User login
Win Whitcomb: Hospitalists Central to Helping Hospitals Meet Performance Goals, Avoid Financial Penalities


After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
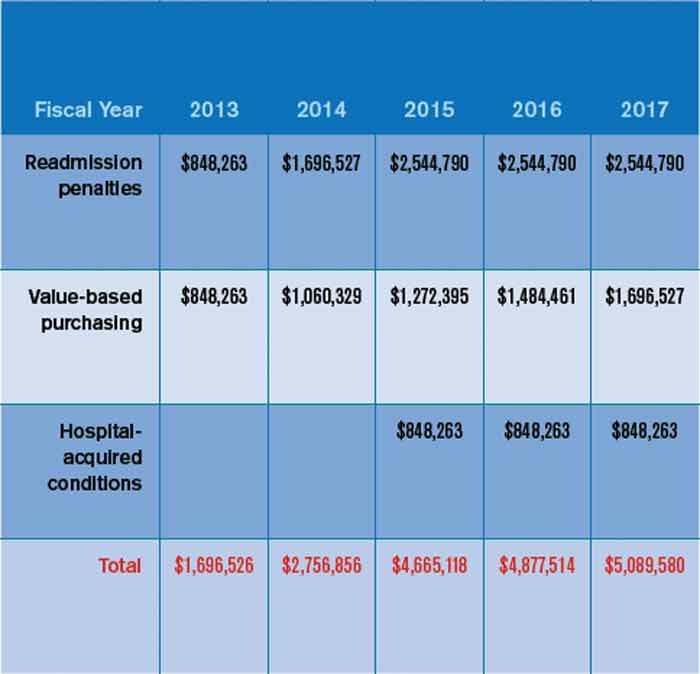
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
After a long wait, the time where quality really matters to the finance department has arrived. Why? Because now a lot of money is on the line based on hospitals’ ability to demonstrate performance on quality, patient safety, and patient satisfaction measures. And there is no physician group more central to the hospital’s performance on these measures than hospitalists.
To make this point, I will discuss the financial implications of three programs that are part of the Affordable Care Act: hospital value-based purchasing (HVBP), readmission penalties, and hospital-acquired conditions (HACs). Although many have found fault with these programs, especially the ones that only penalize hospitals (HACs and readmissions*), the dollars at risk can represent a new business case for hospitalist programs. High-performing hospitalist programs can positively impact their institution’s income statement.
In October 2012, readmissions penalties and VBP payments/penalties went into effect. In October 2014, a 1% penalty for groups in the worst-performing quartile in the HACs will be in force. Taken together, as Table 1 demonstrates, the total payments at risk will grow such that by fiscal-year 2017, 6% of a hospital’s inpatient payments from Medicare will be at risk. To put this in perspective, Table 2 models the dollars at risk for each of the five years beginning in 2013 for the three programs in a hypothetical, 327-bed hospital. While the risk in 2013 is a modest $1.7 million, by 2017, this hospital has more than $5 million at risk.
So where should hospitalists be focusing their efforts with these three programs and the monies that accompany them? First, for those designing incentive compensation for hospitalists, the incentives should address the applicable elements of these programs. Second, the components of VBP will evolve. For example, 2013 VPB payments are based on 70% process measures (a subset of the core measure set for heart failure, myocardial infarction, pneumonia, and surgery) and 30% patient satisfaction measures. In 2015, VBP will add such outcomes measures as central-line-associated bloodstream infections, catheter UTIs, mortality rates, and the new efficiency measure, Medicare spending per beneficiary. Third, readmissions penalties, while encompassing heart failure, myocardial infarction, and pneumonia for fiscal-year 2013 payments, will expand in fiscal-year 2015 to include chronic obstructive pulmonary disease, coronary artery bypass grafting, percutaneous coronary intervention, and other vascular conditions.
While all this can be hard to keep track of, not to mention address in the course of daily patient care, I suggest hospitalists set the following priorities to enable high performance for their hospitals under these programs:
- Catheter UTIs. Work with nursing, the ED, and other areas to ensure that catheters are indicated, insertion is sterile, there is a mechanism for their prompt removal, specimens are collected and handled appropriately, and that “present on admission” is documented if appropriate.
- Central-line-associated bloodstream infections. Ensure your hospital has the systems in place to support the central-line insertion bundle, and that the bundle elements are followed and documented.
- Readmissions. Focus on heart failure, pneumonia, myocardial infarction, and COPD; work with nursing and case management to identify those at high risk for readmission; perform targeted interventions based on that risk (e.g. palliative care or clinical pharmacy consultation); prioritize medication reconciliation; provide timely communication of discharge summary to the next provider of care; and contact the patient soon after discharge to ensure they are following their plan of care.
- Patient satisfaction. Have a system for high performance on the questions comprising the “doctor communication” domain. These are “How often did doctors treat you with courtesy and respect/listen carefully to you/explain things in a way you could understand?”
Medicare’s Message
Clearly, the financial impacts of hospital quality, satisfaction, and safety are growing, conveying the message from the Centers for Medicare & Medicaid Services (CMS) that quality matters, making a business case for quality. Our focus as leaders in hospital systems improvement will only sharpen as we see hospital payments increasingly affected as a direct consequence of our efforts. If that doesn’t get the attention of the finance department, what will?
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
2013: The Year of Quality Improvement
Years ago, hospitalists were introduced as new, efficient options for staffing hospitals. Today, they are known as the quarterbacks for patient care and quality improvement (QI) within the hospital.
This year, hospitalists everywhere can help their hospitals resolve to make 2013 a landmark year for QI. And making time for quality improvement need not be a major investment, nor do you have to “reinvent the wheel” and create your own programs.
SHM’s full menu of QI options gives hospitalists and other caregivers the confidence that their program is field-tested as well as the ability to choose the level of involvement that’s right for them.
For more information, visit www.hospitalmedicine.org/qi.
Years ago, hospitalists were introduced as new, efficient options for staffing hospitals. Today, they are known as the quarterbacks for patient care and quality improvement (QI) within the hospital.
This year, hospitalists everywhere can help their hospitals resolve to make 2013 a landmark year for QI. And making time for quality improvement need not be a major investment, nor do you have to “reinvent the wheel” and create your own programs.
SHM’s full menu of QI options gives hospitalists and other caregivers the confidence that their program is field-tested as well as the ability to choose the level of involvement that’s right for them.
For more information, visit www.hospitalmedicine.org/qi.
Years ago, hospitalists were introduced as new, efficient options for staffing hospitals. Today, they are known as the quarterbacks for patient care and quality improvement (QI) within the hospital.
This year, hospitalists everywhere can help their hospitals resolve to make 2013 a landmark year for QI. And making time for quality improvement need not be a major investment, nor do you have to “reinvent the wheel” and create your own programs.
SHM’s full menu of QI options gives hospitalists and other caregivers the confidence that their program is field-tested as well as the ability to choose the level of involvement that’s right for them.
For more information, visit www.hospitalmedicine.org/qi.
Society for Hospital Medicine Compiles List of Don'ts for Hospitalists
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
Shaun Frost: Call for Transparency in Healthcare Performance Results to Impact Hospitalists

Policymakers believe that publicly reporting healthcare performance results is essential to improving care delivery. In order to achieve a healthcare system that is consistently reliable, the Institute of Medicine (IOM) recently recommended that performance transparency be considered a foundational feature of healthcare systems that seek to constantly, systematically, and seamlessly improve.1 The IOM has suggested strategies (see Table 1, right) for producing readily available information on safety, quality, prices and cost, and health outcomes. As these strategies are being deployed, it is essential that hospitalists consider the impact they will have on their personal practice, key stakeholders, and the patients that they serve.
Performance Data Sources
The accessibility of publicly reported healthcare performance information is increasing rapidly. Among HM practitioners, perhaps the most widely recognized data source is the Centers for Medicare & Medicaid Services’ (CMS) Hospital Compare website (www.hospitalcompare.hhs.gov). According to CMS, its performance information on more than 4,000 hospitals is intended to help patients make decisions about where to seek healthcare, as well as encourage hospitals to improve the quality of care they provide.
The information currently reported is extensive and comprehensive (see Table 2, right). Furthermore, CMS continually adds data as new performance measures are created and validated.
Beyond the federal government, private health insurance companies, consortiums of employer purchasers of healthcare (e.g. the Leapfrog Group), and community collaboratives (e.g. Minnesota Community Measurement in the state of Minnesota) are reporting care provider performance information.
In addition, consumer advocacy groups have entered the picture. Earlier this year, Consumer Reports magazine launched an initiative to rate the quality of hospitals (and cardiac surgery groups) through the publication of patient outcomes (central-line-associated bloodstream infections, surgical site infections, readmissions, complications, mortality), patient experience (communications about medications and discharge, and other markers of satisfaction), and hospital best practices (use of EHR, and the appropriate use of abdominal and chest CT scanning). Consumer Reports also provides a composite hospital safety score, and a 36-page technical manual explaining the strategy and methodology behind their ratings.
Public performance reporting is furthermore becoming big business for healthcare entrepreneurs. Castlight Health, with its $181 million in private capital backing, is viewed by some as the “Travelocity of healthcare.” Castlight calls its searchable databases “transparency portals” that allow consumers to understand, before they visit a care provider, what they will be paying and how the care provider ranks on quality and outcomes.
Finally, numerous unregulated Internet sites that employ methodologically questionable practices are reporting on healthcare performance. Many of these sources collect and publish subjective reports of care experiences, with little or no requirement that the reporter confirm the nature of the relationship that they have with the care provider.
Transparency and Key Stakeholders
The hospital that you work in expects you to know how it performs, and to help it improve in the areas over which you have influence. Hospitals monitor publicly reported data because their futures depend on strong performance. As of October 2012, hospital Medicare reimbursement is linked to publicly reported performance measures that were incorporated into CMS’ value-based purchasing (VBP) initiative. Furthermore, hospital market share will be increasingly dependent on performance transparency as consumers and patients utilize these data to make informed decisions about where to seek high-value healthcare.
Patients have a vested interest in knowing how their care providers perform. A recent study by PricewaterhouseCoopers reported that 72% of consumers ranked provider reputation and personal experience as the top drivers of provider choice.2 Furthermore, employers and patients increasingly are demanding access to care affordability information—an interest driven in large part by the increasing popularity of consumer-directed health insurance plans (CDHPs). Under CDHPs, patients save money on premiums in exchange for higher deductibles that are typically paired with healthcare spending accounts. The intent is to increase consumer engagement and awareness of the cost of routine healthcare expenses while protecting against the cost of catastrophic events. It is estimated that 15% to 20% of people with employer-sponsored health insurance are in high-deductible plans, and many believe CDHPs will soon make up the majority of employer-provided coverage.
Patients interested in knowing how individual doctors perform will soon have increased access to this type of information as well. For example, CMS also produces a Physician Compare website (www.medicare.gov/find-a-doctor) that offers performance information on individual doctors. Currently, Physician Compare has little detailed information. Expect this to change, however, as Medicare moves forward with developing valid and reliable individual physician performance metrics for its Physician Value-Based Payment Modifier (VBPM) program (see “A New Measuring Stick,”).
Under VBPM, doctors will have payment modifiers assigned to their Medicare professional fee claims that will adjust payments based on the value of care that they have delivered historically. For example, it is possible in the future that physicians failing to prescribe ace inhibitors to heart failure patients will be paid less than physicians who universally provide evidence-based, best-practice heart failure care. The measurement period for the calculation of these modifiers begins this year, and hospitalists need to be aware that their performance after this time period might affect the amount of Medicare professional fee reimbursement they receive in the future.
Conclusions
Public performance reporting is a keystone healthcare reform strategy that will influence the behavior and practice patterns of hospitals and hospitalists. Hospitalists should regularly review publicly reported healthcare performance data, and commit to working collaboratively with colleagues to capitalize on improvement opportunities suggested by these data.
Dr. Frost is president of SHM.
References
- Institute of Medicine. Best care at lower cost: The path to continuously learning health care in America. Institute of Medicine website. Available at: http://www.iom.edu/bestcare. Accessed Nov. 24, 2012.
- PricewaterhouseCoopers’ Health Research Institute. Customer experience in healthcare: the moment of truth. PricewaterhouseCoopers website. Available at: http://www.pwc.com/es_MX/mx/publicaciones/archivo/2012-09-customer-experience-healthcare.pdf. Accessed Nov. 25, 2012.
Policymakers believe that publicly reporting healthcare performance results is essential to improving care delivery. In order to achieve a healthcare system that is consistently reliable, the Institute of Medicine (IOM) recently recommended that performance transparency be considered a foundational feature of healthcare systems that seek to constantly, systematically, and seamlessly improve.1 The IOM has suggested strategies (see Table 1, right) for producing readily available information on safety, quality, prices and cost, and health outcomes. As these strategies are being deployed, it is essential that hospitalists consider the impact they will have on their personal practice, key stakeholders, and the patients that they serve.
Performance Data Sources
The accessibility of publicly reported healthcare performance information is increasing rapidly. Among HM practitioners, perhaps the most widely recognized data source is the Centers for Medicare & Medicaid Services’ (CMS) Hospital Compare website (www.hospitalcompare.hhs.gov). According to CMS, its performance information on more than 4,000 hospitals is intended to help patients make decisions about where to seek healthcare, as well as encourage hospitals to improve the quality of care they provide.
The information currently reported is extensive and comprehensive (see Table 2, right). Furthermore, CMS continually adds data as new performance measures are created and validated.
Beyond the federal government, private health insurance companies, consortiums of employer purchasers of healthcare (e.g. the Leapfrog Group), and community collaboratives (e.g. Minnesota Community Measurement in the state of Minnesota) are reporting care provider performance information.
In addition, consumer advocacy groups have entered the picture. Earlier this year, Consumer Reports magazine launched an initiative to rate the quality of hospitals (and cardiac surgery groups) through the publication of patient outcomes (central-line-associated bloodstream infections, surgical site infections, readmissions, complications, mortality), patient experience (communications about medications and discharge, and other markers of satisfaction), and hospital best practices (use of EHR, and the appropriate use of abdominal and chest CT scanning). Consumer Reports also provides a composite hospital safety score, and a 36-page technical manual explaining the strategy and methodology behind their ratings.
Public performance reporting is furthermore becoming big business for healthcare entrepreneurs. Castlight Health, with its $181 million in private capital backing, is viewed by some as the “Travelocity of healthcare.” Castlight calls its searchable databases “transparency portals” that allow consumers to understand, before they visit a care provider, what they will be paying and how the care provider ranks on quality and outcomes.
Finally, numerous unregulated Internet sites that employ methodologically questionable practices are reporting on healthcare performance. Many of these sources collect and publish subjective reports of care experiences, with little or no requirement that the reporter confirm the nature of the relationship that they have with the care provider.
Transparency and Key Stakeholders
The hospital that you work in expects you to know how it performs, and to help it improve in the areas over which you have influence. Hospitals monitor publicly reported data because their futures depend on strong performance. As of October 2012, hospital Medicare reimbursement is linked to publicly reported performance measures that were incorporated into CMS’ value-based purchasing (VBP) initiative. Furthermore, hospital market share will be increasingly dependent on performance transparency as consumers and patients utilize these data to make informed decisions about where to seek high-value healthcare.
Patients have a vested interest in knowing how their care providers perform. A recent study by PricewaterhouseCoopers reported that 72% of consumers ranked provider reputation and personal experience as the top drivers of provider choice.2 Furthermore, employers and patients increasingly are demanding access to care affordability information—an interest driven in large part by the increasing popularity of consumer-directed health insurance plans (CDHPs). Under CDHPs, patients save money on premiums in exchange for higher deductibles that are typically paired with healthcare spending accounts. The intent is to increase consumer engagement and awareness of the cost of routine healthcare expenses while protecting against the cost of catastrophic events. It is estimated that 15% to 20% of people with employer-sponsored health insurance are in high-deductible plans, and many believe CDHPs will soon make up the majority of employer-provided coverage.
Patients interested in knowing how individual doctors perform will soon have increased access to this type of information as well. For example, CMS also produces a Physician Compare website (www.medicare.gov/find-a-doctor) that offers performance information on individual doctors. Currently, Physician Compare has little detailed information. Expect this to change, however, as Medicare moves forward with developing valid and reliable individual physician performance metrics for its Physician Value-Based Payment Modifier (VBPM) program (see “A New Measuring Stick,”).
Under VBPM, doctors will have payment modifiers assigned to their Medicare professional fee claims that will adjust payments based on the value of care that they have delivered historically. For example, it is possible in the future that physicians failing to prescribe ace inhibitors to heart failure patients will be paid less than physicians who universally provide evidence-based, best-practice heart failure care. The measurement period for the calculation of these modifiers begins this year, and hospitalists need to be aware that their performance after this time period might affect the amount of Medicare professional fee reimbursement they receive in the future.
Conclusions
Public performance reporting is a keystone healthcare reform strategy that will influence the behavior and practice patterns of hospitals and hospitalists. Hospitalists should regularly review publicly reported healthcare performance data, and commit to working collaboratively with colleagues to capitalize on improvement opportunities suggested by these data.
Dr. Frost is president of SHM.
References
- Institute of Medicine. Best care at lower cost: The path to continuously learning health care in America. Institute of Medicine website. Available at: http://www.iom.edu/bestcare. Accessed Nov. 24, 2012.
- PricewaterhouseCoopers’ Health Research Institute. Customer experience in healthcare: the moment of truth. PricewaterhouseCoopers website. Available at: http://www.pwc.com/es_MX/mx/publicaciones/archivo/2012-09-customer-experience-healthcare.pdf. Accessed Nov. 25, 2012.
Policymakers believe that publicly reporting healthcare performance results is essential to improving care delivery. In order to achieve a healthcare system that is consistently reliable, the Institute of Medicine (IOM) recently recommended that performance transparency be considered a foundational feature of healthcare systems that seek to constantly, systematically, and seamlessly improve.1 The IOM has suggested strategies (see Table 1, right) for producing readily available information on safety, quality, prices and cost, and health outcomes. As these strategies are being deployed, it is essential that hospitalists consider the impact they will have on their personal practice, key stakeholders, and the patients that they serve.
Performance Data Sources
The accessibility of publicly reported healthcare performance information is increasing rapidly. Among HM practitioners, perhaps the most widely recognized data source is the Centers for Medicare & Medicaid Services’ (CMS) Hospital Compare website (www.hospitalcompare.hhs.gov). According to CMS, its performance information on more than 4,000 hospitals is intended to help patients make decisions about where to seek healthcare, as well as encourage hospitals to improve the quality of care they provide.
The information currently reported is extensive and comprehensive (see Table 2, right). Furthermore, CMS continually adds data as new performance measures are created and validated.
Beyond the federal government, private health insurance companies, consortiums of employer purchasers of healthcare (e.g. the Leapfrog Group), and community collaboratives (e.g. Minnesota Community Measurement in the state of Minnesota) are reporting care provider performance information.
In addition, consumer advocacy groups have entered the picture. Earlier this year, Consumer Reports magazine launched an initiative to rate the quality of hospitals (and cardiac surgery groups) through the publication of patient outcomes (central-line-associated bloodstream infections, surgical site infections, readmissions, complications, mortality), patient experience (communications about medications and discharge, and other markers of satisfaction), and hospital best practices (use of EHR, and the appropriate use of abdominal and chest CT scanning). Consumer Reports also provides a composite hospital safety score, and a 36-page technical manual explaining the strategy and methodology behind their ratings.
Public performance reporting is furthermore becoming big business for healthcare entrepreneurs. Castlight Health, with its $181 million in private capital backing, is viewed by some as the “Travelocity of healthcare.” Castlight calls its searchable databases “transparency portals” that allow consumers to understand, before they visit a care provider, what they will be paying and how the care provider ranks on quality and outcomes.
Finally, numerous unregulated Internet sites that employ methodologically questionable practices are reporting on healthcare performance. Many of these sources collect and publish subjective reports of care experiences, with little or no requirement that the reporter confirm the nature of the relationship that they have with the care provider.
Transparency and Key Stakeholders
The hospital that you work in expects you to know how it performs, and to help it improve in the areas over which you have influence. Hospitals monitor publicly reported data because their futures depend on strong performance. As of October 2012, hospital Medicare reimbursement is linked to publicly reported performance measures that were incorporated into CMS’ value-based purchasing (VBP) initiative. Furthermore, hospital market share will be increasingly dependent on performance transparency as consumers and patients utilize these data to make informed decisions about where to seek high-value healthcare.
Patients have a vested interest in knowing how their care providers perform. A recent study by PricewaterhouseCoopers reported that 72% of consumers ranked provider reputation and personal experience as the top drivers of provider choice.2 Furthermore, employers and patients increasingly are demanding access to care affordability information—an interest driven in large part by the increasing popularity of consumer-directed health insurance plans (CDHPs). Under CDHPs, patients save money on premiums in exchange for higher deductibles that are typically paired with healthcare spending accounts. The intent is to increase consumer engagement and awareness of the cost of routine healthcare expenses while protecting against the cost of catastrophic events. It is estimated that 15% to 20% of people with employer-sponsored health insurance are in high-deductible plans, and many believe CDHPs will soon make up the majority of employer-provided coverage.
Patients interested in knowing how individual doctors perform will soon have increased access to this type of information as well. For example, CMS also produces a Physician Compare website (www.medicare.gov/find-a-doctor) that offers performance information on individual doctors. Currently, Physician Compare has little detailed information. Expect this to change, however, as Medicare moves forward with developing valid and reliable individual physician performance metrics for its Physician Value-Based Payment Modifier (VBPM) program (see “A New Measuring Stick,”).
Under VBPM, doctors will have payment modifiers assigned to their Medicare professional fee claims that will adjust payments based on the value of care that they have delivered historically. For example, it is possible in the future that physicians failing to prescribe ace inhibitors to heart failure patients will be paid less than physicians who universally provide evidence-based, best-practice heart failure care. The measurement period for the calculation of these modifiers begins this year, and hospitalists need to be aware that their performance after this time period might affect the amount of Medicare professional fee reimbursement they receive in the future.
Conclusions
Public performance reporting is a keystone healthcare reform strategy that will influence the behavior and practice patterns of hospitals and hospitalists. Hospitalists should regularly review publicly reported healthcare performance data, and commit to working collaboratively with colleagues to capitalize on improvement opportunities suggested by these data.
Dr. Frost is president of SHM.
References
- Institute of Medicine. Best care at lower cost: The path to continuously learning health care in America. Institute of Medicine website. Available at: http://www.iom.edu/bestcare. Accessed Nov. 24, 2012.
- PricewaterhouseCoopers’ Health Research Institute. Customer experience in healthcare: the moment of truth. PricewaterhouseCoopers website. Available at: http://www.pwc.com/es_MX/mx/publicaciones/archivo/2012-09-customer-experience-healthcare.pdf. Accessed Nov. 25, 2012.
Tailored Health IT Improves VTE Rates
Electronic decision support significantly improves VTE prophylaxis and hospital-acquired VTE rates, according to a new study in the Journal of Hospital Medicine.
The report, "Improving Hospital Venous Thromboembolism Prophylaxis With Electronic Decision Report," saw overall medical service prophylaxis rise to 82.1% from 61.9% (P<0.001) and pharmacologic VTE prophylaxis increase to 74.5% from 59% (P<0.001).
"Healthcare leaders talk about information technology (IT) as a means toward effecting improvements in quality and patient safety and, most of the time, they view that and discuss that in terms of the actual IT system being implemented," says lead author Rohit Bhalla, MD, MPH, associate professor of clinical medicine at Albert Einstein College of Medicine in New York City. "What our intervention really got to was once you've implemented an IT system ... how can it be modified, vis-à-vis decision support, so that it provides an even better result than you get with the product that comes out of the box."
Tailoring a health IT system to improve outcomes requires interdisciplinary work that includes quality officers, physicians, IT staff, and programmers. Hospitalist and fellow author Jason Adelman, MD, MS, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., where the study was conducted, says that the research can help generate future buy-in from physicians who don't value electronic decision support tools.
It can "ease the swallowing of the bitter pill to know that it really makes a difference," Dr. Adelman says. "Don't be up in arms when you're forced to do something a little bit extra, because it really works."
Visit our website for more information about health information technology.
Electronic decision support significantly improves VTE prophylaxis and hospital-acquired VTE rates, according to a new study in the Journal of Hospital Medicine.
The report, "Improving Hospital Venous Thromboembolism Prophylaxis With Electronic Decision Report," saw overall medical service prophylaxis rise to 82.1% from 61.9% (P<0.001) and pharmacologic VTE prophylaxis increase to 74.5% from 59% (P<0.001).
"Healthcare leaders talk about information technology (IT) as a means toward effecting improvements in quality and patient safety and, most of the time, they view that and discuss that in terms of the actual IT system being implemented," says lead author Rohit Bhalla, MD, MPH, associate professor of clinical medicine at Albert Einstein College of Medicine in New York City. "What our intervention really got to was once you've implemented an IT system ... how can it be modified, vis-à-vis decision support, so that it provides an even better result than you get with the product that comes out of the box."
Tailoring a health IT system to improve outcomes requires interdisciplinary work that includes quality officers, physicians, IT staff, and programmers. Hospitalist and fellow author Jason Adelman, MD, MS, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., where the study was conducted, says that the research can help generate future buy-in from physicians who don't value electronic decision support tools.
It can "ease the swallowing of the bitter pill to know that it really makes a difference," Dr. Adelman says. "Don't be up in arms when you're forced to do something a little bit extra, because it really works."
Visit our website for more information about health information technology.
Electronic decision support significantly improves VTE prophylaxis and hospital-acquired VTE rates, according to a new study in the Journal of Hospital Medicine.
The report, "Improving Hospital Venous Thromboembolism Prophylaxis With Electronic Decision Report," saw overall medical service prophylaxis rise to 82.1% from 61.9% (P<0.001) and pharmacologic VTE prophylaxis increase to 74.5% from 59% (P<0.001).
"Healthcare leaders talk about information technology (IT) as a means toward effecting improvements in quality and patient safety and, most of the time, they view that and discuss that in terms of the actual IT system being implemented," says lead author Rohit Bhalla, MD, MPH, associate professor of clinical medicine at Albert Einstein College of Medicine in New York City. "What our intervention really got to was once you've implemented an IT system ... how can it be modified, vis-à-vis decision support, so that it provides an even better result than you get with the product that comes out of the box."
Tailoring a health IT system to improve outcomes requires interdisciplinary work that includes quality officers, physicians, IT staff, and programmers. Hospitalist and fellow author Jason Adelman, MD, MS, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., where the study was conducted, says that the research can help generate future buy-in from physicians who don't value electronic decision support tools.
It can "ease the swallowing of the bitter pill to know that it really makes a difference," Dr. Adelman says. "Don't be up in arms when you're forced to do something a little bit extra, because it really works."
Visit our website for more information about health information technology.
Hospitalists Take Greater Role in Assessing and Treating Pain
A multidisciplinary pain-management research group at Mount Sinai School of Medicine in New York City has been evaluating numerical pain-rating scales, independent predictors of severe pain, their association with patient satisfaction rates, and improved inpatient pain outcomes resulting from targeted interventions with physicians. However, they found that while overall pain scores on medicine floors were lower than for surgical patients, they were also less responsive to the targeted interventions.
The group is piloting a program to promote pain champions in its department of medicine and encourage hospitalists to partner with nurses in focusing on pain assessment and treatment.
David L. Reich, MD, an anesthesiologist at Mount Sinai who leads the pain group, and colleagues recently published results from their research in the American Journal of Medical Quality.1 Pain increasingly will be an issue for hospitals and hospitalists, he says, with two pain-related questions now included on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that is part of the government’s value-based purchasing initiative.
“It is our belief that unrelieved pain is an overall driver of other patient-reported metrics,” Dr. Reich says.
Andrew Dunn, MD, SFHM, head of the hospitalist service at Mount Sinai, acknowledges that medicine floors have been less successful at improving pain management, in part because the patient population is so much more heterogeneous.
“One thing that did not work was to have the pain team join medical rounds. That’s just not systematic or robust enough,” Dr. Dunn says. “We have piloted a program where patients’ pain scores are now delivered twice a day in reports to nurse managers and floor medical directors.”
Consecutive reports of pain scores of 5 or more (on a scale of 0 to 10) trigger consideration of a consultation with either the anesthesiology pain-management service or palliative-care service.
Reference
A multidisciplinary pain-management research group at Mount Sinai School of Medicine in New York City has been evaluating numerical pain-rating scales, independent predictors of severe pain, their association with patient satisfaction rates, and improved inpatient pain outcomes resulting from targeted interventions with physicians. However, they found that while overall pain scores on medicine floors were lower than for surgical patients, they were also less responsive to the targeted interventions.
The group is piloting a program to promote pain champions in its department of medicine and encourage hospitalists to partner with nurses in focusing on pain assessment and treatment.
David L. Reich, MD, an anesthesiologist at Mount Sinai who leads the pain group, and colleagues recently published results from their research in the American Journal of Medical Quality.1 Pain increasingly will be an issue for hospitals and hospitalists, he says, with two pain-related questions now included on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that is part of the government’s value-based purchasing initiative.
“It is our belief that unrelieved pain is an overall driver of other patient-reported metrics,” Dr. Reich says.
Andrew Dunn, MD, SFHM, head of the hospitalist service at Mount Sinai, acknowledges that medicine floors have been less successful at improving pain management, in part because the patient population is so much more heterogeneous.
“One thing that did not work was to have the pain team join medical rounds. That’s just not systematic or robust enough,” Dr. Dunn says. “We have piloted a program where patients’ pain scores are now delivered twice a day in reports to nurse managers and floor medical directors.”
Consecutive reports of pain scores of 5 or more (on a scale of 0 to 10) trigger consideration of a consultation with either the anesthesiology pain-management service or palliative-care service.
Reference
A multidisciplinary pain-management research group at Mount Sinai School of Medicine in New York City has been evaluating numerical pain-rating scales, independent predictors of severe pain, their association with patient satisfaction rates, and improved inpatient pain outcomes resulting from targeted interventions with physicians. However, they found that while overall pain scores on medicine floors were lower than for surgical patients, they were also less responsive to the targeted interventions.
The group is piloting a program to promote pain champions in its department of medicine and encourage hospitalists to partner with nurses in focusing on pain assessment and treatment.
David L. Reich, MD, an anesthesiologist at Mount Sinai who leads the pain group, and colleagues recently published results from their research in the American Journal of Medical Quality.1 Pain increasingly will be an issue for hospitals and hospitalists, he says, with two pain-related questions now included on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey that is part of the government’s value-based purchasing initiative.
“It is our belief that unrelieved pain is an overall driver of other patient-reported metrics,” Dr. Reich says.
Andrew Dunn, MD, SFHM, head of the hospitalist service at Mount Sinai, acknowledges that medicine floors have been less successful at improving pain management, in part because the patient population is so much more heterogeneous.
“One thing that did not work was to have the pain team join medical rounds. That’s just not systematic or robust enough,” Dr. Dunn says. “We have piloted a program where patients’ pain scores are now delivered twice a day in reports to nurse managers and floor medical directors.”
Consecutive reports of pain scores of 5 or more (on a scale of 0 to 10) trigger consideration of a consultation with either the anesthesiology pain-management service or palliative-care service.
Reference
Win Whitcomb: Introducing Neuroquality and Neurosafety

The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
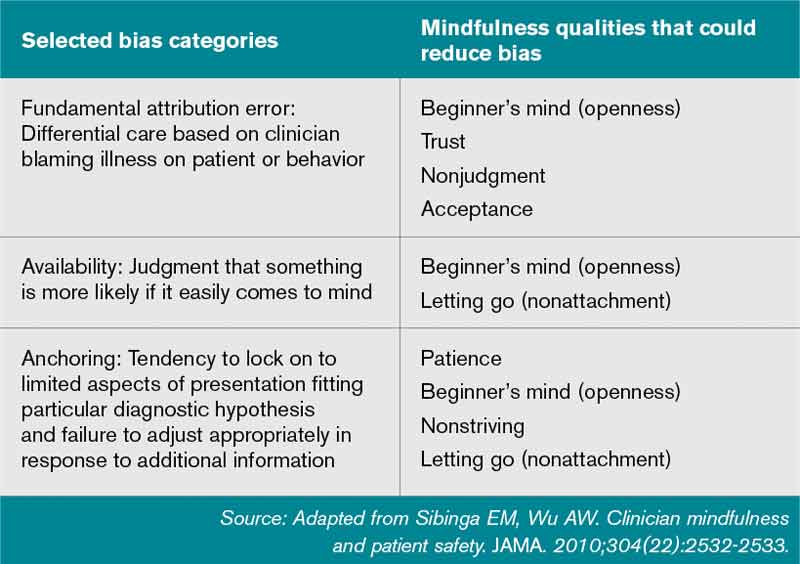
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The prefix “neuro” has become quite popular the last couple of years. We have neuroeconomics, neuroplasticity, neuroergonomics, and, of course, neurohospitalist. The explosion of interest in the brain can be seen in the popular press, television, blogs, and the Journal of the American Medical Association.
I predict that recent breakthroughs in brain science and related fields (cognitive psychology, neurobiology, molecular biology, linguistics, and artificial intelligence, among others) will have a profound impact on the fields of quality improvement (QI) and patient safety, and, consequently on HM. To date, the patient safety movement has focused on systems issues in an effort to reduce harm induced by the healthcare system. I submit that for healthcare to be reliable and error-free in the future, we must leverage the innate strengths of the brain. Here I mention four areas where brain science breakthroughs can enable us to improve patient safety practices.
Diagnostic Error
Patrick Croskerry, an emergency physician and researcher, has described errors in diagnosis as stemming in part from cognitive bias. He offers “de-biasing strategies” as an approach to decreasing diagnostic error.
One of the most powerful de-biasing strategies is metacognition, or awareness of one’s own thinking processes. Closely related to metacognition is mindfulness, defined as the “nonjudgmental awareness of the present moment.” A growing body of literature makes the case that enhancing mindfulness might reduce the impact bias has on diagnostic error.1 Table 1 (right) mentions a subset of bias types and how mindfulness might mitigate them. I’m sure you can think of cases you’ve encountered where bias has affected the diagnostic outcome.
Empathy and Patient Experience
As the focus on patient experience grows, approaches to improving performance on patient satisfaction surveys are proliferating. Whatever technical components you choose to employ, a capacity for caregiver empathy is a crucial underlying factor to a better patient experience. Harvard psychiatrist Helen Riess, MD, points out that we are now beginning to understand the neurobiological basis of empathy. She and others present evidence that we may be able to “up-regulate” empathy through education or cognitive practices.2 Several studies suggest we might be able to realize improved therapeutic relationships between physicians and patients, and they have led to programs, such as the ones at Stanford and Emory universities, that train caregivers to enhance empathy and compassion.
Interruptions and Cognitive Error
It has been customary in high-risk industries to ensure that certain procedures are free of interruptions. There is recognition that disturbances during high-stakes tasks, such as airline takeoff, carry disastrous consequences. We now know that multitasking is a myth and that the brain instead switches between tasks sequentially. But task-switching comes at the high cost of a marked increase in the rate of cognitive error.3 As we learn more, decreasing interruptions or delineating “interruption-free” zones in healthcare could be a way to mitigate an inherent vulnerability in our cognitive abilities.
Fatigue and Medical Error
It is well documented that sleep deprivation correlates with a decline in cognitive
performance in a number of classes of healthcare workers. Fatigue has also increased diagnostic error among residents. A 2011 Sentinel Alert from The Joint Commission creates a standard that healthcare organizations implement a fatigue-management plan to mitigate the potential harm caused by tired professionals.
Most of the approaches to improving outcomes in the hospital have focused on process improvement and systems thinking. But errors also occur due to the thinking process of clinicians. In the book “Brain Rules,” author John Medina argues that schools and businesses create an environment that is less than friendly to the brain, citing current classroom design and cubicles for office workers. As a result, he states, we often have poor educational and business performance. I have little doubt that if Medina spent a few hours in a hospital, he would come to a similar conclusion: We don’t do the brain any favors when it comes to creating a healthy environment for providing safe and reliable care to our patients.
References
- Sibinga EM, Wu AW. Clinician mindfulness and patient safety. JAMA. 2010;304(22):2532-2533.
- Riess H. Empathy in medicine─a neurobiological perspective. JAMA. 2010;304(14):1604-1605.
- Rogers RD, Monsell S. The costs of a predictable switch between simple cognitive tasks. J Exper Psychol. 1995;124(2):207–231.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
The Quality Journey of Hospitalist David J. Yu
Hospitalist David J. Yu, MD, FACP, MBA, SFHM, medical director of the adult inpatient service at Presbyterian Healthcare Services in Albuquerque, N.M., began his quality journey by earning an MBA, then spending a week at University of Toyota in Gardena, Calif., to learn its Lean process-management techniques. He presented a Research, Innovations, and Clinical Vignettes poster at HM12 that outlined the multidisciplinary quality initiative at 453-bed Presbyterian Hospital in Albuquerque.
The project identified problems of throughput, ED diversion, disjointed team rounding, inadequate communication, multiple patient handoffs, low staff morale, and greater-than-expected length of stay (LOS).
“We really dug into the issues on a granular level,” with the participation of finance, nursing, care coordinators, physical therapy, and other staffers alongside the hospitalists, Dr. Yu says. The project ended up changing the practice from a model in which 11 hospitalist teams and five admitting hospitalists cared for patients throughout the hospital’s various floors while carrying caseloads too high to manage optimally. They replaced it with a unit-based rounding model, with hospitalists and care coordinators geographically segregated on units and multidisciplinary rounds to improve the efficiency of team communication (see “A Holy Grail,” July 2012, p. 30).
The group also used data to persuade the hospital’s administration to add hospitalist FTEs. As a result, LOS on two pilot units decreased by nearly half a day, with increased inpatient volume, higher patient satisfaction scores on Press-Ganey surveys, and an estimated net financial benefit of nearly $3.5 million between April 2010 and December 2011—even counting the additional hospitalist FTEs. This model has since spread to all medical units in the hospital.
“We need to be in the business of producing ‘defect-free’ discharges,” Dr. Yu quips. “Every group needs a local solution. But the mantra for this work is standardization....That’s where the leadership of the hospitalist comes in. It’s not, ‘Follow me,’ but ‘Hey, join us in collaborating together to come up with a solution.’
“It has been a two-year journey, and we’re still learning.”
Hospitalist David J. Yu, MD, FACP, MBA, SFHM, medical director of the adult inpatient service at Presbyterian Healthcare Services in Albuquerque, N.M., began his quality journey by earning an MBA, then spending a week at University of Toyota in Gardena, Calif., to learn its Lean process-management techniques. He presented a Research, Innovations, and Clinical Vignettes poster at HM12 that outlined the multidisciplinary quality initiative at 453-bed Presbyterian Hospital in Albuquerque.
The project identified problems of throughput, ED diversion, disjointed team rounding, inadequate communication, multiple patient handoffs, low staff morale, and greater-than-expected length of stay (LOS).
“We really dug into the issues on a granular level,” with the participation of finance, nursing, care coordinators, physical therapy, and other staffers alongside the hospitalists, Dr. Yu says. The project ended up changing the practice from a model in which 11 hospitalist teams and five admitting hospitalists cared for patients throughout the hospital’s various floors while carrying caseloads too high to manage optimally. They replaced it with a unit-based rounding model, with hospitalists and care coordinators geographically segregated on units and multidisciplinary rounds to improve the efficiency of team communication (see “A Holy Grail,” July 2012, p. 30).
The group also used data to persuade the hospital’s administration to add hospitalist FTEs. As a result, LOS on two pilot units decreased by nearly half a day, with increased inpatient volume, higher patient satisfaction scores on Press-Ganey surveys, and an estimated net financial benefit of nearly $3.5 million between April 2010 and December 2011—even counting the additional hospitalist FTEs. This model has since spread to all medical units in the hospital.
“We need to be in the business of producing ‘defect-free’ discharges,” Dr. Yu quips. “Every group needs a local solution. But the mantra for this work is standardization....That’s where the leadership of the hospitalist comes in. It’s not, ‘Follow me,’ but ‘Hey, join us in collaborating together to come up with a solution.’
“It has been a two-year journey, and we’re still learning.”
Hospitalist David J. Yu, MD, FACP, MBA, SFHM, medical director of the adult inpatient service at Presbyterian Healthcare Services in Albuquerque, N.M., began his quality journey by earning an MBA, then spending a week at University of Toyota in Gardena, Calif., to learn its Lean process-management techniques. He presented a Research, Innovations, and Clinical Vignettes poster at HM12 that outlined the multidisciplinary quality initiative at 453-bed Presbyterian Hospital in Albuquerque.
The project identified problems of throughput, ED diversion, disjointed team rounding, inadequate communication, multiple patient handoffs, low staff morale, and greater-than-expected length of stay (LOS).
“We really dug into the issues on a granular level,” with the participation of finance, nursing, care coordinators, physical therapy, and other staffers alongside the hospitalists, Dr. Yu says. The project ended up changing the practice from a model in which 11 hospitalist teams and five admitting hospitalists cared for patients throughout the hospital’s various floors while carrying caseloads too high to manage optimally. They replaced it with a unit-based rounding model, with hospitalists and care coordinators geographically segregated on units and multidisciplinary rounds to improve the efficiency of team communication (see “A Holy Grail,” July 2012, p. 30).
The group also used data to persuade the hospital’s administration to add hospitalist FTEs. As a result, LOS on two pilot units decreased by nearly half a day, with increased inpatient volume, higher patient satisfaction scores on Press-Ganey surveys, and an estimated net financial benefit of nearly $3.5 million between April 2010 and December 2011—even counting the additional hospitalist FTEs. This model has since spread to all medical units in the hospital.
“We need to be in the business of producing ‘defect-free’ discharges,” Dr. Yu quips. “Every group needs a local solution. But the mantra for this work is standardization....That’s where the leadership of the hospitalist comes in. It’s not, ‘Follow me,’ but ‘Hey, join us in collaborating together to come up with a solution.’
“It has been a two-year journey, and we’re still learning.”
Hospitalists' Voices to be Heard on Capitol Hill
Every year, hundreds of thousands of people from all parts of the country travel to Washington, D.C., and visit Congress. Regardless of the organizations they represent, almost all of them have one thing in common: They go to Capitol Hill with an “ask.”
Some ask for a vote on a particular piece of legislation; some request funding for their projects. Regardless, there is almost always an ask.
But hospitalists are different, according to SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, and committee member Brad Flansbaum, DO, MPH, SFHM. They are featured in a new video about “Hospitalists on the Hill,” SHM’s day to meet with members of Congress.
Rather than lobbying or asking for assistance, hospitalists bring solutions to the healthcare problems currently vexing communities throughout the country. By introducing the hospitalist model and its role in quality improvement (QI) to some of the most influential government figures in public health, hospitalists who make the visit to Capitol Hill help to spread some of the best practices in hospital-based healthcare and share their personal experiences at the same time.
“Every constituency that comes in is asking them for something,” Dr. Greeno says in one of the SHM-produced videos. “We don’t ask for anything. We offer. We offer our expertise. We offer to help them make better decisions than they would make otherwise.”
That contribution matters to members of Congress and their healthcare staff. Drs. Greeno and Flansbaum are “Hill Day” veterans who have seen firsthand how legislators and their staff absorb SHM’s message and materials.
“I thought that if we are leaving materials behind, that the minute we walk out of the office, it was going in the trash,” Dr. Greeno says. “That’s not what happens. They read this stuff.”
In 2013, Hospitalists on the Hill will take place May 16, the day before the official start of HM’s annual meeting at the Gaylord National Resort & Convention Center in National Harbor, Md., just a few minutes south of Washington, D.C. The agenda is ambitious, starting with a briefing about what to expect when meeting Congress members on Capitol Hill, followed by a full day of meetings with policymakers, regulators, and their staff.
“We spend our day going back and forth, from the Senate side of the Capitol to the House side of the Capitol, in and out of the office buildings, walking the halls of Congress,” Dr. Greeno says. “It’s a blast. It’s so interesting. And we’re getting a chance to sit down and deliver our message.”
For Dr. Flansbaum, it’s an opportunity to promote action in Washington.
“It really brings government to life,” he says. “You realize that, as bottlenecked as things might be sometimes, things have to get done.”
HM13 attendees can sign-up for Hospitalists on the Hill during annual-meeing registration. For more information, visit www.hospitalmedicine2013.org/onthehill.
Brendon Shank is SHM’s associate vice president of communications.
Every year, hundreds of thousands of people from all parts of the country travel to Washington, D.C., and visit Congress. Regardless of the organizations they represent, almost all of them have one thing in common: They go to Capitol Hill with an “ask.”
Some ask for a vote on a particular piece of legislation; some request funding for their projects. Regardless, there is almost always an ask.
But hospitalists are different, according to SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, and committee member Brad Flansbaum, DO, MPH, SFHM. They are featured in a new video about “Hospitalists on the Hill,” SHM’s day to meet with members of Congress.
Rather than lobbying or asking for assistance, hospitalists bring solutions to the healthcare problems currently vexing communities throughout the country. By introducing the hospitalist model and its role in quality improvement (QI) to some of the most influential government figures in public health, hospitalists who make the visit to Capitol Hill help to spread some of the best practices in hospital-based healthcare and share their personal experiences at the same time.
“Every constituency that comes in is asking them for something,” Dr. Greeno says in one of the SHM-produced videos. “We don’t ask for anything. We offer. We offer our expertise. We offer to help them make better decisions than they would make otherwise.”
That contribution matters to members of Congress and their healthcare staff. Drs. Greeno and Flansbaum are “Hill Day” veterans who have seen firsthand how legislators and their staff absorb SHM’s message and materials.
“I thought that if we are leaving materials behind, that the minute we walk out of the office, it was going in the trash,” Dr. Greeno says. “That’s not what happens. They read this stuff.”
In 2013, Hospitalists on the Hill will take place May 16, the day before the official start of HM’s annual meeting at the Gaylord National Resort & Convention Center in National Harbor, Md., just a few minutes south of Washington, D.C. The agenda is ambitious, starting with a briefing about what to expect when meeting Congress members on Capitol Hill, followed by a full day of meetings with policymakers, regulators, and their staff.
“We spend our day going back and forth, from the Senate side of the Capitol to the House side of the Capitol, in and out of the office buildings, walking the halls of Congress,” Dr. Greeno says. “It’s a blast. It’s so interesting. And we’re getting a chance to sit down and deliver our message.”
For Dr. Flansbaum, it’s an opportunity to promote action in Washington.
“It really brings government to life,” he says. “You realize that, as bottlenecked as things might be sometimes, things have to get done.”
HM13 attendees can sign-up for Hospitalists on the Hill during annual-meeing registration. For more information, visit www.hospitalmedicine2013.org/onthehill.
Brendon Shank is SHM’s associate vice president of communications.
Every year, hundreds of thousands of people from all parts of the country travel to Washington, D.C., and visit Congress. Regardless of the organizations they represent, almost all of them have one thing in common: They go to Capitol Hill with an “ask.”
Some ask for a vote on a particular piece of legislation; some request funding for their projects. Regardless, there is almost always an ask.
But hospitalists are different, according to SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, and committee member Brad Flansbaum, DO, MPH, SFHM. They are featured in a new video about “Hospitalists on the Hill,” SHM’s day to meet with members of Congress.
Rather than lobbying or asking for assistance, hospitalists bring solutions to the healthcare problems currently vexing communities throughout the country. By introducing the hospitalist model and its role in quality improvement (QI) to some of the most influential government figures in public health, hospitalists who make the visit to Capitol Hill help to spread some of the best practices in hospital-based healthcare and share their personal experiences at the same time.
“Every constituency that comes in is asking them for something,” Dr. Greeno says in one of the SHM-produced videos. “We don’t ask for anything. We offer. We offer our expertise. We offer to help them make better decisions than they would make otherwise.”
That contribution matters to members of Congress and their healthcare staff. Drs. Greeno and Flansbaum are “Hill Day” veterans who have seen firsthand how legislators and their staff absorb SHM’s message and materials.
“I thought that if we are leaving materials behind, that the minute we walk out of the office, it was going in the trash,” Dr. Greeno says. “That’s not what happens. They read this stuff.”
In 2013, Hospitalists on the Hill will take place May 16, the day before the official start of HM’s annual meeting at the Gaylord National Resort & Convention Center in National Harbor, Md., just a few minutes south of Washington, D.C. The agenda is ambitious, starting with a briefing about what to expect when meeting Congress members on Capitol Hill, followed by a full day of meetings with policymakers, regulators, and their staff.
“We spend our day going back and forth, from the Senate side of the Capitol to the House side of the Capitol, in and out of the office buildings, walking the halls of Congress,” Dr. Greeno says. “It’s a blast. It’s so interesting. And we’re getting a chance to sit down and deliver our message.”
For Dr. Flansbaum, it’s an opportunity to promote action in Washington.
“It really brings government to life,” he says. “You realize that, as bottlenecked as things might be sometimes, things have to get done.”
HM13 attendees can sign-up for Hospitalists on the Hill during annual-meeing registration. For more information, visit www.hospitalmedicine2013.org/onthehill.
Brendon Shank is SHM’s associate vice president of communications.
Guidelines Help Slash CLABSI Rate by 40% in the ICU
The largest effort to date to tackle central-line-associated bloodstream infections (CLABSIs) has reduced infection rates in ICUs nationwide by 40%, according to preliminary findings from the federal Agency for Healthcare Research and Quality (AHRQ).
AHRQ attributes the decrease to a CLABSI safety checklist from the Comprehensive Unit-Based Safety Program (CUSP) that encourages hospital staff to wash their hands prior to inserting central lines, avoid the femoral site, remove lines when they are no longer needed, and use the antimicrobial agent chlorhexidine to clean the patient's insertion site.
The checklist was developed by Peter Pronovost, MD, PhD, FCCM, and colleagues at Johns Hopkins University in Baltimore, and originally implemented in ICUs statewide in Michigan as the Keystone Project. Since 2009, CUSP has recruited more than 1,000 participating hospitals in 44 states. CUSP collectively reported a decrease to 1.25 from 1.87 CLABSIs per 1,000 central-line days 10-12 months after implementing the program, according to AHRQ [PDF].
The real game-changer for CLABSIs has been the widespread adoption of chlorhexidine as an insertion site disinfectant, says Sanjay Saint, MD, MPH, director of the Veterans Administration at the University of Michigan Patient Safety Enhancement Program in Ann Arbor and professor of medicine at the University of Michigan. Dr. Saint is on the national leadership team of On the CUSP: Stop CAUTI (Catheter-Associated Urinary Tract Infections), an initiative that aims to reduce mean rates of CAUTI infections by 25% in hospitals nationwide.
Although hospitalists don't routinely place central lines, their role in this procedure is growing, both in nonacademic hospitals that lack intensivists and on hospitals' general medicine floors.
"My take-home message for hospitalists: if you are putting in central lines, if you only make one change in practice, is to use chlorhexidine as the site disinfectant," Dr. Saint says.
Visit our website for more information about central-line-associated bloodstream infections.
The largest effort to date to tackle central-line-associated bloodstream infections (CLABSIs) has reduced infection rates in ICUs nationwide by 40%, according to preliminary findings from the federal Agency for Healthcare Research and Quality (AHRQ).
AHRQ attributes the decrease to a CLABSI safety checklist from the Comprehensive Unit-Based Safety Program (CUSP) that encourages hospital staff to wash their hands prior to inserting central lines, avoid the femoral site, remove lines when they are no longer needed, and use the antimicrobial agent chlorhexidine to clean the patient's insertion site.
The checklist was developed by Peter Pronovost, MD, PhD, FCCM, and colleagues at Johns Hopkins University in Baltimore, and originally implemented in ICUs statewide in Michigan as the Keystone Project. Since 2009, CUSP has recruited more than 1,000 participating hospitals in 44 states. CUSP collectively reported a decrease to 1.25 from 1.87 CLABSIs per 1,000 central-line days 10-12 months after implementing the program, according to AHRQ [PDF].
The real game-changer for CLABSIs has been the widespread adoption of chlorhexidine as an insertion site disinfectant, says Sanjay Saint, MD, MPH, director of the Veterans Administration at the University of Michigan Patient Safety Enhancement Program in Ann Arbor and professor of medicine at the University of Michigan. Dr. Saint is on the national leadership team of On the CUSP: Stop CAUTI (Catheter-Associated Urinary Tract Infections), an initiative that aims to reduce mean rates of CAUTI infections by 25% in hospitals nationwide.
Although hospitalists don't routinely place central lines, their role in this procedure is growing, both in nonacademic hospitals that lack intensivists and on hospitals' general medicine floors.
"My take-home message for hospitalists: if you are putting in central lines, if you only make one change in practice, is to use chlorhexidine as the site disinfectant," Dr. Saint says.
Visit our website for more information about central-line-associated bloodstream infections.
The largest effort to date to tackle central-line-associated bloodstream infections (CLABSIs) has reduced infection rates in ICUs nationwide by 40%, according to preliminary findings from the federal Agency for Healthcare Research and Quality (AHRQ).
AHRQ attributes the decrease to a CLABSI safety checklist from the Comprehensive Unit-Based Safety Program (CUSP) that encourages hospital staff to wash their hands prior to inserting central lines, avoid the femoral site, remove lines when they are no longer needed, and use the antimicrobial agent chlorhexidine to clean the patient's insertion site.
The checklist was developed by Peter Pronovost, MD, PhD, FCCM, and colleagues at Johns Hopkins University in Baltimore, and originally implemented in ICUs statewide in Michigan as the Keystone Project. Since 2009, CUSP has recruited more than 1,000 participating hospitals in 44 states. CUSP collectively reported a decrease to 1.25 from 1.87 CLABSIs per 1,000 central-line days 10-12 months after implementing the program, according to AHRQ [PDF].
The real game-changer for CLABSIs has been the widespread adoption of chlorhexidine as an insertion site disinfectant, says Sanjay Saint, MD, MPH, director of the Veterans Administration at the University of Michigan Patient Safety Enhancement Program in Ann Arbor and professor of medicine at the University of Michigan. Dr. Saint is on the national leadership team of On the CUSP: Stop CAUTI (Catheter-Associated Urinary Tract Infections), an initiative that aims to reduce mean rates of CAUTI infections by 25% in hospitals nationwide.
Although hospitalists don't routinely place central lines, their role in this procedure is growing, both in nonacademic hospitals that lack intensivists and on hospitals' general medicine floors.
"My take-home message for hospitalists: if you are putting in central lines, if you only make one change in practice, is to use chlorhexidine as the site disinfectant," Dr. Saint says.
Visit our website for more information about central-line-associated bloodstream infections.