User login
Questions Have Been Raised about Potential Risks from Using Abbott Laboratories' Novel Coronary Stent
(Reuters) - U.S. government scientists have raised questions about the potential risks to patients of heart attacks and blood clots from Abbott Laboratories' novel coronary stent that dissolves after it is implanted.
Abbott is seeking U.S. approval to sell the stent, called Absorb, as an alternative to metal stents currently used in percutaneous coronary intervention. Unlike traditional stents that remain in place after implantation, Absorb is designed to disappear within three years of the procedure.
U.S. Food and Drug Administration staff, in documents released before an advisory panel meets on Tuesday to consider whether to recommend approval of the device, said they would ask the outside experts about data showing more heart attack and stent-related blood clots compared with Abbott's drug-coated metal Xience stent.
FDA said it also will ask the panel to address risks associated with the device when used in smaller arteries.
A large clinical trial released in October concluded that the Absorb stent, which is made of a plastic similar to dissolving sutures, was comparable to Xience in overall safety and effectiveness. Although Xience appeared to be numerically better than Absorb at one year on a variety of secondary measures, the differences were not considered statistically significant.
"These results are from physicians using a new therapy for the first time. Consequently, we expect them to improve with time and experience," said Abbott spokesman Jonathon Hamilton.
In the Absorb III clinical study, patients with small vessels comprised less than 20 percent of the total and experienced relatively low rates of adverse events even though many had known risk factors, including diabetes, Hamilton said.
More than 125,000 patients already have been treated with Absorb in more than 100 countries where it is commercially available.
If approved in the United States, Absorb would compete with Xience, the market-leading stent, and with Medtronic Plc's Resolute stent and Boston Scientific's Synergy and Promus stents. Synergy's polymer coating used to deliver a drug disappears over time, leaving a bare metal stent in place.
Wells Fargo analyst Larry Biegelsen said he expects Absorb to get a positive recommendation from the advisory panel, followed by FDA approval later this year.
"In the U.S., we estimate Absorb will capture about 5 percent of the total drug-eluting stent market, although our estimate may prove conservative if the post-approval data and experience with Absorb improves," Biegelsen wrote in a note to clients.
(Reuters) - U.S. government scientists have raised questions about the potential risks to patients of heart attacks and blood clots from Abbott Laboratories' novel coronary stent that dissolves after it is implanted.
Abbott is seeking U.S. approval to sell the stent, called Absorb, as an alternative to metal stents currently used in percutaneous coronary intervention. Unlike traditional stents that remain in place after implantation, Absorb is designed to disappear within three years of the procedure.
U.S. Food and Drug Administration staff, in documents released before an advisory panel meets on Tuesday to consider whether to recommend approval of the device, said they would ask the outside experts about data showing more heart attack and stent-related blood clots compared with Abbott's drug-coated metal Xience stent.
FDA said it also will ask the panel to address risks associated with the device when used in smaller arteries.
A large clinical trial released in October concluded that the Absorb stent, which is made of a plastic similar to dissolving sutures, was comparable to Xience in overall safety and effectiveness. Although Xience appeared to be numerically better than Absorb at one year on a variety of secondary measures, the differences were not considered statistically significant.
"These results are from physicians using a new therapy for the first time. Consequently, we expect them to improve with time and experience," said Abbott spokesman Jonathon Hamilton.
In the Absorb III clinical study, patients with small vessels comprised less than 20 percent of the total and experienced relatively low rates of adverse events even though many had known risk factors, including diabetes, Hamilton said.
More than 125,000 patients already have been treated with Absorb in more than 100 countries where it is commercially available.
If approved in the United States, Absorb would compete with Xience, the market-leading stent, and with Medtronic Plc's Resolute stent and Boston Scientific's Synergy and Promus stents. Synergy's polymer coating used to deliver a drug disappears over time, leaving a bare metal stent in place.
Wells Fargo analyst Larry Biegelsen said he expects Absorb to get a positive recommendation from the advisory panel, followed by FDA approval later this year.
"In the U.S., we estimate Absorb will capture about 5 percent of the total drug-eluting stent market, although our estimate may prove conservative if the post-approval data and experience with Absorb improves," Biegelsen wrote in a note to clients.
(Reuters) - U.S. government scientists have raised questions about the potential risks to patients of heart attacks and blood clots from Abbott Laboratories' novel coronary stent that dissolves after it is implanted.
Abbott is seeking U.S. approval to sell the stent, called Absorb, as an alternative to metal stents currently used in percutaneous coronary intervention. Unlike traditional stents that remain in place after implantation, Absorb is designed to disappear within three years of the procedure.
U.S. Food and Drug Administration staff, in documents released before an advisory panel meets on Tuesday to consider whether to recommend approval of the device, said they would ask the outside experts about data showing more heart attack and stent-related blood clots compared with Abbott's drug-coated metal Xience stent.
FDA said it also will ask the panel to address risks associated with the device when used in smaller arteries.
A large clinical trial released in October concluded that the Absorb stent, which is made of a plastic similar to dissolving sutures, was comparable to Xience in overall safety and effectiveness. Although Xience appeared to be numerically better than Absorb at one year on a variety of secondary measures, the differences were not considered statistically significant.
"These results are from physicians using a new therapy for the first time. Consequently, we expect them to improve with time and experience," said Abbott spokesman Jonathon Hamilton.
In the Absorb III clinical study, patients with small vessels comprised less than 20 percent of the total and experienced relatively low rates of adverse events even though many had known risk factors, including diabetes, Hamilton said.
More than 125,000 patients already have been treated with Absorb in more than 100 countries where it is commercially available.
If approved in the United States, Absorb would compete with Xience, the market-leading stent, and with Medtronic Plc's Resolute stent and Boston Scientific's Synergy and Promus stents. Synergy's polymer coating used to deliver a drug disappears over time, leaving a bare metal stent in place.
Wells Fargo analyst Larry Biegelsen said he expects Absorb to get a positive recommendation from the advisory panel, followed by FDA approval later this year.
"In the U.S., we estimate Absorb will capture about 5 percent of the total drug-eluting stent market, although our estimate may prove conservative if the post-approval data and experience with Absorb improves," Biegelsen wrote in a note to clients.
Computer models simulate HSCT recovery

Photo by Darren Baker
New research indicates that computer models can simulate the recovery of the immune system in patients undergoing hematopoietic stem cell transplant (HSCT).
The study suggests the possibility of using DNA sequencing and computer modeling to predict which HSCT recipients might suffer complications such as graft-versus-host-disease.
The research was published in Biology of Blood and Marrow Transplantation.
The study builds upon prior research, which showed that the immune system may be modeled as a dynamical system. Dynamical systems are mathematical objects used to model physical phenomena that change over time. These systems can be used to predict future states via observations of past and present states.
Researchers say the ability to predict immune system recovery after HSCT could potentially allow doctors to refine donor selection and better personalize post-transplant care to improve outcomes.
With this in mind, the team sequenced the DNA of 34 HSCT donor-recipient pairs and used the resulting information in a computer model to simulate how the recipient’s T-cell repertoire will recover following transplant.
“This study is the first to simulate the growth of the T-cell repertoire following transplantation using variables that aren’t accounted for in typical HLA donor-recipient matching,” said study author Amir Ahmed Toor, MD, of Virginia Commonwealth University in Richmond.
“Using a larger cohort of patients than in previous studies, we were able to mathematically predict the interactions of these variables, which led to simulations that appear to be very similar to clinically observed post-transplantation T-cell repertoire development.”
Previous research by Dr Toor and his colleagues revealed large variations between donor-recipient minor histocompatibility antigens that could potentially contribute to transplant complications not accounted for by HLA testing.
The models used in the computer simulations were driven by population growth formulas developed from past studies by Dr Toor and his colleagues that revealed distinct patterns of lymphocyte recovery in HSCT recipients.
Using matrix mathematics to develop the simulations, the researchers observed competition among T cells as the T-cell repertoire develops.
This competition leads to certain families of T cells becoming dominant and more numerous, which crowds out weaker T-cell families, causing them to develop later and in fewer numbers.
“We are attempting to account for the many variables that could impact T-cell repertoire development and, in turn, patient outcomes,” Dr Toor said.
“In future studies, we hope to explore the impact of organ-specific antigen expression. The knowledge gained from this research could potentially allow more accurate predictions of which organs could be most affected by graft-versus-host-disease.” ![]()
Photo by Darren Baker
New research indicates that computer models can simulate the recovery of the immune system in patients undergoing hematopoietic stem cell transplant (HSCT).
The study suggests the possibility of using DNA sequencing and computer modeling to predict which HSCT recipients might suffer complications such as graft-versus-host-disease.
The research was published in Biology of Blood and Marrow Transplantation.
The study builds upon prior research, which showed that the immune system may be modeled as a dynamical system. Dynamical systems are mathematical objects used to model physical phenomena that change over time. These systems can be used to predict future states via observations of past and present states.
Researchers say the ability to predict immune system recovery after HSCT could potentially allow doctors to refine donor selection and better personalize post-transplant care to improve outcomes.
With this in mind, the team sequenced the DNA of 34 HSCT donor-recipient pairs and used the resulting information in a computer model to simulate how the recipient’s T-cell repertoire will recover following transplant.
“This study is the first to simulate the growth of the T-cell repertoire following transplantation using variables that aren’t accounted for in typical HLA donor-recipient matching,” said study author Amir Ahmed Toor, MD, of Virginia Commonwealth University in Richmond.
“Using a larger cohort of patients than in previous studies, we were able to mathematically predict the interactions of these variables, which led to simulations that appear to be very similar to clinically observed post-transplantation T-cell repertoire development.”
Previous research by Dr Toor and his colleagues revealed large variations between donor-recipient minor histocompatibility antigens that could potentially contribute to transplant complications not accounted for by HLA testing.
The models used in the computer simulations were driven by population growth formulas developed from past studies by Dr Toor and his colleagues that revealed distinct patterns of lymphocyte recovery in HSCT recipients.
Using matrix mathematics to develop the simulations, the researchers observed competition among T cells as the T-cell repertoire develops.
This competition leads to certain families of T cells becoming dominant and more numerous, which crowds out weaker T-cell families, causing them to develop later and in fewer numbers.
“We are attempting to account for the many variables that could impact T-cell repertoire development and, in turn, patient outcomes,” Dr Toor said.
“In future studies, we hope to explore the impact of organ-specific antigen expression. The knowledge gained from this research could potentially allow more accurate predictions of which organs could be most affected by graft-versus-host-disease.” ![]()
Photo by Darren Baker
New research indicates that computer models can simulate the recovery of the immune system in patients undergoing hematopoietic stem cell transplant (HSCT).
The study suggests the possibility of using DNA sequencing and computer modeling to predict which HSCT recipients might suffer complications such as graft-versus-host-disease.
The research was published in Biology of Blood and Marrow Transplantation.
The study builds upon prior research, which showed that the immune system may be modeled as a dynamical system. Dynamical systems are mathematical objects used to model physical phenomena that change over time. These systems can be used to predict future states via observations of past and present states.
Researchers say the ability to predict immune system recovery after HSCT could potentially allow doctors to refine donor selection and better personalize post-transplant care to improve outcomes.
With this in mind, the team sequenced the DNA of 34 HSCT donor-recipient pairs and used the resulting information in a computer model to simulate how the recipient’s T-cell repertoire will recover following transplant.
“This study is the first to simulate the growth of the T-cell repertoire following transplantation using variables that aren’t accounted for in typical HLA donor-recipient matching,” said study author Amir Ahmed Toor, MD, of Virginia Commonwealth University in Richmond.
“Using a larger cohort of patients than in previous studies, we were able to mathematically predict the interactions of these variables, which led to simulations that appear to be very similar to clinically observed post-transplantation T-cell repertoire development.”
Previous research by Dr Toor and his colleagues revealed large variations between donor-recipient minor histocompatibility antigens that could potentially contribute to transplant complications not accounted for by HLA testing.
The models used in the computer simulations were driven by population growth formulas developed from past studies by Dr Toor and his colleagues that revealed distinct patterns of lymphocyte recovery in HSCT recipients.
Using matrix mathematics to develop the simulations, the researchers observed competition among T cells as the T-cell repertoire develops.
This competition leads to certain families of T cells becoming dominant and more numerous, which crowds out weaker T-cell families, causing them to develop later and in fewer numbers.
“We are attempting to account for the many variables that could impact T-cell repertoire development and, in turn, patient outcomes,” Dr Toor said.
“In future studies, we hope to explore the impact of organ-specific antigen expression. The knowledge gained from this research could potentially allow more accurate predictions of which organs could be most affected by graft-versus-host-disease.” ![]()
Antibody recognizes human plasma cells
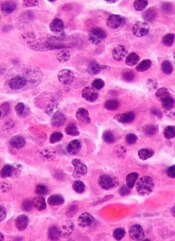
Researchers say they have generated a monoclonal antibody that could have diagnostic and therapeutic applications for multiple myeloma (MM) and other plasma cell disorders.
The team generated this antibody, VLRB MM3, from immunized lampreys, a type of jawless fish.
Experiments with VLRB MM3 showed that it can identify normal plasma cells in samples from healthy donors and malignant plasma cells in samples from patients with MM.
Götz Ehrhardt, PhD, of the University of Toronto in Ontario, Canada, and his colleagues described this work in JCI Insight.
The researchers noted that antibody-secreting plasma cells arise from B-cell precursors and are essential for adaptive immune responses against invading pathogens. Plasma cell dysfunction is associated with autoimmune and neoplastic disorders, including MM.
Surface markers that are specific to plasma cells have not been identified, and antibodies that only recognize these cells have been challenging to generate using conventional systems.
However, Dr Ehrhardt and his colleagues found they could generate a plasma-cell-specific antibody from immunized lampreys.
The researchers injected lamprey larvae with a bone marrow isolate from an MM patient and screened the resulting monoclonal antibodies for those that recognized both malignant and non-malignant plasma cells.
Further characterization of the antibody VLRB MM3 revealed that it is specific to plasma cells and does not recognize other B-cell populations or progenitors.
VLRB MM3 binding was shown to coincide with CD38 dimerization and correlate with and impede the NAD glycohydrolase activity of this glycoprotein.
Considering these findings together, the researchers concluded that VLRB MM3 represents a unique tool that might aid the treatment and diagnosis of plasma cell disorders. ![]()
Researchers say they have generated a monoclonal antibody that could have diagnostic and therapeutic applications for multiple myeloma (MM) and other plasma cell disorders.
The team generated this antibody, VLRB MM3, from immunized lampreys, a type of jawless fish.
Experiments with VLRB MM3 showed that it can identify normal plasma cells in samples from healthy donors and malignant plasma cells in samples from patients with MM.
Götz Ehrhardt, PhD, of the University of Toronto in Ontario, Canada, and his colleagues described this work in JCI Insight.
The researchers noted that antibody-secreting plasma cells arise from B-cell precursors and are essential for adaptive immune responses against invading pathogens. Plasma cell dysfunction is associated with autoimmune and neoplastic disorders, including MM.
Surface markers that are specific to plasma cells have not been identified, and antibodies that only recognize these cells have been challenging to generate using conventional systems.
However, Dr Ehrhardt and his colleagues found they could generate a plasma-cell-specific antibody from immunized lampreys.
The researchers injected lamprey larvae with a bone marrow isolate from an MM patient and screened the resulting monoclonal antibodies for those that recognized both malignant and non-malignant plasma cells.
Further characterization of the antibody VLRB MM3 revealed that it is specific to plasma cells and does not recognize other B-cell populations or progenitors.
VLRB MM3 binding was shown to coincide with CD38 dimerization and correlate with and impede the NAD glycohydrolase activity of this glycoprotein.
Considering these findings together, the researchers concluded that VLRB MM3 represents a unique tool that might aid the treatment and diagnosis of plasma cell disorders. ![]()
Researchers say they have generated a monoclonal antibody that could have diagnostic and therapeutic applications for multiple myeloma (MM) and other plasma cell disorders.
The team generated this antibody, VLRB MM3, from immunized lampreys, a type of jawless fish.
Experiments with VLRB MM3 showed that it can identify normal plasma cells in samples from healthy donors and malignant plasma cells in samples from patients with MM.
Götz Ehrhardt, PhD, of the University of Toronto in Ontario, Canada, and his colleagues described this work in JCI Insight.
The researchers noted that antibody-secreting plasma cells arise from B-cell precursors and are essential for adaptive immune responses against invading pathogens. Plasma cell dysfunction is associated with autoimmune and neoplastic disorders, including MM.
Surface markers that are specific to plasma cells have not been identified, and antibodies that only recognize these cells have been challenging to generate using conventional systems.
However, Dr Ehrhardt and his colleagues found they could generate a plasma-cell-specific antibody from immunized lampreys.
The researchers injected lamprey larvae with a bone marrow isolate from an MM patient and screened the resulting monoclonal antibodies for those that recognized both malignant and non-malignant plasma cells.
Further characterization of the antibody VLRB MM3 revealed that it is specific to plasma cells and does not recognize other B-cell populations or progenitors.
VLRB MM3 binding was shown to coincide with CD38 dimerization and correlate with and impede the NAD glycohydrolase activity of this glycoprotein.
Considering these findings together, the researchers concluded that VLRB MM3 represents a unique tool that might aid the treatment and diagnosis of plasma cell disorders. ![]()
Night of the Living Thrips: An Unusual Outbreak of Thysanoptera Dermatitis
Case Reports
A platoon of 24 US Marines participated in a 1-week outdoor training exercise (February 4–8) at the Marine Corps Training Area Bellows in Oahu, Hawaii. During the last 3 days of training, 15 (62.5%) marines presented to the same primary care provider with what appeared to be diffuse scattered lesions on the face, neck, and dorsal aspect of the hands. All 15 patients reported that they noticed the lesions upon waking up the morning after their second night at the training area. The patients were unable to recollect specific direct arthropod interactions, but they reported the presence of “bugs” in the training area and denied use of any insect repellents, insect nets, or sunscreen. Sleeping arrangements varied from covered vehicles and cots to sleeping bags on the ground, which were laundered independently by each marine and thereby were ruled out as a commonality. The patients denied working with any chemicals or cleansers while in the field. Further questioning of all 15 patients revealed a history of extended contact with live foliage as branches were broken off to build camouflaged sites.
The following week, a second platoon of 20 marines occupied a separate undisturbed portion of the same training area for a similar 1-week training evolution. Manifestation of similar symptoms among members of the second group, who had no contact with the initial 15 patients, supported the likely environmental etiology of the eruptions.
 |
| Figure 1. Numerous well-circumscribed, discrete, pink-red papules diffusely scattered across the face. |
 |
| Figure 2. Papules with classic anemic halos. |
Referral
Two patients from the first group were evaluated at the dermatology clinic at Tripler Army Medical Center (Honolulu, Hawaii) on day 10 of the initial outbreak. Cutaneous examination revealed numerous discrete, pink-red, well-circumscribed, 2- to 4-mm, dome-shaped papules exclusive to exposed areas on the face, neck, and dorsal aspect of the hands (Figures 1 and 2). Anemic halos surrounding the hand papules were noted (Figure 2). A punch biopsy in both patients revealed spongiotic dermatitis with superficial perivascular and interstitial lymphohistiocytic inflammation with eosinophils, suggestive of an arthropod bite (Figure 3). No retained arthropod parts wereidentified. Both patients were treated with triamcinolone ointment twice daily for 7 days with total resolution of the lesions.
Site Survey Results
Five days following the initial presentation of the first outbreak, a daytime site survey of the training area was conducted by a medical entomologist, an environmental health scientist, and a wildlife biologist. Records indicated that prior to the current utilization, the training area had not been used for 9 months. Approximately half of the training area was covered with mixed scrub vegetation and the remainder was clear pavement or sand (clear of vegetation). Feral hogs (Sus scrofa), cats (Felis domesticus), and mongooses (Herpestes javanicus) were observed at the site. Patient interviews and site survey ruled out a number of potential environmental irritants, including contact with fresh or salt water and chemical contaminants in the air or soil.
Because biting insects were suspected as the cause of the eruptions, an overnight entomological survey was conducted 3 weeks after the first outbreak under similar weather conditions and was centered in the area of an Australian pine (Casuarina equisetifolia) forest where most of the marines had slept during training. Mosquitoes (Aedes albopictus and Culex quinquefasciatus) were observed in the area, with an estimated biting rate of 1 to 2 bites per hour. Centipedes (Scolopendra subspinipes) were commonly observed after dark. There was no sign of heavy bird roosting or nesting, which would be a possible source of biting ectoparasites. Other than the Australian pine, notable vegetation present included Christmasberry (Schinus terebinthifolius), koa haole (Leucaena leucocephala), and Chinese banyan (Ficus microcarpa). A survey of the vegetation uncovered no notable insects, and no damage to the leaves of the Chinese banyans, which is typical of thrip infestation, was noted.
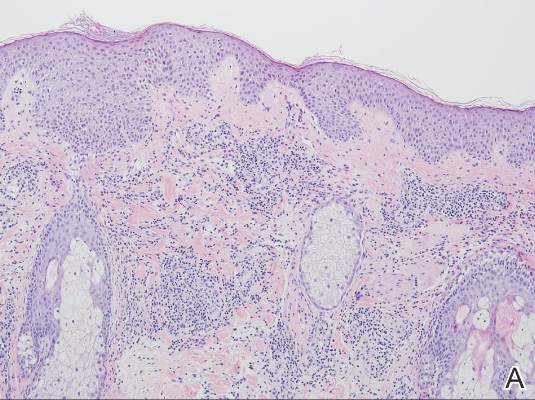 |  |
| Figure 3. Superficial and deep perivascular and interstitial dermatitis (A)(H&E, original magnification ×10) with lymphocytic predominance (B)(H&E, original magnification ×40). | |
After completion of a resource-intensive investigation that included site survey, literature review, detailed patient history including thrips-associated skin manifestations, and thorough consultation with local dermatologists and entomologists, the findings seemingly pointed to thrips as the most likely etiology of the eruption seen in our patients and a diagnosis of Thysanoptera dermatitis was made.
Comment
Thrips are small winged insects in the order Thysanoptera, which comprises more than 5000 identified species ranging in size from 0.5 to 15 mm, though most are approximately 1 mm.1 The insects typically are phytophagous (feeding on plants) and are attracted to humidity and seemingly the sweat of animals and humans.2 Although largely a phytophagous organism, a few published cases of thrips exposure reported papular skin eruptions known as Thysanoptera dermatitis.3-8 Several species of thrips across the globe have been associated with incidental attacks on humans to include “Heliothrips indicus Bagnall, a cotton pest of the Sudan; Thrips imagines Bagnall, reported in Australia; Limothrips cerealium (Haliday), in Germany; Gynaitkothrips uzeli Zimmerman, in Algeria; and other species.”7 In Hawaii, Gynaikothrips ficorum (Cuban laurel thrips) is a common pest of the Chinese banyan tree (F microcarpa) tree.9
A case series reported by Goldstein and Skipworth5 in the late 1960s of military personnel stationed in Oahu described exposure to similar environmental conditions with resultant lesions that were nearly identical to those seen in our patients. The final conclusion of the investigation was that Cuban laurel thrips were the likely etiology, though mites also were considered.5 In a subsequent commentary in 1968, Waisman10 reported similar eruptions in hospitalized patients with further comment regarding the nocturnal occurrence of the bites. Additionally, the eruptions were reported to be short lasting and devoid of discomfort, similar to our patient population.10
Following suit, Aeling6 published a case series in 1974 depicting several service members who presented with symptoms that were nearly identical to the symptoms experienced by our patients as well as those of Goldstein and Skipworth.5 The investigator coined the term hypoanesthetic halos in Hawaii to describe the findings and further reported that Hawaiian dermatologists were familiar with the symptoms and clinical presentation of the disease. Patients in this outbreak had observed small flying insects, similar to the reports from our patients, and postulated that the symptoms occurred secondary to insect bites.6
Since the report by Goldstein and Skipworth5 in 1968, the majority of the literature regarding Thysanoptera dermatitis has largely been in case reports. In 1987, Fishman7 reported the case of a 43-year-old woman who presented with a palm-sized area of grouped red puncta on the lateral neck with the subsequent entrapment and identification of a flower thrips from the patient’s clothing. In 2005, Leigheb et al2 reported the case of a 30-year-old man with an erythematous papular cutaneous eruption on the anterior chest. In this case, the causative etiology was unequivocally confirmed upon identification of the presence of thrips on biopsy.2 In 2006, Guarneri et al1 reported the case of a 59-year-old farmer who had tentatively been diagnosed with delusional parasitosis until persistent presentation to a dermatologist for evaluation enabled the capture and identification of grain thrips. More recently, another case of likely Thysanoptera dermatitis was published in 2012 after a man presented with a slide-mounted thrip from his skin for evaluation as to a potential cause of a recurrent rash he had been experiencing.11 In all of these cases, it was fortunate that a specific organism could be identified for 2 reasons: (1) members of the order Thysanoptera have a biological cycle of only 11 to 36 days, and (2) thrips may go virtually unnoticed by humans, as they are often difficult to see due to their small size.2,12 Perhaps the most extensive report, however, comes from Childers et al8 in a descriptive case series published in 2005. In this report, the investigators provided a thorough detailing of multiple encounters dating back to 1883 through which patients were inadvertently exposed to various species of thrips and subsequently presented with arthropod bites.
Conclusion
The rapid and clustered manner of patient presentation in this case series makes it unique and highlights the need for further consideration of Thysanoptera dermatitis as a potential etiology for an outbreak of a papular eruption. Further reporting may help to better contextualize the true epidemiology of the condition and subsequently may trigger its greater inclusion in the differential diagnosis for a pruritic papular eruption.
Acknowledgments
We would like to extend our appreciation to Amy Spizuoco, DO (New York, New York), for her assistance with the initial diagnosis; Steve Montgomery, PhD (Honolulu, Hawaii), for his assistance with further entomological discussion of potential etiologies; and John R. Gilstad, MD (Honolulu, Hawaii), for contributing his thoughts on the differential diagnosis of the presenting symptoms.
1. Guarneri F, Guarneri C, Mento G, et al. Pseudo‐delusory syndrome caused by Limothrips cerealium. Int J Dermatol. 2006;45:197-199.
2. Leigheb G, Tiberio R, Filosa G, et al. Thysanoptera dermatitis. J Eur Acad Dermatol Venereol. 2005;19:722-724.
3. Williams CB. A blood sucking thrips. The Entomologist. 1921;54:164.
4. Bailey SF. Thrips attacking man. Can Entomol. 1936;68:95-98.
5. Goldstein N, Skipworth GB. Papular eruption secondary to thrips bites. JAMA. 1968;203:53-55.
6. Aeling JL. Hypoanesthetic halos in Hawaii. Cutis. 1974;14:541-544.
7. Fishman HC. Thrips. Arch Dermatol. 1987;123:993.
8. Childers CC, Beshear RJ, Frantz G, et al. A review of thrips species biting man including records in Florida and Georgia between 1986-1997. Florida Entomologist. 2005;88:447-451.
9. Funasaki GY. Studies on the life cycle and propagation technique of Montandoniola moraguesi (Puton)(Heteroptera: Anthocoridae). Proc Hawaii Entomol Soc. 1966;XIX.2:209-211.
10. Waisman M. Thrips bites dermatitis. JAMA. 1968;204:82.
11. Martin J, Richmond A, Davis BM, et al. Thysanoptera dermatitis presenting as folie à deux. Arch Dermatol. 2012;148:864-865.
12. Cooper RG. Dermatitis & conjunctivitis in workers on an ostrich farm following thrips infestation. Indian J Med Res. 2007;125:588-589.
Case Reports
A platoon of 24 US Marines participated in a 1-week outdoor training exercise (February 4–8) at the Marine Corps Training Area Bellows in Oahu, Hawaii. During the last 3 days of training, 15 (62.5%) marines presented to the same primary care provider with what appeared to be diffuse scattered lesions on the face, neck, and dorsal aspect of the hands. All 15 patients reported that they noticed the lesions upon waking up the morning after their second night at the training area. The patients were unable to recollect specific direct arthropod interactions, but they reported the presence of “bugs” in the training area and denied use of any insect repellents, insect nets, or sunscreen. Sleeping arrangements varied from covered vehicles and cots to sleeping bags on the ground, which were laundered independently by each marine and thereby were ruled out as a commonality. The patients denied working with any chemicals or cleansers while in the field. Further questioning of all 15 patients revealed a history of extended contact with live foliage as branches were broken off to build camouflaged sites.
The following week, a second platoon of 20 marines occupied a separate undisturbed portion of the same training area for a similar 1-week training evolution. Manifestation of similar symptoms among members of the second group, who had no contact with the initial 15 patients, supported the likely environmental etiology of the eruptions.
|
| Figure 1. Numerous well-circumscribed, discrete, pink-red papules diffusely scattered across the face. |
|
| Figure 2. Papules with classic anemic halos. |
Referral
Two patients from the first group were evaluated at the dermatology clinic at Tripler Army Medical Center (Honolulu, Hawaii) on day 10 of the initial outbreak. Cutaneous examination revealed numerous discrete, pink-red, well-circumscribed, 2- to 4-mm, dome-shaped papules exclusive to exposed areas on the face, neck, and dorsal aspect of the hands (Figures 1 and 2). Anemic halos surrounding the hand papules were noted (Figure 2). A punch biopsy in both patients revealed spongiotic dermatitis with superficial perivascular and interstitial lymphohistiocytic inflammation with eosinophils, suggestive of an arthropod bite (Figure 3). No retained arthropod parts wereidentified. Both patients were treated with triamcinolone ointment twice daily for 7 days with total resolution of the lesions.
Site Survey Results
Five days following the initial presentation of the first outbreak, a daytime site survey of the training area was conducted by a medical entomologist, an environmental health scientist, and a wildlife biologist. Records indicated that prior to the current utilization, the training area had not been used for 9 months. Approximately half of the training area was covered with mixed scrub vegetation and the remainder was clear pavement or sand (clear of vegetation). Feral hogs (Sus scrofa), cats (Felis domesticus), and mongooses (Herpestes javanicus) were observed at the site. Patient interviews and site survey ruled out a number of potential environmental irritants, including contact with fresh or salt water and chemical contaminants in the air or soil.
Because biting insects were suspected as the cause of the eruptions, an overnight entomological survey was conducted 3 weeks after the first outbreak under similar weather conditions and was centered in the area of an Australian pine (Casuarina equisetifolia) forest where most of the marines had slept during training. Mosquitoes (Aedes albopictus and Culex quinquefasciatus) were observed in the area, with an estimated biting rate of 1 to 2 bites per hour. Centipedes (Scolopendra subspinipes) were commonly observed after dark. There was no sign of heavy bird roosting or nesting, which would be a possible source of biting ectoparasites. Other than the Australian pine, notable vegetation present included Christmasberry (Schinus terebinthifolius), koa haole (Leucaena leucocephala), and Chinese banyan (Ficus microcarpa). A survey of the vegetation uncovered no notable insects, and no damage to the leaves of the Chinese banyans, which is typical of thrip infestation, was noted.
| |
| Figure 3. Superficial and deep perivascular and interstitial dermatitis (A)(H&E, original magnification ×10) with lymphocytic predominance (B)(H&E, original magnification ×40). | |
After completion of a resource-intensive investigation that included site survey, literature review, detailed patient history including thrips-associated skin manifestations, and thorough consultation with local dermatologists and entomologists, the findings seemingly pointed to thrips as the most likely etiology of the eruption seen in our patients and a diagnosis of Thysanoptera dermatitis was made.
Comment
Thrips are small winged insects in the order Thysanoptera, which comprises more than 5000 identified species ranging in size from 0.5 to 15 mm, though most are approximately 1 mm.1 The insects typically are phytophagous (feeding on plants) and are attracted to humidity and seemingly the sweat of animals and humans.2 Although largely a phytophagous organism, a few published cases of thrips exposure reported papular skin eruptions known as Thysanoptera dermatitis.3-8 Several species of thrips across the globe have been associated with incidental attacks on humans to include “Heliothrips indicus Bagnall, a cotton pest of the Sudan; Thrips imagines Bagnall, reported in Australia; Limothrips cerealium (Haliday), in Germany; Gynaitkothrips uzeli Zimmerman, in Algeria; and other species.”7 In Hawaii, Gynaikothrips ficorum (Cuban laurel thrips) is a common pest of the Chinese banyan tree (F microcarpa) tree.9
A case series reported by Goldstein and Skipworth5 in the late 1960s of military personnel stationed in Oahu described exposure to similar environmental conditions with resultant lesions that were nearly identical to those seen in our patients. The final conclusion of the investigation was that Cuban laurel thrips were the likely etiology, though mites also were considered.5 In a subsequent commentary in 1968, Waisman10 reported similar eruptions in hospitalized patients with further comment regarding the nocturnal occurrence of the bites. Additionally, the eruptions were reported to be short lasting and devoid of discomfort, similar to our patient population.10
Following suit, Aeling6 published a case series in 1974 depicting several service members who presented with symptoms that were nearly identical to the symptoms experienced by our patients as well as those of Goldstein and Skipworth.5 The investigator coined the term hypoanesthetic halos in Hawaii to describe the findings and further reported that Hawaiian dermatologists were familiar with the symptoms and clinical presentation of the disease. Patients in this outbreak had observed small flying insects, similar to the reports from our patients, and postulated that the symptoms occurred secondary to insect bites.6
Since the report by Goldstein and Skipworth5 in 1968, the majority of the literature regarding Thysanoptera dermatitis has largely been in case reports. In 1987, Fishman7 reported the case of a 43-year-old woman who presented with a palm-sized area of grouped red puncta on the lateral neck with the subsequent entrapment and identification of a flower thrips from the patient’s clothing. In 2005, Leigheb et al2 reported the case of a 30-year-old man with an erythematous papular cutaneous eruption on the anterior chest. In this case, the causative etiology was unequivocally confirmed upon identification of the presence of thrips on biopsy.2 In 2006, Guarneri et al1 reported the case of a 59-year-old farmer who had tentatively been diagnosed with delusional parasitosis until persistent presentation to a dermatologist for evaluation enabled the capture and identification of grain thrips. More recently, another case of likely Thysanoptera dermatitis was published in 2012 after a man presented with a slide-mounted thrip from his skin for evaluation as to a potential cause of a recurrent rash he had been experiencing.11 In all of these cases, it was fortunate that a specific organism could be identified for 2 reasons: (1) members of the order Thysanoptera have a biological cycle of only 11 to 36 days, and (2) thrips may go virtually unnoticed by humans, as they are often difficult to see due to their small size.2,12 Perhaps the most extensive report, however, comes from Childers et al8 in a descriptive case series published in 2005. In this report, the investigators provided a thorough detailing of multiple encounters dating back to 1883 through which patients were inadvertently exposed to various species of thrips and subsequently presented with arthropod bites.
Conclusion
The rapid and clustered manner of patient presentation in this case series makes it unique and highlights the need for further consideration of Thysanoptera dermatitis as a potential etiology for an outbreak of a papular eruption. Further reporting may help to better contextualize the true epidemiology of the condition and subsequently may trigger its greater inclusion in the differential diagnosis for a pruritic papular eruption.
Acknowledgments
We would like to extend our appreciation to Amy Spizuoco, DO (New York, New York), for her assistance with the initial diagnosis; Steve Montgomery, PhD (Honolulu, Hawaii), for his assistance with further entomological discussion of potential etiologies; and John R. Gilstad, MD (Honolulu, Hawaii), for contributing his thoughts on the differential diagnosis of the presenting symptoms.
Case Reports
A platoon of 24 US Marines participated in a 1-week outdoor training exercise (February 4–8) at the Marine Corps Training Area Bellows in Oahu, Hawaii. During the last 3 days of training, 15 (62.5%) marines presented to the same primary care provider with what appeared to be diffuse scattered lesions on the face, neck, and dorsal aspect of the hands. All 15 patients reported that they noticed the lesions upon waking up the morning after their second night at the training area. The patients were unable to recollect specific direct arthropod interactions, but they reported the presence of “bugs” in the training area and denied use of any insect repellents, insect nets, or sunscreen. Sleeping arrangements varied from covered vehicles and cots to sleeping bags on the ground, which were laundered independently by each marine and thereby were ruled out as a commonality. The patients denied working with any chemicals or cleansers while in the field. Further questioning of all 15 patients revealed a history of extended contact with live foliage as branches were broken off to build camouflaged sites.
The following week, a second platoon of 20 marines occupied a separate undisturbed portion of the same training area for a similar 1-week training evolution. Manifestation of similar symptoms among members of the second group, who had no contact with the initial 15 patients, supported the likely environmental etiology of the eruptions.
|
| Figure 1. Numerous well-circumscribed, discrete, pink-red papules diffusely scattered across the face. |
|
| Figure 2. Papules with classic anemic halos. |
Referral
Two patients from the first group were evaluated at the dermatology clinic at Tripler Army Medical Center (Honolulu, Hawaii) on day 10 of the initial outbreak. Cutaneous examination revealed numerous discrete, pink-red, well-circumscribed, 2- to 4-mm, dome-shaped papules exclusive to exposed areas on the face, neck, and dorsal aspect of the hands (Figures 1 and 2). Anemic halos surrounding the hand papules were noted (Figure 2). A punch biopsy in both patients revealed spongiotic dermatitis with superficial perivascular and interstitial lymphohistiocytic inflammation with eosinophils, suggestive of an arthropod bite (Figure 3). No retained arthropod parts wereidentified. Both patients were treated with triamcinolone ointment twice daily for 7 days with total resolution of the lesions.
Site Survey Results
Five days following the initial presentation of the first outbreak, a daytime site survey of the training area was conducted by a medical entomologist, an environmental health scientist, and a wildlife biologist. Records indicated that prior to the current utilization, the training area had not been used for 9 months. Approximately half of the training area was covered with mixed scrub vegetation and the remainder was clear pavement or sand (clear of vegetation). Feral hogs (Sus scrofa), cats (Felis domesticus), and mongooses (Herpestes javanicus) were observed at the site. Patient interviews and site survey ruled out a number of potential environmental irritants, including contact with fresh or salt water and chemical contaminants in the air or soil.
Because biting insects were suspected as the cause of the eruptions, an overnight entomological survey was conducted 3 weeks after the first outbreak under similar weather conditions and was centered in the area of an Australian pine (Casuarina equisetifolia) forest where most of the marines had slept during training. Mosquitoes (Aedes albopictus and Culex quinquefasciatus) were observed in the area, with an estimated biting rate of 1 to 2 bites per hour. Centipedes (Scolopendra subspinipes) were commonly observed after dark. There was no sign of heavy bird roosting or nesting, which would be a possible source of biting ectoparasites. Other than the Australian pine, notable vegetation present included Christmasberry (Schinus terebinthifolius), koa haole (Leucaena leucocephala), and Chinese banyan (Ficus microcarpa). A survey of the vegetation uncovered no notable insects, and no damage to the leaves of the Chinese banyans, which is typical of thrip infestation, was noted.
| |
| Figure 3. Superficial and deep perivascular and interstitial dermatitis (A)(H&E, original magnification ×10) with lymphocytic predominance (B)(H&E, original magnification ×40). | |
After completion of a resource-intensive investigation that included site survey, literature review, detailed patient history including thrips-associated skin manifestations, and thorough consultation with local dermatologists and entomologists, the findings seemingly pointed to thrips as the most likely etiology of the eruption seen in our patients and a diagnosis of Thysanoptera dermatitis was made.
Comment
Thrips are small winged insects in the order Thysanoptera, which comprises more than 5000 identified species ranging in size from 0.5 to 15 mm, though most are approximately 1 mm.1 The insects typically are phytophagous (feeding on plants) and are attracted to humidity and seemingly the sweat of animals and humans.2 Although largely a phytophagous organism, a few published cases of thrips exposure reported papular skin eruptions known as Thysanoptera dermatitis.3-8 Several species of thrips across the globe have been associated with incidental attacks on humans to include “Heliothrips indicus Bagnall, a cotton pest of the Sudan; Thrips imagines Bagnall, reported in Australia; Limothrips cerealium (Haliday), in Germany; Gynaitkothrips uzeli Zimmerman, in Algeria; and other species.”7 In Hawaii, Gynaikothrips ficorum (Cuban laurel thrips) is a common pest of the Chinese banyan tree (F microcarpa) tree.9
A case series reported by Goldstein and Skipworth5 in the late 1960s of military personnel stationed in Oahu described exposure to similar environmental conditions with resultant lesions that were nearly identical to those seen in our patients. The final conclusion of the investigation was that Cuban laurel thrips were the likely etiology, though mites also were considered.5 In a subsequent commentary in 1968, Waisman10 reported similar eruptions in hospitalized patients with further comment regarding the nocturnal occurrence of the bites. Additionally, the eruptions were reported to be short lasting and devoid of discomfort, similar to our patient population.10
Following suit, Aeling6 published a case series in 1974 depicting several service members who presented with symptoms that were nearly identical to the symptoms experienced by our patients as well as those of Goldstein and Skipworth.5 The investigator coined the term hypoanesthetic halos in Hawaii to describe the findings and further reported that Hawaiian dermatologists were familiar with the symptoms and clinical presentation of the disease. Patients in this outbreak had observed small flying insects, similar to the reports from our patients, and postulated that the symptoms occurred secondary to insect bites.6
Since the report by Goldstein and Skipworth5 in 1968, the majority of the literature regarding Thysanoptera dermatitis has largely been in case reports. In 1987, Fishman7 reported the case of a 43-year-old woman who presented with a palm-sized area of grouped red puncta on the lateral neck with the subsequent entrapment and identification of a flower thrips from the patient’s clothing. In 2005, Leigheb et al2 reported the case of a 30-year-old man with an erythematous papular cutaneous eruption on the anterior chest. In this case, the causative etiology was unequivocally confirmed upon identification of the presence of thrips on biopsy.2 In 2006, Guarneri et al1 reported the case of a 59-year-old farmer who had tentatively been diagnosed with delusional parasitosis until persistent presentation to a dermatologist for evaluation enabled the capture and identification of grain thrips. More recently, another case of likely Thysanoptera dermatitis was published in 2012 after a man presented with a slide-mounted thrip from his skin for evaluation as to a potential cause of a recurrent rash he had been experiencing.11 In all of these cases, it was fortunate that a specific organism could be identified for 2 reasons: (1) members of the order Thysanoptera have a biological cycle of only 11 to 36 days, and (2) thrips may go virtually unnoticed by humans, as they are often difficult to see due to their small size.2,12 Perhaps the most extensive report, however, comes from Childers et al8 in a descriptive case series published in 2005. In this report, the investigators provided a thorough detailing of multiple encounters dating back to 1883 through which patients were inadvertently exposed to various species of thrips and subsequently presented with arthropod bites.
Conclusion
The rapid and clustered manner of patient presentation in this case series makes it unique and highlights the need for further consideration of Thysanoptera dermatitis as a potential etiology for an outbreak of a papular eruption. Further reporting may help to better contextualize the true epidemiology of the condition and subsequently may trigger its greater inclusion in the differential diagnosis for a pruritic papular eruption.
Acknowledgments
We would like to extend our appreciation to Amy Spizuoco, DO (New York, New York), for her assistance with the initial diagnosis; Steve Montgomery, PhD (Honolulu, Hawaii), for his assistance with further entomological discussion of potential etiologies; and John R. Gilstad, MD (Honolulu, Hawaii), for contributing his thoughts on the differential diagnosis of the presenting symptoms.
1. Guarneri F, Guarneri C, Mento G, et al. Pseudo‐delusory syndrome caused by Limothrips cerealium. Int J Dermatol. 2006;45:197-199.
2. Leigheb G, Tiberio R, Filosa G, et al. Thysanoptera dermatitis. J Eur Acad Dermatol Venereol. 2005;19:722-724.
3. Williams CB. A blood sucking thrips. The Entomologist. 1921;54:164.
4. Bailey SF. Thrips attacking man. Can Entomol. 1936;68:95-98.
5. Goldstein N, Skipworth GB. Papular eruption secondary to thrips bites. JAMA. 1968;203:53-55.
6. Aeling JL. Hypoanesthetic halos in Hawaii. Cutis. 1974;14:541-544.
7. Fishman HC. Thrips. Arch Dermatol. 1987;123:993.
8. Childers CC, Beshear RJ, Frantz G, et al. A review of thrips species biting man including records in Florida and Georgia between 1986-1997. Florida Entomologist. 2005;88:447-451.
9. Funasaki GY. Studies on the life cycle and propagation technique of Montandoniola moraguesi (Puton)(Heteroptera: Anthocoridae). Proc Hawaii Entomol Soc. 1966;XIX.2:209-211.
10. Waisman M. Thrips bites dermatitis. JAMA. 1968;204:82.
11. Martin J, Richmond A, Davis BM, et al. Thysanoptera dermatitis presenting as folie à deux. Arch Dermatol. 2012;148:864-865.
12. Cooper RG. Dermatitis & conjunctivitis in workers on an ostrich farm following thrips infestation. Indian J Med Res. 2007;125:588-589.
1. Guarneri F, Guarneri C, Mento G, et al. Pseudo‐delusory syndrome caused by Limothrips cerealium. Int J Dermatol. 2006;45:197-199.
2. Leigheb G, Tiberio R, Filosa G, et al. Thysanoptera dermatitis. J Eur Acad Dermatol Venereol. 2005;19:722-724.
3. Williams CB. A blood sucking thrips. The Entomologist. 1921;54:164.
4. Bailey SF. Thrips attacking man. Can Entomol. 1936;68:95-98.
5. Goldstein N, Skipworth GB. Papular eruption secondary to thrips bites. JAMA. 1968;203:53-55.
6. Aeling JL. Hypoanesthetic halos in Hawaii. Cutis. 1974;14:541-544.
7. Fishman HC. Thrips. Arch Dermatol. 1987;123:993.
8. Childers CC, Beshear RJ, Frantz G, et al. A review of thrips species biting man including records in Florida and Georgia between 1986-1997. Florida Entomologist. 2005;88:447-451.
9. Funasaki GY. Studies on the life cycle and propagation technique of Montandoniola moraguesi (Puton)(Heteroptera: Anthocoridae). Proc Hawaii Entomol Soc. 1966;XIX.2:209-211.
10. Waisman M. Thrips bites dermatitis. JAMA. 1968;204:82.
11. Martin J, Richmond A, Davis BM, et al. Thysanoptera dermatitis presenting as folie à deux. Arch Dermatol. 2012;148:864-865.
12. Cooper RG. Dermatitis & conjunctivitis in workers on an ostrich farm following thrips infestation. Indian J Med Res. 2007;125:588-589.
Practice Points
- Thysanoptera dermatitis presents as a diffuse cutaneous eruption consisting of scattered pruritic papules to exposed skin surfaces.
- The importance of considering the environmental component of a cutaneous eruption via a thorough understanding of local flora and fauna cannot be underestimated.
- The role of a dermatologist in the rapid identification of a cutaneous eruption in the setting of an acute cluster outbreak is of utmost importance to assist with eliminating infectious and environmental public health threats from the differential diagnosis.

Trabectedin found to benefit patients with uterine leiomyosarcoma
SAN DIEGO – Among patients with uterine leiomyosarcoma who underwent prior chemotherapy, treatment with trabectedin resulted in superior disease control, with significantly longer progression-free survival, compared with dacarbazine, a phase III trial showed.
“Trabectedin is an important new treatment option for patients with advanced uterine LMS after anthracycline-containing treatment,” lead study author Dr. Martee L. Hensley said at annual meeting of the Society of Gynecologic Oncology.

Trabectedin, which is marketed by Janssen Products and is also known as ET743, has a novel mechanism of action that “distorts DNA structure resulting in the initiation of DNA repair,” explained Dr. Hensley, a surgical oncologist at Memorial Sloan Kettering Cancer Center, New York. “At the same time it binds and inhibits repair mechanisms, thereby activating apoptosis. In addition, trabectedin inhibits transcriptional activation and can modify the tumor microenvironment.”
ET743-SAR-3007 was the largest randomized, phase III study in soft tissue sarcoma. It found that trabectedin demonstrated a statistically significant improvement in progression-free survival (PFS), compared with dacarbazine (4.2 months vs. 1.5 months; hazard ratio = .55; P less than .001). The results led to FDA approval of trabectedin for the treatment of patients with leiomyosarcoma (LMS) or liposarcoma (LPS), after prior anthracycline therapy. In addition, a previously reported subgroup analysis demonstrated equivalent PFS benefit in patients with either LMS (HR = .56) or LPS HR = .55). However, the majority of that study population (73%) had LMS, and most of those (40%) were uterine LMS. The purpose of the current analysis was the subgroup of patients 232 with uterine LMS who were enrolled in ET743-SAR-3007, which was conducted in 90 sites on four different countries.
Dr. Hensley reported that of the 232 women, 144 were randomized to receive a 24-hour infusion of trabectedin 1.5 mg/m2 every three weeks and 88 to receive a 20- to-120-minute infusion of dacarbazine 1 g/m2 every three weeks. “It’s interesting to note that the vast majority of these patients are enrolling in this study for either a third or fourth-line therapy, and nearly 20% are enrolling for fifth-line therapy for metastatic sarcoma,” she said. The primary endpoint was overall survival, while secondary endpoints were progression-free survival, overall response rate, duration of response, safety, and patient-reported outcomes.
The median number of treatment cycles was four in the trabectedin arm, compared with two in the dacarbazine arm. Nearly 40% of patients in the trabectedin arm received at least six cycles of therapy, compared with 19% in the dacarbazine arm. “There is probably a lack of cumulative toxicity that allows patients that have good disease control to remain trabectedin for a prolonged period of time,” Dr. Hensley said.
The researchers found that in patients with uterine LMS, trabectedin significantly improved progression-free survival, compared with those who received dacarbazine (4.01 months vs. 1.54 months, respectively; HR: .57; P = .0012). “Because progression-free survival can be a soft endpoint, the study was designed to collect radiographic images for central review,” Dr. Hensley said. “That was achieved in 60% of the study population in order to corroborate the PFS endpoint.”
The overall survival benefit observed with trabectedin treatment did not differ from that of dacarbazine (a median of 13.4 months vs. 12.9 months, respectively; HR = .89; P = .5107). Dr. Hensley characterized the overall response rate of both agents as “modest” (11% in the trabectedin arm, vs. 9% in the dacarbazine arm; P = .816).
Median time to response was similar between both arms (about three months) as was median duration of response (about four months for the dacarbazine arm vs. six months for the trabectedin arm). However, she pointed out that those two comparisons were based on a total of 22 patients: seven in the dacarbazine arm and 15 in the trabectedin arm.
Grade 3-4 adverse events such as increased ALT and neutropenia were more common in the trabectedin arm, compared with the dacarbazine arm (69% vs. 42%). There were two treatment-related deaths within 30 days of last dose in the trabectedin arm (1.4%) and no deaths on the dacarbazine arm.
SAN DIEGO – Among patients with uterine leiomyosarcoma who underwent prior chemotherapy, treatment with trabectedin resulted in superior disease control, with significantly longer progression-free survival, compared with dacarbazine, a phase III trial showed.
“Trabectedin is an important new treatment option for patients with advanced uterine LMS after anthracycline-containing treatment,” lead study author Dr. Martee L. Hensley said at annual meeting of the Society of Gynecologic Oncology.
Trabectedin, which is marketed by Janssen Products and is also known as ET743, has a novel mechanism of action that “distorts DNA structure resulting in the initiation of DNA repair,” explained Dr. Hensley, a surgical oncologist at Memorial Sloan Kettering Cancer Center, New York. “At the same time it binds and inhibits repair mechanisms, thereby activating apoptosis. In addition, trabectedin inhibits transcriptional activation and can modify the tumor microenvironment.”
ET743-SAR-3007 was the largest randomized, phase III study in soft tissue sarcoma. It found that trabectedin demonstrated a statistically significant improvement in progression-free survival (PFS), compared with dacarbazine (4.2 months vs. 1.5 months; hazard ratio = .55; P less than .001). The results led to FDA approval of trabectedin for the treatment of patients with leiomyosarcoma (LMS) or liposarcoma (LPS), after prior anthracycline therapy. In addition, a previously reported subgroup analysis demonstrated equivalent PFS benefit in patients with either LMS (HR = .56) or LPS HR = .55). However, the majority of that study population (73%) had LMS, and most of those (40%) were uterine LMS. The purpose of the current analysis was the subgroup of patients 232 with uterine LMS who were enrolled in ET743-SAR-3007, which was conducted in 90 sites on four different countries.
Dr. Hensley reported that of the 232 women, 144 were randomized to receive a 24-hour infusion of trabectedin 1.5 mg/m2 every three weeks and 88 to receive a 20- to-120-minute infusion of dacarbazine 1 g/m2 every three weeks. “It’s interesting to note that the vast majority of these patients are enrolling in this study for either a third or fourth-line therapy, and nearly 20% are enrolling for fifth-line therapy for metastatic sarcoma,” she said. The primary endpoint was overall survival, while secondary endpoints were progression-free survival, overall response rate, duration of response, safety, and patient-reported outcomes.
The median number of treatment cycles was four in the trabectedin arm, compared with two in the dacarbazine arm. Nearly 40% of patients in the trabectedin arm received at least six cycles of therapy, compared with 19% in the dacarbazine arm. “There is probably a lack of cumulative toxicity that allows patients that have good disease control to remain trabectedin for a prolonged period of time,” Dr. Hensley said.
The researchers found that in patients with uterine LMS, trabectedin significantly improved progression-free survival, compared with those who received dacarbazine (4.01 months vs. 1.54 months, respectively; HR: .57; P = .0012). “Because progression-free survival can be a soft endpoint, the study was designed to collect radiographic images for central review,” Dr. Hensley said. “That was achieved in 60% of the study population in order to corroborate the PFS endpoint.”
The overall survival benefit observed with trabectedin treatment did not differ from that of dacarbazine (a median of 13.4 months vs. 12.9 months, respectively; HR = .89; P = .5107). Dr. Hensley characterized the overall response rate of both agents as “modest” (11% in the trabectedin arm, vs. 9% in the dacarbazine arm; P = .816).
Median time to response was similar between both arms (about three months) as was median duration of response (about four months for the dacarbazine arm vs. six months for the trabectedin arm). However, she pointed out that those two comparisons were based on a total of 22 patients: seven in the dacarbazine arm and 15 in the trabectedin arm.
Grade 3-4 adverse events such as increased ALT and neutropenia were more common in the trabectedin arm, compared with the dacarbazine arm (69% vs. 42%). There were two treatment-related deaths within 30 days of last dose in the trabectedin arm (1.4%) and no deaths on the dacarbazine arm.
SAN DIEGO – Among patients with uterine leiomyosarcoma who underwent prior chemotherapy, treatment with trabectedin resulted in superior disease control, with significantly longer progression-free survival, compared with dacarbazine, a phase III trial showed.
“Trabectedin is an important new treatment option for patients with advanced uterine LMS after anthracycline-containing treatment,” lead study author Dr. Martee L. Hensley said at annual meeting of the Society of Gynecologic Oncology.
Trabectedin, which is marketed by Janssen Products and is also known as ET743, has a novel mechanism of action that “distorts DNA structure resulting in the initiation of DNA repair,” explained Dr. Hensley, a surgical oncologist at Memorial Sloan Kettering Cancer Center, New York. “At the same time it binds and inhibits repair mechanisms, thereby activating apoptosis. In addition, trabectedin inhibits transcriptional activation and can modify the tumor microenvironment.”
ET743-SAR-3007 was the largest randomized, phase III study in soft tissue sarcoma. It found that trabectedin demonstrated a statistically significant improvement in progression-free survival (PFS), compared with dacarbazine (4.2 months vs. 1.5 months; hazard ratio = .55; P less than .001). The results led to FDA approval of trabectedin for the treatment of patients with leiomyosarcoma (LMS) or liposarcoma (LPS), after prior anthracycline therapy. In addition, a previously reported subgroup analysis demonstrated equivalent PFS benefit in patients with either LMS (HR = .56) or LPS HR = .55). However, the majority of that study population (73%) had LMS, and most of those (40%) were uterine LMS. The purpose of the current analysis was the subgroup of patients 232 with uterine LMS who were enrolled in ET743-SAR-3007, which was conducted in 90 sites on four different countries.
Dr. Hensley reported that of the 232 women, 144 were randomized to receive a 24-hour infusion of trabectedin 1.5 mg/m2 every three weeks and 88 to receive a 20- to-120-minute infusion of dacarbazine 1 g/m2 every three weeks. “It’s interesting to note that the vast majority of these patients are enrolling in this study for either a third or fourth-line therapy, and nearly 20% are enrolling for fifth-line therapy for metastatic sarcoma,” she said. The primary endpoint was overall survival, while secondary endpoints were progression-free survival, overall response rate, duration of response, safety, and patient-reported outcomes.
The median number of treatment cycles was four in the trabectedin arm, compared with two in the dacarbazine arm. Nearly 40% of patients in the trabectedin arm received at least six cycles of therapy, compared with 19% in the dacarbazine arm. “There is probably a lack of cumulative toxicity that allows patients that have good disease control to remain trabectedin for a prolonged period of time,” Dr. Hensley said.
The researchers found that in patients with uterine LMS, trabectedin significantly improved progression-free survival, compared with those who received dacarbazine (4.01 months vs. 1.54 months, respectively; HR: .57; P = .0012). “Because progression-free survival can be a soft endpoint, the study was designed to collect radiographic images for central review,” Dr. Hensley said. “That was achieved in 60% of the study population in order to corroborate the PFS endpoint.”
The overall survival benefit observed with trabectedin treatment did not differ from that of dacarbazine (a median of 13.4 months vs. 12.9 months, respectively; HR = .89; P = .5107). Dr. Hensley characterized the overall response rate of both agents as “modest” (11% in the trabectedin arm, vs. 9% in the dacarbazine arm; P = .816).
Median time to response was similar between both arms (about three months) as was median duration of response (about four months for the dacarbazine arm vs. six months for the trabectedin arm). However, she pointed out that those two comparisons were based on a total of 22 patients: seven in the dacarbazine arm and 15 in the trabectedin arm.
Grade 3-4 adverse events such as increased ALT and neutropenia were more common in the trabectedin arm, compared with the dacarbazine arm (69% vs. 42%). There were two treatment-related deaths within 30 days of last dose in the trabectedin arm (1.4%) and no deaths on the dacarbazine arm.
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point: Trabectedin is a new treatment option for patients with advanced uterine leiomyosarcoma after anthracycline-containing treatment.
Major finding: In patients with uterine LMS, trabectedin significantly improved progression-free survival, compared with those who received dacarbazine (4.01 months vs. 1.54 months, respectively; HR: .57; P = .0012).
Data source: Results from 144 women who were randomized to receive a 24-hour infusion of trabectedin 1.5 mg/m2 every three weeks, and 88 who received a 20- to-120-minute infusion of dacarbazine 1 g/m2 every three weeks.
Disclosures: Dr. Hensley reported having received consulting and research funding from Janssen Research and Development, LLC. She also disclosed that her spouse is employed by Sanofi.

New SHM Members – April 2016
K. Terrell, MD, Alabama
W. Burt, Arkansas
O. Shill, Arizona
S. Akhtar, MD, California
G. Andonian, California
E. Blecharczy, MD, FAAP, California
P. Febres, MD, California
C. Green, MD, California
C. Ha, California
R. Haile-Meskale, California
M. Hakimipour, MD, California
R. Hanemann, California
S. Khachoyan, California
M. Mahig, MD, California
R. Matson, California
K. McBride, California
M. Miles, BSN, MHA, MS, RN, California
P. Morales, California
J. Tannous, California
N. Aryee Tetteh, California
G. Thompson, California
I. Thomlinson, California
R. Valand, MPH, California
G. L. Wergowske, MD, California
S. Clyne, Colorado
J. Valentin, MD, FACP, Colorado
A. Noonan, APRN, Connecticut
J. Samuel, MD, Connecticut
D. Schillinger, Florida
N. Fobi-Nunga, Georgia
C. Troutman, RN, Georgia
I. Molano, MD, Iowa
Z. Abbas, Illinois
J. Burton, Illinois
F. Chowdhury, Illinois
S. Patel, MD, Illinois
M. Knutson, DO, Indiana
E. Wanas, MD, Indiana
B. E. Bradley, MBChB, Kentucky
T. Jetha, Louisiana
N. Melendez-Rios, MD, Massachusetts
A. Miskiv, Massachusetts
K. Nakashima, MD, Massachusetts
P. Pilegi, ACNP, Massachusetts
E. Shannon, Massachusetts
N. Singh, Massachusetts
R. Thatte, MD, Massachusetts
J. Viola, Massachusetts
J. Bie, CRNP, Maryland
C. Lafeer, Maryland
J. Mignano, Maryland
H. Jarawan, Maine
D. Stein, DO, Maine
S. Franso, MD, Michigan
T. LaBonte, MD, Michigan
D. Malaka, MD, MPH, Michigan
A. Miller, Minnesota
M. Usher, MD, PhD, Minnesota
M. Brinkmeier, MD, Missouri
S. Hassan, Missouri
R. Pitts, MD, Missouri
J. Sorg, MD, Missouri
M. Vaughan, Mississippi
C. Brown, ACMPE, North Carolina
D. Ghiassi, North Carolina
J. Hoffman, North Carolina
C. Norman, MS, PA-C, North Carolina
K. McDonald, MD, Nebraska
Y. Melnikova, MD, New Hampshire
J. Adigun, MD, New Jersey
S. Bhatt, MD, New Jersey
K. Bhavsar, New Jersey
S. Griggs, ANP, New York
G. Jabbour, New York
K. Kang, New York
P. Kayi, MD, New York
C. Lopez, MD, MPH, New York
O. Olafisoye, MD, New York
J. K. Salvani, MD, New York
M. Shinwa, New York
P. Wander, New York
S. Boyle, Ohio
S. Goates, Ohio
A. Hochhausler, MD, Ohio
V. Jayanti, Ohio
D. Kassay, CNP, Ohio
K. Welch, Ohio
J. Retson, CCFP, Ontario
V. Cheng, Pennsylvania
G. Chong, Pennsylvania
J. Hart, MD, Pennsylvania
M. M. Scoulos-Hanson, Pennsylvania
M. Shelkin, DO, Pennsylvania
S. Freeman, Rhode Island
G. Hussain, Rhode Island
R. Ulrich, PA-C, South Carolina
K. Inama, APRN-BC, South Dakota
S. Bray, Saskatchewan
D. E. Adams III, MD, Tennessee
I. Ellis, MD, Tennessee
C. Parrish, Tennessee
K. San, MC, USAR, Tennessee
A. Ahmed, MD, Texas
Z. Conrad, Texas
A. Iqbal, MD, Texas
J. Jamullamudi, MD, Texas
W. Mallot, Texas
C. Okoro, MD, Texas
C. Shy, Texas
P. Vankawala, Texas
L. Walker, Texas
D. Glodowski, MD, Utah
K. Brunson, NP, Virginia
E. Caldwell, Virginia
M. H. Chouindard, MD, Virginia
S. Edwards, MD, Virginia
S. Feldmann, Virginia
D. Kadariya, MBBS, MD, Virginia
J. Lachar, MBBS, MD, Virginia
B. Queen, MD, Virginia
A. M. Shamas, MD, Virginia
A. Wong, MD, Virginia
T. Chang, Washington
E. Gorbacheva, MD, Washington
Z. Li, PA-C, Washington
I. Murray, PA-C, Washington
M. Schaffer, MD, Washington
M. Stolzberg, Washington
K. Miller, MD, Wisconsin
C. Ranheim, MD, Wisconsin
A. Vincent, Wisconsin
J. Yi, DO, West Virginia
K. Han
S. Pannick
Y. Tan
K. Terrell, MD, Alabama
W. Burt, Arkansas
O. Shill, Arizona
S. Akhtar, MD, California
G. Andonian, California
E. Blecharczy, MD, FAAP, California
P. Febres, MD, California
C. Green, MD, California
C. Ha, California
R. Haile-Meskale, California
M. Hakimipour, MD, California
R. Hanemann, California
S. Khachoyan, California
M. Mahig, MD, California
R. Matson, California
K. McBride, California
M. Miles, BSN, MHA, MS, RN, California
P. Morales, California
J. Tannous, California
N. Aryee Tetteh, California
G. Thompson, California
I. Thomlinson, California
R. Valand, MPH, California
G. L. Wergowske, MD, California
S. Clyne, Colorado
J. Valentin, MD, FACP, Colorado
A. Noonan, APRN, Connecticut
J. Samuel, MD, Connecticut
D. Schillinger, Florida
N. Fobi-Nunga, Georgia
C. Troutman, RN, Georgia
I. Molano, MD, Iowa
Z. Abbas, Illinois
J. Burton, Illinois
F. Chowdhury, Illinois
S. Patel, MD, Illinois
M. Knutson, DO, Indiana
E. Wanas, MD, Indiana
B. E. Bradley, MBChB, Kentucky
T. Jetha, Louisiana
N. Melendez-Rios, MD, Massachusetts
A. Miskiv, Massachusetts
K. Nakashima, MD, Massachusetts
P. Pilegi, ACNP, Massachusetts
E. Shannon, Massachusetts
N. Singh, Massachusetts
R. Thatte, MD, Massachusetts
J. Viola, Massachusetts
J. Bie, CRNP, Maryland
C. Lafeer, Maryland
J. Mignano, Maryland
H. Jarawan, Maine
D. Stein, DO, Maine
S. Franso, MD, Michigan
T. LaBonte, MD, Michigan
D. Malaka, MD, MPH, Michigan
A. Miller, Minnesota
M. Usher, MD, PhD, Minnesota
M. Brinkmeier, MD, Missouri
S. Hassan, Missouri
R. Pitts, MD, Missouri
J. Sorg, MD, Missouri
M. Vaughan, Mississippi
C. Brown, ACMPE, North Carolina
D. Ghiassi, North Carolina
J. Hoffman, North Carolina
C. Norman, MS, PA-C, North Carolina
K. McDonald, MD, Nebraska
Y. Melnikova, MD, New Hampshire
J. Adigun, MD, New Jersey
S. Bhatt, MD, New Jersey
K. Bhavsar, New Jersey
S. Griggs, ANP, New York
G. Jabbour, New York
K. Kang, New York
P. Kayi, MD, New York
C. Lopez, MD, MPH, New York
O. Olafisoye, MD, New York
J. K. Salvani, MD, New York
M. Shinwa, New York
P. Wander, New York
S. Boyle, Ohio
S. Goates, Ohio
A. Hochhausler, MD, Ohio
V. Jayanti, Ohio
D. Kassay, CNP, Ohio
K. Welch, Ohio
J. Retson, CCFP, Ontario
V. Cheng, Pennsylvania
G. Chong, Pennsylvania
J. Hart, MD, Pennsylvania
M. M. Scoulos-Hanson, Pennsylvania
M. Shelkin, DO, Pennsylvania
S. Freeman, Rhode Island
G. Hussain, Rhode Island
R. Ulrich, PA-C, South Carolina
K. Inama, APRN-BC, South Dakota
S. Bray, Saskatchewan
D. E. Adams III, MD, Tennessee
I. Ellis, MD, Tennessee
C. Parrish, Tennessee
K. San, MC, USAR, Tennessee
A. Ahmed, MD, Texas
Z. Conrad, Texas
A. Iqbal, MD, Texas
J. Jamullamudi, MD, Texas
W. Mallot, Texas
C. Okoro, MD, Texas
C. Shy, Texas
P. Vankawala, Texas
L. Walker, Texas
D. Glodowski, MD, Utah
K. Brunson, NP, Virginia
E. Caldwell, Virginia
M. H. Chouindard, MD, Virginia
S. Edwards, MD, Virginia
S. Feldmann, Virginia
D. Kadariya, MBBS, MD, Virginia
J. Lachar, MBBS, MD, Virginia
B. Queen, MD, Virginia
A. M. Shamas, MD, Virginia
A. Wong, MD, Virginia
T. Chang, Washington
E. Gorbacheva, MD, Washington
Z. Li, PA-C, Washington
I. Murray, PA-C, Washington
M. Schaffer, MD, Washington
M. Stolzberg, Washington
K. Miller, MD, Wisconsin
C. Ranheim, MD, Wisconsin
A. Vincent, Wisconsin
J. Yi, DO, West Virginia
K. Han
S. Pannick
Y. Tan
K. Terrell, MD, Alabama
W. Burt, Arkansas
O. Shill, Arizona
S. Akhtar, MD, California
G. Andonian, California
E. Blecharczy, MD, FAAP, California
P. Febres, MD, California
C. Green, MD, California
C. Ha, California
R. Haile-Meskale, California
M. Hakimipour, MD, California
R. Hanemann, California
S. Khachoyan, California
M. Mahig, MD, California
R. Matson, California
K. McBride, California
M. Miles, BSN, MHA, MS, RN, California
P. Morales, California
J. Tannous, California
N. Aryee Tetteh, California
G. Thompson, California
I. Thomlinson, California
R. Valand, MPH, California
G. L. Wergowske, MD, California
S. Clyne, Colorado
J. Valentin, MD, FACP, Colorado
A. Noonan, APRN, Connecticut
J. Samuel, MD, Connecticut
D. Schillinger, Florida
N. Fobi-Nunga, Georgia
C. Troutman, RN, Georgia
I. Molano, MD, Iowa
Z. Abbas, Illinois
J. Burton, Illinois
F. Chowdhury, Illinois
S. Patel, MD, Illinois
M. Knutson, DO, Indiana
E. Wanas, MD, Indiana
B. E. Bradley, MBChB, Kentucky
T. Jetha, Louisiana
N. Melendez-Rios, MD, Massachusetts
A. Miskiv, Massachusetts
K. Nakashima, MD, Massachusetts
P. Pilegi, ACNP, Massachusetts
E. Shannon, Massachusetts
N. Singh, Massachusetts
R. Thatte, MD, Massachusetts
J. Viola, Massachusetts
J. Bie, CRNP, Maryland
C. Lafeer, Maryland
J. Mignano, Maryland
H. Jarawan, Maine
D. Stein, DO, Maine
S. Franso, MD, Michigan
T. LaBonte, MD, Michigan
D. Malaka, MD, MPH, Michigan
A. Miller, Minnesota
M. Usher, MD, PhD, Minnesota
M. Brinkmeier, MD, Missouri
S. Hassan, Missouri
R. Pitts, MD, Missouri
J. Sorg, MD, Missouri
M. Vaughan, Mississippi
C. Brown, ACMPE, North Carolina
D. Ghiassi, North Carolina
J. Hoffman, North Carolina
C. Norman, MS, PA-C, North Carolina
K. McDonald, MD, Nebraska
Y. Melnikova, MD, New Hampshire
J. Adigun, MD, New Jersey
S. Bhatt, MD, New Jersey
K. Bhavsar, New Jersey
S. Griggs, ANP, New York
G. Jabbour, New York
K. Kang, New York
P. Kayi, MD, New York
C. Lopez, MD, MPH, New York
O. Olafisoye, MD, New York
J. K. Salvani, MD, New York
M. Shinwa, New York
P. Wander, New York
S. Boyle, Ohio
S. Goates, Ohio
A. Hochhausler, MD, Ohio
V. Jayanti, Ohio
D. Kassay, CNP, Ohio
K. Welch, Ohio
J. Retson, CCFP, Ontario
V. Cheng, Pennsylvania
G. Chong, Pennsylvania
J. Hart, MD, Pennsylvania
M. M. Scoulos-Hanson, Pennsylvania
M. Shelkin, DO, Pennsylvania
S. Freeman, Rhode Island
G. Hussain, Rhode Island
R. Ulrich, PA-C, South Carolina
K. Inama, APRN-BC, South Dakota
S. Bray, Saskatchewan
D. E. Adams III, MD, Tennessee
I. Ellis, MD, Tennessee
C. Parrish, Tennessee
K. San, MC, USAR, Tennessee
A. Ahmed, MD, Texas
Z. Conrad, Texas
A. Iqbal, MD, Texas
J. Jamullamudi, MD, Texas
W. Mallot, Texas
C. Okoro, MD, Texas
C. Shy, Texas
P. Vankawala, Texas
L. Walker, Texas
D. Glodowski, MD, Utah
K. Brunson, NP, Virginia
E. Caldwell, Virginia
M. H. Chouindard, MD, Virginia
S. Edwards, MD, Virginia
S. Feldmann, Virginia
D. Kadariya, MBBS, MD, Virginia
J. Lachar, MBBS, MD, Virginia
B. Queen, MD, Virginia
A. M. Shamas, MD, Virginia
A. Wong, MD, Virginia
T. Chang, Washington
E. Gorbacheva, MD, Washington
Z. Li, PA-C, Washington
I. Murray, PA-C, Washington
M. Schaffer, MD, Washington
M. Stolzberg, Washington
K. Miller, MD, Wisconsin
C. Ranheim, MD, Wisconsin
A. Vincent, Wisconsin
J. Yi, DO, West Virginia
K. Han
S. Pannick
Y. Tan
FDA authorizes new test for Zika virus

Photo by Graham Colm
In response to a request from the US Centers for Disease Control and Prevention (CDC), the US Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for the Trioplex Real-time RT-PCR Assay, a tool that can be used to detect Zika virus.
The assay allows doctors to tell if an individual is infected with chikungunya, dengue, or Zika virus using a single test, instead of having to perform 3 separate tests to identify the infection.
The Trioplex Real-time RT-PCR Assay can be used to detect virus RNA in serum, cerebrospinal fluid, urine, and amniotic fluid specimens.
The CDC hopes this EUA will allow the agency to more rapidly perform testing to detect acute Zika virus infection.
An EUA allows the use of unapproved medical products or unapproved uses of approved medical products in an emergency. The products must be used to diagnose, treat, or prevent serious or life-threatening conditions caused by chemical, biological, radiological, or nuclear threat agents, when there are no adequate alternatives.
The CDC said it will begin distributing the Trioplex Real-time RT-PCR Assay during the next 2 weeks to qualified laboratories in the Laboratory Response Network, an integrated network of domestic and international laboratories that respond to public health emergencies.
The test will not be available in US hospitals or other primary care settings.
Last month, the FDA issued an EUA for a different test used to detect the Zika virus, the Zika IgM Antibody Capture Enzyme-Linked Immunosorbent Assay (Zika MAC-ELISA).
This test was distributed to qualified laboratories in the Laboratory Response Network but was not made available in US hospitals or other primary care settings. ![]()
Photo by Graham Colm
In response to a request from the US Centers for Disease Control and Prevention (CDC), the US Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for the Trioplex Real-time RT-PCR Assay, a tool that can be used to detect Zika virus.
The assay allows doctors to tell if an individual is infected with chikungunya, dengue, or Zika virus using a single test, instead of having to perform 3 separate tests to identify the infection.
The Trioplex Real-time RT-PCR Assay can be used to detect virus RNA in serum, cerebrospinal fluid, urine, and amniotic fluid specimens.
The CDC hopes this EUA will allow the agency to more rapidly perform testing to detect acute Zika virus infection.
An EUA allows the use of unapproved medical products or unapproved uses of approved medical products in an emergency. The products must be used to diagnose, treat, or prevent serious or life-threatening conditions caused by chemical, biological, radiological, or nuclear threat agents, when there are no adequate alternatives.
The CDC said it will begin distributing the Trioplex Real-time RT-PCR Assay during the next 2 weeks to qualified laboratories in the Laboratory Response Network, an integrated network of domestic and international laboratories that respond to public health emergencies.
The test will not be available in US hospitals or other primary care settings.
Last month, the FDA issued an EUA for a different test used to detect the Zika virus, the Zika IgM Antibody Capture Enzyme-Linked Immunosorbent Assay (Zika MAC-ELISA).
This test was distributed to qualified laboratories in the Laboratory Response Network but was not made available in US hospitals or other primary care settings. ![]()
Photo by Graham Colm
In response to a request from the US Centers for Disease Control and Prevention (CDC), the US Food and Drug Administration (FDA) has issued an Emergency Use Authorization (EUA) for the Trioplex Real-time RT-PCR Assay, a tool that can be used to detect Zika virus.
The assay allows doctors to tell if an individual is infected with chikungunya, dengue, or Zika virus using a single test, instead of having to perform 3 separate tests to identify the infection.
The Trioplex Real-time RT-PCR Assay can be used to detect virus RNA in serum, cerebrospinal fluid, urine, and amniotic fluid specimens.
The CDC hopes this EUA will allow the agency to more rapidly perform testing to detect acute Zika virus infection.
An EUA allows the use of unapproved medical products or unapproved uses of approved medical products in an emergency. The products must be used to diagnose, treat, or prevent serious or life-threatening conditions caused by chemical, biological, radiological, or nuclear threat agents, when there are no adequate alternatives.
The CDC said it will begin distributing the Trioplex Real-time RT-PCR Assay during the next 2 weeks to qualified laboratories in the Laboratory Response Network, an integrated network of domestic and international laboratories that respond to public health emergencies.
The test will not be available in US hospitals or other primary care settings.
Last month, the FDA issued an EUA for a different test used to detect the Zika virus, the Zika IgM Antibody Capture Enzyme-Linked Immunosorbent Assay (Zika MAC-ELISA).
This test was distributed to qualified laboratories in the Laboratory Response Network but was not made available in US hospitals or other primary care settings. ![]()
Decline in depression symptoms followed less than standard number of ketamine doses
Ketamine was 80% effective at decreasing depression symptoms, in a study of 100 depression patients who received less frequent and lower total doses of ketamine than are typically administered to treat depression.
Each study participant received no more than one ketamine intravenous infusion per week, with 4.3 having been the average total number of ketamine infusions received by a patient during the study. The frequency with which an infusion was received and the total number of infusions received by a patient were tailored to each patient’s responses to the therapy, according to the study’s author, Dr. Theodore Henderson. This study used a schedule of treatments for patients that differed from the established protocol for ketamine usage as an antidepressant, which is 3 times per week.
Prior to receiving the intravenous ketamine infusions, study participant’s Quick Inventory of Depressive Symptomatology-Self Report (QIDS-SR) score was 17.87 plus or minus 2.8 points, which corresponds to being severely depressed. The QIDS-SR score for each of the 80 study participants who responded to the therapy decreased by 10.8 plus or minus 3.5 points. The QIDS-SR of each of the 20 non-responders to the therapy changed by 0.8 plus or minus 1.8 points.
This study showed “clinical improvement with much fewer infusions for most patients. From a mechanistic standpoint, this can only be possible if ketamine is inducing increased BDNF [brain-derived neurotrophic factor] which leads to lasting changes in synapses, dendrites, and neuronal circuits,” Dr. Henderson said.
The study participants comprised 80 patients with recurrent unipolar depression and 20 patients with recurrent bipolar depression from Neuro-Luminance Ketamine Infusion Centers. Side effects experienced by the patients included elevated blood pressure, nausea, and dizziness, which was very common.
“Further controlled studies of the best clinical methods for ketamine infusion therapy are encouraged.” Dr. Henderson said.
Read the study in Neural Regeneration Research (doi: 10.4103/1673-5374.177708).
Ketamine was 80% effective at decreasing depression symptoms, in a study of 100 depression patients who received less frequent and lower total doses of ketamine than are typically administered to treat depression.
Each study participant received no more than one ketamine intravenous infusion per week, with 4.3 having been the average total number of ketamine infusions received by a patient during the study. The frequency with which an infusion was received and the total number of infusions received by a patient were tailored to each patient’s responses to the therapy, according to the study’s author, Dr. Theodore Henderson. This study used a schedule of treatments for patients that differed from the established protocol for ketamine usage as an antidepressant, which is 3 times per week.
Prior to receiving the intravenous ketamine infusions, study participant’s Quick Inventory of Depressive Symptomatology-Self Report (QIDS-SR) score was 17.87 plus or minus 2.8 points, which corresponds to being severely depressed. The QIDS-SR score for each of the 80 study participants who responded to the therapy decreased by 10.8 plus or minus 3.5 points. The QIDS-SR of each of the 20 non-responders to the therapy changed by 0.8 plus or minus 1.8 points.
This study showed “clinical improvement with much fewer infusions for most patients. From a mechanistic standpoint, this can only be possible if ketamine is inducing increased BDNF [brain-derived neurotrophic factor] which leads to lasting changes in synapses, dendrites, and neuronal circuits,” Dr. Henderson said.
The study participants comprised 80 patients with recurrent unipolar depression and 20 patients with recurrent bipolar depression from Neuro-Luminance Ketamine Infusion Centers. Side effects experienced by the patients included elevated blood pressure, nausea, and dizziness, which was very common.
“Further controlled studies of the best clinical methods for ketamine infusion therapy are encouraged.” Dr. Henderson said.
Read the study in Neural Regeneration Research (doi: 10.4103/1673-5374.177708).
Ketamine was 80% effective at decreasing depression symptoms, in a study of 100 depression patients who received less frequent and lower total doses of ketamine than are typically administered to treat depression.
Each study participant received no more than one ketamine intravenous infusion per week, with 4.3 having been the average total number of ketamine infusions received by a patient during the study. The frequency with which an infusion was received and the total number of infusions received by a patient were tailored to each patient’s responses to the therapy, according to the study’s author, Dr. Theodore Henderson. This study used a schedule of treatments for patients that differed from the established protocol for ketamine usage as an antidepressant, which is 3 times per week.
Prior to receiving the intravenous ketamine infusions, study participant’s Quick Inventory of Depressive Symptomatology-Self Report (QIDS-SR) score was 17.87 plus or minus 2.8 points, which corresponds to being severely depressed. The QIDS-SR score for each of the 80 study participants who responded to the therapy decreased by 10.8 plus or minus 3.5 points. The QIDS-SR of each of the 20 non-responders to the therapy changed by 0.8 plus or minus 1.8 points.
This study showed “clinical improvement with much fewer infusions for most patients. From a mechanistic standpoint, this can only be possible if ketamine is inducing increased BDNF [brain-derived neurotrophic factor] which leads to lasting changes in synapses, dendrites, and neuronal circuits,” Dr. Henderson said.
The study participants comprised 80 patients with recurrent unipolar depression and 20 patients with recurrent bipolar depression from Neuro-Luminance Ketamine Infusion Centers. Side effects experienced by the patients included elevated blood pressure, nausea, and dizziness, which was very common.
“Further controlled studies of the best clinical methods for ketamine infusion therapy are encouraged.” Dr. Henderson said.
Read the study in Neural Regeneration Research (doi: 10.4103/1673-5374.177708).
FROM NEURAL REGENERATION RESEARCH
Getting a leg up on bone comorbidities in lupus
MAUI, HAWAII – Patients with systemic lupus erythematosus (SLE) really need to be placed on bone protection therapy as soon as they start on corticosteroids because their risks of steroid-related osteoporosis and osteonecrosis are so high, Dr. Dafna D. Gladman advised at the 2016 Rheumatology Winter Clinical Symposium.
Investigators for new studies of large cohorts of SLE patients seen at the University of Toronto Lupus Clinic have examined numerous potential predictors of bone comorbidities, but only one independent risk factor emerged: a high cumulative dose of corticosteroids, said Dr. Gladman, professor of medicine and codirector of the clinic.
“The dose of steroids is certainly important. It’s relevant to patient management because we obviously want to try to minimize the amount of steroids that patients with lupus get,” the rheumatologist observed.
The Toronto experience underscores just how common and serious these bone comorbidities are.
Among 1,729 SLE patients in the clinic database, 13.6% developed symptomatic osteonecrosis as defined by clinical symptoms plus positive imaging findings. Overall, 86% were female. The mean age at diagnosis of SLE was 26.6 years, with a mean 8.2-year interval from SLE diagnosis to the first episode of osteonecrosis. The 235 patients with osteonecrosis had a collective 382 affected joints at the time of their first osteonecrosis diagnosis, with an additional 160 joints becoming osteonecrotic later.
Particularly noteworthy was the finding that fully 47% of patients had more than one site involved at the time of their first osteonecrotic event, according to Dr. Gladman.
By far the most frequently affected joints were the hips, followed by knees. Surgery was often required in order to manage the injuries. Indeed, surgery was performed on more than half of osteonecrotic hips, 30% of affected wrists, and 20% of knees.
In a multivariate regression analysis involving 162 SLE patients with osteonecrosis and an equal number of matched controls who had SLE but not osteonecrosis, the only independent predictor of osteonecrosis was a high cumulative dose of corticosteroids; in the osteonecrosis group, it averaged 31 g. Factors that didn’t pan out as predictors included patient age, gender, race, smoking status, current or past use of antimalarial drugs, duration of immunosuppressive therapy, disease severity as reflected by the adjusted mean SLE Disease Activity Index score 3 years prior to osteonecrosis or the last clinic visit, total serum cholesterol, and a history of Raynaud’s, vasculitis, or renal or CNS involvement.
Turning to osteoporosis in SLE patients, Dr. Gladman said that among 286 patients who underwent bone mineral density (BMD) measurement at the time they were first seen in the clinic, 31.5% had an abnormal result. Among the 173 premenopausal females, 17% had a BMD below the lower limit of normal for their age. So did 27% of men below age 50. In postmenopausal women, the prevalences of osteoporosis and osteopenia were 12% and 43%, respectively. One of 10 men over age 50 had osteoporosis, while 8 had low BMD.
Twenty patients had a symptomatic fragility fracture at the time of their BMD test, and, of note, only half of them had an abnormal BMD.
“So the BMD does not actually identify all those patients who are at risk for the adverse outcome of osteoporosis, which will be a fragility fracture,” Dr. Gladman said.
She reported having no financial conflicts of interest regarding her presentation.
MAUI, HAWAII – Patients with systemic lupus erythematosus (SLE) really need to be placed on bone protection therapy as soon as they start on corticosteroids because their risks of steroid-related osteoporosis and osteonecrosis are so high, Dr. Dafna D. Gladman advised at the 2016 Rheumatology Winter Clinical Symposium.
Investigators for new studies of large cohorts of SLE patients seen at the University of Toronto Lupus Clinic have examined numerous potential predictors of bone comorbidities, but only one independent risk factor emerged: a high cumulative dose of corticosteroids, said Dr. Gladman, professor of medicine and codirector of the clinic.
“The dose of steroids is certainly important. It’s relevant to patient management because we obviously want to try to minimize the amount of steroids that patients with lupus get,” the rheumatologist observed.
The Toronto experience underscores just how common and serious these bone comorbidities are.
Among 1,729 SLE patients in the clinic database, 13.6% developed symptomatic osteonecrosis as defined by clinical symptoms plus positive imaging findings. Overall, 86% were female. The mean age at diagnosis of SLE was 26.6 years, with a mean 8.2-year interval from SLE diagnosis to the first episode of osteonecrosis. The 235 patients with osteonecrosis had a collective 382 affected joints at the time of their first osteonecrosis diagnosis, with an additional 160 joints becoming osteonecrotic later.
Particularly noteworthy was the finding that fully 47% of patients had more than one site involved at the time of their first osteonecrotic event, according to Dr. Gladman.
By far the most frequently affected joints were the hips, followed by knees. Surgery was often required in order to manage the injuries. Indeed, surgery was performed on more than half of osteonecrotic hips, 30% of affected wrists, and 20% of knees.
In a multivariate regression analysis involving 162 SLE patients with osteonecrosis and an equal number of matched controls who had SLE but not osteonecrosis, the only independent predictor of osteonecrosis was a high cumulative dose of corticosteroids; in the osteonecrosis group, it averaged 31 g. Factors that didn’t pan out as predictors included patient age, gender, race, smoking status, current or past use of antimalarial drugs, duration of immunosuppressive therapy, disease severity as reflected by the adjusted mean SLE Disease Activity Index score 3 years prior to osteonecrosis or the last clinic visit, total serum cholesterol, and a history of Raynaud’s, vasculitis, or renal or CNS involvement.
Turning to osteoporosis in SLE patients, Dr. Gladman said that among 286 patients who underwent bone mineral density (BMD) measurement at the time they were first seen in the clinic, 31.5% had an abnormal result. Among the 173 premenopausal females, 17% had a BMD below the lower limit of normal for their age. So did 27% of men below age 50. In postmenopausal women, the prevalences of osteoporosis and osteopenia were 12% and 43%, respectively. One of 10 men over age 50 had osteoporosis, while 8 had low BMD.
Twenty patients had a symptomatic fragility fracture at the time of their BMD test, and, of note, only half of them had an abnormal BMD.
“So the BMD does not actually identify all those patients who are at risk for the adverse outcome of osteoporosis, which will be a fragility fracture,” Dr. Gladman said.
She reported having no financial conflicts of interest regarding her presentation.
MAUI, HAWAII – Patients with systemic lupus erythematosus (SLE) really need to be placed on bone protection therapy as soon as they start on corticosteroids because their risks of steroid-related osteoporosis and osteonecrosis are so high, Dr. Dafna D. Gladman advised at the 2016 Rheumatology Winter Clinical Symposium.
Investigators for new studies of large cohorts of SLE patients seen at the University of Toronto Lupus Clinic have examined numerous potential predictors of bone comorbidities, but only one independent risk factor emerged: a high cumulative dose of corticosteroids, said Dr. Gladman, professor of medicine and codirector of the clinic.
“The dose of steroids is certainly important. It’s relevant to patient management because we obviously want to try to minimize the amount of steroids that patients with lupus get,” the rheumatologist observed.
The Toronto experience underscores just how common and serious these bone comorbidities are.
Among 1,729 SLE patients in the clinic database, 13.6% developed symptomatic osteonecrosis as defined by clinical symptoms plus positive imaging findings. Overall, 86% were female. The mean age at diagnosis of SLE was 26.6 years, with a mean 8.2-year interval from SLE diagnosis to the first episode of osteonecrosis. The 235 patients with osteonecrosis had a collective 382 affected joints at the time of their first osteonecrosis diagnosis, with an additional 160 joints becoming osteonecrotic later.
Particularly noteworthy was the finding that fully 47% of patients had more than one site involved at the time of their first osteonecrotic event, according to Dr. Gladman.
By far the most frequently affected joints were the hips, followed by knees. Surgery was often required in order to manage the injuries. Indeed, surgery was performed on more than half of osteonecrotic hips, 30% of affected wrists, and 20% of knees.
In a multivariate regression analysis involving 162 SLE patients with osteonecrosis and an equal number of matched controls who had SLE but not osteonecrosis, the only independent predictor of osteonecrosis was a high cumulative dose of corticosteroids; in the osteonecrosis group, it averaged 31 g. Factors that didn’t pan out as predictors included patient age, gender, race, smoking status, current or past use of antimalarial drugs, duration of immunosuppressive therapy, disease severity as reflected by the adjusted mean SLE Disease Activity Index score 3 years prior to osteonecrosis or the last clinic visit, total serum cholesterol, and a history of Raynaud’s, vasculitis, or renal or CNS involvement.
Turning to osteoporosis in SLE patients, Dr. Gladman said that among 286 patients who underwent bone mineral density (BMD) measurement at the time they were first seen in the clinic, 31.5% had an abnormal result. Among the 173 premenopausal females, 17% had a BMD below the lower limit of normal for their age. So did 27% of men below age 50. In postmenopausal women, the prevalences of osteoporosis and osteopenia were 12% and 43%, respectively. One of 10 men over age 50 had osteoporosis, while 8 had low BMD.
Twenty patients had a symptomatic fragility fracture at the time of their BMD test, and, of note, only half of them had an abnormal BMD.
“So the BMD does not actually identify all those patients who are at risk for the adverse outcome of osteoporosis, which will be a fragility fracture,” Dr. Gladman said.
She reported having no financial conflicts of interest regarding her presentation.
EXPERT ANALYSIS FROM RWCS 2016
FDA rejects ready-to-use bivalirudin formulation

Image by Kevin MacKenzie
The US Food and Drug Administration (FDA) has said it cannot, at present, approve a ready-to-use (RTU) formulation of bivalirudin (Kangio).
The product is a liquid, intravenous formulation of 5 mg/mL of bivalirudin in a 50-mL vial.
It does not require reconstitution before administration.
This RTU bivalirudin is intended for use as an anticoagulant in patients with unstable angina who are undergoing percutaneous transluminal coronary angioplasty.
The drug is also intended for patients undergoing percutaneous coronary intervention (PCI) with provisional use of a glycoprotein IIb/IIIa inhibitor and for patients undergoing PCI who have or are at risk of developing heparin-induced thrombocytopenia and thrombosis syndrome.
The RTU bivalirudin contains the same active ingredient and is designed to be given at the same dose and rate as Angiomax, a lyophilized powder form of bivalirudin that must be reconstituted. The RTU formulation does not require any reconstitution or initial dilution, which is intended to reduce work flow and the risk of dosing errors.
The FDA issued a complete response letter to the company developing the RTU formulation of bivalirudin, Eagle Pharmaceuticals.
The FDA issues complete response letters to communicate that the initial review of an application is complete, but the agency cannot approve the application in its present form and requests additional information.
In its letter to Eagle Pharmaceuticals, the FDA requested further characterization of bivalirudin-related substances in the drug product. The company said it will work directly with the FDA to determine an appropriate path forward to address the comments.
“We are evaluating the FDA’s response and will work closely with the agency to better understand and address their comments regarding Kangio,” said Scott Tarriff, president and chief executive officer of Eagle Pharmaceuticals.
“We remain committed to Kangio as an important new formulation of bivalirudin for intravenous use, offering multiple benefits for patients and caregivers.” ![]()
Image by Kevin MacKenzie
The US Food and Drug Administration (FDA) has said it cannot, at present, approve a ready-to-use (RTU) formulation of bivalirudin (Kangio).
The product is a liquid, intravenous formulation of 5 mg/mL of bivalirudin in a 50-mL vial.
It does not require reconstitution before administration.
This RTU bivalirudin is intended for use as an anticoagulant in patients with unstable angina who are undergoing percutaneous transluminal coronary angioplasty.
The drug is also intended for patients undergoing percutaneous coronary intervention (PCI) with provisional use of a glycoprotein IIb/IIIa inhibitor and for patients undergoing PCI who have or are at risk of developing heparin-induced thrombocytopenia and thrombosis syndrome.
The RTU bivalirudin contains the same active ingredient and is designed to be given at the same dose and rate as Angiomax, a lyophilized powder form of bivalirudin that must be reconstituted. The RTU formulation does not require any reconstitution or initial dilution, which is intended to reduce work flow and the risk of dosing errors.
The FDA issued a complete response letter to the company developing the RTU formulation of bivalirudin, Eagle Pharmaceuticals.
The FDA issues complete response letters to communicate that the initial review of an application is complete, but the agency cannot approve the application in its present form and requests additional information.
In its letter to Eagle Pharmaceuticals, the FDA requested further characterization of bivalirudin-related substances in the drug product. The company said it will work directly with the FDA to determine an appropriate path forward to address the comments.
“We are evaluating the FDA’s response and will work closely with the agency to better understand and address their comments regarding Kangio,” said Scott Tarriff, president and chief executive officer of Eagle Pharmaceuticals.
“We remain committed to Kangio as an important new formulation of bivalirudin for intravenous use, offering multiple benefits for patients and caregivers.” ![]()
Image by Kevin MacKenzie
The US Food and Drug Administration (FDA) has said it cannot, at present, approve a ready-to-use (RTU) formulation of bivalirudin (Kangio).
The product is a liquid, intravenous formulation of 5 mg/mL of bivalirudin in a 50-mL vial.
It does not require reconstitution before administration.
This RTU bivalirudin is intended for use as an anticoagulant in patients with unstable angina who are undergoing percutaneous transluminal coronary angioplasty.
The drug is also intended for patients undergoing percutaneous coronary intervention (PCI) with provisional use of a glycoprotein IIb/IIIa inhibitor and for patients undergoing PCI who have or are at risk of developing heparin-induced thrombocytopenia and thrombosis syndrome.
The RTU bivalirudin contains the same active ingredient and is designed to be given at the same dose and rate as Angiomax, a lyophilized powder form of bivalirudin that must be reconstituted. The RTU formulation does not require any reconstitution or initial dilution, which is intended to reduce work flow and the risk of dosing errors.
The FDA issued a complete response letter to the company developing the RTU formulation of bivalirudin, Eagle Pharmaceuticals.
The FDA issues complete response letters to communicate that the initial review of an application is complete, but the agency cannot approve the application in its present form and requests additional information.
In its letter to Eagle Pharmaceuticals, the FDA requested further characterization of bivalirudin-related substances in the drug product. The company said it will work directly with the FDA to determine an appropriate path forward to address the comments.
“We are evaluating the FDA’s response and will work closely with the agency to better understand and address their comments regarding Kangio,” said Scott Tarriff, president and chief executive officer of Eagle Pharmaceuticals.
“We remain committed to Kangio as an important new formulation of bivalirudin for intravenous use, offering multiple benefits for patients and caregivers.” ![]()