User login
Can online mindfulness and self-compassion training improve quality of life for patients with atopic dermatitis?
, according to results of a small randomized controlled trial in Japan.
“We found that skin disease–specific QOL improved over time with a large effect size,” lead study author Sanae Kishimoto, MHS, MPH, of the School of Public Health, Graduate School of Medicine at Kyoto University and colleagues write in JAMA Dermatology. “These findings suggest that mindfulness and self-compassion training is an effective treatment option for adults with AD.”
A bothersome disease that worsens quality of life
AD, a chronic, relapsing, inflammatory, multifactorial skin disease involving intense itching, affects an estimated 15%-30% of children and 2%-10% of adults, with the incidence increasing in industrialized countries, the authors state.

Measured by disability-adjusted life years, AD has the highest disease burden among skin diseases, and people with AD commonly have anxiety, depression, and sleep problems. Treatments include medications, other skin care, and lifestyle changes. New biologics appear to be effective but are expensive and need to be studied for their long-term safety, the authors add.
“Stress can make the skin worse, but at the same time the skin disease and symptoms cause stress,” Peter A. Lio, MD, who was not involved in the study, told this news organization by email. “This vicious cycle contributes greatly to impairing quality of life.”
A program focused on wise, kind self-care
In the SMiLE study, the authors recruited adults with moderate to severe AD and Dermatology Life Quality Index (DLQI) score above 6 from dermatology clinics and through online announcements over 1 year beginning in July 2019.
Participants averaged 36.3 years of age, 80% were women, and their mean AD duration was 26.6 years. Everyone was allowed to receive usual care during the study, except for dupilumab (a newly marketed drug when the study started), psychotherapy, or other mindfulness training.
The researchers randomly assigned 56 adults to receive mindfulness training in addition to their usual care and 51 to the wait list plus usual care. Those in the training group received eight weekly 90-minute online mindfulness and self-compassion sessions. Each group-based session was conducted at the same time and day of the week and included meditation, informal psychoeducation, inquiry, and a short lecture, along with an optional 1-day silent meditation retreat at week 7 and an optional 2-hour videoconferencing booster session at week 13.
The intervention encouraged a nonjudgmental relationship with stress using mindfulness-based stress reduction (MBSR) and emphasized a compassionate relationship with oneself during suffering using mindful self-compassion (MSC). The program was developed and taught by lead author Dr. Kishimoto, a Japanese licensed clinical psychologist who has a history of AD, the paper notes.
At 13 weeks, after completing electronic assessments, patients in the training group showed greater improvement in the DLQI score than those on the wait list (between-group difference estimate, –6.34; 95% confidence interval, –8.27 to –4.41; P < .001). The standardized effect size (Cohen’s d) at 13 weeks was –1.06 (95% CI, –1.39 to –0.74).
Patients in the training group also improved more in all secondary outcomes: severity, itch- and scratch-related visual analog scales, self-compassion, mindfulness, psychological symptoms, and adherence to dermatologist-advised treatments.
They were also more likely to follow their dermatologist’s medical treatment plans, including moisturizer and topical steroid use.
One serious adverse event, endometrial cancer in one patient, was judged to be unrelated to the intervention.
Online format may give more patients access to treatment
“With relatively limited data in the literature, this particularly well-done, important study is likely to positively shape thinking around this topic,” said Dr. Lio, of the departments of dermatology and pediatrics at Northwestern University, Chicago. “This study nicely demonstrates that an online approach can be effective.
“In theory, these methods or techniques could democratize treatments like this, and open them up to many more patients,” he added. He would like to see partially or entirely automated apps (free of cost), similar to meditation “apps,” to treat patients more cost-effectively.
Dr. Lio explained that excluding participants on dupilumab (Dupixent) makes the results slightly less generalizable to patients with moderate to severe AD, who may have the most serious QOL challenges and who are often candidates for dupilumab.
“However, given that we almost never have all the known variables for a study, we are generally comfortable extrapolating that the intervention would likely be helpful for patients taking dupilumab as well, despite it not being specifically evaluated in that group,” he said.
Susan Massick, MD, of the department of dermatology at the Ohio State University Wexner Medical Center in Columbus, advises clinicians to take a multipronged approach to treating the physical and behavioral components of AD and to embrace therapies beyond prescription medications.
“Self-compassion training is another tool in our toolbox toward finding the right fix for our patients,” Dr. Massick said by email. She was not involved with this research.
“I applaud the focus of this study on behavioral health training as a means toward wellness and improved mindfulness,” she added. “I was impressed by the extent to which these simple measures helped improve the quality of life for patients who used the training.”
U.S. patients can benefit from these findings
“My sense is that AD patients the world over have many similar characteristics and concerns, so I would anticipate that the results would be comparable in a U.S. population,” Dr. Lio said. “Other studies performed in the U.S. also support this line of thinking.”
Although the study involved highly motivated patients in Japan, the suffering that patients with AD experience is universal regardless of race or ethnicity, Dr. Massick said. “Americans may be even more willing to embrace mindfulness and self-compassion training as a path toward better health and wellness.”
The study was funded by the Japan Agency for Medical Research and Development and the Mental Health Okamoto Memorial Foundation, the KDDI Foundation, the Pfizer Health Research Foundation, and the Japan Society for the Promotion of Science.
Dr. Kishimoto and several coauthors report relevant financial relationships with pharmaceutical companies. Dr. Lio reports financial relationships with Sanofi and Regeneron, the joint developers of dupilumab. Dr. Massick reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to results of a small randomized controlled trial in Japan.
“We found that skin disease–specific QOL improved over time with a large effect size,” lead study author Sanae Kishimoto, MHS, MPH, of the School of Public Health, Graduate School of Medicine at Kyoto University and colleagues write in JAMA Dermatology. “These findings suggest that mindfulness and self-compassion training is an effective treatment option for adults with AD.”
A bothersome disease that worsens quality of life
AD, a chronic, relapsing, inflammatory, multifactorial skin disease involving intense itching, affects an estimated 15%-30% of children and 2%-10% of adults, with the incidence increasing in industrialized countries, the authors state.
Measured by disability-adjusted life years, AD has the highest disease burden among skin diseases, and people with AD commonly have anxiety, depression, and sleep problems. Treatments include medications, other skin care, and lifestyle changes. New biologics appear to be effective but are expensive and need to be studied for their long-term safety, the authors add.
“Stress can make the skin worse, but at the same time the skin disease and symptoms cause stress,” Peter A. Lio, MD, who was not involved in the study, told this news organization by email. “This vicious cycle contributes greatly to impairing quality of life.”
A program focused on wise, kind self-care
In the SMiLE study, the authors recruited adults with moderate to severe AD and Dermatology Life Quality Index (DLQI) score above 6 from dermatology clinics and through online announcements over 1 year beginning in July 2019.
Participants averaged 36.3 years of age, 80% were women, and their mean AD duration was 26.6 years. Everyone was allowed to receive usual care during the study, except for dupilumab (a newly marketed drug when the study started), psychotherapy, or other mindfulness training.
The researchers randomly assigned 56 adults to receive mindfulness training in addition to their usual care and 51 to the wait list plus usual care. Those in the training group received eight weekly 90-minute online mindfulness and self-compassion sessions. Each group-based session was conducted at the same time and day of the week and included meditation, informal psychoeducation, inquiry, and a short lecture, along with an optional 1-day silent meditation retreat at week 7 and an optional 2-hour videoconferencing booster session at week 13.
The intervention encouraged a nonjudgmental relationship with stress using mindfulness-based stress reduction (MBSR) and emphasized a compassionate relationship with oneself during suffering using mindful self-compassion (MSC). The program was developed and taught by lead author Dr. Kishimoto, a Japanese licensed clinical psychologist who has a history of AD, the paper notes.
At 13 weeks, after completing electronic assessments, patients in the training group showed greater improvement in the DLQI score than those on the wait list (between-group difference estimate, –6.34; 95% confidence interval, –8.27 to –4.41; P < .001). The standardized effect size (Cohen’s d) at 13 weeks was –1.06 (95% CI, –1.39 to –0.74).
Patients in the training group also improved more in all secondary outcomes: severity, itch- and scratch-related visual analog scales, self-compassion, mindfulness, psychological symptoms, and adherence to dermatologist-advised treatments.
They were also more likely to follow their dermatologist’s medical treatment plans, including moisturizer and topical steroid use.
One serious adverse event, endometrial cancer in one patient, was judged to be unrelated to the intervention.
Online format may give more patients access to treatment
“With relatively limited data in the literature, this particularly well-done, important study is likely to positively shape thinking around this topic,” said Dr. Lio, of the departments of dermatology and pediatrics at Northwestern University, Chicago. “This study nicely demonstrates that an online approach can be effective.
“In theory, these methods or techniques could democratize treatments like this, and open them up to many more patients,” he added. He would like to see partially or entirely automated apps (free of cost), similar to meditation “apps,” to treat patients more cost-effectively.
Dr. Lio explained that excluding participants on dupilumab (Dupixent) makes the results slightly less generalizable to patients with moderate to severe AD, who may have the most serious QOL challenges and who are often candidates for dupilumab.
“However, given that we almost never have all the known variables for a study, we are generally comfortable extrapolating that the intervention would likely be helpful for patients taking dupilumab as well, despite it not being specifically evaluated in that group,” he said.
Susan Massick, MD, of the department of dermatology at the Ohio State University Wexner Medical Center in Columbus, advises clinicians to take a multipronged approach to treating the physical and behavioral components of AD and to embrace therapies beyond prescription medications.
“Self-compassion training is another tool in our toolbox toward finding the right fix for our patients,” Dr. Massick said by email. She was not involved with this research.
“I applaud the focus of this study on behavioral health training as a means toward wellness and improved mindfulness,” she added. “I was impressed by the extent to which these simple measures helped improve the quality of life for patients who used the training.”
U.S. patients can benefit from these findings
“My sense is that AD patients the world over have many similar characteristics and concerns, so I would anticipate that the results would be comparable in a U.S. population,” Dr. Lio said. “Other studies performed in the U.S. also support this line of thinking.”
Although the study involved highly motivated patients in Japan, the suffering that patients with AD experience is universal regardless of race or ethnicity, Dr. Massick said. “Americans may be even more willing to embrace mindfulness and self-compassion training as a path toward better health and wellness.”
The study was funded by the Japan Agency for Medical Research and Development and the Mental Health Okamoto Memorial Foundation, the KDDI Foundation, the Pfizer Health Research Foundation, and the Japan Society for the Promotion of Science.
Dr. Kishimoto and several coauthors report relevant financial relationships with pharmaceutical companies. Dr. Lio reports financial relationships with Sanofi and Regeneron, the joint developers of dupilumab. Dr. Massick reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to results of a small randomized controlled trial in Japan.
“We found that skin disease–specific QOL improved over time with a large effect size,” lead study author Sanae Kishimoto, MHS, MPH, of the School of Public Health, Graduate School of Medicine at Kyoto University and colleagues write in JAMA Dermatology. “These findings suggest that mindfulness and self-compassion training is an effective treatment option for adults with AD.”
A bothersome disease that worsens quality of life
AD, a chronic, relapsing, inflammatory, multifactorial skin disease involving intense itching, affects an estimated 15%-30% of children and 2%-10% of adults, with the incidence increasing in industrialized countries, the authors state.
Measured by disability-adjusted life years, AD has the highest disease burden among skin diseases, and people with AD commonly have anxiety, depression, and sleep problems. Treatments include medications, other skin care, and lifestyle changes. New biologics appear to be effective but are expensive and need to be studied for their long-term safety, the authors add.
“Stress can make the skin worse, but at the same time the skin disease and symptoms cause stress,” Peter A. Lio, MD, who was not involved in the study, told this news organization by email. “This vicious cycle contributes greatly to impairing quality of life.”
A program focused on wise, kind self-care
In the SMiLE study, the authors recruited adults with moderate to severe AD and Dermatology Life Quality Index (DLQI) score above 6 from dermatology clinics and through online announcements over 1 year beginning in July 2019.
Participants averaged 36.3 years of age, 80% were women, and their mean AD duration was 26.6 years. Everyone was allowed to receive usual care during the study, except for dupilumab (a newly marketed drug when the study started), psychotherapy, or other mindfulness training.
The researchers randomly assigned 56 adults to receive mindfulness training in addition to their usual care and 51 to the wait list plus usual care. Those in the training group received eight weekly 90-minute online mindfulness and self-compassion sessions. Each group-based session was conducted at the same time and day of the week and included meditation, informal psychoeducation, inquiry, and a short lecture, along with an optional 1-day silent meditation retreat at week 7 and an optional 2-hour videoconferencing booster session at week 13.
The intervention encouraged a nonjudgmental relationship with stress using mindfulness-based stress reduction (MBSR) and emphasized a compassionate relationship with oneself during suffering using mindful self-compassion (MSC). The program was developed and taught by lead author Dr. Kishimoto, a Japanese licensed clinical psychologist who has a history of AD, the paper notes.
At 13 weeks, after completing electronic assessments, patients in the training group showed greater improvement in the DLQI score than those on the wait list (between-group difference estimate, –6.34; 95% confidence interval, –8.27 to –4.41; P < .001). The standardized effect size (Cohen’s d) at 13 weeks was –1.06 (95% CI, –1.39 to –0.74).
Patients in the training group also improved more in all secondary outcomes: severity, itch- and scratch-related visual analog scales, self-compassion, mindfulness, psychological symptoms, and adherence to dermatologist-advised treatments.
They were also more likely to follow their dermatologist’s medical treatment plans, including moisturizer and topical steroid use.
One serious adverse event, endometrial cancer in one patient, was judged to be unrelated to the intervention.
Online format may give more patients access to treatment
“With relatively limited data in the literature, this particularly well-done, important study is likely to positively shape thinking around this topic,” said Dr. Lio, of the departments of dermatology and pediatrics at Northwestern University, Chicago. “This study nicely demonstrates that an online approach can be effective.
“In theory, these methods or techniques could democratize treatments like this, and open them up to many more patients,” he added. He would like to see partially or entirely automated apps (free of cost), similar to meditation “apps,” to treat patients more cost-effectively.
Dr. Lio explained that excluding participants on dupilumab (Dupixent) makes the results slightly less generalizable to patients with moderate to severe AD, who may have the most serious QOL challenges and who are often candidates for dupilumab.
“However, given that we almost never have all the known variables for a study, we are generally comfortable extrapolating that the intervention would likely be helpful for patients taking dupilumab as well, despite it not being specifically evaluated in that group,” he said.
Susan Massick, MD, of the department of dermatology at the Ohio State University Wexner Medical Center in Columbus, advises clinicians to take a multipronged approach to treating the physical and behavioral components of AD and to embrace therapies beyond prescription medications.
“Self-compassion training is another tool in our toolbox toward finding the right fix for our patients,” Dr. Massick said by email. She was not involved with this research.
“I applaud the focus of this study on behavioral health training as a means toward wellness and improved mindfulness,” she added. “I was impressed by the extent to which these simple measures helped improve the quality of life for patients who used the training.”
U.S. patients can benefit from these findings
“My sense is that AD patients the world over have many similar characteristics and concerns, so I would anticipate that the results would be comparable in a U.S. population,” Dr. Lio said. “Other studies performed in the U.S. also support this line of thinking.”
Although the study involved highly motivated patients in Japan, the suffering that patients with AD experience is universal regardless of race or ethnicity, Dr. Massick said. “Americans may be even more willing to embrace mindfulness and self-compassion training as a path toward better health and wellness.”
The study was funded by the Japan Agency for Medical Research and Development and the Mental Health Okamoto Memorial Foundation, the KDDI Foundation, the Pfizer Health Research Foundation, and the Japan Society for the Promotion of Science.
Dr. Kishimoto and several coauthors report relevant financial relationships with pharmaceutical companies. Dr. Lio reports financial relationships with Sanofi and Regeneron, the joint developers of dupilumab. Dr. Massick reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA DERMATOLOGY
Harmful emotional hit of antidepressants underappreciated
SAN FRANCISCO – , new research shows.
Emotional blunting can be described as feeling emotionally flat and incapable of finding pleasure. The patient may feel less sadness, guilt, or hopelessness, but that may come at the cost of feeling less joy, surprise, and happiness. Some people with SSRI-induced blunting even report caring less about important relationships.

It’s an issue that needs greater attention, study investigator Mujeeb U. Shad, MD, with Valley Health Services and University of Nevada, Las Vegas, said in an interview.
“Patients may come to the clinic and report feeling emotionally and cognitively flat and not be taken seriously by their provider, but they are genuinely reporting something that is happening to them and decreasing their quality of life,” Dr. Shad explained.
The study was presented at the annual meeting of the American Psychiatric Association.
Something ‘missing’
Dr. Shad said that the genesis for the study came from a resident who noticed that many patients receiving SSRIs reported feeling better and not as bothered by the depression, yet, at the same time, they felt something was “missing. Their families would say, ‘You’re better but you’re not the same person.’ ”
To investigate further, the researchers did a “scoping review” of 25 original studies that assessed antidepressant-related emotional blunting. Until now, there hasn’t been a systematic review of this issue, Dr. Shad said.
Ten of the studies looked at the role of SSRIs in emotional blunting, whereas the other 15 looked at serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and second-generation antipsychotic medications.
The results of the review show that emotional blunting is a significant patient-reported concern. It often presents as a subjective complaint of changed personality, feeling a lesser intensity of overall emotions, and the manifestation of not being oneself often attributed to antidepressant use, the researchers found. Emotional blunting was more commonly associated with SSRIs than with the other medications in the studies.
Common clinical strategies to manage antidepressant-induced emotional blunting reported in the literature include dose reduction or switching to a different antidepressant class; however, the literature did not make the distinction between emotional blunting as a primary symptom of depression or an adverse effect of antidepressants.
Dr. Shad said that there is a need to develop valid and reliable measures to assess emotional blunting related to antidepressants.
He noted that optimal patient care should include pre- and posttreatment assessment of emotional blunting. One useful tool is the Oxford Questionnaire on the Emotional Side-Effects of Antidepressants.
Can’t get to the top
Jacob Cross, MD, who wasn’t involved in the study, said that he has seen the impact of antidepressant-related emotional blunting first-hand.
“I’ve had multiple patients report emotional blunting on antidepressant therapy,” Dr. Cross, with the department of psychiatry, Rush Medical College, Chicago, said.
“These patients feel like their emotions are not as high and not as low; so they experience directional improvement, but they’re still not feeling like they can get that top peak emotion. It’s kind of similar to anhedonia. They’re just feeling like a little cut off, like they’re climbing a cliff and just can’t get to that top,” Dr. Cross said.
For a patient with emotional blunting, Dr. Cross said he might “switch to an antidepressant that’s more stimulating like an SNRI from an SSRI. You could also lower the dose and see if that helps, but I usually change the drug class.”
The study had no specific funding. Dr. Shad and Dr. Cross have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , new research shows.
Emotional blunting can be described as feeling emotionally flat and incapable of finding pleasure. The patient may feel less sadness, guilt, or hopelessness, but that may come at the cost of feeling less joy, surprise, and happiness. Some people with SSRI-induced blunting even report caring less about important relationships.
It’s an issue that needs greater attention, study investigator Mujeeb U. Shad, MD, with Valley Health Services and University of Nevada, Las Vegas, said in an interview.
“Patients may come to the clinic and report feeling emotionally and cognitively flat and not be taken seriously by their provider, but they are genuinely reporting something that is happening to them and decreasing their quality of life,” Dr. Shad explained.
The study was presented at the annual meeting of the American Psychiatric Association.
Something ‘missing’
Dr. Shad said that the genesis for the study came from a resident who noticed that many patients receiving SSRIs reported feeling better and not as bothered by the depression, yet, at the same time, they felt something was “missing. Their families would say, ‘You’re better but you’re not the same person.’ ”
To investigate further, the researchers did a “scoping review” of 25 original studies that assessed antidepressant-related emotional blunting. Until now, there hasn’t been a systematic review of this issue, Dr. Shad said.
Ten of the studies looked at the role of SSRIs in emotional blunting, whereas the other 15 looked at serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and second-generation antipsychotic medications.
The results of the review show that emotional blunting is a significant patient-reported concern. It often presents as a subjective complaint of changed personality, feeling a lesser intensity of overall emotions, and the manifestation of not being oneself often attributed to antidepressant use, the researchers found. Emotional blunting was more commonly associated with SSRIs than with the other medications in the studies.
Common clinical strategies to manage antidepressant-induced emotional blunting reported in the literature include dose reduction or switching to a different antidepressant class; however, the literature did not make the distinction between emotional blunting as a primary symptom of depression or an adverse effect of antidepressants.
Dr. Shad said that there is a need to develop valid and reliable measures to assess emotional blunting related to antidepressants.
He noted that optimal patient care should include pre- and posttreatment assessment of emotional blunting. One useful tool is the Oxford Questionnaire on the Emotional Side-Effects of Antidepressants.
Can’t get to the top
Jacob Cross, MD, who wasn’t involved in the study, said that he has seen the impact of antidepressant-related emotional blunting first-hand.
“I’ve had multiple patients report emotional blunting on antidepressant therapy,” Dr. Cross, with the department of psychiatry, Rush Medical College, Chicago, said.
“These patients feel like their emotions are not as high and not as low; so they experience directional improvement, but they’re still not feeling like they can get that top peak emotion. It’s kind of similar to anhedonia. They’re just feeling like a little cut off, like they’re climbing a cliff and just can’t get to that top,” Dr. Cross said.
For a patient with emotional blunting, Dr. Cross said he might “switch to an antidepressant that’s more stimulating like an SNRI from an SSRI. You could also lower the dose and see if that helps, but I usually change the drug class.”
The study had no specific funding. Dr. Shad and Dr. Cross have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , new research shows.
Emotional blunting can be described as feeling emotionally flat and incapable of finding pleasure. The patient may feel less sadness, guilt, or hopelessness, but that may come at the cost of feeling less joy, surprise, and happiness. Some people with SSRI-induced blunting even report caring less about important relationships.
It’s an issue that needs greater attention, study investigator Mujeeb U. Shad, MD, with Valley Health Services and University of Nevada, Las Vegas, said in an interview.
“Patients may come to the clinic and report feeling emotionally and cognitively flat and not be taken seriously by their provider, but they are genuinely reporting something that is happening to them and decreasing their quality of life,” Dr. Shad explained.
The study was presented at the annual meeting of the American Psychiatric Association.
Something ‘missing’
Dr. Shad said that the genesis for the study came from a resident who noticed that many patients receiving SSRIs reported feeling better and not as bothered by the depression, yet, at the same time, they felt something was “missing. Their families would say, ‘You’re better but you’re not the same person.’ ”
To investigate further, the researchers did a “scoping review” of 25 original studies that assessed antidepressant-related emotional blunting. Until now, there hasn’t been a systematic review of this issue, Dr. Shad said.
Ten of the studies looked at the role of SSRIs in emotional blunting, whereas the other 15 looked at serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and second-generation antipsychotic medications.
The results of the review show that emotional blunting is a significant patient-reported concern. It often presents as a subjective complaint of changed personality, feeling a lesser intensity of overall emotions, and the manifestation of not being oneself often attributed to antidepressant use, the researchers found. Emotional blunting was more commonly associated with SSRIs than with the other medications in the studies.
Common clinical strategies to manage antidepressant-induced emotional blunting reported in the literature include dose reduction or switching to a different antidepressant class; however, the literature did not make the distinction between emotional blunting as a primary symptom of depression or an adverse effect of antidepressants.
Dr. Shad said that there is a need to develop valid and reliable measures to assess emotional blunting related to antidepressants.
He noted that optimal patient care should include pre- and posttreatment assessment of emotional blunting. One useful tool is the Oxford Questionnaire on the Emotional Side-Effects of Antidepressants.
Can’t get to the top
Jacob Cross, MD, who wasn’t involved in the study, said that he has seen the impact of antidepressant-related emotional blunting first-hand.
“I’ve had multiple patients report emotional blunting on antidepressant therapy,” Dr. Cross, with the department of psychiatry, Rush Medical College, Chicago, said.
“These patients feel like their emotions are not as high and not as low; so they experience directional improvement, but they’re still not feeling like they can get that top peak emotion. It’s kind of similar to anhedonia. They’re just feeling like a little cut off, like they’re climbing a cliff and just can’t get to that top,” Dr. Cross said.
For a patient with emotional blunting, Dr. Cross said he might “switch to an antidepressant that’s more stimulating like an SNRI from an SSRI. You could also lower the dose and see if that helps, but I usually change the drug class.”
The study had no specific funding. Dr. Shad and Dr. Cross have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
AT APA 2023
Eating disorder apps fall short when it comes to privacy
SAN FRANCISCO –
Federal laws require those handling sensitive health information to have policies and security safeguards in place to protect such information, whether it’s stored on paper or electronically.
“As it stands right now, there’s not enough evidence to support using these apps as an adjunct to clinical care,” study author Theodora O’Leary, a 4th-year medical student at Tufts University, Boston, said in an interview. “We need more research on the efficacy of these apps because right now not enough of them meet HIPAA [standards] and don’t have privacy and security measures.”
The findings were presented at the annual meeting of the American Psychiatric Association.
Eating disorders (EDs) are a common mental health condition affecting almost 1 in 10 Americans over their lifetime. Yet only about a third of patients with an eating disorder receive adequate treatment.
The pandemic saw a rise in eating disorders and in the use of mental health apps “to kind of fill the gap because people couldn’t be seen in person,” said Ms. O’Leary.
Inexpensive and accessible
Smartphone apps have a lot of advantages for patients with an ED. For one thing, they’re relatively inexpensive and accessible; most Americans already own one or more devices on which these apps can be used.
They’re also a feasible means of delivering psychological interventions, which are often recommended for EDs. Among these interventions, cognitive-behavioral therapy (CBT) has the largest evidence base for this condition.
Also, as many individuals with an ED may be reluctant to seek treatment because of stigma and shame, the anonymity afforded by an app could increase access to the help they seek.
But Ms. O’Leary warned the Food and Drug Administration does not regulate these apps, and people are sharing their personal health information on them.
The researchers conducted a review of commercially available eating disorder apps by searching the Apple and Google play stores using key phrases such as “eating disorder,” “anorexia,” and “binge eating disorder.”
They found 16 relevant apps that they added to the publicly available apps already in a database at Tufts, for a total of about 36 that were evaluated in the study (the number fluctuates as apps are deleted.)
They then reviewed the apps using the 105 questions based on the APA’s app evaluation model, which covers categories such as efficacy, privacy, accessibility, and clinical applicability. And they used filters to group apps by characteristics such as function, cost, and features.
The vast majority were self-help apps, which include things like journaling, meditation, and information on CBT. Others were reference apps that provide related definitions and sometimes include surveys to determine, for example, if the user has an eating disorder.
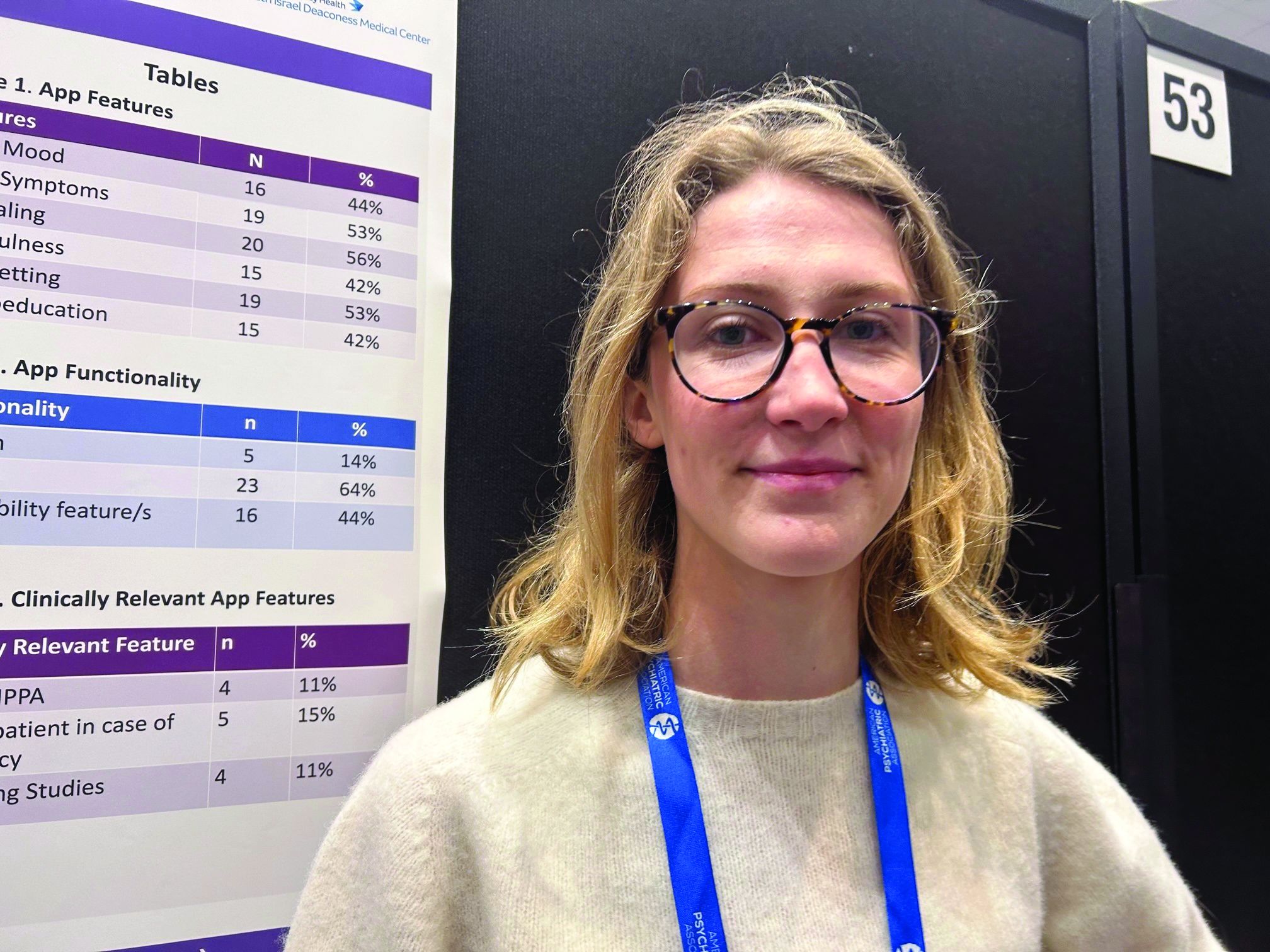
About 44% of the apps track mood, and 53% track symptoms. Some 56% include journaling, 42% mindfulness, 53% goal setting, and 42% psychoeducation.
Hybrid care
Only 5% of apps allow for “hybrid” care. This, explained Ms. O’Leary, is when clinicians use their own app to access patients’ apps, allowing them to track food restrictions and therapies, and make comments.
“The hybrid is viewed as the best form of app”, she said. “It’s almost like an adjunct to clinical care.”
Hybrid apps also tend to have patient safety features, she added. And these apps meet HIPAA standards, which only 11% of the apps in the study did.
Only 15% of apps advised patients to take steps in case of an emergency, and 11% had supporting studies. And where there was supporting research, much of it was funded by the app creators, said Ms. O’Leary.
For example, an app provided by Noom (the weight loss program that promises to help change habits and mindsets around food) “has a bunch of feasibility studies but they’re all funded by Noom”, which can introduce bias, she explained.
None of the apps were created by an accredited health care institution, she noted. “And I think only one app out of all the eating disorder apps we looked at was from a nonprofit.”
About 17% of the apps offer help with a “coach” or “expert”. However, these apps often fail to disclose the definition of a coach or state they’re not a replacement for medical care.
Coaching apps more expensive
Additionally, these coaching apps are often some of the most expensive, said Ms. O’Leary.
Daniel E. Gih, MD, associate professor at the University of Nebraska Medical Center, Omaha, helped start an eating disorders program at the University of Michigan and continues to treat patients with eating disorders. He said the increase in the use of eating disorder apps isn’t surprising as the incidence of these disorders increased in the wake of pandemic restrictions, especially among young people.
“Patients are likely doing more research on their medical conditions and trying to crowdsource information or self-treat,” Dr. Gih said.
It’s unclear whether “shame or just the general lack of specialized eating disorder professionals,” including physicians, is driving some of the interest in these apps, he added.
Dr. Gih stressed eating disorder apps should not only include screening for suicidality, but also explicitly tell patients to seek immediate attention if they show certain signs – for example, fainting, chest pain, or blood in emesis.
“The apps may be giving patients false hope or delaying medical care,” he said. “Apps are likely not sufficient enough to replace a multidisciplinary team with experience and expertise in eating disorders.”
Ms. O’Leary and Dr. Gih report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO –
Federal laws require those handling sensitive health information to have policies and security safeguards in place to protect such information, whether it’s stored on paper or electronically.
“As it stands right now, there’s not enough evidence to support using these apps as an adjunct to clinical care,” study author Theodora O’Leary, a 4th-year medical student at Tufts University, Boston, said in an interview. “We need more research on the efficacy of these apps because right now not enough of them meet HIPAA [standards] and don’t have privacy and security measures.”
The findings were presented at the annual meeting of the American Psychiatric Association.
Eating disorders (EDs) are a common mental health condition affecting almost 1 in 10 Americans over their lifetime. Yet only about a third of patients with an eating disorder receive adequate treatment.
The pandemic saw a rise in eating disorders and in the use of mental health apps “to kind of fill the gap because people couldn’t be seen in person,” said Ms. O’Leary.
Inexpensive and accessible
Smartphone apps have a lot of advantages for patients with an ED. For one thing, they’re relatively inexpensive and accessible; most Americans already own one or more devices on which these apps can be used.
They’re also a feasible means of delivering psychological interventions, which are often recommended for EDs. Among these interventions, cognitive-behavioral therapy (CBT) has the largest evidence base for this condition.
Also, as many individuals with an ED may be reluctant to seek treatment because of stigma and shame, the anonymity afforded by an app could increase access to the help they seek.
But Ms. O’Leary warned the Food and Drug Administration does not regulate these apps, and people are sharing their personal health information on them.
The researchers conducted a review of commercially available eating disorder apps by searching the Apple and Google play stores using key phrases such as “eating disorder,” “anorexia,” and “binge eating disorder.”
They found 16 relevant apps that they added to the publicly available apps already in a database at Tufts, for a total of about 36 that were evaluated in the study (the number fluctuates as apps are deleted.)
They then reviewed the apps using the 105 questions based on the APA’s app evaluation model, which covers categories such as efficacy, privacy, accessibility, and clinical applicability. And they used filters to group apps by characteristics such as function, cost, and features.
The vast majority were self-help apps, which include things like journaling, meditation, and information on CBT. Others were reference apps that provide related definitions and sometimes include surveys to determine, for example, if the user has an eating disorder.
About 44% of the apps track mood, and 53% track symptoms. Some 56% include journaling, 42% mindfulness, 53% goal setting, and 42% psychoeducation.
Hybrid care
Only 5% of apps allow for “hybrid” care. This, explained Ms. O’Leary, is when clinicians use their own app to access patients’ apps, allowing them to track food restrictions and therapies, and make comments.
“The hybrid is viewed as the best form of app”, she said. “It’s almost like an adjunct to clinical care.”
Hybrid apps also tend to have patient safety features, she added. And these apps meet HIPAA standards, which only 11% of the apps in the study did.
Only 15% of apps advised patients to take steps in case of an emergency, and 11% had supporting studies. And where there was supporting research, much of it was funded by the app creators, said Ms. O’Leary.
For example, an app provided by Noom (the weight loss program that promises to help change habits and mindsets around food) “has a bunch of feasibility studies but they’re all funded by Noom”, which can introduce bias, she explained.
None of the apps were created by an accredited health care institution, she noted. “And I think only one app out of all the eating disorder apps we looked at was from a nonprofit.”
About 17% of the apps offer help with a “coach” or “expert”. However, these apps often fail to disclose the definition of a coach or state they’re not a replacement for medical care.
Coaching apps more expensive
Additionally, these coaching apps are often some of the most expensive, said Ms. O’Leary.
Daniel E. Gih, MD, associate professor at the University of Nebraska Medical Center, Omaha, helped start an eating disorders program at the University of Michigan and continues to treat patients with eating disorders. He said the increase in the use of eating disorder apps isn’t surprising as the incidence of these disorders increased in the wake of pandemic restrictions, especially among young people.
“Patients are likely doing more research on their medical conditions and trying to crowdsource information or self-treat,” Dr. Gih said.
It’s unclear whether “shame or just the general lack of specialized eating disorder professionals,” including physicians, is driving some of the interest in these apps, he added.
Dr. Gih stressed eating disorder apps should not only include screening for suicidality, but also explicitly tell patients to seek immediate attention if they show certain signs – for example, fainting, chest pain, or blood in emesis.
“The apps may be giving patients false hope or delaying medical care,” he said. “Apps are likely not sufficient enough to replace a multidisciplinary team with experience and expertise in eating disorders.”
Ms. O’Leary and Dr. Gih report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO –
Federal laws require those handling sensitive health information to have policies and security safeguards in place to protect such information, whether it’s stored on paper or electronically.
“As it stands right now, there’s not enough evidence to support using these apps as an adjunct to clinical care,” study author Theodora O’Leary, a 4th-year medical student at Tufts University, Boston, said in an interview. “We need more research on the efficacy of these apps because right now not enough of them meet HIPAA [standards] and don’t have privacy and security measures.”
The findings were presented at the annual meeting of the American Psychiatric Association.
Eating disorders (EDs) are a common mental health condition affecting almost 1 in 10 Americans over their lifetime. Yet only about a third of patients with an eating disorder receive adequate treatment.
The pandemic saw a rise in eating disorders and in the use of mental health apps “to kind of fill the gap because people couldn’t be seen in person,” said Ms. O’Leary.
Inexpensive and accessible
Smartphone apps have a lot of advantages for patients with an ED. For one thing, they’re relatively inexpensive and accessible; most Americans already own one or more devices on which these apps can be used.
They’re also a feasible means of delivering psychological interventions, which are often recommended for EDs. Among these interventions, cognitive-behavioral therapy (CBT) has the largest evidence base for this condition.
Also, as many individuals with an ED may be reluctant to seek treatment because of stigma and shame, the anonymity afforded by an app could increase access to the help they seek.
But Ms. O’Leary warned the Food and Drug Administration does not regulate these apps, and people are sharing their personal health information on them.
The researchers conducted a review of commercially available eating disorder apps by searching the Apple and Google play stores using key phrases such as “eating disorder,” “anorexia,” and “binge eating disorder.”
They found 16 relevant apps that they added to the publicly available apps already in a database at Tufts, for a total of about 36 that were evaluated in the study (the number fluctuates as apps are deleted.)
They then reviewed the apps using the 105 questions based on the APA’s app evaluation model, which covers categories such as efficacy, privacy, accessibility, and clinical applicability. And they used filters to group apps by characteristics such as function, cost, and features.
The vast majority were self-help apps, which include things like journaling, meditation, and information on CBT. Others were reference apps that provide related definitions and sometimes include surveys to determine, for example, if the user has an eating disorder.
About 44% of the apps track mood, and 53% track symptoms. Some 56% include journaling, 42% mindfulness, 53% goal setting, and 42% psychoeducation.
Hybrid care
Only 5% of apps allow for “hybrid” care. This, explained Ms. O’Leary, is when clinicians use their own app to access patients’ apps, allowing them to track food restrictions and therapies, and make comments.
“The hybrid is viewed as the best form of app”, she said. “It’s almost like an adjunct to clinical care.”
Hybrid apps also tend to have patient safety features, she added. And these apps meet HIPAA standards, which only 11% of the apps in the study did.
Only 15% of apps advised patients to take steps in case of an emergency, and 11% had supporting studies. And where there was supporting research, much of it was funded by the app creators, said Ms. O’Leary.
For example, an app provided by Noom (the weight loss program that promises to help change habits and mindsets around food) “has a bunch of feasibility studies but they’re all funded by Noom”, which can introduce bias, she explained.
None of the apps were created by an accredited health care institution, she noted. “And I think only one app out of all the eating disorder apps we looked at was from a nonprofit.”
About 17% of the apps offer help with a “coach” or “expert”. However, these apps often fail to disclose the definition of a coach or state they’re not a replacement for medical care.
Coaching apps more expensive
Additionally, these coaching apps are often some of the most expensive, said Ms. O’Leary.
Daniel E. Gih, MD, associate professor at the University of Nebraska Medical Center, Omaha, helped start an eating disorders program at the University of Michigan and continues to treat patients with eating disorders. He said the increase in the use of eating disorder apps isn’t surprising as the incidence of these disorders increased in the wake of pandemic restrictions, especially among young people.
“Patients are likely doing more research on their medical conditions and trying to crowdsource information or self-treat,” Dr. Gih said.
It’s unclear whether “shame or just the general lack of specialized eating disorder professionals,” including physicians, is driving some of the interest in these apps, he added.
Dr. Gih stressed eating disorder apps should not only include screening for suicidality, but also explicitly tell patients to seek immediate attention if they show certain signs – for example, fainting, chest pain, or blood in emesis.
“The apps may be giving patients false hope or delaying medical care,” he said. “Apps are likely not sufficient enough to replace a multidisciplinary team with experience and expertise in eating disorders.”
Ms. O’Leary and Dr. Gih report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT APA 2023
Docs can help combat TikTok misinformation on rare psychiatric disorder
SAN FRANCISCO – , new research shows.
These findings, say investigators, underscore the need for mental health professionals to help counter the spread of false information by creating accurate content and posting it on the popular social media platform.

“Health care professionals need to make engaging content to post on social media platforms like YouTube and especially TikTok, to reach wider audiences and combat misinformation about DID,” study investigator Isreal Bladimir Munoz, a fourth-year medical student at University of Texas, Galveston, said in an interview.
The findings were presented at the annual meeting of the American Psychiatric Association.
Popularized by the media
A rare condition affecting less than 1% of the general population, DID involves two or more distinct personality states, along with changes in behavior and memory gaps.
The condition has been popularized in books and the media. Movies such as “Split,” “Psycho,” and “Fight Club” all feature characters with DID.
“These bring awareness about the condition, but also often sensationalize or stigmatize it and reinforce stereotypes,” said Mr. Munoz.
In recent years, social media has become an integral part of everyday life. An estimated 4.2 billion people actively frequent sites such as YouTube, TikTok, Twitter, and Meta.
Although social media allows for instant communication and the opportunity for self-expression, there are mounting concerns about the spread of misinformation and its potential impact on mental health and privacy, said Mr. Munoz.
To evaluate the quality and accuracy of information about DID on social media, investigators analyzed 60 YouTube and 97 TikTok videos on the condition.
To evaluate the reliability and the intent and reliability of videos, researchers used the modified DISCERN instrument and the Global Quality Scale, a five-point rating system.
Using these tools, the researchers determined whether the selected videos were useful, misleading, or neither. Mr. Munoz said videos were classified as useful if they contained accurate information about the condition and its pathogenesis, treatment, and management.
Researchers determined that for YouTube videos, 51.7% were useful, 6.6% were misleading, and 34.7% were neither. About 43.3% of these videos involved interviews, 21.7% were educational, 15% involved personal stories, 8.3% were films/TV programs, 5% were comedy skits, and 3.3% were another content type.
The highest quality YouTube videos were from educational organizations and health care professionals. The least accurate videos came from independent users and film/TV sources.
As for TikTok videos on DID, only 5.2% were useful, 10.3% were misleading, and 41.7% were neither.
The main sources for TikTok videos were independent organizations, whereas podcasts and film/TV were the least common sources.
The findings, said Mr. Munoz, underscore the need for medical professionals to develop high-quality content about DID and post it on TikTok to counter misinformation on social media.
Call to action
In a comment, Howard Y. Liu, MD, a child and adolescent psychiatrist and chair of the department of psychiatry, University of Nebraska, Omaha, described the study as “compelling.”

When it comes to public health messages, it’s important to know what social media people are using. Today’s parents are on Twitter and Facebook, whereas their children are more likely to be checking out YouTube and TikTok, said Dr. Liu, chair of the APA’s Council on Communications.
“TikTok is critical because that’s where all the youth eyeballs are,” he said.
The medical profession needs to engage with the platform to reach this next-generation audience and help stop the spread of misinformation about DID, said Dr. Liu. He noted that the APA is looking into undertaking such an initiative.
The study investigators report no relevant disclosures. Dr. Liu reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , new research shows.
These findings, say investigators, underscore the need for mental health professionals to help counter the spread of false information by creating accurate content and posting it on the popular social media platform.
“Health care professionals need to make engaging content to post on social media platforms like YouTube and especially TikTok, to reach wider audiences and combat misinformation about DID,” study investigator Isreal Bladimir Munoz, a fourth-year medical student at University of Texas, Galveston, said in an interview.
The findings were presented at the annual meeting of the American Psychiatric Association.
Popularized by the media
A rare condition affecting less than 1% of the general population, DID involves two or more distinct personality states, along with changes in behavior and memory gaps.
The condition has been popularized in books and the media. Movies such as “Split,” “Psycho,” and “Fight Club” all feature characters with DID.
“These bring awareness about the condition, but also often sensationalize or stigmatize it and reinforce stereotypes,” said Mr. Munoz.
In recent years, social media has become an integral part of everyday life. An estimated 4.2 billion people actively frequent sites such as YouTube, TikTok, Twitter, and Meta.
Although social media allows for instant communication and the opportunity for self-expression, there are mounting concerns about the spread of misinformation and its potential impact on mental health and privacy, said Mr. Munoz.
To evaluate the quality and accuracy of information about DID on social media, investigators analyzed 60 YouTube and 97 TikTok videos on the condition.
To evaluate the reliability and the intent and reliability of videos, researchers used the modified DISCERN instrument and the Global Quality Scale, a five-point rating system.
Using these tools, the researchers determined whether the selected videos were useful, misleading, or neither. Mr. Munoz said videos were classified as useful if they contained accurate information about the condition and its pathogenesis, treatment, and management.
Researchers determined that for YouTube videos, 51.7% were useful, 6.6% were misleading, and 34.7% were neither. About 43.3% of these videos involved interviews, 21.7% were educational, 15% involved personal stories, 8.3% were films/TV programs, 5% were comedy skits, and 3.3% were another content type.
The highest quality YouTube videos were from educational organizations and health care professionals. The least accurate videos came from independent users and film/TV sources.
As for TikTok videos on DID, only 5.2% were useful, 10.3% were misleading, and 41.7% were neither.
The main sources for TikTok videos were independent organizations, whereas podcasts and film/TV were the least common sources.
The findings, said Mr. Munoz, underscore the need for medical professionals to develop high-quality content about DID and post it on TikTok to counter misinformation on social media.
Call to action
In a comment, Howard Y. Liu, MD, a child and adolescent psychiatrist and chair of the department of psychiatry, University of Nebraska, Omaha, described the study as “compelling.”
When it comes to public health messages, it’s important to know what social media people are using. Today’s parents are on Twitter and Facebook, whereas their children are more likely to be checking out YouTube and TikTok, said Dr. Liu, chair of the APA’s Council on Communications.
“TikTok is critical because that’s where all the youth eyeballs are,” he said.
The medical profession needs to engage with the platform to reach this next-generation audience and help stop the spread of misinformation about DID, said Dr. Liu. He noted that the APA is looking into undertaking such an initiative.
The study investigators report no relevant disclosures. Dr. Liu reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , new research shows.
These findings, say investigators, underscore the need for mental health professionals to help counter the spread of false information by creating accurate content and posting it on the popular social media platform.
“Health care professionals need to make engaging content to post on social media platforms like YouTube and especially TikTok, to reach wider audiences and combat misinformation about DID,” study investigator Isreal Bladimir Munoz, a fourth-year medical student at University of Texas, Galveston, said in an interview.
The findings were presented at the annual meeting of the American Psychiatric Association.
Popularized by the media
A rare condition affecting less than 1% of the general population, DID involves two or more distinct personality states, along with changes in behavior and memory gaps.
The condition has been popularized in books and the media. Movies such as “Split,” “Psycho,” and “Fight Club” all feature characters with DID.
“These bring awareness about the condition, but also often sensationalize or stigmatize it and reinforce stereotypes,” said Mr. Munoz.
In recent years, social media has become an integral part of everyday life. An estimated 4.2 billion people actively frequent sites such as YouTube, TikTok, Twitter, and Meta.
Although social media allows for instant communication and the opportunity for self-expression, there are mounting concerns about the spread of misinformation and its potential impact on mental health and privacy, said Mr. Munoz.
To evaluate the quality and accuracy of information about DID on social media, investigators analyzed 60 YouTube and 97 TikTok videos on the condition.
To evaluate the reliability and the intent and reliability of videos, researchers used the modified DISCERN instrument and the Global Quality Scale, a five-point rating system.
Using these tools, the researchers determined whether the selected videos were useful, misleading, or neither. Mr. Munoz said videos were classified as useful if they contained accurate information about the condition and its pathogenesis, treatment, and management.
Researchers determined that for YouTube videos, 51.7% were useful, 6.6% were misleading, and 34.7% were neither. About 43.3% of these videos involved interviews, 21.7% were educational, 15% involved personal stories, 8.3% were films/TV programs, 5% were comedy skits, and 3.3% were another content type.
The highest quality YouTube videos were from educational organizations and health care professionals. The least accurate videos came from independent users and film/TV sources.
As for TikTok videos on DID, only 5.2% were useful, 10.3% were misleading, and 41.7% were neither.
The main sources for TikTok videos were independent organizations, whereas podcasts and film/TV were the least common sources.
The findings, said Mr. Munoz, underscore the need for medical professionals to develop high-quality content about DID and post it on TikTok to counter misinformation on social media.
Call to action
In a comment, Howard Y. Liu, MD, a child and adolescent psychiatrist and chair of the department of psychiatry, University of Nebraska, Omaha, described the study as “compelling.”
When it comes to public health messages, it’s important to know what social media people are using. Today’s parents are on Twitter and Facebook, whereas their children are more likely to be checking out YouTube and TikTok, said Dr. Liu, chair of the APA’s Council on Communications.
“TikTok is critical because that’s where all the youth eyeballs are,” he said.
The medical profession needs to engage with the platform to reach this next-generation audience and help stop the spread of misinformation about DID, said Dr. Liu. He noted that the APA is looking into undertaking such an initiative.
The study investigators report no relevant disclosures. Dr. Liu reports no relevant disclosures.
A version of this article first appeared on Medscape.com.
AT APA 2023
The family firearm often used in youth suicide
SAN FRANCISCO – , according to results of a novel “psychological autopsy study” of loved ones of youth who died by gun-related suicide.
Yet, families don’t always recognize the danger firearms pose to a young person with suicide risk factors, even when there is a young person in the house with a mental health condition, the data show.
Perhaps most importantly, many parents indicated that they would have removed firearms from the home if it had been suggested by their health care professionals.
The study was presented at the American Psychiatric Association annual meeting.
The message is very clear: Clinicians need to ask about guns and gun safety with patients and families, said study investigator Paul Nestadt, MD, of Johns Hopkins Bloomberg School of Public Health in Baltimore.
“It’s never illegal to ask about gun access and it’s medically relevant. Just do it,” he said during a briefing with reporters.
Grim statistics
Suicide rates have been climbing in the United States for the majority of the past 20 years. Suicide is the second most common cause of death among youth.

Dr. Nestadt noted that overall about 8% of suicide attempts result in death, but when an attempt involves a firearm the percentage jumps astronomically to 90%.
Research has shown that for every 10% increase in household firearms in a given community there is a 27% increase in youth suicide deaths.
“In the world of public health and mental health, we think about having access to firearms as an important risk factor for completed suicide. But in the United States, guns have become an important part of how many Americans see themselves,” Dr. Nestadt told reporters.
Research has shown that half of gun owners say owning a gun is central to their identity and three quarters say it’s essential to their freedom, he noted.
To explore these attitudes further, Dr. Nestadt and colleagues did 11 “psychological autopsy interviews” with the loved ones of nine young people aged 17-21 who died by gun-related suicide. They interviewed six mothers, three fathers, one sibling, and one close friend.
Most of the families had some level of “familial engagement” with firearms, Dr. Nestadt reported.
In more than two-thirds of the families, the youth used a family-owned firearm to commit suicide.
Notably, more than three-quarters of the youth had received mental health care before taking their lives, with many receiving care in the weeks prior to their suicide; 44% had made a prior suicide attempt.
In many cases, parents shared that they had not considered their family-owned firearms to be sources of danger and indicated that had their clinicians expressed concern about the gun in the home, they may have acted to reduce the risk by removing it.
Several also shared that they would have considered using Maryland’s Extreme Risk Protective Order Law if it had existed at the time and they had been made aware of it.
Extreme risk protection order (ERPO) laws, or “red flag laws,” prohibit individuals at risk for harming themselves or others from purchasing or owning a firearm.
Dr. Nestadt said youth suicide interventions “must acknowledge culturally embedded roots of identity formation while rescripting firearms from expressions of family cohesion to instruments that may undermine that cohesion.”
‘Courageous study’
Dr. Nestadt noted that while this study was challenging on many fronts, it took no convincing to get these grieving families to participate.
“They wanted to talk to us, especially because they were hopeful that our work could help prevent future suicides, but also they wanted to talk about their loved ones,” he said.
“When you lose someone to cancer, people give you hugs and flowers. When you lose someone to suicide, people don’t discuss it. Suicide has a stigma to it.”
Briefing moderator Howard Liu, MD, MBA, chair of the department of psychiatry, University of Nebraska Medical Center, Omaha, praised the study team for a “courageous study that really required a tremendous amount of vulnerability from the research team and clearly from the survivors as well.”
This is an “important and timely public health discussion,” said Dr. Liu, chair of the APA Council on Communications.
“We’re all facing this challenge of how do we reduce suicide across all ages, from youth to adults as well. This is a really vital discussion and such an important clue about access and trying to reduce access in a moment of impulsivity,” he added.
The study had no commercial funding. Dr. Nestadt and Dr. Liu report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , according to results of a novel “psychological autopsy study” of loved ones of youth who died by gun-related suicide.
Yet, families don’t always recognize the danger firearms pose to a young person with suicide risk factors, even when there is a young person in the house with a mental health condition, the data show.
Perhaps most importantly, many parents indicated that they would have removed firearms from the home if it had been suggested by their health care professionals.
The study was presented at the American Psychiatric Association annual meeting.
The message is very clear: Clinicians need to ask about guns and gun safety with patients and families, said study investigator Paul Nestadt, MD, of Johns Hopkins Bloomberg School of Public Health in Baltimore.
“It’s never illegal to ask about gun access and it’s medically relevant. Just do it,” he said during a briefing with reporters.
Grim statistics
Suicide rates have been climbing in the United States for the majority of the past 20 years. Suicide is the second most common cause of death among youth.
Dr. Nestadt noted that overall about 8% of suicide attempts result in death, but when an attempt involves a firearm the percentage jumps astronomically to 90%.
Research has shown that for every 10% increase in household firearms in a given community there is a 27% increase in youth suicide deaths.
“In the world of public health and mental health, we think about having access to firearms as an important risk factor for completed suicide. But in the United States, guns have become an important part of how many Americans see themselves,” Dr. Nestadt told reporters.
Research has shown that half of gun owners say owning a gun is central to their identity and three quarters say it’s essential to their freedom, he noted.
To explore these attitudes further, Dr. Nestadt and colleagues did 11 “psychological autopsy interviews” with the loved ones of nine young people aged 17-21 who died by gun-related suicide. They interviewed six mothers, three fathers, one sibling, and one close friend.
Most of the families had some level of “familial engagement” with firearms, Dr. Nestadt reported.
In more than two-thirds of the families, the youth used a family-owned firearm to commit suicide.
Notably, more than three-quarters of the youth had received mental health care before taking their lives, with many receiving care in the weeks prior to their suicide; 44% had made a prior suicide attempt.
In many cases, parents shared that they had not considered their family-owned firearms to be sources of danger and indicated that had their clinicians expressed concern about the gun in the home, they may have acted to reduce the risk by removing it.
Several also shared that they would have considered using Maryland’s Extreme Risk Protective Order Law if it had existed at the time and they had been made aware of it.
Extreme risk protection order (ERPO) laws, or “red flag laws,” prohibit individuals at risk for harming themselves or others from purchasing or owning a firearm.
Dr. Nestadt said youth suicide interventions “must acknowledge culturally embedded roots of identity formation while rescripting firearms from expressions of family cohesion to instruments that may undermine that cohesion.”
‘Courageous study’
Dr. Nestadt noted that while this study was challenging on many fronts, it took no convincing to get these grieving families to participate.
“They wanted to talk to us, especially because they were hopeful that our work could help prevent future suicides, but also they wanted to talk about their loved ones,” he said.
“When you lose someone to cancer, people give you hugs and flowers. When you lose someone to suicide, people don’t discuss it. Suicide has a stigma to it.”
Briefing moderator Howard Liu, MD, MBA, chair of the department of psychiatry, University of Nebraska Medical Center, Omaha, praised the study team for a “courageous study that really required a tremendous amount of vulnerability from the research team and clearly from the survivors as well.”
This is an “important and timely public health discussion,” said Dr. Liu, chair of the APA Council on Communications.
“We’re all facing this challenge of how do we reduce suicide across all ages, from youth to adults as well. This is a really vital discussion and such an important clue about access and trying to reduce access in a moment of impulsivity,” he added.
The study had no commercial funding. Dr. Nestadt and Dr. Liu report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – , according to results of a novel “psychological autopsy study” of loved ones of youth who died by gun-related suicide.
Yet, families don’t always recognize the danger firearms pose to a young person with suicide risk factors, even when there is a young person in the house with a mental health condition, the data show.
Perhaps most importantly, many parents indicated that they would have removed firearms from the home if it had been suggested by their health care professionals.
The study was presented at the American Psychiatric Association annual meeting.
The message is very clear: Clinicians need to ask about guns and gun safety with patients and families, said study investigator Paul Nestadt, MD, of Johns Hopkins Bloomberg School of Public Health in Baltimore.
“It’s never illegal to ask about gun access and it’s medically relevant. Just do it,” he said during a briefing with reporters.
Grim statistics
Suicide rates have been climbing in the United States for the majority of the past 20 years. Suicide is the second most common cause of death among youth.
Dr. Nestadt noted that overall about 8% of suicide attempts result in death, but when an attempt involves a firearm the percentage jumps astronomically to 90%.
Research has shown that for every 10% increase in household firearms in a given community there is a 27% increase in youth suicide deaths.
“In the world of public health and mental health, we think about having access to firearms as an important risk factor for completed suicide. But in the United States, guns have become an important part of how many Americans see themselves,” Dr. Nestadt told reporters.
Research has shown that half of gun owners say owning a gun is central to their identity and three quarters say it’s essential to their freedom, he noted.
To explore these attitudes further, Dr. Nestadt and colleagues did 11 “psychological autopsy interviews” with the loved ones of nine young people aged 17-21 who died by gun-related suicide. They interviewed six mothers, three fathers, one sibling, and one close friend.
Most of the families had some level of “familial engagement” with firearms, Dr. Nestadt reported.
In more than two-thirds of the families, the youth used a family-owned firearm to commit suicide.
Notably, more than three-quarters of the youth had received mental health care before taking their lives, with many receiving care in the weeks prior to their suicide; 44% had made a prior suicide attempt.
In many cases, parents shared that they had not considered their family-owned firearms to be sources of danger and indicated that had their clinicians expressed concern about the gun in the home, they may have acted to reduce the risk by removing it.
Several also shared that they would have considered using Maryland’s Extreme Risk Protective Order Law if it had existed at the time and they had been made aware of it.
Extreme risk protection order (ERPO) laws, or “red flag laws,” prohibit individuals at risk for harming themselves or others from purchasing or owning a firearm.
Dr. Nestadt said youth suicide interventions “must acknowledge culturally embedded roots of identity formation while rescripting firearms from expressions of family cohesion to instruments that may undermine that cohesion.”
‘Courageous study’
Dr. Nestadt noted that while this study was challenging on many fronts, it took no convincing to get these grieving families to participate.
“They wanted to talk to us, especially because they were hopeful that our work could help prevent future suicides, but also they wanted to talk about their loved ones,” he said.
“When you lose someone to cancer, people give you hugs and flowers. When you lose someone to suicide, people don’t discuss it. Suicide has a stigma to it.”
Briefing moderator Howard Liu, MD, MBA, chair of the department of psychiatry, University of Nebraska Medical Center, Omaha, praised the study team for a “courageous study that really required a tremendous amount of vulnerability from the research team and clearly from the survivors as well.”
This is an “important and timely public health discussion,” said Dr. Liu, chair of the APA Council on Communications.
“We’re all facing this challenge of how do we reduce suicide across all ages, from youth to adults as well. This is a really vital discussion and such an important clue about access and trying to reduce access in a moment of impulsivity,” he added.
The study had no commercial funding. Dr. Nestadt and Dr. Liu report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT APA 2023
Black patients most likely to be restrained in EDs, Latino patients least likely
SAN FRANCISCO – .
In contrast, Hispanic/Latino patients were less likely to be restrained than both Black and White patients, researchers reported in a poster presented at the annual meeting of the American Psychiatric Association. The study authors also found that clinicians rarely turned to restraints, using them in just 2,712 of 882,390 ED visits (0.3%) over a 7-year period.
The study doesn’t examine why the disparities exist. But lead author Erika Chang-Sing, a medical student at Yale University, New Haven, Conn., said in an interview that it’s clear that racial bias is the cause of the differences in restraint rates among White, Black, and Hispanics/Latino patients. “We think that there are multiple contributing factors to the higher rates of restraint for Black patients brought to the hospital by police, and all of them are rooted in systemic racism,” she said, adding that “the lower odds of restraint in the Hispanic or Latino group are also rooted in systemic racism and inequity.”
According to Ms. Chang-Sing, researchers launched the study to gain insight into the use of the restraints in the Southeast and to see what’s happening in light of the recent publicizing of killings of Black people by police. Being taken to the hospital by police “might contribute both to the individual patient’s behavior and the health care provider’s assessment of risk in determining whether or not to apply restraints,” she said.
Other research has linked ethnicity to higher rates of restraint use. For example, a 2021 study of 32,054 cases of patients under mandatory psychiatric hold in 11 Massachusetts emergency rooms found that Black (adjusted odds ratio, 1.22) and Hispanic (aOR, 1.45) patients were more likely to be restrained than White patients.
For the new study, researchers retrospectively tracked 885,102 emergency room visits at three North Carolina emergency departments from 2015 to 2022, including 9,130 who were brought in by police and 2,712 who were physically restrained because of the perceived risk of violence. “Providers use restraints, or straps, to secure the patient’s wrists and ankles to the bed,” Ms. Chang-Sing said.
Among all patients, 52.5% were Black, but 66% of those who were restrained were Black. The numbers for White patients were 35.7% and 23.9%, respectively, and 5.7% and 3.2% for Hispanics/Latino patients. Black patients were less likely than White patients to get a psychiatric primary emergency department diagnosis (aOR, 0.67), but those in that category were more likely than their White counterparts to be restrained (aOR, 1.36).
The higher risk of restraint use in Black patients overall disappeared when researchers adjusted their statistics to account for the effects of sex, age, and type of insurance (aOR, 0.86). Ms. Chang-Sing said the study team is reanalyzing the data since they think insurance may not be a confounder.
Why might Hispanic/Latino ethnicity be protective against restraint use? “This may be due to language barriers, fear of law enforcement, and avoidance of the hospital in the first place,” Ms. Chang-Sing said.
Emergency physician Wendy Macias-Konstantopoulos, MD, MPH, MBA, of Harvard Medical School and Massachusetts General Hospital, both in Boston, coauthored the 2021 study on police restraints. In an interview, she said the new findings add to previous research by providing data about the role played by the police who bring patients to the ED. She added that there is no evidence that certain populations simply need more restraints.
What can be done to reduce disparities in restraint use? Mental health teams can make a difference by responding to mental health emergencies, Ms. Chang-Sing said. “These providers can be instrumental in communicating to patients that the intention is to care for them, not to punish them.”
Another strategy is to increase the number of clinics and crisis response centers, she said. Hospital-based crisis response teams can also be helpful, she said. “Because these teams are focused only on behavioral emergencies, they can be more thoughtful in avoiding the use of restraints.”
No study funding was reported. The study authors and Dr. Macias-Konstantopoulos have no disclosures.
SAN FRANCISCO – .
In contrast, Hispanic/Latino patients were less likely to be restrained than both Black and White patients, researchers reported in a poster presented at the annual meeting of the American Psychiatric Association. The study authors also found that clinicians rarely turned to restraints, using them in just 2,712 of 882,390 ED visits (0.3%) over a 7-year period.
The study doesn’t examine why the disparities exist. But lead author Erika Chang-Sing, a medical student at Yale University, New Haven, Conn., said in an interview that it’s clear that racial bias is the cause of the differences in restraint rates among White, Black, and Hispanics/Latino patients. “We think that there are multiple contributing factors to the higher rates of restraint for Black patients brought to the hospital by police, and all of them are rooted in systemic racism,” she said, adding that “the lower odds of restraint in the Hispanic or Latino group are also rooted in systemic racism and inequity.”
According to Ms. Chang-Sing, researchers launched the study to gain insight into the use of the restraints in the Southeast and to see what’s happening in light of the recent publicizing of killings of Black people by police. Being taken to the hospital by police “might contribute both to the individual patient’s behavior and the health care provider’s assessment of risk in determining whether or not to apply restraints,” she said.
Other research has linked ethnicity to higher rates of restraint use. For example, a 2021 study of 32,054 cases of patients under mandatory psychiatric hold in 11 Massachusetts emergency rooms found that Black (adjusted odds ratio, 1.22) and Hispanic (aOR, 1.45) patients were more likely to be restrained than White patients.
For the new study, researchers retrospectively tracked 885,102 emergency room visits at three North Carolina emergency departments from 2015 to 2022, including 9,130 who were brought in by police and 2,712 who were physically restrained because of the perceived risk of violence. “Providers use restraints, or straps, to secure the patient’s wrists and ankles to the bed,” Ms. Chang-Sing said.
Among all patients, 52.5% were Black, but 66% of those who were restrained were Black. The numbers for White patients were 35.7% and 23.9%, respectively, and 5.7% and 3.2% for Hispanics/Latino patients. Black patients were less likely than White patients to get a psychiatric primary emergency department diagnosis (aOR, 0.67), but those in that category were more likely than their White counterparts to be restrained (aOR, 1.36).
The higher risk of restraint use in Black patients overall disappeared when researchers adjusted their statistics to account for the effects of sex, age, and type of insurance (aOR, 0.86). Ms. Chang-Sing said the study team is reanalyzing the data since they think insurance may not be a confounder.
Why might Hispanic/Latino ethnicity be protective against restraint use? “This may be due to language barriers, fear of law enforcement, and avoidance of the hospital in the first place,” Ms. Chang-Sing said.
Emergency physician Wendy Macias-Konstantopoulos, MD, MPH, MBA, of Harvard Medical School and Massachusetts General Hospital, both in Boston, coauthored the 2021 study on police restraints. In an interview, she said the new findings add to previous research by providing data about the role played by the police who bring patients to the ED. She added that there is no evidence that certain populations simply need more restraints.
What can be done to reduce disparities in restraint use? Mental health teams can make a difference by responding to mental health emergencies, Ms. Chang-Sing said. “These providers can be instrumental in communicating to patients that the intention is to care for them, not to punish them.”
Another strategy is to increase the number of clinics and crisis response centers, she said. Hospital-based crisis response teams can also be helpful, she said. “Because these teams are focused only on behavioral emergencies, they can be more thoughtful in avoiding the use of restraints.”
No study funding was reported. The study authors and Dr. Macias-Konstantopoulos have no disclosures.
SAN FRANCISCO – .
In contrast, Hispanic/Latino patients were less likely to be restrained than both Black and White patients, researchers reported in a poster presented at the annual meeting of the American Psychiatric Association. The study authors also found that clinicians rarely turned to restraints, using them in just 2,712 of 882,390 ED visits (0.3%) over a 7-year period.
The study doesn’t examine why the disparities exist. But lead author Erika Chang-Sing, a medical student at Yale University, New Haven, Conn., said in an interview that it’s clear that racial bias is the cause of the differences in restraint rates among White, Black, and Hispanics/Latino patients. “We think that there are multiple contributing factors to the higher rates of restraint for Black patients brought to the hospital by police, and all of them are rooted in systemic racism,” she said, adding that “the lower odds of restraint in the Hispanic or Latino group are also rooted in systemic racism and inequity.”
According to Ms. Chang-Sing, researchers launched the study to gain insight into the use of the restraints in the Southeast and to see what’s happening in light of the recent publicizing of killings of Black people by police. Being taken to the hospital by police “might contribute both to the individual patient’s behavior and the health care provider’s assessment of risk in determining whether or not to apply restraints,” she said.
Other research has linked ethnicity to higher rates of restraint use. For example, a 2021 study of 32,054 cases of patients under mandatory psychiatric hold in 11 Massachusetts emergency rooms found that Black (adjusted odds ratio, 1.22) and Hispanic (aOR, 1.45) patients were more likely to be restrained than White patients.
For the new study, researchers retrospectively tracked 885,102 emergency room visits at three North Carolina emergency departments from 2015 to 2022, including 9,130 who were brought in by police and 2,712 who were physically restrained because of the perceived risk of violence. “Providers use restraints, or straps, to secure the patient’s wrists and ankles to the bed,” Ms. Chang-Sing said.
Among all patients, 52.5% were Black, but 66% of those who were restrained were Black. The numbers for White patients were 35.7% and 23.9%, respectively, and 5.7% and 3.2% for Hispanics/Latino patients. Black patients were less likely than White patients to get a psychiatric primary emergency department diagnosis (aOR, 0.67), but those in that category were more likely than their White counterparts to be restrained (aOR, 1.36).
The higher risk of restraint use in Black patients overall disappeared when researchers adjusted their statistics to account for the effects of sex, age, and type of insurance (aOR, 0.86). Ms. Chang-Sing said the study team is reanalyzing the data since they think insurance may not be a confounder.
Why might Hispanic/Latino ethnicity be protective against restraint use? “This may be due to language barriers, fear of law enforcement, and avoidance of the hospital in the first place,” Ms. Chang-Sing said.
Emergency physician Wendy Macias-Konstantopoulos, MD, MPH, MBA, of Harvard Medical School and Massachusetts General Hospital, both in Boston, coauthored the 2021 study on police restraints. In an interview, she said the new findings add to previous research by providing data about the role played by the police who bring patients to the ED. She added that there is no evidence that certain populations simply need more restraints.
What can be done to reduce disparities in restraint use? Mental health teams can make a difference by responding to mental health emergencies, Ms. Chang-Sing said. “These providers can be instrumental in communicating to patients that the intention is to care for them, not to punish them.”
Another strategy is to increase the number of clinics and crisis response centers, she said. Hospital-based crisis response teams can also be helpful, she said. “Because these teams are focused only on behavioral emergencies, they can be more thoughtful in avoiding the use of restraints.”
No study funding was reported. The study authors and Dr. Macias-Konstantopoulos have no disclosures.
AT APA 2023
Eating disorders in children is a global public health emergency
The high figures are concerning from a public health perspective and highlight the need to implement strategies for preventing eating disorders.
These disorders include anorexia nervosa, bulimia nervosa, binge eating disorder, and eating disorder–not otherwise specified. The prevalence of these disorders in young people has markedly increased globally over the past 50 years. Eating disorders are among the most life-threatening mental disorders; they were responsible for 318 deaths worldwide in 2019.
Because some individuals with eating disorders conceal core symptoms and avoid or delay seeking specialist care because of feelings of embarrassment, stigma, or ambivalence toward treatment, most cases of eating disorders remain undetected and untreated.
Brazilian researchers conducted studies to assess risky behaviors and predisposing factors among young people. The researchers observed that the probability of experiencing eating disorders was higher among young people who had an intense fear of gaining weight, who experienced thin-ideal internalization, who were excessively concerned about food, who experienced compulsive eating episodes, or who used laxatives. As previously reported, most participants in these studies had never sought professional help.
A study conducted in 2020 concluded that the media greatly influences the construction of one’s body image and the creation of aesthetic standards, particularly for adolescents. Adolescents then change their eating patterns and become more vulnerable to mental disorders related to eating.
A group of researchers from several countries, including Brazilians connected to the State University of Londrina, conducted the Global Proportion of Disordered Eating in Children and Adolescents – A Systematic Review and Meta-analysis. The study was coordinated by José Francisco López-Gil, PhD, of the University of Castilla–La Mancha (Spain). The investigators determined the rate of disordered eating among children and adolescents using the SCOFF (Sick, Control, One, Fat, Food) questionnaire, which is the most widely used screening measure for eating disorders.
Methods and results
Four databases were systematically searched (PubMed, Scopus, Web of Science, and the Cochrane Library); date limits were from January 1999 to November 2022. Studies were required to meet the following criteria: participants – studies of community samples of children and adolescents aged 6-18 years – and outcome – disordered eating assessed by the SCOFF questionnaire. The exclusion criteria were studies conducted with young people who had been diagnosed with physical or mental disorders; studies that were published before 1999, because the SCOFF questionnaire was designed in that year; studies in which data were collected during the COVID-19 pandemic, because of the possibility of selection bias; studies that employed data from the same surveys/studies, to avoid duplication; and systematic reviews and/or meta-analyses and qualitative and case studies.
In all, 32 studies, which involved a total of 63,181 participants from 16 countries, were included in the systematic review and meta-analysis, according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. The overall proportion of children and adolescents with disordered eating was 22.36% (95% confidence interval, 18.84%-26.09%; P < .001; n = 63,181). According to the researchers, girls were significantly more likely to report disordered eating (30.03%; 95% CI, 25.61%-34.65%; n = 27,548) than boys (16.98%; 95% CI, 13.46%-20.81%; n = 26,170; P < .001). It was also observed that disordered eating became more elevated with increasing age (B, 0.03; 95% CI, 0-0.06; P = .049) and BMI (B, 0.03; 95% CI, 0.01-0.05; P < .001).
Translation of outcomes
According to the authors, this was the first meta-analysis that comprehensively examined the overall proportion of children and adolescents with disordered eating in terms of gender, mean age, and BMI. They identified 14,856 (22.36%) children and adolescents with disordered eating in the population analyzed (n = 63,181). A relevant consideration made by the researchers is that, in general, disordered eating and eating disorders are not similar. “Not all children and adolescents who reported disordered eating behaviors (for example, selective eating) will necessarily be diagnosed with an eating disorder.” However, disordered eating in childhood or adolescence may predict outcomes associated with eating disorders in early adulthood. “For this reason, this high proportion found is worrisome and calls for urgent action to try to address this situation.”
The study also found that the proportion of children and adolescents with disordered eating was higher among girls than boys. The reasons for the difference in the prevalence with respect to the sex of the participants are not well understood. Boys are presumed to underreport the problem because of the societal perception that these disorders mostly affect girls and because disordered eating has usually been thought by the general population to be exclusive to girls and women. In addition, it has been noted that the current diagnostic criteria for eating disorders fail to detect disordered eating behaviors more commonly observed in boys than girls, such as intensely engaging in muscle mass gain and weight gain with the goal of improving body image satisfaction. On the other hand, the proportion of young people with disordered eating increased with increasing age and BMI. This finding is in line with the scientific literature worldwide.
The study has certain limitations. First, only studies that analyzed disordered eating using the SCOFF questionnaire were included. Second, because of the cross-sectional nature of most of the included studies, a causal relationship cannot be established. Third, owing to the inclusion of binge eating disorder and other eating disorders specified in the DSM-5, there is not enough evidence to support the use of SCOFF in primary care and community-based settings for screening for the range of eating disorders. Fourth, the meta-analysis included studies in which self-report questionnaires were used to assess disordered eating, and consequently, social desirability and recall bias could have influenced the findings.
Quick measures required
Identifying the magnitude of disordered eating and its distribution in at-risk populations is crucial for planning and executing actions aimed at preventing, detecting, and treating them. Eating disorders are a global public health problem that health care professionals, families, and other community members involved in caring for children and adolescents must not ignore, the researchers said. In addition to diagnosed eating disorders, parents, guardians, and health care professionals should be aware of symptoms of disordered eating, which include behaviors such as weight-loss dieting, binge eating, self-induced vomiting, excessive exercise, and the use of laxatives or diuretics without medical prescription.
This article was translated from the Medscape Portuguese Edition. A version of this article appeared on Medscape.com.
The high figures are concerning from a public health perspective and highlight the need to implement strategies for preventing eating disorders.
These disorders include anorexia nervosa, bulimia nervosa, binge eating disorder, and eating disorder–not otherwise specified. The prevalence of these disorders in young people has markedly increased globally over the past 50 years. Eating disorders are among the most life-threatening mental disorders; they were responsible for 318 deaths worldwide in 2019.
Because some individuals with eating disorders conceal core symptoms and avoid or delay seeking specialist care because of feelings of embarrassment, stigma, or ambivalence toward treatment, most cases of eating disorders remain undetected and untreated.
Brazilian researchers conducted studies to assess risky behaviors and predisposing factors among young people. The researchers observed that the probability of experiencing eating disorders was higher among young people who had an intense fear of gaining weight, who experienced thin-ideal internalization, who were excessively concerned about food, who experienced compulsive eating episodes, or who used laxatives. As previously reported, most participants in these studies had never sought professional help.
A study conducted in 2020 concluded that the media greatly influences the construction of one’s body image and the creation of aesthetic standards, particularly for adolescents. Adolescents then change their eating patterns and become more vulnerable to mental disorders related to eating.
A group of researchers from several countries, including Brazilians connected to the State University of Londrina, conducted the Global Proportion of Disordered Eating in Children and Adolescents – A Systematic Review and Meta-analysis. The study was coordinated by José Francisco López-Gil, PhD, of the University of Castilla–La Mancha (Spain). The investigators determined the rate of disordered eating among children and adolescents using the SCOFF (Sick, Control, One, Fat, Food) questionnaire, which is the most widely used screening measure for eating disorders.
Methods and results
Four databases were systematically searched (PubMed, Scopus, Web of Science, and the Cochrane Library); date limits were from January 1999 to November 2022. Studies were required to meet the following criteria: participants – studies of community samples of children and adolescents aged 6-18 years – and outcome – disordered eating assessed by the SCOFF questionnaire. The exclusion criteria were studies conducted with young people who had been diagnosed with physical or mental disorders; studies that were published before 1999, because the SCOFF questionnaire was designed in that year; studies in which data were collected during the COVID-19 pandemic, because of the possibility of selection bias; studies that employed data from the same surveys/studies, to avoid duplication; and systematic reviews and/or meta-analyses and qualitative and case studies.
In all, 32 studies, which involved a total of 63,181 participants from 16 countries, were included in the systematic review and meta-analysis, according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. The overall proportion of children and adolescents with disordered eating was 22.36% (95% confidence interval, 18.84%-26.09%; P < .001; n = 63,181). According to the researchers, girls were significantly more likely to report disordered eating (30.03%; 95% CI, 25.61%-34.65%; n = 27,548) than boys (16.98%; 95% CI, 13.46%-20.81%; n = 26,170; P < .001). It was also observed that disordered eating became more elevated with increasing age (B, 0.03; 95% CI, 0-0.06; P = .049) and BMI (B, 0.03; 95% CI, 0.01-0.05; P < .001).
Translation of outcomes
According to the authors, this was the first meta-analysis that comprehensively examined the overall proportion of children and adolescents with disordered eating in terms of gender, mean age, and BMI. They identified 14,856 (22.36%) children and adolescents with disordered eating in the population analyzed (n = 63,181). A relevant consideration made by the researchers is that, in general, disordered eating and eating disorders are not similar. “Not all children and adolescents who reported disordered eating behaviors (for example, selective eating) will necessarily be diagnosed with an eating disorder.” However, disordered eating in childhood or adolescence may predict outcomes associated with eating disorders in early adulthood. “For this reason, this high proportion found is worrisome and calls for urgent action to try to address this situation.”
The study also found that the proportion of children and adolescents with disordered eating was higher among girls than boys. The reasons for the difference in the prevalence with respect to the sex of the participants are not well understood. Boys are presumed to underreport the problem because of the societal perception that these disorders mostly affect girls and because disordered eating has usually been thought by the general population to be exclusive to girls and women. In addition, it has been noted that the current diagnostic criteria for eating disorders fail to detect disordered eating behaviors more commonly observed in boys than girls, such as intensely engaging in muscle mass gain and weight gain with the goal of improving body image satisfaction. On the other hand, the proportion of young people with disordered eating increased with increasing age and BMI. This finding is in line with the scientific literature worldwide.
The study has certain limitations. First, only studies that analyzed disordered eating using the SCOFF questionnaire were included. Second, because of the cross-sectional nature of most of the included studies, a causal relationship cannot be established. Third, owing to the inclusion of binge eating disorder and other eating disorders specified in the DSM-5, there is not enough evidence to support the use of SCOFF in primary care and community-based settings for screening for the range of eating disorders. Fourth, the meta-analysis included studies in which self-report questionnaires were used to assess disordered eating, and consequently, social desirability and recall bias could have influenced the findings.
Quick measures required
Identifying the magnitude of disordered eating and its distribution in at-risk populations is crucial for planning and executing actions aimed at preventing, detecting, and treating them. Eating disorders are a global public health problem that health care professionals, families, and other community members involved in caring for children and adolescents must not ignore, the researchers said. In addition to diagnosed eating disorders, parents, guardians, and health care professionals should be aware of symptoms of disordered eating, which include behaviors such as weight-loss dieting, binge eating, self-induced vomiting, excessive exercise, and the use of laxatives or diuretics without medical prescription.
This article was translated from the Medscape Portuguese Edition. A version of this article appeared on Medscape.com.
The high figures are concerning from a public health perspective and highlight the need to implement strategies for preventing eating disorders.
These disorders include anorexia nervosa, bulimia nervosa, binge eating disorder, and eating disorder–not otherwise specified. The prevalence of these disorders in young people has markedly increased globally over the past 50 years. Eating disorders are among the most life-threatening mental disorders; they were responsible for 318 deaths worldwide in 2019.
Because some individuals with eating disorders conceal core symptoms and avoid or delay seeking specialist care because of feelings of embarrassment, stigma, or ambivalence toward treatment, most cases of eating disorders remain undetected and untreated.
Brazilian researchers conducted studies to assess risky behaviors and predisposing factors among young people. The researchers observed that the probability of experiencing eating disorders was higher among young people who had an intense fear of gaining weight, who experienced thin-ideal internalization, who were excessively concerned about food, who experienced compulsive eating episodes, or who used laxatives. As previously reported, most participants in these studies had never sought professional help.
A study conducted in 2020 concluded that the media greatly influences the construction of one’s body image and the creation of aesthetic standards, particularly for adolescents. Adolescents then change their eating patterns and become more vulnerable to mental disorders related to eating.
A group of researchers from several countries, including Brazilians connected to the State University of Londrina, conducted the Global Proportion of Disordered Eating in Children and Adolescents – A Systematic Review and Meta-analysis. The study was coordinated by José Francisco López-Gil, PhD, of the University of Castilla–La Mancha (Spain). The investigators determined the rate of disordered eating among children and adolescents using the SCOFF (Sick, Control, One, Fat, Food) questionnaire, which is the most widely used screening measure for eating disorders.
Methods and results
Four databases were systematically searched (PubMed, Scopus, Web of Science, and the Cochrane Library); date limits were from January 1999 to November 2022. Studies were required to meet the following criteria: participants – studies of community samples of children and adolescents aged 6-18 years – and outcome – disordered eating assessed by the SCOFF questionnaire. The exclusion criteria were studies conducted with young people who had been diagnosed with physical or mental disorders; studies that were published before 1999, because the SCOFF questionnaire was designed in that year; studies in which data were collected during the COVID-19 pandemic, because of the possibility of selection bias; studies that employed data from the same surveys/studies, to avoid duplication; and systematic reviews and/or meta-analyses and qualitative and case studies.
In all, 32 studies, which involved a total of 63,181 participants from 16 countries, were included in the systematic review and meta-analysis, according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. The overall proportion of children and adolescents with disordered eating was 22.36% (95% confidence interval, 18.84%-26.09%; P < .001; n = 63,181). According to the researchers, girls were significantly more likely to report disordered eating (30.03%; 95% CI, 25.61%-34.65%; n = 27,548) than boys (16.98%; 95% CI, 13.46%-20.81%; n = 26,170; P < .001). It was also observed that disordered eating became more elevated with increasing age (B, 0.03; 95% CI, 0-0.06; P = .049) and BMI (B, 0.03; 95% CI, 0.01-0.05; P < .001).
Translation of outcomes
According to the authors, this was the first meta-analysis that comprehensively examined the overall proportion of children and adolescents with disordered eating in terms of gender, mean age, and BMI. They identified 14,856 (22.36%) children and adolescents with disordered eating in the population analyzed (n = 63,181). A relevant consideration made by the researchers is that, in general, disordered eating and eating disorders are not similar. “Not all children and adolescents who reported disordered eating behaviors (for example, selective eating) will necessarily be diagnosed with an eating disorder.” However, disordered eating in childhood or adolescence may predict outcomes associated with eating disorders in early adulthood. “For this reason, this high proportion found is worrisome and calls for urgent action to try to address this situation.”
The study also found that the proportion of children and adolescents with disordered eating was higher among girls than boys. The reasons for the difference in the prevalence with respect to the sex of the participants are not well understood. Boys are presumed to underreport the problem because of the societal perception that these disorders mostly affect girls and because disordered eating has usually been thought by the general population to be exclusive to girls and women. In addition, it has been noted that the current diagnostic criteria for eating disorders fail to detect disordered eating behaviors more commonly observed in boys than girls, such as intensely engaging in muscle mass gain and weight gain with the goal of improving body image satisfaction. On the other hand, the proportion of young people with disordered eating increased with increasing age and BMI. This finding is in line with the scientific literature worldwide.
The study has certain limitations. First, only studies that analyzed disordered eating using the SCOFF questionnaire were included. Second, because of the cross-sectional nature of most of the included studies, a causal relationship cannot be established. Third, owing to the inclusion of binge eating disorder and other eating disorders specified in the DSM-5, there is not enough evidence to support the use of SCOFF in primary care and community-based settings for screening for the range of eating disorders. Fourth, the meta-analysis included studies in which self-report questionnaires were used to assess disordered eating, and consequently, social desirability and recall bias could have influenced the findings.
Quick measures required
Identifying the magnitude of disordered eating and its distribution in at-risk populations is crucial for planning and executing actions aimed at preventing, detecting, and treating them. Eating disorders are a global public health problem that health care professionals, families, and other community members involved in caring for children and adolescents must not ignore, the researchers said. In addition to diagnosed eating disorders, parents, guardians, and health care professionals should be aware of symptoms of disordered eating, which include behaviors such as weight-loss dieting, binge eating, self-induced vomiting, excessive exercise, and the use of laxatives or diuretics without medical prescription.
This article was translated from the Medscape Portuguese Edition. A version of this article appeared on Medscape.com.
FROM JAMA PEDIATRICS
Study says casual pot use harmful to teens
Teenagers who use cannabis recreationally are two to three times more likely to have depression and suicidal thoughts than those who don’t use it. And teens who have cannabis use disorder – which means they can’t stop using it despite health and social problems – are four times more likely to have those same thoughts and feelings.
The study was published in JAMA. It looked at information from 68,000 teens in the National Survey on Drug Use and Health.
Marijuana use was also linked to other issues including not doing well in school, skipping school, and getting in trouble with the police. 
“Kids, year by year, have been moving towards a view that marijuana is safe and benign – that’s factually incorrect,” lead author of the study, Ryan Sultan, MD, an assistant professor of clinical psychiatry at Columbia University, New York, told Yahoo Life.
Dr. Sultan said he was surprised that recreational users had a much higher risk of mental health issues. “We typically think of recreational use as not being a concerning behavior.”
The study did not seek to explain the link between mental health problems and cannabis use.
“The more you use it, the more it negatively affects your thinking. That’s increasing the likelihood of depression and more suicidal thoughts,” Dr. Sultan said. “It’s feedback that spirals downward and gets to a place that really concerns us as child psychiatrists.”
Dr. Sultan said parents should talk to their children about marijuana use, depression, and anxiety.
NIDA and American Academy of Child and Adolescent Psychiatry provided funding for the study. One coauthor reported receiving grants and personal fees from several medical and sports organizations. The other authors reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
Teenagers who use cannabis recreationally are two to three times more likely to have depression and suicidal thoughts than those who don’t use it. And teens who have cannabis use disorder – which means they can’t stop using it despite health and social problems – are four times more likely to have those same thoughts and feelings.
The study was published in JAMA. It looked at information from 68,000 teens in the National Survey on Drug Use and Health.
Marijuana use was also linked to other issues including not doing well in school, skipping school, and getting in trouble with the police.
“Kids, year by year, have been moving towards a view that marijuana is safe and benign – that’s factually incorrect,” lead author of the study, Ryan Sultan, MD, an assistant professor of clinical psychiatry at Columbia University, New York, told Yahoo Life.
Dr. Sultan said he was surprised that recreational users had a much higher risk of mental health issues. “We typically think of recreational use as not being a concerning behavior.”
The study did not seek to explain the link between mental health problems and cannabis use.
“The more you use it, the more it negatively affects your thinking. That’s increasing the likelihood of depression and more suicidal thoughts,” Dr. Sultan said. “It’s feedback that spirals downward and gets to a place that really concerns us as child psychiatrists.”
Dr. Sultan said parents should talk to their children about marijuana use, depression, and anxiety.
NIDA and American Academy of Child and Adolescent Psychiatry provided funding for the study. One coauthor reported receiving grants and personal fees from several medical and sports organizations. The other authors reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
Teenagers who use cannabis recreationally are two to three times more likely to have depression and suicidal thoughts than those who don’t use it. And teens who have cannabis use disorder – which means they can’t stop using it despite health and social problems – are four times more likely to have those same thoughts and feelings.
The study was published in JAMA. It looked at information from 68,000 teens in the National Survey on Drug Use and Health.
Marijuana use was also linked to other issues including not doing well in school, skipping school, and getting in trouble with the police.
“Kids, year by year, have been moving towards a view that marijuana is safe and benign – that’s factually incorrect,” lead author of the study, Ryan Sultan, MD, an assistant professor of clinical psychiatry at Columbia University, New York, told Yahoo Life.
Dr. Sultan said he was surprised that recreational users had a much higher risk of mental health issues. “We typically think of recreational use as not being a concerning behavior.”
The study did not seek to explain the link between mental health problems and cannabis use.
“The more you use it, the more it negatively affects your thinking. That’s increasing the likelihood of depression and more suicidal thoughts,” Dr. Sultan said. “It’s feedback that spirals downward and gets to a place that really concerns us as child psychiatrists.”
Dr. Sultan said parents should talk to their children about marijuana use, depression, and anxiety.
NIDA and American Academy of Child and Adolescent Psychiatry provided funding for the study. One coauthor reported receiving grants and personal fees from several medical and sports organizations. The other authors reported no conflicts of interest.
A version of this article first appeared on WebMD.com.
FROM JAMA
Differences in 30-Day Readmission Rates in Older Adults With Dementia
Study 1 Overview (Park et al)
Objective: To compare rates of adverse events and 30-day readmission among patients with dementia who undergo percutaneous coronary intervention (PCI) with those without dementia.
Design: This cohort study used a national database of hospital readmissions developed by the Agency for Healthcare Research and Quality.
Setting and participants: Data from State Inpatient Databases were used to derive this national readmissions database representing 80% of hospitals from 28 states that contribute data. The study included all individuals aged 18 years and older who were identified to have had a PCI procedure in the years 2017 and 2018. International Classification of Diseases, Tenth Revision (ICD-10) codes were used to identify PCI procedures, including drug-eluting stent placement, bare-metal stent placement, and balloon angioplasty, performed in patients who presented with myocardial infarction and unstable angina and those with stable ischemic heart disease. Patients were stratified into those with or without dementia, also defined using ICD-10 codes. A total of 755,406 index hospitalizations were included; 2.3% of the patients had dementia.
Main outcome measures: The primary study outcome was 30-day all-cause readmission, with the cause classified as cardiovascular or noncardiovascular. Secondary outcome measures examined were delirium, in-hospital mortality, cardiac arrest, blood transfusion, acute kidney injury, fall in hospital, length of hospital stay, and other adverse outcomes. Location at discharge was also examined. Other covariates included in the analysis were age, sex, comorbidities, hospital characteristics, primary payer, and median income. For analysis, a propensity score matching algorithm was applied to match patients with and without dementia. Kaplan-Meier curves were used to examine 30-day readmission rates, and a Cox proportional hazards model was used to calculate hazard ratios (HR) for those with and without dementia. For secondary outcomes, logistic regression models were used to calculate odds ratios (OR) of outcomes between those with and without dementia.
Main results: The average age of those with dementia was 78.8 years vs 64.9 years in those without dementia. Women made up 42.8% of those with dementia and 31.3% of those without dementia. Those with dementia also had higher rates of comorbidities, such as heart failure, renal failure, and depression. After propensity score matching, 17,309 and 17,187 patients with and without dementia, respectively, were included. Covariates were balanced between the 2 groups after matching. For the primary outcome, patients with dementia were more likely to be readmitted at 30 days (HR, 1.11; 95% CI, 1.05-1.18; P < .01) when compared to those without dementia. For other adverse outcomes, delirium was significantly more likely to occur for those with dementia (OR, 4.37; 95% CI, 3.69-5.16; P < .01). Patients with dementia were also more likely to die in hospital (OR, 1.15; 95% CI, 1.01-1.30; P = .03), have cardiac arrest (OR, 1.19; 95% CI, 1.01-1.39; P = .04), receive a blood transfusion (OR, 1.17; 95% CI, 1.00-1.36; P = .05), experience acute kidney injury (OR, 1.30; 95% CI, 1.21-1.39; P < .01), and fall in hospital (OR, 2.51; 95% CI, 2.06-3.07; P < .01). Hospital length of stay was higher for those with dementia, with a mean difference of 1.43 days. For discharge location, patients with dementia were more likely to be sent to a skilled nursing facility (30.1% vs 12.2%) and less likely to be discharged home.
Conclusion: Patients with dementia are more likely to experience adverse events, including delirium, mortality, kidney injury, and falls after PCI, and are more likely to be readmitted to the hospital in 30 days compared to those without dementia.
Study 2 Overview (Gilmore-Bykovskyi et al)
Objective: To examine the association between race and 30-day readmissions in Black and non-Hispanic White Medicare beneficiaries with dementia.
Design: This was a retrospective cohort study that used 100% Medicare fee-for service claims data from all hospitalizations between January 1, 2014, and November 30, 2014, for all enrollees with a dementia diagnosis. The claims data were linked to the patient, hospital stay, and hospital factors. Patients with dementia were identified using a validated algorithm that requires an inpatient, skilled nursing facility, home health, or Part B institutional or noninstitutional claim with a qualifying diagnostic code during a 3-year period. Persons enrolled in a health maintenance organization plan were excluded.
Main outcome measures: The primary outcome examined in this study was 30-day all-cause readmission. Self-reported race and ethnic identity was a baseline covariate. Persons who self-reported Black or non-Hispanic White race were included in the study; other categories of race and ethnicity were excluded because of prior evidence suggesting low accuracy of these categories in Medicare claims data. Other covariates included neighborhood disadvantage, measured using the Area Deprivation Index (ADI), and rurality; hospital-level and hospital stay–level characteristics such as for-profit status and number of annual discharges; and individual demographic characteristics and comorbidities. The ADI is constructed using variables of poverty, education, housing, and employment and is represented as a percentile ranking of level of disadvantage. Unadjusted and adjusted analyses of 30-day hospital readmission were conducted. Models using various levels of adjustment were constructed to examine the contributions of the identified covariates to the estimated association between 30-day readmission and race.
Main results: A total of 1,523,142 index hospital stays among 945,481 beneficiaries were included; 215,815 episodes were among Black beneficiaries and 1,307,327 episodes were among non-Hispanic White beneficiaries. Mean age was 81.5 years, and approximately 61% of beneficiaries were female. Black beneficiaries were younger but had higher rates of dual Medicare/Medicaid eligibility and disability; they were also more likely to reside in disadvantaged neighborhoods. Black beneficiaries had a 30-day readmission rate of 24.1% compared with 18.5% in non-Hispanic White beneficiaries (unadjusted OR, 1.37; 95% CI, 1.35-1.39). The differences in outcomes persisted after adjusting for geographic factors, social factors, hospital characteristics, hospital stay factors, demographics, and comorbidities, suggesting that unmeasured underlying racial disparities not included in this model accounted for the differences. The effects of certain variables, such as neighborhood, differed by race; for example, the protective effect of living in a less disadvantaged neighborhood was observed among White beneficiaries but not Black beneficiaries.
Conclusion: Racial and geographic disparities in 30-day readmission rates were observed among Medicare beneficiaries with dementia. Protective effects associated with neighborhood advantage may confer different levels of benefit for people of different race.
Commentary
Adults living with dementia are at higher risk of adverse outcomes across settings. In the first study, by Park et al, among adults who underwent a cardiac procedure (PCI), those with dementia were more likely to experience adverse events compared to those without dementia. These outcomes include increased rates of 30-day readmissions, delirium, cardiac arrest, and falls. These findings are consistent with other studies that found a similar association among patients who underwent other cardiac procedures, such as transcatheter aortic valve replacement.1 Because dementia is a strong predisposing factor for delirium, it is not surprising that delirium is observed across patients who underwent different procedures or hospitalization episodes.2 Because of the potential hazards for inpatients with dementia, hospitals have developed risk-reduction programs, such as those that promote recognition of dementia, and management strategies that reduce the risk of delirium.3 Delirium prevention may also impact other adverse outcomes, such as falls, discharge to institutional care, and readmissions.
Racial disparities in care outcomes have been documented across settings, including hospital4 and hospice care settings.5 In study 2, by Gilmore-Bykovskyi et al, the findings of higher rates of hospital readmission among Black patients when compared to non-Hispanic White patients were not surprising. The central finding of this study is that even when accounting for various levels of factors, including hospital-level, hospital stay–level, individual (demographics, comorbidities), and neighborhood characteristics (disadvantage), the observed disparity diminished but persisted, suggesting that while these various levels of factors contributed to the observed disparity, other unmeasured factors also contributed. Another key finding is that the effect of the various factors examined in this study may affect different subgroups in different ways, suggesting underlying factors, and thus potential solutions to reduce disparities in care outcomes, could differ among subgroups.
Applications for Clinical Practice and System Implementation
These 2 studies add to the literature on factors that can affect 30-day hospital readmission rates in patients with dementia. These data could allow for more robust discussions of what to anticipate when adults with dementia undergo specific procedures, and also further build the case that improvements in care, such as delirium prevention programs, could offer benefits. The observation about racial and ethnic disparities in care outcomes among patients with dementia highlights the continued need to better understand the drivers of these disparities so that hospital systems and policy makers can consider and test possible solutions. Future studies should further disentangle the relationships among the various levels of factors and observed disparities in outcomes, especially for this vulnerable population of adults living with dementia.
Practice Points
- Clinicians should be aware of the additional risks for poor outcomes that dementia confers.
- Awareness of this increased risk will inform discussions of risks and benefits for older adults considered for procedures.
–William W. Hung, MD, MPH
1. Park DY, Sana MK, Shoura S, et al. Readmission and in-hospital outcomes after transcatheter aortic valve replacement in patients with dementia. Cardiovasc Revasc Med. 2023;46:70-77. doi:10.1016/j.carrev.2022.08.016
2. McNicoll L, Pisani MA, Zhang Y, et al. Delirium in the intensive care unit: occurrence and clinical course in older patients. J Am Geriatr Soc. 2003;51(5):591-598. doi:10.1034/j.1600-0579.2003.00201.x
3. Weldingh NM, Mellingsæter MR, Hegna BW, et al. Impact of a dementia-friendly program on detection and management of patients with cognitive impairment and delirium in acute-care hospital units: a controlled clinical trial design. BMC Geriatr. 2022;22(1):266. doi:10.1186/s12877-022-02949-0
4. Hermosura AH, Noonan CJ, Fyfe-Johnson AL, et al. Hospital disparities between native Hawaiian and other pacific islanders and non-Hispanic whites with Alzheimer’s disease and related dementias. J Aging Health. 2020;32(10):1579-1590. doi:10.1177/0898264320945177
5. Zhang Y, Shao H, Zhang M, Li J. Healthcare utilization and mortality after hospice live discharge among Medicare patients with and without Alzheimer’s disease and related dementias. J Gen Intern Med. 2023 Jan 17. doi:10.1007/s11606-023-08031-8
Study 1 Overview (Park et al)
Objective: To compare rates of adverse events and 30-day readmission among patients with dementia who undergo percutaneous coronary intervention (PCI) with those without dementia.
Design: This cohort study used a national database of hospital readmissions developed by the Agency for Healthcare Research and Quality.
Setting and participants: Data from State Inpatient Databases were used to derive this national readmissions database representing 80% of hospitals from 28 states that contribute data. The study included all individuals aged 18 years and older who were identified to have had a PCI procedure in the years 2017 and 2018. International Classification of Diseases, Tenth Revision (ICD-10) codes were used to identify PCI procedures, including drug-eluting stent placement, bare-metal stent placement, and balloon angioplasty, performed in patients who presented with myocardial infarction and unstable angina and those with stable ischemic heart disease. Patients were stratified into those with or without dementia, also defined using ICD-10 codes. A total of 755,406 index hospitalizations were included; 2.3% of the patients had dementia.
Main outcome measures: The primary study outcome was 30-day all-cause readmission, with the cause classified as cardiovascular or noncardiovascular. Secondary outcome measures examined were delirium, in-hospital mortality, cardiac arrest, blood transfusion, acute kidney injury, fall in hospital, length of hospital stay, and other adverse outcomes. Location at discharge was also examined. Other covariates included in the analysis were age, sex, comorbidities, hospital characteristics, primary payer, and median income. For analysis, a propensity score matching algorithm was applied to match patients with and without dementia. Kaplan-Meier curves were used to examine 30-day readmission rates, and a Cox proportional hazards model was used to calculate hazard ratios (HR) for those with and without dementia. For secondary outcomes, logistic regression models were used to calculate odds ratios (OR) of outcomes between those with and without dementia.
Main results: The average age of those with dementia was 78.8 years vs 64.9 years in those without dementia. Women made up 42.8% of those with dementia and 31.3% of those without dementia. Those with dementia also had higher rates of comorbidities, such as heart failure, renal failure, and depression. After propensity score matching, 17,309 and 17,187 patients with and without dementia, respectively, were included. Covariates were balanced between the 2 groups after matching. For the primary outcome, patients with dementia were more likely to be readmitted at 30 days (HR, 1.11; 95% CI, 1.05-1.18; P < .01) when compared to those without dementia. For other adverse outcomes, delirium was significantly more likely to occur for those with dementia (OR, 4.37; 95% CI, 3.69-5.16; P < .01). Patients with dementia were also more likely to die in hospital (OR, 1.15; 95% CI, 1.01-1.30; P = .03), have cardiac arrest (OR, 1.19; 95% CI, 1.01-1.39; P = .04), receive a blood transfusion (OR, 1.17; 95% CI, 1.00-1.36; P = .05), experience acute kidney injury (OR, 1.30; 95% CI, 1.21-1.39; P < .01), and fall in hospital (OR, 2.51; 95% CI, 2.06-3.07; P < .01). Hospital length of stay was higher for those with dementia, with a mean difference of 1.43 days. For discharge location, patients with dementia were more likely to be sent to a skilled nursing facility (30.1% vs 12.2%) and less likely to be discharged home.
Conclusion: Patients with dementia are more likely to experience adverse events, including delirium, mortality, kidney injury, and falls after PCI, and are more likely to be readmitted to the hospital in 30 days compared to those without dementia.
Study 2 Overview (Gilmore-Bykovskyi et al)
Objective: To examine the association between race and 30-day readmissions in Black and non-Hispanic White Medicare beneficiaries with dementia.
Design: This was a retrospective cohort study that used 100% Medicare fee-for service claims data from all hospitalizations between January 1, 2014, and November 30, 2014, for all enrollees with a dementia diagnosis. The claims data were linked to the patient, hospital stay, and hospital factors. Patients with dementia were identified using a validated algorithm that requires an inpatient, skilled nursing facility, home health, or Part B institutional or noninstitutional claim with a qualifying diagnostic code during a 3-year period. Persons enrolled in a health maintenance organization plan were excluded.
Main outcome measures: The primary outcome examined in this study was 30-day all-cause readmission. Self-reported race and ethnic identity was a baseline covariate. Persons who self-reported Black or non-Hispanic White race were included in the study; other categories of race and ethnicity were excluded because of prior evidence suggesting low accuracy of these categories in Medicare claims data. Other covariates included neighborhood disadvantage, measured using the Area Deprivation Index (ADI), and rurality; hospital-level and hospital stay–level characteristics such as for-profit status and number of annual discharges; and individual demographic characteristics and comorbidities. The ADI is constructed using variables of poverty, education, housing, and employment and is represented as a percentile ranking of level of disadvantage. Unadjusted and adjusted analyses of 30-day hospital readmission were conducted. Models using various levels of adjustment were constructed to examine the contributions of the identified covariates to the estimated association between 30-day readmission and race.
Main results: A total of 1,523,142 index hospital stays among 945,481 beneficiaries were included; 215,815 episodes were among Black beneficiaries and 1,307,327 episodes were among non-Hispanic White beneficiaries. Mean age was 81.5 years, and approximately 61% of beneficiaries were female. Black beneficiaries were younger but had higher rates of dual Medicare/Medicaid eligibility and disability; they were also more likely to reside in disadvantaged neighborhoods. Black beneficiaries had a 30-day readmission rate of 24.1% compared with 18.5% in non-Hispanic White beneficiaries (unadjusted OR, 1.37; 95% CI, 1.35-1.39). The differences in outcomes persisted after adjusting for geographic factors, social factors, hospital characteristics, hospital stay factors, demographics, and comorbidities, suggesting that unmeasured underlying racial disparities not included in this model accounted for the differences. The effects of certain variables, such as neighborhood, differed by race; for example, the protective effect of living in a less disadvantaged neighborhood was observed among White beneficiaries but not Black beneficiaries.
Conclusion: Racial and geographic disparities in 30-day readmission rates were observed among Medicare beneficiaries with dementia. Protective effects associated with neighborhood advantage may confer different levels of benefit for people of different race.
Commentary
Adults living with dementia are at higher risk of adverse outcomes across settings. In the first study, by Park et al, among adults who underwent a cardiac procedure (PCI), those with dementia were more likely to experience adverse events compared to those without dementia. These outcomes include increased rates of 30-day readmissions, delirium, cardiac arrest, and falls. These findings are consistent with other studies that found a similar association among patients who underwent other cardiac procedures, such as transcatheter aortic valve replacement.1 Because dementia is a strong predisposing factor for delirium, it is not surprising that delirium is observed across patients who underwent different procedures or hospitalization episodes.2 Because of the potential hazards for inpatients with dementia, hospitals have developed risk-reduction programs, such as those that promote recognition of dementia, and management strategies that reduce the risk of delirium.3 Delirium prevention may also impact other adverse outcomes, such as falls, discharge to institutional care, and readmissions.
Racial disparities in care outcomes have been documented across settings, including hospital4 and hospice care settings.5 In study 2, by Gilmore-Bykovskyi et al, the findings of higher rates of hospital readmission among Black patients when compared to non-Hispanic White patients were not surprising. The central finding of this study is that even when accounting for various levels of factors, including hospital-level, hospital stay–level, individual (demographics, comorbidities), and neighborhood characteristics (disadvantage), the observed disparity diminished but persisted, suggesting that while these various levels of factors contributed to the observed disparity, other unmeasured factors also contributed. Another key finding is that the effect of the various factors examined in this study may affect different subgroups in different ways, suggesting underlying factors, and thus potential solutions to reduce disparities in care outcomes, could differ among subgroups.
Applications for Clinical Practice and System Implementation
These 2 studies add to the literature on factors that can affect 30-day hospital readmission rates in patients with dementia. These data could allow for more robust discussions of what to anticipate when adults with dementia undergo specific procedures, and also further build the case that improvements in care, such as delirium prevention programs, could offer benefits. The observation about racial and ethnic disparities in care outcomes among patients with dementia highlights the continued need to better understand the drivers of these disparities so that hospital systems and policy makers can consider and test possible solutions. Future studies should further disentangle the relationships among the various levels of factors and observed disparities in outcomes, especially for this vulnerable population of adults living with dementia.
Practice Points
- Clinicians should be aware of the additional risks for poor outcomes that dementia confers.
- Awareness of this increased risk will inform discussions of risks and benefits for older adults considered for procedures.
–William W. Hung, MD, MPH
Study 1 Overview (Park et al)
Objective: To compare rates of adverse events and 30-day readmission among patients with dementia who undergo percutaneous coronary intervention (PCI) with those without dementia.
Design: This cohort study used a national database of hospital readmissions developed by the Agency for Healthcare Research and Quality.
Setting and participants: Data from State Inpatient Databases were used to derive this national readmissions database representing 80% of hospitals from 28 states that contribute data. The study included all individuals aged 18 years and older who were identified to have had a PCI procedure in the years 2017 and 2018. International Classification of Diseases, Tenth Revision (ICD-10) codes were used to identify PCI procedures, including drug-eluting stent placement, bare-metal stent placement, and balloon angioplasty, performed in patients who presented with myocardial infarction and unstable angina and those with stable ischemic heart disease. Patients were stratified into those with or without dementia, also defined using ICD-10 codes. A total of 755,406 index hospitalizations were included; 2.3% of the patients had dementia.
Main outcome measures: The primary study outcome was 30-day all-cause readmission, with the cause classified as cardiovascular or noncardiovascular. Secondary outcome measures examined were delirium, in-hospital mortality, cardiac arrest, blood transfusion, acute kidney injury, fall in hospital, length of hospital stay, and other adverse outcomes. Location at discharge was also examined. Other covariates included in the analysis were age, sex, comorbidities, hospital characteristics, primary payer, and median income. For analysis, a propensity score matching algorithm was applied to match patients with and without dementia. Kaplan-Meier curves were used to examine 30-day readmission rates, and a Cox proportional hazards model was used to calculate hazard ratios (HR) for those with and without dementia. For secondary outcomes, logistic regression models were used to calculate odds ratios (OR) of outcomes between those with and without dementia.
Main results: The average age of those with dementia was 78.8 years vs 64.9 years in those without dementia. Women made up 42.8% of those with dementia and 31.3% of those without dementia. Those with dementia also had higher rates of comorbidities, such as heart failure, renal failure, and depression. After propensity score matching, 17,309 and 17,187 patients with and without dementia, respectively, were included. Covariates were balanced between the 2 groups after matching. For the primary outcome, patients with dementia were more likely to be readmitted at 30 days (HR, 1.11; 95% CI, 1.05-1.18; P < .01) when compared to those without dementia. For other adverse outcomes, delirium was significantly more likely to occur for those with dementia (OR, 4.37; 95% CI, 3.69-5.16; P < .01). Patients with dementia were also more likely to die in hospital (OR, 1.15; 95% CI, 1.01-1.30; P = .03), have cardiac arrest (OR, 1.19; 95% CI, 1.01-1.39; P = .04), receive a blood transfusion (OR, 1.17; 95% CI, 1.00-1.36; P = .05), experience acute kidney injury (OR, 1.30; 95% CI, 1.21-1.39; P < .01), and fall in hospital (OR, 2.51; 95% CI, 2.06-3.07; P < .01). Hospital length of stay was higher for those with dementia, with a mean difference of 1.43 days. For discharge location, patients with dementia were more likely to be sent to a skilled nursing facility (30.1% vs 12.2%) and less likely to be discharged home.
Conclusion: Patients with dementia are more likely to experience adverse events, including delirium, mortality, kidney injury, and falls after PCI, and are more likely to be readmitted to the hospital in 30 days compared to those without dementia.
Study 2 Overview (Gilmore-Bykovskyi et al)
Objective: To examine the association between race and 30-day readmissions in Black and non-Hispanic White Medicare beneficiaries with dementia.
Design: This was a retrospective cohort study that used 100% Medicare fee-for service claims data from all hospitalizations between January 1, 2014, and November 30, 2014, for all enrollees with a dementia diagnosis. The claims data were linked to the patient, hospital stay, and hospital factors. Patients with dementia were identified using a validated algorithm that requires an inpatient, skilled nursing facility, home health, or Part B institutional or noninstitutional claim with a qualifying diagnostic code during a 3-year period. Persons enrolled in a health maintenance organization plan were excluded.
Main outcome measures: The primary outcome examined in this study was 30-day all-cause readmission. Self-reported race and ethnic identity was a baseline covariate. Persons who self-reported Black or non-Hispanic White race were included in the study; other categories of race and ethnicity were excluded because of prior evidence suggesting low accuracy of these categories in Medicare claims data. Other covariates included neighborhood disadvantage, measured using the Area Deprivation Index (ADI), and rurality; hospital-level and hospital stay–level characteristics such as for-profit status and number of annual discharges; and individual demographic characteristics and comorbidities. The ADI is constructed using variables of poverty, education, housing, and employment and is represented as a percentile ranking of level of disadvantage. Unadjusted and adjusted analyses of 30-day hospital readmission were conducted. Models using various levels of adjustment were constructed to examine the contributions of the identified covariates to the estimated association between 30-day readmission and race.
Main results: A total of 1,523,142 index hospital stays among 945,481 beneficiaries were included; 215,815 episodes were among Black beneficiaries and 1,307,327 episodes were among non-Hispanic White beneficiaries. Mean age was 81.5 years, and approximately 61% of beneficiaries were female. Black beneficiaries were younger but had higher rates of dual Medicare/Medicaid eligibility and disability; they were also more likely to reside in disadvantaged neighborhoods. Black beneficiaries had a 30-day readmission rate of 24.1% compared with 18.5% in non-Hispanic White beneficiaries (unadjusted OR, 1.37; 95% CI, 1.35-1.39). The differences in outcomes persisted after adjusting for geographic factors, social factors, hospital characteristics, hospital stay factors, demographics, and comorbidities, suggesting that unmeasured underlying racial disparities not included in this model accounted for the differences. The effects of certain variables, such as neighborhood, differed by race; for example, the protective effect of living in a less disadvantaged neighborhood was observed among White beneficiaries but not Black beneficiaries.
Conclusion: Racial and geographic disparities in 30-day readmission rates were observed among Medicare beneficiaries with dementia. Protective effects associated with neighborhood advantage may confer different levels of benefit for people of different race.
Commentary
Adults living with dementia are at higher risk of adverse outcomes across settings. In the first study, by Park et al, among adults who underwent a cardiac procedure (PCI), those with dementia were more likely to experience adverse events compared to those without dementia. These outcomes include increased rates of 30-day readmissions, delirium, cardiac arrest, and falls. These findings are consistent with other studies that found a similar association among patients who underwent other cardiac procedures, such as transcatheter aortic valve replacement.1 Because dementia is a strong predisposing factor for delirium, it is not surprising that delirium is observed across patients who underwent different procedures or hospitalization episodes.2 Because of the potential hazards for inpatients with dementia, hospitals have developed risk-reduction programs, such as those that promote recognition of dementia, and management strategies that reduce the risk of delirium.3 Delirium prevention may also impact other adverse outcomes, such as falls, discharge to institutional care, and readmissions.
Racial disparities in care outcomes have been documented across settings, including hospital4 and hospice care settings.5 In study 2, by Gilmore-Bykovskyi et al, the findings of higher rates of hospital readmission among Black patients when compared to non-Hispanic White patients were not surprising. The central finding of this study is that even when accounting for various levels of factors, including hospital-level, hospital stay–level, individual (demographics, comorbidities), and neighborhood characteristics (disadvantage), the observed disparity diminished but persisted, suggesting that while these various levels of factors contributed to the observed disparity, other unmeasured factors also contributed. Another key finding is that the effect of the various factors examined in this study may affect different subgroups in different ways, suggesting underlying factors, and thus potential solutions to reduce disparities in care outcomes, could differ among subgroups.
Applications for Clinical Practice and System Implementation
These 2 studies add to the literature on factors that can affect 30-day hospital readmission rates in patients with dementia. These data could allow for more robust discussions of what to anticipate when adults with dementia undergo specific procedures, and also further build the case that improvements in care, such as delirium prevention programs, could offer benefits. The observation about racial and ethnic disparities in care outcomes among patients with dementia highlights the continued need to better understand the drivers of these disparities so that hospital systems and policy makers can consider and test possible solutions. Future studies should further disentangle the relationships among the various levels of factors and observed disparities in outcomes, especially for this vulnerable population of adults living with dementia.
Practice Points
- Clinicians should be aware of the additional risks for poor outcomes that dementia confers.
- Awareness of this increased risk will inform discussions of risks and benefits for older adults considered for procedures.
–William W. Hung, MD, MPH
1. Park DY, Sana MK, Shoura S, et al. Readmission and in-hospital outcomes after transcatheter aortic valve replacement in patients with dementia. Cardiovasc Revasc Med. 2023;46:70-77. doi:10.1016/j.carrev.2022.08.016
2. McNicoll L, Pisani MA, Zhang Y, et al. Delirium in the intensive care unit: occurrence and clinical course in older patients. J Am Geriatr Soc. 2003;51(5):591-598. doi:10.1034/j.1600-0579.2003.00201.x
3. Weldingh NM, Mellingsæter MR, Hegna BW, et al. Impact of a dementia-friendly program on detection and management of patients with cognitive impairment and delirium in acute-care hospital units: a controlled clinical trial design. BMC Geriatr. 2022;22(1):266. doi:10.1186/s12877-022-02949-0
4. Hermosura AH, Noonan CJ, Fyfe-Johnson AL, et al. Hospital disparities between native Hawaiian and other pacific islanders and non-Hispanic whites with Alzheimer’s disease and related dementias. J Aging Health. 2020;32(10):1579-1590. doi:10.1177/0898264320945177
5. Zhang Y, Shao H, Zhang M, Li J. Healthcare utilization and mortality after hospice live discharge among Medicare patients with and without Alzheimer’s disease and related dementias. J Gen Intern Med. 2023 Jan 17. doi:10.1007/s11606-023-08031-8
1. Park DY, Sana MK, Shoura S, et al. Readmission and in-hospital outcomes after transcatheter aortic valve replacement in patients with dementia. Cardiovasc Revasc Med. 2023;46:70-77. doi:10.1016/j.carrev.2022.08.016
2. McNicoll L, Pisani MA, Zhang Y, et al. Delirium in the intensive care unit: occurrence and clinical course in older patients. J Am Geriatr Soc. 2003;51(5):591-598. doi:10.1034/j.1600-0579.2003.00201.x
3. Weldingh NM, Mellingsæter MR, Hegna BW, et al. Impact of a dementia-friendly program on detection and management of patients with cognitive impairment and delirium in acute-care hospital units: a controlled clinical trial design. BMC Geriatr. 2022;22(1):266. doi:10.1186/s12877-022-02949-0
4. Hermosura AH, Noonan CJ, Fyfe-Johnson AL, et al. Hospital disparities between native Hawaiian and other pacific islanders and non-Hispanic whites with Alzheimer’s disease and related dementias. J Aging Health. 2020;32(10):1579-1590. doi:10.1177/0898264320945177
5. Zhang Y, Shao H, Zhang M, Li J. Healthcare utilization and mortality after hospice live discharge among Medicare patients with and without Alzheimer’s disease and related dementias. J Gen Intern Med. 2023 Jan 17. doi:10.1007/s11606-023-08031-8
No expiration date for sex
For health professionals, the thought that our parents and grandparents don’t have sex – or didn’t – might be comforting.
The reality is that, for a significant proportion of our older patients, sex has no use-by date. Humans are sexual beings throughout their lives, yet the culture has concealed that fact.
According to Rome, the purpose of sex is to make children. According to Hollywood, sex is only for the young, the healthy, and the beautiful. For the medical profession, sex consists mainly of risks or dysfunctions.
The results of these biases? Sexuality and intimacy are essential elements for quality of life, with clear physical, emotional, and relational benefits.
Let’s look at the data when researchers dared to ask seniors about their sexuality.
We start with the 2015 U.K. national research on sexuality. The study found a link between age and a decline in various aspects of sexual activity – but not a zeroing-out. For example, among men aged 70-79, 59% reported having had sex in the past year, with 19% having intercourse at least twice a month and 18% masturbating at least that often. Above age 80, those numbers dropped to 39%, 6%, and 5%, respectively. The reason behind the declines? A combination of taboo, fear of disease, use of medications or other interventions that disrupt sexual function or cause disfigurement, and a little bit of age itself.
What about women? Among women ages 70-79, 39% said they’d had sex in the past year, with 6% having intercourse at least twice per month and 5% masturbating two times or more monthly. Above age 80, those numbers were 10%, 4.5%, and 1%, respectively. Driving the falloff in women were the same factors as for men, plus the sad reality that many heterosexual women become widowed because their older male partners die earlier.
The male-female difference also reflects lower levels of testosterone in women. And, because women say they value intimacy more than performance, we have two explanations for their lower frequency of masturbation. After all, a lot of intimacy occurs without either intercourse or masturbation.
Surprising and relevant is the amount of distress – or rather, their relative lack thereof – older patients report because of sexual problems. At age 18-44, 11% of U.S. women indicated sexual distress; at age 45-64, the figure was 15%; and at age 65 and up, 9%.
For clinicians, those figures should prompt us to look more closely at alternative forms of sexual expression – those not involving intercourse or masturbation – in the aged, a field physicians typically do not consider.
Although dyspareunia or erectile problems affect many in long-standing relationships, neither is a reason to abstain from sexual pleasure. Indeed, in many couples, oral sex will replace vaginal intercourse, and if urinary, fecal, or flatal incontinence intrude, couples often waive oral sex in favor of more cuddling, kissing, digital stimulation, and other forms of sexual pleasure.
What about the expiry date for sex?
Fascinating research from Nils Beckman, PhD, and colleagues found that the sex drive persists even as people (and men in particular) reach their 100th year. Dr. Beckman’s group interviewed 269 Swedish seniors, all without dementia, at age 97. Sexual desire was affirmed by 27% of men and 5% of women in the survey. Among the men, 32% said they still had sexual thoughts, compared with 18% of women. Meanwhile, 26% of the men and 15% of the women said they missed sexual activity.
What should clinicians do with this information? First, we could start talking about sex with our older patients. According to the 97-year-old Swedes, most want us to! More than 8 in 10 of both women and men in the survey expressed positive views about questions on sexuality. And please don’t be scared to address the subject in the single senior. They, too, can have a sexual or relationship issue and are happy when we raise the subject. They’re not scared to talk about masturbation, either.
When caring for those with chronic diseases, cancer, in the course of physical rehabilitation, and even in the last phase of life, the clinical experience indicates that our patients are happy when we address sexuality and intimacy. Doing so can open the door to the admission of a problem and a corresponding solution, a lubricant or a PDE5 inhibitor.
But sometimes the solution is the conversation itself: Roughly 25% of patients are sufficiently helped simply by talking about sex. Addressing the importance of sexual pleasure is nearly always valuable.
Here are a few ice-breakers I find helpful:
- Did taking this medication change aspects of sexuality? If so, does that bother you?
- Knowing that continuing intimacy is healthy, do you mind if I address that subject?
- We know that aspects of sexuality and intimacy are healthy. Without a partner, some people become sexually isolated. Would you like to talk about that?’
If addressing sexuality has benefits, what about sex itself?
We are gradually learning more about the many short-, intermediate-, and long-term health benefits of solo and joint sexual activity. Short-term benefits include muscle relaxation, pain relief (even, perhaps ironically, for headaches), and better sleep – all pretty valuable for older adults. Examples of intermediate-term benefits include stress relief and less depression. Research from the United States has found that hugging can reduce the concentrations of proinflammatory cytokines, and kissing positively influences cholesterol levels.
Finally, while the long-term benefits of sex might be less relevant for seniors, they do exist.
Among them are delayed onset of dementia and a substantial reduction in cardiovascular and cerebrovascular problems in men. More sex has been linked to longevity, with men benefiting a bit more than women from going through the entire process, including an orgasm, whereas women appear to gain from having a “satisfying” sex life, which does not always require an orgasm.
Let us not forget that these benefits apply to both patients and clinicians alike. Addressing intimacy and sexuality can ease eventual sexual concerns and potentially create a stronger clinician-patient relationship.
Dr. Gianotten, MD is emeritus senior lecturer in medical sexology, Erasmus University Medical Centre, Rotterdam, the Netherlands. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
For health professionals, the thought that our parents and grandparents don’t have sex – or didn’t – might be comforting.
The reality is that, for a significant proportion of our older patients, sex has no use-by date. Humans are sexual beings throughout their lives, yet the culture has concealed that fact.
According to Rome, the purpose of sex is to make children. According to Hollywood, sex is only for the young, the healthy, and the beautiful. For the medical profession, sex consists mainly of risks or dysfunctions.
The results of these biases? Sexuality and intimacy are essential elements for quality of life, with clear physical, emotional, and relational benefits.
Let’s look at the data when researchers dared to ask seniors about their sexuality.
We start with the 2015 U.K. national research on sexuality. The study found a link between age and a decline in various aspects of sexual activity – but not a zeroing-out. For example, among men aged 70-79, 59% reported having had sex in the past year, with 19% having intercourse at least twice a month and 18% masturbating at least that often. Above age 80, those numbers dropped to 39%, 6%, and 5%, respectively. The reason behind the declines? A combination of taboo, fear of disease, use of medications or other interventions that disrupt sexual function or cause disfigurement, and a little bit of age itself.
What about women? Among women ages 70-79, 39% said they’d had sex in the past year, with 6% having intercourse at least twice per month and 5% masturbating two times or more monthly. Above age 80, those numbers were 10%, 4.5%, and 1%, respectively. Driving the falloff in women were the same factors as for men, plus the sad reality that many heterosexual women become widowed because their older male partners die earlier.
The male-female difference also reflects lower levels of testosterone in women. And, because women say they value intimacy more than performance, we have two explanations for their lower frequency of masturbation. After all, a lot of intimacy occurs without either intercourse or masturbation.
Surprising and relevant is the amount of distress – or rather, their relative lack thereof – older patients report because of sexual problems. At age 18-44, 11% of U.S. women indicated sexual distress; at age 45-64, the figure was 15%; and at age 65 and up, 9%.
For clinicians, those figures should prompt us to look more closely at alternative forms of sexual expression – those not involving intercourse or masturbation – in the aged, a field physicians typically do not consider.
Although dyspareunia or erectile problems affect many in long-standing relationships, neither is a reason to abstain from sexual pleasure. Indeed, in many couples, oral sex will replace vaginal intercourse, and if urinary, fecal, or flatal incontinence intrude, couples often waive oral sex in favor of more cuddling, kissing, digital stimulation, and other forms of sexual pleasure.
What about the expiry date for sex?
Fascinating research from Nils Beckman, PhD, and colleagues found that the sex drive persists even as people (and men in particular) reach their 100th year. Dr. Beckman’s group interviewed 269 Swedish seniors, all without dementia, at age 97. Sexual desire was affirmed by 27% of men and 5% of women in the survey. Among the men, 32% said they still had sexual thoughts, compared with 18% of women. Meanwhile, 26% of the men and 15% of the women said they missed sexual activity.
What should clinicians do with this information? First, we could start talking about sex with our older patients. According to the 97-year-old Swedes, most want us to! More than 8 in 10 of both women and men in the survey expressed positive views about questions on sexuality. And please don’t be scared to address the subject in the single senior. They, too, can have a sexual or relationship issue and are happy when we raise the subject. They’re not scared to talk about masturbation, either.
When caring for those with chronic diseases, cancer, in the course of physical rehabilitation, and even in the last phase of life, the clinical experience indicates that our patients are happy when we address sexuality and intimacy. Doing so can open the door to the admission of a problem and a corresponding solution, a lubricant or a PDE5 inhibitor.
But sometimes the solution is the conversation itself: Roughly 25% of patients are sufficiently helped simply by talking about sex. Addressing the importance of sexual pleasure is nearly always valuable.
Here are a few ice-breakers I find helpful:
- Did taking this medication change aspects of sexuality? If so, does that bother you?
- Knowing that continuing intimacy is healthy, do you mind if I address that subject?
- We know that aspects of sexuality and intimacy are healthy. Without a partner, some people become sexually isolated. Would you like to talk about that?’
If addressing sexuality has benefits, what about sex itself?
We are gradually learning more about the many short-, intermediate-, and long-term health benefits of solo and joint sexual activity. Short-term benefits include muscle relaxation, pain relief (even, perhaps ironically, for headaches), and better sleep – all pretty valuable for older adults. Examples of intermediate-term benefits include stress relief and less depression. Research from the United States has found that hugging can reduce the concentrations of proinflammatory cytokines, and kissing positively influences cholesterol levels.
Finally, while the long-term benefits of sex might be less relevant for seniors, they do exist.
Among them are delayed onset of dementia and a substantial reduction in cardiovascular and cerebrovascular problems in men. More sex has been linked to longevity, with men benefiting a bit more than women from going through the entire process, including an orgasm, whereas women appear to gain from having a “satisfying” sex life, which does not always require an orgasm.
Let us not forget that these benefits apply to both patients and clinicians alike. Addressing intimacy and sexuality can ease eventual sexual concerns and potentially create a stronger clinician-patient relationship.
Dr. Gianotten, MD is emeritus senior lecturer in medical sexology, Erasmus University Medical Centre, Rotterdam, the Netherlands. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
For health professionals, the thought that our parents and grandparents don’t have sex – or didn’t – might be comforting.
The reality is that, for a significant proportion of our older patients, sex has no use-by date. Humans are sexual beings throughout their lives, yet the culture has concealed that fact.
According to Rome, the purpose of sex is to make children. According to Hollywood, sex is only for the young, the healthy, and the beautiful. For the medical profession, sex consists mainly of risks or dysfunctions.
The results of these biases? Sexuality and intimacy are essential elements for quality of life, with clear physical, emotional, and relational benefits.
Let’s look at the data when researchers dared to ask seniors about their sexuality.
We start with the 2015 U.K. national research on sexuality. The study found a link between age and a decline in various aspects of sexual activity – but not a zeroing-out. For example, among men aged 70-79, 59% reported having had sex in the past year, with 19% having intercourse at least twice a month and 18% masturbating at least that often. Above age 80, those numbers dropped to 39%, 6%, and 5%, respectively. The reason behind the declines? A combination of taboo, fear of disease, use of medications or other interventions that disrupt sexual function or cause disfigurement, and a little bit of age itself.
What about women? Among women ages 70-79, 39% said they’d had sex in the past year, with 6% having intercourse at least twice per month and 5% masturbating two times or more monthly. Above age 80, those numbers were 10%, 4.5%, and 1%, respectively. Driving the falloff in women were the same factors as for men, plus the sad reality that many heterosexual women become widowed because their older male partners die earlier.
The male-female difference also reflects lower levels of testosterone in women. And, because women say they value intimacy more than performance, we have two explanations for their lower frequency of masturbation. After all, a lot of intimacy occurs without either intercourse or masturbation.
Surprising and relevant is the amount of distress – or rather, their relative lack thereof – older patients report because of sexual problems. At age 18-44, 11% of U.S. women indicated sexual distress; at age 45-64, the figure was 15%; and at age 65 and up, 9%.
For clinicians, those figures should prompt us to look more closely at alternative forms of sexual expression – those not involving intercourse or masturbation – in the aged, a field physicians typically do not consider.
Although dyspareunia or erectile problems affect many in long-standing relationships, neither is a reason to abstain from sexual pleasure. Indeed, in many couples, oral sex will replace vaginal intercourse, and if urinary, fecal, or flatal incontinence intrude, couples often waive oral sex in favor of more cuddling, kissing, digital stimulation, and other forms of sexual pleasure.
What about the expiry date for sex?
Fascinating research from Nils Beckman, PhD, and colleagues found that the sex drive persists even as people (and men in particular) reach their 100th year. Dr. Beckman’s group interviewed 269 Swedish seniors, all without dementia, at age 97. Sexual desire was affirmed by 27% of men and 5% of women in the survey. Among the men, 32% said they still had sexual thoughts, compared with 18% of women. Meanwhile, 26% of the men and 15% of the women said they missed sexual activity.
What should clinicians do with this information? First, we could start talking about sex with our older patients. According to the 97-year-old Swedes, most want us to! More than 8 in 10 of both women and men in the survey expressed positive views about questions on sexuality. And please don’t be scared to address the subject in the single senior. They, too, can have a sexual or relationship issue and are happy when we raise the subject. They’re not scared to talk about masturbation, either.
When caring for those with chronic diseases, cancer, in the course of physical rehabilitation, and even in the last phase of life, the clinical experience indicates that our patients are happy when we address sexuality and intimacy. Doing so can open the door to the admission of a problem and a corresponding solution, a lubricant or a PDE5 inhibitor.
But sometimes the solution is the conversation itself: Roughly 25% of patients are sufficiently helped simply by talking about sex. Addressing the importance of sexual pleasure is nearly always valuable.
Here are a few ice-breakers I find helpful:
- Did taking this medication change aspects of sexuality? If so, does that bother you?
- Knowing that continuing intimacy is healthy, do you mind if I address that subject?
- We know that aspects of sexuality and intimacy are healthy. Without a partner, some people become sexually isolated. Would you like to talk about that?’
If addressing sexuality has benefits, what about sex itself?
We are gradually learning more about the many short-, intermediate-, and long-term health benefits of solo and joint sexual activity. Short-term benefits include muscle relaxation, pain relief (even, perhaps ironically, for headaches), and better sleep – all pretty valuable for older adults. Examples of intermediate-term benefits include stress relief and less depression. Research from the United States has found that hugging can reduce the concentrations of proinflammatory cytokines, and kissing positively influences cholesterol levels.
Finally, while the long-term benefits of sex might be less relevant for seniors, they do exist.
Among them are delayed onset of dementia and a substantial reduction in cardiovascular and cerebrovascular problems in men. More sex has been linked to longevity, with men benefiting a bit more than women from going through the entire process, including an orgasm, whereas women appear to gain from having a “satisfying” sex life, which does not always require an orgasm.
Let us not forget that these benefits apply to both patients and clinicians alike. Addressing intimacy and sexuality can ease eventual sexual concerns and potentially create a stronger clinician-patient relationship.
Dr. Gianotten, MD is emeritus senior lecturer in medical sexology, Erasmus University Medical Centre, Rotterdam, the Netherlands. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.