Cervical screening recommendations do not cover all circumstances
Cervical screening recommendations do not cover all circumstances
Starting cervical cancer screening at age 21 does not necessarily take into account the fact that we are seeing youngsters initiating sexual activity as young as age 9. We obviously see pregnancies early as well. Waiting to screen until age 21, therefore, may cause us to miss the development of high-grade lesions and cervical cancer. As you know, cases in the literature report instances of invasive cancer with first Pap test at age 21. Also, human papillomavirus (HPV) is spread by sexual activity, with the squamous columnar junction more susceptible to infection at a young age.
Recommendations regarding cervical cancer screening for older women also should take into account new sexual partners. Currently, both men and women are living longer and are remarrying or are sexually active with multiple partners. The fact that older women are desiring hormone replacement for vaginal lubrication and dyspareunia shows that they are sexually active even in their late 70s. I believe that the incidence of HPV infection to cervical, vaginal, and vulvar tissue will be increasing as a result.
In an age in which primary care physicians do not have time to perform Pap tests or vaginal, cervical, and vulvar exams because they are overwhelmed with keeping up with patients’ major medical issues is a misunderstanding regarding current recommendations for Pap test screening.
Elizabeth Reinoehl-McClaskey, DO Onley, Virginia
Dr. Einstein responds
Sexual behavior can start early, but this does not lead to cancer. When we screen, we are looking for cancer, not HPV infection, which is quite common in women and men younger than age 21. Also, one might question whether current screening techniques pick up early-onset tumors. Regarding older women, sexual activity and the rate of older women getting cervical cancer should be considered in future guidelines.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Cervical screening recommendations do not cover all circumstances
Starting cervical cancer screening at age 21 does not necessarily take into account the fact that we are seeing youngsters initiating sexual activity as young as age 9. We obviously see pregnancies early as well. Waiting to screen until age 21, therefore, may cause us to miss the development of high-grade lesions and cervical cancer. As you know, cases in the literature report instances of invasive cancer with first Pap test at age 21. Also, human papillomavirus (HPV) is spread by sexual activity, with the squamous columnar junction more susceptible to infection at a young age.
Recommendations regarding cervical cancer screening for older women also should take into account new sexual partners. Currently, both men and women are living longer and are remarrying or are sexually active with multiple partners. The fact that older women are desiring hormone replacement for vaginal lubrication and dyspareunia shows that they are sexually active even in their late 70s. I believe that the incidence of HPV infection to cervical, vaginal, and vulvar tissue will be increasing as a result.
In an age in which primary care physicians do not have time to perform Pap tests or vaginal, cervical, and vulvar exams because they are overwhelmed with keeping up with patients’ major medical issues is a misunderstanding regarding current recommendations for Pap test screening.
Elizabeth Reinoehl-McClaskey, DO Onley, Virginia
Dr. Einstein responds
Sexual behavior can start early, but this does not lead to cancer. When we screen, we are looking for cancer, not HPV infection, which is quite common in women and men younger than age 21. Also, one might question whether current screening techniques pick up early-onset tumors. Regarding older women, sexual activity and the rate of older women getting cervical cancer should be considered in future guidelines.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Cervical screening recommendations do not cover all circumstances
Starting cervical cancer screening at age 21 does not necessarily take into account the fact that we are seeing youngsters initiating sexual activity as young as age 9. We obviously see pregnancies early as well. Waiting to screen until age 21, therefore, may cause us to miss the development of high-grade lesions and cervical cancer. As you know, cases in the literature report instances of invasive cancer with first Pap test at age 21. Also, human papillomavirus (HPV) is spread by sexual activity, with the squamous columnar junction more susceptible to infection at a young age.
Recommendations regarding cervical cancer screening for older women also should take into account new sexual partners. Currently, both men and women are living longer and are remarrying or are sexually active with multiple partners. The fact that older women are desiring hormone replacement for vaginal lubrication and dyspareunia shows that they are sexually active even in their late 70s. I believe that the incidence of HPV infection to cervical, vaginal, and vulvar tissue will be increasing as a result.
In an age in which primary care physicians do not have time to perform Pap tests or vaginal, cervical, and vulvar exams because they are overwhelmed with keeping up with patients’ major medical issues is a misunderstanding regarding current recommendations for Pap test screening.
Elizabeth Reinoehl-McClaskey, DO Onley, Virginia
Dr. Einstein responds
Sexual behavior can start early, but this does not lead to cancer. When we screen, we are looking for cancer, not HPV infection, which is quite common in women and men younger than age 21. Also, one might question whether current screening techniques pick up early-onset tumors. Regarding older women, sexual activity and the rate of older women getting cervical cancer should be considered in future guidelines.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
I want to thank Dr. Barbieri for the introduction to his April editorial in which he states that the “trusted nurse midwife asks you to consult on her patient.” Where I practice (in a large suburb of Kansas with a hospital where more than 5,000 babies are delivered yearly), there is a serious lack of midwives and an even greater lack of physicians to support them. As the co-owner of an independently owned nurse-midwife practice, after losing our collaborating physician, we were unable to secure collaboration from any other group, despite our cesarean delivery rate of 5%, vaginal birth after cesarean success rate of 87%, and chorioamnionitis rate of 0%. Please continue to educate your readers on the benefit to women when all obstetric providers work together.
Julie Gorenc, CNM Lenexa, Kansas
Dr. Barbieri responds
I thank Ms. Gorenc for her support of OBG Management and share her concern about optimizing obstetric care. Given the pending shortage of clinicians, we will need all experienced clinicians to work together to ensure access to high-quality obstetric care. My observation is that many obstetricians are concerned about liability issues that can be associated with coverage of other clinicians, including nurse midwives. The quality of obstetric care and collaboration would be enhanced if our medical tort system could evolve to a “just culture,” ending the “blame and shame” associated with tort litigation.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
I want to thank Dr. Barbieri for the introduction to his April editorial in which he states that the “trusted nurse midwife asks you to consult on her patient.” Where I practice (in a large suburb of Kansas with a hospital where more than 5,000 babies are delivered yearly), there is a serious lack of midwives and an even greater lack of physicians to support them. As the co-owner of an independently owned nurse-midwife practice, after losing our collaborating physician, we were unable to secure collaboration from any other group, despite our cesarean delivery rate of 5%, vaginal birth after cesarean success rate of 87%, and chorioamnionitis rate of 0%. Please continue to educate your readers on the benefit to women when all obstetric providers work together.
Julie Gorenc, CNM Lenexa, Kansas
Dr. Barbieri responds
I thank Ms. Gorenc for her support of OBG Management and share her concern about optimizing obstetric care. Given the pending shortage of clinicians, we will need all experienced clinicians to work together to ensure access to high-quality obstetric care. My observation is that many obstetricians are concerned about liability issues that can be associated with coverage of other clinicians, including nurse midwives. The quality of obstetric care and collaboration would be enhanced if our medical tort system could evolve to a “just culture,” ending the “blame and shame” associated with tort litigation.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Midwife-physician alliance benefits women
I want to thank Dr. Barbieri for the introduction to his April editorial in which he states that the “trusted nurse midwife asks you to consult on her patient.” Where I practice (in a large suburb of Kansas with a hospital where more than 5,000 babies are delivered yearly), there is a serious lack of midwives and an even greater lack of physicians to support them. As the co-owner of an independently owned nurse-midwife practice, after losing our collaborating physician, we were unable to secure collaboration from any other group, despite our cesarean delivery rate of 5%, vaginal birth after cesarean success rate of 87%, and chorioamnionitis rate of 0%. Please continue to educate your readers on the benefit to women when all obstetric providers work together.
Julie Gorenc, CNM Lenexa, Kansas
Dr. Barbieri responds
I thank Ms. Gorenc for her support of OBG Management and share her concern about optimizing obstetric care. Given the pending shortage of clinicians, we will need all experienced clinicians to work together to ensure access to high-quality obstetric care. My observation is that many obstetricians are concerned about liability issues that can be associated with coverage of other clinicians, including nurse midwives. The quality of obstetric care and collaboration would be enhanced if our medical tort system could evolve to a “just culture,” ending the “blame and shame” associated with tort litigation.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Diagnostics company asserts medical and pathology groups prefer cotesting for cervical cancer screening
Diagnostics company asserts medical and pathology groups prefer cotesting for cervical cancer screening
We are concerned about Dr. Wright’s March 2018 gynecologic cancer coverage of US Preventive Services Task Force (USPSTF) screening guidelines for cervical cancer.
The article suggests that draft USPSTF cervical cancer guidelines issued in September 2017 are final when in fact that is not the case. The USPSTF issued draft guidelines in late 2017, butfinal publication is pending USPSTFrevisions in response to submitted public comments. This means that, for now, existing USPSTF guidelines remain in place, and these guidelines clearly recommend cotesting (high-risk HPV and cytology/Pap) in women 30 to 65 years of age every 5 years as an appropriate screening modality, in alignment with the American College of Obstetricians and Gynecologists, the American Society for Colposcopy and Cervical Pathology, and the American Cancer Society, among others.
It is also notable that the proposed USPSTF guidelines have been met with sharp resistance. ACOG, as well as several organizations, including the American Society of Clinical Pathology, American Society of Cytopathology, the American Society for Cytotechnology, the College of American Pathologists, the International Academy of Cytology, and the Papanicolaou Society of Cytopathology, cite concerns with the proposed USPSTF guidelines and continue to argue in favor of cotesting in women 30 to 65 years of age.1,2
We also fear that Dr. Wright may have provided data out of context. For instance, he notes that the USPSTF, in its draft guidelines, found that cotesting increased the number of follow-up tests but did not increase detection of CIN3+ in a decision model. Yet, the USPSTF analysis overrelied on research from European populations (not representative of the US cervical cancer experience) and excluded peer-reviewed data of women in the United States, which clearly shows that HPV-Pap together catches more cervical cancers than either Pap or HPV alone.3
D.P. Alagia, MD, and Harvey W. Kaufman, MD, MBA Quest Diagnostics Madison, New Jersey
Dr. Wright responds
I thank Drs. Alagia and Kaufman for their interest in the work and their comments regarding the USPSTF cervical cancer guidelines. As stated in the article, the USPSTF recommendations are currently in draft form and subject to revision based on public comment. The guidelines are a synthesis of best available evidence and are meant to weigh the benefits and harms of various cervical cancer screening strategies. The recommendations are based in part on simulation modeling that incorporates available evidence and projects the long-term effects of multiple rounds of screening. While the decision models incorporated a large amount of data and were robust in a variety of sensitivity analyses, as with all decision analyses, they are limited by the underlying assumptions utilized in the model. Over the last 2 decades, screening practices for cervical cancer have dramatically shifted. Highlighting the USPSTF draft guidelines was meant to raise awareness among clinicians and policy makers of the evolving role of high-risk HPV testing, either alone or in combination with cytology, as a screening modality for cervical cancer.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
References
American College of Obstetricians and Gynecologists. Leading women’s health care groups issue joint statement on USPSTF draft cervical cancer screening recommendations. September 13, 2017. https://www.acog.org/About-ACOG/News-Room/Statements/2017/Leading-Womens-Health-Care-Groups-Issue-Joint-Statement-on-USPSTF. Accessed July 5, 2018.
Cytopathology Education and Technology Consortium. Response to new USPSTF guidelines for cervical cancer screening. October 2, 2017. https://s3.amazonaws.com/ascpcdn/static/ONELab/pdf/2017/CETC+-USPSTF+Letter+10-2-17.PDF. Accessed July 5, 2018.
Blatt AJ, Kennedy R, Luff RD, Austin RM, Rabin DS. Comparison of cervical cancer screening results among 256,648 women in multiple clinical practices. Cancer Cytopathol. 2015;123:282–288.
Diagnostics company asserts medical and pathology groups prefer cotesting for cervical cancer screening
We are concerned about Dr. Wright’s March 2018 gynecologic cancer coverage of US Preventive Services Task Force (USPSTF) screening guidelines for cervical cancer.
The article suggests that draft USPSTF cervical cancer guidelines issued in September 2017 are final when in fact that is not the case. The USPSTF issued draft guidelines in late 2017, butfinal publication is pending USPSTFrevisions in response to submitted public comments. This means that, for now, existing USPSTF guidelines remain in place, and these guidelines clearly recommend cotesting (high-risk HPV and cytology/Pap) in women 30 to 65 years of age every 5 years as an appropriate screening modality, in alignment with the American College of Obstetricians and Gynecologists, the American Society for Colposcopy and Cervical Pathology, and the American Cancer Society, among others.
It is also notable that the proposed USPSTF guidelines have been met with sharp resistance. ACOG, as well as several organizations, including the American Society of Clinical Pathology, American Society of Cytopathology, the American Society for Cytotechnology, the College of American Pathologists, the International Academy of Cytology, and the Papanicolaou Society of Cytopathology, cite concerns with the proposed USPSTF guidelines and continue to argue in favor of cotesting in women 30 to 65 years of age.1,2
We also fear that Dr. Wright may have provided data out of context. For instance, he notes that the USPSTF, in its draft guidelines, found that cotesting increased the number of follow-up tests but did not increase detection of CIN3+ in a decision model. Yet, the USPSTF analysis overrelied on research from European populations (not representative of the US cervical cancer experience) and excluded peer-reviewed data of women in the United States, which clearly shows that HPV-Pap together catches more cervical cancers than either Pap or HPV alone.3
D.P. Alagia, MD, and Harvey W. Kaufman, MD, MBA Quest Diagnostics Madison, New Jersey
Dr. Wright responds
I thank Drs. Alagia and Kaufman for their interest in the work and their comments regarding the USPSTF cervical cancer guidelines. As stated in the article, the USPSTF recommendations are currently in draft form and subject to revision based on public comment. The guidelines are a synthesis of best available evidence and are meant to weigh the benefits and harms of various cervical cancer screening strategies. The recommendations are based in part on simulation modeling that incorporates available evidence and projects the long-term effects of multiple rounds of screening. While the decision models incorporated a large amount of data and were robust in a variety of sensitivity analyses, as with all decision analyses, they are limited by the underlying assumptions utilized in the model. Over the last 2 decades, screening practices for cervical cancer have dramatically shifted. Highlighting the USPSTF draft guidelines was meant to raise awareness among clinicians and policy makers of the evolving role of high-risk HPV testing, either alone or in combination with cytology, as a screening modality for cervical cancer.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Diagnostics company asserts medical and pathology groups prefer cotesting for cervical cancer screening
We are concerned about Dr. Wright’s March 2018 gynecologic cancer coverage of US Preventive Services Task Force (USPSTF) screening guidelines for cervical cancer.
The article suggests that draft USPSTF cervical cancer guidelines issued in September 2017 are final when in fact that is not the case. The USPSTF issued draft guidelines in late 2017, butfinal publication is pending USPSTFrevisions in response to submitted public comments. This means that, for now, existing USPSTF guidelines remain in place, and these guidelines clearly recommend cotesting (high-risk HPV and cytology/Pap) in women 30 to 65 years of age every 5 years as an appropriate screening modality, in alignment with the American College of Obstetricians and Gynecologists, the American Society for Colposcopy and Cervical Pathology, and the American Cancer Society, among others.
It is also notable that the proposed USPSTF guidelines have been met with sharp resistance. ACOG, as well as several organizations, including the American Society of Clinical Pathology, American Society of Cytopathology, the American Society for Cytotechnology, the College of American Pathologists, the International Academy of Cytology, and the Papanicolaou Society of Cytopathology, cite concerns with the proposed USPSTF guidelines and continue to argue in favor of cotesting in women 30 to 65 years of age.1,2
We also fear that Dr. Wright may have provided data out of context. For instance, he notes that the USPSTF, in its draft guidelines, found that cotesting increased the number of follow-up tests but did not increase detection of CIN3+ in a decision model. Yet, the USPSTF analysis overrelied on research from European populations (not representative of the US cervical cancer experience) and excluded peer-reviewed data of women in the United States, which clearly shows that HPV-Pap together catches more cervical cancers than either Pap or HPV alone.3
D.P. Alagia, MD, and Harvey W. Kaufman, MD, MBA Quest Diagnostics Madison, New Jersey
Dr. Wright responds
I thank Drs. Alagia and Kaufman for their interest in the work and their comments regarding the USPSTF cervical cancer guidelines. As stated in the article, the USPSTF recommendations are currently in draft form and subject to revision based on public comment. The guidelines are a synthesis of best available evidence and are meant to weigh the benefits and harms of various cervical cancer screening strategies. The recommendations are based in part on simulation modeling that incorporates available evidence and projects the long-term effects of multiple rounds of screening. While the decision models incorporated a large amount of data and were robust in a variety of sensitivity analyses, as with all decision analyses, they are limited by the underlying assumptions utilized in the model. Over the last 2 decades, screening practices for cervical cancer have dramatically shifted. Highlighting the USPSTF draft guidelines was meant to raise awareness among clinicians and policy makers of the evolving role of high-risk HPV testing, either alone or in combination with cytology, as a screening modality for cervical cancer.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
References
American College of Obstetricians and Gynecologists. Leading women’s health care groups issue joint statement on USPSTF draft cervical cancer screening recommendations. September 13, 2017. https://www.acog.org/About-ACOG/News-Room/Statements/2017/Leading-Womens-Health-Care-Groups-Issue-Joint-Statement-on-USPSTF. Accessed July 5, 2018.
Cytopathology Education and Technology Consortium. Response to new USPSTF guidelines for cervical cancer screening. October 2, 2017. https://s3.amazonaws.com/ascpcdn/static/ONELab/pdf/2017/CETC+-USPSTF+Letter+10-2-17.PDF. Accessed July 5, 2018.
Blatt AJ, Kennedy R, Luff RD, Austin RM, Rabin DS. Comparison of cervical cancer screening results among 256,648 women in multiple clinical practices. Cancer Cytopathol. 2015;123:282–288.
References
American College of Obstetricians and Gynecologists. Leading women’s health care groups issue joint statement on USPSTF draft cervical cancer screening recommendations. September 13, 2017. https://www.acog.org/About-ACOG/News-Room/Statements/2017/Leading-Womens-Health-Care-Groups-Issue-Joint-Statement-on-USPSTF. Accessed July 5, 2018.
Cytopathology Education and Technology Consortium. Response to new USPSTF guidelines for cervical cancer screening. October 2, 2017. https://s3.amazonaws.com/ascpcdn/static/ONELab/pdf/2017/CETC+-USPSTF+Letter+10-2-17.PDF. Accessed July 5, 2018.
Blatt AJ, Kennedy R, Luff RD, Austin RM, Rabin DS. Comparison of cervical cancer screening results among 256,648 women in multiple clinical practices. Cancer Cytopathol. 2015;123:282–288.
Title X, a bill originally passed in 1970 under President Nixon, is the only federal grant program dedicated to providing family planning services as well as other preventive health care to primarily low-income patients. It is estimated that 70% of patients using Title X services are below the federal poverty level and more than 60% are uninsured or underinsured.1
In 2015 alone, Title X clinics served 3.8 million women, preventing 822,300 unintended pregnancies and 277,800 abortions.2 These clinics provide comprehensive family planning services including information, counseling, and referrals for abortion services. Title X clinics do not use the funding to provide abortion care, and no federal funding from Title X has ever been used to pay for abortions.
FIGURE The American College of Obstetricians and Gynecologists has provided this graphic for easy sharing
Proposed rule changes
The Trump Administration has proposed several new rules for Title X grant recipients.
Here are the main changes3:
There must be a “financial and physical” separation between a clinic that is a Title X grant recipient and a facility where “abortion is a method of family planning.” This would prevent health centers that receive Title X funding from providing abortions at the same facility. This rule would predominantly affect health centers like Planned Parenthood. Although these clinics already have a financial separation from abortion care, there would not be a physical one in most situations and these clinics would lose Title X funding or be forced to stop providing abortion services.
Providers who work at a clinic that receives Title X funding but provides abortions at a completely different facility may be ineligible for ongoing Title X grant money. In the new changes, “funds may not be used…to support the separate abortion business of Title X grant subrecipient.” The changes also propose to “protect Title X providers” from choosing between the health of their patients and their consciences. It plans to do this by removing the requirement to provide abortion counseling and referral and allows “non-directive” counseling.
There would also be a requirement to encourage more parental involvement in minors’ decision making. While clinics already discuss parental involvement, the change would seek to increase the encouragement to young patients to involve parents. Most young patients do involve a parent or guardian in their care; however, many Title X clinics serve young patients who seek care confidentially. Patients seek confidential care due to a multitude of reasons, including history of abuse, lack of trust, and intimate partner violence.
“A Title X project may not perform, promote, refer for, or support abortion as a method of family planning.” Although the rule does not prevent providers from discussing abortions, clinicians could offer little guidance if a patient opts for an abortion. Providers can give a list of “qualified, comprehensive health service providers” but may not disclose which, if any, of the providers perform abortions.
Take action
Title X provides important health care services to low-income, uninsured, and underinsured patients. These proposals put access to comprehensive health care for vulnerable populations at risk. Medical organizations including the American Medical Association and American College of Obstetricians and Gynecologists have made statements against the proposed changes to Title X. As ObGyns, we need to ensure our patients are fully informed and have access to all family planning and preventive health services.
Call or email your local representative and tell them you oppose the changes to Title X. Find your representatives here.
Follow ACOG’s Action Center on protecting Title X, which includes a flyer for your waiting room.
Send a message to the Health and Human Services Secretary. Submit a formal comment through July 31, 2018, on the Federal Registrar website expressing your thoughts with these proposed changes.
References
Title X: Helping ensure access to high-quality care. National family planning website. https://www.nationalfamilyplanning.org/document.doc?id=514. Accessed July 25, 2018.
Publicly Funded Contraceptive Services at U.S. Clinics, 2015. Guttmacher website. https://www.guttmacher.org/article/2018/06/domestic-gag-rule-and-more-administrations-proposed-changes-title-x. Accessed July 25, 2018.
Compliance with statutory program integrity requirements. Federal register website. https://www.federalregister.gov/documents/2018/06/01/2018-11673/compliance-with-statutory-program-integrity-requirements. Accessed July 25, 2018.
Author and Disclosure Information
Dr. Kellogg is Resident, Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts.
Dr. Evans is Assistant Professor, Tufts University School of Medicine; Associate Program Director, Department of Obstetrics and Gynecology, Tufts Medical Center.
The authors report no financial relationships relevant to this article.
Dr. Kellogg is Resident, Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts.
Dr. Evans is Assistant Professor, Tufts University School of Medicine; Associate Program Director, Department of Obstetrics and Gynecology, Tufts Medical Center.
The authors report no financial relationships relevant to this article.
Author and Disclosure Information
Dr. Kellogg is Resident, Department of Obstetrics and Gynecology, Tufts Medical Center, Boston, Massachusetts.
Dr. Evans is Assistant Professor, Tufts University School of Medicine; Associate Program Director, Department of Obstetrics and Gynecology, Tufts Medical Center.
The authors report no financial relationships relevant to this article.
The facts
Title X, a bill originally passed in 1970 under President Nixon, is the only federal grant program dedicated to providing family planning services as well as other preventive health care to primarily low-income patients. It is estimated that 70% of patients using Title X services are below the federal poverty level and more than 60% are uninsured or underinsured.1
In 2015 alone, Title X clinics served 3.8 million women, preventing 822,300 unintended pregnancies and 277,800 abortions.2 These clinics provide comprehensive family planning services including information, counseling, and referrals for abortion services. Title X clinics do not use the funding to provide abortion care, and no federal funding from Title X has ever been used to pay for abortions.
FIGURE The American College of Obstetricians and Gynecologists has provided this graphic for easy sharing
Proposed rule changes
The Trump Administration has proposed several new rules for Title X grant recipients.
Here are the main changes3:
There must be a “financial and physical” separation between a clinic that is a Title X grant recipient and a facility where “abortion is a method of family planning.” This would prevent health centers that receive Title X funding from providing abortions at the same facility. This rule would predominantly affect health centers like Planned Parenthood. Although these clinics already have a financial separation from abortion care, there would not be a physical one in most situations and these clinics would lose Title X funding or be forced to stop providing abortion services.
Providers who work at a clinic that receives Title X funding but provides abortions at a completely different facility may be ineligible for ongoing Title X grant money. In the new changes, “funds may not be used…to support the separate abortion business of Title X grant subrecipient.” The changes also propose to “protect Title X providers” from choosing between the health of their patients and their consciences. It plans to do this by removing the requirement to provide abortion counseling and referral and allows “non-directive” counseling.
There would also be a requirement to encourage more parental involvement in minors’ decision making. While clinics already discuss parental involvement, the change would seek to increase the encouragement to young patients to involve parents. Most young patients do involve a parent or guardian in their care; however, many Title X clinics serve young patients who seek care confidentially. Patients seek confidential care due to a multitude of reasons, including history of abuse, lack of trust, and intimate partner violence.
“A Title X project may not perform, promote, refer for, or support abortion as a method of family planning.” Although the rule does not prevent providers from discussing abortions, clinicians could offer little guidance if a patient opts for an abortion. Providers can give a list of “qualified, comprehensive health service providers” but may not disclose which, if any, of the providers perform abortions.
Take action
Title X provides important health care services to low-income, uninsured, and underinsured patients. These proposals put access to comprehensive health care for vulnerable populations at risk. Medical organizations including the American Medical Association and American College of Obstetricians and Gynecologists have made statements against the proposed changes to Title X. As ObGyns, we need to ensure our patients are fully informed and have access to all family planning and preventive health services.
Call or email your local representative and tell them you oppose the changes to Title X. Find your representatives here.
Follow ACOG’s Action Center on protecting Title X, which includes a flyer for your waiting room.
Send a message to the Health and Human Services Secretary. Submit a formal comment through July 31, 2018, on the Federal Registrar website expressing your thoughts with these proposed changes.
The facts
Title X, a bill originally passed in 1970 under President Nixon, is the only federal grant program dedicated to providing family planning services as well as other preventive health care to primarily low-income patients. It is estimated that 70% of patients using Title X services are below the federal poverty level and more than 60% are uninsured or underinsured.1
In 2015 alone, Title X clinics served 3.8 million women, preventing 822,300 unintended pregnancies and 277,800 abortions.2 These clinics provide comprehensive family planning services including information, counseling, and referrals for abortion services. Title X clinics do not use the funding to provide abortion care, and no federal funding from Title X has ever been used to pay for abortions.
FIGURE The American College of Obstetricians and Gynecologists has provided this graphic for easy sharing
Proposed rule changes
The Trump Administration has proposed several new rules for Title X grant recipients.
Here are the main changes3:
There must be a “financial and physical” separation between a clinic that is a Title X grant recipient and a facility where “abortion is a method of family planning.” This would prevent health centers that receive Title X funding from providing abortions at the same facility. This rule would predominantly affect health centers like Planned Parenthood. Although these clinics already have a financial separation from abortion care, there would not be a physical one in most situations and these clinics would lose Title X funding or be forced to stop providing abortion services.
Providers who work at a clinic that receives Title X funding but provides abortions at a completely different facility may be ineligible for ongoing Title X grant money. In the new changes, “funds may not be used…to support the separate abortion business of Title X grant subrecipient.” The changes also propose to “protect Title X providers” from choosing between the health of their patients and their consciences. It plans to do this by removing the requirement to provide abortion counseling and referral and allows “non-directive” counseling.
There would also be a requirement to encourage more parental involvement in minors’ decision making. While clinics already discuss parental involvement, the change would seek to increase the encouragement to young patients to involve parents. Most young patients do involve a parent or guardian in their care; however, many Title X clinics serve young patients who seek care confidentially. Patients seek confidential care due to a multitude of reasons, including history of abuse, lack of trust, and intimate partner violence.
“A Title X project may not perform, promote, refer for, or support abortion as a method of family planning.” Although the rule does not prevent providers from discussing abortions, clinicians could offer little guidance if a patient opts for an abortion. Providers can give a list of “qualified, comprehensive health service providers” but may not disclose which, if any, of the providers perform abortions.
Take action
Title X provides important health care services to low-income, uninsured, and underinsured patients. These proposals put access to comprehensive health care for vulnerable populations at risk. Medical organizations including the American Medical Association and American College of Obstetricians and Gynecologists have made statements against the proposed changes to Title X. As ObGyns, we need to ensure our patients are fully informed and have access to all family planning and preventive health services.
Call or email your local representative and tell them you oppose the changes to Title X. Find your representatives here.
Follow ACOG’s Action Center on protecting Title X, which includes a flyer for your waiting room.
Send a message to the Health and Human Services Secretary. Submit a formal comment through July 31, 2018, on the Federal Registrar website expressing your thoughts with these proposed changes.
References
Title X: Helping ensure access to high-quality care. National family planning website. https://www.nationalfamilyplanning.org/document.doc?id=514. Accessed July 25, 2018.
Publicly Funded Contraceptive Services at U.S. Clinics, 2015. Guttmacher website. https://www.guttmacher.org/article/2018/06/domestic-gag-rule-and-more-administrations-proposed-changes-title-x. Accessed July 25, 2018.
Compliance with statutory program integrity requirements. Federal register website. https://www.federalregister.gov/documents/2018/06/01/2018-11673/compliance-with-statutory-program-integrity-requirements. Accessed July 25, 2018.
References
Title X: Helping ensure access to high-quality care. National family planning website. https://www.nationalfamilyplanning.org/document.doc?id=514. Accessed July 25, 2018.
Publicly Funded Contraceptive Services at U.S. Clinics, 2015. Guttmacher website. https://www.guttmacher.org/article/2018/06/domestic-gag-rule-and-more-administrations-proposed-changes-title-x. Accessed July 25, 2018.
Compliance with statutory program integrity requirements. Federal register website. https://www.federalregister.gov/documents/2018/06/01/2018-11673/compliance-with-statutory-program-integrity-requirements. Accessed July 25, 2018.
The Food and Drug Administration has approved elagolix (Orilissa) for oral treatment of moderate to severe pain associated with endometriosis, announced AbbVie and Neurocrine Biosciences; this approval makes it the first such treatment in more than a decade. It is expected to be available in the United States in early August.
Elagolix is a gonadotropin-releasing hormone (GnRH) antagonist and the first and only one developed specifically for managing this kind of pain.
The approval is based on two 6-month, randomized, double-blind, placebo-controlled phase 3 trials that compared a total of 952 adult women treated with either elagolix with 734 treated with placebo. All of the women experienced moderate to severe endometriosis pain; their ages ranged from 18 to 49 years.
Of the women in the treatment group, 475 were treated with a 150-mg daily dose, and 477 were treated with a 200-mg twice-daily dose. Both treatment groups showed significantly greater mean reductions in pain – both daily menstrual and nonmenstrual pelvic pain – at 6 months. Furthermore, women in the 200-mg twice-daily group also showed statistically significant greater reductions in pain with sex at 3 months, compared with placebo. Altogether, these represent the three most common kinds of endometriosis pain.
The most concerning adverse event associated with elagolix is dose-dependent decreases in bone mineral density; this effect limits treatment to either 150 mg daily for up to 24 months or 200 mg twice daily for up to 6 months. Bone mineral density loss might not be completely reversible, even with treatment cessation. Common adverse events (occurring in at least 5%) included hot flush/night sweats, headache, and nausea. Elagolix is not recommended for women who are or may be pregnant, have osteoporosis, have severe liver disease, or take strong OATP1B1 inhibitors.
The Food and Drug Administration has approved elagolix (Orilissa) for oral treatment of moderate to severe pain associated with endometriosis, announced AbbVie and Neurocrine Biosciences; this approval makes it the first such treatment in more than a decade. It is expected to be available in the United States in early August.
Elagolix is a gonadotropin-releasing hormone (GnRH) antagonist and the first and only one developed specifically for managing this kind of pain.
The approval is based on two 6-month, randomized, double-blind, placebo-controlled phase 3 trials that compared a total of 952 adult women treated with either elagolix with 734 treated with placebo. All of the women experienced moderate to severe endometriosis pain; their ages ranged from 18 to 49 years.
Of the women in the treatment group, 475 were treated with a 150-mg daily dose, and 477 were treated with a 200-mg twice-daily dose. Both treatment groups showed significantly greater mean reductions in pain – both daily menstrual and nonmenstrual pelvic pain – at 6 months. Furthermore, women in the 200-mg twice-daily group also showed statistically significant greater reductions in pain with sex at 3 months, compared with placebo. Altogether, these represent the three most common kinds of endometriosis pain.
The most concerning adverse event associated with elagolix is dose-dependent decreases in bone mineral density; this effect limits treatment to either 150 mg daily for up to 24 months or 200 mg twice daily for up to 6 months. Bone mineral density loss might not be completely reversible, even with treatment cessation. Common adverse events (occurring in at least 5%) included hot flush/night sweats, headache, and nausea. Elagolix is not recommended for women who are or may be pregnant, have osteoporosis, have severe liver disease, or take strong OATP1B1 inhibitors.
The Food and Drug Administration has approved elagolix (Orilissa) for oral treatment of moderate to severe pain associated with endometriosis, announced AbbVie and Neurocrine Biosciences; this approval makes it the first such treatment in more than a decade. It is expected to be available in the United States in early August.
Elagolix is a gonadotropin-releasing hormone (GnRH) antagonist and the first and only one developed specifically for managing this kind of pain.
The approval is based on two 6-month, randomized, double-blind, placebo-controlled phase 3 trials that compared a total of 952 adult women treated with either elagolix with 734 treated with placebo. All of the women experienced moderate to severe endometriosis pain; their ages ranged from 18 to 49 years.
Of the women in the treatment group, 475 were treated with a 150-mg daily dose, and 477 were treated with a 200-mg twice-daily dose. Both treatment groups showed significantly greater mean reductions in pain – both daily menstrual and nonmenstrual pelvic pain – at 6 months. Furthermore, women in the 200-mg twice-daily group also showed statistically significant greater reductions in pain with sex at 3 months, compared with placebo. Altogether, these represent the three most common kinds of endometriosis pain.
The most concerning adverse event associated with elagolix is dose-dependent decreases in bone mineral density; this effect limits treatment to either 150 mg daily for up to 24 months or 200 mg twice daily for up to 6 months. Bone mineral density loss might not be completely reversible, even with treatment cessation. Common adverse events (occurring in at least 5%) included hot flush/night sweats, headache, and nausea. Elagolix is not recommended for women who are or may be pregnant, have osteoporosis, have severe liver disease, or take strong OATP1B1 inhibitors.
Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistulas (VVFs) are the most common type of urogenital fistulas – approximately three times more common than ureterovaginal fistulas – and can be a debilitating problem for women.
Most of the research published in recent years on VVFs and other urogenital fistulas comes from developing countries where these abnormal communications are a common complication of obstructed labor. In the United States, despite a relative paucity of data, VVFs are known to occur most often as a sequelae of gynecologic surgery, usually hysterectomy. Estimates of the incidence of VVF and other urogenital fistula formation are debated but have ranged from 0.5% or less after simple hysterectomy to as high as 2% after radical hysterectomy. Most VVFs are believed to occur after hysterectomy performed for benign disease, and many – but not all – are caused by inadvertent bladder injury that was not recognized intraoperatively.
Women who have had one or more cesarean deliveries and those who have had prior pelvic or vaginal surgery are at increased risk. In addition, both radiation therapy and inflammation that occur with diseases such as pelvic inflammatory disease or inflammatory bowel disease can negatively affect tissue quality and healing from surgical procedures – and can lead ultimately to the development of urogenital fistulas – although even less is known about incidence in these cases.
Prevention
Intraoperatively, VVFs may best be prevented through careful mobilization of the bladder off the vaginal wall, the use of delayed absorbable sutures (preferably Vicryl sutures), and the use of cystoscopy to assess the bladder for injury. If cystoscopy is not available, retrograde filling with a Foley catheter will still be helpful.
An overly aggressive approach to creating the bladder flap during hysterectomy and other surgeries can increase the risk of devascularization and the subsequent formation of fistulas. When the blood supply is found to have been compromised, affected tissue can be strengthened by oversewing with imbrication. When an inadvertent cystotomy is identified, repair is often best achieved with omental tissue interposed between the bladder and vagina. If there is any doubt about bladder integrity, an interposition graft between the bladder flap and the vaginal cuff will help reduce the incidence of fistula formation. Whenever overlapping suture lines occur (the vaginal cuff and the cystotomy repair), the risk of VVF formation will increase. Other than that using omentum, peritoneal grafts will also work well.
VVF formation may still occur, however, despite recognition and repair of an injury – and despite normal findings on cystoscopy. In patients who have had prior cesarean deliveries or other prior pelvic surgery, for example, tissue devascularization may cause a delayed injury, with the process of tissue necrosis and VVF formation occurring up to a month after surgery. It is important to appreciate the factors that predispose patients to VVF and to anticipate an increased risk, but in many cases of delayed VVF, it’s quite possible that nothing could have been done to prevent the problem.
Work-up
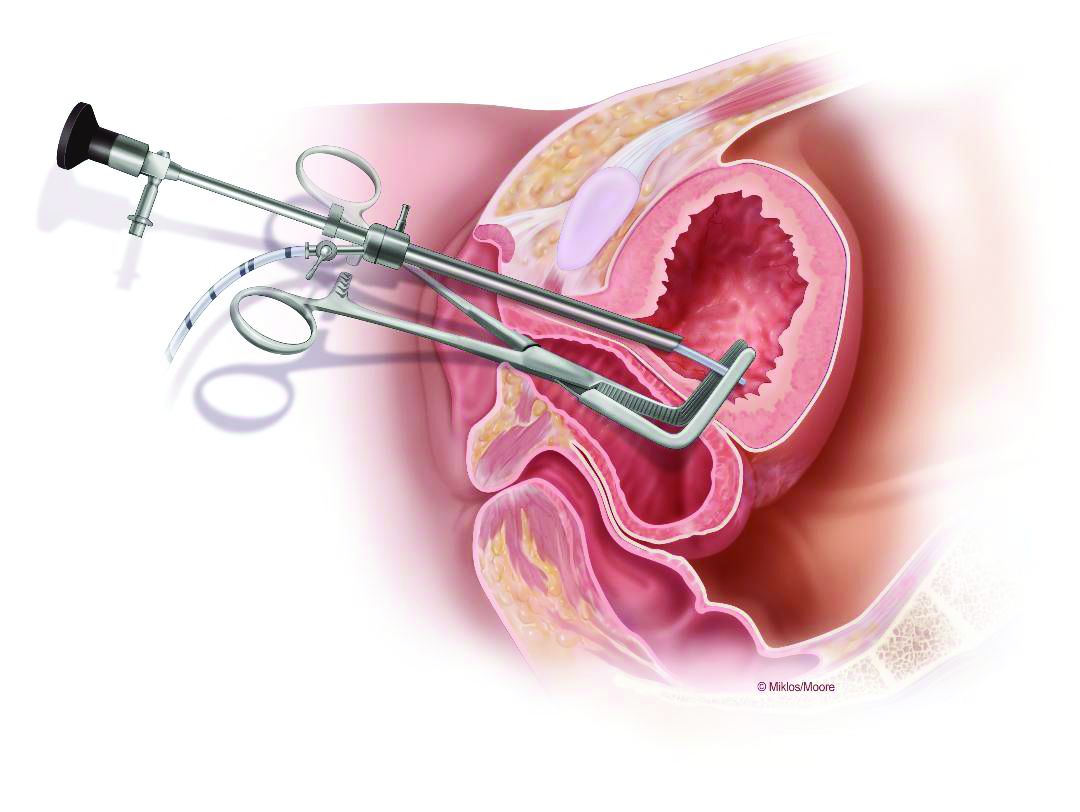
Courtesy of John Miklos, MD
This drawing shows the location of a typical posthysterectomy fistula.
Vesicovaginal fistulas typically present as painless, continuous urine leakage from the vagina. The medical history should include standard questions about pelvic health history and symptom characteristics (in order to exclude hematuria or leakage of fluid other than urine), as well as questions aimed at differentiating symptoms of VVF from other causes of urinary incontinence, such as stress incontinence. In my experience, urine leakage is often incorrectly dismissed as stress incontinence when it is actually VVF. A high index of suspicion will help make an earlier diagnosis. This does not usually change the management, but helps manage the anxiety, expectations, and needs of the patient.
I recommend beginning the work-up for a suspected VVF with a thorough cystoscopic evaluation of the bladder for injury. An irregular appearance of the bladder, signs of inflammation, and poor or absent ureteral efflux are often indicative of VVF in the presence of vaginal leakage. Following cystoscopy, I perform a split speculum examination of the vagina. Most injuries will be on the anterior wall or the apex (cuff). A recently formed fistula may appear as a hole or as a small, red area of granulation tissue with no visible opening.
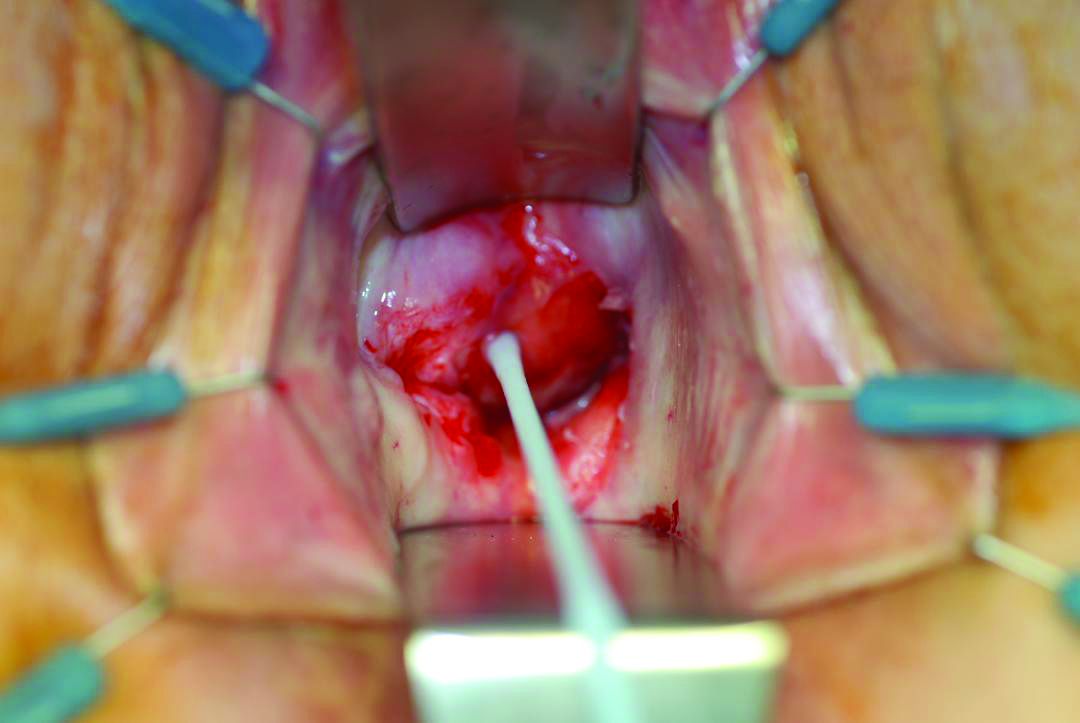
Courtesy of John Miklos, MD
Using a right angle clamp and a cystoscope confirms the fistula.
It can be difficult to visualize the vaginal fistula opening of more mature fistulas; similarly, very small fistulas may be difficult to find because of their size and the anatomy of the vagina. When a prior hysterectomy has led to a fistula, the vaginal fistula opening is typically located in the upper third of the vagina or at the vaginal cuff. If cuff sutures are still intact, this may also make localization of the fistula more difficult.
Leakage in the vagina can sometimes be detected with a retrograde filling of the bladder; other times, it is possible to detect leakage without filling the bladder. In all cases, it’s important to remember that more than one fistula – and more than one fistula type – may be present. A VVF and ureterovaginal fistula will sometimes occur together, which means that abnormal cystoscopy findings in a patient who experiences leakage does not necessarily rule out the presence of a concurrent ureterovaginal fistula.
Phenazopyridine (Pyridium) administered orally will turn the urine orange and can help visualize the leakage of urine into the vagina. When used in combination with the use of blue dye (methylene blue) infused into the bladder, a VVF may be distinguished from a ureterovaginal fistula. To completely evaluate the number and location of fistulas, however, imaging studies are necessary. In my experience, a CT urogram with IV contrast can also help localize ureteral injuries.
Surgical treatment
VVFs can almost always be repaired vaginally. If the fistula is too high in location or too complex, then an abdominal approach, either robotic, laparoscopic, or open, may be necessary. I prefer a vaginal approach to VVF repair whenever feasible because of its straightforward nature, lower morbidity, and high rate of success on the first attempt. Failure rates are between 5% and 20% for each attempt, so more than one surgery may be required. It is not unreasonable to attempt two or three vaginal approach repairs if each successive attempt results in a smaller fistula. A decision to go abdominal must be made based on the chances of a successful vaginal approach and on the patient’s wishes.
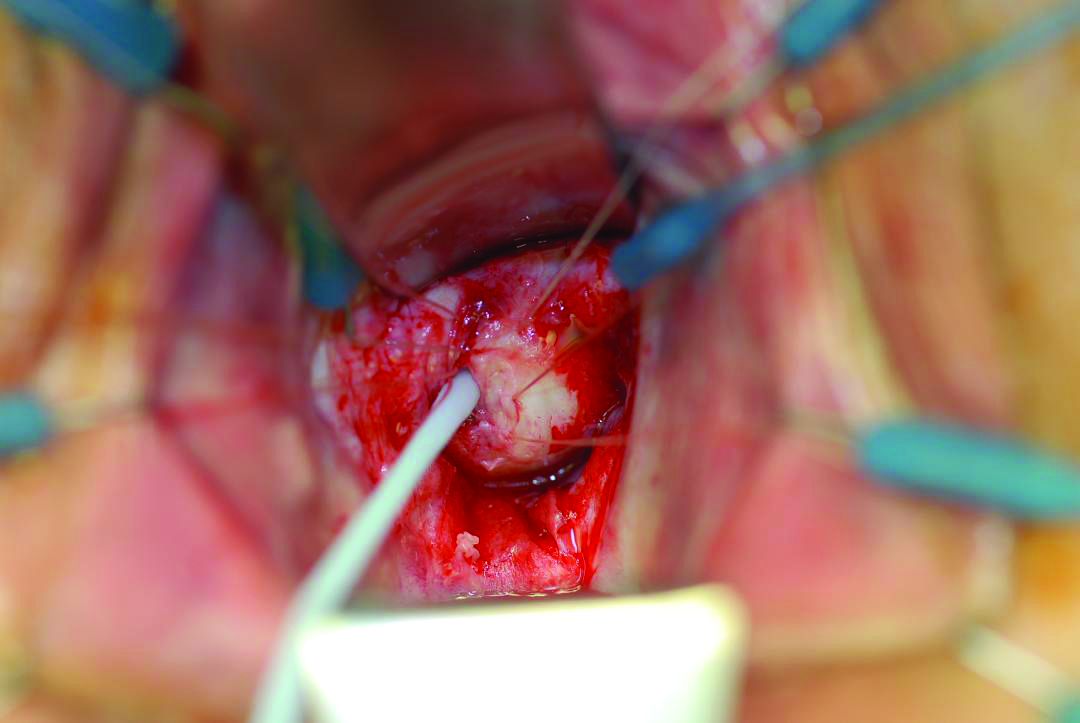
Courtesy of Dionysios Veronikis, MD
A pediatric Foley catheter can be used for traction prior to fistula closure.
Successful fistula repair requires tension-free suture lines, no overlapping suture lines, and good vascular supply to the tissue. The timing of repair has long been controversial, but barring the presence of active pelvic infection, which may require an immediate surgical approach, the timing of fistula repair depends almost solely on the quality of the surrounding tissue. This relates to the need for a good vascular supply.
Early repair can be done if the tissue is pliable and healthy. But in general, if surgery is performed too close to the time of injury, the surrounding tissue will be erythematous and likely to break down with closure. The goal is to wait until the granulation tissue has dissipated and the area is no longer inflamed; after gynecologic surgery, this generally occurs within 6-12 weeks.
Regular vaginal exams about every 2 weeks can be used to monitor progress. During the waiting period, catheterization of the bladder can improve comfort for the patient and may even allow for spontaneous closure of the fistula. In fact, I usually tell patients who are diagnosed with a VVF within the first few weeks after surgery that spontaneous closure is a possible outcome given continuous urinary drainage for up to 30 days, provided that the VVF is small enough. This may be optimistic thinking on the part of the surgeon and the patient, but there is little downside to this approach.
The Latzko technique described in 1992 is still widely used for vaginal repair of VVFs. With this approach, the vaginal epithelium is incised around the fistula, and vaginal epithelial flaps are raised and removed around the fistula tract (in a circle of about 2-3 cm in diameter) for a multilayer approximation of healthy tissues. Several layers are sometimes needed, but in most cases, two layers are sufficient.
In my experience, a modified approach to the traditional Latzko procedure is more successful. Prior to closure, either anterior or posterior to the VVF, a small rim of vaginal epithelium is removed and, on the other side, the epithelium is mobilized at least 1 cm lateral to the fistula on both sides, and about 2 cm distal. This allows for the creation of a small, modified, thumbnail flap that completely patches the fistula closure without tension and without the need for any overlapping suture lines. The key is to secure flap tissue from the side where there appears to be more vaginal tissue. The tissue should be loose; if there appears to be any strain, the repair is likely to fail.
The first layer of closure with delayed absorbable sutures. Some surgeons prefer a running suture instead of interrupted.
There are not enough data from the United States or other developed countries to demonstrate the superiority of this modified approach, but data from the obstetric population in Africa – and my own experience – suggest that it yields better outcomes.
A VVF that is larger may require the use of additional sources of tissue. A graft called the Martius graft, or labial fibrofatty tissue graft, is sometimes used to reinforce repairs of larger fistulas, even those that are high in the vaginal vault. The procedure involves a vertical incision on the inner side of the labium majus and detachment of fibroadipose tissue from its underlying bulbocavernosus muscle. This fat-pad flap is vascularized and thus serves as a pedicled graft. It can be tunneled under the vaginal epithelium to reach the site of closure. The procedure has limited use with the vaginal approach to VVF, but is important to be aware of.
Other sources of grafts or flaps that can sometimes be used with the vaginal approach include the gracilis muscle, the gluteal muscle and peritoneum, and fasciocutaneous tissue from the inner thigh.
The avoidance of overlapping suture lines and multiple layers of closure will help ensure a water-tight closure. If there is any leakage upon testing the integrity of the repair, particularly one that is vaginally approached, such leakage will continue and the repair will have been unsuccessful. In an abdominal surgery for VVF, a small amount of remaining leakage will probably resolve on its own after 10-14 days of catheter placement.
Placement of a Jackson-Pratt (JP) drain is controversial. It has been suggested that a JP drain placed on continuous suction will pull urine out of the bladder and increase the risk of a fistula. I don’t place a JP drain in my repairs as I find them to not be helpful. A cystogram can be done 1 week after repair to confirm healing, but there is some debate about whether or not the procedure is useful at that point. In my experience, if the patient does not have a cystogram and gets postrepair leakage, I have the same information as I would have obtained through a positive finding on a cystogram.
Dr. Garely is chair of obstetrics and gynecology and director of urogynecology and pelvic reconstructive surgery at the South Nassau Communities Hospital, Oceanside, N.Y., and a clinical professor of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai, New York. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Vesicovaginal fistula continues to be the most common form of genitourinary fistula, with resultant diminishment in quality of life secondary to physical and psychosocial distress. While it has been reported that 1 million women in Sub-Saharan Africa have untreated vesicovaginal fistula secondary to obstetric trauma, vesicovaginal fistulas are relatively rare in the United States. Per the United States National Hospital Discharge Survey, in 2007, fewer than 5,000 vesicovaginal fistula repairs were performed out of over 2.3 million procedures involving the female urinary and genital system.
Dr. Charles E. Miller
The rarity of the diagnosis is also reflected in data collected from the English National Health Service, where vesicovaginal fistula occurred in 1 in 788 hysterectomies (although more common in radical hysterectomy, at 1 in 87).
In a recent systematic review and meta-analysis on the management of vesicovaginal fistulas in women following benign gynecologic surgery, Bodner-Adler et al. evaluated 282 full-text articles to identify 124 studies for inclusion (PLoS One. 2017 Feb 22;12[2]:e0171554). Only ten studies involved solely conservative management with prolonged bladder drainage. Dismal success was noted: 8%. Surgery was performed in 96.4% of cases (1379/1430); transvaginal in 39%, transabdominal/transvesical in 36%, laparoscopic/robotic approach in 15%, and transabdominal/transvaginal in 3%. Overall success rate in these surgical cases was 97.98% (95% confidence interval, 96.13%-99.29%); with similar procedural success: transvaginal, 89.96%-97.49%; transabdominal/transvesical, 94.55%-99.18%; and laparoscopic/robotic, 96.85%-99.99%. Studies are very limited comparing the various surgical techniques, with only one study comparing transvaginal, transabdominal, and laparoscopic approaches. Interestingly, in this study, the laparoscopic approach was noted to have the least morbidity (Ou CS et al. J Lapraoendosc Adv Surg Tech A. 2004 Feb;14(1):17-21).
For this edition of the Master Class in Gynecologic Surgery, I have enlisted the assistance of Alan D. Garely, MD, FACOG, FACS, of the Icahn School of Medicine at Mount Sinai, New York. Dr. Garely has served on the board of directors for the American Urogynecologic Society, serves as chair of the gynecology and obstetrics advisory board for the American College of Surgeons, and has published numerous papers and book chapters.
It is a pleasure to welcome Dr. Garely to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL. He has no disclosures related to this column.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
Cervical dysplasia is commonly diagnosed in women who have completed childbearing and don’t desire future fertility. While diagnostic and/or definitive therapy for cervical dysplasia can include hysterectomy, there are important considerations to make when offering this procedure to patients.
Dr. Emma C. Rossi
Pitfalls
Hysterectomy is commonly requested by patients upon learning of cervical dysplasia, particularly if they have chronic human papillomavirus (HPV) infection and have experienced years of frequent surveillance and interventions. They may see hysterectomy as an option to avoid this close surveillance and to be free of their dysplasia. There are two main concerns with offering hysterectomy as the primary surgical option for the management of dysplasia. Firstly, it may not be curative, and secondly, it may be an inadequate excisional procedure, particularly if the patient has occult invasive disease that has not been adequately diagnosed with a loop electrosurgical excision procedure (LEEP) or a cone biopsy procedure.
It is important to counsel these patients that surgery is not a treatment for high-risk HPV infection, which is the underlying etiology of their disease. With that etiology, HPV infection is likely to persist after hysterectomy and they may develop vaginal or vulvar dysplasia. Therefore, the American Society for Colposcopy and Cervical Pathology recommends that cytology and/or high-risk HPV surveillance continue following hysterectomy if that surgery was performed for dysplasia.1 Hysterectomy is not a means to avoid years of surveillance testing. Approximately 10% of women who have hysterectomy for cervical dysplasia develop vaginal dysplasia or cancer after surgery.2,3 This is similar to the likelihood of recurrent dysplasia after an alternative excisional procedure. In my experience, this diagnosis is often met with enormous frustration for the patient who thought that her hysterectomy would be the cure of her HPV-related disease. Thorough colposcopic evaluation of the vagina can be technically challenging after hysterectomy because of difficulty adequately visualizing lesions within the vaginal rugations, particularly within the puckered lateral vaginal fornices, the most common location for dysplasia.3 We will explore the diagnosis and treatment options for vaginal dysplasia further in a future column.
It is critical that, if patients are offered hysterectomy for treatment of cervical dysplasia, they are counseled that it may not be curative, that they will require long-term vaginal surveillance, and that they are at continued risk for vaginal and vulvar cancer.
An additional concern with performing hysterectomy for definitive management of cervical dysplasia is the concern that occult cancer may be missed preoperatively, and that the hysterectomy is inadequate surgical clearance of the disease. Approximately 2%-5% of patients with a high-grade squamous intraepithelial lesion or equivocal Pap test have occult cervical cancer.4 A similar proportion of patients with cervical intraepithelial neoplasia stage III or adenocarcinoma in situ on colposcopy biopsy have invasive carcinoma on evaluation of an excisional specimen.5 The traditional surgical approach has dictated that a modified (type II) or extended (type III) radical hysterectomy be performed in the setting of FIGO stage IA2 or greater cervical cancer. Radical hysterectomies remove parametrial tissue, effectively achieving a wider margin around the primary lesion. This is important because cervical cancer primarily spreads via direct extension.
The appropriate radicality of surgery for microscopic lesions is debated. It has been proposed that for very small, low-risk lesions, a traditional extrafascial hysterectomy or trachelectomy, or possibly even a large conization, may be adequate.6 However, this is controversial, and National Comprehensive Cancer Network guidelines still advocate for radical procedures for these lesions.7 Certainly an excisional procedure (LEEP or cone) should first be performed to define the size and histologic features of the lesion, and ideally, evaluation and counseling with a gynecologic oncologist should be performed prior to offering patients with a stage IA2 or greater lesion an extrafascial hysterectomy. Additionally, a separate decision would need to be made regarding the need for lymphadenectomy, as this is typically recommended for patients with stage IA2 or greater lesions.
Patients should be counseled that, if extrafascial (simple) hysterectomy is chosen as the primary excisional procedure, they may require additional therapy (additional surgery, or radiation and possibly chemotherapy) if cancer is found in the specimen and the parametrial margin is inadequate. Additionally, and of more concern, if the lesion is a bulky lesion extending into the parametrium and not recognized preoperatively, a “cut-through” hysterectomy will be inadvertently performed (in which margins are grossly positive). These situations typically feature heavy blood loss with patients at increased risk for immediate surgical complications. Postoperatively, prognosis is substantially worse for patients who have had a cut-through hysterectomy, compared stage for stage with patients who primarily received a radical procedure with negative margins or primary chemotherapy and radiation.8 Otherwise said, their risk for death is higher if this error is made. Therefore a thorough examination is essential prior to performing hysterectomy for dysplasia. Any suspicion of bulky cancer should be considered a contraindication for proceeding.
Preoperative evaluation
As a rule, no patient should transition directly from cytologic evaluation with Pap screening to hysterectomy. A colposcopic evaluation of the cervix and vagina accompanied with a thorough bimanual rectovaginal examination should always be performed first. Biopsies of the ectocervix and ideally the endocervix should be obtained because the accuracy of histology is greater than that of cytology. For patients with cervical intraepithelial neoplasia stage I lesions, hysterectomy is not appropriate, as these patients have an extremely low risk for the development of cervical cancer, and the risks and costs of hysterectomy are not justified in such a population.
Surgeons should wait at least 6 weeks following conization or LEEP before performing hysterectomy in order to minimize the likelihood of perioperative complications.9
Substituting LEEP or cone with hysterectomy
In general, it is the most prudent approach to first perform a diagnostic excision with LEEP or cone biopsy before proceeding with hysterectomy for definitive surgery. However, there may be some situations in which this is not feasible. In patients whose cervix is very small and flush with the vagina, an excisional procedure may not be technically possible without concern for damage to adjacent structures. In these patients, after a thorough exam has evaluated for gross disease, a hysterectomy may be the only way to adequately diagnose and treat high-grade dysplasia through excision. For patients with limited access to resources, transportation, or a concern for noncompliance with follow-up, surgeons may wish to offer patients primary hysterectomy rather than a staged procedure.
Hysterectomy remains a potential option for treatment of cervical dysplasia. However, patients should be made aware of the risks of undertreatment of occult cancers, the need for long-term surveillance testing, and the risk for future vaginal dysplasia or cancer. Ideally a comprehensive, stepwise assessment from cytology to colposcopy and examination to diagnostic excisional procedure will first take place to proceed safely with this approach.
References
1. Saslow D et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. CA Cancer J Clin. 2012 May-Jun;62(3):147-72.
2. Schockaert S et al. Incidence of vaginal intraepithelial neoplasia after hysterectomy for cervical intraepithelial neoplasia: a retrospective study. Am J Obstet Gynecol. 2008 Aug;199(2):113.e1-5.
3. Kalogirou D et al. Vaginal intraepithelial neoplasia (VAIN) following hysterectomy in patients treated for carcinoma in situ of the cervix. Eur J Gynaecol Oncol. 1997;18(3):188-91.
5. Latif NA et al. Management of adenocarcinoma in situ of the uterine cervix: a comparison of loop electrosurgical excision procedure and cold knife conization. J Low Genit Tract Dis. 2015 Apr;19(2):97-102.
8. Barber HR et al. Operative management of patients previously operated upon for a benign lesion with cervical cancer as a surprise finding. Am J Obstet Gynecol. 1968 Aug 1;101(7):959-65.
9. Sullivan SA et al. Association between timing of cervical excision procedure to minimally invasive hysterectomy and surgical complications. Gynecol Oncol. 2017 Feb;144(2):294-298.
What would the United States look like without Roe v. Wade, the 1973 case that legalized abortion nationwide?
That’s the question now that President Donald Trump has chosen Judge Brett Kavanaugh as his nominee to replace retiring Supreme Court Justice Anthony Kennedy.
trekandshoot/thinkstock
Reversing the landmark case would not automatically make abortion illegal across the country. Instead, it would return the decision about abortion legality to the states, where a patchwork of laws are already in place that render abortion more or less available, largely depending on individual states’ political leanings.
“We think there are 22 states likely to ban abortion without Roe,” because of a combination of factors including existing laws and regulation on the books and the positions of the governor and state legislature, said Amy Myrick, staff attorney at the Center for Reproductive Rights, which represents abortion-rights advocates in court.
“The threat level is very high now,” Ms. Myrick said.
Judge Kavanaugh never opined on Roe v. Wade directly during his tenure on the U.S. District Court in Washington. In his 2006 confirmation hearing for that position, though, he said he would follow Roe v. Wade as a “binding precedent” of the Supreme Court – which lower-court judges are required to do.
Abortion opponents are buoyed by the pick.
“Judge Kavanaugh is an experienced, principled jurist with a strong record of protecting life and constitutional rights,” Marjorie Dannenfelser, president of the Susan B. Anthony List, said in a statement. She spearheaded support for Trump in his presidential campaign after he promised to appoint to the Supreme Court only justices who would overturn Roe v. Wade.
Justice Kennedy, by contrast, was a swing vote on abortion issues. He frequently sided with conservatives to uphold abortion restrictions. However, in key cases in 1992 and 2016, he sided with liberals to uphold Roe’s core finding that the right to abortion is part of a right to privacy that is embedded within the U.S. Constitution.
Even now, with Roe v. Wade’s protections in place, a woman’s ability to access abortion is heavily dependent on where she lives.
According to an analysis by the Guttmacher Institute, a reproductive-rights think tank, 19 states adopted 63 new restrictions on abortion rights and access. At the same time, 21 states adopted 58 measures last year intended to expand access to women’s reproductive health.
Since 2011, states have enacted nearly 1,200 separate abortion restrictions, according to Guttmacher, making these types of laws far more common.
As of now, four states – Louisiana, Mississippi and North and South Dakota – have what are known as abortion “trigger laws.” Those laws – passed long after Roe was handed down – would make abortion illegal if and when the Supreme Court were to say Roe is no more.
“They are designed to make abortion illegal immediately,” said Ms. Myrick.
Another dozen or so states still have abortion bans on the books that predated Roe v. Wade.
Some have been formally blocked by the courts but not repealed. Those bans could, at least in theory, be reinstated, although “someone would have to go into court and ask to lift that injunction,” said Ms. Myrick.
States could simply begin enforcing other bans that were never formally blocked, like one in Alabama that makes abortion providers subject to fines and up to a year in jail.
At the same time, Ms. Myrick said, “there are 20 states where abortion would probably remain safe and legal.”
The path to the high court
Several major challenges to state abortion laws are already in the judicial pipeline. One of these will have to get to the Supreme Court to enable a majority to overturn Roe v. Wade.
“It’s not a question of if, it’s a question of what or when,” said Sarah Lipton-Lubet, vice president for reproductive health and rights at the National Partnership for Women & Families.
The cases fall into three major categories.
The first – and most likely type to result in the court taking a broad look at Roe v. Wade – are “gestational” bans that seek to restrict abortion at a certain point in pregnancy, said Ms. Lipton-Lubet.
Mississippi has a 15-week ban, currently being challenged in federal court; Louisiana enacted a similar ban, but it would take effect only if Mississippi’s law is upheld. Iowa earlier this spring passed a 6-week ban, although that is being challenged in state court under the Iowa Constitution.
The second category involves regulations on abortion providers.
One pending case, for instance, involves an Arkansas law that would effectively ban medication abortions. Finally, there are bans on specific procedures, including several in Texas, Arkansas, and Alabama that would outlaw “dilation and evacuation” abortions, which are the most common type used in the second trimester of pregnancy.
Ms. Myrick and Ms. Lipton-Lubet agree that there is no way to predict which abortion case is likely to reach the high court first.
The case that’s actually closest to the Supreme Court, noted Ms. Myrick, is a challenge to an Indiana law that would outlaw abortion if the woman is seeking it for sex selection or because the fetus could be disabled. A federal appeals court found that law unconstitutional in April.
Many analysts also agree that even with the court’s likely philosophical shift, Roe v. Wade might not actually be overturned at all.
Instead, said Ms. Lipton-Lubet, a more conservative court could “just hollow it out” by allowing restrictive state laws to stand.
“The court cares about things like its own legitimacy,” said Ms. Myrick, “and how often a precedent has been upheld in the past.”
Given that Roe’s central finding – that the decision to have an abortion falls under the constitutional right to privacy – has been upheld three times, even an antiabortion court might be loath to overrule it in its entirety.
KHN’s coverage of women’s health care issues is supported in part by The David and Lucile Packard Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
What would the United States look like without Roe v. Wade, the 1973 case that legalized abortion nationwide?
That’s the question now that President Donald Trump has chosen Judge Brett Kavanaugh as his nominee to replace retiring Supreme Court Justice Anthony Kennedy.
trekandshoot/thinkstock
Reversing the landmark case would not automatically make abortion illegal across the country. Instead, it would return the decision about abortion legality to the states, where a patchwork of laws are already in place that render abortion more or less available, largely depending on individual states’ political leanings.
“We think there are 22 states likely to ban abortion without Roe,” because of a combination of factors including existing laws and regulation on the books and the positions of the governor and state legislature, said Amy Myrick, staff attorney at the Center for Reproductive Rights, which represents abortion-rights advocates in court.
“The threat level is very high now,” Ms. Myrick said.
Judge Kavanaugh never opined on Roe v. Wade directly during his tenure on the U.S. District Court in Washington. In his 2006 confirmation hearing for that position, though, he said he would follow Roe v. Wade as a “binding precedent” of the Supreme Court – which lower-court judges are required to do.
Abortion opponents are buoyed by the pick.
“Judge Kavanaugh is an experienced, principled jurist with a strong record of protecting life and constitutional rights,” Marjorie Dannenfelser, president of the Susan B. Anthony List, said in a statement. She spearheaded support for Trump in his presidential campaign after he promised to appoint to the Supreme Court only justices who would overturn Roe v. Wade.
Justice Kennedy, by contrast, was a swing vote on abortion issues. He frequently sided with conservatives to uphold abortion restrictions. However, in key cases in 1992 and 2016, he sided with liberals to uphold Roe’s core finding that the right to abortion is part of a right to privacy that is embedded within the U.S. Constitution.
Even now, with Roe v. Wade’s protections in place, a woman’s ability to access abortion is heavily dependent on where she lives.
According to an analysis by the Guttmacher Institute, a reproductive-rights think tank, 19 states adopted 63 new restrictions on abortion rights and access. At the same time, 21 states adopted 58 measures last year intended to expand access to women’s reproductive health.
Since 2011, states have enacted nearly 1,200 separate abortion restrictions, according to Guttmacher, making these types of laws far more common.
As of now, four states – Louisiana, Mississippi and North and South Dakota – have what are known as abortion “trigger laws.” Those laws – passed long after Roe was handed down – would make abortion illegal if and when the Supreme Court were to say Roe is no more.
“They are designed to make abortion illegal immediately,” said Ms. Myrick.
Another dozen or so states still have abortion bans on the books that predated Roe v. Wade.
Some have been formally blocked by the courts but not repealed. Those bans could, at least in theory, be reinstated, although “someone would have to go into court and ask to lift that injunction,” said Ms. Myrick.
States could simply begin enforcing other bans that were never formally blocked, like one in Alabama that makes abortion providers subject to fines and up to a year in jail.
At the same time, Ms. Myrick said, “there are 20 states where abortion would probably remain safe and legal.”
The path to the high court
Several major challenges to state abortion laws are already in the judicial pipeline. One of these will have to get to the Supreme Court to enable a majority to overturn Roe v. Wade.
“It’s not a question of if, it’s a question of what or when,” said Sarah Lipton-Lubet, vice president for reproductive health and rights at the National Partnership for Women & Families.
The cases fall into three major categories.
The first – and most likely type to result in the court taking a broad look at Roe v. Wade – are “gestational” bans that seek to restrict abortion at a certain point in pregnancy, said Ms. Lipton-Lubet.
Mississippi has a 15-week ban, currently being challenged in federal court; Louisiana enacted a similar ban, but it would take effect only if Mississippi’s law is upheld. Iowa earlier this spring passed a 6-week ban, although that is being challenged in state court under the Iowa Constitution.
The second category involves regulations on abortion providers.
One pending case, for instance, involves an Arkansas law that would effectively ban medication abortions. Finally, there are bans on specific procedures, including several in Texas, Arkansas, and Alabama that would outlaw “dilation and evacuation” abortions, which are the most common type used in the second trimester of pregnancy.
Ms. Myrick and Ms. Lipton-Lubet agree that there is no way to predict which abortion case is likely to reach the high court first.
The case that’s actually closest to the Supreme Court, noted Ms. Myrick, is a challenge to an Indiana law that would outlaw abortion if the woman is seeking it for sex selection or because the fetus could be disabled. A federal appeals court found that law unconstitutional in April.
Many analysts also agree that even with the court’s likely philosophical shift, Roe v. Wade might not actually be overturned at all.
Instead, said Ms. Lipton-Lubet, a more conservative court could “just hollow it out” by allowing restrictive state laws to stand.
“The court cares about things like its own legitimacy,” said Ms. Myrick, “and how often a precedent has been upheld in the past.”
Given that Roe’s central finding – that the decision to have an abortion falls under the constitutional right to privacy – has been upheld three times, even an antiabortion court might be loath to overrule it in its entirety.
KHN’s coverage of women’s health care issues is supported in part by The David and Lucile Packard Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
What would the United States look like without Roe v. Wade, the 1973 case that legalized abortion nationwide?
That’s the question now that President Donald Trump has chosen Judge Brett Kavanaugh as his nominee to replace retiring Supreme Court Justice Anthony Kennedy.
trekandshoot/thinkstock
Reversing the landmark case would not automatically make abortion illegal across the country. Instead, it would return the decision about abortion legality to the states, where a patchwork of laws are already in place that render abortion more or less available, largely depending on individual states’ political leanings.
“We think there are 22 states likely to ban abortion without Roe,” because of a combination of factors including existing laws and regulation on the books and the positions of the governor and state legislature, said Amy Myrick, staff attorney at the Center for Reproductive Rights, which represents abortion-rights advocates in court.
“The threat level is very high now,” Ms. Myrick said.
Judge Kavanaugh never opined on Roe v. Wade directly during his tenure on the U.S. District Court in Washington. In his 2006 confirmation hearing for that position, though, he said he would follow Roe v. Wade as a “binding precedent” of the Supreme Court – which lower-court judges are required to do.
Abortion opponents are buoyed by the pick.
“Judge Kavanaugh is an experienced, principled jurist with a strong record of protecting life and constitutional rights,” Marjorie Dannenfelser, president of the Susan B. Anthony List, said in a statement. She spearheaded support for Trump in his presidential campaign after he promised to appoint to the Supreme Court only justices who would overturn Roe v. Wade.
Justice Kennedy, by contrast, was a swing vote on abortion issues. He frequently sided with conservatives to uphold abortion restrictions. However, in key cases in 1992 and 2016, he sided with liberals to uphold Roe’s core finding that the right to abortion is part of a right to privacy that is embedded within the U.S. Constitution.
Even now, with Roe v. Wade’s protections in place, a woman’s ability to access abortion is heavily dependent on where she lives.
According to an analysis by the Guttmacher Institute, a reproductive-rights think tank, 19 states adopted 63 new restrictions on abortion rights and access. At the same time, 21 states adopted 58 measures last year intended to expand access to women’s reproductive health.
Since 2011, states have enacted nearly 1,200 separate abortion restrictions, according to Guttmacher, making these types of laws far more common.
As of now, four states – Louisiana, Mississippi and North and South Dakota – have what are known as abortion “trigger laws.” Those laws – passed long after Roe was handed down – would make abortion illegal if and when the Supreme Court were to say Roe is no more.
“They are designed to make abortion illegal immediately,” said Ms. Myrick.
Another dozen or so states still have abortion bans on the books that predated Roe v. Wade.
Some have been formally blocked by the courts but not repealed. Those bans could, at least in theory, be reinstated, although “someone would have to go into court and ask to lift that injunction,” said Ms. Myrick.
States could simply begin enforcing other bans that were never formally blocked, like one in Alabama that makes abortion providers subject to fines and up to a year in jail.
At the same time, Ms. Myrick said, “there are 20 states where abortion would probably remain safe and legal.”
The path to the high court
Several major challenges to state abortion laws are already in the judicial pipeline. One of these will have to get to the Supreme Court to enable a majority to overturn Roe v. Wade.
“It’s not a question of if, it’s a question of what or when,” said Sarah Lipton-Lubet, vice president for reproductive health and rights at the National Partnership for Women & Families.
The cases fall into three major categories.
The first – and most likely type to result in the court taking a broad look at Roe v. Wade – are “gestational” bans that seek to restrict abortion at a certain point in pregnancy, said Ms. Lipton-Lubet.
Mississippi has a 15-week ban, currently being challenged in federal court; Louisiana enacted a similar ban, but it would take effect only if Mississippi’s law is upheld. Iowa earlier this spring passed a 6-week ban, although that is being challenged in state court under the Iowa Constitution.
The second category involves regulations on abortion providers.
One pending case, for instance, involves an Arkansas law that would effectively ban medication abortions. Finally, there are bans on specific procedures, including several in Texas, Arkansas, and Alabama that would outlaw “dilation and evacuation” abortions, which are the most common type used in the second trimester of pregnancy.
Ms. Myrick and Ms. Lipton-Lubet agree that there is no way to predict which abortion case is likely to reach the high court first.
The case that’s actually closest to the Supreme Court, noted Ms. Myrick, is a challenge to an Indiana law that would outlaw abortion if the woman is seeking it for sex selection or because the fetus could be disabled. A federal appeals court found that law unconstitutional in April.
Many analysts also agree that even with the court’s likely philosophical shift, Roe v. Wade might not actually be overturned at all.
Instead, said Ms. Lipton-Lubet, a more conservative court could “just hollow it out” by allowing restrictive state laws to stand.
“The court cares about things like its own legitimacy,” said Ms. Myrick, “and how often a precedent has been upheld in the past.”
Given that Roe’s central finding – that the decision to have an abortion falls under the constitutional right to privacy – has been upheld three times, even an antiabortion court might be loath to overrule it in its entirety.
KHN’s coverage of women’s health care issues is supported in part by The David and Lucile Packard Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Transcutaneous electrical nerve stimulation (TENS) was effective at treating chronic vulvar pain at the vestibule in combination with vaginal diazepam and with placebo in a randomized, double-blind, placebo-controlled trial.
In the TENS/diazepam and TENS/placebo groups, participants reported significant improvements from baseline in pain and sexual functioning by questionnaire and visual analog scale. They also improved in measurements of pelvic floor muscle tone and vestibular nerve fiber current perception threshold.
The study had two groups of 21 women each, all aged 18 years or older and diagnosed (by physical exam) with moderate or severe pelvic floor hypertonic dysfunction. The diazepam was a tablet inserted vaginally daily before bed.
The TENS therapy was also self-administered (after six or seven supervised trial sessions), a recommended three times per week. The device is a 20-mm diameter plastic vaginal probe with gold metallic transversal rings as electrodes, inserted 20 mm, with 30 minutes of electrical stimulation increased slowly until sensation “reached a level described as the maximum tolerable without experiencing pain.” Vulvar pain was assessed on a on a 10-cm visual analog scale and dyspareunia on the Marinoff dyspareunia scale.
At the primary endpoint, the mean change from baseline to 60 days, the diazepam combination improved from 7.5 on the visual scale to 4.7, while the placebo combination improved from 7.2 to 4.3 (P not significant between the groups). Marinoff dyspareunia scores, however, improved from 2.5 to 1.6 and from 2.0 to 1.3, respectively (P less than .01).
Though “very few statistically significant differences in outcomes between the two groups were observed ... our results indicate that diazepam is able to positively change the functions of the pelvic floor muscle often highlighted” in women with vestibulodynia, reported Filippo Murina, MD, of the University of Milan and his coauthors. This conclusion followed from the Marinoff scores and from vaginal surface electromyography. In the latter measure, the diazepam group showed a significantly greater ability to relax the pelvic floor muscle after contraction (3.8 vs. 2.4 microvolts; P = .01), compared with the placebo group.
“We also observed that TENS itself is essential in reducing vulvar pain and the action of diazepam is useful but not decisive. ... It is possible that vaginal diazepam alone is insufficient to resolve the symptoms related to pelvic floor muscle dysfunction, while vaginal diazepam and TENS together provide a synergistic benefit in vestibulodynia patients,” wrote Dr. Murina and his coauthors.
This study was supported by the Associazione Italiana Vulvodinia. The authors declared no conflicts of interest.
Transcutaneous electrical nerve stimulation (TENS) was effective at treating chronic vulvar pain at the vestibule in combination with vaginal diazepam and with placebo in a randomized, double-blind, placebo-controlled trial.
In the TENS/diazepam and TENS/placebo groups, participants reported significant improvements from baseline in pain and sexual functioning by questionnaire and visual analog scale. They also improved in measurements of pelvic floor muscle tone and vestibular nerve fiber current perception threshold.
The study had two groups of 21 women each, all aged 18 years or older and diagnosed (by physical exam) with moderate or severe pelvic floor hypertonic dysfunction. The diazepam was a tablet inserted vaginally daily before bed.
The TENS therapy was also self-administered (after six or seven supervised trial sessions), a recommended three times per week. The device is a 20-mm diameter plastic vaginal probe with gold metallic transversal rings as electrodes, inserted 20 mm, with 30 minutes of electrical stimulation increased slowly until sensation “reached a level described as the maximum tolerable without experiencing pain.” Vulvar pain was assessed on a on a 10-cm visual analog scale and dyspareunia on the Marinoff dyspareunia scale.
At the primary endpoint, the mean change from baseline to 60 days, the diazepam combination improved from 7.5 on the visual scale to 4.7, while the placebo combination improved from 7.2 to 4.3 (P not significant between the groups). Marinoff dyspareunia scores, however, improved from 2.5 to 1.6 and from 2.0 to 1.3, respectively (P less than .01).
Though “very few statistically significant differences in outcomes between the two groups were observed ... our results indicate that diazepam is able to positively change the functions of the pelvic floor muscle often highlighted” in women with vestibulodynia, reported Filippo Murina, MD, of the University of Milan and his coauthors. This conclusion followed from the Marinoff scores and from vaginal surface electromyography. In the latter measure, the diazepam group showed a significantly greater ability to relax the pelvic floor muscle after contraction (3.8 vs. 2.4 microvolts; P = .01), compared with the placebo group.
“We also observed that TENS itself is essential in reducing vulvar pain and the action of diazepam is useful but not decisive. ... It is possible that vaginal diazepam alone is insufficient to resolve the symptoms related to pelvic floor muscle dysfunction, while vaginal diazepam and TENS together provide a synergistic benefit in vestibulodynia patients,” wrote Dr. Murina and his coauthors.
This study was supported by the Associazione Italiana Vulvodinia. The authors declared no conflicts of interest.
Transcutaneous electrical nerve stimulation (TENS) was effective at treating chronic vulvar pain at the vestibule in combination with vaginal diazepam and with placebo in a randomized, double-blind, placebo-controlled trial.
In the TENS/diazepam and TENS/placebo groups, participants reported significant improvements from baseline in pain and sexual functioning by questionnaire and visual analog scale. They also improved in measurements of pelvic floor muscle tone and vestibular nerve fiber current perception threshold.
The study had two groups of 21 women each, all aged 18 years or older and diagnosed (by physical exam) with moderate or severe pelvic floor hypertonic dysfunction. The diazepam was a tablet inserted vaginally daily before bed.
The TENS therapy was also self-administered (after six or seven supervised trial sessions), a recommended three times per week. The device is a 20-mm diameter plastic vaginal probe with gold metallic transversal rings as electrodes, inserted 20 mm, with 30 minutes of electrical stimulation increased slowly until sensation “reached a level described as the maximum tolerable without experiencing pain.” Vulvar pain was assessed on a on a 10-cm visual analog scale and dyspareunia on the Marinoff dyspareunia scale.
At the primary endpoint, the mean change from baseline to 60 days, the diazepam combination improved from 7.5 on the visual scale to 4.7, while the placebo combination improved from 7.2 to 4.3 (P not significant between the groups). Marinoff dyspareunia scores, however, improved from 2.5 to 1.6 and from 2.0 to 1.3, respectively (P less than .01).
Though “very few statistically significant differences in outcomes between the two groups were observed ... our results indicate that diazepam is able to positively change the functions of the pelvic floor muscle often highlighted” in women with vestibulodynia, reported Filippo Murina, MD, of the University of Milan and his coauthors. This conclusion followed from the Marinoff scores and from vaginal surface electromyography. In the latter measure, the diazepam group showed a significantly greater ability to relax the pelvic floor muscle after contraction (3.8 vs. 2.4 microvolts; P = .01), compared with the placebo group.
“We also observed that TENS itself is essential in reducing vulvar pain and the action of diazepam is useful but not decisive. ... It is possible that vaginal diazepam alone is insufficient to resolve the symptoms related to pelvic floor muscle dysfunction, while vaginal diazepam and TENS together provide a synergistic benefit in vestibulodynia patients,” wrote Dr. Murina and his coauthors.
This study was supported by the Associazione Italiana Vulvodinia. The authors declared no conflicts of interest.