User login
Dasatinib activity prominent in subset of GIST patients
Dasatinib might have activity in some subsets of patients with imatinib-resistant gastrointestinal stromal tumors (GISTs), investigators have reported.
The tyrosine kinase inhibitor had a 29% rate of 6-month progression-free survival (PFS) in a nonrandomized, 50-patient study.
That PFS rate was well above the 10% threshold that would have constituted evidence of inactive treatment, but it “fell just short of our goal” of 30% that would have been considered evidence of drug activity, wrote Scott M. Schuetze, MD, PhD, of the department of internal medicine, University of Michigan, Ann Arbor, and his coauthors. The report was published in JAMA Oncology.
It was also higher than the 16% 6-month PFS rate reported in a randomized trial of sunitinib, which was approved for imatinib-resistant GIST treatment in 2006. However, it was lower than the 38% 6-month PFS rate reported for regorafenib, which was approved in 2013 for that indication, the researchers noted.
Exploratory analyses did identify a few biomarker-driven subsets that might particularly benefit from dasatinib therapy. Notably, the 6-month PFS rate was 50% for patients with tumors expressing phosphorylated SRC.
While intriguing, the results of the exploratory analyses are hampered by the small number of patients enrolled in the trial; only 14 patients in the study had phosphorylated SRC.
“Further studies should explore whether activated SRC is a prognostic biomarker of more indolent disease, or is a predictive biomarker of response to tyrosine kinase therapy,” the researchers wrote.
Patients in the study had imatinib refractory GIST. They received dasatinib 70 mg twice daily. They were enrolled in 2008-2009 and followed for at least 5 years.
In addition to previously receiving imatinib, most enrollees (80%) had already been treated with sunitinib as well. The study started before the approval of sunitinib in GIST, but after the approval of regorafenib, the investigators noted.
“Preclinical research suggested that dasatinib had higher potency against mutations in the activation domain of KIT and PDGFRA than imatinib and sunitinib,” the authors recounted.
This trial did provide some evidence in support of that preclinical data: One patient with a specific mutation in PDGFRA exhibited prolonged tumor control.
Bristol-Myers Squibb provided funding for the trial and dasatinib. Dr. Schuetze reported disclosures related to Novartis, Amgen, Janssen, Daiichi-Sankyo, Eli Lilly, and AB Science.
SOURCE: Schuetze SM et al. 2018 Apr 26. doi: 10.1001/jamaoncol.2018.0601.
Dasatinib might have activity in some subsets of patients with imatinib-resistant gastrointestinal stromal tumors (GISTs), investigators have reported.
The tyrosine kinase inhibitor had a 29% rate of 6-month progression-free survival (PFS) in a nonrandomized, 50-patient study.
That PFS rate was well above the 10% threshold that would have constituted evidence of inactive treatment, but it “fell just short of our goal” of 30% that would have been considered evidence of drug activity, wrote Scott M. Schuetze, MD, PhD, of the department of internal medicine, University of Michigan, Ann Arbor, and his coauthors. The report was published in JAMA Oncology.
It was also higher than the 16% 6-month PFS rate reported in a randomized trial of sunitinib, which was approved for imatinib-resistant GIST treatment in 2006. However, it was lower than the 38% 6-month PFS rate reported for regorafenib, which was approved in 2013 for that indication, the researchers noted.
Exploratory analyses did identify a few biomarker-driven subsets that might particularly benefit from dasatinib therapy. Notably, the 6-month PFS rate was 50% for patients with tumors expressing phosphorylated SRC.
While intriguing, the results of the exploratory analyses are hampered by the small number of patients enrolled in the trial; only 14 patients in the study had phosphorylated SRC.
“Further studies should explore whether activated SRC is a prognostic biomarker of more indolent disease, or is a predictive biomarker of response to tyrosine kinase therapy,” the researchers wrote.
Patients in the study had imatinib refractory GIST. They received dasatinib 70 mg twice daily. They were enrolled in 2008-2009 and followed for at least 5 years.
In addition to previously receiving imatinib, most enrollees (80%) had already been treated with sunitinib as well. The study started before the approval of sunitinib in GIST, but after the approval of regorafenib, the investigators noted.
“Preclinical research suggested that dasatinib had higher potency against mutations in the activation domain of KIT and PDGFRA than imatinib and sunitinib,” the authors recounted.
This trial did provide some evidence in support of that preclinical data: One patient with a specific mutation in PDGFRA exhibited prolonged tumor control.
Bristol-Myers Squibb provided funding for the trial and dasatinib. Dr. Schuetze reported disclosures related to Novartis, Amgen, Janssen, Daiichi-Sankyo, Eli Lilly, and AB Science.
SOURCE: Schuetze SM et al. 2018 Apr 26. doi: 10.1001/jamaoncol.2018.0601.
Dasatinib might have activity in some subsets of patients with imatinib-resistant gastrointestinal stromal tumors (GISTs), investigators have reported.
The tyrosine kinase inhibitor had a 29% rate of 6-month progression-free survival (PFS) in a nonrandomized, 50-patient study.
That PFS rate was well above the 10% threshold that would have constituted evidence of inactive treatment, but it “fell just short of our goal” of 30% that would have been considered evidence of drug activity, wrote Scott M. Schuetze, MD, PhD, of the department of internal medicine, University of Michigan, Ann Arbor, and his coauthors. The report was published in JAMA Oncology.
It was also higher than the 16% 6-month PFS rate reported in a randomized trial of sunitinib, which was approved for imatinib-resistant GIST treatment in 2006. However, it was lower than the 38% 6-month PFS rate reported for regorafenib, which was approved in 2013 for that indication, the researchers noted.
Exploratory analyses did identify a few biomarker-driven subsets that might particularly benefit from dasatinib therapy. Notably, the 6-month PFS rate was 50% for patients with tumors expressing phosphorylated SRC.
While intriguing, the results of the exploratory analyses are hampered by the small number of patients enrolled in the trial; only 14 patients in the study had phosphorylated SRC.
“Further studies should explore whether activated SRC is a prognostic biomarker of more indolent disease, or is a predictive biomarker of response to tyrosine kinase therapy,” the researchers wrote.
Patients in the study had imatinib refractory GIST. They received dasatinib 70 mg twice daily. They were enrolled in 2008-2009 and followed for at least 5 years.
In addition to previously receiving imatinib, most enrollees (80%) had already been treated with sunitinib as well. The study started before the approval of sunitinib in GIST, but after the approval of regorafenib, the investigators noted.
“Preclinical research suggested that dasatinib had higher potency against mutations in the activation domain of KIT and PDGFRA than imatinib and sunitinib,” the authors recounted.
This trial did provide some evidence in support of that preclinical data: One patient with a specific mutation in PDGFRA exhibited prolonged tumor control.
Bristol-Myers Squibb provided funding for the trial and dasatinib. Dr. Schuetze reported disclosures related to Novartis, Amgen, Janssen, Daiichi-Sankyo, Eli Lilly, and AB Science.
SOURCE: Schuetze SM et al. 2018 Apr 26. doi: 10.1001/jamaoncol.2018.0601.
FROM JAMA ONCOLOGY
Key clinical point: The efficacy of dasatinib in imatinib-resistant GIST was just short of what investigators considered evidence of an active drug.
Major finding: The estimated rate of 6-month progression-free survival was 29% overall, though it was 50% in one biomarker-defined patient subset.
Study details: A nonrandomized single-arm study of 50 patients with GIST treated with dasatinib 70 mg twice daily.
Disclosures: Bristol-Myers Squibb provided funding for the trial and dasatinib. Dr. Schuetze reported disclosures related to Novartis, Amgen, Janssen, Daiichi-Sankyo, Eli Lilly, and AB Science.
Source: Schuetze SM et al. JAMA Oncol. 2018 Apr 26. doi: 10.1001/jamaoncol.2018.0601.
Early breast cancer: Patients report favorable quality of life after partial breast irradiation
In women with breast cancer undergoing breast-conserving surgery, accelerated partial breast irradiation (APBI) using multicatheter brachytherapy does not negatively affect quality of life, compared with standard whole breast irradiation, investigators have reported.
Patients reported similar quality of life scores for multicatheter brachytherapy–based APBI and whole breast irradiation in the study by the Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO).
Moreover, breast symptom scores were significantly worse for whole-breast radiation, Rebekka Schäfer, MD, of the department of radiation oncology at the University Hospital Würzburg (Germany) and colleagues reported in Lancet Oncology.
“This trial provides further clinical evidence that APBI with interstitial brachytherapy can be considered as an alternative treatment option after breast-conserving surgery for patients with low-risk breast cancer,” Dr. Schäfer and coauthors wrote.
In several previous studies, APBI has been shown to have clinical outcomes equivalent to those of whole breast irradiation in terms of disease recurrence, survival, and treatment side effects, they added.
The quality of life findings in the present report come from long-term follow-up of a randomized, controlled, phase 3 trial conducted at 16 European centers. This study included 1,184 women with early breast cancer randomly who, after receiving breast-conserving surgery, were assigned either to APBI that used multicatheter brachytherapy or to whole breast irradiation.
Women in the study completed validated quality of life questionnaires right before and right after radiotherapy, as well as during follow-up.
A little more than half of the women in each group completed the quality of life questionnaires after the treatment and again at follow-up, investigators said.
Global health status was stable over time in both groups, investigators reported. In the APBI group, global health status score on a scale of 0-100 was 65.6 right after the procedure and 66.2 at 5 years; similarly, scores in the whole breast irradiation group were 64.6 after radiotherapy and 66.0 at 5 years.
The only quality of life difference between arms that investigators characterized as moderately clinically relevant was in breast symptom scores, which were significantly worse in the whole breast radiation group right after radiotherapy (difference of means, 13.6; 95% CI, 9.7-17.5; P less than .0001) and at 3-month follow-up (difference of means, 12.7; 95% CI, 9.8-15.6; P less than .0001).
Emotional functioning, fatigue, and financial difficulty scores in the APBI group were “slightly better” than in the whole breast radiation group right after radiotherapy and at a 3-month follow-up, investigators reported; however, at 5 year follow-up, there were no significant differences between arms in those measures.
“Our findings show that APBI using multicatheter interstitial brachytherapy does not result in clinically significant deterioration of overall quality of life and that the different domains of quality of life after APBI were not worse in comparison with whole breast irradiation in terms of clinically relevant differences,” Dr. Schäfer and colleagues concluded in their report.
Dr. Schäfer reported no conflicts of interest. Coauthors reported disclosures outside of the submitted work including Nucletron Operations BV, Elekta Company, Merck Serono, Novocure, AstraZeneca, and Bristol-Myers Squibb, among others.
SOURCE: Schäfer R et al. Lancet Oncol. 2018 Apr 22. doi: 10.1016/S1470-2045(18)30195-5.
This study by Schäfer and colleagues supports results of earlier and smaller studies showing promising quality of life results following accelerated partial breast irradiation (APBI) using multicatheter brachytherapy, according to Reshma Jagsi, MD.
“The results suggest that for quality of life, multicatheter brachytherapy-based APBI does not adversely affect outcomes, compared with whole breast irradiation,” Dr. Jagsi wrote in an editorial accompanying the article.
In previous trials, APBI using external radiation beam techniques has likewise shown favorable and promising quality of life outcomes.
There are now eagerly anticipated studies of APBI delivered primarily using external beam techniques that have included rigorous collection of quality of life outcomes, Dr. Jagsi added.
Those trials, which include RAPID and RTOG 0413/NSABP B39, will provide additional evidence to consider alongside those of the trial reported by Schäfer and colleagues on behalf of the Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO).
“Together with the results from the GEC-ESTRO trial, results from these trials will be meaningful to the many tens of thousands of women who undergo breast-conserving surgery and adjuvant radiotherapy each year,” Dr. Jagsi wrote.
Reshma Jagsi, MD, is with the department of radiation oncology at the University of Michigan, Ann Arbor. These comments are derived from editorial in Lancet Oncology . Dr. Jagsi reported receiving personal fees from Amgen.
This study by Schäfer and colleagues supports results of earlier and smaller studies showing promising quality of life results following accelerated partial breast irradiation (APBI) using multicatheter brachytherapy, according to Reshma Jagsi, MD.
“The results suggest that for quality of life, multicatheter brachytherapy-based APBI does not adversely affect outcomes, compared with whole breast irradiation,” Dr. Jagsi wrote in an editorial accompanying the article.
In previous trials, APBI using external radiation beam techniques has likewise shown favorable and promising quality of life outcomes.
There are now eagerly anticipated studies of APBI delivered primarily using external beam techniques that have included rigorous collection of quality of life outcomes, Dr. Jagsi added.
Those trials, which include RAPID and RTOG 0413/NSABP B39, will provide additional evidence to consider alongside those of the trial reported by Schäfer and colleagues on behalf of the Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO).
“Together with the results from the GEC-ESTRO trial, results from these trials will be meaningful to the many tens of thousands of women who undergo breast-conserving surgery and adjuvant radiotherapy each year,” Dr. Jagsi wrote.
Reshma Jagsi, MD, is with the department of radiation oncology at the University of Michigan, Ann Arbor. These comments are derived from editorial in Lancet Oncology . Dr. Jagsi reported receiving personal fees from Amgen.
This study by Schäfer and colleagues supports results of earlier and smaller studies showing promising quality of life results following accelerated partial breast irradiation (APBI) using multicatheter brachytherapy, according to Reshma Jagsi, MD.
“The results suggest that for quality of life, multicatheter brachytherapy-based APBI does not adversely affect outcomes, compared with whole breast irradiation,” Dr. Jagsi wrote in an editorial accompanying the article.
In previous trials, APBI using external radiation beam techniques has likewise shown favorable and promising quality of life outcomes.
There are now eagerly anticipated studies of APBI delivered primarily using external beam techniques that have included rigorous collection of quality of life outcomes, Dr. Jagsi added.
Those trials, which include RAPID and RTOG 0413/NSABP B39, will provide additional evidence to consider alongside those of the trial reported by Schäfer and colleagues on behalf of the Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO).
“Together with the results from the GEC-ESTRO trial, results from these trials will be meaningful to the many tens of thousands of women who undergo breast-conserving surgery and adjuvant radiotherapy each year,” Dr. Jagsi wrote.
Reshma Jagsi, MD, is with the department of radiation oncology at the University of Michigan, Ann Arbor. These comments are derived from editorial in Lancet Oncology . Dr. Jagsi reported receiving personal fees from Amgen.
In women with breast cancer undergoing breast-conserving surgery, accelerated partial breast irradiation (APBI) using multicatheter brachytherapy does not negatively affect quality of life, compared with standard whole breast irradiation, investigators have reported.
Patients reported similar quality of life scores for multicatheter brachytherapy–based APBI and whole breast irradiation in the study by the Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO).
Moreover, breast symptom scores were significantly worse for whole-breast radiation, Rebekka Schäfer, MD, of the department of radiation oncology at the University Hospital Würzburg (Germany) and colleagues reported in Lancet Oncology.
“This trial provides further clinical evidence that APBI with interstitial brachytherapy can be considered as an alternative treatment option after breast-conserving surgery for patients with low-risk breast cancer,” Dr. Schäfer and coauthors wrote.
In several previous studies, APBI has been shown to have clinical outcomes equivalent to those of whole breast irradiation in terms of disease recurrence, survival, and treatment side effects, they added.
The quality of life findings in the present report come from long-term follow-up of a randomized, controlled, phase 3 trial conducted at 16 European centers. This study included 1,184 women with early breast cancer randomly who, after receiving breast-conserving surgery, were assigned either to APBI that used multicatheter brachytherapy or to whole breast irradiation.
Women in the study completed validated quality of life questionnaires right before and right after radiotherapy, as well as during follow-up.
A little more than half of the women in each group completed the quality of life questionnaires after the treatment and again at follow-up, investigators said.
Global health status was stable over time in both groups, investigators reported. In the APBI group, global health status score on a scale of 0-100 was 65.6 right after the procedure and 66.2 at 5 years; similarly, scores in the whole breast irradiation group were 64.6 after radiotherapy and 66.0 at 5 years.
The only quality of life difference between arms that investigators characterized as moderately clinically relevant was in breast symptom scores, which were significantly worse in the whole breast radiation group right after radiotherapy (difference of means, 13.6; 95% CI, 9.7-17.5; P less than .0001) and at 3-month follow-up (difference of means, 12.7; 95% CI, 9.8-15.6; P less than .0001).
Emotional functioning, fatigue, and financial difficulty scores in the APBI group were “slightly better” than in the whole breast radiation group right after radiotherapy and at a 3-month follow-up, investigators reported; however, at 5 year follow-up, there were no significant differences between arms in those measures.
“Our findings show that APBI using multicatheter interstitial brachytherapy does not result in clinically significant deterioration of overall quality of life and that the different domains of quality of life after APBI were not worse in comparison with whole breast irradiation in terms of clinically relevant differences,” Dr. Schäfer and colleagues concluded in their report.
Dr. Schäfer reported no conflicts of interest. Coauthors reported disclosures outside of the submitted work including Nucletron Operations BV, Elekta Company, Merck Serono, Novocure, AstraZeneca, and Bristol-Myers Squibb, among others.
SOURCE: Schäfer R et al. Lancet Oncol. 2018 Apr 22. doi: 10.1016/S1470-2045(18)30195-5.
In women with breast cancer undergoing breast-conserving surgery, accelerated partial breast irradiation (APBI) using multicatheter brachytherapy does not negatively affect quality of life, compared with standard whole breast irradiation, investigators have reported.
Patients reported similar quality of life scores for multicatheter brachytherapy–based APBI and whole breast irradiation in the study by the Groupe Européen de Curiethérapie of European Society for Radiotherapy and Oncology (GEC-ESTRO).
Moreover, breast symptom scores were significantly worse for whole-breast radiation, Rebekka Schäfer, MD, of the department of radiation oncology at the University Hospital Würzburg (Germany) and colleagues reported in Lancet Oncology.
“This trial provides further clinical evidence that APBI with interstitial brachytherapy can be considered as an alternative treatment option after breast-conserving surgery for patients with low-risk breast cancer,” Dr. Schäfer and coauthors wrote.
In several previous studies, APBI has been shown to have clinical outcomes equivalent to those of whole breast irradiation in terms of disease recurrence, survival, and treatment side effects, they added.
The quality of life findings in the present report come from long-term follow-up of a randomized, controlled, phase 3 trial conducted at 16 European centers. This study included 1,184 women with early breast cancer randomly who, after receiving breast-conserving surgery, were assigned either to APBI that used multicatheter brachytherapy or to whole breast irradiation.
Women in the study completed validated quality of life questionnaires right before and right after radiotherapy, as well as during follow-up.
A little more than half of the women in each group completed the quality of life questionnaires after the treatment and again at follow-up, investigators said.
Global health status was stable over time in both groups, investigators reported. In the APBI group, global health status score on a scale of 0-100 was 65.6 right after the procedure and 66.2 at 5 years; similarly, scores in the whole breast irradiation group were 64.6 after radiotherapy and 66.0 at 5 years.
The only quality of life difference between arms that investigators characterized as moderately clinically relevant was in breast symptom scores, which were significantly worse in the whole breast radiation group right after radiotherapy (difference of means, 13.6; 95% CI, 9.7-17.5; P less than .0001) and at 3-month follow-up (difference of means, 12.7; 95% CI, 9.8-15.6; P less than .0001).
Emotional functioning, fatigue, and financial difficulty scores in the APBI group were “slightly better” than in the whole breast radiation group right after radiotherapy and at a 3-month follow-up, investigators reported; however, at 5 year follow-up, there were no significant differences between arms in those measures.
“Our findings show that APBI using multicatheter interstitial brachytherapy does not result in clinically significant deterioration of overall quality of life and that the different domains of quality of life after APBI were not worse in comparison with whole breast irradiation in terms of clinically relevant differences,” Dr. Schäfer and colleagues concluded in their report.
Dr. Schäfer reported no conflicts of interest. Coauthors reported disclosures outside of the submitted work including Nucletron Operations BV, Elekta Company, Merck Serono, Novocure, AstraZeneca, and Bristol-Myers Squibb, among others.
SOURCE: Schäfer R et al. Lancet Oncol. 2018 Apr 22. doi: 10.1016/S1470-2045(18)30195-5.
FROM LANCET ONCOLOGY
Key clinical point: Quality of life results support the use of accelerated partial breast irradiation (APBI) using multicatheter brachytherapy as an alternative to whole breast radiation after breast-conserving surgery.
Major finding: Patients reported similar quality of life scores for the two modalities, while breast symptom scores for whole breast radiation were significantly worse right after radiotherapy (difference of means, 13.6; 95% confidence interval, 9.7-17.5; P less than .0001) and at 3-month follow-up (difference of means, 12.7; 95% CI, 9.8-15.6; P less than .0001), compared with those for APBI.
Study details: 5-year quality of life results from a European phase 3 trial including 1,184 women with early breast cancer who, after undergoing breast-conserving surgery, received either whole breast irradiation or APBI using multicatheter brachytherapy.
Disclosures: Authors reported disclosures outside of the submitted work including Nucletron Operations BV, Elekta Company, Merck Serono, Novocure, AstraZeneca, and Bristol-Myers Squibb, among others.
Source: Schäfer R et al. Lancet Oncol. 2018 Apr 22. doi: 10.1016/S1470-2045(18)30195-5.
Stroke patients benefited from CPAP
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
the results of a randomized study suggest.
Obstructive sleep apnea is present in 50%-80% of patients with stroke, previous studies show, and its presence is associated with impaired function and cognition, delirium, and longer rehabilitation time, among other negative impacts, wrote Anupama Gupta, PhD, and her coauthors from the All India Institute of Medical Sciences, New Delhi, in the Journal of Clinical Sleep Medicine. Although multiple trials have shown a positive effect of CPAP on stroke recovery, relatively few investigations have looked specifically at whether the intervention prevents subsequent vascular events.
Patients’ clinical stroke outcomes were categorized in accordance with the Modified Rankin Scale (mRS), which is most widely used to assess disability and dependence outcomes among patients with stroke.
Significantly more patients who were treated with CPAP experienced an improvement in their mRS score by at least 1 point, when assessed at both 6 and 12 months following entrance into the study. Specifically, 53% (16) of patients in the CPAP group had an improvement of at least 1 point in their mRS score at 12 months, compared with 27% (11) of patients who did not use CPAP (P = .03).
“These differences are statistically significant, as well as clinically meaningful and relevant,” Dr. Gupta and her colleagues said in their report.
This finding was consistent with what researchers have seen in some earlier studies of stroke patients who used CPAP, the researchers wrote.
Additionally, CPAP-treated patients had fewer subsequent vascular events, compared with those who did not use CPAP, though the difference did not reach statistical significance. There was only one new vascular event (3.33%) in the CPAP group at 12-month follow-up, versus six events (15%) in the non-CPAP group (P = .23).
Nevertheless, the results provide more evidence for the potential benefit of CPAP in stroke patients with obstructive sleep apnea, the researchers noted.
“Our results indicate that new vascular events may be better prevented – and significantly more patients may make good stroke recovery – with CPAP treatment as compared to only best medical treatment,” Dr. Gupta and her colleagues wrote.
Before the study started, investigators determined that they would have needed 80 patients per arm for a power of 80%. A total of 679 patients were screened, but only 116 reported for polysomnography testing, and of those, 83 had at least moderate obstructive sleep apnea.
Due to a lack of CPAP devices, only 70 of those 83 patients made it all the way to randomization, investigators reported.
Dr. Gupta and her coauthors reported no conflicts of interest related to the study.
SOURCE: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
FROM THE JOURNAL OF CLINICAL SLEEP MEDICINE
Key clinical point: Continuous positive airway pressure (CPAP) treatment may prevent vascular events in patients with stroke who have OSA.
Major finding: There was one vascular event (3.33%) at 12 months for CPAP-treated patients, versus six events (15%) in non-CPAP patients, though the difference was not significant (P = .23).
Study details: A single-blind, randomized, controlled trial including 70 patients with imaging-confirmed first arterial stroke and OSA.
Disclosures: The authors reported no conflicts of interest related to the study.
Source: Gupta A et al. J Clin Sleep Med. 2018 Mar 30. pii:jc-17-00230.
CVD risk high in individuals who once had metabolically healthy obesity
Nearly half of the individuals with MHO developed metabolic syndrome over time, according to the analysis of 6,809 participants followed since the year 2000 in the Multi-Ethnic Study of Atherosclerosis.
Those who developed metabolic syndrome had an increased risk of CVD, compared with those who did not, according to results published in the Journal of the American College of Cardiology.
The results provide new evidence that MHO alone is not a stable or reliable characterization of lower CVD risk, according to Morgana Mongraw-Chaffin, PhD, of the department of epidemiology and prevention at Wake Forest University, Winston-Salem, N.C., and her coauthors.
“Instead, MHO signals an opportunity for weight reduction, and prevention and management of existing metabolic syndrome components should be prioritized,” Dr. Mongraw-Chaffin and her colleagues wrote.
Individuals with MHO, defined in this study as a body mass index of 30 kg/m2 or greater without metabolic syndrome, have a relatively favorable metabolic profile. However, their precise level of CVD risk remains contentious, the investigators noted.
“Although the accumulating evidence is leaning toward the consensus that MHO is not a low-risk state compared with metabolically healthy normal weight, many questions remain about the risk stratification for this group and what causes the heterogeneity seen in the literature,” they wrote.
In this study, 501 out of 1,051 individuals with MHO at baseline (48%) developed metabolic syndrome over a median follow-up of 12.2 years. Moreover, they then had increased odds of CVD (odds ratio, 1.60; 95% confidence interval, 1.14-2.25), compared with individuals who had stable MHO or normal weight.
Duration of metabolic syndrome was linearly associated with CVD risk, with an odds ratio of 0.41 for those with metabolic syndrome at one out of five study visits, 2.19 for metabolic syndrome at two or three visits, and 2.50 for metabolic syndrome at four or five visits, the researchers said.
The results of this study may explain why some previous meta-analyses found individuals with MHO had increased risk, but only with longer duration of follow-up.
“Both transition to metabolic syndrome and longer duration of metabolic syndrome were associated with CVD, indicating that those with MHO may experience a lag in risk while they progress to metabolic syndrome and develop the resultant cardiometabolic risk,” Dr. Mongraw-Chaffin and her coauthors wrote.
The results mean that MHO represents an opportunity for primary prevention of CVD, they added.
“Prevention of incident metabolic syndrome and resulting CVD at the population level will necessitate the prevention of obesity,” they explained in a discussion of the results.
Dr. Mongraw-Chaffin and her associates reported that they had no relevant relationships to disclose.
SOURCE: Mongraw-Chaffin M et al. J Am Coll Cardiol 2018 May 1;71(17):1857-65.
While obesity has inherent adverse effects on cardiometabolic parameters and cardiovascular disease (CVD) risk factors, metabolically healthy obesity (MHO) has emerged as a categorization of obese individuals who may not be at increased CVD risk because of relatively normal levels of lipids, blood pressure, and glucose.
An increasing body of research, however, including the present study by Dr. Mongraw-Chaffin and colleagues, highlights “dangers and long-term outcomes” of the MHO phenotype, Dr. Prakash Deedwania and Dr. Carl J. Lavie wrote in an editorial.
The analysis of 6,809 individuals in the Multi-Ethic Study of Atherosclerosis found that MHO is not a stable condition, as almost one-half of individuals developed metabolic syndrome over 12.2 years of follow-up, they noted.
Moreover, CVD risk was indeed elevated in these individuals with “unstable” MHO.
“Clearly, therefore, prevention of obesity in the first place is most prudent,” Dr. Deedwania and Dr. Lavie said in their editorial. “Prevention of progressive weight gain over time among the overweight and mildly obese is also of high importance to prevent development of metabolic syndrome and subsequent risk of CVD.”
If individuals with MHO can be identified early, the authors said, there is an excellent opportunity for primary prevention through lifestyle changes, including weight loss and regular physical exercise that might prevent MHO from converting to metabolically unhealthy obesity.
“Such population-wide healthy interventions are the only hope of preventing the oncoming tsunami of metabolic syndrome, diabetes, and CVD,” the editorial authors concluded.
Prakash Deedwania, MD, is with the University of California at San Francisco School of Medicine Program at Fresno. Carl J. Lavie, MD, is with the John Ochsner Heart and Vascular Institute, New Orleans, and the University of Queensland in Brisbane, Australia. These comments are derived from their editorial in the Journal of the American College of Cardiology ( 2018 May 1;71[17]:1866-8) . Both authors reported they had no relevant relationships to disclose.
While obesity has inherent adverse effects on cardiometabolic parameters and cardiovascular disease (CVD) risk factors, metabolically healthy obesity (MHO) has emerged as a categorization of obese individuals who may not be at increased CVD risk because of relatively normal levels of lipids, blood pressure, and glucose.
An increasing body of research, however, including the present study by Dr. Mongraw-Chaffin and colleagues, highlights “dangers and long-term outcomes” of the MHO phenotype, Dr. Prakash Deedwania and Dr. Carl J. Lavie wrote in an editorial.
The analysis of 6,809 individuals in the Multi-Ethic Study of Atherosclerosis found that MHO is not a stable condition, as almost one-half of individuals developed metabolic syndrome over 12.2 years of follow-up, they noted.
Moreover, CVD risk was indeed elevated in these individuals with “unstable” MHO.
“Clearly, therefore, prevention of obesity in the first place is most prudent,” Dr. Deedwania and Dr. Lavie said in their editorial. “Prevention of progressive weight gain over time among the overweight and mildly obese is also of high importance to prevent development of metabolic syndrome and subsequent risk of CVD.”
If individuals with MHO can be identified early, the authors said, there is an excellent opportunity for primary prevention through lifestyle changes, including weight loss and regular physical exercise that might prevent MHO from converting to metabolically unhealthy obesity.
“Such population-wide healthy interventions are the only hope of preventing the oncoming tsunami of metabolic syndrome, diabetes, and CVD,” the editorial authors concluded.
Prakash Deedwania, MD, is with the University of California at San Francisco School of Medicine Program at Fresno. Carl J. Lavie, MD, is with the John Ochsner Heart and Vascular Institute, New Orleans, and the University of Queensland in Brisbane, Australia. These comments are derived from their editorial in the Journal of the American College of Cardiology ( 2018 May 1;71[17]:1866-8) . Both authors reported they had no relevant relationships to disclose.
While obesity has inherent adverse effects on cardiometabolic parameters and cardiovascular disease (CVD) risk factors, metabolically healthy obesity (MHO) has emerged as a categorization of obese individuals who may not be at increased CVD risk because of relatively normal levels of lipids, blood pressure, and glucose.
An increasing body of research, however, including the present study by Dr. Mongraw-Chaffin and colleagues, highlights “dangers and long-term outcomes” of the MHO phenotype, Dr. Prakash Deedwania and Dr. Carl J. Lavie wrote in an editorial.
The analysis of 6,809 individuals in the Multi-Ethic Study of Atherosclerosis found that MHO is not a stable condition, as almost one-half of individuals developed metabolic syndrome over 12.2 years of follow-up, they noted.
Moreover, CVD risk was indeed elevated in these individuals with “unstable” MHO.
“Clearly, therefore, prevention of obesity in the first place is most prudent,” Dr. Deedwania and Dr. Lavie said in their editorial. “Prevention of progressive weight gain over time among the overweight and mildly obese is also of high importance to prevent development of metabolic syndrome and subsequent risk of CVD.”
If individuals with MHO can be identified early, the authors said, there is an excellent opportunity for primary prevention through lifestyle changes, including weight loss and regular physical exercise that might prevent MHO from converting to metabolically unhealthy obesity.
“Such population-wide healthy interventions are the only hope of preventing the oncoming tsunami of metabolic syndrome, diabetes, and CVD,” the editorial authors concluded.
Prakash Deedwania, MD, is with the University of California at San Francisco School of Medicine Program at Fresno. Carl J. Lavie, MD, is with the John Ochsner Heart and Vascular Institute, New Orleans, and the University of Queensland in Brisbane, Australia. These comments are derived from their editorial in the Journal of the American College of Cardiology ( 2018 May 1;71[17]:1866-8) . Both authors reported they had no relevant relationships to disclose.
Nearly half of the individuals with MHO developed metabolic syndrome over time, according to the analysis of 6,809 participants followed since the year 2000 in the Multi-Ethnic Study of Atherosclerosis.
Those who developed metabolic syndrome had an increased risk of CVD, compared with those who did not, according to results published in the Journal of the American College of Cardiology.
The results provide new evidence that MHO alone is not a stable or reliable characterization of lower CVD risk, according to Morgana Mongraw-Chaffin, PhD, of the department of epidemiology and prevention at Wake Forest University, Winston-Salem, N.C., and her coauthors.
“Instead, MHO signals an opportunity for weight reduction, and prevention and management of existing metabolic syndrome components should be prioritized,” Dr. Mongraw-Chaffin and her colleagues wrote.
Individuals with MHO, defined in this study as a body mass index of 30 kg/m2 or greater without metabolic syndrome, have a relatively favorable metabolic profile. However, their precise level of CVD risk remains contentious, the investigators noted.
“Although the accumulating evidence is leaning toward the consensus that MHO is not a low-risk state compared with metabolically healthy normal weight, many questions remain about the risk stratification for this group and what causes the heterogeneity seen in the literature,” they wrote.
In this study, 501 out of 1,051 individuals with MHO at baseline (48%) developed metabolic syndrome over a median follow-up of 12.2 years. Moreover, they then had increased odds of CVD (odds ratio, 1.60; 95% confidence interval, 1.14-2.25), compared with individuals who had stable MHO or normal weight.
Duration of metabolic syndrome was linearly associated with CVD risk, with an odds ratio of 0.41 for those with metabolic syndrome at one out of five study visits, 2.19 for metabolic syndrome at two or three visits, and 2.50 for metabolic syndrome at four or five visits, the researchers said.
The results of this study may explain why some previous meta-analyses found individuals with MHO had increased risk, but only with longer duration of follow-up.
“Both transition to metabolic syndrome and longer duration of metabolic syndrome were associated with CVD, indicating that those with MHO may experience a lag in risk while they progress to metabolic syndrome and develop the resultant cardiometabolic risk,” Dr. Mongraw-Chaffin and her coauthors wrote.
The results mean that MHO represents an opportunity for primary prevention of CVD, they added.
“Prevention of incident metabolic syndrome and resulting CVD at the population level will necessitate the prevention of obesity,” they explained in a discussion of the results.
Dr. Mongraw-Chaffin and her associates reported that they had no relevant relationships to disclose.
SOURCE: Mongraw-Chaffin M et al. J Am Coll Cardiol 2018 May 1;71(17):1857-65.
Nearly half of the individuals with MHO developed metabolic syndrome over time, according to the analysis of 6,809 participants followed since the year 2000 in the Multi-Ethnic Study of Atherosclerosis.
Those who developed metabolic syndrome had an increased risk of CVD, compared with those who did not, according to results published in the Journal of the American College of Cardiology.
The results provide new evidence that MHO alone is not a stable or reliable characterization of lower CVD risk, according to Morgana Mongraw-Chaffin, PhD, of the department of epidemiology and prevention at Wake Forest University, Winston-Salem, N.C., and her coauthors.
“Instead, MHO signals an opportunity for weight reduction, and prevention and management of existing metabolic syndrome components should be prioritized,” Dr. Mongraw-Chaffin and her colleagues wrote.
Individuals with MHO, defined in this study as a body mass index of 30 kg/m2 or greater without metabolic syndrome, have a relatively favorable metabolic profile. However, their precise level of CVD risk remains contentious, the investigators noted.
“Although the accumulating evidence is leaning toward the consensus that MHO is not a low-risk state compared with metabolically healthy normal weight, many questions remain about the risk stratification for this group and what causes the heterogeneity seen in the literature,” they wrote.
In this study, 501 out of 1,051 individuals with MHO at baseline (48%) developed metabolic syndrome over a median follow-up of 12.2 years. Moreover, they then had increased odds of CVD (odds ratio, 1.60; 95% confidence interval, 1.14-2.25), compared with individuals who had stable MHO or normal weight.
Duration of metabolic syndrome was linearly associated with CVD risk, with an odds ratio of 0.41 for those with metabolic syndrome at one out of five study visits, 2.19 for metabolic syndrome at two or three visits, and 2.50 for metabolic syndrome at four or five visits, the researchers said.
The results of this study may explain why some previous meta-analyses found individuals with MHO had increased risk, but only with longer duration of follow-up.
“Both transition to metabolic syndrome and longer duration of metabolic syndrome were associated with CVD, indicating that those with MHO may experience a lag in risk while they progress to metabolic syndrome and develop the resultant cardiometabolic risk,” Dr. Mongraw-Chaffin and her coauthors wrote.
The results mean that MHO represents an opportunity for primary prevention of CVD, they added.
“Prevention of incident metabolic syndrome and resulting CVD at the population level will necessitate the prevention of obesity,” they explained in a discussion of the results.
Dr. Mongraw-Chaffin and her associates reported that they had no relevant relationships to disclose.
SOURCE: Mongraw-Chaffin M et al. J Am Coll Cardiol 2018 May 1;71(17):1857-65.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: Metabolically healthy obesity (MHO) was transient and was not a reliable indicator of future risk of cardiovascular disease risk, prompting investigators to recommend weight loss and lifestyle management for any individual with obesity.
Major finding: Nearly half of patients with MHO developed metabolic syndrome over a median follow-up of 12.2 years. They had increased risk of cardiovascular disease, compared with individuals who had stable MHO or normal weight (odds ratio, 1.60, 95% CI, 1.14-2.25).
Study details: Analysis based on data for 6,809 participants in the Multi-Ethnic Study of Atherosclerosis (MESA), a six-center U.S. population-based longitudinal cohort study started in 2000.
Disclosures: The authors reported they had no relevant relationships to disclose.
Source: Mongraw-Chaffin M et al. J Am Coll Cardiol. 2018 May 1;71(17):1857-65.
Meta-analysis finds no link between stroke and sickle cell trait
Those findings contrast with an earlier longitudinal study that found a 1.4-fold risk of ischemic stroke in SCT carriers, the authors noted.
In their study, neither crude stroke incidence rates nor regression analysis indicated a link between SCT and stroke, said first author Hyacinth I. Hyacinth, MD, PhD, MPH, of the Aflac Cancer and Blood Disorder Center, Emory University, Atlanta, and his coauthors.
“The absence of an association between SCT and risk of ischemic stroke was consistent among the cohorts, and suggests that SCT is not an independent genetic risk factor for ischemic stroke among African Americans,” Dr. Hyacinth and his coauthors wrote.
The results may have implications for patient care. In particular, a more thorough evaluation of stroke in a patient with SCT may be warranted, instead of assuming that the SCT is an underlying cause of the stroke, they said.
The meta-analysis included a total of 19,464 subjects from four large, prospective, population-based studies with African American cohorts.
Results of the meta-analysis show that crude incidence of stroke was similar for individuals with SCT, at 2.9 per 1,000 person-years (95% confidence interval, 2.2-4.0), and for those with no SCT, at 3.2 per 1,000 person-years (95% CI, 2.7-3.8).
After adjusting for stroke risk factors, the hazard ratio of stroke independently associated with SCT was 0.80 (95% CI, 0.47-1.35; P = 0.82), results further show.
It’s unclear why this study found no association between SCT and stroke when the earlier population-based study suggested a link between the two. Dr. Hyacinth and his coauthors suggested differences in study methods or proportion of individuals at risk for stroke may account for the divergent findings. They also controlled for left ventricular hypertrophy, while the previous study did not.
“However, in our analysis, adjusting for left ventricular hypertrophy did not change the direction of estimate effects,” they said in the report.
Further study is needed to determine whether or not SCT may be linked to a particular type of stroke. “We were unable to test the association of SCT with ischemic stroke subtypes,” the authors noted.
Dr. Hyacinth and his coauthors reported no conflicts of interest related to the study.
SOURCE: Hyacinth HI et al. JAMA Neurol. 2018 Apr 23. doi:10.1001/jamaneurol.2018.0571
Those findings contrast with an earlier longitudinal study that found a 1.4-fold risk of ischemic stroke in SCT carriers, the authors noted.
In their study, neither crude stroke incidence rates nor regression analysis indicated a link between SCT and stroke, said first author Hyacinth I. Hyacinth, MD, PhD, MPH, of the Aflac Cancer and Blood Disorder Center, Emory University, Atlanta, and his coauthors.
“The absence of an association between SCT and risk of ischemic stroke was consistent among the cohorts, and suggests that SCT is not an independent genetic risk factor for ischemic stroke among African Americans,” Dr. Hyacinth and his coauthors wrote.
The results may have implications for patient care. In particular, a more thorough evaluation of stroke in a patient with SCT may be warranted, instead of assuming that the SCT is an underlying cause of the stroke, they said.
The meta-analysis included a total of 19,464 subjects from four large, prospective, population-based studies with African American cohorts.
Results of the meta-analysis show that crude incidence of stroke was similar for individuals with SCT, at 2.9 per 1,000 person-years (95% confidence interval, 2.2-4.0), and for those with no SCT, at 3.2 per 1,000 person-years (95% CI, 2.7-3.8).
After adjusting for stroke risk factors, the hazard ratio of stroke independently associated with SCT was 0.80 (95% CI, 0.47-1.35; P = 0.82), results further show.
It’s unclear why this study found no association between SCT and stroke when the earlier population-based study suggested a link between the two. Dr. Hyacinth and his coauthors suggested differences in study methods or proportion of individuals at risk for stroke may account for the divergent findings. They also controlled for left ventricular hypertrophy, while the previous study did not.
“However, in our analysis, adjusting for left ventricular hypertrophy did not change the direction of estimate effects,” they said in the report.
Further study is needed to determine whether or not SCT may be linked to a particular type of stroke. “We were unable to test the association of SCT with ischemic stroke subtypes,” the authors noted.
Dr. Hyacinth and his coauthors reported no conflicts of interest related to the study.
SOURCE: Hyacinth HI et al. JAMA Neurol. 2018 Apr 23. doi:10.1001/jamaneurol.2018.0571
Those findings contrast with an earlier longitudinal study that found a 1.4-fold risk of ischemic stroke in SCT carriers, the authors noted.
In their study, neither crude stroke incidence rates nor regression analysis indicated a link between SCT and stroke, said first author Hyacinth I. Hyacinth, MD, PhD, MPH, of the Aflac Cancer and Blood Disorder Center, Emory University, Atlanta, and his coauthors.
“The absence of an association between SCT and risk of ischemic stroke was consistent among the cohorts, and suggests that SCT is not an independent genetic risk factor for ischemic stroke among African Americans,” Dr. Hyacinth and his coauthors wrote.
The results may have implications for patient care. In particular, a more thorough evaluation of stroke in a patient with SCT may be warranted, instead of assuming that the SCT is an underlying cause of the stroke, they said.
The meta-analysis included a total of 19,464 subjects from four large, prospective, population-based studies with African American cohorts.
Results of the meta-analysis show that crude incidence of stroke was similar for individuals with SCT, at 2.9 per 1,000 person-years (95% confidence interval, 2.2-4.0), and for those with no SCT, at 3.2 per 1,000 person-years (95% CI, 2.7-3.8).
After adjusting for stroke risk factors, the hazard ratio of stroke independently associated with SCT was 0.80 (95% CI, 0.47-1.35; P = 0.82), results further show.
It’s unclear why this study found no association between SCT and stroke when the earlier population-based study suggested a link between the two. Dr. Hyacinth and his coauthors suggested differences in study methods or proportion of individuals at risk for stroke may account for the divergent findings. They also controlled for left ventricular hypertrophy, while the previous study did not.
“However, in our analysis, adjusting for left ventricular hypertrophy did not change the direction of estimate effects,” they said in the report.
Further study is needed to determine whether or not SCT may be linked to a particular type of stroke. “We were unable to test the association of SCT with ischemic stroke subtypes,” the authors noted.
Dr. Hyacinth and his coauthors reported no conflicts of interest related to the study.
SOURCE: Hyacinth HI et al. JAMA Neurol. 2018 Apr 23. doi:10.1001/jamaneurol.2018.0571
FROM JAMA NEUROLOGY
Key clinical point: In contrast to results of a previous study, a meta-analysis has found no evidence linking sickle cell trait (SCT) and risk of incident ischemic stroke in African Americans.
Major finding: Crude stroke incidence was not different for SCT versus no SCT. After adjusting for stroke risk factors, the hazard ratio of stroke independently associated with SCT was 0.80 (95% CI, 0.47-1.35; P = .82).
Study details: A meta-analysis of the association between SCT and risk of incident ischemic stroke in four large prospective, population-based studies with African American cohorts (19,464 total subjects).
Disclosures: Authors reported no conflicts of interest related to the study.
Source: Hyacinth HI et al. JAMA Neurol. 2018 Apr 23. doi: 10.1001/jamaneurol.2018.0571.
Artificial pancreas treatment improves glycemic control in T1DM: Meta-analysis
Use of artificial pancreas devices added nearly 2.5 hours of time in near normoglycemia over 24 hours in patients with type 1 diabetes, a meta-analysis of randomized clinical trials showed.
The improvement versus control subjects was primarily because of the favorable effect of the closed loop glucose control systems in the overnight period, authors of the meta-analysis reported in the BMJ.
Both single and dual hormone systems had robust results in the meta-anaysis, said lead researcher Eleni Bekiari, MD, PhD, of Aristotle University of Thessaloniki, Greece, and her coinvestigators.
Results were likewise robust for an analysis restricted to trials conducted under normal living conditions and no remote monitoring, supporting the convenience and ease of use of these systems, according to Dr. Bekiari and her colleagues.
“Overall, our results reflect the progress made over recent decades of extensive research and development in artificial pancreas use,” they wrote.
Despite the findings, more research needs to be done, they added, since the individual clinical trials supporting use of closed-loop systems in type 1 diabetes have included relatively few patients and have had short follow-up durations.
The systematic review and meta-analysis by Dr. Bekiari and her colleagues was based on 40 randomized controlled trials involving a total of 1,027 participants. The primary outcome of the analysis was proportion of time that sensor glucose level was in the normoglycemic range of 3.9-10 mmol/L.
Overall, use of the systems was associated with 140 additional minutes in near normoglycemia over 24 hours, with a 9.62% mean weighted difference (95% confidence interval, 7.54%-11.7%), reported data show.
The favorable effect was even more evident on overnight measures, the investigators said, with a weighted mean difference of 15.15% (95% CI, 12.21%-18.09%).
Results were similar even when the analysis was limited to studies that had a low risk of bias, and also when the analysis was limited to studies of unsupervised patients in normal living conditions, according to Dr. Bekiari and her associates.
Artificial pancreas use also had favorable impacts on time in hyperglycemia over the entire day. Compared with controls, time with glucose concentrations less than 10 mmol/L were shortened by about 2 hours, the investigators said.
Likewise, mean levels of sensor blood glucose over 24 hours fell by 0.48 mmol/L compared with control treatment (95% CI, 0.3-0.66 mmol/L), they reported.
Taken together, these findings suggest artificial pancreas systems are efficacious and safe for patients with type 1 diabetes, the investigators concluded.
“Further research with rigorous studies, cooperation of research groups in terms of outcome reporting, and cost-effectiveness data are required to verify these findings and support adoption of artificial pancreas systems in clinical practice,” they wrote.
Dr. Bekiari reported no disclosures. Her coauthors reported disclosures related to Medtronic, Novo Nordisk, Sanofi, AstraZeneca, Boehringer Ingelheim and others outside of the submitted work.
SOURCE: Bekiai E et al. BMJ 2018;361:k1310.
Closed-loop glucose control systems have much to offer patients, but better evidence will likely be needed to convince policy makers who have increasing demands and scarce resources, Dr. Norman Waugh and his coauthors said in an editorial.
Users of closed-loop systems did spend approximately 10% more time near normoglycemia when compared with control subjects in the present systematic review and meta-analysis of randomized clinical trials by Dr. Bekiari and colleagues.
The overall base of evidence is weak, however, and many studies in the review were low quality, according to Dr. Waugh and his coauthors. Moreover, the trials were short, with the majority lasting 7 days or less, they noted.
The current review does demonstrate that closed-loop systems improve control overnight and reduce the burden of self-management during the day, but it’s unknown if the systems can reduce long-term diabetes complications, according to the editorial authors, and evidence to date is insufficient for policy makers to perform cost-effectiveness analyses.
“We need longer and larger trials, in both adults and children, to compare closed-loop systems with self-management using continuous glucose monitoring,” Dr. Waugh and his colleagues wrote. “These trials should measure HbA1c for modeling the effects on complications, blood glucose variability, hypoglycemia, quality of life, and cost effectiveness.”
Norman Waugh is professor of public health medicine and health technology assessment at the University of Warwick, England. These comments are derived from an editorial by Dr. Waugh and his coauthors BMJ. 2018;361:k1613. doi: 10.1136/bmj.k1613 . They reported advising Roche and Novo Nordisk on matters not related to the topic of this editorial.
Closed-loop glucose control systems have much to offer patients, but better evidence will likely be needed to convince policy makers who have increasing demands and scarce resources, Dr. Norman Waugh and his coauthors said in an editorial.
Users of closed-loop systems did spend approximately 10% more time near normoglycemia when compared with control subjects in the present systematic review and meta-analysis of randomized clinical trials by Dr. Bekiari and colleagues.
The overall base of evidence is weak, however, and many studies in the review were low quality, according to Dr. Waugh and his coauthors. Moreover, the trials were short, with the majority lasting 7 days or less, they noted.
The current review does demonstrate that closed-loop systems improve control overnight and reduce the burden of self-management during the day, but it’s unknown if the systems can reduce long-term diabetes complications, according to the editorial authors, and evidence to date is insufficient for policy makers to perform cost-effectiveness analyses.
“We need longer and larger trials, in both adults and children, to compare closed-loop systems with self-management using continuous glucose monitoring,” Dr. Waugh and his colleagues wrote. “These trials should measure HbA1c for modeling the effects on complications, blood glucose variability, hypoglycemia, quality of life, and cost effectiveness.”
Norman Waugh is professor of public health medicine and health technology assessment at the University of Warwick, England. These comments are derived from an editorial by Dr. Waugh and his coauthors BMJ. 2018;361:k1613. doi: 10.1136/bmj.k1613 . They reported advising Roche and Novo Nordisk on matters not related to the topic of this editorial.
Closed-loop glucose control systems have much to offer patients, but better evidence will likely be needed to convince policy makers who have increasing demands and scarce resources, Dr. Norman Waugh and his coauthors said in an editorial.
Users of closed-loop systems did spend approximately 10% more time near normoglycemia when compared with control subjects in the present systematic review and meta-analysis of randomized clinical trials by Dr. Bekiari and colleagues.
The overall base of evidence is weak, however, and many studies in the review were low quality, according to Dr. Waugh and his coauthors. Moreover, the trials were short, with the majority lasting 7 days or less, they noted.
The current review does demonstrate that closed-loop systems improve control overnight and reduce the burden of self-management during the day, but it’s unknown if the systems can reduce long-term diabetes complications, according to the editorial authors, and evidence to date is insufficient for policy makers to perform cost-effectiveness analyses.
“We need longer and larger trials, in both adults and children, to compare closed-loop systems with self-management using continuous glucose monitoring,” Dr. Waugh and his colleagues wrote. “These trials should measure HbA1c for modeling the effects on complications, blood glucose variability, hypoglycemia, quality of life, and cost effectiveness.”
Norman Waugh is professor of public health medicine and health technology assessment at the University of Warwick, England. These comments are derived from an editorial by Dr. Waugh and his coauthors BMJ. 2018;361:k1613. doi: 10.1136/bmj.k1613 . They reported advising Roche and Novo Nordisk on matters not related to the topic of this editorial.
Use of artificial pancreas devices added nearly 2.5 hours of time in near normoglycemia over 24 hours in patients with type 1 diabetes, a meta-analysis of randomized clinical trials showed.
The improvement versus control subjects was primarily because of the favorable effect of the closed loop glucose control systems in the overnight period, authors of the meta-analysis reported in the BMJ.
Both single and dual hormone systems had robust results in the meta-anaysis, said lead researcher Eleni Bekiari, MD, PhD, of Aristotle University of Thessaloniki, Greece, and her coinvestigators.
Results were likewise robust for an analysis restricted to trials conducted under normal living conditions and no remote monitoring, supporting the convenience and ease of use of these systems, according to Dr. Bekiari and her colleagues.
“Overall, our results reflect the progress made over recent decades of extensive research and development in artificial pancreas use,” they wrote.
Despite the findings, more research needs to be done, they added, since the individual clinical trials supporting use of closed-loop systems in type 1 diabetes have included relatively few patients and have had short follow-up durations.
The systematic review and meta-analysis by Dr. Bekiari and her colleagues was based on 40 randomized controlled trials involving a total of 1,027 participants. The primary outcome of the analysis was proportion of time that sensor glucose level was in the normoglycemic range of 3.9-10 mmol/L.
Overall, use of the systems was associated with 140 additional minutes in near normoglycemia over 24 hours, with a 9.62% mean weighted difference (95% confidence interval, 7.54%-11.7%), reported data show.
The favorable effect was even more evident on overnight measures, the investigators said, with a weighted mean difference of 15.15% (95% CI, 12.21%-18.09%).
Results were similar even when the analysis was limited to studies that had a low risk of bias, and also when the analysis was limited to studies of unsupervised patients in normal living conditions, according to Dr. Bekiari and her associates.
Artificial pancreas use also had favorable impacts on time in hyperglycemia over the entire day. Compared with controls, time with glucose concentrations less than 10 mmol/L were shortened by about 2 hours, the investigators said.
Likewise, mean levels of sensor blood glucose over 24 hours fell by 0.48 mmol/L compared with control treatment (95% CI, 0.3-0.66 mmol/L), they reported.
Taken together, these findings suggest artificial pancreas systems are efficacious and safe for patients with type 1 diabetes, the investigators concluded.
“Further research with rigorous studies, cooperation of research groups in terms of outcome reporting, and cost-effectiveness data are required to verify these findings and support adoption of artificial pancreas systems in clinical practice,” they wrote.
Dr. Bekiari reported no disclosures. Her coauthors reported disclosures related to Medtronic, Novo Nordisk, Sanofi, AstraZeneca, Boehringer Ingelheim and others outside of the submitted work.
SOURCE: Bekiai E et al. BMJ 2018;361:k1310.
Use of artificial pancreas devices added nearly 2.5 hours of time in near normoglycemia over 24 hours in patients with type 1 diabetes, a meta-analysis of randomized clinical trials showed.
The improvement versus control subjects was primarily because of the favorable effect of the closed loop glucose control systems in the overnight period, authors of the meta-analysis reported in the BMJ.
Both single and dual hormone systems had robust results in the meta-anaysis, said lead researcher Eleni Bekiari, MD, PhD, of Aristotle University of Thessaloniki, Greece, and her coinvestigators.
Results were likewise robust for an analysis restricted to trials conducted under normal living conditions and no remote monitoring, supporting the convenience and ease of use of these systems, according to Dr. Bekiari and her colleagues.
“Overall, our results reflect the progress made over recent decades of extensive research and development in artificial pancreas use,” they wrote.
Despite the findings, more research needs to be done, they added, since the individual clinical trials supporting use of closed-loop systems in type 1 diabetes have included relatively few patients and have had short follow-up durations.
The systematic review and meta-analysis by Dr. Bekiari and her colleagues was based on 40 randomized controlled trials involving a total of 1,027 participants. The primary outcome of the analysis was proportion of time that sensor glucose level was in the normoglycemic range of 3.9-10 mmol/L.
Overall, use of the systems was associated with 140 additional minutes in near normoglycemia over 24 hours, with a 9.62% mean weighted difference (95% confidence interval, 7.54%-11.7%), reported data show.
The favorable effect was even more evident on overnight measures, the investigators said, with a weighted mean difference of 15.15% (95% CI, 12.21%-18.09%).
Results were similar even when the analysis was limited to studies that had a low risk of bias, and also when the analysis was limited to studies of unsupervised patients in normal living conditions, according to Dr. Bekiari and her associates.
Artificial pancreas use also had favorable impacts on time in hyperglycemia over the entire day. Compared with controls, time with glucose concentrations less than 10 mmol/L were shortened by about 2 hours, the investigators said.
Likewise, mean levels of sensor blood glucose over 24 hours fell by 0.48 mmol/L compared with control treatment (95% CI, 0.3-0.66 mmol/L), they reported.
Taken together, these findings suggest artificial pancreas systems are efficacious and safe for patients with type 1 diabetes, the investigators concluded.
“Further research with rigorous studies, cooperation of research groups in terms of outcome reporting, and cost-effectiveness data are required to verify these findings and support adoption of artificial pancreas systems in clinical practice,” they wrote.
Dr. Bekiari reported no disclosures. Her coauthors reported disclosures related to Medtronic, Novo Nordisk, Sanofi, AstraZeneca, Boehringer Ingelheim and others outside of the submitted work.
SOURCE: Bekiai E et al. BMJ 2018;361:k1310.
FROM THE BMJ
Key clinical point: In patients with type 1 diabetes, artificial pancreas systems were effective in increasing the amount of time patients spent in the near normoglycemic range.
Major finding: The proportion of time in the near-normoglycemic range was significantly higher both overnight (15.15% mean weighted difference) and over 24 hours (9.62% mean weighted difference) for artificial pancreas versus controls.
Study details: A systematic review and meta-analysis of 40 randomized controlled trials including 1,027 participants.
Disclosures: Authors reported disclosures related to Medtronic, Novo Nordisk, Sanofi, AstraZeneca, Boehringer Ingelheim, and others outside of the submitted work.
Source: Bekiari E et al. BMJ 2018;361:k1310.
24-hour ambulatory BP measurements strongly predict mortality
Ambulatory measurements of blood pressure more strongly predicted all-cause and cardiovascular mortality than did BP measured in the clinic, according to analysis of a large patient registry in Spain.
The results also showed an increased risk of death associated with white coat hypertension and an even stronger association between death and masked hypertension. They were published in the New England Journal of Medicine.
Previous investigations had found that 24-hour ambulatory BP measurements were better predictors of patient outcomes than those obtained in the clinic or at home, but those investigations were small or population based.“In these studies, the number of clinical outcomes was limited, which reduced the ability to assess the predictive value of clinic blood pressure data as compared with ambulatory data,” reported José R. Banegas, MD, of the department of preventive medicine and public health at the Autonomous University of Madrid and his colleagues.
To better define the prognostic value of 24-hour ambulatory blood pressure measurement, Dr. Banegas and his colleagues looked at data on a large cohort of primary care patients in the Spanish Ambulatory Blood Pressure Registry. Their analysis included 63,910 adults recruited to the registry during 2004-2014.
Patients had blood pressure measurements taken in the clinic according to standard procedures. Afterward, they had ambulatory blood pressure monitoring that used an automated device programmed to record BP every 20 minutes during the day and every 30 minutes at night.
They found that overall clinic and ambulatory blood pressure measurements had a relatively similar magnitude of association with all-cause and cardiovascular mortality.
However, clinic systolic pressure lost its predictive power for all-cause mortality after adjustment for 24-hour ambulatory systolic pressure. The hazard ratio for all-cause mortality dropped from 1.54 before the adjustment to 1.02 after the adjustment, Dr. Banegas and his colleagues reported.
By contrast, ambulatory systolic pressure kept its predictive value after accounting for clinical systolic pressure, with a hazard ratio for all-cause mortality of 1.58 before and after the adjustment, they said in the report.
The strongest association with all-cause mortality was found in patients with masked hypertension – normal clinic readings but elevated ambulatory readings. The hazard ratio for all-cause mortality in that group was 2.83 when adjusted for clinic blood pressure, with similar findings reported for cardiovascular mortality.
White coat hypertension was also associated with increased risk of mortality. The finding of elevated clinic BP and normal 24-hour ambulatory BP had a hazard ratio of 1.79 for all-cause mortality after adjustment for clinic BP, results showed.
“In our study, white coat hypertension was not benign, which may be due in part to the higher mean blood pressure over 24 hours in these patients (119.9/71.9 mm Hg vs. 116.6/70.6 mm Hg in normotensive patients; P less than .001) or to their metabolic phenotype,” the investigators wrote.
Lacer Laboratories, the Spanish Society of Hypertension, and some European government agencies supported the study. Dr. Banegas reported grants from Fondo de Investigación Sanitaria and personal fees from Lacer. Coauthors reported disclosures related to Vascular Dynamics USA, Relypsa USA, Novartis Pharma USA, Daiichi Sankyo, Boehringer Ingelheim, Pfizer, Lacer Laboratories Spain, and others.
SOURCE: Banegas JR et al. N Engl J Med. 2018;378:1509-20.
The investigation by Dr. Banegas and colleagues confirms that ambulatory blood pressure monitoring is useful for assessing blood pressure, the most important and treatable factor contributing to death and disability.
The registry study addresses several clinically relevant issues. In particular, ambulatory blood pressure measures more strongly predicted all-cause and cardiovascular mortality as compared with blood pressure measured in the clinic.
Moreover, the highest hazard ratio of death was seen in patients with masked hypertension, or those with normal clinic-measured blood pressure but elevated ambulatory measurements.
Finally, patients with white coat hypertension (elevated clinic but normal ambulatory blood pressure) had a risk of cardiovascular death twice as high as patients with normal clinic and ambulatory values.
The ominous effect of white coat hypertension has been noted by others, and it is probably related to the increasing magnitude (that is, the difference between clinic blood pressure and ambulatory blood pressure) to white coat hypertension with age.
Ambulatory blood pressure monitoring equipment has evolved and is much lighter than in the past, making it more acceptable to patients.
With more patients undergoing ambulatory blood pressure monitoring, several countries established ambulatory monitoring registries, such as the Spanish registry evaluated in this study.
Ultimately, one hopes the results of this registry study would serve as one more spur to providers and device manufacturers to initiate a registry in the United States.
Raymond R. Townsend, MD, is from the University of Pennsylvania, Philadelphia. These comments are based on his editorial that appeared in the New England Journal of Medicine . Dr. Townsend reported disclosures related to Medtronic, AXIO, and CLARUS Therapeutics, among others.
The investigation by Dr. Banegas and colleagues confirms that ambulatory blood pressure monitoring is useful for assessing blood pressure, the most important and treatable factor contributing to death and disability.
The registry study addresses several clinically relevant issues. In particular, ambulatory blood pressure measures more strongly predicted all-cause and cardiovascular mortality as compared with blood pressure measured in the clinic.
Moreover, the highest hazard ratio of death was seen in patients with masked hypertension, or those with normal clinic-measured blood pressure but elevated ambulatory measurements.
Finally, patients with white coat hypertension (elevated clinic but normal ambulatory blood pressure) had a risk of cardiovascular death twice as high as patients with normal clinic and ambulatory values.
The ominous effect of white coat hypertension has been noted by others, and it is probably related to the increasing magnitude (that is, the difference between clinic blood pressure and ambulatory blood pressure) to white coat hypertension with age.
Ambulatory blood pressure monitoring equipment has evolved and is much lighter than in the past, making it more acceptable to patients.
With more patients undergoing ambulatory blood pressure monitoring, several countries established ambulatory monitoring registries, such as the Spanish registry evaluated in this study.
Ultimately, one hopes the results of this registry study would serve as one more spur to providers and device manufacturers to initiate a registry in the United States.
Raymond R. Townsend, MD, is from the University of Pennsylvania, Philadelphia. These comments are based on his editorial that appeared in the New England Journal of Medicine . Dr. Townsend reported disclosures related to Medtronic, AXIO, and CLARUS Therapeutics, among others.
The investigation by Dr. Banegas and colleagues confirms that ambulatory blood pressure monitoring is useful for assessing blood pressure, the most important and treatable factor contributing to death and disability.
The registry study addresses several clinically relevant issues. In particular, ambulatory blood pressure measures more strongly predicted all-cause and cardiovascular mortality as compared with blood pressure measured in the clinic.
Moreover, the highest hazard ratio of death was seen in patients with masked hypertension, or those with normal clinic-measured blood pressure but elevated ambulatory measurements.
Finally, patients with white coat hypertension (elevated clinic but normal ambulatory blood pressure) had a risk of cardiovascular death twice as high as patients with normal clinic and ambulatory values.
The ominous effect of white coat hypertension has been noted by others, and it is probably related to the increasing magnitude (that is, the difference between clinic blood pressure and ambulatory blood pressure) to white coat hypertension with age.
Ambulatory blood pressure monitoring equipment has evolved and is much lighter than in the past, making it more acceptable to patients.
With more patients undergoing ambulatory blood pressure monitoring, several countries established ambulatory monitoring registries, such as the Spanish registry evaluated in this study.
Ultimately, one hopes the results of this registry study would serve as one more spur to providers and device manufacturers to initiate a registry in the United States.
Raymond R. Townsend, MD, is from the University of Pennsylvania, Philadelphia. These comments are based on his editorial that appeared in the New England Journal of Medicine . Dr. Townsend reported disclosures related to Medtronic, AXIO, and CLARUS Therapeutics, among others.
Ambulatory measurements of blood pressure more strongly predicted all-cause and cardiovascular mortality than did BP measured in the clinic, according to analysis of a large patient registry in Spain.
The results also showed an increased risk of death associated with white coat hypertension and an even stronger association between death and masked hypertension. They were published in the New England Journal of Medicine.
Previous investigations had found that 24-hour ambulatory BP measurements were better predictors of patient outcomes than those obtained in the clinic or at home, but those investigations were small or population based.“In these studies, the number of clinical outcomes was limited, which reduced the ability to assess the predictive value of clinic blood pressure data as compared with ambulatory data,” reported José R. Banegas, MD, of the department of preventive medicine and public health at the Autonomous University of Madrid and his colleagues.
To better define the prognostic value of 24-hour ambulatory blood pressure measurement, Dr. Banegas and his colleagues looked at data on a large cohort of primary care patients in the Spanish Ambulatory Blood Pressure Registry. Their analysis included 63,910 adults recruited to the registry during 2004-2014.
Patients had blood pressure measurements taken in the clinic according to standard procedures. Afterward, they had ambulatory blood pressure monitoring that used an automated device programmed to record BP every 20 minutes during the day and every 30 minutes at night.
They found that overall clinic and ambulatory blood pressure measurements had a relatively similar magnitude of association with all-cause and cardiovascular mortality.
However, clinic systolic pressure lost its predictive power for all-cause mortality after adjustment for 24-hour ambulatory systolic pressure. The hazard ratio for all-cause mortality dropped from 1.54 before the adjustment to 1.02 after the adjustment, Dr. Banegas and his colleagues reported.
By contrast, ambulatory systolic pressure kept its predictive value after accounting for clinical systolic pressure, with a hazard ratio for all-cause mortality of 1.58 before and after the adjustment, they said in the report.
The strongest association with all-cause mortality was found in patients with masked hypertension – normal clinic readings but elevated ambulatory readings. The hazard ratio for all-cause mortality in that group was 2.83 when adjusted for clinic blood pressure, with similar findings reported for cardiovascular mortality.
White coat hypertension was also associated with increased risk of mortality. The finding of elevated clinic BP and normal 24-hour ambulatory BP had a hazard ratio of 1.79 for all-cause mortality after adjustment for clinic BP, results showed.
“In our study, white coat hypertension was not benign, which may be due in part to the higher mean blood pressure over 24 hours in these patients (119.9/71.9 mm Hg vs. 116.6/70.6 mm Hg in normotensive patients; P less than .001) or to their metabolic phenotype,” the investigators wrote.
Lacer Laboratories, the Spanish Society of Hypertension, and some European government agencies supported the study. Dr. Banegas reported grants from Fondo de Investigación Sanitaria and personal fees from Lacer. Coauthors reported disclosures related to Vascular Dynamics USA, Relypsa USA, Novartis Pharma USA, Daiichi Sankyo, Boehringer Ingelheim, Pfizer, Lacer Laboratories Spain, and others.
SOURCE: Banegas JR et al. N Engl J Med. 2018;378:1509-20.
Ambulatory measurements of blood pressure more strongly predicted all-cause and cardiovascular mortality than did BP measured in the clinic, according to analysis of a large patient registry in Spain.
The results also showed an increased risk of death associated with white coat hypertension and an even stronger association between death and masked hypertension. They were published in the New England Journal of Medicine.
Previous investigations had found that 24-hour ambulatory BP measurements were better predictors of patient outcomes than those obtained in the clinic or at home, but those investigations were small or population based.“In these studies, the number of clinical outcomes was limited, which reduced the ability to assess the predictive value of clinic blood pressure data as compared with ambulatory data,” reported José R. Banegas, MD, of the department of preventive medicine and public health at the Autonomous University of Madrid and his colleagues.
To better define the prognostic value of 24-hour ambulatory blood pressure measurement, Dr. Banegas and his colleagues looked at data on a large cohort of primary care patients in the Spanish Ambulatory Blood Pressure Registry. Their analysis included 63,910 adults recruited to the registry during 2004-2014.
Patients had blood pressure measurements taken in the clinic according to standard procedures. Afterward, they had ambulatory blood pressure monitoring that used an automated device programmed to record BP every 20 minutes during the day and every 30 minutes at night.
They found that overall clinic and ambulatory blood pressure measurements had a relatively similar magnitude of association with all-cause and cardiovascular mortality.
However, clinic systolic pressure lost its predictive power for all-cause mortality after adjustment for 24-hour ambulatory systolic pressure. The hazard ratio for all-cause mortality dropped from 1.54 before the adjustment to 1.02 after the adjustment, Dr. Banegas and his colleagues reported.
By contrast, ambulatory systolic pressure kept its predictive value after accounting for clinical systolic pressure, with a hazard ratio for all-cause mortality of 1.58 before and after the adjustment, they said in the report.
The strongest association with all-cause mortality was found in patients with masked hypertension – normal clinic readings but elevated ambulatory readings. The hazard ratio for all-cause mortality in that group was 2.83 when adjusted for clinic blood pressure, with similar findings reported for cardiovascular mortality.
White coat hypertension was also associated with increased risk of mortality. The finding of elevated clinic BP and normal 24-hour ambulatory BP had a hazard ratio of 1.79 for all-cause mortality after adjustment for clinic BP, results showed.
“In our study, white coat hypertension was not benign, which may be due in part to the higher mean blood pressure over 24 hours in these patients (119.9/71.9 mm Hg vs. 116.6/70.6 mm Hg in normotensive patients; P less than .001) or to their metabolic phenotype,” the investigators wrote.
Lacer Laboratories, the Spanish Society of Hypertension, and some European government agencies supported the study. Dr. Banegas reported grants from Fondo de Investigación Sanitaria and personal fees from Lacer. Coauthors reported disclosures related to Vascular Dynamics USA, Relypsa USA, Novartis Pharma USA, Daiichi Sankyo, Boehringer Ingelheim, Pfizer, Lacer Laboratories Spain, and others.
SOURCE: Banegas JR et al. N Engl J Med. 2018;378:1509-20.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: Modeling showed a stronger association between ambulatory systolic pressure and all-cause mortality (adjusted HR, 1.58 per 1-SD pressure increase) than between clinic systolic pressure and all-cause mortality (adjusted HR, 1.02).
Study details: Retrospective analysis of mortality from a cohort of 63,910 adults recruited to a registry in Spain during 2004-2014.
Disclosures: Lacer Laboratories, the Spanish Society of Hypertension, and some European government agencies supported the study. Dr. Banegas reported grants from Fondo de Investigación Sanitaria and personal fees from Lacer. Coauthors reported disclosures related to Vascular Dynamics USA, Relypsa USA, Novartis Pharma USA, Daiichi Sankyo, Boehringer Ingelheim, Pfizer, Lacer Laboratories Spain, and others.
Source: Banegas JR et al. N Engl J Med 2018;378:1509-20.
Ibrutinib plus carfilzomib active in relapsed multiple myeloma
In patients with multiple myeloma who had already undergone multiple lines of therapy, the combination of ibrutinib and carfilzomib with or without dexamethasone produced a favorable rate of response and progression-free survival.
Ibrutinib and carfilzomib combination therapy was also associated with manageable safety in the phase 1 results of the ongoing study, investigators wrote in the journal Leukemia & Lymphoma.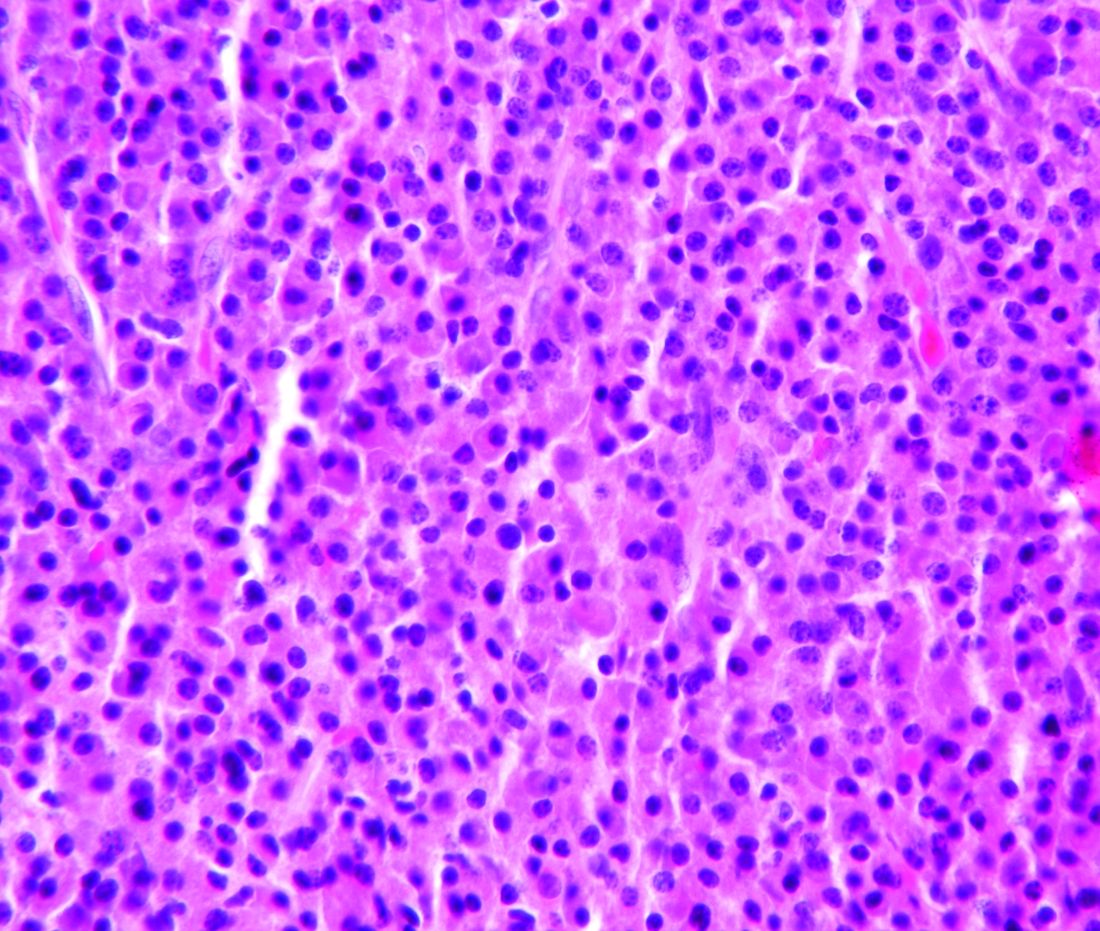
The reported overall response rate in the study was 67%. Median progression-free survival was 7.2 months, which was “encouraging considering the poor outcomes often observed in this group,” Dr. Chari and colleagues wrote.
Carfilzomib, a selective and irreversible proteasome inhibitor, is indicated for patients with previously treated multiple myeloma. Ibrutinib, an orally administered covalent inhibitor of Bruton tyrosine kinase, already has Food and Drug Administration approval for treatment of several B-cell malignancies. Bruton tyrosine kinase is expressed in more than 85% of myeloma tumor cells, according to the researchers, and its signaling may contribute to development of drug resistance.
In an earlier phase 2 study, ibrutinib plus dexamethasone produced a 28% clinical benefit rate and median progression-free survival of 4.6 months. Preclinical data suggest combining ibrutinib and carfilzomib may have a synergistic effect, according to researchers.
To test that hypothesis, Dr. Chari and colleagues conducted a phase 1 dose-finding study including 43 myeloma patients who had previously received at least two lines of therapy, including bortezomib and an immunomodulatory agent. Among those patients, about three-quarters were refractory to bortezomib and one-quarter had high-risk cytogenetics.
A total of 35 patients in the study received ibrutinib and carfilzomib plus dexamethasone; 8 patients received only ibrutinib and carfilzomib.
Key phase 1 results included the 67% response rate, of which 21% had very good partial response and 2% had stringent complete response. No dose-limiting toxicities were observed.
Both carfilzomib and ibrutinib have known cardiac toxicities, but cardiac adverse events in this study did not reach dose-limiting toxicity criteria and were effectively managed by dose reductions or rechallenge, researchers reported.
Hypertension, anemia, pneumonia, fatigue, diarrhea, and thrombocytopenia were the most common grade 3 events observed. “Ultimately, toxicities and/or treatment discontinuations could be attributed to comorbidities, underlying disease factors, or toxicities due to prior therapies,” the researchers wrote.
Enrollment in phase 2b of the study is ongoing.
Dr. Chari received research funding from Pharmacyclics during the study and grants from other companies outside of the study work.
SOURCE: Chari A et al. Leuk Lymphoma. 2018 Apr 4. doi: 10.1080/10428194.2018.1443337.
In patients with multiple myeloma who had already undergone multiple lines of therapy, the combination of ibrutinib and carfilzomib with or without dexamethasone produced a favorable rate of response and progression-free survival.
Ibrutinib and carfilzomib combination therapy was also associated with manageable safety in the phase 1 results of the ongoing study, investigators wrote in the journal Leukemia & Lymphoma.
The reported overall response rate in the study was 67%. Median progression-free survival was 7.2 months, which was “encouraging considering the poor outcomes often observed in this group,” Dr. Chari and colleagues wrote.
Carfilzomib, a selective and irreversible proteasome inhibitor, is indicated for patients with previously treated multiple myeloma. Ibrutinib, an orally administered covalent inhibitor of Bruton tyrosine kinase, already has Food and Drug Administration approval for treatment of several B-cell malignancies. Bruton tyrosine kinase is expressed in more than 85% of myeloma tumor cells, according to the researchers, and its signaling may contribute to development of drug resistance.
In an earlier phase 2 study, ibrutinib plus dexamethasone produced a 28% clinical benefit rate and median progression-free survival of 4.6 months. Preclinical data suggest combining ibrutinib and carfilzomib may have a synergistic effect, according to researchers.
To test that hypothesis, Dr. Chari and colleagues conducted a phase 1 dose-finding study including 43 myeloma patients who had previously received at least two lines of therapy, including bortezomib and an immunomodulatory agent. Among those patients, about three-quarters were refractory to bortezomib and one-quarter had high-risk cytogenetics.
A total of 35 patients in the study received ibrutinib and carfilzomib plus dexamethasone; 8 patients received only ibrutinib and carfilzomib.
Key phase 1 results included the 67% response rate, of which 21% had very good partial response and 2% had stringent complete response. No dose-limiting toxicities were observed.
Both carfilzomib and ibrutinib have known cardiac toxicities, but cardiac adverse events in this study did not reach dose-limiting toxicity criteria and were effectively managed by dose reductions or rechallenge, researchers reported.
Hypertension, anemia, pneumonia, fatigue, diarrhea, and thrombocytopenia were the most common grade 3 events observed. “Ultimately, toxicities and/or treatment discontinuations could be attributed to comorbidities, underlying disease factors, or toxicities due to prior therapies,” the researchers wrote.
Enrollment in phase 2b of the study is ongoing.
Dr. Chari received research funding from Pharmacyclics during the study and grants from other companies outside of the study work.
SOURCE: Chari A et al. Leuk Lymphoma. 2018 Apr 4. doi: 10.1080/10428194.2018.1443337.
In patients with multiple myeloma who had already undergone multiple lines of therapy, the combination of ibrutinib and carfilzomib with or without dexamethasone produced a favorable rate of response and progression-free survival.
Ibrutinib and carfilzomib combination therapy was also associated with manageable safety in the phase 1 results of the ongoing study, investigators wrote in the journal Leukemia & Lymphoma.
The reported overall response rate in the study was 67%. Median progression-free survival was 7.2 months, which was “encouraging considering the poor outcomes often observed in this group,” Dr. Chari and colleagues wrote.
Carfilzomib, a selective and irreversible proteasome inhibitor, is indicated for patients with previously treated multiple myeloma. Ibrutinib, an orally administered covalent inhibitor of Bruton tyrosine kinase, already has Food and Drug Administration approval for treatment of several B-cell malignancies. Bruton tyrosine kinase is expressed in more than 85% of myeloma tumor cells, according to the researchers, and its signaling may contribute to development of drug resistance.
In an earlier phase 2 study, ibrutinib plus dexamethasone produced a 28% clinical benefit rate and median progression-free survival of 4.6 months. Preclinical data suggest combining ibrutinib and carfilzomib may have a synergistic effect, according to researchers.
To test that hypothesis, Dr. Chari and colleagues conducted a phase 1 dose-finding study including 43 myeloma patients who had previously received at least two lines of therapy, including bortezomib and an immunomodulatory agent. Among those patients, about three-quarters were refractory to bortezomib and one-quarter had high-risk cytogenetics.
A total of 35 patients in the study received ibrutinib and carfilzomib plus dexamethasone; 8 patients received only ibrutinib and carfilzomib.
Key phase 1 results included the 67% response rate, of which 21% had very good partial response and 2% had stringent complete response. No dose-limiting toxicities were observed.
Both carfilzomib and ibrutinib have known cardiac toxicities, but cardiac adverse events in this study did not reach dose-limiting toxicity criteria and were effectively managed by dose reductions or rechallenge, researchers reported.
Hypertension, anemia, pneumonia, fatigue, diarrhea, and thrombocytopenia were the most common grade 3 events observed. “Ultimately, toxicities and/or treatment discontinuations could be attributed to comorbidities, underlying disease factors, or toxicities due to prior therapies,” the researchers wrote.
Enrollment in phase 2b of the study is ongoing.
Dr. Chari received research funding from Pharmacyclics during the study and grants from other companies outside of the study work.
SOURCE: Chari A et al. Leuk Lymphoma. 2018 Apr 4. doi: 10.1080/10428194.2018.1443337.
FROM LEUKEMIA & LYMPHOMA
Key clinical point:
Major finding: The overall response rate was 67%, including a 21% very good partial response and 2% stringent complete response.
Study details: A phase 1 dose-finding study including 43 myeloma patients who had previously received at least two lines of therapy.
Disclosures: Dr. Chari received research funding from Pharmacyclics during the study and grants from other companies outside of the study work.
Source: Chari A et al. Leuk Lymphoma. 2018 Apr 4. doi: 10.1080/10428194.2018.1443337.
Statin plus chemo yields encouraging results in poor-risk AML
Patients with poor-risk acute myelogenous leukemia (AML) had promising rates of response and survival following treatment with a statin added to standard chemotherapy, researchers reported.
Pravastatin in combination with idarubicin and cytarabine had a 30% response rate in poor-risk AML patients, according to Anjali S. Advani, MD, of the Taussig Cancer Institute at the Cleveland Clinic, and her coauthors.
Although that response rate did not meet a prespecified threshold for statistical significance, results of the phase 2 study were nevertheless “encouraging” for a group of patients with unfavorable cytogenetics and poor-risk molecular mutations, the researchers wrote. The study was published in Leukemia Research.
The estimated median overall survival was 4.1 months in the phase 2 trial, known as SWOG S0919. About one-quarter of the patients were able to proceed to allogeneic hematopoietic stem cell transplant, and for that group, median overall survival was 27.1 months.
These findings appear to provide further support for the hypothesis that targeting the cholesterol pathway may be a promising approach in patients with AML.
Some previous investigations suggested that AML blasts overexpress genes for lipoprotein receptors and regulatory enzymes, while others showed that these cells import and synthesize cholesterol at levels higher than what is seen in normal progenitor cells. In addition, some AML patients have hypocholesterolemia that usually resolves when they achieve a complete remission.
“These observations suggest that AML cells may require high levels of cholesterol for their survival and that abnormalities in cholesterol homeostasis are necessary for AML cell survival,” the researchers wrote.
This led to a phase 1 trial of pravastatin plus idarubicin/cytarabine, followed by the phase 2 SWOG S0919 trial, which demonstrated a 75% rate of complete response (CR) or complete response with incomplete count recovery (CRi) for the regimen.
The SWOG S0919 study was amended to include the poor-risk AML patients described in the present study. That cohort of 46 patients had a CR/CRi of less than 6 months after their last induction regimen or refractory disease. Many had poor-risk cytogenetics (43%) or one of a number of poor-risk mutations, according to the study report.
Pravastatin, in addition to working on the cholesterol pathway in AML, may also have a therapeutic advantage in patients with FLT3 mutations. Three out of six patients with FLT3 mutations achieved CR/CRi, corroborating earlier preclinical studies and suggesting further study of this specific patient population would be worthwhile, the researchers noted.
The study was supported in part by the National Institutes of Health and Bristol-Myers Squibb. Dr. Advani reported having no financial disclosures but other study authors reported relationships with various pharmaceutical companies.
SOURCE: Advani AS et al. Leuk Res. 2018 Apr;67:17-20.
Patients with poor-risk acute myelogenous leukemia (AML) had promising rates of response and survival following treatment with a statin added to standard chemotherapy, researchers reported.
Pravastatin in combination with idarubicin and cytarabine had a 30% response rate in poor-risk AML patients, according to Anjali S. Advani, MD, of the Taussig Cancer Institute at the Cleveland Clinic, and her coauthors.
Although that response rate did not meet a prespecified threshold for statistical significance, results of the phase 2 study were nevertheless “encouraging” for a group of patients with unfavorable cytogenetics and poor-risk molecular mutations, the researchers wrote. The study was published in Leukemia Research.
The estimated median overall survival was 4.1 months in the phase 2 trial, known as SWOG S0919. About one-quarter of the patients were able to proceed to allogeneic hematopoietic stem cell transplant, and for that group, median overall survival was 27.1 months.
These findings appear to provide further support for the hypothesis that targeting the cholesterol pathway may be a promising approach in patients with AML.
Some previous investigations suggested that AML blasts overexpress genes for lipoprotein receptors and regulatory enzymes, while others showed that these cells import and synthesize cholesterol at levels higher than what is seen in normal progenitor cells. In addition, some AML patients have hypocholesterolemia that usually resolves when they achieve a complete remission.
“These observations suggest that AML cells may require high levels of cholesterol for their survival and that abnormalities in cholesterol homeostasis are necessary for AML cell survival,” the researchers wrote.
This led to a phase 1 trial of pravastatin plus idarubicin/cytarabine, followed by the phase 2 SWOG S0919 trial, which demonstrated a 75% rate of complete response (CR) or complete response with incomplete count recovery (CRi) for the regimen.
The SWOG S0919 study was amended to include the poor-risk AML patients described in the present study. That cohort of 46 patients had a CR/CRi of less than 6 months after their last induction regimen or refractory disease. Many had poor-risk cytogenetics (43%) or one of a number of poor-risk mutations, according to the study report.
Pravastatin, in addition to working on the cholesterol pathway in AML, may also have a therapeutic advantage in patients with FLT3 mutations. Three out of six patients with FLT3 mutations achieved CR/CRi, corroborating earlier preclinical studies and suggesting further study of this specific patient population would be worthwhile, the researchers noted.
The study was supported in part by the National Institutes of Health and Bristol-Myers Squibb. Dr. Advani reported having no financial disclosures but other study authors reported relationships with various pharmaceutical companies.
SOURCE: Advani AS et al. Leuk Res. 2018 Apr;67:17-20.
Patients with poor-risk acute myelogenous leukemia (AML) had promising rates of response and survival following treatment with a statin added to standard chemotherapy, researchers reported.
Pravastatin in combination with idarubicin and cytarabine had a 30% response rate in poor-risk AML patients, according to Anjali S. Advani, MD, of the Taussig Cancer Institute at the Cleveland Clinic, and her coauthors.
Although that response rate did not meet a prespecified threshold for statistical significance, results of the phase 2 study were nevertheless “encouraging” for a group of patients with unfavorable cytogenetics and poor-risk molecular mutations, the researchers wrote. The study was published in Leukemia Research.
The estimated median overall survival was 4.1 months in the phase 2 trial, known as SWOG S0919. About one-quarter of the patients were able to proceed to allogeneic hematopoietic stem cell transplant, and for that group, median overall survival was 27.1 months.
These findings appear to provide further support for the hypothesis that targeting the cholesterol pathway may be a promising approach in patients with AML.
Some previous investigations suggested that AML blasts overexpress genes for lipoprotein receptors and regulatory enzymes, while others showed that these cells import and synthesize cholesterol at levels higher than what is seen in normal progenitor cells. In addition, some AML patients have hypocholesterolemia that usually resolves when they achieve a complete remission.
“These observations suggest that AML cells may require high levels of cholesterol for their survival and that abnormalities in cholesterol homeostasis are necessary for AML cell survival,” the researchers wrote.
This led to a phase 1 trial of pravastatin plus idarubicin/cytarabine, followed by the phase 2 SWOG S0919 trial, which demonstrated a 75% rate of complete response (CR) or complete response with incomplete count recovery (CRi) for the regimen.
The SWOG S0919 study was amended to include the poor-risk AML patients described in the present study. That cohort of 46 patients had a CR/CRi of less than 6 months after their last induction regimen or refractory disease. Many had poor-risk cytogenetics (43%) or one of a number of poor-risk mutations, according to the study report.
Pravastatin, in addition to working on the cholesterol pathway in AML, may also have a therapeutic advantage in patients with FLT3 mutations. Three out of six patients with FLT3 mutations achieved CR/CRi, corroborating earlier preclinical studies and suggesting further study of this specific patient population would be worthwhile, the researchers noted.
The study was supported in part by the National Institutes of Health and Bristol-Myers Squibb. Dr. Advani reported having no financial disclosures but other study authors reported relationships with various pharmaceutical companies.
SOURCE: Advani AS et al. Leuk Res. 2018 Apr;67:17-20.
FROM LEUKEMIA RESEARCH
Key clinical point:
Major finding: Pravastatin in combination with idarubicin and cytarabine had a 30% response rate in poor risk AML patients.
Study details: Results from the poor-risk cohort (n = 46) in SWOG S0919, a phase 2 study.
Disclosures: The research was supported in part by the National Institutes of Health and Bristol-Myers Squibb. Dr. Advani reported having no financial disclosures but other study authors reported relationships with various pharmaceutical companies.
Source: Advani AS et al. Leuk Res. 2018 Apr;67:17-20.
VIDEO: Meta-analysis: Mortality, safety data may favor SGLT2 inhibitors in T2DM
Sodium-glucose cotransporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) agonists were both associated with a lower mortality risk, compared with that seen with dipeptidyl peptidase–4 (DPP-4) inhibitors and in controls, in patients with type 2 diabetes, according to findings from a large network meta-analysis.
In addition, the GLP-1 agonists were associated with a higher risk of adverse events that led to study withdrawal, compared with SGLT2 inhibitors, according to the analysis conducted by Sean L. Zheng, BM BCh, of the department of endocrinology at the Imperial College Healthcare NHS Foundation Trust, London, and his coinvestigators.
“Of the 3 classes tested, SGLT2 inhibition may be preferred over the incretin-based therapies based on their association with lower mortality and their favorable adverse-event profile,” Dr. Zheng and his coinvestigators wrote in a report on the study published in JAMA.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Source: JAMA
For patients with type 2 diabetes who don’t achieve target glycemic control on metformin, Dr. Zheng and his coauthors noted, international guidelines recommend SGLT2 inhibitors or incretin-based treatments as a next step.
However, there has been little exploration of the relative clinical effectiveness of these drug classes, which has led to uncertainty about what treatment approach is optimal. “When no head-to-head trial exists, network meta-analysis can be used to estimate the effect,” the authors wrote.
To compare the efficacy of the drug classes in reducing mortality and cardiovascular outcomes, Dr. Zheng and his colleagues conducted a systematic review and meta-analysis of 236 randomized clinical trials including 176,310 participants.
The primary outcome of the study was all-cause mortality.
Both SGLT2 inhibitors and GLP-1 agonists were associated with significantly lower all-cause mortality than that seen in controls (placebo or no treatment), while DPP-4 inhibitors were not, investigators found in the meta-analysis.
For that endpoint, SGLT2 inhibitors had an absolute risk difference of –1.0%, with a hazard ratio of 0.80, and GLP-1 agonists had an absolute RD of –0.6% and an HR of 0.88. By contrast, DPP-4 inhibitors had an absolute RD of 0.1% and an HR of 1.02, according to the published report.
Moreover, when compared with DPP-4 inhibitors, SGLT2 inhibitors and GLP-1 agonists were associated with reduced all-cause mortality, with an absolute risk difference of –0.9% and –0.5%, respectively, they found.
SGLT2 inhibitors and GLP-1 agonists also were significantly associated with lower cardiovascular mortality than controls were, while SGLT2 inhibitors were significantly associated with lower heart failure event rates versus those seen controls, they also found.
Safety outcomes analysis showed that GLP-1 agonists, compared with SGLT2 inhibitors and DPP-4 inhibitors, had a higher risk of adverse events that led patients to withdraw from the study.
The DPP-4 inhibitors were associated with increased acute pancreatitis risk, according to the safety analysis. “SGLT2 inhibitors were associated with increased risk of genital infections but not urinary tract infections. There was a high degree of heterogeneity for lower-limb amputations driven by the significant increase in events with canagliflozin but neutral effects of empagliflozin,” they said.
“Careful treatment selection may be necessary to minimize these outcomes in at-risk patients,” Dr. Zheng and his coauthors concluded.
One author reported potential conflicts of interest with Roche Diabetes, Dexcom, Medtronics Diabetes, and others. Another was supported by a grant from the British Heart Foundation. No other conflicts were reported.
SOURCE: Zheng SL et al. JAMA. 2018;319(15):1580-91.
Sodium-glucose cotransporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) agonists were both associated with a lower mortality risk, compared with that seen with dipeptidyl peptidase–4 (DPP-4) inhibitors and in controls, in patients with type 2 diabetes, according to findings from a large network meta-analysis.
In addition, the GLP-1 agonists were associated with a higher risk of adverse events that led to study withdrawal, compared with SGLT2 inhibitors, according to the analysis conducted by Sean L. Zheng, BM BCh, of the department of endocrinology at the Imperial College Healthcare NHS Foundation Trust, London, and his coinvestigators.
“Of the 3 classes tested, SGLT2 inhibition may be preferred over the incretin-based therapies based on their association with lower mortality and their favorable adverse-event profile,” Dr. Zheng and his coinvestigators wrote in a report on the study published in JAMA.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Source: JAMA
For patients with type 2 diabetes who don’t achieve target glycemic control on metformin, Dr. Zheng and his coauthors noted, international guidelines recommend SGLT2 inhibitors or incretin-based treatments as a next step.
However, there has been little exploration of the relative clinical effectiveness of these drug classes, which has led to uncertainty about what treatment approach is optimal. “When no head-to-head trial exists, network meta-analysis can be used to estimate the effect,” the authors wrote.
To compare the efficacy of the drug classes in reducing mortality and cardiovascular outcomes, Dr. Zheng and his colleagues conducted a systematic review and meta-analysis of 236 randomized clinical trials including 176,310 participants.
The primary outcome of the study was all-cause mortality.
Both SGLT2 inhibitors and GLP-1 agonists were associated with significantly lower all-cause mortality than that seen in controls (placebo or no treatment), while DPP-4 inhibitors were not, investigators found in the meta-analysis.
For that endpoint, SGLT2 inhibitors had an absolute risk difference of –1.0%, with a hazard ratio of 0.80, and GLP-1 agonists had an absolute RD of –0.6% and an HR of 0.88. By contrast, DPP-4 inhibitors had an absolute RD of 0.1% and an HR of 1.02, according to the published report.
Moreover, when compared with DPP-4 inhibitors, SGLT2 inhibitors and GLP-1 agonists were associated with reduced all-cause mortality, with an absolute risk difference of –0.9% and –0.5%, respectively, they found.
SGLT2 inhibitors and GLP-1 agonists also were significantly associated with lower cardiovascular mortality than controls were, while SGLT2 inhibitors were significantly associated with lower heart failure event rates versus those seen controls, they also found.
Safety outcomes analysis showed that GLP-1 agonists, compared with SGLT2 inhibitors and DPP-4 inhibitors, had a higher risk of adverse events that led patients to withdraw from the study.
The DPP-4 inhibitors were associated with increased acute pancreatitis risk, according to the safety analysis. “SGLT2 inhibitors were associated with increased risk of genital infections but not urinary tract infections. There was a high degree of heterogeneity for lower-limb amputations driven by the significant increase in events with canagliflozin but neutral effects of empagliflozin,” they said.
“Careful treatment selection may be necessary to minimize these outcomes in at-risk patients,” Dr. Zheng and his coauthors concluded.
One author reported potential conflicts of interest with Roche Diabetes, Dexcom, Medtronics Diabetes, and others. Another was supported by a grant from the British Heart Foundation. No other conflicts were reported.
SOURCE: Zheng SL et al. JAMA. 2018;319(15):1580-91.
Sodium-glucose cotransporter 2 (SGLT2) inhibitors and glucagonlike peptide–1 (GLP-1) agonists were both associated with a lower mortality risk, compared with that seen with dipeptidyl peptidase–4 (DPP-4) inhibitors and in controls, in patients with type 2 diabetes, according to findings from a large network meta-analysis.
In addition, the GLP-1 agonists were associated with a higher risk of adverse events that led to study withdrawal, compared with SGLT2 inhibitors, according to the analysis conducted by Sean L. Zheng, BM BCh, of the department of endocrinology at the Imperial College Healthcare NHS Foundation Trust, London, and his coinvestigators.
“Of the 3 classes tested, SGLT2 inhibition may be preferred over the incretin-based therapies based on their association with lower mortality and their favorable adverse-event profile,” Dr. Zheng and his coinvestigators wrote in a report on the study published in JAMA.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Source: JAMA
For patients with type 2 diabetes who don’t achieve target glycemic control on metformin, Dr. Zheng and his coauthors noted, international guidelines recommend SGLT2 inhibitors or incretin-based treatments as a next step.
However, there has been little exploration of the relative clinical effectiveness of these drug classes, which has led to uncertainty about what treatment approach is optimal. “When no head-to-head trial exists, network meta-analysis can be used to estimate the effect,” the authors wrote.
To compare the efficacy of the drug classes in reducing mortality and cardiovascular outcomes, Dr. Zheng and his colleagues conducted a systematic review and meta-analysis of 236 randomized clinical trials including 176,310 participants.
The primary outcome of the study was all-cause mortality.
Both SGLT2 inhibitors and GLP-1 agonists were associated with significantly lower all-cause mortality than that seen in controls (placebo or no treatment), while DPP-4 inhibitors were not, investigators found in the meta-analysis.
For that endpoint, SGLT2 inhibitors had an absolute risk difference of –1.0%, with a hazard ratio of 0.80, and GLP-1 agonists had an absolute RD of –0.6% and an HR of 0.88. By contrast, DPP-4 inhibitors had an absolute RD of 0.1% and an HR of 1.02, according to the published report.
Moreover, when compared with DPP-4 inhibitors, SGLT2 inhibitors and GLP-1 agonists were associated with reduced all-cause mortality, with an absolute risk difference of –0.9% and –0.5%, respectively, they found.
SGLT2 inhibitors and GLP-1 agonists also were significantly associated with lower cardiovascular mortality than controls were, while SGLT2 inhibitors were significantly associated with lower heart failure event rates versus those seen controls, they also found.
Safety outcomes analysis showed that GLP-1 agonists, compared with SGLT2 inhibitors and DPP-4 inhibitors, had a higher risk of adverse events that led patients to withdraw from the study.
The DPP-4 inhibitors were associated with increased acute pancreatitis risk, according to the safety analysis. “SGLT2 inhibitors were associated with increased risk of genital infections but not urinary tract infections. There was a high degree of heterogeneity for lower-limb amputations driven by the significant increase in events with canagliflozin but neutral effects of empagliflozin,” they said.
“Careful treatment selection may be necessary to minimize these outcomes in at-risk patients,” Dr. Zheng and his coauthors concluded.
One author reported potential conflicts of interest with Roche Diabetes, Dexcom, Medtronics Diabetes, and others. Another was supported by a grant from the British Heart Foundation. No other conflicts were reported.
SOURCE: Zheng SL et al. JAMA. 2018;319(15):1580-91.
FROM JAMA
Key clinical point: that were either placebo or no treatment.
Major finding: When compared with DPP-4 inhibitors, SGLT2 inhibitors and GLP-1 agonists were both associated with reduced all-cause mortality, with an absolute risk difference of –0.9% and –0.5%, respectively.
Study details: A systematic review and meta-analysis of 236 randomized clinical trials including 176,310 participants.
Disclosures: One author reported potential conflicts of interest with Roche Diabetes, Dexcom, Medtronics Diabetes, and others. Another was supported by a grant from the British Heart Foundation. No other conflicts were reported.
Source: Zheng SL et al. JAMA. 2018;319(15):1580-91.
