User login
Value-Based Purchasing Model for Medicare Reimbursement Extends to Physicians
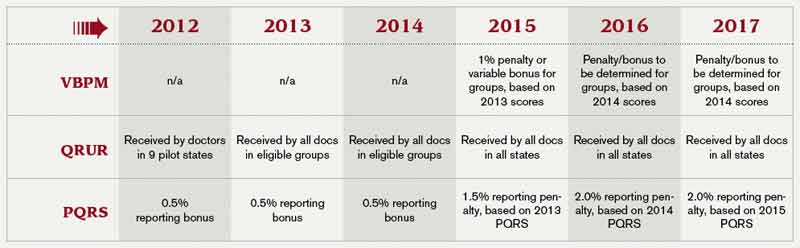
What: The program, authorized by 2010’s Affordable Care Act, extends CMS’ concept of value-based purchasing to the individual physician level. That means a portion of doctors’ Medicare reimbursements will be contingent on scores designed to measure the quality and efficiency of the healthcare they deliver.
How: The program is designed to be budget-neutral, meaning that doctors will be graded on a curve; some will lose a percentage of Medicare reimbursements, while others will gain increased payments. A prerequisite for any bonus will be participation in the Physician Quality Reporting System (PQRS), which carries its own nonparticipation penalties. The PQRS forms the core of the program, with a beefed-up Physician Compare website and the Physician Feedback Program providing public and private report cards, respectively. The latter will consist of confidential Quality and Resource Use Reports (QRURs), based on information from Medicare claims and the PQRS.
Who: At first, the VBPM program will apply to groups of 100 or more eligible professionals, currently defined as physicians, practitioners, and therapists. By 2017, however, all physicians will participate. Those in rural practices, critical-access hospitals, and federally qualified health centers are exempt; ACO participants are exempt for 2015 and 2016.
What: The program, authorized by 2010’s Affordable Care Act, extends CMS’ concept of value-based purchasing to the individual physician level. That means a portion of doctors’ Medicare reimbursements will be contingent on scores designed to measure the quality and efficiency of the healthcare they deliver.
How: The program is designed to be budget-neutral, meaning that doctors will be graded on a curve; some will lose a percentage of Medicare reimbursements, while others will gain increased payments. A prerequisite for any bonus will be participation in the Physician Quality Reporting System (PQRS), which carries its own nonparticipation penalties. The PQRS forms the core of the program, with a beefed-up Physician Compare website and the Physician Feedback Program providing public and private report cards, respectively. The latter will consist of confidential Quality and Resource Use Reports (QRURs), based on information from Medicare claims and the PQRS.
Who: At first, the VBPM program will apply to groups of 100 or more eligible professionals, currently defined as physicians, practitioners, and therapists. By 2017, however, all physicians will participate. Those in rural practices, critical-access hospitals, and federally qualified health centers are exempt; ACO participants are exempt for 2015 and 2016.
What: The program, authorized by 2010’s Affordable Care Act, extends CMS’ concept of value-based purchasing to the individual physician level. That means a portion of doctors’ Medicare reimbursements will be contingent on scores designed to measure the quality and efficiency of the healthcare they deliver.
How: The program is designed to be budget-neutral, meaning that doctors will be graded on a curve; some will lose a percentage of Medicare reimbursements, while others will gain increased payments. A prerequisite for any bonus will be participation in the Physician Quality Reporting System (PQRS), which carries its own nonparticipation penalties. The PQRS forms the core of the program, with a beefed-up Physician Compare website and the Physician Feedback Program providing public and private report cards, respectively. The latter will consist of confidential Quality and Resource Use Reports (QRURs), based on information from Medicare claims and the PQRS.
Who: At first, the VBPM program will apply to groups of 100 or more eligible professionals, currently defined as physicians, practitioners, and therapists. By 2017, however, all physicians will participate. Those in rural practices, critical-access hospitals, and federally qualified health centers are exempt; ACO participants are exempt for 2015 and 2016.
Paying Attention to Detail Critical in Medical Coding
Documentation demands attention to detail. For a patient with abdominal pain, be sure to ask: How long has the patient experienced pain? Is it generalized or in a particular quadrant? Sharp or dull? And does it radiate? And jot down the answers.
“Try to use adjectives that would give specifics regarding the complaint,” says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist at the University of Pennsylvania’s department of medicine. She also suggests hospitalists find out which medications a patient is taking or has taken and indicate whether symptoms have improved or deteriorated. Here’s how Mulholland would document such a case:
Initial hospital admission, level of service:
Code 99223
83-year-old male admitted from the emergency room, complaining of intermittent crampy lower abdominal pain (severe at times), blood in stool and increased weakness for three weeks, worse when getting up or standing. Patient has decreased appetite and progressive shortness of breath. His review of systems is otherwise negative.
Past medical history: Coronary artery disease and hypertension
Family history: Mother with Type 2 diabetes
Social history: Quit smoking 20 years ago
Alert: Blood pressure (90/68), pulse (88), and respiratory (24)
Eyes: Non-icteric
ENT: Dry oral mucosa
Lymphatic: Palpable nodes—right auxilla and right inguinal areas
Lungs: Clear
Cardio: Slight tachycardia, no murmurs, rubs or gallops
Abdomen: Slightly distended, tender on palpation
Skin: Slightly diaphoretic, no rashes or bruising
Neurologic: Cranial nerves intact, alert and conversant
Psychiatric: Anxious
Lab results: Blood in stool, hemoglobin (6.7), serum blood glucose (120), serum sodium (132), serum potassium (4.3), chest X-ray clear (my interpretation). Old records requested.
Assessment: Gastrointestional bleeding, tachycardia, and mild dehydration
Treatment plan: Check hemoglobin and hematocrit every six hours. Also check prothrombin time and partial prothrombin time. Repeat electrolytes in the morning. Order an X-ray of the lower gastrointestinal tract. Type and screen for 2 units of packed red blood cells, and transfuse pending repeat hemoglobin and hematocrit values. Infuse intravenous fluids at 80 cc per minute. Check electrocardiogram. Consult GI regarding endoscopy.
—Susan Kreimer
Documentation demands attention to detail. For a patient with abdominal pain, be sure to ask: How long has the patient experienced pain? Is it generalized or in a particular quadrant? Sharp or dull? And does it radiate? And jot down the answers.
“Try to use adjectives that would give specifics regarding the complaint,” says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist at the University of Pennsylvania’s department of medicine. She also suggests hospitalists find out which medications a patient is taking or has taken and indicate whether symptoms have improved or deteriorated. Here’s how Mulholland would document such a case:
Initial hospital admission, level of service:
Code 99223
83-year-old male admitted from the emergency room, complaining of intermittent crampy lower abdominal pain (severe at times), blood in stool and increased weakness for three weeks, worse when getting up or standing. Patient has decreased appetite and progressive shortness of breath. His review of systems is otherwise negative.
Past medical history: Coronary artery disease and hypertension
Family history: Mother with Type 2 diabetes
Social history: Quit smoking 20 years ago
Alert: Blood pressure (90/68), pulse (88), and respiratory (24)
Eyes: Non-icteric
ENT: Dry oral mucosa
Lymphatic: Palpable nodes—right auxilla and right inguinal areas
Lungs: Clear
Cardio: Slight tachycardia, no murmurs, rubs or gallops
Abdomen: Slightly distended, tender on palpation
Skin: Slightly diaphoretic, no rashes or bruising
Neurologic: Cranial nerves intact, alert and conversant
Psychiatric: Anxious
Lab results: Blood in stool, hemoglobin (6.7), serum blood glucose (120), serum sodium (132), serum potassium (4.3), chest X-ray clear (my interpretation). Old records requested.
Assessment: Gastrointestional bleeding, tachycardia, and mild dehydration
Treatment plan: Check hemoglobin and hematocrit every six hours. Also check prothrombin time and partial prothrombin time. Repeat electrolytes in the morning. Order an X-ray of the lower gastrointestinal tract. Type and screen for 2 units of packed red blood cells, and transfuse pending repeat hemoglobin and hematocrit values. Infuse intravenous fluids at 80 cc per minute. Check electrocardiogram. Consult GI regarding endoscopy.
—Susan Kreimer
Documentation demands attention to detail. For a patient with abdominal pain, be sure to ask: How long has the patient experienced pain? Is it generalized or in a particular quadrant? Sharp or dull? And does it radiate? And jot down the answers.
“Try to use adjectives that would give specifics regarding the complaint,” says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist at the University of Pennsylvania’s department of medicine. She also suggests hospitalists find out which medications a patient is taking or has taken and indicate whether symptoms have improved or deteriorated. Here’s how Mulholland would document such a case:
Initial hospital admission, level of service:
Code 99223
83-year-old male admitted from the emergency room, complaining of intermittent crampy lower abdominal pain (severe at times), blood in stool and increased weakness for three weeks, worse when getting up or standing. Patient has decreased appetite and progressive shortness of breath. His review of systems is otherwise negative.
Past medical history: Coronary artery disease and hypertension
Family history: Mother with Type 2 diabetes
Social history: Quit smoking 20 years ago
Alert: Blood pressure (90/68), pulse (88), and respiratory (24)
Eyes: Non-icteric
ENT: Dry oral mucosa
Lymphatic: Palpable nodes—right auxilla and right inguinal areas
Lungs: Clear
Cardio: Slight tachycardia, no murmurs, rubs or gallops
Abdomen: Slightly distended, tender on palpation
Skin: Slightly diaphoretic, no rashes or bruising
Neurologic: Cranial nerves intact, alert and conversant
Psychiatric: Anxious
Lab results: Blood in stool, hemoglobin (6.7), serum blood glucose (120), serum sodium (132), serum potassium (4.3), chest X-ray clear (my interpretation). Old records requested.
Assessment: Gastrointestional bleeding, tachycardia, and mild dehydration
Treatment plan: Check hemoglobin and hematocrit every six hours. Also check prothrombin time and partial prothrombin time. Repeat electrolytes in the morning. Order an X-ray of the lower gastrointestinal tract. Type and screen for 2 units of packed red blood cells, and transfuse pending repeat hemoglobin and hematocrit values. Infuse intravenous fluids at 80 cc per minute. Check electrocardiogram. Consult GI regarding endoscopy.
—Susan Kreimer
2013: The Year of Quality Improvement
Years ago, hospitalists were introduced as new, efficient options for staffing hospitals. Today, they are known as the quarterbacks for patient care and quality improvement (QI) within the hospital.
This year, hospitalists everywhere can help their hospitals resolve to make 2013 a landmark year for QI. And making time for quality improvement need not be a major investment, nor do you have to “reinvent the wheel” and create your own programs.
SHM’s full menu of QI options gives hospitalists and other caregivers the confidence that their program is field-tested as well as the ability to choose the level of involvement that’s right for them.
For more information, visit www.hospitalmedicine.org/qi.
Years ago, hospitalists were introduced as new, efficient options for staffing hospitals. Today, they are known as the quarterbacks for patient care and quality improvement (QI) within the hospital.
This year, hospitalists everywhere can help their hospitals resolve to make 2013 a landmark year for QI. And making time for quality improvement need not be a major investment, nor do you have to “reinvent the wheel” and create your own programs.
SHM’s full menu of QI options gives hospitalists and other caregivers the confidence that their program is field-tested as well as the ability to choose the level of involvement that’s right for them.
For more information, visit www.hospitalmedicine.org/qi.
Years ago, hospitalists were introduced as new, efficient options for staffing hospitals. Today, they are known as the quarterbacks for patient care and quality improvement (QI) within the hospital.
This year, hospitalists everywhere can help their hospitals resolve to make 2013 a landmark year for QI. And making time for quality improvement need not be a major investment, nor do you have to “reinvent the wheel” and create your own programs.
SHM’s full menu of QI options gives hospitalists and other caregivers the confidence that their program is field-tested as well as the ability to choose the level of involvement that’s right for them.
For more information, visit www.hospitalmedicine.org/qi.
Fellow in Hospital Medicine Spotlight: Amir Jaffer, MD, SFHM

Undergraduate education: Boston University, College of Liberal Arts.
Medical school: Boston University School of Medicine.
Notable: Dr. Jaffer is a pioneer in demonstrating how hospitalists can perform preoperative evaluations. He was the medical director of the IMPACT (Internal Medicine Preoperative Assessment, Consultation, and Treatment) Center at Cleveland Clinic. He is an editor of the recently published “Perioperative Medicine: Medical Consultation and Co-Management”, the first comprehensive reference text focused on perioperative medicine created specifically for hospitalists. Dr. Jaffer’s focus is on perioperative medicine, and he is passionate about anticoagulation and thrombosis; he has served on the panel of the 8th and 9th edition of the American College of Chest Physician’s Antithrombotic Guidelines. In 2010, he received the SHM Award of Excellence in Teaching and was HM10 course director.
FYI: Dr. Jaffer loves to travel with his family. In recent years he’s visited Spain, Australia, and Turkey. He has become more health-conscious and works out four to five times a week.
Quotable: “Being a senior fellow means being a role model for other leaders, hospitalists, residents, and students, and highlighting for them how one can be a leader in education, teamwork, quality, and systems improvement.”
Undergraduate education: Boston University, College of Liberal Arts.
Medical school: Boston University School of Medicine.
Notable: Dr. Jaffer is a pioneer in demonstrating how hospitalists can perform preoperative evaluations. He was the medical director of the IMPACT (Internal Medicine Preoperative Assessment, Consultation, and Treatment) Center at Cleveland Clinic. He is an editor of the recently published “Perioperative Medicine: Medical Consultation and Co-Management”, the first comprehensive reference text focused on perioperative medicine created specifically for hospitalists. Dr. Jaffer’s focus is on perioperative medicine, and he is passionate about anticoagulation and thrombosis; he has served on the panel of the 8th and 9th edition of the American College of Chest Physician’s Antithrombotic Guidelines. In 2010, he received the SHM Award of Excellence in Teaching and was HM10 course director.
FYI: Dr. Jaffer loves to travel with his family. In recent years he’s visited Spain, Australia, and Turkey. He has become more health-conscious and works out four to five times a week.
Quotable: “Being a senior fellow means being a role model for other leaders, hospitalists, residents, and students, and highlighting for them how one can be a leader in education, teamwork, quality, and systems improvement.”
Undergraduate education: Boston University, College of Liberal Arts.
Medical school: Boston University School of Medicine.
Notable: Dr. Jaffer is a pioneer in demonstrating how hospitalists can perform preoperative evaluations. He was the medical director of the IMPACT (Internal Medicine Preoperative Assessment, Consultation, and Treatment) Center at Cleveland Clinic. He is an editor of the recently published “Perioperative Medicine: Medical Consultation and Co-Management”, the first comprehensive reference text focused on perioperative medicine created specifically for hospitalists. Dr. Jaffer’s focus is on perioperative medicine, and he is passionate about anticoagulation and thrombosis; he has served on the panel of the 8th and 9th edition of the American College of Chest Physician’s Antithrombotic Guidelines. In 2010, he received the SHM Award of Excellence in Teaching and was HM10 course director.
FYI: Dr. Jaffer loves to travel with his family. In recent years he’s visited Spain, Australia, and Turkey. He has become more health-conscious and works out four to five times a week.
Quotable: “Being a senior fellow means being a role model for other leaders, hospitalists, residents, and students, and highlighting for them how one can be a leader in education, teamwork, quality, and systems improvement.”
Society for Hospital Medicine Compiles List of Don'ts for Hospitalists
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
Hospitalists Encouraged to Join the Future of Hospital Conversation
This month, hospitalists can play a role in crowdsourcing the future of the community hospital. And one hospitalist is helping to shape the game.
On Jan. 8, the Institute for the Future launched its Future of Hospital foresight game (www.futureofhospital.org). The game will tap the wisdom of healthcare experts, urban planners, technologists, sociologists, local community leaders, social entrepreneurs, and citizens interested in engaging in a thoughtful discussion about future possibilities for community hospitals.
Hospitalist Jason Stein, MD, SFHM, is working with the Institute for the Future to help judge the responses and participation in the online, crowd-sourced game. As an advisor to the Centers for Medicare & Medicaid Services Innovation Center, Dr. Stein is no stranger to new ideas for hospitals. He was one of the co-architects of SHM’s Implementation Guides, which create step-wise approaches for system-level change. He also has been recognized nationally for his work redesigning traditional medical wards into accountable-care units, each featuring unit-based physician teams that conduct structured interdisciplinary bedside rounds (SIBRs).
“This is an exciting way for hospitalists to join a dynamic conversation about how hospitals—and their staff—provide the best care possible to their patients in 21st-century, American healthcare,” Dr. Stein says.
The Future of the Hospital is a game that anyone can play; all that is required is ideas. If others build on those ideas, contributors win points and create award-winning chains of innovation, linking people and their ideas from all over the world.
“Hospitalists have been on the cutting edge of some of the best ideas in healthcare for the last two decades,” Dr. Stein says. “This is an exciting and innovative way for all of us to contribute ideas and leverage our collective experience for the good of our hospitals and patients.”
This month, hospitalists can play a role in crowdsourcing the future of the community hospital. And one hospitalist is helping to shape the game.
On Jan. 8, the Institute for the Future launched its Future of Hospital foresight game (www.futureofhospital.org). The game will tap the wisdom of healthcare experts, urban planners, technologists, sociologists, local community leaders, social entrepreneurs, and citizens interested in engaging in a thoughtful discussion about future possibilities for community hospitals.
Hospitalist Jason Stein, MD, SFHM, is working with the Institute for the Future to help judge the responses and participation in the online, crowd-sourced game. As an advisor to the Centers for Medicare & Medicaid Services Innovation Center, Dr. Stein is no stranger to new ideas for hospitals. He was one of the co-architects of SHM’s Implementation Guides, which create step-wise approaches for system-level change. He also has been recognized nationally for his work redesigning traditional medical wards into accountable-care units, each featuring unit-based physician teams that conduct structured interdisciplinary bedside rounds (SIBRs).
“This is an exciting way for hospitalists to join a dynamic conversation about how hospitals—and their staff—provide the best care possible to their patients in 21st-century, American healthcare,” Dr. Stein says.
The Future of the Hospital is a game that anyone can play; all that is required is ideas. If others build on those ideas, contributors win points and create award-winning chains of innovation, linking people and their ideas from all over the world.
“Hospitalists have been on the cutting edge of some of the best ideas in healthcare for the last two decades,” Dr. Stein says. “This is an exciting and innovative way for all of us to contribute ideas and leverage our collective experience for the good of our hospitals and patients.”
This month, hospitalists can play a role in crowdsourcing the future of the community hospital. And one hospitalist is helping to shape the game.
On Jan. 8, the Institute for the Future launched its Future of Hospital foresight game (www.futureofhospital.org). The game will tap the wisdom of healthcare experts, urban planners, technologists, sociologists, local community leaders, social entrepreneurs, and citizens interested in engaging in a thoughtful discussion about future possibilities for community hospitals.
Hospitalist Jason Stein, MD, SFHM, is working with the Institute for the Future to help judge the responses and participation in the online, crowd-sourced game. As an advisor to the Centers for Medicare & Medicaid Services Innovation Center, Dr. Stein is no stranger to new ideas for hospitals. He was one of the co-architects of SHM’s Implementation Guides, which create step-wise approaches for system-level change. He also has been recognized nationally for his work redesigning traditional medical wards into accountable-care units, each featuring unit-based physician teams that conduct structured interdisciplinary bedside rounds (SIBRs).
“This is an exciting way for hospitalists to join a dynamic conversation about how hospitals—and their staff—provide the best care possible to their patients in 21st-century, American healthcare,” Dr. Stein says.
The Future of the Hospital is a game that anyone can play; all that is required is ideas. If others build on those ideas, contributors win points and create award-winning chains of innovation, linking people and their ideas from all over the world.
“Hospitalists have been on the cutting edge of some of the best ideas in healthcare for the last two decades,” Dr. Stein says. “This is an exciting and innovative way for all of us to contribute ideas and leverage our collective experience for the good of our hospitals and patients.”
HMX Term of the Month: Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)
HCAHPS is a national, standardized survey of hospital patients created to publicly report patients’ perspective of hospital care. The survey asks a random sample of recently discharged patients about important aspects of their hospital experience. The HCAHPS results posted on Medicare’s Hospital Compare website (www.hospitalcompare.hhs.gov) allow consumers to make fair and objective comparisons of hospitals and individual hospitals to state and national benchmarks.
Contributed by HMX user Dr. Patrick Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance and Standards Committee.
HCAHPS is a national, standardized survey of hospital patients created to publicly report patients’ perspective of hospital care. The survey asks a random sample of recently discharged patients about important aspects of their hospital experience. The HCAHPS results posted on Medicare’s Hospital Compare website (www.hospitalcompare.hhs.gov) allow consumers to make fair and objective comparisons of hospitals and individual hospitals to state and national benchmarks.
Contributed by HMX user Dr. Patrick Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance and Standards Committee.
HCAHPS is a national, standardized survey of hospital patients created to publicly report patients’ perspective of hospital care. The survey asks a random sample of recently discharged patients about important aspects of their hospital experience. The HCAHPS results posted on Medicare’s Hospital Compare website (www.hospitalcompare.hhs.gov) allow consumers to make fair and objective comparisons of hospitals and individual hospitals to state and national benchmarks.
Contributed by HMX user Dr. Patrick Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance and Standards Committee.
Medicaid Payments for Some Primary-Care Services Reach Parity with Medicare Levels
On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulation implementing increased Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
Covered Medicaid services include evaluation and management codes between 99201 and 99499 when used by physicians with a specialty designation of family medicine, general internal medicine, or pediatric medicine. CMS also finalized a policy to qualify services provided by subspecialists related to the designated primary-care specialists board-certified by the American Board of Medical Specialties, American Osteopathic Association, and the American Board of Physician Specialties. Advanced-practice clinicians also qualify for the increased payment when services are furnished under a physician’s personal supervision.
In commenting on the proposed rule, SHM stated that hospitalists should qualify for purposes of the increased payment because they are an important part of the “team” of clinicians required to treat many common conditions within the Medicaid population, and that hospitalists often provide the first contact and facilitate an entry point into the comprehensive care network.
CMS agreed.
The codes included in the pay increase will be limited to traditional primary care but also will include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services.
Hospitalists will qualify for the enhanced payment, but it remains somewhat unclear how individual states will handle the increase. State Medicaid agencies could pay physicians based on their self-attestation alone or in conjunction with any other provider enrollment requirements that currently exist in the state. Further, inclusion of a code does not require a state to pay for the service if it is not already covered under the state’s Medicaid program. All other state coverage and payment policy rules related to the services also remain in effect.
Timing of the pay increase also remains unclear. The statute requires that states make higher payments for services provided on or after Jan. 1, 2013, but for many physicians, the higher payment might be longer in coming despite being retroactive to the January deadline. States must submit a State Plan Amendment (SPA) to reflect the fee schedule rate increases by March 31, 2013, and CMS may then take up to 90 days to review and approve the SPA. Therefore, it could be six months or longer before eligible physicians and practitioners receive any of the payment increase.
States will receive an estimated $5.8 billion in 2013 and $6.1 billion in 2014 in federal funds to meet this two-year requirement, unless Congress acts to extend or fund the provision permanently. In response to an SHM suggestion on the potential to extend the increase, CMS will be collecting relevant data on the impact of the pay increase on Medicaid patients.
Even with the remaining uncertainty and timing issues, this is a change in payment policy that presents an important shift in the valuation of primary-care services, including some services provided by hospitalists. Medicaid services are notoriously undervalued, and this increase to providers will certainly have a positive impact on the accessibility of care for patients.
Josh Boswell is SHM’s interim senior manager of government relations.
On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulation implementing increased Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
Covered Medicaid services include evaluation and management codes between 99201 and 99499 when used by physicians with a specialty designation of family medicine, general internal medicine, or pediatric medicine. CMS also finalized a policy to qualify services provided by subspecialists related to the designated primary-care specialists board-certified by the American Board of Medical Specialties, American Osteopathic Association, and the American Board of Physician Specialties. Advanced-practice clinicians also qualify for the increased payment when services are furnished under a physician’s personal supervision.
In commenting on the proposed rule, SHM stated that hospitalists should qualify for purposes of the increased payment because they are an important part of the “team” of clinicians required to treat many common conditions within the Medicaid population, and that hospitalists often provide the first contact and facilitate an entry point into the comprehensive care network.
CMS agreed.
The codes included in the pay increase will be limited to traditional primary care but also will include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services.
Hospitalists will qualify for the enhanced payment, but it remains somewhat unclear how individual states will handle the increase. State Medicaid agencies could pay physicians based on their self-attestation alone or in conjunction with any other provider enrollment requirements that currently exist in the state. Further, inclusion of a code does not require a state to pay for the service if it is not already covered under the state’s Medicaid program. All other state coverage and payment policy rules related to the services also remain in effect.
Timing of the pay increase also remains unclear. The statute requires that states make higher payments for services provided on or after Jan. 1, 2013, but for many physicians, the higher payment might be longer in coming despite being retroactive to the January deadline. States must submit a State Plan Amendment (SPA) to reflect the fee schedule rate increases by March 31, 2013, and CMS may then take up to 90 days to review and approve the SPA. Therefore, it could be six months or longer before eligible physicians and practitioners receive any of the payment increase.
States will receive an estimated $5.8 billion in 2013 and $6.1 billion in 2014 in federal funds to meet this two-year requirement, unless Congress acts to extend or fund the provision permanently. In response to an SHM suggestion on the potential to extend the increase, CMS will be collecting relevant data on the impact of the pay increase on Medicaid patients.
Even with the remaining uncertainty and timing issues, this is a change in payment policy that presents an important shift in the valuation of primary-care services, including some services provided by hospitalists. Medicaid services are notoriously undervalued, and this increase to providers will certainly have a positive impact on the accessibility of care for patients.
Josh Boswell is SHM’s interim senior manager of government relations.
On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulation implementing increased Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
Covered Medicaid services include evaluation and management codes between 99201 and 99499 when used by physicians with a specialty designation of family medicine, general internal medicine, or pediatric medicine. CMS also finalized a policy to qualify services provided by subspecialists related to the designated primary-care specialists board-certified by the American Board of Medical Specialties, American Osteopathic Association, and the American Board of Physician Specialties. Advanced-practice clinicians also qualify for the increased payment when services are furnished under a physician’s personal supervision.
In commenting on the proposed rule, SHM stated that hospitalists should qualify for purposes of the increased payment because they are an important part of the “team” of clinicians required to treat many common conditions within the Medicaid population, and that hospitalists often provide the first contact and facilitate an entry point into the comprehensive care network.
CMS agreed.
The codes included in the pay increase will be limited to traditional primary care but also will include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services.
Hospitalists will qualify for the enhanced payment, but it remains somewhat unclear how individual states will handle the increase. State Medicaid agencies could pay physicians based on their self-attestation alone or in conjunction with any other provider enrollment requirements that currently exist in the state. Further, inclusion of a code does not require a state to pay for the service if it is not already covered under the state’s Medicaid program. All other state coverage and payment policy rules related to the services also remain in effect.
Timing of the pay increase also remains unclear. The statute requires that states make higher payments for services provided on or after Jan. 1, 2013, but for many physicians, the higher payment might be longer in coming despite being retroactive to the January deadline. States must submit a State Plan Amendment (SPA) to reflect the fee schedule rate increases by March 31, 2013, and CMS may then take up to 90 days to review and approve the SPA. Therefore, it could be six months or longer before eligible physicians and practitioners receive any of the payment increase.
States will receive an estimated $5.8 billion in 2013 and $6.1 billion in 2014 in federal funds to meet this two-year requirement, unless Congress acts to extend or fund the provision permanently. In response to an SHM suggestion on the potential to extend the increase, CMS will be collecting relevant data on the impact of the pay increase on Medicaid patients.
Even with the remaining uncertainty and timing issues, this is a change in payment policy that presents an important shift in the valuation of primary-care services, including some services provided by hospitalists. Medicaid services are notoriously undervalued, and this increase to providers will certainly have a positive impact on the accessibility of care for patients.
Josh Boswell is SHM’s interim senior manager of government relations.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Interventions that improve discharge handovers reviewed
- Duration of in-hospital cardiac resuscitation and survival rates
- Early sepsis intervention strategies to decrease mortality risk
- Hypoglycemia linked to increased mortality in critically ill
- Increased bleeding risk for cardiac patients
- Hospital-run vs. anesthesiologist-run preoperative clinics
- Postoperative delirium and cognitive impairment in cardiac patients
- Benefits of resuming anticoagulants after GI bleeding
- Preoperative hyponatremia and risk of perioperative mortality
Systematic Review Highlights Several Interventions That Improve Discharge Handovers
Clinical question: Do interventions to improve patient handovers at discharge have positive effects on patient care?
Background: The transition from hospital to primary care is often suboptimal and has been associated with unfavorable outcomes, including hospital readmission, increased healthcare utilization, and adverse drug events post-discharge. This review sought to characterize different types of interventions aimed at improving discharge handovers and to evaluate their effects.
Study design: Systematic review of randomized controlled trials.
Setting: Studies published from January 1990 to March 2011.
Synopsis: Review of published databases identified 36 randomized controlled studies on interventions to improve discharge handovers. Studies were blindly evaluated by two reviewers on quality, interventions, and outcomes. There was significant heterogeneity in interventions and outcomes; thus, statistical analysis was not possible. Most studies evaluated multicomponent interventions and had more than one outcome measure.
Of the 36 studies reviewed, 25 reported statistically significant improvements in outcomes, including reduced hospital utilization and improved continuity of care. Effective interventions included medication reconciliation; structured discharge information (facilitated by electronic resources); multidisciplinary discharge planning; shared involvement in arranging care between inpatient and outpatient physicians; and Web-based access to discharge information by the outpatient provider.
The complexity of the interventions and the heterogeneity of reported results did not allow for firm conclusions to be drawn regarding which specific interventions had the strongest effects.
Bottom line: Interventions that target the quality and safety of handovers between hospital and outpatient providers at discharge can significantly reduce hospital utilization and improve continuity of care.
Citation: Hesselink G, Schoonhoven L, Barach P, et al. Improving patient handovers from hospital to primary care: a systematic review. Ann Intern Med. 2012;157:417-428.
Longer Duration of In-Hospital Cardiac Resuscitation Associated with Increased Survival
Clinical question: Are prolonged cardiac resuscitation efforts associated with improved outcomes?
Background: There is little evidence or guidelines on how long to maintain resuscitative efforts during in-hospital cardiac arrest, leading to variation in practice. This study characterized patterns of resuscitation duration and relationship to the return of spontaneous circulation and survival to discharge.
Study design: Retrospective observational study.
Setting: Four hundred thirty-five U.S. hospitals reporting data to the American Heart Association’s Get With The Guidelines: Resuscitation registry.
Synopsis: Using duration of resuscitation in nonsurvivors as a surrogate for the tendency of a facility to perform prolonged efforts, hospitals were divided into quartiles. Overall, of 64,339 patients in the registry, 31,198 (48.5%) had return of circulation and 9,912 (15.4%) survived to discharge. Resuscitative efforts in nonsurvivors ranged from a median of 16 to 25 minutes between the lowest and highest quartiles.
There was a stepwise increase in the likelihood for patients to have return of spontaneous circulation and to survive to discharge between each quartile. Specifically, comparing shortest to longest, there was a significant adjusted odds ratio of 1.12 for both the return of circulation (P<0.0001) and survival to discharge (P=0.021). The survival benefit was most apparent for those with pulseless electrical activity or asystole as initial rhythms, as compared to ventricular tachycardia or fibrillation.
Limitations included the study’s observational design, which meant causality could not be determined. Additionally, the study did not account for the quality of resuscitative efforts (e.g. depth of chest compressions, adherence with guidelines), which might have influenced outcomes. Importantly, the study looked at survival to discharge, but it did not evaluate long-term survival or functional status post-discharge, which might better reflect the success of resuscitation.
Bottom line: Prolonged resuscitative efforts were observed to be associated with increased likelihood of return of spontaneous circulation and survival to discharge; this data might provide clinical guidance in determining when to stop resuscitation efforts.
Citation: Goldberger ZD, Chan PS, Berg RA, et al. Duration of resuscitation efforts and survival after in-hospital cardiac arrest: an observational study. Lancet. 2012;380:1473-1481.
Early Sepsis Intervention Strategies Decrease Mortality, Length of Stay, and Cost
Clinical question: For patients with sepsis or septic shock, what is the impact of a real-time comprehensive continuous quality-improvement (QI) initiative on in-hospital mortality, morbidity, and healthcare resource utilization in community and tertiary-care hospitals in the U.S.?
Background: Multiple single-center trials have demonstrated that early sepsis intervention strategies (early goal-directed therapy, resuscitation bundles) improve in-hospital mortality. Little is known about the effectiveness of incorporating these strategies into a real-time continuous QI initiative and implementing interventions across multiple sites simultaneously.
Study design: Pre-post at some sites and concurrent implementation design at other sites.
Setting: Five community and six-tertiary care U.S. hospitals.
Synopsis: The GENeralized Early Sepsis Intervention Strategies (GENESIS) project was a CQI initiative that combined several QI concepts with validated early sepsis interventions known as resuscitation bundles (RB). Continuous QI was implemented on patients with severe sepsis or septic shock in both before and after designs (eight hospitals), and in concurrent designs (three hospitals). The control group was comprised of historical controls treated before GENESIS and patients with incomplete implementation of RB, totaling 1,554 patients. The treatment group included patients treated after GENESIS and those with complete RB compliance, totaling 4,801 patients.
Compared with the control group, patients in the treatment group had a 33% decreased risk of in-hospital mortality (RR 0.67, 95% CI 0.63-0.72), an absolute decrease in hospital length of stay (LOS) by 5.1 days (20.7 days vs. 15.6 days, P<0.001) and a $47,923 reduction in total hospital charges (P<0.001). Limitations included the study design (not a prospective randomized trial), and the possibility of other concurrent unmeasured quality initiatives taking place at the study sites, which might have contributed to improved outcomes.
Bottom line: Early sepsis intervention strategies in the form of a comprehensive continuous QI initiative can decrease mortality, hospital LOS, and cost in both tertiary-care and community hospitals.
Citation: Cannon CM, Holthaus CV, Zubrow MT, et al. The GENESIS project (GENeralized Early Sepsis Intervention Strategies): a multicenter quality improvement collaborative. J Intensive Care Med. 2012; Aug 17. doi:10.1177/0885066612453025.
Hypoglycemia Associated with Increased Mortality in the Critically Ill
Clinical question: Is hypoglycemia associated with mortality in critically ill patients?
Background: Initial studies suggested that intensive glucose control reduces mortality in surgical ICU patients and reduces morbidity in medical ICU patients, but further studies have not supported these findings. Recent literature shows conflicting results on the effects of intense glucose control in critically ill patients.
Study design: Post-hoc analysis of the NICE-SUGAR study database.
Setting: ICUs in 42 hospitals in Australia, New Zealand, and Canada.
Synopsis: The NICE-SUGAR study was a multicenter trial that randomized 6,104 ICU patients to intensive (glucose 80 to 108 mg/dL) or conventional glucose control (≤180 mg/dL). Patients were followed for 90 days or until death, with death being the primary end point. Severe hypoglycemia (<40 mg/dL) was recorded in 6.8% of patients in the intensive glucose control group versus 0.5% in the conventional group. The study showed that intensive glucose control was associated with increased mortality among adult ICU patients.
Using the NICE-SUGAR database, the authors conducted a Cox regression analysis to examine the associations between hypoglycemia and death. A total of 2,714 patients had moderate hypoglycemia (glucose 41 to 70 mg/dL), and 223 patients had severe hypoglycemia. The hazard ratio for mortality was 1.41 (95% CI 1.21-1.62, P<0.001) for patients with moderate hypoglycemia and 2.10 (95% CI 1.59-2.77, P<0.001) for severe hypoglycemia, compared to patients without hypoglycemia.
These findings show a strong association between mortality and hypoglycemia but do not prove causality. Hospitalists caring for ICU patients must be aware that hypoglycemia is associated with mortality and focus on avoiding hypoglycemia. The American Diabetes Association currently recommends a target blood glucose level of 140 to 180 mg/dL for most critically ill patients.
Bottom line: Hypoglycemia (glucose <70 mg/dL) is associated with increased risk of mortality in ICU patients.
Citation: Finfer S, Chittock DR, Su SY, et al. Hypoglycemia and risk of death in critically ill patients. New Engl J Med. 2012;367(12):1108-1118.
Increased Bleeding Risk for Cardiac Patients on Multiple Antithrombotic Drugs
Clinical question: Is there an increased risk of bleeding in atrial fibrillation patients treated with multiple antithrombotic agents following acute myocardial infarction (MI) or percutaneous coronary intervention (PCI)?
Background: Current treatment for atrial fibrillation patients with MI or PCI includes vitamin K antagonist (VKA) therapy to prevent stroke and antiplatelet agents to prevent further coronary events. There are inconsistent findings on the safety and efficacy of combined therapy with VKA, aspirin, and clopidogrel, specifically with regard to bleeding risk.
Study design: Retrospective cohort study.
Setting: Nationwide registry in Denmark.
Synopsis: Using the National Patient Registry in Denmark, 11,480 patients with atrial fibrillation who were admitted for MI or PCI were identified. Patients were grouped by medication regimen, including monotherapy (aspirin, clopidogrel, or VKA), dual therapy (dual antiplatelet or VKA+antiplatelet), or triple therapy (VKA+aspirin+clopidogrel). The primary outcome was nonfatal or fatal bleeding within one year.
Patients receiving triple therapy had the highest rate of bleeding, with a crude incidence of 14.2 events per 100 person-years. Patients treated with VKA+aspirin+clopidogel were significantly more likely than those on VKA+antiplatelet (HR 1.47, 95% CI 1.04-2.08) or dual antiplatelet (HR 2.20, 95% CI 1.58-3.08) treatment to have a bleeding event within 90 days, and similar trends were seen at 90 to 360 days. There was no significant difference in thromboembolic events among patients on VKA+aspirin+clopidogrel versus VKA+antiplatelet therapy.
Only bleeding events that required hospitalization were recorded, which might underestimate the bleeding risks of these regimens. Additionally, INR levels were not determined, which could impact both bleeding and thromboembolic outcomes.
However, this study does suggest that there are significant bleeding risks among patients treated with triple therapy. Hospitalists should weigh the risks of thromboembolic events with bleeding risks in patients with atrial fibrillation and MI/PCI, and only prescribe VKA+aspirin+clopidogrel with these risks in mind.
Bottom line: Immediate and continued bleeding risk is increased in patients with atrial fibrillation admitted with PCI or MI who are placed on triple antithrombotic therapy with VKA+aspirin+clopidogrel.
Citation: Lamberts M, Olesen JB, Ruwald MH, et al. Bleeding after initiation of multiple antithrombotic drugs, including triple therapy, in atrial fibrillation patients following myocardial infarction and coronary intervention. Circulation. 2012;126:1185-1193.
Hospitalist-Run Preoperative Clinic Improves Outcomes in Complex Surgical Patients
Clinical question: Do hospitalist-run preoperative clinics improve outcomes for medically complex patients undergoing noncardiac surgery compared to traditional anesthesiologist-run preoperative clinics?
Background: Studies of perioperative medical consultation have shown inconsistent effects on quality of care, but preoperative medical consultation has only been evaluated in the immediate preoperative period (one day prior to surgery or less). Little is known about the impact of involving hospitalists earlier in the preoperative period.
Study design: Retrospective, pre-post study.
Setting: Veterans Affairs Greater Los Angeles Healthcare System (VAGLAHS).
Synopsis: In July 2004, the VAGLAHS Preoperative Clinic transitioned from being anesthesiologist-run to hospitalist-run. Mid-level providers were trained on preoperative medical assessment, and patients were only evaluated by anesthesia staff on the day of surgery, after they had been deemed medically acceptable for surgery. All patients seen in the clinic from July 2003 to July 2005 were included in the study. Period A included patients evaluated when anesthesia staff supervised the clinic. Period B included patients evaluated during the first year of the hospitalist-run system.
There were 1,101 patients with inpatient surgeries in Period A, and 1,126 patients in Period B. Mean length of stay (LOS) decreased to 5.28 days during the hospitalist-run model from 9.87 days during the anesthesiologist-run model. LOS reductions were most notable in patients with ASA scores of 3 or higher; LOS reductions were not seen in an internal control of surgical patients who were not evaluated in the preoperative clinic. Inpatient mortality was also reduced in Period B compared with Period A, to 4 cases (0.36%) from 14 cases (1.27%) (P=0.0158). Specific processes that led to improved outcomes for patients in Period B could not be identified. The VA study setting might limit the generalizability of the results.
Bottom line: A hospitalist-run preoperative clinic was associated with decreased LOS and inpatient mortality compared with a traditional anesthesiologist-run clinic.
Citation: Vazirani S, Lankarani-Fard A, Lian LJ, Stelzner M, Asch SM. Preoperative processes and outcomes after implementation of a hospitalist-run preoperative clinic. J Hosp Med. 2012 Sep 7. doi:10.1002/jhm.1968.
Delirium after Cardiac Surgery Associated with Prolonged Cognitive Impairment
Clinical question: Is postoperative delirium associated with decreased cognitive function in the first year after cardiac surgery?
Background: In general populations, delirium has been associated with long-term decline in cognitive ability. Delirium and cognitive dysfunction are both common following cardiac surgery, but the effects of postoperative delirium on the trajectory of cognitive function over time is unclear.
Study design: Prospective cohort study.
Setting: Two academic medical centers and a Veterans Administration hospital.
Synopsis: Two hundred twenty-five patients aged 60 or older who were scheduled to undergo coronary artery bypass grafting or valve replacement surgery were included. Patients underwent preoperative assessment cognitive function with the use of the Mini-Mental State Examination (MMSE). Starting on postoperative Day 2, patients underwent daily assessment for delirium. After discharge, cognitive function was reassessed at months one, six, and 12.
Postoperative delirium occurred in 103 patients (46%). Patients with delirium were older, had higher comorbidity scores, and had lower MMSE scores at baseline. Among the overall study population, adjusted MMSE scores dropped 4.6 points from baseline to postoperative Day 2, then were observed to increase by approximately one point per day during postoperative days 3 to 5 with minimal change thereafter. Patients with delirium had greater decrease in cognitive function in the immediate postoperative period compared to patients without delirium (7.7 points vs. 2.1, P<0.001).
Patients without delirium returned to their baseline cognitive ability by one month postoperatively, while patients who had delirium were still making gains up to six months post-operatively, never returning to baseline level of function by one year. Unmeasured confounders and uncertain sensitivity of the MMSE to detect mild cognitive impairment might limit these findings.
Bottom line: Cognitive function decreases in the immediate postoperative period following cardiac surgery. Compared to patients without delirium, patients with delirium experience more dramatic and prolonged cognitive impairment postoperatively, without returning to their preoperative level of cognitive function at one year.
Citation: Saczynski JS, Marcantonio ER, Quach L, et al. Cognitive trajectories after postoperative delirium. New Engl J Med. 2012;367:30-39.
Benefits of Resuming Anticoagulation after GI Bleed Outweigh Risks for Most Patients
Clinical question: In warfarin-treated patients who have experienced gastrointestinal (GI) bleeding, what are the patterns of restarting warfarin therapy and the incidence of thrombosis, recurrent GI bleed, and death in the 90 days following index bleed?
Background: In warfarin-treated patients who experience GI bleeding, warfarin is often temporarily held or permanently discontinued, placing patients at increased risk for developing thromboembolism. Little is known about the risks, benefits, and timing of restarting warfarin in this patient population.
Study design: Retrospective cohort study.
Setting: Kaiser Permanente Colorado.
Synopsis: Using clinical and administrative databases, 442 patients who presented with GI bleeding while receiving warfarin therapy were identified. Patients were grouped by whether they resumed warfarin (n=260, including 41 patients in whom anticoagulation was never interrupted), or did not resume warfarin therapy (n=182) in the 90 days following index GI bleed. Patients with prosthetic heart valves or GI bleeding localized to the rectum/anus were more commonly restarted on warfarin, whereas older patients and those in whom the source of bleeding was not identified were less likely to be restarted on warfarin therapy.
Restarting warfarin therapy after index GI bleed was associated with lower risk of thrombosis (HR 0.05, 95% CI 0.01-0.58) and death from any cause (HR 0.31, 95% CI 0.15-0.62), and it was not associated with a significant increase in risk for recurrent GI bleed (HR 1.32, 95% CI 0.50-3.57).
The authors concluded that for many patients who experience a warfarin-associated GI bleed, the benefits of restarting warfarin therapy outweigh the risks. No conclusions were made regarding the optimal timing of resuming therapy. Limitations included the use of administrative data and inability to determine the potential influence of aspirin use on outcomes.
Bottom line: Resuming warfarin in the 90 days following a warfarin-associated GI bleed is associated with decreased risk of thrombosis and death without increased risk for recurrent GI bleed.
Citation: Witt DM, Delate T, Garcia DA, et al. Risk of thromboembolism, recurrent hemorrhage, and death after warfarin therapy interruption for gastrointestinal tract bleeding. Arch Intern Med. 2012 Sep 12. doi:10.1001/archinternmed.2012.4261.
Preoperative Hyponatremia Associated with Increased Risk for Perioperative Complications and Mortality
Clinical question: Is preoperative hyponatremia an indicator of perioperative morbidity and mortality?
Background: Hyponatremia is a common diagnosis in the hospital setting and is associated with adverse outcomes, even in mild cases. However, it is unclear if this association exists in surgical patients when detected preoperatively.
Study design: Retrospective cohort study.
Setting: Academic and community hospitals participating in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP).
Synopsis: A total of 75,423 adult patients with hyponatremia (sodium <135 mEq/L) who were undergoing major surgery were compared to 888,840 patients with normal preoperative sodium levels over a six-year period. The primary outcome was 30-day mortality. Secondary outcomes included postoperative major coronary events, stroke, wound infection, pneumonia, and length of stay (LOS).
Compared to patients with normal sodium levels, those with preoperative hyponatremia had higher rates of perioperative mortality (5.2% vs. 1.3%; adjusted odds ratio 1.44, 95% CI 1.38-1.50), with increased risk that correlated with increasing severity of hyponatremia. Association with postoperative mortality was particularly strong among hyponatremic patients with ASA scores of 1 or 2 and those undergoing nonemergency surgery.
Patients with preoperative hyponatremia were also found to have increased risk for all postoperative complications evaluated, with the exception of stroke. Limitations included the potential for unmeasured confounders and not being able to account for the role of medications used perioperatively. Research is needed to determine whether correcting preoperative hyponatremia lessens the risk of mortality and other postoperative complications.
Bottom line: Among patients undergoing major surgery, preoperative hyponatremia is a predictor of postoperative 30-day mortality and morbidity.
Citation: Leung AA, McAlister FA, Rogers SO, et al. Preoperative hyponatremia and perioperative complications. Arch Intern Med. 2012;172:1-8.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Interventions that improve discharge handovers reviewed
- Duration of in-hospital cardiac resuscitation and survival rates
- Early sepsis intervention strategies to decrease mortality risk
- Hypoglycemia linked to increased mortality in critically ill
- Increased bleeding risk for cardiac patients
- Hospital-run vs. anesthesiologist-run preoperative clinics
- Postoperative delirium and cognitive impairment in cardiac patients
- Benefits of resuming anticoagulants after GI bleeding
- Preoperative hyponatremia and risk of perioperative mortality
Systematic Review Highlights Several Interventions That Improve Discharge Handovers
Clinical question: Do interventions to improve patient handovers at discharge have positive effects on patient care?
Background: The transition from hospital to primary care is often suboptimal and has been associated with unfavorable outcomes, including hospital readmission, increased healthcare utilization, and adverse drug events post-discharge. This review sought to characterize different types of interventions aimed at improving discharge handovers and to evaluate their effects.
Study design: Systematic review of randomized controlled trials.
Setting: Studies published from January 1990 to March 2011.
Synopsis: Review of published databases identified 36 randomized controlled studies on interventions to improve discharge handovers. Studies were blindly evaluated by two reviewers on quality, interventions, and outcomes. There was significant heterogeneity in interventions and outcomes; thus, statistical analysis was not possible. Most studies evaluated multicomponent interventions and had more than one outcome measure.
Of the 36 studies reviewed, 25 reported statistically significant improvements in outcomes, including reduced hospital utilization and improved continuity of care. Effective interventions included medication reconciliation; structured discharge information (facilitated by electronic resources); multidisciplinary discharge planning; shared involvement in arranging care between inpatient and outpatient physicians; and Web-based access to discharge information by the outpatient provider.
The complexity of the interventions and the heterogeneity of reported results did not allow for firm conclusions to be drawn regarding which specific interventions had the strongest effects.
Bottom line: Interventions that target the quality and safety of handovers between hospital and outpatient providers at discharge can significantly reduce hospital utilization and improve continuity of care.
Citation: Hesselink G, Schoonhoven L, Barach P, et al. Improving patient handovers from hospital to primary care: a systematic review. Ann Intern Med. 2012;157:417-428.
Longer Duration of In-Hospital Cardiac Resuscitation Associated with Increased Survival
Clinical question: Are prolonged cardiac resuscitation efforts associated with improved outcomes?
Background: There is little evidence or guidelines on how long to maintain resuscitative efforts during in-hospital cardiac arrest, leading to variation in practice. This study characterized patterns of resuscitation duration and relationship to the return of spontaneous circulation and survival to discharge.
Study design: Retrospective observational study.
Setting: Four hundred thirty-five U.S. hospitals reporting data to the American Heart Association’s Get With The Guidelines: Resuscitation registry.
Synopsis: Using duration of resuscitation in nonsurvivors as a surrogate for the tendency of a facility to perform prolonged efforts, hospitals were divided into quartiles. Overall, of 64,339 patients in the registry, 31,198 (48.5%) had return of circulation and 9,912 (15.4%) survived to discharge. Resuscitative efforts in nonsurvivors ranged from a median of 16 to 25 minutes between the lowest and highest quartiles.
There was a stepwise increase in the likelihood for patients to have return of spontaneous circulation and to survive to discharge between each quartile. Specifically, comparing shortest to longest, there was a significant adjusted odds ratio of 1.12 for both the return of circulation (P<0.0001) and survival to discharge (P=0.021). The survival benefit was most apparent for those with pulseless electrical activity or asystole as initial rhythms, as compared to ventricular tachycardia or fibrillation.
Limitations included the study’s observational design, which meant causality could not be determined. Additionally, the study did not account for the quality of resuscitative efforts (e.g. depth of chest compressions, adherence with guidelines), which might have influenced outcomes. Importantly, the study looked at survival to discharge, but it did not evaluate long-term survival or functional status post-discharge, which might better reflect the success of resuscitation.
Bottom line: Prolonged resuscitative efforts were observed to be associated with increased likelihood of return of spontaneous circulation and survival to discharge; this data might provide clinical guidance in determining when to stop resuscitation efforts.
Citation: Goldberger ZD, Chan PS, Berg RA, et al. Duration of resuscitation efforts and survival after in-hospital cardiac arrest: an observational study. Lancet. 2012;380:1473-1481.
Early Sepsis Intervention Strategies Decrease Mortality, Length of Stay, and Cost
Clinical question: For patients with sepsis or septic shock, what is the impact of a real-time comprehensive continuous quality-improvement (QI) initiative on in-hospital mortality, morbidity, and healthcare resource utilization in community and tertiary-care hospitals in the U.S.?
Background: Multiple single-center trials have demonstrated that early sepsis intervention strategies (early goal-directed therapy, resuscitation bundles) improve in-hospital mortality. Little is known about the effectiveness of incorporating these strategies into a real-time continuous QI initiative and implementing interventions across multiple sites simultaneously.
Study design: Pre-post at some sites and concurrent implementation design at other sites.
Setting: Five community and six-tertiary care U.S. hospitals.
Synopsis: The GENeralized Early Sepsis Intervention Strategies (GENESIS) project was a CQI initiative that combined several QI concepts with validated early sepsis interventions known as resuscitation bundles (RB). Continuous QI was implemented on patients with severe sepsis or septic shock in both before and after designs (eight hospitals), and in concurrent designs (three hospitals). The control group was comprised of historical controls treated before GENESIS and patients with incomplete implementation of RB, totaling 1,554 patients. The treatment group included patients treated after GENESIS and those with complete RB compliance, totaling 4,801 patients.
Compared with the control group, patients in the treatment group had a 33% decreased risk of in-hospital mortality (RR 0.67, 95% CI 0.63-0.72), an absolute decrease in hospital length of stay (LOS) by 5.1 days (20.7 days vs. 15.6 days, P<0.001) and a $47,923 reduction in total hospital charges (P<0.001). Limitations included the study design (not a prospective randomized trial), and the possibility of other concurrent unmeasured quality initiatives taking place at the study sites, which might have contributed to improved outcomes.
Bottom line: Early sepsis intervention strategies in the form of a comprehensive continuous QI initiative can decrease mortality, hospital LOS, and cost in both tertiary-care and community hospitals.
Citation: Cannon CM, Holthaus CV, Zubrow MT, et al. The GENESIS project (GENeralized Early Sepsis Intervention Strategies): a multicenter quality improvement collaborative. J Intensive Care Med. 2012; Aug 17. doi:10.1177/0885066612453025.
Hypoglycemia Associated with Increased Mortality in the Critically Ill
Clinical question: Is hypoglycemia associated with mortality in critically ill patients?
Background: Initial studies suggested that intensive glucose control reduces mortality in surgical ICU patients and reduces morbidity in medical ICU patients, but further studies have not supported these findings. Recent literature shows conflicting results on the effects of intense glucose control in critically ill patients.
Study design: Post-hoc analysis of the NICE-SUGAR study database.
Setting: ICUs in 42 hospitals in Australia, New Zealand, and Canada.
Synopsis: The NICE-SUGAR study was a multicenter trial that randomized 6,104 ICU patients to intensive (glucose 80 to 108 mg/dL) or conventional glucose control (≤180 mg/dL). Patients were followed for 90 days or until death, with death being the primary end point. Severe hypoglycemia (<40 mg/dL) was recorded in 6.8% of patients in the intensive glucose control group versus 0.5% in the conventional group. The study showed that intensive glucose control was associated with increased mortality among adult ICU patients.
Using the NICE-SUGAR database, the authors conducted a Cox regression analysis to examine the associations between hypoglycemia and death. A total of 2,714 patients had moderate hypoglycemia (glucose 41 to 70 mg/dL), and 223 patients had severe hypoglycemia. The hazard ratio for mortality was 1.41 (95% CI 1.21-1.62, P<0.001) for patients with moderate hypoglycemia and 2.10 (95% CI 1.59-2.77, P<0.001) for severe hypoglycemia, compared to patients without hypoglycemia.
These findings show a strong association between mortality and hypoglycemia but do not prove causality. Hospitalists caring for ICU patients must be aware that hypoglycemia is associated with mortality and focus on avoiding hypoglycemia. The American Diabetes Association currently recommends a target blood glucose level of 140 to 180 mg/dL for most critically ill patients.
Bottom line: Hypoglycemia (glucose <70 mg/dL) is associated with increased risk of mortality in ICU patients.
Citation: Finfer S, Chittock DR, Su SY, et al. Hypoglycemia and risk of death in critically ill patients. New Engl J Med. 2012;367(12):1108-1118.
Increased Bleeding Risk for Cardiac Patients on Multiple Antithrombotic Drugs
Clinical question: Is there an increased risk of bleeding in atrial fibrillation patients treated with multiple antithrombotic agents following acute myocardial infarction (MI) or percutaneous coronary intervention (PCI)?
Background: Current treatment for atrial fibrillation patients with MI or PCI includes vitamin K antagonist (VKA) therapy to prevent stroke and antiplatelet agents to prevent further coronary events. There are inconsistent findings on the safety and efficacy of combined therapy with VKA, aspirin, and clopidogrel, specifically with regard to bleeding risk.
Study design: Retrospective cohort study.
Setting: Nationwide registry in Denmark.
Synopsis: Using the National Patient Registry in Denmark, 11,480 patients with atrial fibrillation who were admitted for MI or PCI were identified. Patients were grouped by medication regimen, including monotherapy (aspirin, clopidogrel, or VKA), dual therapy (dual antiplatelet or VKA+antiplatelet), or triple therapy (VKA+aspirin+clopidogrel). The primary outcome was nonfatal or fatal bleeding within one year.
Patients receiving triple therapy had the highest rate of bleeding, with a crude incidence of 14.2 events per 100 person-years. Patients treated with VKA+aspirin+clopidogel were significantly more likely than those on VKA+antiplatelet (HR 1.47, 95% CI 1.04-2.08) or dual antiplatelet (HR 2.20, 95% CI 1.58-3.08) treatment to have a bleeding event within 90 days, and similar trends were seen at 90 to 360 days. There was no significant difference in thromboembolic events among patients on VKA+aspirin+clopidogrel versus VKA+antiplatelet therapy.
Only bleeding events that required hospitalization were recorded, which might underestimate the bleeding risks of these regimens. Additionally, INR levels were not determined, which could impact both bleeding and thromboembolic outcomes.
However, this study does suggest that there are significant bleeding risks among patients treated with triple therapy. Hospitalists should weigh the risks of thromboembolic events with bleeding risks in patients with atrial fibrillation and MI/PCI, and only prescribe VKA+aspirin+clopidogrel with these risks in mind.
Bottom line: Immediate and continued bleeding risk is increased in patients with atrial fibrillation admitted with PCI or MI who are placed on triple antithrombotic therapy with VKA+aspirin+clopidogrel.
Citation: Lamberts M, Olesen JB, Ruwald MH, et al. Bleeding after initiation of multiple antithrombotic drugs, including triple therapy, in atrial fibrillation patients following myocardial infarction and coronary intervention. Circulation. 2012;126:1185-1193.
Hospitalist-Run Preoperative Clinic Improves Outcomes in Complex Surgical Patients
Clinical question: Do hospitalist-run preoperative clinics improve outcomes for medically complex patients undergoing noncardiac surgery compared to traditional anesthesiologist-run preoperative clinics?
Background: Studies of perioperative medical consultation have shown inconsistent effects on quality of care, but preoperative medical consultation has only been evaluated in the immediate preoperative period (one day prior to surgery or less). Little is known about the impact of involving hospitalists earlier in the preoperative period.
Study design: Retrospective, pre-post study.
Setting: Veterans Affairs Greater Los Angeles Healthcare System (VAGLAHS).
Synopsis: In July 2004, the VAGLAHS Preoperative Clinic transitioned from being anesthesiologist-run to hospitalist-run. Mid-level providers were trained on preoperative medical assessment, and patients were only evaluated by anesthesia staff on the day of surgery, after they had been deemed medically acceptable for surgery. All patients seen in the clinic from July 2003 to July 2005 were included in the study. Period A included patients evaluated when anesthesia staff supervised the clinic. Period B included patients evaluated during the first year of the hospitalist-run system.
There were 1,101 patients with inpatient surgeries in Period A, and 1,126 patients in Period B. Mean length of stay (LOS) decreased to 5.28 days during the hospitalist-run model from 9.87 days during the anesthesiologist-run model. LOS reductions were most notable in patients with ASA scores of 3 or higher; LOS reductions were not seen in an internal control of surgical patients who were not evaluated in the preoperative clinic. Inpatient mortality was also reduced in Period B compared with Period A, to 4 cases (0.36%) from 14 cases (1.27%) (P=0.0158). Specific processes that led to improved outcomes for patients in Period B could not be identified. The VA study setting might limit the generalizability of the results.
Bottom line: A hospitalist-run preoperative clinic was associated with decreased LOS and inpatient mortality compared with a traditional anesthesiologist-run clinic.
Citation: Vazirani S, Lankarani-Fard A, Lian LJ, Stelzner M, Asch SM. Preoperative processes and outcomes after implementation of a hospitalist-run preoperative clinic. J Hosp Med. 2012 Sep 7. doi:10.1002/jhm.1968.
Delirium after Cardiac Surgery Associated with Prolonged Cognitive Impairment
Clinical question: Is postoperative delirium associated with decreased cognitive function in the first year after cardiac surgery?
Background: In general populations, delirium has been associated with long-term decline in cognitive ability. Delirium and cognitive dysfunction are both common following cardiac surgery, but the effects of postoperative delirium on the trajectory of cognitive function over time is unclear.
Study design: Prospective cohort study.
Setting: Two academic medical centers and a Veterans Administration hospital.
Synopsis: Two hundred twenty-five patients aged 60 or older who were scheduled to undergo coronary artery bypass grafting or valve replacement surgery were included. Patients underwent preoperative assessment cognitive function with the use of the Mini-Mental State Examination (MMSE). Starting on postoperative Day 2, patients underwent daily assessment for delirium. After discharge, cognitive function was reassessed at months one, six, and 12.
Postoperative delirium occurred in 103 patients (46%). Patients with delirium were older, had higher comorbidity scores, and had lower MMSE scores at baseline. Among the overall study population, adjusted MMSE scores dropped 4.6 points from baseline to postoperative Day 2, then were observed to increase by approximately one point per day during postoperative days 3 to 5 with minimal change thereafter. Patients with delirium had greater decrease in cognitive function in the immediate postoperative period compared to patients without delirium (7.7 points vs. 2.1, P<0.001).
Patients without delirium returned to their baseline cognitive ability by one month postoperatively, while patients who had delirium were still making gains up to six months post-operatively, never returning to baseline level of function by one year. Unmeasured confounders and uncertain sensitivity of the MMSE to detect mild cognitive impairment might limit these findings.
Bottom line: Cognitive function decreases in the immediate postoperative period following cardiac surgery. Compared to patients without delirium, patients with delirium experience more dramatic and prolonged cognitive impairment postoperatively, without returning to their preoperative level of cognitive function at one year.
Citation: Saczynski JS, Marcantonio ER, Quach L, et al. Cognitive trajectories after postoperative delirium. New Engl J Med. 2012;367:30-39.
Benefits of Resuming Anticoagulation after GI Bleed Outweigh Risks for Most Patients
Clinical question: In warfarin-treated patients who have experienced gastrointestinal (GI) bleeding, what are the patterns of restarting warfarin therapy and the incidence of thrombosis, recurrent GI bleed, and death in the 90 days following index bleed?
Background: In warfarin-treated patients who experience GI bleeding, warfarin is often temporarily held or permanently discontinued, placing patients at increased risk for developing thromboembolism. Little is known about the risks, benefits, and timing of restarting warfarin in this patient population.
Study design: Retrospective cohort study.
Setting: Kaiser Permanente Colorado.
Synopsis: Using clinical and administrative databases, 442 patients who presented with GI bleeding while receiving warfarin therapy were identified. Patients were grouped by whether they resumed warfarin (n=260, including 41 patients in whom anticoagulation was never interrupted), or did not resume warfarin therapy (n=182) in the 90 days following index GI bleed. Patients with prosthetic heart valves or GI bleeding localized to the rectum/anus were more commonly restarted on warfarin, whereas older patients and those in whom the source of bleeding was not identified were less likely to be restarted on warfarin therapy.
Restarting warfarin therapy after index GI bleed was associated with lower risk of thrombosis (HR 0.05, 95% CI 0.01-0.58) and death from any cause (HR 0.31, 95% CI 0.15-0.62), and it was not associated with a significant increase in risk for recurrent GI bleed (HR 1.32, 95% CI 0.50-3.57).
The authors concluded that for many patients who experience a warfarin-associated GI bleed, the benefits of restarting warfarin therapy outweigh the risks. No conclusions were made regarding the optimal timing of resuming therapy. Limitations included the use of administrative data and inability to determine the potential influence of aspirin use on outcomes.
Bottom line: Resuming warfarin in the 90 days following a warfarin-associated GI bleed is associated with decreased risk of thrombosis and death without increased risk for recurrent GI bleed.
Citation: Witt DM, Delate T, Garcia DA, et al. Risk of thromboembolism, recurrent hemorrhage, and death after warfarin therapy interruption for gastrointestinal tract bleeding. Arch Intern Med. 2012 Sep 12. doi:10.1001/archinternmed.2012.4261.
Preoperative Hyponatremia Associated with Increased Risk for Perioperative Complications and Mortality
Clinical question: Is preoperative hyponatremia an indicator of perioperative morbidity and mortality?
Background: Hyponatremia is a common diagnosis in the hospital setting and is associated with adverse outcomes, even in mild cases. However, it is unclear if this association exists in surgical patients when detected preoperatively.
Study design: Retrospective cohort study.
Setting: Academic and community hospitals participating in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP).
Synopsis: A total of 75,423 adult patients with hyponatremia (sodium <135 mEq/L) who were undergoing major surgery were compared to 888,840 patients with normal preoperative sodium levels over a six-year period. The primary outcome was 30-day mortality. Secondary outcomes included postoperative major coronary events, stroke, wound infection, pneumonia, and length of stay (LOS).
Compared to patients with normal sodium levels, those with preoperative hyponatremia had higher rates of perioperative mortality (5.2% vs. 1.3%; adjusted odds ratio 1.44, 95% CI 1.38-1.50), with increased risk that correlated with increasing severity of hyponatremia. Association with postoperative mortality was particularly strong among hyponatremic patients with ASA scores of 1 or 2 and those undergoing nonemergency surgery.
Patients with preoperative hyponatremia were also found to have increased risk for all postoperative complications evaluated, with the exception of stroke. Limitations included the potential for unmeasured confounders and not being able to account for the role of medications used perioperatively. Research is needed to determine whether correcting preoperative hyponatremia lessens the risk of mortality and other postoperative complications.
Bottom line: Among patients undergoing major surgery, preoperative hyponatremia is a predictor of postoperative 30-day mortality and morbidity.
Citation: Leung AA, McAlister FA, Rogers SO, et al. Preoperative hyponatremia and perioperative complications. Arch Intern Med. 2012;172:1-8.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Interventions that improve discharge handovers reviewed
- Duration of in-hospital cardiac resuscitation and survival rates
- Early sepsis intervention strategies to decrease mortality risk
- Hypoglycemia linked to increased mortality in critically ill
- Increased bleeding risk for cardiac patients
- Hospital-run vs. anesthesiologist-run preoperative clinics
- Postoperative delirium and cognitive impairment in cardiac patients
- Benefits of resuming anticoagulants after GI bleeding
- Preoperative hyponatremia and risk of perioperative mortality
Systematic Review Highlights Several Interventions That Improve Discharge Handovers
Clinical question: Do interventions to improve patient handovers at discharge have positive effects on patient care?
Background: The transition from hospital to primary care is often suboptimal and has been associated with unfavorable outcomes, including hospital readmission, increased healthcare utilization, and adverse drug events post-discharge. This review sought to characterize different types of interventions aimed at improving discharge handovers and to evaluate their effects.
Study design: Systematic review of randomized controlled trials.
Setting: Studies published from January 1990 to March 2011.
Synopsis: Review of published databases identified 36 randomized controlled studies on interventions to improve discharge handovers. Studies were blindly evaluated by two reviewers on quality, interventions, and outcomes. There was significant heterogeneity in interventions and outcomes; thus, statistical analysis was not possible. Most studies evaluated multicomponent interventions and had more than one outcome measure.
Of the 36 studies reviewed, 25 reported statistically significant improvements in outcomes, including reduced hospital utilization and improved continuity of care. Effective interventions included medication reconciliation; structured discharge information (facilitated by electronic resources); multidisciplinary discharge planning; shared involvement in arranging care between inpatient and outpatient physicians; and Web-based access to discharge information by the outpatient provider.
The complexity of the interventions and the heterogeneity of reported results did not allow for firm conclusions to be drawn regarding which specific interventions had the strongest effects.
Bottom line: Interventions that target the quality and safety of handovers between hospital and outpatient providers at discharge can significantly reduce hospital utilization and improve continuity of care.
Citation: Hesselink G, Schoonhoven L, Barach P, et al. Improving patient handovers from hospital to primary care: a systematic review. Ann Intern Med. 2012;157:417-428.
Longer Duration of In-Hospital Cardiac Resuscitation Associated with Increased Survival
Clinical question: Are prolonged cardiac resuscitation efforts associated with improved outcomes?
Background: There is little evidence or guidelines on how long to maintain resuscitative efforts during in-hospital cardiac arrest, leading to variation in practice. This study characterized patterns of resuscitation duration and relationship to the return of spontaneous circulation and survival to discharge.
Study design: Retrospective observational study.
Setting: Four hundred thirty-five U.S. hospitals reporting data to the American Heart Association’s Get With The Guidelines: Resuscitation registry.
Synopsis: Using duration of resuscitation in nonsurvivors as a surrogate for the tendency of a facility to perform prolonged efforts, hospitals were divided into quartiles. Overall, of 64,339 patients in the registry, 31,198 (48.5%) had return of circulation and 9,912 (15.4%) survived to discharge. Resuscitative efforts in nonsurvivors ranged from a median of 16 to 25 minutes between the lowest and highest quartiles.
There was a stepwise increase in the likelihood for patients to have return of spontaneous circulation and to survive to discharge between each quartile. Specifically, comparing shortest to longest, there was a significant adjusted odds ratio of 1.12 for both the return of circulation (P<0.0001) and survival to discharge (P=0.021). The survival benefit was most apparent for those with pulseless electrical activity or asystole as initial rhythms, as compared to ventricular tachycardia or fibrillation.
Limitations included the study’s observational design, which meant causality could not be determined. Additionally, the study did not account for the quality of resuscitative efforts (e.g. depth of chest compressions, adherence with guidelines), which might have influenced outcomes. Importantly, the study looked at survival to discharge, but it did not evaluate long-term survival or functional status post-discharge, which might better reflect the success of resuscitation.
Bottom line: Prolonged resuscitative efforts were observed to be associated with increased likelihood of return of spontaneous circulation and survival to discharge; this data might provide clinical guidance in determining when to stop resuscitation efforts.
Citation: Goldberger ZD, Chan PS, Berg RA, et al. Duration of resuscitation efforts and survival after in-hospital cardiac arrest: an observational study. Lancet. 2012;380:1473-1481.
Early Sepsis Intervention Strategies Decrease Mortality, Length of Stay, and Cost
Clinical question: For patients with sepsis or septic shock, what is the impact of a real-time comprehensive continuous quality-improvement (QI) initiative on in-hospital mortality, morbidity, and healthcare resource utilization in community and tertiary-care hospitals in the U.S.?
Background: Multiple single-center trials have demonstrated that early sepsis intervention strategies (early goal-directed therapy, resuscitation bundles) improve in-hospital mortality. Little is known about the effectiveness of incorporating these strategies into a real-time continuous QI initiative and implementing interventions across multiple sites simultaneously.
Study design: Pre-post at some sites and concurrent implementation design at other sites.
Setting: Five community and six-tertiary care U.S. hospitals.
Synopsis: The GENeralized Early Sepsis Intervention Strategies (GENESIS) project was a CQI initiative that combined several QI concepts with validated early sepsis interventions known as resuscitation bundles (RB). Continuous QI was implemented on patients with severe sepsis or septic shock in both before and after designs (eight hospitals), and in concurrent designs (three hospitals). The control group was comprised of historical controls treated before GENESIS and patients with incomplete implementation of RB, totaling 1,554 patients. The treatment group included patients treated after GENESIS and those with complete RB compliance, totaling 4,801 patients.
Compared with the control group, patients in the treatment group had a 33% decreased risk of in-hospital mortality (RR 0.67, 95% CI 0.63-0.72), an absolute decrease in hospital length of stay (LOS) by 5.1 days (20.7 days vs. 15.6 days, P<0.001) and a $47,923 reduction in total hospital charges (P<0.001). Limitations included the study design (not a prospective randomized trial), and the possibility of other concurrent unmeasured quality initiatives taking place at the study sites, which might have contributed to improved outcomes.
Bottom line: Early sepsis intervention strategies in the form of a comprehensive continuous QI initiative can decrease mortality, hospital LOS, and cost in both tertiary-care and community hospitals.
Citation: Cannon CM, Holthaus CV, Zubrow MT, et al. The GENESIS project (GENeralized Early Sepsis Intervention Strategies): a multicenter quality improvement collaborative. J Intensive Care Med. 2012; Aug 17. doi:10.1177/0885066612453025.
Hypoglycemia Associated with Increased Mortality in the Critically Ill
Clinical question: Is hypoglycemia associated with mortality in critically ill patients?
Background: Initial studies suggested that intensive glucose control reduces mortality in surgical ICU patients and reduces morbidity in medical ICU patients, but further studies have not supported these findings. Recent literature shows conflicting results on the effects of intense glucose control in critically ill patients.
Study design: Post-hoc analysis of the NICE-SUGAR study database.
Setting: ICUs in 42 hospitals in Australia, New Zealand, and Canada.
Synopsis: The NICE-SUGAR study was a multicenter trial that randomized 6,104 ICU patients to intensive (glucose 80 to 108 mg/dL) or conventional glucose control (≤180 mg/dL). Patients were followed for 90 days or until death, with death being the primary end point. Severe hypoglycemia (<40 mg/dL) was recorded in 6.8% of patients in the intensive glucose control group versus 0.5% in the conventional group. The study showed that intensive glucose control was associated with increased mortality among adult ICU patients.
Using the NICE-SUGAR database, the authors conducted a Cox regression analysis to examine the associations between hypoglycemia and death. A total of 2,714 patients had moderate hypoglycemia (glucose 41 to 70 mg/dL), and 223 patients had severe hypoglycemia. The hazard ratio for mortality was 1.41 (95% CI 1.21-1.62, P<0.001) for patients with moderate hypoglycemia and 2.10 (95% CI 1.59-2.77, P<0.001) for severe hypoglycemia, compared to patients without hypoglycemia.
These findings show a strong association between mortality and hypoglycemia but do not prove causality. Hospitalists caring for ICU patients must be aware that hypoglycemia is associated with mortality and focus on avoiding hypoglycemia. The American Diabetes Association currently recommends a target blood glucose level of 140 to 180 mg/dL for most critically ill patients.
Bottom line: Hypoglycemia (glucose <70 mg/dL) is associated with increased risk of mortality in ICU patients.
Citation: Finfer S, Chittock DR, Su SY, et al. Hypoglycemia and risk of death in critically ill patients. New Engl J Med. 2012;367(12):1108-1118.
Increased Bleeding Risk for Cardiac Patients on Multiple Antithrombotic Drugs
Clinical question: Is there an increased risk of bleeding in atrial fibrillation patients treated with multiple antithrombotic agents following acute myocardial infarction (MI) or percutaneous coronary intervention (PCI)?
Background: Current treatment for atrial fibrillation patients with MI or PCI includes vitamin K antagonist (VKA) therapy to prevent stroke and antiplatelet agents to prevent further coronary events. There are inconsistent findings on the safety and efficacy of combined therapy with VKA, aspirin, and clopidogrel, specifically with regard to bleeding risk.
Study design: Retrospective cohort study.
Setting: Nationwide registry in Denmark.
Synopsis: Using the National Patient Registry in Denmark, 11,480 patients with atrial fibrillation who were admitted for MI or PCI were identified. Patients were grouped by medication regimen, including monotherapy (aspirin, clopidogrel, or VKA), dual therapy (dual antiplatelet or VKA+antiplatelet), or triple therapy (VKA+aspirin+clopidogrel). The primary outcome was nonfatal or fatal bleeding within one year.
Patients receiving triple therapy had the highest rate of bleeding, with a crude incidence of 14.2 events per 100 person-years. Patients treated with VKA+aspirin+clopidogel were significantly more likely than those on VKA+antiplatelet (HR 1.47, 95% CI 1.04-2.08) or dual antiplatelet (HR 2.20, 95% CI 1.58-3.08) treatment to have a bleeding event within 90 days, and similar trends were seen at 90 to 360 days. There was no significant difference in thromboembolic events among patients on VKA+aspirin+clopidogrel versus VKA+antiplatelet therapy.
Only bleeding events that required hospitalization were recorded, which might underestimate the bleeding risks of these regimens. Additionally, INR levels were not determined, which could impact both bleeding and thromboembolic outcomes.
However, this study does suggest that there are significant bleeding risks among patients treated with triple therapy. Hospitalists should weigh the risks of thromboembolic events with bleeding risks in patients with atrial fibrillation and MI/PCI, and only prescribe VKA+aspirin+clopidogrel with these risks in mind.
Bottom line: Immediate and continued bleeding risk is increased in patients with atrial fibrillation admitted with PCI or MI who are placed on triple antithrombotic therapy with VKA+aspirin+clopidogrel.
Citation: Lamberts M, Olesen JB, Ruwald MH, et al. Bleeding after initiation of multiple antithrombotic drugs, including triple therapy, in atrial fibrillation patients following myocardial infarction and coronary intervention. Circulation. 2012;126:1185-1193.
Hospitalist-Run Preoperative Clinic Improves Outcomes in Complex Surgical Patients
Clinical question: Do hospitalist-run preoperative clinics improve outcomes for medically complex patients undergoing noncardiac surgery compared to traditional anesthesiologist-run preoperative clinics?
Background: Studies of perioperative medical consultation have shown inconsistent effects on quality of care, but preoperative medical consultation has only been evaluated in the immediate preoperative period (one day prior to surgery or less). Little is known about the impact of involving hospitalists earlier in the preoperative period.
Study design: Retrospective, pre-post study.
Setting: Veterans Affairs Greater Los Angeles Healthcare System (VAGLAHS).
Synopsis: In July 2004, the VAGLAHS Preoperative Clinic transitioned from being anesthesiologist-run to hospitalist-run. Mid-level providers were trained on preoperative medical assessment, and patients were only evaluated by anesthesia staff on the day of surgery, after they had been deemed medically acceptable for surgery. All patients seen in the clinic from July 2003 to July 2005 were included in the study. Period A included patients evaluated when anesthesia staff supervised the clinic. Period B included patients evaluated during the first year of the hospitalist-run system.
There were 1,101 patients with inpatient surgeries in Period A, and 1,126 patients in Period B. Mean length of stay (LOS) decreased to 5.28 days during the hospitalist-run model from 9.87 days during the anesthesiologist-run model. LOS reductions were most notable in patients with ASA scores of 3 or higher; LOS reductions were not seen in an internal control of surgical patients who were not evaluated in the preoperative clinic. Inpatient mortality was also reduced in Period B compared with Period A, to 4 cases (0.36%) from 14 cases (1.27%) (P=0.0158). Specific processes that led to improved outcomes for patients in Period B could not be identified. The VA study setting might limit the generalizability of the results.
Bottom line: A hospitalist-run preoperative clinic was associated with decreased LOS and inpatient mortality compared with a traditional anesthesiologist-run clinic.
Citation: Vazirani S, Lankarani-Fard A, Lian LJ, Stelzner M, Asch SM. Preoperative processes and outcomes after implementation of a hospitalist-run preoperative clinic. J Hosp Med. 2012 Sep 7. doi:10.1002/jhm.1968.
Delirium after Cardiac Surgery Associated with Prolonged Cognitive Impairment
Clinical question: Is postoperative delirium associated with decreased cognitive function in the first year after cardiac surgery?
Background: In general populations, delirium has been associated with long-term decline in cognitive ability. Delirium and cognitive dysfunction are both common following cardiac surgery, but the effects of postoperative delirium on the trajectory of cognitive function over time is unclear.
Study design: Prospective cohort study.
Setting: Two academic medical centers and a Veterans Administration hospital.
Synopsis: Two hundred twenty-five patients aged 60 or older who were scheduled to undergo coronary artery bypass grafting or valve replacement surgery were included. Patients underwent preoperative assessment cognitive function with the use of the Mini-Mental State Examination (MMSE). Starting on postoperative Day 2, patients underwent daily assessment for delirium. After discharge, cognitive function was reassessed at months one, six, and 12.
Postoperative delirium occurred in 103 patients (46%). Patients with delirium were older, had higher comorbidity scores, and had lower MMSE scores at baseline. Among the overall study population, adjusted MMSE scores dropped 4.6 points from baseline to postoperative Day 2, then were observed to increase by approximately one point per day during postoperative days 3 to 5 with minimal change thereafter. Patients with delirium had greater decrease in cognitive function in the immediate postoperative period compared to patients without delirium (7.7 points vs. 2.1, P<0.001).
Patients without delirium returned to their baseline cognitive ability by one month postoperatively, while patients who had delirium were still making gains up to six months post-operatively, never returning to baseline level of function by one year. Unmeasured confounders and uncertain sensitivity of the MMSE to detect mild cognitive impairment might limit these findings.
Bottom line: Cognitive function decreases in the immediate postoperative period following cardiac surgery. Compared to patients without delirium, patients with delirium experience more dramatic and prolonged cognitive impairment postoperatively, without returning to their preoperative level of cognitive function at one year.
Citation: Saczynski JS, Marcantonio ER, Quach L, et al. Cognitive trajectories after postoperative delirium. New Engl J Med. 2012;367:30-39.
Benefits of Resuming Anticoagulation after GI Bleed Outweigh Risks for Most Patients
Clinical question: In warfarin-treated patients who have experienced gastrointestinal (GI) bleeding, what are the patterns of restarting warfarin therapy and the incidence of thrombosis, recurrent GI bleed, and death in the 90 days following index bleed?
Background: In warfarin-treated patients who experience GI bleeding, warfarin is often temporarily held or permanently discontinued, placing patients at increased risk for developing thromboembolism. Little is known about the risks, benefits, and timing of restarting warfarin in this patient population.
Study design: Retrospective cohort study.
Setting: Kaiser Permanente Colorado.
Synopsis: Using clinical and administrative databases, 442 patients who presented with GI bleeding while receiving warfarin therapy were identified. Patients were grouped by whether they resumed warfarin (n=260, including 41 patients in whom anticoagulation was never interrupted), or did not resume warfarin therapy (n=182) in the 90 days following index GI bleed. Patients with prosthetic heart valves or GI bleeding localized to the rectum/anus were more commonly restarted on warfarin, whereas older patients and those in whom the source of bleeding was not identified were less likely to be restarted on warfarin therapy.
Restarting warfarin therapy after index GI bleed was associated with lower risk of thrombosis (HR 0.05, 95% CI 0.01-0.58) and death from any cause (HR 0.31, 95% CI 0.15-0.62), and it was not associated with a significant increase in risk for recurrent GI bleed (HR 1.32, 95% CI 0.50-3.57).
The authors concluded that for many patients who experience a warfarin-associated GI bleed, the benefits of restarting warfarin therapy outweigh the risks. No conclusions were made regarding the optimal timing of resuming therapy. Limitations included the use of administrative data and inability to determine the potential influence of aspirin use on outcomes.
Bottom line: Resuming warfarin in the 90 days following a warfarin-associated GI bleed is associated with decreased risk of thrombosis and death without increased risk for recurrent GI bleed.
Citation: Witt DM, Delate T, Garcia DA, et al. Risk of thromboembolism, recurrent hemorrhage, and death after warfarin therapy interruption for gastrointestinal tract bleeding. Arch Intern Med. 2012 Sep 12. doi:10.1001/archinternmed.2012.4261.
Preoperative Hyponatremia Associated with Increased Risk for Perioperative Complications and Mortality
Clinical question: Is preoperative hyponatremia an indicator of perioperative morbidity and mortality?
Background: Hyponatremia is a common diagnosis in the hospital setting and is associated with adverse outcomes, even in mild cases. However, it is unclear if this association exists in surgical patients when detected preoperatively.
Study design: Retrospective cohort study.
Setting: Academic and community hospitals participating in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP).
Synopsis: A total of 75,423 adult patients with hyponatremia (sodium <135 mEq/L) who were undergoing major surgery were compared to 888,840 patients with normal preoperative sodium levels over a six-year period. The primary outcome was 30-day mortality. Secondary outcomes included postoperative major coronary events, stroke, wound infection, pneumonia, and length of stay (LOS).
Compared to patients with normal sodium levels, those with preoperative hyponatremia had higher rates of perioperative mortality (5.2% vs. 1.3%; adjusted odds ratio 1.44, 95% CI 1.38-1.50), with increased risk that correlated with increasing severity of hyponatremia. Association with postoperative mortality was particularly strong among hyponatremic patients with ASA scores of 1 or 2 and those undergoing nonemergency surgery.
Patients with preoperative hyponatremia were also found to have increased risk for all postoperative complications evaluated, with the exception of stroke. Limitations included the potential for unmeasured confounders and not being able to account for the role of medications used perioperatively. Research is needed to determine whether correcting preoperative hyponatremia lessens the risk of mortality and other postoperative complications.
Bottom line: Among patients undergoing major surgery, preoperative hyponatremia is a predictor of postoperative 30-day mortality and morbidity.
Citation: Leung AA, McAlister FA, Rogers SO, et al. Preoperative hyponatremia and perioperative complications. Arch Intern Med. 2012;172:1-8.
Pediatric Hospitalists Trust Their Gut with Serious Infections

Clinical question: How helpful is the “gut feeling” that clinicians might have that a child is more ill than they look?
Background: Timely recognition of serious infections in children is difficult but critical to improved outcomes. Numerous studies have examined clinical criteria and laboratory tests to distinguish viral infections from more serious bacterial infections but have demonstrated mixed results. Clinicians’ subjective impressions of patients continue to drive many care patterns, and the relevance of a gut feeling that something is wrong remains unclear.
Study design: Prospective observational study.
Setting: Primary-care clinics in Flanders, Belgium.
Synopsis: Nearly 4,000 children 0-16 years of age were evaluated after presentation for acute illness in primary-care settings. Clinical features, overall “clinical impression” (serious illness present or absent), and “gut feelings” (present, absent or unsure) that something was wrong were prospectively recorded. Serious infections were defined as hospital admissions for potential bacterial infections.
The presence of a gut feeling significantly increased the risk of serious illness (likelihood ratio 25.5, 95% confidence interval 7.9 to 82.0) and had a consistently higher specificity than clinical impression alone. The overall sensitivity of the gut feeling in this cohort was 61.9% with a specificity of 97.2%, while the positive predictive value was 10.8% and negative predictive value 99.8%. A history of convulsions and parental concerns were independently strongly associated with a positive gut feeling.
Similar to other clinical and laboratory evaluations designed to detect serious illness, the absence of a gut feeling might be the more useful finding from this study. Limitations of the data include an inability to further delve into what gives rise to a gut feeling in clinical practice as well as a moderate level of variance in the multivariate models. Additionally, only 21 children were ultimately admitted to the hospital, which, in conjunction with the subsequent power limitations, highlights the proverbial difficulty of finding that “needle in the haystack.”
Bottom line: The presence or absence of a gut feeling that something is wrong might be an important component of the history in acute childhood illness.
Citation: Van den Bruel A, Thompson M, Buntinx F, Mant D. Clinicians’ gut feeling about serious infections in children: observational study. BMJ. 2012;345:e6144.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: How helpful is the “gut feeling” that clinicians might have that a child is more ill than they look?
Background: Timely recognition of serious infections in children is difficult but critical to improved outcomes. Numerous studies have examined clinical criteria and laboratory tests to distinguish viral infections from more serious bacterial infections but have demonstrated mixed results. Clinicians’ subjective impressions of patients continue to drive many care patterns, and the relevance of a gut feeling that something is wrong remains unclear.
Study design: Prospective observational study.
Setting: Primary-care clinics in Flanders, Belgium.
Synopsis: Nearly 4,000 children 0-16 years of age were evaluated after presentation for acute illness in primary-care settings. Clinical features, overall “clinical impression” (serious illness present or absent), and “gut feelings” (present, absent or unsure) that something was wrong were prospectively recorded. Serious infections were defined as hospital admissions for potential bacterial infections.
The presence of a gut feeling significantly increased the risk of serious illness (likelihood ratio 25.5, 95% confidence interval 7.9 to 82.0) and had a consistently higher specificity than clinical impression alone. The overall sensitivity of the gut feeling in this cohort was 61.9% with a specificity of 97.2%, while the positive predictive value was 10.8% and negative predictive value 99.8%. A history of convulsions and parental concerns were independently strongly associated with a positive gut feeling.
Similar to other clinical and laboratory evaluations designed to detect serious illness, the absence of a gut feeling might be the more useful finding from this study. Limitations of the data include an inability to further delve into what gives rise to a gut feeling in clinical practice as well as a moderate level of variance in the multivariate models. Additionally, only 21 children were ultimately admitted to the hospital, which, in conjunction with the subsequent power limitations, highlights the proverbial difficulty of finding that “needle in the haystack.”
Bottom line: The presence or absence of a gut feeling that something is wrong might be an important component of the history in acute childhood illness.
Citation: Van den Bruel A, Thompson M, Buntinx F, Mant D. Clinicians’ gut feeling about serious infections in children: observational study. BMJ. 2012;345:e6144.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: How helpful is the “gut feeling” that clinicians might have that a child is more ill than they look?
Background: Timely recognition of serious infections in children is difficult but critical to improved outcomes. Numerous studies have examined clinical criteria and laboratory tests to distinguish viral infections from more serious bacterial infections but have demonstrated mixed results. Clinicians’ subjective impressions of patients continue to drive many care patterns, and the relevance of a gut feeling that something is wrong remains unclear.
Study design: Prospective observational study.
Setting: Primary-care clinics in Flanders, Belgium.
Synopsis: Nearly 4,000 children 0-16 years of age were evaluated after presentation for acute illness in primary-care settings. Clinical features, overall “clinical impression” (serious illness present or absent), and “gut feelings” (present, absent or unsure) that something was wrong were prospectively recorded. Serious infections were defined as hospital admissions for potential bacterial infections.
The presence of a gut feeling significantly increased the risk of serious illness (likelihood ratio 25.5, 95% confidence interval 7.9 to 82.0) and had a consistently higher specificity than clinical impression alone. The overall sensitivity of the gut feeling in this cohort was 61.9% with a specificity of 97.2%, while the positive predictive value was 10.8% and negative predictive value 99.8%. A history of convulsions and parental concerns were independently strongly associated with a positive gut feeling.
Similar to other clinical and laboratory evaluations designed to detect serious illness, the absence of a gut feeling might be the more useful finding from this study. Limitations of the data include an inability to further delve into what gives rise to a gut feeling in clinical practice as well as a moderate level of variance in the multivariate models. Additionally, only 21 children were ultimately admitted to the hospital, which, in conjunction with the subsequent power limitations, highlights the proverbial difficulty of finding that “needle in the haystack.”
Bottom line: The presence or absence of a gut feeling that something is wrong might be an important component of the history in acute childhood illness.
Citation: Van den Bruel A, Thompson M, Buntinx F, Mant D. Clinicians’ gut feeling about serious infections in children: observational study. BMJ. 2012;345:e6144.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.