A 6-year-old girl was brought to a pediatric emergency department (ED) in Atlanta by her mother. The mother stated that during the previous hour, she had noticed that her daughter’s face seemed weaker on the right side.
The night before, the child had said, “I can’t blink my eye”; when her mother asked her to demonstrate, the child seemed to be able to blink both eyes appropriately, and she had no further complaints. The next morning, the child complained of the light being too bright and asked to wear her mother’s sunglasses. In the course of the day, she continued to complain of eye discomfort, which she described as “stinging” and “sore.” The mother could see nothing abnormal, but by late afternoon noticed that her daughter’s smile and facial movements were asymmetrical. She immediately took her to the pediatric ED.
The child had no significant medical history and no surgical history. Her vaccination schedule was current, and she denied any recent illnesses. The mother could recall no exposures to infections or tick bites, no rashes, and no trauma to the face or head. The mother and child were visiting Atlanta from northeastern Florida.
The review of systems was negative for headache, fever, chills, rash, earache, sore throat, cough, rhinorrhea, vision changes, weight loss, or change in appetite or disposition. The child was afebrile, and the other vital signs were within normal limits.
Physical examination revealed an alert child who was calm and conversant. Her height was 45” and weight, 43 lb. Otoscopic exam showed normal ears and tympanic membranes with no sign of otitis media or ear pathology. No throat redness, tonsillar enlargement, or lymphadenopathies were noted. Breath sounds were clear, and heart rhythm and rate were regular without murmur.
The patient’s left eye appeared normal, and the right eye was mildly erythematic without drainage or swelling; since corneal abrasion was not suspected, a slit lamp examination was not performed. Upon neurologic examination, right eye ptosis with incomplete lid closure, asymmetrical mouth movement with smile, and a diminished nasal labial fold crease were noted on the right side. When the child was asked to raise her eyebrows and wrinkle her forehead, asymmetrical forehead creases were apparent. All other cranial nerve functions were intact, and motor and sensory responses, including gait and reflexes, were assessed as normal. Unilateral dysfunction of right-sided cranial nerve VII (CN VII), including forehead involvement, was confirmed, consistent with a grade of III to IV on the House-Brackmann (maximum, VI)1,2 facial nerve grading scale.
Based on the rapid onset of unilateral facial nerve paresis (FNP) and an otherwise normal exam, the patient was diagnosed with Bell’s palsy. No further testing was done, and the child was given a dose of oral prednisolone 40 mg in the ED, with a prescription for four more days of oral prednisolone at 15 mg bid. The need for eye protection and lubrication was emphasized to the mother, who was given lubricating eye drops to administer. The mother was also instructed to follow up with the child’s primary care practitioner upon their return to Florida.
The child was seen by her pediatrician three days later. Her facial paresis had not worsened in the interim, and the pediatrician declined to extend the course of corticosteroids or to add an antiviral medication. At the mother’s request, the child was referred to a pediatric otolaryngologist, who saw her the following day and adjusted the treatment plan. The child was prescribed prednisolone elixir 20 mg bid for one week, followed by a tapering dose for the second week. In addition, she was prescribed oral acyclovir 400 mg qid for 10 days. Her mother was instructed to return with the child in one week for audiometry testing.
Discussion Idiopathic FNP, commonly referred to as Bell’s palsy, is defined as an acute unilateral paresis of the facial nerve without detectable underlying cause.3,4 It most commonly occurs among persons ages 15 to 45, with a prevalence rate of 15 to 30 cases per 100,000 persons. The peak incidence of Bell’s palsy is in the fourth decade of life. Diabetic patients and pregnant women are disproportionately affected by idiopathic FNP.2,5 About 8% to 10% of patients will experience a recurrence of Bell’s palsy within 10 years.2,6
Pediatric FNP can be congenital or acquired. Congenital FNP is most often associated with birth trauma and occurs at a rate of 2.1 cases per 1,000 births. Rare genetic syndromes can also manifest with FNP and will most often present with other syndromic anomalies noted at birth.7
Acquired FNP is two to four times less common in children than adults, with an estimated prevalence of 2.7 per 100,000 patients younger than 10. Children account for only a small proportion of subjects in published studies that address diagnosis and management of FNP.3 While the presentation of FNP is much the same in adults and children, some notable differences in etiology exist.2,3,7-9 Infectious, traumatic, or neoplastic causes of FNP are more common among children than adults and must be distinguished from idiopathic FNP.7,9-11
Decisions regarding diagnostic testing, pharmacologic treatment, and referral must be guided by the history and physical exam, neurologic exam, and clinical judgment. Being able to identify or exclude alarming causes of FNP, such as neoplasm, will aid the primary care practitioner in treatment and referral practices for this condition.
Pathophysiology CN VII, the facial nerve, has a broad scope of function that incorporates both sensory and motor pathways. The brachial nerve portion of CN VII controls the muscles of voluntary facial expression. CN VII also autonomically innervates the lacrimal gland and submandibular gland and governs sensation from part of the ear as well as taste from the anterior two-thirds of the tongue.4
The precise pathophysiology involved in FNP remains an area of continuing debate, but infectious, vascular, immunologic, and genetic causes have been hypothesized.7,12 Inflammation and subsequent nerve damage along CN VII caused by an infectious process is thought to be the most likely explanation for the pathogenesis of acquired FNP in both adults and children.5,13
Herpes simplex virus 1 (HSV-1) has been suggested as the virus most commonly linked to FNP in both adults and children, but it is unlikely to be the sole cause.5,6,9 Data from a three-year prospective study of FNP cases in children support a relationship between pediatric FNP and HSV-1 infection.14 Other infectious causes implicated in pediatric FNP are Lyme disease, Epstein-Barr, varicella zoster virus, rubella, coxsackie virus, adenovirus, and otitis media.4,7,9
Presentation, History, and Physical Exam Most children with idiopathic FNP will present with sudden-onset facial asymmetry and may have decreased tearing, loss of the conjunctival reflex (leading to difficulty closing the eye), an inability to hold the lips tightly together, and difficulty keeping food in the mouth. Complaints of otalgia, speech disturbances, hyperacusis, and altered sense of taste are common.2,7 Recent occurrence of an upper respiratory infection is often reported in the history of a pediatric patient with FNP.3,7,15,16
Idiopathic FNP is essentially a diagnosis of exclusion.3,5 A meticulous history must be conducted, including any recent illnesses, trauma to the face or head, vaccines, rashes, and travel. Assessment of the head, eyes, ears, nose, and throat, and a careful neurologic history must be conducted to identify nonidiopathic causes of FNP (see Table 15-7,9). Facial weakness can progress from mild palsy to complete paralysis over one to two weeks5; therefore, a careful history of the progression of facial weakness should be ascertained and documented.5,17
A full neurologic exam is essential. Cranial nerves I through XII should be evaluated; any malfunction of a cranial nerve other than CN VII could be indicative of a tumor or process other than idiopathic FNP. Assessment of facial nerve function is imperative, as this factor is the most important for predicting recovery; it can also aid in formulating a prognosis and directing treatment.5,9,17
The House-Brackmann facial nerve grading system1,2 is considered the gold standard for grading severity of facial paresis9 (see Table 21,2 ). A clear distinction between paresis (partial or incomplete palsy) and paralysis (complete palsy) must be made. Pediatric patients with an incomplete palsy have an improved chance of full recovery.17,18
Any abnormalities in the peripheral neurologic exam should prompt further testing. FNP not involving the forehead musculature, gradual progression of paresis, and weakness in any extremity could be indicative of a central lesion. FNP has been the presenting symptom in various neoplastic processes, including leukemia, cholesteatoma, and astrocytoma.3,7,9
Otitis media is a frequent cause of FNP among children.9-11 Thus, a thorough examination of the ear canal, tympanic membrane, and hearing should be performed. The throat and oropharynx should be inspected, and the parotid gland palpated. Any swelling or abnormalities warrant further investigation.
Lyme disease presenting with FNP is more common in children than adults. This may be related to the increased likelihood for children to be bitten by ticks in the head and neck areas. Frequently, FNP associated with Lyme disease is bilateral—as often as 25% of the time.19 Headache, onset of symptoms during peak Lyme season, or bilateral FNP should raise the clinician’s suspicion for Lyme disease.7,9,19
An accurate assessment of blood pressure is essential, as severe hypertension may be implicated in FNP in children.3,5,7 One literature review reported that hypertension was the origin of FNP in 3% to 17% of affected children.20 Vascular hemorrhage induced by hypertension is thought to cause nerve compression and subsequent FNP.7
A bilateral eye exam is also important. Irritation is likely, and the patient with any suspected corneal abrasion or damage should be referred to an ophthalmologist.6,18
Laboratory Testing and Imaging Diagnostic testing that facilitates the exclusion of known causes of FNP should be considered, as there is no specific laboratory test to confirm the diagnosis. A complete blood count, Lyme titers, cerebrospinal fluid analysis, CT, and/or MRI may be warranted, based on the clinical presentation.7-9 In children in whom Lyme disease is suspected (ie, those living in tick-endemic areas or with recent tick bites), serologic testing should be performed. Lumbar puncture and an evaluation of cerebrospinal fluid may be necessary in cases in which meningitis cannot be excluded.7,9
Specialized diagnostic tests are not routinely recommended for patients with paresis that is improving. Audiometry and evaluation of the stapedial reflex may help guide treatment decisions for patients whose condition is not improving. In children, the presence or return of the stapedial reflex within three weeks of disease onset is predictive of complete recovery.5 In patients who experience complete paralysis or unimproved paresis, results of electrodiagnostic testing (in particular, evoked facial nerve electroneuronography) can help forecast recovery of facial nerve function.5,17
Treatment and Management Treatment for FNP in adults is controversial, and even more so for the pediatric patient. Treatment decisions consist of eye care, corticosteroids, antiviral medications, and appropriate referrals.
Eye care. Eye lubrication and protection should be implemented immediately. Protecting the cornea is paramount; thorough lubrication of the eye is the mainstay of treatment.18 Artificial tears should be used frequently during the day, and an ointment should be applied to the eye at night. Use of eye patches is controversial, as they may actually cause corneal injury.7,9 Taping the eye shut at night may prevent trauma during sleep, but this option must be considered carefully.9,18
Corticosteroids. Early initiation of corticosteroids should be considered for all patients with FNP, including children.2,7,9,17 Studies are inconclusive as to whether steroid therapy is beneficial in children with idiopathic FNP. However, two 2010 reviews of pediatric FNP recommend early initiation of steroids for children with acute-onset FNP, particularly when facial paresis is evaluated at a House-Brackmann grade V or VI.7,9 The American Academy of Family Physicians (AAFP) recommends a tapering course of prednisone for all patients, begun as soon as possible.6 The prednisone dosage for pediatric patients is usually 1.0 mg/kg/d, split into two doses, for six days, followed by a tapering dose for four days.5
Antivirals and antibiotic therapy. When an infectious cause of FNP is known, appropriate antibiotic or antiviral therapy should begin. If the patient lives in or has traveled to an area endemic for Lyme disease, empiric treatment may be appropriate. When Ramsay Hunt syndrome is diagnosed or herpetic lesions are visible, antiviral treatment should be initiated.7
Antiviral therapy for idiopathic FNP is the most controversial of the treatment decisions. In 2001, the American Academy of Neurology concluded that no clear benefit from acyclovir could be ascertained, although it might be effective.13 This was affirmed in a recently updated Cochrane review of antiviral therapy for idiopathic FNP.12 Antiviral therapy alone showed no benefit, compared with placebo; however, combined antiviral and corticosteroid therapy was more effective than placebo alone in recovery outcomes. Antivirals may benefit pediatric patients and should be considered early when the cause of FNP is viral or idiopathic.7,9
Referrals. Initial presentation and course of paresis should guide referral patterns for the pediatric patient presenting with FNP. The American Academy of Pediatrics (AAP) recommends referral to an otolaryngologist for any infant or child with FNP.21 The AAFP recommends referral to a specialist for any patient who does not show improvement within two weeks.6
In patients with complete paralysis, early surgical intervention may be considered, and referral should be made promptly for electrodiagnostic testing and surgical consult. In cases in which otitis media causes FNP, myringotomy and tube insertion are indicated, and appropriate referral should be made.7,9
Outcomes |The prognosis in children with FNP is good, and most will recover completely.2,9-11,22 Idiopathic and infectious etiologies of FNP seem to have the greatest likelihood for complete recovery.10,11,16,17 Recovery appears to be affected by etiology, degree of paresis, and treatment. How these factors coalesce is not fully understood, and up to 20% of children may have mild to moderate residual facial nerve dysfunction.10,11,19,22
The Case Patient The child’s facial nerve function gradually returned over a three-week period, with no residual deficit (see Figures 1a, 1b, and 1c). Results of the audiometry screening on day 10 were normal, showing a positive stapedial reflex. An MRI, performed four months after the initial paralysis to rule out any tumors, yielded normal results.
This case highlights the differing management of pediatric Bell’s palsy among emergency, pediatric, and specialized providers. This child was managed more aggressively under the care of an otolaryngologist with a two-week course of steroids, antiviral medication for 10 days, and a follow-up MRI to rule out any evidence of a tumor. The need for further research to guide practice in the pediatric patient with Bell’s palsy is apparent.
Conclusion FNP in the pediatric population is rare and more likely to have an identifiable cause than among adults. Careful examination should reveal differential diagnoses that warrant treatment and referrals. The main causes of FNP that should not be missed are otitis media, hypertension, varicella zoster virus (Ramsay Hunt syndrome), neoplastic processes, and Lyme disease.
Practitioners should have a high index of suspicion for nonidiopathic causes of FNP when a child has a neurologic exam that includes facial paresis of gradual onset, abnormal function of other cranial nerves, lack of forehead muscle weakness, or peripheral abnormalities. In addition to the history and exam, blood work and radiologic imaging can aid the practitioner in ruling in or out nonidiopathic causes of FNP.
Grading of facial palsy severity using the House-Brackmann scale helps guide prognosis and referral choices. Referral to a specialist in otolaryngology is appropriate and recommended by the AAP. Referral should be made to an ophthalmologist if any suspicion of corneal abrasion exists.
Treatment in children should consist of eye care and steroids. Antiviral therapy should be considered on an individualized basis and when evidence of HSV or varicella exists. Parents should be advised about the importance of eye care in a child with FNP (see Table 35-7,9,17,18,22).
The emotional stress associated with FNP can be significant for both children and adults; fear of lifelong facial deformity can be psychologically debilitating. Yet a favorable prognosis for recovery of facial nerve function can be relayed to anxious parents.
References
1. House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985;93(2): 146-147.
2. Finsterer J. Management of peripheral facial nerve palsy. Eur Arch Otorhinolaryngol. 2008;265(7):743-752.
3. Lunan R, Nagarajan L. Bell’s palsy: a guideline proposal following a review of practice. J Paediatr Child Health. 2008;44(4):219-220.
4. Blosser CG, Reider-Demer M. Neurologic disorders. In: Burns CE, Dunn AM, Brady MA, et al, eds. Pediatric Primary Care. 4th ed. St. Louis: Saunders Elsevier; 2008:634-672.
5. Singhi P, Jain V. Bell’s palsy in children. Semin Pediatr Neurol. 2003;10(4):289-297.
6. Tiemstra JD, Khatkhate N. Bell’s palsy: diagnosis and management. Am Fam Physician. 2007;76(7):997-1002.
7. Lorch M, Teach SJ. Facial nerve palsy: Etiology and approach to diagnosis and treatment. Pediatr Emerg Care. 2010;26(10):763-769.
8. El-Hawrani AS, Eng CY, Ahmed SK, et al. General practitioners’ referral pattern for children with acute facial paralysis. J Laryngol Otol. 2005;119(7):540-542.
9. Shargorodsky J, Lin HW, Gopen Q. Facial nerve palsy in the pediatric population. Clin Pediatr (Phila). 2010;49(5):411-417.
10. Wang CH, Chang YC, Shih HM, et al. Facial palsy in children: emergency department management and outcome. Pediatr Emerg Care. 2010;26(2):121-125.
11. Evans AK, Licameli G, Brietzke S, et al. Pediatric facial nerve paralysis: patients, management and outcomes. Int J Pediatr Otorhinolaryngol. 2005;69(11):1521-1528.
12. Lockhart P, Daly F, Pitkethly M, et al. Antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2009;(4):CD001869.
13. Grogan PM, Gronseth GS. Practice parameter: steroids, acyclovir, and surgery for Bell’s palsy (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56(7):830-836.
14. Khine H, Mayers M, Avner JR, et al. Association between herpes simplex virus-1 infection and idiopathic unilateral facial paralysis in children and adolescents. Pediatr Infect Dis J. 2008;27(5):468-469.
15. Tsai HS, Chang LY, Lu CY, et al. Epidemiology and treatment of Bell’s palsy in children in northern Taiwan. J Microbiol Immunol Infect. 2009;42(4):351-356.
16. Cha CI, Hong CK, Park MS, Yeo SG. Comparison of facial nerve paralysis in adults and children. Yonsei Med J. 2008;49(5):725-734.
17. Linder TE, Abdelkafy W, Cavero-Vanek S. The management of peripheral facial nerve palsy: “paresis” versus “paralysis” and sources of ambiguity in study designs. Otol Neurotol. 2010;31(2):319-327.
18. Rahman I, Sadiq SA. Ophthalmic management of facial nerve palsy: a review. Surv Ophthalmol. 2007;52(2):121-144.
19. Skogman BH, Croner S, Odkvist L. Acute facial palsy in children: a 2-year follow-up with focus on Lyme neuroborreliosis. Int J Pediatr Otorhinolaryngol. 2003;67(6):597-602.
20. Siegler RL, Brewer ED, Corneli HM, Thompson JA. Hypertension first seen as facial paralysis: case reports and review of the literature. Pediatrics. 1991;87(3):387-389.
21. Surgical Advisory Panel, American Academy of Pediatrics. Guidelines for referral to pediatric surgical specialists. Pediatrics. 2002;110(1 pt 1):187-191.
22. Chen WX, Wong V. Prognosis of Bell’s palsy in children: analysis of 29 cases. Brain Dev. 2005; 27(7):504-508.
Author and Disclosure Information
Jan Meires, EdD, FNP, BC, Margaret Corrigan Humphries, RN, BSN, CAPA, FNP-S
Jan Meires, EdD, FNP, BC, Margaret Corrigan Humphries, RN, BSN, CAPA, FNP-S
Author and Disclosure Information
Jan Meires, EdD, FNP, BC, Margaret Corrigan Humphries, RN, BSN, CAPA, FNP-S
A 6-year-old girl was brought to a pediatric emergency department (ED) in Atlanta by her mother. The mother stated that during the previous hour, she had noticed that her daughter’s face seemed weaker on the right side.
The night before, the child had said, “I can’t blink my eye”; when her mother asked her to demonstrate, the child seemed to be able to blink both eyes appropriately, and she had no further complaints. The next morning, the child complained of the light being too bright and asked to wear her mother’s sunglasses. In the course of the day, she continued to complain of eye discomfort, which she described as “stinging” and “sore.” The mother could see nothing abnormal, but by late afternoon noticed that her daughter’s smile and facial movements were asymmetrical. She immediately took her to the pediatric ED.
The child had no significant medical history and no surgical history. Her vaccination schedule was current, and she denied any recent illnesses. The mother could recall no exposures to infections or tick bites, no rashes, and no trauma to the face or head. The mother and child were visiting Atlanta from northeastern Florida.
The review of systems was negative for headache, fever, chills, rash, earache, sore throat, cough, rhinorrhea, vision changes, weight loss, or change in appetite or disposition. The child was afebrile, and the other vital signs were within normal limits.
Physical examination revealed an alert child who was calm and conversant. Her height was 45” and weight, 43 lb. Otoscopic exam showed normal ears and tympanic membranes with no sign of otitis media or ear pathology. No throat redness, tonsillar enlargement, or lymphadenopathies were noted. Breath sounds were clear, and heart rhythm and rate were regular without murmur.
The patient’s left eye appeared normal, and the right eye was mildly erythematic without drainage or swelling; since corneal abrasion was not suspected, a slit lamp examination was not performed. Upon neurologic examination, right eye ptosis with incomplete lid closure, asymmetrical mouth movement with smile, and a diminished nasal labial fold crease were noted on the right side. When the child was asked to raise her eyebrows and wrinkle her forehead, asymmetrical forehead creases were apparent. All other cranial nerve functions were intact, and motor and sensory responses, including gait and reflexes, were assessed as normal. Unilateral dysfunction of right-sided cranial nerve VII (CN VII), including forehead involvement, was confirmed, consistent with a grade of III to IV on the House-Brackmann (maximum, VI)1,2 facial nerve grading scale.
Based on the rapid onset of unilateral facial nerve paresis (FNP) and an otherwise normal exam, the patient was diagnosed with Bell’s palsy. No further testing was done, and the child was given a dose of oral prednisolone 40 mg in the ED, with a prescription for four more days of oral prednisolone at 15 mg bid. The need for eye protection and lubrication was emphasized to the mother, who was given lubricating eye drops to administer. The mother was also instructed to follow up with the child’s primary care practitioner upon their return to Florida.
The child was seen by her pediatrician three days later. Her facial paresis had not worsened in the interim, and the pediatrician declined to extend the course of corticosteroids or to add an antiviral medication. At the mother’s request, the child was referred to a pediatric otolaryngologist, who saw her the following day and adjusted the treatment plan. The child was prescribed prednisolone elixir 20 mg bid for one week, followed by a tapering dose for the second week. In addition, she was prescribed oral acyclovir 400 mg qid for 10 days. Her mother was instructed to return with the child in one week for audiometry testing.
Discussion Idiopathic FNP, commonly referred to as Bell’s palsy, is defined as an acute unilateral paresis of the facial nerve without detectable underlying cause.3,4 It most commonly occurs among persons ages 15 to 45, with a prevalence rate of 15 to 30 cases per 100,000 persons. The peak incidence of Bell’s palsy is in the fourth decade of life. Diabetic patients and pregnant women are disproportionately affected by idiopathic FNP.2,5 About 8% to 10% of patients will experience a recurrence of Bell’s palsy within 10 years.2,6
Pediatric FNP can be congenital or acquired. Congenital FNP is most often associated with birth trauma and occurs at a rate of 2.1 cases per 1,000 births. Rare genetic syndromes can also manifest with FNP and will most often present with other syndromic anomalies noted at birth.7
Acquired FNP is two to four times less common in children than adults, with an estimated prevalence of 2.7 per 100,000 patients younger than 10. Children account for only a small proportion of subjects in published studies that address diagnosis and management of FNP.3 While the presentation of FNP is much the same in adults and children, some notable differences in etiology exist.2,3,7-9 Infectious, traumatic, or neoplastic causes of FNP are more common among children than adults and must be distinguished from idiopathic FNP.7,9-11
Decisions regarding diagnostic testing, pharmacologic treatment, and referral must be guided by the history and physical exam, neurologic exam, and clinical judgment. Being able to identify or exclude alarming causes of FNP, such as neoplasm, will aid the primary care practitioner in treatment and referral practices for this condition.
Pathophysiology CN VII, the facial nerve, has a broad scope of function that incorporates both sensory and motor pathways. The brachial nerve portion of CN VII controls the muscles of voluntary facial expression. CN VII also autonomically innervates the lacrimal gland and submandibular gland and governs sensation from part of the ear as well as taste from the anterior two-thirds of the tongue.4
The precise pathophysiology involved in FNP remains an area of continuing debate, but infectious, vascular, immunologic, and genetic causes have been hypothesized.7,12 Inflammation and subsequent nerve damage along CN VII caused by an infectious process is thought to be the most likely explanation for the pathogenesis of acquired FNP in both adults and children.5,13
Herpes simplex virus 1 (HSV-1) has been suggested as the virus most commonly linked to FNP in both adults and children, but it is unlikely to be the sole cause.5,6,9 Data from a three-year prospective study of FNP cases in children support a relationship between pediatric FNP and HSV-1 infection.14 Other infectious causes implicated in pediatric FNP are Lyme disease, Epstein-Barr, varicella zoster virus, rubella, coxsackie virus, adenovirus, and otitis media.4,7,9
Presentation, History, and Physical Exam Most children with idiopathic FNP will present with sudden-onset facial asymmetry and may have decreased tearing, loss of the conjunctival reflex (leading to difficulty closing the eye), an inability to hold the lips tightly together, and difficulty keeping food in the mouth. Complaints of otalgia, speech disturbances, hyperacusis, and altered sense of taste are common.2,7 Recent occurrence of an upper respiratory infection is often reported in the history of a pediatric patient with FNP.3,7,15,16
Idiopathic FNP is essentially a diagnosis of exclusion.3,5 A meticulous history must be conducted, including any recent illnesses, trauma to the face or head, vaccines, rashes, and travel. Assessment of the head, eyes, ears, nose, and throat, and a careful neurologic history must be conducted to identify nonidiopathic causes of FNP (see Table 15-7,9). Facial weakness can progress from mild palsy to complete paralysis over one to two weeks5; therefore, a careful history of the progression of facial weakness should be ascertained and documented.5,17
A full neurologic exam is essential. Cranial nerves I through XII should be evaluated; any malfunction of a cranial nerve other than CN VII could be indicative of a tumor or process other than idiopathic FNP. Assessment of facial nerve function is imperative, as this factor is the most important for predicting recovery; it can also aid in formulating a prognosis and directing treatment.5,9,17
The House-Brackmann facial nerve grading system1,2 is considered the gold standard for grading severity of facial paresis9 (see Table 21,2 ). A clear distinction between paresis (partial or incomplete palsy) and paralysis (complete palsy) must be made. Pediatric patients with an incomplete palsy have an improved chance of full recovery.17,18
Any abnormalities in the peripheral neurologic exam should prompt further testing. FNP not involving the forehead musculature, gradual progression of paresis, and weakness in any extremity could be indicative of a central lesion. FNP has been the presenting symptom in various neoplastic processes, including leukemia, cholesteatoma, and astrocytoma.3,7,9
Otitis media is a frequent cause of FNP among children.9-11 Thus, a thorough examination of the ear canal, tympanic membrane, and hearing should be performed. The throat and oropharynx should be inspected, and the parotid gland palpated. Any swelling or abnormalities warrant further investigation.
Lyme disease presenting with FNP is more common in children than adults. This may be related to the increased likelihood for children to be bitten by ticks in the head and neck areas. Frequently, FNP associated with Lyme disease is bilateral—as often as 25% of the time.19 Headache, onset of symptoms during peak Lyme season, or bilateral FNP should raise the clinician’s suspicion for Lyme disease.7,9,19
An accurate assessment of blood pressure is essential, as severe hypertension may be implicated in FNP in children.3,5,7 One literature review reported that hypertension was the origin of FNP in 3% to 17% of affected children.20 Vascular hemorrhage induced by hypertension is thought to cause nerve compression and subsequent FNP.7
A bilateral eye exam is also important. Irritation is likely, and the patient with any suspected corneal abrasion or damage should be referred to an ophthalmologist.6,18
Laboratory Testing and Imaging Diagnostic testing that facilitates the exclusion of known causes of FNP should be considered, as there is no specific laboratory test to confirm the diagnosis. A complete blood count, Lyme titers, cerebrospinal fluid analysis, CT, and/or MRI may be warranted, based on the clinical presentation.7-9 In children in whom Lyme disease is suspected (ie, those living in tick-endemic areas or with recent tick bites), serologic testing should be performed. Lumbar puncture and an evaluation of cerebrospinal fluid may be necessary in cases in which meningitis cannot be excluded.7,9
Specialized diagnostic tests are not routinely recommended for patients with paresis that is improving. Audiometry and evaluation of the stapedial reflex may help guide treatment decisions for patients whose condition is not improving. In children, the presence or return of the stapedial reflex within three weeks of disease onset is predictive of complete recovery.5 In patients who experience complete paralysis or unimproved paresis, results of electrodiagnostic testing (in particular, evoked facial nerve electroneuronography) can help forecast recovery of facial nerve function.5,17
Treatment and Management Treatment for FNP in adults is controversial, and even more so for the pediatric patient. Treatment decisions consist of eye care, corticosteroids, antiviral medications, and appropriate referrals.
Eye care. Eye lubrication and protection should be implemented immediately. Protecting the cornea is paramount; thorough lubrication of the eye is the mainstay of treatment.18 Artificial tears should be used frequently during the day, and an ointment should be applied to the eye at night. Use of eye patches is controversial, as they may actually cause corneal injury.7,9 Taping the eye shut at night may prevent trauma during sleep, but this option must be considered carefully.9,18
Corticosteroids. Early initiation of corticosteroids should be considered for all patients with FNP, including children.2,7,9,17 Studies are inconclusive as to whether steroid therapy is beneficial in children with idiopathic FNP. However, two 2010 reviews of pediatric FNP recommend early initiation of steroids for children with acute-onset FNP, particularly when facial paresis is evaluated at a House-Brackmann grade V or VI.7,9 The American Academy of Family Physicians (AAFP) recommends a tapering course of prednisone for all patients, begun as soon as possible.6 The prednisone dosage for pediatric patients is usually 1.0 mg/kg/d, split into two doses, for six days, followed by a tapering dose for four days.5
Antivirals and antibiotic therapy. When an infectious cause of FNP is known, appropriate antibiotic or antiviral therapy should begin. If the patient lives in or has traveled to an area endemic for Lyme disease, empiric treatment may be appropriate. When Ramsay Hunt syndrome is diagnosed or herpetic lesions are visible, antiviral treatment should be initiated.7
Antiviral therapy for idiopathic FNP is the most controversial of the treatment decisions. In 2001, the American Academy of Neurology concluded that no clear benefit from acyclovir could be ascertained, although it might be effective.13 This was affirmed in a recently updated Cochrane review of antiviral therapy for idiopathic FNP.12 Antiviral therapy alone showed no benefit, compared with placebo; however, combined antiviral and corticosteroid therapy was more effective than placebo alone in recovery outcomes. Antivirals may benefit pediatric patients and should be considered early when the cause of FNP is viral or idiopathic.7,9
Referrals. Initial presentation and course of paresis should guide referral patterns for the pediatric patient presenting with FNP. The American Academy of Pediatrics (AAP) recommends referral to an otolaryngologist for any infant or child with FNP.21 The AAFP recommends referral to a specialist for any patient who does not show improvement within two weeks.6
In patients with complete paralysis, early surgical intervention may be considered, and referral should be made promptly for electrodiagnostic testing and surgical consult. In cases in which otitis media causes FNP, myringotomy and tube insertion are indicated, and appropriate referral should be made.7,9
Outcomes |The prognosis in children with FNP is good, and most will recover completely.2,9-11,22 Idiopathic and infectious etiologies of FNP seem to have the greatest likelihood for complete recovery.10,11,16,17 Recovery appears to be affected by etiology, degree of paresis, and treatment. How these factors coalesce is not fully understood, and up to 20% of children may have mild to moderate residual facial nerve dysfunction.10,11,19,22
The Case Patient The child’s facial nerve function gradually returned over a three-week period, with no residual deficit (see Figures 1a, 1b, and 1c). Results of the audiometry screening on day 10 were normal, showing a positive stapedial reflex. An MRI, performed four months after the initial paralysis to rule out any tumors, yielded normal results.
This case highlights the differing management of pediatric Bell’s palsy among emergency, pediatric, and specialized providers. This child was managed more aggressively under the care of an otolaryngologist with a two-week course of steroids, antiviral medication for 10 days, and a follow-up MRI to rule out any evidence of a tumor. The need for further research to guide practice in the pediatric patient with Bell’s palsy is apparent.
Conclusion FNP in the pediatric population is rare and more likely to have an identifiable cause than among adults. Careful examination should reveal differential diagnoses that warrant treatment and referrals. The main causes of FNP that should not be missed are otitis media, hypertension, varicella zoster virus (Ramsay Hunt syndrome), neoplastic processes, and Lyme disease.
Practitioners should have a high index of suspicion for nonidiopathic causes of FNP when a child has a neurologic exam that includes facial paresis of gradual onset, abnormal function of other cranial nerves, lack of forehead muscle weakness, or peripheral abnormalities. In addition to the history and exam, blood work and radiologic imaging can aid the practitioner in ruling in or out nonidiopathic causes of FNP.
Grading of facial palsy severity using the House-Brackmann scale helps guide prognosis and referral choices. Referral to a specialist in otolaryngology is appropriate and recommended by the AAP. Referral should be made to an ophthalmologist if any suspicion of corneal abrasion exists.
Treatment in children should consist of eye care and steroids. Antiviral therapy should be considered on an individualized basis and when evidence of HSV or varicella exists. Parents should be advised about the importance of eye care in a child with FNP (see Table 35-7,9,17,18,22).
The emotional stress associated with FNP can be significant for both children and adults; fear of lifelong facial deformity can be psychologically debilitating. Yet a favorable prognosis for recovery of facial nerve function can be relayed to anxious parents.
A 6-year-old girl was brought to a pediatric emergency department (ED) in Atlanta by her mother. The mother stated that during the previous hour, she had noticed that her daughter’s face seemed weaker on the right side.
The night before, the child had said, “I can’t blink my eye”; when her mother asked her to demonstrate, the child seemed to be able to blink both eyes appropriately, and she had no further complaints. The next morning, the child complained of the light being too bright and asked to wear her mother’s sunglasses. In the course of the day, she continued to complain of eye discomfort, which she described as “stinging” and “sore.” The mother could see nothing abnormal, but by late afternoon noticed that her daughter’s smile and facial movements were asymmetrical. She immediately took her to the pediatric ED.
The child had no significant medical history and no surgical history. Her vaccination schedule was current, and she denied any recent illnesses. The mother could recall no exposures to infections or tick bites, no rashes, and no trauma to the face or head. The mother and child were visiting Atlanta from northeastern Florida.
The review of systems was negative for headache, fever, chills, rash, earache, sore throat, cough, rhinorrhea, vision changes, weight loss, or change in appetite or disposition. The child was afebrile, and the other vital signs were within normal limits.
Physical examination revealed an alert child who was calm and conversant. Her height was 45” and weight, 43 lb. Otoscopic exam showed normal ears and tympanic membranes with no sign of otitis media or ear pathology. No throat redness, tonsillar enlargement, or lymphadenopathies were noted. Breath sounds were clear, and heart rhythm and rate were regular without murmur.
The patient’s left eye appeared normal, and the right eye was mildly erythematic without drainage or swelling; since corneal abrasion was not suspected, a slit lamp examination was not performed. Upon neurologic examination, right eye ptosis with incomplete lid closure, asymmetrical mouth movement with smile, and a diminished nasal labial fold crease were noted on the right side. When the child was asked to raise her eyebrows and wrinkle her forehead, asymmetrical forehead creases were apparent. All other cranial nerve functions were intact, and motor and sensory responses, including gait and reflexes, were assessed as normal. Unilateral dysfunction of right-sided cranial nerve VII (CN VII), including forehead involvement, was confirmed, consistent with a grade of III to IV on the House-Brackmann (maximum, VI)1,2 facial nerve grading scale.
Based on the rapid onset of unilateral facial nerve paresis (FNP) and an otherwise normal exam, the patient was diagnosed with Bell’s palsy. No further testing was done, and the child was given a dose of oral prednisolone 40 mg in the ED, with a prescription for four more days of oral prednisolone at 15 mg bid. The need for eye protection and lubrication was emphasized to the mother, who was given lubricating eye drops to administer. The mother was also instructed to follow up with the child’s primary care practitioner upon their return to Florida.
The child was seen by her pediatrician three days later. Her facial paresis had not worsened in the interim, and the pediatrician declined to extend the course of corticosteroids or to add an antiviral medication. At the mother’s request, the child was referred to a pediatric otolaryngologist, who saw her the following day and adjusted the treatment plan. The child was prescribed prednisolone elixir 20 mg bid for one week, followed by a tapering dose for the second week. In addition, she was prescribed oral acyclovir 400 mg qid for 10 days. Her mother was instructed to return with the child in one week for audiometry testing.
Discussion Idiopathic FNP, commonly referred to as Bell’s palsy, is defined as an acute unilateral paresis of the facial nerve without detectable underlying cause.3,4 It most commonly occurs among persons ages 15 to 45, with a prevalence rate of 15 to 30 cases per 100,000 persons. The peak incidence of Bell’s palsy is in the fourth decade of life. Diabetic patients and pregnant women are disproportionately affected by idiopathic FNP.2,5 About 8% to 10% of patients will experience a recurrence of Bell’s palsy within 10 years.2,6
Pediatric FNP can be congenital or acquired. Congenital FNP is most often associated with birth trauma and occurs at a rate of 2.1 cases per 1,000 births. Rare genetic syndromes can also manifest with FNP and will most often present with other syndromic anomalies noted at birth.7
Acquired FNP is two to four times less common in children than adults, with an estimated prevalence of 2.7 per 100,000 patients younger than 10. Children account for only a small proportion of subjects in published studies that address diagnosis and management of FNP.3 While the presentation of FNP is much the same in adults and children, some notable differences in etiology exist.2,3,7-9 Infectious, traumatic, or neoplastic causes of FNP are more common among children than adults and must be distinguished from idiopathic FNP.7,9-11
Decisions regarding diagnostic testing, pharmacologic treatment, and referral must be guided by the history and physical exam, neurologic exam, and clinical judgment. Being able to identify or exclude alarming causes of FNP, such as neoplasm, will aid the primary care practitioner in treatment and referral practices for this condition.
Pathophysiology CN VII, the facial nerve, has a broad scope of function that incorporates both sensory and motor pathways. The brachial nerve portion of CN VII controls the muscles of voluntary facial expression. CN VII also autonomically innervates the lacrimal gland and submandibular gland and governs sensation from part of the ear as well as taste from the anterior two-thirds of the tongue.4
The precise pathophysiology involved in FNP remains an area of continuing debate, but infectious, vascular, immunologic, and genetic causes have been hypothesized.7,12 Inflammation and subsequent nerve damage along CN VII caused by an infectious process is thought to be the most likely explanation for the pathogenesis of acquired FNP in both adults and children.5,13
Herpes simplex virus 1 (HSV-1) has been suggested as the virus most commonly linked to FNP in both adults and children, but it is unlikely to be the sole cause.5,6,9 Data from a three-year prospective study of FNP cases in children support a relationship between pediatric FNP and HSV-1 infection.14 Other infectious causes implicated in pediatric FNP are Lyme disease, Epstein-Barr, varicella zoster virus, rubella, coxsackie virus, adenovirus, and otitis media.4,7,9
Presentation, History, and Physical Exam Most children with idiopathic FNP will present with sudden-onset facial asymmetry and may have decreased tearing, loss of the conjunctival reflex (leading to difficulty closing the eye), an inability to hold the lips tightly together, and difficulty keeping food in the mouth. Complaints of otalgia, speech disturbances, hyperacusis, and altered sense of taste are common.2,7 Recent occurrence of an upper respiratory infection is often reported in the history of a pediatric patient with FNP.3,7,15,16
Idiopathic FNP is essentially a diagnosis of exclusion.3,5 A meticulous history must be conducted, including any recent illnesses, trauma to the face or head, vaccines, rashes, and travel. Assessment of the head, eyes, ears, nose, and throat, and a careful neurologic history must be conducted to identify nonidiopathic causes of FNP (see Table 15-7,9). Facial weakness can progress from mild palsy to complete paralysis over one to two weeks5; therefore, a careful history of the progression of facial weakness should be ascertained and documented.5,17
A full neurologic exam is essential. Cranial nerves I through XII should be evaluated; any malfunction of a cranial nerve other than CN VII could be indicative of a tumor or process other than idiopathic FNP. Assessment of facial nerve function is imperative, as this factor is the most important for predicting recovery; it can also aid in formulating a prognosis and directing treatment.5,9,17
The House-Brackmann facial nerve grading system1,2 is considered the gold standard for grading severity of facial paresis9 (see Table 21,2 ). A clear distinction between paresis (partial or incomplete palsy) and paralysis (complete palsy) must be made. Pediatric patients with an incomplete palsy have an improved chance of full recovery.17,18
Any abnormalities in the peripheral neurologic exam should prompt further testing. FNP not involving the forehead musculature, gradual progression of paresis, and weakness in any extremity could be indicative of a central lesion. FNP has been the presenting symptom in various neoplastic processes, including leukemia, cholesteatoma, and astrocytoma.3,7,9
Otitis media is a frequent cause of FNP among children.9-11 Thus, a thorough examination of the ear canal, tympanic membrane, and hearing should be performed. The throat and oropharynx should be inspected, and the parotid gland palpated. Any swelling or abnormalities warrant further investigation.
Lyme disease presenting with FNP is more common in children than adults. This may be related to the increased likelihood for children to be bitten by ticks in the head and neck areas. Frequently, FNP associated with Lyme disease is bilateral—as often as 25% of the time.19 Headache, onset of symptoms during peak Lyme season, or bilateral FNP should raise the clinician’s suspicion for Lyme disease.7,9,19
An accurate assessment of blood pressure is essential, as severe hypertension may be implicated in FNP in children.3,5,7 One literature review reported that hypertension was the origin of FNP in 3% to 17% of affected children.20 Vascular hemorrhage induced by hypertension is thought to cause nerve compression and subsequent FNP.7
A bilateral eye exam is also important. Irritation is likely, and the patient with any suspected corneal abrasion or damage should be referred to an ophthalmologist.6,18
Laboratory Testing and Imaging Diagnostic testing that facilitates the exclusion of known causes of FNP should be considered, as there is no specific laboratory test to confirm the diagnosis. A complete blood count, Lyme titers, cerebrospinal fluid analysis, CT, and/or MRI may be warranted, based on the clinical presentation.7-9 In children in whom Lyme disease is suspected (ie, those living in tick-endemic areas or with recent tick bites), serologic testing should be performed. Lumbar puncture and an evaluation of cerebrospinal fluid may be necessary in cases in which meningitis cannot be excluded.7,9
Specialized diagnostic tests are not routinely recommended for patients with paresis that is improving. Audiometry and evaluation of the stapedial reflex may help guide treatment decisions for patients whose condition is not improving. In children, the presence or return of the stapedial reflex within three weeks of disease onset is predictive of complete recovery.5 In patients who experience complete paralysis or unimproved paresis, results of electrodiagnostic testing (in particular, evoked facial nerve electroneuronography) can help forecast recovery of facial nerve function.5,17
Treatment and Management Treatment for FNP in adults is controversial, and even more so for the pediatric patient. Treatment decisions consist of eye care, corticosteroids, antiviral medications, and appropriate referrals.
Eye care. Eye lubrication and protection should be implemented immediately. Protecting the cornea is paramount; thorough lubrication of the eye is the mainstay of treatment.18 Artificial tears should be used frequently during the day, and an ointment should be applied to the eye at night. Use of eye patches is controversial, as they may actually cause corneal injury.7,9 Taping the eye shut at night may prevent trauma during sleep, but this option must be considered carefully.9,18
Corticosteroids. Early initiation of corticosteroids should be considered for all patients with FNP, including children.2,7,9,17 Studies are inconclusive as to whether steroid therapy is beneficial in children with idiopathic FNP. However, two 2010 reviews of pediatric FNP recommend early initiation of steroids for children with acute-onset FNP, particularly when facial paresis is evaluated at a House-Brackmann grade V or VI.7,9 The American Academy of Family Physicians (AAFP) recommends a tapering course of prednisone for all patients, begun as soon as possible.6 The prednisone dosage for pediatric patients is usually 1.0 mg/kg/d, split into two doses, for six days, followed by a tapering dose for four days.5
Antivirals and antibiotic therapy. When an infectious cause of FNP is known, appropriate antibiotic or antiviral therapy should begin. If the patient lives in or has traveled to an area endemic for Lyme disease, empiric treatment may be appropriate. When Ramsay Hunt syndrome is diagnosed or herpetic lesions are visible, antiviral treatment should be initiated.7
Antiviral therapy for idiopathic FNP is the most controversial of the treatment decisions. In 2001, the American Academy of Neurology concluded that no clear benefit from acyclovir could be ascertained, although it might be effective.13 This was affirmed in a recently updated Cochrane review of antiviral therapy for idiopathic FNP.12 Antiviral therapy alone showed no benefit, compared with placebo; however, combined antiviral and corticosteroid therapy was more effective than placebo alone in recovery outcomes. Antivirals may benefit pediatric patients and should be considered early when the cause of FNP is viral or idiopathic.7,9
Referrals. Initial presentation and course of paresis should guide referral patterns for the pediatric patient presenting with FNP. The American Academy of Pediatrics (AAP) recommends referral to an otolaryngologist for any infant or child with FNP.21 The AAFP recommends referral to a specialist for any patient who does not show improvement within two weeks.6
In patients with complete paralysis, early surgical intervention may be considered, and referral should be made promptly for electrodiagnostic testing and surgical consult. In cases in which otitis media causes FNP, myringotomy and tube insertion are indicated, and appropriate referral should be made.7,9
Outcomes |The prognosis in children with FNP is good, and most will recover completely.2,9-11,22 Idiopathic and infectious etiologies of FNP seem to have the greatest likelihood for complete recovery.10,11,16,17 Recovery appears to be affected by etiology, degree of paresis, and treatment. How these factors coalesce is not fully understood, and up to 20% of children may have mild to moderate residual facial nerve dysfunction.10,11,19,22
The Case Patient The child’s facial nerve function gradually returned over a three-week period, with no residual deficit (see Figures 1a, 1b, and 1c). Results of the audiometry screening on day 10 were normal, showing a positive stapedial reflex. An MRI, performed four months after the initial paralysis to rule out any tumors, yielded normal results.
This case highlights the differing management of pediatric Bell’s palsy among emergency, pediatric, and specialized providers. This child was managed more aggressively under the care of an otolaryngologist with a two-week course of steroids, antiviral medication for 10 days, and a follow-up MRI to rule out any evidence of a tumor. The need for further research to guide practice in the pediatric patient with Bell’s palsy is apparent.
Conclusion FNP in the pediatric population is rare and more likely to have an identifiable cause than among adults. Careful examination should reveal differential diagnoses that warrant treatment and referrals. The main causes of FNP that should not be missed are otitis media, hypertension, varicella zoster virus (Ramsay Hunt syndrome), neoplastic processes, and Lyme disease.
Practitioners should have a high index of suspicion for nonidiopathic causes of FNP when a child has a neurologic exam that includes facial paresis of gradual onset, abnormal function of other cranial nerves, lack of forehead muscle weakness, or peripheral abnormalities. In addition to the history and exam, blood work and radiologic imaging can aid the practitioner in ruling in or out nonidiopathic causes of FNP.
Grading of facial palsy severity using the House-Brackmann scale helps guide prognosis and referral choices. Referral to a specialist in otolaryngology is appropriate and recommended by the AAP. Referral should be made to an ophthalmologist if any suspicion of corneal abrasion exists.
Treatment in children should consist of eye care and steroids. Antiviral therapy should be considered on an individualized basis and when evidence of HSV or varicella exists. Parents should be advised about the importance of eye care in a child with FNP (see Table 35-7,9,17,18,22).
The emotional stress associated with FNP can be significant for both children and adults; fear of lifelong facial deformity can be psychologically debilitating. Yet a favorable prognosis for recovery of facial nerve function can be relayed to anxious parents.
References
1. House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985;93(2): 146-147.
2. Finsterer J. Management of peripheral facial nerve palsy. Eur Arch Otorhinolaryngol. 2008;265(7):743-752.
3. Lunan R, Nagarajan L. Bell’s palsy: a guideline proposal following a review of practice. J Paediatr Child Health. 2008;44(4):219-220.
4. Blosser CG, Reider-Demer M. Neurologic disorders. In: Burns CE, Dunn AM, Brady MA, et al, eds. Pediatric Primary Care. 4th ed. St. Louis: Saunders Elsevier; 2008:634-672.
5. Singhi P, Jain V. Bell’s palsy in children. Semin Pediatr Neurol. 2003;10(4):289-297.
6. Tiemstra JD, Khatkhate N. Bell’s palsy: diagnosis and management. Am Fam Physician. 2007;76(7):997-1002.
7. Lorch M, Teach SJ. Facial nerve palsy: Etiology and approach to diagnosis and treatment. Pediatr Emerg Care. 2010;26(10):763-769.
8. El-Hawrani AS, Eng CY, Ahmed SK, et al. General practitioners’ referral pattern for children with acute facial paralysis. J Laryngol Otol. 2005;119(7):540-542.
9. Shargorodsky J, Lin HW, Gopen Q. Facial nerve palsy in the pediatric population. Clin Pediatr (Phila). 2010;49(5):411-417.
10. Wang CH, Chang YC, Shih HM, et al. Facial palsy in children: emergency department management and outcome. Pediatr Emerg Care. 2010;26(2):121-125.
11. Evans AK, Licameli G, Brietzke S, et al. Pediatric facial nerve paralysis: patients, management and outcomes. Int J Pediatr Otorhinolaryngol. 2005;69(11):1521-1528.
12. Lockhart P, Daly F, Pitkethly M, et al. Antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2009;(4):CD001869.
13. Grogan PM, Gronseth GS. Practice parameter: steroids, acyclovir, and surgery for Bell’s palsy (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56(7):830-836.
14. Khine H, Mayers M, Avner JR, et al. Association between herpes simplex virus-1 infection and idiopathic unilateral facial paralysis in children and adolescents. Pediatr Infect Dis J. 2008;27(5):468-469.
15. Tsai HS, Chang LY, Lu CY, et al. Epidemiology and treatment of Bell’s palsy in children in northern Taiwan. J Microbiol Immunol Infect. 2009;42(4):351-356.
16. Cha CI, Hong CK, Park MS, Yeo SG. Comparison of facial nerve paralysis in adults and children. Yonsei Med J. 2008;49(5):725-734.
17. Linder TE, Abdelkafy W, Cavero-Vanek S. The management of peripheral facial nerve palsy: “paresis” versus “paralysis” and sources of ambiguity in study designs. Otol Neurotol. 2010;31(2):319-327.
18. Rahman I, Sadiq SA. Ophthalmic management of facial nerve palsy: a review. Surv Ophthalmol. 2007;52(2):121-144.
19. Skogman BH, Croner S, Odkvist L. Acute facial palsy in children: a 2-year follow-up with focus on Lyme neuroborreliosis. Int J Pediatr Otorhinolaryngol. 2003;67(6):597-602.
20. Siegler RL, Brewer ED, Corneli HM, Thompson JA. Hypertension first seen as facial paralysis: case reports and review of the literature. Pediatrics. 1991;87(3):387-389.
21. Surgical Advisory Panel, American Academy of Pediatrics. Guidelines for referral to pediatric surgical specialists. Pediatrics. 2002;110(1 pt 1):187-191.
22. Chen WX, Wong V. Prognosis of Bell’s palsy in children: analysis of 29 cases. Brain Dev. 2005; 27(7):504-508.
References
1. House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985;93(2): 146-147.
2. Finsterer J. Management of peripheral facial nerve palsy. Eur Arch Otorhinolaryngol. 2008;265(7):743-752.
3. Lunan R, Nagarajan L. Bell’s palsy: a guideline proposal following a review of practice. J Paediatr Child Health. 2008;44(4):219-220.
4. Blosser CG, Reider-Demer M. Neurologic disorders. In: Burns CE, Dunn AM, Brady MA, et al, eds. Pediatric Primary Care. 4th ed. St. Louis: Saunders Elsevier; 2008:634-672.
5. Singhi P, Jain V. Bell’s palsy in children. Semin Pediatr Neurol. 2003;10(4):289-297.
6. Tiemstra JD, Khatkhate N. Bell’s palsy: diagnosis and management. Am Fam Physician. 2007;76(7):997-1002.
7. Lorch M, Teach SJ. Facial nerve palsy: Etiology and approach to diagnosis and treatment. Pediatr Emerg Care. 2010;26(10):763-769.
8. El-Hawrani AS, Eng CY, Ahmed SK, et al. General practitioners’ referral pattern for children with acute facial paralysis. J Laryngol Otol. 2005;119(7):540-542.
9. Shargorodsky J, Lin HW, Gopen Q. Facial nerve palsy in the pediatric population. Clin Pediatr (Phila). 2010;49(5):411-417.
10. Wang CH, Chang YC, Shih HM, et al. Facial palsy in children: emergency department management and outcome. Pediatr Emerg Care. 2010;26(2):121-125.
11. Evans AK, Licameli G, Brietzke S, et al. Pediatric facial nerve paralysis: patients, management and outcomes. Int J Pediatr Otorhinolaryngol. 2005;69(11):1521-1528.
12. Lockhart P, Daly F, Pitkethly M, et al. Antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2009;(4):CD001869.
13. Grogan PM, Gronseth GS. Practice parameter: steroids, acyclovir, and surgery for Bell’s palsy (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56(7):830-836.
14. Khine H, Mayers M, Avner JR, et al. Association between herpes simplex virus-1 infection and idiopathic unilateral facial paralysis in children and adolescents. Pediatr Infect Dis J. 2008;27(5):468-469.
15. Tsai HS, Chang LY, Lu CY, et al. Epidemiology and treatment of Bell’s palsy in children in northern Taiwan. J Microbiol Immunol Infect. 2009;42(4):351-356.
16. Cha CI, Hong CK, Park MS, Yeo SG. Comparison of facial nerve paralysis in adults and children. Yonsei Med J. 2008;49(5):725-734.
17. Linder TE, Abdelkafy W, Cavero-Vanek S. The management of peripheral facial nerve palsy: “paresis” versus “paralysis” and sources of ambiguity in study designs. Otol Neurotol. 2010;31(2):319-327.
18. Rahman I, Sadiq SA. Ophthalmic management of facial nerve palsy: a review. Surv Ophthalmol. 2007;52(2):121-144.
19. Skogman BH, Croner S, Odkvist L. Acute facial palsy in children: a 2-year follow-up with focus on Lyme neuroborreliosis. Int J Pediatr Otorhinolaryngol. 2003;67(6):597-602.
20. Siegler RL, Brewer ED, Corneli HM, Thompson JA. Hypertension first seen as facial paralysis: case reports and review of the literature. Pediatrics. 1991;87(3):387-389.
21. Surgical Advisory Panel, American Academy of Pediatrics. Guidelines for referral to pediatric surgical specialists. Pediatrics. 2002;110(1 pt 1):187-191.
22. Chen WX, Wong V. Prognosis of Bell’s palsy in children: analysis of 29 cases. Brain Dev. 2005; 27(7):504-508.
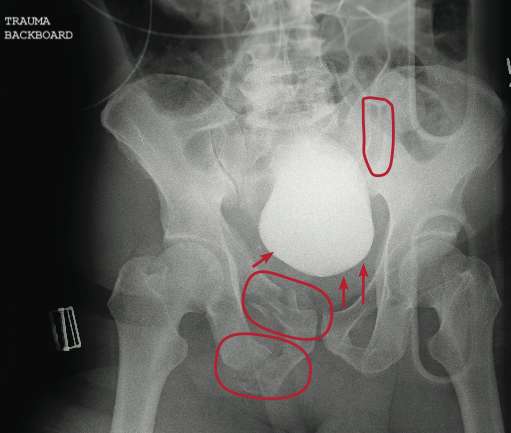
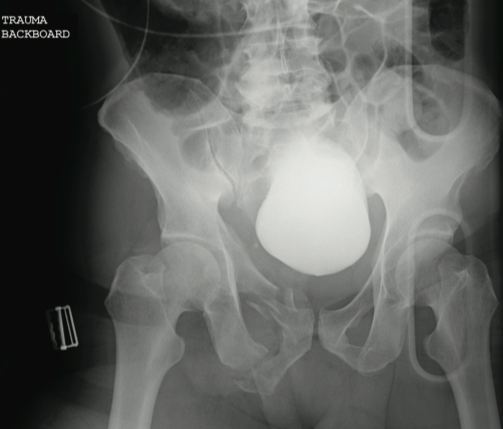
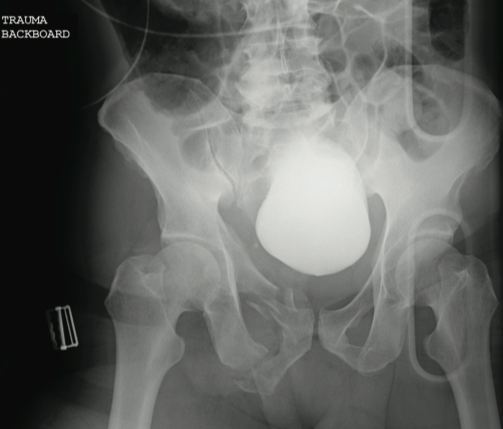
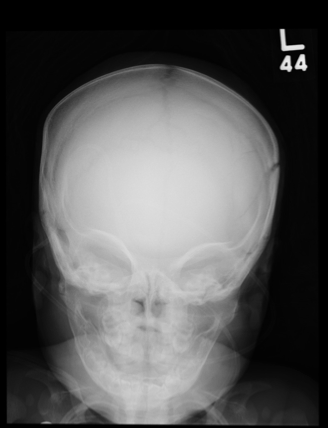
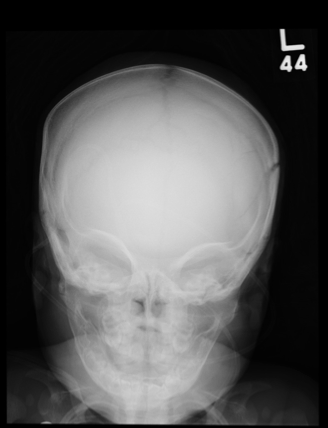
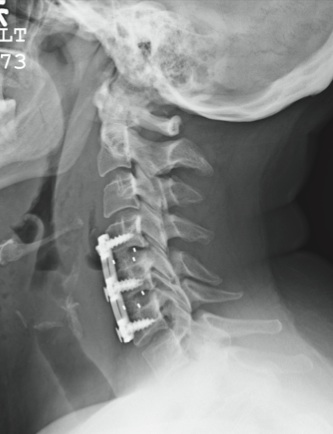
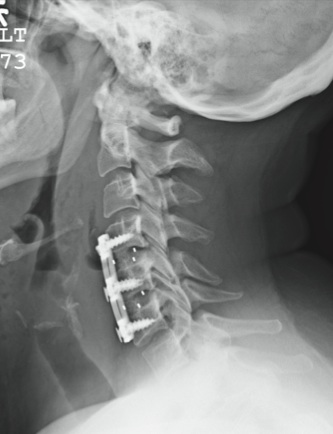
ANSWER The radiograph demonstrates a lucency at the base of the odontoid (C2). In addition, there is a slight posterior subluxation of C1 on C2.
Although these findings were deemed likely to be chronic and old in nature, for completeness, an MRI of the cervical spine was obtained. It did, in fact, confirm the findings to be old.
ANSWER The radiograph demonstrates a lucency at the base of the odontoid (C2). In addition, there is a slight posterior subluxation of C1 on C2.
Although these findings were deemed likely to be chronic and old in nature, for completeness, an MRI of the cervical spine was obtained. It did, in fact, confirm the findings to be old.
ANSWER The radiograph demonstrates a lucency at the base of the odontoid (C2). In addition, there is a slight posterior subluxation of C1 on C2.
Although these findings were deemed likely to be chronic and old in nature, for completeness, an MRI of the cervical spine was obtained. It did, in fact, confirm the findings to be old.
A 72-year-old nursing home resident is sent for evaluation of decreased level of consciousness, nausea, vomiting, and increasing confusion. He denies any recent injury or trauma. His medical history is significant for diabetes, stroke, dementia, atrial fibrillation, and hypertension.
The patient denies any head or neck pain. His vital signs are stable. Overall, aside from reports of occasional confusion, his physical examination is benign. He moves all of his extremities well and appears to have no deficits, including no neck or back tenderness.
In reviewing his lab work, you see his sodium concentration is 126 mEq/L. CT of the head shows only chronic changes. Cervical spine radiographs are also obtained; the lateral view is shown. What is your impression?
For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
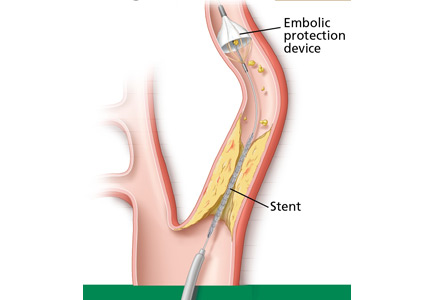
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail shishem@gmail.com
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail shishem@gmail.com
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
Author and Disclosure Information
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail shishem@gmail.com
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
In CREST, stenting and surgery had similar combined rates of stroke, MI, and death when performed by highly qualified interventionalists and surgeons in carefully selected patients.
The risk of periprocedural stroke was higher with stenting; most of those strokes were nonmajor. Both major and nonmajor strokes were associated with decreased quality of life in long-term follow-up.
Endarterectomy was associated with higher rates of periprocedural MI than stenting.
Endarterectomy carried a significantly higher rate of cranial nerve damage than stenting.
The radiograph reveals several findings. First, there are obvious displaced fractures of the right superior and inferior rami bones. There is also a diastatic fracture of the left sacroiliac joint.
Also, as the bladder is full of contrast (probably from a recent cystogram), note how it appears to be displaced to a more superior position than usual. This is second- ary to formation of a pelvic hematoma.
The radiograph reveals several findings. First, there are obvious displaced fractures of the right superior and inferior rami bones. There is also a diastatic fracture of the left sacroiliac joint.
Also, as the bladder is full of contrast (probably from a recent cystogram), note how it appears to be displaced to a more superior position than usual. This is second- ary to formation of a pelvic hematoma.
The radiograph reveals several findings. First, there are obvious displaced fractures of the right superior and inferior rami bones. There is also a diastatic fracture of the left sacroiliac joint.
Also, as the bladder is full of contrast (probably from a recent cystogram), note how it appears to be displaced to a more superior position than usual. This is second- ary to formation of a pelvic hematoma.
A 59-year-old man was struck by a car while walking. He was initially evaluated at another facility, intubated, resuscitated, and stabilized, then transferred to your facility. He is believed to have a severe head injury and possibly other internal injuries.
The man is unresponsive on arrival at your facility. No medical history is available. His vital signs are stable, with a blood pressure of 113/74 mm Hg; heart rate, 101 beats/min; and respiratory rate, 14 breaths/min. Initial Glasgow Coma Scale score is reported as a 3T. It is unclear whether the patient has recently received any sedation.
As you are reviewing the results of testing conducted at both your facility and the facility to which the patient was originally taken, you see a portable pelvic radiograph (shown). What is your impression?
If a patient taking warfarin (Coumadin) or other anticoagulant drug suffers an intracerebral hemorrhage (ICH) and survives, the physician faces the dilemma of whether to resume the anticoagulant. On one hand, the drug was prescribed because the patient was at risk of a thromboembolic event such as stroke or pulmonary embolism. On the other hand, warfarin use may increase the risk of another ICH.
Unfortunately, we have little evidence from clinical trials on which to base the decision. Nevertheless, we believe that in selected patients the potential benefit of resuming anticoagulation outweighs the considerable risk.
In the pages that follow, we summarize when and how anticoagulation therapy should be resumed after ICH.
A DEADLY COMPLICATION OF ANTICOAGULANT THERAPY
Intracranial bleeding is the most feared and the most deadly complication of oral anticoagulant therapy.1 The substantial risks associated with oral anticoagulants likely account for these drugs being underprescribed in patients who have indications for them.2–4
While bleeding is the major risk, not all bleeding events are equally damaging. Extracranial bleeding (eg, gastrointestinal bleeding, hematuria, epistaxis) leads to death or disability in only 3% of cases, whereas intracranial bleeding such as ICH leads to death or disability 76% of cases.5
Even without anticoagulation, ICH is the deadliest form of stroke,6–9 and if the patient has been taking warfarin, the risk of disability and death is substantially higher.6,10 Warfarin has a striking effect on the incidence and outcomes of ICH. While the overall incidence of ICH in the general population is approximately 25 per 100,000 person-years, the incidence in patients on warfarin is exponentially higher, at 2 to 3 per 100 per year, and appears to be increasing.11,12 In addition, once ICH occurs, the risk of death is up to twice as high in those on warfarin.6 The bulk of this effect is likely due to a higher risk of ongoing bleeding after the event.10,13–16
Major risk factors for ICH in patients taking oral anticoagulants include a higher international normalized ratio (INR) and older age.11,17
TWO KEY QUESTIONS
Once a patient is diagnosed with warfarin-related ICH, clinicians typically take urgent measures to restore normal coagulation, hoping to limit ongoing bleeding and improve outcome.18,19
The higher the INR at presentation, the greater the risk of death.6 In addition, in retrospective studies, some authors have noted that earlier correction of the INR is associated with better outcome.14,16
While emergency reversal of warfarin is widely considered standard treatment in the acute phase,20–24 concern persists about its safety in patients at high risk of thromboembolism.
Until the results of clinical trials are available, decisions about whether to reverse and when to resume anticoagulation hinge on two questions:
In the acute phase, how does the risk of further bleeding (hematoma expansion) compare with the short-term risk of thromboembolism?
In the chronic phase, how does the risk of recurrent hemorrhage compare with the excess risk of thromboembolism if the patient does not resume anticoagulation therapy?
ACUTELY, THE RISK OF BLEEDING OUTWEIGHS THAT OF CLOTTING
High risk of hematoma expansion after ICH
Unfortunately, continued bleeding is common after ICH. In patients who present within 3 hours of symptom onset, 26% of hematomas expand more than 33% over the first hour, and another 12% expand this amount over the next 20 hours.6 In warfarin-associated ICH, up to 50% of patients develop this level of hematoma expansion, but it appears to take place over a more prolonged period of time.10,13–16 Over 70% of patients presenting acutely develop at least some amount of expansion within 24 hours.25 Therefore, the risk of hematoma expansion in the first 24 hours is likely so high that patients cannot safely receive anticoagulants during this time frame.
But not all patients are at equal risk of hematoma expansion. Several features are associated with higher risk (Table 1)10,26–40:
A large hematoma volume on presentation is a significant predictor of expansion, possibly reflecting a more severe underlying insult.26,27
Early presentation, especially within 3 hours of symptom onset, also appears to mark those at higher risk, presumably because such patients undergo computed tomography (CT) while still bleeding.26,27
Figure 1. The “spot sign” (arrow), contrast extravasation after contrast-enhanced computed tomography, is associated with a high risk of hematoma expansion.For those on warfarin, a higher INR is a significant predictor, not just of higher risk, but also of a more delayed expansion.10,28
Certain radiographic findings indicate higher risk. One is the “spot sign,” ie, contrast extravasation after contrast-enhanced CT27,29–31 (Figure 1). Apparently, the more spots present, and the denser the contrast, the greater the risk, an observation that has led to a proposed “spot-sign score” that may predict both expansion and poor outcome. 32,41
Given the high risk of hematoma expansion in the early phase, and given our inability to predict hematoma expansion, most authorities recommend immediate reversal of anticoagulation after diagnosis.42–44 Reversal of anticoagulation typically includes intravenous vitamin K, which begins to act within several hours, and repletion of coagulation factors, which act within minutes (prothrombin complex concentrates and recombinant factor VIIa [NovoSeven]) or a few hours (fresh frozen plasma).1
Dosages:
Vitamin K 5 to 10 mg intravenously
Prothrombin complex concentrates 10 to 50 U/kg
Recombinant factor VIIa 40 to 80 μg/kg
Fresh frozen plasma 10 to 50 U/kg.
Risk of thromboembolism after ICH: Ongoing and cumulative
Thromboembolism after ICH is a major concern, for two main reasons.
First, patients on oral anticoagulation typically have a preexisting risk factor and are thus at higher risk of a thromboembolic event, particularly while they are off anticoagulation. Patients with atrial fibrillation or a mechanical valve are at risk of arterial events such as ischemic stroke, whereas patients with a known venous thromboembolic condition such as deep venous thrombosis or pulmonary embolism are at risk of extension of the thrombosis or recurrence of a venous thrombotic event.
Second, ICH itself increases the risk of arterial and venous thromboembolic events. Including patients not previously on anticoagulation, this risk is as high as 7% during the initial hospitalization and 9% during the first 90 days.45,46 Worth noting is that patients who previously received anticoagulant drugs (and who are off this therapy in the acute phase) are at no higher risk of thromboembolism compared with those who never received anticoagulants.45
However, while the risk of hematoma expansion is highest at presentation and then decreases with time, the risk of thromboembolism (particularly venous thromboembolism) is ongoing and cumulative. Arterial thromboembolism is more likely to occur early, within the first week, whereas venous thromboembolism can occur later.45
Overall, studies have estimated the short-term risk of pulmonary embolism to be 1% to 2%, deep venous thrombosis 1% to 4%, myocardial ischemia about 2%, and cerebral ischemia 2% to 3%.45,46 However, when patients are actively screened, the incidence of asymptomatic deep venous thrombosis is found to be as high as 16% in the first 10 days,47 and evidence of myocardial ischemia can be detected in up to 27% of patients.48
Therefore, the risk of hematoma expansion appears to be high and the risk of thromboembolism appears to be low during the first day after ICH. Over the next days, as the risk of hematoma expansion recedes, this ratio shifts.
Studies of in-hospital anticoagulation after ICH
The data on restarting oral anticoagulation in the acute phase are sparse. In practice, clinicians typically start heparinoids in low subcutaneous doses to prevent deep venous thrombosis and, after the first few days or a week, consider increasing to a full anticoagulation dose or starting an oral anticoagulant and subsequently discontinuing the heparin when the INR is in the therapeutic range (see discussion below).
ICH patients in general may benefit from starting prophylactic-dose heparin therapy early. One randomized trial found that starting heparin in a low subcutaneous dose the day after an ICH decreased the risk of thromboembolism without increasing the risk of rebleeding.49 Another study also found no increased risk of rebleeding with early prophylactic-dose subcutaneous heparin.50
As the benefit appears to outweigh the risk, national guidelines suggest starting subcutaneous heparin early in all ICH patients, including those not previously on warfarin.42,43
Commonly used heparinoid regimens include unfractionated heparin 5,000 units subcutaneously twice a day; enoxaparin (Lovenox) 40 mg once a day; and dalteparin (Fragmin) 5,000 units once a day.51 In addition, all patients should receive optimal mechanical thromboprophylaxis, including graduated compression stockings or intermittent pneumatic compression stockings, or both.
LONG-TERM MANAGEMENT: ICH RECURRENCE VS THROMBOEMBOLISM
Risk of ICH recurrence on warfarin is not precisely known
Overall, the risk of ICH recurrence is about 1% at 3 months, and warfarin likely increases this risk.42,52 Unfortunately, the risk of ICH recurrence in patients on anticoagulation therapy after a first ICH is not clear, and no population-based study has clarified this risk. Therefore, the best we can do at present is to try to estimate the risk of recurrent warfarin-related ICH by separately examining two issues:
The risk of ICH recurrence in general
The risk of major bleeding (including ICH) in the general population of patients on warfarin.
The risk of ICH recurrence in general is about 2% to 4% per patient-year.52–54 However, this risk appears to be a function of the underlying vasculopathy. ICH location is often used as a surrogate for underlying cause. Most ICHs in deep hemispheric (basal ganglia, thalamus) or brainstem territories are likely caused by hypertensive vasculopathy, whereas lobar ICH is often associated with cerebral amyloid angiopathy.52–54 Presumably because of this distinction, ICH in a deep location recurs in about 2% of cases per year, compared with 4% for lobar ICH.53 The presence and number of microbleeds on T2-weighted gradient-echo magnetic resonance imaging appear to predict ICH recurrence; microbleeds likely are markers of more severe or widespread underlying vasculopathy.55–57
A genetic risk factor for the recurrence of lobar ICH is apolipoprotein E genotype58; future studies may highlight genetic variations that specifically modify the risk of warfarin-related ICH.59 Unfortunately, there is currently no way to modify the risk of ICH associated with cerebral amyloid angiopathy. On the other hand, in patients with hypertensive hemorrhage, antihypertensive therapy likely reduces the risk of recurrent ICH. One randomized controlled trial showed that such therapy decreased the risk of ICH by more than half.60
The risk of major bleeding in the general population of patients on warfarin may be 2% to 3% per year and is likely higher in the first month.11 The risk is higher in older patients and if the INR rises above 4.0.11,17 For some patients, it is possible to estimate the likelihood of major bleeding using validated decision-support tools that include factors such as age, sex, and medical history.11,61–64
Given the lack of data specifically addressing the risk of ICH recurrence on warfarin, the clinician is left to try to extrapolate this risk from available data using specific patient characteristics that modify the presumed risk. For example, one can combine factors such as ICH location (or better yet, the underlying cause) with decision-support tools that predict the risk of major bleeding. Close control of both blood pressure and the INR appears especially critical for patients receiving anticoagulation after ICH.11,60,65 Still, the risk does not disappear with good INR control, and most patients with anticoagulation-related ICH present with INRs within the therapeutic range.5,10,65
Long-term risk of thromboembolism depends on underlying condition
In the long term, the risk of thromboembolism depends on the reason for which the patient was originally given anticoagulation. In addition, many patients with ICH suffer decreased mobility and are therefore at higher risk of venous thromboembolism than before their event.
Nonvalvular atrial fibrillation is the most common indication for anticoagulation. For these patients, the risk of ischemic stroke is 2% to 5% per year.66,67 The system usually used to stratify this risk is CHADS2, an acronym for five key risk factors:
Congestive heart failure (1 point)
Hypertension (1 point)
Age over 75 (1 point)
Diabetes mellitus (1 point)
Prior stroke or transient ischemic attack (2 points).
The annual risk of stroke ranges from 1.9% (score of 0) to 18.2% (score of 6).68,69 In patients with nonvalvular atrial fibrillation, the excess risk of ischemic stroke without anticoagulation must be weighed against the risk of ICH recurrence.
A mechanical heart valve, another common indication, carries a risk of ischemic stroke of about 4% per year.70 A mechanical valve is traditionally considered an absolute indication for anticoagulation. However, patients with lobar ICH face a risk of recurrence that is greater than 4% per year, and so the risks of resuming anticoagulation may well outweigh the benefits.
Heart failure may be associated with a risk of ischemic stroke of 1% to 4% per year, and this is likely a function of disease severity.71
Venous thromboembolism. The risk of recurrent venous thromboembolism in patients with deep venous thrombosis or pulmonary embolism is around 4% per year.72 Given that ICH itself confers a 2% to 3% risk of these conditions, the rate of recurrence of deep venous thrombosis may well be much higher in those ICH patients who have also already had deep venous thrombosis.
Data on resuming oral anticoagulation after ICH
Several studies have examined the outcomes when oral anticoagulants were resumed after ICH (Table 2),73–76 but experts differ on when these drugs should be resumed (eg, between 1 and 10 days after onset), or even whether they should be resumed at all.19
Notably, an analysis of 52 patients found a high risk of ICH recurrence (and gastrointestinal bleeding) in patients who restarted warfarin, and a high risk of myocardial infarction and ischemic stroke in those who did not restart, with neither strategy demonstrating a clear benefit in the rate of death or disability.73 All patients with a thromboembolic event were being treated for a previous event, suggesting that secondary prevention is a stronger indication for anticoagulation than primary prevention in this population.73
IF AND WHEN TO RESTART
Two major questions to consider are whether the benefits of restarting anticoagulation outweigh the risk, and if so, when and how should anticoagulation be restarted?
Whether to restart anticoagulation
As for the risk-benefit ratio, many think that anticoagulation should be restarted only with extreme caution and possibly only in those with deep ICH or a documented history of thromboembolism.19
In one decision analysis examining whether to restart anticoagulation after ICH in patients with atrial fibrillation, the risk of thromboembolism would need to exceed 7% per year to justify restarting anticoagulation after deep ICH,67 and no risk level was high enough to justify restarting anticoagulation after lobar ICH.
For patients at sufficiently high risk of ICH recurrence, antiplatelet treatment is probably safer, as antiplatelet agents carry a substantially lower risk of bleeding.54,77–79 The American Heart Association comments that for nonvalvular atrial fibrillation, long-term anticoagulation should be avoided after spontaneous lobar ICH, but that antiplatelet agents may be considered. 42 They note that anticoagulation after nonlobar ICH may be considered depending on the indication.42
The decision to restart anticoagulation may also be a function of whether the underlying risk factor is a temporary one. For example, atrial fibrillation or a mechanical heart valve confers a long-term, ongoing risk of arterial thromboembolism, and such patients would not normally be considered for a short course of warfarin therapy. However, isolated deep vein thrombosis may only require anticoagulation for a limited time, such as 3 to 6 months.80 Perhaps for such patients the long-term outcome is maximized with a narrowly defined, temporary course of anticoagulation.
When to restart anticoagulation
As for when to restart, it is not certain how long after symptom onset the risk of ongoing bleeding continues. Clearly, the risk is high on the first day, but small after the first few days.
The European Stroke Initiative recommends that patients with a strong indication for anticoagulation, such as a history of embolic stroke with atrial fibrillation, should be restarted on warfarin after 10 to 14 days, depending on the risk of thromboembolism and ICH recurrence.43
The American Heart Association suggests that, in patients with a very high risk of thromboembolism for whom restarting warfarin is considered, warfarin may be restarted 7 to 10 days after ICH onset.42
The American College of Chest Physicians recommends starting prophylactic-dose heparin the day after an ICH, with no clear guidance on restarting warfarin.81
ALTERNATIVES TO WARFARIN
Alternatives to warfarin that show promise in reducing bleeding risk include factor Xa and direct thrombin inhibitors, which may reduce the risk of thromboembolism to an extent similar to that of warfarin, but with fewer bleeding complications.82
In patients with atrial fibrillation, the direct thrombin inhibitor dabigatran (Pradaxa) was shown to prevent ischemic stroke to a similar or greater degree than warfarin, with fewer bleeding complications.83 Further patient follow-up is under way to ensure that this drug does not cause liver problems, as did a similarly designed predecessor.84
The availability of this and other agents in various stages of development82 will probably not make warfarin extinct. Rather, they may change the “tipping point,” the threshold at which the risk of thromboembolism is high enough to justify the risks associated with restarting warfarin therapy. In addition, clinical decision tools clarifying the individual patient’s risk of thromboembolism vs the risk of ICH recurrence will help physicians tailor the therapy to the patient.
For the moment, in situations in which the decision is difficult, maximizing the use of antiplatelet agents offers the best hope.85
RECOMMENDATIONS IN LIEU OF GUIDELINES
No guideline can broadly cover every clinical scenario. Many factors go into assessing a patient’s risk of hematoma expansion or recurrent hemorrhage (Table 3) and the extent to which anticoagulation can reduce the risk of thromboembolism.
In the short term, most patients with ICH will likely benefit from acute reversal of anticoagulation, followed by gradual reinstitution of prophylactic-dose anticoagulation after the first 24 to 72 hours.
In the long term, many patients with lobar hemorrhage, cerebral amyloid angiopathy, or other risk factors may remain at higher risk of anticoagulant-related ICH recurrence than of fatal or disabling thromboembolic events and would therefore be best managed without anticoagulants. Conversely, those with deep hemispheric ICH, hypertension that can be well controlled, and a high risk of disabling thromboembolism may receive a net benefit from restarting anticoagulation.
Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med2007; 167:1414–1419.
Choudhry NK, Anderson GM, Laupacis A, Ross-Degnan D, Normand SL, Soumerai SB. Impact of adverse events on prescribing warfarin in patients with atrial fibrillation: matched pair analysis. BMJ2006; 332:141–145.
Choudhry NK, Soumerai SB, Normand SL, Ross-Degnan D, Laupacis A, Anderson GM. Warfarin prescribing in atrial fibrillation: the impact of physician, patient, and hospital characteristics. Am J Med2006; 119:607–615.
Fang MC, Go AS, Chang Y, et al. Death and disability from warfarin-associated intracranial and extracranial hemorrhages. Am J Med2007; 120:700–705.
Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med2004; 164:880–884.
Dixon AA, Holness RO, Howes WJ, Garner JB. Spontaneous intracerebral haemorrhage: an analysis of factors affecting prognosis. Can J Neurol Sci1985; 12:267–271.
Broderick JP, Adams HP, Barsan W, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke1999; 30:905–915.
Flibotte JJ, Hagan N, O’Donnell J, Greenberg SM, Rosand J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology2004; 63:1059–1064.
Schulman S, Beyth RJ, Kearon C, Levine MN; American College of Chest Physicians. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):257S–298S.
Flaherty ML, Kissela B, Woo D, et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology2007; 68:116–121.
Lee SB, Manno EM, Layton KF, Wijdicks EF. Progression of warfarin-associated intracerebral hemorrhage after INR normalization with FFP. Neurology2006; 67:1272–1274.
Huttner HB, Schellinger PD, Hartmann M, et al. Hematoma growth and outcome in treated neurocritical care patients with intracerebral hemorrhage related to oral anticoagulant therapy: comparison of acute treatment strategies using vitamin K, fresh frozen plasma, and prothrombin complex concentrates. Stroke2006; 37:1465–1470.
Sjöblom L, Hårdemark HG, Lindgren A, et al. Management and prognostic features of intracerebral hemorrhage during anticoagulant therapy: a Swedish multicenter study. Stroke2001; 32:2567–2574.
Yasaka M, Minematsu K, Naritomi H, Sakata T, Yamaguchi T. Predisposing factors for enlargement of intracerebral hemorrhage in patients treated with warfarin. Thromb Haemost2003; 89:278–283.
Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation2007; 115:2689–2696.
Goldstein JN, Thomas SH, Frontiero V, et al. Timing of fresh frozen plasma administration and rapid correction of coagulopathy in warfarin-related intracerebral hemorrhage. Stroke2006; 37:151–155.
Aguilar MI, Hart RG, Kase CS, et al. Treatment of warfarin-associated intracerebral hemorrhage: literature review and expert opinion. Mayo Clin Proc2007; 82:82–92.
Guidelines on oral anticoagulation: third edition. Br J Haematol1998; 101:374–387.
Baglin TP, Keeling DM, Watson HG; British Committee for Standards in Haematology. Guidelines on oral anticoagulation (warfarin): third edition—2005 update. Br J Haematol2006; 132:277–285.
O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al; British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol2004; 126:11–28.
Baker RI, Coughlin PB, Gallus AS, Harper PL, Salem HH, Wood EM; Warfarin Reversal Consensus Group. Warfarin reversal: consensus guidelines, on behalf of the Australasian Society of Thrombosis and Haemostasis. Med J Aust2004; 181:492–497.
Davis SM, Broderick J, Hennerici M, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology2006; 66:1175–1181.
Broderick JP, Diringer MN, Hill MD, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Determinants of intracerebral hemorrhage growth: an exploratory analysis. Stroke2007; 38:1072–1075.
Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology2007; 68:889–894.
Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of spontaneous intracerebral hemorrhage. Incidence and time course. Stroke1996; 27:1783–1787.
Kim J, Smith A, Hemphill JC, et al. Contrast extravasation on CT predicts mortality in primary intracerebral hemorrhage. AJNR Am J Neuroradiol2008; 29:520–525.
Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebral hemorrhage. Stroke2007; 38:1257–1262.
Barras CD, Tress BM, Christensen S, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Density and shape as CT predictors of intracerebral hemorrhage growth. Stroke2009; 40:1325–1331.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. Systematic characterization of the computed tomography angiography spot sign in primary intracerebral hemorrhage identifies patients at highest risk for hematoma expansion: the spot sign score. Stroke2009; 40:2994–3000.
Fujii Y, Takeuchi S, Sasaki O, Minakawa T, Tanaka R. Multivariate analysis of predictors of hematoma enlargement in spontaneous intracerebral hemorrhage. Stroke1998; 29:1160–1166.
Ederies A, Demchuk A, Chia T, et al. Postcontrast CT extravasation is associated with hematoma expansion in CTA spot negative patients. Stroke2009; 40:1672–1676.
Delgado P, Alvarez-Sabín J, Abilleira S, et al. Plasma d-dimer predicts poor outcome after acute intracerebral hemorrhage. Neurology2006; 67:94–98.
Naidech AM, Jovanovic B, Liebling S, et al. Reduced platelet activity is associated with early clot growth and worse 3-month outcome after intracerebral hemorrhage. Stroke2009; 40:2398–2401.
Silva Y, Leira R, Tejada J, Lainez JM, Castillo J, Dávalos A; Stroke Project, Cerebrovascular Diseases Group of the Spanish Neurological Society. Molecular signatures of vascular injury are associated with early growth of intracerebral hemorrhage. Stroke2005; 36:86–91.
Sansing LH, Messe SR, Cucchiara BL, Cohen SN, Lyden PD, Kasner SE; CHANT Investigators. Prior antiplatelet use does not affect hemorrhage growth or outcome after ICH. Neurology2009; 72:1397–1402.
Moussouttas M, Malhotra R, Fernandez L, et al. Role of antiplatelet agents in hematoma expansion during the acute period of intracerebral hemorrhage. Neurocrit Care2010; 12:24–29.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. The spot sign score in primary intracerebral hemorrhage identifies patients at highest risk of in-hospital mortality and poor outcome among survivors. Stroke2010; 41:54–60.
Broderick J, Connolly S, Feldmann E, et al; American Heart Association; American Stroke Association Stroke Council; High Blood Pressure Research Council; Quality of Care and Outcomes in Research Interdisciplinary Working Group. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke2007; 38:2001–2023.
Steiner T, Kaste M, Forsting M, et al. Recommendations for the management of intracranial haemorrhage - part I: spontaneous intracerebral haemorrhage. The European Stroke Initiative Writing Committee and the Writing Committee for the EUSI Executive Committee. Cerebrovasc Dis2006; 22:294–316.
Steiner T, Rosand J, Diringer M. Intracerebral hemorrhage associated with oral anticoagulant therapy: current practices and unresolved questions. Stroke2006; 37:256–262.
Goldstein JN, Fazen LE, Wendell L, et al. Risk of thromboembolism following acute intracerebral hemorrhage. Neurocrit Care2009; 10:28–34.
Christensen MC, Dawson J, Vincent C. Risk of thromboembolic complications after intracerebral hemorrhage according to ethnicity. Adv Ther2008; 25:831–841.
Lacut K, Bressollette L, Le Gal G, et al; VICTORIAh (Venous Intermittent Compression and Thrombosis Occurrence Related to Intracerebral Acute hemorrhage) Investigators. Prevention of venous thrombosis in patients with acute intracerebral hemorrhage. Neurology2005; 65:865–869.
Diringer MN, Skolnick BE, Mayer SA, et al. Thromboembolic events with recombinant activated factor VII in spontaneous intracerebral hemorrhage: results from the Factor Seven for Acute Hemorrhagic Stroke (FAST) trial. Stroke2010; 41:48–53.
Boeer A, Voth E, Henze T, Prange HW. Early heparin therapy in patients with spontaneous intracerebral haemorrhage. J Neurol Neurosurg Psychiatry1991; 54:466–467.
Dickmann U, Voth E, Schicha H, Henze T, Prange H, Emrich D. Heparin therapy, deep-vein thrombosis and pulmonary embolism after intracerebral hemorrhage. Klin Wochenschr1988; 66:1182–1183.
Geerts WH, Bergqvist D, Pineo GF, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):381S–453S.
Vermeer SE, Algra A, Franke CL, Koudstaal PJ, Rinkel GJ. Long-term prognosis after recovery from primary intracerebral hemorrhage. Neurology2002; 59:205–209.
Bailey RD, Hart RG, Benavente O, Pearce LA. Recurrent brain hemorrhage is more frequent than ischemic stroke after intracranial hemorrhage. Neurology2001; 56:773–777.
Viswanathan A, Rakich SM, Engel C, et al. Antiplatelet use after intracerebral hemorrhage. Neurology2006; 66:206–209.
Greenberg SM, Eng JA, Ning M, Smith EE, Rosand J. Hemorrhage burden predicts recurrent intracerebral hemorrhage after lobar hemorrhage. Stroke2004; 35:1415–1420.
Lee SH, Ryu WS, Roh JK. Cerebral microbleeds are a risk factor for warfarin-related intracerebral hemorrhage. Neurology2009; 72:171–176.
Ueno H, Naka H, Ohshita T, et al. Association between cerebral microbleeds on T2*-weighted MR images and recurrent hemorrhagic stroke in patients treated with warfarin following ischemic stroke. AJNR Am J Neuroradiol2008; 29:1483–1486.
O’Donnell HC, Rosand J, Knudsen KA, et al. Apolipoprotein E genotype and the risk of recurrent lobar intracerebral hemorrhage. N Engl J Med2000; 342:240–245.
Genes for Cerebral Hemorrhage on Anticoagulation (GOCHA) Collaborative Group. Exploiting common genetic variation to make anticoagulation safer. Stroke2009; 40(suppl 3):S64–S66.
Tzourio C, Arima H, Harrap S, et al. APOE genotype, ethnicity, and the risk of cerebral hemorrhage. Neurology2008; 70:1322–1328.
Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med1998; 105:91–99.
Kuijer PM, Hutten BA, Prins MH, Büller HR. Prediction of the risk of bleeding during anticoagulant treatment for venous thromboembolism. Arch Intern Med1999; 159:457–460.
Wess ML, Schauer DP, Johnston JA, et al. Application of a decision support tool for anticoagulation in patients with non-valvular atrial fibrillation. J Gen Intern Med2008; 23:411–417.
Singer DE, Chang Y, Fang MC, et al. Should patient characteristics influence target anticoagulation intensity for stroke prevention in nonvalvular atrial fibrillation? The ATRIA study. Circ Cardiovasc Qual Outcomes2009; 2:297–304.
Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation. Ann Intern Med2004; 141:745–752.
Singer DE, Chang Y, Fang MC, et al. The net clinical benefit of warfarin anticoagulation in atrial fibrillation. Ann Intern Med2009; 151:297–305.
Eckman MH, Rosand J, Knudsen KA, Singer DE, Greenberg SM. Can patients be anticoagulated after intracerebral hemorrhage? A decision analysis. Stroke2003; 34:1710–1716.
Baruch L, Gage BF, Horrow J, et al. Can patients at elevated risk of stroke treated with anticoagulants be further risk stratified?Stroke2007; 38:2459–2463.
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA2001; 285:2864–2870.
Cannegieter SC, Rosendaal FR, Briët E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation1994; 89:635–641.
Freudenberger RS, Hellkamp AS, Halperin JL, et al; SCD-HeFT Investigators. Risk of thromboembolism in heart failure: an analysis from the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Circulation2007; 115:2637–2641.
Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med1996; 125:1–7.
Claassen DO, Kazemi N, Zubkov AY, Wijdicks EF, Rabinstein AA. Restarting anticoagulation therapy after warfarin-associated intracerebral hemorrhage. Arch Neurol2008; 65:1313–1318.
De Vleeschouwer S, Van Calenbergh F, van Loon J, Nuttin B, Goffin J, Plets C. Risk analysis of thrombo-embolic and recurrent bleeding events in the management of intracranial haemorrhage due to oral anticoagulation. Acta Chir Belg2005; 105:268–274.
Butler AC, Tait RC. Restarting anticoagulation in prosthetic heart valve patients after intracranial haemorrhage: a 2-year follow-up. Br J Haematol1998; 103:1064–1066.
Bertram M, Bonsanto M, Hacke W, Schwab S. Managing the therapeutic dilemma: patients with spontaneous intracerebral hemorrhage and urgent need for anticoagulation. J Neurol2000; 247:209–214.
Taylor FC, Cohen H, Ebrahim S. Systematic review of long term anticoagulation or antiplatelet treatment in patients with nonrheumatic atrial fibrillation. BMJ2001; 322:321–326.
Flaherty ML, Tao H, Haverbusch M, et al. Warfarin use leads to larger intracerebral hematomas. Neurology2008; 71:1084–1089.
Sansing LH, Messe SR, Cucchiara BL, Cohen SN, Lyden PD, Kasner SE; CHANT Investigators. Prior antiplatelet use does not affect hemorrhage growth or outcome after ICH. Neurology2009; 72:1397–1402.
Snow V, Qaseem A, Barry P, et al; American College of Physicians; American Academy of Family Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med2007; 146:204–210.
Albers GW, Amarenco P, Easton JD, Sacco RL, Teal PA; merican College of Chest Physicians. Antithrombotic and thrombolytic therapy for ischemic stroke: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):630S–639S.
Hankey GJ, Eikelboom JW. Antithrombotic drugs for patients with ischaemic stroke and transient ischaemic attack to prevent recurrent major vascular events. Lancet Neurol2010; 9:273–284.
Schulman S, Kearon C, Kakkar AK, et al; RE-COVER Study Group. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med2009; 361:2342–2352.
Schulman S, Wåhlander K, Lundström T, Clason SB, Eriksson H; THRIVE III Investigators. Secondary prevention of venous thromboembolism with the oral direct thrombin inhibitor ximelagatran. N Engl J Med2003; 349:1713–1721.
Singer DE, Albers GW, Dalen JE, et al; American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):546S–592S.
Joshua N. Goldstein, MD, PhD Assistant Professor, Department of Emergency Medicine, Massachusetts General Hospital, Boston, MA
Steven M. Greenberg, MD, PhD Director, Hemorrhagic Stroke Research Program, Department of Neurology, and the Vascular Center, Massachusetts General Hospital, Boston, MA
Address: Joshua N. Goldstein, MD, PhD, Department of Emergency Medicine, Massachusetts General Hospital, Zero Emerson Place, Suite 3B, Boston, MA 02114; e-mail jgoldstein@partners.org
Dr. Goldstein has acted as a consultant and a member of advisory committees or review panels for CSL Behring.
Joshua N. Goldstein, MD, PhD Assistant Professor, Department of Emergency Medicine, Massachusetts General Hospital, Boston, MA
Steven M. Greenberg, MD, PhD Director, Hemorrhagic Stroke Research Program, Department of Neurology, and the Vascular Center, Massachusetts General Hospital, Boston, MA
Address: Joshua N. Goldstein, MD, PhD, Department of Emergency Medicine, Massachusetts General Hospital, Zero Emerson Place, Suite 3B, Boston, MA 02114; e-mail jgoldstein@partners.org
Dr. Goldstein has acted as a consultant and a member of advisory committees or review panels for CSL Behring.
Author and Disclosure Information
Joshua N. Goldstein, MD, PhD Assistant Professor, Department of Emergency Medicine, Massachusetts General Hospital, Boston, MA
Steven M. Greenberg, MD, PhD Director, Hemorrhagic Stroke Research Program, Department of Neurology, and the Vascular Center, Massachusetts General Hospital, Boston, MA
Address: Joshua N. Goldstein, MD, PhD, Department of Emergency Medicine, Massachusetts General Hospital, Zero Emerson Place, Suite 3B, Boston, MA 02114; e-mail jgoldstein@partners.org
Dr. Goldstein has acted as a consultant and a member of advisory committees or review panels for CSL Behring.
If a patient taking warfarin (Coumadin) or other anticoagulant drug suffers an intracerebral hemorrhage (ICH) and survives, the physician faces the dilemma of whether to resume the anticoagulant. On one hand, the drug was prescribed because the patient was at risk of a thromboembolic event such as stroke or pulmonary embolism. On the other hand, warfarin use may increase the risk of another ICH.
Unfortunately, we have little evidence from clinical trials on which to base the decision. Nevertheless, we believe that in selected patients the potential benefit of resuming anticoagulation outweighs the considerable risk.
In the pages that follow, we summarize when and how anticoagulation therapy should be resumed after ICH.
A DEADLY COMPLICATION OF ANTICOAGULANT THERAPY
Intracranial bleeding is the most feared and the most deadly complication of oral anticoagulant therapy.1 The substantial risks associated with oral anticoagulants likely account for these drugs being underprescribed in patients who have indications for them.2–4
While bleeding is the major risk, not all bleeding events are equally damaging. Extracranial bleeding (eg, gastrointestinal bleeding, hematuria, epistaxis) leads to death or disability in only 3% of cases, whereas intracranial bleeding such as ICH leads to death or disability 76% of cases.5
Even without anticoagulation, ICH is the deadliest form of stroke,6–9 and if the patient has been taking warfarin, the risk of disability and death is substantially higher.6,10 Warfarin has a striking effect on the incidence and outcomes of ICH. While the overall incidence of ICH in the general population is approximately 25 per 100,000 person-years, the incidence in patients on warfarin is exponentially higher, at 2 to 3 per 100 per year, and appears to be increasing.11,12 In addition, once ICH occurs, the risk of death is up to twice as high in those on warfarin.6 The bulk of this effect is likely due to a higher risk of ongoing bleeding after the event.10,13–16
Major risk factors for ICH in patients taking oral anticoagulants include a higher international normalized ratio (INR) and older age.11,17
TWO KEY QUESTIONS
Once a patient is diagnosed with warfarin-related ICH, clinicians typically take urgent measures to restore normal coagulation, hoping to limit ongoing bleeding and improve outcome.18,19
The higher the INR at presentation, the greater the risk of death.6 In addition, in retrospective studies, some authors have noted that earlier correction of the INR is associated with better outcome.14,16
While emergency reversal of warfarin is widely considered standard treatment in the acute phase,20–24 concern persists about its safety in patients at high risk of thromboembolism.
Until the results of clinical trials are available, decisions about whether to reverse and when to resume anticoagulation hinge on two questions:
In the acute phase, how does the risk of further bleeding (hematoma expansion) compare with the short-term risk of thromboembolism?
In the chronic phase, how does the risk of recurrent hemorrhage compare with the excess risk of thromboembolism if the patient does not resume anticoagulation therapy?
ACUTELY, THE RISK OF BLEEDING OUTWEIGHS THAT OF CLOTTING
High risk of hematoma expansion after ICH
Unfortunately, continued bleeding is common after ICH. In patients who present within 3 hours of symptom onset, 26% of hematomas expand more than 33% over the first hour, and another 12% expand this amount over the next 20 hours.6 In warfarin-associated ICH, up to 50% of patients develop this level of hematoma expansion, but it appears to take place over a more prolonged period of time.10,13–16 Over 70% of patients presenting acutely develop at least some amount of expansion within 24 hours.25 Therefore, the risk of hematoma expansion in the first 24 hours is likely so high that patients cannot safely receive anticoagulants during this time frame.
But not all patients are at equal risk of hematoma expansion. Several features are associated with higher risk (Table 1)10,26–40:
A large hematoma volume on presentation is a significant predictor of expansion, possibly reflecting a more severe underlying insult.26,27
Early presentation, especially within 3 hours of symptom onset, also appears to mark those at higher risk, presumably because such patients undergo computed tomography (CT) while still bleeding.26,27
Figure 1. The “spot sign” (arrow), contrast extravasation after contrast-enhanced computed tomography, is associated with a high risk of hematoma expansion.For those on warfarin, a higher INR is a significant predictor, not just of higher risk, but also of a more delayed expansion.10,28
Certain radiographic findings indicate higher risk. One is the “spot sign,” ie, contrast extravasation after contrast-enhanced CT27,29–31 (Figure 1). Apparently, the more spots present, and the denser the contrast, the greater the risk, an observation that has led to a proposed “spot-sign score” that may predict both expansion and poor outcome. 32,41
Given the high risk of hematoma expansion in the early phase, and given our inability to predict hematoma expansion, most authorities recommend immediate reversal of anticoagulation after diagnosis.42–44 Reversal of anticoagulation typically includes intravenous vitamin K, which begins to act within several hours, and repletion of coagulation factors, which act within minutes (prothrombin complex concentrates and recombinant factor VIIa [NovoSeven]) or a few hours (fresh frozen plasma).1
Dosages:
Vitamin K 5 to 10 mg intravenously
Prothrombin complex concentrates 10 to 50 U/kg
Recombinant factor VIIa 40 to 80 μg/kg
Fresh frozen plasma 10 to 50 U/kg.
Risk of thromboembolism after ICH: Ongoing and cumulative
Thromboembolism after ICH is a major concern, for two main reasons.
First, patients on oral anticoagulation typically have a preexisting risk factor and are thus at higher risk of a thromboembolic event, particularly while they are off anticoagulation. Patients with atrial fibrillation or a mechanical valve are at risk of arterial events such as ischemic stroke, whereas patients with a known venous thromboembolic condition such as deep venous thrombosis or pulmonary embolism are at risk of extension of the thrombosis or recurrence of a venous thrombotic event.
Second, ICH itself increases the risk of arterial and venous thromboembolic events. Including patients not previously on anticoagulation, this risk is as high as 7% during the initial hospitalization and 9% during the first 90 days.45,46 Worth noting is that patients who previously received anticoagulant drugs (and who are off this therapy in the acute phase) are at no higher risk of thromboembolism compared with those who never received anticoagulants.45
However, while the risk of hematoma expansion is highest at presentation and then decreases with time, the risk of thromboembolism (particularly venous thromboembolism) is ongoing and cumulative. Arterial thromboembolism is more likely to occur early, within the first week, whereas venous thromboembolism can occur later.45
Overall, studies have estimated the short-term risk of pulmonary embolism to be 1% to 2%, deep venous thrombosis 1% to 4%, myocardial ischemia about 2%, and cerebral ischemia 2% to 3%.45,46 However, when patients are actively screened, the incidence of asymptomatic deep venous thrombosis is found to be as high as 16% in the first 10 days,47 and evidence of myocardial ischemia can be detected in up to 27% of patients.48
Therefore, the risk of hematoma expansion appears to be high and the risk of thromboembolism appears to be low during the first day after ICH. Over the next days, as the risk of hematoma expansion recedes, this ratio shifts.
Studies of in-hospital anticoagulation after ICH
The data on restarting oral anticoagulation in the acute phase are sparse. In practice, clinicians typically start heparinoids in low subcutaneous doses to prevent deep venous thrombosis and, after the first few days or a week, consider increasing to a full anticoagulation dose or starting an oral anticoagulant and subsequently discontinuing the heparin when the INR is in the therapeutic range (see discussion below).
ICH patients in general may benefit from starting prophylactic-dose heparin therapy early. One randomized trial found that starting heparin in a low subcutaneous dose the day after an ICH decreased the risk of thromboembolism without increasing the risk of rebleeding.49 Another study also found no increased risk of rebleeding with early prophylactic-dose subcutaneous heparin.50
As the benefit appears to outweigh the risk, national guidelines suggest starting subcutaneous heparin early in all ICH patients, including those not previously on warfarin.42,43
Commonly used heparinoid regimens include unfractionated heparin 5,000 units subcutaneously twice a day; enoxaparin (Lovenox) 40 mg once a day; and dalteparin (Fragmin) 5,000 units once a day.51 In addition, all patients should receive optimal mechanical thromboprophylaxis, including graduated compression stockings or intermittent pneumatic compression stockings, or both.
LONG-TERM MANAGEMENT: ICH RECURRENCE VS THROMBOEMBOLISM
Risk of ICH recurrence on warfarin is not precisely known
Overall, the risk of ICH recurrence is about 1% at 3 months, and warfarin likely increases this risk.42,52 Unfortunately, the risk of ICH recurrence in patients on anticoagulation therapy after a first ICH is not clear, and no population-based study has clarified this risk. Therefore, the best we can do at present is to try to estimate the risk of recurrent warfarin-related ICH by separately examining two issues:
The risk of ICH recurrence in general
The risk of major bleeding (including ICH) in the general population of patients on warfarin.
The risk of ICH recurrence in general is about 2% to 4% per patient-year.52–54 However, this risk appears to be a function of the underlying vasculopathy. ICH location is often used as a surrogate for underlying cause. Most ICHs in deep hemispheric (basal ganglia, thalamus) or brainstem territories are likely caused by hypertensive vasculopathy, whereas lobar ICH is often associated with cerebral amyloid angiopathy.52–54 Presumably because of this distinction, ICH in a deep location recurs in about 2% of cases per year, compared with 4% for lobar ICH.53 The presence and number of microbleeds on T2-weighted gradient-echo magnetic resonance imaging appear to predict ICH recurrence; microbleeds likely are markers of more severe or widespread underlying vasculopathy.55–57
A genetic risk factor for the recurrence of lobar ICH is apolipoprotein E genotype58; future studies may highlight genetic variations that specifically modify the risk of warfarin-related ICH.59 Unfortunately, there is currently no way to modify the risk of ICH associated with cerebral amyloid angiopathy. On the other hand, in patients with hypertensive hemorrhage, antihypertensive therapy likely reduces the risk of recurrent ICH. One randomized controlled trial showed that such therapy decreased the risk of ICH by more than half.60
The risk of major bleeding in the general population of patients on warfarin may be 2% to 3% per year and is likely higher in the first month.11 The risk is higher in older patients and if the INR rises above 4.0.11,17 For some patients, it is possible to estimate the likelihood of major bleeding using validated decision-support tools that include factors such as age, sex, and medical history.11,61–64
Given the lack of data specifically addressing the risk of ICH recurrence on warfarin, the clinician is left to try to extrapolate this risk from available data using specific patient characteristics that modify the presumed risk. For example, one can combine factors such as ICH location (or better yet, the underlying cause) with decision-support tools that predict the risk of major bleeding. Close control of both blood pressure and the INR appears especially critical for patients receiving anticoagulation after ICH.11,60,65 Still, the risk does not disappear with good INR control, and most patients with anticoagulation-related ICH present with INRs within the therapeutic range.5,10,65
Long-term risk of thromboembolism depends on underlying condition
In the long term, the risk of thromboembolism depends on the reason for which the patient was originally given anticoagulation. In addition, many patients with ICH suffer decreased mobility and are therefore at higher risk of venous thromboembolism than before their event.
Nonvalvular atrial fibrillation is the most common indication for anticoagulation. For these patients, the risk of ischemic stroke is 2% to 5% per year.66,67 The system usually used to stratify this risk is CHADS2, an acronym for five key risk factors:
Congestive heart failure (1 point)
Hypertension (1 point)
Age over 75 (1 point)
Diabetes mellitus (1 point)
Prior stroke or transient ischemic attack (2 points).
The annual risk of stroke ranges from 1.9% (score of 0) to 18.2% (score of 6).68,69 In patients with nonvalvular atrial fibrillation, the excess risk of ischemic stroke without anticoagulation must be weighed against the risk of ICH recurrence.
A mechanical heart valve, another common indication, carries a risk of ischemic stroke of about 4% per year.70 A mechanical valve is traditionally considered an absolute indication for anticoagulation. However, patients with lobar ICH face a risk of recurrence that is greater than 4% per year, and so the risks of resuming anticoagulation may well outweigh the benefits.
Heart failure may be associated with a risk of ischemic stroke of 1% to 4% per year, and this is likely a function of disease severity.71
Venous thromboembolism. The risk of recurrent venous thromboembolism in patients with deep venous thrombosis or pulmonary embolism is around 4% per year.72 Given that ICH itself confers a 2% to 3% risk of these conditions, the rate of recurrence of deep venous thrombosis may well be much higher in those ICH patients who have also already had deep venous thrombosis.
Data on resuming oral anticoagulation after ICH
Several studies have examined the outcomes when oral anticoagulants were resumed after ICH (Table 2),73–76 but experts differ on when these drugs should be resumed (eg, between 1 and 10 days after onset), or even whether they should be resumed at all.19
Notably, an analysis of 52 patients found a high risk of ICH recurrence (and gastrointestinal bleeding) in patients who restarted warfarin, and a high risk of myocardial infarction and ischemic stroke in those who did not restart, with neither strategy demonstrating a clear benefit in the rate of death or disability.73 All patients with a thromboembolic event were being treated for a previous event, suggesting that secondary prevention is a stronger indication for anticoagulation than primary prevention in this population.73
IF AND WHEN TO RESTART
Two major questions to consider are whether the benefits of restarting anticoagulation outweigh the risk, and if so, when and how should anticoagulation be restarted?
Whether to restart anticoagulation
As for the risk-benefit ratio, many think that anticoagulation should be restarted only with extreme caution and possibly only in those with deep ICH or a documented history of thromboembolism.19
In one decision analysis examining whether to restart anticoagulation after ICH in patients with atrial fibrillation, the risk of thromboembolism would need to exceed 7% per year to justify restarting anticoagulation after deep ICH,67 and no risk level was high enough to justify restarting anticoagulation after lobar ICH.
For patients at sufficiently high risk of ICH recurrence, antiplatelet treatment is probably safer, as antiplatelet agents carry a substantially lower risk of bleeding.54,77–79 The American Heart Association comments that for nonvalvular atrial fibrillation, long-term anticoagulation should be avoided after spontaneous lobar ICH, but that antiplatelet agents may be considered. 42 They note that anticoagulation after nonlobar ICH may be considered depending on the indication.42
The decision to restart anticoagulation may also be a function of whether the underlying risk factor is a temporary one. For example, atrial fibrillation or a mechanical heart valve confers a long-term, ongoing risk of arterial thromboembolism, and such patients would not normally be considered for a short course of warfarin therapy. However, isolated deep vein thrombosis may only require anticoagulation for a limited time, such as 3 to 6 months.80 Perhaps for such patients the long-term outcome is maximized with a narrowly defined, temporary course of anticoagulation.
When to restart anticoagulation
As for when to restart, it is not certain how long after symptom onset the risk of ongoing bleeding continues. Clearly, the risk is high on the first day, but small after the first few days.
The European Stroke Initiative recommends that patients with a strong indication for anticoagulation, such as a history of embolic stroke with atrial fibrillation, should be restarted on warfarin after 10 to 14 days, depending on the risk of thromboembolism and ICH recurrence.43
The American Heart Association suggests that, in patients with a very high risk of thromboembolism for whom restarting warfarin is considered, warfarin may be restarted 7 to 10 days after ICH onset.42
The American College of Chest Physicians recommends starting prophylactic-dose heparin the day after an ICH, with no clear guidance on restarting warfarin.81
ALTERNATIVES TO WARFARIN
Alternatives to warfarin that show promise in reducing bleeding risk include factor Xa and direct thrombin inhibitors, which may reduce the risk of thromboembolism to an extent similar to that of warfarin, but with fewer bleeding complications.82
In patients with atrial fibrillation, the direct thrombin inhibitor dabigatran (Pradaxa) was shown to prevent ischemic stroke to a similar or greater degree than warfarin, with fewer bleeding complications.83 Further patient follow-up is under way to ensure that this drug does not cause liver problems, as did a similarly designed predecessor.84
The availability of this and other agents in various stages of development82 will probably not make warfarin extinct. Rather, they may change the “tipping point,” the threshold at which the risk of thromboembolism is high enough to justify the risks associated with restarting warfarin therapy. In addition, clinical decision tools clarifying the individual patient’s risk of thromboembolism vs the risk of ICH recurrence will help physicians tailor the therapy to the patient.
For the moment, in situations in which the decision is difficult, maximizing the use of antiplatelet agents offers the best hope.85
RECOMMENDATIONS IN LIEU OF GUIDELINES
No guideline can broadly cover every clinical scenario. Many factors go into assessing a patient’s risk of hematoma expansion or recurrent hemorrhage (Table 3) and the extent to which anticoagulation can reduce the risk of thromboembolism.
In the short term, most patients with ICH will likely benefit from acute reversal of anticoagulation, followed by gradual reinstitution of prophylactic-dose anticoagulation after the first 24 to 72 hours.
In the long term, many patients with lobar hemorrhage, cerebral amyloid angiopathy, or other risk factors may remain at higher risk of anticoagulant-related ICH recurrence than of fatal or disabling thromboembolic events and would therefore be best managed without anticoagulants. Conversely, those with deep hemispheric ICH, hypertension that can be well controlled, and a high risk of disabling thromboembolism may receive a net benefit from restarting anticoagulation.
If a patient taking warfarin (Coumadin) or other anticoagulant drug suffers an intracerebral hemorrhage (ICH) and survives, the physician faces the dilemma of whether to resume the anticoagulant. On one hand, the drug was prescribed because the patient was at risk of a thromboembolic event such as stroke or pulmonary embolism. On the other hand, warfarin use may increase the risk of another ICH.
Unfortunately, we have little evidence from clinical trials on which to base the decision. Nevertheless, we believe that in selected patients the potential benefit of resuming anticoagulation outweighs the considerable risk.
In the pages that follow, we summarize when and how anticoagulation therapy should be resumed after ICH.
A DEADLY COMPLICATION OF ANTICOAGULANT THERAPY
Intracranial bleeding is the most feared and the most deadly complication of oral anticoagulant therapy.1 The substantial risks associated with oral anticoagulants likely account for these drugs being underprescribed in patients who have indications for them.2–4
While bleeding is the major risk, not all bleeding events are equally damaging. Extracranial bleeding (eg, gastrointestinal bleeding, hematuria, epistaxis) leads to death or disability in only 3% of cases, whereas intracranial bleeding such as ICH leads to death or disability 76% of cases.5
Even without anticoagulation, ICH is the deadliest form of stroke,6–9 and if the patient has been taking warfarin, the risk of disability and death is substantially higher.6,10 Warfarin has a striking effect on the incidence and outcomes of ICH. While the overall incidence of ICH in the general population is approximately 25 per 100,000 person-years, the incidence in patients on warfarin is exponentially higher, at 2 to 3 per 100 per year, and appears to be increasing.11,12 In addition, once ICH occurs, the risk of death is up to twice as high in those on warfarin.6 The bulk of this effect is likely due to a higher risk of ongoing bleeding after the event.10,13–16
Major risk factors for ICH in patients taking oral anticoagulants include a higher international normalized ratio (INR) and older age.11,17
TWO KEY QUESTIONS
Once a patient is diagnosed with warfarin-related ICH, clinicians typically take urgent measures to restore normal coagulation, hoping to limit ongoing bleeding and improve outcome.18,19
The higher the INR at presentation, the greater the risk of death.6 In addition, in retrospective studies, some authors have noted that earlier correction of the INR is associated with better outcome.14,16
While emergency reversal of warfarin is widely considered standard treatment in the acute phase,20–24 concern persists about its safety in patients at high risk of thromboembolism.
Until the results of clinical trials are available, decisions about whether to reverse and when to resume anticoagulation hinge on two questions:
In the acute phase, how does the risk of further bleeding (hematoma expansion) compare with the short-term risk of thromboembolism?
In the chronic phase, how does the risk of recurrent hemorrhage compare with the excess risk of thromboembolism if the patient does not resume anticoagulation therapy?
ACUTELY, THE RISK OF BLEEDING OUTWEIGHS THAT OF CLOTTING
High risk of hematoma expansion after ICH
Unfortunately, continued bleeding is common after ICH. In patients who present within 3 hours of symptom onset, 26% of hematomas expand more than 33% over the first hour, and another 12% expand this amount over the next 20 hours.6 In warfarin-associated ICH, up to 50% of patients develop this level of hematoma expansion, but it appears to take place over a more prolonged period of time.10,13–16 Over 70% of patients presenting acutely develop at least some amount of expansion within 24 hours.25 Therefore, the risk of hematoma expansion in the first 24 hours is likely so high that patients cannot safely receive anticoagulants during this time frame.
But not all patients are at equal risk of hematoma expansion. Several features are associated with higher risk (Table 1)10,26–40:
A large hematoma volume on presentation is a significant predictor of expansion, possibly reflecting a more severe underlying insult.26,27
Early presentation, especially within 3 hours of symptom onset, also appears to mark those at higher risk, presumably because such patients undergo computed tomography (CT) while still bleeding.26,27
Figure 1. The “spot sign” (arrow), contrast extravasation after contrast-enhanced computed tomography, is associated with a high risk of hematoma expansion.For those on warfarin, a higher INR is a significant predictor, not just of higher risk, but also of a more delayed expansion.10,28
Certain radiographic findings indicate higher risk. One is the “spot sign,” ie, contrast extravasation after contrast-enhanced CT27,29–31 (Figure 1). Apparently, the more spots present, and the denser the contrast, the greater the risk, an observation that has led to a proposed “spot-sign score” that may predict both expansion and poor outcome. 32,41
Given the high risk of hematoma expansion in the early phase, and given our inability to predict hematoma expansion, most authorities recommend immediate reversal of anticoagulation after diagnosis.42–44 Reversal of anticoagulation typically includes intravenous vitamin K, which begins to act within several hours, and repletion of coagulation factors, which act within minutes (prothrombin complex concentrates and recombinant factor VIIa [NovoSeven]) or a few hours (fresh frozen plasma).1
Dosages:
Vitamin K 5 to 10 mg intravenously
Prothrombin complex concentrates 10 to 50 U/kg
Recombinant factor VIIa 40 to 80 μg/kg
Fresh frozen plasma 10 to 50 U/kg.
Risk of thromboembolism after ICH: Ongoing and cumulative
Thromboembolism after ICH is a major concern, for two main reasons.
First, patients on oral anticoagulation typically have a preexisting risk factor and are thus at higher risk of a thromboembolic event, particularly while they are off anticoagulation. Patients with atrial fibrillation or a mechanical valve are at risk of arterial events such as ischemic stroke, whereas patients with a known venous thromboembolic condition such as deep venous thrombosis or pulmonary embolism are at risk of extension of the thrombosis or recurrence of a venous thrombotic event.
Second, ICH itself increases the risk of arterial and venous thromboembolic events. Including patients not previously on anticoagulation, this risk is as high as 7% during the initial hospitalization and 9% during the first 90 days.45,46 Worth noting is that patients who previously received anticoagulant drugs (and who are off this therapy in the acute phase) are at no higher risk of thromboembolism compared with those who never received anticoagulants.45
However, while the risk of hematoma expansion is highest at presentation and then decreases with time, the risk of thromboembolism (particularly venous thromboembolism) is ongoing and cumulative. Arterial thromboembolism is more likely to occur early, within the first week, whereas venous thromboembolism can occur later.45
Overall, studies have estimated the short-term risk of pulmonary embolism to be 1% to 2%, deep venous thrombosis 1% to 4%, myocardial ischemia about 2%, and cerebral ischemia 2% to 3%.45,46 However, when patients are actively screened, the incidence of asymptomatic deep venous thrombosis is found to be as high as 16% in the first 10 days,47 and evidence of myocardial ischemia can be detected in up to 27% of patients.48
Therefore, the risk of hematoma expansion appears to be high and the risk of thromboembolism appears to be low during the first day after ICH. Over the next days, as the risk of hematoma expansion recedes, this ratio shifts.
Studies of in-hospital anticoagulation after ICH
The data on restarting oral anticoagulation in the acute phase are sparse. In practice, clinicians typically start heparinoids in low subcutaneous doses to prevent deep venous thrombosis and, after the first few days or a week, consider increasing to a full anticoagulation dose or starting an oral anticoagulant and subsequently discontinuing the heparin when the INR is in the therapeutic range (see discussion below).
ICH patients in general may benefit from starting prophylactic-dose heparin therapy early. One randomized trial found that starting heparin in a low subcutaneous dose the day after an ICH decreased the risk of thromboembolism without increasing the risk of rebleeding.49 Another study also found no increased risk of rebleeding with early prophylactic-dose subcutaneous heparin.50
As the benefit appears to outweigh the risk, national guidelines suggest starting subcutaneous heparin early in all ICH patients, including those not previously on warfarin.42,43
Commonly used heparinoid regimens include unfractionated heparin 5,000 units subcutaneously twice a day; enoxaparin (Lovenox) 40 mg once a day; and dalteparin (Fragmin) 5,000 units once a day.51 In addition, all patients should receive optimal mechanical thromboprophylaxis, including graduated compression stockings or intermittent pneumatic compression stockings, or both.
LONG-TERM MANAGEMENT: ICH RECURRENCE VS THROMBOEMBOLISM
Risk of ICH recurrence on warfarin is not precisely known
Overall, the risk of ICH recurrence is about 1% at 3 months, and warfarin likely increases this risk.42,52 Unfortunately, the risk of ICH recurrence in patients on anticoagulation therapy after a first ICH is not clear, and no population-based study has clarified this risk. Therefore, the best we can do at present is to try to estimate the risk of recurrent warfarin-related ICH by separately examining two issues:
The risk of ICH recurrence in general
The risk of major bleeding (including ICH) in the general population of patients on warfarin.
The risk of ICH recurrence in general is about 2% to 4% per patient-year.52–54 However, this risk appears to be a function of the underlying vasculopathy. ICH location is often used as a surrogate for underlying cause. Most ICHs in deep hemispheric (basal ganglia, thalamus) or brainstem territories are likely caused by hypertensive vasculopathy, whereas lobar ICH is often associated with cerebral amyloid angiopathy.52–54 Presumably because of this distinction, ICH in a deep location recurs in about 2% of cases per year, compared with 4% for lobar ICH.53 The presence and number of microbleeds on T2-weighted gradient-echo magnetic resonance imaging appear to predict ICH recurrence; microbleeds likely are markers of more severe or widespread underlying vasculopathy.55–57
A genetic risk factor for the recurrence of lobar ICH is apolipoprotein E genotype58; future studies may highlight genetic variations that specifically modify the risk of warfarin-related ICH.59 Unfortunately, there is currently no way to modify the risk of ICH associated with cerebral amyloid angiopathy. On the other hand, in patients with hypertensive hemorrhage, antihypertensive therapy likely reduces the risk of recurrent ICH. One randomized controlled trial showed that such therapy decreased the risk of ICH by more than half.60
The risk of major bleeding in the general population of patients on warfarin may be 2% to 3% per year and is likely higher in the first month.11 The risk is higher in older patients and if the INR rises above 4.0.11,17 For some patients, it is possible to estimate the likelihood of major bleeding using validated decision-support tools that include factors such as age, sex, and medical history.11,61–64
Given the lack of data specifically addressing the risk of ICH recurrence on warfarin, the clinician is left to try to extrapolate this risk from available data using specific patient characteristics that modify the presumed risk. For example, one can combine factors such as ICH location (or better yet, the underlying cause) with decision-support tools that predict the risk of major bleeding. Close control of both blood pressure and the INR appears especially critical for patients receiving anticoagulation after ICH.11,60,65 Still, the risk does not disappear with good INR control, and most patients with anticoagulation-related ICH present with INRs within the therapeutic range.5,10,65
Long-term risk of thromboembolism depends on underlying condition
In the long term, the risk of thromboembolism depends on the reason for which the patient was originally given anticoagulation. In addition, many patients with ICH suffer decreased mobility and are therefore at higher risk of venous thromboembolism than before their event.
Nonvalvular atrial fibrillation is the most common indication for anticoagulation. For these patients, the risk of ischemic stroke is 2% to 5% per year.66,67 The system usually used to stratify this risk is CHADS2, an acronym for five key risk factors:
Congestive heart failure (1 point)
Hypertension (1 point)
Age over 75 (1 point)
Diabetes mellitus (1 point)
Prior stroke or transient ischemic attack (2 points).
The annual risk of stroke ranges from 1.9% (score of 0) to 18.2% (score of 6).68,69 In patients with nonvalvular atrial fibrillation, the excess risk of ischemic stroke without anticoagulation must be weighed against the risk of ICH recurrence.
A mechanical heart valve, another common indication, carries a risk of ischemic stroke of about 4% per year.70 A mechanical valve is traditionally considered an absolute indication for anticoagulation. However, patients with lobar ICH face a risk of recurrence that is greater than 4% per year, and so the risks of resuming anticoagulation may well outweigh the benefits.
Heart failure may be associated with a risk of ischemic stroke of 1% to 4% per year, and this is likely a function of disease severity.71
Venous thromboembolism. The risk of recurrent venous thromboembolism in patients with deep venous thrombosis or pulmonary embolism is around 4% per year.72 Given that ICH itself confers a 2% to 3% risk of these conditions, the rate of recurrence of deep venous thrombosis may well be much higher in those ICH patients who have also already had deep venous thrombosis.
Data on resuming oral anticoagulation after ICH
Several studies have examined the outcomes when oral anticoagulants were resumed after ICH (Table 2),73–76 but experts differ on when these drugs should be resumed (eg, between 1 and 10 days after onset), or even whether they should be resumed at all.19
Notably, an analysis of 52 patients found a high risk of ICH recurrence (and gastrointestinal bleeding) in patients who restarted warfarin, and a high risk of myocardial infarction and ischemic stroke in those who did not restart, with neither strategy demonstrating a clear benefit in the rate of death or disability.73 All patients with a thromboembolic event were being treated for a previous event, suggesting that secondary prevention is a stronger indication for anticoagulation than primary prevention in this population.73
IF AND WHEN TO RESTART
Two major questions to consider are whether the benefits of restarting anticoagulation outweigh the risk, and if so, when and how should anticoagulation be restarted?
Whether to restart anticoagulation
As for the risk-benefit ratio, many think that anticoagulation should be restarted only with extreme caution and possibly only in those with deep ICH or a documented history of thromboembolism.19
In one decision analysis examining whether to restart anticoagulation after ICH in patients with atrial fibrillation, the risk of thromboembolism would need to exceed 7% per year to justify restarting anticoagulation after deep ICH,67 and no risk level was high enough to justify restarting anticoagulation after lobar ICH.
For patients at sufficiently high risk of ICH recurrence, antiplatelet treatment is probably safer, as antiplatelet agents carry a substantially lower risk of bleeding.54,77–79 The American Heart Association comments that for nonvalvular atrial fibrillation, long-term anticoagulation should be avoided after spontaneous lobar ICH, but that antiplatelet agents may be considered. 42 They note that anticoagulation after nonlobar ICH may be considered depending on the indication.42
The decision to restart anticoagulation may also be a function of whether the underlying risk factor is a temporary one. For example, atrial fibrillation or a mechanical heart valve confers a long-term, ongoing risk of arterial thromboembolism, and such patients would not normally be considered for a short course of warfarin therapy. However, isolated deep vein thrombosis may only require anticoagulation for a limited time, such as 3 to 6 months.80 Perhaps for such patients the long-term outcome is maximized with a narrowly defined, temporary course of anticoagulation.
When to restart anticoagulation
As for when to restart, it is not certain how long after symptom onset the risk of ongoing bleeding continues. Clearly, the risk is high on the first day, but small after the first few days.
The European Stroke Initiative recommends that patients with a strong indication for anticoagulation, such as a history of embolic stroke with atrial fibrillation, should be restarted on warfarin after 10 to 14 days, depending on the risk of thromboembolism and ICH recurrence.43
The American Heart Association suggests that, in patients with a very high risk of thromboembolism for whom restarting warfarin is considered, warfarin may be restarted 7 to 10 days after ICH onset.42
The American College of Chest Physicians recommends starting prophylactic-dose heparin the day after an ICH, with no clear guidance on restarting warfarin.81
ALTERNATIVES TO WARFARIN
Alternatives to warfarin that show promise in reducing bleeding risk include factor Xa and direct thrombin inhibitors, which may reduce the risk of thromboembolism to an extent similar to that of warfarin, but with fewer bleeding complications.82
In patients with atrial fibrillation, the direct thrombin inhibitor dabigatran (Pradaxa) was shown to prevent ischemic stroke to a similar or greater degree than warfarin, with fewer bleeding complications.83 Further patient follow-up is under way to ensure that this drug does not cause liver problems, as did a similarly designed predecessor.84
The availability of this and other agents in various stages of development82 will probably not make warfarin extinct. Rather, they may change the “tipping point,” the threshold at which the risk of thromboembolism is high enough to justify the risks associated with restarting warfarin therapy. In addition, clinical decision tools clarifying the individual patient’s risk of thromboembolism vs the risk of ICH recurrence will help physicians tailor the therapy to the patient.
For the moment, in situations in which the decision is difficult, maximizing the use of antiplatelet agents offers the best hope.85
RECOMMENDATIONS IN LIEU OF GUIDELINES
No guideline can broadly cover every clinical scenario. Many factors go into assessing a patient’s risk of hematoma expansion or recurrent hemorrhage (Table 3) and the extent to which anticoagulation can reduce the risk of thromboembolism.
In the short term, most patients with ICH will likely benefit from acute reversal of anticoagulation, followed by gradual reinstitution of prophylactic-dose anticoagulation after the first 24 to 72 hours.
In the long term, many patients with lobar hemorrhage, cerebral amyloid angiopathy, or other risk factors may remain at higher risk of anticoagulant-related ICH recurrence than of fatal or disabling thromboembolic events and would therefore be best managed without anticoagulants. Conversely, those with deep hemispheric ICH, hypertension that can be well controlled, and a high risk of disabling thromboembolism may receive a net benefit from restarting anticoagulation.
Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med2007; 167:1414–1419.
Choudhry NK, Anderson GM, Laupacis A, Ross-Degnan D, Normand SL, Soumerai SB. Impact of adverse events on prescribing warfarin in patients with atrial fibrillation: matched pair analysis. BMJ2006; 332:141–145.
Choudhry NK, Soumerai SB, Normand SL, Ross-Degnan D, Laupacis A, Anderson GM. Warfarin prescribing in atrial fibrillation: the impact of physician, patient, and hospital characteristics. Am J Med2006; 119:607–615.
Fang MC, Go AS, Chang Y, et al. Death and disability from warfarin-associated intracranial and extracranial hemorrhages. Am J Med2007; 120:700–705.
Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med2004; 164:880–884.
Dixon AA, Holness RO, Howes WJ, Garner JB. Spontaneous intracerebral haemorrhage: an analysis of factors affecting prognosis. Can J Neurol Sci1985; 12:267–271.
Broderick JP, Adams HP, Barsan W, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke1999; 30:905–915.
Flibotte JJ, Hagan N, O’Donnell J, Greenberg SM, Rosand J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology2004; 63:1059–1064.
Schulman S, Beyth RJ, Kearon C, Levine MN; American College of Chest Physicians. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):257S–298S.
Flaherty ML, Kissela B, Woo D, et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology2007; 68:116–121.
Lee SB, Manno EM, Layton KF, Wijdicks EF. Progression of warfarin-associated intracerebral hemorrhage after INR normalization with FFP. Neurology2006; 67:1272–1274.
Huttner HB, Schellinger PD, Hartmann M, et al. Hematoma growth and outcome in treated neurocritical care patients with intracerebral hemorrhage related to oral anticoagulant therapy: comparison of acute treatment strategies using vitamin K, fresh frozen plasma, and prothrombin complex concentrates. Stroke2006; 37:1465–1470.
Sjöblom L, Hårdemark HG, Lindgren A, et al. Management and prognostic features of intracerebral hemorrhage during anticoagulant therapy: a Swedish multicenter study. Stroke2001; 32:2567–2574.
Yasaka M, Minematsu K, Naritomi H, Sakata T, Yamaguchi T. Predisposing factors for enlargement of intracerebral hemorrhage in patients treated with warfarin. Thromb Haemost2003; 89:278–283.
Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation2007; 115:2689–2696.
Goldstein JN, Thomas SH, Frontiero V, et al. Timing of fresh frozen plasma administration and rapid correction of coagulopathy in warfarin-related intracerebral hemorrhage. Stroke2006; 37:151–155.
Aguilar MI, Hart RG, Kase CS, et al. Treatment of warfarin-associated intracerebral hemorrhage: literature review and expert opinion. Mayo Clin Proc2007; 82:82–92.
Guidelines on oral anticoagulation: third edition. Br J Haematol1998; 101:374–387.
Baglin TP, Keeling DM, Watson HG; British Committee for Standards in Haematology. Guidelines on oral anticoagulation (warfarin): third edition—2005 update. Br J Haematol2006; 132:277–285.
O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al; British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol2004; 126:11–28.
Baker RI, Coughlin PB, Gallus AS, Harper PL, Salem HH, Wood EM; Warfarin Reversal Consensus Group. Warfarin reversal: consensus guidelines, on behalf of the Australasian Society of Thrombosis and Haemostasis. Med J Aust2004; 181:492–497.
Davis SM, Broderick J, Hennerici M, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology2006; 66:1175–1181.
Broderick JP, Diringer MN, Hill MD, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Determinants of intracerebral hemorrhage growth: an exploratory analysis. Stroke2007; 38:1072–1075.
Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology2007; 68:889–894.
Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of spontaneous intracerebral hemorrhage. Incidence and time course. Stroke1996; 27:1783–1787.
Kim J, Smith A, Hemphill JC, et al. Contrast extravasation on CT predicts mortality in primary intracerebral hemorrhage. AJNR Am J Neuroradiol2008; 29:520–525.
Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebral hemorrhage. Stroke2007; 38:1257–1262.
Barras CD, Tress BM, Christensen S, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Density and shape as CT predictors of intracerebral hemorrhage growth. Stroke2009; 40:1325–1331.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. Systematic characterization of the computed tomography angiography spot sign in primary intracerebral hemorrhage identifies patients at highest risk for hematoma expansion: the spot sign score. Stroke2009; 40:2994–3000.
Fujii Y, Takeuchi S, Sasaki O, Minakawa T, Tanaka R. Multivariate analysis of predictors of hematoma enlargement in spontaneous intracerebral hemorrhage. Stroke1998; 29:1160–1166.
Ederies A, Demchuk A, Chia T, et al. Postcontrast CT extravasation is associated with hematoma expansion in CTA spot negative patients. Stroke2009; 40:1672–1676.
Delgado P, Alvarez-Sabín J, Abilleira S, et al. Plasma d-dimer predicts poor outcome after acute intracerebral hemorrhage. Neurology2006; 67:94–98.
Naidech AM, Jovanovic B, Liebling S, et al. Reduced platelet activity is associated with early clot growth and worse 3-month outcome after intracerebral hemorrhage. Stroke2009; 40:2398–2401.
Silva Y, Leira R, Tejada J, Lainez JM, Castillo J, Dávalos A; Stroke Project, Cerebrovascular Diseases Group of the Spanish Neurological Society. Molecular signatures of vascular injury are associated with early growth of intracerebral hemorrhage. Stroke2005; 36:86–91.
Sansing LH, Messe SR, Cucchiara BL, Cohen SN, Lyden PD, Kasner SE; CHANT Investigators. Prior antiplatelet use does not affect hemorrhage growth or outcome after ICH. Neurology2009; 72:1397–1402.
Moussouttas M, Malhotra R, Fernandez L, et al. Role of antiplatelet agents in hematoma expansion during the acute period of intracerebral hemorrhage. Neurocrit Care2010; 12:24–29.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. The spot sign score in primary intracerebral hemorrhage identifies patients at highest risk of in-hospital mortality and poor outcome among survivors. Stroke2010; 41:54–60.
Broderick J, Connolly S, Feldmann E, et al; American Heart Association; American Stroke Association Stroke Council; High Blood Pressure Research Council; Quality of Care and Outcomes in Research Interdisciplinary Working Group. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke2007; 38:2001–2023.
Steiner T, Kaste M, Forsting M, et al. Recommendations for the management of intracranial haemorrhage - part I: spontaneous intracerebral haemorrhage. The European Stroke Initiative Writing Committee and the Writing Committee for the EUSI Executive Committee. Cerebrovasc Dis2006; 22:294–316.
Steiner T, Rosand J, Diringer M. Intracerebral hemorrhage associated with oral anticoagulant therapy: current practices and unresolved questions. Stroke2006; 37:256–262.
Goldstein JN, Fazen LE, Wendell L, et al. Risk of thromboembolism following acute intracerebral hemorrhage. Neurocrit Care2009; 10:28–34.
Christensen MC, Dawson J, Vincent C. Risk of thromboembolic complications after intracerebral hemorrhage according to ethnicity. Adv Ther2008; 25:831–841.
Lacut K, Bressollette L, Le Gal G, et al; VICTORIAh (Venous Intermittent Compression and Thrombosis Occurrence Related to Intracerebral Acute hemorrhage) Investigators. Prevention of venous thrombosis in patients with acute intracerebral hemorrhage. Neurology2005; 65:865–869.
Diringer MN, Skolnick BE, Mayer SA, et al. Thromboembolic events with recombinant activated factor VII in spontaneous intracerebral hemorrhage: results from the Factor Seven for Acute Hemorrhagic Stroke (FAST) trial. Stroke2010; 41:48–53.
Boeer A, Voth E, Henze T, Prange HW. Early heparin therapy in patients with spontaneous intracerebral haemorrhage. J Neurol Neurosurg Psychiatry1991; 54:466–467.
Dickmann U, Voth E, Schicha H, Henze T, Prange H, Emrich D. Heparin therapy, deep-vein thrombosis and pulmonary embolism after intracerebral hemorrhage. Klin Wochenschr1988; 66:1182–1183.
Geerts WH, Bergqvist D, Pineo GF, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):381S–453S.
Vermeer SE, Algra A, Franke CL, Koudstaal PJ, Rinkel GJ. Long-term prognosis after recovery from primary intracerebral hemorrhage. Neurology2002; 59:205–209.
Bailey RD, Hart RG, Benavente O, Pearce LA. Recurrent brain hemorrhage is more frequent than ischemic stroke after intracranial hemorrhage. Neurology2001; 56:773–777.
Viswanathan A, Rakich SM, Engel C, et al. Antiplatelet use after intracerebral hemorrhage. Neurology2006; 66:206–209.
Greenberg SM, Eng JA, Ning M, Smith EE, Rosand J. Hemorrhage burden predicts recurrent intracerebral hemorrhage after lobar hemorrhage. Stroke2004; 35:1415–1420.
Lee SH, Ryu WS, Roh JK. Cerebral microbleeds are a risk factor for warfarin-related intracerebral hemorrhage. Neurology2009; 72:171–176.
Ueno H, Naka H, Ohshita T, et al. Association between cerebral microbleeds on T2*-weighted MR images and recurrent hemorrhagic stroke in patients treated with warfarin following ischemic stroke. AJNR Am J Neuroradiol2008; 29:1483–1486.
O’Donnell HC, Rosand J, Knudsen KA, et al. Apolipoprotein E genotype and the risk of recurrent lobar intracerebral hemorrhage. N Engl J Med2000; 342:240–245.
Genes for Cerebral Hemorrhage on Anticoagulation (GOCHA) Collaborative Group. Exploiting common genetic variation to make anticoagulation safer. Stroke2009; 40(suppl 3):S64–S66.
Tzourio C, Arima H, Harrap S, et al. APOE genotype, ethnicity, and the risk of cerebral hemorrhage. Neurology2008; 70:1322–1328.
Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med1998; 105:91–99.
Kuijer PM, Hutten BA, Prins MH, Büller HR. Prediction of the risk of bleeding during anticoagulant treatment for venous thromboembolism. Arch Intern Med1999; 159:457–460.
Wess ML, Schauer DP, Johnston JA, et al. Application of a decision support tool for anticoagulation in patients with non-valvular atrial fibrillation. J Gen Intern Med2008; 23:411–417.
Singer DE, Chang Y, Fang MC, et al. Should patient characteristics influence target anticoagulation intensity for stroke prevention in nonvalvular atrial fibrillation? The ATRIA study. Circ Cardiovasc Qual Outcomes2009; 2:297–304.
Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation. Ann Intern Med2004; 141:745–752.
Singer DE, Chang Y, Fang MC, et al. The net clinical benefit of warfarin anticoagulation in atrial fibrillation. Ann Intern Med2009; 151:297–305.
Eckman MH, Rosand J, Knudsen KA, Singer DE, Greenberg SM. Can patients be anticoagulated after intracerebral hemorrhage? A decision analysis. Stroke2003; 34:1710–1716.
Baruch L, Gage BF, Horrow J, et al. Can patients at elevated risk of stroke treated with anticoagulants be further risk stratified?Stroke2007; 38:2459–2463.
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA2001; 285:2864–2870.
Cannegieter SC, Rosendaal FR, Briët E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation1994; 89:635–641.
Freudenberger RS, Hellkamp AS, Halperin JL, et al; SCD-HeFT Investigators. Risk of thromboembolism in heart failure: an analysis from the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Circulation2007; 115:2637–2641.
Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med1996; 125:1–7.
Claassen DO, Kazemi N, Zubkov AY, Wijdicks EF, Rabinstein AA. Restarting anticoagulation therapy after warfarin-associated intracerebral hemorrhage. Arch Neurol2008; 65:1313–1318.
De Vleeschouwer S, Van Calenbergh F, van Loon J, Nuttin B, Goffin J, Plets C. Risk analysis of thrombo-embolic and recurrent bleeding events in the management of intracranial haemorrhage due to oral anticoagulation. Acta Chir Belg2005; 105:268–274.
Butler AC, Tait RC. Restarting anticoagulation in prosthetic heart valve patients after intracranial haemorrhage: a 2-year follow-up. Br J Haematol1998; 103:1064–1066.
Bertram M, Bonsanto M, Hacke W, Schwab S. Managing the therapeutic dilemma: patients with spontaneous intracerebral hemorrhage and urgent need for anticoagulation. J Neurol2000; 247:209–214.
Taylor FC, Cohen H, Ebrahim S. Systematic review of long term anticoagulation or antiplatelet treatment in patients with nonrheumatic atrial fibrillation. BMJ2001; 322:321–326.
Flaherty ML, Tao H, Haverbusch M, et al. Warfarin use leads to larger intracerebral hematomas. Neurology2008; 71:1084–1089.
Sansing LH, Messe SR, Cucchiara BL, Cohen SN, Lyden PD, Kasner SE; CHANT Investigators. Prior antiplatelet use does not affect hemorrhage growth or outcome after ICH. Neurology2009; 72:1397–1402.
Snow V, Qaseem A, Barry P, et al; American College of Physicians; American Academy of Family Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med2007; 146:204–210.
Albers GW, Amarenco P, Easton JD, Sacco RL, Teal PA; merican College of Chest Physicians. Antithrombotic and thrombolytic therapy for ischemic stroke: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):630S–639S.
Hankey GJ, Eikelboom JW. Antithrombotic drugs for patients with ischaemic stroke and transient ischaemic attack to prevent recurrent major vascular events. Lancet Neurol2010; 9:273–284.
Schulman S, Kearon C, Kakkar AK, et al; RE-COVER Study Group. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med2009; 361:2342–2352.
Schulman S, Wåhlander K, Lundström T, Clason SB, Eriksson H; THRIVE III Investigators. Secondary prevention of venous thromboembolism with the oral direct thrombin inhibitor ximelagatran. N Engl J Med2003; 349:1713–1721.
Singer DE, Albers GW, Dalen JE, et al; American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):546S–592S.
Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med2007; 167:1414–1419.
Choudhry NK, Anderson GM, Laupacis A, Ross-Degnan D, Normand SL, Soumerai SB. Impact of adverse events on prescribing warfarin in patients with atrial fibrillation: matched pair analysis. BMJ2006; 332:141–145.
Choudhry NK, Soumerai SB, Normand SL, Ross-Degnan D, Laupacis A, Anderson GM. Warfarin prescribing in atrial fibrillation: the impact of physician, patient, and hospital characteristics. Am J Med2006; 119:607–615.
Fang MC, Go AS, Chang Y, et al. Death and disability from warfarin-associated intracranial and extracranial hemorrhages. Am J Med2007; 120:700–705.
Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med2004; 164:880–884.
Dixon AA, Holness RO, Howes WJ, Garner JB. Spontaneous intracerebral haemorrhage: an analysis of factors affecting prognosis. Can J Neurol Sci1985; 12:267–271.
Broderick JP, Adams HP, Barsan W, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke1999; 30:905–915.
Flibotte JJ, Hagan N, O’Donnell J, Greenberg SM, Rosand J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology2004; 63:1059–1064.
Schulman S, Beyth RJ, Kearon C, Levine MN; American College of Chest Physicians. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):257S–298S.
Flaherty ML, Kissela B, Woo D, et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology2007; 68:116–121.
Lee SB, Manno EM, Layton KF, Wijdicks EF. Progression of warfarin-associated intracerebral hemorrhage after INR normalization with FFP. Neurology2006; 67:1272–1274.
Huttner HB, Schellinger PD, Hartmann M, et al. Hematoma growth and outcome in treated neurocritical care patients with intracerebral hemorrhage related to oral anticoagulant therapy: comparison of acute treatment strategies using vitamin K, fresh frozen plasma, and prothrombin complex concentrates. Stroke2006; 37:1465–1470.
Sjöblom L, Hårdemark HG, Lindgren A, et al. Management and prognostic features of intracerebral hemorrhage during anticoagulant therapy: a Swedish multicenter study. Stroke2001; 32:2567–2574.
Yasaka M, Minematsu K, Naritomi H, Sakata T, Yamaguchi T. Predisposing factors for enlargement of intracerebral hemorrhage in patients treated with warfarin. Thromb Haemost2003; 89:278–283.
Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation2007; 115:2689–2696.
Goldstein JN, Thomas SH, Frontiero V, et al. Timing of fresh frozen plasma administration and rapid correction of coagulopathy in warfarin-related intracerebral hemorrhage. Stroke2006; 37:151–155.
Aguilar MI, Hart RG, Kase CS, et al. Treatment of warfarin-associated intracerebral hemorrhage: literature review and expert opinion. Mayo Clin Proc2007; 82:82–92.
Guidelines on oral anticoagulation: third edition. Br J Haematol1998; 101:374–387.
Baglin TP, Keeling DM, Watson HG; British Committee for Standards in Haematology. Guidelines on oral anticoagulation (warfarin): third edition—2005 update. Br J Haematol2006; 132:277–285.
O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al; British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol2004; 126:11–28.
Baker RI, Coughlin PB, Gallus AS, Harper PL, Salem HH, Wood EM; Warfarin Reversal Consensus Group. Warfarin reversal: consensus guidelines, on behalf of the Australasian Society of Thrombosis and Haemostasis. Med J Aust2004; 181:492–497.
Davis SM, Broderick J, Hennerici M, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology2006; 66:1175–1181.
Broderick JP, Diringer MN, Hill MD, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Determinants of intracerebral hemorrhage growth: an exploratory analysis. Stroke2007; 38:1072–1075.
Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology2007; 68:889–894.
Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of spontaneous intracerebral hemorrhage. Incidence and time course. Stroke1996; 27:1783–1787.
Kim J, Smith A, Hemphill JC, et al. Contrast extravasation on CT predicts mortality in primary intracerebral hemorrhage. AJNR Am J Neuroradiol2008; 29:520–525.
Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebral hemorrhage. Stroke2007; 38:1257–1262.
Barras CD, Tress BM, Christensen S, et al; Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators. Density and shape as CT predictors of intracerebral hemorrhage growth. Stroke2009; 40:1325–1331.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. Systematic characterization of the computed tomography angiography spot sign in primary intracerebral hemorrhage identifies patients at highest risk for hematoma expansion: the spot sign score. Stroke2009; 40:2994–3000.
Fujii Y, Takeuchi S, Sasaki O, Minakawa T, Tanaka R. Multivariate analysis of predictors of hematoma enlargement in spontaneous intracerebral hemorrhage. Stroke1998; 29:1160–1166.
Ederies A, Demchuk A, Chia T, et al. Postcontrast CT extravasation is associated with hematoma expansion in CTA spot negative patients. Stroke2009; 40:1672–1676.
Delgado P, Alvarez-Sabín J, Abilleira S, et al. Plasma d-dimer predicts poor outcome after acute intracerebral hemorrhage. Neurology2006; 67:94–98.
Naidech AM, Jovanovic B, Liebling S, et al. Reduced platelet activity is associated with early clot growth and worse 3-month outcome after intracerebral hemorrhage. Stroke2009; 40:2398–2401.
Silva Y, Leira R, Tejada J, Lainez JM, Castillo J, Dávalos A; Stroke Project, Cerebrovascular Diseases Group of the Spanish Neurological Society. Molecular signatures of vascular injury are associated with early growth of intracerebral hemorrhage. Stroke2005; 36:86–91.
Sansing LH, Messe SR, Cucchiara BL, Cohen SN, Lyden PD, Kasner SE; CHANT Investigators. Prior antiplatelet use does not affect hemorrhage growth or outcome after ICH. Neurology2009; 72:1397–1402.
Moussouttas M, Malhotra R, Fernandez L, et al. Role of antiplatelet agents in hematoma expansion during the acute period of intracerebral hemorrhage. Neurocrit Care2010; 12:24–29.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. The spot sign score in primary intracerebral hemorrhage identifies patients at highest risk of in-hospital mortality and poor outcome among survivors. Stroke2010; 41:54–60.
Broderick J, Connolly S, Feldmann E, et al; American Heart Association; American Stroke Association Stroke Council; High Blood Pressure Research Council; Quality of Care and Outcomes in Research Interdisciplinary Working Group. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke2007; 38:2001–2023.
Steiner T, Kaste M, Forsting M, et al. Recommendations for the management of intracranial haemorrhage - part I: spontaneous intracerebral haemorrhage. The European Stroke Initiative Writing Committee and the Writing Committee for the EUSI Executive Committee. Cerebrovasc Dis2006; 22:294–316.
Steiner T, Rosand J, Diringer M. Intracerebral hemorrhage associated with oral anticoagulant therapy: current practices and unresolved questions. Stroke2006; 37:256–262.
Goldstein JN, Fazen LE, Wendell L, et al. Risk of thromboembolism following acute intracerebral hemorrhage. Neurocrit Care2009; 10:28–34.
Christensen MC, Dawson J, Vincent C. Risk of thromboembolic complications after intracerebral hemorrhage according to ethnicity. Adv Ther2008; 25:831–841.
Lacut K, Bressollette L, Le Gal G, et al; VICTORIAh (Venous Intermittent Compression and Thrombosis Occurrence Related to Intracerebral Acute hemorrhage) Investigators. Prevention of venous thrombosis in patients with acute intracerebral hemorrhage. Neurology2005; 65:865–869.
Diringer MN, Skolnick BE, Mayer SA, et al. Thromboembolic events with recombinant activated factor VII in spontaneous intracerebral hemorrhage: results from the Factor Seven for Acute Hemorrhagic Stroke (FAST) trial. Stroke2010; 41:48–53.
Boeer A, Voth E, Henze T, Prange HW. Early heparin therapy in patients with spontaneous intracerebral haemorrhage. J Neurol Neurosurg Psychiatry1991; 54:466–467.
Dickmann U, Voth E, Schicha H, Henze T, Prange H, Emrich D. Heparin therapy, deep-vein thrombosis and pulmonary embolism after intracerebral hemorrhage. Klin Wochenschr1988; 66:1182–1183.
Geerts WH, Bergqvist D, Pineo GF, et al; American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):381S–453S.
Vermeer SE, Algra A, Franke CL, Koudstaal PJ, Rinkel GJ. Long-term prognosis after recovery from primary intracerebral hemorrhage. Neurology2002; 59:205–209.
Bailey RD, Hart RG, Benavente O, Pearce LA. Recurrent brain hemorrhage is more frequent than ischemic stroke after intracranial hemorrhage. Neurology2001; 56:773–777.
Viswanathan A, Rakich SM, Engel C, et al. Antiplatelet use after intracerebral hemorrhage. Neurology2006; 66:206–209.
Greenberg SM, Eng JA, Ning M, Smith EE, Rosand J. Hemorrhage burden predicts recurrent intracerebral hemorrhage after lobar hemorrhage. Stroke2004; 35:1415–1420.
Lee SH, Ryu WS, Roh JK. Cerebral microbleeds are a risk factor for warfarin-related intracerebral hemorrhage. Neurology2009; 72:171–176.
Ueno H, Naka H, Ohshita T, et al. Association between cerebral microbleeds on T2*-weighted MR images and recurrent hemorrhagic stroke in patients treated with warfarin following ischemic stroke. AJNR Am J Neuroradiol2008; 29:1483–1486.
O’Donnell HC, Rosand J, Knudsen KA, et al. Apolipoprotein E genotype and the risk of recurrent lobar intracerebral hemorrhage. N Engl J Med2000; 342:240–245.
Genes for Cerebral Hemorrhage on Anticoagulation (GOCHA) Collaborative Group. Exploiting common genetic variation to make anticoagulation safer. Stroke2009; 40(suppl 3):S64–S66.
Tzourio C, Arima H, Harrap S, et al. APOE genotype, ethnicity, and the risk of cerebral hemorrhage. Neurology2008; 70:1322–1328.
Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med1998; 105:91–99.
Kuijer PM, Hutten BA, Prins MH, Büller HR. Prediction of the risk of bleeding during anticoagulant treatment for venous thromboembolism. Arch Intern Med1999; 159:457–460.
Wess ML, Schauer DP, Johnston JA, et al. Application of a decision support tool for anticoagulation in patients with non-valvular atrial fibrillation. J Gen Intern Med2008; 23:411–417.
Singer DE, Chang Y, Fang MC, et al. Should patient characteristics influence target anticoagulation intensity for stroke prevention in nonvalvular atrial fibrillation? The ATRIA study. Circ Cardiovasc Qual Outcomes2009; 2:297–304.
Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation. Ann Intern Med2004; 141:745–752.
Singer DE, Chang Y, Fang MC, et al. The net clinical benefit of warfarin anticoagulation in atrial fibrillation. Ann Intern Med2009; 151:297–305.
Eckman MH, Rosand J, Knudsen KA, Singer DE, Greenberg SM. Can patients be anticoagulated after intracerebral hemorrhage? A decision analysis. Stroke2003; 34:1710–1716.
Baruch L, Gage BF, Horrow J, et al. Can patients at elevated risk of stroke treated with anticoagulants be further risk stratified?Stroke2007; 38:2459–2463.
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA2001; 285:2864–2870.
Cannegieter SC, Rosendaal FR, Briët E. Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses. Circulation1994; 89:635–641.
Freudenberger RS, Hellkamp AS, Halperin JL, et al; SCD-HeFT Investigators. Risk of thromboembolism in heart failure: an analysis from the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Circulation2007; 115:2637–2641.
Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med1996; 125:1–7.
Claassen DO, Kazemi N, Zubkov AY, Wijdicks EF, Rabinstein AA. Restarting anticoagulation therapy after warfarin-associated intracerebral hemorrhage. Arch Neurol2008; 65:1313–1318.
De Vleeschouwer S, Van Calenbergh F, van Loon J, Nuttin B, Goffin J, Plets C. Risk analysis of thrombo-embolic and recurrent bleeding events in the management of intracranial haemorrhage due to oral anticoagulation. Acta Chir Belg2005; 105:268–274.
Butler AC, Tait RC. Restarting anticoagulation in prosthetic heart valve patients after intracranial haemorrhage: a 2-year follow-up. Br J Haematol1998; 103:1064–1066.
Bertram M, Bonsanto M, Hacke W, Schwab S. Managing the therapeutic dilemma: patients with spontaneous intracerebral hemorrhage and urgent need for anticoagulation. J Neurol2000; 247:209–214.
Taylor FC, Cohen H, Ebrahim S. Systematic review of long term anticoagulation or antiplatelet treatment in patients with nonrheumatic atrial fibrillation. BMJ2001; 322:321–326.
Flaherty ML, Tao H, Haverbusch M, et al. Warfarin use leads to larger intracerebral hematomas. Neurology2008; 71:1084–1089.
Sansing LH, Messe SR, Cucchiara BL, Cohen SN, Lyden PD, Kasner SE; CHANT Investigators. Prior antiplatelet use does not affect hemorrhage growth or outcome after ICH. Neurology2009; 72:1397–1402.
Snow V, Qaseem A, Barry P, et al; American College of Physicians; American Academy of Family Physicians Panel on Deep Venous Thrombosis/Pulmonary Embolism. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med2007; 146:204–210.
Albers GW, Amarenco P, Easton JD, Sacco RL, Teal PA; merican College of Chest Physicians. Antithrombotic and thrombolytic therapy for ischemic stroke: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):630S–639S.
Hankey GJ, Eikelboom JW. Antithrombotic drugs for patients with ischaemic stroke and transient ischaemic attack to prevent recurrent major vascular events. Lancet Neurol2010; 9:273–284.
Schulman S, Kearon C, Kakkar AK, et al; RE-COVER Study Group. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med2009; 361:2342–2352.
Schulman S, Wåhlander K, Lundström T, Clason SB, Eriksson H; THRIVE III Investigators. Secondary prevention of venous thromboembolism with the oral direct thrombin inhibitor ximelagatran. N Engl J Med2003; 349:1713–1721.
Singer DE, Albers GW, Dalen JE, et al; American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008; 133(suppl 6):546S–592S.
Given the high risk of hematoma expansion in the early phase of acute ICH, most experts recommend reversing anticoagulation immediately.
Many clinicians start subcutaneous heparinoids in low doses 24 to 72 hours after ICH to prevent deep vein thrombosis, and after the first few days or a week, consider either increasing the dose to a full anticoagulation dose or making a transition to oral anticoagulants.
Many patients with lobar hemorrhage or cerebral amyloid angiopathy may remain at higher risk of anticoagulant-related ICH recurrence than thromboembolic events and would therefore be best managed without anticoagulants.
Those with deep hemispheric ICH, hypertension that can be well controlled, and a high risk of disabling thromboembolism may receive net benefit from restarting anticoagulation.
ANSWER The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
ANSWER The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
ANSWER The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
A 24-year-old man who works as a landscaper/tree-cutter presents for evaluation of right shoulder pain after a tree fell on him. He states that he attempted to run away as the tree fell, but it struck him nonetheless. He did not lose consciousness. The tree struck the right side of his body.
The patient’s medical history is unremarkable. He is complaining of right-side back and shoulder pain. Initial vital signs and primary survey appear to be normal.
Secondary survey shows decreased range of motion in the right shoulder, with point tenderness in the scapula. There are no obvious deformities. Distal pulses are strong, and the patient is otherwise neurovascularly intact.
Radiograph of the right shoulder is shown. What is your impression?
ANSWER The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
ANSWER The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
ANSWER The radiograph shows an osseous fragment along the inferior aspect of the glenohumeral joint. Close examination reveals a defect within the scapula itself, most likely consistent with an acute fracture.
A 24-year-old man who works as a landscaper/tree-cutter presents for evaluation of right shoulder pain after a tree fell on him. He states that he attempted to run away as the tree fell, but it struck him nonetheless. He did not lose consciousness. The tree struck the right side of his body.
The patient’s medical history is unremarkable. He is complaining of right-side back and shoulder pain. Initial vital signs and primary survey appear to be normal.
Secondary survey shows decreased range of motion in the right shoulder, with point tenderness in the scapula. There are no obvious deformities. Distal pulses are strong, and the patient is otherwise neurovascularly intact.
Radiograph of the right shoulder is shown. What is your impression?
A 72-year-old man presented to his primary care provider’s office with complaints of peeling skin on his penis and frequent, burning urination. He said he had first noticed redness on his penis about four days earlier, adding that it was growing worse. He was unsure whether he was truly experiencing frequent urination or just more aware of urinating because of the burning pain. He reported no attempts to treat himself, stating that he was “just keeping an eye on it and hoping it would go away.”
The patient’s medical history was limited to hypertension, for which he was taking valsartan, and allergies, for which he took fexofenadine. His surgical history included a tonsillectomy and appendectomy during his early teens. He had no known allergies to any medications.
The patient was married and retired after an executive career. He and his wife split their residence between New York and Florida during seasonal changes and were living in Florida at the time. He reported social drinking (“on rare occasions, these days”) and smoking an occasional cigar. He reported that he showers only once or twice weekly because of dry skin.
The following vital signs were recorded: blood pressure, 110/72 mm Hg; heart rate, 68 beats/min; respirations, 15/min; temperature, 97.8°F; and O2 saturation, 99% on room air. He was 73” tall and weighed 197 lb, with a BMI of 26.
The patient was alert and oriented. His physical exam was overall unremarkable, with the exception of an uncircumcised penis with redness and inflammation on the glans penis and no discharge noted. The reddened area was bright and shiny with a moist appearance and well-defined borders. The man denied any risk for sexually transmitted disease (STD) and denied any penile discharge. He also denied fever, chills, or arthritis.
Urinalysis performed in the office was negative for a urinary tract infection or for elevated glucose. A laboratory report from six months earlier was reviewed; all findings were within normal range, including the blood glucose level, with special attention paid for possible underlying cause; and the prostate-specific antigen (PSA) level, obtained for possible prostatitis or prostate cancer.
The differential diagnosis included eczema or psoriasis, Zoon’s balanitis, penile cancer, balanitis xerotica obliterans (lichen sclerosus), candidiasis balanitis, and circinate balanitis (as occurs in patients with Reiter’s disease; see table1-5). The absence of circumcision and the patient’s report of infrequent bathing raised concern for a hygiene-related etiology; the final diagnosis, made empirically, was candidiasis balanitis. Regarding an underlying cause, the laboratory order included a urine culture, fasting complete blood count, chemistry panel, and PSA level.
The patient was given instructions to wash the affected area twice daily for one week with a lukewarm weak saline solution (1 tablespoon salt/L water),5,6 gently retracting the foreskin; he was also given a topical antifungal cream7 (ketoconazole 2%, although other choices are discussed below), to be applied two to three times daily until his symptoms resolved.6 He was advised to return in one week if the condition did not improve or grew worse5; referral to dermatology would then be considered. The patient was also advised that in the case of a recurrent episode, dermatology would be consulted. The possibility of circumcision was discussed,8 and the patient was given information about the procedure, with referral to a urologist in the area.
Discussion
Balanitis is an inflammation of the glans penis; balanoposthitis involves the foreskin and prepuce.9-11 Balanitis can occur in men of any age, with etiologies varying with a patient’s age. Typical signs and symptoms include redness and swelling of the glans penis or foreskin, itching and/or pain, urethral discharge, phimosis, swollen lymph nodes, ulceration or plaque appearance, and pain on urination.12
In addition to the differential diagnoses mentioned, several additional conditions can be considered in a man with penile lesions. In older men, it is particularly important to investigate such lesions thoroughly, following the patient until the underlying cause is determined and the best treatment choice is selected. Specialists in dermatology and urology can best identify persistent or chronic lesions and make appropriate treatment recommendations, including possible circumcision.
The condition is commonly associated with absence of circumcision, poor hygiene, and phimosis (the inability to retract the foreskin from the glans penis). Accumulation of glandular secretions (smegma) and sloughed epithelial cells under the foreskin can lead to irritation and subsequent infection.
Uncontrolled or poorly controlled diabetes can be implicated in candidiasis infections.1 Other causes and contributing factors include chemical irritants (eg, soaps, lubricating jelly), edematous conditions (including congestive heart failure, cirrhosis, and nephrosis), drug allergies, morbid obesity, and a number of viruses and other pathogens, including those associated with STDs.12
A more detailed laboratory work-up might include the following:
• Serum glucose test (as part of a diabetes screening; in older men, this inflammatory condition can be a presenting sign of diabetes mellitus6)
• Culture of discharge, if any is present
• Serology test for STDs
• Wet mount with potassium hydroxide (for Candida albicans infection)
• Ultrasound, in severe cases or when urinary obstruction is suspected.
Additionally, in chronic cases, the patient should be referred to dermatology or urology for biopsy.5,9 Testing for anaerobes should also be considered for the patient and his sexual partner; if results are positive, treatment with oral metronidazole (400 mg tid for 10 days) is advised.6
In this patient’s case, the test that would best support an in-office diagnosis of candidiasis balanitis is a wet mount with potassium hydroxide. This was not performed at the time of the case patient’s visit, however; the diagnosis was empirically determined.
Management, Including Patient Education
Treatment of candidiasis balanitis involves routinely cleaning the penis and foreskin, as the case patient was instructed; use of soap, an irritant, should be avoided until the condition is resolved.7,10 Appropriate topical antifungal creams include nystatin, ketoconazole, miconazole, clotrimazole, econazole, and terbinafine, applied two to three times daily for at least 10 days; a cream combining an imidazole with 1% hydrocortisone may be effective for patients with significant inflammation.5,6,8,10,13
The patient should be instructed to:
• Keep the area clean and dry
• Wash twice daily with weak saline solution after removing residual medication and before applying fresh medication
• Wear loose cotton underwear
• Avoid sharing towels or cleaning cloths
• Wash personal items and surfaces, if possible, with disinfectant
• Notify sexual partner(s) that they may need treatment
• Discontinue sexual intercourse until infection is resolved
• Continue treatment for 10 to 14 days, even though relief may occur early
• Follow up with the clinician if no improvement is seen within one week
• Consider circumcision, in case of chronic infection.1,2,8,12
Conclusion
It is important to diagnose balanitis correctly, as this condition can affect sexual and urinary function, and its effects should not be underestimated in older men. Differentiating between infectious, noninfectious, premalignant, and malignant lesions will lead to appropriate care and allow early diagnosis or prevention of curable malignancies.
References
1. Singh S, Bunker C. Male genital dermatoses in old age. Age Ageing. 2008;37(5):500-504.
2. Thompson IM, Teichman JM, Elston DM, Sea J. Noninfectious penile lesions. Am Fam Physician. 2010;81(2):167-174.
3. Lane JE, Johnson J. Persistent penile patch. Am Fam Physician. 2008;78(9):1081-1082.
4. Gupta S, Malhotra AK, Ajith C. Lichen sclerosus: role of occlusion of the genital skin in the pathogenesis. Indian J Dermatol Venereol Leprol. 2010;76(1):56-58.
5. British Association for Sexual Health and HIV, Clinical Effectiveness Group. 2008 UK National Guideline on the Management of Balanoposthitis. www.bashh.org/documents/2062. Accessed September 22, 2010.
6. Ashton R, Leppard B. Differential Diagnosis in Dermatology. 3rd ed. London: Radcliffe Publishing Ltd; 2004:321.
7. NHS Institute for Innovation and Improvement. Clinical Knowledge Summaries: Balanitis (June 2009). www.cks.nhs.uk/balanitis/management/scenario_balanitis_adults#-378526. Accessed September 22, 2010.
8. Parker J. Management of common fungal infections in primary care. Nurs Stand. 2009;23(43):42-46.
9. Green MB, Bailey PP. Infectious processes: urinary tract infections and sexually transmitted diseases. In: Buttaro TM, Trybulski J, Bailey PP, Sandberg-Cook J, eds. Primary Care: A Collaborative Practice. 3rd ed. St. Louis, MO: Mosby Elsevier; 2008:576-590.
10. Singh-Behl D, Tomecki KJ. Common skins infections 2009. www.clevelandclinicmeded .com/medicalpubs/diseasemanagement/dermatol ogy/common-skin-infections. Accessed September 22, 2010.
11. Ko WT, Adal KA, Tomecki KJ. Infectious diseases. Med Clin North Am. 1998;82:(5):1001-1031.
12. Morgan K, McCance, KL. Alterations of the reproductive systems. In: McCance KL, Huether SE, eds. Pathophysiology: The Biologic Basis for Disease in Adults and Children. 5th ed. St. Louis, MO: Elsevier Mosby; 2006:805-807.
13. Waugh MA, Evans EG, Nayyar KC, Fong R. Clotrimazole (Canestan) in the treatment of candidal balanitis in men: with incidental observations on diabetic candidal balanoposthitis. Br J Vener Dis. 1978;54(3):184-186.
A 72-year-old man presented to his primary care provider’s office with complaints of peeling skin on his penis and frequent, burning urination. He said he had first noticed redness on his penis about four days earlier, adding that it was growing worse. He was unsure whether he was truly experiencing frequent urination or just more aware of urinating because of the burning pain. He reported no attempts to treat himself, stating that he was “just keeping an eye on it and hoping it would go away.”
The patient’s medical history was limited to hypertension, for which he was taking valsartan, and allergies, for which he took fexofenadine. His surgical history included a tonsillectomy and appendectomy during his early teens. He had no known allergies to any medications.
The patient was married and retired after an executive career. He and his wife split their residence between New York and Florida during seasonal changes and were living in Florida at the time. He reported social drinking (“on rare occasions, these days”) and smoking an occasional cigar. He reported that he showers only once or twice weekly because of dry skin.
The following vital signs were recorded: blood pressure, 110/72 mm Hg; heart rate, 68 beats/min; respirations, 15/min; temperature, 97.8°F; and O2 saturation, 99% on room air. He was 73” tall and weighed 197 lb, with a BMI of 26.
The patient was alert and oriented. His physical exam was overall unremarkable, with the exception of an uncircumcised penis with redness and inflammation on the glans penis and no discharge noted. The reddened area was bright and shiny with a moist appearance and well-defined borders. The man denied any risk for sexually transmitted disease (STD) and denied any penile discharge. He also denied fever, chills, or arthritis.
Urinalysis performed in the office was negative for a urinary tract infection or for elevated glucose. A laboratory report from six months earlier was reviewed; all findings were within normal range, including the blood glucose level, with special attention paid for possible underlying cause; and the prostate-specific antigen (PSA) level, obtained for possible prostatitis or prostate cancer.
The differential diagnosis included eczema or psoriasis, Zoon’s balanitis, penile cancer, balanitis xerotica obliterans (lichen sclerosus), candidiasis balanitis, and circinate balanitis (as occurs in patients with Reiter’s disease; see table1-5). The absence of circumcision and the patient’s report of infrequent bathing raised concern for a hygiene-related etiology; the final diagnosis, made empirically, was candidiasis balanitis. Regarding an underlying cause, the laboratory order included a urine culture, fasting complete blood count, chemistry panel, and PSA level.
The patient was given instructions to wash the affected area twice daily for one week with a lukewarm weak saline solution (1 tablespoon salt/L water),5,6 gently retracting the foreskin; he was also given a topical antifungal cream7 (ketoconazole 2%, although other choices are discussed below), to be applied two to three times daily until his symptoms resolved.6 He was advised to return in one week if the condition did not improve or grew worse5; referral to dermatology would then be considered. The patient was also advised that in the case of a recurrent episode, dermatology would be consulted. The possibility of circumcision was discussed,8 and the patient was given information about the procedure, with referral to a urologist in the area.
Discussion
Balanitis is an inflammation of the glans penis; balanoposthitis involves the foreskin and prepuce.9-11 Balanitis can occur in men of any age, with etiologies varying with a patient’s age. Typical signs and symptoms include redness and swelling of the glans penis or foreskin, itching and/or pain, urethral discharge, phimosis, swollen lymph nodes, ulceration or plaque appearance, and pain on urination.12
In addition to the differential diagnoses mentioned, several additional conditions can be considered in a man with penile lesions. In older men, it is particularly important to investigate such lesions thoroughly, following the patient until the underlying cause is determined and the best treatment choice is selected. Specialists in dermatology and urology can best identify persistent or chronic lesions and make appropriate treatment recommendations, including possible circumcision.
The condition is commonly associated with absence of circumcision, poor hygiene, and phimosis (the inability to retract the foreskin from the glans penis). Accumulation of glandular secretions (smegma) and sloughed epithelial cells under the foreskin can lead to irritation and subsequent infection.
Uncontrolled or poorly controlled diabetes can be implicated in candidiasis infections.1 Other causes and contributing factors include chemical irritants (eg, soaps, lubricating jelly), edematous conditions (including congestive heart failure, cirrhosis, and nephrosis), drug allergies, morbid obesity, and a number of viruses and other pathogens, including those associated with STDs.12
A more detailed laboratory work-up might include the following:
• Serum glucose test (as part of a diabetes screening; in older men, this inflammatory condition can be a presenting sign of diabetes mellitus6)
• Culture of discharge, if any is present
• Serology test for STDs
• Wet mount with potassium hydroxide (for Candida albicans infection)
• Ultrasound, in severe cases or when urinary obstruction is suspected.
Additionally, in chronic cases, the patient should be referred to dermatology or urology for biopsy.5,9 Testing for anaerobes should also be considered for the patient and his sexual partner; if results are positive, treatment with oral metronidazole (400 mg tid for 10 days) is advised.6
In this patient’s case, the test that would best support an in-office diagnosis of candidiasis balanitis is a wet mount with potassium hydroxide. This was not performed at the time of the case patient’s visit, however; the diagnosis was empirically determined.
Management, Including Patient Education
Treatment of candidiasis balanitis involves routinely cleaning the penis and foreskin, as the case patient was instructed; use of soap, an irritant, should be avoided until the condition is resolved.7,10 Appropriate topical antifungal creams include nystatin, ketoconazole, miconazole, clotrimazole, econazole, and terbinafine, applied two to three times daily for at least 10 days; a cream combining an imidazole with 1% hydrocortisone may be effective for patients with significant inflammation.5,6,8,10,13
The patient should be instructed to:
• Keep the area clean and dry
• Wash twice daily with weak saline solution after removing residual medication and before applying fresh medication
• Wear loose cotton underwear
• Avoid sharing towels or cleaning cloths
• Wash personal items and surfaces, if possible, with disinfectant
• Notify sexual partner(s) that they may need treatment
• Discontinue sexual intercourse until infection is resolved
• Continue treatment for 10 to 14 days, even though relief may occur early
• Follow up with the clinician if no improvement is seen within one week
• Consider circumcision, in case of chronic infection.1,2,8,12
Conclusion
It is important to diagnose balanitis correctly, as this condition can affect sexual and urinary function, and its effects should not be underestimated in older men. Differentiating between infectious, noninfectious, premalignant, and malignant lesions will lead to appropriate care and allow early diagnosis or prevention of curable malignancies.
A 72-year-old man presented to his primary care provider’s office with complaints of peeling skin on his penis and frequent, burning urination. He said he had first noticed redness on his penis about four days earlier, adding that it was growing worse. He was unsure whether he was truly experiencing frequent urination or just more aware of urinating because of the burning pain. He reported no attempts to treat himself, stating that he was “just keeping an eye on it and hoping it would go away.”
The patient’s medical history was limited to hypertension, for which he was taking valsartan, and allergies, for which he took fexofenadine. His surgical history included a tonsillectomy and appendectomy during his early teens. He had no known allergies to any medications.
The patient was married and retired after an executive career. He and his wife split their residence between New York and Florida during seasonal changes and were living in Florida at the time. He reported social drinking (“on rare occasions, these days”) and smoking an occasional cigar. He reported that he showers only once or twice weekly because of dry skin.
The following vital signs were recorded: blood pressure, 110/72 mm Hg; heart rate, 68 beats/min; respirations, 15/min; temperature, 97.8°F; and O2 saturation, 99% on room air. He was 73” tall and weighed 197 lb, with a BMI of 26.
The patient was alert and oriented. His physical exam was overall unremarkable, with the exception of an uncircumcised penis with redness and inflammation on the glans penis and no discharge noted. The reddened area was bright and shiny with a moist appearance and well-defined borders. The man denied any risk for sexually transmitted disease (STD) and denied any penile discharge. He also denied fever, chills, or arthritis.
Urinalysis performed in the office was negative for a urinary tract infection or for elevated glucose. A laboratory report from six months earlier was reviewed; all findings were within normal range, including the blood glucose level, with special attention paid for possible underlying cause; and the prostate-specific antigen (PSA) level, obtained for possible prostatitis or prostate cancer.
The differential diagnosis included eczema or psoriasis, Zoon’s balanitis, penile cancer, balanitis xerotica obliterans (lichen sclerosus), candidiasis balanitis, and circinate balanitis (as occurs in patients with Reiter’s disease; see table1-5). The absence of circumcision and the patient’s report of infrequent bathing raised concern for a hygiene-related etiology; the final diagnosis, made empirically, was candidiasis balanitis. Regarding an underlying cause, the laboratory order included a urine culture, fasting complete blood count, chemistry panel, and PSA level.
The patient was given instructions to wash the affected area twice daily for one week with a lukewarm weak saline solution (1 tablespoon salt/L water),5,6 gently retracting the foreskin; he was also given a topical antifungal cream7 (ketoconazole 2%, although other choices are discussed below), to be applied two to three times daily until his symptoms resolved.6 He was advised to return in one week if the condition did not improve or grew worse5; referral to dermatology would then be considered. The patient was also advised that in the case of a recurrent episode, dermatology would be consulted. The possibility of circumcision was discussed,8 and the patient was given information about the procedure, with referral to a urologist in the area.
Discussion
Balanitis is an inflammation of the glans penis; balanoposthitis involves the foreskin and prepuce.9-11 Balanitis can occur in men of any age, with etiologies varying with a patient’s age. Typical signs and symptoms include redness and swelling of the glans penis or foreskin, itching and/or pain, urethral discharge, phimosis, swollen lymph nodes, ulceration or plaque appearance, and pain on urination.12
In addition to the differential diagnoses mentioned, several additional conditions can be considered in a man with penile lesions. In older men, it is particularly important to investigate such lesions thoroughly, following the patient until the underlying cause is determined and the best treatment choice is selected. Specialists in dermatology and urology can best identify persistent or chronic lesions and make appropriate treatment recommendations, including possible circumcision.
The condition is commonly associated with absence of circumcision, poor hygiene, and phimosis (the inability to retract the foreskin from the glans penis). Accumulation of glandular secretions (smegma) and sloughed epithelial cells under the foreskin can lead to irritation and subsequent infection.
Uncontrolled or poorly controlled diabetes can be implicated in candidiasis infections.1 Other causes and contributing factors include chemical irritants (eg, soaps, lubricating jelly), edematous conditions (including congestive heart failure, cirrhosis, and nephrosis), drug allergies, morbid obesity, and a number of viruses and other pathogens, including those associated with STDs.12
A more detailed laboratory work-up might include the following:
• Serum glucose test (as part of a diabetes screening; in older men, this inflammatory condition can be a presenting sign of diabetes mellitus6)
• Culture of discharge, if any is present
• Serology test for STDs
• Wet mount with potassium hydroxide (for Candida albicans infection)
• Ultrasound, in severe cases or when urinary obstruction is suspected.
Additionally, in chronic cases, the patient should be referred to dermatology or urology for biopsy.5,9 Testing for anaerobes should also be considered for the patient and his sexual partner; if results are positive, treatment with oral metronidazole (400 mg tid for 10 days) is advised.6
In this patient’s case, the test that would best support an in-office diagnosis of candidiasis balanitis is a wet mount with potassium hydroxide. This was not performed at the time of the case patient’s visit, however; the diagnosis was empirically determined.
Management, Including Patient Education
Treatment of candidiasis balanitis involves routinely cleaning the penis and foreskin, as the case patient was instructed; use of soap, an irritant, should be avoided until the condition is resolved.7,10 Appropriate topical antifungal creams include nystatin, ketoconazole, miconazole, clotrimazole, econazole, and terbinafine, applied two to three times daily for at least 10 days; a cream combining an imidazole with 1% hydrocortisone may be effective for patients with significant inflammation.5,6,8,10,13
The patient should be instructed to:
• Keep the area clean and dry
• Wash twice daily with weak saline solution after removing residual medication and before applying fresh medication
• Wear loose cotton underwear
• Avoid sharing towels or cleaning cloths
• Wash personal items and surfaces, if possible, with disinfectant
• Notify sexual partner(s) that they may need treatment
• Discontinue sexual intercourse until infection is resolved
• Continue treatment for 10 to 14 days, even though relief may occur early
• Follow up with the clinician if no improvement is seen within one week
• Consider circumcision, in case of chronic infection.1,2,8,12
Conclusion
It is important to diagnose balanitis correctly, as this condition can affect sexual and urinary function, and its effects should not be underestimated in older men. Differentiating between infectious, noninfectious, premalignant, and malignant lesions will lead to appropriate care and allow early diagnosis or prevention of curable malignancies.
References
1. Singh S, Bunker C. Male genital dermatoses in old age. Age Ageing. 2008;37(5):500-504.
2. Thompson IM, Teichman JM, Elston DM, Sea J. Noninfectious penile lesions. Am Fam Physician. 2010;81(2):167-174.
3. Lane JE, Johnson J. Persistent penile patch. Am Fam Physician. 2008;78(9):1081-1082.
4. Gupta S, Malhotra AK, Ajith C. Lichen sclerosus: role of occlusion of the genital skin in the pathogenesis. Indian J Dermatol Venereol Leprol. 2010;76(1):56-58.
5. British Association for Sexual Health and HIV, Clinical Effectiveness Group. 2008 UK National Guideline on the Management of Balanoposthitis. www.bashh.org/documents/2062. Accessed September 22, 2010.
6. Ashton R, Leppard B. Differential Diagnosis in Dermatology. 3rd ed. London: Radcliffe Publishing Ltd; 2004:321.
7. NHS Institute for Innovation and Improvement. Clinical Knowledge Summaries: Balanitis (June 2009). www.cks.nhs.uk/balanitis/management/scenario_balanitis_adults#-378526. Accessed September 22, 2010.
8. Parker J. Management of common fungal infections in primary care. Nurs Stand. 2009;23(43):42-46.
9. Green MB, Bailey PP. Infectious processes: urinary tract infections and sexually transmitted diseases. In: Buttaro TM, Trybulski J, Bailey PP, Sandberg-Cook J, eds. Primary Care: A Collaborative Practice. 3rd ed. St. Louis, MO: Mosby Elsevier; 2008:576-590.
10. Singh-Behl D, Tomecki KJ. Common skins infections 2009. www.clevelandclinicmeded .com/medicalpubs/diseasemanagement/dermatol ogy/common-skin-infections. Accessed September 22, 2010.
11. Ko WT, Adal KA, Tomecki KJ. Infectious diseases. Med Clin North Am. 1998;82:(5):1001-1031.
12. Morgan K, McCance, KL. Alterations of the reproductive systems. In: McCance KL, Huether SE, eds. Pathophysiology: The Biologic Basis for Disease in Adults and Children. 5th ed. St. Louis, MO: Elsevier Mosby; 2006:805-807.
13. Waugh MA, Evans EG, Nayyar KC, Fong R. Clotrimazole (Canestan) in the treatment of candidal balanitis in men: with incidental observations on diabetic candidal balanoposthitis. Br J Vener Dis. 1978;54(3):184-186.
References
1. Singh S, Bunker C. Male genital dermatoses in old age. Age Ageing. 2008;37(5):500-504.
2. Thompson IM, Teichman JM, Elston DM, Sea J. Noninfectious penile lesions. Am Fam Physician. 2010;81(2):167-174.
3. Lane JE, Johnson J. Persistent penile patch. Am Fam Physician. 2008;78(9):1081-1082.
4. Gupta S, Malhotra AK, Ajith C. Lichen sclerosus: role of occlusion of the genital skin in the pathogenesis. Indian J Dermatol Venereol Leprol. 2010;76(1):56-58.
5. British Association for Sexual Health and HIV, Clinical Effectiveness Group. 2008 UK National Guideline on the Management of Balanoposthitis. www.bashh.org/documents/2062. Accessed September 22, 2010.
6. Ashton R, Leppard B. Differential Diagnosis in Dermatology. 3rd ed. London: Radcliffe Publishing Ltd; 2004:321.
7. NHS Institute for Innovation and Improvement. Clinical Knowledge Summaries: Balanitis (June 2009). www.cks.nhs.uk/balanitis/management/scenario_balanitis_adults#-378526. Accessed September 22, 2010.
8. Parker J. Management of common fungal infections in primary care. Nurs Stand. 2009;23(43):42-46.
9. Green MB, Bailey PP. Infectious processes: urinary tract infections and sexually transmitted diseases. In: Buttaro TM, Trybulski J, Bailey PP, Sandberg-Cook J, eds. Primary Care: A Collaborative Practice. 3rd ed. St. Louis, MO: Mosby Elsevier; 2008:576-590.
10. Singh-Behl D, Tomecki KJ. Common skins infections 2009. www.clevelandclinicmeded .com/medicalpubs/diseasemanagement/dermatol ogy/common-skin-infections. Accessed September 22, 2010.
11. Ko WT, Adal KA, Tomecki KJ. Infectious diseases. Med Clin North Am. 1998;82:(5):1001-1031.
12. Morgan K, McCance, KL. Alterations of the reproductive systems. In: McCance KL, Huether SE, eds. Pathophysiology: The Biologic Basis for Disease in Adults and Children. 5th ed. St. Louis, MO: Elsevier Mosby; 2006:805-807.
13. Waugh MA, Evans EG, Nayyar KC, Fong R. Clotrimazole (Canestan) in the treatment of candidal balanitis in men: with incidental observations on diabetic candidal balanoposthitis. Br J Vener Dis. 1978;54(3):184-186.
ANSWER The plain film demonstrates bilateral parietal skull fractures, more evident on the left than right side. Subsequent noncontrast CT of the skull confirmed these fractures, and also showed bilateral subdural hematomas.
Such findings, both clinically and radiographically, are highly worrisome and suggestive of nonaccidental injury (ie, abuse). This unfortunate infant was placed immediately under the care of the Department of Family and Children Services and moved to the pediatric ICU for close monitoring.
ANSWER The plain film demonstrates bilateral parietal skull fractures, more evident on the left than right side. Subsequent noncontrast CT of the skull confirmed these fractures, and also showed bilateral subdural hematomas.
Such findings, both clinically and radiographically, are highly worrisome and suggestive of nonaccidental injury (ie, abuse). This unfortunate infant was placed immediately under the care of the Department of Family and Children Services and moved to the pediatric ICU for close monitoring.
ANSWER The plain film demonstrates bilateral parietal skull fractures, more evident on the left than right side. Subsequent noncontrast CT of the skull confirmed these fractures, and also showed bilateral subdural hematomas.
Such findings, both clinically and radiographically, are highly worrisome and suggestive of nonaccidental injury (ie, abuse). This unfortunate infant was placed immediately under the care of the Department of Family and Children Services and moved to the pediatric ICU for close monitoring.
A 5-month-old girl is brought to your facility for decreased level of consciousness. According to the parents, the infant reportedly fell out of her car seat earlier this morning.
Prenatal history is unremarkable; immunizations are up to date. Initial examination shows a lethargic female infant with vital signs as follows: temperature, 99.7°F; blood pressure, 91/65 mm Hg; heart rate; 180 beats/min; and initial O2 saturation, 86% on room air. Supplemental oxygen and an IV fluid bolus are given, which correct the hypoxia and tachycardia.
Physical exam shows a depressed anterior fontanelle and bilateral periorbital ecchymosis, as well as multiple bruises of varying ages on the face and body. An old scar on the left side of the forehead is noted as well. While still somewhat lethargic, the infant does move all extremities to painful stimuli. A weak cry is present.
Initial radiographs of the chest and skull are obtained; the one of the skull is shown. What is your impression?
ANSWER The patient is status post two-level anterior cervical diskectomy and fusion, with interbody grafts and hardware appearing intact. The radiograph demonstrates significant prevertebral soft-tissue swelling greater than 2 cm over several levels. This results in significant posterior compression of the oropharynx. Such findings are typically seen in patients who develop retropharyngeal hematomas.
This patient was urgently returned to the operating room, where she underwent successful evacuation of a hematoma that was under a moderate amount of pressure. No specific source was identified, which is not uncommon.
ANSWER The patient is status post two-level anterior cervical diskectomy and fusion, with interbody grafts and hardware appearing intact. The radiograph demonstrates significant prevertebral soft-tissue swelling greater than 2 cm over several levels. This results in significant posterior compression of the oropharynx. Such findings are typically seen in patients who develop retropharyngeal hematomas.
This patient was urgently returned to the operating room, where she underwent successful evacuation of a hematoma that was under a moderate amount of pressure. No specific source was identified, which is not uncommon.
The patient made a full recovery.
ANSWER The patient is status post two-level anterior cervical diskectomy and fusion, with interbody grafts and hardware appearing intact. The radiograph demonstrates significant prevertebral soft-tissue swelling greater than 2 cm over several levels. This results in significant posterior compression of the oropharynx. Such findings are typically seen in patients who develop retropharyngeal hematomas.
This patient was urgently returned to the operating room, where she underwent successful evacuation of a hematoma that was under a moderate amount of pressure. No specific source was identified, which is not uncommon.
You receive a call from the nursing staff stating that a postoperative patient is experiencing respiratory distress. The patient is a 41-year-old woman who underwent a two-level anterior cervical diskectomy and fusion yesterday.
There were no problems during the surgery. Earlier this morning, when the patient was examined during rounds, she was experiencing mild dysphagia, and steroids were ordered. Now, the patient says she cannot breathe well unless she is sitting upright. Her vital signs are stable, with an O2 saturation of 93%. Her incision is swollen and appears full.
Stat radiograph of the cervical spine is obtained (shown). What is your impression?
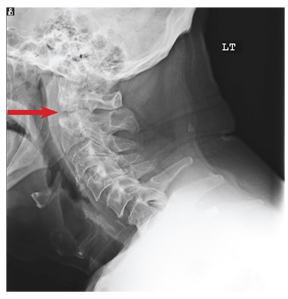


 Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.