User login
Cannabis Use by Veterans and Potential Interactions With Antineoplastic Agents: Analysis and Literature Review
Cannabis Use by Veterans and Potential Interactions With Antineoplastic Agents: Analysis and Literature Review
Cannabis has a long history of use for medicinal and recreational purposes. Research illustrates the potential benefits and increased prevalence of cannabis use in patients with cancer.1 Cannabis products have been shown to possess antineoplastic and palliative activity, improving nociceptive and neuropathic pain in addition to chemotherapy-related nausea and vomiting.2-5 Despite these developments and changing social attitudes toward cannabis, there remains a lack of comprehensive data on patient perspectives regarding its use, especially in regions where cannabis remains illegal. This knowledge gap is notable among veterans undergoing cancer treatment in states where cannabis is prohibited. Up to 57% of veterans report lifetime marijuana use, making it crucial to understand this population’s cannabis use patterns and potential interactions with cancer treatments.6
This observational study sought to determine the prevalence of cannabis use among patients undergoing cancer treatment at the US Department of Veterans Affairs (VA) Memphis Healthcare System and evaluate the potential risks associated with combining cannabis products with anticancer therapies.
METHODS
This prospective observational study identified cannabis use among veterans receiving antineoplastic therapy at the Lt. Col. Luke Weathers Jr. VA Medical Center (WJVAMC) and analyzed potential interactions between cannabis products and their cancer treatments. Participants included adults aged > 18 years undergoing antineoplastic therapy at WJVAMC who consented to the study. Data collection involved a written survey approved by the WJVAMC Institutional Review Board and verbal consent from participants. The survey asked participants about their cannabis use in the previous 90 days, including details on quantity, frequency, and method of consumption (eg, inhalation, oral, topical). No incentives were offered for participation.
Surveys from 50 patients who used cannabis were analyzed and their electronic health records were reviewed for sex, age, diagnosis, and antineoplastic regimen. This information was securely stored. A literature review was conducted using PubMed and the Cochrane Library to explore potential interactions between cannabis and the antineoplastic agents that were prescribed to patients in the study, focusing on toxicity, efficacy, or synergistic effects.
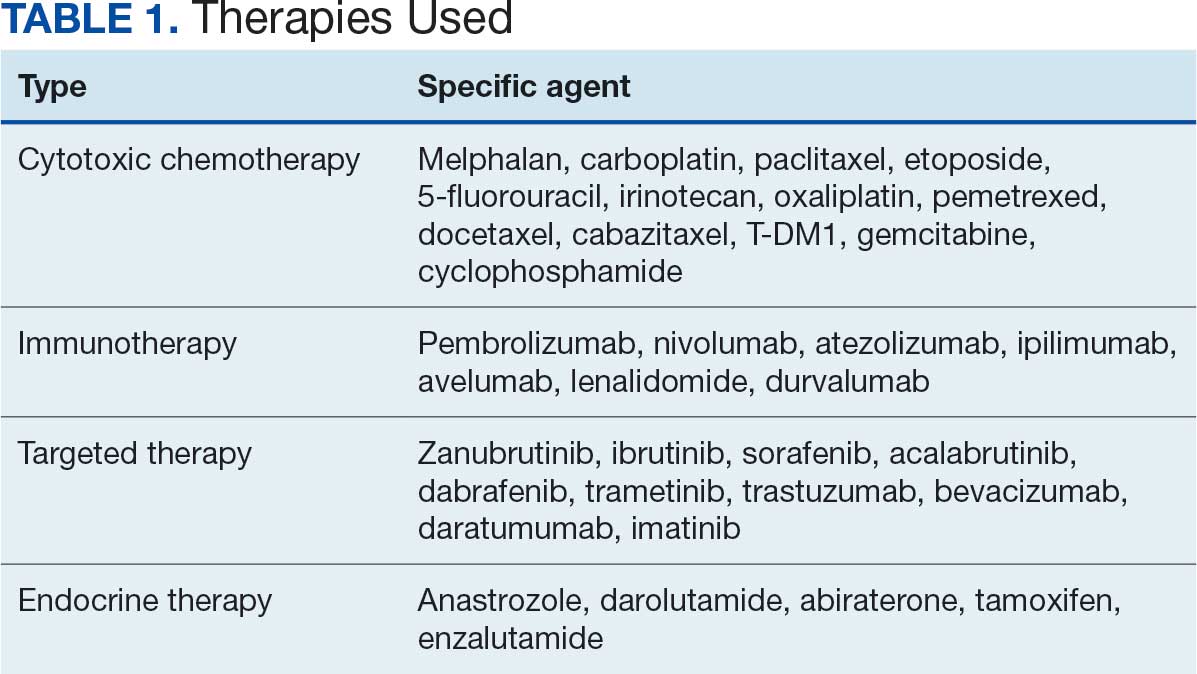
Patients were categorized into 4 groups based on treatment: cytotoxic chemotherapy, immunotherapy, endocrine therapy, and targeted therapy. Patients undergoing multiple types of therapies were included in each applicable category.
RESULTS
A total of 132 patients agreed to participate. Fifty patients (38%) acknowledged using cannabis products within 90 days. The patients that used cannabis products within 90 days of the survey reported the following malignancies: 8 patients (16%) had prostate cancer, 3 patients (6%) had hepatocellular carcinoma, 7 patients (14%) had pancreatic carcinoma, 5 patients (10%) had multiple myeloma, 3 patients (6%) had chronic lymphocytic leukemia, 9 patients (18%) had non-small cell lung cancer, 3 patients (6%) had breast cancer, 3 (6%) patients had bladder cancer, 2 patients (4%) had renal cell carcinoma, 1 (2%) patient had chronic myeloid leukemia, 1 (2%) patient had renal amyloid, 1 patient (2%) had supraglottic squamous cell carcinoma, 1 patient (2%) had esophageal carcinoma, 1 (2%) patient had small cell lung cancer, 1 (2%) patient had gastric cancer, and 1 patient (2%) had follicular lymphoma.
Five (10%) of the cannabis users were female, and 45 (90%) were male. Twenty-nine patients (58%) were aged 66 to 75 years, 16 (32%) were aged 56 to 65 years, 3 (6%) were aged 46 to 55 years, and 2 (4%) were aged 76 to 85 years.
Thirty-five patients (70%) inhaled cannabis as opposed to using it via other formulations or a combination (eg, inhalation and topical). Thirty-eight percent of patients used cannabis once daily, 24% used < 1 daily, and 28% used it ≥ 2 times daily. Five patients (10%) did not report the frequency of their cannabis use. Among the patients who reported cannabis use, 21 (42%) were undergoing cytotoxic chemotherapy, 19 (38%) were undergoing immunotherapy, 12 (24%) were undergoing targeted therapy, and 10 (20%) were undergoing endocrine therapy. Some patients were treated with multiple types of antineoplastic agents and were counted in multiple categories (Table 1).
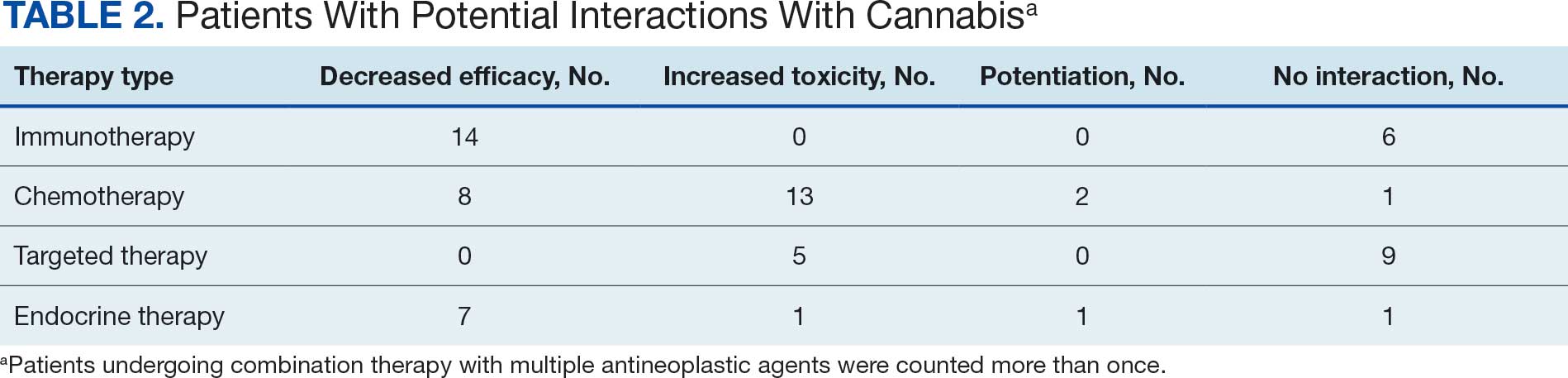
Following a literature review of cannabis and antineoplastic agents, patients were evaluated for the potential effects of cannabis on their treatment. The literature review revealed that 31% of cytotoxic chemotherapy agents received by patients in this study might have increased toxicity, and 19% could have reduced efficacy when combined with cannabis. Among immunotherapy agents received by patients in this study, 70% might have decreased efficacy when combined with cannabis use. For targeted therapies, 35% could have increased toxicity, and 70% of endocrine agents could potentially have decreased efficacy (Table 2).
DISCUSSION
This prospective study corroborates previous research by demonstrating that more than one-third of patients receiving oncology care at WJVAMC use cannabis, most often inhaled. Cannabis use was observed among patients undergoing various cancer therapies, including cytotoxic chemotherapy, immunotherapy, targeted therapy, and endocrine therapy. The most common malignancies among cannabis users at WJVAMC include patients with lung cancer, prostate cancer, pancreatic cancer, and multiple myeloma. Cannabis use in patients with pancreatic cancer and multiple myeloma was significantly out of proportion to their prevalence at WJVAMC. This could potentially be due to their drastic effect on quality of life.
Cannabis use increased the risk of toxicity in patients treated with cytotoxic chemotherapy and targeted therapy. Cannabis use potentially decreased efficacy for patients treated with cytotoxic chemotherapy and/or immunotherapy. Cannabis use did not increase the risk of toxicity or efficacy in patients treated with endocrine therapy.
Antineoplastics/Cannabis Interactions
The potential interactions between cannabis and antineoplastic therapies administered at WJVAMC are worth exploring. While this review aims to shed light on possible interactions, it is important to acknowledge that much of the data is preliminary and derived from in vitro studies. The interactions should be interpreted as potential risks rather than established facts. Additional research is needed to confirm these interactions and effectively guide clinical practices. Understanding these dynamics is essential to optimize patient care and manage the complex interplay between cannabis use and cancer treatment.
Originating from Central Asia, the cannabis plant contains > 400 medicinally relevant compounds, of which about 100 are cannabinoids (CBs). Key CBs are cannabidiol (CBD), a nonpsychoactive compound, and ?-9-tetrahydrocannabinol (THC), a psychoactive compound. THC can make up 20% to 30% of the dry weight of female cannabis flowers.7
CBs act through the endocannabinoid system, involving CB1 and CB2 receptors, endogenous CBs like anandamide (AEA) and 2-arachidonoylglycerol, and various enzymes. These endogenous CBs, derived from arachidonic acid, play roles in cell growth and proliferation.8 In some studies, AEA has induced apoptosis in neuroblastoma cells and inhibited proliferation in breast cancer cells. However, other research suggests AEA may block apoptosis under certain conditions.9
CB receptors are transmembrane proteins that interact with CBs differently depending on tissue type and CB structure. Synthetic CBs are designed to target specific receptors, while natural CBs may act as both agonists and antagonists.10
Cytochrome P450 Metabolism
The human cytochrome P450 (CYP) 3A subfamily affects the metabolism of many therapeutic drugs, including cancer therapeutics.11 The various compositions of cannabis are primarily metabolized by the CYP450 pathway, the same as many cancer-directed pharmacologic treatments. CBs act as both CYP inducers and inhibitors. THC, for example, is a CYP inducer whereas CBD is a CYP inhibitor; both are found in the various compounds available for consumption.12,13 Pharmacology research has suggested potential interactions and effects on established adverse symptoms, but clinical data are lacking, and current research revealing interactions are only recognized in vitro.14
The Antineoplastic Activity of Cannabis
CBs can affect various cancer-related pathways such as PKB, AMPK, CAMKK-ß, mTOR, PDHK, HIF-1 a, and PPAR-γ. Δ-9-THC can selectively induce apoptosis in tumor cells without harming normal cells, though the exact mechanism remains unclear. Promising results from early mouse studies led to a 2006 human study where intracranial Δ-9-THC in patients with recurrent glioma yielded a median survival of 24 weeks, with 2 patients surviving > 1 year.15
In a 2022 review article, Cherkasova et al highlighted potential clinical benefits of cannabis across various cancers. They found that upregulated CB1 receptors in colon cancer might enhance the effect of 5-fluorouracil. However, many studies are preliminary and therefore not definitive.10
Additional research is needed to refine these findings. Challenges include variability in cannabis formulations, the complex tumor microenvironment, and the legal and psychoactive issues surrounding cannabis use. These factors complicate the design of multicenter randomized studies and may deter patients from disclosing cannabis use, thereby hindering efforts to fully understand its therapeutic potential.
Cannabis/Cytotoxic Chemotherapy Interactions
The chemotherapy agents used in this study included carboplatin, paclitaxel, 5-fluorouracil, etoposide, irinotecan, oxaliplatin, pemetrexed, docetaxel, cabazitaxel, T-DM1, gemcitabine, and cyclophosphamide. There is a paucity of research regarding the interactions between cytotoxic chemotherapy and cannabis. Most studies focused on CBD due to its inhibition of the CYP450 pathway, which is used for metabolizing cytotoxic chemotherapies. Through this mechanism, CBD could potentially increase the concentrations of chemotherapeutic agents, enhancing their toxicity.
When combined with irinotecan, cannabis can pose risks. Δ-9-THC undergoes first-pass metabolism in the liver, mediated by the CYP450 system and CYP3A4. The glucuronidation of irinotecan is mediated by uridine diphosphate glycosyltransferase, leading to its recirculation within the hepatic system and potentially increased toxicity due to prolonged drug presence. Cannabis may also compete with drug binding to albumin, altering the plasma concentrations of irinotecan and its conversion to the metabolite SN38.16
Cannabis products can affect chemotherapy levels by interacting with cellular transporters. The MRP1 transporter family, encoded by the ABCC gene family, is expressed mainly in the lung, kidney, skeletal muscle, and hematopoietic stem cells. A 2018 study investigating the effects of THC, CBD, and CBN on MRP1 transporters found that the presence of a cannabis component increased the concentration of vincristine 3-fold. Additional studies suggest the interaction with the CB1 receptor may lead to changes in the expression of MRP1 transporters.17
CBD inhibits the BCRP transporter, which functions as an efflux pump for methotrexate. Consequently, CBD can increase methotrexate levels, potentially enhancing efficacy but also worsening adverse effects.18
In pancreatic cancer, CBD specifically interacts with gemcitabine. CB1 and CB2 receptors are upregulated, and CBD inhibits the GPR55 receptor. These interactions may enhance the antineoplastic effect of gemcitabine, reducing cell cycle progression and growth.19
CBD also interacts with temozolomide (TMZ) by affecting extracellular vesicles used by cells for pro-oncogenic signaling and immune system evasion. Experiments on patient-derived glioblastoma cells, both chemotherapy-resistant and chemotherapy-sensitive, found that CBD increases the formation of extracellular vesicles with reduced levels of miR21 (pro-oncogenic) and elevated levels of miR126 (antioncogenic).20 CBD has also been found to decrease prohibitin levels, a protein associated with TMZ resistance.
In patients with glioblastoma, CBD combined with chemotherapeutic agents like TMZ, carmustine, doxorubicin, and cisplatin has shown increased sensitivity and improved tumor response. CBD is also known to inhibit NF-kB, a pathway that sustains tumor viability despite chemotherapy.21 Additionally, CBD inhibits the P-glycoprotein system, affecting chemotherapy efflux from neoplastic cells.14 In vitro studies have found that CBD is synergistic with bortezomib in inhibiting cancer cell viability. In another glioblastoma model, CBD enhanced the antiproliferative effects of both TMZ and carmustine.14
Different cannabis formulations may vary in how they interact with various cytotoxic chemotherapeutic agents. Some may potentiate the effects of chemotherapy and act synergistically to inhibit tumor growth, while others may lead to increased toxicity.10 More research is needed to determine which formulations, in combination with specific agents and doses, may have significant interactions that warrant adjustments in chemotherapy dosing.
Cannabis/Immunotherapy Interactions
Cannabis is an immunosuppressant. Data suggest the use of cannabis during immunotherapy worsens treatment outcomes in patients with cancer.22 Exogenous (THC) and endogenous (AEA) CBs negatively affect antitumor immunity by impairing the function of tumor-specific T cells via CB2 and by inhibiting the Jak1-STATs signaling in T cells through CNR2. Xiong et al found that THC reduces the therapeutic effect of anti-PD-1 therapy.22
In a prospective observational clinical study, Bar-Sela et al analyzed 102 patients with advanced cancer—of which 68 were cannabis users—that were started on immune checkpoint inhibitor therapy. The study found that cannabis users on anti-PD-1 (nivolumab, pembrolizumab), anti-CTLA-4 (ipilimumab), and anti-PD-L1 (durvalumab, atezolizumab) had a significant decrease in time to treatment progression and overall survival vs cannabis non-users.23 However, a 2023 study by Waissengrin et al found that concomitant use of medical cannabis with pembrolizumab had no harmful effect in advanced non-small cell lung cancer.24 Time to treatment progression of cannabis users did not differ from cannabis nonusers.25
Cannabis/Endocrine Therapy Interactions
In addition to having direct antineoplastic activity on tumor cells, data exist that show how cannabis affects the endocrine system. In animal models, cannabis has been found to suppress the whole hypothalamic-pituitary-adrenal axis as well as other hormones like thyroid, prolactin, and growth hormone. In breast cancer, cannabis competes with estrogen for the estrogen receptor and suppresses growth.26
The endocrine agents used by patients with cancer in this study were antiandrogens like abiraterone, enzalutamide, tamoxifen and anastrozole. Abiraterone is metabolized by CYP450 isoenzymes and uridine diphosphate glycosyltransferases. Cannabis inhibits both processes and therefore may lead to increased toxicities.27 Conversely, enzalutamide is a strong CYP3A inducer, and cannabis use during enzalutamide therapy may significantly increase the toxic effects of cannabis.
There is evidence that molecular pathways involving CB receptors and estrogens overlap, which may lead to interactions when antiestrogens are used in cannabis users with hormone receptor-positive breast cancer.26 In preclinical studies, tamoxifen has been shown to act as an inverse agonist on CB1 and CB2 receptors, though the significance of this finding is unclear. There is no research evaluating the effects of CBs on tamoxifen treatment. However, CBD has been found to potentiate the effectiveness of anastrozole or exemestane in breast cancer cell lines.28 Dobovišek et al demonstrated no inhibitory effect of CBD on the activity of tamoxifen, fulvestrant, or palbociclib in breast cancer cell lines.29 The interactions between hormone receptor-positive breast cancer and cannabinoids are complex, and the clinical significance of these interactions remains difficult to identify.
Cannabis/Targeted Therapy Interactions
The targeted therapies used by patients in this study included zanubrutinib, ibrutinib, sorafenib, acalabrutinib, dabrafenib, trametinib, trastuzumab, bevacizumab, daratumumab, and imatinib. Compared to other classes of cancer treatments, most studies have not demonstrated decreased efficacy or increased toxicity of targeted anticancer drugs when used concomitantly with CBD.29
Trastuzumab is a recombinant humanized monoclonal antibody that targets the proto-oncogene HER2/neu. It is used to treat select patients with metastatic breast cancer. Studies have shown that cannabis use does not attenuate the effectiveness of trastuzumab in HER2-positive and triple-negative breast cancer subtypes.29 One study found that CBD, in combination with chemotherapeutics and Bruton tyrosine kinase inhibitors, such as ibrutinib and zanubrutinib, has synergistic potential for treating diffuse large B-cell lymphoma and mantle cell lymphoma cell lines. This synergy is attributed to the CB1 antagonist activity of cannabis against diffuse large B-cell lymphoma and mantle cell lymphoma cell lines.30,31
Moreover, combining cannabinoids with bevacizumab (a monoclonal anti-VEGF antibody) has been shown to decrease tumor growth and intratumoral hypoxia in clinically relevant human glioblastoma models. This effect is mediated through the downregulation of HIF-1α.32 Long-term studies evaluating the potential harmful or synergistic potential of CBD on targeted anticancer therapy are needed.
CONCLUSIONS
This exploratory study of patients receiving cancer therapy at WJVAMC found a significant prevalence of concurrent cannabis use among patients undergoing antineoplastic treatments. Given that many antineoplastic agents are metabolized by the CYP450 enzyme system, the findings of this study suggest that concurrent cannabis use may pose risks of suboptimal therapeutic outcomes due to potential interactions affecting drug metabolism. These interactions could impact the efficacy and toxicity of the antineoplastic therapies, potentially leading to diminished therapeutic effects or exacerbated adverse reactions.
Patients should be informed regarding the potential decreased efficacy of immunotherapy with concurrent use of cannabis products. They should also be aware of the possibility of increased toxicity with other treatment modalities, though the exact impact on efficacy remains unclear. This highlights the necessity of caution when combining cannabis with prescribed cancer treatments.
While this study identified possible interactions, its data are preliminary and highlight the need for more rigorous research. Future studies should include larger, well-designed cohorts to compare outcomes between cannabis users and nonusers. Such research is essential to fully elucidate the clinical implications of cannabis use during cancer treatment, address the high prevalence of cannabis use among patients with cancer, and mitigate potential risks associated with combining cannabis products with antineoplastic therapies. This will ensure that treatment strategies are optimized for safety and efficacy in this complex patient population.
- Steele G, Arneson T, Zylla D. A comprehensive review of cannabis in patients with cancer: availability in the USA, general efficacy, and safety. Curr Oncol Rep. 2019;21:1-10. doi:10.1007/s11912-019-0757-7
- Brown D, Watson M, Schloss J. Pharmacological evidence of medicinal cannabis in oncology: a systematic review. Support Care Cancer. 2019;27:3195-320. doi:10.1007/s00520-019-04774-5
- Abrams DI. Integrating cannabis into clinical cancer care. Curr Oncol. 2016;23:S8-S14. doi:10.37.47/co.23.3099
- Serafimovska T, Darkovska-Serafimovska M, Stefkov G, Arsova-Sarafinovska Z, Balkanov T. Pharmacotherapeutic considerations for use of cannabinoids to relieve symptoms of nausea and vomiting induced by chemotherapy. Folia Medica (Plovdiv). 2020;62:668-678. doi:10.3897/folmed.62e51478
- Bar-Sela G, Zalman D, Semenysty V, Ballan E. The effects of dosage-controlled cannabis capsules on cancer-related cachexia and anorexia syndrome in advanced cancer patients: pilot study. Integr Cancer Ther. 2019;18:1534735419881498. doi:10.1177/1534735419881498
- Pederson ER, Villarosa-Hurlocker MC, Prince MA. Use of protective behavioral strategies among young adult veteran marijuana users. Cannabis. 2018;1:14-27.
- Schilling S, Melzer R, McCabe PF. Cannabis sativa. Curr Biol. 2020;30:R8-R9. doi:10.1016/j.cub.2019.10.039
- McDougle DR, Kambalyal A, Meling DD, Das A. Endocannabinoids anandamide and 2-arachidonoylglycerol are substrates for human CYP2J2 epoxygenase. J Pharmacol Exp Ther. 2014;351:616-627. doi:10.1124/jpet.114216598
- Movsesyan VA, Stoica BA, Yakovlev AG, et al. Anandamide-induced cell death in primary neuronal cultures: role of calpain and caspase pathways. Cell Death Differ. 2004;11:1121-1132. doi:10.1038/sj.cdd.4401442
- Cherkasova V, Wang B, Gerasymchuk M, Fiselier A, Kovalchuk O, Kovalchuk I. Use of cannabis and cannabinoids for treatment of cancer. Cancers (Basel). 2022;14:5142. doi:10.3390/cancers14205142
- Engels FK, Ten Tije AJ, Baker SD, et al. Effect of cytochrome P450 3A4 inhibition on the pharmacokinetics of docetaxel. Clin Pharmacol Ther. 2004;75:448-454. doi:10.1016/j.clpt.2004.01.001
- Alsherbiny MA, Li CG. Medicinal cannabis-potential drug interactions. Medicines (Basel). 2018;6:3. doi:10.3390/medicines6010003
- Stout SM, Cimino NM. Exogenous cannabinoids as substrates, inhibitors, and inducers of human drug metabolizing enzymes: a systematic review. Drug Metab Rev. 2014;46:86-95. doi:10.3109/03602532.2013.849268
- Opitz BJ, Ostroff ML, Whitman AC. The potential clinical implications and importance of drug interactions between anticancer agents and cannabidiol in patients with cancer. J Pharm Pract. 2020;33:506-512. doi:10.1177/0897190019828920
- Guzmán M, Duarte MJ, Blázquez C, et al. A pilot clinical study of D9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme. Br J Cancer. 2006;95:197-203. doi:10.1038/sj.bjc.6603236
- Kopjar N, Fuchs N, Brcic Karaconji I, et al. High doses of ?9-tetrahydrocannabinol might impair irinotecan chemotherapy: a review of potentially harmful interactions. Clin Drug Investig. 2020;40:775-787. doi:10.1007/s40261-020-00954-y
- Bouquié R, Deslandes G, Mazaré H, et al. Cannabis and anticancer drugs: societal usage and expected pharmacological interactions - a review. Fundam Clin Pharmacol. 2018;32:462-484. doi:10.1111/fcp.12373
- Buchtova T, Lukac D, Skrott Z, Chroma K, Bartek J, Mistrik M. Drug-drug interactions of cannabidiol with standard-of-care chemotherapeutics. Int J Mol Sci. 2023;24:2885. doi:10.3390/ijms24032885
- Sharafi G, He H, Nikfarjam M. Potential use of cannabinoids for the treatment of pancreatic cancer. J Pancreat Cancer. 2019;5:1-7. doi:10.1089/pancan.2018.0019
- Kosgodage US, Uysal-Onganer P, MacLatchy A, et al. Cannabidiol affects extracellular vesicle release, miR21 and miR126, and reduces prohibitin protein in glioblastoma multiforme cells. Transl Oncol. 2019;12:513-522. doi:10.1016/j.tranon.2018.12.004
- Elbaz M, Nasser MW, Ravi J, et al. Modulation of the tumor microenvironment and inhibition of EGF/EGFR pathway: novel anti-tumor mechanisms of cannabidiol in breast cancer. Mol Oncol. 2015;9:906-919. doi:10.1016/j.molonc.2014.12.010
- Xiong X, Chen S, Shen J, et al. Cannabis suppresses anti-tumor immunity by inhibiting JAK/STAT signaling in T cells through CNR2. Signal Transduct Target Ther. 2022;7:99. doi:10.1038/s41392-022-00918-y
- Bar-Sela G, Cohen I, Campisi-Pinto S, et al. Cannabis consumption used by cancer patients during immunotherapy correlates with poor clinical outcome. Cancers (Basel). 2020;12:2447. doi:10.3390/cancers12092447
- Waissengrin B, Leshem Y, Taya M, et al. The use of medical cannabis concomitantly with immune checkpoint inhibitors in non-small cell lung cancer: a sigh of relief? Eur J Cancer. 2023;180:52-61. doi:10.1016/j.ejca.2022.11.022
- Sarsembayeva A, Schicho R. Cannabinoids and the endocannabinoid system in immunotherapy: helpful or harmful? Front Oncol. 2023;13:1296906. doi:10.3389/fonc.2023.1296906
- Kisková T, Mungenast F, Suváková M, Jäger W, Thalhammer T. Future aspects for cannabinoids in breast cancer therapy. Int J Mol Sci. 2019;20:1673. doi:10.3390/ijms20071673
- Woerdenbag HJ, Olinga P, Kok EA, et al. Potential, limitations and risks of cannabis-derived products in cancer treatment. Cancers (Basel). 2023;15:2119. doi:10.3390/cancers15072119
- Almeida CF, Teixeira N, Valente MJ, Vinggaard AM, Correia-da-Silva G, Amaral C. Cannabidiol as a promising adjuvant therapy for estrogen receptor-positive breast tumors: unveiling its benefits with aromatase inhibitors. Cancers (Basel). 2023;15:2517. doi:10.3390/cancers15092517
- Dobovišek L, Novak M, Krstanovic F, Borštnar S, Turnšek TL, Debeljak N. Effect of combining CBD with standard breast cancer therapeutics. Adv Cancer Biol Metastasis. 2022;4:100038. doi:10.1016/j.adcanc.2022.100038
- Strong T, Rauvolfova J, Jackson E, Pham LV, Bryant J. Synergistic effect of cannabidiol with conventional chemotherapy treatment. Blood. 2018;132:5382. doi:10.1182/blood-2018-99-116749
- Maggi F, Morelli MB, Tomassoni D, et al. The effects of cannabidiol via TRPV2 channel in chronic myeloid leukemia cells and its combination with imatinib. Cancer Sci. 2022;113:1235-1249. doi:10.1111/cas.15257
- Obad N, Janji B, Prestegarden L, et al. ATPS-59 improving efficacy of bevacizumab treatment in glioblastoma by targeting hif1 alpha. Neuro Oncol. 2015;17:v31. doi:10.1093/neuonc/nov204.59
Cannabis has a long history of use for medicinal and recreational purposes. Research illustrates the potential benefits and increased prevalence of cannabis use in patients with cancer.1 Cannabis products have been shown to possess antineoplastic and palliative activity, improving nociceptive and neuropathic pain in addition to chemotherapy-related nausea and vomiting.2-5 Despite these developments and changing social attitudes toward cannabis, there remains a lack of comprehensive data on patient perspectives regarding its use, especially in regions where cannabis remains illegal. This knowledge gap is notable among veterans undergoing cancer treatment in states where cannabis is prohibited. Up to 57% of veterans report lifetime marijuana use, making it crucial to understand this population’s cannabis use patterns and potential interactions with cancer treatments.6
This observational study sought to determine the prevalence of cannabis use among patients undergoing cancer treatment at the US Department of Veterans Affairs (VA) Memphis Healthcare System and evaluate the potential risks associated with combining cannabis products with anticancer therapies.
METHODS
This prospective observational study identified cannabis use among veterans receiving antineoplastic therapy at the Lt. Col. Luke Weathers Jr. VA Medical Center (WJVAMC) and analyzed potential interactions between cannabis products and their cancer treatments. Participants included adults aged > 18 years undergoing antineoplastic therapy at WJVAMC who consented to the study. Data collection involved a written survey approved by the WJVAMC Institutional Review Board and verbal consent from participants. The survey asked participants about their cannabis use in the previous 90 days, including details on quantity, frequency, and method of consumption (eg, inhalation, oral, topical). No incentives were offered for participation.
Surveys from 50 patients who used cannabis were analyzed and their electronic health records were reviewed for sex, age, diagnosis, and antineoplastic regimen. This information was securely stored. A literature review was conducted using PubMed and the Cochrane Library to explore potential interactions between cannabis and the antineoplastic agents that were prescribed to patients in the study, focusing on toxicity, efficacy, or synergistic effects.
Patients were categorized into 4 groups based on treatment: cytotoxic chemotherapy, immunotherapy, endocrine therapy, and targeted therapy. Patients undergoing multiple types of therapies were included in each applicable category.
RESULTS
A total of 132 patients agreed to participate. Fifty patients (38%) acknowledged using cannabis products within 90 days. The patients that used cannabis products within 90 days of the survey reported the following malignancies: 8 patients (16%) had prostate cancer, 3 patients (6%) had hepatocellular carcinoma, 7 patients (14%) had pancreatic carcinoma, 5 patients (10%) had multiple myeloma, 3 patients (6%) had chronic lymphocytic leukemia, 9 patients (18%) had non-small cell lung cancer, 3 patients (6%) had breast cancer, 3 (6%) patients had bladder cancer, 2 patients (4%) had renal cell carcinoma, 1 (2%) patient had chronic myeloid leukemia, 1 (2%) patient had renal amyloid, 1 patient (2%) had supraglottic squamous cell carcinoma, 1 patient (2%) had esophageal carcinoma, 1 (2%) patient had small cell lung cancer, 1 (2%) patient had gastric cancer, and 1 patient (2%) had follicular lymphoma.
Five (10%) of the cannabis users were female, and 45 (90%) were male. Twenty-nine patients (58%) were aged 66 to 75 years, 16 (32%) were aged 56 to 65 years, 3 (6%) were aged 46 to 55 years, and 2 (4%) were aged 76 to 85 years.
Thirty-five patients (70%) inhaled cannabis as opposed to using it via other formulations or a combination (eg, inhalation and topical). Thirty-eight percent of patients used cannabis once daily, 24% used < 1 daily, and 28% used it ≥ 2 times daily. Five patients (10%) did not report the frequency of their cannabis use. Among the patients who reported cannabis use, 21 (42%) were undergoing cytotoxic chemotherapy, 19 (38%) were undergoing immunotherapy, 12 (24%) were undergoing targeted therapy, and 10 (20%) were undergoing endocrine therapy. Some patients were treated with multiple types of antineoplastic agents and were counted in multiple categories (Table 1).
Following a literature review of cannabis and antineoplastic agents, patients were evaluated for the potential effects of cannabis on their treatment. The literature review revealed that 31% of cytotoxic chemotherapy agents received by patients in this study might have increased toxicity, and 19% could have reduced efficacy when combined with cannabis. Among immunotherapy agents received by patients in this study, 70% might have decreased efficacy when combined with cannabis use. For targeted therapies, 35% could have increased toxicity, and 70% of endocrine agents could potentially have decreased efficacy (Table 2).
DISCUSSION
This prospective study corroborates previous research by demonstrating that more than one-third of patients receiving oncology care at WJVAMC use cannabis, most often inhaled. Cannabis use was observed among patients undergoing various cancer therapies, including cytotoxic chemotherapy, immunotherapy, targeted therapy, and endocrine therapy. The most common malignancies among cannabis users at WJVAMC include patients with lung cancer, prostate cancer, pancreatic cancer, and multiple myeloma. Cannabis use in patients with pancreatic cancer and multiple myeloma was significantly out of proportion to their prevalence at WJVAMC. This could potentially be due to their drastic effect on quality of life.
Cannabis use increased the risk of toxicity in patients treated with cytotoxic chemotherapy and targeted therapy. Cannabis use potentially decreased efficacy for patients treated with cytotoxic chemotherapy and/or immunotherapy. Cannabis use did not increase the risk of toxicity or efficacy in patients treated with endocrine therapy.
Antineoplastics/Cannabis Interactions
The potential interactions between cannabis and antineoplastic therapies administered at WJVAMC are worth exploring. While this review aims to shed light on possible interactions, it is important to acknowledge that much of the data is preliminary and derived from in vitro studies. The interactions should be interpreted as potential risks rather than established facts. Additional research is needed to confirm these interactions and effectively guide clinical practices. Understanding these dynamics is essential to optimize patient care and manage the complex interplay between cannabis use and cancer treatment.
Originating from Central Asia, the cannabis plant contains > 400 medicinally relevant compounds, of which about 100 are cannabinoids (CBs). Key CBs are cannabidiol (CBD), a nonpsychoactive compound, and ?-9-tetrahydrocannabinol (THC), a psychoactive compound. THC can make up 20% to 30% of the dry weight of female cannabis flowers.7
CBs act through the endocannabinoid system, involving CB1 and CB2 receptors, endogenous CBs like anandamide (AEA) and 2-arachidonoylglycerol, and various enzymes. These endogenous CBs, derived from arachidonic acid, play roles in cell growth and proliferation.8 In some studies, AEA has induced apoptosis in neuroblastoma cells and inhibited proliferation in breast cancer cells. However, other research suggests AEA may block apoptosis under certain conditions.9
CB receptors are transmembrane proteins that interact with CBs differently depending on tissue type and CB structure. Synthetic CBs are designed to target specific receptors, while natural CBs may act as both agonists and antagonists.10
Cytochrome P450 Metabolism
The human cytochrome P450 (CYP) 3A subfamily affects the metabolism of many therapeutic drugs, including cancer therapeutics.11 The various compositions of cannabis are primarily metabolized by the CYP450 pathway, the same as many cancer-directed pharmacologic treatments. CBs act as both CYP inducers and inhibitors. THC, for example, is a CYP inducer whereas CBD is a CYP inhibitor; both are found in the various compounds available for consumption.12,13 Pharmacology research has suggested potential interactions and effects on established adverse symptoms, but clinical data are lacking, and current research revealing interactions are only recognized in vitro.14
The Antineoplastic Activity of Cannabis
CBs can affect various cancer-related pathways such as PKB, AMPK, CAMKK-ß, mTOR, PDHK, HIF-1 a, and PPAR-γ. Δ-9-THC can selectively induce apoptosis in tumor cells without harming normal cells, though the exact mechanism remains unclear. Promising results from early mouse studies led to a 2006 human study where intracranial Δ-9-THC in patients with recurrent glioma yielded a median survival of 24 weeks, with 2 patients surviving > 1 year.15
In a 2022 review article, Cherkasova et al highlighted potential clinical benefits of cannabis across various cancers. They found that upregulated CB1 receptors in colon cancer might enhance the effect of 5-fluorouracil. However, many studies are preliminary and therefore not definitive.10
Additional research is needed to refine these findings. Challenges include variability in cannabis formulations, the complex tumor microenvironment, and the legal and psychoactive issues surrounding cannabis use. These factors complicate the design of multicenter randomized studies and may deter patients from disclosing cannabis use, thereby hindering efforts to fully understand its therapeutic potential.
Cannabis/Cytotoxic Chemotherapy Interactions
The chemotherapy agents used in this study included carboplatin, paclitaxel, 5-fluorouracil, etoposide, irinotecan, oxaliplatin, pemetrexed, docetaxel, cabazitaxel, T-DM1, gemcitabine, and cyclophosphamide. There is a paucity of research regarding the interactions between cytotoxic chemotherapy and cannabis. Most studies focused on CBD due to its inhibition of the CYP450 pathway, which is used for metabolizing cytotoxic chemotherapies. Through this mechanism, CBD could potentially increase the concentrations of chemotherapeutic agents, enhancing their toxicity.
When combined with irinotecan, cannabis can pose risks. Δ-9-THC undergoes first-pass metabolism in the liver, mediated by the CYP450 system and CYP3A4. The glucuronidation of irinotecan is mediated by uridine diphosphate glycosyltransferase, leading to its recirculation within the hepatic system and potentially increased toxicity due to prolonged drug presence. Cannabis may also compete with drug binding to albumin, altering the plasma concentrations of irinotecan and its conversion to the metabolite SN38.16
Cannabis products can affect chemotherapy levels by interacting with cellular transporters. The MRP1 transporter family, encoded by the ABCC gene family, is expressed mainly in the lung, kidney, skeletal muscle, and hematopoietic stem cells. A 2018 study investigating the effects of THC, CBD, and CBN on MRP1 transporters found that the presence of a cannabis component increased the concentration of vincristine 3-fold. Additional studies suggest the interaction with the CB1 receptor may lead to changes in the expression of MRP1 transporters.17
CBD inhibits the BCRP transporter, which functions as an efflux pump for methotrexate. Consequently, CBD can increase methotrexate levels, potentially enhancing efficacy but also worsening adverse effects.18
In pancreatic cancer, CBD specifically interacts with gemcitabine. CB1 and CB2 receptors are upregulated, and CBD inhibits the GPR55 receptor. These interactions may enhance the antineoplastic effect of gemcitabine, reducing cell cycle progression and growth.19
CBD also interacts with temozolomide (TMZ) by affecting extracellular vesicles used by cells for pro-oncogenic signaling and immune system evasion. Experiments on patient-derived glioblastoma cells, both chemotherapy-resistant and chemotherapy-sensitive, found that CBD increases the formation of extracellular vesicles with reduced levels of miR21 (pro-oncogenic) and elevated levels of miR126 (antioncogenic).20 CBD has also been found to decrease prohibitin levels, a protein associated with TMZ resistance.
In patients with glioblastoma, CBD combined with chemotherapeutic agents like TMZ, carmustine, doxorubicin, and cisplatin has shown increased sensitivity and improved tumor response. CBD is also known to inhibit NF-kB, a pathway that sustains tumor viability despite chemotherapy.21 Additionally, CBD inhibits the P-glycoprotein system, affecting chemotherapy efflux from neoplastic cells.14 In vitro studies have found that CBD is synergistic with bortezomib in inhibiting cancer cell viability. In another glioblastoma model, CBD enhanced the antiproliferative effects of both TMZ and carmustine.14
Different cannabis formulations may vary in how they interact with various cytotoxic chemotherapeutic agents. Some may potentiate the effects of chemotherapy and act synergistically to inhibit tumor growth, while others may lead to increased toxicity.10 More research is needed to determine which formulations, in combination with specific agents and doses, may have significant interactions that warrant adjustments in chemotherapy dosing.
Cannabis/Immunotherapy Interactions
Cannabis is an immunosuppressant. Data suggest the use of cannabis during immunotherapy worsens treatment outcomes in patients with cancer.22 Exogenous (THC) and endogenous (AEA) CBs negatively affect antitumor immunity by impairing the function of tumor-specific T cells via CB2 and by inhibiting the Jak1-STATs signaling in T cells through CNR2. Xiong et al found that THC reduces the therapeutic effect of anti-PD-1 therapy.22
In a prospective observational clinical study, Bar-Sela et al analyzed 102 patients with advanced cancer—of which 68 were cannabis users—that were started on immune checkpoint inhibitor therapy. The study found that cannabis users on anti-PD-1 (nivolumab, pembrolizumab), anti-CTLA-4 (ipilimumab), and anti-PD-L1 (durvalumab, atezolizumab) had a significant decrease in time to treatment progression and overall survival vs cannabis non-users.23 However, a 2023 study by Waissengrin et al found that concomitant use of medical cannabis with pembrolizumab had no harmful effect in advanced non-small cell lung cancer.24 Time to treatment progression of cannabis users did not differ from cannabis nonusers.25
Cannabis/Endocrine Therapy Interactions
In addition to having direct antineoplastic activity on tumor cells, data exist that show how cannabis affects the endocrine system. In animal models, cannabis has been found to suppress the whole hypothalamic-pituitary-adrenal axis as well as other hormones like thyroid, prolactin, and growth hormone. In breast cancer, cannabis competes with estrogen for the estrogen receptor and suppresses growth.26
The endocrine agents used by patients with cancer in this study were antiandrogens like abiraterone, enzalutamide, tamoxifen and anastrozole. Abiraterone is metabolized by CYP450 isoenzymes and uridine diphosphate glycosyltransferases. Cannabis inhibits both processes and therefore may lead to increased toxicities.27 Conversely, enzalutamide is a strong CYP3A inducer, and cannabis use during enzalutamide therapy may significantly increase the toxic effects of cannabis.
There is evidence that molecular pathways involving CB receptors and estrogens overlap, which may lead to interactions when antiestrogens are used in cannabis users with hormone receptor-positive breast cancer.26 In preclinical studies, tamoxifen has been shown to act as an inverse agonist on CB1 and CB2 receptors, though the significance of this finding is unclear. There is no research evaluating the effects of CBs on tamoxifen treatment. However, CBD has been found to potentiate the effectiveness of anastrozole or exemestane in breast cancer cell lines.28 Dobovišek et al demonstrated no inhibitory effect of CBD on the activity of tamoxifen, fulvestrant, or palbociclib in breast cancer cell lines.29 The interactions between hormone receptor-positive breast cancer and cannabinoids are complex, and the clinical significance of these interactions remains difficult to identify.
Cannabis/Targeted Therapy Interactions
The targeted therapies used by patients in this study included zanubrutinib, ibrutinib, sorafenib, acalabrutinib, dabrafenib, trametinib, trastuzumab, bevacizumab, daratumumab, and imatinib. Compared to other classes of cancer treatments, most studies have not demonstrated decreased efficacy or increased toxicity of targeted anticancer drugs when used concomitantly with CBD.29
Trastuzumab is a recombinant humanized monoclonal antibody that targets the proto-oncogene HER2/neu. It is used to treat select patients with metastatic breast cancer. Studies have shown that cannabis use does not attenuate the effectiveness of trastuzumab in HER2-positive and triple-negative breast cancer subtypes.29 One study found that CBD, in combination with chemotherapeutics and Bruton tyrosine kinase inhibitors, such as ibrutinib and zanubrutinib, has synergistic potential for treating diffuse large B-cell lymphoma and mantle cell lymphoma cell lines. This synergy is attributed to the CB1 antagonist activity of cannabis against diffuse large B-cell lymphoma and mantle cell lymphoma cell lines.30,31
Moreover, combining cannabinoids with bevacizumab (a monoclonal anti-VEGF antibody) has been shown to decrease tumor growth and intratumoral hypoxia in clinically relevant human glioblastoma models. This effect is mediated through the downregulation of HIF-1α.32 Long-term studies evaluating the potential harmful or synergistic potential of CBD on targeted anticancer therapy are needed.
CONCLUSIONS
This exploratory study of patients receiving cancer therapy at WJVAMC found a significant prevalence of concurrent cannabis use among patients undergoing antineoplastic treatments. Given that many antineoplastic agents are metabolized by the CYP450 enzyme system, the findings of this study suggest that concurrent cannabis use may pose risks of suboptimal therapeutic outcomes due to potential interactions affecting drug metabolism. These interactions could impact the efficacy and toxicity of the antineoplastic therapies, potentially leading to diminished therapeutic effects or exacerbated adverse reactions.
Patients should be informed regarding the potential decreased efficacy of immunotherapy with concurrent use of cannabis products. They should also be aware of the possibility of increased toxicity with other treatment modalities, though the exact impact on efficacy remains unclear. This highlights the necessity of caution when combining cannabis with prescribed cancer treatments.
While this study identified possible interactions, its data are preliminary and highlight the need for more rigorous research. Future studies should include larger, well-designed cohorts to compare outcomes between cannabis users and nonusers. Such research is essential to fully elucidate the clinical implications of cannabis use during cancer treatment, address the high prevalence of cannabis use among patients with cancer, and mitigate potential risks associated with combining cannabis products with antineoplastic therapies. This will ensure that treatment strategies are optimized for safety and efficacy in this complex patient population.
Cannabis has a long history of use for medicinal and recreational purposes. Research illustrates the potential benefits and increased prevalence of cannabis use in patients with cancer.1 Cannabis products have been shown to possess antineoplastic and palliative activity, improving nociceptive and neuropathic pain in addition to chemotherapy-related nausea and vomiting.2-5 Despite these developments and changing social attitudes toward cannabis, there remains a lack of comprehensive data on patient perspectives regarding its use, especially in regions where cannabis remains illegal. This knowledge gap is notable among veterans undergoing cancer treatment in states where cannabis is prohibited. Up to 57% of veterans report lifetime marijuana use, making it crucial to understand this population’s cannabis use patterns and potential interactions with cancer treatments.6
This observational study sought to determine the prevalence of cannabis use among patients undergoing cancer treatment at the US Department of Veterans Affairs (VA) Memphis Healthcare System and evaluate the potential risks associated with combining cannabis products with anticancer therapies.
METHODS
This prospective observational study identified cannabis use among veterans receiving antineoplastic therapy at the Lt. Col. Luke Weathers Jr. VA Medical Center (WJVAMC) and analyzed potential interactions between cannabis products and their cancer treatments. Participants included adults aged > 18 years undergoing antineoplastic therapy at WJVAMC who consented to the study. Data collection involved a written survey approved by the WJVAMC Institutional Review Board and verbal consent from participants. The survey asked participants about their cannabis use in the previous 90 days, including details on quantity, frequency, and method of consumption (eg, inhalation, oral, topical). No incentives were offered for participation.
Surveys from 50 patients who used cannabis were analyzed and their electronic health records were reviewed for sex, age, diagnosis, and antineoplastic regimen. This information was securely stored. A literature review was conducted using PubMed and the Cochrane Library to explore potential interactions between cannabis and the antineoplastic agents that were prescribed to patients in the study, focusing on toxicity, efficacy, or synergistic effects.
Patients were categorized into 4 groups based on treatment: cytotoxic chemotherapy, immunotherapy, endocrine therapy, and targeted therapy. Patients undergoing multiple types of therapies were included in each applicable category.
RESULTS
A total of 132 patients agreed to participate. Fifty patients (38%) acknowledged using cannabis products within 90 days. The patients that used cannabis products within 90 days of the survey reported the following malignancies: 8 patients (16%) had prostate cancer, 3 patients (6%) had hepatocellular carcinoma, 7 patients (14%) had pancreatic carcinoma, 5 patients (10%) had multiple myeloma, 3 patients (6%) had chronic lymphocytic leukemia, 9 patients (18%) had non-small cell lung cancer, 3 patients (6%) had breast cancer, 3 (6%) patients had bladder cancer, 2 patients (4%) had renal cell carcinoma, 1 (2%) patient had chronic myeloid leukemia, 1 (2%) patient had renal amyloid, 1 patient (2%) had supraglottic squamous cell carcinoma, 1 patient (2%) had esophageal carcinoma, 1 (2%) patient had small cell lung cancer, 1 (2%) patient had gastric cancer, and 1 patient (2%) had follicular lymphoma.
Five (10%) of the cannabis users were female, and 45 (90%) were male. Twenty-nine patients (58%) were aged 66 to 75 years, 16 (32%) were aged 56 to 65 years, 3 (6%) were aged 46 to 55 years, and 2 (4%) were aged 76 to 85 years.
Thirty-five patients (70%) inhaled cannabis as opposed to using it via other formulations or a combination (eg, inhalation and topical). Thirty-eight percent of patients used cannabis once daily, 24% used < 1 daily, and 28% used it ≥ 2 times daily. Five patients (10%) did not report the frequency of their cannabis use. Among the patients who reported cannabis use, 21 (42%) were undergoing cytotoxic chemotherapy, 19 (38%) were undergoing immunotherapy, 12 (24%) were undergoing targeted therapy, and 10 (20%) were undergoing endocrine therapy. Some patients were treated with multiple types of antineoplastic agents and were counted in multiple categories (Table 1).
Following a literature review of cannabis and antineoplastic agents, patients were evaluated for the potential effects of cannabis on their treatment. The literature review revealed that 31% of cytotoxic chemotherapy agents received by patients in this study might have increased toxicity, and 19% could have reduced efficacy when combined with cannabis. Among immunotherapy agents received by patients in this study, 70% might have decreased efficacy when combined with cannabis use. For targeted therapies, 35% could have increased toxicity, and 70% of endocrine agents could potentially have decreased efficacy (Table 2).
DISCUSSION
This prospective study corroborates previous research by demonstrating that more than one-third of patients receiving oncology care at WJVAMC use cannabis, most often inhaled. Cannabis use was observed among patients undergoing various cancer therapies, including cytotoxic chemotherapy, immunotherapy, targeted therapy, and endocrine therapy. The most common malignancies among cannabis users at WJVAMC include patients with lung cancer, prostate cancer, pancreatic cancer, and multiple myeloma. Cannabis use in patients with pancreatic cancer and multiple myeloma was significantly out of proportion to their prevalence at WJVAMC. This could potentially be due to their drastic effect on quality of life.
Cannabis use increased the risk of toxicity in patients treated with cytotoxic chemotherapy and targeted therapy. Cannabis use potentially decreased efficacy for patients treated with cytotoxic chemotherapy and/or immunotherapy. Cannabis use did not increase the risk of toxicity or efficacy in patients treated with endocrine therapy.
Antineoplastics/Cannabis Interactions
The potential interactions between cannabis and antineoplastic therapies administered at WJVAMC are worth exploring. While this review aims to shed light on possible interactions, it is important to acknowledge that much of the data is preliminary and derived from in vitro studies. The interactions should be interpreted as potential risks rather than established facts. Additional research is needed to confirm these interactions and effectively guide clinical practices. Understanding these dynamics is essential to optimize patient care and manage the complex interplay between cannabis use and cancer treatment.
Originating from Central Asia, the cannabis plant contains > 400 medicinally relevant compounds, of which about 100 are cannabinoids (CBs). Key CBs are cannabidiol (CBD), a nonpsychoactive compound, and ?-9-tetrahydrocannabinol (THC), a psychoactive compound. THC can make up 20% to 30% of the dry weight of female cannabis flowers.7
CBs act through the endocannabinoid system, involving CB1 and CB2 receptors, endogenous CBs like anandamide (AEA) and 2-arachidonoylglycerol, and various enzymes. These endogenous CBs, derived from arachidonic acid, play roles in cell growth and proliferation.8 In some studies, AEA has induced apoptosis in neuroblastoma cells and inhibited proliferation in breast cancer cells. However, other research suggests AEA may block apoptosis under certain conditions.9
CB receptors are transmembrane proteins that interact with CBs differently depending on tissue type and CB structure. Synthetic CBs are designed to target specific receptors, while natural CBs may act as both agonists and antagonists.10
Cytochrome P450 Metabolism
The human cytochrome P450 (CYP) 3A subfamily affects the metabolism of many therapeutic drugs, including cancer therapeutics.11 The various compositions of cannabis are primarily metabolized by the CYP450 pathway, the same as many cancer-directed pharmacologic treatments. CBs act as both CYP inducers and inhibitors. THC, for example, is a CYP inducer whereas CBD is a CYP inhibitor; both are found in the various compounds available for consumption.12,13 Pharmacology research has suggested potential interactions and effects on established adverse symptoms, but clinical data are lacking, and current research revealing interactions are only recognized in vitro.14
The Antineoplastic Activity of Cannabis
CBs can affect various cancer-related pathways such as PKB, AMPK, CAMKK-ß, mTOR, PDHK, HIF-1 a, and PPAR-γ. Δ-9-THC can selectively induce apoptosis in tumor cells without harming normal cells, though the exact mechanism remains unclear. Promising results from early mouse studies led to a 2006 human study where intracranial Δ-9-THC in patients with recurrent glioma yielded a median survival of 24 weeks, with 2 patients surviving > 1 year.15
In a 2022 review article, Cherkasova et al highlighted potential clinical benefits of cannabis across various cancers. They found that upregulated CB1 receptors in colon cancer might enhance the effect of 5-fluorouracil. However, many studies are preliminary and therefore not definitive.10
Additional research is needed to refine these findings. Challenges include variability in cannabis formulations, the complex tumor microenvironment, and the legal and psychoactive issues surrounding cannabis use. These factors complicate the design of multicenter randomized studies and may deter patients from disclosing cannabis use, thereby hindering efforts to fully understand its therapeutic potential.
Cannabis/Cytotoxic Chemotherapy Interactions
The chemotherapy agents used in this study included carboplatin, paclitaxel, 5-fluorouracil, etoposide, irinotecan, oxaliplatin, pemetrexed, docetaxel, cabazitaxel, T-DM1, gemcitabine, and cyclophosphamide. There is a paucity of research regarding the interactions between cytotoxic chemotherapy and cannabis. Most studies focused on CBD due to its inhibition of the CYP450 pathway, which is used for metabolizing cytotoxic chemotherapies. Through this mechanism, CBD could potentially increase the concentrations of chemotherapeutic agents, enhancing their toxicity.
When combined with irinotecan, cannabis can pose risks. Δ-9-THC undergoes first-pass metabolism in the liver, mediated by the CYP450 system and CYP3A4. The glucuronidation of irinotecan is mediated by uridine diphosphate glycosyltransferase, leading to its recirculation within the hepatic system and potentially increased toxicity due to prolonged drug presence. Cannabis may also compete with drug binding to albumin, altering the plasma concentrations of irinotecan and its conversion to the metabolite SN38.16
Cannabis products can affect chemotherapy levels by interacting with cellular transporters. The MRP1 transporter family, encoded by the ABCC gene family, is expressed mainly in the lung, kidney, skeletal muscle, and hematopoietic stem cells. A 2018 study investigating the effects of THC, CBD, and CBN on MRP1 transporters found that the presence of a cannabis component increased the concentration of vincristine 3-fold. Additional studies suggest the interaction with the CB1 receptor may lead to changes in the expression of MRP1 transporters.17
CBD inhibits the BCRP transporter, which functions as an efflux pump for methotrexate. Consequently, CBD can increase methotrexate levels, potentially enhancing efficacy but also worsening adverse effects.18
In pancreatic cancer, CBD specifically interacts with gemcitabine. CB1 and CB2 receptors are upregulated, and CBD inhibits the GPR55 receptor. These interactions may enhance the antineoplastic effect of gemcitabine, reducing cell cycle progression and growth.19
CBD also interacts with temozolomide (TMZ) by affecting extracellular vesicles used by cells for pro-oncogenic signaling and immune system evasion. Experiments on patient-derived glioblastoma cells, both chemotherapy-resistant and chemotherapy-sensitive, found that CBD increases the formation of extracellular vesicles with reduced levels of miR21 (pro-oncogenic) and elevated levels of miR126 (antioncogenic).20 CBD has also been found to decrease prohibitin levels, a protein associated with TMZ resistance.
In patients with glioblastoma, CBD combined with chemotherapeutic agents like TMZ, carmustine, doxorubicin, and cisplatin has shown increased sensitivity and improved tumor response. CBD is also known to inhibit NF-kB, a pathway that sustains tumor viability despite chemotherapy.21 Additionally, CBD inhibits the P-glycoprotein system, affecting chemotherapy efflux from neoplastic cells.14 In vitro studies have found that CBD is synergistic with bortezomib in inhibiting cancer cell viability. In another glioblastoma model, CBD enhanced the antiproliferative effects of both TMZ and carmustine.14
Different cannabis formulations may vary in how they interact with various cytotoxic chemotherapeutic agents. Some may potentiate the effects of chemotherapy and act synergistically to inhibit tumor growth, while others may lead to increased toxicity.10 More research is needed to determine which formulations, in combination with specific agents and doses, may have significant interactions that warrant adjustments in chemotherapy dosing.
Cannabis/Immunotherapy Interactions
Cannabis is an immunosuppressant. Data suggest the use of cannabis during immunotherapy worsens treatment outcomes in patients with cancer.22 Exogenous (THC) and endogenous (AEA) CBs negatively affect antitumor immunity by impairing the function of tumor-specific T cells via CB2 and by inhibiting the Jak1-STATs signaling in T cells through CNR2. Xiong et al found that THC reduces the therapeutic effect of anti-PD-1 therapy.22
In a prospective observational clinical study, Bar-Sela et al analyzed 102 patients with advanced cancer—of which 68 were cannabis users—that were started on immune checkpoint inhibitor therapy. The study found that cannabis users on anti-PD-1 (nivolumab, pembrolizumab), anti-CTLA-4 (ipilimumab), and anti-PD-L1 (durvalumab, atezolizumab) had a significant decrease in time to treatment progression and overall survival vs cannabis non-users.23 However, a 2023 study by Waissengrin et al found that concomitant use of medical cannabis with pembrolizumab had no harmful effect in advanced non-small cell lung cancer.24 Time to treatment progression of cannabis users did not differ from cannabis nonusers.25
Cannabis/Endocrine Therapy Interactions
In addition to having direct antineoplastic activity on tumor cells, data exist that show how cannabis affects the endocrine system. In animal models, cannabis has been found to suppress the whole hypothalamic-pituitary-adrenal axis as well as other hormones like thyroid, prolactin, and growth hormone. In breast cancer, cannabis competes with estrogen for the estrogen receptor and suppresses growth.26
The endocrine agents used by patients with cancer in this study were antiandrogens like abiraterone, enzalutamide, tamoxifen and anastrozole. Abiraterone is metabolized by CYP450 isoenzymes and uridine diphosphate glycosyltransferases. Cannabis inhibits both processes and therefore may lead to increased toxicities.27 Conversely, enzalutamide is a strong CYP3A inducer, and cannabis use during enzalutamide therapy may significantly increase the toxic effects of cannabis.
There is evidence that molecular pathways involving CB receptors and estrogens overlap, which may lead to interactions when antiestrogens are used in cannabis users with hormone receptor-positive breast cancer.26 In preclinical studies, tamoxifen has been shown to act as an inverse agonist on CB1 and CB2 receptors, though the significance of this finding is unclear. There is no research evaluating the effects of CBs on tamoxifen treatment. However, CBD has been found to potentiate the effectiveness of anastrozole or exemestane in breast cancer cell lines.28 Dobovišek et al demonstrated no inhibitory effect of CBD on the activity of tamoxifen, fulvestrant, or palbociclib in breast cancer cell lines.29 The interactions between hormone receptor-positive breast cancer and cannabinoids are complex, and the clinical significance of these interactions remains difficult to identify.
Cannabis/Targeted Therapy Interactions
The targeted therapies used by patients in this study included zanubrutinib, ibrutinib, sorafenib, acalabrutinib, dabrafenib, trametinib, trastuzumab, bevacizumab, daratumumab, and imatinib. Compared to other classes of cancer treatments, most studies have not demonstrated decreased efficacy or increased toxicity of targeted anticancer drugs when used concomitantly with CBD.29
Trastuzumab is a recombinant humanized monoclonal antibody that targets the proto-oncogene HER2/neu. It is used to treat select patients with metastatic breast cancer. Studies have shown that cannabis use does not attenuate the effectiveness of trastuzumab in HER2-positive and triple-negative breast cancer subtypes.29 One study found that CBD, in combination with chemotherapeutics and Bruton tyrosine kinase inhibitors, such as ibrutinib and zanubrutinib, has synergistic potential for treating diffuse large B-cell lymphoma and mantle cell lymphoma cell lines. This synergy is attributed to the CB1 antagonist activity of cannabis against diffuse large B-cell lymphoma and mantle cell lymphoma cell lines.30,31
Moreover, combining cannabinoids with bevacizumab (a monoclonal anti-VEGF antibody) has been shown to decrease tumor growth and intratumoral hypoxia in clinically relevant human glioblastoma models. This effect is mediated through the downregulation of HIF-1α.32 Long-term studies evaluating the potential harmful or synergistic potential of CBD on targeted anticancer therapy are needed.
CONCLUSIONS
This exploratory study of patients receiving cancer therapy at WJVAMC found a significant prevalence of concurrent cannabis use among patients undergoing antineoplastic treatments. Given that many antineoplastic agents are metabolized by the CYP450 enzyme system, the findings of this study suggest that concurrent cannabis use may pose risks of suboptimal therapeutic outcomes due to potential interactions affecting drug metabolism. These interactions could impact the efficacy and toxicity of the antineoplastic therapies, potentially leading to diminished therapeutic effects or exacerbated adverse reactions.
Patients should be informed regarding the potential decreased efficacy of immunotherapy with concurrent use of cannabis products. They should also be aware of the possibility of increased toxicity with other treatment modalities, though the exact impact on efficacy remains unclear. This highlights the necessity of caution when combining cannabis with prescribed cancer treatments.
While this study identified possible interactions, its data are preliminary and highlight the need for more rigorous research. Future studies should include larger, well-designed cohorts to compare outcomes between cannabis users and nonusers. Such research is essential to fully elucidate the clinical implications of cannabis use during cancer treatment, address the high prevalence of cannabis use among patients with cancer, and mitigate potential risks associated with combining cannabis products with antineoplastic therapies. This will ensure that treatment strategies are optimized for safety and efficacy in this complex patient population.
- Steele G, Arneson T, Zylla D. A comprehensive review of cannabis in patients with cancer: availability in the USA, general efficacy, and safety. Curr Oncol Rep. 2019;21:1-10. doi:10.1007/s11912-019-0757-7
- Brown D, Watson M, Schloss J. Pharmacological evidence of medicinal cannabis in oncology: a systematic review. Support Care Cancer. 2019;27:3195-320. doi:10.1007/s00520-019-04774-5
- Abrams DI. Integrating cannabis into clinical cancer care. Curr Oncol. 2016;23:S8-S14. doi:10.37.47/co.23.3099
- Serafimovska T, Darkovska-Serafimovska M, Stefkov G, Arsova-Sarafinovska Z, Balkanov T. Pharmacotherapeutic considerations for use of cannabinoids to relieve symptoms of nausea and vomiting induced by chemotherapy. Folia Medica (Plovdiv). 2020;62:668-678. doi:10.3897/folmed.62e51478
- Bar-Sela G, Zalman D, Semenysty V, Ballan E. The effects of dosage-controlled cannabis capsules on cancer-related cachexia and anorexia syndrome in advanced cancer patients: pilot study. Integr Cancer Ther. 2019;18:1534735419881498. doi:10.1177/1534735419881498
- Pederson ER, Villarosa-Hurlocker MC, Prince MA. Use of protective behavioral strategies among young adult veteran marijuana users. Cannabis. 2018;1:14-27.
- Schilling S, Melzer R, McCabe PF. Cannabis sativa. Curr Biol. 2020;30:R8-R9. doi:10.1016/j.cub.2019.10.039
- McDougle DR, Kambalyal A, Meling DD, Das A. Endocannabinoids anandamide and 2-arachidonoylglycerol are substrates for human CYP2J2 epoxygenase. J Pharmacol Exp Ther. 2014;351:616-627. doi:10.1124/jpet.114216598
- Movsesyan VA, Stoica BA, Yakovlev AG, et al. Anandamide-induced cell death in primary neuronal cultures: role of calpain and caspase pathways. Cell Death Differ. 2004;11:1121-1132. doi:10.1038/sj.cdd.4401442
- Cherkasova V, Wang B, Gerasymchuk M, Fiselier A, Kovalchuk O, Kovalchuk I. Use of cannabis and cannabinoids for treatment of cancer. Cancers (Basel). 2022;14:5142. doi:10.3390/cancers14205142
- Engels FK, Ten Tije AJ, Baker SD, et al. Effect of cytochrome P450 3A4 inhibition on the pharmacokinetics of docetaxel. Clin Pharmacol Ther. 2004;75:448-454. doi:10.1016/j.clpt.2004.01.001
- Alsherbiny MA, Li CG. Medicinal cannabis-potential drug interactions. Medicines (Basel). 2018;6:3. doi:10.3390/medicines6010003
- Stout SM, Cimino NM. Exogenous cannabinoids as substrates, inhibitors, and inducers of human drug metabolizing enzymes: a systematic review. Drug Metab Rev. 2014;46:86-95. doi:10.3109/03602532.2013.849268
- Opitz BJ, Ostroff ML, Whitman AC. The potential clinical implications and importance of drug interactions between anticancer agents and cannabidiol in patients with cancer. J Pharm Pract. 2020;33:506-512. doi:10.1177/0897190019828920
- Guzmán M, Duarte MJ, Blázquez C, et al. A pilot clinical study of D9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme. Br J Cancer. 2006;95:197-203. doi:10.1038/sj.bjc.6603236
- Kopjar N, Fuchs N, Brcic Karaconji I, et al. High doses of ?9-tetrahydrocannabinol might impair irinotecan chemotherapy: a review of potentially harmful interactions. Clin Drug Investig. 2020;40:775-787. doi:10.1007/s40261-020-00954-y
- Bouquié R, Deslandes G, Mazaré H, et al. Cannabis and anticancer drugs: societal usage and expected pharmacological interactions - a review. Fundam Clin Pharmacol. 2018;32:462-484. doi:10.1111/fcp.12373
- Buchtova T, Lukac D, Skrott Z, Chroma K, Bartek J, Mistrik M. Drug-drug interactions of cannabidiol with standard-of-care chemotherapeutics. Int J Mol Sci. 2023;24:2885. doi:10.3390/ijms24032885
- Sharafi G, He H, Nikfarjam M. Potential use of cannabinoids for the treatment of pancreatic cancer. J Pancreat Cancer. 2019;5:1-7. doi:10.1089/pancan.2018.0019
- Kosgodage US, Uysal-Onganer P, MacLatchy A, et al. Cannabidiol affects extracellular vesicle release, miR21 and miR126, and reduces prohibitin protein in glioblastoma multiforme cells. Transl Oncol. 2019;12:513-522. doi:10.1016/j.tranon.2018.12.004
- Elbaz M, Nasser MW, Ravi J, et al. Modulation of the tumor microenvironment and inhibition of EGF/EGFR pathway: novel anti-tumor mechanisms of cannabidiol in breast cancer. Mol Oncol. 2015;9:906-919. doi:10.1016/j.molonc.2014.12.010
- Xiong X, Chen S, Shen J, et al. Cannabis suppresses anti-tumor immunity by inhibiting JAK/STAT signaling in T cells through CNR2. Signal Transduct Target Ther. 2022;7:99. doi:10.1038/s41392-022-00918-y
- Bar-Sela G, Cohen I, Campisi-Pinto S, et al. Cannabis consumption used by cancer patients during immunotherapy correlates with poor clinical outcome. Cancers (Basel). 2020;12:2447. doi:10.3390/cancers12092447
- Waissengrin B, Leshem Y, Taya M, et al. The use of medical cannabis concomitantly with immune checkpoint inhibitors in non-small cell lung cancer: a sigh of relief? Eur J Cancer. 2023;180:52-61. doi:10.1016/j.ejca.2022.11.022
- Sarsembayeva A, Schicho R. Cannabinoids and the endocannabinoid system in immunotherapy: helpful or harmful? Front Oncol. 2023;13:1296906. doi:10.3389/fonc.2023.1296906
- Kisková T, Mungenast F, Suváková M, Jäger W, Thalhammer T. Future aspects for cannabinoids in breast cancer therapy. Int J Mol Sci. 2019;20:1673. doi:10.3390/ijms20071673
- Woerdenbag HJ, Olinga P, Kok EA, et al. Potential, limitations and risks of cannabis-derived products in cancer treatment. Cancers (Basel). 2023;15:2119. doi:10.3390/cancers15072119
- Almeida CF, Teixeira N, Valente MJ, Vinggaard AM, Correia-da-Silva G, Amaral C. Cannabidiol as a promising adjuvant therapy for estrogen receptor-positive breast tumors: unveiling its benefits with aromatase inhibitors. Cancers (Basel). 2023;15:2517. doi:10.3390/cancers15092517
- Dobovišek L, Novak M, Krstanovic F, Borštnar S, Turnšek TL, Debeljak N. Effect of combining CBD with standard breast cancer therapeutics. Adv Cancer Biol Metastasis. 2022;4:100038. doi:10.1016/j.adcanc.2022.100038
- Strong T, Rauvolfova J, Jackson E, Pham LV, Bryant J. Synergistic effect of cannabidiol with conventional chemotherapy treatment. Blood. 2018;132:5382. doi:10.1182/blood-2018-99-116749
- Maggi F, Morelli MB, Tomassoni D, et al. The effects of cannabidiol via TRPV2 channel in chronic myeloid leukemia cells and its combination with imatinib. Cancer Sci. 2022;113:1235-1249. doi:10.1111/cas.15257
- Obad N, Janji B, Prestegarden L, et al. ATPS-59 improving efficacy of bevacizumab treatment in glioblastoma by targeting hif1 alpha. Neuro Oncol. 2015;17:v31. doi:10.1093/neuonc/nov204.59
- Steele G, Arneson T, Zylla D. A comprehensive review of cannabis in patients with cancer: availability in the USA, general efficacy, and safety. Curr Oncol Rep. 2019;21:1-10. doi:10.1007/s11912-019-0757-7
- Brown D, Watson M, Schloss J. Pharmacological evidence of medicinal cannabis in oncology: a systematic review. Support Care Cancer. 2019;27:3195-320. doi:10.1007/s00520-019-04774-5
- Abrams DI. Integrating cannabis into clinical cancer care. Curr Oncol. 2016;23:S8-S14. doi:10.37.47/co.23.3099
- Serafimovska T, Darkovska-Serafimovska M, Stefkov G, Arsova-Sarafinovska Z, Balkanov T. Pharmacotherapeutic considerations for use of cannabinoids to relieve symptoms of nausea and vomiting induced by chemotherapy. Folia Medica (Plovdiv). 2020;62:668-678. doi:10.3897/folmed.62e51478
- Bar-Sela G, Zalman D, Semenysty V, Ballan E. The effects of dosage-controlled cannabis capsules on cancer-related cachexia and anorexia syndrome in advanced cancer patients: pilot study. Integr Cancer Ther. 2019;18:1534735419881498. doi:10.1177/1534735419881498
- Pederson ER, Villarosa-Hurlocker MC, Prince MA. Use of protective behavioral strategies among young adult veteran marijuana users. Cannabis. 2018;1:14-27.
- Schilling S, Melzer R, McCabe PF. Cannabis sativa. Curr Biol. 2020;30:R8-R9. doi:10.1016/j.cub.2019.10.039
- McDougle DR, Kambalyal A, Meling DD, Das A. Endocannabinoids anandamide and 2-arachidonoylglycerol are substrates for human CYP2J2 epoxygenase. J Pharmacol Exp Ther. 2014;351:616-627. doi:10.1124/jpet.114216598
- Movsesyan VA, Stoica BA, Yakovlev AG, et al. Anandamide-induced cell death in primary neuronal cultures: role of calpain and caspase pathways. Cell Death Differ. 2004;11:1121-1132. doi:10.1038/sj.cdd.4401442
- Cherkasova V, Wang B, Gerasymchuk M, Fiselier A, Kovalchuk O, Kovalchuk I. Use of cannabis and cannabinoids for treatment of cancer. Cancers (Basel). 2022;14:5142. doi:10.3390/cancers14205142
- Engels FK, Ten Tije AJ, Baker SD, et al. Effect of cytochrome P450 3A4 inhibition on the pharmacokinetics of docetaxel. Clin Pharmacol Ther. 2004;75:448-454. doi:10.1016/j.clpt.2004.01.001
- Alsherbiny MA, Li CG. Medicinal cannabis-potential drug interactions. Medicines (Basel). 2018;6:3. doi:10.3390/medicines6010003
- Stout SM, Cimino NM. Exogenous cannabinoids as substrates, inhibitors, and inducers of human drug metabolizing enzymes: a systematic review. Drug Metab Rev. 2014;46:86-95. doi:10.3109/03602532.2013.849268
- Opitz BJ, Ostroff ML, Whitman AC. The potential clinical implications and importance of drug interactions between anticancer agents and cannabidiol in patients with cancer. J Pharm Pract. 2020;33:506-512. doi:10.1177/0897190019828920
- Guzmán M, Duarte MJ, Blázquez C, et al. A pilot clinical study of D9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme. Br J Cancer. 2006;95:197-203. doi:10.1038/sj.bjc.6603236
- Kopjar N, Fuchs N, Brcic Karaconji I, et al. High doses of ?9-tetrahydrocannabinol might impair irinotecan chemotherapy: a review of potentially harmful interactions. Clin Drug Investig. 2020;40:775-787. doi:10.1007/s40261-020-00954-y
- Bouquié R, Deslandes G, Mazaré H, et al. Cannabis and anticancer drugs: societal usage and expected pharmacological interactions - a review. Fundam Clin Pharmacol. 2018;32:462-484. doi:10.1111/fcp.12373
- Buchtova T, Lukac D, Skrott Z, Chroma K, Bartek J, Mistrik M. Drug-drug interactions of cannabidiol with standard-of-care chemotherapeutics. Int J Mol Sci. 2023;24:2885. doi:10.3390/ijms24032885
- Sharafi G, He H, Nikfarjam M. Potential use of cannabinoids for the treatment of pancreatic cancer. J Pancreat Cancer. 2019;5:1-7. doi:10.1089/pancan.2018.0019
- Kosgodage US, Uysal-Onganer P, MacLatchy A, et al. Cannabidiol affects extracellular vesicle release, miR21 and miR126, and reduces prohibitin protein in glioblastoma multiforme cells. Transl Oncol. 2019;12:513-522. doi:10.1016/j.tranon.2018.12.004
- Elbaz M, Nasser MW, Ravi J, et al. Modulation of the tumor microenvironment and inhibition of EGF/EGFR pathway: novel anti-tumor mechanisms of cannabidiol in breast cancer. Mol Oncol. 2015;9:906-919. doi:10.1016/j.molonc.2014.12.010
- Xiong X, Chen S, Shen J, et al. Cannabis suppresses anti-tumor immunity by inhibiting JAK/STAT signaling in T cells through CNR2. Signal Transduct Target Ther. 2022;7:99. doi:10.1038/s41392-022-00918-y
- Bar-Sela G, Cohen I, Campisi-Pinto S, et al. Cannabis consumption used by cancer patients during immunotherapy correlates with poor clinical outcome. Cancers (Basel). 2020;12:2447. doi:10.3390/cancers12092447
- Waissengrin B, Leshem Y, Taya M, et al. The use of medical cannabis concomitantly with immune checkpoint inhibitors in non-small cell lung cancer: a sigh of relief? Eur J Cancer. 2023;180:52-61. doi:10.1016/j.ejca.2022.11.022
- Sarsembayeva A, Schicho R. Cannabinoids and the endocannabinoid system in immunotherapy: helpful or harmful? Front Oncol. 2023;13:1296906. doi:10.3389/fonc.2023.1296906
- Kisková T, Mungenast F, Suváková M, Jäger W, Thalhammer T. Future aspects for cannabinoids in breast cancer therapy. Int J Mol Sci. 2019;20:1673. doi:10.3390/ijms20071673
- Woerdenbag HJ, Olinga P, Kok EA, et al. Potential, limitations and risks of cannabis-derived products in cancer treatment. Cancers (Basel). 2023;15:2119. doi:10.3390/cancers15072119
- Almeida CF, Teixeira N, Valente MJ, Vinggaard AM, Correia-da-Silva G, Amaral C. Cannabidiol as a promising adjuvant therapy for estrogen receptor-positive breast tumors: unveiling its benefits with aromatase inhibitors. Cancers (Basel). 2023;15:2517. doi:10.3390/cancers15092517
- Dobovišek L, Novak M, Krstanovic F, Borštnar S, Turnšek TL, Debeljak N. Effect of combining CBD with standard breast cancer therapeutics. Adv Cancer Biol Metastasis. 2022;4:100038. doi:10.1016/j.adcanc.2022.100038
- Strong T, Rauvolfova J, Jackson E, Pham LV, Bryant J. Synergistic effect of cannabidiol with conventional chemotherapy treatment. Blood. 2018;132:5382. doi:10.1182/blood-2018-99-116749
- Maggi F, Morelli MB, Tomassoni D, et al. The effects of cannabidiol via TRPV2 channel in chronic myeloid leukemia cells and its combination with imatinib. Cancer Sci. 2022;113:1235-1249. doi:10.1111/cas.15257
- Obad N, Janji B, Prestegarden L, et al. ATPS-59 improving efficacy of bevacizumab treatment in glioblastoma by targeting hif1 alpha. Neuro Oncol. 2015;17:v31. doi:10.1093/neuonc/nov204.59
Cannabis Use by Veterans and Potential Interactions With Antineoplastic Agents: Analysis and Literature Review
Cannabis Use by Veterans and Potential Interactions With Antineoplastic Agents: Analysis and Literature Review

Early Outcomes of Stereotactic Body Radiotherapy for Localized Prostate Cancer: A Retrospective Analysis
Early Outcomes of Stereotactic Body Radiotherapy for Localized Prostate Cancer: A Retrospective Analysis
Prostate cancer is the most common cancer in US males, with an estimated 313,780 new cases and 35,770 deaths in 2025.1 Several treatment options are available for localized prostate cancer that have similar outcomes, including active surveillance for low-risk cancers, surgery, or radiotherapy.2,3 Conventional fractionation radiotherapy (CFRT) with 40 to 45 fractions over 8 to 9 weeks has been used for decades. Over the past 2 decades, moderate hypofractionation schedules with 2.4 to 3.4 Gy per fraction over 20 to 28 fractions have become standard, as many noninferiority randomized clinical trials (RCTs) such as CHHiP (UK),4 PROFIT (Canada and Europe),5 NRG Oncology RTOG 0415 (US),6 HYPRO (Netherlands),7,8 and HYPO-RT-PC (Sweden and Denmark),9 have shown the noninferiority of moderately hypofractionated radiotherapy compared with CFRT. Notably, most of these noninferiority studies primarily included patients with low- or intermediate-risk prostate cancer, except for the HYPO-RT-PC trial,9 which also included patients with intermediate- and high-risk prostate cancer.
These noninferiority studies, along with technological advances in radiotherapy, such as intensity-modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT), and image-guided radiotherapy (IGRT), paved the path to ultrahypofractionated stereotactic body radiotherapy (SBRT) that is delivered in 5 fractions of ≥ 6 Gy. This high dose per fraction may have a radiobiologic advantage over conventional fractionation. The relatively low a/ß ratio of prostate cancer, estimated to be between 1 and 2, suggests that tumor cells may be particularly sensitive to the high doses per fraction delivered in SBRT.10-13 Compared with CFRT, SBRT-induced tumor cell death may also be mediated through different pathways; this pathway appears to be generated in a dose-dependent manner, particularly with doses > 8 Gy per fraction.14,15 Additionally, the higher a/ß ratio for the surrounding organs at risk, such as the bladder and rectum, theoretically allows for an improved therapeutic ratio window that maximizes tumor control while minimizing damage to healthy tissues.
A substantial body of evidence from prospective studies and meta-analyses supports the use of SBRT for localized prostate cancer. HYPO-RT-PC, a significant phase 3 noninferiority study, enrolled 1200 patients with intermediate (89%) and high-risk (11%) prostate cancer randomized between 2 arms, including CFRT to 78 Gy in 39 fractions and SBRT to 42.7 Gy in 7 fractions, treated 3 days weekly. After a median follow-up of 60 months, the estimated 5-year biochemical relapse-free survival rate was 84% in both groups.9 This trial was notable because it was the first randomized study to demonstrate that SBRT was noninferior to CFRT in intermediate- and high-risk prostate cancer patients. Another pivotal phase 3 trial, the PACE-B study, enrolled 874 patients to compare SBRT (36.25 Gy to the prostate gland, with a secondary dose of 40 Gy to the gross tumor volume where applicable, in 5 fractions) with CFRT (78 Gy in 39 fractions) and moderately hypofractionated radiotherapy (HFRT) (62 Gy in 20 fractions) in patients with low- or intermediate-risk prostate cancer. With a 74-month median follow-up, the study reported 5-year biochemical free rates of 94.6% for CFRT and 95.8% for SBRT, confirming the noninferiority of SBRT to CFRT.15
SBRT offers short, effective, and convenient treatment to many patients with localized prostate cancer. While previous guidelines were more restrictive, the March 2026 National Comprehensive Cancer Network (NCCN) guidelines now list SBRT as a preferred treatment modality for high-risk prostate cancer.16
Given the growing body of evidence supporting the efficacy and safety of SBRT, we implemented an SBRT program in 2014 at a tertiary care center for veterans. This retrospective study was undertaken to evaluate the early efficacy and toxicity of SBRT in patients with localized prostate cancer treated at our institution, including patients across all risk stratifications.
METHODS
We identified 242 patients diagnosed with prostate cancer who underwent SBRT treatment between November 2014 and October 2024 at Overland Park Veterans Affairs Radiation Oncology Clinic. For the final analysis, 46 patients with < 2 years of follow-up and 22 patients who died from causes other than prostate cancer were excluded, resulting in a cohort of 174 patients with ≥ 24-month follow-up.
Treatment
Patients eligible for staging underwent imaging according to NCCN guidelines, including computed tomography (CT) of the abdomen and pelvis, bone scintigraphy, or, in recent years, prostate-specific membrane antigen positron emission tomography, primarily used for unfavorable intermediate-risk (UIR) and high-risk (HR) cancers. Patients with a negative staging work-up for nodal or skeletal disease were included. Prior to planning the CT simulation, patients were given bowel preparation instructions, including a low-fiber and low-gas-producing diet, simethicone, and enemas, the night before and morning of the simulation. Patients were instructed to arrive with a comfortably full bladder, having not voided for 2 to 3 hours prior to the procedure. At Kansas City Veterans Affairs Medical Center (KCVAMC), SBRT treatment was generally restricted to patients with a baseline American Urological Association symptom score of 15 to 20 out of 35 and a prostate gland size < 80 mL to minimize the risk of acute urinary toxicity. We did not use intraprostatic fiducials, hydrogel rectal spacers, or intravenous contrast agents for planning CT simulation.
Patients were placed in a supine position, and a vacuum bag was used for immobilization. Following the CT simulation, the images were transferred to the Eclipse treatment planning system. The clinical target volume (CTV) encompassed the prostate and the proximal 1.0 cm of the seminal vesicles for Gleason score (GS) 1 to 2, and the entire seminal vesicle was included for GS 3 to 5, which is consistent with KCVAMC practice and established safety protocols. The planning target volume (PTV) was created by uniformly expanding the CTV by 5 to 7 mm, except for the posterior margin, which was limited to 3 to 5 mm. When elective nodal radiotherapy was planned for HR prostate cancer, the pelvic field for CT simulation started at the L-2 upper border, with the lower border extending to the lesser trochanter. The pelvic nodes were delineated per Radiation Therapy Oncology Group (RTOG) guidelines.17 The CTV nodes (CTVn), including common iliac, external and internal iliac nodes, obturator, and presacral nodes, were created by uniformly expanding the CTVn by 2 to 3 mm. Slice-by-slice corrections were made to avoid bowel overlap in these patients.
The use of androgen deprivation therapy (ADT) for a duration of 6 to 24 months was prescribed for patients with UIR or HR prostate cancer per NCCN guidelines.16 The prescribed dose to the PTV was 36.25 to 40 Gy (40 Gy was mostly used as a boost to the dominant lesion) in 5 fractions, with each fraction ranging from 7.25 to 8 Gy. For elective nodal radiotherapy in patients at HR, the prescribed dose was 25 Gy in 5 fractions. All patients were planned for VMAT, which aims to deliver ≥ 95% of the prescription dose to 95% of the PTV. Once the physician approved the treatment plan and physics quality assessment was completed, treatments commenced on an every-other-day schedule. Patients received the same bowel preparation instructions for each treatment as for the planning CT simulation. Daily treatment accuracy was confirmed via daily 3-dimensional cone-beam CT (CBCT) for IGRT. No fiducials or hydrogel rectal spacers were used.
Follow-up Schedule and Toxicity Assessment
Follow-up assessments were conducted 4 to 6 weeks after radiation therapy and then repeated every 6 months for 2 to 5 years, and annually thereafter. At each follow-up visit, patients were evaluated for genitourinary (GU) and gastrointestinal (GI) toxicity, according to RTOG toxicity criteria. Prostate-specific antigen (PSA) levels were monitored; in patients receiving ADT, testosterone levels were also checked.
Statistical Analysis
Biochemical failure was defined using the Phoenix definition (nadir PSA + 2 ng/mL). Differences between dose cohorts were assessed using the log-rank test for survival outcomes and X2 testing for categorical variables. GU and GI toxicities were summarized as cumulative incidences of RTOG grade ≥ II events. Statistical significance was set at P < .05.
RESULTS
One hundred seventy-four patients were included in the retrospective review. Patients had a median follow-up of 45 months (range, 24-111) (Figure). The median age at treatment was 74 years (range, 51-88), and the median pretreatment PSA level was 11.9 ng/mL (range, 0.6-69.5). Twenty-six patients (14.9%) had a GS 1, 77 (44.3%) had GS 2, 41 (23.6%) had GS 3, 18 (10.3%) had GS 4, and 12 (6.9%) had GS 5. Fifty-one patients (29.3%) received elective pelvic nodal radiotherapy, and 93 patients (53.4%) received ADT (Table 1).
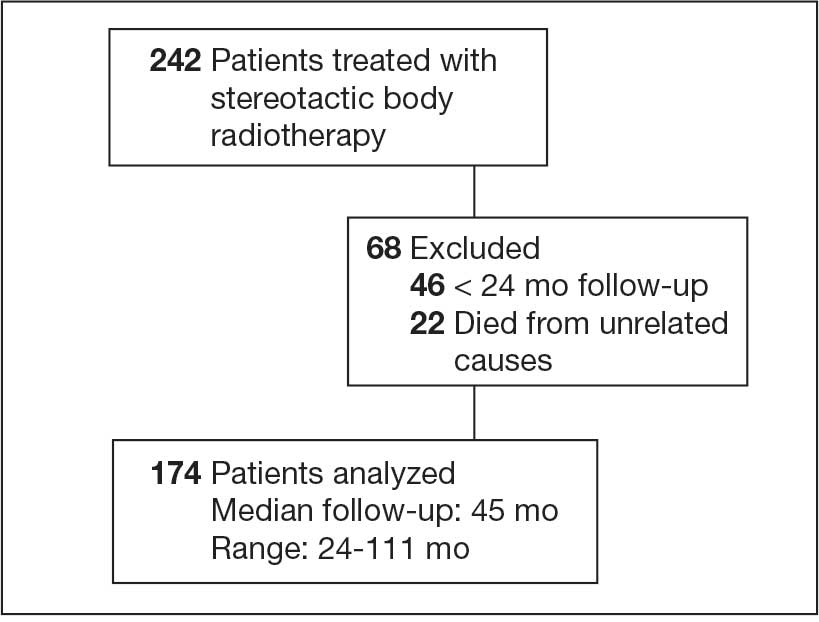
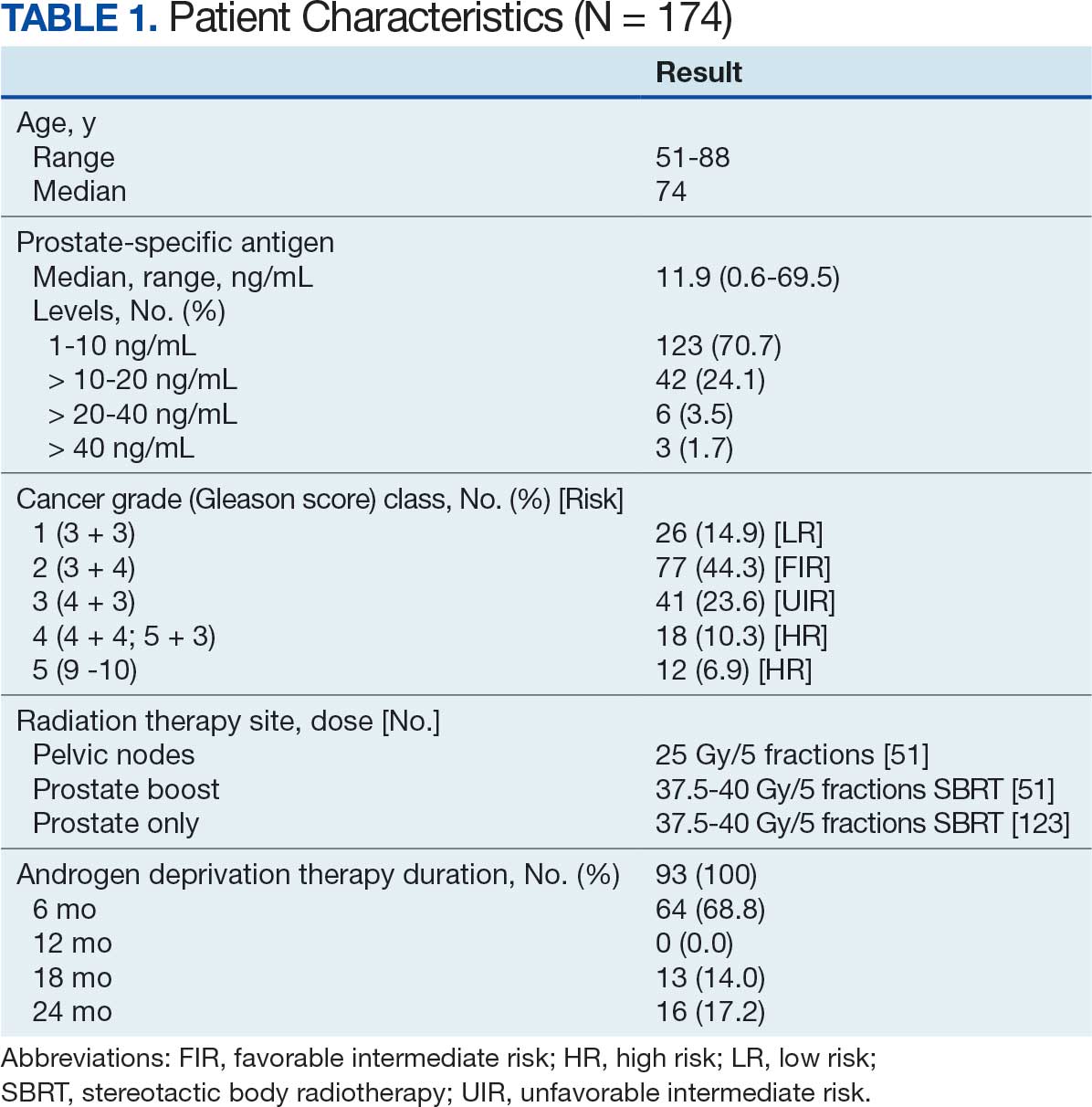
At 24 months follow-up, 6 patients (3.4%) had biochemical failures. One patient died from metastatic prostate cancer, and 5 patients are living with biochemical failure (Table 2). The actuarial 5-year overall survival (OS) rate was 99.4%, and the 5-year disease-free survival (DFS) rate was 96.6%. We performed a subanalysis comparing outcomes of the 36.25 Gy vs 40 Gy SBRT cohorts. There was no statistically significant difference in DFS, OS, or the cumulative incidence of grade II/III toxicity between patients treated with 40 Gy vs 36.25 Gy. Outcomes stratified by NCCN risk groups (low, intermediate, high/very high) are detailed in Table 3. As expected, DFS was slightly lower in the high-risk group, but overall disease control remained high across all stratifications.
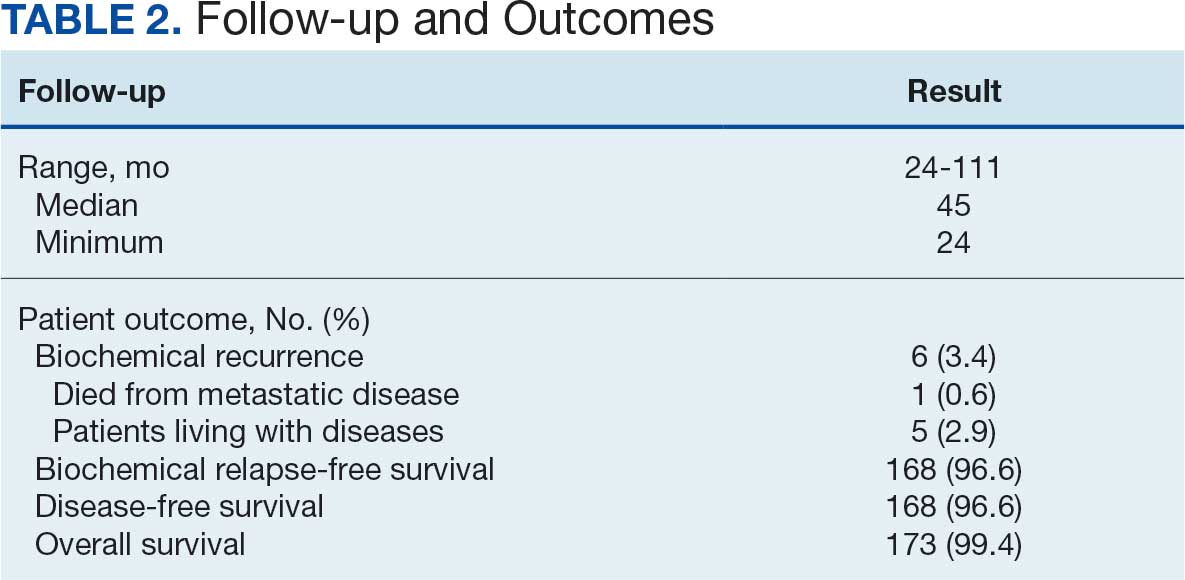
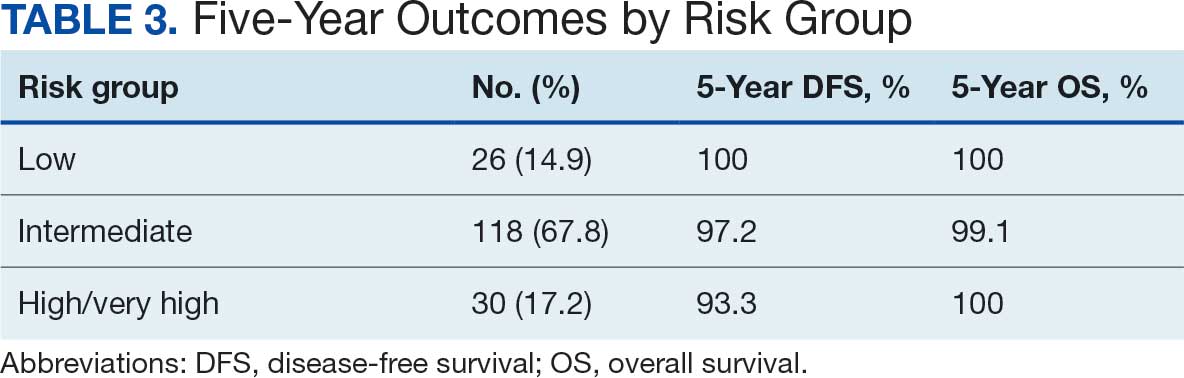
The cumulative incidence of RTOG grade II and higher GU toxicity was 28.2% (Table 4). This included 46 patients (26.4%) with grade II GU toxicity and 2 patients (1.2%) who developed grade III GU complications (1 requiring self-catheterization and another a suprapubic catheter for urinary retention). One patient (0.6%) treated with a 40 Gy dose regimen experienced a grade IV GU complication in the form of a rectovesical fistula necessitating surgical intervention.
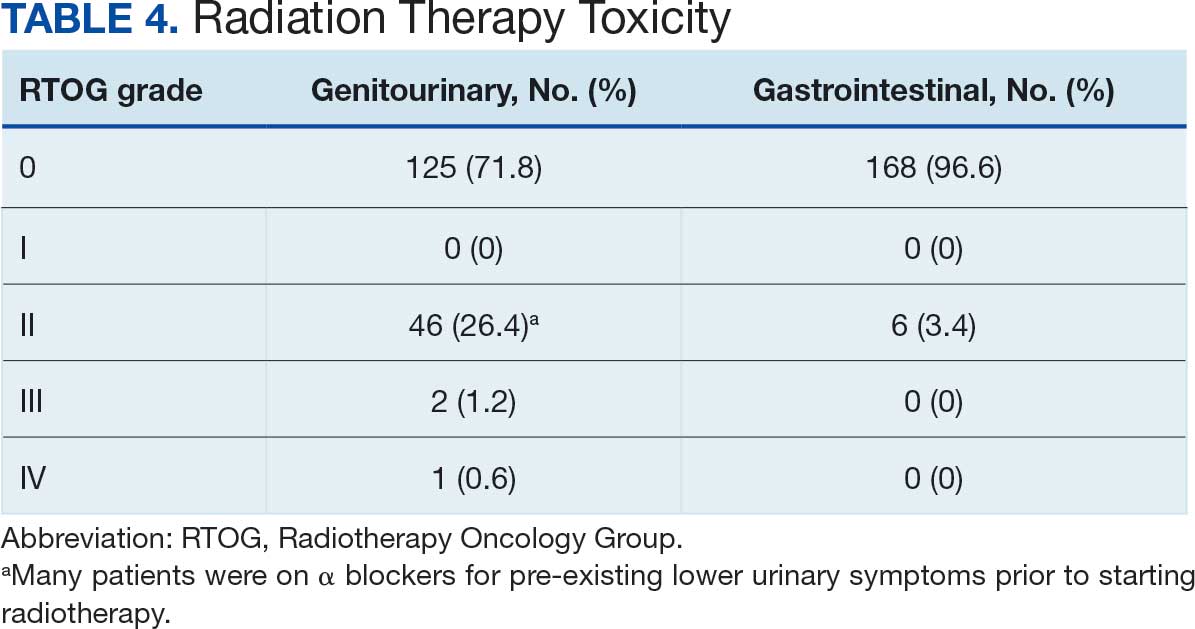
The cumulative incidence of RTOG grade II or higher GI toxicity was 3.4%, and no grade III or IV gastrointestinal toxicities were observed during the follow-up period. Importantly, intraprostatic fiducials, hydrogel rectal spacers, or intravenous contrast were not routinely used in this cohort of patients.
The high rates of actuarial 5-year DFS and OS observed suggest a favorable initial response to the SBRT regimen employed at KCVAMC. However, given the potential for late recurrence in patients with prostate cancer, longer follow-up is essential to determine the durability of these outcomes. The observed GU toxicity rate of 28.2% for grade II and higher events warrants careful consideration and compares with other published data on SBRT for prostate cancer.15 The occurrence of a grade IV rectovesical fistula, although rare, is a notable adverse event that warrants discussion in the context of the treatment approach. The low incidence of grade II or higher GI toxicity is an encouraging finding, particularly given that hydrogel rectal spacers are not routinely used to minimize rectal exposure.
DISCUSSION
The primary objective of this retrospective study was to evaluate the outcomes of SBRT for patients with localized prostate cancer treated at KCVAMC and to compare these results with those reported in the literature. Our findings demonstrate promising intermediate-term efficacy, with an estimated 5-year DFS of 96.6% and OS of 99.4% at a median follow-up of 45 months. Furthermore, the observed toxicity profile appears acceptable, with a cumulative grade II and higher GU toxicity rate of 28.2% and a grade II or higher GI toxicity rate of 3.4%. Notably, these outcomes were achieved without the routine use of intraprostatic fiducials or hydrogel rectal spacers.
Two pivotal randomized phase 3 trials have established the noninferiority of ultrahypofractionated radiotherapy (UHRT) with SBRT over conventional fractionation. The HYPO-RT-PC trial compared SBRT (42.7 Gy in 7 fractions) with conventional fractionation (78 Gy in 39 fractions) in intermediate- and high-risk patients with prostate cancer and reported a 5-year biochemical relapse-free survival of 84% in both arms.9 The PACE-B trial, which included patients at low- and intermediate-risk, compared SBRT (36.25 Gy in 5 fractions) with conventional or moderate HFRT and reported a 5-year biochemical control rate of 95.8% in the SBRT arm and 94.6% in the control arm.15
A comprehensive review and meta-analysis of 7 phase 3 studies involving 6795 patients compared different radiotherapy regimens, namely, UHRT, HFRT, and CFRT, and reported that after 5 years, the DFS rates were 85.1% for CFRT, 86% for HFRT, and 85% for UHRT, with no significant difference in toxicity among the 3 different treatment approaches.18 This suggests that shorter, more intense radiotherapy schedules (UHRT and HFRT) may be as effective and safe as traditional, longer courses of radiation.
There are multiple published nonrandomized prospective trials in which thousands of patients with extreme hypofractionation have been treated with different doses, fractions, and techniques. While heterogeneity and limited long-term follow-up in the existing evidence are acknowledged, these data suggest that prostate SBRT provides appropriate biochemical control with few high-grade toxicities, supporting its ongoing global use and justifying further prospective investigations. Comparative data are shown in Table 5. Several ongoing studies are evaluating noninferiority, superiority, and cost-effectiveness using different methodologies (Table 6).9,15,19-24
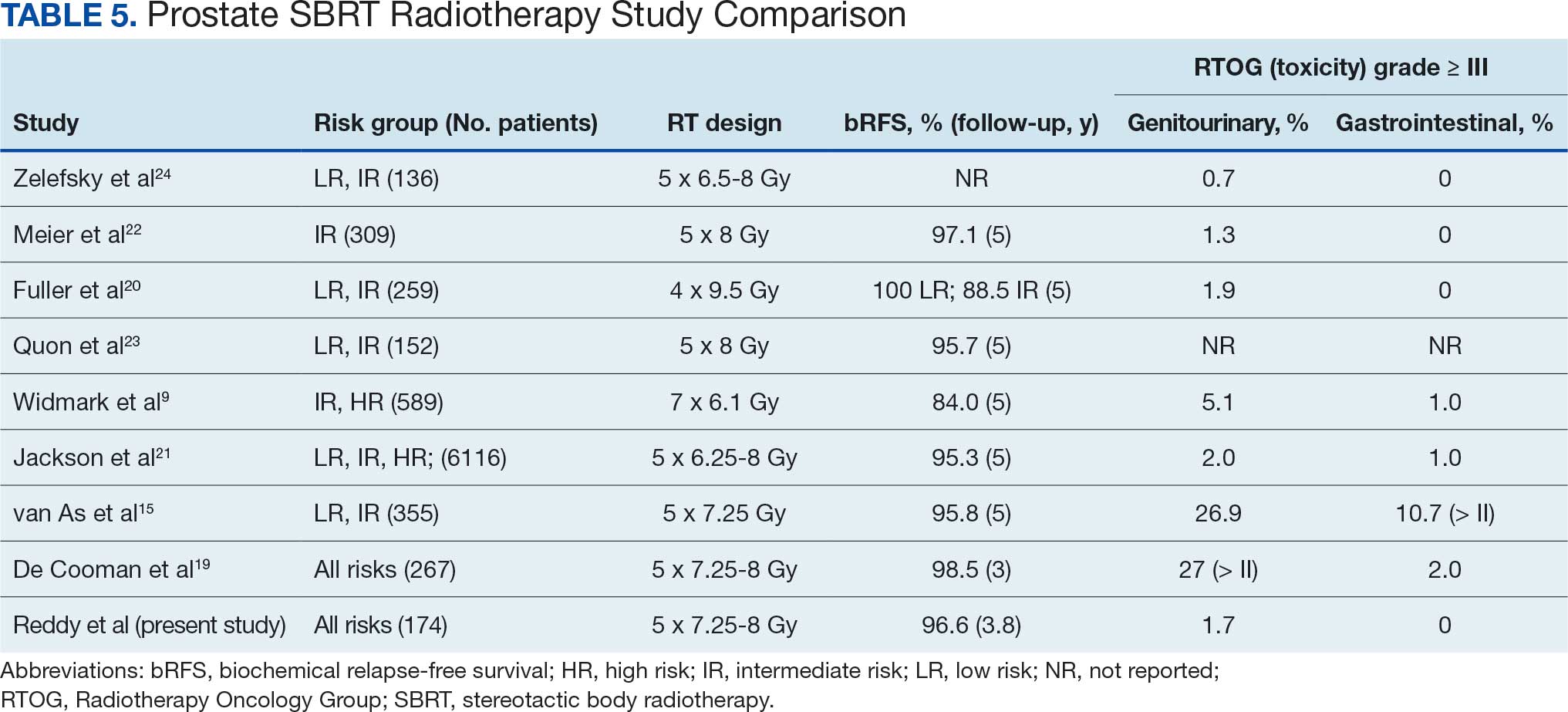
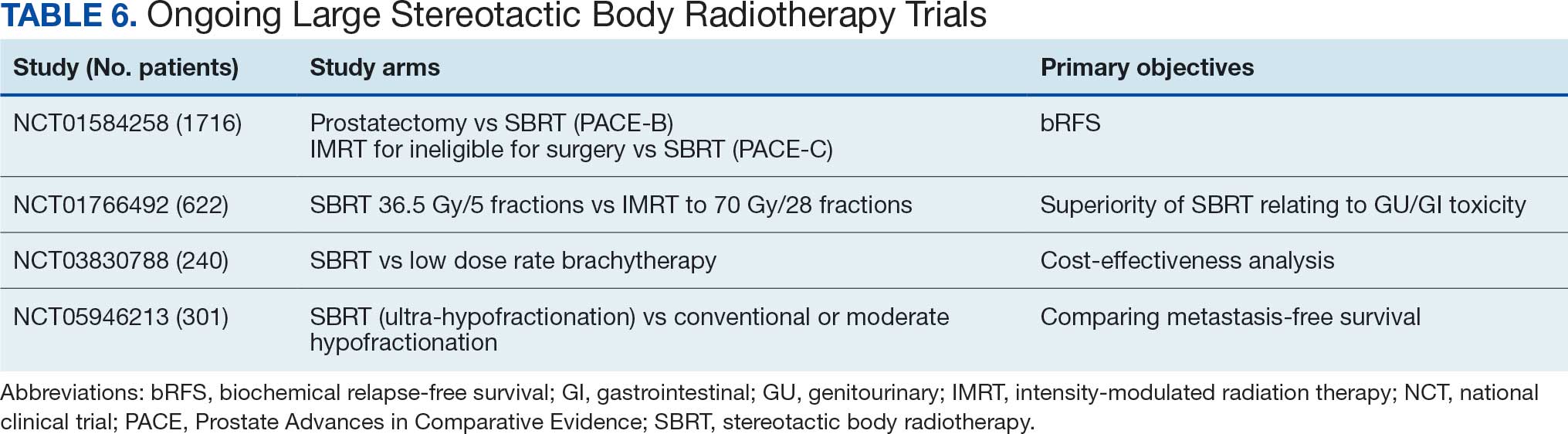
This study’s efficacy outcomes, particularly the high DFS rate, are consistent with the findings from these landmark trials, suggesting that the SBRT regimen used at KCVAMC is effective in achieving early disease control despite 17.2% of patients having high-risk disease. The GU toxicity observed in this study, with a 28.2% rate of grade II or higher events, is also comparable with the 26.9% reported in the 5-fraction SBRT arm of the PACE-B trial, which had a longer median follow-up of 74 months.15 It is important to note that a portion of these grade II events occurred in patients who were already on a blockers for pre-existing lower urinary tract symptoms before starting radiotherapy, which may inflate the observed cumulative acute toxicity score.
A critical comparison is how SBRT toxicity aligns with moderate hypofractionation (eg, 60 Gy in 20 fractions or 70 Gy in 28 fractions as reported by others).4,6 Our observed grade III and higher GU toxicity rate (1.7%) and grade III and higher GI toxicity rate (0%) are highly favorable when compared with historical moderate hypofractionation data, which typically report grade III GU toxicity in the range of 2% to 3% and grade III GI toxicity around 1% to 2%. This suggests that despite the higher dose per fraction, SBRT does not necessarily lead to increased severe acute toxicity, potentially offering a superior therapeutic ratio for GI and GU sparing.
However, the occurrence of a grade IV rectovesical fistula in 1 patient (0.6%)—who received the 40 Gy dose—was a serious complication that warrants careful consideration. This rare, but severe, complication in the higher dose cohort underscores the potential for increased organ-at-risk toxicity, particularly in the absence of a hydrogel rectal spacer, which is designed to mitigate high-dose rectal exposure. While the overall rate of significant GU toxicity remains low, this event highlights the potential risks associated with SBRT. Hydrogel rectal spacers are designed to increase the distance between the prostate and the rectum, which can reduce the rectal radiation dose and potentially mitigate the risk of such fistulas. The low rate of grade II or worse GI toxicity (3.4%) in our study is noteworthy, especially considering that hydrogel spacers were not routinely used. This finding aligns with the 2.5% GI toxicity rate reported in the SBRT arm of the PACE-B trial, suggesting that careful treatment planning and delivery techniques, such as VMAT-IMRT and daily CBCT for IGRT, may contribute to minimizing GI toxicity even without the use of rectal spacers.15 The exclusive use of 3-dimensional CBCT for IGRT in our study, without the use of fiducial markers, suggests that accurate target localization can be achieved with this approach, contributing to the observed efficacy and reduced toxicity.
Strengths and Limitations
This study’s retrospective, single-center design may have introduced selection bias. The median follow-up of 45 months, while substantial, is still relatively short for assessing very late toxicities and long-term oncologic outcomes in prostate cancer, which is known for late recurrences. Additionally, the lack of a direct comparison group within KCVAMC limits the ability to definitively attribute the observed outcomes solely to SBRT treatment. However, the strengths of this study include the inclusion of a consecutive series of veteran patients with localized prostate cancer across all risk categories, providing a real-world perspective on SBRT outcomes in a diverse patient population. Furthermore, the detailed assessment of efficacy and toxicity via standardized RTOG criteria enhances the comparability of our findings with those of other published prospective studies, despite the retrospective nature of the data.
CONCLUSIONS
This single-institution retrospective analysis revealed that short-term SBRT (36.25 to 40 Gy in 5 fractions), with a minimum follow-up of 24 months and a median follow-up of 45 months, for localized prostate cancer, including patients at HR, is associated with promising early efficacy and acceptable toxicity, even in the absence of routine fiducial or hydrogel spacer use. The favorable actuarial 5-year DFS and OS rates, coupled with a manageable toxicity profile, suggest that SBRT is a safe and convenient treatment option for many patients with localized prostate cancer. However, a longer follow-up is necessary to confirm these findings and fully characterize the long-term efficacy and toxicity of this SBRT regimen. Nevertheless, the results contribute to the growing body of evidence suggesting that SBRT is a safe and convenient treatment option for many patients with localized prostate cancer.
- Siegel RL, Kratzer TB, Giaquinto AN, et al. Cancer statistics, 2025. CA Cancer J Clin. 2025;75:10-45. doi:10.3322/caac.21871
- Donovan JL, Hamdy FC, Lane JA, et al. Patient-reported outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. 2016;375:1425-1437. doi:10.1056/NEJMoa1606221
- Hamdy FC, Donovan JL, Lane JA, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375:1415-1424. doi:10.1056/NEJMoa1606220
- Dearnaley D, Syndikus I, Mossop H, et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016;17:1047-1060. doi:10.1016/S1470-2045(16)30102-4
- Catton CN, Lukka H, Gu CS, et al. Randomized trial of a hypofractionated radiation regimen for the treatment of localized prostate cancer. J Clin Oncol. 2017;35:1884-1890. doi:10.1200/JCO.2016.71.7397
- Lee WR, Dignam JJ, Amin MB, et al. Long-term analysis of NRG Oncology RTOG 0415: a randomized phase III noninferiority study comparing two fractionation schedules in patients with low-risk prostate cancer. J Clin Oncol. 2024;42:2377-2381. doi:10.1200/JCO.23.02445
- de Vries KC, Wortel RC, Oomen-de Hoop E, et al. Hypofractionated versus conventionally fractionated radiation therapy for patients with intermediate- or high-risk, localized, prostate cancer: 7-year outcomes from the randomized, multicenter, open-label, phase 3 HYPRO trial. Int J Radiat Oncol Biol Phys. 2020;106:108-115. doi:10.1016/j.ijrobp.2019.09.007
- Incrocci L, Wortel RC, Alemayehu WG, et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with localised prostate cancer (HYPRO): final efficacy results from a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2016;17:1061-1069. doi:10.1016/S1470-2045(16)30070-5
- Widmark A, Gunnlaugsson A, Beckman L, et al. Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial. Lancet. 2019;394:385-395. doi:10.1016/S0140-6736(19)31131-6
- Brenner DJ, Hall EJ. Fractionation and protraction for radiotherapy of prostate carcinoma. Int J Radiat Oncol Biol Phys. 1999;43:1095-101. doi:10.1016/s0360-3016(98)00438-6
- Dasu A. Is the alpha/beta value for prostate tumours low enough to be safely used in clinical trials? Clin Oncol (R Coll Radiol). 2007;19:289-301. doi:10.1016/j.clon.2007.02.007
- Garcia-Barros M, Paris F, Cordon-Cardo C, et al. Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science. 2003;300:1155-1159. doi:10.1126/science.1082504
- Gulliford S, Hall E, Dearnaley D. Hypofractionation trials and radiobiology of prostate cancer. Oncoscience. 2017;4:27-28. doi:10.18632/oncoscience.347
- Fuks Z, Kolesnick R. Engaging the vascular component of the tumor response. Cancer Cell. 2005;8:89-91. doi:10.1016/j.ccr.2005.07.014
- van As N, Griffin C, Tree A, et al. Phase 3 Trial of stereotactic body radiotherapy in localized prostate cancer. N Engl J Med. Oct 17 2024;391:1413-1425. doi:10.1056/NEJMoa2403365
- National Comprehensive Cancer Network. NCCN Guidelines Version 5. 2026 Prostate Cancer. Accessed March 24, 2026. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
- Lawton CA, Michalski J, El-Naqa I, et al. RTOG GU radiation oncology specialists reach consensus on pelvic lymph node volumes for high-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2009;74:383-387. doi:10.1016/j.ijrobp.2008.08.002
- Lehrer EJ, Kishan AU, Yu JB, et al. Ultrahypofractionated versus hypofractionated and conventionally fractionated radiation therapy for localized prostate cancer: a systematic review and meta-analysis of phase III randomized trials. Radiother Oncol. 2020;148:235-242. doi:10.1016/j.radonc.2020.04.037
- De Cooman B, Debacker T, Adams T, et al. Stereotactic body radiotherapy (SBRT) as a treatment for localized prostate cancer: a retrospective analysis. Radiat Oncol. 2025;20:25. doi:10.1186/s13014-025-02598-8
- Fuller DB, Falchook AD, Crabtree T, et al. Phase 2 multicenter trial of heterogeneous-dosing stereotactic body radiotherapy for low- and intermediate-risk prostate cancer: 5-year outcomes. Eur Urol Oncol. 2018;1:540-547. doi:10.1016/j.euo.2018.06.013
- Jackson WC, Silva J, Hartman HE, et al. Stereotactic body radiation therapy for localized prostate cancer: a systematic review and meta-analysis of over 6,000 patients treated on prospective studies. Int J Radiat Oncol Biol Phys. 2019;104:778-789. doi:10.1016/j.ijrobp.2019.03.051
- Meier RM, Bloch DA, Cotrutz C, et al. Multicenter trial of stereotactic body radiation therapy for low- and intermediate-risk prostate cancer: survival and toxicity endpoints. nt J Radiat Oncol Biol Phys. 2018;102:296-303. doi:10.1016/j.ijrobp.2018.05.040
- Quon HC, Ong A, Cheung P, et al. Once-weekly versus every-other-day stereotactic body radiotherapy in patients with prostate cancer (PATRIOT): a phase 2 randomized trial. Radiother Oncol. 2018;127:206-212. doi:10.1016/j.radonc.2018.02.029
- Zelefsky MJ, Kollmeier M, McBride S, et al. Five-year outcomes of a phase 1 dose-escalation study using stereotactic body radiosurgery for patients with low-risk and intermediate-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2019;104:42-49. doi:10.1016/j.ijrobp.2018.12.045
Prostate cancer is the most common cancer in US males, with an estimated 313,780 new cases and 35,770 deaths in 2025.1 Several treatment options are available for localized prostate cancer that have similar outcomes, including active surveillance for low-risk cancers, surgery, or radiotherapy.2,3 Conventional fractionation radiotherapy (CFRT) with 40 to 45 fractions over 8 to 9 weeks has been used for decades. Over the past 2 decades, moderate hypofractionation schedules with 2.4 to 3.4 Gy per fraction over 20 to 28 fractions have become standard, as many noninferiority randomized clinical trials (RCTs) such as CHHiP (UK),4 PROFIT (Canada and Europe),5 NRG Oncology RTOG 0415 (US),6 HYPRO (Netherlands),7,8 and HYPO-RT-PC (Sweden and Denmark),9 have shown the noninferiority of moderately hypofractionated radiotherapy compared with CFRT. Notably, most of these noninferiority studies primarily included patients with low- or intermediate-risk prostate cancer, except for the HYPO-RT-PC trial,9 which also included patients with intermediate- and high-risk prostate cancer.
These noninferiority studies, along with technological advances in radiotherapy, such as intensity-modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT), and image-guided radiotherapy (IGRT), paved the path to ultrahypofractionated stereotactic body radiotherapy (SBRT) that is delivered in 5 fractions of ≥ 6 Gy. This high dose per fraction may have a radiobiologic advantage over conventional fractionation. The relatively low a/ß ratio of prostate cancer, estimated to be between 1 and 2, suggests that tumor cells may be particularly sensitive to the high doses per fraction delivered in SBRT.10-13 Compared with CFRT, SBRT-induced tumor cell death may also be mediated through different pathways; this pathway appears to be generated in a dose-dependent manner, particularly with doses > 8 Gy per fraction.14,15 Additionally, the higher a/ß ratio for the surrounding organs at risk, such as the bladder and rectum, theoretically allows for an improved therapeutic ratio window that maximizes tumor control while minimizing damage to healthy tissues.
A substantial body of evidence from prospective studies and meta-analyses supports the use of SBRT for localized prostate cancer. HYPO-RT-PC, a significant phase 3 noninferiority study, enrolled 1200 patients with intermediate (89%) and high-risk (11%) prostate cancer randomized between 2 arms, including CFRT to 78 Gy in 39 fractions and SBRT to 42.7 Gy in 7 fractions, treated 3 days weekly. After a median follow-up of 60 months, the estimated 5-year biochemical relapse-free survival rate was 84% in both groups.9 This trial was notable because it was the first randomized study to demonstrate that SBRT was noninferior to CFRT in intermediate- and high-risk prostate cancer patients. Another pivotal phase 3 trial, the PACE-B study, enrolled 874 patients to compare SBRT (36.25 Gy to the prostate gland, with a secondary dose of 40 Gy to the gross tumor volume where applicable, in 5 fractions) with CFRT (78 Gy in 39 fractions) and moderately hypofractionated radiotherapy (HFRT) (62 Gy in 20 fractions) in patients with low- or intermediate-risk prostate cancer. With a 74-month median follow-up, the study reported 5-year biochemical free rates of 94.6% for CFRT and 95.8% for SBRT, confirming the noninferiority of SBRT to CFRT.15
SBRT offers short, effective, and convenient treatment to many patients with localized prostate cancer. While previous guidelines were more restrictive, the March 2026 National Comprehensive Cancer Network (NCCN) guidelines now list SBRT as a preferred treatment modality for high-risk prostate cancer.16
Given the growing body of evidence supporting the efficacy and safety of SBRT, we implemented an SBRT program in 2014 at a tertiary care center for veterans. This retrospective study was undertaken to evaluate the early efficacy and toxicity of SBRT in patients with localized prostate cancer treated at our institution, including patients across all risk stratifications.
METHODS
We identified 242 patients diagnosed with prostate cancer who underwent SBRT treatment between November 2014 and October 2024 at Overland Park Veterans Affairs Radiation Oncology Clinic. For the final analysis, 46 patients with < 2 years of follow-up and 22 patients who died from causes other than prostate cancer were excluded, resulting in a cohort of 174 patients with ≥ 24-month follow-up.
Treatment
Patients eligible for staging underwent imaging according to NCCN guidelines, including computed tomography (CT) of the abdomen and pelvis, bone scintigraphy, or, in recent years, prostate-specific membrane antigen positron emission tomography, primarily used for unfavorable intermediate-risk (UIR) and high-risk (HR) cancers. Patients with a negative staging work-up for nodal or skeletal disease were included. Prior to planning the CT simulation, patients were given bowel preparation instructions, including a low-fiber and low-gas-producing diet, simethicone, and enemas, the night before and morning of the simulation. Patients were instructed to arrive with a comfortably full bladder, having not voided for 2 to 3 hours prior to the procedure. At Kansas City Veterans Affairs Medical Center (KCVAMC), SBRT treatment was generally restricted to patients with a baseline American Urological Association symptom score of 15 to 20 out of 35 and a prostate gland size < 80 mL to minimize the risk of acute urinary toxicity. We did not use intraprostatic fiducials, hydrogel rectal spacers, or intravenous contrast agents for planning CT simulation.
Patients were placed in a supine position, and a vacuum bag was used for immobilization. Following the CT simulation, the images were transferred to the Eclipse treatment planning system. The clinical target volume (CTV) encompassed the prostate and the proximal 1.0 cm of the seminal vesicles for Gleason score (GS) 1 to 2, and the entire seminal vesicle was included for GS 3 to 5, which is consistent with KCVAMC practice and established safety protocols. The planning target volume (PTV) was created by uniformly expanding the CTV by 5 to 7 mm, except for the posterior margin, which was limited to 3 to 5 mm. When elective nodal radiotherapy was planned for HR prostate cancer, the pelvic field for CT simulation started at the L-2 upper border, with the lower border extending to the lesser trochanter. The pelvic nodes were delineated per Radiation Therapy Oncology Group (RTOG) guidelines.17 The CTV nodes (CTVn), including common iliac, external and internal iliac nodes, obturator, and presacral nodes, were created by uniformly expanding the CTVn by 2 to 3 mm. Slice-by-slice corrections were made to avoid bowel overlap in these patients.
The use of androgen deprivation therapy (ADT) for a duration of 6 to 24 months was prescribed for patients with UIR or HR prostate cancer per NCCN guidelines.16 The prescribed dose to the PTV was 36.25 to 40 Gy (40 Gy was mostly used as a boost to the dominant lesion) in 5 fractions, with each fraction ranging from 7.25 to 8 Gy. For elective nodal radiotherapy in patients at HR, the prescribed dose was 25 Gy in 5 fractions. All patients were planned for VMAT, which aims to deliver ≥ 95% of the prescription dose to 95% of the PTV. Once the physician approved the treatment plan and physics quality assessment was completed, treatments commenced on an every-other-day schedule. Patients received the same bowel preparation instructions for each treatment as for the planning CT simulation. Daily treatment accuracy was confirmed via daily 3-dimensional cone-beam CT (CBCT) for IGRT. No fiducials or hydrogel rectal spacers were used.
Follow-up Schedule and Toxicity Assessment
Follow-up assessments were conducted 4 to 6 weeks after radiation therapy and then repeated every 6 months for 2 to 5 years, and annually thereafter. At each follow-up visit, patients were evaluated for genitourinary (GU) and gastrointestinal (GI) toxicity, according to RTOG toxicity criteria. Prostate-specific antigen (PSA) levels were monitored; in patients receiving ADT, testosterone levels were also checked.
Statistical Analysis
Biochemical failure was defined using the Phoenix definition (nadir PSA + 2 ng/mL). Differences between dose cohorts were assessed using the log-rank test for survival outcomes and X2 testing for categorical variables. GU and GI toxicities were summarized as cumulative incidences of RTOG grade ≥ II events. Statistical significance was set at P < .05.
RESULTS
One hundred seventy-four patients were included in the retrospective review. Patients had a median follow-up of 45 months (range, 24-111) (Figure). The median age at treatment was 74 years (range, 51-88), and the median pretreatment PSA level was 11.9 ng/mL (range, 0.6-69.5). Twenty-six patients (14.9%) had a GS 1, 77 (44.3%) had GS 2, 41 (23.6%) had GS 3, 18 (10.3%) had GS 4, and 12 (6.9%) had GS 5. Fifty-one patients (29.3%) received elective pelvic nodal radiotherapy, and 93 patients (53.4%) received ADT (Table 1).
At 24 months follow-up, 6 patients (3.4%) had biochemical failures. One patient died from metastatic prostate cancer, and 5 patients are living with biochemical failure (Table 2). The actuarial 5-year overall survival (OS) rate was 99.4%, and the 5-year disease-free survival (DFS) rate was 96.6%. We performed a subanalysis comparing outcomes of the 36.25 Gy vs 40 Gy SBRT cohorts. There was no statistically significant difference in DFS, OS, or the cumulative incidence of grade II/III toxicity between patients treated with 40 Gy vs 36.25 Gy. Outcomes stratified by NCCN risk groups (low, intermediate, high/very high) are detailed in Table 3. As expected, DFS was slightly lower in the high-risk group, but overall disease control remained high across all stratifications.
The cumulative incidence of RTOG grade II and higher GU toxicity was 28.2% (Table 4). This included 46 patients (26.4%) with grade II GU toxicity and 2 patients (1.2%) who developed grade III GU complications (1 requiring self-catheterization and another a suprapubic catheter for urinary retention). One patient (0.6%) treated with a 40 Gy dose regimen experienced a grade IV GU complication in the form of a rectovesical fistula necessitating surgical intervention.
The cumulative incidence of RTOG grade II or higher GI toxicity was 3.4%, and no grade III or IV gastrointestinal toxicities were observed during the follow-up period. Importantly, intraprostatic fiducials, hydrogel rectal spacers, or intravenous contrast were not routinely used in this cohort of patients.
The high rates of actuarial 5-year DFS and OS observed suggest a favorable initial response to the SBRT regimen employed at KCVAMC. However, given the potential for late recurrence in patients with prostate cancer, longer follow-up is essential to determine the durability of these outcomes. The observed GU toxicity rate of 28.2% for grade II and higher events warrants careful consideration and compares with other published data on SBRT for prostate cancer.15 The occurrence of a grade IV rectovesical fistula, although rare, is a notable adverse event that warrants discussion in the context of the treatment approach. The low incidence of grade II or higher GI toxicity is an encouraging finding, particularly given that hydrogel rectal spacers are not routinely used to minimize rectal exposure.
DISCUSSION
The primary objective of this retrospective study was to evaluate the outcomes of SBRT for patients with localized prostate cancer treated at KCVAMC and to compare these results with those reported in the literature. Our findings demonstrate promising intermediate-term efficacy, with an estimated 5-year DFS of 96.6% and OS of 99.4% at a median follow-up of 45 months. Furthermore, the observed toxicity profile appears acceptable, with a cumulative grade II and higher GU toxicity rate of 28.2% and a grade II or higher GI toxicity rate of 3.4%. Notably, these outcomes were achieved without the routine use of intraprostatic fiducials or hydrogel rectal spacers.
Two pivotal randomized phase 3 trials have established the noninferiority of ultrahypofractionated radiotherapy (UHRT) with SBRT over conventional fractionation. The HYPO-RT-PC trial compared SBRT (42.7 Gy in 7 fractions) with conventional fractionation (78 Gy in 39 fractions) in intermediate- and high-risk patients with prostate cancer and reported a 5-year biochemical relapse-free survival of 84% in both arms.9 The PACE-B trial, which included patients at low- and intermediate-risk, compared SBRT (36.25 Gy in 5 fractions) with conventional or moderate HFRT and reported a 5-year biochemical control rate of 95.8% in the SBRT arm and 94.6% in the control arm.15
A comprehensive review and meta-analysis of 7 phase 3 studies involving 6795 patients compared different radiotherapy regimens, namely, UHRT, HFRT, and CFRT, and reported that after 5 years, the DFS rates were 85.1% for CFRT, 86% for HFRT, and 85% for UHRT, with no significant difference in toxicity among the 3 different treatment approaches.18 This suggests that shorter, more intense radiotherapy schedules (UHRT and HFRT) may be as effective and safe as traditional, longer courses of radiation.
There are multiple published nonrandomized prospective trials in which thousands of patients with extreme hypofractionation have been treated with different doses, fractions, and techniques. While heterogeneity and limited long-term follow-up in the existing evidence are acknowledged, these data suggest that prostate SBRT provides appropriate biochemical control with few high-grade toxicities, supporting its ongoing global use and justifying further prospective investigations. Comparative data are shown in Table 5. Several ongoing studies are evaluating noninferiority, superiority, and cost-effectiveness using different methodologies (Table 6).9,15,19-24
This study’s efficacy outcomes, particularly the high DFS rate, are consistent with the findings from these landmark trials, suggesting that the SBRT regimen used at KCVAMC is effective in achieving early disease control despite 17.2% of patients having high-risk disease. The GU toxicity observed in this study, with a 28.2% rate of grade II or higher events, is also comparable with the 26.9% reported in the 5-fraction SBRT arm of the PACE-B trial, which had a longer median follow-up of 74 months.15 It is important to note that a portion of these grade II events occurred in patients who were already on a blockers for pre-existing lower urinary tract symptoms before starting radiotherapy, which may inflate the observed cumulative acute toxicity score.
A critical comparison is how SBRT toxicity aligns with moderate hypofractionation (eg, 60 Gy in 20 fractions or 70 Gy in 28 fractions as reported by others).4,6 Our observed grade III and higher GU toxicity rate (1.7%) and grade III and higher GI toxicity rate (0%) are highly favorable when compared with historical moderate hypofractionation data, which typically report grade III GU toxicity in the range of 2% to 3% and grade III GI toxicity around 1% to 2%. This suggests that despite the higher dose per fraction, SBRT does not necessarily lead to increased severe acute toxicity, potentially offering a superior therapeutic ratio for GI and GU sparing.
However, the occurrence of a grade IV rectovesical fistula in 1 patient (0.6%)—who received the 40 Gy dose—was a serious complication that warrants careful consideration. This rare, but severe, complication in the higher dose cohort underscores the potential for increased organ-at-risk toxicity, particularly in the absence of a hydrogel rectal spacer, which is designed to mitigate high-dose rectal exposure. While the overall rate of significant GU toxicity remains low, this event highlights the potential risks associated with SBRT. Hydrogel rectal spacers are designed to increase the distance between the prostate and the rectum, which can reduce the rectal radiation dose and potentially mitigate the risk of such fistulas. The low rate of grade II or worse GI toxicity (3.4%) in our study is noteworthy, especially considering that hydrogel spacers were not routinely used. This finding aligns with the 2.5% GI toxicity rate reported in the SBRT arm of the PACE-B trial, suggesting that careful treatment planning and delivery techniques, such as VMAT-IMRT and daily CBCT for IGRT, may contribute to minimizing GI toxicity even without the use of rectal spacers.15 The exclusive use of 3-dimensional CBCT for IGRT in our study, without the use of fiducial markers, suggests that accurate target localization can be achieved with this approach, contributing to the observed efficacy and reduced toxicity.
Strengths and Limitations
This study’s retrospective, single-center design may have introduced selection bias. The median follow-up of 45 months, while substantial, is still relatively short for assessing very late toxicities and long-term oncologic outcomes in prostate cancer, which is known for late recurrences. Additionally, the lack of a direct comparison group within KCVAMC limits the ability to definitively attribute the observed outcomes solely to SBRT treatment. However, the strengths of this study include the inclusion of a consecutive series of veteran patients with localized prostate cancer across all risk categories, providing a real-world perspective on SBRT outcomes in a diverse patient population. Furthermore, the detailed assessment of efficacy and toxicity via standardized RTOG criteria enhances the comparability of our findings with those of other published prospective studies, despite the retrospective nature of the data.
CONCLUSIONS
This single-institution retrospective analysis revealed that short-term SBRT (36.25 to 40 Gy in 5 fractions), with a minimum follow-up of 24 months and a median follow-up of 45 months, for localized prostate cancer, including patients at HR, is associated with promising early efficacy and acceptable toxicity, even in the absence of routine fiducial or hydrogel spacer use. The favorable actuarial 5-year DFS and OS rates, coupled with a manageable toxicity profile, suggest that SBRT is a safe and convenient treatment option for many patients with localized prostate cancer. However, a longer follow-up is necessary to confirm these findings and fully characterize the long-term efficacy and toxicity of this SBRT regimen. Nevertheless, the results contribute to the growing body of evidence suggesting that SBRT is a safe and convenient treatment option for many patients with localized prostate cancer.
Prostate cancer is the most common cancer in US males, with an estimated 313,780 new cases and 35,770 deaths in 2025.1 Several treatment options are available for localized prostate cancer that have similar outcomes, including active surveillance for low-risk cancers, surgery, or radiotherapy.2,3 Conventional fractionation radiotherapy (CFRT) with 40 to 45 fractions over 8 to 9 weeks has been used for decades. Over the past 2 decades, moderate hypofractionation schedules with 2.4 to 3.4 Gy per fraction over 20 to 28 fractions have become standard, as many noninferiority randomized clinical trials (RCTs) such as CHHiP (UK),4 PROFIT (Canada and Europe),5 NRG Oncology RTOG 0415 (US),6 HYPRO (Netherlands),7,8 and HYPO-RT-PC (Sweden and Denmark),9 have shown the noninferiority of moderately hypofractionated radiotherapy compared with CFRT. Notably, most of these noninferiority studies primarily included patients with low- or intermediate-risk prostate cancer, except for the HYPO-RT-PC trial,9 which also included patients with intermediate- and high-risk prostate cancer.
These noninferiority studies, along with technological advances in radiotherapy, such as intensity-modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT), and image-guided radiotherapy (IGRT), paved the path to ultrahypofractionated stereotactic body radiotherapy (SBRT) that is delivered in 5 fractions of ≥ 6 Gy. This high dose per fraction may have a radiobiologic advantage over conventional fractionation. The relatively low a/ß ratio of prostate cancer, estimated to be between 1 and 2, suggests that tumor cells may be particularly sensitive to the high doses per fraction delivered in SBRT.10-13 Compared with CFRT, SBRT-induced tumor cell death may also be mediated through different pathways; this pathway appears to be generated in a dose-dependent manner, particularly with doses > 8 Gy per fraction.14,15 Additionally, the higher a/ß ratio for the surrounding organs at risk, such as the bladder and rectum, theoretically allows for an improved therapeutic ratio window that maximizes tumor control while minimizing damage to healthy tissues.
A substantial body of evidence from prospective studies and meta-analyses supports the use of SBRT for localized prostate cancer. HYPO-RT-PC, a significant phase 3 noninferiority study, enrolled 1200 patients with intermediate (89%) and high-risk (11%) prostate cancer randomized between 2 arms, including CFRT to 78 Gy in 39 fractions and SBRT to 42.7 Gy in 7 fractions, treated 3 days weekly. After a median follow-up of 60 months, the estimated 5-year biochemical relapse-free survival rate was 84% in both groups.9 This trial was notable because it was the first randomized study to demonstrate that SBRT was noninferior to CFRT in intermediate- and high-risk prostate cancer patients. Another pivotal phase 3 trial, the PACE-B study, enrolled 874 patients to compare SBRT (36.25 Gy to the prostate gland, with a secondary dose of 40 Gy to the gross tumor volume where applicable, in 5 fractions) with CFRT (78 Gy in 39 fractions) and moderately hypofractionated radiotherapy (HFRT) (62 Gy in 20 fractions) in patients with low- or intermediate-risk prostate cancer. With a 74-month median follow-up, the study reported 5-year biochemical free rates of 94.6% for CFRT and 95.8% for SBRT, confirming the noninferiority of SBRT to CFRT.15
SBRT offers short, effective, and convenient treatment to many patients with localized prostate cancer. While previous guidelines were more restrictive, the March 2026 National Comprehensive Cancer Network (NCCN) guidelines now list SBRT as a preferred treatment modality for high-risk prostate cancer.16
Given the growing body of evidence supporting the efficacy and safety of SBRT, we implemented an SBRT program in 2014 at a tertiary care center for veterans. This retrospective study was undertaken to evaluate the early efficacy and toxicity of SBRT in patients with localized prostate cancer treated at our institution, including patients across all risk stratifications.
METHODS
We identified 242 patients diagnosed with prostate cancer who underwent SBRT treatment between November 2014 and October 2024 at Overland Park Veterans Affairs Radiation Oncology Clinic. For the final analysis, 46 patients with < 2 years of follow-up and 22 patients who died from causes other than prostate cancer were excluded, resulting in a cohort of 174 patients with ≥ 24-month follow-up.
Treatment
Patients eligible for staging underwent imaging according to NCCN guidelines, including computed tomography (CT) of the abdomen and pelvis, bone scintigraphy, or, in recent years, prostate-specific membrane antigen positron emission tomography, primarily used for unfavorable intermediate-risk (UIR) and high-risk (HR) cancers. Patients with a negative staging work-up for nodal or skeletal disease were included. Prior to planning the CT simulation, patients were given bowel preparation instructions, including a low-fiber and low-gas-producing diet, simethicone, and enemas, the night before and morning of the simulation. Patients were instructed to arrive with a comfortably full bladder, having not voided for 2 to 3 hours prior to the procedure. At Kansas City Veterans Affairs Medical Center (KCVAMC), SBRT treatment was generally restricted to patients with a baseline American Urological Association symptom score of 15 to 20 out of 35 and a prostate gland size < 80 mL to minimize the risk of acute urinary toxicity. We did not use intraprostatic fiducials, hydrogel rectal spacers, or intravenous contrast agents for planning CT simulation.
Patients were placed in a supine position, and a vacuum bag was used for immobilization. Following the CT simulation, the images were transferred to the Eclipse treatment planning system. The clinical target volume (CTV) encompassed the prostate and the proximal 1.0 cm of the seminal vesicles for Gleason score (GS) 1 to 2, and the entire seminal vesicle was included for GS 3 to 5, which is consistent with KCVAMC practice and established safety protocols. The planning target volume (PTV) was created by uniformly expanding the CTV by 5 to 7 mm, except for the posterior margin, which was limited to 3 to 5 mm. When elective nodal radiotherapy was planned for HR prostate cancer, the pelvic field for CT simulation started at the L-2 upper border, with the lower border extending to the lesser trochanter. The pelvic nodes were delineated per Radiation Therapy Oncology Group (RTOG) guidelines.17 The CTV nodes (CTVn), including common iliac, external and internal iliac nodes, obturator, and presacral nodes, were created by uniformly expanding the CTVn by 2 to 3 mm. Slice-by-slice corrections were made to avoid bowel overlap in these patients.
The use of androgen deprivation therapy (ADT) for a duration of 6 to 24 months was prescribed for patients with UIR or HR prostate cancer per NCCN guidelines.16 The prescribed dose to the PTV was 36.25 to 40 Gy (40 Gy was mostly used as a boost to the dominant lesion) in 5 fractions, with each fraction ranging from 7.25 to 8 Gy. For elective nodal radiotherapy in patients at HR, the prescribed dose was 25 Gy in 5 fractions. All patients were planned for VMAT, which aims to deliver ≥ 95% of the prescription dose to 95% of the PTV. Once the physician approved the treatment plan and physics quality assessment was completed, treatments commenced on an every-other-day schedule. Patients received the same bowel preparation instructions for each treatment as for the planning CT simulation. Daily treatment accuracy was confirmed via daily 3-dimensional cone-beam CT (CBCT) for IGRT. No fiducials or hydrogel rectal spacers were used.
Follow-up Schedule and Toxicity Assessment
Follow-up assessments were conducted 4 to 6 weeks after radiation therapy and then repeated every 6 months for 2 to 5 years, and annually thereafter. At each follow-up visit, patients were evaluated for genitourinary (GU) and gastrointestinal (GI) toxicity, according to RTOG toxicity criteria. Prostate-specific antigen (PSA) levels were monitored; in patients receiving ADT, testosterone levels were also checked.
Statistical Analysis
Biochemical failure was defined using the Phoenix definition (nadir PSA + 2 ng/mL). Differences between dose cohorts were assessed using the log-rank test for survival outcomes and X2 testing for categorical variables. GU and GI toxicities were summarized as cumulative incidences of RTOG grade ≥ II events. Statistical significance was set at P < .05.
RESULTS
One hundred seventy-four patients were included in the retrospective review. Patients had a median follow-up of 45 months (range, 24-111) (Figure). The median age at treatment was 74 years (range, 51-88), and the median pretreatment PSA level was 11.9 ng/mL (range, 0.6-69.5). Twenty-six patients (14.9%) had a GS 1, 77 (44.3%) had GS 2, 41 (23.6%) had GS 3, 18 (10.3%) had GS 4, and 12 (6.9%) had GS 5. Fifty-one patients (29.3%) received elective pelvic nodal radiotherapy, and 93 patients (53.4%) received ADT (Table 1).
At 24 months follow-up, 6 patients (3.4%) had biochemical failures. One patient died from metastatic prostate cancer, and 5 patients are living with biochemical failure (Table 2). The actuarial 5-year overall survival (OS) rate was 99.4%, and the 5-year disease-free survival (DFS) rate was 96.6%. We performed a subanalysis comparing outcomes of the 36.25 Gy vs 40 Gy SBRT cohorts. There was no statistically significant difference in DFS, OS, or the cumulative incidence of grade II/III toxicity between patients treated with 40 Gy vs 36.25 Gy. Outcomes stratified by NCCN risk groups (low, intermediate, high/very high) are detailed in Table 3. As expected, DFS was slightly lower in the high-risk group, but overall disease control remained high across all stratifications.
The cumulative incidence of RTOG grade II and higher GU toxicity was 28.2% (Table 4). This included 46 patients (26.4%) with grade II GU toxicity and 2 patients (1.2%) who developed grade III GU complications (1 requiring self-catheterization and another a suprapubic catheter for urinary retention). One patient (0.6%) treated with a 40 Gy dose regimen experienced a grade IV GU complication in the form of a rectovesical fistula necessitating surgical intervention.
The cumulative incidence of RTOG grade II or higher GI toxicity was 3.4%, and no grade III or IV gastrointestinal toxicities were observed during the follow-up period. Importantly, intraprostatic fiducials, hydrogel rectal spacers, or intravenous contrast were not routinely used in this cohort of patients.
The high rates of actuarial 5-year DFS and OS observed suggest a favorable initial response to the SBRT regimen employed at KCVAMC. However, given the potential for late recurrence in patients with prostate cancer, longer follow-up is essential to determine the durability of these outcomes. The observed GU toxicity rate of 28.2% for grade II and higher events warrants careful consideration and compares with other published data on SBRT for prostate cancer.15 The occurrence of a grade IV rectovesical fistula, although rare, is a notable adverse event that warrants discussion in the context of the treatment approach. The low incidence of grade II or higher GI toxicity is an encouraging finding, particularly given that hydrogel rectal spacers are not routinely used to minimize rectal exposure.
DISCUSSION
The primary objective of this retrospective study was to evaluate the outcomes of SBRT for patients with localized prostate cancer treated at KCVAMC and to compare these results with those reported in the literature. Our findings demonstrate promising intermediate-term efficacy, with an estimated 5-year DFS of 96.6% and OS of 99.4% at a median follow-up of 45 months. Furthermore, the observed toxicity profile appears acceptable, with a cumulative grade II and higher GU toxicity rate of 28.2% and a grade II or higher GI toxicity rate of 3.4%. Notably, these outcomes were achieved without the routine use of intraprostatic fiducials or hydrogel rectal spacers.
Two pivotal randomized phase 3 trials have established the noninferiority of ultrahypofractionated radiotherapy (UHRT) with SBRT over conventional fractionation. The HYPO-RT-PC trial compared SBRT (42.7 Gy in 7 fractions) with conventional fractionation (78 Gy in 39 fractions) in intermediate- and high-risk patients with prostate cancer and reported a 5-year biochemical relapse-free survival of 84% in both arms.9 The PACE-B trial, which included patients at low- and intermediate-risk, compared SBRT (36.25 Gy in 5 fractions) with conventional or moderate HFRT and reported a 5-year biochemical control rate of 95.8% in the SBRT arm and 94.6% in the control arm.15
A comprehensive review and meta-analysis of 7 phase 3 studies involving 6795 patients compared different radiotherapy regimens, namely, UHRT, HFRT, and CFRT, and reported that after 5 years, the DFS rates were 85.1% for CFRT, 86% for HFRT, and 85% for UHRT, with no significant difference in toxicity among the 3 different treatment approaches.18 This suggests that shorter, more intense radiotherapy schedules (UHRT and HFRT) may be as effective and safe as traditional, longer courses of radiation.
There are multiple published nonrandomized prospective trials in which thousands of patients with extreme hypofractionation have been treated with different doses, fractions, and techniques. While heterogeneity and limited long-term follow-up in the existing evidence are acknowledged, these data suggest that prostate SBRT provides appropriate biochemical control with few high-grade toxicities, supporting its ongoing global use and justifying further prospective investigations. Comparative data are shown in Table 5. Several ongoing studies are evaluating noninferiority, superiority, and cost-effectiveness using different methodologies (Table 6).9,15,19-24
This study’s efficacy outcomes, particularly the high DFS rate, are consistent with the findings from these landmark trials, suggesting that the SBRT regimen used at KCVAMC is effective in achieving early disease control despite 17.2% of patients having high-risk disease. The GU toxicity observed in this study, with a 28.2% rate of grade II or higher events, is also comparable with the 26.9% reported in the 5-fraction SBRT arm of the PACE-B trial, which had a longer median follow-up of 74 months.15 It is important to note that a portion of these grade II events occurred in patients who were already on a blockers for pre-existing lower urinary tract symptoms before starting radiotherapy, which may inflate the observed cumulative acute toxicity score.
A critical comparison is how SBRT toxicity aligns with moderate hypofractionation (eg, 60 Gy in 20 fractions or 70 Gy in 28 fractions as reported by others).4,6 Our observed grade III and higher GU toxicity rate (1.7%) and grade III and higher GI toxicity rate (0%) are highly favorable when compared with historical moderate hypofractionation data, which typically report grade III GU toxicity in the range of 2% to 3% and grade III GI toxicity around 1% to 2%. This suggests that despite the higher dose per fraction, SBRT does not necessarily lead to increased severe acute toxicity, potentially offering a superior therapeutic ratio for GI and GU sparing.
However, the occurrence of a grade IV rectovesical fistula in 1 patient (0.6%)—who received the 40 Gy dose—was a serious complication that warrants careful consideration. This rare, but severe, complication in the higher dose cohort underscores the potential for increased organ-at-risk toxicity, particularly in the absence of a hydrogel rectal spacer, which is designed to mitigate high-dose rectal exposure. While the overall rate of significant GU toxicity remains low, this event highlights the potential risks associated with SBRT. Hydrogel rectal spacers are designed to increase the distance between the prostate and the rectum, which can reduce the rectal radiation dose and potentially mitigate the risk of such fistulas. The low rate of grade II or worse GI toxicity (3.4%) in our study is noteworthy, especially considering that hydrogel spacers were not routinely used. This finding aligns with the 2.5% GI toxicity rate reported in the SBRT arm of the PACE-B trial, suggesting that careful treatment planning and delivery techniques, such as VMAT-IMRT and daily CBCT for IGRT, may contribute to minimizing GI toxicity even without the use of rectal spacers.15 The exclusive use of 3-dimensional CBCT for IGRT in our study, without the use of fiducial markers, suggests that accurate target localization can be achieved with this approach, contributing to the observed efficacy and reduced toxicity.
Strengths and Limitations
This study’s retrospective, single-center design may have introduced selection bias. The median follow-up of 45 months, while substantial, is still relatively short for assessing very late toxicities and long-term oncologic outcomes in prostate cancer, which is known for late recurrences. Additionally, the lack of a direct comparison group within KCVAMC limits the ability to definitively attribute the observed outcomes solely to SBRT treatment. However, the strengths of this study include the inclusion of a consecutive series of veteran patients with localized prostate cancer across all risk categories, providing a real-world perspective on SBRT outcomes in a diverse patient population. Furthermore, the detailed assessment of efficacy and toxicity via standardized RTOG criteria enhances the comparability of our findings with those of other published prospective studies, despite the retrospective nature of the data.
CONCLUSIONS
This single-institution retrospective analysis revealed that short-term SBRT (36.25 to 40 Gy in 5 fractions), with a minimum follow-up of 24 months and a median follow-up of 45 months, for localized prostate cancer, including patients at HR, is associated with promising early efficacy and acceptable toxicity, even in the absence of routine fiducial or hydrogel spacer use. The favorable actuarial 5-year DFS and OS rates, coupled with a manageable toxicity profile, suggest that SBRT is a safe and convenient treatment option for many patients with localized prostate cancer. However, a longer follow-up is necessary to confirm these findings and fully characterize the long-term efficacy and toxicity of this SBRT regimen. Nevertheless, the results contribute to the growing body of evidence suggesting that SBRT is a safe and convenient treatment option for many patients with localized prostate cancer.
- Siegel RL, Kratzer TB, Giaquinto AN, et al. Cancer statistics, 2025. CA Cancer J Clin. 2025;75:10-45. doi:10.3322/caac.21871
- Donovan JL, Hamdy FC, Lane JA, et al. Patient-reported outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. 2016;375:1425-1437. doi:10.1056/NEJMoa1606221
- Hamdy FC, Donovan JL, Lane JA, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375:1415-1424. doi:10.1056/NEJMoa1606220
- Dearnaley D, Syndikus I, Mossop H, et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016;17:1047-1060. doi:10.1016/S1470-2045(16)30102-4
- Catton CN, Lukka H, Gu CS, et al. Randomized trial of a hypofractionated radiation regimen for the treatment of localized prostate cancer. J Clin Oncol. 2017;35:1884-1890. doi:10.1200/JCO.2016.71.7397
- Lee WR, Dignam JJ, Amin MB, et al. Long-term analysis of NRG Oncology RTOG 0415: a randomized phase III noninferiority study comparing two fractionation schedules in patients with low-risk prostate cancer. J Clin Oncol. 2024;42:2377-2381. doi:10.1200/JCO.23.02445
- de Vries KC, Wortel RC, Oomen-de Hoop E, et al. Hypofractionated versus conventionally fractionated radiation therapy for patients with intermediate- or high-risk, localized, prostate cancer: 7-year outcomes from the randomized, multicenter, open-label, phase 3 HYPRO trial. Int J Radiat Oncol Biol Phys. 2020;106:108-115. doi:10.1016/j.ijrobp.2019.09.007
- Incrocci L, Wortel RC, Alemayehu WG, et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with localised prostate cancer (HYPRO): final efficacy results from a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2016;17:1061-1069. doi:10.1016/S1470-2045(16)30070-5
- Widmark A, Gunnlaugsson A, Beckman L, et al. Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial. Lancet. 2019;394:385-395. doi:10.1016/S0140-6736(19)31131-6
- Brenner DJ, Hall EJ. Fractionation and protraction for radiotherapy of prostate carcinoma. Int J Radiat Oncol Biol Phys. 1999;43:1095-101. doi:10.1016/s0360-3016(98)00438-6
- Dasu A. Is the alpha/beta value for prostate tumours low enough to be safely used in clinical trials? Clin Oncol (R Coll Radiol). 2007;19:289-301. doi:10.1016/j.clon.2007.02.007
- Garcia-Barros M, Paris F, Cordon-Cardo C, et al. Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science. 2003;300:1155-1159. doi:10.1126/science.1082504
- Gulliford S, Hall E, Dearnaley D. Hypofractionation trials and radiobiology of prostate cancer. Oncoscience. 2017;4:27-28. doi:10.18632/oncoscience.347
- Fuks Z, Kolesnick R. Engaging the vascular component of the tumor response. Cancer Cell. 2005;8:89-91. doi:10.1016/j.ccr.2005.07.014
- van As N, Griffin C, Tree A, et al. Phase 3 Trial of stereotactic body radiotherapy in localized prostate cancer. N Engl J Med. Oct 17 2024;391:1413-1425. doi:10.1056/NEJMoa2403365
- National Comprehensive Cancer Network. NCCN Guidelines Version 5. 2026 Prostate Cancer. Accessed March 24, 2026. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
- Lawton CA, Michalski J, El-Naqa I, et al. RTOG GU radiation oncology specialists reach consensus on pelvic lymph node volumes for high-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2009;74:383-387. doi:10.1016/j.ijrobp.2008.08.002
- Lehrer EJ, Kishan AU, Yu JB, et al. Ultrahypofractionated versus hypofractionated and conventionally fractionated radiation therapy for localized prostate cancer: a systematic review and meta-analysis of phase III randomized trials. Radiother Oncol. 2020;148:235-242. doi:10.1016/j.radonc.2020.04.037
- De Cooman B, Debacker T, Adams T, et al. Stereotactic body radiotherapy (SBRT) as a treatment for localized prostate cancer: a retrospective analysis. Radiat Oncol. 2025;20:25. doi:10.1186/s13014-025-02598-8
- Fuller DB, Falchook AD, Crabtree T, et al. Phase 2 multicenter trial of heterogeneous-dosing stereotactic body radiotherapy for low- and intermediate-risk prostate cancer: 5-year outcomes. Eur Urol Oncol. 2018;1:540-547. doi:10.1016/j.euo.2018.06.013
- Jackson WC, Silva J, Hartman HE, et al. Stereotactic body radiation therapy for localized prostate cancer: a systematic review and meta-analysis of over 6,000 patients treated on prospective studies. Int J Radiat Oncol Biol Phys. 2019;104:778-789. doi:10.1016/j.ijrobp.2019.03.051
- Meier RM, Bloch DA, Cotrutz C, et al. Multicenter trial of stereotactic body radiation therapy for low- and intermediate-risk prostate cancer: survival and toxicity endpoints. nt J Radiat Oncol Biol Phys. 2018;102:296-303. doi:10.1016/j.ijrobp.2018.05.040
- Quon HC, Ong A, Cheung P, et al. Once-weekly versus every-other-day stereotactic body radiotherapy in patients with prostate cancer (PATRIOT): a phase 2 randomized trial. Radiother Oncol. 2018;127:206-212. doi:10.1016/j.radonc.2018.02.029
- Zelefsky MJ, Kollmeier M, McBride S, et al. Five-year outcomes of a phase 1 dose-escalation study using stereotactic body radiosurgery for patients with low-risk and intermediate-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2019;104:42-49. doi:10.1016/j.ijrobp.2018.12.045
- Siegel RL, Kratzer TB, Giaquinto AN, et al. Cancer statistics, 2025. CA Cancer J Clin. 2025;75:10-45. doi:10.3322/caac.21871
- Donovan JL, Hamdy FC, Lane JA, et al. Patient-reported outcomes after monitoring, surgery, or radiotherapy for prostate cancer. N Engl J Med. 2016;375:1425-1437. doi:10.1056/NEJMoa1606221
- Hamdy FC, Donovan JL, Lane JA, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375:1415-1424. doi:10.1056/NEJMoa1606220
- Dearnaley D, Syndikus I, Mossop H, et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016;17:1047-1060. doi:10.1016/S1470-2045(16)30102-4
- Catton CN, Lukka H, Gu CS, et al. Randomized trial of a hypofractionated radiation regimen for the treatment of localized prostate cancer. J Clin Oncol. 2017;35:1884-1890. doi:10.1200/JCO.2016.71.7397
- Lee WR, Dignam JJ, Amin MB, et al. Long-term analysis of NRG Oncology RTOG 0415: a randomized phase III noninferiority study comparing two fractionation schedules in patients with low-risk prostate cancer. J Clin Oncol. 2024;42:2377-2381. doi:10.1200/JCO.23.02445
- de Vries KC, Wortel RC, Oomen-de Hoop E, et al. Hypofractionated versus conventionally fractionated radiation therapy for patients with intermediate- or high-risk, localized, prostate cancer: 7-year outcomes from the randomized, multicenter, open-label, phase 3 HYPRO trial. Int J Radiat Oncol Biol Phys. 2020;106:108-115. doi:10.1016/j.ijrobp.2019.09.007
- Incrocci L, Wortel RC, Alemayehu WG, et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with localised prostate cancer (HYPRO): final efficacy results from a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2016;17:1061-1069. doi:10.1016/S1470-2045(16)30070-5
- Widmark A, Gunnlaugsson A, Beckman L, et al. Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial. Lancet. 2019;394:385-395. doi:10.1016/S0140-6736(19)31131-6
- Brenner DJ, Hall EJ. Fractionation and protraction for radiotherapy of prostate carcinoma. Int J Radiat Oncol Biol Phys. 1999;43:1095-101. doi:10.1016/s0360-3016(98)00438-6
- Dasu A. Is the alpha/beta value for prostate tumours low enough to be safely used in clinical trials? Clin Oncol (R Coll Radiol). 2007;19:289-301. doi:10.1016/j.clon.2007.02.007
- Garcia-Barros M, Paris F, Cordon-Cardo C, et al. Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science. 2003;300:1155-1159. doi:10.1126/science.1082504
- Gulliford S, Hall E, Dearnaley D. Hypofractionation trials and radiobiology of prostate cancer. Oncoscience. 2017;4:27-28. doi:10.18632/oncoscience.347
- Fuks Z, Kolesnick R. Engaging the vascular component of the tumor response. Cancer Cell. 2005;8:89-91. doi:10.1016/j.ccr.2005.07.014
- van As N, Griffin C, Tree A, et al. Phase 3 Trial of stereotactic body radiotherapy in localized prostate cancer. N Engl J Med. Oct 17 2024;391:1413-1425. doi:10.1056/NEJMoa2403365
- National Comprehensive Cancer Network. NCCN Guidelines Version 5. 2026 Prostate Cancer. Accessed March 24, 2026. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
- Lawton CA, Michalski J, El-Naqa I, et al. RTOG GU radiation oncology specialists reach consensus on pelvic lymph node volumes for high-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2009;74:383-387. doi:10.1016/j.ijrobp.2008.08.002
- Lehrer EJ, Kishan AU, Yu JB, et al. Ultrahypofractionated versus hypofractionated and conventionally fractionated radiation therapy for localized prostate cancer: a systematic review and meta-analysis of phase III randomized trials. Radiother Oncol. 2020;148:235-242. doi:10.1016/j.radonc.2020.04.037
- De Cooman B, Debacker T, Adams T, et al. Stereotactic body radiotherapy (SBRT) as a treatment for localized prostate cancer: a retrospective analysis. Radiat Oncol. 2025;20:25. doi:10.1186/s13014-025-02598-8
- Fuller DB, Falchook AD, Crabtree T, et al. Phase 2 multicenter trial of heterogeneous-dosing stereotactic body radiotherapy for low- and intermediate-risk prostate cancer: 5-year outcomes. Eur Urol Oncol. 2018;1:540-547. doi:10.1016/j.euo.2018.06.013
- Jackson WC, Silva J, Hartman HE, et al. Stereotactic body radiation therapy for localized prostate cancer: a systematic review and meta-analysis of over 6,000 patients treated on prospective studies. Int J Radiat Oncol Biol Phys. 2019;104:778-789. doi:10.1016/j.ijrobp.2019.03.051
- Meier RM, Bloch DA, Cotrutz C, et al. Multicenter trial of stereotactic body radiation therapy for low- and intermediate-risk prostate cancer: survival and toxicity endpoints. nt J Radiat Oncol Biol Phys. 2018;102:296-303. doi:10.1016/j.ijrobp.2018.05.040
- Quon HC, Ong A, Cheung P, et al. Once-weekly versus every-other-day stereotactic body radiotherapy in patients with prostate cancer (PATRIOT): a phase 2 randomized trial. Radiother Oncol. 2018;127:206-212. doi:10.1016/j.radonc.2018.02.029
- Zelefsky MJ, Kollmeier M, McBride S, et al. Five-year outcomes of a phase 1 dose-escalation study using stereotactic body radiosurgery for patients with low-risk and intermediate-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2019;104:42-49. doi:10.1016/j.ijrobp.2018.12.045
Early Outcomes of Stereotactic Body Radiotherapy for Localized Prostate Cancer: A Retrospective Analysis
Early Outcomes of Stereotactic Body Radiotherapy for Localized Prostate Cancer: A Retrospective Analysis

Capturing Pathology Workload Associated With Precision Oncology
Capturing Pathology Workload Associated With Precision Oncology
Precision oncology (PO) is cancer treatment individualized to the special characteristics of a patient’s tumor. It has become standard care for most patients with advanced cancer. Advances in molecular cell biology and immunology have identified numerous targets and many therapies have been developed as a result. Molecular testing and targeted therapy are typically covered by insurance, even when inflation-adjusted price growth is considered.1 Barriers remain, however, and pathologists are uniquely qualified to address some of the challenges.2
Most US laboratories do not perform molecular diagnostic tests for PO, particularly comprehensive evaluation of multiple targets by next-generation sequencing, or other techniques. Instead, these tests are sent to reference laboratories. The workload associated with referral testing is an obstacle to increased use of such tests. Despite guideline recommendations, a minority of indicated tests are performed.3 This is true even when testing costs are covered by clinical trials or grants, such as those in the Veterans Health Administration (VHA).
The main characteristic of successful PO programs is a multidisciplinary commitment, including pathology involvement in molecular tumor boards and assistance with test selection, tissue collection, and result interpretation.2 This, however, adds to the workload for the pathology department, an underappreciated phenomenon in the context of pathology workforce shortages.4
Workforce shortages impact all occupations in the laboratory setting. Though the shortage of medical technologists in clinical pathology laboratories has repeatedly been identified as critical at the VHA as well as in the private sector, the same cannot be said for staff shortages in anatomic pathology laboratories. Thus, the hospital laboratory divisions are concerned with biopsy or resection tissue specimens as opposed to the bodily fluid specimens that predominate in clinical laboratories.5 The lack of accurate data on histopathology technicians and technologists has precluded the degree of recognition seen for medical technologists. In labor statistics, these occupations are often obscured by inclusion with other jobs in broad categories such as medical and clinical laboratory technologists and technicians.6 Vacancy—the principal metric used to assess medical laboratory workforce shortage—fails to account for positions that are eventually eliminated after remaining vacant for prolonged periods, positions not replaced as a result of ambitious efficiency measures, or positions that were never created due to insufficient funding, reasons for administrative disapproval, or coverage by laboratory professionals working extra shifts or second jobs.7
Increased demand for pathologists is suggested by a 42% increase in workload per pathologist over the last decade, while a shortage is suggested by decreases in absolute and population-adjusted numbers of pathologists.8,9 An influx of pathologists is not an expected remedy due to the global decline in medical graduates pursuing careers in the field.8
Approximations for required labor and potential revenue generation are necessary to justify creation of pathology positions. This work mostly has gone uncaptured due to the limitations of Current Procedural Terminology (CPT) codes. Few laboratories have consistently used the 88363, 88325, and G0452 CPT codes. The pathology clinical consultation CPT codes (80503-80506) released in 2022 enhance acquisition of this work. The new codes replace 80500 and 80502 and allow for more precise identification of any work requiring medical judgment that a pathologist does at the request of another qualified health care professional (HCP) or as required by federal or state regulation.
The codes can be used to bill for associated time spent reviewing health records, communicating with other HCPs, placing orders, and documentation. An HCP can bill according to level of medical decision-making (MDM) or time spent by the consulting pathologist. Code 80503 can be billed for 5 to 20 minutes of a pathologist's time, 80504 for 21 to 40 minutes, 80505 for 41 to 60 minutes, and 80506 for each additional 30 minutes after the first hour. Levels of MDM (low, moderate, and high) are defined as for other evaluation and management services. A consultation report must be generated and contain documentation of the consultation request, pathologist interpretation, and justification for the level of service associated with the chosen code. Relative value units (RVUs) and reimbursement associated with each as well as other consultation-related codes are available in Table 1.
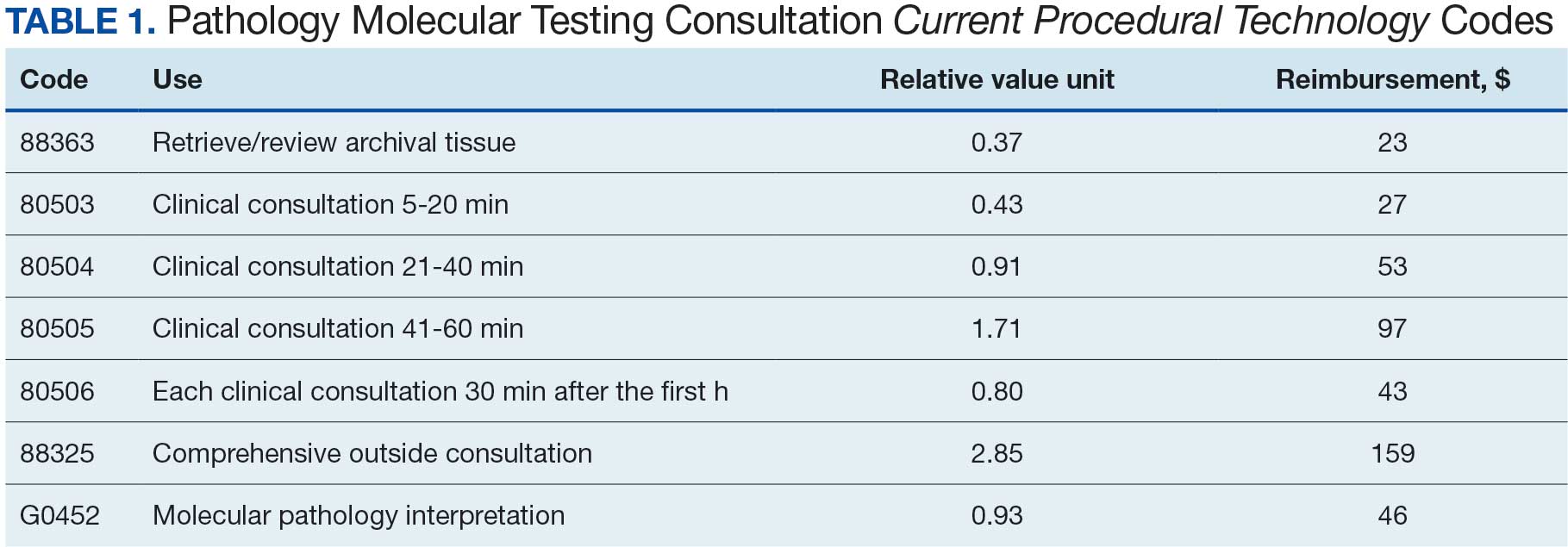
This article outlines how the pathology time investment associated with anatomic pathology molecular testing at the Kansas City Veterans Affairs Medical Center (KCVAMC) can be captured using the consultation process and new CPT codes. Staff included 4 pathologists, 3 histotechnologists, 1 histology supervisor, 1 grossing room technician, and 1 cytotechnologist, 1 cytology technician.
METHODS
The AP molecular testing consultation process at the KCVAMC was mapped, with the average time measured for each step (Figure). AP records for 2021 were reviewed to determine the number of AP molecular send out tests. Cumulative time investment was calculated in hours and a theoretical number of RVUs was calculated using the new pathology clinical consultation CPT codes (80503-80506). This theoretical number of RVUs was compared with the total AP RVUs generated in 2021 to determine a potential increase in RVUs with use of the new CPT codes to capture pathology work associated with AP molecular testing consultations.
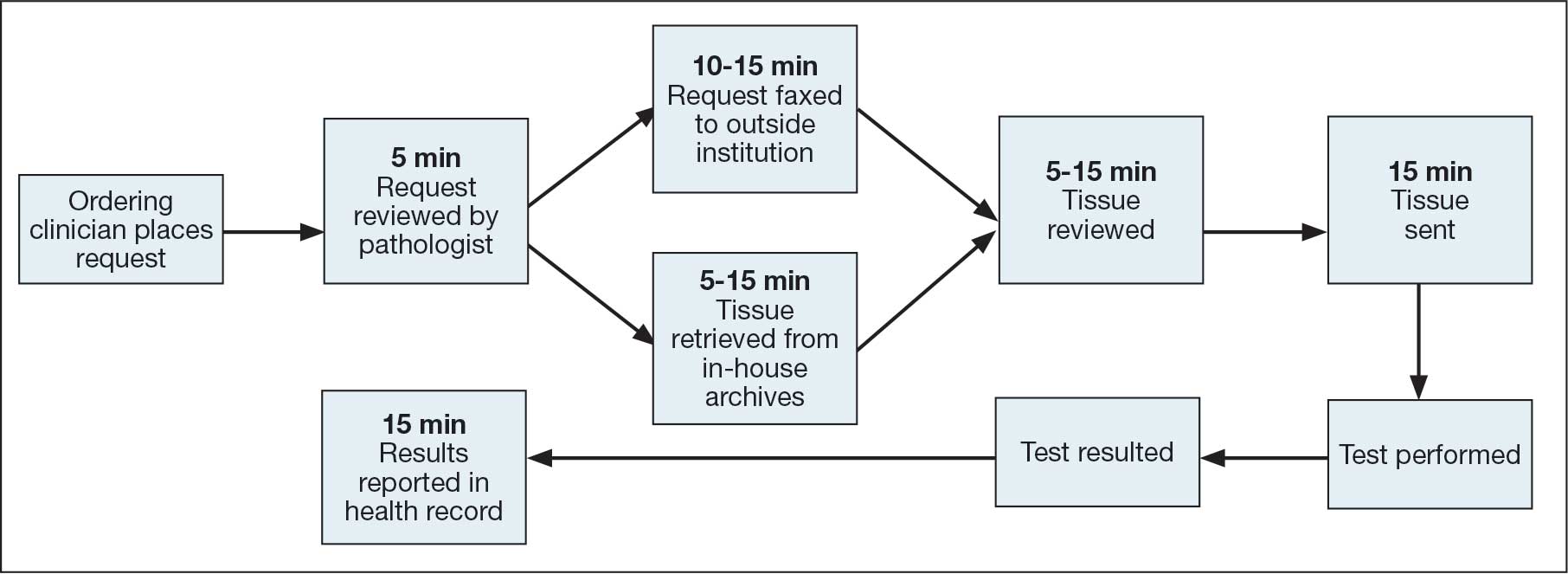
RESULTS
From 2021 to 2023, there were 21,021 AP cases at the KCVAMC. Basal cell carcinomas and squamous cell carcinomas of the skin were excluded because they comprise most cancer cases but almost never necessitate AP molecular test consultations. A total of 2118 cancer cases were included, representing 10.1% of all cases. Ancillary AP molecular send-out tests were performed on 1338 (6.4%) cases. Since ancillary tissue tests are requested by consultation at the KCVAMC, this resulted in 1338 consultations (Table 2).
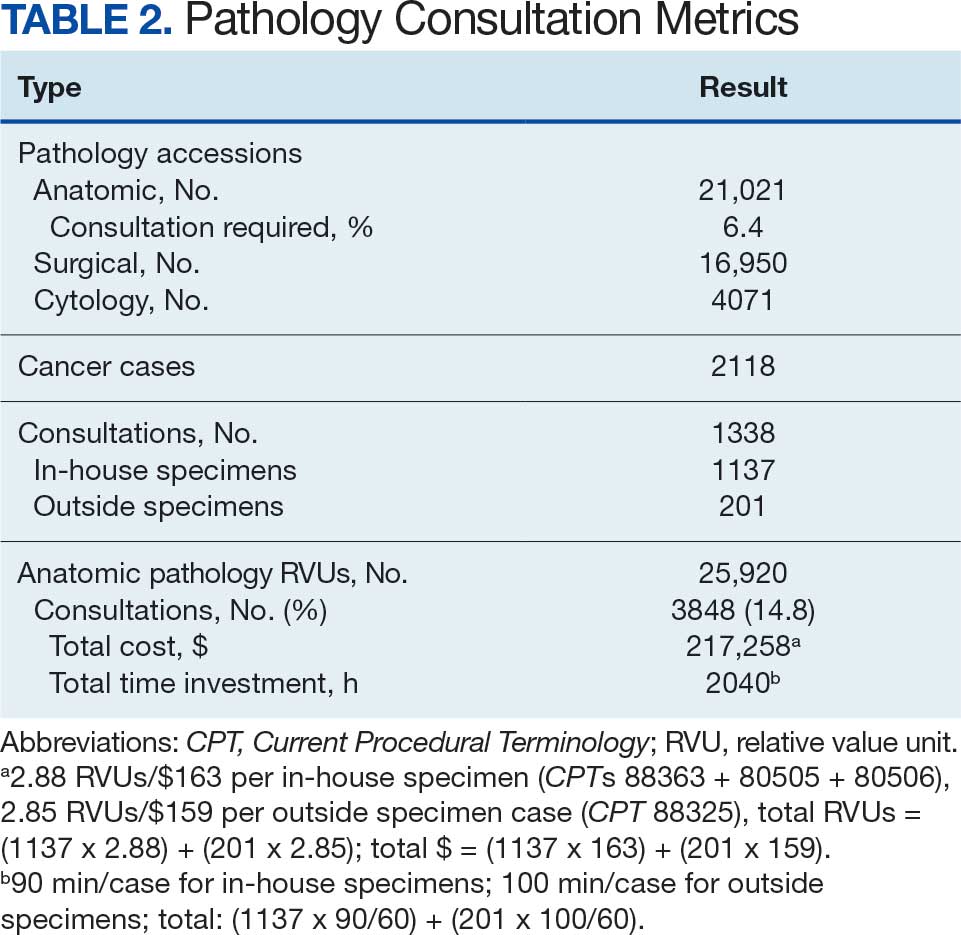
The time to complete a consultation was measured by calculating the mean time required to complete each step (Table 3). With in-house specimen consultations requiring 90 minutes each and outside specimen consultations requiring 100 minutes each, a total of 2040 hours of pathology staff time was necessary to complete associated consultations. Billing for this time with the new pathology clinical consultation CPT codes would generate 3847 RVUs, which would have equated to 14.8% (3847/25,920) of the anatomic pathology RVUs.
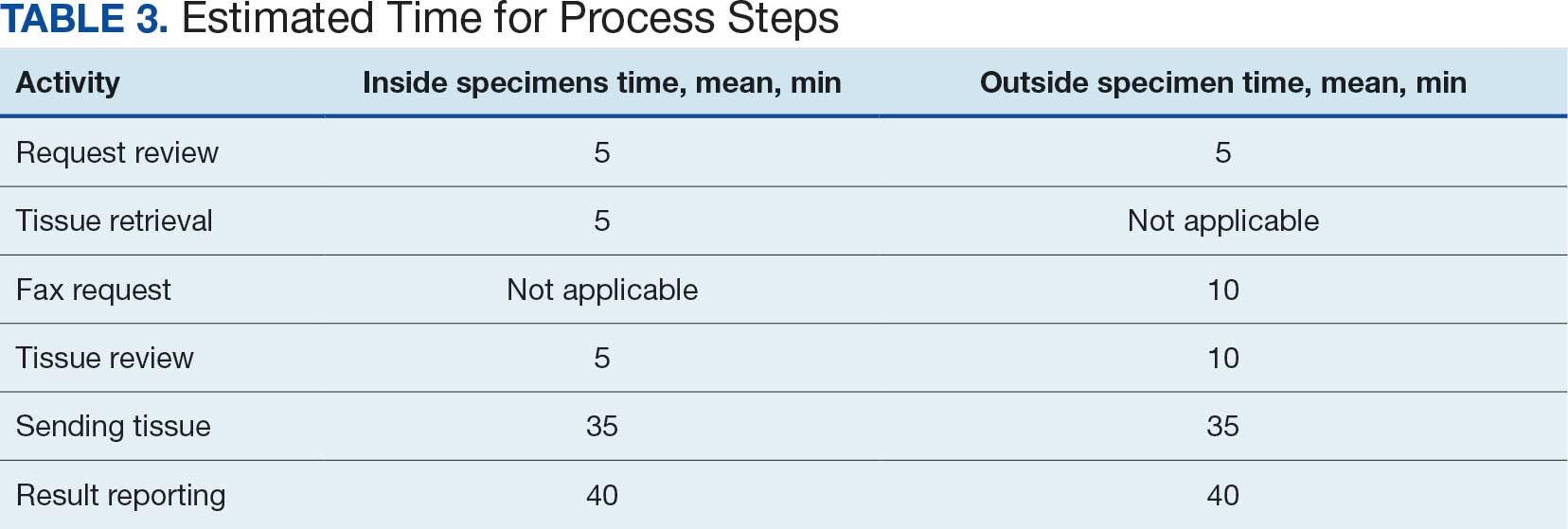
DISCUSSION
When considering the lengths of time for tasks associated with each consultation, it is important to remember that the volume (2-3 daily), was insufficient to meaningfully benefit from batching. Thus, waiting to perform a particular task until it was needed for multiple cases reduced the inefficiency associated with starting and switching between tasks. Both the Computerized Patient Record System and VistA had to be reopened, reauthenticated, and reloaded for each step that required use of the health record, printer, or fax machine. Faxes also required waiting for transmission and printed confirmation of successful transmission. As a result, the time values denoted for each step are likely underestimated, as the effect of interruptions is significant and not reflected in the estimates recorded.10
This analysis has demonstrated that PO entails a significant amount of work for pathology departments. To determine and maintain appropriate staffing models, this work must be captured and reimbursed. Unlike other pathology work, which is performed in-house and reimbursed for the associated test, a significant proportion of PO testing is sent out. Even if more reliable assays are developed, the physical processes of sending out samples and reporting test results cannot be outsourced. Independent and commensurate reimbursement methods are necessary to allow for this work and PO.
CMS included new pathology clinical consultation codes that may be used to bill for some of this work according to the 2022 physician fee schedule due to advocacy work by the College of American Pathologists and the American Medical Association CPT editorial panel.11
CONCLUSIONS
This analysis found that adoption of PO may present a significant amount of additional work for pathology departments. To determine and maintain appropriate staffing models, work completed by pathologists in this manner must be recorded and reimbursed. Pathologists need to be trained and encouraged to use these CPT codes and bill for the work described in this article. The increased revenue will allow for additional positions to alleviate the burdens imposed by understaffing so that pathology can function as a facilitator of PO rather than as a barrier to it.
- Wilson LE, Greiner MA, Altomare I, et al. Rapid rise in the cost of targeted cancer therapies for Medicare patients with solid tumors from 2006 to 2015. J Geriatr Oncol. 2021;12:375-380. doi:10.1016/j.jgo.2020.11.007
- Ersek JL, Black LJ, Thompson MA, et al. Implementing precision medicine programs and clinical trials in the community-based oncology practice: barriers and best practices. Am Soc Clin Oncol Educ Book. 2018;38:188-196. doi:10.1200/EDBK_200633
- Inal C, Yilmaz E, Cheng H, et al. Effect of reflex testing by pathologists on molecular testing rates in lung cancer patients: experience from a community-based academic center. J Clin Oncol. 2014;32:8098. doi:10.1200/jco.2014.32.15_suppl.8098
- Robboy SJ, Gupta S, Crawford JM, et al. The pathologist workforce in the United States: II. an interactive modeling tool for analyzing future qualitative and quantitative staffing demands for services. Arch Pathol Lab Med. 2015;139:1413-1430. doi:10.5858/arpa.2014-0559-OA
- OIG determination of Veterans Health Administration’s occupational staffing shortages fiscal year 2021. Department of Veterans Affairs OIG. September 28, 2021. Accessed January 30, 2026. https://www.oversight.gov/report/VA/OIG-determination-veterans-health-administrations-occupational-staffing-shortages-fiscal
- Zanto S, Cremeans L, Deutsch-Keahey D, et al. Addressing the clinical laboratory workforce shortage. The American Society for Clinical Laboratory Science. July 2, 2020. Accessed January 30, 2026. https://ascls.org/addressing-the-clinical-laboratory-workforce-shortage/
- Bennett A, Garcia E, Schulze M, et al. Building a laboratory workforce to meet the future: ASCP Task Force on the Laboratory Professionals Workforce. Am J Clin Pathol. 2014;141:154-167. doi:10.1309/AJCPIV2OG8TEGHHZ
- Fielder T, Watts F, Howden C, et al. Why choose a pathology career? Arch Pathol Lab Med. 2022;146:903-910. doi:10.5858/arpa.2021-0118-OA
- Metter DM, Colgan TJ, Leung ST, et al. Trends in the US and Canadian pathologist workforces from 2007 to 2017. JAMA Netw Open. 2019;2:e194337. doi:10.1001/jamanetworkopen.2019.4337
- Schulte B. Work interruptions can cost you 6 hours a day. An efficiency expert explains how to avoid them. The Washington Post. June 1, 2015. Accessed January 30, 2026. https://www.washingtonpost.com/news/inspired-life/wp/2015/06/01/interruptions-at-work-can-cost-you-up-to-6-hours-a-day-heres-how-to-avoid-them/
- Fiegl C. Medicare adopts new clinical consult billing codes. College of American Pathologists Today. December 2021. Accessed January 30, 2026. https://www.captodayonline.com/medicare-adopts-new-clinical-consult-billing-code
Precision oncology (PO) is cancer treatment individualized to the special characteristics of a patient’s tumor. It has become standard care for most patients with advanced cancer. Advances in molecular cell biology and immunology have identified numerous targets and many therapies have been developed as a result. Molecular testing and targeted therapy are typically covered by insurance, even when inflation-adjusted price growth is considered.1 Barriers remain, however, and pathologists are uniquely qualified to address some of the challenges.2
Most US laboratories do not perform molecular diagnostic tests for PO, particularly comprehensive evaluation of multiple targets by next-generation sequencing, or other techniques. Instead, these tests are sent to reference laboratories. The workload associated with referral testing is an obstacle to increased use of such tests. Despite guideline recommendations, a minority of indicated tests are performed.3 This is true even when testing costs are covered by clinical trials or grants, such as those in the Veterans Health Administration (VHA).
The main characteristic of successful PO programs is a multidisciplinary commitment, including pathology involvement in molecular tumor boards and assistance with test selection, tissue collection, and result interpretation.2 This, however, adds to the workload for the pathology department, an underappreciated phenomenon in the context of pathology workforce shortages.4
Workforce shortages impact all occupations in the laboratory setting. Though the shortage of medical technologists in clinical pathology laboratories has repeatedly been identified as critical at the VHA as well as in the private sector, the same cannot be said for staff shortages in anatomic pathology laboratories. Thus, the hospital laboratory divisions are concerned with biopsy or resection tissue specimens as opposed to the bodily fluid specimens that predominate in clinical laboratories.5 The lack of accurate data on histopathology technicians and technologists has precluded the degree of recognition seen for medical technologists. In labor statistics, these occupations are often obscured by inclusion with other jobs in broad categories such as medical and clinical laboratory technologists and technicians.6 Vacancy—the principal metric used to assess medical laboratory workforce shortage—fails to account for positions that are eventually eliminated after remaining vacant for prolonged periods, positions not replaced as a result of ambitious efficiency measures, or positions that were never created due to insufficient funding, reasons for administrative disapproval, or coverage by laboratory professionals working extra shifts or second jobs.7
Increased demand for pathologists is suggested by a 42% increase in workload per pathologist over the last decade, while a shortage is suggested by decreases in absolute and population-adjusted numbers of pathologists.8,9 An influx of pathologists is not an expected remedy due to the global decline in medical graduates pursuing careers in the field.8
Approximations for required labor and potential revenue generation are necessary to justify creation of pathology positions. This work mostly has gone uncaptured due to the limitations of Current Procedural Terminology (CPT) codes. Few laboratories have consistently used the 88363, 88325, and G0452 CPT codes. The pathology clinical consultation CPT codes (80503-80506) released in 2022 enhance acquisition of this work. The new codes replace 80500 and 80502 and allow for more precise identification of any work requiring medical judgment that a pathologist does at the request of another qualified health care professional (HCP) or as required by federal or state regulation.
The codes can be used to bill for associated time spent reviewing health records, communicating with other HCPs, placing orders, and documentation. An HCP can bill according to level of medical decision-making (MDM) or time spent by the consulting pathologist. Code 80503 can be billed for 5 to 20 minutes of a pathologist's time, 80504 for 21 to 40 minutes, 80505 for 41 to 60 minutes, and 80506 for each additional 30 minutes after the first hour. Levels of MDM (low, moderate, and high) are defined as for other evaluation and management services. A consultation report must be generated and contain documentation of the consultation request, pathologist interpretation, and justification for the level of service associated with the chosen code. Relative value units (RVUs) and reimbursement associated with each as well as other consultation-related codes are available in Table 1.
This article outlines how the pathology time investment associated with anatomic pathology molecular testing at the Kansas City Veterans Affairs Medical Center (KCVAMC) can be captured using the consultation process and new CPT codes. Staff included 4 pathologists, 3 histotechnologists, 1 histology supervisor, 1 grossing room technician, and 1 cytotechnologist, 1 cytology technician.
METHODS
The AP molecular testing consultation process at the KCVAMC was mapped, with the average time measured for each step (Figure). AP records for 2021 were reviewed to determine the number of AP molecular send out tests. Cumulative time investment was calculated in hours and a theoretical number of RVUs was calculated using the new pathology clinical consultation CPT codes (80503-80506). This theoretical number of RVUs was compared with the total AP RVUs generated in 2021 to determine a potential increase in RVUs with use of the new CPT codes to capture pathology work associated with AP molecular testing consultations.
RESULTS
From 2021 to 2023, there were 21,021 AP cases at the KCVAMC. Basal cell carcinomas and squamous cell carcinomas of the skin were excluded because they comprise most cancer cases but almost never necessitate AP molecular test consultations. A total of 2118 cancer cases were included, representing 10.1% of all cases. Ancillary AP molecular send-out tests were performed on 1338 (6.4%) cases. Since ancillary tissue tests are requested by consultation at the KCVAMC, this resulted in 1338 consultations (Table 2).
The time to complete a consultation was measured by calculating the mean time required to complete each step (Table 3). With in-house specimen consultations requiring 90 minutes each and outside specimen consultations requiring 100 minutes each, a total of 2040 hours of pathology staff time was necessary to complete associated consultations. Billing for this time with the new pathology clinical consultation CPT codes would generate 3847 RVUs, which would have equated to 14.8% (3847/25,920) of the anatomic pathology RVUs.
DISCUSSION
When considering the lengths of time for tasks associated with each consultation, it is important to remember that the volume (2-3 daily), was insufficient to meaningfully benefit from batching. Thus, waiting to perform a particular task until it was needed for multiple cases reduced the inefficiency associated with starting and switching between tasks. Both the Computerized Patient Record System and VistA had to be reopened, reauthenticated, and reloaded for each step that required use of the health record, printer, or fax machine. Faxes also required waiting for transmission and printed confirmation of successful transmission. As a result, the time values denoted for each step are likely underestimated, as the effect of interruptions is significant and not reflected in the estimates recorded.10
This analysis has demonstrated that PO entails a significant amount of work for pathology departments. To determine and maintain appropriate staffing models, this work must be captured and reimbursed. Unlike other pathology work, which is performed in-house and reimbursed for the associated test, a significant proportion of PO testing is sent out. Even if more reliable assays are developed, the physical processes of sending out samples and reporting test results cannot be outsourced. Independent and commensurate reimbursement methods are necessary to allow for this work and PO.
CMS included new pathology clinical consultation codes that may be used to bill for some of this work according to the 2022 physician fee schedule due to advocacy work by the College of American Pathologists and the American Medical Association CPT editorial panel.11
CONCLUSIONS
This analysis found that adoption of PO may present a significant amount of additional work for pathology departments. To determine and maintain appropriate staffing models, work completed by pathologists in this manner must be recorded and reimbursed. Pathologists need to be trained and encouraged to use these CPT codes and bill for the work described in this article. The increased revenue will allow for additional positions to alleviate the burdens imposed by understaffing so that pathology can function as a facilitator of PO rather than as a barrier to it.
Precision oncology (PO) is cancer treatment individualized to the special characteristics of a patient’s tumor. It has become standard care for most patients with advanced cancer. Advances in molecular cell biology and immunology have identified numerous targets and many therapies have been developed as a result. Molecular testing and targeted therapy are typically covered by insurance, even when inflation-adjusted price growth is considered.1 Barriers remain, however, and pathologists are uniquely qualified to address some of the challenges.2
Most US laboratories do not perform molecular diagnostic tests for PO, particularly comprehensive evaluation of multiple targets by next-generation sequencing, or other techniques. Instead, these tests are sent to reference laboratories. The workload associated with referral testing is an obstacle to increased use of such tests. Despite guideline recommendations, a minority of indicated tests are performed.3 This is true even when testing costs are covered by clinical trials or grants, such as those in the Veterans Health Administration (VHA).
The main characteristic of successful PO programs is a multidisciplinary commitment, including pathology involvement in molecular tumor boards and assistance with test selection, tissue collection, and result interpretation.2 This, however, adds to the workload for the pathology department, an underappreciated phenomenon in the context of pathology workforce shortages.4
Workforce shortages impact all occupations in the laboratory setting. Though the shortage of medical technologists in clinical pathology laboratories has repeatedly been identified as critical at the VHA as well as in the private sector, the same cannot be said for staff shortages in anatomic pathology laboratories. Thus, the hospital laboratory divisions are concerned with biopsy or resection tissue specimens as opposed to the bodily fluid specimens that predominate in clinical laboratories.5 The lack of accurate data on histopathology technicians and technologists has precluded the degree of recognition seen for medical technologists. In labor statistics, these occupations are often obscured by inclusion with other jobs in broad categories such as medical and clinical laboratory technologists and technicians.6 Vacancy—the principal metric used to assess medical laboratory workforce shortage—fails to account for positions that are eventually eliminated after remaining vacant for prolonged periods, positions not replaced as a result of ambitious efficiency measures, or positions that were never created due to insufficient funding, reasons for administrative disapproval, or coverage by laboratory professionals working extra shifts or second jobs.7
Increased demand for pathologists is suggested by a 42% increase in workload per pathologist over the last decade, while a shortage is suggested by decreases in absolute and population-adjusted numbers of pathologists.8,9 An influx of pathologists is not an expected remedy due to the global decline in medical graduates pursuing careers in the field.8
Approximations for required labor and potential revenue generation are necessary to justify creation of pathology positions. This work mostly has gone uncaptured due to the limitations of Current Procedural Terminology (CPT) codes. Few laboratories have consistently used the 88363, 88325, and G0452 CPT codes. The pathology clinical consultation CPT codes (80503-80506) released in 2022 enhance acquisition of this work. The new codes replace 80500 and 80502 and allow for more precise identification of any work requiring medical judgment that a pathologist does at the request of another qualified health care professional (HCP) or as required by federal or state regulation.
The codes can be used to bill for associated time spent reviewing health records, communicating with other HCPs, placing orders, and documentation. An HCP can bill according to level of medical decision-making (MDM) or time spent by the consulting pathologist. Code 80503 can be billed for 5 to 20 minutes of a pathologist's time, 80504 for 21 to 40 minutes, 80505 for 41 to 60 minutes, and 80506 for each additional 30 minutes after the first hour. Levels of MDM (low, moderate, and high) are defined as for other evaluation and management services. A consultation report must be generated and contain documentation of the consultation request, pathologist interpretation, and justification for the level of service associated with the chosen code. Relative value units (RVUs) and reimbursement associated with each as well as other consultation-related codes are available in Table 1.
This article outlines how the pathology time investment associated with anatomic pathology molecular testing at the Kansas City Veterans Affairs Medical Center (KCVAMC) can be captured using the consultation process and new CPT codes. Staff included 4 pathologists, 3 histotechnologists, 1 histology supervisor, 1 grossing room technician, and 1 cytotechnologist, 1 cytology technician.
METHODS
The AP molecular testing consultation process at the KCVAMC was mapped, with the average time measured for each step (Figure). AP records for 2021 were reviewed to determine the number of AP molecular send out tests. Cumulative time investment was calculated in hours and a theoretical number of RVUs was calculated using the new pathology clinical consultation CPT codes (80503-80506). This theoretical number of RVUs was compared with the total AP RVUs generated in 2021 to determine a potential increase in RVUs with use of the new CPT codes to capture pathology work associated with AP molecular testing consultations.
RESULTS
From 2021 to 2023, there were 21,021 AP cases at the KCVAMC. Basal cell carcinomas and squamous cell carcinomas of the skin were excluded because they comprise most cancer cases but almost never necessitate AP molecular test consultations. A total of 2118 cancer cases were included, representing 10.1% of all cases. Ancillary AP molecular send-out tests were performed on 1338 (6.4%) cases. Since ancillary tissue tests are requested by consultation at the KCVAMC, this resulted in 1338 consultations (Table 2).
The time to complete a consultation was measured by calculating the mean time required to complete each step (Table 3). With in-house specimen consultations requiring 90 minutes each and outside specimen consultations requiring 100 minutes each, a total of 2040 hours of pathology staff time was necessary to complete associated consultations. Billing for this time with the new pathology clinical consultation CPT codes would generate 3847 RVUs, which would have equated to 14.8% (3847/25,920) of the anatomic pathology RVUs.
DISCUSSION
When considering the lengths of time for tasks associated with each consultation, it is important to remember that the volume (2-3 daily), was insufficient to meaningfully benefit from batching. Thus, waiting to perform a particular task until it was needed for multiple cases reduced the inefficiency associated with starting and switching between tasks. Both the Computerized Patient Record System and VistA had to be reopened, reauthenticated, and reloaded for each step that required use of the health record, printer, or fax machine. Faxes also required waiting for transmission and printed confirmation of successful transmission. As a result, the time values denoted for each step are likely underestimated, as the effect of interruptions is significant and not reflected in the estimates recorded.10
This analysis has demonstrated that PO entails a significant amount of work for pathology departments. To determine and maintain appropriate staffing models, this work must be captured and reimbursed. Unlike other pathology work, which is performed in-house and reimbursed for the associated test, a significant proportion of PO testing is sent out. Even if more reliable assays are developed, the physical processes of sending out samples and reporting test results cannot be outsourced. Independent and commensurate reimbursement methods are necessary to allow for this work and PO.
CMS included new pathology clinical consultation codes that may be used to bill for some of this work according to the 2022 physician fee schedule due to advocacy work by the College of American Pathologists and the American Medical Association CPT editorial panel.11
CONCLUSIONS
This analysis found that adoption of PO may present a significant amount of additional work for pathology departments. To determine and maintain appropriate staffing models, work completed by pathologists in this manner must be recorded and reimbursed. Pathologists need to be trained and encouraged to use these CPT codes and bill for the work described in this article. The increased revenue will allow for additional positions to alleviate the burdens imposed by understaffing so that pathology can function as a facilitator of PO rather than as a barrier to it.
- Wilson LE, Greiner MA, Altomare I, et al. Rapid rise in the cost of targeted cancer therapies for Medicare patients with solid tumors from 2006 to 2015. J Geriatr Oncol. 2021;12:375-380. doi:10.1016/j.jgo.2020.11.007
- Ersek JL, Black LJ, Thompson MA, et al. Implementing precision medicine programs and clinical trials in the community-based oncology practice: barriers and best practices. Am Soc Clin Oncol Educ Book. 2018;38:188-196. doi:10.1200/EDBK_200633
- Inal C, Yilmaz E, Cheng H, et al. Effect of reflex testing by pathologists on molecular testing rates in lung cancer patients: experience from a community-based academic center. J Clin Oncol. 2014;32:8098. doi:10.1200/jco.2014.32.15_suppl.8098
- Robboy SJ, Gupta S, Crawford JM, et al. The pathologist workforce in the United States: II. an interactive modeling tool for analyzing future qualitative and quantitative staffing demands for services. Arch Pathol Lab Med. 2015;139:1413-1430. doi:10.5858/arpa.2014-0559-OA
- OIG determination of Veterans Health Administration’s occupational staffing shortages fiscal year 2021. Department of Veterans Affairs OIG. September 28, 2021. Accessed January 30, 2026. https://www.oversight.gov/report/VA/OIG-determination-veterans-health-administrations-occupational-staffing-shortages-fiscal
- Zanto S, Cremeans L, Deutsch-Keahey D, et al. Addressing the clinical laboratory workforce shortage. The American Society for Clinical Laboratory Science. July 2, 2020. Accessed January 30, 2026. https://ascls.org/addressing-the-clinical-laboratory-workforce-shortage/
- Bennett A, Garcia E, Schulze M, et al. Building a laboratory workforce to meet the future: ASCP Task Force on the Laboratory Professionals Workforce. Am J Clin Pathol. 2014;141:154-167. doi:10.1309/AJCPIV2OG8TEGHHZ
- Fielder T, Watts F, Howden C, et al. Why choose a pathology career? Arch Pathol Lab Med. 2022;146:903-910. doi:10.5858/arpa.2021-0118-OA
- Metter DM, Colgan TJ, Leung ST, et al. Trends in the US and Canadian pathologist workforces from 2007 to 2017. JAMA Netw Open. 2019;2:e194337. doi:10.1001/jamanetworkopen.2019.4337
- Schulte B. Work interruptions can cost you 6 hours a day. An efficiency expert explains how to avoid them. The Washington Post. June 1, 2015. Accessed January 30, 2026. https://www.washingtonpost.com/news/inspired-life/wp/2015/06/01/interruptions-at-work-can-cost-you-up-to-6-hours-a-day-heres-how-to-avoid-them/
- Fiegl C. Medicare adopts new clinical consult billing codes. College of American Pathologists Today. December 2021. Accessed January 30, 2026. https://www.captodayonline.com/medicare-adopts-new-clinical-consult-billing-code
- Wilson LE, Greiner MA, Altomare I, et al. Rapid rise in the cost of targeted cancer therapies for Medicare patients with solid tumors from 2006 to 2015. J Geriatr Oncol. 2021;12:375-380. doi:10.1016/j.jgo.2020.11.007
- Ersek JL, Black LJ, Thompson MA, et al. Implementing precision medicine programs and clinical trials in the community-based oncology practice: barriers and best practices. Am Soc Clin Oncol Educ Book. 2018;38:188-196. doi:10.1200/EDBK_200633
- Inal C, Yilmaz E, Cheng H, et al. Effect of reflex testing by pathologists on molecular testing rates in lung cancer patients: experience from a community-based academic center. J Clin Oncol. 2014;32:8098. doi:10.1200/jco.2014.32.15_suppl.8098
- Robboy SJ, Gupta S, Crawford JM, et al. The pathologist workforce in the United States: II. an interactive modeling tool for analyzing future qualitative and quantitative staffing demands for services. Arch Pathol Lab Med. 2015;139:1413-1430. doi:10.5858/arpa.2014-0559-OA
- OIG determination of Veterans Health Administration’s occupational staffing shortages fiscal year 2021. Department of Veterans Affairs OIG. September 28, 2021. Accessed January 30, 2026. https://www.oversight.gov/report/VA/OIG-determination-veterans-health-administrations-occupational-staffing-shortages-fiscal
- Zanto S, Cremeans L, Deutsch-Keahey D, et al. Addressing the clinical laboratory workforce shortage. The American Society for Clinical Laboratory Science. July 2, 2020. Accessed January 30, 2026. https://ascls.org/addressing-the-clinical-laboratory-workforce-shortage/
- Bennett A, Garcia E, Schulze M, et al. Building a laboratory workforce to meet the future: ASCP Task Force on the Laboratory Professionals Workforce. Am J Clin Pathol. 2014;141:154-167. doi:10.1309/AJCPIV2OG8TEGHHZ
- Fielder T, Watts F, Howden C, et al. Why choose a pathology career? Arch Pathol Lab Med. 2022;146:903-910. doi:10.5858/arpa.2021-0118-OA
- Metter DM, Colgan TJ, Leung ST, et al. Trends in the US and Canadian pathologist workforces from 2007 to 2017. JAMA Netw Open. 2019;2:e194337. doi:10.1001/jamanetworkopen.2019.4337
- Schulte B. Work interruptions can cost you 6 hours a day. An efficiency expert explains how to avoid them. The Washington Post. June 1, 2015. Accessed January 30, 2026. https://www.washingtonpost.com/news/inspired-life/wp/2015/06/01/interruptions-at-work-can-cost-you-up-to-6-hours-a-day-heres-how-to-avoid-them/
- Fiegl C. Medicare adopts new clinical consult billing codes. College of American Pathologists Today. December 2021. Accessed January 30, 2026. https://www.captodayonline.com/medicare-adopts-new-clinical-consult-billing-code
Capturing Pathology Workload Associated With Precision Oncology
Capturing Pathology Workload Associated With Precision Oncology
Investigating Real-World Tolerance and Dose Reductions of Oncology Multikinase Inhibitors in a VA Population
Investigating Real-World Tolerance and Dose Reductions of Oncology Multikinase Inhibitors in a VA Population
The US Department of Veterans Affairs (VA) annually treats around 450,000 veterans with cancer and diagnoses an additional 56,000.1,2 Oral multikinase inhibitors (MKIs) are widely used as targeted therapies for many different malignancies. Despite the ease of oral administration, these agents are often accompanied by significant adverse effects (AEs) and drug-drug interactions.3,4 Common AEs include hypertension, cutaneous reactions, gastrointestinal disturbances, proteinuria, and fatigue. Some serious outcomes that may occur are myocardial infarction, thrombosis, nephrotic syndrome, hemorrhage, hepatotoxicity, and gastrointestinal events.5,6 Due to poor tolerability of these AEs, dose reductions, frequent therapy holds, and discontinuation of therapy may occur.
The US Food and Drug Administration recognizes dosing challenges with novel therapies and has created the Oncology Center of Excellence (OCE) Project Optimus initiative to reform dose optimization in oncology drug development. The initiative aims to shift the focus from establishing dose regimens based on the maximum tolerated doses of cytotoxic chemotherapeutics to an emphasis on maximum efficacy, safety, and tolerability, which better reflect real-world dosing.7,8
MKIs can be challenging to manage because of the frequent toxicity-related dose reductions, interruptions, and discontinuations. In a multicenter retrospective study, Schnadig et al investigated dosing characteristics of first-line sunitinib for advanced renal cell carcinoma (RCC) and found that, among 114 patients who experienced AEs while taking sunitinib, 39.5% had dose reductions, 5.3% delayed therapy, 18.4% required additional supportive medications, and 22.8% discontinued sunitinib.9 Overall survival and median progression-free survival of these patients were lower than reported by Motzer et al in a phase 3 clinical trial.10 Schnadig et al concluded that patients treated with sunitinib for RCC in the community setting required more frequent dose reductions and had less time on therapy compared with patients in clinical trials, which ultimately impacted clinical outcomes.9
At the VA North Texas Health Care System (VANTHCS), patients with cancer have difficulty tolerating MKIs and often require dose alterations and/or discontinuation because of drug intolerance rather than discontinuation due to progression. Frequent dose adjustments for toxicity management can place more strain on patients and health care resources because of additional appointments, clinician time, and emergency department visits. Escalating drug costs can also cause concern when prescription doses are unused or changed frequently.
To capture and quantify prescribing practices and dose adjustments, this study evaluated the tolerability of MKIs at VANTHCS. This analysis may also guide clinicians in the selection of starting doses as well as dose titration expectations to optimize MKI therapy.
METHODS
This single-center, retrospective chart review analyzed patients receiving oral oncology MKIs for various malignancies at VANTHCS between January 1, 2014, and October 31, 2024. Participants included adults aged ≥ 18 years with a prescription for axitinib, cabozantinib, lenvatinib, pazopanib, regorafenib, sorafenib, or sunitinib initiated by the hematology/oncology service at VANTHCS. Patients were included if they had follow-up documentation with the hematology/oncology service and/or other VANTHCS clinicians outlining their course of therapy after MKI initiation. Patients were excluded if they did not have sufficient follow-up documentation (eg, transferred care to a non-VA health care practitioner [HCP], moved to another VA health care system), were enrolled in clinical trials, or were prescribed an MKI from a Care in the Community (CITC) prescriber. Electronic health record review and data collection were performed using the VA Computerized Patient Record System and Research Electronic Data Capture. Data were collected from the time of initiation to cessation of therapy and included information regarding therapy changes, progressive disease, and date of death, when available. Data collected included age, sex, race, comorbidities, date of death, type of malignancy and subtypes, cancer stage, MKI used (ie, drug, dose, frequency, schedule, and indication), dates of medication changes (ie, start, adjustment, hold, discontinuation), concurrent antineoplastic treatments, and AEs documented at times of dose change or interruption.
The primary outcome was MKI tolerance determined using relative dose intensity (RDI) and mean and median time on therapy. Two methods are used to calculate RDI that vary in how they approach time on therapy as outlined in Hawn et al.11 This study used method 2, which accounts for holds in therapy by comparing the actual duration of treatment with the duration expected according to treatment protocol. Method 1 compares the prescribed dose with the administered dose and does not adjust for holds.11 Using method 2, the RDI in this study was calculated by dividing the total actual dose given by the total indicated dose for the malignancy being treated, which accounts for duration of treatment.

The total actual dose was the strength, frequency, and days on therapy for each time frame of treatment multiplied together. This method accounted for all dose adjustments and time periods of treatment holds, including patient self-adjustments, prescriber-directed adjustments, and nonadherence determined by HCP documentation and/or prescription data. Similarly, the indicated total dose was calculated by multiplying the indicated strength, frequency, and all days that treatment should have occurred (time from start to finish). Indicated doses were derived from the prescribing information for each malignancy with the exception of sunitinib, for which the off-label dose of 37.5 mg daily was considered a full dose.12,13 The total indicated dose for axitinib was calculated by considering the dose escalation schedule from the prescribing information.
Patients who required dose reductions due to renal/hepatic impairments or drug-drug interactions had their total indicated dose calculated using dose adjustments listed in the prescribing information. The mean RDI for each MKI agent was calculated by averaging the RDI for each prescription. The overall combined mean RDI included the means of all the MKIs reviewed to avoid skewing the results toward an MKI with more prescriptions. RDIs were also calculated for each cancer type for each agent. Additional descriptive secondary outcomes included rates of AEs and adjustments in doses.
RESULTS
Electronic data extraction identified 278 patients with 366 MKI prescriptions, of which 108 veterans with 158 MKI prescriptions were excluded. The top reason for exclusion was patients managed through CITC. Ultimately, 170 veterans with 208 MKI prescriptions managed by the VANTHCS hematology/oncology clinic were included (Table 1). Among patients receiving MKIs, the mean age was 72.7 years, 98% were male, and 99% had metastatic disease.
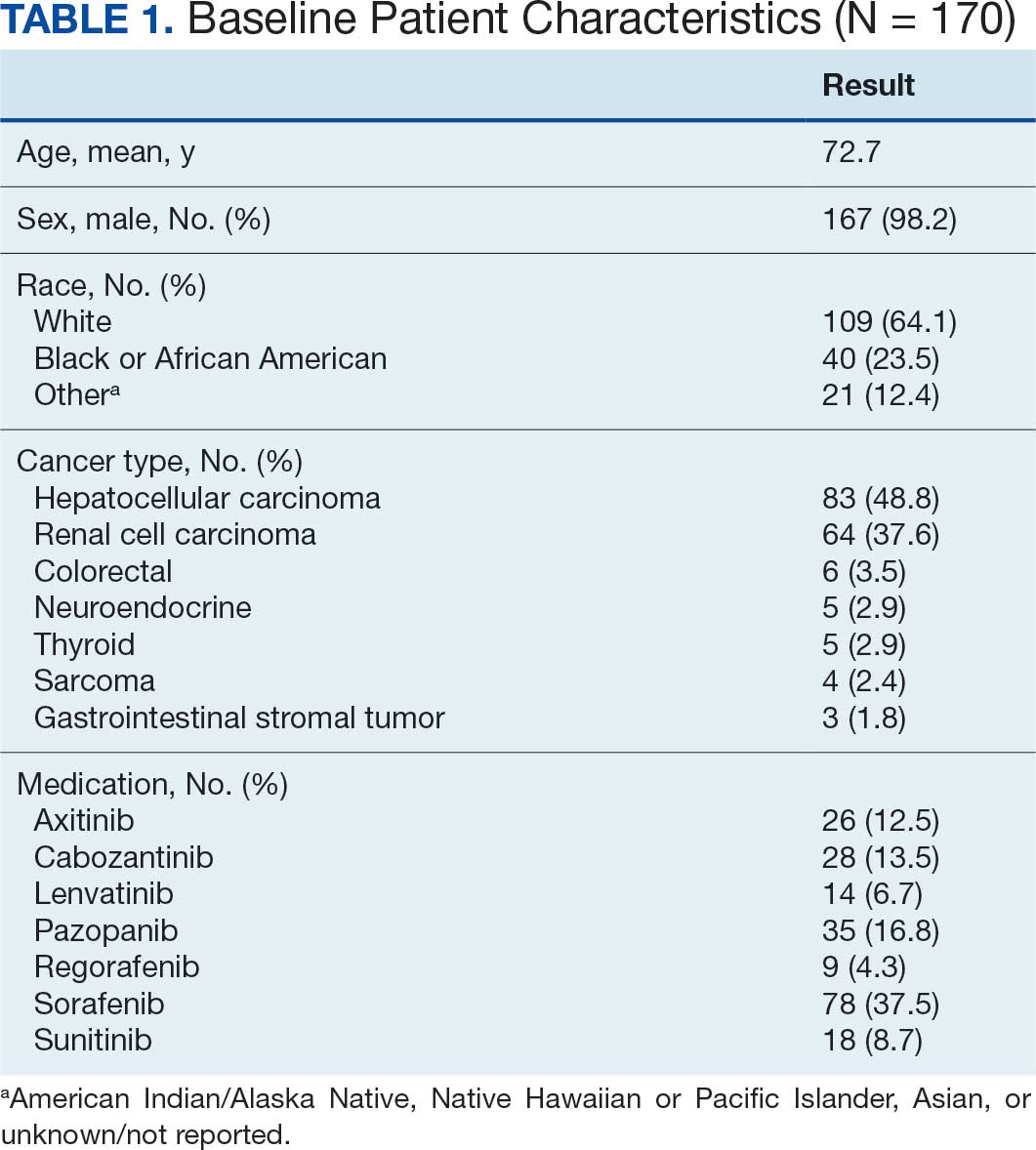
The overall combined mean MKI RDI was 67.5% using method 2 and ranged from 85.5% for sunitinib to 49.0% for sorafenib (Figure 1). Additional information regarding mean and median RDIs using method 2 is shown in Figure 1 and further subdivided by cancer type in Table 2. Median RDIs overall were similar to mean RDIs for most agents. Figure 2 indicates the mean and median time on therapy, reflecting time on therapy excluding days therapy was held. The overall combined mean and median days on therapy for all MKIs were 155 days and 95 days, respectively. Mean time on therapy depended on the agent used and ranged from 35 days (regorafenib) to 237 days (cabozantinib).
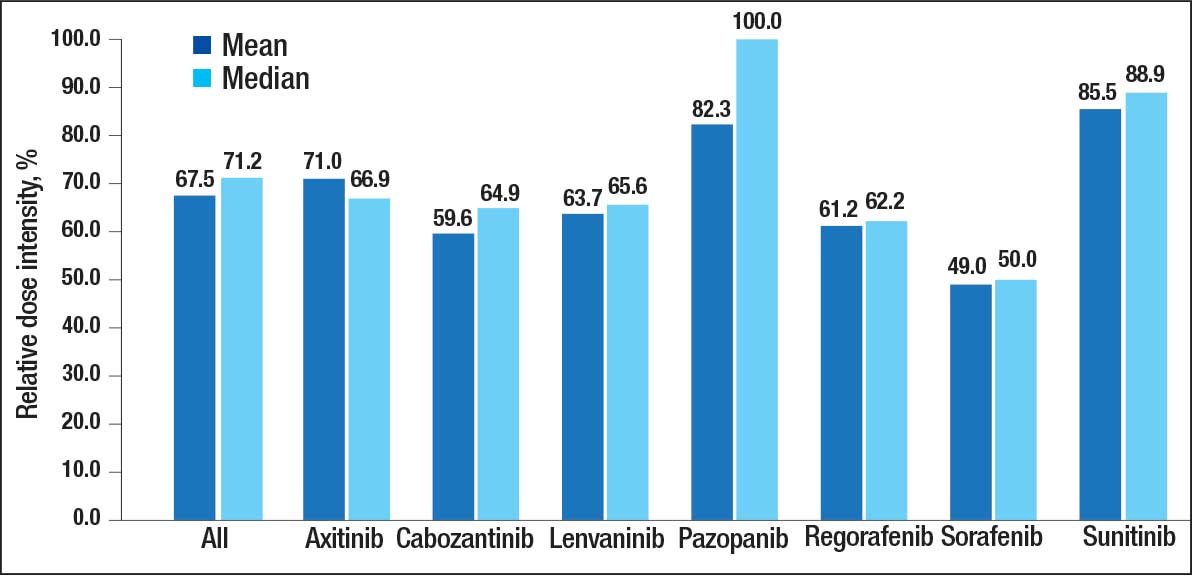
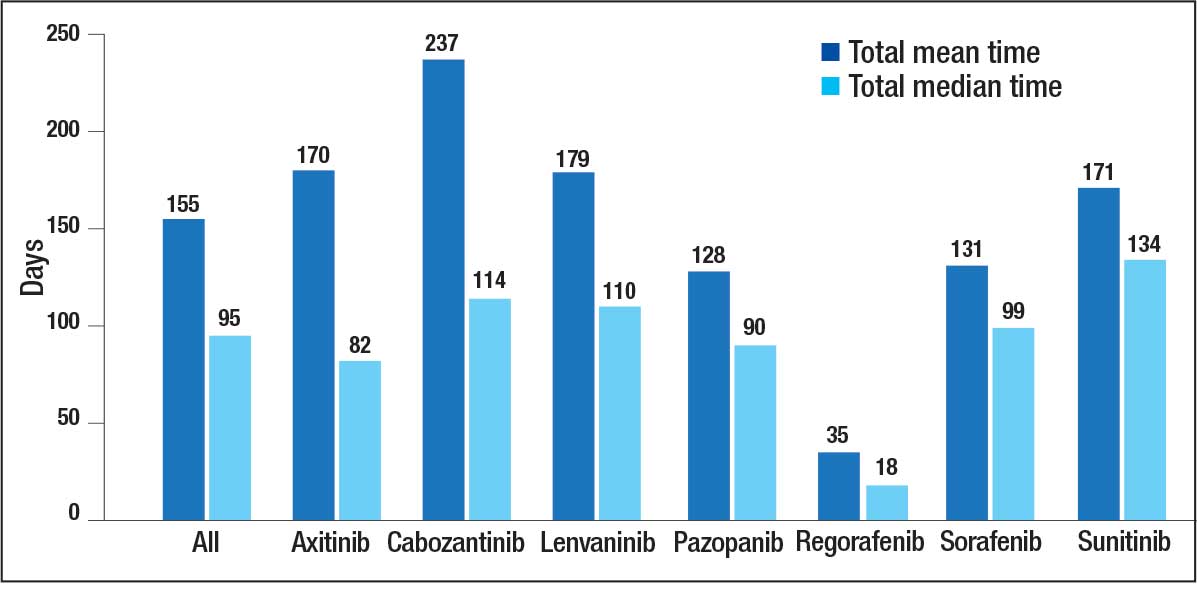
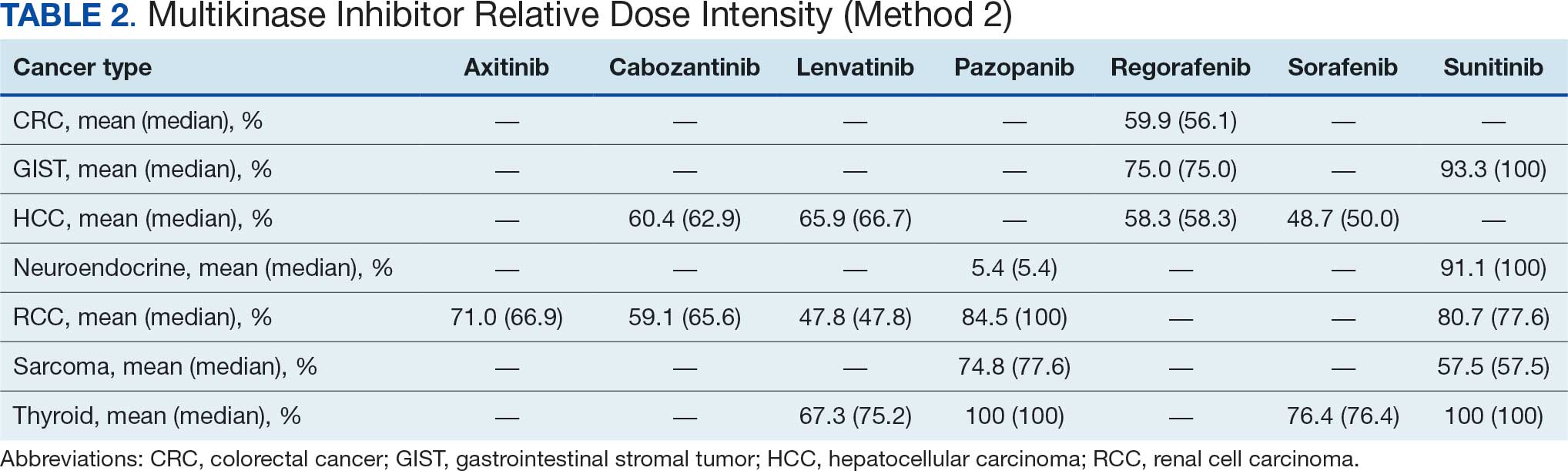
Of 208 MKI prescriptions, 127 (61.1%) were initiated at a reduced dose due to baseline concerns for tolerance such as performance status, frailty, and prior intolerance of other treatments. Eighty-one prescriptions (38.9%) were initiated at their indicated doses. Ninety prescriptions (43.3%) required dose reductions during treatment. Some MKI prescriptions had multiple dose increases and decreases, which is why RDI more accurately reflects dose adjustments. A total of 376 AEs that contributed to a dose adjustment, hold, or discontinuation occurred across all MKI prescriptions. The most common AEs were 82 failure-to-thrive events (21.8%) (fatigue, malaise, loss of appetite, reduced mobility, global decline), 79 gastrointestinal events (21.0%) (nausea, vomiting, diarrhea, abdominal pain), 62 dermatologic events (16.5%) (rash, hand-foot skin reactions, allergic response), 61 hepatic dysfunction events (16.2%) (liver enzyme elevations, hyperbilirubinemia), 40 cardiovascular events (10.6%) (hypertension, heart failure exacerbations, edema), and 33 renal dysfunction events (8.8%) (acute kidney injury, proteinuria) (Appendix 1).
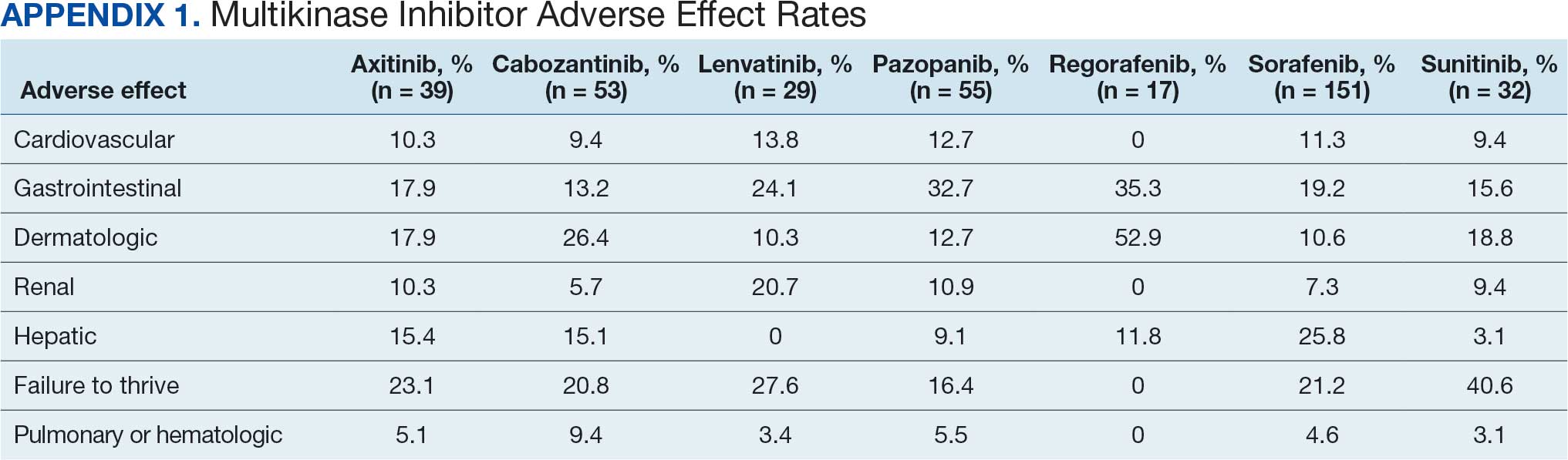
DISCUSSION
The mean RDI of MKI prescriptions used in the veteran population at VANTHCS was about two-thirds of the indicated dose. These results indicate that most veterans required dose reductions and/or holds due to concerns over initial tolerance/performance status, worsening clinical condition, and/or intolerable AEs attributed to treatment. A retrospective study conducted by Denduluri et al suggested that an RDI of < 85% is a clinically meaningful reduction for traditional chemotherapy based on previous literature.14 However, it is less clear what RDI should be expected specifically for MKIs in real-world populations. The MKI phase 3 approval trials in RCC for axitinib, lenvatinib, and sunitinib found median RDIs of 89.4%, 69.6% to 70.4%, and 83.9%, respectively. Each trial cited dose reductions most commonly as the result of treatment-related AEs.15,16
Studies on the impact of RDIs on survival outcomes found that higher RDIs may improve overall and progression-free survival. Retrospective studies inspecting lenvatinib in hepatocellular carcinoma (HCC) indicated that an RDI > 70% in the initial 4 weeks resulted in favorable survival outcomes.17 Similarly, a retrospective study investigating sunitinib in RCC found that an RDI > 60% conferred favorable survival outcomes.18 Alghamdi et al noted that patients taking sorafenib for HCC who had RDI > 50% had a favorable trend in survival characteristics. Interestingly, the study found an RDI of 50% to 75% appeared to have better survival than an RDI > 75%.19 The authors of these studies hypothesized that additional dose reductions allowed for longer total time on therapy due to improved tolerability.17-19
This analysis found that the RDIs for most MKI agents at VANTHCS were < 85% and lower than the RDIs found in other review articles and phase 3 trials, with the exceptions of pazopanib in thyroid cancer and sunitinib in gastrointestinal stromal tumor (GIST), thyroid cancer, and neuroendocrine cancer. The reasons for the lower RDIs in this study are likely multifactorial, reflecting patient population characteristics, off-label dosing practices, and HCP experiences with these agents. Many veterans have chronic comorbidities that could contribute to reduced performance status and ability to tolerate these therapies. Despite attempts to preemptively reduce doses for patients and account for potential impaired tolerance, there were patients who required further dose reductions in our study.
Failure to thrive was the most common AE leading to dose adjustment or discontinuation, which illustrates the extensive effects these agents have on patient functioning in a real-world population. Notably though, the RDI for sunitinib was higher in this population because about half of patients were dosed using the off-label recommendation, whereas the prescribing information recommends a more intensive 6-week dosing cycle for certain cancer types.12,13,20 Sorafenib was also often dose-adjusted based on a pharmacokinetic study of sorafenib in renal/hepatic dysfunction, and the RDI likely reflects the off-label prescribing pattern.21
Patients with thyroid cancer were found to have higher RDIs compared with those receiving the same agents for other cancer types. Improved tolerability of MKIs in thyroid cancer may be due to a generally more tolerable disease course. Thyroid cancer is the most common cancer in individuals aged < 40 years, a population that is often more robust with fewer comorbidities. Moreover, the 5-year relative survival rate for thyroid cancer remains > 98%.22 This rate is in contrast to those for other cancer types such as HCC, with a 5-year relative survival rate of only 15%.23
It is challenging to compare the mean and median times on therapy found in this study with those in current literature, as this review included multiple different cancer types for each agent. However, the numbers are generally lower than durations of therapy found across the different disease states and further emphasize the difficulty in tolerating MKIs in the VANTHCS population. Regorafenib had a short duration of time on therapy, which highlights the importance of trials like ReDOS and initiatives such as OCE Project Optimus in helping improve tolerance.7,8,24
Comparing our results with other studies proved challenging because the RDI calculation methods were not specified. Calculating RDIs in this study using method 1, which does not account for holds, resulted in higher RDIs (Appendix 2). Using method 1, all MKIs had RDIs < 85%, except for pazopanib in thyroid cancer (100%) and RCC (87.9%), and sunitinib in GIST (93.6%), thyroid cancer (100%), and neuroendocrine cancer (93.7%). Notably, using method 1 increased the RDI for pazopanib in neuroendocrine cancer from 5.4% to 50.0%. The low RDI was attributed to a single veteran with a long hold duration, which demonstrates the discrepancy that can occur between the 2 methods.
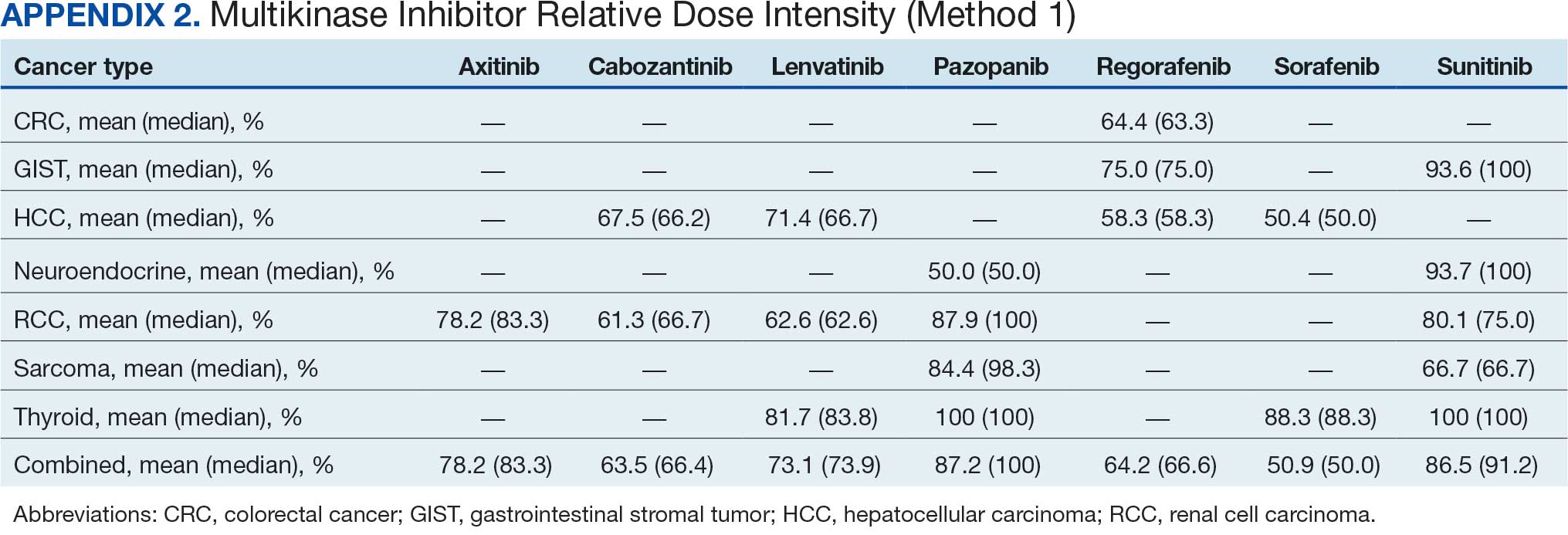
Limitations
The retrospective design, lack of survival outcomes, and difficulty comparing results with other literature were limitations of this study. Because survival outcomes were not evaluated, future research should seek to investigate how RDIs and dose adjustments made among MKIs can affect survival outcomes in real-world populations. This veteran population with cancer often had multiple chronic comorbidities, which may have contributed to difficulty tolerating MKIs and could have impacted results. Disease-related factors may have influenced the poor tolerance of the MKIs and were not specifically accounted for. Adjustment for comorbidities was not possible because of discrepancies and/or incomplete diagnosis codes and Eastern Cooperative Oncology Group performance status scores documented in patient charts. Therefore, we decided not to report these findings due to potential inaccuracies.
CONCLUSIONS
Results of this study demonstrate that oncology MKI agents used at VANTHCS were difficult for patients to tolerate, leading to suboptimal dosing compared with indicated doses established in clinical trials and prescribing information. Clinicians may use these data to help guide clinical decision-making whenever initiating and managing MKI agents in this population. These findings reinforce that MKI agents are often difficult to tolerate in real-world practice, and indicated doses are often not achieved. Further studies should aim to investigate the effect that various RDIs have on overall survival. Further investigation into different dosing schemes for MKIs to improve tolerability and longer-term use may also prove beneficial.
This analysis may help guide clinicians to carefully approach dosing MKI agents in the veteran population. Given the RDI and AEs, more clinicians may consider starting at lower than indicated doses with the goal to titrate up as tolerated. Additionally, the results highlight the importance of considering palliative care consults and ensuring appropriate supportive care agents are preemptively engaged and adjusted as needed. Approaching dosing and titrations cautiously may help reduce the burden of management on the health care system.
- Frequently asked questions. VA National Oncology Program. 2025. Accessed December 15, 2025. https://www.cancer.va.gov/CANCER/faqs.html
- Torez L. Reigniting the cancer moonshot to beat cancer. VA News. April 20, 2023. Accessed April 6, 2026. https://news.va.gov/118378/reigniting-the-cancer-moonshot-to-beat-cancer
- Shah NN, Casella E, Capozzi D, et al. Improving the safety of oral chemotherapy at an academic medical center. J Oncol Pract. 2016;12:e71-e76. doi:10.1200/JOP.2015.007260
- Hussaarts KGAM, Veerman GDM, Jansman FGA, et al. Clinically relevant drug interactions with multikinase inhibitors: a review. Ther Adv Med Oncol. 2019;11:1758835918818347. doi:10.1177/1758835918818347
- Shyam Sunder S, Sharma UC, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8:262. doi:10.1038/s41392-023-01469-6
- Thomson RJ, Moshirfar M, Ronquillo Y. Tyrosine kinase inhibitors. In: StatPearls [Internet]. StatPearls Publishing; updated July 18, 2023. Accessed December 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK563322/
- Project Optimus. US Food and Drug Administration. Updated December 6, 2024. Accessed December 15, 2025. https://www.fda.gov/about-fda/oncology-center-excellence/project-optimus
- Optimizing the dosage of human prescription drugs and biological products for the treatment of oncologic diseases: Guidance for Industry. Docket number FDA-2022-D-2827. US Food and Drug Administration. August 2024. Accessed December 15, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/optimizing-dosage-human-prescription-drugs-and-biological-products-treatment-oncologic-diseases
- Schnadig ID, Hutson TE, Chung H, et al. Dosing patterns, toxicity, and outcomes in patients treated with first-line sunitinib for advanced renal cell carcinoma in community-based practices. Clin Genitourin Cancer. 2014;12:413-421. doi:10.1016/j.clgc.2014.06.015
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115-124. doi:10.1056/nejmoa065044
- Hawn C, Bansal D. Relative dose intensity in oncology trials: a discussion of two approaches. PharmaSUG. 2024. Accessed April 6, 2026. https://pharmasug.org/proceedings/2024/ST/PharmaSUG-2024-ST-297.pdf
- George S, Merriam P, Maki RG, et al. Multicenter phase II trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009;27:3154-3160. doi:10.1200/jco.2008.20.9890
- George S, Blay JY, Casali PG, et al. Clinical evaluation of continuous daily dosing of sunitinib malate in patients with advanced gastrointestinal stromal tumour after imatinib failure. Eur J Cancer. 2009;45:1959-1968. doi:10.1016/j.ejca.2009.02.011
- Denduluri N, Patt DA, Wang Y, et al. Dose delays, dose reductions, and relative dose intensity in patients with cancer who received adjuvant or neoadjuvant chemotherapy in community oncology practices. J Natl Compr Canc Netw. 2015;13:1383-1393. doi:10.6004/jnccn.2015.0166
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380:1103-1115. doi:10.1056/nejmoa1816047
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384:1289-1300. doi:10.1056/nejmoa2035716
- Kirino S, Tsuchiya K, Kurosaki M, et al. Relative dose intensity over the first four weeks of lenvatinib therapy is a factor of favorable response and overall survival in patients with unresectable hepatocellular carcinoma. PloS One. 2020;15:e0231828. doi:10.1371/journal.pone.0231828
- Ishihara H, Takagi T, Kondo T, et al. Decreased relative dose intensity during the early phase of treatment impacts the therapeutic efficacy of sunitinib in metastatic renal cell carcinoma. Jpn J Clin Oncol. 2018;48:667-672. doi:10.1093/jjco/hyy078
- Alghamdi MA, Amaro CP, Lee-Ying R, et al. Effect of sorafenib starting dose and dose intensity on survival in patients with hepatocellular carcinoma: results from a Canadian Multicenter Database. Cancer Med. 2020;9:4918-4928. doi:10.1002/cam4.3228
- Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006;295:2516-2524. doi:10.1001/jama.295.21.2516
- Miller AA, Murry DJ, Owzar K, et al. Phase I and pharmacokinetic study of sorafenib in patients with hepatic or renal dysfunction: CALGB 60301. J Clin Oncol. 2009;27:1800-1805. doi:10.1200/jco.2008.20.0931
- Boucai L, Zafereo M, Cabanillas ME. Thyroid cancer: a review. JAMA. 2024;331:425-435. doi:10.1001/jama.2023.26348
- Amin N, Anwar J, Sulaiman A, et al. Hepatocellular carcinoma: a comprehensive review. Diseases. 2025;13:207. doi:10.3390/diseases13070207
- Bekaii-Saab TS, Ou FS, Ahn DH, et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): a randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019;20:1070-1082. doi:10.1016/s1470-2045(19)30272-4
The US Department of Veterans Affairs (VA) annually treats around 450,000 veterans with cancer and diagnoses an additional 56,000.1,2 Oral multikinase inhibitors (MKIs) are widely used as targeted therapies for many different malignancies. Despite the ease of oral administration, these agents are often accompanied by significant adverse effects (AEs) and drug-drug interactions.3,4 Common AEs include hypertension, cutaneous reactions, gastrointestinal disturbances, proteinuria, and fatigue. Some serious outcomes that may occur are myocardial infarction, thrombosis, nephrotic syndrome, hemorrhage, hepatotoxicity, and gastrointestinal events.5,6 Due to poor tolerability of these AEs, dose reductions, frequent therapy holds, and discontinuation of therapy may occur.
The US Food and Drug Administration recognizes dosing challenges with novel therapies and has created the Oncology Center of Excellence (OCE) Project Optimus initiative to reform dose optimization in oncology drug development. The initiative aims to shift the focus from establishing dose regimens based on the maximum tolerated doses of cytotoxic chemotherapeutics to an emphasis on maximum efficacy, safety, and tolerability, which better reflect real-world dosing.7,8
MKIs can be challenging to manage because of the frequent toxicity-related dose reductions, interruptions, and discontinuations. In a multicenter retrospective study, Schnadig et al investigated dosing characteristics of first-line sunitinib for advanced renal cell carcinoma (RCC) and found that, among 114 patients who experienced AEs while taking sunitinib, 39.5% had dose reductions, 5.3% delayed therapy, 18.4% required additional supportive medications, and 22.8% discontinued sunitinib.9 Overall survival and median progression-free survival of these patients were lower than reported by Motzer et al in a phase 3 clinical trial.10 Schnadig et al concluded that patients treated with sunitinib for RCC in the community setting required more frequent dose reductions and had less time on therapy compared with patients in clinical trials, which ultimately impacted clinical outcomes.9
At the VA North Texas Health Care System (VANTHCS), patients with cancer have difficulty tolerating MKIs and often require dose alterations and/or discontinuation because of drug intolerance rather than discontinuation due to progression. Frequent dose adjustments for toxicity management can place more strain on patients and health care resources because of additional appointments, clinician time, and emergency department visits. Escalating drug costs can also cause concern when prescription doses are unused or changed frequently.
To capture and quantify prescribing practices and dose adjustments, this study evaluated the tolerability of MKIs at VANTHCS. This analysis may also guide clinicians in the selection of starting doses as well as dose titration expectations to optimize MKI therapy.
METHODS
This single-center, retrospective chart review analyzed patients receiving oral oncology MKIs for various malignancies at VANTHCS between January 1, 2014, and October 31, 2024. Participants included adults aged ≥ 18 years with a prescription for axitinib, cabozantinib, lenvatinib, pazopanib, regorafenib, sorafenib, or sunitinib initiated by the hematology/oncology service at VANTHCS. Patients were included if they had follow-up documentation with the hematology/oncology service and/or other VANTHCS clinicians outlining their course of therapy after MKI initiation. Patients were excluded if they did not have sufficient follow-up documentation (eg, transferred care to a non-VA health care practitioner [HCP], moved to another VA health care system), were enrolled in clinical trials, or were prescribed an MKI from a Care in the Community (CITC) prescriber. Electronic health record review and data collection were performed using the VA Computerized Patient Record System and Research Electronic Data Capture. Data were collected from the time of initiation to cessation of therapy and included information regarding therapy changes, progressive disease, and date of death, when available. Data collected included age, sex, race, comorbidities, date of death, type of malignancy and subtypes, cancer stage, MKI used (ie, drug, dose, frequency, schedule, and indication), dates of medication changes (ie, start, adjustment, hold, discontinuation), concurrent antineoplastic treatments, and AEs documented at times of dose change or interruption.
The primary outcome was MKI tolerance determined using relative dose intensity (RDI) and mean and median time on therapy. Two methods are used to calculate RDI that vary in how they approach time on therapy as outlined in Hawn et al.11 This study used method 2, which accounts for holds in therapy by comparing the actual duration of treatment with the duration expected according to treatment protocol. Method 1 compares the prescribed dose with the administered dose and does not adjust for holds.11 Using method 2, the RDI in this study was calculated by dividing the total actual dose given by the total indicated dose for the malignancy being treated, which accounts for duration of treatment.
The total actual dose was the strength, frequency, and days on therapy for each time frame of treatment multiplied together. This method accounted for all dose adjustments and time periods of treatment holds, including patient self-adjustments, prescriber-directed adjustments, and nonadherence determined by HCP documentation and/or prescription data. Similarly, the indicated total dose was calculated by multiplying the indicated strength, frequency, and all days that treatment should have occurred (time from start to finish). Indicated doses were derived from the prescribing information for each malignancy with the exception of sunitinib, for which the off-label dose of 37.5 mg daily was considered a full dose.12,13 The total indicated dose for axitinib was calculated by considering the dose escalation schedule from the prescribing information.
Patients who required dose reductions due to renal/hepatic impairments or drug-drug interactions had their total indicated dose calculated using dose adjustments listed in the prescribing information. The mean RDI for each MKI agent was calculated by averaging the RDI for each prescription. The overall combined mean RDI included the means of all the MKIs reviewed to avoid skewing the results toward an MKI with more prescriptions. RDIs were also calculated for each cancer type for each agent. Additional descriptive secondary outcomes included rates of AEs and adjustments in doses.
RESULTS
Electronic data extraction identified 278 patients with 366 MKI prescriptions, of which 108 veterans with 158 MKI prescriptions were excluded. The top reason for exclusion was patients managed through CITC. Ultimately, 170 veterans with 208 MKI prescriptions managed by the VANTHCS hematology/oncology clinic were included (Table 1). Among patients receiving MKIs, the mean age was 72.7 years, 98% were male, and 99% had metastatic disease.
The overall combined mean MKI RDI was 67.5% using method 2 and ranged from 85.5% for sunitinib to 49.0% for sorafenib (Figure 1). Additional information regarding mean and median RDIs using method 2 is shown in Figure 1 and further subdivided by cancer type in Table 2. Median RDIs overall were similar to mean RDIs for most agents. Figure 2 indicates the mean and median time on therapy, reflecting time on therapy excluding days therapy was held. The overall combined mean and median days on therapy for all MKIs were 155 days and 95 days, respectively. Mean time on therapy depended on the agent used and ranged from 35 days (regorafenib) to 237 days (cabozantinib).
Of 208 MKI prescriptions, 127 (61.1%) were initiated at a reduced dose due to baseline concerns for tolerance such as performance status, frailty, and prior intolerance of other treatments. Eighty-one prescriptions (38.9%) were initiated at their indicated doses. Ninety prescriptions (43.3%) required dose reductions during treatment. Some MKI prescriptions had multiple dose increases and decreases, which is why RDI more accurately reflects dose adjustments. A total of 376 AEs that contributed to a dose adjustment, hold, or discontinuation occurred across all MKI prescriptions. The most common AEs were 82 failure-to-thrive events (21.8%) (fatigue, malaise, loss of appetite, reduced mobility, global decline), 79 gastrointestinal events (21.0%) (nausea, vomiting, diarrhea, abdominal pain), 62 dermatologic events (16.5%) (rash, hand-foot skin reactions, allergic response), 61 hepatic dysfunction events (16.2%) (liver enzyme elevations, hyperbilirubinemia), 40 cardiovascular events (10.6%) (hypertension, heart failure exacerbations, edema), and 33 renal dysfunction events (8.8%) (acute kidney injury, proteinuria) (Appendix 1).
DISCUSSION
The mean RDI of MKI prescriptions used in the veteran population at VANTHCS was about two-thirds of the indicated dose. These results indicate that most veterans required dose reductions and/or holds due to concerns over initial tolerance/performance status, worsening clinical condition, and/or intolerable AEs attributed to treatment. A retrospective study conducted by Denduluri et al suggested that an RDI of < 85% is a clinically meaningful reduction for traditional chemotherapy based on previous literature.14 However, it is less clear what RDI should be expected specifically for MKIs in real-world populations. The MKI phase 3 approval trials in RCC for axitinib, lenvatinib, and sunitinib found median RDIs of 89.4%, 69.6% to 70.4%, and 83.9%, respectively. Each trial cited dose reductions most commonly as the result of treatment-related AEs.15,16
Studies on the impact of RDIs on survival outcomes found that higher RDIs may improve overall and progression-free survival. Retrospective studies inspecting lenvatinib in hepatocellular carcinoma (HCC) indicated that an RDI > 70% in the initial 4 weeks resulted in favorable survival outcomes.17 Similarly, a retrospective study investigating sunitinib in RCC found that an RDI > 60% conferred favorable survival outcomes.18 Alghamdi et al noted that patients taking sorafenib for HCC who had RDI > 50% had a favorable trend in survival characteristics. Interestingly, the study found an RDI of 50% to 75% appeared to have better survival than an RDI > 75%.19 The authors of these studies hypothesized that additional dose reductions allowed for longer total time on therapy due to improved tolerability.17-19
This analysis found that the RDIs for most MKI agents at VANTHCS were < 85% and lower than the RDIs found in other review articles and phase 3 trials, with the exceptions of pazopanib in thyroid cancer and sunitinib in gastrointestinal stromal tumor (GIST), thyroid cancer, and neuroendocrine cancer. The reasons for the lower RDIs in this study are likely multifactorial, reflecting patient population characteristics, off-label dosing practices, and HCP experiences with these agents. Many veterans have chronic comorbidities that could contribute to reduced performance status and ability to tolerate these therapies. Despite attempts to preemptively reduce doses for patients and account for potential impaired tolerance, there were patients who required further dose reductions in our study.
Failure to thrive was the most common AE leading to dose adjustment or discontinuation, which illustrates the extensive effects these agents have on patient functioning in a real-world population. Notably though, the RDI for sunitinib was higher in this population because about half of patients were dosed using the off-label recommendation, whereas the prescribing information recommends a more intensive 6-week dosing cycle for certain cancer types.12,13,20 Sorafenib was also often dose-adjusted based on a pharmacokinetic study of sorafenib in renal/hepatic dysfunction, and the RDI likely reflects the off-label prescribing pattern.21
Patients with thyroid cancer were found to have higher RDIs compared with those receiving the same agents for other cancer types. Improved tolerability of MKIs in thyroid cancer may be due to a generally more tolerable disease course. Thyroid cancer is the most common cancer in individuals aged < 40 years, a population that is often more robust with fewer comorbidities. Moreover, the 5-year relative survival rate for thyroid cancer remains > 98%.22 This rate is in contrast to those for other cancer types such as HCC, with a 5-year relative survival rate of only 15%.23
It is challenging to compare the mean and median times on therapy found in this study with those in current literature, as this review included multiple different cancer types for each agent. However, the numbers are generally lower than durations of therapy found across the different disease states and further emphasize the difficulty in tolerating MKIs in the VANTHCS population. Regorafenib had a short duration of time on therapy, which highlights the importance of trials like ReDOS and initiatives such as OCE Project Optimus in helping improve tolerance.7,8,24
Comparing our results with other studies proved challenging because the RDI calculation methods were not specified. Calculating RDIs in this study using method 1, which does not account for holds, resulted in higher RDIs (Appendix 2). Using method 1, all MKIs had RDIs < 85%, except for pazopanib in thyroid cancer (100%) and RCC (87.9%), and sunitinib in GIST (93.6%), thyroid cancer (100%), and neuroendocrine cancer (93.7%). Notably, using method 1 increased the RDI for pazopanib in neuroendocrine cancer from 5.4% to 50.0%. The low RDI was attributed to a single veteran with a long hold duration, which demonstrates the discrepancy that can occur between the 2 methods.
Limitations
The retrospective design, lack of survival outcomes, and difficulty comparing results with other literature were limitations of this study. Because survival outcomes were not evaluated, future research should seek to investigate how RDIs and dose adjustments made among MKIs can affect survival outcomes in real-world populations. This veteran population with cancer often had multiple chronic comorbidities, which may have contributed to difficulty tolerating MKIs and could have impacted results. Disease-related factors may have influenced the poor tolerance of the MKIs and were not specifically accounted for. Adjustment for comorbidities was not possible because of discrepancies and/or incomplete diagnosis codes and Eastern Cooperative Oncology Group performance status scores documented in patient charts. Therefore, we decided not to report these findings due to potential inaccuracies.
CONCLUSIONS
Results of this study demonstrate that oncology MKI agents used at VANTHCS were difficult for patients to tolerate, leading to suboptimal dosing compared with indicated doses established in clinical trials and prescribing information. Clinicians may use these data to help guide clinical decision-making whenever initiating and managing MKI agents in this population. These findings reinforce that MKI agents are often difficult to tolerate in real-world practice, and indicated doses are often not achieved. Further studies should aim to investigate the effect that various RDIs have on overall survival. Further investigation into different dosing schemes for MKIs to improve tolerability and longer-term use may also prove beneficial.
This analysis may help guide clinicians to carefully approach dosing MKI agents in the veteran population. Given the RDI and AEs, more clinicians may consider starting at lower than indicated doses with the goal to titrate up as tolerated. Additionally, the results highlight the importance of considering palliative care consults and ensuring appropriate supportive care agents are preemptively engaged and adjusted as needed. Approaching dosing and titrations cautiously may help reduce the burden of management on the health care system.
The US Department of Veterans Affairs (VA) annually treats around 450,000 veterans with cancer and diagnoses an additional 56,000.1,2 Oral multikinase inhibitors (MKIs) are widely used as targeted therapies for many different malignancies. Despite the ease of oral administration, these agents are often accompanied by significant adverse effects (AEs) and drug-drug interactions.3,4 Common AEs include hypertension, cutaneous reactions, gastrointestinal disturbances, proteinuria, and fatigue. Some serious outcomes that may occur are myocardial infarction, thrombosis, nephrotic syndrome, hemorrhage, hepatotoxicity, and gastrointestinal events.5,6 Due to poor tolerability of these AEs, dose reductions, frequent therapy holds, and discontinuation of therapy may occur.
The US Food and Drug Administration recognizes dosing challenges with novel therapies and has created the Oncology Center of Excellence (OCE) Project Optimus initiative to reform dose optimization in oncology drug development. The initiative aims to shift the focus from establishing dose regimens based on the maximum tolerated doses of cytotoxic chemotherapeutics to an emphasis on maximum efficacy, safety, and tolerability, which better reflect real-world dosing.7,8
MKIs can be challenging to manage because of the frequent toxicity-related dose reductions, interruptions, and discontinuations. In a multicenter retrospective study, Schnadig et al investigated dosing characteristics of first-line sunitinib for advanced renal cell carcinoma (RCC) and found that, among 114 patients who experienced AEs while taking sunitinib, 39.5% had dose reductions, 5.3% delayed therapy, 18.4% required additional supportive medications, and 22.8% discontinued sunitinib.9 Overall survival and median progression-free survival of these patients were lower than reported by Motzer et al in a phase 3 clinical trial.10 Schnadig et al concluded that patients treated with sunitinib for RCC in the community setting required more frequent dose reductions and had less time on therapy compared with patients in clinical trials, which ultimately impacted clinical outcomes.9
At the VA North Texas Health Care System (VANTHCS), patients with cancer have difficulty tolerating MKIs and often require dose alterations and/or discontinuation because of drug intolerance rather than discontinuation due to progression. Frequent dose adjustments for toxicity management can place more strain on patients and health care resources because of additional appointments, clinician time, and emergency department visits. Escalating drug costs can also cause concern when prescription doses are unused or changed frequently.
To capture and quantify prescribing practices and dose adjustments, this study evaluated the tolerability of MKIs at VANTHCS. This analysis may also guide clinicians in the selection of starting doses as well as dose titration expectations to optimize MKI therapy.
METHODS
This single-center, retrospective chart review analyzed patients receiving oral oncology MKIs for various malignancies at VANTHCS between January 1, 2014, and October 31, 2024. Participants included adults aged ≥ 18 years with a prescription for axitinib, cabozantinib, lenvatinib, pazopanib, regorafenib, sorafenib, or sunitinib initiated by the hematology/oncology service at VANTHCS. Patients were included if they had follow-up documentation with the hematology/oncology service and/or other VANTHCS clinicians outlining their course of therapy after MKI initiation. Patients were excluded if they did not have sufficient follow-up documentation (eg, transferred care to a non-VA health care practitioner [HCP], moved to another VA health care system), were enrolled in clinical trials, or were prescribed an MKI from a Care in the Community (CITC) prescriber. Electronic health record review and data collection were performed using the VA Computerized Patient Record System and Research Electronic Data Capture. Data were collected from the time of initiation to cessation of therapy and included information regarding therapy changes, progressive disease, and date of death, when available. Data collected included age, sex, race, comorbidities, date of death, type of malignancy and subtypes, cancer stage, MKI used (ie, drug, dose, frequency, schedule, and indication), dates of medication changes (ie, start, adjustment, hold, discontinuation), concurrent antineoplastic treatments, and AEs documented at times of dose change or interruption.
The primary outcome was MKI tolerance determined using relative dose intensity (RDI) and mean and median time on therapy. Two methods are used to calculate RDI that vary in how they approach time on therapy as outlined in Hawn et al.11 This study used method 2, which accounts for holds in therapy by comparing the actual duration of treatment with the duration expected according to treatment protocol. Method 1 compares the prescribed dose with the administered dose and does not adjust for holds.11 Using method 2, the RDI in this study was calculated by dividing the total actual dose given by the total indicated dose for the malignancy being treated, which accounts for duration of treatment.
The total actual dose was the strength, frequency, and days on therapy for each time frame of treatment multiplied together. This method accounted for all dose adjustments and time periods of treatment holds, including patient self-adjustments, prescriber-directed adjustments, and nonadherence determined by HCP documentation and/or prescription data. Similarly, the indicated total dose was calculated by multiplying the indicated strength, frequency, and all days that treatment should have occurred (time from start to finish). Indicated doses were derived from the prescribing information for each malignancy with the exception of sunitinib, for which the off-label dose of 37.5 mg daily was considered a full dose.12,13 The total indicated dose for axitinib was calculated by considering the dose escalation schedule from the prescribing information.
Patients who required dose reductions due to renal/hepatic impairments or drug-drug interactions had their total indicated dose calculated using dose adjustments listed in the prescribing information. The mean RDI for each MKI agent was calculated by averaging the RDI for each prescription. The overall combined mean RDI included the means of all the MKIs reviewed to avoid skewing the results toward an MKI with more prescriptions. RDIs were also calculated for each cancer type for each agent. Additional descriptive secondary outcomes included rates of AEs and adjustments in doses.
RESULTS
Electronic data extraction identified 278 patients with 366 MKI prescriptions, of which 108 veterans with 158 MKI prescriptions were excluded. The top reason for exclusion was patients managed through CITC. Ultimately, 170 veterans with 208 MKI prescriptions managed by the VANTHCS hematology/oncology clinic were included (Table 1). Among patients receiving MKIs, the mean age was 72.7 years, 98% were male, and 99% had metastatic disease.
The overall combined mean MKI RDI was 67.5% using method 2 and ranged from 85.5% for sunitinib to 49.0% for sorafenib (Figure 1). Additional information regarding mean and median RDIs using method 2 is shown in Figure 1 and further subdivided by cancer type in Table 2. Median RDIs overall were similar to mean RDIs for most agents. Figure 2 indicates the mean and median time on therapy, reflecting time on therapy excluding days therapy was held. The overall combined mean and median days on therapy for all MKIs were 155 days and 95 days, respectively. Mean time on therapy depended on the agent used and ranged from 35 days (regorafenib) to 237 days (cabozantinib).
Of 208 MKI prescriptions, 127 (61.1%) were initiated at a reduced dose due to baseline concerns for tolerance such as performance status, frailty, and prior intolerance of other treatments. Eighty-one prescriptions (38.9%) were initiated at their indicated doses. Ninety prescriptions (43.3%) required dose reductions during treatment. Some MKI prescriptions had multiple dose increases and decreases, which is why RDI more accurately reflects dose adjustments. A total of 376 AEs that contributed to a dose adjustment, hold, or discontinuation occurred across all MKI prescriptions. The most common AEs were 82 failure-to-thrive events (21.8%) (fatigue, malaise, loss of appetite, reduced mobility, global decline), 79 gastrointestinal events (21.0%) (nausea, vomiting, diarrhea, abdominal pain), 62 dermatologic events (16.5%) (rash, hand-foot skin reactions, allergic response), 61 hepatic dysfunction events (16.2%) (liver enzyme elevations, hyperbilirubinemia), 40 cardiovascular events (10.6%) (hypertension, heart failure exacerbations, edema), and 33 renal dysfunction events (8.8%) (acute kidney injury, proteinuria) (Appendix 1).
DISCUSSION
The mean RDI of MKI prescriptions used in the veteran population at VANTHCS was about two-thirds of the indicated dose. These results indicate that most veterans required dose reductions and/or holds due to concerns over initial tolerance/performance status, worsening clinical condition, and/or intolerable AEs attributed to treatment. A retrospective study conducted by Denduluri et al suggested that an RDI of < 85% is a clinically meaningful reduction for traditional chemotherapy based on previous literature.14 However, it is less clear what RDI should be expected specifically for MKIs in real-world populations. The MKI phase 3 approval trials in RCC for axitinib, lenvatinib, and sunitinib found median RDIs of 89.4%, 69.6% to 70.4%, and 83.9%, respectively. Each trial cited dose reductions most commonly as the result of treatment-related AEs.15,16
Studies on the impact of RDIs on survival outcomes found that higher RDIs may improve overall and progression-free survival. Retrospective studies inspecting lenvatinib in hepatocellular carcinoma (HCC) indicated that an RDI > 70% in the initial 4 weeks resulted in favorable survival outcomes.17 Similarly, a retrospective study investigating sunitinib in RCC found that an RDI > 60% conferred favorable survival outcomes.18 Alghamdi et al noted that patients taking sorafenib for HCC who had RDI > 50% had a favorable trend in survival characteristics. Interestingly, the study found an RDI of 50% to 75% appeared to have better survival than an RDI > 75%.19 The authors of these studies hypothesized that additional dose reductions allowed for longer total time on therapy due to improved tolerability.17-19
This analysis found that the RDIs for most MKI agents at VANTHCS were < 85% and lower than the RDIs found in other review articles and phase 3 trials, with the exceptions of pazopanib in thyroid cancer and sunitinib in gastrointestinal stromal tumor (GIST), thyroid cancer, and neuroendocrine cancer. The reasons for the lower RDIs in this study are likely multifactorial, reflecting patient population characteristics, off-label dosing practices, and HCP experiences with these agents. Many veterans have chronic comorbidities that could contribute to reduced performance status and ability to tolerate these therapies. Despite attempts to preemptively reduce doses for patients and account for potential impaired tolerance, there were patients who required further dose reductions in our study.
Failure to thrive was the most common AE leading to dose adjustment or discontinuation, which illustrates the extensive effects these agents have on patient functioning in a real-world population. Notably though, the RDI for sunitinib was higher in this population because about half of patients were dosed using the off-label recommendation, whereas the prescribing information recommends a more intensive 6-week dosing cycle for certain cancer types.12,13,20 Sorafenib was also often dose-adjusted based on a pharmacokinetic study of sorafenib in renal/hepatic dysfunction, and the RDI likely reflects the off-label prescribing pattern.21
Patients with thyroid cancer were found to have higher RDIs compared with those receiving the same agents for other cancer types. Improved tolerability of MKIs in thyroid cancer may be due to a generally more tolerable disease course. Thyroid cancer is the most common cancer in individuals aged < 40 years, a population that is often more robust with fewer comorbidities. Moreover, the 5-year relative survival rate for thyroid cancer remains > 98%.22 This rate is in contrast to those for other cancer types such as HCC, with a 5-year relative survival rate of only 15%.23
It is challenging to compare the mean and median times on therapy found in this study with those in current literature, as this review included multiple different cancer types for each agent. However, the numbers are generally lower than durations of therapy found across the different disease states and further emphasize the difficulty in tolerating MKIs in the VANTHCS population. Regorafenib had a short duration of time on therapy, which highlights the importance of trials like ReDOS and initiatives such as OCE Project Optimus in helping improve tolerance.7,8,24
Comparing our results with other studies proved challenging because the RDI calculation methods were not specified. Calculating RDIs in this study using method 1, which does not account for holds, resulted in higher RDIs (Appendix 2). Using method 1, all MKIs had RDIs < 85%, except for pazopanib in thyroid cancer (100%) and RCC (87.9%), and sunitinib in GIST (93.6%), thyroid cancer (100%), and neuroendocrine cancer (93.7%). Notably, using method 1 increased the RDI for pazopanib in neuroendocrine cancer from 5.4% to 50.0%. The low RDI was attributed to a single veteran with a long hold duration, which demonstrates the discrepancy that can occur between the 2 methods.
Limitations
The retrospective design, lack of survival outcomes, and difficulty comparing results with other literature were limitations of this study. Because survival outcomes were not evaluated, future research should seek to investigate how RDIs and dose adjustments made among MKIs can affect survival outcomes in real-world populations. This veteran population with cancer often had multiple chronic comorbidities, which may have contributed to difficulty tolerating MKIs and could have impacted results. Disease-related factors may have influenced the poor tolerance of the MKIs and were not specifically accounted for. Adjustment for comorbidities was not possible because of discrepancies and/or incomplete diagnosis codes and Eastern Cooperative Oncology Group performance status scores documented in patient charts. Therefore, we decided not to report these findings due to potential inaccuracies.
CONCLUSIONS
Results of this study demonstrate that oncology MKI agents used at VANTHCS were difficult for patients to tolerate, leading to suboptimal dosing compared with indicated doses established in clinical trials and prescribing information. Clinicians may use these data to help guide clinical decision-making whenever initiating and managing MKI agents in this population. These findings reinforce that MKI agents are often difficult to tolerate in real-world practice, and indicated doses are often not achieved. Further studies should aim to investigate the effect that various RDIs have on overall survival. Further investigation into different dosing schemes for MKIs to improve tolerability and longer-term use may also prove beneficial.
This analysis may help guide clinicians to carefully approach dosing MKI agents in the veteran population. Given the RDI and AEs, more clinicians may consider starting at lower than indicated doses with the goal to titrate up as tolerated. Additionally, the results highlight the importance of considering palliative care consults and ensuring appropriate supportive care agents are preemptively engaged and adjusted as needed. Approaching dosing and titrations cautiously may help reduce the burden of management on the health care system.
- Frequently asked questions. VA National Oncology Program. 2025. Accessed December 15, 2025. https://www.cancer.va.gov/CANCER/faqs.html
- Torez L. Reigniting the cancer moonshot to beat cancer. VA News. April 20, 2023. Accessed April 6, 2026. https://news.va.gov/118378/reigniting-the-cancer-moonshot-to-beat-cancer
- Shah NN, Casella E, Capozzi D, et al. Improving the safety of oral chemotherapy at an academic medical center. J Oncol Pract. 2016;12:e71-e76. doi:10.1200/JOP.2015.007260
- Hussaarts KGAM, Veerman GDM, Jansman FGA, et al. Clinically relevant drug interactions with multikinase inhibitors: a review. Ther Adv Med Oncol. 2019;11:1758835918818347. doi:10.1177/1758835918818347
- Shyam Sunder S, Sharma UC, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8:262. doi:10.1038/s41392-023-01469-6
- Thomson RJ, Moshirfar M, Ronquillo Y. Tyrosine kinase inhibitors. In: StatPearls [Internet]. StatPearls Publishing; updated July 18, 2023. Accessed December 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK563322/
- Project Optimus. US Food and Drug Administration. Updated December 6, 2024. Accessed December 15, 2025. https://www.fda.gov/about-fda/oncology-center-excellence/project-optimus
- Optimizing the dosage of human prescription drugs and biological products for the treatment of oncologic diseases: Guidance for Industry. Docket number FDA-2022-D-2827. US Food and Drug Administration. August 2024. Accessed December 15, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/optimizing-dosage-human-prescription-drugs-and-biological-products-treatment-oncologic-diseases
- Schnadig ID, Hutson TE, Chung H, et al. Dosing patterns, toxicity, and outcomes in patients treated with first-line sunitinib for advanced renal cell carcinoma in community-based practices. Clin Genitourin Cancer. 2014;12:413-421. doi:10.1016/j.clgc.2014.06.015
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115-124. doi:10.1056/nejmoa065044
- Hawn C, Bansal D. Relative dose intensity in oncology trials: a discussion of two approaches. PharmaSUG. 2024. Accessed April 6, 2026. https://pharmasug.org/proceedings/2024/ST/PharmaSUG-2024-ST-297.pdf
- George S, Merriam P, Maki RG, et al. Multicenter phase II trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009;27:3154-3160. doi:10.1200/jco.2008.20.9890
- George S, Blay JY, Casali PG, et al. Clinical evaluation of continuous daily dosing of sunitinib malate in patients with advanced gastrointestinal stromal tumour after imatinib failure. Eur J Cancer. 2009;45:1959-1968. doi:10.1016/j.ejca.2009.02.011
- Denduluri N, Patt DA, Wang Y, et al. Dose delays, dose reductions, and relative dose intensity in patients with cancer who received adjuvant or neoadjuvant chemotherapy in community oncology practices. J Natl Compr Canc Netw. 2015;13:1383-1393. doi:10.6004/jnccn.2015.0166
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380:1103-1115. doi:10.1056/nejmoa1816047
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384:1289-1300. doi:10.1056/nejmoa2035716
- Kirino S, Tsuchiya K, Kurosaki M, et al. Relative dose intensity over the first four weeks of lenvatinib therapy is a factor of favorable response and overall survival in patients with unresectable hepatocellular carcinoma. PloS One. 2020;15:e0231828. doi:10.1371/journal.pone.0231828
- Ishihara H, Takagi T, Kondo T, et al. Decreased relative dose intensity during the early phase of treatment impacts the therapeutic efficacy of sunitinib in metastatic renal cell carcinoma. Jpn J Clin Oncol. 2018;48:667-672. doi:10.1093/jjco/hyy078
- Alghamdi MA, Amaro CP, Lee-Ying R, et al. Effect of sorafenib starting dose and dose intensity on survival in patients with hepatocellular carcinoma: results from a Canadian Multicenter Database. Cancer Med. 2020;9:4918-4928. doi:10.1002/cam4.3228
- Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006;295:2516-2524. doi:10.1001/jama.295.21.2516
- Miller AA, Murry DJ, Owzar K, et al. Phase I and pharmacokinetic study of sorafenib in patients with hepatic or renal dysfunction: CALGB 60301. J Clin Oncol. 2009;27:1800-1805. doi:10.1200/jco.2008.20.0931
- Boucai L, Zafereo M, Cabanillas ME. Thyroid cancer: a review. JAMA. 2024;331:425-435. doi:10.1001/jama.2023.26348
- Amin N, Anwar J, Sulaiman A, et al. Hepatocellular carcinoma: a comprehensive review. Diseases. 2025;13:207. doi:10.3390/diseases13070207
- Bekaii-Saab TS, Ou FS, Ahn DH, et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): a randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019;20:1070-1082. doi:10.1016/s1470-2045(19)30272-4
- Frequently asked questions. VA National Oncology Program. 2025. Accessed December 15, 2025. https://www.cancer.va.gov/CANCER/faqs.html
- Torez L. Reigniting the cancer moonshot to beat cancer. VA News. April 20, 2023. Accessed April 6, 2026. https://news.va.gov/118378/reigniting-the-cancer-moonshot-to-beat-cancer
- Shah NN, Casella E, Capozzi D, et al. Improving the safety of oral chemotherapy at an academic medical center. J Oncol Pract. 2016;12:e71-e76. doi:10.1200/JOP.2015.007260
- Hussaarts KGAM, Veerman GDM, Jansman FGA, et al. Clinically relevant drug interactions with multikinase inhibitors: a review. Ther Adv Med Oncol. 2019;11:1758835918818347. doi:10.1177/1758835918818347
- Shyam Sunder S, Sharma UC, Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. 2023;8:262. doi:10.1038/s41392-023-01469-6
- Thomson RJ, Moshirfar M, Ronquillo Y. Tyrosine kinase inhibitors. In: StatPearls [Internet]. StatPearls Publishing; updated July 18, 2023. Accessed December 15, 2025. https://www.ncbi.nlm.nih.gov/books/NBK563322/
- Project Optimus. US Food and Drug Administration. Updated December 6, 2024. Accessed December 15, 2025. https://www.fda.gov/about-fda/oncology-center-excellence/project-optimus
- Optimizing the dosage of human prescription drugs and biological products for the treatment of oncologic diseases: Guidance for Industry. Docket number FDA-2022-D-2827. US Food and Drug Administration. August 2024. Accessed December 15, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/optimizing-dosage-human-prescription-drugs-and-biological-products-treatment-oncologic-diseases
- Schnadig ID, Hutson TE, Chung H, et al. Dosing patterns, toxicity, and outcomes in patients treated with first-line sunitinib for advanced renal cell carcinoma in community-based practices. Clin Genitourin Cancer. 2014;12:413-421. doi:10.1016/j.clgc.2014.06.015
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115-124. doi:10.1056/nejmoa065044
- Hawn C, Bansal D. Relative dose intensity in oncology trials: a discussion of two approaches. PharmaSUG. 2024. Accessed April 6, 2026. https://pharmasug.org/proceedings/2024/ST/PharmaSUG-2024-ST-297.pdf
- George S, Merriam P, Maki RG, et al. Multicenter phase II trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009;27:3154-3160. doi:10.1200/jco.2008.20.9890
- George S, Blay JY, Casali PG, et al. Clinical evaluation of continuous daily dosing of sunitinib malate in patients with advanced gastrointestinal stromal tumour after imatinib failure. Eur J Cancer. 2009;45:1959-1968. doi:10.1016/j.ejca.2009.02.011
- Denduluri N, Patt DA, Wang Y, et al. Dose delays, dose reductions, and relative dose intensity in patients with cancer who received adjuvant or neoadjuvant chemotherapy in community oncology practices. J Natl Compr Canc Netw. 2015;13:1383-1393. doi:10.6004/jnccn.2015.0166
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380:1103-1115. doi:10.1056/nejmoa1816047
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384:1289-1300. doi:10.1056/nejmoa2035716
- Kirino S, Tsuchiya K, Kurosaki M, et al. Relative dose intensity over the first four weeks of lenvatinib therapy is a factor of favorable response and overall survival in patients with unresectable hepatocellular carcinoma. PloS One. 2020;15:e0231828. doi:10.1371/journal.pone.0231828
- Ishihara H, Takagi T, Kondo T, et al. Decreased relative dose intensity during the early phase of treatment impacts the therapeutic efficacy of sunitinib in metastatic renal cell carcinoma. Jpn J Clin Oncol. 2018;48:667-672. doi:10.1093/jjco/hyy078
- Alghamdi MA, Amaro CP, Lee-Ying R, et al. Effect of sorafenib starting dose and dose intensity on survival in patients with hepatocellular carcinoma: results from a Canadian Multicenter Database. Cancer Med. 2020;9:4918-4928. doi:10.1002/cam4.3228
- Motzer RJ, Rini BI, Bukowski RM, et al. Sunitinib in patients with metastatic renal cell carcinoma. JAMA. 2006;295:2516-2524. doi:10.1001/jama.295.21.2516
- Miller AA, Murry DJ, Owzar K, et al. Phase I and pharmacokinetic study of sorafenib in patients with hepatic or renal dysfunction: CALGB 60301. J Clin Oncol. 2009;27:1800-1805. doi:10.1200/jco.2008.20.0931
- Boucai L, Zafereo M, Cabanillas ME. Thyroid cancer: a review. JAMA. 2024;331:425-435. doi:10.1001/jama.2023.26348
- Amin N, Anwar J, Sulaiman A, et al. Hepatocellular carcinoma: a comprehensive review. Diseases. 2025;13:207. doi:10.3390/diseases13070207
- Bekaii-Saab TS, Ou FS, Ahn DH, et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): a randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019;20:1070-1082. doi:10.1016/s1470-2045(19)30272-4
Investigating Real-World Tolerance and Dose Reductions of Oncology Multikinase Inhibitors in a VA Population
Investigating Real-World Tolerance and Dose Reductions of Oncology Multikinase Inhibitors in a VA Population
Alignment of ChatGPT Responses With AAD Guidelines for Cutaneous Melanoma
Alignment of ChatGPT Responses With AAD Guidelines for Cutaneous Melanoma
To the Editor:
ChatGPT (OpenAI), a popular large language model that generates responses to user queries, has attracted substantial attention as a potential resource for patient education.1 While prior studies have shown that ChatGPT can provide reliable and general patient information, its alignment with the American Academy of Dermatology’s (AAD’s) guidelines for primary cutaneous melanoma (CM) compared to evidence in the recent literature has not been evaluated.2,3 In this study, we compared ChatGPT’s responses to the 25 evidence-based questions utilized by the AAD to establish its 2019 recommendations for primary CM. Because the 2019 AAD guidelines included literature only through April 2017, we conducted an additional search (May 2017–February 2024) to assess ChatGPT’s alignment with more recent evidence not captured in the guidelines.
On April 17, 2024, 2 authors (D.P. and A.F.) prompted ChatGPT with 25 evidence-based questions from the 2019 AAD guidelines for the management of primary CM.4 ChatGPT’s responses were compared with the AAD’s published recommendations and were cross-referenced with responses gathered from our own search of PubMed articles indexed for MEDLINE using the phrase melanoma (cutaneous) and treatment, which included studies from May 2017 to February 2024.
ChatGPT’s answers to 23 of the questions aligned with the AAD’s guidelines (Table 1); in instances when the guidelines were inconclusive regarding pathology, the model provided recommendations supported by our contemporary PubMed literature search. Of the 3 questions related to CM pathology, the AAD guidelines had sufficient evidence to provide recommendations for 2 questions. The first question evaluated the clinical information necessary to help the pathologist improve diagnosis (Table 2). ChatGPT’s response to one question about staged excision and Mohs micrographic surgery for melanoma in situ did not align with the AAD guidelines (Table 3).
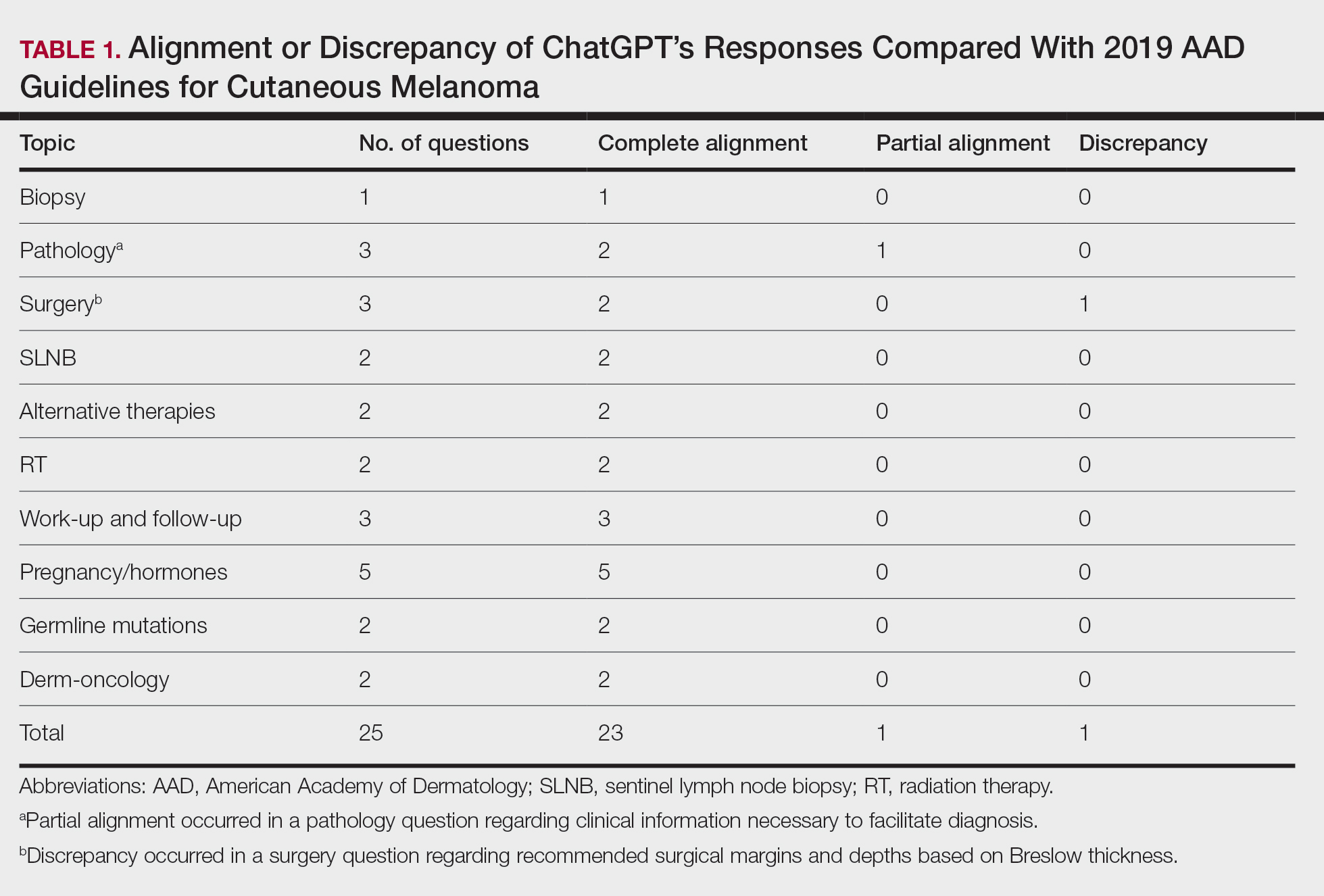
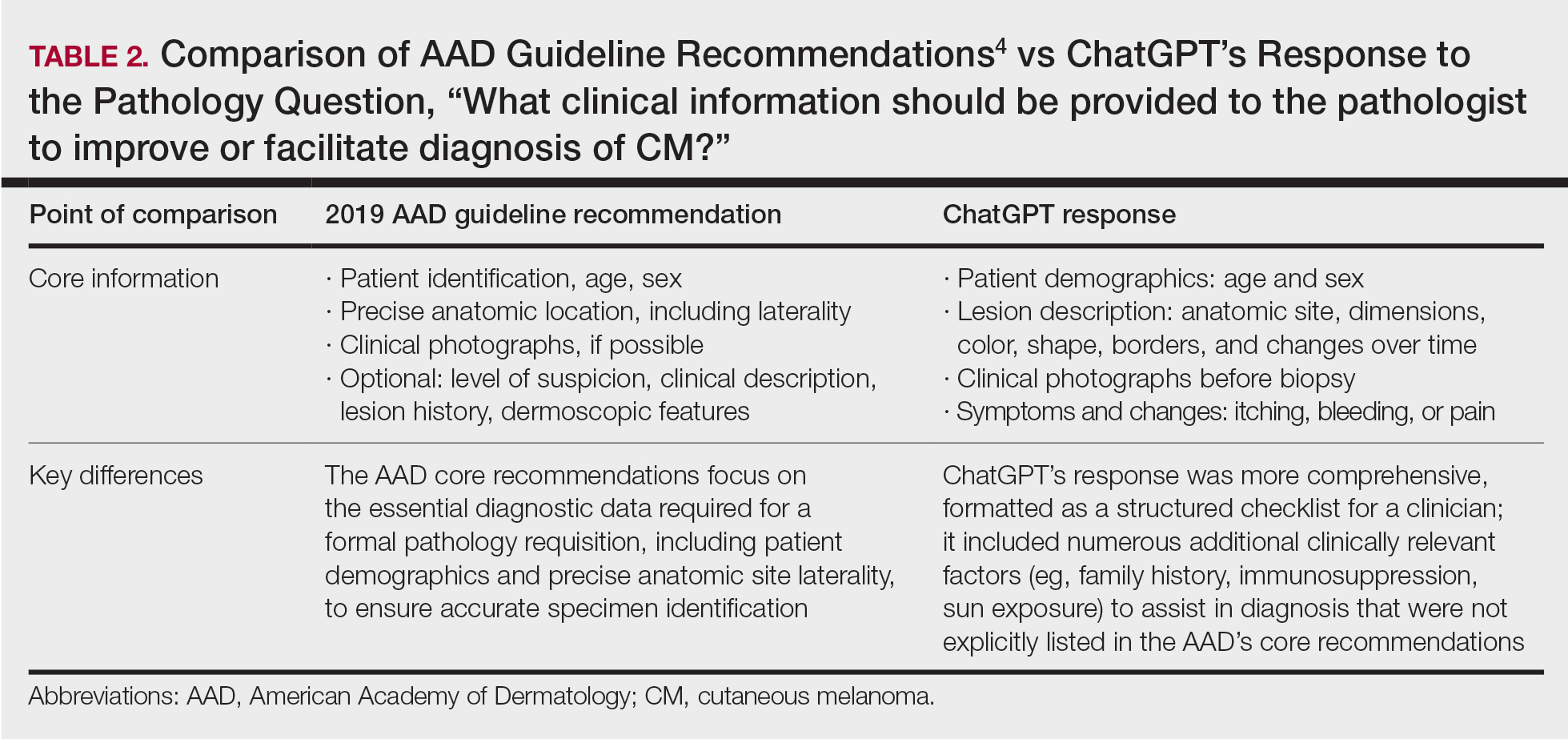
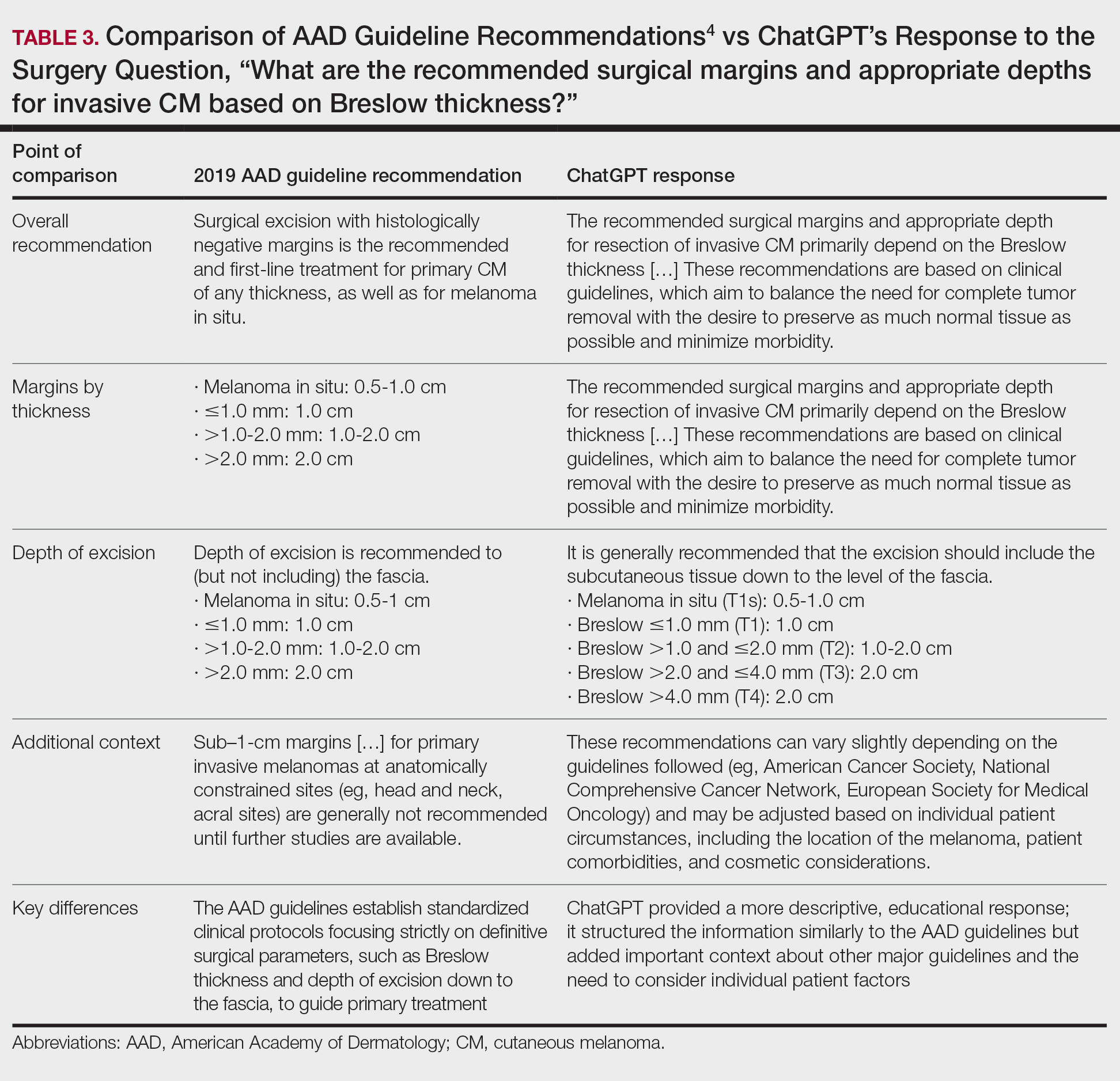
Our results showed that ChatGPT provided comprehensive responses aligned with current evidence on CM treatment, except for one surgery question for which its response differed from the AAD guidelines. Our findings are consistent with an observational study that reported board-certified dermatologists rated ChatGPT’s responses on melanoma-related questions as 4.88 on a scale of 1 to 5 (1 indicated completely inaccurate information, 5 indicated complete accuracy for clinical sufficiency in practice). The authors also found that ChatGPT gave vague advice, such as to “get regular skin exams,” which is less specific than dermatologists’ recommendations for annual, biannual, or more frequent examinations.5 ChatGPT’s limitations in offering comprehensive answers for some questions aligned with our findings, specifically the omission of key information in the surgical-related question, highlighting the challenge of relying on AI for nuanced clinical guidance.
We found that ChatGPT considered immunosuppression an important risk factor for CM. Similarly, a 2023 cohort study of 93 patients with melanoma and a history of immunosuppression reported that these patients had a higher risk for CM compared with a control group from the National Cancer Institute’s Surveillance, Epidemiology and End Results Program (standardized incidence ratio, 1.53; 95% CI, 1.12-2.04), indicating that incidence of CM in immunocompromised patients was 53% higher than an age- and sex-matched population cohort.6
Our findings also demonstrated that both ChatGPT’s responses and the AAD guidelines aligned in indicating that evidence linking pregnancy to an increased risk for CM remains inconclusive and that pregnant women should still undergo surveillance. A 2022 retrospective cohort study of 1406 women comparing pregnancy-associated melanoma to non–pregnancy-associated CM had no difference in overall survival (hazard ratio, 0.75; 95% CI, 0.54-1.05).7 However, tumor thickness (2.01-4.00 mm) was greater in postpartum cases compared with cases in nonpregnant women (odds ratio, 1.75; 95% CI, 1.03-2.98), suggesting that pregnancy may affect tumor characteristics.7 These findings underscore the importance of using AI tools such as ChatGPT as a supplement to—rather than as a replacement for—expert clinical judgment and up-to-date medical guidelines.
- Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2:E0000198.
- Roster K, Kann RB, Farabi B, et al. Readability and health literacy scores for ChatGPT-generated dermatology public education materials: cross-sectional analysis of sunscreen and melanoma questions. JMIR Dermatol. 2024;7:E50163.
- Dihan Q, Chauhan M, Eleiwa T, et al. Using large language models to generate educational materials on childhood glaucoma. Am J Ophthalmol. 2024;265:28-38.
- Swetter SM, Tsao H, Bichakjian CK, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2019;80:208-250.
- Young JN, O’Hagan R, Poplausky D, et al. The utility of ChatGPT in generating patient-facing and clinical responses for melanoma. J Am Acad Dermatol. 2023;89:602-604.
- Killeen TF, Shanley R, Ramesh V, et al. Malignant melanoma in a retrospective cohort of immunocompromised patients: a statistical and pathologic analysis. Cancers (Basel). 2023;15:3600.
- Kiuru M, Li Q, Zhu G, et al. Melanoma in women of childbearing age and in pregnancy in California, 1994-2015: a population-based cohort study. J Eur Acad Dermatol Venereol. 2022;36:2025-2035.
To the Editor:
ChatGPT (OpenAI), a popular large language model that generates responses to user queries, has attracted substantial attention as a potential resource for patient education.1 While prior studies have shown that ChatGPT can provide reliable and general patient information, its alignment with the American Academy of Dermatology’s (AAD’s) guidelines for primary cutaneous melanoma (CM) compared to evidence in the recent literature has not been evaluated.2,3 In this study, we compared ChatGPT’s responses to the 25 evidence-based questions utilized by the AAD to establish its 2019 recommendations for primary CM. Because the 2019 AAD guidelines included literature only through April 2017, we conducted an additional search (May 2017–February 2024) to assess ChatGPT’s alignment with more recent evidence not captured in the guidelines.
On April 17, 2024, 2 authors (D.P. and A.F.) prompted ChatGPT with 25 evidence-based questions from the 2019 AAD guidelines for the management of primary CM.4 ChatGPT’s responses were compared with the AAD’s published recommendations and were cross-referenced with responses gathered from our own search of PubMed articles indexed for MEDLINE using the phrase melanoma (cutaneous) and treatment, which included studies from May 2017 to February 2024.
ChatGPT’s answers to 23 of the questions aligned with the AAD’s guidelines (Table 1); in instances when the guidelines were inconclusive regarding pathology, the model provided recommendations supported by our contemporary PubMed literature search. Of the 3 questions related to CM pathology, the AAD guidelines had sufficient evidence to provide recommendations for 2 questions. The first question evaluated the clinical information necessary to help the pathologist improve diagnosis (Table 2). ChatGPT’s response to one question about staged excision and Mohs micrographic surgery for melanoma in situ did not align with the AAD guidelines (Table 3).
Our results showed that ChatGPT provided comprehensive responses aligned with current evidence on CM treatment, except for one surgery question for which its response differed from the AAD guidelines. Our findings are consistent with an observational study that reported board-certified dermatologists rated ChatGPT’s responses on melanoma-related questions as 4.88 on a scale of 1 to 5 (1 indicated completely inaccurate information, 5 indicated complete accuracy for clinical sufficiency in practice). The authors also found that ChatGPT gave vague advice, such as to “get regular skin exams,” which is less specific than dermatologists’ recommendations for annual, biannual, or more frequent examinations.5 ChatGPT’s limitations in offering comprehensive answers for some questions aligned with our findings, specifically the omission of key information in the surgical-related question, highlighting the challenge of relying on AI for nuanced clinical guidance.
We found that ChatGPT considered immunosuppression an important risk factor for CM. Similarly, a 2023 cohort study of 93 patients with melanoma and a history of immunosuppression reported that these patients had a higher risk for CM compared with a control group from the National Cancer Institute’s Surveillance, Epidemiology and End Results Program (standardized incidence ratio, 1.53; 95% CI, 1.12-2.04), indicating that incidence of CM in immunocompromised patients was 53% higher than an age- and sex-matched population cohort.6
Our findings also demonstrated that both ChatGPT’s responses and the AAD guidelines aligned in indicating that evidence linking pregnancy to an increased risk for CM remains inconclusive and that pregnant women should still undergo surveillance. A 2022 retrospective cohort study of 1406 women comparing pregnancy-associated melanoma to non–pregnancy-associated CM had no difference in overall survival (hazard ratio, 0.75; 95% CI, 0.54-1.05).7 However, tumor thickness (2.01-4.00 mm) was greater in postpartum cases compared with cases in nonpregnant women (odds ratio, 1.75; 95% CI, 1.03-2.98), suggesting that pregnancy may affect tumor characteristics.7 These findings underscore the importance of using AI tools such as ChatGPT as a supplement to—rather than as a replacement for—expert clinical judgment and up-to-date medical guidelines.
To the Editor:
ChatGPT (OpenAI), a popular large language model that generates responses to user queries, has attracted substantial attention as a potential resource for patient education.1 While prior studies have shown that ChatGPT can provide reliable and general patient information, its alignment with the American Academy of Dermatology’s (AAD’s) guidelines for primary cutaneous melanoma (CM) compared to evidence in the recent literature has not been evaluated.2,3 In this study, we compared ChatGPT’s responses to the 25 evidence-based questions utilized by the AAD to establish its 2019 recommendations for primary CM. Because the 2019 AAD guidelines included literature only through April 2017, we conducted an additional search (May 2017–February 2024) to assess ChatGPT’s alignment with more recent evidence not captured in the guidelines.
On April 17, 2024, 2 authors (D.P. and A.F.) prompted ChatGPT with 25 evidence-based questions from the 2019 AAD guidelines for the management of primary CM.4 ChatGPT’s responses were compared with the AAD’s published recommendations and were cross-referenced with responses gathered from our own search of PubMed articles indexed for MEDLINE using the phrase melanoma (cutaneous) and treatment, which included studies from May 2017 to February 2024.
ChatGPT’s answers to 23 of the questions aligned with the AAD’s guidelines (Table 1); in instances when the guidelines were inconclusive regarding pathology, the model provided recommendations supported by our contemporary PubMed literature search. Of the 3 questions related to CM pathology, the AAD guidelines had sufficient evidence to provide recommendations for 2 questions. The first question evaluated the clinical information necessary to help the pathologist improve diagnosis (Table 2). ChatGPT’s response to one question about staged excision and Mohs micrographic surgery for melanoma in situ did not align with the AAD guidelines (Table 3).
Our results showed that ChatGPT provided comprehensive responses aligned with current evidence on CM treatment, except for one surgery question for which its response differed from the AAD guidelines. Our findings are consistent with an observational study that reported board-certified dermatologists rated ChatGPT’s responses on melanoma-related questions as 4.88 on a scale of 1 to 5 (1 indicated completely inaccurate information, 5 indicated complete accuracy for clinical sufficiency in practice). The authors also found that ChatGPT gave vague advice, such as to “get regular skin exams,” which is less specific than dermatologists’ recommendations for annual, biannual, or more frequent examinations.5 ChatGPT’s limitations in offering comprehensive answers for some questions aligned with our findings, specifically the omission of key information in the surgical-related question, highlighting the challenge of relying on AI for nuanced clinical guidance.
We found that ChatGPT considered immunosuppression an important risk factor for CM. Similarly, a 2023 cohort study of 93 patients with melanoma and a history of immunosuppression reported that these patients had a higher risk for CM compared with a control group from the National Cancer Institute’s Surveillance, Epidemiology and End Results Program (standardized incidence ratio, 1.53; 95% CI, 1.12-2.04), indicating that incidence of CM in immunocompromised patients was 53% higher than an age- and sex-matched population cohort.6
Our findings also demonstrated that both ChatGPT’s responses and the AAD guidelines aligned in indicating that evidence linking pregnancy to an increased risk for CM remains inconclusive and that pregnant women should still undergo surveillance. A 2022 retrospective cohort study of 1406 women comparing pregnancy-associated melanoma to non–pregnancy-associated CM had no difference in overall survival (hazard ratio, 0.75; 95% CI, 0.54-1.05).7 However, tumor thickness (2.01-4.00 mm) was greater in postpartum cases compared with cases in nonpregnant women (odds ratio, 1.75; 95% CI, 1.03-2.98), suggesting that pregnancy may affect tumor characteristics.7 These findings underscore the importance of using AI tools such as ChatGPT as a supplement to—rather than as a replacement for—expert clinical judgment and up-to-date medical guidelines.
- Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2:E0000198.
- Roster K, Kann RB, Farabi B, et al. Readability and health literacy scores for ChatGPT-generated dermatology public education materials: cross-sectional analysis of sunscreen and melanoma questions. JMIR Dermatol. 2024;7:E50163.
- Dihan Q, Chauhan M, Eleiwa T, et al. Using large language models to generate educational materials on childhood glaucoma. Am J Ophthalmol. 2024;265:28-38.
- Swetter SM, Tsao H, Bichakjian CK, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2019;80:208-250.
- Young JN, O’Hagan R, Poplausky D, et al. The utility of ChatGPT in generating patient-facing and clinical responses for melanoma. J Am Acad Dermatol. 2023;89:602-604.
- Killeen TF, Shanley R, Ramesh V, et al. Malignant melanoma in a retrospective cohort of immunocompromised patients: a statistical and pathologic analysis. Cancers (Basel). 2023;15:3600.
- Kiuru M, Li Q, Zhu G, et al. Melanoma in women of childbearing age and in pregnancy in California, 1994-2015: a population-based cohort study. J Eur Acad Dermatol Venereol. 2022;36:2025-2035.
- Kung TH, Cheatham M, Medenilla A, et al. Performance of ChatGPT on USMLE: potential for AI-assisted medical education using large language models. PLOS Digit Health. 2023;2:E0000198.
- Roster K, Kann RB, Farabi B, et al. Readability and health literacy scores for ChatGPT-generated dermatology public education materials: cross-sectional analysis of sunscreen and melanoma questions. JMIR Dermatol. 2024;7:E50163.
- Dihan Q, Chauhan M, Eleiwa T, et al. Using large language models to generate educational materials on childhood glaucoma. Am J Ophthalmol. 2024;265:28-38.
- Swetter SM, Tsao H, Bichakjian CK, et al. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol. 2019;80:208-250.
- Young JN, O’Hagan R, Poplausky D, et al. The utility of ChatGPT in generating patient-facing and clinical responses for melanoma. J Am Acad Dermatol. 2023;89:602-604.
- Killeen TF, Shanley R, Ramesh V, et al. Malignant melanoma in a retrospective cohort of immunocompromised patients: a statistical and pathologic analysis. Cancers (Basel). 2023;15:3600.
- Kiuru M, Li Q, Zhu G, et al. Melanoma in women of childbearing age and in pregnancy in California, 1994-2015: a population-based cohort study. J Eur Acad Dermatol Venereol. 2022;36:2025-2035.
Alignment of ChatGPT Responses With AAD Guidelines for Cutaneous Melanoma
Alignment of ChatGPT Responses With AAD Guidelines for Cutaneous Melanoma
PRACTICE POINTS
- ChatGPT provides structured, educational-style responses with broad contextual detail but may omit key clinical nuances such as specific surgical considerations, including staged excision or Mohs micrographic surgery for melanoma in situ.
- Large language models should be viewed as a tool to supplement expert clinical judgment and established guidelines rather than as a standalone replacement for dermatologic decision-making.

Predictors of Lidocaine Volume Used During Mohs Micrographic Surgery
Predictors of Lidocaine Volume Used During Mohs Micrographic Surgery
To the Editor:
Mohs micrographic surgery (MMS) is performed in stages and often requires repeated administration of a local anesthetic, most commonly lidocaine. While generally safe, lidocaine administration carries the potential for cumulative toxicity, particularly in patients who have large or multiple lesions or medical comorbidities or who require extensive repair. Current safety guidelines suggest upper limits of 7 mg/kg (or 500 mg) of lidocaine with epinephrine and 4.5 mg/kg (or 300 mg) without epinephrine for adults.1 However, concerns have been raised about the relevance of these thresholds to MMS, in which anesthetic administration may be prolonged, cumulative, and influenced by surgical complexity.2-5 While clinical experience often guides anesthetic planning, limited data exist identifying predictors of lidocaine use during MMS.
We performed an institutional review board–approved retrospective chart review of 149 patients who underwent 170 MMS procedures at a single academic dermatologic surgery center between July 2022 and June 2023. The aim of our study was to identify clinical and surgical predictors of lidocaine volume used during MMS. All procedures were performed by board-certified dermatologic surgeons (including A.J.). All patients received 1% lidocaine with epinephrine as the primary anesthetic agent. We collected patient demographic variables (age, sex, race, weight), procedural characteristics (anatomic site, number of Mohs stages, skin cancer type, number of surgical sites treated in one day, preoperative and postoperative lesion size, surgeon, repair type), comorbid conditions (hypertension, diabetes), and time from diagnosis to surgery. Data were extracted from the institutional REDCap system. We used t tests and analysis of variance for categorical variables and linear regression for continuous predictors, with statistical significance set at P<.05.
Baseline characteristics of the study patients are outlined in Table 1. The mean (SD) age was 74.2 (9.4) years, and most patients (98.7% [147/149]) were White. The mean (SD) weight was 83.1 (19.1) kg. Most lesions were either basal cell carcinoma (BCC)(50.6%) or squamous cell carcinoma (SCC)(44.1%), with 5.3% of lesions representing melanoma. The mean (SD) total lidocaine volume administered was 11.8 (8.3) mL. The majority (123/149 [72.4%]) of cases required one Mohs stage, but a subset required multiple stages, with a maximum of 5.
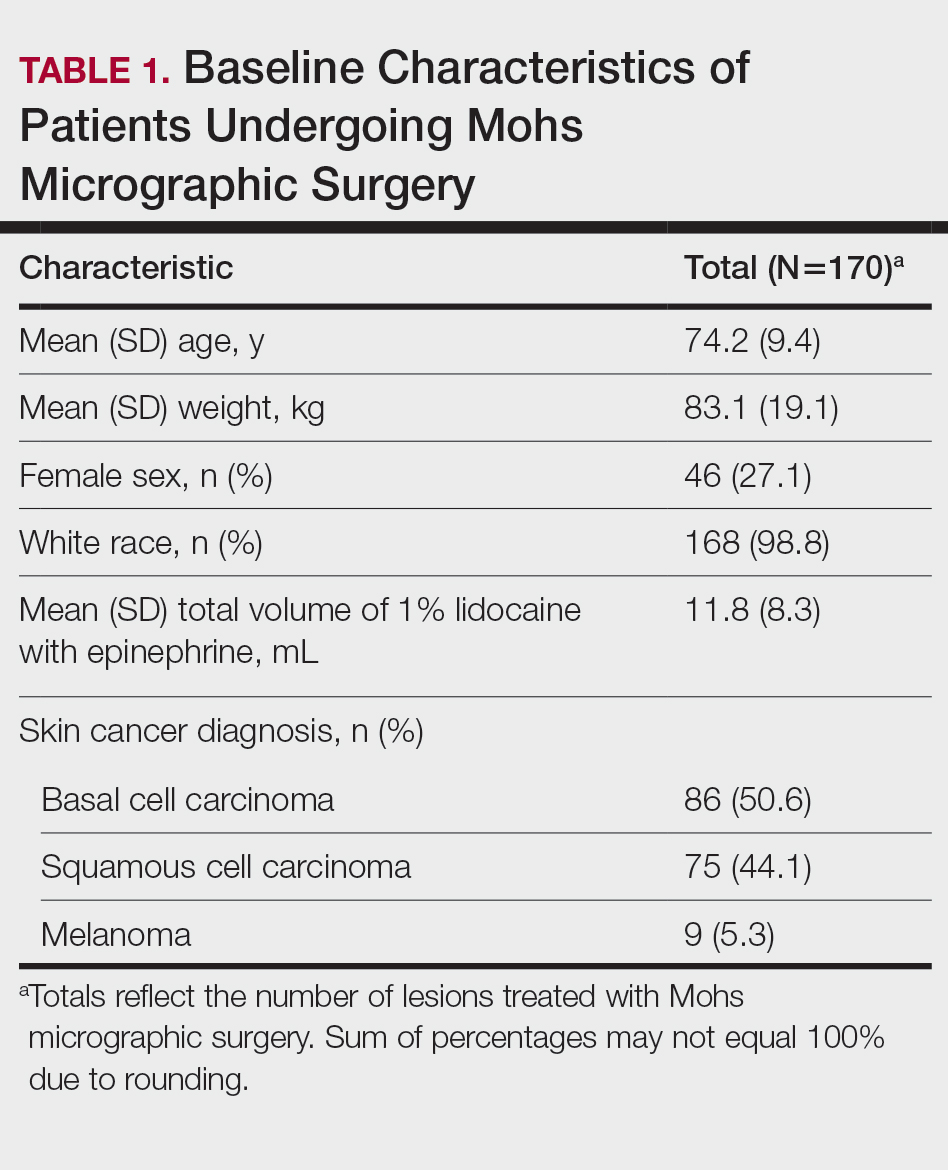
Several procedural and patient factors were significantly associated with the volume of lidocaine used. As expected, lesion size strongly influenced lidocaine volume. Both preoperative and postoperative lesion sizes were highly significant linear predictors (R2=0.28 and 0.41, respectively; P<.001), and postoperative lesion size demonstrated the strongest correlation of all tested variables. Patient weight was also significantly associated with lidocaine use (R2=.03, P=.0202), though the proportion of explained variance was modest. The operating surgeon also was significantly associated with lidocaine use (P=.006), suggesting potential variation in anesthetic technique or threshold for reinfiltration. The number of surgical sites treated in a single session also was significantly associated with greater lidocaine volume (P<.001).
Skin cancer type was a notable categorical predictor. Melanomas required substantially more lidocaine than BCCs or SCCs, with a mean (SD) volume of 25.6 (12.1) mL compared with 10.8 (6.0) mL for BCC and 11.4 (8.8) mL for SCC (P<.001). This difference may reflect disparities in surgical margin requirements, tumor depth, or intraoperative technique. While lesion location and number of stages were not statistically significant overall, mean lidocaine volumes trended higher in lesions on the trunk (18.2 mL) and in procedures requiring 3 or more stages (up to 22.0 mL for a single 4-stage case), though small sample sizes limited the ability to detect statistically significant differences in these subgroups. Detailed comparisons are presented in Table 2.
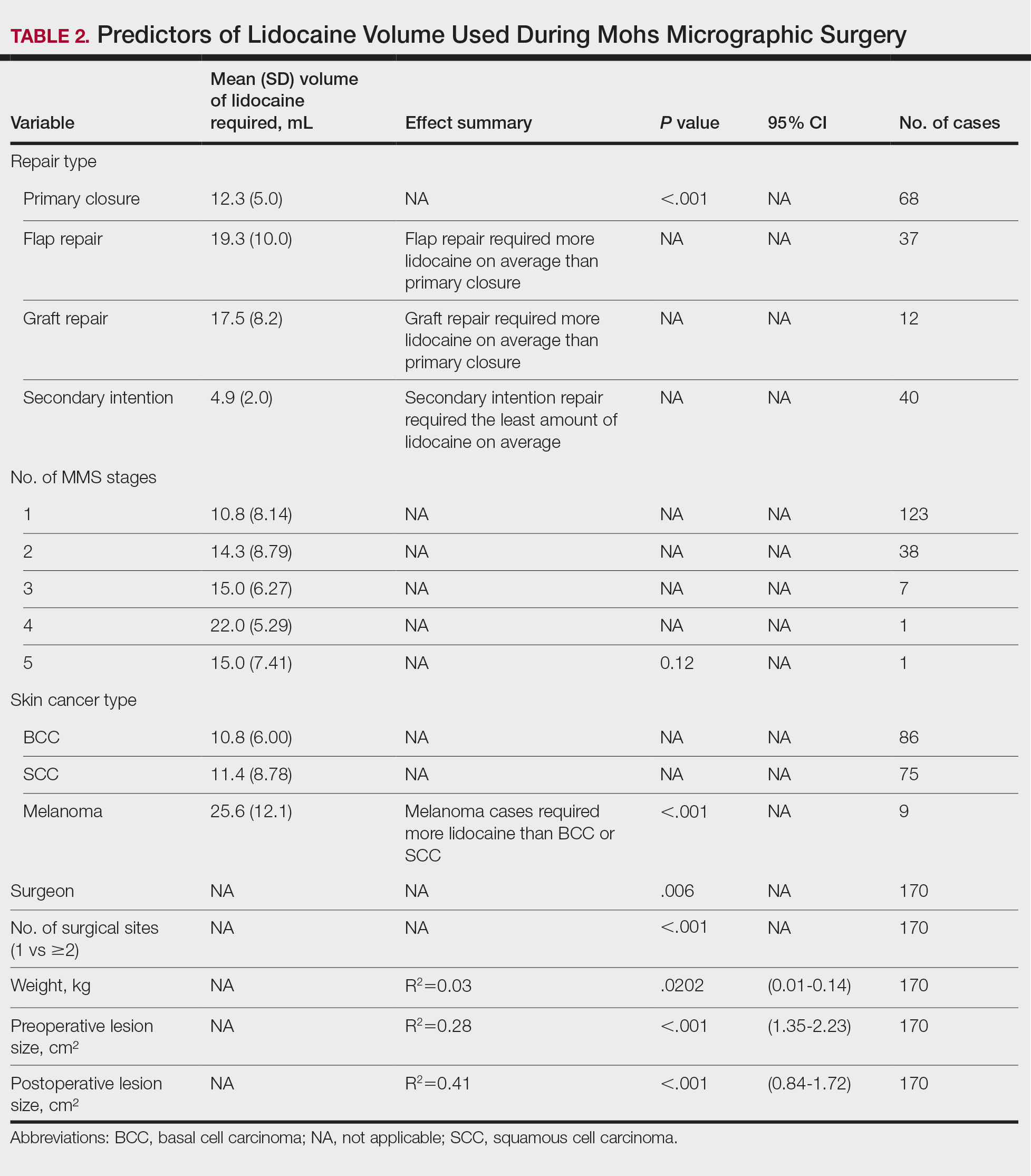
Wound repair type also was significantly associated with lidocaine volume requirements. Primary closures required a mean (SD) volume of 12.3 (5.0) mL, whereas flap repairs required 19.3 (10.0) mL and graft repairs required 17.5 (8.2) mL. Secondary-intention healing used the lowest lidocaine volumes (mean [SD], 4.9 [2.0] mL). Differences across repair types were statistically significant (analysis of variance, P<.001). These findings indicate that more complex reconstructions, such as flaps and grafts, are associated with higher anesthetic needs when compared with primary closures or secondary-intention healing.
Several other predictors, including age, time from diagnosis to surgery, and comorbid conditions such as hypertension or diabetes, were not significantly associated with anesthetic volume in our cohort. Time from diagnosis to surgery ranged widely but did not correlate with lesion size or lidocaine use, possibly due to scheduling variability or biopsy technique.
These findings offer practical implications for clinical planning. While most MMS cases fall well within safe limits for lidocaine administration, some patients—particularly those with melanoma, large lesions, or multiple surgical sites—may approach thresholds at which further monitoring or dose tracking becomes relevant. Anticipating higher anesthetic requirements may help surgical teams plan procedure length, anesthesia restocking, or sequencing of multisite cases. Our analysis also showed that the type of wound repair meaningfully influences anesthetic use, with flap and graft repairs requiring substantially higher lidocaine volumes than primary closures and secondary-intention healing. Considering both tumor characteristics and the planned reconstruction may therefore improve the accuracy of anesthetic forecasting during preoperative planning.
We also observed surgeon-level variation in lidocaine volume despite standardized tumor types and case complexity. This suggests a role for individual technique (eg, depth of field block, number of reinfiltrations) and highlights the need for ongoing education around anesthetic optimization.
Our study was limited by its retrospective design, single-institution setting, and demographically homogeneous population. With 98.8% of patients identifying as White, generalizability to skin of color populations may be limited. In addition, lidocaine metabolism may vary across patient factors not captured here (eg, hepatic or renal function). Finally, although lidocaine volume was the outcome of interest, we did not measure patient-reported pain control, which may further clarify anesthetic adequacy. Nonetheless, our analysis demonstrated that routinely available clinical and procedural data can predict lidocaine volume requirements with reasonable reliability. Although no patient in our cohort approached the maximum recommended lidocaine dose, understanding these predictors may help anticipate scenarios nearing maximum dosing thresholds. In future studies, integrating weight-based thresholds (eg, mL/kg received) or serum lidocaine levels may improve safety monitoring and validate toxicity thresholds in complex cases.
In conclusion, we identified several key factors that predict lidocaine volume during MMS, including lesion size, melanoma diagnosis, number of surgical sites, patient weight, planned reconstruction type, and the operating surgeon. Among these factors, melanoma cases required more than twice the volume of lidocaine compared to BCC and SCC cases, and flap and graft repairs demonstrated the highest anesthetic requirements among closure types. Taken together, these findings reinforce the need for advanced anesthetic planning in aggressive, anatomically complex, or reconstruction-intensive cases and may support more informed intraoperative decision-making.
- Kouba DJ, LoPiccolo MC, Alam M, et al. Guidelines for the use of local anesthesia in office-based dermatologic surgery. J Am Acad Dermatol. 2016;74:1201-1219. doi:10.1016/j.jaad.2016.01.022
- Wang A, Grushchak S, Kaul S, et al. Toxicity of infiltrative lidocaine in dermatologic surgery: are current limits valid? Dermatol Pract Concept. 2021;11:e2021120. doi:10.5826/dpc.1104a120
- Patrinely JR Jr, Darragh C, Frank N, et al. Risk of adverse events due to high volumes of local anesthesia during Mohs micrographic surgery. Arch Dermatol Res. 2021;313:679-684. doi:10.1007/s00403-020-02155-1
- Butterwick KJ, Goldman MP, Sriprachya-Anunt S. Lidocaine levels during the first two hours of infiltration of dilute anesthetic solution for tumescent liposuction: rapid versus slow delivery. Dermatol Surg. 1999;25:681-685. doi:10.1046/j.1524-4725.1999.98275.x
- Flanagan K, McLean R, Goldberg D. Is it time to redefine lidocaine administration guidelines in Mohs surgery? J Drugs Dermatol. 2020;19:433.
To the Editor:
Mohs micrographic surgery (MMS) is performed in stages and often requires repeated administration of a local anesthetic, most commonly lidocaine. While generally safe, lidocaine administration carries the potential for cumulative toxicity, particularly in patients who have large or multiple lesions or medical comorbidities or who require extensive repair. Current safety guidelines suggest upper limits of 7 mg/kg (or 500 mg) of lidocaine with epinephrine and 4.5 mg/kg (or 300 mg) without epinephrine for adults.1 However, concerns have been raised about the relevance of these thresholds to MMS, in which anesthetic administration may be prolonged, cumulative, and influenced by surgical complexity.2-5 While clinical experience often guides anesthetic planning, limited data exist identifying predictors of lidocaine use during MMS.
We performed an institutional review board–approved retrospective chart review of 149 patients who underwent 170 MMS procedures at a single academic dermatologic surgery center between July 2022 and June 2023. The aim of our study was to identify clinical and surgical predictors of lidocaine volume used during MMS. All procedures were performed by board-certified dermatologic surgeons (including A.J.). All patients received 1% lidocaine with epinephrine as the primary anesthetic agent. We collected patient demographic variables (age, sex, race, weight), procedural characteristics (anatomic site, number of Mohs stages, skin cancer type, number of surgical sites treated in one day, preoperative and postoperative lesion size, surgeon, repair type), comorbid conditions (hypertension, diabetes), and time from diagnosis to surgery. Data were extracted from the institutional REDCap system. We used t tests and analysis of variance for categorical variables and linear regression for continuous predictors, with statistical significance set at P<.05.
Baseline characteristics of the study patients are outlined in Table 1. The mean (SD) age was 74.2 (9.4) years, and most patients (98.7% [147/149]) were White. The mean (SD) weight was 83.1 (19.1) kg. Most lesions were either basal cell carcinoma (BCC)(50.6%) or squamous cell carcinoma (SCC)(44.1%), with 5.3% of lesions representing melanoma. The mean (SD) total lidocaine volume administered was 11.8 (8.3) mL. The majority (123/149 [72.4%]) of cases required one Mohs stage, but a subset required multiple stages, with a maximum of 5.
Several procedural and patient factors were significantly associated with the volume of lidocaine used. As expected, lesion size strongly influenced lidocaine volume. Both preoperative and postoperative lesion sizes were highly significant linear predictors (R2=0.28 and 0.41, respectively; P<.001), and postoperative lesion size demonstrated the strongest correlation of all tested variables. Patient weight was also significantly associated with lidocaine use (R2=.03, P=.0202), though the proportion of explained variance was modest. The operating surgeon also was significantly associated with lidocaine use (P=.006), suggesting potential variation in anesthetic technique or threshold for reinfiltration. The number of surgical sites treated in a single session also was significantly associated with greater lidocaine volume (P<.001).
Skin cancer type was a notable categorical predictor. Melanomas required substantially more lidocaine than BCCs or SCCs, with a mean (SD) volume of 25.6 (12.1) mL compared with 10.8 (6.0) mL for BCC and 11.4 (8.8) mL for SCC (P<.001). This difference may reflect disparities in surgical margin requirements, tumor depth, or intraoperative technique. While lesion location and number of stages were not statistically significant overall, mean lidocaine volumes trended higher in lesions on the trunk (18.2 mL) and in procedures requiring 3 or more stages (up to 22.0 mL for a single 4-stage case), though small sample sizes limited the ability to detect statistically significant differences in these subgroups. Detailed comparisons are presented in Table 2.
Wound repair type also was significantly associated with lidocaine volume requirements. Primary closures required a mean (SD) volume of 12.3 (5.0) mL, whereas flap repairs required 19.3 (10.0) mL and graft repairs required 17.5 (8.2) mL. Secondary-intention healing used the lowest lidocaine volumes (mean [SD], 4.9 [2.0] mL). Differences across repair types were statistically significant (analysis of variance, P<.001). These findings indicate that more complex reconstructions, such as flaps and grafts, are associated with higher anesthetic needs when compared with primary closures or secondary-intention healing.
Several other predictors, including age, time from diagnosis to surgery, and comorbid conditions such as hypertension or diabetes, were not significantly associated with anesthetic volume in our cohort. Time from diagnosis to surgery ranged widely but did not correlate with lesion size or lidocaine use, possibly due to scheduling variability or biopsy technique.
These findings offer practical implications for clinical planning. While most MMS cases fall well within safe limits for lidocaine administration, some patients—particularly those with melanoma, large lesions, or multiple surgical sites—may approach thresholds at which further monitoring or dose tracking becomes relevant. Anticipating higher anesthetic requirements may help surgical teams plan procedure length, anesthesia restocking, or sequencing of multisite cases. Our analysis also showed that the type of wound repair meaningfully influences anesthetic use, with flap and graft repairs requiring substantially higher lidocaine volumes than primary closures and secondary-intention healing. Considering both tumor characteristics and the planned reconstruction may therefore improve the accuracy of anesthetic forecasting during preoperative planning.
We also observed surgeon-level variation in lidocaine volume despite standardized tumor types and case complexity. This suggests a role for individual technique (eg, depth of field block, number of reinfiltrations) and highlights the need for ongoing education around anesthetic optimization.
Our study was limited by its retrospective design, single-institution setting, and demographically homogeneous population. With 98.8% of patients identifying as White, generalizability to skin of color populations may be limited. In addition, lidocaine metabolism may vary across patient factors not captured here (eg, hepatic or renal function). Finally, although lidocaine volume was the outcome of interest, we did not measure patient-reported pain control, which may further clarify anesthetic adequacy. Nonetheless, our analysis demonstrated that routinely available clinical and procedural data can predict lidocaine volume requirements with reasonable reliability. Although no patient in our cohort approached the maximum recommended lidocaine dose, understanding these predictors may help anticipate scenarios nearing maximum dosing thresholds. In future studies, integrating weight-based thresholds (eg, mL/kg received) or serum lidocaine levels may improve safety monitoring and validate toxicity thresholds in complex cases.
In conclusion, we identified several key factors that predict lidocaine volume during MMS, including lesion size, melanoma diagnosis, number of surgical sites, patient weight, planned reconstruction type, and the operating surgeon. Among these factors, melanoma cases required more than twice the volume of lidocaine compared to BCC and SCC cases, and flap and graft repairs demonstrated the highest anesthetic requirements among closure types. Taken together, these findings reinforce the need for advanced anesthetic planning in aggressive, anatomically complex, or reconstruction-intensive cases and may support more informed intraoperative decision-making.
To the Editor:
Mohs micrographic surgery (MMS) is performed in stages and often requires repeated administration of a local anesthetic, most commonly lidocaine. While generally safe, lidocaine administration carries the potential for cumulative toxicity, particularly in patients who have large or multiple lesions or medical comorbidities or who require extensive repair. Current safety guidelines suggest upper limits of 7 mg/kg (or 500 mg) of lidocaine with epinephrine and 4.5 mg/kg (or 300 mg) without epinephrine for adults.1 However, concerns have been raised about the relevance of these thresholds to MMS, in which anesthetic administration may be prolonged, cumulative, and influenced by surgical complexity.2-5 While clinical experience often guides anesthetic planning, limited data exist identifying predictors of lidocaine use during MMS.
We performed an institutional review board–approved retrospective chart review of 149 patients who underwent 170 MMS procedures at a single academic dermatologic surgery center between July 2022 and June 2023. The aim of our study was to identify clinical and surgical predictors of lidocaine volume used during MMS. All procedures were performed by board-certified dermatologic surgeons (including A.J.). All patients received 1% lidocaine with epinephrine as the primary anesthetic agent. We collected patient demographic variables (age, sex, race, weight), procedural characteristics (anatomic site, number of Mohs stages, skin cancer type, number of surgical sites treated in one day, preoperative and postoperative lesion size, surgeon, repair type), comorbid conditions (hypertension, diabetes), and time from diagnosis to surgery. Data were extracted from the institutional REDCap system. We used t tests and analysis of variance for categorical variables and linear regression for continuous predictors, with statistical significance set at P<.05.
Baseline characteristics of the study patients are outlined in Table 1. The mean (SD) age was 74.2 (9.4) years, and most patients (98.7% [147/149]) were White. The mean (SD) weight was 83.1 (19.1) kg. Most lesions were either basal cell carcinoma (BCC)(50.6%) or squamous cell carcinoma (SCC)(44.1%), with 5.3% of lesions representing melanoma. The mean (SD) total lidocaine volume administered was 11.8 (8.3) mL. The majority (123/149 [72.4%]) of cases required one Mohs stage, but a subset required multiple stages, with a maximum of 5.
Several procedural and patient factors were significantly associated with the volume of lidocaine used. As expected, lesion size strongly influenced lidocaine volume. Both preoperative and postoperative lesion sizes were highly significant linear predictors (R2=0.28 and 0.41, respectively; P<.001), and postoperative lesion size demonstrated the strongest correlation of all tested variables. Patient weight was also significantly associated with lidocaine use (R2=.03, P=.0202), though the proportion of explained variance was modest. The operating surgeon also was significantly associated with lidocaine use (P=.006), suggesting potential variation in anesthetic technique or threshold for reinfiltration. The number of surgical sites treated in a single session also was significantly associated with greater lidocaine volume (P<.001).
Skin cancer type was a notable categorical predictor. Melanomas required substantially more lidocaine than BCCs or SCCs, with a mean (SD) volume of 25.6 (12.1) mL compared with 10.8 (6.0) mL for BCC and 11.4 (8.8) mL for SCC (P<.001). This difference may reflect disparities in surgical margin requirements, tumor depth, or intraoperative technique. While lesion location and number of stages were not statistically significant overall, mean lidocaine volumes trended higher in lesions on the trunk (18.2 mL) and in procedures requiring 3 or more stages (up to 22.0 mL for a single 4-stage case), though small sample sizes limited the ability to detect statistically significant differences in these subgroups. Detailed comparisons are presented in Table 2.
Wound repair type also was significantly associated with lidocaine volume requirements. Primary closures required a mean (SD) volume of 12.3 (5.0) mL, whereas flap repairs required 19.3 (10.0) mL and graft repairs required 17.5 (8.2) mL. Secondary-intention healing used the lowest lidocaine volumes (mean [SD], 4.9 [2.0] mL). Differences across repair types were statistically significant (analysis of variance, P<.001). These findings indicate that more complex reconstructions, such as flaps and grafts, are associated with higher anesthetic needs when compared with primary closures or secondary-intention healing.
Several other predictors, including age, time from diagnosis to surgery, and comorbid conditions such as hypertension or diabetes, were not significantly associated with anesthetic volume in our cohort. Time from diagnosis to surgery ranged widely but did not correlate with lesion size or lidocaine use, possibly due to scheduling variability or biopsy technique.
These findings offer practical implications for clinical planning. While most MMS cases fall well within safe limits for lidocaine administration, some patients—particularly those with melanoma, large lesions, or multiple surgical sites—may approach thresholds at which further monitoring or dose tracking becomes relevant. Anticipating higher anesthetic requirements may help surgical teams plan procedure length, anesthesia restocking, or sequencing of multisite cases. Our analysis also showed that the type of wound repair meaningfully influences anesthetic use, with flap and graft repairs requiring substantially higher lidocaine volumes than primary closures and secondary-intention healing. Considering both tumor characteristics and the planned reconstruction may therefore improve the accuracy of anesthetic forecasting during preoperative planning.
We also observed surgeon-level variation in lidocaine volume despite standardized tumor types and case complexity. This suggests a role for individual technique (eg, depth of field block, number of reinfiltrations) and highlights the need for ongoing education around anesthetic optimization.
Our study was limited by its retrospective design, single-institution setting, and demographically homogeneous population. With 98.8% of patients identifying as White, generalizability to skin of color populations may be limited. In addition, lidocaine metabolism may vary across patient factors not captured here (eg, hepatic or renal function). Finally, although lidocaine volume was the outcome of interest, we did not measure patient-reported pain control, which may further clarify anesthetic adequacy. Nonetheless, our analysis demonstrated that routinely available clinical and procedural data can predict lidocaine volume requirements with reasonable reliability. Although no patient in our cohort approached the maximum recommended lidocaine dose, understanding these predictors may help anticipate scenarios nearing maximum dosing thresholds. In future studies, integrating weight-based thresholds (eg, mL/kg received) or serum lidocaine levels may improve safety monitoring and validate toxicity thresholds in complex cases.
In conclusion, we identified several key factors that predict lidocaine volume during MMS, including lesion size, melanoma diagnosis, number of surgical sites, patient weight, planned reconstruction type, and the operating surgeon. Among these factors, melanoma cases required more than twice the volume of lidocaine compared to BCC and SCC cases, and flap and graft repairs demonstrated the highest anesthetic requirements among closure types. Taken together, these findings reinforce the need for advanced anesthetic planning in aggressive, anatomically complex, or reconstruction-intensive cases and may support more informed intraoperative decision-making.
- Kouba DJ, LoPiccolo MC, Alam M, et al. Guidelines for the use of local anesthesia in office-based dermatologic surgery. J Am Acad Dermatol. 2016;74:1201-1219. doi:10.1016/j.jaad.2016.01.022
- Wang A, Grushchak S, Kaul S, et al. Toxicity of infiltrative lidocaine in dermatologic surgery: are current limits valid? Dermatol Pract Concept. 2021;11:e2021120. doi:10.5826/dpc.1104a120
- Patrinely JR Jr, Darragh C, Frank N, et al. Risk of adverse events due to high volumes of local anesthesia during Mohs micrographic surgery. Arch Dermatol Res. 2021;313:679-684. doi:10.1007/s00403-020-02155-1
- Butterwick KJ, Goldman MP, Sriprachya-Anunt S. Lidocaine levels during the first two hours of infiltration of dilute anesthetic solution for tumescent liposuction: rapid versus slow delivery. Dermatol Surg. 1999;25:681-685. doi:10.1046/j.1524-4725.1999.98275.x
- Flanagan K, McLean R, Goldberg D. Is it time to redefine lidocaine administration guidelines in Mohs surgery? J Drugs Dermatol. 2020;19:433.
- Kouba DJ, LoPiccolo MC, Alam M, et al. Guidelines for the use of local anesthesia in office-based dermatologic surgery. J Am Acad Dermatol. 2016;74:1201-1219. doi:10.1016/j.jaad.2016.01.022
- Wang A, Grushchak S, Kaul S, et al. Toxicity of infiltrative lidocaine in dermatologic surgery: are current limits valid? Dermatol Pract Concept. 2021;11:e2021120. doi:10.5826/dpc.1104a120
- Patrinely JR Jr, Darragh C, Frank N, et al. Risk of adverse events due to high volumes of local anesthesia during Mohs micrographic surgery. Arch Dermatol Res. 2021;313:679-684. doi:10.1007/s00403-020-02155-1
- Butterwick KJ, Goldman MP, Sriprachya-Anunt S. Lidocaine levels during the first two hours of infiltration of dilute anesthetic solution for tumescent liposuction: rapid versus slow delivery. Dermatol Surg. 1999;25:681-685. doi:10.1046/j.1524-4725.1999.98275.x
- Flanagan K, McLean R, Goldberg D. Is it time to redefine lidocaine administration guidelines in Mohs surgery? J Drugs Dermatol. 2020;19:433.
Predictors of Lidocaine Volume Used During Mohs Micrographic Surgery
Predictors of Lidocaine Volume Used During Mohs Micrographic Surgery
Practice Points
- Larger lesion size, melanoma diagnosis, and multiple surgical sites are associated with higher lidocaine volume requirements during Mohs micrographic surgery.
- Melanomas required more than twice the average lidocaine volume compared with basal cell carcinomas and squamous cell carcinomas.
- Flap and graft repairs require substantially more lidocaine than primary closures, while secondary-intention healing uses the least, making reconstruction type an important predictor of total anesthetic needs.

Severe Cutaneous Adverse Reactions in the Setting of Antineoplastic Therapy: A Single-Institution Retrospective Study
Severe Cutaneous Adverse Reactions in the Setting of Antineoplastic Therapy: A Single-Institution Retrospective Study
To the Editor:
Severe cutaneous adverse reactions (SCARs) are rare, life-threatening reactions that include acute generalized exanthematous pustulosis (AGEP), drug reaction with eosinophilia and systemic symptoms (DRESS), and Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN).1 In addition to being associated with commonly implicated medications, SCARs also may occur in the setting of antineoplastic therapy.2,3 Although antineoplastic-associated SCARs have been described, diagnosis can be difficult due to varying latency periods and atypical clinical features, such as those observed with BRAF inhibitor–related DRESS during immunotherapy.4 Severe cutaneous adverse reactions can increase morbidity and mortality in the oncologic patient population due to both the clinical sequelae from the cutaneous reaction and the potential to interrupt cancer treatment.
The aim of this study was to evaluate the clinical characteristics, outcomes, and impact on cancer treatment among patients diagnosed with a SCAR while receiving active therapy for malignancy. We conducted a retrospective chart review of electronic medical records at Yale New Haven Hospital (New Haven, Connecticut) from 2013 to 2023, identifying patients receiving antineoplastic therapy who were diagnosed with a SCAR. Cases were identified through a search of the electronic medical record performed by the joint data analytics team using the keywords DRESS, SJS, TEN, AGEP, and generalized bullous fixed drug eruption, along with spelling variations (both abbreviations and full terms), in addition to manual review by one of the authors (K.V.) of the inpatient dermatology consultation log and dermatopathology database. Only patients for whom an antineoplastic agent was identified as a high-probability culprit by the dermatology and/or oncology teams were included.
In total, 20 patients (11 female, 9 male) were identified as having an antineoplastic-associated SCAR. All patients had metastatic or advanced disease. We identified 2 (10%) cases of AGEP, 16 (80%) cases of DRESS, and 3 (15%) cases of SJS/TEN. One patient on immunotherapy had 2 distinct SCARs (AGEP, DRESS) at different time points. Table 1 describes patient and SCAR characteristics as well as impact on cancer treatment. The median (interquartile range [IQR]) latency period for AGEP was 7.5 (4-11) days. The median (IQR) latency period for 13 of the 16 (81%) DRESS cases was 14 (10-32) days. For 3 DRESS cases with a potential second-hit phenomenon in the setting of current or antecedent immunotherapy,5 the median (IQR) latency period was 122 (96-426) days for the immunotherapy drug and 28 (21-52) days for the drug culprit. The median (IQR) latency period for SJS/TEN was 23 (20-27) days.
Patients received treatment with combination systemic corticosteroids and topical corticosteroids in 13 (65%) cases, systemic corticosteroid monotherapy in 6 (30%) cases, or combination systemic corticosteroids and etanercept in 1 (5%) case. All patients experienced resolution of the SCAR and survived to hospital discharge. Most (17/20 [85%]) patients experienced interruption or discontinuation of cancer treatment. Table 2 describes the implicated antineoplastic therapies, which included chemotherapy (3 DRESS, 1 SJS/TEN), hormonal therapy (1 DRESS), immunotherapy (1 AGEP, 4 DRESS), and targeted therapy (1 AGEP, 8 DRESS, 2 SJS/TEN).
Limitations of this study include the retrospective study design, the small sample size, and the challenge of drug culprit identification in oncologic patients on multiple high-probability medications.
Though rare, SCARs can be encountered in patients on antineoplastic therapy with a wide range of drug culprits. In our cohort, SCARs occurred with various antineoplastic agents, including chemotherapy, hormonal therapy, immunotherapy, and targeted therapy. The most common antineoplastic-associated SCAR was DRESS, which had the widest latency period in the setting of a potential second-hit phenomenon with another drug culprit. Although we did not observe any cases of SJS/TEN in the immunotherapy category, it is important to consider progressive immunotherapy-related mucocutaneous eruption in the differential diagnosis. Fortunately, all patients survived to hospital discharge and experienced SCAR resolution with systemic treatment; however, most patients experienced interruption of cancer therapy, which has the potential to affect oncologic outcomes. This interruption is not uncommon, as rechallenge of an antineoplastic agent in patients with a therapy-related SCAR generally is not recommended. The awareness and prompt management of SCARs in a patient on treatment for malignancy are critical in order to minimize negative outcomes in this vulnerable patient population.
- Duong TA, Valeyrie-Allanore L, Wolkenstein P, et al. Severe cutaneous adverse reactions to drugs. Lancet. 2017;390: 1996-2011.
- Chen CB, Wu MY, Ng CY, et al. Severe cutaneous adverse reactions induced by targeted anticancer therapies and immunotherapies. Cancer Manag Res. 2018;10:1259-1273.
- Ng CY, Chen CB, Wu MY, et al. Anticancer drugs induced severe adverse cutaneous drug reactions: an updated review on the risks associated with anticancer targeted therapy or immunotherapies. J Immunol Res. 2018;2018:5376476.
- Maloney NJ, Rana J, Yang JJ, et al. Clinical features of druginduced hypersensitivity syndrome to BRAF inhibitors with and without previous immune checkpoint inhibition: a review. Support Care Cancer. 2022;30:2839-2851.
- Hammond S, Olsson-Brown A, Grice S, et al. Does immune checkpoint inhibitor therapy increase the frequency of adverse reactions to concomitant medications? Clin Exp Allergy. 2022;52:600-603.
To the Editor:
Severe cutaneous adverse reactions (SCARs) are rare, life-threatening reactions that include acute generalized exanthematous pustulosis (AGEP), drug reaction with eosinophilia and systemic symptoms (DRESS), and Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN).1 In addition to being associated with commonly implicated medications, SCARs also may occur in the setting of antineoplastic therapy.2,3 Although antineoplastic-associated SCARs have been described, diagnosis can be difficult due to varying latency periods and atypical clinical features, such as those observed with BRAF inhibitor–related DRESS during immunotherapy.4 Severe cutaneous adverse reactions can increase morbidity and mortality in the oncologic patient population due to both the clinical sequelae from the cutaneous reaction and the potential to interrupt cancer treatment.
The aim of this study was to evaluate the clinical characteristics, outcomes, and impact on cancer treatment among patients diagnosed with a SCAR while receiving active therapy for malignancy. We conducted a retrospective chart review of electronic medical records at Yale New Haven Hospital (New Haven, Connecticut) from 2013 to 2023, identifying patients receiving antineoplastic therapy who were diagnosed with a SCAR. Cases were identified through a search of the electronic medical record performed by the joint data analytics team using the keywords DRESS, SJS, TEN, AGEP, and generalized bullous fixed drug eruption, along with spelling variations (both abbreviations and full terms), in addition to manual review by one of the authors (K.V.) of the inpatient dermatology consultation log and dermatopathology database. Only patients for whom an antineoplastic agent was identified as a high-probability culprit by the dermatology and/or oncology teams were included.
In total, 20 patients (11 female, 9 male) were identified as having an antineoplastic-associated SCAR. All patients had metastatic or advanced disease. We identified 2 (10%) cases of AGEP, 16 (80%) cases of DRESS, and 3 (15%) cases of SJS/TEN. One patient on immunotherapy had 2 distinct SCARs (AGEP, DRESS) at different time points. Table 1 describes patient and SCAR characteristics as well as impact on cancer treatment. The median (interquartile range [IQR]) latency period for AGEP was 7.5 (4-11) days. The median (IQR) latency period for 13 of the 16 (81%) DRESS cases was 14 (10-32) days. For 3 DRESS cases with a potential second-hit phenomenon in the setting of current or antecedent immunotherapy,5 the median (IQR) latency period was 122 (96-426) days for the immunotherapy drug and 28 (21-52) days for the drug culprit. The median (IQR) latency period for SJS/TEN was 23 (20-27) days.
Patients received treatment with combination systemic corticosteroids and topical corticosteroids in 13 (65%) cases, systemic corticosteroid monotherapy in 6 (30%) cases, or combination systemic corticosteroids and etanercept in 1 (5%) case. All patients experienced resolution of the SCAR and survived to hospital discharge. Most (17/20 [85%]) patients experienced interruption or discontinuation of cancer treatment. Table 2 describes the implicated antineoplastic therapies, which included chemotherapy (3 DRESS, 1 SJS/TEN), hormonal therapy (1 DRESS), immunotherapy (1 AGEP, 4 DRESS), and targeted therapy (1 AGEP, 8 DRESS, 2 SJS/TEN).
Limitations of this study include the retrospective study design, the small sample size, and the challenge of drug culprit identification in oncologic patients on multiple high-probability medications.
Though rare, SCARs can be encountered in patients on antineoplastic therapy with a wide range of drug culprits. In our cohort, SCARs occurred with various antineoplastic agents, including chemotherapy, hormonal therapy, immunotherapy, and targeted therapy. The most common antineoplastic-associated SCAR was DRESS, which had the widest latency period in the setting of a potential second-hit phenomenon with another drug culprit. Although we did not observe any cases of SJS/TEN in the immunotherapy category, it is important to consider progressive immunotherapy-related mucocutaneous eruption in the differential diagnosis. Fortunately, all patients survived to hospital discharge and experienced SCAR resolution with systemic treatment; however, most patients experienced interruption of cancer therapy, which has the potential to affect oncologic outcomes. This interruption is not uncommon, as rechallenge of an antineoplastic agent in patients with a therapy-related SCAR generally is not recommended. The awareness and prompt management of SCARs in a patient on treatment for malignancy are critical in order to minimize negative outcomes in this vulnerable patient population.
To the Editor:
Severe cutaneous adverse reactions (SCARs) are rare, life-threatening reactions that include acute generalized exanthematous pustulosis (AGEP), drug reaction with eosinophilia and systemic symptoms (DRESS), and Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN).1 In addition to being associated with commonly implicated medications, SCARs also may occur in the setting of antineoplastic therapy.2,3 Although antineoplastic-associated SCARs have been described, diagnosis can be difficult due to varying latency periods and atypical clinical features, such as those observed with BRAF inhibitor–related DRESS during immunotherapy.4 Severe cutaneous adverse reactions can increase morbidity and mortality in the oncologic patient population due to both the clinical sequelae from the cutaneous reaction and the potential to interrupt cancer treatment.
The aim of this study was to evaluate the clinical characteristics, outcomes, and impact on cancer treatment among patients diagnosed with a SCAR while receiving active therapy for malignancy. We conducted a retrospective chart review of electronic medical records at Yale New Haven Hospital (New Haven, Connecticut) from 2013 to 2023, identifying patients receiving antineoplastic therapy who were diagnosed with a SCAR. Cases were identified through a search of the electronic medical record performed by the joint data analytics team using the keywords DRESS, SJS, TEN, AGEP, and generalized bullous fixed drug eruption, along with spelling variations (both abbreviations and full terms), in addition to manual review by one of the authors (K.V.) of the inpatient dermatology consultation log and dermatopathology database. Only patients for whom an antineoplastic agent was identified as a high-probability culprit by the dermatology and/or oncology teams were included.
In total, 20 patients (11 female, 9 male) were identified as having an antineoplastic-associated SCAR. All patients had metastatic or advanced disease. We identified 2 (10%) cases of AGEP, 16 (80%) cases of DRESS, and 3 (15%) cases of SJS/TEN. One patient on immunotherapy had 2 distinct SCARs (AGEP, DRESS) at different time points. Table 1 describes patient and SCAR characteristics as well as impact on cancer treatment. The median (interquartile range [IQR]) latency period for AGEP was 7.5 (4-11) days. The median (IQR) latency period for 13 of the 16 (81%) DRESS cases was 14 (10-32) days. For 3 DRESS cases with a potential second-hit phenomenon in the setting of current or antecedent immunotherapy,5 the median (IQR) latency period was 122 (96-426) days for the immunotherapy drug and 28 (21-52) days for the drug culprit. The median (IQR) latency period for SJS/TEN was 23 (20-27) days.
Patients received treatment with combination systemic corticosteroids and topical corticosteroids in 13 (65%) cases, systemic corticosteroid monotherapy in 6 (30%) cases, or combination systemic corticosteroids and etanercept in 1 (5%) case. All patients experienced resolution of the SCAR and survived to hospital discharge. Most (17/20 [85%]) patients experienced interruption or discontinuation of cancer treatment. Table 2 describes the implicated antineoplastic therapies, which included chemotherapy (3 DRESS, 1 SJS/TEN), hormonal therapy (1 DRESS), immunotherapy (1 AGEP, 4 DRESS), and targeted therapy (1 AGEP, 8 DRESS, 2 SJS/TEN).
Limitations of this study include the retrospective study design, the small sample size, and the challenge of drug culprit identification in oncologic patients on multiple high-probability medications.
Though rare, SCARs can be encountered in patients on antineoplastic therapy with a wide range of drug culprits. In our cohort, SCARs occurred with various antineoplastic agents, including chemotherapy, hormonal therapy, immunotherapy, and targeted therapy. The most common antineoplastic-associated SCAR was DRESS, which had the widest latency period in the setting of a potential second-hit phenomenon with another drug culprit. Although we did not observe any cases of SJS/TEN in the immunotherapy category, it is important to consider progressive immunotherapy-related mucocutaneous eruption in the differential diagnosis. Fortunately, all patients survived to hospital discharge and experienced SCAR resolution with systemic treatment; however, most patients experienced interruption of cancer therapy, which has the potential to affect oncologic outcomes. This interruption is not uncommon, as rechallenge of an antineoplastic agent in patients with a therapy-related SCAR generally is not recommended. The awareness and prompt management of SCARs in a patient on treatment for malignancy are critical in order to minimize negative outcomes in this vulnerable patient population.
- Duong TA, Valeyrie-Allanore L, Wolkenstein P, et al. Severe cutaneous adverse reactions to drugs. Lancet. 2017;390: 1996-2011.
- Chen CB, Wu MY, Ng CY, et al. Severe cutaneous adverse reactions induced by targeted anticancer therapies and immunotherapies. Cancer Manag Res. 2018;10:1259-1273.
- Ng CY, Chen CB, Wu MY, et al. Anticancer drugs induced severe adverse cutaneous drug reactions: an updated review on the risks associated with anticancer targeted therapy or immunotherapies. J Immunol Res. 2018;2018:5376476.
- Maloney NJ, Rana J, Yang JJ, et al. Clinical features of druginduced hypersensitivity syndrome to BRAF inhibitors with and without previous immune checkpoint inhibition: a review. Support Care Cancer. 2022;30:2839-2851.
- Hammond S, Olsson-Brown A, Grice S, et al. Does immune checkpoint inhibitor therapy increase the frequency of adverse reactions to concomitant medications? Clin Exp Allergy. 2022;52:600-603.
- Duong TA, Valeyrie-Allanore L, Wolkenstein P, et al. Severe cutaneous adverse reactions to drugs. Lancet. 2017;390: 1996-2011.
- Chen CB, Wu MY, Ng CY, et al. Severe cutaneous adverse reactions induced by targeted anticancer therapies and immunotherapies. Cancer Manag Res. 2018;10:1259-1273.
- Ng CY, Chen CB, Wu MY, et al. Anticancer drugs induced severe adverse cutaneous drug reactions: an updated review on the risks associated with anticancer targeted therapy or immunotherapies. J Immunol Res. 2018;2018:5376476.
- Maloney NJ, Rana J, Yang JJ, et al. Clinical features of druginduced hypersensitivity syndrome to BRAF inhibitors with and without previous immune checkpoint inhibition: a review. Support Care Cancer. 2022;30:2839-2851.
- Hammond S, Olsson-Brown A, Grice S, et al. Does immune checkpoint inhibitor therapy increase the frequency of adverse reactions to concomitant medications? Clin Exp Allergy. 2022;52:600-603.
Severe Cutaneous Adverse Reactions in the Setting of Antineoplastic Therapy: A Single-Institution Retrospective Study
Severe Cutaneous Adverse Reactions in the Setting of Antineoplastic Therapy: A Single-Institution Retrospective Study
Practice Points
- Clinicians should be aware of the occurrence of severe cutaneous adverse reactions (SCARs) in patients on antineoplastic therapy to prevent delays in treatment and improve patient outcomes.
- Rapid initiation of treatment can be effective in resolving SCARs and ensuring full recovery.
- Close coordination between dermatology and oncology teams is crucial to manage SCARs while minimizing cancer treatment interruptions.
Adverse Events Associated With At-Home Microcurrent Facial Devices
Adverse Events Associated With At-Home Microcurrent Facial Devices
To the Editor:
At-home microcurrent facial devices have gained rapid popularity for cosmetic rejuvenation, promising improvements in skin tone, contour, and collagen production.¹ In particular, the post–COVID-19 era has seen a surge in at-home beauty practices driven by social media influence, with the global microcurrent facial market estimated at $372.9 million in 2022 and projected to grow at a compound annual growth rate of 7.3% through 2030.1 Microcurrent devices deliver low-level electrical currents to the skin and underlying muscles. Given the limited exploration of the long-term safety, we aimed to collate existing data and identify trends in reports of adverse events (AEs) associated with these microcurrent devices.
On April 15, 2025, the US Food and Drug Administration’s Manufacturer and User Facility Device Experience (MAUDE) database was queried for medical device reports from January 1, 2013, through March 31, 2025, using product names and keywords including NuFACE, TheraFace, FOREO, and microcurrent device. Search terms were limited to brands for which complaint data existed in the MAUDE database at the time of query. To ensure accuracy, reports were manually reviewed to eliminate duplicates and irrelevant entries.
A total of 28 unique AE reports associated with at-home microcurrent devices were identified (eTable). The majority involved NuFACE devices (ie, NuFACE Trinity, NuFACE Mini, and NuFACE Trinity+)(NuFACE)(n=25), followed by the TheraFace PRO (Therabody, Inc)(n=2) and the FOREO BEAR (FOREO)(n=1). The most frequently documented AEs associated with the NuFACE devices included arrhythmia (7/25 [28%]), pain (6/25 [24%]), dizziness (4/25 [16%]), headache (4/25 [16%]), and inflammation (4/25 [16%]). There was 1 (4%) case of retinal detachment. The TheraFace PRO was associated with device overheating (2/2 [100%]), and the FOREO BEAR was associated with facial deformity/disfigurement (1/1 [100%]).
While microcurrent therapy is widely marketed to consumers through social media influencers and at-home beauty platforms,1 randomized controlled trials (RCTs) evaluating AEs related to use of this technology are lacking, possibly due to nonstringent regulation of nonprescription cosmetic devices.² Contrary to our findings, RCTs of microcurrent devices have reported minimal or no AEs; for instance, an RCT evaluating 56 participants treated 5 times weekly for 12 weeks with a microcurrent device that was not included in our analysis reported only mild erythema in all experimental group participants.2 In another RCT of 30 participants, 15 of whom were treated with a microcurrent device and 15 with placebo for 30 minutes once daily over a period of 10 days, no AEs were reported.3 A cohort analysis of 34 patients also provided preliminary evidence supporting the use of microcurrent therapy for chronic back and neck pain, beyond its cosmetic applications.4 Despite the lack of reported AEs in the literature, there is a notable absence of large-scale, rigorous studies on this topic.
Our analysis was subject to the limitations of the MAUDE database, in which reports of severe AEs are more likely to be reported than transient ones. Additionally, the small sample size and lack of a known denominator make it difficult to compare frequencies of AEs among different microcurrent tools. The products chosen for this study were the select few that reported complaint data, but there is a large existing market of devices that may be associated with AEs that have yet to be reported, potentially because of their novelty.
Our findings suggest that, despite their over-the-counter availability, microcurrent facial devices may carry major risks—particularly in at-home settings. While short-term studies have highlighted potential benefits, the small sample sizes and limited follow-up make it difficult to comprehensively characterize long-term safety risks. Among available studies on microcurrent beauty treatments, the longest follow-up was only 12 weeks.2 Our findings support the need for further large-scale and longitudinal studies to evaluate both the efficacy and safety of at-home microcurrent therapy, especially with increasing consumer interest. The diversity of the products available adds to the challenge of broad safety guidelines, in addition to the lack of long-term clinical studies.
- Microcurrent Facial Market Size, Growth & Trends Report 2030. Grand View Research. Published 2023. Accessed March 3, 2026. https://www.grandviewresearch.com/industry-analysis/microcurrent-facial-market-report
- Bu P, Duan R, Luo J, et al. Development of home beauty devices for facial rejuvenation: establishment of efficacy evaluation system. Clin Cosmet Investig Dermatol. 2024;17:553-563.
- Jain S, Arora M. Effect of microcurrent facial muscle toning on fine wrinkles & firmness of face. IAMR J Physiother. 2012;1:13-19.
- Armstrong K, Gokal R, Chevalier A, et al. Microcurrent point stimulation applied to lower back acupuncture points for the treatment of nonspecific neck pain. J Altern Complement Med. 2017;23:295-299.
To the Editor:
At-home microcurrent facial devices have gained rapid popularity for cosmetic rejuvenation, promising improvements in skin tone, contour, and collagen production.¹ In particular, the post–COVID-19 era has seen a surge in at-home beauty practices driven by social media influence, with the global microcurrent facial market estimated at $372.9 million in 2022 and projected to grow at a compound annual growth rate of 7.3% through 2030.1 Microcurrent devices deliver low-level electrical currents to the skin and underlying muscles. Given the limited exploration of the long-term safety, we aimed to collate existing data and identify trends in reports of adverse events (AEs) associated with these microcurrent devices.
On April 15, 2025, the US Food and Drug Administration’s Manufacturer and User Facility Device Experience (MAUDE) database was queried for medical device reports from January 1, 2013, through March 31, 2025, using product names and keywords including NuFACE, TheraFace, FOREO, and microcurrent device. Search terms were limited to brands for which complaint data existed in the MAUDE database at the time of query. To ensure accuracy, reports were manually reviewed to eliminate duplicates and irrelevant entries.
A total of 28 unique AE reports associated with at-home microcurrent devices were identified (eTable). The majority involved NuFACE devices (ie, NuFACE Trinity, NuFACE Mini, and NuFACE Trinity+)(NuFACE)(n=25), followed by the TheraFace PRO (Therabody, Inc)(n=2) and the FOREO BEAR (FOREO)(n=1). The most frequently documented AEs associated with the NuFACE devices included arrhythmia (7/25 [28%]), pain (6/25 [24%]), dizziness (4/25 [16%]), headache (4/25 [16%]), and inflammation (4/25 [16%]). There was 1 (4%) case of retinal detachment. The TheraFace PRO was associated with device overheating (2/2 [100%]), and the FOREO BEAR was associated with facial deformity/disfigurement (1/1 [100%]).
While microcurrent therapy is widely marketed to consumers through social media influencers and at-home beauty platforms,1 randomized controlled trials (RCTs) evaluating AEs related to use of this technology are lacking, possibly due to nonstringent regulation of nonprescription cosmetic devices.² Contrary to our findings, RCTs of microcurrent devices have reported minimal or no AEs; for instance, an RCT evaluating 56 participants treated 5 times weekly for 12 weeks with a microcurrent device that was not included in our analysis reported only mild erythema in all experimental group participants.2 In another RCT of 30 participants, 15 of whom were treated with a microcurrent device and 15 with placebo for 30 minutes once daily over a period of 10 days, no AEs were reported.3 A cohort analysis of 34 patients also provided preliminary evidence supporting the use of microcurrent therapy for chronic back and neck pain, beyond its cosmetic applications.4 Despite the lack of reported AEs in the literature, there is a notable absence of large-scale, rigorous studies on this topic.
Our analysis was subject to the limitations of the MAUDE database, in which reports of severe AEs are more likely to be reported than transient ones. Additionally, the small sample size and lack of a known denominator make it difficult to compare frequencies of AEs among different microcurrent tools. The products chosen for this study were the select few that reported complaint data, but there is a large existing market of devices that may be associated with AEs that have yet to be reported, potentially because of their novelty.
Our findings suggest that, despite their over-the-counter availability, microcurrent facial devices may carry major risks—particularly in at-home settings. While short-term studies have highlighted potential benefits, the small sample sizes and limited follow-up make it difficult to comprehensively characterize long-term safety risks. Among available studies on microcurrent beauty treatments, the longest follow-up was only 12 weeks.2 Our findings support the need for further large-scale and longitudinal studies to evaluate both the efficacy and safety of at-home microcurrent therapy, especially with increasing consumer interest. The diversity of the products available adds to the challenge of broad safety guidelines, in addition to the lack of long-term clinical studies.
To the Editor:
At-home microcurrent facial devices have gained rapid popularity for cosmetic rejuvenation, promising improvements in skin tone, contour, and collagen production.¹ In particular, the post–COVID-19 era has seen a surge in at-home beauty practices driven by social media influence, with the global microcurrent facial market estimated at $372.9 million in 2022 and projected to grow at a compound annual growth rate of 7.3% through 2030.1 Microcurrent devices deliver low-level electrical currents to the skin and underlying muscles. Given the limited exploration of the long-term safety, we aimed to collate existing data and identify trends in reports of adverse events (AEs) associated with these microcurrent devices.
On April 15, 2025, the US Food and Drug Administration’s Manufacturer and User Facility Device Experience (MAUDE) database was queried for medical device reports from January 1, 2013, through March 31, 2025, using product names and keywords including NuFACE, TheraFace, FOREO, and microcurrent device. Search terms were limited to brands for which complaint data existed in the MAUDE database at the time of query. To ensure accuracy, reports were manually reviewed to eliminate duplicates and irrelevant entries.
A total of 28 unique AE reports associated with at-home microcurrent devices were identified (eTable). The majority involved NuFACE devices (ie, NuFACE Trinity, NuFACE Mini, and NuFACE Trinity+)(NuFACE)(n=25), followed by the TheraFace PRO (Therabody, Inc)(n=2) and the FOREO BEAR (FOREO)(n=1). The most frequently documented AEs associated with the NuFACE devices included arrhythmia (7/25 [28%]), pain (6/25 [24%]), dizziness (4/25 [16%]), headache (4/25 [16%]), and inflammation (4/25 [16%]). There was 1 (4%) case of retinal detachment. The TheraFace PRO was associated with device overheating (2/2 [100%]), and the FOREO BEAR was associated with facial deformity/disfigurement (1/1 [100%]).
While microcurrent therapy is widely marketed to consumers through social media influencers and at-home beauty platforms,1 randomized controlled trials (RCTs) evaluating AEs related to use of this technology are lacking, possibly due to nonstringent regulation of nonprescription cosmetic devices.² Contrary to our findings, RCTs of microcurrent devices have reported minimal or no AEs; for instance, an RCT evaluating 56 participants treated 5 times weekly for 12 weeks with a microcurrent device that was not included in our analysis reported only mild erythema in all experimental group participants.2 In another RCT of 30 participants, 15 of whom were treated with a microcurrent device and 15 with placebo for 30 minutes once daily over a period of 10 days, no AEs were reported.3 A cohort analysis of 34 patients also provided preliminary evidence supporting the use of microcurrent therapy for chronic back and neck pain, beyond its cosmetic applications.4 Despite the lack of reported AEs in the literature, there is a notable absence of large-scale, rigorous studies on this topic.
Our analysis was subject to the limitations of the MAUDE database, in which reports of severe AEs are more likely to be reported than transient ones. Additionally, the small sample size and lack of a known denominator make it difficult to compare frequencies of AEs among different microcurrent tools. The products chosen for this study were the select few that reported complaint data, but there is a large existing market of devices that may be associated with AEs that have yet to be reported, potentially because of their novelty.
Our findings suggest that, despite their over-the-counter availability, microcurrent facial devices may carry major risks—particularly in at-home settings. While short-term studies have highlighted potential benefits, the small sample sizes and limited follow-up make it difficult to comprehensively characterize long-term safety risks. Among available studies on microcurrent beauty treatments, the longest follow-up was only 12 weeks.2 Our findings support the need for further large-scale and longitudinal studies to evaluate both the efficacy and safety of at-home microcurrent therapy, especially with increasing consumer interest. The diversity of the products available adds to the challenge of broad safety guidelines, in addition to the lack of long-term clinical studies.
- Microcurrent Facial Market Size, Growth & Trends Report 2030. Grand View Research. Published 2023. Accessed March 3, 2026. https://www.grandviewresearch.com/industry-analysis/microcurrent-facial-market-report
- Bu P, Duan R, Luo J, et al. Development of home beauty devices for facial rejuvenation: establishment of efficacy evaluation system. Clin Cosmet Investig Dermatol. 2024;17:553-563.
- Jain S, Arora M. Effect of microcurrent facial muscle toning on fine wrinkles & firmness of face. IAMR J Physiother. 2012;1:13-19.
- Armstrong K, Gokal R, Chevalier A, et al. Microcurrent point stimulation applied to lower back acupuncture points for the treatment of nonspecific neck pain. J Altern Complement Med. 2017;23:295-299.
- Microcurrent Facial Market Size, Growth & Trends Report 2030. Grand View Research. Published 2023. Accessed March 3, 2026. https://www.grandviewresearch.com/industry-analysis/microcurrent-facial-market-report
- Bu P, Duan R, Luo J, et al. Development of home beauty devices for facial rejuvenation: establishment of efficacy evaluation system. Clin Cosmet Investig Dermatol. 2024;17:553-563.
- Jain S, Arora M. Effect of microcurrent facial muscle toning on fine wrinkles & firmness of face. IAMR J Physiother. 2012;1:13-19.
- Armstrong K, Gokal R, Chevalier A, et al. Microcurrent point stimulation applied to lower back acupuncture points for the treatment of nonspecific neck pain. J Altern Complement Med. 2017;23:295-299.
Adverse Events Associated With At-Home Microcurrent Facial Devices
Adverse Events Associated With At-Home Microcurrent Facial Devices
PRACTICE POINTS
- At-home microcurrent facial devices have been associated with serious adverse events, including arrhythmia, pain, dizziness, and retinal detachment, based on US Food and Drug Administration Manufacturer and User Facility Device Experience database reports, underscoring the importance of counseling patients about potential risks prior to use.
- Existing randomized controlled trials of microcurrent devices are limited by small sample sizes and short follow-up periods (maximum 12 weeks), making it difficult to characterize the long-term safety profile of these increasingly popular devices.
- Dermatologists should be aware that the largely unregulated at-home microcurrent device market lacks robust, large-scale safety data. Patients, particularly those with cardiac conditions or implanted electrical devices, should be advised to consult a physician before use.

Predictors of Unplanned Postoperative Visits in a Veterans Affairs Hand Surgery Practice
Predictors of Unplanned Postoperative Visits in a Veterans Affairs Hand Surgery Practice
Patients make unplanned appointments after elective soft tissue hand surgery for real or perceived complications when they experience pain, anxiety, or fear. Unplanned appointments can create travel and financial burdens for patients and families. These appointments take time away from scheduled appointments and can contribute to late arrivals and delays in other clinics. Unscheduled appointments contribute to poor access when staff are diverted from scheduled appointments. If predictive factors can be identified, unplanned appointments may either be ameliorated or avoided with better perioperative risk management or education.
Methods
The US Department of Veterans Affairs (VA) North Florida/South Georgia Veterans Health System (NFSGVAHS) and University of Florida Institutional Review Board approved a retrospective chart review of all plastic surgery cases performed at the Malcom Randall VA Medical Center (MRVAMC) and Lake City VAMC operating rooms from July 1, 2018, through December 31, 2019, and January 1, 2021, through June 30, 2022 (nonurgent surgeries were discouraged during the COVID-19 pandemic). Elective soft tissue hand surgery cases were identified based on the operative description found in the Surgical Service Surgeon Staffing Report reviewed monthly by the Service Chief. Potential indicators of unplanned visits were recorded, including age; sex; diagnosis of diabetes, depression, anxiety, or posttraumatic stress disorder (PTSD); current smoking status; and residential zip code. We used the first 3 digits of the patients’ zip codes, which indicate region, as an estimate of proximity to the MRVAMC, which has a 50-county catchment area across North Florida and South Georgia. Diagnoses were found on the “problem list” from the electronic health record documented in the history and physical examinations before surgery. Clinic notes were examined for 3 months postsurgery to identify unplanned postoperative visits and the reason for the appointment. A χ2 analysis was conducted using Excel Version 2402. P < .05 was used to determine whether age (> 60 years), sex, proximity to MRVAMC, diabetes, smoking, depression, anxiety, or PTSD were statistically significant independent risk factors for these appointments.
Results
A total of 1009 elective soft tissue hand surgeries at MRVAMC were reviewed. The patients median age was 61 years. Patients included 173 women (17.1%) and 836 men (82.9%). Eighty-one patients (8.0%) returned for unplanned visits. Age (P = .82); proximity to MRVAMC (P = .34); and diabetes (P = .60), smoking (P = .55), anxiety (P = .33), or PTSD (P = .37) were not statistically significant predictors of unplanned appointments. Depression diagnosis (P = .04) and female sex (P = .03) were found to be independent risk factors for an unplanned appointment (Table 1). The most common indication for the requested appointment was pain-related, followed closely by noninfectious wound concerns and persistent symptoms (Table 2).
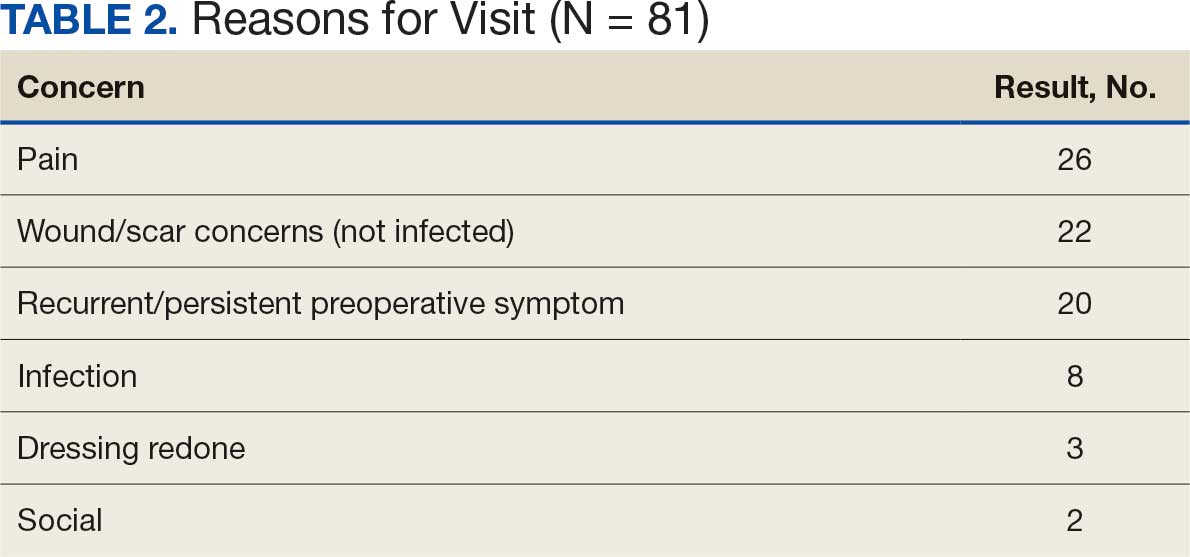
Discussion
Improved access, quality, and efficiency for patients are goals for the VA.1-3 The MRVAMC Plastic and Hand Surgery service provides care for the NFSGVAHS and receives an average of 15 to 20 consultation requests daily. The Veterans Health Administration is frequently challenged by staff shortages, and surgical services struggle to respond to consultation requests and treat patients within reasonable time frames.4,5
The objective of this study was to identify risk factors for unplanned postoperative appointments following elective hand surgery. Unplanned appointments prevent scheduled patients from being seen on time and contribute to backlogs and delays. When patients schedule multiple appointments on the same day, delays in the first clinic’s scheduled appointments create delays for the second and third clinics. Hand surgery clinics can provide a better experience for patients and staff by identifying and mitigating factors prompting unplanned visits.
We anticipated that wound complications would prompt unscheduled visits. Diabetes is a known risk factor for wound healing complications after plastic and hand surgery.6,7 A hemoglobin A1c (HbA1c) screening protocol used by the NFSGVAHS plastic surgery service since 2015 to identify poorly controlled patients with diabetes before surgery may partially explain this finding.8 We did not find a statistically significant difference between patients with diabetes and patients without diabetes for scheduling unplanned appointments. The plastic surgery service does not perform elective hand surgery unless the patient’s HbA1c level is < 9%, or violate the flexor sheath unless HbA1c level is < 8%. However, Zhuang et al found an increase in soft tissue infections after hand surgery with HbA1c levels ≥ 7%.9
Smoking is a potential factor in postoperative hand surgery complications.10,11 Lans et al found an increased incidence of 30-day emergency room visits in current and former smokers after outpatient upper extremity fracture surgery.12 The MRVAMC Plastic Surgery Service counsels patients about the risk of skin necrosis and delayed wound healing, but does not cancel cases or obtain laboratory values to verify abstinence in patients undergoing hand surgery. The VA has multiple resources available for patients interested in smoking cessation through mental health services.13
MRVAMC patients have been known to resist returning for scheduled appointments due to the costs or availability of transportation. We suspected that patients who lived further from MRVAMC would be less likely to return for unscheduled visits. We used the first 3 digits of the patients’ mailing zip code to estimate residential proximity to MRVAMC. An acknowledged limitation to this approach is that some veterans have primary addresses in other regions but still spend significant time in the MRVAMC catchment area and use the facility for their health care during the winter months. These “snowbirds” might reside near the facility despite having official addresses that are more distant. Additionally, there was no increased risk of unplanned visits after hand surgery in patients aged > 61 years (the median age of study participants) (P = .82). Dependence on a third party for transportation in older veterans could impact this finding.
Based on the observation that most patients needed reassurance rather than an intervention when they returned for unscheduled appointments, diagnoses of depression, anxiety, and PTSD were evaluated as separate predictive factors. In previous research, anxiety was found to be a risk factor for problematic recovery following carpal tunnel surgery.14 In the current study, depression was found to be a statistically significant predictor of unscheduled postoperative appointments (P = .04), while anxiety (P = .33) and PTSD (P = .37) were not statistically significant predictors. This is consistent with other studies that have found preexisting depression can predict complications after hand surgery.15,16 Vranceanu et al found that depression predicted pain intensity and disability after elective hand surgery.16 Similarly, Oflazoglu et al found a 12% incidence of depression based on the Patient Health Questionnaire-9 in new and returning hand patients who presented to an academic practice.17 They suggest patients should be assessed at all levels of care and that those with poor responses to surgical or nonsurgical management should be evaluated for depression. MRVAMC has a large mental health service consisting of psychiatrists, psychologists, addiction specialists, social workers, and homeless outreach, and patients tend to already have a diagnosis and mental health practitioner when they present to the clinic.
Recent studies found that wound problems, pain, and stiffness were the most common reasons for return visits.18,19 Shetty et al identified younger age, worse preoperative pain scores, and poor access to transportation as predictors of preventable emergency room visits, which generate higher health care expenditures than an office visit.19 Our study’s top reasons for appointments (pain, wound/scar concerns, persistent symptoms) can be addressed with additional presurgery patient and family education. Additionally, clinicians encourage nonnarcotic pain management strategies including anti-inflammatories, acetaminophen, elevation, splinting, and hand therapy, and the hospital employs experienced, fellowship-trained anesthesia block faculty who help limit perioperative narcotic use. Patients are advised that pain can be used to guide them through the postoperative recovery by preventing overuse and alerting them to a problem that would be masked with narcotics, and long-standing problems such as chronic nerve compressions may continue to cause pain after surgery.
Patients and families can be given consistent and repetitive verbal and written information, instructions, and expectations at the initial consultation, preoperative appointment, and on the day of surgery. Postoperatively, outside their scheduled appointments, patients are encouraged to use the My HealtheVet secure messaging system or call the clinic to access an experienced registered nurse before making a long drive. Access to virtual or phone visits can reduce emergent in-person visits in a VA population.20
Ozdag et al found that 42% of patients who had elective carpal tunnel surgery made unplanned electronic messages or phone contact within 2 weeks postsurgery. The authors point out the uncompensated administrative burden on the staff answering these messages and suggest pre-empting the contacts with more up-front education regarding postoperative pain expectations and management strategies.21
Fisher et al found that attending hand therapy reduced the number of emergency department visits in postoperative infection cases.22 At MRVAMC, a postoperative emergency department visit for a patient prompts an urgent unplanned appointment to the plastic surgery clinic, often on the same day. The MRVAMC occupational therapy clinic employed 3 on-site certified hand therapists during the study period. Because all hand surgery patients at the clinic receive hand therapy on the same day as their first postoperative appointment, attendance at hand therapy was not evaluated as a predictor of unplanned visits. Scheduled hand therapy is another point of contact where the clinic can provide reassurance and patient education.
While females made up 17.1% of the patients in this study, they constituted 12.5% of all veterans in Florida in fiscal year 2023.23 This study found that women were more likely to present for unplanned postoperative appointments (P = .03). This is consistent with existing literature which has found that women are higher users of health care and office-based appointments.24,25 This finding suggests the need for further study into whether our methods of communicating instructions to female patients undergoing plastic surgery may not be optimal.
Strengths and Limitations
As a retrospective review, the authors used information documented by multiple different health care practitioners, including trainees. The electronic medical record problem lists and templates provide consistency of information; however, less seasoned clinicians may interpret what they see and hear differently from more experienced clinicians in the postoperative setting. This study occurred in one part of the country with demographics that may not mirror other VA systems or the general population. The authors hope this study can be a starting point for other health care facilities to investigate ways to minimize the burden of unscheduled appointments. A strength of the study is that it was conducted within a closed system, as patients tend to stay within the VA system and documentation and communication among clinicians, even outside the immediate facility, are easily accessed through the electronic health record.
Conclusions
This study found that depression diagnosis and female sex are statistically significant predictors of unplanned postoperative visits after elective soft tissue hand surgery. More effective patient education during the preoperative period, particularly in patients with depression, may be warranted.
- Apaydin EA, Paige NM, Begashaw MM, et al. Veterans Health Administration (VA) vs. non-VA healthcare quality: a systematic review. J Gen Intern Med. 2023;38:2179-2188. doi:10.1007/s11606-023-08207-2
- Blegen M, Ko J, Salzman G, et al. Comparing quality of surgical care between the US Department of Veterans Affairs and non-Veterans Affairs settings: a systematic review. J Am Coll Surg. 2023;237:352-361. doi:10.1097/XCS.0000000000000720
- Valsangkar NP, Eppstein AC, Lawson RA, et al. Effect of lean processes on surgical wait times and efficiency in a tertiary care veterans affairs medical center. JAMA Surg. 2017;152:42-47. doi:10.1001/jamasurg.2016.2808
- National Association of Veterans Affairs Physicians and Dentists. Physicians remain at top of staffing shortage in VA. NAVAPD. December 20, 2023. Accessed March 16, 2026. https://www.navapd.org/news/physicians-remain-at-top-of-staffing-shortage-in-va
- OIG Determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2024. Veterans Affairs Office of Inspector General. August 7, 2024. Accessed February 4, 2026. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-0
- Goltsman D, Morrison KA, Ascherman JA. Defining the association between diabetes and plastic surgery outcomes: an analysis of nearly 40,000 patients. Plast Reconstr Surg Glob Open. 2017;5:e1461. doi:10.1097/GOX.0000000000001461 7.
- Cox CT, Sierra S, Egan A, et al. Elevated hemoglobin A1c and the risk of postoperative complications in elective hand and upper extremity surgery. Cureus. 2023;15:e48373. doi:10.7759/cureus.48373
- Coady-Fariborzian L, Anstead C. HbA1c and infection in diabetic elective hand surgery: a Veterans Affair Medical Center experience 2012-2018. Hand (NY). 2023;18:994-998. doi:10.1177/1558944720937363<
- Zhuang T, Shapiro LM, Fogel N, et al. Perioperative laboratory markers as risk factors for surgical site infection after elective hand surgery. J Hand Surg Am. 2021;46:675-684. doi:10.1016/j.jhsa.2021.04.001
- Cho BH, Aziz KT, Giladi AM. The impact of smoking on early postoperative complications in hand surgery. J Hand Surg Am. 2021;46:336.e1-336.e11. doi:10.1016/j.jhsa.2020.07.01411.
- Del Core MA, Ahn J, Golden AS, et al. Effect of smoking on short-term postoperative complications after elective upper extremity surgery. Hand (N Y). 2022;17:231-238. doi:10.1177/1558944720926638
- Lans J, Beagles CB, Watkins IT, et al. Unplanned postoperative emergency department visits after upper extremity fracture surgery. J Orthop Trauma. 2025;39:22-27. doi:10.1097/BOT.0000000000002925
- Tobacco and health - how to quit. US Dept of Veterans Affairs. Updated October 29, 2025. Accessed February 4, 2026. https://www.mentalhealth.va.gov/quit-tobacco/how-to-quit.asp
- Ryan C, Miner H, Ramachandran S, et al. General anxiety is associated with problematic initial recovery after carpal tunnel release. Clin Orthop Relat Res. 2022;480:1576-1581. doi:10.1097/CORR.0000000000002115
- Crijns TJ, Bernstein DN, Ring D, et al. Depression and pain interference correlate with physical function in patients recovering from hand surgery. Hand (N Y). 2019;14:830-835. doi:10.1177/1558944718777814
- Vranceanu AM, Jupiter JB, Mudgal CS, et al. Predictors of pain intensity and disability after minor hand surgery. J Hand Surg Am. 2010;35:956-960. doi:10.1016/j.jhsa.2010.02.00117.
- Oflazoglu K, Mellema JJ, Menendez ME, et al. Prevalence of and factors associated with major depression in patients with upper extremity conditions. J Hand Surg Am. 2016;41:263-269. doi:10.1016/j.jhsa.2015.11.019
- Townsend CB, Henry TW, Lutsky KF, et al. Unplanned office visits following outpatient hand surgery. Hand (N Y). 2022;17:1264-1268. doi:10.1177/15589447211028932
- Shetty PN, Guarino GM, Zhang G, et al. Risk factors for preventable emergency department use after outpatient hand surgery. J Hand Surg Am. 2022;47:855-864. doi:10.1016/j.jhsa.2022.05.012
- Sommers-Olson B, Christianson J, Neumann T, et al. Reducing nonemergent visits to the emergency department in a Veterans Affairs multistate system. J Emerg Nurs. 2023;49:539-545. doi:10.1016/j.jen.2023.02.010
- Ozdag Y, Manzar S, El Koussaify J, et al. Unplanned postoperative phone calls and electronic messages for patients with and without opioid prescriptions after carpal tunnel release. J Hand Surg Glob Online. 2024;6:363-368. doi:10.1016/j.jhsg.2024.02.006
- Fisher AH, Gandhi J, Nelson Z, et al. Immediate interventions after surgery to reduce readmission for upper extremity infections. Ann Plast Surg. 2022;88:S163-S169. doi:10.1097/SAP.0000000000003141
- Florida Department of Veterans Affairs Fast Facts. Florida Department of Veterans Affairs. Accessed February 4, 2026. https://floridavets.org/our-veterans/profilefast-facts/
- Bertakis KD, Azari R, Helms LJ, et al. Gender differences in the utilization of health care services. J Fam Pract. 2000;49:147-152.
- Ashman JJ, Santo L, Okeyode T. Characteristics of office-based physician visits, 2018. NCHS Data Brief. 2021;408:1-8.
Patients make unplanned appointments after elective soft tissue hand surgery for real or perceived complications when they experience pain, anxiety, or fear. Unplanned appointments can create travel and financial burdens for patients and families. These appointments take time away from scheduled appointments and can contribute to late arrivals and delays in other clinics. Unscheduled appointments contribute to poor access when staff are diverted from scheduled appointments. If predictive factors can be identified, unplanned appointments may either be ameliorated or avoided with better perioperative risk management or education.
Methods
The US Department of Veterans Affairs (VA) North Florida/South Georgia Veterans Health System (NFSGVAHS) and University of Florida Institutional Review Board approved a retrospective chart review of all plastic surgery cases performed at the Malcom Randall VA Medical Center (MRVAMC) and Lake City VAMC operating rooms from July 1, 2018, through December 31, 2019, and January 1, 2021, through June 30, 2022 (nonurgent surgeries were discouraged during the COVID-19 pandemic). Elective soft tissue hand surgery cases were identified based on the operative description found in the Surgical Service Surgeon Staffing Report reviewed monthly by the Service Chief. Potential indicators of unplanned visits were recorded, including age; sex; diagnosis of diabetes, depression, anxiety, or posttraumatic stress disorder (PTSD); current smoking status; and residential zip code. We used the first 3 digits of the patients’ zip codes, which indicate region, as an estimate of proximity to the MRVAMC, which has a 50-county catchment area across North Florida and South Georgia. Diagnoses were found on the “problem list” from the electronic health record documented in the history and physical examinations before surgery. Clinic notes were examined for 3 months postsurgery to identify unplanned postoperative visits and the reason for the appointment. A χ2 analysis was conducted using Excel Version 2402. P < .05 was used to determine whether age (> 60 years), sex, proximity to MRVAMC, diabetes, smoking, depression, anxiety, or PTSD were statistically significant independent risk factors for these appointments.
Results
A total of 1009 elective soft tissue hand surgeries at MRVAMC were reviewed. The patients median age was 61 years. Patients included 173 women (17.1%) and 836 men (82.9%). Eighty-one patients (8.0%) returned for unplanned visits. Age (P = .82); proximity to MRVAMC (P = .34); and diabetes (P = .60), smoking (P = .55), anxiety (P = .33), or PTSD (P = .37) were not statistically significant predictors of unplanned appointments. Depression diagnosis (P = .04) and female sex (P = .03) were found to be independent risk factors for an unplanned appointment (Table 1). The most common indication for the requested appointment was pain-related, followed closely by noninfectious wound concerns and persistent symptoms (Table 2).
Discussion
Improved access, quality, and efficiency for patients are goals for the VA.1-3 The MRVAMC Plastic and Hand Surgery service provides care for the NFSGVAHS and receives an average of 15 to 20 consultation requests daily. The Veterans Health Administration is frequently challenged by staff shortages, and surgical services struggle to respond to consultation requests and treat patients within reasonable time frames.4,5
The objective of this study was to identify risk factors for unplanned postoperative appointments following elective hand surgery. Unplanned appointments prevent scheduled patients from being seen on time and contribute to backlogs and delays. When patients schedule multiple appointments on the same day, delays in the first clinic’s scheduled appointments create delays for the second and third clinics. Hand surgery clinics can provide a better experience for patients and staff by identifying and mitigating factors prompting unplanned visits.
We anticipated that wound complications would prompt unscheduled visits. Diabetes is a known risk factor for wound healing complications after plastic and hand surgery.6,7 A hemoglobin A1c (HbA1c) screening protocol used by the NFSGVAHS plastic surgery service since 2015 to identify poorly controlled patients with diabetes before surgery may partially explain this finding.8 We did not find a statistically significant difference between patients with diabetes and patients without diabetes for scheduling unplanned appointments. The plastic surgery service does not perform elective hand surgery unless the patient’s HbA1c level is < 9%, or violate the flexor sheath unless HbA1c level is < 8%. However, Zhuang et al found an increase in soft tissue infections after hand surgery with HbA1c levels ≥ 7%.9
Smoking is a potential factor in postoperative hand surgery complications.10,11 Lans et al found an increased incidence of 30-day emergency room visits in current and former smokers after outpatient upper extremity fracture surgery.12 The MRVAMC Plastic Surgery Service counsels patients about the risk of skin necrosis and delayed wound healing, but does not cancel cases or obtain laboratory values to verify abstinence in patients undergoing hand surgery. The VA has multiple resources available for patients interested in smoking cessation through mental health services.13
MRVAMC patients have been known to resist returning for scheduled appointments due to the costs or availability of transportation. We suspected that patients who lived further from MRVAMC would be less likely to return for unscheduled visits. We used the first 3 digits of the patients’ mailing zip code to estimate residential proximity to MRVAMC. An acknowledged limitation to this approach is that some veterans have primary addresses in other regions but still spend significant time in the MRVAMC catchment area and use the facility for their health care during the winter months. These “snowbirds” might reside near the facility despite having official addresses that are more distant. Additionally, there was no increased risk of unplanned visits after hand surgery in patients aged > 61 years (the median age of study participants) (P = .82). Dependence on a third party for transportation in older veterans could impact this finding.
Based on the observation that most patients needed reassurance rather than an intervention when they returned for unscheduled appointments, diagnoses of depression, anxiety, and PTSD were evaluated as separate predictive factors. In previous research, anxiety was found to be a risk factor for problematic recovery following carpal tunnel surgery.14 In the current study, depression was found to be a statistically significant predictor of unscheduled postoperative appointments (P = .04), while anxiety (P = .33) and PTSD (P = .37) were not statistically significant predictors. This is consistent with other studies that have found preexisting depression can predict complications after hand surgery.15,16 Vranceanu et al found that depression predicted pain intensity and disability after elective hand surgery.16 Similarly, Oflazoglu et al found a 12% incidence of depression based on the Patient Health Questionnaire-9 in new and returning hand patients who presented to an academic practice.17 They suggest patients should be assessed at all levels of care and that those with poor responses to surgical or nonsurgical management should be evaluated for depression. MRVAMC has a large mental health service consisting of psychiatrists, psychologists, addiction specialists, social workers, and homeless outreach, and patients tend to already have a diagnosis and mental health practitioner when they present to the clinic.
Recent studies found that wound problems, pain, and stiffness were the most common reasons for return visits.18,19 Shetty et al identified younger age, worse preoperative pain scores, and poor access to transportation as predictors of preventable emergency room visits, which generate higher health care expenditures than an office visit.19 Our study’s top reasons for appointments (pain, wound/scar concerns, persistent symptoms) can be addressed with additional presurgery patient and family education. Additionally, clinicians encourage nonnarcotic pain management strategies including anti-inflammatories, acetaminophen, elevation, splinting, and hand therapy, and the hospital employs experienced, fellowship-trained anesthesia block faculty who help limit perioperative narcotic use. Patients are advised that pain can be used to guide them through the postoperative recovery by preventing overuse and alerting them to a problem that would be masked with narcotics, and long-standing problems such as chronic nerve compressions may continue to cause pain after surgery.
Patients and families can be given consistent and repetitive verbal and written information, instructions, and expectations at the initial consultation, preoperative appointment, and on the day of surgery. Postoperatively, outside their scheduled appointments, patients are encouraged to use the My HealtheVet secure messaging system or call the clinic to access an experienced registered nurse before making a long drive. Access to virtual or phone visits can reduce emergent in-person visits in a VA population.20
Ozdag et al found that 42% of patients who had elective carpal tunnel surgery made unplanned electronic messages or phone contact within 2 weeks postsurgery. The authors point out the uncompensated administrative burden on the staff answering these messages and suggest pre-empting the contacts with more up-front education regarding postoperative pain expectations and management strategies.21
Fisher et al found that attending hand therapy reduced the number of emergency department visits in postoperative infection cases.22 At MRVAMC, a postoperative emergency department visit for a patient prompts an urgent unplanned appointment to the plastic surgery clinic, often on the same day. The MRVAMC occupational therapy clinic employed 3 on-site certified hand therapists during the study period. Because all hand surgery patients at the clinic receive hand therapy on the same day as their first postoperative appointment, attendance at hand therapy was not evaluated as a predictor of unplanned visits. Scheduled hand therapy is another point of contact where the clinic can provide reassurance and patient education.
While females made up 17.1% of the patients in this study, they constituted 12.5% of all veterans in Florida in fiscal year 2023.23 This study found that women were more likely to present for unplanned postoperative appointments (P = .03). This is consistent with existing literature which has found that women are higher users of health care and office-based appointments.24,25 This finding suggests the need for further study into whether our methods of communicating instructions to female patients undergoing plastic surgery may not be optimal.
Strengths and Limitations
As a retrospective review, the authors used information documented by multiple different health care practitioners, including trainees. The electronic medical record problem lists and templates provide consistency of information; however, less seasoned clinicians may interpret what they see and hear differently from more experienced clinicians in the postoperative setting. This study occurred in one part of the country with demographics that may not mirror other VA systems or the general population. The authors hope this study can be a starting point for other health care facilities to investigate ways to minimize the burden of unscheduled appointments. A strength of the study is that it was conducted within a closed system, as patients tend to stay within the VA system and documentation and communication among clinicians, even outside the immediate facility, are easily accessed through the electronic health record.
Conclusions
This study found that depression diagnosis and female sex are statistically significant predictors of unplanned postoperative visits after elective soft tissue hand surgery. More effective patient education during the preoperative period, particularly in patients with depression, may be warranted.
Patients make unplanned appointments after elective soft tissue hand surgery for real or perceived complications when they experience pain, anxiety, or fear. Unplanned appointments can create travel and financial burdens for patients and families. These appointments take time away from scheduled appointments and can contribute to late arrivals and delays in other clinics. Unscheduled appointments contribute to poor access when staff are diverted from scheduled appointments. If predictive factors can be identified, unplanned appointments may either be ameliorated or avoided with better perioperative risk management or education.
Methods
The US Department of Veterans Affairs (VA) North Florida/South Georgia Veterans Health System (NFSGVAHS) and University of Florida Institutional Review Board approved a retrospective chart review of all plastic surgery cases performed at the Malcom Randall VA Medical Center (MRVAMC) and Lake City VAMC operating rooms from July 1, 2018, through December 31, 2019, and January 1, 2021, through June 30, 2022 (nonurgent surgeries were discouraged during the COVID-19 pandemic). Elective soft tissue hand surgery cases were identified based on the operative description found in the Surgical Service Surgeon Staffing Report reviewed monthly by the Service Chief. Potential indicators of unplanned visits were recorded, including age; sex; diagnosis of diabetes, depression, anxiety, or posttraumatic stress disorder (PTSD); current smoking status; and residential zip code. We used the first 3 digits of the patients’ zip codes, which indicate region, as an estimate of proximity to the MRVAMC, which has a 50-county catchment area across North Florida and South Georgia. Diagnoses were found on the “problem list” from the electronic health record documented in the history and physical examinations before surgery. Clinic notes were examined for 3 months postsurgery to identify unplanned postoperative visits and the reason for the appointment. A χ2 analysis was conducted using Excel Version 2402. P < .05 was used to determine whether age (> 60 years), sex, proximity to MRVAMC, diabetes, smoking, depression, anxiety, or PTSD were statistically significant independent risk factors for these appointments.
Results
A total of 1009 elective soft tissue hand surgeries at MRVAMC were reviewed. The patients median age was 61 years. Patients included 173 women (17.1%) and 836 men (82.9%). Eighty-one patients (8.0%) returned for unplanned visits. Age (P = .82); proximity to MRVAMC (P = .34); and diabetes (P = .60), smoking (P = .55), anxiety (P = .33), or PTSD (P = .37) were not statistically significant predictors of unplanned appointments. Depression diagnosis (P = .04) and female sex (P = .03) were found to be independent risk factors for an unplanned appointment (Table 1). The most common indication for the requested appointment was pain-related, followed closely by noninfectious wound concerns and persistent symptoms (Table 2).
Discussion
Improved access, quality, and efficiency for patients are goals for the VA.1-3 The MRVAMC Plastic and Hand Surgery service provides care for the NFSGVAHS and receives an average of 15 to 20 consultation requests daily. The Veterans Health Administration is frequently challenged by staff shortages, and surgical services struggle to respond to consultation requests and treat patients within reasonable time frames.4,5
The objective of this study was to identify risk factors for unplanned postoperative appointments following elective hand surgery. Unplanned appointments prevent scheduled patients from being seen on time and contribute to backlogs and delays. When patients schedule multiple appointments on the same day, delays in the first clinic’s scheduled appointments create delays for the second and third clinics. Hand surgery clinics can provide a better experience for patients and staff by identifying and mitigating factors prompting unplanned visits.
We anticipated that wound complications would prompt unscheduled visits. Diabetes is a known risk factor for wound healing complications after plastic and hand surgery.6,7 A hemoglobin A1c (HbA1c) screening protocol used by the NFSGVAHS plastic surgery service since 2015 to identify poorly controlled patients with diabetes before surgery may partially explain this finding.8 We did not find a statistically significant difference between patients with diabetes and patients without diabetes for scheduling unplanned appointments. The plastic surgery service does not perform elective hand surgery unless the patient’s HbA1c level is < 9%, or violate the flexor sheath unless HbA1c level is < 8%. However, Zhuang et al found an increase in soft tissue infections after hand surgery with HbA1c levels ≥ 7%.9
Smoking is a potential factor in postoperative hand surgery complications.10,11 Lans et al found an increased incidence of 30-day emergency room visits in current and former smokers after outpatient upper extremity fracture surgery.12 The MRVAMC Plastic Surgery Service counsels patients about the risk of skin necrosis and delayed wound healing, but does not cancel cases or obtain laboratory values to verify abstinence in patients undergoing hand surgery. The VA has multiple resources available for patients interested in smoking cessation through mental health services.13
MRVAMC patients have been known to resist returning for scheduled appointments due to the costs or availability of transportation. We suspected that patients who lived further from MRVAMC would be less likely to return for unscheduled visits. We used the first 3 digits of the patients’ mailing zip code to estimate residential proximity to MRVAMC. An acknowledged limitation to this approach is that some veterans have primary addresses in other regions but still spend significant time in the MRVAMC catchment area and use the facility for their health care during the winter months. These “snowbirds” might reside near the facility despite having official addresses that are more distant. Additionally, there was no increased risk of unplanned visits after hand surgery in patients aged > 61 years (the median age of study participants) (P = .82). Dependence on a third party for transportation in older veterans could impact this finding.
Based on the observation that most patients needed reassurance rather than an intervention when they returned for unscheduled appointments, diagnoses of depression, anxiety, and PTSD were evaluated as separate predictive factors. In previous research, anxiety was found to be a risk factor for problematic recovery following carpal tunnel surgery.14 In the current study, depression was found to be a statistically significant predictor of unscheduled postoperative appointments (P = .04), while anxiety (P = .33) and PTSD (P = .37) were not statistically significant predictors. This is consistent with other studies that have found preexisting depression can predict complications after hand surgery.15,16 Vranceanu et al found that depression predicted pain intensity and disability after elective hand surgery.16 Similarly, Oflazoglu et al found a 12% incidence of depression based on the Patient Health Questionnaire-9 in new and returning hand patients who presented to an academic practice.17 They suggest patients should be assessed at all levels of care and that those with poor responses to surgical or nonsurgical management should be evaluated for depression. MRVAMC has a large mental health service consisting of psychiatrists, psychologists, addiction specialists, social workers, and homeless outreach, and patients tend to already have a diagnosis and mental health practitioner when they present to the clinic.
Recent studies found that wound problems, pain, and stiffness were the most common reasons for return visits.18,19 Shetty et al identified younger age, worse preoperative pain scores, and poor access to transportation as predictors of preventable emergency room visits, which generate higher health care expenditures than an office visit.19 Our study’s top reasons for appointments (pain, wound/scar concerns, persistent symptoms) can be addressed with additional presurgery patient and family education. Additionally, clinicians encourage nonnarcotic pain management strategies including anti-inflammatories, acetaminophen, elevation, splinting, and hand therapy, and the hospital employs experienced, fellowship-trained anesthesia block faculty who help limit perioperative narcotic use. Patients are advised that pain can be used to guide them through the postoperative recovery by preventing overuse and alerting them to a problem that would be masked with narcotics, and long-standing problems such as chronic nerve compressions may continue to cause pain after surgery.
Patients and families can be given consistent and repetitive verbal and written information, instructions, and expectations at the initial consultation, preoperative appointment, and on the day of surgery. Postoperatively, outside their scheduled appointments, patients are encouraged to use the My HealtheVet secure messaging system or call the clinic to access an experienced registered nurse before making a long drive. Access to virtual or phone visits can reduce emergent in-person visits in a VA population.20
Ozdag et al found that 42% of patients who had elective carpal tunnel surgery made unplanned electronic messages or phone contact within 2 weeks postsurgery. The authors point out the uncompensated administrative burden on the staff answering these messages and suggest pre-empting the contacts with more up-front education regarding postoperative pain expectations and management strategies.21
Fisher et al found that attending hand therapy reduced the number of emergency department visits in postoperative infection cases.22 At MRVAMC, a postoperative emergency department visit for a patient prompts an urgent unplanned appointment to the plastic surgery clinic, often on the same day. The MRVAMC occupational therapy clinic employed 3 on-site certified hand therapists during the study period. Because all hand surgery patients at the clinic receive hand therapy on the same day as their first postoperative appointment, attendance at hand therapy was not evaluated as a predictor of unplanned visits. Scheduled hand therapy is another point of contact where the clinic can provide reassurance and patient education.
While females made up 17.1% of the patients in this study, they constituted 12.5% of all veterans in Florida in fiscal year 2023.23 This study found that women were more likely to present for unplanned postoperative appointments (P = .03). This is consistent with existing literature which has found that women are higher users of health care and office-based appointments.24,25 This finding suggests the need for further study into whether our methods of communicating instructions to female patients undergoing plastic surgery may not be optimal.
Strengths and Limitations
As a retrospective review, the authors used information documented by multiple different health care practitioners, including trainees. The electronic medical record problem lists and templates provide consistency of information; however, less seasoned clinicians may interpret what they see and hear differently from more experienced clinicians in the postoperative setting. This study occurred in one part of the country with demographics that may not mirror other VA systems or the general population. The authors hope this study can be a starting point for other health care facilities to investigate ways to minimize the burden of unscheduled appointments. A strength of the study is that it was conducted within a closed system, as patients tend to stay within the VA system and documentation and communication among clinicians, even outside the immediate facility, are easily accessed through the electronic health record.
Conclusions
This study found that depression diagnosis and female sex are statistically significant predictors of unplanned postoperative visits after elective soft tissue hand surgery. More effective patient education during the preoperative period, particularly in patients with depression, may be warranted.
- Apaydin EA, Paige NM, Begashaw MM, et al. Veterans Health Administration (VA) vs. non-VA healthcare quality: a systematic review. J Gen Intern Med. 2023;38:2179-2188. doi:10.1007/s11606-023-08207-2
- Blegen M, Ko J, Salzman G, et al. Comparing quality of surgical care between the US Department of Veterans Affairs and non-Veterans Affairs settings: a systematic review. J Am Coll Surg. 2023;237:352-361. doi:10.1097/XCS.0000000000000720
- Valsangkar NP, Eppstein AC, Lawson RA, et al. Effect of lean processes on surgical wait times and efficiency in a tertiary care veterans affairs medical center. JAMA Surg. 2017;152:42-47. doi:10.1001/jamasurg.2016.2808
- National Association of Veterans Affairs Physicians and Dentists. Physicians remain at top of staffing shortage in VA. NAVAPD. December 20, 2023. Accessed March 16, 2026. https://www.navapd.org/news/physicians-remain-at-top-of-staffing-shortage-in-va
- OIG Determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2024. Veterans Affairs Office of Inspector General. August 7, 2024. Accessed February 4, 2026. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-0
- Goltsman D, Morrison KA, Ascherman JA. Defining the association between diabetes and plastic surgery outcomes: an analysis of nearly 40,000 patients. Plast Reconstr Surg Glob Open. 2017;5:e1461. doi:10.1097/GOX.0000000000001461 7.
- Cox CT, Sierra S, Egan A, et al. Elevated hemoglobin A1c and the risk of postoperative complications in elective hand and upper extremity surgery. Cureus. 2023;15:e48373. doi:10.7759/cureus.48373
- Coady-Fariborzian L, Anstead C. HbA1c and infection in diabetic elective hand surgery: a Veterans Affair Medical Center experience 2012-2018. Hand (NY). 2023;18:994-998. doi:10.1177/1558944720937363<
- Zhuang T, Shapiro LM, Fogel N, et al. Perioperative laboratory markers as risk factors for surgical site infection after elective hand surgery. J Hand Surg Am. 2021;46:675-684. doi:10.1016/j.jhsa.2021.04.001
- Cho BH, Aziz KT, Giladi AM. The impact of smoking on early postoperative complications in hand surgery. J Hand Surg Am. 2021;46:336.e1-336.e11. doi:10.1016/j.jhsa.2020.07.01411.
- Del Core MA, Ahn J, Golden AS, et al. Effect of smoking on short-term postoperative complications after elective upper extremity surgery. Hand (N Y). 2022;17:231-238. doi:10.1177/1558944720926638
- Lans J, Beagles CB, Watkins IT, et al. Unplanned postoperative emergency department visits after upper extremity fracture surgery. J Orthop Trauma. 2025;39:22-27. doi:10.1097/BOT.0000000000002925
- Tobacco and health - how to quit. US Dept of Veterans Affairs. Updated October 29, 2025. Accessed February 4, 2026. https://www.mentalhealth.va.gov/quit-tobacco/how-to-quit.asp
- Ryan C, Miner H, Ramachandran S, et al. General anxiety is associated with problematic initial recovery after carpal tunnel release. Clin Orthop Relat Res. 2022;480:1576-1581. doi:10.1097/CORR.0000000000002115
- Crijns TJ, Bernstein DN, Ring D, et al. Depression and pain interference correlate with physical function in patients recovering from hand surgery. Hand (N Y). 2019;14:830-835. doi:10.1177/1558944718777814
- Vranceanu AM, Jupiter JB, Mudgal CS, et al. Predictors of pain intensity and disability after minor hand surgery. J Hand Surg Am. 2010;35:956-960. doi:10.1016/j.jhsa.2010.02.00117.
- Oflazoglu K, Mellema JJ, Menendez ME, et al. Prevalence of and factors associated with major depression in patients with upper extremity conditions. J Hand Surg Am. 2016;41:263-269. doi:10.1016/j.jhsa.2015.11.019
- Townsend CB, Henry TW, Lutsky KF, et al. Unplanned office visits following outpatient hand surgery. Hand (N Y). 2022;17:1264-1268. doi:10.1177/15589447211028932
- Shetty PN, Guarino GM, Zhang G, et al. Risk factors for preventable emergency department use after outpatient hand surgery. J Hand Surg Am. 2022;47:855-864. doi:10.1016/j.jhsa.2022.05.012
- Sommers-Olson B, Christianson J, Neumann T, et al. Reducing nonemergent visits to the emergency department in a Veterans Affairs multistate system. J Emerg Nurs. 2023;49:539-545. doi:10.1016/j.jen.2023.02.010
- Ozdag Y, Manzar S, El Koussaify J, et al. Unplanned postoperative phone calls and electronic messages for patients with and without opioid prescriptions after carpal tunnel release. J Hand Surg Glob Online. 2024;6:363-368. doi:10.1016/j.jhsg.2024.02.006
- Fisher AH, Gandhi J, Nelson Z, et al. Immediate interventions after surgery to reduce readmission for upper extremity infections. Ann Plast Surg. 2022;88:S163-S169. doi:10.1097/SAP.0000000000003141
- Florida Department of Veterans Affairs Fast Facts. Florida Department of Veterans Affairs. Accessed February 4, 2026. https://floridavets.org/our-veterans/profilefast-facts/
- Bertakis KD, Azari R, Helms LJ, et al. Gender differences in the utilization of health care services. J Fam Pract. 2000;49:147-152.
- Ashman JJ, Santo L, Okeyode T. Characteristics of office-based physician visits, 2018. NCHS Data Brief. 2021;408:1-8.
- Apaydin EA, Paige NM, Begashaw MM, et al. Veterans Health Administration (VA) vs. non-VA healthcare quality: a systematic review. J Gen Intern Med. 2023;38:2179-2188. doi:10.1007/s11606-023-08207-2
- Blegen M, Ko J, Salzman G, et al. Comparing quality of surgical care between the US Department of Veterans Affairs and non-Veterans Affairs settings: a systematic review. J Am Coll Surg. 2023;237:352-361. doi:10.1097/XCS.0000000000000720
- Valsangkar NP, Eppstein AC, Lawson RA, et al. Effect of lean processes on surgical wait times and efficiency in a tertiary care veterans affairs medical center. JAMA Surg. 2017;152:42-47. doi:10.1001/jamasurg.2016.2808
- National Association of Veterans Affairs Physicians and Dentists. Physicians remain at top of staffing shortage in VA. NAVAPD. December 20, 2023. Accessed March 16, 2026. https://www.navapd.org/news/physicians-remain-at-top-of-staffing-shortage-in-va
- OIG Determination of Veterans Health Administration’s severe occupational staffing shortages fiscal year 2024. Veterans Affairs Office of Inspector General. August 7, 2024. Accessed February 4, 2026. https://www.vaoig.gov/reports/national-healthcare-review/oig-determination-veterans-health-administrations-severe-0
- Goltsman D, Morrison KA, Ascherman JA. Defining the association between diabetes and plastic surgery outcomes: an analysis of nearly 40,000 patients. Plast Reconstr Surg Glob Open. 2017;5:e1461. doi:10.1097/GOX.0000000000001461 7.
- Cox CT, Sierra S, Egan A, et al. Elevated hemoglobin A1c and the risk of postoperative complications in elective hand and upper extremity surgery. Cureus. 2023;15:e48373. doi:10.7759/cureus.48373
- Coady-Fariborzian L, Anstead C. HbA1c and infection in diabetic elective hand surgery: a Veterans Affair Medical Center experience 2012-2018. Hand (NY). 2023;18:994-998. doi:10.1177/1558944720937363<
- Zhuang T, Shapiro LM, Fogel N, et al. Perioperative laboratory markers as risk factors for surgical site infection after elective hand surgery. J Hand Surg Am. 2021;46:675-684. doi:10.1016/j.jhsa.2021.04.001
- Cho BH, Aziz KT, Giladi AM. The impact of smoking on early postoperative complications in hand surgery. J Hand Surg Am. 2021;46:336.e1-336.e11. doi:10.1016/j.jhsa.2020.07.01411.
- Del Core MA, Ahn J, Golden AS, et al. Effect of smoking on short-term postoperative complications after elective upper extremity surgery. Hand (N Y). 2022;17:231-238. doi:10.1177/1558944720926638
- Lans J, Beagles CB, Watkins IT, et al. Unplanned postoperative emergency department visits after upper extremity fracture surgery. J Orthop Trauma. 2025;39:22-27. doi:10.1097/BOT.0000000000002925
- Tobacco and health - how to quit. US Dept of Veterans Affairs. Updated October 29, 2025. Accessed February 4, 2026. https://www.mentalhealth.va.gov/quit-tobacco/how-to-quit.asp
- Ryan C, Miner H, Ramachandran S, et al. General anxiety is associated with problematic initial recovery after carpal tunnel release. Clin Orthop Relat Res. 2022;480:1576-1581. doi:10.1097/CORR.0000000000002115
- Crijns TJ, Bernstein DN, Ring D, et al. Depression and pain interference correlate with physical function in patients recovering from hand surgery. Hand (N Y). 2019;14:830-835. doi:10.1177/1558944718777814
- Vranceanu AM, Jupiter JB, Mudgal CS, et al. Predictors of pain intensity and disability after minor hand surgery. J Hand Surg Am. 2010;35:956-960. doi:10.1016/j.jhsa.2010.02.00117.
- Oflazoglu K, Mellema JJ, Menendez ME, et al. Prevalence of and factors associated with major depression in patients with upper extremity conditions. J Hand Surg Am. 2016;41:263-269. doi:10.1016/j.jhsa.2015.11.019
- Townsend CB, Henry TW, Lutsky KF, et al. Unplanned office visits following outpatient hand surgery. Hand (N Y). 2022;17:1264-1268. doi:10.1177/15589447211028932
- Shetty PN, Guarino GM, Zhang G, et al. Risk factors for preventable emergency department use after outpatient hand surgery. J Hand Surg Am. 2022;47:855-864. doi:10.1016/j.jhsa.2022.05.012
- Sommers-Olson B, Christianson J, Neumann T, et al. Reducing nonemergent visits to the emergency department in a Veterans Affairs multistate system. J Emerg Nurs. 2023;49:539-545. doi:10.1016/j.jen.2023.02.010
- Ozdag Y, Manzar S, El Koussaify J, et al. Unplanned postoperative phone calls and electronic messages for patients with and without opioid prescriptions after carpal tunnel release. J Hand Surg Glob Online. 2024;6:363-368. doi:10.1016/j.jhsg.2024.02.006
- Fisher AH, Gandhi J, Nelson Z, et al. Immediate interventions after surgery to reduce readmission for upper extremity infections. Ann Plast Surg. 2022;88:S163-S169. doi:10.1097/SAP.0000000000003141
- Florida Department of Veterans Affairs Fast Facts. Florida Department of Veterans Affairs. Accessed February 4, 2026. https://floridavets.org/our-veterans/profilefast-facts/
- Bertakis KD, Azari R, Helms LJ, et al. Gender differences in the utilization of health care services. J Fam Pract. 2000;49:147-152.
- Ashman JJ, Santo L, Okeyode T. Characteristics of office-based physician visits, 2018. NCHS Data Brief. 2021;408:1-8.
Predictors of Unplanned Postoperative Visits in a Veterans Affairs Hand Surgery Practice
Predictors of Unplanned Postoperative Visits in a Veterans Affairs Hand Surgery Practice

Mental Health Prescribers’ Perceptions of Patients With Substance Use Disorders and Harm Reduction Services
Mental Health Prescribers’ Perceptions of Patients With Substance Use Disorders and Harm Reduction Services
The Public Health and Welfare Act of 1988 prohibited the use of federal funds to “provide individuals with hypodermic needles or syringes so that such individuals may use illegal drugs.”1 Although the Act included the caveat that the US Surgeon General may determine that “a demonstration needle exchange program would be effective in reducing drug abuse,” and thus federal funds could be used, the legislation prohibited federal, state, and local agencies from funding syringe services programs (SSPs). SSPs use various harm reduction tools to improve public safety and reduce the potential harmful consequences of risky behaviors, similar to how using a seat belt while driving reduces the risk of injury or death.2 SSPs are rooted in evidence-based practices, and several studies, according to the Centers for Disease Control and Prevention, have found that people who use drugs (PWUDs) who use community-based SSPs are 5 times more likely to enter treatment than those who do not use these programs. Additionally, these programs have shown an estimated 50% reduction in HIV and hepatitis C infections.3
Amid a 2015 HIV outbreak in Indiana among individuals sharing needles for injection drug use, Congress passed an omnibus spending bill that partially lifted the federal funding restriction. Federal funds now may be used for operational costs that support SSPs but may not be used to purchase syringes themselves.4
Following the 2015 legislation, federal agencies began implementing SSPs. The Veterans Health Administration (VHA) established SSPs at 3 medical centers in 2017.5 Veterans who participated in the programs were able to access supplies (eg, syringes, fentanyl test strips, wound care kits, and condoms) through donations to US Department of Veterans Affairs (VA) medical centers (VAMCs). The success of these programs laid the foundation for the VHA to implement SSPs nationally. VHA SSPs provided access to naloxone (an opioid overdose reversal medication), fentanyl test strips, condoms, sterile syringe distribution, testing for blood-borne viruses, HIV pre-exposure prophylaxis, as well as educational materials and resources, and low-barrier access to drug treatment (eg, medications for opioid use disorder [OUD]).
In 2020, the Biden Administration outlined 7 drug policy priorities, which included enhancing evidence-based harm reduction efforts. 6 This policy also discussed mandates for federal agencies to remove barriers to federal funding for purchasing syringes and other harm reduction supplies. The VHA responded to the policy by publishing guidance that recommended VAMCs develop and/or ensure veterans have access to harm reduction services in the community, where state law is not legally more stringent.7
In 2025 the Trump administration Statement of Drug Policy Priorities encouraged local jurisdictions to increase the availability of drug test strips and naloxone.8 These significant policy shifts moved SSPs from being housed mostly in local public health departments and community-based organizations to also being available at health care facilities. 9 VAMCs have unique opportunities to provide universal health care that includes both prevention services and other medical management to PWUD.
One study assessed staff perceptions of PWUD at a VAMC in preparation for a training program about harm reduction. The results indicated an overall positive staff perception of PWUD, although only the Drug and Drug Problems Perceptions Questionnaire (DDPPQ) was administered, which assessed comfort of working with this population and not explicitly the use of harm reduction.10 Another study interviewed clinical pharmacists, primary care clinicians, social workers, and directors of addiction and mental health services to determine barriers and facilitators (ie, potential opportunities to promote change) to implementing harm reduction at the VHA. The study identified barriers to be a lack of knowledge, time, and comfort, while suggesting opportunities for improvement were engagement of champions, communication and educational strategies, and adaptation of existing infrastructure.11
While these findings are insightful for the VHA to disseminate a harm reduction program, there remains a gap in assessing staff willingness to provide harm reduction services. Evidence on harm reduction services among veterans is limited and more research is needed to better understand the role of these services and acceptance among enrolled veterans and VHA staff. Specifically, more research is needed on health care practitioners’ (HCPs) perceptions of harm reduction use.
Mental health care practitioners frequently treat patients with substance use disorders (SUDs), making them an ideal initial cohort to assess willingness to provide harm reduction to this population. By analyzing mental HCPs’ perceptions, additional interventions could be identified, implemented, and evaluated to improve their willingness to provide harm reduction tools.
This project focused on mental health clinicians with prescribing privileges: physicians (allopathic and osteopathic physicians), nurse practitioners, physician assistants, and clinical pharmacist practitioners. Mental health prescribers were selected because they are uniquely positioned at the intersection of prevention and treatment in drug use. Furthermore, mental health prescribers at the VAMCs included in this study are usually the primary point of entry to SUD clinics. This mixed-methods study used an anonymous online survey and voluntary postsurvey discussions with mental health care prescribers to elaborate on their beliefs and attitudes, providing deeper insight into their responses regarding harm reduction.
Methods
This project was conducted by the Veterans Integrated Services Network (VISN) 5 academic detailing team. VISN 5 serves veterans from economically and demographically diverse areas in Maryland; Washington, DC; West Virginia; and portions of Virginia, Pennsylvania, Ohio, and Kentucky. VAMCs in Baltimore, Maryland, and Washington, DC, serve a largely urban population while the 4 West Virginia facilities in Martinsburg, Huntington, Beckley, and Clarksburg, serve a largely rural population. West Virginia has been the epicenter of the opioid crisis and consistently has the highest drug overdose deaths per capita in the United States.12 Among cities, Baltimore, Maryland, has the highest number of drug overdose deaths per capita with 174.1 per 100,000 people.12,13
At the time of this project, the 6 VISN 5 VAMCs had established overdose education and naloxone distribution (OEND) programs. Although OEND programs have existed since 2013, VISN 5 SSPs and harm reduction services that provided fentanyl test strips were only available at the Martinsburg, Beckley, and Huntington VAMCs. All 6 VAMCs had substance use treatment programs with a variety of inpatient and outpatient mental health services. The Washington, DC and Baltimore VAMCs had opioid treatment programs that provided methadone maintenance.
The VISN 5 academic detailing team consists of 7 clinical pharmacists. These academic detailers plan annual systematic interventions to provide medical knowledge translation services on health-related campaigns. Academic detailers are trained in change management and motivational interviewing. They uniquely facilitate conversations with HCPs on various topics or campaigns, aiming for quality improvement and behavioral change through positive relationships and sharing resources.14 Academic detailing conversations and relationships with HCPs involve assessing and understanding HCP behaviors, including barriers and readiness to change to align with the goal of improving patient outcomes. Academic detailing has improved practice behaviors around providing OEND in VHA.15
To prepare for a harm reduction campaign, the academic detailers sought to gain insight from target VISN 5 mental health prescribers. Figure 1 outlines the project timeline, which started with emails inviting mental health prescribers to complete an anonymous online survey. Academic detailers from each site emailed mental health prescribers who completed the survey to determine interest in expanding on survey findings. Mental health prescribers who completed the survey could participate in a postsurvey discussion.

Surveys
Between January 29, 2024, and February 22, 2024, the academic detailers emailed facility mental health prescribers (N = 156) a link to an anonymous 15-question survey. The email informed recipients of the survey’s purpose: to gain a better understanding of prescriber perceptions of veterans with SUD and harm reduction programs and their willingness to provide harm reduction tools, to better determine interventions that could be implemented.
The survey collected prescriber demographic data and their perceptions of PWUD and harm reduction tools and education. Survey questions were extrapolated from validated surveys (eg, DDPPQ) and survey-based implicit association test.16,17 The survey used multiple choice and 5-point Likert scale questions. Mental health prescribers were asked about their role at the VHA, years in practice, medical center affiliation, type of SUDs treated (eg, opioid, stimulant, alcohol, cannabis, or other), and whether they had previously met with academic detailers about harm reduction.
Respondents read statements about patients with or without SUD and provided Likert scale responses describing their regard, level of comfort, and preferences. The survey included Likert scale questions about respondents’ comfort in providing harm reduction education and supplies. Respondents also noted whether they believed harm reduction reduced substance use, harm reduction tools encourage people with SUD to continue using drugs, and whether HCPs can impact clinical change.
Postsurvey interviews with predetermined questions were conducted in-person or via video conference with ≥ 1 prescriber at each VAMC by an academic detailer. The postsurvey discussion offered an opportunity for respondents to further elaborate and describe previous experiences and current beliefs that may affect their attitudes toward people with SUD and their views on harm reduction. Participants received no compensation for survey completion or interviews.
Analysis
The Washington VAMC Institutional Review Board reviewed and approved this project as quality improvement with potential publication. No inferential statistics were calculated. Survey participant demographics were reported using frequencies and proportions reported for categorical variables. Notes from follow-up interviews were analyzed using the Prosci Awareness, Desire, Knowledge, Ability, and Reinforcement (ADKAR) Model for Change Management.18 This framework is used by academic detailers to determine a prescriber’s stage of change, which helps select the appropriate resources to move the clinician along a change framework. Completed postsurvey interview sheets, including notes written by the academic detailer, were analyzed by the project lead (NJ) who reviewed each interview sheet and analysis with the academic detailer who led the discussion.
Results
Sixty-six respondents completed the online survey (42% response rate), and 7 mental health prescribers participated in a postsurvey discussion. Thirty-one participants (47%) were physicians and 17 (26%) were in practice for > 20 years. Response rates reflected the size of mental health staff at each VAMC at the time of the survey: 17 respondents (26%) worked at each of the Martinsburg and Baltimore VAMCs, with fewer at the other VAMCs (Table 1). Alcohol use disorder was the most commonly reported SUD treated (n = 62; 33%), followed by cannabis use disorder (n = 40; 21%), OUD (n = 38; 20%), and stimulant use disorder (n = 37; 20%).
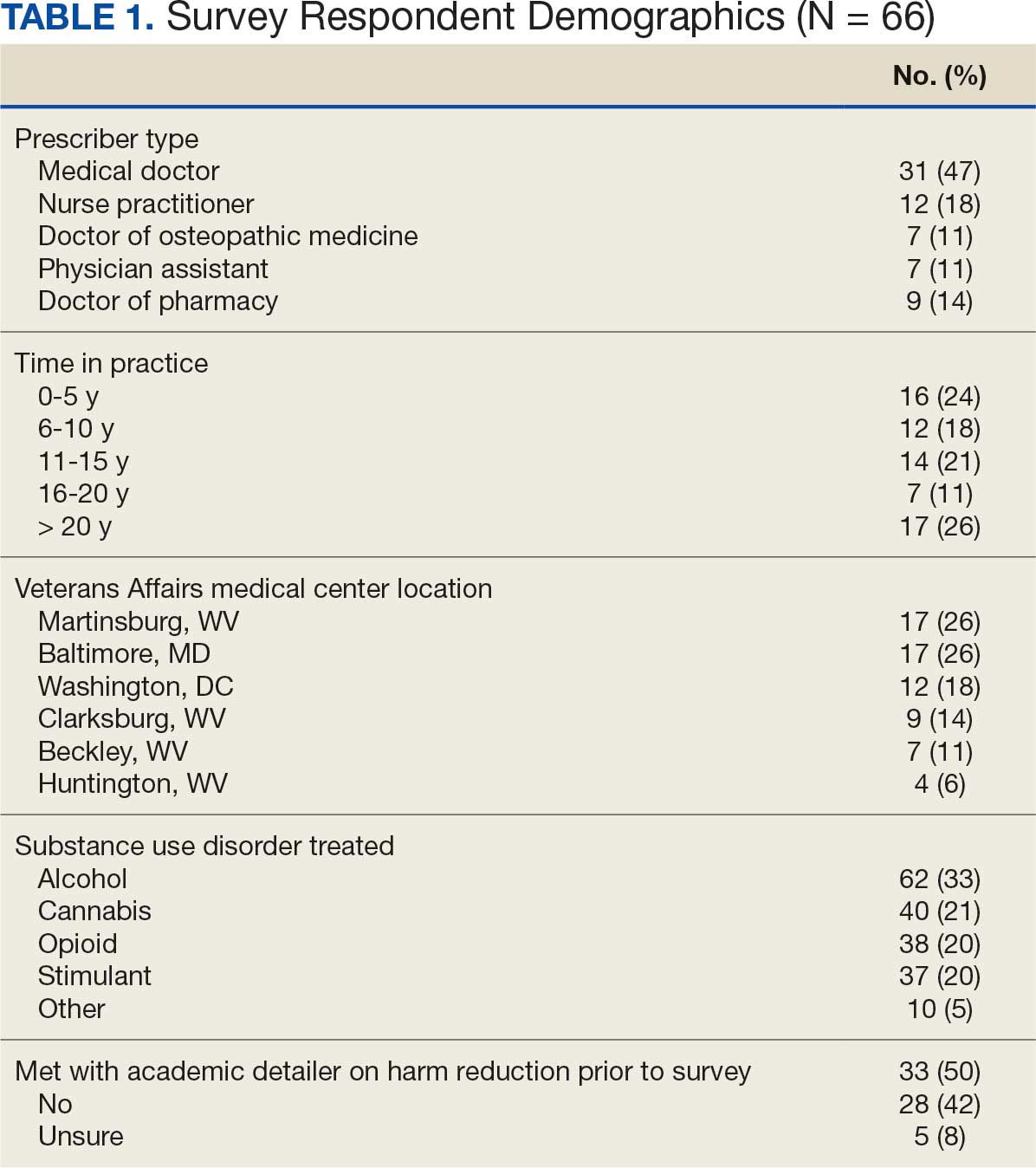
Respondents felt comfortable and confident educating patients on ways to reduce harm related to substance use (91%; mean [SD], 4.24 [0.84]). Most prescribers surveyed (97%; mean [SD], 1.59 [0.68]) disagreed or strongly disagreed that harm reduction encourages patients with SUD to continue using drugs, and all prescribers surveyed disagreed that there is nothing they can do to encourage harm reduction. Survey results were mixed for personal comfort in working with people with SUD vs people without SUD (Figure 2). Respondents were most willing to provide naloxone (95%; mean [SD], 4.71 [0.78]), compared to fentanyl test strips (61%; mean [SD], 3.61 [1.41]) or syringes (39%; mean [SD], 3.18 [1.39]). Respondents were neutral or least willing to provide syringes (Figure 3).
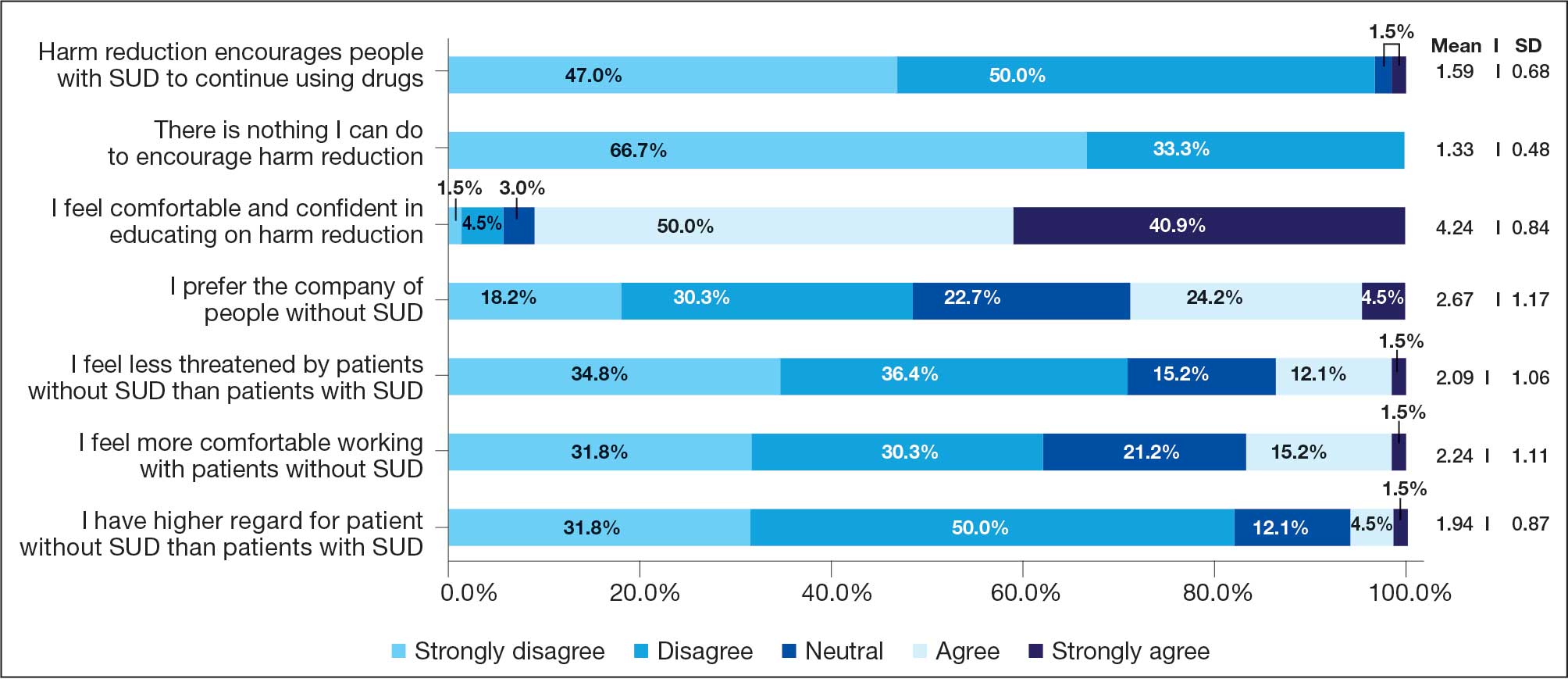
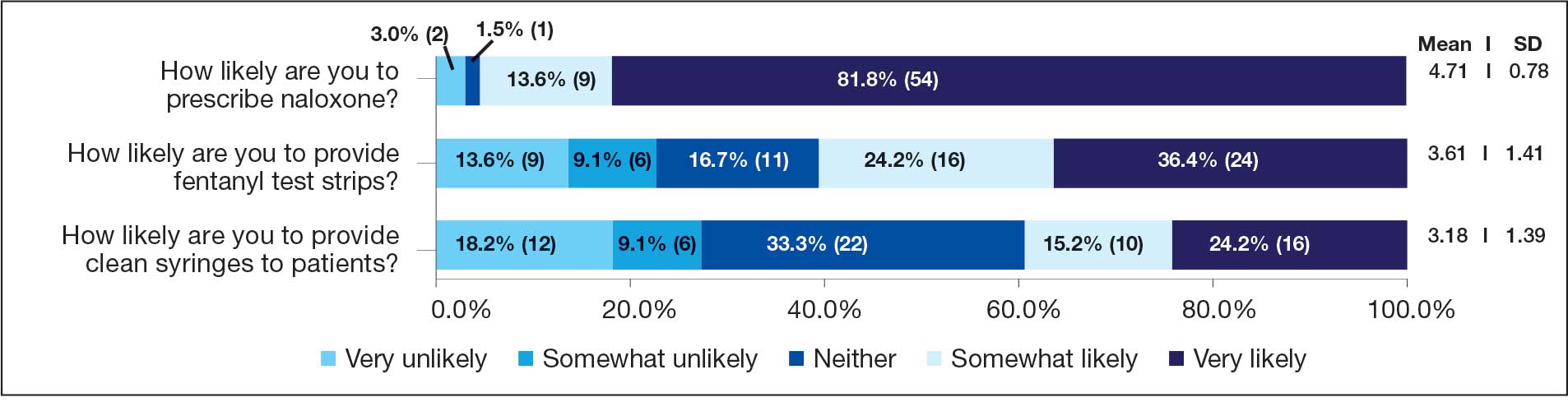
Seven postsurvey interviews were completed between academic detailers and mental health clinicians across the 6 VAMCs. Respondents included 1 physician assistant, 1 nurse practitioner, 1 pharmacist, and 4 physicians. Notes were analyzed using the ADKAR Change Competency Model to organize clinician stages of change (Table 2).
Barriers identified by interviewees included lack of mobile services, lack of confidence and awareness of the availability of harm reduction at their respective medical center, lack of time to discuss harm reduction, negative sentiments toward providing SUD-related harm reduction, discomfort with harm reduction products, and lack of knowledge and time to learn about harm reduction services. Opportunities identified to drive change in practice included additional time allotted during patient appointments, educational discussions and presentations to increase knowledge of and comfort with harm reduction tools, a clear clinical patient care workflow and process for harm reduction services, and reinforcement strategies to recognize success.
Discussion
This project investigated mental health prescribers’ perceptions of harm reduction at VAMCs in West Virginia, Maryland, and Washington, DC. While previous studies have demonstrated the efficacy of harm reduction tools, there is a lack of research on HCPs willingness to use these resources. This study suggests that while most respondents feel confident in and see the value of offering harm reduction resources to patients, a disparity exists between which resources HCPs are more likely to use and factors that would further enhance their ability to integrate harm reduction into practice. The follow-up interviews provided additional insight into the survey results.
Most respondents met the awareness and desire stage and moved to the knowledge, ability, or reinforcement ADKAR stage. It would be reasonable to extrapolate that most of the respondents felt comfortable with and were very likely to offer certain harm reduction tools. In the ADKAR interview analysis, the most common factors needed to drive change included having more time during patient appointments, additional education, clear processes for harm reduction services, and reinforcement strategies to sustain change. Respondents noted that harm reduction discussions took extra time in their already limited appointments with patients, which may have limited time for discussions surrounding all other mental health concerns. These discussions often necessitate in-depth conversations to accurately understand the patients’ needs. Given HCP time constraints, they may view harm reduction as lower in urgency and priority relative to other concerns. While most respondents were in the reinforcement phase, it is important to note the ADKAR model is fluid, and therefore an HCP could move forward or backward. This movement can be noted in the postsurvey interviews where, for example, prescriber 6 was determined to be in the reinforcement stage since they had already discussed harm reduction with patients. However, prescriber 6 also noted a barrier of unfamiliarity with local laws, which could shift them to the ADKAR knowledge stage.
Respondents noted that education through didactic sessions could lead to better incorporation of harm reduction into patient care. While harm reduction has evidence supporting its effectiveness, the respondents noted willingness to discuss harm reduction when treatment fails or the patient refuses treatment or referrals. Respondents expressed mixed opinions on use of harm reduction tools among patients with SUDs as some prescribers viewed harm reduction as part of a treatment plan and others viewed a return to drug use as a failure of treatment. Furthermore, respondents expressed hesitancy surrounding certain harm reduction tools, such as fentanyl test strips or syringes, and perceived these supplies as intended for medical use rather than harm reduction. HCPs may feel uncomfortable offering these supplies for drug use, despite their use for reducing risk.
Most responses were received from VAMCs with large mental health substance use programs. Respondents at larger, urban facilities (Washington, DC, and Baltimore, Maryland) expressed more hesitancy around using harm reduction tools despite having more harm reduction resources available compared to smaller or rural sites. These results align with previous studies that found no difference in prescribers providing medications for OUD in rural and urban VAMCs, showing urban sites, despite more resources, are not more willing to provide harm reduction or other addiction services.19 This evidence might indicate that urban sites may not use available resources (eg, methadone clinics) or that rural sites can provide just as robust medications for OUD care as urban sites.
Follow-up interview analysis indicated that HCPs lack knowledge of certain harm reduction tools. One-on-one peer discussions, like academic detailing, can facilitate discussions around a prescriber’s role in harm reduction, address gaps in knowledge by sharing what is available at the facilities for harm reduction, and suggest conversation points to help prescribers start harm reduction discussions with patients unwilling to begin treatment. Additionally, academic detailing can connect prescribers to available resources in the community to provide pragmatic approaches and suggestions. A clear and consistent treatment process may reduce barriers by reassuring prescribers they have support and by providing consistent directions so that prescribers do not waste time.
Reinforcement is important for sustaining change. VAMCs could consider positive feedback and other evidence-based reinforcement strategies (eg, social recognition, continuing education) to communicate that these changes are noticed and appreciated.20 Late adopters may also be influenced by seeing positive feedback and results for peers. Systematic changes can be the catalyst for and sustain individual change.
Shifting perceptions and adopting change may be challenging, especially for SUD, which can be highly stigmatized. Promotion of successful change should be multifaceted and include both system and individual approaches. VHA systemic changes that could contribute to positive change include provision of time and access to SUD treatment training, a clear and sustainable treatment process, and reinforcement by recognizing success. In addition, facility leadership could provide support through dedicated time and resources during the workday for SUD treatment and harm reduction training. Support could empower HCPs and convey leadership support for harm reduction. This dedicated time could be used for didactic lecture sessions or individual meetings with academic detailers who can tailor discussions to the prescriber’s practice.
Strengths and Limitations
This survey included prescribers from a range of mental health care practice settings (eg, inpatient, outpatient clinic, rural, urban) and varied years of experience. This variety resulted in diverse perspectives and knowledge bases. Postsurvey interviews allowed academic detailers to gain deeper insight into answers in the survey, which can guide future interventions. Postsurvey interviews and application of the ADKAR model provided additional viewpoints on harm reduction.
A limitation of this project is the absence of an assessment of respondents’ harm reduction knowledge accuracy. Although respondents reported confidence in discussing harm reduction with patients, the survey did not assess whether their knowledge was accurate. Additionally, the survey did not ask about the availability of syringes and test strips at the prescribers’ VAMC, which could explain discrepancies in responses between naloxone and other forms of harm reduction (drug test strips and syringes were not available to all HCPs in the VISN). This lack of availability may have skewed responses. West Virginia SSPs, for example, were closed following legislative changes, which may contribute to stigma.21
Not all respondents were asked to do a follow-up interview, which limited the perspectives included in this study. Each site had ≥ 1 follow-up interview to limit the academic detailer’s workload. The initial survey included the phrase clean syringe, which can be stigmatizing and insinuate that PWUD are not clean. The preferred term would have been sterile syringe.22
Conclusions
This survey of mental health prescribers found that most respondents are comfortable treating patients with SUD and confident in educating patients on harm reduction. Additionally, most respondents were more willing to provide naloxone vs fentanyl test strips or sterile syringes. A lack of time and awareness was the most frequently cited barrier to harm reduction services. As the VHA continues to expand access to harm reduction programs, which have proven to increase treatment rates and reduce disease, it will be imperative for HCPs, including mental health prescribers, to recognize the benefit of these programs for veterans with SUD. Future interventions should be designed and evaluated in collaboration with all HCPs and patients. This project determined ways to promote change for prescribers, but it will be important for further research to continue those conversations and incorporate patient perspectives.
- Use of funds to supply hypodermic needles or syringes for illegal drug use; prohibition, 42 USC § 300ee-5 (1988). Accessed January 5, 2026. https://www.law.cornell.edu /uscode/text/42/300ee-5
- OD2A Case Study: Harm Reduction. Centers for Disease Control and Prevention. June 9, 2025. Accessed January 5, 2026. https://www.cdc.gov/overdose-prevention/php /od2a/harm-reduction.html
- Strengthening Syringe Services Programs (SSPs). Centers for Disease Control and Prevention. March 20, 2024. Accessed January 5, 2026. https://www.cdc.gov/hepatitis -syringe-services/php/about/index.html
- Weinmeyer R. Needle exchange programs’ status in US politics. AMA J Ethics. 2016;18:252-257. doi:10.1001/journalofethics.2016.18.3.hlaw1-1603
- Rife-Pennington T, Dinges E, Ho MQ. Implementing syringe services programs within the Veterans Health Administration: facility experiences and next steps. J Am Pharm Assoc (2003). 2023;63:234-240. doi:10.1016/j.japh.2022.10.019
- The Biden-Harris Administration’s Statement of Drug Policy Priorities for Year One. Executive Office of the President, Office of National Drug Control Policy. April 1, 2021. Accessed January 5, 2026. https://bidenwhitehouse.archives.gov/wp-content/uploads/2021/03/BidenHarris -Statement-of-Drug-Policy-Priorities-April-1.pdf
- HIV - for veterans and the public syringe services programs. US Department of Veterans Affairs. Updated August 16, 2021. Accessed January 5, 2026. https://www.hiv .va.gov/patient/ssp.asp
- Trump Administration’s Statement of Drug Policy Priorities. White House. April 1, 2025. Accessed January 7, 2026. https://www.whitehouse.gov/wp-content /uploads/2025/04/2025-Trump-Administration-Drug-Policy -Priorities.pdf
- Health Centers and Syringe Services Programs. National Health Care for the Homeless Council. May 2023. Accessed January 5, 2026. https://nhchc.org/wp-content /uploads/2023/06/Health-Centers-SSPs-Final.pdf
- Lynch RD, Biederman DJ, Silva S, Demasi K. A syringe service program within a federal system: foundations for implementation. J Addict Nurs. 2021;32:152-158. doi:10.1097/JAN.0000000000000402
- Harvey LH, Sliwinski SK, Flike K, et al. The integration of harm reduction services in the Veterans Health Administration (VHA): a qualitative analysis of barriers and facilitators. J Addict Dis. 2024;42:326-334. doi:10.1080/10550887.2023.2210021
- Drug Overdose Death Rates. National Center for Drug Abuse Statistics. Accessed January 5, 2026. https:// drugabusestatistics.org/drug-overdose-deaths
- Ng G. New database shows Baltimore greatly devastated by opioid epidemic. Updated August 21, 2023. Accessed January 5, 2026. https://www.wbaltv.com/article/opioid -epidemic-database-baltimore-deaths/44869671
- Introductory Guide to Academic Detailing. National Resource Center for Academic Detailing. 2017. Accessed January 5, 2026. https://www.narcad.org /uploads/5/7/9/5/57955981/introductory_guide_to_ad.pdf
- Zhang J. Can educational outreach improve experts’ decision making? Evidence from a national opioid academic detailing program. SSRN. 2023;4297398. doi:10.2139/ssrn.4297398
- Watson H, Maclaren W, Kerr S. Staff attitudes towards working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206- 215. doi:10.1111/j.1360-0443.2006.01686.x
- Dahl RA, Vakkalanka JP, Harland KK, Radke J. Investigating healthcare provider bias toward patients who use drugs using a survey-based implicit association test: pilot study. J Addict Med. 2022;16:557-562. doi:10.1097/ADM.0000000000000970
- Hiatt JM, Creasey TJ. Change Management: The People Side of Change. Prosci Learning Center Publications; 2012.
- Wyse JJ, Shull S, Lindner S, et al. Access to medications for opioid use disorder in rural versus urban Veterans Health Administration facilities. J Gen Intern Med. 2023;38:1871-1876. doi:10.1007/s11606-023-08027-4
- Mostofian F, Ruban C, Simunovic N, Bhandari M. Changing physician behavior: what works?. Am J Manag Care. 2015;21(1):75-84.
- Bergdorf-Smith K, Bridge Initiative for S&T Policy, Leadership, and Communications. Syringe Service Programs and HIV Prevention in West Virginia. West Virginia University. February 5, 2024. Accessed January 5, 2026. https:// scitechpolicy.wvu.edu/science-and-technology-notes -articles/2024/02/05/syringe-service-programs-and-hiv -prevention-in-west-virginia
- Brunsdon N. Stop saying ‘clean’. Injecting Advice. February 7, 2011. Accessed January 5, 2026. https:// injectingadvice.com/stop-saying-clean/
The Public Health and Welfare Act of 1988 prohibited the use of federal funds to “provide individuals with hypodermic needles or syringes so that such individuals may use illegal drugs.”1 Although the Act included the caveat that the US Surgeon General may determine that “a demonstration needle exchange program would be effective in reducing drug abuse,” and thus federal funds could be used, the legislation prohibited federal, state, and local agencies from funding syringe services programs (SSPs). SSPs use various harm reduction tools to improve public safety and reduce the potential harmful consequences of risky behaviors, similar to how using a seat belt while driving reduces the risk of injury or death.2 SSPs are rooted in evidence-based practices, and several studies, according to the Centers for Disease Control and Prevention, have found that people who use drugs (PWUDs) who use community-based SSPs are 5 times more likely to enter treatment than those who do not use these programs. Additionally, these programs have shown an estimated 50% reduction in HIV and hepatitis C infections.3
Amid a 2015 HIV outbreak in Indiana among individuals sharing needles for injection drug use, Congress passed an omnibus spending bill that partially lifted the federal funding restriction. Federal funds now may be used for operational costs that support SSPs but may not be used to purchase syringes themselves.4
Following the 2015 legislation, federal agencies began implementing SSPs. The Veterans Health Administration (VHA) established SSPs at 3 medical centers in 2017.5 Veterans who participated in the programs were able to access supplies (eg, syringes, fentanyl test strips, wound care kits, and condoms) through donations to US Department of Veterans Affairs (VA) medical centers (VAMCs). The success of these programs laid the foundation for the VHA to implement SSPs nationally. VHA SSPs provided access to naloxone (an opioid overdose reversal medication), fentanyl test strips, condoms, sterile syringe distribution, testing for blood-borne viruses, HIV pre-exposure prophylaxis, as well as educational materials and resources, and low-barrier access to drug treatment (eg, medications for opioid use disorder [OUD]).
In 2020, the Biden Administration outlined 7 drug policy priorities, which included enhancing evidence-based harm reduction efforts. 6 This policy also discussed mandates for federal agencies to remove barriers to federal funding for purchasing syringes and other harm reduction supplies. The VHA responded to the policy by publishing guidance that recommended VAMCs develop and/or ensure veterans have access to harm reduction services in the community, where state law is not legally more stringent.7
In 2025 the Trump administration Statement of Drug Policy Priorities encouraged local jurisdictions to increase the availability of drug test strips and naloxone.8 These significant policy shifts moved SSPs from being housed mostly in local public health departments and community-based organizations to also being available at health care facilities. 9 VAMCs have unique opportunities to provide universal health care that includes both prevention services and other medical management to PWUD.
One study assessed staff perceptions of PWUD at a VAMC in preparation for a training program about harm reduction. The results indicated an overall positive staff perception of PWUD, although only the Drug and Drug Problems Perceptions Questionnaire (DDPPQ) was administered, which assessed comfort of working with this population and not explicitly the use of harm reduction.10 Another study interviewed clinical pharmacists, primary care clinicians, social workers, and directors of addiction and mental health services to determine barriers and facilitators (ie, potential opportunities to promote change) to implementing harm reduction at the VHA. The study identified barriers to be a lack of knowledge, time, and comfort, while suggesting opportunities for improvement were engagement of champions, communication and educational strategies, and adaptation of existing infrastructure.11
While these findings are insightful for the VHA to disseminate a harm reduction program, there remains a gap in assessing staff willingness to provide harm reduction services. Evidence on harm reduction services among veterans is limited and more research is needed to better understand the role of these services and acceptance among enrolled veterans and VHA staff. Specifically, more research is needed on health care practitioners’ (HCPs) perceptions of harm reduction use.
Mental health care practitioners frequently treat patients with substance use disorders (SUDs), making them an ideal initial cohort to assess willingness to provide harm reduction to this population. By analyzing mental HCPs’ perceptions, additional interventions could be identified, implemented, and evaluated to improve their willingness to provide harm reduction tools.
This project focused on mental health clinicians with prescribing privileges: physicians (allopathic and osteopathic physicians), nurse practitioners, physician assistants, and clinical pharmacist practitioners. Mental health prescribers were selected because they are uniquely positioned at the intersection of prevention and treatment in drug use. Furthermore, mental health prescribers at the VAMCs included in this study are usually the primary point of entry to SUD clinics. This mixed-methods study used an anonymous online survey and voluntary postsurvey discussions with mental health care prescribers to elaborate on their beliefs and attitudes, providing deeper insight into their responses regarding harm reduction.
Methods
This project was conducted by the Veterans Integrated Services Network (VISN) 5 academic detailing team. VISN 5 serves veterans from economically and demographically diverse areas in Maryland; Washington, DC; West Virginia; and portions of Virginia, Pennsylvania, Ohio, and Kentucky. VAMCs in Baltimore, Maryland, and Washington, DC, serve a largely urban population while the 4 West Virginia facilities in Martinsburg, Huntington, Beckley, and Clarksburg, serve a largely rural population. West Virginia has been the epicenter of the opioid crisis and consistently has the highest drug overdose deaths per capita in the United States.12 Among cities, Baltimore, Maryland, has the highest number of drug overdose deaths per capita with 174.1 per 100,000 people.12,13
At the time of this project, the 6 VISN 5 VAMCs had established overdose education and naloxone distribution (OEND) programs. Although OEND programs have existed since 2013, VISN 5 SSPs and harm reduction services that provided fentanyl test strips were only available at the Martinsburg, Beckley, and Huntington VAMCs. All 6 VAMCs had substance use treatment programs with a variety of inpatient and outpatient mental health services. The Washington, DC and Baltimore VAMCs had opioid treatment programs that provided methadone maintenance.
The VISN 5 academic detailing team consists of 7 clinical pharmacists. These academic detailers plan annual systematic interventions to provide medical knowledge translation services on health-related campaigns. Academic detailers are trained in change management and motivational interviewing. They uniquely facilitate conversations with HCPs on various topics or campaigns, aiming for quality improvement and behavioral change through positive relationships and sharing resources.14 Academic detailing conversations and relationships with HCPs involve assessing and understanding HCP behaviors, including barriers and readiness to change to align with the goal of improving patient outcomes. Academic detailing has improved practice behaviors around providing OEND in VHA.15
To prepare for a harm reduction campaign, the academic detailers sought to gain insight from target VISN 5 mental health prescribers. Figure 1 outlines the project timeline, which started with emails inviting mental health prescribers to complete an anonymous online survey. Academic detailers from each site emailed mental health prescribers who completed the survey to determine interest in expanding on survey findings. Mental health prescribers who completed the survey could participate in a postsurvey discussion.
Surveys
Between January 29, 2024, and February 22, 2024, the academic detailers emailed facility mental health prescribers (N = 156) a link to an anonymous 15-question survey. The email informed recipients of the survey’s purpose: to gain a better understanding of prescriber perceptions of veterans with SUD and harm reduction programs and their willingness to provide harm reduction tools, to better determine interventions that could be implemented.
The survey collected prescriber demographic data and their perceptions of PWUD and harm reduction tools and education. Survey questions were extrapolated from validated surveys (eg, DDPPQ) and survey-based implicit association test.16,17 The survey used multiple choice and 5-point Likert scale questions. Mental health prescribers were asked about their role at the VHA, years in practice, medical center affiliation, type of SUDs treated (eg, opioid, stimulant, alcohol, cannabis, or other), and whether they had previously met with academic detailers about harm reduction.
Respondents read statements about patients with or without SUD and provided Likert scale responses describing their regard, level of comfort, and preferences. The survey included Likert scale questions about respondents’ comfort in providing harm reduction education and supplies. Respondents also noted whether they believed harm reduction reduced substance use, harm reduction tools encourage people with SUD to continue using drugs, and whether HCPs can impact clinical change.
Postsurvey interviews with predetermined questions were conducted in-person or via video conference with ≥ 1 prescriber at each VAMC by an academic detailer. The postsurvey discussion offered an opportunity for respondents to further elaborate and describe previous experiences and current beliefs that may affect their attitudes toward people with SUD and their views on harm reduction. Participants received no compensation for survey completion or interviews.
Analysis
The Washington VAMC Institutional Review Board reviewed and approved this project as quality improvement with potential publication. No inferential statistics were calculated. Survey participant demographics were reported using frequencies and proportions reported for categorical variables. Notes from follow-up interviews were analyzed using the Prosci Awareness, Desire, Knowledge, Ability, and Reinforcement (ADKAR) Model for Change Management.18 This framework is used by academic detailers to determine a prescriber’s stage of change, which helps select the appropriate resources to move the clinician along a change framework. Completed postsurvey interview sheets, including notes written by the academic detailer, were analyzed by the project lead (NJ) who reviewed each interview sheet and analysis with the academic detailer who led the discussion.
Results
Sixty-six respondents completed the online survey (42% response rate), and 7 mental health prescribers participated in a postsurvey discussion. Thirty-one participants (47%) were physicians and 17 (26%) were in practice for > 20 years. Response rates reflected the size of mental health staff at each VAMC at the time of the survey: 17 respondents (26%) worked at each of the Martinsburg and Baltimore VAMCs, with fewer at the other VAMCs (Table 1). Alcohol use disorder was the most commonly reported SUD treated (n = 62; 33%), followed by cannabis use disorder (n = 40; 21%), OUD (n = 38; 20%), and stimulant use disorder (n = 37; 20%).
Respondents felt comfortable and confident educating patients on ways to reduce harm related to substance use (91%; mean [SD], 4.24 [0.84]). Most prescribers surveyed (97%; mean [SD], 1.59 [0.68]) disagreed or strongly disagreed that harm reduction encourages patients with SUD to continue using drugs, and all prescribers surveyed disagreed that there is nothing they can do to encourage harm reduction. Survey results were mixed for personal comfort in working with people with SUD vs people without SUD (Figure 2). Respondents were most willing to provide naloxone (95%; mean [SD], 4.71 [0.78]), compared to fentanyl test strips (61%; mean [SD], 3.61 [1.41]) or syringes (39%; mean [SD], 3.18 [1.39]). Respondents were neutral or least willing to provide syringes (Figure 3).
Seven postsurvey interviews were completed between academic detailers and mental health clinicians across the 6 VAMCs. Respondents included 1 physician assistant, 1 nurse practitioner, 1 pharmacist, and 4 physicians. Notes were analyzed using the ADKAR Change Competency Model to organize clinician stages of change (Table 2).
Barriers identified by interviewees included lack of mobile services, lack of confidence and awareness of the availability of harm reduction at their respective medical center, lack of time to discuss harm reduction, negative sentiments toward providing SUD-related harm reduction, discomfort with harm reduction products, and lack of knowledge and time to learn about harm reduction services. Opportunities identified to drive change in practice included additional time allotted during patient appointments, educational discussions and presentations to increase knowledge of and comfort with harm reduction tools, a clear clinical patient care workflow and process for harm reduction services, and reinforcement strategies to recognize success.
Discussion
This project investigated mental health prescribers’ perceptions of harm reduction at VAMCs in West Virginia, Maryland, and Washington, DC. While previous studies have demonstrated the efficacy of harm reduction tools, there is a lack of research on HCPs willingness to use these resources. This study suggests that while most respondents feel confident in and see the value of offering harm reduction resources to patients, a disparity exists between which resources HCPs are more likely to use and factors that would further enhance their ability to integrate harm reduction into practice. The follow-up interviews provided additional insight into the survey results.
Most respondents met the awareness and desire stage and moved to the knowledge, ability, or reinforcement ADKAR stage. It would be reasonable to extrapolate that most of the respondents felt comfortable with and were very likely to offer certain harm reduction tools. In the ADKAR interview analysis, the most common factors needed to drive change included having more time during patient appointments, additional education, clear processes for harm reduction services, and reinforcement strategies to sustain change. Respondents noted that harm reduction discussions took extra time in their already limited appointments with patients, which may have limited time for discussions surrounding all other mental health concerns. These discussions often necessitate in-depth conversations to accurately understand the patients’ needs. Given HCP time constraints, they may view harm reduction as lower in urgency and priority relative to other concerns. While most respondents were in the reinforcement phase, it is important to note the ADKAR model is fluid, and therefore an HCP could move forward or backward. This movement can be noted in the postsurvey interviews where, for example, prescriber 6 was determined to be in the reinforcement stage since they had already discussed harm reduction with patients. However, prescriber 6 also noted a barrier of unfamiliarity with local laws, which could shift them to the ADKAR knowledge stage.
Respondents noted that education through didactic sessions could lead to better incorporation of harm reduction into patient care. While harm reduction has evidence supporting its effectiveness, the respondents noted willingness to discuss harm reduction when treatment fails or the patient refuses treatment or referrals. Respondents expressed mixed opinions on use of harm reduction tools among patients with SUDs as some prescribers viewed harm reduction as part of a treatment plan and others viewed a return to drug use as a failure of treatment. Furthermore, respondents expressed hesitancy surrounding certain harm reduction tools, such as fentanyl test strips or syringes, and perceived these supplies as intended for medical use rather than harm reduction. HCPs may feel uncomfortable offering these supplies for drug use, despite their use for reducing risk.
Most responses were received from VAMCs with large mental health substance use programs. Respondents at larger, urban facilities (Washington, DC, and Baltimore, Maryland) expressed more hesitancy around using harm reduction tools despite having more harm reduction resources available compared to smaller or rural sites. These results align with previous studies that found no difference in prescribers providing medications for OUD in rural and urban VAMCs, showing urban sites, despite more resources, are not more willing to provide harm reduction or other addiction services.19 This evidence might indicate that urban sites may not use available resources (eg, methadone clinics) or that rural sites can provide just as robust medications for OUD care as urban sites.
Follow-up interview analysis indicated that HCPs lack knowledge of certain harm reduction tools. One-on-one peer discussions, like academic detailing, can facilitate discussions around a prescriber’s role in harm reduction, address gaps in knowledge by sharing what is available at the facilities for harm reduction, and suggest conversation points to help prescribers start harm reduction discussions with patients unwilling to begin treatment. Additionally, academic detailing can connect prescribers to available resources in the community to provide pragmatic approaches and suggestions. A clear and consistent treatment process may reduce barriers by reassuring prescribers they have support and by providing consistent directions so that prescribers do not waste time.
Reinforcement is important for sustaining change. VAMCs could consider positive feedback and other evidence-based reinforcement strategies (eg, social recognition, continuing education) to communicate that these changes are noticed and appreciated.20 Late adopters may also be influenced by seeing positive feedback and results for peers. Systematic changes can be the catalyst for and sustain individual change.
Shifting perceptions and adopting change may be challenging, especially for SUD, which can be highly stigmatized. Promotion of successful change should be multifaceted and include both system and individual approaches. VHA systemic changes that could contribute to positive change include provision of time and access to SUD treatment training, a clear and sustainable treatment process, and reinforcement by recognizing success. In addition, facility leadership could provide support through dedicated time and resources during the workday for SUD treatment and harm reduction training. Support could empower HCPs and convey leadership support for harm reduction. This dedicated time could be used for didactic lecture sessions or individual meetings with academic detailers who can tailor discussions to the prescriber’s practice.
Strengths and Limitations
This survey included prescribers from a range of mental health care practice settings (eg, inpatient, outpatient clinic, rural, urban) and varied years of experience. This variety resulted in diverse perspectives and knowledge bases. Postsurvey interviews allowed academic detailers to gain deeper insight into answers in the survey, which can guide future interventions. Postsurvey interviews and application of the ADKAR model provided additional viewpoints on harm reduction.
A limitation of this project is the absence of an assessment of respondents’ harm reduction knowledge accuracy. Although respondents reported confidence in discussing harm reduction with patients, the survey did not assess whether their knowledge was accurate. Additionally, the survey did not ask about the availability of syringes and test strips at the prescribers’ VAMC, which could explain discrepancies in responses between naloxone and other forms of harm reduction (drug test strips and syringes were not available to all HCPs in the VISN). This lack of availability may have skewed responses. West Virginia SSPs, for example, were closed following legislative changes, which may contribute to stigma.21
Not all respondents were asked to do a follow-up interview, which limited the perspectives included in this study. Each site had ≥ 1 follow-up interview to limit the academic detailer’s workload. The initial survey included the phrase clean syringe, which can be stigmatizing and insinuate that PWUD are not clean. The preferred term would have been sterile syringe.22
Conclusions
This survey of mental health prescribers found that most respondents are comfortable treating patients with SUD and confident in educating patients on harm reduction. Additionally, most respondents were more willing to provide naloxone vs fentanyl test strips or sterile syringes. A lack of time and awareness was the most frequently cited barrier to harm reduction services. As the VHA continues to expand access to harm reduction programs, which have proven to increase treatment rates and reduce disease, it will be imperative for HCPs, including mental health prescribers, to recognize the benefit of these programs for veterans with SUD. Future interventions should be designed and evaluated in collaboration with all HCPs and patients. This project determined ways to promote change for prescribers, but it will be important for further research to continue those conversations and incorporate patient perspectives.
The Public Health and Welfare Act of 1988 prohibited the use of federal funds to “provide individuals with hypodermic needles or syringes so that such individuals may use illegal drugs.”1 Although the Act included the caveat that the US Surgeon General may determine that “a demonstration needle exchange program would be effective in reducing drug abuse,” and thus federal funds could be used, the legislation prohibited federal, state, and local agencies from funding syringe services programs (SSPs). SSPs use various harm reduction tools to improve public safety and reduce the potential harmful consequences of risky behaviors, similar to how using a seat belt while driving reduces the risk of injury or death.2 SSPs are rooted in evidence-based practices, and several studies, according to the Centers for Disease Control and Prevention, have found that people who use drugs (PWUDs) who use community-based SSPs are 5 times more likely to enter treatment than those who do not use these programs. Additionally, these programs have shown an estimated 50% reduction in HIV and hepatitis C infections.3
Amid a 2015 HIV outbreak in Indiana among individuals sharing needles for injection drug use, Congress passed an omnibus spending bill that partially lifted the federal funding restriction. Federal funds now may be used for operational costs that support SSPs but may not be used to purchase syringes themselves.4
Following the 2015 legislation, federal agencies began implementing SSPs. The Veterans Health Administration (VHA) established SSPs at 3 medical centers in 2017.5 Veterans who participated in the programs were able to access supplies (eg, syringes, fentanyl test strips, wound care kits, and condoms) through donations to US Department of Veterans Affairs (VA) medical centers (VAMCs). The success of these programs laid the foundation for the VHA to implement SSPs nationally. VHA SSPs provided access to naloxone (an opioid overdose reversal medication), fentanyl test strips, condoms, sterile syringe distribution, testing for blood-borne viruses, HIV pre-exposure prophylaxis, as well as educational materials and resources, and low-barrier access to drug treatment (eg, medications for opioid use disorder [OUD]).
In 2020, the Biden Administration outlined 7 drug policy priorities, which included enhancing evidence-based harm reduction efforts. 6 This policy also discussed mandates for federal agencies to remove barriers to federal funding for purchasing syringes and other harm reduction supplies. The VHA responded to the policy by publishing guidance that recommended VAMCs develop and/or ensure veterans have access to harm reduction services in the community, where state law is not legally more stringent.7
In 2025 the Trump administration Statement of Drug Policy Priorities encouraged local jurisdictions to increase the availability of drug test strips and naloxone.8 These significant policy shifts moved SSPs from being housed mostly in local public health departments and community-based organizations to also being available at health care facilities. 9 VAMCs have unique opportunities to provide universal health care that includes both prevention services and other medical management to PWUD.
One study assessed staff perceptions of PWUD at a VAMC in preparation for a training program about harm reduction. The results indicated an overall positive staff perception of PWUD, although only the Drug and Drug Problems Perceptions Questionnaire (DDPPQ) was administered, which assessed comfort of working with this population and not explicitly the use of harm reduction.10 Another study interviewed clinical pharmacists, primary care clinicians, social workers, and directors of addiction and mental health services to determine barriers and facilitators (ie, potential opportunities to promote change) to implementing harm reduction at the VHA. The study identified barriers to be a lack of knowledge, time, and comfort, while suggesting opportunities for improvement were engagement of champions, communication and educational strategies, and adaptation of existing infrastructure.11
While these findings are insightful for the VHA to disseminate a harm reduction program, there remains a gap in assessing staff willingness to provide harm reduction services. Evidence on harm reduction services among veterans is limited and more research is needed to better understand the role of these services and acceptance among enrolled veterans and VHA staff. Specifically, more research is needed on health care practitioners’ (HCPs) perceptions of harm reduction use.
Mental health care practitioners frequently treat patients with substance use disorders (SUDs), making them an ideal initial cohort to assess willingness to provide harm reduction to this population. By analyzing mental HCPs’ perceptions, additional interventions could be identified, implemented, and evaluated to improve their willingness to provide harm reduction tools.
This project focused on mental health clinicians with prescribing privileges: physicians (allopathic and osteopathic physicians), nurse practitioners, physician assistants, and clinical pharmacist practitioners. Mental health prescribers were selected because they are uniquely positioned at the intersection of prevention and treatment in drug use. Furthermore, mental health prescribers at the VAMCs included in this study are usually the primary point of entry to SUD clinics. This mixed-methods study used an anonymous online survey and voluntary postsurvey discussions with mental health care prescribers to elaborate on their beliefs and attitudes, providing deeper insight into their responses regarding harm reduction.
Methods
This project was conducted by the Veterans Integrated Services Network (VISN) 5 academic detailing team. VISN 5 serves veterans from economically and demographically diverse areas in Maryland; Washington, DC; West Virginia; and portions of Virginia, Pennsylvania, Ohio, and Kentucky. VAMCs in Baltimore, Maryland, and Washington, DC, serve a largely urban population while the 4 West Virginia facilities in Martinsburg, Huntington, Beckley, and Clarksburg, serve a largely rural population. West Virginia has been the epicenter of the opioid crisis and consistently has the highest drug overdose deaths per capita in the United States.12 Among cities, Baltimore, Maryland, has the highest number of drug overdose deaths per capita with 174.1 per 100,000 people.12,13
At the time of this project, the 6 VISN 5 VAMCs had established overdose education and naloxone distribution (OEND) programs. Although OEND programs have existed since 2013, VISN 5 SSPs and harm reduction services that provided fentanyl test strips were only available at the Martinsburg, Beckley, and Huntington VAMCs. All 6 VAMCs had substance use treatment programs with a variety of inpatient and outpatient mental health services. The Washington, DC and Baltimore VAMCs had opioid treatment programs that provided methadone maintenance.
The VISN 5 academic detailing team consists of 7 clinical pharmacists. These academic detailers plan annual systematic interventions to provide medical knowledge translation services on health-related campaigns. Academic detailers are trained in change management and motivational interviewing. They uniquely facilitate conversations with HCPs on various topics or campaigns, aiming for quality improvement and behavioral change through positive relationships and sharing resources.14 Academic detailing conversations and relationships with HCPs involve assessing and understanding HCP behaviors, including barriers and readiness to change to align with the goal of improving patient outcomes. Academic detailing has improved practice behaviors around providing OEND in VHA.15
To prepare for a harm reduction campaign, the academic detailers sought to gain insight from target VISN 5 mental health prescribers. Figure 1 outlines the project timeline, which started with emails inviting mental health prescribers to complete an anonymous online survey. Academic detailers from each site emailed mental health prescribers who completed the survey to determine interest in expanding on survey findings. Mental health prescribers who completed the survey could participate in a postsurvey discussion.
Surveys
Between January 29, 2024, and February 22, 2024, the academic detailers emailed facility mental health prescribers (N = 156) a link to an anonymous 15-question survey. The email informed recipients of the survey’s purpose: to gain a better understanding of prescriber perceptions of veterans with SUD and harm reduction programs and their willingness to provide harm reduction tools, to better determine interventions that could be implemented.
The survey collected prescriber demographic data and their perceptions of PWUD and harm reduction tools and education. Survey questions were extrapolated from validated surveys (eg, DDPPQ) and survey-based implicit association test.16,17 The survey used multiple choice and 5-point Likert scale questions. Mental health prescribers were asked about their role at the VHA, years in practice, medical center affiliation, type of SUDs treated (eg, opioid, stimulant, alcohol, cannabis, or other), and whether they had previously met with academic detailers about harm reduction.
Respondents read statements about patients with or without SUD and provided Likert scale responses describing their regard, level of comfort, and preferences. The survey included Likert scale questions about respondents’ comfort in providing harm reduction education and supplies. Respondents also noted whether they believed harm reduction reduced substance use, harm reduction tools encourage people with SUD to continue using drugs, and whether HCPs can impact clinical change.
Postsurvey interviews with predetermined questions were conducted in-person or via video conference with ≥ 1 prescriber at each VAMC by an academic detailer. The postsurvey discussion offered an opportunity for respondents to further elaborate and describe previous experiences and current beliefs that may affect their attitudes toward people with SUD and their views on harm reduction. Participants received no compensation for survey completion or interviews.
Analysis
The Washington VAMC Institutional Review Board reviewed and approved this project as quality improvement with potential publication. No inferential statistics were calculated. Survey participant demographics were reported using frequencies and proportions reported for categorical variables. Notes from follow-up interviews were analyzed using the Prosci Awareness, Desire, Knowledge, Ability, and Reinforcement (ADKAR) Model for Change Management.18 This framework is used by academic detailers to determine a prescriber’s stage of change, which helps select the appropriate resources to move the clinician along a change framework. Completed postsurvey interview sheets, including notes written by the academic detailer, were analyzed by the project lead (NJ) who reviewed each interview sheet and analysis with the academic detailer who led the discussion.
Results
Sixty-six respondents completed the online survey (42% response rate), and 7 mental health prescribers participated in a postsurvey discussion. Thirty-one participants (47%) were physicians and 17 (26%) were in practice for > 20 years. Response rates reflected the size of mental health staff at each VAMC at the time of the survey: 17 respondents (26%) worked at each of the Martinsburg and Baltimore VAMCs, with fewer at the other VAMCs (Table 1). Alcohol use disorder was the most commonly reported SUD treated (n = 62; 33%), followed by cannabis use disorder (n = 40; 21%), OUD (n = 38; 20%), and stimulant use disorder (n = 37; 20%).
Respondents felt comfortable and confident educating patients on ways to reduce harm related to substance use (91%; mean [SD], 4.24 [0.84]). Most prescribers surveyed (97%; mean [SD], 1.59 [0.68]) disagreed or strongly disagreed that harm reduction encourages patients with SUD to continue using drugs, and all prescribers surveyed disagreed that there is nothing they can do to encourage harm reduction. Survey results were mixed for personal comfort in working with people with SUD vs people without SUD (Figure 2). Respondents were most willing to provide naloxone (95%; mean [SD], 4.71 [0.78]), compared to fentanyl test strips (61%; mean [SD], 3.61 [1.41]) or syringes (39%; mean [SD], 3.18 [1.39]). Respondents were neutral or least willing to provide syringes (Figure 3).
Seven postsurvey interviews were completed between academic detailers and mental health clinicians across the 6 VAMCs. Respondents included 1 physician assistant, 1 nurse practitioner, 1 pharmacist, and 4 physicians. Notes were analyzed using the ADKAR Change Competency Model to organize clinician stages of change (Table 2).
Barriers identified by interviewees included lack of mobile services, lack of confidence and awareness of the availability of harm reduction at their respective medical center, lack of time to discuss harm reduction, negative sentiments toward providing SUD-related harm reduction, discomfort with harm reduction products, and lack of knowledge and time to learn about harm reduction services. Opportunities identified to drive change in practice included additional time allotted during patient appointments, educational discussions and presentations to increase knowledge of and comfort with harm reduction tools, a clear clinical patient care workflow and process for harm reduction services, and reinforcement strategies to recognize success.
Discussion
This project investigated mental health prescribers’ perceptions of harm reduction at VAMCs in West Virginia, Maryland, and Washington, DC. While previous studies have demonstrated the efficacy of harm reduction tools, there is a lack of research on HCPs willingness to use these resources. This study suggests that while most respondents feel confident in and see the value of offering harm reduction resources to patients, a disparity exists between which resources HCPs are more likely to use and factors that would further enhance their ability to integrate harm reduction into practice. The follow-up interviews provided additional insight into the survey results.
Most respondents met the awareness and desire stage and moved to the knowledge, ability, or reinforcement ADKAR stage. It would be reasonable to extrapolate that most of the respondents felt comfortable with and were very likely to offer certain harm reduction tools. In the ADKAR interview analysis, the most common factors needed to drive change included having more time during patient appointments, additional education, clear processes for harm reduction services, and reinforcement strategies to sustain change. Respondents noted that harm reduction discussions took extra time in their already limited appointments with patients, which may have limited time for discussions surrounding all other mental health concerns. These discussions often necessitate in-depth conversations to accurately understand the patients’ needs. Given HCP time constraints, they may view harm reduction as lower in urgency and priority relative to other concerns. While most respondents were in the reinforcement phase, it is important to note the ADKAR model is fluid, and therefore an HCP could move forward or backward. This movement can be noted in the postsurvey interviews where, for example, prescriber 6 was determined to be in the reinforcement stage since they had already discussed harm reduction with patients. However, prescriber 6 also noted a barrier of unfamiliarity with local laws, which could shift them to the ADKAR knowledge stage.
Respondents noted that education through didactic sessions could lead to better incorporation of harm reduction into patient care. While harm reduction has evidence supporting its effectiveness, the respondents noted willingness to discuss harm reduction when treatment fails or the patient refuses treatment or referrals. Respondents expressed mixed opinions on use of harm reduction tools among patients with SUDs as some prescribers viewed harm reduction as part of a treatment plan and others viewed a return to drug use as a failure of treatment. Furthermore, respondents expressed hesitancy surrounding certain harm reduction tools, such as fentanyl test strips or syringes, and perceived these supplies as intended for medical use rather than harm reduction. HCPs may feel uncomfortable offering these supplies for drug use, despite their use for reducing risk.
Most responses were received from VAMCs with large mental health substance use programs. Respondents at larger, urban facilities (Washington, DC, and Baltimore, Maryland) expressed more hesitancy around using harm reduction tools despite having more harm reduction resources available compared to smaller or rural sites. These results align with previous studies that found no difference in prescribers providing medications for OUD in rural and urban VAMCs, showing urban sites, despite more resources, are not more willing to provide harm reduction or other addiction services.19 This evidence might indicate that urban sites may not use available resources (eg, methadone clinics) or that rural sites can provide just as robust medications for OUD care as urban sites.
Follow-up interview analysis indicated that HCPs lack knowledge of certain harm reduction tools. One-on-one peer discussions, like academic detailing, can facilitate discussions around a prescriber’s role in harm reduction, address gaps in knowledge by sharing what is available at the facilities for harm reduction, and suggest conversation points to help prescribers start harm reduction discussions with patients unwilling to begin treatment. Additionally, academic detailing can connect prescribers to available resources in the community to provide pragmatic approaches and suggestions. A clear and consistent treatment process may reduce barriers by reassuring prescribers they have support and by providing consistent directions so that prescribers do not waste time.
Reinforcement is important for sustaining change. VAMCs could consider positive feedback and other evidence-based reinforcement strategies (eg, social recognition, continuing education) to communicate that these changes are noticed and appreciated.20 Late adopters may also be influenced by seeing positive feedback and results for peers. Systematic changes can be the catalyst for and sustain individual change.
Shifting perceptions and adopting change may be challenging, especially for SUD, which can be highly stigmatized. Promotion of successful change should be multifaceted and include both system and individual approaches. VHA systemic changes that could contribute to positive change include provision of time and access to SUD treatment training, a clear and sustainable treatment process, and reinforcement by recognizing success. In addition, facility leadership could provide support through dedicated time and resources during the workday for SUD treatment and harm reduction training. Support could empower HCPs and convey leadership support for harm reduction. This dedicated time could be used for didactic lecture sessions or individual meetings with academic detailers who can tailor discussions to the prescriber’s practice.
Strengths and Limitations
This survey included prescribers from a range of mental health care practice settings (eg, inpatient, outpatient clinic, rural, urban) and varied years of experience. This variety resulted in diverse perspectives and knowledge bases. Postsurvey interviews allowed academic detailers to gain deeper insight into answers in the survey, which can guide future interventions. Postsurvey interviews and application of the ADKAR model provided additional viewpoints on harm reduction.
A limitation of this project is the absence of an assessment of respondents’ harm reduction knowledge accuracy. Although respondents reported confidence in discussing harm reduction with patients, the survey did not assess whether their knowledge was accurate. Additionally, the survey did not ask about the availability of syringes and test strips at the prescribers’ VAMC, which could explain discrepancies in responses between naloxone and other forms of harm reduction (drug test strips and syringes were not available to all HCPs in the VISN). This lack of availability may have skewed responses. West Virginia SSPs, for example, were closed following legislative changes, which may contribute to stigma.21
Not all respondents were asked to do a follow-up interview, which limited the perspectives included in this study. Each site had ≥ 1 follow-up interview to limit the academic detailer’s workload. The initial survey included the phrase clean syringe, which can be stigmatizing and insinuate that PWUD are not clean. The preferred term would have been sterile syringe.22
Conclusions
This survey of mental health prescribers found that most respondents are comfortable treating patients with SUD and confident in educating patients on harm reduction. Additionally, most respondents were more willing to provide naloxone vs fentanyl test strips or sterile syringes. A lack of time and awareness was the most frequently cited barrier to harm reduction services. As the VHA continues to expand access to harm reduction programs, which have proven to increase treatment rates and reduce disease, it will be imperative for HCPs, including mental health prescribers, to recognize the benefit of these programs for veterans with SUD. Future interventions should be designed and evaluated in collaboration with all HCPs and patients. This project determined ways to promote change for prescribers, but it will be important for further research to continue those conversations and incorporate patient perspectives.
- Use of funds to supply hypodermic needles or syringes for illegal drug use; prohibition, 42 USC § 300ee-5 (1988). Accessed January 5, 2026. https://www.law.cornell.edu /uscode/text/42/300ee-5
- OD2A Case Study: Harm Reduction. Centers for Disease Control and Prevention. June 9, 2025. Accessed January 5, 2026. https://www.cdc.gov/overdose-prevention/php /od2a/harm-reduction.html
- Strengthening Syringe Services Programs (SSPs). Centers for Disease Control and Prevention. March 20, 2024. Accessed January 5, 2026. https://www.cdc.gov/hepatitis -syringe-services/php/about/index.html
- Weinmeyer R. Needle exchange programs’ status in US politics. AMA J Ethics. 2016;18:252-257. doi:10.1001/journalofethics.2016.18.3.hlaw1-1603
- Rife-Pennington T, Dinges E, Ho MQ. Implementing syringe services programs within the Veterans Health Administration: facility experiences and next steps. J Am Pharm Assoc (2003). 2023;63:234-240. doi:10.1016/j.japh.2022.10.019
- The Biden-Harris Administration’s Statement of Drug Policy Priorities for Year One. Executive Office of the President, Office of National Drug Control Policy. April 1, 2021. Accessed January 5, 2026. https://bidenwhitehouse.archives.gov/wp-content/uploads/2021/03/BidenHarris -Statement-of-Drug-Policy-Priorities-April-1.pdf
- HIV - for veterans and the public syringe services programs. US Department of Veterans Affairs. Updated August 16, 2021. Accessed January 5, 2026. https://www.hiv .va.gov/patient/ssp.asp
- Trump Administration’s Statement of Drug Policy Priorities. White House. April 1, 2025. Accessed January 7, 2026. https://www.whitehouse.gov/wp-content /uploads/2025/04/2025-Trump-Administration-Drug-Policy -Priorities.pdf
- Health Centers and Syringe Services Programs. National Health Care for the Homeless Council. May 2023. Accessed January 5, 2026. https://nhchc.org/wp-content /uploads/2023/06/Health-Centers-SSPs-Final.pdf
- Lynch RD, Biederman DJ, Silva S, Demasi K. A syringe service program within a federal system: foundations for implementation. J Addict Nurs. 2021;32:152-158. doi:10.1097/JAN.0000000000000402
- Harvey LH, Sliwinski SK, Flike K, et al. The integration of harm reduction services in the Veterans Health Administration (VHA): a qualitative analysis of barriers and facilitators. J Addict Dis. 2024;42:326-334. doi:10.1080/10550887.2023.2210021
- Drug Overdose Death Rates. National Center for Drug Abuse Statistics. Accessed January 5, 2026. https:// drugabusestatistics.org/drug-overdose-deaths
- Ng G. New database shows Baltimore greatly devastated by opioid epidemic. Updated August 21, 2023. Accessed January 5, 2026. https://www.wbaltv.com/article/opioid -epidemic-database-baltimore-deaths/44869671
- Introductory Guide to Academic Detailing. National Resource Center for Academic Detailing. 2017. Accessed January 5, 2026. https://www.narcad.org /uploads/5/7/9/5/57955981/introductory_guide_to_ad.pdf
- Zhang J. Can educational outreach improve experts’ decision making? Evidence from a national opioid academic detailing program. SSRN. 2023;4297398. doi:10.2139/ssrn.4297398
- Watson H, Maclaren W, Kerr S. Staff attitudes towards working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206- 215. doi:10.1111/j.1360-0443.2006.01686.x
- Dahl RA, Vakkalanka JP, Harland KK, Radke J. Investigating healthcare provider bias toward patients who use drugs using a survey-based implicit association test: pilot study. J Addict Med. 2022;16:557-562. doi:10.1097/ADM.0000000000000970
- Hiatt JM, Creasey TJ. Change Management: The People Side of Change. Prosci Learning Center Publications; 2012.
- Wyse JJ, Shull S, Lindner S, et al. Access to medications for opioid use disorder in rural versus urban Veterans Health Administration facilities. J Gen Intern Med. 2023;38:1871-1876. doi:10.1007/s11606-023-08027-4
- Mostofian F, Ruban C, Simunovic N, Bhandari M. Changing physician behavior: what works?. Am J Manag Care. 2015;21(1):75-84.
- Bergdorf-Smith K, Bridge Initiative for S&T Policy, Leadership, and Communications. Syringe Service Programs and HIV Prevention in West Virginia. West Virginia University. February 5, 2024. Accessed January 5, 2026. https:// scitechpolicy.wvu.edu/science-and-technology-notes -articles/2024/02/05/syringe-service-programs-and-hiv -prevention-in-west-virginia
- Brunsdon N. Stop saying ‘clean’. Injecting Advice. February 7, 2011. Accessed January 5, 2026. https:// injectingadvice.com/stop-saying-clean/
- Use of funds to supply hypodermic needles or syringes for illegal drug use; prohibition, 42 USC § 300ee-5 (1988). Accessed January 5, 2026. https://www.law.cornell.edu /uscode/text/42/300ee-5
- OD2A Case Study: Harm Reduction. Centers for Disease Control and Prevention. June 9, 2025. Accessed January 5, 2026. https://www.cdc.gov/overdose-prevention/php /od2a/harm-reduction.html
- Strengthening Syringe Services Programs (SSPs). Centers for Disease Control and Prevention. March 20, 2024. Accessed January 5, 2026. https://www.cdc.gov/hepatitis -syringe-services/php/about/index.html
- Weinmeyer R. Needle exchange programs’ status in US politics. AMA J Ethics. 2016;18:252-257. doi:10.1001/journalofethics.2016.18.3.hlaw1-1603
- Rife-Pennington T, Dinges E, Ho MQ. Implementing syringe services programs within the Veterans Health Administration: facility experiences and next steps. J Am Pharm Assoc (2003). 2023;63:234-240. doi:10.1016/j.japh.2022.10.019
- The Biden-Harris Administration’s Statement of Drug Policy Priorities for Year One. Executive Office of the President, Office of National Drug Control Policy. April 1, 2021. Accessed January 5, 2026. https://bidenwhitehouse.archives.gov/wp-content/uploads/2021/03/BidenHarris -Statement-of-Drug-Policy-Priorities-April-1.pdf
- HIV - for veterans and the public syringe services programs. US Department of Veterans Affairs. Updated August 16, 2021. Accessed January 5, 2026. https://www.hiv .va.gov/patient/ssp.asp
- Trump Administration’s Statement of Drug Policy Priorities. White House. April 1, 2025. Accessed January 7, 2026. https://www.whitehouse.gov/wp-content /uploads/2025/04/2025-Trump-Administration-Drug-Policy -Priorities.pdf
- Health Centers and Syringe Services Programs. National Health Care for the Homeless Council. May 2023. Accessed January 5, 2026. https://nhchc.org/wp-content /uploads/2023/06/Health-Centers-SSPs-Final.pdf
- Lynch RD, Biederman DJ, Silva S, Demasi K. A syringe service program within a federal system: foundations for implementation. J Addict Nurs. 2021;32:152-158. doi:10.1097/JAN.0000000000000402
- Harvey LH, Sliwinski SK, Flike K, et al. The integration of harm reduction services in the Veterans Health Administration (VHA): a qualitative analysis of barriers and facilitators. J Addict Dis. 2024;42:326-334. doi:10.1080/10550887.2023.2210021
- Drug Overdose Death Rates. National Center for Drug Abuse Statistics. Accessed January 5, 2026. https:// drugabusestatistics.org/drug-overdose-deaths
- Ng G. New database shows Baltimore greatly devastated by opioid epidemic. Updated August 21, 2023. Accessed January 5, 2026. https://www.wbaltv.com/article/opioid -epidemic-database-baltimore-deaths/44869671
- Introductory Guide to Academic Detailing. National Resource Center for Academic Detailing. 2017. Accessed January 5, 2026. https://www.narcad.org /uploads/5/7/9/5/57955981/introductory_guide_to_ad.pdf
- Zhang J. Can educational outreach improve experts’ decision making? Evidence from a national opioid academic detailing program. SSRN. 2023;4297398. doi:10.2139/ssrn.4297398
- Watson H, Maclaren W, Kerr S. Staff attitudes towards working with drug users: development of the Drug Problems Perceptions Questionnaire. Addiction. 2007;102:206- 215. doi:10.1111/j.1360-0443.2006.01686.x
- Dahl RA, Vakkalanka JP, Harland KK, Radke J. Investigating healthcare provider bias toward patients who use drugs using a survey-based implicit association test: pilot study. J Addict Med. 2022;16:557-562. doi:10.1097/ADM.0000000000000970
- Hiatt JM, Creasey TJ. Change Management: The People Side of Change. Prosci Learning Center Publications; 2012.
- Wyse JJ, Shull S, Lindner S, et al. Access to medications for opioid use disorder in rural versus urban Veterans Health Administration facilities. J Gen Intern Med. 2023;38:1871-1876. doi:10.1007/s11606-023-08027-4
- Mostofian F, Ruban C, Simunovic N, Bhandari M. Changing physician behavior: what works?. Am J Manag Care. 2015;21(1):75-84.
- Bergdorf-Smith K, Bridge Initiative for S&T Policy, Leadership, and Communications. Syringe Service Programs and HIV Prevention in West Virginia. West Virginia University. February 5, 2024. Accessed January 5, 2026. https:// scitechpolicy.wvu.edu/science-and-technology-notes -articles/2024/02/05/syringe-service-programs-and-hiv -prevention-in-west-virginia
- Brunsdon N. Stop saying ‘clean’. Injecting Advice. February 7, 2011. Accessed January 5, 2026. https:// injectingadvice.com/stop-saying-clean/
Mental Health Prescribers’ Perceptions of Patients With Substance Use Disorders and Harm Reduction Services
Mental Health Prescribers’ Perceptions of Patients With Substance Use Disorders and Harm Reduction Services