User login
Dietary changes to microbiome may improve lung function
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT CHEST 2023
Semaglutide win in HFpEF with obesity regardless of ejection fraction: STEP-HFpEF
CLEVELAND – independently of baseline left-ventricular ejection fraction (LVEF).
The finding comes from a prespecified secondary analysis of the STEP-HFpEF trial of more than 500 nondiabetic patients with obesity and HF with an initial LVEF of 45% or greater.
They suggest that for patients with the obesity phenotype of HFpEF, semaglutide (Wegovy) could potentially join SGLT2 inhibitors on the short list of meds with consistent treatment effects whether LVEF is mildly reduced, preserved, or in the normal range.
That would distinguish the drug, a glucagon-like peptide-1 (GLP-1) receptor agonist, from mineralocorticoid receptor antagonists (MRA), sacubitril-valsartan (Entresto), and other renin-angiotensin-system inhibitors (RASi), whose benefits tend to taper off with rising LVEF.
The patients assigned to semaglutide showed significant improvement in both primary endpoints – change in Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS) and change in body weight at 52 weeks – whether their baseline LVEF was 45%-49%, 50%-59%, or 60% or greater.
Results were similar for improvements in 6-minute walk distance (6MWD) and levels of NT-terminal pro–brain natriuretic peptide (NT-proBNP) and C-reactive protein, observed Javed Butler, MD, when presenting the analysis at the annual meeting of the Heart Failure Society of America, Cleveland.
Dr. Butler, of Baylor Scott and White Research Institute, Dallas, and the University of Mississippi, Jackson, is also lead author of the study, which was published on the same day in the Journal of the American College of Cardiology.
In his presentation, Dr. Butler singled out the NT-proBNP finding as “very meaningful” with respect to understanding potential mechanisms of the drug effects observed in the trial.
For example, people with obesity tend to have lower than average natriuretic peptide levels that “actually go up a bit” when they lose weight, he observed. But in the trial, “we saw a reduction in NT-proBNP in spite of the weight loss,” regardless of LVEF category.
John McMurray, MD, University of Glasgow, the invited discussant for Dr. Butler’s presentation, agreed that it raises the question whether weight loss was the sole semaglutide effect responsible for the improvement in heart failure status and biomarkers. The accompanying NT-proBNP reductions – when the opposite might otherwise have been expected – may point to a possible mechanism of action that is “something more than just weight loss,” he said. “If that were the case, it becomes very important, because it means that this treatment might do good things in non-obese patients or might do good things in patients with other types of heart failure.”
‘Vital reassurance’
More definitive trials are needed “to clarify safety and efficacy of obesity-targeted therapeutics in HF across the ejection fraction spectrum,” according to an accompanying editorial).
Still, the STEP-HFpEF analysis “strengthens the role of GLP-1 [receptor agonists] to ameliorate health status” for patients with obesity and HF with mildly reduced or preserved ejection fraction, write Muthiah Vaduganathan, MD, MPH, and John W. Ostrominski, MD, Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Its findings “provide vital reassurance” on semaglutide safety and efficacy in HF with below-normal LVEF and “tentatively support the existence of a more general, LVEF-independent, obesity-related HF phenotype capable of favorable modification with incretin-based therapies.”
The lack of heterogeneity in treatment effects across LVEF subgroups “is not surprising,” but “the findings reinforce that the benefits of this therapy in those meeting trial criteria do not vary by left ventricular ejection fraction,” Gregg C. Fonarow, MD, University of California, Los Angeles, Medical Center, said in an interview.
It remains unknown, however, “whether the improvement in health status, functional status, and reduced inflammation” will translate to reduced risk of cardiovascular death or HF hospitalization, said Dr. Fonarow, who isn’t connected to STEP-HFpEF.
It’s a question for future studies, he agreed, whether semaglutide would confer similar benefits for patients with obesity and HF with LVEF less than 45% or in non-obese HF patients.
Dr. McMurray proposed that future GLP-1 receptor agonist heart-failure trials should include non-obese patients to determine whether the effects seen in STEP-HFpEF were due to something more than weight loss. Trials in patients with obesity and HF with reduced LVEF would also be important.
“If it turns out just to be about weight loss, then we need to think about the alternatives,” including diet, exercise, and bariatric surgery but also, potentially, weight-loss drugs other than semaglutide, he said.
No heterogeneity by LVEF
STEP-HFpEF randomly assigned 529 patients free of diabetes with an LVEF greater than or equal to 45%, a body mass index (BMI) of at least 30 kg/m2, and NYHA functional status of 2-4 to either a placebo injection or 2.4-mg semaglutide subcutaneously once a week (the dose used for weight reduction) atop standard care.
As previously reported, those assigned to semaglutide showed significant improvements at 1 year in symptoms and in physical limitation, per changes in KCCQ-CSS, and weight loss, compared with the control group. Their exercise capacity, as measured by 6MWD, also improved.
The more weight patients lost while taking semaglutide, the better their KCCQ-CSS and 6MWD outcomes, a prior secondary analysis suggested. But the STEP-HFpEF researchers said weight loss did not appear to explain all of their gains, compared with usual care.
For the current analysis, the 263 patients assigned to receive semaglutide and 266 control patients were divided into three groups by baseline LVEF and compared for the same outcomes.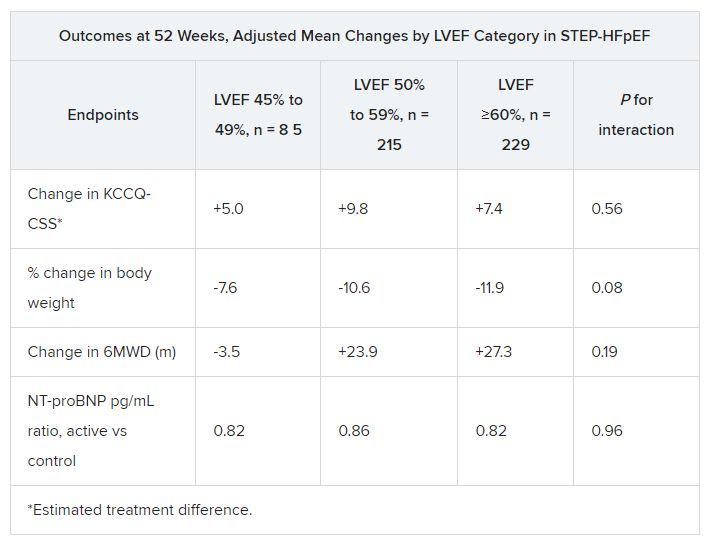
The semaglutide group, compared with control patients, also showed a significantly increased hierarchical composite win ratio, 1.72 (95% CI, 1.37-2.15; P < .001), that was consistent across LVEF categories and that accounted for all-cause mortality, HF events, KCCQ-CSS and 6MWD changes, and change in CRP.
Limitations make it hard to generalize the results, the authors caution. Well over 90% of the participants were White patients, for example, and the overall trial was not powered to show subgroup differences.
Given the many patients with HFpEF who have a cardiometabolic phenotype and are with overweight or obesity, write Dr. Butler and colleagues, their treatment approach “may ultimately include combination therapy with SGLT2 inhibitors and GLP-1 receptor agonists, given their non-overlapping and complementary mechanisms of action.”
Dr. Fonarow noted that both MRAs and sacubitril-valsartan offer clinical benefits for patients with HF and LVEF “in the 41%-60% range” that are evident “across BMI categories.”
So it’s likely, he said, that those medications as well as SGLT2 inhibitors will be used along with GLP-1 receptor agonists for patients with HFpEF and obesity.
STEP-HFpEF was funded by Novo Nordisk. Dr. Butler and the other authors disclose consulting for many companies, a list of which can be found in the report. Dr. Fonarow reports consulting for multiple companies. Dr. McMurray discloses consulting for AstraZeneca. Dr. Ostrominski reports no relevant disclosures. Dr. Vaduganathan discloses receiving grant support, serving on advisory boards, or speaking for multiple companies and serving on committees for studies sponsored by AstraZeneca, Galmed, Novartis, Bayer AG, Occlutech, and Impulse Dynamics.
A version of this article appeared on Medscape.com.
CLEVELAND – independently of baseline left-ventricular ejection fraction (LVEF).
The finding comes from a prespecified secondary analysis of the STEP-HFpEF trial of more than 500 nondiabetic patients with obesity and HF with an initial LVEF of 45% or greater.
They suggest that for patients with the obesity phenotype of HFpEF, semaglutide (Wegovy) could potentially join SGLT2 inhibitors on the short list of meds with consistent treatment effects whether LVEF is mildly reduced, preserved, or in the normal range.
That would distinguish the drug, a glucagon-like peptide-1 (GLP-1) receptor agonist, from mineralocorticoid receptor antagonists (MRA), sacubitril-valsartan (Entresto), and other renin-angiotensin-system inhibitors (RASi), whose benefits tend to taper off with rising LVEF.
The patients assigned to semaglutide showed significant improvement in both primary endpoints – change in Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS) and change in body weight at 52 weeks – whether their baseline LVEF was 45%-49%, 50%-59%, or 60% or greater.
Results were similar for improvements in 6-minute walk distance (6MWD) and levels of NT-terminal pro–brain natriuretic peptide (NT-proBNP) and C-reactive protein, observed Javed Butler, MD, when presenting the analysis at the annual meeting of the Heart Failure Society of America, Cleveland.
Dr. Butler, of Baylor Scott and White Research Institute, Dallas, and the University of Mississippi, Jackson, is also lead author of the study, which was published on the same day in the Journal of the American College of Cardiology.
In his presentation, Dr. Butler singled out the NT-proBNP finding as “very meaningful” with respect to understanding potential mechanisms of the drug effects observed in the trial.
For example, people with obesity tend to have lower than average natriuretic peptide levels that “actually go up a bit” when they lose weight, he observed. But in the trial, “we saw a reduction in NT-proBNP in spite of the weight loss,” regardless of LVEF category.
John McMurray, MD, University of Glasgow, the invited discussant for Dr. Butler’s presentation, agreed that it raises the question whether weight loss was the sole semaglutide effect responsible for the improvement in heart failure status and biomarkers. The accompanying NT-proBNP reductions – when the opposite might otherwise have been expected – may point to a possible mechanism of action that is “something more than just weight loss,” he said. “If that were the case, it becomes very important, because it means that this treatment might do good things in non-obese patients or might do good things in patients with other types of heart failure.”
‘Vital reassurance’
More definitive trials are needed “to clarify safety and efficacy of obesity-targeted therapeutics in HF across the ejection fraction spectrum,” according to an accompanying editorial).
Still, the STEP-HFpEF analysis “strengthens the role of GLP-1 [receptor agonists] to ameliorate health status” for patients with obesity and HF with mildly reduced or preserved ejection fraction, write Muthiah Vaduganathan, MD, MPH, and John W. Ostrominski, MD, Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Its findings “provide vital reassurance” on semaglutide safety and efficacy in HF with below-normal LVEF and “tentatively support the existence of a more general, LVEF-independent, obesity-related HF phenotype capable of favorable modification with incretin-based therapies.”
The lack of heterogeneity in treatment effects across LVEF subgroups “is not surprising,” but “the findings reinforce that the benefits of this therapy in those meeting trial criteria do not vary by left ventricular ejection fraction,” Gregg C. Fonarow, MD, University of California, Los Angeles, Medical Center, said in an interview.
It remains unknown, however, “whether the improvement in health status, functional status, and reduced inflammation” will translate to reduced risk of cardiovascular death or HF hospitalization, said Dr. Fonarow, who isn’t connected to STEP-HFpEF.
It’s a question for future studies, he agreed, whether semaglutide would confer similar benefits for patients with obesity and HF with LVEF less than 45% or in non-obese HF patients.
Dr. McMurray proposed that future GLP-1 receptor agonist heart-failure trials should include non-obese patients to determine whether the effects seen in STEP-HFpEF were due to something more than weight loss. Trials in patients with obesity and HF with reduced LVEF would also be important.
“If it turns out just to be about weight loss, then we need to think about the alternatives,” including diet, exercise, and bariatric surgery but also, potentially, weight-loss drugs other than semaglutide, he said.
No heterogeneity by LVEF
STEP-HFpEF randomly assigned 529 patients free of diabetes with an LVEF greater than or equal to 45%, a body mass index (BMI) of at least 30 kg/m2, and NYHA functional status of 2-4 to either a placebo injection or 2.4-mg semaglutide subcutaneously once a week (the dose used for weight reduction) atop standard care.
As previously reported, those assigned to semaglutide showed significant improvements at 1 year in symptoms and in physical limitation, per changes in KCCQ-CSS, and weight loss, compared with the control group. Their exercise capacity, as measured by 6MWD, also improved.
The more weight patients lost while taking semaglutide, the better their KCCQ-CSS and 6MWD outcomes, a prior secondary analysis suggested. But the STEP-HFpEF researchers said weight loss did not appear to explain all of their gains, compared with usual care.
For the current analysis, the 263 patients assigned to receive semaglutide and 266 control patients were divided into three groups by baseline LVEF and compared for the same outcomes.
The semaglutide group, compared with control patients, also showed a significantly increased hierarchical composite win ratio, 1.72 (95% CI, 1.37-2.15; P < .001), that was consistent across LVEF categories and that accounted for all-cause mortality, HF events, KCCQ-CSS and 6MWD changes, and change in CRP.
Limitations make it hard to generalize the results, the authors caution. Well over 90% of the participants were White patients, for example, and the overall trial was not powered to show subgroup differences.
Given the many patients with HFpEF who have a cardiometabolic phenotype and are with overweight or obesity, write Dr. Butler and colleagues, their treatment approach “may ultimately include combination therapy with SGLT2 inhibitors and GLP-1 receptor agonists, given their non-overlapping and complementary mechanisms of action.”
Dr. Fonarow noted that both MRAs and sacubitril-valsartan offer clinical benefits for patients with HF and LVEF “in the 41%-60% range” that are evident “across BMI categories.”
So it’s likely, he said, that those medications as well as SGLT2 inhibitors will be used along with GLP-1 receptor agonists for patients with HFpEF and obesity.
STEP-HFpEF was funded by Novo Nordisk. Dr. Butler and the other authors disclose consulting for many companies, a list of which can be found in the report. Dr. Fonarow reports consulting for multiple companies. Dr. McMurray discloses consulting for AstraZeneca. Dr. Ostrominski reports no relevant disclosures. Dr. Vaduganathan discloses receiving grant support, serving on advisory boards, or speaking for multiple companies and serving on committees for studies sponsored by AstraZeneca, Galmed, Novartis, Bayer AG, Occlutech, and Impulse Dynamics.
A version of this article appeared on Medscape.com.
CLEVELAND – independently of baseline left-ventricular ejection fraction (LVEF).
The finding comes from a prespecified secondary analysis of the STEP-HFpEF trial of more than 500 nondiabetic patients with obesity and HF with an initial LVEF of 45% or greater.
They suggest that for patients with the obesity phenotype of HFpEF, semaglutide (Wegovy) could potentially join SGLT2 inhibitors on the short list of meds with consistent treatment effects whether LVEF is mildly reduced, preserved, or in the normal range.
That would distinguish the drug, a glucagon-like peptide-1 (GLP-1) receptor agonist, from mineralocorticoid receptor antagonists (MRA), sacubitril-valsartan (Entresto), and other renin-angiotensin-system inhibitors (RASi), whose benefits tend to taper off with rising LVEF.
The patients assigned to semaglutide showed significant improvement in both primary endpoints – change in Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS) and change in body weight at 52 weeks – whether their baseline LVEF was 45%-49%, 50%-59%, or 60% or greater.
Results were similar for improvements in 6-minute walk distance (6MWD) and levels of NT-terminal pro–brain natriuretic peptide (NT-proBNP) and C-reactive protein, observed Javed Butler, MD, when presenting the analysis at the annual meeting of the Heart Failure Society of America, Cleveland.
Dr. Butler, of Baylor Scott and White Research Institute, Dallas, and the University of Mississippi, Jackson, is also lead author of the study, which was published on the same day in the Journal of the American College of Cardiology.
In his presentation, Dr. Butler singled out the NT-proBNP finding as “very meaningful” with respect to understanding potential mechanisms of the drug effects observed in the trial.
For example, people with obesity tend to have lower than average natriuretic peptide levels that “actually go up a bit” when they lose weight, he observed. But in the trial, “we saw a reduction in NT-proBNP in spite of the weight loss,” regardless of LVEF category.
John McMurray, MD, University of Glasgow, the invited discussant for Dr. Butler’s presentation, agreed that it raises the question whether weight loss was the sole semaglutide effect responsible for the improvement in heart failure status and biomarkers. The accompanying NT-proBNP reductions – when the opposite might otherwise have been expected – may point to a possible mechanism of action that is “something more than just weight loss,” he said. “If that were the case, it becomes very important, because it means that this treatment might do good things in non-obese patients or might do good things in patients with other types of heart failure.”
‘Vital reassurance’
More definitive trials are needed “to clarify safety and efficacy of obesity-targeted therapeutics in HF across the ejection fraction spectrum,” according to an accompanying editorial).
Still, the STEP-HFpEF analysis “strengthens the role of GLP-1 [receptor agonists] to ameliorate health status” for patients with obesity and HF with mildly reduced or preserved ejection fraction, write Muthiah Vaduganathan, MD, MPH, and John W. Ostrominski, MD, Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Its findings “provide vital reassurance” on semaglutide safety and efficacy in HF with below-normal LVEF and “tentatively support the existence of a more general, LVEF-independent, obesity-related HF phenotype capable of favorable modification with incretin-based therapies.”
The lack of heterogeneity in treatment effects across LVEF subgroups “is not surprising,” but “the findings reinforce that the benefits of this therapy in those meeting trial criteria do not vary by left ventricular ejection fraction,” Gregg C. Fonarow, MD, University of California, Los Angeles, Medical Center, said in an interview.
It remains unknown, however, “whether the improvement in health status, functional status, and reduced inflammation” will translate to reduced risk of cardiovascular death or HF hospitalization, said Dr. Fonarow, who isn’t connected to STEP-HFpEF.
It’s a question for future studies, he agreed, whether semaglutide would confer similar benefits for patients with obesity and HF with LVEF less than 45% or in non-obese HF patients.
Dr. McMurray proposed that future GLP-1 receptor agonist heart-failure trials should include non-obese patients to determine whether the effects seen in STEP-HFpEF were due to something more than weight loss. Trials in patients with obesity and HF with reduced LVEF would also be important.
“If it turns out just to be about weight loss, then we need to think about the alternatives,” including diet, exercise, and bariatric surgery but also, potentially, weight-loss drugs other than semaglutide, he said.
No heterogeneity by LVEF
STEP-HFpEF randomly assigned 529 patients free of diabetes with an LVEF greater than or equal to 45%, a body mass index (BMI) of at least 30 kg/m2, and NYHA functional status of 2-4 to either a placebo injection or 2.4-mg semaglutide subcutaneously once a week (the dose used for weight reduction) atop standard care.
As previously reported, those assigned to semaglutide showed significant improvements at 1 year in symptoms and in physical limitation, per changes in KCCQ-CSS, and weight loss, compared with the control group. Their exercise capacity, as measured by 6MWD, also improved.
The more weight patients lost while taking semaglutide, the better their KCCQ-CSS and 6MWD outcomes, a prior secondary analysis suggested. But the STEP-HFpEF researchers said weight loss did not appear to explain all of their gains, compared with usual care.
For the current analysis, the 263 patients assigned to receive semaglutide and 266 control patients were divided into three groups by baseline LVEF and compared for the same outcomes.
The semaglutide group, compared with control patients, also showed a significantly increased hierarchical composite win ratio, 1.72 (95% CI, 1.37-2.15; P < .001), that was consistent across LVEF categories and that accounted for all-cause mortality, HF events, KCCQ-CSS and 6MWD changes, and change in CRP.
Limitations make it hard to generalize the results, the authors caution. Well over 90% of the participants were White patients, for example, and the overall trial was not powered to show subgroup differences.
Given the many patients with HFpEF who have a cardiometabolic phenotype and are with overweight or obesity, write Dr. Butler and colleagues, their treatment approach “may ultimately include combination therapy with SGLT2 inhibitors and GLP-1 receptor agonists, given their non-overlapping and complementary mechanisms of action.”
Dr. Fonarow noted that both MRAs and sacubitril-valsartan offer clinical benefits for patients with HF and LVEF “in the 41%-60% range” that are evident “across BMI categories.”
So it’s likely, he said, that those medications as well as SGLT2 inhibitors will be used along with GLP-1 receptor agonists for patients with HFpEF and obesity.
STEP-HFpEF was funded by Novo Nordisk. Dr. Butler and the other authors disclose consulting for many companies, a list of which can be found in the report. Dr. Fonarow reports consulting for multiple companies. Dr. McMurray discloses consulting for AstraZeneca. Dr. Ostrominski reports no relevant disclosures. Dr. Vaduganathan discloses receiving grant support, serving on advisory boards, or speaking for multiple companies and serving on committees for studies sponsored by AstraZeneca, Galmed, Novartis, Bayer AG, Occlutech, and Impulse Dynamics.
A version of this article appeared on Medscape.com.
AT HFSA 2023
IPF pipeline crowded with new drug candidates
With the emergence of pirfenidone and nintedanib over the past decade or so, pulmonologists now have at their disposal two breakthrough antifibrotic agents for the treatment of idiopathic pulmonary fibrosis.

But these two drugs have a number of shortcomings that a host of investigative agents are aiming to address. For one, while pirfenidone and nintedanib have been shown to slow disease progression and improve symptoms, they don’t stop or reverse the disease. Also, a large number of patients with IPF don’t tolerate these drugs well. And, their high cost is a barrier for many patients.
in terms of therapies or interventions that have better efficacy, better long-term tolerability, and that improve symptoms and quality of life for our patients with IPF disease,” said Joyce Lee, MD, associate professor of medicine–pulmonary at the University of Colorado at Denver, Aurora, and senior medical adviser for research and health care quality for the Pulmonary Fibrosis Foundation.
The National Institutes of Health estimates that more than 30,000 new cases of IPF are diagnosed in the United States annually, and as many as 3 million people have the disease worldwide. The 5-year survival rate is less than 40% after diagnosis. Bloomberg News reported that more than 80 pharmaceutical companies are working on IPF treatments. iHealthcareAnalyst estimates the global market for IPF will reach $10.1 billion by 2029 thanks to rapidly increasing prevalence and incidence with age, premium-priced drugs, and rapid approval of new treatments.
The perils of phase 3 studies
A search on ClinicalTrials.gov turned up 89 investigative IPF treatments in human trials. However, the search for alternatives can be perilous. “In the field, we have gotten used to promising phase 2 studies that failed in the phase 3 stage of development,” Dr. Lee said. “I don’t hold my breath these days just in terms of trying to predict whether or not the efficacy will be present in the phase 3 clinical trial.”
Three notable phase 3 flops include the ISABELA 1 and 2 trials of the autotaxin inhibitor ziritaxestat, which failed to meet their primary endpoint and were halted early (JAMA. 2023;329:1567-78). The phase 3 ZEPHYRUS-1 trial failed to show any benefit of pamrevlumab to improve percent predicted force vital capacity (ppFVC) at week 48, causing discontinuation of a second phase 3 trial. The phase 3 STARSCAPE-OLE study of intravenous recombinant human pentraxin-2 was terminated earlier this year when the sponsor, Hoffmann-LaRoche, decided it was unable to meet its primary objective (NCT04594707).
In the meantime, these six other phase 3 programs in IPF are still in the field:
Anlotinib. A phase 2 and 3 trial in China is evaluating 1-year outcomes of once-daily oral anlotinib for treatment of IPF/progressive fibrosis-interstitial lung disease (PF-ILDS) (NCT05828953). Anlotinib is a tyrosine kinase inhibitor (TKI) that targets four factors: vascular endothelial growth factor receptor (VEGR), fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptors (PDGFR), and c-kit. It’s approved in China as a third-line therapy for non–small cell lung cancer (NSCLC).
BI 101550. Enrollment in the FIBRONEER-IPF trial commenced last fall (NCT05321069), with completion scheduled for late next year. BI 1015550 is an oral phosphodiesterase 4B (PDE4B) inhibitor. FIBRONEER-ILD is a separate phase 3 trial in fibrosing idiopathic lung disease (NCT05321082). In both trials, the primary endpoint is the absolute change from baseline in FVC at week 52.
BMS-986278. Results of a phase 2 trial showed that twice-daily treatment with oral BMS-986278 60 mg over 26 weeks reduced the rate of decline in ppFVC by 69% vs. placebo. The phase 3 ALOFT trial has been approved but hasn’t yet started recruiting patients (NCT06003426). BMS-986278 is a lysophosphatidic acid receptor 1 (LPA1) antagonist.
Lanxoprazole. Commonly used to treat and prevent gastrointestinal problems like stomach ulcers and esophagitis, this oral proton pump inhibitor (PPI) is the focus of a trial in the United Kingdom evaluating if PPIs can slow the progression of IPF (NCT04965298).
N-acetylcysteine (NAC). The PRECISIONS trial is evaluating the effect of NAC plus standard-of-care treatment in IPF patients who have the TOLLIP rs3750910 TT genotype (NCT04300920). Participants receive 600 mg NAC orally or matched placebo three times daily for 24 months. Trial completion is scheduled for 2025.
Treprostinil. Already approved to treat pulmonary arterial hypertension and pulmonary hypertension associated with interstitial lung disease, inhaled Treprostinil is the subject of the TETON 1 and 2 trials evaluating its impact on ppFVC after 52 weeks of treatment (NCT04708782, NCT05255991).
Phase 2 candidates
The primary endpoint in most of the phase 2 trials is change in ppFVC capacity from baseline to week 24. The following investigative therapies are in phase 2 trials:
Bexotegrast (PLN-74809), an oral, small molecule, dual-selective inhibitor of alphav/beta6 and alphav/beta1 (NCT04396756).
BBT-877, described as a potent autotaxin (ATX) inhibitor, demonstrated its ability to inhibit lysophosphatidic acid (LPA) production by as much as 90 percent (NCT05483907).
CC-90001, an oral, once-daily c-Jun N-terminal kinases (JNK) inhibitor. JNKs have been implicated in the underlying mechanisms of fibrosis, including epithelial cell death, inflammation and polarization of profibrotic macrophages, fibroblast activation, and collagen production (NCT03142191).
C21 targets the underlying fibrosis in IPF by stimulating the protective arm of the renin-angiotensin system. It also has an upstream effect by promoting alveolar repair by which it can reduce fibrosis formation, stabilize disease, and increase lung capacity (NCT04533022).
CSL312 (garadacimab) is a humanized anti-FXIIa monoclonal antibody administrated intravenously (NCT05130970).
Cudetaxestat, a noncompetitive autotaxin inhibitor (NCT05373914).
Bersiposocin/DWN12088, an inhibitor of prolyl-tRNA synthetase 1 (PARS1), which is suspected to control the pathologic accumulation of collagen containing high amounts of proline in fibrotic diseases (NCT05389215).
ENV-101, a small-molecule inhibitor of the Hedgehog (Hh) signaling pathway, which plays a key role in IPF. This agent was originally developed to target Hh-driven cancers (NCT04968574).
GKT137831 (setanaxib) inhibits nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX) isoforms. (NCT03865927).
HZN-825, a lysophosphatidic acid receptor 1 (LPAR1) antagonist. (NCT05032066)
Ifetroban, a potent and selective thromboxane-prostanoid receptor (TPr) antagonist, which exhibits a high affinity for TPr on platelets, vascular and airway smooth muscle, and fibroblasts, and lacks agonistic activity (NCT05571059).
INS018_055, a small-molecule, oral antifibrotic candidate notable for being the first entirely AI-generated drug to enter phase 2 trials. Trial enrollment started in October (NCT05975983, NCT05983920)
Jaktinib dihydrochloride monohydrate, an oral JAK1, JAK2, and JAK3 inhibitor (NCT04312594).
Leramistat, an anti–tumor necrosis factor (TNF) agent (NCT05951296).
LTP001, an oral, selectively deuterated form of pirfenidone designed to retain the antifibrotic and anti-inflammatory activity of pirfenidone with a differentiated pharmacokinetic profile (NCT05497284, NCT05321420).
ME-015 (suplatast tosilate) aims to stabilize ion channels in the neuronal endings in the lungs that mediate IPF-related cough (NCT05983471).
Nalbuphine, a small-molecule, dual-mechanism treatment for chronic cough in IPF. It acts as both a mu opioid receptor antagonist and a kappa opioid receptor agonist (NCT05964335). The CANAL trial, complete last year, is evaluating an extended-release formulation (NCT04030026).
NP-120 (ifenprodil), a small-molecule N-methyl-D-aspartate (NMDA) receptor antagonist, specifically targets the NMDA-type subunit 2B (GluN2B) (NCT04318704).
Orvepitant, a selective antagonist for the NK₁ receptor, is being evaluated to treat IPF-related cough (NCT05815089).
RXC007 (zelasudil), a Rho-associated coiled-coil–containing protein kinase 2 (ROCK2) selective inhibitor, was granted FDA orphan drug designation in August 2023 (NCT05570058).
Saracatinib, a selective Src kinase inhibitor originally developed for oncological indications (NCT04598919).
SHR-1906, an intravenous treatment, inhibits binding of a target protein to a variety of cytokines and growth factors, affects downstream signaling pathways, and reduces cell proliferation and migration (NCT05722964).
TTI-101, an oral, small-molecule inhibitor of signal transducer and activator of transcription (STAT3), which has been found to accumulate in the lungs of IPF patients (NCT05671835).
VAY736 (lanalumab), a BAFF-R inhibitor (NCT03287414).
Vixarelimab, a human monoclonal oncastatin M receptor beta antibody (NCT05785624).
Some investigative programs, however, didn’t make it out of phase 2. The trial evaluating inhaled GB0139, a selective functional antagonist of G-protein–coupled receptor 84, which plays a key role in fibrosis, failed to meet its primary endpoint (NCT03832946). Likewise, oral GLPG1205 failed to show a significant difference in FVC decline vs. placebo (NCT03725852). The program to develop SAR156597, also known as romilkimab, was halted (NCT02345070). ND-L02-s0201n, an siRNA oligonucleotide drug designed to inhibit heat shock protein 47 (HSP47), which regulates collagen synthesis and secretion that causes fibrosis, didn’t show the expected efficacy (NCT03538301).
Phase 1 trials
No fewer than 27 phase 1 trials are evaluating investigative treatments for IPF, many in the early phase or not yet recruiting. According to GlobalData, phase 1 drugs for IPF have a 66% chance of moving onto phase 2. Among the advanced phase 1 trials that have gained corporate backing are:
9MW3811, an anti–interleukin-11 monoclonal antibody IV injection (NCT05912049).
ANG-3070, an oral tyrosine kinase inhibitor targeting platelet-derived growth factor (PDGFR) alpha and beta (NCT05387785).
C106, an angiotensin II type 2 receptor agonist (NCT05427253).
HuL001, which targets alpha-enolase (NCT04540770).
LTI-03, a Caveolin-1 (Cav1)-related peptide designed to restore Cav1 expression in lung tissue (NCT05954988).
ORIN1001, a first-in-class small molecule that selectively blocks the inositol requiring enzyme 1alphase (IRE1) RNAse and blocks X-box binding protein 1 (XBP1) activation (NCT04643769).
PRS-220 is an orally inhaled anticalin protein targeting connective tissue growth factor (CTGF) (NTC05473533).
TRK-250, a single-strand, long-chain nucleic acid that selectively suppresses expression of transforming growth factor-beta 1 (TGF-beta1) protein (NCT03727802).
“While we have therapies that we’re able to give patients, we need to do more and we need to do better,” Dr. Lee said. “We’re all hopeful the next phase 3 clinical trial will be something that will help change the treatment paradigm for our patients. We’re very patient, and hopefully those that are interested in improving this treatment landscape will continue to persist.”
Dr. Lee disclosed financial relationships with Boehringer Ingelheim, Pliant Therapeutics, Blade Therapeutics, United Therapeutics, Eleven P15. and Avalyn Pharma.
With the emergence of pirfenidone and nintedanib over the past decade or so, pulmonologists now have at their disposal two breakthrough antifibrotic agents for the treatment of idiopathic pulmonary fibrosis.
But these two drugs have a number of shortcomings that a host of investigative agents are aiming to address. For one, while pirfenidone and nintedanib have been shown to slow disease progression and improve symptoms, they don’t stop or reverse the disease. Also, a large number of patients with IPF don’t tolerate these drugs well. And, their high cost is a barrier for many patients.
in terms of therapies or interventions that have better efficacy, better long-term tolerability, and that improve symptoms and quality of life for our patients with IPF disease,” said Joyce Lee, MD, associate professor of medicine–pulmonary at the University of Colorado at Denver, Aurora, and senior medical adviser for research and health care quality for the Pulmonary Fibrosis Foundation.
The National Institutes of Health estimates that more than 30,000 new cases of IPF are diagnosed in the United States annually, and as many as 3 million people have the disease worldwide. The 5-year survival rate is less than 40% after diagnosis. Bloomberg News reported that more than 80 pharmaceutical companies are working on IPF treatments. iHealthcareAnalyst estimates the global market for IPF will reach $10.1 billion by 2029 thanks to rapidly increasing prevalence and incidence with age, premium-priced drugs, and rapid approval of new treatments.
The perils of phase 3 studies
A search on ClinicalTrials.gov turned up 89 investigative IPF treatments in human trials. However, the search for alternatives can be perilous. “In the field, we have gotten used to promising phase 2 studies that failed in the phase 3 stage of development,” Dr. Lee said. “I don’t hold my breath these days just in terms of trying to predict whether or not the efficacy will be present in the phase 3 clinical trial.”
Three notable phase 3 flops include the ISABELA 1 and 2 trials of the autotaxin inhibitor ziritaxestat, which failed to meet their primary endpoint and were halted early (JAMA. 2023;329:1567-78). The phase 3 ZEPHYRUS-1 trial failed to show any benefit of pamrevlumab to improve percent predicted force vital capacity (ppFVC) at week 48, causing discontinuation of a second phase 3 trial. The phase 3 STARSCAPE-OLE study of intravenous recombinant human pentraxin-2 was terminated earlier this year when the sponsor, Hoffmann-LaRoche, decided it was unable to meet its primary objective (NCT04594707).
In the meantime, these six other phase 3 programs in IPF are still in the field:
Anlotinib. A phase 2 and 3 trial in China is evaluating 1-year outcomes of once-daily oral anlotinib for treatment of IPF/progressive fibrosis-interstitial lung disease (PF-ILDS) (NCT05828953). Anlotinib is a tyrosine kinase inhibitor (TKI) that targets four factors: vascular endothelial growth factor receptor (VEGR), fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptors (PDGFR), and c-kit. It’s approved in China as a third-line therapy for non–small cell lung cancer (NSCLC).
BI 101550. Enrollment in the FIBRONEER-IPF trial commenced last fall (NCT05321069), with completion scheduled for late next year. BI 1015550 is an oral phosphodiesterase 4B (PDE4B) inhibitor. FIBRONEER-ILD is a separate phase 3 trial in fibrosing idiopathic lung disease (NCT05321082). In both trials, the primary endpoint is the absolute change from baseline in FVC at week 52.
BMS-986278. Results of a phase 2 trial showed that twice-daily treatment with oral BMS-986278 60 mg over 26 weeks reduced the rate of decline in ppFVC by 69% vs. placebo. The phase 3 ALOFT trial has been approved but hasn’t yet started recruiting patients (NCT06003426). BMS-986278 is a lysophosphatidic acid receptor 1 (LPA1) antagonist.
Lanxoprazole. Commonly used to treat and prevent gastrointestinal problems like stomach ulcers and esophagitis, this oral proton pump inhibitor (PPI) is the focus of a trial in the United Kingdom evaluating if PPIs can slow the progression of IPF (NCT04965298).
N-acetylcysteine (NAC). The PRECISIONS trial is evaluating the effect of NAC plus standard-of-care treatment in IPF patients who have the TOLLIP rs3750910 TT genotype (NCT04300920). Participants receive 600 mg NAC orally or matched placebo three times daily for 24 months. Trial completion is scheduled for 2025.
Treprostinil. Already approved to treat pulmonary arterial hypertension and pulmonary hypertension associated with interstitial lung disease, inhaled Treprostinil is the subject of the TETON 1 and 2 trials evaluating its impact on ppFVC after 52 weeks of treatment (NCT04708782, NCT05255991).
Phase 2 candidates
The primary endpoint in most of the phase 2 trials is change in ppFVC capacity from baseline to week 24. The following investigative therapies are in phase 2 trials:
Bexotegrast (PLN-74809), an oral, small molecule, dual-selective inhibitor of alphav/beta6 and alphav/beta1 (NCT04396756).
BBT-877, described as a potent autotaxin (ATX) inhibitor, demonstrated its ability to inhibit lysophosphatidic acid (LPA) production by as much as 90 percent (NCT05483907).
CC-90001, an oral, once-daily c-Jun N-terminal kinases (JNK) inhibitor. JNKs have been implicated in the underlying mechanisms of fibrosis, including epithelial cell death, inflammation and polarization of profibrotic macrophages, fibroblast activation, and collagen production (NCT03142191).
C21 targets the underlying fibrosis in IPF by stimulating the protective arm of the renin-angiotensin system. It also has an upstream effect by promoting alveolar repair by which it can reduce fibrosis formation, stabilize disease, and increase lung capacity (NCT04533022).
CSL312 (garadacimab) is a humanized anti-FXIIa monoclonal antibody administrated intravenously (NCT05130970).
Cudetaxestat, a noncompetitive autotaxin inhibitor (NCT05373914).
Bersiposocin/DWN12088, an inhibitor of prolyl-tRNA synthetase 1 (PARS1), which is suspected to control the pathologic accumulation of collagen containing high amounts of proline in fibrotic diseases (NCT05389215).
ENV-101, a small-molecule inhibitor of the Hedgehog (Hh) signaling pathway, which plays a key role in IPF. This agent was originally developed to target Hh-driven cancers (NCT04968574).
GKT137831 (setanaxib) inhibits nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX) isoforms. (NCT03865927).
HZN-825, a lysophosphatidic acid receptor 1 (LPAR1) antagonist. (NCT05032066)
Ifetroban, a potent and selective thromboxane-prostanoid receptor (TPr) antagonist, which exhibits a high affinity for TPr on platelets, vascular and airway smooth muscle, and fibroblasts, and lacks agonistic activity (NCT05571059).
INS018_055, a small-molecule, oral antifibrotic candidate notable for being the first entirely AI-generated drug to enter phase 2 trials. Trial enrollment started in October (NCT05975983, NCT05983920)
Jaktinib dihydrochloride monohydrate, an oral JAK1, JAK2, and JAK3 inhibitor (NCT04312594).
Leramistat, an anti–tumor necrosis factor (TNF) agent (NCT05951296).
LTP001, an oral, selectively deuterated form of pirfenidone designed to retain the antifibrotic and anti-inflammatory activity of pirfenidone with a differentiated pharmacokinetic profile (NCT05497284, NCT05321420).
ME-015 (suplatast tosilate) aims to stabilize ion channels in the neuronal endings in the lungs that mediate IPF-related cough (NCT05983471).
Nalbuphine, a small-molecule, dual-mechanism treatment for chronic cough in IPF. It acts as both a mu opioid receptor antagonist and a kappa opioid receptor agonist (NCT05964335). The CANAL trial, complete last year, is evaluating an extended-release formulation (NCT04030026).
NP-120 (ifenprodil), a small-molecule N-methyl-D-aspartate (NMDA) receptor antagonist, specifically targets the NMDA-type subunit 2B (GluN2B) (NCT04318704).
Orvepitant, a selective antagonist for the NK₁ receptor, is being evaluated to treat IPF-related cough (NCT05815089).
RXC007 (zelasudil), a Rho-associated coiled-coil–containing protein kinase 2 (ROCK2) selective inhibitor, was granted FDA orphan drug designation in August 2023 (NCT05570058).
Saracatinib, a selective Src kinase inhibitor originally developed for oncological indications (NCT04598919).
SHR-1906, an intravenous treatment, inhibits binding of a target protein to a variety of cytokines and growth factors, affects downstream signaling pathways, and reduces cell proliferation and migration (NCT05722964).
TTI-101, an oral, small-molecule inhibitor of signal transducer and activator of transcription (STAT3), which has been found to accumulate in the lungs of IPF patients (NCT05671835).
VAY736 (lanalumab), a BAFF-R inhibitor (NCT03287414).
Vixarelimab, a human monoclonal oncastatin M receptor beta antibody (NCT05785624).
Some investigative programs, however, didn’t make it out of phase 2. The trial evaluating inhaled GB0139, a selective functional antagonist of G-protein–coupled receptor 84, which plays a key role in fibrosis, failed to meet its primary endpoint (NCT03832946). Likewise, oral GLPG1205 failed to show a significant difference in FVC decline vs. placebo (NCT03725852). The program to develop SAR156597, also known as romilkimab, was halted (NCT02345070). ND-L02-s0201n, an siRNA oligonucleotide drug designed to inhibit heat shock protein 47 (HSP47), which regulates collagen synthesis and secretion that causes fibrosis, didn’t show the expected efficacy (NCT03538301).
Phase 1 trials
No fewer than 27 phase 1 trials are evaluating investigative treatments for IPF, many in the early phase or not yet recruiting. According to GlobalData, phase 1 drugs for IPF have a 66% chance of moving onto phase 2. Among the advanced phase 1 trials that have gained corporate backing are:
9MW3811, an anti–interleukin-11 monoclonal antibody IV injection (NCT05912049).
ANG-3070, an oral tyrosine kinase inhibitor targeting platelet-derived growth factor (PDGFR) alpha and beta (NCT05387785).
C106, an angiotensin II type 2 receptor agonist (NCT05427253).
HuL001, which targets alpha-enolase (NCT04540770).
LTI-03, a Caveolin-1 (Cav1)-related peptide designed to restore Cav1 expression in lung tissue (NCT05954988).
ORIN1001, a first-in-class small molecule that selectively blocks the inositol requiring enzyme 1alphase (IRE1) RNAse and blocks X-box binding protein 1 (XBP1) activation (NCT04643769).
PRS-220 is an orally inhaled anticalin protein targeting connective tissue growth factor (CTGF) (NTC05473533).
TRK-250, a single-strand, long-chain nucleic acid that selectively suppresses expression of transforming growth factor-beta 1 (TGF-beta1) protein (NCT03727802).
“While we have therapies that we’re able to give patients, we need to do more and we need to do better,” Dr. Lee said. “We’re all hopeful the next phase 3 clinical trial will be something that will help change the treatment paradigm for our patients. We’re very patient, and hopefully those that are interested in improving this treatment landscape will continue to persist.”
Dr. Lee disclosed financial relationships with Boehringer Ingelheim, Pliant Therapeutics, Blade Therapeutics, United Therapeutics, Eleven P15. and Avalyn Pharma.
With the emergence of pirfenidone and nintedanib over the past decade or so, pulmonologists now have at their disposal two breakthrough antifibrotic agents for the treatment of idiopathic pulmonary fibrosis.
But these two drugs have a number of shortcomings that a host of investigative agents are aiming to address. For one, while pirfenidone and nintedanib have been shown to slow disease progression and improve symptoms, they don’t stop or reverse the disease. Also, a large number of patients with IPF don’t tolerate these drugs well. And, their high cost is a barrier for many patients.
in terms of therapies or interventions that have better efficacy, better long-term tolerability, and that improve symptoms and quality of life for our patients with IPF disease,” said Joyce Lee, MD, associate professor of medicine–pulmonary at the University of Colorado at Denver, Aurora, and senior medical adviser for research and health care quality for the Pulmonary Fibrosis Foundation.
The National Institutes of Health estimates that more than 30,000 new cases of IPF are diagnosed in the United States annually, and as many as 3 million people have the disease worldwide. The 5-year survival rate is less than 40% after diagnosis. Bloomberg News reported that more than 80 pharmaceutical companies are working on IPF treatments. iHealthcareAnalyst estimates the global market for IPF will reach $10.1 billion by 2029 thanks to rapidly increasing prevalence and incidence with age, premium-priced drugs, and rapid approval of new treatments.
The perils of phase 3 studies
A search on ClinicalTrials.gov turned up 89 investigative IPF treatments in human trials. However, the search for alternatives can be perilous. “In the field, we have gotten used to promising phase 2 studies that failed in the phase 3 stage of development,” Dr. Lee said. “I don’t hold my breath these days just in terms of trying to predict whether or not the efficacy will be present in the phase 3 clinical trial.”
Three notable phase 3 flops include the ISABELA 1 and 2 trials of the autotaxin inhibitor ziritaxestat, which failed to meet their primary endpoint and were halted early (JAMA. 2023;329:1567-78). The phase 3 ZEPHYRUS-1 trial failed to show any benefit of pamrevlumab to improve percent predicted force vital capacity (ppFVC) at week 48, causing discontinuation of a second phase 3 trial. The phase 3 STARSCAPE-OLE study of intravenous recombinant human pentraxin-2 was terminated earlier this year when the sponsor, Hoffmann-LaRoche, decided it was unable to meet its primary objective (NCT04594707).
In the meantime, these six other phase 3 programs in IPF are still in the field:
Anlotinib. A phase 2 and 3 trial in China is evaluating 1-year outcomes of once-daily oral anlotinib for treatment of IPF/progressive fibrosis-interstitial lung disease (PF-ILDS) (NCT05828953). Anlotinib is a tyrosine kinase inhibitor (TKI) that targets four factors: vascular endothelial growth factor receptor (VEGR), fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptors (PDGFR), and c-kit. It’s approved in China as a third-line therapy for non–small cell lung cancer (NSCLC).
BI 101550. Enrollment in the FIBRONEER-IPF trial commenced last fall (NCT05321069), with completion scheduled for late next year. BI 1015550 is an oral phosphodiesterase 4B (PDE4B) inhibitor. FIBRONEER-ILD is a separate phase 3 trial in fibrosing idiopathic lung disease (NCT05321082). In both trials, the primary endpoint is the absolute change from baseline in FVC at week 52.
BMS-986278. Results of a phase 2 trial showed that twice-daily treatment with oral BMS-986278 60 mg over 26 weeks reduced the rate of decline in ppFVC by 69% vs. placebo. The phase 3 ALOFT trial has been approved but hasn’t yet started recruiting patients (NCT06003426). BMS-986278 is a lysophosphatidic acid receptor 1 (LPA1) antagonist.
Lanxoprazole. Commonly used to treat and prevent gastrointestinal problems like stomach ulcers and esophagitis, this oral proton pump inhibitor (PPI) is the focus of a trial in the United Kingdom evaluating if PPIs can slow the progression of IPF (NCT04965298).
N-acetylcysteine (NAC). The PRECISIONS trial is evaluating the effect of NAC plus standard-of-care treatment in IPF patients who have the TOLLIP rs3750910 TT genotype (NCT04300920). Participants receive 600 mg NAC orally or matched placebo three times daily for 24 months. Trial completion is scheduled for 2025.
Treprostinil. Already approved to treat pulmonary arterial hypertension and pulmonary hypertension associated with interstitial lung disease, inhaled Treprostinil is the subject of the TETON 1 and 2 trials evaluating its impact on ppFVC after 52 weeks of treatment (NCT04708782, NCT05255991).
Phase 2 candidates
The primary endpoint in most of the phase 2 trials is change in ppFVC capacity from baseline to week 24. The following investigative therapies are in phase 2 trials:
Bexotegrast (PLN-74809), an oral, small molecule, dual-selective inhibitor of alphav/beta6 and alphav/beta1 (NCT04396756).
BBT-877, described as a potent autotaxin (ATX) inhibitor, demonstrated its ability to inhibit lysophosphatidic acid (LPA) production by as much as 90 percent (NCT05483907).
CC-90001, an oral, once-daily c-Jun N-terminal kinases (JNK) inhibitor. JNKs have been implicated in the underlying mechanisms of fibrosis, including epithelial cell death, inflammation and polarization of profibrotic macrophages, fibroblast activation, and collagen production (NCT03142191).
C21 targets the underlying fibrosis in IPF by stimulating the protective arm of the renin-angiotensin system. It also has an upstream effect by promoting alveolar repair by which it can reduce fibrosis formation, stabilize disease, and increase lung capacity (NCT04533022).
CSL312 (garadacimab) is a humanized anti-FXIIa monoclonal antibody administrated intravenously (NCT05130970).
Cudetaxestat, a noncompetitive autotaxin inhibitor (NCT05373914).
Bersiposocin/DWN12088, an inhibitor of prolyl-tRNA synthetase 1 (PARS1), which is suspected to control the pathologic accumulation of collagen containing high amounts of proline in fibrotic diseases (NCT05389215).
ENV-101, a small-molecule inhibitor of the Hedgehog (Hh) signaling pathway, which plays a key role in IPF. This agent was originally developed to target Hh-driven cancers (NCT04968574).
GKT137831 (setanaxib) inhibits nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX) isoforms. (NCT03865927).
HZN-825, a lysophosphatidic acid receptor 1 (LPAR1) antagonist. (NCT05032066)
Ifetroban, a potent and selective thromboxane-prostanoid receptor (TPr) antagonist, which exhibits a high affinity for TPr on platelets, vascular and airway smooth muscle, and fibroblasts, and lacks agonistic activity (NCT05571059).
INS018_055, a small-molecule, oral antifibrotic candidate notable for being the first entirely AI-generated drug to enter phase 2 trials. Trial enrollment started in October (NCT05975983, NCT05983920)
Jaktinib dihydrochloride monohydrate, an oral JAK1, JAK2, and JAK3 inhibitor (NCT04312594).
Leramistat, an anti–tumor necrosis factor (TNF) agent (NCT05951296).
LTP001, an oral, selectively deuterated form of pirfenidone designed to retain the antifibrotic and anti-inflammatory activity of pirfenidone with a differentiated pharmacokinetic profile (NCT05497284, NCT05321420).
ME-015 (suplatast tosilate) aims to stabilize ion channels in the neuronal endings in the lungs that mediate IPF-related cough (NCT05983471).
Nalbuphine, a small-molecule, dual-mechanism treatment for chronic cough in IPF. It acts as both a mu opioid receptor antagonist and a kappa opioid receptor agonist (NCT05964335). The CANAL trial, complete last year, is evaluating an extended-release formulation (NCT04030026).
NP-120 (ifenprodil), a small-molecule N-methyl-D-aspartate (NMDA) receptor antagonist, specifically targets the NMDA-type subunit 2B (GluN2B) (NCT04318704).
Orvepitant, a selective antagonist for the NK₁ receptor, is being evaluated to treat IPF-related cough (NCT05815089).
RXC007 (zelasudil), a Rho-associated coiled-coil–containing protein kinase 2 (ROCK2) selective inhibitor, was granted FDA orphan drug designation in August 2023 (NCT05570058).
Saracatinib, a selective Src kinase inhibitor originally developed for oncological indications (NCT04598919).
SHR-1906, an intravenous treatment, inhibits binding of a target protein to a variety of cytokines and growth factors, affects downstream signaling pathways, and reduces cell proliferation and migration (NCT05722964).
TTI-101, an oral, small-molecule inhibitor of signal transducer and activator of transcription (STAT3), which has been found to accumulate in the lungs of IPF patients (NCT05671835).
VAY736 (lanalumab), a BAFF-R inhibitor (NCT03287414).
Vixarelimab, a human monoclonal oncastatin M receptor beta antibody (NCT05785624).
Some investigative programs, however, didn’t make it out of phase 2. The trial evaluating inhaled GB0139, a selective functional antagonist of G-protein–coupled receptor 84, which plays a key role in fibrosis, failed to meet its primary endpoint (NCT03832946). Likewise, oral GLPG1205 failed to show a significant difference in FVC decline vs. placebo (NCT03725852). The program to develop SAR156597, also known as romilkimab, was halted (NCT02345070). ND-L02-s0201n, an siRNA oligonucleotide drug designed to inhibit heat shock protein 47 (HSP47), which regulates collagen synthesis and secretion that causes fibrosis, didn’t show the expected efficacy (NCT03538301).
Phase 1 trials
No fewer than 27 phase 1 trials are evaluating investigative treatments for IPF, many in the early phase or not yet recruiting. According to GlobalData, phase 1 drugs for IPF have a 66% chance of moving onto phase 2. Among the advanced phase 1 trials that have gained corporate backing are:
9MW3811, an anti–interleukin-11 monoclonal antibody IV injection (NCT05912049).
ANG-3070, an oral tyrosine kinase inhibitor targeting platelet-derived growth factor (PDGFR) alpha and beta (NCT05387785).
C106, an angiotensin II type 2 receptor agonist (NCT05427253).
HuL001, which targets alpha-enolase (NCT04540770).
LTI-03, a Caveolin-1 (Cav1)-related peptide designed to restore Cav1 expression in lung tissue (NCT05954988).
ORIN1001, a first-in-class small molecule that selectively blocks the inositol requiring enzyme 1alphase (IRE1) RNAse and blocks X-box binding protein 1 (XBP1) activation (NCT04643769).
PRS-220 is an orally inhaled anticalin protein targeting connective tissue growth factor (CTGF) (NTC05473533).
TRK-250, a single-strand, long-chain nucleic acid that selectively suppresses expression of transforming growth factor-beta 1 (TGF-beta1) protein (NCT03727802).
“While we have therapies that we’re able to give patients, we need to do more and we need to do better,” Dr. Lee said. “We’re all hopeful the next phase 3 clinical trial will be something that will help change the treatment paradigm for our patients. We’re very patient, and hopefully those that are interested in improving this treatment landscape will continue to persist.”
Dr. Lee disclosed financial relationships with Boehringer Ingelheim, Pliant Therapeutics, Blade Therapeutics, United Therapeutics, Eleven P15. and Avalyn Pharma.
Short, long-lasting bronchodilators similar for exacerbated COPD
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
AT CHEST 2023
Take two pills and make a donation
I was a resident, on morning rounds. The attending neurologist was young and ambitious (weren’t we all once?), trying to get the hospital to help him fund a research program in his subspecialty of interest.
One of the patients we saw that morning was a locally known successful businessman who’d been admitted, fortunately not for anything too serious.

My attending took the history, verifying the one I’d presented, and examined the gentleman. He then made some teaching points and explained the care plan to the patient.
Pretty standard up to that point.
After answering questions, however, the attending suddenly went into a sales pitch on his new research program, asking the guy for a financial donation, and giving him the card for the person at his office handling the funding.
I don’t remember anymore if he repeated that with other patients, but even now it still leaves a bad taste in my mouth. As a resident I wasn’t in a position to criticize him, nor did I want to endanger my own standing in the program by talking to someone higher up.
He was, fortunately, the only attending I ever worked with who did that. It still stands out in my mind, perhaps as an example of what not to do, and sometimes I still think about it.
Perhaps I’m naive, but I assumed he was an aberration. Apparently not, as the American College of Physicians recently issued a position paper advising its members not to ask patients for donations to the doctor’s workplace. There’s actually an acronym, GPF (Grateful Patient Fundraising) for this.
I understand a lot of these doctors are in academics and need funding for research and other programs. I know that a lot of good comes from this research, and I fully support it.
But this seems to be a bad way of doing it. Standing at the bedside on that long-ago morning, I remember thinking the patient (who looked kind of surprised) was going to wonder if this was a vague sort of hint: You’ll get better care if you pay up. Or a veiled threat that you may not get decent care if you don’t. I have no idea if he donated.
There must be a better way to get funding than hitting up a patient as part of the care plan. Perhaps discharge materials might include a brochure about how to make a donation, if interested. Or the ubiquitous portal might have a “donate” box in the task bar.
If the patient were to initiate this on his own, I wouldn’t have an issue with it. He gets out of the hospital, is grateful for his care, and calls the physician’s office to say he’d like to make a donation to whatever his program is (or just goes online to do it). That’s fine. I’ve even had the occasional patient call my office to say they’d like to make a donation to my favorite charity, and I give them a list of various neurology research foundations (none of which I’m affiliated with, for the record).
But to actively solicit donations from someone under your care is tasteless and inappropriate. It creates a conflict of interest for both parties.
The patient may believe he’ll get better care, and is obligated to keep giving – or else. The physician may feel like he’s stuck going beyond what’s really needed, ordering unnecessary tests and such to keep the financial VIP happy. And what happens if the big donor patient calls in because he hurt his ankle and needs a Percocet refill that another doctor won’t give him?
The statement by the ACP is appropriate. The only thing that bothers me about it is that it had to be made at all.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I was a resident, on morning rounds. The attending neurologist was young and ambitious (weren’t we all once?), trying to get the hospital to help him fund a research program in his subspecialty of interest.
One of the patients we saw that morning was a locally known successful businessman who’d been admitted, fortunately not for anything too serious.
My attending took the history, verifying the one I’d presented, and examined the gentleman. He then made some teaching points and explained the care plan to the patient.
Pretty standard up to that point.
After answering questions, however, the attending suddenly went into a sales pitch on his new research program, asking the guy for a financial donation, and giving him the card for the person at his office handling the funding.
I don’t remember anymore if he repeated that with other patients, but even now it still leaves a bad taste in my mouth. As a resident I wasn’t in a position to criticize him, nor did I want to endanger my own standing in the program by talking to someone higher up.
He was, fortunately, the only attending I ever worked with who did that. It still stands out in my mind, perhaps as an example of what not to do, and sometimes I still think about it.
Perhaps I’m naive, but I assumed he was an aberration. Apparently not, as the American College of Physicians recently issued a position paper advising its members not to ask patients for donations to the doctor’s workplace. There’s actually an acronym, GPF (Grateful Patient Fundraising) for this.
I understand a lot of these doctors are in academics and need funding for research and other programs. I know that a lot of good comes from this research, and I fully support it.
But this seems to be a bad way of doing it. Standing at the bedside on that long-ago morning, I remember thinking the patient (who looked kind of surprised) was going to wonder if this was a vague sort of hint: You’ll get better care if you pay up. Or a veiled threat that you may not get decent care if you don’t. I have no idea if he donated.
There must be a better way to get funding than hitting up a patient as part of the care plan. Perhaps discharge materials might include a brochure about how to make a donation, if interested. Or the ubiquitous portal might have a “donate” box in the task bar.
If the patient were to initiate this on his own, I wouldn’t have an issue with it. He gets out of the hospital, is grateful for his care, and calls the physician’s office to say he’d like to make a donation to whatever his program is (or just goes online to do it). That’s fine. I’ve even had the occasional patient call my office to say they’d like to make a donation to my favorite charity, and I give them a list of various neurology research foundations (none of which I’m affiliated with, for the record).
But to actively solicit donations from someone under your care is tasteless and inappropriate. It creates a conflict of interest for both parties.
The patient may believe he’ll get better care, and is obligated to keep giving – or else. The physician may feel like he’s stuck going beyond what’s really needed, ordering unnecessary tests and such to keep the financial VIP happy. And what happens if the big donor patient calls in because he hurt his ankle and needs a Percocet refill that another doctor won’t give him?
The statement by the ACP is appropriate. The only thing that bothers me about it is that it had to be made at all.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I was a resident, on morning rounds. The attending neurologist was young and ambitious (weren’t we all once?), trying to get the hospital to help him fund a research program in his subspecialty of interest.
One of the patients we saw that morning was a locally known successful businessman who’d been admitted, fortunately not for anything too serious.
My attending took the history, verifying the one I’d presented, and examined the gentleman. He then made some teaching points and explained the care plan to the patient.
Pretty standard up to that point.
After answering questions, however, the attending suddenly went into a sales pitch on his new research program, asking the guy for a financial donation, and giving him the card for the person at his office handling the funding.
I don’t remember anymore if he repeated that with other patients, but even now it still leaves a bad taste in my mouth. As a resident I wasn’t in a position to criticize him, nor did I want to endanger my own standing in the program by talking to someone higher up.
He was, fortunately, the only attending I ever worked with who did that. It still stands out in my mind, perhaps as an example of what not to do, and sometimes I still think about it.
Perhaps I’m naive, but I assumed he was an aberration. Apparently not, as the American College of Physicians recently issued a position paper advising its members not to ask patients for donations to the doctor’s workplace. There’s actually an acronym, GPF (Grateful Patient Fundraising) for this.
I understand a lot of these doctors are in academics and need funding for research and other programs. I know that a lot of good comes from this research, and I fully support it.
But this seems to be a bad way of doing it. Standing at the bedside on that long-ago morning, I remember thinking the patient (who looked kind of surprised) was going to wonder if this was a vague sort of hint: You’ll get better care if you pay up. Or a veiled threat that you may not get decent care if you don’t. I have no idea if he donated.
There must be a better way to get funding than hitting up a patient as part of the care plan. Perhaps discharge materials might include a brochure about how to make a donation, if interested. Or the ubiquitous portal might have a “donate” box in the task bar.
If the patient were to initiate this on his own, I wouldn’t have an issue with it. He gets out of the hospital, is grateful for his care, and calls the physician’s office to say he’d like to make a donation to whatever his program is (or just goes online to do it). That’s fine. I’ve even had the occasional patient call my office to say they’d like to make a donation to my favorite charity, and I give them a list of various neurology research foundations (none of which I’m affiliated with, for the record).
But to actively solicit donations from someone under your care is tasteless and inappropriate. It creates a conflict of interest for both parties.
The patient may believe he’ll get better care, and is obligated to keep giving – or else. The physician may feel like he’s stuck going beyond what’s really needed, ordering unnecessary tests and such to keep the financial VIP happy. And what happens if the big donor patient calls in because he hurt his ankle and needs a Percocet refill that another doctor won’t give him?
The statement by the ACP is appropriate. The only thing that bothers me about it is that it had to be made at all.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Sleep irregularity
In discussions between health care providers and patients, the words “regularity” and “irregularity” come up primarily in reference to either constipation or menstrual cycles. However, the participants in a recent panel convened by the National Sleep Foundation think we should also be discussing irregularity when we are discussing sleep with our patients.
The sleep experts on the panel began by considering 40,000 papers that directly or tangentially dealt with the topic of irregular sleep patterns. The reviewers uncovered numerous references to an association between sleep irregularity and a wide variety of adverse health outcomes, including obesity and metabolic disorders, hypertension and other cardiovascular disorders, and elevations in several inflammatory markers. Not surprisingly, the investigators also found an abundance of references supporting an association between irregular sleep and a suite of mental health problems, including depression, mood disorders, lower self esteem, poor academic performance, and deficits in attention. For example, several of the studies the panel reviewed found that in college students, GPA was lower when their sleep pattern was irregular. There were some papers that found no significant association between irregular sleep and other adverse health outcomes, but none of the studies demonstrated an association with better or improved health outcomes.

There is currently no universally accepted definition of an irregular sleep pattern. The experts pointed to some papers that used a standard deviation of 1 hour from the patient’s usual bed time determined by averaging over an interval measured in weeks. You and I shouldn’t be surprised that irregular sleep is unhealthy, but the breadth of the panel’s findings is impressive.
Although it has been long in coming, sleep is finally beginning to get some attention by the media. The focus is usually on the optimal number of hours we need each night. This panel’s findings suggest that total sleep time is only part of the story, and may even be less important than the regularity of our sleep patterns.
For those of us in pediatrics, the place where irregularity raises its ugly head is with teenagers and weekends. Although the numbers are far from clear, the question remains of how effective is catch-up sleep after a week of too-early mornings and too-late bedtimes for the chronically under-slept adolescent.
In some studies in which patients had the demonstrable effects of sleep deprivation (e.g., metabolic and cardiovascular) there was some improvement when weekend sleep was extended by 1 or 2 hours, but none beyond 2 hours.
The panel’s findings, while certainly significant, merely add weight and nuance to the existing evidence of importance of sleep and the damage done by sleep deprivation. As one of the panel members has said, “Sleep is the third pillar of health, equally important as diet and exercise, if not more.” However, this message is not getting out, or at least it is not being heeded. Like obesity, our efforts as advisers to our patients isn’t working. Unfortunately, this is because our advice is often whispered and given halfheartedly.
There was some evidence of improvement as a result of the pandemic, when those fortunate enough to be able to work from home were taking advantage of the flexibility in their schedules and getting more sleep. But health care providers certainly can’t take responsibility for what was an accident of nature.
Those of you who have been reading Letters from Maine for the last 3 decades may tire of my beating the tired horse of sleep deprivation. But I will not be deterred. I see very little evidence among health care professionals in taking the importance of sleep seriously. Sure, they may include it buried in the list of potential contributors to their patient’s complaint, but I see very little effort to move it higher on their list of priorities and almost no movement toward making substantive recommendations and then reinforcing them with follow-up.
Like obesity, sleep deprivation is a societal problem. We can lay some of the blame on Thomas Edison, but Until that time you will continue to read columns like this one when I encounter significant studies on the importance of sleep.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
In discussions between health care providers and patients, the words “regularity” and “irregularity” come up primarily in reference to either constipation or menstrual cycles. However, the participants in a recent panel convened by the National Sleep Foundation think we should also be discussing irregularity when we are discussing sleep with our patients.
The sleep experts on the panel began by considering 40,000 papers that directly or tangentially dealt with the topic of irregular sleep patterns. The reviewers uncovered numerous references to an association between sleep irregularity and a wide variety of adverse health outcomes, including obesity and metabolic disorders, hypertension and other cardiovascular disorders, and elevations in several inflammatory markers. Not surprisingly, the investigators also found an abundance of references supporting an association between irregular sleep and a suite of mental health problems, including depression, mood disorders, lower self esteem, poor academic performance, and deficits in attention. For example, several of the studies the panel reviewed found that in college students, GPA was lower when their sleep pattern was irregular. There were some papers that found no significant association between irregular sleep and other adverse health outcomes, but none of the studies demonstrated an association with better or improved health outcomes.
There is currently no universally accepted definition of an irregular sleep pattern. The experts pointed to some papers that used a standard deviation of 1 hour from the patient’s usual bed time determined by averaging over an interval measured in weeks. You and I shouldn’t be surprised that irregular sleep is unhealthy, but the breadth of the panel’s findings is impressive.
Although it has been long in coming, sleep is finally beginning to get some attention by the media. The focus is usually on the optimal number of hours we need each night. This panel’s findings suggest that total sleep time is only part of the story, and may even be less important than the regularity of our sleep patterns.
For those of us in pediatrics, the place where irregularity raises its ugly head is with teenagers and weekends. Although the numbers are far from clear, the question remains of how effective is catch-up sleep after a week of too-early mornings and too-late bedtimes for the chronically under-slept adolescent.
In some studies in which patients had the demonstrable effects of sleep deprivation (e.g., metabolic and cardiovascular) there was some improvement when weekend sleep was extended by 1 or 2 hours, but none beyond 2 hours.
The panel’s findings, while certainly significant, merely add weight and nuance to the existing evidence of importance of sleep and the damage done by sleep deprivation. As one of the panel members has said, “Sleep is the third pillar of health, equally important as diet and exercise, if not more.” However, this message is not getting out, or at least it is not being heeded. Like obesity, our efforts as advisers to our patients isn’t working. Unfortunately, this is because our advice is often whispered and given halfheartedly.
There was some evidence of improvement as a result of the pandemic, when those fortunate enough to be able to work from home were taking advantage of the flexibility in their schedules and getting more sleep. But health care providers certainly can’t take responsibility for what was an accident of nature.
Those of you who have been reading Letters from Maine for the last 3 decades may tire of my beating the tired horse of sleep deprivation. But I will not be deterred. I see very little evidence among health care professionals in taking the importance of sleep seriously. Sure, they may include it buried in the list of potential contributors to their patient’s complaint, but I see very little effort to move it higher on their list of priorities and almost no movement toward making substantive recommendations and then reinforcing them with follow-up.
Like obesity, sleep deprivation is a societal problem. We can lay some of the blame on Thomas Edison, but Until that time you will continue to read columns like this one when I encounter significant studies on the importance of sleep.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
In discussions between health care providers and patients, the words “regularity” and “irregularity” come up primarily in reference to either constipation or menstrual cycles. However, the participants in a recent panel convened by the National Sleep Foundation think we should also be discussing irregularity when we are discussing sleep with our patients.
The sleep experts on the panel began by considering 40,000 papers that directly or tangentially dealt with the topic of irregular sleep patterns. The reviewers uncovered numerous references to an association between sleep irregularity and a wide variety of adverse health outcomes, including obesity and metabolic disorders, hypertension and other cardiovascular disorders, and elevations in several inflammatory markers. Not surprisingly, the investigators also found an abundance of references supporting an association between irregular sleep and a suite of mental health problems, including depression, mood disorders, lower self esteem, poor academic performance, and deficits in attention. For example, several of the studies the panel reviewed found that in college students, GPA was lower when their sleep pattern was irregular. There were some papers that found no significant association between irregular sleep and other adverse health outcomes, but none of the studies demonstrated an association with better or improved health outcomes.
There is currently no universally accepted definition of an irregular sleep pattern. The experts pointed to some papers that used a standard deviation of 1 hour from the patient’s usual bed time determined by averaging over an interval measured in weeks. You and I shouldn’t be surprised that irregular sleep is unhealthy, but the breadth of the panel’s findings is impressive.
Although it has been long in coming, sleep is finally beginning to get some attention by the media. The focus is usually on the optimal number of hours we need each night. This panel’s findings suggest that total sleep time is only part of the story, and may even be less important than the regularity of our sleep patterns.
For those of us in pediatrics, the place where irregularity raises its ugly head is with teenagers and weekends. Although the numbers are far from clear, the question remains of how effective is catch-up sleep after a week of too-early mornings and too-late bedtimes for the chronically under-slept adolescent.
In some studies in which patients had the demonstrable effects of sleep deprivation (e.g., metabolic and cardiovascular) there was some improvement when weekend sleep was extended by 1 or 2 hours, but none beyond 2 hours.
The panel’s findings, while certainly significant, merely add weight and nuance to the existing evidence of importance of sleep and the damage done by sleep deprivation. As one of the panel members has said, “Sleep is the third pillar of health, equally important as diet and exercise, if not more.” However, this message is not getting out, or at least it is not being heeded. Like obesity, our efforts as advisers to our patients isn’t working. Unfortunately, this is because our advice is often whispered and given halfheartedly.
There was some evidence of improvement as a result of the pandemic, when those fortunate enough to be able to work from home were taking advantage of the flexibility in their schedules and getting more sleep. But health care providers certainly can’t take responsibility for what was an accident of nature.
Those of you who have been reading Letters from Maine for the last 3 decades may tire of my beating the tired horse of sleep deprivation. But I will not be deterred. I see very little evidence among health care professionals in taking the importance of sleep seriously. Sure, they may include it buried in the list of potential contributors to their patient’s complaint, but I see very little effort to move it higher on their list of priorities and almost no movement toward making substantive recommendations and then reinforcing them with follow-up.
Like obesity, sleep deprivation is a societal problem. We can lay some of the blame on Thomas Edison, but Until that time you will continue to read columns like this one when I encounter significant studies on the importance of sleep.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Burnout in medical profession higher among women, younger clinicians
The poster child for a burned-out physician is a young woman practicing in primary care, according to a new study of more than 1,300 clinicians.
The study, published in JAMA Network Open. investigated patterns in physician burnout among 1,373 physicians at Massachusetts General Physicians Organization, a hospital-owned group practice. It assessed burnout in 3 years: 2017, 2019, and 2021.
Respondents were queried about their satisfaction with their career and compensation, as well as their well-being, administrative workload, and leadership and diversity.
Female physicians exhibited a higher burnout rate than male physicians (odds ratio, 1.47; 95% confidence interval, 1.02-2.12), while among primary care physicians (PCPs), the burnout rate was almost three times higher than among those in internal medicine (OR, 2.82; 95% CI, 1.76-4.50). Among physicians with 30 or more years of experience, the burnout rate was lower than among those with 10 years of experience or less (OR, 0.21; 95% CI, 0.13-0.35).
The fact that burnout disproportionately affects female physicians could reflect the additional household and family obligations women are often expected to handle, as well as their desire to form relationships with their patients, according to Timothy Hoff, PhD, a professor of management, healthcare systems, and health policy at Northeastern University, Boston.
“Female physicians tend to practice differently than their male counterparts,” said Dr. Hoff, who studies primary care. “They may focus more on the relational aspects of care, and that could lead to a higher rate of burnout.”
The study used the Maslach Burnout Inventory and three burnout subscales: exhaustion, cynicism, and reduced personal efficacy. The cohort was composed of 50% men, 67% White respondents, and 87% non-Hispanic respondents. A little over two-thirds of physicians had from 11 to 20 years of experience.
About 93% of those surveyed responded; by comparison, response rates were between 27% and 32% in previous analyses of physician burnout, the study authors say. They attribute this high participation rate to the fact that they compensated each participant with $850, more than is usually offered.
Hilton Gomes, MD, a partner at a concierge primary care practice in Miami – who has been practicing medicine for more than 15 years – said the increased rates of burnout among his younger colleagues are partly the result of a recent shift in what is considered the ideal work-life balance.
“Younger generations of doctors enter the profession with a strong desire for a better work-life balance. Unfortunately, medicine does not typically lend itself to achieving this balance,” he said.
Dr. Gomes recalled a time in medical school when he tried to visit his former pediatrician, who couldn’t be found at home.
“His wife informed me that he was tending to an urgent sick visit at the hospital, while his wife had to deal with their own grandson’s fracture being treated at urgent care,” Dr. Gomes said. “This illustrates, in my experience, how older generations of physicians accepted the demands of the profession as part of their commitment, and this often involved putting our own families second.”
Dr. Gomes, like many other PCPs who have converted to concierge medicine, previously worked at a practice where he saw nearly two dozen patients a day for a maximum of 15 minutes each.
“The structure of managed care often results in primary care physicians spending less time with patients and more time on paperwork, which is not the reason why physicians enter the field of medicine,” Dr. Gomes said.
Physicians are not alone in their feelings of physical and mental exhaustion. In the Medscape Physician Assistant Burnout Report 2023, 16% of respondents said the burnout they experienced was so severe that they were thinking of leaving medicine.
In 2022, PCP burnout cost the United States $260 million in excess health care expenditures. Burnout has also increased rates of physician suicide over the past 50 years and has led to a rise in medical errors.
Physicians say that programs that teach them to perform yoga and take deep breaths – which are offered by their employers – are not the solution.
“We sort of know what the realities of physician burnout are now; the imperative is to address it,” Dr. Hoff said. “We need studies that focus on the concepts of sustainability.”
The study was funded by the Massachusetts General Physicians Organization. A coauthor reports receiving a grant from the American Heart Association. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
The poster child for a burned-out physician is a young woman practicing in primary care, according to a new study of more than 1,300 clinicians.
The study, published in JAMA Network Open. investigated patterns in physician burnout among 1,373 physicians at Massachusetts General Physicians Organization, a hospital-owned group practice. It assessed burnout in 3 years: 2017, 2019, and 2021.
Respondents were queried about their satisfaction with their career and compensation, as well as their well-being, administrative workload, and leadership and diversity.
Female physicians exhibited a higher burnout rate than male physicians (odds ratio, 1.47; 95% confidence interval, 1.02-2.12), while among primary care physicians (PCPs), the burnout rate was almost three times higher than among those in internal medicine (OR, 2.82; 95% CI, 1.76-4.50). Among physicians with 30 or more years of experience, the burnout rate was lower than among those with 10 years of experience or less (OR, 0.21; 95% CI, 0.13-0.35).
The fact that burnout disproportionately affects female physicians could reflect the additional household and family obligations women are often expected to handle, as well as their desire to form relationships with their patients, according to Timothy Hoff, PhD, a professor of management, healthcare systems, and health policy at Northeastern University, Boston.
“Female physicians tend to practice differently than their male counterparts,” said Dr. Hoff, who studies primary care. “They may focus more on the relational aspects of care, and that could lead to a higher rate of burnout.”
The study used the Maslach Burnout Inventory and three burnout subscales: exhaustion, cynicism, and reduced personal efficacy. The cohort was composed of 50% men, 67% White respondents, and 87% non-Hispanic respondents. A little over two-thirds of physicians had from 11 to 20 years of experience.
About 93% of those surveyed responded; by comparison, response rates were between 27% and 32% in previous analyses of physician burnout, the study authors say. They attribute this high participation rate to the fact that they compensated each participant with $850, more than is usually offered.
Hilton Gomes, MD, a partner at a concierge primary care practice in Miami – who has been practicing medicine for more than 15 years – said the increased rates of burnout among his younger colleagues are partly the result of a recent shift in what is considered the ideal work-life balance.
“Younger generations of doctors enter the profession with a strong desire for a better work-life balance. Unfortunately, medicine does not typically lend itself to achieving this balance,” he said.
Dr. Gomes recalled a time in medical school when he tried to visit his former pediatrician, who couldn’t be found at home.
“His wife informed me that he was tending to an urgent sick visit at the hospital, while his wife had to deal with their own grandson’s fracture being treated at urgent care,” Dr. Gomes said. “This illustrates, in my experience, how older generations of physicians accepted the demands of the profession as part of their commitment, and this often involved putting our own families second.”
Dr. Gomes, like many other PCPs who have converted to concierge medicine, previously worked at a practice where he saw nearly two dozen patients a day for a maximum of 15 minutes each.
“The structure of managed care often results in primary care physicians spending less time with patients and more time on paperwork, which is not the reason why physicians enter the field of medicine,” Dr. Gomes said.
Physicians are not alone in their feelings of physical and mental exhaustion. In the Medscape Physician Assistant Burnout Report 2023, 16% of respondents said the burnout they experienced was so severe that they were thinking of leaving medicine.
In 2022, PCP burnout cost the United States $260 million in excess health care expenditures. Burnout has also increased rates of physician suicide over the past 50 years and has led to a rise in medical errors.
Physicians say that programs that teach them to perform yoga and take deep breaths – which are offered by their employers – are not the solution.
“We sort of know what the realities of physician burnout are now; the imperative is to address it,” Dr. Hoff said. “We need studies that focus on the concepts of sustainability.”
The study was funded by the Massachusetts General Physicians Organization. A coauthor reports receiving a grant from the American Heart Association. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
The poster child for a burned-out physician is a young woman practicing in primary care, according to a new study of more than 1,300 clinicians.
The study, published in JAMA Network Open. investigated patterns in physician burnout among 1,373 physicians at Massachusetts General Physicians Organization, a hospital-owned group practice. It assessed burnout in 3 years: 2017, 2019, and 2021.
Respondents were queried about their satisfaction with their career and compensation, as well as their well-being, administrative workload, and leadership and diversity.
Female physicians exhibited a higher burnout rate than male physicians (odds ratio, 1.47; 95% confidence interval, 1.02-2.12), while among primary care physicians (PCPs), the burnout rate was almost three times higher than among those in internal medicine (OR, 2.82; 95% CI, 1.76-4.50). Among physicians with 30 or more years of experience, the burnout rate was lower than among those with 10 years of experience or less (OR, 0.21; 95% CI, 0.13-0.35).
The fact that burnout disproportionately affects female physicians could reflect the additional household and family obligations women are often expected to handle, as well as their desire to form relationships with their patients, according to Timothy Hoff, PhD, a professor of management, healthcare systems, and health policy at Northeastern University, Boston.
“Female physicians tend to practice differently than their male counterparts,” said Dr. Hoff, who studies primary care. “They may focus more on the relational aspects of care, and that could lead to a higher rate of burnout.”
The study used the Maslach Burnout Inventory and three burnout subscales: exhaustion, cynicism, and reduced personal efficacy. The cohort was composed of 50% men, 67% White respondents, and 87% non-Hispanic respondents. A little over two-thirds of physicians had from 11 to 20 years of experience.
About 93% of those surveyed responded; by comparison, response rates were between 27% and 32% in previous analyses of physician burnout, the study authors say. They attribute this high participation rate to the fact that they compensated each participant with $850, more than is usually offered.
Hilton Gomes, MD, a partner at a concierge primary care practice in Miami – who has been practicing medicine for more than 15 years – said the increased rates of burnout among his younger colleagues are partly the result of a recent shift in what is considered the ideal work-life balance.
“Younger generations of doctors enter the profession with a strong desire for a better work-life balance. Unfortunately, medicine does not typically lend itself to achieving this balance,” he said.
Dr. Gomes recalled a time in medical school when he tried to visit his former pediatrician, who couldn’t be found at home.
“His wife informed me that he was tending to an urgent sick visit at the hospital, while his wife had to deal with their own grandson’s fracture being treated at urgent care,” Dr. Gomes said. “This illustrates, in my experience, how older generations of physicians accepted the demands of the profession as part of their commitment, and this often involved putting our own families second.”
Dr. Gomes, like many other PCPs who have converted to concierge medicine, previously worked at a practice where he saw nearly two dozen patients a day for a maximum of 15 minutes each.
“The structure of managed care often results in primary care physicians spending less time with patients and more time on paperwork, which is not the reason why physicians enter the field of medicine,” Dr. Gomes said.
Physicians are not alone in their feelings of physical and mental exhaustion. In the Medscape Physician Assistant Burnout Report 2023, 16% of respondents said the burnout they experienced was so severe that they were thinking of leaving medicine.
In 2022, PCP burnout cost the United States $260 million in excess health care expenditures. Burnout has also increased rates of physician suicide over the past 50 years and has led to a rise in medical errors.
Physicians say that programs that teach them to perform yoga and take deep breaths – which are offered by their employers – are not the solution.
“We sort of know what the realities of physician burnout are now; the imperative is to address it,” Dr. Hoff said. “We need studies that focus on the concepts of sustainability.”
The study was funded by the Massachusetts General Physicians Organization. A coauthor reports receiving a grant from the American Heart Association. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
MASLD linked to increased risk for various clinical outcomes
TOPLINE:
Metabolic dysfunction–associated steatotic liver disease (MASLD) significantly raises the risk for cardiovascular, metabolic, oncologic, and other outcomes, a new meta-analysis suggests.
METHODOLOGY:
- Researchers conducted a comprehensive meta-analysis of studies to investigate longitudinal clinical outcomes associated with MASLD, previously known as nonalcoholic fatty liver disease.
- They identified 129 original studies that evaluated the longitudinal risks for incident clinical outcomes in patients with MASLD vs those without the disease.
- Investigators calculated pooled risk estimates for clinical outcomes in patients with MASLD and those without MASLD, with MASLD being diagnosed by imaging, biopsy, blood tests, or ICD codes.
TAKEAWAY:
- MASLD was associated with a significant increased risk for cardiovascular disease outcomes (hazard ratio, 1.43), metabolic outcomes such as incident hypertension (HR, 1.75), prediabetes (HR, 1.69), diabetes (HR, 2.56), metabolic syndrome (HR, 2.57), chronic kidney disease (HR, 1.38), and various liver-related outcomes (HR, 3.92).
- Patients with advanced MASLD had a significantly greater risk (P = .02) of developing diabetes than did their peers with less severe MASLD (HR, 1.63), compared with persons without MASLD.
- MASLD was also associated with all cancers (HR, 1.54); the highest risk was seen for hepatocellular carcinoma (HR, 4.37).
- Subgroup analyses stratified by sex found no significant differences in the risks observed between men and women with MASLD.
IN PRACTICE:
“It is imperative to understand that MASLD is a complex and multifaceted condition that requires a comprehensive approach to recognition and treatment beyond that of the hepatologist alone,” the authors wrote. “The growing prevalence of MASLD will remain a major global health threat that requires effective disease management frameworks to be put in place.”
SOURCE:
The study, with co–first authors Kai En Chan and Elden Yen Hng Ong, National University of Singapore, was published online in Clinical Gastroenterology and Hepatology.
LIMITATIONS:
The results depend on the validity of the original studies, and residual confounding factors may have biased the reported results. The study is also limited in its inclusion of large population-based studies using ICD codes that may result in misclassification bias. There was no examination of longitudinal outcomes in patients with histologically confirmed MASLD.
DISCLOSURES:
The study had no funding. Some authors reported research support, consulting fees, or stock options from pharmaceutical companies.
A version of this article appeared on Medscape.com.
TOPLINE:
Metabolic dysfunction–associated steatotic liver disease (MASLD) significantly raises the risk for cardiovascular, metabolic, oncologic, and other outcomes, a new meta-analysis suggests.
METHODOLOGY:
- Researchers conducted a comprehensive meta-analysis of studies to investigate longitudinal clinical outcomes associated with MASLD, previously known as nonalcoholic fatty liver disease.
- They identified 129 original studies that evaluated the longitudinal risks for incident clinical outcomes in patients with MASLD vs those without the disease.
- Investigators calculated pooled risk estimates for clinical outcomes in patients with MASLD and those without MASLD, with MASLD being diagnosed by imaging, biopsy, blood tests, or ICD codes.
TAKEAWAY:
- MASLD was associated with a significant increased risk for cardiovascular disease outcomes (hazard ratio, 1.43), metabolic outcomes such as incident hypertension (HR, 1.75), prediabetes (HR, 1.69), diabetes (HR, 2.56), metabolic syndrome (HR, 2.57), chronic kidney disease (HR, 1.38), and various liver-related outcomes (HR, 3.92).
- Patients with advanced MASLD had a significantly greater risk (P = .02) of developing diabetes than did their peers with less severe MASLD (HR, 1.63), compared with persons without MASLD.
- MASLD was also associated with all cancers (HR, 1.54); the highest risk was seen for hepatocellular carcinoma (HR, 4.37).
- Subgroup analyses stratified by sex found no significant differences in the risks observed between men and women with MASLD.
IN PRACTICE:
“It is imperative to understand that MASLD is a complex and multifaceted condition that requires a comprehensive approach to recognition and treatment beyond that of the hepatologist alone,” the authors wrote. “The growing prevalence of MASLD will remain a major global health threat that requires effective disease management frameworks to be put in place.”
SOURCE:
The study, with co–first authors Kai En Chan and Elden Yen Hng Ong, National University of Singapore, was published online in Clinical Gastroenterology and Hepatology.
LIMITATIONS:
The results depend on the validity of the original studies, and residual confounding factors may have biased the reported results. The study is also limited in its inclusion of large population-based studies using ICD codes that may result in misclassification bias. There was no examination of longitudinal outcomes in patients with histologically confirmed MASLD.
DISCLOSURES:
The study had no funding. Some authors reported research support, consulting fees, or stock options from pharmaceutical companies.
A version of this article appeared on Medscape.com.
TOPLINE:
Metabolic dysfunction–associated steatotic liver disease (MASLD) significantly raises the risk for cardiovascular, metabolic, oncologic, and other outcomes, a new meta-analysis suggests.
METHODOLOGY:
- Researchers conducted a comprehensive meta-analysis of studies to investigate longitudinal clinical outcomes associated with MASLD, previously known as nonalcoholic fatty liver disease.
- They identified 129 original studies that evaluated the longitudinal risks for incident clinical outcomes in patients with MASLD vs those without the disease.
- Investigators calculated pooled risk estimates for clinical outcomes in patients with MASLD and those without MASLD, with MASLD being diagnosed by imaging, biopsy, blood tests, or ICD codes.
TAKEAWAY:
- MASLD was associated with a significant increased risk for cardiovascular disease outcomes (hazard ratio, 1.43), metabolic outcomes such as incident hypertension (HR, 1.75), prediabetes (HR, 1.69), diabetes (HR, 2.56), metabolic syndrome (HR, 2.57), chronic kidney disease (HR, 1.38), and various liver-related outcomes (HR, 3.92).
- Patients with advanced MASLD had a significantly greater risk (P = .02) of developing diabetes than did their peers with less severe MASLD (HR, 1.63), compared with persons without MASLD.
- MASLD was also associated with all cancers (HR, 1.54); the highest risk was seen for hepatocellular carcinoma (HR, 4.37).
- Subgroup analyses stratified by sex found no significant differences in the risks observed between men and women with MASLD.
IN PRACTICE:
“It is imperative to understand that MASLD is a complex and multifaceted condition that requires a comprehensive approach to recognition and treatment beyond that of the hepatologist alone,” the authors wrote. “The growing prevalence of MASLD will remain a major global health threat that requires effective disease management frameworks to be put in place.”
SOURCE:
The study, with co–first authors Kai En Chan and Elden Yen Hng Ong, National University of Singapore, was published online in Clinical Gastroenterology and Hepatology.
LIMITATIONS:
The results depend on the validity of the original studies, and residual confounding factors may have biased the reported results. The study is also limited in its inclusion of large population-based studies using ICD codes that may result in misclassification bias. There was no examination of longitudinal outcomes in patients with histologically confirmed MASLD.
DISCLOSURES:
The study had no funding. Some authors reported research support, consulting fees, or stock options from pharmaceutical companies.
A version of this article appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Home-based exercise benefits patients with PAD
TOPLINE:
Compared with supervised treadmill workouts at a gym, which is considered first-line therapy for walking impairment in lower extremity peripheral artery disease (PAD), exercising at home significantly improves 6-minute walking (6MW) distance, but not maximal treadmill walking distance, results of a new meta-analysis show.
METHODOLOGY:
- The analysis included five randomized clinical trials with a total of 719 participants, mean age 68.6 years, all led by researchers at Northwestern University, Chicago, that compared either supervised treadmill or home-based walking exercise with a nonexercise control group in people with PAD (defined as Ankle Brachial Index ≤ 0.90).
- All trials measured 6-minute walk (6MW) distance (walking as far as possible in 6 minutes), treadmill walking performance, and outcomes from the Walking Impairment Questionnaire (WIQ), which includes distance, walking speed, and stair-climbing domains, at baseline and at 6 months.
- Supervised treadmill exercise interventions included three individualized exercise sessions per week with an exercise physiologist at an exercise center, and home-based exercises involved walking near home 5 days per week, both for up to 50 minutes per session.
TAKEAWAY:
- After adjusting for study, age, sex, race, smoking, history of myocardial infarction, heart failure, and baseline 6MW distance, the study found both exercise interventions were better than nonexercise controls for 6MW distance.
- Compared with supervised treadmill exercise, home-based walking was associated with significantly improved mean 6MW distance (31.8 m vs. 55.6 m; adjusted between-group difference: −23.8 m; 95% confidence interval, −44.0 to −3.6; P = .021), and significantly improved WIQ walking speed score.
- However, home-based walking was associated with significantly less improvement in maximal treadmill walking distance, compared with supervised treadmill exercise (adjusted between-group difference: 132.5 m; 95% CI, 72.1-192.9; P < .001).
IN PRACTICE:
Home-based walking exercise “circumvents” barriers to accessing supervised exercise such as having to travel to a facility, said the authors, who noted the new data “demonstrated a large and consistent effect of home-based walking exercise on improved 6MW distance and also significantly improved the WIQ walking speed score, compared with supervised treadmill exercise.”
SOURCE:
The study was conducted by Neela D. Thangada, MD, Northwestern University, Chicago, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
Data were combined from different randomized clinical trials that were led by one investigative team, and reported comparisons were not prespecified. Comparisons between supervised and home-based exercise lacked statistical power for the WIQ distance and stair-climbing measures.
DISCLOSURES:
The study was sponsored by the National Center for Research Resources and the National Heart, Lung, and Blood Institute of the National Institutes of Health. Dr. Thangada reports no relevant financial relationships. Disclosures for study coauthors can be found with the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
Compared with supervised treadmill workouts at a gym, which is considered first-line therapy for walking impairment in lower extremity peripheral artery disease (PAD), exercising at home significantly improves 6-minute walking (6MW) distance, but not maximal treadmill walking distance, results of a new meta-analysis show.
METHODOLOGY:
- The analysis included five randomized clinical trials with a total of 719 participants, mean age 68.6 years, all led by researchers at Northwestern University, Chicago, that compared either supervised treadmill or home-based walking exercise with a nonexercise control group in people with PAD (defined as Ankle Brachial Index ≤ 0.90).
- All trials measured 6-minute walk (6MW) distance (walking as far as possible in 6 minutes), treadmill walking performance, and outcomes from the Walking Impairment Questionnaire (WIQ), which includes distance, walking speed, and stair-climbing domains, at baseline and at 6 months.
- Supervised treadmill exercise interventions included three individualized exercise sessions per week with an exercise physiologist at an exercise center, and home-based exercises involved walking near home 5 days per week, both for up to 50 minutes per session.
TAKEAWAY:
- After adjusting for study, age, sex, race, smoking, history of myocardial infarction, heart failure, and baseline 6MW distance, the study found both exercise interventions were better than nonexercise controls for 6MW distance.
- Compared with supervised treadmill exercise, home-based walking was associated with significantly improved mean 6MW distance (31.8 m vs. 55.6 m; adjusted between-group difference: −23.8 m; 95% confidence interval, −44.0 to −3.6; P = .021), and significantly improved WIQ walking speed score.
- However, home-based walking was associated with significantly less improvement in maximal treadmill walking distance, compared with supervised treadmill exercise (adjusted between-group difference: 132.5 m; 95% CI, 72.1-192.9; P < .001).
IN PRACTICE:
Home-based walking exercise “circumvents” barriers to accessing supervised exercise such as having to travel to a facility, said the authors, who noted the new data “demonstrated a large and consistent effect of home-based walking exercise on improved 6MW distance and also significantly improved the WIQ walking speed score, compared with supervised treadmill exercise.”
SOURCE:
The study was conducted by Neela D. Thangada, MD, Northwestern University, Chicago, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
Data were combined from different randomized clinical trials that were led by one investigative team, and reported comparisons were not prespecified. Comparisons between supervised and home-based exercise lacked statistical power for the WIQ distance and stair-climbing measures.
DISCLOSURES:
The study was sponsored by the National Center for Research Resources and the National Heart, Lung, and Blood Institute of the National Institutes of Health. Dr. Thangada reports no relevant financial relationships. Disclosures for study coauthors can be found with the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
Compared with supervised treadmill workouts at a gym, which is considered first-line therapy for walking impairment in lower extremity peripheral artery disease (PAD), exercising at home significantly improves 6-minute walking (6MW) distance, but not maximal treadmill walking distance, results of a new meta-analysis show.
METHODOLOGY:
- The analysis included five randomized clinical trials with a total of 719 participants, mean age 68.6 years, all led by researchers at Northwestern University, Chicago, that compared either supervised treadmill or home-based walking exercise with a nonexercise control group in people with PAD (defined as Ankle Brachial Index ≤ 0.90).
- All trials measured 6-minute walk (6MW) distance (walking as far as possible in 6 minutes), treadmill walking performance, and outcomes from the Walking Impairment Questionnaire (WIQ), which includes distance, walking speed, and stair-climbing domains, at baseline and at 6 months.
- Supervised treadmill exercise interventions included three individualized exercise sessions per week with an exercise physiologist at an exercise center, and home-based exercises involved walking near home 5 days per week, both for up to 50 minutes per session.
TAKEAWAY:
- After adjusting for study, age, sex, race, smoking, history of myocardial infarction, heart failure, and baseline 6MW distance, the study found both exercise interventions were better than nonexercise controls for 6MW distance.
- Compared with supervised treadmill exercise, home-based walking was associated with significantly improved mean 6MW distance (31.8 m vs. 55.6 m; adjusted between-group difference: −23.8 m; 95% confidence interval, −44.0 to −3.6; P = .021), and significantly improved WIQ walking speed score.
- However, home-based walking was associated with significantly less improvement in maximal treadmill walking distance, compared with supervised treadmill exercise (adjusted between-group difference: 132.5 m; 95% CI, 72.1-192.9; P < .001).
IN PRACTICE:
Home-based walking exercise “circumvents” barriers to accessing supervised exercise such as having to travel to a facility, said the authors, who noted the new data “demonstrated a large and consistent effect of home-based walking exercise on improved 6MW distance and also significantly improved the WIQ walking speed score, compared with supervised treadmill exercise.”
SOURCE:
The study was conducted by Neela D. Thangada, MD, Northwestern University, Chicago, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
Data were combined from different randomized clinical trials that were led by one investigative team, and reported comparisons were not prespecified. Comparisons between supervised and home-based exercise lacked statistical power for the WIQ distance and stair-climbing measures.
DISCLOSURES:
The study was sponsored by the National Center for Research Resources and the National Heart, Lung, and Blood Institute of the National Institutes of Health. Dr. Thangada reports no relevant financial relationships. Disclosures for study coauthors can be found with the original article.
A version of this article first appeared on Medscape.com.
A new clue into the cause, spread of Parkinson’s disease?
.
While defects in mitochondrial functions and in mitochondrial DNA have been implicated in PD in the past, the current study demonstrates “for the first time how damaged mitochondrial DNA can underlie the mechanisms of PD initiation and spread in brain,” lead investigator Shohreh Issazadeh-Navikas, PhD, with the University of Copenhagen, told this news organization.
“This has direct implication for clinical diagnosis” – if damaged mtDNA can be detected in blood, it could serve as an early biomarker for disease, she explained.
The study was published online in Molecular Psychiatry.
“Infectious-like” spread of PD pathology
In earlier work, the researchers identified dysregulated interferon-beta (IFN-beta) signaling as a “top candidate pathway” associated with sporadic PD and its progression to PD with dementia (PDD).
In mice PD models that were deficient in IFN-beta signaling, the investigators showed that neuronal IFN-beta is required to maintain mitochondrial homeostasis and metabolism.
Lack of neuronal IFN-beta or disruption of its downstream signaling causes the accumulation of damaged mitochondria with excessive oxidative stress and insufficient adenosine triphosphate production.
In the current study, using postmortem brain tissue samples from patients with sporadic PD, they confirmed that there were deletions of mtDNA in the medial frontal gyrus, a region implicated in cognitive impairments in PD, suggesting a potential role of damaged mtDNA in disease pathophysiology.
They also identified mtDNA deletions in a “hotspot” in complex I respiratory chain subunits that were associated with dysregulation of oxidative stress and DNA damage response pathways in cohorts with sporadic PD and PDD.
They confirmed the contribution of mtDNA damage to PD pathology in the PD mouse models. They showed that lack of neuronal IFN-beta signaling leads to oxidative damage and mutations in mtDNA in neurons, which are subsequently released outside the neurons.
Injecting damaged mtDNA into mouse brain induced PDD-like behavioral symptoms, including neuropsychiatric, motor, and cognitive impairments. It also caused neurodegeneration in brain regions distant from the injection site, suggesting that damaged mtDNA triggers spread of PDD characteristics in an “infectious-like” manner, the researchers report.
Further study revealed that the mechanism through which damaged mtDNA causes pathology in healthy neurons involves dual activation of Toll-like receptor (TLR) 9 and 4 pathways, leading to increased oxidative stress and neuronal cell death, respectively.
“Our proteomic analysis of extracellular vesicles containing damaged mtDNA identified the TLR4 activator, ribosomal protein S3, as a key protein involved in recognizing and extruding damaged mtDNA,” the investigators write.
In the future they plan to investigate how mtDNA damage can serve as a predictive marker for different disease stages and progression and to explore potential therapeutic strategies aimed at restoring normal mitochondrial function to rectify the mitochondrial dysfunctions implicated in PD.
Making a comeback?
Commenting on the research for this news organization, James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, noted that the role of mitochondria in PD is “like a starlet that burst onto the scene in the 80s, faded into obscurity, and through diligence and continued research has moved beyond being a solid character actor and is reemerging as a force to reckon with.
“This paper only adds to the allure that mitochondria may have in contributing to PD by providing evidence of a novel process by which mitochondria may be not only contributing to PD and loss of dopamine neurons but may play a larger role in the subsequent effects that many people with PD experience – dementia,” Dr. Beck said.
He noted that the authors identified several proteins as facilitating the neurodegeneration that is wrought by damaged mitochondrial DNA.
“These could be potential targets for future drug development. In addition, this work implicates alterations in immune signaling and drugs in development to target inflammatory responses may also bring ancillary benefit,” Dr. Beck said.
However, he said, “while very interesting findings, this is really the first effort that demonstrates how damaged mitochondrial DNA may contribute to neurodegeneration in the context of PD and PD dementia. Further work needs to validate these findings as well as to elucidate mechanisms underlying the propagation of the mitochondrial DNA from cell to cell.”
Funding for this research was provided by the European Union’s Horizon 2020 Research and Innovation Program, the Lundbeck Foundation, and the Danish Council for Independent Research–Medicine. Dr. Issazadeh-Navikas and Dr. Beck have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
.
While defects in mitochondrial functions and in mitochondrial DNA have been implicated in PD in the past, the current study demonstrates “for the first time how damaged mitochondrial DNA can underlie the mechanisms of PD initiation and spread in brain,” lead investigator Shohreh Issazadeh-Navikas, PhD, with the University of Copenhagen, told this news organization.
“This has direct implication for clinical diagnosis” – if damaged mtDNA can be detected in blood, it could serve as an early biomarker for disease, she explained.
The study was published online in Molecular Psychiatry.
“Infectious-like” spread of PD pathology
In earlier work, the researchers identified dysregulated interferon-beta (IFN-beta) signaling as a “top candidate pathway” associated with sporadic PD and its progression to PD with dementia (PDD).
In mice PD models that were deficient in IFN-beta signaling, the investigators showed that neuronal IFN-beta is required to maintain mitochondrial homeostasis and metabolism.
Lack of neuronal IFN-beta or disruption of its downstream signaling causes the accumulation of damaged mitochondria with excessive oxidative stress and insufficient adenosine triphosphate production.
In the current study, using postmortem brain tissue samples from patients with sporadic PD, they confirmed that there were deletions of mtDNA in the medial frontal gyrus, a region implicated in cognitive impairments in PD, suggesting a potential role of damaged mtDNA in disease pathophysiology.
They also identified mtDNA deletions in a “hotspot” in complex I respiratory chain subunits that were associated with dysregulation of oxidative stress and DNA damage response pathways in cohorts with sporadic PD and PDD.
They confirmed the contribution of mtDNA damage to PD pathology in the PD mouse models. They showed that lack of neuronal IFN-beta signaling leads to oxidative damage and mutations in mtDNA in neurons, which are subsequently released outside the neurons.
Injecting damaged mtDNA into mouse brain induced PDD-like behavioral symptoms, including neuropsychiatric, motor, and cognitive impairments. It also caused neurodegeneration in brain regions distant from the injection site, suggesting that damaged mtDNA triggers spread of PDD characteristics in an “infectious-like” manner, the researchers report.
Further study revealed that the mechanism through which damaged mtDNA causes pathology in healthy neurons involves dual activation of Toll-like receptor (TLR) 9 and 4 pathways, leading to increased oxidative stress and neuronal cell death, respectively.
“Our proteomic analysis of extracellular vesicles containing damaged mtDNA identified the TLR4 activator, ribosomal protein S3, as a key protein involved in recognizing and extruding damaged mtDNA,” the investigators write.
In the future they plan to investigate how mtDNA damage can serve as a predictive marker for different disease stages and progression and to explore potential therapeutic strategies aimed at restoring normal mitochondrial function to rectify the mitochondrial dysfunctions implicated in PD.
Making a comeback?
Commenting on the research for this news organization, James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, noted that the role of mitochondria in PD is “like a starlet that burst onto the scene in the 80s, faded into obscurity, and through diligence and continued research has moved beyond being a solid character actor and is reemerging as a force to reckon with.
“This paper only adds to the allure that mitochondria may have in contributing to PD by providing evidence of a novel process by which mitochondria may be not only contributing to PD and loss of dopamine neurons but may play a larger role in the subsequent effects that many people with PD experience – dementia,” Dr. Beck said.
He noted that the authors identified several proteins as facilitating the neurodegeneration that is wrought by damaged mitochondrial DNA.
“These could be potential targets for future drug development. In addition, this work implicates alterations in immune signaling and drugs in development to target inflammatory responses may also bring ancillary benefit,” Dr. Beck said.
However, he said, “while very interesting findings, this is really the first effort that demonstrates how damaged mitochondrial DNA may contribute to neurodegeneration in the context of PD and PD dementia. Further work needs to validate these findings as well as to elucidate mechanisms underlying the propagation of the mitochondrial DNA from cell to cell.”
Funding for this research was provided by the European Union’s Horizon 2020 Research and Innovation Program, the Lundbeck Foundation, and the Danish Council for Independent Research–Medicine. Dr. Issazadeh-Navikas and Dr. Beck have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
.
While defects in mitochondrial functions and in mitochondrial DNA have been implicated in PD in the past, the current study demonstrates “for the first time how damaged mitochondrial DNA can underlie the mechanisms of PD initiation and spread in brain,” lead investigator Shohreh Issazadeh-Navikas, PhD, with the University of Copenhagen, told this news organization.
“This has direct implication for clinical diagnosis” – if damaged mtDNA can be detected in blood, it could serve as an early biomarker for disease, she explained.
The study was published online in Molecular Psychiatry.
“Infectious-like” spread of PD pathology
In earlier work, the researchers identified dysregulated interferon-beta (IFN-beta) signaling as a “top candidate pathway” associated with sporadic PD and its progression to PD with dementia (PDD).
In mice PD models that were deficient in IFN-beta signaling, the investigators showed that neuronal IFN-beta is required to maintain mitochondrial homeostasis and metabolism.
Lack of neuronal IFN-beta or disruption of its downstream signaling causes the accumulation of damaged mitochondria with excessive oxidative stress and insufficient adenosine triphosphate production.
In the current study, using postmortem brain tissue samples from patients with sporadic PD, they confirmed that there were deletions of mtDNA in the medial frontal gyrus, a region implicated in cognitive impairments in PD, suggesting a potential role of damaged mtDNA in disease pathophysiology.
They also identified mtDNA deletions in a “hotspot” in complex I respiratory chain subunits that were associated with dysregulation of oxidative stress and DNA damage response pathways in cohorts with sporadic PD and PDD.
They confirmed the contribution of mtDNA damage to PD pathology in the PD mouse models. They showed that lack of neuronal IFN-beta signaling leads to oxidative damage and mutations in mtDNA in neurons, which are subsequently released outside the neurons.
Injecting damaged mtDNA into mouse brain induced PDD-like behavioral symptoms, including neuropsychiatric, motor, and cognitive impairments. It also caused neurodegeneration in brain regions distant from the injection site, suggesting that damaged mtDNA triggers spread of PDD characteristics in an “infectious-like” manner, the researchers report.
Further study revealed that the mechanism through which damaged mtDNA causes pathology in healthy neurons involves dual activation of Toll-like receptor (TLR) 9 and 4 pathways, leading to increased oxidative stress and neuronal cell death, respectively.
“Our proteomic analysis of extracellular vesicles containing damaged mtDNA identified the TLR4 activator, ribosomal protein S3, as a key protein involved in recognizing and extruding damaged mtDNA,” the investigators write.
In the future they plan to investigate how mtDNA damage can serve as a predictive marker for different disease stages and progression and to explore potential therapeutic strategies aimed at restoring normal mitochondrial function to rectify the mitochondrial dysfunctions implicated in PD.
Making a comeback?
Commenting on the research for this news organization, James Beck, PhD, chief scientific officer at the Parkinson’s Foundation, noted that the role of mitochondria in PD is “like a starlet that burst onto the scene in the 80s, faded into obscurity, and through diligence and continued research has moved beyond being a solid character actor and is reemerging as a force to reckon with.
“This paper only adds to the allure that mitochondria may have in contributing to PD by providing evidence of a novel process by which mitochondria may be not only contributing to PD and loss of dopamine neurons but may play a larger role in the subsequent effects that many people with PD experience – dementia,” Dr. Beck said.
He noted that the authors identified several proteins as facilitating the neurodegeneration that is wrought by damaged mitochondrial DNA.
“These could be potential targets for future drug development. In addition, this work implicates alterations in immune signaling and drugs in development to target inflammatory responses may also bring ancillary benefit,” Dr. Beck said.
However, he said, “while very interesting findings, this is really the first effort that demonstrates how damaged mitochondrial DNA may contribute to neurodegeneration in the context of PD and PD dementia. Further work needs to validate these findings as well as to elucidate mechanisms underlying the propagation of the mitochondrial DNA from cell to cell.”
Funding for this research was provided by the European Union’s Horizon 2020 Research and Innovation Program, the Lundbeck Foundation, and the Danish Council for Independent Research–Medicine. Dr. Issazadeh-Navikas and Dr. Beck have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM MOLECULAR PSYCHIATRY