User login
Meta-analysis identifies the biologic and small-molecule therapies associated with infection risk in PsA
Key clinical point: The risk for infections in patients with psoriatic arthritis (PsA) did not increase with most biologic and small-molecule therapies, except bimekizumab, apremilast, and 30 mg upadacitinib.
Major finding: In patients with PsA, bimekizumab (relative risk [RR] 14.23; 95% CI 1.97-102.60), apremilast (RR 1.41; 95% CI 1.08-1.83) and 30 mg upadacitinib (RR 1.37; 95% CI 1.05-1.80) led to a significantly higher risk of infections compared to placebo, with 30 mg upadacitinib vs placebo also increasing the risk for serious infections (RR 3.66; 95% CI 1.43-9.38).
Study details: Findings are from a network meta-analysis of 94 randomized controlled trials including 54,369 patients with PsA or psoriasis who were treated with 14 biologics, five small molecules, or placebo.
Disclosures: This study was partly funded by grants from the National Taiwan University Hospital and Chang Gung Memorial Hospital. HY Chiu and YH Huang declared receiving speaking fees or honoraria from, serving as principal investigator for, or having other ties with various sources.
Source: Chiu HY et al. Comparative short-term risks of infection and serious infection in patients receiving biologic and small-molecule therapies for psoriasis and psoriatic arthritis: A systemic review and network meta-analysis of randomized controlled trials. Ther Adv Chronic Dis. 2023;14:20406223231206225. (Oct 27). doi: 10.1177/20406223231206225
Key clinical point: The risk for infections in patients with psoriatic arthritis (PsA) did not increase with most biologic and small-molecule therapies, except bimekizumab, apremilast, and 30 mg upadacitinib.
Major finding: In patients with PsA, bimekizumab (relative risk [RR] 14.23; 95% CI 1.97-102.60), apremilast (RR 1.41; 95% CI 1.08-1.83) and 30 mg upadacitinib (RR 1.37; 95% CI 1.05-1.80) led to a significantly higher risk of infections compared to placebo, with 30 mg upadacitinib vs placebo also increasing the risk for serious infections (RR 3.66; 95% CI 1.43-9.38).
Study details: Findings are from a network meta-analysis of 94 randomized controlled trials including 54,369 patients with PsA or psoriasis who were treated with 14 biologics, five small molecules, or placebo.
Disclosures: This study was partly funded by grants from the National Taiwan University Hospital and Chang Gung Memorial Hospital. HY Chiu and YH Huang declared receiving speaking fees or honoraria from, serving as principal investigator for, or having other ties with various sources.
Source: Chiu HY et al. Comparative short-term risks of infection and serious infection in patients receiving biologic and small-molecule therapies for psoriasis and psoriatic arthritis: A systemic review and network meta-analysis of randomized controlled trials. Ther Adv Chronic Dis. 2023;14:20406223231206225. (Oct 27). doi: 10.1177/20406223231206225
Key clinical point: The risk for infections in patients with psoriatic arthritis (PsA) did not increase with most biologic and small-molecule therapies, except bimekizumab, apremilast, and 30 mg upadacitinib.
Major finding: In patients with PsA, bimekizumab (relative risk [RR] 14.23; 95% CI 1.97-102.60), apremilast (RR 1.41; 95% CI 1.08-1.83) and 30 mg upadacitinib (RR 1.37; 95% CI 1.05-1.80) led to a significantly higher risk of infections compared to placebo, with 30 mg upadacitinib vs placebo also increasing the risk for serious infections (RR 3.66; 95% CI 1.43-9.38).
Study details: Findings are from a network meta-analysis of 94 randomized controlled trials including 54,369 patients with PsA or psoriasis who were treated with 14 biologics, five small molecules, or placebo.
Disclosures: This study was partly funded by grants from the National Taiwan University Hospital and Chang Gung Memorial Hospital. HY Chiu and YH Huang declared receiving speaking fees or honoraria from, serving as principal investigator for, or having other ties with various sources.
Source: Chiu HY et al. Comparative short-term risks of infection and serious infection in patients receiving biologic and small-molecule therapies for psoriasis and psoriatic arthritis: A systemic review and network meta-analysis of randomized controlled trials. Ther Adv Chronic Dis. 2023;14:20406223231206225. (Oct 27). doi: 10.1177/20406223231206225
PsA tied to increased risk of depressive symptoms and functional impairment
Key clinical point: A diagnosis of psoriatic arthritis (PsA) significantly increased the odds of functional impairment and the prevalence of depressive symptoms in patients with psoriatic disease.
Major finding: A diagnosis of PsA was associated with increased odds of functional impairment in everyday life (odds ratio [OR] 9.56, P = .005) and the presence of moderate-to-severe depressive symptoms (OR 2.69, P = .046).
Study details: Findings are from a cross-sectional study including 300 patients with psoriatic disease, of whom 189 patients had PsA.
Disclosures: This study was partly sponsored by Novartis Pharma GmbH, Germany. Some authors declared receiving speaker honoraria, travel grants, or research funding from or having other ties with various sources, including Novartis. The other authors declared no conflicts of interest.
Source: Frede N et al. Psoriasis and psoriatic arthritis have a major impact on quality of life and depressive symptoms: A cross-sectional study of 300 patients. Rheumatol Ther. 2023 (Oct 15). doi: 10.1007/s40744-023-00602-9
Key clinical point: A diagnosis of psoriatic arthritis (PsA) significantly increased the odds of functional impairment and the prevalence of depressive symptoms in patients with psoriatic disease.
Major finding: A diagnosis of PsA was associated with increased odds of functional impairment in everyday life (odds ratio [OR] 9.56, P = .005) and the presence of moderate-to-severe depressive symptoms (OR 2.69, P = .046).
Study details: Findings are from a cross-sectional study including 300 patients with psoriatic disease, of whom 189 patients had PsA.
Disclosures: This study was partly sponsored by Novartis Pharma GmbH, Germany. Some authors declared receiving speaker honoraria, travel grants, or research funding from or having other ties with various sources, including Novartis. The other authors declared no conflicts of interest.
Source: Frede N et al. Psoriasis and psoriatic arthritis have a major impact on quality of life and depressive symptoms: A cross-sectional study of 300 patients. Rheumatol Ther. 2023 (Oct 15). doi: 10.1007/s40744-023-00602-9
Key clinical point: A diagnosis of psoriatic arthritis (PsA) significantly increased the odds of functional impairment and the prevalence of depressive symptoms in patients with psoriatic disease.
Major finding: A diagnosis of PsA was associated with increased odds of functional impairment in everyday life (odds ratio [OR] 9.56, P = .005) and the presence of moderate-to-severe depressive symptoms (OR 2.69, P = .046).
Study details: Findings are from a cross-sectional study including 300 patients with psoriatic disease, of whom 189 patients had PsA.
Disclosures: This study was partly sponsored by Novartis Pharma GmbH, Germany. Some authors declared receiving speaker honoraria, travel grants, or research funding from or having other ties with various sources, including Novartis. The other authors declared no conflicts of interest.
Source: Frede N et al. Psoriasis and psoriatic arthritis have a major impact on quality of life and depressive symptoms: A cross-sectional study of 300 patients. Rheumatol Ther. 2023 (Oct 15). doi: 10.1007/s40744-023-00602-9
Cathepsin K and G levels in serum and synovial fluid hold diagnostic potential in PsA
Key clinical point: Patients with psoriatic arthritis (PsA) had higher levels of cathepsins G and K in the serum and synovial fluid than patients with gonarthrosis or control individuals having no physical findings related to their internal organs, skin, or joints.
Major finding: Cathepsin G and cathepsin K levels in the serum (P < .01) and synovial fluid (P < .02) were significantly higher in the PsA group than in the gonarthrosis or control group. Serum cathepsin G levels > 6 ng/mL and serum cathepsin K levels > 0.86 ng/mL showed 100% diagnostic accuracy in distinguishing patients with PsA from control individuals and patients with gonarthrosis, respectively, whereas synovial fluid cathepsin G levels > 2 ng/mL showed 100% accuracy in distinguishing PsA from gonarthrosis.
Study details: This retrospective case-control study included 156 patients having PsA with synovial effusion, 50 patients with gonarthrosis, and 30 control individuals.
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Popova-Belova SD et al. Serum and synovial levels of cathepsin G and cathepsin K in patients with psoriatic arthritis and their correlation with disease activity indices. Diagnostics (Basel). 2023;13(20):3250 (Oct 19). doi: 10.3390/diagnostics13203250
Key clinical point: Patients with psoriatic arthritis (PsA) had higher levels of cathepsins G and K in the serum and synovial fluid than patients with gonarthrosis or control individuals having no physical findings related to their internal organs, skin, or joints.
Major finding: Cathepsin G and cathepsin K levels in the serum (P < .01) and synovial fluid (P < .02) were significantly higher in the PsA group than in the gonarthrosis or control group. Serum cathepsin G levels > 6 ng/mL and serum cathepsin K levels > 0.86 ng/mL showed 100% diagnostic accuracy in distinguishing patients with PsA from control individuals and patients with gonarthrosis, respectively, whereas synovial fluid cathepsin G levels > 2 ng/mL showed 100% accuracy in distinguishing PsA from gonarthrosis.
Study details: This retrospective case-control study included 156 patients having PsA with synovial effusion, 50 patients with gonarthrosis, and 30 control individuals.
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Popova-Belova SD et al. Serum and synovial levels of cathepsin G and cathepsin K in patients with psoriatic arthritis and their correlation with disease activity indices. Diagnostics (Basel). 2023;13(20):3250 (Oct 19). doi: 10.3390/diagnostics13203250
Key clinical point: Patients with psoriatic arthritis (PsA) had higher levels of cathepsins G and K in the serum and synovial fluid than patients with gonarthrosis or control individuals having no physical findings related to their internal organs, skin, or joints.
Major finding: Cathepsin G and cathepsin K levels in the serum (P < .01) and synovial fluid (P < .02) were significantly higher in the PsA group than in the gonarthrosis or control group. Serum cathepsin G levels > 6 ng/mL and serum cathepsin K levels > 0.86 ng/mL showed 100% diagnostic accuracy in distinguishing patients with PsA from control individuals and patients with gonarthrosis, respectively, whereas synovial fluid cathepsin G levels > 2 ng/mL showed 100% accuracy in distinguishing PsA from gonarthrosis.
Study details: This retrospective case-control study included 156 patients having PsA with synovial effusion, 50 patients with gonarthrosis, and 30 control individuals.
Disclosures: This study did not receive any external funding. The authors declared no conflicts of interest.
Source: Popova-Belova SD et al. Serum and synovial levels of cathepsin G and cathepsin K in patients with psoriatic arthritis and their correlation with disease activity indices. Diagnostics (Basel). 2023;13(20):3250 (Oct 19). doi: 10.3390/diagnostics13203250
Tildrakizumab may check the progression to PsA in psoriatic patients
Key clinical point: Tildrakizumab was able to reduce the occurrence of psoriatic arthritis (PsA) in patients with psoriasis by improving nailfold bleeding (NFB) and capillary enlargement, which are well-known risk factors for the development of PsA.
Major finding: NFB (hazard ratio [HR] 2.92; P = .003) and capillary enlargement (HR 4.61; P < .0001) were recognized as risk factors for PsA development; however, both conditions improved significantly after 1 month of tildrakizumab initiation, with the improvements being sustained up to 13 months (all P < .01). Therefore, tildrakizumab treatment significantly reduced the risk for PsA (HR 0.06; P = .007) in patients with psoriasis.
Study details: Findings are from a prospective cohort study which included 246 patients with psoriasis vulgaris having no prior exposure to systemic treatments and topical treatments for distal interphalangeal joints and nails who received either tildrakizumab (n = 20) or topical agents (n = 226).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Fukasawa T et al. The optimal use of tildrakizumab in the elderly via improvement of Treg function and its preventive effect of psoriatic arthritis. Front Immunol. 2023;14:1286251. (Oct 19) doi: 10.3389/fimmu.2023.1286251
Key clinical point: Tildrakizumab was able to reduce the occurrence of psoriatic arthritis (PsA) in patients with psoriasis by improving nailfold bleeding (NFB) and capillary enlargement, which are well-known risk factors for the development of PsA.
Major finding: NFB (hazard ratio [HR] 2.92; P = .003) and capillary enlargement (HR 4.61; P < .0001) were recognized as risk factors for PsA development; however, both conditions improved significantly after 1 month of tildrakizumab initiation, with the improvements being sustained up to 13 months (all P < .01). Therefore, tildrakizumab treatment significantly reduced the risk for PsA (HR 0.06; P = .007) in patients with psoriasis.
Study details: Findings are from a prospective cohort study which included 246 patients with psoriasis vulgaris having no prior exposure to systemic treatments and topical treatments for distal interphalangeal joints and nails who received either tildrakizumab (n = 20) or topical agents (n = 226).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Fukasawa T et al. The optimal use of tildrakizumab in the elderly via improvement of Treg function and its preventive effect of psoriatic arthritis. Front Immunol. 2023;14:1286251. (Oct 19) doi: 10.3389/fimmu.2023.1286251
Key clinical point: Tildrakizumab was able to reduce the occurrence of psoriatic arthritis (PsA) in patients with psoriasis by improving nailfold bleeding (NFB) and capillary enlargement, which are well-known risk factors for the development of PsA.
Major finding: NFB (hazard ratio [HR] 2.92; P = .003) and capillary enlargement (HR 4.61; P < .0001) were recognized as risk factors for PsA development; however, both conditions improved significantly after 1 month of tildrakizumab initiation, with the improvements being sustained up to 13 months (all P < .01). Therefore, tildrakizumab treatment significantly reduced the risk for PsA (HR 0.06; P = .007) in patients with psoriasis.
Study details: Findings are from a prospective cohort study which included 246 patients with psoriasis vulgaris having no prior exposure to systemic treatments and topical treatments for distal interphalangeal joints and nails who received either tildrakizumab (n = 20) or topical agents (n = 226).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Fukasawa T et al. The optimal use of tildrakizumab in the elderly via improvement of Treg function and its preventive effect of psoriatic arthritis. Front Immunol. 2023;14:1286251. (Oct 19) doi: 10.3389/fimmu.2023.1286251
Ixekizumab improves disease signs and symptoms in patients with severe PsA
Key clinical point: Treatment with ixekizumab for 24 weeks improved disease activity outcomes without causing any new adverse events (AE) in patients with severe peripheral psoriatic arthritis (PsA).
Major finding: At week 24, a significantly higher proportion of patients with severe PsA receiving ixekizumab every 4 weeks and ixekizumab every 2 weeks vs placebo achieved ≥20% improvement in the American College of Rheumatology scores (63.3% and 60.4% vs 24.5%, P ≤ .001). No new AE were reported.
Study details: Findings are from a post hoc analysis of the SPIRIT-P1 trial including 204 patients with severe peripheral PsA who received ixekizumab, adalimumab, or placebo for 24 weeks.
Disclosures: This study was funded by Eli Lilly and Company. Four authors declared being employees or stockholders of Eli Lilly Japan KK, Lilly Deutschland GmbH, or Eli Lilly and Company. The other authors declared ties with various sources, including Eli Lilly.
Source: Kameda H et al. Ixekizumab efficacy in patients with severe peripheral psoriatic arthritis: A post hoc analysis of a phase 3, randomized, double-blind, placebo-controlled study (SPIRIT-P1). Rheumatol Ther. 2023 (Oct 19). doi: 10.1007/s40744-023-00605-6
Key clinical point: Treatment with ixekizumab for 24 weeks improved disease activity outcomes without causing any new adverse events (AE) in patients with severe peripheral psoriatic arthritis (PsA).
Major finding: At week 24, a significantly higher proportion of patients with severe PsA receiving ixekizumab every 4 weeks and ixekizumab every 2 weeks vs placebo achieved ≥20% improvement in the American College of Rheumatology scores (63.3% and 60.4% vs 24.5%, P ≤ .001). No new AE were reported.
Study details: Findings are from a post hoc analysis of the SPIRIT-P1 trial including 204 patients with severe peripheral PsA who received ixekizumab, adalimumab, or placebo for 24 weeks.
Disclosures: This study was funded by Eli Lilly and Company. Four authors declared being employees or stockholders of Eli Lilly Japan KK, Lilly Deutschland GmbH, or Eli Lilly and Company. The other authors declared ties with various sources, including Eli Lilly.
Source: Kameda H et al. Ixekizumab efficacy in patients with severe peripheral psoriatic arthritis: A post hoc analysis of a phase 3, randomized, double-blind, placebo-controlled study (SPIRIT-P1). Rheumatol Ther. 2023 (Oct 19). doi: 10.1007/s40744-023-00605-6
Key clinical point: Treatment with ixekizumab for 24 weeks improved disease activity outcomes without causing any new adverse events (AE) in patients with severe peripheral psoriatic arthritis (PsA).
Major finding: At week 24, a significantly higher proportion of patients with severe PsA receiving ixekizumab every 4 weeks and ixekizumab every 2 weeks vs placebo achieved ≥20% improvement in the American College of Rheumatology scores (63.3% and 60.4% vs 24.5%, P ≤ .001). No new AE were reported.
Study details: Findings are from a post hoc analysis of the SPIRIT-P1 trial including 204 patients with severe peripheral PsA who received ixekizumab, adalimumab, or placebo for 24 weeks.
Disclosures: This study was funded by Eli Lilly and Company. Four authors declared being employees or stockholders of Eli Lilly Japan KK, Lilly Deutschland GmbH, or Eli Lilly and Company. The other authors declared ties with various sources, including Eli Lilly.
Source: Kameda H et al. Ixekizumab efficacy in patients with severe peripheral psoriatic arthritis: A post hoc analysis of a phase 3, randomized, double-blind, placebo-controlled study (SPIRIT-P1). Rheumatol Ther. 2023 (Oct 19). doi: 10.1007/s40744-023-00605-6
Real-world study shows favorable efficacy-safety profile of dual targeted therapy in refractory PsA
Key clinical point: Dual targeted therapy (DTT) combining two biological disease-modifying antirheumatic drugs (bDMARD) or targeted synthetic (ts) DMARD led to satisfactory clinical improvements and no serious adverse events in patients with difficult-to-treat refractory psoriatic arthritis (PsA).
Major finding: At a median exposure of 14.86 months, the DTT retention rate in patients with PsA was 42.8%, with 40.0% and 53.3% of patients achieving remission or low activity and major clinical improvements, respectively. Treatment discontinuation due to adverse events was reported in one patient with PsA and multiple comorbidities.
Study details: Findings are from an observational, retrospective, cross-sectional study including patients with refractory PsA (n = 14) or spondyloarthritis (n = 22) who simultaneously received two bDMARD or tsDMARD with different therapeutic targets.
Disclosures: This study did not receive any funding. R García-Vicuña declared receiving educational grants, research grants, consultancies, speaking fees, or support for attending meetings from various sources.
Source: Valero-Martinez C et al. Dual targeted therapy in patients with psoriatic arthritis and spondyloarthritis: A real-world multicenter experience from Spain. Front Immunol. 2023;14:1283251 (Oct 23). doi: 10.3389/fimmu.2023.1283251
Key clinical point: Dual targeted therapy (DTT) combining two biological disease-modifying antirheumatic drugs (bDMARD) or targeted synthetic (ts) DMARD led to satisfactory clinical improvements and no serious adverse events in patients with difficult-to-treat refractory psoriatic arthritis (PsA).
Major finding: At a median exposure of 14.86 months, the DTT retention rate in patients with PsA was 42.8%, with 40.0% and 53.3% of patients achieving remission or low activity and major clinical improvements, respectively. Treatment discontinuation due to adverse events was reported in one patient with PsA and multiple comorbidities.
Study details: Findings are from an observational, retrospective, cross-sectional study including patients with refractory PsA (n = 14) or spondyloarthritis (n = 22) who simultaneously received two bDMARD or tsDMARD with different therapeutic targets.
Disclosures: This study did not receive any funding. R García-Vicuña declared receiving educational grants, research grants, consultancies, speaking fees, or support for attending meetings from various sources.
Source: Valero-Martinez C et al. Dual targeted therapy in patients with psoriatic arthritis and spondyloarthritis: A real-world multicenter experience from Spain. Front Immunol. 2023;14:1283251 (Oct 23). doi: 10.3389/fimmu.2023.1283251
Key clinical point: Dual targeted therapy (DTT) combining two biological disease-modifying antirheumatic drugs (bDMARD) or targeted synthetic (ts) DMARD led to satisfactory clinical improvements and no serious adverse events in patients with difficult-to-treat refractory psoriatic arthritis (PsA).
Major finding: At a median exposure of 14.86 months, the DTT retention rate in patients with PsA was 42.8%, with 40.0% and 53.3% of patients achieving remission or low activity and major clinical improvements, respectively. Treatment discontinuation due to adverse events was reported in one patient with PsA and multiple comorbidities.
Study details: Findings are from an observational, retrospective, cross-sectional study including patients with refractory PsA (n = 14) or spondyloarthritis (n = 22) who simultaneously received two bDMARD or tsDMARD with different therapeutic targets.
Disclosures: This study did not receive any funding. R García-Vicuña declared receiving educational grants, research grants, consultancies, speaking fees, or support for attending meetings from various sources.
Source: Valero-Martinez C et al. Dual targeted therapy in patients with psoriatic arthritis and spondyloarthritis: A real-world multicenter experience from Spain. Front Immunol. 2023;14:1283251 (Oct 23). doi: 10.3389/fimmu.2023.1283251
Predictors of minimal disease activity achievement in upadacitinib-treated PsA
Key clinical point: This real-world study validated the efficacy of upadacitinib and elucidated the variables influencing the attainment of minimal disease activity (MDA) in response to upadacitinib therapy in patients with psoriatic arthritis (PsA).
Major finding: At week 24, nearly half (47%) of the patients treated with upadacitinib achieved MDA, with males (odds ratio [OR] 2.54; P = .043), patients naive to biologic disease-modifying antirheumatic drugs (OR 4.13; P = .013), and patients with high baseline C-reactive protein levels (OR 2.49; P = .046) having higher odds of achieving MDA.
Study details: Findings are from the preliminary results of the ongoing UPREAL-PsA study including 126 patients with peripheral or axial PsA who received 15 mg upadacitinib once daily.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Luchetti Gentiloni MM et al. Upadacitinib effectiveness and factors associated with minimal disease activity achievement in patients with psoriatic arthritis: Preliminary data of a real-life multicenter study. Arthritis Res Ther. 2023;25:196. (Oct 11). doi: 10.1186/s13075-023-03182-9
Key clinical point: This real-world study validated the efficacy of upadacitinib and elucidated the variables influencing the attainment of minimal disease activity (MDA) in response to upadacitinib therapy in patients with psoriatic arthritis (PsA).
Major finding: At week 24, nearly half (47%) of the patients treated with upadacitinib achieved MDA, with males (odds ratio [OR] 2.54; P = .043), patients naive to biologic disease-modifying antirheumatic drugs (OR 4.13; P = .013), and patients with high baseline C-reactive protein levels (OR 2.49; P = .046) having higher odds of achieving MDA.
Study details: Findings are from the preliminary results of the ongoing UPREAL-PsA study including 126 patients with peripheral or axial PsA who received 15 mg upadacitinib once daily.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Luchetti Gentiloni MM et al. Upadacitinib effectiveness and factors associated with minimal disease activity achievement in patients with psoriatic arthritis: Preliminary data of a real-life multicenter study. Arthritis Res Ther. 2023;25:196. (Oct 11). doi: 10.1186/s13075-023-03182-9
Key clinical point: This real-world study validated the efficacy of upadacitinib and elucidated the variables influencing the attainment of minimal disease activity (MDA) in response to upadacitinib therapy in patients with psoriatic arthritis (PsA).
Major finding: At week 24, nearly half (47%) of the patients treated with upadacitinib achieved MDA, with males (odds ratio [OR] 2.54; P = .043), patients naive to biologic disease-modifying antirheumatic drugs (OR 4.13; P = .013), and patients with high baseline C-reactive protein levels (OR 2.49; P = .046) having higher odds of achieving MDA.
Study details: Findings are from the preliminary results of the ongoing UPREAL-PsA study including 126 patients with peripheral or axial PsA who received 15 mg upadacitinib once daily.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Luchetti Gentiloni MM et al. Upadacitinib effectiveness and factors associated with minimal disease activity achievement in patients with psoriatic arthritis: Preliminary data of a real-life multicenter study. Arthritis Res Ther. 2023;25:196. (Oct 11). doi: 10.1186/s13075-023-03182-9
Apremilast beats placebo in early PsA affecting few joints
SAN DIEGO – Patients with early oligoarticular psoriatic arthritis (PsA) who took apremilast (Otezla) had more than double the response rate of placebo-treated patients by 16 weeks in a double-blind and randomized phase 4 study.
Oligoarticular PsA can significantly affect quality of life even though few joints are affected, and there’s a lack of relevant clinical data to guide treatment, said rheumatologist Philip J. Mease, MD, of the University of Washington and Swedish Medical Center, Seattle, who reported the results in a presentation at the annual meeting of the American College of Rheumatology.
The findings of the study, called FOREMOST, support the use of the drug in mild PsA, Alexis Ogdie, MD, director of the Penn Psoriatic Arthritis Clinic and the Penn Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, said in an interview. Dr. Ogdie, who was not involved with the research, noted that rheumatologists commonly prescribe apremilast for mild PsA, although previous research has focused on severe PsA cases.
By 16 weeks, 33.9% of 203 who received apremilast and 16% of 105 who received placebo (difference, 18.5%; 95% confidence interval, 8.9-28.1; P = .0008) met the trial’s primary outcome, a modified version of minimal disease activity score (MDA-Joints), which required attainment of 1 or fewer swollen and/or tender joints plus three of five additional criteria (psoriasis body surface area of 3% or less, a patient pain visual analog scale assessment of 15 mm or less out of 0-100 mm, a patient global assessment of 20 mm or less out of 0-100 mm, a Health Assessment Questionnaire-Disability Index score of 0.5 or less, and a Leeds Enthesitis Index score of 1 or less). The primary analysis was conducted only in joints affected at baseline.
The researchers recruited patients with 2-4 swollen and/or tender joints out of a total of 66-68 joints assessed; most patients (87%) randomized in the study had 4 or fewer active joints at baseline. The patients had a mean age of 50.9. The mean duration of PsA was 9.9 months, and 39.9% of patients were taking a conventional disease-modifying antirheumatic drug.
In a clinically important outcome, the percentage who had a patient-reported pain response improvement defined as “significant” reached 31.4% with placebo, compared with 48.8% for apremilast (difference, 17.7%; 95% CI, 6.0-29.4; P = .0044), and the percentage who reached a patient-reported pain response defined as “major” totaled 19.1% for placebo vs. 41.3% for apremilast (difference, 22.3%; 95% CI, 11.7-32.9; P = .002).
In an exploratory analysis of all joints, the percentages meeting MDA-Joints criteria for response were 7.9% with placebo and 21.3% with apremilast (difference, 13.6%; 95% CI, 5.9-21.4; P = .0028. Focusing on this exploratory analysis, Dr. Ogdie noted that examination of all joints is “more consistent” with the understanding of disease activity than only looking at the initial joints that had disease activity.
A post-hoc analysis among subjects with 2-4 affected joints found rates similar to the primary endpoint analysis: MDA-Joints response rates were reached by 34.4% of those who took apremilast and by 17.2% of those who took placebo.
When asked about the relatively low response rate for apremilast, Dr. Ogdie said the drug is “a really mild medication, which is why it belongs in the mild disease population. That’s balanced by the fact that it has a pretty good safety profile,” especially compared with the alternative of methotrexate, she said.
Almost all patients can tolerate apremilast, she said, although they may experience nausea or diarrhea. (The study found that adverse events were as expected for apremilast, and the drug was well tolerated.) Blood labs aren’t necessary, she added, as they are in patients taking methotrexate.
As for cost, apremilast is a highly expensive drug, especially when compared to methotrexate, which costs pennies per tablet at some pharmacies. Amgen, the manufacturer of apremilast, lists the price as $4,600 a month. Still, insurers generally cover apremilast, Dr. Ogdie said.
The study was sponsored by Amgen. Dr. Mease reported financial relationships with many pharmaceutical companies, including Amgen. Many other coauthors reported financial relationships with Amgen and other pharmaceutical companies or were employees of Amgen. Dr. Ogdie reported having multiple consulting relationships with pharmaceutical companies, including Amgen, and receiving grant funding from multiple companies as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Psoriasis Foundation, Rheumatology Research Foundation, and Forward Databank.
SAN DIEGO – Patients with early oligoarticular psoriatic arthritis (PsA) who took apremilast (Otezla) had more than double the response rate of placebo-treated patients by 16 weeks in a double-blind and randomized phase 4 study.
Oligoarticular PsA can significantly affect quality of life even though few joints are affected, and there’s a lack of relevant clinical data to guide treatment, said rheumatologist Philip J. Mease, MD, of the University of Washington and Swedish Medical Center, Seattle, who reported the results in a presentation at the annual meeting of the American College of Rheumatology.
The findings of the study, called FOREMOST, support the use of the drug in mild PsA, Alexis Ogdie, MD, director of the Penn Psoriatic Arthritis Clinic and the Penn Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, said in an interview. Dr. Ogdie, who was not involved with the research, noted that rheumatologists commonly prescribe apremilast for mild PsA, although previous research has focused on severe PsA cases.
By 16 weeks, 33.9% of 203 who received apremilast and 16% of 105 who received placebo (difference, 18.5%; 95% confidence interval, 8.9-28.1; P = .0008) met the trial’s primary outcome, a modified version of minimal disease activity score (MDA-Joints), which required attainment of 1 or fewer swollen and/or tender joints plus three of five additional criteria (psoriasis body surface area of 3% or less, a patient pain visual analog scale assessment of 15 mm or less out of 0-100 mm, a patient global assessment of 20 mm or less out of 0-100 mm, a Health Assessment Questionnaire-Disability Index score of 0.5 or less, and a Leeds Enthesitis Index score of 1 or less). The primary analysis was conducted only in joints affected at baseline.
The researchers recruited patients with 2-4 swollen and/or tender joints out of a total of 66-68 joints assessed; most patients (87%) randomized in the study had 4 or fewer active joints at baseline. The patients had a mean age of 50.9. The mean duration of PsA was 9.9 months, and 39.9% of patients were taking a conventional disease-modifying antirheumatic drug.
In a clinically important outcome, the percentage who had a patient-reported pain response improvement defined as “significant” reached 31.4% with placebo, compared with 48.8% for apremilast (difference, 17.7%; 95% CI, 6.0-29.4; P = .0044), and the percentage who reached a patient-reported pain response defined as “major” totaled 19.1% for placebo vs. 41.3% for apremilast (difference, 22.3%; 95% CI, 11.7-32.9; P = .002).
In an exploratory analysis of all joints, the percentages meeting MDA-Joints criteria for response were 7.9% with placebo and 21.3% with apremilast (difference, 13.6%; 95% CI, 5.9-21.4; P = .0028. Focusing on this exploratory analysis, Dr. Ogdie noted that examination of all joints is “more consistent” with the understanding of disease activity than only looking at the initial joints that had disease activity.
A post-hoc analysis among subjects with 2-4 affected joints found rates similar to the primary endpoint analysis: MDA-Joints response rates were reached by 34.4% of those who took apremilast and by 17.2% of those who took placebo.
When asked about the relatively low response rate for apremilast, Dr. Ogdie said the drug is “a really mild medication, which is why it belongs in the mild disease population. That’s balanced by the fact that it has a pretty good safety profile,” especially compared with the alternative of methotrexate, she said.
Almost all patients can tolerate apremilast, she said, although they may experience nausea or diarrhea. (The study found that adverse events were as expected for apremilast, and the drug was well tolerated.) Blood labs aren’t necessary, she added, as they are in patients taking methotrexate.
As for cost, apremilast is a highly expensive drug, especially when compared to methotrexate, which costs pennies per tablet at some pharmacies. Amgen, the manufacturer of apremilast, lists the price as $4,600 a month. Still, insurers generally cover apremilast, Dr. Ogdie said.
The study was sponsored by Amgen. Dr. Mease reported financial relationships with many pharmaceutical companies, including Amgen. Many other coauthors reported financial relationships with Amgen and other pharmaceutical companies or were employees of Amgen. Dr. Ogdie reported having multiple consulting relationships with pharmaceutical companies, including Amgen, and receiving grant funding from multiple companies as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Psoriasis Foundation, Rheumatology Research Foundation, and Forward Databank.
SAN DIEGO – Patients with early oligoarticular psoriatic arthritis (PsA) who took apremilast (Otezla) had more than double the response rate of placebo-treated patients by 16 weeks in a double-blind and randomized phase 4 study.
Oligoarticular PsA can significantly affect quality of life even though few joints are affected, and there’s a lack of relevant clinical data to guide treatment, said rheumatologist Philip J. Mease, MD, of the University of Washington and Swedish Medical Center, Seattle, who reported the results in a presentation at the annual meeting of the American College of Rheumatology.
The findings of the study, called FOREMOST, support the use of the drug in mild PsA, Alexis Ogdie, MD, director of the Penn Psoriatic Arthritis Clinic and the Penn Center for Clinical Epidemiology and Biostatistics at the University of Pennsylvania, Philadelphia, said in an interview. Dr. Ogdie, who was not involved with the research, noted that rheumatologists commonly prescribe apremilast for mild PsA, although previous research has focused on severe PsA cases.
By 16 weeks, 33.9% of 203 who received apremilast and 16% of 105 who received placebo (difference, 18.5%; 95% confidence interval, 8.9-28.1; P = .0008) met the trial’s primary outcome, a modified version of minimal disease activity score (MDA-Joints), which required attainment of 1 or fewer swollen and/or tender joints plus three of five additional criteria (psoriasis body surface area of 3% or less, a patient pain visual analog scale assessment of 15 mm or less out of 0-100 mm, a patient global assessment of 20 mm or less out of 0-100 mm, a Health Assessment Questionnaire-Disability Index score of 0.5 or less, and a Leeds Enthesitis Index score of 1 or less). The primary analysis was conducted only in joints affected at baseline.
The researchers recruited patients with 2-4 swollen and/or tender joints out of a total of 66-68 joints assessed; most patients (87%) randomized in the study had 4 or fewer active joints at baseline. The patients had a mean age of 50.9. The mean duration of PsA was 9.9 months, and 39.9% of patients were taking a conventional disease-modifying antirheumatic drug.
In a clinically important outcome, the percentage who had a patient-reported pain response improvement defined as “significant” reached 31.4% with placebo, compared with 48.8% for apremilast (difference, 17.7%; 95% CI, 6.0-29.4; P = .0044), and the percentage who reached a patient-reported pain response defined as “major” totaled 19.1% for placebo vs. 41.3% for apremilast (difference, 22.3%; 95% CI, 11.7-32.9; P = .002).
In an exploratory analysis of all joints, the percentages meeting MDA-Joints criteria for response were 7.9% with placebo and 21.3% with apremilast (difference, 13.6%; 95% CI, 5.9-21.4; P = .0028. Focusing on this exploratory analysis, Dr. Ogdie noted that examination of all joints is “more consistent” with the understanding of disease activity than only looking at the initial joints that had disease activity.
A post-hoc analysis among subjects with 2-4 affected joints found rates similar to the primary endpoint analysis: MDA-Joints response rates were reached by 34.4% of those who took apremilast and by 17.2% of those who took placebo.
When asked about the relatively low response rate for apremilast, Dr. Ogdie said the drug is “a really mild medication, which is why it belongs in the mild disease population. That’s balanced by the fact that it has a pretty good safety profile,” especially compared with the alternative of methotrexate, she said.
Almost all patients can tolerate apremilast, she said, although they may experience nausea or diarrhea. (The study found that adverse events were as expected for apremilast, and the drug was well tolerated.) Blood labs aren’t necessary, she added, as they are in patients taking methotrexate.
As for cost, apremilast is a highly expensive drug, especially when compared to methotrexate, which costs pennies per tablet at some pharmacies. Amgen, the manufacturer of apremilast, lists the price as $4,600 a month. Still, insurers generally cover apremilast, Dr. Ogdie said.
The study was sponsored by Amgen. Dr. Mease reported financial relationships with many pharmaceutical companies, including Amgen. Many other coauthors reported financial relationships with Amgen and other pharmaceutical companies or were employees of Amgen. Dr. Ogdie reported having multiple consulting relationships with pharmaceutical companies, including Amgen, and receiving grant funding from multiple companies as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Psoriasis Foundation, Rheumatology Research Foundation, and Forward Databank.
AT ACR 2023
TNF blockers not associated with poorer pregnancy outcomes
SAN DIEGO – Continuing a tumor necrosis factor inhibitor (TNFi) during pregnancy does not increase risk of worse fetal or obstetric outcomes, according to new research presented at the annual meeting of the American College of Rheumatology.
Patients who continued a TNFi also had fewer severe infections requiring hospitalization, compared with those who stopped taking the medication during their pregnancy.
“The main message is that patients continuing were not doing worse than the patients stopping. It’s an important clinical message for rheumatologists who are not really confident in dealing with these drugs during pregnancy,” said Anna Moltó, MD, PhD, a rheumatologist at Cochin Hospital, Paris, who led the research. “It adds to the data that it seems to be safe,” she added in an interview.
Previous research, largely from pregnant patients with inflammatory bowel disease, suggests that taking a TNFi during pregnancy is safe, and 2020 ACR guidelines conditionally recommend continuing therapy prior to and during pregnancy; however, many people still stop taking the drugs during pregnancy for fear of potentially harming the fetus.
To better understand how TNFi use affected pregnancy outcomes, Dr. Moltó and colleagues analyzed data from a French nationwide health insurance database to identify adult women with chronic rheumatic inflammatory disease. All women included in the cohort had a singleton pregnancy between 2008 and 2017 and were taking a TNFi upon pregnancy diagnosis.
Patients who restarted TNFi after initially pausing because of pregnancy were included in the continuation group.
Researchers identified more than 2,000 pregnancies, including 1,503 in individuals with spondyloarthritis and 579 individuals with rheumatoid arthritis. Patients were, on average, 31 years old and were diagnosed with a rheumatic disease 4 years prior to their pregnancy.
About 72% (n = 1,497) discontinued TNFi after learning they were pregnant, and 584 individuals continued treatment. Dr. Moltó noted that data from more recent years might have captured lower discontinuation rates among pregnant individuals, but those data were not available for the study.
There was no difference in unfavorable obstetrical or infant outcomes, including spontaneous abortion, preeclampsia, gestational diabetes, major congenital malformation, and severe infection of the infant requiring hospitalization. Somewhat surprisingly, the data showed that women who discontinued a TNFi were more likely to be hospitalized for infection either during their pregnancy or up to 6 weeks after delivery, compared with those who continued therapy (1.3% vs. 0.2%, respectively).
Dr. Moltó is currently looking into what could be behind this counterintuitive result, but she hypothesizes that patients who had stopped TNFi may have been taking more glucocorticoids.
“At our institution, there is generally a comfort level with continuing TNF inhibitors during pregnancy, at least until about 36 weeks,” said Sara K. Tedeschi, MD, MPH, a rheumatologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, both in Boston. Sometimes, there is concern for risk of infection to the infant, depending on the type of TNFi being used, she added during a press conference.
“I think that these are really informative and supportive data to let women know that they probably have a really good chance of doing very well during the pregnancy if they continue” their TNFi, said Dr. Tedeschi, who was not involved with the study.
TNF discontinuation on the decline
In a related study, researchers at McGill University, Montreal, found that TNFi discontinuation prior to pregnancy had decreased over time in individuals with chronic inflammatory diseases.
Using a database of U.S. insurance claims, they identified 3,372 women with RA, ankylosing spondylitis (AS), psoriasis/psoriatic arthritis (PsA), and/or inflammatory bowel disease (IBD) who previously used a TNFi and gave birth between 2011 and 2019. A patient was considered to have used a TNFi if she had filled a prescription or had an infusion procedure insurance claim within 12 weeks before the gestational period or anytime during pregnancy. Researchers did not have time-specific data to account for women who stopped treatment at pregnancy diagnosis.
Nearly half (47%) of all identified pregnancies were in individuals with IBD, and the rest included patients with RA (24%), psoriasis or PsA (16%), AS (3%), or more than one diagnosis (10%).
In total, 14% of women discontinued TNFi use in the 12 weeks before becoming pregnant and did not restart. From 2011 to 2013, 19% of patients stopped their TNFi, but this proportion decreased overtime, with 10% of patients stopping therapy from 2017 to 2019 (P < .0001).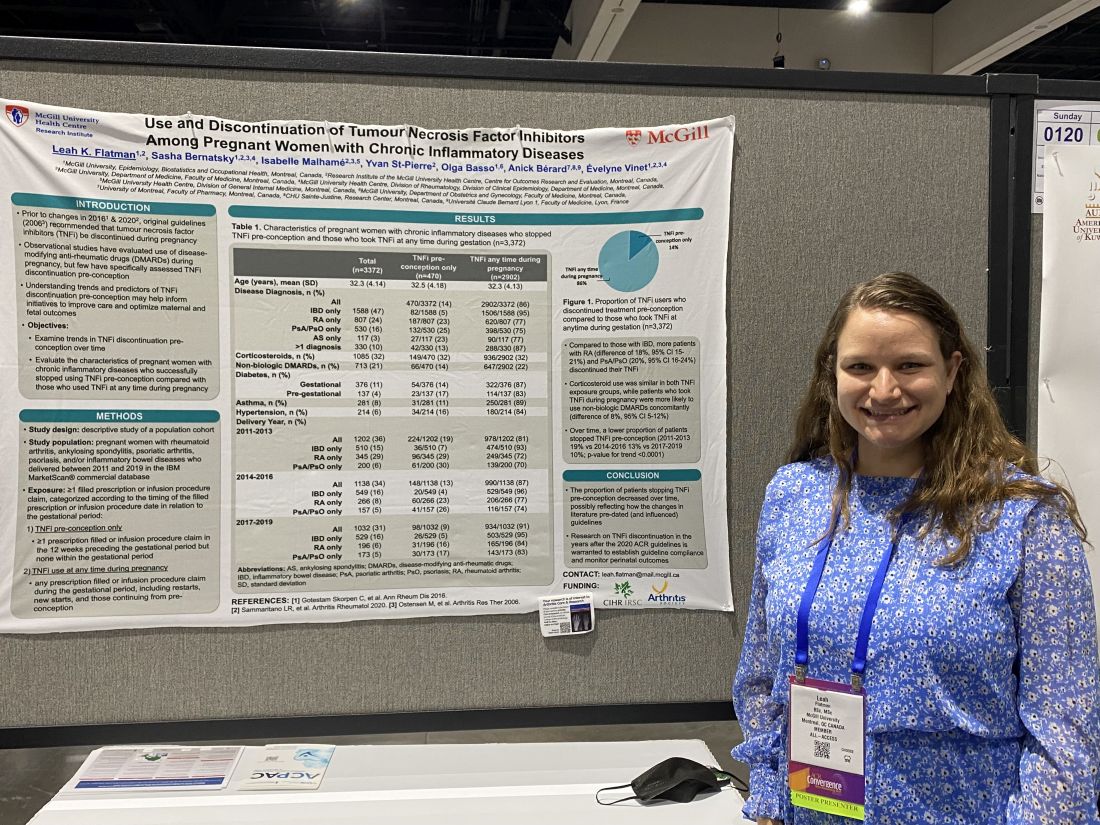
This decline “possibly reflects the increase in real-world evidence about the safety of TNFi in pregnancy. That research, in turn, led to new guidelines recommending the continuation of TNFi during pregnancy,” first author Leah Flatman, a PhD candidate in epidemiology at McGill, said in an interview. “I think we can see this potentially as good news.”
More patients with RA, psoriasis/PsA, and AS discontinued TNFi therapy prior to conception (23%-25%), compared with those with IBD (5%).
Ms. Flatman noted that her study and Moltó’s study complement each other by providing data on individuals stopping TNFi prior to conception versus those stopping treatment after pregnancy diagnosis.
“These findings demonstrate that continuing TNFi during pregnancy appears not to be associated with an increase in adverse obstetrical or infant outcomes,” Ms. Flatman said of Dr. Moltó’s study. “As guidelines currently recommend continuing TNFi, studies like this help demonstrate that the guideline changes do not appear to be associated with an increase in adverse events.”
Dr. Moltó and Ms. Flatman disclosed no relevant financial relationships. Dr. Tedeschi has worked as a consultant for Novartis.
A version of this article appeared on Medscape.com.
SAN DIEGO – Continuing a tumor necrosis factor inhibitor (TNFi) during pregnancy does not increase risk of worse fetal or obstetric outcomes, according to new research presented at the annual meeting of the American College of Rheumatology.
Patients who continued a TNFi also had fewer severe infections requiring hospitalization, compared with those who stopped taking the medication during their pregnancy.
“The main message is that patients continuing were not doing worse than the patients stopping. It’s an important clinical message for rheumatologists who are not really confident in dealing with these drugs during pregnancy,” said Anna Moltó, MD, PhD, a rheumatologist at Cochin Hospital, Paris, who led the research. “It adds to the data that it seems to be safe,” she added in an interview.
Previous research, largely from pregnant patients with inflammatory bowel disease, suggests that taking a TNFi during pregnancy is safe, and 2020 ACR guidelines conditionally recommend continuing therapy prior to and during pregnancy; however, many people still stop taking the drugs during pregnancy for fear of potentially harming the fetus.
To better understand how TNFi use affected pregnancy outcomes, Dr. Moltó and colleagues analyzed data from a French nationwide health insurance database to identify adult women with chronic rheumatic inflammatory disease. All women included in the cohort had a singleton pregnancy between 2008 and 2017 and were taking a TNFi upon pregnancy diagnosis.
Patients who restarted TNFi after initially pausing because of pregnancy were included in the continuation group.
Researchers identified more than 2,000 pregnancies, including 1,503 in individuals with spondyloarthritis and 579 individuals with rheumatoid arthritis. Patients were, on average, 31 years old and were diagnosed with a rheumatic disease 4 years prior to their pregnancy.
About 72% (n = 1,497) discontinued TNFi after learning they were pregnant, and 584 individuals continued treatment. Dr. Moltó noted that data from more recent years might have captured lower discontinuation rates among pregnant individuals, but those data were not available for the study.
There was no difference in unfavorable obstetrical or infant outcomes, including spontaneous abortion, preeclampsia, gestational diabetes, major congenital malformation, and severe infection of the infant requiring hospitalization. Somewhat surprisingly, the data showed that women who discontinued a TNFi were more likely to be hospitalized for infection either during their pregnancy or up to 6 weeks after delivery, compared with those who continued therapy (1.3% vs. 0.2%, respectively).
Dr. Moltó is currently looking into what could be behind this counterintuitive result, but she hypothesizes that patients who had stopped TNFi may have been taking more glucocorticoids.
“At our institution, there is generally a comfort level with continuing TNF inhibitors during pregnancy, at least until about 36 weeks,” said Sara K. Tedeschi, MD, MPH, a rheumatologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, both in Boston. Sometimes, there is concern for risk of infection to the infant, depending on the type of TNFi being used, she added during a press conference.
“I think that these are really informative and supportive data to let women know that they probably have a really good chance of doing very well during the pregnancy if they continue” their TNFi, said Dr. Tedeschi, who was not involved with the study.
TNF discontinuation on the decline
In a related study, researchers at McGill University, Montreal, found that TNFi discontinuation prior to pregnancy had decreased over time in individuals with chronic inflammatory diseases.
Using a database of U.S. insurance claims, they identified 3,372 women with RA, ankylosing spondylitis (AS), psoriasis/psoriatic arthritis (PsA), and/or inflammatory bowel disease (IBD) who previously used a TNFi and gave birth between 2011 and 2019. A patient was considered to have used a TNFi if she had filled a prescription or had an infusion procedure insurance claim within 12 weeks before the gestational period or anytime during pregnancy. Researchers did not have time-specific data to account for women who stopped treatment at pregnancy diagnosis.
Nearly half (47%) of all identified pregnancies were in individuals with IBD, and the rest included patients with RA (24%), psoriasis or PsA (16%), AS (3%), or more than one diagnosis (10%).
In total, 14% of women discontinued TNFi use in the 12 weeks before becoming pregnant and did not restart. From 2011 to 2013, 19% of patients stopped their TNFi, but this proportion decreased overtime, with 10% of patients stopping therapy from 2017 to 2019 (P < .0001).
This decline “possibly reflects the increase in real-world evidence about the safety of TNFi in pregnancy. That research, in turn, led to new guidelines recommending the continuation of TNFi during pregnancy,” first author Leah Flatman, a PhD candidate in epidemiology at McGill, said in an interview. “I think we can see this potentially as good news.”
More patients with RA, psoriasis/PsA, and AS discontinued TNFi therapy prior to conception (23%-25%), compared with those with IBD (5%).
Ms. Flatman noted that her study and Moltó’s study complement each other by providing data on individuals stopping TNFi prior to conception versus those stopping treatment after pregnancy diagnosis.
“These findings demonstrate that continuing TNFi during pregnancy appears not to be associated with an increase in adverse obstetrical or infant outcomes,” Ms. Flatman said of Dr. Moltó’s study. “As guidelines currently recommend continuing TNFi, studies like this help demonstrate that the guideline changes do not appear to be associated with an increase in adverse events.”
Dr. Moltó and Ms. Flatman disclosed no relevant financial relationships. Dr. Tedeschi has worked as a consultant for Novartis.
A version of this article appeared on Medscape.com.
SAN DIEGO – Continuing a tumor necrosis factor inhibitor (TNFi) during pregnancy does not increase risk of worse fetal or obstetric outcomes, according to new research presented at the annual meeting of the American College of Rheumatology.
Patients who continued a TNFi also had fewer severe infections requiring hospitalization, compared with those who stopped taking the medication during their pregnancy.
“The main message is that patients continuing were not doing worse than the patients stopping. It’s an important clinical message for rheumatologists who are not really confident in dealing with these drugs during pregnancy,” said Anna Moltó, MD, PhD, a rheumatologist at Cochin Hospital, Paris, who led the research. “It adds to the data that it seems to be safe,” she added in an interview.
Previous research, largely from pregnant patients with inflammatory bowel disease, suggests that taking a TNFi during pregnancy is safe, and 2020 ACR guidelines conditionally recommend continuing therapy prior to and during pregnancy; however, many people still stop taking the drugs during pregnancy for fear of potentially harming the fetus.
To better understand how TNFi use affected pregnancy outcomes, Dr. Moltó and colleagues analyzed data from a French nationwide health insurance database to identify adult women with chronic rheumatic inflammatory disease. All women included in the cohort had a singleton pregnancy between 2008 and 2017 and were taking a TNFi upon pregnancy diagnosis.
Patients who restarted TNFi after initially pausing because of pregnancy were included in the continuation group.
Researchers identified more than 2,000 pregnancies, including 1,503 in individuals with spondyloarthritis and 579 individuals with rheumatoid arthritis. Patients were, on average, 31 years old and were diagnosed with a rheumatic disease 4 years prior to their pregnancy.
About 72% (n = 1,497) discontinued TNFi after learning they were pregnant, and 584 individuals continued treatment. Dr. Moltó noted that data from more recent years might have captured lower discontinuation rates among pregnant individuals, but those data were not available for the study.
There was no difference in unfavorable obstetrical or infant outcomes, including spontaneous abortion, preeclampsia, gestational diabetes, major congenital malformation, and severe infection of the infant requiring hospitalization. Somewhat surprisingly, the data showed that women who discontinued a TNFi were more likely to be hospitalized for infection either during their pregnancy or up to 6 weeks after delivery, compared with those who continued therapy (1.3% vs. 0.2%, respectively).
Dr. Moltó is currently looking into what could be behind this counterintuitive result, but she hypothesizes that patients who had stopped TNFi may have been taking more glucocorticoids.
“At our institution, there is generally a comfort level with continuing TNF inhibitors during pregnancy, at least until about 36 weeks,” said Sara K. Tedeschi, MD, MPH, a rheumatologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, both in Boston. Sometimes, there is concern for risk of infection to the infant, depending on the type of TNFi being used, she added during a press conference.
“I think that these are really informative and supportive data to let women know that they probably have a really good chance of doing very well during the pregnancy if they continue” their TNFi, said Dr. Tedeschi, who was not involved with the study.
TNF discontinuation on the decline
In a related study, researchers at McGill University, Montreal, found that TNFi discontinuation prior to pregnancy had decreased over time in individuals with chronic inflammatory diseases.
Using a database of U.S. insurance claims, they identified 3,372 women with RA, ankylosing spondylitis (AS), psoriasis/psoriatic arthritis (PsA), and/or inflammatory bowel disease (IBD) who previously used a TNFi and gave birth between 2011 and 2019. A patient was considered to have used a TNFi if she had filled a prescription or had an infusion procedure insurance claim within 12 weeks before the gestational period or anytime during pregnancy. Researchers did not have time-specific data to account for women who stopped treatment at pregnancy diagnosis.
Nearly half (47%) of all identified pregnancies were in individuals with IBD, and the rest included patients with RA (24%), psoriasis or PsA (16%), AS (3%), or more than one diagnosis (10%).
In total, 14% of women discontinued TNFi use in the 12 weeks before becoming pregnant and did not restart. From 2011 to 2013, 19% of patients stopped their TNFi, but this proportion decreased overtime, with 10% of patients stopping therapy from 2017 to 2019 (P < .0001).
This decline “possibly reflects the increase in real-world evidence about the safety of TNFi in pregnancy. That research, in turn, led to new guidelines recommending the continuation of TNFi during pregnancy,” first author Leah Flatman, a PhD candidate in epidemiology at McGill, said in an interview. “I think we can see this potentially as good news.”
More patients with RA, psoriasis/PsA, and AS discontinued TNFi therapy prior to conception (23%-25%), compared with those with IBD (5%).
Ms. Flatman noted that her study and Moltó’s study complement each other by providing data on individuals stopping TNFi prior to conception versus those stopping treatment after pregnancy diagnosis.
“These findings demonstrate that continuing TNFi during pregnancy appears not to be associated with an increase in adverse obstetrical or infant outcomes,” Ms. Flatman said of Dr. Moltó’s study. “As guidelines currently recommend continuing TNFi, studies like this help demonstrate that the guideline changes do not appear to be associated with an increase in adverse events.”
Dr. Moltó and Ms. Flatman disclosed no relevant financial relationships. Dr. Tedeschi has worked as a consultant for Novartis.
A version of this article appeared on Medscape.com.
AT ACR 2023
The challenges of palmoplantar pustulosis and other acral psoriatic disease
WASHINGTON – The approval last year of the interleukin (IL)-36 receptor antagonist spesolimab for treating generalized pustular psoriasis flares brightened the treatment landscape for this rare condition, and a recently published phase 2 study suggests a potential role of spesolimab for flare prevention. , according to speakers at the annual research symposium of the National Psoriasis Foundation.
“The IL-36 receptor antagonists don’t seem to be quite the answer for [palmoplantar pustulosis] that they are for generalized pustular psoriasis [GPP],” Megan H. Noe, MD, MPH, assistant professor of dermatology at Harvard Medical School and a dermatologist at Brigham and Women’s Hospital, Boston, said at the meeting.
Psoriasis affecting the hands and feet – both pustular and nonpustular – has a higher impact on quality of life and higher functional disability than does non-acral psoriasis, is less responsive to treatment, and has a “very confusing nomenclature” that complicates research and thus management, said Jason Ezra Hawkes, MD, a dermatologist in Rocklin, Calif., and former faculty member of several departments of dermatology. Both he and Dr. Noe spoke during a tough-to-treat session at the NPF meeting.
IL-17 and IL-23 blockade, as well as tumor necrosis factor (TNF) inhibition, are effective overall for palmoplantar psoriasis (nonpustular), but in general, responses are lower than for plaque psoriasis. Apremilast (Otezla), a phosphodiesterase-4 inhibitor, has some efficacy for pustular variants, but for hyperkeratotic variants it “does not perform as well as more selective inhibition of IL-17 and IL-23 blockade,” he said.

In general, ”what’s happening in the acral sites is different from an immune perspective than what’s happening in the non-acral sites,” and more research utilizing a clearer, descriptive nomenclature is needed to tease out differing immunophenotypes, explained Dr. Hawkes, who has led multiple clinical trials of treatments for psoriasis and other inflammatory skin conditions.
Palmoplantar pustulosis, and a word on generalized disease
Dermatologists are using a variety of treatments for palmoplantar pustulosis, with no clear first-line choices, Dr. Noe said. In a case series of almost 200 patients with palmoplantar pustulosis across 20 dermatology practices, published in JAMA Dermatology, 35% of patients received a systemic therapy prescription at their initial encounter – most commonly acitretin, followed by methotrexate and phototherapy. “Biologics were used, but use was varied and not as often as with oral agents,” said Dr. Noe, a coauthor of the study.
TNF blockers led to improvements ranging from 57% to 84%, depending on the agent, in a 2020 retrospective study of patients with palmoplantar pustulosis or acrodermatitis continua of Hallopeau, Dr. Noe noted. However, rates of complete clearance were only 20%-29%.
Apremilast showed modest efficacy after 5 months of treatment, with 62% of patients achieving at least a 50% improvement in the Palmoplantar Pustulosis Psoriasis Area and Severity Index (PPPASI) in a 2021 open-label, phase 2 study involving 21 patients. “This may represent a potential treatment option,” Dr. Noe said. “It’s something, but not what we’re used to seeing in our plaque psoriasis patients.”
A 2021 phase 2a, double-blind, randomized, placebo-controlled study of spesolimab in patients with palmoplantar pustulosis, meanwhile, failed to meet its primary endpoint, with only 32% of patients achieving a 50% improvement at 16 weeks, compared with 24% of patients in the placebo arm. And a recently published network meta-analysis found that none of the five drugs studied in seven randomized controlled trials – biologic or oral – was more effective than placebo for clearance or improvement of palmoplantar pustulosis.
The spesolimab (Spevigo) results have been disappointing considering the biologic’s newfound efficacy and role as the first Food and Drug Administration–approved therapy for generalized pustular disease, according to Dr. Noe. The ability of a single 900-mg intravenous dose of the IL-36 receptor antagonist to completely clear pustules at 1 week in 54% of patients with generalized disease, compared with 6% of the placebo group, was “groundbreaking,” she said, referring to results of the pivotal trial published in the New England Journal of Medicine.
And given that “preventing GPP flares is ultimately what we want,” she said, more good news was reported this year in The Lancet: The finding from an international, randomized, placebo-controlled study that high-dose subcutaneous spesolimab significantly reduced the risk of a flare over 48 weeks. “There are lots of ongoing studies right now to understand the best way to dose spesolimab,” she said.
Moreover, another IL-36 receptor antagonist, imsidolimab, is being investigated in a phase 3 trial for generalized pustular disease, she noted. A phase 2, open-label study of patients with GPP found that “more than half of patients were very much improved at 4 weeks, and some patients started showing improvement at day 3,” Dr. Noe said.
An area of research she is interested in is the potential for Janus kinase (JAK) inhibitors as a treatment for palmoplantar pustulosis. For pustulosis on the hands and feet, recent case reports describing the efficacy of JAK inhibitors have caught her eye. “Right now, all we have is this case report data, mostly with tofacitinib, but I think it’s exciting,” she said, noting a recently published report in the British Journal of Dermatology.
Palmoplantar psoriasis
Pustular psoriatic disease can be localized to the hand and/or feet only, or can co-occur with generalized pustular disease, just as palmoplantar psoriasis can be localized to the hands and/or feet or, more commonly, can co-occur with widespread plaque psoriasis. Research has shown, Dr. Hawkes said, that with both types of acral disease, many patients have or have had plaque psoriasis outside of acral sites.
The nomenclature and acronyms for palmoplantar psoriatic disease have complicated patient education, communication, and research, Dr. Hawkes said. Does PPP refer to palmoplantar psoriasis, or palmoplantar pustulosis, for instance? What is the difference between palmoplantar pustulosis (coined PPP) and palmoplantar pustular psoriasis (referred to as PPPP)?
What if disease is only on the hands, only on the feet, or only on the backs of the hands? And at what point is disease not classified as palmoplantar psoriasis, but plaque psoriasis with involvement of the hands and feet? Inconsistencies and lack of clarification lead to “confusing” literature, he said.
Heterogeneity in populations across trials resulting from “inconsistent categorization and phenotype inclusion” may partly account for the recalcitrance to treatment reported in the literature, he said. Misdiagnosis as psoriasis in cases of localized disease (confusion with eczema, for instance), and the fact that hands and feet are subject to increased trauma and injury, compared with non-acral sites, are also at play.
Trials may also allow insufficient time for improvement, compared with non-acral sites. “What we’ve learned about the hands and feet is that it takes a much longer time for disease to improve,” Dr. Hawkes said, so primary endpoints must take this into account.
There is unique immunologic signaling in palmoplantar disease that differs from the predominant signaling in traditional plaque psoriasis, he emphasized, and “mixed immunophenotypes” that need to be unraveled.
Dr. Hawkes disclosed ties with AbbVie, Arcutis, Bristol-Myers Squibb, Boehringer Ingelheim, Janssen, LEO, Lilly, Novartis, Pfizer, Regeneron, Sanofi, Sun Pharma, and UCB. Dr. Noe disclosed ties to Bristol-Myers Squibb and Boehringer Ingelheim.
WASHINGTON – The approval last year of the interleukin (IL)-36 receptor antagonist spesolimab for treating generalized pustular psoriasis flares brightened the treatment landscape for this rare condition, and a recently published phase 2 study suggests a potential role of spesolimab for flare prevention. , according to speakers at the annual research symposium of the National Psoriasis Foundation.
“The IL-36 receptor antagonists don’t seem to be quite the answer for [palmoplantar pustulosis] that they are for generalized pustular psoriasis [GPP],” Megan H. Noe, MD, MPH, assistant professor of dermatology at Harvard Medical School and a dermatologist at Brigham and Women’s Hospital, Boston, said at the meeting.
Psoriasis affecting the hands and feet – both pustular and nonpustular – has a higher impact on quality of life and higher functional disability than does non-acral psoriasis, is less responsive to treatment, and has a “very confusing nomenclature” that complicates research and thus management, said Jason Ezra Hawkes, MD, a dermatologist in Rocklin, Calif., and former faculty member of several departments of dermatology. Both he and Dr. Noe spoke during a tough-to-treat session at the NPF meeting.
IL-17 and IL-23 blockade, as well as tumor necrosis factor (TNF) inhibition, are effective overall for palmoplantar psoriasis (nonpustular), but in general, responses are lower than for plaque psoriasis. Apremilast (Otezla), a phosphodiesterase-4 inhibitor, has some efficacy for pustular variants, but for hyperkeratotic variants it “does not perform as well as more selective inhibition of IL-17 and IL-23 blockade,” he said.
In general, ”what’s happening in the acral sites is different from an immune perspective than what’s happening in the non-acral sites,” and more research utilizing a clearer, descriptive nomenclature is needed to tease out differing immunophenotypes, explained Dr. Hawkes, who has led multiple clinical trials of treatments for psoriasis and other inflammatory skin conditions.
Palmoplantar pustulosis, and a word on generalized disease
Dermatologists are using a variety of treatments for palmoplantar pustulosis, with no clear first-line choices, Dr. Noe said. In a case series of almost 200 patients with palmoplantar pustulosis across 20 dermatology practices, published in JAMA Dermatology, 35% of patients received a systemic therapy prescription at their initial encounter – most commonly acitretin, followed by methotrexate and phototherapy. “Biologics were used, but use was varied and not as often as with oral agents,” said Dr. Noe, a coauthor of the study.
TNF blockers led to improvements ranging from 57% to 84%, depending on the agent, in a 2020 retrospective study of patients with palmoplantar pustulosis or acrodermatitis continua of Hallopeau, Dr. Noe noted. However, rates of complete clearance were only 20%-29%.
Apremilast showed modest efficacy after 5 months of treatment, with 62% of patients achieving at least a 50% improvement in the Palmoplantar Pustulosis Psoriasis Area and Severity Index (PPPASI) in a 2021 open-label, phase 2 study involving 21 patients. “This may represent a potential treatment option,” Dr. Noe said. “It’s something, but not what we’re used to seeing in our plaque psoriasis patients.”
A 2021 phase 2a, double-blind, randomized, placebo-controlled study of spesolimab in patients with palmoplantar pustulosis, meanwhile, failed to meet its primary endpoint, with only 32% of patients achieving a 50% improvement at 16 weeks, compared with 24% of patients in the placebo arm. And a recently published network meta-analysis found that none of the five drugs studied in seven randomized controlled trials – biologic or oral – was more effective than placebo for clearance or improvement of palmoplantar pustulosis.
The spesolimab (Spevigo) results have been disappointing considering the biologic’s newfound efficacy and role as the first Food and Drug Administration–approved therapy for generalized pustular disease, according to Dr. Noe. The ability of a single 900-mg intravenous dose of the IL-36 receptor antagonist to completely clear pustules at 1 week in 54% of patients with generalized disease, compared with 6% of the placebo group, was “groundbreaking,” she said, referring to results of the pivotal trial published in the New England Journal of Medicine.
And given that “preventing GPP flares is ultimately what we want,” she said, more good news was reported this year in The Lancet: The finding from an international, randomized, placebo-controlled study that high-dose subcutaneous spesolimab significantly reduced the risk of a flare over 48 weeks. “There are lots of ongoing studies right now to understand the best way to dose spesolimab,” she said.
Moreover, another IL-36 receptor antagonist, imsidolimab, is being investigated in a phase 3 trial for generalized pustular disease, she noted. A phase 2, open-label study of patients with GPP found that “more than half of patients were very much improved at 4 weeks, and some patients started showing improvement at day 3,” Dr. Noe said.
An area of research she is interested in is the potential for Janus kinase (JAK) inhibitors as a treatment for palmoplantar pustulosis. For pustulosis on the hands and feet, recent case reports describing the efficacy of JAK inhibitors have caught her eye. “Right now, all we have is this case report data, mostly with tofacitinib, but I think it’s exciting,” she said, noting a recently published report in the British Journal of Dermatology.
Palmoplantar psoriasis
Pustular psoriatic disease can be localized to the hand and/or feet only, or can co-occur with generalized pustular disease, just as palmoplantar psoriasis can be localized to the hands and/or feet or, more commonly, can co-occur with widespread plaque psoriasis. Research has shown, Dr. Hawkes said, that with both types of acral disease, many patients have or have had plaque psoriasis outside of acral sites.
The nomenclature and acronyms for palmoplantar psoriatic disease have complicated patient education, communication, and research, Dr. Hawkes said. Does PPP refer to palmoplantar psoriasis, or palmoplantar pustulosis, for instance? What is the difference between palmoplantar pustulosis (coined PPP) and palmoplantar pustular psoriasis (referred to as PPPP)?
What if disease is only on the hands, only on the feet, or only on the backs of the hands? And at what point is disease not classified as palmoplantar psoriasis, but plaque psoriasis with involvement of the hands and feet? Inconsistencies and lack of clarification lead to “confusing” literature, he said.
Heterogeneity in populations across trials resulting from “inconsistent categorization and phenotype inclusion” may partly account for the recalcitrance to treatment reported in the literature, he said. Misdiagnosis as psoriasis in cases of localized disease (confusion with eczema, for instance), and the fact that hands and feet are subject to increased trauma and injury, compared with non-acral sites, are also at play.
Trials may also allow insufficient time for improvement, compared with non-acral sites. “What we’ve learned about the hands and feet is that it takes a much longer time for disease to improve,” Dr. Hawkes said, so primary endpoints must take this into account.
There is unique immunologic signaling in palmoplantar disease that differs from the predominant signaling in traditional plaque psoriasis, he emphasized, and “mixed immunophenotypes” that need to be unraveled.
Dr. Hawkes disclosed ties with AbbVie, Arcutis, Bristol-Myers Squibb, Boehringer Ingelheim, Janssen, LEO, Lilly, Novartis, Pfizer, Regeneron, Sanofi, Sun Pharma, and UCB. Dr. Noe disclosed ties to Bristol-Myers Squibb and Boehringer Ingelheim.
WASHINGTON – The approval last year of the interleukin (IL)-36 receptor antagonist spesolimab for treating generalized pustular psoriasis flares brightened the treatment landscape for this rare condition, and a recently published phase 2 study suggests a potential role of spesolimab for flare prevention. , according to speakers at the annual research symposium of the National Psoriasis Foundation.
“The IL-36 receptor antagonists don’t seem to be quite the answer for [palmoplantar pustulosis] that they are for generalized pustular psoriasis [GPP],” Megan H. Noe, MD, MPH, assistant professor of dermatology at Harvard Medical School and a dermatologist at Brigham and Women’s Hospital, Boston, said at the meeting.
Psoriasis affecting the hands and feet – both pustular and nonpustular – has a higher impact on quality of life and higher functional disability than does non-acral psoriasis, is less responsive to treatment, and has a “very confusing nomenclature” that complicates research and thus management, said Jason Ezra Hawkes, MD, a dermatologist in Rocklin, Calif., and former faculty member of several departments of dermatology. Both he and Dr. Noe spoke during a tough-to-treat session at the NPF meeting.
IL-17 and IL-23 blockade, as well as tumor necrosis factor (TNF) inhibition, are effective overall for palmoplantar psoriasis (nonpustular), but in general, responses are lower than for plaque psoriasis. Apremilast (Otezla), a phosphodiesterase-4 inhibitor, has some efficacy for pustular variants, but for hyperkeratotic variants it “does not perform as well as more selective inhibition of IL-17 and IL-23 blockade,” he said.
In general, ”what’s happening in the acral sites is different from an immune perspective than what’s happening in the non-acral sites,” and more research utilizing a clearer, descriptive nomenclature is needed to tease out differing immunophenotypes, explained Dr. Hawkes, who has led multiple clinical trials of treatments for psoriasis and other inflammatory skin conditions.
Palmoplantar pustulosis, and a word on generalized disease
Dermatologists are using a variety of treatments for palmoplantar pustulosis, with no clear first-line choices, Dr. Noe said. In a case series of almost 200 patients with palmoplantar pustulosis across 20 dermatology practices, published in JAMA Dermatology, 35% of patients received a systemic therapy prescription at their initial encounter – most commonly acitretin, followed by methotrexate and phototherapy. “Biologics were used, but use was varied and not as often as with oral agents,” said Dr. Noe, a coauthor of the study.
TNF blockers led to improvements ranging from 57% to 84%, depending on the agent, in a 2020 retrospective study of patients with palmoplantar pustulosis or acrodermatitis continua of Hallopeau, Dr. Noe noted. However, rates of complete clearance were only 20%-29%.
Apremilast showed modest efficacy after 5 months of treatment, with 62% of patients achieving at least a 50% improvement in the Palmoplantar Pustulosis Psoriasis Area and Severity Index (PPPASI) in a 2021 open-label, phase 2 study involving 21 patients. “This may represent a potential treatment option,” Dr. Noe said. “It’s something, but not what we’re used to seeing in our plaque psoriasis patients.”
A 2021 phase 2a, double-blind, randomized, placebo-controlled study of spesolimab in patients with palmoplantar pustulosis, meanwhile, failed to meet its primary endpoint, with only 32% of patients achieving a 50% improvement at 16 weeks, compared with 24% of patients in the placebo arm. And a recently published network meta-analysis found that none of the five drugs studied in seven randomized controlled trials – biologic or oral – was more effective than placebo for clearance or improvement of palmoplantar pustulosis.
The spesolimab (Spevigo) results have been disappointing considering the biologic’s newfound efficacy and role as the first Food and Drug Administration–approved therapy for generalized pustular disease, according to Dr. Noe. The ability of a single 900-mg intravenous dose of the IL-36 receptor antagonist to completely clear pustules at 1 week in 54% of patients with generalized disease, compared with 6% of the placebo group, was “groundbreaking,” she said, referring to results of the pivotal trial published in the New England Journal of Medicine.
And given that “preventing GPP flares is ultimately what we want,” she said, more good news was reported this year in The Lancet: The finding from an international, randomized, placebo-controlled study that high-dose subcutaneous spesolimab significantly reduced the risk of a flare over 48 weeks. “There are lots of ongoing studies right now to understand the best way to dose spesolimab,” she said.
Moreover, another IL-36 receptor antagonist, imsidolimab, is being investigated in a phase 3 trial for generalized pustular disease, she noted. A phase 2, open-label study of patients with GPP found that “more than half of patients were very much improved at 4 weeks, and some patients started showing improvement at day 3,” Dr. Noe said.
An area of research she is interested in is the potential for Janus kinase (JAK) inhibitors as a treatment for palmoplantar pustulosis. For pustulosis on the hands and feet, recent case reports describing the efficacy of JAK inhibitors have caught her eye. “Right now, all we have is this case report data, mostly with tofacitinib, but I think it’s exciting,” she said, noting a recently published report in the British Journal of Dermatology.
Palmoplantar psoriasis
Pustular psoriatic disease can be localized to the hand and/or feet only, or can co-occur with generalized pustular disease, just as palmoplantar psoriasis can be localized to the hands and/or feet or, more commonly, can co-occur with widespread plaque psoriasis. Research has shown, Dr. Hawkes said, that with both types of acral disease, many patients have or have had plaque psoriasis outside of acral sites.
The nomenclature and acronyms for palmoplantar psoriatic disease have complicated patient education, communication, and research, Dr. Hawkes said. Does PPP refer to palmoplantar psoriasis, or palmoplantar pustulosis, for instance? What is the difference between palmoplantar pustulosis (coined PPP) and palmoplantar pustular psoriasis (referred to as PPPP)?
What if disease is only on the hands, only on the feet, or only on the backs of the hands? And at what point is disease not classified as palmoplantar psoriasis, but plaque psoriasis with involvement of the hands and feet? Inconsistencies and lack of clarification lead to “confusing” literature, he said.
Heterogeneity in populations across trials resulting from “inconsistent categorization and phenotype inclusion” may partly account for the recalcitrance to treatment reported in the literature, he said. Misdiagnosis as psoriasis in cases of localized disease (confusion with eczema, for instance), and the fact that hands and feet are subject to increased trauma and injury, compared with non-acral sites, are also at play.
Trials may also allow insufficient time for improvement, compared with non-acral sites. “What we’ve learned about the hands and feet is that it takes a much longer time for disease to improve,” Dr. Hawkes said, so primary endpoints must take this into account.
There is unique immunologic signaling in palmoplantar disease that differs from the predominant signaling in traditional plaque psoriasis, he emphasized, and “mixed immunophenotypes” that need to be unraveled.
Dr. Hawkes disclosed ties with AbbVie, Arcutis, Bristol-Myers Squibb, Boehringer Ingelheim, Janssen, LEO, Lilly, Novartis, Pfizer, Regeneron, Sanofi, Sun Pharma, and UCB. Dr. Noe disclosed ties to Bristol-Myers Squibb and Boehringer Ingelheim.
AT THE NPF RESEARCH SYMPOSIUM 2023