User login
Mouse model replicates aggressive AML subtype

Researchers have developed a mouse model of an aggressive type of acute myeloid leukemia (AML) that, they believe, accurately replicates the human form of the disease.
The model replicates AML with co-occurring mutations in FLT3 and DNMT3A.
The researchers said they found that mice with Flt3-ITD and inducible deletion of Dnmt3a developed a rapidly lethal, completely penetrant, and transplantable AML of normal karyotype.
The team described this work in Cancer Discovery.
“Our goal was to create a model that was faithful to the human form of the disease that can be used for preclinical testing of potential cures,” said study author H. Leighton Grimes, PhD, of Cincinnati Children’s Hospital Medical Center in Ohio.
“Previous models were slow, difficult to analyze, and did not accurately represent the human disease. This model is rapid, fully penetrant, and completely spontaneous. We hope that it will open the way for other researchers to join us in attacking this particularly lethal AML subtype.”
Dr Grimes and his colleagues said they were able to look at the disease in a new way with the help of a powerful new core facility utilizing analytical tools related to single-cell RNA sequencing. The team used complementary single-cell analyses to identify the core leukemia-causing stem cells of the tumor.
“Before, researchers were comparing the gene expression patterns of one AML subtype to either normal cells or other AML subtypes,” said study author Sara Meyer, PhD, a fellow in the Grimes lab.
“That approach made it difficult to tease out the specific impact of Dnmt3a mutation. Instead, we isolated the variables and studied only human and murine AML with Flt3 mutation. Comparing Flt3-mutant AML with and without Dnmt3a mutation allowed us to more finely identify those patterns that were specific to the Dnmt3a mutation.”
With that more detailed understanding, the researchers gained new insights into the contributions of the Dnmt3a mutation to the disease.
First, their work confirms suspicions that low-level Dnmt3a activity is cancer-causing. Moreover, they discovered that reduced Dnmt3a function allows genes that are normally expressed only at early development stages of blood cell formation to continue expression at later stages, leading to the development of AML.
The researchers also found that, in mouse tumor cells, rescuing expression of Dnmt3a reversed the leukemia phenotypes and gene expression. But they said more research is warranted to determine if rescuing normal levels of DNMT3A function is a viable method for treating human AML.
The team also identified several potential treatment targets that are unique to this type of AML. In future studies, they plan to proceed with testing potential therapies. ![]()
Researchers have developed a mouse model of an aggressive type of acute myeloid leukemia (AML) that, they believe, accurately replicates the human form of the disease.
The model replicates AML with co-occurring mutations in FLT3 and DNMT3A.
The researchers said they found that mice with Flt3-ITD and inducible deletion of Dnmt3a developed a rapidly lethal, completely penetrant, and transplantable AML of normal karyotype.
The team described this work in Cancer Discovery.
“Our goal was to create a model that was faithful to the human form of the disease that can be used for preclinical testing of potential cures,” said study author H. Leighton Grimes, PhD, of Cincinnati Children’s Hospital Medical Center in Ohio.
“Previous models were slow, difficult to analyze, and did not accurately represent the human disease. This model is rapid, fully penetrant, and completely spontaneous. We hope that it will open the way for other researchers to join us in attacking this particularly lethal AML subtype.”
Dr Grimes and his colleagues said they were able to look at the disease in a new way with the help of a powerful new core facility utilizing analytical tools related to single-cell RNA sequencing. The team used complementary single-cell analyses to identify the core leukemia-causing stem cells of the tumor.
“Before, researchers were comparing the gene expression patterns of one AML subtype to either normal cells or other AML subtypes,” said study author Sara Meyer, PhD, a fellow in the Grimes lab.
“That approach made it difficult to tease out the specific impact of Dnmt3a mutation. Instead, we isolated the variables and studied only human and murine AML with Flt3 mutation. Comparing Flt3-mutant AML with and without Dnmt3a mutation allowed us to more finely identify those patterns that were specific to the Dnmt3a mutation.”
With that more detailed understanding, the researchers gained new insights into the contributions of the Dnmt3a mutation to the disease.
First, their work confirms suspicions that low-level Dnmt3a activity is cancer-causing. Moreover, they discovered that reduced Dnmt3a function allows genes that are normally expressed only at early development stages of blood cell formation to continue expression at later stages, leading to the development of AML.
The researchers also found that, in mouse tumor cells, rescuing expression of Dnmt3a reversed the leukemia phenotypes and gene expression. But they said more research is warranted to determine if rescuing normal levels of DNMT3A function is a viable method for treating human AML.
The team also identified several potential treatment targets that are unique to this type of AML. In future studies, they plan to proceed with testing potential therapies. ![]()
Researchers have developed a mouse model of an aggressive type of acute myeloid leukemia (AML) that, they believe, accurately replicates the human form of the disease.
The model replicates AML with co-occurring mutations in FLT3 and DNMT3A.
The researchers said they found that mice with Flt3-ITD and inducible deletion of Dnmt3a developed a rapidly lethal, completely penetrant, and transplantable AML of normal karyotype.
The team described this work in Cancer Discovery.
“Our goal was to create a model that was faithful to the human form of the disease that can be used for preclinical testing of potential cures,” said study author H. Leighton Grimes, PhD, of Cincinnati Children’s Hospital Medical Center in Ohio.
“Previous models were slow, difficult to analyze, and did not accurately represent the human disease. This model is rapid, fully penetrant, and completely spontaneous. We hope that it will open the way for other researchers to join us in attacking this particularly lethal AML subtype.”
Dr Grimes and his colleagues said they were able to look at the disease in a new way with the help of a powerful new core facility utilizing analytical tools related to single-cell RNA sequencing. The team used complementary single-cell analyses to identify the core leukemia-causing stem cells of the tumor.
“Before, researchers were comparing the gene expression patterns of one AML subtype to either normal cells or other AML subtypes,” said study author Sara Meyer, PhD, a fellow in the Grimes lab.
“That approach made it difficult to tease out the specific impact of Dnmt3a mutation. Instead, we isolated the variables and studied only human and murine AML with Flt3 mutation. Comparing Flt3-mutant AML with and without Dnmt3a mutation allowed us to more finely identify those patterns that were specific to the Dnmt3a mutation.”
With that more detailed understanding, the researchers gained new insights into the contributions of the Dnmt3a mutation to the disease.
First, their work confirms suspicions that low-level Dnmt3a activity is cancer-causing. Moreover, they discovered that reduced Dnmt3a function allows genes that are normally expressed only at early development stages of blood cell formation to continue expression at later stages, leading to the development of AML.
The researchers also found that, in mouse tumor cells, rescuing expression of Dnmt3a reversed the leukemia phenotypes and gene expression. But they said more research is warranted to determine if rescuing normal levels of DNMT3A function is a viable method for treating human AML.
The team also identified several potential treatment targets that are unique to this type of AML. In future studies, they plan to proceed with testing potential therapies. ![]()
FDA OKs use of test to screen blood donations for Zika virus
The US Food and Drug Administration (FDA) is allowing the use of an investigational test to screen blood donations for Zika virus.
The test, known as the cobas® Zika test, has not been granted FDA clearance or approval, but it may be used under an investigational new drug application protocol for screening donated blood in areas with active, mosquito-borne transmission of Zika virus.
This means the test can be used by US blood screening laboratories, but the laboratories will need to be enrolled in and contracted into a clinical trial for the test, as specified and agreed with the FDA’s Center for Biologics Evaluation and Research.
By authorizing use of the cobas® Zika test, the FDA is allowing blood establishments in Puerto Rico—a US territory with local, mosquito-borne transmission of the Zika virus—to resume collecting donations of whole blood and blood components.
“The availability of an investigational test to screen donated blood for Zika virus is an important step forward in maintaining the safety of the nation’s blood supply, especially for those US territories already experiencing active transmission,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“In the future, should Zika virus transmission occur in other areas, blood collection establishments will be able to continue to collect blood and use the investigational screening test, minimizing disruption to the blood supply.”
About the test
The cobas® Zika test is a qualitative in vitro nucleic acid screening test for the direct detection of Zika virus RNA in plasma specimens from individual human
blood donors.
The test is based on fully automated sample preparation (nucleic acid extraction and purification), followed by PCR amplification and detection.
The cobas® Zika test is manufactured by Roche and is intended for use with Roche’s cobas® 6800/8800 Systems.
The cobas® 6800/8800 Systems consist of the sample supply module, the transfer module, the processing module, and the analytic module. Automated data management is performed by the cobas® 6800/8800 software, which assigns test results for all tests as non-reactive, reactive, or invalid.
“The cobas® Zika test has been specifically designed utilizing the generic cobas® omni Utility Channel on the cobas® 6800/8800 Systems,” said Roland Diggelmann, chief operating officer of Roche Diagnostics.
“These fully automated, high-volume systems provide solutions for blood services to detect the virus and ensure that potentially infected blood units are not made available for transfusion.”
Test availability
Initially, the cobas® Zika test will be deployed to screen blood donations collected locally in Puerto Rico. It is expected that this testing will enable the
reinstatement of the blood services in Puerto Rico and reduce the reliance of blood importation from other areas in the US.
The second stage of deployment for the cobas® Zika test will be to prepare for screening of blood donations collected by blood services in the southern US.
In addition, Roche said it is working with regulators around the world to determine the path forward to implement the cobas® Zika test for blood screening.
Implications for Puerto Rico
On February 16, the FDA issued a guidance for US blood establishments to reduce the risk of transfusion-transmitted Zika virus. In the guidance, the FDA recommended that areas with active transmission of Zika virus obtain whole blood and blood components from areas without active transmission of the virus.
As a result, local blood collection in Puerto Rico was suspended. On March 7, the Department of Health and Human Services announced that it arranged for shipments of blood products from the continental US to Puerto Rico.
The FDA guidance also states that establishments in areas with active Zika transmission may collect locally if a licensed or investigational test for screening donated blood is available.
Once screening of blood donations for Zika virus using the cobas® Zika test begins, blood establishments in Puerto Rico may resume collecting donations of whole blood and blood components. However, the FDA’s recommendations for Zika blood donor deferrals remain in place. ![]()
The US Food and Drug Administration (FDA) is allowing the use of an investigational test to screen blood donations for Zika virus.
The test, known as the cobas® Zika test, has not been granted FDA clearance or approval, but it may be used under an investigational new drug application protocol for screening donated blood in areas with active, mosquito-borne transmission of Zika virus.
This means the test can be used by US blood screening laboratories, but the laboratories will need to be enrolled in and contracted into a clinical trial for the test, as specified and agreed with the FDA’s Center for Biologics Evaluation and Research.
By authorizing use of the cobas® Zika test, the FDA is allowing blood establishments in Puerto Rico—a US territory with local, mosquito-borne transmission of the Zika virus—to resume collecting donations of whole blood and blood components.
“The availability of an investigational test to screen donated blood for Zika virus is an important step forward in maintaining the safety of the nation’s blood supply, especially for those US territories already experiencing active transmission,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“In the future, should Zika virus transmission occur in other areas, blood collection establishments will be able to continue to collect blood and use the investigational screening test, minimizing disruption to the blood supply.”
About the test
The cobas® Zika test is a qualitative in vitro nucleic acid screening test for the direct detection of Zika virus RNA in plasma specimens from individual human
blood donors.
The test is based on fully automated sample preparation (nucleic acid extraction and purification), followed by PCR amplification and detection.
The cobas® Zika test is manufactured by Roche and is intended for use with Roche’s cobas® 6800/8800 Systems.
The cobas® 6800/8800 Systems consist of the sample supply module, the transfer module, the processing module, and the analytic module. Automated data management is performed by the cobas® 6800/8800 software, which assigns test results for all tests as non-reactive, reactive, or invalid.
“The cobas® Zika test has been specifically designed utilizing the generic cobas® omni Utility Channel on the cobas® 6800/8800 Systems,” said Roland Diggelmann, chief operating officer of Roche Diagnostics.
“These fully automated, high-volume systems provide solutions for blood services to detect the virus and ensure that potentially infected blood units are not made available for transfusion.”
Test availability
Initially, the cobas® Zika test will be deployed to screen blood donations collected locally in Puerto Rico. It is expected that this testing will enable the
reinstatement of the blood services in Puerto Rico and reduce the reliance of blood importation from other areas in the US.
The second stage of deployment for the cobas® Zika test will be to prepare for screening of blood donations collected by blood services in the southern US.
In addition, Roche said it is working with regulators around the world to determine the path forward to implement the cobas® Zika test for blood screening.
Implications for Puerto Rico
On February 16, the FDA issued a guidance for US blood establishments to reduce the risk of transfusion-transmitted Zika virus. In the guidance, the FDA recommended that areas with active transmission of Zika virus obtain whole blood and blood components from areas without active transmission of the virus.
As a result, local blood collection in Puerto Rico was suspended. On March 7, the Department of Health and Human Services announced that it arranged for shipments of blood products from the continental US to Puerto Rico.
The FDA guidance also states that establishments in areas with active Zika transmission may collect locally if a licensed or investigational test for screening donated blood is available.
Once screening of blood donations for Zika virus using the cobas® Zika test begins, blood establishments in Puerto Rico may resume collecting donations of whole blood and blood components. However, the FDA’s recommendations for Zika blood donor deferrals remain in place. ![]()
The US Food and Drug Administration (FDA) is allowing the use of an investigational test to screen blood donations for Zika virus.
The test, known as the cobas® Zika test, has not been granted FDA clearance or approval, but it may be used under an investigational new drug application protocol for screening donated blood in areas with active, mosquito-borne transmission of Zika virus.
This means the test can be used by US blood screening laboratories, but the laboratories will need to be enrolled in and contracted into a clinical trial for the test, as specified and agreed with the FDA’s Center for Biologics Evaluation and Research.
By authorizing use of the cobas® Zika test, the FDA is allowing blood establishments in Puerto Rico—a US territory with local, mosquito-borne transmission of the Zika virus—to resume collecting donations of whole blood and blood components.
“The availability of an investigational test to screen donated blood for Zika virus is an important step forward in maintaining the safety of the nation’s blood supply, especially for those US territories already experiencing active transmission,” said Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research.
“In the future, should Zika virus transmission occur in other areas, blood collection establishments will be able to continue to collect blood and use the investigational screening test, minimizing disruption to the blood supply.”
About the test
The cobas® Zika test is a qualitative in vitro nucleic acid screening test for the direct detection of Zika virus RNA in plasma specimens from individual human
blood donors.
The test is based on fully automated sample preparation (nucleic acid extraction and purification), followed by PCR amplification and detection.
The cobas® Zika test is manufactured by Roche and is intended for use with Roche’s cobas® 6800/8800 Systems.
The cobas® 6800/8800 Systems consist of the sample supply module, the transfer module, the processing module, and the analytic module. Automated data management is performed by the cobas® 6800/8800 software, which assigns test results for all tests as non-reactive, reactive, or invalid.
“The cobas® Zika test has been specifically designed utilizing the generic cobas® omni Utility Channel on the cobas® 6800/8800 Systems,” said Roland Diggelmann, chief operating officer of Roche Diagnostics.
“These fully automated, high-volume systems provide solutions for blood services to detect the virus and ensure that potentially infected blood units are not made available for transfusion.”
Test availability
Initially, the cobas® Zika test will be deployed to screen blood donations collected locally in Puerto Rico. It is expected that this testing will enable the
reinstatement of the blood services in Puerto Rico and reduce the reliance of blood importation from other areas in the US.
The second stage of deployment for the cobas® Zika test will be to prepare for screening of blood donations collected by blood services in the southern US.
In addition, Roche said it is working with regulators around the world to determine the path forward to implement the cobas® Zika test for blood screening.
Implications for Puerto Rico
On February 16, the FDA issued a guidance for US blood establishments to reduce the risk of transfusion-transmitted Zika virus. In the guidance, the FDA recommended that areas with active transmission of Zika virus obtain whole blood and blood components from areas without active transmission of the virus.
As a result, local blood collection in Puerto Rico was suspended. On March 7, the Department of Health and Human Services announced that it arranged for shipments of blood products from the continental US to Puerto Rico.
The FDA guidance also states that establishments in areas with active Zika transmission may collect locally if a licensed or investigational test for screening donated blood is available.
Once screening of blood donations for Zika virus using the cobas® Zika test begins, blood establishments in Puerto Rico may resume collecting donations of whole blood and blood components. However, the FDA’s recommendations for Zika blood donor deferrals remain in place. ![]()
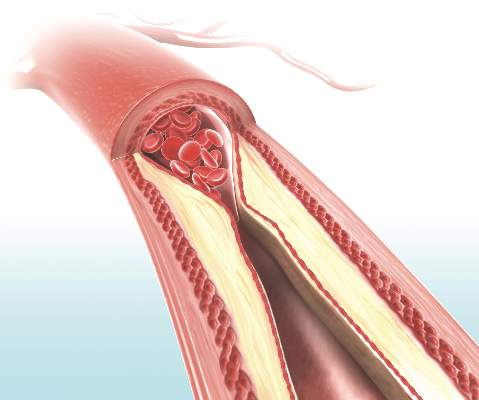
Only ‘early’ estradiol limits atherosclerosis progression
Hormone therapy – estradiol with or without progesterone – only limits the progression of subclinical atherosclerosis if it is initiated within 6 years of menopause onset, according to a report published online March 30 in the New England Journal of Medicine.
The “hormone-timing hypothesis” posits that hormone therapy’s beneficial effects on atherosclerosis depend on the timing of initiating that therapy relative to menopause. To test this hypothesis, researchers began the ELITE study (Early versus Late Intervention Trial with Estradiol) in 2002, using serial noninvasive measurements of carotid-artery intima-media thickness (CIMT) as a marker of atherosclerosis progression.

Several other studies since 2002 have reported that the timing hypothesis appears to be valid, wrote Dr. Howard N. Hodis of the Atherosclerosis Research Unit, University of Southern California, Los Angeles, and his associates.
Their single-center trial involved 643 healthy postmenopausal women who had no diabetes and no evidence of cardiovascular disease at baseline, and who were randomly assigned to receive either daily oral estradiol or a matching placebo for 5 years. Women who had an intact uterus and took active estradiol also received a 4% micronized progesterone vaginal gel, while those who had an intact uterus and took placebo also received a matching placebo gel.
The participants were stratified according to the number of years they were past menopause: less than 6 years (271 women in the “early” group) or more than 10 years (372 in the “late” group).
A total of 137 women in the early group and 186 women in the late group were assigned to active estradiol, while 134 women in the early group and 186 women in the late group were assigned to placebo. As expected, serum estradiol levels were at least 3 times higher among women assigned to active treatment, compared with those assigned to placebo.
The primary outcome – the effect of hormone therapy on CIMT progression – differed by timing of the initiation of treatment. In the “early” group, the mean CIMT progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo.
In contrast, in the “late” group, the rates of CIMT progression were not significantly different between estradiol and placebo, the investigators wrote (N Engl J Med. 2016;374:1221-31. doi: 10.1056/NEJMoa1505241).
This beneficial effect remained significant in a sensitivity analysis restricted only to study participants who showed at least 80% adherence to their assigned treatment. The benefit also remained significant in a post-hoc analysis comparing women who took estradiol alone against those who took estradiol plus progestogen, as well as in a separate analysis comparing women who used lipid-lowering and/or hypertensive medications against those who did not.
The findings add further evidence in favor of the hormone timing hypothesis. The effect of estradiol therapy on CIMT progression was significantly modified by time since menopause (P = .007 for the interaction), the researchers wrote.
Cardiac computer tomography (CT) was used as a different method of assessing coronary atherosclerosis in a subgroup of 167 women in the early group (88 receiving estradiol and 79 receiving placebo) and 214 in the late group (101 receiving estradiol and 113 receiving placebo). The timing of estradiol treatment did not affect coronary artery calcium and other cardiac CT measures. This is consistent with previous reports that hormone therapy has no significant effect on established lesions in the coronary arteries, the researchers wrote.
The ELITE trial was funded by the National Institute on Aging. Dr. Hodis reported having no relevant financial disclosures; two of his associates reported ties to GE and TherapeuticsMD.
Despite the favorable effect of estrogen on atherosclerosis in early postmenopausal women in the ELITE trial, the relevance of these results to clinical coronary heart disease events remains questionable. The trial assessed only surrogate measures of coronary heart disease and was not designed or powered to assess clinical events. The occurrence of myocardial infarction and stroke involves not only atherosclerotic plaque formation but also plaque rupture and thrombosis. Any changes in these latter two phenomena would not be captured by the CIMT measurements in ELITE — a point of particular interest, given that postmenopausal hormone therapy may promote thrombosis and inflammation. A final caution is that the available clinical data in support of the timing hypothesis are suggestive but inconsistent.
Guidelines from various professional organizations currently caution against using postmenopausal hormone therapy for the purpose of preventing cardiovascular events. Although the ELITE trial results support the hypothesis that postmenopausal hormone therapy may have more favorable effects on atherosclerosis when initiated soon after menopause, extrapolation of these results to clinical events would be premature, and the present guidance remains prudent.
Dr. John F. Keaney, Jr., is at the University of Massachusetts, Worcester and is an associate editor at the New England Journal of Medicine, and Dr. Caren G. Solomon is a deputy editor at the New England Journal of Medicine. They reported having no relevant financial disclosures. These remarks are adapted from an accompanying editorial (N Engl J Med. 2016 Mar 30. doi: 10.1056/NEJMe1602846).
Despite the favorable effect of estrogen on atherosclerosis in early postmenopausal women in the ELITE trial, the relevance of these results to clinical coronary heart disease events remains questionable. The trial assessed only surrogate measures of coronary heart disease and was not designed or powered to assess clinical events. The occurrence of myocardial infarction and stroke involves not only atherosclerotic plaque formation but also plaque rupture and thrombosis. Any changes in these latter two phenomena would not be captured by the CIMT measurements in ELITE — a point of particular interest, given that postmenopausal hormone therapy may promote thrombosis and inflammation. A final caution is that the available clinical data in support of the timing hypothesis are suggestive but inconsistent.
Guidelines from various professional organizations currently caution against using postmenopausal hormone therapy for the purpose of preventing cardiovascular events. Although the ELITE trial results support the hypothesis that postmenopausal hormone therapy may have more favorable effects on atherosclerosis when initiated soon after menopause, extrapolation of these results to clinical events would be premature, and the present guidance remains prudent.
Dr. John F. Keaney, Jr., is at the University of Massachusetts, Worcester and is an associate editor at the New England Journal of Medicine, and Dr. Caren G. Solomon is a deputy editor at the New England Journal of Medicine. They reported having no relevant financial disclosures. These remarks are adapted from an accompanying editorial (N Engl J Med. 2016 Mar 30. doi: 10.1056/NEJMe1602846).
Despite the favorable effect of estrogen on atherosclerosis in early postmenopausal women in the ELITE trial, the relevance of these results to clinical coronary heart disease events remains questionable. The trial assessed only surrogate measures of coronary heart disease and was not designed or powered to assess clinical events. The occurrence of myocardial infarction and stroke involves not only atherosclerotic plaque formation but also plaque rupture and thrombosis. Any changes in these latter two phenomena would not be captured by the CIMT measurements in ELITE — a point of particular interest, given that postmenopausal hormone therapy may promote thrombosis and inflammation. A final caution is that the available clinical data in support of the timing hypothesis are suggestive but inconsistent.
Guidelines from various professional organizations currently caution against using postmenopausal hormone therapy for the purpose of preventing cardiovascular events. Although the ELITE trial results support the hypothesis that postmenopausal hormone therapy may have more favorable effects on atherosclerosis when initiated soon after menopause, extrapolation of these results to clinical events would be premature, and the present guidance remains prudent.
Dr. John F. Keaney, Jr., is at the University of Massachusetts, Worcester and is an associate editor at the New England Journal of Medicine, and Dr. Caren G. Solomon is a deputy editor at the New England Journal of Medicine. They reported having no relevant financial disclosures. These remarks are adapted from an accompanying editorial (N Engl J Med. 2016 Mar 30. doi: 10.1056/NEJMe1602846).
Hormone therapy – estradiol with or without progesterone – only limits the progression of subclinical atherosclerosis if it is initiated within 6 years of menopause onset, according to a report published online March 30 in the New England Journal of Medicine.
The “hormone-timing hypothesis” posits that hormone therapy’s beneficial effects on atherosclerosis depend on the timing of initiating that therapy relative to menopause. To test this hypothesis, researchers began the ELITE study (Early versus Late Intervention Trial with Estradiol) in 2002, using serial noninvasive measurements of carotid-artery intima-media thickness (CIMT) as a marker of atherosclerosis progression.
Several other studies since 2002 have reported that the timing hypothesis appears to be valid, wrote Dr. Howard N. Hodis of the Atherosclerosis Research Unit, University of Southern California, Los Angeles, and his associates.
Their single-center trial involved 643 healthy postmenopausal women who had no diabetes and no evidence of cardiovascular disease at baseline, and who were randomly assigned to receive either daily oral estradiol or a matching placebo for 5 years. Women who had an intact uterus and took active estradiol also received a 4% micronized progesterone vaginal gel, while those who had an intact uterus and took placebo also received a matching placebo gel.
The participants were stratified according to the number of years they were past menopause: less than 6 years (271 women in the “early” group) or more than 10 years (372 in the “late” group).
A total of 137 women in the early group and 186 women in the late group were assigned to active estradiol, while 134 women in the early group and 186 women in the late group were assigned to placebo. As expected, serum estradiol levels were at least 3 times higher among women assigned to active treatment, compared with those assigned to placebo.
The primary outcome – the effect of hormone therapy on CIMT progression – differed by timing of the initiation of treatment. In the “early” group, the mean CIMT progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo.
In contrast, in the “late” group, the rates of CIMT progression were not significantly different between estradiol and placebo, the investigators wrote (N Engl J Med. 2016;374:1221-31. doi: 10.1056/NEJMoa1505241).
This beneficial effect remained significant in a sensitivity analysis restricted only to study participants who showed at least 80% adherence to their assigned treatment. The benefit also remained significant in a post-hoc analysis comparing women who took estradiol alone against those who took estradiol plus progestogen, as well as in a separate analysis comparing women who used lipid-lowering and/or hypertensive medications against those who did not.
The findings add further evidence in favor of the hormone timing hypothesis. The effect of estradiol therapy on CIMT progression was significantly modified by time since menopause (P = .007 for the interaction), the researchers wrote.
Cardiac computer tomography (CT) was used as a different method of assessing coronary atherosclerosis in a subgroup of 167 women in the early group (88 receiving estradiol and 79 receiving placebo) and 214 in the late group (101 receiving estradiol and 113 receiving placebo). The timing of estradiol treatment did not affect coronary artery calcium and other cardiac CT measures. This is consistent with previous reports that hormone therapy has no significant effect on established lesions in the coronary arteries, the researchers wrote.
The ELITE trial was funded by the National Institute on Aging. Dr. Hodis reported having no relevant financial disclosures; two of his associates reported ties to GE and TherapeuticsMD.
Hormone therapy – estradiol with or without progesterone – only limits the progression of subclinical atherosclerosis if it is initiated within 6 years of menopause onset, according to a report published online March 30 in the New England Journal of Medicine.
The “hormone-timing hypothesis” posits that hormone therapy’s beneficial effects on atherosclerosis depend on the timing of initiating that therapy relative to menopause. To test this hypothesis, researchers began the ELITE study (Early versus Late Intervention Trial with Estradiol) in 2002, using serial noninvasive measurements of carotid-artery intima-media thickness (CIMT) as a marker of atherosclerosis progression.
Several other studies since 2002 have reported that the timing hypothesis appears to be valid, wrote Dr. Howard N. Hodis of the Atherosclerosis Research Unit, University of Southern California, Los Angeles, and his associates.
Their single-center trial involved 643 healthy postmenopausal women who had no diabetes and no evidence of cardiovascular disease at baseline, and who were randomly assigned to receive either daily oral estradiol or a matching placebo for 5 years. Women who had an intact uterus and took active estradiol also received a 4% micronized progesterone vaginal gel, while those who had an intact uterus and took placebo also received a matching placebo gel.
The participants were stratified according to the number of years they were past menopause: less than 6 years (271 women in the “early” group) or more than 10 years (372 in the “late” group).
A total of 137 women in the early group and 186 women in the late group were assigned to active estradiol, while 134 women in the early group and 186 women in the late group were assigned to placebo. As expected, serum estradiol levels were at least 3 times higher among women assigned to active treatment, compared with those assigned to placebo.
The primary outcome – the effect of hormone therapy on CIMT progression – differed by timing of the initiation of treatment. In the “early” group, the mean CIMT progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo.
In contrast, in the “late” group, the rates of CIMT progression were not significantly different between estradiol and placebo, the investigators wrote (N Engl J Med. 2016;374:1221-31. doi: 10.1056/NEJMoa1505241).
This beneficial effect remained significant in a sensitivity analysis restricted only to study participants who showed at least 80% adherence to their assigned treatment. The benefit also remained significant in a post-hoc analysis comparing women who took estradiol alone against those who took estradiol plus progestogen, as well as in a separate analysis comparing women who used lipid-lowering and/or hypertensive medications against those who did not.
The findings add further evidence in favor of the hormone timing hypothesis. The effect of estradiol therapy on CIMT progression was significantly modified by time since menopause (P = .007 for the interaction), the researchers wrote.
Cardiac computer tomography (CT) was used as a different method of assessing coronary atherosclerosis in a subgroup of 167 women in the early group (88 receiving estradiol and 79 receiving placebo) and 214 in the late group (101 receiving estradiol and 113 receiving placebo). The timing of estradiol treatment did not affect coronary artery calcium and other cardiac CT measures. This is consistent with previous reports that hormone therapy has no significant effect on established lesions in the coronary arteries, the researchers wrote.
The ELITE trial was funded by the National Institute on Aging. Dr. Hodis reported having no relevant financial disclosures; two of his associates reported ties to GE and TherapeuticsMD.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Estradiol only limits the progression of subclinical atherosclerosis if it is initiated within 6 years of menopause, not later.
Major finding: The mean CIMT progression rate was decreased by 0.0034 mm per year with estradiol, compared with placebo, but only in women who initiated hormone therapy within 6 years of menopause onset.
Data source: A single-center randomized, double-blind, placebo-controlled trial involving 643 healthy postmenopausal women treated for 5 years.
Disclosures: The ELITE trial was funded by the National Institute on Aging. Dr. Hodis reported having no relevant financial disclosures; two of his associates reported ties to GE and TherapeuticsMD.
Can the Mediterranean Diet Reduce the Risk of Hip Fracture?
Eating a Mediterranean diet full of fruits, vegetables, fish, nuts, legumes, and whole grains is associated with a slightly lower risk of hip fracture in women, according to a study published online ahead of print in JAMA Internal Medicine.
Researchers analyzed data on diet and fracture risk in more than 90,000 postmenopausal women (average age, 63.6 years) who were followed for an average of almost 16 years. Diet quality and adherence were assessed by scores on 4 scales: the alternate Mediterranean Diet (aMED); the Healthy Eating Index 2010 (HEI-2010); the Alternate Healthy Eating Index 2010 (AHEI-2010); and the Dietary Approaches to Stop Hypertension (DASH) diet.
Women who scored the highest for adherence to a Mediterranean diet were at lower risk for hip fractures, although the absolute risk reduction was 0.29%. There was no association between a Mediterranean diet and total fracture risk.
A higher HEI-2010 or DASH score was inversely related to the risk of hip fracture, but the finding was not statistically significant. There was no association between HEI-2010, DASH and total fracture risk. The highest scores for AHEI-2010 were not significantly associated with hip or total fracture risk.
Suggested Reading
Haring B, Crandall CJ, Wu C, et al. Dietary patterns and fractures in postmenopausal women: results from the women's health initiative. JAMA Intern Med. 2016 Mar 28. [Epub ahead of print]
Eating a Mediterranean diet full of fruits, vegetables, fish, nuts, legumes, and whole grains is associated with a slightly lower risk of hip fracture in women, according to a study published online ahead of print in JAMA Internal Medicine.
Researchers analyzed data on diet and fracture risk in more than 90,000 postmenopausal women (average age, 63.6 years) who were followed for an average of almost 16 years. Diet quality and adherence were assessed by scores on 4 scales: the alternate Mediterranean Diet (aMED); the Healthy Eating Index 2010 (HEI-2010); the Alternate Healthy Eating Index 2010 (AHEI-2010); and the Dietary Approaches to Stop Hypertension (DASH) diet.
Women who scored the highest for adherence to a Mediterranean diet were at lower risk for hip fractures, although the absolute risk reduction was 0.29%. There was no association between a Mediterranean diet and total fracture risk.
A higher HEI-2010 or DASH score was inversely related to the risk of hip fracture, but the finding was not statistically significant. There was no association between HEI-2010, DASH and total fracture risk. The highest scores for AHEI-2010 were not significantly associated with hip or total fracture risk.
Eating a Mediterranean diet full of fruits, vegetables, fish, nuts, legumes, and whole grains is associated with a slightly lower risk of hip fracture in women, according to a study published online ahead of print in JAMA Internal Medicine.
Researchers analyzed data on diet and fracture risk in more than 90,000 postmenopausal women (average age, 63.6 years) who were followed for an average of almost 16 years. Diet quality and adherence were assessed by scores on 4 scales: the alternate Mediterranean Diet (aMED); the Healthy Eating Index 2010 (HEI-2010); the Alternate Healthy Eating Index 2010 (AHEI-2010); and the Dietary Approaches to Stop Hypertension (DASH) diet.
Women who scored the highest for adherence to a Mediterranean diet were at lower risk for hip fractures, although the absolute risk reduction was 0.29%. There was no association between a Mediterranean diet and total fracture risk.
A higher HEI-2010 or DASH score was inversely related to the risk of hip fracture, but the finding was not statistically significant. There was no association between HEI-2010, DASH and total fracture risk. The highest scores for AHEI-2010 were not significantly associated with hip or total fracture risk.
Suggested Reading
Haring B, Crandall CJ, Wu C, et al. Dietary patterns and fractures in postmenopausal women: results from the women's health initiative. JAMA Intern Med. 2016 Mar 28. [Epub ahead of print]
Suggested Reading
Haring B, Crandall CJ, Wu C, et al. Dietary patterns and fractures in postmenopausal women: results from the women's health initiative. JAMA Intern Med. 2016 Mar 28. [Epub ahead of print]
Rate of Tommy John Surgeries in Young Athletes Is on the Rise
An increasing number of adolescents are undergoing ulnar lateral ligament (UCL) surgery to repair a pitching-related elbow injury, according to a study published online ahead of print in the March issue of the American Journal of Sports Medicine.
Analyzing a database of all ambulatory discharges in New York state, researchers found that 444 patients underwent surgery to repair their UCL between 2002 and 2011. The median age of study participants was 21; most were male.
The total volume of UCL surgeries increased nearly 200% during that time, while the number of UCL reconstructions per 100,000 people tripled from 0.15 to 0.45. Almost all of the growth occurred in two age groups, 17- to 18-year-olds and 19- to 20-year-olds. Patients who had private insurance were 25 times more likely to undergo UCL construction than those with Medicaid.
Suggested Reading
Hodgins JL, Vitale M, Arons RR, et al. Epidemiology of Medial Ulnar Collateral Ligament Reconstruction. Am J Sports Med. 2016 Mar;44(3):729-34. [Epub ahead of print].
An increasing number of adolescents are undergoing ulnar lateral ligament (UCL) surgery to repair a pitching-related elbow injury, according to a study published online ahead of print in the March issue of the American Journal of Sports Medicine.
Analyzing a database of all ambulatory discharges in New York state, researchers found that 444 patients underwent surgery to repair their UCL between 2002 and 2011. The median age of study participants was 21; most were male.
The total volume of UCL surgeries increased nearly 200% during that time, while the number of UCL reconstructions per 100,000 people tripled from 0.15 to 0.45. Almost all of the growth occurred in two age groups, 17- to 18-year-olds and 19- to 20-year-olds. Patients who had private insurance were 25 times more likely to undergo UCL construction than those with Medicaid.
An increasing number of adolescents are undergoing ulnar lateral ligament (UCL) surgery to repair a pitching-related elbow injury, according to a study published online ahead of print in the March issue of the American Journal of Sports Medicine.
Analyzing a database of all ambulatory discharges in New York state, researchers found that 444 patients underwent surgery to repair their UCL between 2002 and 2011. The median age of study participants was 21; most were male.
The total volume of UCL surgeries increased nearly 200% during that time, while the number of UCL reconstructions per 100,000 people tripled from 0.15 to 0.45. Almost all of the growth occurred in two age groups, 17- to 18-year-olds and 19- to 20-year-olds. Patients who had private insurance were 25 times more likely to undergo UCL construction than those with Medicaid.
Suggested Reading
Hodgins JL, Vitale M, Arons RR, et al. Epidemiology of Medial Ulnar Collateral Ligament Reconstruction. Am J Sports Med. 2016 Mar;44(3):729-34. [Epub ahead of print].
Suggested Reading
Hodgins JL, Vitale M, Arons RR, et al. Epidemiology of Medial Ulnar Collateral Ligament Reconstruction. Am J Sports Med. 2016 Mar;44(3):729-34. [Epub ahead of print].
ADHD Medications Are Linked to Diminished Bone Density in Young Patients
Children and adolescents who take medication for attention-deficit hyperactivity disorder (ADHD) show decreased bone density, according to a large cross-sectional study presented at the 2016 Annual Meeting of the American Academy of Orthopaedic Surgeons in Orlando.
Researchers identified 5,315 pediatric patients in the Center for Disease Control and Prevention’s National Health and Nutrition Examination Survey (NHANES) and compared children who were taking an ADHD medication (methylphenidate, desmethylphenidate, dextroamphetamine, atomoxetine, or lisdexamfetamine) with those who were not.
Children taking ADHD medication had lower bone mineral density in the femur, femoral neck, and lumbar spine. Approximately 25% of survey participants who were taking ADHD medication met criteria for osteopenia.
Researchers were able to rule out other potential causes of low bone density in these children, including age, sex, race/ethnicity, and poverty levels. However, the study did not include information on dose, duration of use, or changes in therapy because of the limitations of the NHANES survey data.
Children and adolescents who take medication for attention-deficit hyperactivity disorder (ADHD) show decreased bone density, according to a large cross-sectional study presented at the 2016 Annual Meeting of the American Academy of Orthopaedic Surgeons in Orlando.
Researchers identified 5,315 pediatric patients in the Center for Disease Control and Prevention’s National Health and Nutrition Examination Survey (NHANES) and compared children who were taking an ADHD medication (methylphenidate, desmethylphenidate, dextroamphetamine, atomoxetine, or lisdexamfetamine) with those who were not.
Children taking ADHD medication had lower bone mineral density in the femur, femoral neck, and lumbar spine. Approximately 25% of survey participants who were taking ADHD medication met criteria for osteopenia.
Researchers were able to rule out other potential causes of low bone density in these children, including age, sex, race/ethnicity, and poverty levels. However, the study did not include information on dose, duration of use, or changes in therapy because of the limitations of the NHANES survey data.
Children and adolescents who take medication for attention-deficit hyperactivity disorder (ADHD) show decreased bone density, according to a large cross-sectional study presented at the 2016 Annual Meeting of the American Academy of Orthopaedic Surgeons in Orlando.
Researchers identified 5,315 pediatric patients in the Center for Disease Control and Prevention’s National Health and Nutrition Examination Survey (NHANES) and compared children who were taking an ADHD medication (methylphenidate, desmethylphenidate, dextroamphetamine, atomoxetine, or lisdexamfetamine) with those who were not.
Children taking ADHD medication had lower bone mineral density in the femur, femoral neck, and lumbar spine. Approximately 25% of survey participants who were taking ADHD medication met criteria for osteopenia.
Researchers were able to rule out other potential causes of low bone density in these children, including age, sex, race/ethnicity, and poverty levels. However, the study did not include information on dose, duration of use, or changes in therapy because of the limitations of the NHANES survey data.
April 2016 Quiz 2
Q2: ANSWER: D
Critique
This series of endoscopic findings shows changes consistent with inflammation of the cuff.
Up to 20%-30% of patients with ulcerative colitis ultimately require colectomy due to medically refractory colitis or to the development of dysplasia. A total abdominal protocolectomy with ileal pouch anal anastomosis has become the surgical procedure of choice for most ulcerative colitis patients who require surgery.
There are both early and late complications of this type of surgery. Late complications include anastomotic stricture, pouchitis, abscesses, inflammation of the cuff or cuffitis, and functional difficulties such as irritable pouch syndrome, anal pain, and pouch stasis. Patients may also present with inflammation of the pouch and the prepouch ileum that is consistent with Crohn’s disease. Endoscopy can help to narrow down the differential diagnosis of these pouch complications.

In this series of photos the prepouch ileum has no inflammation. The pouch also has no ulcerations or evidence of pouchitis or Crohn’s disease. The cuff is inflamed consistent with a diagnosis of cuffitis. If the inflammation becomes difficult to manage, immunosuppressive therapy may be required but at this point it is reasonable to start with topical therapy to the inflamed area.
Reference
- Li, Y. Shen, B. Evaluating pouch problems. Gastroenterology Clinics North Am. 2012;41:355-78.
- Shen, G. Diagnosis and management of post-operative ileal pouch disorders. Clin Colon Rectal Surg. 2010;23:259-68.
Q2: ANSWER: D
Critique
This series of endoscopic findings shows changes consistent with inflammation of the cuff.
Up to 20%-30% of patients with ulcerative colitis ultimately require colectomy due to medically refractory colitis or to the development of dysplasia. A total abdominal protocolectomy with ileal pouch anal anastomosis has become the surgical procedure of choice for most ulcerative colitis patients who require surgery.
There are both early and late complications of this type of surgery. Late complications include anastomotic stricture, pouchitis, abscesses, inflammation of the cuff or cuffitis, and functional difficulties such as irritable pouch syndrome, anal pain, and pouch stasis. Patients may also present with inflammation of the pouch and the prepouch ileum that is consistent with Crohn’s disease. Endoscopy can help to narrow down the differential diagnosis of these pouch complications.
In this series of photos the prepouch ileum has no inflammation. The pouch also has no ulcerations or evidence of pouchitis or Crohn’s disease. The cuff is inflamed consistent with a diagnosis of cuffitis. If the inflammation becomes difficult to manage, immunosuppressive therapy may be required but at this point it is reasonable to start with topical therapy to the inflamed area.
Reference
- Li, Y. Shen, B. Evaluating pouch problems. Gastroenterology Clinics North Am. 2012;41:355-78.
- Shen, G. Diagnosis and management of post-operative ileal pouch disorders. Clin Colon Rectal Surg. 2010;23:259-68.
Q2: ANSWER: D
Critique
This series of endoscopic findings shows changes consistent with inflammation of the cuff.
Up to 20%-30% of patients with ulcerative colitis ultimately require colectomy due to medically refractory colitis or to the development of dysplasia. A total abdominal protocolectomy with ileal pouch anal anastomosis has become the surgical procedure of choice for most ulcerative colitis patients who require surgery.
There are both early and late complications of this type of surgery. Late complications include anastomotic stricture, pouchitis, abscesses, inflammation of the cuff or cuffitis, and functional difficulties such as irritable pouch syndrome, anal pain, and pouch stasis. Patients may also present with inflammation of the pouch and the prepouch ileum that is consistent with Crohn’s disease. Endoscopy can help to narrow down the differential diagnosis of these pouch complications.
In this series of photos the prepouch ileum has no inflammation. The pouch also has no ulcerations or evidence of pouchitis or Crohn’s disease. The cuff is inflamed consistent with a diagnosis of cuffitis. If the inflammation becomes difficult to manage, immunosuppressive therapy may be required but at this point it is reasonable to start with topical therapy to the inflamed area.
Reference
- Li, Y. Shen, B. Evaluating pouch problems. Gastroenterology Clinics North Am. 2012;41:355-78.
- Shen, G. Diagnosis and management of post-operative ileal pouch disorders. Clin Colon Rectal Surg. 2010;23:259-68.
Why the AMA is (now) worth joining

Until recently, I was not a member of the American Medical Association (AMA). For the past 30 years, I chose not to join because I was troubled by the organization’s direction and the way it seemed to be dominated by special interests. But things have changed—and so has its focus.
The AMA has a new strategy entitled, “A vision for a healthier nation.” Well aligned with the needs of family physicians, the campaign addresses 3 specific areas: better patient health, smarter medical training, and sustainable practices.
Better patient health. The AMA is partnering with several public health-oriented organizations, including the Centers for Disease Control and Prevention, to reach out to individuals with diabetes, cardiovascular disease, and cardiac risk factors to promote primary and secondary prevention strategies at a population level. This is a very different posture than the AMA assumed in the early 20th century, when it was more likely to resist public health programs.
Smarter medical training. Under the direction of family physician Susan Skochelak, MD, MPH, group vice president for medical education, the AMA has provided grant funding to 31 US medical schools to assist with curricular redesign and innovation to train physicians to be effective leaders in the health care system of the future.
Sustainable practices. This area houses what is perhaps the AMA’s most meaningful new program for primary care clinicians. Under the leadership of general internist Christine A. Sinsky, MD, PhD, vice president for professional satisfaction, the AMA has developed a suite of Web tools to help physicians improve the quality and efficiency of their clinical practices.
Specifically, the AMA is offering the STEPS Forward program, a collection of interactive, educational modules developed by physicians for physicians to help address common practice challenges and to achieve the quadruple aim of a better patient experience, better population health, lower overall costs, and improved professional satisfaction.1 The 27 modules are self-directed, group learning exercises that encompass a wide range of thorny issues we deal with on a daily basis. A sampling of topics includes: preparing your practice for change, revenue cycle management, synchronized prescription renewals, and creating a strong team culture.
Programs like these are evidence that the new AMA is a different organization from the one I chose not to join for the past 30 years. I am now a member. Check it out; it might be time for you to join, too.
1. STEPS Forward Series and CME Accreditation. American Medical Association Web site. Available at http://www.ama-assn.org/ama/pub/about-ama/strategic-focus/physician-practices/steps-forward.page. Accessed March 16, 2016.
Until recently, I was not a member of the American Medical Association (AMA). For the past 30 years, I chose not to join because I was troubled by the organization’s direction and the way it seemed to be dominated by special interests. But things have changed—and so has its focus.
The AMA has a new strategy entitled, “A vision for a healthier nation.” Well aligned with the needs of family physicians, the campaign addresses 3 specific areas: better patient health, smarter medical training, and sustainable practices.
Better patient health. The AMA is partnering with several public health-oriented organizations, including the Centers for Disease Control and Prevention, to reach out to individuals with diabetes, cardiovascular disease, and cardiac risk factors to promote primary and secondary prevention strategies at a population level. This is a very different posture than the AMA assumed in the early 20th century, when it was more likely to resist public health programs.
Smarter medical training. Under the direction of family physician Susan Skochelak, MD, MPH, group vice president for medical education, the AMA has provided grant funding to 31 US medical schools to assist with curricular redesign and innovation to train physicians to be effective leaders in the health care system of the future.
Sustainable practices. This area houses what is perhaps the AMA’s most meaningful new program for primary care clinicians. Under the leadership of general internist Christine A. Sinsky, MD, PhD, vice president for professional satisfaction, the AMA has developed a suite of Web tools to help physicians improve the quality and efficiency of their clinical practices.
Specifically, the AMA is offering the STEPS Forward program, a collection of interactive, educational modules developed by physicians for physicians to help address common practice challenges and to achieve the quadruple aim of a better patient experience, better population health, lower overall costs, and improved professional satisfaction.1 The 27 modules are self-directed, group learning exercises that encompass a wide range of thorny issues we deal with on a daily basis. A sampling of topics includes: preparing your practice for change, revenue cycle management, synchronized prescription renewals, and creating a strong team culture.
Programs like these are evidence that the new AMA is a different organization from the one I chose not to join for the past 30 years. I am now a member. Check it out; it might be time for you to join, too.
Until recently, I was not a member of the American Medical Association (AMA). For the past 30 years, I chose not to join because I was troubled by the organization’s direction and the way it seemed to be dominated by special interests. But things have changed—and so has its focus.
The AMA has a new strategy entitled, “A vision for a healthier nation.” Well aligned with the needs of family physicians, the campaign addresses 3 specific areas: better patient health, smarter medical training, and sustainable practices.
Better patient health. The AMA is partnering with several public health-oriented organizations, including the Centers for Disease Control and Prevention, to reach out to individuals with diabetes, cardiovascular disease, and cardiac risk factors to promote primary and secondary prevention strategies at a population level. This is a very different posture than the AMA assumed in the early 20th century, when it was more likely to resist public health programs.
Smarter medical training. Under the direction of family physician Susan Skochelak, MD, MPH, group vice president for medical education, the AMA has provided grant funding to 31 US medical schools to assist with curricular redesign and innovation to train physicians to be effective leaders in the health care system of the future.
Sustainable practices. This area houses what is perhaps the AMA’s most meaningful new program for primary care clinicians. Under the leadership of general internist Christine A. Sinsky, MD, PhD, vice president for professional satisfaction, the AMA has developed a suite of Web tools to help physicians improve the quality and efficiency of their clinical practices.
Specifically, the AMA is offering the STEPS Forward program, a collection of interactive, educational modules developed by physicians for physicians to help address common practice challenges and to achieve the quadruple aim of a better patient experience, better population health, lower overall costs, and improved professional satisfaction.1 The 27 modules are self-directed, group learning exercises that encompass a wide range of thorny issues we deal with on a daily basis. A sampling of topics includes: preparing your practice for change, revenue cycle management, synchronized prescription renewals, and creating a strong team culture.
Programs like these are evidence that the new AMA is a different organization from the one I chose not to join for the past 30 years. I am now a member. Check it out; it might be time for you to join, too.
1. STEPS Forward Series and CME Accreditation. American Medical Association Web site. Available at http://www.ama-assn.org/ama/pub/about-ama/strategic-focus/physician-practices/steps-forward.page. Accessed March 16, 2016.
1. STEPS Forward Series and CME Accreditation. American Medical Association Web site. Available at http://www.ama-assn.org/ama/pub/about-ama/strategic-focus/physician-practices/steps-forward.page. Accessed March 16, 2016.
Flamin’ hots
If you have been practicing for a while, you’re probably old enough to remember the Life cereal commercial that featured Mikey, the “he likes it” kid, who would eat anything. It was falsely rumored that he died from eating too many Pop Rocks candy with soda pop, causing his stomach to explode. Although there was no truth to any of it, it was the rumor of the day. Well, today there is a new snack on the block that is sending many children and teens to the emergency department.

Flamin’ Hots characterize several brands of chips in which the snacks are covered in a chili pepper mixture. As the name implies, the chips are very hot, which only adds to the excitement associated with them. But we have seen an increase in ED visits by teens for severe abdominal pain and red stools.
If you examine the label, it lists “natural flavors,” which is the industry’s code word for their secret formula. In fact, nowhere on the label is chili or any other spicy seasoning listed. Even more interesting is that you can’t find anywhere on the Internet what makes Flamin’ Hot chips so hot. There is evidence to support that red pepper and chili peppers are related to gastric ulcers (Crit Rev Food Sci Nutr. 2006;46[4]:275-328).
Examining the food label, one might be misled into thinking it’s is actually a reasonable snack. The serving size is listed as 21 pieces, but the likelihood that anyone stops at 21 pieces is small. In fact, there are reports that there is an addictive component. As the chili pepper hits the stomach, it causes pain, which causes a release of endorphins. This leads to a feeling of pleasure, which in turns encourages the person to want more chips, hence the ingestion of multiple bags prior to the trip to the ED.

There have been many warnings of the deleterious effects of the chips. In 2011 California, and soon after that Illinois, banned it from schools, stating it was unhealthy. Many schools since then have followed suit. But despite all the hype, kids are eating them by the dozen. Although there are no data to support that there is a cause and effect relationship with Flamin’ Hots and ulcers, it is safe to assume with the number of ED visits and the diet of the average teen, that at least gastritis is an issue.
Beyond stomach pain, prolonged intake of spicy hot snacks will contribute to high cholesterol and obesity. Many children are under the false assumption that because they don’t eat big meals, they are eating well. But because so many of these unhealthy snacks are empty calories and increase fat intake (N Engl J Med. 2006 Apr 13;354[15]:1601-13), children’s body mass indices continue to rise. Informing parents about the harmful effect is important so they can monitor intake as well as encourage healthier snacks. Understanding how to read a food label is another important thing to teach during well visits so that parents can understand how much fat is in these snacks and can adjust accordingly.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
If you have been practicing for a while, you’re probably old enough to remember the Life cereal commercial that featured Mikey, the “he likes it” kid, who would eat anything. It was falsely rumored that he died from eating too many Pop Rocks candy with soda pop, causing his stomach to explode. Although there was no truth to any of it, it was the rumor of the day. Well, today there is a new snack on the block that is sending many children and teens to the emergency department.
Flamin’ Hots characterize several brands of chips in which the snacks are covered in a chili pepper mixture. As the name implies, the chips are very hot, which only adds to the excitement associated with them. But we have seen an increase in ED visits by teens for severe abdominal pain and red stools.
If you examine the label, it lists “natural flavors,” which is the industry’s code word for their secret formula. In fact, nowhere on the label is chili or any other spicy seasoning listed. Even more interesting is that you can’t find anywhere on the Internet what makes Flamin’ Hot chips so hot. There is evidence to support that red pepper and chili peppers are related to gastric ulcers (Crit Rev Food Sci Nutr. 2006;46[4]:275-328).
Examining the food label, one might be misled into thinking it’s is actually a reasonable snack. The serving size is listed as 21 pieces, but the likelihood that anyone stops at 21 pieces is small. In fact, there are reports that there is an addictive component. As the chili pepper hits the stomach, it causes pain, which causes a release of endorphins. This leads to a feeling of pleasure, which in turns encourages the person to want more chips, hence the ingestion of multiple bags prior to the trip to the ED.
There have been many warnings of the deleterious effects of the chips. In 2011 California, and soon after that Illinois, banned it from schools, stating it was unhealthy. Many schools since then have followed suit. But despite all the hype, kids are eating them by the dozen. Although there are no data to support that there is a cause and effect relationship with Flamin’ Hots and ulcers, it is safe to assume with the number of ED visits and the diet of the average teen, that at least gastritis is an issue.
Beyond stomach pain, prolonged intake of spicy hot snacks will contribute to high cholesterol and obesity. Many children are under the false assumption that because they don’t eat big meals, they are eating well. But because so many of these unhealthy snacks are empty calories and increase fat intake (N Engl J Med. 2006 Apr 13;354[15]:1601-13), children’s body mass indices continue to rise. Informing parents about the harmful effect is important so they can monitor intake as well as encourage healthier snacks. Understanding how to read a food label is another important thing to teach during well visits so that parents can understand how much fat is in these snacks and can adjust accordingly.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
If you have been practicing for a while, you’re probably old enough to remember the Life cereal commercial that featured Mikey, the “he likes it” kid, who would eat anything. It was falsely rumored that he died from eating too many Pop Rocks candy with soda pop, causing his stomach to explode. Although there was no truth to any of it, it was the rumor of the day. Well, today there is a new snack on the block that is sending many children and teens to the emergency department.
Flamin’ Hots characterize several brands of chips in which the snacks are covered in a chili pepper mixture. As the name implies, the chips are very hot, which only adds to the excitement associated with them. But we have seen an increase in ED visits by teens for severe abdominal pain and red stools.
If you examine the label, it lists “natural flavors,” which is the industry’s code word for their secret formula. In fact, nowhere on the label is chili or any other spicy seasoning listed. Even more interesting is that you can’t find anywhere on the Internet what makes Flamin’ Hot chips so hot. There is evidence to support that red pepper and chili peppers are related to gastric ulcers (Crit Rev Food Sci Nutr. 2006;46[4]:275-328).
Examining the food label, one might be misled into thinking it’s is actually a reasonable snack. The serving size is listed as 21 pieces, but the likelihood that anyone stops at 21 pieces is small. In fact, there are reports that there is an addictive component. As the chili pepper hits the stomach, it causes pain, which causes a release of endorphins. This leads to a feeling of pleasure, which in turns encourages the person to want more chips, hence the ingestion of multiple bags prior to the trip to the ED.
There have been many warnings of the deleterious effects of the chips. In 2011 California, and soon after that Illinois, banned it from schools, stating it was unhealthy. Many schools since then have followed suit. But despite all the hype, kids are eating them by the dozen. Although there are no data to support that there is a cause and effect relationship with Flamin’ Hots and ulcers, it is safe to assume with the number of ED visits and the diet of the average teen, that at least gastritis is an issue.
Beyond stomach pain, prolonged intake of spicy hot snacks will contribute to high cholesterol and obesity. Many children are under the false assumption that because they don’t eat big meals, they are eating well. But because so many of these unhealthy snacks are empty calories and increase fat intake (N Engl J Med. 2006 Apr 13;354[15]:1601-13), children’s body mass indices continue to rise. Informing parents about the harmful effect is important so they can monitor intake as well as encourage healthier snacks. Understanding how to read a food label is another important thing to teach during well visits so that parents can understand how much fat is in these snacks and can adjust accordingly.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.

Biologics for Psoriasis

Review the PDF of the fact sheet on biologics for psoriasis with board-relevant, easy-to-review material. This month's fact sheet discusses the current US Food and Drug Administration–approved biologic medications for psoriasis and psoriatic arthritis, including the mechanism of action, dosing, and side effects.
Practice Questions
1. Which biologic is administered as an intravenous infusion?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
2. Which biologic is dosed based on body weight?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
3. Which biologic has been shown to worsen existing Crohn disease?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
4. Which biologic is a fusion protein?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
5. Which biologic has been shown to cause reversible posterior leukoencephalopathy syndrome?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
Answers to practice questions provided on next page
Practice Question Answers
1. Which biologic is administered as an intravenous infusion?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
2. Which biologic is dosed based on body weight?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
3. Which biologic has been shown to worsen existing Crohn disease?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
4. Which biologic is a fusion protein?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
5. Which biologic has been shown to cause reversible posterior leukoencephalopathy syndrome?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
Review the PDF of the fact sheet on biologics for psoriasis with board-relevant, easy-to-review material. This month's fact sheet discusses the current US Food and Drug Administration–approved biologic medications for psoriasis and psoriatic arthritis, including the mechanism of action, dosing, and side effects.
Practice Questions
1. Which biologic is administered as an intravenous infusion?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
2. Which biologic is dosed based on body weight?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
3. Which biologic has been shown to worsen existing Crohn disease?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
4. Which biologic is a fusion protein?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
5. Which biologic has been shown to cause reversible posterior leukoencephalopathy syndrome?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
Answers to practice questions provided on next page
Practice Question Answers
1. Which biologic is administered as an intravenous infusion?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
2. Which biologic is dosed based on body weight?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
3. Which biologic has been shown to worsen existing Crohn disease?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
4. Which biologic is a fusion protein?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
5. Which biologic has been shown to cause reversible posterior leukoencephalopathy syndrome?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
Review the PDF of the fact sheet on biologics for psoriasis with board-relevant, easy-to-review material. This month's fact sheet discusses the current US Food and Drug Administration–approved biologic medications for psoriasis and psoriatic arthritis, including the mechanism of action, dosing, and side effects.
Practice Questions
1. Which biologic is administered as an intravenous infusion?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
2. Which biologic is dosed based on body weight?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
3. Which biologic has been shown to worsen existing Crohn disease?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
4. Which biologic is a fusion protein?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
5. Which biologic has been shown to cause reversible posterior leukoencephalopathy syndrome?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
Answers to practice questions provided on next page
Practice Question Answers
1. Which biologic is administered as an intravenous infusion?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
2. Which biologic is dosed based on body weight?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
3. Which biologic has been shown to worsen existing Crohn disease?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
4. Which biologic is a fusion protein?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
5. Which biologic has been shown to cause reversible posterior leukoencephalopathy syndrome?
a. adalimumab
b. etanercept
c. infliximab
d. secukinumab
e. ustekinumab
