User login
SCAI releases first definition of cardiogenic shock
LAS VEGAS – The Society for Cardiovascular Angiography & Interventions released on May 19 the first-ever classification scheme for cardiogenic shock, dividing the condition into five severity levels.

The expert consensus panel that devised the new definition and classification model hopes it will spearhead a reset of research into the management of cardiogenic shock so that clinicians can assess interventions and introduce them into practice in a more precise, reproducible, and systematic way, Srihari S. Naidu, MD, said while presenting the proposal at the society’s annual scientific sessions.
The writing panel’s hope is that the new definition will “drive earlier recognition of shock and at a more precise stage to guide appropriate and timely escalation of care” and to “better define prospectively the value of mechanical circulatory support, extracorporeal membrane oxygenation, and other therapies,” said Dr. Naidu, chair of the writing group, as well as professor of medicine at New York Medical College and director of the cardiac catheterization laboratory at Westchester Medical Center, both in Valhalla, N.Y.

At the core of the classification scheme are the definitions for five strata of disease, which start at stage A, the “at-risk” patients before shock onset, and progress through stage B, “beginning”; stage C, “classic”; stage D, “deteriorating”; and stage E, “extremis,” which defines a patient with circulatory collapse (Catheter Cardiovasc Interv. 2019 May 19; doi: 10.1002/ccd.28329). Another key element of the classification model is the cardiac arrest “modifier,” designated by a subscripted letter A, which identifies patients who have had a cardiac arrest, regardless of duration. So a patient could be a stage BA, which identifies a patient with clinical evidence of relative hypotension or tachycardia without hypoperfusion and with a history of cardiac arrest.
The statement also itemizes several biomarkers and hemodynamic measurements that need regular, serial monitoring, such as blood lactate and right arterial pressure. Although the document leaves specific, defining values for some of these measures vaguely defined – the intent is that future research will fill in these gaps – the overall message is that clinicians caring for cardiogenic shock patients “need to be aggressive and look for these things,” Dr. Naidu said in a video interview.
“Until we agree on a definition of cardiogenic shock, we can’t go anywhere,” commented Larry S. Dean, MD, professor of medicine at and director of the Regional Heart Center of the University of Washington in Seattle. “There are a lot of conflicting data out there, and until we have a shared definition, we can’t advance our practice. We need to start looking at shock patients in a more precise way.”
“Without a clear definition of cardiogenic shock we will never improve patient outcomes. Every shock trial must define shock. If investigators just say ‘patients were in shock,’ I don’t know what that means,” noted Navin K. Kapur, MD, director of the Interventional Research Laboratories at Tufts Medical Center in Boston and a member of the writing panel.

Dr. Naidu and others on the panel highlighted the need to now validate the classification scheme’s ability to consistently categorize patients and predict their disease trajectories. They have begun the validation process with a 10,000-patient database of “all-comers” with cardiogenic shock maintained by the Mayo Clinic. Full results from this analysis will be out soon, but Dr. Naidu revealed in passing that it successfully provided validation of the proposed scheme.
The new definition received endorsements from the American College of Cardiology, the American Heart Association, the Society of Critical Care Medicine, and the Society of Thoracic Surgeons.
Dr. Naidu had no disclosures.
LAS VEGAS – The Society for Cardiovascular Angiography & Interventions released on May 19 the first-ever classification scheme for cardiogenic shock, dividing the condition into five severity levels.
The expert consensus panel that devised the new definition and classification model hopes it will spearhead a reset of research into the management of cardiogenic shock so that clinicians can assess interventions and introduce them into practice in a more precise, reproducible, and systematic way, Srihari S. Naidu, MD, said while presenting the proposal at the society’s annual scientific sessions.
The writing panel’s hope is that the new definition will “drive earlier recognition of shock and at a more precise stage to guide appropriate and timely escalation of care” and to “better define prospectively the value of mechanical circulatory support, extracorporeal membrane oxygenation, and other therapies,” said Dr. Naidu, chair of the writing group, as well as professor of medicine at New York Medical College and director of the cardiac catheterization laboratory at Westchester Medical Center, both in Valhalla, N.Y.
At the core of the classification scheme are the definitions for five strata of disease, which start at stage A, the “at-risk” patients before shock onset, and progress through stage B, “beginning”; stage C, “classic”; stage D, “deteriorating”; and stage E, “extremis,” which defines a patient with circulatory collapse (Catheter Cardiovasc Interv. 2019 May 19; doi: 10.1002/ccd.28329). Another key element of the classification model is the cardiac arrest “modifier,” designated by a subscripted letter A, which identifies patients who have had a cardiac arrest, regardless of duration. So a patient could be a stage BA, which identifies a patient with clinical evidence of relative hypotension or tachycardia without hypoperfusion and with a history of cardiac arrest.
The statement also itemizes several biomarkers and hemodynamic measurements that need regular, serial monitoring, such as blood lactate and right arterial pressure. Although the document leaves specific, defining values for some of these measures vaguely defined – the intent is that future research will fill in these gaps – the overall message is that clinicians caring for cardiogenic shock patients “need to be aggressive and look for these things,” Dr. Naidu said in a video interview.
“Until we agree on a definition of cardiogenic shock, we can’t go anywhere,” commented Larry S. Dean, MD, professor of medicine at and director of the Regional Heart Center of the University of Washington in Seattle. “There are a lot of conflicting data out there, and until we have a shared definition, we can’t advance our practice. We need to start looking at shock patients in a more precise way.”
“Without a clear definition of cardiogenic shock we will never improve patient outcomes. Every shock trial must define shock. If investigators just say ‘patients were in shock,’ I don’t know what that means,” noted Navin K. Kapur, MD, director of the Interventional Research Laboratories at Tufts Medical Center in Boston and a member of the writing panel.
Dr. Naidu and others on the panel highlighted the need to now validate the classification scheme’s ability to consistently categorize patients and predict their disease trajectories. They have begun the validation process with a 10,000-patient database of “all-comers” with cardiogenic shock maintained by the Mayo Clinic. Full results from this analysis will be out soon, but Dr. Naidu revealed in passing that it successfully provided validation of the proposed scheme.
The new definition received endorsements from the American College of Cardiology, the American Heart Association, the Society of Critical Care Medicine, and the Society of Thoracic Surgeons.
Dr. Naidu had no disclosures.
LAS VEGAS – The Society for Cardiovascular Angiography & Interventions released on May 19 the first-ever classification scheme for cardiogenic shock, dividing the condition into five severity levels.
The expert consensus panel that devised the new definition and classification model hopes it will spearhead a reset of research into the management of cardiogenic shock so that clinicians can assess interventions and introduce them into practice in a more precise, reproducible, and systematic way, Srihari S. Naidu, MD, said while presenting the proposal at the society’s annual scientific sessions.
The writing panel’s hope is that the new definition will “drive earlier recognition of shock and at a more precise stage to guide appropriate and timely escalation of care” and to “better define prospectively the value of mechanical circulatory support, extracorporeal membrane oxygenation, and other therapies,” said Dr. Naidu, chair of the writing group, as well as professor of medicine at New York Medical College and director of the cardiac catheterization laboratory at Westchester Medical Center, both in Valhalla, N.Y.
At the core of the classification scheme are the definitions for five strata of disease, which start at stage A, the “at-risk” patients before shock onset, and progress through stage B, “beginning”; stage C, “classic”; stage D, “deteriorating”; and stage E, “extremis,” which defines a patient with circulatory collapse (Catheter Cardiovasc Interv. 2019 May 19; doi: 10.1002/ccd.28329). Another key element of the classification model is the cardiac arrest “modifier,” designated by a subscripted letter A, which identifies patients who have had a cardiac arrest, regardless of duration. So a patient could be a stage BA, which identifies a patient with clinical evidence of relative hypotension or tachycardia without hypoperfusion and with a history of cardiac arrest.
The statement also itemizes several biomarkers and hemodynamic measurements that need regular, serial monitoring, such as blood lactate and right arterial pressure. Although the document leaves specific, defining values for some of these measures vaguely defined – the intent is that future research will fill in these gaps – the overall message is that clinicians caring for cardiogenic shock patients “need to be aggressive and look for these things,” Dr. Naidu said in a video interview.
“Until we agree on a definition of cardiogenic shock, we can’t go anywhere,” commented Larry S. Dean, MD, professor of medicine at and director of the Regional Heart Center of the University of Washington in Seattle. “There are a lot of conflicting data out there, and until we have a shared definition, we can’t advance our practice. We need to start looking at shock patients in a more precise way.”
“Without a clear definition of cardiogenic shock we will never improve patient outcomes. Every shock trial must define shock. If investigators just say ‘patients were in shock,’ I don’t know what that means,” noted Navin K. Kapur, MD, director of the Interventional Research Laboratories at Tufts Medical Center in Boston and a member of the writing panel.
Dr. Naidu and others on the panel highlighted the need to now validate the classification scheme’s ability to consistently categorize patients and predict their disease trajectories. They have begun the validation process with a 10,000-patient database of “all-comers” with cardiogenic shock maintained by the Mayo Clinic. Full results from this analysis will be out soon, but Dr. Naidu revealed in passing that it successfully provided validation of the proposed scheme.
The new definition received endorsements from the American College of Cardiology, the American Heart Association, the Society of Critical Care Medicine, and the Society of Thoracic Surgeons.
Dr. Naidu had no disclosures.
REPORTING FROM SCAI 2019
CABANA: Heart failure patients got biggest bang from AFib ablation
SAN FRANCISCO – Catheter ablation of atrial fibrillation (AFib) in the roughly one-third of patients with heart failure enrolled in the CABANA multicenter, randomized trial produced striking, statistically significant improvements both in the study’s primary, combined endpoint and in all-cause mortality in intention-to-treat analyses.

These findings, from prespecified secondary analyses, contrasted with the study’s overall result, which showed no benefit in the primary endpoint analysis in the total study population of 2,204 patients with AFib (JAMA. 2019 Apr 2;321[13]:1261-74). They are also at odds with the primary endpoint result in the two-thirds of enrolled patients without heart failure, which showed no significant between-group differences in these two outcome measures among the patients assigned to the catheter ablation arm and the study’s control, which was medical management arm.
Among the 778 AFib patients enrolled in CABANA with any form of heart failure (35% of the total study enrollment), the incidence of the study’s primary endpoint – the combined rate of death, disabling stroke, serious bleeding, or cardiac arrest during a median follow-up of slightly more than 4 years – was 36% lower among the catheter-ablated heart failure patients than in the heart failure patients assigned to medical treatment, according to an intention-to-treat analysis, which was a statistically significant difference. The incidence of all-cause mortality during follow-up was 43% lower in the ablated heart failure patients, compared with the controls, Douglas L. Packer, MD, said at the annual scientific sessions of the Heart Rhythm Society.
In contrast, among enrolled patients without heart failure, the intention-to-treat primary endpoint was 6% higher in the ablated patients, and all-cause mortality was a relative 27% higher, although neither difference was statistically significant.
It’s a “little surprising” that the results showed this much benefit in the patients with heart failure, said Dr. Packer, professor of medicine at the Mayo Clinic in Rochester, Minn., and lead investigator of the CABANA (Catheter Ablation vs Anti-Arrhythmic Drug Therapy for Atrial Fibrillation) trial. “I think these data confirm the results of the CASTLE-AF trial, but without some of the glitches some people have cited” about that study, such as concerns about a high level of patient selection in CASTLE-AF and its relatively modest number of enrolled patients, he said in an interview.
The CASTLE-AF (Catheter Ablation vs. Standard Conventional Treatment in Patients With LV Dysfunction and AF) study, run entirely in patients with heart failure with reduced ejection fraction and AFib, showed a statistically significant improvement in patient survival and heart failure hospitalization after catheter ablation compared with medical management (N Engl J Med. 2018 Feb 1;378[5]:417-27). Prior to the CASTLE-AF report, results from several other small studies (J Interv Card Electrophysiol. 2018 Oct;53[1]:19-29), as well as those from the AATAC trial (Circulation. 2016 Apr 26;133[17]:1637-44), also showed consistent evidence for benefit from catheter ablation in patients with heart failure and AFib, noted CABANA coinvestigator Jonathan P. Piccini, MD, during a separate talk at the meeting.
“The improvement of cardiovascular outcomes with ablation in patients with heart failure and AFib is consistent across multiple trials, at least with respect to heart failure with reduced ejection fraction” concluded Dr. Piccini, a cardiac electrophysiologist at Duke University in Durham, N.C.
As a result of the new heart failure analysis, “I think the guidelines will change,” predicted Dr. Packer, with catheter ablation receiving a firmer endorsement for patients with heart failure the next time U.S. guidelines for heart failure and AFib management are updated. The findings say “there is substantial benefit of catheter ablation in heart failure patients, but I don’t think our findings lessen the utility of ablation in patients without heart failure,” he stressed. Even patients without heart failure showed reduction in AFib burden and improvement in quality of life that were similar to what was seen in the heart failure patients.
The new report from CABANA of benefit from AFib catheter ablation in patients with heart failure “absolutely advances the evidence,” commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago. “A number of us were quite circumspect about this based on the CASTLE-AF data, but the new CABANA analyses have addressed our anxiety that the CASTLE-AF results were just by chance.” The new CABANA analyses “may not confirm CASTLE-AF, but it enriches the conversation and makes it possible that we are seeing benefit in some patients with heart failure who get ablated.”
Dr. Yancy, who chaired the most recent update to the U.S. heart failure management guideline (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803) stopped short of saying that the cumulative evidence now supports a guideline change, but he acknowledged in an interview that the evidence could legitimately influence practice. Catheter ablation should now be “strongly considered” in patients with heart failure and AFib, he said, although he also had three qualifications for opting for this approach: Patients must already be on guideline-directed medical therapy for their heart failure, the catheter ablation needs to be performed by an experienced and skilled operator, and follow-up surveillance must focus on both the patient’s AFib and heart failure. “It’s absolutely appropriate to consider catheter ablation” for heart failure patients, but the evidence is not yet there for guideline change, Dr. Yancy concluded.
It remains uncertain why catheter ablation of AFib should be more effective in patients with heart failure than in those without. Dr. Packer speculated that one reason may be the heart rate reduction that AFib ablation produces may especially benefit heart failure patients. An additional helpful effect of ablation in heart failure patients may be reducing heart rate variability. Another notable finding of the new analysis was that 79% of patients with heart failure in CABANA had heart failure with preserved ejection fraction, with a left ventricular ejection fraction of at least 50%. “Getting rid of AFib in patients with heart failure with preserved ejection fraction will be more important than we have thought,” Dr. Packer said.
Other new CABANA analyses presented for the first time in separate talks at the meeting also showed that, while catheter ablation had no meaningful difference in effect on outcomes based on the sex of patients, both age and minority ethnic and racial status appeared to make a substantial difference. For CABANA’s primary endpoint, catheter ablation was especially effective for improving outcomes in patients 64 years old or younger, and the analysis showed a signal of possibly worse outcomes in patients who were at least 75 years old. The “substantially” better outcomes in minority-group patients represented the largest between-group difference among subgroups seen in CABANA and is a “big deal,” said Dr. Packer, who predicted that future catheter ablation use will likely rise in patients with heart failure, in younger patients, and in minority patients.
Dr. Piccini noted that, “it’s possible that CABANA identified some patient subgroups that do really well after ablation, but the problem is that, in the United States, we now often don’t treat” minority patients or those with reduced left ventricular ejection fractions with ablation, according to recent registry findings.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and/or received research funding from these four companies, as well as numerous drug and device companies, and has a financial interest in a licensed AFib mapping technology. Dr. Piccini has ties Boston Scientific, Medtronic, and numerous other drug and device companies, and disclosed an unspecified relationship with GlaxoSmithKline. Dr. Yancy disclosed an unspecified relationship with Abbott Laboratories.
SOURCE: Packer DL. Heart Rhythm 2019, Abstract S-AB14-06.
SAN FRANCISCO – Catheter ablation of atrial fibrillation (AFib) in the roughly one-third of patients with heart failure enrolled in the CABANA multicenter, randomized trial produced striking, statistically significant improvements both in the study’s primary, combined endpoint and in all-cause mortality in intention-to-treat analyses.
These findings, from prespecified secondary analyses, contrasted with the study’s overall result, which showed no benefit in the primary endpoint analysis in the total study population of 2,204 patients with AFib (JAMA. 2019 Apr 2;321[13]:1261-74). They are also at odds with the primary endpoint result in the two-thirds of enrolled patients without heart failure, which showed no significant between-group differences in these two outcome measures among the patients assigned to the catheter ablation arm and the study’s control, which was medical management arm.
Among the 778 AFib patients enrolled in CABANA with any form of heart failure (35% of the total study enrollment), the incidence of the study’s primary endpoint – the combined rate of death, disabling stroke, serious bleeding, or cardiac arrest during a median follow-up of slightly more than 4 years – was 36% lower among the catheter-ablated heart failure patients than in the heart failure patients assigned to medical treatment, according to an intention-to-treat analysis, which was a statistically significant difference. The incidence of all-cause mortality during follow-up was 43% lower in the ablated heart failure patients, compared with the controls, Douglas L. Packer, MD, said at the annual scientific sessions of the Heart Rhythm Society.
In contrast, among enrolled patients without heart failure, the intention-to-treat primary endpoint was 6% higher in the ablated patients, and all-cause mortality was a relative 27% higher, although neither difference was statistically significant.
It’s a “little surprising” that the results showed this much benefit in the patients with heart failure, said Dr. Packer, professor of medicine at the Mayo Clinic in Rochester, Minn., and lead investigator of the CABANA (Catheter Ablation vs Anti-Arrhythmic Drug Therapy for Atrial Fibrillation) trial. “I think these data confirm the results of the CASTLE-AF trial, but without some of the glitches some people have cited” about that study, such as concerns about a high level of patient selection in CASTLE-AF and its relatively modest number of enrolled patients, he said in an interview.
The CASTLE-AF (Catheter Ablation vs. Standard Conventional Treatment in Patients With LV Dysfunction and AF) study, run entirely in patients with heart failure with reduced ejection fraction and AFib, showed a statistically significant improvement in patient survival and heart failure hospitalization after catheter ablation compared with medical management (N Engl J Med. 2018 Feb 1;378[5]:417-27). Prior to the CASTLE-AF report, results from several other small studies (J Interv Card Electrophysiol. 2018 Oct;53[1]:19-29), as well as those from the AATAC trial (Circulation. 2016 Apr 26;133[17]:1637-44), also showed consistent evidence for benefit from catheter ablation in patients with heart failure and AFib, noted CABANA coinvestigator Jonathan P. Piccini, MD, during a separate talk at the meeting.
“The improvement of cardiovascular outcomes with ablation in patients with heart failure and AFib is consistent across multiple trials, at least with respect to heart failure with reduced ejection fraction” concluded Dr. Piccini, a cardiac electrophysiologist at Duke University in Durham, N.C.
As a result of the new heart failure analysis, “I think the guidelines will change,” predicted Dr. Packer, with catheter ablation receiving a firmer endorsement for patients with heart failure the next time U.S. guidelines for heart failure and AFib management are updated. The findings say “there is substantial benefit of catheter ablation in heart failure patients, but I don’t think our findings lessen the utility of ablation in patients without heart failure,” he stressed. Even patients without heart failure showed reduction in AFib burden and improvement in quality of life that were similar to what was seen in the heart failure patients.
The new report from CABANA of benefit from AFib catheter ablation in patients with heart failure “absolutely advances the evidence,” commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago. “A number of us were quite circumspect about this based on the CASTLE-AF data, but the new CABANA analyses have addressed our anxiety that the CASTLE-AF results were just by chance.” The new CABANA analyses “may not confirm CASTLE-AF, but it enriches the conversation and makes it possible that we are seeing benefit in some patients with heart failure who get ablated.”
Dr. Yancy, who chaired the most recent update to the U.S. heart failure management guideline (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803) stopped short of saying that the cumulative evidence now supports a guideline change, but he acknowledged in an interview that the evidence could legitimately influence practice. Catheter ablation should now be “strongly considered” in patients with heart failure and AFib, he said, although he also had three qualifications for opting for this approach: Patients must already be on guideline-directed medical therapy for their heart failure, the catheter ablation needs to be performed by an experienced and skilled operator, and follow-up surveillance must focus on both the patient’s AFib and heart failure. “It’s absolutely appropriate to consider catheter ablation” for heart failure patients, but the evidence is not yet there for guideline change, Dr. Yancy concluded.
It remains uncertain why catheter ablation of AFib should be more effective in patients with heart failure than in those without. Dr. Packer speculated that one reason may be the heart rate reduction that AFib ablation produces may especially benefit heart failure patients. An additional helpful effect of ablation in heart failure patients may be reducing heart rate variability. Another notable finding of the new analysis was that 79% of patients with heart failure in CABANA had heart failure with preserved ejection fraction, with a left ventricular ejection fraction of at least 50%. “Getting rid of AFib in patients with heart failure with preserved ejection fraction will be more important than we have thought,” Dr. Packer said.
Other new CABANA analyses presented for the first time in separate talks at the meeting also showed that, while catheter ablation had no meaningful difference in effect on outcomes based on the sex of patients, both age and minority ethnic and racial status appeared to make a substantial difference. For CABANA’s primary endpoint, catheter ablation was especially effective for improving outcomes in patients 64 years old or younger, and the analysis showed a signal of possibly worse outcomes in patients who were at least 75 years old. The “substantially” better outcomes in minority-group patients represented the largest between-group difference among subgroups seen in CABANA and is a “big deal,” said Dr. Packer, who predicted that future catheter ablation use will likely rise in patients with heart failure, in younger patients, and in minority patients.
Dr. Piccini noted that, “it’s possible that CABANA identified some patient subgroups that do really well after ablation, but the problem is that, in the United States, we now often don’t treat” minority patients or those with reduced left ventricular ejection fractions with ablation, according to recent registry findings.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and/or received research funding from these four companies, as well as numerous drug and device companies, and has a financial interest in a licensed AFib mapping technology. Dr. Piccini has ties Boston Scientific, Medtronic, and numerous other drug and device companies, and disclosed an unspecified relationship with GlaxoSmithKline. Dr. Yancy disclosed an unspecified relationship with Abbott Laboratories.
SOURCE: Packer DL. Heart Rhythm 2019, Abstract S-AB14-06.
SAN FRANCISCO – Catheter ablation of atrial fibrillation (AFib) in the roughly one-third of patients with heart failure enrolled in the CABANA multicenter, randomized trial produced striking, statistically significant improvements both in the study’s primary, combined endpoint and in all-cause mortality in intention-to-treat analyses.
These findings, from prespecified secondary analyses, contrasted with the study’s overall result, which showed no benefit in the primary endpoint analysis in the total study population of 2,204 patients with AFib (JAMA. 2019 Apr 2;321[13]:1261-74). They are also at odds with the primary endpoint result in the two-thirds of enrolled patients without heart failure, which showed no significant between-group differences in these two outcome measures among the patients assigned to the catheter ablation arm and the study’s control, which was medical management arm.
Among the 778 AFib patients enrolled in CABANA with any form of heart failure (35% of the total study enrollment), the incidence of the study’s primary endpoint – the combined rate of death, disabling stroke, serious bleeding, or cardiac arrest during a median follow-up of slightly more than 4 years – was 36% lower among the catheter-ablated heart failure patients than in the heart failure patients assigned to medical treatment, according to an intention-to-treat analysis, which was a statistically significant difference. The incidence of all-cause mortality during follow-up was 43% lower in the ablated heart failure patients, compared with the controls, Douglas L. Packer, MD, said at the annual scientific sessions of the Heart Rhythm Society.
In contrast, among enrolled patients without heart failure, the intention-to-treat primary endpoint was 6% higher in the ablated patients, and all-cause mortality was a relative 27% higher, although neither difference was statistically significant.
It’s a “little surprising” that the results showed this much benefit in the patients with heart failure, said Dr. Packer, professor of medicine at the Mayo Clinic in Rochester, Minn., and lead investigator of the CABANA (Catheter Ablation vs Anti-Arrhythmic Drug Therapy for Atrial Fibrillation) trial. “I think these data confirm the results of the CASTLE-AF trial, but without some of the glitches some people have cited” about that study, such as concerns about a high level of patient selection in CASTLE-AF and its relatively modest number of enrolled patients, he said in an interview.
The CASTLE-AF (Catheter Ablation vs. Standard Conventional Treatment in Patients With LV Dysfunction and AF) study, run entirely in patients with heart failure with reduced ejection fraction and AFib, showed a statistically significant improvement in patient survival and heart failure hospitalization after catheter ablation compared with medical management (N Engl J Med. 2018 Feb 1;378[5]:417-27). Prior to the CASTLE-AF report, results from several other small studies (J Interv Card Electrophysiol. 2018 Oct;53[1]:19-29), as well as those from the AATAC trial (Circulation. 2016 Apr 26;133[17]:1637-44), also showed consistent evidence for benefit from catheter ablation in patients with heart failure and AFib, noted CABANA coinvestigator Jonathan P. Piccini, MD, during a separate talk at the meeting.
“The improvement of cardiovascular outcomes with ablation in patients with heart failure and AFib is consistent across multiple trials, at least with respect to heart failure with reduced ejection fraction” concluded Dr. Piccini, a cardiac electrophysiologist at Duke University in Durham, N.C.
As a result of the new heart failure analysis, “I think the guidelines will change,” predicted Dr. Packer, with catheter ablation receiving a firmer endorsement for patients with heart failure the next time U.S. guidelines for heart failure and AFib management are updated. The findings say “there is substantial benefit of catheter ablation in heart failure patients, but I don’t think our findings lessen the utility of ablation in patients without heart failure,” he stressed. Even patients without heart failure showed reduction in AFib burden and improvement in quality of life that were similar to what was seen in the heart failure patients.
The new report from CABANA of benefit from AFib catheter ablation in patients with heart failure “absolutely advances the evidence,” commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago. “A number of us were quite circumspect about this based on the CASTLE-AF data, but the new CABANA analyses have addressed our anxiety that the CASTLE-AF results were just by chance.” The new CABANA analyses “may not confirm CASTLE-AF, but it enriches the conversation and makes it possible that we are seeing benefit in some patients with heart failure who get ablated.”
Dr. Yancy, who chaired the most recent update to the U.S. heart failure management guideline (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803) stopped short of saying that the cumulative evidence now supports a guideline change, but he acknowledged in an interview that the evidence could legitimately influence practice. Catheter ablation should now be “strongly considered” in patients with heart failure and AFib, he said, although he also had three qualifications for opting for this approach: Patients must already be on guideline-directed medical therapy for their heart failure, the catheter ablation needs to be performed by an experienced and skilled operator, and follow-up surveillance must focus on both the patient’s AFib and heart failure. “It’s absolutely appropriate to consider catheter ablation” for heart failure patients, but the evidence is not yet there for guideline change, Dr. Yancy concluded.
It remains uncertain why catheter ablation of AFib should be more effective in patients with heart failure than in those without. Dr. Packer speculated that one reason may be the heart rate reduction that AFib ablation produces may especially benefit heart failure patients. An additional helpful effect of ablation in heart failure patients may be reducing heart rate variability. Another notable finding of the new analysis was that 79% of patients with heart failure in CABANA had heart failure with preserved ejection fraction, with a left ventricular ejection fraction of at least 50%. “Getting rid of AFib in patients with heart failure with preserved ejection fraction will be more important than we have thought,” Dr. Packer said.
Other new CABANA analyses presented for the first time in separate talks at the meeting also showed that, while catheter ablation had no meaningful difference in effect on outcomes based on the sex of patients, both age and minority ethnic and racial status appeared to make a substantial difference. For CABANA’s primary endpoint, catheter ablation was especially effective for improving outcomes in patients 64 years old or younger, and the analysis showed a signal of possibly worse outcomes in patients who were at least 75 years old. The “substantially” better outcomes in minority-group patients represented the largest between-group difference among subgroups seen in CABANA and is a “big deal,” said Dr. Packer, who predicted that future catheter ablation use will likely rise in patients with heart failure, in younger patients, and in minority patients.
Dr. Piccini noted that, “it’s possible that CABANA identified some patient subgroups that do really well after ablation, but the problem is that, in the United States, we now often don’t treat” minority patients or those with reduced left ventricular ejection fractions with ablation, according to recent registry findings.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and/or received research funding from these four companies, as well as numerous drug and device companies, and has a financial interest in a licensed AFib mapping technology. Dr. Piccini has ties Boston Scientific, Medtronic, and numerous other drug and device companies, and disclosed an unspecified relationship with GlaxoSmithKline. Dr. Yancy disclosed an unspecified relationship with Abbott Laboratories.
SOURCE: Packer DL. Heart Rhythm 2019, Abstract S-AB14-06.
REPORTING FROM HEART RHYTHM 2019
Key clinical point: Catheter ablation for atrial fibrillation is especially effective in patients with heart failure.
Major finding: Heart failure patients treated with catheter ablation had a 36% relative cut in the primary endpoint, compared with control patients.
Study details: CABANA, a multicenter, randomized trial with 2,204 patients, including 778 patients with heart failure.
Disclosures: CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and/or received research funding from these four companies, as well as numerous drug and device companies, and has a financial interest in a licensed AFib mapping technology. Source: Packer DL. Heart Rhythm 2019, Abstract S-AB14-06.
Stroke policy recommendations incorporate advances in endovascular therapy
Stroke centers need to collaborate within their regions to assure best practices and optimal access to comprehensive stroke centers as well as newly-designated thrombectomy-capable stroke centers, according to an updated policy statement from the American Stroke Association published in Stroke.

Opeolu Adeoye, MD, associate professor of emergency medicine and neurosurgery at the University of Cincinnati – and chair of the policy statement writing group – and coauthors updated the ASA’s 2005 recommendations for policy makers and public health care agencies to reflect current evidence, the increased availability of endovascular therapy, and new stroke center certifications.
“We have seen monumental advancements in acute stroke care over the past 14 years, and our concept of a comprehensive stroke system of care has evolved as a result,” Dr. Adeoye said in a news release.
While a recommendation to support the initiation of stroke prevention regimens remains unchanged from the 2005 recommendations, the 2019 update emphasizes a need to support long-term adherence to such regimens. To that end, researchers should examine the potential benefits of stroke prevention efforts that incorporate social media, gamification, and other technologies and principles to promote healthy behavior, the authors suggested. Furthermore, technology may allow for the passive surveillance of baseline behaviors and enable researchers to track changes in behavior over time.
Thrombectomy-capable centers
Thrombectomy-capable stroke centers, which have capabilities between those of primary stroke centers and comprehensive stroke centers, provide a relatively new level of acute stroke care. In communities that do not otherwise have access to thrombectomy, these centers play a clear role. In communities with comprehensive stroke centers, their role “is more controversial, and routing plans for patients with a suspected LVO [large vessel occlusion] should always seek the center of highest capability when travel time differences are short,” the statement says.
Timely parenchymal and arterial imaging via CT or MRI are needed to identify the subset of patients who may benefit from thrombectomy. All centers managing stroke patients should develop a plan for the definitive identification and treatment of these patients. Imaging techniques that assess penumbral patterns to identify candidates for endovascular therapy between 6 and 24 hours after patients were last known to be normal “merit broader adoption,” the statement says.
Hospitals without thrombectomy capability should have transfer protocols to allow the rapid treatment of these patients to hospitals with the appropriate level of care. In rural facilities that lack 24/7 imaging and radiology capabilities, this may mean rapid transfer of patients with clinically suspected LVO to hospitals where their work-up may be expedited.
To improve process, centers providing thrombectomy should rigorously track patient flow at all time points from presentation to imaging to intervention. Reperfusion rates, procedural complications, and patient clinical outcomes must be tracked and reported.
Travel times
Triage paradigms and protocols should be developed to ensure that emergency medical service (EMS) providers are able to rapidly identify all patients with a known or suspected stroke and to assess them with a validated and standardized instrument for stroke screening such as FAST (Face, Arm, Speech, Time), Los Angeles Prehospital Stroke Screen, or Cincinnati Prehospital Stroke Scale.
In prehospital patients who screen positive for suspected stroke, a standard prehospital stroke severity assessment tool such as the Cincinnati Stroke Triage Assessment Tool, Rapid Arterial Occlusion Evaluation, Los Angeles Motor Scale, or Field Assessment Stroke Triage for Emergency Destination should be used. “Further research is needed to establish the most effective prehospital stroke severity triage scale,” the authors noted. In all cases, EMS should notify hospitals that a stroke patient is en route.
“When there are several intravenous alteplase–capable hospitals in a well-defined geographic region, extra transportation times to reach a facility capable of endovascular thrombectomy should be limited to no more than 15 minutes in patients with a prehospital stroke severity score suggestive of LVO,” according to the recommendations. “When several hospital options exist within similar travel times, EMS should seek care at the facility capable of offering the highest level of stroke care. Further research is needed to establish travel time parameters for hospital bypass in cases of prehospital suspicion of LVO.”
Outcomes and discharge
Centers should track various treatment and patient outcomes, and all patients discharged to their homes should have appropriate follow-up with specialized stroke services and primary care and be screened for postacute complications.
Government institutions should standardize the organization of stroke care, ensure that stroke patients receive timely care at appropriate hospitals, and facilitate access to secondary prevention and rehabilitation resources after stroke, the authors wrote.
“Programs geared at further improving the knowledge of the public, encouraging primordial and primary prevention, advancing and facilitating acute therapy, improving secondary prevention and recovery from stroke, and reducing disparities in stroke care should be actively developed in a coordinated and collaborative fashion by providers and policymakers at the local, state, and national levels,” the authors concluded. “Such efforts will continue to mitigate the effects of stroke on society.”
Dr. Adeoye had no disclosures. Some coauthors reported research grants and consultant or advisory board positions.
SOURCE: Adeoye O et al. Stroke. 2019 May 20. doi: 10.1161/STR.0000000000000173.
When determining where to transport a patient with stroke, uncertainty about the patient’s diagnosis and eligibility for thrombectomy is a necessary consideration, said Robert A. Harrington, MD, of Stanford University (Calif.), in an accompanying editorial.
In lieu of better data, stroke systems should follow the recommendation of the Mission: Lifeline Severity-based Stroke Triage Algorithm for emergency medical services to avoid more than 15 minutes of additional travel time to transport a patient to a center that can perform endovascular therapy when the patient may be eligible for intravenous tissue plasminogen activator (tPA), said Dr. Harrington.
Delays in initiating tPA could lead to some patients not receiving treatment. “Some patients with suspected LVO [large vessel occlusion] either will not have thrombectomy or will not be eligible for it, and they also run the risk of not receiving any acute reperfusion therapy. Consequently, transport algorithms and models must take into account the uncertainty in prehospital diagnosis when considering the most appropriate facility,” he said.
Forthcoming acute stroke guidelines “will recommend intravenous tPA for all eligible subjects” because administration of tPA before endovascular thrombectomy does not appear to be harmful, Dr. Harrington noted.
Ultimately, approaches to routing patients may vary by region. “It is up to local and regional communities ... to define how best to implement these elements into a stroke system of care that meets their needs and resources and to define the types of hospitals that should qualify as points of entry for patients with suspected LVO strokes,” Dr. Harrington said.
A group convened by the American Heart Association and American Stroke Association is drafting further guiding principles for stroke systems of care in various regional settings.
Dr. Harrington is president-elect of the American Heart Association. He reported receiving research grants from AstraZeneca and Bristol-Myers Squibb.
When determining where to transport a patient with stroke, uncertainty about the patient’s diagnosis and eligibility for thrombectomy is a necessary consideration, said Robert A. Harrington, MD, of Stanford University (Calif.), in an accompanying editorial.
In lieu of better data, stroke systems should follow the recommendation of the Mission: Lifeline Severity-based Stroke Triage Algorithm for emergency medical services to avoid more than 15 minutes of additional travel time to transport a patient to a center that can perform endovascular therapy when the patient may be eligible for intravenous tissue plasminogen activator (tPA), said Dr. Harrington.
Delays in initiating tPA could lead to some patients not receiving treatment. “Some patients with suspected LVO [large vessel occlusion] either will not have thrombectomy or will not be eligible for it, and they also run the risk of not receiving any acute reperfusion therapy. Consequently, transport algorithms and models must take into account the uncertainty in prehospital diagnosis when considering the most appropriate facility,” he said.
Forthcoming acute stroke guidelines “will recommend intravenous tPA for all eligible subjects” because administration of tPA before endovascular thrombectomy does not appear to be harmful, Dr. Harrington noted.
Ultimately, approaches to routing patients may vary by region. “It is up to local and regional communities ... to define how best to implement these elements into a stroke system of care that meets their needs and resources and to define the types of hospitals that should qualify as points of entry for patients with suspected LVO strokes,” Dr. Harrington said.
A group convened by the American Heart Association and American Stroke Association is drafting further guiding principles for stroke systems of care in various regional settings.
Dr. Harrington is president-elect of the American Heart Association. He reported receiving research grants from AstraZeneca and Bristol-Myers Squibb.
When determining where to transport a patient with stroke, uncertainty about the patient’s diagnosis and eligibility for thrombectomy is a necessary consideration, said Robert A. Harrington, MD, of Stanford University (Calif.), in an accompanying editorial.
In lieu of better data, stroke systems should follow the recommendation of the Mission: Lifeline Severity-based Stroke Triage Algorithm for emergency medical services to avoid more than 15 minutes of additional travel time to transport a patient to a center that can perform endovascular therapy when the patient may be eligible for intravenous tissue plasminogen activator (tPA), said Dr. Harrington.
Delays in initiating tPA could lead to some patients not receiving treatment. “Some patients with suspected LVO [large vessel occlusion] either will not have thrombectomy or will not be eligible for it, and they also run the risk of not receiving any acute reperfusion therapy. Consequently, transport algorithms and models must take into account the uncertainty in prehospital diagnosis when considering the most appropriate facility,” he said.
Forthcoming acute stroke guidelines “will recommend intravenous tPA for all eligible subjects” because administration of tPA before endovascular thrombectomy does not appear to be harmful, Dr. Harrington noted.
Ultimately, approaches to routing patients may vary by region. “It is up to local and regional communities ... to define how best to implement these elements into a stroke system of care that meets their needs and resources and to define the types of hospitals that should qualify as points of entry for patients with suspected LVO strokes,” Dr. Harrington said.
A group convened by the American Heart Association and American Stroke Association is drafting further guiding principles for stroke systems of care in various regional settings.
Dr. Harrington is president-elect of the American Heart Association. He reported receiving research grants from AstraZeneca and Bristol-Myers Squibb.
Stroke centers need to collaborate within their regions to assure best practices and optimal access to comprehensive stroke centers as well as newly-designated thrombectomy-capable stroke centers, according to an updated policy statement from the American Stroke Association published in Stroke.
Opeolu Adeoye, MD, associate professor of emergency medicine and neurosurgery at the University of Cincinnati – and chair of the policy statement writing group – and coauthors updated the ASA’s 2005 recommendations for policy makers and public health care agencies to reflect current evidence, the increased availability of endovascular therapy, and new stroke center certifications.
“We have seen monumental advancements in acute stroke care over the past 14 years, and our concept of a comprehensive stroke system of care has evolved as a result,” Dr. Adeoye said in a news release.
While a recommendation to support the initiation of stroke prevention regimens remains unchanged from the 2005 recommendations, the 2019 update emphasizes a need to support long-term adherence to such regimens. To that end, researchers should examine the potential benefits of stroke prevention efforts that incorporate social media, gamification, and other technologies and principles to promote healthy behavior, the authors suggested. Furthermore, technology may allow for the passive surveillance of baseline behaviors and enable researchers to track changes in behavior over time.
Thrombectomy-capable centers
Thrombectomy-capable stroke centers, which have capabilities between those of primary stroke centers and comprehensive stroke centers, provide a relatively new level of acute stroke care. In communities that do not otherwise have access to thrombectomy, these centers play a clear role. In communities with comprehensive stroke centers, their role “is more controversial, and routing plans for patients with a suspected LVO [large vessel occlusion] should always seek the center of highest capability when travel time differences are short,” the statement says.
Timely parenchymal and arterial imaging via CT or MRI are needed to identify the subset of patients who may benefit from thrombectomy. All centers managing stroke patients should develop a plan for the definitive identification and treatment of these patients. Imaging techniques that assess penumbral patterns to identify candidates for endovascular therapy between 6 and 24 hours after patients were last known to be normal “merit broader adoption,” the statement says.
Hospitals without thrombectomy capability should have transfer protocols to allow the rapid treatment of these patients to hospitals with the appropriate level of care. In rural facilities that lack 24/7 imaging and radiology capabilities, this may mean rapid transfer of patients with clinically suspected LVO to hospitals where their work-up may be expedited.
To improve process, centers providing thrombectomy should rigorously track patient flow at all time points from presentation to imaging to intervention. Reperfusion rates, procedural complications, and patient clinical outcomes must be tracked and reported.
Travel times
Triage paradigms and protocols should be developed to ensure that emergency medical service (EMS) providers are able to rapidly identify all patients with a known or suspected stroke and to assess them with a validated and standardized instrument for stroke screening such as FAST (Face, Arm, Speech, Time), Los Angeles Prehospital Stroke Screen, or Cincinnati Prehospital Stroke Scale.
In prehospital patients who screen positive for suspected stroke, a standard prehospital stroke severity assessment tool such as the Cincinnati Stroke Triage Assessment Tool, Rapid Arterial Occlusion Evaluation, Los Angeles Motor Scale, or Field Assessment Stroke Triage for Emergency Destination should be used. “Further research is needed to establish the most effective prehospital stroke severity triage scale,” the authors noted. In all cases, EMS should notify hospitals that a stroke patient is en route.
“When there are several intravenous alteplase–capable hospitals in a well-defined geographic region, extra transportation times to reach a facility capable of endovascular thrombectomy should be limited to no more than 15 minutes in patients with a prehospital stroke severity score suggestive of LVO,” according to the recommendations. “When several hospital options exist within similar travel times, EMS should seek care at the facility capable of offering the highest level of stroke care. Further research is needed to establish travel time parameters for hospital bypass in cases of prehospital suspicion of LVO.”
Outcomes and discharge
Centers should track various treatment and patient outcomes, and all patients discharged to their homes should have appropriate follow-up with specialized stroke services and primary care and be screened for postacute complications.
Government institutions should standardize the organization of stroke care, ensure that stroke patients receive timely care at appropriate hospitals, and facilitate access to secondary prevention and rehabilitation resources after stroke, the authors wrote.
“Programs geared at further improving the knowledge of the public, encouraging primordial and primary prevention, advancing and facilitating acute therapy, improving secondary prevention and recovery from stroke, and reducing disparities in stroke care should be actively developed in a coordinated and collaborative fashion by providers and policymakers at the local, state, and national levels,” the authors concluded. “Such efforts will continue to mitigate the effects of stroke on society.”
Dr. Adeoye had no disclosures. Some coauthors reported research grants and consultant or advisory board positions.
SOURCE: Adeoye O et al. Stroke. 2019 May 20. doi: 10.1161/STR.0000000000000173.
Stroke centers need to collaborate within their regions to assure best practices and optimal access to comprehensive stroke centers as well as newly-designated thrombectomy-capable stroke centers, according to an updated policy statement from the American Stroke Association published in Stroke.
Opeolu Adeoye, MD, associate professor of emergency medicine and neurosurgery at the University of Cincinnati – and chair of the policy statement writing group – and coauthors updated the ASA’s 2005 recommendations for policy makers and public health care agencies to reflect current evidence, the increased availability of endovascular therapy, and new stroke center certifications.
“We have seen monumental advancements in acute stroke care over the past 14 years, and our concept of a comprehensive stroke system of care has evolved as a result,” Dr. Adeoye said in a news release.
While a recommendation to support the initiation of stroke prevention regimens remains unchanged from the 2005 recommendations, the 2019 update emphasizes a need to support long-term adherence to such regimens. To that end, researchers should examine the potential benefits of stroke prevention efforts that incorporate social media, gamification, and other technologies and principles to promote healthy behavior, the authors suggested. Furthermore, technology may allow for the passive surveillance of baseline behaviors and enable researchers to track changes in behavior over time.
Thrombectomy-capable centers
Thrombectomy-capable stroke centers, which have capabilities between those of primary stroke centers and comprehensive stroke centers, provide a relatively new level of acute stroke care. In communities that do not otherwise have access to thrombectomy, these centers play a clear role. In communities with comprehensive stroke centers, their role “is more controversial, and routing plans for patients with a suspected LVO [large vessel occlusion] should always seek the center of highest capability when travel time differences are short,” the statement says.
Timely parenchymal and arterial imaging via CT or MRI are needed to identify the subset of patients who may benefit from thrombectomy. All centers managing stroke patients should develop a plan for the definitive identification and treatment of these patients. Imaging techniques that assess penumbral patterns to identify candidates for endovascular therapy between 6 and 24 hours after patients were last known to be normal “merit broader adoption,” the statement says.
Hospitals without thrombectomy capability should have transfer protocols to allow the rapid treatment of these patients to hospitals with the appropriate level of care. In rural facilities that lack 24/7 imaging and radiology capabilities, this may mean rapid transfer of patients with clinically suspected LVO to hospitals where their work-up may be expedited.
To improve process, centers providing thrombectomy should rigorously track patient flow at all time points from presentation to imaging to intervention. Reperfusion rates, procedural complications, and patient clinical outcomes must be tracked and reported.
Travel times
Triage paradigms and protocols should be developed to ensure that emergency medical service (EMS) providers are able to rapidly identify all patients with a known or suspected stroke and to assess them with a validated and standardized instrument for stroke screening such as FAST (Face, Arm, Speech, Time), Los Angeles Prehospital Stroke Screen, or Cincinnati Prehospital Stroke Scale.
In prehospital patients who screen positive for suspected stroke, a standard prehospital stroke severity assessment tool such as the Cincinnati Stroke Triage Assessment Tool, Rapid Arterial Occlusion Evaluation, Los Angeles Motor Scale, or Field Assessment Stroke Triage for Emergency Destination should be used. “Further research is needed to establish the most effective prehospital stroke severity triage scale,” the authors noted. In all cases, EMS should notify hospitals that a stroke patient is en route.
“When there are several intravenous alteplase–capable hospitals in a well-defined geographic region, extra transportation times to reach a facility capable of endovascular thrombectomy should be limited to no more than 15 minutes in patients with a prehospital stroke severity score suggestive of LVO,” according to the recommendations. “When several hospital options exist within similar travel times, EMS should seek care at the facility capable of offering the highest level of stroke care. Further research is needed to establish travel time parameters for hospital bypass in cases of prehospital suspicion of LVO.”
Outcomes and discharge
Centers should track various treatment and patient outcomes, and all patients discharged to their homes should have appropriate follow-up with specialized stroke services and primary care and be screened for postacute complications.
Government institutions should standardize the organization of stroke care, ensure that stroke patients receive timely care at appropriate hospitals, and facilitate access to secondary prevention and rehabilitation resources after stroke, the authors wrote.
“Programs geared at further improving the knowledge of the public, encouraging primordial and primary prevention, advancing and facilitating acute therapy, improving secondary prevention and recovery from stroke, and reducing disparities in stroke care should be actively developed in a coordinated and collaborative fashion by providers and policymakers at the local, state, and national levels,” the authors concluded. “Such efforts will continue to mitigate the effects of stroke on society.”
Dr. Adeoye had no disclosures. Some coauthors reported research grants and consultant or advisory board positions.
SOURCE: Adeoye O et al. Stroke. 2019 May 20. doi: 10.1161/STR.0000000000000173.
FROM STROKE
New risk score predicts cardiac-device infection
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
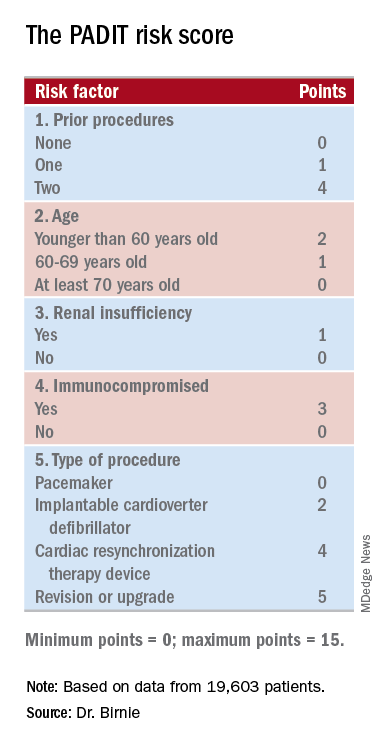
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
REPORTING FROM HEART RHYTHM 2019
Key clinical point: Researchers have devised a five-item scoring formula to predict a patient’s risk for infection from an cardiac rhythm–device procedure.
Major finding: The risk score had an optimism-corrected concordance statistic of 0.704.
Study details: Investigators developed the risk score using data from PADIT, a multicenter, randomized trial with 19,603 patients.
Disclosures: PADIT received no commercial funding. Dr. Birnie had no relevant disclosures.
Source: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.

Respiratory effects may account for worse survival in women undergoing DTA and TAAA repair
Women undergoing open descending thoracic aortic aneurysm (DTA) and open thoracoabdominal aortic aneurysm (TAAA) repair are not at greater risk for operative mortality than their male counterparts. However, they are at significantly greater risk for major adverse events and have significantly lower 5-year survival, according to the results of a single institution database review of 738 surgery patients.
From May 1997 to June 2017, there were 462 men (59%) and 321 women (41%) who underwent open repair of DTA or TAAA, according to Leonard N. Girardi, MD, and colleagues from Weill Cornell Medicine, New York, who performed the study published in the Journal of Vascular Surgery. The researchers used logistic regression and Cox regression analyses to assess the effect of sex on perioperative and long-term outcomes.
Demographically, women were significantly older (67.6 years vs. 62.6 years), with a significantly higher incidence of chronic obstructive pulmonary disease (47.0% vs. 35.7%) and a significantly greater percentage of patients with a forced expiratory volume in 1 second less than 50% (28.3% vs 18.2%). Degenerative aneurysms were significantly more common in women (61.7% vs. 41.6%), whereas chronic dissections significantly predominated in men (42.4% vs. 23.1%). Operative mortality was not significantly different between women and men (5.6% vs. 6.2%); however, women were significantly more likely to require a tracheostomy after surgery (10.6% vs. 5.0%).
Logistic regression found that being a woman was an independent risk factor for a composite of major adverse events (odds ratio, 2.68) and need for tracheostomy (OR, 3.73). In addition, women had significantly worse 5-year survival than men undergoing DTA or TAAA repair (59.7% vs. 66.2%, P =.025). There was no difference in overall survival between 1997-2007 and 2008-2017.
“Women and men undergoing TAAA repair have significant and consistent differences in preoperative characteristics. Despite these differences, operative mortality is similar between the two groups. However, women are at significantly increased risk of [major adverse events], especially respiratory failure, because of those differences in risk factors, including age, pulmonary function, and aneurysm etiology,” the researchers concluded.
The authors reported that they had no conflicts of interest.
SOURCE: Girardi LN et al. J Vasc Surg 2019;69:1028-35.
Women undergoing open descending thoracic aortic aneurysm (DTA) and open thoracoabdominal aortic aneurysm (TAAA) repair are not at greater risk for operative mortality than their male counterparts. However, they are at significantly greater risk for major adverse events and have significantly lower 5-year survival, according to the results of a single institution database review of 738 surgery patients.
From May 1997 to June 2017, there were 462 men (59%) and 321 women (41%) who underwent open repair of DTA or TAAA, according to Leonard N. Girardi, MD, and colleagues from Weill Cornell Medicine, New York, who performed the study published in the Journal of Vascular Surgery. The researchers used logistic regression and Cox regression analyses to assess the effect of sex on perioperative and long-term outcomes.
Demographically, women were significantly older (67.6 years vs. 62.6 years), with a significantly higher incidence of chronic obstructive pulmonary disease (47.0% vs. 35.7%) and a significantly greater percentage of patients with a forced expiratory volume in 1 second less than 50% (28.3% vs 18.2%). Degenerative aneurysms were significantly more common in women (61.7% vs. 41.6%), whereas chronic dissections significantly predominated in men (42.4% vs. 23.1%). Operative mortality was not significantly different between women and men (5.6% vs. 6.2%); however, women were significantly more likely to require a tracheostomy after surgery (10.6% vs. 5.0%).
Logistic regression found that being a woman was an independent risk factor for a composite of major adverse events (odds ratio, 2.68) and need for tracheostomy (OR, 3.73). In addition, women had significantly worse 5-year survival than men undergoing DTA or TAAA repair (59.7% vs. 66.2%, P =.025). There was no difference in overall survival between 1997-2007 and 2008-2017.
“Women and men undergoing TAAA repair have significant and consistent differences in preoperative characteristics. Despite these differences, operative mortality is similar between the two groups. However, women are at significantly increased risk of [major adverse events], especially respiratory failure, because of those differences in risk factors, including age, pulmonary function, and aneurysm etiology,” the researchers concluded.
The authors reported that they had no conflicts of interest.
SOURCE: Girardi LN et al. J Vasc Surg 2019;69:1028-35.
Women undergoing open descending thoracic aortic aneurysm (DTA) and open thoracoabdominal aortic aneurysm (TAAA) repair are not at greater risk for operative mortality than their male counterparts. However, they are at significantly greater risk for major adverse events and have significantly lower 5-year survival, according to the results of a single institution database review of 738 surgery patients.
From May 1997 to June 2017, there were 462 men (59%) and 321 women (41%) who underwent open repair of DTA or TAAA, according to Leonard N. Girardi, MD, and colleagues from Weill Cornell Medicine, New York, who performed the study published in the Journal of Vascular Surgery. The researchers used logistic regression and Cox regression analyses to assess the effect of sex on perioperative and long-term outcomes.
Demographically, women were significantly older (67.6 years vs. 62.6 years), with a significantly higher incidence of chronic obstructive pulmonary disease (47.0% vs. 35.7%) and a significantly greater percentage of patients with a forced expiratory volume in 1 second less than 50% (28.3% vs 18.2%). Degenerative aneurysms were significantly more common in women (61.7% vs. 41.6%), whereas chronic dissections significantly predominated in men (42.4% vs. 23.1%). Operative mortality was not significantly different between women and men (5.6% vs. 6.2%); however, women were significantly more likely to require a tracheostomy after surgery (10.6% vs. 5.0%).
Logistic regression found that being a woman was an independent risk factor for a composite of major adverse events (odds ratio, 2.68) and need for tracheostomy (OR, 3.73). In addition, women had significantly worse 5-year survival than men undergoing DTA or TAAA repair (59.7% vs. 66.2%, P =.025). There was no difference in overall survival between 1997-2007 and 2008-2017.
“Women and men undergoing TAAA repair have significant and consistent differences in preoperative characteristics. Despite these differences, operative mortality is similar between the two groups. However, women are at significantly increased risk of [major adverse events], especially respiratory failure, because of those differences in risk factors, including age, pulmonary function, and aneurysm etiology,” the researchers concluded.
The authors reported that they had no conflicts of interest.
SOURCE: Girardi LN et al. J Vasc Surg 2019;69:1028-35.
FROM THE JOURNAL OF VASCULAR SURGERY
TAVR for bicuspid aortic stenosis gets selective thumbs up
NEW ORLEANS – Results of the largest-ever analysis of TAVR in patients with bicuspid aortic stenosis indicate that key 30-day and 1-year outcomes are similar to those of propensity-matched TAVR patients with tricuspid disease, Raj R. Makkar, MD, said at the annual meeting of the American College of Cardiology.
“Select bicuspid anatomy is amenable to TAVR with current-generation, balloon-expandable TAVR technology with acceptable clinical outcomes. These data provide an argument for TAVR to be a reasonable alternative for bicuspid AS [aortic stenosis] patients who are at intermediate or high risk for surgical aortic valve replacement, which are the patients that are enrolled in this registry, and provide a sound basis to conduct a randomized clinical trial in young patients with bicuspid AS who are at low risk for surgery,” declared Dr. Makkar, director of interventional cardiology and the cardiac catheterization laboratory at Cedars-Sinai Medical Center in Los Angeles.
The landmark randomized trials of TAVR versus SAVR (surgical aortic valve replacement) that established TAVR as the preferred treatment for patients with severe aortic stenosis who are at high, intermediate, or low surgical risk systematically excluded patients with bicuspid AS, even though bicuspid anatomy is common, particularly in younger patients with AS.
Despite the absence of supportive randomized trial data, TAVR is being done for bicuspid AS. To learn how patients with bicuspid disease have fared, Dr. Makkar and coinvestigators analyzed the real-world Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy (STS/ACC TVT) Registry of all patients who underwent TAVR with the balloon-expandable Sapien 3 stent in the United States during 2015-2018. They compared outcomes in 2,691 patients with high or intermediate surgical risk who underwent TAVR for bicuspid AS to an equal number of patients who had TAVR for tricuspid disease, with the two groups being propensity-matched across 25 variables.
Key outcomes were reassuringly similar in the two groups. For example, 30-day and 1-year all-cause mortality rates were 2.6% and 10.8% in patients with bicuspid valves and similar, at 2.5% and 12.1%, in those with tricuspid AS. Paravalvular leak rates at 30 days and 1 year were similar in the two groups. The Kansas City Cardiomyopathy Questionnaire scores, reflecting quality of life, improved dramatically – by nearly 30 points – from pre-TAVR baseline in both groups. The proportion of patients who were New York Heart Association functional class III or IV improved from nearly 85% at baseline to about 8% at 30 days and 1 year, again with no significant difference between the bicuspid and tricuspid AS groups. And there were other benefits, too.
“Despite the concerns regarding optimal expansion of these valves in a bicuspid anatomy, what we observed here was a significant and similar reduction in mean gradients and increase in valve area, both in the bicuspid and tricuspid AS patients. So there was no impact of bicuspid anatomy as seen here in terms of valve hemodynamics,” according to the cardiologist.
Conversion from TAVR to open surgery was required in 0.9% of bicuspid and 0.4% of tricuspid AS patients. Rates of aortic dissection and need for aortic valve reintervention were similarly low in both groups.
The 30-day stroke rate was significantly higher in the bicuspid patients – 2.4% versus 1.6% – but by 1 year there was no significant between-group difference, with stroke rates of 3.4% in the bicuspid and 3.1% in the tricuspid TAVR patients.
“I’d like to point out that more than 75% of strokes occurred in the first 3 days. These are periprocedural strokes, and there was no difference in the time distribution of strokes between the bicuspid and tricuspid groups,” Dr. Makkar said.
These stroke data make a compelling case for the routine use of cerebral protection devices in patients undergoing TAVR, something which now occurs in less than 10% of cases nationally, he continued.
“I would argue that, based on these data, it would be wise for us to use cerebral protection devices, especially when we are doing TAVR in patients with bicuspid AS, because their valves tend to be more heavily calcified than is often the case in tricuspid AS,” Dr. Makkar said.
Discussant Mayra Guerrero, MD, of the Mayo Clinic in Rochester, Minn., took issue with Dr. Makkar’s comment regarding the need for a randomized trial of TAVR in bicuspid AS patients with low surgical risk.
“Do we really need a randomized trial when we see in real-world experience with more than 2,600 patients that the outcomes are fairly similar?” she asked.
Affirmative, Dr. Makkar responded, in light of the fact that the STS/ACC TVT Registry doesn’t include low–surgical risk, typically relatively young bicuspid AS TAVR patients.
“I would say that these data are reassuring and encouraging, but we must not get carried away. I think that would be the important message that I must give,” Dr. Makkar replied. “I think for patients who are high risk and who are intermediate risk, with STS scores of what they were here – 5 and more – I think it’s reasonable to consider them for TAVR based upon CT anatomy. For young patients, as I concluded, I think we must do a randomized clinical trial to definitely establish the safety and efficacy in these patients.”
Dr. Makkar reported receiving research grants from and serving as a consultant to Edwards Lifesciences, which supported the study, as well as Abbott, Medtronic, and Boston Scientific.
bjancin@mdedge.com
SOURCE: Makkar RR. ACC 19, 404-15. Late-breaking clinical trials
NEW ORLEANS – Results of the largest-ever analysis of TAVR in patients with bicuspid aortic stenosis indicate that key 30-day and 1-year outcomes are similar to those of propensity-matched TAVR patients with tricuspid disease, Raj R. Makkar, MD, said at the annual meeting of the American College of Cardiology.
“Select bicuspid anatomy is amenable to TAVR with current-generation, balloon-expandable TAVR technology with acceptable clinical outcomes. These data provide an argument for TAVR to be a reasonable alternative for bicuspid AS [aortic stenosis] patients who are at intermediate or high risk for surgical aortic valve replacement, which are the patients that are enrolled in this registry, and provide a sound basis to conduct a randomized clinical trial in young patients with bicuspid AS who are at low risk for surgery,” declared Dr. Makkar, director of interventional cardiology and the cardiac catheterization laboratory at Cedars-Sinai Medical Center in Los Angeles.
The landmark randomized trials of TAVR versus SAVR (surgical aortic valve replacement) that established TAVR as the preferred treatment for patients with severe aortic stenosis who are at high, intermediate, or low surgical risk systematically excluded patients with bicuspid AS, even though bicuspid anatomy is common, particularly in younger patients with AS.
Despite the absence of supportive randomized trial data, TAVR is being done for bicuspid AS. To learn how patients with bicuspid disease have fared, Dr. Makkar and coinvestigators analyzed the real-world Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy (STS/ACC TVT) Registry of all patients who underwent TAVR with the balloon-expandable Sapien 3 stent in the United States during 2015-2018. They compared outcomes in 2,691 patients with high or intermediate surgical risk who underwent TAVR for bicuspid AS to an equal number of patients who had TAVR for tricuspid disease, with the two groups being propensity-matched across 25 variables.
Key outcomes were reassuringly similar in the two groups. For example, 30-day and 1-year all-cause mortality rates were 2.6% and 10.8% in patients with bicuspid valves and similar, at 2.5% and 12.1%, in those with tricuspid AS. Paravalvular leak rates at 30 days and 1 year were similar in the two groups. The Kansas City Cardiomyopathy Questionnaire scores, reflecting quality of life, improved dramatically – by nearly 30 points – from pre-TAVR baseline in both groups. The proportion of patients who were New York Heart Association functional class III or IV improved from nearly 85% at baseline to about 8% at 30 days and 1 year, again with no significant difference between the bicuspid and tricuspid AS groups. And there were other benefits, too.
“Despite the concerns regarding optimal expansion of these valves in a bicuspid anatomy, what we observed here was a significant and similar reduction in mean gradients and increase in valve area, both in the bicuspid and tricuspid AS patients. So there was no impact of bicuspid anatomy as seen here in terms of valve hemodynamics,” according to the cardiologist.
Conversion from TAVR to open surgery was required in 0.9% of bicuspid and 0.4% of tricuspid AS patients. Rates of aortic dissection and need for aortic valve reintervention were similarly low in both groups.
The 30-day stroke rate was significantly higher in the bicuspid patients – 2.4% versus 1.6% – but by 1 year there was no significant between-group difference, with stroke rates of 3.4% in the bicuspid and 3.1% in the tricuspid TAVR patients.
“I’d like to point out that more than 75% of strokes occurred in the first 3 days. These are periprocedural strokes, and there was no difference in the time distribution of strokes between the bicuspid and tricuspid groups,” Dr. Makkar said.
These stroke data make a compelling case for the routine use of cerebral protection devices in patients undergoing TAVR, something which now occurs in less than 10% of cases nationally, he continued.
“I would argue that, based on these data, it would be wise for us to use cerebral protection devices, especially when we are doing TAVR in patients with bicuspid AS, because their valves tend to be more heavily calcified than is often the case in tricuspid AS,” Dr. Makkar said.
Discussant Mayra Guerrero, MD, of the Mayo Clinic in Rochester, Minn., took issue with Dr. Makkar’s comment regarding the need for a randomized trial of TAVR in bicuspid AS patients with low surgical risk.
“Do we really need a randomized trial when we see in real-world experience with more than 2,600 patients that the outcomes are fairly similar?” she asked.
Affirmative, Dr. Makkar responded, in light of the fact that the STS/ACC TVT Registry doesn’t include low–surgical risk, typically relatively young bicuspid AS TAVR patients.
“I would say that these data are reassuring and encouraging, but we must not get carried away. I think that would be the important message that I must give,” Dr. Makkar replied. “I think for patients who are high risk and who are intermediate risk, with STS scores of what they were here – 5 and more – I think it’s reasonable to consider them for TAVR based upon CT anatomy. For young patients, as I concluded, I think we must do a randomized clinical trial to definitely establish the safety and efficacy in these patients.”
Dr. Makkar reported receiving research grants from and serving as a consultant to Edwards Lifesciences, which supported the study, as well as Abbott, Medtronic, and Boston Scientific.
bjancin@mdedge.com
SOURCE: Makkar RR. ACC 19, 404-15. Late-breaking clinical trials
NEW ORLEANS – Results of the largest-ever analysis of TAVR in patients with bicuspid aortic stenosis indicate that key 30-day and 1-year outcomes are similar to those of propensity-matched TAVR patients with tricuspid disease, Raj R. Makkar, MD, said at the annual meeting of the American College of Cardiology.
“Select bicuspid anatomy is amenable to TAVR with current-generation, balloon-expandable TAVR technology with acceptable clinical outcomes. These data provide an argument for TAVR to be a reasonable alternative for bicuspid AS [aortic stenosis] patients who are at intermediate or high risk for surgical aortic valve replacement, which are the patients that are enrolled in this registry, and provide a sound basis to conduct a randomized clinical trial in young patients with bicuspid AS who are at low risk for surgery,” declared Dr. Makkar, director of interventional cardiology and the cardiac catheterization laboratory at Cedars-Sinai Medical Center in Los Angeles.
The landmark randomized trials of TAVR versus SAVR (surgical aortic valve replacement) that established TAVR as the preferred treatment for patients with severe aortic stenosis who are at high, intermediate, or low surgical risk systematically excluded patients with bicuspid AS, even though bicuspid anatomy is common, particularly in younger patients with AS.
Despite the absence of supportive randomized trial data, TAVR is being done for bicuspid AS. To learn how patients with bicuspid disease have fared, Dr. Makkar and coinvestigators analyzed the real-world Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy (STS/ACC TVT) Registry of all patients who underwent TAVR with the balloon-expandable Sapien 3 stent in the United States during 2015-2018. They compared outcomes in 2,691 patients with high or intermediate surgical risk who underwent TAVR for bicuspid AS to an equal number of patients who had TAVR for tricuspid disease, with the two groups being propensity-matched across 25 variables.
Key outcomes were reassuringly similar in the two groups. For example, 30-day and 1-year all-cause mortality rates were 2.6% and 10.8% in patients with bicuspid valves and similar, at 2.5% and 12.1%, in those with tricuspid AS. Paravalvular leak rates at 30 days and 1 year were similar in the two groups. The Kansas City Cardiomyopathy Questionnaire scores, reflecting quality of life, improved dramatically – by nearly 30 points – from pre-TAVR baseline in both groups. The proportion of patients who were New York Heart Association functional class III or IV improved from nearly 85% at baseline to about 8% at 30 days and 1 year, again with no significant difference between the bicuspid and tricuspid AS groups. And there were other benefits, too.
“Despite the concerns regarding optimal expansion of these valves in a bicuspid anatomy, what we observed here was a significant and similar reduction in mean gradients and increase in valve area, both in the bicuspid and tricuspid AS patients. So there was no impact of bicuspid anatomy as seen here in terms of valve hemodynamics,” according to the cardiologist.
Conversion from TAVR to open surgery was required in 0.9% of bicuspid and 0.4% of tricuspid AS patients. Rates of aortic dissection and need for aortic valve reintervention were similarly low in both groups.
The 30-day stroke rate was significantly higher in the bicuspid patients – 2.4% versus 1.6% – but by 1 year there was no significant between-group difference, with stroke rates of 3.4% in the bicuspid and 3.1% in the tricuspid TAVR patients.
“I’d like to point out that more than 75% of strokes occurred in the first 3 days. These are periprocedural strokes, and there was no difference in the time distribution of strokes between the bicuspid and tricuspid groups,” Dr. Makkar said.
These stroke data make a compelling case for the routine use of cerebral protection devices in patients undergoing TAVR, something which now occurs in less than 10% of cases nationally, he continued.
“I would argue that, based on these data, it would be wise for us to use cerebral protection devices, especially when we are doing TAVR in patients with bicuspid AS, because their valves tend to be more heavily calcified than is often the case in tricuspid AS,” Dr. Makkar said.
Discussant Mayra Guerrero, MD, of the Mayo Clinic in Rochester, Minn., took issue with Dr. Makkar’s comment regarding the need for a randomized trial of TAVR in bicuspid AS patients with low surgical risk.
“Do we really need a randomized trial when we see in real-world experience with more than 2,600 patients that the outcomes are fairly similar?” she asked.
Affirmative, Dr. Makkar responded, in light of the fact that the STS/ACC TVT Registry doesn’t include low–surgical risk, typically relatively young bicuspid AS TAVR patients.
“I would say that these data are reassuring and encouraging, but we must not get carried away. I think that would be the important message that I must give,” Dr. Makkar replied. “I think for patients who are high risk and who are intermediate risk, with STS scores of what they were here – 5 and more – I think it’s reasonable to consider them for TAVR based upon CT anatomy. For young patients, as I concluded, I think we must do a randomized clinical trial to definitely establish the safety and efficacy in these patients.”
Dr. Makkar reported receiving research grants from and serving as a consultant to Edwards Lifesciences, which supported the study, as well as Abbott, Medtronic, and Boston Scientific.
bjancin@mdedge.com
SOURCE: Makkar RR. ACC 19, 404-15. Late-breaking clinical trials
REPORTING FROM ACC 19
Unrecognized focal stenosis after angiographically successful PCI

Moreover, in 82% of DEFINE PCI participants with post-PCI residual ischemia as defined by instantaneous wave-free ratio (iFR) with pullback evaluation of the whole coronary vessel, the impaired physiology was due to an angiographically unrecognized focal stenosis that’s usually potentially treatable, Allen Jeremias, MD, observed in presenting the DEFINE PCI results at the annual meeting of the American College of Cardiology.
“We estimated that if all residual focal lesions could be treated with additional PCI, the rate of significant ischemia could theoretically be reduced from 24% to 5%, said Dr. Jeremias, director of the physiology core laboratory at the Cardiovascular Research Foundation in New York.
Post-PCI ischemia has been associated with recurrent angina and repeat PCI. The 24% prevalence of residual impaired physiology and ischemia despite a successful angiographic result may seem startlingly high to some, but it really shouldn’t be, according to Dr. Jeremias, who is also director of interventional cardiology research and associate director of the cardiac catheterization laboratory at St. Francis Hospital in Roslyn, N.Y.
“There are a lot of physiologic studies looking at FFR [fractional flow reserve] before PCI to determine if we should do it. And we learned how unreliable the angiogram is to make those decisions. So I think obviously we shouldn’t be surprised if the angiogram afterwards is just as unreliable,” he said.
DEFINE PCI was a prospective observational study of 500 patients who underwent PCI for stable or unstable angina at 27 U.S. and European sites. An iFR was done prior to PCI in all vessels with an angiographic lesion severity of 40% or more. Participating interventionalists performed angiographically guided PCI and confirmed their procedural success with post-PCI angiography before the patient left the cath lab. They also performed an iFR manual pullback interrogation of the entire treated vessel. Although the iFR data are linked to the angiographic images via a technology known as co-registration, the operators were blinded to the iFR results, which along with the angiograms were interpreted in a core laboratory. All patients received guideline-directed medical therapy.
The iFR improved on average from 0.69 pre-PCI to 0.93 post treatment. To put that in perspective, an iFR value of 0.89 or less defines hemodynamically significant ischemia.
Residual physiologic impairment post PCI was deemed due to a missed focal stenosis in 82% of cases and to diffuse atherosclerotic disease in the other 18%. Untreated focal lesions were located within the stent in 38% of cases, proximally in 31%, and distal to the stent in the remainder.
Dr. Jeremias said the investigators looked in vain for possible predictors of post-PCI residual impaired physiology. Post-PCI angiographic results were poorly correlated with iFR. For example, 30% of patients with a residual diameter stenosis of 50% or more had a post-PCI iFR of 0.89 or less, as did 21% of those with a residual diameter stenosis of less than 50%, a nonsignificant difference. Moreover, there were no procedural predictors of poor physiologic outcome.
“I don’t think that the answer is more angiograms or procedural changes guided by the angiogram, but rather guiding of the procedure with physiology and also intravascular imaging,” the cardiologist said.
Session cochair J. Dawn Abbott, MD, an interventional cardiologist at Brown University in Providence, R.I., said DEFINE PCI “really brings up the importance of co-registration of iFR, be it with optical coherence tomography or angiography, because we need the information together. If we can’t see these lesions on the angiogram, we need to be doing more complicated combined physiology and anatomy.”
“This is a very interesting study that I think generates a lot of provocative information,” said discussant John J. Warner, MD.
“It certainly challenges, once again, our definition of angiographic success.” The key remaining question is whether additional PCI addressing the residual focal stenoses causing ischemia will result in improved clinical outcomes, added Dr. Warner, an interventional cardiologist and CEO of the University of Texas Southwestern Medical Center Hospitals, Dallas.
Dr. Jeremias noted that DEFINE PCI participants are in the process of being followed through 12 months to see the impact of residual ischemia on recurrent angina, major adverse cardiovascular events, and quality of life. Moreover, a large randomized trial known as DEFINE GPS (Guided Physiologic Stenting) will soon get underway. Participants will be randomized to unblinded iFR-guided therapy with pullback in order to optimize the physiologic result or to conventional angiographically guided PCI. This trial will define the clinical value of PCI with iFR pullback and should answer the question of whether the more important iFR number is the magnitude of the iFR gain achieved via revascularization or the absolute iFR number achieved at the end.
DEFINE PCI and DEFINE GPS are funded by Volcano/Philips. Dr. Jeremias reported serving as a consultant to that company and a handful of others.
SOURCE: Jeremias A. ACC 19 Abstract 408-10.
Moreover, in 82% of DEFINE PCI participants with post-PCI residual ischemia as defined by instantaneous wave-free ratio (iFR) with pullback evaluation of the whole coronary vessel, the impaired physiology was due to an angiographically unrecognized focal stenosis that’s usually potentially treatable, Allen Jeremias, MD, observed in presenting the DEFINE PCI results at the annual meeting of the American College of Cardiology.
“We estimated that if all residual focal lesions could be treated with additional PCI, the rate of significant ischemia could theoretically be reduced from 24% to 5%, said Dr. Jeremias, director of the physiology core laboratory at the Cardiovascular Research Foundation in New York.
Post-PCI ischemia has been associated with recurrent angina and repeat PCI. The 24% prevalence of residual impaired physiology and ischemia despite a successful angiographic result may seem startlingly high to some, but it really shouldn’t be, according to Dr. Jeremias, who is also director of interventional cardiology research and associate director of the cardiac catheterization laboratory at St. Francis Hospital in Roslyn, N.Y.
“There are a lot of physiologic studies looking at FFR [fractional flow reserve] before PCI to determine if we should do it. And we learned how unreliable the angiogram is to make those decisions. So I think obviously we shouldn’t be surprised if the angiogram afterwards is just as unreliable,” he said.
DEFINE PCI was a prospective observational study of 500 patients who underwent PCI for stable or unstable angina at 27 U.S. and European sites. An iFR was done prior to PCI in all vessels with an angiographic lesion severity of 40% or more. Participating interventionalists performed angiographically guided PCI and confirmed their procedural success with post-PCI angiography before the patient left the cath lab. They also performed an iFR manual pullback interrogation of the entire treated vessel. Although the iFR data are linked to the angiographic images via a technology known as co-registration, the operators were blinded to the iFR results, which along with the angiograms were interpreted in a core laboratory. All patients received guideline-directed medical therapy.
The iFR improved on average from 0.69 pre-PCI to 0.93 post treatment. To put that in perspective, an iFR value of 0.89 or less defines hemodynamically significant ischemia.
Residual physiologic impairment post PCI was deemed due to a missed focal stenosis in 82% of cases and to diffuse atherosclerotic disease in the other 18%. Untreated focal lesions were located within the stent in 38% of cases, proximally in 31%, and distal to the stent in the remainder.
Dr. Jeremias said the investigators looked in vain for possible predictors of post-PCI residual impaired physiology. Post-PCI angiographic results were poorly correlated with iFR. For example, 30% of patients with a residual diameter stenosis of 50% or more had a post-PCI iFR of 0.89 or less, as did 21% of those with a residual diameter stenosis of less than 50%, a nonsignificant difference. Moreover, there were no procedural predictors of poor physiologic outcome.
“I don’t think that the answer is more angiograms or procedural changes guided by the angiogram, but rather guiding of the procedure with physiology and also intravascular imaging,” the cardiologist said.
Session cochair J. Dawn Abbott, MD, an interventional cardiologist at Brown University in Providence, R.I., said DEFINE PCI “really brings up the importance of co-registration of iFR, be it with optical coherence tomography or angiography, because we need the information together. If we can’t see these lesions on the angiogram, we need to be doing more complicated combined physiology and anatomy.”
“This is a very interesting study that I think generates a lot of provocative information,” said discussant John J. Warner, MD.
“It certainly challenges, once again, our definition of angiographic success.” The key remaining question is whether additional PCI addressing the residual focal stenoses causing ischemia will result in improved clinical outcomes, added Dr. Warner, an interventional cardiologist and CEO of the University of Texas Southwestern Medical Center Hospitals, Dallas.
Dr. Jeremias noted that DEFINE PCI participants are in the process of being followed through 12 months to see the impact of residual ischemia on recurrent angina, major adverse cardiovascular events, and quality of life. Moreover, a large randomized trial known as DEFINE GPS (Guided Physiologic Stenting) will soon get underway. Participants will be randomized to unblinded iFR-guided therapy with pullback in order to optimize the physiologic result or to conventional angiographically guided PCI. This trial will define the clinical value of PCI with iFR pullback and should answer the question of whether the more important iFR number is the magnitude of the iFR gain achieved via revascularization or the absolute iFR number achieved at the end.
DEFINE PCI and DEFINE GPS are funded by Volcano/Philips. Dr. Jeremias reported serving as a consultant to that company and a handful of others.
SOURCE: Jeremias A. ACC 19 Abstract 408-10.
Moreover, in 82% of DEFINE PCI participants with post-PCI residual ischemia as defined by instantaneous wave-free ratio (iFR) with pullback evaluation of the whole coronary vessel, the impaired physiology was due to an angiographically unrecognized focal stenosis that’s usually potentially treatable, Allen Jeremias, MD, observed in presenting the DEFINE PCI results at the annual meeting of the American College of Cardiology.
“We estimated that if all residual focal lesions could be treated with additional PCI, the rate of significant ischemia could theoretically be reduced from 24% to 5%, said Dr. Jeremias, director of the physiology core laboratory at the Cardiovascular Research Foundation in New York.
Post-PCI ischemia has been associated with recurrent angina and repeat PCI. The 24% prevalence of residual impaired physiology and ischemia despite a successful angiographic result may seem startlingly high to some, but it really shouldn’t be, according to Dr. Jeremias, who is also director of interventional cardiology research and associate director of the cardiac catheterization laboratory at St. Francis Hospital in Roslyn, N.Y.
“There are a lot of physiologic studies looking at FFR [fractional flow reserve] before PCI to determine if we should do it. And we learned how unreliable the angiogram is to make those decisions. So I think obviously we shouldn’t be surprised if the angiogram afterwards is just as unreliable,” he said.
DEFINE PCI was a prospective observational study of 500 patients who underwent PCI for stable or unstable angina at 27 U.S. and European sites. An iFR was done prior to PCI in all vessels with an angiographic lesion severity of 40% or more. Participating interventionalists performed angiographically guided PCI and confirmed their procedural success with post-PCI angiography before the patient left the cath lab. They also performed an iFR manual pullback interrogation of the entire treated vessel. Although the iFR data are linked to the angiographic images via a technology known as co-registration, the operators were blinded to the iFR results, which along with the angiograms were interpreted in a core laboratory. All patients received guideline-directed medical therapy.
The iFR improved on average from 0.69 pre-PCI to 0.93 post treatment. To put that in perspective, an iFR value of 0.89 or less defines hemodynamically significant ischemia.
Residual physiologic impairment post PCI was deemed due to a missed focal stenosis in 82% of cases and to diffuse atherosclerotic disease in the other 18%. Untreated focal lesions were located within the stent in 38% of cases, proximally in 31%, and distal to the stent in the remainder.
Dr. Jeremias said the investigators looked in vain for possible predictors of post-PCI residual impaired physiology. Post-PCI angiographic results were poorly correlated with iFR. For example, 30% of patients with a residual diameter stenosis of 50% or more had a post-PCI iFR of 0.89 or less, as did 21% of those with a residual diameter stenosis of less than 50%, a nonsignificant difference. Moreover, there were no procedural predictors of poor physiologic outcome.
“I don’t think that the answer is more angiograms or procedural changes guided by the angiogram, but rather guiding of the procedure with physiology and also intravascular imaging,” the cardiologist said.
Session cochair J. Dawn Abbott, MD, an interventional cardiologist at Brown University in Providence, R.I., said DEFINE PCI “really brings up the importance of co-registration of iFR, be it with optical coherence tomography or angiography, because we need the information together. If we can’t see these lesions on the angiogram, we need to be doing more complicated combined physiology and anatomy.”
“This is a very interesting study that I think generates a lot of provocative information,” said discussant John J. Warner, MD.
“It certainly challenges, once again, our definition of angiographic success.” The key remaining question is whether additional PCI addressing the residual focal stenoses causing ischemia will result in improved clinical outcomes, added Dr. Warner, an interventional cardiologist and CEO of the University of Texas Southwestern Medical Center Hospitals, Dallas.
Dr. Jeremias noted that DEFINE PCI participants are in the process of being followed through 12 months to see the impact of residual ischemia on recurrent angina, major adverse cardiovascular events, and quality of life. Moreover, a large randomized trial known as DEFINE GPS (Guided Physiologic Stenting) will soon get underway. Participants will be randomized to unblinded iFR-guided therapy with pullback in order to optimize the physiologic result or to conventional angiographically guided PCI. This trial will define the clinical value of PCI with iFR pullback and should answer the question of whether the more important iFR number is the magnitude of the iFR gain achieved via revascularization or the absolute iFR number achieved at the end.
DEFINE PCI and DEFINE GPS are funded by Volcano/Philips. Dr. Jeremias reported serving as a consultant to that company and a handful of others.
SOURCE: Jeremias A. ACC 19 Abstract 408-10.
REPORTING FROM ACC 19
Noninvasive FFRCT called ADVANCE in chest pain assessment
NEW ORLEANS – Fractional flow reserve derived noninvasively from coronary CT angiography showed clinical merit as a practical tool for evaluation of chest pain at 1 year of follow-up in the ADVANCE registry, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.

In ADVANCE, a fractional flow reserve value greater than 0.80 derived from CT angiography, or FFRCT, was associated with a significantly lower rate of cardiovascular death or MI at 1 year than in patients with an FFRCT of 0.80 or lower, according to Dr. Patel, professor of medicine and chief of the division of cardiology at Duke University, Durham, N.C.
“The lower rates of revascularization and clinical events in patients with FFRCT who were managed conservatively provide reassurance regarding this clinical strategy if you were to put it into your practice,” he observed.
ADVANCE is in an international, real-world, prospective registry of more than 5,000 patients in Europe, Japan, and North America. All had clinically suspected ischemic coronary artery disease (CAD). They also had at least 30% atherosclerosis documented on coronary CT angiography as a trigger for noninvasive assessment of FFR calculated from computational fluid dynamics. The idea behind FFRCT is that by combining the anatomic information provided by CT angiography with the physiological, functional data from FFR, the result is a better guide to need for revascularization of true obstructive CAD than with conventional invasive coronary angiography alone. Indeed, FFRCT could eventually prove to be a cost-effective gatekeeper to the cardiac catheterization laboratory by cutting down on high rates of invasive coronary angiography for nonactionable CAD.
That point was suggested by the previously reported 90-day outcomes of the ADVANCE registry, the cardiologist explained. Participating physicians first classified patients and made a revascularization/no-revascularization management plan on the basis of the core laboratory CT angiography results alone. But when they received the FFRCT results, they reclassified patients and changed the management plan in 67% of cases. That’s because the prevalence of nonobstructive CAD was 44% in patients with an FFRCT greater than 0.80 in all coronary arteries, compared with just 14% in those with an FFRCT of 0.80 or less. As a result, 72% of patients with an FFRCT of 0.80 or less underwent revascularization, while the vast majority of patients with an FFRCT greater than 0.80 were initially managed conservatively (Eur Heart J. 2018 Nov 1;39[41]:3701-11).
The 1-year outcomes from ADVANCE as presented by Dr. Patel showed low rates of major adverse cardiovascular events overall. Of note, the composite endpoint of cardiovascular death or MI occurred significantly more often in patients with an FFRCT of 0.80 or less, by a margin of 0.8% versus 0.2%, for a 320% increased relative risk. The patients with a FFRCT greater than 0.80 continued to have a much lower revascularization rate from 90 days through 1 year: 5.8% versus 38.4% in the lower-FFRCT group. And 93% of patients placed on medical therapy alone after receiving their FFRCT results remained on medical therapy without revascularization or a major adverse cardiovascular event at 1 year.
Discussant Matthew J. Budoff, MD, commented that it’s time to move beyond observational studies and conduct randomized trials of an FFRCT-based screening strategy in patients with clinical suspicion of obstructive CAD.
“We want to understand the enormous advantages of having FFR-like data before we take patients to the cath lab. And I do think that adding physiology to the anatomy is going to be the approach that we’re going to be predominantly using in the future,” said Dr. Budoff, professor of medicine at the University of California, Los Angeles.
Dr. Patel noted that the ongoing, randomized, 2,100-patient PRECISE study is directed at determining in a more definitive way the clinical and cost-effectiveness of an FFRCT strategy.
The ADVANCE registry is funded by HeartFlow. Dr. Patel reported receiving research grants from that company and several others, as well as the National Institutes of Health. He serves on advisory boards for Bayer, Janssen, and Amgen.
Simultaneous with Dr. Patel’s presentation at ACC 2019, the 1-year ADVANCE registry results were published online (JACC Cardiovasc Imag. 2019 Mar 17. doi: 10.1016/j.jcmg.2019.03.003).
NEW ORLEANS – Fractional flow reserve derived noninvasively from coronary CT angiography showed clinical merit as a practical tool for evaluation of chest pain at 1 year of follow-up in the ADVANCE registry, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.
In ADVANCE, a fractional flow reserve value greater than 0.80 derived from CT angiography, or FFRCT, was associated with a significantly lower rate of cardiovascular death or MI at 1 year than in patients with an FFRCT of 0.80 or lower, according to Dr. Patel, professor of medicine and chief of the division of cardiology at Duke University, Durham, N.C.
“The lower rates of revascularization and clinical events in patients with FFRCT who were managed conservatively provide reassurance regarding this clinical strategy if you were to put it into your practice,” he observed.
ADVANCE is in an international, real-world, prospective registry of more than 5,000 patients in Europe, Japan, and North America. All had clinically suspected ischemic coronary artery disease (CAD). They also had at least 30% atherosclerosis documented on coronary CT angiography as a trigger for noninvasive assessment of FFR calculated from computational fluid dynamics. The idea behind FFRCT is that by combining the anatomic information provided by CT angiography with the physiological, functional data from FFR, the result is a better guide to need for revascularization of true obstructive CAD than with conventional invasive coronary angiography alone. Indeed, FFRCT could eventually prove to be a cost-effective gatekeeper to the cardiac catheterization laboratory by cutting down on high rates of invasive coronary angiography for nonactionable CAD.
That point was suggested by the previously reported 90-day outcomes of the ADVANCE registry, the cardiologist explained. Participating physicians first classified patients and made a revascularization/no-revascularization management plan on the basis of the core laboratory CT angiography results alone. But when they received the FFRCT results, they reclassified patients and changed the management plan in 67% of cases. That’s because the prevalence of nonobstructive CAD was 44% in patients with an FFRCT greater than 0.80 in all coronary arteries, compared with just 14% in those with an FFRCT of 0.80 or less. As a result, 72% of patients with an FFRCT of 0.80 or less underwent revascularization, while the vast majority of patients with an FFRCT greater than 0.80 were initially managed conservatively (Eur Heart J. 2018 Nov 1;39[41]:3701-11).
The 1-year outcomes from ADVANCE as presented by Dr. Patel showed low rates of major adverse cardiovascular events overall. Of note, the composite endpoint of cardiovascular death or MI occurred significantly more often in patients with an FFRCT of 0.80 or less, by a margin of 0.8% versus 0.2%, for a 320% increased relative risk. The patients with a FFRCT greater than 0.80 continued to have a much lower revascularization rate from 90 days through 1 year: 5.8% versus 38.4% in the lower-FFRCT group. And 93% of patients placed on medical therapy alone after receiving their FFRCT results remained on medical therapy without revascularization or a major adverse cardiovascular event at 1 year.
Discussant Matthew J. Budoff, MD, commented that it’s time to move beyond observational studies and conduct randomized trials of an FFRCT-based screening strategy in patients with clinical suspicion of obstructive CAD.
“We want to understand the enormous advantages of having FFR-like data before we take patients to the cath lab. And I do think that adding physiology to the anatomy is going to be the approach that we’re going to be predominantly using in the future,” said Dr. Budoff, professor of medicine at the University of California, Los Angeles.
Dr. Patel noted that the ongoing, randomized, 2,100-patient PRECISE study is directed at determining in a more definitive way the clinical and cost-effectiveness of an FFRCT strategy.
The ADVANCE registry is funded by HeartFlow. Dr. Patel reported receiving research grants from that company and several others, as well as the National Institutes of Health. He serves on advisory boards for Bayer, Janssen, and Amgen.
Simultaneous with Dr. Patel’s presentation at ACC 2019, the 1-year ADVANCE registry results were published online (JACC Cardiovasc Imag. 2019 Mar 17. doi: 10.1016/j.jcmg.2019.03.003).
NEW ORLEANS – Fractional flow reserve derived noninvasively from coronary CT angiography showed clinical merit as a practical tool for evaluation of chest pain at 1 year of follow-up in the ADVANCE registry, Manesh R. Patel, MD, reported at the annual meeting of the American College of Cardiology.
In ADVANCE, a fractional flow reserve value greater than 0.80 derived from CT angiography, or FFRCT, was associated with a significantly lower rate of cardiovascular death or MI at 1 year than in patients with an FFRCT of 0.80 or lower, according to Dr. Patel, professor of medicine and chief of the division of cardiology at Duke University, Durham, N.C.
“The lower rates of revascularization and clinical events in patients with FFRCT who were managed conservatively provide reassurance regarding this clinical strategy if you were to put it into your practice,” he observed.
ADVANCE is in an international, real-world, prospective registry of more than 5,000 patients in Europe, Japan, and North America. All had clinically suspected ischemic coronary artery disease (CAD). They also had at least 30% atherosclerosis documented on coronary CT angiography as a trigger for noninvasive assessment of FFR calculated from computational fluid dynamics. The idea behind FFRCT is that by combining the anatomic information provided by CT angiography with the physiological, functional data from FFR, the result is a better guide to need for revascularization of true obstructive CAD than with conventional invasive coronary angiography alone. Indeed, FFRCT could eventually prove to be a cost-effective gatekeeper to the cardiac catheterization laboratory by cutting down on high rates of invasive coronary angiography for nonactionable CAD.
That point was suggested by the previously reported 90-day outcomes of the ADVANCE registry, the cardiologist explained. Participating physicians first classified patients and made a revascularization/no-revascularization management plan on the basis of the core laboratory CT angiography results alone. But when they received the FFRCT results, they reclassified patients and changed the management plan in 67% of cases. That’s because the prevalence of nonobstructive CAD was 44% in patients with an FFRCT greater than 0.80 in all coronary arteries, compared with just 14% in those with an FFRCT of 0.80 or less. As a result, 72% of patients with an FFRCT of 0.80 or less underwent revascularization, while the vast majority of patients with an FFRCT greater than 0.80 were initially managed conservatively (Eur Heart J. 2018 Nov 1;39[41]:3701-11).
The 1-year outcomes from ADVANCE as presented by Dr. Patel showed low rates of major adverse cardiovascular events overall. Of note, the composite endpoint of cardiovascular death or MI occurred significantly more often in patients with an FFRCT of 0.80 or less, by a margin of 0.8% versus 0.2%, for a 320% increased relative risk. The patients with a FFRCT greater than 0.80 continued to have a much lower revascularization rate from 90 days through 1 year: 5.8% versus 38.4% in the lower-FFRCT group. And 93% of patients placed on medical therapy alone after receiving their FFRCT results remained on medical therapy without revascularization or a major adverse cardiovascular event at 1 year.
Discussant Matthew J. Budoff, MD, commented that it’s time to move beyond observational studies and conduct randomized trials of an FFRCT-based screening strategy in patients with clinical suspicion of obstructive CAD.
“We want to understand the enormous advantages of having FFR-like data before we take patients to the cath lab. And I do think that adding physiology to the anatomy is going to be the approach that we’re going to be predominantly using in the future,” said Dr. Budoff, professor of medicine at the University of California, Los Angeles.
Dr. Patel noted that the ongoing, randomized, 2,100-patient PRECISE study is directed at determining in a more definitive way the clinical and cost-effectiveness of an FFRCT strategy.
The ADVANCE registry is funded by HeartFlow. Dr. Patel reported receiving research grants from that company and several others, as well as the National Institutes of Health. He serves on advisory boards for Bayer, Janssen, and Amgen.
Simultaneous with Dr. Patel’s presentation at ACC 2019, the 1-year ADVANCE registry results were published online (JACC Cardiovasc Imag. 2019 Mar 17. doi: 10.1016/j.jcmg.2019.03.003).
REPORTING FROM ACC 19
Medical societies endorse tiered certification for U.S. heart-valve care
![]()
The centerpiece of the integrated model is a certification process that would designate appropriate hospitals as “Comprehensive (Level I)” or “Primary (Level II)” valve centers to serve as the designated U.S. sites for performing repair or replacement of aortic and mitral valves by transcatheter or open-surgery procedures.
The consensus document, written by a panel of mostly interventional cardiologists or heart surgeons and published in Journal of the American College of Cardiology, cited the success of similar accreditation and tiered systems that have become fixtures in United States for the delivery of care for trauma, stroke, cancer, bariatric surgery, and percutaneous coronary intervention for acute ST-segment elevation MI.
The focus of the consensus document is to “initiate a discussion regarding whether a regionalized, tiered system of care for patients with [valvular heart disease (VHD)] that accounts for the differences in valve center expertise, experience, and resources constitutes a more rational delivery model than one left to expand continuously without direction,” the panel wrote.
Under the proposal, a key component of every designated valve center would be a multidisciplinary clinical team, staffed at minimum with an interventional cardiologist, a cardiac surgeon, echocardiographic and radiographic imaging specialists, a specialist in heart failure, a person with valve expertise, nurse practitioners, a cardiovascular anesthesiologist, a program navigator, and a data manager. Valve centers also would need to enroll patients in registries, perform research, education, and training, and collect data using carefully selected performance metrics.
The document addresses case-volume minimums, a topic that’s been tricky for leaders in the heart-valve field to reconcile as they try to balance volume thresholds against having valve procedures readily available and convenient for rural or remote patients.
“The primary motivation behind volume recommendations is not to exclude centers but rather to serve as one metric in the identification of centers that are most capable of providing certain services,” the consensus statement explained. “Volumes alone are not necessarily the best surrogate for quality, but a volume-outcome association does exist for many cardiac procedures.”
Recent proof of this relationship for transcatheter aortic valve replacement appeared in an article published earlier in April; the article reviewed 30-day mortality outcomes for more than 113,000 U.S. patients who underwent this procedure and showed that centers with the lowest procedure volumes also had the highest mortality rate (New Engl J Med. 2019 April 3. doi: 10.1056/NEJMsa1901109).
But the document also qualified its support of and the role for volume minimums, highlighting that case volume is an inadequate surrogate for program quality, especially when considered in isolation. “The proposed concept of system care for VHD patients is not conceived to deny individuals and institutions the opportunity to provide services, nor should it be perceived to impede the ability of a committed center to achieve its strategic goals. Rather, it is intended to focus more on outcomes and not simply on procedural volumes.”
The launch by the Joint Commission of a Comprehensive Cardiac Advanced Certification program in January 2017, which included VHD care, is a step toward that goal, but “there is a great deal of detailed work ahead to realize the goal of this proposal,” according to the consensus document.
The consensus statement was issued by the American Association for Thoracic Surgery, the American College of Cardiology, the American Society of Echocardiography, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons.
SOURCE: Nishimura RA et al. J Amer Coll Cardiol. 2019 April 19. doi: 10.1016/j.jacc.2018.10.007.
![]()
The centerpiece of the integrated model is a certification process that would designate appropriate hospitals as “Comprehensive (Level I)” or “Primary (Level II)” valve centers to serve as the designated U.S. sites for performing repair or replacement of aortic and mitral valves by transcatheter or open-surgery procedures.
The consensus document, written by a panel of mostly interventional cardiologists or heart surgeons and published in Journal of the American College of Cardiology, cited the success of similar accreditation and tiered systems that have become fixtures in United States for the delivery of care for trauma, stroke, cancer, bariatric surgery, and percutaneous coronary intervention for acute ST-segment elevation MI.
The focus of the consensus document is to “initiate a discussion regarding whether a regionalized, tiered system of care for patients with [valvular heart disease (VHD)] that accounts for the differences in valve center expertise, experience, and resources constitutes a more rational delivery model than one left to expand continuously without direction,” the panel wrote.
Under the proposal, a key component of every designated valve center would be a multidisciplinary clinical team, staffed at minimum with an interventional cardiologist, a cardiac surgeon, echocardiographic and radiographic imaging specialists, a specialist in heart failure, a person with valve expertise, nurse practitioners, a cardiovascular anesthesiologist, a program navigator, and a data manager. Valve centers also would need to enroll patients in registries, perform research, education, and training, and collect data using carefully selected performance metrics.
The document addresses case-volume minimums, a topic that’s been tricky for leaders in the heart-valve field to reconcile as they try to balance volume thresholds against having valve procedures readily available and convenient for rural or remote patients.
“The primary motivation behind volume recommendations is not to exclude centers but rather to serve as one metric in the identification of centers that are most capable of providing certain services,” the consensus statement explained. “Volumes alone are not necessarily the best surrogate for quality, but a volume-outcome association does exist for many cardiac procedures.”
Recent proof of this relationship for transcatheter aortic valve replacement appeared in an article published earlier in April; the article reviewed 30-day mortality outcomes for more than 113,000 U.S. patients who underwent this procedure and showed that centers with the lowest procedure volumes also had the highest mortality rate (New Engl J Med. 2019 April 3. doi: 10.1056/NEJMsa1901109).
But the document also qualified its support of and the role for volume minimums, highlighting that case volume is an inadequate surrogate for program quality, especially when considered in isolation. “The proposed concept of system care for VHD patients is not conceived to deny individuals and institutions the opportunity to provide services, nor should it be perceived to impede the ability of a committed center to achieve its strategic goals. Rather, it is intended to focus more on outcomes and not simply on procedural volumes.”
The launch by the Joint Commission of a Comprehensive Cardiac Advanced Certification program in January 2017, which included VHD care, is a step toward that goal, but “there is a great deal of detailed work ahead to realize the goal of this proposal,” according to the consensus document.
The consensus statement was issued by the American Association for Thoracic Surgery, the American College of Cardiology, the American Society of Echocardiography, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons.
SOURCE: Nishimura RA et al. J Amer Coll Cardiol. 2019 April 19. doi: 10.1016/j.jacc.2018.10.007.
![]()
The centerpiece of the integrated model is a certification process that would designate appropriate hospitals as “Comprehensive (Level I)” or “Primary (Level II)” valve centers to serve as the designated U.S. sites for performing repair or replacement of aortic and mitral valves by transcatheter or open-surgery procedures.
The consensus document, written by a panel of mostly interventional cardiologists or heart surgeons and published in Journal of the American College of Cardiology, cited the success of similar accreditation and tiered systems that have become fixtures in United States for the delivery of care for trauma, stroke, cancer, bariatric surgery, and percutaneous coronary intervention for acute ST-segment elevation MI.
The focus of the consensus document is to “initiate a discussion regarding whether a regionalized, tiered system of care for patients with [valvular heart disease (VHD)] that accounts for the differences in valve center expertise, experience, and resources constitutes a more rational delivery model than one left to expand continuously without direction,” the panel wrote.
Under the proposal, a key component of every designated valve center would be a multidisciplinary clinical team, staffed at minimum with an interventional cardiologist, a cardiac surgeon, echocardiographic and radiographic imaging specialists, a specialist in heart failure, a person with valve expertise, nurse practitioners, a cardiovascular anesthesiologist, a program navigator, and a data manager. Valve centers also would need to enroll patients in registries, perform research, education, and training, and collect data using carefully selected performance metrics.
The document addresses case-volume minimums, a topic that’s been tricky for leaders in the heart-valve field to reconcile as they try to balance volume thresholds against having valve procedures readily available and convenient for rural or remote patients.
“The primary motivation behind volume recommendations is not to exclude centers but rather to serve as one metric in the identification of centers that are most capable of providing certain services,” the consensus statement explained. “Volumes alone are not necessarily the best surrogate for quality, but a volume-outcome association does exist for many cardiac procedures.”
Recent proof of this relationship for transcatheter aortic valve replacement appeared in an article published earlier in April; the article reviewed 30-day mortality outcomes for more than 113,000 U.S. patients who underwent this procedure and showed that centers with the lowest procedure volumes also had the highest mortality rate (New Engl J Med. 2019 April 3. doi: 10.1056/NEJMsa1901109).
But the document also qualified its support of and the role for volume minimums, highlighting that case volume is an inadequate surrogate for program quality, especially when considered in isolation. “The proposed concept of system care for VHD patients is not conceived to deny individuals and institutions the opportunity to provide services, nor should it be perceived to impede the ability of a committed center to achieve its strategic goals. Rather, it is intended to focus more on outcomes and not simply on procedural volumes.”
The launch by the Joint Commission of a Comprehensive Cardiac Advanced Certification program in January 2017, which included VHD care, is a step toward that goal, but “there is a great deal of detailed work ahead to realize the goal of this proposal,” according to the consensus document.
The consensus statement was issued by the American Association for Thoracic Surgery, the American College of Cardiology, the American Society of Echocardiography, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons.
SOURCE: Nishimura RA et al. J Amer Coll Cardiol. 2019 April 19. doi: 10.1016/j.jacc.2018.10.007.
FROM JACC
PCI reduces mortality after STEMI in older adults
The use of percutaneous coronary intervention after ST-segment elevation myocardial infarction is increasing in older adults, and is associated with significantly lower in-hospital mortality, new research has found.
“Our study shows that the rates of utilization of PCI in older patients with STEMI and cardiogenic shock is rising. This rise has been paralleled by an equivalent decline in unadjusted mortality rates,” Abdulla A. Damluji, MD, and his coinvestigators wrote in an analysis published in the Journal of the American College of Cardiology.
They looked at outcomes of 317,728 cases of STEMI with cardiogenic shock during 1999-2013, of which 35% occurred in individuals aged 75 years or above.
Over the study period, the proportion of adults aged 75 years and over who underwent percutaneous coronary intervention after STEMI increased from 27% in 1999 to 56% in 2013. At the same time, in-hospital mortality rates in those patients declined from 64% in 1999 to 46% in 2013. Both differences were significant at P less than 0.001.
PCI more than halved the mortality associated with STEMI in older adults, even after adjustment for propensity score, and this was seen across all four U.S. Census Bureau regions in the analysis.
However, mortality rates were slightly higher in patients who underwent percutaneous coronary intervention and had a bleeding event, compared with those who did not have a bleeding event.
There were some significant differences in the prevalence of cardiovascular risk factors and noncardiovascular diagnoses between those who underwent percutaneous coronary intervention and those who did not. There was around a 20% higher prevalence of obesity, but a lower prevalence of valvular heart disease and heart failure, in individuals who were treated with percutaneous coronary intervention than among those who were not.
Older adults who received percutaneous coronary intervention also had a significantly lower disease burden compared with older adults who did not, and were more likely to be younger, male, and not an underrepresented minority.
“Despite the improvement in survival associated with early revascularization as reported by these studies, many older adults with multiple chronic conditions, worse disease burden, and possibly limited life expectancy as assessed by interventional cardiologists do not receive early revascularization with PCI,” wrote Dr. Damluji of Sinai Hospital of Baltimore and Johns Hopkins University, and his coauthors.
“This study was aimed to address this important selection bias by implementing different methods of propensity matching to understand the influence of early revascularization adjusting for demographic, clinical, and hospital characteristics between older adults with early revascularization versus those without revascularization.”
The study was partly supported by the Jane and Stanley F. Rodbell family. Three authors declared support from the National Institute on Aging. Two authors declared funding from private industry and one declared pharmaceutical stocks. No other conflicts of interest were declared.
SOURCE: Damluji A et al. J Am Coll Cardiol. 2019 Apr;73(15):1890-900.
Despite recent advances in early revascularization approaches, such as increasing availability and improved safety profile, which have seen a decrease in mortality rates after cardiogenic shock, many of the studies of these advances have excluded elderly patients. This limits the generalizability of the results.
This study is the largest analysis so far to explore the outcomes of cardiogenic shock and percutaneous coronary intervention in older adults. The authors have used a propensity score adjustment in an attempt to account for potentially confounding baseline characteristics, and shown significantly lower mortality after PCI.
However, the analysis is subject to the usual limitations of observational studies. In particular is the fact that patients with cardiogenic shock represent a spectrum of risk, comorbidities, degrees of disease, and coronary anatomy. These comorbid conditions could therefore have affected the selection decision for revascularization, and therefore outcomes. The challenge still remains also to identify older patients who are more likely to benefit from revascularization after STEMI.
Dr. Eliano P. Navarese is from Interventional Cardiology and Cardiovascular Medicine, Mater Dei Hospital and SIRIO MEDICINE Research Network, Italy. Dr. Sunil V. Rao is from the faculty of medicine at the University of Alberta, Edmonton. Dr. Mitchell W. Krucoff is from Duke University Medical Center/Duke Clinical Research Institute, Durham, N.C. These comments are adapted from their editorial (J Am Coll Cardiol. 2019 Apr;73(15):1901-4). No conflicts of interest were declared.
Despite recent advances in early revascularization approaches, such as increasing availability and improved safety profile, which have seen a decrease in mortality rates after cardiogenic shock, many of the studies of these advances have excluded elderly patients. This limits the generalizability of the results.
This study is the largest analysis so far to explore the outcomes of cardiogenic shock and percutaneous coronary intervention in older adults. The authors have used a propensity score adjustment in an attempt to account for potentially confounding baseline characteristics, and shown significantly lower mortality after PCI.
However, the analysis is subject to the usual limitations of observational studies. In particular is the fact that patients with cardiogenic shock represent a spectrum of risk, comorbidities, degrees of disease, and coronary anatomy. These comorbid conditions could therefore have affected the selection decision for revascularization, and therefore outcomes. The challenge still remains also to identify older patients who are more likely to benefit from revascularization after STEMI.
Dr. Eliano P. Navarese is from Interventional Cardiology and Cardiovascular Medicine, Mater Dei Hospital and SIRIO MEDICINE Research Network, Italy. Dr. Sunil V. Rao is from the faculty of medicine at the University of Alberta, Edmonton. Dr. Mitchell W. Krucoff is from Duke University Medical Center/Duke Clinical Research Institute, Durham, N.C. These comments are adapted from their editorial (J Am Coll Cardiol. 2019 Apr;73(15):1901-4). No conflicts of interest were declared.
Despite recent advances in early revascularization approaches, such as increasing availability and improved safety profile, which have seen a decrease in mortality rates after cardiogenic shock, many of the studies of these advances have excluded elderly patients. This limits the generalizability of the results.
This study is the largest analysis so far to explore the outcomes of cardiogenic shock and percutaneous coronary intervention in older adults. The authors have used a propensity score adjustment in an attempt to account for potentially confounding baseline characteristics, and shown significantly lower mortality after PCI.
However, the analysis is subject to the usual limitations of observational studies. In particular is the fact that patients with cardiogenic shock represent a spectrum of risk, comorbidities, degrees of disease, and coronary anatomy. These comorbid conditions could therefore have affected the selection decision for revascularization, and therefore outcomes. The challenge still remains also to identify older patients who are more likely to benefit from revascularization after STEMI.
Dr. Eliano P. Navarese is from Interventional Cardiology and Cardiovascular Medicine, Mater Dei Hospital and SIRIO MEDICINE Research Network, Italy. Dr. Sunil V. Rao is from the faculty of medicine at the University of Alberta, Edmonton. Dr. Mitchell W. Krucoff is from Duke University Medical Center/Duke Clinical Research Institute, Durham, N.C. These comments are adapted from their editorial (J Am Coll Cardiol. 2019 Apr;73(15):1901-4). No conflicts of interest were declared.
The use of percutaneous coronary intervention after ST-segment elevation myocardial infarction is increasing in older adults, and is associated with significantly lower in-hospital mortality, new research has found.
“Our study shows that the rates of utilization of PCI in older patients with STEMI and cardiogenic shock is rising. This rise has been paralleled by an equivalent decline in unadjusted mortality rates,” Abdulla A. Damluji, MD, and his coinvestigators wrote in an analysis published in the Journal of the American College of Cardiology.
They looked at outcomes of 317,728 cases of STEMI with cardiogenic shock during 1999-2013, of which 35% occurred in individuals aged 75 years or above.
Over the study period, the proportion of adults aged 75 years and over who underwent percutaneous coronary intervention after STEMI increased from 27% in 1999 to 56% in 2013. At the same time, in-hospital mortality rates in those patients declined from 64% in 1999 to 46% in 2013. Both differences were significant at P less than 0.001.
PCI more than halved the mortality associated with STEMI in older adults, even after adjustment for propensity score, and this was seen across all four U.S. Census Bureau regions in the analysis.
However, mortality rates were slightly higher in patients who underwent percutaneous coronary intervention and had a bleeding event, compared with those who did not have a bleeding event.
There were some significant differences in the prevalence of cardiovascular risk factors and noncardiovascular diagnoses between those who underwent percutaneous coronary intervention and those who did not. There was around a 20% higher prevalence of obesity, but a lower prevalence of valvular heart disease and heart failure, in individuals who were treated with percutaneous coronary intervention than among those who were not.
Older adults who received percutaneous coronary intervention also had a significantly lower disease burden compared with older adults who did not, and were more likely to be younger, male, and not an underrepresented minority.
“Despite the improvement in survival associated with early revascularization as reported by these studies, many older adults with multiple chronic conditions, worse disease burden, and possibly limited life expectancy as assessed by interventional cardiologists do not receive early revascularization with PCI,” wrote Dr. Damluji of Sinai Hospital of Baltimore and Johns Hopkins University, and his coauthors.
“This study was aimed to address this important selection bias by implementing different methods of propensity matching to understand the influence of early revascularization adjusting for demographic, clinical, and hospital characteristics between older adults with early revascularization versus those without revascularization.”
The study was partly supported by the Jane and Stanley F. Rodbell family. Three authors declared support from the National Institute on Aging. Two authors declared funding from private industry and one declared pharmaceutical stocks. No other conflicts of interest were declared.
SOURCE: Damluji A et al. J Am Coll Cardiol. 2019 Apr;73(15):1890-900.
The use of percutaneous coronary intervention after ST-segment elevation myocardial infarction is increasing in older adults, and is associated with significantly lower in-hospital mortality, new research has found.
“Our study shows that the rates of utilization of PCI in older patients with STEMI and cardiogenic shock is rising. This rise has been paralleled by an equivalent decline in unadjusted mortality rates,” Abdulla A. Damluji, MD, and his coinvestigators wrote in an analysis published in the Journal of the American College of Cardiology.
They looked at outcomes of 317,728 cases of STEMI with cardiogenic shock during 1999-2013, of which 35% occurred in individuals aged 75 years or above.
Over the study period, the proportion of adults aged 75 years and over who underwent percutaneous coronary intervention after STEMI increased from 27% in 1999 to 56% in 2013. At the same time, in-hospital mortality rates in those patients declined from 64% in 1999 to 46% in 2013. Both differences were significant at P less than 0.001.
PCI more than halved the mortality associated with STEMI in older adults, even after adjustment for propensity score, and this was seen across all four U.S. Census Bureau regions in the analysis.
However, mortality rates were slightly higher in patients who underwent percutaneous coronary intervention and had a bleeding event, compared with those who did not have a bleeding event.
There were some significant differences in the prevalence of cardiovascular risk factors and noncardiovascular diagnoses between those who underwent percutaneous coronary intervention and those who did not. There was around a 20% higher prevalence of obesity, but a lower prevalence of valvular heart disease and heart failure, in individuals who were treated with percutaneous coronary intervention than among those who were not.
Older adults who received percutaneous coronary intervention also had a significantly lower disease burden compared with older adults who did not, and were more likely to be younger, male, and not an underrepresented minority.
“Despite the improvement in survival associated with early revascularization as reported by these studies, many older adults with multiple chronic conditions, worse disease burden, and possibly limited life expectancy as assessed by interventional cardiologists do not receive early revascularization with PCI,” wrote Dr. Damluji of Sinai Hospital of Baltimore and Johns Hopkins University, and his coauthors.
“This study was aimed to address this important selection bias by implementing different methods of propensity matching to understand the influence of early revascularization adjusting for demographic, clinical, and hospital characteristics between older adults with early revascularization versus those without revascularization.”
The study was partly supported by the Jane and Stanley F. Rodbell family. Three authors declared support from the National Institute on Aging. Two authors declared funding from private industry and one declared pharmaceutical stocks. No other conflicts of interest were declared.
SOURCE: Damluji A et al. J Am Coll Cardiol. 2019 Apr;73(15):1890-900.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY