User login
Accountable Care Organizations (ACO) Gain Popularity with Physicians in Wake of Added Incentives, Revised Federal Rules
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
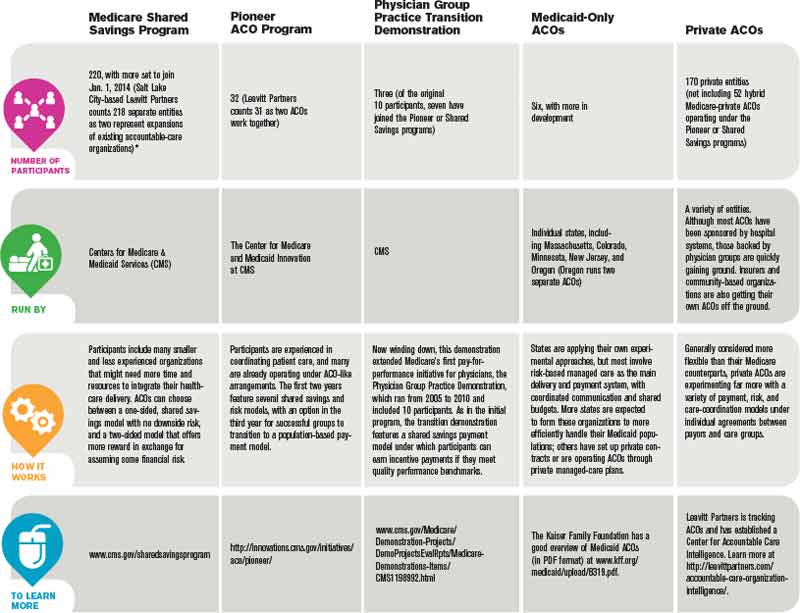
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.

—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”

Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.

—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.

Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.
Reference
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.
—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”
Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.
—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.
Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.
Reference
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.
—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”
Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.
—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.
Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.
Reference
The Future of ACOs Remains Cloudy
Experts disagree on what a sustainable accountable-care organization (ACO) will look like in the future. The shared savings model currently dominates the ACO landscape, but David Muhlestein, an analyst with Washington, D.C.-based healthcare consulting firm Leavitt Partners, says his firm’s interviews with participants suggest that very few see the approach as the best long-term answer. Some believe those capitated models of the 1990s—the much-despised HMOs with their narrowly defined networks and global payments to provider groups—could make a comeback in a slightly altered form. Others feel strongly that a bundled payment model, which provides more flexibility in where patients can go for care, will instead dominate. A few providers have even suggested that the shared savings experiment will eventually revert back to a fee-for-service approach.

—David Muhlestein, analyst, Leavitt Partners, Washington, D.C.
SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says bundled payments and shared savings alone are unlikely to deliver optimal value within the integrated care structure.
“There’s just not enough incentive, and the organization that’s taking risk doesn’t have enough flexibility in terms of how they use resources,” says Dr. Greeno, chief medical officer of Cogent HMG. The real improvements, Dr. Greeno says, might not come until ACOs assume a more capitated structure in which they accept global risk and are given unfettered freedom in how they allocate payments. In the meantime, he says, Medicare could be simply trying to encourage organizations “to start dipping their toe in the water of integrated care.”
John Pilotte, director of performance-based payment policy in the Center for Medicare at CMS, agreed that one major aim of its Shared Savings Program is to provide a “new avenue for providers to work together to better coordinate care for Medicare fee-for-service beneficiaries, and to move away from volume-based incentives and to recognize and reward them for improving the quality and efficiency and effectiveness of the care they deliver.”
Muhlestein says his firm has spoken with many organizations that are carefully monitoring how the current ACOs are faring. “Right now, the ACOs that have formed are people who want to forge their own trail,” he says. “There are many more providers that want to follow some path, and they want to follow a path that has some evidence that it has been successful.”
The more paths that are taken, he says, the greater the likelihood that one or more will achieve success. And although healthcare analysts often talk about success in terms of controlling costs, Muhlestein says, quality improvement (QI) and better outcomes alone could prove alluring to would-be ACOs.
“Even if we don’t see a moderation in cost growth, but we do see an improvement in quality, there is the chance that the model could still stick around, because that’s enough,” he says. “Even if we’re paying the same amount, we’re getting better results, so our value has improved.”
Regardless of how the ACO experiment plays out, Dr. Greeno says, it represents a fundamental shift toward a more integrated, pay-for-performance healthcare system that will not be optional for providers in the near future.
“Everyone is going to be asked to perform at a higher level, and there’s going to be tremendous pressure on hospitalists to lead that performance,” he says. “My advice would be to embrace it—it’s a great opportunity to bring value to the healthcare system.” TH
Bryn Nelson is a freelance medical writer in Seattle.
Experts disagree on what a sustainable accountable-care organization (ACO) will look like in the future. The shared savings model currently dominates the ACO landscape, but David Muhlestein, an analyst with Washington, D.C.-based healthcare consulting firm Leavitt Partners, says his firm’s interviews with participants suggest that very few see the approach as the best long-term answer. Some believe those capitated models of the 1990s—the much-despised HMOs with their narrowly defined networks and global payments to provider groups—could make a comeback in a slightly altered form. Others feel strongly that a bundled payment model, which provides more flexibility in where patients can go for care, will instead dominate. A few providers have even suggested that the shared savings experiment will eventually revert back to a fee-for-service approach.
—David Muhlestein, analyst, Leavitt Partners, Washington, D.C.
SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says bundled payments and shared savings alone are unlikely to deliver optimal value within the integrated care structure.
“There’s just not enough incentive, and the organization that’s taking risk doesn’t have enough flexibility in terms of how they use resources,” says Dr. Greeno, chief medical officer of Cogent HMG. The real improvements, Dr. Greeno says, might not come until ACOs assume a more capitated structure in which they accept global risk and are given unfettered freedom in how they allocate payments. In the meantime, he says, Medicare could be simply trying to encourage organizations “to start dipping their toe in the water of integrated care.”
John Pilotte, director of performance-based payment policy in the Center for Medicare at CMS, agreed that one major aim of its Shared Savings Program is to provide a “new avenue for providers to work together to better coordinate care for Medicare fee-for-service beneficiaries, and to move away from volume-based incentives and to recognize and reward them for improving the quality and efficiency and effectiveness of the care they deliver.”
Muhlestein says his firm has spoken with many organizations that are carefully monitoring how the current ACOs are faring. “Right now, the ACOs that have formed are people who want to forge their own trail,” he says. “There are many more providers that want to follow some path, and they want to follow a path that has some evidence that it has been successful.”
The more paths that are taken, he says, the greater the likelihood that one or more will achieve success. And although healthcare analysts often talk about success in terms of controlling costs, Muhlestein says, quality improvement (QI) and better outcomes alone could prove alluring to would-be ACOs.
“Even if we don’t see a moderation in cost growth, but we do see an improvement in quality, there is the chance that the model could still stick around, because that’s enough,” he says. “Even if we’re paying the same amount, we’re getting better results, so our value has improved.”
Regardless of how the ACO experiment plays out, Dr. Greeno says, it represents a fundamental shift toward a more integrated, pay-for-performance healthcare system that will not be optional for providers in the near future.
“Everyone is going to be asked to perform at a higher level, and there’s going to be tremendous pressure on hospitalists to lead that performance,” he says. “My advice would be to embrace it—it’s a great opportunity to bring value to the healthcare system.” TH
Bryn Nelson is a freelance medical writer in Seattle.
Experts disagree on what a sustainable accountable-care organization (ACO) will look like in the future. The shared savings model currently dominates the ACO landscape, but David Muhlestein, an analyst with Washington, D.C.-based healthcare consulting firm Leavitt Partners, says his firm’s interviews with participants suggest that very few see the approach as the best long-term answer. Some believe those capitated models of the 1990s—the much-despised HMOs with their narrowly defined networks and global payments to provider groups—could make a comeback in a slightly altered form. Others feel strongly that a bundled payment model, which provides more flexibility in where patients can go for care, will instead dominate. A few providers have even suggested that the shared savings experiment will eventually revert back to a fee-for-service approach.
—David Muhlestein, analyst, Leavitt Partners, Washington, D.C.
SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says bundled payments and shared savings alone are unlikely to deliver optimal value within the integrated care structure.
“There’s just not enough incentive, and the organization that’s taking risk doesn’t have enough flexibility in terms of how they use resources,” says Dr. Greeno, chief medical officer of Cogent HMG. The real improvements, Dr. Greeno says, might not come until ACOs assume a more capitated structure in which they accept global risk and are given unfettered freedom in how they allocate payments. In the meantime, he says, Medicare could be simply trying to encourage organizations “to start dipping their toe in the water of integrated care.”
John Pilotte, director of performance-based payment policy in the Center for Medicare at CMS, agreed that one major aim of its Shared Savings Program is to provide a “new avenue for providers to work together to better coordinate care for Medicare fee-for-service beneficiaries, and to move away from volume-based incentives and to recognize and reward them for improving the quality and efficiency and effectiveness of the care they deliver.”
Muhlestein says his firm has spoken with many organizations that are carefully monitoring how the current ACOs are faring. “Right now, the ACOs that have formed are people who want to forge their own trail,” he says. “There are many more providers that want to follow some path, and they want to follow a path that has some evidence that it has been successful.”
The more paths that are taken, he says, the greater the likelihood that one or more will achieve success. And although healthcare analysts often talk about success in terms of controlling costs, Muhlestein says, quality improvement (QI) and better outcomes alone could prove alluring to would-be ACOs.
“Even if we don’t see a moderation in cost growth, but we do see an improvement in quality, there is the chance that the model could still stick around, because that’s enough,” he says. “Even if we’re paying the same amount, we’re getting better results, so our value has improved.”
Regardless of how the ACO experiment plays out, Dr. Greeno says, it represents a fundamental shift toward a more integrated, pay-for-performance healthcare system that will not be optional for providers in the near future.
“Everyone is going to be asked to perform at a higher level, and there’s going to be tremendous pressure on hospitalists to lead that performance,” he says. “My advice would be to embrace it—it’s a great opportunity to bring value to the healthcare system.” TH
Bryn Nelson is a freelance medical writer in Seattle.
SHM Sections Adds Global Health and Human Rights Category
SHM Sections offer opportunities for members to connect with communities of their peers who share specialties or interests. At present, SHM Sections include:
- Med-Peds
- International
- Global Health and Human Rights
- Rural Hospitalists
- Practice Administrators
SHM Section of the Month
Seeing as how the focused-practice pathway for hospitalists is a first of its kind for physician credentialing boards, the ABIM is planning a “fairly significant” research effort tracking participants’ experience, Dr. Holmboe says.
Global Health and Human Rights is one of the newest SHM Sections, and represents a growing passion among hospitalists as increasing numbers of internal-medicine physicians express interest in overseas placements in resource-limited settings. SHM also recognizes the need for mentored training in global health.
Over the last decade, interest in global health has grown significantly amongst trainees, faculty, and staff. Current priorities for global health include: health-system strengthening, workforce training, QI and patient safety. These priorities align to core strengths of hospital medicine, which is therefore well suited to meet these global health challenges.
For more information about this and other Sections, visit www.hospitalmedicine.org/membership.
SHM Sections offer opportunities for members to connect with communities of their peers who share specialties or interests. At present, SHM Sections include:
- Med-Peds
- International
- Global Health and Human Rights
- Rural Hospitalists
- Practice Administrators
SHM Section of the Month
Seeing as how the focused-practice pathway for hospitalists is a first of its kind for physician credentialing boards, the ABIM is planning a “fairly significant” research effort tracking participants’ experience, Dr. Holmboe says.
Global Health and Human Rights is one of the newest SHM Sections, and represents a growing passion among hospitalists as increasing numbers of internal-medicine physicians express interest in overseas placements in resource-limited settings. SHM also recognizes the need for mentored training in global health.
Over the last decade, interest in global health has grown significantly amongst trainees, faculty, and staff. Current priorities for global health include: health-system strengthening, workforce training, QI and patient safety. These priorities align to core strengths of hospital medicine, which is therefore well suited to meet these global health challenges.
For more information about this and other Sections, visit www.hospitalmedicine.org/membership.
SHM Sections offer opportunities for members to connect with communities of their peers who share specialties or interests. At present, SHM Sections include:
- Med-Peds
- International
- Global Health and Human Rights
- Rural Hospitalists
- Practice Administrators
SHM Section of the Month
Seeing as how the focused-practice pathway for hospitalists is a first of its kind for physician credentialing boards, the ABIM is planning a “fairly significant” research effort tracking participants’ experience, Dr. Holmboe says.
Global Health and Human Rights is one of the newest SHM Sections, and represents a growing passion among hospitalists as increasing numbers of internal-medicine physicians express interest in overseas placements in resource-limited settings. SHM also recognizes the need for mentored training in global health.
Over the last decade, interest in global health has grown significantly amongst trainees, faculty, and staff. Current priorities for global health include: health-system strengthening, workforce training, QI and patient safety. These priorities align to core strengths of hospital medicine, which is therefore well suited to meet these global health challenges.
For more information about this and other Sections, visit www.hospitalmedicine.org/membership.
Digital Diagnostic Tools Unpopular with Patients, Study Finds
A recent study from the University of Missouri to explore how patients react to physicians’ use of computerized clinical decision support systems finds that these devices could leave patients feeling ignored and dissatisfied with their medical care, potentially increasing noncompliance with treatment while distracting physicians from the patient encounter.1
“Patients may be concerned that the decision aids reduce their face-to-face time with physicians,” says lead author Victoria Shaffer, PhD, assistant professor of health and psychological sciences at the University of Missouri. She recommends incorporating computerized systems as teaching tools to engage patients and help them understand their diagnoses and recommendations. “Anything physicians or nurses can do to humanize the process may make patients more comfortable,” she says.
The study presented participants with written descriptions of hypothetical physician-patient encounters, with the physician using unaided judgment, pursuing advice from a medical expert, or using computerized clinical decision support. Physicians using the latter were viewed as less capable, but participants also were less likely to assign those physicians responsibility for negative outcomes.
A concurrent study from Missouri, part of a $14 million project funded by the Centers for Medicare & Medicaid Services (CMS) to reduce avoidable rehospitalizations of nursing home residents, suggests that sophisticated information technology (IT) can lead to more robust and integrated communication strategies among clinical staff, as well as better-coordinated care.2 Nursing informatics expert Gregory Alexander found that nursing homes with IT used it to help make clinical decisions, electronically track patient care, and securely relay medical information.
References
- Shaffer VA, Probst CA, Merkle EC, Arkes HR, Mitchell AM. Why do patients derogate physicians who use a computer-based diagnostic support system? Med Decis Making. 2013;33(1):108-118.
- Alexander GL, Steege LM, Pasupathy KS, Wise K. Case studies of IT sophistication in nursing homes: a mixed method approach to examine communication strategies about pressure ulcer prevention practices. SciVerse website. Available at: http://www.sciencedirect.com/science/article/pii/S0169814112001229. Accessed March 10, 2013.
A recent study from the University of Missouri to explore how patients react to physicians’ use of computerized clinical decision support systems finds that these devices could leave patients feeling ignored and dissatisfied with their medical care, potentially increasing noncompliance with treatment while distracting physicians from the patient encounter.1
“Patients may be concerned that the decision aids reduce their face-to-face time with physicians,” says lead author Victoria Shaffer, PhD, assistant professor of health and psychological sciences at the University of Missouri. She recommends incorporating computerized systems as teaching tools to engage patients and help them understand their diagnoses and recommendations. “Anything physicians or nurses can do to humanize the process may make patients more comfortable,” she says.
The study presented participants with written descriptions of hypothetical physician-patient encounters, with the physician using unaided judgment, pursuing advice from a medical expert, or using computerized clinical decision support. Physicians using the latter were viewed as less capable, but participants also were less likely to assign those physicians responsibility for negative outcomes.
A concurrent study from Missouri, part of a $14 million project funded by the Centers for Medicare & Medicaid Services (CMS) to reduce avoidable rehospitalizations of nursing home residents, suggests that sophisticated information technology (IT) can lead to more robust and integrated communication strategies among clinical staff, as well as better-coordinated care.2 Nursing informatics expert Gregory Alexander found that nursing homes with IT used it to help make clinical decisions, electronically track patient care, and securely relay medical information.
References
- Shaffer VA, Probst CA, Merkle EC, Arkes HR, Mitchell AM. Why do patients derogate physicians who use a computer-based diagnostic support system? Med Decis Making. 2013;33(1):108-118.
- Alexander GL, Steege LM, Pasupathy KS, Wise K. Case studies of IT sophistication in nursing homes: a mixed method approach to examine communication strategies about pressure ulcer prevention practices. SciVerse website. Available at: http://www.sciencedirect.com/science/article/pii/S0169814112001229. Accessed March 10, 2013.
A recent study from the University of Missouri to explore how patients react to physicians’ use of computerized clinical decision support systems finds that these devices could leave patients feeling ignored and dissatisfied with their medical care, potentially increasing noncompliance with treatment while distracting physicians from the patient encounter.1
“Patients may be concerned that the decision aids reduce their face-to-face time with physicians,” says lead author Victoria Shaffer, PhD, assistant professor of health and psychological sciences at the University of Missouri. She recommends incorporating computerized systems as teaching tools to engage patients and help them understand their diagnoses and recommendations. “Anything physicians or nurses can do to humanize the process may make patients more comfortable,” she says.
The study presented participants with written descriptions of hypothetical physician-patient encounters, with the physician using unaided judgment, pursuing advice from a medical expert, or using computerized clinical decision support. Physicians using the latter were viewed as less capable, but participants also were less likely to assign those physicians responsibility for negative outcomes.
A concurrent study from Missouri, part of a $14 million project funded by the Centers for Medicare & Medicaid Services (CMS) to reduce avoidable rehospitalizations of nursing home residents, suggests that sophisticated information technology (IT) can lead to more robust and integrated communication strategies among clinical staff, as well as better-coordinated care.2 Nursing informatics expert Gregory Alexander found that nursing homes with IT used it to help make clinical decisions, electronically track patient care, and securely relay medical information.
References
- Shaffer VA, Probst CA, Merkle EC, Arkes HR, Mitchell AM. Why do patients derogate physicians who use a computer-based diagnostic support system? Med Decis Making. 2013;33(1):108-118.
- Alexander GL, Steege LM, Pasupathy KS, Wise K. Case studies of IT sophistication in nursing homes: a mixed method approach to examine communication strategies about pressure ulcer prevention practices. SciVerse website. Available at: http://www.sciencedirect.com/science/article/pii/S0169814112001229. Accessed March 10, 2013.
National Medicare Readmissions Study Identifies Little Progress
A new Dartmouth Atlas Project study of Medicare 30-day hospital readmissions found that rates essentially stayed the same (15.9% for medical discharges) between 2008 and 2010. But readmission rates varied widely across regions, with medical discharges at 18.1% in Bronx, N.Y., versus 11.4% in Ogden, Utah.
The report, The Revolving Door: A Report on U.S. Hospital Readmissions, also incorporates results from in-depth interviews with patients and providers.1 It sheds light on why so many patients (1 in 6 medical and 1 in 8 surgical discharges) end up back in the hospital so soon—and what hospitals, physicians, nurses, and others are doing to limit avoidable readmissions.
An online interactive map (available at www.rwjf.org) displays the Dartmouth data on 30-day readmissions by hospital referral region.
The research was supported and publicized by the Robert Wood Johnson Foundation of Princeton, N.J., which has a number of other efforts under way to address readmissions. Another recent study supported by the foundation’s Nurse Faculty Scholars Program found that increased nurse-to-patient staffing ratios and good working environments for nurses were associated with significantly reduced 30-day readmissions.2
The foundation recently named the five winners of its “Transitions to Better Care” video contest, in which hospitals and health systems submitted short films to highlight innovative local practices to improve care transitions before, during, and after discharge. Check out the winning videos by searching “contest” at rwjf.org.
References
- The Dartmouth Atlas of Health Care. The Revolving Door: A Report on U.S. Hospital Readmissions. The Dartmouth Atlas of Health Care website. Available at: http://www.dartmouthatlas.org/pages/readmissions2013. Accessed March 10, 2013.
- McHugh M, Ma C. Hospital nursing and 30-day readmissions among Medicare patients with heart failure, acute myocardial infarction, and pneumonia. Med Care. 2013;51(1):52-59.
A new Dartmouth Atlas Project study of Medicare 30-day hospital readmissions found that rates essentially stayed the same (15.9% for medical discharges) between 2008 and 2010. But readmission rates varied widely across regions, with medical discharges at 18.1% in Bronx, N.Y., versus 11.4% in Ogden, Utah.
The report, The Revolving Door: A Report on U.S. Hospital Readmissions, also incorporates results from in-depth interviews with patients and providers.1 It sheds light on why so many patients (1 in 6 medical and 1 in 8 surgical discharges) end up back in the hospital so soon—and what hospitals, physicians, nurses, and others are doing to limit avoidable readmissions.
An online interactive map (available at www.rwjf.org) displays the Dartmouth data on 30-day readmissions by hospital referral region.
The research was supported and publicized by the Robert Wood Johnson Foundation of Princeton, N.J., which has a number of other efforts under way to address readmissions. Another recent study supported by the foundation’s Nurse Faculty Scholars Program found that increased nurse-to-patient staffing ratios and good working environments for nurses were associated with significantly reduced 30-day readmissions.2
The foundation recently named the five winners of its “Transitions to Better Care” video contest, in which hospitals and health systems submitted short films to highlight innovative local practices to improve care transitions before, during, and after discharge. Check out the winning videos by searching “contest” at rwjf.org.
References
- The Dartmouth Atlas of Health Care. The Revolving Door: A Report on U.S. Hospital Readmissions. The Dartmouth Atlas of Health Care website. Available at: http://www.dartmouthatlas.org/pages/readmissions2013. Accessed March 10, 2013.
- McHugh M, Ma C. Hospital nursing and 30-day readmissions among Medicare patients with heart failure, acute myocardial infarction, and pneumonia. Med Care. 2013;51(1):52-59.
A new Dartmouth Atlas Project study of Medicare 30-day hospital readmissions found that rates essentially stayed the same (15.9% for medical discharges) between 2008 and 2010. But readmission rates varied widely across regions, with medical discharges at 18.1% in Bronx, N.Y., versus 11.4% in Ogden, Utah.
The report, The Revolving Door: A Report on U.S. Hospital Readmissions, also incorporates results from in-depth interviews with patients and providers.1 It sheds light on why so many patients (1 in 6 medical and 1 in 8 surgical discharges) end up back in the hospital so soon—and what hospitals, physicians, nurses, and others are doing to limit avoidable readmissions.
An online interactive map (available at www.rwjf.org) displays the Dartmouth data on 30-day readmissions by hospital referral region.
The research was supported and publicized by the Robert Wood Johnson Foundation of Princeton, N.J., which has a number of other efforts under way to address readmissions. Another recent study supported by the foundation’s Nurse Faculty Scholars Program found that increased nurse-to-patient staffing ratios and good working environments for nurses were associated with significantly reduced 30-day readmissions.2
The foundation recently named the five winners of its “Transitions to Better Care” video contest, in which hospitals and health systems submitted short films to highlight innovative local practices to improve care transitions before, during, and after discharge. Check out the winning videos by searching “contest” at rwjf.org.
References
- The Dartmouth Atlas of Health Care. The Revolving Door: A Report on U.S. Hospital Readmissions. The Dartmouth Atlas of Health Care website. Available at: http://www.dartmouthatlas.org/pages/readmissions2013. Accessed March 10, 2013.
- McHugh M, Ma C. Hospital nursing and 30-day readmissions among Medicare patients with heart failure, acute myocardial infarction, and pneumonia. Med Care. 2013;51(1):52-59.
Society of Hospital Medicine Launches Online Training Program for Hospitalists
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)
Hospital Medicine Advocates Aid in Securing $10 Million for National Quality Forum
Hospitalists on the Hill
WHEN: May 16, 2013
WHERE: Washington, D.C.
HOW: Register today at www.hospitalmedicine2013.org/onthehill Space is limited.
The American Taxpayer Relief Act, which was signed into law Jan. 3 to stave off the fiscal cliff, contained a little-mentioned provision that reauthorized $10 million in Medicare funding for the National Quality Forum (NQF). Hospitalists, taking on the role of policy advocates, helped secure this reauthorization and score a victory for national quality-improvement (QI) efforts.
The NQF is a nonprofit organization established to create consensus around national priorities and measures for performing reporting and improvement in healthcare. It receives funding through a variety of sources ranging from public funds, private organizations and membership dues. Since 2009, it has received $10 million annually from a U.S. Department of Health and Human Services contract. That contract, a significant portion of NQF funding, was set to end in 2012.
The Stand for Quality coalition, composed of healthcare organizations supportive of the NQF, helps ensure that Congress sustains funding and support of performance measurement reporting and QI. SHM historically has been a strong proponent of the NQF, pitching in at the start of Stand for Quality four years ago this month. As it became clear that the federal contract for the NQF was not likely to be renewed by Congress for the 2013 calendar year, the member organizations of Stand for Quality were asked to step up to the plate in any way they could.
Jumping at the opportunity to assist, SHM linked hospitalists to their members of Congress in support of the NQF. Through members of SHM's Public Policy and Performance Measurement and Reporting committees, SHM connected with congressional offices and urged them to join a sign-on letter from the office of U.S. Sen. Mark Begich (D-Alaska) office in support of continued NQF funding. Letters between members of Congress are a way that legislators internally lobby on behalf of a particular issue. Hearing from their constituents can help persuade a legislator to act.
Sharing professional expertise also can inform a legislator's decisions. SHM members have a wealth of specialized knowledge and experiences that greatly benefit health policy discussions. In December 2012, SHM was asked to join NQF staffers and several other organizations on Capitol Hill for visits with select members of Congress, including several physician-legislators. These meetings were designed to raise the profile of the important work NQF is doing for QI and to make sure that NQF funding was not forgotten in any debt deal.
Mangla Gulati, MD, FACP, FHM, a hospitalist and SHM member, participated in these visits on behalf of hospital medicine and provided much-needed physician input on the importance of NQF's work.
The benefits of in-person visits are mutual: Members of Congress learn more about the real-life effects of a particular policy and, according to Dr. Gulati, "the visits to the Hill were a very valuable experience and shed a whole new light on the challenges we face in medicine."
Taken together, these advocacy tactics—coalition-building, contacting congressional offices, and in-person visits in Washington—were crucial to securing NQF's funding reauthorization and are critical tools for the advocacy work at SHM. The most concrete and impactful advocacy includes positioning hospitalists on the front line and sharing their perspectives and experiences with policymakers and their staffs.
We hope you'll heed this call and join SHM in Washington, D.C., May 16 for Hospitalists on the Hill, part of SHM's annual meeting. For more information and to register, go to www.hospitalmedicine2013.org/onthehill.
Joshua Lapps is SHM's government relations specialist.
Hospitalists on the Hill
WHEN: May 16, 2013
WHERE: Washington, D.C.
HOW: Register today at www.hospitalmedicine2013.org/onthehill Space is limited.
The American Taxpayer Relief Act, which was signed into law Jan. 3 to stave off the fiscal cliff, contained a little-mentioned provision that reauthorized $10 million in Medicare funding for the National Quality Forum (NQF). Hospitalists, taking on the role of policy advocates, helped secure this reauthorization and score a victory for national quality-improvement (QI) efforts.
The NQF is a nonprofit organization established to create consensus around national priorities and measures for performing reporting and improvement in healthcare. It receives funding through a variety of sources ranging from public funds, private organizations and membership dues. Since 2009, it has received $10 million annually from a U.S. Department of Health and Human Services contract. That contract, a significant portion of NQF funding, was set to end in 2012.
The Stand for Quality coalition, composed of healthcare organizations supportive of the NQF, helps ensure that Congress sustains funding and support of performance measurement reporting and QI. SHM historically has been a strong proponent of the NQF, pitching in at the start of Stand for Quality four years ago this month. As it became clear that the federal contract for the NQF was not likely to be renewed by Congress for the 2013 calendar year, the member organizations of Stand for Quality were asked to step up to the plate in any way they could.
Jumping at the opportunity to assist, SHM linked hospitalists to their members of Congress in support of the NQF. Through members of SHM's Public Policy and Performance Measurement and Reporting committees, SHM connected with congressional offices and urged them to join a sign-on letter from the office of U.S. Sen. Mark Begich (D-Alaska) office in support of continued NQF funding. Letters between members of Congress are a way that legislators internally lobby on behalf of a particular issue. Hearing from their constituents can help persuade a legislator to act.
Sharing professional expertise also can inform a legislator's decisions. SHM members have a wealth of specialized knowledge and experiences that greatly benefit health policy discussions. In December 2012, SHM was asked to join NQF staffers and several other organizations on Capitol Hill for visits with select members of Congress, including several physician-legislators. These meetings were designed to raise the profile of the important work NQF is doing for QI and to make sure that NQF funding was not forgotten in any debt deal.
Mangla Gulati, MD, FACP, FHM, a hospitalist and SHM member, participated in these visits on behalf of hospital medicine and provided much-needed physician input on the importance of NQF's work.
The benefits of in-person visits are mutual: Members of Congress learn more about the real-life effects of a particular policy and, according to Dr. Gulati, "the visits to the Hill were a very valuable experience and shed a whole new light on the challenges we face in medicine."
Taken together, these advocacy tactics—coalition-building, contacting congressional offices, and in-person visits in Washington—were crucial to securing NQF's funding reauthorization and are critical tools for the advocacy work at SHM. The most concrete and impactful advocacy includes positioning hospitalists on the front line and sharing their perspectives and experiences with policymakers and their staffs.
We hope you'll heed this call and join SHM in Washington, D.C., May 16 for Hospitalists on the Hill, part of SHM's annual meeting. For more information and to register, go to www.hospitalmedicine2013.org/onthehill.
Joshua Lapps is SHM's government relations specialist.
Hospitalists on the Hill
WHEN: May 16, 2013
WHERE: Washington, D.C.
HOW: Register today at www.hospitalmedicine2013.org/onthehill Space is limited.
The American Taxpayer Relief Act, which was signed into law Jan. 3 to stave off the fiscal cliff, contained a little-mentioned provision that reauthorized $10 million in Medicare funding for the National Quality Forum (NQF). Hospitalists, taking on the role of policy advocates, helped secure this reauthorization and score a victory for national quality-improvement (QI) efforts.
The NQF is a nonprofit organization established to create consensus around national priorities and measures for performing reporting and improvement in healthcare. It receives funding through a variety of sources ranging from public funds, private organizations and membership dues. Since 2009, it has received $10 million annually from a U.S. Department of Health and Human Services contract. That contract, a significant portion of NQF funding, was set to end in 2012.
The Stand for Quality coalition, composed of healthcare organizations supportive of the NQF, helps ensure that Congress sustains funding and support of performance measurement reporting and QI. SHM historically has been a strong proponent of the NQF, pitching in at the start of Stand for Quality four years ago this month. As it became clear that the federal contract for the NQF was not likely to be renewed by Congress for the 2013 calendar year, the member organizations of Stand for Quality were asked to step up to the plate in any way they could.
Jumping at the opportunity to assist, SHM linked hospitalists to their members of Congress in support of the NQF. Through members of SHM's Public Policy and Performance Measurement and Reporting committees, SHM connected with congressional offices and urged them to join a sign-on letter from the office of U.S. Sen. Mark Begich (D-Alaska) office in support of continued NQF funding. Letters between members of Congress are a way that legislators internally lobby on behalf of a particular issue. Hearing from their constituents can help persuade a legislator to act.
Sharing professional expertise also can inform a legislator's decisions. SHM members have a wealth of specialized knowledge and experiences that greatly benefit health policy discussions. In December 2012, SHM was asked to join NQF staffers and several other organizations on Capitol Hill for visits with select members of Congress, including several physician-legislators. These meetings were designed to raise the profile of the important work NQF is doing for QI and to make sure that NQF funding was not forgotten in any debt deal.
Mangla Gulati, MD, FACP, FHM, a hospitalist and SHM member, participated in these visits on behalf of hospital medicine and provided much-needed physician input on the importance of NQF's work.
The benefits of in-person visits are mutual: Members of Congress learn more about the real-life effects of a particular policy and, according to Dr. Gulati, "the visits to the Hill were a very valuable experience and shed a whole new light on the challenges we face in medicine."
Taken together, these advocacy tactics—coalition-building, contacting congressional offices, and in-person visits in Washington—were crucial to securing NQF's funding reauthorization and are critical tools for the advocacy work at SHM. The most concrete and impactful advocacy includes positioning hospitalists on the front line and sharing their perspectives and experiences with policymakers and their staffs.
We hope you'll heed this call and join SHM in Washington, D.C., May 16 for Hospitalists on the Hill, part of SHM's annual meeting. For more information and to register, go to www.hospitalmedicine2013.org/onthehill.
Joshua Lapps is SHM's government relations specialist.
HMX Term of the Month: Achievement Points
Awarded to a hospital by comparing an individual hospital’s performance measure rates during a certain period with all hospitals’ rates during the baseline period.
Awarded to a hospital by comparing an individual hospital’s performance measure rates during a certain period with all hospitals’ rates during the baseline period.
Awarded to a hospital by comparing an individual hospital’s performance measure rates during a certain period with all hospitals’ rates during the baseline period.
Win Whitcomb: Hospital Value-Based Purchasing Program Adds Measure in Efficiency Domain

HVBP’s First Efficiency Measure
Move over, cost, LOS—make room for ‘Medicare spending per beneficiary’
The unwritten rule in hospitalist circles is that lower cost and length of stay (LOS) mean higher efficiency, with hospitalists (me included) often pointing to one or both of these as a yardstick of performance in the efficiency domain. But if we lower hospital length of stay and costs while shifting costs to post-hospital care, have we solved anything?
This very question was raised by Kuo and Goodwin’s observational study that revealed that decreased hospital costs and LOS were offset by higher utilization and costs after discharge under hospitalist care.1
Efficiency As a Domain of Quality
Using the Institute of Medicine’s (IOM) six domains of quality as a framework (see Table 1, right), the Centers for Medicare & Medicaid Services’ (CMS) Hospital Value-Based Purchasing (HVBP) program seeks to encourage enhanced quality in all of the IOM domains. For HVBP 2015, we see the addition of the first measure in the domain of efficiency.
You may be saying to yourself, “It’s only 2013. Why should I worry about HVBP 2015?” Here’s why: The measurement periods for HVBP 2015 are May to December 2011 (baseline) and May to December 2013 (performance). Hospitals can succeed under HVBP if they demonstrate improvement from baseline or attainment, which indicates maintenance of a high level of performance despite no substantial improvement from baseline. Medicare spending per beneficiary (MSPB) will make up 20% of the 2015 HVBP incentive pool for hospitals.
Medicare Spending Per Beneficiary Instead of Costs or LOS
Why did CMS choose to use MSPB as a measure and not simply hospital costs or length of stay? Measuring efficiency of hospital care has proven to be a sticky wicket. If one simply measures and rewards decreased hospital costs and/or length of stay (which you might legitimately argue is exactly what the current DRG system does by paying a case rate to the hospital), one runs the risk of shifting costs to settings beyond the four walls of the hospital, or even fueling higher rates of hospital readmissions. Also, physician costs and other costs (therapy, home care) are not accounted for; they are accounted for under MSPB (described below). Finally, hospital costs and LOS vary substantially across regions and by severity of illness of the patients being analyzed. This makes it difficult to compare, for example, LOS in California versus Massachusetts.
The MSPB is designed to be a comprehensive and equitable metric:
- It seeks to eliminate cost-shifting among settings by widening the time period from three days prior to 30 days post-inpatient-care episode;
- It looks at the full cost of care by including expenses from both Medicare Part A (hospital) and Part B (doctors, PT, OT, home health, others);
- It incorporates risk adjustment by taking into account differences in patient health status; and
- It seeks to level the playing field by using a price standardization methodology that factors in geographic payment differences in wages, practice costs, and payments for indirect medical education and disproportionate share hospitals (those that treat large numbers of the indigent population).
Driving High Performance in Medicare Spending Per Beneficiary
Hospitalists straddle the Part A and Part B elements of Medicare; they have one foot in the hospital and one foot in the physician practice world. They should be able to improve their hospitals’ performance under the MSPB yardstick. Since the performance measurement period starts in May, now is the time to sharpen your focus on MSPB.
Here are the top priorities for MSPB that I recommend for hospitalists:
Reduction of marginally beneficial resource utilization. This is a process of analyzing resource (e.g. pharmacy, radiology, laboratory, blood products) utilization for the purpose of minimizing costly practices that do not benefit the patient. This is an essential practice of a high-functioning hospitalist program. Through its participation in the Choosing Wisely campaign (see “Stop! Think Twice Before You Order,” p. 46), SHM has helped hospitalists have conversations about these practices with patients.
Hospital throughput. Work on “front end” throughput with the ED by having a process in place to quickly evaluate and facilitate potential admissions. Work with case management to assure timely (and early in the day) discharges.
Safe-discharge processes. We reviewed key elements of a safe discharge last month and provided a link to SHM’s Project BOOST (www.hospitalmedicine.org/boost). From the MSPB perspective: A safe discharge minimizes exorbitant spending after discharge.
Documentation integrity. Because MSPB is risk-adjusted, the more the record reflects patient severity of illness, the better your hospital will perform, all else being equal. Work collaboratively with your documentation integrity professionals!
Much of the success of the HM specialty has been built on the tenet that the hospitalist model delivers efficient inpatient care. In the coming years, the specialty’s contribution will increasingly be gauged by the MSPB measure.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
HVBP’s First Efficiency Measure
Move over, cost, LOS—make room for ‘Medicare spending per beneficiary’
The unwritten rule in hospitalist circles is that lower cost and length of stay (LOS) mean higher efficiency, with hospitalists (me included) often pointing to one or both of these as a yardstick of performance in the efficiency domain. But if we lower hospital length of stay and costs while shifting costs to post-hospital care, have we solved anything?
This very question was raised by Kuo and Goodwin’s observational study that revealed that decreased hospital costs and LOS were offset by higher utilization and costs after discharge under hospitalist care.1
Efficiency As a Domain of Quality
Using the Institute of Medicine’s (IOM) six domains of quality as a framework (see Table 1, right), the Centers for Medicare & Medicaid Services’ (CMS) Hospital Value-Based Purchasing (HVBP) program seeks to encourage enhanced quality in all of the IOM domains. For HVBP 2015, we see the addition of the first measure in the domain of efficiency.
You may be saying to yourself, “It’s only 2013. Why should I worry about HVBP 2015?” Here’s why: The measurement periods for HVBP 2015 are May to December 2011 (baseline) and May to December 2013 (performance). Hospitals can succeed under HVBP if they demonstrate improvement from baseline or attainment, which indicates maintenance of a high level of performance despite no substantial improvement from baseline. Medicare spending per beneficiary (MSPB) will make up 20% of the 2015 HVBP incentive pool for hospitals.
Medicare Spending Per Beneficiary Instead of Costs or LOS
Why did CMS choose to use MSPB as a measure and not simply hospital costs or length of stay? Measuring efficiency of hospital care has proven to be a sticky wicket. If one simply measures and rewards decreased hospital costs and/or length of stay (which you might legitimately argue is exactly what the current DRG system does by paying a case rate to the hospital), one runs the risk of shifting costs to settings beyond the four walls of the hospital, or even fueling higher rates of hospital readmissions. Also, physician costs and other costs (therapy, home care) are not accounted for; they are accounted for under MSPB (described below). Finally, hospital costs and LOS vary substantially across regions and by severity of illness of the patients being analyzed. This makes it difficult to compare, for example, LOS in California versus Massachusetts.
The MSPB is designed to be a comprehensive and equitable metric:
- It seeks to eliminate cost-shifting among settings by widening the time period from three days prior to 30 days post-inpatient-care episode;
- It looks at the full cost of care by including expenses from both Medicare Part A (hospital) and Part B (doctors, PT, OT, home health, others);
- It incorporates risk adjustment by taking into account differences in patient health status; and
- It seeks to level the playing field by using a price standardization methodology that factors in geographic payment differences in wages, practice costs, and payments for indirect medical education and disproportionate share hospitals (those that treat large numbers of the indigent population).
Driving High Performance in Medicare Spending Per Beneficiary
Hospitalists straddle the Part A and Part B elements of Medicare; they have one foot in the hospital and one foot in the physician practice world. They should be able to improve their hospitals’ performance under the MSPB yardstick. Since the performance measurement period starts in May, now is the time to sharpen your focus on MSPB.
Here are the top priorities for MSPB that I recommend for hospitalists:
Reduction of marginally beneficial resource utilization. This is a process of analyzing resource (e.g. pharmacy, radiology, laboratory, blood products) utilization for the purpose of minimizing costly practices that do not benefit the patient. This is an essential practice of a high-functioning hospitalist program. Through its participation in the Choosing Wisely campaign (see “Stop! Think Twice Before You Order,” p. 46), SHM has helped hospitalists have conversations about these practices with patients.
Hospital throughput. Work on “front end” throughput with the ED by having a process in place to quickly evaluate and facilitate potential admissions. Work with case management to assure timely (and early in the day) discharges.
Safe-discharge processes. We reviewed key elements of a safe discharge last month and provided a link to SHM’s Project BOOST (www.hospitalmedicine.org/boost). From the MSPB perspective: A safe discharge minimizes exorbitant spending after discharge.
Documentation integrity. Because MSPB is risk-adjusted, the more the record reflects patient severity of illness, the better your hospital will perform, all else being equal. Work collaboratively with your documentation integrity professionals!
Much of the success of the HM specialty has been built on the tenet that the hospitalist model delivers efficient inpatient care. In the coming years, the specialty’s contribution will increasingly be gauged by the MSPB measure.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
HVBP’s First Efficiency Measure
Move over, cost, LOS—make room for ‘Medicare spending per beneficiary’
The unwritten rule in hospitalist circles is that lower cost and length of stay (LOS) mean higher efficiency, with hospitalists (me included) often pointing to one or both of these as a yardstick of performance in the efficiency domain. But if we lower hospital length of stay and costs while shifting costs to post-hospital care, have we solved anything?
This very question was raised by Kuo and Goodwin’s observational study that revealed that decreased hospital costs and LOS were offset by higher utilization and costs after discharge under hospitalist care.1
Efficiency As a Domain of Quality
Using the Institute of Medicine’s (IOM) six domains of quality as a framework (see Table 1, right), the Centers for Medicare & Medicaid Services’ (CMS) Hospital Value-Based Purchasing (HVBP) program seeks to encourage enhanced quality in all of the IOM domains. For HVBP 2015, we see the addition of the first measure in the domain of efficiency.
You may be saying to yourself, “It’s only 2013. Why should I worry about HVBP 2015?” Here’s why: The measurement periods for HVBP 2015 are May to December 2011 (baseline) and May to December 2013 (performance). Hospitals can succeed under HVBP if they demonstrate improvement from baseline or attainment, which indicates maintenance of a high level of performance despite no substantial improvement from baseline. Medicare spending per beneficiary (MSPB) will make up 20% of the 2015 HVBP incentive pool for hospitals.
Medicare Spending Per Beneficiary Instead of Costs or LOS
Why did CMS choose to use MSPB as a measure and not simply hospital costs or length of stay? Measuring efficiency of hospital care has proven to be a sticky wicket. If one simply measures and rewards decreased hospital costs and/or length of stay (which you might legitimately argue is exactly what the current DRG system does by paying a case rate to the hospital), one runs the risk of shifting costs to settings beyond the four walls of the hospital, or even fueling higher rates of hospital readmissions. Also, physician costs and other costs (therapy, home care) are not accounted for; they are accounted for under MSPB (described below). Finally, hospital costs and LOS vary substantially across regions and by severity of illness of the patients being analyzed. This makes it difficult to compare, for example, LOS in California versus Massachusetts.
The MSPB is designed to be a comprehensive and equitable metric:
- It seeks to eliminate cost-shifting among settings by widening the time period from three days prior to 30 days post-inpatient-care episode;
- It looks at the full cost of care by including expenses from both Medicare Part A (hospital) and Part B (doctors, PT, OT, home health, others);
- It incorporates risk adjustment by taking into account differences in patient health status; and
- It seeks to level the playing field by using a price standardization methodology that factors in geographic payment differences in wages, practice costs, and payments for indirect medical education and disproportionate share hospitals (those that treat large numbers of the indigent population).
Driving High Performance in Medicare Spending Per Beneficiary
Hospitalists straddle the Part A and Part B elements of Medicare; they have one foot in the hospital and one foot in the physician practice world. They should be able to improve their hospitals’ performance under the MSPB yardstick. Since the performance measurement period starts in May, now is the time to sharpen your focus on MSPB.
Here are the top priorities for MSPB that I recommend for hospitalists:
Reduction of marginally beneficial resource utilization. This is a process of analyzing resource (e.g. pharmacy, radiology, laboratory, blood products) utilization for the purpose of minimizing costly practices that do not benefit the patient. This is an essential practice of a high-functioning hospitalist program. Through its participation in the Choosing Wisely campaign (see “Stop! Think Twice Before You Order,” p. 46), SHM has helped hospitalists have conversations about these practices with patients.
Hospital throughput. Work on “front end” throughput with the ED by having a process in place to quickly evaluate and facilitate potential admissions. Work with case management to assure timely (and early in the day) discharges.
Safe-discharge processes. We reviewed key elements of a safe discharge last month and provided a link to SHM’s Project BOOST (www.hospitalmedicine.org/boost). From the MSPB perspective: A safe discharge minimizes exorbitant spending after discharge.
Documentation integrity. Because MSPB is risk-adjusted, the more the record reflects patient severity of illness, the better your hospital will perform, all else being equal. Work collaboratively with your documentation integrity professionals!
Much of the success of the HM specialty has been built on the tenet that the hospitalist model delivers efficient inpatient care. In the coming years, the specialty’s contribution will increasingly be gauged by the MSPB measure.
Reference
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at wfwhit@comcast.net.
Choosing Wisely Campaign Initiatives Grounded in Tenets of Hospital Medicine

The Choosing Wisely campaign is focused on better decision-making, improved quality, and decreased healthcare costs. Such focus on efficiency and cost-effectiveness also was part of the initial motivation for developing hospital medicine, says one of HM’s pioneering doctors.
Robert Wachter, MD, MHM, who heads the division of hospital medicine at the University of California at San Francisco, compares the current national obsession about healthcare waste with the medical quality and patient safety movements of the past decade.
“It’s the right time, the right message, and the right messenger,” says Dr. Wachter, who also chairs the American Board of Internal Medicine and sits on the board of the ABIM Foundation. “We’re a little scared about raised expectations. Delivering on them is going to be more difficult, even, than patient safety was, because ultimately it will require curtailing some income streams. You can’t reach the final outcome of cutting costs in healthcare without someone making less money.”
Dr. Wachter expects the medical community to hear “similar kinds of drumbeats about waste” from every corner of healthcare. “I think hospitalists should be active and enthusiastic partners in the Choosing Wisely campaign,” he says, “and leaders in American healthcare’s efforts to figure out how to purge waste from the system and decrease unnecessary expense.
The Choosing Wisely campaign is focused on better decision-making, improved quality, and decreased healthcare costs. Such focus on efficiency and cost-effectiveness also was part of the initial motivation for developing hospital medicine, says one of HM’s pioneering doctors.
Robert Wachter, MD, MHM, who heads the division of hospital medicine at the University of California at San Francisco, compares the current national obsession about healthcare waste with the medical quality and patient safety movements of the past decade.
“It’s the right time, the right message, and the right messenger,” says Dr. Wachter, who also chairs the American Board of Internal Medicine and sits on the board of the ABIM Foundation. “We’re a little scared about raised expectations. Delivering on them is going to be more difficult, even, than patient safety was, because ultimately it will require curtailing some income streams. You can’t reach the final outcome of cutting costs in healthcare without someone making less money.”
Dr. Wachter expects the medical community to hear “similar kinds of drumbeats about waste” from every corner of healthcare. “I think hospitalists should be active and enthusiastic partners in the Choosing Wisely campaign,” he says, “and leaders in American healthcare’s efforts to figure out how to purge waste from the system and decrease unnecessary expense.
The Choosing Wisely campaign is focused on better decision-making, improved quality, and decreased healthcare costs. Such focus on efficiency and cost-effectiveness also was part of the initial motivation for developing hospital medicine, says one of HM’s pioneering doctors.
Robert Wachter, MD, MHM, who heads the division of hospital medicine at the University of California at San Francisco, compares the current national obsession about healthcare waste with the medical quality and patient safety movements of the past decade.
“It’s the right time, the right message, and the right messenger,” says Dr. Wachter, who also chairs the American Board of Internal Medicine and sits on the board of the ABIM Foundation. “We’re a little scared about raised expectations. Delivering on them is going to be more difficult, even, than patient safety was, because ultimately it will require curtailing some income streams. You can’t reach the final outcome of cutting costs in healthcare without someone making less money.”
Dr. Wachter expects the medical community to hear “similar kinds of drumbeats about waste” from every corner of healthcare. “I think hospitalists should be active and enthusiastic partners in the Choosing Wisely campaign,” he says, “and leaders in American healthcare’s efforts to figure out how to purge waste from the system and decrease unnecessary expense.