User login
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
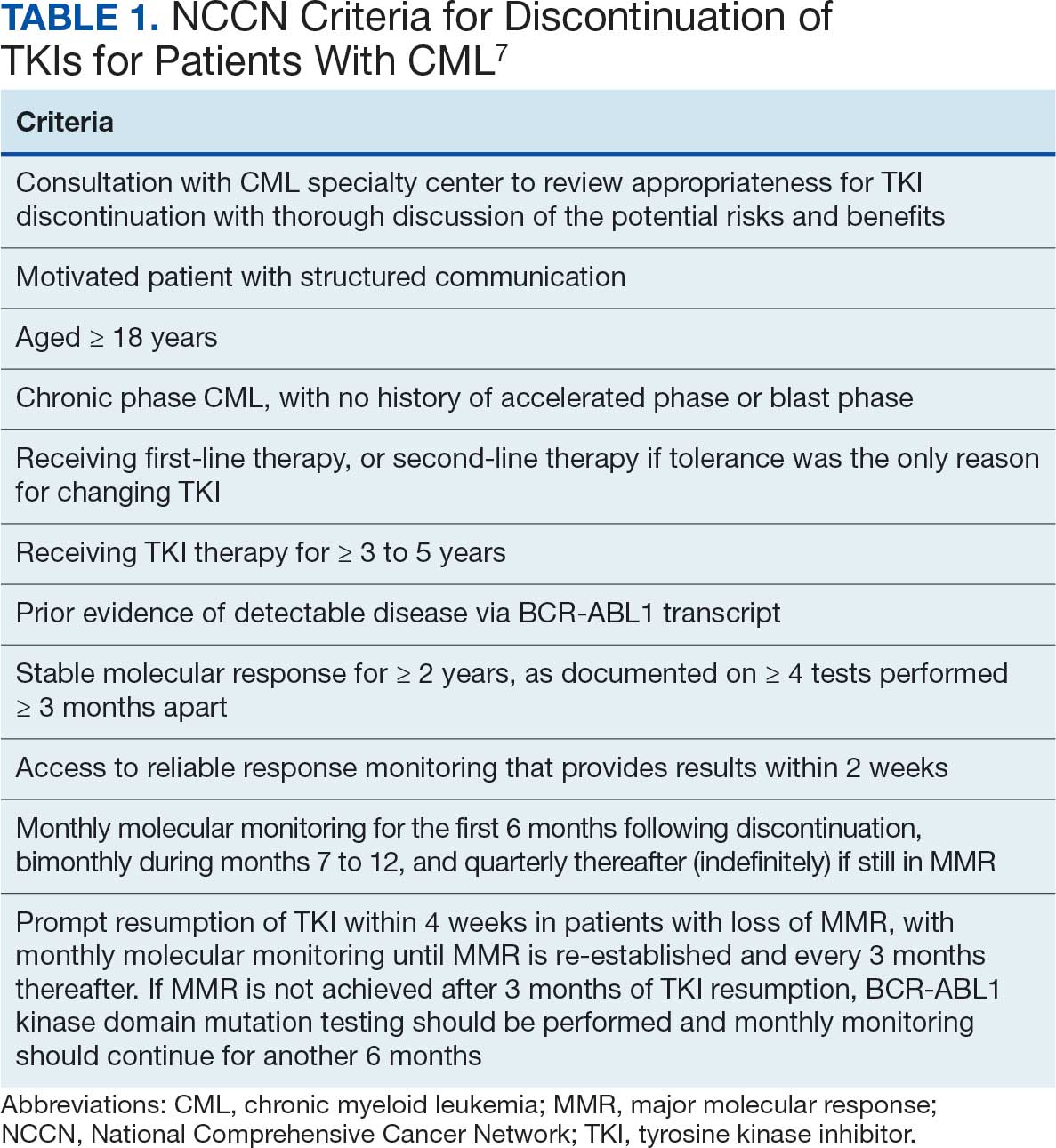
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
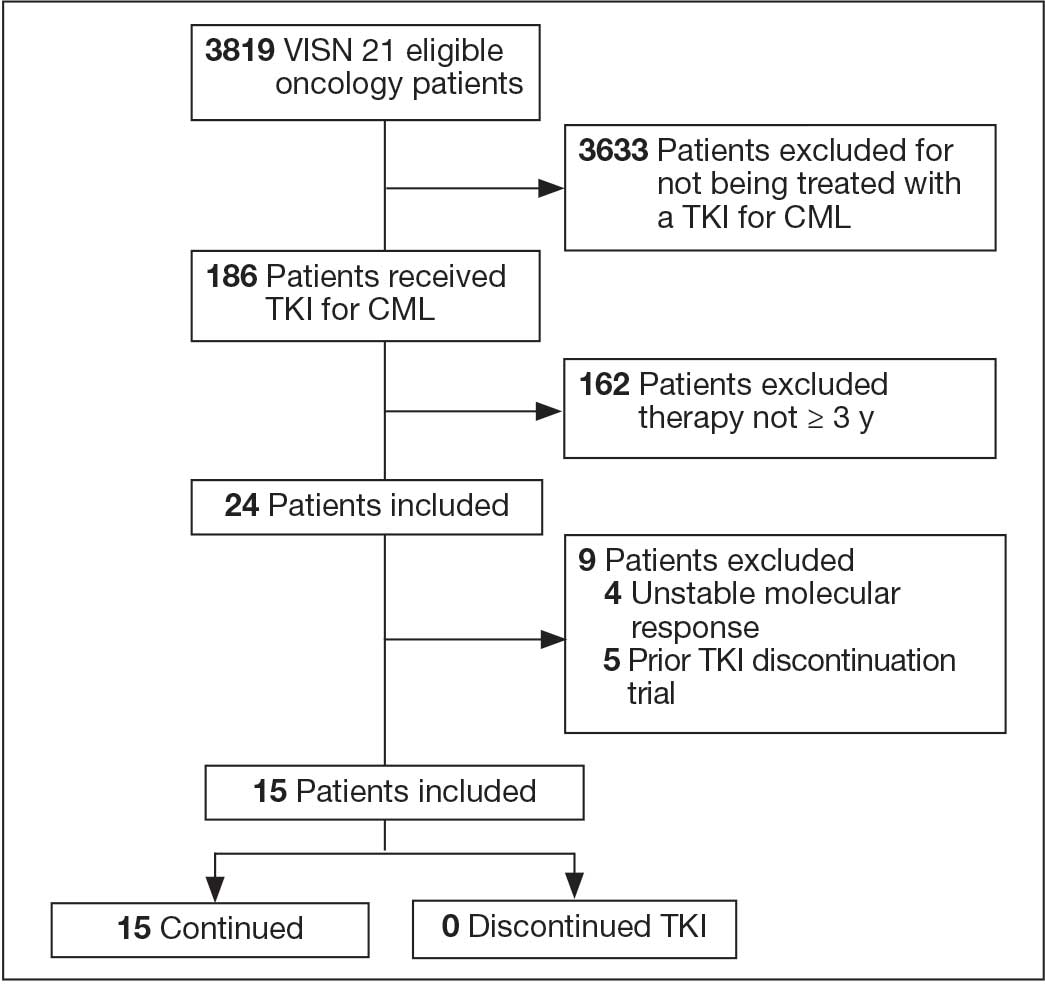
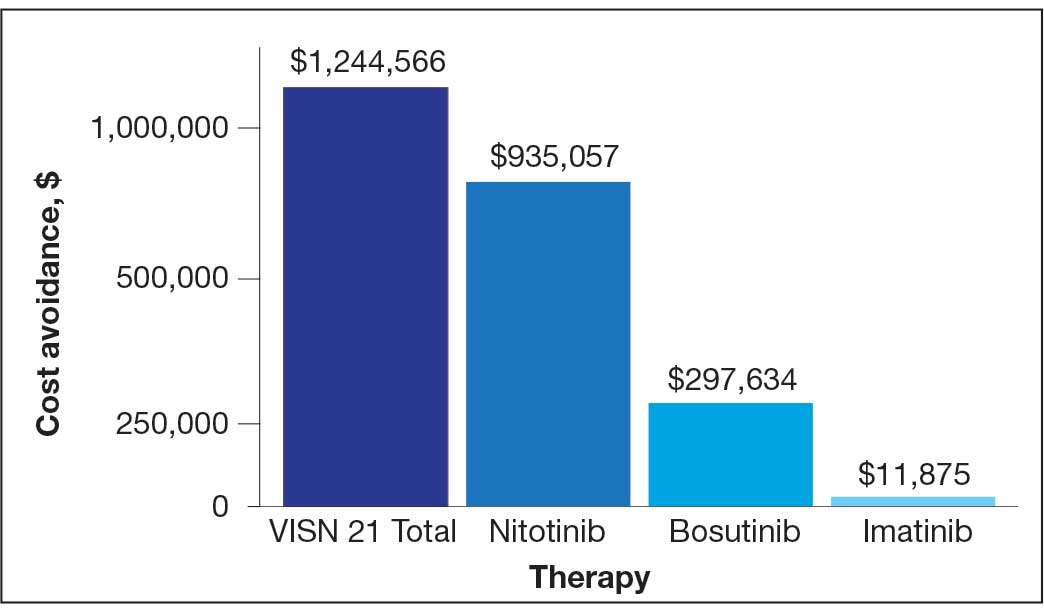
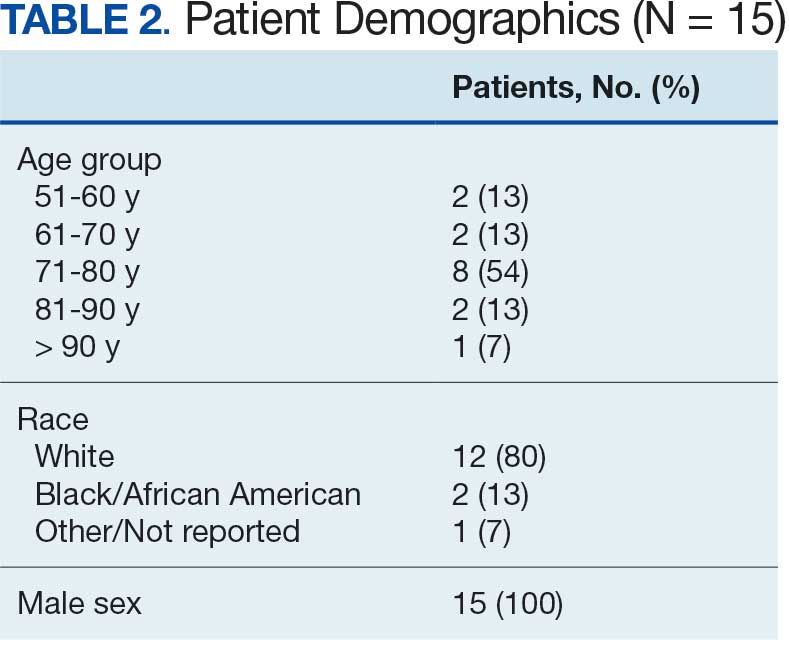
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
AVAHO Regional Meeting Addresses Complex World of Peripheral T-Cell Lymphoma
AVAHO Regional Meeting Addresses Complex World of Peripheral T-Cell Lymphoma
SAN FRANCISCO – Peripheral T-cell lymphoma (PTCL) accounts for 4% of mature non-Hodgkin lymphoma cases in the US, or only about 4000 cases a year. While the number of patients is small, however, treatment for PTCL is complex due to wide variations in subtypes and survival rates, a hematologist-oncologist said at the March 21 Association of VA Hematology/Oncology (AVAHO) regional meeting on lymphoma.
Weiyun Ai, MD, PhD, a clinical professor of medicine at University of California, San Francisco who specializes in lymphoma, explained that there are multiple subtypes of PTCL based on their location within the body. Ai discussed a 2008 analysis of North American cases of PTCL and natural killer/T-cell lymphoma from 1990-2002, of which:
34% were PTCL, not otherwise specified;
16% were angioimmunoblastic T-cell lymphoma (AITL);
16% were anaplastic large cell lymphoma (ALCL), anaplastic lymphoma kinase (ALK)-positive;
7.8% were ALCL, ALK-negative;
5.8% were enteropathy-type;
5.4% were primary cutaneous ALCL; and
5.1% were extranodal natural killer/T-cell lymphoma, nasal type.
The remaining cases were adult T-cell leukemia/lymphoma, hepatosplenic, subcutaneous panniculitis-like, and unclassified.
International Prognostic Index Predicts Outcomes
“The subtype with the best outcome is ALCL, ALK-positive with a 5-year overall survival rate of 70% followed by ALK-negative ALCL at 50%, and all the other common subtypes at 30%,” Ai said.
Ai outlined the International Prognostic Index (IPI), a tool to predict clinical outcomes in patients with aggressive non-Hodgkin lymphoma based on risk factors. IPI assigns worse scores to patients aged > 60 years; patients who have higher (worse) performance scores, higher lactate dehydrogenase (LDH) levels, and more extranodal sites; and patients at stages III-IV.
First-Line Therapy: Consider Subtypes and CD30 Levels
Subtypes and CD30 expression levels are important factors in choosing therapy, Ai said, and 2019’s landmark ECHELON-2 study (updated in 2022) defines the standard.
Newly diagnosed patients who strongly express CD30 (ie, those with both types of ALCL) are recommended to be treated with A+CHP (brentuximab vedotin [BV] plus cyclophosphamide, doxorubicin, and prednisone).
Combination therapy of cyclophosphamide, doxorubicin, hydroxydaunorubicin, vincristine, and prednisone (CHOP) was the prior standard of care until the ECHELON-2 study, Ai said.
That trial, which randomized 452 patients with untreated PTCL (CD30 ≥ 10%) to A+CHP or CHOP, found that 5-year progression-free rates were 51.4% vs 43.0%, respectively (hazard ratio [HR], 0.70; 95% CI, 0.53-0.91). Five-year overall survival rates were 70.1% vs. 61.0%, respectively (HR, 0.72; 95% CI, 0.53-0.99).
The threshold CD30 level at which to turn to A+CHP—1%, 5%, or 10%—“is kind of a dealer’s choice,” Ai said. Her own cutoff is 1%.
“If they're < 1%, I tend not to do it,” Ai said. “It's usually much more expensive, as you can imagine.”
If CD30 < 1%, Ai recommends CHOP or, in younger patients, CHOP plus etoposide (CHOEP).
Follow-up treatments include autologous stem cell transplant (ASCT) and observation/maintenance, depending on factors such as subtype, fitness, and remission.
Transplant: Still Relevant
When ECHELON-2 was released, some clinicians wondered if ASCT was still warranted, Ai said. A posthoc exploratory analysis found a 62% reduction in relative risk for progression in patients who underwent transplants after reaching complete remission with A+CHP.
The findings provide support for transplant, she said.
For transplant-ineligible patients, a small analysis of BV and CHP followed by BV maintenance showed a progression-free survival curve that appeared to plateau after 18-24 months.
“You don't see this kind of curve very often. I was quite impressed,” Ai said. “If the patient is willing and able, I will give them BV cycles.”
Ai discloses relationships with ADC, AbbVie, Acrotech, Kite, and Kyowa Kirin.
SAN FRANCISCO – Peripheral T-cell lymphoma (PTCL) accounts for 4% of mature non-Hodgkin lymphoma cases in the US, or only about 4000 cases a year. While the number of patients is small, however, treatment for PTCL is complex due to wide variations in subtypes and survival rates, a hematologist-oncologist said at the March 21 Association of VA Hematology/Oncology (AVAHO) regional meeting on lymphoma.
Weiyun Ai, MD, PhD, a clinical professor of medicine at University of California, San Francisco who specializes in lymphoma, explained that there are multiple subtypes of PTCL based on their location within the body. Ai discussed a 2008 analysis of North American cases of PTCL and natural killer/T-cell lymphoma from 1990-2002, of which:
34% were PTCL, not otherwise specified;
16% were angioimmunoblastic T-cell lymphoma (AITL);
16% were anaplastic large cell lymphoma (ALCL), anaplastic lymphoma kinase (ALK)-positive;
7.8% were ALCL, ALK-negative;
5.8% were enteropathy-type;
5.4% were primary cutaneous ALCL; and
5.1% were extranodal natural killer/T-cell lymphoma, nasal type.
The remaining cases were adult T-cell leukemia/lymphoma, hepatosplenic, subcutaneous panniculitis-like, and unclassified.
International Prognostic Index Predicts Outcomes
“The subtype with the best outcome is ALCL, ALK-positive with a 5-year overall survival rate of 70% followed by ALK-negative ALCL at 50%, and all the other common subtypes at 30%,” Ai said.
Ai outlined the International Prognostic Index (IPI), a tool to predict clinical outcomes in patients with aggressive non-Hodgkin lymphoma based on risk factors. IPI assigns worse scores to patients aged > 60 years; patients who have higher (worse) performance scores, higher lactate dehydrogenase (LDH) levels, and more extranodal sites; and patients at stages III-IV.
First-Line Therapy: Consider Subtypes and CD30 Levels
Subtypes and CD30 expression levels are important factors in choosing therapy, Ai said, and 2019’s landmark ECHELON-2 study (updated in 2022) defines the standard.
Newly diagnosed patients who strongly express CD30 (ie, those with both types of ALCL) are recommended to be treated with A+CHP (brentuximab vedotin [BV] plus cyclophosphamide, doxorubicin, and prednisone).
Combination therapy of cyclophosphamide, doxorubicin, hydroxydaunorubicin, vincristine, and prednisone (CHOP) was the prior standard of care until the ECHELON-2 study, Ai said.
That trial, which randomized 452 patients with untreated PTCL (CD30 ≥ 10%) to A+CHP or CHOP, found that 5-year progression-free rates were 51.4% vs 43.0%, respectively (hazard ratio [HR], 0.70; 95% CI, 0.53-0.91). Five-year overall survival rates were 70.1% vs. 61.0%, respectively (HR, 0.72; 95% CI, 0.53-0.99).
The threshold CD30 level at which to turn to A+CHP—1%, 5%, or 10%—“is kind of a dealer’s choice,” Ai said. Her own cutoff is 1%.
“If they're < 1%, I tend not to do it,” Ai said. “It's usually much more expensive, as you can imagine.”
If CD30 < 1%, Ai recommends CHOP or, in younger patients, CHOP plus etoposide (CHOEP).
Follow-up treatments include autologous stem cell transplant (ASCT) and observation/maintenance, depending on factors such as subtype, fitness, and remission.
Transplant: Still Relevant
When ECHELON-2 was released, some clinicians wondered if ASCT was still warranted, Ai said. A posthoc exploratory analysis found a 62% reduction in relative risk for progression in patients who underwent transplants after reaching complete remission with A+CHP.
The findings provide support for transplant, she said.
For transplant-ineligible patients, a small analysis of BV and CHP followed by BV maintenance showed a progression-free survival curve that appeared to plateau after 18-24 months.
“You don't see this kind of curve very often. I was quite impressed,” Ai said. “If the patient is willing and able, I will give them BV cycles.”
Ai discloses relationships with ADC, AbbVie, Acrotech, Kite, and Kyowa Kirin.
SAN FRANCISCO – Peripheral T-cell lymphoma (PTCL) accounts for 4% of mature non-Hodgkin lymphoma cases in the US, or only about 4000 cases a year. While the number of patients is small, however, treatment for PTCL is complex due to wide variations in subtypes and survival rates, a hematologist-oncologist said at the March 21 Association of VA Hematology/Oncology (AVAHO) regional meeting on lymphoma.
Weiyun Ai, MD, PhD, a clinical professor of medicine at University of California, San Francisco who specializes in lymphoma, explained that there are multiple subtypes of PTCL based on their location within the body. Ai discussed a 2008 analysis of North American cases of PTCL and natural killer/T-cell lymphoma from 1990-2002, of which:
34% were PTCL, not otherwise specified;
16% were angioimmunoblastic T-cell lymphoma (AITL);
16% were anaplastic large cell lymphoma (ALCL), anaplastic lymphoma kinase (ALK)-positive;
7.8% were ALCL, ALK-negative;
5.8% were enteropathy-type;
5.4% were primary cutaneous ALCL; and
5.1% were extranodal natural killer/T-cell lymphoma, nasal type.
The remaining cases were adult T-cell leukemia/lymphoma, hepatosplenic, subcutaneous panniculitis-like, and unclassified.
International Prognostic Index Predicts Outcomes
“The subtype with the best outcome is ALCL, ALK-positive with a 5-year overall survival rate of 70% followed by ALK-negative ALCL at 50%, and all the other common subtypes at 30%,” Ai said.
Ai outlined the International Prognostic Index (IPI), a tool to predict clinical outcomes in patients with aggressive non-Hodgkin lymphoma based on risk factors. IPI assigns worse scores to patients aged > 60 years; patients who have higher (worse) performance scores, higher lactate dehydrogenase (LDH) levels, and more extranodal sites; and patients at stages III-IV.
First-Line Therapy: Consider Subtypes and CD30 Levels
Subtypes and CD30 expression levels are important factors in choosing therapy, Ai said, and 2019’s landmark ECHELON-2 study (updated in 2022) defines the standard.
Newly diagnosed patients who strongly express CD30 (ie, those with both types of ALCL) are recommended to be treated with A+CHP (brentuximab vedotin [BV] plus cyclophosphamide, doxorubicin, and prednisone).
Combination therapy of cyclophosphamide, doxorubicin, hydroxydaunorubicin, vincristine, and prednisone (CHOP) was the prior standard of care until the ECHELON-2 study, Ai said.
That trial, which randomized 452 patients with untreated PTCL (CD30 ≥ 10%) to A+CHP or CHOP, found that 5-year progression-free rates were 51.4% vs 43.0%, respectively (hazard ratio [HR], 0.70; 95% CI, 0.53-0.91). Five-year overall survival rates were 70.1% vs. 61.0%, respectively (HR, 0.72; 95% CI, 0.53-0.99).
The threshold CD30 level at which to turn to A+CHP—1%, 5%, or 10%—“is kind of a dealer’s choice,” Ai said. Her own cutoff is 1%.
“If they're < 1%, I tend not to do it,” Ai said. “It's usually much more expensive, as you can imagine.”
If CD30 < 1%, Ai recommends CHOP or, in younger patients, CHOP plus etoposide (CHOEP).
Follow-up treatments include autologous stem cell transplant (ASCT) and observation/maintenance, depending on factors such as subtype, fitness, and remission.
Transplant: Still Relevant
When ECHELON-2 was released, some clinicians wondered if ASCT was still warranted, Ai said. A posthoc exploratory analysis found a 62% reduction in relative risk for progression in patients who underwent transplants after reaching complete remission with A+CHP.
The findings provide support for transplant, she said.
For transplant-ineligible patients, a small analysis of BV and CHP followed by BV maintenance showed a progression-free survival curve that appeared to plateau after 18-24 months.
“You don't see this kind of curve very often. I was quite impressed,” Ai said. “If the patient is willing and able, I will give them BV cycles.”
Ai discloses relationships with ADC, AbbVie, Acrotech, Kite, and Kyowa Kirin.
AVAHO Regional Meeting Addresses Complex World of Peripheral T-Cell Lymphoma
AVAHO Regional Meeting Addresses Complex World of Peripheral T-Cell Lymphoma
Agent Orange Exposure Increases Lymphoma Risk in Million Veteran Program Cohort
TOPLINE: Agent Orange exposure was associated with a 26% to 71% increased risk for multiple lymphoid cancers in veterans enrolled in the US Department of Veterans Affairs (VA) Million Veterans Program (MVP), while genetic predisposition independently raised risk by 12% to 81% across different lymphoma subtypes. A case-controlled analysis of 255,155 veterans found no significant interaction between genetic risk scores and Agent Orange exposure.
METHODOLOGY:
A case-control study included 255,155 non-Hispanic White veterans (median age 67 years, 92.5% male) enrolled in the VA MVP with genotype and Agent Orange exposure data.
Researchers analyzed five lymphoid malignant neoplasm subtypes: chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma diagnosed from January 1965 through June 2024.
Agent Orange exposure was determined through self-reported survey responses, while polygenic risk scores were derived from genome-wide association studies of lymphoid malignant neoplasms.
Analysis included adjustments for age at enrollment, sex, and the first 10 genetic principal components in logistic regression models evaluating Agent Orange exposure, polygenic risk scores, and their potential interaction.
TAKEAWAY:
Agent Orange exposure significantly increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% CI, 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores were independently associated with all lymphoma subtypes, with strongest associations for chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93) and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
Analysis in African American participants showed similar associations for multiple myeloma with both Agent Orange exposure (OR, 1.56; 95% CI, 1.18-2.07) and polygenic risk scores (OR, 1.31; 95% CI, 1.15-1.49).
According to the researchers, no significant polygenic risk score and Agent Orange exposure interactions were observed for any lymphoma subtype.
IN PRACTICE: "Our study addressed the public health concerns surrounding Agent Orange exposure and lymphoid malignant neoplasms, finding that both Agent Orange exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation," wrote the authors of the study.
SOURCE: The study was led by researchers at the University of California, Irvine and the Tibor Rubin Veterans Affairs Medical Center, Long Beach, Californiaand was published online on August 13 in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest case-control study of Agent Orange exposure and lymphoid malignant neoplasm risk, the power to detect interaction associations in specific subtypes might be limited. Self-reported Agent Orange exposure data may have introduced survival bias, particularly in aggressive subtypes, as patients with aggressive tumors may have died before joining the MVP. Additionally, about half of the patients were diagnosed with lymphoid malignant neoplasms before self-reporting Agent Orange exposure, potentially introducing recall bias.
DISCLOSURES: The research was supported by a Veterans Affairs Career Development Award Xueyi Teng, PhD, received grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Agent Orange exposure was associated with a 26% to 71% increased risk for multiple lymphoid cancers in veterans enrolled in the US Department of Veterans Affairs (VA) Million Veterans Program (MVP), while genetic predisposition independently raised risk by 12% to 81% across different lymphoma subtypes. A case-controlled analysis of 255,155 veterans found no significant interaction between genetic risk scores and Agent Orange exposure.
METHODOLOGY:
A case-control study included 255,155 non-Hispanic White veterans (median age 67 years, 92.5% male) enrolled in the VA MVP with genotype and Agent Orange exposure data.
Researchers analyzed five lymphoid malignant neoplasm subtypes: chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma diagnosed from January 1965 through June 2024.
Agent Orange exposure was determined through self-reported survey responses, while polygenic risk scores were derived from genome-wide association studies of lymphoid malignant neoplasms.
Analysis included adjustments for age at enrollment, sex, and the first 10 genetic principal components in logistic regression models evaluating Agent Orange exposure, polygenic risk scores, and their potential interaction.
TAKEAWAY:
Agent Orange exposure significantly increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% CI, 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores were independently associated with all lymphoma subtypes, with strongest associations for chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93) and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
Analysis in African American participants showed similar associations for multiple myeloma with both Agent Orange exposure (OR, 1.56; 95% CI, 1.18-2.07) and polygenic risk scores (OR, 1.31; 95% CI, 1.15-1.49).
According to the researchers, no significant polygenic risk score and Agent Orange exposure interactions were observed for any lymphoma subtype.
IN PRACTICE: "Our study addressed the public health concerns surrounding Agent Orange exposure and lymphoid malignant neoplasms, finding that both Agent Orange exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation," wrote the authors of the study.
SOURCE: The study was led by researchers at the University of California, Irvine and the Tibor Rubin Veterans Affairs Medical Center, Long Beach, Californiaand was published online on August 13 in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest case-control study of Agent Orange exposure and lymphoid malignant neoplasm risk, the power to detect interaction associations in specific subtypes might be limited. Self-reported Agent Orange exposure data may have introduced survival bias, particularly in aggressive subtypes, as patients with aggressive tumors may have died before joining the MVP. Additionally, about half of the patients were diagnosed with lymphoid malignant neoplasms before self-reporting Agent Orange exposure, potentially introducing recall bias.
DISCLOSURES: The research was supported by a Veterans Affairs Career Development Award Xueyi Teng, PhD, received grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Agent Orange exposure was associated with a 26% to 71% increased risk for multiple lymphoid cancers in veterans enrolled in the US Department of Veterans Affairs (VA) Million Veterans Program (MVP), while genetic predisposition independently raised risk by 12% to 81% across different lymphoma subtypes. A case-controlled analysis of 255,155 veterans found no significant interaction between genetic risk scores and Agent Orange exposure.
METHODOLOGY:
A case-control study included 255,155 non-Hispanic White veterans (median age 67 years, 92.5% male) enrolled in the VA MVP with genotype and Agent Orange exposure data.
Researchers analyzed five lymphoid malignant neoplasm subtypes: chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma diagnosed from January 1965 through June 2024.
Agent Orange exposure was determined through self-reported survey responses, while polygenic risk scores were derived from genome-wide association studies of lymphoid malignant neoplasms.
Analysis included adjustments for age at enrollment, sex, and the first 10 genetic principal components in logistic regression models evaluating Agent Orange exposure, polygenic risk scores, and their potential interaction.
TAKEAWAY:
Agent Orange exposure significantly increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% CI, 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores were independently associated with all lymphoma subtypes, with strongest associations for chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93) and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
Analysis in African American participants showed similar associations for multiple myeloma with both Agent Orange exposure (OR, 1.56; 95% CI, 1.18-2.07) and polygenic risk scores (OR, 1.31; 95% CI, 1.15-1.49).
According to the researchers, no significant polygenic risk score and Agent Orange exposure interactions were observed for any lymphoma subtype.
IN PRACTICE: "Our study addressed the public health concerns surrounding Agent Orange exposure and lymphoid malignant neoplasms, finding that both Agent Orange exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation," wrote the authors of the study.
SOURCE: The study was led by researchers at the University of California, Irvine and the Tibor Rubin Veterans Affairs Medical Center, Long Beach, Californiaand was published online on August 13 in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest case-control study of Agent Orange exposure and lymphoid malignant neoplasm risk, the power to detect interaction associations in specific subtypes might be limited. Self-reported Agent Orange exposure data may have introduced survival bias, particularly in aggressive subtypes, as patients with aggressive tumors may have died before joining the MVP. Additionally, about half of the patients were diagnosed with lymphoid malignant neoplasms before self-reporting Agent Orange exposure, potentially introducing recall bias.
DISCLOSURES: The research was supported by a Veterans Affairs Career Development Award Xueyi Teng, PhD, received grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A Case Report on Bortezomib-Induced Hypotension: Rare Adverse Effect in Proteasome Inhibitor Therapy
Case Presentation
A 75-year-old man with chronic kidney disease, hypertension and diabetes mellitus presented with acute kidney injury (creatinine 5.2 from baseline 4.2) and a two-week history of increased urinary frequency. Labs revealed high anion gap metabolic acidosis, proteinuria, hematuria, pyuria, and acute on chronic anemia. He was diagnosed with kappa light chain nephropathy and multiple myeloma with 32% plasma cells on bone marrow biopsy. He began treatment with bortezomib, cyclophosphamide, and dexamethasone (Cy- BorD). Three days after cyclophosphamide and five days after bortezomib, the patient developed persistent hypotension with systolic BP in the 50s, unresponsive to fluids and Trendelenburg position. Due to end-stage renal disease with anuria, fluid resuscitation was limited. He required norepinephrine and was transferred to the ICU. Given instability, hemodialysis was deferred, and continuous renal replacement therapy was initiated. Shock evaluation included a CT abdomen showing enteritis versus ileus; however, infectious workup was negative. Cardiogenic shock was ruled out with a serial echocardiogram showing normal ejection fractions of 59-67% without significant valvular disease. The workup for adrenal insufficiency was negative. After the exclusion of other potential causes of shock, severe refractory hypotension was attributed to bortezomib toxicity.Hypotension is a known adverse effect of bortezomib. Orthostatic hypotension may occur in 8 to 9% of patients, and rarely, patients may experience heart failure, conduction disorders and arrhythmias, or cardiogenic shock. The pathologic mechanism of this toxicity is still poorly understood. Proposed mechanisms include direct endothelial toxicity as evidenced by thrombotic microangiopathy or impairment of sympathetic and parasympathetic nerve fibres. Most commonly, patients experience neurotoxicity, which may manifest as autonomic dysfunction or peripheral neuropathy. Cardiovascular complications are typically reversible. Our patient’s cardiac function remained within normal limits; therefore, his persistent hypotension was felt to be the result of direct toxicity from bortezomib rather than cardiogenic shock. Ultimately, blood pressure did improve, and vasopressors were discontinued. However, he continued to have orthostatic hypotension and continued to require supportive fludrocortisone, midodrine, and pyridostigmine. Goals of care have been discussed, and he wished to continue pursuing restorative care, with a plan for transition to carfilzomib versus daratumumab outpatient.
Case Presentation
A 75-year-old man with chronic kidney disease, hypertension and diabetes mellitus presented with acute kidney injury (creatinine 5.2 from baseline 4.2) and a two-week history of increased urinary frequency. Labs revealed high anion gap metabolic acidosis, proteinuria, hematuria, pyuria, and acute on chronic anemia. He was diagnosed with kappa light chain nephropathy and multiple myeloma with 32% plasma cells on bone marrow biopsy. He began treatment with bortezomib, cyclophosphamide, and dexamethasone (Cy- BorD). Three days after cyclophosphamide and five days after bortezomib, the patient developed persistent hypotension with systolic BP in the 50s, unresponsive to fluids and Trendelenburg position. Due to end-stage renal disease with anuria, fluid resuscitation was limited. He required norepinephrine and was transferred to the ICU. Given instability, hemodialysis was deferred, and continuous renal replacement therapy was initiated. Shock evaluation included a CT abdomen showing enteritis versus ileus; however, infectious workup was negative. Cardiogenic shock was ruled out with a serial echocardiogram showing normal ejection fractions of 59-67% without significant valvular disease. The workup for adrenal insufficiency was negative. After the exclusion of other potential causes of shock, severe refractory hypotension was attributed to bortezomib toxicity.Hypotension is a known adverse effect of bortezomib. Orthostatic hypotension may occur in 8 to 9% of patients, and rarely, patients may experience heart failure, conduction disorders and arrhythmias, or cardiogenic shock. The pathologic mechanism of this toxicity is still poorly understood. Proposed mechanisms include direct endothelial toxicity as evidenced by thrombotic microangiopathy or impairment of sympathetic and parasympathetic nerve fibres. Most commonly, patients experience neurotoxicity, which may manifest as autonomic dysfunction or peripheral neuropathy. Cardiovascular complications are typically reversible. Our patient’s cardiac function remained within normal limits; therefore, his persistent hypotension was felt to be the result of direct toxicity from bortezomib rather than cardiogenic shock. Ultimately, blood pressure did improve, and vasopressors were discontinued. However, he continued to have orthostatic hypotension and continued to require supportive fludrocortisone, midodrine, and pyridostigmine. Goals of care have been discussed, and he wished to continue pursuing restorative care, with a plan for transition to carfilzomib versus daratumumab outpatient.
Case Presentation
A 75-year-old man with chronic kidney disease, hypertension and diabetes mellitus presented with acute kidney injury (creatinine 5.2 from baseline 4.2) and a two-week history of increased urinary frequency. Labs revealed high anion gap metabolic acidosis, proteinuria, hematuria, pyuria, and acute on chronic anemia. He was diagnosed with kappa light chain nephropathy and multiple myeloma with 32% plasma cells on bone marrow biopsy. He began treatment with bortezomib, cyclophosphamide, and dexamethasone (Cy- BorD). Three days after cyclophosphamide and five days after bortezomib, the patient developed persistent hypotension with systolic BP in the 50s, unresponsive to fluids and Trendelenburg position. Due to end-stage renal disease with anuria, fluid resuscitation was limited. He required norepinephrine and was transferred to the ICU. Given instability, hemodialysis was deferred, and continuous renal replacement therapy was initiated. Shock evaluation included a CT abdomen showing enteritis versus ileus; however, infectious workup was negative. Cardiogenic shock was ruled out with a serial echocardiogram showing normal ejection fractions of 59-67% without significant valvular disease. The workup for adrenal insufficiency was negative. After the exclusion of other potential causes of shock, severe refractory hypotension was attributed to bortezomib toxicity.Hypotension is a known adverse effect of bortezomib. Orthostatic hypotension may occur in 8 to 9% of patients, and rarely, patients may experience heart failure, conduction disorders and arrhythmias, or cardiogenic shock. The pathologic mechanism of this toxicity is still poorly understood. Proposed mechanisms include direct endothelial toxicity as evidenced by thrombotic microangiopathy or impairment of sympathetic and parasympathetic nerve fibres. Most commonly, patients experience neurotoxicity, which may manifest as autonomic dysfunction or peripheral neuropathy. Cardiovascular complications are typically reversible. Our patient’s cardiac function remained within normal limits; therefore, his persistent hypotension was felt to be the result of direct toxicity from bortezomib rather than cardiogenic shock. Ultimately, blood pressure did improve, and vasopressors were discontinued. However, he continued to have orthostatic hypotension and continued to require supportive fludrocortisone, midodrine, and pyridostigmine. Goals of care have been discussed, and he wished to continue pursuing restorative care, with a plan for transition to carfilzomib versus daratumumab outpatient.
An Uncommon Presentation of Marginal Zone Lymphoma Involving the Sciatic Foramen
Background
Marginal zone lymphoma (MZL) is an indolent B-cell non-Hodgkin lymphoma most commonly arising in mucosal, nodal, or splenic tissues. While extranodal presentations are recognized, involvement of the sciatic foramen is exceedingly rare. We present a unique case of stage IV MZL with primary involvement of the left sciatic foramen, identified incidentally during urologic evaluation.
Case Presentation
A 74-year-old male patient was referred for hematologic evaluation after imaging revealed a left sciatic foraminal mass during work-up for elevated PSA. CT abdomen/pelvis revealed a 4.7 cm mass in the left sciatic foramen. Follow-up PET-CT confirmed hypermetabolic activity in the mass, with additional areas of uptake in the right ilium and pleural- pericardial regions. The patient was asymptomatic and denied B-symptoms. CT-guided biopsy of the sciatic mass revealed low-grade B-cell lymphoma. Flow cytometry showed a CD20-positive, CD5-negative, CD10-negative, lambda light chain–restricted population consistent with marginal zone lymphoma. Laboratory studies demonstrated iron deficiency anemia, with otherwise unremarkable counts and chemistries. He was started on monotherapy with rituximab for four cycles. He tolerated treatment well. Interval PET imaging in April 2025 showed stable disease in the sciatic foramen and mild improvement in pleural- pericardial uptake. He is planned to start obinutuzumab in the upcoming month.
Discussion
This case illustrates a rare anatomic presentation of MZL, likely representing primary sciatic foramen involvement. The presence of additional PETavid lesions complicates staging, raising consideration of stage I vs. III/IV disease. Biopsy was limited to the sciatic lesion, and no bone marrow sampling was performed. Given the patient’s excellent performance status, absence of symptoms, and low tumor burden, single-agent rituximab was chosen initially in accordance with NCCN guidelines.
Conclusions
Sciatic foramen involvement by MZL is an extremely rare occurrence and may mimic more common soft tissue or neurogenic tumors radiographically. This case underscores the importance of biopsy for diagnosis and the value of multidisciplinary care. In the veteran population, such incidental findings on imaging warrant comprehensive evaluation, particularly in atypical anatomical sites.
Background
Marginal zone lymphoma (MZL) is an indolent B-cell non-Hodgkin lymphoma most commonly arising in mucosal, nodal, or splenic tissues. While extranodal presentations are recognized, involvement of the sciatic foramen is exceedingly rare. We present a unique case of stage IV MZL with primary involvement of the left sciatic foramen, identified incidentally during urologic evaluation.
Case Presentation
A 74-year-old male patient was referred for hematologic evaluation after imaging revealed a left sciatic foraminal mass during work-up for elevated PSA. CT abdomen/pelvis revealed a 4.7 cm mass in the left sciatic foramen. Follow-up PET-CT confirmed hypermetabolic activity in the mass, with additional areas of uptake in the right ilium and pleural- pericardial regions. The patient was asymptomatic and denied B-symptoms. CT-guided biopsy of the sciatic mass revealed low-grade B-cell lymphoma. Flow cytometry showed a CD20-positive, CD5-negative, CD10-negative, lambda light chain–restricted population consistent with marginal zone lymphoma. Laboratory studies demonstrated iron deficiency anemia, with otherwise unremarkable counts and chemistries. He was started on monotherapy with rituximab for four cycles. He tolerated treatment well. Interval PET imaging in April 2025 showed stable disease in the sciatic foramen and mild improvement in pleural- pericardial uptake. He is planned to start obinutuzumab in the upcoming month.
Discussion
This case illustrates a rare anatomic presentation of MZL, likely representing primary sciatic foramen involvement. The presence of additional PETavid lesions complicates staging, raising consideration of stage I vs. III/IV disease. Biopsy was limited to the sciatic lesion, and no bone marrow sampling was performed. Given the patient’s excellent performance status, absence of symptoms, and low tumor burden, single-agent rituximab was chosen initially in accordance with NCCN guidelines.
Conclusions
Sciatic foramen involvement by MZL is an extremely rare occurrence and may mimic more common soft tissue or neurogenic tumors radiographically. This case underscores the importance of biopsy for diagnosis and the value of multidisciplinary care. In the veteran population, such incidental findings on imaging warrant comprehensive evaluation, particularly in atypical anatomical sites.
Background
Marginal zone lymphoma (MZL) is an indolent B-cell non-Hodgkin lymphoma most commonly arising in mucosal, nodal, or splenic tissues. While extranodal presentations are recognized, involvement of the sciatic foramen is exceedingly rare. We present a unique case of stage IV MZL with primary involvement of the left sciatic foramen, identified incidentally during urologic evaluation.
Case Presentation
A 74-year-old male patient was referred for hematologic evaluation after imaging revealed a left sciatic foraminal mass during work-up for elevated PSA. CT abdomen/pelvis revealed a 4.7 cm mass in the left sciatic foramen. Follow-up PET-CT confirmed hypermetabolic activity in the mass, with additional areas of uptake in the right ilium and pleural- pericardial regions. The patient was asymptomatic and denied B-symptoms. CT-guided biopsy of the sciatic mass revealed low-grade B-cell lymphoma. Flow cytometry showed a CD20-positive, CD5-negative, CD10-negative, lambda light chain–restricted population consistent with marginal zone lymphoma. Laboratory studies demonstrated iron deficiency anemia, with otherwise unremarkable counts and chemistries. He was started on monotherapy with rituximab for four cycles. He tolerated treatment well. Interval PET imaging in April 2025 showed stable disease in the sciatic foramen and mild improvement in pleural- pericardial uptake. He is planned to start obinutuzumab in the upcoming month.
Discussion
This case illustrates a rare anatomic presentation of MZL, likely representing primary sciatic foramen involvement. The presence of additional PETavid lesions complicates staging, raising consideration of stage I vs. III/IV disease. Biopsy was limited to the sciatic lesion, and no bone marrow sampling was performed. Given the patient’s excellent performance status, absence of symptoms, and low tumor burden, single-agent rituximab was chosen initially in accordance with NCCN guidelines.
Conclusions
Sciatic foramen involvement by MZL is an extremely rare occurrence and may mimic more common soft tissue or neurogenic tumors radiographically. This case underscores the importance of biopsy for diagnosis and the value of multidisciplinary care. In the veteran population, such incidental findings on imaging warrant comprehensive evaluation, particularly in atypical anatomical sites.
Agent Orange Exposure and Genetic Factors Independently Raise Risk for Multiple Lymphoma Types
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: A large-scale case-control study using the Million Veteran Program (MVP) found The study found independent associations of both genetic predisposition and Agent Orange (AO) exposure for several lymphoid malignant neoplasm subtypes.
METHODOLOGY:
A case-control study included 255,155 US veterans enrolled in the MVP with available genotype, Agent Orange exposure information, and lymphoid malignant neoplasm diagnosis from January 1, 1965, through June T1, 2024.
Analysis focused on non-Hispanic White veterans (median age 67 years; 92.5% male) due to ancestry distribution requirements for genome-wide association studies data availability.
Researchers excluded 628 samples across all lymphoid malignant neoplasm groups and 61,343 control samples due to unavailability of AO exposure information.
Investigators analyzed risk for chronic lymphocytic leukemia, diffuse large B-cell lymphoma, follicular lymphoma, marginal zone lymphoma, and multiple myeloma as primary outcomes.
TAKEAWAY:
Agent Orange exposure was associated with increased risk for chronic lymphocytic leukemia (odds ratio [OR], 1.61; 95% confidence interval [CI], 1.40-1.84), diffuse large B-cell lymphoma (OR, 1.26; 95% CI, 1.03-1.53), follicular lymphoma (OR, 1.71; 95% CI, 1.39-2.11), and multiple myeloma (OR, 1.58; 95% CI, 1.35-1.86).
Polygenic risk scores showed significant associations with all subtypes: chronic lymphocytic leukemia (OR, 1.81; 95% CI, 1.70-1.93), diffuse large B-cell lymphoma (OR, 1.12; 95% CI, 1.02-1.21), follicular lymphoma (OR, 1.33; 95% CI, 1.21-1.47), marginal zone lymphoma (OR, 1.17; 95% CI, 1.04-1.32), and multiple myeloma (OR, 1.41; 95% CI, 1.31-1.52).
No significant polygenic risk score and AO exposure interactions were observed in the development of any lymphoid malignant neoplasm subtypes.
The researchers found independent associations of both genetic predisposition and Agent Orange exposure on several lymphoid malignant neoplasm subtypes.
IN PRACTICE:
"Our study addressed the public health concerns surrounding AO exposure and lymphoid malignant neoplasms, finding that both AO exposure and polygenic risk are independently associated with disease, suggesting potentially distinct and additive pathways that merit further investigation,” the authors wrote.
SOURCE: The study was led by Xueyi Teng, PhD, Department of Biological Chemistry, School of Medicine, University of California in Irvine, and Helen Ma, MD, Tibor Rubin Veterans Affairs Medical Center in Long Beach. It was published online in JAMA Network Open.
LIMITATIONS: According to the authors, while this represents the largest study of Agent Orange exposure and genetic risk in lymphoid malignant neoplasm development, the power to find interaction associations in specific subtypes might be limited. Self-reported AO exposure may have introduced survival bias, especially in aggressive subtypes, as patients with aggressive tumors might have died before joining the MVP. Additionally, approximately half of the patients were diagnosed with lymphoid malignant neoplasm before self-reporting AO exposure in the survey, potentially introducing recall bias.
DISCLOSURES: Xueyi Teng, PhD, reported receiving grants from the George E. Hewitt Foundation for Medical Research Postdoc Fellowship during the conduct of the study. The research was supported by grant MVPOOO and Veterans Affairs Career Development Award 1IK2CX002437-O1A1. No other disclosures were reported.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Study Investigates Non-Hodgkin Lymphoma in Air Force Missileers
Individuals working near intercontinental ballistic missiles (ICBMs), may be at higher risk of developing non-Hodgkin lymphoma (NHL) according to a preprint analysis conducted on missileers at Malmstrom Air Force Base in Montana. The study, which has not undergone peer review, found higher rates of NHL diagnosis at younger ages compared with the general population. The study also found a statistically significant increase in NHL diagnoses among older missileers, with such rates surpassing expected benchmarks.
The findings build on anecdotal and evidentiary data gathered in the last 50-plus years, including from the Torchlight Initiative, established in 2023 to collect self-reported cancer diagnoses and related fatalities from personnel and family members associated with the ICBM community.
The report shows patterns that “warranted a detailed statistical analysis,” leading to a granular examination of the registry and categorization of the data by cancer type, geographical location, and specific demographics. This narrowed the focus to 18 missileers who served at Malmstrom and were diagnosed with NHL.
In 2001, the Air Force Institute for Operational Health did a site evaluation and sampled for potential chemical and biological contaminants at Malmstrom following various reports of cancers from missileers, including 2 who died after being diagnosed with NHL. In a 2005 review, the Air Force said, “there is not sufficient evidence to consider the possibility of a cancer clustering to justify further investigation.”
In 2022, Lt. Col. Daniel Sebeck, a vice commander of Space Delta 8 in Colorado who served at Malmstrom and a close friend and fellow missileer were diagnosed with NHL. Sebeck discovered 36 cancer cases among missileers who had been stationed at Malmstrom. Ten developed NHL, 2 developed Hodgkin lymphoma, and 24 developed another form of cancer. The Air Force has acknowledged the concerns.
In 2023, US Air Force School of Aerospace Medicine (USAFSAM) approved the Missile Community Cancer Study (MCCS) to assess “specific cancer concerns raised by missile community members across related career fields and also examines the possibility of clusters of non-Hodgkin’s lymphoma at intercontinental ballistic missile bases.” The study compares 14 common cancers in the general population with that of missile-related career fields. The USAFSAM is reviewing records from former and current Missile Community members on active duty from 1976-2010, as well as state and national cancer data from multiple registries.
Early results from the MCCS suggested elevated rates of some cancers—mainly breast and prostate cancer—among missileers, maintainers, and other ICMB-related job positions, which aligns with other national cancer data.
At a June 2024 AFGSC town hall, officials announced that missileers would now have their information submitted to the Defense Occupational and Environmental Health Readiness System (DOEHRS), a Pentagon database for reporting occupational and exposure hazards.
"This info from DOEHRS flows into the recently developed Individual Longitudinal Exposure Record, a system that compiles occupational and environmental health data throughout a person's career," Lt. Col. John Severns, a spokesperson for Air Force Global Strike Command, said. DOEHRS, which has tracked Air Force records since 2010, allows US Department of Defense and US Department of Veterans Affairs clinical staff to access the information.
MCCS considers potential PCB exposures an occupational hazard. The Air Force says researchers are working with the System Program Offices and leadership to determine the timeframe of PCB removal from bases.
The lack of incontrovertible evidence connecting workplace toxins to NHL has often stymied patients and their family members from receiving appropriate benefits. An “informal talk” in April led by Rep. Mark Takano (D-CA) and Sen. Richard Blumenthal (D-CT) focused on exposures to hazardous materials at US military bases. Participants included various advocacy groups like the Torchlight Initiative, the Invisible Enemy, and Burn Pits 360.
More than a dozen veterans spoke about serving at military bases where they were exposed to a variety of harmful substances, and issues they faced in receiving coverage. David Crete, a veteran and chairman of The Invisible Enemy, said, “I am asking Congress to please allow us to get the benefits every other veteran earned. We are not asking to be special but to be treated equal.”
Rep. Takano called for greater focus on toxic exposures at US military bases: “We must push back against the idea that service members are only in harm’s way in war zones.”
Individuals working near intercontinental ballistic missiles (ICBMs), may be at higher risk of developing non-Hodgkin lymphoma (NHL) according to a preprint analysis conducted on missileers at Malmstrom Air Force Base in Montana. The study, which has not undergone peer review, found higher rates of NHL diagnosis at younger ages compared with the general population. The study also found a statistically significant increase in NHL diagnoses among older missileers, with such rates surpassing expected benchmarks.
The findings build on anecdotal and evidentiary data gathered in the last 50-plus years, including from the Torchlight Initiative, established in 2023 to collect self-reported cancer diagnoses and related fatalities from personnel and family members associated with the ICBM community.
The report shows patterns that “warranted a detailed statistical analysis,” leading to a granular examination of the registry and categorization of the data by cancer type, geographical location, and specific demographics. This narrowed the focus to 18 missileers who served at Malmstrom and were diagnosed with NHL.
In 2001, the Air Force Institute for Operational Health did a site evaluation and sampled for potential chemical and biological contaminants at Malmstrom following various reports of cancers from missileers, including 2 who died after being diagnosed with NHL. In a 2005 review, the Air Force said, “there is not sufficient evidence to consider the possibility of a cancer clustering to justify further investigation.”
In 2022, Lt. Col. Daniel Sebeck, a vice commander of Space Delta 8 in Colorado who served at Malmstrom and a close friend and fellow missileer were diagnosed with NHL. Sebeck discovered 36 cancer cases among missileers who had been stationed at Malmstrom. Ten developed NHL, 2 developed Hodgkin lymphoma, and 24 developed another form of cancer. The Air Force has acknowledged the concerns.
In 2023, US Air Force School of Aerospace Medicine (USAFSAM) approved the Missile Community Cancer Study (MCCS) to assess “specific cancer concerns raised by missile community members across related career fields and also examines the possibility of clusters of non-Hodgkin’s lymphoma at intercontinental ballistic missile bases.” The study compares 14 common cancers in the general population with that of missile-related career fields. The USAFSAM is reviewing records from former and current Missile Community members on active duty from 1976-2010, as well as state and national cancer data from multiple registries.
Early results from the MCCS suggested elevated rates of some cancers—mainly breast and prostate cancer—among missileers, maintainers, and other ICMB-related job positions, which aligns with other national cancer data.
At a June 2024 AFGSC town hall, officials announced that missileers would now have their information submitted to the Defense Occupational and Environmental Health Readiness System (DOEHRS), a Pentagon database for reporting occupational and exposure hazards.
"This info from DOEHRS flows into the recently developed Individual Longitudinal Exposure Record, a system that compiles occupational and environmental health data throughout a person's career," Lt. Col. John Severns, a spokesperson for Air Force Global Strike Command, said. DOEHRS, which has tracked Air Force records since 2010, allows US Department of Defense and US Department of Veterans Affairs clinical staff to access the information.
MCCS considers potential PCB exposures an occupational hazard. The Air Force says researchers are working with the System Program Offices and leadership to determine the timeframe of PCB removal from bases.
The lack of incontrovertible evidence connecting workplace toxins to NHL has often stymied patients and their family members from receiving appropriate benefits. An “informal talk” in April led by Rep. Mark Takano (D-CA) and Sen. Richard Blumenthal (D-CT) focused on exposures to hazardous materials at US military bases. Participants included various advocacy groups like the Torchlight Initiative, the Invisible Enemy, and Burn Pits 360.
More than a dozen veterans spoke about serving at military bases where they were exposed to a variety of harmful substances, and issues they faced in receiving coverage. David Crete, a veteran and chairman of The Invisible Enemy, said, “I am asking Congress to please allow us to get the benefits every other veteran earned. We are not asking to be special but to be treated equal.”
Rep. Takano called for greater focus on toxic exposures at US military bases: “We must push back against the idea that service members are only in harm’s way in war zones.”
Individuals working near intercontinental ballistic missiles (ICBMs), may be at higher risk of developing non-Hodgkin lymphoma (NHL) according to a preprint analysis conducted on missileers at Malmstrom Air Force Base in Montana. The study, which has not undergone peer review, found higher rates of NHL diagnosis at younger ages compared with the general population. The study also found a statistically significant increase in NHL diagnoses among older missileers, with such rates surpassing expected benchmarks.
The findings build on anecdotal and evidentiary data gathered in the last 50-plus years, including from the Torchlight Initiative, established in 2023 to collect self-reported cancer diagnoses and related fatalities from personnel and family members associated with the ICBM community.
The report shows patterns that “warranted a detailed statistical analysis,” leading to a granular examination of the registry and categorization of the data by cancer type, geographical location, and specific demographics. This narrowed the focus to 18 missileers who served at Malmstrom and were diagnosed with NHL.
In 2001, the Air Force Institute for Operational Health did a site evaluation and sampled for potential chemical and biological contaminants at Malmstrom following various reports of cancers from missileers, including 2 who died after being diagnosed with NHL. In a 2005 review, the Air Force said, “there is not sufficient evidence to consider the possibility of a cancer clustering to justify further investigation.”
In 2022, Lt. Col. Daniel Sebeck, a vice commander of Space Delta 8 in Colorado who served at Malmstrom and a close friend and fellow missileer were diagnosed with NHL. Sebeck discovered 36 cancer cases among missileers who had been stationed at Malmstrom. Ten developed NHL, 2 developed Hodgkin lymphoma, and 24 developed another form of cancer. The Air Force has acknowledged the concerns.
In 2023, US Air Force School of Aerospace Medicine (USAFSAM) approved the Missile Community Cancer Study (MCCS) to assess “specific cancer concerns raised by missile community members across related career fields and also examines the possibility of clusters of non-Hodgkin’s lymphoma at intercontinental ballistic missile bases.” The study compares 14 common cancers in the general population with that of missile-related career fields. The USAFSAM is reviewing records from former and current Missile Community members on active duty from 1976-2010, as well as state and national cancer data from multiple registries.
Early results from the MCCS suggested elevated rates of some cancers—mainly breast and prostate cancer—among missileers, maintainers, and other ICMB-related job positions, which aligns with other national cancer data.
At a June 2024 AFGSC town hall, officials announced that missileers would now have their information submitted to the Defense Occupational and Environmental Health Readiness System (DOEHRS), a Pentagon database for reporting occupational and exposure hazards.
"This info from DOEHRS flows into the recently developed Individual Longitudinal Exposure Record, a system that compiles occupational and environmental health data throughout a person's career," Lt. Col. John Severns, a spokesperson for Air Force Global Strike Command, said. DOEHRS, which has tracked Air Force records since 2010, allows US Department of Defense and US Department of Veterans Affairs clinical staff to access the information.
MCCS considers potential PCB exposures an occupational hazard. The Air Force says researchers are working with the System Program Offices and leadership to determine the timeframe of PCB removal from bases.
The lack of incontrovertible evidence connecting workplace toxins to NHL has often stymied patients and their family members from receiving appropriate benefits. An “informal talk” in April led by Rep. Mark Takano (D-CA) and Sen. Richard Blumenthal (D-CT) focused on exposures to hazardous materials at US military bases. Participants included various advocacy groups like the Torchlight Initiative, the Invisible Enemy, and Burn Pits 360.
More than a dozen veterans spoke about serving at military bases where they were exposed to a variety of harmful substances, and issues they faced in receiving coverage. David Crete, a veteran and chairman of The Invisible Enemy, said, “I am asking Congress to please allow us to get the benefits every other veteran earned. We are not asking to be special but to be treated equal.”
Rep. Takano called for greater focus on toxic exposures at US military bases: “We must push back against the idea that service members are only in harm’s way in war zones.”
 visual information does not imply or constitute DoD endorsement.")
RVD With Weekly Bortezomib Has a Favorable Toxicity and Effectiveness Profile in a Large Cohort of US Veterans With Multiple Myeloma
Background
Lenalidomide, bortezomib, and dexamethasone (RVD) is standard triplet induction for fit newly-diagnosed myeloma (NDMM) patients, with response rate (RR)>90%. A 21-day cycle with bortezomib given days 1, 4, 8, and 11 (2x/w) is standard. However, up to 80% of patients develop neuropathy. Weekly bortezomib dosing (1x/w), subcutaneous route, and 28- to 35-day cycle length may optimize tolerance. We present an effectiveness and toxicity analysis of Veterans who received RVD with 1x/w and 2x/w bortezomib for NDMM.
Methods
The VA Corporate Data Warehouse identified 1499 Veterans with NDMM given RVD ≤42 days of treatment start. 840 Veterans were grouped for initial analysis based on criteria: 1) lenalidomide and ≥ 3 bortezomib doses during cycle 1; 2) ≥6 mean days between bortezomib treatments=1x/w); and 3) number of lenalidomide days informed cycle length (21d, 28d, or 35d; default 7-day rest). Investigators reviewed algorithm results to finalize group assignments. Endpoints included depth of response, time to next treatment (TTNT), overall survival (OS), and neuropathy. Neuropathy was defined as use of neuropathy medications and neuropathy ICD-10 codes.
Results
Our algorithm correctly assigned 82% of 840 cycle 1 RVD schedules. The largest groups were 21d 1x/w (n=291), 21d 2x/w (n=193), 28d 1x/w (n=188), and 28d 2x/w (n=82). Median age was 68.3; 53% were non-Hispanic White. Demographics and ISS stage of groups were similar. 30% underwent autologous transplant. Tolerability. Median number of bortezomib doses ranged from 22.5-25.5 (p=0.57). Neuropathy favored 1x/w, 17.7 vs 30.2% (p=0.0001) and was highest (34.7%) in 21d 2x/w. Effectiveness. Response was assessable for 28% of patients. RR (72%, p=0.68) and median TTNT (19.3 months, p=0.20) were similar, including 1x/w vs 2x/w comparison (p=0.79). 21d regimens optimized TTNT (21.4 vs 13.9 months, p=0.045) and trended to better OS (73 vs 65 months, p=0.06).
Conclusions
1x/w RVD preserved effectiveness compared to “standard” RVD in a large Veteran cohort. 1x/w reduced neuropathy incidence. 28d regimens demonstrated inferior longer-term outcomes. Certain endpoints, such as RR and neuropathy, appear underestimated due to data source limitations. 21d 1x/w RVD optimizes effectiveness, tolerability, and administration and should be considered for broader utilization in Veterans with NDMM.
Background
Lenalidomide, bortezomib, and dexamethasone (RVD) is standard triplet induction for fit newly-diagnosed myeloma (NDMM) patients, with response rate (RR)>90%. A 21-day cycle with bortezomib given days 1, 4, 8, and 11 (2x/w) is standard. However, up to 80% of patients develop neuropathy. Weekly bortezomib dosing (1x/w), subcutaneous route, and 28- to 35-day cycle length may optimize tolerance. We present an effectiveness and toxicity analysis of Veterans who received RVD with 1x/w and 2x/w bortezomib for NDMM.
Methods
The VA Corporate Data Warehouse identified 1499 Veterans with NDMM given RVD ≤42 days of treatment start. 840 Veterans were grouped for initial analysis based on criteria: 1) lenalidomide and ≥ 3 bortezomib doses during cycle 1; 2) ≥6 mean days between bortezomib treatments=1x/w); and 3) number of lenalidomide days informed cycle length (21d, 28d, or 35d; default 7-day rest). Investigators reviewed algorithm results to finalize group assignments. Endpoints included depth of response, time to next treatment (TTNT), overall survival (OS), and neuropathy. Neuropathy was defined as use of neuropathy medications and neuropathy ICD-10 codes.
Results
Our algorithm correctly assigned 82% of 840 cycle 1 RVD schedules. The largest groups were 21d 1x/w (n=291), 21d 2x/w (n=193), 28d 1x/w (n=188), and 28d 2x/w (n=82). Median age was 68.3; 53% were non-Hispanic White. Demographics and ISS stage of groups were similar. 30% underwent autologous transplant. Tolerability. Median number of bortezomib doses ranged from 22.5-25.5 (p=0.57). Neuropathy favored 1x/w, 17.7 vs 30.2% (p=0.0001) and was highest (34.7%) in 21d 2x/w. Effectiveness. Response was assessable for 28% of patients. RR (72%, p=0.68) and median TTNT (19.3 months, p=0.20) were similar, including 1x/w vs 2x/w comparison (p=0.79). 21d regimens optimized TTNT (21.4 vs 13.9 months, p=0.045) and trended to better OS (73 vs 65 months, p=0.06).
Conclusions
1x/w RVD preserved effectiveness compared to “standard” RVD in a large Veteran cohort. 1x/w reduced neuropathy incidence. 28d regimens demonstrated inferior longer-term outcomes. Certain endpoints, such as RR and neuropathy, appear underestimated due to data source limitations. 21d 1x/w RVD optimizes effectiveness, tolerability, and administration and should be considered for broader utilization in Veterans with NDMM.
Background
Lenalidomide, bortezomib, and dexamethasone (RVD) is standard triplet induction for fit newly-diagnosed myeloma (NDMM) patients, with response rate (RR)>90%. A 21-day cycle with bortezomib given days 1, 4, 8, and 11 (2x/w) is standard. However, up to 80% of patients develop neuropathy. Weekly bortezomib dosing (1x/w), subcutaneous route, and 28- to 35-day cycle length may optimize tolerance. We present an effectiveness and toxicity analysis of Veterans who received RVD with 1x/w and 2x/w bortezomib for NDMM.
Methods
The VA Corporate Data Warehouse identified 1499 Veterans with NDMM given RVD ≤42 days of treatment start. 840 Veterans were grouped for initial analysis based on criteria: 1) lenalidomide and ≥ 3 bortezomib doses during cycle 1; 2) ≥6 mean days between bortezomib treatments=1x/w); and 3) number of lenalidomide days informed cycle length (21d, 28d, or 35d; default 7-day rest). Investigators reviewed algorithm results to finalize group assignments. Endpoints included depth of response, time to next treatment (TTNT), overall survival (OS), and neuropathy. Neuropathy was defined as use of neuropathy medications and neuropathy ICD-10 codes.
Results
Our algorithm correctly assigned 82% of 840 cycle 1 RVD schedules. The largest groups were 21d 1x/w (n=291), 21d 2x/w (n=193), 28d 1x/w (n=188), and 28d 2x/w (n=82). Median age was 68.3; 53% were non-Hispanic White. Demographics and ISS stage of groups were similar. 30% underwent autologous transplant. Tolerability. Median number of bortezomib doses ranged from 22.5-25.5 (p=0.57). Neuropathy favored 1x/w, 17.7 vs 30.2% (p=0.0001) and was highest (34.7%) in 21d 2x/w. Effectiveness. Response was assessable for 28% of patients. RR (72%, p=0.68) and median TTNT (19.3 months, p=0.20) were similar, including 1x/w vs 2x/w comparison (p=0.79). 21d regimens optimized TTNT (21.4 vs 13.9 months, p=0.045) and trended to better OS (73 vs 65 months, p=0.06).
Conclusions
1x/w RVD preserved effectiveness compared to “standard” RVD in a large Veteran cohort. 1x/w reduced neuropathy incidence. 28d regimens demonstrated inferior longer-term outcomes. Certain endpoints, such as RR and neuropathy, appear underestimated due to data source limitations. 21d 1x/w RVD optimizes effectiveness, tolerability, and administration and should be considered for broader utilization in Veterans with NDMM.
Chronic Myeloid Leukemia Presenting as Priapism: A Rare and Acute Initial Presentation in a Young Male
Introduction
Priapism, defined as a prolonged and often painful penile erection without sexual arousal, constitutes a urological emergency requiring immediate intervention. While commonly associated with conditions like sickle cell anemia and certain medications, malignancy-related priapism is rare and frequently overlooked. Herein, we present a unique case of a 31-year-old male with no significant medical history, who developed persistent priapism as the initial presentation of chronic myeloid leukemia (CML).
Case Presentation
A 31-year-old male without significant medical history, presented to the emergency department with painless priapism, was evaluated by urology and discharged home with precautions. He returned the following day with persistent, now painful priapism. Upon examination, his vital signs were stable. Urology performed aspiration and injection with Sudafed, resulting in mild symptom improvement. Laboratory findings revealed elevated white blood cell count (563.64 k/mcL), anemia (hemoglobin 8.4 g/dL), and a peripheral blood smear showed immature circulating cells with blast forms. He was transferred to a tertiary care center where conservative management addressed bleeding from the penile injection site, with subsequent treatment including leukapheresis and hydroxyurea for cytoreduction. Imaging revealed severe splenomegaly (36 cm) with abdominal mass effect. Peripheral flow cytometry didn’t show malignancy, but cytogenetic analysis showed a BCR/ABL1 fusion gene, confirming chronic myeloid leukemia (CML). Bone marrow biopsy showed hypercellularity without increased blasts. Treatment with dasatinib reduced the white count to 52,000 k/mcL, and was discharged home.
Discussion
Priapism is a urological emergency necessitating immediate intervention to prevent erectile dysfunction and permanent impotence. Management aims to achieve detumescence and typically involves methods such as irrigation or injection of vasoconstrictors into the penis. Malignancy-associated priapism (MAP) often results from venous obstruction due to hyperviscosity. Studies show that CML accounts for approximately 50% cases presenting with MAP, predominantly affecting younger individuals with a mean onset around 27 years of age. Priapism can occur before, during, or after treatment initiation or splenectomy in these patients. Providers should keep a high threshold of suspicion for MAP in patients with no other risk factors as prompt identification and treatment are needed to avoid permanent injury.
Introduction
Priapism, defined as a prolonged and often painful penile erection without sexual arousal, constitutes a urological emergency requiring immediate intervention. While commonly associated with conditions like sickle cell anemia and certain medications, malignancy-related priapism is rare and frequently overlooked. Herein, we present a unique case of a 31-year-old male with no significant medical history, who developed persistent priapism as the initial presentation of chronic myeloid leukemia (CML).
Case Presentation
A 31-year-old male without significant medical history, presented to the emergency department with painless priapism, was evaluated by urology and discharged home with precautions. He returned the following day with persistent, now painful priapism. Upon examination, his vital signs were stable. Urology performed aspiration and injection with Sudafed, resulting in mild symptom improvement. Laboratory findings revealed elevated white blood cell count (563.64 k/mcL), anemia (hemoglobin 8.4 g/dL), and a peripheral blood smear showed immature circulating cells with blast forms. He was transferred to a tertiary care center where conservative management addressed bleeding from the penile injection site, with subsequent treatment including leukapheresis and hydroxyurea for cytoreduction. Imaging revealed severe splenomegaly (36 cm) with abdominal mass effect. Peripheral flow cytometry didn’t show malignancy, but cytogenetic analysis showed a BCR/ABL1 fusion gene, confirming chronic myeloid leukemia (CML). Bone marrow biopsy showed hypercellularity without increased blasts. Treatment with dasatinib reduced the white count to 52,000 k/mcL, and was discharged home.
Discussion
Priapism is a urological emergency necessitating immediate intervention to prevent erectile dysfunction and permanent impotence. Management aims to achieve detumescence and typically involves methods such as irrigation or injection of vasoconstrictors into the penis. Malignancy-associated priapism (MAP) often results from venous obstruction due to hyperviscosity. Studies show that CML accounts for approximately 50% cases presenting with MAP, predominantly affecting younger individuals with a mean onset around 27 years of age. Priapism can occur before, during, or after treatment initiation or splenectomy in these patients. Providers should keep a high threshold of suspicion for MAP in patients with no other risk factors as prompt identification and treatment are needed to avoid permanent injury.
Introduction
Priapism, defined as a prolonged and often painful penile erection without sexual arousal, constitutes a urological emergency requiring immediate intervention. While commonly associated with conditions like sickle cell anemia and certain medications, malignancy-related priapism is rare and frequently overlooked. Herein, we present a unique case of a 31-year-old male with no significant medical history, who developed persistent priapism as the initial presentation of chronic myeloid leukemia (CML).
Case Presentation
A 31-year-old male without significant medical history, presented to the emergency department with painless priapism, was evaluated by urology and discharged home with precautions. He returned the following day with persistent, now painful priapism. Upon examination, his vital signs were stable. Urology performed aspiration and injection with Sudafed, resulting in mild symptom improvement. Laboratory findings revealed elevated white blood cell count (563.64 k/mcL), anemia (hemoglobin 8.4 g/dL), and a peripheral blood smear showed immature circulating cells with blast forms. He was transferred to a tertiary care center where conservative management addressed bleeding from the penile injection site, with subsequent treatment including leukapheresis and hydroxyurea for cytoreduction. Imaging revealed severe splenomegaly (36 cm) with abdominal mass effect. Peripheral flow cytometry didn’t show malignancy, but cytogenetic analysis showed a BCR/ABL1 fusion gene, confirming chronic myeloid leukemia (CML). Bone marrow biopsy showed hypercellularity without increased blasts. Treatment with dasatinib reduced the white count to 52,000 k/mcL, and was discharged home.
Discussion
Priapism is a urological emergency necessitating immediate intervention to prevent erectile dysfunction and permanent impotence. Management aims to achieve detumescence and typically involves methods such as irrigation or injection of vasoconstrictors into the penis. Malignancy-associated priapism (MAP) often results from venous obstruction due to hyperviscosity. Studies show that CML accounts for approximately 50% cases presenting with MAP, predominantly affecting younger individuals with a mean onset around 27 years of age. Priapism can occur before, during, or after treatment initiation or splenectomy in these patients. Providers should keep a high threshold of suspicion for MAP in patients with no other risk factors as prompt identification and treatment are needed to avoid permanent injury.
The First Female Patient in the Veteran Affairs System to Receive Chimeric Antigen Receptors (CAR) T-cell Therapy for Refractory Multiple Myeloma and the Role of CAR T-cell Therapy in Penta-refractory Disease
Background
In 2024, the first two veterans, both from the Michael E. DeBakey Veteran Affairs (VA) Medical Center, received chimeric antigen receptors (CAR) T-cell therapy for refractory multiple myeloma through the Tennessee Valley Healthcare System (TVHS). Currently, TVHS is the only VA where this treatment is available. One of these patients also had penta-refractory multiple myeloma (P-RMM), which is associated with significantly worse progression-free survival and overall survival (OS) (Gill et al, 2021). P-RMM is defined as resistance to at least two immunomodulatory drugs, two different proteasome inhibitors, and one CD38 monoclonal antibody.
Case Presentation
A 71-year-old female veteran was diagnosed with high-risk multiple myeloma and received induction therapy with carfilzomib, lenalidomide, and dexamethasone in 2017. She underwent autologous stem cell transplant (SCT) in 4/2018. The veteran subsequently received maintenance therapy with lenalidomide, bortezomib, and dexamethasone. Her disease recurred in 1/2022. The patient then received two more lines of treatments with daratumumab and pomalidomide followed by selinexor. She had another autologous SCT in 5/2023, to which she was refractory. Her fifth line therapy included addition of bortezomib to her selinexor regimen. She eventually underwent CAR T-cell therapy at THVS on 5/1/2024 with good tolerance of therapy. At her follow-up visit, the patient had significant response to CAR T-cell treatment, based on her symptoms and improvement in free light chains and serum protein electrophoresis.
Discussion
CAR T-cell therapy is one of the newest and most cutting-edge therapies for patients with refractory multiple myeloma. Access to this therapy has been limited throughout the country. However, as shown by our case, this life-saving treatment is now available to patients within the VA. According to a retrospective study on P-RMM patients, the OS in patients who received B-cell maturation antigen (BCMA) targeted therapy was significantly higher than in those who did not (17 vs. 6 months, p < 0.0001). Among the BCMA-targeted therapies, CAR T-cell therapy is associated with the highest OS (29 months) compared to antibody-drug conjugates and bispecific T-cell engagers (Atrash et al, 2023). Thus, accessibility to CAR T-cell therapy was essential in our patient with P-RMM in ensuring her best survival outcomes.
Background
In 2024, the first two veterans, both from the Michael E. DeBakey Veteran Affairs (VA) Medical Center, received chimeric antigen receptors (CAR) T-cell therapy for refractory multiple myeloma through the Tennessee Valley Healthcare System (TVHS). Currently, TVHS is the only VA where this treatment is available. One of these patients also had penta-refractory multiple myeloma (P-RMM), which is associated with significantly worse progression-free survival and overall survival (OS) (Gill et al, 2021). P-RMM is defined as resistance to at least two immunomodulatory drugs, two different proteasome inhibitors, and one CD38 monoclonal antibody.
Case Presentation
A 71-year-old female veteran was diagnosed with high-risk multiple myeloma and received induction therapy with carfilzomib, lenalidomide, and dexamethasone in 2017. She underwent autologous stem cell transplant (SCT) in 4/2018. The veteran subsequently received maintenance therapy with lenalidomide, bortezomib, and dexamethasone. Her disease recurred in 1/2022. The patient then received two more lines of treatments with daratumumab and pomalidomide followed by selinexor. She had another autologous SCT in 5/2023, to which she was refractory. Her fifth line therapy included addition of bortezomib to her selinexor regimen. She eventually underwent CAR T-cell therapy at THVS on 5/1/2024 with good tolerance of therapy. At her follow-up visit, the patient had significant response to CAR T-cell treatment, based on her symptoms and improvement in free light chains and serum protein electrophoresis.
Discussion
CAR T-cell therapy is one of the newest and most cutting-edge therapies for patients with refractory multiple myeloma. Access to this therapy has been limited throughout the country. However, as shown by our case, this life-saving treatment is now available to patients within the VA. According to a retrospective study on P-RMM patients, the OS in patients who received B-cell maturation antigen (BCMA) targeted therapy was significantly higher than in those who did not (17 vs. 6 months, p < 0.0001). Among the BCMA-targeted therapies, CAR T-cell therapy is associated with the highest OS (29 months) compared to antibody-drug conjugates and bispecific T-cell engagers (Atrash et al, 2023). Thus, accessibility to CAR T-cell therapy was essential in our patient with P-RMM in ensuring her best survival outcomes.
Background
In 2024, the first two veterans, both from the Michael E. DeBakey Veteran Affairs (VA) Medical Center, received chimeric antigen receptors (CAR) T-cell therapy for refractory multiple myeloma through the Tennessee Valley Healthcare System (TVHS). Currently, TVHS is the only VA where this treatment is available. One of these patients also had penta-refractory multiple myeloma (P-RMM), which is associated with significantly worse progression-free survival and overall survival (OS) (Gill et al, 2021). P-RMM is defined as resistance to at least two immunomodulatory drugs, two different proteasome inhibitors, and one CD38 monoclonal antibody.
Case Presentation
A 71-year-old female veteran was diagnosed with high-risk multiple myeloma and received induction therapy with carfilzomib, lenalidomide, and dexamethasone in 2017. She underwent autologous stem cell transplant (SCT) in 4/2018. The veteran subsequently received maintenance therapy with lenalidomide, bortezomib, and dexamethasone. Her disease recurred in 1/2022. The patient then received two more lines of treatments with daratumumab and pomalidomide followed by selinexor. She had another autologous SCT in 5/2023, to which she was refractory. Her fifth line therapy included addition of bortezomib to her selinexor regimen. She eventually underwent CAR T-cell therapy at THVS on 5/1/2024 with good tolerance of therapy. At her follow-up visit, the patient had significant response to CAR T-cell treatment, based on her symptoms and improvement in free light chains and serum protein electrophoresis.
Discussion
CAR T-cell therapy is one of the newest and most cutting-edge therapies for patients with refractory multiple myeloma. Access to this therapy has been limited throughout the country. However, as shown by our case, this life-saving treatment is now available to patients within the VA. According to a retrospective study on P-RMM patients, the OS in patients who received B-cell maturation antigen (BCMA) targeted therapy was significantly higher than in those who did not (17 vs. 6 months, p < 0.0001). Among the BCMA-targeted therapies, CAR T-cell therapy is associated with the highest OS (29 months) compared to antibody-drug conjugates and bispecific T-cell engagers (Atrash et al, 2023). Thus, accessibility to CAR T-cell therapy was essential in our patient with P-RMM in ensuring her best survival outcomes.