User login
U.S. adults report depression at record rates: Survey
In a survey, 29% of adults said they had been diagnosed with depression during their lifetime, and 18% said they currently have depression or are being treated for it. Those rates are up from the baseline 2015 rates of 20% of people ever having depression and 11% of people with a current diagnosis.
Depression had been steadily rising before the pandemic, and the Gallup analysts wrote that “social isolation, loneliness, fear of infection, psychological exhaustion (particularly among frontline responders such as health care workers), elevated substance abuse, and disruptions in mental health services have all likely played a role” in the increase.
“The fact that Americans are more depressed and struggling after this time of incredible stress and isolation is perhaps not surprising,” American Psychiatric Association president Rebecca Brendel, MD, told CNN. “There are lingering effects on our health, especially our mental health, from the past 3 years that disrupted everything we knew.”
The new estimates are based on online survey responses collected in February from 5,167 adults in the United States who answered the questions:
- Has a doctor or nurse ever told you that you have depression?
- Do you currently have or are you currently being treated for depression?
Depression, which is also called major depressive disorder, is a treatable illness that negatively affects how someone feels, thinks, and acts. The symptoms can be both emotional (such as sadness or loss of interest in activities) and physical (such as fatigue or slowed movements or speech).
The latest study found that depression rates increased the most among women, young adults, Black people, and Hispanic people. For the first time, more Black and Hispanic people than White people reported ever being diagnosed with depression. The lifetime depression rate among Black people was 34%, compared with 31% for Hispanic people and 29% for White people.
The rate of lifetime depression among women jumped 10 percentage points in the past 5 years, to 37%, in February, the survey results showed. About 1 in 4 women said they currently had depression or were being treated for it, up 6 percentage points compared with 5 years ago.
When responses were analyzed by age, those 18-44 years old were the most likely to report ever being diagnosed with depression or currently having the illness. About one-third of younger adults have ever been diagnosed, and more than 1 in 5 said they currently have depression.
Dr. Brendel said awareness and reduced stigma could be adding to the rising rates of depression.
“We’re making it easier to talk about mental health and looking at it as part of our overall wellness, just like physical health,” she said. “People are aware of depression, and people are seeking help for it.”
If you or someone you know needs help, dial 988 for support from the national Suicide & Crisis Lifeline. It’s free, confidential, and available 24 hours a day, 7 days a week. You can also visit 988lifeline.org and choose the chat feature.
A version of this article first appeared on Medscape.com.
In a survey, 29% of adults said they had been diagnosed with depression during their lifetime, and 18% said they currently have depression or are being treated for it. Those rates are up from the baseline 2015 rates of 20% of people ever having depression and 11% of people with a current diagnosis.
Depression had been steadily rising before the pandemic, and the Gallup analysts wrote that “social isolation, loneliness, fear of infection, psychological exhaustion (particularly among frontline responders such as health care workers), elevated substance abuse, and disruptions in mental health services have all likely played a role” in the increase.
“The fact that Americans are more depressed and struggling after this time of incredible stress and isolation is perhaps not surprising,” American Psychiatric Association president Rebecca Brendel, MD, told CNN. “There are lingering effects on our health, especially our mental health, from the past 3 years that disrupted everything we knew.”
The new estimates are based on online survey responses collected in February from 5,167 adults in the United States who answered the questions:
- Has a doctor or nurse ever told you that you have depression?
- Do you currently have or are you currently being treated for depression?
Depression, which is also called major depressive disorder, is a treatable illness that negatively affects how someone feels, thinks, and acts. The symptoms can be both emotional (such as sadness or loss of interest in activities) and physical (such as fatigue or slowed movements or speech).
The latest study found that depression rates increased the most among women, young adults, Black people, and Hispanic people. For the first time, more Black and Hispanic people than White people reported ever being diagnosed with depression. The lifetime depression rate among Black people was 34%, compared with 31% for Hispanic people and 29% for White people.
The rate of lifetime depression among women jumped 10 percentage points in the past 5 years, to 37%, in February, the survey results showed. About 1 in 4 women said they currently had depression or were being treated for it, up 6 percentage points compared with 5 years ago.
When responses were analyzed by age, those 18-44 years old were the most likely to report ever being diagnosed with depression or currently having the illness. About one-third of younger adults have ever been diagnosed, and more than 1 in 5 said they currently have depression.
Dr. Brendel said awareness and reduced stigma could be adding to the rising rates of depression.
“We’re making it easier to talk about mental health and looking at it as part of our overall wellness, just like physical health,” she said. “People are aware of depression, and people are seeking help for it.”
If you or someone you know needs help, dial 988 for support from the national Suicide & Crisis Lifeline. It’s free, confidential, and available 24 hours a day, 7 days a week. You can also visit 988lifeline.org and choose the chat feature.
A version of this article first appeared on Medscape.com.
In a survey, 29% of adults said they had been diagnosed with depression during their lifetime, and 18% said they currently have depression or are being treated for it. Those rates are up from the baseline 2015 rates of 20% of people ever having depression and 11% of people with a current diagnosis.
Depression had been steadily rising before the pandemic, and the Gallup analysts wrote that “social isolation, loneliness, fear of infection, psychological exhaustion (particularly among frontline responders such as health care workers), elevated substance abuse, and disruptions in mental health services have all likely played a role” in the increase.
“The fact that Americans are more depressed and struggling after this time of incredible stress and isolation is perhaps not surprising,” American Psychiatric Association president Rebecca Brendel, MD, told CNN. “There are lingering effects on our health, especially our mental health, from the past 3 years that disrupted everything we knew.”
The new estimates are based on online survey responses collected in February from 5,167 adults in the United States who answered the questions:
- Has a doctor or nurse ever told you that you have depression?
- Do you currently have or are you currently being treated for depression?
Depression, which is also called major depressive disorder, is a treatable illness that negatively affects how someone feels, thinks, and acts. The symptoms can be both emotional (such as sadness or loss of interest in activities) and physical (such as fatigue or slowed movements or speech).
The latest study found that depression rates increased the most among women, young adults, Black people, and Hispanic people. For the first time, more Black and Hispanic people than White people reported ever being diagnosed with depression. The lifetime depression rate among Black people was 34%, compared with 31% for Hispanic people and 29% for White people.
The rate of lifetime depression among women jumped 10 percentage points in the past 5 years, to 37%, in February, the survey results showed. About 1 in 4 women said they currently had depression or were being treated for it, up 6 percentage points compared with 5 years ago.
When responses were analyzed by age, those 18-44 years old were the most likely to report ever being diagnosed with depression or currently having the illness. About one-third of younger adults have ever been diagnosed, and more than 1 in 5 said they currently have depression.
Dr. Brendel said awareness and reduced stigma could be adding to the rising rates of depression.
“We’re making it easier to talk about mental health and looking at it as part of our overall wellness, just like physical health,” she said. “People are aware of depression, and people are seeking help for it.”
If you or someone you know needs help, dial 988 for support from the national Suicide & Crisis Lifeline. It’s free, confidential, and available 24 hours a day, 7 days a week. You can also visit 988lifeline.org and choose the chat feature.
A version of this article first appeared on Medscape.com.
Overcoming death anxiety: Understanding our lives and legacies
Disappointment – “I failed this exam, my life is ruined” or regret – “I am getting a divorce, I wasted so much of my life.” Patients present with a wide variety of complaints that can be understood as a form of death anxiety.
Fundamentally, patients come to see us to understand and explain their lives. One can reinterpret this as a patient asking, “If I died today, would my life have been good enough?” or “When I die, how will I look back at this moment in time and judge the choices I made?”
Other patients come to us attempting to use the same maladaptive defenses that did not serve them well in the past in the hopes of achieving a new outcome that will validate their lives. While it may be understandable that a child dissociates when facing abuse, hoping that this defense mechanism – as an adult – will work, it is unlikely to be fruitful and will certainly not validate or repair the past. This hope to repair one’s past can be interpreted as a fear of death – “I cannot die without correcting this.” This psychic conflict can intensify if one does not adopt a more adaptive understanding of his or her life.

Death anxiety is the feeling associated with the finality of life. Not only is life final, but a constant reminder of that fact is the idea that any one moment is final. Other than in science fiction, one cannot return to a prior moment and repair the past in the hope of a better future. Time goes only in one direction and death is the natural outcome of all life.
Death may have some evolutionary purpose that encourages the promotion of newer and more fitter genes, but one doesn’t have to consider its origin and reason to admit death’s constancy throughout humanity. People die and that is an anxiety-provoking fact of life. Death anxiety can feel especially tangible in our connected world. In a world of constant news, it can feel – for many people – that if your house wasn’t displaced because of global warming or that you are not a war refugee, you don’t deserve to be seen and heard.
This can be a particularly strong feeling for and among physicians, who don’t think that the mental health challenges generated by their own tough circumstances deserve to be labeled a mental disorder, so they designate themselves as having “burnout”1 – as they don’t deserve the sympathy of having the clinically significant impairments of “depression.” Our traumas don’t seem important enough to deserve notice, and thus we may feel like we could die without ever having truly mattered.

This can also be applied in the reverse fashion. Certain individuals, like celebrities, live such extravagant lives that our simpler achievements can feel futile in comparison. While the neighbor’s grass has always felt greener, we are now constantly exposed to perfectly manicured lawns on social media. When compounded, the idea that our successes and our pains are both simultaneously irrelevant can lead one to have very palpable death anxiety – my life will never matter if none of the things I do matter, or my life will never matter because I will never achieve the requisite number of “likes” or “views” on social media required to believe that one’s life was worth living.
A way of alleviating death anxiety can be through the concept of legacy, or what we leave behind. How will people remember me? Will people remember me, or will I disappear like a shadow into the distant memory of my near and dear ones? The idea of being forgotten or lost to memory is intolerable to some and can be a strong driving force to “make a name” for oneself. For those who crave fame, whether a celebrity or a generous alumnus, part of this is likely related to remaining well known after death. After all, one can argue that you are not truly dead as long as you continue to live in the memory and/or genes of others.
Legacy thus serves as a form of posthumous transitional object; a way of calming our fears about how we will be remembered. For many, reconciling their feelings towards their legacy is an avenue to tame death anxiety.
A case study
The case of Mr. B illustrates this. As a 72-year-old male with a long history of generalized anxiety, he once had a nightmare as a child, similar to the plot of Sleeping Beauty. In his dream, he walks up a spiral staircase in a castle and touches the spindle on a spinning wheel, thus ending his life. The dream was vivid and marked him.
His fear of death has subsequently reared its head throughout his life. In more recent years, he has suffered from cardiovascular disease. Although he is now quite stable on his current cardiac medications, he is constantly fearful that he will experience a cardiac event while asleep and suddenly die. He is so anxious about not waking up in the morning that falling asleep is nearly impossible.
Mr. B is single, with no close family besides a sister who lives in another state. He has a dog and few friends. He worries about what will happen to his dog if he doesn’t wake up in the morning, but perhaps most distressing to him is “there’s so much left for me to do, I have so much to write!” As an accomplished author, he continues to write, and hopes to publish many more novels in his lifetime. It is unsurprising that someone without a strong social network may fear death and feel pressured to somehow make a mark on the world before the curtain falls. It is scary to think that even without us, life goes on.
By bringing to Mr. B’s attention that his ever-present anxiety is rooted in fear of death, he was able to gain more insight into his own defensive behaviors. By confronting his death anxiety and processing his definition of a life well lived together in therapy, he’s acknowledged his lack of social connection as demoralizing, and has made significant strides to remedy this. He’s been able to focus on a more fulfilling life day to day, with less emphasis on his to-do list and aspirations. Instead, he’s connected more with his faith and members of his church. He’s gotten close to several neighbors and enjoys long dinners with them on his back patio.
At a recent meeting, he confessed that he feels “lighter” and not as fearful about sudden cardiac death, and thus has noticed that his overall anxiety has diminished greatly. He concluded that experiencing meaningful relationships in the present moment would give him greater joy than spending his remaining time engaged in preserving a future identity for himself. It seems elementary, but if we look within, we may find that we all suffer similarly: How much of our daily actions, thoughts, and fears are tied to the looming threat of death?
Conclusion
While modern psychiatry continues to advance with better understandings of our neurobiology, improved knowledge of pathophysiological processes of mental illness, and expanding discovery of novel pharmacotherapeutics, the modern psychiatrist should not forget fundamental truths of behavior and humanity that were once the staple of psychiatry.
Death anxiety is one of those truths; it is the ultimate stressor that we will all face and should be regular study and practice for psychiatrists. In this article, we explored some of those facets most meaningful to us but recommend you expand your study to the many more available.
Patients often come to physicians seeking validation of their lives or trying to use the same maladaptive defense mechanisms that did not serve them well in the past to achieve a better outcome.
In today’s world, death anxiety can feel palpable due to the constant exposure to global news and social media that can make us feel irrelevant. However, legacy, or what we leave behind, can serve as a way to alleviate death anxiety. For many, reconciling their feelings toward their legacy is an avenue to tame death anxiety. Therapy can help individuals gain insight into their defensive behaviors and process their definition of a life well lived. By focusing on a life worth living, individuals can alleviate their death anxiety and gain a sense of fulfillment.
Dr. Akkoor is a psychiatry resident at the University of California, San Diego. She is interested in immigrant mental health, ethics, consultation-liaison psychiatry, and medical education. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Badre and Dr. Akkoor have no conflicts of interest.
Reference
1. Badre N. Burnout: A concept that rebrands mental illness for professionals. Clinical Psychiatry News. 2020 Mar 5.
Disappointment – “I failed this exam, my life is ruined” or regret – “I am getting a divorce, I wasted so much of my life.” Patients present with a wide variety of complaints that can be understood as a form of death anxiety.
Fundamentally, patients come to see us to understand and explain their lives. One can reinterpret this as a patient asking, “If I died today, would my life have been good enough?” or “When I die, how will I look back at this moment in time and judge the choices I made?”
Other patients come to us attempting to use the same maladaptive defenses that did not serve them well in the past in the hopes of achieving a new outcome that will validate their lives. While it may be understandable that a child dissociates when facing abuse, hoping that this defense mechanism – as an adult – will work, it is unlikely to be fruitful and will certainly not validate or repair the past. This hope to repair one’s past can be interpreted as a fear of death – “I cannot die without correcting this.” This psychic conflict can intensify if one does not adopt a more adaptive understanding of his or her life.
Death anxiety is the feeling associated with the finality of life. Not only is life final, but a constant reminder of that fact is the idea that any one moment is final. Other than in science fiction, one cannot return to a prior moment and repair the past in the hope of a better future. Time goes only in one direction and death is the natural outcome of all life.
Death may have some evolutionary purpose that encourages the promotion of newer and more fitter genes, but one doesn’t have to consider its origin and reason to admit death’s constancy throughout humanity. People die and that is an anxiety-provoking fact of life. Death anxiety can feel especially tangible in our connected world. In a world of constant news, it can feel – for many people – that if your house wasn’t displaced because of global warming or that you are not a war refugee, you don’t deserve to be seen and heard.
This can be a particularly strong feeling for and among physicians, who don’t think that the mental health challenges generated by their own tough circumstances deserve to be labeled a mental disorder, so they designate themselves as having “burnout”1 – as they don’t deserve the sympathy of having the clinically significant impairments of “depression.” Our traumas don’t seem important enough to deserve notice, and thus we may feel like we could die without ever having truly mattered.
This can also be applied in the reverse fashion. Certain individuals, like celebrities, live such extravagant lives that our simpler achievements can feel futile in comparison. While the neighbor’s grass has always felt greener, we are now constantly exposed to perfectly manicured lawns on social media. When compounded, the idea that our successes and our pains are both simultaneously irrelevant can lead one to have very palpable death anxiety – my life will never matter if none of the things I do matter, or my life will never matter because I will never achieve the requisite number of “likes” or “views” on social media required to believe that one’s life was worth living.
A way of alleviating death anxiety can be through the concept of legacy, or what we leave behind. How will people remember me? Will people remember me, or will I disappear like a shadow into the distant memory of my near and dear ones? The idea of being forgotten or lost to memory is intolerable to some and can be a strong driving force to “make a name” for oneself. For those who crave fame, whether a celebrity or a generous alumnus, part of this is likely related to remaining well known after death. After all, one can argue that you are not truly dead as long as you continue to live in the memory and/or genes of others.
Legacy thus serves as a form of posthumous transitional object; a way of calming our fears about how we will be remembered. For many, reconciling their feelings towards their legacy is an avenue to tame death anxiety.
A case study
The case of Mr. B illustrates this. As a 72-year-old male with a long history of generalized anxiety, he once had a nightmare as a child, similar to the plot of Sleeping Beauty. In his dream, he walks up a spiral staircase in a castle and touches the spindle on a spinning wheel, thus ending his life. The dream was vivid and marked him.
His fear of death has subsequently reared its head throughout his life. In more recent years, he has suffered from cardiovascular disease. Although he is now quite stable on his current cardiac medications, he is constantly fearful that he will experience a cardiac event while asleep and suddenly die. He is so anxious about not waking up in the morning that falling asleep is nearly impossible.
Mr. B is single, with no close family besides a sister who lives in another state. He has a dog and few friends. He worries about what will happen to his dog if he doesn’t wake up in the morning, but perhaps most distressing to him is “there’s so much left for me to do, I have so much to write!” As an accomplished author, he continues to write, and hopes to publish many more novels in his lifetime. It is unsurprising that someone without a strong social network may fear death and feel pressured to somehow make a mark on the world before the curtain falls. It is scary to think that even without us, life goes on.
By bringing to Mr. B’s attention that his ever-present anxiety is rooted in fear of death, he was able to gain more insight into his own defensive behaviors. By confronting his death anxiety and processing his definition of a life well lived together in therapy, he’s acknowledged his lack of social connection as demoralizing, and has made significant strides to remedy this. He’s been able to focus on a more fulfilling life day to day, with less emphasis on his to-do list and aspirations. Instead, he’s connected more with his faith and members of his church. He’s gotten close to several neighbors and enjoys long dinners with them on his back patio.
At a recent meeting, he confessed that he feels “lighter” and not as fearful about sudden cardiac death, and thus has noticed that his overall anxiety has diminished greatly. He concluded that experiencing meaningful relationships in the present moment would give him greater joy than spending his remaining time engaged in preserving a future identity for himself. It seems elementary, but if we look within, we may find that we all suffer similarly: How much of our daily actions, thoughts, and fears are tied to the looming threat of death?
Conclusion
While modern psychiatry continues to advance with better understandings of our neurobiology, improved knowledge of pathophysiological processes of mental illness, and expanding discovery of novel pharmacotherapeutics, the modern psychiatrist should not forget fundamental truths of behavior and humanity that were once the staple of psychiatry.
Death anxiety is one of those truths; it is the ultimate stressor that we will all face and should be regular study and practice for psychiatrists. In this article, we explored some of those facets most meaningful to us but recommend you expand your study to the many more available.
Patients often come to physicians seeking validation of their lives or trying to use the same maladaptive defense mechanisms that did not serve them well in the past to achieve a better outcome.
In today’s world, death anxiety can feel palpable due to the constant exposure to global news and social media that can make us feel irrelevant. However, legacy, or what we leave behind, can serve as a way to alleviate death anxiety. For many, reconciling their feelings toward their legacy is an avenue to tame death anxiety. Therapy can help individuals gain insight into their defensive behaviors and process their definition of a life well lived. By focusing on a life worth living, individuals can alleviate their death anxiety and gain a sense of fulfillment.
Dr. Akkoor is a psychiatry resident at the University of California, San Diego. She is interested in immigrant mental health, ethics, consultation-liaison psychiatry, and medical education. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Badre and Dr. Akkoor have no conflicts of interest.
Reference
1. Badre N. Burnout: A concept that rebrands mental illness for professionals. Clinical Psychiatry News. 2020 Mar 5.
Disappointment – “I failed this exam, my life is ruined” or regret – “I am getting a divorce, I wasted so much of my life.” Patients present with a wide variety of complaints that can be understood as a form of death anxiety.
Fundamentally, patients come to see us to understand and explain their lives. One can reinterpret this as a patient asking, “If I died today, would my life have been good enough?” or “When I die, how will I look back at this moment in time and judge the choices I made?”
Other patients come to us attempting to use the same maladaptive defenses that did not serve them well in the past in the hopes of achieving a new outcome that will validate their lives. While it may be understandable that a child dissociates when facing abuse, hoping that this defense mechanism – as an adult – will work, it is unlikely to be fruitful and will certainly not validate or repair the past. This hope to repair one’s past can be interpreted as a fear of death – “I cannot die without correcting this.” This psychic conflict can intensify if one does not adopt a more adaptive understanding of his or her life.
Death anxiety is the feeling associated with the finality of life. Not only is life final, but a constant reminder of that fact is the idea that any one moment is final. Other than in science fiction, one cannot return to a prior moment and repair the past in the hope of a better future. Time goes only in one direction and death is the natural outcome of all life.
Death may have some evolutionary purpose that encourages the promotion of newer and more fitter genes, but one doesn’t have to consider its origin and reason to admit death’s constancy throughout humanity. People die and that is an anxiety-provoking fact of life. Death anxiety can feel especially tangible in our connected world. In a world of constant news, it can feel – for many people – that if your house wasn’t displaced because of global warming or that you are not a war refugee, you don’t deserve to be seen and heard.
This can be a particularly strong feeling for and among physicians, who don’t think that the mental health challenges generated by their own tough circumstances deserve to be labeled a mental disorder, so they designate themselves as having “burnout”1 – as they don’t deserve the sympathy of having the clinically significant impairments of “depression.” Our traumas don’t seem important enough to deserve notice, and thus we may feel like we could die without ever having truly mattered.
This can also be applied in the reverse fashion. Certain individuals, like celebrities, live such extravagant lives that our simpler achievements can feel futile in comparison. While the neighbor’s grass has always felt greener, we are now constantly exposed to perfectly manicured lawns on social media. When compounded, the idea that our successes and our pains are both simultaneously irrelevant can lead one to have very palpable death anxiety – my life will never matter if none of the things I do matter, or my life will never matter because I will never achieve the requisite number of “likes” or “views” on social media required to believe that one’s life was worth living.
A way of alleviating death anxiety can be through the concept of legacy, or what we leave behind. How will people remember me? Will people remember me, or will I disappear like a shadow into the distant memory of my near and dear ones? The idea of being forgotten or lost to memory is intolerable to some and can be a strong driving force to “make a name” for oneself. For those who crave fame, whether a celebrity or a generous alumnus, part of this is likely related to remaining well known after death. After all, one can argue that you are not truly dead as long as you continue to live in the memory and/or genes of others.
Legacy thus serves as a form of posthumous transitional object; a way of calming our fears about how we will be remembered. For many, reconciling their feelings towards their legacy is an avenue to tame death anxiety.
A case study
The case of Mr. B illustrates this. As a 72-year-old male with a long history of generalized anxiety, he once had a nightmare as a child, similar to the plot of Sleeping Beauty. In his dream, he walks up a spiral staircase in a castle and touches the spindle on a spinning wheel, thus ending his life. The dream was vivid and marked him.
His fear of death has subsequently reared its head throughout his life. In more recent years, he has suffered from cardiovascular disease. Although he is now quite stable on his current cardiac medications, he is constantly fearful that he will experience a cardiac event while asleep and suddenly die. He is so anxious about not waking up in the morning that falling asleep is nearly impossible.
Mr. B is single, with no close family besides a sister who lives in another state. He has a dog and few friends. He worries about what will happen to his dog if he doesn’t wake up in the morning, but perhaps most distressing to him is “there’s so much left for me to do, I have so much to write!” As an accomplished author, he continues to write, and hopes to publish many more novels in his lifetime. It is unsurprising that someone without a strong social network may fear death and feel pressured to somehow make a mark on the world before the curtain falls. It is scary to think that even without us, life goes on.
By bringing to Mr. B’s attention that his ever-present anxiety is rooted in fear of death, he was able to gain more insight into his own defensive behaviors. By confronting his death anxiety and processing his definition of a life well lived together in therapy, he’s acknowledged his lack of social connection as demoralizing, and has made significant strides to remedy this. He’s been able to focus on a more fulfilling life day to day, with less emphasis on his to-do list and aspirations. Instead, he’s connected more with his faith and members of his church. He’s gotten close to several neighbors and enjoys long dinners with them on his back patio.
At a recent meeting, he confessed that he feels “lighter” and not as fearful about sudden cardiac death, and thus has noticed that his overall anxiety has diminished greatly. He concluded that experiencing meaningful relationships in the present moment would give him greater joy than spending his remaining time engaged in preserving a future identity for himself. It seems elementary, but if we look within, we may find that we all suffer similarly: How much of our daily actions, thoughts, and fears are tied to the looming threat of death?
Conclusion
While modern psychiatry continues to advance with better understandings of our neurobiology, improved knowledge of pathophysiological processes of mental illness, and expanding discovery of novel pharmacotherapeutics, the modern psychiatrist should not forget fundamental truths of behavior and humanity that were once the staple of psychiatry.
Death anxiety is one of those truths; it is the ultimate stressor that we will all face and should be regular study and practice for psychiatrists. In this article, we explored some of those facets most meaningful to us but recommend you expand your study to the many more available.
Patients often come to physicians seeking validation of their lives or trying to use the same maladaptive defense mechanisms that did not serve them well in the past to achieve a better outcome.
In today’s world, death anxiety can feel palpable due to the constant exposure to global news and social media that can make us feel irrelevant. However, legacy, or what we leave behind, can serve as a way to alleviate death anxiety. For many, reconciling their feelings toward their legacy is an avenue to tame death anxiety. Therapy can help individuals gain insight into their defensive behaviors and process their definition of a life well lived. By focusing on a life worth living, individuals can alleviate their death anxiety and gain a sense of fulfillment.
Dr. Akkoor is a psychiatry resident at the University of California, San Diego. She is interested in immigrant mental health, ethics, consultation-liaison psychiatry, and medical education. Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com. Dr. Badre and Dr. Akkoor have no conflicts of interest.
Reference
1. Badre N. Burnout: A concept that rebrands mental illness for professionals. Clinical Psychiatry News. 2020 Mar 5.
FDA moves to curb misuse of ADHD meds
“The current prescribing information for some prescription stimulants does not provide up-to-date warnings about the harms of misuse and abuse, and particularly that most individuals who misuse prescription stimulants get their drugs from other family members or peers,” the FDA said in a drug safety communication.![]()
Going forward, updated drug labels will clearly state that patients should never share their prescription stimulants with anyone, and the boxed warning will describe the risks of misuse, abuse, addiction, and overdose consistently for all medicines in the class, the FDA said.
The boxed warning will also advise heath care professionals to monitor patients closely for signs and symptoms of misuse, abuse, and addiction.
Patient medication guides will be updated to educate patients and caregivers about these risks.
The FDA encourages prescribers to assess patient risk of misuse, abuse, and addiction before prescribing a stimulant and to counsel patients not to share the medication.
Friends and family
A recent literature review by the FDA found that friends and family members are the most common source of prescription stimulant misuse and abuse (nonmedical use). Estimates of such use range from 56% to 80%.
Misuse/abuse of a patient’s own prescription make up 10%-20% of people who report nonmedical stimulant use.
Less commonly reported sources include drug dealers or strangers (4%-7% of people who report nonmedical use) and the Internet (1%-2%).
The groups at highest risk for misuse/abuse of prescription stimulants are young adults aged 18-25 years, college students, and adolescents and young adults who have been diagnosed with ADHD, the FDA said.
Recent data from the Centers for Disease Control and Prevention show that during the first year of the COVID-19 pandemic, prescriptions for stimulants increased 10% among older children and adults.
A version of this article first appeared on Medscape.com.
“The current prescribing information for some prescription stimulants does not provide up-to-date warnings about the harms of misuse and abuse, and particularly that most individuals who misuse prescription stimulants get their drugs from other family members or peers,” the FDA said in a drug safety communication.![]()
Going forward, updated drug labels will clearly state that patients should never share their prescription stimulants with anyone, and the boxed warning will describe the risks of misuse, abuse, addiction, and overdose consistently for all medicines in the class, the FDA said.
The boxed warning will also advise heath care professionals to monitor patients closely for signs and symptoms of misuse, abuse, and addiction.
Patient medication guides will be updated to educate patients and caregivers about these risks.
The FDA encourages prescribers to assess patient risk of misuse, abuse, and addiction before prescribing a stimulant and to counsel patients not to share the medication.
Friends and family
A recent literature review by the FDA found that friends and family members are the most common source of prescription stimulant misuse and abuse (nonmedical use). Estimates of such use range from 56% to 80%.
Misuse/abuse of a patient’s own prescription make up 10%-20% of people who report nonmedical stimulant use.
Less commonly reported sources include drug dealers or strangers (4%-7% of people who report nonmedical use) and the Internet (1%-2%).
The groups at highest risk for misuse/abuse of prescription stimulants are young adults aged 18-25 years, college students, and adolescents and young adults who have been diagnosed with ADHD, the FDA said.
Recent data from the Centers for Disease Control and Prevention show that during the first year of the COVID-19 pandemic, prescriptions for stimulants increased 10% among older children and adults.
A version of this article first appeared on Medscape.com.
“The current prescribing information for some prescription stimulants does not provide up-to-date warnings about the harms of misuse and abuse, and particularly that most individuals who misuse prescription stimulants get their drugs from other family members or peers,” the FDA said in a drug safety communication.![]()
Going forward, updated drug labels will clearly state that patients should never share their prescription stimulants with anyone, and the boxed warning will describe the risks of misuse, abuse, addiction, and overdose consistently for all medicines in the class, the FDA said.
The boxed warning will also advise heath care professionals to monitor patients closely for signs and symptoms of misuse, abuse, and addiction.
Patient medication guides will be updated to educate patients and caregivers about these risks.
The FDA encourages prescribers to assess patient risk of misuse, abuse, and addiction before prescribing a stimulant and to counsel patients not to share the medication.
Friends and family
A recent literature review by the FDA found that friends and family members are the most common source of prescription stimulant misuse and abuse (nonmedical use). Estimates of such use range from 56% to 80%.
Misuse/abuse of a patient’s own prescription make up 10%-20% of people who report nonmedical stimulant use.
Less commonly reported sources include drug dealers or strangers (4%-7% of people who report nonmedical use) and the Internet (1%-2%).
The groups at highest risk for misuse/abuse of prescription stimulants are young adults aged 18-25 years, college students, and adolescents and young adults who have been diagnosed with ADHD, the FDA said.
Recent data from the Centers for Disease Control and Prevention show that during the first year of the COVID-19 pandemic, prescriptions for stimulants increased 10% among older children and adults.
A version of this article first appeared on Medscape.com.
Anxiety high among Americans, national poll shows
results of a national mental health poll conducted by the American Psychiatric Association (APA) show.
“There is a lot of worry in the world right now about economic uncertainty, about violence, about how we’re going to come out of this period of time,” APA President Rebecca W. Brendel, MD, JD, said during an APA press briefing announcing the latest poll results.
Brendel said the results are an important reminder and opportunity for psychiatrists to put their finger on the pulse of Americans’ mental health.
“If 70% of people are feeling unsafe, we need to come up with individual and also society-based solutions to help people move forward so that we can see a brighter future and not experience so much anxiety,” she added.
The poll was conducted between April 20 and 22, 2023, among a nationally representative sample of 2,201 adults. The analysis also tracks data from a poll conducted between April 23 and 24, 2022, among a sample of 2,210 adults.
Overall, nearly two in five adults (37%) reported feeling more anxious than they were at this time last year, which is higher than in 2022 (32%) but lower than in 2021 (41%) and 2020 (62%).
About one-third (30%) of adults said they have consulted a mental health care professional, a slight uptick from 2022.
Other issues keeping Americans up at night include keeping their identity safe (68%), their health (66%), paying bills or expenses (65%), climate change (59%), the opioid epidemic (50%) and the impact of emerging technology on day-to-day life (45%).
Half of respondents reported they would be likely to consider a mental health treatment involving cannabis or marijuana, while most said they would be unlikely to consider a treatment involving psychedelics (59%) or ketamine (56%).
Two-thirds (68%) of American adults reported that their children and teenagers have more mental health problems than they did a decade ago.
More than 50% of parents are concerned about their children’s technology use (59%) and mental state (55%), and 31% have encountered difficulty scheduling appointments with mental health professionals for their children.
More than three-quarters (78%) of U.S. adults believe mental health affects physical health and that untreated mental illness has a significant negative effect on families (78%). About two-thirds (64%) believe untreated mental illness harms the economy.
One in three adults (34%) would not vote for a candidate for elected office who has a mental illness – up 7% from 2022.
“The majority of the public understands something we’ve been saying for a long time: Your mental health is about your health,” Saul Levin, MD, MPA, chief executive officer and medical director at the American Psychiatric Association, said in the release.
“It’s contingent upon us as a field to continue to spread that message, and that those who are experiencing mental health concerns aren’t alone and that there are ways to receive help,” Dr. Levin added.
A version of this article originally appeared on Medscape.com.
results of a national mental health poll conducted by the American Psychiatric Association (APA) show.
“There is a lot of worry in the world right now about economic uncertainty, about violence, about how we’re going to come out of this period of time,” APA President Rebecca W. Brendel, MD, JD, said during an APA press briefing announcing the latest poll results.
Brendel said the results are an important reminder and opportunity for psychiatrists to put their finger on the pulse of Americans’ mental health.
“If 70% of people are feeling unsafe, we need to come up with individual and also society-based solutions to help people move forward so that we can see a brighter future and not experience so much anxiety,” she added.
The poll was conducted between April 20 and 22, 2023, among a nationally representative sample of 2,201 adults. The analysis also tracks data from a poll conducted between April 23 and 24, 2022, among a sample of 2,210 adults.
Overall, nearly two in five adults (37%) reported feeling more anxious than they were at this time last year, which is higher than in 2022 (32%) but lower than in 2021 (41%) and 2020 (62%).
About one-third (30%) of adults said they have consulted a mental health care professional, a slight uptick from 2022.
Other issues keeping Americans up at night include keeping their identity safe (68%), their health (66%), paying bills or expenses (65%), climate change (59%), the opioid epidemic (50%) and the impact of emerging technology on day-to-day life (45%).
Half of respondents reported they would be likely to consider a mental health treatment involving cannabis or marijuana, while most said they would be unlikely to consider a treatment involving psychedelics (59%) or ketamine (56%).
Two-thirds (68%) of American adults reported that their children and teenagers have more mental health problems than they did a decade ago.
More than 50% of parents are concerned about their children’s technology use (59%) and mental state (55%), and 31% have encountered difficulty scheduling appointments with mental health professionals for their children.
More than three-quarters (78%) of U.S. adults believe mental health affects physical health and that untreated mental illness has a significant negative effect on families (78%). About two-thirds (64%) believe untreated mental illness harms the economy.
One in three adults (34%) would not vote for a candidate for elected office who has a mental illness – up 7% from 2022.
“The majority of the public understands something we’ve been saying for a long time: Your mental health is about your health,” Saul Levin, MD, MPA, chief executive officer and medical director at the American Psychiatric Association, said in the release.
“It’s contingent upon us as a field to continue to spread that message, and that those who are experiencing mental health concerns aren’t alone and that there are ways to receive help,” Dr. Levin added.
A version of this article originally appeared on Medscape.com.
results of a national mental health poll conducted by the American Psychiatric Association (APA) show.
“There is a lot of worry in the world right now about economic uncertainty, about violence, about how we’re going to come out of this period of time,” APA President Rebecca W. Brendel, MD, JD, said during an APA press briefing announcing the latest poll results.
Brendel said the results are an important reminder and opportunity for psychiatrists to put their finger on the pulse of Americans’ mental health.
“If 70% of people are feeling unsafe, we need to come up with individual and also society-based solutions to help people move forward so that we can see a brighter future and not experience so much anxiety,” she added.
The poll was conducted between April 20 and 22, 2023, among a nationally representative sample of 2,201 adults. The analysis also tracks data from a poll conducted between April 23 and 24, 2022, among a sample of 2,210 adults.
Overall, nearly two in five adults (37%) reported feeling more anxious than they were at this time last year, which is higher than in 2022 (32%) but lower than in 2021 (41%) and 2020 (62%).
About one-third (30%) of adults said they have consulted a mental health care professional, a slight uptick from 2022.
Other issues keeping Americans up at night include keeping their identity safe (68%), their health (66%), paying bills or expenses (65%), climate change (59%), the opioid epidemic (50%) and the impact of emerging technology on day-to-day life (45%).
Half of respondents reported they would be likely to consider a mental health treatment involving cannabis or marijuana, while most said they would be unlikely to consider a treatment involving psychedelics (59%) or ketamine (56%).
Two-thirds (68%) of American adults reported that their children and teenagers have more mental health problems than they did a decade ago.
More than 50% of parents are concerned about their children’s technology use (59%) and mental state (55%), and 31% have encountered difficulty scheduling appointments with mental health professionals for their children.
More than three-quarters (78%) of U.S. adults believe mental health affects physical health and that untreated mental illness has a significant negative effect on families (78%). About two-thirds (64%) believe untreated mental illness harms the economy.
One in three adults (34%) would not vote for a candidate for elected office who has a mental illness – up 7% from 2022.
“The majority of the public understands something we’ve been saying for a long time: Your mental health is about your health,” Saul Levin, MD, MPA, chief executive officer and medical director at the American Psychiatric Association, said in the release.
“It’s contingent upon us as a field to continue to spread that message, and that those who are experiencing mental health concerns aren’t alone and that there are ways to receive help,” Dr. Levin added.
A version of this article originally appeared on Medscape.com.
Mental health promotion
May is Mental Health Awareness Month, providing us a chance to go beyond discussing the screening, diagnosis, and evidence-based treatments for the mental illnesses of youth. The World Health Organization defines good mental health as “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her own community.” While the science of mental health promotion and disease prevention in childhood and adolescence is relatively young, there are several discrete domains in which you can follow and support your patient’s developing mental health. This begins with the well-being of new parents, and then moves into how parents are helping their children to develop skills to manage their basic daily needs and impulses, their thoughts and feelings, their stresses and their relationships. With a little support from you, parents can confidently help their children develop the foundations for good mental health.
First year of life: Parental mental health

Perhaps the strongest risk factor for serious mental illness in childhood and adulthood is parental neglect during the first year of life, and neglect in the first several months of life is the most commonly reported form of child abuse. Infant neglect is associated with parental depression (and other mental illnesses), parental substance use, and a parent’s own experience of childhood abuse or neglect. Neglect is more common with teenaged parents and parents living in poverty. Pediatricians are uniquely connected to families during the first year of a child’s life. The American Academy of Pediatrics recommends screening new mothers for depression at 1-, 2-, 4-, and 6-month infant check-ups with the Edinburgh Postnatal Depression Screen. Even without a positive screen, new parents may need the fortifications of extra community support to adapt to the changes parenthood brings.
At checkups, ask (both) parents how they are managing the stresses of a new baby. Are they getting restful sleep? Do they have social supports? Are they connected to a community (friends, extended family, faith) or isolated? Are they developing confidence as parents or feeling overwhelmed? Simple guidance, such as “sleep when the baby sleeps” and reassurance that taking good care of themselves is taking good care of the baby is always helpful. Sometimes you will need to refer for treatment or to community supports. Have your list of online and in-person resources at the ready to provide parents with these prescriptions. Supporting parental mental health and adjustment in the first year of life is possibly the most important building block for their child’s future mental health.
Toddlers and up: Emotional literacy
Emotional literacy (sometimes called “emotional intelligence”) is the capacity to recognize, identify, and manage feelings in oneself and in others. This skill begins to develop in infancy when parents respond to their baby’s cries with attunement, feeding or changing them if needed, and at other times simply reflecting their feelings and soothing them with movement, singing, or quiet talking. As children grow, so does their range of feelings, and their (cognitive) capacity to identify and manage them. Parents support this development by being available whenever their young children experience strong emotions, calmly listening, and acknowledging their discomfort. Parents can offer words for describing those feelings, and even be curious with their young children where in their bodies they are feeling them, how they can stay patient while the feeling passes or things they might be able to do to feel better. Parents may want to remove their child’s distress, but staying calm, curious, and present while helping their child to manage it will build their child’s emotional health. Parents can nurture this development in a less intense way by reading books about feelings together and noticing and identifying feelings in other children or in cartoon characters.
School-age children: Adding mindfulness
While a child’s cognitive development unfolds naturally, school-age children can cultivate awareness of their thoughts. This becomes possible after awareness of feelings and parents can help their older children consider whether something they are experiencing is a thought, a feeling, or a fact. They do so in the same way they helped their child develop emotional literacy: By responding with calm, curiosity, and confidence every time their child comes to them in distress (especially mild distress, like boredom!) or with a challenge or a question. With a difficult situation, parents start by helping their child to identify thoughts and feelings before impulsively acting on them. Parents can help children identify what’s in their control, try different approaches, and be flexible if their first efforts don’t work. Children need to learn that failing at things is how we learn and grow. Just like learning to ride a bike, it builds their frustration tolerance, their knowledge that they can do difficult things, and that distress subsides. These are critical building blocks for adolescence, when the challenges become greater and they manage them more independently.

Learning “mindfulness” (a practice that cultivates nonjudgmental awareness of one’s own thoughts, feelings, and sensations) can help children (and parents) to cultivate quiet self-awareness outside of moments of difficulty. “Stop, Breathe, and Think” and “Mindful gNATs” are two free apps that are recommended by the American Academy of Child and Adolescent Psychiatry for children (and their parents) to use to practice this awareness of thoughts and feelings.
Early and later adolescence: Stress management skills
Building on this awareness of thoughts and emotions, adolescents develop adaptive coping skills by facing challenges with the support of their parents nearby. Parents should still be ready to respond to charged emotional moments with calm and curiosity, validating their child’s distress while helping them to consider healthy responses. Helping their teenager to describe their experience, differentiating feelings from thoughts (and facts), and considering different choices within their control is foundational to resilience in adulthood. Parents also help their teenagers by reminding them of the need for good self-care (sleep, exercise, nutrition), nourishing social relationships, and protecting time for rest and recharging activities. Sometimes, parents will think with their teenager about why they are engaged in an activity that is stressful, whether it is authentically important to them, and why. Adolescents should be deepening their sense of identity, interests, talents, and even values, and stressful moments are rich opportunities to do so, with the support of caring adults. Without intentionally building these skills, adolescents will be more prone to managing stress with avoidance or unhealthy coping, such as excessive eating, video gaming, drugs, or alcohol.
Infancy and up: Behavioral healthy habits (sleep, physical activity, nutrition, and screen time)
Healthy habits sound simple, but establishing them is not always easy. The idea of a habit is that it makes managing something challenging or important more automatic, and thus easier and more reliable. Many of the same habits that promote physical health in adulthood also promote mental health: adequate, restful sleep; daily physical activity; a nutritious diet and a healthy relationship with food; and managing screen time in a developmentally appropriate way. Infants depend entirely on their parents for regulation of these behaviors. As their children grow, parents will adapt these routines so that their children are gradually regulating these needs and activities more independently. In each of these areas, children need clear expectations and routines, consistent consequences and positive feedback, and the modeling and patient support of their parents. Educate parents about what good sleep hygiene looks like at each age. Discuss ways to support regular physical activity, especially as a family. Ask the parents about nutrition, including how they manage picky eating; how many family meals they enjoy together; and whether food is ever used to manage boredom or distress. Finally, talk with parents about a developmentally appropriate approach to rules and expectations around screen time and the importance of using family-based rules. Establishing expectations and routines during early childhood means children learn how good it feels to have restful sleep, regular exercise, and happy, healthy family meals. In adolescence, parents can then focus on helping their children to manage temptation, challenge, disappointment, and frustration more independently.
Infancy and up: Relational health
Children develop the skills needed for healthy relationships at home, and they are connected to all of the skills described above. Children need attuned, responsive, and reliable parenting to build a capacity for trust of others, to learn how to communicate honestly and effectively, to learn to expect and offer compassion and respect, and to learn how to handle disagreement and conflict. They learn these skills by watching their parents and by developing the emotional, cognitive, and behavioral healthy habits with their parents’ help. They need a consistently safe and responsive environment at home. They need parents who are attuned and flexible, while maintaining routines and high expectations. They need parents who make time for them when they are sad or struggling, and make time for joy, play, and mindless fun. While a detailed assessment of how the family is functioning may go beyond a check-up, you can ask about those routines that build healthy habits (family mealtime, sleep routines, screen time rules), communication style, and what the family enjoys doing together. Learning about how a family is building these healthy habits and how connected they are to one another can give you a clear snapshot of how well a child may be doing on their mental health growth curve, and what areas might benefit from more active guidance and support.
Dr. Swick is physician in chief at Ohana Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
May is Mental Health Awareness Month, providing us a chance to go beyond discussing the screening, diagnosis, and evidence-based treatments for the mental illnesses of youth. The World Health Organization defines good mental health as “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her own community.” While the science of mental health promotion and disease prevention in childhood and adolescence is relatively young, there are several discrete domains in which you can follow and support your patient’s developing mental health. This begins with the well-being of new parents, and then moves into how parents are helping their children to develop skills to manage their basic daily needs and impulses, their thoughts and feelings, their stresses and their relationships. With a little support from you, parents can confidently help their children develop the foundations for good mental health.
First year of life: Parental mental health
Perhaps the strongest risk factor for serious mental illness in childhood and adulthood is parental neglect during the first year of life, and neglect in the first several months of life is the most commonly reported form of child abuse. Infant neglect is associated with parental depression (and other mental illnesses), parental substance use, and a parent’s own experience of childhood abuse or neglect. Neglect is more common with teenaged parents and parents living in poverty. Pediatricians are uniquely connected to families during the first year of a child’s life. The American Academy of Pediatrics recommends screening new mothers for depression at 1-, 2-, 4-, and 6-month infant check-ups with the Edinburgh Postnatal Depression Screen. Even without a positive screen, new parents may need the fortifications of extra community support to adapt to the changes parenthood brings.
At checkups, ask (both) parents how they are managing the stresses of a new baby. Are they getting restful sleep? Do they have social supports? Are they connected to a community (friends, extended family, faith) or isolated? Are they developing confidence as parents or feeling overwhelmed? Simple guidance, such as “sleep when the baby sleeps” and reassurance that taking good care of themselves is taking good care of the baby is always helpful. Sometimes you will need to refer for treatment or to community supports. Have your list of online and in-person resources at the ready to provide parents with these prescriptions. Supporting parental mental health and adjustment in the first year of life is possibly the most important building block for their child’s future mental health.
Toddlers and up: Emotional literacy
Emotional literacy (sometimes called “emotional intelligence”) is the capacity to recognize, identify, and manage feelings in oneself and in others. This skill begins to develop in infancy when parents respond to their baby’s cries with attunement, feeding or changing them if needed, and at other times simply reflecting their feelings and soothing them with movement, singing, or quiet talking. As children grow, so does their range of feelings, and their (cognitive) capacity to identify and manage them. Parents support this development by being available whenever their young children experience strong emotions, calmly listening, and acknowledging their discomfort. Parents can offer words for describing those feelings, and even be curious with their young children where in their bodies they are feeling them, how they can stay patient while the feeling passes or things they might be able to do to feel better. Parents may want to remove their child’s distress, but staying calm, curious, and present while helping their child to manage it will build their child’s emotional health. Parents can nurture this development in a less intense way by reading books about feelings together and noticing and identifying feelings in other children or in cartoon characters.
School-age children: Adding mindfulness
While a child’s cognitive development unfolds naturally, school-age children can cultivate awareness of their thoughts. This becomes possible after awareness of feelings and parents can help their older children consider whether something they are experiencing is a thought, a feeling, or a fact. They do so in the same way they helped their child develop emotional literacy: By responding with calm, curiosity, and confidence every time their child comes to them in distress (especially mild distress, like boredom!) or with a challenge or a question. With a difficult situation, parents start by helping their child to identify thoughts and feelings before impulsively acting on them. Parents can help children identify what’s in their control, try different approaches, and be flexible if their first efforts don’t work. Children need to learn that failing at things is how we learn and grow. Just like learning to ride a bike, it builds their frustration tolerance, their knowledge that they can do difficult things, and that distress subsides. These are critical building blocks for adolescence, when the challenges become greater and they manage them more independently.
Learning “mindfulness” (a practice that cultivates nonjudgmental awareness of one’s own thoughts, feelings, and sensations) can help children (and parents) to cultivate quiet self-awareness outside of moments of difficulty. “Stop, Breathe, and Think” and “Mindful gNATs” are two free apps that are recommended by the American Academy of Child and Adolescent Psychiatry for children (and their parents) to use to practice this awareness of thoughts and feelings.
Early and later adolescence: Stress management skills
Building on this awareness of thoughts and emotions, adolescents develop adaptive coping skills by facing challenges with the support of their parents nearby. Parents should still be ready to respond to charged emotional moments with calm and curiosity, validating their child’s distress while helping them to consider healthy responses. Helping their teenager to describe their experience, differentiating feelings from thoughts (and facts), and considering different choices within their control is foundational to resilience in adulthood. Parents also help their teenagers by reminding them of the need for good self-care (sleep, exercise, nutrition), nourishing social relationships, and protecting time for rest and recharging activities. Sometimes, parents will think with their teenager about why they are engaged in an activity that is stressful, whether it is authentically important to them, and why. Adolescents should be deepening their sense of identity, interests, talents, and even values, and stressful moments are rich opportunities to do so, with the support of caring adults. Without intentionally building these skills, adolescents will be more prone to managing stress with avoidance or unhealthy coping, such as excessive eating, video gaming, drugs, or alcohol.
Infancy and up: Behavioral healthy habits (sleep, physical activity, nutrition, and screen time)
Healthy habits sound simple, but establishing them is not always easy. The idea of a habit is that it makes managing something challenging or important more automatic, and thus easier and more reliable. Many of the same habits that promote physical health in adulthood also promote mental health: adequate, restful sleep; daily physical activity; a nutritious diet and a healthy relationship with food; and managing screen time in a developmentally appropriate way. Infants depend entirely on their parents for regulation of these behaviors. As their children grow, parents will adapt these routines so that their children are gradually regulating these needs and activities more independently. In each of these areas, children need clear expectations and routines, consistent consequences and positive feedback, and the modeling and patient support of their parents. Educate parents about what good sleep hygiene looks like at each age. Discuss ways to support regular physical activity, especially as a family. Ask the parents about nutrition, including how they manage picky eating; how many family meals they enjoy together; and whether food is ever used to manage boredom or distress. Finally, talk with parents about a developmentally appropriate approach to rules and expectations around screen time and the importance of using family-based rules. Establishing expectations and routines during early childhood means children learn how good it feels to have restful sleep, regular exercise, and happy, healthy family meals. In adolescence, parents can then focus on helping their children to manage temptation, challenge, disappointment, and frustration more independently.
Infancy and up: Relational health
Children develop the skills needed for healthy relationships at home, and they are connected to all of the skills described above. Children need attuned, responsive, and reliable parenting to build a capacity for trust of others, to learn how to communicate honestly and effectively, to learn to expect and offer compassion and respect, and to learn how to handle disagreement and conflict. They learn these skills by watching their parents and by developing the emotional, cognitive, and behavioral healthy habits with their parents’ help. They need a consistently safe and responsive environment at home. They need parents who are attuned and flexible, while maintaining routines and high expectations. They need parents who make time for them when they are sad or struggling, and make time for joy, play, and mindless fun. While a detailed assessment of how the family is functioning may go beyond a check-up, you can ask about those routines that build healthy habits (family mealtime, sleep routines, screen time rules), communication style, and what the family enjoys doing together. Learning about how a family is building these healthy habits and how connected they are to one another can give you a clear snapshot of how well a child may be doing on their mental health growth curve, and what areas might benefit from more active guidance and support.
Dr. Swick is physician in chief at Ohana Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
May is Mental Health Awareness Month, providing us a chance to go beyond discussing the screening, diagnosis, and evidence-based treatments for the mental illnesses of youth. The World Health Organization defines good mental health as “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her own community.” While the science of mental health promotion and disease prevention in childhood and adolescence is relatively young, there are several discrete domains in which you can follow and support your patient’s developing mental health. This begins with the well-being of new parents, and then moves into how parents are helping their children to develop skills to manage their basic daily needs and impulses, their thoughts and feelings, their stresses and their relationships. With a little support from you, parents can confidently help their children develop the foundations for good mental health.
First year of life: Parental mental health
Perhaps the strongest risk factor for serious mental illness in childhood and adulthood is parental neglect during the first year of life, and neglect in the first several months of life is the most commonly reported form of child abuse. Infant neglect is associated with parental depression (and other mental illnesses), parental substance use, and a parent’s own experience of childhood abuse or neglect. Neglect is more common with teenaged parents and parents living in poverty. Pediatricians are uniquely connected to families during the first year of a child’s life. The American Academy of Pediatrics recommends screening new mothers for depression at 1-, 2-, 4-, and 6-month infant check-ups with the Edinburgh Postnatal Depression Screen. Even without a positive screen, new parents may need the fortifications of extra community support to adapt to the changes parenthood brings.
At checkups, ask (both) parents how they are managing the stresses of a new baby. Are they getting restful sleep? Do they have social supports? Are they connected to a community (friends, extended family, faith) or isolated? Are they developing confidence as parents or feeling overwhelmed? Simple guidance, such as “sleep when the baby sleeps” and reassurance that taking good care of themselves is taking good care of the baby is always helpful. Sometimes you will need to refer for treatment or to community supports. Have your list of online and in-person resources at the ready to provide parents with these prescriptions. Supporting parental mental health and adjustment in the first year of life is possibly the most important building block for their child’s future mental health.
Toddlers and up: Emotional literacy
Emotional literacy (sometimes called “emotional intelligence”) is the capacity to recognize, identify, and manage feelings in oneself and in others. This skill begins to develop in infancy when parents respond to their baby’s cries with attunement, feeding or changing them if needed, and at other times simply reflecting their feelings and soothing them with movement, singing, or quiet talking. As children grow, so does their range of feelings, and their (cognitive) capacity to identify and manage them. Parents support this development by being available whenever their young children experience strong emotions, calmly listening, and acknowledging their discomfort. Parents can offer words for describing those feelings, and even be curious with their young children where in their bodies they are feeling them, how they can stay patient while the feeling passes or things they might be able to do to feel better. Parents may want to remove their child’s distress, but staying calm, curious, and present while helping their child to manage it will build their child’s emotional health. Parents can nurture this development in a less intense way by reading books about feelings together and noticing and identifying feelings in other children or in cartoon characters.
School-age children: Adding mindfulness
While a child’s cognitive development unfolds naturally, school-age children can cultivate awareness of their thoughts. This becomes possible after awareness of feelings and parents can help their older children consider whether something they are experiencing is a thought, a feeling, or a fact. They do so in the same way they helped their child develop emotional literacy: By responding with calm, curiosity, and confidence every time their child comes to them in distress (especially mild distress, like boredom!) or with a challenge or a question. With a difficult situation, parents start by helping their child to identify thoughts and feelings before impulsively acting on them. Parents can help children identify what’s in their control, try different approaches, and be flexible if their first efforts don’t work. Children need to learn that failing at things is how we learn and grow. Just like learning to ride a bike, it builds their frustration tolerance, their knowledge that they can do difficult things, and that distress subsides. These are critical building blocks for adolescence, when the challenges become greater and they manage them more independently.
Learning “mindfulness” (a practice that cultivates nonjudgmental awareness of one’s own thoughts, feelings, and sensations) can help children (and parents) to cultivate quiet self-awareness outside of moments of difficulty. “Stop, Breathe, and Think” and “Mindful gNATs” are two free apps that are recommended by the American Academy of Child and Adolescent Psychiatry for children (and their parents) to use to practice this awareness of thoughts and feelings.
Early and later adolescence: Stress management skills
Building on this awareness of thoughts and emotions, adolescents develop adaptive coping skills by facing challenges with the support of their parents nearby. Parents should still be ready to respond to charged emotional moments with calm and curiosity, validating their child’s distress while helping them to consider healthy responses. Helping their teenager to describe their experience, differentiating feelings from thoughts (and facts), and considering different choices within their control is foundational to resilience in adulthood. Parents also help their teenagers by reminding them of the need for good self-care (sleep, exercise, nutrition), nourishing social relationships, and protecting time for rest and recharging activities. Sometimes, parents will think with their teenager about why they are engaged in an activity that is stressful, whether it is authentically important to them, and why. Adolescents should be deepening their sense of identity, interests, talents, and even values, and stressful moments are rich opportunities to do so, with the support of caring adults. Without intentionally building these skills, adolescents will be more prone to managing stress with avoidance or unhealthy coping, such as excessive eating, video gaming, drugs, or alcohol.
Infancy and up: Behavioral healthy habits (sleep, physical activity, nutrition, and screen time)
Healthy habits sound simple, but establishing them is not always easy. The idea of a habit is that it makes managing something challenging or important more automatic, and thus easier and more reliable. Many of the same habits that promote physical health in adulthood also promote mental health: adequate, restful sleep; daily physical activity; a nutritious diet and a healthy relationship with food; and managing screen time in a developmentally appropriate way. Infants depend entirely on their parents for regulation of these behaviors. As their children grow, parents will adapt these routines so that their children are gradually regulating these needs and activities more independently. In each of these areas, children need clear expectations and routines, consistent consequences and positive feedback, and the modeling and patient support of their parents. Educate parents about what good sleep hygiene looks like at each age. Discuss ways to support regular physical activity, especially as a family. Ask the parents about nutrition, including how they manage picky eating; how many family meals they enjoy together; and whether food is ever used to manage boredom or distress. Finally, talk with parents about a developmentally appropriate approach to rules and expectations around screen time and the importance of using family-based rules. Establishing expectations and routines during early childhood means children learn how good it feels to have restful sleep, regular exercise, and happy, healthy family meals. In adolescence, parents can then focus on helping their children to manage temptation, challenge, disappointment, and frustration more independently.
Infancy and up: Relational health
Children develop the skills needed for healthy relationships at home, and they are connected to all of the skills described above. Children need attuned, responsive, and reliable parenting to build a capacity for trust of others, to learn how to communicate honestly and effectively, to learn to expect and offer compassion and respect, and to learn how to handle disagreement and conflict. They learn these skills by watching their parents and by developing the emotional, cognitive, and behavioral healthy habits with their parents’ help. They need a consistently safe and responsive environment at home. They need parents who are attuned and flexible, while maintaining routines and high expectations. They need parents who make time for them when they are sad or struggling, and make time for joy, play, and mindless fun. While a detailed assessment of how the family is functioning may go beyond a check-up, you can ask about those routines that build healthy habits (family mealtime, sleep routines, screen time rules), communication style, and what the family enjoys doing together. Learning about how a family is building these healthy habits and how connected they are to one another can give you a clear snapshot of how well a child may be doing on their mental health growth curve, and what areas might benefit from more active guidance and support.
Dr. Swick is physician in chief at Ohana Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
Young men at highest schizophrenia risk from cannabis abuse
A new study confirms the robust link between cannabis use and schizophrenia among men and women but suggests that young men may be especially susceptible to schizophrenia from cannabis abuse.
Of note,

“The entanglement of substance use disorders and mental illnesses is a major public health issue, requiring urgent action and support for people who need it,” study coauthor Nora Volkow, MD, director of the National Institute on Drug Abuse, said in a news release.
“As access to potent cannabis products continues to expand, it is crucial that we also expand prevention, screening, and treatment for people who may experience mental illnesses associated with cannabis use,” Dr. Volkow added.
The study was published online in Psychological Medicine.
A modifiable risk factor
The researchers analyzed Danish registry data spanning 5 decades and representing more than 6.9 million people in Denmark to estimate the population-level percentage of schizophrenia cases attributable to CUD.
A total of 60,563 participants were diagnosed with CUD. Three-quarters of cases were in men; there were 45,327 incident cases of schizophrenia during the study period.
The overall adjusted hazard ratio for CUD on schizophrenia was slightly higher among males than females (aHR, 2.42 vs. 2.02); however, among those aged 16 to 20 years, the adjusted incidence risk ratio for males was more than twice that for females (aIRR, 3.84 vs. 1.81).
The researchers estimate that, in 2021, about 15% of schizophrenia cases among males aged 16-49 could have been avoided by preventing CUD, compared with 4% among females in this age range.
For young men aged 21-30, the proportion of preventable schizophrenia cases related to CUD may be as high as 30%, the authors reported.
“Alongside the increasing evidence that CUD is a modifiable risk factor for schizophrenia, our findings underscore the importance of evidence-based strategies to regulate cannabis use and to effectively prevent, screen for, and treat CUD as well as schizophrenia,” the researchers wrote.
Legalization sends the wrong message
In a press statement, lead investigator Carsten Hjorthøj, PhD, with the University of Copenhagen, noted that “increases in the legalization of cannabis over the past few decades have made it one of the most frequently used psychoactive substances in the world, while also decreasing the public’s perception of its harm. This study adds to our growing understanding that cannabis use is not harmless, and that risks are not fixed at one point in time.”
In a prior study, Dr. Hjorthøj and colleagues found that the proportion of new schizophrenia cases attributable to CUD has consistently increased over the past 20 years.
“In my view, the association is most likely causative, at least to a large extent,” Dr. Hjorthøj said at the time this research was published.
“It is of course nearly impossible to use epidemiological studies to actually prove causation, but all the numbers behave exactly in the way that would be expected under the theory of causation,” Dr. Hjorthøj added.
The study received no specific funding. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study confirms the robust link between cannabis use and schizophrenia among men and women but suggests that young men may be especially susceptible to schizophrenia from cannabis abuse.
Of note,
“The entanglement of substance use disorders and mental illnesses is a major public health issue, requiring urgent action and support for people who need it,” study coauthor Nora Volkow, MD, director of the National Institute on Drug Abuse, said in a news release.
“As access to potent cannabis products continues to expand, it is crucial that we also expand prevention, screening, and treatment for people who may experience mental illnesses associated with cannabis use,” Dr. Volkow added.
The study was published online in Psychological Medicine.
A modifiable risk factor
The researchers analyzed Danish registry data spanning 5 decades and representing more than 6.9 million people in Denmark to estimate the population-level percentage of schizophrenia cases attributable to CUD.
A total of 60,563 participants were diagnosed with CUD. Three-quarters of cases were in men; there were 45,327 incident cases of schizophrenia during the study period.
The overall adjusted hazard ratio for CUD on schizophrenia was slightly higher among males than females (aHR, 2.42 vs. 2.02); however, among those aged 16 to 20 years, the adjusted incidence risk ratio for males was more than twice that for females (aIRR, 3.84 vs. 1.81).
The researchers estimate that, in 2021, about 15% of schizophrenia cases among males aged 16-49 could have been avoided by preventing CUD, compared with 4% among females in this age range.
For young men aged 21-30, the proportion of preventable schizophrenia cases related to CUD may be as high as 30%, the authors reported.
“Alongside the increasing evidence that CUD is a modifiable risk factor for schizophrenia, our findings underscore the importance of evidence-based strategies to regulate cannabis use and to effectively prevent, screen for, and treat CUD as well as schizophrenia,” the researchers wrote.
Legalization sends the wrong message
In a press statement, lead investigator Carsten Hjorthøj, PhD, with the University of Copenhagen, noted that “increases in the legalization of cannabis over the past few decades have made it one of the most frequently used psychoactive substances in the world, while also decreasing the public’s perception of its harm. This study adds to our growing understanding that cannabis use is not harmless, and that risks are not fixed at one point in time.”
In a prior study, Dr. Hjorthøj and colleagues found that the proportion of new schizophrenia cases attributable to CUD has consistently increased over the past 20 years.
“In my view, the association is most likely causative, at least to a large extent,” Dr. Hjorthøj said at the time this research was published.
“It is of course nearly impossible to use epidemiological studies to actually prove causation, but all the numbers behave exactly in the way that would be expected under the theory of causation,” Dr. Hjorthøj added.
The study received no specific funding. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study confirms the robust link between cannabis use and schizophrenia among men and women but suggests that young men may be especially susceptible to schizophrenia from cannabis abuse.
Of note,
“The entanglement of substance use disorders and mental illnesses is a major public health issue, requiring urgent action and support for people who need it,” study coauthor Nora Volkow, MD, director of the National Institute on Drug Abuse, said in a news release.
“As access to potent cannabis products continues to expand, it is crucial that we also expand prevention, screening, and treatment for people who may experience mental illnesses associated with cannabis use,” Dr. Volkow added.
The study was published online in Psychological Medicine.
A modifiable risk factor
The researchers analyzed Danish registry data spanning 5 decades and representing more than 6.9 million people in Denmark to estimate the population-level percentage of schizophrenia cases attributable to CUD.
A total of 60,563 participants were diagnosed with CUD. Three-quarters of cases were in men; there were 45,327 incident cases of schizophrenia during the study period.
The overall adjusted hazard ratio for CUD on schizophrenia was slightly higher among males than females (aHR, 2.42 vs. 2.02); however, among those aged 16 to 20 years, the adjusted incidence risk ratio for males was more than twice that for females (aIRR, 3.84 vs. 1.81).
The researchers estimate that, in 2021, about 15% of schizophrenia cases among males aged 16-49 could have been avoided by preventing CUD, compared with 4% among females in this age range.
For young men aged 21-30, the proportion of preventable schizophrenia cases related to CUD may be as high as 30%, the authors reported.
“Alongside the increasing evidence that CUD is a modifiable risk factor for schizophrenia, our findings underscore the importance of evidence-based strategies to regulate cannabis use and to effectively prevent, screen for, and treat CUD as well as schizophrenia,” the researchers wrote.
Legalization sends the wrong message
In a press statement, lead investigator Carsten Hjorthøj, PhD, with the University of Copenhagen, noted that “increases in the legalization of cannabis over the past few decades have made it one of the most frequently used psychoactive substances in the world, while also decreasing the public’s perception of its harm. This study adds to our growing understanding that cannabis use is not harmless, and that risks are not fixed at one point in time.”
In a prior study, Dr. Hjorthøj and colleagues found that the proportion of new schizophrenia cases attributable to CUD has consistently increased over the past 20 years.
“In my view, the association is most likely causative, at least to a large extent,” Dr. Hjorthøj said at the time this research was published.
“It is of course nearly impossible to use epidemiological studies to actually prove causation, but all the numbers behave exactly in the way that would be expected under the theory of causation,” Dr. Hjorthøj added.
The study received no specific funding. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PSYCHOLOGICAL MEDICINE
Integrating mental health and primary care: From dipping a toe to taking a plunge
In case anybody hasn’t noticed, the good ole days are long gone in which pediatric patients with mental health challenges could be simply referred out to be promptly assessed and treated by specialists. Due to a shortage of psychiatrists coupled with large increases in the number of youth presenting with emotional-behavioral difficulties, primary care clinicians are now called upon to fill in much of this gap, with professional organizations like the AAP articulating that .1

To meet this need, new models of integrated or collaborative care between primary care and mental health clinicians have been attempted and tested. While these initiatives have certainly been a welcome advance to many pediatricians, the large numbers of different models and initiatives out there have made for a rather confusing landscape that many busy primary care clinicians have found difficult to navigate.
In an attempt to offer some guidance on the subject, the American Academy of Child and Adolescent Psychiatry recently published a clinical update on pediatric collaborative care.2 The report is rich with resources and ideas. One of the main points of the document is that there are different levels of integration that exist. Kind of like the situation with recycling and household waste reduction, it is possible to make valuable improvements at any level of participation, although evidence suggests that more extensive efforts offer the most benefits. At one end of the spectrum, psychiatrists and primary care clinicians maintain separate practices and medical records and occasionally discuss mutual patients. Middle levels may include “colocation” with mental health and primary care professionals sharing a building and/or being part of the same overall system but continuing to work mainly independently. At the highest levels of integration, there is a coordinated and collaborative team that supports an intentional system of care with consistent communication about individual patients and general workflows. These approaches vary in the amount that the following four core areas of integrated care are incorporated.
- Direct service. Many integrated care initiatives heavily rely on the services of an on-site mental health care manager or behavioral health consultant who can provide a number of important functions such as overseeing of the integrated care program, conducting brief therapy with youth and parents, overseeing mental health screenings at the clinic, and providing general mental health promotion guidance.
- Care coordination. Helping patients and families find needed mental health, social services, and educational resources is a key component of integrated care. This task can fall to the practice’s behavioral health consultant, if there is one, but more general care coordinators can also be trained for this important role. The University of Washington’s Center for Advancing Integrated Mental Health Solutions has some published guidelines in this area.3
- Consultation. More advanced integrated care models often have established relationships to specific child psychiatric clinicians who are able to meet with the primary care team to discuss cases and general approaches to various problems. Alternatively, a number of states have implemented what are called Child Psychiatry Access Programs that give primary care clinicians a phone number to an organization (often affiliated with an academic medical center) that can provide quick and even immediate access to a child psychiatry provider for specific questions. Recent federal grants have led to many if not most states now having one of these programs in place, and a website listing these programs and their contact information is available.4
- Education. As mental health training was traditionally not part of a typical pediatrics residency, there have been a number of strategies introduced to help primary care clinicians increase their proficiency and comfort level when it comes to assessing and treating emotional-behavioral problems. These include specific conferences, online programs, and case-based training through mechanisms like the ECHO program.5,6 The AAP itself has released a number of toolkits and training materials related to mental health care that are available.7
The report also outlines some obstacles that continue to get in the way of more extensive integrative care efforts. Chief among them are financial concerns, including how to pay for what often are traditionally nonbillable efforts, particularly those that involve the communication of two expensive health care professionals. Some improvements have been made, however, such as the creation of some relatively new codes (such as 99451 and 99452) that can be submitted by both a primary care and mental health professional when there is a consultation that occurs that does not involve an actual face-to-face encounter.
One area that, in my view, has not received the level of attention it deserves when it comes to integrated care is the degree to which these programs have the potential not only to improve the care of children and adolescents already struggling with mental health challenges but also to serve as a powerful prevention tool to lower the risk of being diagnosed with a psychiatric disorder in the future and generally to improve levels of well-being. Thus far, however, research on various integrated programs has shown promising results that indicate that overall care for patients with mental health challenges improves.8 Further, when it comes to costs, there is some evidence to suggest that some of the biggest financial gains associated with integrated care has to do with reduced nonpsychiatric medical expenses of patients.9 This, then, suggests that practices that participate in capitated or accountable care organization structures could particularly benefit both clinically and financially from these collaborations.
If your practice has been challenged with the level of mental health care you are now expected to provide and has been contemplating even some small moves toward integrated care, now may the time to put those thoughts into action.
References
1. Foy JM et al. American Academy of Pediatrics policy statement. Mental health competencies for pediatric practice. Pediatrics. 2019;144(5):e20192757.
2. AACAP Committee on Collaborative and Integrated Care and AACAP Committee on Quality Issues. Clinical update: Collaborative mental health care for children and adolescents in pediatric primary care. J Am Acad Child Adolesc Psychiatry. 2023;62(2):91-119.
3. Behavioral health care managers. AIMS Center, University of Washington. Accessed May 5, 2023. Available at https://aims.uw.edu/online-bhcm-modules.
4. National Network of Child Psychiatry Access Programs. Accessed May 5, 2023. Available at https://www.nncpap.org/.
5. Project Echo Programs. Accessed May 5, 2023. https://hsc.unm.edu/echo.
6. Project TEACH. Accessed May 5, 2023. https://projectteachny.org.
7. Earls MF et al. Addressing mental health concerns in pediatrics: A practical resource toolkit for clinicians, 2nd edition. Itasca, Ill.: American Academy of Pediatrics, 2021.
8. Asarnow JR et al. Integrated medical-behavioral care compared with usual primary care for child and adolescent behavioral health: A meta analysis. JAMA Pediatr. 2015;169(10):929-37.
9. Unutzer J et al. Long-term costs effects of collaborative care for late-life depression. Am J Manag Care. 2008.14(2):95-100.
Dr. Rettew is a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland. His latest book is “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
In case anybody hasn’t noticed, the good ole days are long gone in which pediatric patients with mental health challenges could be simply referred out to be promptly assessed and treated by specialists. Due to a shortage of psychiatrists coupled with large increases in the number of youth presenting with emotional-behavioral difficulties, primary care clinicians are now called upon to fill in much of this gap, with professional organizations like the AAP articulating that .1
To meet this need, new models of integrated or collaborative care between primary care and mental health clinicians have been attempted and tested. While these initiatives have certainly been a welcome advance to many pediatricians, the large numbers of different models and initiatives out there have made for a rather confusing landscape that many busy primary care clinicians have found difficult to navigate.
In an attempt to offer some guidance on the subject, the American Academy of Child and Adolescent Psychiatry recently published a clinical update on pediatric collaborative care.2 The report is rich with resources and ideas. One of the main points of the document is that there are different levels of integration that exist. Kind of like the situation with recycling and household waste reduction, it is possible to make valuable improvements at any level of participation, although evidence suggests that more extensive efforts offer the most benefits. At one end of the spectrum, psychiatrists and primary care clinicians maintain separate practices and medical records and occasionally discuss mutual patients. Middle levels may include “colocation” with mental health and primary care professionals sharing a building and/or being part of the same overall system but continuing to work mainly independently. At the highest levels of integration, there is a coordinated and collaborative team that supports an intentional system of care with consistent communication about individual patients and general workflows. These approaches vary in the amount that the following four core areas of integrated care are incorporated.
- Direct service. Many integrated care initiatives heavily rely on the services of an on-site mental health care manager or behavioral health consultant who can provide a number of important functions such as overseeing of the integrated care program, conducting brief therapy with youth and parents, overseeing mental health screenings at the clinic, and providing general mental health promotion guidance.
- Care coordination. Helping patients and families find needed mental health, social services, and educational resources is a key component of integrated care. This task can fall to the practice’s behavioral health consultant, if there is one, but more general care coordinators can also be trained for this important role. The University of Washington’s Center for Advancing Integrated Mental Health Solutions has some published guidelines in this area.3
- Consultation. More advanced integrated care models often have established relationships to specific child psychiatric clinicians who are able to meet with the primary care team to discuss cases and general approaches to various problems. Alternatively, a number of states have implemented what are called Child Psychiatry Access Programs that give primary care clinicians a phone number to an organization (often affiliated with an academic medical center) that can provide quick and even immediate access to a child psychiatry provider for specific questions. Recent federal grants have led to many if not most states now having one of these programs in place, and a website listing these programs and their contact information is available.4
- Education. As mental health training was traditionally not part of a typical pediatrics residency, there have been a number of strategies introduced to help primary care clinicians increase their proficiency and comfort level when it comes to assessing and treating emotional-behavioral problems. These include specific conferences, online programs, and case-based training through mechanisms like the ECHO program.5,6 The AAP itself has released a number of toolkits and training materials related to mental health care that are available.7
The report also outlines some obstacles that continue to get in the way of more extensive integrative care efforts. Chief among them are financial concerns, including how to pay for what often are traditionally nonbillable efforts, particularly those that involve the communication of two expensive health care professionals. Some improvements have been made, however, such as the creation of some relatively new codes (such as 99451 and 99452) that can be submitted by both a primary care and mental health professional when there is a consultation that occurs that does not involve an actual face-to-face encounter.
One area that, in my view, has not received the level of attention it deserves when it comes to integrated care is the degree to which these programs have the potential not only to improve the care of children and adolescents already struggling with mental health challenges but also to serve as a powerful prevention tool to lower the risk of being diagnosed with a psychiatric disorder in the future and generally to improve levels of well-being. Thus far, however, research on various integrated programs has shown promising results that indicate that overall care for patients with mental health challenges improves.8 Further, when it comes to costs, there is some evidence to suggest that some of the biggest financial gains associated with integrated care has to do with reduced nonpsychiatric medical expenses of patients.9 This, then, suggests that practices that participate in capitated or accountable care organization structures could particularly benefit both clinically and financially from these collaborations.
If your practice has been challenged with the level of mental health care you are now expected to provide and has been contemplating even some small moves toward integrated care, now may the time to put those thoughts into action.
References
1. Foy JM et al. American Academy of Pediatrics policy statement. Mental health competencies for pediatric practice. Pediatrics. 2019;144(5):e20192757.
2. AACAP Committee on Collaborative and Integrated Care and AACAP Committee on Quality Issues. Clinical update: Collaborative mental health care for children and adolescents in pediatric primary care. J Am Acad Child Adolesc Psychiatry. 2023;62(2):91-119.
3. Behavioral health care managers. AIMS Center, University of Washington. Accessed May 5, 2023. Available at https://aims.uw.edu/online-bhcm-modules.
4. National Network of Child Psychiatry Access Programs. Accessed May 5, 2023. Available at https://www.nncpap.org/.
5. Project Echo Programs. Accessed May 5, 2023. https://hsc.unm.edu/echo.
6. Project TEACH. Accessed May 5, 2023. https://projectteachny.org.
7. Earls MF et al. Addressing mental health concerns in pediatrics: A practical resource toolkit for clinicians, 2nd edition. Itasca, Ill.: American Academy of Pediatrics, 2021.
8. Asarnow JR et al. Integrated medical-behavioral care compared with usual primary care for child and adolescent behavioral health: A meta analysis. JAMA Pediatr. 2015;169(10):929-37.
9. Unutzer J et al. Long-term costs effects of collaborative care for late-life depression. Am J Manag Care. 2008.14(2):95-100.
Dr. Rettew is a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland. His latest book is “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
In case anybody hasn’t noticed, the good ole days are long gone in which pediatric patients with mental health challenges could be simply referred out to be promptly assessed and treated by specialists. Due to a shortage of psychiatrists coupled with large increases in the number of youth presenting with emotional-behavioral difficulties, primary care clinicians are now called upon to fill in much of this gap, with professional organizations like the AAP articulating that .1
To meet this need, new models of integrated or collaborative care between primary care and mental health clinicians have been attempted and tested. While these initiatives have certainly been a welcome advance to many pediatricians, the large numbers of different models and initiatives out there have made for a rather confusing landscape that many busy primary care clinicians have found difficult to navigate.
In an attempt to offer some guidance on the subject, the American Academy of Child and Adolescent Psychiatry recently published a clinical update on pediatric collaborative care.2 The report is rich with resources and ideas. One of the main points of the document is that there are different levels of integration that exist. Kind of like the situation with recycling and household waste reduction, it is possible to make valuable improvements at any level of participation, although evidence suggests that more extensive efforts offer the most benefits. At one end of the spectrum, psychiatrists and primary care clinicians maintain separate practices and medical records and occasionally discuss mutual patients. Middle levels may include “colocation” with mental health and primary care professionals sharing a building and/or being part of the same overall system but continuing to work mainly independently. At the highest levels of integration, there is a coordinated and collaborative team that supports an intentional system of care with consistent communication about individual patients and general workflows. These approaches vary in the amount that the following four core areas of integrated care are incorporated.
- Direct service. Many integrated care initiatives heavily rely on the services of an on-site mental health care manager or behavioral health consultant who can provide a number of important functions such as overseeing of the integrated care program, conducting brief therapy with youth and parents, overseeing mental health screenings at the clinic, and providing general mental health promotion guidance.
- Care coordination. Helping patients and families find needed mental health, social services, and educational resources is a key component of integrated care. This task can fall to the practice’s behavioral health consultant, if there is one, but more general care coordinators can also be trained for this important role. The University of Washington’s Center for Advancing Integrated Mental Health Solutions has some published guidelines in this area.3
- Consultation. More advanced integrated care models often have established relationships to specific child psychiatric clinicians who are able to meet with the primary care team to discuss cases and general approaches to various problems. Alternatively, a number of states have implemented what are called Child Psychiatry Access Programs that give primary care clinicians a phone number to an organization (often affiliated with an academic medical center) that can provide quick and even immediate access to a child psychiatry provider for specific questions. Recent federal grants have led to many if not most states now having one of these programs in place, and a website listing these programs and their contact information is available.4
- Education. As mental health training was traditionally not part of a typical pediatrics residency, there have been a number of strategies introduced to help primary care clinicians increase their proficiency and comfort level when it comes to assessing and treating emotional-behavioral problems. These include specific conferences, online programs, and case-based training through mechanisms like the ECHO program.5,6 The AAP itself has released a number of toolkits and training materials related to mental health care that are available.7
The report also outlines some obstacles that continue to get in the way of more extensive integrative care efforts. Chief among them are financial concerns, including how to pay for what often are traditionally nonbillable efforts, particularly those that involve the communication of two expensive health care professionals. Some improvements have been made, however, such as the creation of some relatively new codes (such as 99451 and 99452) that can be submitted by both a primary care and mental health professional when there is a consultation that occurs that does not involve an actual face-to-face encounter.
One area that, in my view, has not received the level of attention it deserves when it comes to integrated care is the degree to which these programs have the potential not only to improve the care of children and adolescents already struggling with mental health challenges but also to serve as a powerful prevention tool to lower the risk of being diagnosed with a psychiatric disorder in the future and generally to improve levels of well-being. Thus far, however, research on various integrated programs has shown promising results that indicate that overall care for patients with mental health challenges improves.8 Further, when it comes to costs, there is some evidence to suggest that some of the biggest financial gains associated with integrated care has to do with reduced nonpsychiatric medical expenses of patients.9 This, then, suggests that practices that participate in capitated or accountable care organization structures could particularly benefit both clinically and financially from these collaborations.
If your practice has been challenged with the level of mental health care you are now expected to provide and has been contemplating even some small moves toward integrated care, now may the time to put those thoughts into action.
References
1. Foy JM et al. American Academy of Pediatrics policy statement. Mental health competencies for pediatric practice. Pediatrics. 2019;144(5):e20192757.
2. AACAP Committee on Collaborative and Integrated Care and AACAP Committee on Quality Issues. Clinical update: Collaborative mental health care for children and adolescents in pediatric primary care. J Am Acad Child Adolesc Psychiatry. 2023;62(2):91-119.
3. Behavioral health care managers. AIMS Center, University of Washington. Accessed May 5, 2023. Available at https://aims.uw.edu/online-bhcm-modules.
4. National Network of Child Psychiatry Access Programs. Accessed May 5, 2023. Available at https://www.nncpap.org/.
5. Project Echo Programs. Accessed May 5, 2023. https://hsc.unm.edu/echo.
6. Project TEACH. Accessed May 5, 2023. https://projectteachny.org.
7. Earls MF et al. Addressing mental health concerns in pediatrics: A practical resource toolkit for clinicians, 2nd edition. Itasca, Ill.: American Academy of Pediatrics, 2021.
8. Asarnow JR et al. Integrated medical-behavioral care compared with usual primary care for child and adolescent behavioral health: A meta analysis. JAMA Pediatr. 2015;169(10):929-37.
9. Unutzer J et al. Long-term costs effects of collaborative care for late-life depression. Am J Manag Care. 2008.14(2):95-100.
Dr. Rettew is a child and adolescent psychiatrist with Lane County Behavioral Health in Eugene, Ore., and Oregon Health & Science University, Portland. His latest book is “Parenting Made Complicated: What Science Really Knows about the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Widespread prescribing of stimulants with other CNS-active meds
Investigators analyzed prescription drug claims for over 9.1 million U.S. adults over a 1-year period and found that 276,223 (3%) had used a schedule II stimulant, such as methylphenidate and amphetamines, during that time. Of these 276,223 patients, 45% combined these agents with one or more additional CNS-active drugs and almost 25% were simultaneously using two or more additional CNS-active drugs.
Close to half of the stimulant users were taking an antidepressant, while close to one-third filled prescriptions for anxiolytic/sedative/hypnotic meditations, and one-fifth received opioid prescriptions.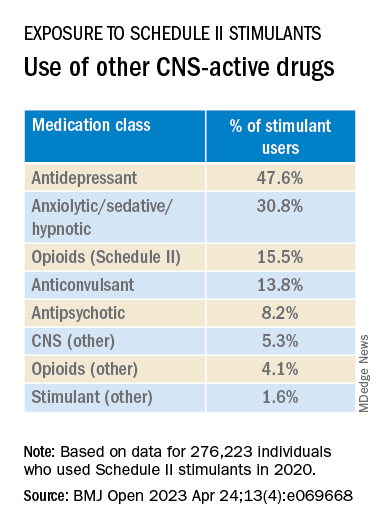
The widespread, often off-label use of these stimulants in combination therapy with antidepressants, anxiolytics, opioids, and other psychoactive drugs, “reveals new patterns of utilization beyond the approved use of stimulants as monotherapy for ADHD, but because there are so few studies of these kinds of combination therapy, both the advantages and additional risks [of this type of prescribing] remain unknown,” study investigator Thomas J. Moore, AB, faculty associate in epidemiology, Johns Hopkins Bloomberg School of Public Health and Johns Hopkins Medicine, Baltimore, told this news organization.
The study was published online in BMJ Open.
‘Dangerous’ substances
Amphetamines and methylphenidate are CNS stimulants that have been in use for almost a century. Like opioids and barbiturates, they’re considered “dangerous” and classified as schedule II Controlled Substances because of their high potential for abuse.
Over many years, these stimulants have been used for multiple purposes, including nasal congestion, narcolepsy, appetite suppression, binge eating, depression, senile behavior, lethargy, and ADHD, the researchers note.
Observational studies suggest medical use of these agents has been increasing in the United States. The investigators conducted previous research that revealed a 79% increase from 2013 to 2018 in the number of adults who self-report their use. The current study, said Mr. Moore, explores how these stimulants are being used.
For the study, data was extracted from the MarketScan 2019 and 2020 Commercial Claims and Encounters Databases, focusing on 9.1 million adults aged 19-64 years who were continuously enrolled in an included commercial benefit plan from Oct. 1, 2019 to Dec. 31, 2020.
The primary outcome consisted of an outpatient prescription claim, service date, and days’ supply for the CNS-active drugs.
The researchers defined “combination-2” therapy as 60 or more days of combination treatment with a schedule II stimulant and at least one additional CNS-active drug. “Combination-3” therapy was defined as the addition of at least two additional CNS-active drugs.
The researchers used service date and days’ supply to examine the number of stimulant and other CNS-active drugs for each of the days of 2020.
CNS-active drug classes included antidepressants, anxiolytics/sedatives/hypnotics, antipsychotics, opioids, anticonvulsants, and other CNS-active drugs.
Prescribing cascade
Of the total number of adults enrolled, 3% (n = 276,223) were taking schedule II stimulants during 2020, with a median of 8 (interquartile range, 4-11) prescriptions. These drugs provided 227 (IQR, 110-322) treatment days of exposure.
Among those taking stimulants 45.5% combined the use of at least one additional CNS-active drug for a median of 213 (IQR, 126-301) treatment days; and 24.3% used at least two additional CNS-active drugs for a median of 182 (IQR, 108-276) days.
“Clinicians should beware of the prescribing cascade. Sometimes it begins with an antidepressant that causes too much sedation, so a stimulant gets added, which leads to insomnia, so alprazolam gets added to the mix,” Mr. Moore said.
He cautioned that this “leaves a patient with multiple drugs, all with discontinuation effects of different kinds and clashing effects.”
These new findings, the investigators note, “add new public health concerns to those raised by our previous study. ... this more-detailed profile reveals several new patterns.”
Most patients become “long-term users” once treatment has started, with 75% continuing for a 1-year period.
“This underscores the possible risks of nonmedical use and dependence that have warranted the classification of these drugs as having high potential for psychological or physical dependence and their prominent appearance in toxicology drug rankings of fatal overdose cases,” they write.
They note that the data “do not indicate which intervention may have come first – a stimulant added to compensate for excess sedation from the benzodiazepine, or the alprazolam added to calm excessive CNS stimulation and/or insomnia from the stimulants or other drugs.”
Several limitations cited by the authors include the fact that, although the population encompassed 9.1 million people, it “may not represent all commercially insured adults,” and it doesn’t include people who aren’t covered by commercial insurance.
Moreover, the MarketScan dataset included up to four diagnosis codes for each outpatient and emergency department encounter; therefore, it was not possible to directly link the diagnoses to specific prescription drug claims, and thus the diagnoses were not evaluated.
“Since many providers will not accept a drug claim for a schedule II stimulant without an on-label diagnosis of ADHD,” the authors suspect that “large numbers of this diagnosis were present.”
Complex prescribing regimens
Mark Olfson, MD, MPH, professor of psychiatry, medicine, and law and professor of epidemiology, Columbia University Irving Medical Center, New York, said the report “highlights the pharmacological complexity of adults who are treated with stimulants.”

Dr. Olfson, who is a research psychiatrist at the New York State Psychiatric Institute, New York, and was not involved with the study, observed there is “evidence to support stimulants as an adjunctive therapy for treatment-resistant unipolar depression in older adults.”
However, he added, “this indication is unlikely to fully explain the high proportion of nonelderly, stimulant-treated adults who also receive antidepressants.”
These new findings “call for research to increase our understanding of the clinical contexts that motivate these complex prescribing regimens as well as their effectiveness and safety,” said Dr. Olfson.
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors. Mr. Moore declares no relevant financial relationships. Coauthor G. Caleb Alexander, MD, is past chair and a current member of the Food and Drug Administration’s Peripheral and Central Nervous System Advisory Committee; is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation, for whom he has served as a paid expert witness; and is a past member of OptumRx’s National P&T Committee. Dr. Olfson declares no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators analyzed prescription drug claims for over 9.1 million U.S. adults over a 1-year period and found that 276,223 (3%) had used a schedule II stimulant, such as methylphenidate and amphetamines, during that time. Of these 276,223 patients, 45% combined these agents with one or more additional CNS-active drugs and almost 25% were simultaneously using two or more additional CNS-active drugs.
Close to half of the stimulant users were taking an antidepressant, while close to one-third filled prescriptions for anxiolytic/sedative/hypnotic meditations, and one-fifth received opioid prescriptions.
The widespread, often off-label use of these stimulants in combination therapy with antidepressants, anxiolytics, opioids, and other psychoactive drugs, “reveals new patterns of utilization beyond the approved use of stimulants as monotherapy for ADHD, but because there are so few studies of these kinds of combination therapy, both the advantages and additional risks [of this type of prescribing] remain unknown,” study investigator Thomas J. Moore, AB, faculty associate in epidemiology, Johns Hopkins Bloomberg School of Public Health and Johns Hopkins Medicine, Baltimore, told this news organization.
The study was published online in BMJ Open.
‘Dangerous’ substances
Amphetamines and methylphenidate are CNS stimulants that have been in use for almost a century. Like opioids and barbiturates, they’re considered “dangerous” and classified as schedule II Controlled Substances because of their high potential for abuse.
Over many years, these stimulants have been used for multiple purposes, including nasal congestion, narcolepsy, appetite suppression, binge eating, depression, senile behavior, lethargy, and ADHD, the researchers note.
Observational studies suggest medical use of these agents has been increasing in the United States. The investigators conducted previous research that revealed a 79% increase from 2013 to 2018 in the number of adults who self-report their use. The current study, said Mr. Moore, explores how these stimulants are being used.
For the study, data was extracted from the MarketScan 2019 and 2020 Commercial Claims and Encounters Databases, focusing on 9.1 million adults aged 19-64 years who were continuously enrolled in an included commercial benefit plan from Oct. 1, 2019 to Dec. 31, 2020.
The primary outcome consisted of an outpatient prescription claim, service date, and days’ supply for the CNS-active drugs.
The researchers defined “combination-2” therapy as 60 or more days of combination treatment with a schedule II stimulant and at least one additional CNS-active drug. “Combination-3” therapy was defined as the addition of at least two additional CNS-active drugs.
The researchers used service date and days’ supply to examine the number of stimulant and other CNS-active drugs for each of the days of 2020.
CNS-active drug classes included antidepressants, anxiolytics/sedatives/hypnotics, antipsychotics, opioids, anticonvulsants, and other CNS-active drugs.
Prescribing cascade
Of the total number of adults enrolled, 3% (n = 276,223) were taking schedule II stimulants during 2020, with a median of 8 (interquartile range, 4-11) prescriptions. These drugs provided 227 (IQR, 110-322) treatment days of exposure.
Among those taking stimulants 45.5% combined the use of at least one additional CNS-active drug for a median of 213 (IQR, 126-301) treatment days; and 24.3% used at least two additional CNS-active drugs for a median of 182 (IQR, 108-276) days.
“Clinicians should beware of the prescribing cascade. Sometimes it begins with an antidepressant that causes too much sedation, so a stimulant gets added, which leads to insomnia, so alprazolam gets added to the mix,” Mr. Moore said.
He cautioned that this “leaves a patient with multiple drugs, all with discontinuation effects of different kinds and clashing effects.”
These new findings, the investigators note, “add new public health concerns to those raised by our previous study. ... this more-detailed profile reveals several new patterns.”
Most patients become “long-term users” once treatment has started, with 75% continuing for a 1-year period.
“This underscores the possible risks of nonmedical use and dependence that have warranted the classification of these drugs as having high potential for psychological or physical dependence and their prominent appearance in toxicology drug rankings of fatal overdose cases,” they write.
They note that the data “do not indicate which intervention may have come first – a stimulant added to compensate for excess sedation from the benzodiazepine, or the alprazolam added to calm excessive CNS stimulation and/or insomnia from the stimulants or other drugs.”
Several limitations cited by the authors include the fact that, although the population encompassed 9.1 million people, it “may not represent all commercially insured adults,” and it doesn’t include people who aren’t covered by commercial insurance.
Moreover, the MarketScan dataset included up to four diagnosis codes for each outpatient and emergency department encounter; therefore, it was not possible to directly link the diagnoses to specific prescription drug claims, and thus the diagnoses were not evaluated.
“Since many providers will not accept a drug claim for a schedule II stimulant without an on-label diagnosis of ADHD,” the authors suspect that “large numbers of this diagnosis were present.”
Complex prescribing regimens
Mark Olfson, MD, MPH, professor of psychiatry, medicine, and law and professor of epidemiology, Columbia University Irving Medical Center, New York, said the report “highlights the pharmacological complexity of adults who are treated with stimulants.”
Dr. Olfson, who is a research psychiatrist at the New York State Psychiatric Institute, New York, and was not involved with the study, observed there is “evidence to support stimulants as an adjunctive therapy for treatment-resistant unipolar depression in older adults.”
However, he added, “this indication is unlikely to fully explain the high proportion of nonelderly, stimulant-treated adults who also receive antidepressants.”
These new findings “call for research to increase our understanding of the clinical contexts that motivate these complex prescribing regimens as well as their effectiveness and safety,” said Dr. Olfson.
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors. Mr. Moore declares no relevant financial relationships. Coauthor G. Caleb Alexander, MD, is past chair and a current member of the Food and Drug Administration’s Peripheral and Central Nervous System Advisory Committee; is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation, for whom he has served as a paid expert witness; and is a past member of OptumRx’s National P&T Committee. Dr. Olfson declares no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators analyzed prescription drug claims for over 9.1 million U.S. adults over a 1-year period and found that 276,223 (3%) had used a schedule II stimulant, such as methylphenidate and amphetamines, during that time. Of these 276,223 patients, 45% combined these agents with one or more additional CNS-active drugs and almost 25% were simultaneously using two or more additional CNS-active drugs.
Close to half of the stimulant users were taking an antidepressant, while close to one-third filled prescriptions for anxiolytic/sedative/hypnotic meditations, and one-fifth received opioid prescriptions.
The widespread, often off-label use of these stimulants in combination therapy with antidepressants, anxiolytics, opioids, and other psychoactive drugs, “reveals new patterns of utilization beyond the approved use of stimulants as monotherapy for ADHD, but because there are so few studies of these kinds of combination therapy, both the advantages and additional risks [of this type of prescribing] remain unknown,” study investigator Thomas J. Moore, AB, faculty associate in epidemiology, Johns Hopkins Bloomberg School of Public Health and Johns Hopkins Medicine, Baltimore, told this news organization.
The study was published online in BMJ Open.
‘Dangerous’ substances
Amphetamines and methylphenidate are CNS stimulants that have been in use for almost a century. Like opioids and barbiturates, they’re considered “dangerous” and classified as schedule II Controlled Substances because of their high potential for abuse.
Over many years, these stimulants have been used for multiple purposes, including nasal congestion, narcolepsy, appetite suppression, binge eating, depression, senile behavior, lethargy, and ADHD, the researchers note.
Observational studies suggest medical use of these agents has been increasing in the United States. The investigators conducted previous research that revealed a 79% increase from 2013 to 2018 in the number of adults who self-report their use. The current study, said Mr. Moore, explores how these stimulants are being used.
For the study, data was extracted from the MarketScan 2019 and 2020 Commercial Claims and Encounters Databases, focusing on 9.1 million adults aged 19-64 years who were continuously enrolled in an included commercial benefit plan from Oct. 1, 2019 to Dec. 31, 2020.
The primary outcome consisted of an outpatient prescription claim, service date, and days’ supply for the CNS-active drugs.
The researchers defined “combination-2” therapy as 60 or more days of combination treatment with a schedule II stimulant and at least one additional CNS-active drug. “Combination-3” therapy was defined as the addition of at least two additional CNS-active drugs.
The researchers used service date and days’ supply to examine the number of stimulant and other CNS-active drugs for each of the days of 2020.
CNS-active drug classes included antidepressants, anxiolytics/sedatives/hypnotics, antipsychotics, opioids, anticonvulsants, and other CNS-active drugs.
Prescribing cascade
Of the total number of adults enrolled, 3% (n = 276,223) were taking schedule II stimulants during 2020, with a median of 8 (interquartile range, 4-11) prescriptions. These drugs provided 227 (IQR, 110-322) treatment days of exposure.
Among those taking stimulants 45.5% combined the use of at least one additional CNS-active drug for a median of 213 (IQR, 126-301) treatment days; and 24.3% used at least two additional CNS-active drugs for a median of 182 (IQR, 108-276) days.
“Clinicians should beware of the prescribing cascade. Sometimes it begins with an antidepressant that causes too much sedation, so a stimulant gets added, which leads to insomnia, so alprazolam gets added to the mix,” Mr. Moore said.
He cautioned that this “leaves a patient with multiple drugs, all with discontinuation effects of different kinds and clashing effects.”
These new findings, the investigators note, “add new public health concerns to those raised by our previous study. ... this more-detailed profile reveals several new patterns.”
Most patients become “long-term users” once treatment has started, with 75% continuing for a 1-year period.
“This underscores the possible risks of nonmedical use and dependence that have warranted the classification of these drugs as having high potential for psychological or physical dependence and their prominent appearance in toxicology drug rankings of fatal overdose cases,” they write.
They note that the data “do not indicate which intervention may have come first – a stimulant added to compensate for excess sedation from the benzodiazepine, or the alprazolam added to calm excessive CNS stimulation and/or insomnia from the stimulants or other drugs.”
Several limitations cited by the authors include the fact that, although the population encompassed 9.1 million people, it “may not represent all commercially insured adults,” and it doesn’t include people who aren’t covered by commercial insurance.
Moreover, the MarketScan dataset included up to four diagnosis codes for each outpatient and emergency department encounter; therefore, it was not possible to directly link the diagnoses to specific prescription drug claims, and thus the diagnoses were not evaluated.
“Since many providers will not accept a drug claim for a schedule II stimulant without an on-label diagnosis of ADHD,” the authors suspect that “large numbers of this diagnosis were present.”
Complex prescribing regimens
Mark Olfson, MD, MPH, professor of psychiatry, medicine, and law and professor of epidemiology, Columbia University Irving Medical Center, New York, said the report “highlights the pharmacological complexity of adults who are treated with stimulants.”
Dr. Olfson, who is a research psychiatrist at the New York State Psychiatric Institute, New York, and was not involved with the study, observed there is “evidence to support stimulants as an adjunctive therapy for treatment-resistant unipolar depression in older adults.”
However, he added, “this indication is unlikely to fully explain the high proportion of nonelderly, stimulant-treated adults who also receive antidepressants.”
These new findings “call for research to increase our understanding of the clinical contexts that motivate these complex prescribing regimens as well as their effectiveness and safety,” said Dr. Olfson.
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors. Mr. Moore declares no relevant financial relationships. Coauthor G. Caleb Alexander, MD, is past chair and a current member of the Food and Drug Administration’s Peripheral and Central Nervous System Advisory Committee; is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation, for whom he has served as a paid expert witness; and is a past member of OptumRx’s National P&T Committee. Dr. Olfson declares no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM BMJ OPEN
Most children with ADHD are not receiving treatment
Just more than one-third (34.8%) had received either treatment.
Researchers, led by Mark Olfson, MD, MPH, Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law and professor of epidemiology at New York State Psychiatric Institute and Columbia University Department of Psychiatry, New York, also found that girls were much less likely to get medications.
In this cross-sectional sample taken from 11, 723 children in the Adolescent Brain and Cognitive Development Study, 1,206 children aged 9 and 10 years had parent-reported ADHD, and of those children, 15.7% of boys and 7% of girls were currently receiving ADHD medications. The parents reported the children met ADHD criteria according to the Diagnostic and Statistical Manual of Mental Disorders.
Findings were published online in JAMA Network Open.
Diagnoses have doubled but treatment numbers lag
Report authors noted that the percentage of U.S. children whose parents report their child has been diagnosed with ADHD has nearly doubled over 2 decades from 5.5% in 1999 to 9.8% in 2018. That has led to misperceptions among professionals and the public that the disorder is overdiagnosed and overtreated, the authors wrote.
However, they wrote, “a focus on the increasing numbers of children treated for ADHD does not give a sense of what fraction of children in the population with ADHD receive treatment.”
Higher uptake at lower income and education levels
Researchers also found that, contrary to popular belief, children with ADHD from families with lower educational levels and lower income were more likely than those with higher educational levels and higher incomes to have received outpatient mental health care.
Among children with ADHD whose parents did not have a high school education, 32.2% of children were receiving medications while among children of parents with a bachelor’s degree 11.5% received medications.
Among children from families with incomes of less than $25 000, 36.5% were receiving outpatient mental health care, compared with 20.1% of those from families with incomes of $75,000 or more.
“These patterns suggest that attitudinal rather than socioeconomic factors often impede the flow of children with ADHD into treatment,” they wrote.
Black children less likely to receive medications
The researchers found that substantially more White children (14.8% [104 of 759]) than Black children (9.4% [22 of 206]), received medication, a finding consistent with previous research.
“Population-based racial and ethnic gradients exist in prescriptions for stimulants and other controlled substances, with the highest rates in majority-White areas,” the authors wrote. “As a result of structural racism, Black parents’ perspectives might further influence ADHD management decisions through mistrust in clinicians and concerns over safety and efficacy of stimulants.”
“Physician efforts to recognize and manage their own implicit biases, together with patient-centered clinical approaches that promote shared decision-making,” might help narrow the treatment gap, the authors wrote. That includes talking with Black parents about their knowledge and beliefs concerning managing ADHD, they added.
Confirming diagnosis critical
The authors noted that not all children with parent-reported ADHD need treatment or would benefit from it.
Lenard Adler, MD, director of the adult ADHD program and professor of Psychiatry and Child and Adolescent Psychiatry at New York University Langone Health, who was not part of the current study, said this research emphasizes the urgency of clinical diagnosis.
Dr. Adler was part of a team of researchers that found similar low numbers for treatment among adults with ADHD.
The current results highlight that “we want to get the diagnosis correct so that people who receive a diagnosis actually have it and, if they do, that they have access to care. Because the consequences for not having treatment for ADHD are significant,” Dr. Adler said.
He urged physicians who diagnose ADHD to make follow-up part of the care plan or these treatment gaps will persist.
The authors wrote that the results suggest a need to increase availability for mental health services and better communicate symptoms among parents, teachers, and primary care providers.
The authors declare no relevant financial relationships. Dr. Adler has consulted with Supernus Pharmaceuticals and Otsuka Pharmaceuticals, has done research with Takeda, and has received royalty payments from NYU for licensing of ADHD training materials.
Just more than one-third (34.8%) had received either treatment.
Researchers, led by Mark Olfson, MD, MPH, Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law and professor of epidemiology at New York State Psychiatric Institute and Columbia University Department of Psychiatry, New York, also found that girls were much less likely to get medications.
In this cross-sectional sample taken from 11, 723 children in the Adolescent Brain and Cognitive Development Study, 1,206 children aged 9 and 10 years had parent-reported ADHD, and of those children, 15.7% of boys and 7% of girls were currently receiving ADHD medications. The parents reported the children met ADHD criteria according to the Diagnostic and Statistical Manual of Mental Disorders.
Findings were published online in JAMA Network Open.
Diagnoses have doubled but treatment numbers lag
Report authors noted that the percentage of U.S. children whose parents report their child has been diagnosed with ADHD has nearly doubled over 2 decades from 5.5% in 1999 to 9.8% in 2018. That has led to misperceptions among professionals and the public that the disorder is overdiagnosed and overtreated, the authors wrote.
However, they wrote, “a focus on the increasing numbers of children treated for ADHD does not give a sense of what fraction of children in the population with ADHD receive treatment.”
Higher uptake at lower income and education levels
Researchers also found that, contrary to popular belief, children with ADHD from families with lower educational levels and lower income were more likely than those with higher educational levels and higher incomes to have received outpatient mental health care.
Among children with ADHD whose parents did not have a high school education, 32.2% of children were receiving medications while among children of parents with a bachelor’s degree 11.5% received medications.
Among children from families with incomes of less than $25 000, 36.5% were receiving outpatient mental health care, compared with 20.1% of those from families with incomes of $75,000 or more.
“These patterns suggest that attitudinal rather than socioeconomic factors often impede the flow of children with ADHD into treatment,” they wrote.
Black children less likely to receive medications
The researchers found that substantially more White children (14.8% [104 of 759]) than Black children (9.4% [22 of 206]), received medication, a finding consistent with previous research.
“Population-based racial and ethnic gradients exist in prescriptions for stimulants and other controlled substances, with the highest rates in majority-White areas,” the authors wrote. “As a result of structural racism, Black parents’ perspectives might further influence ADHD management decisions through mistrust in clinicians and concerns over safety and efficacy of stimulants.”
“Physician efforts to recognize and manage their own implicit biases, together with patient-centered clinical approaches that promote shared decision-making,” might help narrow the treatment gap, the authors wrote. That includes talking with Black parents about their knowledge and beliefs concerning managing ADHD, they added.
Confirming diagnosis critical
The authors noted that not all children with parent-reported ADHD need treatment or would benefit from it.
Lenard Adler, MD, director of the adult ADHD program and professor of Psychiatry and Child and Adolescent Psychiatry at New York University Langone Health, who was not part of the current study, said this research emphasizes the urgency of clinical diagnosis.
Dr. Adler was part of a team of researchers that found similar low numbers for treatment among adults with ADHD.
The current results highlight that “we want to get the diagnosis correct so that people who receive a diagnosis actually have it and, if they do, that they have access to care. Because the consequences for not having treatment for ADHD are significant,” Dr. Adler said.
He urged physicians who diagnose ADHD to make follow-up part of the care plan or these treatment gaps will persist.
The authors wrote that the results suggest a need to increase availability for mental health services and better communicate symptoms among parents, teachers, and primary care providers.
The authors declare no relevant financial relationships. Dr. Adler has consulted with Supernus Pharmaceuticals and Otsuka Pharmaceuticals, has done research with Takeda, and has received royalty payments from NYU for licensing of ADHD training materials.
Just more than one-third (34.8%) had received either treatment.
Researchers, led by Mark Olfson, MD, MPH, Elizabeth K. Dollard Professor of Psychiatry, Medicine and Law and professor of epidemiology at New York State Psychiatric Institute and Columbia University Department of Psychiatry, New York, also found that girls were much less likely to get medications.
In this cross-sectional sample taken from 11, 723 children in the Adolescent Brain and Cognitive Development Study, 1,206 children aged 9 and 10 years had parent-reported ADHD, and of those children, 15.7% of boys and 7% of girls were currently receiving ADHD medications. The parents reported the children met ADHD criteria according to the Diagnostic and Statistical Manual of Mental Disorders.
Findings were published online in JAMA Network Open.
Diagnoses have doubled but treatment numbers lag
Report authors noted that the percentage of U.S. children whose parents report their child has been diagnosed with ADHD has nearly doubled over 2 decades from 5.5% in 1999 to 9.8% in 2018. That has led to misperceptions among professionals and the public that the disorder is overdiagnosed and overtreated, the authors wrote.
However, they wrote, “a focus on the increasing numbers of children treated for ADHD does not give a sense of what fraction of children in the population with ADHD receive treatment.”
Higher uptake at lower income and education levels
Researchers also found that, contrary to popular belief, children with ADHD from families with lower educational levels and lower income were more likely than those with higher educational levels and higher incomes to have received outpatient mental health care.
Among children with ADHD whose parents did not have a high school education, 32.2% of children were receiving medications while among children of parents with a bachelor’s degree 11.5% received medications.
Among children from families with incomes of less than $25 000, 36.5% were receiving outpatient mental health care, compared with 20.1% of those from families with incomes of $75,000 or more.
“These patterns suggest that attitudinal rather than socioeconomic factors often impede the flow of children with ADHD into treatment,” they wrote.
Black children less likely to receive medications
The researchers found that substantially more White children (14.8% [104 of 759]) than Black children (9.4% [22 of 206]), received medication, a finding consistent with previous research.
“Population-based racial and ethnic gradients exist in prescriptions for stimulants and other controlled substances, with the highest rates in majority-White areas,” the authors wrote. “As a result of structural racism, Black parents’ perspectives might further influence ADHD management decisions through mistrust in clinicians and concerns over safety and efficacy of stimulants.”
“Physician efforts to recognize and manage their own implicit biases, together with patient-centered clinical approaches that promote shared decision-making,” might help narrow the treatment gap, the authors wrote. That includes talking with Black parents about their knowledge and beliefs concerning managing ADHD, they added.
Confirming diagnosis critical
The authors noted that not all children with parent-reported ADHD need treatment or would benefit from it.
Lenard Adler, MD, director of the adult ADHD program and professor of Psychiatry and Child and Adolescent Psychiatry at New York University Langone Health, who was not part of the current study, said this research emphasizes the urgency of clinical diagnosis.
Dr. Adler was part of a team of researchers that found similar low numbers for treatment among adults with ADHD.
The current results highlight that “we want to get the diagnosis correct so that people who receive a diagnosis actually have it and, if they do, that they have access to care. Because the consequences for not having treatment for ADHD are significant,” Dr. Adler said.
He urged physicians who diagnose ADHD to make follow-up part of the care plan or these treatment gaps will persist.
The authors wrote that the results suggest a need to increase availability for mental health services and better communicate symptoms among parents, teachers, and primary care providers.
The authors declare no relevant financial relationships. Dr. Adler has consulted with Supernus Pharmaceuticals and Otsuka Pharmaceuticals, has done research with Takeda, and has received royalty payments from NYU for licensing of ADHD training materials.
FROM JAMA NETWORK OPEN
Long-term impact of childhood trauma explained
WASHINGTON –
“We already knew childhood trauma is associated with the later development of depressive and anxiety disorders, but it’s been unclear what makes sufferers of early trauma more likely to develop these psychiatric conditions,” study investigator Erika Kuzminskaite, PhD candidate, department of psychiatry, Amsterdam University Medical Center (UMC), the Netherlands, told this news organization.
“The evidence now points to unbalanced stress systems as a possible cause of this vulnerability, and now the most important question is, how we can develop preventive interventions,” she added.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Elevated cortisol, inflammation
The study included 2,779 adults from the Netherlands Study of Depression and Anxiety (NESDA). Two thirds of participants were female.
Participants retrospectively reported childhood trauma, defined as emotional, physical, or sexual abuse or emotional or physical neglect, before the age of 18 years. Severe trauma was defined as multiple types or increased frequency of abuse.
Of the total cohort, 48% reported experiencing some childhood trauma – 21% reported severe trauma, 27% reported mild trauma, and 42% reported no childhood trauma.
Among those with trauma, 89% had a current or remitted anxiety or depressive disorder, and 11% had no psychiatric sequelae. Among participants who reported no trauma, 68% had a current or remitted disorder, and 32% had no psychiatric disorders.
At baseline, researchers assessed markers of major bodily stress systems, including the hypothalamic-pituitary-adrenal (HPA) axis, the immune-inflammatory system, and the autonomic nervous system (ANS). They examined these markers separately and cumulatively.
In one model, investigators found that levels of cortisol and inflammation were significantly elevated in those with severe childhood trauma compared to those with no childhood trauma. The effects were largest for the cumulative markers for HPA-axis, inflammation, and all stress system markers (Cohen’s d = 0.23, 0.12, and 0.25, respectively). There was no association with ANS markers.
The results were partially explained by lifestyle, said Ms. Kuzminskaite, who noted that people with severe childhood trauma tend to have a higher body mass index, smoke more, and have other unhealthy habits that may represent a “coping” mechanism for trauma.
Those who experienced childhood trauma also have higher rates of other disorders, including asthma, diabetes, and cardiovascular disease. Ms. Kuzminskaite noted that people with childhood trauma have at least double the risk of cancer in later life.
When researchers adjusted for lifestyle factors and chronic conditions, the association for cortisol was reduced and that for inflammation disappeared. However, the cumulative inflammatory markers remained significant.
Another model examined lipopolysaccharide-stimulated (LPS) immune-inflammatory markers by childhood trauma severity. This provides a more “dynamic” measure of stress systems than looking only at static circulating levels in the blood, as was done in the first model, said Ms. Kuzminskaite.
“These levels should theoretically be more affected by experiences such as childhood trauma and they are also less sensitive to lifestyle.”
Here, researchers found significant positive associations with childhood trauma, especially severe trauma, after adjusting for lifestyle and health-related covariates (cumulative index d = 0.19).
“Almost all people with childhood trauma, especially severe trauma, had LPS-stimulated cytokines upregulated,” said Ms. Kuzminskaite. “So again, there is this dysregulation of immune system functioning in these subjects.”
And again, the strongest effect was for the cumulative index of all cytokines, she said.
Personalized interventions
Ms. Kuzminskaite noted the importance of learning the impact of early trauma on stress responses. “The goal is to eventually have personalized interventions for people with depression or anxiety related to childhood trauma, or even preventative interventions. If we know, for example, something is going wrong with a patient’s stress systems, we can suggest some therapeutic targets.”
Investigators in Amsterdam are examining the efficacy of mifepristone, which blocks progesterone and is used along with misoprostol for medication abortions and to treat high blood sugar. “The drug is supposed to reset the stress system functioning,” said Ms. Kuzminskaite.
It’s still important to target unhealthy lifestyle habits “that are really impacting the functioning of the stress systems,” she said. Lifestyle interventions could improve the efficacy of treatments for depression, for example, she added.
Luana Marques, PhD, associate professor, department of psychiatry, Harvard Medical School, Boston, said such research is important.
“It reveals the potentially extensive and long-lasting impact of childhood trauma on functioning. The findings underscore the importance of equipping at-risk and trauma-exposed youth with evidence-based skills for managing stress,” she said.
No conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
WASHINGTON –
“We already knew childhood trauma is associated with the later development of depressive and anxiety disorders, but it’s been unclear what makes sufferers of early trauma more likely to develop these psychiatric conditions,” study investigator Erika Kuzminskaite, PhD candidate, department of psychiatry, Amsterdam University Medical Center (UMC), the Netherlands, told this news organization.
“The evidence now points to unbalanced stress systems as a possible cause of this vulnerability, and now the most important question is, how we can develop preventive interventions,” she added.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Elevated cortisol, inflammation
The study included 2,779 adults from the Netherlands Study of Depression and Anxiety (NESDA). Two thirds of participants were female.
Participants retrospectively reported childhood trauma, defined as emotional, physical, or sexual abuse or emotional or physical neglect, before the age of 18 years. Severe trauma was defined as multiple types or increased frequency of abuse.
Of the total cohort, 48% reported experiencing some childhood trauma – 21% reported severe trauma, 27% reported mild trauma, and 42% reported no childhood trauma.
Among those with trauma, 89% had a current or remitted anxiety or depressive disorder, and 11% had no psychiatric sequelae. Among participants who reported no trauma, 68% had a current or remitted disorder, and 32% had no psychiatric disorders.
At baseline, researchers assessed markers of major bodily stress systems, including the hypothalamic-pituitary-adrenal (HPA) axis, the immune-inflammatory system, and the autonomic nervous system (ANS). They examined these markers separately and cumulatively.
In one model, investigators found that levels of cortisol and inflammation were significantly elevated in those with severe childhood trauma compared to those with no childhood trauma. The effects were largest for the cumulative markers for HPA-axis, inflammation, and all stress system markers (Cohen’s d = 0.23, 0.12, and 0.25, respectively). There was no association with ANS markers.
The results were partially explained by lifestyle, said Ms. Kuzminskaite, who noted that people with severe childhood trauma tend to have a higher body mass index, smoke more, and have other unhealthy habits that may represent a “coping” mechanism for trauma.
Those who experienced childhood trauma also have higher rates of other disorders, including asthma, diabetes, and cardiovascular disease. Ms. Kuzminskaite noted that people with childhood trauma have at least double the risk of cancer in later life.
When researchers adjusted for lifestyle factors and chronic conditions, the association for cortisol was reduced and that for inflammation disappeared. However, the cumulative inflammatory markers remained significant.
Another model examined lipopolysaccharide-stimulated (LPS) immune-inflammatory markers by childhood trauma severity. This provides a more “dynamic” measure of stress systems than looking only at static circulating levels in the blood, as was done in the first model, said Ms. Kuzminskaite.
“These levels should theoretically be more affected by experiences such as childhood trauma and they are also less sensitive to lifestyle.”
Here, researchers found significant positive associations with childhood trauma, especially severe trauma, after adjusting for lifestyle and health-related covariates (cumulative index d = 0.19).
“Almost all people with childhood trauma, especially severe trauma, had LPS-stimulated cytokines upregulated,” said Ms. Kuzminskaite. “So again, there is this dysregulation of immune system functioning in these subjects.”
And again, the strongest effect was for the cumulative index of all cytokines, she said.
Personalized interventions
Ms. Kuzminskaite noted the importance of learning the impact of early trauma on stress responses. “The goal is to eventually have personalized interventions for people with depression or anxiety related to childhood trauma, or even preventative interventions. If we know, for example, something is going wrong with a patient’s stress systems, we can suggest some therapeutic targets.”
Investigators in Amsterdam are examining the efficacy of mifepristone, which blocks progesterone and is used along with misoprostol for medication abortions and to treat high blood sugar. “The drug is supposed to reset the stress system functioning,” said Ms. Kuzminskaite.
It’s still important to target unhealthy lifestyle habits “that are really impacting the functioning of the stress systems,” she said. Lifestyle interventions could improve the efficacy of treatments for depression, for example, she added.
Luana Marques, PhD, associate professor, department of psychiatry, Harvard Medical School, Boston, said such research is important.
“It reveals the potentially extensive and long-lasting impact of childhood trauma on functioning. The findings underscore the importance of equipping at-risk and trauma-exposed youth with evidence-based skills for managing stress,” she said.
No conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
WASHINGTON –
“We already knew childhood trauma is associated with the later development of depressive and anxiety disorders, but it’s been unclear what makes sufferers of early trauma more likely to develop these psychiatric conditions,” study investigator Erika Kuzminskaite, PhD candidate, department of psychiatry, Amsterdam University Medical Center (UMC), the Netherlands, told this news organization.
“The evidence now points to unbalanced stress systems as a possible cause of this vulnerability, and now the most important question is, how we can develop preventive interventions,” she added.
The findings were presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Elevated cortisol, inflammation
The study included 2,779 adults from the Netherlands Study of Depression and Anxiety (NESDA). Two thirds of participants were female.
Participants retrospectively reported childhood trauma, defined as emotional, physical, or sexual abuse or emotional or physical neglect, before the age of 18 years. Severe trauma was defined as multiple types or increased frequency of abuse.
Of the total cohort, 48% reported experiencing some childhood trauma – 21% reported severe trauma, 27% reported mild trauma, and 42% reported no childhood trauma.
Among those with trauma, 89% had a current or remitted anxiety or depressive disorder, and 11% had no psychiatric sequelae. Among participants who reported no trauma, 68% had a current or remitted disorder, and 32% had no psychiatric disorders.
At baseline, researchers assessed markers of major bodily stress systems, including the hypothalamic-pituitary-adrenal (HPA) axis, the immune-inflammatory system, and the autonomic nervous system (ANS). They examined these markers separately and cumulatively.
In one model, investigators found that levels of cortisol and inflammation were significantly elevated in those with severe childhood trauma compared to those with no childhood trauma. The effects were largest for the cumulative markers for HPA-axis, inflammation, and all stress system markers (Cohen’s d = 0.23, 0.12, and 0.25, respectively). There was no association with ANS markers.
The results were partially explained by lifestyle, said Ms. Kuzminskaite, who noted that people with severe childhood trauma tend to have a higher body mass index, smoke more, and have other unhealthy habits that may represent a “coping” mechanism for trauma.
Those who experienced childhood trauma also have higher rates of other disorders, including asthma, diabetes, and cardiovascular disease. Ms. Kuzminskaite noted that people with childhood trauma have at least double the risk of cancer in later life.
When researchers adjusted for lifestyle factors and chronic conditions, the association for cortisol was reduced and that for inflammation disappeared. However, the cumulative inflammatory markers remained significant.
Another model examined lipopolysaccharide-stimulated (LPS) immune-inflammatory markers by childhood trauma severity. This provides a more “dynamic” measure of stress systems than looking only at static circulating levels in the blood, as was done in the first model, said Ms. Kuzminskaite.
“These levels should theoretically be more affected by experiences such as childhood trauma and they are also less sensitive to lifestyle.”
Here, researchers found significant positive associations with childhood trauma, especially severe trauma, after adjusting for lifestyle and health-related covariates (cumulative index d = 0.19).
“Almost all people with childhood trauma, especially severe trauma, had LPS-stimulated cytokines upregulated,” said Ms. Kuzminskaite. “So again, there is this dysregulation of immune system functioning in these subjects.”
And again, the strongest effect was for the cumulative index of all cytokines, she said.
Personalized interventions
Ms. Kuzminskaite noted the importance of learning the impact of early trauma on stress responses. “The goal is to eventually have personalized interventions for people with depression or anxiety related to childhood trauma, or even preventative interventions. If we know, for example, something is going wrong with a patient’s stress systems, we can suggest some therapeutic targets.”
Investigators in Amsterdam are examining the efficacy of mifepristone, which blocks progesterone and is used along with misoprostol for medication abortions and to treat high blood sugar. “The drug is supposed to reset the stress system functioning,” said Ms. Kuzminskaite.
It’s still important to target unhealthy lifestyle habits “that are really impacting the functioning of the stress systems,” she said. Lifestyle interventions could improve the efficacy of treatments for depression, for example, she added.
Luana Marques, PhD, associate professor, department of psychiatry, Harvard Medical School, Boston, said such research is important.
“It reveals the potentially extensive and long-lasting impact of childhood trauma on functioning. The findings underscore the importance of equipping at-risk and trauma-exposed youth with evidence-based skills for managing stress,” she said.
No conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
AT ADAA 2023