User login
Institute of Medicine Report Examines Medical Misdiagnoses

Authors of the IOM’s “Improving Diagnosis in Health Care” report cite problems in communication and limitations in electronic health records behind inaccurate and delayed diagnoses, concluding that the problem of diagnostic errors generally has not been adequately studied.1
“This problem is significant and serious. Yet we don’t know for sure how often it occurs, how serious it is, or how much it costs,” said the IOM committee’s chair, John Ball, MD, of the American College of Physicians, in a prepared statement. The report concludes there is no easy fix for the problem of diagnostic errors, which are a leading cause of adverse events in hospitals and of malpractice lawsuits for hospitalists, but calls for a major reassessment of the diagnostic process.2
Hospitalist Mangla Gulati, MD, FACP, SFHM, assistant chief medical officer at the University of Maryland Medical Center in Baltimore, says hospitalists would be remiss if they failed to take a closer look at the IOM report. “Diagnostic error is something we haven’t much talked about in medicine,” Dr. Gulati says. “Part of the goal of this report is to actually include the patient in those conversations.” Patients who are rehospitalized, she says, may have been given an incorrect initial diagnosis that was never rectified, or there may have been a failure to communicate important information.
“How many tests do we order where results come back after a patient leaves the hospital?” asks Kedar Mate, MD, senior vice president at the Institute for Healthcare Improvement and a hospitalist at Weill Cornell Medicine in New York City. “How many in-hospital diagnoses are made without all of the available information from outside providers?”
One simple intervention hospitalists could do immediately, he says, is to start tracking all important tests ordered for patients on a board in the medical team’s meeting room, only removing them from the board when results have been checked and communicated to the patient and outpatient provider.
References
- National Academies of Sciences, Engineering, and Medicine. Improving Diagnosis in Health Care. Washington, DC: The National Academies Press. 2015.
- Saber Tehrani AS, Lee HW, Mathews SC, et al. 25-year summary of U.S. malpractice claims for diagnostic errors 1986–2010: An analysis from the National Practitioner Data Bank. BMJ Qual Saf. 2013 Aug; 22(8):672–680.
Authors of the IOM’s “Improving Diagnosis in Health Care” report cite problems in communication and limitations in electronic health records behind inaccurate and delayed diagnoses, concluding that the problem of diagnostic errors generally has not been adequately studied.1
“This problem is significant and serious. Yet we don’t know for sure how often it occurs, how serious it is, or how much it costs,” said the IOM committee’s chair, John Ball, MD, of the American College of Physicians, in a prepared statement. The report concludes there is no easy fix for the problem of diagnostic errors, which are a leading cause of adverse events in hospitals and of malpractice lawsuits for hospitalists, but calls for a major reassessment of the diagnostic process.2
Hospitalist Mangla Gulati, MD, FACP, SFHM, assistant chief medical officer at the University of Maryland Medical Center in Baltimore, says hospitalists would be remiss if they failed to take a closer look at the IOM report. “Diagnostic error is something we haven’t much talked about in medicine,” Dr. Gulati says. “Part of the goal of this report is to actually include the patient in those conversations.” Patients who are rehospitalized, she says, may have been given an incorrect initial diagnosis that was never rectified, or there may have been a failure to communicate important information.
“How many tests do we order where results come back after a patient leaves the hospital?” asks Kedar Mate, MD, senior vice president at the Institute for Healthcare Improvement and a hospitalist at Weill Cornell Medicine in New York City. “How many in-hospital diagnoses are made without all of the available information from outside providers?”
One simple intervention hospitalists could do immediately, he says, is to start tracking all important tests ordered for patients on a board in the medical team’s meeting room, only removing them from the board when results have been checked and communicated to the patient and outpatient provider.
References
- National Academies of Sciences, Engineering, and Medicine. Improving Diagnosis in Health Care. Washington, DC: The National Academies Press. 2015.
- Saber Tehrani AS, Lee HW, Mathews SC, et al. 25-year summary of U.S. malpractice claims for diagnostic errors 1986–2010: An analysis from the National Practitioner Data Bank. BMJ Qual Saf. 2013 Aug; 22(8):672–680.
Authors of the IOM’s “Improving Diagnosis in Health Care” report cite problems in communication and limitations in electronic health records behind inaccurate and delayed diagnoses, concluding that the problem of diagnostic errors generally has not been adequately studied.1
“This problem is significant and serious. Yet we don’t know for sure how often it occurs, how serious it is, or how much it costs,” said the IOM committee’s chair, John Ball, MD, of the American College of Physicians, in a prepared statement. The report concludes there is no easy fix for the problem of diagnostic errors, which are a leading cause of adverse events in hospitals and of malpractice lawsuits for hospitalists, but calls for a major reassessment of the diagnostic process.2
Hospitalist Mangla Gulati, MD, FACP, SFHM, assistant chief medical officer at the University of Maryland Medical Center in Baltimore, says hospitalists would be remiss if they failed to take a closer look at the IOM report. “Diagnostic error is something we haven’t much talked about in medicine,” Dr. Gulati says. “Part of the goal of this report is to actually include the patient in those conversations.” Patients who are rehospitalized, she says, may have been given an incorrect initial diagnosis that was never rectified, or there may have been a failure to communicate important information.
“How many tests do we order where results come back after a patient leaves the hospital?” asks Kedar Mate, MD, senior vice president at the Institute for Healthcare Improvement and a hospitalist at Weill Cornell Medicine in New York City. “How many in-hospital diagnoses are made without all of the available information from outside providers?”
One simple intervention hospitalists could do immediately, he says, is to start tracking all important tests ordered for patients on a board in the medical team’s meeting room, only removing them from the board when results have been checked and communicated to the patient and outpatient provider.
References
- National Academies of Sciences, Engineering, and Medicine. Improving Diagnosis in Health Care. Washington, DC: The National Academies Press. 2015.
- Saber Tehrani AS, Lee HW, Mathews SC, et al. 25-year summary of U.S. malpractice claims for diagnostic errors 1986–2010: An analysis from the National Practitioner Data Bank. BMJ Qual Saf. 2013 Aug; 22(8):672–680.
Quality Improvement Initiative Targets Sepsis
A quality improvement (QI) initiative at University Hospital in Salt Lake City aims to save lives and cut hospital costs by reducing inpatient sepsis mortality.
Program co-leaders, hospitalists Devin Horton, MD, and Kencee Graves, MD, of University Hospital, launched the initiative as a pilot program last October. They began by surveying hospital house staff and nurses on their ability to recognize and define six different sepsis syndromes from clinical vignettes. A total of 136 surveyed residents recognized the correct condition only 56% of the time, and 280 surveyed nurses only did so 17% of the time. The hospitalists determined that better education about sepsis was crucial.
“We developed a robust teaching program for nurses and residents using Septris, an online educational game from Stanford University,” Dr. Horton says. The team also developed technology that can recognize worsening vital signs in a patient and automatically trigger an alert to a charge nurse or rapid response team.
The team’s Modified Early Warning System (MEWS) for recognizing sepsis is similar to the Early Warning and Response System (EWRS) system used at the University of Pennsylvania Health System and the University of California San Diego, and draws on other hospitals’ sepsis systems. Dr. Horton says one difference in their system is the involvement of nursing aides who take vital signs, enter them real-time into electronic health records (EHR), and receive prompts from abnormal vital signs to retake all vitals and confirm abnormal results. It also incorporates EHR decision support tools, including links to pre-populated medical order panels, such as for the ordering of tests for lactate and blood cultures.
“Severe sepsis is often quoted as the number one cause of mortality among hospitalized patients, with a rate up to 10 times that of acute myocardial infarction,” Dr. Horton explains. “The one treatment that consistently decreases mortality is timely administration of antibiotics. But, in order for a patient to be given timely antibiotics, the nurse or resident must first recognize that the patient has sepsis.”
“This is one of the biggest and most far-reaching improvement initiatives that has been done at our institution,” says Robert Pendleton, MD, chief quality officer at University Hospital. Dr. Horton says he predicts the program will “save 50 lives and $1 million per year.”
For more information, contact him at: devin.horton@hsc.utah.edu.
A quality improvement (QI) initiative at University Hospital in Salt Lake City aims to save lives and cut hospital costs by reducing inpatient sepsis mortality.
Program co-leaders, hospitalists Devin Horton, MD, and Kencee Graves, MD, of University Hospital, launched the initiative as a pilot program last October. They began by surveying hospital house staff and nurses on their ability to recognize and define six different sepsis syndromes from clinical vignettes. A total of 136 surveyed residents recognized the correct condition only 56% of the time, and 280 surveyed nurses only did so 17% of the time. The hospitalists determined that better education about sepsis was crucial.
“We developed a robust teaching program for nurses and residents using Septris, an online educational game from Stanford University,” Dr. Horton says. The team also developed technology that can recognize worsening vital signs in a patient and automatically trigger an alert to a charge nurse or rapid response team.
The team’s Modified Early Warning System (MEWS) for recognizing sepsis is similar to the Early Warning and Response System (EWRS) system used at the University of Pennsylvania Health System and the University of California San Diego, and draws on other hospitals’ sepsis systems. Dr. Horton says one difference in their system is the involvement of nursing aides who take vital signs, enter them real-time into electronic health records (EHR), and receive prompts from abnormal vital signs to retake all vitals and confirm abnormal results. It also incorporates EHR decision support tools, including links to pre-populated medical order panels, such as for the ordering of tests for lactate and blood cultures.
“Severe sepsis is often quoted as the number one cause of mortality among hospitalized patients, with a rate up to 10 times that of acute myocardial infarction,” Dr. Horton explains. “The one treatment that consistently decreases mortality is timely administration of antibiotics. But, in order for a patient to be given timely antibiotics, the nurse or resident must first recognize that the patient has sepsis.”
“This is one of the biggest and most far-reaching improvement initiatives that has been done at our institution,” says Robert Pendleton, MD, chief quality officer at University Hospital. Dr. Horton says he predicts the program will “save 50 lives and $1 million per year.”
For more information, contact him at: devin.horton@hsc.utah.edu.
A quality improvement (QI) initiative at University Hospital in Salt Lake City aims to save lives and cut hospital costs by reducing inpatient sepsis mortality.
Program co-leaders, hospitalists Devin Horton, MD, and Kencee Graves, MD, of University Hospital, launched the initiative as a pilot program last October. They began by surveying hospital house staff and nurses on their ability to recognize and define six different sepsis syndromes from clinical vignettes. A total of 136 surveyed residents recognized the correct condition only 56% of the time, and 280 surveyed nurses only did so 17% of the time. The hospitalists determined that better education about sepsis was crucial.
“We developed a robust teaching program for nurses and residents using Septris, an online educational game from Stanford University,” Dr. Horton says. The team also developed technology that can recognize worsening vital signs in a patient and automatically trigger an alert to a charge nurse or rapid response team.
The team’s Modified Early Warning System (MEWS) for recognizing sepsis is similar to the Early Warning and Response System (EWRS) system used at the University of Pennsylvania Health System and the University of California San Diego, and draws on other hospitals’ sepsis systems. Dr. Horton says one difference in their system is the involvement of nursing aides who take vital signs, enter them real-time into electronic health records (EHR), and receive prompts from abnormal vital signs to retake all vitals and confirm abnormal results. It also incorporates EHR decision support tools, including links to pre-populated medical order panels, such as for the ordering of tests for lactate and blood cultures.
“Severe sepsis is often quoted as the number one cause of mortality among hospitalized patients, with a rate up to 10 times that of acute myocardial infarction,” Dr. Horton explains. “The one treatment that consistently decreases mortality is timely administration of antibiotics. But, in order for a patient to be given timely antibiotics, the nurse or resident must first recognize that the patient has sepsis.”
“This is one of the biggest and most far-reaching improvement initiatives that has been done at our institution,” says Robert Pendleton, MD, chief quality officer at University Hospital. Dr. Horton says he predicts the program will “save 50 lives and $1 million per year.”
For more information, contact him at: devin.horton@hsc.utah.edu.
Early Mobility Program
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
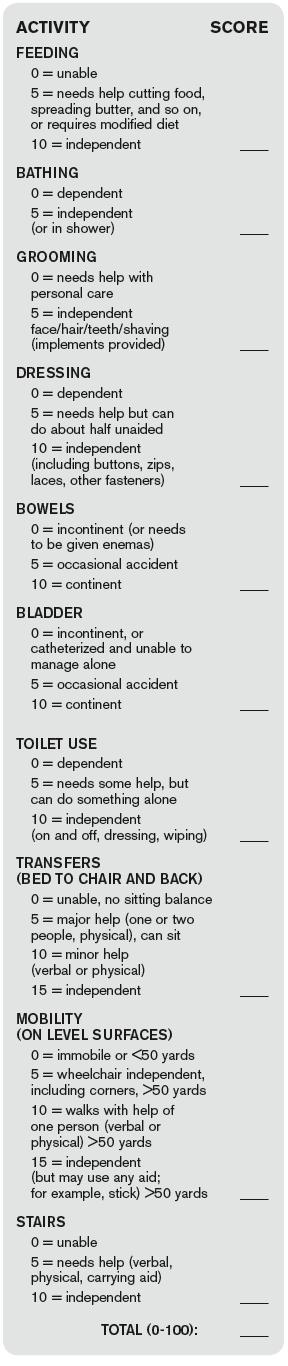
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.


References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.
References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.
References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
Thombosis Management Demands Balanced Approach
The delicate balance involved in providing hospitalized patients with needed anticoagulant, anti-platelet, and thrombolytic therapies for stroke and possible cardiac complications, while minimizing bleed risks, was explored by several speakers at the University of California San Francisco’s annual Management of the Hospitalized Patient conference.
“These are dynamic issues and they’re moving all the time,” said Tracy Minichiello, MD, a former hospitalist who now runs Anticoagulation and Thrombosis Services at the San Francisco VA Medical Center. Dosing and monitoring choices for physicians have grown more complicated with the new oral anticoagulants (apixaban, dabigatran, and rivaroxaban), and Dr. Minichiello said another balancing act is emerging in hospitals trying to avoid unnecessary and wasteful treatments.
“There is interest on both sides of that question,” Dr. Minichiello said, adding that the stakes are high. “We don’t want to miss the diagnosis of pulmonary embolisms, which can be difficult to catch. But now there’s more discussion
of the other side of the issue—overdiagnosis and overtreatment—where we’re also trying to avoid, for example, overuse of CT scans.”

Another major thrust of Dr. Minichiello’s presentations involved bridging therapies, the application of a parenteral, short-acting anticoagulant therapy during the temporary interruption of warfarin anticoagulation for an invasive procedure. Bridging decreases stroke and embolism risk but comes with an increased risk for bleeding.
“Full intensity bridging therapy for anticoagulation potentially can do more harm than good,” she said, noting a dearth of data to support mortality benefits of bridging therapy.
Literature increasingly recommends that hospitalists be more selective about the use of bridging therapies that might have been employed reflexively in the past, Dr. Minichiello noted. “[Hospitalists] must be mindful of the risks and benefits,” she said. Physicians should also think twice about concomitant antiplatelet therapy, like aspirin with anticoagulants. “We need to work collaboratively with our cardiology colleagues when a patient is on two or three of these therapies,” she said. “Recommendations in this area are in evolution.”
Elise Bouchard, MD, an internist at Centre Maria-Chapdelaine in Dolbeau-Mistassini, Québec, attended Dr. Minichiello’s breakout session on challenging cases.
“I learned that we shouldn’t use aspirin with Coumadin or other anticoagulants, except for cases like acute coronary syndrome,”
Dr. Bouchard said. She also explained that a number of her patients with cancer, for example, need anticoagulation treatment and hate getting another injection, so she tries to offer the oral anticoagulants whenever possible.
Dr. Minichiello works with hospitalists at the San Francisco VA who seek consults around performing procedures, choosing anticoagulants, and determining when to restart treatments.
“Most hospitalists don’t have access to a service like ours, although they might be able to call on a hematology consult service [or pharmacist],” she said. She suggested that hospitalists trying to develop their own evidenced-based protocols use websites like the University of Washington’s Anticoagulation Services website, or the American Society of Health System Pharmacists’ Anticoagulation Resource Center.
The delicate balance involved in providing hospitalized patients with needed anticoagulant, anti-platelet, and thrombolytic therapies for stroke and possible cardiac complications, while minimizing bleed risks, was explored by several speakers at the University of California San Francisco’s annual Management of the Hospitalized Patient conference.
“These are dynamic issues and they’re moving all the time,” said Tracy Minichiello, MD, a former hospitalist who now runs Anticoagulation and Thrombosis Services at the San Francisco VA Medical Center. Dosing and monitoring choices for physicians have grown more complicated with the new oral anticoagulants (apixaban, dabigatran, and rivaroxaban), and Dr. Minichiello said another balancing act is emerging in hospitals trying to avoid unnecessary and wasteful treatments.
“There is interest on both sides of that question,” Dr. Minichiello said, adding that the stakes are high. “We don’t want to miss the diagnosis of pulmonary embolisms, which can be difficult to catch. But now there’s more discussion
of the other side of the issue—overdiagnosis and overtreatment—where we’re also trying to avoid, for example, overuse of CT scans.”
Another major thrust of Dr. Minichiello’s presentations involved bridging therapies, the application of a parenteral, short-acting anticoagulant therapy during the temporary interruption of warfarin anticoagulation for an invasive procedure. Bridging decreases stroke and embolism risk but comes with an increased risk for bleeding.
“Full intensity bridging therapy for anticoagulation potentially can do more harm than good,” she said, noting a dearth of data to support mortality benefits of bridging therapy.
Literature increasingly recommends that hospitalists be more selective about the use of bridging therapies that might have been employed reflexively in the past, Dr. Minichiello noted. “[Hospitalists] must be mindful of the risks and benefits,” she said. Physicians should also think twice about concomitant antiplatelet therapy, like aspirin with anticoagulants. “We need to work collaboratively with our cardiology colleagues when a patient is on two or three of these therapies,” she said. “Recommendations in this area are in evolution.”
Elise Bouchard, MD, an internist at Centre Maria-Chapdelaine in Dolbeau-Mistassini, Québec, attended Dr. Minichiello’s breakout session on challenging cases.
“I learned that we shouldn’t use aspirin with Coumadin or other anticoagulants, except for cases like acute coronary syndrome,”
Dr. Bouchard said. She also explained that a number of her patients with cancer, for example, need anticoagulation treatment and hate getting another injection, so she tries to offer the oral anticoagulants whenever possible.
Dr. Minichiello works with hospitalists at the San Francisco VA who seek consults around performing procedures, choosing anticoagulants, and determining when to restart treatments.
“Most hospitalists don’t have access to a service like ours, although they might be able to call on a hematology consult service [or pharmacist],” she said. She suggested that hospitalists trying to develop their own evidenced-based protocols use websites like the University of Washington’s Anticoagulation Services website, or the American Society of Health System Pharmacists’ Anticoagulation Resource Center.
The delicate balance involved in providing hospitalized patients with needed anticoagulant, anti-platelet, and thrombolytic therapies for stroke and possible cardiac complications, while minimizing bleed risks, was explored by several speakers at the University of California San Francisco’s annual Management of the Hospitalized Patient conference.
“These are dynamic issues and they’re moving all the time,” said Tracy Minichiello, MD, a former hospitalist who now runs Anticoagulation and Thrombosis Services at the San Francisco VA Medical Center. Dosing and monitoring choices for physicians have grown more complicated with the new oral anticoagulants (apixaban, dabigatran, and rivaroxaban), and Dr. Minichiello said another balancing act is emerging in hospitals trying to avoid unnecessary and wasteful treatments.
“There is interest on both sides of that question,” Dr. Minichiello said, adding that the stakes are high. “We don’t want to miss the diagnosis of pulmonary embolisms, which can be difficult to catch. But now there’s more discussion
of the other side of the issue—overdiagnosis and overtreatment—where we’re also trying to avoid, for example, overuse of CT scans.”
Another major thrust of Dr. Minichiello’s presentations involved bridging therapies, the application of a parenteral, short-acting anticoagulant therapy during the temporary interruption of warfarin anticoagulation for an invasive procedure. Bridging decreases stroke and embolism risk but comes with an increased risk for bleeding.
“Full intensity bridging therapy for anticoagulation potentially can do more harm than good,” she said, noting a dearth of data to support mortality benefits of bridging therapy.
Literature increasingly recommends that hospitalists be more selective about the use of bridging therapies that might have been employed reflexively in the past, Dr. Minichiello noted. “[Hospitalists] must be mindful of the risks and benefits,” she said. Physicians should also think twice about concomitant antiplatelet therapy, like aspirin with anticoagulants. “We need to work collaboratively with our cardiology colleagues when a patient is on two or three of these therapies,” she said. “Recommendations in this area are in evolution.”
Elise Bouchard, MD, an internist at Centre Maria-Chapdelaine in Dolbeau-Mistassini, Québec, attended Dr. Minichiello’s breakout session on challenging cases.
“I learned that we shouldn’t use aspirin with Coumadin or other anticoagulants, except for cases like acute coronary syndrome,”
Dr. Bouchard said. She also explained that a number of her patients with cancer, for example, need anticoagulation treatment and hate getting another injection, so she tries to offer the oral anticoagulants whenever possible.
Dr. Minichiello works with hospitalists at the San Francisco VA who seek consults around performing procedures, choosing anticoagulants, and determining when to restart treatments.
“Most hospitalists don’t have access to a service like ours, although they might be able to call on a hematology consult service [or pharmacist],” she said. She suggested that hospitalists trying to develop their own evidenced-based protocols use websites like the University of Washington’s Anticoagulation Services website, or the American Society of Health System Pharmacists’ Anticoagulation Resource Center.
Limiting Full-Contact Practice Reduces Football Concussions
WASHINGTON, DC—Limiting the amount of full-contact tackling that occurs in high school football practice reduces the rate of sports-related concussions among the athletes, according to a prospective study.
“Something as simple as saying they can’t tackle all the time, limiting the amount of minutes each month, reduced the incidence,” said Timothy A. McGuine, PhD, Senior Scientist at the University of Wisconsin, Madison, at the American Academy of Pediatrics Annual Meeting.
“The majority of sports-related concussions sustained in high school football practice occurred during full-contact activities,” he said. “The rate of sports-related concussions sustained in high school football practice was more than twice as high in the two seasons prior to a rule change limiting the amount and duration of full-contact activities.”
Testing a Tackle-Limiting Rule
In their study, Dr. McGuine and his associates tested the effects of a tackle-limiting rule implemented in 2014 in a state interscholastic athletic association for all players in grades 9 through 12. The rule prohibited full-contact play during the first practice week, and full contact was defined as “drills or game situations that occur at game speed when full tackles are made at a competitive pace and players are taken to the ground.” The players engaged in full-contact play for as long as 75 minutes total during the second week of practice and for a maximum of 60 min/week for all subsequent weeks in the practice season. The rule did not apply to games.
For data on the two years before the rule change, 2,081 athletes with a mean age of 16 reported their concussion history in the 2012 season, which included 36 schools, and the 2013 season, which included 18 schools. In 2014, licensed athletic trainers recorded the incidence and severity of each sports-related concussion for the 945 players at 26 schools. During all three seasons, almost half the concussions (46%) occurred during tackling. Although the overall rate of concussions dropped from 1.57 per 1,000 athletic exposures in the combined 2012 and 2013 seasons to 1.28 per 1,000 athletic exposures in the 2014 season, the difference was not significant. During the 2012 and 2013 seasons combined, 206 players (9%) sustained 211 concussions, compared with 67 players (7%) with 70 concussions in 2014.
The difference in concussions occurring during practice, however, did differ significantly before and after the rule change. The rate of concussions during practice in 2014 was 0.33 concussions per 1,000 athletic exposures, compared with 0.76 concussions per 1,000 exposures in the 2012 and 2013 seasons. Twelve of 15 concussions in 2014 practices occurred during full-contact practices, a rate of 0.57 per 1,000 exposures, and 82 of 86 concussions in the 2012 and 2013 seasons occurred during full contact practices, a rate of 0.87 per 1,000 exposures.
The investigators observed no difference in concussion rate during the games following the rule change. The 2014 rate of concussions during games was 5.74 per 1,000 exposures, compared with 5.81 per 1,000 exposures in the combined 2012 and 2013 seasons. The severity of concussions sustained before and after the rule change also did not differ, and athletes’ years of football-playing experience had no effect on the concussion incidence in 2014.
To Tackle or Not to Tackle?
Despite the relationship between full-contact play and concussions, Dr. McGuine said that he would not support banning tackling from football.
“I think the benefits of the sport far outweigh the risks,” Dr. McGuine said. “Concussions particularly have transcended a sports issue and become a public health issue and have become political, and I’m very much against legislators, policy makers, [and] associations making blanket rules without the evidence to back those,” he said. “There are lingering long-term effects from all orthopedic injuries, but we’re focusing on concussions.”
Equipment modification is unlikely to make much difference in concussion rates either, said Dr. McGuine, whose previous study on football helmets found that the brand and model did not influence concussion risk. “Concussions are multifactorial,” he said. “We can’t just limit the amount of force transmitted to the brain and say we’re going to stop these injuries from occurring.”
One important strategy for reducing concussions is increasing parents’ and athletes’ awareness about multiple injuries and about ways to reduce the risk, Dr. McGuine said.
“Concussions are like any other injury [such as] ankle sprains, knee injuries and surgeries, [and] shoulder dislocations,” he said. “If you have one, you’re more susceptible to having another one, as opposed to somebody who never had that injury, so the problems are repeat injuries and lingering injuries.” Any of these injuries can have a lasting effect on a young athlete’s quality of life, Dr. McGuine added.
Another way to decrease the incidence of concussions is to enforce rules against leading, or lowering, athletes’ heads during tackling.
“A big issue now is penalizing players for leading with their head and face, but I think we need to be consistent there, too,” Dr. McGuine said. “We can’t penalize defensive players for lowering their helmet if we’re not going to penalize running backs and wide receivers.”
—Tara Haelle
WASHINGTON, DC—Limiting the amount of full-contact tackling that occurs in high school football practice reduces the rate of sports-related concussions among the athletes, according to a prospective study.
“Something as simple as saying they can’t tackle all the time, limiting the amount of minutes each month, reduced the incidence,” said Timothy A. McGuine, PhD, Senior Scientist at the University of Wisconsin, Madison, at the American Academy of Pediatrics Annual Meeting.
“The majority of sports-related concussions sustained in high school football practice occurred during full-contact activities,” he said. “The rate of sports-related concussions sustained in high school football practice was more than twice as high in the two seasons prior to a rule change limiting the amount and duration of full-contact activities.”
Testing a Tackle-Limiting Rule
In their study, Dr. McGuine and his associates tested the effects of a tackle-limiting rule implemented in 2014 in a state interscholastic athletic association for all players in grades 9 through 12. The rule prohibited full-contact play during the first practice week, and full contact was defined as “drills or game situations that occur at game speed when full tackles are made at a competitive pace and players are taken to the ground.” The players engaged in full-contact play for as long as 75 minutes total during the second week of practice and for a maximum of 60 min/week for all subsequent weeks in the practice season. The rule did not apply to games.
For data on the two years before the rule change, 2,081 athletes with a mean age of 16 reported their concussion history in the 2012 season, which included 36 schools, and the 2013 season, which included 18 schools. In 2014, licensed athletic trainers recorded the incidence and severity of each sports-related concussion for the 945 players at 26 schools. During all three seasons, almost half the concussions (46%) occurred during tackling. Although the overall rate of concussions dropped from 1.57 per 1,000 athletic exposures in the combined 2012 and 2013 seasons to 1.28 per 1,000 athletic exposures in the 2014 season, the difference was not significant. During the 2012 and 2013 seasons combined, 206 players (9%) sustained 211 concussions, compared with 67 players (7%) with 70 concussions in 2014.
The difference in concussions occurring during practice, however, did differ significantly before and after the rule change. The rate of concussions during practice in 2014 was 0.33 concussions per 1,000 athletic exposures, compared with 0.76 concussions per 1,000 exposures in the 2012 and 2013 seasons. Twelve of 15 concussions in 2014 practices occurred during full-contact practices, a rate of 0.57 per 1,000 exposures, and 82 of 86 concussions in the 2012 and 2013 seasons occurred during full contact practices, a rate of 0.87 per 1,000 exposures.
The investigators observed no difference in concussion rate during the games following the rule change. The 2014 rate of concussions during games was 5.74 per 1,000 exposures, compared with 5.81 per 1,000 exposures in the combined 2012 and 2013 seasons. The severity of concussions sustained before and after the rule change also did not differ, and athletes’ years of football-playing experience had no effect on the concussion incidence in 2014.
To Tackle or Not to Tackle?
Despite the relationship between full-contact play and concussions, Dr. McGuine said that he would not support banning tackling from football.
“I think the benefits of the sport far outweigh the risks,” Dr. McGuine said. “Concussions particularly have transcended a sports issue and become a public health issue and have become political, and I’m very much against legislators, policy makers, [and] associations making blanket rules without the evidence to back those,” he said. “There are lingering long-term effects from all orthopedic injuries, but we’re focusing on concussions.”
Equipment modification is unlikely to make much difference in concussion rates either, said Dr. McGuine, whose previous study on football helmets found that the brand and model did not influence concussion risk. “Concussions are multifactorial,” he said. “We can’t just limit the amount of force transmitted to the brain and say we’re going to stop these injuries from occurring.”
One important strategy for reducing concussions is increasing parents’ and athletes’ awareness about multiple injuries and about ways to reduce the risk, Dr. McGuine said.
“Concussions are like any other injury [such as] ankle sprains, knee injuries and surgeries, [and] shoulder dislocations,” he said. “If you have one, you’re more susceptible to having another one, as opposed to somebody who never had that injury, so the problems are repeat injuries and lingering injuries.” Any of these injuries can have a lasting effect on a young athlete’s quality of life, Dr. McGuine added.
Another way to decrease the incidence of concussions is to enforce rules against leading, or lowering, athletes’ heads during tackling.
“A big issue now is penalizing players for leading with their head and face, but I think we need to be consistent there, too,” Dr. McGuine said. “We can’t penalize defensive players for lowering their helmet if we’re not going to penalize running backs and wide receivers.”
—Tara Haelle
WASHINGTON, DC—Limiting the amount of full-contact tackling that occurs in high school football practice reduces the rate of sports-related concussions among the athletes, according to a prospective study.
“Something as simple as saying they can’t tackle all the time, limiting the amount of minutes each month, reduced the incidence,” said Timothy A. McGuine, PhD, Senior Scientist at the University of Wisconsin, Madison, at the American Academy of Pediatrics Annual Meeting.
“The majority of sports-related concussions sustained in high school football practice occurred during full-contact activities,” he said. “The rate of sports-related concussions sustained in high school football practice was more than twice as high in the two seasons prior to a rule change limiting the amount and duration of full-contact activities.”
Testing a Tackle-Limiting Rule
In their study, Dr. McGuine and his associates tested the effects of a tackle-limiting rule implemented in 2014 in a state interscholastic athletic association for all players in grades 9 through 12. The rule prohibited full-contact play during the first practice week, and full contact was defined as “drills or game situations that occur at game speed when full tackles are made at a competitive pace and players are taken to the ground.” The players engaged in full-contact play for as long as 75 minutes total during the second week of practice and for a maximum of 60 min/week for all subsequent weeks in the practice season. The rule did not apply to games.
For data on the two years before the rule change, 2,081 athletes with a mean age of 16 reported their concussion history in the 2012 season, which included 36 schools, and the 2013 season, which included 18 schools. In 2014, licensed athletic trainers recorded the incidence and severity of each sports-related concussion for the 945 players at 26 schools. During all three seasons, almost half the concussions (46%) occurred during tackling. Although the overall rate of concussions dropped from 1.57 per 1,000 athletic exposures in the combined 2012 and 2013 seasons to 1.28 per 1,000 athletic exposures in the 2014 season, the difference was not significant. During the 2012 and 2013 seasons combined, 206 players (9%) sustained 211 concussions, compared with 67 players (7%) with 70 concussions in 2014.
The difference in concussions occurring during practice, however, did differ significantly before and after the rule change. The rate of concussions during practice in 2014 was 0.33 concussions per 1,000 athletic exposures, compared with 0.76 concussions per 1,000 exposures in the 2012 and 2013 seasons. Twelve of 15 concussions in 2014 practices occurred during full-contact practices, a rate of 0.57 per 1,000 exposures, and 82 of 86 concussions in the 2012 and 2013 seasons occurred during full contact practices, a rate of 0.87 per 1,000 exposures.
The investigators observed no difference in concussion rate during the games following the rule change. The 2014 rate of concussions during games was 5.74 per 1,000 exposures, compared with 5.81 per 1,000 exposures in the combined 2012 and 2013 seasons. The severity of concussions sustained before and after the rule change also did not differ, and athletes’ years of football-playing experience had no effect on the concussion incidence in 2014.
To Tackle or Not to Tackle?
Despite the relationship between full-contact play and concussions, Dr. McGuine said that he would not support banning tackling from football.
“I think the benefits of the sport far outweigh the risks,” Dr. McGuine said. “Concussions particularly have transcended a sports issue and become a public health issue and have become political, and I’m very much against legislators, policy makers, [and] associations making blanket rules without the evidence to back those,” he said. “There are lingering long-term effects from all orthopedic injuries, but we’re focusing on concussions.”
Equipment modification is unlikely to make much difference in concussion rates either, said Dr. McGuine, whose previous study on football helmets found that the brand and model did not influence concussion risk. “Concussions are multifactorial,” he said. “We can’t just limit the amount of force transmitted to the brain and say we’re going to stop these injuries from occurring.”
One important strategy for reducing concussions is increasing parents’ and athletes’ awareness about multiple injuries and about ways to reduce the risk, Dr. McGuine said.
“Concussions are like any other injury [such as] ankle sprains, knee injuries and surgeries, [and] shoulder dislocations,” he said. “If you have one, you’re more susceptible to having another one, as opposed to somebody who never had that injury, so the problems are repeat injuries and lingering injuries.” Any of these injuries can have a lasting effect on a young athlete’s quality of life, Dr. McGuine added.
Another way to decrease the incidence of concussions is to enforce rules against leading, or lowering, athletes’ heads during tackling.
“A big issue now is penalizing players for leading with their head and face, but I think we need to be consistent there, too,” Dr. McGuine said. “We can’t penalize defensive players for lowering their helmet if we’re not going to penalize running backs and wide receivers.”
—Tara Haelle
Liver Transplant Only Cure for Some Inpatients with Cirrhosis

Bilal Hameed, MD, assistant professor of medicine in the division of gastroenterology at the University of California San Francisco, reviewed a wide range of serious and life-threatening medical complications resulting from cirrhosis during the annual UCSF Management of the Hospitalized Patient conference.
Recurring complications of cirrhosis can include ascites, acute variceal and portal hypertensive bleeds, hepatic encephalopathy, bacterial peritonitis, acute renal failure, sepsis, and a host of other infections. In many cases, options for treatment are limited, because the patient develops decompensated cirrhosis.

Poor prognosis makes it important to urge these patients to get on a liver transplantation list, sooner rather than later, Dr. Hameed told hospitalists attending his small group session.
“Liver transplantation has changed this field,” he said. “Call us to see if your patient might be a candidate.”
Unlike transplant lists for kidneys and some other organs, on which patients must wait for their turn, liver transplants are assigned based on need, as reflected in the patient’s Model for End-Stage Liver Disease (MELD) score, an objective clinical scale derived from blood values.
“Patients do really well on transplants, with 60% survival at 10 years,” he said. He also noted that patients with advanced, decompensated disease who do not find a place on the transplant list might instead be candidates for palliative care or hospice referral.
Many conditions, such as infections, can still be managed with timely treatment, returning the patient back to baseline.
“The risk of infection is very high. Starting antibiotics early can help,” Dr. Hameed said.
And for conditions where fluid volume is an issue, including spontaneous bacterial peritonitis, hypernatremia, or intrinsic renal disease, albumin is recommended as the evidence-based treatment of choice. “Please don’t overtransfuse these patients,” he said.
Jeannie Yip, MD, a nocturnist at Kaiser Foundation Hospital in Oakland, Calif., said that she frequently admits these kinds of patients to her hospital. For her, Dr. Hameed’s albumin recommendation was the most important lesson.
“I was still using IV fluids in patients coming in with volume depletion, to rule out acute renal failure. It’s always a dilemma if you have a hypotensive patient with low sodium and low blood pressure who tells you, ‘I haven’t eaten for a week,’” she explained. “It’s been hard for me not to give them fluids. But after listening to this talk, I see that I should give albumin instead.”
Bilal Hameed, MD, assistant professor of medicine in the division of gastroenterology at the University of California San Francisco, reviewed a wide range of serious and life-threatening medical complications resulting from cirrhosis during the annual UCSF Management of the Hospitalized Patient conference.
Recurring complications of cirrhosis can include ascites, acute variceal and portal hypertensive bleeds, hepatic encephalopathy, bacterial peritonitis, acute renal failure, sepsis, and a host of other infections. In many cases, options for treatment are limited, because the patient develops decompensated cirrhosis.
Poor prognosis makes it important to urge these patients to get on a liver transplantation list, sooner rather than later, Dr. Hameed told hospitalists attending his small group session.
“Liver transplantation has changed this field,” he said. “Call us to see if your patient might be a candidate.”
Unlike transplant lists for kidneys and some other organs, on which patients must wait for their turn, liver transplants are assigned based on need, as reflected in the patient’s Model for End-Stage Liver Disease (MELD) score, an objective clinical scale derived from blood values.
“Patients do really well on transplants, with 60% survival at 10 years,” he said. He also noted that patients with advanced, decompensated disease who do not find a place on the transplant list might instead be candidates for palliative care or hospice referral.
Many conditions, such as infections, can still be managed with timely treatment, returning the patient back to baseline.
“The risk of infection is very high. Starting antibiotics early can help,” Dr. Hameed said.
And for conditions where fluid volume is an issue, including spontaneous bacterial peritonitis, hypernatremia, or intrinsic renal disease, albumin is recommended as the evidence-based treatment of choice. “Please don’t overtransfuse these patients,” he said.
Jeannie Yip, MD, a nocturnist at Kaiser Foundation Hospital in Oakland, Calif., said that she frequently admits these kinds of patients to her hospital. For her, Dr. Hameed’s albumin recommendation was the most important lesson.
“I was still using IV fluids in patients coming in with volume depletion, to rule out acute renal failure. It’s always a dilemma if you have a hypotensive patient with low sodium and low blood pressure who tells you, ‘I haven’t eaten for a week,’” she explained. “It’s been hard for me not to give them fluids. But after listening to this talk, I see that I should give albumin instead.”
Bilal Hameed, MD, assistant professor of medicine in the division of gastroenterology at the University of California San Francisco, reviewed a wide range of serious and life-threatening medical complications resulting from cirrhosis during the annual UCSF Management of the Hospitalized Patient conference.
Recurring complications of cirrhosis can include ascites, acute variceal and portal hypertensive bleeds, hepatic encephalopathy, bacterial peritonitis, acute renal failure, sepsis, and a host of other infections. In many cases, options for treatment are limited, because the patient develops decompensated cirrhosis.
Poor prognosis makes it important to urge these patients to get on a liver transplantation list, sooner rather than later, Dr. Hameed told hospitalists attending his small group session.
“Liver transplantation has changed this field,” he said. “Call us to see if your patient might be a candidate.”
Unlike transplant lists for kidneys and some other organs, on which patients must wait for their turn, liver transplants are assigned based on need, as reflected in the patient’s Model for End-Stage Liver Disease (MELD) score, an objective clinical scale derived from blood values.
“Patients do really well on transplants, with 60% survival at 10 years,” he said. He also noted that patients with advanced, decompensated disease who do not find a place on the transplant list might instead be candidates for palliative care or hospice referral.
Many conditions, such as infections, can still be managed with timely treatment, returning the patient back to baseline.
“The risk of infection is very high. Starting antibiotics early can help,” Dr. Hameed said.
And for conditions where fluid volume is an issue, including spontaneous bacterial peritonitis, hypernatremia, or intrinsic renal disease, albumin is recommended as the evidence-based treatment of choice. “Please don’t overtransfuse these patients,” he said.
Jeannie Yip, MD, a nocturnist at Kaiser Foundation Hospital in Oakland, Calif., said that she frequently admits these kinds of patients to her hospital. For her, Dr. Hameed’s albumin recommendation was the most important lesson.
“I was still using IV fluids in patients coming in with volume depletion, to rule out acute renal failure. It’s always a dilemma if you have a hypotensive patient with low sodium and low blood pressure who tells you, ‘I haven’t eaten for a week,’” she explained. “It’s been hard for me not to give them fluids. But after listening to this talk, I see that I should give albumin instead.”
Quality of Healthcare Systems Depends on People Caring Within
The experience I describe here is an acute illness that my family experienced. Aside from the actual illness, most of the story will not sound surprising or unique to most of you. It is a story about traversing the medical system to get care for my mom, an elderly patient with Alzheimer’s, over the course of three weeks. It is a story about miscommunications and fumbled handoffs, and complex insurance and payments systems that drive decision-making.
In this column, I aim only to describe our experience, which was both predictable and disappointing, within the healthcare system that we all own.
The Background
Sheila is a 76-year-old Caucasian female with a history of well-controlled hypertension and hyperlipidemia and moderate-stage Alzheimer’s disease, diagnosed about six years ago. She has resided in an assisted living facility for about three years and is still relatively independent in her activities of daily living (ADLs). She has remained relatively healthy and active despite her continuously progressive Alzheimer’s.
Her acute illness started when she developed diarrhea that was moderate in volume and frequency. Over the course of several days, the diarrhea significantly affected her sleep and activities, and she became more confused and essentially confined to her room. By day five, she was visibly dehydrated, with dry, cracked lips and skin tenting. Her daughter, Tara, brought her to the ED in the hospital at which her PCP was on staff. During the eight-hour ED stay, Sheila was rehydrated and was able to keep oral fluids down. Her blood work was normal, although the staff were unable to collect a stool sample. Sheila was discharged with instructions to see her PCP within a few days. No one from the ED contacted the PCP, and no one was able to set up a follow-up appointment.
The next day the diarrhea continued, so Tara contacted the PCP. The office staff noted that their next available appointment was in five days. Tara took that appointment and continued to help her mom with symptom management. Over the next several days, the diarrhea continued and the dehydration worsened again, so Tara took her back to the same ED, where they reassured her that the labs were normal, sent a stool sample off for testing, rehydrated her, and sent her home again. On the discharge paperwork, the ED physician noted that they had “set up home health nursing” and instructed a follow-up with Sheila’s PCP.
The next day, Tara contacted the PCP to check on the upcoming appointment, get advice on what to do, and see when the home health nurse would arrive. The PCP office confirmed the upcoming appointment in two days, told her to continue what she was doing, and said they did not know anything of the home health order and that she should contact the ED to clarify. When she contacted the ED, staff there told her the PCP would have to order the home health; Tara then called the PCP again, and he said he could not order home health, given the fact that he had not yet seen Sheila or her ED record. Tara asked a logical question, “But don’t you have the ED records? That is your hospital, right?”
The same cycle ensued over the next few days—now two weeks into the illness—and Sheila started to require increasing assistance with all of her ADLs, including toileting and showering, along with constant supervision to ensure hydration. The family pieced together as much help as possible. Several days later, on a Thursday night, the dehydration was again obvious, so Tara took her to another ED, given the lack of assistance received from the first two ED visits. In this ED, after evaluation, they admitted Sheila for observation. The family again pieced together 24/7 coverage for the hospital stay. The next day, Sheila continued to have diarrhea, now with vomiting. The ED hydrated her and relieved her vomiting and diarrhea with medications.
Because she was in observation, the hospitalist informed the family that he had written a discharge order. The family requested more time, given the fact that she was extremely confused, was hallucinating, and had not kept anything down by mouth; the hospitalist then changed Sheila to inpatient status for ongoing care. By Saturday, the vomiting and diarrhea were much better controlled with medications, but she had not taken anything by mouth other than a few sips of liquid. She was given a regular diet and kept a few bites down. The rounding hospitalist (the third in three days) told Tara he had consulted gastroenterology but that they were no longer needed and Sheila could be discharged. Tara requested that they fulfill the GI consult instead of discharging Sheila, given the length of time of the illness (now almost three weeks), the fact that she was nowhere near her baseline status, and the lack of diagnosis.
In the meantime, when one of the nurses from the assisted living facility called Tara to check on Sheila, she pointed out that she had noticed her mother’s Alzheimer’s medication “looked different” starting about three weeks ago, which coincided with the onset of the diarrhea. With this information, the GI consultant took a good history, looked at the imaging and lab testing, and told the family he strongly suspected the diarrhea had been caused by a change to generic from brand name, a decision that had been made due to the cost of brand name. He recommended stopping the medication, and, if no improvement was seen in the diarrhea within 48 hours, he would expand his workup.
The next day, a Sunday, the same hospitalist rounded early and wrote discharge orders. When Tara’s sister, Michelle, arrived, the nurse told her of the discharge order. Michelle asked another logical question: “But do we know what is wrong with her yet? Has the diarrhea stopped?” The nurse recounted “only a few bowel movements” over the course of the night and no vomiting. Michelle pleaded with the nurse to at least see if her mom could tolerate breakfast before discharge. She then talked to the hospitalist, who recounted that Sheila had told him that morning that she had not had any diarrhea all night. Michelle asked another logical question, “But you know she has Alzheimer’s, right?”
Sheila did well with breakfast, and, after several hours without diarrhea, she was discharged back to her assisted living facility with Michelle. The PCP never called, home health was never ordered, and the low-cost medication was still on her discharge paperwork.
Bottom Line
Throughout all this, my sisters asked me and others so many logical questions during the three-week illness, such as “Don’t they review the medication list before a patient goes home?” and “Why didn’t the ED contact the PCP? He works in the same hospital, right?” Being hundreds of miles away, and knowing both how the system should work and how it does work, I found it sobering to see all the typical breakdowns happening to my own family. I felt disappointed and dismayed, but not the least bit surprised.
The one person who truly made a difference was the nurse at the assisted living facility, who used common sense (“The medication looks different”) and compassion (“Hi, just calling to check on Sheila”) to help us determine what was wrong. She saved us all additional diagnostic tests and unnecessary visits.
As a chief quality officer, I talk incessantly about systems approaches to improving quality and safety, but while I know how impactful reliable systems can be on good outcomes, the system will only ever be as good as the people caring within.

The experience I describe here is an acute illness that my family experienced. Aside from the actual illness, most of the story will not sound surprising or unique to most of you. It is a story about traversing the medical system to get care for my mom, an elderly patient with Alzheimer’s, over the course of three weeks. It is a story about miscommunications and fumbled handoffs, and complex insurance and payments systems that drive decision-making.
In this column, I aim only to describe our experience, which was both predictable and disappointing, within the healthcare system that we all own.
The Background
Sheila is a 76-year-old Caucasian female with a history of well-controlled hypertension and hyperlipidemia and moderate-stage Alzheimer’s disease, diagnosed about six years ago. She has resided in an assisted living facility for about three years and is still relatively independent in her activities of daily living (ADLs). She has remained relatively healthy and active despite her continuously progressive Alzheimer’s.
Her acute illness started when she developed diarrhea that was moderate in volume and frequency. Over the course of several days, the diarrhea significantly affected her sleep and activities, and she became more confused and essentially confined to her room. By day five, she was visibly dehydrated, with dry, cracked lips and skin tenting. Her daughter, Tara, brought her to the ED in the hospital at which her PCP was on staff. During the eight-hour ED stay, Sheila was rehydrated and was able to keep oral fluids down. Her blood work was normal, although the staff were unable to collect a stool sample. Sheila was discharged with instructions to see her PCP within a few days. No one from the ED contacted the PCP, and no one was able to set up a follow-up appointment.
The next day the diarrhea continued, so Tara contacted the PCP. The office staff noted that their next available appointment was in five days. Tara took that appointment and continued to help her mom with symptom management. Over the next several days, the diarrhea continued and the dehydration worsened again, so Tara took her back to the same ED, where they reassured her that the labs were normal, sent a stool sample off for testing, rehydrated her, and sent her home again. On the discharge paperwork, the ED physician noted that they had “set up home health nursing” and instructed a follow-up with Sheila’s PCP.
The next day, Tara contacted the PCP to check on the upcoming appointment, get advice on what to do, and see when the home health nurse would arrive. The PCP office confirmed the upcoming appointment in two days, told her to continue what she was doing, and said they did not know anything of the home health order and that she should contact the ED to clarify. When she contacted the ED, staff there told her the PCP would have to order the home health; Tara then called the PCP again, and he said he could not order home health, given the fact that he had not yet seen Sheila or her ED record. Tara asked a logical question, “But don’t you have the ED records? That is your hospital, right?”
The same cycle ensued over the next few days—now two weeks into the illness—and Sheila started to require increasing assistance with all of her ADLs, including toileting and showering, along with constant supervision to ensure hydration. The family pieced together as much help as possible. Several days later, on a Thursday night, the dehydration was again obvious, so Tara took her to another ED, given the lack of assistance received from the first two ED visits. In this ED, after evaluation, they admitted Sheila for observation. The family again pieced together 24/7 coverage for the hospital stay. The next day, Sheila continued to have diarrhea, now with vomiting. The ED hydrated her and relieved her vomiting and diarrhea with medications.
Because she was in observation, the hospitalist informed the family that he had written a discharge order. The family requested more time, given the fact that she was extremely confused, was hallucinating, and had not kept anything down by mouth; the hospitalist then changed Sheila to inpatient status for ongoing care. By Saturday, the vomiting and diarrhea were much better controlled with medications, but she had not taken anything by mouth other than a few sips of liquid. She was given a regular diet and kept a few bites down. The rounding hospitalist (the third in three days) told Tara he had consulted gastroenterology but that they were no longer needed and Sheila could be discharged. Tara requested that they fulfill the GI consult instead of discharging Sheila, given the length of time of the illness (now almost three weeks), the fact that she was nowhere near her baseline status, and the lack of diagnosis.
In the meantime, when one of the nurses from the assisted living facility called Tara to check on Sheila, she pointed out that she had noticed her mother’s Alzheimer’s medication “looked different” starting about three weeks ago, which coincided with the onset of the diarrhea. With this information, the GI consultant took a good history, looked at the imaging and lab testing, and told the family he strongly suspected the diarrhea had been caused by a change to generic from brand name, a decision that had been made due to the cost of brand name. He recommended stopping the medication, and, if no improvement was seen in the diarrhea within 48 hours, he would expand his workup.
The next day, a Sunday, the same hospitalist rounded early and wrote discharge orders. When Tara’s sister, Michelle, arrived, the nurse told her of the discharge order. Michelle asked another logical question: “But do we know what is wrong with her yet? Has the diarrhea stopped?” The nurse recounted “only a few bowel movements” over the course of the night and no vomiting. Michelle pleaded with the nurse to at least see if her mom could tolerate breakfast before discharge. She then talked to the hospitalist, who recounted that Sheila had told him that morning that she had not had any diarrhea all night. Michelle asked another logical question, “But you know she has Alzheimer’s, right?”
Sheila did well with breakfast, and, after several hours without diarrhea, she was discharged back to her assisted living facility with Michelle. The PCP never called, home health was never ordered, and the low-cost medication was still on her discharge paperwork.
Bottom Line
Throughout all this, my sisters asked me and others so many logical questions during the three-week illness, such as “Don’t they review the medication list before a patient goes home?” and “Why didn’t the ED contact the PCP? He works in the same hospital, right?” Being hundreds of miles away, and knowing both how the system should work and how it does work, I found it sobering to see all the typical breakdowns happening to my own family. I felt disappointed and dismayed, but not the least bit surprised.
The one person who truly made a difference was the nurse at the assisted living facility, who used common sense (“The medication looks different”) and compassion (“Hi, just calling to check on Sheila”) to help us determine what was wrong. She saved us all additional diagnostic tests and unnecessary visits.
As a chief quality officer, I talk incessantly about systems approaches to improving quality and safety, but while I know how impactful reliable systems can be on good outcomes, the system will only ever be as good as the people caring within.
The experience I describe here is an acute illness that my family experienced. Aside from the actual illness, most of the story will not sound surprising or unique to most of you. It is a story about traversing the medical system to get care for my mom, an elderly patient with Alzheimer’s, over the course of three weeks. It is a story about miscommunications and fumbled handoffs, and complex insurance and payments systems that drive decision-making.
In this column, I aim only to describe our experience, which was both predictable and disappointing, within the healthcare system that we all own.
The Background
Sheila is a 76-year-old Caucasian female with a history of well-controlled hypertension and hyperlipidemia and moderate-stage Alzheimer’s disease, diagnosed about six years ago. She has resided in an assisted living facility for about three years and is still relatively independent in her activities of daily living (ADLs). She has remained relatively healthy and active despite her continuously progressive Alzheimer’s.
Her acute illness started when she developed diarrhea that was moderate in volume and frequency. Over the course of several days, the diarrhea significantly affected her sleep and activities, and she became more confused and essentially confined to her room. By day five, she was visibly dehydrated, with dry, cracked lips and skin tenting. Her daughter, Tara, brought her to the ED in the hospital at which her PCP was on staff. During the eight-hour ED stay, Sheila was rehydrated and was able to keep oral fluids down. Her blood work was normal, although the staff were unable to collect a stool sample. Sheila was discharged with instructions to see her PCP within a few days. No one from the ED contacted the PCP, and no one was able to set up a follow-up appointment.
The next day the diarrhea continued, so Tara contacted the PCP. The office staff noted that their next available appointment was in five days. Tara took that appointment and continued to help her mom with symptom management. Over the next several days, the diarrhea continued and the dehydration worsened again, so Tara took her back to the same ED, where they reassured her that the labs were normal, sent a stool sample off for testing, rehydrated her, and sent her home again. On the discharge paperwork, the ED physician noted that they had “set up home health nursing” and instructed a follow-up with Sheila’s PCP.
The next day, Tara contacted the PCP to check on the upcoming appointment, get advice on what to do, and see when the home health nurse would arrive. The PCP office confirmed the upcoming appointment in two days, told her to continue what she was doing, and said they did not know anything of the home health order and that she should contact the ED to clarify. When she contacted the ED, staff there told her the PCP would have to order the home health; Tara then called the PCP again, and he said he could not order home health, given the fact that he had not yet seen Sheila or her ED record. Tara asked a logical question, “But don’t you have the ED records? That is your hospital, right?”
The same cycle ensued over the next few days—now two weeks into the illness—and Sheila started to require increasing assistance with all of her ADLs, including toileting and showering, along with constant supervision to ensure hydration. The family pieced together as much help as possible. Several days later, on a Thursday night, the dehydration was again obvious, so Tara took her to another ED, given the lack of assistance received from the first two ED visits. In this ED, after evaluation, they admitted Sheila for observation. The family again pieced together 24/7 coverage for the hospital stay. The next day, Sheila continued to have diarrhea, now with vomiting. The ED hydrated her and relieved her vomiting and diarrhea with medications.
Because she was in observation, the hospitalist informed the family that he had written a discharge order. The family requested more time, given the fact that she was extremely confused, was hallucinating, and had not kept anything down by mouth; the hospitalist then changed Sheila to inpatient status for ongoing care. By Saturday, the vomiting and diarrhea were much better controlled with medications, but she had not taken anything by mouth other than a few sips of liquid. She was given a regular diet and kept a few bites down. The rounding hospitalist (the third in three days) told Tara he had consulted gastroenterology but that they were no longer needed and Sheila could be discharged. Tara requested that they fulfill the GI consult instead of discharging Sheila, given the length of time of the illness (now almost three weeks), the fact that she was nowhere near her baseline status, and the lack of diagnosis.
In the meantime, when one of the nurses from the assisted living facility called Tara to check on Sheila, she pointed out that she had noticed her mother’s Alzheimer’s medication “looked different” starting about three weeks ago, which coincided with the onset of the diarrhea. With this information, the GI consultant took a good history, looked at the imaging and lab testing, and told the family he strongly suspected the diarrhea had been caused by a change to generic from brand name, a decision that had been made due to the cost of brand name. He recommended stopping the medication, and, if no improvement was seen in the diarrhea within 48 hours, he would expand his workup.
The next day, a Sunday, the same hospitalist rounded early and wrote discharge orders. When Tara’s sister, Michelle, arrived, the nurse told her of the discharge order. Michelle asked another logical question: “But do we know what is wrong with her yet? Has the diarrhea stopped?” The nurse recounted “only a few bowel movements” over the course of the night and no vomiting. Michelle pleaded with the nurse to at least see if her mom could tolerate breakfast before discharge. She then talked to the hospitalist, who recounted that Sheila had told him that morning that she had not had any diarrhea all night. Michelle asked another logical question, “But you know she has Alzheimer’s, right?”
Sheila did well with breakfast, and, after several hours without diarrhea, she was discharged back to her assisted living facility with Michelle. The PCP never called, home health was never ordered, and the low-cost medication was still on her discharge paperwork.
Bottom Line
Throughout all this, my sisters asked me and others so many logical questions during the three-week illness, such as “Don’t they review the medication list before a patient goes home?” and “Why didn’t the ED contact the PCP? He works in the same hospital, right?” Being hundreds of miles away, and knowing both how the system should work and how it does work, I found it sobering to see all the typical breakdowns happening to my own family. I felt disappointed and dismayed, but not the least bit surprised.
The one person who truly made a difference was the nurse at the assisted living facility, who used common sense (“The medication looks different”) and compassion (“Hi, just calling to check on Sheila”) to help us determine what was wrong. She saved us all additional diagnostic tests and unnecessary visits.
As a chief quality officer, I talk incessantly about systems approaches to improving quality and safety, but while I know how impactful reliable systems can be on good outcomes, the system will only ever be as good as the people caring within.
Poor Continuity of Patient Care Increases Work for Hospitalist Groups

I think every hospitalist group should diligently try to maximize hospitalist-patient continuity, but many seem to adopt schedules and other operational practices that erode it. Let’s walk through the issue of continuity, starting with some history.
Inpatient Continuity in Old Healthcare System
Proudly carrying a pager nearly the size of a loaf of bread and wearing a white shirt and pants with Converse All Stars, I served as a hospital orderly in the 1970s. This position involved things like getting patients out of bed, placing Foley catheters, performing chest compressions during codes, and transporting the bodies of the deceased to the morgue. I really enjoyed the work, and the experience serves as one of my historical frames of reference for how hospital care has evolved since then.
The way I remember it, nearly everyone at the hospital worked a predictable schedule. RN staffing was the same each day; it didn’t vary based on census. Each full-time RN worked five shifts a week, eight hours each. Most or all would work alternate weekends and would have two compensatory days off during the following work week. This resulted in terrific continuity between nurse and patient, and the long length of stays meant patients and nurses got to know one another really well.
Continuity Takes a Hit
But things have changed. Nurse-patient continuity seems to have declined significantly as a result of two main forces: the hospital’s efforts to reduce staffing costs by varying nurse staffing to match daily patient volume, and nurses’ desire for a wide variety of work schedules. Asking a bedside nurse in today’s hospital whether the patient’s confusion, diarrhea, or appetite is meaningfully different today than yesterday typically yields the same reply. “This is my first day with the patient; I’ll have to look at the chart.”
I couldn’t find many research articles or editorials regarding hospital nurse-patient continuity from one day to the next. But several researchers seem to have begun studying this issue and have recently published a proposed framework for assessing it, and I found one study showing it wasn’t correlated with rates of pressure ulcers.1,2.
My anecdotal experience tells me continuity between the patient and caregivers of all stripes matters a lot. Research will be valuable in helping us to better understand its most significant costs and benefits, but I’m already convinced “Continuity is King” and should be one of the most important factors in the design of work schedules and patient allocation models for nurses and hospitalists alike.
While some might say we should wait for randomized trials of continuity to determine its importance, I’m inclined to see it like the authors of “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials.” As a ding against those who insist on research data when common sense may be sufficient, they concluded “…that everyone might benefit if the most radical protagonists of evidence-based medicine organised and participated in a double-blind, randomised, placebo-controlled, crossover trial of the parachute.3
Continuity and Hospitalists
On top of what I see as erosion in nurse-patient continuity, the arrival of hospitalists disrupted doctor-patient continuity across the inpatient and outpatient setting. While there was significant concern about this when our field first took off in the 1990s, it seems to be getting a great deal less attention over the last few years. In many hospitalist groups I work with, it is one of the last factors considered when creating a work schedule. Factors that are examined include the following:
- Solely for provider convenience, a group might regularly schedule a provider for only two or three consecutive daytime shifts, or sometimes only single days;
- Groups that use unit-based hospital (a.k.a. “geographic”) staffing might have a patient transfer to a different attending hospitalist solely as a result of moving to a room in a different nursing unit; and
- As part of morning load leveling, some groups reassign existing patients to a new hospitalist.
I think all groups should work hard to avoid doing these things. And while I seem to be a real outlier on this one, I think the benefits of a separate daytime hospitalist admitter shift are not worth the cost of having different doctors always do the admission and first follow-up visit. Most groups should consider moving the admitter into an additional rounder position and allocating daytime admissions across all hospitalists.
One study found that hospitalist discontinuity was not associated with adverse events, and another found it was associated with higher length of stay for selected diagnoses.4,5 But there is too little research to draw hard conclusions. I’m convinced poor continuity increases the possibility of handoff-related errors, likely results in lower patient satisfaction, and increases the overall work of the hospitalist group, because more providers have to take the time to get to know the patient.
Although there will always be some tension between terrific continuity and a sustainable hospitalist lifestyle—a person can work only so many consecutive days before wearing out—every group should thoughtfully consider whether they are doing everything reasonable to maximize continuity. After all, continuity is king.

References
- Stifter J, Yao Y, Lopez KC, Khokhar A, Wilkie DJ, Keenan GM. Proposing a new conceptual model and an exemplar measure using health information technology to examine the impact of relational nurse continuity on hospital-acquired pressure ulcers. ANS Adv Nurs Sci. 2015;38(3):241-251.
- Stifter J, Yao Y, Lodhi MK, et al. Nurse continuity and hospital-acquired pressure ulcers: a comparative analysis using an electronic health record “big data” set. Nurs Res. 2015;64(5):361-371.
- Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ. 2003;327(7429):1459-1461.
- O’Leary KJ, Turner J, Christensen N, et al. The effect of hospitalist discontinuity on adverse events. J Hosp Med. 2015;10(3):147-151.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
I think every hospitalist group should diligently try to maximize hospitalist-patient continuity, but many seem to adopt schedules and other operational practices that erode it. Let’s walk through the issue of continuity, starting with some history.
Inpatient Continuity in Old Healthcare System
Proudly carrying a pager nearly the size of a loaf of bread and wearing a white shirt and pants with Converse All Stars, I served as a hospital orderly in the 1970s. This position involved things like getting patients out of bed, placing Foley catheters, performing chest compressions during codes, and transporting the bodies of the deceased to the morgue. I really enjoyed the work, and the experience serves as one of my historical frames of reference for how hospital care has evolved since then.
The way I remember it, nearly everyone at the hospital worked a predictable schedule. RN staffing was the same each day; it didn’t vary based on census. Each full-time RN worked five shifts a week, eight hours each. Most or all would work alternate weekends and would have two compensatory days off during the following work week. This resulted in terrific continuity between nurse and patient, and the long length of stays meant patients and nurses got to know one another really well.
Continuity Takes a Hit
But things have changed. Nurse-patient continuity seems to have declined significantly as a result of two main forces: the hospital’s efforts to reduce staffing costs by varying nurse staffing to match daily patient volume, and nurses’ desire for a wide variety of work schedules. Asking a bedside nurse in today’s hospital whether the patient’s confusion, diarrhea, or appetite is meaningfully different today than yesterday typically yields the same reply. “This is my first day with the patient; I’ll have to look at the chart.”
I couldn’t find many research articles or editorials regarding hospital nurse-patient continuity from one day to the next. But several researchers seem to have begun studying this issue and have recently published a proposed framework for assessing it, and I found one study showing it wasn’t correlated with rates of pressure ulcers.1,2.
My anecdotal experience tells me continuity between the patient and caregivers of all stripes matters a lot. Research will be valuable in helping us to better understand its most significant costs and benefits, but I’m already convinced “Continuity is King” and should be one of the most important factors in the design of work schedules and patient allocation models for nurses and hospitalists alike.
While some might say we should wait for randomized trials of continuity to determine its importance, I’m inclined to see it like the authors of “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials.” As a ding against those who insist on research data when common sense may be sufficient, they concluded “…that everyone might benefit if the most radical protagonists of evidence-based medicine organised and participated in a double-blind, randomised, placebo-controlled, crossover trial of the parachute.3
Continuity and Hospitalists
On top of what I see as erosion in nurse-patient continuity, the arrival of hospitalists disrupted doctor-patient continuity across the inpatient and outpatient setting. While there was significant concern about this when our field first took off in the 1990s, it seems to be getting a great deal less attention over the last few years. In many hospitalist groups I work with, it is one of the last factors considered when creating a work schedule. Factors that are examined include the following:
- Solely for provider convenience, a group might regularly schedule a provider for only two or three consecutive daytime shifts, or sometimes only single days;
- Groups that use unit-based hospital (a.k.a. “geographic”) staffing might have a patient transfer to a different attending hospitalist solely as a result of moving to a room in a different nursing unit; and
- As part of morning load leveling, some groups reassign existing patients to a new hospitalist.
I think all groups should work hard to avoid doing these things. And while I seem to be a real outlier on this one, I think the benefits of a separate daytime hospitalist admitter shift are not worth the cost of having different doctors always do the admission and first follow-up visit. Most groups should consider moving the admitter into an additional rounder position and allocating daytime admissions across all hospitalists.
One study found that hospitalist discontinuity was not associated with adverse events, and another found it was associated with higher length of stay for selected diagnoses.4,5 But there is too little research to draw hard conclusions. I’m convinced poor continuity increases the possibility of handoff-related errors, likely results in lower patient satisfaction, and increases the overall work of the hospitalist group, because more providers have to take the time to get to know the patient.
Although there will always be some tension between terrific continuity and a sustainable hospitalist lifestyle—a person can work only so many consecutive days before wearing out—every group should thoughtfully consider whether they are doing everything reasonable to maximize continuity. After all, continuity is king.
References
- Stifter J, Yao Y, Lopez KC, Khokhar A, Wilkie DJ, Keenan GM. Proposing a new conceptual model and an exemplar measure using health information technology to examine the impact of relational nurse continuity on hospital-acquired pressure ulcers. ANS Adv Nurs Sci. 2015;38(3):241-251.
- Stifter J, Yao Y, Lodhi MK, et al. Nurse continuity and hospital-acquired pressure ulcers: a comparative analysis using an electronic health record “big data” set. Nurs Res. 2015;64(5):361-371.
- Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ. 2003;327(7429):1459-1461.
- O’Leary KJ, Turner J, Christensen N, et al. The effect of hospitalist discontinuity on adverse events. J Hosp Med. 2015;10(3):147-151.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
I think every hospitalist group should diligently try to maximize hospitalist-patient continuity, but many seem to adopt schedules and other operational practices that erode it. Let’s walk through the issue of continuity, starting with some history.
Inpatient Continuity in Old Healthcare System
Proudly carrying a pager nearly the size of a loaf of bread and wearing a white shirt and pants with Converse All Stars, I served as a hospital orderly in the 1970s. This position involved things like getting patients out of bed, placing Foley catheters, performing chest compressions during codes, and transporting the bodies of the deceased to the morgue. I really enjoyed the work, and the experience serves as one of my historical frames of reference for how hospital care has evolved since then.
The way I remember it, nearly everyone at the hospital worked a predictable schedule. RN staffing was the same each day; it didn’t vary based on census. Each full-time RN worked five shifts a week, eight hours each. Most or all would work alternate weekends and would have two compensatory days off during the following work week. This resulted in terrific continuity between nurse and patient, and the long length of stays meant patients and nurses got to know one another really well.
Continuity Takes a Hit
But things have changed. Nurse-patient continuity seems to have declined significantly as a result of two main forces: the hospital’s efforts to reduce staffing costs by varying nurse staffing to match daily patient volume, and nurses’ desire for a wide variety of work schedules. Asking a bedside nurse in today’s hospital whether the patient’s confusion, diarrhea, or appetite is meaningfully different today than yesterday typically yields the same reply. “This is my first day with the patient; I’ll have to look at the chart.”
I couldn’t find many research articles or editorials regarding hospital nurse-patient continuity from one day to the next. But several researchers seem to have begun studying this issue and have recently published a proposed framework for assessing it, and I found one study showing it wasn’t correlated with rates of pressure ulcers.1,2.
My anecdotal experience tells me continuity between the patient and caregivers of all stripes matters a lot. Research will be valuable in helping us to better understand its most significant costs and benefits, but I’m already convinced “Continuity is King” and should be one of the most important factors in the design of work schedules and patient allocation models for nurses and hospitalists alike.
While some might say we should wait for randomized trials of continuity to determine its importance, I’m inclined to see it like the authors of “Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials.” As a ding against those who insist on research data when common sense may be sufficient, they concluded “…that everyone might benefit if the most radical protagonists of evidence-based medicine organised and participated in a double-blind, randomised, placebo-controlled, crossover trial of the parachute.3
Continuity and Hospitalists
On top of what I see as erosion in nurse-patient continuity, the arrival of hospitalists disrupted doctor-patient continuity across the inpatient and outpatient setting. While there was significant concern about this when our field first took off in the 1990s, it seems to be getting a great deal less attention over the last few years. In many hospitalist groups I work with, it is one of the last factors considered when creating a work schedule. Factors that are examined include the following:
- Solely for provider convenience, a group might regularly schedule a provider for only two or three consecutive daytime shifts, or sometimes only single days;
- Groups that use unit-based hospital (a.k.a. “geographic”) staffing might have a patient transfer to a different attending hospitalist solely as a result of moving to a room in a different nursing unit; and
- As part of morning load leveling, some groups reassign existing patients to a new hospitalist.
I think all groups should work hard to avoid doing these things. And while I seem to be a real outlier on this one, I think the benefits of a separate daytime hospitalist admitter shift are not worth the cost of having different doctors always do the admission and first follow-up visit. Most groups should consider moving the admitter into an additional rounder position and allocating daytime admissions across all hospitalists.
One study found that hospitalist discontinuity was not associated with adverse events, and another found it was associated with higher length of stay for selected diagnoses.4,5 But there is too little research to draw hard conclusions. I’m convinced poor continuity increases the possibility of handoff-related errors, likely results in lower patient satisfaction, and increases the overall work of the hospitalist group, because more providers have to take the time to get to know the patient.
Although there will always be some tension between terrific continuity and a sustainable hospitalist lifestyle—a person can work only so many consecutive days before wearing out—every group should thoughtfully consider whether they are doing everything reasonable to maximize continuity. After all, continuity is king.
References
- Stifter J, Yao Y, Lopez KC, Khokhar A, Wilkie DJ, Keenan GM. Proposing a new conceptual model and an exemplar measure using health information technology to examine the impact of relational nurse continuity on hospital-acquired pressure ulcers. ANS Adv Nurs Sci. 2015;38(3):241-251.
- Stifter J, Yao Y, Lodhi MK, et al. Nurse continuity and hospital-acquired pressure ulcers: a comparative analysis using an electronic health record “big data” set. Nurs Res. 2015;64(5):361-371.
- Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ. 2003;327(7429):1459-1461.
- O’Leary KJ, Turner J, Christensen N, et al. The effect of hospitalist discontinuity on adverse events. J Hosp Med. 2015;10(3):147-151.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
Microemboli May Play a Role in Certain Migraine Auras
The prevalence and frequency of interictal microembolic signals (MES) are higher in migraineurs with higher cortical dysfunction (HCD) during aura, compared with migraineurs without HCD during aura and with healthy controls, according to a study published online ahead of print September 29 in Cephalalgia.
Jasna Zidverc-Trajkovi´c, MD, a neurologist at the Neurology Clinic of the Clinical Center of Serbia in Belgrade, and her colleagues used transcranial Doppler ultrasound to test their hypothesis that the complexity of migraine aura depends on hypoperfusion caused by microemboli that occur in different regions of the brain. The goal was to evaluate the prevalence and clinical impact of interictal MES in migraineurs with HCD during aura.
The investigators enrolled 34 individuals with migraine who experienced language and memory impairment during aura (HCD group), 31 patients who had migraine with only visual or visual and somatosensory symptoms during aura (control group I), and 34 healthy individuals (control group II). A Doppler instrument was used to detect microemboli, and the researchers also compared demographic data, disease features, and the detection of MES between these groups, as well as the predictors of HCD during the aura.
MES Predicted HCD
The duration of aura (34.71 ±18.05 minutes vs 23.87 ±13.64 minutes) was significantly longer, and the frequency of aura per year (16.29 ±14.21 vs 10.10 ±11.00) was significantly higher in the HCD group, compared with control group I. The presence of somatosensory symptoms during the aura was significantly higher in the HCD group as well.
A binary logistic regression analysis identified three independent predictors of HCD occurrence in patients with migraine aura. These predictors were longer duration of the aura, presence of somatosensory symptoms during the aura, and positive MES detection.
MES were interictally detected in 29% of patients with migraine who experienced migraines with HCD during the aura, but in only 3% of participants with visual or somatosensory aura. In addition, the number of detected MES in a single patient was as high as 85 among patients in the HCD group, compared with eight that were detected in other examined patients and healthy controls.
Stroke-Risk Stratification
The detection of MES and investigation of the origin of microembolism could be a valuable tool for screening individuals with migraine with aura for ischemic stroke risk, as well as investigating links between migraine with aura and ischemic stroke, said Dr. Zidverc-Trajkovi´c.
The investigators speculated that in patients who have memory and language impairment during migraine aura, the cerebral cortex may be affected by cortical spreading depression in regions beyond the occipital lobe, and microemboli may trigger cortical spreading depression. This sequence of events, in turn, might contribute to the pathophysiology of migraine aura.
“Further research should include analysis of the influence of microemboli on the neuron–glial interaction or the network modulation and pathophysiology of cortical spreading depression,” the investigators said.
MES Was Recorded Outside Migraine Attacks
“Cortical spreading depression has been shown to occur in humans in ischemic stroke, severe traumatic brain lesions, and following hypoxia, and the scientifically relevant question is how spreading depression is triggered in patients who suffer from migraines with aura,” said Hans-Christoph Diener, MD, PhD, Chair of the Department of Neurology at the University of Duisburg-Essen in Germany, in an accompanying editorial. “The current study proposes that microemboli are a potential trigger.
“Microembolic signals, or MES, were detected in 29.4% of patients with higher cortical aura, which was much higher than in the other two groups,” he added. “But what does this finding implicate? The nature of MES is unknown in patients without atherosclerotic plaques, and one assumed mechanism is right–left shunt either through a patent foramen ovale or through pulmonary shunts. Patent foramen ovale is associated with a higher prevalence of migraine with aura.
“The major shortcoming of the study is the recording of MES outside migraine attacks. It is difficult to understand how MES occurring outside migraine attacks should play a role in the rare events of complex auras, and many of the assumptions and implications of the authors in the discussion are not supported by scientific evidence,” said Dr. Diener.
“In summary, this is an interesting observation with very limited relationship to the pathophysiology of migraine aura, and further research is needed,” Dr. Diener concluded.
—Roxanne Nelson
Suggested Reading
Diener HC. What triggers migraine aura? Cephalalgia. 2015 Sep 28 [Epub ahead of print].
Petrusic I, Podgorac A, Zidverc-Trajkovic J, et al. Do interictal microembolic signals play a role in higher cortical dysfunction during migraine aura? Cephalalgia. 2015 Sep 29 [Epub ahead of print].
The prevalence and frequency of interictal microembolic signals (MES) are higher in migraineurs with higher cortical dysfunction (HCD) during aura, compared with migraineurs without HCD during aura and with healthy controls, according to a study published online ahead of print September 29 in Cephalalgia.
Jasna Zidverc-Trajkovi´c, MD, a neurologist at the Neurology Clinic of the Clinical Center of Serbia in Belgrade, and her colleagues used transcranial Doppler ultrasound to test their hypothesis that the complexity of migraine aura depends on hypoperfusion caused by microemboli that occur in different regions of the brain. The goal was to evaluate the prevalence and clinical impact of interictal MES in migraineurs with HCD during aura.
The investigators enrolled 34 individuals with migraine who experienced language and memory impairment during aura (HCD group), 31 patients who had migraine with only visual or visual and somatosensory symptoms during aura (control group I), and 34 healthy individuals (control group II). A Doppler instrument was used to detect microemboli, and the researchers also compared demographic data, disease features, and the detection of MES between these groups, as well as the predictors of HCD during the aura.
MES Predicted HCD
The duration of aura (34.71 ±18.05 minutes vs 23.87 ±13.64 minutes) was significantly longer, and the frequency of aura per year (16.29 ±14.21 vs 10.10 ±11.00) was significantly higher in the HCD group, compared with control group I. The presence of somatosensory symptoms during the aura was significantly higher in the HCD group as well.
A binary logistic regression analysis identified three independent predictors of HCD occurrence in patients with migraine aura. These predictors were longer duration of the aura, presence of somatosensory symptoms during the aura, and positive MES detection.
MES were interictally detected in 29% of patients with migraine who experienced migraines with HCD during the aura, but in only 3% of participants with visual or somatosensory aura. In addition, the number of detected MES in a single patient was as high as 85 among patients in the HCD group, compared with eight that were detected in other examined patients and healthy controls.
Stroke-Risk Stratification
The detection of MES and investigation of the origin of microembolism could be a valuable tool for screening individuals with migraine with aura for ischemic stroke risk, as well as investigating links between migraine with aura and ischemic stroke, said Dr. Zidverc-Trajkovi´c.
The investigators speculated that in patients who have memory and language impairment during migraine aura, the cerebral cortex may be affected by cortical spreading depression in regions beyond the occipital lobe, and microemboli may trigger cortical spreading depression. This sequence of events, in turn, might contribute to the pathophysiology of migraine aura.
“Further research should include analysis of the influence of microemboli on the neuron–glial interaction or the network modulation and pathophysiology of cortical spreading depression,” the investigators said.
MES Was Recorded Outside Migraine Attacks
“Cortical spreading depression has been shown to occur in humans in ischemic stroke, severe traumatic brain lesions, and following hypoxia, and the scientifically relevant question is how spreading depression is triggered in patients who suffer from migraines with aura,” said Hans-Christoph Diener, MD, PhD, Chair of the Department of Neurology at the University of Duisburg-Essen in Germany, in an accompanying editorial. “The current study proposes that microemboli are a potential trigger.
“Microembolic signals, or MES, were detected in 29.4% of patients with higher cortical aura, which was much higher than in the other two groups,” he added. “But what does this finding implicate? The nature of MES is unknown in patients without atherosclerotic plaques, and one assumed mechanism is right–left shunt either through a patent foramen ovale or through pulmonary shunts. Patent foramen ovale is associated with a higher prevalence of migraine with aura.
“The major shortcoming of the study is the recording of MES outside migraine attacks. It is difficult to understand how MES occurring outside migraine attacks should play a role in the rare events of complex auras, and many of the assumptions and implications of the authors in the discussion are not supported by scientific evidence,” said Dr. Diener.
“In summary, this is an interesting observation with very limited relationship to the pathophysiology of migraine aura, and further research is needed,” Dr. Diener concluded.
—Roxanne Nelson
The prevalence and frequency of interictal microembolic signals (MES) are higher in migraineurs with higher cortical dysfunction (HCD) during aura, compared with migraineurs without HCD during aura and with healthy controls, according to a study published online ahead of print September 29 in Cephalalgia.
Jasna Zidverc-Trajkovi´c, MD, a neurologist at the Neurology Clinic of the Clinical Center of Serbia in Belgrade, and her colleagues used transcranial Doppler ultrasound to test their hypothesis that the complexity of migraine aura depends on hypoperfusion caused by microemboli that occur in different regions of the brain. The goal was to evaluate the prevalence and clinical impact of interictal MES in migraineurs with HCD during aura.
The investigators enrolled 34 individuals with migraine who experienced language and memory impairment during aura (HCD group), 31 patients who had migraine with only visual or visual and somatosensory symptoms during aura (control group I), and 34 healthy individuals (control group II). A Doppler instrument was used to detect microemboli, and the researchers also compared demographic data, disease features, and the detection of MES between these groups, as well as the predictors of HCD during the aura.
MES Predicted HCD
The duration of aura (34.71 ±18.05 minutes vs 23.87 ±13.64 minutes) was significantly longer, and the frequency of aura per year (16.29 ±14.21 vs 10.10 ±11.00) was significantly higher in the HCD group, compared with control group I. The presence of somatosensory symptoms during the aura was significantly higher in the HCD group as well.
A binary logistic regression analysis identified three independent predictors of HCD occurrence in patients with migraine aura. These predictors were longer duration of the aura, presence of somatosensory symptoms during the aura, and positive MES detection.
MES were interictally detected in 29% of patients with migraine who experienced migraines with HCD during the aura, but in only 3% of participants with visual or somatosensory aura. In addition, the number of detected MES in a single patient was as high as 85 among patients in the HCD group, compared with eight that were detected in other examined patients and healthy controls.
Stroke-Risk Stratification
The detection of MES and investigation of the origin of microembolism could be a valuable tool for screening individuals with migraine with aura for ischemic stroke risk, as well as investigating links between migraine with aura and ischemic stroke, said Dr. Zidverc-Trajkovi´c.
The investigators speculated that in patients who have memory and language impairment during migraine aura, the cerebral cortex may be affected by cortical spreading depression in regions beyond the occipital lobe, and microemboli may trigger cortical spreading depression. This sequence of events, in turn, might contribute to the pathophysiology of migraine aura.
“Further research should include analysis of the influence of microemboli on the neuron–glial interaction or the network modulation and pathophysiology of cortical spreading depression,” the investigators said.
MES Was Recorded Outside Migraine Attacks
“Cortical spreading depression has been shown to occur in humans in ischemic stroke, severe traumatic brain lesions, and following hypoxia, and the scientifically relevant question is how spreading depression is triggered in patients who suffer from migraines with aura,” said Hans-Christoph Diener, MD, PhD, Chair of the Department of Neurology at the University of Duisburg-Essen in Germany, in an accompanying editorial. “The current study proposes that microemboli are a potential trigger.
“Microembolic signals, or MES, were detected in 29.4% of patients with higher cortical aura, which was much higher than in the other two groups,” he added. “But what does this finding implicate? The nature of MES is unknown in patients without atherosclerotic plaques, and one assumed mechanism is right–left shunt either through a patent foramen ovale or through pulmonary shunts. Patent foramen ovale is associated with a higher prevalence of migraine with aura.
“The major shortcoming of the study is the recording of MES outside migraine attacks. It is difficult to understand how MES occurring outside migraine attacks should play a role in the rare events of complex auras, and many of the assumptions and implications of the authors in the discussion are not supported by scientific evidence,” said Dr. Diener.
“In summary, this is an interesting observation with very limited relationship to the pathophysiology of migraine aura, and further research is needed,” Dr. Diener concluded.
—Roxanne Nelson
Suggested Reading
Diener HC. What triggers migraine aura? Cephalalgia. 2015 Sep 28 [Epub ahead of print].
Petrusic I, Podgorac A, Zidverc-Trajkovic J, et al. Do interictal microembolic signals play a role in higher cortical dysfunction during migraine aura? Cephalalgia. 2015 Sep 29 [Epub ahead of print].
Suggested Reading
Diener HC. What triggers migraine aura? Cephalalgia. 2015 Sep 28 [Epub ahead of print].
Petrusic I, Podgorac A, Zidverc-Trajkovic J, et al. Do interictal microembolic signals play a role in higher cortical dysfunction during migraine aura? Cephalalgia. 2015 Sep 29 [Epub ahead of print].
Make the Diagnosis - December 2015
Diagnosis: Henoch-Schönlein purpura
Henoch-Schönlein purpura (HSP), also known as immunoglobulin A (IgA) vasculitis, is characterized by palpable purpura, abdominal pain, renal disease, arthritis and/or arthralgia. HSP affects all ages, but is most common in children (the mean age of onset is between six and seven years of age). It also has a slight predilection for males, as well as whites and Asians. Patients are more likely to present during the fall, winter, and spring. It is thought that HSP may be associated with infections that are more prevalent during these times of the year.
Patients typically have purpura and joint or abdominal pain, although some may present without significant skin manifestations or pain. The rash associated with HSP may appear as erythematous macules or papules that coalesce and evolve into palpable purpura with petechiae, ecchymoses, and/or subcutaneous edema. The skin is typically affected in areas that are more dependent or experience more pressure, such as the lower extremities or buttocks. A more diffuse distribution across the entire body can be seen in those who are nonambulatory.

The arthritis associated with HSP usually affects the lower extremities, and it is oligoarticular, nondeforming, and transient, with prominent swelling and tenderness. Gastrointestinal involvement may manifest as nausea, vomiting, abdominal pain, transient paralytic ileus, hemorrhage, bowel ischemia, intussusception (rare in adults), and/or bowel perforation. These symptoms tend to develop 1 week after the rash, but there are reports of gastrointestinal complaints preceding all other manifestations of HSP.
Additionally, there can be renal involvement, which is more common in adults. These patients may experience hematuria with or without red blood cell casts, nephrotic range proteinuria, and/or elevated serum creatinine. Other less common symptoms that have been reported in patients with HSP include scrotal pain and swelling, headaches, seizures, ataxia, central and peripheral neuropathies, impaired lung diffusion capacity, keratitis, and uveitis.
The diagnosis of HSP is classically based upon clinical presentation. The diagnosis may be complicated in cases in which patients do not present with classic signs, such as palpable purpura of the lower extremities and buttocks. In these situations, a biopsy of the skin or kidney may aid in the diagnosis.
The differential diagnosis for HSP includes acute hemorrhagic edema of infancy, coagulopathies, hemolytic uremic syndrome, hypersensitivity vasculitis, IgA nephropathy, immune thrombocytopenia purpura, juvenile idiopathic arthritis, reactive arthritis, rheumatic fever, small vessel vasculitis, and systemic lupus erythematosus.
The etiology of HSP is unclear. Most believe that it is an immune-mediated vasculitis with genetic and environmental influences. In HSP, there is leukocytoclastic vasculitis with deposition of IgA immune complexes, complement component 3 (C3), and fibrin in the affected vessel walls. Small vessels within the papillary dermis are usually present with an inflammatory infiltrate of neutrophils and monocytes.
The treatment of HSP usually consists of supportive care, since most patients will recover spontaneously. Therefore, hydration, rest, and pain relief are essential. Other treatment modalities may be required for more severe or extensive HSP and its complications.
Our patient’s biopsy results were consistent with a leukocytoclastic vasculitis. His biopsy revealed an inflammatory infiltrate of lymphocytes, neutrophils, and nuclear dust with extravasation of erythrocytes and fibrin in the walls of small blood vessels, along with prominent papillary dermal edema and subepidermal vesiculation. Direct immunofluorescence was positive for IgA, C3, and fibrinogen in upper dermal blood vessels. The patient also had renal involvement that was confirmed with a renal biopsy.
This case and photos are courtesy of Tanya Greywal, University of California, San Diego, and Dr. Brooke Resh Sateesh, San Diego Family Dermatology.
Dr. Bilu Martin is in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit your case for possible publication, send an email to dermnews@frontlinemedcom.com.
Diagnosis: Henoch-Schönlein purpura
Henoch-Schönlein purpura (HSP), also known as immunoglobulin A (IgA) vasculitis, is characterized by palpable purpura, abdominal pain, renal disease, arthritis and/or arthralgia. HSP affects all ages, but is most common in children (the mean age of onset is between six and seven years of age). It also has a slight predilection for males, as well as whites and Asians. Patients are more likely to present during the fall, winter, and spring. It is thought that HSP may be associated with infections that are more prevalent during these times of the year.
Patients typically have purpura and joint or abdominal pain, although some may present without significant skin manifestations or pain. The rash associated with HSP may appear as erythematous macules or papules that coalesce and evolve into palpable purpura with petechiae, ecchymoses, and/or subcutaneous edema. The skin is typically affected in areas that are more dependent or experience more pressure, such as the lower extremities or buttocks. A more diffuse distribution across the entire body can be seen in those who are nonambulatory.
The arthritis associated with HSP usually affects the lower extremities, and it is oligoarticular, nondeforming, and transient, with prominent swelling and tenderness. Gastrointestinal involvement may manifest as nausea, vomiting, abdominal pain, transient paralytic ileus, hemorrhage, bowel ischemia, intussusception (rare in adults), and/or bowel perforation. These symptoms tend to develop 1 week after the rash, but there are reports of gastrointestinal complaints preceding all other manifestations of HSP.
Additionally, there can be renal involvement, which is more common in adults. These patients may experience hematuria with or without red blood cell casts, nephrotic range proteinuria, and/or elevated serum creatinine. Other less common symptoms that have been reported in patients with HSP include scrotal pain and swelling, headaches, seizures, ataxia, central and peripheral neuropathies, impaired lung diffusion capacity, keratitis, and uveitis.
The diagnosis of HSP is classically based upon clinical presentation. The diagnosis may be complicated in cases in which patients do not present with classic signs, such as palpable purpura of the lower extremities and buttocks. In these situations, a biopsy of the skin or kidney may aid in the diagnosis.
The differential diagnosis for HSP includes acute hemorrhagic edema of infancy, coagulopathies, hemolytic uremic syndrome, hypersensitivity vasculitis, IgA nephropathy, immune thrombocytopenia purpura, juvenile idiopathic arthritis, reactive arthritis, rheumatic fever, small vessel vasculitis, and systemic lupus erythematosus.
The etiology of HSP is unclear. Most believe that it is an immune-mediated vasculitis with genetic and environmental influences. In HSP, there is leukocytoclastic vasculitis with deposition of IgA immune complexes, complement component 3 (C3), and fibrin in the affected vessel walls. Small vessels within the papillary dermis are usually present with an inflammatory infiltrate of neutrophils and monocytes.
The treatment of HSP usually consists of supportive care, since most patients will recover spontaneously. Therefore, hydration, rest, and pain relief are essential. Other treatment modalities may be required for more severe or extensive HSP and its complications.
Our patient’s biopsy results were consistent with a leukocytoclastic vasculitis. His biopsy revealed an inflammatory infiltrate of lymphocytes, neutrophils, and nuclear dust with extravasation of erythrocytes and fibrin in the walls of small blood vessels, along with prominent papillary dermal edema and subepidermal vesiculation. Direct immunofluorescence was positive for IgA, C3, and fibrinogen in upper dermal blood vessels. The patient also had renal involvement that was confirmed with a renal biopsy.
This case and photos are courtesy of Tanya Greywal, University of California, San Diego, and Dr. Brooke Resh Sateesh, San Diego Family Dermatology.
Dr. Bilu Martin is in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit your case for possible publication, send an email to dermnews@frontlinemedcom.com.
Diagnosis: Henoch-Schönlein purpura
Henoch-Schönlein purpura (HSP), also known as immunoglobulin A (IgA) vasculitis, is characterized by palpable purpura, abdominal pain, renal disease, arthritis and/or arthralgia. HSP affects all ages, but is most common in children (the mean age of onset is between six and seven years of age). It also has a slight predilection for males, as well as whites and Asians. Patients are more likely to present during the fall, winter, and spring. It is thought that HSP may be associated with infections that are more prevalent during these times of the year.
Patients typically have purpura and joint or abdominal pain, although some may present without significant skin manifestations or pain. The rash associated with HSP may appear as erythematous macules or papules that coalesce and evolve into palpable purpura with petechiae, ecchymoses, and/or subcutaneous edema. The skin is typically affected in areas that are more dependent or experience more pressure, such as the lower extremities or buttocks. A more diffuse distribution across the entire body can be seen in those who are nonambulatory.
The arthritis associated with HSP usually affects the lower extremities, and it is oligoarticular, nondeforming, and transient, with prominent swelling and tenderness. Gastrointestinal involvement may manifest as nausea, vomiting, abdominal pain, transient paralytic ileus, hemorrhage, bowel ischemia, intussusception (rare in adults), and/or bowel perforation. These symptoms tend to develop 1 week after the rash, but there are reports of gastrointestinal complaints preceding all other manifestations of HSP.
Additionally, there can be renal involvement, which is more common in adults. These patients may experience hematuria with or without red blood cell casts, nephrotic range proteinuria, and/or elevated serum creatinine. Other less common symptoms that have been reported in patients with HSP include scrotal pain and swelling, headaches, seizures, ataxia, central and peripheral neuropathies, impaired lung diffusion capacity, keratitis, and uveitis.
The diagnosis of HSP is classically based upon clinical presentation. The diagnosis may be complicated in cases in which patients do not present with classic signs, such as palpable purpura of the lower extremities and buttocks. In these situations, a biopsy of the skin or kidney may aid in the diagnosis.
The differential diagnosis for HSP includes acute hemorrhagic edema of infancy, coagulopathies, hemolytic uremic syndrome, hypersensitivity vasculitis, IgA nephropathy, immune thrombocytopenia purpura, juvenile idiopathic arthritis, reactive arthritis, rheumatic fever, small vessel vasculitis, and systemic lupus erythematosus.
The etiology of HSP is unclear. Most believe that it is an immune-mediated vasculitis with genetic and environmental influences. In HSP, there is leukocytoclastic vasculitis with deposition of IgA immune complexes, complement component 3 (C3), and fibrin in the affected vessel walls. Small vessels within the papillary dermis are usually present with an inflammatory infiltrate of neutrophils and monocytes.
The treatment of HSP usually consists of supportive care, since most patients will recover spontaneously. Therefore, hydration, rest, and pain relief are essential. Other treatment modalities may be required for more severe or extensive HSP and its complications.
Our patient’s biopsy results were consistent with a leukocytoclastic vasculitis. His biopsy revealed an inflammatory infiltrate of lymphocytes, neutrophils, and nuclear dust with extravasation of erythrocytes and fibrin in the walls of small blood vessels, along with prominent papillary dermal edema and subepidermal vesiculation. Direct immunofluorescence was positive for IgA, C3, and fibrinogen in upper dermal blood vessels. The patient also had renal involvement that was confirmed with a renal biopsy.
This case and photos are courtesy of Tanya Greywal, University of California, San Diego, and Dr. Brooke Resh Sateesh, San Diego Family Dermatology.
Dr. Bilu Martin is in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit your case for possible publication, send an email to dermnews@frontlinemedcom.com.

A 40-year-old male with no significant past medical history presented for progressive asymptomatic blisters on the feet, and erythematous lesions on the arms, legs, and trunk. His symptoms began with edema of the feet after a long flight to the Philippines. After a few days, erosions and bullae began forming on his dorsal feet. He was initially evaluated in the Philippines by his primary care physician,who treated him with antibiotics. The patient soon developed pruritic red bumps on his forearms and trunk. The patient was later seen in the emergency department in the United States. At that time, his physical exam was significant for large bullae on a dusky base on the bilateral dorsal feet, and scattered erythematous papules and violaceous macules with dusky centers on the legs, arms, and trunk.
