User login
Bridging the Gap Between Inpatient and Outpatient Care
The Olin E. Teague Veterans’ Center (OETVC) in Temple, Texas, is a teaching hospital with 189 beds that provides patients access to medical, surgical, and specialty care. In 2022, 116,359 veterans received care at OETVC and 5393 inpatient admissions were noted. The inpatient ward consists of 3 teaching teams staffed by an attending physician, a second-year internal medicine resident, and 2 to 3 interns while hospitalists staff the 3 nonteaching teams. OETVC residents receive training on both routine and complex medical problems.
Each day, teaching teams discharge patients. With the complexity of discharges, there is always a risk of patients not following up with their primary care physicians, potential issues with filling medications, confusion about new medication regiments, and even potential postdischarge questions. In 1990, Holloway and colleagues evaluated potential risk factors for readmission among veterans. This study found that discharge from a geriatrics or intermediate care bed, chronic disease diagnosis, ≥ 2 procedures performed, increasing age, and distance from a veterans affairs medical center were risk factors.1
Several community hospital studies have evaluated readmission risk factors. One from 2000 noted that patients with more hospitalizations, lower mental health function, a diagnosis of chronic obstructive pulmonary disorder, and increased satisfaction with access to emergency care were associated with increased readmission in 90 days.2 Due to the readmission risks, OETVC decided to construct a program that would help these patients successfully transition from inpatient to outpatient care while establishing means to discuss their care with a physician for reassurance and guidance.
TRANSITION OF CARE PROGRAM
Transition of care programs have been implemented and evaluated in many institutions. A 2017 systematic review of transition of care programs supported the use of tailored discharge planning and postdischarge phone calls to reduce hospital readmission, noting that 6 studies demonstrated a statistically significant reduction in 30-day readmission rate.3 Another study found that pharmacy involvement in the transition of care reduced medication-related problems following discharge.4
Program Goals
The foundational goal of our program was to bridge the gap between inpatient and outpatient medicine. We hoped to improve patient adherence with their discharge regimens, improve access to primary care physicians, and improve discharge follow-up. Since hospitalization can be overwhelming, we hoped to capture potential barriers to medical care postdischarge when patients return home while decreasing hospital readmissions. Our second- and third-year resident physicians spend as much time as needed going through the patient’s course of illness throughout their hospitalization and treatment plans to ensure their understanding and potential success.
This program benefits residents by providing medical education and patient communication opportunities. Residents must review the patient’s clinical trajectory before calling them. In this process, residents develop an understanding of routine and complex illness scripts, or pathways of common illnesses. They also prepare for potential questions about the hospitalization, new medications, and follow-up care. Lastly, residents can focus on communication skills. Without the time pressures of returning to a busy rotation, the residents spend as much time discussing the hospital course and ensuring patient understanding as needed.
Program Description
At the beginning of each week, second- and third-year residents review the list of discharges from the 3 teaching teams. The list is generated by a medical service management analyst. The residents review patient records for inpatient services, laboratory results, medication changes, and proposed follow-up plans designed by the admission team prior to their phone call. The resident is also responsible for reviewing and reconciling discharge instructions and orders. Then, the resident calls the patient and reviews their hospitalization. If a patient does not answer, the resident leaves a voicemail that complies with the Health Insurance Portability and Accountability Act.
When patients answer the call, the resident follows a script (Appendix). Residents are encouraged to ask patients open-ended questions and address any new needs. They also discuss changes in symptoms, medications, functional status, and remind the patient about follow-up appointments. If imaging or specific orders were missed at discharge, the residents notify the chief resident, lead hospitalist, or deputy associate chief of staff for medical service. If additional laboratory tests need to be ordered, the resident devises a follow-up plan. If needed, specialty referrals can be placed. When residents feel there are multiple items that need to be addressed or if they notice any major concerns, they can recommend the patient present to the emergency department for evaluation. The chief resident, lead hospitalist, and deputy associate chair for medical service are available to assist with discussions about complex medical situations or new concerning symptoms. Residents document their encounters in the Computerized Patient Record System health record and any tests that need follow-up. This differs from the standard of care follow-up programs, which are conducted by primary care medicine nurses and do not fully discuss the hospitalization.
Implementation
This program was implemented as a 1-week elective for interested residents and part of the clinic rotation. The internal medicine medical service analyst pulls all discharges on Friday, which are then provided to the residents. The residents on rotation work through the discharges and find teaching team patients to follow up with and call.
Findings
Implementation of this program has yielded many benefits. The reminder of the importance of a primary care appointment has motivated patients to continue following up on an outpatient basis. Residents were also able to capture lapses in patient understanding. Residents could answer forgotten questions and help patients understand their admission pathology without time pressures. Residents have identified patients with hypoglycemia due to changed insulin regimens, set up specialist follow-up appointments, and provided additional education facilitating adherence. Additionally, several residents have expressed satisfaction with the ability to practice their communication skills. Others appreciated contributing to future patient successes.
While the focus on this article has been to share the program description, we have tabulated preliminary data. In January 2023, there were 239 internal medicine admissions; 158 admissions (66%) were teaching team patients, and 97 patients (61%) were called by a resident and spoken to regarding their care. There were 24 teaching team readmissions within 30 days, and 10 (42%) received a follow-up phone call. Eighty-one admitted patients were treated by nonteaching teams, 10 (12%) of whom were readmissions. Comparing 30-day readmission rates, 10 nonteaching team patients (12%), 10 teaching team patients (6.3%) who talk to a resident in the transition of care program were readmitted, and 24 teaching team patients who did not talk to a resident (10%) were readmitted.
DISCUSSION
The OETVC transition of care program was planned, formulated, and implemented without modeling after any other projects or institutions. This program aimed to utilize our residents as resources for patients.
Transition of care is defined as steps taken in a clinical encounter to assist with the coordination and continuity of patient care transferring between locations or levels of care.5 A 2018 study evaluating the utility of transition of care programs on adults aged ≥ 60 years found a reduction in rehospitalization rates, increased use of primary care services, and potential reduction in home health usage.6
In 2021, Johns Hopkins University School of Medicine implemented a program after polling residents and discovering their awareness of gaps in the transition of care.7 In 2002, pharmacists evaluated the impact of follow-up telephone calls to recently hospitalized patients. This group of pharmacists found that these calls were associated with increased patient satisfaction, resolution of medication-related problems and fewer emergency department returns.8
Our program differs from other transition of care programs in that resident physicians made the follow-up calls to patients. Residents could address all aspects of medical care, including new symptoms, new prescriptions, adverse events, and risk factors for readmission, or order new imaging and medications when appropriate. In the program, residents called all patients discharged after receiving care within their team. Calls were not based on risk assessments. The residents were able to speak with 61% of discharged patients. When readmission rates were compared between patients who received a resident follow-up phone call and those who did not, patients receiving the resident phone call were readmitted at a lower rate: 6.3% vs 10%, respectively.
While our data suggest a potential trend of decreased readmission, more follow-up over a longer period may be needed. We believe this program can benefit patients and our model can act as a template for other institutions interested in starting their own programs.
Challenges
Although our process is efficient, there have been some challenges. The discharge is created by the medical service management analyst and then sent to the chief resident, but there was concern that the list could be missed if either individual was unavailable. The chairperson for the department of medicine and their secretary are now involved in the process. To reduce unanswered telephone calls, residents use OETVC phones. Health Insurance Portability and Accountability Act-compliant voicemails providing a time for a follow-up call were implemented. As a result, veterans have answered their phones more regularly and are more aware of calls. Orders are generally placed by the chief resident, lead hospitalist, or chair of the medical service to ensure follow-up because residents are on rotation for 1 week at a time. Access to a physician also allows patients to discuss items unrelated to their hospitalization, introducing new symptoms, or situations requiring a resident to act with limited data.
CONCLUSIONS
The transition of care follow-up program described in this article may be beneficial for both internal medicine residents and patients. Second- and third-year residents are developing a better understanding of the trajectory of many illnesses and are given the opportunity to retrospectively analyze what they would do differently based on knowledge gained from their chart reviews. They are also given the opportunity to work on communication skills and explain courses of illnesses to patients in an easy-to-understand format without time constraints. Patients now have access to a physician following discharge to discuss any concerns with their hospitalization, condition, and follow-up. This program will continue to address barriers to care and adapt to improve the success of care transitions.
1. Holloway JJ, Medendorp SV, Bromberg J. Risk factors for early readmission among veterans. Health Serv Res. 1990;25(1 Pt 2):213-237.
2. Smith DM, Giobbie-Hurder A, Weinberger M, et al. Predicting non-elective hospital readmissions: a multi-site study. Department of Veterans Affairs Cooperative Study Group on Primary Care and Readmissions. J Clin Epidemiol. 2000;53(11):1113-1118. doi:10.1016/s0895-4356(00)00236-5
3. Kamermayer AK, Leasure AR, Anderson L. The Effectiveness of Transitions-of-Care Interventions in Reducing Hospital Readmissions and Mortality: A Systematic Review. Dimens Crit Care Nurs. 2017;36(6):311-316. doi:10.1097/DCC.0000000000000266
4. Daliri S, Hugtenburg JG, Ter Riet G, et al. The effect of a pharmacy-led transitional care program on medication-related problems post-discharge: A before-After prospective study. PLoS One. 2019;14(3):e0213593. Published 2019 Mar 12. doi:10.1371/journal.pone.0213593
5. Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003;51(4):549-555. doi:10.1046/j.1532-5415.2003.51185.x
6. Weeks LE, Macdonald M, Helwig M, Bishop A, Martin-Misener R, Iduye D. The impact of transitional care programs on health services utilization among community-dwelling older adults and their caregivers: a systematic review protocol of quantitative evidence. JBI Database System Rev Implement Rep. 2016;14(3):26-34. doi:10.11124/JBISRIR-2016-2568
7. Sheikh F, Gathecha E, Arbaje AI, Christmas C. Internal Medicine Residents’ Views About Care Transitions: Results of an Educational Intervention. J Med Educ Curric Dev. 2021;8:2382120520988590. Published 2021 Jan 20. doi:10.1177/2382120520988590
8. Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Dis Mon. 2002;48(4):239-248. doi:10.1016/s0011-5029(02)90031-3
The Olin E. Teague Veterans’ Center (OETVC) in Temple, Texas, is a teaching hospital with 189 beds that provides patients access to medical, surgical, and specialty care. In 2022, 116,359 veterans received care at OETVC and 5393 inpatient admissions were noted. The inpatient ward consists of 3 teaching teams staffed by an attending physician, a second-year internal medicine resident, and 2 to 3 interns while hospitalists staff the 3 nonteaching teams. OETVC residents receive training on both routine and complex medical problems.
Each day, teaching teams discharge patients. With the complexity of discharges, there is always a risk of patients not following up with their primary care physicians, potential issues with filling medications, confusion about new medication regiments, and even potential postdischarge questions. In 1990, Holloway and colleagues evaluated potential risk factors for readmission among veterans. This study found that discharge from a geriatrics or intermediate care bed, chronic disease diagnosis, ≥ 2 procedures performed, increasing age, and distance from a veterans affairs medical center were risk factors.1
Several community hospital studies have evaluated readmission risk factors. One from 2000 noted that patients with more hospitalizations, lower mental health function, a diagnosis of chronic obstructive pulmonary disorder, and increased satisfaction with access to emergency care were associated with increased readmission in 90 days.2 Due to the readmission risks, OETVC decided to construct a program that would help these patients successfully transition from inpatient to outpatient care while establishing means to discuss their care with a physician for reassurance and guidance.
TRANSITION OF CARE PROGRAM
Transition of care programs have been implemented and evaluated in many institutions. A 2017 systematic review of transition of care programs supported the use of tailored discharge planning and postdischarge phone calls to reduce hospital readmission, noting that 6 studies demonstrated a statistically significant reduction in 30-day readmission rate.3 Another study found that pharmacy involvement in the transition of care reduced medication-related problems following discharge.4
Program Goals
The foundational goal of our program was to bridge the gap between inpatient and outpatient medicine. We hoped to improve patient adherence with their discharge regimens, improve access to primary care physicians, and improve discharge follow-up. Since hospitalization can be overwhelming, we hoped to capture potential barriers to medical care postdischarge when patients return home while decreasing hospital readmissions. Our second- and third-year resident physicians spend as much time as needed going through the patient’s course of illness throughout their hospitalization and treatment plans to ensure their understanding and potential success.
This program benefits residents by providing medical education and patient communication opportunities. Residents must review the patient’s clinical trajectory before calling them. In this process, residents develop an understanding of routine and complex illness scripts, or pathways of common illnesses. They also prepare for potential questions about the hospitalization, new medications, and follow-up care. Lastly, residents can focus on communication skills. Without the time pressures of returning to a busy rotation, the residents spend as much time discussing the hospital course and ensuring patient understanding as needed.
Program Description
At the beginning of each week, second- and third-year residents review the list of discharges from the 3 teaching teams. The list is generated by a medical service management analyst. The residents review patient records for inpatient services, laboratory results, medication changes, and proposed follow-up plans designed by the admission team prior to their phone call. The resident is also responsible for reviewing and reconciling discharge instructions and orders. Then, the resident calls the patient and reviews their hospitalization. If a patient does not answer, the resident leaves a voicemail that complies with the Health Insurance Portability and Accountability Act.
When patients answer the call, the resident follows a script (Appendix). Residents are encouraged to ask patients open-ended questions and address any new needs. They also discuss changes in symptoms, medications, functional status, and remind the patient about follow-up appointments. If imaging or specific orders were missed at discharge, the residents notify the chief resident, lead hospitalist, or deputy associate chief of staff for medical service. If additional laboratory tests need to be ordered, the resident devises a follow-up plan. If needed, specialty referrals can be placed. When residents feel there are multiple items that need to be addressed or if they notice any major concerns, they can recommend the patient present to the emergency department for evaluation. The chief resident, lead hospitalist, and deputy associate chair for medical service are available to assist with discussions about complex medical situations or new concerning symptoms. Residents document their encounters in the Computerized Patient Record System health record and any tests that need follow-up. This differs from the standard of care follow-up programs, which are conducted by primary care medicine nurses and do not fully discuss the hospitalization.
Implementation
This program was implemented as a 1-week elective for interested residents and part of the clinic rotation. The internal medicine medical service analyst pulls all discharges on Friday, which are then provided to the residents. The residents on rotation work through the discharges and find teaching team patients to follow up with and call.
Findings
Implementation of this program has yielded many benefits. The reminder of the importance of a primary care appointment has motivated patients to continue following up on an outpatient basis. Residents were also able to capture lapses in patient understanding. Residents could answer forgotten questions and help patients understand their admission pathology without time pressures. Residents have identified patients with hypoglycemia due to changed insulin regimens, set up specialist follow-up appointments, and provided additional education facilitating adherence. Additionally, several residents have expressed satisfaction with the ability to practice their communication skills. Others appreciated contributing to future patient successes.
While the focus on this article has been to share the program description, we have tabulated preliminary data. In January 2023, there were 239 internal medicine admissions; 158 admissions (66%) were teaching team patients, and 97 patients (61%) were called by a resident and spoken to regarding their care. There were 24 teaching team readmissions within 30 days, and 10 (42%) received a follow-up phone call. Eighty-one admitted patients were treated by nonteaching teams, 10 (12%) of whom were readmissions. Comparing 30-day readmission rates, 10 nonteaching team patients (12%), 10 teaching team patients (6.3%) who talk to a resident in the transition of care program were readmitted, and 24 teaching team patients who did not talk to a resident (10%) were readmitted.
DISCUSSION
The OETVC transition of care program was planned, formulated, and implemented without modeling after any other projects or institutions. This program aimed to utilize our residents as resources for patients.
Transition of care is defined as steps taken in a clinical encounter to assist with the coordination and continuity of patient care transferring between locations or levels of care.5 A 2018 study evaluating the utility of transition of care programs on adults aged ≥ 60 years found a reduction in rehospitalization rates, increased use of primary care services, and potential reduction in home health usage.6
In 2021, Johns Hopkins University School of Medicine implemented a program after polling residents and discovering their awareness of gaps in the transition of care.7 In 2002, pharmacists evaluated the impact of follow-up telephone calls to recently hospitalized patients. This group of pharmacists found that these calls were associated with increased patient satisfaction, resolution of medication-related problems and fewer emergency department returns.8
Our program differs from other transition of care programs in that resident physicians made the follow-up calls to patients. Residents could address all aspects of medical care, including new symptoms, new prescriptions, adverse events, and risk factors for readmission, or order new imaging and medications when appropriate. In the program, residents called all patients discharged after receiving care within their team. Calls were not based on risk assessments. The residents were able to speak with 61% of discharged patients. When readmission rates were compared between patients who received a resident follow-up phone call and those who did not, patients receiving the resident phone call were readmitted at a lower rate: 6.3% vs 10%, respectively.
While our data suggest a potential trend of decreased readmission, more follow-up over a longer period may be needed. We believe this program can benefit patients and our model can act as a template for other institutions interested in starting their own programs.
Challenges
Although our process is efficient, there have been some challenges. The discharge is created by the medical service management analyst and then sent to the chief resident, but there was concern that the list could be missed if either individual was unavailable. The chairperson for the department of medicine and their secretary are now involved in the process. To reduce unanswered telephone calls, residents use OETVC phones. Health Insurance Portability and Accountability Act-compliant voicemails providing a time for a follow-up call were implemented. As a result, veterans have answered their phones more regularly and are more aware of calls. Orders are generally placed by the chief resident, lead hospitalist, or chair of the medical service to ensure follow-up because residents are on rotation for 1 week at a time. Access to a physician also allows patients to discuss items unrelated to their hospitalization, introducing new symptoms, or situations requiring a resident to act with limited data.
CONCLUSIONS
The transition of care follow-up program described in this article may be beneficial for both internal medicine residents and patients. Second- and third-year residents are developing a better understanding of the trajectory of many illnesses and are given the opportunity to retrospectively analyze what they would do differently based on knowledge gained from their chart reviews. They are also given the opportunity to work on communication skills and explain courses of illnesses to patients in an easy-to-understand format without time constraints. Patients now have access to a physician following discharge to discuss any concerns with their hospitalization, condition, and follow-up. This program will continue to address barriers to care and adapt to improve the success of care transitions.
The Olin E. Teague Veterans’ Center (OETVC) in Temple, Texas, is a teaching hospital with 189 beds that provides patients access to medical, surgical, and specialty care. In 2022, 116,359 veterans received care at OETVC and 5393 inpatient admissions were noted. The inpatient ward consists of 3 teaching teams staffed by an attending physician, a second-year internal medicine resident, and 2 to 3 interns while hospitalists staff the 3 nonteaching teams. OETVC residents receive training on both routine and complex medical problems.
Each day, teaching teams discharge patients. With the complexity of discharges, there is always a risk of patients not following up with their primary care physicians, potential issues with filling medications, confusion about new medication regiments, and even potential postdischarge questions. In 1990, Holloway and colleagues evaluated potential risk factors for readmission among veterans. This study found that discharge from a geriatrics or intermediate care bed, chronic disease diagnosis, ≥ 2 procedures performed, increasing age, and distance from a veterans affairs medical center were risk factors.1
Several community hospital studies have evaluated readmission risk factors. One from 2000 noted that patients with more hospitalizations, lower mental health function, a diagnosis of chronic obstructive pulmonary disorder, and increased satisfaction with access to emergency care were associated with increased readmission in 90 days.2 Due to the readmission risks, OETVC decided to construct a program that would help these patients successfully transition from inpatient to outpatient care while establishing means to discuss their care with a physician for reassurance and guidance.
TRANSITION OF CARE PROGRAM
Transition of care programs have been implemented and evaluated in many institutions. A 2017 systematic review of transition of care programs supported the use of tailored discharge planning and postdischarge phone calls to reduce hospital readmission, noting that 6 studies demonstrated a statistically significant reduction in 30-day readmission rate.3 Another study found that pharmacy involvement in the transition of care reduced medication-related problems following discharge.4
Program Goals
The foundational goal of our program was to bridge the gap between inpatient and outpatient medicine. We hoped to improve patient adherence with their discharge regimens, improve access to primary care physicians, and improve discharge follow-up. Since hospitalization can be overwhelming, we hoped to capture potential barriers to medical care postdischarge when patients return home while decreasing hospital readmissions. Our second- and third-year resident physicians spend as much time as needed going through the patient’s course of illness throughout their hospitalization and treatment plans to ensure their understanding and potential success.
This program benefits residents by providing medical education and patient communication opportunities. Residents must review the patient’s clinical trajectory before calling them. In this process, residents develop an understanding of routine and complex illness scripts, or pathways of common illnesses. They also prepare for potential questions about the hospitalization, new medications, and follow-up care. Lastly, residents can focus on communication skills. Without the time pressures of returning to a busy rotation, the residents spend as much time discussing the hospital course and ensuring patient understanding as needed.
Program Description
At the beginning of each week, second- and third-year residents review the list of discharges from the 3 teaching teams. The list is generated by a medical service management analyst. The residents review patient records for inpatient services, laboratory results, medication changes, and proposed follow-up plans designed by the admission team prior to their phone call. The resident is also responsible for reviewing and reconciling discharge instructions and orders. Then, the resident calls the patient and reviews their hospitalization. If a patient does not answer, the resident leaves a voicemail that complies with the Health Insurance Portability and Accountability Act.
When patients answer the call, the resident follows a script (Appendix). Residents are encouraged to ask patients open-ended questions and address any new needs. They also discuss changes in symptoms, medications, functional status, and remind the patient about follow-up appointments. If imaging or specific orders were missed at discharge, the residents notify the chief resident, lead hospitalist, or deputy associate chief of staff for medical service. If additional laboratory tests need to be ordered, the resident devises a follow-up plan. If needed, specialty referrals can be placed. When residents feel there are multiple items that need to be addressed or if they notice any major concerns, they can recommend the patient present to the emergency department for evaluation. The chief resident, lead hospitalist, and deputy associate chair for medical service are available to assist with discussions about complex medical situations or new concerning symptoms. Residents document their encounters in the Computerized Patient Record System health record and any tests that need follow-up. This differs from the standard of care follow-up programs, which are conducted by primary care medicine nurses and do not fully discuss the hospitalization.
Implementation
This program was implemented as a 1-week elective for interested residents and part of the clinic rotation. The internal medicine medical service analyst pulls all discharges on Friday, which are then provided to the residents. The residents on rotation work through the discharges and find teaching team patients to follow up with and call.
Findings
Implementation of this program has yielded many benefits. The reminder of the importance of a primary care appointment has motivated patients to continue following up on an outpatient basis. Residents were also able to capture lapses in patient understanding. Residents could answer forgotten questions and help patients understand their admission pathology without time pressures. Residents have identified patients with hypoglycemia due to changed insulin regimens, set up specialist follow-up appointments, and provided additional education facilitating adherence. Additionally, several residents have expressed satisfaction with the ability to practice their communication skills. Others appreciated contributing to future patient successes.
While the focus on this article has been to share the program description, we have tabulated preliminary data. In January 2023, there were 239 internal medicine admissions; 158 admissions (66%) were teaching team patients, and 97 patients (61%) were called by a resident and spoken to regarding their care. There were 24 teaching team readmissions within 30 days, and 10 (42%) received a follow-up phone call. Eighty-one admitted patients were treated by nonteaching teams, 10 (12%) of whom were readmissions. Comparing 30-day readmission rates, 10 nonteaching team patients (12%), 10 teaching team patients (6.3%) who talk to a resident in the transition of care program were readmitted, and 24 teaching team patients who did not talk to a resident (10%) were readmitted.
DISCUSSION
The OETVC transition of care program was planned, formulated, and implemented without modeling after any other projects or institutions. This program aimed to utilize our residents as resources for patients.
Transition of care is defined as steps taken in a clinical encounter to assist with the coordination and continuity of patient care transferring between locations or levels of care.5 A 2018 study evaluating the utility of transition of care programs on adults aged ≥ 60 years found a reduction in rehospitalization rates, increased use of primary care services, and potential reduction in home health usage.6
In 2021, Johns Hopkins University School of Medicine implemented a program after polling residents and discovering their awareness of gaps in the transition of care.7 In 2002, pharmacists evaluated the impact of follow-up telephone calls to recently hospitalized patients. This group of pharmacists found that these calls were associated with increased patient satisfaction, resolution of medication-related problems and fewer emergency department returns.8
Our program differs from other transition of care programs in that resident physicians made the follow-up calls to patients. Residents could address all aspects of medical care, including new symptoms, new prescriptions, adverse events, and risk factors for readmission, or order new imaging and medications when appropriate. In the program, residents called all patients discharged after receiving care within their team. Calls were not based on risk assessments. The residents were able to speak with 61% of discharged patients. When readmission rates were compared between patients who received a resident follow-up phone call and those who did not, patients receiving the resident phone call were readmitted at a lower rate: 6.3% vs 10%, respectively.
While our data suggest a potential trend of decreased readmission, more follow-up over a longer period may be needed. We believe this program can benefit patients and our model can act as a template for other institutions interested in starting their own programs.
Challenges
Although our process is efficient, there have been some challenges. The discharge is created by the medical service management analyst and then sent to the chief resident, but there was concern that the list could be missed if either individual was unavailable. The chairperson for the department of medicine and their secretary are now involved in the process. To reduce unanswered telephone calls, residents use OETVC phones. Health Insurance Portability and Accountability Act-compliant voicemails providing a time for a follow-up call were implemented. As a result, veterans have answered their phones more regularly and are more aware of calls. Orders are generally placed by the chief resident, lead hospitalist, or chair of the medical service to ensure follow-up because residents are on rotation for 1 week at a time. Access to a physician also allows patients to discuss items unrelated to their hospitalization, introducing new symptoms, or situations requiring a resident to act with limited data.
CONCLUSIONS
The transition of care follow-up program described in this article may be beneficial for both internal medicine residents and patients. Second- and third-year residents are developing a better understanding of the trajectory of many illnesses and are given the opportunity to retrospectively analyze what they would do differently based on knowledge gained from their chart reviews. They are also given the opportunity to work on communication skills and explain courses of illnesses to patients in an easy-to-understand format without time constraints. Patients now have access to a physician following discharge to discuss any concerns with their hospitalization, condition, and follow-up. This program will continue to address barriers to care and adapt to improve the success of care transitions.
1. Holloway JJ, Medendorp SV, Bromberg J. Risk factors for early readmission among veterans. Health Serv Res. 1990;25(1 Pt 2):213-237.
2. Smith DM, Giobbie-Hurder A, Weinberger M, et al. Predicting non-elective hospital readmissions: a multi-site study. Department of Veterans Affairs Cooperative Study Group on Primary Care and Readmissions. J Clin Epidemiol. 2000;53(11):1113-1118. doi:10.1016/s0895-4356(00)00236-5
3. Kamermayer AK, Leasure AR, Anderson L. The Effectiveness of Transitions-of-Care Interventions in Reducing Hospital Readmissions and Mortality: A Systematic Review. Dimens Crit Care Nurs. 2017;36(6):311-316. doi:10.1097/DCC.0000000000000266
4. Daliri S, Hugtenburg JG, Ter Riet G, et al. The effect of a pharmacy-led transitional care program on medication-related problems post-discharge: A before-After prospective study. PLoS One. 2019;14(3):e0213593. Published 2019 Mar 12. doi:10.1371/journal.pone.0213593
5. Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003;51(4):549-555. doi:10.1046/j.1532-5415.2003.51185.x
6. Weeks LE, Macdonald M, Helwig M, Bishop A, Martin-Misener R, Iduye D. The impact of transitional care programs on health services utilization among community-dwelling older adults and their caregivers: a systematic review protocol of quantitative evidence. JBI Database System Rev Implement Rep. 2016;14(3):26-34. doi:10.11124/JBISRIR-2016-2568
7. Sheikh F, Gathecha E, Arbaje AI, Christmas C. Internal Medicine Residents’ Views About Care Transitions: Results of an Educational Intervention. J Med Educ Curric Dev. 2021;8:2382120520988590. Published 2021 Jan 20. doi:10.1177/2382120520988590
8. Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Dis Mon. 2002;48(4):239-248. doi:10.1016/s0011-5029(02)90031-3
1. Holloway JJ, Medendorp SV, Bromberg J. Risk factors for early readmission among veterans. Health Serv Res. 1990;25(1 Pt 2):213-237.
2. Smith DM, Giobbie-Hurder A, Weinberger M, et al. Predicting non-elective hospital readmissions: a multi-site study. Department of Veterans Affairs Cooperative Study Group on Primary Care and Readmissions. J Clin Epidemiol. 2000;53(11):1113-1118. doi:10.1016/s0895-4356(00)00236-5
3. Kamermayer AK, Leasure AR, Anderson L. The Effectiveness of Transitions-of-Care Interventions in Reducing Hospital Readmissions and Mortality: A Systematic Review. Dimens Crit Care Nurs. 2017;36(6):311-316. doi:10.1097/DCC.0000000000000266
4. Daliri S, Hugtenburg JG, Ter Riet G, et al. The effect of a pharmacy-led transitional care program on medication-related problems post-discharge: A before-After prospective study. PLoS One. 2019;14(3):e0213593. Published 2019 Mar 12. doi:10.1371/journal.pone.0213593
5. Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003;51(4):549-555. doi:10.1046/j.1532-5415.2003.51185.x
6. Weeks LE, Macdonald M, Helwig M, Bishop A, Martin-Misener R, Iduye D. The impact of transitional care programs on health services utilization among community-dwelling older adults and their caregivers: a systematic review protocol of quantitative evidence. JBI Database System Rev Implement Rep. 2016;14(3):26-34. doi:10.11124/JBISRIR-2016-2568
7. Sheikh F, Gathecha E, Arbaje AI, Christmas C. Internal Medicine Residents’ Views About Care Transitions: Results of an Educational Intervention. J Med Educ Curric Dev. 2021;8:2382120520988590. Published 2021 Jan 20. doi:10.1177/2382120520988590
8. Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Dis Mon. 2002;48(4):239-248. doi:10.1016/s0011-5029(02)90031-3
Role of JAK2 in Polycythemia Vera

How does the presence of the JAK2 V617F mutation affect the diagnosis and classification of myeloproliferative neoplasms?
Dr. Richard: The JAK2 V617F mutation is found in > 90% of patients with polycythemia vera (PV). The remaining patients with PV have mutations in a different portion of the JAK2 gene. Since JAK2 mutations are found in virtually all patients with PV, having the mutation helps make the diagnosis, but does not carry prognostic significance. Some studies suggest that the allele burden of the mutated JAK2 V617F could be used to identify aggressive disease, but that finding is not universally accepted across all health care entities or practitioners. Variations in acceptance may be due to factors such as evolution of knowledge based on the latest evidence, clinical practice variability and priorities, availability of testing, and complexity of disease management.
This is not true of the 2 other classical myeloproliferative neoplasms (MPNs) that we see commonly in our clinics: essential thrombocytosis (ET) and myelofibrosis (MF). The CALR mutation can be seen in patients with ET and MF and signals a less aggressive form of the disease.
The presence of JAK2 V617F is critical for prognosis. Although it does not directly help to inform the patient of what to expect, identifying the mutation provides us with important information about the patient’s prognosis, which helps guide treatment decisions such as the intensity of therapy and monitoring for thrombotic events.
What are the potential implications of the JAK2 V617F mutation in the treatment of PV?
Dr. Richard: The discovery of the JAK2 V617F mutation in MPNs in 2005 led to the hope that perhaps there would be targeted therapy that could result in disease remissions. We had all hoped that the spectacular responses observed in patients with chronic myelogenous leukemia (CML) treated with imatinib could be replicated with JAK2 inhibitors. It turned out that blocking JAK2 was insufficient to reverse the disease. Studies are still ongoing whether drugs that can decrease the JAK2 V617F allele burden could be used to achieve a type of remission. Perhaps combination therapies will need to be developed.
I am hopeful that in the future we do see advancements that provide improved diagnosis and monitoring to help facilitate early detection, personalized treatment approaches to offer more effective and well tolerated therapies, risk stratification and prognostication to help identify higher risk progression, combination therapies to possibly improve efficacy and adherence, and novel therapeutic targets to help discover new treatments and provide improved outcomes.
How can JAK2 V617F lead to 3 different forms of myeloproliferative neoplasms?
Dr. Richard: The short answer is no one knows exactly. The phenotypic differences between PV and the other 2 MPN variants are most likely determined by the integration of other signaling pathways that are activated by the corresponding driver mutation, and interactions with other mutations. What also seems to matter is the sequence in which the individual mutations are acquired.
There have been documented cases of post-polycythemic leukemia that no longer have the JAK2 V617F mutation. However, at some point that mutation was lost, and the cells acquired other driver mutations that resulted in leukemia.
What we do know now is that there are several potential interactions that can coexist with JAK2 V617F. There is MPL mutation, which contributes to disease pathogenesis and thrombotic risk. Independent of JAK2 V617F pathways is CALR mutation, which is another driver of MPNs. In addition are other JAK mutations, epigenetic alterations, and microenvironmental factors. All of these have the potential to influence clinical manifestations by impacting clinical outcomes, affecting expression patterns and signaling inflammation within the bone marrow microenvironment.
Are there any ongoing research efforts or clinical trials exploring targeted therapies that specifically address the JAK2 V617F mutation in patients with PV?
Dr. Richard: The ongoing research efforts to address JAK2-targeted therapies are looking at options like novel JAK inhibitors, combination therapies, resistance mechanisms, improved safety profiles, biomarker identification, exploring new indications, and preclinical studies that involve the development and testing of new JAK inhibitors.
Other JAK2-targeted therapies continue to be in development. At this time, we have ruxolitinib, pacritinib, fedratinib, and momelotinib. None of them appear to be a magic bullet the way imatinib was with CML. Perhaps a better disease comparison is chronic lymphocytic leukemia (CLL). In CLL, targeted therapies against Bruton tyrosine kinase and BCL2 are being combined to result in many years of disease control. JAK2 inhibition may need to be combined with another active drug, perhaps against a mutation or pathway that has not yet been identified.
How does the presence of the JAK2 V617F mutation affect the diagnosis and classification of myeloproliferative neoplasms?
Dr. Richard: The JAK2 V617F mutation is found in > 90% of patients with polycythemia vera (PV). The remaining patients with PV have mutations in a different portion of the JAK2 gene. Since JAK2 mutations are found in virtually all patients with PV, having the mutation helps make the diagnosis, but does not carry prognostic significance. Some studies suggest that the allele burden of the mutated JAK2 V617F could be used to identify aggressive disease, but that finding is not universally accepted across all health care entities or practitioners. Variations in acceptance may be due to factors such as evolution of knowledge based on the latest evidence, clinical practice variability and priorities, availability of testing, and complexity of disease management.
This is not true of the 2 other classical myeloproliferative neoplasms (MPNs) that we see commonly in our clinics: essential thrombocytosis (ET) and myelofibrosis (MF). The CALR mutation can be seen in patients with ET and MF and signals a less aggressive form of the disease.
The presence of JAK2 V617F is critical for prognosis. Although it does not directly help to inform the patient of what to expect, identifying the mutation provides us with important information about the patient’s prognosis, which helps guide treatment decisions such as the intensity of therapy and monitoring for thrombotic events.
What are the potential implications of the JAK2 V617F mutation in the treatment of PV?
Dr. Richard: The discovery of the JAK2 V617F mutation in MPNs in 2005 led to the hope that perhaps there would be targeted therapy that could result in disease remissions. We had all hoped that the spectacular responses observed in patients with chronic myelogenous leukemia (CML) treated with imatinib could be replicated with JAK2 inhibitors. It turned out that blocking JAK2 was insufficient to reverse the disease. Studies are still ongoing whether drugs that can decrease the JAK2 V617F allele burden could be used to achieve a type of remission. Perhaps combination therapies will need to be developed.
I am hopeful that in the future we do see advancements that provide improved diagnosis and monitoring to help facilitate early detection, personalized treatment approaches to offer more effective and well tolerated therapies, risk stratification and prognostication to help identify higher risk progression, combination therapies to possibly improve efficacy and adherence, and novel therapeutic targets to help discover new treatments and provide improved outcomes.
How can JAK2 V617F lead to 3 different forms of myeloproliferative neoplasms?
Dr. Richard: The short answer is no one knows exactly. The phenotypic differences between PV and the other 2 MPN variants are most likely determined by the integration of other signaling pathways that are activated by the corresponding driver mutation, and interactions with other mutations. What also seems to matter is the sequence in which the individual mutations are acquired.
There have been documented cases of post-polycythemic leukemia that no longer have the JAK2 V617F mutation. However, at some point that mutation was lost, and the cells acquired other driver mutations that resulted in leukemia.
What we do know now is that there are several potential interactions that can coexist with JAK2 V617F. There is MPL mutation, which contributes to disease pathogenesis and thrombotic risk. Independent of JAK2 V617F pathways is CALR mutation, which is another driver of MPNs. In addition are other JAK mutations, epigenetic alterations, and microenvironmental factors. All of these have the potential to influence clinical manifestations by impacting clinical outcomes, affecting expression patterns and signaling inflammation within the bone marrow microenvironment.
Are there any ongoing research efforts or clinical trials exploring targeted therapies that specifically address the JAK2 V617F mutation in patients with PV?
Dr. Richard: The ongoing research efforts to address JAK2-targeted therapies are looking at options like novel JAK inhibitors, combination therapies, resistance mechanisms, improved safety profiles, biomarker identification, exploring new indications, and preclinical studies that involve the development and testing of new JAK inhibitors.
Other JAK2-targeted therapies continue to be in development. At this time, we have ruxolitinib, pacritinib, fedratinib, and momelotinib. None of them appear to be a magic bullet the way imatinib was with CML. Perhaps a better disease comparison is chronic lymphocytic leukemia (CLL). In CLL, targeted therapies against Bruton tyrosine kinase and BCL2 are being combined to result in many years of disease control. JAK2 inhibition may need to be combined with another active drug, perhaps against a mutation or pathway that has not yet been identified.
How does the presence of the JAK2 V617F mutation affect the diagnosis and classification of myeloproliferative neoplasms?
Dr. Richard: The JAK2 V617F mutation is found in > 90% of patients with polycythemia vera (PV). The remaining patients with PV have mutations in a different portion of the JAK2 gene. Since JAK2 mutations are found in virtually all patients with PV, having the mutation helps make the diagnosis, but does not carry prognostic significance. Some studies suggest that the allele burden of the mutated JAK2 V617F could be used to identify aggressive disease, but that finding is not universally accepted across all health care entities or practitioners. Variations in acceptance may be due to factors such as evolution of knowledge based on the latest evidence, clinical practice variability and priorities, availability of testing, and complexity of disease management.
This is not true of the 2 other classical myeloproliferative neoplasms (MPNs) that we see commonly in our clinics: essential thrombocytosis (ET) and myelofibrosis (MF). The CALR mutation can be seen in patients with ET and MF and signals a less aggressive form of the disease.
The presence of JAK2 V617F is critical for prognosis. Although it does not directly help to inform the patient of what to expect, identifying the mutation provides us with important information about the patient’s prognosis, which helps guide treatment decisions such as the intensity of therapy and monitoring for thrombotic events.
What are the potential implications of the JAK2 V617F mutation in the treatment of PV?
Dr. Richard: The discovery of the JAK2 V617F mutation in MPNs in 2005 led to the hope that perhaps there would be targeted therapy that could result in disease remissions. We had all hoped that the spectacular responses observed in patients with chronic myelogenous leukemia (CML) treated with imatinib could be replicated with JAK2 inhibitors. It turned out that blocking JAK2 was insufficient to reverse the disease. Studies are still ongoing whether drugs that can decrease the JAK2 V617F allele burden could be used to achieve a type of remission. Perhaps combination therapies will need to be developed.
I am hopeful that in the future we do see advancements that provide improved diagnosis and monitoring to help facilitate early detection, personalized treatment approaches to offer more effective and well tolerated therapies, risk stratification and prognostication to help identify higher risk progression, combination therapies to possibly improve efficacy and adherence, and novel therapeutic targets to help discover new treatments and provide improved outcomes.
How can JAK2 V617F lead to 3 different forms of myeloproliferative neoplasms?
Dr. Richard: The short answer is no one knows exactly. The phenotypic differences between PV and the other 2 MPN variants are most likely determined by the integration of other signaling pathways that are activated by the corresponding driver mutation, and interactions with other mutations. What also seems to matter is the sequence in which the individual mutations are acquired.
There have been documented cases of post-polycythemic leukemia that no longer have the JAK2 V617F mutation. However, at some point that mutation was lost, and the cells acquired other driver mutations that resulted in leukemia.
What we do know now is that there are several potential interactions that can coexist with JAK2 V617F. There is MPL mutation, which contributes to disease pathogenesis and thrombotic risk. Independent of JAK2 V617F pathways is CALR mutation, which is another driver of MPNs. In addition are other JAK mutations, epigenetic alterations, and microenvironmental factors. All of these have the potential to influence clinical manifestations by impacting clinical outcomes, affecting expression patterns and signaling inflammation within the bone marrow microenvironment.
Are there any ongoing research efforts or clinical trials exploring targeted therapies that specifically address the JAK2 V617F mutation in patients with PV?
Dr. Richard: The ongoing research efforts to address JAK2-targeted therapies are looking at options like novel JAK inhibitors, combination therapies, resistance mechanisms, improved safety profiles, biomarker identification, exploring new indications, and preclinical studies that involve the development and testing of new JAK inhibitors.
Other JAK2-targeted therapies continue to be in development. At this time, we have ruxolitinib, pacritinib, fedratinib, and momelotinib. None of them appear to be a magic bullet the way imatinib was with CML. Perhaps a better disease comparison is chronic lymphocytic leukemia (CLL). In CLL, targeted therapies against Bruton tyrosine kinase and BCL2 are being combined to result in many years of disease control. JAK2 inhibition may need to be combined with another active drug, perhaps against a mutation or pathway that has not yet been identified.
Discussing a Silent Problem: Communicating Effectively About Lipid Risks and Management
This transcript has been edited for clarity.
Jorge Plutzky, MD: Hi. I'm Dr Jorge Plutzky, director of preventive cardiology at the Brigham and Women's Hospital, and in that setting I direct our lipid clinic. I'm pleased to be here today to talk about how we communicate about cholesterol. And I'm pleased to be able to do that today with a patient of mine, Brian McMahon.
Brian, thank you for being here.
Brian McMahon: Thank you, Doctor.
Plutzky: Why don't you tell people listening how we came to connect in the first place.
McMahon: Well, it was around statins. I had been prescribed one probably 10 years ago, and I had an adverse reaction to it — a violent reaction. And the doctor just told me to stop taking it. So I did. And I never asked another question.
And then 10 years later, my GP in Connecticut said, "You should go get a calcium score exam. Insurance doesn't cover it. It's 90 bucks, and it'll be the best 90 bucks you ever spent." And then the numbers were not good. That led me to come and talk to you about what do I do now? What are my options? I had an adverse reaction to statins. I didn't think I could even take them.
Plutzky: That's so important. Really, the failure was in your physician not getting that initial follow-up: Okay, so you had this reaction; what are the potential explanations for that, and what could be the next steps?
It really should not fall upon you as a patient to have to push that. But in fact, when people are better educated about the issues in our system, sometimes you do have to be your own advocate and ask, "What's next?" And it's important for us in communicating these issues during that first encounter, which might be with a primary care physician or a cardiologist, but more often it's with a primary care physician.
We're more motivated when someone's already had an event — secondary prevention. Let's not have another one because the patient has now been through something scary: a heart attack or a stent or even bypass surgery or a stroke. Those really motivate people. But even in that setting, we often find that patients don't necessarily stay on treatment or don't necessarily get treated aggressively enough to the right LDL level.
So that becomes important to set the stage early about why we are doing this, and let's come up with options that are safe, usually well tolerated, and have been extensively studied.
McMahon: I think the key is that it is a silent killer, so you don't feel bad, you don't have a rash, you don't have a scratch. It's not painful, but it could kill you. But the very fact that it's just that the statin doesn't agree with you — that was a real mess, in my estimation.
Plutzky: Often in settings of primary prevention, you're trying to conjure up the future for someone, saying, "You know what? If we don't do something, we're going to run into issues." But those patients don't feel bad. You're right that it is silent, but that's where the huge opportunity exists: early intervention — identifying what that risk is and how many different options we have, like if someone doesn't succeed on or has an issue with a statin. We know that's uncommon, but people often do well with some of these other alternatives, including just a different statin, which was the case with you.
McMahon: Right. And I had no idea that that was even available to me. That was an eye-opener, that there are options available to me, that I can find different things that work; but for goodness' sake, you should be on it.
Plutzky: Yes, we often have patients do well on a statin. Some patients really can't take a statin.
We'll go through a couple different options. I often will lay out for people who think they're having an issue with the statin that there are three possibilities: One, it's not the statin, because in the clinical trials we see people who quit the placebo as often as they quit the statin. Sharing that with patients matters. It's possible that what one felt wasn't even related to the statin. Two, sometimes reactions are statin specific. We try a different statin and then someone does well. Sometimes that may be influenced by the fact that we've laid out the data and explained to a patient, "We know that statins are safe, effective, and well tolerated, and here's the benefit for you down the road."
Is that part of why that second statin now works? It's hard to know. I've had many physician patients who say, "I didn't feel great on that one, but now I'm on a different statin and I'm feeling, much better." So, everyone reacts differently.
McMahon: I love that you walked me into it too. It wasn't just, "Here's 20 mg. We started at 5 mg, then we went to 10 mg, now we're at 20 mg." You took the time to say, "I hear you and I heard what happened to you. So, let's walk into this." I lost 10 years of taking statins, which would have put me in a different place.
Plutzky: The fact is that the first dose of the statin has the biggest impact on reducing your LDL. And then as you titrate it up, which we do all the time — we have with you — the effect on the lowering of LDL is less impactful. That's why it can be a way in with people to say, "Let's start with this low dose." At least they're on something. And people often say, "Wow! I really feel completely fine on this." There are people who either just can't take a statin at all or who, once they're on the statin, aren't getting to a low enough or appropriate LDL number, and it's good to have those alternatives.
One of them is specifically theoretically designed for people who think they've had muscle issues with statin. Your issues were different, but bempedoic acid is an alternative. And even going beyond that, we now have injectable medicines that really are very effective at bringing down LDL.
When people hear injections, they're like, "Oh my gosh, I don't want to take an injection," but explain to people how easy it is to do those injections. It's basically just a pen against your skin. That really reduces their fear and their anxiety. But it's important to realize that we do have many tools for lowering LDL. If someone runs into a problem with the statin that you can't overcome, then it's important to move on.
So we should recognize how important it is to lower LDL. Realizing how many tools we have allows people to begin working through the process where the objective is: I want to get my LDL down, and if we can do it with a statin, then we're taking advantage of all this data we have about their benefits. But if that turns out not to work for a given patient, even after trying and explaining things, then let's move on. But let's get to that ultimate goal of lowering LDL as one component of risk.
I think there's nothing more empowering for the person you're dealing with than to share with them what it is that you know; that you know, based upon medical science and clinical trials, what that rationale is, because no one is trying to hurt themselves. If someone comes in who doesn't want to take a statin, it's not because they're trying to have a heart attack. They're not trying to hurt themselves. There's some barrier to what's motivating them, to what's keeping them from this therapy. We just have to better communicate what the goal is and what the basis is for pursuing this, and then finding your way through the woods of saying, "Well, that worked great and we've made it" vs "We've run into something, so let's go on a different path."
McMahon: I think that to me was the light-bulb moment, which was that experience with statin: Don't take it anymore. And then 10 years go by and now I'm in trouble. And then I find out that there is a wealth of opportunities. There are so many arrows in your quiver — not to make a Cupid joke, but there are so many arrows available to fix this, and I didn't know it. Now I do.
Plutzky: Yes, it's empowering. I think there's a challenge for us as caregivers to more broadly share what we know so that people are motivated and empowered to say, "I want to get treated. I want to do better. And I understand the extent to which this is a risk for me if I don't do better."
McMahon: Right.
Plutzky: So often there's a family history associated with that, too. Sometimes when I'm communicating with patients the idea of "You need to do this," especially patients with young kids, I'm communicating, "How you eat and your activity level is sending a very powerful message to your kids."
McMahon: Yes.
Plutzky: We're trying to eat healthy. We're more oriented toward vegetables. We're being active. Let's go for a walk. Let's go for a family run. Let's have a sport that we do together. Or even just the kids seeing you leave the house to say, "I'm off." "Where are you going, Dad?" "I'm going to play tennis." "Can I come with you?" And then…
McMahon: It creates a lifestyle.
Plutzky: Yes.
McMahon: Well, it comes back to: You have one heart.
Plutzky: Yes. Well, it's been a pleasure to have a chance to discuss what are really important topics. I mean, this is really impactful. Far beyond just your experience, it's the chance for other people to realize that these are issues that need to be recognized, dealt with; that people need to be empowered; and that ultimately it comes down to us about how to better communicate.
I'm always very focused on how can a patient know what I know and what I think matters based upon evidence, data, clinical trials. How do we share that and share that in very limited time windows? It's been a privilege to work with you, Brian, in a clinical setting, and I'm very appreciative of your taking the time to join us today.
McMahon: Thank you for getting me on the right path. I'm grateful.
Plutzky: Well, you've done that for yourself. Good talking to you.
McMahon: Likewise.
Jorge Plutzky, MD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: Altimmune; Boehringer Ingelheim; Esperion; New Amsterdam; Novo Nordisk
Received research grant from: Boehringer Ingelheim; Novartis
Serve(d) on clinical trial committee for: Esperion; Novo Nordisk
Brian McMahon has disclosed no relevant financial relationships.
This transcript has been edited for clarity.
Jorge Plutzky, MD: Hi. I'm Dr Jorge Plutzky, director of preventive cardiology at the Brigham and Women's Hospital, and in that setting I direct our lipid clinic. I'm pleased to be here today to talk about how we communicate about cholesterol. And I'm pleased to be able to do that today with a patient of mine, Brian McMahon.
Brian, thank you for being here.
Brian McMahon: Thank you, Doctor.
Plutzky: Why don't you tell people listening how we came to connect in the first place.
McMahon: Well, it was around statins. I had been prescribed one probably 10 years ago, and I had an adverse reaction to it — a violent reaction. And the doctor just told me to stop taking it. So I did. And I never asked another question.
And then 10 years later, my GP in Connecticut said, "You should go get a calcium score exam. Insurance doesn't cover it. It's 90 bucks, and it'll be the best 90 bucks you ever spent." And then the numbers were not good. That led me to come and talk to you about what do I do now? What are my options? I had an adverse reaction to statins. I didn't think I could even take them.
Plutzky: That's so important. Really, the failure was in your physician not getting that initial follow-up: Okay, so you had this reaction; what are the potential explanations for that, and what could be the next steps?
It really should not fall upon you as a patient to have to push that. But in fact, when people are better educated about the issues in our system, sometimes you do have to be your own advocate and ask, "What's next?" And it's important for us in communicating these issues during that first encounter, which might be with a primary care physician or a cardiologist, but more often it's with a primary care physician.
We're more motivated when someone's already had an event — secondary prevention. Let's not have another one because the patient has now been through something scary: a heart attack or a stent or even bypass surgery or a stroke. Those really motivate people. But even in that setting, we often find that patients don't necessarily stay on treatment or don't necessarily get treated aggressively enough to the right LDL level.
So that becomes important to set the stage early about why we are doing this, and let's come up with options that are safe, usually well tolerated, and have been extensively studied.
McMahon: I think the key is that it is a silent killer, so you don't feel bad, you don't have a rash, you don't have a scratch. It's not painful, but it could kill you. But the very fact that it's just that the statin doesn't agree with you — that was a real mess, in my estimation.
Plutzky: Often in settings of primary prevention, you're trying to conjure up the future for someone, saying, "You know what? If we don't do something, we're going to run into issues." But those patients don't feel bad. You're right that it is silent, but that's where the huge opportunity exists: early intervention — identifying what that risk is and how many different options we have, like if someone doesn't succeed on or has an issue with a statin. We know that's uncommon, but people often do well with some of these other alternatives, including just a different statin, which was the case with you.
McMahon: Right. And I had no idea that that was even available to me. That was an eye-opener, that there are options available to me, that I can find different things that work; but for goodness' sake, you should be on it.
Plutzky: Yes, we often have patients do well on a statin. Some patients really can't take a statin.
We'll go through a couple different options. I often will lay out for people who think they're having an issue with the statin that there are three possibilities: One, it's not the statin, because in the clinical trials we see people who quit the placebo as often as they quit the statin. Sharing that with patients matters. It's possible that what one felt wasn't even related to the statin. Two, sometimes reactions are statin specific. We try a different statin and then someone does well. Sometimes that may be influenced by the fact that we've laid out the data and explained to a patient, "We know that statins are safe, effective, and well tolerated, and here's the benefit for you down the road."
Is that part of why that second statin now works? It's hard to know. I've had many physician patients who say, "I didn't feel great on that one, but now I'm on a different statin and I'm feeling, much better." So, everyone reacts differently.
McMahon: I love that you walked me into it too. It wasn't just, "Here's 20 mg. We started at 5 mg, then we went to 10 mg, now we're at 20 mg." You took the time to say, "I hear you and I heard what happened to you. So, let's walk into this." I lost 10 years of taking statins, which would have put me in a different place.
Plutzky: The fact is that the first dose of the statin has the biggest impact on reducing your LDL. And then as you titrate it up, which we do all the time — we have with you — the effect on the lowering of LDL is less impactful. That's why it can be a way in with people to say, "Let's start with this low dose." At least they're on something. And people often say, "Wow! I really feel completely fine on this." There are people who either just can't take a statin at all or who, once they're on the statin, aren't getting to a low enough or appropriate LDL number, and it's good to have those alternatives.
One of them is specifically theoretically designed for people who think they've had muscle issues with statin. Your issues were different, but bempedoic acid is an alternative. And even going beyond that, we now have injectable medicines that really are very effective at bringing down LDL.
When people hear injections, they're like, "Oh my gosh, I don't want to take an injection," but explain to people how easy it is to do those injections. It's basically just a pen against your skin. That really reduces their fear and their anxiety. But it's important to realize that we do have many tools for lowering LDL. If someone runs into a problem with the statin that you can't overcome, then it's important to move on.
So we should recognize how important it is to lower LDL. Realizing how many tools we have allows people to begin working through the process where the objective is: I want to get my LDL down, and if we can do it with a statin, then we're taking advantage of all this data we have about their benefits. But if that turns out not to work for a given patient, even after trying and explaining things, then let's move on. But let's get to that ultimate goal of lowering LDL as one component of risk.
I think there's nothing more empowering for the person you're dealing with than to share with them what it is that you know; that you know, based upon medical science and clinical trials, what that rationale is, because no one is trying to hurt themselves. If someone comes in who doesn't want to take a statin, it's not because they're trying to have a heart attack. They're not trying to hurt themselves. There's some barrier to what's motivating them, to what's keeping them from this therapy. We just have to better communicate what the goal is and what the basis is for pursuing this, and then finding your way through the woods of saying, "Well, that worked great and we've made it" vs "We've run into something, so let's go on a different path."
McMahon: I think that to me was the light-bulb moment, which was that experience with statin: Don't take it anymore. And then 10 years go by and now I'm in trouble. And then I find out that there is a wealth of opportunities. There are so many arrows in your quiver — not to make a Cupid joke, but there are so many arrows available to fix this, and I didn't know it. Now I do.
Plutzky: Yes, it's empowering. I think there's a challenge for us as caregivers to more broadly share what we know so that people are motivated and empowered to say, "I want to get treated. I want to do better. And I understand the extent to which this is a risk for me if I don't do better."
McMahon: Right.
Plutzky: So often there's a family history associated with that, too. Sometimes when I'm communicating with patients the idea of "You need to do this," especially patients with young kids, I'm communicating, "How you eat and your activity level is sending a very powerful message to your kids."
McMahon: Yes.
Plutzky: We're trying to eat healthy. We're more oriented toward vegetables. We're being active. Let's go for a walk. Let's go for a family run. Let's have a sport that we do together. Or even just the kids seeing you leave the house to say, "I'm off." "Where are you going, Dad?" "I'm going to play tennis." "Can I come with you?" And then…
McMahon: It creates a lifestyle.
Plutzky: Yes.
McMahon: Well, it comes back to: You have one heart.
Plutzky: Yes. Well, it's been a pleasure to have a chance to discuss what are really important topics. I mean, this is really impactful. Far beyond just your experience, it's the chance for other people to realize that these are issues that need to be recognized, dealt with; that people need to be empowered; and that ultimately it comes down to us about how to better communicate.
I'm always very focused on how can a patient know what I know and what I think matters based upon evidence, data, clinical trials. How do we share that and share that in very limited time windows? It's been a privilege to work with you, Brian, in a clinical setting, and I'm very appreciative of your taking the time to join us today.
McMahon: Thank you for getting me on the right path. I'm grateful.
Plutzky: Well, you've done that for yourself. Good talking to you.
McMahon: Likewise.
Jorge Plutzky, MD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: Altimmune; Boehringer Ingelheim; Esperion; New Amsterdam; Novo Nordisk
Received research grant from: Boehringer Ingelheim; Novartis
Serve(d) on clinical trial committee for: Esperion; Novo Nordisk
Brian McMahon has disclosed no relevant financial relationships.
This transcript has been edited for clarity.
Jorge Plutzky, MD: Hi. I'm Dr Jorge Plutzky, director of preventive cardiology at the Brigham and Women's Hospital, and in that setting I direct our lipid clinic. I'm pleased to be here today to talk about how we communicate about cholesterol. And I'm pleased to be able to do that today with a patient of mine, Brian McMahon.
Brian, thank you for being here.
Brian McMahon: Thank you, Doctor.
Plutzky: Why don't you tell people listening how we came to connect in the first place.
McMahon: Well, it was around statins. I had been prescribed one probably 10 years ago, and I had an adverse reaction to it — a violent reaction. And the doctor just told me to stop taking it. So I did. And I never asked another question.
And then 10 years later, my GP in Connecticut said, "You should go get a calcium score exam. Insurance doesn't cover it. It's 90 bucks, and it'll be the best 90 bucks you ever spent." And then the numbers were not good. That led me to come and talk to you about what do I do now? What are my options? I had an adverse reaction to statins. I didn't think I could even take them.
Plutzky: That's so important. Really, the failure was in your physician not getting that initial follow-up: Okay, so you had this reaction; what are the potential explanations for that, and what could be the next steps?
It really should not fall upon you as a patient to have to push that. But in fact, when people are better educated about the issues in our system, sometimes you do have to be your own advocate and ask, "What's next?" And it's important for us in communicating these issues during that first encounter, which might be with a primary care physician or a cardiologist, but more often it's with a primary care physician.
We're more motivated when someone's already had an event — secondary prevention. Let's not have another one because the patient has now been through something scary: a heart attack or a stent or even bypass surgery or a stroke. Those really motivate people. But even in that setting, we often find that patients don't necessarily stay on treatment or don't necessarily get treated aggressively enough to the right LDL level.
So that becomes important to set the stage early about why we are doing this, and let's come up with options that are safe, usually well tolerated, and have been extensively studied.
McMahon: I think the key is that it is a silent killer, so you don't feel bad, you don't have a rash, you don't have a scratch. It's not painful, but it could kill you. But the very fact that it's just that the statin doesn't agree with you — that was a real mess, in my estimation.
Plutzky: Often in settings of primary prevention, you're trying to conjure up the future for someone, saying, "You know what? If we don't do something, we're going to run into issues." But those patients don't feel bad. You're right that it is silent, but that's where the huge opportunity exists: early intervention — identifying what that risk is and how many different options we have, like if someone doesn't succeed on or has an issue with a statin. We know that's uncommon, but people often do well with some of these other alternatives, including just a different statin, which was the case with you.
McMahon: Right. And I had no idea that that was even available to me. That was an eye-opener, that there are options available to me, that I can find different things that work; but for goodness' sake, you should be on it.
Plutzky: Yes, we often have patients do well on a statin. Some patients really can't take a statin.
We'll go through a couple different options. I often will lay out for people who think they're having an issue with the statin that there are three possibilities: One, it's not the statin, because in the clinical trials we see people who quit the placebo as often as they quit the statin. Sharing that with patients matters. It's possible that what one felt wasn't even related to the statin. Two, sometimes reactions are statin specific. We try a different statin and then someone does well. Sometimes that may be influenced by the fact that we've laid out the data and explained to a patient, "We know that statins are safe, effective, and well tolerated, and here's the benefit for you down the road."
Is that part of why that second statin now works? It's hard to know. I've had many physician patients who say, "I didn't feel great on that one, but now I'm on a different statin and I'm feeling, much better." So, everyone reacts differently.
McMahon: I love that you walked me into it too. It wasn't just, "Here's 20 mg. We started at 5 mg, then we went to 10 mg, now we're at 20 mg." You took the time to say, "I hear you and I heard what happened to you. So, let's walk into this." I lost 10 years of taking statins, which would have put me in a different place.
Plutzky: The fact is that the first dose of the statin has the biggest impact on reducing your LDL. And then as you titrate it up, which we do all the time — we have with you — the effect on the lowering of LDL is less impactful. That's why it can be a way in with people to say, "Let's start with this low dose." At least they're on something. And people often say, "Wow! I really feel completely fine on this." There are people who either just can't take a statin at all or who, once they're on the statin, aren't getting to a low enough or appropriate LDL number, and it's good to have those alternatives.
One of them is specifically theoretically designed for people who think they've had muscle issues with statin. Your issues were different, but bempedoic acid is an alternative. And even going beyond that, we now have injectable medicines that really are very effective at bringing down LDL.
When people hear injections, they're like, "Oh my gosh, I don't want to take an injection," but explain to people how easy it is to do those injections. It's basically just a pen against your skin. That really reduces their fear and their anxiety. But it's important to realize that we do have many tools for lowering LDL. If someone runs into a problem with the statin that you can't overcome, then it's important to move on.
So we should recognize how important it is to lower LDL. Realizing how many tools we have allows people to begin working through the process where the objective is: I want to get my LDL down, and if we can do it with a statin, then we're taking advantage of all this data we have about their benefits. But if that turns out not to work for a given patient, even after trying and explaining things, then let's move on. But let's get to that ultimate goal of lowering LDL as one component of risk.
I think there's nothing more empowering for the person you're dealing with than to share with them what it is that you know; that you know, based upon medical science and clinical trials, what that rationale is, because no one is trying to hurt themselves. If someone comes in who doesn't want to take a statin, it's not because they're trying to have a heart attack. They're not trying to hurt themselves. There's some barrier to what's motivating them, to what's keeping them from this therapy. We just have to better communicate what the goal is and what the basis is for pursuing this, and then finding your way through the woods of saying, "Well, that worked great and we've made it" vs "We've run into something, so let's go on a different path."
McMahon: I think that to me was the light-bulb moment, which was that experience with statin: Don't take it anymore. And then 10 years go by and now I'm in trouble. And then I find out that there is a wealth of opportunities. There are so many arrows in your quiver — not to make a Cupid joke, but there are so many arrows available to fix this, and I didn't know it. Now I do.
Plutzky: Yes, it's empowering. I think there's a challenge for us as caregivers to more broadly share what we know so that people are motivated and empowered to say, "I want to get treated. I want to do better. And I understand the extent to which this is a risk for me if I don't do better."
McMahon: Right.
Plutzky: So often there's a family history associated with that, too. Sometimes when I'm communicating with patients the idea of "You need to do this," especially patients with young kids, I'm communicating, "How you eat and your activity level is sending a very powerful message to your kids."
McMahon: Yes.
Plutzky: We're trying to eat healthy. We're more oriented toward vegetables. We're being active. Let's go for a walk. Let's go for a family run. Let's have a sport that we do together. Or even just the kids seeing you leave the house to say, "I'm off." "Where are you going, Dad?" "I'm going to play tennis." "Can I come with you?" And then…
McMahon: It creates a lifestyle.
Plutzky: Yes.
McMahon: Well, it comes back to: You have one heart.
Plutzky: Yes. Well, it's been a pleasure to have a chance to discuss what are really important topics. I mean, this is really impactful. Far beyond just your experience, it's the chance for other people to realize that these are issues that need to be recognized, dealt with; that people need to be empowered; and that ultimately it comes down to us about how to better communicate.
I'm always very focused on how can a patient know what I know and what I think matters based upon evidence, data, clinical trials. How do we share that and share that in very limited time windows? It's been a privilege to work with you, Brian, in a clinical setting, and I'm very appreciative of your taking the time to join us today.
McMahon: Thank you for getting me on the right path. I'm grateful.
Plutzky: Well, you've done that for yourself. Good talking to you.
McMahon: Likewise.
Jorge Plutzky, MD, has disclosed the following relevant financial relationships:
Serve(d) as a consultant for: Altimmune; Boehringer Ingelheim; Esperion; New Amsterdam; Novo Nordisk
Received research grant from: Boehringer Ingelheim; Novartis
Serve(d) on clinical trial committee for: Esperion; Novo Nordisk
Brian McMahon has disclosed no relevant financial relationships.

Recalcitrant Folliculitis Decalvans Treatment Outcomes With Biologics and Small Molecule Inhibitors
Folliculitis decalvans (FD) is classified as a rare primary neutrophilic cicatricial alopecia occurring predominantly in middle-aged adults. Although the true etiology is still unknown, the pathogenesis behind the inflammatory follicular lesions stems from possible Staphylococcus aureus infection and an impaired host immune system in response to released superantigens. 1 The clinical severity of this inflammatory scalp disorder can range from mild to severe and debilitating. Multiple treatment regimens have been developed with the goal of maintaining full remission. We provide a summary of tumor necrosis factor (TNF) inhibitors, Janus kinase (JAK) inhibitors, phosphodiesterase 4 (PDE4) inhibitors, and monoclonal antibodies being utilized for patients with therapy-recalcitrant FD.
Methods
We conducted a PubMed, Medline, and Google Scholar search for the terms refractory FD, recalcitrant FD, or therapy-resistant FD to identify articles published in English from 1998 to 2022. Articles that reported recalcitrant cases and subsequent therapy with TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies were included. Articles were excluded if recalcitrant cases were not clearly defined. Remission was defined as no recurrence in lesions or pustules or as a reduction in the inflammatory process with stabilization upon continuation or discontinuation of the therapy regimen. Two reviewers (T.F. and K.U.) independently searched for and screened each report.
Results
Treatment of recalcitrant FD with biologics or small molecule inhibitors was discussed in 9 studies with a combined total of 35 patients.2-10 The treatment regimens included TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies (Table).
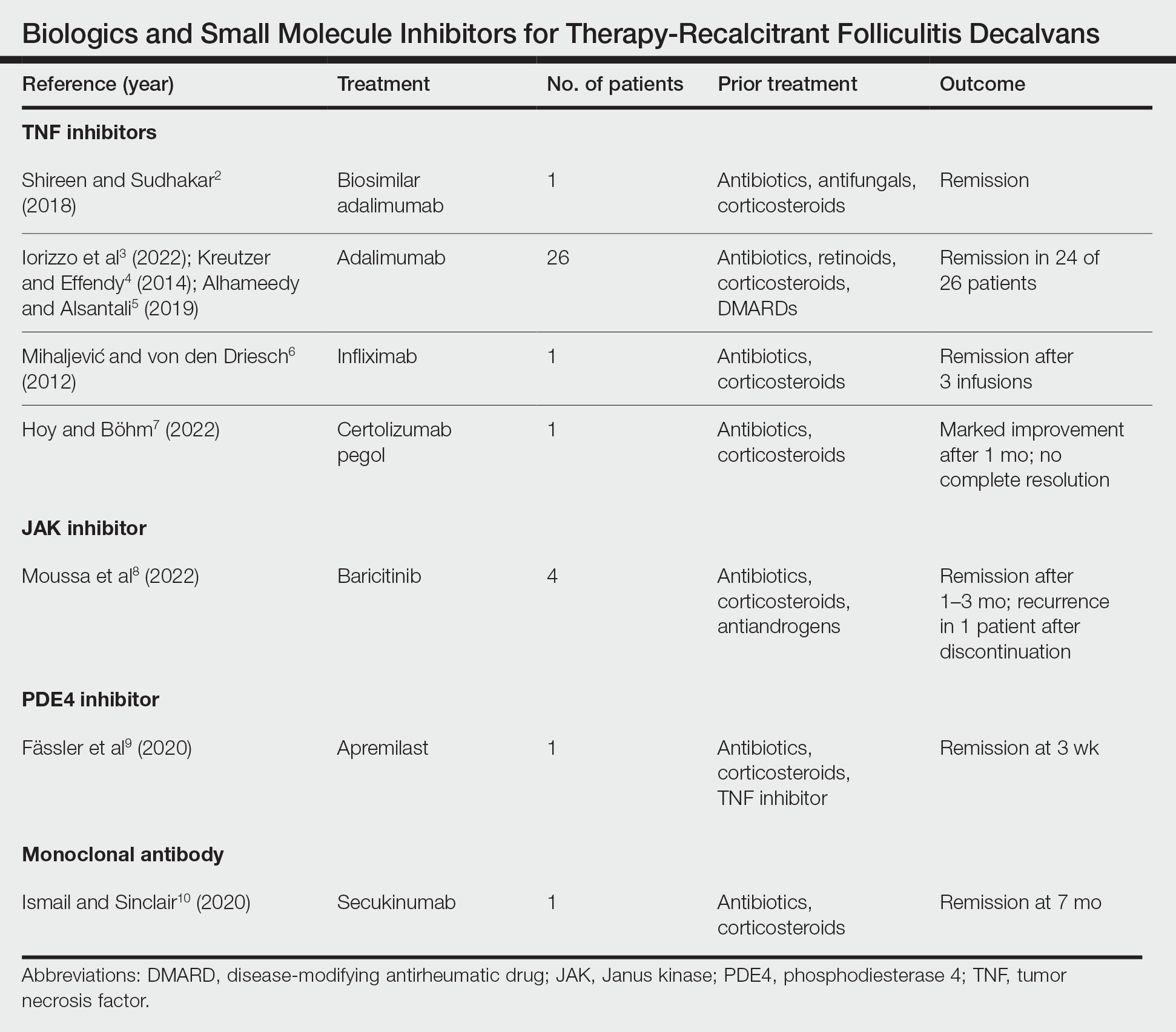
The TNF inhibitors were utilized in 6 reports with a combined total of 29 patients. Treatments included adalimumab or biosimilar adalimumab (27/29 patients), infliximab (1/29 patients), and certolizumab pegol (1/29 patients). Remission was reported in 26 of 29 cases. There were 2 nonresponders to adalimumab and marked improvement with certolizumab pegol without complete resolution. The use of the JAK inhibitor baricitinib in 4 patients resulted in remission. In all 4 patients, baricitinib was used with concurrent treatments, and remission was achieved in an average of 2.25 months. The use of a PDE4 inhibitor, apremilast, was reported in 1 case; remission was achieved in 3 weeks. Secukinumab, a monoclonal antibody that targets IL-17, was utilized in 1 patient. Marked improvement was seen after 2 months, with complete remission in 7 months.
Comment
Traditional treatment regimens for FD most often include a combination of topical and oral antibiotics; isotretinoin; and oral, topical, or intralesional corticosteroids. In the past, interventions typically were suppressive as opposed to curative; however, recent treatment advancements have shown promise in achieving lasting remission.
Most reports targeting treatment-resistant FD involved the use of TNF inhibitors, including adalimumab, biosimilar adalimumab, infliximab, and certolizumab pegol. Adalimumab was the most frequently used TNF inhibitor, with 24 of 26 treated patients achieving remission. Adalimumab may have been used the most in the treatment of FD because TNF is pronounced in other neutrophilic dermatoses that have been successfully treated with TNF inhibitors. It has been reported that adalimumab needs to be continued, as stoppage or interruption led to relapse.3
Although there are few reports of the use of JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies for FD, these treatment modalities show promise, as their use led to marked improvement or lasting remission with ongoing treatment. The use of the PDE4 inhibitor apremilast displayed the most rapid improvement of any of the reviewed treatments, with remission achieved in just 3 weeks.9 The rapid success of apremilast may be attributed to the inhibitory effect on neutrophils.
Miguel-Gómez et al11 provided a therapeutic protocol for FD based on the severity of disease (N=60). The protocol included rifampicin plus clindamycin for the treatment of severe disease, as 90.5% (19/21) of resistant cases showed clinical response, with remission of 5 months’ duration. Although this may be acceptable for some patients, others may require an alternative approach. Tietze et al12 showed that rifampicin and clindamycin had the lowest success rate for long-term remission, with 8 of 10 patients relapsing within 2 to 4 months. In addition, the emergence of antimicrobial resistance remains a major concern in the treatment of FD. Upon the review of the most recent reports of successful treatment of therapy-resistant FD, biologics and small molecule inhibitors have shown remission extending through a 12-month follow-up period. We suggest considering the addition of biologics and small molecule inhibitors to the treatment protocol for severe or resistant disease.
Limitations—In the articles reviewed, the definition of remission was inconsistent among authors—some characterized it as no recurrence in lesions or pustules and some as a reduction in the inflammatory process. True duration of remission was difficult to assess from case reports, as follow-up periods varied prior to publication. The studies included in this review consisted mainly of small sample sizes owing to the rarity of FD, and consequently, strength of evidence is lacking. Inherent to the nature of systematic reviews, publication bias may have occurred. Lastly, several studies were impacted by difficulty in obtaining optimal treatment due to financial hardship, and regimens were adjusted accordingly.
Conclusion
The relapsing nature of FD leads to frustration and poor quality of life for patients. There is a paucity of data to guide treatment when FD remains recalcitrant to traditional therapy. Therapies such as TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies have shown success in the treatment of this often difficult-to-treat disease. Small sample sizes in reports discussing treatment for resistant cases as well as conflicting results make it challenging to draw conclusions about treatment efficacy. Larger studies are needed to understand the long-term outcomes of treatment options. Regardless, disease severity, patient history, patient preferences, and treatment goals can guide the selection of therapeutic options.
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Shireen F, Sudhakar A. A case of isotretinoin therapy-refractory folliculitis decalvans treated successfully with biosimilar adalimumab (Exemptia). Int J Trichology. 2018;10:240-241.
- Iorizzo M, Starace M, Vano-Galvan S, et al. Refractory folliculitis decalvans treated with adalimumab: a case series of 23 patients. J Am Acad Dermatol. 2022;87:666-669. doi:10.1016/j.jaad.2022.02.044
- Kreutzer K, Effendy I. Therapy-resistant folliculitis decalvans and lichen planopilaris successfully treated with adalimumab. J Dtsch Dermatol Ges. 2014;12:74-76. doi:10.1111/ddg.12224
- Alhameedy MM, Alsantali AM. Therapy-recalcitrant folliculitis decalvans controlled successfully with adalimumab. Int J Trichology. 2019;11:241-243. doi:10.4103/ijt.ijt_92_19
- Mihaljevic´ N, von den Driesch P. Successful use of infliximab in a patient with recalcitrant folliculitis decalvans. J Dtsch Dermatol Ges. 2012;10:589-590. doi:10.1111/j.1610-0387.2012.07972.x
- Hoy M, Böhm M. Therapy-refractory folliculitis decalvans treated with certolizumab pegol. Int J Dermatol. 2022;61:e26-e28. doi:10.1111/ijd.15914
- Moussa A, Asfour L, Eisman S, et al. Successful treatment of folliculitis decalvans with baricitinib: a case series. Australas J Dermatol. 2022;63:279-281. doi:10.1111/ajd.13786
- Fässler M, Radonjic-Hoesli S, Feldmeyer L, et al. Successful treatment of refractory folliculitis decalvans with apremilast. JAAD Case Rep. 2020;6:1079-1081. doi:10.1016/j.jdcr.2020.08.019
- Ismail FF, Sinclair R. Successful treatment of refractory folliculitis decalvans with secukinumab. Australas J Dermatol. 2020;61:165-166. doi:10.1111/ajd.13190
- Miguel-Gómez L, Rodrigues-Barata AR, Molina-Ruiz A, et al. Folliculitis decalvans: effectiveness of therapies and prognostic factors in a multicenter series of 60 patients with long-term follow-up. J Am Acad Dermatol. 2018;79:878-883. doi:10.1016/j.jaad.2018.05.1240
- Tietze JK, Heppt MV, von Preußen A, et al. Oral isotretinoin as the most effective treatment in folliculitis decalvans: a retrospective comparison of different treatment regimens in 28 patients. J Eur Acad Dermatol Venereol. 2015;29:1816-1821. doi:10.1111/jdv.13052
Folliculitis decalvans (FD) is classified as a rare primary neutrophilic cicatricial alopecia occurring predominantly in middle-aged adults. Although the true etiology is still unknown, the pathogenesis behind the inflammatory follicular lesions stems from possible Staphylococcus aureus infection and an impaired host immune system in response to released superantigens. 1 The clinical severity of this inflammatory scalp disorder can range from mild to severe and debilitating. Multiple treatment regimens have been developed with the goal of maintaining full remission. We provide a summary of tumor necrosis factor (TNF) inhibitors, Janus kinase (JAK) inhibitors, phosphodiesterase 4 (PDE4) inhibitors, and monoclonal antibodies being utilized for patients with therapy-recalcitrant FD.
Methods
We conducted a PubMed, Medline, and Google Scholar search for the terms refractory FD, recalcitrant FD, or therapy-resistant FD to identify articles published in English from 1998 to 2022. Articles that reported recalcitrant cases and subsequent therapy with TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies were included. Articles were excluded if recalcitrant cases were not clearly defined. Remission was defined as no recurrence in lesions or pustules or as a reduction in the inflammatory process with stabilization upon continuation or discontinuation of the therapy regimen. Two reviewers (T.F. and K.U.) independently searched for and screened each report.
Results
Treatment of recalcitrant FD with biologics or small molecule inhibitors was discussed in 9 studies with a combined total of 35 patients.2-10 The treatment regimens included TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies (Table).
The TNF inhibitors were utilized in 6 reports with a combined total of 29 patients. Treatments included adalimumab or biosimilar adalimumab (27/29 patients), infliximab (1/29 patients), and certolizumab pegol (1/29 patients). Remission was reported in 26 of 29 cases. There were 2 nonresponders to adalimumab and marked improvement with certolizumab pegol without complete resolution. The use of the JAK inhibitor baricitinib in 4 patients resulted in remission. In all 4 patients, baricitinib was used with concurrent treatments, and remission was achieved in an average of 2.25 months. The use of a PDE4 inhibitor, apremilast, was reported in 1 case; remission was achieved in 3 weeks. Secukinumab, a monoclonal antibody that targets IL-17, was utilized in 1 patient. Marked improvement was seen after 2 months, with complete remission in 7 months.
Comment
Traditional treatment regimens for FD most often include a combination of topical and oral antibiotics; isotretinoin; and oral, topical, or intralesional corticosteroids. In the past, interventions typically were suppressive as opposed to curative; however, recent treatment advancements have shown promise in achieving lasting remission.
Most reports targeting treatment-resistant FD involved the use of TNF inhibitors, including adalimumab, biosimilar adalimumab, infliximab, and certolizumab pegol. Adalimumab was the most frequently used TNF inhibitor, with 24 of 26 treated patients achieving remission. Adalimumab may have been used the most in the treatment of FD because TNF is pronounced in other neutrophilic dermatoses that have been successfully treated with TNF inhibitors. It has been reported that adalimumab needs to be continued, as stoppage or interruption led to relapse.3
Although there are few reports of the use of JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies for FD, these treatment modalities show promise, as their use led to marked improvement or lasting remission with ongoing treatment. The use of the PDE4 inhibitor apremilast displayed the most rapid improvement of any of the reviewed treatments, with remission achieved in just 3 weeks.9 The rapid success of apremilast may be attributed to the inhibitory effect on neutrophils.
Miguel-Gómez et al11 provided a therapeutic protocol for FD based on the severity of disease (N=60). The protocol included rifampicin plus clindamycin for the treatment of severe disease, as 90.5% (19/21) of resistant cases showed clinical response, with remission of 5 months’ duration. Although this may be acceptable for some patients, others may require an alternative approach. Tietze et al12 showed that rifampicin and clindamycin had the lowest success rate for long-term remission, with 8 of 10 patients relapsing within 2 to 4 months. In addition, the emergence of antimicrobial resistance remains a major concern in the treatment of FD. Upon the review of the most recent reports of successful treatment of therapy-resistant FD, biologics and small molecule inhibitors have shown remission extending through a 12-month follow-up period. We suggest considering the addition of biologics and small molecule inhibitors to the treatment protocol for severe or resistant disease.
Limitations—In the articles reviewed, the definition of remission was inconsistent among authors—some characterized it as no recurrence in lesions or pustules and some as a reduction in the inflammatory process. True duration of remission was difficult to assess from case reports, as follow-up periods varied prior to publication. The studies included in this review consisted mainly of small sample sizes owing to the rarity of FD, and consequently, strength of evidence is lacking. Inherent to the nature of systematic reviews, publication bias may have occurred. Lastly, several studies were impacted by difficulty in obtaining optimal treatment due to financial hardship, and regimens were adjusted accordingly.
Conclusion
The relapsing nature of FD leads to frustration and poor quality of life for patients. There is a paucity of data to guide treatment when FD remains recalcitrant to traditional therapy. Therapies such as TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies have shown success in the treatment of this often difficult-to-treat disease. Small sample sizes in reports discussing treatment for resistant cases as well as conflicting results make it challenging to draw conclusions about treatment efficacy. Larger studies are needed to understand the long-term outcomes of treatment options. Regardless, disease severity, patient history, patient preferences, and treatment goals can guide the selection of therapeutic options.
Folliculitis decalvans (FD) is classified as a rare primary neutrophilic cicatricial alopecia occurring predominantly in middle-aged adults. Although the true etiology is still unknown, the pathogenesis behind the inflammatory follicular lesions stems from possible Staphylococcus aureus infection and an impaired host immune system in response to released superantigens. 1 The clinical severity of this inflammatory scalp disorder can range from mild to severe and debilitating. Multiple treatment regimens have been developed with the goal of maintaining full remission. We provide a summary of tumor necrosis factor (TNF) inhibitors, Janus kinase (JAK) inhibitors, phosphodiesterase 4 (PDE4) inhibitors, and monoclonal antibodies being utilized for patients with therapy-recalcitrant FD.
Methods
We conducted a PubMed, Medline, and Google Scholar search for the terms refractory FD, recalcitrant FD, or therapy-resistant FD to identify articles published in English from 1998 to 2022. Articles that reported recalcitrant cases and subsequent therapy with TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies were included. Articles were excluded if recalcitrant cases were not clearly defined. Remission was defined as no recurrence in lesions or pustules or as a reduction in the inflammatory process with stabilization upon continuation or discontinuation of the therapy regimen. Two reviewers (T.F. and K.U.) independently searched for and screened each report.
Results
Treatment of recalcitrant FD with biologics or small molecule inhibitors was discussed in 9 studies with a combined total of 35 patients.2-10 The treatment regimens included TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies (Table).
The TNF inhibitors were utilized in 6 reports with a combined total of 29 patients. Treatments included adalimumab or biosimilar adalimumab (27/29 patients), infliximab (1/29 patients), and certolizumab pegol (1/29 patients). Remission was reported in 26 of 29 cases. There were 2 nonresponders to adalimumab and marked improvement with certolizumab pegol without complete resolution. The use of the JAK inhibitor baricitinib in 4 patients resulted in remission. In all 4 patients, baricitinib was used with concurrent treatments, and remission was achieved in an average of 2.25 months. The use of a PDE4 inhibitor, apremilast, was reported in 1 case; remission was achieved in 3 weeks. Secukinumab, a monoclonal antibody that targets IL-17, was utilized in 1 patient. Marked improvement was seen after 2 months, with complete remission in 7 months.
Comment
Traditional treatment regimens for FD most often include a combination of topical and oral antibiotics; isotretinoin; and oral, topical, or intralesional corticosteroids. In the past, interventions typically were suppressive as opposed to curative; however, recent treatment advancements have shown promise in achieving lasting remission.
Most reports targeting treatment-resistant FD involved the use of TNF inhibitors, including adalimumab, biosimilar adalimumab, infliximab, and certolizumab pegol. Adalimumab was the most frequently used TNF inhibitor, with 24 of 26 treated patients achieving remission. Adalimumab may have been used the most in the treatment of FD because TNF is pronounced in other neutrophilic dermatoses that have been successfully treated with TNF inhibitors. It has been reported that adalimumab needs to be continued, as stoppage or interruption led to relapse.3
Although there are few reports of the use of JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies for FD, these treatment modalities show promise, as their use led to marked improvement or lasting remission with ongoing treatment. The use of the PDE4 inhibitor apremilast displayed the most rapid improvement of any of the reviewed treatments, with remission achieved in just 3 weeks.9 The rapid success of apremilast may be attributed to the inhibitory effect on neutrophils.
Miguel-Gómez et al11 provided a therapeutic protocol for FD based on the severity of disease (N=60). The protocol included rifampicin plus clindamycin for the treatment of severe disease, as 90.5% (19/21) of resistant cases showed clinical response, with remission of 5 months’ duration. Although this may be acceptable for some patients, others may require an alternative approach. Tietze et al12 showed that rifampicin and clindamycin had the lowest success rate for long-term remission, with 8 of 10 patients relapsing within 2 to 4 months. In addition, the emergence of antimicrobial resistance remains a major concern in the treatment of FD. Upon the review of the most recent reports of successful treatment of therapy-resistant FD, biologics and small molecule inhibitors have shown remission extending through a 12-month follow-up period. We suggest considering the addition of biologics and small molecule inhibitors to the treatment protocol for severe or resistant disease.
Limitations—In the articles reviewed, the definition of remission was inconsistent among authors—some characterized it as no recurrence in lesions or pustules and some as a reduction in the inflammatory process. True duration of remission was difficult to assess from case reports, as follow-up periods varied prior to publication. The studies included in this review consisted mainly of small sample sizes owing to the rarity of FD, and consequently, strength of evidence is lacking. Inherent to the nature of systematic reviews, publication bias may have occurred. Lastly, several studies were impacted by difficulty in obtaining optimal treatment due to financial hardship, and regimens were adjusted accordingly.
Conclusion
The relapsing nature of FD leads to frustration and poor quality of life for patients. There is a paucity of data to guide treatment when FD remains recalcitrant to traditional therapy. Therapies such as TNF inhibitors, JAK inhibitors, PDE4 inhibitors, and monoclonal antibodies have shown success in the treatment of this often difficult-to-treat disease. Small sample sizes in reports discussing treatment for resistant cases as well as conflicting results make it challenging to draw conclusions about treatment efficacy. Larger studies are needed to understand the long-term outcomes of treatment options. Regardless, disease severity, patient history, patient preferences, and treatment goals can guide the selection of therapeutic options.
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Shireen F, Sudhakar A. A case of isotretinoin therapy-refractory folliculitis decalvans treated successfully with biosimilar adalimumab (Exemptia). Int J Trichology. 2018;10:240-241.
- Iorizzo M, Starace M, Vano-Galvan S, et al. Refractory folliculitis decalvans treated with adalimumab: a case series of 23 patients. J Am Acad Dermatol. 2022;87:666-669. doi:10.1016/j.jaad.2022.02.044
- Kreutzer K, Effendy I. Therapy-resistant folliculitis decalvans and lichen planopilaris successfully treated with adalimumab. J Dtsch Dermatol Ges. 2014;12:74-76. doi:10.1111/ddg.12224
- Alhameedy MM, Alsantali AM. Therapy-recalcitrant folliculitis decalvans controlled successfully with adalimumab. Int J Trichology. 2019;11:241-243. doi:10.4103/ijt.ijt_92_19
- Mihaljevic´ N, von den Driesch P. Successful use of infliximab in a patient with recalcitrant folliculitis decalvans. J Dtsch Dermatol Ges. 2012;10:589-590. doi:10.1111/j.1610-0387.2012.07972.x
- Hoy M, Böhm M. Therapy-refractory folliculitis decalvans treated with certolizumab pegol. Int J Dermatol. 2022;61:e26-e28. doi:10.1111/ijd.15914
- Moussa A, Asfour L, Eisman S, et al. Successful treatment of folliculitis decalvans with baricitinib: a case series. Australas J Dermatol. 2022;63:279-281. doi:10.1111/ajd.13786
- Fässler M, Radonjic-Hoesli S, Feldmeyer L, et al. Successful treatment of refractory folliculitis decalvans with apremilast. JAAD Case Rep. 2020;6:1079-1081. doi:10.1016/j.jdcr.2020.08.019
- Ismail FF, Sinclair R. Successful treatment of refractory folliculitis decalvans with secukinumab. Australas J Dermatol. 2020;61:165-166. doi:10.1111/ajd.13190
- Miguel-Gómez L, Rodrigues-Barata AR, Molina-Ruiz A, et al. Folliculitis decalvans: effectiveness of therapies and prognostic factors in a multicenter series of 60 patients with long-term follow-up. J Am Acad Dermatol. 2018;79:878-883. doi:10.1016/j.jaad.2018.05.1240
- Tietze JK, Heppt MV, von Preußen A, et al. Oral isotretinoin as the most effective treatment in folliculitis decalvans: a retrospective comparison of different treatment regimens in 28 patients. J Eur Acad Dermatol Venereol. 2015;29:1816-1821. doi:10.1111/jdv.13052
- Otberg N, Kang H, Alzolibani AA, et al. Folliculitis decalvans. Dermatol Ther. 2008;21:238-244. doi:10.1111/j.1529-8019.2008.00204.x
- Shireen F, Sudhakar A. A case of isotretinoin therapy-refractory folliculitis decalvans treated successfully with biosimilar adalimumab (Exemptia). Int J Trichology. 2018;10:240-241.
- Iorizzo M, Starace M, Vano-Galvan S, et al. Refractory folliculitis decalvans treated with adalimumab: a case series of 23 patients. J Am Acad Dermatol. 2022;87:666-669. doi:10.1016/j.jaad.2022.02.044
- Kreutzer K, Effendy I. Therapy-resistant folliculitis decalvans and lichen planopilaris successfully treated with adalimumab. J Dtsch Dermatol Ges. 2014;12:74-76. doi:10.1111/ddg.12224
- Alhameedy MM, Alsantali AM. Therapy-recalcitrant folliculitis decalvans controlled successfully with adalimumab. Int J Trichology. 2019;11:241-243. doi:10.4103/ijt.ijt_92_19
- Mihaljevic´ N, von den Driesch P. Successful use of infliximab in a patient with recalcitrant folliculitis decalvans. J Dtsch Dermatol Ges. 2012;10:589-590. doi:10.1111/j.1610-0387.2012.07972.x
- Hoy M, Böhm M. Therapy-refractory folliculitis decalvans treated with certolizumab pegol. Int J Dermatol. 2022;61:e26-e28. doi:10.1111/ijd.15914
- Moussa A, Asfour L, Eisman S, et al. Successful treatment of folliculitis decalvans with baricitinib: a case series. Australas J Dermatol. 2022;63:279-281. doi:10.1111/ajd.13786
- Fässler M, Radonjic-Hoesli S, Feldmeyer L, et al. Successful treatment of refractory folliculitis decalvans with apremilast. JAAD Case Rep. 2020;6:1079-1081. doi:10.1016/j.jdcr.2020.08.019
- Ismail FF, Sinclair R. Successful treatment of refractory folliculitis decalvans with secukinumab. Australas J Dermatol. 2020;61:165-166. doi:10.1111/ajd.13190
- Miguel-Gómez L, Rodrigues-Barata AR, Molina-Ruiz A, et al. Folliculitis decalvans: effectiveness of therapies and prognostic factors in a multicenter series of 60 patients with long-term follow-up. J Am Acad Dermatol. 2018;79:878-883. doi:10.1016/j.jaad.2018.05.1240
- Tietze JK, Heppt MV, von Preußen A, et al. Oral isotretinoin as the most effective treatment in folliculitis decalvans: a retrospective comparison of different treatment regimens in 28 patients. J Eur Acad Dermatol Venereol. 2015;29:1816-1821. doi:10.1111/jdv.13052
Practice Points
- Tumor necrosis factor inhibitors, Janus kinase inhibitors, phosphodiesterase 4 inhibitors, and monoclonal antibodies have shown success in the treatment of folliculitis decalvans resistant to traditional therapies.
- The true etiology of folliculitis decalvans is still unknown, but possible factors include Staphylococcus aureus infection and an impaired host immune system, which may benefit from treatment with biologics and small molecule inhibitors.
Commentary: Transition from Psoriasis to PsA and New Drug Analyses, June 2024

In regard to treatment, bimekizumab is a new monoclonal antibody that dually targets interleukin (IL)-17A and IL-17F and is highly efficacious for the treatment of psoriasis. In a meta-analysis of four placebo-controlled randomized clinical trials that included 1323 patients with PsA (age 18 years or older), of whom 853 received bimekizumab, Su and colleagues demonstrated that bimekizumab led to a significantly higher response rate for minimal disease activity (risk ratio [RR] 4.188; P < .001) and a 70% or greater improvement in the American College of Rheumatology (ACR) criteria (RR 7.932; P < .0001) when compared with placebo. Bimekizumab was superior to placebo in achieving ACR20/50/70 response at a dose of 160 mg. The risk for treatment-emergent adverse events was modestly higher with bimekizumab vs placebo (RR 1.423; P = .023), whereas the risk for serious cancers, upper respiratory tract infection, injection site reactions, and pharyngitis was similar for both. Thus, bimekizumab is an efficacious agent for the treatment of PsA. Future head-to-head studies will help clinicians determine the role of this drug in the management of PsA.
Not all patients respond equally well to targeted therapies, and the so-called challenging-to-treat patients are being increasingly described. Kivitz and colleagues recently described the efficacy of secukinumab, a monoclonal antibody targeting IL-17A, in these challenging-to-treat patients from the United States. In a post hoc subgroup analysis of four phase 3 studies that included 279 patients, they demonstrated that patients receiving 300 mg secukinumab and 150 mg with a loading dose had a higher rate of achieving the ACR20 response (59.7% and 43.4%, respectively) vs 15.6% for placebo (both P < .0001). The Psoriasis Area and Severity Index 90 response was 47.1% and 22.2%, respectively, vs 5.3% (both P < .05). Thus, secukinumab is efficacious in more challenging-to-treat patients. However, such patients need to be better characterized so that effective treatment strategies to achieve a state of low disease activity may be implemented.
In regard to treatment, bimekizumab is a new monoclonal antibody that dually targets interleukin (IL)-17A and IL-17F and is highly efficacious for the treatment of psoriasis. In a meta-analysis of four placebo-controlled randomized clinical trials that included 1323 patients with PsA (age 18 years or older), of whom 853 received bimekizumab, Su and colleagues demonstrated that bimekizumab led to a significantly higher response rate for minimal disease activity (risk ratio [RR] 4.188; P < .001) and a 70% or greater improvement in the American College of Rheumatology (ACR) criteria (RR 7.932; P < .0001) when compared with placebo. Bimekizumab was superior to placebo in achieving ACR20/50/70 response at a dose of 160 mg. The risk for treatment-emergent adverse events was modestly higher with bimekizumab vs placebo (RR 1.423; P = .023), whereas the risk for serious cancers, upper respiratory tract infection, injection site reactions, and pharyngitis was similar for both. Thus, bimekizumab is an efficacious agent for the treatment of PsA. Future head-to-head studies will help clinicians determine the role of this drug in the management of PsA.
Not all patients respond equally well to targeted therapies, and the so-called challenging-to-treat patients are being increasingly described. Kivitz and colleagues recently described the efficacy of secukinumab, a monoclonal antibody targeting IL-17A, in these challenging-to-treat patients from the United States. In a post hoc subgroup analysis of four phase 3 studies that included 279 patients, they demonstrated that patients receiving 300 mg secukinumab and 150 mg with a loading dose had a higher rate of achieving the ACR20 response (59.7% and 43.4%, respectively) vs 15.6% for placebo (both P < .0001). The Psoriasis Area and Severity Index 90 response was 47.1% and 22.2%, respectively, vs 5.3% (both P < .05). Thus, secukinumab is efficacious in more challenging-to-treat patients. However, such patients need to be better characterized so that effective treatment strategies to achieve a state of low disease activity may be implemented.
In regard to treatment, bimekizumab is a new monoclonal antibody that dually targets interleukin (IL)-17A and IL-17F and is highly efficacious for the treatment of psoriasis. In a meta-analysis of four placebo-controlled randomized clinical trials that included 1323 patients with PsA (age 18 years or older), of whom 853 received bimekizumab, Su and colleagues demonstrated that bimekizumab led to a significantly higher response rate for minimal disease activity (risk ratio [RR] 4.188; P < .001) and a 70% or greater improvement in the American College of Rheumatology (ACR) criteria (RR 7.932; P < .0001) when compared with placebo. Bimekizumab was superior to placebo in achieving ACR20/50/70 response at a dose of 160 mg. The risk for treatment-emergent adverse events was modestly higher with bimekizumab vs placebo (RR 1.423; P = .023), whereas the risk for serious cancers, upper respiratory tract infection, injection site reactions, and pharyngitis was similar for both. Thus, bimekizumab is an efficacious agent for the treatment of PsA. Future head-to-head studies will help clinicians determine the role of this drug in the management of PsA.
Not all patients respond equally well to targeted therapies, and the so-called challenging-to-treat patients are being increasingly described. Kivitz and colleagues recently described the efficacy of secukinumab, a monoclonal antibody targeting IL-17A, in these challenging-to-treat patients from the United States. In a post hoc subgroup analysis of four phase 3 studies that included 279 patients, they demonstrated that patients receiving 300 mg secukinumab and 150 mg with a loading dose had a higher rate of achieving the ACR20 response (59.7% and 43.4%, respectively) vs 15.6% for placebo (both P < .0001). The Psoriasis Area and Severity Index 90 response was 47.1% and 22.2%, respectively, vs 5.3% (both P < .05). Thus, secukinumab is efficacious in more challenging-to-treat patients. However, such patients need to be better characterized so that effective treatment strategies to achieve a state of low disease activity may be implemented.
Commentary: Looking at Migraine Treatment in a Comprehensive Way, June 2024

Migraine care requires a comprehensive approach. Identifying and avoiding triggers is a key component of patient-directed self-care. For many migraine patients, preventive therapy can substantially improve their quality of life. Yet, even with the best migraine prevention plan, many patients experience occasional migraines and require therapy for acute symptom relief. When it comes to selecting therapies for acute migraine treatment, criteria include efficacy, fast action, long duration of action, low risk for rebound symptoms, minimal side effects, and patient safety. Prescription therapies and therapies used in a medical setting include new calcitonin gene-related peptide (CGRP) receptor antagonists as well as antihistamines, antiemetics, neuroleptics, and triptans that have been used for years.
A study published in The Journal of Headache and Pain in April 2024 examined migraine symptom relief with the use of Nurtec OTD (rimegepant), one of the recently approved CGRP receptor antagonists. This post hoc subgroup analysis of a large double-blind randomized phase 3 clinical trial included 1075 participants, of whom 538 took 75 mg rimegepant and 537 took placebo to treat a single migraine episode. According to the analysis, rimegepant outperformed placebo on measures of freedom from the most bothersome symptom, pain relief at 2 hours post-dose, ability to function normally at 2 hours post-dose, use of rescue medication within 24 hours post-dose, and sustained pain freedom up to 48 hours post-dose. Treatment-emergent adverse events were assessed using EEG, vital signs, and laboratory tests. There was no notable difference in the incidence of adverse events between the rimegepant group and the placebo group, and no drug-related adverse events were reported.
This result is similar to that of previous studies which have demonstrated the significant efficacy of CGRP receptor blockers on acute migraine symptoms, including pain, bothersome symptoms, and nausea when compared with placebo.1
A study published in the May 2024 issue of Pediatric Emergency Care examined the efficacy of prochlorperazine monotherapy or prochlorperazine combined with diphenhydramine for the treatment of acute migraine in the pediatric emergency department. This retrospective study included 1683 patients who were treated with either prochlorperazine monotherapy or diphenhydramine co-administered with prochlorperazine. The authors reported that the need for additional therapy, the 72-hour return visit rates, and the admission rates were equal for both groups. They reported that, overall, 13% of the patients required additional therapy, 16.7% were admitted, and 5.3% returned within 72 hours. Extrapyramidal side effects were reported in 2.4% of patients in the prochlorperazine group, while none of the patients in the prochlorperazine/diphenhydramine group reported extrapyramidal side effects. This difference in side-effect incidence should not be interpreted as a protective effect of diphenhydramine but could be an indication that adding diphenhydramine did not increase the risk for extrapyramidal side effects.
A study published in the April 2024 issue of Headache examined the efficacy of parenteral agents on acute migraine in the emergency room setting. The data analysis included 97 studies. The authors examined the efficacy of these medications and various combinations:
- •diphenhydramine (intravenous);
- •trimethobenzamide (intramuscular);
- •granisetron (intravenous);
- •valproate (intravenous);
- •neuroleptics (intravenous):
- ◦prochlorperazine,
- ◦chlorpromazine,
- ◦haloperidol,
- ◦droperidol,
- ◦methotrimeprazine; and
- •dihydroergotamine (intravenous, intramuscular, or subcutaneous);
- •ketorolac (intravenous); and
- •magnesium sulfate (intravenous).
Each of these therapies was shown to improve migraine symptoms. According to the authors, "the majority of the parenteral agents commonly available to treat patients with migraine headaches in emergency settings was shown to be effective in providing pain relief." They recommended combination therapy or monotherapy of either neuroleptics or metoclopramide as first-line treatment options for treating acute migraine pain and acknowledged that these therapies carry an increased risk for extrapyramidal side effects.
According to a study published in 2015 in Cephalgia, there were 1.2 million migraine visits to US emergency departments in 2010.2 With emerging preventive and acute treatments, it is possible that these numbers could decrease. However, the need for self-administration of acute migraine treatment and for migraine care in the emergency room setting is not likely to go away. The results regarding efficacy and safety of acute migraine therapies are encouraging, as patients who are experiencing migraine need acute therapy for distressing symptoms and do not always have many available options. Patients who can use prescription treatment may need to try a few different therapies before learning which acute migraine treatment is the most effective and which treatment causes the fewest side effects for them personally. Migraine patients who need care in the emergency room can experience speedy and effective relief with most available therapies.
Additional References
1. Pak K, Kim J, Lee GH, et al. Effectiveness of calcitonin gene-related peptide receptor antagonists for migraine treatment: a meta-analysis. Eur Neurol. 2022;85(3):195-201. doi: 10.1159/000521697 Source
2. Friedman BW, West J, Vinson DR, et al. Current management of migraine in US emergency departments: An analysis of the National Hospital Ambulatory Medical Care Survey. Cephalalgia. 2015;35(4):301-309. doi: 10.1177/0333102414539055 Source
Migraine care requires a comprehensive approach. Identifying and avoiding triggers is a key component of patient-directed self-care. For many migraine patients, preventive therapy can substantially improve their quality of life. Yet, even with the best migraine prevention plan, many patients experience occasional migraines and require therapy for acute symptom relief. When it comes to selecting therapies for acute migraine treatment, criteria include efficacy, fast action, long duration of action, low risk for rebound symptoms, minimal side effects, and patient safety. Prescription therapies and therapies used in a medical setting include new calcitonin gene-related peptide (CGRP) receptor antagonists as well as antihistamines, antiemetics, neuroleptics, and triptans that have been used for years.
A study published in The Journal of Headache and Pain in April 2024 examined migraine symptom relief with the use of Nurtec OTD (rimegepant), one of the recently approved CGRP receptor antagonists. This post hoc subgroup analysis of a large double-blind randomized phase 3 clinical trial included 1075 participants, of whom 538 took 75 mg rimegepant and 537 took placebo to treat a single migraine episode. According to the analysis, rimegepant outperformed placebo on measures of freedom from the most bothersome symptom, pain relief at 2 hours post-dose, ability to function normally at 2 hours post-dose, use of rescue medication within 24 hours post-dose, and sustained pain freedom up to 48 hours post-dose. Treatment-emergent adverse events were assessed using EEG, vital signs, and laboratory tests. There was no notable difference in the incidence of adverse events between the rimegepant group and the placebo group, and no drug-related adverse events were reported.
This result is similar to that of previous studies which have demonstrated the significant efficacy of CGRP receptor blockers on acute migraine symptoms, including pain, bothersome symptoms, and nausea when compared with placebo.1
A study published in the May 2024 issue of Pediatric Emergency Care examined the efficacy of prochlorperazine monotherapy or prochlorperazine combined with diphenhydramine for the treatment of acute migraine in the pediatric emergency department. This retrospective study included 1683 patients who were treated with either prochlorperazine monotherapy or diphenhydramine co-administered with prochlorperazine. The authors reported that the need for additional therapy, the 72-hour return visit rates, and the admission rates were equal for both groups. They reported that, overall, 13% of the patients required additional therapy, 16.7% were admitted, and 5.3% returned within 72 hours. Extrapyramidal side effects were reported in 2.4% of patients in the prochlorperazine group, while none of the patients in the prochlorperazine/diphenhydramine group reported extrapyramidal side effects. This difference in side-effect incidence should not be interpreted as a protective effect of diphenhydramine but could be an indication that adding diphenhydramine did not increase the risk for extrapyramidal side effects.
A study published in the April 2024 issue of Headache examined the efficacy of parenteral agents on acute migraine in the emergency room setting. The data analysis included 97 studies. The authors examined the efficacy of these medications and various combinations:
- •diphenhydramine (intravenous);
- •trimethobenzamide (intramuscular);
- •granisetron (intravenous);
- •valproate (intravenous);
- •neuroleptics (intravenous):
- ◦prochlorperazine,
- ◦chlorpromazine,
- ◦haloperidol,
- ◦droperidol,
- ◦methotrimeprazine; and
- •dihydroergotamine (intravenous, intramuscular, or subcutaneous);
- •ketorolac (intravenous); and
- •magnesium sulfate (intravenous).
Each of these therapies was shown to improve migraine symptoms. According to the authors, "the majority of the parenteral agents commonly available to treat patients with migraine headaches in emergency settings was shown to be effective in providing pain relief." They recommended combination therapy or monotherapy of either neuroleptics or metoclopramide as first-line treatment options for treating acute migraine pain and acknowledged that these therapies carry an increased risk for extrapyramidal side effects.
According to a study published in 2015 in Cephalgia, there were 1.2 million migraine visits to US emergency departments in 2010.2 With emerging preventive and acute treatments, it is possible that these numbers could decrease. However, the need for self-administration of acute migraine treatment and for migraine care in the emergency room setting is not likely to go away. The results regarding efficacy and safety of acute migraine therapies are encouraging, as patients who are experiencing migraine need acute therapy for distressing symptoms and do not always have many available options. Patients who can use prescription treatment may need to try a few different therapies before learning which acute migraine treatment is the most effective and which treatment causes the fewest side effects for them personally. Migraine patients who need care in the emergency room can experience speedy and effective relief with most available therapies.
Additional References
1. Pak K, Kim J, Lee GH, et al. Effectiveness of calcitonin gene-related peptide receptor antagonists for migraine treatment: a meta-analysis. Eur Neurol. 2022;85(3):195-201. doi: 10.1159/000521697 Source
2. Friedman BW, West J, Vinson DR, et al. Current management of migraine in US emergency departments: An analysis of the National Hospital Ambulatory Medical Care Survey. Cephalalgia. 2015;35(4):301-309. doi: 10.1177/0333102414539055 Source
Migraine care requires a comprehensive approach. Identifying and avoiding triggers is a key component of patient-directed self-care. For many migraine patients, preventive therapy can substantially improve their quality of life. Yet, even with the best migraine prevention plan, many patients experience occasional migraines and require therapy for acute symptom relief. When it comes to selecting therapies for acute migraine treatment, criteria include efficacy, fast action, long duration of action, low risk for rebound symptoms, minimal side effects, and patient safety. Prescription therapies and therapies used in a medical setting include new calcitonin gene-related peptide (CGRP) receptor antagonists as well as antihistamines, antiemetics, neuroleptics, and triptans that have been used for years.
A study published in The Journal of Headache and Pain in April 2024 examined migraine symptom relief with the use of Nurtec OTD (rimegepant), one of the recently approved CGRP receptor antagonists. This post hoc subgroup analysis of a large double-blind randomized phase 3 clinical trial included 1075 participants, of whom 538 took 75 mg rimegepant and 537 took placebo to treat a single migraine episode. According to the analysis, rimegepant outperformed placebo on measures of freedom from the most bothersome symptom, pain relief at 2 hours post-dose, ability to function normally at 2 hours post-dose, use of rescue medication within 24 hours post-dose, and sustained pain freedom up to 48 hours post-dose. Treatment-emergent adverse events were assessed using EEG, vital signs, and laboratory tests. There was no notable difference in the incidence of adverse events between the rimegepant group and the placebo group, and no drug-related adverse events were reported.
This result is similar to that of previous studies which have demonstrated the significant efficacy of CGRP receptor blockers on acute migraine symptoms, including pain, bothersome symptoms, and nausea when compared with placebo.1
A study published in the May 2024 issue of Pediatric Emergency Care examined the efficacy of prochlorperazine monotherapy or prochlorperazine combined with diphenhydramine for the treatment of acute migraine in the pediatric emergency department. This retrospective study included 1683 patients who were treated with either prochlorperazine monotherapy or diphenhydramine co-administered with prochlorperazine. The authors reported that the need for additional therapy, the 72-hour return visit rates, and the admission rates were equal for both groups. They reported that, overall, 13% of the patients required additional therapy, 16.7% were admitted, and 5.3% returned within 72 hours. Extrapyramidal side effects were reported in 2.4% of patients in the prochlorperazine group, while none of the patients in the prochlorperazine/diphenhydramine group reported extrapyramidal side effects. This difference in side-effect incidence should not be interpreted as a protective effect of diphenhydramine but could be an indication that adding diphenhydramine did not increase the risk for extrapyramidal side effects.
A study published in the April 2024 issue of Headache examined the efficacy of parenteral agents on acute migraine in the emergency room setting. The data analysis included 97 studies. The authors examined the efficacy of these medications and various combinations:
- •diphenhydramine (intravenous);
- •trimethobenzamide (intramuscular);
- •granisetron (intravenous);
- •valproate (intravenous);
- •neuroleptics (intravenous):
- ◦prochlorperazine,
- ◦chlorpromazine,
- ◦haloperidol,
- ◦droperidol,
- ◦methotrimeprazine; and
- •dihydroergotamine (intravenous, intramuscular, or subcutaneous);
- •ketorolac (intravenous); and
- •magnesium sulfate (intravenous).
Each of these therapies was shown to improve migraine symptoms. According to the authors, "the majority of the parenteral agents commonly available to treat patients with migraine headaches in emergency settings was shown to be effective in providing pain relief." They recommended combination therapy or monotherapy of either neuroleptics or metoclopramide as first-line treatment options for treating acute migraine pain and acknowledged that these therapies carry an increased risk for extrapyramidal side effects.
According to a study published in 2015 in Cephalgia, there were 1.2 million migraine visits to US emergency departments in 2010.2 With emerging preventive and acute treatments, it is possible that these numbers could decrease. However, the need for self-administration of acute migraine treatment and for migraine care in the emergency room setting is not likely to go away. The results regarding efficacy and safety of acute migraine therapies are encouraging, as patients who are experiencing migraine need acute therapy for distressing symptoms and do not always have many available options. Patients who can use prescription treatment may need to try a few different therapies before learning which acute migraine treatment is the most effective and which treatment causes the fewest side effects for them personally. Migraine patients who need care in the emergency room can experience speedy and effective relief with most available therapies.
Additional References
1. Pak K, Kim J, Lee GH, et al. Effectiveness of calcitonin gene-related peptide receptor antagonists for migraine treatment: a meta-analysis. Eur Neurol. 2022;85(3):195-201. doi: 10.1159/000521697 Source
2. Friedman BW, West J, Vinson DR, et al. Current management of migraine in US emergency departments: An analysis of the National Hospital Ambulatory Medical Care Survey. Cephalalgia. 2015;35(4):301-309. doi: 10.1177/0333102414539055 Source
Surgical Pearls and Wellness Tips From the American Academy of Dermatology Annual Meeting
Attendees of the 2024 American Academy of Dermatology annual meeting in San Diego, California, were eager to delve into the latest trends and advancements in dermatology and dermatologic surgery. This article provides a few key takeaways for residents from a range of engaging sessions, with an emphasis on procedural dermatology and physician health and well-being.
Practical Applications of Surgical Enhancements
In an informative session dedicated to dermatologic surgeons and their patients, “Simple Tricks and Practical Tips to Optimize the Surgical Experience for You and Your Patients,” attendees learned practical tips for enhancing the surgical experience. The discussion spanned various aspects of surgery, from managing preoperative anxiety with anxiolytics such as midazolam to the strategic use of skin hooks for delicate tissue manipulation. Midazolam is fast acting and its use is tailored to patient factors such as weight, hepatic function, and prior use. An innovative anxiety management algorithm combining “talkesethesia” with other methods such as anodynes and benzodiazepines underscored the importance of a calm patient in successful surgical outcomes. Talkesthesia involves engaging patients in soothing and distracting conversation throughout the procedure. This technique can include discussing nonmedical topics of interest with the patient—such as their hobbies, family, or favorite movies—to divert their attention from the surgical process and reduce anxiety. By creating a friendly and reassuring atmosphere, talkesthesia helps to establish trust between the patient and the medical team, ultimately contributing to a more relaxed and cooperative patient.1
The utility of skin hooks also was discussed, with an emphasis on their role in ensuring gentle tissue handling. The modified buried vertical mattress technique was discussed for its added benefits in wound approximation and strength. Emphasis was placed on the importance of maintaining a clear surgical field by electrocautery to ensure optimal visibility.
Focusing on the treatment of skin cancer, curettage alone was touted as a viable alternative to electrodesiccation and curettage, especially in reducing postoperative hypopigmentation while maintaining high cure rates. This method was shown to be effective in treating basal cell carcinoma and well-differentiated squamous cell carcinoma.2,3
Suturing techniques such as pulley, purse-string, and buried sutures offer efficiencies in time, cost, and improved healing in high-tension areas. These methods can contribute to postsurgical aesthetic and functional outcomes. Additionally, Dr. Desiree Ratner shared her tips for painless local anesthesia techniques, emphasizing the importance of patient comfort through methods such as slow injection and buffering of lidocaine. The next time you give a local anesthetic, try this technique to minimize pain: using a 30-gauge needle, hold the syringe with the bevel up, insert only the bevel into the skin (needle tip goes into the papillary dermis), and numb superficially around the periphery using as little volume as possible. Keep pressure slow and steady without moving the needle, then insert the needle only in previously anesthetized areas, numbing deeply only after the entire periphery has been anesthetized.
The session concluded with the recommendation to provide patients with a goody bag containing postoperative supplies. This thoughtful gesture not only enhances patient satisfaction but also addresses the practical aspect of postsurgery care, offering an inexpensive yet impactful way to ensure patients have the necessary supplies for their recovery.
Take-Home Point—This session distilled essential surgical enhancements into practical applications, emphasizing the importance of anxiety management, delicate tissue handling, innovative suturing techniques, and thoughtful patient care postsurgery. The overarching message highlighted the synergy between technical skill and patient-centric approaches in optimizing surgical outcomes, underscoring the significance of attention to detail in every aspect of patient care, from preoperative preparation to postoperative recovery.
Optimizing Safety and Ergonomics in Surgical Practices
Understanding the dynamics of surgical plume is crucial to safety in the operating room. The carcinogenic risk associated with surgical smoke is not trivial: exposure to the plume generated by monopolar electrocautery in a single day can be equivalent to smoking approximately 30 cigarettes, and a surgeon’s lifetime cancer risk from polycyclic aromatic hydrocarbons exposure is alarmingly high.4 To mitigate these risks, several strategies were recommended, including using lower-energy settings, choosing indirect or bipolar cautery, and ensuring efficient room ventilation with HEPA (high-efficiency particulate absorbing) filters to turn over air frequently. Additionally, employing the use of smoke evacuators and suction devices with proper filters can reduce particulate matter in the operating room.
The importance of the surgeon’s posture during procedures also was emphasized for ergonomic benefits and to minimize fatigue. Maintaining a neutral stance with the core and glutes engaged, standing on the balls of the feet, and aligning the table height to keep the hands at the lower chest level were recommended; this not only helps in reducing strain but also in maintaining precision during surgical tasks.
The surgeons on the panel also highlighted the novel use of hydrocolloid dressings with tattoo lasers, electrodesiccation and curettage for treating rhinophyma, and purse-string closure for chest defects as evolving practices to enhance outcomes and safety.
The session offered valuable insights into suturing techniques, advocating for the use of deep sutures—ideally Monocryl (Ethicon US, LLC)—for superficial closures and fast-absorbing gut sutures for patients who are not expected to return for suture removal. Keith LeBlanc Jr, MD, shared one of his favorite tricks for suturing fragile, sun-damaged skin on the forearm in elderly patients: apply adhesive skin closures aligned parallel to the suture line, then suture through them for extra support. This can help ensure a more secure closure.
In situations when no deep sutures are required, such as on the hair-bearing scalp, large bites through the galea using monofilament nonabsorbable sutures for up to 14 days or staples can offer favorable closures and enhanced hemostasis. Tranexamic acid has emerged as a versatile hemostatic agent—available in multiple forms ranging from direct injection to topical applications—and is cost-effective, enhancing its accessibility in various surgical settings.
A high proportion of patients are taken aback by the length of the scar following removal of what they perceive as a small skin cancer. Leslie Storey, MD, cleverly recommended using the back of a glove to mark surgical planning, giving the patient a visual guide for anticipating the size of the excision. This is a simple yet effective approach to enhance patient understanding and informed consent.
Lastly, the notion that “patients remember you if you don’t cause them pain” resonated deeply, underlining the importance of gentle techniques such as pinching the suture rather than pushing the wound edges together and asking assistants to maintain tension without obstructing the field. In the words of Seth Matarasso, MD: “If you pain ‘em, you won’t retain ‘em!”
Take-Home Point—The take-home message from the session was a comprehensive approach to surgical excellence that aligns technical proficiency with a strong emphasis on safety, patient comfort, and operative efficiency. Surgeons were advised to adopt practices that reduce the risks associated with surgical plume, maintain ergonomic discipline, and apply innovative suturing techniques to enhance patient outcomes. Compassionate patient care, innovative use of materials and methods, and a commitment to continual learning and adaptation of new evidence-based practices are paramount for the modern surgeon.
Approaches for Facial Reconstruction
The intricacies of multisubunit facial reconstruction were explored in a session that blended the pursuit of aesthetic harmony with functional restoration, “Simplifying the Complex: Reconstructing Multisubunit Defects.” The session began with an introduction to flap design principles, emphasizing the importance of thorough defect analysis and the strategic design of flaps. A key objective within this framework is the integration of the flap within existing cosmetic subunits to avoid unwanted effects such as unintended eyebrow elevation.
The concept of tissue reservoirs was discussed,focusing on regions such as the glabella as potential sources for skin recruitment. This then transitioned into a nuanced discussion on incision planning, underscoring the significance of aligning incision lines with relaxed skin tension lines to enhance healing and minimize scarring.
The topic of delayed reconstruction also was introduced as a deliberate tactic for high-risk tumor management. This approach allows for an in-depth pathologic examination and provides patients with more time for psychological adjustment, which may be particularly important for those with complex medical histories or those who require staged surgical interventions.
In a thorough examination of flap design techniques, the session highlighted the bilobed transposition flap as a versatile choice for nasal reconstruction, particularly apt for the distal third of the nose due to its design that harnesses skin from nonadjacent areas. Accompanying this was an exploration of Zitelli modifications, which enhance the bilobed flap by reducing issues such as pincushioning through a moderated rotation angle and the strategic incorporation of a Burow triangle.
Finally, the interpolated paranasal flap was discussed. This technique is designed to reduce the risk for cheek asymmetry and is suitable for patients with generous donor sites; however, this method requires diligent evaluation to avoid complications such as external nasal valve collapse.
Take-Home Point—This session highlighted approaches in facial reconstruction, emphasizing the necessity of strategic flap design and meticulous incision planning to maintain aesthetic harmony and functional integrity.
Strategies for Improving Physician Well-Being
Evidence-based recommendations to support physicians’ well-being are crucial as the health care system becomes increasingly demanding. Instead of focusing on aspects of the health care system that frequently are outside of physicians’ control, the session “A Realistic and Evidence-Based Roadmap for Thriving in Life and Career” discussed many practical, self-empowering tools and strategies to lead a happier and healthier life—both personally and professionally.
The speakers cautioned against the concept of an “unlimited ceiling” for achieving a certain goal, where an unlimited amount of time and energy is allowed to be dedicated to a given task over a period of time. They highlighted the potential consequences of this approach, such as stress, dissatisfaction, and ultimately burnout. The speakers explored the concept of well-being as a continuous journey rather than a destination, emphasizing that it is not the opposite of burnout. To promote well-being, the speakers advocated for utilizing concepts rooted in positive psychology to empower the individual rather than longing for a different environment. They hypothesized that changing one’s life can be accomplished by changing one’s mind, independent of the environment.
The roadmap for physician well-being, as presented by clinical psychologist Amy MacDonald, PsyD, commenced with urging the audience to introspect on situations and experiences, categorizing them into “feel good” and “feel bad” buckets. For every feel-good event, Dr. MacDonald proposed 5 mental exercises for optimized well-being: (1) control/increase: evaluate whether one can control or increase the frequency of the event; (2) consider: reflect on why this event feels good and explore other aspects to gain any additional joy from the event; (3) share: recognize that some feel goods are more joyous when shared; (4) value: connect the feel-good experiences with personal core values, as research shows value affirmations can buffer neuroendocrine and psychological stress responses; and (5) savor: deliberately relish each small or notable feel-good moment.
Similarly, after labeling an event as a feel-bad experience, Dr. MacDonald encouraged the audience to go through mental exercises to strengthen their well-being journey; however, before proceeding, she highlighted the importance of arming ourselves with self-compassion. The 5 mental exercises to address feel bads include (1) solve: assess whether we have control over the situation and attempt to make changes if possible; (2) reframe: explore new perspectives and assess assumptions without minimizing the situation; (3) connect: embrace the positive impact of safe human connections on our stress response; (4) reflect: search curiously using a compassionate lens for any existing patterns of reactions; and (5) accept and pivot: allow thoughts and feelings to exist and pivot to values-based engagement without waiting for the environment to change. Consistently seeking and appreciating feel goods while addressing rather than suppressing the feel bads can lead to joyful satisfaction and overall well-being.
Additional pearls for optimizing physician well-being included accurately labeling emotions rather than lumping them into an overarching theme (eg, stressed), avoiding comparisons with others, choosing courage over comfort, celebrating vulnerability, and embracing the ability to say no to prioritize engagements aligned with one’s purpose and values. Additional resources were shared for further reading, including Emotional Agility by Susan David, Daring Greatly and Rising Strong by Brené Brown, and Self-Compassion by Kristin Neff.
Take-Home Point—This lecture highlighted key strategies for physicians to improve their well-being, emphasizing self-empowerment and practical tools over external circumstances. It distinguished between productive and destructive influences on satisfaction, and emphasized decision-making aligned with personal values. The concept of well-being as a journey, not a destination, was central, encouraging positive psychology and self-reflection to enhance fulfillment. By focusing on amplifying feel-good experiences and addressing feel-bad experiences with resilience, the lecture advocated for internal over external change, offering a pathway to a balanced and satisfying professional and personal life for physicians.
Final Thoughts
The recent American Academy of Dermatology meeting offered valuable insights and practical pearls to enhance surgical practices and promote physician well-being, in addition to a wide range of topics beyond what is mentioned in this article. From optimizing surgical techniques to prioritizing patient care and safety, the sessions underscored the importance of continuous learning and adaptation in the ever-evolving field of dermatology. As we reflect on the lessons learned and the camaraderie shared during this gathering, let us carry forward these teachings to improve patient outcomes, foster innovation, and cultivate resilience in our pursuit of excellence. Together, we can continue to push the boundaries of dermatologic care while nurturing our own well-being and that of our colleagues, ensuring a brighter future for both patients and practitioners alike.
Acknowledgments—Sultan H. Qiblawi, MD, MBA; Eva Shelton, MD; and Christy T. Behnam, MD (all from Madison, Wisconsin), shared their insights and key takeaways from American Academy of Dermatology lecturers, which enriched the content of this article.
- Hills LS. Putting patients at ease with conversation. J Med Pract Manage. 2006;22:168-170.
- Barlow JO, Zalla MJ, Kyle A, et al. Treatment of basal cell carcinoma with curettage alone. J Am Acad Dermatol. 2006;54:1039-1045.
- Yakish K, Graham J, Hossler EW. Efficacy of curettage alone for invasive cutaneous squamous cell carcinoma: a retrospective cohort study. J Am Acad Dermatol. 2017;77:582-584.
- Shah NR. Commentary on: “surgical smoke—a health hazard in the operating theatre: a study to quantify exposure and a survey of the use of smoke extractor systems in UK plastic surgery units.”Ann Med Surg (Lond). 2012;1:23-24.
Attendees of the 2024 American Academy of Dermatology annual meeting in San Diego, California, were eager to delve into the latest trends and advancements in dermatology and dermatologic surgery. This article provides a few key takeaways for residents from a range of engaging sessions, with an emphasis on procedural dermatology and physician health and well-being.
Practical Applications of Surgical Enhancements
In an informative session dedicated to dermatologic surgeons and their patients, “Simple Tricks and Practical Tips to Optimize the Surgical Experience for You and Your Patients,” attendees learned practical tips for enhancing the surgical experience. The discussion spanned various aspects of surgery, from managing preoperative anxiety with anxiolytics such as midazolam to the strategic use of skin hooks for delicate tissue manipulation. Midazolam is fast acting and its use is tailored to patient factors such as weight, hepatic function, and prior use. An innovative anxiety management algorithm combining “talkesethesia” with other methods such as anodynes and benzodiazepines underscored the importance of a calm patient in successful surgical outcomes. Talkesthesia involves engaging patients in soothing and distracting conversation throughout the procedure. This technique can include discussing nonmedical topics of interest with the patient—such as their hobbies, family, or favorite movies—to divert their attention from the surgical process and reduce anxiety. By creating a friendly and reassuring atmosphere, talkesthesia helps to establish trust between the patient and the medical team, ultimately contributing to a more relaxed and cooperative patient.1
The utility of skin hooks also was discussed, with an emphasis on their role in ensuring gentle tissue handling. The modified buried vertical mattress technique was discussed for its added benefits in wound approximation and strength. Emphasis was placed on the importance of maintaining a clear surgical field by electrocautery to ensure optimal visibility.
Focusing on the treatment of skin cancer, curettage alone was touted as a viable alternative to electrodesiccation and curettage, especially in reducing postoperative hypopigmentation while maintaining high cure rates. This method was shown to be effective in treating basal cell carcinoma and well-differentiated squamous cell carcinoma.2,3
Suturing techniques such as pulley, purse-string, and buried sutures offer efficiencies in time, cost, and improved healing in high-tension areas. These methods can contribute to postsurgical aesthetic and functional outcomes. Additionally, Dr. Desiree Ratner shared her tips for painless local anesthesia techniques, emphasizing the importance of patient comfort through methods such as slow injection and buffering of lidocaine. The next time you give a local anesthetic, try this technique to minimize pain: using a 30-gauge needle, hold the syringe with the bevel up, insert only the bevel into the skin (needle tip goes into the papillary dermis), and numb superficially around the periphery using as little volume as possible. Keep pressure slow and steady without moving the needle, then insert the needle only in previously anesthetized areas, numbing deeply only after the entire periphery has been anesthetized.
The session concluded with the recommendation to provide patients with a goody bag containing postoperative supplies. This thoughtful gesture not only enhances patient satisfaction but also addresses the practical aspect of postsurgery care, offering an inexpensive yet impactful way to ensure patients have the necessary supplies for their recovery.
Take-Home Point—This session distilled essential surgical enhancements into practical applications, emphasizing the importance of anxiety management, delicate tissue handling, innovative suturing techniques, and thoughtful patient care postsurgery. The overarching message highlighted the synergy between technical skill and patient-centric approaches in optimizing surgical outcomes, underscoring the significance of attention to detail in every aspect of patient care, from preoperative preparation to postoperative recovery.
Optimizing Safety and Ergonomics in Surgical Practices
Understanding the dynamics of surgical plume is crucial to safety in the operating room. The carcinogenic risk associated with surgical smoke is not trivial: exposure to the plume generated by monopolar electrocautery in a single day can be equivalent to smoking approximately 30 cigarettes, and a surgeon’s lifetime cancer risk from polycyclic aromatic hydrocarbons exposure is alarmingly high.4 To mitigate these risks, several strategies were recommended, including using lower-energy settings, choosing indirect or bipolar cautery, and ensuring efficient room ventilation with HEPA (high-efficiency particulate absorbing) filters to turn over air frequently. Additionally, employing the use of smoke evacuators and suction devices with proper filters can reduce particulate matter in the operating room.
The importance of the surgeon’s posture during procedures also was emphasized for ergonomic benefits and to minimize fatigue. Maintaining a neutral stance with the core and glutes engaged, standing on the balls of the feet, and aligning the table height to keep the hands at the lower chest level were recommended; this not only helps in reducing strain but also in maintaining precision during surgical tasks.
The surgeons on the panel also highlighted the novel use of hydrocolloid dressings with tattoo lasers, electrodesiccation and curettage for treating rhinophyma, and purse-string closure for chest defects as evolving practices to enhance outcomes and safety.
The session offered valuable insights into suturing techniques, advocating for the use of deep sutures—ideally Monocryl (Ethicon US, LLC)—for superficial closures and fast-absorbing gut sutures for patients who are not expected to return for suture removal. Keith LeBlanc Jr, MD, shared one of his favorite tricks for suturing fragile, sun-damaged skin on the forearm in elderly patients: apply adhesive skin closures aligned parallel to the suture line, then suture through them for extra support. This can help ensure a more secure closure.
In situations when no deep sutures are required, such as on the hair-bearing scalp, large bites through the galea using monofilament nonabsorbable sutures for up to 14 days or staples can offer favorable closures and enhanced hemostasis. Tranexamic acid has emerged as a versatile hemostatic agent—available in multiple forms ranging from direct injection to topical applications—and is cost-effective, enhancing its accessibility in various surgical settings.
A high proportion of patients are taken aback by the length of the scar following removal of what they perceive as a small skin cancer. Leslie Storey, MD, cleverly recommended using the back of a glove to mark surgical planning, giving the patient a visual guide for anticipating the size of the excision. This is a simple yet effective approach to enhance patient understanding and informed consent.
Lastly, the notion that “patients remember you if you don’t cause them pain” resonated deeply, underlining the importance of gentle techniques such as pinching the suture rather than pushing the wound edges together and asking assistants to maintain tension without obstructing the field. In the words of Seth Matarasso, MD: “If you pain ‘em, you won’t retain ‘em!”
Take-Home Point—The take-home message from the session was a comprehensive approach to surgical excellence that aligns technical proficiency with a strong emphasis on safety, patient comfort, and operative efficiency. Surgeons were advised to adopt practices that reduce the risks associated with surgical plume, maintain ergonomic discipline, and apply innovative suturing techniques to enhance patient outcomes. Compassionate patient care, innovative use of materials and methods, and a commitment to continual learning and adaptation of new evidence-based practices are paramount for the modern surgeon.
Approaches for Facial Reconstruction
The intricacies of multisubunit facial reconstruction were explored in a session that blended the pursuit of aesthetic harmony with functional restoration, “Simplifying the Complex: Reconstructing Multisubunit Defects.” The session began with an introduction to flap design principles, emphasizing the importance of thorough defect analysis and the strategic design of flaps. A key objective within this framework is the integration of the flap within existing cosmetic subunits to avoid unwanted effects such as unintended eyebrow elevation.
The concept of tissue reservoirs was discussed,focusing on regions such as the glabella as potential sources for skin recruitment. This then transitioned into a nuanced discussion on incision planning, underscoring the significance of aligning incision lines with relaxed skin tension lines to enhance healing and minimize scarring.
The topic of delayed reconstruction also was introduced as a deliberate tactic for high-risk tumor management. This approach allows for an in-depth pathologic examination and provides patients with more time for psychological adjustment, which may be particularly important for those with complex medical histories or those who require staged surgical interventions.
In a thorough examination of flap design techniques, the session highlighted the bilobed transposition flap as a versatile choice for nasal reconstruction, particularly apt for the distal third of the nose due to its design that harnesses skin from nonadjacent areas. Accompanying this was an exploration of Zitelli modifications, which enhance the bilobed flap by reducing issues such as pincushioning through a moderated rotation angle and the strategic incorporation of a Burow triangle.
Finally, the interpolated paranasal flap was discussed. This technique is designed to reduce the risk for cheek asymmetry and is suitable for patients with generous donor sites; however, this method requires diligent evaluation to avoid complications such as external nasal valve collapse.
Take-Home Point—This session highlighted approaches in facial reconstruction, emphasizing the necessity of strategic flap design and meticulous incision planning to maintain aesthetic harmony and functional integrity.
Strategies for Improving Physician Well-Being
Evidence-based recommendations to support physicians’ well-being are crucial as the health care system becomes increasingly demanding. Instead of focusing on aspects of the health care system that frequently are outside of physicians’ control, the session “A Realistic and Evidence-Based Roadmap for Thriving in Life and Career” discussed many practical, self-empowering tools and strategies to lead a happier and healthier life—both personally and professionally.
The speakers cautioned against the concept of an “unlimited ceiling” for achieving a certain goal, where an unlimited amount of time and energy is allowed to be dedicated to a given task over a period of time. They highlighted the potential consequences of this approach, such as stress, dissatisfaction, and ultimately burnout. The speakers explored the concept of well-being as a continuous journey rather than a destination, emphasizing that it is not the opposite of burnout. To promote well-being, the speakers advocated for utilizing concepts rooted in positive psychology to empower the individual rather than longing for a different environment. They hypothesized that changing one’s life can be accomplished by changing one’s mind, independent of the environment.
The roadmap for physician well-being, as presented by clinical psychologist Amy MacDonald, PsyD, commenced with urging the audience to introspect on situations and experiences, categorizing them into “feel good” and “feel bad” buckets. For every feel-good event, Dr. MacDonald proposed 5 mental exercises for optimized well-being: (1) control/increase: evaluate whether one can control or increase the frequency of the event; (2) consider: reflect on why this event feels good and explore other aspects to gain any additional joy from the event; (3) share: recognize that some feel goods are more joyous when shared; (4) value: connect the feel-good experiences with personal core values, as research shows value affirmations can buffer neuroendocrine and psychological stress responses; and (5) savor: deliberately relish each small or notable feel-good moment.
Similarly, after labeling an event as a feel-bad experience, Dr. MacDonald encouraged the audience to go through mental exercises to strengthen their well-being journey; however, before proceeding, she highlighted the importance of arming ourselves with self-compassion. The 5 mental exercises to address feel bads include (1) solve: assess whether we have control over the situation and attempt to make changes if possible; (2) reframe: explore new perspectives and assess assumptions without minimizing the situation; (3) connect: embrace the positive impact of safe human connections on our stress response; (4) reflect: search curiously using a compassionate lens for any existing patterns of reactions; and (5) accept and pivot: allow thoughts and feelings to exist and pivot to values-based engagement without waiting for the environment to change. Consistently seeking and appreciating feel goods while addressing rather than suppressing the feel bads can lead to joyful satisfaction and overall well-being.
Additional pearls for optimizing physician well-being included accurately labeling emotions rather than lumping them into an overarching theme (eg, stressed), avoiding comparisons with others, choosing courage over comfort, celebrating vulnerability, and embracing the ability to say no to prioritize engagements aligned with one’s purpose and values. Additional resources were shared for further reading, including Emotional Agility by Susan David, Daring Greatly and Rising Strong by Brené Brown, and Self-Compassion by Kristin Neff.
Take-Home Point—This lecture highlighted key strategies for physicians to improve their well-being, emphasizing self-empowerment and practical tools over external circumstances. It distinguished between productive and destructive influences on satisfaction, and emphasized decision-making aligned with personal values. The concept of well-being as a journey, not a destination, was central, encouraging positive psychology and self-reflection to enhance fulfillment. By focusing on amplifying feel-good experiences and addressing feel-bad experiences with resilience, the lecture advocated for internal over external change, offering a pathway to a balanced and satisfying professional and personal life for physicians.
Final Thoughts
The recent American Academy of Dermatology meeting offered valuable insights and practical pearls to enhance surgical practices and promote physician well-being, in addition to a wide range of topics beyond what is mentioned in this article. From optimizing surgical techniques to prioritizing patient care and safety, the sessions underscored the importance of continuous learning and adaptation in the ever-evolving field of dermatology. As we reflect on the lessons learned and the camaraderie shared during this gathering, let us carry forward these teachings to improve patient outcomes, foster innovation, and cultivate resilience in our pursuit of excellence. Together, we can continue to push the boundaries of dermatologic care while nurturing our own well-being and that of our colleagues, ensuring a brighter future for both patients and practitioners alike.
Acknowledgments—Sultan H. Qiblawi, MD, MBA; Eva Shelton, MD; and Christy T. Behnam, MD (all from Madison, Wisconsin), shared their insights and key takeaways from American Academy of Dermatology lecturers, which enriched the content of this article.
Attendees of the 2024 American Academy of Dermatology annual meeting in San Diego, California, were eager to delve into the latest trends and advancements in dermatology and dermatologic surgery. This article provides a few key takeaways for residents from a range of engaging sessions, with an emphasis on procedural dermatology and physician health and well-being.
Practical Applications of Surgical Enhancements
In an informative session dedicated to dermatologic surgeons and their patients, “Simple Tricks and Practical Tips to Optimize the Surgical Experience for You and Your Patients,” attendees learned practical tips for enhancing the surgical experience. The discussion spanned various aspects of surgery, from managing preoperative anxiety with anxiolytics such as midazolam to the strategic use of skin hooks for delicate tissue manipulation. Midazolam is fast acting and its use is tailored to patient factors such as weight, hepatic function, and prior use. An innovative anxiety management algorithm combining “talkesethesia” with other methods such as anodynes and benzodiazepines underscored the importance of a calm patient in successful surgical outcomes. Talkesthesia involves engaging patients in soothing and distracting conversation throughout the procedure. This technique can include discussing nonmedical topics of interest with the patient—such as their hobbies, family, or favorite movies—to divert their attention from the surgical process and reduce anxiety. By creating a friendly and reassuring atmosphere, talkesthesia helps to establish trust between the patient and the medical team, ultimately contributing to a more relaxed and cooperative patient.1
The utility of skin hooks also was discussed, with an emphasis on their role in ensuring gentle tissue handling. The modified buried vertical mattress technique was discussed for its added benefits in wound approximation and strength. Emphasis was placed on the importance of maintaining a clear surgical field by electrocautery to ensure optimal visibility.
Focusing on the treatment of skin cancer, curettage alone was touted as a viable alternative to electrodesiccation and curettage, especially in reducing postoperative hypopigmentation while maintaining high cure rates. This method was shown to be effective in treating basal cell carcinoma and well-differentiated squamous cell carcinoma.2,3
Suturing techniques such as pulley, purse-string, and buried sutures offer efficiencies in time, cost, and improved healing in high-tension areas. These methods can contribute to postsurgical aesthetic and functional outcomes. Additionally, Dr. Desiree Ratner shared her tips for painless local anesthesia techniques, emphasizing the importance of patient comfort through methods such as slow injection and buffering of lidocaine. The next time you give a local anesthetic, try this technique to minimize pain: using a 30-gauge needle, hold the syringe with the bevel up, insert only the bevel into the skin (needle tip goes into the papillary dermis), and numb superficially around the periphery using as little volume as possible. Keep pressure slow and steady without moving the needle, then insert the needle only in previously anesthetized areas, numbing deeply only after the entire periphery has been anesthetized.
The session concluded with the recommendation to provide patients with a goody bag containing postoperative supplies. This thoughtful gesture not only enhances patient satisfaction but also addresses the practical aspect of postsurgery care, offering an inexpensive yet impactful way to ensure patients have the necessary supplies for their recovery.
Take-Home Point—This session distilled essential surgical enhancements into practical applications, emphasizing the importance of anxiety management, delicate tissue handling, innovative suturing techniques, and thoughtful patient care postsurgery. The overarching message highlighted the synergy between technical skill and patient-centric approaches in optimizing surgical outcomes, underscoring the significance of attention to detail in every aspect of patient care, from preoperative preparation to postoperative recovery.
Optimizing Safety and Ergonomics in Surgical Practices
Understanding the dynamics of surgical plume is crucial to safety in the operating room. The carcinogenic risk associated with surgical smoke is not trivial: exposure to the plume generated by monopolar electrocautery in a single day can be equivalent to smoking approximately 30 cigarettes, and a surgeon’s lifetime cancer risk from polycyclic aromatic hydrocarbons exposure is alarmingly high.4 To mitigate these risks, several strategies were recommended, including using lower-energy settings, choosing indirect or bipolar cautery, and ensuring efficient room ventilation with HEPA (high-efficiency particulate absorbing) filters to turn over air frequently. Additionally, employing the use of smoke evacuators and suction devices with proper filters can reduce particulate matter in the operating room.
The importance of the surgeon’s posture during procedures also was emphasized for ergonomic benefits and to minimize fatigue. Maintaining a neutral stance with the core and glutes engaged, standing on the balls of the feet, and aligning the table height to keep the hands at the lower chest level were recommended; this not only helps in reducing strain but also in maintaining precision during surgical tasks.
The surgeons on the panel also highlighted the novel use of hydrocolloid dressings with tattoo lasers, electrodesiccation and curettage for treating rhinophyma, and purse-string closure for chest defects as evolving practices to enhance outcomes and safety.
The session offered valuable insights into suturing techniques, advocating for the use of deep sutures—ideally Monocryl (Ethicon US, LLC)—for superficial closures and fast-absorbing gut sutures for patients who are not expected to return for suture removal. Keith LeBlanc Jr, MD, shared one of his favorite tricks for suturing fragile, sun-damaged skin on the forearm in elderly patients: apply adhesive skin closures aligned parallel to the suture line, then suture through them for extra support. This can help ensure a more secure closure.
In situations when no deep sutures are required, such as on the hair-bearing scalp, large bites through the galea using monofilament nonabsorbable sutures for up to 14 days or staples can offer favorable closures and enhanced hemostasis. Tranexamic acid has emerged as a versatile hemostatic agent—available in multiple forms ranging from direct injection to topical applications—and is cost-effective, enhancing its accessibility in various surgical settings.
A high proportion of patients are taken aback by the length of the scar following removal of what they perceive as a small skin cancer. Leslie Storey, MD, cleverly recommended using the back of a glove to mark surgical planning, giving the patient a visual guide for anticipating the size of the excision. This is a simple yet effective approach to enhance patient understanding and informed consent.
Lastly, the notion that “patients remember you if you don’t cause them pain” resonated deeply, underlining the importance of gentle techniques such as pinching the suture rather than pushing the wound edges together and asking assistants to maintain tension without obstructing the field. In the words of Seth Matarasso, MD: “If you pain ‘em, you won’t retain ‘em!”
Take-Home Point—The take-home message from the session was a comprehensive approach to surgical excellence that aligns technical proficiency with a strong emphasis on safety, patient comfort, and operative efficiency. Surgeons were advised to adopt practices that reduce the risks associated with surgical plume, maintain ergonomic discipline, and apply innovative suturing techniques to enhance patient outcomes. Compassionate patient care, innovative use of materials and methods, and a commitment to continual learning and adaptation of new evidence-based practices are paramount for the modern surgeon.
Approaches for Facial Reconstruction
The intricacies of multisubunit facial reconstruction were explored in a session that blended the pursuit of aesthetic harmony with functional restoration, “Simplifying the Complex: Reconstructing Multisubunit Defects.” The session began with an introduction to flap design principles, emphasizing the importance of thorough defect analysis and the strategic design of flaps. A key objective within this framework is the integration of the flap within existing cosmetic subunits to avoid unwanted effects such as unintended eyebrow elevation.
The concept of tissue reservoirs was discussed,focusing on regions such as the glabella as potential sources for skin recruitment. This then transitioned into a nuanced discussion on incision planning, underscoring the significance of aligning incision lines with relaxed skin tension lines to enhance healing and minimize scarring.
The topic of delayed reconstruction also was introduced as a deliberate tactic for high-risk tumor management. This approach allows for an in-depth pathologic examination and provides patients with more time for psychological adjustment, which may be particularly important for those with complex medical histories or those who require staged surgical interventions.
In a thorough examination of flap design techniques, the session highlighted the bilobed transposition flap as a versatile choice for nasal reconstruction, particularly apt for the distal third of the nose due to its design that harnesses skin from nonadjacent areas. Accompanying this was an exploration of Zitelli modifications, which enhance the bilobed flap by reducing issues such as pincushioning through a moderated rotation angle and the strategic incorporation of a Burow triangle.
Finally, the interpolated paranasal flap was discussed. This technique is designed to reduce the risk for cheek asymmetry and is suitable for patients with generous donor sites; however, this method requires diligent evaluation to avoid complications such as external nasal valve collapse.
Take-Home Point—This session highlighted approaches in facial reconstruction, emphasizing the necessity of strategic flap design and meticulous incision planning to maintain aesthetic harmony and functional integrity.
Strategies for Improving Physician Well-Being
Evidence-based recommendations to support physicians’ well-being are crucial as the health care system becomes increasingly demanding. Instead of focusing on aspects of the health care system that frequently are outside of physicians’ control, the session “A Realistic and Evidence-Based Roadmap for Thriving in Life and Career” discussed many practical, self-empowering tools and strategies to lead a happier and healthier life—both personally and professionally.
The speakers cautioned against the concept of an “unlimited ceiling” for achieving a certain goal, where an unlimited amount of time and energy is allowed to be dedicated to a given task over a period of time. They highlighted the potential consequences of this approach, such as stress, dissatisfaction, and ultimately burnout. The speakers explored the concept of well-being as a continuous journey rather than a destination, emphasizing that it is not the opposite of burnout. To promote well-being, the speakers advocated for utilizing concepts rooted in positive psychology to empower the individual rather than longing for a different environment. They hypothesized that changing one’s life can be accomplished by changing one’s mind, independent of the environment.
The roadmap for physician well-being, as presented by clinical psychologist Amy MacDonald, PsyD, commenced with urging the audience to introspect on situations and experiences, categorizing them into “feel good” and “feel bad” buckets. For every feel-good event, Dr. MacDonald proposed 5 mental exercises for optimized well-being: (1) control/increase: evaluate whether one can control or increase the frequency of the event; (2) consider: reflect on why this event feels good and explore other aspects to gain any additional joy from the event; (3) share: recognize that some feel goods are more joyous when shared; (4) value: connect the feel-good experiences with personal core values, as research shows value affirmations can buffer neuroendocrine and psychological stress responses; and (5) savor: deliberately relish each small or notable feel-good moment.
Similarly, after labeling an event as a feel-bad experience, Dr. MacDonald encouraged the audience to go through mental exercises to strengthen their well-being journey; however, before proceeding, she highlighted the importance of arming ourselves with self-compassion. The 5 mental exercises to address feel bads include (1) solve: assess whether we have control over the situation and attempt to make changes if possible; (2) reframe: explore new perspectives and assess assumptions without minimizing the situation; (3) connect: embrace the positive impact of safe human connections on our stress response; (4) reflect: search curiously using a compassionate lens for any existing patterns of reactions; and (5) accept and pivot: allow thoughts and feelings to exist and pivot to values-based engagement without waiting for the environment to change. Consistently seeking and appreciating feel goods while addressing rather than suppressing the feel bads can lead to joyful satisfaction and overall well-being.
Additional pearls for optimizing physician well-being included accurately labeling emotions rather than lumping them into an overarching theme (eg, stressed), avoiding comparisons with others, choosing courage over comfort, celebrating vulnerability, and embracing the ability to say no to prioritize engagements aligned with one’s purpose and values. Additional resources were shared for further reading, including Emotional Agility by Susan David, Daring Greatly and Rising Strong by Brené Brown, and Self-Compassion by Kristin Neff.
Take-Home Point—This lecture highlighted key strategies for physicians to improve their well-being, emphasizing self-empowerment and practical tools over external circumstances. It distinguished between productive and destructive influences on satisfaction, and emphasized decision-making aligned with personal values. The concept of well-being as a journey, not a destination, was central, encouraging positive psychology and self-reflection to enhance fulfillment. By focusing on amplifying feel-good experiences and addressing feel-bad experiences with resilience, the lecture advocated for internal over external change, offering a pathway to a balanced and satisfying professional and personal life for physicians.
Final Thoughts
The recent American Academy of Dermatology meeting offered valuable insights and practical pearls to enhance surgical practices and promote physician well-being, in addition to a wide range of topics beyond what is mentioned in this article. From optimizing surgical techniques to prioritizing patient care and safety, the sessions underscored the importance of continuous learning and adaptation in the ever-evolving field of dermatology. As we reflect on the lessons learned and the camaraderie shared during this gathering, let us carry forward these teachings to improve patient outcomes, foster innovation, and cultivate resilience in our pursuit of excellence. Together, we can continue to push the boundaries of dermatologic care while nurturing our own well-being and that of our colleagues, ensuring a brighter future for both patients and practitioners alike.
Acknowledgments—Sultan H. Qiblawi, MD, MBA; Eva Shelton, MD; and Christy T. Behnam, MD (all from Madison, Wisconsin), shared their insights and key takeaways from American Academy of Dermatology lecturers, which enriched the content of this article.
- Hills LS. Putting patients at ease with conversation. J Med Pract Manage. 2006;22:168-170.
- Barlow JO, Zalla MJ, Kyle A, et al. Treatment of basal cell carcinoma with curettage alone. J Am Acad Dermatol. 2006;54:1039-1045.
- Yakish K, Graham J, Hossler EW. Efficacy of curettage alone for invasive cutaneous squamous cell carcinoma: a retrospective cohort study. J Am Acad Dermatol. 2017;77:582-584.
- Shah NR. Commentary on: “surgical smoke—a health hazard in the operating theatre: a study to quantify exposure and a survey of the use of smoke extractor systems in UK plastic surgery units.”Ann Med Surg (Lond). 2012;1:23-24.
- Hills LS. Putting patients at ease with conversation. J Med Pract Manage. 2006;22:168-170.
- Barlow JO, Zalla MJ, Kyle A, et al. Treatment of basal cell carcinoma with curettage alone. J Am Acad Dermatol. 2006;54:1039-1045.
- Yakish K, Graham J, Hossler EW. Efficacy of curettage alone for invasive cutaneous squamous cell carcinoma: a retrospective cohort study. J Am Acad Dermatol. 2017;77:582-584.
- Shah NR. Commentary on: “surgical smoke—a health hazard in the operating theatre: a study to quantify exposure and a survey of the use of smoke extractor systems in UK plastic surgery units.”Ann Med Surg (Lond). 2012;1:23-24.
RESIDENT PEARLS
- By protecting yourself and ensuring your own longevity as a practicing physician, you will be better able to care for your patients over the long term. Focus on self-empowerment and positive psychology for a balanced life.
- Protect yourself from surgical plume by using smoke evacuators and ensuring proper room ventilation with HEPA (high-efficiency particulate absorbing) filters whenever possible. Stick to low-energy settings for electrocautery.
- During surgical procedures, maintain a neutral posture, keep your core and glutes engaged, and adjust the table height to reduce strain and improve precision.

Commentary: Aspirin, Childbirth, and Everolimus in BC, June 2024

The postpartum period represents a possibly vulnerable time window for development of new cancers with metastatic potential. Studies in young-onset breast cancer have shown a postpartum diagnosis up to 10 years after childbirth associated with adverse breast cancer survival outcomes.4 Women with germline BRCA1/2 pathogenic variants have a higher risk of developing breast cancer at a younger age compared to the general population.5 A prospective cohort study that included 903 women with germline BRCA1/2 mutations diagnosed with stage I-III breast cancer at age ≤ 45 years investigated whether time since childbirth and time since breast cancer diagnosis were associated with mortality in this population (
The mechanisms involved in development of endocrine therapy (ET) resistance are complex and may include changes in hormone signaling, alterations in growth factor signaling pathway components, and appearance of resistant clonal populations.6 Prior studies have shown efficacy with the mammalian target of rapamycin (mTOR) inhibitor everolimus in combination with various ET backbones. However, the sequencing of these combinations in current clinical practice has shifted in light of significant therapeutic advancements in this space.7 A retrospective observational study including 161 patients with advanced hormone receptor–positive (HR+)/ human epidermal growth factor receptor–2 negative (HER2-) breast cancer treated with everolimus plus ET (exemestane, fulvestrant, tamoxifen) reported outcomes on the real-world use of these regimens after progression on cyclin-dependent kinase (CDK) 4/6 inhibitor therapy (Sánchez-Bayona et al). At a median follow-up of 15 months, the estimated median progression-free survival (PFS) was 6.0 months (95% CI 5.3-7.8 months); PFS was longer among those with previous CDK4/6 inhibitor use lasting >18 months (8.7 months; 95% CI 6.6-11.3 months), patients without visceral disease (8.0 months; 95% CI 5.8-10.5 months), and those who were chemotherapy-naive in the advanced setting (7.2 months; 95% CI 5.9-8.4 months). These data support a role for everolimus plus ET as a treatment option post–CDK4/6 inhibitor treatment for selected patient populations, including those whose tumors lack targetable somatic mutations (such as PIK3CA and ESR1 mutations), and may provide meaningful clinical benefit in this setting.
Additional References
- Rothwell PM, Wilson M, Price JF, et al. Effect of daily aspirin on risk of cancer metastasis: A study of incident cancers during randomised controlled trials. Lancet. 2012;379:1591-601. doi: 10.1016/S0140-6736(12)60209-8 Source
- Okada S, Morimoto T, Ogawa H, et al, and the JPAD Trial Investigators. Effect of aspirin on cancer chemoprevention in Japanese patients with type 2 diabetes: 10-year observational follow-up of a randomized controlled trial. Diabetes Care. 2018;41:1757-1764. doi: 10.2337/dc18-0368 Source
- Burn J, Sheth H, Elliott F, et al, on behalf of the CAPP2 Investigators. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: A double-blind, randomised, placebo-controlled trial. Lancet. 2020;395:1855-1863. doi: 10.1016/S0140-6736(20)30366-4 Source
- Shao C, Yu Z, Xiao J, et al. Prognosis of pregnancy-associated breast cancer: A meta-analysis. BMC Cancer. 2020;20:746. doi: 10.1186/s12885-020-07248-8 Source
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317:2402-2416. doi: 10.1001/jama.2017.7112 Source
- Hanker AB, Sudhan DR, Arteaga CL. Overcoming endocrine resistance in breast cancer. Cancer Cell. 2020;37:496-513. doi: 10.1016/j.ccell.2020.03.009 Source
- Kornblum N, Zhao F, Manola J, et al. Randomized phase II trial of fulvestrant plus everolimus or placebo in postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer resistant to aromatase inhibitor therapy: Results of PrE0102. J Clin Oncol. 2018;36:1556-1563. doi: 10.1200/JCO.2017.76.9331 Source
The postpartum period represents a possibly vulnerable time window for development of new cancers with metastatic potential. Studies in young-onset breast cancer have shown a postpartum diagnosis up to 10 years after childbirth associated with adverse breast cancer survival outcomes.4 Women with germline BRCA1/2 pathogenic variants have a higher risk of developing breast cancer at a younger age compared to the general population.5 A prospective cohort study that included 903 women with germline BRCA1/2 mutations diagnosed with stage I-III breast cancer at age ≤ 45 years investigated whether time since childbirth and time since breast cancer diagnosis were associated with mortality in this population (
The mechanisms involved in development of endocrine therapy (ET) resistance are complex and may include changes in hormone signaling, alterations in growth factor signaling pathway components, and appearance of resistant clonal populations.6 Prior studies have shown efficacy with the mammalian target of rapamycin (mTOR) inhibitor everolimus in combination with various ET backbones. However, the sequencing of these combinations in current clinical practice has shifted in light of significant therapeutic advancements in this space.7 A retrospective observational study including 161 patients with advanced hormone receptor–positive (HR+)/ human epidermal growth factor receptor–2 negative (HER2-) breast cancer treated with everolimus plus ET (exemestane, fulvestrant, tamoxifen) reported outcomes on the real-world use of these regimens after progression on cyclin-dependent kinase (CDK) 4/6 inhibitor therapy (Sánchez-Bayona et al). At a median follow-up of 15 months, the estimated median progression-free survival (PFS) was 6.0 months (95% CI 5.3-7.8 months); PFS was longer among those with previous CDK4/6 inhibitor use lasting >18 months (8.7 months; 95% CI 6.6-11.3 months), patients without visceral disease (8.0 months; 95% CI 5.8-10.5 months), and those who were chemotherapy-naive in the advanced setting (7.2 months; 95% CI 5.9-8.4 months). These data support a role for everolimus plus ET as a treatment option post–CDK4/6 inhibitor treatment for selected patient populations, including those whose tumors lack targetable somatic mutations (such as PIK3CA and ESR1 mutations), and may provide meaningful clinical benefit in this setting.
Additional References
- Rothwell PM, Wilson M, Price JF, et al. Effect of daily aspirin on risk of cancer metastasis: A study of incident cancers during randomised controlled trials. Lancet. 2012;379:1591-601. doi: 10.1016/S0140-6736(12)60209-8 Source
- Okada S, Morimoto T, Ogawa H, et al, and the JPAD Trial Investigators. Effect of aspirin on cancer chemoprevention in Japanese patients with type 2 diabetes: 10-year observational follow-up of a randomized controlled trial. Diabetes Care. 2018;41:1757-1764. doi: 10.2337/dc18-0368 Source
- Burn J, Sheth H, Elliott F, et al, on behalf of the CAPP2 Investigators. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: A double-blind, randomised, placebo-controlled trial. Lancet. 2020;395:1855-1863. doi: 10.1016/S0140-6736(20)30366-4 Source
- Shao C, Yu Z, Xiao J, et al. Prognosis of pregnancy-associated breast cancer: A meta-analysis. BMC Cancer. 2020;20:746. doi: 10.1186/s12885-020-07248-8 Source
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317:2402-2416. doi: 10.1001/jama.2017.7112 Source
- Hanker AB, Sudhan DR, Arteaga CL. Overcoming endocrine resistance in breast cancer. Cancer Cell. 2020;37:496-513. doi: 10.1016/j.ccell.2020.03.009 Source
- Kornblum N, Zhao F, Manola J, et al. Randomized phase II trial of fulvestrant plus everolimus or placebo in postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer resistant to aromatase inhibitor therapy: Results of PrE0102. J Clin Oncol. 2018;36:1556-1563. doi: 10.1200/JCO.2017.76.9331 Source
The postpartum period represents a possibly vulnerable time window for development of new cancers with metastatic potential. Studies in young-onset breast cancer have shown a postpartum diagnosis up to 10 years after childbirth associated with adverse breast cancer survival outcomes.4 Women with germline BRCA1/2 pathogenic variants have a higher risk of developing breast cancer at a younger age compared to the general population.5 A prospective cohort study that included 903 women with germline BRCA1/2 mutations diagnosed with stage I-III breast cancer at age ≤ 45 years investigated whether time since childbirth and time since breast cancer diagnosis were associated with mortality in this population (
The mechanisms involved in development of endocrine therapy (ET) resistance are complex and may include changes in hormone signaling, alterations in growth factor signaling pathway components, and appearance of resistant clonal populations.6 Prior studies have shown efficacy with the mammalian target of rapamycin (mTOR) inhibitor everolimus in combination with various ET backbones. However, the sequencing of these combinations in current clinical practice has shifted in light of significant therapeutic advancements in this space.7 A retrospective observational study including 161 patients with advanced hormone receptor–positive (HR+)/ human epidermal growth factor receptor–2 negative (HER2-) breast cancer treated with everolimus plus ET (exemestane, fulvestrant, tamoxifen) reported outcomes on the real-world use of these regimens after progression on cyclin-dependent kinase (CDK) 4/6 inhibitor therapy (Sánchez-Bayona et al). At a median follow-up of 15 months, the estimated median progression-free survival (PFS) was 6.0 months (95% CI 5.3-7.8 months); PFS was longer among those with previous CDK4/6 inhibitor use lasting >18 months (8.7 months; 95% CI 6.6-11.3 months), patients without visceral disease (8.0 months; 95% CI 5.8-10.5 months), and those who were chemotherapy-naive in the advanced setting (7.2 months; 95% CI 5.9-8.4 months). These data support a role for everolimus plus ET as a treatment option post–CDK4/6 inhibitor treatment for selected patient populations, including those whose tumors lack targetable somatic mutations (such as PIK3CA and ESR1 mutations), and may provide meaningful clinical benefit in this setting.
Additional References
- Rothwell PM, Wilson M, Price JF, et al. Effect of daily aspirin on risk of cancer metastasis: A study of incident cancers during randomised controlled trials. Lancet. 2012;379:1591-601. doi: 10.1016/S0140-6736(12)60209-8 Source
- Okada S, Morimoto T, Ogawa H, et al, and the JPAD Trial Investigators. Effect of aspirin on cancer chemoprevention in Japanese patients with type 2 diabetes: 10-year observational follow-up of a randomized controlled trial. Diabetes Care. 2018;41:1757-1764. doi: 10.2337/dc18-0368 Source
- Burn J, Sheth H, Elliott F, et al, on behalf of the CAPP2 Investigators. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: A double-blind, randomised, placebo-controlled trial. Lancet. 2020;395:1855-1863. doi: 10.1016/S0140-6736(20)30366-4 Source
- Shao C, Yu Z, Xiao J, et al. Prognosis of pregnancy-associated breast cancer: A meta-analysis. BMC Cancer. 2020;20:746. doi: 10.1186/s12885-020-07248-8 Source
- Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317:2402-2416. doi: 10.1001/jama.2017.7112 Source
- Hanker AB, Sudhan DR, Arteaga CL. Overcoming endocrine resistance in breast cancer. Cancer Cell. 2020;37:496-513. doi: 10.1016/j.ccell.2020.03.009 Source
- Kornblum N, Zhao F, Manola J, et al. Randomized phase II trial of fulvestrant plus everolimus or placebo in postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer resistant to aromatase inhibitor therapy: Results of PrE0102. J Clin Oncol. 2018;36:1556-1563. doi: 10.1200/JCO.2017.76.9331 Source
Transient Symmetric Blanching Macules on a Background of Reticulate Erythema
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
The Diagnosis: BASCULE Syndrome
The patient had previously been thought to have livedo reticularis by primary care. Repeat antinuclear antibody (ANA) testing was positive (1:1280 homogeneous [reflexive titers all negative]). However, upon dermatologic evaluation, the manifestation of the rash in addition to onset occurring with postural changes challenged the livedo reticularis diagnosis. Extensive research and consultation with dermatologic colleagues led to the diagnosis of the rare entity BASCULE syndrome. BASCULE (Bier anemic spots, cyanosis, and urticarialike eruption) syndrome was described by Bessis et al1 in 2016. It is a rare condition but may be underreported.2 It is a benign pediatric disorder in the vascular acrosyndrome family that is characterized by underlying vasomotor dysfunction in distal regions of the body. Raynaud phenomenon is a widely known member of this family. As seen in our patient, it typically presents on the distal legs and feet with numerous irregular hypopigmented macules on a cyanotic background. Red-orange papules may appear on the hypopigmented macules and often are pruritic. Lesions on the distal upper extremities are less common, and a case involving the trunk has been reported.3 Onset generally begins within a couple of minutes of standing or mechanical compression of the lower legs, with full reversal of symptoms occurring within minutes of laying down or walking. Commonly reported associated symptoms include tenderness, pruritus, edema, and pain; however, the cutaneous lesions may be asymptomatic. The condition tends to affect adolescents, as seen in our patient; however, there have been reports in infants as young as 3 months to adults aged 19 years.2
The pathophysiology behind BASCULE syndrome remains unclear but is believed to be centered around the role of physiologic venous stasis that occurs when standing. The hypoxia secondary to stasis is thought to induce amplified vasoconstriction of arterioles. These responses are further exaggerated due to absence of venoarteriolar reflexes in dermal ascending arterioles, leading to Bier spots.2 The role of mast cells and eosinophils remains unclear. It is a clinical diagnosis without clear histologic findings; therefore, biopsy was not pursued in our patient.
Although BASCULE syndrome is a benign entity, it is imperative that it be recognized to avoid a time consuming, expensive, and anxiety-producing diagnostic workup, as occurred in our patient. Although not a manifestation of systemic disease, BASCULE syndrome may be associated with orthostatic hypotension in up to 20% of cases.2,4 Therefore, these patients should undergo orthostatic testing, including the tilt table test. In our patient, these manifestations were not appreciated.
There are no current guidelines for effective treatment of BASCULE syndrome. Given the possible role of mast cells in the condition, H1 antihistamines are proposed as first-line treatment. Desloratadine (10 mg/d for 7 days) has been found to be associated with improvement of pruritus. However, a recent literature review found little evidence to support the use of H1 antihistamines for resolution of other symptoms.2
The differential diagnosis includes livedo reticularis, Bier spots, Sneddon syndrome, and urticarial vasculitis. Livedo reticularis presents as distinct, netlike, blue-erythematousviolaceous discoloration, which differs from the distinct orange-red macules in BASCULE syndrome.5 In addition to distinct variances in dermatologic presentation, livedo reticularis typically is associated with cold exposure as a causative agent, with cold avoidance as the treatment for this benign and often transient condition.6 This phenomenon was not appreciated in our patient. Livedo reticularis commonly occurs with antiphospholipid syndrome.5 This association in combination with our patient's positive ANA findings and her mother's history of miscarriages resulted in the misdiagnosis as livedo reticularis.
Bier spots manifest as white macules with surrounding erythema and typically present in young adults. When first described in the literature, it was debated if BASCULE syndrome was simply another manifestation of Bier spots or postural orthostatic intolerance,4 as there was a large consensus that postural orthostatic intolerance was associated with BASCULE syndrome, with the majority of patients not meeting criteria for the condition. Heymann4 addressed the differences in BASCULE manifestations vs typical Bier spots. The author extended the syndrome to include cyanosis, an urticarialike eruption of red-orange macules with central papules located centrally, pruritus, tenderness, and partial or diffuse edema, in addition to Bier spots.4
Sneddon syndrome is a rare progressive disorder that affects small- to medium-sized blood vessels resulting in multiple episodes of ischemia in the brain. Skin manifestations of these repeated strokes are similar to livedo reticularis, typically manifesting as livedo racemosa—irregular reticular patterns of skin mottling with reddish-blue hues.6 However, Sneddon syndrome is more generalized and widespread and differs from BASCULE syndrome in shape and histologic findings. Our patient presented with findings on the legs, which is more characteristic of livedo reticularis vs livedo racemosa. Our patient experienced resolution upon laying down and sitting, and Sneddon syndrome persists beyond postural changes. Furthermore, patients with Sneddon syndrome present with neurologic symptoms such as prodromal headaches.6
Urticarial vasculitis was ruled out in our patient because of the duration of symptoms as well as the spatial changes. Urticarial vasculitis is a rare skin condition characterized by chronic recurring urticarial lesions that may persist for more than a day. This condition typically presents in middle-aged women and rarely in children. Urticarial vasculitis is thought to be immune-complex mediated, but its cause is largely unknown. It is a common manifestation of underlying conditions such as systemic lupus erythematosus.6 Our patient had a positive ANA and possible autoimmune history from her mother; however, urticarial vasculitis does not present transiently on the legs or in the rash pattern appreciated in our patient.
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
- Bessis D, Jeziorski E, Rigau V, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome: a new entity? Br J Dermatol. 2016;175:218-220. doi:10.1111/bjd.14589
- Baurens N, Briand C, Giovannini-Chami L, et al. Case report, practices survey and literature review of an under-recognized pediatric vascular disorder: the BASCULE syndrome. Front Pediatr. 2022;10:849914. doi:10.3389/fped.2022.849914
- Jiménez-Gallo D, Collantes-Rodríguez C, Ossorio-García L, et al. Bier anaemic spots, cyanosis with urticaria-like eruption (BASCULE) syndrome on trunk and upper limbs. Pediatr Dermatol. 2018;35:E313-E315. doi:10.1111/pde.13558
- Heymann WR. BASCULE syndrome: is something brewing with Bier spots? Dermatology World Insights and Inquiries. September 7, 2022. https://www.aad.org/dw/dw-insights-and-inquiries/archive/2022/bascule-syndrome
- Sajjan VV, Lunge S, Swamy MB, et al. Livedo reticularis: a review of the literature. Indian Dermatol Online J. 2015;6:315-321. doi:10.4103/2229-5178.164493
- Gu SL, Jorizzo JL. Urticarial vasculitis. Int J Womens Dermatol. 2021;7:290-297. doi:10.1016/j.ijwd.2021.01.021
An 11-year-old girl was referred to the dermatology clinic for evaluation of a rash on the legs and feet of 1 year’s duration. The rash appeared every time she was standing for longer than 10 to 15 minutes and resolved when sitting or laying down. After the initial onset, the rash did not spread to other body areas but became more prominent in appearance. The patient endorsed intense pruritus associated with the rash. A review of systems was negative for fever, headaches, history of blood clots, and joint pain. She did not have any known medical conditions or take any medications. The patient’s mother reported that the patient experienced episodes of leg numbness while sitting in vehicles from 6 to 10 years of age. There was no family history of rheumatologic, hematologic, or cardiac conditions. The patient’s mother had experienced 2 miscarriages but denied any other obstetric complications. The patient had 1 sibling who was unaffected. Physical examination revealed reticulate erythema on the calves with scattered regions of blanching and evanescent pink macules as well as dermatographism.
One month prior to presenting to dermatology, the patient was evaluated by rheumatology, endocrinology, and hematology. Laboratory workup completed at age 3 years included antinuclear antibody, anticardiolipin antibody, and antithrombin III activity; factor V Leiden; cryoglobulins; quantitation (human chorionic gonadotropin); proteins S and C activity; antineutrophil cytoplasmic antibody screen; thyroid studies; prothrombin time; and partial thromboplastin time. All laboratory results were within reference range.
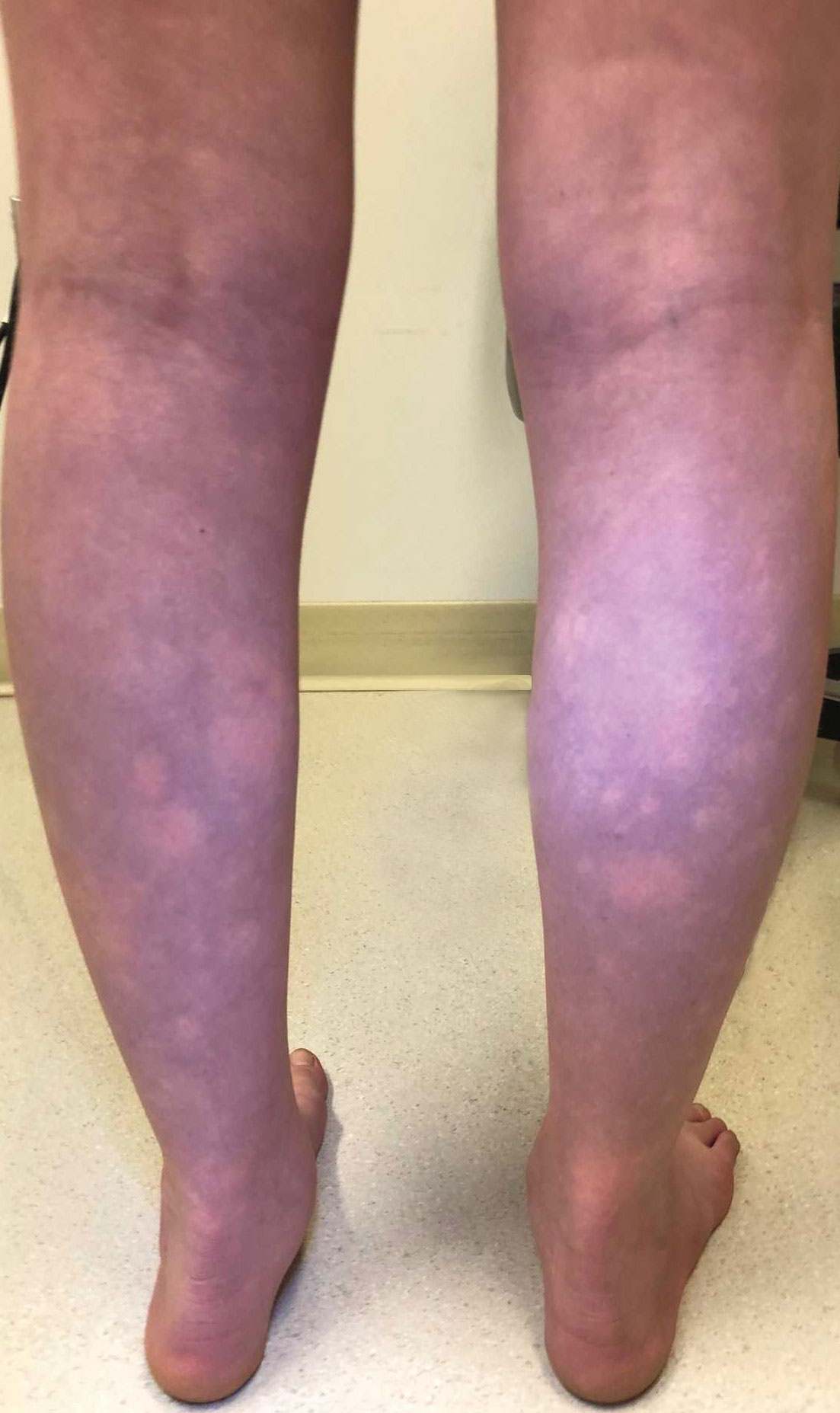

Diphenhydramine and Prochlorperazine Combo Not Associated With Migraine Treatment Failure
Key clinical point: The odds of treatment failure were not increased, and no extrapyramidal adverse events were reported in pediatric patients with migraine when diphenhydramine was coadministered with prochlorperazine in an emergency department (ED) setting.
Major finding: The administration of diphenhydramine plus prochlorperazine vs prochlorperazine alone was not associated with increased odds of additional migraine therapy (P = .347), hospitalization rates (P = .425), and 72-hour return visit rates (P = .271). None of the patients in the diphenhydramine plus prochlorperazine group experienced extrapyramidal adverse events, while 2.4% of patients in prochlorperazine group experienced extrapyramidal adverse events.
Study details: Findings are from a retrospective cohort study that included 1683 pediatric patients with migraine presenting to the ED who received diphenhydramine plus prochlorperazine (n = 1215) or prochlorperazine only (n = 468).
Disclosures: This study did not disclose any funding source. The authors declared no conflicts of interest.
Source: Naeem S, Lozano JM, Ruiz Castaneda AM, Lowe D. Diphenhydramine and migraine treatment failure in pediatric patients receiving prochlorperazine. Pediatr Emerg Care. 2024 (May 9). doi: 10.1097/PEC.0000000000003202 Source
Key clinical point: The odds of treatment failure were not increased, and no extrapyramidal adverse events were reported in pediatric patients with migraine when diphenhydramine was coadministered with prochlorperazine in an emergency department (ED) setting.
Major finding: The administration of diphenhydramine plus prochlorperazine vs prochlorperazine alone was not associated with increased odds of additional migraine therapy (P = .347), hospitalization rates (P = .425), and 72-hour return visit rates (P = .271). None of the patients in the diphenhydramine plus prochlorperazine group experienced extrapyramidal adverse events, while 2.4% of patients in prochlorperazine group experienced extrapyramidal adverse events.
Study details: Findings are from a retrospective cohort study that included 1683 pediatric patients with migraine presenting to the ED who received diphenhydramine plus prochlorperazine (n = 1215) or prochlorperazine only (n = 468).
Disclosures: This study did not disclose any funding source. The authors declared no conflicts of interest.
Source: Naeem S, Lozano JM, Ruiz Castaneda AM, Lowe D. Diphenhydramine and migraine treatment failure in pediatric patients receiving prochlorperazine. Pediatr Emerg Care. 2024 (May 9). doi: 10.1097/PEC.0000000000003202 Source
Key clinical point: The odds of treatment failure were not increased, and no extrapyramidal adverse events were reported in pediatric patients with migraine when diphenhydramine was coadministered with prochlorperazine in an emergency department (ED) setting.
Major finding: The administration of diphenhydramine plus prochlorperazine vs prochlorperazine alone was not associated with increased odds of additional migraine therapy (P = .347), hospitalization rates (P = .425), and 72-hour return visit rates (P = .271). None of the patients in the diphenhydramine plus prochlorperazine group experienced extrapyramidal adverse events, while 2.4% of patients in prochlorperazine group experienced extrapyramidal adverse events.
Study details: Findings are from a retrospective cohort study that included 1683 pediatric patients with migraine presenting to the ED who received diphenhydramine plus prochlorperazine (n = 1215) or prochlorperazine only (n = 468).
Disclosures: This study did not disclose any funding source. The authors declared no conflicts of interest.
Source: Naeem S, Lozano JM, Ruiz Castaneda AM, Lowe D. Diphenhydramine and migraine treatment failure in pediatric patients receiving prochlorperazine. Pediatr Emerg Care. 2024 (May 9). doi: 10.1097/PEC.0000000000003202 Source