User login
Advice Issued on Including Patient Representatives in Research
New recommendations from the European League Against Rheumatism provide structure to the growing practice of including patient representatives in research projects.
The recommendations should be useful not only within the European League Against Rheumatism (EULAR) but also to other medical researchers, Maarten P. T. de Wit of Vrije Universiteit Medical Centre, Amsterdam, and his associates reported. EULAR convened a 16-member task force that crafted eight recommendations to promote inclusion of the patient perspective in EULAR-funded scientific research.
Their paper was published online in advance of publication in Annals of the Rheumatic Diseases (doi:10.1136/ard.2010.135129).
Some previous reports suggest that the benefits of including patient representatives in research outweigh the drawbacks. Although including one or more patient representatives has become "usual practice" in EULAR scientific projects, the League’s standardized procedures previously have not described how best to do this, the task force said.
They defined patient research partners as "persons with a relevant disease who operate as active research team members on an equal basis with professional researchers, adding the benefit of their experiential knowledge to any phase of the project."
Including patient research partners can help prevent mismatches between patient preferences and the focus of research, lead to more patient-oriented research agendas, empower patients, and build trust between patient organizations and medical institutions, data suggest.
The task force of three rheumatologists, one rheumatologist/epidemiologist, two allied health professionals, two research organization representatives, and eight patient research partners from six countries reviewed the literature and met twice to develop the recommendations, which were then evaluated by 28 patient representatives and 53 health professionals.
First, the task force strongly recommended that clinical researchers and groups that are developing guidelines or recommendations work with patient research partners, and that other researchers consider patient participation. Patients’ experiential knowledge is important even for laboratory-based research, and researchers who do not include patient partners should justify that decision, they said.
Second, patient participation should be considered for all phases of a research project and is essential in the early stages of research when critical decisions about the protocol and project are made. If this recommendation is not followed, investigators should explain why when publishing results. The group of experts that reviewed the recommendations diverged a bit in their approval of this recommendation, with 27 of 28 patients (96%) agreeing with it compared with only 43 of 53 professionals (81%).
Third, each project should include at least two patient research partners. There’s no solid evidence to support this, but it adds to the team’s diversity and supports the patient partners, and provides a substitute if one patient is absent due to rheumatic illness. This recommendation also drew more support from patients in the group of experts, winning agreement from 26 patients (93%) compared with 36 professionals (68%). Rates of agreement on the other recommendations did not differ significantly between patients and professionals.
Fourth, give potential patient research partners a clear description of the minimum requirements for the position and clarify the roles of the patient partners and the principal investigator.
Fifth, take into account the patient’s communication skills, motivation, and attitude when selecting patient research partners. Having a critical but constructive and proactive attitude is ideal. Academic training is not necessary and a medical background might even be undesirable, though some familiarity with medical terminology helps. "Thinking like an outsider is crucial to provide experiential knowledge," the task force said.
Sixth, a good attitude, good communication, and good support from the principal investigator are crucial for the full participation of patient partners. These skills to create a safe and respectful environment for patient partners may not come naturally to researchers, who should learn these skills or get training.
Seventh, give patient partners the information and training they need to participate, including awareness of ethical issues such as confidentiality, privacy, and legislation.
Eighth, recognize the contributions of patient research partners, which is usually voluntary work.
Research teams that incorporate these recommendations should evaluate the barriers to their implementation and the benefits of working with patient partners to add to the meager literature on these subjects, the task force said.
The authors reported having no relevant conflicts of interest.
New recommendations from the European League Against Rheumatism provide structure to the growing practice of including patient representatives in research projects.
The recommendations should be useful not only within the European League Against Rheumatism (EULAR) but also to other medical researchers, Maarten P. T. de Wit of Vrije Universiteit Medical Centre, Amsterdam, and his associates reported. EULAR convened a 16-member task force that crafted eight recommendations to promote inclusion of the patient perspective in EULAR-funded scientific research.
Their paper was published online in advance of publication in Annals of the Rheumatic Diseases (doi:10.1136/ard.2010.135129).
Some previous reports suggest that the benefits of including patient representatives in research outweigh the drawbacks. Although including one or more patient representatives has become "usual practice" in EULAR scientific projects, the League’s standardized procedures previously have not described how best to do this, the task force said.
They defined patient research partners as "persons with a relevant disease who operate as active research team members on an equal basis with professional researchers, adding the benefit of their experiential knowledge to any phase of the project."
Including patient research partners can help prevent mismatches between patient preferences and the focus of research, lead to more patient-oriented research agendas, empower patients, and build trust between patient organizations and medical institutions, data suggest.
The task force of three rheumatologists, one rheumatologist/epidemiologist, two allied health professionals, two research organization representatives, and eight patient research partners from six countries reviewed the literature and met twice to develop the recommendations, which were then evaluated by 28 patient representatives and 53 health professionals.
First, the task force strongly recommended that clinical researchers and groups that are developing guidelines or recommendations work with patient research partners, and that other researchers consider patient participation. Patients’ experiential knowledge is important even for laboratory-based research, and researchers who do not include patient partners should justify that decision, they said.
Second, patient participation should be considered for all phases of a research project and is essential in the early stages of research when critical decisions about the protocol and project are made. If this recommendation is not followed, investigators should explain why when publishing results. The group of experts that reviewed the recommendations diverged a bit in their approval of this recommendation, with 27 of 28 patients (96%) agreeing with it compared with only 43 of 53 professionals (81%).
Third, each project should include at least two patient research partners. There’s no solid evidence to support this, but it adds to the team’s diversity and supports the patient partners, and provides a substitute if one patient is absent due to rheumatic illness. This recommendation also drew more support from patients in the group of experts, winning agreement from 26 patients (93%) compared with 36 professionals (68%). Rates of agreement on the other recommendations did not differ significantly between patients and professionals.
Fourth, give potential patient research partners a clear description of the minimum requirements for the position and clarify the roles of the patient partners and the principal investigator.
Fifth, take into account the patient’s communication skills, motivation, and attitude when selecting patient research partners. Having a critical but constructive and proactive attitude is ideal. Academic training is not necessary and a medical background might even be undesirable, though some familiarity with medical terminology helps. "Thinking like an outsider is crucial to provide experiential knowledge," the task force said.
Sixth, a good attitude, good communication, and good support from the principal investigator are crucial for the full participation of patient partners. These skills to create a safe and respectful environment for patient partners may not come naturally to researchers, who should learn these skills or get training.
Seventh, give patient partners the information and training they need to participate, including awareness of ethical issues such as confidentiality, privacy, and legislation.
Eighth, recognize the contributions of patient research partners, which is usually voluntary work.
Research teams that incorporate these recommendations should evaluate the barriers to their implementation and the benefits of working with patient partners to add to the meager literature on these subjects, the task force said.
The authors reported having no relevant conflicts of interest.
New recommendations from the European League Against Rheumatism provide structure to the growing practice of including patient representatives in research projects.
The recommendations should be useful not only within the European League Against Rheumatism (EULAR) but also to other medical researchers, Maarten P. T. de Wit of Vrije Universiteit Medical Centre, Amsterdam, and his associates reported. EULAR convened a 16-member task force that crafted eight recommendations to promote inclusion of the patient perspective in EULAR-funded scientific research.
Their paper was published online in advance of publication in Annals of the Rheumatic Diseases (doi:10.1136/ard.2010.135129).
Some previous reports suggest that the benefits of including patient representatives in research outweigh the drawbacks. Although including one or more patient representatives has become "usual practice" in EULAR scientific projects, the League’s standardized procedures previously have not described how best to do this, the task force said.
They defined patient research partners as "persons with a relevant disease who operate as active research team members on an equal basis with professional researchers, adding the benefit of their experiential knowledge to any phase of the project."
Including patient research partners can help prevent mismatches between patient preferences and the focus of research, lead to more patient-oriented research agendas, empower patients, and build trust between patient organizations and medical institutions, data suggest.
The task force of three rheumatologists, one rheumatologist/epidemiologist, two allied health professionals, two research organization representatives, and eight patient research partners from six countries reviewed the literature and met twice to develop the recommendations, which were then evaluated by 28 patient representatives and 53 health professionals.
First, the task force strongly recommended that clinical researchers and groups that are developing guidelines or recommendations work with patient research partners, and that other researchers consider patient participation. Patients’ experiential knowledge is important even for laboratory-based research, and researchers who do not include patient partners should justify that decision, they said.
Second, patient participation should be considered for all phases of a research project and is essential in the early stages of research when critical decisions about the protocol and project are made. If this recommendation is not followed, investigators should explain why when publishing results. The group of experts that reviewed the recommendations diverged a bit in their approval of this recommendation, with 27 of 28 patients (96%) agreeing with it compared with only 43 of 53 professionals (81%).
Third, each project should include at least two patient research partners. There’s no solid evidence to support this, but it adds to the team’s diversity and supports the patient partners, and provides a substitute if one patient is absent due to rheumatic illness. This recommendation also drew more support from patients in the group of experts, winning agreement from 26 patients (93%) compared with 36 professionals (68%). Rates of agreement on the other recommendations did not differ significantly between patients and professionals.
Fourth, give potential patient research partners a clear description of the minimum requirements for the position and clarify the roles of the patient partners and the principal investigator.
Fifth, take into account the patient’s communication skills, motivation, and attitude when selecting patient research partners. Having a critical but constructive and proactive attitude is ideal. Academic training is not necessary and a medical background might even be undesirable, though some familiarity with medical terminology helps. "Thinking like an outsider is crucial to provide experiential knowledge," the task force said.
Sixth, a good attitude, good communication, and good support from the principal investigator are crucial for the full participation of patient partners. These skills to create a safe and respectful environment for patient partners may not come naturally to researchers, who should learn these skills or get training.
Seventh, give patient partners the information and training they need to participate, including awareness of ethical issues such as confidentiality, privacy, and legislation.
Eighth, recognize the contributions of patient research partners, which is usually voluntary work.
Research teams that incorporate these recommendations should evaluate the barriers to their implementation and the benefits of working with patient partners to add to the meager literature on these subjects, the task force said.
The authors reported having no relevant conflicts of interest.
FROM THE ANNALS OF THE RHEUMATIC DISEASES
Major Finding: Eight recommendations from the European League Against Rheumatism specify how and why to include patient representatives in research projects.
Data Source: Expert consensus formed by a task force of 16 health care workers, researchers, and patients, with the recommendations evaluated by an expert panel of 28 patients and 53 medical and research professionals.
Disclosures: The authors reported having no relevant conflicts of interest.
Site Compares Hospitals' Rates of Early Elective Deliveries
The latest salvo in the battle to eliminate unnecessary deliveries before 39 weeks gestation is a Web site that lets expectant mothers compare individual hospital rates of early elective deliveries.
An annual survey by the Leapfrog Group found 57,000 early deliveries by induction or scheduled C-section for nonmedical reasons at 773 U.S. hospitals that provided data. Rates varied between hospitals by more than 100-fold. In Ohio, for example, early elective delivery rates ranged from 0.3% to 32% among the 36 hospitals reporting.
The Leapfrog Group is a project of employers that buy health insurance for employees, such as General Motors and the Boeing Company. View the survey findings.
"This is a matter of great national concern," Leapfrog chief executive officer Leah Binder said in a telephone press conference. "There are thousands of babies in neonatal intensive care units who shouldn’t be there today."
Babies need at least 39 weeks of gestation to fully develop the brain and lungs. Babies delivered before term (40 weeks or later) for nonmedical reasons are more likely to need intensive care and breathing assistance, to develop infections, and to die, previous studies have shown. Elective C-sections increase risks for mothers and affect options for future deliveries. Delivery before 39 weeks is not justified unless there is a medical indication for early delivery, Dr. Alan R. Fleischman said in the teleconference.
"Gestational dating can be grossly inaccurate, even off by as much as 2 weeks, so unindicated inductions and scheduled cesarean sections can have serious consequences, even possibly resulting in a premature birth – a baby born before 37 weeks," said Dr. Fleischman, medical director of the March of Dimes. "Every week counts," since a third of fetal development occurs in the last 5 weeks of pregnancy.
He and Barbara Rudolph, Ph.D., Leapfrog’s senior science director, will host two free national webinars in February for health care workers to promote a quality improvement toolkit for eliminating early elective deliveries; they are scheduled for Feb. 15 from noon to 1 p.m., Eastern time, and Feb. 17 from 3 p.m. to 4 p.m. For more information, contact Leapfrog’s Melissa Danforth at mdanforth@leapfroggroup.org.
The "Less than 39 weeks toolkit," developed by the March of Dimes with the California Department of Health and the California Maternal Quality Care Collaborative, is available for free online. It includes a literature review about the risks of early elective delivery, a step-by-step guide for hospital leaders who want to eliminate early elective deliveries, a guide for measuring and tracking quality improvement, sample forms and case studies, and educational tools for clinicians, staff, and patients.
The Leapfrog data comprised a minimum of 100 births from each hospital that reported, with early elective deliveries ascertained from those. The methodology was developed by the Joint Commission and does not cover all births in 2010 at each hospital.
Rates of elective deliveries between 37 and 39 full weeks of gestation ranged from less than 5% to more than 40% at individual hospitals. There is no national benchmark for an acceptable rate of early elective delivery, so Leapfrog tapped an expert panel to say that 12% or less would be acceptable. Half of the reporting hospitals in the survey hit that benchmark and 29% reported rates below 5%, so Leapfrog will lower its acceptable rate for 2011 to 5%, Ms. Binder said.
Not all hospitals were surveyed, and many who were did not respond. In Alabama, for example, 101 hospitals declined to respond and 5 said the survey did not apply to them. The four hospitals that responded reported early elective delivery rates of 13%-24%. Rates can vary greatly on local levels too. At Los Angeles hospitals, rates ranged from 4% to 29%, and in Boston, from less than 1% to 27%.
Women need to demand that hospitals disclose their early elective delivery rate in order to make informed decisions about where to give birth, Maureen Corry of the advocacy group Childbirth Connection said in the teleconference.
Her organization commissioned a poll of 1,573 women delivering in U.S. hospitals in 2005 (the Listening to Mothers II survey) and found that 1 in 3 mothers reported labor induced by artificial means. Reasons reported for induction were caregiver concern that they were overdue (25%), maternal health problems (19%), the mother’s desire to finish the pregnancy (19%), and caregiver concern about the size of the baby (17%), Ms. Corry said.
Guidelines by the American College of Obstetricians and Gynecologists have long opposed elective early deliveries and say that a large size is not an indication for early elective delivery, Dr. Fleishman said. "It’s more than just education that’s needed. It is a commitment on the part of the hospital to set up specific guidelines and policies to empower those people who are taking the requests of doctors who are initiating inductions or scheduling cesareans to question, to have forms and a peer review process," he said.
Attention to early elective deliveries has been ratcheting up as rates increase despite evidence of the potential harm associated with the practice. In 2010, the Joint Commission, an accrediting body, added elective deliveries to its core measures of health care quality.
Centers for Disease Control and Prevention data show that the average time U.S. fetuses spend in the womb has decreased by 7 days since 1992, according to a Dec. 26, 2010 report by California Watch, a project of the nonprofit Center for Investigational Reporting. Between 1990 and 2006, deliveries at 36 weeks increased by approximately 30% and deliveries at 37 or 38 weeks increased by 40%. There are now more U.S. babies born at 39 weeks than at full term (40 weeks or later), the report said.
C-section deliveries are more common at for-profit hospitals, according to a separate report by California Watch on Sept. 11, 2010. The Leapfrog report did not analyze the data by type of hospital.
National statistics show that between 1990 and 2006, the rate of labor induction increased from 9% to 23% of deliveries, and the C-section rate hit a high of 32%, Leapfrog’s Dr. Rudolph said.
The Leapfrog Group, the March of Dimes, and Childbirth Connection issued a "call to action" in response to the survey findings. Four of the largest U.S. health insurers – Aetna, CIGNA, UnitedHealthcare, and Wellpoint – will conduct a campaign to educate expectant mothers about the importance of a full gestation and the wisdom of comparing elective delivery rates in their local hospitals, Ms. Binder said.
Ms. Binder, Dr. Rudolph, Dr. Fleischman, and Ms. Corry work for organizations advocating improved health and medical practices for pregnant women and infants.
The latest salvo in the battle to eliminate unnecessary deliveries before 39 weeks gestation is a Web site that lets expectant mothers compare individual hospital rates of early elective deliveries.
An annual survey by the Leapfrog Group found 57,000 early deliveries by induction or scheduled C-section for nonmedical reasons at 773 U.S. hospitals that provided data. Rates varied between hospitals by more than 100-fold. In Ohio, for example, early elective delivery rates ranged from 0.3% to 32% among the 36 hospitals reporting.
The Leapfrog Group is a project of employers that buy health insurance for employees, such as General Motors and the Boeing Company. View the survey findings.
"This is a matter of great national concern," Leapfrog chief executive officer Leah Binder said in a telephone press conference. "There are thousands of babies in neonatal intensive care units who shouldn’t be there today."
Babies need at least 39 weeks of gestation to fully develop the brain and lungs. Babies delivered before term (40 weeks or later) for nonmedical reasons are more likely to need intensive care and breathing assistance, to develop infections, and to die, previous studies have shown. Elective C-sections increase risks for mothers and affect options for future deliveries. Delivery before 39 weeks is not justified unless there is a medical indication for early delivery, Dr. Alan R. Fleischman said in the teleconference.
"Gestational dating can be grossly inaccurate, even off by as much as 2 weeks, so unindicated inductions and scheduled cesarean sections can have serious consequences, even possibly resulting in a premature birth – a baby born before 37 weeks," said Dr. Fleischman, medical director of the March of Dimes. "Every week counts," since a third of fetal development occurs in the last 5 weeks of pregnancy.
He and Barbara Rudolph, Ph.D., Leapfrog’s senior science director, will host two free national webinars in February for health care workers to promote a quality improvement toolkit for eliminating early elective deliveries; they are scheduled for Feb. 15 from noon to 1 p.m., Eastern time, and Feb. 17 from 3 p.m. to 4 p.m. For more information, contact Leapfrog’s Melissa Danforth at mdanforth@leapfroggroup.org.
The "Less than 39 weeks toolkit," developed by the March of Dimes with the California Department of Health and the California Maternal Quality Care Collaborative, is available for free online. It includes a literature review about the risks of early elective delivery, a step-by-step guide for hospital leaders who want to eliminate early elective deliveries, a guide for measuring and tracking quality improvement, sample forms and case studies, and educational tools for clinicians, staff, and patients.
The Leapfrog data comprised a minimum of 100 births from each hospital that reported, with early elective deliveries ascertained from those. The methodology was developed by the Joint Commission and does not cover all births in 2010 at each hospital.
Rates of elective deliveries between 37 and 39 full weeks of gestation ranged from less than 5% to more than 40% at individual hospitals. There is no national benchmark for an acceptable rate of early elective delivery, so Leapfrog tapped an expert panel to say that 12% or less would be acceptable. Half of the reporting hospitals in the survey hit that benchmark and 29% reported rates below 5%, so Leapfrog will lower its acceptable rate for 2011 to 5%, Ms. Binder said.
Not all hospitals were surveyed, and many who were did not respond. In Alabama, for example, 101 hospitals declined to respond and 5 said the survey did not apply to them. The four hospitals that responded reported early elective delivery rates of 13%-24%. Rates can vary greatly on local levels too. At Los Angeles hospitals, rates ranged from 4% to 29%, and in Boston, from less than 1% to 27%.
Women need to demand that hospitals disclose their early elective delivery rate in order to make informed decisions about where to give birth, Maureen Corry of the advocacy group Childbirth Connection said in the teleconference.
Her organization commissioned a poll of 1,573 women delivering in U.S. hospitals in 2005 (the Listening to Mothers II survey) and found that 1 in 3 mothers reported labor induced by artificial means. Reasons reported for induction were caregiver concern that they were overdue (25%), maternal health problems (19%), the mother’s desire to finish the pregnancy (19%), and caregiver concern about the size of the baby (17%), Ms. Corry said.
Guidelines by the American College of Obstetricians and Gynecologists have long opposed elective early deliveries and say that a large size is not an indication for early elective delivery, Dr. Fleishman said. "It’s more than just education that’s needed. It is a commitment on the part of the hospital to set up specific guidelines and policies to empower those people who are taking the requests of doctors who are initiating inductions or scheduling cesareans to question, to have forms and a peer review process," he said.
Attention to early elective deliveries has been ratcheting up as rates increase despite evidence of the potential harm associated with the practice. In 2010, the Joint Commission, an accrediting body, added elective deliveries to its core measures of health care quality.
Centers for Disease Control and Prevention data show that the average time U.S. fetuses spend in the womb has decreased by 7 days since 1992, according to a Dec. 26, 2010 report by California Watch, a project of the nonprofit Center for Investigational Reporting. Between 1990 and 2006, deliveries at 36 weeks increased by approximately 30% and deliveries at 37 or 38 weeks increased by 40%. There are now more U.S. babies born at 39 weeks than at full term (40 weeks or later), the report said.
C-section deliveries are more common at for-profit hospitals, according to a separate report by California Watch on Sept. 11, 2010. The Leapfrog report did not analyze the data by type of hospital.
National statistics show that between 1990 and 2006, the rate of labor induction increased from 9% to 23% of deliveries, and the C-section rate hit a high of 32%, Leapfrog’s Dr. Rudolph said.
The Leapfrog Group, the March of Dimes, and Childbirth Connection issued a "call to action" in response to the survey findings. Four of the largest U.S. health insurers – Aetna, CIGNA, UnitedHealthcare, and Wellpoint – will conduct a campaign to educate expectant mothers about the importance of a full gestation and the wisdom of comparing elective delivery rates in their local hospitals, Ms. Binder said.
Ms. Binder, Dr. Rudolph, Dr. Fleischman, and Ms. Corry work for organizations advocating improved health and medical practices for pregnant women and infants.
The latest salvo in the battle to eliminate unnecessary deliveries before 39 weeks gestation is a Web site that lets expectant mothers compare individual hospital rates of early elective deliveries.
An annual survey by the Leapfrog Group found 57,000 early deliveries by induction or scheduled C-section for nonmedical reasons at 773 U.S. hospitals that provided data. Rates varied between hospitals by more than 100-fold. In Ohio, for example, early elective delivery rates ranged from 0.3% to 32% among the 36 hospitals reporting.
The Leapfrog Group is a project of employers that buy health insurance for employees, such as General Motors and the Boeing Company. View the survey findings.
"This is a matter of great national concern," Leapfrog chief executive officer Leah Binder said in a telephone press conference. "There are thousands of babies in neonatal intensive care units who shouldn’t be there today."
Babies need at least 39 weeks of gestation to fully develop the brain and lungs. Babies delivered before term (40 weeks or later) for nonmedical reasons are more likely to need intensive care and breathing assistance, to develop infections, and to die, previous studies have shown. Elective C-sections increase risks for mothers and affect options for future deliveries. Delivery before 39 weeks is not justified unless there is a medical indication for early delivery, Dr. Alan R. Fleischman said in the teleconference.
"Gestational dating can be grossly inaccurate, even off by as much as 2 weeks, so unindicated inductions and scheduled cesarean sections can have serious consequences, even possibly resulting in a premature birth – a baby born before 37 weeks," said Dr. Fleischman, medical director of the March of Dimes. "Every week counts," since a third of fetal development occurs in the last 5 weeks of pregnancy.
He and Barbara Rudolph, Ph.D., Leapfrog’s senior science director, will host two free national webinars in February for health care workers to promote a quality improvement toolkit for eliminating early elective deliveries; they are scheduled for Feb. 15 from noon to 1 p.m., Eastern time, and Feb. 17 from 3 p.m. to 4 p.m. For more information, contact Leapfrog’s Melissa Danforth at mdanforth@leapfroggroup.org.
The "Less than 39 weeks toolkit," developed by the March of Dimes with the California Department of Health and the California Maternal Quality Care Collaborative, is available for free online. It includes a literature review about the risks of early elective delivery, a step-by-step guide for hospital leaders who want to eliminate early elective deliveries, a guide for measuring and tracking quality improvement, sample forms and case studies, and educational tools for clinicians, staff, and patients.
The Leapfrog data comprised a minimum of 100 births from each hospital that reported, with early elective deliveries ascertained from those. The methodology was developed by the Joint Commission and does not cover all births in 2010 at each hospital.
Rates of elective deliveries between 37 and 39 full weeks of gestation ranged from less than 5% to more than 40% at individual hospitals. There is no national benchmark for an acceptable rate of early elective delivery, so Leapfrog tapped an expert panel to say that 12% or less would be acceptable. Half of the reporting hospitals in the survey hit that benchmark and 29% reported rates below 5%, so Leapfrog will lower its acceptable rate for 2011 to 5%, Ms. Binder said.
Not all hospitals were surveyed, and many who were did not respond. In Alabama, for example, 101 hospitals declined to respond and 5 said the survey did not apply to them. The four hospitals that responded reported early elective delivery rates of 13%-24%. Rates can vary greatly on local levels too. At Los Angeles hospitals, rates ranged from 4% to 29%, and in Boston, from less than 1% to 27%.
Women need to demand that hospitals disclose their early elective delivery rate in order to make informed decisions about where to give birth, Maureen Corry of the advocacy group Childbirth Connection said in the teleconference.
Her organization commissioned a poll of 1,573 women delivering in U.S. hospitals in 2005 (the Listening to Mothers II survey) and found that 1 in 3 mothers reported labor induced by artificial means. Reasons reported for induction were caregiver concern that they were overdue (25%), maternal health problems (19%), the mother’s desire to finish the pregnancy (19%), and caregiver concern about the size of the baby (17%), Ms. Corry said.
Guidelines by the American College of Obstetricians and Gynecologists have long opposed elective early deliveries and say that a large size is not an indication for early elective delivery, Dr. Fleishman said. "It’s more than just education that’s needed. It is a commitment on the part of the hospital to set up specific guidelines and policies to empower those people who are taking the requests of doctors who are initiating inductions or scheduling cesareans to question, to have forms and a peer review process," he said.
Attention to early elective deliveries has been ratcheting up as rates increase despite evidence of the potential harm associated with the practice. In 2010, the Joint Commission, an accrediting body, added elective deliveries to its core measures of health care quality.
Centers for Disease Control and Prevention data show that the average time U.S. fetuses spend in the womb has decreased by 7 days since 1992, according to a Dec. 26, 2010 report by California Watch, a project of the nonprofit Center for Investigational Reporting. Between 1990 and 2006, deliveries at 36 weeks increased by approximately 30% and deliveries at 37 or 38 weeks increased by 40%. There are now more U.S. babies born at 39 weeks than at full term (40 weeks or later), the report said.
C-section deliveries are more common at for-profit hospitals, according to a separate report by California Watch on Sept. 11, 2010. The Leapfrog report did not analyze the data by type of hospital.
National statistics show that between 1990 and 2006, the rate of labor induction increased from 9% to 23% of deliveries, and the C-section rate hit a high of 32%, Leapfrog’s Dr. Rudolph said.
The Leapfrog Group, the March of Dimes, and Childbirth Connection issued a "call to action" in response to the survey findings. Four of the largest U.S. health insurers – Aetna, CIGNA, UnitedHealthcare, and Wellpoint – will conduct a campaign to educate expectant mothers about the importance of a full gestation and the wisdom of comparing elective delivery rates in their local hospitals, Ms. Binder said.
Ms. Binder, Dr. Rudolph, Dr. Fleischman, and Ms. Corry work for organizations advocating improved health and medical practices for pregnant women and infants.
Site Compares Hospitals' Rates of Early Elective Deliveries
The latest salvo in the battle to eliminate unnecessary deliveries before 39 weeks gestation is a Web site that lets expectant mothers compare individual hospital rates of early elective deliveries.
An annual survey by the Leapfrog Group found 57,000 early deliveries by induction or scheduled C-section for nonmedical reasons at 773 U.S. hospitals that provided data. Rates varied between hospitals by more than 100-fold. In Ohio, for example, early elective delivery rates ranged from 0.3% to 32% among the 36 hospitals reporting.
The Leapfrog Group is a project of employers that buy health insurance for employees, such as General Motors and the Boeing Company. View the survey findings.
"This is a matter of great national concern," Leapfrog chief executive officer Leah Binder said in a telephone press conference. "There are thousands of babies in neonatal intensive care units who shouldn’t be there today."
Babies need at least 39 weeks of gestation to fully develop the brain and lungs. Babies delivered before term (40 weeks or later) for nonmedical reasons are more likely to need intensive care and breathing assistance, to develop infections, and to die, previous studies have shown. Elective C-sections increase risks for mothers and affect options for future deliveries. Delivery before 39 weeks is not justified unless there is a medical indication for early delivery, Dr. Alan R. Fleischman said in the teleconference.
"Gestational dating can be grossly inaccurate, even off by as much as 2 weeks, so unindicated inductions and scheduled cesarean sections can have serious consequences, even possibly resulting in a premature birth – a baby born before 37 weeks," said Dr. Fleischman, medical director of the March of Dimes. "Every week counts," since a third of fetal development occurs in the last 5 weeks of pregnancy.
He and Barbara Rudolph, Ph.D., Leapfrog’s senior science director, will host two free national webinars in February for health care workers to promote a quality improvement toolkit for eliminating early elective deliveries; they are scheduled for Feb. 15 from noon to 1 p.m., Eastern time, and Feb. 17 from 3 p.m. to 4 p.m. For more information, contact Leapfrog’s Melissa Danforth at mdanforth@leapfroggroup.org.
The "Less than 39 weeks toolkit," developed by the March of Dimes with the California Department of Health and the California Maternal Quality Care Collaborative, is available for free online. It includes a literature review about the risks of early elective delivery, a step-by-step guide for hospital leaders who want to eliminate early elective deliveries, a guide for measuring and tracking quality improvement, sample forms and case studies, and educational tools for clinicians, staff, and patients.
The Leapfrog data comprised a minimum of 100 births from each hospital that reported, with early elective deliveries ascertained from those. The methodology was developed by the Joint Commission and does not cover all births in 2010 at each hospital.
Rates of elective deliveries between 37 and 39 full weeks of gestation ranged from less than 5% to more than 40% at individual hospitals. There is no national benchmark for an acceptable rate of early elective delivery, so Leapfrog tapped an expert panel to say that 12% or less would be acceptable. Half of the reporting hospitals in the survey hit that benchmark and 29% reported rates below 5%, so Leapfrog will lower its acceptable rate for 2011 to 5%, Ms. Binder said.
Not all hospitals were surveyed, and many who were did not respond. In Alabama, for example, 101 hospitals declined to respond and 5 said the survey did not apply to them. The four hospitals that responded reported early elective delivery rates of 13%-24%. Rates can vary greatly on local levels too. At Los Angeles hospitals, rates ranged from 4% to 29%, and in Boston, from less than 1% to 27%.
Women need to demand that hospitals disclose their early elective delivery rate in order to make informed decisions about where to give birth, Maureen Corry of the advocacy group Childbirth Connection said in the teleconference.
Her organization commissioned a poll of 1,573 women delivering in U.S. hospitals in 2005 (the Listening to Mothers II survey) and found that 1 in 3 mothers reported labor induced by artificial means. Reasons reported for induction were caregiver concern that they were overdue (25%), maternal health problems (19%), the mother’s desire to finish the pregnancy (19%), and caregiver concern about the size of the baby (17%), Ms. Corry said.
Guidelines by the American College of Obstetricians and Gynecologists have long opposed elective early deliveries and say that a large size is not an indication for early elective delivery, Dr. Fleishman said. "It’s more than just education that’s needed. It is a commitment on the part of the hospital to set up specific guidelines and policies to empower those people who are taking the requests of doctors who are initiating inductions or scheduling cesareans to question, to have forms and a peer review process," he said.
Attention to early elective deliveries has been ratcheting up as rates increase despite evidence of the potential harm associated with the practice. In 2010, the Joint Commission, an accrediting body, added elective deliveries to its core measures of health care quality.
Centers for Disease Control and Prevention data show that the average time U.S. fetuses spend in the womb has decreased by 7 days since 1992, according to a Dec. 26, 2010 report by California Watch, a project of the nonprofit Center for Investigational Reporting. Between 1990 and 2006, deliveries at 36 weeks increased by approximately 30% and deliveries at 37 or 38 weeks increased by 40%. There are now more U.S. babies born at 39 weeks than at full term (40 weeks or later), the report said.
C-section deliveries are more common at for-profit hospitals, according to a separate report by California Watch on Sept. 11, 2010. The Leapfrog report did not analyze the data by type of hospital.
National statistics show that between 1990 and 2006, the rate of labor induction increased from 9% to 23% of deliveries, and the C-section rate hit a high of 32%, Leapfrog’s Dr. Rudolph said.
The Leapfrog Group, the March of Dimes, and Childbirth Connection issued a "call to action" in response to the survey findings. Four of the largest U.S. health insurers – Aetna, CIGNA, UnitedHealthcare, and Wellpoint – will conduct a campaign to educate expectant mothers about the importance of a full gestation and the wisdom of comparing elective delivery rates in their local hospitals, Ms. Binder said.
Ms. Binder, Dr. Rudolph, Dr. Fleischman, and Ms. Corry work for organizations advocating improved health and medical practices for pregnant women and infants.
The latest salvo in the battle to eliminate unnecessary deliveries before 39 weeks gestation is a Web site that lets expectant mothers compare individual hospital rates of early elective deliveries.
An annual survey by the Leapfrog Group found 57,000 early deliveries by induction or scheduled C-section for nonmedical reasons at 773 U.S. hospitals that provided data. Rates varied between hospitals by more than 100-fold. In Ohio, for example, early elective delivery rates ranged from 0.3% to 32% among the 36 hospitals reporting.
The Leapfrog Group is a project of employers that buy health insurance for employees, such as General Motors and the Boeing Company. View the survey findings.
"This is a matter of great national concern," Leapfrog chief executive officer Leah Binder said in a telephone press conference. "There are thousands of babies in neonatal intensive care units who shouldn’t be there today."
Babies need at least 39 weeks of gestation to fully develop the brain and lungs. Babies delivered before term (40 weeks or later) for nonmedical reasons are more likely to need intensive care and breathing assistance, to develop infections, and to die, previous studies have shown. Elective C-sections increase risks for mothers and affect options for future deliveries. Delivery before 39 weeks is not justified unless there is a medical indication for early delivery, Dr. Alan R. Fleischman said in the teleconference.
"Gestational dating can be grossly inaccurate, even off by as much as 2 weeks, so unindicated inductions and scheduled cesarean sections can have serious consequences, even possibly resulting in a premature birth – a baby born before 37 weeks," said Dr. Fleischman, medical director of the March of Dimes. "Every week counts," since a third of fetal development occurs in the last 5 weeks of pregnancy.
He and Barbara Rudolph, Ph.D., Leapfrog’s senior science director, will host two free national webinars in February for health care workers to promote a quality improvement toolkit for eliminating early elective deliveries; they are scheduled for Feb. 15 from noon to 1 p.m., Eastern time, and Feb. 17 from 3 p.m. to 4 p.m. For more information, contact Leapfrog’s Melissa Danforth at mdanforth@leapfroggroup.org.
The "Less than 39 weeks toolkit," developed by the March of Dimes with the California Department of Health and the California Maternal Quality Care Collaborative, is available for free online. It includes a literature review about the risks of early elective delivery, a step-by-step guide for hospital leaders who want to eliminate early elective deliveries, a guide for measuring and tracking quality improvement, sample forms and case studies, and educational tools for clinicians, staff, and patients.
The Leapfrog data comprised a minimum of 100 births from each hospital that reported, with early elective deliveries ascertained from those. The methodology was developed by the Joint Commission and does not cover all births in 2010 at each hospital.
Rates of elective deliveries between 37 and 39 full weeks of gestation ranged from less than 5% to more than 40% at individual hospitals. There is no national benchmark for an acceptable rate of early elective delivery, so Leapfrog tapped an expert panel to say that 12% or less would be acceptable. Half of the reporting hospitals in the survey hit that benchmark and 29% reported rates below 5%, so Leapfrog will lower its acceptable rate for 2011 to 5%, Ms. Binder said.
Not all hospitals were surveyed, and many who were did not respond. In Alabama, for example, 101 hospitals declined to respond and 5 said the survey did not apply to them. The four hospitals that responded reported early elective delivery rates of 13%-24%. Rates can vary greatly on local levels too. At Los Angeles hospitals, rates ranged from 4% to 29%, and in Boston, from less than 1% to 27%.
Women need to demand that hospitals disclose their early elective delivery rate in order to make informed decisions about where to give birth, Maureen Corry of the advocacy group Childbirth Connection said in the teleconference.
Her organization commissioned a poll of 1,573 women delivering in U.S. hospitals in 2005 (the Listening to Mothers II survey) and found that 1 in 3 mothers reported labor induced by artificial means. Reasons reported for induction were caregiver concern that they were overdue (25%), maternal health problems (19%), the mother’s desire to finish the pregnancy (19%), and caregiver concern about the size of the baby (17%), Ms. Corry said.
Guidelines by the American College of Obstetricians and Gynecologists have long opposed elective early deliveries and say that a large size is not an indication for early elective delivery, Dr. Fleishman said. "It’s more than just education that’s needed. It is a commitment on the part of the hospital to set up specific guidelines and policies to empower those people who are taking the requests of doctors who are initiating inductions or scheduling cesareans to question, to have forms and a peer review process," he said.
Attention to early elective deliveries has been ratcheting up as rates increase despite evidence of the potential harm associated with the practice. In 2010, the Joint Commission, an accrediting body, added elective deliveries to its core measures of health care quality.
Centers for Disease Control and Prevention data show that the average time U.S. fetuses spend in the womb has decreased by 7 days since 1992, according to a Dec. 26, 2010 report by California Watch, a project of the nonprofit Center for Investigational Reporting. Between 1990 and 2006, deliveries at 36 weeks increased by approximately 30% and deliveries at 37 or 38 weeks increased by 40%. There are now more U.S. babies born at 39 weeks than at full term (40 weeks or later), the report said.
C-section deliveries are more common at for-profit hospitals, according to a separate report by California Watch on Sept. 11, 2010. The Leapfrog report did not analyze the data by type of hospital.
National statistics show that between 1990 and 2006, the rate of labor induction increased from 9% to 23% of deliveries, and the C-section rate hit a high of 32%, Leapfrog’s Dr. Rudolph said.
The Leapfrog Group, the March of Dimes, and Childbirth Connection issued a "call to action" in response to the survey findings. Four of the largest U.S. health insurers – Aetna, CIGNA, UnitedHealthcare, and Wellpoint – will conduct a campaign to educate expectant mothers about the importance of a full gestation and the wisdom of comparing elective delivery rates in their local hospitals, Ms. Binder said.
Ms. Binder, Dr. Rudolph, Dr. Fleischman, and Ms. Corry work for organizations advocating improved health and medical practices for pregnant women and infants.
The latest salvo in the battle to eliminate unnecessary deliveries before 39 weeks gestation is a Web site that lets expectant mothers compare individual hospital rates of early elective deliveries.
An annual survey by the Leapfrog Group found 57,000 early deliveries by induction or scheduled C-section for nonmedical reasons at 773 U.S. hospitals that provided data. Rates varied between hospitals by more than 100-fold. In Ohio, for example, early elective delivery rates ranged from 0.3% to 32% among the 36 hospitals reporting.
The Leapfrog Group is a project of employers that buy health insurance for employees, such as General Motors and the Boeing Company. View the survey findings.
"This is a matter of great national concern," Leapfrog chief executive officer Leah Binder said in a telephone press conference. "There are thousands of babies in neonatal intensive care units who shouldn’t be there today."
Babies need at least 39 weeks of gestation to fully develop the brain and lungs. Babies delivered before term (40 weeks or later) for nonmedical reasons are more likely to need intensive care and breathing assistance, to develop infections, and to die, previous studies have shown. Elective C-sections increase risks for mothers and affect options for future deliveries. Delivery before 39 weeks is not justified unless there is a medical indication for early delivery, Dr. Alan R. Fleischman said in the teleconference.
"Gestational dating can be grossly inaccurate, even off by as much as 2 weeks, so unindicated inductions and scheduled cesarean sections can have serious consequences, even possibly resulting in a premature birth – a baby born before 37 weeks," said Dr. Fleischman, medical director of the March of Dimes. "Every week counts," since a third of fetal development occurs in the last 5 weeks of pregnancy.
He and Barbara Rudolph, Ph.D., Leapfrog’s senior science director, will host two free national webinars in February for health care workers to promote a quality improvement toolkit for eliminating early elective deliveries; they are scheduled for Feb. 15 from noon to 1 p.m., Eastern time, and Feb. 17 from 3 p.m. to 4 p.m. For more information, contact Leapfrog’s Melissa Danforth at mdanforth@leapfroggroup.org.
The "Less than 39 weeks toolkit," developed by the March of Dimes with the California Department of Health and the California Maternal Quality Care Collaborative, is available for free online. It includes a literature review about the risks of early elective delivery, a step-by-step guide for hospital leaders who want to eliminate early elective deliveries, a guide for measuring and tracking quality improvement, sample forms and case studies, and educational tools for clinicians, staff, and patients.
The Leapfrog data comprised a minimum of 100 births from each hospital that reported, with early elective deliveries ascertained from those. The methodology was developed by the Joint Commission and does not cover all births in 2010 at each hospital.
Rates of elective deliveries between 37 and 39 full weeks of gestation ranged from less than 5% to more than 40% at individual hospitals. There is no national benchmark for an acceptable rate of early elective delivery, so Leapfrog tapped an expert panel to say that 12% or less would be acceptable. Half of the reporting hospitals in the survey hit that benchmark and 29% reported rates below 5%, so Leapfrog will lower its acceptable rate for 2011 to 5%, Ms. Binder said.
Not all hospitals were surveyed, and many who were did not respond. In Alabama, for example, 101 hospitals declined to respond and 5 said the survey did not apply to them. The four hospitals that responded reported early elective delivery rates of 13%-24%. Rates can vary greatly on local levels too. At Los Angeles hospitals, rates ranged from 4% to 29%, and in Boston, from less than 1% to 27%.
Women need to demand that hospitals disclose their early elective delivery rate in order to make informed decisions about where to give birth, Maureen Corry of the advocacy group Childbirth Connection said in the teleconference.
Her organization commissioned a poll of 1,573 women delivering in U.S. hospitals in 2005 (the Listening to Mothers II survey) and found that 1 in 3 mothers reported labor induced by artificial means. Reasons reported for induction were caregiver concern that they were overdue (25%), maternal health problems (19%), the mother’s desire to finish the pregnancy (19%), and caregiver concern about the size of the baby (17%), Ms. Corry said.
Guidelines by the American College of Obstetricians and Gynecologists have long opposed elective early deliveries and say that a large size is not an indication for early elective delivery, Dr. Fleishman said. "It’s more than just education that’s needed. It is a commitment on the part of the hospital to set up specific guidelines and policies to empower those people who are taking the requests of doctors who are initiating inductions or scheduling cesareans to question, to have forms and a peer review process," he said.
Attention to early elective deliveries has been ratcheting up as rates increase despite evidence of the potential harm associated with the practice. In 2010, the Joint Commission, an accrediting body, added elective deliveries to its core measures of health care quality.
Centers for Disease Control and Prevention data show that the average time U.S. fetuses spend in the womb has decreased by 7 days since 1992, according to a Dec. 26, 2010 report by California Watch, a project of the nonprofit Center for Investigational Reporting. Between 1990 and 2006, deliveries at 36 weeks increased by approximately 30% and deliveries at 37 or 38 weeks increased by 40%. There are now more U.S. babies born at 39 weeks than at full term (40 weeks or later), the report said.
C-section deliveries are more common at for-profit hospitals, according to a separate report by California Watch on Sept. 11, 2010. The Leapfrog report did not analyze the data by type of hospital.
National statistics show that between 1990 and 2006, the rate of labor induction increased from 9% to 23% of deliveries, and the C-section rate hit a high of 32%, Leapfrog’s Dr. Rudolph said.
The Leapfrog Group, the March of Dimes, and Childbirth Connection issued a "call to action" in response to the survey findings. Four of the largest U.S. health insurers – Aetna, CIGNA, UnitedHealthcare, and Wellpoint – will conduct a campaign to educate expectant mothers about the importance of a full gestation and the wisdom of comparing elective delivery rates in their local hospitals, Ms. Binder said.
Ms. Binder, Dr. Rudolph, Dr. Fleischman, and Ms. Corry work for organizations advocating improved health and medical practices for pregnant women and infants.
Major Finding: For the first time, the public can compare rates of early elective deliveries among individual hospitals. Rates ranged from below 1% to more than 40%.
Data Source: Online publication of birth data voluntarily reported by 773 U.S. hospitals in an annual survey by the Leapfrog Group.
Disclosures: Ms. Binder, Dr. Rudolph, Dr. Fleischman, and Ms. Corry work for organizations advocating improved health and medical practices for pregnant women and infants.
Imaging Slightly Better at Identifying Early RA Progression
Two imaging modalities independently predicted progressive joint erosion in patients with early rheumatoid arthritis as a group, but the tests performed only slightly better than did clinical and demographic variables for individual prognoses, judging from findings of a 1-year study published in Annals of the Rheumatic Diseases.
Among 79 patients who completed quarterly follow-ups with a battery of imaging and nonimaging measures, 53 (67%) showed erosive progression. On a group level, results of ultrasound grey-scale (USGS) findings of inflammation and magnetic resonance images showing bone marrow edema each were significant predictors that erosive disease progression would be detected by MRI.
Patients with USGS inflammation in the dominant wrist were twice as likely to develop erosive progression and patients with MRI bone marrow edema in the dominant wrist were 28% more likely to develop erosive progression compared with patients without these imaging findings, Dr. Pernille Bøyesen and associates reported (Ann. Rheum. Dis. 2011;70:176-9 [doi: 10.1136/ard.2009.126953]).
On an individual level, however, the imaging modalities were not dramatically better than clinical and demographic variables to predict erosive progression of early RA. USGS inflammation, synovitis on MRI, and bone marrow edema that was visible on MRI performed slightly better than using antibody to cyclic citrullinated protein, rheumatoid factor, and disease activity score based on a 28-joint count, reported Dr. Bøyesen of Diakonhjemmet Hospital, Oslo.
USGS inflammation was the best of 12 imaging modalities and measures of disease severity in identifying patients at risk of developing erosions on MRI, with a sensitivity of 78%, a specificity of 55%, a positive likelihood ration of 1.75, and accuracy of 70%.
Future studies are needed using composite indices of disease progression, including modern imaging modalities, to determine their value as predictors of an individual patient’s likelihood of disease progression, the investigators concluded.
The study appears to be the first to confirm previous data suggesting that measuring inflammation by ultrasound can help predict subsequent joint damage, they noted. The findings also confirmed previous data identifying bone marrow edema on MRI as an independent predictor of joint damage.
Other imaging modalities in the study included digital x-ray radiogrammetry (DXR) of cortical bone mineral density in the hand. Results showed only trends toward higher levels of synovitis on MRI and bone density loss on DXR in patients with erosive progression of disease at 1 year. The findings did not support previous studies that reported cortical hand bone mineral density to be independently predictive of erosive progression, perhaps due to the small size of the study, Dr. Bøyesen added.
Given the comprehensive comparison of imaging modalities in the study, however, 84 patients can be considered a large number, the investigators noted.
The multivariate analyses controlled for the effects of age, sex, and other independent variables.
The investigators declared having no conflicts of interest. The study was funded by the Eastern Norway Regional Health Authority, the Research Council of Norway, the Norwegian Rheumatism Association, the Norwegian Women Public Health Association, the Grethe Harbitz Legacy, and the Marie and Else Mustad Legacy.
Two imaging modalities independently predicted progressive joint erosion in patients with early rheumatoid arthritis as a group, but the tests performed only slightly better than did clinical and demographic variables for individual prognoses, judging from findings of a 1-year study published in Annals of the Rheumatic Diseases.
Among 79 patients who completed quarterly follow-ups with a battery of imaging and nonimaging measures, 53 (67%) showed erosive progression. On a group level, results of ultrasound grey-scale (USGS) findings of inflammation and magnetic resonance images showing bone marrow edema each were significant predictors that erosive disease progression would be detected by MRI.
Patients with USGS inflammation in the dominant wrist were twice as likely to develop erosive progression and patients with MRI bone marrow edema in the dominant wrist were 28% more likely to develop erosive progression compared with patients without these imaging findings, Dr. Pernille Bøyesen and associates reported (Ann. Rheum. Dis. 2011;70:176-9 [doi: 10.1136/ard.2009.126953]).
On an individual level, however, the imaging modalities were not dramatically better than clinical and demographic variables to predict erosive progression of early RA. USGS inflammation, synovitis on MRI, and bone marrow edema that was visible on MRI performed slightly better than using antibody to cyclic citrullinated protein, rheumatoid factor, and disease activity score based on a 28-joint count, reported Dr. Bøyesen of Diakonhjemmet Hospital, Oslo.
USGS inflammation was the best of 12 imaging modalities and measures of disease severity in identifying patients at risk of developing erosions on MRI, with a sensitivity of 78%, a specificity of 55%, a positive likelihood ration of 1.75, and accuracy of 70%.
Future studies are needed using composite indices of disease progression, including modern imaging modalities, to determine their value as predictors of an individual patient’s likelihood of disease progression, the investigators concluded.
The study appears to be the first to confirm previous data suggesting that measuring inflammation by ultrasound can help predict subsequent joint damage, they noted. The findings also confirmed previous data identifying bone marrow edema on MRI as an independent predictor of joint damage.
Other imaging modalities in the study included digital x-ray radiogrammetry (DXR) of cortical bone mineral density in the hand. Results showed only trends toward higher levels of synovitis on MRI and bone density loss on DXR in patients with erosive progression of disease at 1 year. The findings did not support previous studies that reported cortical hand bone mineral density to be independently predictive of erosive progression, perhaps due to the small size of the study, Dr. Bøyesen added.
Given the comprehensive comparison of imaging modalities in the study, however, 84 patients can be considered a large number, the investigators noted.
The multivariate analyses controlled for the effects of age, sex, and other independent variables.
The investigators declared having no conflicts of interest. The study was funded by the Eastern Norway Regional Health Authority, the Research Council of Norway, the Norwegian Rheumatism Association, the Norwegian Women Public Health Association, the Grethe Harbitz Legacy, and the Marie and Else Mustad Legacy.
Two imaging modalities independently predicted progressive joint erosion in patients with early rheumatoid arthritis as a group, but the tests performed only slightly better than did clinical and demographic variables for individual prognoses, judging from findings of a 1-year study published in Annals of the Rheumatic Diseases.
Among 79 patients who completed quarterly follow-ups with a battery of imaging and nonimaging measures, 53 (67%) showed erosive progression. On a group level, results of ultrasound grey-scale (USGS) findings of inflammation and magnetic resonance images showing bone marrow edema each were significant predictors that erosive disease progression would be detected by MRI.
Patients with USGS inflammation in the dominant wrist were twice as likely to develop erosive progression and patients with MRI bone marrow edema in the dominant wrist were 28% more likely to develop erosive progression compared with patients without these imaging findings, Dr. Pernille Bøyesen and associates reported (Ann. Rheum. Dis. 2011;70:176-9 [doi: 10.1136/ard.2009.126953]).
On an individual level, however, the imaging modalities were not dramatically better than clinical and demographic variables to predict erosive progression of early RA. USGS inflammation, synovitis on MRI, and bone marrow edema that was visible on MRI performed slightly better than using antibody to cyclic citrullinated protein, rheumatoid factor, and disease activity score based on a 28-joint count, reported Dr. Bøyesen of Diakonhjemmet Hospital, Oslo.
USGS inflammation was the best of 12 imaging modalities and measures of disease severity in identifying patients at risk of developing erosions on MRI, with a sensitivity of 78%, a specificity of 55%, a positive likelihood ration of 1.75, and accuracy of 70%.
Future studies are needed using composite indices of disease progression, including modern imaging modalities, to determine their value as predictors of an individual patient’s likelihood of disease progression, the investigators concluded.
The study appears to be the first to confirm previous data suggesting that measuring inflammation by ultrasound can help predict subsequent joint damage, they noted. The findings also confirmed previous data identifying bone marrow edema on MRI as an independent predictor of joint damage.
Other imaging modalities in the study included digital x-ray radiogrammetry (DXR) of cortical bone mineral density in the hand. Results showed only trends toward higher levels of synovitis on MRI and bone density loss on DXR in patients with erosive progression of disease at 1 year. The findings did not support previous studies that reported cortical hand bone mineral density to be independently predictive of erosive progression, perhaps due to the small size of the study, Dr. Bøyesen added.
Given the comprehensive comparison of imaging modalities in the study, however, 84 patients can be considered a large number, the investigators noted.
The multivariate analyses controlled for the effects of age, sex, and other independent variables.
The investigators declared having no conflicts of interest. The study was funded by the Eastern Norway Regional Health Authority, the Research Council of Norway, the Norwegian Rheumatism Association, the Norwegian Women Public Health Association, the Grethe Harbitz Legacy, and the Marie and Else Mustad Legacy.
FROM ANNALS OF THE RHEUMATIC DISEASES
Federal Guidelines for Osteoporosis Screening Updated
New federal recommendations on screening for osteoporosis provide more detail on when to screen women younger than age 65 years and – for the first time – point to a lack of data for screening decisions in men.
The U.S. Preventive Services Task Force updated its 2002 recommendations on osteoporosis screening to call for routine screening in all women aged 65 years or older and in any younger women whose fracture risk is equal to or greater than that of a 65-year-old white woman who has no additional risk factors (equivalent to a 9.3% or greater risk of fracture within 10 years). Previously, women younger than 65 years would be screened if they were at least 60 years old with risk factors for fracture.
The new recommendations were posted on the USPSTF Web site and published online by the Annals of Internal Medicine on Jan. 18.
For the first time, the USPSTF evaluated the evidence for osteoporosis screening in men and found insufficient evidence to form any recommendation, Dr. Ned Colange, chair of the USPSTF, said in an interview. There’s not enough evidence to recommend osteoporosis screening or treatment in men with no prior osteoporotic fractures, and "there’s certainly not enough evidence to say, ‘Don’t’ do it," he said.
"While there’s not a call to action, that’s an important call for research," added Dr. Colange, who is president and CEO of the Colorado Trust Foundation, Denver.
In women, the recommendations do not say to stop osteoporosis screening at any specific age because the risk of fractures continues to increase with advancing age, and the minimal potential harms of treatment remain small. Clinicians who are considering treating older patients with significant morbidity should take into account data showing that the benefits of osteoporosis treatment emerge 18-24 months after starting treatment.
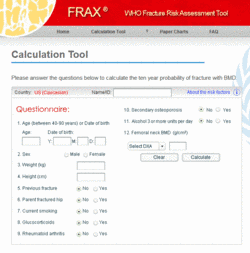
To predict an individual’s risk for osteoporotic fracture, the USPSTF used the online FRAX tool, developed by the World Health Organization and the National Osteoporosis Foundation.
"The nice thing about the FRAX calculator is, the patient herself can determine that risk. It’s available online. It uses measures that the woman should know," Dr. Colange said. "The clinician can do it, but the patient herself could do it as well."
The FRAX tool estimates 10-year fracture risk based on easily obtained information such as age, body mass index (BMI), parental fracture history, and tobacco or alcohol use. It asks about results of dual-energy x-ray absorptiometry scans but does not require this information to calculate fracture risk.
Younger women can reach the new threshold for screening because of various risk factors. For example, a white woman would qualify for screening if she is 50 years old, smokes, drinks alcohol daily, has a BMI less than 21, and has a parental history of fracture. A 55-year-old white woman would need only a parental fracture history to warrant osteoporosis screening. A 60-year-old white woman who smokes and drinks alcohol daily would fit the 10-year-risk profile for screening (Ann. Intern. Med. 2011 Jan 18 [doi:]).
White women are more likely than women of other races or ethnic backgrounds to develop osteoporosis and fractures. Although there are fewer data on nonwhite women, the USPSTF recommended screening all women at age 65 years because the consequences of failing to identify and treat low bone-mineral density are considerable, the potential risks of treatment are small, and it’s unclear if there’s a better strategy for screening nonwhite women.
There are not enough data to recommend when to rescreen women without osteoporosis on their initial screen, the USPSTF stated, but at least a 2-year interval would be needed to assess a change in bone density and perhaps longer for better prediction of fracture risk.
The new recommendations are based on a 2010 review of studies published since 2002 by a team at the University of Oregon Health and Science University’s Evidence-Based Practice Center in Portland.
An estimated 12 million Americans aged 50 years or older will have osteoporosis in 2012. Among postmenopausal women, 15% will develop a hip fracture during their lifetime, 25% will develop a vertebral deformity, and osteoporotic fractures of any kind will affect 50%.
For clinicians, the biggest change in the new screening recommendations may be the need to calculate the 10-year fracture risk in women aged younger than 65, two experts suggested in interviews.
"They will need to know what tools are out there to be able to figure out whether a younger person is at equal to or greater risk than a 65-year-old woman with no addition risk factors," Dr. Carolyn J. Crandall said.
The online FRAX calculator that was used by the USPSTF is a "really good tool" for this purpose, said Dr. Crandall. "Clinicians will have to access that tool in their clinics, which means they will either need Internet access at some point, or else they can download versions that are available for iPhone, or print versions that are available."
Dr. Edward S. Leib also commended inclusion of the FRAX tool in the guidelines, but cautioned that it has some weaknesses that were discussed at a November 2010 "position development conference" conducted jointly by the International Osteoporosis Foundation and the International Society for Clinical Densitometry.
Some important risk factors that could affect the 10-year fracture risk would not necessarily be reflected in the FRAX calculation, he said. In addition, the FRAX tool is based on an international model, and although it included U.S. databases, the calculations may not reflect risks in regional populations.
"For example, in a retrospective review of our population of 15,000 postmenopausal women having bone density studies over the past 10 years, we did not find a correlation between history of fracturing and parental history of hip fractures," he said.
Both Dr. Crandall and Dr. Leib also commended the USPSTF for acknowledging the need for more research in men, but Dr. Leib had hoped for more guidance. "It is known that the fracture risk in men who are age 75 is about equivalent to women who are age 65. I would have hoped that the USPSTF would have recommended screening at that age" despite the lack of primary prevention trials, he said.
Dr. Crandall is professor of medicine at the University of California, Los Angeles. She said she has no pertinent conflicts of interest. Dr. Leib is professor of medicine at the University of Vermont, Burlington.He said he has no pertinent conflicts of interest.
For clinicians, the biggest change in the new screening recommendations may be the need to calculate the 10-year fracture risk in women aged younger than 65, two experts suggested in interviews.
"They will need to know what tools are out there to be able to figure out whether a younger person is at equal to or greater risk than a 65-year-old woman with no addition risk factors," Dr. Carolyn J. Crandall said.
The online FRAX calculator that was used by the USPSTF is a "really good tool" for this purpose, said Dr. Crandall. "Clinicians will have to access that tool in their clinics, which means they will either need Internet access at some point, or else they can download versions that are available for iPhone, or print versions that are available."
Dr. Edward S. Leib also commended inclusion of the FRAX tool in the guidelines, but cautioned that it has some weaknesses that were discussed at a November 2010 "position development conference" conducted jointly by the International Osteoporosis Foundation and the International Society for Clinical Densitometry.
Some important risk factors that could affect the 10-year fracture risk would not necessarily be reflected in the FRAX calculation, he said. In addition, the FRAX tool is based on an international model, and although it included U.S. databases, the calculations may not reflect risks in regional populations.
"For example, in a retrospective review of our population of 15,000 postmenopausal women having bone density studies over the past 10 years, we did not find a correlation between history of fracturing and parental history of hip fractures," he said.
Both Dr. Crandall and Dr. Leib also commended the USPSTF for acknowledging the need for more research in men, but Dr. Leib had hoped for more guidance. "It is known that the fracture risk in men who are age 75 is about equivalent to women who are age 65. I would have hoped that the USPSTF would have recommended screening at that age" despite the lack of primary prevention trials, he said.
Dr. Crandall is professor of medicine at the University of California, Los Angeles. She said she has no pertinent conflicts of interest. Dr. Leib is professor of medicine at the University of Vermont, Burlington.He said he has no pertinent conflicts of interest.
For clinicians, the biggest change in the new screening recommendations may be the need to calculate the 10-year fracture risk in women aged younger than 65, two experts suggested in interviews.
"They will need to know what tools are out there to be able to figure out whether a younger person is at equal to or greater risk than a 65-year-old woman with no addition risk factors," Dr. Carolyn J. Crandall said.
The online FRAX calculator that was used by the USPSTF is a "really good tool" for this purpose, said Dr. Crandall. "Clinicians will have to access that tool in their clinics, which means they will either need Internet access at some point, or else they can download versions that are available for iPhone, or print versions that are available."
Dr. Edward S. Leib also commended inclusion of the FRAX tool in the guidelines, but cautioned that it has some weaknesses that were discussed at a November 2010 "position development conference" conducted jointly by the International Osteoporosis Foundation and the International Society for Clinical Densitometry.
Some important risk factors that could affect the 10-year fracture risk would not necessarily be reflected in the FRAX calculation, he said. In addition, the FRAX tool is based on an international model, and although it included U.S. databases, the calculations may not reflect risks in regional populations.
"For example, in a retrospective review of our population of 15,000 postmenopausal women having bone density studies over the past 10 years, we did not find a correlation between history of fracturing and parental history of hip fractures," he said.
Both Dr. Crandall and Dr. Leib also commended the USPSTF for acknowledging the need for more research in men, but Dr. Leib had hoped for more guidance. "It is known that the fracture risk in men who are age 75 is about equivalent to women who are age 65. I would have hoped that the USPSTF would have recommended screening at that age" despite the lack of primary prevention trials, he said.
Dr. Crandall is professor of medicine at the University of California, Los Angeles. She said she has no pertinent conflicts of interest. Dr. Leib is professor of medicine at the University of Vermont, Burlington.He said he has no pertinent conflicts of interest.
New federal recommendations on screening for osteoporosis provide more detail on when to screen women younger than age 65 years and – for the first time – point to a lack of data for screening decisions in men.
The U.S. Preventive Services Task Force updated its 2002 recommendations on osteoporosis screening to call for routine screening in all women aged 65 years or older and in any younger women whose fracture risk is equal to or greater than that of a 65-year-old white woman who has no additional risk factors (equivalent to a 9.3% or greater risk of fracture within 10 years). Previously, women younger than 65 years would be screened if they were at least 60 years old with risk factors for fracture.
The new recommendations were posted on the USPSTF Web site and published online by the Annals of Internal Medicine on Jan. 18.
For the first time, the USPSTF evaluated the evidence for osteoporosis screening in men and found insufficient evidence to form any recommendation, Dr. Ned Colange, chair of the USPSTF, said in an interview. There’s not enough evidence to recommend osteoporosis screening or treatment in men with no prior osteoporotic fractures, and "there’s certainly not enough evidence to say, ‘Don’t’ do it," he said.
"While there’s not a call to action, that’s an important call for research," added Dr. Colange, who is president and CEO of the Colorado Trust Foundation, Denver.
In women, the recommendations do not say to stop osteoporosis screening at any specific age because the risk of fractures continues to increase with advancing age, and the minimal potential harms of treatment remain small. Clinicians who are considering treating older patients with significant morbidity should take into account data showing that the benefits of osteoporosis treatment emerge 18-24 months after starting treatment.
To predict an individual’s risk for osteoporotic fracture, the USPSTF used the online FRAX tool, developed by the World Health Organization and the National Osteoporosis Foundation.
"The nice thing about the FRAX calculator is, the patient herself can determine that risk. It’s available online. It uses measures that the woman should know," Dr. Colange said. "The clinician can do it, but the patient herself could do it as well."
The FRAX tool estimates 10-year fracture risk based on easily obtained information such as age, body mass index (BMI), parental fracture history, and tobacco or alcohol use. It asks about results of dual-energy x-ray absorptiometry scans but does not require this information to calculate fracture risk.
Younger women can reach the new threshold for screening because of various risk factors. For example, a white woman would qualify for screening if she is 50 years old, smokes, drinks alcohol daily, has a BMI less than 21, and has a parental history of fracture. A 55-year-old white woman would need only a parental fracture history to warrant osteoporosis screening. A 60-year-old white woman who smokes and drinks alcohol daily would fit the 10-year-risk profile for screening (Ann. Intern. Med. 2011 Jan 18 [doi:]).
White women are more likely than women of other races or ethnic backgrounds to develop osteoporosis and fractures. Although there are fewer data on nonwhite women, the USPSTF recommended screening all women at age 65 years because the consequences of failing to identify and treat low bone-mineral density are considerable, the potential risks of treatment are small, and it’s unclear if there’s a better strategy for screening nonwhite women.
There are not enough data to recommend when to rescreen women without osteoporosis on their initial screen, the USPSTF stated, but at least a 2-year interval would be needed to assess a change in bone density and perhaps longer for better prediction of fracture risk.
The new recommendations are based on a 2010 review of studies published since 2002 by a team at the University of Oregon Health and Science University’s Evidence-Based Practice Center in Portland.
An estimated 12 million Americans aged 50 years or older will have osteoporosis in 2012. Among postmenopausal women, 15% will develop a hip fracture during their lifetime, 25% will develop a vertebral deformity, and osteoporotic fractures of any kind will affect 50%.
New federal recommendations on screening for osteoporosis provide more detail on when to screen women younger than age 65 years and – for the first time – point to a lack of data for screening decisions in men.
The U.S. Preventive Services Task Force updated its 2002 recommendations on osteoporosis screening to call for routine screening in all women aged 65 years or older and in any younger women whose fracture risk is equal to or greater than that of a 65-year-old white woman who has no additional risk factors (equivalent to a 9.3% or greater risk of fracture within 10 years). Previously, women younger than 65 years would be screened if they were at least 60 years old with risk factors for fracture.
The new recommendations were posted on the USPSTF Web site and published online by the Annals of Internal Medicine on Jan. 18.
For the first time, the USPSTF evaluated the evidence for osteoporosis screening in men and found insufficient evidence to form any recommendation, Dr. Ned Colange, chair of the USPSTF, said in an interview. There’s not enough evidence to recommend osteoporosis screening or treatment in men with no prior osteoporotic fractures, and "there’s certainly not enough evidence to say, ‘Don’t’ do it," he said.
"While there’s not a call to action, that’s an important call for research," added Dr. Colange, who is president and CEO of the Colorado Trust Foundation, Denver.
In women, the recommendations do not say to stop osteoporosis screening at any specific age because the risk of fractures continues to increase with advancing age, and the minimal potential harms of treatment remain small. Clinicians who are considering treating older patients with significant morbidity should take into account data showing that the benefits of osteoporosis treatment emerge 18-24 months after starting treatment.
To predict an individual’s risk for osteoporotic fracture, the USPSTF used the online FRAX tool, developed by the World Health Organization and the National Osteoporosis Foundation.
"The nice thing about the FRAX calculator is, the patient herself can determine that risk. It’s available online. It uses measures that the woman should know," Dr. Colange said. "The clinician can do it, but the patient herself could do it as well."
The FRAX tool estimates 10-year fracture risk based on easily obtained information such as age, body mass index (BMI), parental fracture history, and tobacco or alcohol use. It asks about results of dual-energy x-ray absorptiometry scans but does not require this information to calculate fracture risk.
Younger women can reach the new threshold for screening because of various risk factors. For example, a white woman would qualify for screening if she is 50 years old, smokes, drinks alcohol daily, has a BMI less than 21, and has a parental history of fracture. A 55-year-old white woman would need only a parental fracture history to warrant osteoporosis screening. A 60-year-old white woman who smokes and drinks alcohol daily would fit the 10-year-risk profile for screening (Ann. Intern. Med. 2011 Jan 18 [doi:]).
White women are more likely than women of other races or ethnic backgrounds to develop osteoporosis and fractures. Although there are fewer data on nonwhite women, the USPSTF recommended screening all women at age 65 years because the consequences of failing to identify and treat low bone-mineral density are considerable, the potential risks of treatment are small, and it’s unclear if there’s a better strategy for screening nonwhite women.
There are not enough data to recommend when to rescreen women without osteoporosis on their initial screen, the USPSTF stated, but at least a 2-year interval would be needed to assess a change in bone density and perhaps longer for better prediction of fracture risk.
The new recommendations are based on a 2010 review of studies published since 2002 by a team at the University of Oregon Health and Science University’s Evidence-Based Practice Center in Portland.
An estimated 12 million Americans aged 50 years or older will have osteoporosis in 2012. Among postmenopausal women, 15% will develop a hip fracture during their lifetime, 25% will develop a vertebral deformity, and osteoporotic fractures of any kind will affect 50%.
Infection Odds Higher With Some Anti-TNF Agents
Patients taking monoclonal anti–tumor necrosis factor antibody therapy were more likely than those on soluble anti-TNF receptor therapy to develop opportunistic infections, other than tuberculosis, in a study of a French national registry.
Of the three anti-TNF agents used in France in 2004-2007, infliximab was associated with an 18-fold increased risk and adalimumab was associated with a 10-fold increased risk for nontuberculosis opportunistic infection, compared with etanercept, Dr. Dominique Salmon-Ceron and her associates reported.
The findings were published online on Dec. 21, 2010. A higher incidence of opportunistic infection with infliximab or adalimumab, compared with etanercept, did not reach statistical significance because of the rarity of the infections. But the findings are supported by previous reports from the Food and Drug Administration, a Spanish registry, a study of 21 Japanese patients, and other accounts of a greater risk for opportunistic infection with infliximab, compared with etanercept, the investigators noted (Ann. Rheum. Dis. 2010 Dec. 21 [doi:10.1136/ard.2010.137422]).
The study also identified a third risk factor: treatment with more than 10 mg/day of oral steroids or IV steroid boluses during the year before a diagnosis of non-TB opportunistic infection. Previous studies also identified this risk factor in patients with rheumatoid arthritis or systemic lupus erythematosus, so the current analysis "strengthens the need to avoid high doses of steroids for patients receiving anti-TNF agents," reported Dr. Salmon-Ceron, who is professor of infectious diseases at Université René Descartes, Paris, as well as a member of the staff at of Hôpital Cochin in that city.
The data in the study come from the 3-year French RATIO (Research Axed on Tolerance of Biotherapies) registry and involved all cases in France of opportunistic infections in patients receiving anti-TNF agents for any reason. The case-control analysis matched each of the 43 case patients (with a total of 45 opportunistic infections) with 3 control patients who took anti-TNF agents without developing opportunistic infections.
Patients had been treated with anti-TNF agents for RA (26), spondyloarthritides (3), inflammatory colitis (8), psoriasis (1), or other problems (5). Four were on etanercept, 10 received adalimumab, and 39 were on infliximab.
Using reports from pharmaceutical companies, the investigators estimated a total of 57,711 patient-years of use of anti-TNF therapy during the study period. They calculated an annual incidence of opportunistic infection in patients receiving anti-TNF agents as 152 per 100,000 patient-years, after adjusting for age and sex.
Differences in the incidence of opportunistic infection differed by anti-TNF agent, but the differences were not statistically significant (7 per 100,000 patient-years with etanercept, 62 per 100,000 patient-years with adalimumab, and 291 per 100,000 patient-years with infliximab). Because the opportunistic infections were rare, the confidence intervals were large and prevented statistical significance in comparisons.
Dr. Salmon-Ceron and her associates previously reported analyses of the same database showing that TB is the most common opportunistic infection in patients on anti-TNF agents, and that these therapies increased the risk for Legionella pneumophila pneumonia. They excluded those two infections from the current study to look at the risk for other infections.
The non-TB opportunistic infections were diverse and severe. Ten of the 43 patients required treatment in the intensive care unit, and 4 died. RATIO followed patients for 3 years from the diagnosis of opportunistic infection. An expert committee of three infectious disease specialists validated the diagnoses of opportunistic infection.
Bacterial infections accounted for a third of the opportunistic infections, including four with listeriosis, four with nocardiosis, four with atypical mycobacteriosis, and three with non-typhoid salmonellosis.
Of the 43 cases, 18 were viral infections, including 8 with severe herpes zoster, 3 with varicella, 3 with extensive herpes simplex, and 4 with disseminated cytomegalovirus infections.
In all, 10 cases were fungal infections, including 5 with pneumocystosis, 3 with invasive aspergillosis, and 2 with cryptococcosis.
Two cases were parasitic infections, both with leishmaniasis.
The anti-TNF therapy was stopped when opportunistic infection developed in all but one patient with pneumocystosis who remained on infliximab and recovered. Seventeen patients resumed anti-TNF therapy (usually the same one) after treating the opportunistic infection for a median of 1.7 months. Three relapses of opportunistic infections occurred, two among the 17 patients who resumed anti-TNF therapy and one among the 26 patients who did not restart anti-TNF agents.
Some of Dr. Salmon-Ceron's coauthors have been consultants or speakers for Abbott, Schering Plough, UCB, or Wyeth. The study was funded by Abbott, Schering Plough, Wyeth, and INSERM (Institut National de la Santé et de la Recherche Mèdicale).
Patients taking monoclonal anti–tumor necrosis factor antibody therapy were more likely than those on soluble anti-TNF receptor therapy to develop opportunistic infections, other than tuberculosis, in a study of a French national registry.
Of the three anti-TNF agents used in France in 2004-2007, infliximab was associated with an 18-fold increased risk and adalimumab was associated with a 10-fold increased risk for nontuberculosis opportunistic infection, compared with etanercept, Dr. Dominique Salmon-Ceron and her associates reported.
The findings were published online on Dec. 21, 2010. A higher incidence of opportunistic infection with infliximab or adalimumab, compared with etanercept, did not reach statistical significance because of the rarity of the infections. But the findings are supported by previous reports from the Food and Drug Administration, a Spanish registry, a study of 21 Japanese patients, and other accounts of a greater risk for opportunistic infection with infliximab, compared with etanercept, the investigators noted (Ann. Rheum. Dis. 2010 Dec. 21 [doi:10.1136/ard.2010.137422]).
The study also identified a third risk factor: treatment with more than 10 mg/day of oral steroids or IV steroid boluses during the year before a diagnosis of non-TB opportunistic infection. Previous studies also identified this risk factor in patients with rheumatoid arthritis or systemic lupus erythematosus, so the current analysis "strengthens the need to avoid high doses of steroids for patients receiving anti-TNF agents," reported Dr. Salmon-Ceron, who is professor of infectious diseases at Université René Descartes, Paris, as well as a member of the staff at of Hôpital Cochin in that city.
The data in the study come from the 3-year French RATIO (Research Axed on Tolerance of Biotherapies) registry and involved all cases in France of opportunistic infections in patients receiving anti-TNF agents for any reason. The case-control analysis matched each of the 43 case patients (with a total of 45 opportunistic infections) with 3 control patients who took anti-TNF agents without developing opportunistic infections.
Patients had been treated with anti-TNF agents for RA (26), spondyloarthritides (3), inflammatory colitis (8), psoriasis (1), or other problems (5). Four were on etanercept, 10 received adalimumab, and 39 were on infliximab.
Using reports from pharmaceutical companies, the investigators estimated a total of 57,711 patient-years of use of anti-TNF therapy during the study period. They calculated an annual incidence of opportunistic infection in patients receiving anti-TNF agents as 152 per 100,000 patient-years, after adjusting for age and sex.
Differences in the incidence of opportunistic infection differed by anti-TNF agent, but the differences were not statistically significant (7 per 100,000 patient-years with etanercept, 62 per 100,000 patient-years with adalimumab, and 291 per 100,000 patient-years with infliximab). Because the opportunistic infections were rare, the confidence intervals were large and prevented statistical significance in comparisons.
Dr. Salmon-Ceron and her associates previously reported analyses of the same database showing that TB is the most common opportunistic infection in patients on anti-TNF agents, and that these therapies increased the risk for Legionella pneumophila pneumonia. They excluded those two infections from the current study to look at the risk for other infections.
The non-TB opportunistic infections were diverse and severe. Ten of the 43 patients required treatment in the intensive care unit, and 4 died. RATIO followed patients for 3 years from the diagnosis of opportunistic infection. An expert committee of three infectious disease specialists validated the diagnoses of opportunistic infection.
Bacterial infections accounted for a third of the opportunistic infections, including four with listeriosis, four with nocardiosis, four with atypical mycobacteriosis, and three with non-typhoid salmonellosis.
Of the 43 cases, 18 were viral infections, including 8 with severe herpes zoster, 3 with varicella, 3 with extensive herpes simplex, and 4 with disseminated cytomegalovirus infections.
In all, 10 cases were fungal infections, including 5 with pneumocystosis, 3 with invasive aspergillosis, and 2 with cryptococcosis.
Two cases were parasitic infections, both with leishmaniasis.
The anti-TNF therapy was stopped when opportunistic infection developed in all but one patient with pneumocystosis who remained on infliximab and recovered. Seventeen patients resumed anti-TNF therapy (usually the same one) after treating the opportunistic infection for a median of 1.7 months. Three relapses of opportunistic infections occurred, two among the 17 patients who resumed anti-TNF therapy and one among the 26 patients who did not restart anti-TNF agents.
Some of Dr. Salmon-Ceron's coauthors have been consultants or speakers for Abbott, Schering Plough, UCB, or Wyeth. The study was funded by Abbott, Schering Plough, Wyeth, and INSERM (Institut National de la Santé et de la Recherche Mèdicale).
Patients taking monoclonal anti–tumor necrosis factor antibody therapy were more likely than those on soluble anti-TNF receptor therapy to develop opportunistic infections, other than tuberculosis, in a study of a French national registry.
Of the three anti-TNF agents used in France in 2004-2007, infliximab was associated with an 18-fold increased risk and adalimumab was associated with a 10-fold increased risk for nontuberculosis opportunistic infection, compared with etanercept, Dr. Dominique Salmon-Ceron and her associates reported.
The findings were published online on Dec. 21, 2010. A higher incidence of opportunistic infection with infliximab or adalimumab, compared with etanercept, did not reach statistical significance because of the rarity of the infections. But the findings are supported by previous reports from the Food and Drug Administration, a Spanish registry, a study of 21 Japanese patients, and other accounts of a greater risk for opportunistic infection with infliximab, compared with etanercept, the investigators noted (Ann. Rheum. Dis. 2010 Dec. 21 [doi:10.1136/ard.2010.137422]).
The study also identified a third risk factor: treatment with more than 10 mg/day of oral steroids or IV steroid boluses during the year before a diagnosis of non-TB opportunistic infection. Previous studies also identified this risk factor in patients with rheumatoid arthritis or systemic lupus erythematosus, so the current analysis "strengthens the need to avoid high doses of steroids for patients receiving anti-TNF agents," reported Dr. Salmon-Ceron, who is professor of infectious diseases at Université René Descartes, Paris, as well as a member of the staff at of Hôpital Cochin in that city.
The data in the study come from the 3-year French RATIO (Research Axed on Tolerance of Biotherapies) registry and involved all cases in France of opportunistic infections in patients receiving anti-TNF agents for any reason. The case-control analysis matched each of the 43 case patients (with a total of 45 opportunistic infections) with 3 control patients who took anti-TNF agents without developing opportunistic infections.
Patients had been treated with anti-TNF agents for RA (26), spondyloarthritides (3), inflammatory colitis (8), psoriasis (1), or other problems (5). Four were on etanercept, 10 received adalimumab, and 39 were on infliximab.
Using reports from pharmaceutical companies, the investigators estimated a total of 57,711 patient-years of use of anti-TNF therapy during the study period. They calculated an annual incidence of opportunistic infection in patients receiving anti-TNF agents as 152 per 100,000 patient-years, after adjusting for age and sex.
Differences in the incidence of opportunistic infection differed by anti-TNF agent, but the differences were not statistically significant (7 per 100,000 patient-years with etanercept, 62 per 100,000 patient-years with adalimumab, and 291 per 100,000 patient-years with infliximab). Because the opportunistic infections were rare, the confidence intervals were large and prevented statistical significance in comparisons.
Dr. Salmon-Ceron and her associates previously reported analyses of the same database showing that TB is the most common opportunistic infection in patients on anti-TNF agents, and that these therapies increased the risk for Legionella pneumophila pneumonia. They excluded those two infections from the current study to look at the risk for other infections.
The non-TB opportunistic infections were diverse and severe. Ten of the 43 patients required treatment in the intensive care unit, and 4 died. RATIO followed patients for 3 years from the diagnosis of opportunistic infection. An expert committee of three infectious disease specialists validated the diagnoses of opportunistic infection.
Bacterial infections accounted for a third of the opportunistic infections, including four with listeriosis, four with nocardiosis, four with atypical mycobacteriosis, and three with non-typhoid salmonellosis.
Of the 43 cases, 18 were viral infections, including 8 with severe herpes zoster, 3 with varicella, 3 with extensive herpes simplex, and 4 with disseminated cytomegalovirus infections.
In all, 10 cases were fungal infections, including 5 with pneumocystosis, 3 with invasive aspergillosis, and 2 with cryptococcosis.
Two cases were parasitic infections, both with leishmaniasis.
The anti-TNF therapy was stopped when opportunistic infection developed in all but one patient with pneumocystosis who remained on infliximab and recovered. Seventeen patients resumed anti-TNF therapy (usually the same one) after treating the opportunistic infection for a median of 1.7 months. Three relapses of opportunistic infections occurred, two among the 17 patients who resumed anti-TNF therapy and one among the 26 patients who did not restart anti-TNF agents.
Some of Dr. Salmon-Ceron's coauthors have been consultants or speakers for Abbott, Schering Plough, UCB, or Wyeth. The study was funded by Abbott, Schering Plough, Wyeth, and INSERM (Institut National de la Santé et de la Recherche Mèdicale).
FROM THE ANNALS OF RHEUMATIC DISEASES
Major Finding: Opportunistic infections other than tuberculosis were 18 times more likely in patients on infliximab and 10 times more likely in patients on adalimumab, compared with patients on etanercept.
Data Source: A study of a French national registry of all patients with opportunistic infections while they were on anti-TNF agents, and case-control analysis of 43 patients with 45 non-TB opportunistic infections and 3 matched control patients without infection on anti-TNF agents.
Disclosures: Some of Dr. Salmon-Ceron's coauthors have been consultants or speakers for Abbott, Schering Plough, UCB, or Wyeth. The study was funded by Abbott, Schering Plough, Wyeth, and INSERM (Institut National de la Santé et de la Recherche Mèdicale (INSERM).
Opportunistic Infection Odds Higher With Some Anti-TNF Agents
Patients taking monoclonal anti–tumor necrosis factor antibody therapy were more likely than those on soluble anti-TNF receptor therapy to develop opportunistic infections, other than tuberculosis, in a study of a French national registry.
Of the three anti-TNF agents used in France in 2004-2007, infliximab was associated with an 18-fold increased risk and adalimumab was associated with a 10-fold increased risk for nontuberculosis opportunistic infection, compared with etanercept, Dr. Dominique Salmon-Ceron and her associates reported. The findings were published online on Dec. 21, 2010. A higher incidence of opportunistic infection with infliximab or adalimumab, compared with etanercept, did not reach statistical significance because of the rarity of the infections. But the findings are supported by previous reports from the Food and Drug Administration, a Spanish registry, a study of 21 Japanese patients, and other accounts of a greater risk for opportunistic infection with infliximab, compared with etanercept, the investigators noted (Ann. Rheum. Dis. 2010 Dec. 21 [doi:10.1136/ard.2010.137422]).
The study also identified a third risk factor: treatment with more than 10 mg/day of oral steroids or IV steroid boluses during the year before a diagnosis of non-TB opportunistic infection. Previous studies also identified this risk factor in patients with rheumatoid arthritis or systemic lupus erythematosus, so the current analysis “strengthens the need to avoid high doses of steroids for patients receiving anti-TNF agents,” reported Dr. Salmon-Ceron, who is professor of infectious diseases at Université René Descartes, Paris, as well as a member of the staff at of Hôpital Cochin in that city.
The data in the study come from the 3-year French RATIO (Research Axed on Tolerance of Biotherapies) registry and involved all cases in France of opportunistic infections in patients receiving anti-TNF agents for any reason. The case-control analysis matched each of the 43 case patients (with a total of 45 opportunistic infections) with 3 control patients who took anti-TNF agents without developing opportunistic infections.
Patients had been treated with anti-TNF agents for RA (26), spondyloarthritides (3), inflammatory colitis (8), psoriasis (1), or other problems (5). Four were on etanercept, 10 received adalimumab, and 39 were on infliximab.
Using reports from pharmaceutical companies, the investigators estimated a total of 57,711 patient-years of use of anti-TNF therapy during the study period. They calculated an annual incidence of opportunistic infection in patients receiving anti-TNF agents as 152 per 100,000 patient-years, after adjusting for age and sex.
Differences in the incidence of opportunistic infection differed by anti-TNF agent, but the differences were not statistically significant (7 per 100,000 patient-years with etanercept, 62 per 100,000 patient-years with adalimumab, and 291 per 100,000 patient-years with infliximab). Because the opportunistic infections were rare, the confidence intervals were large and prevented statistical significance in comparisons.
Dr. Salmon-Ceron and her associates previously reported analyses of the same database showing that TB is the most common opportunistic infection in patients on anti-TNF agents, and that these therapies increased the risk for Legionella pneumophila pneumonia. They excluded those two infections from the current study to look at the risk for other infections.
The non-TB opportunistic infections were diverse and severe. Ten of the 43 patients required treatment in the intensive care unit, and 4 died. RATIO followed patients for 3 years from the diagnosis of opportunistic infection. An expert committee of three infectious disease specialists validated the diagnoses of opportunistic infection.
Bacterial infections accounted for a third of the opportunistic infections, including four with listeriosis, four with nocardiosis, four with atypical mycobacteriosis, and three with non-typhoid salmonellosis.
Of the 43 cases, 18 were viral infections, including 8 with severe herpes zoster, 3 with varicella, 3 with extensive herpes simplex, and 4 with disseminated cytomegalovirus infections.
In all, 10 cases were fungal infections, including 5 with pneumocystosis, 3 with invasive aspergillosis, and 2 with cryptococcosis.
Two cases were parasitic infections, both with leishmaniasis.
The anti-TNF therapy was stopped when opportunistic infection developed in all but one patient with pneumocystosis who remained on infliximab and recovered. Seventeen patients resumed anti-TNF therapy (usually the same one) after treating the opportunistic infection for a median of 1.7 months. Three relapses of opportunistic infections occurred, two among the 17 patients who resumed anti-TNF therapy and one among the 26 patients who did not restart anti-TNF agents.
Some of Dr. Salmon-Ceron’s coauthors have been consultants or speakers for Abbott, Schering Plough, UCB, or Wyeth. The study was funded by Abbott, Schering Plough, Wyeth, and INSERM (Institut National de la Santé et de la Recherche Médicale).
Patients taking monoclonal anti–tumor necrosis factor antibody therapy were more likely than those on soluble anti-TNF receptor therapy to develop opportunistic infections, other than tuberculosis, in a study of a French national registry.
Of the three anti-TNF agents used in France in 2004-2007, infliximab was associated with an 18-fold increased risk and adalimumab was associated with a 10-fold increased risk for nontuberculosis opportunistic infection, compared with etanercept, Dr. Dominique Salmon-Ceron and her associates reported. The findings were published online on Dec. 21, 2010. A higher incidence of opportunistic infection with infliximab or adalimumab, compared with etanercept, did not reach statistical significance because of the rarity of the infections. But the findings are supported by previous reports from the Food and Drug Administration, a Spanish registry, a study of 21 Japanese patients, and other accounts of a greater risk for opportunistic infection with infliximab, compared with etanercept, the investigators noted (Ann. Rheum. Dis. 2010 Dec. 21 [doi:10.1136/ard.2010.137422]).
The study also identified a third risk factor: treatment with more than 10 mg/day of oral steroids or IV steroid boluses during the year before a diagnosis of non-TB opportunistic infection. Previous studies also identified this risk factor in patients with rheumatoid arthritis or systemic lupus erythematosus, so the current analysis “strengthens the need to avoid high doses of steroids for patients receiving anti-TNF agents,” reported Dr. Salmon-Ceron, who is professor of infectious diseases at Université René Descartes, Paris, as well as a member of the staff at of Hôpital Cochin in that city.
The data in the study come from the 3-year French RATIO (Research Axed on Tolerance of Biotherapies) registry and involved all cases in France of opportunistic infections in patients receiving anti-TNF agents for any reason. The case-control analysis matched each of the 43 case patients (with a total of 45 opportunistic infections) with 3 control patients who took anti-TNF agents without developing opportunistic infections.
Patients had been treated with anti-TNF agents for RA (26), spondyloarthritides (3), inflammatory colitis (8), psoriasis (1), or other problems (5). Four were on etanercept, 10 received adalimumab, and 39 were on infliximab.
Using reports from pharmaceutical companies, the investigators estimated a total of 57,711 patient-years of use of anti-TNF therapy during the study period. They calculated an annual incidence of opportunistic infection in patients receiving anti-TNF agents as 152 per 100,000 patient-years, after adjusting for age and sex.
Differences in the incidence of opportunistic infection differed by anti-TNF agent, but the differences were not statistically significant (7 per 100,000 patient-years with etanercept, 62 per 100,000 patient-years with adalimumab, and 291 per 100,000 patient-years with infliximab). Because the opportunistic infections were rare, the confidence intervals were large and prevented statistical significance in comparisons.
Dr. Salmon-Ceron and her associates previously reported analyses of the same database showing that TB is the most common opportunistic infection in patients on anti-TNF agents, and that these therapies increased the risk for Legionella pneumophila pneumonia. They excluded those two infections from the current study to look at the risk for other infections.
The non-TB opportunistic infections were diverse and severe. Ten of the 43 patients required treatment in the intensive care unit, and 4 died. RATIO followed patients for 3 years from the diagnosis of opportunistic infection. An expert committee of three infectious disease specialists validated the diagnoses of opportunistic infection.
Bacterial infections accounted for a third of the opportunistic infections, including four with listeriosis, four with nocardiosis, four with atypical mycobacteriosis, and three with non-typhoid salmonellosis.
Of the 43 cases, 18 were viral infections, including 8 with severe herpes zoster, 3 with varicella, 3 with extensive herpes simplex, and 4 with disseminated cytomegalovirus infections.
In all, 10 cases were fungal infections, including 5 with pneumocystosis, 3 with invasive aspergillosis, and 2 with cryptococcosis.
Two cases were parasitic infections, both with leishmaniasis.
The anti-TNF therapy was stopped when opportunistic infection developed in all but one patient with pneumocystosis who remained on infliximab and recovered. Seventeen patients resumed anti-TNF therapy (usually the same one) after treating the opportunistic infection for a median of 1.7 months. Three relapses of opportunistic infections occurred, two among the 17 patients who resumed anti-TNF therapy and one among the 26 patients who did not restart anti-TNF agents.
Some of Dr. Salmon-Ceron’s coauthors have been consultants or speakers for Abbott, Schering Plough, UCB, or Wyeth. The study was funded by Abbott, Schering Plough, Wyeth, and INSERM (Institut National de la Santé et de la Recherche Médicale).
Patients taking monoclonal anti–tumor necrosis factor antibody therapy were more likely than those on soluble anti-TNF receptor therapy to develop opportunistic infections, other than tuberculosis, in a study of a French national registry.
Of the three anti-TNF agents used in France in 2004-2007, infliximab was associated with an 18-fold increased risk and adalimumab was associated with a 10-fold increased risk for nontuberculosis opportunistic infection, compared with etanercept, Dr. Dominique Salmon-Ceron and her associates reported. The findings were published online on Dec. 21, 2010. A higher incidence of opportunistic infection with infliximab or adalimumab, compared with etanercept, did not reach statistical significance because of the rarity of the infections. But the findings are supported by previous reports from the Food and Drug Administration, a Spanish registry, a study of 21 Japanese patients, and other accounts of a greater risk for opportunistic infection with infliximab, compared with etanercept, the investigators noted (Ann. Rheum. Dis. 2010 Dec. 21 [doi:10.1136/ard.2010.137422]).
The study also identified a third risk factor: treatment with more than 10 mg/day of oral steroids or IV steroid boluses during the year before a diagnosis of non-TB opportunistic infection. Previous studies also identified this risk factor in patients with rheumatoid arthritis or systemic lupus erythematosus, so the current analysis “strengthens the need to avoid high doses of steroids for patients receiving anti-TNF agents,” reported Dr. Salmon-Ceron, who is professor of infectious diseases at Université René Descartes, Paris, as well as a member of the staff at of Hôpital Cochin in that city.
The data in the study come from the 3-year French RATIO (Research Axed on Tolerance of Biotherapies) registry and involved all cases in France of opportunistic infections in patients receiving anti-TNF agents for any reason. The case-control analysis matched each of the 43 case patients (with a total of 45 opportunistic infections) with 3 control patients who took anti-TNF agents without developing opportunistic infections.
Patients had been treated with anti-TNF agents for RA (26), spondyloarthritides (3), inflammatory colitis (8), psoriasis (1), or other problems (5). Four were on etanercept, 10 received adalimumab, and 39 were on infliximab.
Using reports from pharmaceutical companies, the investigators estimated a total of 57,711 patient-years of use of anti-TNF therapy during the study period. They calculated an annual incidence of opportunistic infection in patients receiving anti-TNF agents as 152 per 100,000 patient-years, after adjusting for age and sex.
Differences in the incidence of opportunistic infection differed by anti-TNF agent, but the differences were not statistically significant (7 per 100,000 patient-years with etanercept, 62 per 100,000 patient-years with adalimumab, and 291 per 100,000 patient-years with infliximab). Because the opportunistic infections were rare, the confidence intervals were large and prevented statistical significance in comparisons.
Dr. Salmon-Ceron and her associates previously reported analyses of the same database showing that TB is the most common opportunistic infection in patients on anti-TNF agents, and that these therapies increased the risk for Legionella pneumophila pneumonia. They excluded those two infections from the current study to look at the risk for other infections.
The non-TB opportunistic infections were diverse and severe. Ten of the 43 patients required treatment in the intensive care unit, and 4 died. RATIO followed patients for 3 years from the diagnosis of opportunistic infection. An expert committee of three infectious disease specialists validated the diagnoses of opportunistic infection.
Bacterial infections accounted for a third of the opportunistic infections, including four with listeriosis, four with nocardiosis, four with atypical mycobacteriosis, and three with non-typhoid salmonellosis.
Of the 43 cases, 18 were viral infections, including 8 with severe herpes zoster, 3 with varicella, 3 with extensive herpes simplex, and 4 with disseminated cytomegalovirus infections.
In all, 10 cases were fungal infections, including 5 with pneumocystosis, 3 with invasive aspergillosis, and 2 with cryptococcosis.
Two cases were parasitic infections, both with leishmaniasis.
The anti-TNF therapy was stopped when opportunistic infection developed in all but one patient with pneumocystosis who remained on infliximab and recovered. Seventeen patients resumed anti-TNF therapy (usually the same one) after treating the opportunistic infection for a median of 1.7 months. Three relapses of opportunistic infections occurred, two among the 17 patients who resumed anti-TNF therapy and one among the 26 patients who did not restart anti-TNF agents.
Some of Dr. Salmon-Ceron’s coauthors have been consultants or speakers for Abbott, Schering Plough, UCB, or Wyeth. The study was funded by Abbott, Schering Plough, Wyeth, and INSERM (Institut National de la Santé et de la Recherche Médicale).
Major Finding:
Opportunistic infections other than tuberculosis were 18 times more likely in
patients on infliximab and 10 times more likely in patients on adalimumab,
compared with patients on etanercept.
Data Source: A study
of a French national registry of all patients with opportunistic infections
while they were on anti-TNF agents, and case-control analysis of 43 patients
with 45 non-TB opportunistic infections and 3 matched control patients without
infection on anti-TNF agents.
Disclosures: Some
of Dr. Salmon-Ceron’s coauthors have been consultants or speakers for Abbott,
Schering Plough, UCB, or Wyeth. The study was funded by Abbott, Schering
Plough, Wyeth, and INSERM (Institut National de la Santé et de la Recherche
Médicale (INSERM).
Statin Didn't Lessen Atherosclerosis in Lupus
Atorvastatin therapy did not improve subclinical measures of atherosclerosis or disease activity, compared with placebo, in a 2-year, randomized, double-blind study of 200 adults with systemic lupus erythematosus published in Annals of the Rheumatic Diseases.
The results surprised the investigators because atorvastatin had seemed to be an ideal choice to interrupt the accelerated atherosclerosis seen in SLE, reported Dr. Michelle A. Petri.
Previous studies had shown some potential benefits from the anti-inflammatory effects of statins in other autoimmune diseases, including rheumatoid arthritis and multiple sclerosis. Findings from one small study of pravastatin in patients with SLE found that it reduced total cholesterol and LDL cholesterol levels but did not reduce C-reactive protein levels.
In the current study, there was no significant difference between patients who were randomized to 40 mg/day atorvastatin or placebo in progression of coronary artery calcium, carotid intima media thickness, or carotid plaque. There also were no significant differences between groups in measures of disease activity, inflammation, or endothelial cell activation, reported Dr. Petri, professor of medicine at Johns Hopkins University, Baltimore, and her associates (Ann. Rheum. Dis. 2011 Dec. 21 [doi:10.1136/ard.2010.136762]).
The atorvastatin group, however, was more likely to develop elevations in liver function tests, even as late as 18 months into the study.
The lack of any evidence of an anti-inflammatory benefit from the statin suggests that something besides statins should be considered to manage the accelerated atherosclerosis of SLE, the investigators suggested. Patients with SLE and hyperlipidemia should continue to be treated with statins and other lipid-lowering medications, they added, but with closer monitoring of liver function tests even if the statin dosage doesn’t change, reported Dr. Petri, who is also the director of lupus center at Johns Hopkins as well as director of the Hopkins Lupus Cohort.
At the start of the study, the groups were similar and none of the patients had taken statins for at least 3 months. They underwent helical CT scanning to assess coronary artery calcium and carotid duplex to assess carotid intima media thickness and carotid plaque. These tests were repeated at the 2-year follow-up. Records of disease activity in the 2 years prior to starting the study were compared with quarterly measures of disease activity during the study.
In all, 96 patients on atorvastatin and 91 on placebo completed the study.
At baseline, 42% of patients in the atorvastatin group and 43% in the placebo group had coronary artery calcium. Carotid plaque was seen in 20% of the atorvastatin group and 15% of the placebo group, a difference that was not statistically significant.
Coronary artery calcium scores changed in 51% of those on atorvastatin and in 54% of those on placebo, with no significant differences between groups in the proportions whose scores increased or decreased, or by how much. All patients with carotid plaque at baseline also had it at follow-up. Among patients without carotid plaque at baseline, 25% in the atorvastatin group and 23% on placebo progressed to having plaque at follow-up.
The mean carotid intima media thickness was 0.59 mm in the atorvastatin group and 0.57 mm in the placebo group at baseline, and 0.66 mm in both groups after 2 years. In a post hoc analysis of the proportions of patients in whom carotid intima media thickness improved, stayed the same, or got worse, results favored atorvastatin, the investigators noted.
Changes in levels of total cholesterol and lipoprotein differed significantly between groups. In the atorvastatin group, total cholesterol decreased by 31 mg/dL (or 17%), compared with an increase in the placebo group of 6 mg/dL (or 3%). In the atorvastatin group, lipoprotein levels increased by 8 mg/dL (or 12%), compared with a decrease in the placebo group of 7 mg/dL (or 10%).
Disease activity was measured using the Safety of Estrogens in Lupus: National Assessment revision of the SLE Disease Activity Index.
Dr. Petri was formerly an advisor and speaker for Pfizer, which markets atorvastatin. None of her coauthors had conflicts of interest. The study was funded by the Alliance for Lupus Research, the Arthritis Foundation, the Hopkins Lupus Cohort, and the National Center for Research Resources.
Atorvastatin therapy did not improve subclinical measures of atherosclerosis or disease activity, compared with placebo, in a 2-year, randomized, double-blind study of 200 adults with systemic lupus erythematosus published in Annals of the Rheumatic Diseases.
The results surprised the investigators because atorvastatin had seemed to be an ideal choice to interrupt the accelerated atherosclerosis seen in SLE, reported Dr. Michelle A. Petri.
Previous studies had shown some potential benefits from the anti-inflammatory effects of statins in other autoimmune diseases, including rheumatoid arthritis and multiple sclerosis. Findings from one small study of pravastatin in patients with SLE found that it reduced total cholesterol and LDL cholesterol levels but did not reduce C-reactive protein levels.
In the current study, there was no significant difference between patients who were randomized to 40 mg/day atorvastatin or placebo in progression of coronary artery calcium, carotid intima media thickness, or carotid plaque. There also were no significant differences between groups in measures of disease activity, inflammation, or endothelial cell activation, reported Dr. Petri, professor of medicine at Johns Hopkins University, Baltimore, and her associates (Ann. Rheum. Dis. 2011 Dec. 21 [doi:10.1136/ard.2010.136762]).
The atorvastatin group, however, was more likely to develop elevations in liver function tests, even as late as 18 months into the study.
The lack of any evidence of an anti-inflammatory benefit from the statin suggests that something besides statins should be considered to manage the accelerated atherosclerosis of SLE, the investigators suggested. Patients with SLE and hyperlipidemia should continue to be treated with statins and other lipid-lowering medications, they added, but with closer monitoring of liver function tests even if the statin dosage doesn’t change, reported Dr. Petri, who is also the director of lupus center at Johns Hopkins as well as director of the Hopkins Lupus Cohort.
At the start of the study, the groups were similar and none of the patients had taken statins for at least 3 months. They underwent helical CT scanning to assess coronary artery calcium and carotid duplex to assess carotid intima media thickness and carotid plaque. These tests were repeated at the 2-year follow-up. Records of disease activity in the 2 years prior to starting the study were compared with quarterly measures of disease activity during the study.
In all, 96 patients on atorvastatin and 91 on placebo completed the study.
At baseline, 42% of patients in the atorvastatin group and 43% in the placebo group had coronary artery calcium. Carotid plaque was seen in 20% of the atorvastatin group and 15% of the placebo group, a difference that was not statistically significant.
Coronary artery calcium scores changed in 51% of those on atorvastatin and in 54% of those on placebo, with no significant differences between groups in the proportions whose scores increased or decreased, or by how much. All patients with carotid plaque at baseline also had it at follow-up. Among patients without carotid plaque at baseline, 25% in the atorvastatin group and 23% on placebo progressed to having plaque at follow-up.
The mean carotid intima media thickness was 0.59 mm in the atorvastatin group and 0.57 mm in the placebo group at baseline, and 0.66 mm in both groups after 2 years. In a post hoc analysis of the proportions of patients in whom carotid intima media thickness improved, stayed the same, or got worse, results favored atorvastatin, the investigators noted.
Changes in levels of total cholesterol and lipoprotein differed significantly between groups. In the atorvastatin group, total cholesterol decreased by 31 mg/dL (or 17%), compared with an increase in the placebo group of 6 mg/dL (or 3%). In the atorvastatin group, lipoprotein levels increased by 8 mg/dL (or 12%), compared with a decrease in the placebo group of 7 mg/dL (or 10%).
Disease activity was measured using the Safety of Estrogens in Lupus: National Assessment revision of the SLE Disease Activity Index.
Dr. Petri was formerly an advisor and speaker for Pfizer, which markets atorvastatin. None of her coauthors had conflicts of interest. The study was funded by the Alliance for Lupus Research, the Arthritis Foundation, the Hopkins Lupus Cohort, and the National Center for Research Resources.
Atorvastatin therapy did not improve subclinical measures of atherosclerosis or disease activity, compared with placebo, in a 2-year, randomized, double-blind study of 200 adults with systemic lupus erythematosus published in Annals of the Rheumatic Diseases.
The results surprised the investigators because atorvastatin had seemed to be an ideal choice to interrupt the accelerated atherosclerosis seen in SLE, reported Dr. Michelle A. Petri.
Previous studies had shown some potential benefits from the anti-inflammatory effects of statins in other autoimmune diseases, including rheumatoid arthritis and multiple sclerosis. Findings from one small study of pravastatin in patients with SLE found that it reduced total cholesterol and LDL cholesterol levels but did not reduce C-reactive protein levels.
In the current study, there was no significant difference between patients who were randomized to 40 mg/day atorvastatin or placebo in progression of coronary artery calcium, carotid intima media thickness, or carotid plaque. There also were no significant differences between groups in measures of disease activity, inflammation, or endothelial cell activation, reported Dr. Petri, professor of medicine at Johns Hopkins University, Baltimore, and her associates (Ann. Rheum. Dis. 2011 Dec. 21 [doi:10.1136/ard.2010.136762]).
The atorvastatin group, however, was more likely to develop elevations in liver function tests, even as late as 18 months into the study.
The lack of any evidence of an anti-inflammatory benefit from the statin suggests that something besides statins should be considered to manage the accelerated atherosclerosis of SLE, the investigators suggested. Patients with SLE and hyperlipidemia should continue to be treated with statins and other lipid-lowering medications, they added, but with closer monitoring of liver function tests even if the statin dosage doesn’t change, reported Dr. Petri, who is also the director of lupus center at Johns Hopkins as well as director of the Hopkins Lupus Cohort.
At the start of the study, the groups were similar and none of the patients had taken statins for at least 3 months. They underwent helical CT scanning to assess coronary artery calcium and carotid duplex to assess carotid intima media thickness and carotid plaque. These tests were repeated at the 2-year follow-up. Records of disease activity in the 2 years prior to starting the study were compared with quarterly measures of disease activity during the study.
In all, 96 patients on atorvastatin and 91 on placebo completed the study.
At baseline, 42% of patients in the atorvastatin group and 43% in the placebo group had coronary artery calcium. Carotid plaque was seen in 20% of the atorvastatin group and 15% of the placebo group, a difference that was not statistically significant.
Coronary artery calcium scores changed in 51% of those on atorvastatin and in 54% of those on placebo, with no significant differences between groups in the proportions whose scores increased or decreased, or by how much. All patients with carotid plaque at baseline also had it at follow-up. Among patients without carotid plaque at baseline, 25% in the atorvastatin group and 23% on placebo progressed to having plaque at follow-up.
The mean carotid intima media thickness was 0.59 mm in the atorvastatin group and 0.57 mm in the placebo group at baseline, and 0.66 mm in both groups after 2 years. In a post hoc analysis of the proportions of patients in whom carotid intima media thickness improved, stayed the same, or got worse, results favored atorvastatin, the investigators noted.
Changes in levels of total cholesterol and lipoprotein differed significantly between groups. In the atorvastatin group, total cholesterol decreased by 31 mg/dL (or 17%), compared with an increase in the placebo group of 6 mg/dL (or 3%). In the atorvastatin group, lipoprotein levels increased by 8 mg/dL (or 12%), compared with a decrease in the placebo group of 7 mg/dL (or 10%).
Disease activity was measured using the Safety of Estrogens in Lupus: National Assessment revision of the SLE Disease Activity Index.
Dr. Petri was formerly an advisor and speaker for Pfizer, which markets atorvastatin. None of her coauthors had conflicts of interest. The study was funded by the Alliance for Lupus Research, the Arthritis Foundation, the Hopkins Lupus Cohort, and the National Center for Research Resources.
NSAIDs All Associated With Cardiovascular Risk
Each of seven NSAIDs was associated with significantly increased risk for MI, stroke, or death from cardiovascular disease, compared with placebo, in the most comprehensive meta-analysis of the subject so far.

The relative risks with any individual NSAID, compared with placebo, often were double, triple, or quadruple the risk with placebo, the study found. The absolute numbers of MIs and other cardiovascular outcomes were small, but the network meta-analysis design of the study "provides the best available evidence on the safety of this class of drugs," Dr. Sven Trelle and his associates reported.
Contrary to some previous reports, the current study also found no suggestion that this increased cardiovascular risk is specific to cyclo-oxygenase-2 (COX-2) inhibitors. Therefore the use of all NSAIDs – and the over-the-counter availability of some of them – should be reconsidered, Dr. Trelle stated in a report published online by BMJ (Jan. 11, 2011;342:c7086[doi/10.1136/bmj.c7086]).
Dr. Trelle of the University of Bern, Switzerland, acknowledged that therapeutic options for chronic musculoskeletal pain are limited, but cautioned that "cardiovascular risk needs to be taken into account when prescribing" any NSAID.
The meta-analysis included any large, randomized controlled trials comparing any NSAID with other NSAIDs or placebo. Data were available for naproxen, ibuprofen, diclofenac, celecoxib, etoricoxib, rofecoxib, and lumiracoxib. The risk for a cardiovascular event had to increase by more than 30% to be considered significant.
Overall, naproxen appeared to be the least harmful NSAID in terms of cardiovascular outcomes. Risks were greatest with ibuprofen, diclofenac, etoricoxib, and lumiracoxib.
Four NSAIDs were associated with significantly increased risk for myocardial infarction (the primary outcome in the current analysis) in 29 of the trials that reported 554 MIs. The relative risk for MI doubled with rofecoxib or lumiracoxib, was 35% higher with celecoxib, and was 61% higher with ibuprofen, compared with placebo. Evidence was lacking for increased MI risk with the other three NSAIDs.
Among secondary outcomes, stroke risk increased with all NSAIDs in 26 trials that reported 377 strokes. The increased risk was significant with four of the drugs, roughly doubling with naproxen and tripling with ibuprofen, diclofenac, etoricoxib, or lumiracoxib, compared with placebo.
Twenty-six trials reported 312 deaths from cardiovascular disease, accounting for 46% of all deaths in the trials. All NSAIDs except naproxen were associated with higher risk for cardiovascular death, which increased by 58% with rofecoxib, roughly doubled with ibuprofen, celecoxib, or lumiracoxib, and increased approximately fourfold with diclofenac or etoricoxib, compared with placebo.
All the NSAIDs were associated with increased risk for death from any cause, compared with placebo, and the increase was significant for all except naproxen. There were 676 deaths from any cause in 28 trials, and the risk of death roughly doubled with any of the other six NSAIDs.
Looking at a composite of nonfatal MI, nonfatal stroke, or cardiovascular death in 30 trials that reported 1,091 composite events, the risk increased with all the NSAIDs and increased significantly with all but naproxen. The odds for the composite outcome increased 43% with celecoxib, 44% with rofecoxib, 53% with etoricoxib, 60% with diclofenac, and more than doubled with lumiracoxib or ibuprofen.
An estimated 5% of all visits to U.S. physicians are related to prescribing NSAIDs, which are considered the cornerstone for managing the pain of osteoarthritis and other painful conditions. Rofecoxib, a COX-2 inhibitor, was withdrawn from the market in 2004 after a randomized, placebo-controlled trial found its use was associated with increased cardiovascular risk. The Food and Drug Administration has since denied approval of etoricoxib because of an inadequate risk-benefit profile.
Debate about the safety of NSAIDs has continued despite several conventional meta-analyses that could not integrate all available randomized evidence. That’s the strength of the network meta-analysis, which allowed a unified analysis of all the large trials while respecting randomization, according to Dr. Trelle.
Because of the low absolute numbers of events, more than 100,000 patients would need to be followed in a trial for at least a year to evaluate the cardiovascular safety of an NSAID, which is unlikely to happen, he added.
The Swiss National Science Foundation funded the study. The investigators reporting having no conflicts of interest.
The cardiotoxicity of NSAIDs is particularly worrisome because many patients have both cardiovascular disease and musculoskeletal disease, Wayne A. Ray, Ph.D., noted in an editorial accompanying Dr. Trelle’s study.
What Dr. Trelle’s study adds to the existing literature on NSAIDs is the potentially powerful technique known as network meta-analysis, which can extract more information from the data when certain assumptions are met, compared with traditional analyses, he wrote. The strength of the technique is that it uses all of the data, but it has some inherent weaknesses that should inspire caution when interpreting estimates based on indirect comparisons, explained Dr. Ray.
For example, no large, placebo-controlled trials compared etoricoxib vs. placebo. Risks of etoricoxib vs. placebo were estimated based on a chain of direct comparisons in separate trials – etoricoxib vs. diclofenac; diclofenac vs. rofecoxib or celecoxib, and finally rofecoxib or celecoxib vs. placebo.
Based on all the studies, what are the best strategies for clinicians who are considering NSAIDs for patients at high risk of cardiovascular disease? Avoid COX-2 inhibitors, especially in higher doses, Dr. Ray advised. Avoid diclofenac. Remember that ibuprofen may attenuate the antiplatelet effects of aspirin.
For now, naproxen seems to be the safest NSAID in terms of cardiovascular risk. More information on the relative cardiovascular safety of three NSAIDs should become available after conclusion of the ongoing Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen (PRECISION) trial.
With any NSAID, consider also prescribing gastroprotective drugs.
NSAIDs are not the only option for treatment of musculoskeletal symptoms. Clinicians also prescribe paracetamol, low-dose opioid analgesics, and newer drugs, but without large-scale comparison studies, it’s impossible to tell which is best for both efficacy and safety, Dr. Ray wrote in the online issue of BMJ.
"Perhaps it is time for a larger, more systematic evaluation of a broader range of alternatives," he suggested.
Wayne A. Ray, Ph.D., is a professor and director of pharmacoepidemiology at Vanderbilt University, Nashville, Tenn. Dr. Ray reports that he has received financial support from Pfizer, was a paid expert witness in a lawsuit by the state of Texas against Merck, and is a paid expert in an insurance company action against the maker of Prempro.
The cardiotoxicity of NSAIDs is particularly worrisome because many patients have both cardiovascular disease and musculoskeletal disease, Wayne A. Ray, Ph.D., noted in an editorial accompanying Dr. Trelle’s study.
What Dr. Trelle’s study adds to the existing literature on NSAIDs is the potentially powerful technique known as network meta-analysis, which can extract more information from the data when certain assumptions are met, compared with traditional analyses, he wrote. The strength of the technique is that it uses all of the data, but it has some inherent weaknesses that should inspire caution when interpreting estimates based on indirect comparisons, explained Dr. Ray.
For example, no large, placebo-controlled trials compared etoricoxib vs. placebo. Risks of etoricoxib vs. placebo were estimated based on a chain of direct comparisons in separate trials – etoricoxib vs. diclofenac; diclofenac vs. rofecoxib or celecoxib, and finally rofecoxib or celecoxib vs. placebo.
Based on all the studies, what are the best strategies for clinicians who are considering NSAIDs for patients at high risk of cardiovascular disease? Avoid COX-2 inhibitors, especially in higher doses, Dr. Ray advised. Avoid diclofenac. Remember that ibuprofen may attenuate the antiplatelet effects of aspirin.
For now, naproxen seems to be the safest NSAID in terms of cardiovascular risk. More information on the relative cardiovascular safety of three NSAIDs should become available after conclusion of the ongoing Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen (PRECISION) trial.
With any NSAID, consider also prescribing gastroprotective drugs.
NSAIDs are not the only option for treatment of musculoskeletal symptoms. Clinicians also prescribe paracetamol, low-dose opioid analgesics, and newer drugs, but without large-scale comparison studies, it’s impossible to tell which is best for both efficacy and safety, Dr. Ray wrote in the online issue of BMJ.
"Perhaps it is time for a larger, more systematic evaluation of a broader range of alternatives," he suggested.
Wayne A. Ray, Ph.D., is a professor and director of pharmacoepidemiology at Vanderbilt University, Nashville, Tenn. Dr. Ray reports that he has received financial support from Pfizer, was a paid expert witness in a lawsuit by the state of Texas against Merck, and is a paid expert in an insurance company action against the maker of Prempro.
The cardiotoxicity of NSAIDs is particularly worrisome because many patients have both cardiovascular disease and musculoskeletal disease, Wayne A. Ray, Ph.D., noted in an editorial accompanying Dr. Trelle’s study.
What Dr. Trelle’s study adds to the existing literature on NSAIDs is the potentially powerful technique known as network meta-analysis, which can extract more information from the data when certain assumptions are met, compared with traditional analyses, he wrote. The strength of the technique is that it uses all of the data, but it has some inherent weaknesses that should inspire caution when interpreting estimates based on indirect comparisons, explained Dr. Ray.
For example, no large, placebo-controlled trials compared etoricoxib vs. placebo. Risks of etoricoxib vs. placebo were estimated based on a chain of direct comparisons in separate trials – etoricoxib vs. diclofenac; diclofenac vs. rofecoxib or celecoxib, and finally rofecoxib or celecoxib vs. placebo.
Based on all the studies, what are the best strategies for clinicians who are considering NSAIDs for patients at high risk of cardiovascular disease? Avoid COX-2 inhibitors, especially in higher doses, Dr. Ray advised. Avoid diclofenac. Remember that ibuprofen may attenuate the antiplatelet effects of aspirin.
For now, naproxen seems to be the safest NSAID in terms of cardiovascular risk. More information on the relative cardiovascular safety of three NSAIDs should become available after conclusion of the ongoing Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen (PRECISION) trial.
With any NSAID, consider also prescribing gastroprotective drugs.
NSAIDs are not the only option for treatment of musculoskeletal symptoms. Clinicians also prescribe paracetamol, low-dose opioid analgesics, and newer drugs, but without large-scale comparison studies, it’s impossible to tell which is best for both efficacy and safety, Dr. Ray wrote in the online issue of BMJ.
"Perhaps it is time for a larger, more systematic evaluation of a broader range of alternatives," he suggested.
Wayne A. Ray, Ph.D., is a professor and director of pharmacoepidemiology at Vanderbilt University, Nashville, Tenn. Dr. Ray reports that he has received financial support from Pfizer, was a paid expert witness in a lawsuit by the state of Texas against Merck, and is a paid expert in an insurance company action against the maker of Prempro.
Each of seven NSAIDs was associated with significantly increased risk for MI, stroke, or death from cardiovascular disease, compared with placebo, in the most comprehensive meta-analysis of the subject so far.
The relative risks with any individual NSAID, compared with placebo, often were double, triple, or quadruple the risk with placebo, the study found. The absolute numbers of MIs and other cardiovascular outcomes were small, but the network meta-analysis design of the study "provides the best available evidence on the safety of this class of drugs," Dr. Sven Trelle and his associates reported.
Contrary to some previous reports, the current study also found no suggestion that this increased cardiovascular risk is specific to cyclo-oxygenase-2 (COX-2) inhibitors. Therefore the use of all NSAIDs – and the over-the-counter availability of some of them – should be reconsidered, Dr. Trelle stated in a report published online by BMJ (Jan. 11, 2011;342:c7086[doi/10.1136/bmj.c7086]).
Dr. Trelle of the University of Bern, Switzerland, acknowledged that therapeutic options for chronic musculoskeletal pain are limited, but cautioned that "cardiovascular risk needs to be taken into account when prescribing" any NSAID.
The meta-analysis included any large, randomized controlled trials comparing any NSAID with other NSAIDs or placebo. Data were available for naproxen, ibuprofen, diclofenac, celecoxib, etoricoxib, rofecoxib, and lumiracoxib. The risk for a cardiovascular event had to increase by more than 30% to be considered significant.
Overall, naproxen appeared to be the least harmful NSAID in terms of cardiovascular outcomes. Risks were greatest with ibuprofen, diclofenac, etoricoxib, and lumiracoxib.
Four NSAIDs were associated with significantly increased risk for myocardial infarction (the primary outcome in the current analysis) in 29 of the trials that reported 554 MIs. The relative risk for MI doubled with rofecoxib or lumiracoxib, was 35% higher with celecoxib, and was 61% higher with ibuprofen, compared with placebo. Evidence was lacking for increased MI risk with the other three NSAIDs.
Among secondary outcomes, stroke risk increased with all NSAIDs in 26 trials that reported 377 strokes. The increased risk was significant with four of the drugs, roughly doubling with naproxen and tripling with ibuprofen, diclofenac, etoricoxib, or lumiracoxib, compared with placebo.
Twenty-six trials reported 312 deaths from cardiovascular disease, accounting for 46% of all deaths in the trials. All NSAIDs except naproxen were associated with higher risk for cardiovascular death, which increased by 58% with rofecoxib, roughly doubled with ibuprofen, celecoxib, or lumiracoxib, and increased approximately fourfold with diclofenac or etoricoxib, compared with placebo.
All the NSAIDs were associated with increased risk for death from any cause, compared with placebo, and the increase was significant for all except naproxen. There were 676 deaths from any cause in 28 trials, and the risk of death roughly doubled with any of the other six NSAIDs.
Looking at a composite of nonfatal MI, nonfatal stroke, or cardiovascular death in 30 trials that reported 1,091 composite events, the risk increased with all the NSAIDs and increased significantly with all but naproxen. The odds for the composite outcome increased 43% with celecoxib, 44% with rofecoxib, 53% with etoricoxib, 60% with diclofenac, and more than doubled with lumiracoxib or ibuprofen.
An estimated 5% of all visits to U.S. physicians are related to prescribing NSAIDs, which are considered the cornerstone for managing the pain of osteoarthritis and other painful conditions. Rofecoxib, a COX-2 inhibitor, was withdrawn from the market in 2004 after a randomized, placebo-controlled trial found its use was associated with increased cardiovascular risk. The Food and Drug Administration has since denied approval of etoricoxib because of an inadequate risk-benefit profile.
Debate about the safety of NSAIDs has continued despite several conventional meta-analyses that could not integrate all available randomized evidence. That’s the strength of the network meta-analysis, which allowed a unified analysis of all the large trials while respecting randomization, according to Dr. Trelle.
Because of the low absolute numbers of events, more than 100,000 patients would need to be followed in a trial for at least a year to evaluate the cardiovascular safety of an NSAID, which is unlikely to happen, he added.
The Swiss National Science Foundation funded the study. The investigators reporting having no conflicts of interest.
Each of seven NSAIDs was associated with significantly increased risk for MI, stroke, or death from cardiovascular disease, compared with placebo, in the most comprehensive meta-analysis of the subject so far.
The relative risks with any individual NSAID, compared with placebo, often were double, triple, or quadruple the risk with placebo, the study found. The absolute numbers of MIs and other cardiovascular outcomes were small, but the network meta-analysis design of the study "provides the best available evidence on the safety of this class of drugs," Dr. Sven Trelle and his associates reported.
Contrary to some previous reports, the current study also found no suggestion that this increased cardiovascular risk is specific to cyclo-oxygenase-2 (COX-2) inhibitors. Therefore the use of all NSAIDs – and the over-the-counter availability of some of them – should be reconsidered, Dr. Trelle stated in a report published online by BMJ (Jan. 11, 2011;342:c7086[doi/10.1136/bmj.c7086]).
Dr. Trelle of the University of Bern, Switzerland, acknowledged that therapeutic options for chronic musculoskeletal pain are limited, but cautioned that "cardiovascular risk needs to be taken into account when prescribing" any NSAID.
The meta-analysis included any large, randomized controlled trials comparing any NSAID with other NSAIDs or placebo. Data were available for naproxen, ibuprofen, diclofenac, celecoxib, etoricoxib, rofecoxib, and lumiracoxib. The risk for a cardiovascular event had to increase by more than 30% to be considered significant.
Overall, naproxen appeared to be the least harmful NSAID in terms of cardiovascular outcomes. Risks were greatest with ibuprofen, diclofenac, etoricoxib, and lumiracoxib.
Four NSAIDs were associated with significantly increased risk for myocardial infarction (the primary outcome in the current analysis) in 29 of the trials that reported 554 MIs. The relative risk for MI doubled with rofecoxib or lumiracoxib, was 35% higher with celecoxib, and was 61% higher with ibuprofen, compared with placebo. Evidence was lacking for increased MI risk with the other three NSAIDs.
Among secondary outcomes, stroke risk increased with all NSAIDs in 26 trials that reported 377 strokes. The increased risk was significant with four of the drugs, roughly doubling with naproxen and tripling with ibuprofen, diclofenac, etoricoxib, or lumiracoxib, compared with placebo.
Twenty-six trials reported 312 deaths from cardiovascular disease, accounting for 46% of all deaths in the trials. All NSAIDs except naproxen were associated with higher risk for cardiovascular death, which increased by 58% with rofecoxib, roughly doubled with ibuprofen, celecoxib, or lumiracoxib, and increased approximately fourfold with diclofenac or etoricoxib, compared with placebo.
All the NSAIDs were associated with increased risk for death from any cause, compared with placebo, and the increase was significant for all except naproxen. There were 676 deaths from any cause in 28 trials, and the risk of death roughly doubled with any of the other six NSAIDs.
Looking at a composite of nonfatal MI, nonfatal stroke, or cardiovascular death in 30 trials that reported 1,091 composite events, the risk increased with all the NSAIDs and increased significantly with all but naproxen. The odds for the composite outcome increased 43% with celecoxib, 44% with rofecoxib, 53% with etoricoxib, 60% with diclofenac, and more than doubled with lumiracoxib or ibuprofen.
An estimated 5% of all visits to U.S. physicians are related to prescribing NSAIDs, which are considered the cornerstone for managing the pain of osteoarthritis and other painful conditions. Rofecoxib, a COX-2 inhibitor, was withdrawn from the market in 2004 after a randomized, placebo-controlled trial found its use was associated with increased cardiovascular risk. The Food and Drug Administration has since denied approval of etoricoxib because of an inadequate risk-benefit profile.
Debate about the safety of NSAIDs has continued despite several conventional meta-analyses that could not integrate all available randomized evidence. That’s the strength of the network meta-analysis, which allowed a unified analysis of all the large trials while respecting randomization, according to Dr. Trelle.
Because of the low absolute numbers of events, more than 100,000 patients would need to be followed in a trial for at least a year to evaluate the cardiovascular safety of an NSAID, which is unlikely to happen, he added.
The Swiss National Science Foundation funded the study. The investigators reporting having no conflicts of interest.
FROM BMJ
NSAIDs All Associated With Cardiovascular Risk
Each of seven NSAIDs was associated with significantly increased risk for MI, stroke, or death from cardiovascular disease, compared with placebo, in the most comprehensive meta-analysis of the subject so far.

The relative risks with any individual NSAID, compared with placebo, often were double, triple, or quadruple the risk with placebo, the study found. The absolute numbers of MIs and other cardiovascular outcomes were small, but the network meta-analysis design of the study "provides the best available evidence on the safety of this class of drugs," Dr. Sven Trelle and his associates reported.
Contrary to some previous reports, the current study also found no suggestion that this increased cardiovascular risk is specific to cyclo-oxygenase-2 (COX-2) inhibitors. Therefore the use of all NSAIDs – and the over-the-counter availability of some of them – should be reconsidered, Dr. Trelle stated in a report published online by BMJ (Jan. 11, 2011;342:c7086[doi/10.1136/bmj.c7086]).
Dr. Trelle of the University of Bern, Switzerland, acknowledged that therapeutic options for chronic musculoskeletal pain are limited, but cautioned that "cardiovascular risk needs to be taken into account when prescribing" any NSAID.
The meta-analysis included any large, randomized controlled trials comparing any NSAID with other NSAIDs or placebo. Data were available for naproxen, ibuprofen, diclofenac, celecoxib, etoricoxib, rofecoxib, and lumiracoxib. The risk for a cardiovascular event had to increase by more than 30% to be considered significant.
Overall, naproxen appeared to be the least harmful NSAID in terms of cardiovascular outcomes. Risks were greatest with ibuprofen, diclofenac, etoricoxib, and lumiracoxib.
Four NSAIDs were associated with significantly increased risk for myocardial infarction (the primary outcome in the current analysis) in 29 of the trials that reported 554 MIs. The relative risk for MI doubled with rofecoxib or lumiracoxib, was 35% higher with celecoxib, and was 61% higher with ibuprofen, compared with placebo. Evidence was lacking for increased MI risk with the other three NSAIDs.
Among secondary outcomes, stroke risk increased with all NSAIDs in 26 trials that reported 377 strokes. The increased risk was significant with four of the drugs, roughly doubling with naproxen and tripling with ibuprofen, diclofenac, etoricoxib, or lumiracoxib, compared with placebo.
Twenty-six trials reported 312 deaths from cardiovascular disease, accounting for 46% of all deaths in the trials. All NSAIDs except naproxen were associated with higher risk for cardiovascular death, which increased by 58% with rofecoxib, roughly doubled with ibuprofen, celecoxib, or lumiracoxib, and increased approximately fourfold with diclofenac or etoricoxib, compared with placebo.
All the NSAIDs were associated with increased risk for death from any cause, compared with placebo, and the increase was significant for all except naproxen. There were 676 deaths from any cause in 28 trials, and the risk of death roughly doubled with any of the other six NSAIDs.
Looking at a composite of nonfatal MI, nonfatal stroke, or cardiovascular death in 30 trials that reported 1,091 composite events, the risk increased with all the NSAIDs and increased significantly with all but naproxen. The odds for the composite outcome increased 43% with celecoxib, 44% with rofecoxib, 53% with etoricoxib, 60% with diclofenac, and more than doubled with lumiracoxib or ibuprofen.
An estimated 5% of all visits to U.S. physicians are related to prescribing NSAIDs, which are considered the cornerstone for managing the pain of osteoarthritis and other painful conditions. Rofecoxib, a COX-2 inhibitor, was withdrawn from the market in 2004 after a randomized, placebo-controlled trial found its use was associated with increased cardiovascular risk. The Food and Drug Administration has since denied approval of etoricoxib because of an inadequate risk-benefit profile.
Debate about the safety of NSAIDs has continued despite several conventional meta-analyses that could not integrate all available randomized evidence. That’s the strength of the network meta-analysis, which allowed a unified analysis of all the large trials while respecting randomization, according to Dr. Trelle.
Because of the low absolute numbers of events, more than 100,000 patients would need to be followed in a trial for at least a year to evaluate the cardiovascular safety of an NSAID, which is unlikely to happen, he added.
The Swiss National Science Foundation funded the study. The investigators reporting having no conflicts of interest.
The cardiotoxicity of NSAIDs is particularly worrisome because many patients have both cardiovascular disease and musculoskeletal disease, Wayne A. Ray, Ph.D., noted in an editorial accompanying Dr. Trelle’s study.
What Dr. Trelle’s study adds to the existing literature on NSAIDs is the potentially powerful technique known as network meta-analysis, which can extract more information from the data when certain assumptions are met, compared with traditional analyses, he wrote. The strength of the technique is that it uses all of the data, but it has some inherent weaknesses that should inspire caution when interpreting estimates based on indirect comparisons, explained Dr. Ray.
For example, no large, placebo-controlled trials compared etoricoxib vs. placebo. Risks of etoricoxib vs. placebo were estimated based on a chain of direct comparisons in separate trials – etoricoxib vs. diclofenac; diclofenac vs. rofecoxib or celecoxib, and finally rofecoxib or celecoxib vs. placebo.
Based on all the studies, what are the best strategies for clinicians who are considering NSAIDs for patients at high risk of cardiovascular disease? Avoid COX-2 inhibitors, especially in higher doses, Dr. Ray advised. Avoid diclofenac. Remember that ibuprofen may attenuate the antiplatelet effects of aspirin.
For now, naproxen seems to be the safest NSAID in terms of cardiovascular risk. More information on the relative cardiovascular safety of three NSAIDs should become available after conclusion of the ongoing Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen (PRECISION) trial.
With any NSAID, consider also prescribing gastroprotective drugs.
NSAIDs are not the only option for treatment of musculoskeletal symptoms. Clinicians also prescribe paracetamol, low-dose opioid analgesics, and newer drugs, but without large-scale comparison studies, it’s impossible to tell which is best for both efficacy and safety, Dr. Ray wrote in the online issue of BMJ.
"Perhaps it is time for a larger, more systematic evaluation of a broader range of alternatives," he suggested.
Wayne A. Ray, Ph.D., is a professor and director of pharmacoepidemiology at Vanderbilt University, Nashville, Tenn. Dr. Ray reports that he has received financial support from Pfizer, was a paid expert witness in a lawsuit by the state of Texas against Merck, and is a paid expert in an insurance company action against the maker of Prempro.
The cardiotoxicity of NSAIDs is particularly worrisome because many patients have both cardiovascular disease and musculoskeletal disease, Wayne A. Ray, Ph.D., noted in an editorial accompanying Dr. Trelle’s study.
What Dr. Trelle’s study adds to the existing literature on NSAIDs is the potentially powerful technique known as network meta-analysis, which can extract more information from the data when certain assumptions are met, compared with traditional analyses, he wrote. The strength of the technique is that it uses all of the data, but it has some inherent weaknesses that should inspire caution when interpreting estimates based on indirect comparisons, explained Dr. Ray.
For example, no large, placebo-controlled trials compared etoricoxib vs. placebo. Risks of etoricoxib vs. placebo were estimated based on a chain of direct comparisons in separate trials – etoricoxib vs. diclofenac; diclofenac vs. rofecoxib or celecoxib, and finally rofecoxib or celecoxib vs. placebo.
Based on all the studies, what are the best strategies for clinicians who are considering NSAIDs for patients at high risk of cardiovascular disease? Avoid COX-2 inhibitors, especially in higher doses, Dr. Ray advised. Avoid diclofenac. Remember that ibuprofen may attenuate the antiplatelet effects of aspirin.
For now, naproxen seems to be the safest NSAID in terms of cardiovascular risk. More information on the relative cardiovascular safety of three NSAIDs should become available after conclusion of the ongoing Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen (PRECISION) trial.
With any NSAID, consider also prescribing gastroprotective drugs.
NSAIDs are not the only option for treatment of musculoskeletal symptoms. Clinicians also prescribe paracetamol, low-dose opioid analgesics, and newer drugs, but without large-scale comparison studies, it’s impossible to tell which is best for both efficacy and safety, Dr. Ray wrote in the online issue of BMJ.
"Perhaps it is time for a larger, more systematic evaluation of a broader range of alternatives," he suggested.
Wayne A. Ray, Ph.D., is a professor and director of pharmacoepidemiology at Vanderbilt University, Nashville, Tenn. Dr. Ray reports that he has received financial support from Pfizer, was a paid expert witness in a lawsuit by the state of Texas against Merck, and is a paid expert in an insurance company action against the maker of Prempro.
The cardiotoxicity of NSAIDs is particularly worrisome because many patients have both cardiovascular disease and musculoskeletal disease, Wayne A. Ray, Ph.D., noted in an editorial accompanying Dr. Trelle’s study.
What Dr. Trelle’s study adds to the existing literature on NSAIDs is the potentially powerful technique known as network meta-analysis, which can extract more information from the data when certain assumptions are met, compared with traditional analyses, he wrote. The strength of the technique is that it uses all of the data, but it has some inherent weaknesses that should inspire caution when interpreting estimates based on indirect comparisons, explained Dr. Ray.
For example, no large, placebo-controlled trials compared etoricoxib vs. placebo. Risks of etoricoxib vs. placebo were estimated based on a chain of direct comparisons in separate trials – etoricoxib vs. diclofenac; diclofenac vs. rofecoxib or celecoxib, and finally rofecoxib or celecoxib vs. placebo.
Based on all the studies, what are the best strategies for clinicians who are considering NSAIDs for patients at high risk of cardiovascular disease? Avoid COX-2 inhibitors, especially in higher doses, Dr. Ray advised. Avoid diclofenac. Remember that ibuprofen may attenuate the antiplatelet effects of aspirin.
For now, naproxen seems to be the safest NSAID in terms of cardiovascular risk. More information on the relative cardiovascular safety of three NSAIDs should become available after conclusion of the ongoing Prospective Randomized Evaluation of Celecoxib Integrated Safety vs. Ibuprofen or Naproxen (PRECISION) trial.
With any NSAID, consider also prescribing gastroprotective drugs.
NSAIDs are not the only option for treatment of musculoskeletal symptoms. Clinicians also prescribe paracetamol, low-dose opioid analgesics, and newer drugs, but without large-scale comparison studies, it’s impossible to tell which is best for both efficacy and safety, Dr. Ray wrote in the online issue of BMJ.
"Perhaps it is time for a larger, more systematic evaluation of a broader range of alternatives," he suggested.
Wayne A. Ray, Ph.D., is a professor and director of pharmacoepidemiology at Vanderbilt University, Nashville, Tenn. Dr. Ray reports that he has received financial support from Pfizer, was a paid expert witness in a lawsuit by the state of Texas against Merck, and is a paid expert in an insurance company action against the maker of Prempro.
Each of seven NSAIDs was associated with significantly increased risk for MI, stroke, or death from cardiovascular disease, compared with placebo, in the most comprehensive meta-analysis of the subject so far.
The relative risks with any individual NSAID, compared with placebo, often were double, triple, or quadruple the risk with placebo, the study found. The absolute numbers of MIs and other cardiovascular outcomes were small, but the network meta-analysis design of the study "provides the best available evidence on the safety of this class of drugs," Dr. Sven Trelle and his associates reported.
Contrary to some previous reports, the current study also found no suggestion that this increased cardiovascular risk is specific to cyclo-oxygenase-2 (COX-2) inhibitors. Therefore the use of all NSAIDs – and the over-the-counter availability of some of them – should be reconsidered, Dr. Trelle stated in a report published online by BMJ (Jan. 11, 2011;342:c7086[doi/10.1136/bmj.c7086]).
Dr. Trelle of the University of Bern, Switzerland, acknowledged that therapeutic options for chronic musculoskeletal pain are limited, but cautioned that "cardiovascular risk needs to be taken into account when prescribing" any NSAID.
The meta-analysis included any large, randomized controlled trials comparing any NSAID with other NSAIDs or placebo. Data were available for naproxen, ibuprofen, diclofenac, celecoxib, etoricoxib, rofecoxib, and lumiracoxib. The risk for a cardiovascular event had to increase by more than 30% to be considered significant.
Overall, naproxen appeared to be the least harmful NSAID in terms of cardiovascular outcomes. Risks were greatest with ibuprofen, diclofenac, etoricoxib, and lumiracoxib.
Four NSAIDs were associated with significantly increased risk for myocardial infarction (the primary outcome in the current analysis) in 29 of the trials that reported 554 MIs. The relative risk for MI doubled with rofecoxib or lumiracoxib, was 35% higher with celecoxib, and was 61% higher with ibuprofen, compared with placebo. Evidence was lacking for increased MI risk with the other three NSAIDs.
Among secondary outcomes, stroke risk increased with all NSAIDs in 26 trials that reported 377 strokes. The increased risk was significant with four of the drugs, roughly doubling with naproxen and tripling with ibuprofen, diclofenac, etoricoxib, or lumiracoxib, compared with placebo.
Twenty-six trials reported 312 deaths from cardiovascular disease, accounting for 46% of all deaths in the trials. All NSAIDs except naproxen were associated with higher risk for cardiovascular death, which increased by 58% with rofecoxib, roughly doubled with ibuprofen, celecoxib, or lumiracoxib, and increased approximately fourfold with diclofenac or etoricoxib, compared with placebo.
All the NSAIDs were associated with increased risk for death from any cause, compared with placebo, and the increase was significant for all except naproxen. There were 676 deaths from any cause in 28 trials, and the risk of death roughly doubled with any of the other six NSAIDs.
Looking at a composite of nonfatal MI, nonfatal stroke, or cardiovascular death in 30 trials that reported 1,091 composite events, the risk increased with all the NSAIDs and increased significantly with all but naproxen. The odds for the composite outcome increased 43% with celecoxib, 44% with rofecoxib, 53% with etoricoxib, 60% with diclofenac, and more than doubled with lumiracoxib or ibuprofen.
An estimated 5% of all visits to U.S. physicians are related to prescribing NSAIDs, which are considered the cornerstone for managing the pain of osteoarthritis and other painful conditions. Rofecoxib, a COX-2 inhibitor, was withdrawn from the market in 2004 after a randomized, placebo-controlled trial found its use was associated with increased cardiovascular risk. The Food and Drug Administration has since denied approval of etoricoxib because of an inadequate risk-benefit profile.
Debate about the safety of NSAIDs has continued despite several conventional meta-analyses that could not integrate all available randomized evidence. That’s the strength of the network meta-analysis, which allowed a unified analysis of all the large trials while respecting randomization, according to Dr. Trelle.
Because of the low absolute numbers of events, more than 100,000 patients would need to be followed in a trial for at least a year to evaluate the cardiovascular safety of an NSAID, which is unlikely to happen, he added.
The Swiss National Science Foundation funded the study. The investigators reporting having no conflicts of interest.
Each of seven NSAIDs was associated with significantly increased risk for MI, stroke, or death from cardiovascular disease, compared with placebo, in the most comprehensive meta-analysis of the subject so far.
The relative risks with any individual NSAID, compared with placebo, often were double, triple, or quadruple the risk with placebo, the study found. The absolute numbers of MIs and other cardiovascular outcomes were small, but the network meta-analysis design of the study "provides the best available evidence on the safety of this class of drugs," Dr. Sven Trelle and his associates reported.
Contrary to some previous reports, the current study also found no suggestion that this increased cardiovascular risk is specific to cyclo-oxygenase-2 (COX-2) inhibitors. Therefore the use of all NSAIDs – and the over-the-counter availability of some of them – should be reconsidered, Dr. Trelle stated in a report published online by BMJ (Jan. 11, 2011;342:c7086[doi/10.1136/bmj.c7086]).
Dr. Trelle of the University of Bern, Switzerland, acknowledged that therapeutic options for chronic musculoskeletal pain are limited, but cautioned that "cardiovascular risk needs to be taken into account when prescribing" any NSAID.
The meta-analysis included any large, randomized controlled trials comparing any NSAID with other NSAIDs or placebo. Data were available for naproxen, ibuprofen, diclofenac, celecoxib, etoricoxib, rofecoxib, and lumiracoxib. The risk for a cardiovascular event had to increase by more than 30% to be considered significant.
Overall, naproxen appeared to be the least harmful NSAID in terms of cardiovascular outcomes. Risks were greatest with ibuprofen, diclofenac, etoricoxib, and lumiracoxib.
Four NSAIDs were associated with significantly increased risk for myocardial infarction (the primary outcome in the current analysis) in 29 of the trials that reported 554 MIs. The relative risk for MI doubled with rofecoxib or lumiracoxib, was 35% higher with celecoxib, and was 61% higher with ibuprofen, compared with placebo. Evidence was lacking for increased MI risk with the other three NSAIDs.
Among secondary outcomes, stroke risk increased with all NSAIDs in 26 trials that reported 377 strokes. The increased risk was significant with four of the drugs, roughly doubling with naproxen and tripling with ibuprofen, diclofenac, etoricoxib, or lumiracoxib, compared with placebo.
Twenty-six trials reported 312 deaths from cardiovascular disease, accounting for 46% of all deaths in the trials. All NSAIDs except naproxen were associated with higher risk for cardiovascular death, which increased by 58% with rofecoxib, roughly doubled with ibuprofen, celecoxib, or lumiracoxib, and increased approximately fourfold with diclofenac or etoricoxib, compared with placebo.
All the NSAIDs were associated with increased risk for death from any cause, compared with placebo, and the increase was significant for all except naproxen. There were 676 deaths from any cause in 28 trials, and the risk of death roughly doubled with any of the other six NSAIDs.
Looking at a composite of nonfatal MI, nonfatal stroke, or cardiovascular death in 30 trials that reported 1,091 composite events, the risk increased with all the NSAIDs and increased significantly with all but naproxen. The odds for the composite outcome increased 43% with celecoxib, 44% with rofecoxib, 53% with etoricoxib, 60% with diclofenac, and more than doubled with lumiracoxib or ibuprofen.
An estimated 5% of all visits to U.S. physicians are related to prescribing NSAIDs, which are considered the cornerstone for managing the pain of osteoarthritis and other painful conditions. Rofecoxib, a COX-2 inhibitor, was withdrawn from the market in 2004 after a randomized, placebo-controlled trial found its use was associated with increased cardiovascular risk. The Food and Drug Administration has since denied approval of etoricoxib because of an inadequate risk-benefit profile.
Debate about the safety of NSAIDs has continued despite several conventional meta-analyses that could not integrate all available randomized evidence. That’s the strength of the network meta-analysis, which allowed a unified analysis of all the large trials while respecting randomization, according to Dr. Trelle.
Because of the low absolute numbers of events, more than 100,000 patients would need to be followed in a trial for at least a year to evaluate the cardiovascular safety of an NSAID, which is unlikely to happen, he added.
The Swiss National Science Foundation funded the study. The investigators reporting having no conflicts of interest.
FROM BMJ
Major Finding: Each of seven NSAIDs was associated with significantly increased risk for MI, stroke, or death from cardiovascular disease, compared with placebo.
Data Source: Network meta-analysis of 31 large, randomized controlled trials comparing any NSAID with other NSAIDs or placebo in 116,429 patients with 117,218 patient-years of follow-up.
Disclosures: The Swiss National Science Foundation funded the study. The investigators reported having no conflicts of interest.