User login
PAS: Early antibiotics linked to later overweight
SAN DIEGO – The use of oral antibiotics before 4 years of age was associated with a significantly increased risk of later overweight in a large cohort study.
“Antibiotics may provide a physician-modifiable risk factor for obesity prevention in early childhood,” Dr. Elizabeth Dawson-Hahn said at the annual meeting of the Pediatric Academic Societies.

The study included 4,938 children born at Group Health Cooperative, the Seattle-based integrated health care system. Their electronic medical records indicated that 3,533 of them, or 72%, filled one or more prescriptions for oral antibiotics at ages 0-47 months. In this group, 53% were less than 12 months old at the time of their first oral antibiotic exposure, while the rest were 12-47 months old.
At ages 48-59 months, roughly 12% of all study participants were overweight, as defined by a body mass index at or above the 85th percentile. The prevalence was similar regardless of whether a child was exposed to early oral antibiotics. However, the groups with and without early antibiotic exposure differed in key ways, including a more than threefold higher prevalence of childhood asthma in those with early antibiotic exposure.
In a prespecified logistic regression analysis adjusted for sex, Medicaid status, childhood asthma, race, maternal antibiotic exposure during pregnancy, delivery type, and birth weight, each course of oral antibiotics a child received up to 47 months of age was associated with a 3% increased likelihood of being overweight at 48-59 months – and children who got early oral antibiotics received a mean of 3.7 courses by age 47 months. Thus, early antibiotic exposure was associated on average with a significant 11% increased risk of later overweight (P = .005), reported Dr. Dawson-Hahn, a general pediatrics fellow at the University of Washington, Seattle.
The increased risk of overweight related to early antibiotics was concentrated in the children who received the medications in infancy. In another logistic regression analysis, children who got oral antibiotics prior to age 12 months were at an adjusted 20% increased risk of being overweight at ages 48-59 months, compared with children who didn’t receive oral antibiotics before 48 months of age. In contrast, the risk of overweight in kids who received oral antibiotics at ages 12-47 months wasn’t significantly different from the risk in the unexposed group.
Future studies should explore the mechanism of the observed relationship between early antibiotic exposure and later overweight, Dr. Dawson-Hahn said. One leading hypothesis is that the early exposure alters the composition of the developing gut microbiome. Antibiotics have been used for decades as a means of boosting the weight of livestock, she noted.
Dr. Dawson-Hahn said she is planning to reanalyze the data set to see if weight gain differed depending upon the type of antibiotic involved in an early exposure. More than 80% of children with early antibiotic exposure received amoxicillin.
One audience member noted that just because the health plan’s electronic pharmacy records show a prescription for oral antibiotics was filled doesn’t mean the child took the full course. Dr. Dawson-Hahn agreed, but noted that her study findings are consistent with the results of prior studies by other investigators in the past 2 years, which typically relied upon parental recall of antibiotic exposure.
“We thought documented prescription fill would be an improvement over that,” she added.
Dr. Dawson-Hahn’s study was funded by a Hearst Foundation Fellowship Award and a Ruth L. Kirschstein National Research Service Award. She reported having no relevant financial conflicts.
SAN DIEGO – The use of oral antibiotics before 4 years of age was associated with a significantly increased risk of later overweight in a large cohort study.
“Antibiotics may provide a physician-modifiable risk factor for obesity prevention in early childhood,” Dr. Elizabeth Dawson-Hahn said at the annual meeting of the Pediatric Academic Societies.
The study included 4,938 children born at Group Health Cooperative, the Seattle-based integrated health care system. Their electronic medical records indicated that 3,533 of them, or 72%, filled one or more prescriptions for oral antibiotics at ages 0-47 months. In this group, 53% were less than 12 months old at the time of their first oral antibiotic exposure, while the rest were 12-47 months old.
At ages 48-59 months, roughly 12% of all study participants were overweight, as defined by a body mass index at or above the 85th percentile. The prevalence was similar regardless of whether a child was exposed to early oral antibiotics. However, the groups with and without early antibiotic exposure differed in key ways, including a more than threefold higher prevalence of childhood asthma in those with early antibiotic exposure.
In a prespecified logistic regression analysis adjusted for sex, Medicaid status, childhood asthma, race, maternal antibiotic exposure during pregnancy, delivery type, and birth weight, each course of oral antibiotics a child received up to 47 months of age was associated with a 3% increased likelihood of being overweight at 48-59 months – and children who got early oral antibiotics received a mean of 3.7 courses by age 47 months. Thus, early antibiotic exposure was associated on average with a significant 11% increased risk of later overweight (P = .005), reported Dr. Dawson-Hahn, a general pediatrics fellow at the University of Washington, Seattle.
The increased risk of overweight related to early antibiotics was concentrated in the children who received the medications in infancy. In another logistic regression analysis, children who got oral antibiotics prior to age 12 months were at an adjusted 20% increased risk of being overweight at ages 48-59 months, compared with children who didn’t receive oral antibiotics before 48 months of age. In contrast, the risk of overweight in kids who received oral antibiotics at ages 12-47 months wasn’t significantly different from the risk in the unexposed group.
Future studies should explore the mechanism of the observed relationship between early antibiotic exposure and later overweight, Dr. Dawson-Hahn said. One leading hypothesis is that the early exposure alters the composition of the developing gut microbiome. Antibiotics have been used for decades as a means of boosting the weight of livestock, she noted.
Dr. Dawson-Hahn said she is planning to reanalyze the data set to see if weight gain differed depending upon the type of antibiotic involved in an early exposure. More than 80% of children with early antibiotic exposure received amoxicillin.
One audience member noted that just because the health plan’s electronic pharmacy records show a prescription for oral antibiotics was filled doesn’t mean the child took the full course. Dr. Dawson-Hahn agreed, but noted that her study findings are consistent with the results of prior studies by other investigators in the past 2 years, which typically relied upon parental recall of antibiotic exposure.
“We thought documented prescription fill would be an improvement over that,” she added.
Dr. Dawson-Hahn’s study was funded by a Hearst Foundation Fellowship Award and a Ruth L. Kirschstein National Research Service Award. She reported having no relevant financial conflicts.
SAN DIEGO – The use of oral antibiotics before 4 years of age was associated with a significantly increased risk of later overweight in a large cohort study.
“Antibiotics may provide a physician-modifiable risk factor for obesity prevention in early childhood,” Dr. Elizabeth Dawson-Hahn said at the annual meeting of the Pediatric Academic Societies.
The study included 4,938 children born at Group Health Cooperative, the Seattle-based integrated health care system. Their electronic medical records indicated that 3,533 of them, or 72%, filled one or more prescriptions for oral antibiotics at ages 0-47 months. In this group, 53% were less than 12 months old at the time of their first oral antibiotic exposure, while the rest were 12-47 months old.
At ages 48-59 months, roughly 12% of all study participants were overweight, as defined by a body mass index at or above the 85th percentile. The prevalence was similar regardless of whether a child was exposed to early oral antibiotics. However, the groups with and without early antibiotic exposure differed in key ways, including a more than threefold higher prevalence of childhood asthma in those with early antibiotic exposure.
In a prespecified logistic regression analysis adjusted for sex, Medicaid status, childhood asthma, race, maternal antibiotic exposure during pregnancy, delivery type, and birth weight, each course of oral antibiotics a child received up to 47 months of age was associated with a 3% increased likelihood of being overweight at 48-59 months – and children who got early oral antibiotics received a mean of 3.7 courses by age 47 months. Thus, early antibiotic exposure was associated on average with a significant 11% increased risk of later overweight (P = .005), reported Dr. Dawson-Hahn, a general pediatrics fellow at the University of Washington, Seattle.
The increased risk of overweight related to early antibiotics was concentrated in the children who received the medications in infancy. In another logistic regression analysis, children who got oral antibiotics prior to age 12 months were at an adjusted 20% increased risk of being overweight at ages 48-59 months, compared with children who didn’t receive oral antibiotics before 48 months of age. In contrast, the risk of overweight in kids who received oral antibiotics at ages 12-47 months wasn’t significantly different from the risk in the unexposed group.
Future studies should explore the mechanism of the observed relationship between early antibiotic exposure and later overweight, Dr. Dawson-Hahn said. One leading hypothesis is that the early exposure alters the composition of the developing gut microbiome. Antibiotics have been used for decades as a means of boosting the weight of livestock, she noted.
Dr. Dawson-Hahn said she is planning to reanalyze the data set to see if weight gain differed depending upon the type of antibiotic involved in an early exposure. More than 80% of children with early antibiotic exposure received amoxicillin.
One audience member noted that just because the health plan’s electronic pharmacy records show a prescription for oral antibiotics was filled doesn’t mean the child took the full course. Dr. Dawson-Hahn agreed, but noted that her study findings are consistent with the results of prior studies by other investigators in the past 2 years, which typically relied upon parental recall of antibiotic exposure.
“We thought documented prescription fill would be an improvement over that,” she added.
Dr. Dawson-Hahn’s study was funded by a Hearst Foundation Fellowship Award and a Ruth L. Kirschstein National Research Service Award. She reported having no relevant financial conflicts.
AT THE PAS ANNUAL MEETING
Key clinical point: Children who received oral antibiotics prior to 48 months of age were more likely to be overweight at ages 48-59 months.
Major finding: For each course of oral antibiotics a child received during 0-47 months of age, the odds of being at or above the 85th percentile for body mass index at 48-59 months increased by 3%.
Data source: A retrospective cohort study including 4,938 children whose families belonged to a large integrated health plan.
Disclosures: Dr. Dawson-Hahn’s study was funded by a Hearst Foundation Fellowship Award and a Ruth L. Kirschstein National Research Service Award. She reported having no relevant financial conflicts.

AAS: Suicidal ideation common, underrecognized in prisoners
ATLANTA – One-third of a large sample of male state prison inmates reported some level of suicidal ideation in the first-ever study to examine the applicability of Joiner’s interpersonal theory of suicide in a correctional setting.
That’s a high rate, especially since the study participants hadn’t been red-flagged by prison officials for any indication of increased suicidality. By comparison, studies conducted in the general population outside of a prison setting have placed the prevalence of suicidal ideation at 2%-10%, Jon Mandracchia, Ph.D., noted at the annual conference of the American Association of Suicidology.
His study earned the Young Investigator of the Year Award from the American Foundation for Suicide Prevention.

Suicide is a serious problem in correctional settings. According to the Bureau of Justice Statistics, suicide is the number-one cause of death in jails, accounting for 29% of all mortality in that setting. In prisons, suicide accounts for 6.2% of all deaths, making it the fourth most common cause of mortality, said Dr. Mandracchia of the University of Southern Mississippi, Hattiesburg.
Prison officials realize suicide is a major problem. Guards, nurses, and other staff have been trained to be on the lookout for suicidality and are quick to ask inmates if they’ve been thinking about harming themselves, but the answer is virtually always no.
“Prison is a harsh place. You can’t live in prison if you’re seen as a potential victim or target by other inmates,” Dr. Mandracchia said. “You’re not going to admit to anything that might possibly be perceived as weakness, whether it’s true or just in your mind.”
The interpersonal theory of suicide, introduced by Thomas Joiner, Ph.D., a decade ago, has generated enormous interest among suicide researchers because of its simplicity and ready testability. Indeed, much of this year’s AAS conference was devoted to studies examining the theory’s validity in various populations.
The theory holds that, for suicide attempts to occur, three elements are necessary. In Dr. Joiner’s terminology, an individual must simultaneously experience thwarted belongingness and perceived burdensomeness, which together generate suicidal ideation. To move from ideation to action, however, a third component must be present: acquired capability, the ability to overcome the powerful, innate urge to survive. Acquired capability is often achieved through desensitization to trauma or pain.
Prison is an environment rife with thwarted belongingness and perceived burdensomeness. Prisoners are removed from their family and friends, hence the thwarted belongingness. They also often feel that they’ve become a burden to their family because they’re not providing income and often ask their families for money to buy snacks. Moreover, they are constantly reminded that they are a burden on society. Dr. Mandracchia hypothesized that, if the interpersonal theory of suicide is valid in a prison population, then prisoners who score high on measures of thwarted belongingness and perceived burdensomeness should have the highest levels of suicidal ideation.
That’s exactly what he found in his study of 399 male inmates in Mississippi state prisons. For his measurement tools, he used the Beck Scale for Suicide Ideation and the Interpersonal Needs Questionnaire, which features separate scales to look at perceived burdensomeness and thwarted belongingness. In addition, he employed the Center for Epidemiological Studies Depression Scale and the hopelessness scale from the Depression Hopelessness Suicide Screening Form, a tool developed specifically for use in criminal offenders. He measured inmates’ levels of depression and hopelessness to be able to control for those two factors in his analysis, since they are traditionally viewed as risk factors for suicide but aren’t central to the Joiner model.
Dr. Mandracchia found a strong dose-response effect between thwarted belongingness and perceived burdensomeness and suicidal ideation among the inmates, all of whom participated in the study voluntarily. Inmates who scored in the top tertiles for both thwarted belongingness and perceived burdensomeness had the greatest amount of suicidal ideation, while those in the middle tertiles had mid-range levels of suicidal ideation on the Beck scale.
Dr. Mandracchia highlighted several practical implications of the study findings in terms of suicidality assessment and management in prison populations. For example, instead of asking inmates, “How are you feeling?” and “Are you thinking of hurting yourself?” as prison staff routinely do now, they should instead be on the lookout for inmates who complain that they are a burden to their family or feel particularly isolated. This ought to reduce the traditionally extremely high false-positive and false-negative rates for detection of suicidality in correctional institutions, he said.
In terms of implications for management, Dr. Mandracchia said that he is trying to convince prison officials to limit their use of suicide watch.
“They don’t know what else to do, so when they’re concerned about someone they remove them and lock them in isolation until they’re safe. That’s often counterproductive. It takes the inmates away from their support system,” he said.
Mental health professionals working in prison settings also could try to boost inmates’ sense of belongingness, perhaps by encouraging them to join one of the prosocial groups that exist in prisons. Staying in touch with friends and family by writing letters is another means of increasing belongingness. Perceived burdensomeness can be addressed through cognitive behavioral therapy aimed at helping inmates gain a more accurate picture of how much of a burden they are to others, Dr. Mandracchia added.
He is planning a longitudinal study to identify measures that predict actual future suicidal behavior among prison inmates, but acknowledged there are challenges to doing this work.
“When you start doing mental health research in prisons, you quickly realize that no one wants you there. Not the staff, not the inmates,” he said.
Dr. Mandracchia reported having no financial conflicts regarding this study, which was conducted free of commercial support.
ATLANTA – One-third of a large sample of male state prison inmates reported some level of suicidal ideation in the first-ever study to examine the applicability of Joiner’s interpersonal theory of suicide in a correctional setting.
That’s a high rate, especially since the study participants hadn’t been red-flagged by prison officials for any indication of increased suicidality. By comparison, studies conducted in the general population outside of a prison setting have placed the prevalence of suicidal ideation at 2%-10%, Jon Mandracchia, Ph.D., noted at the annual conference of the American Association of Suicidology.
His study earned the Young Investigator of the Year Award from the American Foundation for Suicide Prevention.
Suicide is a serious problem in correctional settings. According to the Bureau of Justice Statistics, suicide is the number-one cause of death in jails, accounting for 29% of all mortality in that setting. In prisons, suicide accounts for 6.2% of all deaths, making it the fourth most common cause of mortality, said Dr. Mandracchia of the University of Southern Mississippi, Hattiesburg.
Prison officials realize suicide is a major problem. Guards, nurses, and other staff have been trained to be on the lookout for suicidality and are quick to ask inmates if they’ve been thinking about harming themselves, but the answer is virtually always no.
“Prison is a harsh place. You can’t live in prison if you’re seen as a potential victim or target by other inmates,” Dr. Mandracchia said. “You’re not going to admit to anything that might possibly be perceived as weakness, whether it’s true or just in your mind.”
The interpersonal theory of suicide, introduced by Thomas Joiner, Ph.D., a decade ago, has generated enormous interest among suicide researchers because of its simplicity and ready testability. Indeed, much of this year’s AAS conference was devoted to studies examining the theory’s validity in various populations.
The theory holds that, for suicide attempts to occur, three elements are necessary. In Dr. Joiner’s terminology, an individual must simultaneously experience thwarted belongingness and perceived burdensomeness, which together generate suicidal ideation. To move from ideation to action, however, a third component must be present: acquired capability, the ability to overcome the powerful, innate urge to survive. Acquired capability is often achieved through desensitization to trauma or pain.
Prison is an environment rife with thwarted belongingness and perceived burdensomeness. Prisoners are removed from their family and friends, hence the thwarted belongingness. They also often feel that they’ve become a burden to their family because they’re not providing income and often ask their families for money to buy snacks. Moreover, they are constantly reminded that they are a burden on society. Dr. Mandracchia hypothesized that, if the interpersonal theory of suicide is valid in a prison population, then prisoners who score high on measures of thwarted belongingness and perceived burdensomeness should have the highest levels of suicidal ideation.
That’s exactly what he found in his study of 399 male inmates in Mississippi state prisons. For his measurement tools, he used the Beck Scale for Suicide Ideation and the Interpersonal Needs Questionnaire, which features separate scales to look at perceived burdensomeness and thwarted belongingness. In addition, he employed the Center for Epidemiological Studies Depression Scale and the hopelessness scale from the Depression Hopelessness Suicide Screening Form, a tool developed specifically for use in criminal offenders. He measured inmates’ levels of depression and hopelessness to be able to control for those two factors in his analysis, since they are traditionally viewed as risk factors for suicide but aren’t central to the Joiner model.
Dr. Mandracchia found a strong dose-response effect between thwarted belongingness and perceived burdensomeness and suicidal ideation among the inmates, all of whom participated in the study voluntarily. Inmates who scored in the top tertiles for both thwarted belongingness and perceived burdensomeness had the greatest amount of suicidal ideation, while those in the middle tertiles had mid-range levels of suicidal ideation on the Beck scale.
Dr. Mandracchia highlighted several practical implications of the study findings in terms of suicidality assessment and management in prison populations. For example, instead of asking inmates, “How are you feeling?” and “Are you thinking of hurting yourself?” as prison staff routinely do now, they should instead be on the lookout for inmates who complain that they are a burden to their family or feel particularly isolated. This ought to reduce the traditionally extremely high false-positive and false-negative rates for detection of suicidality in correctional institutions, he said.
In terms of implications for management, Dr. Mandracchia said that he is trying to convince prison officials to limit their use of suicide watch.
“They don’t know what else to do, so when they’re concerned about someone they remove them and lock them in isolation until they’re safe. That’s often counterproductive. It takes the inmates away from their support system,” he said.
Mental health professionals working in prison settings also could try to boost inmates’ sense of belongingness, perhaps by encouraging them to join one of the prosocial groups that exist in prisons. Staying in touch with friends and family by writing letters is another means of increasing belongingness. Perceived burdensomeness can be addressed through cognitive behavioral therapy aimed at helping inmates gain a more accurate picture of how much of a burden they are to others, Dr. Mandracchia added.
He is planning a longitudinal study to identify measures that predict actual future suicidal behavior among prison inmates, but acknowledged there are challenges to doing this work.
“When you start doing mental health research in prisons, you quickly realize that no one wants you there. Not the staff, not the inmates,” he said.
Dr. Mandracchia reported having no financial conflicts regarding this study, which was conducted free of commercial support.
ATLANTA – One-third of a large sample of male state prison inmates reported some level of suicidal ideation in the first-ever study to examine the applicability of Joiner’s interpersonal theory of suicide in a correctional setting.
That’s a high rate, especially since the study participants hadn’t been red-flagged by prison officials for any indication of increased suicidality. By comparison, studies conducted in the general population outside of a prison setting have placed the prevalence of suicidal ideation at 2%-10%, Jon Mandracchia, Ph.D., noted at the annual conference of the American Association of Suicidology.
His study earned the Young Investigator of the Year Award from the American Foundation for Suicide Prevention.
Suicide is a serious problem in correctional settings. According to the Bureau of Justice Statistics, suicide is the number-one cause of death in jails, accounting for 29% of all mortality in that setting. In prisons, suicide accounts for 6.2% of all deaths, making it the fourth most common cause of mortality, said Dr. Mandracchia of the University of Southern Mississippi, Hattiesburg.
Prison officials realize suicide is a major problem. Guards, nurses, and other staff have been trained to be on the lookout for suicidality and are quick to ask inmates if they’ve been thinking about harming themselves, but the answer is virtually always no.
“Prison is a harsh place. You can’t live in prison if you’re seen as a potential victim or target by other inmates,” Dr. Mandracchia said. “You’re not going to admit to anything that might possibly be perceived as weakness, whether it’s true or just in your mind.”
The interpersonal theory of suicide, introduced by Thomas Joiner, Ph.D., a decade ago, has generated enormous interest among suicide researchers because of its simplicity and ready testability. Indeed, much of this year’s AAS conference was devoted to studies examining the theory’s validity in various populations.
The theory holds that, for suicide attempts to occur, three elements are necessary. In Dr. Joiner’s terminology, an individual must simultaneously experience thwarted belongingness and perceived burdensomeness, which together generate suicidal ideation. To move from ideation to action, however, a third component must be present: acquired capability, the ability to overcome the powerful, innate urge to survive. Acquired capability is often achieved through desensitization to trauma or pain.
Prison is an environment rife with thwarted belongingness and perceived burdensomeness. Prisoners are removed from their family and friends, hence the thwarted belongingness. They also often feel that they’ve become a burden to their family because they’re not providing income and often ask their families for money to buy snacks. Moreover, they are constantly reminded that they are a burden on society. Dr. Mandracchia hypothesized that, if the interpersonal theory of suicide is valid in a prison population, then prisoners who score high on measures of thwarted belongingness and perceived burdensomeness should have the highest levels of suicidal ideation.
That’s exactly what he found in his study of 399 male inmates in Mississippi state prisons. For his measurement tools, he used the Beck Scale for Suicide Ideation and the Interpersonal Needs Questionnaire, which features separate scales to look at perceived burdensomeness and thwarted belongingness. In addition, he employed the Center for Epidemiological Studies Depression Scale and the hopelessness scale from the Depression Hopelessness Suicide Screening Form, a tool developed specifically for use in criminal offenders. He measured inmates’ levels of depression and hopelessness to be able to control for those two factors in his analysis, since they are traditionally viewed as risk factors for suicide but aren’t central to the Joiner model.
Dr. Mandracchia found a strong dose-response effect between thwarted belongingness and perceived burdensomeness and suicidal ideation among the inmates, all of whom participated in the study voluntarily. Inmates who scored in the top tertiles for both thwarted belongingness and perceived burdensomeness had the greatest amount of suicidal ideation, while those in the middle tertiles had mid-range levels of suicidal ideation on the Beck scale.
Dr. Mandracchia highlighted several practical implications of the study findings in terms of suicidality assessment and management in prison populations. For example, instead of asking inmates, “How are you feeling?” and “Are you thinking of hurting yourself?” as prison staff routinely do now, they should instead be on the lookout for inmates who complain that they are a burden to their family or feel particularly isolated. This ought to reduce the traditionally extremely high false-positive and false-negative rates for detection of suicidality in correctional institutions, he said.
In terms of implications for management, Dr. Mandracchia said that he is trying to convince prison officials to limit their use of suicide watch.
“They don’t know what else to do, so when they’re concerned about someone they remove them and lock them in isolation until they’re safe. That’s often counterproductive. It takes the inmates away from their support system,” he said.
Mental health professionals working in prison settings also could try to boost inmates’ sense of belongingness, perhaps by encouraging them to join one of the prosocial groups that exist in prisons. Staying in touch with friends and family by writing letters is another means of increasing belongingness. Perceived burdensomeness can be addressed through cognitive behavioral therapy aimed at helping inmates gain a more accurate picture of how much of a burden they are to others, Dr. Mandracchia added.
He is planning a longitudinal study to identify measures that predict actual future suicidal behavior among prison inmates, but acknowledged there are challenges to doing this work.
“When you start doing mental health research in prisons, you quickly realize that no one wants you there. Not the staff, not the inmates,” he said.
Dr. Mandracchia reported having no financial conflicts regarding this study, which was conducted free of commercial support.
AT THE ANNUAL AAS CONFERENCE
Key clinical point: 33% of adult male state prison inmates showed some degree of suicidal ideation upon structured testing.
Major finding: Consistent with Joiner’s interpersonal theory of suicide, the higher an inmate’s scores in the domains of thwarted belongingness and perceived burdensomeness, the greater his degree of suicidal ideation.
Data source: This cross-sectional observational study included 399 adult male inmates in Mississippi’s state prisons.
Disclosures: The presenter reported having no financial conflicts regarding this study, which was conducted free of commercial support.

Testosterone therapy has neutral cardiovascular effects
SAN DIEGO– Testosterone therapy for men with low serum testosterone had no impact one way or another on cardiovascular risk in a large, community-based study.
“Testosterone therapy is not associated with any deleterious or beneficial effect on cardiovascular outcomes. But our study does reinforce that it’s very important to go back to the basics and try to manage the traditional risk factors that are known predictors of adverse outcomes,” Dr. Zuber Ali said at the annual meeting of the American College of Cardiology.

The cardiovascular impact of testosterone therapy in men with low serum levels is a controversial subject. Early studies reported cardioprotective benefits; however, at least three more recent studies found adverse effects, and the Food and Drug Administration recently issued a request that manufacturers of approved testosterone products revise their product labeling to include a new black box warning of “a possible increased cardiovascular risk associated with testosterone use.”
“Given these conflicting reports, we wanted to look at our experience in a large, community-based health care system,” explained Dr. Ali of the Aurora University of Wisconsin Medical Group in Milwaukee.
He presented a retrospective cohort study of 7,245 men, mean age 54 years, with a low baseline total testosterone level below 300 ng/dL who were followed during 2011-2014.
The combined rate of the composite outcome comprising all-cause mortality, acute MI, and stroke was 5.5% in men who received testosterone therapy, compared with 6.7% in those who did not. This translated into a statistically significant unadjusted 29% relative risk reduction in favor of testosterone therapy. However, upon adjusting for differences in baseline cardiovascular risk factors, the relative risk advantage for testosterone therapy dropped from 29% to 20%, which was no longer statistically significant.
This cardiovascular-neutral result was confirmed in a separate analysis in which 3,155 of the men on testosterone therapy were paired one to one with an equal number of controls who were propensity-matched on the basis of demographics and cardiovascular risk factors, including diabetes, atrial fibrillation, and chronic kidney disease. During a mean 1.8 years of follow-up, the composite outcome occurred in 1.7% of the testosterone therapy group and 2.2% of matched controls, a nonsignificant difference.
In a multivariate analysis, the significant predictors of cardiovascular outcomes proved to be dyslipidemia, age, length of follow-up, a history of acute MI or stroke/TIA, and smoking. Testosterone therapy didn’t make the list, according to Dr. Ali.
One audience member commented that while these data are reassuring up to a point, 1.8 years of follow-up is not very long from a cardiovascular risk perspective. Dr. Ali agreed, adding that he and his coinvestigators are continuing to follow these men and will be gathering longer-term data. But so far, at least, there is no signal of increased cardiovascular risk.
In issuing its request for a label change, the FDA also required manufacturers of approved testosterone products to conduct a well-designed clinical trial, either separately or in collaboration, to specifically address the question of possible cardiovascular risk. While Dr. Ali welcomed this development because it should finally provide definitive answers, he noted that no such study has begun, and long-term outcome data are years away. In the interim, he added, data such as he presented are probably the best that can be expected in terms of providing guidance on risks and benefits for physician/patient treatment decision making.
Dr. Ali reported having no financial conflicts regarding this study, which was conducted free of commercial support.
SAN DIEGO– Testosterone therapy for men with low serum testosterone had no impact one way or another on cardiovascular risk in a large, community-based study.
“Testosterone therapy is not associated with any deleterious or beneficial effect on cardiovascular outcomes. But our study does reinforce that it’s very important to go back to the basics and try to manage the traditional risk factors that are known predictors of adverse outcomes,” Dr. Zuber Ali said at the annual meeting of the American College of Cardiology.
The cardiovascular impact of testosterone therapy in men with low serum levels is a controversial subject. Early studies reported cardioprotective benefits; however, at least three more recent studies found adverse effects, and the Food and Drug Administration recently issued a request that manufacturers of approved testosterone products revise their product labeling to include a new black box warning of “a possible increased cardiovascular risk associated with testosterone use.”
“Given these conflicting reports, we wanted to look at our experience in a large, community-based health care system,” explained Dr. Ali of the Aurora University of Wisconsin Medical Group in Milwaukee.
He presented a retrospective cohort study of 7,245 men, mean age 54 years, with a low baseline total testosterone level below 300 ng/dL who were followed during 2011-2014.
The combined rate of the composite outcome comprising all-cause mortality, acute MI, and stroke was 5.5% in men who received testosterone therapy, compared with 6.7% in those who did not. This translated into a statistically significant unadjusted 29% relative risk reduction in favor of testosterone therapy. However, upon adjusting for differences in baseline cardiovascular risk factors, the relative risk advantage for testosterone therapy dropped from 29% to 20%, which was no longer statistically significant.
This cardiovascular-neutral result was confirmed in a separate analysis in which 3,155 of the men on testosterone therapy were paired one to one with an equal number of controls who were propensity-matched on the basis of demographics and cardiovascular risk factors, including diabetes, atrial fibrillation, and chronic kidney disease. During a mean 1.8 years of follow-up, the composite outcome occurred in 1.7% of the testosterone therapy group and 2.2% of matched controls, a nonsignificant difference.
In a multivariate analysis, the significant predictors of cardiovascular outcomes proved to be dyslipidemia, age, length of follow-up, a history of acute MI or stroke/TIA, and smoking. Testosterone therapy didn’t make the list, according to Dr. Ali.
One audience member commented that while these data are reassuring up to a point, 1.8 years of follow-up is not very long from a cardiovascular risk perspective. Dr. Ali agreed, adding that he and his coinvestigators are continuing to follow these men and will be gathering longer-term data. But so far, at least, there is no signal of increased cardiovascular risk.
In issuing its request for a label change, the FDA also required manufacturers of approved testosterone products to conduct a well-designed clinical trial, either separately or in collaboration, to specifically address the question of possible cardiovascular risk. While Dr. Ali welcomed this development because it should finally provide definitive answers, he noted that no such study has begun, and long-term outcome data are years away. In the interim, he added, data such as he presented are probably the best that can be expected in terms of providing guidance on risks and benefits for physician/patient treatment decision making.
Dr. Ali reported having no financial conflicts regarding this study, which was conducted free of commercial support.
SAN DIEGO– Testosterone therapy for men with low serum testosterone had no impact one way or another on cardiovascular risk in a large, community-based study.
“Testosterone therapy is not associated with any deleterious or beneficial effect on cardiovascular outcomes. But our study does reinforce that it’s very important to go back to the basics and try to manage the traditional risk factors that are known predictors of adverse outcomes,” Dr. Zuber Ali said at the annual meeting of the American College of Cardiology.
The cardiovascular impact of testosterone therapy in men with low serum levels is a controversial subject. Early studies reported cardioprotective benefits; however, at least three more recent studies found adverse effects, and the Food and Drug Administration recently issued a request that manufacturers of approved testosterone products revise their product labeling to include a new black box warning of “a possible increased cardiovascular risk associated with testosterone use.”
“Given these conflicting reports, we wanted to look at our experience in a large, community-based health care system,” explained Dr. Ali of the Aurora University of Wisconsin Medical Group in Milwaukee.
He presented a retrospective cohort study of 7,245 men, mean age 54 years, with a low baseline total testosterone level below 300 ng/dL who were followed during 2011-2014.
The combined rate of the composite outcome comprising all-cause mortality, acute MI, and stroke was 5.5% in men who received testosterone therapy, compared with 6.7% in those who did not. This translated into a statistically significant unadjusted 29% relative risk reduction in favor of testosterone therapy. However, upon adjusting for differences in baseline cardiovascular risk factors, the relative risk advantage for testosterone therapy dropped from 29% to 20%, which was no longer statistically significant.
This cardiovascular-neutral result was confirmed in a separate analysis in which 3,155 of the men on testosterone therapy were paired one to one with an equal number of controls who were propensity-matched on the basis of demographics and cardiovascular risk factors, including diabetes, atrial fibrillation, and chronic kidney disease. During a mean 1.8 years of follow-up, the composite outcome occurred in 1.7% of the testosterone therapy group and 2.2% of matched controls, a nonsignificant difference.
In a multivariate analysis, the significant predictors of cardiovascular outcomes proved to be dyslipidemia, age, length of follow-up, a history of acute MI or stroke/TIA, and smoking. Testosterone therapy didn’t make the list, according to Dr. Ali.
One audience member commented that while these data are reassuring up to a point, 1.8 years of follow-up is not very long from a cardiovascular risk perspective. Dr. Ali agreed, adding that he and his coinvestigators are continuing to follow these men and will be gathering longer-term data. But so far, at least, there is no signal of increased cardiovascular risk.
In issuing its request for a label change, the FDA also required manufacturers of approved testosterone products to conduct a well-designed clinical trial, either separately or in collaboration, to specifically address the question of possible cardiovascular risk. While Dr. Ali welcomed this development because it should finally provide definitive answers, he noted that no such study has begun, and long-term outcome data are years away. In the interim, he added, data such as he presented are probably the best that can be expected in terms of providing guidance on risks and benefits for physician/patient treatment decision making.
Dr. Ali reported having no financial conflicts regarding this study, which was conducted free of commercial support.
AT ACC 15
Key clinical point: Testosterone therapy for men with low serum testosterone had no significant impact on their cardiovascular event rate.
Major finding: The incidence of the composite outcome of all-cause mortality, acute MI, or stroke during a mean 1.8 years of follow-up was 1.7% in men on testosterone therapy and 2.2% in propensity-matched controls, a nonsignificant difference.
Data source: A retrospective cohort study in 7,245 men with low serum testosterone.
Disclosures: The presenter reported having no financial conflicts regarding this study, which was conducted free of commercial support.

AAS: Preventing suicide clusters on college campuses
ATLANTA– A landmark study of newspaper coverage of suicides provides empirical support for media guidelines aimed at minimizing the likelihood of suicide clusters among college students.
“Given the prevalence of suicide on college campuses, and the associated risk of suicide contagion and clustering, it’s imperative that colleges develop effective and comprehensive postvention programs,” Madelyn S. Gould, Ph.D., said at the annual conference of the American Association of Suicidology.

According to the Centers for Disease Control and Prevention, suicide is the No. 2 cause of death among college students, with roughly 1,100 completed suicides occurring annually, noted Dr. Gould, professor of epidemiology in psychiatry at Columbia University, New York, and the New York State Psychiatric Institute.
Suicide contagion is the process by which direct or indirect knowledge of one suicide facilitates subsequent suicide. Dr. Gould was the lead investigator in a national study that examined the role of newspaper coverage of suicide as a contributor to suicide clusters among 13- to 20-year-olds. The retrospective, population-based, case-control study included 48 communities in which suicide clusters occurred during 1988-1996 – before the arrival of social media. The control group consisted of 95 matched communities in which a youth suicide was not followed by a suicide cluster.
The key finding: The more sensational the newspaper coverage of suicides as evidenced by a greater number of stories, front page placement, and more details about the suicidal individual and act, the greater the likelihood of subsequent suicide clusters (Lancet Psychiatry 2014;1:34-43).
Dr. Gould highlighted what she considers a seminal study led by Dr. Thomas Niederkrotenthaler of the Medical University of Vienna. The investigators analyzed the content of nearly 500 suicide-related Austrian print media articles and demonstrated that while sensational and/or repetitive coverage of suicides was associated with a subsequent increase in suicide, stories about mastery-of-crisis – that is, articles about individuals with suicidal ideation who adopted coping strategies other than suicidal behavior when faced with adverse circumstances – were associated with a decreased suicide rate (Br. J. Psychiatry 2010;197:234-43). Dr. Niederkrotenthaler calls it “the Papageno effect,” after a lovesick character in Mozart’s opera “The Magic Flute” whose planned suicide is averted by three child spirits who remind him of alternatives to death.
Dr. Gould noted that emotions also can be spread through the social media, as was made evident by the Facebook’s News Feed Experiment. In this massive study, investigators in Facebook’s research department manipulated the emotional content of the Facebook News Feed for 689,003 Facebook members. When exposure to friends’ positive emotional content in their news feed was reduced, subjects produced fewer positive and more negative posts. When exposure to negative content in the news feed was reduced, the result was more positive and fewer negative posts (Proc. Natl. Acad. Sci. USA 2014;11:8788-90).
The Higher Education Mental Health Alliance has disseminated a comprehensive suicide postvention guide for colleges. It includes specific recommendations aimed at limiting suicide contagion on campuses. The guide includes recommended media guidelines in the wake of suicide, emphasizes the importance of addressing common and counterproductive myths about suicide, and provides tips on how to shape students’ desire to “do something” in the aftermath of a student suicide while at the same time balancing that constructive urge against the needs of mourners.
Guidance regarding how to encourage responsible social networking in the aftermath of a suicide is available from the Suicide Prevention Research Center, Dr. Gould continued.
Up to half of college students with suicidal ideation choose not to share that information with anyone.
“There are a lot of vulnerable students on campuses. Consider implementing the American Foundation for Suicide Prevention’s anonymous online Interactive Screening Program,” she said.
Dr. Gould’s suicide cluster study was funded by the National Institute of Mental Health and the American Foundation for Suicide Prevention. She reported receiving royalties as coauthor of the Columbia-Suicide Severity Rating Scale.
ATLANTA– A landmark study of newspaper coverage of suicides provides empirical support for media guidelines aimed at minimizing the likelihood of suicide clusters among college students.
“Given the prevalence of suicide on college campuses, and the associated risk of suicide contagion and clustering, it’s imperative that colleges develop effective and comprehensive postvention programs,” Madelyn S. Gould, Ph.D., said at the annual conference of the American Association of Suicidology.
According to the Centers for Disease Control and Prevention, suicide is the No. 2 cause of death among college students, with roughly 1,100 completed suicides occurring annually, noted Dr. Gould, professor of epidemiology in psychiatry at Columbia University, New York, and the New York State Psychiatric Institute.
Suicide contagion is the process by which direct or indirect knowledge of one suicide facilitates subsequent suicide. Dr. Gould was the lead investigator in a national study that examined the role of newspaper coverage of suicide as a contributor to suicide clusters among 13- to 20-year-olds. The retrospective, population-based, case-control study included 48 communities in which suicide clusters occurred during 1988-1996 – before the arrival of social media. The control group consisted of 95 matched communities in which a youth suicide was not followed by a suicide cluster.
The key finding: The more sensational the newspaper coverage of suicides as evidenced by a greater number of stories, front page placement, and more details about the suicidal individual and act, the greater the likelihood of subsequent suicide clusters (Lancet Psychiatry 2014;1:34-43).
Dr. Gould highlighted what she considers a seminal study led by Dr. Thomas Niederkrotenthaler of the Medical University of Vienna. The investigators analyzed the content of nearly 500 suicide-related Austrian print media articles and demonstrated that while sensational and/or repetitive coverage of suicides was associated with a subsequent increase in suicide, stories about mastery-of-crisis – that is, articles about individuals with suicidal ideation who adopted coping strategies other than suicidal behavior when faced with adverse circumstances – were associated with a decreased suicide rate (Br. J. Psychiatry 2010;197:234-43). Dr. Niederkrotenthaler calls it “the Papageno effect,” after a lovesick character in Mozart’s opera “The Magic Flute” whose planned suicide is averted by three child spirits who remind him of alternatives to death.
Dr. Gould noted that emotions also can be spread through the social media, as was made evident by the Facebook’s News Feed Experiment. In this massive study, investigators in Facebook’s research department manipulated the emotional content of the Facebook News Feed for 689,003 Facebook members. When exposure to friends’ positive emotional content in their news feed was reduced, subjects produced fewer positive and more negative posts. When exposure to negative content in the news feed was reduced, the result was more positive and fewer negative posts (Proc. Natl. Acad. Sci. USA 2014;11:8788-90).
The Higher Education Mental Health Alliance has disseminated a comprehensive suicide postvention guide for colleges. It includes specific recommendations aimed at limiting suicide contagion on campuses. The guide includes recommended media guidelines in the wake of suicide, emphasizes the importance of addressing common and counterproductive myths about suicide, and provides tips on how to shape students’ desire to “do something” in the aftermath of a student suicide while at the same time balancing that constructive urge against the needs of mourners.
Guidance regarding how to encourage responsible social networking in the aftermath of a suicide is available from the Suicide Prevention Research Center, Dr. Gould continued.
Up to half of college students with suicidal ideation choose not to share that information with anyone.
“There are a lot of vulnerable students on campuses. Consider implementing the American Foundation for Suicide Prevention’s anonymous online Interactive Screening Program,” she said.
Dr. Gould’s suicide cluster study was funded by the National Institute of Mental Health and the American Foundation for Suicide Prevention. She reported receiving royalties as coauthor of the Columbia-Suicide Severity Rating Scale.
ATLANTA– A landmark study of newspaper coverage of suicides provides empirical support for media guidelines aimed at minimizing the likelihood of suicide clusters among college students.
“Given the prevalence of suicide on college campuses, and the associated risk of suicide contagion and clustering, it’s imperative that colleges develop effective and comprehensive postvention programs,” Madelyn S. Gould, Ph.D., said at the annual conference of the American Association of Suicidology.
According to the Centers for Disease Control and Prevention, suicide is the No. 2 cause of death among college students, with roughly 1,100 completed suicides occurring annually, noted Dr. Gould, professor of epidemiology in psychiatry at Columbia University, New York, and the New York State Psychiatric Institute.
Suicide contagion is the process by which direct or indirect knowledge of one suicide facilitates subsequent suicide. Dr. Gould was the lead investigator in a national study that examined the role of newspaper coverage of suicide as a contributor to suicide clusters among 13- to 20-year-olds. The retrospective, population-based, case-control study included 48 communities in which suicide clusters occurred during 1988-1996 – before the arrival of social media. The control group consisted of 95 matched communities in which a youth suicide was not followed by a suicide cluster.
The key finding: The more sensational the newspaper coverage of suicides as evidenced by a greater number of stories, front page placement, and more details about the suicidal individual and act, the greater the likelihood of subsequent suicide clusters (Lancet Psychiatry 2014;1:34-43).
Dr. Gould highlighted what she considers a seminal study led by Dr. Thomas Niederkrotenthaler of the Medical University of Vienna. The investigators analyzed the content of nearly 500 suicide-related Austrian print media articles and demonstrated that while sensational and/or repetitive coverage of suicides was associated with a subsequent increase in suicide, stories about mastery-of-crisis – that is, articles about individuals with suicidal ideation who adopted coping strategies other than suicidal behavior when faced with adverse circumstances – were associated with a decreased suicide rate (Br. J. Psychiatry 2010;197:234-43). Dr. Niederkrotenthaler calls it “the Papageno effect,” after a lovesick character in Mozart’s opera “The Magic Flute” whose planned suicide is averted by three child spirits who remind him of alternatives to death.
Dr. Gould noted that emotions also can be spread through the social media, as was made evident by the Facebook’s News Feed Experiment. In this massive study, investigators in Facebook’s research department manipulated the emotional content of the Facebook News Feed for 689,003 Facebook members. When exposure to friends’ positive emotional content in their news feed was reduced, subjects produced fewer positive and more negative posts. When exposure to negative content in the news feed was reduced, the result was more positive and fewer negative posts (Proc. Natl. Acad. Sci. USA 2014;11:8788-90).
The Higher Education Mental Health Alliance has disseminated a comprehensive suicide postvention guide for colleges. It includes specific recommendations aimed at limiting suicide contagion on campuses. The guide includes recommended media guidelines in the wake of suicide, emphasizes the importance of addressing common and counterproductive myths about suicide, and provides tips on how to shape students’ desire to “do something” in the aftermath of a student suicide while at the same time balancing that constructive urge against the needs of mourners.
Guidance regarding how to encourage responsible social networking in the aftermath of a suicide is available from the Suicide Prevention Research Center, Dr. Gould continued.
Up to half of college students with suicidal ideation choose not to share that information with anyone.
“There are a lot of vulnerable students on campuses. Consider implementing the American Foundation for Suicide Prevention’s anonymous online Interactive Screening Program,” she said.
Dr. Gould’s suicide cluster study was funded by the National Institute of Mental Health and the American Foundation for Suicide Prevention. She reported receiving royalties as coauthor of the Columbia-Suicide Severity Rating Scale.
EXPERT ANALYSIS FROM THE ANNUAL AAS CONFERENCE

Novel agent lowers LDL more than ezetimibe
SAN DIEGO– ETC-1002, an oral LDL-lowering drug with a novel mechanism of action, decreased LDL by up to 30% more than did ezetimibe in a large phase IIb study.
The 348-patient trial also showed that ETC-1002 and ezetimibe are additive in their LDL-lowering effects, with the combination reducing LDL levels by up to 48%, compared with baseline, Dr. Paul Thompson reported at the annual meeting of the American College of Cardiology.

Importantly, the investigational drug and ezetimibe, which is marketed in the United States as Zetia, showed similarly favorable safety and tolerability profiles. And ETC-1002 proved equally effective at LDL-lowering in statin-intolerant and -tolerant patients, noted Dr. Thompson, director of cardiology at Hartford (Conn.) Hospital and professor of medicine at the University of Connecticut, Storrs.
ETC-1002 is a first-in-class oral modulator of the enzymes adenosine triphosphate citrate lyase and adenosine monophosphate–activated protein kinase. These dual mechanisms of action cause the liver to take up LDL cholesterol from the blood.
Asked how he sees the drug potentially fitting into the dyslipidemia treatment landscape, which could soon include the eagerly anticipated, super-potent LDL-lowering proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, Dr. Thompson pointed out that there have been no cardiovascular outcome studies of ETC-1002.
“Without outcomes data in terms of survival, I’d say ETC-1002 will be an additional drug in our armamentarium for treating high cholesterol levels. And so far, we’ve generally seen that reductions in LDL cholesterol result in reductions in clinical events. I would think that this drug would be a way to treat statin-intolerant or -tolerant patients in combination with ezetimibe or alone. And where it fits in will depend somewhat on the cost of the medication,” he said.
The double-blind, phase IIb study randomized 177 hypercholesterolemic patients with muscle-related statin intolerance and 171 without statin intolerance to 12 weeks of once-daily ETC-1002 at 120 mg or 180 mg, ezetimibe at 10 mg, the combination of ETC-1002 at 120 mg plus ezetimibe 10 mg, or ETC-1002 at 180 and ezetimibe 10 mg.
ETC-1002 at the lower dose reduced LDL by a mean of 27% from a baseline of 165 mg/dL. The 180-mg dose decreased LDL by 30%. In contrast, ezetimibe monotherapy lowered LDL by 21%, a significantly lesser effect than with either dose of ETC-1002. The effects of combination therapy were additive: ETC-1002 at 120 mg plus ezetimibe reduced LDL by 43%, compared with baseline, while ETC-1002 at 180 mg plus ezetimibe 10 mg lowered LDL by 48%.
ETC-1002 also improved other atherogenic lipids and markers of systemic inflammation. For example, apolipoprotein B decreased by 30% with ETC-1002 at 120 mg, 40% with ETC-1002 at 180 mg, and 10% with ezetimibe at 10 mg. Similarly, C-reactive protein levels fell by 30% and 40% with low- and higher-dose ETC-1002, compared with a 10% reduction with ezetimibe.
Muscle-related complaints were several-fold more common in the group with a history of statin intolerance as defined by the Food and Drug Administration – namely, muscle-related intolerance to at least two statins, including one at the lowest approved dose. However, rates of discontinuation from drug-related adverse events were similarly low at 3%-8% across the five treatment arms.
“I think the take-home message is that the safety profile of the drug looks good,” the cardiologist said.
No significant changes were seen in body weight, blood glucose levels, or blood pressure during the 12-week study.
Dr. Thompson reported receiving a research grant from Esperion Therapeutics, the study sponsor. He serves as a consultant to AstraZeneca, Merck, and Sanofi-Aventis.
SAN DIEGO– ETC-1002, an oral LDL-lowering drug with a novel mechanism of action, decreased LDL by up to 30% more than did ezetimibe in a large phase IIb study.
The 348-patient trial also showed that ETC-1002 and ezetimibe are additive in their LDL-lowering effects, with the combination reducing LDL levels by up to 48%, compared with baseline, Dr. Paul Thompson reported at the annual meeting of the American College of Cardiology.
Importantly, the investigational drug and ezetimibe, which is marketed in the United States as Zetia, showed similarly favorable safety and tolerability profiles. And ETC-1002 proved equally effective at LDL-lowering in statin-intolerant and -tolerant patients, noted Dr. Thompson, director of cardiology at Hartford (Conn.) Hospital and professor of medicine at the University of Connecticut, Storrs.
ETC-1002 is a first-in-class oral modulator of the enzymes adenosine triphosphate citrate lyase and adenosine monophosphate–activated protein kinase. These dual mechanisms of action cause the liver to take up LDL cholesterol from the blood.
Asked how he sees the drug potentially fitting into the dyslipidemia treatment landscape, which could soon include the eagerly anticipated, super-potent LDL-lowering proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, Dr. Thompson pointed out that there have been no cardiovascular outcome studies of ETC-1002.
“Without outcomes data in terms of survival, I’d say ETC-1002 will be an additional drug in our armamentarium for treating high cholesterol levels. And so far, we’ve generally seen that reductions in LDL cholesterol result in reductions in clinical events. I would think that this drug would be a way to treat statin-intolerant or -tolerant patients in combination with ezetimibe or alone. And where it fits in will depend somewhat on the cost of the medication,” he said.
The double-blind, phase IIb study randomized 177 hypercholesterolemic patients with muscle-related statin intolerance and 171 without statin intolerance to 12 weeks of once-daily ETC-1002 at 120 mg or 180 mg, ezetimibe at 10 mg, the combination of ETC-1002 at 120 mg plus ezetimibe 10 mg, or ETC-1002 at 180 and ezetimibe 10 mg.
ETC-1002 at the lower dose reduced LDL by a mean of 27% from a baseline of 165 mg/dL. The 180-mg dose decreased LDL by 30%. In contrast, ezetimibe monotherapy lowered LDL by 21%, a significantly lesser effect than with either dose of ETC-1002. The effects of combination therapy were additive: ETC-1002 at 120 mg plus ezetimibe reduced LDL by 43%, compared with baseline, while ETC-1002 at 180 mg plus ezetimibe 10 mg lowered LDL by 48%.
ETC-1002 also improved other atherogenic lipids and markers of systemic inflammation. For example, apolipoprotein B decreased by 30% with ETC-1002 at 120 mg, 40% with ETC-1002 at 180 mg, and 10% with ezetimibe at 10 mg. Similarly, C-reactive protein levels fell by 30% and 40% with low- and higher-dose ETC-1002, compared with a 10% reduction with ezetimibe.
Muscle-related complaints were several-fold more common in the group with a history of statin intolerance as defined by the Food and Drug Administration – namely, muscle-related intolerance to at least two statins, including one at the lowest approved dose. However, rates of discontinuation from drug-related adverse events were similarly low at 3%-8% across the five treatment arms.
“I think the take-home message is that the safety profile of the drug looks good,” the cardiologist said.
No significant changes were seen in body weight, blood glucose levels, or blood pressure during the 12-week study.
Dr. Thompson reported receiving a research grant from Esperion Therapeutics, the study sponsor. He serves as a consultant to AstraZeneca, Merck, and Sanofi-Aventis.
SAN DIEGO– ETC-1002, an oral LDL-lowering drug with a novel mechanism of action, decreased LDL by up to 30% more than did ezetimibe in a large phase IIb study.
The 348-patient trial also showed that ETC-1002 and ezetimibe are additive in their LDL-lowering effects, with the combination reducing LDL levels by up to 48%, compared with baseline, Dr. Paul Thompson reported at the annual meeting of the American College of Cardiology.
Importantly, the investigational drug and ezetimibe, which is marketed in the United States as Zetia, showed similarly favorable safety and tolerability profiles. And ETC-1002 proved equally effective at LDL-lowering in statin-intolerant and -tolerant patients, noted Dr. Thompson, director of cardiology at Hartford (Conn.) Hospital and professor of medicine at the University of Connecticut, Storrs.
ETC-1002 is a first-in-class oral modulator of the enzymes adenosine triphosphate citrate lyase and adenosine monophosphate–activated protein kinase. These dual mechanisms of action cause the liver to take up LDL cholesterol from the blood.
Asked how he sees the drug potentially fitting into the dyslipidemia treatment landscape, which could soon include the eagerly anticipated, super-potent LDL-lowering proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, Dr. Thompson pointed out that there have been no cardiovascular outcome studies of ETC-1002.
“Without outcomes data in terms of survival, I’d say ETC-1002 will be an additional drug in our armamentarium for treating high cholesterol levels. And so far, we’ve generally seen that reductions in LDL cholesterol result in reductions in clinical events. I would think that this drug would be a way to treat statin-intolerant or -tolerant patients in combination with ezetimibe or alone. And where it fits in will depend somewhat on the cost of the medication,” he said.
The double-blind, phase IIb study randomized 177 hypercholesterolemic patients with muscle-related statin intolerance and 171 without statin intolerance to 12 weeks of once-daily ETC-1002 at 120 mg or 180 mg, ezetimibe at 10 mg, the combination of ETC-1002 at 120 mg plus ezetimibe 10 mg, or ETC-1002 at 180 and ezetimibe 10 mg.
ETC-1002 at the lower dose reduced LDL by a mean of 27% from a baseline of 165 mg/dL. The 180-mg dose decreased LDL by 30%. In contrast, ezetimibe monotherapy lowered LDL by 21%, a significantly lesser effect than with either dose of ETC-1002. The effects of combination therapy were additive: ETC-1002 at 120 mg plus ezetimibe reduced LDL by 43%, compared with baseline, while ETC-1002 at 180 mg plus ezetimibe 10 mg lowered LDL by 48%.
ETC-1002 also improved other atherogenic lipids and markers of systemic inflammation. For example, apolipoprotein B decreased by 30% with ETC-1002 at 120 mg, 40% with ETC-1002 at 180 mg, and 10% with ezetimibe at 10 mg. Similarly, C-reactive protein levels fell by 30% and 40% with low- and higher-dose ETC-1002, compared with a 10% reduction with ezetimibe.
Muscle-related complaints were several-fold more common in the group with a history of statin intolerance as defined by the Food and Drug Administration – namely, muscle-related intolerance to at least two statins, including one at the lowest approved dose. However, rates of discontinuation from drug-related adverse events were similarly low at 3%-8% across the five treatment arms.
“I think the take-home message is that the safety profile of the drug looks good,” the cardiologist said.
No significant changes were seen in body weight, blood glucose levels, or blood pressure during the 12-week study.
Dr. Thompson reported receiving a research grant from Esperion Therapeutics, the study sponsor. He serves as a consultant to AstraZeneca, Merck, and Sanofi-Aventis.
AT ACC 15
Key clinical point: A novel investigational LDL cholesterol–lowering agent showed greater lipid lowering than did ezetimibe along with similar safety and tolerability.
Major finding: ETC-1002 at 180 mg once daily lowered LDL by a mean of 30%, while ezetimibe at 10 mg/day decreased LDL by 21%.
Data source: This phase IIb, double-blind, randomized, 12-week trial included 348 hypercholesterolemic patients, roughly half with a history of statin intolerance.
Disclosures: The study presenter received a research grant from Esperion Therapeutics, which sponsored the trial.

AAAAI: Grass allergy tablets show favorable NNT
HOUSTON – The number needed to treat with Timothy grass sublingual immunotherapy tablets for allergic rhinitis to achieve a clinically meaningful response is 7.9, Dr. Stephen R. Durham reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
What the low number needed to treat (NNT) means in this instance is that, on average, 7.9 children or adults with Timothy grass–induced allergic rhinitis with or without conjunctivitis would need to be treated with Merck’s sublingual immunotherapy tablet (SLIT) rather than placebo daily for 3 years in order for 1 additional patient to obtain sustained benefit. Sustained benefit was defined as at least 50% well days for the entire grass pollen season during each of the 3 treatment years plus the subsequent 2 years of no treatment, explained Dr. Durham of Royal Brompton and Harefield Hospitals and Imperial College, London.

A ‘well day’ was considered as a day with no use of open-label rescue medication and in which the worst score recorded was ‘none’ or ‘mild’ for each of the four nasal and two ocular symptoms measured. This NNT analysis was based upon pooled data from six pivotal randomized, double-blind, phase III, placebo-controlled clinical trials totaling 3,094 patients, Dr. Durham added.
A separate analysis of the same pooled data using a different definition of favorable response – that is, a total combined daily symptom and daily medication score of 3 or less during the entire grass pollen season during the 3 treatment years, plus the following 2 no-treatment years – yielded an NNT of 9.4. The maximum total daily symptom score during any given year was 18, while the maximum daily medication score per year was 30-36, depending upon whether the participant was a child or adult, and whether the study was conducted in Europe or the United States.
The risk-benefit ratio of SLIT for allergic rhinitis in the pooled analysis was favorable as reflected in a number needed to harm of 303, with harm defined as a treatment-related systemic allergic reaction. When the NNH was recalculated using epinephrine usage as the harmful endpoint, the NNH was closely similar at 305.
Merck’s Timothy grass SLIT, marketed as Grastek, is FDA-approved for treatment of allergic rhinitis in adults and children as young as 5 years of age.
Dr. Durham reported receiving research grants and serving as a consultant to Merck, ALK, and Stallergenes. The NNT analysis was funded by Merck, and the phase III clinical trials on which the analysis was based were supported by ALK and Merck.
HOUSTON – The number needed to treat with Timothy grass sublingual immunotherapy tablets for allergic rhinitis to achieve a clinically meaningful response is 7.9, Dr. Stephen R. Durham reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
What the low number needed to treat (NNT) means in this instance is that, on average, 7.9 children or adults with Timothy grass–induced allergic rhinitis with or without conjunctivitis would need to be treated with Merck’s sublingual immunotherapy tablet (SLIT) rather than placebo daily for 3 years in order for 1 additional patient to obtain sustained benefit. Sustained benefit was defined as at least 50% well days for the entire grass pollen season during each of the 3 treatment years plus the subsequent 2 years of no treatment, explained Dr. Durham of Royal Brompton and Harefield Hospitals and Imperial College, London.
A ‘well day’ was considered as a day with no use of open-label rescue medication and in which the worst score recorded was ‘none’ or ‘mild’ for each of the four nasal and two ocular symptoms measured. This NNT analysis was based upon pooled data from six pivotal randomized, double-blind, phase III, placebo-controlled clinical trials totaling 3,094 patients, Dr. Durham added.
A separate analysis of the same pooled data using a different definition of favorable response – that is, a total combined daily symptom and daily medication score of 3 or less during the entire grass pollen season during the 3 treatment years, plus the following 2 no-treatment years – yielded an NNT of 9.4. The maximum total daily symptom score during any given year was 18, while the maximum daily medication score per year was 30-36, depending upon whether the participant was a child or adult, and whether the study was conducted in Europe or the United States.
The risk-benefit ratio of SLIT for allergic rhinitis in the pooled analysis was favorable as reflected in a number needed to harm of 303, with harm defined as a treatment-related systemic allergic reaction. When the NNH was recalculated using epinephrine usage as the harmful endpoint, the NNH was closely similar at 305.
Merck’s Timothy grass SLIT, marketed as Grastek, is FDA-approved for treatment of allergic rhinitis in adults and children as young as 5 years of age.
Dr. Durham reported receiving research grants and serving as a consultant to Merck, ALK, and Stallergenes. The NNT analysis was funded by Merck, and the phase III clinical trials on which the analysis was based were supported by ALK and Merck.
HOUSTON – The number needed to treat with Timothy grass sublingual immunotherapy tablets for allergic rhinitis to achieve a clinically meaningful response is 7.9, Dr. Stephen R. Durham reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
What the low number needed to treat (NNT) means in this instance is that, on average, 7.9 children or adults with Timothy grass–induced allergic rhinitis with or without conjunctivitis would need to be treated with Merck’s sublingual immunotherapy tablet (SLIT) rather than placebo daily for 3 years in order for 1 additional patient to obtain sustained benefit. Sustained benefit was defined as at least 50% well days for the entire grass pollen season during each of the 3 treatment years plus the subsequent 2 years of no treatment, explained Dr. Durham of Royal Brompton and Harefield Hospitals and Imperial College, London.
A ‘well day’ was considered as a day with no use of open-label rescue medication and in which the worst score recorded was ‘none’ or ‘mild’ for each of the four nasal and two ocular symptoms measured. This NNT analysis was based upon pooled data from six pivotal randomized, double-blind, phase III, placebo-controlled clinical trials totaling 3,094 patients, Dr. Durham added.
A separate analysis of the same pooled data using a different definition of favorable response – that is, a total combined daily symptom and daily medication score of 3 or less during the entire grass pollen season during the 3 treatment years, plus the following 2 no-treatment years – yielded an NNT of 9.4. The maximum total daily symptom score during any given year was 18, while the maximum daily medication score per year was 30-36, depending upon whether the participant was a child or adult, and whether the study was conducted in Europe or the United States.
The risk-benefit ratio of SLIT for allergic rhinitis in the pooled analysis was favorable as reflected in a number needed to harm of 303, with harm defined as a treatment-related systemic allergic reaction. When the NNH was recalculated using epinephrine usage as the harmful endpoint, the NNH was closely similar at 305.
Merck’s Timothy grass SLIT, marketed as Grastek, is FDA-approved for treatment of allergic rhinitis in adults and children as young as 5 years of age.
Dr. Durham reported receiving research grants and serving as a consultant to Merck, ALK, and Stallergenes. The NNT analysis was funded by Merck, and the phase III clinical trials on which the analysis was based were supported by ALK and Merck.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: The number of allergic rhinitis patients who need to be treated with Timothy grass immunotherapy tablets to obtain a sustained clinically important response is 7.9.
Major finding: For every 7.9 patients who took the sublingual immunotherapy tablets rather than placebo daily for 3 years, one additional patient experienced ‘well days’ for the entire grass pollen season during those 3 years, along with the next 2 years of no treatment.
Data source: This analysis was based upon six pivotal phase III, randomized, double-blind, placebo-controlled clinical trials totaling 3,094 adults and children with allergic rhinitis.
Disclosures: This NNT analysis was sponsored by Merck. The presenter reported receiving a research grant from the company.

AAS: Brief therapy reduces repeat self-harm
ATLANTA – The strongest evidence to date that brief psychological therapy is effective in reducing repetition of acts of self-harm comes from a new Cochrane Collaboration meta-analysis.
Current guidelines on management of self-harm provided by the United Kingdom’s National Institute for Health and Care Excellence (NICE) state that psychological therapy “may” prevent recurrent self-harm, but this guidance relied upon limited evidence. The new Cochrane Collaboration review, based on 18 randomized controlled trials, greatly strengthens support for that conclusion, Dr. Keith Hawton said at the annual meeting of the American Association of Suicidology.

“And I’ve got to add, of course, that psychological therapy may be at least as effective in terms of other important outcomes,” observed Dr. Hawton, lead author of the soon-to-be published Cochrane meta-analysis. Dr. Hawton is professor of psychiatry and director of the Centre for Suicide Research at the University of Oxford (England).
The meta-analysis included 11 randomized trials of brief psychological therapy or treatment as usual in adults in which the primary outcome was repetition of self-harm during 6 months of follow-up. There were 146 such events in 663 patients who underwent psychological therapy, compared with 176 events in 640 controls, for an adjusted 43% relative risk reduction.
In 10 trials featuring 12 months of follow-up, some of which were also included in the 6-month analysis, there were 263 events in 1,101 psychotherapy recipients, compared with 308 events in 1,131 controls. That translates into a statistically significant 20% relative risk reduction favoring brief psychotherapy.
Depression scores at last follow-up were significantly lower in the psychotherapy recipients, compared with treatment as usual. So were hopelessness and suicidal ideation scores.
Nine suicides occurred among 1,169 patients randomized to psychotherapy, vs. 15 in 1,185 controls. Although this represents a 34% relative risk reduction, the difference wasn’t significant, because suicide was such a rare event, even in these high-risk patients who – as documented in the Multicentre Study of Self Harm in England – have a 50-fold greater risk of death by suicide in the year following a self-harm event than the risk in the general population.
“This illustrates the problem in using suicide as an outcome, even when you stack up a lot of studies,” Dr. Hawton noted.
The trials in the meta-analysis were conducted throughout the world, so “treatment as usual” in the control arm varied from study to study. But even in the United Kingdom, where the NICE guidelines state that all self-harm patients who present to a hospital should receive a psychosocial assessment, including an evaluation of their needs and risks, a 32-hospital study showed that only 60% of self-harm patients actually get such an assessment, the psychiatrist said.
A variety of forms of brief psychological therapy for self-harm were employed in the randomized trials. Most involved short-term cognitive-behavioral therapy, problem-solving therapy, or dialectical behavior therapy. Components shared by the various regimens included engagement; a careful examination of the process associated with an individual’s self-harm; problem-solving; cognitive therapy to address the patient’s problems, thoughts, images, and core beliefs; and ongoing monitoring of depression, hopelessness, and thoughts of self-harm.
“The self-harm population is very heterogeneous. There’s a wide range of problems and needs. Brief psychological therapy isn’t suitable for all patients. We’ve estimated that about 30% could benefit from this approach,” according to Dr. Hawton.
Based in part upon the Cochrane Collaboration analysis, the local directors of health services across England and Wales recently have received guidance that brief psychological therapy is to be made available routinely to patients seen by self-harm mental health programs, he added.
Self-harm is defined in the United Kingdom as intentional nonfatal self-poisoning or self-injury regardless of the degree of suicidal intent.
Looking ahead, Dr. Hawton cited several developments that show promise as potential new therapies for self-harm patients.
“Mindfulness has achieved great success in recent years, particularly based on very impressive impacts in people with relapsing depression. This is clearly an area that’s going to be developed in relation to the self- harm population. In fact, there is already work going on,” he said.
Similarly, randomized studies are underway evaluating ketamine and its analogs for acute suicidality based upon the highly favorable results reported in treating severe depression.
Internet and mobile telephone–based interventions for self-harm patients are “proliferating” at the moment, Dr. Hawton said.
“One of the issues is how to individualize therapy through these approaches,” he noted.
Dr. Hawton’s research is funded by the National Institute for Health Research. He reported having no financial conflicts.
ATLANTA – The strongest evidence to date that brief psychological therapy is effective in reducing repetition of acts of self-harm comes from a new Cochrane Collaboration meta-analysis.
Current guidelines on management of self-harm provided by the United Kingdom’s National Institute for Health and Care Excellence (NICE) state that psychological therapy “may” prevent recurrent self-harm, but this guidance relied upon limited evidence. The new Cochrane Collaboration review, based on 18 randomized controlled trials, greatly strengthens support for that conclusion, Dr. Keith Hawton said at the annual meeting of the American Association of Suicidology.
“And I’ve got to add, of course, that psychological therapy may be at least as effective in terms of other important outcomes,” observed Dr. Hawton, lead author of the soon-to-be published Cochrane meta-analysis. Dr. Hawton is professor of psychiatry and director of the Centre for Suicide Research at the University of Oxford (England).
The meta-analysis included 11 randomized trials of brief psychological therapy or treatment as usual in adults in which the primary outcome was repetition of self-harm during 6 months of follow-up. There were 146 such events in 663 patients who underwent psychological therapy, compared with 176 events in 640 controls, for an adjusted 43% relative risk reduction.
In 10 trials featuring 12 months of follow-up, some of which were also included in the 6-month analysis, there were 263 events in 1,101 psychotherapy recipients, compared with 308 events in 1,131 controls. That translates into a statistically significant 20% relative risk reduction favoring brief psychotherapy.
Depression scores at last follow-up were significantly lower in the psychotherapy recipients, compared with treatment as usual. So were hopelessness and suicidal ideation scores.
Nine suicides occurred among 1,169 patients randomized to psychotherapy, vs. 15 in 1,185 controls. Although this represents a 34% relative risk reduction, the difference wasn’t significant, because suicide was such a rare event, even in these high-risk patients who – as documented in the Multicentre Study of Self Harm in England – have a 50-fold greater risk of death by suicide in the year following a self-harm event than the risk in the general population.
“This illustrates the problem in using suicide as an outcome, even when you stack up a lot of studies,” Dr. Hawton noted.
The trials in the meta-analysis were conducted throughout the world, so “treatment as usual” in the control arm varied from study to study. But even in the United Kingdom, where the NICE guidelines state that all self-harm patients who present to a hospital should receive a psychosocial assessment, including an evaluation of their needs and risks, a 32-hospital study showed that only 60% of self-harm patients actually get such an assessment, the psychiatrist said.
A variety of forms of brief psychological therapy for self-harm were employed in the randomized trials. Most involved short-term cognitive-behavioral therapy, problem-solving therapy, or dialectical behavior therapy. Components shared by the various regimens included engagement; a careful examination of the process associated with an individual’s self-harm; problem-solving; cognitive therapy to address the patient’s problems, thoughts, images, and core beliefs; and ongoing monitoring of depression, hopelessness, and thoughts of self-harm.
“The self-harm population is very heterogeneous. There’s a wide range of problems and needs. Brief psychological therapy isn’t suitable for all patients. We’ve estimated that about 30% could benefit from this approach,” according to Dr. Hawton.
Based in part upon the Cochrane Collaboration analysis, the local directors of health services across England and Wales recently have received guidance that brief psychological therapy is to be made available routinely to patients seen by self-harm mental health programs, he added.
Self-harm is defined in the United Kingdom as intentional nonfatal self-poisoning or self-injury regardless of the degree of suicidal intent.
Looking ahead, Dr. Hawton cited several developments that show promise as potential new therapies for self-harm patients.
“Mindfulness has achieved great success in recent years, particularly based on very impressive impacts in people with relapsing depression. This is clearly an area that’s going to be developed in relation to the self- harm population. In fact, there is already work going on,” he said.
Similarly, randomized studies are underway evaluating ketamine and its analogs for acute suicidality based upon the highly favorable results reported in treating severe depression.
Internet and mobile telephone–based interventions for self-harm patients are “proliferating” at the moment, Dr. Hawton said.
“One of the issues is how to individualize therapy through these approaches,” he noted.
Dr. Hawton’s research is funded by the National Institute for Health Research. He reported having no financial conflicts.
ATLANTA – The strongest evidence to date that brief psychological therapy is effective in reducing repetition of acts of self-harm comes from a new Cochrane Collaboration meta-analysis.
Current guidelines on management of self-harm provided by the United Kingdom’s National Institute for Health and Care Excellence (NICE) state that psychological therapy “may” prevent recurrent self-harm, but this guidance relied upon limited evidence. The new Cochrane Collaboration review, based on 18 randomized controlled trials, greatly strengthens support for that conclusion, Dr. Keith Hawton said at the annual meeting of the American Association of Suicidology.
“And I’ve got to add, of course, that psychological therapy may be at least as effective in terms of other important outcomes,” observed Dr. Hawton, lead author of the soon-to-be published Cochrane meta-analysis. Dr. Hawton is professor of psychiatry and director of the Centre for Suicide Research at the University of Oxford (England).
The meta-analysis included 11 randomized trials of brief psychological therapy or treatment as usual in adults in which the primary outcome was repetition of self-harm during 6 months of follow-up. There were 146 such events in 663 patients who underwent psychological therapy, compared with 176 events in 640 controls, for an adjusted 43% relative risk reduction.
In 10 trials featuring 12 months of follow-up, some of which were also included in the 6-month analysis, there were 263 events in 1,101 psychotherapy recipients, compared with 308 events in 1,131 controls. That translates into a statistically significant 20% relative risk reduction favoring brief psychotherapy.
Depression scores at last follow-up were significantly lower in the psychotherapy recipients, compared with treatment as usual. So were hopelessness and suicidal ideation scores.
Nine suicides occurred among 1,169 patients randomized to psychotherapy, vs. 15 in 1,185 controls. Although this represents a 34% relative risk reduction, the difference wasn’t significant, because suicide was such a rare event, even in these high-risk patients who – as documented in the Multicentre Study of Self Harm in England – have a 50-fold greater risk of death by suicide in the year following a self-harm event than the risk in the general population.
“This illustrates the problem in using suicide as an outcome, even when you stack up a lot of studies,” Dr. Hawton noted.
The trials in the meta-analysis were conducted throughout the world, so “treatment as usual” in the control arm varied from study to study. But even in the United Kingdom, where the NICE guidelines state that all self-harm patients who present to a hospital should receive a psychosocial assessment, including an evaluation of their needs and risks, a 32-hospital study showed that only 60% of self-harm patients actually get such an assessment, the psychiatrist said.
A variety of forms of brief psychological therapy for self-harm were employed in the randomized trials. Most involved short-term cognitive-behavioral therapy, problem-solving therapy, or dialectical behavior therapy. Components shared by the various regimens included engagement; a careful examination of the process associated with an individual’s self-harm; problem-solving; cognitive therapy to address the patient’s problems, thoughts, images, and core beliefs; and ongoing monitoring of depression, hopelessness, and thoughts of self-harm.
“The self-harm population is very heterogeneous. There’s a wide range of problems and needs. Brief psychological therapy isn’t suitable for all patients. We’ve estimated that about 30% could benefit from this approach,” according to Dr. Hawton.
Based in part upon the Cochrane Collaboration analysis, the local directors of health services across England and Wales recently have received guidance that brief psychological therapy is to be made available routinely to patients seen by self-harm mental health programs, he added.
Self-harm is defined in the United Kingdom as intentional nonfatal self-poisoning or self-injury regardless of the degree of suicidal intent.
Looking ahead, Dr. Hawton cited several developments that show promise as potential new therapies for self-harm patients.
“Mindfulness has achieved great success in recent years, particularly based on very impressive impacts in people with relapsing depression. This is clearly an area that’s going to be developed in relation to the self- harm population. In fact, there is already work going on,” he said.
Similarly, randomized studies are underway evaluating ketamine and its analogs for acute suicidality based upon the highly favorable results reported in treating severe depression.
Internet and mobile telephone–based interventions for self-harm patients are “proliferating” at the moment, Dr. Hawton said.
“One of the issues is how to individualize therapy through these approaches,” he noted.
Dr. Hawton’s research is funded by the National Institute for Health Research. He reported having no financial conflicts.
AT THE ANNUAL AAS CONFERENCE
Key clinical point: Patients who underwent a course of brief psychological therapy after presenting to a hospital with self-harm were 20% less likely to have a repeat episode in the next 12 months than were those who received treatment as usual.
Major finding: Repeated self-harm events occurred within 1 year in 263 of 1,101 psychotherapy recipients, compared with 308 of 1,131 controls.
Data source: A Cochrane Collaboration meta-analysis of 18 randomized, controlled trials.
Disclosures: The U.K. National Institute for Health Research supported the study. The presenter reported having no financial conflicts.

How to forestall heart failure by 15 years
SAN DIEGO– Men and women who are able to prevent or delay onset of hypertension, obesity, and diabetes beyond age 45 years can expect to reap a major benefit: living for 11-15 years longer without heart failure, according to a novel study featuring more than 500,000 person-years of follow-up.
“We’re interested in thinking about risk in a different way. Traditionally, risk has been thought of in terms of how different risk factors lead to increased chances for heart failure. Instead, we’re interested in thinking about how preventing the development of risk factors leads to increased longevity and extension of heart failure–free survival. It’s a much more powerful message when you’re talking to patients in their 30s or 40s to say that they’ll be able to live 11-15 years longer without heart failure if they can avoid developing these three risk factors,” Dr. Faraz S. Ahmad explained at the annual meeting of the American College of Cardiology.

He presented an analysis of pooled data from four large studies with adjudicated heart failure outcomes. The analysis, conducted as part of the Cardiovascular Lifetime Risk Pooling Project, included a total of 19,429 subjects with a median 21.3 years of follow-up, during which 1,677 participants were diagnosed with incident heart failure.
This analysis quantified the association between prevalent hypertension, diabetes, and/or obesity with heart failure–free and overall survival, beginning at age 45 years and with 50 years of subsequent follow-up, noted Dr. Ahmad, a cardiology fellow at Northwestern University, Chicago.
Among men with none of the three key risk factors at age 45 years, the multivariate-adjusted risk of subsequently developing heart failure was reduced by 73%, compared with that of men with all three risk factors present. Women with none of the three risk factors enjoyed an 85% relative risk reduction.
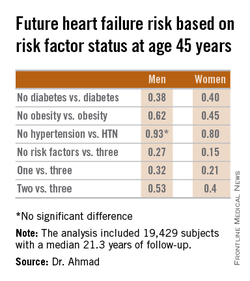
Among men who developed heart failure, those with diabetes by age 45 years were diagnosed with heart failure 8.6 years earlier than were those without diabetes at age 45 years. Among women with diabetes at age 45 years, heart failure was diagnosed when they were 10.6 years younger than in those without diabetes were.
These data take on added weight in light of projections regarding the future of heart failure in the United States. At present, there are an estimated 825,000 new cases of heart failure per year. The disease prevalence is 5.1 million. The annual cost is $31 billion and is expected to climb by 126% over the next 20 years, Dr. Ahmad said.
The four studies upon which this lifetime risk analysis was based were the Framingham Heart Study, the Framingham Offspring Study, the Atherosclerosis Risk in Communities study, and the Chicago Heart Association Detection Project in Industry. Together they included 509,650 person-years of follow-up. All four studies were funded by the National Heart, Lung, and Blood Institute, as was this analysis. Dr. Ahmad reported having no financial conflicts.
SAN DIEGO– Men and women who are able to prevent or delay onset of hypertension, obesity, and diabetes beyond age 45 years can expect to reap a major benefit: living for 11-15 years longer without heart failure, according to a novel study featuring more than 500,000 person-years of follow-up.
“We’re interested in thinking about risk in a different way. Traditionally, risk has been thought of in terms of how different risk factors lead to increased chances for heart failure. Instead, we’re interested in thinking about how preventing the development of risk factors leads to increased longevity and extension of heart failure–free survival. It’s a much more powerful message when you’re talking to patients in their 30s or 40s to say that they’ll be able to live 11-15 years longer without heart failure if they can avoid developing these three risk factors,” Dr. Faraz S. Ahmad explained at the annual meeting of the American College of Cardiology.
He presented an analysis of pooled data from four large studies with adjudicated heart failure outcomes. The analysis, conducted as part of the Cardiovascular Lifetime Risk Pooling Project, included a total of 19,429 subjects with a median 21.3 years of follow-up, during which 1,677 participants were diagnosed with incident heart failure.
This analysis quantified the association between prevalent hypertension, diabetes, and/or obesity with heart failure–free and overall survival, beginning at age 45 years and with 50 years of subsequent follow-up, noted Dr. Ahmad, a cardiology fellow at Northwestern University, Chicago.
Among men with none of the three key risk factors at age 45 years, the multivariate-adjusted risk of subsequently developing heart failure was reduced by 73%, compared with that of men with all three risk factors present. Women with none of the three risk factors enjoyed an 85% relative risk reduction.
Among men who developed heart failure, those with diabetes by age 45 years were diagnosed with heart failure 8.6 years earlier than were those without diabetes at age 45 years. Among women with diabetes at age 45 years, heart failure was diagnosed when they were 10.6 years younger than in those without diabetes were.
These data take on added weight in light of projections regarding the future of heart failure in the United States. At present, there are an estimated 825,000 new cases of heart failure per year. The disease prevalence is 5.1 million. The annual cost is $31 billion and is expected to climb by 126% over the next 20 years, Dr. Ahmad said.
The four studies upon which this lifetime risk analysis was based were the Framingham Heart Study, the Framingham Offspring Study, the Atherosclerosis Risk in Communities study, and the Chicago Heart Association Detection Project in Industry. Together they included 509,650 person-years of follow-up. All four studies were funded by the National Heart, Lung, and Blood Institute, as was this analysis. Dr. Ahmad reported having no financial conflicts.
SAN DIEGO– Men and women who are able to prevent or delay onset of hypertension, obesity, and diabetes beyond age 45 years can expect to reap a major benefit: living for 11-15 years longer without heart failure, according to a novel study featuring more than 500,000 person-years of follow-up.
“We’re interested in thinking about risk in a different way. Traditionally, risk has been thought of in terms of how different risk factors lead to increased chances for heart failure. Instead, we’re interested in thinking about how preventing the development of risk factors leads to increased longevity and extension of heart failure–free survival. It’s a much more powerful message when you’re talking to patients in their 30s or 40s to say that they’ll be able to live 11-15 years longer without heart failure if they can avoid developing these three risk factors,” Dr. Faraz S. Ahmad explained at the annual meeting of the American College of Cardiology.
He presented an analysis of pooled data from four large studies with adjudicated heart failure outcomes. The analysis, conducted as part of the Cardiovascular Lifetime Risk Pooling Project, included a total of 19,429 subjects with a median 21.3 years of follow-up, during which 1,677 participants were diagnosed with incident heart failure.
This analysis quantified the association between prevalent hypertension, diabetes, and/or obesity with heart failure–free and overall survival, beginning at age 45 years and with 50 years of subsequent follow-up, noted Dr. Ahmad, a cardiology fellow at Northwestern University, Chicago.
Among men with none of the three key risk factors at age 45 years, the multivariate-adjusted risk of subsequently developing heart failure was reduced by 73%, compared with that of men with all three risk factors present. Women with none of the three risk factors enjoyed an 85% relative risk reduction.
Among men who developed heart failure, those with diabetes by age 45 years were diagnosed with heart failure 8.6 years earlier than were those without diabetes at age 45 years. Among women with diabetes at age 45 years, heart failure was diagnosed when they were 10.6 years younger than in those without diabetes were.
These data take on added weight in light of projections regarding the future of heart failure in the United States. At present, there are an estimated 825,000 new cases of heart failure per year. The disease prevalence is 5.1 million. The annual cost is $31 billion and is expected to climb by 126% over the next 20 years, Dr. Ahmad said.
The four studies upon which this lifetime risk analysis was based were the Framingham Heart Study, the Framingham Offspring Study, the Atherosclerosis Risk in Communities study, and the Chicago Heart Association Detection Project in Industry. Together they included 509,650 person-years of follow-up. All four studies were funded by the National Heart, Lung, and Blood Institute, as was this analysis. Dr. Ahmad reported having no financial conflicts.
AT ACC 15
Key clinical point: Individuals who remain free of hypertension, obesity, and diabetes at age 45 years can expect to enjoy an extra 11-15 years of heart failure–free survival.
Major finding: The lifetime risk of developing heart failure in men without hypertension, obesity, and diabetes at age 45 years was reduced by 73%, compared with the risk in men having all three risk factors at that age. In women free of the three risk factors at age 45 years, the relative risk reduction was 85%.
Data source: This pooled analysis of data from four major studies included 19,429 subjects with 509,650 person-years of follow-up, during which 1,677 participants were newly diagnosed with heart failure.
Disclosures: This analysis was supported by the National Heart, Lung, and Blood Institute. The presenter reported having no financial conflicts.

Screen for acute stress disorder in ACS patients
SAN DIEGO – Screening for acute stress disorder with depression upon hospital admission for acute coronary syndrome enables physicians to identify a subgroup of ACS patients at increased risk for in-hospital mortality, Dr. Edina Cenko reported at the annual meeting of the American College of Cardiology.
“It’s a simple, quick test that’s easy to do in clinical practice, and it identifies a group of ACS patients who warrant special attention. It’s important for physicians to do because most deaths in ACS patients occur before arrival at the hospital or in-hospital,” said Dr. Cenko of the University of Bologna (Italy).

She presented a study of 5,880 patients enrolled in the International Survey of Acute Coronary Syndromes in Transitional Countries, all of whom had survived day 1 following admission for ACS at seven Serbian hospitals during 2009-2014. They were screened for acute stress disorder (ASD) and depression upon admission.
Patients who met the inclusion criteria for ASD due to a traumatic event occurring within 4 weeks prior to their ACS and who also had at least mild depression upon admission as indicated by a score of 8 or more out of a possible 27 points on the Patient Health Questionnaire-9 had a significantly higher subsequent in-hospital mortality: 10.7% compared with 8.1%.
The prevalence of ASD with depression was 51% in patients with ST-elevation MI compared with 67% in those with non–ST-elevation ACS. Upon statistical adjustment for these and other clinical and demographic factors, patients with ASD plus depression were 68% more likely to die in-hospital. Upon further adjustment for the use of guideline-recommended medications and percutaneous coronary intervention, the ASD/depression group remained at 35% increased risk of in-hospital mortality.
Dr. Cenko explained that this study was conducted in Serbia because the nation’s turbulent history in recent decades made for an enriched population of individuals with ASD.
Acute stress disorder was introduced as a new diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. The diagnosis was created for patients who met most of the criteria for posttraumatic stress disorder except their duration of symptoms was insufficient because the traumatic event had taken place too recently to qualify for PTSD. The diagnosis of ASD is included in DSM-5 as well.
The physician-investigators in the international registry identified ACS patients as having ASD if they had experienced a traumatic event within 4 weeks preceding the ACS and about which they were experiencing intrusive thoughts, memories, or nightmares, avoidance of situations that reminded them about the traumatic event, and increased arousal as typically manifest in insomnia and/or irritability.
Dr. Cenko reported having no financial conflicts regarding her study.
SAN DIEGO – Screening for acute stress disorder with depression upon hospital admission for acute coronary syndrome enables physicians to identify a subgroup of ACS patients at increased risk for in-hospital mortality, Dr. Edina Cenko reported at the annual meeting of the American College of Cardiology.
“It’s a simple, quick test that’s easy to do in clinical practice, and it identifies a group of ACS patients who warrant special attention. It’s important for physicians to do because most deaths in ACS patients occur before arrival at the hospital or in-hospital,” said Dr. Cenko of the University of Bologna (Italy).
She presented a study of 5,880 patients enrolled in the International Survey of Acute Coronary Syndromes in Transitional Countries, all of whom had survived day 1 following admission for ACS at seven Serbian hospitals during 2009-2014. They were screened for acute stress disorder (ASD) and depression upon admission.
Patients who met the inclusion criteria for ASD due to a traumatic event occurring within 4 weeks prior to their ACS and who also had at least mild depression upon admission as indicated by a score of 8 or more out of a possible 27 points on the Patient Health Questionnaire-9 had a significantly higher subsequent in-hospital mortality: 10.7% compared with 8.1%.
The prevalence of ASD with depression was 51% in patients with ST-elevation MI compared with 67% in those with non–ST-elevation ACS. Upon statistical adjustment for these and other clinical and demographic factors, patients with ASD plus depression were 68% more likely to die in-hospital. Upon further adjustment for the use of guideline-recommended medications and percutaneous coronary intervention, the ASD/depression group remained at 35% increased risk of in-hospital mortality.
Dr. Cenko explained that this study was conducted in Serbia because the nation’s turbulent history in recent decades made for an enriched population of individuals with ASD.
Acute stress disorder was introduced as a new diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. The diagnosis was created for patients who met most of the criteria for posttraumatic stress disorder except their duration of symptoms was insufficient because the traumatic event had taken place too recently to qualify for PTSD. The diagnosis of ASD is included in DSM-5 as well.
The physician-investigators in the international registry identified ACS patients as having ASD if they had experienced a traumatic event within 4 weeks preceding the ACS and about which they were experiencing intrusive thoughts, memories, or nightmares, avoidance of situations that reminded them about the traumatic event, and increased arousal as typically manifest in insomnia and/or irritability.
Dr. Cenko reported having no financial conflicts regarding her study.
SAN DIEGO – Screening for acute stress disorder with depression upon hospital admission for acute coronary syndrome enables physicians to identify a subgroup of ACS patients at increased risk for in-hospital mortality, Dr. Edina Cenko reported at the annual meeting of the American College of Cardiology.
“It’s a simple, quick test that’s easy to do in clinical practice, and it identifies a group of ACS patients who warrant special attention. It’s important for physicians to do because most deaths in ACS patients occur before arrival at the hospital or in-hospital,” said Dr. Cenko of the University of Bologna (Italy).
She presented a study of 5,880 patients enrolled in the International Survey of Acute Coronary Syndromes in Transitional Countries, all of whom had survived day 1 following admission for ACS at seven Serbian hospitals during 2009-2014. They were screened for acute stress disorder (ASD) and depression upon admission.
Patients who met the inclusion criteria for ASD due to a traumatic event occurring within 4 weeks prior to their ACS and who also had at least mild depression upon admission as indicated by a score of 8 or more out of a possible 27 points on the Patient Health Questionnaire-9 had a significantly higher subsequent in-hospital mortality: 10.7% compared with 8.1%.
The prevalence of ASD with depression was 51% in patients with ST-elevation MI compared with 67% in those with non–ST-elevation ACS. Upon statistical adjustment for these and other clinical and demographic factors, patients with ASD plus depression were 68% more likely to die in-hospital. Upon further adjustment for the use of guideline-recommended medications and percutaneous coronary intervention, the ASD/depression group remained at 35% increased risk of in-hospital mortality.
Dr. Cenko explained that this study was conducted in Serbia because the nation’s turbulent history in recent decades made for an enriched population of individuals with ASD.
Acute stress disorder was introduced as a new diagnosis in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. The diagnosis was created for patients who met most of the criteria for posttraumatic stress disorder except their duration of symptoms was insufficient because the traumatic event had taken place too recently to qualify for PTSD. The diagnosis of ASD is included in DSM-5 as well.
The physician-investigators in the international registry identified ACS patients as having ASD if they had experienced a traumatic event within 4 weeks preceding the ACS and about which they were experiencing intrusive thoughts, memories, or nightmares, avoidance of situations that reminded them about the traumatic event, and increased arousal as typically manifest in insomnia and/or irritability.
Dr. Cenko reported having no financial conflicts regarding her study.
AT ACC 15
Key clinical point: Acute coronary syndrome patients who meet criteria for acute stress disorder along with at least mild depression are at increased risk for in-hospital mortality.
Major finding: In-hospital mortality occurred in 10.7% of ACS patients with acute stress disorder plus depression compared with 8.1% of unaffected ACS patients.
Data source: A study of 5,880 participants in the International Survey of Acute Coronary Syndromes in Transitional Countries.
Disclosures: The presenter reported having no financial conflicts regarding this study, which was conducted free of commercial funding.

Send kids home 2 hours after food challenge testing
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: Food-allergic children who don’t experience a severe immediate reaction following double-blind, placebo-controlled food challenges can safely be discharged home 2 hours post-testing.
Major finding: No severe late reactions occurred in a large cohort of children who underwent double-blind, placebo-controlled food challenges with cow’s milk, cashew, peanut, egg, and hazelnut.
Data source: This retrospective study included 1,142 Dutch children who underwent double-blind, placebo-controlled food challenges at a university clinic.
Disclosures: The presenter reported no conflicts of interest with regard to this university-supported study.
