User login
FDA approves brexanolone for postpartum depression
The Food and Drug Administration on March 19 approved the first medication specifically for the treatment of postpartum depression.

The drug, brexanolone (Zulresso), is to be administered as a single continuous 60-hour infusion for each episode of postpartum depression. . By binding to GABA A receptors, brexanolone increases receptor functionality. The recommended maximum dose of brexanolone is 90 µg/kg/h, and the infusion includes three dosing phases.
Brexanolone provides “an important new treatment option,” said Tiffany Farchione, MD, acting director of the division of psychiatry products in the FDA’s Center for Drug Evaluation and Research, in a press release. “Because of concerns about serious risks, including excessive sedation or sudden loss of consciousness during administration, Zulresso has been approved with a Risk Evaluation and Mitigation Strategy (REMS) and is only available to patients through a restricted distribution program at certified health care facilities where the health care provider can carefully monitor the patient.”
The approval was based on results of three phase 3 trials, which were double-blind, randomized, and placebo-controlled studies in which the primary efficacy endpoint was a change in baseline 60 hours after the start of the infusion on the Hamilton Depression Rating Scale (HAM-D). In all two of the trials, known as Hummingbird 202B and 202C, brexanolone’s impact on the patients’ HAM-D scores was greater than that of placebo, the FDA reported in briefing document released late last year. In addition, the impact of brexanolone on postpartum depression proved both rapid and durable.
Side effects observed in about 3% of the brexanolone patients included dizziness, dry mouth, fatigue, headache, infusion site pain, somnolence, and loss of consciousness. The FDA’s concern about loss of consciousness led the agency to recommend a REMS protocol before a hearing of its Psychopharmacologic Drugs Advisory and Drug Safety and Risk Management Advisory panels late last year. The Zulresso REMS Program will require that the drug be administered by a clinician in a health care facility that is certified. Patients will have to be monitored for excessive sedation and “sudden loss of consciousness and have continuous pulse oximetry monitoring (monitors oxygen levels in the blood),” the FDA said. Another requirement is that patients who receive the infusion will have to be accompanied while interacting with their children. Patients will be advised not to drive, operate machinery or engage in other dangerous activities until they feel totally alert. Those requirements will be addressed in a boxed warning.
The drug should be either adjusted or discontinued for patients whose postpartum depression becomes worse or for those experience suicidal thoughts and behaviors after taking brexanolone, the agency said.
Some physicians use antidepressants to treat postpartum depression, but their effectiveness is limited, according to the FDA. Interventions such as electroconvulsive therapy and psychotherapy also are used, but getting results can several weeks.
The symptoms of postpartum depression are indistinguishable from major depressive disorder, but “the timing of its onset has led to its recognition as potentially unique illness,” the FDA said. Postpartum depression in the United States affects up to 12% of births. In the developed world, suicide is the most common cause of maternal death after childbirth. This suicide risk makes postpartum depression a condition that is life-threatening. In addition, the condition has “profound negative effects on the maternal-infant bond and later infant development,” the FDA said.
SAGE Therapeutics, developer of brexanolone, secured the approval through the FDA’s breakthrough therapy designation process.
Heidi Splete contributed to this article.
The Food and Drug Administration on March 19 approved the first medication specifically for the treatment of postpartum depression.
The drug, brexanolone (Zulresso), is to be administered as a single continuous 60-hour infusion for each episode of postpartum depression. . By binding to GABA A receptors, brexanolone increases receptor functionality. The recommended maximum dose of brexanolone is 90 µg/kg/h, and the infusion includes three dosing phases.
Brexanolone provides “an important new treatment option,” said Tiffany Farchione, MD, acting director of the division of psychiatry products in the FDA’s Center for Drug Evaluation and Research, in a press release. “Because of concerns about serious risks, including excessive sedation or sudden loss of consciousness during administration, Zulresso has been approved with a Risk Evaluation and Mitigation Strategy (REMS) and is only available to patients through a restricted distribution program at certified health care facilities where the health care provider can carefully monitor the patient.”
The approval was based on results of three phase 3 trials, which were double-blind, randomized, and placebo-controlled studies in which the primary efficacy endpoint was a change in baseline 60 hours after the start of the infusion on the Hamilton Depression Rating Scale (HAM-D). In all two of the trials, known as Hummingbird 202B and 202C, brexanolone’s impact on the patients’ HAM-D scores was greater than that of placebo, the FDA reported in briefing document released late last year. In addition, the impact of brexanolone on postpartum depression proved both rapid and durable.
Side effects observed in about 3% of the brexanolone patients included dizziness, dry mouth, fatigue, headache, infusion site pain, somnolence, and loss of consciousness. The FDA’s concern about loss of consciousness led the agency to recommend a REMS protocol before a hearing of its Psychopharmacologic Drugs Advisory and Drug Safety and Risk Management Advisory panels late last year. The Zulresso REMS Program will require that the drug be administered by a clinician in a health care facility that is certified. Patients will have to be monitored for excessive sedation and “sudden loss of consciousness and have continuous pulse oximetry monitoring (monitors oxygen levels in the blood),” the FDA said. Another requirement is that patients who receive the infusion will have to be accompanied while interacting with their children. Patients will be advised not to drive, operate machinery or engage in other dangerous activities until they feel totally alert. Those requirements will be addressed in a boxed warning.
The drug should be either adjusted or discontinued for patients whose postpartum depression becomes worse or for those experience suicidal thoughts and behaviors after taking brexanolone, the agency said.
Some physicians use antidepressants to treat postpartum depression, but their effectiveness is limited, according to the FDA. Interventions such as electroconvulsive therapy and psychotherapy also are used, but getting results can several weeks.
The symptoms of postpartum depression are indistinguishable from major depressive disorder, but “the timing of its onset has led to its recognition as potentially unique illness,” the FDA said. Postpartum depression in the United States affects up to 12% of births. In the developed world, suicide is the most common cause of maternal death after childbirth. This suicide risk makes postpartum depression a condition that is life-threatening. In addition, the condition has “profound negative effects on the maternal-infant bond and later infant development,” the FDA said.
SAGE Therapeutics, developer of brexanolone, secured the approval through the FDA’s breakthrough therapy designation process.
Heidi Splete contributed to this article.
The Food and Drug Administration on March 19 approved the first medication specifically for the treatment of postpartum depression.
The drug, brexanolone (Zulresso), is to be administered as a single continuous 60-hour infusion for each episode of postpartum depression. . By binding to GABA A receptors, brexanolone increases receptor functionality. The recommended maximum dose of brexanolone is 90 µg/kg/h, and the infusion includes three dosing phases.
Brexanolone provides “an important new treatment option,” said Tiffany Farchione, MD, acting director of the division of psychiatry products in the FDA’s Center for Drug Evaluation and Research, in a press release. “Because of concerns about serious risks, including excessive sedation or sudden loss of consciousness during administration, Zulresso has been approved with a Risk Evaluation and Mitigation Strategy (REMS) and is only available to patients through a restricted distribution program at certified health care facilities where the health care provider can carefully monitor the patient.”
The approval was based on results of three phase 3 trials, which were double-blind, randomized, and placebo-controlled studies in which the primary efficacy endpoint was a change in baseline 60 hours after the start of the infusion on the Hamilton Depression Rating Scale (HAM-D). In all two of the trials, known as Hummingbird 202B and 202C, brexanolone’s impact on the patients’ HAM-D scores was greater than that of placebo, the FDA reported in briefing document released late last year. In addition, the impact of brexanolone on postpartum depression proved both rapid and durable.
Side effects observed in about 3% of the brexanolone patients included dizziness, dry mouth, fatigue, headache, infusion site pain, somnolence, and loss of consciousness. The FDA’s concern about loss of consciousness led the agency to recommend a REMS protocol before a hearing of its Psychopharmacologic Drugs Advisory and Drug Safety and Risk Management Advisory panels late last year. The Zulresso REMS Program will require that the drug be administered by a clinician in a health care facility that is certified. Patients will have to be monitored for excessive sedation and “sudden loss of consciousness and have continuous pulse oximetry monitoring (monitors oxygen levels in the blood),” the FDA said. Another requirement is that patients who receive the infusion will have to be accompanied while interacting with their children. Patients will be advised not to drive, operate machinery or engage in other dangerous activities until they feel totally alert. Those requirements will be addressed in a boxed warning.
The drug should be either adjusted or discontinued for patients whose postpartum depression becomes worse or for those experience suicidal thoughts and behaviors after taking brexanolone, the agency said.
Some physicians use antidepressants to treat postpartum depression, but their effectiveness is limited, according to the FDA. Interventions such as electroconvulsive therapy and psychotherapy also are used, but getting results can several weeks.
The symptoms of postpartum depression are indistinguishable from major depressive disorder, but “the timing of its onset has led to its recognition as potentially unique illness,” the FDA said. Postpartum depression in the United States affects up to 12% of births. In the developed world, suicide is the most common cause of maternal death after childbirth. This suicide risk makes postpartum depression a condition that is life-threatening. In addition, the condition has “profound negative effects on the maternal-infant bond and later infant development,” the FDA said.
SAGE Therapeutics, developer of brexanolone, secured the approval through the FDA’s breakthrough therapy designation process.
Heidi Splete contributed to this article.
For Latino patients, mental illness often goes untreated
Intergenerational trauma, attitudes can allow cycles of depression, anxiety to continue

The stigma tied to mental illness can be particularly difficult to overcome for people of Latin American descent, writes Concepción de León in El Espace, a column in the New York Times focused on news and culture relevant to Latinx communities. Sometimes those seeking help run into familiar mantras. “Let me know if any of these sound familiar: 'Boys don’t cry. We don’t air family business. You have to be strong. Turn to God.' These refrains (all of which I’ve heard at least once...) are just some of the responses that people dealing with mental health challenges in Latino communities have come to know well,” Ms. de León wrote. The unequal access to mental health services and health insurance that is a reality for some Latinos compounds the problem. The result is that mental illness can go untreated. Indeed, according to Ms. de León, Latinos, who are just as likely to suffer from a mental illness as non-Hispanic whites, are half as likely to seek treatment. Adriana Alejandre, a Latina who is a licensed marriage and family therapist in Los Angeles, is seeking to change that statistic. Through her podcast, Latinx Therapy, she seeks to spread the word that seeking therapy for mental illness is a positive step. There’s a long way to go, partly because Latino communities tend to value the group over the individual. “The downfall is that people suffer in silence,” said Ms. Alejandre. Therapy is important for some Latinos, according to Ms. Alejandre, because of intergenerational trauma that “allows the cycle to continue – whether it’s trauma, whether it’s depression, anxiety, domestic violence.” Ms. de León said one strategy she used for more than 1 year while she was in therapy was to set boundaries by not sharing what she was doing with family members. Ms. Alejandre said. “But the system will not change if someone does not initiate the change.” The New York Times.
Some state governments are seeking to make mental health services more available. The proposed budget of democratic Gov. Tony Evers of Wisconsin aims to allocate $22 million in mental health funding to school districts in the state to pay for social workers, psychologists, counselors, and nurses. The money would come on top of the $3 million designated by his predecessor and continues the efforts in Wisconsin to give children with mental health problems more access to needed help. The proposed budget also would add $7 million to a state program that works with local health agencies with the goal of providing mental health services for students and would allocate about $2.5 million annually for school staff training. The news is welcome to school districts across Wisconsin. “Schools are struggling to meet all of those [mental health] needs. I think there is an understanding that this is really something we need to be addressing,” said Joanne Juhnke, policy director at Wisconsin Family Ties, which helps families with children who have mental health challenges. Post Crescent, part of the USA Today network.
In Pennsylvania, the state Supreme Court is set to rule on whether those who provide mental health treatment to people addicted to illicit drugs can be free from prosecution. Right now, they are not. As reported in the Legal Intelligence, the case concerns two physicians at a drug addiction treatment facility who treated a man with an opioid addiction. In July 2018, a three-judge Superior Court panel upheld that physicians should not have liability protections under the Mental Health Procedures Act (MHPA). The ruling reversed a lower court decision. The Superior Court judges sympathized with the view that treatment of mental illness in drug treatment facilities be given more legal leeway. Whether that leeway remains in place depends on the Supreme Court. If judges decide no, physicians who recognize signs of mental illness in patients being treated for drug addiction would treat the illness at the risk of subsequent liability. The case has again raised the issue of whether alcoholism and drug dependency should be considered mental illnesses. “We don’t believe it was the intended purpose of the MPHA to include drug addiction. Our concern is we don’t want hospitals or rehab facilities just having patients be seen by psychiatrists in order to invoke the MHPA,” said Patrick Mintzer, the lawyer who will argue the cases before the court. A counter view came from Jack Panella, one of the three Superior Court judges. In his decision, he wrote: “In light of current scientific research, as well as the recent addition of ‘addiction disorders’ to the American Psychiatric Association’s Diagnostic and Statistical Manual–5, we suggest that the Department of Human Services revise this definition.” The Legal Intelligence.
An op-ed in the Des Moines Register applauds republican Gov. Kim Reynolds for introducing two bills that are aimed at expanding mental health services to children and family in Iowa. “After decades of discussion and growing public support, these two bills take a huge step toward establishing a children’s mental health system,” wrote guest columnists Erin Drinnin of the United Way of Central Iowa and Kim Scorza of Seasons Center for Behavioral Health. The two also serve as cochairs of the Coalition to Advance Mental Health in Iowa for Kids (CAMHI4Kids), which includes more than 50 organizations. “Just like building a house requires a sturdy foundation, these bills are an important first step toward creating a structure for children’s mental well-being. In particular, CAMHI4Kids appreciates that these bills establish a voice and a seat for children and families at a regional level, using a system that is already in place,” wrote Ms. Drinnin and Ms. Scorza. The legislation would spell out the core services that would be available regardless of location in Iowa. The services would be geared toward children, rather than adults, reflecting the different mental health needs of children. “These important steps would finally sew together a patchwork of care that families currently must navigate with little direction. If a child is hurt on the playground, a caregiver knows to follow a clear path of care to help that child recover. But for a caregiver who is concerned about a child’s mental health, they often don’t know where to turn for help and must seek out services that might not exist in their community,” wrote Ms. Drinnin and Ms. Scorza. In Iowa, 80,000 children have a diagnosed serious emotional disturbance. About half of children aged 14 years and older with mental illness drop out of high school, and 70% of youth in Iowa’s juvenile justice system have a mental illness. “We are proud that Iowa is working together in a bipartisan way to ensure that our kids have the best start for future success,” wrote Ms. Drinnin and Ms. Scorza. Des Moines Register.
Bill Reilly is the peer support program manager for Bert Nash Community Mental Health Center in Douglas County, Kan. His mental health troubles began in childhood and led to stints in alcohol rehabilitation and mental hospitals, and he tried to end his life several times. But Mr. Reilly now offers his experience to those in trouble. “Those [experiences] can be viewed as a negative until you turn that conversation around and ask, ‘How can this be helpful to another person?’ And to me, that’s where the urgency comes into the work that we’re doing because a clinical relationship is one thing, but a peer support relationship is something different.” He was speaking in support of an initiative that seeks to train and place peer support people in hospital emergency departments in Kansas. The initiative is being spearheaded by Bob Tryanski, Douglas County director of behavioral health projects. “In addition to giving folks the opportunity to have the work experience in an environment where we need peer support, we would wrap around those peers with training, professional development, with coaching and support in an ongoing way,” Mr. Tryanski said, “so that they could become real, robust, huge resources, not just to the emergency department but in our community.” If approved, hiring and training of peers would begin in April, with the goal of having six people in place in emergency rooms by the summer and hiring an additional six people by year end. LJWorld.com.
Intergenerational trauma, attitudes can allow cycles of depression, anxiety to continue
Intergenerational trauma, attitudes can allow cycles of depression, anxiety to continue
The stigma tied to mental illness can be particularly difficult to overcome for people of Latin American descent, writes Concepción de León in El Espace, a column in the New York Times focused on news and culture relevant to Latinx communities. Sometimes those seeking help run into familiar mantras. “Let me know if any of these sound familiar: 'Boys don’t cry. We don’t air family business. You have to be strong. Turn to God.' These refrains (all of which I’ve heard at least once...) are just some of the responses that people dealing with mental health challenges in Latino communities have come to know well,” Ms. de León wrote. The unequal access to mental health services and health insurance that is a reality for some Latinos compounds the problem. The result is that mental illness can go untreated. Indeed, according to Ms. de León, Latinos, who are just as likely to suffer from a mental illness as non-Hispanic whites, are half as likely to seek treatment. Adriana Alejandre, a Latina who is a licensed marriage and family therapist in Los Angeles, is seeking to change that statistic. Through her podcast, Latinx Therapy, she seeks to spread the word that seeking therapy for mental illness is a positive step. There’s a long way to go, partly because Latino communities tend to value the group over the individual. “The downfall is that people suffer in silence,” said Ms. Alejandre. Therapy is important for some Latinos, according to Ms. Alejandre, because of intergenerational trauma that “allows the cycle to continue – whether it’s trauma, whether it’s depression, anxiety, domestic violence.” Ms. de León said one strategy she used for more than 1 year while she was in therapy was to set boundaries by not sharing what she was doing with family members. Ms. Alejandre said. “But the system will not change if someone does not initiate the change.” The New York Times.
Some state governments are seeking to make mental health services more available. The proposed budget of democratic Gov. Tony Evers of Wisconsin aims to allocate $22 million in mental health funding to school districts in the state to pay for social workers, psychologists, counselors, and nurses. The money would come on top of the $3 million designated by his predecessor and continues the efforts in Wisconsin to give children with mental health problems more access to needed help. The proposed budget also would add $7 million to a state program that works with local health agencies with the goal of providing mental health services for students and would allocate about $2.5 million annually for school staff training. The news is welcome to school districts across Wisconsin. “Schools are struggling to meet all of those [mental health] needs. I think there is an understanding that this is really something we need to be addressing,” said Joanne Juhnke, policy director at Wisconsin Family Ties, which helps families with children who have mental health challenges. Post Crescent, part of the USA Today network.
In Pennsylvania, the state Supreme Court is set to rule on whether those who provide mental health treatment to people addicted to illicit drugs can be free from prosecution. Right now, they are not. As reported in the Legal Intelligence, the case concerns two physicians at a drug addiction treatment facility who treated a man with an opioid addiction. In July 2018, a three-judge Superior Court panel upheld that physicians should not have liability protections under the Mental Health Procedures Act (MHPA). The ruling reversed a lower court decision. The Superior Court judges sympathized with the view that treatment of mental illness in drug treatment facilities be given more legal leeway. Whether that leeway remains in place depends on the Supreme Court. If judges decide no, physicians who recognize signs of mental illness in patients being treated for drug addiction would treat the illness at the risk of subsequent liability. The case has again raised the issue of whether alcoholism and drug dependency should be considered mental illnesses. “We don’t believe it was the intended purpose of the MPHA to include drug addiction. Our concern is we don’t want hospitals or rehab facilities just having patients be seen by psychiatrists in order to invoke the MHPA,” said Patrick Mintzer, the lawyer who will argue the cases before the court. A counter view came from Jack Panella, one of the three Superior Court judges. In his decision, he wrote: “In light of current scientific research, as well as the recent addition of ‘addiction disorders’ to the American Psychiatric Association’s Diagnostic and Statistical Manual–5, we suggest that the Department of Human Services revise this definition.” The Legal Intelligence.
An op-ed in the Des Moines Register applauds republican Gov. Kim Reynolds for introducing two bills that are aimed at expanding mental health services to children and family in Iowa. “After decades of discussion and growing public support, these two bills take a huge step toward establishing a children’s mental health system,” wrote guest columnists Erin Drinnin of the United Way of Central Iowa and Kim Scorza of Seasons Center for Behavioral Health. The two also serve as cochairs of the Coalition to Advance Mental Health in Iowa for Kids (CAMHI4Kids), which includes more than 50 organizations. “Just like building a house requires a sturdy foundation, these bills are an important first step toward creating a structure for children’s mental well-being. In particular, CAMHI4Kids appreciates that these bills establish a voice and a seat for children and families at a regional level, using a system that is already in place,” wrote Ms. Drinnin and Ms. Scorza. The legislation would spell out the core services that would be available regardless of location in Iowa. The services would be geared toward children, rather than adults, reflecting the different mental health needs of children. “These important steps would finally sew together a patchwork of care that families currently must navigate with little direction. If a child is hurt on the playground, a caregiver knows to follow a clear path of care to help that child recover. But for a caregiver who is concerned about a child’s mental health, they often don’t know where to turn for help and must seek out services that might not exist in their community,” wrote Ms. Drinnin and Ms. Scorza. In Iowa, 80,000 children have a diagnosed serious emotional disturbance. About half of children aged 14 years and older with mental illness drop out of high school, and 70% of youth in Iowa’s juvenile justice system have a mental illness. “We are proud that Iowa is working together in a bipartisan way to ensure that our kids have the best start for future success,” wrote Ms. Drinnin and Ms. Scorza. Des Moines Register.
Bill Reilly is the peer support program manager for Bert Nash Community Mental Health Center in Douglas County, Kan. His mental health troubles began in childhood and led to stints in alcohol rehabilitation and mental hospitals, and he tried to end his life several times. But Mr. Reilly now offers his experience to those in trouble. “Those [experiences] can be viewed as a negative until you turn that conversation around and ask, ‘How can this be helpful to another person?’ And to me, that’s where the urgency comes into the work that we’re doing because a clinical relationship is one thing, but a peer support relationship is something different.” He was speaking in support of an initiative that seeks to train and place peer support people in hospital emergency departments in Kansas. The initiative is being spearheaded by Bob Tryanski, Douglas County director of behavioral health projects. “In addition to giving folks the opportunity to have the work experience in an environment where we need peer support, we would wrap around those peers with training, professional development, with coaching and support in an ongoing way,” Mr. Tryanski said, “so that they could become real, robust, huge resources, not just to the emergency department but in our community.” If approved, hiring and training of peers would begin in April, with the goal of having six people in place in emergency rooms by the summer and hiring an additional six people by year end. LJWorld.com.
The stigma tied to mental illness can be particularly difficult to overcome for people of Latin American descent, writes Concepción de León in El Espace, a column in the New York Times focused on news and culture relevant to Latinx communities. Sometimes those seeking help run into familiar mantras. “Let me know if any of these sound familiar: 'Boys don’t cry. We don’t air family business. You have to be strong. Turn to God.' These refrains (all of which I’ve heard at least once...) are just some of the responses that people dealing with mental health challenges in Latino communities have come to know well,” Ms. de León wrote. The unequal access to mental health services and health insurance that is a reality for some Latinos compounds the problem. The result is that mental illness can go untreated. Indeed, according to Ms. de León, Latinos, who are just as likely to suffer from a mental illness as non-Hispanic whites, are half as likely to seek treatment. Adriana Alejandre, a Latina who is a licensed marriage and family therapist in Los Angeles, is seeking to change that statistic. Through her podcast, Latinx Therapy, she seeks to spread the word that seeking therapy for mental illness is a positive step. There’s a long way to go, partly because Latino communities tend to value the group over the individual. “The downfall is that people suffer in silence,” said Ms. Alejandre. Therapy is important for some Latinos, according to Ms. Alejandre, because of intergenerational trauma that “allows the cycle to continue – whether it’s trauma, whether it’s depression, anxiety, domestic violence.” Ms. de León said one strategy she used for more than 1 year while she was in therapy was to set boundaries by not sharing what she was doing with family members. Ms. Alejandre said. “But the system will not change if someone does not initiate the change.” The New York Times.
Some state governments are seeking to make mental health services more available. The proposed budget of democratic Gov. Tony Evers of Wisconsin aims to allocate $22 million in mental health funding to school districts in the state to pay for social workers, psychologists, counselors, and nurses. The money would come on top of the $3 million designated by his predecessor and continues the efforts in Wisconsin to give children with mental health problems more access to needed help. The proposed budget also would add $7 million to a state program that works with local health agencies with the goal of providing mental health services for students and would allocate about $2.5 million annually for school staff training. The news is welcome to school districts across Wisconsin. “Schools are struggling to meet all of those [mental health] needs. I think there is an understanding that this is really something we need to be addressing,” said Joanne Juhnke, policy director at Wisconsin Family Ties, which helps families with children who have mental health challenges. Post Crescent, part of the USA Today network.
In Pennsylvania, the state Supreme Court is set to rule on whether those who provide mental health treatment to people addicted to illicit drugs can be free from prosecution. Right now, they are not. As reported in the Legal Intelligence, the case concerns two physicians at a drug addiction treatment facility who treated a man with an opioid addiction. In July 2018, a three-judge Superior Court panel upheld that physicians should not have liability protections under the Mental Health Procedures Act (MHPA). The ruling reversed a lower court decision. The Superior Court judges sympathized with the view that treatment of mental illness in drug treatment facilities be given more legal leeway. Whether that leeway remains in place depends on the Supreme Court. If judges decide no, physicians who recognize signs of mental illness in patients being treated for drug addiction would treat the illness at the risk of subsequent liability. The case has again raised the issue of whether alcoholism and drug dependency should be considered mental illnesses. “We don’t believe it was the intended purpose of the MPHA to include drug addiction. Our concern is we don’t want hospitals or rehab facilities just having patients be seen by psychiatrists in order to invoke the MHPA,” said Patrick Mintzer, the lawyer who will argue the cases before the court. A counter view came from Jack Panella, one of the three Superior Court judges. In his decision, he wrote: “In light of current scientific research, as well as the recent addition of ‘addiction disorders’ to the American Psychiatric Association’s Diagnostic and Statistical Manual–5, we suggest that the Department of Human Services revise this definition.” The Legal Intelligence.
An op-ed in the Des Moines Register applauds republican Gov. Kim Reynolds for introducing two bills that are aimed at expanding mental health services to children and family in Iowa. “After decades of discussion and growing public support, these two bills take a huge step toward establishing a children’s mental health system,” wrote guest columnists Erin Drinnin of the United Way of Central Iowa and Kim Scorza of Seasons Center for Behavioral Health. The two also serve as cochairs of the Coalition to Advance Mental Health in Iowa for Kids (CAMHI4Kids), which includes more than 50 organizations. “Just like building a house requires a sturdy foundation, these bills are an important first step toward creating a structure for children’s mental well-being. In particular, CAMHI4Kids appreciates that these bills establish a voice and a seat for children and families at a regional level, using a system that is already in place,” wrote Ms. Drinnin and Ms. Scorza. The legislation would spell out the core services that would be available regardless of location in Iowa. The services would be geared toward children, rather than adults, reflecting the different mental health needs of children. “These important steps would finally sew together a patchwork of care that families currently must navigate with little direction. If a child is hurt on the playground, a caregiver knows to follow a clear path of care to help that child recover. But for a caregiver who is concerned about a child’s mental health, they often don’t know where to turn for help and must seek out services that might not exist in their community,” wrote Ms. Drinnin and Ms. Scorza. In Iowa, 80,000 children have a diagnosed serious emotional disturbance. About half of children aged 14 years and older with mental illness drop out of high school, and 70% of youth in Iowa’s juvenile justice system have a mental illness. “We are proud that Iowa is working together in a bipartisan way to ensure that our kids have the best start for future success,” wrote Ms. Drinnin and Ms. Scorza. Des Moines Register.
Bill Reilly is the peer support program manager for Bert Nash Community Mental Health Center in Douglas County, Kan. His mental health troubles began in childhood and led to stints in alcohol rehabilitation and mental hospitals, and he tried to end his life several times. But Mr. Reilly now offers his experience to those in trouble. “Those [experiences] can be viewed as a negative until you turn that conversation around and ask, ‘How can this be helpful to another person?’ And to me, that’s where the urgency comes into the work that we’re doing because a clinical relationship is one thing, but a peer support relationship is something different.” He was speaking in support of an initiative that seeks to train and place peer support people in hospital emergency departments in Kansas. The initiative is being spearheaded by Bob Tryanski, Douglas County director of behavioral health projects. “In addition to giving folks the opportunity to have the work experience in an environment where we need peer support, we would wrap around those peers with training, professional development, with coaching and support in an ongoing way,” Mr. Tryanski said, “so that they could become real, robust, huge resources, not just to the emergency department but in our community.” If approved, hiring and training of peers would begin in April, with the goal of having six people in place in emergency rooms by the summer and hiring an additional six people by year end. LJWorld.com.
Up-close view of climate change proves sobering
Dr. Carl Bell steps away from American College of Psychiatrists meeting and gets a jolt
It used to be difficult to conceive of writing about climate change in light of the illnesses we psychiatrists treat. But talking about climate change has become unavoidable. Sometimes, it seems that things weigh heavy on my heart, and I have to write about them – especially when it is serious.

David Alan Pollack, MD, has been talking about climate change for some years now, and while I understood his concern, I had yet to see the psychological effects up close and personal. After all, I live in Chicago, and we are surrounded by concrete and asphalt.
Thankfully, I also travel, and I get a chance to get into nature. While in Hawaii at the American College of Psychiatrists annual meeting in February, I went snorkeling in Hanauma Bay. I saw coral and fish. The problem is I have a very vivid memories of snorkeling in that exact same nature preserve, which also was a Marine Life Conservation District in 1972 while I was attending the American Psychiatric Association annual meeting.
The contrast between the two experiences leaves me with a glum, sad, disappointed, heart-broken feeling because it was an intimate and personal experience with climate change. In 1972, I saw every type of coral imaginable: brain coral, club finger coral, elk coral, great star coral, pillar coral, staghorn coral, table coral, and tube coral. If I remember correctly, there were corky sea fingers and sea fans, but not sea turtles. In 1972, I saw bigeyefish, damselfish, doctorfish, filefish, goatfish, gobies, hogfish, lemon butterflyfish, lizardfish, parrottfish, porcupinefish, pufferfish, queen angelfish, rock beauties, sergeant majors, soldierfish, spot-tail spot-tail butterflyfish, Spanish hogfish, squirrelfish, tangs, trunkfish, or any bluehead or yellowhead wrasses.
In 2019, I saw two pieces of coral less that 9 inches in diameter and not a single sea urchin. There were maybe three types of tropical fish that I was unfamiliar with seeing. The difference between what I saw in 1972 and what I saw in 2019 was like the difference between the rain forest in Puerto Rico and the dunes of the Sahara Desert.
Sure, I have heard David talk about the mental health effects of climate change on stress, anxiety, and depression, and I have always thought that he was right. But to see climate change up close and personal is a sobering experience. I apologize to them for being part of the system and process that is destroying the planet – and leaving them with a hot mess.
At this point, it seems to me that we cannot just try to save the planet by being better stewards of our garbage and pointing out measurable indicators of climate change. We need to actively rather than passively try to save the planet. Of course, the question is who will pay for the active efforts to depollute Earth. From what I saw for myself in Hanauma Bay, I don’t think we have much time. So I am hoping that more people will take the issue of climate change seriously.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit in Chicago, clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago, former president/CEO of Community Mental Health Council, and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago. Check out Dr. Bell’s new book, “Fetal Alcohol Exposure in the African-American Community,” at https://thirdworldpressfoundation.org/product/pre-order-fetal-alcohol-exposure-in-the-african-american-community/.
Dr. Carl Bell steps away from American College of Psychiatrists meeting and gets a jolt
Dr. Carl Bell steps away from American College of Psychiatrists meeting and gets a jolt
It used to be difficult to conceive of writing about climate change in light of the illnesses we psychiatrists treat. But talking about climate change has become unavoidable. Sometimes, it seems that things weigh heavy on my heart, and I have to write about them – especially when it is serious.
David Alan Pollack, MD, has been talking about climate change for some years now, and while I understood his concern, I had yet to see the psychological effects up close and personal. After all, I live in Chicago, and we are surrounded by concrete and asphalt.
Thankfully, I also travel, and I get a chance to get into nature. While in Hawaii at the American College of Psychiatrists annual meeting in February, I went snorkeling in Hanauma Bay. I saw coral and fish. The problem is I have a very vivid memories of snorkeling in that exact same nature preserve, which also was a Marine Life Conservation District in 1972 while I was attending the American Psychiatric Association annual meeting.
The contrast between the two experiences leaves me with a glum, sad, disappointed, heart-broken feeling because it was an intimate and personal experience with climate change. In 1972, I saw every type of coral imaginable: brain coral, club finger coral, elk coral, great star coral, pillar coral, staghorn coral, table coral, and tube coral. If I remember correctly, there were corky sea fingers and sea fans, but not sea turtles. In 1972, I saw bigeyefish, damselfish, doctorfish, filefish, goatfish, gobies, hogfish, lemon butterflyfish, lizardfish, parrottfish, porcupinefish, pufferfish, queen angelfish, rock beauties, sergeant majors, soldierfish, spot-tail spot-tail butterflyfish, Spanish hogfish, squirrelfish, tangs, trunkfish, or any bluehead or yellowhead wrasses.
In 2019, I saw two pieces of coral less that 9 inches in diameter and not a single sea urchin. There were maybe three types of tropical fish that I was unfamiliar with seeing. The difference between what I saw in 1972 and what I saw in 2019 was like the difference between the rain forest in Puerto Rico and the dunes of the Sahara Desert.
Sure, I have heard David talk about the mental health effects of climate change on stress, anxiety, and depression, and I have always thought that he was right. But to see climate change up close and personal is a sobering experience. I apologize to them for being part of the system and process that is destroying the planet – and leaving them with a hot mess.
At this point, it seems to me that we cannot just try to save the planet by being better stewards of our garbage and pointing out measurable indicators of climate change. We need to actively rather than passively try to save the planet. Of course, the question is who will pay for the active efforts to depollute Earth. From what I saw for myself in Hanauma Bay, I don’t think we have much time. So I am hoping that more people will take the issue of climate change seriously.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit in Chicago, clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago, former president/CEO of Community Mental Health Council, and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago. Check out Dr. Bell’s new book, “Fetal Alcohol Exposure in the African-American Community,” at https://thirdworldpressfoundation.org/product/pre-order-fetal-alcohol-exposure-in-the-african-american-community/.
It used to be difficult to conceive of writing about climate change in light of the illnesses we psychiatrists treat. But talking about climate change has become unavoidable. Sometimes, it seems that things weigh heavy on my heart, and I have to write about them – especially when it is serious.
David Alan Pollack, MD, has been talking about climate change for some years now, and while I understood his concern, I had yet to see the psychological effects up close and personal. After all, I live in Chicago, and we are surrounded by concrete and asphalt.
Thankfully, I also travel, and I get a chance to get into nature. While in Hawaii at the American College of Psychiatrists annual meeting in February, I went snorkeling in Hanauma Bay. I saw coral and fish. The problem is I have a very vivid memories of snorkeling in that exact same nature preserve, which also was a Marine Life Conservation District in 1972 while I was attending the American Psychiatric Association annual meeting.
The contrast between the two experiences leaves me with a glum, sad, disappointed, heart-broken feeling because it was an intimate and personal experience with climate change. In 1972, I saw every type of coral imaginable: brain coral, club finger coral, elk coral, great star coral, pillar coral, staghorn coral, table coral, and tube coral. If I remember correctly, there were corky sea fingers and sea fans, but not sea turtles. In 1972, I saw bigeyefish, damselfish, doctorfish, filefish, goatfish, gobies, hogfish, lemon butterflyfish, lizardfish, parrottfish, porcupinefish, pufferfish, queen angelfish, rock beauties, sergeant majors, soldierfish, spot-tail spot-tail butterflyfish, Spanish hogfish, squirrelfish, tangs, trunkfish, or any bluehead or yellowhead wrasses.
In 2019, I saw two pieces of coral less that 9 inches in diameter and not a single sea urchin. There were maybe three types of tropical fish that I was unfamiliar with seeing. The difference between what I saw in 1972 and what I saw in 2019 was like the difference between the rain forest in Puerto Rico and the dunes of the Sahara Desert.
Sure, I have heard David talk about the mental health effects of climate change on stress, anxiety, and depression, and I have always thought that he was right. But to see climate change up close and personal is a sobering experience. I apologize to them for being part of the system and process that is destroying the planet – and leaving them with a hot mess.
At this point, it seems to me that we cannot just try to save the planet by being better stewards of our garbage and pointing out measurable indicators of climate change. We need to actively rather than passively try to save the planet. Of course, the question is who will pay for the active efforts to depollute Earth. From what I saw for myself in Hanauma Bay, I don’t think we have much time. So I am hoping that more people will take the issue of climate change seriously.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit in Chicago, clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago, former president/CEO of Community Mental Health Council, and former director of the Institute for Juvenile Research (birthplace of child psychiatry), also in Chicago. Check out Dr. Bell’s new book, “Fetal Alcohol Exposure in the African-American Community,” at https://thirdworldpressfoundation.org/product/pre-order-fetal-alcohol-exposure-in-the-african-american-community/.
‘The birth of a mother is a complex process’
Softening the blow to women and families of severe perinatal, postpartum psychiatric disorders
Editor’s Note: Alison M. Heru, MD, the Families in Psychiatry columnist, invited Dr. Reinstein to address this topic.
“But this was not what I expected!” That’s a statement I have heard from countless new mothers.

Women often envision pregnancy and the postpartum period as a time of pure joy. The glow of an expectant woman and the excitement of the arrival of a new baby masks the reality that many women struggle emotionally when transitioning to motherhood. Like the birth of a child, the birth of a mother is a complex process. Upholding the myth that all women seamlessly transform into mothers can have devastating effects and hinder access to mental health care.
As a psychiatrist working on a women’s inpatient unit with a perinatal program, I treat women at times of crisis. What may have begun as mild anxiety or depression sometimes quickly spirals into severe psychiatric illness. The sheer force of these severe perinatal and postpartum psychiatric disorders often leaves women and families shocked and confused, wondering what happened to their crumbled dreams of early motherhood.
What must general psychiatrists know about perinatal and postpartum psychiatric disorders? Why is maternal mental health so important? What are the barriers to treatment for these women? How can general psychiatrists best support and treat these new mothers and their families?
What data show
Maternal depression is now known to be one of the most common complications of pregnancy. Studies have suggested that about 11% of women experience depression during pregnancy1 and approximately 17% of women are depressed in the postpartum period.2 Perinatal generalized anxiety disorder has been shown to have a prevalence of 8.5%-10.5% during pregnancy with a wider variance post partum.3 Approximately 3% of women in the general community develop PTSD symptoms following childbirth.4 Research suggests that about 2% of women develop obsessive-compulsive disorder symptoms in the postpartum period.5 Postpartum psychosis, a rare but potentially devastating illness, occurs after 0.1%-0.2% of births.6
Importance of maternal mental health
There is a growing body of literature supporting both obstetric and pediatric adverse outcomes related to untreated psychiatric illness. Untreated maternal depression has been associated with obstetric complications, such as preterm delivery, preeclampsia, low birth weight, as well as the child’s developing cognitive function.7 Anxiety during pregnancy has been associated with both a shorter gestational period and adverse implications for fetal neurodevelopment.

These adverse effects were found to be even more potent in “pregnancy anxiety,” or anxiety specifically focused on the pregnancy, the birth experience, and the transition to motherhood.8 The psychotic symptoms occurring during postpartum psychosis can jeopardize the lives of both a woman and her child and carries a 4% risk of infanticide.9 Although there are limited data about the long-term effects of postpartum obsessive-compulsive disorders and PTSD, it is reasonable to assume that they might carry negative long-term implications for the mother and possibly her child.
Barriers to treatment
Despite the significant rates of mental illness, pregnant and new mothers often face barriers to receiving treatment. Many psychiatrists are hesitant to prescribe psychiatric medication to pregnant women because of concerns about teratogenic potential of psychiatric medications; similar concerns exist for newborn babies when prescribing medications to lactating mothers. In addition, the field of reproductive psychiatry is evolving at a rapid pace, making it difficult for busy psychiatrists to keep up with the ever-growing literature.
Also, it is hard to imagine a population that has more barriers to attending outpatient appointments. For many new mothers, the exhaustion and all-consuming work involved with taking care of a newborn are insurmountable barriers to obtaining mental health care. In addition, despite the awareness that new mothers often are more emotional, families can be slow to recognize the developing severity of a psychiatric illness during the peripartum and postpartum periods.
Supporting and treating new mothers
As general psychiatrists, there are several ways to directly help these women.
1. Expect the expected. Even in women with no prior psychiatric history, a significant percentage of expectant and postpartum women will develop acute psychiatric symptoms. Learn about the different presentations and treatments of perinatal and postpartum psychiatric disorders. For example, a woman might have thoughts of harming her baby in both postpartum psychosis and obsessive-compulsive disorder. However, the acuity and treatment of these two conditions drastically differ.
2. Learn more about psychiatric medications. Several apps and websites are available to psychiatrists to learn about the safety profile of psychiatric medications, such as Reprotox.org, mothertobaby.org, lactmed, and womensmentalhealth.org. Many medications are considered to be relatively safe during pregnancy and breastfeeding. It is important for psychiatrists to appreciate the risks when choosing not to prescribe to pregnant and postpartum women. Sometimes a known risk of a specific medication may be preferable to the unknown risk of leaving a woman susceptible to a severe psychiatric decompensation.
3. Involve all members of the family. A mother’s mental health has significant implications for the entire family. Psychoeducation for the family as well as frequent family sessions are key tools when treating this population. In addition, prescribing to pregnant women provides the opportunity for a psychiatrist to refine skills in joint decision making; it is crucial to involve both a patient and her spouse when discussing psychiatric medications.
4. Provide ready access and collaborate care. It is important to understand the potential rapid onset of psychiatric symptoms during the pregnancy and postpartum period. Psychiatrists should be prepared to collaborate care with other specialties. It is important to establish relationships with community psychotherapists specializing in maternal mental health, pediatricians, as well as obstetricians.
5. Learn when to seek a higher level of care. Although many women with perinatal and postpartum psychiatric symptoms can be managed as outpatients, women at times need a higher level of care. Similar to general psychiatry, women who are acutely suicidal or homicidal or have a sudden onset of psychotic and manic symptoms all should be evaluated immediately for inpatient hospitalization. Women with less severe symptoms but who require a higher level of care than typically offered in standard outpatient treatment should be candidates for partial hospitalization programs.
General intensive programs usually can accommodate these women, but it is ideal to refer this population to perinatal intensive programs. Postpartum Support International (postpartum.net) lists the nationwide inpatient and partial perinatal programs as well as regional and local services. An example of inpatient perinatal care is the women’s unit at Zucker Hillside Hospital (Northwell Health System, Glen Oaks, N.Y.), which houses an inpatient perinatal program. As a psychiatrist on the unit, I treat acute symptoms such as depression, anxiety, psychosis, mania, and catatonia that occur during the perinatal and postpartum periods. Given the severity of symptoms, I use a wide range of psychiatric medications with the possibility of electroconvulsive therapy when indicated. Psychotherapy staff on the unit offer specialized perinatal, mothers, and dialectical behavioral therapy groups. Breast pumps are available for women who wish to breastfeed. Accommodations are made for babies and children to visit their mother when clinically appropriate. Once discharged, women often are referred to Zucker Hillside’s own perinatal outpatient clinic for continued treatment. Similar models exist in select inpatient units as well as an increasing number of partial programs across the United States.
Conclusion
Psychiatric care for pregnant and new mothers can be challenging, but it is also immensely rewarding. Restoring a mother’s mental health usually leads to increased emotional stability for her entire family. Given the prevalence of maternal mental health disorders, psychiatrists in nearly every setting will encounter this population of women. With dedicated time devoted to reviewing the literature and learning about local resources, psychiatrists can feel comfortable treating women throughout the childbearing experience.
References
1. J Affect Disord. 2017 Sep;219:86-92.
2. J Psychiatr Res. 2018 Sep;104:235-48.
3. J Womens Health. (Larchmt). 2015 Sep;24(9):762-70.
4. Clin Psychol Rev. 2014 Jul;34(5):389-401.
5. Compr Psychiatry. 2009 Nov-Dec;50(6):503-9.
6. Int Rev Psychiatry. 2003 Aug;15(3):231-42.
7. Clin Obstet Gynecol. 2018 Sep;61(3):533-43.
8. Curr Opinion Psychiatry. 2012 Mar;25(2):141-8.
9. Am J Psychiatry. 2009 Apr;166(4):405-8.
Dr. Reinstein is a psychiatry attending at Zucker Hillside Hospital. Her clinical interests include reproductive psychiatry and family therapy, with a specific focus on maternal mental health. Dr. Reinstein completed her adult psychiatry residency training at Montefiore Hospital/Albert Einstein College of Medicine, New York, after graduating from the Albert Einstein College of Medicine and Yeshiva University, New York, with a BA in biology. She is one of the recipients of the 4th Annual Resident Recognition Award for Excellence in Family Oriented Care.
Softening the blow to women and families of severe perinatal, postpartum psychiatric disorders
Softening the blow to women and families of severe perinatal, postpartum psychiatric disorders
Editor’s Note: Alison M. Heru, MD, the Families in Psychiatry columnist, invited Dr. Reinstein to address this topic.
“But this was not what I expected!” That’s a statement I have heard from countless new mothers.
Women often envision pregnancy and the postpartum period as a time of pure joy. The glow of an expectant woman and the excitement of the arrival of a new baby masks the reality that many women struggle emotionally when transitioning to motherhood. Like the birth of a child, the birth of a mother is a complex process. Upholding the myth that all women seamlessly transform into mothers can have devastating effects and hinder access to mental health care.
As a psychiatrist working on a women’s inpatient unit with a perinatal program, I treat women at times of crisis. What may have begun as mild anxiety or depression sometimes quickly spirals into severe psychiatric illness. The sheer force of these severe perinatal and postpartum psychiatric disorders often leaves women and families shocked and confused, wondering what happened to their crumbled dreams of early motherhood.
What must general psychiatrists know about perinatal and postpartum psychiatric disorders? Why is maternal mental health so important? What are the barriers to treatment for these women? How can general psychiatrists best support and treat these new mothers and their families?
What data show
Maternal depression is now known to be one of the most common complications of pregnancy. Studies have suggested that about 11% of women experience depression during pregnancy1 and approximately 17% of women are depressed in the postpartum period.2 Perinatal generalized anxiety disorder has been shown to have a prevalence of 8.5%-10.5% during pregnancy with a wider variance post partum.3 Approximately 3% of women in the general community develop PTSD symptoms following childbirth.4 Research suggests that about 2% of women develop obsessive-compulsive disorder symptoms in the postpartum period.5 Postpartum psychosis, a rare but potentially devastating illness, occurs after 0.1%-0.2% of births.6
Importance of maternal mental health
There is a growing body of literature supporting both obstetric and pediatric adverse outcomes related to untreated psychiatric illness. Untreated maternal depression has been associated with obstetric complications, such as preterm delivery, preeclampsia, low birth weight, as well as the child’s developing cognitive function.7 Anxiety during pregnancy has been associated with both a shorter gestational period and adverse implications for fetal neurodevelopment.
These adverse effects were found to be even more potent in “pregnancy anxiety,” or anxiety specifically focused on the pregnancy, the birth experience, and the transition to motherhood.8 The psychotic symptoms occurring during postpartum psychosis can jeopardize the lives of both a woman and her child and carries a 4% risk of infanticide.9 Although there are limited data about the long-term effects of postpartum obsessive-compulsive disorders and PTSD, it is reasonable to assume that they might carry negative long-term implications for the mother and possibly her child.
Barriers to treatment
Despite the significant rates of mental illness, pregnant and new mothers often face barriers to receiving treatment. Many psychiatrists are hesitant to prescribe psychiatric medication to pregnant women because of concerns about teratogenic potential of psychiatric medications; similar concerns exist for newborn babies when prescribing medications to lactating mothers. In addition, the field of reproductive psychiatry is evolving at a rapid pace, making it difficult for busy psychiatrists to keep up with the ever-growing literature.
Also, it is hard to imagine a population that has more barriers to attending outpatient appointments. For many new mothers, the exhaustion and all-consuming work involved with taking care of a newborn are insurmountable barriers to obtaining mental health care. In addition, despite the awareness that new mothers often are more emotional, families can be slow to recognize the developing severity of a psychiatric illness during the peripartum and postpartum periods.
Supporting and treating new mothers
As general psychiatrists, there are several ways to directly help these women.
1. Expect the expected. Even in women with no prior psychiatric history, a significant percentage of expectant and postpartum women will develop acute psychiatric symptoms. Learn about the different presentations and treatments of perinatal and postpartum psychiatric disorders. For example, a woman might have thoughts of harming her baby in both postpartum psychosis and obsessive-compulsive disorder. However, the acuity and treatment of these two conditions drastically differ.
2. Learn more about psychiatric medications. Several apps and websites are available to psychiatrists to learn about the safety profile of psychiatric medications, such as Reprotox.org, mothertobaby.org, lactmed, and womensmentalhealth.org. Many medications are considered to be relatively safe during pregnancy and breastfeeding. It is important for psychiatrists to appreciate the risks when choosing not to prescribe to pregnant and postpartum women. Sometimes a known risk of a specific medication may be preferable to the unknown risk of leaving a woman susceptible to a severe psychiatric decompensation.
3. Involve all members of the family. A mother’s mental health has significant implications for the entire family. Psychoeducation for the family as well as frequent family sessions are key tools when treating this population. In addition, prescribing to pregnant women provides the opportunity for a psychiatrist to refine skills in joint decision making; it is crucial to involve both a patient and her spouse when discussing psychiatric medications.
4. Provide ready access and collaborate care. It is important to understand the potential rapid onset of psychiatric symptoms during the pregnancy and postpartum period. Psychiatrists should be prepared to collaborate care with other specialties. It is important to establish relationships with community psychotherapists specializing in maternal mental health, pediatricians, as well as obstetricians.
5. Learn when to seek a higher level of care. Although many women with perinatal and postpartum psychiatric symptoms can be managed as outpatients, women at times need a higher level of care. Similar to general psychiatry, women who are acutely suicidal or homicidal or have a sudden onset of psychotic and manic symptoms all should be evaluated immediately for inpatient hospitalization. Women with less severe symptoms but who require a higher level of care than typically offered in standard outpatient treatment should be candidates for partial hospitalization programs.
General intensive programs usually can accommodate these women, but it is ideal to refer this population to perinatal intensive programs. Postpartum Support International (postpartum.net) lists the nationwide inpatient and partial perinatal programs as well as regional and local services. An example of inpatient perinatal care is the women’s unit at Zucker Hillside Hospital (Northwell Health System, Glen Oaks, N.Y.), which houses an inpatient perinatal program. As a psychiatrist on the unit, I treat acute symptoms such as depression, anxiety, psychosis, mania, and catatonia that occur during the perinatal and postpartum periods. Given the severity of symptoms, I use a wide range of psychiatric medications with the possibility of electroconvulsive therapy when indicated. Psychotherapy staff on the unit offer specialized perinatal, mothers, and dialectical behavioral therapy groups. Breast pumps are available for women who wish to breastfeed. Accommodations are made for babies and children to visit their mother when clinically appropriate. Once discharged, women often are referred to Zucker Hillside’s own perinatal outpatient clinic for continued treatment. Similar models exist in select inpatient units as well as an increasing number of partial programs across the United States.
Conclusion
Psychiatric care for pregnant and new mothers can be challenging, but it is also immensely rewarding. Restoring a mother’s mental health usually leads to increased emotional stability for her entire family. Given the prevalence of maternal mental health disorders, psychiatrists in nearly every setting will encounter this population of women. With dedicated time devoted to reviewing the literature and learning about local resources, psychiatrists can feel comfortable treating women throughout the childbearing experience.
References
1. J Affect Disord. 2017 Sep;219:86-92.
2. J Psychiatr Res. 2018 Sep;104:235-48.
3. J Womens Health. (Larchmt). 2015 Sep;24(9):762-70.
4. Clin Psychol Rev. 2014 Jul;34(5):389-401.
5. Compr Psychiatry. 2009 Nov-Dec;50(6):503-9.
6. Int Rev Psychiatry. 2003 Aug;15(3):231-42.
7. Clin Obstet Gynecol. 2018 Sep;61(3):533-43.
8. Curr Opinion Psychiatry. 2012 Mar;25(2):141-8.
9. Am J Psychiatry. 2009 Apr;166(4):405-8.
Dr. Reinstein is a psychiatry attending at Zucker Hillside Hospital. Her clinical interests include reproductive psychiatry and family therapy, with a specific focus on maternal mental health. Dr. Reinstein completed her adult psychiatry residency training at Montefiore Hospital/Albert Einstein College of Medicine, New York, after graduating from the Albert Einstein College of Medicine and Yeshiva University, New York, with a BA in biology. She is one of the recipients of the 4th Annual Resident Recognition Award for Excellence in Family Oriented Care.
Editor’s Note: Alison M. Heru, MD, the Families in Psychiatry columnist, invited Dr. Reinstein to address this topic.
“But this was not what I expected!” That’s a statement I have heard from countless new mothers.
Women often envision pregnancy and the postpartum period as a time of pure joy. The glow of an expectant woman and the excitement of the arrival of a new baby masks the reality that many women struggle emotionally when transitioning to motherhood. Like the birth of a child, the birth of a mother is a complex process. Upholding the myth that all women seamlessly transform into mothers can have devastating effects and hinder access to mental health care.
As a psychiatrist working on a women’s inpatient unit with a perinatal program, I treat women at times of crisis. What may have begun as mild anxiety or depression sometimes quickly spirals into severe psychiatric illness. The sheer force of these severe perinatal and postpartum psychiatric disorders often leaves women and families shocked and confused, wondering what happened to their crumbled dreams of early motherhood.
What must general psychiatrists know about perinatal and postpartum psychiatric disorders? Why is maternal mental health so important? What are the barriers to treatment for these women? How can general psychiatrists best support and treat these new mothers and their families?
What data show
Maternal depression is now known to be one of the most common complications of pregnancy. Studies have suggested that about 11% of women experience depression during pregnancy1 and approximately 17% of women are depressed in the postpartum period.2 Perinatal generalized anxiety disorder has been shown to have a prevalence of 8.5%-10.5% during pregnancy with a wider variance post partum.3 Approximately 3% of women in the general community develop PTSD symptoms following childbirth.4 Research suggests that about 2% of women develop obsessive-compulsive disorder symptoms in the postpartum period.5 Postpartum psychosis, a rare but potentially devastating illness, occurs after 0.1%-0.2% of births.6
Importance of maternal mental health
There is a growing body of literature supporting both obstetric and pediatric adverse outcomes related to untreated psychiatric illness. Untreated maternal depression has been associated with obstetric complications, such as preterm delivery, preeclampsia, low birth weight, as well as the child’s developing cognitive function.7 Anxiety during pregnancy has been associated with both a shorter gestational period and adverse implications for fetal neurodevelopment.
These adverse effects were found to be even more potent in “pregnancy anxiety,” or anxiety specifically focused on the pregnancy, the birth experience, and the transition to motherhood.8 The psychotic symptoms occurring during postpartum psychosis can jeopardize the lives of both a woman and her child and carries a 4% risk of infanticide.9 Although there are limited data about the long-term effects of postpartum obsessive-compulsive disorders and PTSD, it is reasonable to assume that they might carry negative long-term implications for the mother and possibly her child.
Barriers to treatment
Despite the significant rates of mental illness, pregnant and new mothers often face barriers to receiving treatment. Many psychiatrists are hesitant to prescribe psychiatric medication to pregnant women because of concerns about teratogenic potential of psychiatric medications; similar concerns exist for newborn babies when prescribing medications to lactating mothers. In addition, the field of reproductive psychiatry is evolving at a rapid pace, making it difficult for busy psychiatrists to keep up with the ever-growing literature.
Also, it is hard to imagine a population that has more barriers to attending outpatient appointments. For many new mothers, the exhaustion and all-consuming work involved with taking care of a newborn are insurmountable barriers to obtaining mental health care. In addition, despite the awareness that new mothers often are more emotional, families can be slow to recognize the developing severity of a psychiatric illness during the peripartum and postpartum periods.
Supporting and treating new mothers
As general psychiatrists, there are several ways to directly help these women.
1. Expect the expected. Even in women with no prior psychiatric history, a significant percentage of expectant and postpartum women will develop acute psychiatric symptoms. Learn about the different presentations and treatments of perinatal and postpartum psychiatric disorders. For example, a woman might have thoughts of harming her baby in both postpartum psychosis and obsessive-compulsive disorder. However, the acuity and treatment of these two conditions drastically differ.
2. Learn more about psychiatric medications. Several apps and websites are available to psychiatrists to learn about the safety profile of psychiatric medications, such as Reprotox.org, mothertobaby.org, lactmed, and womensmentalhealth.org. Many medications are considered to be relatively safe during pregnancy and breastfeeding. It is important for psychiatrists to appreciate the risks when choosing not to prescribe to pregnant and postpartum women. Sometimes a known risk of a specific medication may be preferable to the unknown risk of leaving a woman susceptible to a severe psychiatric decompensation.
3. Involve all members of the family. A mother’s mental health has significant implications for the entire family. Psychoeducation for the family as well as frequent family sessions are key tools when treating this population. In addition, prescribing to pregnant women provides the opportunity for a psychiatrist to refine skills in joint decision making; it is crucial to involve both a patient and her spouse when discussing psychiatric medications.
4. Provide ready access and collaborate care. It is important to understand the potential rapid onset of psychiatric symptoms during the pregnancy and postpartum period. Psychiatrists should be prepared to collaborate care with other specialties. It is important to establish relationships with community psychotherapists specializing in maternal mental health, pediatricians, as well as obstetricians.
5. Learn when to seek a higher level of care. Although many women with perinatal and postpartum psychiatric symptoms can be managed as outpatients, women at times need a higher level of care. Similar to general psychiatry, women who are acutely suicidal or homicidal or have a sudden onset of psychotic and manic symptoms all should be evaluated immediately for inpatient hospitalization. Women with less severe symptoms but who require a higher level of care than typically offered in standard outpatient treatment should be candidates for partial hospitalization programs.
General intensive programs usually can accommodate these women, but it is ideal to refer this population to perinatal intensive programs. Postpartum Support International (postpartum.net) lists the nationwide inpatient and partial perinatal programs as well as regional and local services. An example of inpatient perinatal care is the women’s unit at Zucker Hillside Hospital (Northwell Health System, Glen Oaks, N.Y.), which houses an inpatient perinatal program. As a psychiatrist on the unit, I treat acute symptoms such as depression, anxiety, psychosis, mania, and catatonia that occur during the perinatal and postpartum periods. Given the severity of symptoms, I use a wide range of psychiatric medications with the possibility of electroconvulsive therapy when indicated. Psychotherapy staff on the unit offer specialized perinatal, mothers, and dialectical behavioral therapy groups. Breast pumps are available for women who wish to breastfeed. Accommodations are made for babies and children to visit their mother when clinically appropriate. Once discharged, women often are referred to Zucker Hillside’s own perinatal outpatient clinic for continued treatment. Similar models exist in select inpatient units as well as an increasing number of partial programs across the United States.
Conclusion
Psychiatric care for pregnant and new mothers can be challenging, but it is also immensely rewarding. Restoring a mother’s mental health usually leads to increased emotional stability for her entire family. Given the prevalence of maternal mental health disorders, psychiatrists in nearly every setting will encounter this population of women. With dedicated time devoted to reviewing the literature and learning about local resources, psychiatrists can feel comfortable treating women throughout the childbearing experience.
References
1. J Affect Disord. 2017 Sep;219:86-92.
2. J Psychiatr Res. 2018 Sep;104:235-48.
3. J Womens Health. (Larchmt). 2015 Sep;24(9):762-70.
4. Clin Psychol Rev. 2014 Jul;34(5):389-401.
5. Compr Psychiatry. 2009 Nov-Dec;50(6):503-9.
6. Int Rev Psychiatry. 2003 Aug;15(3):231-42.
7. Clin Obstet Gynecol. 2018 Sep;61(3):533-43.
8. Curr Opinion Psychiatry. 2012 Mar;25(2):141-8.
9. Am J Psychiatry. 2009 Apr;166(4):405-8.
Dr. Reinstein is a psychiatry attending at Zucker Hillside Hospital. Her clinical interests include reproductive psychiatry and family therapy, with a specific focus on maternal mental health. Dr. Reinstein completed her adult psychiatry residency training at Montefiore Hospital/Albert Einstein College of Medicine, New York, after graduating from the Albert Einstein College of Medicine and Yeshiva University, New York, with a BA in biology. She is one of the recipients of the 4th Annual Resident Recognition Award for Excellence in Family Oriented Care.
Effects of Insomnia and Depression on CPAP Adherence in a Military Population
Continuous positive airway pressure therapy (CPAP) is the first-line treatment for obstructive sleep apnea (OSA) recommended by the American College of Physicians and the American Academy of Sleep Medicine.1,2 CPAP reduces the apnea hypopnea index (AHI), improves oxyhemoglobin desaturation, and reduces cortical arousals associated with apneic/hypopneic events.3 Despite being an effective treatment for OSA, a significant limitation of CPAP is treatment adherence. Factors associated with CPAP adherence include disease and patient characteristics, perceived self-efficacy, treatment titration procedure, device technology factors, adverse effects, and psychosocial factors.4
Recent studies suggest that insomnia and depression may be associated with OSA. According to a review by Luyster and colleagues, insomnia is present in 39% to 58% of patients with OSA.5 Since OSA may disturb sleep by the number of nightly awakenings, OSA may cause or worsen insomnia. Furthermore, insomnia may exacerbate sleep apnea thus impeding the effectiveness of sleep apnea treatment.
In some studies, the presence of insomnia symptoms prior to initiating CPAP treatment has been found to be associated with reduced CPAP adherence. For example, in 2010, Wickwire and colleagues found that there was a negative association with the average nightly minutes of CPAP use for those patients with OSA that reported symptoms of sleep maintenance insomnia.6 This was not found for those patients with OSA who reported symptoms of sleep onset insomnia or reported no insomnia at all. In another study by Pieh and colleagues, self-reported insomnia symptoms were predictive of CPAP adherence (defined as < 4 hours use/night) at a 6-month follow-up.7 However, results from a separate study indicated that insomnia was not associated with 6-month CPAP adherence.8
Depressive symptoms are commonly reported by patients with OSA, and higher rates of depressive symptomatology in patients with OSA have been observed in a number of prevalence studies when compared with the general population.9,10 Between 15% and 56% of patients with OSA are diagnosed with a depressive disorder compared with 6.6% of the general population.11 OSA may be causally related with depression or coexist as a separate disorder. Apnea severity has been shown to exacerbate depressive symptoms, and treatment with CPAP can improve depressive symptoms.12,13 Unfortunately, depression has been found to reduce CPAP adherence. For example, Law and colleagues found that depression was independently associated with poorer adherence during home-based auto-PAP titration.14 Furthermore, in a study by Gurlanick and colleagues, depressive symptoms were independently associated with reduced CPAP adherence in surgical patients with OSA.15
To the best of our knowledge, the combined impact of both insomnia and depression on CPAP adherence has not been investigated. In military populations this may be especially important as CPAP adherence has been reported to be worse in military patients with posttraumatic stress disorder (PTSD) and other psychiatric disorders, and there are increasing rates of insomnia and OSA in the military.16,17 We hypothesize that active-duty and retired military patients with self-reported insomnia and depression will have reduced short and long-term CPAP adherence.
Methods
This is a retrospective cohort study that reviewed charts of active-duty and retired military members diagnosed with OSA by the Sleep Medicine Clinic at Naval Medical Center San Diego in California using a home sleep test (HST). The HSTs were interpreted by board-certified physicians in sleep medicine. Prior to the HST, all patients completed a sleep questionnaire that included self-reports of daytime sleepiness, using the Epworth Sleepiness Scale (ESS), depression using the Center for Epidemiologic Studies Depression Scale (CES-D) and insomnia using the Insomnia Severity Index (ISI).
The study population included active-duty and veteran patients diagnosed with OSA who chose treatment with a CPAP and attended the sleep clinic’s OSA educational class, which discussed the diagnosis and treatment of OSA. Inclusion criteria were patients aged > 18 years and diagnosed with OSA at the Naval Medical Center San Diego sleep lab between June 2014 and June 2015.
The study population was stratified into 4 groups: (1) those with OSA but no self-reported depression or insomnia; (2) those with OSA and self-reported depression but no insomnia; (3) those with OSA and insomnia but no depression; and (4) those with OSA and self-reported depression and insomnia. Charts were excluded from the review if there were incomplete data or if the patient selected an alternative treatment for OSA, such as an oral appliance. A total of 120 charts were included in the final review. This study was approved by the Naval Medical Center San Diego Institutional Review Board.
Data Collection
Data collected included the individual’s age, sex, minimum oxygen saturation during sleep, body mass index (BMI), height, weight, ESS score at time of diagnosis, date of HST, and date of attendance at the clinic’s OSA group treatment class. Diagnosis of OSA was based on the patient’s ≥ 5 AHI. OSA severity was divided into mild (AHI 5-14), moderate (AHI 15-29), or severe (AHI ≥ 30). A patient with a CES-D score > 14 was considered to have clinically significant depression, and a patient with an ISI score of > 14 was considered to have clinically significant insomnia. ISI is a reliable and valid instrument to quantify perceived insomnia severity.18 The CES-D was used only as an indicator of symptoms relating to depression, not to clinically diagnose depression. It also has been used extensively to investigate levels of depression without a psychiatric diagnosis.19
Follow-up CPAP adherence was collected at 3- and 12-month intervals after the date of the patient’s OSA treatment group class and included AHI, median pressure setting, median days used, average time used per night, and percentage of days used for more than 4 hours for the previous 30 days. Data were obtained through Sleep Data and ResMed websites, which receive patient adherence data directly from the patient’s CPAP device. Patients were considered to be adherent with CPAP usage based on the Medicare definition: Use of the CPAP device > 4 hours per night for at least 70% of nights during a 30-day period). The 3-month time frame was used as a short interval because that is when patients are seen in the pulmonary clinic for their initial follow-up appointment. Patients are seen again at 12 months because durable medical equipment supplies must be reordered after 12 months, which requires a patient visit.
Statistical Analysis
Linear regression methods were used to characterize any potential relationships between the predictor variables and the target outcome variables associated with CPAP adherence at 3 and 12 months. Scatterplots were produced to assess whether linear structure was sufficient to characterize any detectable relationships, or whether there existed more complex, nonlinear relationships. The best-fitting linear regression line was examined in relation to the confidence bands of the corresponding LOESS line to determine whether a more complicated model structure was needed to capture the relationship.
Standard tests of assumptions required for these methods were also carried out: QQ plots of residuals to test for normality, the Durbin-Watson test for independence of residuals, and the nonconstant variance score test for heteroskedasticity (ie, Breusch-Pagan test). The results of these assumptions tests are reported only in cases in which the assumptions were revealed to be untenable. In cases in which suspicious outlying observations may have biased analyses, robust versions of the corresponding models were constructed. In no cases did the resulting conclusions change; only the results of the original analysis are reported. All analyses were carried out in R (R Foundation, r-project.org). Statistical significance was defined as P < .05.
Results
Our study population was predominately male (90%) with a median age of 41 years (range 22-65) and BMI of 29.8 (range 7.7-57.2)(Table 1). 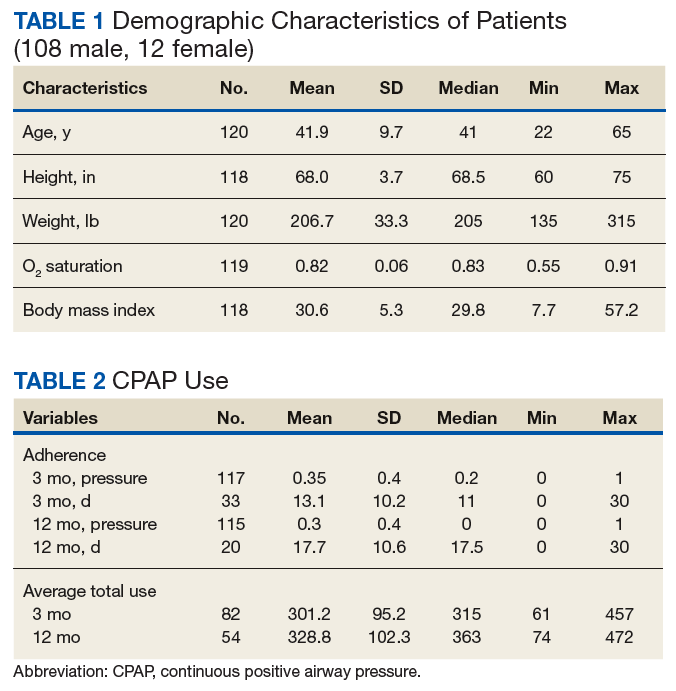
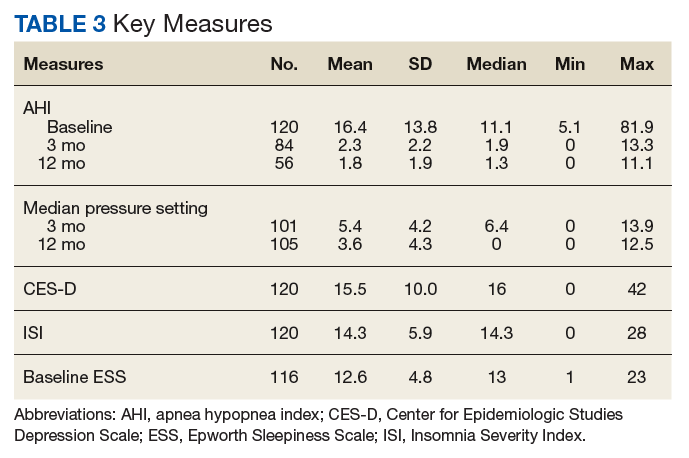
Predictors of CPAP Adherence
OSA severity, as measured by the AHI, was the only promising predictor of CPAP use at 3 months (b, 2.128; t80, 2.854; P = .005; adjusted R2, 0.081). The severity of self-reported daytime sleepiness prior to a diagnosis of OSA, as measured by the ESS, did not predict 3-month CPAP adherence (b, 0.688; t77, 0.300; P = .765; adjusted R2, -0.012). Self-reported depression as measured by the CES-D also did not predict CPAP use at 3 months (b, -0.078; t80, -0.014; P = .941; adjusted R2, -0.012). Similarly, self-reported insomnia, as measured by the ISI, did not predict 3-month CPAP adherence (b, 1.765; t80, 0.939; P = .350; adjusted R2, -0.001). Furthermore, a model that incorporated both depression and insomnia proved no better at accounting for variation in 3-month CPAP use (R2, -0.012). Demographic variables, such as age, sex, or BMI did not predict 3-month CPAP adherence (all Ps > .20). Finally, median CPAP pressure approached statistical significance as a predictor of 3-month CPAP adherence (b, 9.493; t66, 1.881; P = .064; adjusted R2, 0.037) (Figure 1). 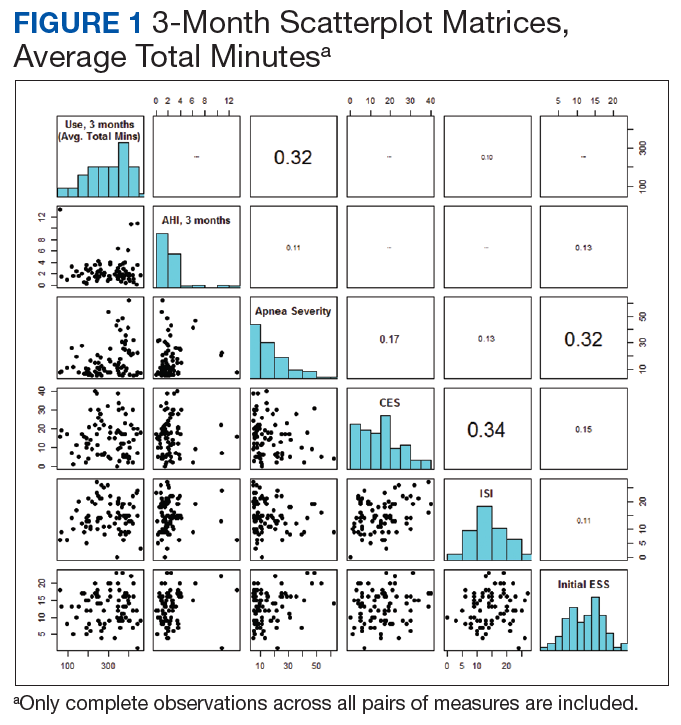
CPAP Use at 12 months
The results for CPAP use at 12 months mirrored the results for 3 months with one main exception: OSA severity, as measured by the AHI, did not predict CPAP use at 12 months (b, 1.158; t52, 1.245; P = .219; adjusted R2, 0.010). Neither adding a quadratic predictor nor log transforming the AHI values produced a better model (R2, -0.0007 vs R2, 0.0089, respectively). The severity of self-reported daytime sleepiness, as measured by the ESS, did not predict 12-month CPAP adherence (b, -2.201; t50, -0.752; P = .456; adjusted R2 = -0.0086). Self-reported depression as measured by the CES-D also did not predict CPAP use at 12 months (b, 0.034, t52, 0.022; P = .983; adjusted R2, -0.092). Self-reported insomnia, as measured by the ISI, also did not predict 12-month CPAP adherence (b, 1.765; t80, 0.939; P = .350; adjusted R2 = -0.001). Furthermore, a model that incorporated both depression and insomnia proved no better at accounting for variation in 12-month CPAP use, (R2, -0.0298). 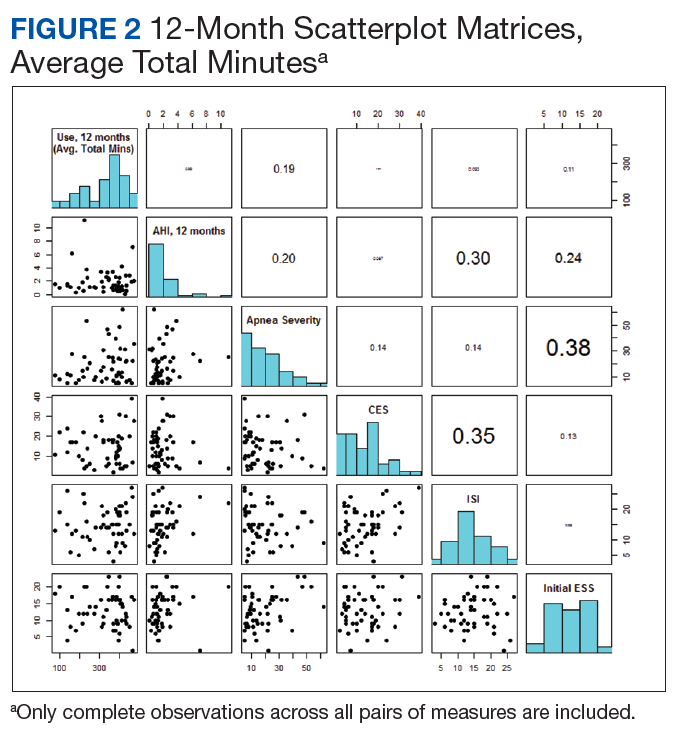
Discussion
Our study did not provide evidence that self-reported depressive and insomnia symptoms, as measured by the CES-D and ISI, can serve as useful predictors of short and long-term CPAP adherence in a sample of active-duty and retired military. OSA severity, as measured by the AHI, was the only promising predictor of CPAP adherence at 3 months.
Insomnia has been shown to improve with the use of CPAP. In a pilot study, Krakow and colleagues investigated the use of CPAP, oral appliances, or bilateral turbinectomy on patients with OSA and chronic insomnia.20 Objective measures of insomnia improved with 1 night of CPAP titration. Björnsdóttir and colleagues evaluated the long-term effects of positive airway pressure (PAP) treatment on 705 adults with middle insomnia.21 They found after 2 years of PAP treatment combined with cognitive behavioral therapy for insomnia, patients had reduced symptoms of middle insomnia. It is possible that persistent insomnia is associated with more severe OSA which was not studied in our population.22
As reported in other studies, it is possible that patients with depressive symptoms can improve with CPAP use, suggesting that depression and CPAP use are not totally unrelated. Edwards and colleagues studied the impact of CPAP on depressive symptoms in men and woman. They found that depressive symptoms are common in OSA and markedly improve with CPAP.23 Bopparaju and colleagues found a high prevalence of anxiety and depression in patients with OSA but did not influence CPAP adherence.24
The results of this study differ from some previous findings where depression was found to predict CPAP adherence.10 This may be due in part to differences in the type of instrument used to assess depression. Wells and colleagues found that baseline depressive symptoms did not correlate with CPAP adherence and that patients with greater CPAP adherence had improvement in OSA and depressive symptoms.25 Furthermore, patients with residual OSA symptoms using CPAP had more depressive symptoms, suggesting that it is the improvement in OSA symptoms that may be correlated with the improvement in depressive symptoms. Although soldiers with PTSD may have reduced CPAP adherence, use of CPAP is associated with improvement in PTSD symptoms.11,26
Limitations
This study had several limitations, including a small sample size. Study patients were also from a single institution, and the majority of patients had mild-to-moderate OSA. A multicenter prospective study with a larger sample size that included more severe patients with OSA may have shown different results. The participants in this study were limited to members from the active-duty and retired military population. The findings in this population may not be transferrable to the general public. Another study limitation was that the ISI and the CES-D were only administered prior to the initiation of CPAP. If the CES-D and ISI were administered at the 3- and 12-month follow-up visits, we could determine whether short and long-term CPAP improved these symptoms or whether there was no association between CPAP adherence with insomnia and depressive symptoms. Another limitation is that we did not have access to information about potential PTSD symptomatology, which has been associated with reduced CPAP adherence and is more common in a military and veteran population.11
Conclusion
This study found little evidence that symptoms of depression and insomnia are useful predictors of CPAP adherence, in either short- or long-term use, in an active-duty and retired military sample. Although these were not found to be predictors of CPAP adherence, further research will be necessary to determine whether CPAP adherence improves symptoms of depression and insomnia in military and veteran populations. Apnea severity did predict CPAP adherence in the short term, but not for any length of time beyond 3 months. More research is needed to explore strategies to improve CPAP adherence in military populations.
1. Qaseem A, Holty JE, Owens DK, Dallas P, Starkey M, Shekelle P; Clinical Guidelines Committee of the American College of Physicians. Management of obstructive sleep apnea in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2013;159(7):471-483.
2. Epstein LJ, Kristo D, Strollo PJ, et al; Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263-276.
3. Gay P, Weaver T, Loube D, Iber C; Positive Airway Pressure Task Force; Standards of Practice Committee; American Academy of Sleep Medicine. Evaluation of positive airway pressure treatment for sleep-related breathing disorders in adults. Sleep. 2006;29(3):381-401.
4. Sawyer AM, Gooneratne NS, Marcus CL, Ofer D, Richards KC, Weaver T. A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep Med Rev. 2011;15(6):343-356.
5. Luyster FS; Buysse DJ; Strollo PJ. Comorbid insomnia and obstructive sleep apnea: challenges for clinical practice and research. J Clin Sleep Med. 2010;6(2):196-204.
6. Wickwire EM, Smith MT, Birnbaum S, Collop NA. Sleep maintenance insomnia complaints predict poor CPAP adherence: a clinical case series. Sleep Med. 2010;11(8):772-776
7. Pieh C, Bach M, Popp R, et al. Insomnia symptoms influence CPAP compliance. Sleep Breath. 2013;17(1):99-104.
8. Nguyên XL, Chaskalovic J, Rakotonanahary D, Fleury B. Insomnia symptoms and CPAP compliance in OSAS patients: a descriptive study using data mining methods. Sleep Med. 2010;11(8):777-784.
9. Yilmaz E, Sedky K, Bennett DS. The relationship between depressive symptoms and obstructive sleep apnea in pediatric populations: a meta-analysis. J Clin Sleep Med. 2013;9(11):1213-1220.
10. Chen YH, Keller JK, Kang JH, Hsieh HJ, Lin HC. Obstructive sleep apnea and the subsequent risk of depressive disorder: a population-based follow-up study. J Clin Sleep Med. 2013;9(5):417-423.
11. Kessler RC, Berglund P, Demler O, et al; National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003:289(23):3095-3105
12. Harris M, Glozier N, Ratnavadivel R, Grunstein RR. Obstructive sleep apnea and depression. Sleep Med Rev. 2009;13(6):437-444.
13. Schwartz D, Kohler W, Karatinos G. Symptoms of depression in individuals with obstructive sleep apnea may be amendable to treatment with continuous positive airway pressure. Chest. 2005;128(3):1304-1309
14. Law M, Naughton M, Ho S, Roebuck T, Dabscheck E. Depression may reduce adherence during CPAP titration trial. J Clin Sleep Med. 2014;10(2):163-169.
15. Guralnick AS, Pant M, Minhaj M, Sweitzer BJ, Mokhlesi B. CPAP adherence in patients with newly diagnosed obstructive sleep apnea prior to elective surgery. J Clin Sleep Med. 2012;8(5):501-506
16. Collen JF, Lettieri CJ, Hoffman M. The impact of posttraumatic stress disorder on CPAP adherence in patients with obstructive sleep apnea. J Clin Sleep Med. 2012;8(6):667-672.
17. Caldwell A, Knapik JJ, Lieberman HR. Trends and factors associated with insomnia and sleep apnea in all United States military service members from 2005 to 2014. J Sleep Res. 2017;26(5):665-670.
18. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297-307.
19. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychological Measurement. 1977;1(3):385-401.
20. Krakow B, Melendrez D, Lee SA, Warner TD, Clark JO, Sklar D. Refractory insomnia and sleep-disordered breathing: a pilot study. Sleep Breath. 2004;8(1):15-29.
21. Björnsdóttir E, Janson C, Sigurdsson JF, et al. Symptoms of insomnia among patients with obstructive sleep apnea before and after two years of positive airway pressure treatment. Sleep. 2013;36(12):1901-1909.
22. Glidewell RN, Renn BN, Roby E, Orr WC. Predictors and patterns of insomnia symptoms in OSA before and after PAP therapy. Sleep Med. 2014;15(8):899-905.
23. Edwards C, Mukherjee S, Simpson L, Palmer LJ, Almeida OP, Hillman DR. Depressive symptoms before and after treatment of obstructive sleep apnea in men and women. J Clin Sleep Med. 2015;11(9):1029-1038.
24. Bopparaju S, Casturi L, Guntupalli B, Surani S, Subramanian S. Anxiety and depression in obstructive sleep apnea: Effect of CPAP therapy and influence on CPAP compliance. Presented at: American College of Chest Physicians Annual Meeting, October 31-November 05, 2009; San Diego, CA. Chest. 2009;136(4, meeting abstracts):71S.
25. Wells RD, Freedland KE, Carney RM, Duntley SP, Stepanski EJ. Adherence, reports of benefits, and depression among patients treated with continuous positive airway pressure. Psychosom Med. 2007;69(5):449-454.
26. Orr JE, Smales C, Alexander TH, et al. Treatment of OSA with CPAP is associated with improvement in PTSD symptoms among veterans. J Clin Sleep Med. 2017;13(1):57-63.
Continuous positive airway pressure therapy (CPAP) is the first-line treatment for obstructive sleep apnea (OSA) recommended by the American College of Physicians and the American Academy of Sleep Medicine.1,2 CPAP reduces the apnea hypopnea index (AHI), improves oxyhemoglobin desaturation, and reduces cortical arousals associated with apneic/hypopneic events.3 Despite being an effective treatment for OSA, a significant limitation of CPAP is treatment adherence. Factors associated with CPAP adherence include disease and patient characteristics, perceived self-efficacy, treatment titration procedure, device technology factors, adverse effects, and psychosocial factors.4
Recent studies suggest that insomnia and depression may be associated with OSA. According to a review by Luyster and colleagues, insomnia is present in 39% to 58% of patients with OSA.5 Since OSA may disturb sleep by the number of nightly awakenings, OSA may cause or worsen insomnia. Furthermore, insomnia may exacerbate sleep apnea thus impeding the effectiveness of sleep apnea treatment.
In some studies, the presence of insomnia symptoms prior to initiating CPAP treatment has been found to be associated with reduced CPAP adherence. For example, in 2010, Wickwire and colleagues found that there was a negative association with the average nightly minutes of CPAP use for those patients with OSA that reported symptoms of sleep maintenance insomnia.6 This was not found for those patients with OSA who reported symptoms of sleep onset insomnia or reported no insomnia at all. In another study by Pieh and colleagues, self-reported insomnia symptoms were predictive of CPAP adherence (defined as < 4 hours use/night) at a 6-month follow-up.7 However, results from a separate study indicated that insomnia was not associated with 6-month CPAP adherence.8
Depressive symptoms are commonly reported by patients with OSA, and higher rates of depressive symptomatology in patients with OSA have been observed in a number of prevalence studies when compared with the general population.9,10 Between 15% and 56% of patients with OSA are diagnosed with a depressive disorder compared with 6.6% of the general population.11 OSA may be causally related with depression or coexist as a separate disorder. Apnea severity has been shown to exacerbate depressive symptoms, and treatment with CPAP can improve depressive symptoms.12,13 Unfortunately, depression has been found to reduce CPAP adherence. For example, Law and colleagues found that depression was independently associated with poorer adherence during home-based auto-PAP titration.14 Furthermore, in a study by Gurlanick and colleagues, depressive symptoms were independently associated with reduced CPAP adherence in surgical patients with OSA.15
To the best of our knowledge, the combined impact of both insomnia and depression on CPAP adherence has not been investigated. In military populations this may be especially important as CPAP adherence has been reported to be worse in military patients with posttraumatic stress disorder (PTSD) and other psychiatric disorders, and there are increasing rates of insomnia and OSA in the military.16,17 We hypothesize that active-duty and retired military patients with self-reported insomnia and depression will have reduced short and long-term CPAP adherence.
Methods
This is a retrospective cohort study that reviewed charts of active-duty and retired military members diagnosed with OSA by the Sleep Medicine Clinic at Naval Medical Center San Diego in California using a home sleep test (HST). The HSTs were interpreted by board-certified physicians in sleep medicine. Prior to the HST, all patients completed a sleep questionnaire that included self-reports of daytime sleepiness, using the Epworth Sleepiness Scale (ESS), depression using the Center for Epidemiologic Studies Depression Scale (CES-D) and insomnia using the Insomnia Severity Index (ISI).
The study population included active-duty and veteran patients diagnosed with OSA who chose treatment with a CPAP and attended the sleep clinic’s OSA educational class, which discussed the diagnosis and treatment of OSA. Inclusion criteria were patients aged > 18 years and diagnosed with OSA at the Naval Medical Center San Diego sleep lab between June 2014 and June 2015.
The study population was stratified into 4 groups: (1) those with OSA but no self-reported depression or insomnia; (2) those with OSA and self-reported depression but no insomnia; (3) those with OSA and insomnia but no depression; and (4) those with OSA and self-reported depression and insomnia. Charts were excluded from the review if there were incomplete data or if the patient selected an alternative treatment for OSA, such as an oral appliance. A total of 120 charts were included in the final review. This study was approved by the Naval Medical Center San Diego Institutional Review Board.
Data Collection
Data collected included the individual’s age, sex, minimum oxygen saturation during sleep, body mass index (BMI), height, weight, ESS score at time of diagnosis, date of HST, and date of attendance at the clinic’s OSA group treatment class. Diagnosis of OSA was based on the patient’s ≥ 5 AHI. OSA severity was divided into mild (AHI 5-14), moderate (AHI 15-29), or severe (AHI ≥ 30). A patient with a CES-D score > 14 was considered to have clinically significant depression, and a patient with an ISI score of > 14 was considered to have clinically significant insomnia. ISI is a reliable and valid instrument to quantify perceived insomnia severity.18 The CES-D was used only as an indicator of symptoms relating to depression, not to clinically diagnose depression. It also has been used extensively to investigate levels of depression without a psychiatric diagnosis.19
Follow-up CPAP adherence was collected at 3- and 12-month intervals after the date of the patient’s OSA treatment group class and included AHI, median pressure setting, median days used, average time used per night, and percentage of days used for more than 4 hours for the previous 30 days. Data were obtained through Sleep Data and ResMed websites, which receive patient adherence data directly from the patient’s CPAP device. Patients were considered to be adherent with CPAP usage based on the Medicare definition: Use of the CPAP device > 4 hours per night for at least 70% of nights during a 30-day period). The 3-month time frame was used as a short interval because that is when patients are seen in the pulmonary clinic for their initial follow-up appointment. Patients are seen again at 12 months because durable medical equipment supplies must be reordered after 12 months, which requires a patient visit.
Statistical Analysis
Linear regression methods were used to characterize any potential relationships between the predictor variables and the target outcome variables associated with CPAP adherence at 3 and 12 months. Scatterplots were produced to assess whether linear structure was sufficient to characterize any detectable relationships, or whether there existed more complex, nonlinear relationships. The best-fitting linear regression line was examined in relation to the confidence bands of the corresponding LOESS line to determine whether a more complicated model structure was needed to capture the relationship.
Standard tests of assumptions required for these methods were also carried out: QQ plots of residuals to test for normality, the Durbin-Watson test for independence of residuals, and the nonconstant variance score test for heteroskedasticity (ie, Breusch-Pagan test). The results of these assumptions tests are reported only in cases in which the assumptions were revealed to be untenable. In cases in which suspicious outlying observations may have biased analyses, robust versions of the corresponding models were constructed. In no cases did the resulting conclusions change; only the results of the original analysis are reported. All analyses were carried out in R (R Foundation, r-project.org). Statistical significance was defined as P < .05.
Results
Our study population was predominately male (90%) with a median age of 41 years (range 22-65) and BMI of 29.8 (range 7.7-57.2)(Table 1).
Predictors of CPAP Adherence
OSA severity, as measured by the AHI, was the only promising predictor of CPAP use at 3 months (b, 2.128; t80, 2.854; P = .005; adjusted R2, 0.081). The severity of self-reported daytime sleepiness prior to a diagnosis of OSA, as measured by the ESS, did not predict 3-month CPAP adherence (b, 0.688; t77, 0.300; P = .765; adjusted R2, -0.012). Self-reported depression as measured by the CES-D also did not predict CPAP use at 3 months (b, -0.078; t80, -0.014; P = .941; adjusted R2, -0.012). Similarly, self-reported insomnia, as measured by the ISI, did not predict 3-month CPAP adherence (b, 1.765; t80, 0.939; P = .350; adjusted R2, -0.001). Furthermore, a model that incorporated both depression and insomnia proved no better at accounting for variation in 3-month CPAP use (R2, -0.012). Demographic variables, such as age, sex, or BMI did not predict 3-month CPAP adherence (all Ps > .20). Finally, median CPAP pressure approached statistical significance as a predictor of 3-month CPAP adherence (b, 9.493; t66, 1.881; P = .064; adjusted R2, 0.037) (Figure 1).
CPAP Use at 12 months
The results for CPAP use at 12 months mirrored the results for 3 months with one main exception: OSA severity, as measured by the AHI, did not predict CPAP use at 12 months (b, 1.158; t52, 1.245; P = .219; adjusted R2, 0.010). Neither adding a quadratic predictor nor log transforming the AHI values produced a better model (R2, -0.0007 vs R2, 0.0089, respectively). The severity of self-reported daytime sleepiness, as measured by the ESS, did not predict 12-month CPAP adherence (b, -2.201; t50, -0.752; P = .456; adjusted R2 = -0.0086). Self-reported depression as measured by the CES-D also did not predict CPAP use at 12 months (b, 0.034, t52, 0.022; P = .983; adjusted R2, -0.092). Self-reported insomnia, as measured by the ISI, also did not predict 12-month CPAP adherence (b, 1.765; t80, 0.939; P = .350; adjusted R2 = -0.001). Furthermore, a model that incorporated both depression and insomnia proved no better at accounting for variation in 12-month CPAP use, (R2, -0.0298).
Discussion
Our study did not provide evidence that self-reported depressive and insomnia symptoms, as measured by the CES-D and ISI, can serve as useful predictors of short and long-term CPAP adherence in a sample of active-duty and retired military. OSA severity, as measured by the AHI, was the only promising predictor of CPAP adherence at 3 months.
Insomnia has been shown to improve with the use of CPAP. In a pilot study, Krakow and colleagues investigated the use of CPAP, oral appliances, or bilateral turbinectomy on patients with OSA and chronic insomnia.20 Objective measures of insomnia improved with 1 night of CPAP titration. Björnsdóttir and colleagues evaluated the long-term effects of positive airway pressure (PAP) treatment on 705 adults with middle insomnia.21 They found after 2 years of PAP treatment combined with cognitive behavioral therapy for insomnia, patients had reduced symptoms of middle insomnia. It is possible that persistent insomnia is associated with more severe OSA which was not studied in our population.22
As reported in other studies, it is possible that patients with depressive symptoms can improve with CPAP use, suggesting that depression and CPAP use are not totally unrelated. Edwards and colleagues studied the impact of CPAP on depressive symptoms in men and woman. They found that depressive symptoms are common in OSA and markedly improve with CPAP.23 Bopparaju and colleagues found a high prevalence of anxiety and depression in patients with OSA but did not influence CPAP adherence.24
The results of this study differ from some previous findings where depression was found to predict CPAP adherence.10 This may be due in part to differences in the type of instrument used to assess depression. Wells and colleagues found that baseline depressive symptoms did not correlate with CPAP adherence and that patients with greater CPAP adherence had improvement in OSA and depressive symptoms.25 Furthermore, patients with residual OSA symptoms using CPAP had more depressive symptoms, suggesting that it is the improvement in OSA symptoms that may be correlated with the improvement in depressive symptoms. Although soldiers with PTSD may have reduced CPAP adherence, use of CPAP is associated with improvement in PTSD symptoms.11,26
Limitations
This study had several limitations, including a small sample size. Study patients were also from a single institution, and the majority of patients had mild-to-moderate OSA. A multicenter prospective study with a larger sample size that included more severe patients with OSA may have shown different results. The participants in this study were limited to members from the active-duty and retired military population. The findings in this population may not be transferrable to the general public. Another study limitation was that the ISI and the CES-D were only administered prior to the initiation of CPAP. If the CES-D and ISI were administered at the 3- and 12-month follow-up visits, we could determine whether short and long-term CPAP improved these symptoms or whether there was no association between CPAP adherence with insomnia and depressive symptoms. Another limitation is that we did not have access to information about potential PTSD symptomatology, which has been associated with reduced CPAP adherence and is more common in a military and veteran population.11
Conclusion
This study found little evidence that symptoms of depression and insomnia are useful predictors of CPAP adherence, in either short- or long-term use, in an active-duty and retired military sample. Although these were not found to be predictors of CPAP adherence, further research will be necessary to determine whether CPAP adherence improves symptoms of depression and insomnia in military and veteran populations. Apnea severity did predict CPAP adherence in the short term, but not for any length of time beyond 3 months. More research is needed to explore strategies to improve CPAP adherence in military populations.
Continuous positive airway pressure therapy (CPAP) is the first-line treatment for obstructive sleep apnea (OSA) recommended by the American College of Physicians and the American Academy of Sleep Medicine.1,2 CPAP reduces the apnea hypopnea index (AHI), improves oxyhemoglobin desaturation, and reduces cortical arousals associated with apneic/hypopneic events.3 Despite being an effective treatment for OSA, a significant limitation of CPAP is treatment adherence. Factors associated with CPAP adherence include disease and patient characteristics, perceived self-efficacy, treatment titration procedure, device technology factors, adverse effects, and psychosocial factors.4
Recent studies suggest that insomnia and depression may be associated with OSA. According to a review by Luyster and colleagues, insomnia is present in 39% to 58% of patients with OSA.5 Since OSA may disturb sleep by the number of nightly awakenings, OSA may cause or worsen insomnia. Furthermore, insomnia may exacerbate sleep apnea thus impeding the effectiveness of sleep apnea treatment.
In some studies, the presence of insomnia symptoms prior to initiating CPAP treatment has been found to be associated with reduced CPAP adherence. For example, in 2010, Wickwire and colleagues found that there was a negative association with the average nightly minutes of CPAP use for those patients with OSA that reported symptoms of sleep maintenance insomnia.6 This was not found for those patients with OSA who reported symptoms of sleep onset insomnia or reported no insomnia at all. In another study by Pieh and colleagues, self-reported insomnia symptoms were predictive of CPAP adherence (defined as < 4 hours use/night) at a 6-month follow-up.7 However, results from a separate study indicated that insomnia was not associated with 6-month CPAP adherence.8
Depressive symptoms are commonly reported by patients with OSA, and higher rates of depressive symptomatology in patients with OSA have been observed in a number of prevalence studies when compared with the general population.9,10 Between 15% and 56% of patients with OSA are diagnosed with a depressive disorder compared with 6.6% of the general population.11 OSA may be causally related with depression or coexist as a separate disorder. Apnea severity has been shown to exacerbate depressive symptoms, and treatment with CPAP can improve depressive symptoms.12,13 Unfortunately, depression has been found to reduce CPAP adherence. For example, Law and colleagues found that depression was independently associated with poorer adherence during home-based auto-PAP titration.14 Furthermore, in a study by Gurlanick and colleagues, depressive symptoms were independently associated with reduced CPAP adherence in surgical patients with OSA.15
To the best of our knowledge, the combined impact of both insomnia and depression on CPAP adherence has not been investigated. In military populations this may be especially important as CPAP adherence has been reported to be worse in military patients with posttraumatic stress disorder (PTSD) and other psychiatric disorders, and there are increasing rates of insomnia and OSA in the military.16,17 We hypothesize that active-duty and retired military patients with self-reported insomnia and depression will have reduced short and long-term CPAP adherence.
Methods
This is a retrospective cohort study that reviewed charts of active-duty and retired military members diagnosed with OSA by the Sleep Medicine Clinic at Naval Medical Center San Diego in California using a home sleep test (HST). The HSTs were interpreted by board-certified physicians in sleep medicine. Prior to the HST, all patients completed a sleep questionnaire that included self-reports of daytime sleepiness, using the Epworth Sleepiness Scale (ESS), depression using the Center for Epidemiologic Studies Depression Scale (CES-D) and insomnia using the Insomnia Severity Index (ISI).
The study population included active-duty and veteran patients diagnosed with OSA who chose treatment with a CPAP and attended the sleep clinic’s OSA educational class, which discussed the diagnosis and treatment of OSA. Inclusion criteria were patients aged > 18 years and diagnosed with OSA at the Naval Medical Center San Diego sleep lab between June 2014 and June 2015.
The study population was stratified into 4 groups: (1) those with OSA but no self-reported depression or insomnia; (2) those with OSA and self-reported depression but no insomnia; (3) those with OSA and insomnia but no depression; and (4) those with OSA and self-reported depression and insomnia. Charts were excluded from the review if there were incomplete data or if the patient selected an alternative treatment for OSA, such as an oral appliance. A total of 120 charts were included in the final review. This study was approved by the Naval Medical Center San Diego Institutional Review Board.
Data Collection
Data collected included the individual’s age, sex, minimum oxygen saturation during sleep, body mass index (BMI), height, weight, ESS score at time of diagnosis, date of HST, and date of attendance at the clinic’s OSA group treatment class. Diagnosis of OSA was based on the patient’s ≥ 5 AHI. OSA severity was divided into mild (AHI 5-14), moderate (AHI 15-29), or severe (AHI ≥ 30). A patient with a CES-D score > 14 was considered to have clinically significant depression, and a patient with an ISI score of > 14 was considered to have clinically significant insomnia. ISI is a reliable and valid instrument to quantify perceived insomnia severity.18 The CES-D was used only as an indicator of symptoms relating to depression, not to clinically diagnose depression. It also has been used extensively to investigate levels of depression without a psychiatric diagnosis.19
Follow-up CPAP adherence was collected at 3- and 12-month intervals after the date of the patient’s OSA treatment group class and included AHI, median pressure setting, median days used, average time used per night, and percentage of days used for more than 4 hours for the previous 30 days. Data were obtained through Sleep Data and ResMed websites, which receive patient adherence data directly from the patient’s CPAP device. Patients were considered to be adherent with CPAP usage based on the Medicare definition: Use of the CPAP device > 4 hours per night for at least 70% of nights during a 30-day period). The 3-month time frame was used as a short interval because that is when patients are seen in the pulmonary clinic for their initial follow-up appointment. Patients are seen again at 12 months because durable medical equipment supplies must be reordered after 12 months, which requires a patient visit.
Statistical Analysis
Linear regression methods were used to characterize any potential relationships between the predictor variables and the target outcome variables associated with CPAP adherence at 3 and 12 months. Scatterplots were produced to assess whether linear structure was sufficient to characterize any detectable relationships, or whether there existed more complex, nonlinear relationships. The best-fitting linear regression line was examined in relation to the confidence bands of the corresponding LOESS line to determine whether a more complicated model structure was needed to capture the relationship.
Standard tests of assumptions required for these methods were also carried out: QQ plots of residuals to test for normality, the Durbin-Watson test for independence of residuals, and the nonconstant variance score test for heteroskedasticity (ie, Breusch-Pagan test). The results of these assumptions tests are reported only in cases in which the assumptions were revealed to be untenable. In cases in which suspicious outlying observations may have biased analyses, robust versions of the corresponding models were constructed. In no cases did the resulting conclusions change; only the results of the original analysis are reported. All analyses were carried out in R (R Foundation, r-project.org). Statistical significance was defined as P < .05.
Results
Our study population was predominately male (90%) with a median age of 41 years (range 22-65) and BMI of 29.8 (range 7.7-57.2)(Table 1).
Predictors of CPAP Adherence
OSA severity, as measured by the AHI, was the only promising predictor of CPAP use at 3 months (b, 2.128; t80, 2.854; P = .005; adjusted R2, 0.081). The severity of self-reported daytime sleepiness prior to a diagnosis of OSA, as measured by the ESS, did not predict 3-month CPAP adherence (b, 0.688; t77, 0.300; P = .765; adjusted R2, -0.012). Self-reported depression as measured by the CES-D also did not predict CPAP use at 3 months (b, -0.078; t80, -0.014; P = .941; adjusted R2, -0.012). Similarly, self-reported insomnia, as measured by the ISI, did not predict 3-month CPAP adherence (b, 1.765; t80, 0.939; P = .350; adjusted R2, -0.001). Furthermore, a model that incorporated both depression and insomnia proved no better at accounting for variation in 3-month CPAP use (R2, -0.012). Demographic variables, such as age, sex, or BMI did not predict 3-month CPAP adherence (all Ps > .20). Finally, median CPAP pressure approached statistical significance as a predictor of 3-month CPAP adherence (b, 9.493; t66, 1.881; P = .064; adjusted R2, 0.037) (Figure 1).
CPAP Use at 12 months
The results for CPAP use at 12 months mirrored the results for 3 months with one main exception: OSA severity, as measured by the AHI, did not predict CPAP use at 12 months (b, 1.158; t52, 1.245; P = .219; adjusted R2, 0.010). Neither adding a quadratic predictor nor log transforming the AHI values produced a better model (R2, -0.0007 vs R2, 0.0089, respectively). The severity of self-reported daytime sleepiness, as measured by the ESS, did not predict 12-month CPAP adherence (b, -2.201; t50, -0.752; P = .456; adjusted R2 = -0.0086). Self-reported depression as measured by the CES-D also did not predict CPAP use at 12 months (b, 0.034, t52, 0.022; P = .983; adjusted R2, -0.092). Self-reported insomnia, as measured by the ISI, also did not predict 12-month CPAP adherence (b, 1.765; t80, 0.939; P = .350; adjusted R2 = -0.001). Furthermore, a model that incorporated both depression and insomnia proved no better at accounting for variation in 12-month CPAP use, (R2, -0.0298).
Discussion
Our study did not provide evidence that self-reported depressive and insomnia symptoms, as measured by the CES-D and ISI, can serve as useful predictors of short and long-term CPAP adherence in a sample of active-duty and retired military. OSA severity, as measured by the AHI, was the only promising predictor of CPAP adherence at 3 months.
Insomnia has been shown to improve with the use of CPAP. In a pilot study, Krakow and colleagues investigated the use of CPAP, oral appliances, or bilateral turbinectomy on patients with OSA and chronic insomnia.20 Objective measures of insomnia improved with 1 night of CPAP titration. Björnsdóttir and colleagues evaluated the long-term effects of positive airway pressure (PAP) treatment on 705 adults with middle insomnia.21 They found after 2 years of PAP treatment combined with cognitive behavioral therapy for insomnia, patients had reduced symptoms of middle insomnia. It is possible that persistent insomnia is associated with more severe OSA which was not studied in our population.22
As reported in other studies, it is possible that patients with depressive symptoms can improve with CPAP use, suggesting that depression and CPAP use are not totally unrelated. Edwards and colleagues studied the impact of CPAP on depressive symptoms in men and woman. They found that depressive symptoms are common in OSA and markedly improve with CPAP.23 Bopparaju and colleagues found a high prevalence of anxiety and depression in patients with OSA but did not influence CPAP adherence.24
The results of this study differ from some previous findings where depression was found to predict CPAP adherence.10 This may be due in part to differences in the type of instrument used to assess depression. Wells and colleagues found that baseline depressive symptoms did not correlate with CPAP adherence and that patients with greater CPAP adherence had improvement in OSA and depressive symptoms.25 Furthermore, patients with residual OSA symptoms using CPAP had more depressive symptoms, suggesting that it is the improvement in OSA symptoms that may be correlated with the improvement in depressive symptoms. Although soldiers with PTSD may have reduced CPAP adherence, use of CPAP is associated with improvement in PTSD symptoms.11,26
Limitations
This study had several limitations, including a small sample size. Study patients were also from a single institution, and the majority of patients had mild-to-moderate OSA. A multicenter prospective study with a larger sample size that included more severe patients with OSA may have shown different results. The participants in this study were limited to members from the active-duty and retired military population. The findings in this population may not be transferrable to the general public. Another study limitation was that the ISI and the CES-D were only administered prior to the initiation of CPAP. If the CES-D and ISI were administered at the 3- and 12-month follow-up visits, we could determine whether short and long-term CPAP improved these symptoms or whether there was no association between CPAP adherence with insomnia and depressive symptoms. Another limitation is that we did not have access to information about potential PTSD symptomatology, which has been associated with reduced CPAP adherence and is more common in a military and veteran population.11
Conclusion
This study found little evidence that symptoms of depression and insomnia are useful predictors of CPAP adherence, in either short- or long-term use, in an active-duty and retired military sample. Although these were not found to be predictors of CPAP adherence, further research will be necessary to determine whether CPAP adherence improves symptoms of depression and insomnia in military and veteran populations. Apnea severity did predict CPAP adherence in the short term, but not for any length of time beyond 3 months. More research is needed to explore strategies to improve CPAP adherence in military populations.
1. Qaseem A, Holty JE, Owens DK, Dallas P, Starkey M, Shekelle P; Clinical Guidelines Committee of the American College of Physicians. Management of obstructive sleep apnea in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2013;159(7):471-483.
2. Epstein LJ, Kristo D, Strollo PJ, et al; Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263-276.
3. Gay P, Weaver T, Loube D, Iber C; Positive Airway Pressure Task Force; Standards of Practice Committee; American Academy of Sleep Medicine. Evaluation of positive airway pressure treatment for sleep-related breathing disorders in adults. Sleep. 2006;29(3):381-401.
4. Sawyer AM, Gooneratne NS, Marcus CL, Ofer D, Richards KC, Weaver T. A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep Med Rev. 2011;15(6):343-356.
5. Luyster FS; Buysse DJ; Strollo PJ. Comorbid insomnia and obstructive sleep apnea: challenges for clinical practice and research. J Clin Sleep Med. 2010;6(2):196-204.
6. Wickwire EM, Smith MT, Birnbaum S, Collop NA. Sleep maintenance insomnia complaints predict poor CPAP adherence: a clinical case series. Sleep Med. 2010;11(8):772-776
7. Pieh C, Bach M, Popp R, et al. Insomnia symptoms influence CPAP compliance. Sleep Breath. 2013;17(1):99-104.
8. Nguyên XL, Chaskalovic J, Rakotonanahary D, Fleury B. Insomnia symptoms and CPAP compliance in OSAS patients: a descriptive study using data mining methods. Sleep Med. 2010;11(8):777-784.
9. Yilmaz E, Sedky K, Bennett DS. The relationship between depressive symptoms and obstructive sleep apnea in pediatric populations: a meta-analysis. J Clin Sleep Med. 2013;9(11):1213-1220.
10. Chen YH, Keller JK, Kang JH, Hsieh HJ, Lin HC. Obstructive sleep apnea and the subsequent risk of depressive disorder: a population-based follow-up study. J Clin Sleep Med. 2013;9(5):417-423.
11. Kessler RC, Berglund P, Demler O, et al; National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003:289(23):3095-3105
12. Harris M, Glozier N, Ratnavadivel R, Grunstein RR. Obstructive sleep apnea and depression. Sleep Med Rev. 2009;13(6):437-444.
13. Schwartz D, Kohler W, Karatinos G. Symptoms of depression in individuals with obstructive sleep apnea may be amendable to treatment with continuous positive airway pressure. Chest. 2005;128(3):1304-1309
14. Law M, Naughton M, Ho S, Roebuck T, Dabscheck E. Depression may reduce adherence during CPAP titration trial. J Clin Sleep Med. 2014;10(2):163-169.
15. Guralnick AS, Pant M, Minhaj M, Sweitzer BJ, Mokhlesi B. CPAP adherence in patients with newly diagnosed obstructive sleep apnea prior to elective surgery. J Clin Sleep Med. 2012;8(5):501-506
16. Collen JF, Lettieri CJ, Hoffman M. The impact of posttraumatic stress disorder on CPAP adherence in patients with obstructive sleep apnea. J Clin Sleep Med. 2012;8(6):667-672.
17. Caldwell A, Knapik JJ, Lieberman HR. Trends and factors associated with insomnia and sleep apnea in all United States military service members from 2005 to 2014. J Sleep Res. 2017;26(5):665-670.
18. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297-307.
19. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychological Measurement. 1977;1(3):385-401.
20. Krakow B, Melendrez D, Lee SA, Warner TD, Clark JO, Sklar D. Refractory insomnia and sleep-disordered breathing: a pilot study. Sleep Breath. 2004;8(1):15-29.
21. Björnsdóttir E, Janson C, Sigurdsson JF, et al. Symptoms of insomnia among patients with obstructive sleep apnea before and after two years of positive airway pressure treatment. Sleep. 2013;36(12):1901-1909.
22. Glidewell RN, Renn BN, Roby E, Orr WC. Predictors and patterns of insomnia symptoms in OSA before and after PAP therapy. Sleep Med. 2014;15(8):899-905.
23. Edwards C, Mukherjee S, Simpson L, Palmer LJ, Almeida OP, Hillman DR. Depressive symptoms before and after treatment of obstructive sleep apnea in men and women. J Clin Sleep Med. 2015;11(9):1029-1038.
24. Bopparaju S, Casturi L, Guntupalli B, Surani S, Subramanian S. Anxiety and depression in obstructive sleep apnea: Effect of CPAP therapy and influence on CPAP compliance. Presented at: American College of Chest Physicians Annual Meeting, October 31-November 05, 2009; San Diego, CA. Chest. 2009;136(4, meeting abstracts):71S.
25. Wells RD, Freedland KE, Carney RM, Duntley SP, Stepanski EJ. Adherence, reports of benefits, and depression among patients treated with continuous positive airway pressure. Psychosom Med. 2007;69(5):449-454.
26. Orr JE, Smales C, Alexander TH, et al. Treatment of OSA with CPAP is associated with improvement in PTSD symptoms among veterans. J Clin Sleep Med. 2017;13(1):57-63.
1. Qaseem A, Holty JE, Owens DK, Dallas P, Starkey M, Shekelle P; Clinical Guidelines Committee of the American College of Physicians. Management of obstructive sleep apnea in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2013;159(7):471-483.
2. Epstein LJ, Kristo D, Strollo PJ, et al; Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263-276.
3. Gay P, Weaver T, Loube D, Iber C; Positive Airway Pressure Task Force; Standards of Practice Committee; American Academy of Sleep Medicine. Evaluation of positive airway pressure treatment for sleep-related breathing disorders in adults. Sleep. 2006;29(3):381-401.
4. Sawyer AM, Gooneratne NS, Marcus CL, Ofer D, Richards KC, Weaver T. A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep Med Rev. 2011;15(6):343-356.
5. Luyster FS; Buysse DJ; Strollo PJ. Comorbid insomnia and obstructive sleep apnea: challenges for clinical practice and research. J Clin Sleep Med. 2010;6(2):196-204.
6. Wickwire EM, Smith MT, Birnbaum S, Collop NA. Sleep maintenance insomnia complaints predict poor CPAP adherence: a clinical case series. Sleep Med. 2010;11(8):772-776
7. Pieh C, Bach M, Popp R, et al. Insomnia symptoms influence CPAP compliance. Sleep Breath. 2013;17(1):99-104.
8. Nguyên XL, Chaskalovic J, Rakotonanahary D, Fleury B. Insomnia symptoms and CPAP compliance in OSAS patients: a descriptive study using data mining methods. Sleep Med. 2010;11(8):777-784.
9. Yilmaz E, Sedky K, Bennett DS. The relationship between depressive symptoms and obstructive sleep apnea in pediatric populations: a meta-analysis. J Clin Sleep Med. 2013;9(11):1213-1220.
10. Chen YH, Keller JK, Kang JH, Hsieh HJ, Lin HC. Obstructive sleep apnea and the subsequent risk of depressive disorder: a population-based follow-up study. J Clin Sleep Med. 2013;9(5):417-423.
11. Kessler RC, Berglund P, Demler O, et al; National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003:289(23):3095-3105
12. Harris M, Glozier N, Ratnavadivel R, Grunstein RR. Obstructive sleep apnea and depression. Sleep Med Rev. 2009;13(6):437-444.
13. Schwartz D, Kohler W, Karatinos G. Symptoms of depression in individuals with obstructive sleep apnea may be amendable to treatment with continuous positive airway pressure. Chest. 2005;128(3):1304-1309
14. Law M, Naughton M, Ho S, Roebuck T, Dabscheck E. Depression may reduce adherence during CPAP titration trial. J Clin Sleep Med. 2014;10(2):163-169.
15. Guralnick AS, Pant M, Minhaj M, Sweitzer BJ, Mokhlesi B. CPAP adherence in patients with newly diagnosed obstructive sleep apnea prior to elective surgery. J Clin Sleep Med. 2012;8(5):501-506
16. Collen JF, Lettieri CJ, Hoffman M. The impact of posttraumatic stress disorder on CPAP adherence in patients with obstructive sleep apnea. J Clin Sleep Med. 2012;8(6):667-672.
17. Caldwell A, Knapik JJ, Lieberman HR. Trends and factors associated with insomnia and sleep apnea in all United States military service members from 2005 to 2014. J Sleep Res. 2017;26(5):665-670.
18. Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297-307.
19. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychological Measurement. 1977;1(3):385-401.
20. Krakow B, Melendrez D, Lee SA, Warner TD, Clark JO, Sklar D. Refractory insomnia and sleep-disordered breathing: a pilot study. Sleep Breath. 2004;8(1):15-29.
21. Björnsdóttir E, Janson C, Sigurdsson JF, et al. Symptoms of insomnia among patients with obstructive sleep apnea before and after two years of positive airway pressure treatment. Sleep. 2013;36(12):1901-1909.
22. Glidewell RN, Renn BN, Roby E, Orr WC. Predictors and patterns of insomnia symptoms in OSA before and after PAP therapy. Sleep Med. 2014;15(8):899-905.
23. Edwards C, Mukherjee S, Simpson L, Palmer LJ, Almeida OP, Hillman DR. Depressive symptoms before and after treatment of obstructive sleep apnea in men and women. J Clin Sleep Med. 2015;11(9):1029-1038.
24. Bopparaju S, Casturi L, Guntupalli B, Surani S, Subramanian S. Anxiety and depression in obstructive sleep apnea: Effect of CPAP therapy and influence on CPAP compliance. Presented at: American College of Chest Physicians Annual Meeting, October 31-November 05, 2009; San Diego, CA. Chest. 2009;136(4, meeting abstracts):71S.
25. Wells RD, Freedland KE, Carney RM, Duntley SP, Stepanski EJ. Adherence, reports of benefits, and depression among patients treated with continuous positive airway pressure. Psychosom Med. 2007;69(5):449-454.
26. Orr JE, Smales C, Alexander TH, et al. Treatment of OSA with CPAP is associated with improvement in PTSD symptoms among veterans. J Clin Sleep Med. 2017;13(1):57-63.
In utero infections raise risk for autism
Children whose mothers experienced any type of infection during pregnancy were nearly 80 times more likely to be diagnosed with autism than those whose mothers did not have infections, based on data from more than one million children in Sweden.

Although previous studies have shown associations between specific infections in utero and specific conditions, such as schizophrenia, “Whether maternal infection and inflammation can alter fetal neurodevelopment to a degree that imparts risk for a broad spectrum of psychopathologic conditions across the child’s lifetime is unknown,” wrote Benjamin J. S. al-Haddad, MD, formerly of Seattle Children’s Hospital, Washington, currently with Doctors without Borders,Katiola, Côte d’Ivoire, and his colleagues.
In a study published In JAMA Psychiatry, the researchers followed 1,791,520 children (48.6% girls) born between Jan. 1, 1973, and Dec. 31, 2014, for up to 41 years using population-based registry data.
Overall, researchers found a 79% increased risk of an autism diagnosis (hazard ratio 1.79) and a 24% increased risk of a depression diagnosis (HR 1.24) for individuals exposed to any maternal infection in utero compared with those not exposed.
Similar increases in risk appeared when the data were broken down by type of infection. Hazard ratios for an autism diagnosis were 1.81 for exposure to a severe maternal infection and 1.89 for a maternal urinary tract infection; hazard ratios for depression were 1.24 and 1.30, respectively, for severe maternal infection and maternal urinary tract infection.
No increased risk in bipolar disorder, or other psychoses including schizophrenia were observed.
The findings were limited by several factors including the inclusion only of infections diagnosed in a hospital setting, and thus may not be generalizable to infections diagnosed in an outpatient setting, the researchers noted. However, the results “amplify the urgency to better understand the role of maternal infection during pregnancy on fetal brain development and suggest that prevention of infection (such as by influenza vaccination) or anti-inflammatory therapies may be important strategies for the primary prevention of some portion of autism and depression,” they said.
The researchers had no conflicts to disclose. The study was funded by grants from several organizations including the National Institutes of Health.
SOURCE: al-Haddad BJS et al. JAMA Psychiatry. doi:10.1001/jamapsychiatry.2019.0029.
Children whose mothers experienced any type of infection during pregnancy were nearly 80 times more likely to be diagnosed with autism than those whose mothers did not have infections, based on data from more than one million children in Sweden.
Although previous studies have shown associations between specific infections in utero and specific conditions, such as schizophrenia, “Whether maternal infection and inflammation can alter fetal neurodevelopment to a degree that imparts risk for a broad spectrum of psychopathologic conditions across the child’s lifetime is unknown,” wrote Benjamin J. S. al-Haddad, MD, formerly of Seattle Children’s Hospital, Washington, currently with Doctors without Borders,Katiola, Côte d’Ivoire, and his colleagues.
In a study published In JAMA Psychiatry, the researchers followed 1,791,520 children (48.6% girls) born between Jan. 1, 1973, and Dec. 31, 2014, for up to 41 years using population-based registry data.
Overall, researchers found a 79% increased risk of an autism diagnosis (hazard ratio 1.79) and a 24% increased risk of a depression diagnosis (HR 1.24) for individuals exposed to any maternal infection in utero compared with those not exposed.
Similar increases in risk appeared when the data were broken down by type of infection. Hazard ratios for an autism diagnosis were 1.81 for exposure to a severe maternal infection and 1.89 for a maternal urinary tract infection; hazard ratios for depression were 1.24 and 1.30, respectively, for severe maternal infection and maternal urinary tract infection.
No increased risk in bipolar disorder, or other psychoses including schizophrenia were observed.
The findings were limited by several factors including the inclusion only of infections diagnosed in a hospital setting, and thus may not be generalizable to infections diagnosed in an outpatient setting, the researchers noted. However, the results “amplify the urgency to better understand the role of maternal infection during pregnancy on fetal brain development and suggest that prevention of infection (such as by influenza vaccination) or anti-inflammatory therapies may be important strategies for the primary prevention of some portion of autism and depression,” they said.
The researchers had no conflicts to disclose. The study was funded by grants from several organizations including the National Institutes of Health.
SOURCE: al-Haddad BJS et al. JAMA Psychiatry. doi:10.1001/jamapsychiatry.2019.0029.
Children whose mothers experienced any type of infection during pregnancy were nearly 80 times more likely to be diagnosed with autism than those whose mothers did not have infections, based on data from more than one million children in Sweden.
Although previous studies have shown associations between specific infections in utero and specific conditions, such as schizophrenia, “Whether maternal infection and inflammation can alter fetal neurodevelopment to a degree that imparts risk for a broad spectrum of psychopathologic conditions across the child’s lifetime is unknown,” wrote Benjamin J. S. al-Haddad, MD, formerly of Seattle Children’s Hospital, Washington, currently with Doctors without Borders,Katiola, Côte d’Ivoire, and his colleagues.
In a study published In JAMA Psychiatry, the researchers followed 1,791,520 children (48.6% girls) born between Jan. 1, 1973, and Dec. 31, 2014, for up to 41 years using population-based registry data.
Overall, researchers found a 79% increased risk of an autism diagnosis (hazard ratio 1.79) and a 24% increased risk of a depression diagnosis (HR 1.24) for individuals exposed to any maternal infection in utero compared with those not exposed.
Similar increases in risk appeared when the data were broken down by type of infection. Hazard ratios for an autism diagnosis were 1.81 for exposure to a severe maternal infection and 1.89 for a maternal urinary tract infection; hazard ratios for depression were 1.24 and 1.30, respectively, for severe maternal infection and maternal urinary tract infection.
No increased risk in bipolar disorder, or other psychoses including schizophrenia were observed.
The findings were limited by several factors including the inclusion only of infections diagnosed in a hospital setting, and thus may not be generalizable to infections diagnosed in an outpatient setting, the researchers noted. However, the results “amplify the urgency to better understand the role of maternal infection during pregnancy on fetal brain development and suggest that prevention of infection (such as by influenza vaccination) or anti-inflammatory therapies may be important strategies for the primary prevention of some portion of autism and depression,” they said.
The researchers had no conflicts to disclose. The study was funded by grants from several organizations including the National Institutes of Health.
SOURCE: al-Haddad BJS et al. JAMA Psychiatry. doi:10.1001/jamapsychiatry.2019.0029.
FROM JAMA PSYCHIATRY
Anxiety, depression compromise believability of drug-allergy testing
SAN FRANCISCO – Less than 4% of people who undergo drug-allergy testing are positive and need to avoid the drug in the future, but many patients who undergo drug-allergy testing and have a negative result cling to their allergic status and struggle with letting go.

New findings suggest that preexisting anxiety or depression plays a role in some people who refuse to believe a negative drug-allergy result, which suggests that these people may need a more tailored intervention to drug-allergy testing and its aftermath, including some type of behavioral intervention.
“Underlying anxiety and depression may reduce the effectiveness of negative drug-allergy evaluation and functional delabeling,” Christine Rukasin, MD, said while presenting a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “In the future, tailored drug-allergy evaluation, behavioral interventions, targeted follow-up communication, and patient education appear necessary to improve the sustained effectiveness of a negative drug-allergy and functional delabeling,” said Dr. Rukasin, an allergy immunology physician at Vanderbilt University in Nashville, Tenn.
The results showed that some people who undergo drug allergy testing “have a high anxiety state and don’t feel comfortable regardless of their test result,” she said in an interview. “This is not where one size fits all. We usually perform a single, oral drug challenge and then pronounce the person free of allergy if the result was negative. We need to better anticipate how effective a drug evaluation will be for someone; will they believe the result?” Individual patients, especially those with diagnosed anxiety or depression, may need multiple challenge tests, both oral and skin, before they believe a negative result, and they may also need referral to a behavioral health specialist, she said.
Dr. Rukasin and her associates ran their study with 100 people who underwent assessment at the Vanderbilt drug-allergy clinic and completed a set of questionnaires. The range of suspected drug allergies included 40% with a suspected reaction to penicillin, 22% to a sulfa-containing drug, 17% to a cephalosporin, 8% to another antibiotic, 7% to an NSAID, and the remainder to other drugs. The 100 participants included 57 people without diagnosed anxiety or depression, 31 diagnosed with anxiety, and 33 diagnosed with depression; some patients had diagnoses for both anxiety and depression.
The questionnaire results from before and after drug-allergy testing showed an apparent association between anxiety, depression, and a decreased willingness to believe the results of a negative drug-allergy test. For example, when posed with the prospect of finding out they were not allergic to the tested drug, 24% of the people with anxiety and 20% of those with depression said that they still would not take the medication if it were prescribed to them, compared with 7% of those without anxiety or depression who gave this response.
Many patients who come to the drug-allergy clinic are scared and worried. “We want to dig deeper, to better help these patients,” Dr. Rukasin said. This is the first reported study to evaluate anxiety in the setting of drug-allergy testing. Further insight into ways to improve the effectiveness of drug-allergy testing hopefully will come from additional analysis of the findings.
Dr. Rukasin had no relevant financial disclosures.
SOURCE: Rukasin C et al. J Allergy Clin Immunol. 2019 Feb;143(2):AB428.
SAN FRANCISCO – Less than 4% of people who undergo drug-allergy testing are positive and need to avoid the drug in the future, but many patients who undergo drug-allergy testing and have a negative result cling to their allergic status and struggle with letting go.
New findings suggest that preexisting anxiety or depression plays a role in some people who refuse to believe a negative drug-allergy result, which suggests that these people may need a more tailored intervention to drug-allergy testing and its aftermath, including some type of behavioral intervention.
“Underlying anxiety and depression may reduce the effectiveness of negative drug-allergy evaluation and functional delabeling,” Christine Rukasin, MD, said while presenting a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “In the future, tailored drug-allergy evaluation, behavioral interventions, targeted follow-up communication, and patient education appear necessary to improve the sustained effectiveness of a negative drug-allergy and functional delabeling,” said Dr. Rukasin, an allergy immunology physician at Vanderbilt University in Nashville, Tenn.
The results showed that some people who undergo drug allergy testing “have a high anxiety state and don’t feel comfortable regardless of their test result,” she said in an interview. “This is not where one size fits all. We usually perform a single, oral drug challenge and then pronounce the person free of allergy if the result was negative. We need to better anticipate how effective a drug evaluation will be for someone; will they believe the result?” Individual patients, especially those with diagnosed anxiety or depression, may need multiple challenge tests, both oral and skin, before they believe a negative result, and they may also need referral to a behavioral health specialist, she said.
Dr. Rukasin and her associates ran their study with 100 people who underwent assessment at the Vanderbilt drug-allergy clinic and completed a set of questionnaires. The range of suspected drug allergies included 40% with a suspected reaction to penicillin, 22% to a sulfa-containing drug, 17% to a cephalosporin, 8% to another antibiotic, 7% to an NSAID, and the remainder to other drugs. The 100 participants included 57 people without diagnosed anxiety or depression, 31 diagnosed with anxiety, and 33 diagnosed with depression; some patients had diagnoses for both anxiety and depression.
The questionnaire results from before and after drug-allergy testing showed an apparent association between anxiety, depression, and a decreased willingness to believe the results of a negative drug-allergy test. For example, when posed with the prospect of finding out they were not allergic to the tested drug, 24% of the people with anxiety and 20% of those with depression said that they still would not take the medication if it were prescribed to them, compared with 7% of those without anxiety or depression who gave this response.
Many patients who come to the drug-allergy clinic are scared and worried. “We want to dig deeper, to better help these patients,” Dr. Rukasin said. This is the first reported study to evaluate anxiety in the setting of drug-allergy testing. Further insight into ways to improve the effectiveness of drug-allergy testing hopefully will come from additional analysis of the findings.
Dr. Rukasin had no relevant financial disclosures.
SOURCE: Rukasin C et al. J Allergy Clin Immunol. 2019 Feb;143(2):AB428.
SAN FRANCISCO – Less than 4% of people who undergo drug-allergy testing are positive and need to avoid the drug in the future, but many patients who undergo drug-allergy testing and have a negative result cling to their allergic status and struggle with letting go.
New findings suggest that preexisting anxiety or depression plays a role in some people who refuse to believe a negative drug-allergy result, which suggests that these people may need a more tailored intervention to drug-allergy testing and its aftermath, including some type of behavioral intervention.
“Underlying anxiety and depression may reduce the effectiveness of negative drug-allergy evaluation and functional delabeling,” Christine Rukasin, MD, said while presenting a poster at the annual meeting of the American Academy of Allergy, Asthma, and Immunology. “In the future, tailored drug-allergy evaluation, behavioral interventions, targeted follow-up communication, and patient education appear necessary to improve the sustained effectiveness of a negative drug-allergy and functional delabeling,” said Dr. Rukasin, an allergy immunology physician at Vanderbilt University in Nashville, Tenn.
The results showed that some people who undergo drug allergy testing “have a high anxiety state and don’t feel comfortable regardless of their test result,” she said in an interview. “This is not where one size fits all. We usually perform a single, oral drug challenge and then pronounce the person free of allergy if the result was negative. We need to better anticipate how effective a drug evaluation will be for someone; will they believe the result?” Individual patients, especially those with diagnosed anxiety or depression, may need multiple challenge tests, both oral and skin, before they believe a negative result, and they may also need referral to a behavioral health specialist, she said.
Dr. Rukasin and her associates ran their study with 100 people who underwent assessment at the Vanderbilt drug-allergy clinic and completed a set of questionnaires. The range of suspected drug allergies included 40% with a suspected reaction to penicillin, 22% to a sulfa-containing drug, 17% to a cephalosporin, 8% to another antibiotic, 7% to an NSAID, and the remainder to other drugs. The 100 participants included 57 people without diagnosed anxiety or depression, 31 diagnosed with anxiety, and 33 diagnosed with depression; some patients had diagnoses for both anxiety and depression.
The questionnaire results from before and after drug-allergy testing showed an apparent association between anxiety, depression, and a decreased willingness to believe the results of a negative drug-allergy test. For example, when posed with the prospect of finding out they were not allergic to the tested drug, 24% of the people with anxiety and 20% of those with depression said that they still would not take the medication if it were prescribed to them, compared with 7% of those without anxiety or depression who gave this response.
Many patients who come to the drug-allergy clinic are scared and worried. “We want to dig deeper, to better help these patients,” Dr. Rukasin said. This is the first reported study to evaluate anxiety in the setting of drug-allergy testing. Further insight into ways to improve the effectiveness of drug-allergy testing hopefully will come from additional analysis of the findings.
Dr. Rukasin had no relevant financial disclosures.
SOURCE: Rukasin C et al. J Allergy Clin Immunol. 2019 Feb;143(2):AB428.
REPORTING FROM AAAAI 2019
fMRI might help differentiate MDD and bipolar disorder
The hippocampal functional connectivity (FC) found in patients with major depressive disorder is different from the FC found in patients with bipolar disorder, an analysis of functional MRI data shows.
“ Ahmed Ameen Fateh and his associates wrote in Psychiatry Research: Neuroimaging.
Mr. Fateh and his associates recruited 29 participants with depression and 30 with bipolar disorder, from a mental health center of Chengdu, Sichuan, China. An additional 30 healthy controls were recruited through advertisements, reported Mr. Fateh, a doctoral student at the University of Electronic Science and Technology of China, Chengdu.
Using one-way analysis of variance, the investigators looked at possible differences in the participants’ hippocampal FC. The results showed that some regions exhibited significant differences in the hippocampal FC among the patients with major depression and bipolar disorder.
If their results could be replicated, the researchers wrote, “such differences may yield future trends towards improving the clinical differentiation between these two types of depression with significant therapeutic and prognostic implications.”
SOURCE: Fateh AA et al. Psychiatry Res Neuroimaging. 2019 Jan 12. doi: 10.1016/j.pscychresns.2019.01.004.
The hippocampal functional connectivity (FC) found in patients with major depressive disorder is different from the FC found in patients with bipolar disorder, an analysis of functional MRI data shows.
“ Ahmed Ameen Fateh and his associates wrote in Psychiatry Research: Neuroimaging.
Mr. Fateh and his associates recruited 29 participants with depression and 30 with bipolar disorder, from a mental health center of Chengdu, Sichuan, China. An additional 30 healthy controls were recruited through advertisements, reported Mr. Fateh, a doctoral student at the University of Electronic Science and Technology of China, Chengdu.
Using one-way analysis of variance, the investigators looked at possible differences in the participants’ hippocampal FC. The results showed that some regions exhibited significant differences in the hippocampal FC among the patients with major depression and bipolar disorder.
If their results could be replicated, the researchers wrote, “such differences may yield future trends towards improving the clinical differentiation between these two types of depression with significant therapeutic and prognostic implications.”
SOURCE: Fateh AA et al. Psychiatry Res Neuroimaging. 2019 Jan 12. doi: 10.1016/j.pscychresns.2019.01.004.
The hippocampal functional connectivity (FC) found in patients with major depressive disorder is different from the FC found in patients with bipolar disorder, an analysis of functional MRI data shows.
“ Ahmed Ameen Fateh and his associates wrote in Psychiatry Research: Neuroimaging.
Mr. Fateh and his associates recruited 29 participants with depression and 30 with bipolar disorder, from a mental health center of Chengdu, Sichuan, China. An additional 30 healthy controls were recruited through advertisements, reported Mr. Fateh, a doctoral student at the University of Electronic Science and Technology of China, Chengdu.
Using one-way analysis of variance, the investigators looked at possible differences in the participants’ hippocampal FC. The results showed that some regions exhibited significant differences in the hippocampal FC among the patients with major depression and bipolar disorder.
If their results could be replicated, the researchers wrote, “such differences may yield future trends towards improving the clinical differentiation between these two types of depression with significant therapeutic and prognostic implications.”
SOURCE: Fateh AA et al. Psychiatry Res Neuroimaging. 2019 Jan 12. doi: 10.1016/j.pscychresns.2019.01.004.
FROM PSYCHIATRY RESEARCH: NEUROIMAGING
Police department offers mental health care for officers
Police officers often are criticized for the way they respond to people with serious mental illness. A police department in Florida is addressing this issue by hiring a licensed clinical psychologist and making her available to officers on a 24/7 basis, an ABC-TV affiliate reported. “The goal is they come in, they work on what they need to; we get them right, we get them good so that they can go back out and do what they need to do – and then they check in as needed,” Brandy Benson, PsyD, said in the report. The meetings take place in her office and not the police station, which allows officers to maintain confidentiality. Each officer is allotted a set number of free sessions for each issue that is fueling their distress. Issues can range from depression to anxiety to marital problems. The aim is prevention – not reaction to whatever has happened. Getting at the root cause can prevent spillover on the job, which in turn, can prove disastrous for officers, the people they serve, and their families. “It’s okay to go through those emotions, but you don’t want to tie those emotions up because sooner or later it’s going to pop and we want to make sure we address that issue before it goes ‘pop,’ ” said St. Petersburg Police Chief Anthony Holloway. WFTS-TV, Tampa Bay, Fla.

Two women have embarked on their self-described “joy tour” to raise awareness about suicide prevention. Shontice McKenzie and Cedrica Mitchell are on the road with the intention of visiting every state, according to an article on thefix.com, a website that focuses on addiction and recovery. The tour is the brainchild of Ms. McKenzie and is funded by her nonprofit H.U.M.A.N.I.T.Y. 360. During their month-long extended stops in Virginia, North Carolina, South Carolina, Georgia, Florida, and a just-completed stay in Alabama, the women are speaking and providing positive outlets to those in turmoil and contemplating suicide, thefix reported, based on a post on al.com. The choice of Alabama as one of the first stops on the planned nationwide tour was deliberate. The suicide rate in the state has been higher than the national average for nearly 3 decades – 16.2/100,000, compared with 13.9/100,000 nationally. Suicide is the second-leading cause of death of those aged 10-14 years in Alabama. Ms. McKenzie and Ms. Mitchell want to see the stigma surrounding mental illness removed. “We have met so many families who are still in denial about a family member who completed the act of suicide because they don’t want the backlash from the public,” Ms. McKenzie said. “They should have received more support around the topic. Then we can prevent suicides. That’s what the Joy Tour is about.” The end of each state visit includes what the two call a “joy jam” – a free event where people can eat, get information on mental health resources in their area, and learn how to incorporate mental health care into their everyday lives. The tour is slated to wrap up in 2023 in Hawaii. Thefix.com.
An editorial in the Winston-Salem (N.C.) Journal has backed a recently introduced bill in the state legislature that would open the door for mental health screenings for public school students. “This legislation is a worthwhile step in tackling the problem of school shootings as well as other problems that can arise among our children. It should work well in conjunction with other efforts, such as increased school security and gun-law reform,” the paper’s editorial board wrote. The bill would trigger a study by the North Carolina Department of Health and Human Services to come up with a screening system that would identify school children at risk of harming themselves or others. The idea is that all students would be screened initially. “We have nothing that determines if a child has a mental health concern ... to the point they could be contemplating harming themselves or others,” said state Rep. John Torbett, the bill’s main sponsor. “This bill would bring smart people together for determining the appropriate criteria.” One of the bill’s cosponsors, Rep. Debra Forsyth, said school counselors tell her that most of their time is spent dealing with students with emotional and mental issues. “When we were studying the impact of [math and reading standards] a few years back, many parents complained about emotional stress in very young children, so issues can obviously arise at an early age,” Ms. Forsyth said in the article. “Our children are facing pressures from all sides – increased testing, peer pressure, and economic difficulties. They’re not receiving the best resources we could provide. It’s about time they received a helping hand.” Winston-Salem Journal.
A mental health facility has opened in southeast Fresno, Calif., that seeks to provide a bridge for people experiencing a mental health crisis and need a place to live, according to a report by ABC affiliate KFSN. The $5 million, 12,000-square-foot, 16-bed facility is an alternative to hospitalization, said Gerardo Puga-Cervantes, an administrator at the facility. “A facility like this creates a stepping-stone that’s closer to the ones before and after, so when a person is making that pathway toward recovery, it’s not a Grand Canyon they have to leap to get that recovery. It’s really a clear pathway,” said Fresno County Behavioral Health Director Dawan Utecht. The facility, called the Fresno Crisis Residential Treatment Center, will provide psychiatric support to residents and will aim to serve hundreds of people each year. To get into the center, patients must be referred by the county’s behavioral health department. Next, the department hopes to provide residential housing for those who leave the facility. ABC30 Action News/KFSN-TV.

A former dairy farm reincarnated as a school called Green Chimneys in Putnam County, N.Y., is helping children with special needs find solace, the New York Times reported. Aside from usual pigs and goats, the farm’s denizens include more exotic critters, such as camels, an emu, peacocks, miniature horses and donkeys, owls, falcons, and a condor. “Green Chimneys’ approach focuses on an awareness of how trauma impacts human and animal lives, that a healing setting can benefit both, and that there is a broader parallel between human, animal, environmental, and societal well-being,” according to the school’s website. The article describes the experience of 8-year-old Xander DeLeon, who was diagnosed with attention-deficit/hyperactivity disorder and dyslexia, and experienced rages and absences while attending a charter school in Manhattan. Now he is pulling down As and Bs. “The school staff tell him that he won’t be able to work on the farm if he doesn’t continue to do well in school,” said Leslie DeLeon, Xander’s mother. The philosophy is that caring for animals can be a means to confidence and social skills for emotionally challenged children. The day and residential facility now has two campuses in Brewster and Carmel, N.Y., more than 240 students, and about the same number of animals. “There has been a lot of research on pets at home and how healthy it is in the past 10 years,” said Steven Klee, PhD, director of clinical and medical services at Green Chimneys. Yet, as he first became aware of the use of animal intervention for special-needs children, even he was skeptical. “When you have traditional training as a psychologist, you never think about doing anything outside of the office,” Dr. Klee said. But Dr. Klee was converted. “Animals in a sense are purer, more consistent, more accepting. You are kind to the animals; they show their appreciation.” New York Times.
Police officers often are criticized for the way they respond to people with serious mental illness. A police department in Florida is addressing this issue by hiring a licensed clinical psychologist and making her available to officers on a 24/7 basis, an ABC-TV affiliate reported. “The goal is they come in, they work on what they need to; we get them right, we get them good so that they can go back out and do what they need to do – and then they check in as needed,” Brandy Benson, PsyD, said in the report. The meetings take place in her office and not the police station, which allows officers to maintain confidentiality. Each officer is allotted a set number of free sessions for each issue that is fueling their distress. Issues can range from depression to anxiety to marital problems. The aim is prevention – not reaction to whatever has happened. Getting at the root cause can prevent spillover on the job, which in turn, can prove disastrous for officers, the people they serve, and their families. “It’s okay to go through those emotions, but you don’t want to tie those emotions up because sooner or later it’s going to pop and we want to make sure we address that issue before it goes ‘pop,’ ” said St. Petersburg Police Chief Anthony Holloway. WFTS-TV, Tampa Bay, Fla.
Two women have embarked on their self-described “joy tour” to raise awareness about suicide prevention. Shontice McKenzie and Cedrica Mitchell are on the road with the intention of visiting every state, according to an article on thefix.com, a website that focuses on addiction and recovery. The tour is the brainchild of Ms. McKenzie and is funded by her nonprofit H.U.M.A.N.I.T.Y. 360. During their month-long extended stops in Virginia, North Carolina, South Carolina, Georgia, Florida, and a just-completed stay in Alabama, the women are speaking and providing positive outlets to those in turmoil and contemplating suicide, thefix reported, based on a post on al.com. The choice of Alabama as one of the first stops on the planned nationwide tour was deliberate. The suicide rate in the state has been higher than the national average for nearly 3 decades – 16.2/100,000, compared with 13.9/100,000 nationally. Suicide is the second-leading cause of death of those aged 10-14 years in Alabama. Ms. McKenzie and Ms. Mitchell want to see the stigma surrounding mental illness removed. “We have met so many families who are still in denial about a family member who completed the act of suicide because they don’t want the backlash from the public,” Ms. McKenzie said. “They should have received more support around the topic. Then we can prevent suicides. That’s what the Joy Tour is about.” The end of each state visit includes what the two call a “joy jam” – a free event where people can eat, get information on mental health resources in their area, and learn how to incorporate mental health care into their everyday lives. The tour is slated to wrap up in 2023 in Hawaii. Thefix.com.
An editorial in the Winston-Salem (N.C.) Journal has backed a recently introduced bill in the state legislature that would open the door for mental health screenings for public school students. “This legislation is a worthwhile step in tackling the problem of school shootings as well as other problems that can arise among our children. It should work well in conjunction with other efforts, such as increased school security and gun-law reform,” the paper’s editorial board wrote. The bill would trigger a study by the North Carolina Department of Health and Human Services to come up with a screening system that would identify school children at risk of harming themselves or others. The idea is that all students would be screened initially. “We have nothing that determines if a child has a mental health concern ... to the point they could be contemplating harming themselves or others,” said state Rep. John Torbett, the bill’s main sponsor. “This bill would bring smart people together for determining the appropriate criteria.” One of the bill’s cosponsors, Rep. Debra Forsyth, said school counselors tell her that most of their time is spent dealing with students with emotional and mental issues. “When we were studying the impact of [math and reading standards] a few years back, many parents complained about emotional stress in very young children, so issues can obviously arise at an early age,” Ms. Forsyth said in the article. “Our children are facing pressures from all sides – increased testing, peer pressure, and economic difficulties. They’re not receiving the best resources we could provide. It’s about time they received a helping hand.” Winston-Salem Journal.
A mental health facility has opened in southeast Fresno, Calif., that seeks to provide a bridge for people experiencing a mental health crisis and need a place to live, according to a report by ABC affiliate KFSN. The $5 million, 12,000-square-foot, 16-bed facility is an alternative to hospitalization, said Gerardo Puga-Cervantes, an administrator at the facility. “A facility like this creates a stepping-stone that’s closer to the ones before and after, so when a person is making that pathway toward recovery, it’s not a Grand Canyon they have to leap to get that recovery. It’s really a clear pathway,” said Fresno County Behavioral Health Director Dawan Utecht. The facility, called the Fresno Crisis Residential Treatment Center, will provide psychiatric support to residents and will aim to serve hundreds of people each year. To get into the center, patients must be referred by the county’s behavioral health department. Next, the department hopes to provide residential housing for those who leave the facility. ABC30 Action News/KFSN-TV.
A former dairy farm reincarnated as a school called Green Chimneys in Putnam County, N.Y., is helping children with special needs find solace, the New York Times reported. Aside from usual pigs and goats, the farm’s denizens include more exotic critters, such as camels, an emu, peacocks, miniature horses and donkeys, owls, falcons, and a condor. “Green Chimneys’ approach focuses on an awareness of how trauma impacts human and animal lives, that a healing setting can benefit both, and that there is a broader parallel between human, animal, environmental, and societal well-being,” according to the school’s website. The article describes the experience of 8-year-old Xander DeLeon, who was diagnosed with attention-deficit/hyperactivity disorder and dyslexia, and experienced rages and absences while attending a charter school in Manhattan. Now he is pulling down As and Bs. “The school staff tell him that he won’t be able to work on the farm if he doesn’t continue to do well in school,” said Leslie DeLeon, Xander’s mother. The philosophy is that caring for animals can be a means to confidence and social skills for emotionally challenged children. The day and residential facility now has two campuses in Brewster and Carmel, N.Y., more than 240 students, and about the same number of animals. “There has been a lot of research on pets at home and how healthy it is in the past 10 years,” said Steven Klee, PhD, director of clinical and medical services at Green Chimneys. Yet, as he first became aware of the use of animal intervention for special-needs children, even he was skeptical. “When you have traditional training as a psychologist, you never think about doing anything outside of the office,” Dr. Klee said. But Dr. Klee was converted. “Animals in a sense are purer, more consistent, more accepting. You are kind to the animals; they show their appreciation.” New York Times.
Police officers often are criticized for the way they respond to people with serious mental illness. A police department in Florida is addressing this issue by hiring a licensed clinical psychologist and making her available to officers on a 24/7 basis, an ABC-TV affiliate reported. “The goal is they come in, they work on what they need to; we get them right, we get them good so that they can go back out and do what they need to do – and then they check in as needed,” Brandy Benson, PsyD, said in the report. The meetings take place in her office and not the police station, which allows officers to maintain confidentiality. Each officer is allotted a set number of free sessions for each issue that is fueling their distress. Issues can range from depression to anxiety to marital problems. The aim is prevention – not reaction to whatever has happened. Getting at the root cause can prevent spillover on the job, which in turn, can prove disastrous for officers, the people they serve, and their families. “It’s okay to go through those emotions, but you don’t want to tie those emotions up because sooner or later it’s going to pop and we want to make sure we address that issue before it goes ‘pop,’ ” said St. Petersburg Police Chief Anthony Holloway. WFTS-TV, Tampa Bay, Fla.
Two women have embarked on their self-described “joy tour” to raise awareness about suicide prevention. Shontice McKenzie and Cedrica Mitchell are on the road with the intention of visiting every state, according to an article on thefix.com, a website that focuses on addiction and recovery. The tour is the brainchild of Ms. McKenzie and is funded by her nonprofit H.U.M.A.N.I.T.Y. 360. During their month-long extended stops in Virginia, North Carolina, South Carolina, Georgia, Florida, and a just-completed stay in Alabama, the women are speaking and providing positive outlets to those in turmoil and contemplating suicide, thefix reported, based on a post on al.com. The choice of Alabama as one of the first stops on the planned nationwide tour was deliberate. The suicide rate in the state has been higher than the national average for nearly 3 decades – 16.2/100,000, compared with 13.9/100,000 nationally. Suicide is the second-leading cause of death of those aged 10-14 years in Alabama. Ms. McKenzie and Ms. Mitchell want to see the stigma surrounding mental illness removed. “We have met so many families who are still in denial about a family member who completed the act of suicide because they don’t want the backlash from the public,” Ms. McKenzie said. “They should have received more support around the topic. Then we can prevent suicides. That’s what the Joy Tour is about.” The end of each state visit includes what the two call a “joy jam” – a free event where people can eat, get information on mental health resources in their area, and learn how to incorporate mental health care into their everyday lives. The tour is slated to wrap up in 2023 in Hawaii. Thefix.com.
An editorial in the Winston-Salem (N.C.) Journal has backed a recently introduced bill in the state legislature that would open the door for mental health screenings for public school students. “This legislation is a worthwhile step in tackling the problem of school shootings as well as other problems that can arise among our children. It should work well in conjunction with other efforts, such as increased school security and gun-law reform,” the paper’s editorial board wrote. The bill would trigger a study by the North Carolina Department of Health and Human Services to come up with a screening system that would identify school children at risk of harming themselves or others. The idea is that all students would be screened initially. “We have nothing that determines if a child has a mental health concern ... to the point they could be contemplating harming themselves or others,” said state Rep. John Torbett, the bill’s main sponsor. “This bill would bring smart people together for determining the appropriate criteria.” One of the bill’s cosponsors, Rep. Debra Forsyth, said school counselors tell her that most of their time is spent dealing with students with emotional and mental issues. “When we were studying the impact of [math and reading standards] a few years back, many parents complained about emotional stress in very young children, so issues can obviously arise at an early age,” Ms. Forsyth said in the article. “Our children are facing pressures from all sides – increased testing, peer pressure, and economic difficulties. They’re not receiving the best resources we could provide. It’s about time they received a helping hand.” Winston-Salem Journal.
A mental health facility has opened in southeast Fresno, Calif., that seeks to provide a bridge for people experiencing a mental health crisis and need a place to live, according to a report by ABC affiliate KFSN. The $5 million, 12,000-square-foot, 16-bed facility is an alternative to hospitalization, said Gerardo Puga-Cervantes, an administrator at the facility. “A facility like this creates a stepping-stone that’s closer to the ones before and after, so when a person is making that pathway toward recovery, it’s not a Grand Canyon they have to leap to get that recovery. It’s really a clear pathway,” said Fresno County Behavioral Health Director Dawan Utecht. The facility, called the Fresno Crisis Residential Treatment Center, will provide psychiatric support to residents and will aim to serve hundreds of people each year. To get into the center, patients must be referred by the county’s behavioral health department. Next, the department hopes to provide residential housing for those who leave the facility. ABC30 Action News/KFSN-TV.
A former dairy farm reincarnated as a school called Green Chimneys in Putnam County, N.Y., is helping children with special needs find solace, the New York Times reported. Aside from usual pigs and goats, the farm’s denizens include more exotic critters, such as camels, an emu, peacocks, miniature horses and donkeys, owls, falcons, and a condor. “Green Chimneys’ approach focuses on an awareness of how trauma impacts human and animal lives, that a healing setting can benefit both, and that there is a broader parallel between human, animal, environmental, and societal well-being,” according to the school’s website. The article describes the experience of 8-year-old Xander DeLeon, who was diagnosed with attention-deficit/hyperactivity disorder and dyslexia, and experienced rages and absences while attending a charter school in Manhattan. Now he is pulling down As and Bs. “The school staff tell him that he won’t be able to work on the farm if he doesn’t continue to do well in school,” said Leslie DeLeon, Xander’s mother. The philosophy is that caring for animals can be a means to confidence and social skills for emotionally challenged children. The day and residential facility now has two campuses in Brewster and Carmel, N.Y., more than 240 students, and about the same number of animals. “There has been a lot of research on pets at home and how healthy it is in the past 10 years,” said Steven Klee, PhD, director of clinical and medical services at Green Chimneys. Yet, as he first became aware of the use of animal intervention for special-needs children, even he was skeptical. “When you have traditional training as a psychologist, you never think about doing anything outside of the office,” Dr. Klee said. But Dr. Klee was converted. “Animals in a sense are purer, more consistent, more accepting. You are kind to the animals; they show their appreciation.” New York Times.
IV ketamine, intranasal esketamine likely to ‘happily coexist’
Dr. Steven Levine offers perspective on how the FDA approval will affect patients, practice
Q: Why is this a “banner day” for psychiatry?
A: This is truly the first new option for depression in 60 years. The selective serotonin reuptake inhibitors (SSRIs) developed in the mid-’80s were not truly new, not much different from the monoamine oxidase inhibitors (MAOI) and tricyclic antidepressants. In fact, they work much like watered-down MAOIs. Esketamine works by a truly novel mechanism.
Even though it constitutes a relatively new treatment, ketamine is a very old medicine, and we probably know more about the pharmacology and mechanisms in depression than for the SSRIs.
The idea of SSRIs working by increasing levels of neurotransmitters like serotonin has never held water. We never really believed that, but for people who respond to them – and many are helped – what is really happening weeks to months down the line is that these drugs increase the plasticity of the brain. Depression, like other mental health conditions, disrupts connections between important brain regions, reducing the number, function, and quality of the connections, and we believe SSRIs improve these.
Ketamine does these same things by a different route and much, much more quickly.
Q: What is esketamine’s method of action, and how long will a dose last?
A: Ketamine and esketamine bind to and block glutamate N-methyl-D-aspartate (NMDA) receptors. This leads to the release of several chemical messengers, the result of which increases the production of neurotrophic factors, in particular brain-derived neurotrophic factor (BDNF), that play a key role in healing damaged connections in the brain. A single dose of esketamine would only be expected to relieve depression symptoms for days, up to a week or 2. Multiple doses over the first few weeks can extend the durability of response to several weeks and sometimes months.
It is not true for every patient, but some do have improvement within 2-4 hours that correlates with physiologic changes. Others can be later responders and require up to 6 exposures.
Q: The FDA approval requires those who administer the drug to complete special training and meet licensure requirements. Is this realistic for small practices?
A: Initially, not every psychiatrist will be able to offer esketamine, and I think it might be beyond the reach of small practices, and that’s probably okay. Enough people and enough centers will be able to offer it to meet the initial demand.
Q: Is esketamine “better” than ketamine infusions? With the approved drug available, will ketamine infusion clinics still have a place?
A: There are major pros with this. The FDA approval takes out of the gray area of off-label administration. It will most likely be covered by insurance now – a huge advantage that will put this in the reach of so many patients who haven’t been able to access this treatment.
I think that, because there are advantages and disadvantages for both IV ketamine and nasal esketamine, they will happily coexist for years to come. However, because nasal esketamine will likely be restricted to prescription by psychiatrists, it may have more impact on non-psychiatrist-led practices. In this way,
Dr. Steven Levine is the founder of Actify Neurotherapies, which operates nine clinics providing ketamine treatment for depression.
Dr. Steven Levine offers perspective on how the FDA approval will affect patients, practice
Dr. Steven Levine offers perspective on how the FDA approval will affect patients, practice
Q: Why is this a “banner day” for psychiatry?
A: This is truly the first new option for depression in 60 years. The selective serotonin reuptake inhibitors (SSRIs) developed in the mid-’80s were not truly new, not much different from the monoamine oxidase inhibitors (MAOI) and tricyclic antidepressants. In fact, they work much like watered-down MAOIs. Esketamine works by a truly novel mechanism.
Even though it constitutes a relatively new treatment, ketamine is a very old medicine, and we probably know more about the pharmacology and mechanisms in depression than for the SSRIs.
The idea of SSRIs working by increasing levels of neurotransmitters like serotonin has never held water. We never really believed that, but for people who respond to them – and many are helped – what is really happening weeks to months down the line is that these drugs increase the plasticity of the brain. Depression, like other mental health conditions, disrupts connections between important brain regions, reducing the number, function, and quality of the connections, and we believe SSRIs improve these.
Ketamine does these same things by a different route and much, much more quickly.
Q: What is esketamine’s method of action, and how long will a dose last?
A: Ketamine and esketamine bind to and block glutamate N-methyl-D-aspartate (NMDA) receptors. This leads to the release of several chemical messengers, the result of which increases the production of neurotrophic factors, in particular brain-derived neurotrophic factor (BDNF), that play a key role in healing damaged connections in the brain. A single dose of esketamine would only be expected to relieve depression symptoms for days, up to a week or 2. Multiple doses over the first few weeks can extend the durability of response to several weeks and sometimes months.
It is not true for every patient, but some do have improvement within 2-4 hours that correlates with physiologic changes. Others can be later responders and require up to 6 exposures.
Q: The FDA approval requires those who administer the drug to complete special training and meet licensure requirements. Is this realistic for small practices?
A: Initially, not every psychiatrist will be able to offer esketamine, and I think it might be beyond the reach of small practices, and that’s probably okay. Enough people and enough centers will be able to offer it to meet the initial demand.
Q: Is esketamine “better” than ketamine infusions? With the approved drug available, will ketamine infusion clinics still have a place?
A: There are major pros with this. The FDA approval takes out of the gray area of off-label administration. It will most likely be covered by insurance now – a huge advantage that will put this in the reach of so many patients who haven’t been able to access this treatment.
I think that, because there are advantages and disadvantages for both IV ketamine and nasal esketamine, they will happily coexist for years to come. However, because nasal esketamine will likely be restricted to prescription by psychiatrists, it may have more impact on non-psychiatrist-led practices. In this way,
Dr. Steven Levine is the founder of Actify Neurotherapies, which operates nine clinics providing ketamine treatment for depression.
Q: Why is this a “banner day” for psychiatry?
A: This is truly the first new option for depression in 60 years. The selective serotonin reuptake inhibitors (SSRIs) developed in the mid-’80s were not truly new, not much different from the monoamine oxidase inhibitors (MAOI) and tricyclic antidepressants. In fact, they work much like watered-down MAOIs. Esketamine works by a truly novel mechanism.
Even though it constitutes a relatively new treatment, ketamine is a very old medicine, and we probably know more about the pharmacology and mechanisms in depression than for the SSRIs.
The idea of SSRIs working by increasing levels of neurotransmitters like serotonin has never held water. We never really believed that, but for people who respond to them – and many are helped – what is really happening weeks to months down the line is that these drugs increase the plasticity of the brain. Depression, like other mental health conditions, disrupts connections between important brain regions, reducing the number, function, and quality of the connections, and we believe SSRIs improve these.
Ketamine does these same things by a different route and much, much more quickly.
Q: What is esketamine’s method of action, and how long will a dose last?
A: Ketamine and esketamine bind to and block glutamate N-methyl-D-aspartate (NMDA) receptors. This leads to the release of several chemical messengers, the result of which increases the production of neurotrophic factors, in particular brain-derived neurotrophic factor (BDNF), that play a key role in healing damaged connections in the brain. A single dose of esketamine would only be expected to relieve depression symptoms for days, up to a week or 2. Multiple doses over the first few weeks can extend the durability of response to several weeks and sometimes months.
It is not true for every patient, but some do have improvement within 2-4 hours that correlates with physiologic changes. Others can be later responders and require up to 6 exposures.
Q: The FDA approval requires those who administer the drug to complete special training and meet licensure requirements. Is this realistic for small practices?
A: Initially, not every psychiatrist will be able to offer esketamine, and I think it might be beyond the reach of small practices, and that’s probably okay. Enough people and enough centers will be able to offer it to meet the initial demand.
Q: Is esketamine “better” than ketamine infusions? With the approved drug available, will ketamine infusion clinics still have a place?
A: There are major pros with this. The FDA approval takes out of the gray area of off-label administration. It will most likely be covered by insurance now – a huge advantage that will put this in the reach of so many patients who haven’t been able to access this treatment.
I think that, because there are advantages and disadvantages for both IV ketamine and nasal esketamine, they will happily coexist for years to come. However, because nasal esketamine will likely be restricted to prescription by psychiatrists, it may have more impact on non-psychiatrist-led practices. In this way,
Dr. Steven Levine is the founder of Actify Neurotherapies, which operates nine clinics providing ketamine treatment for depression.