User login
Are You Ready to Work?
Physicians generally have little experience hunting for jobs. After more than a decade of education and training, graduating residents are in their late 20s—or older—when they begin searching for full-time work, and many struggle with the transition. The following seasonal tips will help you find your first hospitalist job. For more details, check out The Hospitalist's “Resident’s Corner.”
July-September
- Choose a mentor. Find an experienced hospitalist who can provide valuable feedback during your job search.
- Choose your senior-year electives carefully. Focus on areas of weakness, or areas that are pertinent to HM (e.g., infectious disease, cardiology, neurology, critical-care medicine).
- Create or update your curriculum vitae and cover letter. Edit your words carefully; spelling errors or typos in documents are costly.
- • Request letters of recommendation. Think hard about who you want before asking for a letter, as these typically carry a lot of weight in the interview selection process. Although program directors, chiefs of medicine, and hospitalists can be good choices, it is important to choose people who know you well, as they tend to generate a more personal and powerful letter.
October-December
- Start your job search by applying for desired positions. Hospitalists are in high demand; check out these sites for openings: SHM’s Career Center; classified ad sections in the Journal of Hospital Medicine; general medicine journals and The Hospitalist; and hospitals and HM groups of interest. Even if they are not advertising, contact them personally.
- Research potential employers. Prepare appropriate interview questions.
- Bring extra copies of your updated CV and look sharp. Shine your shoes. Is it time to replace the suit you used to apply for residency?
- Send a thank-you note or e-mail to the person(s) you interviewed with.
January-March
- When you receive an offer, it’s time to review the contract and negotiate terms. Don’t hesitate to ask for clarification of unclear points. You might want to have a lawyer review the contract.
- Register for your board examination.
- Apply for state medical licensure. This process varies by state, but it can take several months to complete, especially if you are applying in a state other than where you trained.
- Apply for hospital credentials.
April-June
- Moving to a different city or state can be exciting—and stressful. Talk to your new co-workers to get a feel for the city and recommendations for places to live. Some employers are very helpful with a move; some provide new hires with a real estate agent. Moving expenses often are covered as a condition of employment, but it depends on your contract.
- Consider taking a vacation to either further explore relocation options or to simply relax. You might need time to unwind as your residency concludes. Some future hospitalists like to use this time to intensify their board review; others cringe at the thought.
Dr. Grant is a hospitalist at the University of Michigan Health System in Ann Arbor. Dr. Warren-Marzola is a hospitalist at St. Luke’s Hospital in Toledo, Ohio. Both are members of SHM’s Young Physicians Committee.
Physicians generally have little experience hunting for jobs. After more than a decade of education and training, graduating residents are in their late 20s—or older—when they begin searching for full-time work, and many struggle with the transition. The following seasonal tips will help you find your first hospitalist job. For more details, check out The Hospitalist's “Resident’s Corner.”
July-September
- Choose a mentor. Find an experienced hospitalist who can provide valuable feedback during your job search.
- Choose your senior-year electives carefully. Focus on areas of weakness, or areas that are pertinent to HM (e.g., infectious disease, cardiology, neurology, critical-care medicine).
- Create or update your curriculum vitae and cover letter. Edit your words carefully; spelling errors or typos in documents are costly.
- • Request letters of recommendation. Think hard about who you want before asking for a letter, as these typically carry a lot of weight in the interview selection process. Although program directors, chiefs of medicine, and hospitalists can be good choices, it is important to choose people who know you well, as they tend to generate a more personal and powerful letter.
October-December
- Start your job search by applying for desired positions. Hospitalists are in high demand; check out these sites for openings: SHM’s Career Center; classified ad sections in the Journal of Hospital Medicine; general medicine journals and The Hospitalist; and hospitals and HM groups of interest. Even if they are not advertising, contact them personally.
- Research potential employers. Prepare appropriate interview questions.
- Bring extra copies of your updated CV and look sharp. Shine your shoes. Is it time to replace the suit you used to apply for residency?
- Send a thank-you note or e-mail to the person(s) you interviewed with.
January-March
- When you receive an offer, it’s time to review the contract and negotiate terms. Don’t hesitate to ask for clarification of unclear points. You might want to have a lawyer review the contract.
- Register for your board examination.
- Apply for state medical licensure. This process varies by state, but it can take several months to complete, especially if you are applying in a state other than where you trained.
- Apply for hospital credentials.
April-June
- Moving to a different city or state can be exciting—and stressful. Talk to your new co-workers to get a feel for the city and recommendations for places to live. Some employers are very helpful with a move; some provide new hires with a real estate agent. Moving expenses often are covered as a condition of employment, but it depends on your contract.
- Consider taking a vacation to either further explore relocation options or to simply relax. You might need time to unwind as your residency concludes. Some future hospitalists like to use this time to intensify their board review; others cringe at the thought.
Dr. Grant is a hospitalist at the University of Michigan Health System in Ann Arbor. Dr. Warren-Marzola is a hospitalist at St. Luke’s Hospital in Toledo, Ohio. Both are members of SHM’s Young Physicians Committee.
Physicians generally have little experience hunting for jobs. After more than a decade of education and training, graduating residents are in their late 20s—or older—when they begin searching for full-time work, and many struggle with the transition. The following seasonal tips will help you find your first hospitalist job. For more details, check out The Hospitalist's “Resident’s Corner.”
July-September
- Choose a mentor. Find an experienced hospitalist who can provide valuable feedback during your job search.
- Choose your senior-year electives carefully. Focus on areas of weakness, or areas that are pertinent to HM (e.g., infectious disease, cardiology, neurology, critical-care medicine).
- Create or update your curriculum vitae and cover letter. Edit your words carefully; spelling errors or typos in documents are costly.
- • Request letters of recommendation. Think hard about who you want before asking for a letter, as these typically carry a lot of weight in the interview selection process. Although program directors, chiefs of medicine, and hospitalists can be good choices, it is important to choose people who know you well, as they tend to generate a more personal and powerful letter.
October-December
- Start your job search by applying for desired positions. Hospitalists are in high demand; check out these sites for openings: SHM’s Career Center; classified ad sections in the Journal of Hospital Medicine; general medicine journals and The Hospitalist; and hospitals and HM groups of interest. Even if they are not advertising, contact them personally.
- Research potential employers. Prepare appropriate interview questions.
- Bring extra copies of your updated CV and look sharp. Shine your shoes. Is it time to replace the suit you used to apply for residency?
- Send a thank-you note or e-mail to the person(s) you interviewed with.
January-March
- When you receive an offer, it’s time to review the contract and negotiate terms. Don’t hesitate to ask for clarification of unclear points. You might want to have a lawyer review the contract.
- Register for your board examination.
- Apply for state medical licensure. This process varies by state, but it can take several months to complete, especially if you are applying in a state other than where you trained.
- Apply for hospital credentials.
April-June
- Moving to a different city or state can be exciting—and stressful. Talk to your new co-workers to get a feel for the city and recommendations for places to live. Some employers are very helpful with a move; some provide new hires with a real estate agent. Moving expenses often are covered as a condition of employment, but it depends on your contract.
- Consider taking a vacation to either further explore relocation options or to simply relax. You might need time to unwind as your residency concludes. Some future hospitalists like to use this time to intensify their board review; others cringe at the thought.
Dr. Grant is a hospitalist at the University of Michigan Health System in Ann Arbor. Dr. Warren-Marzola is a hospitalist at St. Luke’s Hospital in Toledo, Ohio. Both are members of SHM’s Young Physicians Committee.
Hospitals Look to Future with White House Deal
The 10-year, $155 billion revenue cut that the nation's hospitals agreed to this summer to help President Obama push his healthcare reform package through has elicited mixed reactions as stakeholders debate whether reimbursement cuts in the short term will pay off in the long run. And while some hospitalists worry that hospitals might cut support to HM groups, the head of the American Hospital Association (AHA) says the deal was a smart move—one that creates an opportunity for hospitalists to further prove their worth.
Rich Umbdenstock, FACHE, president and CEO of the AHA, says some estimates had hospitals absorbing north of $300 billion in cuts from Medicare reimbursement. “We think that overall, although they are significant reductions, they’re not nearly as onerous or as far-reaching as what the president and the House were proposing,” Umbdenstock says. “As tough as it will be for all of us to navigate this, we believe we have limited the impact to a manageable amount.”
Managing that deficit is an area in which HM leaders can help their respective institutions, Umbdenstock adds.
More than 90% of HM groups receive hospital support from their institutions, according to SHM’s 2007-2008 "Bi-Annual Survey on the State of the Hospital Medicine Movement." “It’s a reality that has some HM groups nervous that the cuts will reduce hospital subsidies. When this money disappears, hospitals are going to have to make some very difficult decisions,” says hospitalist Marc Westle, DO, FACP, CPE, president and managing partner of Asheville Hospital Group in North Carolina. “Something will have to give.”
Umbdenstock sees opportunity in the challenge. And while acknowledging that QI won’t be an HM-centric concern in the coming years, SHM and rank-and-file hospitalists can lead the charge. “We’ve got to get better at understanding what gives us the best positive impact, the best return on information,” Umbdenstock says. “Given the role hospitalists play, they’ll be an increasingly important constituency to further the understanding of where those efficiencies … can be found. They’re on our front lines.”
The White House and hospital groups agreed to $103 billion in savings from delayed increases in Medicare payments, $50 billion from cutting charity care compensation, and $2 billion from readmission rates. Healthcare economists already have argued that the agreement will have less impact than some fear. Mark Pauly, PhD, professor of healthcare management at The Wharton School at the University of Pennsylvania, says hospitals operating on thin margins might suffer from upfront costs, but are likely to profit more when health insurance creates more “paying customers in the long run.”
The 10-year, $155 billion revenue cut that the nation's hospitals agreed to this summer to help President Obama push his healthcare reform package through has elicited mixed reactions as stakeholders debate whether reimbursement cuts in the short term will pay off in the long run. And while some hospitalists worry that hospitals might cut support to HM groups, the head of the American Hospital Association (AHA) says the deal was a smart move—one that creates an opportunity for hospitalists to further prove their worth.
Rich Umbdenstock, FACHE, president and CEO of the AHA, says some estimates had hospitals absorbing north of $300 billion in cuts from Medicare reimbursement. “We think that overall, although they are significant reductions, they’re not nearly as onerous or as far-reaching as what the president and the House were proposing,” Umbdenstock says. “As tough as it will be for all of us to navigate this, we believe we have limited the impact to a manageable amount.”
Managing that deficit is an area in which HM leaders can help their respective institutions, Umbdenstock adds.
More than 90% of HM groups receive hospital support from their institutions, according to SHM’s 2007-2008 "Bi-Annual Survey on the State of the Hospital Medicine Movement." “It’s a reality that has some HM groups nervous that the cuts will reduce hospital subsidies. When this money disappears, hospitals are going to have to make some very difficult decisions,” says hospitalist Marc Westle, DO, FACP, CPE, president and managing partner of Asheville Hospital Group in North Carolina. “Something will have to give.”
Umbdenstock sees opportunity in the challenge. And while acknowledging that QI won’t be an HM-centric concern in the coming years, SHM and rank-and-file hospitalists can lead the charge. “We’ve got to get better at understanding what gives us the best positive impact, the best return on information,” Umbdenstock says. “Given the role hospitalists play, they’ll be an increasingly important constituency to further the understanding of where those efficiencies … can be found. They’re on our front lines.”
The White House and hospital groups agreed to $103 billion in savings from delayed increases in Medicare payments, $50 billion from cutting charity care compensation, and $2 billion from readmission rates. Healthcare economists already have argued that the agreement will have less impact than some fear. Mark Pauly, PhD, professor of healthcare management at The Wharton School at the University of Pennsylvania, says hospitals operating on thin margins might suffer from upfront costs, but are likely to profit more when health insurance creates more “paying customers in the long run.”
The 10-year, $155 billion revenue cut that the nation's hospitals agreed to this summer to help President Obama push his healthcare reform package through has elicited mixed reactions as stakeholders debate whether reimbursement cuts in the short term will pay off in the long run. And while some hospitalists worry that hospitals might cut support to HM groups, the head of the American Hospital Association (AHA) says the deal was a smart move—one that creates an opportunity for hospitalists to further prove their worth.
Rich Umbdenstock, FACHE, president and CEO of the AHA, says some estimates had hospitals absorbing north of $300 billion in cuts from Medicare reimbursement. “We think that overall, although they are significant reductions, they’re not nearly as onerous or as far-reaching as what the president and the House were proposing,” Umbdenstock says. “As tough as it will be for all of us to navigate this, we believe we have limited the impact to a manageable amount.”
Managing that deficit is an area in which HM leaders can help their respective institutions, Umbdenstock adds.
More than 90% of HM groups receive hospital support from their institutions, according to SHM’s 2007-2008 "Bi-Annual Survey on the State of the Hospital Medicine Movement." “It’s a reality that has some HM groups nervous that the cuts will reduce hospital subsidies. When this money disappears, hospitals are going to have to make some very difficult decisions,” says hospitalist Marc Westle, DO, FACP, CPE, president and managing partner of Asheville Hospital Group in North Carolina. “Something will have to give.”
Umbdenstock sees opportunity in the challenge. And while acknowledging that QI won’t be an HM-centric concern in the coming years, SHM and rank-and-file hospitalists can lead the charge. “We’ve got to get better at understanding what gives us the best positive impact, the best return on information,” Umbdenstock says. “Given the role hospitalists play, they’ll be an increasingly important constituency to further the understanding of where those efficiencies … can be found. They’re on our front lines.”
The White House and hospital groups agreed to $103 billion in savings from delayed increases in Medicare payments, $50 billion from cutting charity care compensation, and $2 billion from readmission rates. Healthcare economists already have argued that the agreement will have less impact than some fear. Mark Pauly, PhD, professor of healthcare management at The Wharton School at the University of Pennsylvania, says hospitals operating on thin margins might suffer from upfront costs, but are likely to profit more when health insurance creates more “paying customers in the long run.”
Dirty Laundry?
You do it hundreds of times a year: After a long day of rounds and face-to-face encounters with patients, you walk back to your office and hang up your lab coat. But should you put the same lab coat on tomorrow?
Maybe not, according to the American Medical Association (AMA), which sponsored a discussion forum last month on whether lab coats and certain articles of clothing should be banned to help prevent the spread of methicillin-resistant Staphylococcus aureus and clostridium difficile. The discussion comes two years after the British National Health System instituted a policy banning neckties, white coats, and long sleeves because of the clothing’s potential to spread hospital-acquired infections. The Centers for Disease Control and Prevention estimates more than 2 million Americans contract hospital-acquired infections every year; more than 5% of those cases result in death.
But is the risk for real?
Armando Paez, MD, a hospitalist and infectious-disease specialist at Tufts University’s School of Medicine in Boston, says there is little evidence to show clothing can help spread disease. Nevertheless, he says hospitals should consider laundry policies as a precautionary measure. “Short sleeves are good because you can wash your hands and forearms from patient to patient,” Dr. Paez says. “You can’t do that with the sleeve of a lab coat. … Unless they run a study to compare physicians not wearing white coats versus the ones who do, we will never know. But there are a lot of variables that would need to be controlled to run that experiment.”
Erik DeLue, MD, MBA, FHM, a medical director of the hospitalist program at Virtua Memorial Hospital in Mount Holly, N.J., sees hospitalists adopting scrubs in the future because they are easier to clean and maintain. “We give everyone three lab coats and I know that people aren’t washing them,” he says. “People wash their shirts every day; why do they wash their lab coats once or twice a week?”
Both hospitalists acknowledge that a physician in a lab coat is iconic and beneficial to the healthcare profession. Dr. Paez says his geriatric patients are especially receptive to professional dress. “Traditionally, the white coat still has a large effect on the patient’s mind,” he says.
That said, if the AMA decides to hang up the lab coats, both doctors say their services would follow the guidelines. “While we don’t have great evidence, it’s just common sense,” Dr. DeLue says.
You do it hundreds of times a year: After a long day of rounds and face-to-face encounters with patients, you walk back to your office and hang up your lab coat. But should you put the same lab coat on tomorrow?
Maybe not, according to the American Medical Association (AMA), which sponsored a discussion forum last month on whether lab coats and certain articles of clothing should be banned to help prevent the spread of methicillin-resistant Staphylococcus aureus and clostridium difficile. The discussion comes two years after the British National Health System instituted a policy banning neckties, white coats, and long sleeves because of the clothing’s potential to spread hospital-acquired infections. The Centers for Disease Control and Prevention estimates more than 2 million Americans contract hospital-acquired infections every year; more than 5% of those cases result in death.
But is the risk for real?
Armando Paez, MD, a hospitalist and infectious-disease specialist at Tufts University’s School of Medicine in Boston, says there is little evidence to show clothing can help spread disease. Nevertheless, he says hospitals should consider laundry policies as a precautionary measure. “Short sleeves are good because you can wash your hands and forearms from patient to patient,” Dr. Paez says. “You can’t do that with the sleeve of a lab coat. … Unless they run a study to compare physicians not wearing white coats versus the ones who do, we will never know. But there are a lot of variables that would need to be controlled to run that experiment.”
Erik DeLue, MD, MBA, FHM, a medical director of the hospitalist program at Virtua Memorial Hospital in Mount Holly, N.J., sees hospitalists adopting scrubs in the future because they are easier to clean and maintain. “We give everyone three lab coats and I know that people aren’t washing them,” he says. “People wash their shirts every day; why do they wash their lab coats once or twice a week?”
Both hospitalists acknowledge that a physician in a lab coat is iconic and beneficial to the healthcare profession. Dr. Paez says his geriatric patients are especially receptive to professional dress. “Traditionally, the white coat still has a large effect on the patient’s mind,” he says.
That said, if the AMA decides to hang up the lab coats, both doctors say their services would follow the guidelines. “While we don’t have great evidence, it’s just common sense,” Dr. DeLue says.
You do it hundreds of times a year: After a long day of rounds and face-to-face encounters with patients, you walk back to your office and hang up your lab coat. But should you put the same lab coat on tomorrow?
Maybe not, according to the American Medical Association (AMA), which sponsored a discussion forum last month on whether lab coats and certain articles of clothing should be banned to help prevent the spread of methicillin-resistant Staphylococcus aureus and clostridium difficile. The discussion comes two years after the British National Health System instituted a policy banning neckties, white coats, and long sleeves because of the clothing’s potential to spread hospital-acquired infections. The Centers for Disease Control and Prevention estimates more than 2 million Americans contract hospital-acquired infections every year; more than 5% of those cases result in death.
But is the risk for real?
Armando Paez, MD, a hospitalist and infectious-disease specialist at Tufts University’s School of Medicine in Boston, says there is little evidence to show clothing can help spread disease. Nevertheless, he says hospitals should consider laundry policies as a precautionary measure. “Short sleeves are good because you can wash your hands and forearms from patient to patient,” Dr. Paez says. “You can’t do that with the sleeve of a lab coat. … Unless they run a study to compare physicians not wearing white coats versus the ones who do, we will never know. But there are a lot of variables that would need to be controlled to run that experiment.”
Erik DeLue, MD, MBA, FHM, a medical director of the hospitalist program at Virtua Memorial Hospital in Mount Holly, N.J., sees hospitalists adopting scrubs in the future because they are easier to clean and maintain. “We give everyone three lab coats and I know that people aren’t washing them,” he says. “People wash their shirts every day; why do they wash their lab coats once or twice a week?”
Both hospitalists acknowledge that a physician in a lab coat is iconic and beneficial to the healthcare profession. Dr. Paez says his geriatric patients are especially receptive to professional dress. “Traditionally, the white coat still has a large effect on the patient’s mind,” he says.
That said, if the AMA decides to hang up the lab coats, both doctors say their services would follow the guidelines. “While we don’t have great evidence, it’s just common sense,” Dr. DeLue says.
Nice to Meet You
Susan Connelly of Fruitland Park, Fla., is a volunteer at her local community hospital who until recently had never heard of a hospitalist. One day, she entered a hospital room and, as she regularly did with patients she visited, asked if there was anything the man in the bed needed.
“I want to know where my doctor is,” the patient said.
“You mean your doctor hasn’t seen you?” Connelly asked.
“No,” he said. “I’m not even sure he knows I’m here.”
Somewhat incredulous, Connelly retrieved the hospital’s physician handbook and helped the patient look up his physician’s phone number. “I didn’t think too much about it,” she says. But the following week, when she appeared at the hospital to volunteer, a supervisor called her into the office. The supervisor asked Connelly about the incident and gently admonished her for encouraging the patient to call his primary-care physician (PCP), as “a hospitalist is working with him now.”
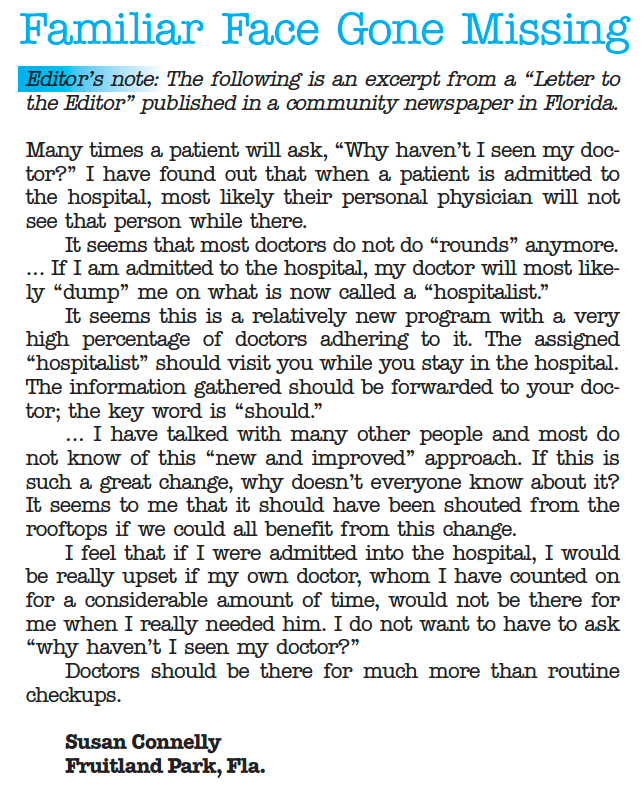
“A what? I had never even heard the term,” Connelly says. She asked her fellow volunteers, known as patient representatives at her hospital, if they had ever heard of a hospitalist. One had, but only because her husband had been admitted for a hospital stay. Concerned, Connelly wrote letters to the editors of two local newspapers. Both were published (see Figure 2, “Familiar Face Gone Missing,” p. 30).
—Robert Centor, MD, associate dean of medicine, University of Alabama at Birmingham
“If I am admitted to the hospital, my doctor will most likely ‘dump’ me on what is now called a ‘hospitalist,’ ” she wrote. “Information gathered [by the hospitalist] should be forwarded to your doctor; the key word is ‘should.’ Why develop this long-term relationship with a doctor, if when you really need him, he is not there for you and you are dealing with a stranger?”
Why indeed?
It might not happen with every new admission, but patient fears are a reality. The uncertainty of a hospital stay, a new physician, and new medications can take their toll on the human psyche. Patients are upset with their PCP, the hospital, the system; many times it’s the hospitalist who feels the brunt of their anger. Not only do hospitalists have to calm a patient worried about PCP disconnect, but they also have to reassure the patient that they will be attentive to their needs, provide a high quality of care during the hospital stay, and communicate with their PCP about diagnoses, medications, and follow-up care. Hospitalists should weave in some of the documented plusses a hospitalist brings to the table: shorter length of stays, greater patient access and availability, and improved quality of care.
Although some patients might view hospitalists as “strangers,” HM physicians can learn methods to ease patient anxiety and answer tough questions from patients about the role they play in hospital care.
Restore Confidence
Simple conversations can help hospitalists defuse patient dissatisfaction. When a patient asks why their PCP won’t be seeing them in the hospital, it’s best to begin with a reassuring approach. For example, introduce yourself and say you have reviewed the case with their PCP. You can include key information from their medical history and recent hospitalizations, if appropriate.
Robert Centor, MD, a hospitalist and associate dean of medicine at the University of Alabama at Birmingham, suggests a few other key behaviors for initial patient visits. He finds a way to make appropriate physical contact by taking a pulse, checking the heart and lungs, or patting a shoulder to clearly embody the role of the physician in charge.
“And pull up a chair,” he says. “If there is no chair, bring in a chair. But sit down—always.”
Dr. Centor also recommends a transparent approach, “especially in hospital medicine,” he explains. “Be explicit about what you’re thinking, what you’re doing, and why you’re doing it.”1
Transparency can protect you as it informs and comforts patients and their families. For instance, “hospitalized patients are probably hearing from every relative they have and half the friends they have,” Dr. Centor says. “If one of those people is a physician, they may be second-guessing you. You can overcome their wariness by remembering that this is all about bedside manner and the explanations you give them, including discharge instructions.”
Dr. Centor says your bedside manner needs to fit your personality. When you talk to a patient, use language that matches your personality. You can adopt someone else’s introductory script; just make sure to modify it to fit your work environment (see “Strategies to Ease Patient Concerns,” p. 29).
“What Is This?”
Earlier this year, CJ Clarke of Leesburg, Fla., underwent a colonoscopy screening at a local doctor’s office. She had been kept on warfarin (Coumadin) to prevent complications, but after she bled for four days from a puncture sustained during the procedure, she went to the ED. She was admitted, but it wasn’t until the following afternoon that she learned that hospitalists—not her PCP— would be taking care of her.
“This totally unknown guy came in and said he would be filling in for my doctor and communicating with [my PCP],” Clarke says. “It was a weekend, and it turns out the first hospitalist was a substitute hospitalist, so then I got another hospitalist. The first one was subbing for the first hospitalist. I wasn’t exactly mad, but I thought, what is this?”
Clarke thought the first hospitalist was knowledgeable; she took comfort in that. “But the second one was extremely knowledgeable and explained the differences between Coumadin and heparin. He really knew his stuff. He talked to my cardiologist when she came in,” Clarke says. “The only thing that I was sorry about was that my primary didn’t seem to get the information very rapidly.”
Care coordination is a vital step in the discharge process, especially when patients think the flow of information between a hospital and a PCP is immediate and seamless. When Clarke was discharged and she returned home, she scheduled an appointment with her PCP. “When I first called, my [PCP] had not even heard I had been admitted,” Clarke says. But by the time she visited the PCP, “she knew everything. … I think it would have been good if sometime during that five-day hospitalization, she had been told—not afterward. Not that she would have come in, because that is not her policy, but just to know she knew.”
HM’s Role: Extended Education
Many HM groups have designated policies for educating patients and assuaging their fears. Because some PCPs might feel left out of the loop when hospitalists care for their patients, these strategies go beyond patient education.
One of the first steps is to involve PCPs in meaningful ways in their patients’ hospital care. When a patient is particularly angered by his PCP’s absence, invite the PCP to visit, or call the PCP more often and let the patient know you’re doing so. As proposed by Bob Wachter, MD, professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World,” and Steven Pantilat, MD, FHM, professor of clinical medicine in the division of hospital medicine at UCSF, and a former SHM president, “the PCP can endorse the hospitalist model and the individual hospitalist, notice subtle findings that differ from the patient’s baseline, and help clarify patient preferences regarding difficult situations by drawing on their previous relationship with the patient. This visit may also benefit the PCP by providing insights into the patient’s illness, personality, or social support that he or she was unaware of previously.”2,3
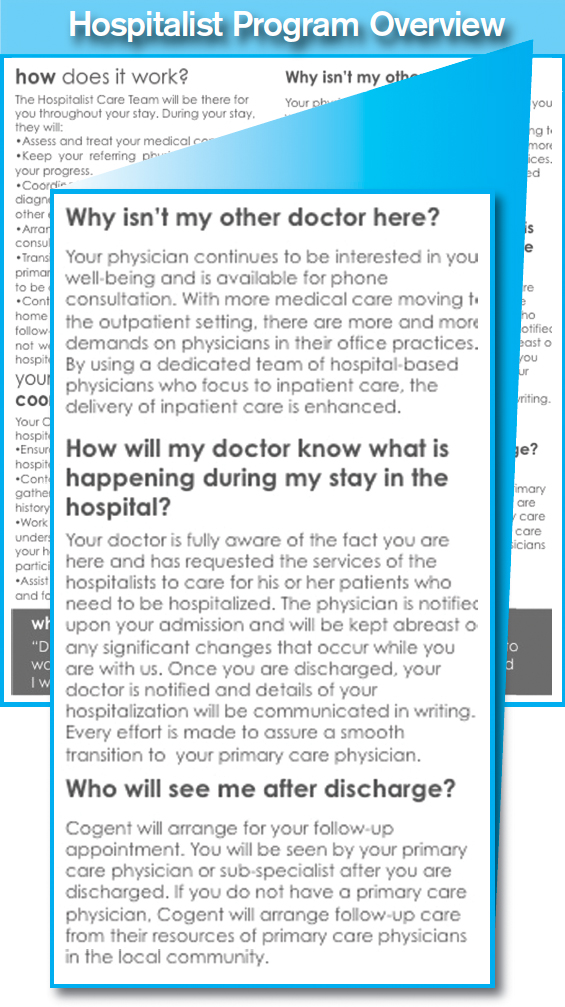
Cogent Healthcare uses an outreach program to calm patient fears and connect with PCPs. The Brentwood, Tenn.-based hospitalist company distributes patient education pamphlets to the PCPs with whom they work, and distributes a flier on admission to show patients the photographs and names of their HM team (see “Make Patient Education A Priority,” p. 29).
Hospitalist training in this arena helps prepare physicians for a potentially uncomfortable work environment. “We need to stress in residency training the specific issue of helping make the patient feel comfortable when their own doctor is not seeing them in the hospital,” Dr. Centor says. “Most young hospitalists right out of their residencies have not experienced primary-care practice, and, so far, we don’t know how to get around that.”
Hospitalist groups also should consider broad initiatives to bring hospitalists together with patient representatives and other volunteers who work with patients. If volunteers are ignored in the educational outreach process, it could exacerbate patients’ negative reactions. Teach volunteers what hospitalists are, their benefit to care delivery, and their value in upholding the mission of quality HM. TH
Andrea Sattinger is a freelance writer based in North Carolina.
References
- Centor RM. A hospitalist inpatient system does not improve patient care outcomes. Arch Intern Med. 2008;168(12):1257-1258.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002;48(4):281-290.
- Wachter RM, Pantilat SZ. The “continuity visit” and the hospitalist model of care. Dis Mon. 2002;48(4): 267-272.
Image Source: PETRI ARTTURI ASIKAINEN / GETTY IMAGES
Susan Connelly of Fruitland Park, Fla., is a volunteer at her local community hospital who until recently had never heard of a hospitalist. One day, she entered a hospital room and, as she regularly did with patients she visited, asked if there was anything the man in the bed needed.
“I want to know where my doctor is,” the patient said.
“You mean your doctor hasn’t seen you?” Connelly asked.
“No,” he said. “I’m not even sure he knows I’m here.”
Somewhat incredulous, Connelly retrieved the hospital’s physician handbook and helped the patient look up his physician’s phone number. “I didn’t think too much about it,” she says. But the following week, when she appeared at the hospital to volunteer, a supervisor called her into the office. The supervisor asked Connelly about the incident and gently admonished her for encouraging the patient to call his primary-care physician (PCP), as “a hospitalist is working with him now.”
“A what? I had never even heard the term,” Connelly says. She asked her fellow volunteers, known as patient representatives at her hospital, if they had ever heard of a hospitalist. One had, but only because her husband had been admitted for a hospital stay. Concerned, Connelly wrote letters to the editors of two local newspapers. Both were published (see Figure 2, “Familiar Face Gone Missing,” p. 30).
—Robert Centor, MD, associate dean of medicine, University of Alabama at Birmingham
“If I am admitted to the hospital, my doctor will most likely ‘dump’ me on what is now called a ‘hospitalist,’ ” she wrote. “Information gathered [by the hospitalist] should be forwarded to your doctor; the key word is ‘should.’ Why develop this long-term relationship with a doctor, if when you really need him, he is not there for you and you are dealing with a stranger?”
Why indeed?
It might not happen with every new admission, but patient fears are a reality. The uncertainty of a hospital stay, a new physician, and new medications can take their toll on the human psyche. Patients are upset with their PCP, the hospital, the system; many times it’s the hospitalist who feels the brunt of their anger. Not only do hospitalists have to calm a patient worried about PCP disconnect, but they also have to reassure the patient that they will be attentive to their needs, provide a high quality of care during the hospital stay, and communicate with their PCP about diagnoses, medications, and follow-up care. Hospitalists should weave in some of the documented plusses a hospitalist brings to the table: shorter length of stays, greater patient access and availability, and improved quality of care.
Although some patients might view hospitalists as “strangers,” HM physicians can learn methods to ease patient anxiety and answer tough questions from patients about the role they play in hospital care.
Restore Confidence
Simple conversations can help hospitalists defuse patient dissatisfaction. When a patient asks why their PCP won’t be seeing them in the hospital, it’s best to begin with a reassuring approach. For example, introduce yourself and say you have reviewed the case with their PCP. You can include key information from their medical history and recent hospitalizations, if appropriate.
Robert Centor, MD, a hospitalist and associate dean of medicine at the University of Alabama at Birmingham, suggests a few other key behaviors for initial patient visits. He finds a way to make appropriate physical contact by taking a pulse, checking the heart and lungs, or patting a shoulder to clearly embody the role of the physician in charge.
“And pull up a chair,” he says. “If there is no chair, bring in a chair. But sit down—always.”
Dr. Centor also recommends a transparent approach, “especially in hospital medicine,” he explains. “Be explicit about what you’re thinking, what you’re doing, and why you’re doing it.”1
Transparency can protect you as it informs and comforts patients and their families. For instance, “hospitalized patients are probably hearing from every relative they have and half the friends they have,” Dr. Centor says. “If one of those people is a physician, they may be second-guessing you. You can overcome their wariness by remembering that this is all about bedside manner and the explanations you give them, including discharge instructions.”
Dr. Centor says your bedside manner needs to fit your personality. When you talk to a patient, use language that matches your personality. You can adopt someone else’s introductory script; just make sure to modify it to fit your work environment (see “Strategies to Ease Patient Concerns,” p. 29).
“What Is This?”
Earlier this year, CJ Clarke of Leesburg, Fla., underwent a colonoscopy screening at a local doctor’s office. She had been kept on warfarin (Coumadin) to prevent complications, but after she bled for four days from a puncture sustained during the procedure, she went to the ED. She was admitted, but it wasn’t until the following afternoon that she learned that hospitalists—not her PCP— would be taking care of her.
“This totally unknown guy came in and said he would be filling in for my doctor and communicating with [my PCP],” Clarke says. “It was a weekend, and it turns out the first hospitalist was a substitute hospitalist, so then I got another hospitalist. The first one was subbing for the first hospitalist. I wasn’t exactly mad, but I thought, what is this?”
Clarke thought the first hospitalist was knowledgeable; she took comfort in that. “But the second one was extremely knowledgeable and explained the differences between Coumadin and heparin. He really knew his stuff. He talked to my cardiologist when she came in,” Clarke says. “The only thing that I was sorry about was that my primary didn’t seem to get the information very rapidly.”
Care coordination is a vital step in the discharge process, especially when patients think the flow of information between a hospital and a PCP is immediate and seamless. When Clarke was discharged and she returned home, she scheduled an appointment with her PCP. “When I first called, my [PCP] had not even heard I had been admitted,” Clarke says. But by the time she visited the PCP, “she knew everything. … I think it would have been good if sometime during that five-day hospitalization, she had been told—not afterward. Not that she would have come in, because that is not her policy, but just to know she knew.”
HM’s Role: Extended Education
Many HM groups have designated policies for educating patients and assuaging their fears. Because some PCPs might feel left out of the loop when hospitalists care for their patients, these strategies go beyond patient education.
One of the first steps is to involve PCPs in meaningful ways in their patients’ hospital care. When a patient is particularly angered by his PCP’s absence, invite the PCP to visit, or call the PCP more often and let the patient know you’re doing so. As proposed by Bob Wachter, MD, professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World,” and Steven Pantilat, MD, FHM, professor of clinical medicine in the division of hospital medicine at UCSF, and a former SHM president, “the PCP can endorse the hospitalist model and the individual hospitalist, notice subtle findings that differ from the patient’s baseline, and help clarify patient preferences regarding difficult situations by drawing on their previous relationship with the patient. This visit may also benefit the PCP by providing insights into the patient’s illness, personality, or social support that he or she was unaware of previously.”2,3
Cogent Healthcare uses an outreach program to calm patient fears and connect with PCPs. The Brentwood, Tenn.-based hospitalist company distributes patient education pamphlets to the PCPs with whom they work, and distributes a flier on admission to show patients the photographs and names of their HM team (see “Make Patient Education A Priority,” p. 29).
Hospitalist training in this arena helps prepare physicians for a potentially uncomfortable work environment. “We need to stress in residency training the specific issue of helping make the patient feel comfortable when their own doctor is not seeing them in the hospital,” Dr. Centor says. “Most young hospitalists right out of their residencies have not experienced primary-care practice, and, so far, we don’t know how to get around that.”
Hospitalist groups also should consider broad initiatives to bring hospitalists together with patient representatives and other volunteers who work with patients. If volunteers are ignored in the educational outreach process, it could exacerbate patients’ negative reactions. Teach volunteers what hospitalists are, their benefit to care delivery, and their value in upholding the mission of quality HM. TH
Andrea Sattinger is a freelance writer based in North Carolina.
References
- Centor RM. A hospitalist inpatient system does not improve patient care outcomes. Arch Intern Med. 2008;168(12):1257-1258.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002;48(4):281-290.
- Wachter RM, Pantilat SZ. The “continuity visit” and the hospitalist model of care. Dis Mon. 2002;48(4): 267-272.
Image Source: PETRI ARTTURI ASIKAINEN / GETTY IMAGES
Susan Connelly of Fruitland Park, Fla., is a volunteer at her local community hospital who until recently had never heard of a hospitalist. One day, she entered a hospital room and, as she regularly did with patients she visited, asked if there was anything the man in the bed needed.
“I want to know where my doctor is,” the patient said.
“You mean your doctor hasn’t seen you?” Connelly asked.
“No,” he said. “I’m not even sure he knows I’m here.”
Somewhat incredulous, Connelly retrieved the hospital’s physician handbook and helped the patient look up his physician’s phone number. “I didn’t think too much about it,” she says. But the following week, when she appeared at the hospital to volunteer, a supervisor called her into the office. The supervisor asked Connelly about the incident and gently admonished her for encouraging the patient to call his primary-care physician (PCP), as “a hospitalist is working with him now.”
“A what? I had never even heard the term,” Connelly says. She asked her fellow volunteers, known as patient representatives at her hospital, if they had ever heard of a hospitalist. One had, but only because her husband had been admitted for a hospital stay. Concerned, Connelly wrote letters to the editors of two local newspapers. Both were published (see Figure 2, “Familiar Face Gone Missing,” p. 30).
—Robert Centor, MD, associate dean of medicine, University of Alabama at Birmingham
“If I am admitted to the hospital, my doctor will most likely ‘dump’ me on what is now called a ‘hospitalist,’ ” she wrote. “Information gathered [by the hospitalist] should be forwarded to your doctor; the key word is ‘should.’ Why develop this long-term relationship with a doctor, if when you really need him, he is not there for you and you are dealing with a stranger?”
Why indeed?
It might not happen with every new admission, but patient fears are a reality. The uncertainty of a hospital stay, a new physician, and new medications can take their toll on the human psyche. Patients are upset with their PCP, the hospital, the system; many times it’s the hospitalist who feels the brunt of their anger. Not only do hospitalists have to calm a patient worried about PCP disconnect, but they also have to reassure the patient that they will be attentive to their needs, provide a high quality of care during the hospital stay, and communicate with their PCP about diagnoses, medications, and follow-up care. Hospitalists should weave in some of the documented plusses a hospitalist brings to the table: shorter length of stays, greater patient access and availability, and improved quality of care.
Although some patients might view hospitalists as “strangers,” HM physicians can learn methods to ease patient anxiety and answer tough questions from patients about the role they play in hospital care.
Restore Confidence
Simple conversations can help hospitalists defuse patient dissatisfaction. When a patient asks why their PCP won’t be seeing them in the hospital, it’s best to begin with a reassuring approach. For example, introduce yourself and say you have reviewed the case with their PCP. You can include key information from their medical history and recent hospitalizations, if appropriate.
Robert Centor, MD, a hospitalist and associate dean of medicine at the University of Alabama at Birmingham, suggests a few other key behaviors for initial patient visits. He finds a way to make appropriate physical contact by taking a pulse, checking the heart and lungs, or patting a shoulder to clearly embody the role of the physician in charge.
“And pull up a chair,” he says. “If there is no chair, bring in a chair. But sit down—always.”
Dr. Centor also recommends a transparent approach, “especially in hospital medicine,” he explains. “Be explicit about what you’re thinking, what you’re doing, and why you’re doing it.”1
Transparency can protect you as it informs and comforts patients and their families. For instance, “hospitalized patients are probably hearing from every relative they have and half the friends they have,” Dr. Centor says. “If one of those people is a physician, they may be second-guessing you. You can overcome their wariness by remembering that this is all about bedside manner and the explanations you give them, including discharge instructions.”
Dr. Centor says your bedside manner needs to fit your personality. When you talk to a patient, use language that matches your personality. You can adopt someone else’s introductory script; just make sure to modify it to fit your work environment (see “Strategies to Ease Patient Concerns,” p. 29).
“What Is This?”
Earlier this year, CJ Clarke of Leesburg, Fla., underwent a colonoscopy screening at a local doctor’s office. She had been kept on warfarin (Coumadin) to prevent complications, but after she bled for four days from a puncture sustained during the procedure, she went to the ED. She was admitted, but it wasn’t until the following afternoon that she learned that hospitalists—not her PCP— would be taking care of her.
“This totally unknown guy came in and said he would be filling in for my doctor and communicating with [my PCP],” Clarke says. “It was a weekend, and it turns out the first hospitalist was a substitute hospitalist, so then I got another hospitalist. The first one was subbing for the first hospitalist. I wasn’t exactly mad, but I thought, what is this?”
Clarke thought the first hospitalist was knowledgeable; she took comfort in that. “But the second one was extremely knowledgeable and explained the differences between Coumadin and heparin. He really knew his stuff. He talked to my cardiologist when she came in,” Clarke says. “The only thing that I was sorry about was that my primary didn’t seem to get the information very rapidly.”
Care coordination is a vital step in the discharge process, especially when patients think the flow of information between a hospital and a PCP is immediate and seamless. When Clarke was discharged and she returned home, she scheduled an appointment with her PCP. “When I first called, my [PCP] had not even heard I had been admitted,” Clarke says. But by the time she visited the PCP, “she knew everything. … I think it would have been good if sometime during that five-day hospitalization, she had been told—not afterward. Not that she would have come in, because that is not her policy, but just to know she knew.”
HM’s Role: Extended Education
Many HM groups have designated policies for educating patients and assuaging their fears. Because some PCPs might feel left out of the loop when hospitalists care for their patients, these strategies go beyond patient education.
One of the first steps is to involve PCPs in meaningful ways in their patients’ hospital care. When a patient is particularly angered by his PCP’s absence, invite the PCP to visit, or call the PCP more often and let the patient know you’re doing so. As proposed by Bob Wachter, MD, professor and chief of the division of hospital medicine at the University of California at San Francisco, a former SHM president, and author of the blog “Wachter’s World,” and Steven Pantilat, MD, FHM, professor of clinical medicine in the division of hospital medicine at UCSF, and a former SHM president, “the PCP can endorse the hospitalist model and the individual hospitalist, notice subtle findings that differ from the patient’s baseline, and help clarify patient preferences regarding difficult situations by drawing on their previous relationship with the patient. This visit may also benefit the PCP by providing insights into the patient’s illness, personality, or social support that he or she was unaware of previously.”2,3
Cogent Healthcare uses an outreach program to calm patient fears and connect with PCPs. The Brentwood, Tenn.-based hospitalist company distributes patient education pamphlets to the PCPs with whom they work, and distributes a flier on admission to show patients the photographs and names of their HM team (see “Make Patient Education A Priority,” p. 29).
Hospitalist training in this arena helps prepare physicians for a potentially uncomfortable work environment. “We need to stress in residency training the specific issue of helping make the patient feel comfortable when their own doctor is not seeing them in the hospital,” Dr. Centor says. “Most young hospitalists right out of their residencies have not experienced primary-care practice, and, so far, we don’t know how to get around that.”
Hospitalist groups also should consider broad initiatives to bring hospitalists together with patient representatives and other volunteers who work with patients. If volunteers are ignored in the educational outreach process, it could exacerbate patients’ negative reactions. Teach volunteers what hospitalists are, their benefit to care delivery, and their value in upholding the mission of quality HM. TH
Andrea Sattinger is a freelance writer based in North Carolina.
References
- Centor RM. A hospitalist inpatient system does not improve patient care outcomes. Arch Intern Med. 2008;168(12):1257-1258.
- Lo B. Ethical and policy implications of hospitalist systems. Dis Mon. 2002;48(4):281-290.
- Wachter RM, Pantilat SZ. The “continuity visit” and the hospitalist model of care. Dis Mon. 2002;48(4): 267-272.
Image Source: PETRI ARTTURI ASIKAINEN / GETTY IMAGES
Digital Dilemma
This spring, before Sentara Norfolk General Hospital in Virginia went live with eCare, its electronic health record (EHR) system, hospitalist Ryan Van Gomple, MD, would admit patients using the same system physicians have used for decades: hastily scrawled patient history notes, paper orders, and phone dictation. But eCare’s introduction—and subsequent tweaking in the past few months—has brought a radical transition to the 543-bed tertiary-care facility. Dr. Van Gomple and other hospitalists at institutions on similar systems can enter and access a patient’s data using desktop computers, handheld devices like Blackberrys or iPhones—even their personal laptops at home.
“One of the advantages is we can go back … not only with notes from the hospital stay; a lot of people are doing outpatient notes in the system, so you can start to piece together a total picture of a person’s medical care,” says Dr. Van Gomple, a hospitalist with Sentara Medical Group. “That’s one of the big goals of [EHR]—to have a streamlined system. One of the challenges is, How do you connect with different systems? That’s a great question.”
Dr. Van Gomple might not have the answer, but thanks to ambitious goals laid out by President Obama, the topic is in the national spotlight and already has nearly $20 billion in stimulus money scheduled for release in July 2010. Digitizing healthcare records to create a more efficient care delivery system—through improved record keeping, shortened patient length of stay (LOS), and increased ED throughput—isn’t a new idea. Hospitals have struggled for more than a decade with the EHR question, debating whether they should—not to mention how they would—create a computerized system to input patient records into a database that is accessible in real time to hospitalists, nurses, primary-care physicians, insurers, and so on. There have been long-stalled discussions on how to settle privacy concerns that arise from electronic records (see “EHR Upgrade Faces Privacy, Communication Obstacles,” p. 27). Still, a multi-billion-dollar federal pledge has created a moment in time to take EHR beyond the discussion phase.

The Office of the National Coordinator of Health Information Technology (ONCHIT) is empowered to shepherd this process. David Blumenthal, MD, MPP, the director of the Institute for Health Policy, a joint effort of Massachusetts General Hospital and Partners Healthcare System, has been named as ONCHIT’s head. Money to entice hospitals to invest in EHR is part of the American Recovery and Reinvestment Act of 2009. And with Congress hammering out the details of healthcare reform legislation, a sharper focus has been placed on the potential efficiencies EHR can offer.
Money and attention aren’t the only keys to this puzzle, however. IT advocates, medical information officers, and HM group leaders say the government spotlight is a wonderful springboard, but they also say physician involvement in implementing the EHR technology is a must and will spur more hospitals to adopt the systems. Less than 8% of U.S. hospitals have EHR in at least one unit, the New England Journal of Medicine reported earlier this year.1 Just 1.5% of hospitals have a comprehensive system in all of their units.
“There are so many barriers getting to where our country really needs to get,” says Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass. “One of the big issues is the meaningful use, and how do you actually set criteria for your using electronic health records the right way? If you look at the big picture, you’re talking about so many clinical practices. … How do you write criteria that are meaningful to all those different settings? The government has an enormous challenge.”
Efficiency: HM Cornerstone
David Yu, MD, FHM, works at a hospital with paperless capability and sees on a daily basis how streamlined health records have a practical effect on a hospitalist’s workload and efficiency. Dr. Yu, medical director of hospitalist services at 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale, is one of EHR’s most passionate advocates.
Decatur Memorial uses GE Healthcare’s Centricity system, which allows hospitalists to “download automatically into our physical history with the click of a button,” says Dr. Yu, a member of Team Hospitalist. “As you’re downloading, you’re accessing the information. It’s literally the same as you driving to the patient’s primary-care physician’s office, pulling the chart, and looking at it.”
Dr. Yu and those who support EHR say it streamlines intakes, discharges, and handoffs, which in turn reduce throughput and length of stay—statistics often cited to prove HM’s value to the hospital administration. The rush for implementation takes on added urgency considering that less than half of 0.5% of hospitals are fully paperless, meaning they have interdepartmental systems that can communicate with each other, according to HIMMS Analytics.
Obama and other healthcare reform advocates envision a day not far in the future when all of America’s hospitals will be connected through a national health records system. Databases in hospitals and physician offices and other healthcare providers will communicate with each other. It will make such health records as X-rays and lab test results a portable commodity, which, in theory, will provide faster and more accurate information for both patients and their providers.
One of the economic stimulus plan’s most important features is its “clarity of purpose,” Dr. Blumenthal wrote in the New England Journal of Medicine earlier this year. “Congress apparently sees [health IT]—computers, software, Internet connection, telemedicine—not as an end in itself, but as a means of improving the quality of healthcare, the health of populations, and the efficiency of healthcare systems.”2
Proactive Approach
Obama has pushed EHR implementation as one of many solutions to the skyrocketing costs of healthcare, saying earlier this year that he is committed to “the immediate investments necessary to ensure that within five years, all of America’s medical records are computerized.” Even so, the EHR upgrade remains only a grand outline, one missing the details that will determine the future. There is time, of course. The first funding through the stimulus bill won’t be available until next summer.
Dr. Blumenthal’s office is crafting an interoperability plan in combination with a pair of still-forming advisory boards: a health information policy committee and a health standards committee. The stimulus bill also promises increased federal reimbursement payments for hospitals with meaningful use of certified EHR. First, the government has to define what is meaningful and, as Dr. Stanley points out, the definition will have different meanings to different sectors of the $2.2 trillion-per-year healthcare industry.
Once those definitions are set, there is a timetable for additional reimbursement and a one-time bonus of $2 million for institutions that implement “meaningful use.” There also will be escalating Medicare penalties for institutions that fail to show the kind of technological progress federal officials are looking for.
But even if those standards are set, it doesn’t guarantee hospitals will buy the technology that vendors are selling. Many in the HM field argue that the next step is the most important one.
“Physician adoption of electronic health records is the central, critical issue this industry is facing over the next few years,” says Todd Johnson, president of Salar Inc., a Baltimore-based firm that develops software applications for clinical documentation. “There are a lot of really bright people working on criteria that make electronic health records good tools. However, there doesn’t seem to be an organized body focused on the EHR adoption issues. Anybody can buy all these tools, but if you ultimately can’t get the right people to use them at the right time, the investment doesn’t yield much, right?”
Johnson, who thinks the federal focus on EHR technology is a main driver behind his firm’s 25% sales growth spurt in the first six months of 2009, says physicians have to be a driving force in the EMR implementation process or the system will fail. Take the industry’s classic cautionary tale: Cedars-Sinai Medical Center in Los Angeles. The oft-innovative institution made national headlines in 2002 when it scrapped a three-month-old, $34 million computerized physician order entry (CPOE) system after more than 400 doctors demanded it be shelved.
“The right thing to do is really steer the discussion to physician adoption,” Johnson says. “Make sure that physicians have a choice. Every hospital—and rightly so—wants to see the benefit of their investment in electronic medical records. If physicians don’t have a voice in what will or won’t work, purchasing decisions will be made without them. And that’s not a great thing. Hospital leadership needs to be cognizant of that.”
Dr. Stanley thinks hospitalists should take a proactive approach to EHR implementation at their hospitals. Many potential issues could be solved if hospitalists take an active role earlier in the process.
“As tedious as those early meetings are,” Dr. Stanley says, “that’s where the big planning and decisions get made. The problem is most people think of it as tedious and boring because they don’t appreciate the technology.”
What’s Ahead
Technology integration is the next step. A handful of companies offer complete EHR platforms, including industry leaders Epic, Meditech, Cerner Corp., GE Healthcare, and McKesson Corp. Specialty firms, such as Johnson’s Salar, offer ancillary and support software and hardware.
Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the stimulus funding dedicated to technology will be better served if it focuses on incentives beyond hospitals. Dr. Rogers and others want to see guidelines to create incentives for IT vendors to offer user-friendly systems designed to further medical efficiency goals.
“If this needed technology was developed and proven, the needs for carrots and sticks for adoption would be far less,” Dr. Rogers and several of his peers wrote in an unpublished letter to the NEJM. “Rather than focusing primarily on adoption of systems that have serious limitations … a bill that requires improvements in existing technologies would have much more impact in improving the quality of healthcare.”
Even before that happens, full-scale implementation of these systems will be a costly project that requires a long-term relationship with a vendor. Dr. Van Gomple’s hospital system, Sentara Healthcare, has budgeted $235 million over 10 years for its EHR implementation, according to Bert Reese, senior vice president and chief information officer. His accountants tell him to expect roughly $50 million to be subsidized by the stimulus package. The money is helpful, but not enough for a hospital or system that still needs to find another $185 million.
“The stimulus is nice to get things going,” Reese says. “But if you as an organization think that will cover the cost, you’ll never get going.”
Reese says Sentara’s return on investment at full implementation—roughly five years from now—will be about $35 million per year in savings. He suggests organizations view the investment through a long-term profit goal in order to show the value over an extended timeframe. Otherwise, some C-suites will be scared off by the initial outlay, failing to see the value of efficiency, cost savings, and improved patient care.
“It’s not an IT project,” Reese says. “It’s a clinical project.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. N Engl J Med. 2009;360(11):1141-1143.
- Blumenthal D. Stimulating the adoption of health information technology. N Engl J Med. 2009;360(15):1477-1479.
- Liebovitz, D. Health care information technology: a cloud around the silver lining? Arch Intern Med. 2009;169(10):924-926.
Image Source: ILLUSTRATION / ALICIA BUELOW
This spring, before Sentara Norfolk General Hospital in Virginia went live with eCare, its electronic health record (EHR) system, hospitalist Ryan Van Gomple, MD, would admit patients using the same system physicians have used for decades: hastily scrawled patient history notes, paper orders, and phone dictation. But eCare’s introduction—and subsequent tweaking in the past few months—has brought a radical transition to the 543-bed tertiary-care facility. Dr. Van Gomple and other hospitalists at institutions on similar systems can enter and access a patient’s data using desktop computers, handheld devices like Blackberrys or iPhones—even their personal laptops at home.
“One of the advantages is we can go back … not only with notes from the hospital stay; a lot of people are doing outpatient notes in the system, so you can start to piece together a total picture of a person’s medical care,” says Dr. Van Gomple, a hospitalist with Sentara Medical Group. “That’s one of the big goals of [EHR]—to have a streamlined system. One of the challenges is, How do you connect with different systems? That’s a great question.”
Dr. Van Gomple might not have the answer, but thanks to ambitious goals laid out by President Obama, the topic is in the national spotlight and already has nearly $20 billion in stimulus money scheduled for release in July 2010. Digitizing healthcare records to create a more efficient care delivery system—through improved record keeping, shortened patient length of stay (LOS), and increased ED throughput—isn’t a new idea. Hospitals have struggled for more than a decade with the EHR question, debating whether they should—not to mention how they would—create a computerized system to input patient records into a database that is accessible in real time to hospitalists, nurses, primary-care physicians, insurers, and so on. There have been long-stalled discussions on how to settle privacy concerns that arise from electronic records (see “EHR Upgrade Faces Privacy, Communication Obstacles,” p. 27). Still, a multi-billion-dollar federal pledge has created a moment in time to take EHR beyond the discussion phase.
The Office of the National Coordinator of Health Information Technology (ONCHIT) is empowered to shepherd this process. David Blumenthal, MD, MPP, the director of the Institute for Health Policy, a joint effort of Massachusetts General Hospital and Partners Healthcare System, has been named as ONCHIT’s head. Money to entice hospitals to invest in EHR is part of the American Recovery and Reinvestment Act of 2009. And with Congress hammering out the details of healthcare reform legislation, a sharper focus has been placed on the potential efficiencies EHR can offer.
Money and attention aren’t the only keys to this puzzle, however. IT advocates, medical information officers, and HM group leaders say the government spotlight is a wonderful springboard, but they also say physician involvement in implementing the EHR technology is a must and will spur more hospitals to adopt the systems. Less than 8% of U.S. hospitals have EHR in at least one unit, the New England Journal of Medicine reported earlier this year.1 Just 1.5% of hospitals have a comprehensive system in all of their units.
“There are so many barriers getting to where our country really needs to get,” says Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass. “One of the big issues is the meaningful use, and how do you actually set criteria for your using electronic health records the right way? If you look at the big picture, you’re talking about so many clinical practices. … How do you write criteria that are meaningful to all those different settings? The government has an enormous challenge.”
Efficiency: HM Cornerstone
David Yu, MD, FHM, works at a hospital with paperless capability and sees on a daily basis how streamlined health records have a practical effect on a hospitalist’s workload and efficiency. Dr. Yu, medical director of hospitalist services at 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale, is one of EHR’s most passionate advocates.
Decatur Memorial uses GE Healthcare’s Centricity system, which allows hospitalists to “download automatically into our physical history with the click of a button,” says Dr. Yu, a member of Team Hospitalist. “As you’re downloading, you’re accessing the information. It’s literally the same as you driving to the patient’s primary-care physician’s office, pulling the chart, and looking at it.”
Dr. Yu and those who support EHR say it streamlines intakes, discharges, and handoffs, which in turn reduce throughput and length of stay—statistics often cited to prove HM’s value to the hospital administration. The rush for implementation takes on added urgency considering that less than half of 0.5% of hospitals are fully paperless, meaning they have interdepartmental systems that can communicate with each other, according to HIMMS Analytics.
Obama and other healthcare reform advocates envision a day not far in the future when all of America’s hospitals will be connected through a national health records system. Databases in hospitals and physician offices and other healthcare providers will communicate with each other. It will make such health records as X-rays and lab test results a portable commodity, which, in theory, will provide faster and more accurate information for both patients and their providers.
One of the economic stimulus plan’s most important features is its “clarity of purpose,” Dr. Blumenthal wrote in the New England Journal of Medicine earlier this year. “Congress apparently sees [health IT]—computers, software, Internet connection, telemedicine—not as an end in itself, but as a means of improving the quality of healthcare, the health of populations, and the efficiency of healthcare systems.”2
Proactive Approach
Obama has pushed EHR implementation as one of many solutions to the skyrocketing costs of healthcare, saying earlier this year that he is committed to “the immediate investments necessary to ensure that within five years, all of America’s medical records are computerized.” Even so, the EHR upgrade remains only a grand outline, one missing the details that will determine the future. There is time, of course. The first funding through the stimulus bill won’t be available until next summer.
Dr. Blumenthal’s office is crafting an interoperability plan in combination with a pair of still-forming advisory boards: a health information policy committee and a health standards committee. The stimulus bill also promises increased federal reimbursement payments for hospitals with meaningful use of certified EHR. First, the government has to define what is meaningful and, as Dr. Stanley points out, the definition will have different meanings to different sectors of the $2.2 trillion-per-year healthcare industry.
Once those definitions are set, there is a timetable for additional reimbursement and a one-time bonus of $2 million for institutions that implement “meaningful use.” There also will be escalating Medicare penalties for institutions that fail to show the kind of technological progress federal officials are looking for.
But even if those standards are set, it doesn’t guarantee hospitals will buy the technology that vendors are selling. Many in the HM field argue that the next step is the most important one.
“Physician adoption of electronic health records is the central, critical issue this industry is facing over the next few years,” says Todd Johnson, president of Salar Inc., a Baltimore-based firm that develops software applications for clinical documentation. “There are a lot of really bright people working on criteria that make electronic health records good tools. However, there doesn’t seem to be an organized body focused on the EHR adoption issues. Anybody can buy all these tools, but if you ultimately can’t get the right people to use them at the right time, the investment doesn’t yield much, right?”
Johnson, who thinks the federal focus on EHR technology is a main driver behind his firm’s 25% sales growth spurt in the first six months of 2009, says physicians have to be a driving force in the EMR implementation process or the system will fail. Take the industry’s classic cautionary tale: Cedars-Sinai Medical Center in Los Angeles. The oft-innovative institution made national headlines in 2002 when it scrapped a three-month-old, $34 million computerized physician order entry (CPOE) system after more than 400 doctors demanded it be shelved.
“The right thing to do is really steer the discussion to physician adoption,” Johnson says. “Make sure that physicians have a choice. Every hospital—and rightly so—wants to see the benefit of their investment in electronic medical records. If physicians don’t have a voice in what will or won’t work, purchasing decisions will be made without them. And that’s not a great thing. Hospital leadership needs to be cognizant of that.”
Dr. Stanley thinks hospitalists should take a proactive approach to EHR implementation at their hospitals. Many potential issues could be solved if hospitalists take an active role earlier in the process.
“As tedious as those early meetings are,” Dr. Stanley says, “that’s where the big planning and decisions get made. The problem is most people think of it as tedious and boring because they don’t appreciate the technology.”
What’s Ahead
Technology integration is the next step. A handful of companies offer complete EHR platforms, including industry leaders Epic, Meditech, Cerner Corp., GE Healthcare, and McKesson Corp. Specialty firms, such as Johnson’s Salar, offer ancillary and support software and hardware.
Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the stimulus funding dedicated to technology will be better served if it focuses on incentives beyond hospitals. Dr. Rogers and others want to see guidelines to create incentives for IT vendors to offer user-friendly systems designed to further medical efficiency goals.
“If this needed technology was developed and proven, the needs for carrots and sticks for adoption would be far less,” Dr. Rogers and several of his peers wrote in an unpublished letter to the NEJM. “Rather than focusing primarily on adoption of systems that have serious limitations … a bill that requires improvements in existing technologies would have much more impact in improving the quality of healthcare.”
Even before that happens, full-scale implementation of these systems will be a costly project that requires a long-term relationship with a vendor. Dr. Van Gomple’s hospital system, Sentara Healthcare, has budgeted $235 million over 10 years for its EHR implementation, according to Bert Reese, senior vice president and chief information officer. His accountants tell him to expect roughly $50 million to be subsidized by the stimulus package. The money is helpful, but not enough for a hospital or system that still needs to find another $185 million.
“The stimulus is nice to get things going,” Reese says. “But if you as an organization think that will cover the cost, you’ll never get going.”
Reese says Sentara’s return on investment at full implementation—roughly five years from now—will be about $35 million per year in savings. He suggests organizations view the investment through a long-term profit goal in order to show the value over an extended timeframe. Otherwise, some C-suites will be scared off by the initial outlay, failing to see the value of efficiency, cost savings, and improved patient care.
“It’s not an IT project,” Reese says. “It’s a clinical project.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. N Engl J Med. 2009;360(11):1141-1143.
- Blumenthal D. Stimulating the adoption of health information technology. N Engl J Med. 2009;360(15):1477-1479.
- Liebovitz, D. Health care information technology: a cloud around the silver lining? Arch Intern Med. 2009;169(10):924-926.
Image Source: ILLUSTRATION / ALICIA BUELOW
This spring, before Sentara Norfolk General Hospital in Virginia went live with eCare, its electronic health record (EHR) system, hospitalist Ryan Van Gomple, MD, would admit patients using the same system physicians have used for decades: hastily scrawled patient history notes, paper orders, and phone dictation. But eCare’s introduction—and subsequent tweaking in the past few months—has brought a radical transition to the 543-bed tertiary-care facility. Dr. Van Gomple and other hospitalists at institutions on similar systems can enter and access a patient’s data using desktop computers, handheld devices like Blackberrys or iPhones—even their personal laptops at home.
“One of the advantages is we can go back … not only with notes from the hospital stay; a lot of people are doing outpatient notes in the system, so you can start to piece together a total picture of a person’s medical care,” says Dr. Van Gomple, a hospitalist with Sentara Medical Group. “That’s one of the big goals of [EHR]—to have a streamlined system. One of the challenges is, How do you connect with different systems? That’s a great question.”
Dr. Van Gomple might not have the answer, but thanks to ambitious goals laid out by President Obama, the topic is in the national spotlight and already has nearly $20 billion in stimulus money scheduled for release in July 2010. Digitizing healthcare records to create a more efficient care delivery system—through improved record keeping, shortened patient length of stay (LOS), and increased ED throughput—isn’t a new idea. Hospitals have struggled for more than a decade with the EHR question, debating whether they should—not to mention how they would—create a computerized system to input patient records into a database that is accessible in real time to hospitalists, nurses, primary-care physicians, insurers, and so on. There have been long-stalled discussions on how to settle privacy concerns that arise from electronic records (see “EHR Upgrade Faces Privacy, Communication Obstacles,” p. 27). Still, a multi-billion-dollar federal pledge has created a moment in time to take EHR beyond the discussion phase.
The Office of the National Coordinator of Health Information Technology (ONCHIT) is empowered to shepherd this process. David Blumenthal, MD, MPP, the director of the Institute for Health Policy, a joint effort of Massachusetts General Hospital and Partners Healthcare System, has been named as ONCHIT’s head. Money to entice hospitals to invest in EHR is part of the American Recovery and Reinvestment Act of 2009. And with Congress hammering out the details of healthcare reform legislation, a sharper focus has been placed on the potential efficiencies EHR can offer.
Money and attention aren’t the only keys to this puzzle, however. IT advocates, medical information officers, and HM group leaders say the government spotlight is a wonderful springboard, but they also say physician involvement in implementing the EHR technology is a must and will spur more hospitals to adopt the systems. Less than 8% of U.S. hospitals have EHR in at least one unit, the New England Journal of Medicine reported earlier this year.1 Just 1.5% of hospitals have a comprehensive system in all of their units.
“There are so many barriers getting to where our country really needs to get,” says Dirk Stanley, MD, MPH, a hospitalist and chief medical informatics officer at Cooley Dickinson Hospital in Northampton, Mass. “One of the big issues is the meaningful use, and how do you actually set criteria for your using electronic health records the right way? If you look at the big picture, you’re talking about so many clinical practices. … How do you write criteria that are meaningful to all those different settings? The government has an enormous challenge.”
Efficiency: HM Cornerstone
David Yu, MD, FHM, works at a hospital with paperless capability and sees on a daily basis how streamlined health records have a practical effect on a hospitalist’s workload and efficiency. Dr. Yu, medical director of hospitalist services at 372-bed Decatur Memorial Hospital in Decatur, Ill., and clinical assistant professor of family and community medicine at Southern Illinois University School of Medicine in Carbondale, is one of EHR’s most passionate advocates.
Decatur Memorial uses GE Healthcare’s Centricity system, which allows hospitalists to “download automatically into our physical history with the click of a button,” says Dr. Yu, a member of Team Hospitalist. “As you’re downloading, you’re accessing the information. It’s literally the same as you driving to the patient’s primary-care physician’s office, pulling the chart, and looking at it.”
Dr. Yu and those who support EHR say it streamlines intakes, discharges, and handoffs, which in turn reduce throughput and length of stay—statistics often cited to prove HM’s value to the hospital administration. The rush for implementation takes on added urgency considering that less than half of 0.5% of hospitals are fully paperless, meaning they have interdepartmental systems that can communicate with each other, according to HIMMS Analytics.
Obama and other healthcare reform advocates envision a day not far in the future when all of America’s hospitals will be connected through a national health records system. Databases in hospitals and physician offices and other healthcare providers will communicate with each other. It will make such health records as X-rays and lab test results a portable commodity, which, in theory, will provide faster and more accurate information for both patients and their providers.
One of the economic stimulus plan’s most important features is its “clarity of purpose,” Dr. Blumenthal wrote in the New England Journal of Medicine earlier this year. “Congress apparently sees [health IT]—computers, software, Internet connection, telemedicine—not as an end in itself, but as a means of improving the quality of healthcare, the health of populations, and the efficiency of healthcare systems.”2
Proactive Approach
Obama has pushed EHR implementation as one of many solutions to the skyrocketing costs of healthcare, saying earlier this year that he is committed to “the immediate investments necessary to ensure that within five years, all of America’s medical records are computerized.” Even so, the EHR upgrade remains only a grand outline, one missing the details that will determine the future. There is time, of course. The first funding through the stimulus bill won’t be available until next summer.
Dr. Blumenthal’s office is crafting an interoperability plan in combination with a pair of still-forming advisory boards: a health information policy committee and a health standards committee. The stimulus bill also promises increased federal reimbursement payments for hospitals with meaningful use of certified EHR. First, the government has to define what is meaningful and, as Dr. Stanley points out, the definition will have different meanings to different sectors of the $2.2 trillion-per-year healthcare industry.
Once those definitions are set, there is a timetable for additional reimbursement and a one-time bonus of $2 million for institutions that implement “meaningful use.” There also will be escalating Medicare penalties for institutions that fail to show the kind of technological progress federal officials are looking for.
But even if those standards are set, it doesn’t guarantee hospitals will buy the technology that vendors are selling. Many in the HM field argue that the next step is the most important one.
“Physician adoption of electronic health records is the central, critical issue this industry is facing over the next few years,” says Todd Johnson, president of Salar Inc., a Baltimore-based firm that develops software applications for clinical documentation. “There are a lot of really bright people working on criteria that make electronic health records good tools. However, there doesn’t seem to be an organized body focused on the EHR adoption issues. Anybody can buy all these tools, but if you ultimately can’t get the right people to use them at the right time, the investment doesn’t yield much, right?”
Johnson, who thinks the federal focus on EHR technology is a main driver behind his firm’s 25% sales growth spurt in the first six months of 2009, says physicians have to be a driving force in the EMR implementation process or the system will fail. Take the industry’s classic cautionary tale: Cedars-Sinai Medical Center in Los Angeles. The oft-innovative institution made national headlines in 2002 when it scrapped a three-month-old, $34 million computerized physician order entry (CPOE) system after more than 400 doctors demanded it be shelved.
“The right thing to do is really steer the discussion to physician adoption,” Johnson says. “Make sure that physicians have a choice. Every hospital—and rightly so—wants to see the benefit of their investment in electronic medical records. If physicians don’t have a voice in what will or won’t work, purchasing decisions will be made without them. And that’s not a great thing. Hospital leadership needs to be cognizant of that.”
Dr. Stanley thinks hospitalists should take a proactive approach to EHR implementation at their hospitals. Many potential issues could be solved if hospitalists take an active role earlier in the process.
“As tedious as those early meetings are,” Dr. Stanley says, “that’s where the big planning and decisions get made. The problem is most people think of it as tedious and boring because they don’t appreciate the technology.”
What’s Ahead
Technology integration is the next step. A handful of companies offer complete EHR platforms, including industry leaders Epic, Meditech, Cerner Corp., GE Healthcare, and McKesson Corp. Specialty firms, such as Johnson’s Salar, offer ancillary and support software and hardware.
Kendall Rogers, MD, assistant professor at the University of New Mexico School of Medicine and chair of SHM’s IT Task Force, says the stimulus funding dedicated to technology will be better served if it focuses on incentives beyond hospitals. Dr. Rogers and others want to see guidelines to create incentives for IT vendors to offer user-friendly systems designed to further medical efficiency goals.
“If this needed technology was developed and proven, the needs for carrots and sticks for adoption would be far less,” Dr. Rogers and several of his peers wrote in an unpublished letter to the NEJM. “Rather than focusing primarily on adoption of systems that have serious limitations … a bill that requires improvements in existing technologies would have much more impact in improving the quality of healthcare.”
Even before that happens, full-scale implementation of these systems will be a costly project that requires a long-term relationship with a vendor. Dr. Van Gomple’s hospital system, Sentara Healthcare, has budgeted $235 million over 10 years for its EHR implementation, according to Bert Reese, senior vice president and chief information officer. His accountants tell him to expect roughly $50 million to be subsidized by the stimulus package. The money is helpful, but not enough for a hospital or system that still needs to find another $185 million.
“The stimulus is nice to get things going,” Reese says. “But if you as an organization think that will cover the cost, you’ll never get going.”
Reese says Sentara’s return on investment at full implementation—roughly five years from now—will be about $35 million per year in savings. He suggests organizations view the investment through a long-term profit goal in order to show the value over an extended timeframe. Otherwise, some C-suites will be scared off by the initial outlay, failing to see the value of efficiency, cost savings, and improved patient care.
“It’s not an IT project,” Reese says. “It’s a clinical project.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Hamel MB, Drazen JM, Epstein AM. The growth of hospitalists and the changing face of primary care. N Engl J Med. 2009;360(11):1141-1143.
- Blumenthal D. Stimulating the adoption of health information technology. N Engl J Med. 2009;360(15):1477-1479.
- Liebovitz, D. Health care information technology: a cloud around the silver lining? Arch Intern Med. 2009;169(10):924-926.
Image Source: ILLUSTRATION / ALICIA BUELOW
Role Refinement

Physician assistants (PAs) and nurse practitioners (NPs), which I will refer to as non-physician providers (NPPs), are popular members of hospitalist practices and have a lot to offer. I think HM groups without NPPs should think about whether adding them would be valuable.
My experience suggests there are many different ways NPPs can contribute to an effective practice. But the optimal NPP role, one that is good for patient care, economically sound for the practice, and satisfying for both the NPP and the MD hospitalists, varies significantly from one practice to the next. I’ve worked with a number of practices that fail to achieve all these goals for a variety of reasons, but a common theme is that the MD hospitalists seem to think the NPPs have been provided for free. As a result, the MDs, and perhaps to some degree the NPPs, feel little or no obligation to develop the optimal NPP job description.
A popular role for NPPs is one very similar to that of the MD hospitalist (e.g., the NPP has a team of patients and rounds and admits daily). That might work well, but for reasons I’ve discussed previously (see “The 411 on NPPs,” September 2008, p. 61), many practices should at least consider other roles for NPPs. One alternative would be to have the NPP work an afternoon-to-night shift (e.g., 3 to 11 p.m.) to handle admissions and “crosscover.” Another option is for the NPP to essentially “own” a component of the practice, such as medical consults for orthopedic patients.
Whatever role is chosen, it must be one that provides the NPP career satisfaction. Over the last few years, I’ve had the pleasure of connecting with Ryan Genzink, PA-C, at various SHM meetings. He essentially is a career hospitalist, and I’ve found him to be a thoughtful guy. At HM09 in Chicago, he and I spoke for a while about NPP roles that provide value and career satisfaction. So I’ve invited him to share his thoughts here.
(Editor’s note: The following is written by Ryan Genzink, PA-C, of Hospitalists of West Michigan in Grand Rapids. He is the AAPA medical liaison to SHM.)
Dr. Nelson correctly observes that while NPPs can be beneficial to HM, there is no “one size fits all” model. However, I think finding the right model for your group sometimes is presented as being more difficult than it really needs to be. Over the years, I have had the opportunity to talk with a number of physicians, PAs, and NPs who work in HM. While models vary, those identified as successful seem to share some common elements.
My story is typical of a lot of PAs working in HM. When I was hired in 2000, my hospital was addressing a workforce shortage. Medical resident workloads were capped, private attending physicians wanted help admitting patients, and the ED was anxious to transfer admitted patients. The hospital was intent on not making our patients wait.
I joined a small group of PAs whose job description included addressing these issues. Like the residents we worked alongside, we took initial calls from the ED, performed histories and physicals, then staffed those with our attending physicians. As a new graduate, I was green and enthusiastic.
The hospitalists were fairly new to working with PAs, too. They had spent years teaching residents, but PAs had joined the group only a year prior. Even so, the group had developed a successful supervision model based on their experiences teaching residents. Patients I saw were cared for by attendings who reviewed the history, asked key questions, performed essential exam elements, and gave the final word on the treatment plan. Teaching naturally flowed from these interactions.
This model continues today. And like the interns who needed less attending input as they transitioned into chief residents, I also required less physician input over time. As our professional relationship grew, the hospitalists became more familiar with my work and exam skills, and I became proficient with our common treatment plans. We functioned together as a team. Of course, this process was no small investment on the part of the hospitalists I worked with. It took time—sometimes with detailed discussions of treatment protocols, or re-examining the patient together to make sure our exams were on the same page. Nonetheless, I think all involved agree the payoff was worth the effort. For our physicians, it made the transition from a resident-based program to one staffed with NPPs favorable. Granted, a residency program has different goals, but because the NPPs don’t rotate off service every six weeks, there is more time to develop collaborative, professional relationships. The investment the attending physicians made stuck.
As work volume increased, PAs in our group expanded into other roles. Our two academic rounding teams, each consisting of one hospitalist and a few residents, added a third team staffed with a hospitalist and a PA. When the residents left, all three teams were staffed with a physician and a PA. NPs later joined the group. And while NPs had slightly different state supervision rules, they functioned in the same roles as the PAs in our facility.
This team approach to rounding works well for our group. The hospitalists and NPPs work together to care for a set group of patients. The hospitalist and the NPP meet in the morning to divide the workload based on acuity, geographic location, and urgency. Sharing a common patient load helps with the common hospitalist dilemma of having to be in two places at the same time. I can see a patient who is ready for discharge (e.g., their ride is on the way), allowing my attending to dedicate his time to another patient’s family conference. In every case, the physician is involved. It is the extent of the involvement that varies. This model gives us flexibility and offers availability to our common patients.
Again, this is one of many successful models. Some, including Dr. Nelson, have suggested that a successful integration model might limit NPPs’ role in the group so that they can have ownership (e.g., post-op consult services). I think there is some merit to this, but this system also has potential unintended consequences.
When we look at what makes hospitalists successful at caring for post-operative patients, we often cite the experience gained from the wide variety of complex medical problems that we address on a daily basis. It is our frequent experience with patients with chronic heart failure that helps us identify the patient in early fluid overload. Our knowledge of diabetic ketoacidosis improves our routine diabetes management.
In my experience, rarely does a patient present with a single, narrowly defined problem. I think that limiting NPPs to the care of specific patient problems will result in limiting their effectiveness and possibly decrease their job satisfaction. I also think HM groups can err on the side of having unrealistic expectations for NPPs. Some groups have them perform the same role as an attending—with an NPP taking the spot of an off-service attending, and vice versa. This can work, if the NPP is experienced. Few would expect a new intern to perform like an attending. Conversely, restricting an NPP to collecting labs and paperwork is not an efficient use of resources.
As Dr. Nelson suggests, successful NPP integration depends on physician leaders being dedicated to the collaborative model and understanding that NPP success is tied to group success. And while admittedly not a perfect test, when in doubt about how an NPP could function in your group, I think asking if a resident would work in the same role is a good starting point. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Physician assistants (PAs) and nurse practitioners (NPs), which I will refer to as non-physician providers (NPPs), are popular members of hospitalist practices and have a lot to offer. I think HM groups without NPPs should think about whether adding them would be valuable.
My experience suggests there are many different ways NPPs can contribute to an effective practice. But the optimal NPP role, one that is good for patient care, economically sound for the practice, and satisfying for both the NPP and the MD hospitalists, varies significantly from one practice to the next. I’ve worked with a number of practices that fail to achieve all these goals for a variety of reasons, but a common theme is that the MD hospitalists seem to think the NPPs have been provided for free. As a result, the MDs, and perhaps to some degree the NPPs, feel little or no obligation to develop the optimal NPP job description.
A popular role for NPPs is one very similar to that of the MD hospitalist (e.g., the NPP has a team of patients and rounds and admits daily). That might work well, but for reasons I’ve discussed previously (see “The 411 on NPPs,” September 2008, p. 61), many practices should at least consider other roles for NPPs. One alternative would be to have the NPP work an afternoon-to-night shift (e.g., 3 to 11 p.m.) to handle admissions and “crosscover.” Another option is for the NPP to essentially “own” a component of the practice, such as medical consults for orthopedic patients.
Whatever role is chosen, it must be one that provides the NPP career satisfaction. Over the last few years, I’ve had the pleasure of connecting with Ryan Genzink, PA-C, at various SHM meetings. He essentially is a career hospitalist, and I’ve found him to be a thoughtful guy. At HM09 in Chicago, he and I spoke for a while about NPP roles that provide value and career satisfaction. So I’ve invited him to share his thoughts here.
(Editor’s note: The following is written by Ryan Genzink, PA-C, of Hospitalists of West Michigan in Grand Rapids. He is the AAPA medical liaison to SHM.)
Dr. Nelson correctly observes that while NPPs can be beneficial to HM, there is no “one size fits all” model. However, I think finding the right model for your group sometimes is presented as being more difficult than it really needs to be. Over the years, I have had the opportunity to talk with a number of physicians, PAs, and NPs who work in HM. While models vary, those identified as successful seem to share some common elements.
My story is typical of a lot of PAs working in HM. When I was hired in 2000, my hospital was addressing a workforce shortage. Medical resident workloads were capped, private attending physicians wanted help admitting patients, and the ED was anxious to transfer admitted patients. The hospital was intent on not making our patients wait.
I joined a small group of PAs whose job description included addressing these issues. Like the residents we worked alongside, we took initial calls from the ED, performed histories and physicals, then staffed those with our attending physicians. As a new graduate, I was green and enthusiastic.
The hospitalists were fairly new to working with PAs, too. They had spent years teaching residents, but PAs had joined the group only a year prior. Even so, the group had developed a successful supervision model based on their experiences teaching residents. Patients I saw were cared for by attendings who reviewed the history, asked key questions, performed essential exam elements, and gave the final word on the treatment plan. Teaching naturally flowed from these interactions.
This model continues today. And like the interns who needed less attending input as they transitioned into chief residents, I also required less physician input over time. As our professional relationship grew, the hospitalists became more familiar with my work and exam skills, and I became proficient with our common treatment plans. We functioned together as a team. Of course, this process was no small investment on the part of the hospitalists I worked with. It took time—sometimes with detailed discussions of treatment protocols, or re-examining the patient together to make sure our exams were on the same page. Nonetheless, I think all involved agree the payoff was worth the effort. For our physicians, it made the transition from a resident-based program to one staffed with NPPs favorable. Granted, a residency program has different goals, but because the NPPs don’t rotate off service every six weeks, there is more time to develop collaborative, professional relationships. The investment the attending physicians made stuck.
As work volume increased, PAs in our group expanded into other roles. Our two academic rounding teams, each consisting of one hospitalist and a few residents, added a third team staffed with a hospitalist and a PA. When the residents left, all three teams were staffed with a physician and a PA. NPs later joined the group. And while NPs had slightly different state supervision rules, they functioned in the same roles as the PAs in our facility.
This team approach to rounding works well for our group. The hospitalists and NPPs work together to care for a set group of patients. The hospitalist and the NPP meet in the morning to divide the workload based on acuity, geographic location, and urgency. Sharing a common patient load helps with the common hospitalist dilemma of having to be in two places at the same time. I can see a patient who is ready for discharge (e.g., their ride is on the way), allowing my attending to dedicate his time to another patient’s family conference. In every case, the physician is involved. It is the extent of the involvement that varies. This model gives us flexibility and offers availability to our common patients.
Again, this is one of many successful models. Some, including Dr. Nelson, have suggested that a successful integration model might limit NPPs’ role in the group so that they can have ownership (e.g., post-op consult services). I think there is some merit to this, but this system also has potential unintended consequences.
When we look at what makes hospitalists successful at caring for post-operative patients, we often cite the experience gained from the wide variety of complex medical problems that we address on a daily basis. It is our frequent experience with patients with chronic heart failure that helps us identify the patient in early fluid overload. Our knowledge of diabetic ketoacidosis improves our routine diabetes management.
In my experience, rarely does a patient present with a single, narrowly defined problem. I think that limiting NPPs to the care of specific patient problems will result in limiting their effectiveness and possibly decrease their job satisfaction. I also think HM groups can err on the side of having unrealistic expectations for NPPs. Some groups have them perform the same role as an attending—with an NPP taking the spot of an off-service attending, and vice versa. This can work, if the NPP is experienced. Few would expect a new intern to perform like an attending. Conversely, restricting an NPP to collecting labs and paperwork is not an efficient use of resources.
As Dr. Nelson suggests, successful NPP integration depends on physician leaders being dedicated to the collaborative model and understanding that NPP success is tied to group success. And while admittedly not a perfect test, when in doubt about how an NPP could function in your group, I think asking if a resident would work in the same role is a good starting point. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Physician assistants (PAs) and nurse practitioners (NPs), which I will refer to as non-physician providers (NPPs), are popular members of hospitalist practices and have a lot to offer. I think HM groups without NPPs should think about whether adding them would be valuable.
My experience suggests there are many different ways NPPs can contribute to an effective practice. But the optimal NPP role, one that is good for patient care, economically sound for the practice, and satisfying for both the NPP and the MD hospitalists, varies significantly from one practice to the next. I’ve worked with a number of practices that fail to achieve all these goals for a variety of reasons, but a common theme is that the MD hospitalists seem to think the NPPs have been provided for free. As a result, the MDs, and perhaps to some degree the NPPs, feel little or no obligation to develop the optimal NPP job description.
A popular role for NPPs is one very similar to that of the MD hospitalist (e.g., the NPP has a team of patients and rounds and admits daily). That might work well, but for reasons I’ve discussed previously (see “The 411 on NPPs,” September 2008, p. 61), many practices should at least consider other roles for NPPs. One alternative would be to have the NPP work an afternoon-to-night shift (e.g., 3 to 11 p.m.) to handle admissions and “crosscover.” Another option is for the NPP to essentially “own” a component of the practice, such as medical consults for orthopedic patients.
Whatever role is chosen, it must be one that provides the NPP career satisfaction. Over the last few years, I’ve had the pleasure of connecting with Ryan Genzink, PA-C, at various SHM meetings. He essentially is a career hospitalist, and I’ve found him to be a thoughtful guy. At HM09 in Chicago, he and I spoke for a while about NPP roles that provide value and career satisfaction. So I’ve invited him to share his thoughts here.
(Editor’s note: The following is written by Ryan Genzink, PA-C, of Hospitalists of West Michigan in Grand Rapids. He is the AAPA medical liaison to SHM.)
Dr. Nelson correctly observes that while NPPs can be beneficial to HM, there is no “one size fits all” model. However, I think finding the right model for your group sometimes is presented as being more difficult than it really needs to be. Over the years, I have had the opportunity to talk with a number of physicians, PAs, and NPs who work in HM. While models vary, those identified as successful seem to share some common elements.
My story is typical of a lot of PAs working in HM. When I was hired in 2000, my hospital was addressing a workforce shortage. Medical resident workloads were capped, private attending physicians wanted help admitting patients, and the ED was anxious to transfer admitted patients. The hospital was intent on not making our patients wait.
I joined a small group of PAs whose job description included addressing these issues. Like the residents we worked alongside, we took initial calls from the ED, performed histories and physicals, then staffed those with our attending physicians. As a new graduate, I was green and enthusiastic.
The hospitalists were fairly new to working with PAs, too. They had spent years teaching residents, but PAs had joined the group only a year prior. Even so, the group had developed a successful supervision model based on their experiences teaching residents. Patients I saw were cared for by attendings who reviewed the history, asked key questions, performed essential exam elements, and gave the final word on the treatment plan. Teaching naturally flowed from these interactions.
This model continues today. And like the interns who needed less attending input as they transitioned into chief residents, I also required less physician input over time. As our professional relationship grew, the hospitalists became more familiar with my work and exam skills, and I became proficient with our common treatment plans. We functioned together as a team. Of course, this process was no small investment on the part of the hospitalists I worked with. It took time—sometimes with detailed discussions of treatment protocols, or re-examining the patient together to make sure our exams were on the same page. Nonetheless, I think all involved agree the payoff was worth the effort. For our physicians, it made the transition from a resident-based program to one staffed with NPPs favorable. Granted, a residency program has different goals, but because the NPPs don’t rotate off service every six weeks, there is more time to develop collaborative, professional relationships. The investment the attending physicians made stuck.
As work volume increased, PAs in our group expanded into other roles. Our two academic rounding teams, each consisting of one hospitalist and a few residents, added a third team staffed with a hospitalist and a PA. When the residents left, all three teams were staffed with a physician and a PA. NPs later joined the group. And while NPs had slightly different state supervision rules, they functioned in the same roles as the PAs in our facility.
This team approach to rounding works well for our group. The hospitalists and NPPs work together to care for a set group of patients. The hospitalist and the NPP meet in the morning to divide the workload based on acuity, geographic location, and urgency. Sharing a common patient load helps with the common hospitalist dilemma of having to be in two places at the same time. I can see a patient who is ready for discharge (e.g., their ride is on the way), allowing my attending to dedicate his time to another patient’s family conference. In every case, the physician is involved. It is the extent of the involvement that varies. This model gives us flexibility and offers availability to our common patients.
Again, this is one of many successful models. Some, including Dr. Nelson, have suggested that a successful integration model might limit NPPs’ role in the group so that they can have ownership (e.g., post-op consult services). I think there is some merit to this, but this system also has potential unintended consequences.
When we look at what makes hospitalists successful at caring for post-operative patients, we often cite the experience gained from the wide variety of complex medical problems that we address on a daily basis. It is our frequent experience with patients with chronic heart failure that helps us identify the patient in early fluid overload. Our knowledge of diabetic ketoacidosis improves our routine diabetes management.
In my experience, rarely does a patient present with a single, narrowly defined problem. I think that limiting NPPs to the care of specific patient problems will result in limiting their effectiveness and possibly decrease their job satisfaction. I also think HM groups can err on the side of having unrealistic expectations for NPPs. Some groups have them perform the same role as an attending—with an NPP taking the spot of an off-service attending, and vice versa. This can work, if the NPP is experienced. Few would expect a new intern to perform like an attending. Conversely, restricting an NPP to collecting labs and paperwork is not an efficient use of resources.
As Dr. Nelson suggests, successful NPP integration depends on physician leaders being dedicated to the collaborative model and understanding that NPP success is tied to group success. And while admittedly not a perfect test, when in doubt about how an NPP could function in your group, I think asking if a resident would work in the same role is a good starting point. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Only Fools Rush In

Irecently bought an Apple computer. This is newsworthy because I am a lifelong PC user, and because I suffer from a genetic inability to adopt new technologies. In fact, I’m so old-school that only the graceless act of brandishing my credit card kept me from being unceremoniously escorted out of the store by Apple “specialists” for scaring off iPod-yearning tweens. Even then I wasn’t allowed to linger post-purchase.
After racing home, I eagerly slipped the 24 inches of iMac splendor out of its slick, mod-ish packaging and set it up on my desk. Thoughts of newfound cachet danced in my head as I peeled off my black “dad” socks and Tevas. It was clear to me that, as advertised, this sleek beauty was going to transform me from a doddering old Luddite into one of those trendy hipsters so keyed into the pulse of society. And it promised to be easier … and better.
What followed reminded me that the gospel of technology could sometimes preach a false god. It took but a few keystrokes to find myself grappling with a new operating system—it looked like Windows but felt like closed doors. Things that I can do effortlessly on my PC—navigate through files, open Web browsers, access my Outlook account, PowerPoint—seemed to take extra steps, new steps, or unknown steps.
Eventually, I was able figure most of this out, but in the end I was left with the very un-sating realization that the Mac wasn’t really any better than my PC. It was cooler, that’s for sure—even my wife took a renewed interest in me. However, after that cool factor quickly chilled, I was left with the queasy feeling that I had just dropped thousands of dollars on a machine that didn’t really function any better than my old machine. And in some cases, it functioned worse.
Fool’s Gold?
Like my new iMac, electronic health records (EHR) are touted as the technological savior of healthcare—if you invest in the rhetoric coming out of Washington. As our legislators struggle to figure out ways to shoehorn 50 million more Americans into the “insured” category, stave off the growing epidemic of medical errors, and improve the general quality of care, digitizing our health records is a commonly noted panacea. And EHR, it’s promised, somehow will do all of this while conveniently reducing the skyrocketing costs of healthcare.
My hospital is on the verge of siphoning tens of millions of dollars of government stimulus funding and hospital capital into the purchase of a major EHR upgrade. This system aims to seamlessly integrate our inpatient and outpatient billing, documentation, lab, and ordering systems into one neatly packaged, computer-driven solution. I’m left wondering if my iMac experience is an augur of how this will play out on a grand stage.
In the spirit of full disclosure, I fully support automating healthcare as much as possible and sit on numerous committees at my institution charged with doing just that. Further, I believe it will be a salve to many of our efficiency, quality, and patient safety issues. However, I worry that in solving some problems, these new technological cure-alls will simply introduce other, unanticipated problems.
Several years ago, my hospital introduced several systems and technological applications aimed at improving quality, safety, and efficiency. One of these is called “rounds reports.” These very handy, printable documents are a terrific idea and a great example of simplified workflow. The doctor simply prints out a one-page summary of the patient’s 24-hour vital signs, medications, and labs, and uses that as the template for their daily note.
As promised, it’s a time-saver. The problem is that this new technology harbors insidious flaws that prey on the frailties of human nature by introducing new portals for error. For example, the report makes it simple to not reconcile medications daily. The time-honored and time-intensive manner of writing all the meds on a progress note is indeed cumbersome, but it has the added effect of forcing the provider to think about each medication—the utility, the dosage, the effects of the failing kidney on the dosage. Automation of this process removes this small but critical safety check. Sure, diligent providers can overcome this by paying close attention to the printout, but human nature dictates that we don’t always do it. In fact, we employed automation to save this type of time in the first place.
The rounds report also helpfully displays the vital signs and blood sugars for the past 24 hours, reducing the time the harried hospitalist has to spend looking these up and writing them down. However, the report doesn’t print out every vital sign and blood-sugar level; it provides a range. Again, it is possible to access these individual levels, but the post-EHR provider, lured by simplification, often doesn’t take the extra step to go to the separate program to gather these numbers. This shortcut enhances efficiency at the expense of having complete data, a scenario that can breed bad outcomes.
More Efficient Doesn’t Mean Better
Then there is the catch-22 of electronic imaging reports. It is impressive how quickly a chest X-ray gets read and reported electronically in my hospital. The downside, of course, is that today’s techno-doc can rely on the written report without reviewing the actual image. We’ve again, in not reviewing the films personally, removed an important safety check.
The point is that while mechanization offers great potential, it is easy to overlook the downside. Many physicians are not as tech-savvy as their kids and likely will struggle with these newfangled devices. For them, this will not simplify their workflow, but rather it will bog them down. These gizmos also are extremely expensive, and many small clinics and rural hospitals will struggle to afford these upgrades, even with taxpayer support. And let’s not overlook the myriad unforeseen hiccups these new systems will breed.
None of this is to say we shouldn’t embrace our “Jetsons”-like future. In fact, I’d counter that we must, and now is the opportune time. Still, I get nervous when I read stories of the endless EHR potential that omit or gloss over the probable limitations. The key will be to adopt these systems in ways that augment their strengths while mitigating their weaknesses. This must include achieving the delicate balance of usability, efficiency, and safety.
Otherwise, we might find that the technological apple will keep the doctors away. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Irecently bought an Apple computer. This is newsworthy because I am a lifelong PC user, and because I suffer from a genetic inability to adopt new technologies. In fact, I’m so old-school that only the graceless act of brandishing my credit card kept me from being unceremoniously escorted out of the store by Apple “specialists” for scaring off iPod-yearning tweens. Even then I wasn’t allowed to linger post-purchase.
After racing home, I eagerly slipped the 24 inches of iMac splendor out of its slick, mod-ish packaging and set it up on my desk. Thoughts of newfound cachet danced in my head as I peeled off my black “dad” socks and Tevas. It was clear to me that, as advertised, this sleek beauty was going to transform me from a doddering old Luddite into one of those trendy hipsters so keyed into the pulse of society. And it promised to be easier … and better.
What followed reminded me that the gospel of technology could sometimes preach a false god. It took but a few keystrokes to find myself grappling with a new operating system—it looked like Windows but felt like closed doors. Things that I can do effortlessly on my PC—navigate through files, open Web browsers, access my Outlook account, PowerPoint—seemed to take extra steps, new steps, or unknown steps.
Eventually, I was able figure most of this out, but in the end I was left with the very un-sating realization that the Mac wasn’t really any better than my PC. It was cooler, that’s for sure—even my wife took a renewed interest in me. However, after that cool factor quickly chilled, I was left with the queasy feeling that I had just dropped thousands of dollars on a machine that didn’t really function any better than my old machine. And in some cases, it functioned worse.
Fool’s Gold?
Like my new iMac, electronic health records (EHR) are touted as the technological savior of healthcare—if you invest in the rhetoric coming out of Washington. As our legislators struggle to figure out ways to shoehorn 50 million more Americans into the “insured” category, stave off the growing epidemic of medical errors, and improve the general quality of care, digitizing our health records is a commonly noted panacea. And EHR, it’s promised, somehow will do all of this while conveniently reducing the skyrocketing costs of healthcare.
My hospital is on the verge of siphoning tens of millions of dollars of government stimulus funding and hospital capital into the purchase of a major EHR upgrade. This system aims to seamlessly integrate our inpatient and outpatient billing, documentation, lab, and ordering systems into one neatly packaged, computer-driven solution. I’m left wondering if my iMac experience is an augur of how this will play out on a grand stage.
In the spirit of full disclosure, I fully support automating healthcare as much as possible and sit on numerous committees at my institution charged with doing just that. Further, I believe it will be a salve to many of our efficiency, quality, and patient safety issues. However, I worry that in solving some problems, these new technological cure-alls will simply introduce other, unanticipated problems.
Several years ago, my hospital introduced several systems and technological applications aimed at improving quality, safety, and efficiency. One of these is called “rounds reports.” These very handy, printable documents are a terrific idea and a great example of simplified workflow. The doctor simply prints out a one-page summary of the patient’s 24-hour vital signs, medications, and labs, and uses that as the template for their daily note.
As promised, it’s a time-saver. The problem is that this new technology harbors insidious flaws that prey on the frailties of human nature by introducing new portals for error. For example, the report makes it simple to not reconcile medications daily. The time-honored and time-intensive manner of writing all the meds on a progress note is indeed cumbersome, but it has the added effect of forcing the provider to think about each medication—the utility, the dosage, the effects of the failing kidney on the dosage. Automation of this process removes this small but critical safety check. Sure, diligent providers can overcome this by paying close attention to the printout, but human nature dictates that we don’t always do it. In fact, we employed automation to save this type of time in the first place.
The rounds report also helpfully displays the vital signs and blood sugars for the past 24 hours, reducing the time the harried hospitalist has to spend looking these up and writing them down. However, the report doesn’t print out every vital sign and blood-sugar level; it provides a range. Again, it is possible to access these individual levels, but the post-EHR provider, lured by simplification, often doesn’t take the extra step to go to the separate program to gather these numbers. This shortcut enhances efficiency at the expense of having complete data, a scenario that can breed bad outcomes.
More Efficient Doesn’t Mean Better
Then there is the catch-22 of electronic imaging reports. It is impressive how quickly a chest X-ray gets read and reported electronically in my hospital. The downside, of course, is that today’s techno-doc can rely on the written report without reviewing the actual image. We’ve again, in not reviewing the films personally, removed an important safety check.
The point is that while mechanization offers great potential, it is easy to overlook the downside. Many physicians are not as tech-savvy as their kids and likely will struggle with these newfangled devices. For them, this will not simplify their workflow, but rather it will bog them down. These gizmos also are extremely expensive, and many small clinics and rural hospitals will struggle to afford these upgrades, even with taxpayer support. And let’s not overlook the myriad unforeseen hiccups these new systems will breed.
None of this is to say we shouldn’t embrace our “Jetsons”-like future. In fact, I’d counter that we must, and now is the opportune time. Still, I get nervous when I read stories of the endless EHR potential that omit or gloss over the probable limitations. The key will be to adopt these systems in ways that augment their strengths while mitigating their weaknesses. This must include achieving the delicate balance of usability, efficiency, and safety.
Otherwise, we might find that the technological apple will keep the doctors away. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Irecently bought an Apple computer. This is newsworthy because I am a lifelong PC user, and because I suffer from a genetic inability to adopt new technologies. In fact, I’m so old-school that only the graceless act of brandishing my credit card kept me from being unceremoniously escorted out of the store by Apple “specialists” for scaring off iPod-yearning tweens. Even then I wasn’t allowed to linger post-purchase.
After racing home, I eagerly slipped the 24 inches of iMac splendor out of its slick, mod-ish packaging and set it up on my desk. Thoughts of newfound cachet danced in my head as I peeled off my black “dad” socks and Tevas. It was clear to me that, as advertised, this sleek beauty was going to transform me from a doddering old Luddite into one of those trendy hipsters so keyed into the pulse of society. And it promised to be easier … and better.
What followed reminded me that the gospel of technology could sometimes preach a false god. It took but a few keystrokes to find myself grappling with a new operating system—it looked like Windows but felt like closed doors. Things that I can do effortlessly on my PC—navigate through files, open Web browsers, access my Outlook account, PowerPoint—seemed to take extra steps, new steps, or unknown steps.
Eventually, I was able figure most of this out, but in the end I was left with the very un-sating realization that the Mac wasn’t really any better than my PC. It was cooler, that’s for sure—even my wife took a renewed interest in me. However, after that cool factor quickly chilled, I was left with the queasy feeling that I had just dropped thousands of dollars on a machine that didn’t really function any better than my old machine. And in some cases, it functioned worse.
Fool’s Gold?
Like my new iMac, electronic health records (EHR) are touted as the technological savior of healthcare—if you invest in the rhetoric coming out of Washington. As our legislators struggle to figure out ways to shoehorn 50 million more Americans into the “insured” category, stave off the growing epidemic of medical errors, and improve the general quality of care, digitizing our health records is a commonly noted panacea. And EHR, it’s promised, somehow will do all of this while conveniently reducing the skyrocketing costs of healthcare.
My hospital is on the verge of siphoning tens of millions of dollars of government stimulus funding and hospital capital into the purchase of a major EHR upgrade. This system aims to seamlessly integrate our inpatient and outpatient billing, documentation, lab, and ordering systems into one neatly packaged, computer-driven solution. I’m left wondering if my iMac experience is an augur of how this will play out on a grand stage.
In the spirit of full disclosure, I fully support automating healthcare as much as possible and sit on numerous committees at my institution charged with doing just that. Further, I believe it will be a salve to many of our efficiency, quality, and patient safety issues. However, I worry that in solving some problems, these new technological cure-alls will simply introduce other, unanticipated problems.
Several years ago, my hospital introduced several systems and technological applications aimed at improving quality, safety, and efficiency. One of these is called “rounds reports.” These very handy, printable documents are a terrific idea and a great example of simplified workflow. The doctor simply prints out a one-page summary of the patient’s 24-hour vital signs, medications, and labs, and uses that as the template for their daily note.
As promised, it’s a time-saver. The problem is that this new technology harbors insidious flaws that prey on the frailties of human nature by introducing new portals for error. For example, the report makes it simple to not reconcile medications daily. The time-honored and time-intensive manner of writing all the meds on a progress note is indeed cumbersome, but it has the added effect of forcing the provider to think about each medication—the utility, the dosage, the effects of the failing kidney on the dosage. Automation of this process removes this small but critical safety check. Sure, diligent providers can overcome this by paying close attention to the printout, but human nature dictates that we don’t always do it. In fact, we employed automation to save this type of time in the first place.
The rounds report also helpfully displays the vital signs and blood sugars for the past 24 hours, reducing the time the harried hospitalist has to spend looking these up and writing them down. However, the report doesn’t print out every vital sign and blood-sugar level; it provides a range. Again, it is possible to access these individual levels, but the post-EHR provider, lured by simplification, often doesn’t take the extra step to go to the separate program to gather these numbers. This shortcut enhances efficiency at the expense of having complete data, a scenario that can breed bad outcomes.
More Efficient Doesn’t Mean Better
Then there is the catch-22 of electronic imaging reports. It is impressive how quickly a chest X-ray gets read and reported electronically in my hospital. The downside, of course, is that today’s techno-doc can rely on the written report without reviewing the actual image. We’ve again, in not reviewing the films personally, removed an important safety check.
The point is that while mechanization offers great potential, it is easy to overlook the downside. Many physicians are not as tech-savvy as their kids and likely will struggle with these newfangled devices. For them, this will not simplify their workflow, but rather it will bog them down. These gizmos also are extremely expensive, and many small clinics and rural hospitals will struggle to afford these upgrades, even with taxpayer support. And let’s not overlook the myriad unforeseen hiccups these new systems will breed.
None of this is to say we shouldn’t embrace our “Jetsons”-like future. In fact, I’d counter that we must, and now is the opportune time. Still, I get nervous when I read stories of the endless EHR potential that omit or gloss over the probable limitations. The key will be to adopt these systems in ways that augment their strengths while mitigating their weaknesses. This must include achieving the delicate balance of usability, efficiency, and safety.
Otherwise, we might find that the technological apple will keep the doctors away. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
What Are They Doing (to Me) in D.C.?

Idon’t know about you, but sometimes I feel as if we are living in an era of information overload when it comes to all of the ideas that are spilling out of Washington and elsewhere under the sobriquet of “healthcare reform.” I thought we should take a few minutes and try to bring all these proposals into focus.
There is an ideal, almost a nirvana, that is being sought. This would include access with a very big “A” to include most, if not all, Americans, and would recognize key differences in patients (comorbidities), and would incentivize value (e.g., quality and cost), and promote evidence-based medicine (EBM) instead of the usual and customary.
That is a far cry from the system that we currently function in. The reality of today is much simpler, at least for the payment part of the system. A hospital or a doctor does something specific, such as a procedure or a visit, and whoever provides the care submits the bill. It is finite and usually involves a small group of individuals or facilities. Because it is simple and to the point, it allows small hospitals and the generally fragmented physician practices to be in the game.
Unfortunately, this system of payment and reward has not led us to the outcomes or performance that our country’s leaders or businesses, and more and more our patients, think we should be getting for our $2.2 trillion. Part of this is due to the fragmentation and variability in how healthcare currently is delivered. More unfortunate is the reality of the disconnect between patients and providers, and the complexity of care. In most healthcare communities, patients can wander through the course of their care to many providers and facilities, most of which have no common information system or business relationship.
One solution that is being considered in Washington is bundling. When policy wonks talk about bundling of payment for an episode of care, they are envisioning a world in which whoever is paying for care (Medicare, insurers, etc.) can pay one fee that would encompass the care provided by all providers, all facilities, and over a broad timeframe (e.g., hospitalization, then 30 days post-discharge). That might work for Mayo in southern Minnesota, Geisinger in northeast Pennsylvania, or Kaiser in Northern California, but just how would it work in the vast majority of places in the U.S.?
If a patient’s care involves two or three separate facilities or a number of providers in the hospital, and it spans as many as 30 days after discharge, how would you assign responsibility for flaws in the patient’s care or the need for additional services? And where is the patient responsibility in all of this?
Knowing all of this, is Congress really ready to write new regulations and pivot 180 degrees on the current system? Glenn Steele, CEO of Geisinger Health System and a recognized leader in a forward-thinking organization, has said, “We probably ought to have a system where we can be innovative, rather than just a new set of rules.”
Baby Steps
In some ways, healthcare reform already is moving forward. The Centers for Medicare and Medicaid Services (CMS) has enacted “never events” in an attempt to improve performance by withholding payment for incidents Medicare thinks just shouldn’t happen (e.g., wrong-side surgery, some hospital-acquired infections).
In addition, 14 communities are ready to perform three-year “comparative effectiveness” trials to attempt to coordinate care among disparate sectors of the healthcare continuum. The research model is looking for ways to deliver optimum care in less-organized sectors of healthcare.
In January, CMS announced site selections for the Acute Care Episode (ACE) demonstration project. ACE is a new, hospital-based demonstration that will test the use of a bundled payment for both hospital and physician services for a select set of inpatient episodes of care. The goal is to improve the quality of care delivered through Medicare fee-for-service. Baptist Health System in San Antonio; Oklahoma Heart Hospital LLC in Oklahoma City; Exempla Saint Joseph Hospital in Denver; Hillcrest Medical Center in Tulsa, Okla.; and Lovelace Health System in Albuquerque, N.M., will participate in the demonstration.
But even when we are just at the beginning of field-testing ideas to improve the delivery of care, all signs point to a major healthcare reform bill coming out of Congress this year. How can they know what will work when the demonstration projects are just starting? How can they anticipate the unintended consequences of wholesale reform? Well, that’s just what Congress can—and does—do. We will all be left to figure out the details on the fly.
The temperature seems to be getting turned up a notch with every healthcare blog and Web posting. When the public and legislators read what Atul Gawande, MD, MPH, wrote in The New Yorker and then it is quoted by the president, suddenly it seems that everyone knows that care is much more expensive in McAllen, Texas, than in nearby El Paso, albeit with worse outcomes. The solution is almost anything that purports to reduce unnecessary variability and ties payment to performance.
Prospective vs. Retrospective Payment
To allow yourself to have a broad context of payment reform, think of “prospective” and “retrospective” payment as two options for a new payment paradigm. Don’t roll your eyes; this stuff is material to how we earn our living.
A prospective system might drastically alter what we have now, by throwing out fee-for-service and no longer paying by the unit of the visit or the procedure, and instead using a global fee (e.g., bundling) that is geared more toward efficiency and effectiveness (i.e., use of resources and better outcomes).
On the other hand, a retrospective system might continue to pay a modified fee-for-service fee (i.e., lower than current reimbursement) with a “significant” bonus for performance (e.g., lower readmission rate, fewer visits to the ED) and improved measureable quality. Of course, this can be “new money” for quality or part of a holdback after upfront fees have been lowered.
In any event, we are probably entering an era in which hospitals and physicians will need to think of themselves as part of a “supply chain” and not just think “I did my job, so pay me.” And during this whole reshuffling of the healthcare deck, there might be calls to remove some of the inequities that have been cobbled onto the Medicare and insurance systems. For example, currently there are significant geographic disparities in Medicare reimbursement (e.g., surgery in Mississippi often is reimbursed at 50% of the same procedure in New York City or Los Angeles). And there are significant payment disparities between medical and surgical specialties and primary-care providers that the Resource-Based Relative Value Scale (RBRVS) system has certainly not corrected.
Integration Hurdles
The small percentage of hospitals, physicians, and patients who currently are in an integrated system probably will have a smoother ride into healthcare’s new future. It is easier for Kaiser or Geisinger or HealthPartners in Minnesota to take on all of the business challenges and risks of accountability for performance and rewards for efficiency. But what about most of the rest of us?
Well, it looks as if we will need to be linked together by contracts and business relationships, by information transfer and management, and we will need strong, forward-thinking, innovative leadership. And we’ll need some trust in each other and our institutions going forward. Equally important, our patients will need to step up and into this new world. If providers and facilities are required to perform better, then patients have to stay in their contracted systems. To have accountability, patients must participate actively.
Some of you might be old enough to remember the last time integration of physicians and hospitals was all the rage. In the 1990s, the driving force was to achieve “economies of scale” and to meet the challenges of managed care with an integrated entity. Most of these attempts were expensive failures.
In 2010, the drive to integration might be the radical reworking of a payment system that is based on a global fee, a system that produces the highest quality at the lowest cost.
One caveat is that significant integration might not be possible. Do hospitals have the expertise and capacity to employ physicians to efficiently deliver care? In this recession, is the capital available to purchase and implement the information systems crucial to integrated care?
Prepared for Change
I profess to have no expertise as a prognosticator, but I do expect some significant changes to come out of Washington in 2009. The common wisdom is that we are currently spending enough in the aggregate to provide all Americans with access to healthcare, and to get better performance and less variability. That seems to mean shaping a new system.
SHM supports changes in payment methodologies that improve the quality and value of healthcare services, align incentives, and promote better clinical outcomes. We believe that healthcare pricing and quality should be transparent to patients and purchasers. We have supported the PQRI, hospital value-based purchasing, and loosening of restrictions on gainsharing between facilities and providers.
Hospitalists are positioned well. We practice in groups and often are aligned with many others in our medical staffs, and with our hospitals’ roles in our communities. We already are thinking about the value equation and trying to balance resources and performance. We are young, adaptable, and less entrenched. And we are new and have less to lose.
I am confident we can be helpful in shaping the future and can thrive in most any new environment. But hold on tight: The future is getting here way ahead of schedule. TH
Dr. Wellikson is CEO of SHM.
Idon’t know about you, but sometimes I feel as if we are living in an era of information overload when it comes to all of the ideas that are spilling out of Washington and elsewhere under the sobriquet of “healthcare reform.” I thought we should take a few minutes and try to bring all these proposals into focus.
There is an ideal, almost a nirvana, that is being sought. This would include access with a very big “A” to include most, if not all, Americans, and would recognize key differences in patients (comorbidities), and would incentivize value (e.g., quality and cost), and promote evidence-based medicine (EBM) instead of the usual and customary.
That is a far cry from the system that we currently function in. The reality of today is much simpler, at least for the payment part of the system. A hospital or a doctor does something specific, such as a procedure or a visit, and whoever provides the care submits the bill. It is finite and usually involves a small group of individuals or facilities. Because it is simple and to the point, it allows small hospitals and the generally fragmented physician practices to be in the game.
Unfortunately, this system of payment and reward has not led us to the outcomes or performance that our country’s leaders or businesses, and more and more our patients, think we should be getting for our $2.2 trillion. Part of this is due to the fragmentation and variability in how healthcare currently is delivered. More unfortunate is the reality of the disconnect between patients and providers, and the complexity of care. In most healthcare communities, patients can wander through the course of their care to many providers and facilities, most of which have no common information system or business relationship.
One solution that is being considered in Washington is bundling. When policy wonks talk about bundling of payment for an episode of care, they are envisioning a world in which whoever is paying for care (Medicare, insurers, etc.) can pay one fee that would encompass the care provided by all providers, all facilities, and over a broad timeframe (e.g., hospitalization, then 30 days post-discharge). That might work for Mayo in southern Minnesota, Geisinger in northeast Pennsylvania, or Kaiser in Northern California, but just how would it work in the vast majority of places in the U.S.?
If a patient’s care involves two or three separate facilities or a number of providers in the hospital, and it spans as many as 30 days after discharge, how would you assign responsibility for flaws in the patient’s care or the need for additional services? And where is the patient responsibility in all of this?
Knowing all of this, is Congress really ready to write new regulations and pivot 180 degrees on the current system? Glenn Steele, CEO of Geisinger Health System and a recognized leader in a forward-thinking organization, has said, “We probably ought to have a system where we can be innovative, rather than just a new set of rules.”
Baby Steps
In some ways, healthcare reform already is moving forward. The Centers for Medicare and Medicaid Services (CMS) has enacted “never events” in an attempt to improve performance by withholding payment for incidents Medicare thinks just shouldn’t happen (e.g., wrong-side surgery, some hospital-acquired infections).
In addition, 14 communities are ready to perform three-year “comparative effectiveness” trials to attempt to coordinate care among disparate sectors of the healthcare continuum. The research model is looking for ways to deliver optimum care in less-organized sectors of healthcare.
In January, CMS announced site selections for the Acute Care Episode (ACE) demonstration project. ACE is a new, hospital-based demonstration that will test the use of a bundled payment for both hospital and physician services for a select set of inpatient episodes of care. The goal is to improve the quality of care delivered through Medicare fee-for-service. Baptist Health System in San Antonio; Oklahoma Heart Hospital LLC in Oklahoma City; Exempla Saint Joseph Hospital in Denver; Hillcrest Medical Center in Tulsa, Okla.; and Lovelace Health System in Albuquerque, N.M., will participate in the demonstration.
But even when we are just at the beginning of field-testing ideas to improve the delivery of care, all signs point to a major healthcare reform bill coming out of Congress this year. How can they know what will work when the demonstration projects are just starting? How can they anticipate the unintended consequences of wholesale reform? Well, that’s just what Congress can—and does—do. We will all be left to figure out the details on the fly.
The temperature seems to be getting turned up a notch with every healthcare blog and Web posting. When the public and legislators read what Atul Gawande, MD, MPH, wrote in The New Yorker and then it is quoted by the president, suddenly it seems that everyone knows that care is much more expensive in McAllen, Texas, than in nearby El Paso, albeit with worse outcomes. The solution is almost anything that purports to reduce unnecessary variability and ties payment to performance.
Prospective vs. Retrospective Payment
To allow yourself to have a broad context of payment reform, think of “prospective” and “retrospective” payment as two options for a new payment paradigm. Don’t roll your eyes; this stuff is material to how we earn our living.
A prospective system might drastically alter what we have now, by throwing out fee-for-service and no longer paying by the unit of the visit or the procedure, and instead using a global fee (e.g., bundling) that is geared more toward efficiency and effectiveness (i.e., use of resources and better outcomes).
On the other hand, a retrospective system might continue to pay a modified fee-for-service fee (i.e., lower than current reimbursement) with a “significant” bonus for performance (e.g., lower readmission rate, fewer visits to the ED) and improved measureable quality. Of course, this can be “new money” for quality or part of a holdback after upfront fees have been lowered.
In any event, we are probably entering an era in which hospitals and physicians will need to think of themselves as part of a “supply chain” and not just think “I did my job, so pay me.” And during this whole reshuffling of the healthcare deck, there might be calls to remove some of the inequities that have been cobbled onto the Medicare and insurance systems. For example, currently there are significant geographic disparities in Medicare reimbursement (e.g., surgery in Mississippi often is reimbursed at 50% of the same procedure in New York City or Los Angeles). And there are significant payment disparities between medical and surgical specialties and primary-care providers that the Resource-Based Relative Value Scale (RBRVS) system has certainly not corrected.
Integration Hurdles
The small percentage of hospitals, physicians, and patients who currently are in an integrated system probably will have a smoother ride into healthcare’s new future. It is easier for Kaiser or Geisinger or HealthPartners in Minnesota to take on all of the business challenges and risks of accountability for performance and rewards for efficiency. But what about most of the rest of us?
Well, it looks as if we will need to be linked together by contracts and business relationships, by information transfer and management, and we will need strong, forward-thinking, innovative leadership. And we’ll need some trust in each other and our institutions going forward. Equally important, our patients will need to step up and into this new world. If providers and facilities are required to perform better, then patients have to stay in their contracted systems. To have accountability, patients must participate actively.
Some of you might be old enough to remember the last time integration of physicians and hospitals was all the rage. In the 1990s, the driving force was to achieve “economies of scale” and to meet the challenges of managed care with an integrated entity. Most of these attempts were expensive failures.
In 2010, the drive to integration might be the radical reworking of a payment system that is based on a global fee, a system that produces the highest quality at the lowest cost.
One caveat is that significant integration might not be possible. Do hospitals have the expertise and capacity to employ physicians to efficiently deliver care? In this recession, is the capital available to purchase and implement the information systems crucial to integrated care?
Prepared for Change
I profess to have no expertise as a prognosticator, but I do expect some significant changes to come out of Washington in 2009. The common wisdom is that we are currently spending enough in the aggregate to provide all Americans with access to healthcare, and to get better performance and less variability. That seems to mean shaping a new system.
SHM supports changes in payment methodologies that improve the quality and value of healthcare services, align incentives, and promote better clinical outcomes. We believe that healthcare pricing and quality should be transparent to patients and purchasers. We have supported the PQRI, hospital value-based purchasing, and loosening of restrictions on gainsharing between facilities and providers.
Hospitalists are positioned well. We practice in groups and often are aligned with many others in our medical staffs, and with our hospitals’ roles in our communities. We already are thinking about the value equation and trying to balance resources and performance. We are young, adaptable, and less entrenched. And we are new and have less to lose.
I am confident we can be helpful in shaping the future and can thrive in most any new environment. But hold on tight: The future is getting here way ahead of schedule. TH
Dr. Wellikson is CEO of SHM.
Idon’t know about you, but sometimes I feel as if we are living in an era of information overload when it comes to all of the ideas that are spilling out of Washington and elsewhere under the sobriquet of “healthcare reform.” I thought we should take a few minutes and try to bring all these proposals into focus.
There is an ideal, almost a nirvana, that is being sought. This would include access with a very big “A” to include most, if not all, Americans, and would recognize key differences in patients (comorbidities), and would incentivize value (e.g., quality and cost), and promote evidence-based medicine (EBM) instead of the usual and customary.
That is a far cry from the system that we currently function in. The reality of today is much simpler, at least for the payment part of the system. A hospital or a doctor does something specific, such as a procedure or a visit, and whoever provides the care submits the bill. It is finite and usually involves a small group of individuals or facilities. Because it is simple and to the point, it allows small hospitals and the generally fragmented physician practices to be in the game.
Unfortunately, this system of payment and reward has not led us to the outcomes or performance that our country’s leaders or businesses, and more and more our patients, think we should be getting for our $2.2 trillion. Part of this is due to the fragmentation and variability in how healthcare currently is delivered. More unfortunate is the reality of the disconnect between patients and providers, and the complexity of care. In most healthcare communities, patients can wander through the course of their care to many providers and facilities, most of which have no common information system or business relationship.
One solution that is being considered in Washington is bundling. When policy wonks talk about bundling of payment for an episode of care, they are envisioning a world in which whoever is paying for care (Medicare, insurers, etc.) can pay one fee that would encompass the care provided by all providers, all facilities, and over a broad timeframe (e.g., hospitalization, then 30 days post-discharge). That might work for Mayo in southern Minnesota, Geisinger in northeast Pennsylvania, or Kaiser in Northern California, but just how would it work in the vast majority of places in the U.S.?
If a patient’s care involves two or three separate facilities or a number of providers in the hospital, and it spans as many as 30 days after discharge, how would you assign responsibility for flaws in the patient’s care or the need for additional services? And where is the patient responsibility in all of this?
Knowing all of this, is Congress really ready to write new regulations and pivot 180 degrees on the current system? Glenn Steele, CEO of Geisinger Health System and a recognized leader in a forward-thinking organization, has said, “We probably ought to have a system where we can be innovative, rather than just a new set of rules.”
Baby Steps
In some ways, healthcare reform already is moving forward. The Centers for Medicare and Medicaid Services (CMS) has enacted “never events” in an attempt to improve performance by withholding payment for incidents Medicare thinks just shouldn’t happen (e.g., wrong-side surgery, some hospital-acquired infections).
In addition, 14 communities are ready to perform three-year “comparative effectiveness” trials to attempt to coordinate care among disparate sectors of the healthcare continuum. The research model is looking for ways to deliver optimum care in less-organized sectors of healthcare.
In January, CMS announced site selections for the Acute Care Episode (ACE) demonstration project. ACE is a new, hospital-based demonstration that will test the use of a bundled payment for both hospital and physician services for a select set of inpatient episodes of care. The goal is to improve the quality of care delivered through Medicare fee-for-service. Baptist Health System in San Antonio; Oklahoma Heart Hospital LLC in Oklahoma City; Exempla Saint Joseph Hospital in Denver; Hillcrest Medical Center in Tulsa, Okla.; and Lovelace Health System in Albuquerque, N.M., will participate in the demonstration.
But even when we are just at the beginning of field-testing ideas to improve the delivery of care, all signs point to a major healthcare reform bill coming out of Congress this year. How can they know what will work when the demonstration projects are just starting? How can they anticipate the unintended consequences of wholesale reform? Well, that’s just what Congress can—and does—do. We will all be left to figure out the details on the fly.
The temperature seems to be getting turned up a notch with every healthcare blog and Web posting. When the public and legislators read what Atul Gawande, MD, MPH, wrote in The New Yorker and then it is quoted by the president, suddenly it seems that everyone knows that care is much more expensive in McAllen, Texas, than in nearby El Paso, albeit with worse outcomes. The solution is almost anything that purports to reduce unnecessary variability and ties payment to performance.
Prospective vs. Retrospective Payment
To allow yourself to have a broad context of payment reform, think of “prospective” and “retrospective” payment as two options for a new payment paradigm. Don’t roll your eyes; this stuff is material to how we earn our living.
A prospective system might drastically alter what we have now, by throwing out fee-for-service and no longer paying by the unit of the visit or the procedure, and instead using a global fee (e.g., bundling) that is geared more toward efficiency and effectiveness (i.e., use of resources and better outcomes).
On the other hand, a retrospective system might continue to pay a modified fee-for-service fee (i.e., lower than current reimbursement) with a “significant” bonus for performance (e.g., lower readmission rate, fewer visits to the ED) and improved measureable quality. Of course, this can be “new money” for quality or part of a holdback after upfront fees have been lowered.
In any event, we are probably entering an era in which hospitals and physicians will need to think of themselves as part of a “supply chain” and not just think “I did my job, so pay me.” And during this whole reshuffling of the healthcare deck, there might be calls to remove some of the inequities that have been cobbled onto the Medicare and insurance systems. For example, currently there are significant geographic disparities in Medicare reimbursement (e.g., surgery in Mississippi often is reimbursed at 50% of the same procedure in New York City or Los Angeles). And there are significant payment disparities between medical and surgical specialties and primary-care providers that the Resource-Based Relative Value Scale (RBRVS) system has certainly not corrected.
Integration Hurdles
The small percentage of hospitals, physicians, and patients who currently are in an integrated system probably will have a smoother ride into healthcare’s new future. It is easier for Kaiser or Geisinger or HealthPartners in Minnesota to take on all of the business challenges and risks of accountability for performance and rewards for efficiency. But what about most of the rest of us?
Well, it looks as if we will need to be linked together by contracts and business relationships, by information transfer and management, and we will need strong, forward-thinking, innovative leadership. And we’ll need some trust in each other and our institutions going forward. Equally important, our patients will need to step up and into this new world. If providers and facilities are required to perform better, then patients have to stay in their contracted systems. To have accountability, patients must participate actively.
Some of you might be old enough to remember the last time integration of physicians and hospitals was all the rage. In the 1990s, the driving force was to achieve “economies of scale” and to meet the challenges of managed care with an integrated entity. Most of these attempts were expensive failures.
In 2010, the drive to integration might be the radical reworking of a payment system that is based on a global fee, a system that produces the highest quality at the lowest cost.
One caveat is that significant integration might not be possible. Do hospitals have the expertise and capacity to employ physicians to efficiently deliver care? In this recession, is the capital available to purchase and implement the information systems crucial to integrated care?
Prepared for Change
I profess to have no expertise as a prognosticator, but I do expect some significant changes to come out of Washington in 2009. The common wisdom is that we are currently spending enough in the aggregate to provide all Americans with access to healthcare, and to get better performance and less variability. That seems to mean shaping a new system.
SHM supports changes in payment methodologies that improve the quality and value of healthcare services, align incentives, and promote better clinical outcomes. We believe that healthcare pricing and quality should be transparent to patients and purchasers. We have supported the PQRI, hospital value-based purchasing, and loosening of restrictions on gainsharing between facilities and providers.
Hospitalists are positioned well. We practice in groups and often are aligned with many others in our medical staffs, and with our hospitals’ roles in our communities. We already are thinking about the value equation and trying to balance resources and performance. We are young, adaptable, and less entrenched. And we are new and have less to lose.
I am confident we can be helpful in shaping the future and can thrive in most any new environment. But hold on tight: The future is getting here way ahead of schedule. TH
Dr. Wellikson is CEO of SHM.
Psych Solutions
Kenneth Duckworth, MD, medical director at Vinfen Corporation in Boston, recalls the frustration he felt when inpatient hospital staff would release his psychiatric patients without contacting him. The lack of communication often led to gaps in his patients’ records and left him scrambling to learn more about the circumstances of the hospitalization.
Those experiences are among the reasons Dr. Duckworth, a triple-board-certified psychiatrist and medical director of the National Alliance on Mental Illness (NAMI), was pleased to hear The Joint Commission had released its Hospital-Based Inpatient Psychiatric Services, or HBIPS, measure set. And he’s not alone. HBIPS provides standardized measures for psychiatric services where previously none existed, and it gives hospitals the ability to use their data as a basis for national comparison.
Ann Watt, associate director, division of quality measurement and research at the Joint Commission, says although it’s still early, the measures seem to be working. “While we don’t have any actual data, we have received positive feedback,” she says. “It seems like the field has accepted them well.”
Standard of Care Guidelines
Comprised of seven main measures that the commission released in October 2008, HBIPS is the result of a determined effort by the nation’s psychiatry leaders, says Noel Mazade, PhD, executive director of the National Association of State Mental Health Program Directors’ Research Institute Inc. HBIPS is available to hospitals accredited under the Comprehensive Accreditation Manual for Hospitals (CAMH), says Celeste Milton, associate project director at the commission’s Department of Quality Measurement. Free-standing psychiatric hospitals and acute-care hospitals with psychiatric units can use the HBIPS measure set to help meet performance requirements under the commission’s ORYX initiative (www. jointcommission.org/AccreditationPrograms/Hospitals/ORYX/).
The Joint Commission’s final HBIPS measure set, which went into effect with Oct. 1, 2008, discharges, followed more than three years’ of field review, public comment, and pilot testing by 196 hospitals across the country. HBIPS’ seven measures address:
—Tim Lineberry, MD, medical director, Mayo Clinic Psychiatric Hospital, Rochester, Minn.
- Admission screening;
- Hours of physical restraint;
- Hours of seclusion;
- Patients discharged on multiple antipsychotic medications;
- Patients discharged on multiple antipsychotic medications with appropriate justification;
- Post-discharge plan creation; and
- Post-discharge plans transmitted to the next level of care provider.
“These are all areas that are of interest to NAMI,” Dr. Duckworth says. “We still have a long way to go, but it’s definitely a step in the right direction.”
The measure set’s effect on psychiatric hospitalists will depend on physicians’ responsibilities at the facilities where they work, Milton says. For example, a psychiatric hospitalist may be asked to screen a patient at admission for violence risk, substance abuse, psychological trauma history, and strengths, such as personal motivation and family involvement (HBIPS Measure 1). Another qualified psychiatric practitioner, such as a psychiatrist, registered nurse, physician’s assistant, or social worker, could perform the screening, she says.
The measures are intended to help unify the screening process used by psychiatric hospitalists; however, traditional hospitalists could be called on to perform a face-to-face evaluation of a patient placed in physical restraint or held in seclusion (Measures 2 and 3). As a result of the evaluation, hospitalists could be asked to write orders to discontinue or renew physical restraint or seclusion, Milton says. The feedback the Joint Commission has received shows psychiatric hospitalists are using the measures. They are most likely to be in charge of managing a patient’s medications and could play a role in documenting appropriate justification for placing a patient on more than one antipsychotic medication at discharge (Measures 4 and 5). Depending on the scope of practice, traditional hospitalists who discharge patients might be responsible for determining a final discharge diagnosis, discharge medications, and next-level-of-care recommendations (Measures 6 and 7). The provider at the next level of care could be an inpatient or outpatient clinician or entity, Milton says.
How It Works
The HBIPS data collection process is similar to other ORYX processes; however, this is the first time the Joint Commission has created a measure set for psychiatric services, says Dr. Mazade, who worked directly with the commission to develop HBIPS. Hospitals using HBIPS will submit data from patients’ medical records to their ORYX vendor. The vendor will submit performance measures to the hospital and the commission, which will provide hospitals with feedback on measure performance, Dr. Mazade says. Initially, the commission will supply acute-care and psychiatric hospitals the option of using HBIPS to meet current ORYX performance measurement requirements, although Dr. Mazade says he expects the commission will eventually mandate use of the measures.
The commission says data collection, analysis, and performance reporting is running behind schedule. Once the commission report is received, hospitals should share the message with their medical staff, Milton says. “This feedback will be useful to all staff involved in patient care to help them improve their practice,” she explains. “The purpose of an initial screening, including a trauma history, is to help the practitioner formulate an individual treatment plan based on information obtained during the initial screening.”
Tim Lineberry, MD, medical director at the Mayo Clinic Psychiatric Hospital in Rochester, Minn., says each HBIPS measure is composed of sub-elements. For example, the assessment measure includes admission screening for violence risk, substance abuse, trauma history, and patient strengths, such as motivation and family involvement. These elements create a more complete picture of the patient and might improve the initial assessment. By improving initial assessment, experts in the field hope hospital staff will be able to better identify problems, Dr. Lineberry says.
“We are all working for improvement in care,” says Dr. Lineberry, noting the Mayo Clinic was one of the pilot sites. “HBIPS is part of that effort.”
Time Is of the Essence
Many of the standards represent areas in which there is consensus among psychiatrists about the need for change, says Anand Pandya, MD, a psychiatric hospitalist and director of inpatient psychiatry at Cedars-Sinai Medical Center in Los Angeles. Many psychiatrists recognize there is a need to improve communication between inpatient psychiatric services and follow-up outpatient providers, Dr. Pandya says. However, a clear consensus has not been reached regarding the standards of tracking patients who take multiple antipsychotic medications, Dr. Pandya says.
“With the low average length of stay in inpatient psychiatric units, it is common for patients to continue a cross-taper between medications after discharge,” Dr. Pandya says. “For most antipsychotic medications, there is insufficient data to determine how fast or slow to cross-taper. I worry that these standards may send the unintentional message that these cross-tapers should be completed quickly during the course of a brief inpatient stay.”
Data suggest individuals using lithium should be tapered off the drug as slowly as possible—probably over months rather than weeks, Dr. Pandya says. “I am concerned that tracking data regarding patients on multiple antipsychotic medications may create incentives to change practice in a sub-optimal direction for some cases,” he says.
Dr. Duckworth also acknowledges patients’ length of stay is getting shorter. Psychiatric hospitalists are under a great deal of pressure to “get people patched up in too short a period of time,” he says. “They really do need more time. There is a temptation to use more than one antipsychotic medication, but people really should not be given two antipsychotic medications unless someone has performed a thoughtful assessment.”
On Board with HBIPS
While HBIPS covers areas of care important to many, the details of implementing the measure set might be challenging, Dr. Lineberry says. The requirements increase the documentation burden for physicians, nurses, and allied health professionals, such as social workers and therapists. Hospitals using electronic medical records might have to modify their records to meet the requirements. And with the new measure comes new, significant personnel costs to audit and collect the data, he says.
“For psychiatric hospitalists who are using HBIPS, it will be helpful to look at the measures from a multidisciplinary standpoint,” Dr. Lineberry says. “Approach HBIPS as a team. Look at the process and see how it works, then adapt it to fit in with your current workflow.”
As of July, more than 274 psychiatric hospitals and psychiatric units had implemented the HBIPS measures. “We don’t usually have numbers until at least six months after,” Milton says, noting the commission is eager to receive quantitative data and report back to the participating hospitals.
Milton anticipates the Joint Commission will submit the HBIPS measure set to the National Quality Forum (NQF) for consideration and endorsement. Although she anticipates the measures will receive NQF endorsement sometime this year, an exact timeline has not been established, she says. The Joint Commission will work closely with the NQF to ensure the HBIPS measure set receives endorsement, and will make necessary modifications that may be required, Milton says.
Once HBIPS receives NQF endorsement, HBIPS data will be publicly reported following the first two quarters of data collection, Milton says. Data on each hospital will be available at www.qualitycheck.org. TH
Gina Gotsill is a freelance medical writer in California. Freelance writer Chris Haliskoe contributed to this report.
Image Source: TIM TEEBKEN/PHOTODISC
Kenneth Duckworth, MD, medical director at Vinfen Corporation in Boston, recalls the frustration he felt when inpatient hospital staff would release his psychiatric patients without contacting him. The lack of communication often led to gaps in his patients’ records and left him scrambling to learn more about the circumstances of the hospitalization.
Those experiences are among the reasons Dr. Duckworth, a triple-board-certified psychiatrist and medical director of the National Alliance on Mental Illness (NAMI), was pleased to hear The Joint Commission had released its Hospital-Based Inpatient Psychiatric Services, or HBIPS, measure set. And he’s not alone. HBIPS provides standardized measures for psychiatric services where previously none existed, and it gives hospitals the ability to use their data as a basis for national comparison.
Ann Watt, associate director, division of quality measurement and research at the Joint Commission, says although it’s still early, the measures seem to be working. “While we don’t have any actual data, we have received positive feedback,” she says. “It seems like the field has accepted them well.”
Standard of Care Guidelines
Comprised of seven main measures that the commission released in October 2008, HBIPS is the result of a determined effort by the nation’s psychiatry leaders, says Noel Mazade, PhD, executive director of the National Association of State Mental Health Program Directors’ Research Institute Inc. HBIPS is available to hospitals accredited under the Comprehensive Accreditation Manual for Hospitals (CAMH), says Celeste Milton, associate project director at the commission’s Department of Quality Measurement. Free-standing psychiatric hospitals and acute-care hospitals with psychiatric units can use the HBIPS measure set to help meet performance requirements under the commission’s ORYX initiative (www. jointcommission.org/AccreditationPrograms/Hospitals/ORYX/).
The Joint Commission’s final HBIPS measure set, which went into effect with Oct. 1, 2008, discharges, followed more than three years’ of field review, public comment, and pilot testing by 196 hospitals across the country. HBIPS’ seven measures address:
—Tim Lineberry, MD, medical director, Mayo Clinic Psychiatric Hospital, Rochester, Minn.
- Admission screening;
- Hours of physical restraint;
- Hours of seclusion;
- Patients discharged on multiple antipsychotic medications;
- Patients discharged on multiple antipsychotic medications with appropriate justification;
- Post-discharge plan creation; and
- Post-discharge plans transmitted to the next level of care provider.
“These are all areas that are of interest to NAMI,” Dr. Duckworth says. “We still have a long way to go, but it’s definitely a step in the right direction.”
The measure set’s effect on psychiatric hospitalists will depend on physicians’ responsibilities at the facilities where they work, Milton says. For example, a psychiatric hospitalist may be asked to screen a patient at admission for violence risk, substance abuse, psychological trauma history, and strengths, such as personal motivation and family involvement (HBIPS Measure 1). Another qualified psychiatric practitioner, such as a psychiatrist, registered nurse, physician’s assistant, or social worker, could perform the screening, she says.
The measures are intended to help unify the screening process used by psychiatric hospitalists; however, traditional hospitalists could be called on to perform a face-to-face evaluation of a patient placed in physical restraint or held in seclusion (Measures 2 and 3). As a result of the evaluation, hospitalists could be asked to write orders to discontinue or renew physical restraint or seclusion, Milton says. The feedback the Joint Commission has received shows psychiatric hospitalists are using the measures. They are most likely to be in charge of managing a patient’s medications and could play a role in documenting appropriate justification for placing a patient on more than one antipsychotic medication at discharge (Measures 4 and 5). Depending on the scope of practice, traditional hospitalists who discharge patients might be responsible for determining a final discharge diagnosis, discharge medications, and next-level-of-care recommendations (Measures 6 and 7). The provider at the next level of care could be an inpatient or outpatient clinician or entity, Milton says.
How It Works
The HBIPS data collection process is similar to other ORYX processes; however, this is the first time the Joint Commission has created a measure set for psychiatric services, says Dr. Mazade, who worked directly with the commission to develop HBIPS. Hospitals using HBIPS will submit data from patients’ medical records to their ORYX vendor. The vendor will submit performance measures to the hospital and the commission, which will provide hospitals with feedback on measure performance, Dr. Mazade says. Initially, the commission will supply acute-care and psychiatric hospitals the option of using HBIPS to meet current ORYX performance measurement requirements, although Dr. Mazade says he expects the commission will eventually mandate use of the measures.
The commission says data collection, analysis, and performance reporting is running behind schedule. Once the commission report is received, hospitals should share the message with their medical staff, Milton says. “This feedback will be useful to all staff involved in patient care to help them improve their practice,” she explains. “The purpose of an initial screening, including a trauma history, is to help the practitioner formulate an individual treatment plan based on information obtained during the initial screening.”
Tim Lineberry, MD, medical director at the Mayo Clinic Psychiatric Hospital in Rochester, Minn., says each HBIPS measure is composed of sub-elements. For example, the assessment measure includes admission screening for violence risk, substance abuse, trauma history, and patient strengths, such as motivation and family involvement. These elements create a more complete picture of the patient and might improve the initial assessment. By improving initial assessment, experts in the field hope hospital staff will be able to better identify problems, Dr. Lineberry says.
“We are all working for improvement in care,” says Dr. Lineberry, noting the Mayo Clinic was one of the pilot sites. “HBIPS is part of that effort.”
Time Is of the Essence
Many of the standards represent areas in which there is consensus among psychiatrists about the need for change, says Anand Pandya, MD, a psychiatric hospitalist and director of inpatient psychiatry at Cedars-Sinai Medical Center in Los Angeles. Many psychiatrists recognize there is a need to improve communication between inpatient psychiatric services and follow-up outpatient providers, Dr. Pandya says. However, a clear consensus has not been reached regarding the standards of tracking patients who take multiple antipsychotic medications, Dr. Pandya says.
“With the low average length of stay in inpatient psychiatric units, it is common for patients to continue a cross-taper between medications after discharge,” Dr. Pandya says. “For most antipsychotic medications, there is insufficient data to determine how fast or slow to cross-taper. I worry that these standards may send the unintentional message that these cross-tapers should be completed quickly during the course of a brief inpatient stay.”
Data suggest individuals using lithium should be tapered off the drug as slowly as possible—probably over months rather than weeks, Dr. Pandya says. “I am concerned that tracking data regarding patients on multiple antipsychotic medications may create incentives to change practice in a sub-optimal direction for some cases,” he says.
Dr. Duckworth also acknowledges patients’ length of stay is getting shorter. Psychiatric hospitalists are under a great deal of pressure to “get people patched up in too short a period of time,” he says. “They really do need more time. There is a temptation to use more than one antipsychotic medication, but people really should not be given two antipsychotic medications unless someone has performed a thoughtful assessment.”
On Board with HBIPS
While HBIPS covers areas of care important to many, the details of implementing the measure set might be challenging, Dr. Lineberry says. The requirements increase the documentation burden for physicians, nurses, and allied health professionals, such as social workers and therapists. Hospitals using electronic medical records might have to modify their records to meet the requirements. And with the new measure comes new, significant personnel costs to audit and collect the data, he says.
“For psychiatric hospitalists who are using HBIPS, it will be helpful to look at the measures from a multidisciplinary standpoint,” Dr. Lineberry says. “Approach HBIPS as a team. Look at the process and see how it works, then adapt it to fit in with your current workflow.”
As of July, more than 274 psychiatric hospitals and psychiatric units had implemented the HBIPS measures. “We don’t usually have numbers until at least six months after,” Milton says, noting the commission is eager to receive quantitative data and report back to the participating hospitals.
Milton anticipates the Joint Commission will submit the HBIPS measure set to the National Quality Forum (NQF) for consideration and endorsement. Although she anticipates the measures will receive NQF endorsement sometime this year, an exact timeline has not been established, she says. The Joint Commission will work closely with the NQF to ensure the HBIPS measure set receives endorsement, and will make necessary modifications that may be required, Milton says.
Once HBIPS receives NQF endorsement, HBIPS data will be publicly reported following the first two quarters of data collection, Milton says. Data on each hospital will be available at www.qualitycheck.org. TH
Gina Gotsill is a freelance medical writer in California. Freelance writer Chris Haliskoe contributed to this report.
Image Source: TIM TEEBKEN/PHOTODISC
Kenneth Duckworth, MD, medical director at Vinfen Corporation in Boston, recalls the frustration he felt when inpatient hospital staff would release his psychiatric patients without contacting him. The lack of communication often led to gaps in his patients’ records and left him scrambling to learn more about the circumstances of the hospitalization.
Those experiences are among the reasons Dr. Duckworth, a triple-board-certified psychiatrist and medical director of the National Alliance on Mental Illness (NAMI), was pleased to hear The Joint Commission had released its Hospital-Based Inpatient Psychiatric Services, or HBIPS, measure set. And he’s not alone. HBIPS provides standardized measures for psychiatric services where previously none existed, and it gives hospitals the ability to use their data as a basis for national comparison.
Ann Watt, associate director, division of quality measurement and research at the Joint Commission, says although it’s still early, the measures seem to be working. “While we don’t have any actual data, we have received positive feedback,” she says. “It seems like the field has accepted them well.”
Standard of Care Guidelines
Comprised of seven main measures that the commission released in October 2008, HBIPS is the result of a determined effort by the nation’s psychiatry leaders, says Noel Mazade, PhD, executive director of the National Association of State Mental Health Program Directors’ Research Institute Inc. HBIPS is available to hospitals accredited under the Comprehensive Accreditation Manual for Hospitals (CAMH), says Celeste Milton, associate project director at the commission’s Department of Quality Measurement. Free-standing psychiatric hospitals and acute-care hospitals with psychiatric units can use the HBIPS measure set to help meet performance requirements under the commission’s ORYX initiative (www. jointcommission.org/AccreditationPrograms/Hospitals/ORYX/).
The Joint Commission’s final HBIPS measure set, which went into effect with Oct. 1, 2008, discharges, followed more than three years’ of field review, public comment, and pilot testing by 196 hospitals across the country. HBIPS’ seven measures address:
—Tim Lineberry, MD, medical director, Mayo Clinic Psychiatric Hospital, Rochester, Minn.
- Admission screening;
- Hours of physical restraint;
- Hours of seclusion;
- Patients discharged on multiple antipsychotic medications;
- Patients discharged on multiple antipsychotic medications with appropriate justification;
- Post-discharge plan creation; and
- Post-discharge plans transmitted to the next level of care provider.
“These are all areas that are of interest to NAMI,” Dr. Duckworth says. “We still have a long way to go, but it’s definitely a step in the right direction.”
The measure set’s effect on psychiatric hospitalists will depend on physicians’ responsibilities at the facilities where they work, Milton says. For example, a psychiatric hospitalist may be asked to screen a patient at admission for violence risk, substance abuse, psychological trauma history, and strengths, such as personal motivation and family involvement (HBIPS Measure 1). Another qualified psychiatric practitioner, such as a psychiatrist, registered nurse, physician’s assistant, or social worker, could perform the screening, she says.
The measures are intended to help unify the screening process used by psychiatric hospitalists; however, traditional hospitalists could be called on to perform a face-to-face evaluation of a patient placed in physical restraint or held in seclusion (Measures 2 and 3). As a result of the evaluation, hospitalists could be asked to write orders to discontinue or renew physical restraint or seclusion, Milton says. The feedback the Joint Commission has received shows psychiatric hospitalists are using the measures. They are most likely to be in charge of managing a patient’s medications and could play a role in documenting appropriate justification for placing a patient on more than one antipsychotic medication at discharge (Measures 4 and 5). Depending on the scope of practice, traditional hospitalists who discharge patients might be responsible for determining a final discharge diagnosis, discharge medications, and next-level-of-care recommendations (Measures 6 and 7). The provider at the next level of care could be an inpatient or outpatient clinician or entity, Milton says.
How It Works
The HBIPS data collection process is similar to other ORYX processes; however, this is the first time the Joint Commission has created a measure set for psychiatric services, says Dr. Mazade, who worked directly with the commission to develop HBIPS. Hospitals using HBIPS will submit data from patients’ medical records to their ORYX vendor. The vendor will submit performance measures to the hospital and the commission, which will provide hospitals with feedback on measure performance, Dr. Mazade says. Initially, the commission will supply acute-care and psychiatric hospitals the option of using HBIPS to meet current ORYX performance measurement requirements, although Dr. Mazade says he expects the commission will eventually mandate use of the measures.
The commission says data collection, analysis, and performance reporting is running behind schedule. Once the commission report is received, hospitals should share the message with their medical staff, Milton says. “This feedback will be useful to all staff involved in patient care to help them improve their practice,” she explains. “The purpose of an initial screening, including a trauma history, is to help the practitioner formulate an individual treatment plan based on information obtained during the initial screening.”
Tim Lineberry, MD, medical director at the Mayo Clinic Psychiatric Hospital in Rochester, Minn., says each HBIPS measure is composed of sub-elements. For example, the assessment measure includes admission screening for violence risk, substance abuse, trauma history, and patient strengths, such as motivation and family involvement. These elements create a more complete picture of the patient and might improve the initial assessment. By improving initial assessment, experts in the field hope hospital staff will be able to better identify problems, Dr. Lineberry says.
“We are all working for improvement in care,” says Dr. Lineberry, noting the Mayo Clinic was one of the pilot sites. “HBIPS is part of that effort.”
Time Is of the Essence
Many of the standards represent areas in which there is consensus among psychiatrists about the need for change, says Anand Pandya, MD, a psychiatric hospitalist and director of inpatient psychiatry at Cedars-Sinai Medical Center in Los Angeles. Many psychiatrists recognize there is a need to improve communication between inpatient psychiatric services and follow-up outpatient providers, Dr. Pandya says. However, a clear consensus has not been reached regarding the standards of tracking patients who take multiple antipsychotic medications, Dr. Pandya says.
“With the low average length of stay in inpatient psychiatric units, it is common for patients to continue a cross-taper between medications after discharge,” Dr. Pandya says. “For most antipsychotic medications, there is insufficient data to determine how fast or slow to cross-taper. I worry that these standards may send the unintentional message that these cross-tapers should be completed quickly during the course of a brief inpatient stay.”
Data suggest individuals using lithium should be tapered off the drug as slowly as possible—probably over months rather than weeks, Dr. Pandya says. “I am concerned that tracking data regarding patients on multiple antipsychotic medications may create incentives to change practice in a sub-optimal direction for some cases,” he says.
Dr. Duckworth also acknowledges patients’ length of stay is getting shorter. Psychiatric hospitalists are under a great deal of pressure to “get people patched up in too short a period of time,” he says. “They really do need more time. There is a temptation to use more than one antipsychotic medication, but people really should not be given two antipsychotic medications unless someone has performed a thoughtful assessment.”
On Board with HBIPS
While HBIPS covers areas of care important to many, the details of implementing the measure set might be challenging, Dr. Lineberry says. The requirements increase the documentation burden for physicians, nurses, and allied health professionals, such as social workers and therapists. Hospitals using electronic medical records might have to modify their records to meet the requirements. And with the new measure comes new, significant personnel costs to audit and collect the data, he says.
“For psychiatric hospitalists who are using HBIPS, it will be helpful to look at the measures from a multidisciplinary standpoint,” Dr. Lineberry says. “Approach HBIPS as a team. Look at the process and see how it works, then adapt it to fit in with your current workflow.”
As of July, more than 274 psychiatric hospitals and psychiatric units had implemented the HBIPS measures. “We don’t usually have numbers until at least six months after,” Milton says, noting the commission is eager to receive quantitative data and report back to the participating hospitals.
Milton anticipates the Joint Commission will submit the HBIPS measure set to the National Quality Forum (NQF) for consideration and endorsement. Although she anticipates the measures will receive NQF endorsement sometime this year, an exact timeline has not been established, she says. The Joint Commission will work closely with the NQF to ensure the HBIPS measure set receives endorsement, and will make necessary modifications that may be required, Milton says.
Once HBIPS receives NQF endorsement, HBIPS data will be publicly reported following the first two quarters of data collection, Milton says. Data on each hospital will be available at www.qualitycheck.org. TH
Gina Gotsill is a freelance medical writer in California. Freelance writer Chris Haliskoe contributed to this report.
Image Source: TIM TEEBKEN/PHOTODISC
How do I keep my elderly patients from falling?
Case
An 85-year-old man with peripheral vascular disease, coronary artery disease, congestive heart failure, dementia, a history of falls, and atrial fibrillation, which was being treated with warfarin, was admitted for a left transmetatarsal amputation. On postoperative day two, the patient slipped as he was getting out of bed to use the bathroom. He hit his head on his IV pole, and a CT scan demonstrated an acute right subdural hemorrhage. He subsequently suffered eight months of delirium before passing away at a skilled nursing facility. How could this incident have been prevented?
Background
Hospitalization represents a vulnerable time for elderly people. The presence of acute illness, an unfamiliar environment, and the frequent addition of new medications predispose an elderly patient to such iatrogenic hazards of hospitalization as falls, pressure ulcers, and delirium.1 Inpatient falls are the most common type of adverse hospital event, accounting for 70% of all inpatient accidents.2 Thirty percent to 40% of inpatient falls result in injury, with 4% to 6% resulting in serious harm.2 Interestingly, 55% of falls occur in patients 60 or younger, but 60% of falls resulting in moderate to severe injury occur in those 70 and older.3
A fall is a seminal event in the life of an elderly person. Even a fall without injury can initiate a vicious circle that begins with a fear of falling and is followed by a self-restriction of mobility, which commonly results in a decline in function.4 Functional decline in the elderly has been shown to predict mortality and nursing home placement.5
Inpatient falls are thought to occur via a complex interplay between medications, inherent patient susceptibilities, and hospital environmental hazards (see Figure 1, below).
Risk Factors
Medication prescription for the hospitalized elderly patient is perhaps the area where the hospitalist can have the greatest impact in reducing a patient’s fall risk. The most common medications thought to predispose community dwelling elders to falls are psychotropic drugs: neuroleptics, sedatives, hypnotics, antidepressants, and benzodiazepines.6
Limited studies of hospitalized patients indicate similar drugs as culprits. Passaro et al demonstrated that benzodiazepines with a half-life <24 hours (e.g., lorazepam and oxazepam) were strongly associated with falls even after correcting for multiple confounders.7 Furthermore, multivariate logistic regression revealed that the use of other psychotropic drugs in addition to benzodiazepines (OR 2.3; 95% CI, 1.6–3.2) was strongly associated with an increased risk of falls. Taking more than five medications also increased a patient’s fall risk (OR 1.6; 95% CI, 1.02–2.6). Thus, the judicious prescription of medications—aimed at decreasing the number and dosage of medications an elderly patient takes—is essential to minimizing the risk for falls.
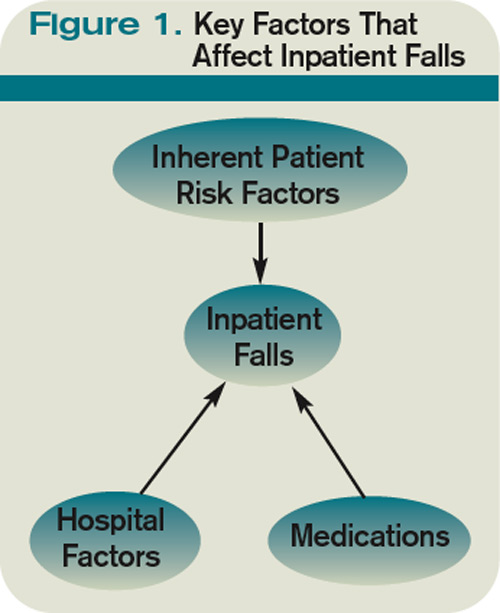
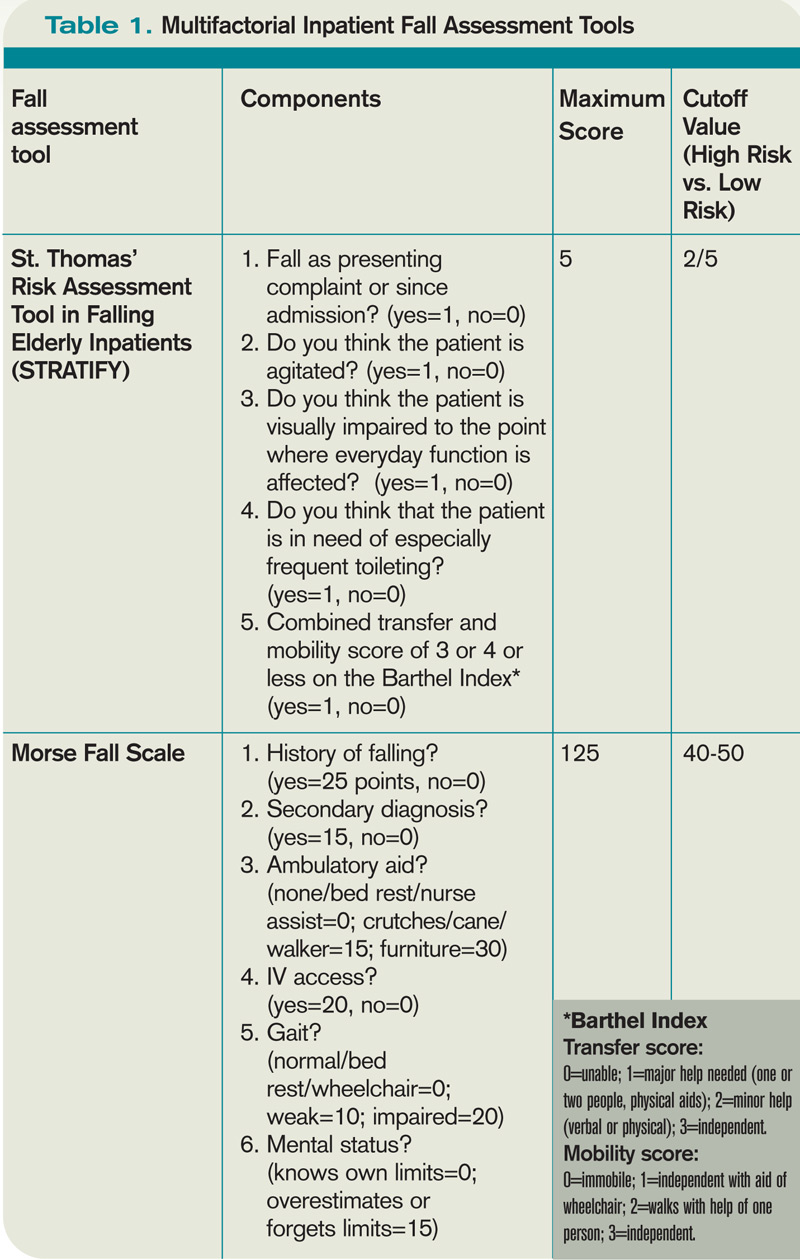
Several studies conducted in hospitalized elderly patients have repeatedly demonstrated a core group of inherent patient risk factors for falls: delirium, agitation or impaired judgment, burden of comorbidity, gait instability or lower-extremity weakness, urinary incontinence or frequency, and a history of falls.2,3,8 These risk factors are targeted as part of most inpatient fall prevention programs, as discussed below.
Several environmental hazards have been known to increase the risk of falls and injury. These include high patient-to-nurse ratio, inappropriate use of bedrails, wet floors, and lack of assistance with ambulation and toileting. The most studied of these is assistance with ambulation and toileting. Hitcho et al demonstrated that as many as 50% of falls are toileting-related.3 The study also showed that only 42% of patients who fell and used an assistive device at home had a fall in the hospital. As many as 85% of patients were not assisted with a device or person at the time of a fall.2 Unassisted falls are associated with increased injury risk (adjusted OR 1.70; 95% CI, 1.23-2.36).
Consistent with this, increased patient-to-nurse ratios are keenly associated with an increased risk of falls. Essentially, a patient whose nurse had more than five patients was 2.6 times more likely to fall than a patient whose nurse had five or fewer patients (95% CI, 1.6 to 4.1). Based on this data, hospitals have invested in low-to-the-floor beds and alarms for beds and chairs. Placing patients on a regular toileting schedule, avoiding medications that cause urinary incontinence, and attention to bowel regimens have become standard components of hospital fall prevention programs. Even though these issues have long been thought to be the purview of nurses and support staff, hospitalist involvement and awareness are crucial to ensuring that these issues are consistently addressed and enforced for every at-risk patient.
Inpatient Fall Prevention
Inpatient falls are similar to other geriatric syndromes and are multifactorial in etiology. Studies that report a decrease in the number of falls identify patients at the highest risk for falls and target multiple risk factors simultaneously.
Several inpatient fall risk assessment tools have been developed. The most widely used and validated in the acute hospital setting are the Morse Falls Scale and St. Thomas’ Risk Assessment Tool in Falling Elderly Inpatients (STRATIFY) (see Table 1, p. 24).9 Both tools incorporate the risk factors identified above—namely, the presence of cognitive or sensory deficits, environmental hazards, history of falls, lower-extremity or gait instability/weakness, and level of comorbidity to create a score. Higher scores are associated with increased fall risk. The scales have demonstrated sensitivities and specificities of 70% to 96% and 50% to 85%, respectively, depending on the population tested and the cutoff scores used.
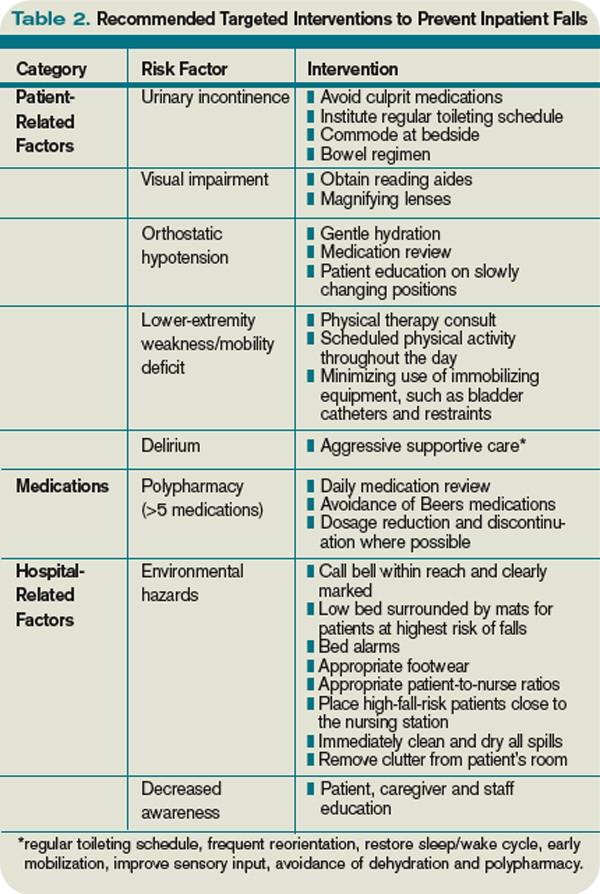

In 2004, Healey et al published the results of one of the few successful randomized, controlled fall-prevention trials in an acute-care setting.10 Pairs of identical hospital units were randomized to intervention and control groups. The sample size was 3,386 patients, with a mean length of stay of 19 days.1 As part of the intervention group, a fall-risk assessment was performed on admission. Patients were screened for deficits in visual acuity (identify a pen, key, or watch from a distance of 2 meters), polypharmacy, orthostatic hypotension, mobility deficits, appropriate bedrail use, footwear safety, bed height, distance of patient from nursing station, loose cables, wet floors, and availability of the nurse call bell.
Interventions for patients who were identified as high fall risks included ophthalmology/optician referral for those for whom reading aides could not be procured, medication review, adjustment of bed rails, and physical therapy. Patients with a history of falls were placed close to nursing stations. Environmental hazards were removed. Patients with orthostatic hypotension were educated on slowly changing body position. Call lights were moved to within easy reach. No additional money was allocated for this study, but by performing these simple interventions, the authors were able to decrease the relative risk of falls by 29% (RR 0.71, 95% CI 0.55–0.90, P=0.006). The incidence of injuries sustained as a result of falling, however, was unchanged.
Two large, prospective studies with historical controls involving 3,000 to 7,000 patients over the course of three years and incorporating similar interventions also demonstrated a decrease in the number of falls.11,12 Fonda and his colleagues were able to demonstrate a 77% reduction in the number of falls resulting in serious injuries.
Even though these studies are promising, a recent cluster-randomized, multifactorial intervention trial involving almost 4,000 patients on a dozen medical floors did not demonstrate a reduction in the incidence of falls or falls with injury.13 Several differences exist between the two randomized trials. In the latter trial, by Cumming et al, a study nurse reviewed the care plan of all of the patients on the intervention wards and made recommendations.13 Also, the study was designed so that each patient on the intervention wards received the intervention, regardless of their fall risk. Additionally, the study period was a mere three months. In the Healey trial, the nurses on the intervention units implemented targeted risk reduction for patients at high risk, and the study period was a full year.
Back to the Case
Our patient had several risk factors for falls on admission. A targeted fall risk assessment on admission would have identified him as high-risk, with a Morse score of 95 given his dementia (15 points), impaired gait status post-transmetatarsal amputation (20 points), secondary diagnoses (multiple comorbidities, 15 points) and history of falls (25 points), and presence of an IV (20 points). The STRATIFY risk assessment tool would have produced similar results.
Frequent toileting assistance, early mobilization, medication review, and environmental modification might have prevented his fall (see Table 2, pg. 24).
Bottom Line
Focused assessment of patients on admission can identify those at risk for falls. Multifactorial inpatient fall-prevention strategies have been shown to reduce the rate of falls in inpatients without increasing costs. TH
Dr. Ölveczky is a geriatric nocturnist in the hospital medicine program, division of medicine, at Beth Israel Deaconess Medical Center in Boston.
References
- Fernandez HM, Callahan KE, Likourezos A, Leipzig RM. House staff member awareness of older inpatients’ risks for hazards of hospitalization. Arch Intern Med. 2008;168(4):390-396.
- Krauss MJ, Evanoff B, Hitcho E, et al. A case control study of patient, medication, and care-related risk factors for inpatient falls. J Gen Intern Med. 2005;20(2):116-122.
- Hitcho EB, Krauss MJ, Birge S, et al. Characteristics and circumstances of falls in a hospital setting: a prospective analysis. J Gen Intern Med. 2004;19(7):732-739.
- Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348(1):42-49.
- Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332(9):556-561.
- Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc. 1999;47(1):30-39.
- Passaro A, Volpato S, Romagnoni F, Manzoli N, Zuliani G, Fellin R. Benzodiazepines with different half-life and falling in a hospitalized population: The GIFA study. Gruppo Italiano di Farmacovigilanza nell'Anziano. J Clin Epidemiol. 2000;53(12):1222-1229.
- Oliver D, Daly F, Martin FC, McMurdo ME. Risk factors and risk assessment tools for falls in hospital in-patients: a systematic review. Age Ageing. 2004;33(2):122-130.
- Scott V, Votova K, Scanlan A, Close J. Multifactorial and functional mobility assessment tools for fall risk among older adults in community, home-support, long-term and acute care settings. Age Ageing. 2007;36(2):130-139.
- Healey F, Monro A, Cockram A, Adams V, Heseltine D. Using targeted risk factor reduction to prevent falls in older in-patients: a randomised controlled trial. Age Ageing. 2004;33(4):390-395.
- Fonda D, Cook J, Sandler V, Bailey M. Sustained reduction in serious fall-related injuries in older people in hospital. Med J Aust. 2006;184(8):379-382.
- Von Renteln-Kruse W, Krause T. Incidence of in-hospital falls in geriatric patients before and after the introduction of an interdisciplinary team-based fall-prevention intervention. J Am Geriatr Soc. 2007;55(12):2068-2074.
- Cumming RG, Sherrington C, Lord SR, et al. Cluster randomised trial of a targeted multifactorial intervention to prevent falls among older people in hospital. BMJ. 2008;336(7647):758-760.
- Oliver D, Britton M, Seed P, Martin FC, Hopper AH. Development and evaluation of evidence based risk assessment tool (STRATIFY) to predict which elderly inpatients will fall: case-control and cohort studies. BMJ. 1997;315(7115):1049-1053.
Case
An 85-year-old man with peripheral vascular disease, coronary artery disease, congestive heart failure, dementia, a history of falls, and atrial fibrillation, which was being treated with warfarin, was admitted for a left transmetatarsal amputation. On postoperative day two, the patient slipped as he was getting out of bed to use the bathroom. He hit his head on his IV pole, and a CT scan demonstrated an acute right subdural hemorrhage. He subsequently suffered eight months of delirium before passing away at a skilled nursing facility. How could this incident have been prevented?
Background
Hospitalization represents a vulnerable time for elderly people. The presence of acute illness, an unfamiliar environment, and the frequent addition of new medications predispose an elderly patient to such iatrogenic hazards of hospitalization as falls, pressure ulcers, and delirium.1 Inpatient falls are the most common type of adverse hospital event, accounting for 70% of all inpatient accidents.2 Thirty percent to 40% of inpatient falls result in injury, with 4% to 6% resulting in serious harm.2 Interestingly, 55% of falls occur in patients 60 or younger, but 60% of falls resulting in moderate to severe injury occur in those 70 and older.3
A fall is a seminal event in the life of an elderly person. Even a fall without injury can initiate a vicious circle that begins with a fear of falling and is followed by a self-restriction of mobility, which commonly results in a decline in function.4 Functional decline in the elderly has been shown to predict mortality and nursing home placement.5
Inpatient falls are thought to occur via a complex interplay between medications, inherent patient susceptibilities, and hospital environmental hazards (see Figure 1, below).
Risk Factors
Medication prescription for the hospitalized elderly patient is perhaps the area where the hospitalist can have the greatest impact in reducing a patient’s fall risk. The most common medications thought to predispose community dwelling elders to falls are psychotropic drugs: neuroleptics, sedatives, hypnotics, antidepressants, and benzodiazepines.6
Limited studies of hospitalized patients indicate similar drugs as culprits. Passaro et al demonstrated that benzodiazepines with a half-life <24 hours (e.g., lorazepam and oxazepam) were strongly associated with falls even after correcting for multiple confounders.7 Furthermore, multivariate logistic regression revealed that the use of other psychotropic drugs in addition to benzodiazepines (OR 2.3; 95% CI, 1.6–3.2) was strongly associated with an increased risk of falls. Taking more than five medications also increased a patient’s fall risk (OR 1.6; 95% CI, 1.02–2.6). Thus, the judicious prescription of medications—aimed at decreasing the number and dosage of medications an elderly patient takes—is essential to minimizing the risk for falls.
Several studies conducted in hospitalized elderly patients have repeatedly demonstrated a core group of inherent patient risk factors for falls: delirium, agitation or impaired judgment, burden of comorbidity, gait instability or lower-extremity weakness, urinary incontinence or frequency, and a history of falls.2,3,8 These risk factors are targeted as part of most inpatient fall prevention programs, as discussed below.
Several environmental hazards have been known to increase the risk of falls and injury. These include high patient-to-nurse ratio, inappropriate use of bedrails, wet floors, and lack of assistance with ambulation and toileting. The most studied of these is assistance with ambulation and toileting. Hitcho et al demonstrated that as many as 50% of falls are toileting-related.3 The study also showed that only 42% of patients who fell and used an assistive device at home had a fall in the hospital. As many as 85% of patients were not assisted with a device or person at the time of a fall.2 Unassisted falls are associated with increased injury risk (adjusted OR 1.70; 95% CI, 1.23-2.36).
Consistent with this, increased patient-to-nurse ratios are keenly associated with an increased risk of falls. Essentially, a patient whose nurse had more than five patients was 2.6 times more likely to fall than a patient whose nurse had five or fewer patients (95% CI, 1.6 to 4.1). Based on this data, hospitals have invested in low-to-the-floor beds and alarms for beds and chairs. Placing patients on a regular toileting schedule, avoiding medications that cause urinary incontinence, and attention to bowel regimens have become standard components of hospital fall prevention programs. Even though these issues have long been thought to be the purview of nurses and support staff, hospitalist involvement and awareness are crucial to ensuring that these issues are consistently addressed and enforced for every at-risk patient.
Inpatient Fall Prevention
Inpatient falls are similar to other geriatric syndromes and are multifactorial in etiology. Studies that report a decrease in the number of falls identify patients at the highest risk for falls and target multiple risk factors simultaneously.
Several inpatient fall risk assessment tools have been developed. The most widely used and validated in the acute hospital setting are the Morse Falls Scale and St. Thomas’ Risk Assessment Tool in Falling Elderly Inpatients (STRATIFY) (see Table 1, p. 24).9 Both tools incorporate the risk factors identified above—namely, the presence of cognitive or sensory deficits, environmental hazards, history of falls, lower-extremity or gait instability/weakness, and level of comorbidity to create a score. Higher scores are associated with increased fall risk. The scales have demonstrated sensitivities and specificities of 70% to 96% and 50% to 85%, respectively, depending on the population tested and the cutoff scores used.
In 2004, Healey et al published the results of one of the few successful randomized, controlled fall-prevention trials in an acute-care setting.10 Pairs of identical hospital units were randomized to intervention and control groups. The sample size was 3,386 patients, with a mean length of stay of 19 days.1 As part of the intervention group, a fall-risk assessment was performed on admission. Patients were screened for deficits in visual acuity (identify a pen, key, or watch from a distance of 2 meters), polypharmacy, orthostatic hypotension, mobility deficits, appropriate bedrail use, footwear safety, bed height, distance of patient from nursing station, loose cables, wet floors, and availability of the nurse call bell.
Interventions for patients who were identified as high fall risks included ophthalmology/optician referral for those for whom reading aides could not be procured, medication review, adjustment of bed rails, and physical therapy. Patients with a history of falls were placed close to nursing stations. Environmental hazards were removed. Patients with orthostatic hypotension were educated on slowly changing body position. Call lights were moved to within easy reach. No additional money was allocated for this study, but by performing these simple interventions, the authors were able to decrease the relative risk of falls by 29% (RR 0.71, 95% CI 0.55–0.90, P=0.006). The incidence of injuries sustained as a result of falling, however, was unchanged.
Two large, prospective studies with historical controls involving 3,000 to 7,000 patients over the course of three years and incorporating similar interventions also demonstrated a decrease in the number of falls.11,12 Fonda and his colleagues were able to demonstrate a 77% reduction in the number of falls resulting in serious injuries.
Even though these studies are promising, a recent cluster-randomized, multifactorial intervention trial involving almost 4,000 patients on a dozen medical floors did not demonstrate a reduction in the incidence of falls or falls with injury.13 Several differences exist between the two randomized trials. In the latter trial, by Cumming et al, a study nurse reviewed the care plan of all of the patients on the intervention wards and made recommendations.13 Also, the study was designed so that each patient on the intervention wards received the intervention, regardless of their fall risk. Additionally, the study period was a mere three months. In the Healey trial, the nurses on the intervention units implemented targeted risk reduction for patients at high risk, and the study period was a full year.
Back to the Case
Our patient had several risk factors for falls on admission. A targeted fall risk assessment on admission would have identified him as high-risk, with a Morse score of 95 given his dementia (15 points), impaired gait status post-transmetatarsal amputation (20 points), secondary diagnoses (multiple comorbidities, 15 points) and history of falls (25 points), and presence of an IV (20 points). The STRATIFY risk assessment tool would have produced similar results.
Frequent toileting assistance, early mobilization, medication review, and environmental modification might have prevented his fall (see Table 2, pg. 24).
Bottom Line
Focused assessment of patients on admission can identify those at risk for falls. Multifactorial inpatient fall-prevention strategies have been shown to reduce the rate of falls in inpatients without increasing costs. TH
Dr. Ölveczky is a geriatric nocturnist in the hospital medicine program, division of medicine, at Beth Israel Deaconess Medical Center in Boston.
References
- Fernandez HM, Callahan KE, Likourezos A, Leipzig RM. House staff member awareness of older inpatients’ risks for hazards of hospitalization. Arch Intern Med. 2008;168(4):390-396.
- Krauss MJ, Evanoff B, Hitcho E, et al. A case control study of patient, medication, and care-related risk factors for inpatient falls. J Gen Intern Med. 2005;20(2):116-122.
- Hitcho EB, Krauss MJ, Birge S, et al. Characteristics and circumstances of falls in a hospital setting: a prospective analysis. J Gen Intern Med. 2004;19(7):732-739.
- Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348(1):42-49.
- Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332(9):556-561.
- Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc. 1999;47(1):30-39.
- Passaro A, Volpato S, Romagnoni F, Manzoli N, Zuliani G, Fellin R. Benzodiazepines with different half-life and falling in a hospitalized population: The GIFA study. Gruppo Italiano di Farmacovigilanza nell'Anziano. J Clin Epidemiol. 2000;53(12):1222-1229.
- Oliver D, Daly F, Martin FC, McMurdo ME. Risk factors and risk assessment tools for falls in hospital in-patients: a systematic review. Age Ageing. 2004;33(2):122-130.
- Scott V, Votova K, Scanlan A, Close J. Multifactorial and functional mobility assessment tools for fall risk among older adults in community, home-support, long-term and acute care settings. Age Ageing. 2007;36(2):130-139.
- Healey F, Monro A, Cockram A, Adams V, Heseltine D. Using targeted risk factor reduction to prevent falls in older in-patients: a randomised controlled trial. Age Ageing. 2004;33(4):390-395.
- Fonda D, Cook J, Sandler V, Bailey M. Sustained reduction in serious fall-related injuries in older people in hospital. Med J Aust. 2006;184(8):379-382.
- Von Renteln-Kruse W, Krause T. Incidence of in-hospital falls in geriatric patients before and after the introduction of an interdisciplinary team-based fall-prevention intervention. J Am Geriatr Soc. 2007;55(12):2068-2074.
- Cumming RG, Sherrington C, Lord SR, et al. Cluster randomised trial of a targeted multifactorial intervention to prevent falls among older people in hospital. BMJ. 2008;336(7647):758-760.
- Oliver D, Britton M, Seed P, Martin FC, Hopper AH. Development and evaluation of evidence based risk assessment tool (STRATIFY) to predict which elderly inpatients will fall: case-control and cohort studies. BMJ. 1997;315(7115):1049-1053.
Case
An 85-year-old man with peripheral vascular disease, coronary artery disease, congestive heart failure, dementia, a history of falls, and atrial fibrillation, which was being treated with warfarin, was admitted for a left transmetatarsal amputation. On postoperative day two, the patient slipped as he was getting out of bed to use the bathroom. He hit his head on his IV pole, and a CT scan demonstrated an acute right subdural hemorrhage. He subsequently suffered eight months of delirium before passing away at a skilled nursing facility. How could this incident have been prevented?
Background
Hospitalization represents a vulnerable time for elderly people. The presence of acute illness, an unfamiliar environment, and the frequent addition of new medications predispose an elderly patient to such iatrogenic hazards of hospitalization as falls, pressure ulcers, and delirium.1 Inpatient falls are the most common type of adverse hospital event, accounting for 70% of all inpatient accidents.2 Thirty percent to 40% of inpatient falls result in injury, with 4% to 6% resulting in serious harm.2 Interestingly, 55% of falls occur in patients 60 or younger, but 60% of falls resulting in moderate to severe injury occur in those 70 and older.3
A fall is a seminal event in the life of an elderly person. Even a fall without injury can initiate a vicious circle that begins with a fear of falling and is followed by a self-restriction of mobility, which commonly results in a decline in function.4 Functional decline in the elderly has been shown to predict mortality and nursing home placement.5
Inpatient falls are thought to occur via a complex interplay between medications, inherent patient susceptibilities, and hospital environmental hazards (see Figure 1, below).
Risk Factors
Medication prescription for the hospitalized elderly patient is perhaps the area where the hospitalist can have the greatest impact in reducing a patient’s fall risk. The most common medications thought to predispose community dwelling elders to falls are psychotropic drugs: neuroleptics, sedatives, hypnotics, antidepressants, and benzodiazepines.6
Limited studies of hospitalized patients indicate similar drugs as culprits. Passaro et al demonstrated that benzodiazepines with a half-life <24 hours (e.g., lorazepam and oxazepam) were strongly associated with falls even after correcting for multiple confounders.7 Furthermore, multivariate logistic regression revealed that the use of other psychotropic drugs in addition to benzodiazepines (OR 2.3; 95% CI, 1.6–3.2) was strongly associated with an increased risk of falls. Taking more than five medications also increased a patient’s fall risk (OR 1.6; 95% CI, 1.02–2.6). Thus, the judicious prescription of medications—aimed at decreasing the number and dosage of medications an elderly patient takes—is essential to minimizing the risk for falls.
Several studies conducted in hospitalized elderly patients have repeatedly demonstrated a core group of inherent patient risk factors for falls: delirium, agitation or impaired judgment, burden of comorbidity, gait instability or lower-extremity weakness, urinary incontinence or frequency, and a history of falls.2,3,8 These risk factors are targeted as part of most inpatient fall prevention programs, as discussed below.
Several environmental hazards have been known to increase the risk of falls and injury. These include high patient-to-nurse ratio, inappropriate use of bedrails, wet floors, and lack of assistance with ambulation and toileting. The most studied of these is assistance with ambulation and toileting. Hitcho et al demonstrated that as many as 50% of falls are toileting-related.3 The study also showed that only 42% of patients who fell and used an assistive device at home had a fall in the hospital. As many as 85% of patients were not assisted with a device or person at the time of a fall.2 Unassisted falls are associated with increased injury risk (adjusted OR 1.70; 95% CI, 1.23-2.36).
Consistent with this, increased patient-to-nurse ratios are keenly associated with an increased risk of falls. Essentially, a patient whose nurse had more than five patients was 2.6 times more likely to fall than a patient whose nurse had five or fewer patients (95% CI, 1.6 to 4.1). Based on this data, hospitals have invested in low-to-the-floor beds and alarms for beds and chairs. Placing patients on a regular toileting schedule, avoiding medications that cause urinary incontinence, and attention to bowel regimens have become standard components of hospital fall prevention programs. Even though these issues have long been thought to be the purview of nurses and support staff, hospitalist involvement and awareness are crucial to ensuring that these issues are consistently addressed and enforced for every at-risk patient.
Inpatient Fall Prevention
Inpatient falls are similar to other geriatric syndromes and are multifactorial in etiology. Studies that report a decrease in the number of falls identify patients at the highest risk for falls and target multiple risk factors simultaneously.
Several inpatient fall risk assessment tools have been developed. The most widely used and validated in the acute hospital setting are the Morse Falls Scale and St. Thomas’ Risk Assessment Tool in Falling Elderly Inpatients (STRATIFY) (see Table 1, p. 24).9 Both tools incorporate the risk factors identified above—namely, the presence of cognitive or sensory deficits, environmental hazards, history of falls, lower-extremity or gait instability/weakness, and level of comorbidity to create a score. Higher scores are associated with increased fall risk. The scales have demonstrated sensitivities and specificities of 70% to 96% and 50% to 85%, respectively, depending on the population tested and the cutoff scores used.
In 2004, Healey et al published the results of one of the few successful randomized, controlled fall-prevention trials in an acute-care setting.10 Pairs of identical hospital units were randomized to intervention and control groups. The sample size was 3,386 patients, with a mean length of stay of 19 days.1 As part of the intervention group, a fall-risk assessment was performed on admission. Patients were screened for deficits in visual acuity (identify a pen, key, or watch from a distance of 2 meters), polypharmacy, orthostatic hypotension, mobility deficits, appropriate bedrail use, footwear safety, bed height, distance of patient from nursing station, loose cables, wet floors, and availability of the nurse call bell.
Interventions for patients who were identified as high fall risks included ophthalmology/optician referral for those for whom reading aides could not be procured, medication review, adjustment of bed rails, and physical therapy. Patients with a history of falls were placed close to nursing stations. Environmental hazards were removed. Patients with orthostatic hypotension were educated on slowly changing body position. Call lights were moved to within easy reach. No additional money was allocated for this study, but by performing these simple interventions, the authors were able to decrease the relative risk of falls by 29% (RR 0.71, 95% CI 0.55–0.90, P=0.006). The incidence of injuries sustained as a result of falling, however, was unchanged.
Two large, prospective studies with historical controls involving 3,000 to 7,000 patients over the course of three years and incorporating similar interventions also demonstrated a decrease in the number of falls.11,12 Fonda and his colleagues were able to demonstrate a 77% reduction in the number of falls resulting in serious injuries.
Even though these studies are promising, a recent cluster-randomized, multifactorial intervention trial involving almost 4,000 patients on a dozen medical floors did not demonstrate a reduction in the incidence of falls or falls with injury.13 Several differences exist between the two randomized trials. In the latter trial, by Cumming et al, a study nurse reviewed the care plan of all of the patients on the intervention wards and made recommendations.13 Also, the study was designed so that each patient on the intervention wards received the intervention, regardless of their fall risk. Additionally, the study period was a mere three months. In the Healey trial, the nurses on the intervention units implemented targeted risk reduction for patients at high risk, and the study period was a full year.
Back to the Case
Our patient had several risk factors for falls on admission. A targeted fall risk assessment on admission would have identified him as high-risk, with a Morse score of 95 given his dementia (15 points), impaired gait status post-transmetatarsal amputation (20 points), secondary diagnoses (multiple comorbidities, 15 points) and history of falls (25 points), and presence of an IV (20 points). The STRATIFY risk assessment tool would have produced similar results.
Frequent toileting assistance, early mobilization, medication review, and environmental modification might have prevented his fall (see Table 2, pg. 24).
Bottom Line
Focused assessment of patients on admission can identify those at risk for falls. Multifactorial inpatient fall-prevention strategies have been shown to reduce the rate of falls in inpatients without increasing costs. TH
Dr. Ölveczky is a geriatric nocturnist in the hospital medicine program, division of medicine, at Beth Israel Deaconess Medical Center in Boston.
References
- Fernandez HM, Callahan KE, Likourezos A, Leipzig RM. House staff member awareness of older inpatients’ risks for hazards of hospitalization. Arch Intern Med. 2008;168(4):390-396.
- Krauss MJ, Evanoff B, Hitcho E, et al. A case control study of patient, medication, and care-related risk factors for inpatient falls. J Gen Intern Med. 2005;20(2):116-122.
- Hitcho EB, Krauss MJ, Birge S, et al. Characteristics and circumstances of falls in a hospital setting: a prospective analysis. J Gen Intern Med. 2004;19(7):732-739.
- Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348(1):42-49.
- Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332(9):556-561.
- Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc. 1999;47(1):30-39.
- Passaro A, Volpato S, Romagnoni F, Manzoli N, Zuliani G, Fellin R. Benzodiazepines with different half-life and falling in a hospitalized population: The GIFA study. Gruppo Italiano di Farmacovigilanza nell'Anziano. J Clin Epidemiol. 2000;53(12):1222-1229.
- Oliver D, Daly F, Martin FC, McMurdo ME. Risk factors and risk assessment tools for falls in hospital in-patients: a systematic review. Age Ageing. 2004;33(2):122-130.
- Scott V, Votova K, Scanlan A, Close J. Multifactorial and functional mobility assessment tools for fall risk among older adults in community, home-support, long-term and acute care settings. Age Ageing. 2007;36(2):130-139.
- Healey F, Monro A, Cockram A, Adams V, Heseltine D. Using targeted risk factor reduction to prevent falls in older in-patients: a randomised controlled trial. Age Ageing. 2004;33(4):390-395.
- Fonda D, Cook J, Sandler V, Bailey M. Sustained reduction in serious fall-related injuries in older people in hospital. Med J Aust. 2006;184(8):379-382.
- Von Renteln-Kruse W, Krause T. Incidence of in-hospital falls in geriatric patients before and after the introduction of an interdisciplinary team-based fall-prevention intervention. J Am Geriatr Soc. 2007;55(12):2068-2074.
- Cumming RG, Sherrington C, Lord SR, et al. Cluster randomised trial of a targeted multifactorial intervention to prevent falls among older people in hospital. BMJ. 2008;336(7647):758-760.
- Oliver D, Britton M, Seed P, Martin FC, Hopper AH. Development and evaluation of evidence based risk assessment tool (STRATIFY) to predict which elderly inpatients will fall: case-control and cohort studies. BMJ. 1997;315(7115):1049-1053.