Did you know you can honor a family member, friend, or colleague whose life has been touched by GI research through a gift to the AGA Research Foundation? Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit.
Giving now or later. Any charitable gift can be made in honor or memory of someone.
A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax. A cash gift of $5,000 or more qualifies for membership in the AGA Supporter Circle.
A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly a percentage of your estate will pass to the AGA Research Foundation in honor of your loved one. A gift in your will of $50,000 or more qualifies for membership in the AGA Legacy Society, which recognizes the foundation’s most generous individual donors.
Named commentary section funds. You can support a commentary section in a specific AGA journal to honor or memorialize a loved one. This can be established with a gift of $100,000 over the course of 5 years or through an estate gift. The AGA Institute Publications Committee will work with you to provide name recognition for the commentary section in a specific AGA journal for five years. All content and editing will be conducted by the editorial board of the journal.
Your Next Step
An honorary gift is a wonderful way to acknowledge someone’s vision for the future. To learn more about ways to recognize your honoree, visit our website at www.foundation.gastro.org.
Did you know you can honor a family member, friend, or colleague whose life has been touched by GI research through a gift to the AGA Research Foundation? Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit.
Giving now or later. Any charitable gift can be made in honor or memory of someone.
A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax. A cash gift of $5,000 or more qualifies for membership in the AGA Supporter Circle.
A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly a percentage of your estate will pass to the AGA Research Foundation in honor of your loved one. A gift in your will of $50,000 or more qualifies for membership in the AGA Legacy Society, which recognizes the foundation’s most generous individual donors.
Named commentary section funds. You can support a commentary section in a specific AGA journal to honor or memorialize a loved one. This can be established with a gift of $100,000 over the course of 5 years or through an estate gift. The AGA Institute Publications Committee will work with you to provide name recognition for the commentary section in a specific AGA journal for five years. All content and editing will be conducted by the editorial board of the journal.
Your Next Step
An honorary gift is a wonderful way to acknowledge someone’s vision for the future. To learn more about ways to recognize your honoree, visit our website at www.foundation.gastro.org.
Did you know you can honor a family member, friend, or colleague whose life has been touched by GI research through a gift to the AGA Research Foundation? Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit.
Giving now or later. Any charitable gift can be made in honor or memory of someone.
A gift today. An outright gift will help fund the AGA Research Awards Program. Your gift will assist in furthering basic digestive disease research which can ultimately advance research into all digestive diseases. The financial benefits include an income tax deduction and possible elimination of capital gains tax. A cash gift of $5,000 or more qualifies for membership in the AGA Supporter Circle.
A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly a percentage of your estate will pass to the AGA Research Foundation in honor of your loved one. A gift in your will of $50,000 or more qualifies for membership in the AGA Legacy Society, which recognizes the foundation’s most generous individual donors.
Named commentary section funds. You can support a commentary section in a specific AGA journal to honor or memorialize a loved one. This can be established with a gift of $100,000 over the course of 5 years or through an estate gift. The AGA Institute Publications Committee will work with you to provide name recognition for the commentary section in a specific AGA journal for five years. All content and editing will be conducted by the editorial board of the journal.
Your Next Step
An honorary gift is a wonderful way to acknowledge someone’s vision for the future. To learn more about ways to recognize your honoree, visit our website at www.foundation.gastro.org.
Lung cancer stands as the leading cause of cancer-related deaths globally, with its prevalence casting a long and challenging shadow. The most important risk factor for lung cancer is tobacco use, a relationship strongly substantiated by data. The impact of smoking cessation to reduce lung cancer incidence is underscored by the US Preventive Services Task Force, which mandates that smoking cessation services be an integral component of lung cancer screening programs.
However, beneath the surface of this overarching concern lies a web of factors contributing to racial and ethnic disparities in smoking cessation. Cultural intricacies play a pivotal role in shaping these disparities. Despite higher instances of light or intermediate smoking, racially ethnic minority groups in the general population often face greater challenges in achieving smoking cessation, as highlighted by Bacio, et al. Adding another layer to this complex scenario is the profound impact of sustained smoking during cancer treatment. Research suggests that for individuals diagnosed with lung cancer, smoking cessation can markedly boost treatment efficacy, reduce the risk of secondary tumors, and even double the chances of survival.1
A study by Harris, et al. delving into the preferences of current smokers within a lung cancer screening setting uncovered noteworthy insights.2 White participants exhibited a fourfold greater likelihood of favoring a digital format for receiving smoking cessation information, while their Black counterparts expressed a preference for face-to-face support, phone assistance, or printed materials.
Moreover, a meta-analysis conducted by Jabari, et al. sheds light on the efficacy of culturally targeted smoking interventions.3 This comprehensive review describes a dual-level approach to tailoring smoking cessation health interventions: surface and deep. Surface adaptations encompass elements like language and imagery, which aim to enhance the acceptability of interventions within specific communities. Simultaneously, deep-tailored elements identify culturally significant factors that can fundamentally influence the behavior of the target population. The findings of this meta-analysis reveal that the integration of culturally tailored components into standard interventions significantly enhances their efficacy in facilitating smoking cessation.
In conclusion, sustained smoking cessation is a crucial element in combating the global burden of lung cancer. Recognizing the importance of individualized approaches in health care, it is imperative to tailor smoking cessation communications and interventions to diverse cultural influences and socioeconomic factors. Culturally tailored smoking cessation programs that account for nuances specific to each community have the potential to significantly enhance their effectiveness. This necessitates a shift towards individualized smoking cessation care, with a targeted focus on increasing cessation rates among racial and ethnic minority groups. In doing so, we take a step closer to a more equitable landscape in the battle against lung cancer.
Lung cancer stands as the leading cause of cancer-related deaths globally, with its prevalence casting a long and challenging shadow. The most important risk factor for lung cancer is tobacco use, a relationship strongly substantiated by data. The impact of smoking cessation to reduce lung cancer incidence is underscored by the US Preventive Services Task Force, which mandates that smoking cessation services be an integral component of lung cancer screening programs.
However, beneath the surface of this overarching concern lies a web of factors contributing to racial and ethnic disparities in smoking cessation. Cultural intricacies play a pivotal role in shaping these disparities. Despite higher instances of light or intermediate smoking, racially ethnic minority groups in the general population often face greater challenges in achieving smoking cessation, as highlighted by Bacio, et al. Adding another layer to this complex scenario is the profound impact of sustained smoking during cancer treatment. Research suggests that for individuals diagnosed with lung cancer, smoking cessation can markedly boost treatment efficacy, reduce the risk of secondary tumors, and even double the chances of survival.1
A study by Harris, et al. delving into the preferences of current smokers within a lung cancer screening setting uncovered noteworthy insights.2 White participants exhibited a fourfold greater likelihood of favoring a digital format for receiving smoking cessation information, while their Black counterparts expressed a preference for face-to-face support, phone assistance, or printed materials.
Moreover, a meta-analysis conducted by Jabari, et al. sheds light on the efficacy of culturally targeted smoking interventions.3 This comprehensive review describes a dual-level approach to tailoring smoking cessation health interventions: surface and deep. Surface adaptations encompass elements like language and imagery, which aim to enhance the acceptability of interventions within specific communities. Simultaneously, deep-tailored elements identify culturally significant factors that can fundamentally influence the behavior of the target population. The findings of this meta-analysis reveal that the integration of culturally tailored components into standard interventions significantly enhances their efficacy in facilitating smoking cessation.
In conclusion, sustained smoking cessation is a crucial element in combating the global burden of lung cancer. Recognizing the importance of individualized approaches in health care, it is imperative to tailor smoking cessation communications and interventions to diverse cultural influences and socioeconomic factors. Culturally tailored smoking cessation programs that account for nuances specific to each community have the potential to significantly enhance their effectiveness. This necessitates a shift towards individualized smoking cessation care, with a targeted focus on increasing cessation rates among racial and ethnic minority groups. In doing so, we take a step closer to a more equitable landscape in the battle against lung cancer.
References
1. Dresler et al. Lung Cancer. 2003.
2. J Cancer Educ. 2018;33[5].
3. Addiction. 2023.
Thoracic Oncology And Chest Procedures Network
Lung Cancer Section
Stella Ogake, MD, FCCP
Lung cancer stands as the leading cause of cancer-related deaths globally, with its prevalence casting a long and challenging shadow. The most important risk factor for lung cancer is tobacco use, a relationship strongly substantiated by data. The impact of smoking cessation to reduce lung cancer incidence is underscored by the US Preventive Services Task Force, which mandates that smoking cessation services be an integral component of lung cancer screening programs.
However, beneath the surface of this overarching concern lies a web of factors contributing to racial and ethnic disparities in smoking cessation. Cultural intricacies play a pivotal role in shaping these disparities. Despite higher instances of light or intermediate smoking, racially ethnic minority groups in the general population often face greater challenges in achieving smoking cessation, as highlighted by Bacio, et al. Adding another layer to this complex scenario is the profound impact of sustained smoking during cancer treatment. Research suggests that for individuals diagnosed with lung cancer, smoking cessation can markedly boost treatment efficacy, reduce the risk of secondary tumors, and even double the chances of survival.1
A study by Harris, et al. delving into the preferences of current smokers within a lung cancer screening setting uncovered noteworthy insights.2 White participants exhibited a fourfold greater likelihood of favoring a digital format for receiving smoking cessation information, while their Black counterparts expressed a preference for face-to-face support, phone assistance, or printed materials.
Moreover, a meta-analysis conducted by Jabari, et al. sheds light on the efficacy of culturally targeted smoking interventions.3 This comprehensive review describes a dual-level approach to tailoring smoking cessation health interventions: surface and deep. Surface adaptations encompass elements like language and imagery, which aim to enhance the acceptability of interventions within specific communities. Simultaneously, deep-tailored elements identify culturally significant factors that can fundamentally influence the behavior of the target population. The findings of this meta-analysis reveal that the integration of culturally tailored components into standard interventions significantly enhances their efficacy in facilitating smoking cessation.
In conclusion, sustained smoking cessation is a crucial element in combating the global burden of lung cancer. Recognizing the importance of individualized approaches in health care, it is imperative to tailor smoking cessation communications and interventions to diverse cultural influences and socioeconomic factors. Culturally tailored smoking cessation programs that account for nuances specific to each community have the potential to significantly enhance their effectiveness. This necessitates a shift towards individualized smoking cessation care, with a targeted focus on increasing cessation rates among racial and ethnic minority groups. In doing so, we take a step closer to a more equitable landscape in the battle against lung cancer.
Q:Are there interventions that can be readily implemented to improve sleep quality for hospitalized patients?
Dr. Arora: A patient’s first night in the hospital is probably not the night to liberalize sleep; you’re still figuring out whether they’re stable. But by the second or third day, you should be questioning—do you need vitals at night? Do you need a 4 AM blood draw?
We did an intervention called SIESTA that included both staff education about batching care and system-wide, electronic health record-based interventions to remind clinicians that as patients get better, you can deintensify their care. And we’re currently doing a randomized controlled trial of educating and empowering patients to ask their teams to help them get better sleep.
Q: Does hospital sleep deprivation affect patients after discharge?
Dr. Arora: Absolutely. “Posthospital syndrome” is the idea that 30 days after discharge, you’re vulnerable to getting readmitted – not because of the disease you came in with, but something else. And people who report sleep complaints in the hospital are more likely to be readmitted.
When people are acutely sleep deprived, their blood pressure is higher. Their blood sugar is higher. Their cytokine response and immune function are blunted. And our work shows that sleep deficits from the hospital continue even when you go home. Fatigue becomes a very real issue. And when you’re super fatigued, are you going to want to do your physical therapy? Will you be able to take care of yourself? Will you be able to learn and understand your discharge instructions?
We have such a huge gap to improve sleep. It’s of interest to people, but they are struggling with how to do it. And that’s where I think empowering frontline clinicians to take the lead is a great project for people to take on.
Vineet Arora, MD, MAPP, is the Dean for Medical Education at the University of Chicago and an academic hospitalist who specializes in the quality, safety, and experience of care delivered to hospitalized adults.
Q:Are there interventions that can be readily implemented to improve sleep quality for hospitalized patients?
Dr. Arora: A patient’s first night in the hospital is probably not the night to liberalize sleep; you’re still figuring out whether they’re stable. But by the second or third day, you should be questioning—do you need vitals at night? Do you need a 4 AM blood draw?
We did an intervention called SIESTA that included both staff education about batching care and system-wide, electronic health record-based interventions to remind clinicians that as patients get better, you can deintensify their care. And we’re currently doing a randomized controlled trial of educating and empowering patients to ask their teams to help them get better sleep.
Q: Does hospital sleep deprivation affect patients after discharge?
Dr. Arora: Absolutely. “Posthospital syndrome” is the idea that 30 days after discharge, you’re vulnerable to getting readmitted – not because of the disease you came in with, but something else. And people who report sleep complaints in the hospital are more likely to be readmitted.
When people are acutely sleep deprived, their blood pressure is higher. Their blood sugar is higher. Their cytokine response and immune function are blunted. And our work shows that sleep deficits from the hospital continue even when you go home. Fatigue becomes a very real issue. And when you’re super fatigued, are you going to want to do your physical therapy? Will you be able to take care of yourself? Will you be able to learn and understand your discharge instructions?
We have such a huge gap to improve sleep. It’s of interest to people, but they are struggling with how to do it. And that’s where I think empowering frontline clinicians to take the lead is a great project for people to take on.
Vineet Arora, MD, MAPP, is the Dean for Medical Education at the University of Chicago and an academic hospitalist who specializes in the quality, safety, and experience of care delivered to hospitalized adults.
Sleep Medicine Network
Nonrespiratory Sleep Section
Dr. Vineet Arora
Q:Are there interventions that can be readily implemented to improve sleep quality for hospitalized patients?
Dr. Arora: A patient’s first night in the hospital is probably not the night to liberalize sleep; you’re still figuring out whether they’re stable. But by the second or third day, you should be questioning—do you need vitals at night? Do you need a 4 AM blood draw?
We did an intervention called SIESTA that included both staff education about batching care and system-wide, electronic health record-based interventions to remind clinicians that as patients get better, you can deintensify their care. And we’re currently doing a randomized controlled trial of educating and empowering patients to ask their teams to help them get better sleep.
Q: Does hospital sleep deprivation affect patients after discharge?
Dr. Arora: Absolutely. “Posthospital syndrome” is the idea that 30 days after discharge, you’re vulnerable to getting readmitted – not because of the disease you came in with, but something else. And people who report sleep complaints in the hospital are more likely to be readmitted.
When people are acutely sleep deprived, their blood pressure is higher. Their blood sugar is higher. Their cytokine response and immune function are blunted. And our work shows that sleep deficits from the hospital continue even when you go home. Fatigue becomes a very real issue. And when you’re super fatigued, are you going to want to do your physical therapy? Will you be able to take care of yourself? Will you be able to learn and understand your discharge instructions?
We have such a huge gap to improve sleep. It’s of interest to people, but they are struggling with how to do it. And that’s where I think empowering frontline clinicians to take the lead is a great project for people to take on.
Vineet Arora, MD, MAPP, is the Dean for Medical Education at the University of Chicago and an academic hospitalist who specializes in the quality, safety, and experience of care delivered to hospitalized adults.
For providers caring for critically ill patients, navigating death and dying in the intensive care unit (ICU) with proficiency and empathy is essential. Approximately 20% of deaths in the United States occur during or shortly after a stay in the ICU and approximately 40% of ICU deaths involve withdrawal of artificial life support (WOALS) or compassionate extubation.
This is a complex process that may involve advanced communication with family, expertise in mechanical ventilation, vasopressors, dialysis, and complex symptom management. Importantly, surrogate medical decision-making for a critically ill patient can be a challenging experience associated with anxiety and depression. How the team approaches WOALS can make a difference to both patients and decision-makers. Unfortunately, there is striking variation in practice and lack of guidance in navigating issues that arise at end-of-life in the ICU. One study of 2,814 hospitals in the US with ICU beds found that 52% had intensivists while 48% did not.2 This highlights the importance of developing resources focusing on end-of-life care in the ICU setting regardless of the providers’ educational training.
Important elements could include the role for protocol-based WOALS, use of oxygen, selection and dosing strategy of comfort-focused medications, establishing expectations, and addressing uncertainties. This would be meaningful in providing effective, ethical end-of-life care based on evidence-based strategies. While death may be unavoidable, a thoughtful approach can allow providers to bring dignity to the dying process and lessen the burden of an already difficult experience for patients and families alike.
References
1. Curtis JR, et al. Am J Respir Crit Care Med. 2012;186[7]:587-592.
2. Halpern NA, et al. Crit Care Med. 2019;47[4]:517-525.
For providers caring for critically ill patients, navigating death and dying in the intensive care unit (ICU) with proficiency and empathy is essential. Approximately 20% of deaths in the United States occur during or shortly after a stay in the ICU and approximately 40% of ICU deaths involve withdrawal of artificial life support (WOALS) or compassionate extubation.
This is a complex process that may involve advanced communication with family, expertise in mechanical ventilation, vasopressors, dialysis, and complex symptom management. Importantly, surrogate medical decision-making for a critically ill patient can be a challenging experience associated with anxiety and depression. How the team approaches WOALS can make a difference to both patients and decision-makers. Unfortunately, there is striking variation in practice and lack of guidance in navigating issues that arise at end-of-life in the ICU. One study of 2,814 hospitals in the US with ICU beds found that 52% had intensivists while 48% did not.2 This highlights the importance of developing resources focusing on end-of-life care in the ICU setting regardless of the providers’ educational training.
Important elements could include the role for protocol-based WOALS, use of oxygen, selection and dosing strategy of comfort-focused medications, establishing expectations, and addressing uncertainties. This would be meaningful in providing effective, ethical end-of-life care based on evidence-based strategies. While death may be unavoidable, a thoughtful approach can allow providers to bring dignity to the dying process and lessen the burden of an already difficult experience for patients and families alike.
References
1. Curtis JR, et al. Am J Respir Crit Care Med. 2012;186[7]:587-592.
2. Halpern NA, et al. Crit Care Med. 2019;47[4]:517-525.
Critical Care Network
Palliative and End-of-Life Care Section
Angela Birdwell, DO, MA
For providers caring for critically ill patients, navigating death and dying in the intensive care unit (ICU) with proficiency and empathy is essential. Approximately 20% of deaths in the United States occur during or shortly after a stay in the ICU and approximately 40% of ICU deaths involve withdrawal of artificial life support (WOALS) or compassionate extubation.
This is a complex process that may involve advanced communication with family, expertise in mechanical ventilation, vasopressors, dialysis, and complex symptom management. Importantly, surrogate medical decision-making for a critically ill patient can be a challenging experience associated with anxiety and depression. How the team approaches WOALS can make a difference to both patients and decision-makers. Unfortunately, there is striking variation in practice and lack of guidance in navigating issues that arise at end-of-life in the ICU. One study of 2,814 hospitals in the US with ICU beds found that 52% had intensivists while 48% did not.2 This highlights the importance of developing resources focusing on end-of-life care in the ICU setting regardless of the providers’ educational training.
Important elements could include the role for protocol-based WOALS, use of oxygen, selection and dosing strategy of comfort-focused medications, establishing expectations, and addressing uncertainties. This would be meaningful in providing effective, ethical end-of-life care based on evidence-based strategies. While death may be unavoidable, a thoughtful approach can allow providers to bring dignity to the dying process and lessen the burden of an already difficult experience for patients and families alike.
References
1. Curtis JR, et al. Am J Respir Crit Care Med. 2012;186[7]:587-592.
2. Halpern NA, et al. Crit Care Med. 2019;47[4]:517-525.
Viral infections frequently cause acute respiratory failure requiring ICU admission. In the United States, influenza causes over 50,000 deaths annually and SARS-CoV2 resulted in 170,000 hospitalizations in December 2023 alone.1 2 RSV lacks precise incidence data due to inconsistent testing but is increasingly implicated in respiratory failure.
Patients with underlying pulmonary comorbidities are at increased risk of severe infection. RSV induces bronchospasm and increases the risk for severe infection in patients with obstructive lung disease.3 Additionally, COPD patients with viral respiratory infections have higher rates of ICU admission, mechanical ventilation, and death compared with similar patients admitted for other etiologies.4
Diagnosis typically is achieved with nasopharyngeal PCR swabs. Positive viral swabs correlate with higher ICU admission and ventilation rates in patients with COPD.4 Coinfection with multiple respiratory viruses leads to higher mortality rates and bacterial and fungal coinfection further increases morbidity and mortality.5
Treatment includes respiratory support with noninvasive ventilation and high-flow nasal cannula, reducing the need for mechanical ventilation.6 Inhaled bronchodilators are particularly beneficial in patients with RSV infection.5 Oseltamivir reduces mortality in severe influenza cases, while remdesivir shows efficacy in SARS-CoV2 infection not requiring invasive ventilation.7 Severe SARS-CoV2 infection can be treated with immunomodulators. However, their availability is limited. Corticosteroids reduce mortality and mechanical ventilation in patients with SARS-CoV2; however, their use is associated with worse outcomes in influenza and RSV.7 8
Vaccination remains crucial for prevention of severe disease. RSV vaccination, in addition to influenza and SARS-CoV2 immunization, presents an opportunity to reduce morbidity and mortality.
References
1. Troeger C, et al. Lancet Infect Dis. 2018;18[11]:1191-1210.
2. WHO COVID-19 Epidemiological Update, 2024.
3. Coussement J, et al. Chest. 2022;161[6]:1475-1484.
4. Mulpuru S, et al. Influenza Other Respir Viruses. 2022;16[6]:1172-1182.
5. Saura O, et al. Expert Rev Anti Infect Ther. 2022;20[12]:1537-1550.
6. Inglis R, Ayebale E, Schultz MJ. Curr Opin Crit Care. 2019;25[1]:45-53.
7. O’Driscoll LS, Martin-Loeches I. Semin Respir Crit Care Med. 2021;42[6]:771-787.
Viral infections frequently cause acute respiratory failure requiring ICU admission. In the United States, influenza causes over 50,000 deaths annually and SARS-CoV2 resulted in 170,000 hospitalizations in December 2023 alone.1 2 RSV lacks precise incidence data due to inconsistent testing but is increasingly implicated in respiratory failure.
Patients with underlying pulmonary comorbidities are at increased risk of severe infection. RSV induces bronchospasm and increases the risk for severe infection in patients with obstructive lung disease.3 Additionally, COPD patients with viral respiratory infections have higher rates of ICU admission, mechanical ventilation, and death compared with similar patients admitted for other etiologies.4
Diagnosis typically is achieved with nasopharyngeal PCR swabs. Positive viral swabs correlate with higher ICU admission and ventilation rates in patients with COPD.4 Coinfection with multiple respiratory viruses leads to higher mortality rates and bacterial and fungal coinfection further increases morbidity and mortality.5
Treatment includes respiratory support with noninvasive ventilation and high-flow nasal cannula, reducing the need for mechanical ventilation.6 Inhaled bronchodilators are particularly beneficial in patients with RSV infection.5 Oseltamivir reduces mortality in severe influenza cases, while remdesivir shows efficacy in SARS-CoV2 infection not requiring invasive ventilation.7 Severe SARS-CoV2 infection can be treated with immunomodulators. However, their availability is limited. Corticosteroids reduce mortality and mechanical ventilation in patients with SARS-CoV2; however, their use is associated with worse outcomes in influenza and RSV.7 8
Vaccination remains crucial for prevention of severe disease. RSV vaccination, in addition to influenza and SARS-CoV2 immunization, presents an opportunity to reduce morbidity and mortality.
References
1. Troeger C, et al. Lancet Infect Dis. 2018;18[11]:1191-1210.
2. WHO COVID-19 Epidemiological Update, 2024.
3. Coussement J, et al. Chest. 2022;161[6]:1475-1484.
4. Mulpuru S, et al. Influenza Other Respir Viruses. 2022;16[6]:1172-1182.
5. Saura O, et al. Expert Rev Anti Infect Ther. 2022;20[12]:1537-1550.
6. Inglis R, Ayebale E, Schultz MJ. Curr Opin Crit Care. 2019;25[1]:45-53.
7. O’Driscoll LS, Martin-Loeches I. Semin Respir Crit Care Med. 2021;42[6]:771-787.
8. Bhimraj, A et al. Clin Inf Dis. 2022.
Chest Infections and Disaster Response Network
Disaster Response and Global Health Section
Zein Kattih, MD
Kathryn Hughes, MD
Brian Tran, MD
Viral infections frequently cause acute respiratory failure requiring ICU admission. In the United States, influenza causes over 50,000 deaths annually and SARS-CoV2 resulted in 170,000 hospitalizations in December 2023 alone.1 2 RSV lacks precise incidence data due to inconsistent testing but is increasingly implicated in respiratory failure.
Patients with underlying pulmonary comorbidities are at increased risk of severe infection. RSV induces bronchospasm and increases the risk for severe infection in patients with obstructive lung disease.3 Additionally, COPD patients with viral respiratory infections have higher rates of ICU admission, mechanical ventilation, and death compared with similar patients admitted for other etiologies.4
Diagnosis typically is achieved with nasopharyngeal PCR swabs. Positive viral swabs correlate with higher ICU admission and ventilation rates in patients with COPD.4 Coinfection with multiple respiratory viruses leads to higher mortality rates and bacterial and fungal coinfection further increases morbidity and mortality.5
Treatment includes respiratory support with noninvasive ventilation and high-flow nasal cannula, reducing the need for mechanical ventilation.6 Inhaled bronchodilators are particularly beneficial in patients with RSV infection.5 Oseltamivir reduces mortality in severe influenza cases, while remdesivir shows efficacy in SARS-CoV2 infection not requiring invasive ventilation.7 Severe SARS-CoV2 infection can be treated with immunomodulators. However, their availability is limited. Corticosteroids reduce mortality and mechanical ventilation in patients with SARS-CoV2; however, their use is associated with worse outcomes in influenza and RSV.7 8
Vaccination remains crucial for prevention of severe disease. RSV vaccination, in addition to influenza and SARS-CoV2 immunization, presents an opportunity to reduce morbidity and mortality.
References
1. Troeger C, et al. Lancet Infect Dis. 2018;18[11]:1191-1210.
2. WHO COVID-19 Epidemiological Update, 2024.
3. Coussement J, et al. Chest. 2022;161[6]:1475-1484.
4. Mulpuru S, et al. Influenza Other Respir Viruses. 2022;16[6]:1172-1182.
5. Saura O, et al. Expert Rev Anti Infect Ther. 2022;20[12]:1537-1550.
6. Inglis R, Ayebale E, Schultz MJ. Curr Opin Crit Care. 2019;25[1]:45-53.
7. O’Driscoll LS, Martin-Loeches I. Semin Respir Crit Care Med. 2021;42[6]:771-787.
Remodeling of airways and destruction of parenchyma by immune and inflammatory mechanisms are the leading cause of lung function decline in patients with COPD. Type 2 inflammation has been recognized as an important phenotypic pathway in asthma. However, its role in COPD has been much less clear, which had been largely associated with innate immune response.1
Activation of Interleukin (IL)-25, IL-33, thymic stromal lymphopoietin (TSLP) produces type 2 cytokines IL-4, IL-5, and IL-13, either by binding to ILC2 or by direct Th2 cells resulting in elevated eosinophils in sputum, lungs, and blood, as well as fractional exhaled nitric oxide.2 The combined inflammation from this pathway underpins the pathological changes seen in airway mucosa, causing mucous hypersecretion and hyperresponsiveness.
Prior trials delineating the role of biologics, such as mepolizumab and benralizumab, showed variable results with possible benefit of add-on biologics on the annual COPD exacerbations among patients with eosinophilic phenotype of COPD.3
More recently, the BOREAS trial evaluated the role of dupilumab as an add-on therapy for patients with type 2 inflammation-driven COPD established using blood eosinophil count of at least 300/mL at initial screening.4 Dupilumab is a human monoclonal antibody that blocks combined IL-4 and IL-13 pathways with a broader effect on the type 2 inflammation. It included patients with moderate to severe exacerbations despite maximal triple inhaler therapy with blood eosinophilia. Patients with asthma were excluded. This 52-week trial showed reduction in annual moderate to severe COPD exacerbations, sustained lung function improvement as measured by prebronchodilator FEV1, and improvement in patient-reported respiratory symptoms.4 Evaluation of sustainability of these results with therapy step-down approaches should be explored.
Remodeling of airways and destruction of parenchyma by immune and inflammatory mechanisms are the leading cause of lung function decline in patients with COPD. Type 2 inflammation has been recognized as an important phenotypic pathway in asthma. However, its role in COPD has been much less clear, which had been largely associated with innate immune response.1
Activation of Interleukin (IL)-25, IL-33, thymic stromal lymphopoietin (TSLP) produces type 2 cytokines IL-4, IL-5, and IL-13, either by binding to ILC2 or by direct Th2 cells resulting in elevated eosinophils in sputum, lungs, and blood, as well as fractional exhaled nitric oxide.2 The combined inflammation from this pathway underpins the pathological changes seen in airway mucosa, causing mucous hypersecretion and hyperresponsiveness.
Prior trials delineating the role of biologics, such as mepolizumab and benralizumab, showed variable results with possible benefit of add-on biologics on the annual COPD exacerbations among patients with eosinophilic phenotype of COPD.3
More recently, the BOREAS trial evaluated the role of dupilumab as an add-on therapy for patients with type 2 inflammation-driven COPD established using blood eosinophil count of at least 300/mL at initial screening.4 Dupilumab is a human monoclonal antibody that blocks combined IL-4 and IL-13 pathways with a broader effect on the type 2 inflammation. It included patients with moderate to severe exacerbations despite maximal triple inhaler therapy with blood eosinophilia. Patients with asthma were excluded. This 52-week trial showed reduction in annual moderate to severe COPD exacerbations, sustained lung function improvement as measured by prebronchodilator FEV1, and improvement in patient-reported respiratory symptoms.4 Evaluation of sustainability of these results with therapy step-down approaches should be explored.
References
1. Scanlon & McKenzie, 2012.
2. Brusselle et al, 2013.
3. Pavord et al, 2017.
4. Bhatt et al, 2023.
Airways Disorders Network
Asthma and COPD Section
Maria Azhar, MD
Abdullah Alismail, PhD, RRT, FCCP
Raghav Gupta, MD, FCCP
Remodeling of airways and destruction of parenchyma by immune and inflammatory mechanisms are the leading cause of lung function decline in patients with COPD. Type 2 inflammation has been recognized as an important phenotypic pathway in asthma. However, its role in COPD has been much less clear, which had been largely associated with innate immune response.1
Activation of Interleukin (IL)-25, IL-33, thymic stromal lymphopoietin (TSLP) produces type 2 cytokines IL-4, IL-5, and IL-13, either by binding to ILC2 or by direct Th2 cells resulting in elevated eosinophils in sputum, lungs, and blood, as well as fractional exhaled nitric oxide.2 The combined inflammation from this pathway underpins the pathological changes seen in airway mucosa, causing mucous hypersecretion and hyperresponsiveness.
Prior trials delineating the role of biologics, such as mepolizumab and benralizumab, showed variable results with possible benefit of add-on biologics on the annual COPD exacerbations among patients with eosinophilic phenotype of COPD.3
More recently, the BOREAS trial evaluated the role of dupilumab as an add-on therapy for patients with type 2 inflammation-driven COPD established using blood eosinophil count of at least 300/mL at initial screening.4 Dupilumab is a human monoclonal antibody that blocks combined IL-4 and IL-13 pathways with a broader effect on the type 2 inflammation. It included patients with moderate to severe exacerbations despite maximal triple inhaler therapy with blood eosinophilia. Patients with asthma were excluded. This 52-week trial showed reduction in annual moderate to severe COPD exacerbations, sustained lung function improvement as measured by prebronchodilator FEV1, and improvement in patient-reported respiratory symptoms.4 Evaluation of sustainability of these results with therapy step-down approaches should be explored.
Learn about the LGBTQ+ at CHEST, Respiratory Care, and Women in Chest Medicine Interest Groups
The value of member community is highly prized at CHEST. In order to provide supportive and engaging spaces where members can convene, share resources, and learn from other members who share similar lived experiences and interests, we were proud to add Interest Groups to our member offerings in 2023.
The introduction of Interest Groups has proven to be an effective way to organically connect CHEST members with shared interests and passions. Membership in one of these groups allows for networking in a smaller setting, with the goals of supporting career development and enriching an individual’s professional path.
CHEST
Dr. Margaret Pisani
CHEST
Dr. Kevin O'Neil
CHEST
Dr. Mauricio Danckers To learn more about the three existing Interest Groups, we spoke with each group’s chair: Margaret Pisani, MD, FCCP, Chair of the Women in Chest Medicine Interest Group; Kevin O’Neil, MD, FCCP, Chair of the Respiratory Care Interest Group; and Mauricio Danckers, MD, FCCP, Chair of the LGBTQ+ at CHEST Interest Group.
1) Tell us about the key issues that your Interest Group is trying to address and who should join this group.
Mauricio Danckers: Our LGBTQ+ community continues to be the target of unrelenting discrimination. Current disparities toward sexual and gender-diverse individuals persistently hinder their personal and professional growth. There are several key issues currently affecting the LGBTQ+ community; among those are ongoing health care disparities, lack of education of our providers on LGBTQ+ health issues, underrepresentation of scientific research in the LGBTQ+ community, and scarce opportunities for mentorship and networking among LGBTQ+ health professionals. Our Interest Group seeks to provide a space to work together to overcome these shortcomings. Through the exchange of ideas, the opportunity for interprofessional collaborations, resource development and dissemination, scholar productivity, organic mentoring, and patient and provider advocacy, we seek to create change and better serve the LGBTQ+ identity in our CHEST community.
Anyone who is ready to make a change for the LGBTQ+ community, their care, and their well-being is encouraged to join. Self-identification as a member of the LGBTQ+ community is not a prerequisite for joining our group. We welcome individuals committed to advancing gender-affirming health, wellness, and education approaches to reduce health disparities.
Kevin O’Neil: The Respiratory Care Interest Group is invested in a number of focus areas, including improving collaboration between pulmonary/critical care/sleep physicians and respiratory care providers with a goal of improved and more efficient patient care, addressing critical shortages in the respiratory therapist (RT) workforce in collaboration with respiratory care organizations by identifying and supporting strategies to grow the workforce, and promoting wellness in all members of the community by providing tools and resources to mitigate stress and reduce burnout.
This Interest Group is for any CHEST member with an interest in respiratory care education or care delivery.
Margaret Pisani: The Women in Chest Medicine Interest Group has two overarching goals. The first is focused on ensuring that content around sex as a biologic variable and the impact of gender—as they relate to lung disease and critical care—are addressed in the educational activities of CHEST. The second is to provide mentorship and aid with career advancement for women in pulmonary, critical care, and sleep medicine (PCCSM) who are members of CHEST.
Anyone who does research on the impact of sex and gender as biologic variables—and the importance of these variables in lung disease—is welcome in this Interest Group. Persons who would like to be involved in mentoring the next generation of women and junior members who would like to learn more about how to be active at CHEST are also encouraged to join.
2) What motivated you to lead an Interest Group?
Danckers: My path in medicine as an LGBTQ+ individual has been unique and personal. It has opened the opportunity to witness the urgency of the changes needed to serve our LGBTQ+ community better. I wanted to lead this Interest Group to connect to other members interested in advancing health care equity for LGBTQ+ individuals, to inspire one another to achieve major changes in LGBTQ+ health education, and to ignite an educational and social initiative supported by CHEST to witness the LGBTQ+ medical community thriving while grounded on mentoring and advocacy.
O’Neil: I’ve been a CHEST member for more than 35 years and involved with respiratory care almost as long. The relationship between pulmonary/critical care physicians and RTs is unique, and RTs are critically important to my ability to care for my patients. I am committed to facilitating opportunities for collaboration between the two groups.
Pisani: I am motivated by my passion to ensure we are providing the best possible education to our members and patients and supporting the next generation of leaders in the PCCSM community.
3) What are the goals for your Interest Group in 2024?
Danckers: 2024 will be an exciting year, no doubt about it! Our goals for 2024 are: 1) to connect talented individuals with professional goals that align with the ones from the Interest Group and CHEST, 2) to increase the presence of the LGBTQ+ identity representation in our CHEST scientific meetings and educational offerings, 3) to build a resource platform for LGBTQ+ health education with the innovative approach CHEST is known to provide, and 4) to provide venues to inspire and support scholarly work within the LGBTQ+ community.
O’Neil: Growing the Interest Group membership and increasing opportunities for RTs to participate in CHEST activities by providing a landing space for new RT members are key initiatives for us. We are also hoping to increase the visibility of the Interest Group through events at the annual meeting, educational offerings, and other opportunities as they arise. We will also focus on improving communication between CHEST and other respiratory organizations.
Pisani: We are focused on ensuring that sex and gender topics are addressed during scientific presentations when relevant to research and patient care and developing resources on specific topics where there is data regarding the impact of sex and gender in lung disease.
Learn about the LGBTQ+ at CHEST, Respiratory Care, and Women in Chest Medicine Interest Groups
Learn about the LGBTQ+ at CHEST, Respiratory Care, and Women in Chest Medicine Interest Groups
The value of member community is highly prized at CHEST. In order to provide supportive and engaging spaces where members can convene, share resources, and learn from other members who share similar lived experiences and interests, we were proud to add Interest Groups to our member offerings in 2023.
The introduction of Interest Groups has proven to be an effective way to organically connect CHEST members with shared interests and passions. Membership in one of these groups allows for networking in a smaller setting, with the goals of supporting career development and enriching an individual’s professional path.
CHEST
Dr. Margaret Pisani
CHEST
Dr. Kevin O'Neil
CHEST
Dr. Mauricio Danckers To learn more about the three existing Interest Groups, we spoke with each group’s chair: Margaret Pisani, MD, FCCP, Chair of the Women in Chest Medicine Interest Group; Kevin O’Neil, MD, FCCP, Chair of the Respiratory Care Interest Group; and Mauricio Danckers, MD, FCCP, Chair of the LGBTQ+ at CHEST Interest Group.
1) Tell us about the key issues that your Interest Group is trying to address and who should join this group.
Mauricio Danckers: Our LGBTQ+ community continues to be the target of unrelenting discrimination. Current disparities toward sexual and gender-diverse individuals persistently hinder their personal and professional growth. There are several key issues currently affecting the LGBTQ+ community; among those are ongoing health care disparities, lack of education of our providers on LGBTQ+ health issues, underrepresentation of scientific research in the LGBTQ+ community, and scarce opportunities for mentorship and networking among LGBTQ+ health professionals. Our Interest Group seeks to provide a space to work together to overcome these shortcomings. Through the exchange of ideas, the opportunity for interprofessional collaborations, resource development and dissemination, scholar productivity, organic mentoring, and patient and provider advocacy, we seek to create change and better serve the LGBTQ+ identity in our CHEST community.
Anyone who is ready to make a change for the LGBTQ+ community, their care, and their well-being is encouraged to join. Self-identification as a member of the LGBTQ+ community is not a prerequisite for joining our group. We welcome individuals committed to advancing gender-affirming health, wellness, and education approaches to reduce health disparities.
Kevin O’Neil: The Respiratory Care Interest Group is invested in a number of focus areas, including improving collaboration between pulmonary/critical care/sleep physicians and respiratory care providers with a goal of improved and more efficient patient care, addressing critical shortages in the respiratory therapist (RT) workforce in collaboration with respiratory care organizations by identifying and supporting strategies to grow the workforce, and promoting wellness in all members of the community by providing tools and resources to mitigate stress and reduce burnout.
This Interest Group is for any CHEST member with an interest in respiratory care education or care delivery.
Margaret Pisani: The Women in Chest Medicine Interest Group has two overarching goals. The first is focused on ensuring that content around sex as a biologic variable and the impact of gender—as they relate to lung disease and critical care—are addressed in the educational activities of CHEST. The second is to provide mentorship and aid with career advancement for women in pulmonary, critical care, and sleep medicine (PCCSM) who are members of CHEST.
Anyone who does research on the impact of sex and gender as biologic variables—and the importance of these variables in lung disease—is welcome in this Interest Group. Persons who would like to be involved in mentoring the next generation of women and junior members who would like to learn more about how to be active at CHEST are also encouraged to join.
2) What motivated you to lead an Interest Group?
Danckers: My path in medicine as an LGBTQ+ individual has been unique and personal. It has opened the opportunity to witness the urgency of the changes needed to serve our LGBTQ+ community better. I wanted to lead this Interest Group to connect to other members interested in advancing health care equity for LGBTQ+ individuals, to inspire one another to achieve major changes in LGBTQ+ health education, and to ignite an educational and social initiative supported by CHEST to witness the LGBTQ+ medical community thriving while grounded on mentoring and advocacy.
O’Neil: I’ve been a CHEST member for more than 35 years and involved with respiratory care almost as long. The relationship between pulmonary/critical care physicians and RTs is unique, and RTs are critically important to my ability to care for my patients. I am committed to facilitating opportunities for collaboration between the two groups.
Pisani: I am motivated by my passion to ensure we are providing the best possible education to our members and patients and supporting the next generation of leaders in the PCCSM community.
3) What are the goals for your Interest Group in 2024?
Danckers: 2024 will be an exciting year, no doubt about it! Our goals for 2024 are: 1) to connect talented individuals with professional goals that align with the ones from the Interest Group and CHEST, 2) to increase the presence of the LGBTQ+ identity representation in our CHEST scientific meetings and educational offerings, 3) to build a resource platform for LGBTQ+ health education with the innovative approach CHEST is known to provide, and 4) to provide venues to inspire and support scholarly work within the LGBTQ+ community.
O’Neil: Growing the Interest Group membership and increasing opportunities for RTs to participate in CHEST activities by providing a landing space for new RT members are key initiatives for us. We are also hoping to increase the visibility of the Interest Group through events at the annual meeting, educational offerings, and other opportunities as they arise. We will also focus on improving communication between CHEST and other respiratory organizations.
Pisani: We are focused on ensuring that sex and gender topics are addressed during scientific presentations when relevant to research and patient care and developing resources on specific topics where there is data regarding the impact of sex and gender in lung disease.
The value of member community is highly prized at CHEST. In order to provide supportive and engaging spaces where members can convene, share resources, and learn from other members who share similar lived experiences and interests, we were proud to add Interest Groups to our member offerings in 2023.
The introduction of Interest Groups has proven to be an effective way to organically connect CHEST members with shared interests and passions. Membership in one of these groups allows for networking in a smaller setting, with the goals of supporting career development and enriching an individual’s professional path.
CHEST
Dr. Margaret Pisani
CHEST
Dr. Kevin O'Neil
CHEST
Dr. Mauricio Danckers To learn more about the three existing Interest Groups, we spoke with each group’s chair: Margaret Pisani, MD, FCCP, Chair of the Women in Chest Medicine Interest Group; Kevin O’Neil, MD, FCCP, Chair of the Respiratory Care Interest Group; and Mauricio Danckers, MD, FCCP, Chair of the LGBTQ+ at CHEST Interest Group.
1) Tell us about the key issues that your Interest Group is trying to address and who should join this group.
Mauricio Danckers: Our LGBTQ+ community continues to be the target of unrelenting discrimination. Current disparities toward sexual and gender-diverse individuals persistently hinder their personal and professional growth. There are several key issues currently affecting the LGBTQ+ community; among those are ongoing health care disparities, lack of education of our providers on LGBTQ+ health issues, underrepresentation of scientific research in the LGBTQ+ community, and scarce opportunities for mentorship and networking among LGBTQ+ health professionals. Our Interest Group seeks to provide a space to work together to overcome these shortcomings. Through the exchange of ideas, the opportunity for interprofessional collaborations, resource development and dissemination, scholar productivity, organic mentoring, and patient and provider advocacy, we seek to create change and better serve the LGBTQ+ identity in our CHEST community.
Anyone who is ready to make a change for the LGBTQ+ community, their care, and their well-being is encouraged to join. Self-identification as a member of the LGBTQ+ community is not a prerequisite for joining our group. We welcome individuals committed to advancing gender-affirming health, wellness, and education approaches to reduce health disparities.
Kevin O’Neil: The Respiratory Care Interest Group is invested in a number of focus areas, including improving collaboration between pulmonary/critical care/sleep physicians and respiratory care providers with a goal of improved and more efficient patient care, addressing critical shortages in the respiratory therapist (RT) workforce in collaboration with respiratory care organizations by identifying and supporting strategies to grow the workforce, and promoting wellness in all members of the community by providing tools and resources to mitigate stress and reduce burnout.
This Interest Group is for any CHEST member with an interest in respiratory care education or care delivery.
Margaret Pisani: The Women in Chest Medicine Interest Group has two overarching goals. The first is focused on ensuring that content around sex as a biologic variable and the impact of gender—as they relate to lung disease and critical care—are addressed in the educational activities of CHEST. The second is to provide mentorship and aid with career advancement for women in pulmonary, critical care, and sleep medicine (PCCSM) who are members of CHEST.
Anyone who does research on the impact of sex and gender as biologic variables—and the importance of these variables in lung disease—is welcome in this Interest Group. Persons who would like to be involved in mentoring the next generation of women and junior members who would like to learn more about how to be active at CHEST are also encouraged to join.
2) What motivated you to lead an Interest Group?
Danckers: My path in medicine as an LGBTQ+ individual has been unique and personal. It has opened the opportunity to witness the urgency of the changes needed to serve our LGBTQ+ community better. I wanted to lead this Interest Group to connect to other members interested in advancing health care equity for LGBTQ+ individuals, to inspire one another to achieve major changes in LGBTQ+ health education, and to ignite an educational and social initiative supported by CHEST to witness the LGBTQ+ medical community thriving while grounded on mentoring and advocacy.
O’Neil: I’ve been a CHEST member for more than 35 years and involved with respiratory care almost as long. The relationship between pulmonary/critical care physicians and RTs is unique, and RTs are critically important to my ability to care for my patients. I am committed to facilitating opportunities for collaboration between the two groups.
Pisani: I am motivated by my passion to ensure we are providing the best possible education to our members and patients and supporting the next generation of leaders in the PCCSM community.
3) What are the goals for your Interest Group in 2024?
Danckers: 2024 will be an exciting year, no doubt about it! Our goals for 2024 are: 1) to connect talented individuals with professional goals that align with the ones from the Interest Group and CHEST, 2) to increase the presence of the LGBTQ+ identity representation in our CHEST scientific meetings and educational offerings, 3) to build a resource platform for LGBTQ+ health education with the innovative approach CHEST is known to provide, and 4) to provide venues to inspire and support scholarly work within the LGBTQ+ community.
O’Neil: Growing the Interest Group membership and increasing opportunities for RTs to participate in CHEST activities by providing a landing space for new RT members are key initiatives for us. We are also hoping to increase the visibility of the Interest Group through events at the annual meeting, educational offerings, and other opportunities as they arise. We will also focus on improving communication between CHEST and other respiratory organizations.
Pisani: We are focused on ensuring that sex and gender topics are addressed during scientific presentations when relevant to research and patient care and developing resources on specific topics where there is data regarding the impact of sex and gender in lung disease.
As the President of the American College of Chest Physicians (CHEST), I have the privilege of regularly addressing CHEST members through a quarterly column where I can share updates and expand on topics that we hold in high regard.
Dr. Jack D. Buckley
As such, I’d like to focus on the CHEST commitment to social responsibility and the work we have done and will continue to do throughout this year and beyond.
In 2023, under the leadership of my predecessor, Doreen Addrizzo-Harris, MD, FCCP, CHEST made strong changes to our organizational focus, including cementing Social Responsibility as a formal pillar of CHEST. In addition to our other four pillars—Education, People, Products, and Growth—this new pillar is a sign of our stronger commitment to be more explicit in our aspirations, measure our success, and move the bar higher.
As part of the new social responsibility pillar, CHEST philanthropy evolved from what was known as the CHEST Foundation and defined a new giving strategy that reflects our organizational commitment to clinical research, community impact, support for the profession, and fostering education. Through growth in our research support and furthering community impact, 2024 will be a strong year of providing grant support aligned to this new giving strategy.
In addition, we formalized how CHEST will pursue our new social responsibility pillar. In 2023, we articulated our organizational values—Community, Inclusivity, Innovation, Advocacy, and Integrity—which will serve as a consistent reminder of who we are as an organization and guide us in decisions as we pursue our mission.
Led by these values, CHEST will use its voice and capabilities to promote change that equitably impacts our community. In 2024 specifically, the organization looks forward to engaging actively with social responsibility by expanding volunteer opportunities local to CHEST headquarters and in conjunction with the location of the annual meeting.
It is also my hope that 2024 will be known as a year of member input, starring feedback from none other than you, our members.
For those who recall my address from the Opening Session at CHEST 2023, I very much encourage you to reach out to share with me your thoughts, your CHEST experience, and more at president@chestnet.org. I look forward to having this regular touchpoint with all of you, and I welcome your input on topics you’d like to hear more on.
As the President of the American College of Chest Physicians (CHEST), I have the privilege of regularly addressing CHEST members through a quarterly column where I can share updates and expand on topics that we hold in high regard.
Dr. Jack D. Buckley
As such, I’d like to focus on the CHEST commitment to social responsibility and the work we have done and will continue to do throughout this year and beyond.
In 2023, under the leadership of my predecessor, Doreen Addrizzo-Harris, MD, FCCP, CHEST made strong changes to our organizational focus, including cementing Social Responsibility as a formal pillar of CHEST. In addition to our other four pillars—Education, People, Products, and Growth—this new pillar is a sign of our stronger commitment to be more explicit in our aspirations, measure our success, and move the bar higher.
As part of the new social responsibility pillar, CHEST philanthropy evolved from what was known as the CHEST Foundation and defined a new giving strategy that reflects our organizational commitment to clinical research, community impact, support for the profession, and fostering education. Through growth in our research support and furthering community impact, 2024 will be a strong year of providing grant support aligned to this new giving strategy.
In addition, we formalized how CHEST will pursue our new social responsibility pillar. In 2023, we articulated our organizational values—Community, Inclusivity, Innovation, Advocacy, and Integrity—which will serve as a consistent reminder of who we are as an organization and guide us in decisions as we pursue our mission.
Led by these values, CHEST will use its voice and capabilities to promote change that equitably impacts our community. In 2024 specifically, the organization looks forward to engaging actively with social responsibility by expanding volunteer opportunities local to CHEST headquarters and in conjunction with the location of the annual meeting.
It is also my hope that 2024 will be known as a year of member input, starring feedback from none other than you, our members.
For those who recall my address from the Opening Session at CHEST 2023, I very much encourage you to reach out to share with me your thoughts, your CHEST experience, and more at president@chestnet.org. I look forward to having this regular touchpoint with all of you, and I welcome your input on topics you’d like to hear more on.
Until next time,
Jack D. Buckley, MD, MPH, FCCP
As the President of the American College of Chest Physicians (CHEST), I have the privilege of regularly addressing CHEST members through a quarterly column where I can share updates and expand on topics that we hold in high regard.
Dr. Jack D. Buckley
As such, I’d like to focus on the CHEST commitment to social responsibility and the work we have done and will continue to do throughout this year and beyond.
In 2023, under the leadership of my predecessor, Doreen Addrizzo-Harris, MD, FCCP, CHEST made strong changes to our organizational focus, including cementing Social Responsibility as a formal pillar of CHEST. In addition to our other four pillars—Education, People, Products, and Growth—this new pillar is a sign of our stronger commitment to be more explicit in our aspirations, measure our success, and move the bar higher.
As part of the new social responsibility pillar, CHEST philanthropy evolved from what was known as the CHEST Foundation and defined a new giving strategy that reflects our organizational commitment to clinical research, community impact, support for the profession, and fostering education. Through growth in our research support and furthering community impact, 2024 will be a strong year of providing grant support aligned to this new giving strategy.
In addition, we formalized how CHEST will pursue our new social responsibility pillar. In 2023, we articulated our organizational values—Community, Inclusivity, Innovation, Advocacy, and Integrity—which will serve as a consistent reminder of who we are as an organization and guide us in decisions as we pursue our mission.
Led by these values, CHEST will use its voice and capabilities to promote change that equitably impacts our community. In 2024 specifically, the organization looks forward to engaging actively with social responsibility by expanding volunteer opportunities local to CHEST headquarters and in conjunction with the location of the annual meeting.
It is also my hope that 2024 will be known as a year of member input, starring feedback from none other than you, our members.
For those who recall my address from the Opening Session at CHEST 2023, I very much encourage you to reach out to share with me your thoughts, your CHEST experience, and more at president@chestnet.org. I look forward to having this regular touchpoint with all of you, and I welcome your input on topics you’d like to hear more on.
Bedside-focused cardiac ultrasound assessment, or cardiac point-of-care ultrasound (POCUS), has become common in intensive care units throughout the US and the world. Many clinicians argue a POCUS cardiac assessment should be completed in most hypotensive patients and all cases of undifferentiated shock.
However, obtaining images adequate for decision making via standard transthoracic echo (TTE) is not possible in a significant number of patients; as high as 30% of critically ill patients, according to The American Society of Echocardiography (ASE) guidelines.1 Factors common to critically ill patients, such as invasive mechanical ventilation, external dressings, and limited mobility, contribute to poor image acquisition.
CHEST
Dr. Kevin Proud
In almost all these cases, the factors limiting image acquisition can be eliminated by utilizing a transesophageal approach. In a recent study, researchers were able to demonstrate that adding transesophageal echocardiography (TEE) to TTE in critically ill patients yielded a new diagnosis or a change in management about 45% of the time.2
Using transesophageal ultrasound for a focused cardiac assessment in hemodynamically unstable patients is not new—and is often referred to as rescue TEE or resuscitative TEE. A broader term, transesophageal ultrasound, has also been used to include sonographic evaluation of the lungs in patients with poor acoustic windows. At my institution, we use the term critical care TEE to define TEE performed by a noncardiology-trained intensivist in an intubated critically ill patient.
Regardless of the term, the use of transesophageal ultrasound by the noncardiologist in the ICU appears to be a developing trend. As with other uses of POCUS, ultrasound machines continue to be able to “do more” at a lower price point. In 2024, several cart-based ultrasound machines are compatible with transesophageal probes and contain software packages capable of common cardiac measurements.
Despite this growing interest, intensivists are likely to encounter barriers to implementing critical care TEE. Our division recently implemented adding TEE to our practice. Our practice involves two separate systems: a Veterans Administration hospital and a university-based county hospital. Our division has integrated the use of TEE in the medical ICU at both institutions. Having navigated the process at both institutions, I can offer some guidance in navigating barriers.
The development of a critical care TEE program must start with a strong base in transthoracic cardiac POCUS, at least for the foreseeable future. Having a strong background in TTE gives learners a solid foundation in cardiac anatomy, cardiac function, and ultrasound properties. Obtaining testamur status or board certification in critical care echocardiography is not an absolute must but is a definite benefit. Having significant experience in TTE image acquisition and interpretation will flatten the learning curve for TEE. Interestingly, image acquisition in TEE is often easier than in TTE, so the paradigm of learning TTE before TEE may reverse in the years to come.
Two barriers often work together to create a vicious cycle that stops the development of a TEE program at its start. These barriers include the lack of training and lack of equipment, specifically a TEE probe. Those who do not understand the value of TEE may ask, “Why purchase equipment for a procedure that you do not yet know how to do?” The opposite question can also be asked, “Why get trained to do something you don’t have the equipment to perform?”
My best advice to break this cycle is to “dive in” to whichever barrier seems easier to overcome first. I started with obtaining knowledge and training. Obtaining training and education in a procedure that is historically not done in your specialty is challenging but is not impossible. It takes a combination of high levels of self-motivation and at least one colleague with the training to support you. I approached a cardiac anesthesiologist, whom I knew from the surgical ICU. Cardiologists can also be a resource, but working with cardiac anesthesiologists offers several advantages. TEEs done by cardiac anesthesiologists are similar to those done in ICU patients (ie, all patients are intubated and sedated). The procedures are also scheduled several days in advance, making it easier to integrate training into your daily work schedule. Lastly, the TEE probe remains in place for several hours, so repeating the probe manipulations again as a learner does not add additional risk to the patient. In my case, we somewhat arbitrarily agreed that I participate in 25 TEE exams. (CME courses, both online and in-person simulation, exist and greatly supplement self-study.)
Obtaining equipment is also a common barrier, though this has become less restrictive in the last several years. As previously mentioned, many cart-based ultrasound machines can accommodate a TEE probe. This changes the request from purchasing a new machine to “just a probe.” Despite the higher cost than most other probes, those in charge of purchasing are often more open to purchasing “a probe” than to purchasing an ultrasound machine.
Additionally, the purchasing decision regarding probes may fall to a different person than it does for an ultrasound machine. If available, POCUS image archiving into the medical record can help offset the cost of equipment, both by increasing revenue via billing and by demonstrating that equipment is being used. If initially declined, continue to ask and work to integrate the purchase into the next year’s budget. Inquire about the process of making a formal request and follow that process. This will often involve obtaining a quote or quotes from the ultrasound manufacturer(s).
Keep in mind that the probe will require a special storage cabinet specifically designed for TEE probes. It is prudent to include this in budget requests. If needed, the echocardiography lab can be a useful resource for additional information regarding the cabinet requirements. It is strongly recommended to discuss TEE probe models with sterile processing before any purchasing. If options are available, it is wise to choose a model the hospital already uses, as the cleaning protocol is well established. Our unit purchased a model that did not have an established protocol, which took nearly 6 months to develop. If probe options are limited, involving sterile processing early to start developing a protocol will help decrease delays.
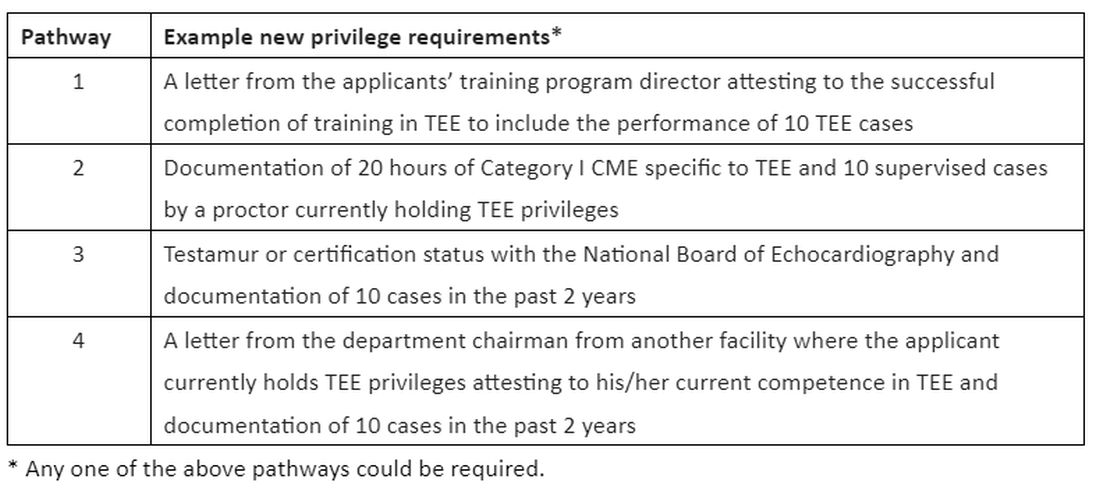
Obtaining hospital privileges is also a common barrier, though this may not be as challenging as expected. Hospitals typically have well-outlined policies on obtaining privileges for established procedures. One of our hospital systems had four different options; the most straightforward required 20 hours of CME specific to TEE and 10 supervised cases by a proctor currently holding TEE privileges (see Table 1).
Discussions about obtaining privileges should involve your division chief, chair of medicine, and the cardiology division chief. Clearly outlining the plan to perform this procedure only in critically ill patients who are already intubated for other reasons made these conversations go much more smoothly. In the development of delineation of privileges, we used the term critical care TEE to clearly define this patient population. During these conversations, highlight the safety of the procedure; ASE guidelines3 estimate a severe complication rate of less than 1 in 10,000 cases and explain the anticipated benefits to critically ill patients.
In conclusion, at an institution that is already adept at the use of POCUS in the ICU, the additional of critical care TEE within 1 to 2 years is a very realistic achievement. It will undoubtedly require patience, persistence, and self-motivation, but the barriers are becoming smaller every day. Stay motivated!
Dr. Proud is Associate Professor of Medicine, Division of Pulmonary and Critical Care Medicine, Pulmonary and Critical Care Medicine Program Director, UT Health San Antonio.
References:
1. Porter TR, Abdelmoneim S, Belcik FT, et al. Guidelines for the cardiac sonographer in the performance of contrast echocardiography: a focused update from the American Society of Echocardiography. J Am Soc Echocardiogr. 2024;27(8):797-810.
2. Si X, Ma J, Cao DY, et al. Transesophageal echocardiography instead or in addition to transthoracic echocardiography in evaluating haemodynamic problems in intubated critically ill patients. Ann Transl Med. 2020;8(12):785.
3. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a cmprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardioraphy and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26(9):921-964.
Bedside-focused cardiac ultrasound assessment, or cardiac point-of-care ultrasound (POCUS), has become common in intensive care units throughout the US and the world. Many clinicians argue a POCUS cardiac assessment should be completed in most hypotensive patients and all cases of undifferentiated shock.
However, obtaining images adequate for decision making via standard transthoracic echo (TTE) is not possible in a significant number of patients; as high as 30% of critically ill patients, according to The American Society of Echocardiography (ASE) guidelines.1 Factors common to critically ill patients, such as invasive mechanical ventilation, external dressings, and limited mobility, contribute to poor image acquisition.
CHEST
Dr. Kevin Proud
In almost all these cases, the factors limiting image acquisition can be eliminated by utilizing a transesophageal approach. In a recent study, researchers were able to demonstrate that adding transesophageal echocardiography (TEE) to TTE in critically ill patients yielded a new diagnosis or a change in management about 45% of the time.2
Using transesophageal ultrasound for a focused cardiac assessment in hemodynamically unstable patients is not new—and is often referred to as rescue TEE or resuscitative TEE. A broader term, transesophageal ultrasound, has also been used to include sonographic evaluation of the lungs in patients with poor acoustic windows. At my institution, we use the term critical care TEE to define TEE performed by a noncardiology-trained intensivist in an intubated critically ill patient.
Regardless of the term, the use of transesophageal ultrasound by the noncardiologist in the ICU appears to be a developing trend. As with other uses of POCUS, ultrasound machines continue to be able to “do more” at a lower price point. In 2024, several cart-based ultrasound machines are compatible with transesophageal probes and contain software packages capable of common cardiac measurements.
Despite this growing interest, intensivists are likely to encounter barriers to implementing critical care TEE. Our division recently implemented adding TEE to our practice. Our practice involves two separate systems: a Veterans Administration hospital and a university-based county hospital. Our division has integrated the use of TEE in the medical ICU at both institutions. Having navigated the process at both institutions, I can offer some guidance in navigating barriers.
The development of a critical care TEE program must start with a strong base in transthoracic cardiac POCUS, at least for the foreseeable future. Having a strong background in TTE gives learners a solid foundation in cardiac anatomy, cardiac function, and ultrasound properties. Obtaining testamur status or board certification in critical care echocardiography is not an absolute must but is a definite benefit. Having significant experience in TTE image acquisition and interpretation will flatten the learning curve for TEE. Interestingly, image acquisition in TEE is often easier than in TTE, so the paradigm of learning TTE before TEE may reverse in the years to come.
Two barriers often work together to create a vicious cycle that stops the development of a TEE program at its start. These barriers include the lack of training and lack of equipment, specifically a TEE probe. Those who do not understand the value of TEE may ask, “Why purchase equipment for a procedure that you do not yet know how to do?” The opposite question can also be asked, “Why get trained to do something you don’t have the equipment to perform?”
My best advice to break this cycle is to “dive in” to whichever barrier seems easier to overcome first. I started with obtaining knowledge and training. Obtaining training and education in a procedure that is historically not done in your specialty is challenging but is not impossible. It takes a combination of high levels of self-motivation and at least one colleague with the training to support you. I approached a cardiac anesthesiologist, whom I knew from the surgical ICU. Cardiologists can also be a resource, but working with cardiac anesthesiologists offers several advantages. TEEs done by cardiac anesthesiologists are similar to those done in ICU patients (ie, all patients are intubated and sedated). The procedures are also scheduled several days in advance, making it easier to integrate training into your daily work schedule. Lastly, the TEE probe remains in place for several hours, so repeating the probe manipulations again as a learner does not add additional risk to the patient. In my case, we somewhat arbitrarily agreed that I participate in 25 TEE exams. (CME courses, both online and in-person simulation, exist and greatly supplement self-study.)
Obtaining equipment is also a common barrier, though this has become less restrictive in the last several years. As previously mentioned, many cart-based ultrasound machines can accommodate a TEE probe. This changes the request from purchasing a new machine to “just a probe.” Despite the higher cost than most other probes, those in charge of purchasing are often more open to purchasing “a probe” than to purchasing an ultrasound machine.
Additionally, the purchasing decision regarding probes may fall to a different person than it does for an ultrasound machine. If available, POCUS image archiving into the medical record can help offset the cost of equipment, both by increasing revenue via billing and by demonstrating that equipment is being used. If initially declined, continue to ask and work to integrate the purchase into the next year’s budget. Inquire about the process of making a formal request and follow that process. This will often involve obtaining a quote or quotes from the ultrasound manufacturer(s).
Keep in mind that the probe will require a special storage cabinet specifically designed for TEE probes. It is prudent to include this in budget requests. If needed, the echocardiography lab can be a useful resource for additional information regarding the cabinet requirements. It is strongly recommended to discuss TEE probe models with sterile processing before any purchasing. If options are available, it is wise to choose a model the hospital already uses, as the cleaning protocol is well established. Our unit purchased a model that did not have an established protocol, which took nearly 6 months to develop. If probe options are limited, involving sterile processing early to start developing a protocol will help decrease delays.
Obtaining hospital privileges is also a common barrier, though this may not be as challenging as expected. Hospitals typically have well-outlined policies on obtaining privileges for established procedures. One of our hospital systems had four different options; the most straightforward required 20 hours of CME specific to TEE and 10 supervised cases by a proctor currently holding TEE privileges (see Table 1).
Discussions about obtaining privileges should involve your division chief, chair of medicine, and the cardiology division chief. Clearly outlining the plan to perform this procedure only in critically ill patients who are already intubated for other reasons made these conversations go much more smoothly. In the development of delineation of privileges, we used the term critical care TEE to clearly define this patient population. During these conversations, highlight the safety of the procedure; ASE guidelines3 estimate a severe complication rate of less than 1 in 10,000 cases and explain the anticipated benefits to critically ill patients.
In conclusion, at an institution that is already adept at the use of POCUS in the ICU, the additional of critical care TEE within 1 to 2 years is a very realistic achievement. It will undoubtedly require patience, persistence, and self-motivation, but the barriers are becoming smaller every day. Stay motivated!
Dr. Proud is Associate Professor of Medicine, Division of Pulmonary and Critical Care Medicine, Pulmonary and Critical Care Medicine Program Director, UT Health San Antonio.
References:
1. Porter TR, Abdelmoneim S, Belcik FT, et al. Guidelines for the cardiac sonographer in the performance of contrast echocardiography: a focused update from the American Society of Echocardiography. J Am Soc Echocardiogr. 2024;27(8):797-810.
2. Si X, Ma J, Cao DY, et al. Transesophageal echocardiography instead or in addition to transthoracic echocardiography in evaluating haemodynamic problems in intubated critically ill patients. Ann Transl Med. 2020;8(12):785.
3. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a cmprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardioraphy and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26(9):921-964.
Bedside-focused cardiac ultrasound assessment, or cardiac point-of-care ultrasound (POCUS), has become common in intensive care units throughout the US and the world. Many clinicians argue a POCUS cardiac assessment should be completed in most hypotensive patients and all cases of undifferentiated shock.
However, obtaining images adequate for decision making via standard transthoracic echo (TTE) is not possible in a significant number of patients; as high as 30% of critically ill patients, according to The American Society of Echocardiography (ASE) guidelines.1 Factors common to critically ill patients, such as invasive mechanical ventilation, external dressings, and limited mobility, contribute to poor image acquisition.
CHEST
Dr. Kevin Proud
In almost all these cases, the factors limiting image acquisition can be eliminated by utilizing a transesophageal approach. In a recent study, researchers were able to demonstrate that adding transesophageal echocardiography (TEE) to TTE in critically ill patients yielded a new diagnosis or a change in management about 45% of the time.2
Using transesophageal ultrasound for a focused cardiac assessment in hemodynamically unstable patients is not new—and is often referred to as rescue TEE or resuscitative TEE. A broader term, transesophageal ultrasound, has also been used to include sonographic evaluation of the lungs in patients with poor acoustic windows. At my institution, we use the term critical care TEE to define TEE performed by a noncardiology-trained intensivist in an intubated critically ill patient.
Regardless of the term, the use of transesophageal ultrasound by the noncardiologist in the ICU appears to be a developing trend. As with other uses of POCUS, ultrasound machines continue to be able to “do more” at a lower price point. In 2024, several cart-based ultrasound machines are compatible with transesophageal probes and contain software packages capable of common cardiac measurements.
Despite this growing interest, intensivists are likely to encounter barriers to implementing critical care TEE. Our division recently implemented adding TEE to our practice. Our practice involves two separate systems: a Veterans Administration hospital and a university-based county hospital. Our division has integrated the use of TEE in the medical ICU at both institutions. Having navigated the process at both institutions, I can offer some guidance in navigating barriers.
The development of a critical care TEE program must start with a strong base in transthoracic cardiac POCUS, at least for the foreseeable future. Having a strong background in TTE gives learners a solid foundation in cardiac anatomy, cardiac function, and ultrasound properties. Obtaining testamur status or board certification in critical care echocardiography is not an absolute must but is a definite benefit. Having significant experience in TTE image acquisition and interpretation will flatten the learning curve for TEE. Interestingly, image acquisition in TEE is often easier than in TTE, so the paradigm of learning TTE before TEE may reverse in the years to come.
Two barriers often work together to create a vicious cycle that stops the development of a TEE program at its start. These barriers include the lack of training and lack of equipment, specifically a TEE probe. Those who do not understand the value of TEE may ask, “Why purchase equipment for a procedure that you do not yet know how to do?” The opposite question can also be asked, “Why get trained to do something you don’t have the equipment to perform?”
My best advice to break this cycle is to “dive in” to whichever barrier seems easier to overcome first. I started with obtaining knowledge and training. Obtaining training and education in a procedure that is historically not done in your specialty is challenging but is not impossible. It takes a combination of high levels of self-motivation and at least one colleague with the training to support you. I approached a cardiac anesthesiologist, whom I knew from the surgical ICU. Cardiologists can also be a resource, but working with cardiac anesthesiologists offers several advantages. TEEs done by cardiac anesthesiologists are similar to those done in ICU patients (ie, all patients are intubated and sedated). The procedures are also scheduled several days in advance, making it easier to integrate training into your daily work schedule. Lastly, the TEE probe remains in place for several hours, so repeating the probe manipulations again as a learner does not add additional risk to the patient. In my case, we somewhat arbitrarily agreed that I participate in 25 TEE exams. (CME courses, both online and in-person simulation, exist and greatly supplement self-study.)
Obtaining equipment is also a common barrier, though this has become less restrictive in the last several years. As previously mentioned, many cart-based ultrasound machines can accommodate a TEE probe. This changes the request from purchasing a new machine to “just a probe.” Despite the higher cost than most other probes, those in charge of purchasing are often more open to purchasing “a probe” than to purchasing an ultrasound machine.
Additionally, the purchasing decision regarding probes may fall to a different person than it does for an ultrasound machine. If available, POCUS image archiving into the medical record can help offset the cost of equipment, both by increasing revenue via billing and by demonstrating that equipment is being used. If initially declined, continue to ask and work to integrate the purchase into the next year’s budget. Inquire about the process of making a formal request and follow that process. This will often involve obtaining a quote or quotes from the ultrasound manufacturer(s).
Keep in mind that the probe will require a special storage cabinet specifically designed for TEE probes. It is prudent to include this in budget requests. If needed, the echocardiography lab can be a useful resource for additional information regarding the cabinet requirements. It is strongly recommended to discuss TEE probe models with sterile processing before any purchasing. If options are available, it is wise to choose a model the hospital already uses, as the cleaning protocol is well established. Our unit purchased a model that did not have an established protocol, which took nearly 6 months to develop. If probe options are limited, involving sterile processing early to start developing a protocol will help decrease delays.
Obtaining hospital privileges is also a common barrier, though this may not be as challenging as expected. Hospitals typically have well-outlined policies on obtaining privileges for established procedures. One of our hospital systems had four different options; the most straightforward required 20 hours of CME specific to TEE and 10 supervised cases by a proctor currently holding TEE privileges (see Table 1).
Discussions about obtaining privileges should involve your division chief, chair of medicine, and the cardiology division chief. Clearly outlining the plan to perform this procedure only in critically ill patients who are already intubated for other reasons made these conversations go much more smoothly. In the development of delineation of privileges, we used the term critical care TEE to clearly define this patient population. During these conversations, highlight the safety of the procedure; ASE guidelines3 estimate a severe complication rate of less than 1 in 10,000 cases and explain the anticipated benefits to critically ill patients.
In conclusion, at an institution that is already adept at the use of POCUS in the ICU, the additional of critical care TEE within 1 to 2 years is a very realistic achievement. It will undoubtedly require patience, persistence, and self-motivation, but the barriers are becoming smaller every day. Stay motivated!
Dr. Proud is Associate Professor of Medicine, Division of Pulmonary and Critical Care Medicine, Pulmonary and Critical Care Medicine Program Director, UT Health San Antonio.
References:
1. Porter TR, Abdelmoneim S, Belcik FT, et al. Guidelines for the cardiac sonographer in the performance of contrast echocardiography: a focused update from the American Society of Echocardiography. J Am Soc Echocardiogr. 2024;27(8):797-810.
2. Si X, Ma J, Cao DY, et al. Transesophageal echocardiography instead or in addition to transthoracic echocardiography in evaluating haemodynamic problems in intubated critically ill patients. Ann Transl Med. 2020;8(12):785.
3. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a cmprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardioraphy and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26(9):921-964.
The American Academy of Sleep Medicine recently published its position statement reaffirming its support of utilizing permanent Standard Time (ST) as opposed to Daylight Saving Time (DST).1 DST usually occurs on the second Sunday in March when we “spring forward” by advancing the clock by 1 hour. The analogous “fall back” on the first Sunday in November refers to reversion back to the original ST, which is more synchronous with the sun’s natural pattern of rise and fall.
Subodh K. Arora, MD
The earliest argument for DST practice dates back to the 1700s when Benjamin Franklin wrote a satirical piece in the Journal of Paris suggesting that advancing the clock to rise earlier in the summer would lead to economization in candle usage and save significant resources for Parisians. The modern version of this assertion infers that increased daylight in the evening will lead to increased consumer activity and work productivity with consequent economic benefits. Interestingly, the adoption of DST has demonstrated the opposite—a reduction in work productivity and economic losses.2 Another often-cited claim is that increased daylight in the evening could lead to fewer motor vehicle accidents. However, the reality is that DST is associated with more frequent car accidents in the morning.
The greatest drawback of DST is that, initially, it leads to sleep deprivation and chronically drives asynchronization between the circadian clock and the social clock. Humans synchronize their internal clock based on several factors, including light, temperature, feeding, and social habits. However, light is the strongest exogenous factor that regulates the internal clock. Light inhibits secretion of melatonin, an endogenous hormone that promotes sleep onset. While there is some individual variation in circadian patterns, exposure to bright light in the morning leads to increased physical, mental, and goal-directed activity.
Conversely, darkness or reduced light exposure in the evening hours promotes decreased activity and sleep onset via melatonin release. DST disrupts this natural process by promoting increased light exposure in the evening. This desynchronizes solar light from our internal clocks, causing a relative phase delay. Acutely, patients experience a form of imposed social jet lag. They lose an hour of sleep due to diminished sleep opportunity, as work and social obligations are typically not altered to allow for a later awakening. With recurrent delays, this lends to a pattern of chronic sleep deprivation which has significant health consequences.
Losing an hour of sleep opportunity as the clock advances in spring has dire consequences. The transition to DST is associated with increased cardiovascular events, including myocardial infarction, stroke, and admissions for acute atrial fibrillation.3 4 5 A large body of work has shown that acute reduction of sleep is associated with higher sympathetic tone, compromised immunity, and increased inflammation. Further, cognitive consequences can ensue in the form of altered situational awareness, increased risky behavior, and worse reaction time—which manifest as increased motor vehicle accidents, injuries, and fatalities.6 Emergency room visits and bounce-back admissions, medical errors and injuries, and missed appointments increase following the switch to DST.7 Psychiatric outcomes, including deaths due to suicide and overdose, are worse with the spring transition.8
Jennifer L. Creamer, MD
Is the problem with DST merely limited to springtime, when we lose an hour of sleep? Not quite. During the “fall back” period, despite theoretically gaining an hour of sleep opportunity, people exhibit evidence of sleep disruption, psychiatric issues, traffic accidents, and inflammatory bowel disease exacerbations. These consequences likely stem from a discordance between circadian and social time, which leads to an earlier awakening based on circadian physiology as opposed to the clock time.
The acute impact of changing our sleep patterns during transitions in clock time may be appreciated more readily, but the damage is much more insidious. Chronic exposure to light in the late evening creates a state of enhanced arousal when the body should be winding down. The chronic incongruency between clock and solar time leads to dyssynchrony in our usual functions, such as food intake, social and physical activity, and basal temperature. Consequently, there is an impetus to fall asleep later. This leads to an accumulation of sleep debt and its associated negative consequences in the general, already chronically sleep-deprived population. This is especially impactful to adolescents and young adults who tend to have a delay in their sleep and wake patterns and, yet, are socially bound to early morning awakenings for school or work.
The scientific evidence behind the health risk and benefit profile of DST and ST is incontrovertible and in favor of ST. The hallmark of appropriate sleep habits involves consistency and appropriate duration. Changing timing forward or backward increases the likelihood of an alteration of the baseline established sleep and circadian consistency.
Unfortunately, despite multiple polls demonstrating the populace’s dislike of DST, repeat attempts to codify DST and negate ST persist. The latest initiative, the Sunshine Protection Act, which promised permanent DST, was passed by the US Senate but was thankfully foiled by Congress in 2022. The act of setting a time is not one that should be taken lightly or in isolation because there are significant, long-lasting health, safety, and socioeconomic consequences of this decision. Practically, this entails a concerted effort from all major economies since consistency is essential for trade and geopolitical relations. China, Japan, and India don’t practice DST. The European Parliament voted successfully to abolish DST in the European Union in 2019 with a plan to implement ST in 2021. Implementation has yet to be successful due to interruptions from the COVID-19 pandemic as well as the current economic and political climate in Europe. Political or theoretical political victories should not supersede the health and safety of an elected official’s constituents. As a medical community, we should continue to use our collective voice to encourage our representatives to vote in ways that positively affect our patients’ health outcomes.
References:
1. Rishi MA, et al. JCSM. 2024;20(1):121.
2. Gibson M, et al. Rev Econ Stat. 2018;100(5):783.
3. Jansky I, et al. N Engl J Med. 2008;359(18):1966.
4. Sipilia J, et al. Sleep Med. 2016;27-28:20.
5. Chudow JJ, et al. Sleep Med. 2020;69:155.
6. Fritz J, et al. Curr Biol. 2020;30(4):729.
7. Ferrazzi E, et al. J Biol Rhythms. 2018;33(5):555-564.
8. Berk M, et al. Sleep Biol Rhythms. 2008;6(1):22.
The American Academy of Sleep Medicine recently published its position statement reaffirming its support of utilizing permanent Standard Time (ST) as opposed to Daylight Saving Time (DST).1 DST usually occurs on the second Sunday in March when we “spring forward” by advancing the clock by 1 hour. The analogous “fall back” on the first Sunday in November refers to reversion back to the original ST, which is more synchronous with the sun’s natural pattern of rise and fall.
Subodh K. Arora, MD
The earliest argument for DST practice dates back to the 1700s when Benjamin Franklin wrote a satirical piece in the Journal of Paris suggesting that advancing the clock to rise earlier in the summer would lead to economization in candle usage and save significant resources for Parisians. The modern version of this assertion infers that increased daylight in the evening will lead to increased consumer activity and work productivity with consequent economic benefits. Interestingly, the adoption of DST has demonstrated the opposite—a reduction in work productivity and economic losses.2 Another often-cited claim is that increased daylight in the evening could lead to fewer motor vehicle accidents. However, the reality is that DST is associated with more frequent car accidents in the morning.
The greatest drawback of DST is that, initially, it leads to sleep deprivation and chronically drives asynchronization between the circadian clock and the social clock. Humans synchronize their internal clock based on several factors, including light, temperature, feeding, and social habits. However, light is the strongest exogenous factor that regulates the internal clock. Light inhibits secretion of melatonin, an endogenous hormone that promotes sleep onset. While there is some individual variation in circadian patterns, exposure to bright light in the morning leads to increased physical, mental, and goal-directed activity.
Conversely, darkness or reduced light exposure in the evening hours promotes decreased activity and sleep onset via melatonin release. DST disrupts this natural process by promoting increased light exposure in the evening. This desynchronizes solar light from our internal clocks, causing a relative phase delay. Acutely, patients experience a form of imposed social jet lag. They lose an hour of sleep due to diminished sleep opportunity, as work and social obligations are typically not altered to allow for a later awakening. With recurrent delays, this lends to a pattern of chronic sleep deprivation which has significant health consequences.
Losing an hour of sleep opportunity as the clock advances in spring has dire consequences. The transition to DST is associated with increased cardiovascular events, including myocardial infarction, stroke, and admissions for acute atrial fibrillation.3 4 5 A large body of work has shown that acute reduction of sleep is associated with higher sympathetic tone, compromised immunity, and increased inflammation. Further, cognitive consequences can ensue in the form of altered situational awareness, increased risky behavior, and worse reaction time—which manifest as increased motor vehicle accidents, injuries, and fatalities.6 Emergency room visits and bounce-back admissions, medical errors and injuries, and missed appointments increase following the switch to DST.7 Psychiatric outcomes, including deaths due to suicide and overdose, are worse with the spring transition.8
Jennifer L. Creamer, MD
Is the problem with DST merely limited to springtime, when we lose an hour of sleep? Not quite. During the “fall back” period, despite theoretically gaining an hour of sleep opportunity, people exhibit evidence of sleep disruption, psychiatric issues, traffic accidents, and inflammatory bowel disease exacerbations. These consequences likely stem from a discordance between circadian and social time, which leads to an earlier awakening based on circadian physiology as opposed to the clock time.
The acute impact of changing our sleep patterns during transitions in clock time may be appreciated more readily, but the damage is much more insidious. Chronic exposure to light in the late evening creates a state of enhanced arousal when the body should be winding down. The chronic incongruency between clock and solar time leads to dyssynchrony in our usual functions, such as food intake, social and physical activity, and basal temperature. Consequently, there is an impetus to fall asleep later. This leads to an accumulation of sleep debt and its associated negative consequences in the general, already chronically sleep-deprived population. This is especially impactful to adolescents and young adults who tend to have a delay in their sleep and wake patterns and, yet, are socially bound to early morning awakenings for school or work.
The scientific evidence behind the health risk and benefit profile of DST and ST is incontrovertible and in favor of ST. The hallmark of appropriate sleep habits involves consistency and appropriate duration. Changing timing forward or backward increases the likelihood of an alteration of the baseline established sleep and circadian consistency.
Unfortunately, despite multiple polls demonstrating the populace’s dislike of DST, repeat attempts to codify DST and negate ST persist. The latest initiative, the Sunshine Protection Act, which promised permanent DST, was passed by the US Senate but was thankfully foiled by Congress in 2022. The act of setting a time is not one that should be taken lightly or in isolation because there are significant, long-lasting health, safety, and socioeconomic consequences of this decision. Practically, this entails a concerted effort from all major economies since consistency is essential for trade and geopolitical relations. China, Japan, and India don’t practice DST. The European Parliament voted successfully to abolish DST in the European Union in 2019 with a plan to implement ST in 2021. Implementation has yet to be successful due to interruptions from the COVID-19 pandemic as well as the current economic and political climate in Europe. Political or theoretical political victories should not supersede the health and safety of an elected official’s constituents. As a medical community, we should continue to use our collective voice to encourage our representatives to vote in ways that positively affect our patients’ health outcomes.
References:
1. Rishi MA, et al. JCSM. 2024;20(1):121.
2. Gibson M, et al. Rev Econ Stat. 2018;100(5):783.
3. Jansky I, et al. N Engl J Med. 2008;359(18):1966.
4. Sipilia J, et al. Sleep Med. 2016;27-28:20.
5. Chudow JJ, et al. Sleep Med. 2020;69:155.
6. Fritz J, et al. Curr Biol. 2020;30(4):729.
7. Ferrazzi E, et al. J Biol Rhythms. 2018;33(5):555-564.
8. Berk M, et al. Sleep Biol Rhythms. 2008;6(1):22.
The American Academy of Sleep Medicine recently published its position statement reaffirming its support of utilizing permanent Standard Time (ST) as opposed to Daylight Saving Time (DST).1 DST usually occurs on the second Sunday in March when we “spring forward” by advancing the clock by 1 hour. The analogous “fall back” on the first Sunday in November refers to reversion back to the original ST, which is more synchronous with the sun’s natural pattern of rise and fall.
Subodh K. Arora, MD
The earliest argument for DST practice dates back to the 1700s when Benjamin Franklin wrote a satirical piece in the Journal of Paris suggesting that advancing the clock to rise earlier in the summer would lead to economization in candle usage and save significant resources for Parisians. The modern version of this assertion infers that increased daylight in the evening will lead to increased consumer activity and work productivity with consequent economic benefits. Interestingly, the adoption of DST has demonstrated the opposite—a reduction in work productivity and economic losses.2 Another often-cited claim is that increased daylight in the evening could lead to fewer motor vehicle accidents. However, the reality is that DST is associated with more frequent car accidents in the morning.
The greatest drawback of DST is that, initially, it leads to sleep deprivation and chronically drives asynchronization between the circadian clock and the social clock. Humans synchronize their internal clock based on several factors, including light, temperature, feeding, and social habits. However, light is the strongest exogenous factor that regulates the internal clock. Light inhibits secretion of melatonin, an endogenous hormone that promotes sleep onset. While there is some individual variation in circadian patterns, exposure to bright light in the morning leads to increased physical, mental, and goal-directed activity.
Conversely, darkness or reduced light exposure in the evening hours promotes decreased activity and sleep onset via melatonin release. DST disrupts this natural process by promoting increased light exposure in the evening. This desynchronizes solar light from our internal clocks, causing a relative phase delay. Acutely, patients experience a form of imposed social jet lag. They lose an hour of sleep due to diminished sleep opportunity, as work and social obligations are typically not altered to allow for a later awakening. With recurrent delays, this lends to a pattern of chronic sleep deprivation which has significant health consequences.
Losing an hour of sleep opportunity as the clock advances in spring has dire consequences. The transition to DST is associated with increased cardiovascular events, including myocardial infarction, stroke, and admissions for acute atrial fibrillation.3 4 5 A large body of work has shown that acute reduction of sleep is associated with higher sympathetic tone, compromised immunity, and increased inflammation. Further, cognitive consequences can ensue in the form of altered situational awareness, increased risky behavior, and worse reaction time—which manifest as increased motor vehicle accidents, injuries, and fatalities.6 Emergency room visits and bounce-back admissions, medical errors and injuries, and missed appointments increase following the switch to DST.7 Psychiatric outcomes, including deaths due to suicide and overdose, are worse with the spring transition.8
Jennifer L. Creamer, MD
Is the problem with DST merely limited to springtime, when we lose an hour of sleep? Not quite. During the “fall back” period, despite theoretically gaining an hour of sleep opportunity, people exhibit evidence of sleep disruption, psychiatric issues, traffic accidents, and inflammatory bowel disease exacerbations. These consequences likely stem from a discordance between circadian and social time, which leads to an earlier awakening based on circadian physiology as opposed to the clock time.
The acute impact of changing our sleep patterns during transitions in clock time may be appreciated more readily, but the damage is much more insidious. Chronic exposure to light in the late evening creates a state of enhanced arousal when the body should be winding down. The chronic incongruency between clock and solar time leads to dyssynchrony in our usual functions, such as food intake, social and physical activity, and basal temperature. Consequently, there is an impetus to fall asleep later. This leads to an accumulation of sleep debt and its associated negative consequences in the general, already chronically sleep-deprived population. This is especially impactful to adolescents and young adults who tend to have a delay in their sleep and wake patterns and, yet, are socially bound to early morning awakenings for school or work.
The scientific evidence behind the health risk and benefit profile of DST and ST is incontrovertible and in favor of ST. The hallmark of appropriate sleep habits involves consistency and appropriate duration. Changing timing forward or backward increases the likelihood of an alteration of the baseline established sleep and circadian consistency.
Unfortunately, despite multiple polls demonstrating the populace’s dislike of DST, repeat attempts to codify DST and negate ST persist. The latest initiative, the Sunshine Protection Act, which promised permanent DST, was passed by the US Senate but was thankfully foiled by Congress in 2022. The act of setting a time is not one that should be taken lightly or in isolation because there are significant, long-lasting health, safety, and socioeconomic consequences of this decision. Practically, this entails a concerted effort from all major economies since consistency is essential for trade and geopolitical relations. China, Japan, and India don’t practice DST. The European Parliament voted successfully to abolish DST in the European Union in 2019 with a plan to implement ST in 2021. Implementation has yet to be successful due to interruptions from the COVID-19 pandemic as well as the current economic and political climate in Europe. Political or theoretical political victories should not supersede the health and safety of an elected official’s constituents. As a medical community, we should continue to use our collective voice to encourage our representatives to vote in ways that positively affect our patients’ health outcomes.
References:
1. Rishi MA, et al. JCSM. 2024;20(1):121.
2. Gibson M, et al. Rev Econ Stat. 2018;100(5):783.
3. Jansky I, et al. N Engl J Med. 2008;359(18):1966.
4. Sipilia J, et al. Sleep Med. 2016;27-28:20.
5. Chudow JJ, et al. Sleep Med. 2020;69:155.
6. Fritz J, et al. Curr Biol. 2020;30(4):729.
7. Ferrazzi E, et al. J Biol Rhythms. 2018;33(5):555-564.
8. Berk M, et al. Sleep Biol Rhythms. 2008;6(1):22.