23 years, I know the hierarchical approach,” Facklam says. “But the times are changing. As medicine becomes broader and more difficult to manage, it has to become more of a team approach. If you look at the data, there won’t be enough physicians in the near future. PAs and NPs can help fill that need.”
Crystal Therrien, MS, ACNP-BC
Workplace: UMass Medical Center encompasses three campuses in central Massachusetts, including University, Memorial, and Marlborough. The hospital medicine division covers all three campuses with 40 to 45 FTEs of physicians and 20 of APPs. Therrien has been with the department since October 2009—her first job after completing NP training—and assumed her leadership role in June 2012.
Responsibilities: Therrien supervises the UMass hospital medicine division’s Affiliate Practitioner Group. She works with physicians on the executive council, coordinates the medicine service, and coordinates cross-coverage with other services in the hospital, including urology, neurology, surgery, GI, interventional radiology, and bone marrow transplants.
Hospitalist staff work 12-hour shifts, providing 24-hour coverage in the hospital, with one physician and two APPs scheduled at night.
“Because we are available 24-7 in house, I work closely with our scheduler. There is also a lot of coordination with subspecialty services in the hospital and on the observation unit,” she says. “I’m also responsible for interviewing and hiring AP candidates, including credentialing, and with the mentorship program. I chair the rapid response program and host our monthly staff meetings,” which involve both business and didactic presentations. She also serves on the hospital’s NP advisory council.
Before Therrien became the lead NP, her predecessor was assigned at 5% administrative.
“I started out 25% administrative because the program has expanded so quickly,” she says, noting that now she is 50% clinic and 50% administrative. “To be a good leader, I think I need to keep my feet on the ground in patient care.”
The story: Therrien worked as an EMT, a volunteer firefighter, and an ED tech before pursuing a degree in nursing.
“I grew up in a house where my dad was a firefighter and my mom was an EMT,” she says. “We were taught the importance of helping others and being selfless. I always had a leadership mentality.”
Therrien credits her physician colleagues for their commitment and support.
“It can be a little more difficult outside of our department,” she says. “They don’t always understand my role. Some of the attendings have not worked with affiliated providers before, but they have worked with residents. So there’s an interesting dynamic for them to learn how to work with us.”
Kimberly Eisenstock, MD, FHM, the clinical chief of hospital medicine, says that when she was looking for someone new to lead the affiliated practitioners, she wanted “a leader who understood their training and where they could be best utilized. Crystal volunteered. Boy, did she! She was the most experienced and enthusiastic candidate, with the most people-oriented skills.”
Dr. Eisenstock says she doesn’t start new roles or programs for the affiliated practitioners without getting the green light from Therrien.
“Crystal now represents the voice for how the division decides to employ APPs and the strategies we use to fill various roles,” she says. TH
Larry Beresford is a freelance writer in Alameda, Calif.
How NPs, PAs Can Prepare for Greater Leadership Roles
Michael Huckabee, MPAS, PhD, PA-C, is director of the Division of Physician Assistant Education at the University of Nebraska Medical Center in Omaha, where he trains both entry-level students and mid-career practitioners pursuing distance learning.
“When PAs are group leaders, they need to have the ability and orientation to involve all of their physicians in decision making,” Huckabee says. “This is a collaborative model of leadership. A term we use in leadership training is called ‘persuasive mapping’—the ability to influence others through reasoning to do something greater.”
What does Huckabee look for in students who might have a knack for leadership but could use a nudge in that direction?
“It’s a person who is somewhat gregarious and who builds strong relationships with others. They come to him or her for advice and ideas. But also with some level of humility—aware and accepting of personal limitations. These are the folks where we can say, ‘Let’s talk about your leadership skills and where we can strengthen you to be better prepared for the opportunities that can come up,’” he explains.
Huckabee says PAs need to get their names into consideration for opportunities on hospital committees such as pharmacy, credentialing, or ethics.
“You have to be well-versed about where you fit as a professional, relative to other advanced practitioners, and how the system works,” he says. “You have to be at the table, looking for opportunities to move the organization forward.”
Laurie Benton, PhD, MPAS, PA-C, RN, DFAAPA, who is the system director of advanced practice professionals for the Baylor Scott & White Health in Dallas, offers some additional advice for PAs and NPs who would like to rise to positions of leadership in their hospital groups or health systems.
“I recommend taking as many leadership classes as your facility offers,” she says. “Also consider taking outside leadership courses and even getting a second degree in business.”
Benton also says NPs and PAs should get involved in state and national professional and specialty associations. For example, the National Commission on Certification of Physician Assistants now offers a certificate of added qualifications in hospital medicine.
“That is where you will learn a great deal about laws that govern PAs and upcoming legislation that could affect what PAs are allowed to do and how they get paid,” she says, as well as the credentialing and boarding of PAs and NPs, which vary from state to state and from hospital to hospital.
—Larry Beresford
Since hospital medicine’s early days, hospitalist physicians have worked alongside physician assistants (PAs) and nurse practitioners (NPs). Some PAs and NPs have ascended to positions of leadership in their HM groups or health systems, in some cases even supervising the physicians.
The Hospitalist connected with six PA and NP leaders in hospital medicine to discuss their career paths as well as the nature and scope of their jobs. They described leadership as a complex, multidimensional concept, with often more of a collaborative model than a clear-cut supervisory relationship with clinicians. Most said they don’t try to be the “boss” of their group and have found ways to impact key decisions.
They also emphasized that PAs and NPs bring special skills and perspectives to team building. Many have supplemented frontline clinical experience with leadership training. And when it comes to decision making, their responsibilities can include hiring, scheduling, training, mentoring, information technology, quality improvement, and other essential functions of the group.
Edwin Lopez, MBA, PA-C
Workplace: St. Elizabeth is a 25-bed critical-access hospital serving a semi-rural bedroom community of 11,000 people an hour southeast of Seattle. It belongs to the nine-hospital CHI Franciscan Health system, and the HM group includes four physicians and four PAs providing 24-hour coverage. The physicians and PAs work in paired teams in the hospital and an 80-bed skilled nursing facility (SNF) across the street. Lopez heads St. Elizabeth’s HM group and is associate medical director of the SNF.
Background: Lopez graduated from the PA program at the University of Washington in 1982 and spent seven years as a PA with a cardiothoracic surgery practice in Tacoma. Then he established his own firm providing PA staffing services for six cardiac surgery programs in western Washington. In 1997, he co-founded an MD/PA hospitalist service covering three hospitals for a Seattle insurance company. That program grew into a larger group that was acquired by CHI Franciscan.
Lopez took time off to earn his MBA in health policy at the University of Washington and Harvard Kennedy School in Boston.
Eight years ago as part of an acquisition, CHI Franciscan asked Lopez to launch an HM program at St. Elizabeth. From the start, he developed the program as a collaborative model. The HM group now covers almost 90% of hospital admissions, manages the ICU, takes calls to admit patients from the ED, and rounds daily on patients in a small hospital that doesn’t have access to a lot of medical specialists.
St. Elizabeth’s has since flourished to become one of the health system’s top performers on quality metrics like HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) scores. However, Lopez admits readmission rates remain high. He noticed that a big part of the readmission problem was coming from the facility across the street, so he proposed the HM group start providing daily coverage to the SNF. In the group’s first year covering the SNF, the hospital’s readmission rate dropped to 5% from 35%.
Listen: Edwin Lopez, PA-C, discusses post-acute Care in the U.S. health system
Responsibilities: Lopez spends roughly half his time seeing patients, which he considers the most satisfying half. The other half is managing and setting clinical and administrative direction for the group.
“My responsibility is to ensure that there is appropriate physician and PA coverage 24-7 in both facilities,” he says, adding he also handles hiring and personnel issue. “We have an understanding here. I help guide, mentor, and direct the team, with the support of our regional medical director.”
The story: Lopez credits his current position to Joe Wilczek, a visionary CEO who came to the health system 18 years ago and retired in 2015.
“Joe and Franciscan’s chief medical officer and system director of hospital medicine came to me and said, ‘We’d like you to go over there and see what you can do at St. Elizabeth.’ There was a definite mandate, with markers they wanted me to reach. They said, ‘If you succeed, we will build you a new hospital building.’”
The new building opened in 2012.
Lopez says he has spent much of his career in quiet oblivion.
“It took five or six years here before people started noticing that our quality and performance were among the highest in the system,” he says. “For my entire 33-year career in medicine, I was never driven by the money. I grew up believing in service and got into medicine to make a difference, to leave a place better than I found it.”
He occasionally fields questions about his role as a PA group leader, which he tries to overcome by building trust, just as he overcame initial resistance to the hospital medicine program at St. Elizabeth from community physicians.
“I am very clear, we as a team are very clear, that we’re all worker bees here. We build strong relationships. We consider ourselves family,” he says. “When family issues come up, we need to sit down and talk about them, even when it may be uncomfortable.”
Laurie Benton, RN, MPAS, PhD, PA-C, DFAAPA
Workplace: Baylor Scott & White Health is the largest nonprofit health system in Texas, with 46 hospitals and 500 multispecialty clinics. Scott & White Memorial Hospital is a 636-bed specialty care and teaching hospital. Its hospital medicine program includes 40 physicians and 34 NP/PAs caring for an average daily census of 240 patients. They cover an observation service, consult service, and long-term acute-care service.
Background: Benton has a PhD in health administration. She has practiced hospital medicine at Scott & White Memorial Hospital since 2000 and before that at Emanuel Hospital in Portland, Ore. Currently an orthopedic hospitalist PA, she has worked in cardiothoracic surgery, critical care, and nephrology settings.
She became the system director for APPs in September 2013. In that role, she leads and represents 428 APPs, including hospitalist, intensivist, and cardiology PAs, in the system’s 26-hospital Central Region. She sits on the board of directors of the American Academy of Physician Assistants and has been on workforce committees for the National Commission on Certification of Physician Assistants and on the CME committee of the National Kidney Foundation.
Responsibilities: Benton coordinates everything, including PAs, advanced practice nurses, and nurse anesthetists, in settings across the healthcare continuum.
“I was appointed by our hospital medicine board and administration to be the APP leader. I report to the chief medical officer,” she says. “But I still see patients; it’s my passion. I’m not ready to give it up completely.”
Benton’s schedule includes two 10-hour clinical shifts per week. The other three days she works on administrative tasks. She attends board meetings as well as regular meetings with the system’s top executives and officers, including the chair of the board and the senior vice president for medical affairs.
“I have a seat on staff credentialing, benefits, and compensation committees, and I’m part of continuing medical education and disaster planning. Pretty much any of the committees we have here, I’m invited to be on,” she says. “I make sure I’m up-to-date on all of the new regulations and have information on any policies that have to do with APPs.”
The story: Benton says her PA training, including mentorship from Edwin Lopez, placed a strong emphasis on helping students develop leadership skills and interests.
“While I was working in nephrology, my supervising physician mentored me and encouraged me to move forward with my education,” she says. Along the way, she participated in a yearlong executive-education program and taught at the University of Texas McCombs School of Business. “Right off, it was not easy because while people saw me as a very strong, very confident provider, they didn’t see me as an administrator. When I worked with administrators, they were speaking a different language. I’d speak medicine, and they’d speak administration. It took a while to learn how to communicate with them.”
She says non-physician professionals traditionally have reported up through a physician and “never had their own voice. … Now that we have our leadership ladder here, it’s still new to some administrators,” she says. “I want to make sure PAs are part of the solution to high-quality healthcare.
“When I’m at the leadership table, we’re working together. The physicians respect my opinion, giving me the opportunity to interact like anyone else at the table.”
Catherine Boyd, MS, PA-C
Workplace: Essex is a private hospitalist group founded in 2007 by James Tollman, MD, FHM, who remains its CEO. It has 34 clinical members, including 16 physicians, 12 PAs, and six NPs. It began providing hospitalist medical care to several hospitals on Massachusetts’ North Shore under contract, then to a psychiatric hospital and a detox treatment center. In recent years, it has expanded into the post-acute arena, providing coverage to 14 SNFs, which now constitute the majority of its business. It also is active with two accountable-care organization networks.
Background: After three years as a respiratory therapist, Boyd enrolled in a PA program at Massachusetts College of Pharmacy and Health Sciences. After graduating in 2005, she worked as a hospitalist and intensivist, including as team leader for the medical emergency team at Lahey Health & Medical Center in Burlington, Mass., and in the PACE (Program of All-Inclusive Care for the Elderly) Internal Medical Department with Partners HealthCare until mid-2014, when she was invited to join Essex.
Responsibilities: “This job is not one thing; I dabble in everything,” says Boyd, who describes herself as the group’s chief operating officer for professional affairs. “I provide direct supervision to our PAs and NPs but also to our independent contractors, including moonlighting physicians. And I help to supervise the full-time physicians.”
She works on system issues, on-site training and mentorship, and implementation of a new electronic health record (EHR) and charge capture system while trying to improve bed flow and quality and decrease clinicians’ job frustrations. She also monitors developments in Medicare regulations.
“I check in with every one of our full-time providers weekly, and I try to offset some of the minutiae of their workday so that they can focus on their patients,” she explains. “Dr. Tollman and I feel that we bring a healthy work-lifestyle balance to the group. We encourage that in our staff. If they are happy in their jobs, it makes quality of care better.”
Boyd also maintains a clinical practice as a hospitalist, with her clinical duties flexing up and down based on patient demand and management needs.
The story: When Boyd was a respiratory therapist at a small community hospital, she worked one-on-one with a physician assistant who inspired her to change careers.
“I really liked what she did. As a PA, I worked to broaden my skill set on a critical care service for seven years,” she says. “But then my two kids got older and I wanted a more flexible schedule. Dr. Tollman came across my résumé when he was looking for a clinician to run operations for Essex.”
Building on 10 years of clinical experience, Boyd has tried to earn the trust of the other clinicians.
“They know they can come to me with questions. I like to think I practice active listening. When there is a problem, I do a case review and try to get all the facts,” she says. “When you earn their trust, the credentials tend to fall away, especially with the doctors I work with on a daily basis.”
Daniel Ladd, PA-C, DFAAPA
Workplace: Founded in 1993 as Hospitalists of Northern Michigan, iNDIGO Health Partners is one of the country’s largest private hospitalist companies, employing 150 physicians, PAs, and NPs who practice at seven hospitals across the state. The program also provides nighttime hospitalist services via telehealth and pediatric hospital medicine. It recently added 10 post-acute providers to work in SNFs and assisted living facilities.
Background: While working as a nurse’s aide, meeting and being inspired by some of the earliest PAs in Michigan, Ladd pursued PA training at Mercy College in Detroit. After graduating in 1984, he was hired by a cardiology practice at Detroit Medical Center. When he moved upstate to Traverse City in 1997, he landed a position as lead PA at another cardiology practice, acting as its liaison to PAs in the hospital. He joined iNDIGO in 2006.
“Jim Levy, one of the first PA hospitalists in Michigan, was an integral part of founding iNDIGO and now is our vice president of human resources,” Ladd says. “He asked me to join iNDIGO, and I jumped at the chance. Hospital medicine was a new opportunity for me and one with more opportunities for PAs to advance than cardiology.”
In 2009, when the company reorganized, the firm’s leadership recognized the need to establish a liaison group as a buffer between the providers and the company. Ladd became president of its new board of managers.
“From there, my position evolved to what it is today,” he says.
Levy calls Ladd a role model and leader, with great credibility among site program directors, hospital CMOs, and providers.
Responsibilities: Ladd gave up his clinical practice as a hospitalist in 2014 in response to growing management responsibilities.
“I do and I don’t miss it,” he says. “I miss the camaraderie of clinical practice, the foxhole mentality on the front lines. But I feel where I am now that I am able to help our providers give better care.
“Concretely, what I do is to help our practitioners and our medical directors at the clinical sites, some of whom are PAs and NPs, supporting them with leadership and education. I listen to their issues, translating and bringing to bear the resources of our company.”
Those resources include staffing, working conditions, office space, and the application of mobile medical technology for billing and clinical decision support.
“A lot of my communication is via email. I feel I am able to make a point without being inflammatory, by stating my purpose—the rationale for my position—and asking for what I need,” Ladd says. “This role is very accepted at iNDIGO. The corollary is that physician leaders who report to me are also comfortable in our relationship. It’s not about me being a PA and them being physicians but about us being colleagues in medicine.
“I’m in a position where I understand their world and am able to help them.”
The story: Encouraged by what he calls “visionary” leaders, Ladd has taken a number of steps to ascend to his current position as chief clinical officer.
“Even going back to the Boy Scouts, I was always one to step forward and volunteer for leadership,” he says. “I was president of my PA class in college and involved with the state association of PAs, as well as taking leadership training through the American Academy of Physician Assistants. I had the good fortune to be hired by a brilliant cardiologist at Detroit Medical Center. … He was the first to encourage me to be not just an excellent clinician but also a leader. He got me involved in implementing the EHR and in medication reconciliation. He promoted me as a PA to his patients and allowed me to become the face of our clinical practice, running the clinical side of the practice.”
Ladd also credits iNDIGO’s leaders for an approach of hiring the best people regardless of degree.
“If they happen to be PAs, great. The company’s vision is to have people with vision and skills to lead, not just based on credentials,” he says. “They established that as a baseline, and now it’s the culture here. We have PAs who are key drivers of the efficiency of this program.”
It hasn’t eliminated the occasional “I’m the physician, I’m delegating to you, and you have to do what I say,” Ladd admits. But he knows handling those situations is part of his job as a practice leader.
“It requires patience and understanding and the ability to see the issue from multiple perspectives,” he says, “and then synthesize all of that into a reasonable solution for all concerned.”
Arnold Facklam III, MSN, FNP-BC, FHM
Workplace: United Memorial has 100 beds and is part of the four-hospital Rochester Regional Health System. Kaleida Health has four acute-care hospitals in western New York. Based an hour apart, they compete, but both now get hospitalist services from Infinity Health Hospitalists of Western New York, a hospitalist group of 30 to 35 providers privately owned by local hospitalist John Patti, MD.
Background: Facklam has been a nocturnist since 2009, when he completed an NP program at D’Youville College in Buffalo. He worked 15 to 17 night shifts a month, first at Kaleida’s DeGraff Memorial Hospital and then at United Memorial, starting in 2013 as a per diem and vacation fill-in, then full-time since 2015. He now works for Infinity Health Hospitalists.
While working as a hospitalist, Facklam became involved with the MSO of Kaleida Health, starting on its Advanced Practice Provider Committee, which represents more than 600 NPs and PAs. Now chair of the committee, he leads change in the scope of practice for NPs and PAs and acts as liaison between APPs and the hospitals and health system.
Responsibilities: As a full-time nocturnist, Facklam has to squeeze in time for his role as director of advanced practice providers. He offers guidance and oversight, under the direction of the vice president of medical affairs, to all NPs, PAs, nurse midwives, and nurse anesthetists. He also is in charge of its rapid response and code blue team coverage at night, plus provides clinical education to family practice medical students and residents overnight in the hospital. He has worked on hospital quality improvement projects since 2012.
Facklam, who acknowledges type A personality tendencies, also maintains two to three night shifts per month at Kaleida’s Millard Suburban Hospital.
In 2012, he became a member, eventually a voting member, of Kaleida’s system-wide MSO Medical Executive Committee, which is responsible for rule making, disciplinary action, and the provision of medical care within the system.
“The MSO is the mechanism for accountability for professional practice,” he says. He is also active in SHM’s NP/PA Committee and now sits on SHM’s Public Policy Committee.
The story: “Working as a nocturnist has given me the flexibility to look into advanced management training,” he says, including Six Sigma green belt course work and certificate training. While at DeGraff, he heard about a call for membership on the NP/PA committee.
“They quickly realized the benefits of having someone with a background like mine on board,” he said. “As a nocturnist, I started going to more meetings and getting involved when the easier thing to do might have been to drive home and go to bed.”
Along the way, he learned a lot about hospital systems and how they work.
“Having been in healthcare for 23 years, I know the hierarchical approach,” Facklam says. “But the times are changing. As medicine becomes broader and more difficult to manage, it has to become more of a team approach. If you look at the data, there won’t be enough physicians in the near future. PAs and NPs can help fill that need.”
Crystal Therrien, MS, ACNP-BC
Workplace: UMass Medical Center encompasses three campuses in central Massachusetts, including University, Memorial, and Marlborough. The hospital medicine division covers all three campuses with 40 to 45 FTEs of physicians and 20 of APPs. Therrien has been with the department since October 2009—her first job after completing NP training—and assumed her leadership role in June 2012.
Responsibilities: Therrien supervises the UMass hospital medicine division’s Affiliate Practitioner Group. She works with physicians on the executive council, coordinates the medicine service, and coordinates cross-coverage with other services in the hospital, including urology, neurology, surgery, GI, interventional radiology, and bone marrow transplants.
Hospitalist staff work 12-hour shifts, providing 24-hour coverage in the hospital, with one physician and two APPs scheduled at night.
“Because we are available 24-7 in house, I work closely with our scheduler. There is also a lot of coordination with subspecialty services in the hospital and on the observation unit,” she says. “I’m also responsible for interviewing and hiring AP candidates, including credentialing, and with the mentorship program. I chair the rapid response program and host our monthly staff meetings,” which involve both business and didactic presentations. She also serves on the hospital’s NP advisory council.
Before Therrien became the lead NP, her predecessor was assigned at 5% administrative.
“I started out 25% administrative because the program has expanded so quickly,” she says, noting that now she is 50% clinic and 50% administrative. “To be a good leader, I think I need to keep my feet on the ground in patient care.”
The story: Therrien worked as an EMT, a volunteer firefighter, and an ED tech before pursuing a degree in nursing.
“I grew up in a house where my dad was a firefighter and my mom was an EMT,” she says. “We were taught the importance of helping others and being selfless. I always had a leadership mentality.”
Therrien credits her physician colleagues for their commitment and support.
“It can be a little more difficult outside of our department,” she says. “They don’t always understand my role. Some of the attendings have not worked with affiliated providers before, but they have worked with residents. So there’s an interesting dynamic for them to learn how to work with us.”
Kimberly Eisenstock, MD, FHM, the clinical chief of hospital medicine, says that when she was looking for someone new to lead the affiliated practitioners, she wanted “a leader who understood their training and where they could be best utilized. Crystal volunteered. Boy, did she! She was the most experienced and enthusiastic candidate, with the most people-oriented skills.”
Dr. Eisenstock says she doesn’t start new roles or programs for the affiliated practitioners without getting the green light from Therrien.
“Crystal now represents the voice for how the division decides to employ APPs and the strategies we use to fill various roles,” she says. TH
Larry Beresford is a freelance writer in Alameda, Calif.
How NPs, PAs Can Prepare for Greater Leadership Roles
Michael Huckabee, MPAS, PhD, PA-C, is director of the Division of Physician Assistant Education at the University of Nebraska Medical Center in Omaha, where he trains both entry-level students and mid-career practitioners pursuing distance learning.
“When PAs are group leaders, they need to have the ability and orientation to involve all of their physicians in decision making,” Huckabee says. “This is a collaborative model of leadership. A term we use in leadership training is called ‘persuasive mapping’—the ability to influence others through reasoning to do something greater.”
What does Huckabee look for in students who might have a knack for leadership but could use a nudge in that direction?
“It’s a person who is somewhat gregarious and who builds strong relationships with others. They come to him or her for advice and ideas. But also with some level of humility—aware and accepting of personal limitations. These are the folks where we can say, ‘Let’s talk about your leadership skills and where we can strengthen you to be better prepared for the opportunities that can come up,’” he explains.
Huckabee says PAs need to get their names into consideration for opportunities on hospital committees such as pharmacy, credentialing, or ethics.
“You have to be well-versed about where you fit as a professional, relative to other advanced practitioners, and how the system works,” he says. “You have to be at the table, looking for opportunities to move the organization forward.”
Laurie Benton, PhD, MPAS, PA-C, RN, DFAAPA, who is the system director of advanced practice professionals for the Baylor Scott & White Health in Dallas, offers some additional advice for PAs and NPs who would like to rise to positions of leadership in their hospital groups or health systems.
“I recommend taking as many leadership classes as your facility offers,” she says. “Also consider taking outside leadership courses and even getting a second degree in business.”
Benton also says NPs and PAs should get involved in state and national professional and specialty associations. For example, the National Commission on Certification of Physician Assistants now offers a certificate of added qualifications in hospital medicine.
“That is where you will learn a great deal about laws that govern PAs and upcoming legislation that could affect what PAs are allowed to do and how they get paid,” she says, as well as the credentialing and boarding of PAs and NPs, which vary from state to state and from hospital to hospital.
—Larry Beresford

Research Shows Link Between EHR and Physician Burnout
Hospitalists’ struggles with the promise and pitfalls of the electronic health record (EHR) can also impinge on their personal satisfaction with their jobs.
The EHR has been identified as a major contributor to physician burnout. Research conducted in 2013 by the RAND Corporation and the American Medical Association (AMA) identified EHRs as the leading cause of physician dissatisfaction, emotional fatigue, depersonalization, and lost enthusiasm for the job.1 The MEMO study found that increased numbers of EHR functions in primary-care settings were associated with physician-reported stress, burnout, and desire to leave the practice.2 Daniel Roberts, MD, FHM, and colleagues found that more than half of hospitalists (52.3%) were affected by burnout, although rates were not higher than in outpatient settings.3
“It’s not fair to blame all physician burnout on the EHR, but the EHR has enabled others to place new demands on physicians and their practices,” says Christine Sinsky, MD, a former hospitalist and current vice president of professional satisfaction for AMA. “The current state of EHR technology appears to worsen professional satisfaction in multiple ways, resulting in reduced face time with patients and more time spent on data-entry functions.”
Dr. Sinsky says her association is trying to address the problem, both with advocacy to delay or revise government requirements for EHR adoption and through its STEPS Forward initiative to help physicians and their staffs redesign medical practices to minimize stress in a changing healthcare environment.
The AMA/RAND research did not break out hospital medicine specifically, although it identified high rates of job dissatisfaction for internists.
Jonathan Pell, MD, hospitalist and assistant professor of medicine at the University of Colorado in Denver, says more research is needed to connect the dots between the EHR and hospitalists’ job satisfaction.
“It makes me wonder, does the EHR affect hospitalists differently than it does outpatient doctors?” he says. “More hospitals and health systems are starting to survey physicians regarding their job satisfaction.”
Dr. Pell also points to computerized physician order entry as a related contributor to job stress.
What Can the Hospitalist Do?
“I’m a believer in the EHR,” says R.J. Bunnell, MD, hospitalist at the 321-bed McKay-Dee Hospital in Ogden, Utah, and physician champion for EHR implementation at Salt Lake City–based Intermountain Healthcare. “We have the potential to reduce medical errors and decrease the burden on physicians, eventually providing unique decision support tools.”
Dr. Bunnell says many of the issues with EHR stem from the complex designs of the systems and cumbersome data collection.
“The practice of medicine is getting more complex year by year, with more regulatory oversight and well-intentioned—but poorly designed—mandates,” he says. “Physicians spend less one-on-one time with their patients and feel they no longer have power over their jobs.”
Dr. Bunnell helped plan implementation of the Intermountain EHR, including its rollout at McKay-Dee last fall.
“We had a positive response to going electronic here,” he says. “Part of it was just the inefficiency of how we did things before, where physicians were already spending 60% of their day on documenting. We started working with our vendor in 2013 to set things up. The team was very proactive, and we spent more than a year on staff training. There’s always a steep learning curve, but it has gone better here than other places.”
Poor rollout and lack of physician involvement in system design can be major contributors to EHR burnout, he adds.
“But for hospitalists, going forward, this is the kind of thing where our specialty could really shine—creating specialized roles for ourselves as agents of change,” Dr. Bunnell says. “If we as physicians don’t recognize the drivers behind these mandates, we’ll just continue to react to them. My hope is that … we will embrace the change, get involved, and find ways to use these tools to fulfill their promise.” TH
Larry Beresford is a freelance writer in California.
References
- Friedberg MW, Chen PG, Van Busum KR, et al. Research report: factors affecting physician professional satisfaction and their implications for patient care, health systems, and health policy. Santa Monica, CA: Rand Corporation, 2013.
- Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care: results from the MEMO Study. J Am Med Inform Assoc. 2014;21(e1): e100-106.
- Roberts DL, Shanafelt TD, Dyrbye LN, West CP. A national comparison of burnout and work-life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176-181.
Hospitalists’ struggles with the promise and pitfalls of the electronic health record (EHR) can also impinge on their personal satisfaction with their jobs.
The EHR has been identified as a major contributor to physician burnout. Research conducted in 2013 by the RAND Corporation and the American Medical Association (AMA) identified EHRs as the leading cause of physician dissatisfaction, emotional fatigue, depersonalization, and lost enthusiasm for the job.1 The MEMO study found that increased numbers of EHR functions in primary-care settings were associated with physician-reported stress, burnout, and desire to leave the practice.2 Daniel Roberts, MD, FHM, and colleagues found that more than half of hospitalists (52.3%) were affected by burnout, although rates were not higher than in outpatient settings.3
“It’s not fair to blame all physician burnout on the EHR, but the EHR has enabled others to place new demands on physicians and their practices,” says Christine Sinsky, MD, a former hospitalist and current vice president of professional satisfaction for AMA. “The current state of EHR technology appears to worsen professional satisfaction in multiple ways, resulting in reduced face time with patients and more time spent on data-entry functions.”
Dr. Sinsky says her association is trying to address the problem, both with advocacy to delay or revise government requirements for EHR adoption and through its STEPS Forward initiative to help physicians and their staffs redesign medical practices to minimize stress in a changing healthcare environment.
The AMA/RAND research did not break out hospital medicine specifically, although it identified high rates of job dissatisfaction for internists.
Jonathan Pell, MD, hospitalist and assistant professor of medicine at the University of Colorado in Denver, says more research is needed to connect the dots between the EHR and hospitalists’ job satisfaction.
“It makes me wonder, does the EHR affect hospitalists differently than it does outpatient doctors?” he says. “More hospitals and health systems are starting to survey physicians regarding their job satisfaction.”
Dr. Pell also points to computerized physician order entry as a related contributor to job stress.
What Can the Hospitalist Do?
“I’m a believer in the EHR,” says R.J. Bunnell, MD, hospitalist at the 321-bed McKay-Dee Hospital in Ogden, Utah, and physician champion for EHR implementation at Salt Lake City–based Intermountain Healthcare. “We have the potential to reduce medical errors and decrease the burden on physicians, eventually providing unique decision support tools.”
Dr. Bunnell says many of the issues with EHR stem from the complex designs of the systems and cumbersome data collection.
“The practice of medicine is getting more complex year by year, with more regulatory oversight and well-intentioned—but poorly designed—mandates,” he says. “Physicians spend less one-on-one time with their patients and feel they no longer have power over their jobs.”
Dr. Bunnell helped plan implementation of the Intermountain EHR, including its rollout at McKay-Dee last fall.
“We had a positive response to going electronic here,” he says. “Part of it was just the inefficiency of how we did things before, where physicians were already spending 60% of their day on documenting. We started working with our vendor in 2013 to set things up. The team was very proactive, and we spent more than a year on staff training. There’s always a steep learning curve, but it has gone better here than other places.”
Poor rollout and lack of physician involvement in system design can be major contributors to EHR burnout, he adds.
“But for hospitalists, going forward, this is the kind of thing where our specialty could really shine—creating specialized roles for ourselves as agents of change,” Dr. Bunnell says. “If we as physicians don’t recognize the drivers behind these mandates, we’ll just continue to react to them. My hope is that … we will embrace the change, get involved, and find ways to use these tools to fulfill their promise.” TH
Larry Beresford is a freelance writer in California.
References
- Friedberg MW, Chen PG, Van Busum KR, et al. Research report: factors affecting physician professional satisfaction and their implications for patient care, health systems, and health policy. Santa Monica, CA: Rand Corporation, 2013.
- Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care: results from the MEMO Study. J Am Med Inform Assoc. 2014;21(e1): e100-106.
- Roberts DL, Shanafelt TD, Dyrbye LN, West CP. A national comparison of burnout and work-life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176-181.
Hospitalists’ struggles with the promise and pitfalls of the electronic health record (EHR) can also impinge on their personal satisfaction with their jobs.
The EHR has been identified as a major contributor to physician burnout. Research conducted in 2013 by the RAND Corporation and the American Medical Association (AMA) identified EHRs as the leading cause of physician dissatisfaction, emotional fatigue, depersonalization, and lost enthusiasm for the job.1 The MEMO study found that increased numbers of EHR functions in primary-care settings were associated with physician-reported stress, burnout, and desire to leave the practice.2 Daniel Roberts, MD, FHM, and colleagues found that more than half of hospitalists (52.3%) were affected by burnout, although rates were not higher than in outpatient settings.3
“It’s not fair to blame all physician burnout on the EHR, but the EHR has enabled others to place new demands on physicians and their practices,” says Christine Sinsky, MD, a former hospitalist and current vice president of professional satisfaction for AMA. “The current state of EHR technology appears to worsen professional satisfaction in multiple ways, resulting in reduced face time with patients and more time spent on data-entry functions.”
Dr. Sinsky says her association is trying to address the problem, both with advocacy to delay or revise government requirements for EHR adoption and through its STEPS Forward initiative to help physicians and their staffs redesign medical practices to minimize stress in a changing healthcare environment.
The AMA/RAND research did not break out hospital medicine specifically, although it identified high rates of job dissatisfaction for internists.
Jonathan Pell, MD, hospitalist and assistant professor of medicine at the University of Colorado in Denver, says more research is needed to connect the dots between the EHR and hospitalists’ job satisfaction.
“It makes me wonder, does the EHR affect hospitalists differently than it does outpatient doctors?” he says. “More hospitals and health systems are starting to survey physicians regarding their job satisfaction.”
Dr. Pell also points to computerized physician order entry as a related contributor to job stress.
What Can the Hospitalist Do?
“I’m a believer in the EHR,” says R.J. Bunnell, MD, hospitalist at the 321-bed McKay-Dee Hospital in Ogden, Utah, and physician champion for EHR implementation at Salt Lake City–based Intermountain Healthcare. “We have the potential to reduce medical errors and decrease the burden on physicians, eventually providing unique decision support tools.”
Dr. Bunnell says many of the issues with EHR stem from the complex designs of the systems and cumbersome data collection.
“The practice of medicine is getting more complex year by year, with more regulatory oversight and well-intentioned—but poorly designed—mandates,” he says. “Physicians spend less one-on-one time with their patients and feel they no longer have power over their jobs.”
Dr. Bunnell helped plan implementation of the Intermountain EHR, including its rollout at McKay-Dee last fall.
“We had a positive response to going electronic here,” he says. “Part of it was just the inefficiency of how we did things before, where physicians were already spending 60% of their day on documenting. We started working with our vendor in 2013 to set things up. The team was very proactive, and we spent more than a year on staff training. There’s always a steep learning curve, but it has gone better here than other places.”
Poor rollout and lack of physician involvement in system design can be major contributors to EHR burnout, he adds.
“But for hospitalists, going forward, this is the kind of thing where our specialty could really shine—creating specialized roles for ourselves as agents of change,” Dr. Bunnell says. “If we as physicians don’t recognize the drivers behind these mandates, we’ll just continue to react to them. My hope is that … we will embrace the change, get involved, and find ways to use these tools to fulfill their promise.” TH
Larry Beresford is a freelance writer in California.
References
- Friedberg MW, Chen PG, Van Busum KR, et al. Research report: factors affecting physician professional satisfaction and their implications for patient care, health systems, and health policy. Santa Monica, CA: Rand Corporation, 2013.
- Babbott S, Manwell LB, Brown R, et al. Electronic medical records and physician stress in primary care: results from the MEMO Study. J Am Med Inform Assoc. 2014;21(e1): e100-106.
- Roberts DL, Shanafelt TD, Dyrbye LN, West CP. A national comparison of burnout and work-life balance among internal medicine hospitalists and outpatient general internists. J Hosp Med. 2014;9(3):176-181.