User login
New Treatment Target for Hypothyroid Elderly
ESTES PARK, COLO. – The latest major guidelines on management of hypothyroidism create a new, looser treatment target for older patients.
“This is a departure from the message we’ve given many times in the past. Elderly people seem to tolerate slight degrees of hypothyroidism and may actually benefit from it,” Dr. Michael T. McDermott said at a conference on internal medicine sponsored by the University of Colorado.
The American Thyroid Association guidelines issued late last year (Thyroid. 2014 Dec;24[12]:1670-75) raise the target serum TSH to 4-6 mIU/L in hypothyroid individuals age 70 or older. The target serum TSH in nonelderly, nonpregnant patients remains unchanged at 0.5-4.5 mIU/L, noted Dr. McDermott, professor of medicine and director of endocrinology and diabetes practice at the University of Colorado Hospital, Aurora.
“The slightly higher TSH treatment target in elderly patients is very heavily evidence-based. Studies showed that people over age 70 often did worse if their TSH was maintained in the low end of the normal range, and that people whose TSH was maintained up to about 6 mIU/L didn’t seem to have any adverse effects from that. It’s kind of a moving target: we’ll probably see the data reevaluated over time. But I think it’s clear that normal elderly people have a normal TSH that’s slightly higher,” according to the endocrinologist.
The starting dose of levothyroxine (LT4) in older patients is 25-50 mcg/day. The TSH level should be rechecked after 6 weeks in patients with overt hypothyroidism and 6-10 weeks in those with subclinical hypothyroidism, with LT4 then being titrated in the elderly until it’s in the 4-6 mIU/L range.
Speaking of subclinical hypothyroidism, which is defined by an elevated TSH but a normal free T4 level, four studies now show the same thing: While subclinical hypothyroidism is independently associated with increased cardiovascular mortality in patients under age 65, it does not carry any increased cardiovascular mortality risk in older individuals. The first of these studies, a meta-analysis of 15 clinical trials totalling 2,531 subclinically hypothyroid patients and more than 26,000 controls, found a 37% increase in cardiovascular mortality in patients younger than 65 with subclinical hypothyroidism, but no increase in older people with the disorder (J Clin Endocrinol Metab. 2008 Aug;93[8]:2998-3007).
“We don’t know why that is, but it’s the reason the recommended TSH range when treating people for subclinical or overt hypothyroidism has now changed in people over age 70,” Dr. McDermott explained.
The consensus recommendations of the American Thyroid Association and the American Association of Clinical Endocrinologists advise treatment of subclinical hypothyroidism involving a TSH level greater than 10.0 mIU/L. In patients with lesser elevations of TSH, however, clinical judgment is critical in deciding whether to treat or monitor.
“If the person has symptoms, treatment is very reasonable. You should know, however, that one-third of people who have a TSH of 4.5-10.0 mIU/L will have a normal TSH 1 year later if you don’t treat them. So if they’re not symptomatic you may usually monitor these patients,” he said.
While LT4 remains the treatment of choice for hypothyroidism, 16% of patients have persistent symptoms despite optimal LT4 therapy. They appear to benefit from a combination of LT4 and liothyronine (LT3) given in a 10:1 ratio. Because LT3 lasts for only about 8 hours, it’s best administered twice daily. Thyroid tests should be obtained before the medication is taken because triiodothyronine (T3) levels rise abruptly in response to a dose.
Dr. McDermott reported having no financial conflicts of interest.
ESTES PARK, COLO. – The latest major guidelines on management of hypothyroidism create a new, looser treatment target for older patients.
“This is a departure from the message we’ve given many times in the past. Elderly people seem to tolerate slight degrees of hypothyroidism and may actually benefit from it,” Dr. Michael T. McDermott said at a conference on internal medicine sponsored by the University of Colorado.
The American Thyroid Association guidelines issued late last year (Thyroid. 2014 Dec;24[12]:1670-75) raise the target serum TSH to 4-6 mIU/L in hypothyroid individuals age 70 or older. The target serum TSH in nonelderly, nonpregnant patients remains unchanged at 0.5-4.5 mIU/L, noted Dr. McDermott, professor of medicine and director of endocrinology and diabetes practice at the University of Colorado Hospital, Aurora.
“The slightly higher TSH treatment target in elderly patients is very heavily evidence-based. Studies showed that people over age 70 often did worse if their TSH was maintained in the low end of the normal range, and that people whose TSH was maintained up to about 6 mIU/L didn’t seem to have any adverse effects from that. It’s kind of a moving target: we’ll probably see the data reevaluated over time. But I think it’s clear that normal elderly people have a normal TSH that’s slightly higher,” according to the endocrinologist.
The starting dose of levothyroxine (LT4) in older patients is 25-50 mcg/day. The TSH level should be rechecked after 6 weeks in patients with overt hypothyroidism and 6-10 weeks in those with subclinical hypothyroidism, with LT4 then being titrated in the elderly until it’s in the 4-6 mIU/L range.
Speaking of subclinical hypothyroidism, which is defined by an elevated TSH but a normal free T4 level, four studies now show the same thing: While subclinical hypothyroidism is independently associated with increased cardiovascular mortality in patients under age 65, it does not carry any increased cardiovascular mortality risk in older individuals. The first of these studies, a meta-analysis of 15 clinical trials totalling 2,531 subclinically hypothyroid patients and more than 26,000 controls, found a 37% increase in cardiovascular mortality in patients younger than 65 with subclinical hypothyroidism, but no increase in older people with the disorder (J Clin Endocrinol Metab. 2008 Aug;93[8]:2998-3007).
“We don’t know why that is, but it’s the reason the recommended TSH range when treating people for subclinical or overt hypothyroidism has now changed in people over age 70,” Dr. McDermott explained.
The consensus recommendations of the American Thyroid Association and the American Association of Clinical Endocrinologists advise treatment of subclinical hypothyroidism involving a TSH level greater than 10.0 mIU/L. In patients with lesser elevations of TSH, however, clinical judgment is critical in deciding whether to treat or monitor.
“If the person has symptoms, treatment is very reasonable. You should know, however, that one-third of people who have a TSH of 4.5-10.0 mIU/L will have a normal TSH 1 year later if you don’t treat them. So if they’re not symptomatic you may usually monitor these patients,” he said.
While LT4 remains the treatment of choice for hypothyroidism, 16% of patients have persistent symptoms despite optimal LT4 therapy. They appear to benefit from a combination of LT4 and liothyronine (LT3) given in a 10:1 ratio. Because LT3 lasts for only about 8 hours, it’s best administered twice daily. Thyroid tests should be obtained before the medication is taken because triiodothyronine (T3) levels rise abruptly in response to a dose.
Dr. McDermott reported having no financial conflicts of interest.
ESTES PARK, COLO. – The latest major guidelines on management of hypothyroidism create a new, looser treatment target for older patients.
“This is a departure from the message we’ve given many times in the past. Elderly people seem to tolerate slight degrees of hypothyroidism and may actually benefit from it,” Dr. Michael T. McDermott said at a conference on internal medicine sponsored by the University of Colorado.
The American Thyroid Association guidelines issued late last year (Thyroid. 2014 Dec;24[12]:1670-75) raise the target serum TSH to 4-6 mIU/L in hypothyroid individuals age 70 or older. The target serum TSH in nonelderly, nonpregnant patients remains unchanged at 0.5-4.5 mIU/L, noted Dr. McDermott, professor of medicine and director of endocrinology and diabetes practice at the University of Colorado Hospital, Aurora.
“The slightly higher TSH treatment target in elderly patients is very heavily evidence-based. Studies showed that people over age 70 often did worse if their TSH was maintained in the low end of the normal range, and that people whose TSH was maintained up to about 6 mIU/L didn’t seem to have any adverse effects from that. It’s kind of a moving target: we’ll probably see the data reevaluated over time. But I think it’s clear that normal elderly people have a normal TSH that’s slightly higher,” according to the endocrinologist.
The starting dose of levothyroxine (LT4) in older patients is 25-50 mcg/day. The TSH level should be rechecked after 6 weeks in patients with overt hypothyroidism and 6-10 weeks in those with subclinical hypothyroidism, with LT4 then being titrated in the elderly until it’s in the 4-6 mIU/L range.
Speaking of subclinical hypothyroidism, which is defined by an elevated TSH but a normal free T4 level, four studies now show the same thing: While subclinical hypothyroidism is independently associated with increased cardiovascular mortality in patients under age 65, it does not carry any increased cardiovascular mortality risk in older individuals. The first of these studies, a meta-analysis of 15 clinical trials totalling 2,531 subclinically hypothyroid patients and more than 26,000 controls, found a 37% increase in cardiovascular mortality in patients younger than 65 with subclinical hypothyroidism, but no increase in older people with the disorder (J Clin Endocrinol Metab. 2008 Aug;93[8]:2998-3007).
“We don’t know why that is, but it’s the reason the recommended TSH range when treating people for subclinical or overt hypothyroidism has now changed in people over age 70,” Dr. McDermott explained.
The consensus recommendations of the American Thyroid Association and the American Association of Clinical Endocrinologists advise treatment of subclinical hypothyroidism involving a TSH level greater than 10.0 mIU/L. In patients with lesser elevations of TSH, however, clinical judgment is critical in deciding whether to treat or monitor.
“If the person has symptoms, treatment is very reasonable. You should know, however, that one-third of people who have a TSH of 4.5-10.0 mIU/L will have a normal TSH 1 year later if you don’t treat them. So if they’re not symptomatic you may usually monitor these patients,” he said.
While LT4 remains the treatment of choice for hypothyroidism, 16% of patients have persistent symptoms despite optimal LT4 therapy. They appear to benefit from a combination of LT4 and liothyronine (LT3) given in a 10:1 ratio. Because LT3 lasts for only about 8 hours, it’s best administered twice daily. Thyroid tests should be obtained before the medication is taken because triiodothyronine (T3) levels rise abruptly in response to a dose.
Dr. McDermott reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
New treatment target for hypothyroid elderly
ESTES PARK, COLO. – The latest major guidelines on management of hypothyroidism create a new, looser treatment target for older patients.
“This is a departure from the message we’ve given many times in the past. Elderly people seem to tolerate slight degrees of hypothyroidism and may actually benefit from it,” Dr. Michael T. McDermott said at a conference on internal medicine sponsored by the University of Colorado.
The American Thyroid Association guidelines issued late last year (Thyroid. 2014 Dec;24[12]:1670-75) raise the target serum TSH to 4-6 mIU/L in hypothyroid individuals age 70 or older. The target serum TSH in nonelderly, nonpregnant patients remains unchanged at 0.5-4.5 mIU/L, noted Dr. McDermott, professor of medicine and director of endocrinology and diabetes practice at the University of Colorado Hospital, Aurora.
“The slightly higher TSH treatment target in elderly patients is very heavily evidence-based. Studies showed that people over age 70 often did worse if their TSH was maintained in the low end of the normal range, and that people whose TSH was maintained up to about 6 mIU/L didn’t seem to have any adverse effects from that. It’s kind of a moving target: we’ll probably see the data reevaluated over time. But I think it’s clear that normal elderly people have a normal TSH that’s slightly higher,” according to the endocrinologist.
The starting dose of levothyroxine (LT4) in older patients is 25-50 mcg/day. The TSH level should be rechecked after 6 weeks in patients with overt hypothyroidism and 6-10 weeks in those with subclinical hypothyroidism, with LT4 then being titrated in the elderly until it’s in the 4-6 mIU/L range.
Speaking of subclinical hypothyroidism, which is defined by an elevated TSH but a normal free T4 level, four studies now show the same thing: While subclinical hypothyroidism is independently associated with increased cardiovascular mortality in patients under age 65, it does not carry any increased cardiovascular mortality risk in older individuals. The first of these studies, a meta-analysis of 15 clinical trials totalling 2,531 subclinically hypothyroid patients and more than 26,000 controls, found a 37% increase in cardiovascular mortality in patients younger than 65 with subclinical hypothyroidism, but no increase in older people with the disorder (J Clin Endocrinol Metab. 2008 Aug;93[8]:2998-3007).
“We don’t know why that is, but it’s the reason the recommended TSH range when treating people for subclinical or overt hypothyroidism has now changed in people over age 70,” Dr. McDermott explained.
The consensus recommendations of the American Thyroid Association and the American Association of Clinical Endocrinologists advise treatment of subclinical hypothyroidism involving a TSH level greater than 10.0 mIU/L. In patients with lesser elevations of TSH, however, clinical judgment is critical in deciding whether to treat or monitor.
“If the person has symptoms, treatment is very reasonable. You should know, however, that one-third of people who have a TSH of 4.5-10.0 mIU/L will have a normal TSH 1 year later if you don’t treat them. So if they’re not symptomatic you may usually monitor these patients,” he said.
While LT4 remains the treatment of choice for hypothyroidism, 16% of patients have persistent symptoms despite optimal LT4 therapy. They appear to benefit from a combination of LT4 and liothyronine (LT3) given in a 10:1 ratio. Because LT3 lasts for only about 8 hours, it’s best administered twice daily. Thyroid tests should be obtained before the medication is taken because triiodothyronine (T3) levels rise abruptly in response to a dose.
Dr. McDermott reported having no financial conflicts of interest.
ESTES PARK, COLO. – The latest major guidelines on management of hypothyroidism create a new, looser treatment target for older patients.
“This is a departure from the message we’ve given many times in the past. Elderly people seem to tolerate slight degrees of hypothyroidism and may actually benefit from it,” Dr. Michael T. McDermott said at a conference on internal medicine sponsored by the University of Colorado.
The American Thyroid Association guidelines issued late last year (Thyroid. 2014 Dec;24[12]:1670-75) raise the target serum TSH to 4-6 mIU/L in hypothyroid individuals age 70 or older. The target serum TSH in nonelderly, nonpregnant patients remains unchanged at 0.5-4.5 mIU/L, noted Dr. McDermott, professor of medicine and director of endocrinology and diabetes practice at the University of Colorado Hospital, Aurora.
“The slightly higher TSH treatment target in elderly patients is very heavily evidence-based. Studies showed that people over age 70 often did worse if their TSH was maintained in the low end of the normal range, and that people whose TSH was maintained up to about 6 mIU/L didn’t seem to have any adverse effects from that. It’s kind of a moving target: we’ll probably see the data reevaluated over time. But I think it’s clear that normal elderly people have a normal TSH that’s slightly higher,” according to the endocrinologist.
The starting dose of levothyroxine (LT4) in older patients is 25-50 mcg/day. The TSH level should be rechecked after 6 weeks in patients with overt hypothyroidism and 6-10 weeks in those with subclinical hypothyroidism, with LT4 then being titrated in the elderly until it’s in the 4-6 mIU/L range.
Speaking of subclinical hypothyroidism, which is defined by an elevated TSH but a normal free T4 level, four studies now show the same thing: While subclinical hypothyroidism is independently associated with increased cardiovascular mortality in patients under age 65, it does not carry any increased cardiovascular mortality risk in older individuals. The first of these studies, a meta-analysis of 15 clinical trials totalling 2,531 subclinically hypothyroid patients and more than 26,000 controls, found a 37% increase in cardiovascular mortality in patients younger than 65 with subclinical hypothyroidism, but no increase in older people with the disorder (J Clin Endocrinol Metab. 2008 Aug;93[8]:2998-3007).
“We don’t know why that is, but it’s the reason the recommended TSH range when treating people for subclinical or overt hypothyroidism has now changed in people over age 70,” Dr. McDermott explained.
The consensus recommendations of the American Thyroid Association and the American Association of Clinical Endocrinologists advise treatment of subclinical hypothyroidism involving a TSH level greater than 10.0 mIU/L. In patients with lesser elevations of TSH, however, clinical judgment is critical in deciding whether to treat or monitor.
“If the person has symptoms, treatment is very reasonable. You should know, however, that one-third of people who have a TSH of 4.5-10.0 mIU/L will have a normal TSH 1 year later if you don’t treat them. So if they’re not symptomatic you may usually monitor these patients,” he said.
While LT4 remains the treatment of choice for hypothyroidism, 16% of patients have persistent symptoms despite optimal LT4 therapy. They appear to benefit from a combination of LT4 and liothyronine (LT3) given in a 10:1 ratio. Because LT3 lasts for only about 8 hours, it’s best administered twice daily. Thyroid tests should be obtained before the medication is taken because triiodothyronine (T3) levels rise abruptly in response to a dose.
Dr. McDermott reported having no financial conflicts of interest.
ESTES PARK, COLO. – The latest major guidelines on management of hypothyroidism create a new, looser treatment target for older patients.
“This is a departure from the message we’ve given many times in the past. Elderly people seem to tolerate slight degrees of hypothyroidism and may actually benefit from it,” Dr. Michael T. McDermott said at a conference on internal medicine sponsored by the University of Colorado.
The American Thyroid Association guidelines issued late last year (Thyroid. 2014 Dec;24[12]:1670-75) raise the target serum TSH to 4-6 mIU/L in hypothyroid individuals age 70 or older. The target serum TSH in nonelderly, nonpregnant patients remains unchanged at 0.5-4.5 mIU/L, noted Dr. McDermott, professor of medicine and director of endocrinology and diabetes practice at the University of Colorado Hospital, Aurora.
“The slightly higher TSH treatment target in elderly patients is very heavily evidence-based. Studies showed that people over age 70 often did worse if their TSH was maintained in the low end of the normal range, and that people whose TSH was maintained up to about 6 mIU/L didn’t seem to have any adverse effects from that. It’s kind of a moving target: we’ll probably see the data reevaluated over time. But I think it’s clear that normal elderly people have a normal TSH that’s slightly higher,” according to the endocrinologist.
The starting dose of levothyroxine (LT4) in older patients is 25-50 mcg/day. The TSH level should be rechecked after 6 weeks in patients with overt hypothyroidism and 6-10 weeks in those with subclinical hypothyroidism, with LT4 then being titrated in the elderly until it’s in the 4-6 mIU/L range.
Speaking of subclinical hypothyroidism, which is defined by an elevated TSH but a normal free T4 level, four studies now show the same thing: While subclinical hypothyroidism is independently associated with increased cardiovascular mortality in patients under age 65, it does not carry any increased cardiovascular mortality risk in older individuals. The first of these studies, a meta-analysis of 15 clinical trials totalling 2,531 subclinically hypothyroid patients and more than 26,000 controls, found a 37% increase in cardiovascular mortality in patients younger than 65 with subclinical hypothyroidism, but no increase in older people with the disorder (J Clin Endocrinol Metab. 2008 Aug;93[8]:2998-3007).
“We don’t know why that is, but it’s the reason the recommended TSH range when treating people for subclinical or overt hypothyroidism has now changed in people over age 70,” Dr. McDermott explained.
The consensus recommendations of the American Thyroid Association and the American Association of Clinical Endocrinologists advise treatment of subclinical hypothyroidism involving a TSH level greater than 10.0 mIU/L. In patients with lesser elevations of TSH, however, clinical judgment is critical in deciding whether to treat or monitor.
“If the person has symptoms, treatment is very reasonable. You should know, however, that one-third of people who have a TSH of 4.5-10.0 mIU/L will have a normal TSH 1 year later if you don’t treat them. So if they’re not symptomatic you may usually monitor these patients,” he said.
While LT4 remains the treatment of choice for hypothyroidism, 16% of patients have persistent symptoms despite optimal LT4 therapy. They appear to benefit from a combination of LT4 and liothyronine (LT3) given in a 10:1 ratio. Because LT3 lasts for only about 8 hours, it’s best administered twice daily. Thyroid tests should be obtained before the medication is taken because triiodothyronine (T3) levels rise abruptly in response to a dose.
Dr. McDermott reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
Testosterone regimen may affect cardiovascular risk
ESTES PARK, COLO. – The delivery route of testosterone therapy in men with hypogonadism has emerged as a new issue in the still-developing story of the therapy’s cardiovascular safety.
A retrospective cohort study of more than 544,000 men in the United States and England who initiated testosterone therapy concluded that the associated cardiovascular risk varied significantly with the dosage form prescribed.

Testosterone by injection inevitably results in pharmacologic hormone levels. Study participants who initiated testosterone injections had a significant 26% increase in the 1-year risk of the composite endpoint of myocardial infarction, unstable angina, or stroke, compared with men using testosterone gels, which generally achieve physiologic levels. The testosterone injectors also had a 34% increase in 1-year all-cause mortality and a 16% increase in all-cause hospitalizations.
In all, 27% of the men received testosterone injections, 56% gels, and 7% patches. Outcomes did not differ between men on the gels and those on testosterone patches (JAMA Intern Med. 2015 Jul 1;175[7]:1187-96).
“This study has made our VA hospital – and VAs across the country – relook at what they’re covering as far as testosterone therapy,” Dr. Margaret E. Wierman said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wierman, who wrote the editorial accompanying the JAMA study, acknowledged the inherent limitations of an epidemiologic study such as this, which can’t prove cause-and-effect. Nonetheless, the study’s strengths, including its sheer size, make it deserving of attention. And the findings raise legitimate concerns about the huge increase in testosterone prescribing in recent years in the U.S. and elsewhere, said Dr. Wierman, who is chief of endocrinology at the Denver VA Medical Center and professor of medicine, physiology and biophysics at the university (JAMA Intern Med. 2015;175[7]:1197-8).
Those concerns were brought to the fore in what she termed an “alarming” Food and Drug Administration report issued last year. The FDA determined that during 2010-2013, testosterone prescriptions in the U.S. jumped by 76% to 2.3 million annually. Disturbingly, hypogonadism was documented in only 50% of patient charts. One quarter of the men didn’t have a baseline testosterone measurement, and 21% never had a follow-up level checked after going on the hormone therapy.
“It shows there’s a lot of charlatanism out there, and a lot of abuse,” she commented.
The FDA also found that 57% of men being prescribed testosterone were also prescribed cardiac medications, suggesting they are at increased cardiovascular risk. Yet the cardiovascular safety of testosterone therapy remains an open question, with all eyes now on the 800-subject, randomized, placebo-controlled, National Institute on Aging–sponsored Testosterone Trial in Older Men, due to report results next year.
In the interim, Dr. Wierman’s take-home message on testosterone, based on her decades of work in the field, is simple: Too little is bad; it is manifest in a variety of physical, psychologic, and sexual symptoms, many of which are related to aging and aren’t sensitive or specific to hypogonadism. Too much is bad as well, posing potential risks of accelerated growth of undiagnosed prostate cancer, tissue edema in patients with cardiac, liver, or renal disease, gynecomastia, erythrocytosis, sleep apnea, stimulation of platelet aggregation, and possibly an increase in cardiovascular events.
The virtues of the middle path were recently underscored in a study of 3,690 community-dwelling Australian men ages 70-89. Over the course of up to 9 years of follow-up, death rates were lower in men in the middle quartiles for testosterone than in those with low or high levels (J Clin Endocrinol Metab. 2014 Jan;99[1]:E9-18).
“This suggests that there may be side effects of pushing testosterone up above the physiologic range, at least in some sets of men,” according to Dr. Wierman.
She fully supports the Endocrine Society’s recommendations to treat men with both signs and symptoms of hypogonadism and documented low testosterone due to a known disorder, and to target physiologic testosterone levels.
“Usually you can find out what the cause is. I want to be a hormone detective. I want to find out what the cause is because if I can reverse the cause, I’d rather have the testosterone level come up on its own,” the endocrinologist said.
Of course, the cause isn’t always reversible. For example, high-dose narcotic therapy is one of the most common causes of acquired central hypogonadism in VA hospitals.
“There are a lot of wounded young men coming back from the war who have horrible osteoporosis and metabolic syndrome who are on narcotics and can’t get off them, and who are not getting testosterone and should be on it,” she said.
There has been a major change in thinking with regard to late-onset hypogonadism, also known as andropause, a disorder that has served as the rationale for much testosterone prescribing. Fifteen years, ago based on data from the Baltimore Longitudinal Study on Aging, it was thought that up to 30% of older men have andropause; however, that conclusion was based solely on testosterone levels, with no consideration of signs and symptoms.
More recently, European investigators used an appropriately more rigorous definition of andropause: that is, a serum total testosterone level below 320 ng/mL plus at least three sexual symptoms, such as low sexual desire, poor morning erection, and erectile dysfunction. By this definition, the prevalence of andropause is much lower, a maximum of 3%-5%. And it’s influenced by advancing age, body mass index, and comorbid conditions (N Engl J Med. 2010 Jul 8;363[2]:123-35).
“The 30% prevalence figure that’s out there is just wrong,” Dr. Wierman stressed. “There may be a diagnosis of late-onset hypogonadism – it’s a diagnosis of exclusion – but it’s much lower.”
In a follow-up study, the same European researchers showed that weight loss in middle-aged and older men was associated with a proportional increase in serum testosterone and sex-hormone binding globulin, while weight gain brought a proportional drop in testosterone and SHBG (Eur J Endocrinol. 2013 Feb 20;168[3]:445-55).
Dr. Wierman said this study contains an important lesson for everyday clinical practice: In overweight older men with low-normal testosterone levels in the 200-250 ng/mL range, the primary recommendation should be diet and lifestyle modification aimed at achieving weight loss, not testosterone therapy. Successful weight loss will boost their testosterone level, improve comorbid obstructive sleep apnea, enhance their cardiovascular and metabolic fitness, and in some cases improve erectile dysfunction, although she was quick to add that low testosterone is “actually a pretty modest cause” of erectile dysfunction.
The number-one cause of erectile dysfunction is poor vascular plumbing as predicted by hypertension and hyperlipidemia. Neurogenic causes are number two and are predicted by chronic back injury, diabetes, and vitamin B12 deficiency. Hormonal causes are next, followed by performance anxiety and other psychogenic issues, and lastly iatrogenic causes involving medication side effects.
Dr. Wierman reported that she is coprincipal investigator for a clinical trial on neuroendocrine dysfunction during rehabilitation after traumatic brain injury funded by the Colorado Brain Trust. Abbvie donates the testosterone gel and placebo utilized in the study.
ESTES PARK, COLO. – The delivery route of testosterone therapy in men with hypogonadism has emerged as a new issue in the still-developing story of the therapy’s cardiovascular safety.
A retrospective cohort study of more than 544,000 men in the United States and England who initiated testosterone therapy concluded that the associated cardiovascular risk varied significantly with the dosage form prescribed.
Testosterone by injection inevitably results in pharmacologic hormone levels. Study participants who initiated testosterone injections had a significant 26% increase in the 1-year risk of the composite endpoint of myocardial infarction, unstable angina, or stroke, compared with men using testosterone gels, which generally achieve physiologic levels. The testosterone injectors also had a 34% increase in 1-year all-cause mortality and a 16% increase in all-cause hospitalizations.
In all, 27% of the men received testosterone injections, 56% gels, and 7% patches. Outcomes did not differ between men on the gels and those on testosterone patches (JAMA Intern Med. 2015 Jul 1;175[7]:1187-96).
“This study has made our VA hospital – and VAs across the country – relook at what they’re covering as far as testosterone therapy,” Dr. Margaret E. Wierman said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wierman, who wrote the editorial accompanying the JAMA study, acknowledged the inherent limitations of an epidemiologic study such as this, which can’t prove cause-and-effect. Nonetheless, the study’s strengths, including its sheer size, make it deserving of attention. And the findings raise legitimate concerns about the huge increase in testosterone prescribing in recent years in the U.S. and elsewhere, said Dr. Wierman, who is chief of endocrinology at the Denver VA Medical Center and professor of medicine, physiology and biophysics at the university (JAMA Intern Med. 2015;175[7]:1197-8).
Those concerns were brought to the fore in what she termed an “alarming” Food and Drug Administration report issued last year. The FDA determined that during 2010-2013, testosterone prescriptions in the U.S. jumped by 76% to 2.3 million annually. Disturbingly, hypogonadism was documented in only 50% of patient charts. One quarter of the men didn’t have a baseline testosterone measurement, and 21% never had a follow-up level checked after going on the hormone therapy.
“It shows there’s a lot of charlatanism out there, and a lot of abuse,” she commented.
The FDA also found that 57% of men being prescribed testosterone were also prescribed cardiac medications, suggesting they are at increased cardiovascular risk. Yet the cardiovascular safety of testosterone therapy remains an open question, with all eyes now on the 800-subject, randomized, placebo-controlled, National Institute on Aging–sponsored Testosterone Trial in Older Men, due to report results next year.
In the interim, Dr. Wierman’s take-home message on testosterone, based on her decades of work in the field, is simple: Too little is bad; it is manifest in a variety of physical, psychologic, and sexual symptoms, many of which are related to aging and aren’t sensitive or specific to hypogonadism. Too much is bad as well, posing potential risks of accelerated growth of undiagnosed prostate cancer, tissue edema in patients with cardiac, liver, or renal disease, gynecomastia, erythrocytosis, sleep apnea, stimulation of platelet aggregation, and possibly an increase in cardiovascular events.
The virtues of the middle path were recently underscored in a study of 3,690 community-dwelling Australian men ages 70-89. Over the course of up to 9 years of follow-up, death rates were lower in men in the middle quartiles for testosterone than in those with low or high levels (J Clin Endocrinol Metab. 2014 Jan;99[1]:E9-18).
“This suggests that there may be side effects of pushing testosterone up above the physiologic range, at least in some sets of men,” according to Dr. Wierman.
She fully supports the Endocrine Society’s recommendations to treat men with both signs and symptoms of hypogonadism and documented low testosterone due to a known disorder, and to target physiologic testosterone levels.
“Usually you can find out what the cause is. I want to be a hormone detective. I want to find out what the cause is because if I can reverse the cause, I’d rather have the testosterone level come up on its own,” the endocrinologist said.
Of course, the cause isn’t always reversible. For example, high-dose narcotic therapy is one of the most common causes of acquired central hypogonadism in VA hospitals.
“There are a lot of wounded young men coming back from the war who have horrible osteoporosis and metabolic syndrome who are on narcotics and can’t get off them, and who are not getting testosterone and should be on it,” she said.
There has been a major change in thinking with regard to late-onset hypogonadism, also known as andropause, a disorder that has served as the rationale for much testosterone prescribing. Fifteen years, ago based on data from the Baltimore Longitudinal Study on Aging, it was thought that up to 30% of older men have andropause; however, that conclusion was based solely on testosterone levels, with no consideration of signs and symptoms.
More recently, European investigators used an appropriately more rigorous definition of andropause: that is, a serum total testosterone level below 320 ng/mL plus at least three sexual symptoms, such as low sexual desire, poor morning erection, and erectile dysfunction. By this definition, the prevalence of andropause is much lower, a maximum of 3%-5%. And it’s influenced by advancing age, body mass index, and comorbid conditions (N Engl J Med. 2010 Jul 8;363[2]:123-35).
“The 30% prevalence figure that’s out there is just wrong,” Dr. Wierman stressed. “There may be a diagnosis of late-onset hypogonadism – it’s a diagnosis of exclusion – but it’s much lower.”
In a follow-up study, the same European researchers showed that weight loss in middle-aged and older men was associated with a proportional increase in serum testosterone and sex-hormone binding globulin, while weight gain brought a proportional drop in testosterone and SHBG (Eur J Endocrinol. 2013 Feb 20;168[3]:445-55).
Dr. Wierman said this study contains an important lesson for everyday clinical practice: In overweight older men with low-normal testosterone levels in the 200-250 ng/mL range, the primary recommendation should be diet and lifestyle modification aimed at achieving weight loss, not testosterone therapy. Successful weight loss will boost their testosterone level, improve comorbid obstructive sleep apnea, enhance their cardiovascular and metabolic fitness, and in some cases improve erectile dysfunction, although she was quick to add that low testosterone is “actually a pretty modest cause” of erectile dysfunction.
The number-one cause of erectile dysfunction is poor vascular plumbing as predicted by hypertension and hyperlipidemia. Neurogenic causes are number two and are predicted by chronic back injury, diabetes, and vitamin B12 deficiency. Hormonal causes are next, followed by performance anxiety and other psychogenic issues, and lastly iatrogenic causes involving medication side effects.
Dr. Wierman reported that she is coprincipal investigator for a clinical trial on neuroendocrine dysfunction during rehabilitation after traumatic brain injury funded by the Colorado Brain Trust. Abbvie donates the testosterone gel and placebo utilized in the study.
ESTES PARK, COLO. – The delivery route of testosterone therapy in men with hypogonadism has emerged as a new issue in the still-developing story of the therapy’s cardiovascular safety.
A retrospective cohort study of more than 544,000 men in the United States and England who initiated testosterone therapy concluded that the associated cardiovascular risk varied significantly with the dosage form prescribed.
Testosterone by injection inevitably results in pharmacologic hormone levels. Study participants who initiated testosterone injections had a significant 26% increase in the 1-year risk of the composite endpoint of myocardial infarction, unstable angina, or stroke, compared with men using testosterone gels, which generally achieve physiologic levels. The testosterone injectors also had a 34% increase in 1-year all-cause mortality and a 16% increase in all-cause hospitalizations.
In all, 27% of the men received testosterone injections, 56% gels, and 7% patches. Outcomes did not differ between men on the gels and those on testosterone patches (JAMA Intern Med. 2015 Jul 1;175[7]:1187-96).
“This study has made our VA hospital – and VAs across the country – relook at what they’re covering as far as testosterone therapy,” Dr. Margaret E. Wierman said at a conference on internal medicine sponsored by the University of Colorado.
Dr. Wierman, who wrote the editorial accompanying the JAMA study, acknowledged the inherent limitations of an epidemiologic study such as this, which can’t prove cause-and-effect. Nonetheless, the study’s strengths, including its sheer size, make it deserving of attention. And the findings raise legitimate concerns about the huge increase in testosterone prescribing in recent years in the U.S. and elsewhere, said Dr. Wierman, who is chief of endocrinology at the Denver VA Medical Center and professor of medicine, physiology and biophysics at the university (JAMA Intern Med. 2015;175[7]:1197-8).
Those concerns were brought to the fore in what she termed an “alarming” Food and Drug Administration report issued last year. The FDA determined that during 2010-2013, testosterone prescriptions in the U.S. jumped by 76% to 2.3 million annually. Disturbingly, hypogonadism was documented in only 50% of patient charts. One quarter of the men didn’t have a baseline testosterone measurement, and 21% never had a follow-up level checked after going on the hormone therapy.
“It shows there’s a lot of charlatanism out there, and a lot of abuse,” she commented.
The FDA also found that 57% of men being prescribed testosterone were also prescribed cardiac medications, suggesting they are at increased cardiovascular risk. Yet the cardiovascular safety of testosterone therapy remains an open question, with all eyes now on the 800-subject, randomized, placebo-controlled, National Institute on Aging–sponsored Testosterone Trial in Older Men, due to report results next year.
In the interim, Dr. Wierman’s take-home message on testosterone, based on her decades of work in the field, is simple: Too little is bad; it is manifest in a variety of physical, psychologic, and sexual symptoms, many of which are related to aging and aren’t sensitive or specific to hypogonadism. Too much is bad as well, posing potential risks of accelerated growth of undiagnosed prostate cancer, tissue edema in patients with cardiac, liver, or renal disease, gynecomastia, erythrocytosis, sleep apnea, stimulation of platelet aggregation, and possibly an increase in cardiovascular events.
The virtues of the middle path were recently underscored in a study of 3,690 community-dwelling Australian men ages 70-89. Over the course of up to 9 years of follow-up, death rates were lower in men in the middle quartiles for testosterone than in those with low or high levels (J Clin Endocrinol Metab. 2014 Jan;99[1]:E9-18).
“This suggests that there may be side effects of pushing testosterone up above the physiologic range, at least in some sets of men,” according to Dr. Wierman.
She fully supports the Endocrine Society’s recommendations to treat men with both signs and symptoms of hypogonadism and documented low testosterone due to a known disorder, and to target physiologic testosterone levels.
“Usually you can find out what the cause is. I want to be a hormone detective. I want to find out what the cause is because if I can reverse the cause, I’d rather have the testosterone level come up on its own,” the endocrinologist said.
Of course, the cause isn’t always reversible. For example, high-dose narcotic therapy is one of the most common causes of acquired central hypogonadism in VA hospitals.
“There are a lot of wounded young men coming back from the war who have horrible osteoporosis and metabolic syndrome who are on narcotics and can’t get off them, and who are not getting testosterone and should be on it,” she said.
There has been a major change in thinking with regard to late-onset hypogonadism, also known as andropause, a disorder that has served as the rationale for much testosterone prescribing. Fifteen years, ago based on data from the Baltimore Longitudinal Study on Aging, it was thought that up to 30% of older men have andropause; however, that conclusion was based solely on testosterone levels, with no consideration of signs and symptoms.
More recently, European investigators used an appropriately more rigorous definition of andropause: that is, a serum total testosterone level below 320 ng/mL plus at least three sexual symptoms, such as low sexual desire, poor morning erection, and erectile dysfunction. By this definition, the prevalence of andropause is much lower, a maximum of 3%-5%. And it’s influenced by advancing age, body mass index, and comorbid conditions (N Engl J Med. 2010 Jul 8;363[2]:123-35).
“The 30% prevalence figure that’s out there is just wrong,” Dr. Wierman stressed. “There may be a diagnosis of late-onset hypogonadism – it’s a diagnosis of exclusion – but it’s much lower.”
In a follow-up study, the same European researchers showed that weight loss in middle-aged and older men was associated with a proportional increase in serum testosterone and sex-hormone binding globulin, while weight gain brought a proportional drop in testosterone and SHBG (Eur J Endocrinol. 2013 Feb 20;168[3]:445-55).
Dr. Wierman said this study contains an important lesson for everyday clinical practice: In overweight older men with low-normal testosterone levels in the 200-250 ng/mL range, the primary recommendation should be diet and lifestyle modification aimed at achieving weight loss, not testosterone therapy. Successful weight loss will boost their testosterone level, improve comorbid obstructive sleep apnea, enhance their cardiovascular and metabolic fitness, and in some cases improve erectile dysfunction, although she was quick to add that low testosterone is “actually a pretty modest cause” of erectile dysfunction.
The number-one cause of erectile dysfunction is poor vascular plumbing as predicted by hypertension and hyperlipidemia. Neurogenic causes are number two and are predicted by chronic back injury, diabetes, and vitamin B12 deficiency. Hormonal causes are next, followed by performance anxiety and other psychogenic issues, and lastly iatrogenic causes involving medication side effects.
Dr. Wierman reported that she is coprincipal investigator for a clinical trial on neuroendocrine dysfunction during rehabilitation after traumatic brain injury funded by the Colorado Brain Trust. Abbvie donates the testosterone gel and placebo utilized in the study.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Sexual abuse history may promote migraine transformation
VALENCIA, SPAIN – A history of childhood sexual abuse is nearly fourfold more common among chronic migraine patients than in those with episodic migraine, Dr. Brad Torphy reported at the International Headache Congress.
This association raises the possibility that prior sexual abuse is a contributing factor in the transformation from episodic migraine – defined as fewer than 15 headache days per month – to the more serious and difficult-to-treat chronic migraine, which entails headaches on 15 or more days monthly, said Dr. Torphy of Diamond Headache Clinic in Chicago.
“The clinical implications of these findings, and what I’m stressing, is the importance of intervention – such as psychological counseling – in episodic migraine patients who have a history of abuse. The other key point is that patients who have episodic migraine may warrant more aggressive therapy, including going on preventive medications sooner, if they have a history of sexual abuse, because they’re probably at risk for progression to chronic migraine,” he said in an interview at the meeting.
Dr. Torphy presented a retrospective study of all new patients seen at the Diamond Headache Clinic during the final 4 months of last year. The new-patient questionnaire includes a section about past sexual abuse. Such a history was reported by 6 (4.4%) of the 135 episodic migraine patients, compared with 30 (15.5%) of the 194 patients with chronic migraine.
“What made me think about doing this study is that at the Diamond Clinic every week we have a meeting with our psychology group, and it just seemed like week after week so many patients had these horrifying stories of their childhood. I thought there must be a connection between that history of sexual abuse and progression to chronic migraine,” he said.
He added that, based upon his experience in the clinic, he suspects that the true proportion of patients with a positive history for sexual abuse is considerably higher than the rates the new-patient questionnaire would suggest.
“A lot of factors would lead to that being a very low number. It’s the patient’s first visit, and it’s a paper questionnaire so patients may not be comfortable checking that box when they don’t know who’s going to see the results. I’ve had cases where patients shared with me only after two or three visits that, yes, I do have that history. I think it’s underreported across the board,” Dr. Torphy continued.
In his review of the literature he found that other investigators have tended either to lump together all kinds of abuse – physical, emotional, and sexual – in analyzing an association with migraine, or if they looked at sexual abuse in particular it was in association with all types of chronic pain, not specifically migraine.
The meeting was sponsored by the International Headache Society and the American Headache Society. Dr. Torphy reported no financial conflicts.
VALENCIA, SPAIN – A history of childhood sexual abuse is nearly fourfold more common among chronic migraine patients than in those with episodic migraine, Dr. Brad Torphy reported at the International Headache Congress.
This association raises the possibility that prior sexual abuse is a contributing factor in the transformation from episodic migraine – defined as fewer than 15 headache days per month – to the more serious and difficult-to-treat chronic migraine, which entails headaches on 15 or more days monthly, said Dr. Torphy of Diamond Headache Clinic in Chicago.
“The clinical implications of these findings, and what I’m stressing, is the importance of intervention – such as psychological counseling – in episodic migraine patients who have a history of abuse. The other key point is that patients who have episodic migraine may warrant more aggressive therapy, including going on preventive medications sooner, if they have a history of sexual abuse, because they’re probably at risk for progression to chronic migraine,” he said in an interview at the meeting.
Dr. Torphy presented a retrospective study of all new patients seen at the Diamond Headache Clinic during the final 4 months of last year. The new-patient questionnaire includes a section about past sexual abuse. Such a history was reported by 6 (4.4%) of the 135 episodic migraine patients, compared with 30 (15.5%) of the 194 patients with chronic migraine.
“What made me think about doing this study is that at the Diamond Clinic every week we have a meeting with our psychology group, and it just seemed like week after week so many patients had these horrifying stories of their childhood. I thought there must be a connection between that history of sexual abuse and progression to chronic migraine,” he said.
He added that, based upon his experience in the clinic, he suspects that the true proportion of patients with a positive history for sexual abuse is considerably higher than the rates the new-patient questionnaire would suggest.
“A lot of factors would lead to that being a very low number. It’s the patient’s first visit, and it’s a paper questionnaire so patients may not be comfortable checking that box when they don’t know who’s going to see the results. I’ve had cases where patients shared with me only after two or three visits that, yes, I do have that history. I think it’s underreported across the board,” Dr. Torphy continued.
In his review of the literature he found that other investigators have tended either to lump together all kinds of abuse – physical, emotional, and sexual – in analyzing an association with migraine, or if they looked at sexual abuse in particular it was in association with all types of chronic pain, not specifically migraine.
The meeting was sponsored by the International Headache Society and the American Headache Society. Dr. Torphy reported no financial conflicts.
VALENCIA, SPAIN – A history of childhood sexual abuse is nearly fourfold more common among chronic migraine patients than in those with episodic migraine, Dr. Brad Torphy reported at the International Headache Congress.
This association raises the possibility that prior sexual abuse is a contributing factor in the transformation from episodic migraine – defined as fewer than 15 headache days per month – to the more serious and difficult-to-treat chronic migraine, which entails headaches on 15 or more days monthly, said Dr. Torphy of Diamond Headache Clinic in Chicago.
“The clinical implications of these findings, and what I’m stressing, is the importance of intervention – such as psychological counseling – in episodic migraine patients who have a history of abuse. The other key point is that patients who have episodic migraine may warrant more aggressive therapy, including going on preventive medications sooner, if they have a history of sexual abuse, because they’re probably at risk for progression to chronic migraine,” he said in an interview at the meeting.
Dr. Torphy presented a retrospective study of all new patients seen at the Diamond Headache Clinic during the final 4 months of last year. The new-patient questionnaire includes a section about past sexual abuse. Such a history was reported by 6 (4.4%) of the 135 episodic migraine patients, compared with 30 (15.5%) of the 194 patients with chronic migraine.
“What made me think about doing this study is that at the Diamond Clinic every week we have a meeting with our psychology group, and it just seemed like week after week so many patients had these horrifying stories of their childhood. I thought there must be a connection between that history of sexual abuse and progression to chronic migraine,” he said.
He added that, based upon his experience in the clinic, he suspects that the true proportion of patients with a positive history for sexual abuse is considerably higher than the rates the new-patient questionnaire would suggest.
“A lot of factors would lead to that being a very low number. It’s the patient’s first visit, and it’s a paper questionnaire so patients may not be comfortable checking that box when they don’t know who’s going to see the results. I’ve had cases where patients shared with me only after two or three visits that, yes, I do have that history. I think it’s underreported across the board,” Dr. Torphy continued.
In his review of the literature he found that other investigators have tended either to lump together all kinds of abuse – physical, emotional, and sexual – in analyzing an association with migraine, or if they looked at sexual abuse in particular it was in association with all types of chronic pain, not specifically migraine.
The meeting was sponsored by the International Headache Society and the American Headache Society. Dr. Torphy reported no financial conflicts.
AT IHC 2015
Key clinical point: Episodic migraine patients with a history of childhood sexual abuse may be at increased risk of transformation to chronic migraine.
Major finding: A history of childhood sexual abuse was self-reported by 4.4% of episodic migraine patients, compared with 15.5% chronic migraineurs.
Data source: A retrospective chart review of 329 consecutive migraine patients seen at a specialized headache clinic.
Disclosures: The presenter reported no financial conflicts.
New era ahead in spondyloarthritis therapy
DENVER – The emerging new era in the treatment of spondyloarthritis is combined blockade of tumor necrosis factor–alpha (TNF-alpha) and interleukin-17 using a bispecific antibody, Dr. Siba P. Raychaudhuri predicted at the annual meeting of the Spondyloarthritis Research and Treatment Network.
“This is the next generation of antibody therapies for spondyloarthritis,” said Dr. Raychaudhuri, a rheumatologist at the University of California, Davis.

This novel approach has a sound theoretical basis. Moreover, studies in mouse models, including models of rheumatoid arthritis (Arthritis Rheumatol. 2015 Jan;67[1]:51-62), have been positive. And proprietary bispecific anti-TNF-alpha/IL-17 antibodies are now in phase I and phase II clinical trials for various forms of spondyloarthritis, he noted.
The impetus for development of this new therapy is widespread agreement that while TNF inhibition has been a step forward in the treatment of axial spondyloarthritis, the efficacy is less than hoped for with these potent and costly agents.
“Things have been sort of gray for almost the last 10 years. All the evidence suggests we’re not getting full efficacy with anti-TNF therapy. We’re getting stuck at about a 60% ASAS 20 response,” he observed.
The explanation for this merely middling success rate appears to be that TNF inhibition induces a counterregulatory uptick in the IL-17 pathway. And in animal models, IL-17 is a key mediator of joint inflammation and destruction.
Dr. Raychaudhuri noted that brodalumab, an investigational human monoclonal antibody directed against IL-17 receptor A, has been shown “reasonably effective” in a phase II study in patients with psoriatic arthritis, which is part of the spondyloarthritis family of autoimmune diseases, achieving an ACR 20 response rate of 39% at week 12 in the high-dose arm (N Engl J Med. 2014 Jun 12;370[24]:2295-306).
The expectation is that by inhibiting both TNF-alpha and IL-17 using a bispecific protein composed of fragments of two different monoclonal antibodies, the result will be reduced growth and differentiation of proinflammatory T cells, decreased T cell migration, and synergistic clinical efficacy, compared with what’s attainable by addressing either target alone.
Dr. Raychaudhuri reported receiving research grants from or serving as a consultant to Abbott, Amgen, Celgene, UCB, and Janssen Biotech.
DENVER – The emerging new era in the treatment of spondyloarthritis is combined blockade of tumor necrosis factor–alpha (TNF-alpha) and interleukin-17 using a bispecific antibody, Dr. Siba P. Raychaudhuri predicted at the annual meeting of the Spondyloarthritis Research and Treatment Network.
“This is the next generation of antibody therapies for spondyloarthritis,” said Dr. Raychaudhuri, a rheumatologist at the University of California, Davis.
This novel approach has a sound theoretical basis. Moreover, studies in mouse models, including models of rheumatoid arthritis (Arthritis Rheumatol. 2015 Jan;67[1]:51-62), have been positive. And proprietary bispecific anti-TNF-alpha/IL-17 antibodies are now in phase I and phase II clinical trials for various forms of spondyloarthritis, he noted.
The impetus for development of this new therapy is widespread agreement that while TNF inhibition has been a step forward in the treatment of axial spondyloarthritis, the efficacy is less than hoped for with these potent and costly agents.
“Things have been sort of gray for almost the last 10 years. All the evidence suggests we’re not getting full efficacy with anti-TNF therapy. We’re getting stuck at about a 60% ASAS 20 response,” he observed.
The explanation for this merely middling success rate appears to be that TNF inhibition induces a counterregulatory uptick in the IL-17 pathway. And in animal models, IL-17 is a key mediator of joint inflammation and destruction.
Dr. Raychaudhuri noted that brodalumab, an investigational human monoclonal antibody directed against IL-17 receptor A, has been shown “reasonably effective” in a phase II study in patients with psoriatic arthritis, which is part of the spondyloarthritis family of autoimmune diseases, achieving an ACR 20 response rate of 39% at week 12 in the high-dose arm (N Engl J Med. 2014 Jun 12;370[24]:2295-306).
The expectation is that by inhibiting both TNF-alpha and IL-17 using a bispecific protein composed of fragments of two different monoclonal antibodies, the result will be reduced growth and differentiation of proinflammatory T cells, decreased T cell migration, and synergistic clinical efficacy, compared with what’s attainable by addressing either target alone.
Dr. Raychaudhuri reported receiving research grants from or serving as a consultant to Abbott, Amgen, Celgene, UCB, and Janssen Biotech.
DENVER – The emerging new era in the treatment of spondyloarthritis is combined blockade of tumor necrosis factor–alpha (TNF-alpha) and interleukin-17 using a bispecific antibody, Dr. Siba P. Raychaudhuri predicted at the annual meeting of the Spondyloarthritis Research and Treatment Network.
“This is the next generation of antibody therapies for spondyloarthritis,” said Dr. Raychaudhuri, a rheumatologist at the University of California, Davis.
This novel approach has a sound theoretical basis. Moreover, studies in mouse models, including models of rheumatoid arthritis (Arthritis Rheumatol. 2015 Jan;67[1]:51-62), have been positive. And proprietary bispecific anti-TNF-alpha/IL-17 antibodies are now in phase I and phase II clinical trials for various forms of spondyloarthritis, he noted.
The impetus for development of this new therapy is widespread agreement that while TNF inhibition has been a step forward in the treatment of axial spondyloarthritis, the efficacy is less than hoped for with these potent and costly agents.
“Things have been sort of gray for almost the last 10 years. All the evidence suggests we’re not getting full efficacy with anti-TNF therapy. We’re getting stuck at about a 60% ASAS 20 response,” he observed.
The explanation for this merely middling success rate appears to be that TNF inhibition induces a counterregulatory uptick in the IL-17 pathway. And in animal models, IL-17 is a key mediator of joint inflammation and destruction.
Dr. Raychaudhuri noted that brodalumab, an investigational human monoclonal antibody directed against IL-17 receptor A, has been shown “reasonably effective” in a phase II study in patients with psoriatic arthritis, which is part of the spondyloarthritis family of autoimmune diseases, achieving an ACR 20 response rate of 39% at week 12 in the high-dose arm (N Engl J Med. 2014 Jun 12;370[24]:2295-306).
The expectation is that by inhibiting both TNF-alpha and IL-17 using a bispecific protein composed of fragments of two different monoclonal antibodies, the result will be reduced growth and differentiation of proinflammatory T cells, decreased T cell migration, and synergistic clinical efficacy, compared with what’s attainable by addressing either target alone.
Dr. Raychaudhuri reported receiving research grants from or serving as a consultant to Abbott, Amgen, Celgene, UCB, and Janssen Biotech.
EXPERT ANALYSIS FROM THE 2015 SPARTAN ANNUAL MEETING

New spondyloarthritis criteria in the works
DENVER – The Spondyloarthritis Research and Treatment Network has voted decisively to create new classification criteria for axial spondyloarthritis, including both ankylosing spondylitis and nonradiographic axial spondyloarthritis.
Following the vote, in which 64% of SPARTAN members attending the group’s annual meeting voted that “this is the right time to proceed,” comoderator Dr. Liron Caplan declared, “This is a very strong push. We’ll need to begin work on our proposal immediately.”

The detailed proposal will contain the justification for new classification criteria as well as outline how SPARTAN will go about creating the criteria in an evidence-based manner with input and financing from industry and patient support groups. The proposal needs to be filed by next March in order to be considered for roughly $135,000 in joint funding from the American College of Rheumatology and the European League Against Rheumatism.
A major impetus for the ambitious project was a frank conversation SPARTAN officers had in the Spring of 2014 with officials at the Food and Drug Administration. The rheumatologists sought an explanation for the FDA’s seemingly counterintuitive rejection of adalimumab (Humira) and certolizumab pegol (Cimzia) for treatment of nonradiographic axial spondyloarthritis (nr-axSpA) on the basis of the very same randomized, controlled trials that earlier resulted in approval for that indication by the European Medicines Agency.
The FDA representatives deemed the Assessment of SpondyloArthritis Society (ASAS) classification criteria (Ann Rheum Dis. 2009;68:777-83) used in those and other SpA trials to be overly broad. They felt the ASAS criteria lack sufficient sensitivity and specificity to ensure that large numbers of patients with fibromyalgia – a far more common disorder – wouldn’t be misclassified as having SpA and treated inappropriately with biologics, which aren’t effective in fibromyalgia, explained Dr. John D. Reveille, professor and vice-chair of rheumatology at the University of Texas, Houston, who attended the meeting.
“The only physicians who can prescribe an approved anti-TNF drug or other biologic in Europe are rheumatologists. The reason the FDA was nervous about approving drugs using the ASAS criteria is because any physician in the U.S. can prescribe those drugs once they’re approved. So the authorities made a regulatory decision about who the people are who are educated or not educated in the diagnosis and management of patients with SpA,” according to Dr. Michael H. Weisman, chair and director of rheumatology at Cedars-Sinai Medical Center in Los Angeles.
Dr. Caplan of the University of Colorado, Denver, observed that developing new and improved criteria for SpA will be a multiyear endeavor. A top goal is to shed light on the natural history of nr-axSpA, about which almost nothing is known. This will probably entail developing a sizable cohort of patients with nr-axSpA, following them for 5 years or so to see who develops ankylosing spondylitis, then looking back to identify reliable predictors.

The SPARTAN vote was preceded by a formal debate on the merits of replacing the ASAS criteria. Dr. Muhammad Asim Khan, professor of medicine at Case Western Reserve University, Cleveland, who 30 years ago was a pioneer in the concept of spondylitic disease without x-ray evidence of sacroiliitis, argued that the ASAS criteria aren’t adequately doing what disease classification criteria are supposed to do: provide a simple, clear means of identifying a homogeneous population for clinical trials. By letting in substantial numbers of patients with fibromyalgia, the criteria water down the clinical outcomes of investigational therapies for SpA.

The opposing argument was provided by ASAS representative Dr. Filip Van den Bosch. He conceded the ASAS classification criteria “aren’t perfect,” but over time they have become familiar to rheumatologists worldwide.
“Modifying the criteria will lead to years of uncertainty,” argued Dr. Van den Bosch, professor of rheumatology at Ghent (Belgium) University.
If, as some have proposed, SPARTAN were to tighten the ASAS criteria by insisting that a patient lacking x-ray evidence of sacroiliitis must possess three or four SpA features instead of the two now required, the result would be a drastic reduction in the sensitivity of the criteria, he continued.
“The challenge of making a correct diagnosis of axSpA cannot be solved by modifying the ASAS criteria. I cannot think of a new SpA feature that’s been identified in the last 5 years that could be added on top of what’s already in there,” the rheumatologist said.
What’s needed, he added, is a concerted effort to better educate physicians about axSpA, including interpretation of spinal x-rays and MRIs, the disease’s signs and symptoms, and how to differentiate SpA from other disorders that cause back pain.
While nearly two-thirds of the SPARTAN membership voted in favor of developing new classification criteria, some prominent voices were raised in dissent.
“I agree with Filip,” said Dr. Weisman. “The problem is not with the criteria, it’s who’s using them.”

Dr. Robert D. Inman, professor of medicine at the University of Toronto, predicted “it’s an exercise in futility” to try to come up with a single set of classification criteria that will provide the high degree of sensitivity that patients and clinicians want so that people who present with early axSpA are not missed while at the same time providing the maximum specificity that payers and regulatory officials seek.
Dr. Sindhu Johnson, who as cochair of the ACR Classification Criteria Subcommittee has shepherded the development of new criteria for a number of rheumatologic diseases, offered the SPARTAN group some practical tips. Because European studies tend to be comprised of monoethnic cohorts, the ACR will look favorably upon a successful SPARTAN effort to incorporate African Americans, Asians, Native Americans, and other minorities in their study cohorts. And SPARTAN should be open and receptive to critical feedback from stakeholders during the criteria development process.
“Get buy in. There’s no point in developing criteria that are extremely rigorous scientifically but that the global community feels are useless, that use tests they don’t have access to. This is one of the criticisms around the Sjögren’s criteria: they require ophthalmologic testing and salivary gland biopsy, and for rheumatologists – even academic rheumatologists at recruiting centers for clinical trials – they don’t have access to this, or it takes too much time. You need to come up with something pragmatic to get buy in,” advised Dr. Johnson of the University of Toronto.
By the way, she added, if the project wins ACR and EULAR funding it can only be named an ACR/EULAR product. “No other organization can be named in the headline,” according to Dr. Johnson.
DENVER – The Spondyloarthritis Research and Treatment Network has voted decisively to create new classification criteria for axial spondyloarthritis, including both ankylosing spondylitis and nonradiographic axial spondyloarthritis.
Following the vote, in which 64% of SPARTAN members attending the group’s annual meeting voted that “this is the right time to proceed,” comoderator Dr. Liron Caplan declared, “This is a very strong push. We’ll need to begin work on our proposal immediately.”
The detailed proposal will contain the justification for new classification criteria as well as outline how SPARTAN will go about creating the criteria in an evidence-based manner with input and financing from industry and patient support groups. The proposal needs to be filed by next March in order to be considered for roughly $135,000 in joint funding from the American College of Rheumatology and the European League Against Rheumatism.
A major impetus for the ambitious project was a frank conversation SPARTAN officers had in the Spring of 2014 with officials at the Food and Drug Administration. The rheumatologists sought an explanation for the FDA’s seemingly counterintuitive rejection of adalimumab (Humira) and certolizumab pegol (Cimzia) for treatment of nonradiographic axial spondyloarthritis (nr-axSpA) on the basis of the very same randomized, controlled trials that earlier resulted in approval for that indication by the European Medicines Agency.
The FDA representatives deemed the Assessment of SpondyloArthritis Society (ASAS) classification criteria (Ann Rheum Dis. 2009;68:777-83) used in those and other SpA trials to be overly broad. They felt the ASAS criteria lack sufficient sensitivity and specificity to ensure that large numbers of patients with fibromyalgia – a far more common disorder – wouldn’t be misclassified as having SpA and treated inappropriately with biologics, which aren’t effective in fibromyalgia, explained Dr. John D. Reveille, professor and vice-chair of rheumatology at the University of Texas, Houston, who attended the meeting.
“The only physicians who can prescribe an approved anti-TNF drug or other biologic in Europe are rheumatologists. The reason the FDA was nervous about approving drugs using the ASAS criteria is because any physician in the U.S. can prescribe those drugs once they’re approved. So the authorities made a regulatory decision about who the people are who are educated or not educated in the diagnosis and management of patients with SpA,” according to Dr. Michael H. Weisman, chair and director of rheumatology at Cedars-Sinai Medical Center in Los Angeles.
Dr. Caplan of the University of Colorado, Denver, observed that developing new and improved criteria for SpA will be a multiyear endeavor. A top goal is to shed light on the natural history of nr-axSpA, about which almost nothing is known. This will probably entail developing a sizable cohort of patients with nr-axSpA, following them for 5 years or so to see who develops ankylosing spondylitis, then looking back to identify reliable predictors.
The SPARTAN vote was preceded by a formal debate on the merits of replacing the ASAS criteria. Dr. Muhammad Asim Khan, professor of medicine at Case Western Reserve University, Cleveland, who 30 years ago was a pioneer in the concept of spondylitic disease without x-ray evidence of sacroiliitis, argued that the ASAS criteria aren’t adequately doing what disease classification criteria are supposed to do: provide a simple, clear means of identifying a homogeneous population for clinical trials. By letting in substantial numbers of patients with fibromyalgia, the criteria water down the clinical outcomes of investigational therapies for SpA.
The opposing argument was provided by ASAS representative Dr. Filip Van den Bosch. He conceded the ASAS classification criteria “aren’t perfect,” but over time they have become familiar to rheumatologists worldwide.
“Modifying the criteria will lead to years of uncertainty,” argued Dr. Van den Bosch, professor of rheumatology at Ghent (Belgium) University.
If, as some have proposed, SPARTAN were to tighten the ASAS criteria by insisting that a patient lacking x-ray evidence of sacroiliitis must possess three or four SpA features instead of the two now required, the result would be a drastic reduction in the sensitivity of the criteria, he continued.
“The challenge of making a correct diagnosis of axSpA cannot be solved by modifying the ASAS criteria. I cannot think of a new SpA feature that’s been identified in the last 5 years that could be added on top of what’s already in there,” the rheumatologist said.
What’s needed, he added, is a concerted effort to better educate physicians about axSpA, including interpretation of spinal x-rays and MRIs, the disease’s signs and symptoms, and how to differentiate SpA from other disorders that cause back pain.
While nearly two-thirds of the SPARTAN membership voted in favor of developing new classification criteria, some prominent voices were raised in dissent.
“I agree with Filip,” said Dr. Weisman. “The problem is not with the criteria, it’s who’s using them.”
Dr. Robert D. Inman, professor of medicine at the University of Toronto, predicted “it’s an exercise in futility” to try to come up with a single set of classification criteria that will provide the high degree of sensitivity that patients and clinicians want so that people who present with early axSpA are not missed while at the same time providing the maximum specificity that payers and regulatory officials seek.
Dr. Sindhu Johnson, who as cochair of the ACR Classification Criteria Subcommittee has shepherded the development of new criteria for a number of rheumatologic diseases, offered the SPARTAN group some practical tips. Because European studies tend to be comprised of monoethnic cohorts, the ACR will look favorably upon a successful SPARTAN effort to incorporate African Americans, Asians, Native Americans, and other minorities in their study cohorts. And SPARTAN should be open and receptive to critical feedback from stakeholders during the criteria development process.
“Get buy in. There’s no point in developing criteria that are extremely rigorous scientifically but that the global community feels are useless, that use tests they don’t have access to. This is one of the criticisms around the Sjögren’s criteria: they require ophthalmologic testing and salivary gland biopsy, and for rheumatologists – even academic rheumatologists at recruiting centers for clinical trials – they don’t have access to this, or it takes too much time. You need to come up with something pragmatic to get buy in,” advised Dr. Johnson of the University of Toronto.
By the way, she added, if the project wins ACR and EULAR funding it can only be named an ACR/EULAR product. “No other organization can be named in the headline,” according to Dr. Johnson.
DENVER – The Spondyloarthritis Research and Treatment Network has voted decisively to create new classification criteria for axial spondyloarthritis, including both ankylosing spondylitis and nonradiographic axial spondyloarthritis.
Following the vote, in which 64% of SPARTAN members attending the group’s annual meeting voted that “this is the right time to proceed,” comoderator Dr. Liron Caplan declared, “This is a very strong push. We’ll need to begin work on our proposal immediately.”
The detailed proposal will contain the justification for new classification criteria as well as outline how SPARTAN will go about creating the criteria in an evidence-based manner with input and financing from industry and patient support groups. The proposal needs to be filed by next March in order to be considered for roughly $135,000 in joint funding from the American College of Rheumatology and the European League Against Rheumatism.
A major impetus for the ambitious project was a frank conversation SPARTAN officers had in the Spring of 2014 with officials at the Food and Drug Administration. The rheumatologists sought an explanation for the FDA’s seemingly counterintuitive rejection of adalimumab (Humira) and certolizumab pegol (Cimzia) for treatment of nonradiographic axial spondyloarthritis (nr-axSpA) on the basis of the very same randomized, controlled trials that earlier resulted in approval for that indication by the European Medicines Agency.
The FDA representatives deemed the Assessment of SpondyloArthritis Society (ASAS) classification criteria (Ann Rheum Dis. 2009;68:777-83) used in those and other SpA trials to be overly broad. They felt the ASAS criteria lack sufficient sensitivity and specificity to ensure that large numbers of patients with fibromyalgia – a far more common disorder – wouldn’t be misclassified as having SpA and treated inappropriately with biologics, which aren’t effective in fibromyalgia, explained Dr. John D. Reveille, professor and vice-chair of rheumatology at the University of Texas, Houston, who attended the meeting.
“The only physicians who can prescribe an approved anti-TNF drug or other biologic in Europe are rheumatologists. The reason the FDA was nervous about approving drugs using the ASAS criteria is because any physician in the U.S. can prescribe those drugs once they’re approved. So the authorities made a regulatory decision about who the people are who are educated or not educated in the diagnosis and management of patients with SpA,” according to Dr. Michael H. Weisman, chair and director of rheumatology at Cedars-Sinai Medical Center in Los Angeles.
Dr. Caplan of the University of Colorado, Denver, observed that developing new and improved criteria for SpA will be a multiyear endeavor. A top goal is to shed light on the natural history of nr-axSpA, about which almost nothing is known. This will probably entail developing a sizable cohort of patients with nr-axSpA, following them for 5 years or so to see who develops ankylosing spondylitis, then looking back to identify reliable predictors.
The SPARTAN vote was preceded by a formal debate on the merits of replacing the ASAS criteria. Dr. Muhammad Asim Khan, professor of medicine at Case Western Reserve University, Cleveland, who 30 years ago was a pioneer in the concept of spondylitic disease without x-ray evidence of sacroiliitis, argued that the ASAS criteria aren’t adequately doing what disease classification criteria are supposed to do: provide a simple, clear means of identifying a homogeneous population for clinical trials. By letting in substantial numbers of patients with fibromyalgia, the criteria water down the clinical outcomes of investigational therapies for SpA.
The opposing argument was provided by ASAS representative Dr. Filip Van den Bosch. He conceded the ASAS classification criteria “aren’t perfect,” but over time they have become familiar to rheumatologists worldwide.
“Modifying the criteria will lead to years of uncertainty,” argued Dr. Van den Bosch, professor of rheumatology at Ghent (Belgium) University.
If, as some have proposed, SPARTAN were to tighten the ASAS criteria by insisting that a patient lacking x-ray evidence of sacroiliitis must possess three or four SpA features instead of the two now required, the result would be a drastic reduction in the sensitivity of the criteria, he continued.
“The challenge of making a correct diagnosis of axSpA cannot be solved by modifying the ASAS criteria. I cannot think of a new SpA feature that’s been identified in the last 5 years that could be added on top of what’s already in there,” the rheumatologist said.
What’s needed, he added, is a concerted effort to better educate physicians about axSpA, including interpretation of spinal x-rays and MRIs, the disease’s signs and symptoms, and how to differentiate SpA from other disorders that cause back pain.
While nearly two-thirds of the SPARTAN membership voted in favor of developing new classification criteria, some prominent voices were raised in dissent.
“I agree with Filip,” said Dr. Weisman. “The problem is not with the criteria, it’s who’s using them.”
Dr. Robert D. Inman, professor of medicine at the University of Toronto, predicted “it’s an exercise in futility” to try to come up with a single set of classification criteria that will provide the high degree of sensitivity that patients and clinicians want so that people who present with early axSpA are not missed while at the same time providing the maximum specificity that payers and regulatory officials seek.
Dr. Sindhu Johnson, who as cochair of the ACR Classification Criteria Subcommittee has shepherded the development of new criteria for a number of rheumatologic diseases, offered the SPARTAN group some practical tips. Because European studies tend to be comprised of monoethnic cohorts, the ACR will look favorably upon a successful SPARTAN effort to incorporate African Americans, Asians, Native Americans, and other minorities in their study cohorts. And SPARTAN should be open and receptive to critical feedback from stakeholders during the criteria development process.
“Get buy in. There’s no point in developing criteria that are extremely rigorous scientifically but that the global community feels are useless, that use tests they don’t have access to. This is one of the criticisms around the Sjögren’s criteria: they require ophthalmologic testing and salivary gland biopsy, and for rheumatologists – even academic rheumatologists at recruiting centers for clinical trials – they don’t have access to this, or it takes too much time. You need to come up with something pragmatic to get buy in,” advised Dr. Johnson of the University of Toronto.
By the way, she added, if the project wins ACR and EULAR funding it can only be named an ACR/EULAR product. “No other organization can be named in the headline,” according to Dr. Johnson.
AT THE 2015 SPARTAN ANNUAL MEETING

Effective primary care screen identified for axial spondyloarthritis
DENVER – Spondyloarthritis experts have zeroed in on a simple and effective screening and referral strategy for nonrheumatologists to use in deciding which patients with chronic low back pain to send to rheumatologists for definitive diagnosis and treatment of axial spondyloarthritis.
The goal is to reduce the unacceptably long delay to diagnosis of axial spondyloarthritis – on average, 7 years – without flooding rheumatologists with enormous numbers of patients who have mechanical low back pain, a vastly more common yet generally self-limited condition, Dr. Abhijeet Danve explained at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).

He presented a systematic review of seven studies that examined various screening and referral strategies in the diagnosis of axial spondyloarthritis (axSpA). The studies totaled more than 3,300 patients with chronic low back pain.
Two key conclusions jumped out from this structured review: One, simple referral strategies and considerably more complex approaches work equally well, resulting in 35%-45% of referred patients ultimately being diagnosed by a rheumatologist as having axSpA.
And two, one strategy emerged on balance as the clear winner: “In our opinion, referring patients with chronic low back pain for more than 3 months, age of onset less than 45 years, and who meet one of three criteria – inflammatory back pain, HLA- [human leukocyte antigen] B27-positivity, or sacroiliitis on imaging – to a rheumatologist for assessment of possible axSpA would be convenient, practical, and widely acceptable,” according to Dr. Danve of Yale University, New Haven, Conn.
The more of these three criteria a patient possessed, the greater the rate of rheumatologist-diagnosed axSpa. If, for example, a patient under age 45 years with a history of low back pain for more than 3 months had classic inflammatory back pain but was HLA-B27-negative and didn’t show sacroiliitis on imaging, the rate of a confirmed diagnosis of axSpa was 25%. The axSpa diagnosis rate rose to 45% with two positive criteria and jumped to 75% in those who met all three criteria.
With appropriate application of any of the strategies evaluated in the systematic review, rheumatologists can expect to see two to three people with chronic low back pain in order to identify one patient with axSpA, he added.
SPARTAN is gearing up for a major educational initiative aimed at primary care physicians, orthopedists, physical therapists, and chiropractors. The goal is to improve early recognition of possible axSpA and bring affected patients to rheumatologists for definitive diagnosis and specialized care. Of note, Dr. Danve’s senior coinvestigator in the referral strategy study was Dr. Atul Deodhar, SPARTAN chair and professor of medicine and medical director of rheumatology clinics at Oregon Health and Science University, Portland.
DENVER – Spondyloarthritis experts have zeroed in on a simple and effective screening and referral strategy for nonrheumatologists to use in deciding which patients with chronic low back pain to send to rheumatologists for definitive diagnosis and treatment of axial spondyloarthritis.
The goal is to reduce the unacceptably long delay to diagnosis of axial spondyloarthritis – on average, 7 years – without flooding rheumatologists with enormous numbers of patients who have mechanical low back pain, a vastly more common yet generally self-limited condition, Dr. Abhijeet Danve explained at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
He presented a systematic review of seven studies that examined various screening and referral strategies in the diagnosis of axial spondyloarthritis (axSpA). The studies totaled more than 3,300 patients with chronic low back pain.
Two key conclusions jumped out from this structured review: One, simple referral strategies and considerably more complex approaches work equally well, resulting in 35%-45% of referred patients ultimately being diagnosed by a rheumatologist as having axSpA.
And two, one strategy emerged on balance as the clear winner: “In our opinion, referring patients with chronic low back pain for more than 3 months, age of onset less than 45 years, and who meet one of three criteria – inflammatory back pain, HLA- [human leukocyte antigen] B27-positivity, or sacroiliitis on imaging – to a rheumatologist for assessment of possible axSpA would be convenient, practical, and widely acceptable,” according to Dr. Danve of Yale University, New Haven, Conn.
The more of these three criteria a patient possessed, the greater the rate of rheumatologist-diagnosed axSpa. If, for example, a patient under age 45 years with a history of low back pain for more than 3 months had classic inflammatory back pain but was HLA-B27-negative and didn’t show sacroiliitis on imaging, the rate of a confirmed diagnosis of axSpa was 25%. The axSpa diagnosis rate rose to 45% with two positive criteria and jumped to 75% in those who met all three criteria.
With appropriate application of any of the strategies evaluated in the systematic review, rheumatologists can expect to see two to three people with chronic low back pain in order to identify one patient with axSpA, he added.
SPARTAN is gearing up for a major educational initiative aimed at primary care physicians, orthopedists, physical therapists, and chiropractors. The goal is to improve early recognition of possible axSpA and bring affected patients to rheumatologists for definitive diagnosis and specialized care. Of note, Dr. Danve’s senior coinvestigator in the referral strategy study was Dr. Atul Deodhar, SPARTAN chair and professor of medicine and medical director of rheumatology clinics at Oregon Health and Science University, Portland.
DENVER – Spondyloarthritis experts have zeroed in on a simple and effective screening and referral strategy for nonrheumatologists to use in deciding which patients with chronic low back pain to send to rheumatologists for definitive diagnosis and treatment of axial spondyloarthritis.
The goal is to reduce the unacceptably long delay to diagnosis of axial spondyloarthritis – on average, 7 years – without flooding rheumatologists with enormous numbers of patients who have mechanical low back pain, a vastly more common yet generally self-limited condition, Dr. Abhijeet Danve explained at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
He presented a systematic review of seven studies that examined various screening and referral strategies in the diagnosis of axial spondyloarthritis (axSpA). The studies totaled more than 3,300 patients with chronic low back pain.
Two key conclusions jumped out from this structured review: One, simple referral strategies and considerably more complex approaches work equally well, resulting in 35%-45% of referred patients ultimately being diagnosed by a rheumatologist as having axSpA.
And two, one strategy emerged on balance as the clear winner: “In our opinion, referring patients with chronic low back pain for more than 3 months, age of onset less than 45 years, and who meet one of three criteria – inflammatory back pain, HLA- [human leukocyte antigen] B27-positivity, or sacroiliitis on imaging – to a rheumatologist for assessment of possible axSpA would be convenient, practical, and widely acceptable,” according to Dr. Danve of Yale University, New Haven, Conn.
The more of these three criteria a patient possessed, the greater the rate of rheumatologist-diagnosed axSpa. If, for example, a patient under age 45 years with a history of low back pain for more than 3 months had classic inflammatory back pain but was HLA-B27-negative and didn’t show sacroiliitis on imaging, the rate of a confirmed diagnosis of axSpa was 25%. The axSpa diagnosis rate rose to 45% with two positive criteria and jumped to 75% in those who met all three criteria.
With appropriate application of any of the strategies evaluated in the systematic review, rheumatologists can expect to see two to three people with chronic low back pain in order to identify one patient with axSpA, he added.
SPARTAN is gearing up for a major educational initiative aimed at primary care physicians, orthopedists, physical therapists, and chiropractors. The goal is to improve early recognition of possible axSpA and bring affected patients to rheumatologists for definitive diagnosis and specialized care. Of note, Dr. Danve’s senior coinvestigator in the referral strategy study was Dr. Atul Deodhar, SPARTAN chair and professor of medicine and medical director of rheumatology clinics at Oregon Health and Science University, Portland.
EXPERT ANALYSIS FROM THE 2015 SPARTAN ANNUAL MEETING

New shingles vaccine delivers whopping efficacy
ESTES PARK, COLO. – The investigational HZ/su vaccine looks like it could be the herpes zoster vaccine of the future for older adults, Dr. Laura P. Hurley said at a conference on internal medicine sponsored by the University of Colorado.
The vaccine demonstrated unprecedented efficacy in the recently reported international ZOE-50 study, which featured 15,411 participants aged 50 years and older who were randomized to either vaccine or placebo.

During a mean 3.2 years of follow-up, the vaccine efficacy was 97.2% for prevention of herpes zoster in adults aged 50 and older. Herpes zoster occurred in 6 subjects in the vaccine group and 210 in the placebo arm. That’s an incidence rate of 0.3 versus 9.1 cases per 1,000 person-years (N Engl J Med. 2015 May 28;372[22]:2087-96).
The HZ/su vaccine, a subunit vaccine containing varicella-zoster virus glycoprotein E and a proprietary adjuvant system, crushed the current Zostavax vaccine in terms of vaccine efficacy in all older-age subgroups based upon comparative data from the earlier large placebo-controlled trials of Zostavax. Efficacy of the HZ/su vaccine was independent of age and was as good in persons over age 70 – the age group where the incidence of herpes zoster and its complications is highest – as in the 50- to 59-year-olds, noted Dr. Hurley, a general internist and vaccination researcher at the university.
Follow-up in ZOE-50 is ongoing and planned for at least 10 years in order to determine the duration of protection. Thus far, however, there is no signal of waning efficacy. In contrast, a recent study of nearly 7,000 Zostavax recipients showed that its efficacy declined over time and remained statistically significant only through year 8 post vaccination (Clin Infect Dis. 2015 Mar 15;60[6]:900-9), she observed.
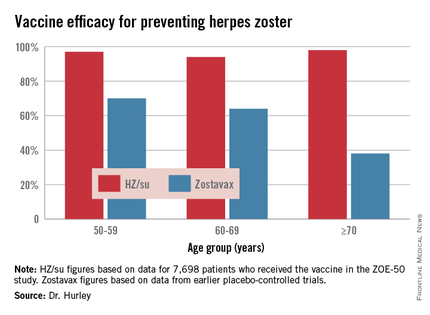
Dr. Hurley described another big advantage of the investigational vaccine, in addition to its almost-too-good-to-be-true efficacy: the fact that, unlike Zostavax, it’s not a live-virus vaccine. That means it doesn’t require freezer storage, thereby removing a major impediment to convenient vaccination. It also means it can potentially be safe for use in immunocompromised patients. Such patients were excluded from ZOE-50 but are the focus of ongoing studies conducted in patients with hematologic and solid organ malignancies, as well as renal transplant recipients.
The HZ/su vaccine has two major drawbacks. One is that it’s delivered in a series of two intramuscular doses with the injections given 2 months apart. “A two-shot series always creates problems with implementation,” according to Dr. Hurley.
The other shortcoming is the high rate of local and systemic reactions during the first week post vaccination. Most of the reactions were mild to moderate in severity and lasted only 1 or 2 days.
“Patients who had a large local reaction to the first shot and were asked to come back 2 months later for the second might be less inclined to do so,” the physician said.
The HZ/su vaccine is being developed by GlaxoSmithKline. Dr. Hurley reported having no financial conflicts of interest.
ESTES PARK, COLO. – The investigational HZ/su vaccine looks like it could be the herpes zoster vaccine of the future for older adults, Dr. Laura P. Hurley said at a conference on internal medicine sponsored by the University of Colorado.
The vaccine demonstrated unprecedented efficacy in the recently reported international ZOE-50 study, which featured 15,411 participants aged 50 years and older who were randomized to either vaccine or placebo.
During a mean 3.2 years of follow-up, the vaccine efficacy was 97.2% for prevention of herpes zoster in adults aged 50 and older. Herpes zoster occurred in 6 subjects in the vaccine group and 210 in the placebo arm. That’s an incidence rate of 0.3 versus 9.1 cases per 1,000 person-years (N Engl J Med. 2015 May 28;372[22]:2087-96).
The HZ/su vaccine, a subunit vaccine containing varicella-zoster virus glycoprotein E and a proprietary adjuvant system, crushed the current Zostavax vaccine in terms of vaccine efficacy in all older-age subgroups based upon comparative data from the earlier large placebo-controlled trials of Zostavax. Efficacy of the HZ/su vaccine was independent of age and was as good in persons over age 70 – the age group where the incidence of herpes zoster and its complications is highest – as in the 50- to 59-year-olds, noted Dr. Hurley, a general internist and vaccination researcher at the university.
Follow-up in ZOE-50 is ongoing and planned for at least 10 years in order to determine the duration of protection. Thus far, however, there is no signal of waning efficacy. In contrast, a recent study of nearly 7,000 Zostavax recipients showed that its efficacy declined over time and remained statistically significant only through year 8 post vaccination (Clin Infect Dis. 2015 Mar 15;60[6]:900-9), she observed.
Dr. Hurley described another big advantage of the investigational vaccine, in addition to its almost-too-good-to-be-true efficacy: the fact that, unlike Zostavax, it’s not a live-virus vaccine. That means it doesn’t require freezer storage, thereby removing a major impediment to convenient vaccination. It also means it can potentially be safe for use in immunocompromised patients. Such patients were excluded from ZOE-50 but are the focus of ongoing studies conducted in patients with hematologic and solid organ malignancies, as well as renal transplant recipients.
The HZ/su vaccine has two major drawbacks. One is that it’s delivered in a series of two intramuscular doses with the injections given 2 months apart. “A two-shot series always creates problems with implementation,” according to Dr. Hurley.
The other shortcoming is the high rate of local and systemic reactions during the first week post vaccination. Most of the reactions were mild to moderate in severity and lasted only 1 or 2 days.
“Patients who had a large local reaction to the first shot and were asked to come back 2 months later for the second might be less inclined to do so,” the physician said.
The HZ/su vaccine is being developed by GlaxoSmithKline. Dr. Hurley reported having no financial conflicts of interest.
ESTES PARK, COLO. – The investigational HZ/su vaccine looks like it could be the herpes zoster vaccine of the future for older adults, Dr. Laura P. Hurley said at a conference on internal medicine sponsored by the University of Colorado.
The vaccine demonstrated unprecedented efficacy in the recently reported international ZOE-50 study, which featured 15,411 participants aged 50 years and older who were randomized to either vaccine or placebo.
During a mean 3.2 years of follow-up, the vaccine efficacy was 97.2% for prevention of herpes zoster in adults aged 50 and older. Herpes zoster occurred in 6 subjects in the vaccine group and 210 in the placebo arm. That’s an incidence rate of 0.3 versus 9.1 cases per 1,000 person-years (N Engl J Med. 2015 May 28;372[22]:2087-96).
The HZ/su vaccine, a subunit vaccine containing varicella-zoster virus glycoprotein E and a proprietary adjuvant system, crushed the current Zostavax vaccine in terms of vaccine efficacy in all older-age subgroups based upon comparative data from the earlier large placebo-controlled trials of Zostavax. Efficacy of the HZ/su vaccine was independent of age and was as good in persons over age 70 – the age group where the incidence of herpes zoster and its complications is highest – as in the 50- to 59-year-olds, noted Dr. Hurley, a general internist and vaccination researcher at the university.
Follow-up in ZOE-50 is ongoing and planned for at least 10 years in order to determine the duration of protection. Thus far, however, there is no signal of waning efficacy. In contrast, a recent study of nearly 7,000 Zostavax recipients showed that its efficacy declined over time and remained statistically significant only through year 8 post vaccination (Clin Infect Dis. 2015 Mar 15;60[6]:900-9), she observed.
Dr. Hurley described another big advantage of the investigational vaccine, in addition to its almost-too-good-to-be-true efficacy: the fact that, unlike Zostavax, it’s not a live-virus vaccine. That means it doesn’t require freezer storage, thereby removing a major impediment to convenient vaccination. It also means it can potentially be safe for use in immunocompromised patients. Such patients were excluded from ZOE-50 but are the focus of ongoing studies conducted in patients with hematologic and solid organ malignancies, as well as renal transplant recipients.
The HZ/su vaccine has two major drawbacks. One is that it’s delivered in a series of two intramuscular doses with the injections given 2 months apart. “A two-shot series always creates problems with implementation,” according to Dr. Hurley.
The other shortcoming is the high rate of local and systemic reactions during the first week post vaccination. Most of the reactions were mild to moderate in severity and lasted only 1 or 2 days.
“Patients who had a large local reaction to the first shot and were asked to come back 2 months later for the second might be less inclined to do so,” the physician said.
The HZ/su vaccine is being developed by GlaxoSmithKline. Dr. Hurley reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Nocturnal Back Pain Suggests Systemic Disorder
ESTES PARK, COLO. – When a patient presents with low back pain, the single most important question to ask is this: “Are you having nocturnal pain or pain that’s unrelieved by rest?
“I really, really like this question. Most low back pain is nonspecific. Less than 5% of patients (with low back pain) have serious systemic pathology, but that’s the 5% we can’t afford to miss initially. This question gets at a key red flag for systemic disease,” Dr. Robert W. Janson explained at a conference on internal medicine sponsored by the University of Colorado.

“If you have mechanical low back pain, when you rest you feel good, just like with osteoarthritis. So if you’re writhing all night or unable to find a comfortable position, then you’re usually in that 5%. It’s inflammatory, metastatic, infectious, a fracture, or acute nerve compression,” said Dr. Janson, chief of rheumatology at the Denver VA Medical Center.
Other red flags for systemic disease include unexplained weight loss, fevers, or sweats; age over 50 years; low back pain present for longer than 6 weeks; or pain that’s unresponsive to treatment. A history of cancer, osteoporosis, corticosteroid therapy, abdominal aortic aneurysm, bowel or bladder symptoms, intravenous drug abuse, skin or urinary tract infection, morning stiffness lasting more than an hour, or sensory or motor loss are additional red flags.
Dr. Janson noted that these are essentially the same criteria the American College of Radiology uses in its 2011 recommendations on the appropriateness of obtaining a lumbar MRI.
Differentiating between mechanical low pain and the far less common inflammatory back pain, or axial spondyloarthropathy, is crucial because the prognosis and treatment are so different.
Inflammatory back pain is typically insidious in onset, relieved by exercise, frequently associated with nocturnal pain, entails more than 60 minutes of morning stiffness, and begins prior to age 40. In contrast, mechanical back pain can begin at any age, is acute in onset, exacerbated by exercise, doesn’t involve nighttime pain, and typically features less than 30 minutes of morning stiffness.
Most mechanical low back pain is self-limited and resolves within 4 weeks. It is characterized by abnormal back flexion, whereas patients with inflammatory back pain lose back mobility in all planes. They also frequently have sacroiliac joint tenderness and reduced chest expansion; patients with mechanical low back pain do not. Neurologic deficits are unusual in patients with spondyloarthropathies, since they are typically young individuals without disc disease.
Dr. Janson reported having no financial conflicts regarding his presentation.
ESTES PARK, COLO. – When a patient presents with low back pain, the single most important question to ask is this: “Are you having nocturnal pain or pain that’s unrelieved by rest?
“I really, really like this question. Most low back pain is nonspecific. Less than 5% of patients (with low back pain) have serious systemic pathology, but that’s the 5% we can’t afford to miss initially. This question gets at a key red flag for systemic disease,” Dr. Robert W. Janson explained at a conference on internal medicine sponsored by the University of Colorado.
“If you have mechanical low back pain, when you rest you feel good, just like with osteoarthritis. So if you’re writhing all night or unable to find a comfortable position, then you’re usually in that 5%. It’s inflammatory, metastatic, infectious, a fracture, or acute nerve compression,” said Dr. Janson, chief of rheumatology at the Denver VA Medical Center.
Other red flags for systemic disease include unexplained weight loss, fevers, or sweats; age over 50 years; low back pain present for longer than 6 weeks; or pain that’s unresponsive to treatment. A history of cancer, osteoporosis, corticosteroid therapy, abdominal aortic aneurysm, bowel or bladder symptoms, intravenous drug abuse, skin or urinary tract infection, morning stiffness lasting more than an hour, or sensory or motor loss are additional red flags.
Dr. Janson noted that these are essentially the same criteria the American College of Radiology uses in its 2011 recommendations on the appropriateness of obtaining a lumbar MRI.
Differentiating between mechanical low pain and the far less common inflammatory back pain, or axial spondyloarthropathy, is crucial because the prognosis and treatment are so different.
Inflammatory back pain is typically insidious in onset, relieved by exercise, frequently associated with nocturnal pain, entails more than 60 minutes of morning stiffness, and begins prior to age 40. In contrast, mechanical back pain can begin at any age, is acute in onset, exacerbated by exercise, doesn’t involve nighttime pain, and typically features less than 30 minutes of morning stiffness.
Most mechanical low back pain is self-limited and resolves within 4 weeks. It is characterized by abnormal back flexion, whereas patients with inflammatory back pain lose back mobility in all planes. They also frequently have sacroiliac joint tenderness and reduced chest expansion; patients with mechanical low back pain do not. Neurologic deficits are unusual in patients with spondyloarthropathies, since they are typically young individuals without disc disease.
Dr. Janson reported having no financial conflicts regarding his presentation.
ESTES PARK, COLO. – When a patient presents with low back pain, the single most important question to ask is this: “Are you having nocturnal pain or pain that’s unrelieved by rest?
“I really, really like this question. Most low back pain is nonspecific. Less than 5% of patients (with low back pain) have serious systemic pathology, but that’s the 5% we can’t afford to miss initially. This question gets at a key red flag for systemic disease,” Dr. Robert W. Janson explained at a conference on internal medicine sponsored by the University of Colorado.
“If you have mechanical low back pain, when you rest you feel good, just like with osteoarthritis. So if you’re writhing all night or unable to find a comfortable position, then you’re usually in that 5%. It’s inflammatory, metastatic, infectious, a fracture, or acute nerve compression,” said Dr. Janson, chief of rheumatology at the Denver VA Medical Center.
Other red flags for systemic disease include unexplained weight loss, fevers, or sweats; age over 50 years; low back pain present for longer than 6 weeks; or pain that’s unresponsive to treatment. A history of cancer, osteoporosis, corticosteroid therapy, abdominal aortic aneurysm, bowel or bladder symptoms, intravenous drug abuse, skin or urinary tract infection, morning stiffness lasting more than an hour, or sensory or motor loss are additional red flags.
Dr. Janson noted that these are essentially the same criteria the American College of Radiology uses in its 2011 recommendations on the appropriateness of obtaining a lumbar MRI.
Differentiating between mechanical low pain and the far less common inflammatory back pain, or axial spondyloarthropathy, is crucial because the prognosis and treatment are so different.
Inflammatory back pain is typically insidious in onset, relieved by exercise, frequently associated with nocturnal pain, entails more than 60 minutes of morning stiffness, and begins prior to age 40. In contrast, mechanical back pain can begin at any age, is acute in onset, exacerbated by exercise, doesn’t involve nighttime pain, and typically features less than 30 minutes of morning stiffness.
Most mechanical low back pain is self-limited and resolves within 4 weeks. It is characterized by abnormal back flexion, whereas patients with inflammatory back pain lose back mobility in all planes. They also frequently have sacroiliac joint tenderness and reduced chest expansion; patients with mechanical low back pain do not. Neurologic deficits are unusual in patients with spondyloarthropathies, since they are typically young individuals without disc disease.
Dr. Janson reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM

Nocturnal back pain suggests systemic disorder
ESTES PARK, COLO. – When a patient presents with low back pain, the single most important question to ask is this: “Are you having nocturnal pain or pain that’s unrelieved by rest?
“I really, really like this question. Most low back pain is nonspecific. Less than 5% of patients (with low back pain) have serious systemic pathology, but that’s the 5% we can’t afford to miss initially. This question gets at a key red flag for systemic disease,” Dr. Robert W. Janson explained at a conference on internal medicine sponsored by the University of Colorado.

“If you have mechanical low back pain, when you rest you feel good, just like with osteoarthritis. So if you’re writhing all night or unable to find a comfortable position, then you’re usually in that 5%. It’s inflammatory, metastatic, infectious, a fracture, or acute nerve compression,” said Dr. Janson, chief of rheumatology at the Denver VA Medical Center.
Other red flags for systemic disease include unexplained weight loss, fevers, or sweats; age over 50 years; low back pain present for longer than 6 weeks; or pain that’s unresponsive to treatment. A history of cancer, osteoporosis, corticosteroid therapy, abdominal aortic aneurysm, bowel or bladder symptoms, intravenous drug abuse, skin or urinary tract infection, morning stiffness lasting more than an hour, or sensory or motor loss are additional red flags.
Dr. Janson noted that these are essentially the same criteria the American College of Radiology uses in its 2011 recommendations on the appropriateness of obtaining a lumbar MRI.
Differentiating between mechanical low pain and the far less common inflammatory back pain, or axial spondyloarthropathy, is crucial because the prognosis and treatment are so different.
Inflammatory back pain is typically insidious in onset, relieved by exercise, frequently associated with nocturnal pain, entails more than 60 minutes of morning stiffness, and begins prior to age 40. In contrast, mechanical back pain can begin at any age, is acute in onset, exacerbated by exercise, doesn’t involve nighttime pain, and typically features less than 30 minutes of morning stiffness.
Most mechanical low back pain is self-limited and resolves within 4 weeks. It is characterized by abnormal back flexion, whereas patients with inflammatory back pain lose back mobility in all planes. They also frequently have sacroiliac joint tenderness and reduced chest expansion; patients with mechanical low back pain do not. Neurologic deficits are unusual in patients with spondyloarthropathies, since they are typically young individuals without disc disease.
Dr. Janson reported having no financial conflicts regarding his presentation.
ESTES PARK, COLO. – When a patient presents with low back pain, the single most important question to ask is this: “Are you having nocturnal pain or pain that’s unrelieved by rest?
“I really, really like this question. Most low back pain is nonspecific. Less than 5% of patients (with low back pain) have serious systemic pathology, but that’s the 5% we can’t afford to miss initially. This question gets at a key red flag for systemic disease,” Dr. Robert W. Janson explained at a conference on internal medicine sponsored by the University of Colorado.
“If you have mechanical low back pain, when you rest you feel good, just like with osteoarthritis. So if you’re writhing all night or unable to find a comfortable position, then you’re usually in that 5%. It’s inflammatory, metastatic, infectious, a fracture, or acute nerve compression,” said Dr. Janson, chief of rheumatology at the Denver VA Medical Center.
Other red flags for systemic disease include unexplained weight loss, fevers, or sweats; age over 50 years; low back pain present for longer than 6 weeks; or pain that’s unresponsive to treatment. A history of cancer, osteoporosis, corticosteroid therapy, abdominal aortic aneurysm, bowel or bladder symptoms, intravenous drug abuse, skin or urinary tract infection, morning stiffness lasting more than an hour, or sensory or motor loss are additional red flags.
Dr. Janson noted that these are essentially the same criteria the American College of Radiology uses in its 2011 recommendations on the appropriateness of obtaining a lumbar MRI.
Differentiating between mechanical low pain and the far less common inflammatory back pain, or axial spondyloarthropathy, is crucial because the prognosis and treatment are so different.
Inflammatory back pain is typically insidious in onset, relieved by exercise, frequently associated with nocturnal pain, entails more than 60 minutes of morning stiffness, and begins prior to age 40. In contrast, mechanical back pain can begin at any age, is acute in onset, exacerbated by exercise, doesn’t involve nighttime pain, and typically features less than 30 minutes of morning stiffness.
Most mechanical low back pain is self-limited and resolves within 4 weeks. It is characterized by abnormal back flexion, whereas patients with inflammatory back pain lose back mobility in all planes. They also frequently have sacroiliac joint tenderness and reduced chest expansion; patients with mechanical low back pain do not. Neurologic deficits are unusual in patients with spondyloarthropathies, since they are typically young individuals without disc disease.
Dr. Janson reported having no financial conflicts regarding his presentation.
ESTES PARK, COLO. – When a patient presents with low back pain, the single most important question to ask is this: “Are you having nocturnal pain or pain that’s unrelieved by rest?
“I really, really like this question. Most low back pain is nonspecific. Less than 5% of patients (with low back pain) have serious systemic pathology, but that’s the 5% we can’t afford to miss initially. This question gets at a key red flag for systemic disease,” Dr. Robert W. Janson explained at a conference on internal medicine sponsored by the University of Colorado.
“If you have mechanical low back pain, when you rest you feel good, just like with osteoarthritis. So if you’re writhing all night or unable to find a comfortable position, then you’re usually in that 5%. It’s inflammatory, metastatic, infectious, a fracture, or acute nerve compression,” said Dr. Janson, chief of rheumatology at the Denver VA Medical Center.
Other red flags for systemic disease include unexplained weight loss, fevers, or sweats; age over 50 years; low back pain present for longer than 6 weeks; or pain that’s unresponsive to treatment. A history of cancer, osteoporosis, corticosteroid therapy, abdominal aortic aneurysm, bowel or bladder symptoms, intravenous drug abuse, skin or urinary tract infection, morning stiffness lasting more than an hour, or sensory or motor loss are additional red flags.
Dr. Janson noted that these are essentially the same criteria the American College of Radiology uses in its 2011 recommendations on the appropriateness of obtaining a lumbar MRI.
Differentiating between mechanical low pain and the far less common inflammatory back pain, or axial spondyloarthropathy, is crucial because the prognosis and treatment are so different.
Inflammatory back pain is typically insidious in onset, relieved by exercise, frequently associated with nocturnal pain, entails more than 60 minutes of morning stiffness, and begins prior to age 40. In contrast, mechanical back pain can begin at any age, is acute in onset, exacerbated by exercise, doesn’t involve nighttime pain, and typically features less than 30 minutes of morning stiffness.
Most mechanical low back pain is self-limited and resolves within 4 weeks. It is characterized by abnormal back flexion, whereas patients with inflammatory back pain lose back mobility in all planes. They also frequently have sacroiliac joint tenderness and reduced chest expansion; patients with mechanical low back pain do not. Neurologic deficits are unusual in patients with spondyloarthropathies, since they are typically young individuals without disc disease.
Dr. Janson reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM THE ANNUAL INTERNAL MEDICINE PROGRAM
