User login
Which antidiabetic for elderly patients? It depends on their CV risk
SAN FRANCISCO – SGLT2 inhibitors did a better job than GLP-1 receptor agonists at preventing heart failure hospitalizations in elderly patients with type 2 diabetes, but at the cost of more strokes, myocardial infarctions, and deaths among those without preexisting cardiovascular disease, according to Harvard University investigators.
Using Medicare claims data and propensity scoring, they matched 43,609 elderly patients who started a sodium-glucose cotransporter 2 (SGLT2) inhibitor for type 2 diabetes, 77% of whom were taking canagliflozin (Invokana), to 43,609 who started a glucagonlike peptide–1 (GLP-1)–receptor agonist, 60% of whom were taking liraglutide (Victoza).
Patients were paired by age, comorbidities, diabetes severity, and dozens of other variables, more than 120 in all. The data window ran from April 2013 through December 2016.
The idea was to compare the drugs directly in order to help clinicians decide which class to choose for older patients as second-line therapy, an important consideration at a time when there’s not much guidance specifically for the elderly, and manufacturers are issuing dueling placebo-controlled trials.
Both classes have shown cardiovascular benefits, but studies were mostly in younger people with preexisting cardiovascular disease (CVD). “The comparative impact of these agents in the older population has not yet been established,” lead investigator Elisabetta Patorno, MD, DrPH, of Harvard University, Boston, said at the annual scientific sessions of the American Diabetes Association.
General themes are emerging from Dr. Patorno’s work; it seems that deciding between the two classes has a lot to do with whether the main concern is heart failure or cardiovascular events. Even so, she said, it’s too early to incorporate the observations into guidelines. The analysis is ongoing, and there are plans to compare impacts on renal disease and other problems.
In the meantime, she and her colleagues found that initiating an SGLT2 inhibitor versus a GLP-1 receptor agonist in the elderly was associated with a 34% decreased risk of heart failure hospitalization (2.5 fewer hospitalizations per 1,000 patient years), with an even larger drop among people who had preexisting CVD.
There was, however, a 41% increased risk of lower limb amputations (0.8 more events per 1,000 patient years) and a 62% increase in diabetic ketoacidosis (DKA, 1 more event), problems previously associated with the class.
Results were comparable – fewer heart failure hospitalizations but more amputations and DKA – when SGLT2 initiation was compared to initiation with dipeptidyl peptidase-4 (DPP-4) inhibitors, another second-line option for type 2 diabetes that includes sitagliptin (Januvia), among others.
There was a 25% increased relative risk of the composite primary outcome of myocardial infarction, stroke, and all-cause mortality when patients without baseline CVD were started on an SGLT2 inhibitor instead of a GLP-1 receptor agonist (3.7 more events per 1,000 patient years). There was no increased risk among patients who already had CVD.
SGLT2 initiation actually had a protective effect, compared with dipeptidyl peptidase-4 inhibitors, with a 23% decreased risk of the composite outcome (6.5 fewer events) among patients both with and without baseline CVD. The findings were all statistically significant.
The average age in the study was 71.5 years; 45% of the subjects were men; 40% had a history of cardiovascular disease; and 60% were on metformin and 24% on insulin at study entry.
The work was funded by the National Institutes of Health. Dr. Patorno disclosed research grants form Boehringer Ingelheim and GlaxoSmithKline. Other investigators reported relationships with numerous pharmaceutical companies.
SAN FRANCISCO – SGLT2 inhibitors did a better job than GLP-1 receptor agonists at preventing heart failure hospitalizations in elderly patients with type 2 diabetes, but at the cost of more strokes, myocardial infarctions, and deaths among those without preexisting cardiovascular disease, according to Harvard University investigators.
Using Medicare claims data and propensity scoring, they matched 43,609 elderly patients who started a sodium-glucose cotransporter 2 (SGLT2) inhibitor for type 2 diabetes, 77% of whom were taking canagliflozin (Invokana), to 43,609 who started a glucagonlike peptide–1 (GLP-1)–receptor agonist, 60% of whom were taking liraglutide (Victoza).
Patients were paired by age, comorbidities, diabetes severity, and dozens of other variables, more than 120 in all. The data window ran from April 2013 through December 2016.
The idea was to compare the drugs directly in order to help clinicians decide which class to choose for older patients as second-line therapy, an important consideration at a time when there’s not much guidance specifically for the elderly, and manufacturers are issuing dueling placebo-controlled trials.
Both classes have shown cardiovascular benefits, but studies were mostly in younger people with preexisting cardiovascular disease (CVD). “The comparative impact of these agents in the older population has not yet been established,” lead investigator Elisabetta Patorno, MD, DrPH, of Harvard University, Boston, said at the annual scientific sessions of the American Diabetes Association.
General themes are emerging from Dr. Patorno’s work; it seems that deciding between the two classes has a lot to do with whether the main concern is heart failure or cardiovascular events. Even so, she said, it’s too early to incorporate the observations into guidelines. The analysis is ongoing, and there are plans to compare impacts on renal disease and other problems.
In the meantime, she and her colleagues found that initiating an SGLT2 inhibitor versus a GLP-1 receptor agonist in the elderly was associated with a 34% decreased risk of heart failure hospitalization (2.5 fewer hospitalizations per 1,000 patient years), with an even larger drop among people who had preexisting CVD.
There was, however, a 41% increased risk of lower limb amputations (0.8 more events per 1,000 patient years) and a 62% increase in diabetic ketoacidosis (DKA, 1 more event), problems previously associated with the class.
Results were comparable – fewer heart failure hospitalizations but more amputations and DKA – when SGLT2 initiation was compared to initiation with dipeptidyl peptidase-4 (DPP-4) inhibitors, another second-line option for type 2 diabetes that includes sitagliptin (Januvia), among others.
There was a 25% increased relative risk of the composite primary outcome of myocardial infarction, stroke, and all-cause mortality when patients without baseline CVD were started on an SGLT2 inhibitor instead of a GLP-1 receptor agonist (3.7 more events per 1,000 patient years). There was no increased risk among patients who already had CVD.
SGLT2 initiation actually had a protective effect, compared with dipeptidyl peptidase-4 inhibitors, with a 23% decreased risk of the composite outcome (6.5 fewer events) among patients both with and without baseline CVD. The findings were all statistically significant.
The average age in the study was 71.5 years; 45% of the subjects were men; 40% had a history of cardiovascular disease; and 60% were on metformin and 24% on insulin at study entry.
The work was funded by the National Institutes of Health. Dr. Patorno disclosed research grants form Boehringer Ingelheim and GlaxoSmithKline. Other investigators reported relationships with numerous pharmaceutical companies.
SAN FRANCISCO – SGLT2 inhibitors did a better job than GLP-1 receptor agonists at preventing heart failure hospitalizations in elderly patients with type 2 diabetes, but at the cost of more strokes, myocardial infarctions, and deaths among those without preexisting cardiovascular disease, according to Harvard University investigators.
Using Medicare claims data and propensity scoring, they matched 43,609 elderly patients who started a sodium-glucose cotransporter 2 (SGLT2) inhibitor for type 2 diabetes, 77% of whom were taking canagliflozin (Invokana), to 43,609 who started a glucagonlike peptide–1 (GLP-1)–receptor agonist, 60% of whom were taking liraglutide (Victoza).
Patients were paired by age, comorbidities, diabetes severity, and dozens of other variables, more than 120 in all. The data window ran from April 2013 through December 2016.
The idea was to compare the drugs directly in order to help clinicians decide which class to choose for older patients as second-line therapy, an important consideration at a time when there’s not much guidance specifically for the elderly, and manufacturers are issuing dueling placebo-controlled trials.
Both classes have shown cardiovascular benefits, but studies were mostly in younger people with preexisting cardiovascular disease (CVD). “The comparative impact of these agents in the older population has not yet been established,” lead investigator Elisabetta Patorno, MD, DrPH, of Harvard University, Boston, said at the annual scientific sessions of the American Diabetes Association.
General themes are emerging from Dr. Patorno’s work; it seems that deciding between the two classes has a lot to do with whether the main concern is heart failure or cardiovascular events. Even so, she said, it’s too early to incorporate the observations into guidelines. The analysis is ongoing, and there are plans to compare impacts on renal disease and other problems.
In the meantime, she and her colleagues found that initiating an SGLT2 inhibitor versus a GLP-1 receptor agonist in the elderly was associated with a 34% decreased risk of heart failure hospitalization (2.5 fewer hospitalizations per 1,000 patient years), with an even larger drop among people who had preexisting CVD.
There was, however, a 41% increased risk of lower limb amputations (0.8 more events per 1,000 patient years) and a 62% increase in diabetic ketoacidosis (DKA, 1 more event), problems previously associated with the class.
Results were comparable – fewer heart failure hospitalizations but more amputations and DKA – when SGLT2 initiation was compared to initiation with dipeptidyl peptidase-4 (DPP-4) inhibitors, another second-line option for type 2 diabetes that includes sitagliptin (Januvia), among others.
There was a 25% increased relative risk of the composite primary outcome of myocardial infarction, stroke, and all-cause mortality when patients without baseline CVD were started on an SGLT2 inhibitor instead of a GLP-1 receptor agonist (3.7 more events per 1,000 patient years). There was no increased risk among patients who already had CVD.
SGLT2 initiation actually had a protective effect, compared with dipeptidyl peptidase-4 inhibitors, with a 23% decreased risk of the composite outcome (6.5 fewer events) among patients both with and without baseline CVD. The findings were all statistically significant.
The average age in the study was 71.5 years; 45% of the subjects were men; 40% had a history of cardiovascular disease; and 60% were on metformin and 24% on insulin at study entry.
The work was funded by the National Institutes of Health. Dr. Patorno disclosed research grants form Boehringer Ingelheim and GlaxoSmithKline. Other investigators reported relationships with numerous pharmaceutical companies.
REPORTING FROM ADA 2019
Pivotal trial shows HFrEF benefits from baroreceptor stimulation
SAN FRANCISCO – Baroreflex activation therapy met all four of its primary endpoints in its U.S. pivotal trial of 264 patients with advanced heart failure with reduced ejection fraction who were ineligible for cardiac resynchronization therapy.

The results showed that ongoing baroreflex activation therapy (BAT) via a single, stimulating electrode surgically placed on a patient’s carotid artery led to statistically significant and clinically meaningful improvements in quality of life and functional capacity while also reducing the level of a biomarker of heart failure severity in patients already on guideline-directed medical therapy, Michael R. Zile, MD, said at the annual scientific sessions of the Heart Rhythm Society. He estimated that the device is appropriate for perhaps a third or more of patients with heart failure with reduced ejection fraction (HFrEF), specifically patients with New York Heart Association functional class III disease who are not candidates for treatment with cardiac resynchronization therapy (CRT) and with a blood level of N-terminal pro–brain natriuretic peptide (NT-proBNP) of less than 1,600 pg/mL, a cutoff that excludes patients with very severe class III HFrEF and focuses on those who benefited in the study.
“To our knowledge, this is the first successful pivotal trial of device-based neuromodulation therapy in HFrEF patients,” said Dr. Zile, professor of medicine at the Medical University of South Carolina in Charleston. “We think that BAT fills an unmet need” in a large number of HFrEF patients. He stressed that the placement of the single, 2-mm, unilateral electrode on the baroreceptor-containing carotid sinus is an “extremely safe and simple” surgery. The electrode attaches to a small, subcutaneously placed generator.
Dr. Zile attributed the treatment’s success, in contrast to a prior, failed attempt to treat HFrEF by vagus nerve stimulation (J Am Coll Cardiol. 2016 Jul 12;68[2]:147-56) to BAT’s action via the patient’s brain, which processes the afferent signal it receives from stimulation to in turn inhibit sympathetic activation and upregulate parasympathetic innervation, with both actions benefiting HFrEF patients. “The integrated autonomic balance is the real difference with this device,” he said. Other helpful effects from BAT are reduced heart rate, reduced cardiac remodeling, increased vasodilation, a decrease in elevated blood pressure, increased diuresis, and a drop in renin secretion. The pivotal trial built on findings from a phase 2 study (JACC Heart Fail. 2015 Jun;3[6]:487-96).
The BeAT-HF (Barostim Neo - Baroreflex Activation Therapy for Heart Failure) trial enrolled patients with class III HFrEF with a left ventricular ejection fraction of 35% or less and a 6-minute walk distance of 150-400 m, who were ineligible for CRT, on optimal medical therapy, and who had an elevated NT-proBNP level. After the study randomized 271 patients to either BAT or ongoing medical therapy only (without use of a sham procedure or sham BAT), the results showed a statistically significant benefit for three of the four primary endpoints. Patients treated with BAT for 6 months had statistically significant and clinically meaningful improvements in their quality of life scores as measured on the Minnesota Living With Heart Failure Questionnaire, in their function as measured by the 6-min walk distance, and in the treatment’s safety, based on the combined rate of major adverse neurological and cardiovascular events, which occurred in 6% of patients treated with BAT, which was significantly better than the study’s prespecified performance goal of 15%.
However, for the fourth primary endpoint – reduction in blood levels of NT-proBNP – the BAT-treated patients showed no significant improvement, compared with the controls. The design of BeAT-HF called for consultation with the Food and Drug Administration in such a situation, and further data analysis showed that the problem may have been that some enrolled patients entered with extremely elevated levels of this biomarker. The agency authorized an added protocol that randomized 102 additional patients that matched the initial cohort but had a requirement for an NT-proBNP level of less than 1,600 pg/mL. The 6-month outcomes of these patients were combined with the previously determined outcomes for 162 of the original 271 patients who entered with NT-proBNP levels within the specified limit, producing a total, final study group of 264 patients, of whom 120 received BAT and completed 6-month follow-up, and 125 received medical therapy only and had 6-month follow-up. These patients averaged about 63 years of age, and 20% were women. On average they were on four heart failure medications, and more than three-quarters also had an implanted cardiac device.
The results from an analysis of this cohort showed a statistically significant, 25% relative reduction in blood levels of NT-proBNP in the BAT patients, compared with the controls, and it also confirmed statistically significant and meaningful improvements in quality of life and function on BAT, compared with controls. The 14-point average improvement in the quality of life score in BAT patients, compared with the controls, on the Minnesota Living With Heart Failure Questionnaire was nearly triple the point improvement that’s considered clinically meaningful and hence was “very convincing” about the treatment’s efficacy, noted Dr. Zile, who is also director of cardiology at the VA Medical Center in Charleston. The 25% drop in average NT-proBNP levels “predicts a marked reduction in morbidity and mortality.” He added that researchers have developed a percutaneous, transcatheter method for placing the carotid electrode that will soon undergo clinical testing.
These results “reconfirm the safety of BAT,” but are limited by a relatively short follow-up of 6 months, no data on survival benefit, and by not having echocardiographic data on possible cardiac remodeling, commented Sanjeev Saksena, MD, medical director of the Electrophysiology Research Foundation in Warren, N.J.
BeAT-HF was sponsored by CVRx, the company developing the baroreflex activation device. Dr. Zile has been a consultant to CVRx and to Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, Lilly, Merck, and Novartis. Dr. Saksena had no disclosures.
SOURCE: Zile MR. Heart Rhythm 2019, Abstract, S-LBCT01-04.
The results that Dr. Zile reported are obviously very promising. It was a huge step forward when researchers identified medical treatments that can safely manipulate the autonomic nervous system in patients with heart failure with reduced ejection fraction. Now we are asking what else we can do because we have run into limits on what we can accomplish with drugs alone. The BeAT-HF study is a step in that direction.

Andrew D. Krahn, MD, is professor of medicine and head of cardiology at the University of British Columbia and St. Paul’s Hospital in Vancouver. He has been a consultant to Medtronic and he has received research funding from Boston Scientific and Medtronic. He made these comments as a discussant for BeAT-HF.
The results that Dr. Zile reported are obviously very promising. It was a huge step forward when researchers identified medical treatments that can safely manipulate the autonomic nervous system in patients with heart failure with reduced ejection fraction. Now we are asking what else we can do because we have run into limits on what we can accomplish with drugs alone. The BeAT-HF study is a step in that direction.
Andrew D. Krahn, MD, is professor of medicine and head of cardiology at the University of British Columbia and St. Paul’s Hospital in Vancouver. He has been a consultant to Medtronic and he has received research funding from Boston Scientific and Medtronic. He made these comments as a discussant for BeAT-HF.
The results that Dr. Zile reported are obviously very promising. It was a huge step forward when researchers identified medical treatments that can safely manipulate the autonomic nervous system in patients with heart failure with reduced ejection fraction. Now we are asking what else we can do because we have run into limits on what we can accomplish with drugs alone. The BeAT-HF study is a step in that direction.
Andrew D. Krahn, MD, is professor of medicine and head of cardiology at the University of British Columbia and St. Paul’s Hospital in Vancouver. He has been a consultant to Medtronic and he has received research funding from Boston Scientific and Medtronic. He made these comments as a discussant for BeAT-HF.
SAN FRANCISCO – Baroreflex activation therapy met all four of its primary endpoints in its U.S. pivotal trial of 264 patients with advanced heart failure with reduced ejection fraction who were ineligible for cardiac resynchronization therapy.
The results showed that ongoing baroreflex activation therapy (BAT) via a single, stimulating electrode surgically placed on a patient’s carotid artery led to statistically significant and clinically meaningful improvements in quality of life and functional capacity while also reducing the level of a biomarker of heart failure severity in patients already on guideline-directed medical therapy, Michael R. Zile, MD, said at the annual scientific sessions of the Heart Rhythm Society. He estimated that the device is appropriate for perhaps a third or more of patients with heart failure with reduced ejection fraction (HFrEF), specifically patients with New York Heart Association functional class III disease who are not candidates for treatment with cardiac resynchronization therapy (CRT) and with a blood level of N-terminal pro–brain natriuretic peptide (NT-proBNP) of less than 1,600 pg/mL, a cutoff that excludes patients with very severe class III HFrEF and focuses on those who benefited in the study.
“To our knowledge, this is the first successful pivotal trial of device-based neuromodulation therapy in HFrEF patients,” said Dr. Zile, professor of medicine at the Medical University of South Carolina in Charleston. “We think that BAT fills an unmet need” in a large number of HFrEF patients. He stressed that the placement of the single, 2-mm, unilateral electrode on the baroreceptor-containing carotid sinus is an “extremely safe and simple” surgery. The electrode attaches to a small, subcutaneously placed generator.
Dr. Zile attributed the treatment’s success, in contrast to a prior, failed attempt to treat HFrEF by vagus nerve stimulation (J Am Coll Cardiol. 2016 Jul 12;68[2]:147-56) to BAT’s action via the patient’s brain, which processes the afferent signal it receives from stimulation to in turn inhibit sympathetic activation and upregulate parasympathetic innervation, with both actions benefiting HFrEF patients. “The integrated autonomic balance is the real difference with this device,” he said. Other helpful effects from BAT are reduced heart rate, reduced cardiac remodeling, increased vasodilation, a decrease in elevated blood pressure, increased diuresis, and a drop in renin secretion. The pivotal trial built on findings from a phase 2 study (JACC Heart Fail. 2015 Jun;3[6]:487-96).
The BeAT-HF (Barostim Neo - Baroreflex Activation Therapy for Heart Failure) trial enrolled patients with class III HFrEF with a left ventricular ejection fraction of 35% or less and a 6-minute walk distance of 150-400 m, who were ineligible for CRT, on optimal medical therapy, and who had an elevated NT-proBNP level. After the study randomized 271 patients to either BAT or ongoing medical therapy only (without use of a sham procedure or sham BAT), the results showed a statistically significant benefit for three of the four primary endpoints. Patients treated with BAT for 6 months had statistically significant and clinically meaningful improvements in their quality of life scores as measured on the Minnesota Living With Heart Failure Questionnaire, in their function as measured by the 6-min walk distance, and in the treatment’s safety, based on the combined rate of major adverse neurological and cardiovascular events, which occurred in 6% of patients treated with BAT, which was significantly better than the study’s prespecified performance goal of 15%.
However, for the fourth primary endpoint – reduction in blood levels of NT-proBNP – the BAT-treated patients showed no significant improvement, compared with the controls. The design of BeAT-HF called for consultation with the Food and Drug Administration in such a situation, and further data analysis showed that the problem may have been that some enrolled patients entered with extremely elevated levels of this biomarker. The agency authorized an added protocol that randomized 102 additional patients that matched the initial cohort but had a requirement for an NT-proBNP level of less than 1,600 pg/mL. The 6-month outcomes of these patients were combined with the previously determined outcomes for 162 of the original 271 patients who entered with NT-proBNP levels within the specified limit, producing a total, final study group of 264 patients, of whom 120 received BAT and completed 6-month follow-up, and 125 received medical therapy only and had 6-month follow-up. These patients averaged about 63 years of age, and 20% were women. On average they were on four heart failure medications, and more than three-quarters also had an implanted cardiac device.
The results from an analysis of this cohort showed a statistically significant, 25% relative reduction in blood levels of NT-proBNP in the BAT patients, compared with the controls, and it also confirmed statistically significant and meaningful improvements in quality of life and function on BAT, compared with controls. The 14-point average improvement in the quality of life score in BAT patients, compared with the controls, on the Minnesota Living With Heart Failure Questionnaire was nearly triple the point improvement that’s considered clinically meaningful and hence was “very convincing” about the treatment’s efficacy, noted Dr. Zile, who is also director of cardiology at the VA Medical Center in Charleston. The 25% drop in average NT-proBNP levels “predicts a marked reduction in morbidity and mortality.” He added that researchers have developed a percutaneous, transcatheter method for placing the carotid electrode that will soon undergo clinical testing.
These results “reconfirm the safety of BAT,” but are limited by a relatively short follow-up of 6 months, no data on survival benefit, and by not having echocardiographic data on possible cardiac remodeling, commented Sanjeev Saksena, MD, medical director of the Electrophysiology Research Foundation in Warren, N.J.
BeAT-HF was sponsored by CVRx, the company developing the baroreflex activation device. Dr. Zile has been a consultant to CVRx and to Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, Lilly, Merck, and Novartis. Dr. Saksena had no disclosures.
SOURCE: Zile MR. Heart Rhythm 2019, Abstract, S-LBCT01-04.
SAN FRANCISCO – Baroreflex activation therapy met all four of its primary endpoints in its U.S. pivotal trial of 264 patients with advanced heart failure with reduced ejection fraction who were ineligible for cardiac resynchronization therapy.
The results showed that ongoing baroreflex activation therapy (BAT) via a single, stimulating electrode surgically placed on a patient’s carotid artery led to statistically significant and clinically meaningful improvements in quality of life and functional capacity while also reducing the level of a biomarker of heart failure severity in patients already on guideline-directed medical therapy, Michael R. Zile, MD, said at the annual scientific sessions of the Heart Rhythm Society. He estimated that the device is appropriate for perhaps a third or more of patients with heart failure with reduced ejection fraction (HFrEF), specifically patients with New York Heart Association functional class III disease who are not candidates for treatment with cardiac resynchronization therapy (CRT) and with a blood level of N-terminal pro–brain natriuretic peptide (NT-proBNP) of less than 1,600 pg/mL, a cutoff that excludes patients with very severe class III HFrEF and focuses on those who benefited in the study.
“To our knowledge, this is the first successful pivotal trial of device-based neuromodulation therapy in HFrEF patients,” said Dr. Zile, professor of medicine at the Medical University of South Carolina in Charleston. “We think that BAT fills an unmet need” in a large number of HFrEF patients. He stressed that the placement of the single, 2-mm, unilateral electrode on the baroreceptor-containing carotid sinus is an “extremely safe and simple” surgery. The electrode attaches to a small, subcutaneously placed generator.
Dr. Zile attributed the treatment’s success, in contrast to a prior, failed attempt to treat HFrEF by vagus nerve stimulation (J Am Coll Cardiol. 2016 Jul 12;68[2]:147-56) to BAT’s action via the patient’s brain, which processes the afferent signal it receives from stimulation to in turn inhibit sympathetic activation and upregulate parasympathetic innervation, with both actions benefiting HFrEF patients. “The integrated autonomic balance is the real difference with this device,” he said. Other helpful effects from BAT are reduced heart rate, reduced cardiac remodeling, increased vasodilation, a decrease in elevated blood pressure, increased diuresis, and a drop in renin secretion. The pivotal trial built on findings from a phase 2 study (JACC Heart Fail. 2015 Jun;3[6]:487-96).
The BeAT-HF (Barostim Neo - Baroreflex Activation Therapy for Heart Failure) trial enrolled patients with class III HFrEF with a left ventricular ejection fraction of 35% or less and a 6-minute walk distance of 150-400 m, who were ineligible for CRT, on optimal medical therapy, and who had an elevated NT-proBNP level. After the study randomized 271 patients to either BAT or ongoing medical therapy only (without use of a sham procedure or sham BAT), the results showed a statistically significant benefit for three of the four primary endpoints. Patients treated with BAT for 6 months had statistically significant and clinically meaningful improvements in their quality of life scores as measured on the Minnesota Living With Heart Failure Questionnaire, in their function as measured by the 6-min walk distance, and in the treatment’s safety, based on the combined rate of major adverse neurological and cardiovascular events, which occurred in 6% of patients treated with BAT, which was significantly better than the study’s prespecified performance goal of 15%.
However, for the fourth primary endpoint – reduction in blood levels of NT-proBNP – the BAT-treated patients showed no significant improvement, compared with the controls. The design of BeAT-HF called for consultation with the Food and Drug Administration in such a situation, and further data analysis showed that the problem may have been that some enrolled patients entered with extremely elevated levels of this biomarker. The agency authorized an added protocol that randomized 102 additional patients that matched the initial cohort but had a requirement for an NT-proBNP level of less than 1,600 pg/mL. The 6-month outcomes of these patients were combined with the previously determined outcomes for 162 of the original 271 patients who entered with NT-proBNP levels within the specified limit, producing a total, final study group of 264 patients, of whom 120 received BAT and completed 6-month follow-up, and 125 received medical therapy only and had 6-month follow-up. These patients averaged about 63 years of age, and 20% were women. On average they were on four heart failure medications, and more than three-quarters also had an implanted cardiac device.
The results from an analysis of this cohort showed a statistically significant, 25% relative reduction in blood levels of NT-proBNP in the BAT patients, compared with the controls, and it also confirmed statistically significant and meaningful improvements in quality of life and function on BAT, compared with controls. The 14-point average improvement in the quality of life score in BAT patients, compared with the controls, on the Minnesota Living With Heart Failure Questionnaire was nearly triple the point improvement that’s considered clinically meaningful and hence was “very convincing” about the treatment’s efficacy, noted Dr. Zile, who is also director of cardiology at the VA Medical Center in Charleston. The 25% drop in average NT-proBNP levels “predicts a marked reduction in morbidity and mortality.” He added that researchers have developed a percutaneous, transcatheter method for placing the carotid electrode that will soon undergo clinical testing.
These results “reconfirm the safety of BAT,” but are limited by a relatively short follow-up of 6 months, no data on survival benefit, and by not having echocardiographic data on possible cardiac remodeling, commented Sanjeev Saksena, MD, medical director of the Electrophysiology Research Foundation in Warren, N.J.
BeAT-HF was sponsored by CVRx, the company developing the baroreflex activation device. Dr. Zile has been a consultant to CVRx and to Abbott, AstraZeneca, Bayer, Bristol-Myers Squibb, Lilly, Merck, and Novartis. Dr. Saksena had no disclosures.
SOURCE: Zile MR. Heart Rhythm 2019, Abstract, S-LBCT01-04.
REPORTING FROM HEART RHYTHM 2019
MADIT-CHIC: CRT aids patients with chemotherapy-induced cardiomyopathy
SAN FRANCISCO – Patients with cardiomyopathy secondary to cancer chemotherapy who qualified for cardiac resynchronization therapy (CRT) by having a wide QRS interval showed a virtually uniform, positive response to this treatment in a multicenter study with 30 patients.
This is the first time this therapy has been prospectively assessed in this patient population.
The results “show for the first time that patients with chemotherapy-induced cardiomyopathy [CHIC] who meet criteria for CRT show significant improvement in left ventricular function and clinical symptoms in the short term” during follow-up of 6 months, Jagmeet P. Singh, MD, said at the annual scientific sessions of the Heart Rhythm Society.
Dr. Singh acknowledged that, with 30 patients, the study was small, uncontrolled, had a brief follow-up of 6 months, and was highly selective. It took collaborating investigators at 12 U.S. centers more than 3.5 years to find the 30 participating patients, who had to meet very specific criteria designed to identify true CHIC. Nonetheless, Dr. Singh considered the results convincing enough to shift practice.
Based on the results, “I would certainly feel comfortable using CRT in patients with CHIC,” said Dr. Singh, associate chief of cardiology at Massachusetts General Hospital and professor of medicine at Harvard Medical School, both in Boston. “If a patient has CHIC with a wide QRS interval and evidence for a conduction defect on their ECG, they are a great candidate for CRT. The results highlight that there is a cohort of patients who develop cardiomyopathy after chemotherapy, and these patients are often written off” and until now have generally received little follow-up for their potential development of cardiomyopathy. Dr. Singh expressed hope that the recent emergence of cardio-oncology as a subspecialty will focus attention on CHIC patients.
The MADIT-CHIC (Multicenter Automatic Defibrillator Implantation Trial – Chemotherapy-Induced Cardiomyopathy) study enrolled patients with a history of exposure to a cancer chemotherapy regimen known to cause cardiomyopathy who had no history of heart failure prior to the chemotherapy. All patients had developed clinically apparent heart failure (New York Heart Association functional class II, III, or IV) at least 6 months after completing chemotherapy, had no other apparent cause of the cardiomyopathy as ascertained by a cardio-oncologist, and were on guideline-directed medical therapy. Enrolled patients also had to have a class I or II indication for CRT, with a left ventricular ejection fraction of 35% or less, a QRS interval of at least 120 milliseconds, sinus rhythm and left bundle branch block, or no left bundle branch block and a QRS of at least 150 milliseconds.
Just over three-quarters of the patients had received an anthracycline drug, and 73% had a history of breast cancer, 20% a history of leukemia or lymphoma, and 7% had a history of sarcoma. The patients averaged 64 years of age, and 87% were women. CRT placement occurred 18-256 months after the end of chemotherapy, with a median of 188 months.
The study’s primary endpoint was the change in left ventricular ejection fraction after 6 months, which increased from an average of 28% at baseline to 39% at follow-up, a statistically significant change. Ejection fraction increased in 29 of the 30 patients, with one patient showing a flat response to CRT. Cardiac function and geometry significantly improved by seven other measures, including left ventricular mass and left atrial volume, and the improved ejection fraction was consistent across several subgroup analyses. Patients’ NYHA functional class improved by at least one level in 41% of patients, and 83% of the patients stopped showing clinical features of heart failure after 6 months on CRT.
MADIT-CHIC received funding from Boston Scientific. Dr. Singh has been a consultant to Abbott, Back Beat, Biotronik, Boston Scientific, EBR, Impulse Dynamics, Medtronic, Microport, St. Jude, and Toray, and he has received research support from Abbott and Boston Scientific.
SOURCE: Singh JP et al. HRS 2019, Abstract S-LBCT02-04.
No guideline currently addresses using cardiac resynchronization therapy to treat chemotherapy-induced cardiomyopathy. The findings from MADIT-CHIC showed a striking benefit from treatment with cardiac resynchronization therapy of a magnitude we would expect to see in patients with nonischemic cardiomyopathy. Patients showed improvements in all measures of cardiac performance.
It appears that CHIC can take as long as decades to appear in a patient, but we now need to have a high level of suspicion for this complication. We need to come up with better ways to monitor development of CHIC in patients who have received cancer chemotherapy so that we can give eligible patients this beneficial treatment. We can be optimistic about the potential for benefit from CRT in these patients.
Kenneth A. Ellenbogen, MD , is chief of cardiology and a professor of medicine at Virginia Commonwealth University in Richmond, Va. He has been a consultant to Boston Scientific, Medtronic, and St. Jude; he has received honoraria from Biotronik; and he has received research funding from Boston Scientific and Medtronic. He made these comments as the designated discussant for the MADIT-CHIC report.
No guideline currently addresses using cardiac resynchronization therapy to treat chemotherapy-induced cardiomyopathy. The findings from MADIT-CHIC showed a striking benefit from treatment with cardiac resynchronization therapy of a magnitude we would expect to see in patients with nonischemic cardiomyopathy. Patients showed improvements in all measures of cardiac performance.
It appears that CHIC can take as long as decades to appear in a patient, but we now need to have a high level of suspicion for this complication. We need to come up with better ways to monitor development of CHIC in patients who have received cancer chemotherapy so that we can give eligible patients this beneficial treatment. We can be optimistic about the potential for benefit from CRT in these patients.
Kenneth A. Ellenbogen, MD , is chief of cardiology and a professor of medicine at Virginia Commonwealth University in Richmond, Va. He has been a consultant to Boston Scientific, Medtronic, and St. Jude; he has received honoraria from Biotronik; and he has received research funding from Boston Scientific and Medtronic. He made these comments as the designated discussant for the MADIT-CHIC report.
No guideline currently addresses using cardiac resynchronization therapy to treat chemotherapy-induced cardiomyopathy. The findings from MADIT-CHIC showed a striking benefit from treatment with cardiac resynchronization therapy of a magnitude we would expect to see in patients with nonischemic cardiomyopathy. Patients showed improvements in all measures of cardiac performance.
It appears that CHIC can take as long as decades to appear in a patient, but we now need to have a high level of suspicion for this complication. We need to come up with better ways to monitor development of CHIC in patients who have received cancer chemotherapy so that we can give eligible patients this beneficial treatment. We can be optimistic about the potential for benefit from CRT in these patients.
Kenneth A. Ellenbogen, MD , is chief of cardiology and a professor of medicine at Virginia Commonwealth University in Richmond, Va. He has been a consultant to Boston Scientific, Medtronic, and St. Jude; he has received honoraria from Biotronik; and he has received research funding from Boston Scientific and Medtronic. He made these comments as the designated discussant for the MADIT-CHIC report.
SAN FRANCISCO – Patients with cardiomyopathy secondary to cancer chemotherapy who qualified for cardiac resynchronization therapy (CRT) by having a wide QRS interval showed a virtually uniform, positive response to this treatment in a multicenter study with 30 patients.
This is the first time this therapy has been prospectively assessed in this patient population.
The results “show for the first time that patients with chemotherapy-induced cardiomyopathy [CHIC] who meet criteria for CRT show significant improvement in left ventricular function and clinical symptoms in the short term” during follow-up of 6 months, Jagmeet P. Singh, MD, said at the annual scientific sessions of the Heart Rhythm Society.
Dr. Singh acknowledged that, with 30 patients, the study was small, uncontrolled, had a brief follow-up of 6 months, and was highly selective. It took collaborating investigators at 12 U.S. centers more than 3.5 years to find the 30 participating patients, who had to meet very specific criteria designed to identify true CHIC. Nonetheless, Dr. Singh considered the results convincing enough to shift practice.
Based on the results, “I would certainly feel comfortable using CRT in patients with CHIC,” said Dr. Singh, associate chief of cardiology at Massachusetts General Hospital and professor of medicine at Harvard Medical School, both in Boston. “If a patient has CHIC with a wide QRS interval and evidence for a conduction defect on their ECG, they are a great candidate for CRT. The results highlight that there is a cohort of patients who develop cardiomyopathy after chemotherapy, and these patients are often written off” and until now have generally received little follow-up for their potential development of cardiomyopathy. Dr. Singh expressed hope that the recent emergence of cardio-oncology as a subspecialty will focus attention on CHIC patients.
The MADIT-CHIC (Multicenter Automatic Defibrillator Implantation Trial – Chemotherapy-Induced Cardiomyopathy) study enrolled patients with a history of exposure to a cancer chemotherapy regimen known to cause cardiomyopathy who had no history of heart failure prior to the chemotherapy. All patients had developed clinically apparent heart failure (New York Heart Association functional class II, III, or IV) at least 6 months after completing chemotherapy, had no other apparent cause of the cardiomyopathy as ascertained by a cardio-oncologist, and were on guideline-directed medical therapy. Enrolled patients also had to have a class I or II indication for CRT, with a left ventricular ejection fraction of 35% or less, a QRS interval of at least 120 milliseconds, sinus rhythm and left bundle branch block, or no left bundle branch block and a QRS of at least 150 milliseconds.
Just over three-quarters of the patients had received an anthracycline drug, and 73% had a history of breast cancer, 20% a history of leukemia or lymphoma, and 7% had a history of sarcoma. The patients averaged 64 years of age, and 87% were women. CRT placement occurred 18-256 months after the end of chemotherapy, with a median of 188 months.
The study’s primary endpoint was the change in left ventricular ejection fraction after 6 months, which increased from an average of 28% at baseline to 39% at follow-up, a statistically significant change. Ejection fraction increased in 29 of the 30 patients, with one patient showing a flat response to CRT. Cardiac function and geometry significantly improved by seven other measures, including left ventricular mass and left atrial volume, and the improved ejection fraction was consistent across several subgroup analyses. Patients’ NYHA functional class improved by at least one level in 41% of patients, and 83% of the patients stopped showing clinical features of heart failure after 6 months on CRT.
MADIT-CHIC received funding from Boston Scientific. Dr. Singh has been a consultant to Abbott, Back Beat, Biotronik, Boston Scientific, EBR, Impulse Dynamics, Medtronic, Microport, St. Jude, and Toray, and he has received research support from Abbott and Boston Scientific.
SOURCE: Singh JP et al. HRS 2019, Abstract S-LBCT02-04.
SAN FRANCISCO – Patients with cardiomyopathy secondary to cancer chemotherapy who qualified for cardiac resynchronization therapy (CRT) by having a wide QRS interval showed a virtually uniform, positive response to this treatment in a multicenter study with 30 patients.
This is the first time this therapy has been prospectively assessed in this patient population.
The results “show for the first time that patients with chemotherapy-induced cardiomyopathy [CHIC] who meet criteria for CRT show significant improvement in left ventricular function and clinical symptoms in the short term” during follow-up of 6 months, Jagmeet P. Singh, MD, said at the annual scientific sessions of the Heart Rhythm Society.
Dr. Singh acknowledged that, with 30 patients, the study was small, uncontrolled, had a brief follow-up of 6 months, and was highly selective. It took collaborating investigators at 12 U.S. centers more than 3.5 years to find the 30 participating patients, who had to meet very specific criteria designed to identify true CHIC. Nonetheless, Dr. Singh considered the results convincing enough to shift practice.
Based on the results, “I would certainly feel comfortable using CRT in patients with CHIC,” said Dr. Singh, associate chief of cardiology at Massachusetts General Hospital and professor of medicine at Harvard Medical School, both in Boston. “If a patient has CHIC with a wide QRS interval and evidence for a conduction defect on their ECG, they are a great candidate for CRT. The results highlight that there is a cohort of patients who develop cardiomyopathy after chemotherapy, and these patients are often written off” and until now have generally received little follow-up for their potential development of cardiomyopathy. Dr. Singh expressed hope that the recent emergence of cardio-oncology as a subspecialty will focus attention on CHIC patients.
The MADIT-CHIC (Multicenter Automatic Defibrillator Implantation Trial – Chemotherapy-Induced Cardiomyopathy) study enrolled patients with a history of exposure to a cancer chemotherapy regimen known to cause cardiomyopathy who had no history of heart failure prior to the chemotherapy. All patients had developed clinically apparent heart failure (New York Heart Association functional class II, III, or IV) at least 6 months after completing chemotherapy, had no other apparent cause of the cardiomyopathy as ascertained by a cardio-oncologist, and were on guideline-directed medical therapy. Enrolled patients also had to have a class I or II indication for CRT, with a left ventricular ejection fraction of 35% or less, a QRS interval of at least 120 milliseconds, sinus rhythm and left bundle branch block, or no left bundle branch block and a QRS of at least 150 milliseconds.
Just over three-quarters of the patients had received an anthracycline drug, and 73% had a history of breast cancer, 20% a history of leukemia or lymphoma, and 7% had a history of sarcoma. The patients averaged 64 years of age, and 87% were women. CRT placement occurred 18-256 months after the end of chemotherapy, with a median of 188 months.
The study’s primary endpoint was the change in left ventricular ejection fraction after 6 months, which increased from an average of 28% at baseline to 39% at follow-up, a statistically significant change. Ejection fraction increased in 29 of the 30 patients, with one patient showing a flat response to CRT. Cardiac function and geometry significantly improved by seven other measures, including left ventricular mass and left atrial volume, and the improved ejection fraction was consistent across several subgroup analyses. Patients’ NYHA functional class improved by at least one level in 41% of patients, and 83% of the patients stopped showing clinical features of heart failure after 6 months on CRT.
MADIT-CHIC received funding from Boston Scientific. Dr. Singh has been a consultant to Abbott, Back Beat, Biotronik, Boston Scientific, EBR, Impulse Dynamics, Medtronic, Microport, St. Jude, and Toray, and he has received research support from Abbott and Boston Scientific.
SOURCE: Singh JP et al. HRS 2019, Abstract S-LBCT02-04.
REPORTING FROM HEART RHYTHM 2019
FDA updates warning about Impella RP System
The Food and Drug Administration has reported that the higher postapproval mortality rates seen with Abiomed’s Impella RP System seem concentrated in a certain subgroup of patients only, according to a letter to health care providers.

The letter updates one from February regarding the observation of higher postapproval mortality rates with the temporary right heart pump.
This subgroup, which did not qualify for premarket clinical studies, was more likely to have been in cardiogenic shock for longer than 48 hours, experienced a cardiac arrest, or suffered a preimplant hypoxic or ischemic neurologic event prior to receiving the device, the FDA suggested in this new letter to health care providers. The 30-day survival rate in this subgroup within a postapproval study (PAS) was 10.7% (3 out of 28), while that among patients who would have qualified for the premarket clinical studies was 64.3% (9 of 14), according to the most recent interim results of that study. The rate among patients who would have qualified for premarket studies is similar to that seen among those premarket studies (73.4%); the overall 30-day survival rate in this PAS was 28.6%.
The FDA said that, based on these analyses, it still believes the benefits outweigh the risks when the Impella RP System is “used for the currently approved indication in appropriately selected patients.”
The FDA advises that health care providers review the device’s revised labeling, which now includes a checklist to help understand which patients could benefit the most. It also advises providers to promptly report any adverse events through MedWatch, which can help the FDA identify and understand the risks associated with the Impella RP System.
More information can be found in the FDA’s letter to health care providers, which is available on the FDA website.
The Food and Drug Administration has reported that the higher postapproval mortality rates seen with Abiomed’s Impella RP System seem concentrated in a certain subgroup of patients only, according to a letter to health care providers.
The letter updates one from February regarding the observation of higher postapproval mortality rates with the temporary right heart pump.
This subgroup, which did not qualify for premarket clinical studies, was more likely to have been in cardiogenic shock for longer than 48 hours, experienced a cardiac arrest, or suffered a preimplant hypoxic or ischemic neurologic event prior to receiving the device, the FDA suggested in this new letter to health care providers. The 30-day survival rate in this subgroup within a postapproval study (PAS) was 10.7% (3 out of 28), while that among patients who would have qualified for the premarket clinical studies was 64.3% (9 of 14), according to the most recent interim results of that study. The rate among patients who would have qualified for premarket studies is similar to that seen among those premarket studies (73.4%); the overall 30-day survival rate in this PAS was 28.6%.
The FDA said that, based on these analyses, it still believes the benefits outweigh the risks when the Impella RP System is “used for the currently approved indication in appropriately selected patients.”
The FDA advises that health care providers review the device’s revised labeling, which now includes a checklist to help understand which patients could benefit the most. It also advises providers to promptly report any adverse events through MedWatch, which can help the FDA identify and understand the risks associated with the Impella RP System.
More information can be found in the FDA’s letter to health care providers, which is available on the FDA website.
The Food and Drug Administration has reported that the higher postapproval mortality rates seen with Abiomed’s Impella RP System seem concentrated in a certain subgroup of patients only, according to a letter to health care providers.
The letter updates one from February regarding the observation of higher postapproval mortality rates with the temporary right heart pump.
This subgroup, which did not qualify for premarket clinical studies, was more likely to have been in cardiogenic shock for longer than 48 hours, experienced a cardiac arrest, or suffered a preimplant hypoxic or ischemic neurologic event prior to receiving the device, the FDA suggested in this new letter to health care providers. The 30-day survival rate in this subgroup within a postapproval study (PAS) was 10.7% (3 out of 28), while that among patients who would have qualified for the premarket clinical studies was 64.3% (9 of 14), according to the most recent interim results of that study. The rate among patients who would have qualified for premarket studies is similar to that seen among those premarket studies (73.4%); the overall 30-day survival rate in this PAS was 28.6%.
The FDA said that, based on these analyses, it still believes the benefits outweigh the risks when the Impella RP System is “used for the currently approved indication in appropriately selected patients.”
The FDA advises that health care providers review the device’s revised labeling, which now includes a checklist to help understand which patients could benefit the most. It also advises providers to promptly report any adverse events through MedWatch, which can help the FDA identify and understand the risks associated with the Impella RP System.
More information can be found in the FDA’s letter to health care providers, which is available on the FDA website.
SCAI releases first definition of cardiogenic shock
LAS VEGAS – The Society for Cardiovascular Angiography & Interventions released on May 19 the first-ever classification scheme for cardiogenic shock, dividing the condition into five severity levels.

The expert consensus panel that devised the new definition and classification model hopes it will spearhead a reset of research into the management of cardiogenic shock so that clinicians can assess interventions and introduce them into practice in a more precise, reproducible, and systematic way, Srihari S. Naidu, MD, said while presenting the proposal at the society’s annual scientific sessions.
The writing panel’s hope is that the new definition will “drive earlier recognition of shock and at a more precise stage to guide appropriate and timely escalation of care” and to “better define prospectively the value of mechanical circulatory support, extracorporeal membrane oxygenation, and other therapies,” said Dr. Naidu, chair of the writing group, as well as professor of medicine at New York Medical College and director of the cardiac catheterization laboratory at Westchester Medical Center, both in Valhalla, N.Y.

At the core of the classification scheme are the definitions for five strata of disease, which start at stage A, the “at-risk” patients before shock onset, and progress through stage B, “beginning”; stage C, “classic”; stage D, “deteriorating”; and stage E, “extremis,” which defines a patient with circulatory collapse (Catheter Cardiovasc Interv. 2019 May 19; doi: 10.1002/ccd.28329). Another key element of the classification model is the cardiac arrest “modifier,” designated by a subscripted letter A, which identifies patients who have had a cardiac arrest, regardless of duration. So a patient could be a stage BA, which identifies a patient with clinical evidence of relative hypotension or tachycardia without hypoperfusion and with a history of cardiac arrest.

The statement also itemizes several biomarkers and hemodynamic measurements that need regular, serial monitoring, such as blood lactate and right arterial pressure. Although the document leaves specific, defining values for some of these measures vaguely defined – the intent is that future research will fill in these gaps – the overall message is that clinicians caring for cardiogenic shock patients “need to be aggressive and look for these things,” Dr. Naidu said in a video interview.
“Until we agree on a definition of cardiogenic shock, we can’t go anywhere,” commented Larry S. Dean, MD, professor of medicine at and director of the Regional Heart Center of the University of Washington in Seattle. “There are a lot of conflicting data out there, and until we have a shared definition, we can’t advance our practice. We need to start looking at shock patients in a more precise way.”
“Without a clear definition of cardiogenic shock we will never improve patient outcomes. Every shock trial must define shock. If investigators just say ‘patients were in shock,’ I don’t know what that means,” noted Navin K. Kapur, MD, director of the Interventional Research Laboratories at Tufts Medical Center in Boston and a member of the writing panel.

Dr. Naidu and others on the panel highlighted the need to now validate the classification scheme’s ability to consistently categorize patients and predict their disease trajectories. They have begun the validation process with a 10,000-patient database of “all-comers” with cardiogenic shock maintained by the Mayo Clinic. Full results from this analysis will be out soon, but Dr. Naidu revealed in passing that it successfully provided validation of the proposed scheme.
The new definition received endorsements from the American College of Cardiology, the American Heart Association, the Society of Critical Care Medicine, and the Society of Thoracic Surgeons.
Dr. Naidu had no disclosures.
LAS VEGAS – The Society for Cardiovascular Angiography & Interventions released on May 19 the first-ever classification scheme for cardiogenic shock, dividing the condition into five severity levels.
The expert consensus panel that devised the new definition and classification model hopes it will spearhead a reset of research into the management of cardiogenic shock so that clinicians can assess interventions and introduce them into practice in a more precise, reproducible, and systematic way, Srihari S. Naidu, MD, said while presenting the proposal at the society’s annual scientific sessions.
The writing panel’s hope is that the new definition will “drive earlier recognition of shock and at a more precise stage to guide appropriate and timely escalation of care” and to “better define prospectively the value of mechanical circulatory support, extracorporeal membrane oxygenation, and other therapies,” said Dr. Naidu, chair of the writing group, as well as professor of medicine at New York Medical College and director of the cardiac catheterization laboratory at Westchester Medical Center, both in Valhalla, N.Y.
At the core of the classification scheme are the definitions for five strata of disease, which start at stage A, the “at-risk” patients before shock onset, and progress through stage B, “beginning”; stage C, “classic”; stage D, “deteriorating”; and stage E, “extremis,” which defines a patient with circulatory collapse (Catheter Cardiovasc Interv. 2019 May 19; doi: 10.1002/ccd.28329). Another key element of the classification model is the cardiac arrest “modifier,” designated by a subscripted letter A, which identifies patients who have had a cardiac arrest, regardless of duration. So a patient could be a stage BA, which identifies a patient with clinical evidence of relative hypotension or tachycardia without hypoperfusion and with a history of cardiac arrest.
The statement also itemizes several biomarkers and hemodynamic measurements that need regular, serial monitoring, such as blood lactate and right arterial pressure. Although the document leaves specific, defining values for some of these measures vaguely defined – the intent is that future research will fill in these gaps – the overall message is that clinicians caring for cardiogenic shock patients “need to be aggressive and look for these things,” Dr. Naidu said in a video interview.
“Until we agree on a definition of cardiogenic shock, we can’t go anywhere,” commented Larry S. Dean, MD, professor of medicine at and director of the Regional Heart Center of the University of Washington in Seattle. “There are a lot of conflicting data out there, and until we have a shared definition, we can’t advance our practice. We need to start looking at shock patients in a more precise way.”
“Without a clear definition of cardiogenic shock we will never improve patient outcomes. Every shock trial must define shock. If investigators just say ‘patients were in shock,’ I don’t know what that means,” noted Navin K. Kapur, MD, director of the Interventional Research Laboratories at Tufts Medical Center in Boston and a member of the writing panel.
Dr. Naidu and others on the panel highlighted the need to now validate the classification scheme’s ability to consistently categorize patients and predict their disease trajectories. They have begun the validation process with a 10,000-patient database of “all-comers” with cardiogenic shock maintained by the Mayo Clinic. Full results from this analysis will be out soon, but Dr. Naidu revealed in passing that it successfully provided validation of the proposed scheme.
The new definition received endorsements from the American College of Cardiology, the American Heart Association, the Society of Critical Care Medicine, and the Society of Thoracic Surgeons.
Dr. Naidu had no disclosures.
LAS VEGAS – The Society for Cardiovascular Angiography & Interventions released on May 19 the first-ever classification scheme for cardiogenic shock, dividing the condition into five severity levels.
The expert consensus panel that devised the new definition and classification model hopes it will spearhead a reset of research into the management of cardiogenic shock so that clinicians can assess interventions and introduce them into practice in a more precise, reproducible, and systematic way, Srihari S. Naidu, MD, said while presenting the proposal at the society’s annual scientific sessions.
The writing panel’s hope is that the new definition will “drive earlier recognition of shock and at a more precise stage to guide appropriate and timely escalation of care” and to “better define prospectively the value of mechanical circulatory support, extracorporeal membrane oxygenation, and other therapies,” said Dr. Naidu, chair of the writing group, as well as professor of medicine at New York Medical College and director of the cardiac catheterization laboratory at Westchester Medical Center, both in Valhalla, N.Y.
At the core of the classification scheme are the definitions for five strata of disease, which start at stage A, the “at-risk” patients before shock onset, and progress through stage B, “beginning”; stage C, “classic”; stage D, “deteriorating”; and stage E, “extremis,” which defines a patient with circulatory collapse (Catheter Cardiovasc Interv. 2019 May 19; doi: 10.1002/ccd.28329). Another key element of the classification model is the cardiac arrest “modifier,” designated by a subscripted letter A, which identifies patients who have had a cardiac arrest, regardless of duration. So a patient could be a stage BA, which identifies a patient with clinical evidence of relative hypotension or tachycardia without hypoperfusion and with a history of cardiac arrest.
The statement also itemizes several biomarkers and hemodynamic measurements that need regular, serial monitoring, such as blood lactate and right arterial pressure. Although the document leaves specific, defining values for some of these measures vaguely defined – the intent is that future research will fill in these gaps – the overall message is that clinicians caring for cardiogenic shock patients “need to be aggressive and look for these things,” Dr. Naidu said in a video interview.
“Until we agree on a definition of cardiogenic shock, we can’t go anywhere,” commented Larry S. Dean, MD, professor of medicine at and director of the Regional Heart Center of the University of Washington in Seattle. “There are a lot of conflicting data out there, and until we have a shared definition, we can’t advance our practice. We need to start looking at shock patients in a more precise way.”
“Without a clear definition of cardiogenic shock we will never improve patient outcomes. Every shock trial must define shock. If investigators just say ‘patients were in shock,’ I don’t know what that means,” noted Navin K. Kapur, MD, director of the Interventional Research Laboratories at Tufts Medical Center in Boston and a member of the writing panel.
Dr. Naidu and others on the panel highlighted the need to now validate the classification scheme’s ability to consistently categorize patients and predict their disease trajectories. They have begun the validation process with a 10,000-patient database of “all-comers” with cardiogenic shock maintained by the Mayo Clinic. Full results from this analysis will be out soon, but Dr. Naidu revealed in passing that it successfully provided validation of the proposed scheme.
The new definition received endorsements from the American College of Cardiology, the American Heart Association, the Society of Critical Care Medicine, and the Society of Thoracic Surgeons.
Dr. Naidu had no disclosures.
REPORTING FROM SCAI 2019
CABANA: Heart failure patients got biggest bang from AFib ablation
SAN FRANCISCO – Catheter ablation of atrial fibrillation (AFib) in the roughly one-third of patients with heart failure enrolled in the CABANA multicenter, randomized trial produced striking, statistically significant improvements both in the study’s primary, combined endpoint and in all-cause mortality in intention-to-treat analyses.

These findings, from prespecified secondary analyses, contrasted with the study’s overall result, which showed no benefit in the primary endpoint analysis in the total study population of 2,204 patients with AFib (JAMA. 2019 Apr 2;321[13]:1261-74). They are also at odds with the primary endpoint result in the two-thirds of enrolled patients without heart failure, which showed no significant between-group differences in these two outcome measures among the patients assigned to the catheter ablation arm and the study’s control, which was medical management arm.
Among the 778 AFib patients enrolled in CABANA with any form of heart failure (35% of the total study enrollment), the incidence of the study’s primary endpoint – the combined rate of death, disabling stroke, serious bleeding, or cardiac arrest during a median follow-up of slightly more than 4 years – was 36% lower among the catheter-ablated heart failure patients than in the heart failure patients assigned to medical treatment, according to an intention-to-treat analysis, which was a statistically significant difference. The incidence of all-cause mortality during follow-up was 43% lower in the ablated heart failure patients, compared with the controls, Douglas L. Packer, MD, said at the annual scientific sessions of the Heart Rhythm Society.
In contrast, among enrolled patients without heart failure, the intention-to-treat primary endpoint was 6% higher in the ablated patients, and all-cause mortality was a relative 27% higher, although neither difference was statistically significant.
It’s a “little surprising” that the results showed this much benefit in the patients with heart failure, said Dr. Packer, professor of medicine at the Mayo Clinic in Rochester, Minn., and lead investigator of the CABANA (Catheter Ablation vs Anti-Arrhythmic Drug Therapy for Atrial Fibrillation) trial. “I think these data confirm the results of the CASTLE-AF trial, but without some of the glitches some people have cited” about that study, such as concerns about a high level of patient selection in CASTLE-AF and its relatively modest number of enrolled patients, he said in an interview.

The CASTLE-AF (Catheter Ablation vs. Standard Conventional Treatment in Patients With LV Dysfunction and AF) study, run entirely in patients with heart failure with reduced ejection fraction and AFib, showed a statistically significant improvement in patient survival and heart failure hospitalization after catheter ablation compared with medical management (N Engl J Med. 2018 Feb 1;378[5]:417-27). Prior to the CASTLE-AF report, results from several other small studies (J Interv Card Electrophysiol. 2018 Oct;53[1]:19-29), as well as those from the AATAC trial (Circulation. 2016 Apr 26;133[17]:1637-44), also showed consistent evidence for benefit from catheter ablation in patients with heart failure and AFib, noted CABANA coinvestigator Jonathan P. Piccini, MD, during a separate talk at the meeting.
“The improvement of cardiovascular outcomes with ablation in patients with heart failure and AFib is consistent across multiple trials, at least with respect to heart failure with reduced ejection fraction” concluded Dr. Piccini, a cardiac electrophysiologist at Duke University in Durham, N.C.
As a result of the new heart failure analysis, “I think the guidelines will change,” predicted Dr. Packer, with catheter ablation receiving a firmer endorsement for patients with heart failure the next time U.S. guidelines for heart failure and AFib management are updated. The findings say “there is substantial benefit of catheter ablation in heart failure patients, but I don’t think our findings lessen the utility of ablation in patients without heart failure,” he stressed. Even patients without heart failure showed reduction in AFib burden and improvement in quality of life that were similar to what was seen in the heart failure patients.
The new report from CABANA of benefit from AFib catheter ablation in patients with heart failure “absolutely advances the evidence,” commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago. “A number of us were quite circumspect about this based on the CASTLE-AF data, but the new CABANA analyses have addressed our anxiety that the CASTLE-AF results were just by chance.” The new CABANA analyses “may not confirm CASTLE-AF, but it enriches the conversation and makes it possible that we are seeing benefit in some patients with heart failure who get ablated.”

Dr. Yancy, who chaired the most recent update to the U.S. heart failure management guideline (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803) stopped short of saying that the cumulative evidence now supports a guideline change, but he acknowledged in an interview that the evidence could legitimately influence practice. Catheter ablation should now be “strongly considered” in patients with heart failure and AFib, he said, although he also had three qualifications for opting for this approach: Patients must already be on guideline-directed medical therapy for their heart failure, the catheter ablation needs to be performed by an experienced and skilled operator, and follow-up surveillance must focus on both the patient’s AFib and heart failure. “It’s absolutely appropriate to consider catheter ablation” for heart failure patients, but the evidence is not yet there for guideline change, Dr. Yancy concluded.
It remains uncertain why catheter ablation of AFib should be more effective in patients with heart failure than in those without. Dr. Packer speculated that one reason may be the heart rate reduction that AFib ablation produces may especially benefit heart failure patients. An additional helpful effect of ablation in heart failure patients may be reducing heart rate variability. Another notable finding of the new analysis was that 79% of patients with heart failure in CABANA had heart failure with preserved ejection fraction, with a left ventricular ejection fraction of at least 50%. “Getting rid of AFib in patients with heart failure with preserved ejection fraction will be more important than we have thought,” Dr. Packer said.
Other new CABANA analyses presented for the first time in separate talks at the meeting also showed that, while catheter ablation had no meaningful difference in effect on outcomes based on the sex of patients, both age and minority ethnic and racial status appeared to make a substantial difference. For CABANA’s primary endpoint, catheter ablation was especially effective for improving outcomes in patients 64 years old or younger, and the analysis showed a signal of possibly worse outcomes in patients who were at least 75 years old. The “substantially” better outcomes in minority-group patients represented the largest between-group difference among subgroups seen in CABANA and is a “big deal,” said Dr. Packer, who predicted that future catheter ablation use will likely rise in patients with heart failure, in younger patients, and in minority patients.
Dr. Piccini noted that, “it’s possible that CABANA identified some patient subgroups that do really well after ablation, but the problem is that, in the United States, we now often don’t treat” minority patients or those with reduced left ventricular ejection fractions with ablation, according to recent registry findings.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and/or received research funding from these four companies, as well as numerous drug and device companies, and has a financial interest in a licensed AFib mapping technology. Dr. Piccini has ties Boston Scientific, Medtronic, and numerous other drug and device companies, and disclosed an unspecified relationship with GlaxoSmithKline. Dr. Yancy disclosed an unspecified relationship with Abbott Laboratories.
SOURCE: Packer DL. Heart Rhythm 2019, Abstract S-AB14-06.
SAN FRANCISCO – Catheter ablation of atrial fibrillation (AFib) in the roughly one-third of patients with heart failure enrolled in the CABANA multicenter, randomized trial produced striking, statistically significant improvements both in the study’s primary, combined endpoint and in all-cause mortality in intention-to-treat analyses.
These findings, from prespecified secondary analyses, contrasted with the study’s overall result, which showed no benefit in the primary endpoint analysis in the total study population of 2,204 patients with AFib (JAMA. 2019 Apr 2;321[13]:1261-74). They are also at odds with the primary endpoint result in the two-thirds of enrolled patients without heart failure, which showed no significant between-group differences in these two outcome measures among the patients assigned to the catheter ablation arm and the study’s control, which was medical management arm.
Among the 778 AFib patients enrolled in CABANA with any form of heart failure (35% of the total study enrollment), the incidence of the study’s primary endpoint – the combined rate of death, disabling stroke, serious bleeding, or cardiac arrest during a median follow-up of slightly more than 4 years – was 36% lower among the catheter-ablated heart failure patients than in the heart failure patients assigned to medical treatment, according to an intention-to-treat analysis, which was a statistically significant difference. The incidence of all-cause mortality during follow-up was 43% lower in the ablated heart failure patients, compared with the controls, Douglas L. Packer, MD, said at the annual scientific sessions of the Heart Rhythm Society.
In contrast, among enrolled patients without heart failure, the intention-to-treat primary endpoint was 6% higher in the ablated patients, and all-cause mortality was a relative 27% higher, although neither difference was statistically significant.
It’s a “little surprising” that the results showed this much benefit in the patients with heart failure, said Dr. Packer, professor of medicine at the Mayo Clinic in Rochester, Minn., and lead investigator of the CABANA (Catheter Ablation vs Anti-Arrhythmic Drug Therapy for Atrial Fibrillation) trial. “I think these data confirm the results of the CASTLE-AF trial, but without some of the glitches some people have cited” about that study, such as concerns about a high level of patient selection in CASTLE-AF and its relatively modest number of enrolled patients, he said in an interview.
The CASTLE-AF (Catheter Ablation vs. Standard Conventional Treatment in Patients With LV Dysfunction and AF) study, run entirely in patients with heart failure with reduced ejection fraction and AFib, showed a statistically significant improvement in patient survival and heart failure hospitalization after catheter ablation compared with medical management (N Engl J Med. 2018 Feb 1;378[5]:417-27). Prior to the CASTLE-AF report, results from several other small studies (J Interv Card Electrophysiol. 2018 Oct;53[1]:19-29), as well as those from the AATAC trial (Circulation. 2016 Apr 26;133[17]:1637-44), also showed consistent evidence for benefit from catheter ablation in patients with heart failure and AFib, noted CABANA coinvestigator Jonathan P. Piccini, MD, during a separate talk at the meeting.
“The improvement of cardiovascular outcomes with ablation in patients with heart failure and AFib is consistent across multiple trials, at least with respect to heart failure with reduced ejection fraction” concluded Dr. Piccini, a cardiac electrophysiologist at Duke University in Durham, N.C.
As a result of the new heart failure analysis, “I think the guidelines will change,” predicted Dr. Packer, with catheter ablation receiving a firmer endorsement for patients with heart failure the next time U.S. guidelines for heart failure and AFib management are updated. The findings say “there is substantial benefit of catheter ablation in heart failure patients, but I don’t think our findings lessen the utility of ablation in patients without heart failure,” he stressed. Even patients without heart failure showed reduction in AFib burden and improvement in quality of life that were similar to what was seen in the heart failure patients.
The new report from CABANA of benefit from AFib catheter ablation in patients with heart failure “absolutely advances the evidence,” commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago. “A number of us were quite circumspect about this based on the CASTLE-AF data, but the new CABANA analyses have addressed our anxiety that the CASTLE-AF results were just by chance.” The new CABANA analyses “may not confirm CASTLE-AF, but it enriches the conversation and makes it possible that we are seeing benefit in some patients with heart failure who get ablated.”
Dr. Yancy, who chaired the most recent update to the U.S. heart failure management guideline (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803) stopped short of saying that the cumulative evidence now supports a guideline change, but he acknowledged in an interview that the evidence could legitimately influence practice. Catheter ablation should now be “strongly considered” in patients with heart failure and AFib, he said, although he also had three qualifications for opting for this approach: Patients must already be on guideline-directed medical therapy for their heart failure, the catheter ablation needs to be performed by an experienced and skilled operator, and follow-up surveillance must focus on both the patient’s AFib and heart failure. “It’s absolutely appropriate to consider catheter ablation” for heart failure patients, but the evidence is not yet there for guideline change, Dr. Yancy concluded.
It remains uncertain why catheter ablation of AFib should be more effective in patients with heart failure than in those without. Dr. Packer speculated that one reason may be the heart rate reduction that AFib ablation produces may especially benefit heart failure patients. An additional helpful effect of ablation in heart failure patients may be reducing heart rate variability. Another notable finding of the new analysis was that 79% of patients with heart failure in CABANA had heart failure with preserved ejection fraction, with a left ventricular ejection fraction of at least 50%. “Getting rid of AFib in patients with heart failure with preserved ejection fraction will be more important than we have thought,” Dr. Packer said.
Other new CABANA analyses presented for the first time in separate talks at the meeting also showed that, while catheter ablation had no meaningful difference in effect on outcomes based on the sex of patients, both age and minority ethnic and racial status appeared to make a substantial difference. For CABANA’s primary endpoint, catheter ablation was especially effective for improving outcomes in patients 64 years old or younger, and the analysis showed a signal of possibly worse outcomes in patients who were at least 75 years old. The “substantially” better outcomes in minority-group patients represented the largest between-group difference among subgroups seen in CABANA and is a “big deal,” said Dr. Packer, who predicted that future catheter ablation use will likely rise in patients with heart failure, in younger patients, and in minority patients.
Dr. Piccini noted that, “it’s possible that CABANA identified some patient subgroups that do really well after ablation, but the problem is that, in the United States, we now often don’t treat” minority patients or those with reduced left ventricular ejection fractions with ablation, according to recent registry findings.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and/or received research funding from these four companies, as well as numerous drug and device companies, and has a financial interest in a licensed AFib mapping technology. Dr. Piccini has ties Boston Scientific, Medtronic, and numerous other drug and device companies, and disclosed an unspecified relationship with GlaxoSmithKline. Dr. Yancy disclosed an unspecified relationship with Abbott Laboratories.
SOURCE: Packer DL. Heart Rhythm 2019, Abstract S-AB14-06.
SAN FRANCISCO – Catheter ablation of atrial fibrillation (AFib) in the roughly one-third of patients with heart failure enrolled in the CABANA multicenter, randomized trial produced striking, statistically significant improvements both in the study’s primary, combined endpoint and in all-cause mortality in intention-to-treat analyses.
These findings, from prespecified secondary analyses, contrasted with the study’s overall result, which showed no benefit in the primary endpoint analysis in the total study population of 2,204 patients with AFib (JAMA. 2019 Apr 2;321[13]:1261-74). They are also at odds with the primary endpoint result in the two-thirds of enrolled patients without heart failure, which showed no significant between-group differences in these two outcome measures among the patients assigned to the catheter ablation arm and the study’s control, which was medical management arm.
Among the 778 AFib patients enrolled in CABANA with any form of heart failure (35% of the total study enrollment), the incidence of the study’s primary endpoint – the combined rate of death, disabling stroke, serious bleeding, or cardiac arrest during a median follow-up of slightly more than 4 years – was 36% lower among the catheter-ablated heart failure patients than in the heart failure patients assigned to medical treatment, according to an intention-to-treat analysis, which was a statistically significant difference. The incidence of all-cause mortality during follow-up was 43% lower in the ablated heart failure patients, compared with the controls, Douglas L. Packer, MD, said at the annual scientific sessions of the Heart Rhythm Society.
In contrast, among enrolled patients without heart failure, the intention-to-treat primary endpoint was 6% higher in the ablated patients, and all-cause mortality was a relative 27% higher, although neither difference was statistically significant.
It’s a “little surprising” that the results showed this much benefit in the patients with heart failure, said Dr. Packer, professor of medicine at the Mayo Clinic in Rochester, Minn., and lead investigator of the CABANA (Catheter Ablation vs Anti-Arrhythmic Drug Therapy for Atrial Fibrillation) trial. “I think these data confirm the results of the CASTLE-AF trial, but without some of the glitches some people have cited” about that study, such as concerns about a high level of patient selection in CASTLE-AF and its relatively modest number of enrolled patients, he said in an interview.
The CASTLE-AF (Catheter Ablation vs. Standard Conventional Treatment in Patients With LV Dysfunction and AF) study, run entirely in patients with heart failure with reduced ejection fraction and AFib, showed a statistically significant improvement in patient survival and heart failure hospitalization after catheter ablation compared with medical management (N Engl J Med. 2018 Feb 1;378[5]:417-27). Prior to the CASTLE-AF report, results from several other small studies (J Interv Card Electrophysiol. 2018 Oct;53[1]:19-29), as well as those from the AATAC trial (Circulation. 2016 Apr 26;133[17]:1637-44), also showed consistent evidence for benefit from catheter ablation in patients with heart failure and AFib, noted CABANA coinvestigator Jonathan P. Piccini, MD, during a separate talk at the meeting.
“The improvement of cardiovascular outcomes with ablation in patients with heart failure and AFib is consistent across multiple trials, at least with respect to heart failure with reduced ejection fraction” concluded Dr. Piccini, a cardiac electrophysiologist at Duke University in Durham, N.C.
As a result of the new heart failure analysis, “I think the guidelines will change,” predicted Dr. Packer, with catheter ablation receiving a firmer endorsement for patients with heart failure the next time U.S. guidelines for heart failure and AFib management are updated. The findings say “there is substantial benefit of catheter ablation in heart failure patients, but I don’t think our findings lessen the utility of ablation in patients without heart failure,” he stressed. Even patients without heart failure showed reduction in AFib burden and improvement in quality of life that were similar to what was seen in the heart failure patients.
The new report from CABANA of benefit from AFib catheter ablation in patients with heart failure “absolutely advances the evidence,” commented Clyde W. Yancy, MD, professor of medicine and chief of cardiology at Northwestern University in Chicago. “A number of us were quite circumspect about this based on the CASTLE-AF data, but the new CABANA analyses have addressed our anxiety that the CASTLE-AF results were just by chance.” The new CABANA analyses “may not confirm CASTLE-AF, but it enriches the conversation and makes it possible that we are seeing benefit in some patients with heart failure who get ablated.”
Dr. Yancy, who chaired the most recent update to the U.S. heart failure management guideline (J Am Coll Cardiol. 2017 Aug 8;70[6]:776-803) stopped short of saying that the cumulative evidence now supports a guideline change, but he acknowledged in an interview that the evidence could legitimately influence practice. Catheter ablation should now be “strongly considered” in patients with heart failure and AFib, he said, although he also had three qualifications for opting for this approach: Patients must already be on guideline-directed medical therapy for their heart failure, the catheter ablation needs to be performed by an experienced and skilled operator, and follow-up surveillance must focus on both the patient’s AFib and heart failure. “It’s absolutely appropriate to consider catheter ablation” for heart failure patients, but the evidence is not yet there for guideline change, Dr. Yancy concluded.
It remains uncertain why catheter ablation of AFib should be more effective in patients with heart failure than in those without. Dr. Packer speculated that one reason may be the heart rate reduction that AFib ablation produces may especially benefit heart failure patients. An additional helpful effect of ablation in heart failure patients may be reducing heart rate variability. Another notable finding of the new analysis was that 79% of patients with heart failure in CABANA had heart failure with preserved ejection fraction, with a left ventricular ejection fraction of at least 50%. “Getting rid of AFib in patients with heart failure with preserved ejection fraction will be more important than we have thought,” Dr. Packer said.
Other new CABANA analyses presented for the first time in separate talks at the meeting also showed that, while catheter ablation had no meaningful difference in effect on outcomes based on the sex of patients, both age and minority ethnic and racial status appeared to make a substantial difference. For CABANA’s primary endpoint, catheter ablation was especially effective for improving outcomes in patients 64 years old or younger, and the analysis showed a signal of possibly worse outcomes in patients who were at least 75 years old. The “substantially” better outcomes in minority-group patients represented the largest between-group difference among subgroups seen in CABANA and is a “big deal,” said Dr. Packer, who predicted that future catheter ablation use will likely rise in patients with heart failure, in younger patients, and in minority patients.
Dr. Piccini noted that, “it’s possible that CABANA identified some patient subgroups that do really well after ablation, but the problem is that, in the United States, we now often don’t treat” minority patients or those with reduced left ventricular ejection fractions with ablation, according to recent registry findings.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and/or received research funding from these four companies, as well as numerous drug and device companies, and has a financial interest in a licensed AFib mapping technology. Dr. Piccini has ties Boston Scientific, Medtronic, and numerous other drug and device companies, and disclosed an unspecified relationship with GlaxoSmithKline. Dr. Yancy disclosed an unspecified relationship with Abbott Laboratories.
SOURCE: Packer DL. Heart Rhythm 2019, Abstract S-AB14-06.
REPORTING FROM HEART RHYTHM 2019
Key clinical point: Catheter ablation for atrial fibrillation is especially effective in patients with heart failure.
Major finding: Heart failure patients treated with catheter ablation had a 36% relative cut in the primary endpoint, compared with control patients.
Study details: CABANA, a multicenter, randomized trial with 2,204 patients, including 778 patients with heart failure.
Disclosures: CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and/or received research funding from these four companies, as well as numerous drug and device companies, and has a financial interest in a licensed AFib mapping technology. Source: Packer DL. Heart Rhythm 2019, Abstract S-AB14-06.
BMI in male teens predicts cardiomyopathy risk
and their risk increased as body mass index increased, according to the results of a nationwide, prospective, registry-based cohort study from Sweden.
The association was strongest for dilated cardiomyopathy, wrote Josefina Robertson, MD, and associates at the University of Gothenburg (Sweden). Over a median of 27 years of follow-up, the risk for dilated cardiomyopathy in adulthood was approximately 38% greater when adolescent body mass index was 22.5-25.0 kg/m2, using a lean but not underweight BMI (18.5-20.0 kg/m2) as the reference group. The increase in risk for dilated cardiomyopathy continued to rise with adolescent BMI and exceeded 700% at a BMI over 35.
The rate of hospitalizations for heart failure caused by cardiomyopathy more than doubled in Sweden from 1987 to 2006, the researchers noted. Adolescent obesity is strongly linked to early heart failure, but few studies have assessed whether adiposity as measured by BMI is associated with cardiomyopathy, and none have confirmed diagnostic validity or looked at subtypes of cardiomyopathy.
“The already marked importance of weight control in youth is further strengthened by [our] findings,” the researchers wrote, “as well as greater evidence for obesity as a potential important cause of adverse cardiac remodeling independent of clinically evident ischemic heart disease.”
The study included 1,668,893 male adolescents who had enlisted for military service in Sweden between 1969 and 2005, when compulsory enlistment ended. It excluded women and the small proportion of men lacking weight or height data. A total of 4,477 cases of cardiomyopathy were diagnosed during follow-up, 59% were dilated cardiomyopathy, 15% were hypertrophic cardiomyopathy, and 11% were alcohol or drug-related cardiomyopathy.
The link between even slightly elevated BMI and dilated cardiomyopathy did not depend on age, year, location, or baseline comorbidities. For each unit increase in BMI, the adjusted risk of dilated cardiomyopathy rose by approximately 15%, the risk of hypertrophic cardiomyopathy rose by 9%, and the risk for drug- or alcohol-related cardiomyopathy rose by 10%. Estimated risks were generally similar after controlling for blood pressure, cardiorespiratory fitness, muscle strength, parents’ level of education, and alcohol or substance use disorders.
Funders included the Swedish government; Swedish Research Council; Swedish Heart and Lung Foundation; and Swedish Council for Health, Working Life, and Welfare. The researchers reported having no conflicts of interest.
SOURCE: Robertson J et al. Circulation. 2019 May 20.
and their risk increased as body mass index increased, according to the results of a nationwide, prospective, registry-based cohort study from Sweden.
The association was strongest for dilated cardiomyopathy, wrote Josefina Robertson, MD, and associates at the University of Gothenburg (Sweden). Over a median of 27 years of follow-up, the risk for dilated cardiomyopathy in adulthood was approximately 38% greater when adolescent body mass index was 22.5-25.0 kg/m2, using a lean but not underweight BMI (18.5-20.0 kg/m2) as the reference group. The increase in risk for dilated cardiomyopathy continued to rise with adolescent BMI and exceeded 700% at a BMI over 35.
The rate of hospitalizations for heart failure caused by cardiomyopathy more than doubled in Sweden from 1987 to 2006, the researchers noted. Adolescent obesity is strongly linked to early heart failure, but few studies have assessed whether adiposity as measured by BMI is associated with cardiomyopathy, and none have confirmed diagnostic validity or looked at subtypes of cardiomyopathy.
“The already marked importance of weight control in youth is further strengthened by [our] findings,” the researchers wrote, “as well as greater evidence for obesity as a potential important cause of adverse cardiac remodeling independent of clinically evident ischemic heart disease.”
The study included 1,668,893 male adolescents who had enlisted for military service in Sweden between 1969 and 2005, when compulsory enlistment ended. It excluded women and the small proportion of men lacking weight or height data. A total of 4,477 cases of cardiomyopathy were diagnosed during follow-up, 59% were dilated cardiomyopathy, 15% were hypertrophic cardiomyopathy, and 11% were alcohol or drug-related cardiomyopathy.
The link between even slightly elevated BMI and dilated cardiomyopathy did not depend on age, year, location, or baseline comorbidities. For each unit increase in BMI, the adjusted risk of dilated cardiomyopathy rose by approximately 15%, the risk of hypertrophic cardiomyopathy rose by 9%, and the risk for drug- or alcohol-related cardiomyopathy rose by 10%. Estimated risks were generally similar after controlling for blood pressure, cardiorespiratory fitness, muscle strength, parents’ level of education, and alcohol or substance use disorders.
Funders included the Swedish government; Swedish Research Council; Swedish Heart and Lung Foundation; and Swedish Council for Health, Working Life, and Welfare. The researchers reported having no conflicts of interest.
SOURCE: Robertson J et al. Circulation. 2019 May 20.
and their risk increased as body mass index increased, according to the results of a nationwide, prospective, registry-based cohort study from Sweden.
The association was strongest for dilated cardiomyopathy, wrote Josefina Robertson, MD, and associates at the University of Gothenburg (Sweden). Over a median of 27 years of follow-up, the risk for dilated cardiomyopathy in adulthood was approximately 38% greater when adolescent body mass index was 22.5-25.0 kg/m2, using a lean but not underweight BMI (18.5-20.0 kg/m2) as the reference group. The increase in risk for dilated cardiomyopathy continued to rise with adolescent BMI and exceeded 700% at a BMI over 35.
The rate of hospitalizations for heart failure caused by cardiomyopathy more than doubled in Sweden from 1987 to 2006, the researchers noted. Adolescent obesity is strongly linked to early heart failure, but few studies have assessed whether adiposity as measured by BMI is associated with cardiomyopathy, and none have confirmed diagnostic validity or looked at subtypes of cardiomyopathy.
“The already marked importance of weight control in youth is further strengthened by [our] findings,” the researchers wrote, “as well as greater evidence for obesity as a potential important cause of adverse cardiac remodeling independent of clinically evident ischemic heart disease.”
The study included 1,668,893 male adolescents who had enlisted for military service in Sweden between 1969 and 2005, when compulsory enlistment ended. It excluded women and the small proportion of men lacking weight or height data. A total of 4,477 cases of cardiomyopathy were diagnosed during follow-up, 59% were dilated cardiomyopathy, 15% were hypertrophic cardiomyopathy, and 11% were alcohol or drug-related cardiomyopathy.
The link between even slightly elevated BMI and dilated cardiomyopathy did not depend on age, year, location, or baseline comorbidities. For each unit increase in BMI, the adjusted risk of dilated cardiomyopathy rose by approximately 15%, the risk of hypertrophic cardiomyopathy rose by 9%, and the risk for drug- or alcohol-related cardiomyopathy rose by 10%. Estimated risks were generally similar after controlling for blood pressure, cardiorespiratory fitness, muscle strength, parents’ level of education, and alcohol or substance use disorders.
Funders included the Swedish government; Swedish Research Council; Swedish Heart and Lung Foundation; and Swedish Council for Health, Working Life, and Welfare. The researchers reported having no conflicts of interest.
SOURCE: Robertson J et al. Circulation. 2019 May 20.
FROM CIRCULATION
Key clinical point: Overweight in male teens predicts subsequent cardiomyopathy. The association increases with BMI and is strongest for dilated cardiomyopathy.
Major finding: Over a median of 27 years of follow-up, the hazard ratio for dilated cardiomyopathy in adulthood was 1.38 when adolescent body mass index was 22.5-25.0 kg/m2, using a BMI of 18.5-20.0 as the reference group. At a BMI over 35, the hazard ratio reached 8.11.
Study details: A nationwide, prospective registry cohort study of 1.67 million adolescent males in Sweden.
Disclosures: Funders included the Swedish government; Swedish Research Council; Swedish Heart and Lung Foundation; and Swedish Council for Health, Working Life and Welfare. The researchers reported having no conflicts of interest.
New risk score predicts cardiac-device infection
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
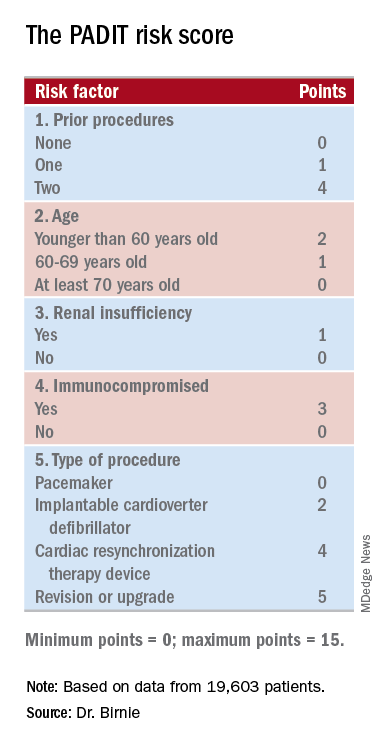
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.

“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
I like this new infection risk score. It addresses a very clinically relevant issue. It’s important for the electrophysiology community to better understand how to best manage infections related to cardiac rhythm devices and ideally prevent them from happening.
I’m not a big fan of risk scores in general because they can sometimes detract from independent thinking about how to manage a patient. However, it is also helpful to have this type of risk-assessment information when discussing management options with a patient.
The PADIT risk score may also help identify which patients could potentially benefit the most from an antibiotic-eluting envelope when receiving an implanted cardiac-rhythm device. Recently reported results from WRAP-IT showed that routinely using envelopes cut the incidence of major infections by a relative 40%, but in absolute terms, the number needed to treat with the envelop to prevent one major infection was about 200 patients, a big number given the high cost of the envelope (N Engl J Med. 2019 May 16;380[20]:1895-905). It is therefore very interesting to think about using the PADIT risk score to better target an effective but expensive preventive measure like an antibiotic-eluting envelop to patients at the highest risk for infection.
Ulrika Birgersdotter-Green, MD , professor of medicine and director of pacemaker and ICD services at the University of California, San Diego, made these comments as a designated discussant for the report. She has been a consultant to and received honoraria from Abbott, Boston Scientific, and Medtronic.
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
SAN FRANCISCO – Researchers have devised a five-item scoring formula to quantify the risk for infection in patients undergoing placement, revision, or removal of a cardiac-rhythm device based on data from nearly 20,000 patients enrolled in a recent infection-prophylaxis trial.
The risk score can help identify patients who might benefit from intensified antibiotic prophylaxis, and it can also help during shared decision making with patients to better understand the risk a patient faces from infection, compared with their predicted device benefit, David H. Birnie, MD, said at the annual scientific sessions of the Heart Rhythm Society.
The new risk score produced a concordance statistic, the area under the receiver-operator characteristic curve, of 0.704. It showed that, although it could use further validation, the score as it currently stands has substantial predictive value, said Dr. Birnie, professor of medicine at the University of Ottawa and deputy chief of cardiology at the University of Ottawa Heart Institute. “It’s certainly better than anything we have now,” he said in a video interview.
Dr. Birnie and his associates used data they collected on baseline characteristics and infection outcomes of the 19,603 patients enrolled in PADIT (Prevention of Arrhythmia Device Infection Trial) who underwent a rhythm-device procedure at 1 of 28 participating Canadian centers. The primary aim of PADIT was to assess the safety and efficacy of an intensified antibiotic-prophylaxis regimen, compared with a standard regimen of a cefazolin infusion just before the procedure. The study’s primary endpoint was the incidence of hospitalization for device infection during 1-year follow-up, and while the intensified prophylactic regimen linked with a 23% relative reduction in the hospitalization rate, compared with standard treatment, the difference was not statistically significant (J Am Coll Cardiol. 2018 Dec 18;72[24]:3098-109).
The researchers analyzed the baseline patient data and the blindly adjudicated infection outcomes and identified five factors that were independently associated with an increased infection rate. They organized the five factors and produced a formula they call the PADIT score (see chart). Those five factors are: prior procedures (the greater the number the greater the risk), age (which unexpectedly had an inverse relationship with infection incidence), depressed renal function, immuno-compromised status, and type of procedure. A patient can potentially score 0-15 points.
Among the PADIT patients a score of 0 correlated with about a 0.3% rate of hospitalization for a device-related infection during 1 year of follow-up, a score of 5 with about a 1.1% rate, a score of 6 with about a 1.8% rate, and a score of seven or more with a 3.4% infection rate over the following year. About 5% of patients had a score of 7 or more, and roughly another 5% had a score of 5 or 6, Dr. Birnie said. At his center, clinicians have begun routinely calculating scores for patients scheduled for an arrhythmia-device procedure, and they are considering routinely administering added antibiotic prophylaxis to patients with a preprocedural score of 6 or higher. They may also use the score to determine whether to use the antibacterial envelope recently reported to prevent cardiac-device infections (N Engl J Med. 2019 May 16;380[20]:1895-905).
“It’s very easy for patients to get to a PADIT score of 7 or higher,” Dr. Birnie noted. As an example, he cited a common patient, an 85-year-old with renal dysfunction who is under consideration for a second replacement of an implantable cardioverter defibrillator. The patient would score 1 point for renal insufficiency, 2 points for the type of device, and 4 points for having a prior history of two devices, and the consequent 3.4% risk for infection might counterbalance the potential benefit this elderly patient could expect from the new device. The score will be very important for targeting treatment, shared decision making, and selection of patients for future intervention trials, he concluded.
“I think this risk score will change practice by giving clinicians a better idea of a patient’s risk for infection,” commented Fred M. Kusumoto, MD, professor of medicine at the Mayo Medical School, Rochester, Minn., and director of heart rhythm services at the Mayo Clinic in Jacksonville, Fla. The PADIT score will help identify patients for whom leaving a device in place is a better option than taking it out because of their infection risk. The risk score could also help improve the cost effectiveness of preventive treatments, such as antibiotic-eluting envelopes, by targeting treatment to higher-risk patients, Dr. Kusumoto said during a press briefing.
SOURCE: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.
REPORTING FROM HEART RHYTHM 2019
Key clinical point: Researchers have devised a five-item scoring formula to predict a patient’s risk for infection from an cardiac rhythm–device procedure.
Major finding: The risk score had an optimism-corrected concordance statistic of 0.704.
Study details: Investigators developed the risk score using data from PADIT, a multicenter, randomized trial with 19,603 patients.
Disclosures: PADIT received no commercial funding. Dr. Birnie had no relevant disclosures.
Source: Birnie DH. Heart Rhythm 2019, Absract S-LCT02-01.

Severe OSA increases cardiovascular risk after surgery
Unrecognized severe obstructive sleep apnea is a risk factor for cardiovascular complications after major noncardiac surgery, according to a study published in JAMA.
The researchers state that perioperative mismanagement of obstructive sleep apnea can lead to serious medical consequences. “General anesthetics, sedatives, and postoperative analgesics are potent respiratory depressants that relax the upper airway dilator muscles and impair ventilatory response to hypoxemia and hypercapnia. Each of these events exacerbates [obstructive sleep apnea] and may predispose patients to postoperative cardiovascular complications,” said researchers who conducted the The Postoperative vascular complications in unrecognised Obstructive Sleep apnoea (POSA) study (NCT01494181).
They undertook a prospective observational cohort study involving 1,218 patients undergoing major noncardiac surgery, who were already considered at high risk of postoperative cardiovascular events – having, for example, a history of coronary artery disease, stroke, diabetes, or renal impairment. However, none had a prior diagnosis of obstructive sleep apnea.
Preoperative sleep monitoring revealed that two-thirds of the cohort had unrecognized and untreated obstructive sleep apnea, including 11.2% with severe obstructive sleep apnea.
At 30 days after surgery, patients with obstructive sleep apnea had a 49% higher risk of the primary outcome of myocardial injury, cardiac death, heart failure, thromboembolism, atrial fibrillation, or stroke, compared with those without obstructive sleep apnea.
However, this association was largely due to a significant 2.23-fold higher risk among patients with severe obstructive sleep apnea, while those with only moderate or mild sleep apnea did not show a significant increased risk of cardiovascular complications.
Patients in this study with severe obstructive sleep apnea had a 13-fold higher risk of cardiac death, 80% higher risk of myocardial injury, more than sixfold higher risk of heart failure, and nearly fourfold higher risk of atrial fibrillation.
Researchers also saw an association between obstructive sleep apnea and increased risk of infective outcomes, unplanned tracheal intubation, postoperative lung ventilation, and readmission to the ICU.
The majority of patients received nocturnal oximetry monitoring during their first 3 nights after surgery. This revealed that patients without obstructive sleep apnea had significant increases in oxygen desaturation index during their first night after surgery, while those with sleep apnea did not return to their baseline oxygen desaturation index until the third night after surgery.
“Despite a substantial decrease in ODI [oxygen desaturation index] with oxygen therapy in patients with OSA during the first 3 postoperative nights, supplemental oxygen did not modify the association between OSA and postoperative cardiovascular event,” wrote Matthew T.V. Chan, MD, of Chinese University of Hong Kong, Prince of Wales Hospital, and coauthors.
Given that the events were associated with longer durations of severe oxyhemoglobin desaturation, more aggressive interventions such as positive airway pressure or oral appliances may be required, they noted.
“However, high-level evidence demonstrating the effect of these measures on perioperative outcomes is lacking [and] further clinical trials are now required to test if additional monitoring or alternative interventions would reduce the risk,” they wrote.
The study was supported by the Health and Medical Research Fund (Hong Kong), National Healthcare Group–Khoo Teck Puat Hospital, University Health Network Foundation, University of Malaya, Malaysian Society of Anaesthesiologists, Auckland Medical Research Foundation, and ResMed. One author declared grants from private industry and a patent pending on an obstructive sleep apnea risk questionnaire used in the study.
SOURCE: Chan M et al. JAMA 2019;321[18]:1788-98. doi: 10.1001/jama.2019.4783.
This study is large, prospective, and rigorous and adds important new information to the puzzle of the impact of sleep apnea on postoperative risk, Dennis Auckley, MD, and Stavros Memtsoudis, MD, wrote in an editorial accompanying this study. The study focused on predetermined clinically significant and measurable events, used standardized and objective sleep apnea testing, and attempted to control for many of the confounders that might have influenced outcomes.
The results suggest that obstructive sleep apnea should be recognized as a major perioperative risk factor, and it should receive the same attention and optimization efforts as comorbidities such as diabetes.
Dr. Auckley is from the division of pulmonary, critical care and sleep medicine at MetroHealth Medical Center, Case Western Reserve University, Cleveland, and Dr. Memtsoudis is clinical professor of anesthesiology at Cornell University, New York. These comments are adapted from an editorial (JAMA 2019;231[18]:1775-6). Both declared board and executive positions with the Society of Anesthesia and Sleep Medicine. Dr. Auckley declared research funding from Medtronic, and Dr. Memtsoudis declared personal fees from Teikoku and Sandoz.
This study is large, prospective, and rigorous and adds important new information to the puzzle of the impact of sleep apnea on postoperative risk, Dennis Auckley, MD, and Stavros Memtsoudis, MD, wrote in an editorial accompanying this study. The study focused on predetermined clinically significant and measurable events, used standardized and objective sleep apnea testing, and attempted to control for many of the confounders that might have influenced outcomes.
The results suggest that obstructive sleep apnea should be recognized as a major perioperative risk factor, and it should receive the same attention and optimization efforts as comorbidities such as diabetes.
Dr. Auckley is from the division of pulmonary, critical care and sleep medicine at MetroHealth Medical Center, Case Western Reserve University, Cleveland, and Dr. Memtsoudis is clinical professor of anesthesiology at Cornell University, New York. These comments are adapted from an editorial (JAMA 2019;231[18]:1775-6). Both declared board and executive positions with the Society of Anesthesia and Sleep Medicine. Dr. Auckley declared research funding from Medtronic, and Dr. Memtsoudis declared personal fees from Teikoku and Sandoz.
This study is large, prospective, and rigorous and adds important new information to the puzzle of the impact of sleep apnea on postoperative risk, Dennis Auckley, MD, and Stavros Memtsoudis, MD, wrote in an editorial accompanying this study. The study focused on predetermined clinically significant and measurable events, used standardized and objective sleep apnea testing, and attempted to control for many of the confounders that might have influenced outcomes.
The results suggest that obstructive sleep apnea should be recognized as a major perioperative risk factor, and it should receive the same attention and optimization efforts as comorbidities such as diabetes.
Dr. Auckley is from the division of pulmonary, critical care and sleep medicine at MetroHealth Medical Center, Case Western Reserve University, Cleveland, and Dr. Memtsoudis is clinical professor of anesthesiology at Cornell University, New York. These comments are adapted from an editorial (JAMA 2019;231[18]:1775-6). Both declared board and executive positions with the Society of Anesthesia and Sleep Medicine. Dr. Auckley declared research funding from Medtronic, and Dr. Memtsoudis declared personal fees from Teikoku and Sandoz.
Unrecognized severe obstructive sleep apnea is a risk factor for cardiovascular complications after major noncardiac surgery, according to a study published in JAMA.
The researchers state that perioperative mismanagement of obstructive sleep apnea can lead to serious medical consequences. “General anesthetics, sedatives, and postoperative analgesics are potent respiratory depressants that relax the upper airway dilator muscles and impair ventilatory response to hypoxemia and hypercapnia. Each of these events exacerbates [obstructive sleep apnea] and may predispose patients to postoperative cardiovascular complications,” said researchers who conducted the The Postoperative vascular complications in unrecognised Obstructive Sleep apnoea (POSA) study (NCT01494181).
They undertook a prospective observational cohort study involving 1,218 patients undergoing major noncardiac surgery, who were already considered at high risk of postoperative cardiovascular events – having, for example, a history of coronary artery disease, stroke, diabetes, or renal impairment. However, none had a prior diagnosis of obstructive sleep apnea.
Preoperative sleep monitoring revealed that two-thirds of the cohort had unrecognized and untreated obstructive sleep apnea, including 11.2% with severe obstructive sleep apnea.
At 30 days after surgery, patients with obstructive sleep apnea had a 49% higher risk of the primary outcome of myocardial injury, cardiac death, heart failure, thromboembolism, atrial fibrillation, or stroke, compared with those without obstructive sleep apnea.
However, this association was largely due to a significant 2.23-fold higher risk among patients with severe obstructive sleep apnea, while those with only moderate or mild sleep apnea did not show a significant increased risk of cardiovascular complications.
Patients in this study with severe obstructive sleep apnea had a 13-fold higher risk of cardiac death, 80% higher risk of myocardial injury, more than sixfold higher risk of heart failure, and nearly fourfold higher risk of atrial fibrillation.
Researchers also saw an association between obstructive sleep apnea and increased risk of infective outcomes, unplanned tracheal intubation, postoperative lung ventilation, and readmission to the ICU.
The majority of patients received nocturnal oximetry monitoring during their first 3 nights after surgery. This revealed that patients without obstructive sleep apnea had significant increases in oxygen desaturation index during their first night after surgery, while those with sleep apnea did not return to their baseline oxygen desaturation index until the third night after surgery.
“Despite a substantial decrease in ODI [oxygen desaturation index] with oxygen therapy in patients with OSA during the first 3 postoperative nights, supplemental oxygen did not modify the association between OSA and postoperative cardiovascular event,” wrote Matthew T.V. Chan, MD, of Chinese University of Hong Kong, Prince of Wales Hospital, and coauthors.
Given that the events were associated with longer durations of severe oxyhemoglobin desaturation, more aggressive interventions such as positive airway pressure or oral appliances may be required, they noted.
“However, high-level evidence demonstrating the effect of these measures on perioperative outcomes is lacking [and] further clinical trials are now required to test if additional monitoring or alternative interventions would reduce the risk,” they wrote.
The study was supported by the Health and Medical Research Fund (Hong Kong), National Healthcare Group–Khoo Teck Puat Hospital, University Health Network Foundation, University of Malaya, Malaysian Society of Anaesthesiologists, Auckland Medical Research Foundation, and ResMed. One author declared grants from private industry and a patent pending on an obstructive sleep apnea risk questionnaire used in the study.
SOURCE: Chan M et al. JAMA 2019;321[18]:1788-98. doi: 10.1001/jama.2019.4783.
Unrecognized severe obstructive sleep apnea is a risk factor for cardiovascular complications after major noncardiac surgery, according to a study published in JAMA.
The researchers state that perioperative mismanagement of obstructive sleep apnea can lead to serious medical consequences. “General anesthetics, sedatives, and postoperative analgesics are potent respiratory depressants that relax the upper airway dilator muscles and impair ventilatory response to hypoxemia and hypercapnia. Each of these events exacerbates [obstructive sleep apnea] and may predispose patients to postoperative cardiovascular complications,” said researchers who conducted the The Postoperative vascular complications in unrecognised Obstructive Sleep apnoea (POSA) study (NCT01494181).
They undertook a prospective observational cohort study involving 1,218 patients undergoing major noncardiac surgery, who were already considered at high risk of postoperative cardiovascular events – having, for example, a history of coronary artery disease, stroke, diabetes, or renal impairment. However, none had a prior diagnosis of obstructive sleep apnea.
Preoperative sleep monitoring revealed that two-thirds of the cohort had unrecognized and untreated obstructive sleep apnea, including 11.2% with severe obstructive sleep apnea.
At 30 days after surgery, patients with obstructive sleep apnea had a 49% higher risk of the primary outcome of myocardial injury, cardiac death, heart failure, thromboembolism, atrial fibrillation, or stroke, compared with those without obstructive sleep apnea.
However, this association was largely due to a significant 2.23-fold higher risk among patients with severe obstructive sleep apnea, while those with only moderate or mild sleep apnea did not show a significant increased risk of cardiovascular complications.
Patients in this study with severe obstructive sleep apnea had a 13-fold higher risk of cardiac death, 80% higher risk of myocardial injury, more than sixfold higher risk of heart failure, and nearly fourfold higher risk of atrial fibrillation.
Researchers also saw an association between obstructive sleep apnea and increased risk of infective outcomes, unplanned tracheal intubation, postoperative lung ventilation, and readmission to the ICU.
The majority of patients received nocturnal oximetry monitoring during their first 3 nights after surgery. This revealed that patients without obstructive sleep apnea had significant increases in oxygen desaturation index during their first night after surgery, while those with sleep apnea did not return to their baseline oxygen desaturation index until the third night after surgery.
“Despite a substantial decrease in ODI [oxygen desaturation index] with oxygen therapy in patients with OSA during the first 3 postoperative nights, supplemental oxygen did not modify the association between OSA and postoperative cardiovascular event,” wrote Matthew T.V. Chan, MD, of Chinese University of Hong Kong, Prince of Wales Hospital, and coauthors.
Given that the events were associated with longer durations of severe oxyhemoglobin desaturation, more aggressive interventions such as positive airway pressure or oral appliances may be required, they noted.
“However, high-level evidence demonstrating the effect of these measures on perioperative outcomes is lacking [and] further clinical trials are now required to test if additional monitoring or alternative interventions would reduce the risk,” they wrote.
The study was supported by the Health and Medical Research Fund (Hong Kong), National Healthcare Group–Khoo Teck Puat Hospital, University Health Network Foundation, University of Malaya, Malaysian Society of Anaesthesiologists, Auckland Medical Research Foundation, and ResMed. One author declared grants from private industry and a patent pending on an obstructive sleep apnea risk questionnaire used in the study.
SOURCE: Chan M et al. JAMA 2019;321[18]:1788-98. doi: 10.1001/jama.2019.4783.
FROM JAMA
Arsenic exposure increases risk of left ventricular hypertrophy
Young Native Americans had increased left ventricular thickness and left ventricular hypertrophy after being exposed to arsenic, and had a greater risk if they showed signs of prehypertension or hypertension, according to recent research.

“The stronger association in subjects with elevated blood pressure suggests that individuals with preclinical heart disease might be more prone to the toxic effects of arsenic on the heart,” Gernot Pichler, MD, PhD, a cardiologist at Hospital Hietzing/Heart Center Clinic Floridsdorf in Vienna, stated in a press release.
Dr. Pichler and colleagues evaluated 1,337 individuals (mean age, 31 years; 61% female) in the Strong Heart Family Study, an extension of the Strong Heart Study that was designed to study cardiovascular disease in Native Americans. The researchers noted that, while the studies were not originally intended to evaluate arsenic exposure in these populations, “the importance of studying arsenic was recognized overtime as increasing evidence supported the role of arsenic in cardiovascular disease and the relatively high arsenic exposure in tribal communities, compared to other general populations in the United States.”
Arsenic exposure was determined through the sum of inorganic and methylated arsenic concentrations in urine, and researchers used transthoracic ECG at baseline and follow-up to compare left ventricular geometry and function. The mean follow-up was 5.6 years and baseline median sum of inorganic and methylated arsenic concentrations in urine was 4.24 (interquartile range, 2.82-6.90) mcg/g creatinine.
Prevalence of left ventricular hypertrophy was 4.6% overall, and the odds ratio of left ventricular hypertrophy per 100% increase in arsenic in the urine was 1.47 (95% confidence interval, 1.05-2.08) overall and 1.58 for individuals with prehypertension or hypertension (95% CI, 1.04-2.41).
“People drinking water from private wells, which are not regulated, need to be aware that arsenic may increase the risk for cardiovascular disease,” said Dr. Pichler. “Testing those wells is a critical first step to take action and prevent exposure.”
Prospective and cross-sectional analyses both showed changes in left ventricular geometry – such as in the left atrial systolic diameter, interventricular septum, and left ventricular posterior wall thickness and mass index – were associated with exposure to arsenic. In addition, left ventricular function factors such as isovolumic relaxation time and stroke volume were also affected by arsenic exposure. However, the researchers noted that their study was limited by a single method of arsenic exposure and having no long-term follow-up for participants.
“The study raises the question of whether the changes in heart structure are reversible if exposure is reduced. Some changes have occurred in water sources in the study communities, and it will be important to check the potential health impact of reducing arsenic exposure,” said Dr. Pichler.
This study was funded by the National Institute of Health Sciences and grants from the National Heart, Lung, and Blood Institute. The authors reported no relevant conflicts of interest.
SOURCE: Pichler G et al. Circ Cardiovasc Imaging. 2019 May 1. doi: 10.1161/CIRCIMAGING.119.009018.
The results from Pichler et al. show the effects of recent arsenic exposure on left ventricular (LV) hypertrophy, but other questions remain as to the long-term effects of arsenic and its interactions with other environmental metals, Rajiv Chowdhury, MBBS, PhD, and Kim van Daalen, BSc, MPhil, wrote in a related editorial.
It has been established that chronic, low to moderate inorganic arsenic exposure may be linked to cardiovascular disease (CVD) and risk factors such as hypertension and diabetes, but it is unclear how different exposure pathways contribute as well as what pathophysiological mechanisms contribute to CVD, and whether arsenic directly or indirectly contributes to cardiac functioning or a worse cardiometabolic profile, respectively, they wrote.
While the results contribute to the understanding of arsenic exposure through drinking water and its relationship to LV function and geometry, urinary arsenic reflects recent exposure and cannot measure arsenic exposure over a period of time. The study also does not account for an individual’s CVD risk or LV functioning/geometry with daily exposure to co-occurring environmental metals, particularly heavy metals, together with arsenic. Factors such as genetics, age, gender, and nutrition also impact an individual’s reaction to arsenic, and studies should be able to differentiate inorganic arsenic obtained from food and other sources.
While “this elegant analysis ... helps to clarify the observational associations of [arsenic] with LV geometry and function, it stimulates further complimentary work,” they wrote. “Such studies would be essential since CVD remains the single leading cause of adult premature death worldwide, and millions of individuals globally are exposed to arsenic and other metal contaminants.”
Dr. Chowdhury and Dr. Daalen are from the cardiovascular epidemiology unit in the department of public health and primary care at the University of Cambridge (England).
The results from Pichler et al. show the effects of recent arsenic exposure on left ventricular (LV) hypertrophy, but other questions remain as to the long-term effects of arsenic and its interactions with other environmental metals, Rajiv Chowdhury, MBBS, PhD, and Kim van Daalen, BSc, MPhil, wrote in a related editorial.
It has been established that chronic, low to moderate inorganic arsenic exposure may be linked to cardiovascular disease (CVD) and risk factors such as hypertension and diabetes, but it is unclear how different exposure pathways contribute as well as what pathophysiological mechanisms contribute to CVD, and whether arsenic directly or indirectly contributes to cardiac functioning or a worse cardiometabolic profile, respectively, they wrote.
While the results contribute to the understanding of arsenic exposure through drinking water and its relationship to LV function and geometry, urinary arsenic reflects recent exposure and cannot measure arsenic exposure over a period of time. The study also does not account for an individual’s CVD risk or LV functioning/geometry with daily exposure to co-occurring environmental metals, particularly heavy metals, together with arsenic. Factors such as genetics, age, gender, and nutrition also impact an individual’s reaction to arsenic, and studies should be able to differentiate inorganic arsenic obtained from food and other sources.
While “this elegant analysis ... helps to clarify the observational associations of [arsenic] with LV geometry and function, it stimulates further complimentary work,” they wrote. “Such studies would be essential since CVD remains the single leading cause of adult premature death worldwide, and millions of individuals globally are exposed to arsenic and other metal contaminants.”
Dr. Chowdhury and Dr. Daalen are from the cardiovascular epidemiology unit in the department of public health and primary care at the University of Cambridge (England).
The results from Pichler et al. show the effects of recent arsenic exposure on left ventricular (LV) hypertrophy, but other questions remain as to the long-term effects of arsenic and its interactions with other environmental metals, Rajiv Chowdhury, MBBS, PhD, and Kim van Daalen, BSc, MPhil, wrote in a related editorial.
It has been established that chronic, low to moderate inorganic arsenic exposure may be linked to cardiovascular disease (CVD) and risk factors such as hypertension and diabetes, but it is unclear how different exposure pathways contribute as well as what pathophysiological mechanisms contribute to CVD, and whether arsenic directly or indirectly contributes to cardiac functioning or a worse cardiometabolic profile, respectively, they wrote.
While the results contribute to the understanding of arsenic exposure through drinking water and its relationship to LV function and geometry, urinary arsenic reflects recent exposure and cannot measure arsenic exposure over a period of time. The study also does not account for an individual’s CVD risk or LV functioning/geometry with daily exposure to co-occurring environmental metals, particularly heavy metals, together with arsenic. Factors such as genetics, age, gender, and nutrition also impact an individual’s reaction to arsenic, and studies should be able to differentiate inorganic arsenic obtained from food and other sources.
While “this elegant analysis ... helps to clarify the observational associations of [arsenic] with LV geometry and function, it stimulates further complimentary work,” they wrote. “Such studies would be essential since CVD remains the single leading cause of adult premature death worldwide, and millions of individuals globally are exposed to arsenic and other metal contaminants.”
Dr. Chowdhury and Dr. Daalen are from the cardiovascular epidemiology unit in the department of public health and primary care at the University of Cambridge (England).
Young Native Americans had increased left ventricular thickness and left ventricular hypertrophy after being exposed to arsenic, and had a greater risk if they showed signs of prehypertension or hypertension, according to recent research.
“The stronger association in subjects with elevated blood pressure suggests that individuals with preclinical heart disease might be more prone to the toxic effects of arsenic on the heart,” Gernot Pichler, MD, PhD, a cardiologist at Hospital Hietzing/Heart Center Clinic Floridsdorf in Vienna, stated in a press release.
Dr. Pichler and colleagues evaluated 1,337 individuals (mean age, 31 years; 61% female) in the Strong Heart Family Study, an extension of the Strong Heart Study that was designed to study cardiovascular disease in Native Americans. The researchers noted that, while the studies were not originally intended to evaluate arsenic exposure in these populations, “the importance of studying arsenic was recognized overtime as increasing evidence supported the role of arsenic in cardiovascular disease and the relatively high arsenic exposure in tribal communities, compared to other general populations in the United States.”
Arsenic exposure was determined through the sum of inorganic and methylated arsenic concentrations in urine, and researchers used transthoracic ECG at baseline and follow-up to compare left ventricular geometry and function. The mean follow-up was 5.6 years and baseline median sum of inorganic and methylated arsenic concentrations in urine was 4.24 (interquartile range, 2.82-6.90) mcg/g creatinine.
Prevalence of left ventricular hypertrophy was 4.6% overall, and the odds ratio of left ventricular hypertrophy per 100% increase in arsenic in the urine was 1.47 (95% confidence interval, 1.05-2.08) overall and 1.58 for individuals with prehypertension or hypertension (95% CI, 1.04-2.41).
“People drinking water from private wells, which are not regulated, need to be aware that arsenic may increase the risk for cardiovascular disease,” said Dr. Pichler. “Testing those wells is a critical first step to take action and prevent exposure.”
Prospective and cross-sectional analyses both showed changes in left ventricular geometry – such as in the left atrial systolic diameter, interventricular septum, and left ventricular posterior wall thickness and mass index – were associated with exposure to arsenic. In addition, left ventricular function factors such as isovolumic relaxation time and stroke volume were also affected by arsenic exposure. However, the researchers noted that their study was limited by a single method of arsenic exposure and having no long-term follow-up for participants.
“The study raises the question of whether the changes in heart structure are reversible if exposure is reduced. Some changes have occurred in water sources in the study communities, and it will be important to check the potential health impact of reducing arsenic exposure,” said Dr. Pichler.
This study was funded by the National Institute of Health Sciences and grants from the National Heart, Lung, and Blood Institute. The authors reported no relevant conflicts of interest.
SOURCE: Pichler G et al. Circ Cardiovasc Imaging. 2019 May 1. doi: 10.1161/CIRCIMAGING.119.009018.
Young Native Americans had increased left ventricular thickness and left ventricular hypertrophy after being exposed to arsenic, and had a greater risk if they showed signs of prehypertension or hypertension, according to recent research.
“The stronger association in subjects with elevated blood pressure suggests that individuals with preclinical heart disease might be more prone to the toxic effects of arsenic on the heart,” Gernot Pichler, MD, PhD, a cardiologist at Hospital Hietzing/Heart Center Clinic Floridsdorf in Vienna, stated in a press release.
Dr. Pichler and colleagues evaluated 1,337 individuals (mean age, 31 years; 61% female) in the Strong Heart Family Study, an extension of the Strong Heart Study that was designed to study cardiovascular disease in Native Americans. The researchers noted that, while the studies were not originally intended to evaluate arsenic exposure in these populations, “the importance of studying arsenic was recognized overtime as increasing evidence supported the role of arsenic in cardiovascular disease and the relatively high arsenic exposure in tribal communities, compared to other general populations in the United States.”
Arsenic exposure was determined through the sum of inorganic and methylated arsenic concentrations in urine, and researchers used transthoracic ECG at baseline and follow-up to compare left ventricular geometry and function. The mean follow-up was 5.6 years and baseline median sum of inorganic and methylated arsenic concentrations in urine was 4.24 (interquartile range, 2.82-6.90) mcg/g creatinine.
Prevalence of left ventricular hypertrophy was 4.6% overall, and the odds ratio of left ventricular hypertrophy per 100% increase in arsenic in the urine was 1.47 (95% confidence interval, 1.05-2.08) overall and 1.58 for individuals with prehypertension or hypertension (95% CI, 1.04-2.41).
“People drinking water from private wells, which are not regulated, need to be aware that arsenic may increase the risk for cardiovascular disease,” said Dr. Pichler. “Testing those wells is a critical first step to take action and prevent exposure.”
Prospective and cross-sectional analyses both showed changes in left ventricular geometry – such as in the left atrial systolic diameter, interventricular septum, and left ventricular posterior wall thickness and mass index – were associated with exposure to arsenic. In addition, left ventricular function factors such as isovolumic relaxation time and stroke volume were also affected by arsenic exposure. However, the researchers noted that their study was limited by a single method of arsenic exposure and having no long-term follow-up for participants.
“The study raises the question of whether the changes in heart structure are reversible if exposure is reduced. Some changes have occurred in water sources in the study communities, and it will be important to check the potential health impact of reducing arsenic exposure,” said Dr. Pichler.
This study was funded by the National Institute of Health Sciences and grants from the National Heart, Lung, and Blood Institute. The authors reported no relevant conflicts of interest.
SOURCE: Pichler G et al. Circ Cardiovasc Imaging. 2019 May 1. doi: 10.1161/CIRCIMAGING.119.009018.
FROM CIRCULATION: CARDIOVASCULAR IMAGING