User login
The Development of a Comprehensive Wound Care Fellowship Curriculum
The Development of a Comprehensive Wound Care Fellowship Curriculum
Often disguised as comorbid conditions, nonhealing and chronic wounds have emerged as a silent epidemic that affects about 6.5 million Americans.1-3 In 2023, estimated US wound care costs were $126.86 billion.4 About 1% to 2% of individuals worldwide will experience a chronic wound in their lifetime. The Veterans Health Administration reported 277,000 inpatient and outpatient encounters for ulcers in 2011, including chronic ulcers of the lower extremity due to diabetes, venous disease, or arterial disease.5 Associated costs of chronic wounds are expected to increase as the populations of developed countries age.6 Effective treatment of chronic wounds requires a nuanced understanding of complex wound pathophysiology, best practices in interdisciplinary and multidisciplinary wound care, and advanced wound care technologies.7,8
The typical 4-year medical school curriculum, followed by residency, offers little in the way of formal didactic training in wound care.9,10 Without specialized and advanced fellowship training dedicated to wound care, health care will lack specialists prepared to manage complex wounds. As a result, wound care-related difficulties may be exacerbated by prolonged recovery time, increased costs, productivity loss, and increased mortality risk.8 Wound care is a growing field of study and practice, and there is a critical need for rigorous training, research, and quality improvement efforts to enhance outcomes for patients with nonhealing wounds.5
One of the most direct ways to address the need for more physicians with specialty training in wound medicine is to implement a comprehensive training curriculum for advanced wound care practice. Although specialized advanced wound care fellowships are available, the curricula primarily detail rotation names and areas for practice without accompanying competencies, milestones, or entrustable professional activities.11 Furthermore, wound care is not recognized as a subspecialty by the Accreditation Council for Graduate Medical Education (ACGME).
This article synthesized the literature and integrated innovative, evidence-based practices into a curriculum for a formal advanced fellowship training program. To our knowledge, no comprehensive wound care curriculum is publicly available that includes rotations, competencies, milestones, entrustable professional activities, and 360-degree evaluation forms.
Program Development
The advanced wound care fellowship program started in January 2014 at the Michael E. DeBakey Veterans Affairs Medical Center in affiliation with the Baylor College of Medicine. The fellowship program was originally designed for geriatrics fellows to extend the 1-year fellowship for an additional year to learn wound care. It has been adjusted to address formal program goals and objectives, competencies, milestones, entrustable professional activities, and evaluations, with the goal of developing an example curriculum for wound care fellowships across specialties. Although the ACGME does not recognize a wound care subspecialty, this curriculum complies with the ACGME 1-year fellowship common program requirements.12,13
Scoping Review
A scoping literature review of Google Scholar and PubMed was performed using the medical subject heading terms “wound care + curriculum” and “wound + care + curriculum” to find advanced wound care medical training, fellowship programs, boards, and related ACGME-accredited specialty curricula. The local wound care fellowship program was initially implemented based on an informal literature review by faculty and their respective contributions to curriculum (ie, process establishing wound care-specific competency domains in accordance with ACGME accreditation competency requirements of 1-year fellowships). 12,13 Standing program practice-based competencies and activities were examined and determined to align with best practices. This scoping review considered additional competencies, competency domains, and entrustable professional activities of reputable wound care fellowship training programs (eg, University of Chicago at Illinois and Wake Forest School of Medicine),8,11,14 a specialty wound care board (American Board of Wound Medicine and Surgery),15 an international wound specialist professional society (European Union of Medical Specialists), 16 and recommended curriculum guidelines for wound care residency programs.17 ACGME-accredited specialty and subspecialty milestones professional activities were examined, including vascular surgery,18 plastic surgery,19 dermatology, 20 foot and ankle,21 orthopedic surgery,22 spinal cord injury,23 and geriatric medicine.24
The competencies, milestones, and entrustable professional activities were compiled and redundancies were eliminated. Wound care specialists from geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy examined the findings and suggested eliminating redundancies, irrelevant content, and content that fell below the minimal expected level of competence for an advanced medical specialist in wound care. An expert consensus meeting further refined items presented to the panel before unanimous consensus resulted in the final set of curriculum competencies, milestones, and entrustable professional activities.
Training Program Feedback
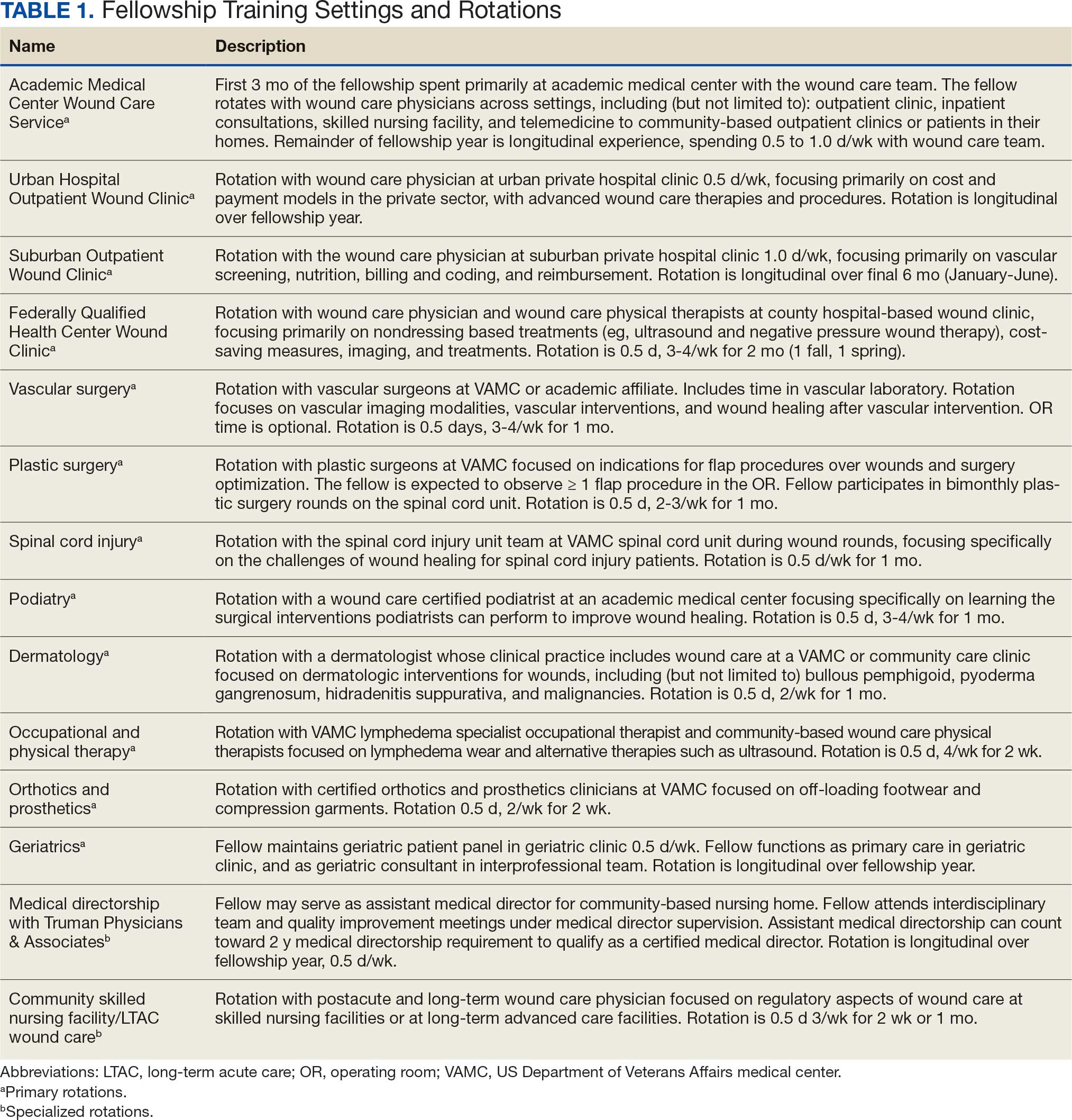
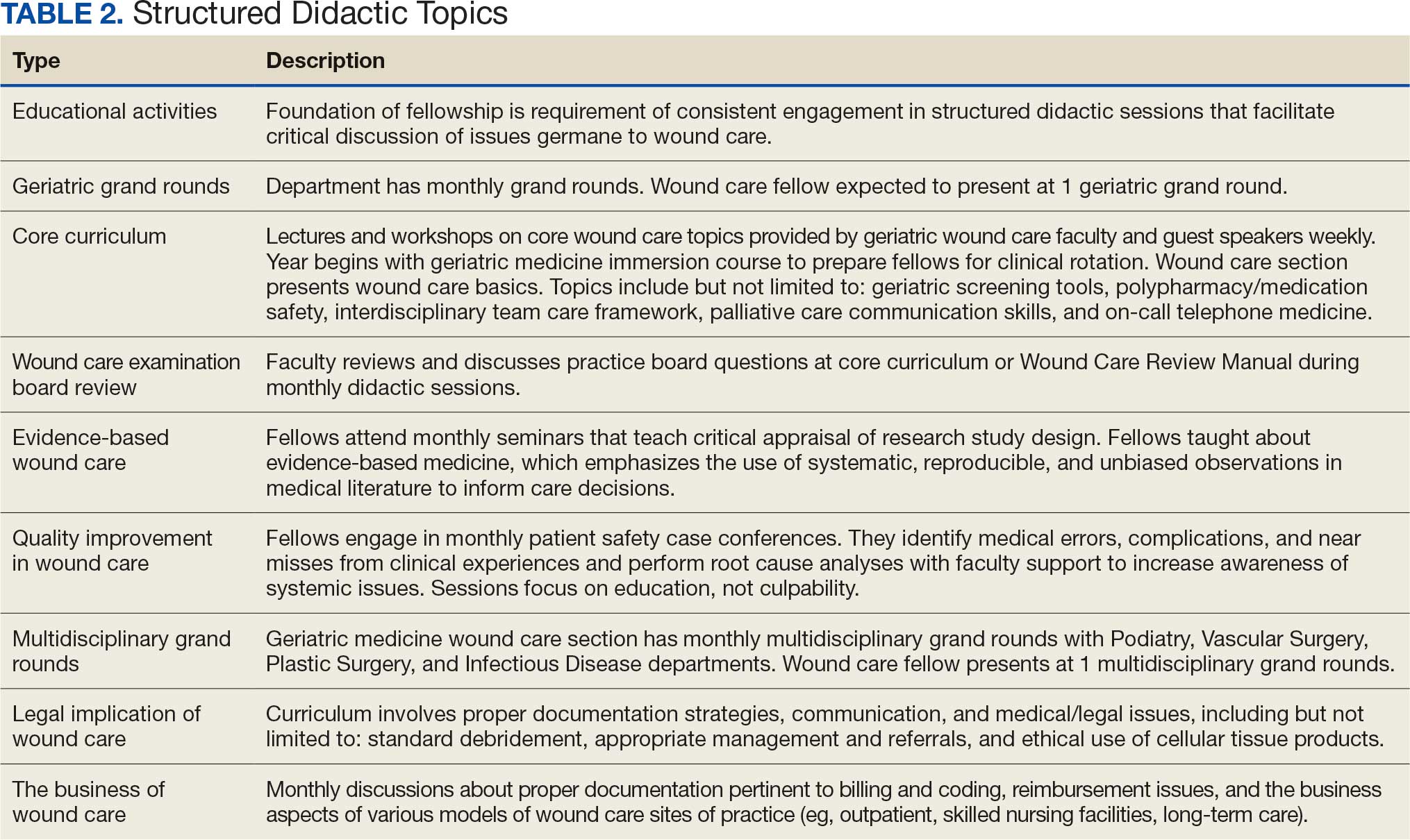
We developed a comprehensive wound care curriculum for an advanced physician fellowship training program based on the streamlined competencies, milestones, and entrustable professional activities (Appendix). Multiple wound care experts from various interdisciplinary backgrounds reached consensus to establish this fellowship curriculum as adaptable for use across training settings. The training program is 12 core rotations and 2 elective rotations (Table 1). Additionally, we developed wound care evaluation forms for faculty-, peer-, and self-assessment of trainees which were adapted from an evidence-based 360-degree evaluation template.25 Suggestions for structured, advanced didactics are in Table 2.
Seventeen fellows have successfully matriculated through the wound care training program. Although wound care certification is not required to work as a wound care specialist, after completion of this fellowship, graduates are able to sit for a wound care certification examination. The American Board of Wound Medicine and Surgery (ABWMS) and the American Board of Wound Management (ABWM) allow physicians to take a certification examination after 1 year of a dedicated wound fellowship program, instead of the typical wound care practice experience ≥ 3 years.
The Clinical Wound Care Fellowship Program collected data for program improvement, and 15 alumni responded (response rate, 88%) to a survey using a 5-point Likert scale. Respondents indicated high mean scores for overall satisfaction (4.7), instructional methods (4.7), program enjoyment (4.7), teaching materials (4.6), and relevance (4.6). All respondents indicated that the fellowship prepared them for a career in wound care as well as their current employment, and 13 of 15 (87%) reported they obtained immediate relevant postfellowship wound care positions and stated that the fellowship prepared them for their current roles. Nine respondents (69%) reported that they were engaged in wound care ≥ 26% of work time. Six respondents (46%) worked in private practice, 3 (23%) at academic medical centers, and 2 (15%) at government- funded hospitals. Four respondents indicated they were board certified in wound care. Program alumni are currently involved in scholarly activities, including 8 in quality improvement and 3 in research.
Discussion
An easily accessible, comprehensive wound care fellowship curriculum has not been previously developed or published. This limited the sources that informed this curriculum. However, the developmental process for this curriculum was robust, as the authors reviewed previously published materials related to wound care, including: 1) descriptive overviews of wound care fellowships; 2) details of month-long rotations for medical students and residents; and 3) practices of the specific environment in which this curriculum was created. Confidence in the practical nature of the curriculum can be assumed, as the experts involved in the development process represented diverse physician specializations, including geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy.
Most wound care clinicians have not completed a formal comprehensive fellowship program. Instead, due to the lack of a comprehensive training curriculum, clinicians have had to use various continuing medical education programs and practice in a wound care setting for ≥ 3 years to be eligible for certification in the specialty. This curriculum will help academic medical centers develop their own fellowship programs, enabling new wound care clinicians to attain certifications more efficiently. As more fellowship programs develop, the goal would be to obtain recognition as an ACGME specialty and standardize the training and competencies for graduates of wound care fellowships.
Conclusions
As new wound care fellowships develop, wound care may become formally acknowledged as its own specialty within medicine and surgery. This will provide wound care with a voice at the national level, particularly in an era of value-based care. Wound care clinicians will be able to advocate for specialty-specific quality metrics and avoid potential penalization for not meeting quality metrics that are irrelevant to wound care.
- Fife CE, Eckert KA, Carter MJ. Publicly Reported wound healing rates: the fantasy and the reality. Adv Wound Care (New Rochelle). 2018;7:77-94. doi:10.1089/wound.2017.0743
- Fife CE, Carter MJ, Walker D. Why is it so hard to do the right thing in wound care?. Wound Repair Regen. 2010;18:154-158. doi:10.1111/j.1524-475X.2010.00571.x
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771. doi:10.1111/j.1524-475X.2009.00543.x
- Queen D, Harding K. What’s the true costs of wounds faced by different healthcare systems around the world?. Int Wound J. 2023;20:3935-3938. doi:10.1111/iwj.14491
- Greer N, Foman N, Dorrian J, et al. Advanced Wound Care Therapies for Non-Healing Diabetic, Venous, and Arterial Ulcers: A Systematic Review [Internet]. US Dept of Veterans Affairs; November 2012. https://www.ncbi.nlm.nih.gov/books/NBK132238/
- Simman R, McNevin AJ. Pursuing the path to specialized wound care: the ABWMS perspective. Todays Wound Clin. 2017;8:10,12.
- Shahin ES, Dassen T, Halfens RJ. Pressure ulcer prevalence in intensive care patients: a cross-sectional study. J Eval Clin Pract. 2008;14:563-568. doi:10.1111/j.1365-2753.2007.00918.x
- Ennis WJ, Valdes W, Meneses P. Wound care specialization: a proposal for a comprehensive fellowship program. Wound Repair Regen. 2004;12:120-128. doi:10.1111/j.1067-1927.2004.012203.x
- Patel NP, Granick MS. Wound education: American medical students are inadequately trained in wound care. Ann Plast Surg. 2007;59:53-55. doi:10.1097/SAP.0b013e31802dd43b
- Patel NP, Granick MS, Kanakaris NK, et al. Comparison of wound education in medical schools in the United States, United Kingdom, and Germany. Eplasty. 2008;8:e8.
- Ennis WJ. Wound care specialization: the current status and future plans to move wound care into the medical community. Adv Wound Care (New Rochelle). 2012;1:184- 188. doi:10.1089/wound.2011.0346
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (fellowship). Updated September 3, 2025. Accessed January 15, 2026. https://www.acgme.org/globalassets/pfassets /programrequirements/2025-reformatted-requirements/cprfellowship_2025_reformatted.pdf
- Accreditation Council for Graduate Medical Education. Program directors’ guide to the common program requirements (fellowship). Updated December 2025. Accessed May 27, 2026. https://www .acgme.org/globalassets/pdfs/guide-to-the-common -program-requirements-fellowship.pdf
- Curriculum overview - wound care and hyperbaric medicine fellowship. Wake Forest University School of Medicine. 2026. Accessed January 5, 2026. https://school .wakehealth.edu/Education-and-Training/Residencies -and-Fellowships/Wound-Care-and-Hyperbaric-Medicine -Fellowship/Curriculum-Overview
- Curriculum overview - American Board of Wound Medicine and Surgery. Core Curriculum for Fellowships in Wound Care. American Board of Wound Medicine and Surgery. 2022. Accessed January 5, 2026. https://abwms.org /curriculum-overview/
- European Wound Management Association. EWMA Wound healing curriculum for physicians. February 13, 2017. Accessed January 15, 2026. https://ewma.org /wp-content/uploads/2024/02/ETR-TF-Wound-Healing -UEMS-approved.pdf
- Accreditation Council for Graduate Medical Education. Recommended Curriculum Guidelines for Family Medicine Residents. Accessed January 5, 2026. https://www.aafp .org/dam/AAFP/documents/medical_education_residency /program_directors/Wound_Care.pdf
- Accreditation Council for Graduate Medical Education. Vascular Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /VascularSurgeryMilestones2.0.pdf
- Accreditation Council for Graduate Medical Education. Plastic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/PlasticSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Dermatology Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /DermatologyMilestones.pdf
- Accreditation Council for Graduate Medical Education. The Foot and Ankle Milestone Project a joint initiative of the Accreditation Council for Graduate Medical Education and the American Board of Orthopaedic Surgery. July 2015. Accessed January 5, 2026. https://www.acgme.org /Portals/0/PDFs/Milestones/FootandAnkleMilestones.pdf
- Accreditation Council for Graduate Medical Education. Orthopaedic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /OrthopaedicSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Spinal Cord Injury Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/SpinalCordInjuryMedicineMilestones.pdf
- Accreditation Council for Graduate Medical Education. Geriatric Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /GeriatricMedicineMilestones.pdf
- Goldhamer ME, Baker K, Anne Rigg DW, et al. Development and implementation of multi-source assessment tools for ACGME residents and fellows. MedEDPORTAL. 2014. Accessed May 14, 2026. doi:10.15766/mep_2374-8265.9839
Often disguised as comorbid conditions, nonhealing and chronic wounds have emerged as a silent epidemic that affects about 6.5 million Americans.1-3 In 2023, estimated US wound care costs were $126.86 billion.4 About 1% to 2% of individuals worldwide will experience a chronic wound in their lifetime. The Veterans Health Administration reported 277,000 inpatient and outpatient encounters for ulcers in 2011, including chronic ulcers of the lower extremity due to diabetes, venous disease, or arterial disease.5 Associated costs of chronic wounds are expected to increase as the populations of developed countries age.6 Effective treatment of chronic wounds requires a nuanced understanding of complex wound pathophysiology, best practices in interdisciplinary and multidisciplinary wound care, and advanced wound care technologies.7,8
The typical 4-year medical school curriculum, followed by residency, offers little in the way of formal didactic training in wound care.9,10 Without specialized and advanced fellowship training dedicated to wound care, health care will lack specialists prepared to manage complex wounds. As a result, wound care-related difficulties may be exacerbated by prolonged recovery time, increased costs, productivity loss, and increased mortality risk.8 Wound care is a growing field of study and practice, and there is a critical need for rigorous training, research, and quality improvement efforts to enhance outcomes for patients with nonhealing wounds.5
One of the most direct ways to address the need for more physicians with specialty training in wound medicine is to implement a comprehensive training curriculum for advanced wound care practice. Although specialized advanced wound care fellowships are available, the curricula primarily detail rotation names and areas for practice without accompanying competencies, milestones, or entrustable professional activities.11 Furthermore, wound care is not recognized as a subspecialty by the Accreditation Council for Graduate Medical Education (ACGME).
This article synthesized the literature and integrated innovative, evidence-based practices into a curriculum for a formal advanced fellowship training program. To our knowledge, no comprehensive wound care curriculum is publicly available that includes rotations, competencies, milestones, entrustable professional activities, and 360-degree evaluation forms.
Program Development
The advanced wound care fellowship program started in January 2014 at the Michael E. DeBakey Veterans Affairs Medical Center in affiliation with the Baylor College of Medicine. The fellowship program was originally designed for geriatrics fellows to extend the 1-year fellowship for an additional year to learn wound care. It has been adjusted to address formal program goals and objectives, competencies, milestones, entrustable professional activities, and evaluations, with the goal of developing an example curriculum for wound care fellowships across specialties. Although the ACGME does not recognize a wound care subspecialty, this curriculum complies with the ACGME 1-year fellowship common program requirements.12,13
Scoping Review
A scoping literature review of Google Scholar and PubMed was performed using the medical subject heading terms “wound care + curriculum” and “wound + care + curriculum” to find advanced wound care medical training, fellowship programs, boards, and related ACGME-accredited specialty curricula. The local wound care fellowship program was initially implemented based on an informal literature review by faculty and their respective contributions to curriculum (ie, process establishing wound care-specific competency domains in accordance with ACGME accreditation competency requirements of 1-year fellowships). 12,13 Standing program practice-based competencies and activities were examined and determined to align with best practices. This scoping review considered additional competencies, competency domains, and entrustable professional activities of reputable wound care fellowship training programs (eg, University of Chicago at Illinois and Wake Forest School of Medicine),8,11,14 a specialty wound care board (American Board of Wound Medicine and Surgery),15 an international wound specialist professional society (European Union of Medical Specialists), 16 and recommended curriculum guidelines for wound care residency programs.17 ACGME-accredited specialty and subspecialty milestones professional activities were examined, including vascular surgery,18 plastic surgery,19 dermatology, 20 foot and ankle,21 orthopedic surgery,22 spinal cord injury,23 and geriatric medicine.24
The competencies, milestones, and entrustable professional activities were compiled and redundancies were eliminated. Wound care specialists from geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy examined the findings and suggested eliminating redundancies, irrelevant content, and content that fell below the minimal expected level of competence for an advanced medical specialist in wound care. An expert consensus meeting further refined items presented to the panel before unanimous consensus resulted in the final set of curriculum competencies, milestones, and entrustable professional activities.
Training Program Feedback
We developed a comprehensive wound care curriculum for an advanced physician fellowship training program based on the streamlined competencies, milestones, and entrustable professional activities (Appendix). Multiple wound care experts from various interdisciplinary backgrounds reached consensus to establish this fellowship curriculum as adaptable for use across training settings. The training program is 12 core rotations and 2 elective rotations (Table 1). Additionally, we developed wound care evaluation forms for faculty-, peer-, and self-assessment of trainees which were adapted from an evidence-based 360-degree evaluation template.25 Suggestions for structured, advanced didactics are in Table 2.
Seventeen fellows have successfully matriculated through the wound care training program. Although wound care certification is not required to work as a wound care specialist, after completion of this fellowship, graduates are able to sit for a wound care certification examination. The American Board of Wound Medicine and Surgery (ABWMS) and the American Board of Wound Management (ABWM) allow physicians to take a certification examination after 1 year of a dedicated wound fellowship program, instead of the typical wound care practice experience ≥ 3 years.
The Clinical Wound Care Fellowship Program collected data for program improvement, and 15 alumni responded (response rate, 88%) to a survey using a 5-point Likert scale. Respondents indicated high mean scores for overall satisfaction (4.7), instructional methods (4.7), program enjoyment (4.7), teaching materials (4.6), and relevance (4.6). All respondents indicated that the fellowship prepared them for a career in wound care as well as their current employment, and 13 of 15 (87%) reported they obtained immediate relevant postfellowship wound care positions and stated that the fellowship prepared them for their current roles. Nine respondents (69%) reported that they were engaged in wound care ≥ 26% of work time. Six respondents (46%) worked in private practice, 3 (23%) at academic medical centers, and 2 (15%) at government- funded hospitals. Four respondents indicated they were board certified in wound care. Program alumni are currently involved in scholarly activities, including 8 in quality improvement and 3 in research.
Discussion
An easily accessible, comprehensive wound care fellowship curriculum has not been previously developed or published. This limited the sources that informed this curriculum. However, the developmental process for this curriculum was robust, as the authors reviewed previously published materials related to wound care, including: 1) descriptive overviews of wound care fellowships; 2) details of month-long rotations for medical students and residents; and 3) practices of the specific environment in which this curriculum was created. Confidence in the practical nature of the curriculum can be assumed, as the experts involved in the development process represented diverse physician specializations, including geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy.
Most wound care clinicians have not completed a formal comprehensive fellowship program. Instead, due to the lack of a comprehensive training curriculum, clinicians have had to use various continuing medical education programs and practice in a wound care setting for ≥ 3 years to be eligible for certification in the specialty. This curriculum will help academic medical centers develop their own fellowship programs, enabling new wound care clinicians to attain certifications more efficiently. As more fellowship programs develop, the goal would be to obtain recognition as an ACGME specialty and standardize the training and competencies for graduates of wound care fellowships.
Conclusions
As new wound care fellowships develop, wound care may become formally acknowledged as its own specialty within medicine and surgery. This will provide wound care with a voice at the national level, particularly in an era of value-based care. Wound care clinicians will be able to advocate for specialty-specific quality metrics and avoid potential penalization for not meeting quality metrics that are irrelevant to wound care.
Often disguised as comorbid conditions, nonhealing and chronic wounds have emerged as a silent epidemic that affects about 6.5 million Americans.1-3 In 2023, estimated US wound care costs were $126.86 billion.4 About 1% to 2% of individuals worldwide will experience a chronic wound in their lifetime. The Veterans Health Administration reported 277,000 inpatient and outpatient encounters for ulcers in 2011, including chronic ulcers of the lower extremity due to diabetes, venous disease, or arterial disease.5 Associated costs of chronic wounds are expected to increase as the populations of developed countries age.6 Effective treatment of chronic wounds requires a nuanced understanding of complex wound pathophysiology, best practices in interdisciplinary and multidisciplinary wound care, and advanced wound care technologies.7,8
The typical 4-year medical school curriculum, followed by residency, offers little in the way of formal didactic training in wound care.9,10 Without specialized and advanced fellowship training dedicated to wound care, health care will lack specialists prepared to manage complex wounds. As a result, wound care-related difficulties may be exacerbated by prolonged recovery time, increased costs, productivity loss, and increased mortality risk.8 Wound care is a growing field of study and practice, and there is a critical need for rigorous training, research, and quality improvement efforts to enhance outcomes for patients with nonhealing wounds.5
One of the most direct ways to address the need for more physicians with specialty training in wound medicine is to implement a comprehensive training curriculum for advanced wound care practice. Although specialized advanced wound care fellowships are available, the curricula primarily detail rotation names and areas for practice without accompanying competencies, milestones, or entrustable professional activities.11 Furthermore, wound care is not recognized as a subspecialty by the Accreditation Council for Graduate Medical Education (ACGME).
This article synthesized the literature and integrated innovative, evidence-based practices into a curriculum for a formal advanced fellowship training program. To our knowledge, no comprehensive wound care curriculum is publicly available that includes rotations, competencies, milestones, entrustable professional activities, and 360-degree evaluation forms.
Program Development
The advanced wound care fellowship program started in January 2014 at the Michael E. DeBakey Veterans Affairs Medical Center in affiliation with the Baylor College of Medicine. The fellowship program was originally designed for geriatrics fellows to extend the 1-year fellowship for an additional year to learn wound care. It has been adjusted to address formal program goals and objectives, competencies, milestones, entrustable professional activities, and evaluations, with the goal of developing an example curriculum for wound care fellowships across specialties. Although the ACGME does not recognize a wound care subspecialty, this curriculum complies with the ACGME 1-year fellowship common program requirements.12,13
Scoping Review
A scoping literature review of Google Scholar and PubMed was performed using the medical subject heading terms “wound care + curriculum” and “wound + care + curriculum” to find advanced wound care medical training, fellowship programs, boards, and related ACGME-accredited specialty curricula. The local wound care fellowship program was initially implemented based on an informal literature review by faculty and their respective contributions to curriculum (ie, process establishing wound care-specific competency domains in accordance with ACGME accreditation competency requirements of 1-year fellowships). 12,13 Standing program practice-based competencies and activities were examined and determined to align with best practices. This scoping review considered additional competencies, competency domains, and entrustable professional activities of reputable wound care fellowship training programs (eg, University of Chicago at Illinois and Wake Forest School of Medicine),8,11,14 a specialty wound care board (American Board of Wound Medicine and Surgery),15 an international wound specialist professional society (European Union of Medical Specialists), 16 and recommended curriculum guidelines for wound care residency programs.17 ACGME-accredited specialty and subspecialty milestones professional activities were examined, including vascular surgery,18 plastic surgery,19 dermatology, 20 foot and ankle,21 orthopedic surgery,22 spinal cord injury,23 and geriatric medicine.24
The competencies, milestones, and entrustable professional activities were compiled and redundancies were eliminated. Wound care specialists from geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy examined the findings and suggested eliminating redundancies, irrelevant content, and content that fell below the minimal expected level of competence for an advanced medical specialist in wound care. An expert consensus meeting further refined items presented to the panel before unanimous consensus resulted in the final set of curriculum competencies, milestones, and entrustable professional activities.
Training Program Feedback
We developed a comprehensive wound care curriculum for an advanced physician fellowship training program based on the streamlined competencies, milestones, and entrustable professional activities (Appendix). Multiple wound care experts from various interdisciplinary backgrounds reached consensus to establish this fellowship curriculum as adaptable for use across training settings. The training program is 12 core rotations and 2 elective rotations (Table 1). Additionally, we developed wound care evaluation forms for faculty-, peer-, and self-assessment of trainees which were adapted from an evidence-based 360-degree evaluation template.25 Suggestions for structured, advanced didactics are in Table 2.
Seventeen fellows have successfully matriculated through the wound care training program. Although wound care certification is not required to work as a wound care specialist, after completion of this fellowship, graduates are able to sit for a wound care certification examination. The American Board of Wound Medicine and Surgery (ABWMS) and the American Board of Wound Management (ABWM) allow physicians to take a certification examination after 1 year of a dedicated wound fellowship program, instead of the typical wound care practice experience ≥ 3 years.
The Clinical Wound Care Fellowship Program collected data for program improvement, and 15 alumni responded (response rate, 88%) to a survey using a 5-point Likert scale. Respondents indicated high mean scores for overall satisfaction (4.7), instructional methods (4.7), program enjoyment (4.7), teaching materials (4.6), and relevance (4.6). All respondents indicated that the fellowship prepared them for a career in wound care as well as their current employment, and 13 of 15 (87%) reported they obtained immediate relevant postfellowship wound care positions and stated that the fellowship prepared them for their current roles. Nine respondents (69%) reported that they were engaged in wound care ≥ 26% of work time. Six respondents (46%) worked in private practice, 3 (23%) at academic medical centers, and 2 (15%) at government- funded hospitals. Four respondents indicated they were board certified in wound care. Program alumni are currently involved in scholarly activities, including 8 in quality improvement and 3 in research.
Discussion
An easily accessible, comprehensive wound care fellowship curriculum has not been previously developed or published. This limited the sources that informed this curriculum. However, the developmental process for this curriculum was robust, as the authors reviewed previously published materials related to wound care, including: 1) descriptive overviews of wound care fellowships; 2) details of month-long rotations for medical students and residents; and 3) practices of the specific environment in which this curriculum was created. Confidence in the practical nature of the curriculum can be assumed, as the experts involved in the development process represented diverse physician specializations, including geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy.
Most wound care clinicians have not completed a formal comprehensive fellowship program. Instead, due to the lack of a comprehensive training curriculum, clinicians have had to use various continuing medical education programs and practice in a wound care setting for ≥ 3 years to be eligible for certification in the specialty. This curriculum will help academic medical centers develop their own fellowship programs, enabling new wound care clinicians to attain certifications more efficiently. As more fellowship programs develop, the goal would be to obtain recognition as an ACGME specialty and standardize the training and competencies for graduates of wound care fellowships.
Conclusions
As new wound care fellowships develop, wound care may become formally acknowledged as its own specialty within medicine and surgery. This will provide wound care with a voice at the national level, particularly in an era of value-based care. Wound care clinicians will be able to advocate for specialty-specific quality metrics and avoid potential penalization for not meeting quality metrics that are irrelevant to wound care.
- Fife CE, Eckert KA, Carter MJ. Publicly Reported wound healing rates: the fantasy and the reality. Adv Wound Care (New Rochelle). 2018;7:77-94. doi:10.1089/wound.2017.0743
- Fife CE, Carter MJ, Walker D. Why is it so hard to do the right thing in wound care?. Wound Repair Regen. 2010;18:154-158. doi:10.1111/j.1524-475X.2010.00571.x
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771. doi:10.1111/j.1524-475X.2009.00543.x
- Queen D, Harding K. What’s the true costs of wounds faced by different healthcare systems around the world?. Int Wound J. 2023;20:3935-3938. doi:10.1111/iwj.14491
- Greer N, Foman N, Dorrian J, et al. Advanced Wound Care Therapies for Non-Healing Diabetic, Venous, and Arterial Ulcers: A Systematic Review [Internet]. US Dept of Veterans Affairs; November 2012. https://www.ncbi.nlm.nih.gov/books/NBK132238/
- Simman R, McNevin AJ. Pursuing the path to specialized wound care: the ABWMS perspective. Todays Wound Clin. 2017;8:10,12.
- Shahin ES, Dassen T, Halfens RJ. Pressure ulcer prevalence in intensive care patients: a cross-sectional study. J Eval Clin Pract. 2008;14:563-568. doi:10.1111/j.1365-2753.2007.00918.x
- Ennis WJ, Valdes W, Meneses P. Wound care specialization: a proposal for a comprehensive fellowship program. Wound Repair Regen. 2004;12:120-128. doi:10.1111/j.1067-1927.2004.012203.x
- Patel NP, Granick MS. Wound education: American medical students are inadequately trained in wound care. Ann Plast Surg. 2007;59:53-55. doi:10.1097/SAP.0b013e31802dd43b
- Patel NP, Granick MS, Kanakaris NK, et al. Comparison of wound education in medical schools in the United States, United Kingdom, and Germany. Eplasty. 2008;8:e8.
- Ennis WJ. Wound care specialization: the current status and future plans to move wound care into the medical community. Adv Wound Care (New Rochelle). 2012;1:184- 188. doi:10.1089/wound.2011.0346
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (fellowship). Updated September 3, 2025. Accessed January 15, 2026. https://www.acgme.org/globalassets/pfassets /programrequirements/2025-reformatted-requirements/cprfellowship_2025_reformatted.pdf
- Accreditation Council for Graduate Medical Education. Program directors’ guide to the common program requirements (fellowship). Updated December 2025. Accessed May 27, 2026. https://www .acgme.org/globalassets/pdfs/guide-to-the-common -program-requirements-fellowship.pdf
- Curriculum overview - wound care and hyperbaric medicine fellowship. Wake Forest University School of Medicine. 2026. Accessed January 5, 2026. https://school .wakehealth.edu/Education-and-Training/Residencies -and-Fellowships/Wound-Care-and-Hyperbaric-Medicine -Fellowship/Curriculum-Overview
- Curriculum overview - American Board of Wound Medicine and Surgery. Core Curriculum for Fellowships in Wound Care. American Board of Wound Medicine and Surgery. 2022. Accessed January 5, 2026. https://abwms.org /curriculum-overview/
- European Wound Management Association. EWMA Wound healing curriculum for physicians. February 13, 2017. Accessed January 15, 2026. https://ewma.org /wp-content/uploads/2024/02/ETR-TF-Wound-Healing -UEMS-approved.pdf
- Accreditation Council for Graduate Medical Education. Recommended Curriculum Guidelines for Family Medicine Residents. Accessed January 5, 2026. https://www.aafp .org/dam/AAFP/documents/medical_education_residency /program_directors/Wound_Care.pdf
- Accreditation Council for Graduate Medical Education. Vascular Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /VascularSurgeryMilestones2.0.pdf
- Accreditation Council for Graduate Medical Education. Plastic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/PlasticSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Dermatology Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /DermatologyMilestones.pdf
- Accreditation Council for Graduate Medical Education. The Foot and Ankle Milestone Project a joint initiative of the Accreditation Council for Graduate Medical Education and the American Board of Orthopaedic Surgery. July 2015. Accessed January 5, 2026. https://www.acgme.org /Portals/0/PDFs/Milestones/FootandAnkleMilestones.pdf
- Accreditation Council for Graduate Medical Education. Orthopaedic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /OrthopaedicSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Spinal Cord Injury Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/SpinalCordInjuryMedicineMilestones.pdf
- Accreditation Council for Graduate Medical Education. Geriatric Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /GeriatricMedicineMilestones.pdf
- Goldhamer ME, Baker K, Anne Rigg DW, et al. Development and implementation of multi-source assessment tools for ACGME residents and fellows. MedEDPORTAL. 2014. Accessed May 14, 2026. doi:10.15766/mep_2374-8265.9839
- Fife CE, Eckert KA, Carter MJ. Publicly Reported wound healing rates: the fantasy and the reality. Adv Wound Care (New Rochelle). 2018;7:77-94. doi:10.1089/wound.2017.0743
- Fife CE, Carter MJ, Walker D. Why is it so hard to do the right thing in wound care?. Wound Repair Regen. 2010;18:154-158. doi:10.1111/j.1524-475X.2010.00571.x
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771. doi:10.1111/j.1524-475X.2009.00543.x
- Queen D, Harding K. What’s the true costs of wounds faced by different healthcare systems around the world?. Int Wound J. 2023;20:3935-3938. doi:10.1111/iwj.14491
- Greer N, Foman N, Dorrian J, et al. Advanced Wound Care Therapies for Non-Healing Diabetic, Venous, and Arterial Ulcers: A Systematic Review [Internet]. US Dept of Veterans Affairs; November 2012. https://www.ncbi.nlm.nih.gov/books/NBK132238/
- Simman R, McNevin AJ. Pursuing the path to specialized wound care: the ABWMS perspective. Todays Wound Clin. 2017;8:10,12.
- Shahin ES, Dassen T, Halfens RJ. Pressure ulcer prevalence in intensive care patients: a cross-sectional study. J Eval Clin Pract. 2008;14:563-568. doi:10.1111/j.1365-2753.2007.00918.x
- Ennis WJ, Valdes W, Meneses P. Wound care specialization: a proposal for a comprehensive fellowship program. Wound Repair Regen. 2004;12:120-128. doi:10.1111/j.1067-1927.2004.012203.x
- Patel NP, Granick MS. Wound education: American medical students are inadequately trained in wound care. Ann Plast Surg. 2007;59:53-55. doi:10.1097/SAP.0b013e31802dd43b
- Patel NP, Granick MS, Kanakaris NK, et al. Comparison of wound education in medical schools in the United States, United Kingdom, and Germany. Eplasty. 2008;8:e8.
- Ennis WJ. Wound care specialization: the current status and future plans to move wound care into the medical community. Adv Wound Care (New Rochelle). 2012;1:184- 188. doi:10.1089/wound.2011.0346
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (fellowship). Updated September 3, 2025. Accessed January 15, 2026. https://www.acgme.org/globalassets/pfassets /programrequirements/2025-reformatted-requirements/cprfellowship_2025_reformatted.pdf
- Accreditation Council for Graduate Medical Education. Program directors’ guide to the common program requirements (fellowship). Updated December 2025. Accessed May 27, 2026. https://www .acgme.org/globalassets/pdfs/guide-to-the-common -program-requirements-fellowship.pdf
- Curriculum overview - wound care and hyperbaric medicine fellowship. Wake Forest University School of Medicine. 2026. Accessed January 5, 2026. https://school .wakehealth.edu/Education-and-Training/Residencies -and-Fellowships/Wound-Care-and-Hyperbaric-Medicine -Fellowship/Curriculum-Overview
- Curriculum overview - American Board of Wound Medicine and Surgery. Core Curriculum for Fellowships in Wound Care. American Board of Wound Medicine and Surgery. 2022. Accessed January 5, 2026. https://abwms.org /curriculum-overview/
- European Wound Management Association. EWMA Wound healing curriculum for physicians. February 13, 2017. Accessed January 15, 2026. https://ewma.org /wp-content/uploads/2024/02/ETR-TF-Wound-Healing -UEMS-approved.pdf
- Accreditation Council for Graduate Medical Education. Recommended Curriculum Guidelines for Family Medicine Residents. Accessed January 5, 2026. https://www.aafp .org/dam/AAFP/documents/medical_education_residency /program_directors/Wound_Care.pdf
- Accreditation Council for Graduate Medical Education. Vascular Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /VascularSurgeryMilestones2.0.pdf
- Accreditation Council for Graduate Medical Education. Plastic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/PlasticSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Dermatology Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /DermatologyMilestones.pdf
- Accreditation Council for Graduate Medical Education. The Foot and Ankle Milestone Project a joint initiative of the Accreditation Council for Graduate Medical Education and the American Board of Orthopaedic Surgery. July 2015. Accessed January 5, 2026. https://www.acgme.org /Portals/0/PDFs/Milestones/FootandAnkleMilestones.pdf
- Accreditation Council for Graduate Medical Education. Orthopaedic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /OrthopaedicSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Spinal Cord Injury Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/SpinalCordInjuryMedicineMilestones.pdf
- Accreditation Council for Graduate Medical Education. Geriatric Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /GeriatricMedicineMilestones.pdf
- Goldhamer ME, Baker K, Anne Rigg DW, et al. Development and implementation of multi-source assessment tools for ACGME residents and fellows. MedEDPORTAL. 2014. Accessed May 14, 2026. doi:10.15766/mep_2374-8265.9839
The Development of a Comprehensive Wound Care Fellowship Curriculum
The Development of a Comprehensive Wound Care Fellowship Curriculum


Medical Education and Firearm-Related Deaths
For the third straight year, firearms killed more children and teens than any other cause, including motor vehicle crashes and cancer. The population-wide toll taken by guns is equally as discouraging. Finally, this elephant in the room is getting some attention from the medical community, but the voices asking for change have most recently been coming from medical students who feel that gun violence deserves to be given a larger role in their education. It’s unclear why this plea is coming from the younger end of the medical community. It may be that, unlike most of their older instructors, these 18- to 25-year-olds have grown up under the growing threat of school shootings and become uncomfortably accustomed to active shooter drills.
Should We Look to Medical School for Answers?
But, does the medical community need to take gun violence more seriously than the rest of the population? What should our response look like? To answer those questions we need to take several steps back to view the bigger picture.

Is the medical community more responsible for this current situation than any other segment of the population? Do physicians bear any more culpability than publishers who sell gun-related magazines? Since its inception pediatrics has taken on the role of advocate for children and their health and well-being. But, is there more we can and should do other than turn up the volume on our advocacy?
While still taking the longer view, let’s ask ourselves what the role of medical school should be. Not just with respect to gun violence but in producing physicians and healthcare providers. We are approaching a crisis in primary care as it loses appeal with physicians at both ends of the age continuum. It could be because it pays poorly — certainly in relation to the cost of medical school — or because the awareness that if done well primary care requires a commitment that is difficult to square with many individuals’ lifestyle expectations.
Is the traditional medical school the right place to be training primary care providers? Medical school is currently aimed at broad and deep exposure. The student will be exposed to the all the diseases to which he or she might be seeing anywhere in the world and at the same time will have learned the mechanisms down to the cellular level that lies behind that pathology. Does a primary care pediatrician practicing in a small city or suburbia need that depth of training? He or she might benefit from some breadth. But maybe it should be focused on socioeconomic and geographic population the doctor is likely to see. This is particularly true for gun-related deaths.
Returning our attention to gun violence and its relation to healthcare, let’s ask ourselves what role the traditional medical school should play. Should it be a breeding ground for gun control advocates? When physicians speak people tend to listen but our effectiveness on issues such as immunizations and gun control has not been what many have hoped for. The supply of guns available to the public in this country is staggering and certainly contributes to gun-related injuries and death. However, I’m afraid that making a significant dent in that supply, given our political history and current climate, is an issue whose ship has sailed.
On the other hand, as gun advocates are often quoted as saying, “it’s not guns that kill, it’s people.” We don’t need to go into to the fallacy of this argument, but it gives us a starting point from which a medical school might focus its efforts on addressing the fallout from gun violence. A curriculum that begins with a presentation of the grizzly statistics and moves on to research about gun-related mental health issues and the social environments that breed violence makes good sense. Recanting the depressing history of how our society got to this place, in which guns outnumber people, should be part of the undergraduate curriculum.
Addressing the specifics of gun safety and suicide prevention in general with families and individuals would be more appropriate during clinical specialty training.
How big a chunk of the curriculum should be committed to gun violence and its fallout? Some of the call for change seems to be suggesting a semester-long course. However, we must accept the reality that instructional time in medical school is a finite asset. Although gunshots are the leading cause of death in children, how effective will even the most cleverly crafted curriculum be in moving the needle on the embarrassing data?
Given what is known about the problem, a day, or at most a week would be sufficient in class time. This could include personal presentations by victims or family members. I’m sure there are some who would see that as insufficient. But I see it as realistic. For the large urban schools, observing an evening shift in the trauma unit of an ER could be a potent addition.
Beyond this, a commitment by the school to host seminars and workshops devoted to gun violence could be an important component. It might also be helpful for a school or training program to promote the habit of whenever an instructor is introducing a potentially fatal disease to the students for the first time, he or she would begin with “To put this in perspective, you should remember that xxx thousand children die of gunshot wounds every year.”
Unfortunately, like obesity, gun-related deaths and injuries are the result of our society’s failure to muster the political will to act in our best interest as a nation. The medical community is left to clean up the collateral damage. There is always more that we could do, but we must be thoughtful in how we invest our energies in the effort.
Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
For the third straight year, firearms killed more children and teens than any other cause, including motor vehicle crashes and cancer. The population-wide toll taken by guns is equally as discouraging. Finally, this elephant in the room is getting some attention from the medical community, but the voices asking for change have most recently been coming from medical students who feel that gun violence deserves to be given a larger role in their education. It’s unclear why this plea is coming from the younger end of the medical community. It may be that, unlike most of their older instructors, these 18- to 25-year-olds have grown up under the growing threat of school shootings and become uncomfortably accustomed to active shooter drills.
Should We Look to Medical School for Answers?
But, does the medical community need to take gun violence more seriously than the rest of the population? What should our response look like? To answer those questions we need to take several steps back to view the bigger picture.
Is the medical community more responsible for this current situation than any other segment of the population? Do physicians bear any more culpability than publishers who sell gun-related magazines? Since its inception pediatrics has taken on the role of advocate for children and their health and well-being. But, is there more we can and should do other than turn up the volume on our advocacy?
While still taking the longer view, let’s ask ourselves what the role of medical school should be. Not just with respect to gun violence but in producing physicians and healthcare providers. We are approaching a crisis in primary care as it loses appeal with physicians at both ends of the age continuum. It could be because it pays poorly — certainly in relation to the cost of medical school — or because the awareness that if done well primary care requires a commitment that is difficult to square with many individuals’ lifestyle expectations.
Is the traditional medical school the right place to be training primary care providers? Medical school is currently aimed at broad and deep exposure. The student will be exposed to the all the diseases to which he or she might be seeing anywhere in the world and at the same time will have learned the mechanisms down to the cellular level that lies behind that pathology. Does a primary care pediatrician practicing in a small city or suburbia need that depth of training? He or she might benefit from some breadth. But maybe it should be focused on socioeconomic and geographic population the doctor is likely to see. This is particularly true for gun-related deaths.
Returning our attention to gun violence and its relation to healthcare, let’s ask ourselves what role the traditional medical school should play. Should it be a breeding ground for gun control advocates? When physicians speak people tend to listen but our effectiveness on issues such as immunizations and gun control has not been what many have hoped for. The supply of guns available to the public in this country is staggering and certainly contributes to gun-related injuries and death. However, I’m afraid that making a significant dent in that supply, given our political history and current climate, is an issue whose ship has sailed.
On the other hand, as gun advocates are often quoted as saying, “it’s not guns that kill, it’s people.” We don’t need to go into to the fallacy of this argument, but it gives us a starting point from which a medical school might focus its efforts on addressing the fallout from gun violence. A curriculum that begins with a presentation of the grizzly statistics and moves on to research about gun-related mental health issues and the social environments that breed violence makes good sense. Recanting the depressing history of how our society got to this place, in which guns outnumber people, should be part of the undergraduate curriculum.
Addressing the specifics of gun safety and suicide prevention in general with families and individuals would be more appropriate during clinical specialty training.
How big a chunk of the curriculum should be committed to gun violence and its fallout? Some of the call for change seems to be suggesting a semester-long course. However, we must accept the reality that instructional time in medical school is a finite asset. Although gunshots are the leading cause of death in children, how effective will even the most cleverly crafted curriculum be in moving the needle on the embarrassing data?
Given what is known about the problem, a day, or at most a week would be sufficient in class time. This could include personal presentations by victims or family members. I’m sure there are some who would see that as insufficient. But I see it as realistic. For the large urban schools, observing an evening shift in the trauma unit of an ER could be a potent addition.
Beyond this, a commitment by the school to host seminars and workshops devoted to gun violence could be an important component. It might also be helpful for a school or training program to promote the habit of whenever an instructor is introducing a potentially fatal disease to the students for the first time, he or she would begin with “To put this in perspective, you should remember that xxx thousand children die of gunshot wounds every year.”
Unfortunately, like obesity, gun-related deaths and injuries are the result of our society’s failure to muster the political will to act in our best interest as a nation. The medical community is left to clean up the collateral damage. There is always more that we could do, but we must be thoughtful in how we invest our energies in the effort.
Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
For the third straight year, firearms killed more children and teens than any other cause, including motor vehicle crashes and cancer. The population-wide toll taken by guns is equally as discouraging. Finally, this elephant in the room is getting some attention from the medical community, but the voices asking for change have most recently been coming from medical students who feel that gun violence deserves to be given a larger role in their education. It’s unclear why this plea is coming from the younger end of the medical community. It may be that, unlike most of their older instructors, these 18- to 25-year-olds have grown up under the growing threat of school shootings and become uncomfortably accustomed to active shooter drills.
Should We Look to Medical School for Answers?
But, does the medical community need to take gun violence more seriously than the rest of the population? What should our response look like? To answer those questions we need to take several steps back to view the bigger picture.
Is the medical community more responsible for this current situation than any other segment of the population? Do physicians bear any more culpability than publishers who sell gun-related magazines? Since its inception pediatrics has taken on the role of advocate for children and their health and well-being. But, is there more we can and should do other than turn up the volume on our advocacy?
While still taking the longer view, let’s ask ourselves what the role of medical school should be. Not just with respect to gun violence but in producing physicians and healthcare providers. We are approaching a crisis in primary care as it loses appeal with physicians at both ends of the age continuum. It could be because it pays poorly — certainly in relation to the cost of medical school — or because the awareness that if done well primary care requires a commitment that is difficult to square with many individuals’ lifestyle expectations.
Is the traditional medical school the right place to be training primary care providers? Medical school is currently aimed at broad and deep exposure. The student will be exposed to the all the diseases to which he or she might be seeing anywhere in the world and at the same time will have learned the mechanisms down to the cellular level that lies behind that pathology. Does a primary care pediatrician practicing in a small city or suburbia need that depth of training? He or she might benefit from some breadth. But maybe it should be focused on socioeconomic and geographic population the doctor is likely to see. This is particularly true for gun-related deaths.
Returning our attention to gun violence and its relation to healthcare, let’s ask ourselves what role the traditional medical school should play. Should it be a breeding ground for gun control advocates? When physicians speak people tend to listen but our effectiveness on issues such as immunizations and gun control has not been what many have hoped for. The supply of guns available to the public in this country is staggering and certainly contributes to gun-related injuries and death. However, I’m afraid that making a significant dent in that supply, given our political history and current climate, is an issue whose ship has sailed.
On the other hand, as gun advocates are often quoted as saying, “it’s not guns that kill, it’s people.” We don’t need to go into to the fallacy of this argument, but it gives us a starting point from which a medical school might focus its efforts on addressing the fallout from gun violence. A curriculum that begins with a presentation of the grizzly statistics and moves on to research about gun-related mental health issues and the social environments that breed violence makes good sense. Recanting the depressing history of how our society got to this place, in which guns outnumber people, should be part of the undergraduate curriculum.
Addressing the specifics of gun safety and suicide prevention in general with families and individuals would be more appropriate during clinical specialty training.
How big a chunk of the curriculum should be committed to gun violence and its fallout? Some of the call for change seems to be suggesting a semester-long course. However, we must accept the reality that instructional time in medical school is a finite asset. Although gunshots are the leading cause of death in children, how effective will even the most cleverly crafted curriculum be in moving the needle on the embarrassing data?
Given what is known about the problem, a day, or at most a week would be sufficient in class time. This could include personal presentations by victims or family members. I’m sure there are some who would see that as insufficient. But I see it as realistic. For the large urban schools, observing an evening shift in the trauma unit of an ER could be a potent addition.
Beyond this, a commitment by the school to host seminars and workshops devoted to gun violence could be an important component. It might also be helpful for a school or training program to promote the habit of whenever an instructor is introducing a potentially fatal disease to the students for the first time, he or she would begin with “To put this in perspective, you should remember that xxx thousand children die of gunshot wounds every year.”
Unfortunately, like obesity, gun-related deaths and injuries are the result of our society’s failure to muster the political will to act in our best interest as a nation. The medical community is left to clean up the collateral damage. There is always more that we could do, but we must be thoughtful in how we invest our energies in the effort.
Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Study Supports Pediatric Concussion Management Approach
“With that result, it means we don’t need to change management protocols” depending on the cause of the concussion, study author Andrée-Anne Ledoux, PhD, a scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Ontario, Canada, said in an interview. “That’s kind of good news. We’re applying the right management protocols with them.”
The data were published on December 4 in JAMA Network Open.
Secondary Analysis
The results stem from a planned secondary analysis of the prospective Predicting and Preventing Postconcussive Problems in Pediatrics study. Conducted from August 2013 to June 2015 at nine pediatric emergency departments in Canada, it included children of different ages (5 to < 18 years), genders, demographic characteristics, and comorbidities. All participants had a concussion.
The secondary analysis focused on study participants who were aged 5-12 years and had presented within 48 hours of injury. The primary outcome was symptom change, which was defined as current ratings minus preinjury ratings, across time (1, 2, 4, 8, and 12 weeks), measured using the Post-Concussion Symptom Inventory.
No significant differences in postinjury recovery curves were found between participants with sport-related concussions (SRC) and those with non-SRC. The latter injuries resulted from causes such as falls and objects dropped on heads. SRC and non-SRC showed a nonlinear association with time, with symptoms decreasing over time.
Perhaps surprisingly, the researchers also reported a higher rate of persisting symptoms after concussion (PSAC) following limited contact sports than following contact sports such as hockey, soccer, rugby, lacrosse, and football. Limited contact sports include activities such as bicycling, horseback riding, tobogganing, gymnastics, and cheerleading.
This finding suggests that the management of SRC may not require distinct strategies based on sports classification, the researchers wrote. “Instead, it may be more appropriate for clinicians to consider the specific dynamics of the activity, such as velocity and risk of falls from heights. This nuanced perspective can aid in assessing the likelihood of persisting symptoms.” The researchers urged more investigation of this question. “A larger sample with more information on injury height and velocity would be required to confirm whether an association exists.”
In addition, the researchers cited guidelines that include a recommendation for a gradual return to low to moderate physical and cognitive activity starting 24-48 hours after a concussion at a level that does not result in recurrence or exacerbation of symptoms.
“Children do need to return to their lives. They need to return to school,” said Ledoux. “They can have accommodations while they return to school, but just returning to school has huge benefits because you’re reintegrating the child into their typical lifestyle and socialization as well.”
A potential limitation of the study was its reliance on participants who had been seen in emergency departments and thus may have been experiencing more intense symptoms than those seen elsewhere.
The researchers also excluded cases of concussion resulting from assaults and motor vehicle crashes. This decision may explain why they didn’t reproduce the previous observation that patients with SRC tended to recover faster than those with concussions from other causes.
Injuries resulting from assaults and motor vehicle crashes can involve damage beyond concussions, Ledoux said. Including these cases would not allow for an apples-to-apples comparison of SRC and non-SRC.
‘Don’t Cocoon Kids’
The authors of an accompanying editorial wrote that the researchers had done “a beautiful job highlighting this important nuance.” Noncontact sports with seemingly little risk “actually carry substantial risks when one imagines the high-impact forces that can occur with a fall from height, albeit rare,” Scott Zuckerman, MD, MPH, assistant professor of neurological surgery at Vanderbilt University Medical Center, Nashville, Tennessee, and colleagues wrote.
The new analysis suggests a need to rethink a “somewhat archaic way of classifying sport risk, which may oversimplify how we categorize risk of brain and spine injuries.”
The commentary also noted how the researchers used the term PSAC to describe lingering symptoms instead of more widely used terms like “persistent postconcussive symptoms” or “postconcussive syndrome.”
“These traditional terms often connote a permanent syndrome or assumption that the concussion itself is solely responsible for 100% of symptoms, which can be harmful to a patient’s recovery,” the editorialists wrote. “Conversely, PSAC offers room for the clinician to discuss how other causes may be maintaining, magnifying, or mimicking concussion symptoms.”
Commenting on the findings, Richard Figler, MD, an orthopedic surgeon at the Cleveland Clinic, Cleveland, praised the researchers for addressing concussion in younger children, a field in which little research has been conducted. The research supports the current approaches to treatment. The approach has shifted toward easing children quickly and safely back into normal routines. “We don’t cocoon kids. We don’t send them to dark rooms,” Figler added.
He also commended the researchers’ decision to examine data about concussions linked to limited contact sports. In contact sports, participants may be more likely to anticipate and prepare for a hit. That’s not the case with injuries sustained in limited contact sports.
“Dodgeball is basically a sucker punch. That’s why these kids have so many concussions,” said Figler. “They typically don’t see the ball coming, or they can’t get out of the way, and they can’t tense themselves to take that blow.”
The Predicting and Preventing Postconcussive Problems in Pediatrics study was funded by the Canadian Institutes of Health Research and the Canadian Institutes of Health Research-Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team. Ledoux reported receiving grants from the Children’s Hospital of Eastern Ontario Foundation, Ontario Brain Institute, and University of Ottawa Brain and Mind Research Institute. She received nonfinancial support from Mobio Interactive outside the submitted work. Zuckerman reported receiving personal fees from the National Football League and Medtronic outside the submitted work. Figler had no relevant financial disclosures.
A version of this article appeared on Medscape.com.
“With that result, it means we don’t need to change management protocols” depending on the cause of the concussion, study author Andrée-Anne Ledoux, PhD, a scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Ontario, Canada, said in an interview. “That’s kind of good news. We’re applying the right management protocols with them.”
The data were published on December 4 in JAMA Network Open.
Secondary Analysis
The results stem from a planned secondary analysis of the prospective Predicting and Preventing Postconcussive Problems in Pediatrics study. Conducted from August 2013 to June 2015 at nine pediatric emergency departments in Canada, it included children of different ages (5 to < 18 years), genders, demographic characteristics, and comorbidities. All participants had a concussion.
The secondary analysis focused on study participants who were aged 5-12 years and had presented within 48 hours of injury. The primary outcome was symptom change, which was defined as current ratings minus preinjury ratings, across time (1, 2, 4, 8, and 12 weeks), measured using the Post-Concussion Symptom Inventory.
No significant differences in postinjury recovery curves were found between participants with sport-related concussions (SRC) and those with non-SRC. The latter injuries resulted from causes such as falls and objects dropped on heads. SRC and non-SRC showed a nonlinear association with time, with symptoms decreasing over time.
Perhaps surprisingly, the researchers also reported a higher rate of persisting symptoms after concussion (PSAC) following limited contact sports than following contact sports such as hockey, soccer, rugby, lacrosse, and football. Limited contact sports include activities such as bicycling, horseback riding, tobogganing, gymnastics, and cheerleading.
This finding suggests that the management of SRC may not require distinct strategies based on sports classification, the researchers wrote. “Instead, it may be more appropriate for clinicians to consider the specific dynamics of the activity, such as velocity and risk of falls from heights. This nuanced perspective can aid in assessing the likelihood of persisting symptoms.” The researchers urged more investigation of this question. “A larger sample with more information on injury height and velocity would be required to confirm whether an association exists.”
In addition, the researchers cited guidelines that include a recommendation for a gradual return to low to moderate physical and cognitive activity starting 24-48 hours after a concussion at a level that does not result in recurrence or exacerbation of symptoms.
“Children do need to return to their lives. They need to return to school,” said Ledoux. “They can have accommodations while they return to school, but just returning to school has huge benefits because you’re reintegrating the child into their typical lifestyle and socialization as well.”
A potential limitation of the study was its reliance on participants who had been seen in emergency departments and thus may have been experiencing more intense symptoms than those seen elsewhere.
The researchers also excluded cases of concussion resulting from assaults and motor vehicle crashes. This decision may explain why they didn’t reproduce the previous observation that patients with SRC tended to recover faster than those with concussions from other causes.
Injuries resulting from assaults and motor vehicle crashes can involve damage beyond concussions, Ledoux said. Including these cases would not allow for an apples-to-apples comparison of SRC and non-SRC.
‘Don’t Cocoon Kids’
The authors of an accompanying editorial wrote that the researchers had done “a beautiful job highlighting this important nuance.” Noncontact sports with seemingly little risk “actually carry substantial risks when one imagines the high-impact forces that can occur with a fall from height, albeit rare,” Scott Zuckerman, MD, MPH, assistant professor of neurological surgery at Vanderbilt University Medical Center, Nashville, Tennessee, and colleagues wrote.
The new analysis suggests a need to rethink a “somewhat archaic way of classifying sport risk, which may oversimplify how we categorize risk of brain and spine injuries.”
The commentary also noted how the researchers used the term PSAC to describe lingering symptoms instead of more widely used terms like “persistent postconcussive symptoms” or “postconcussive syndrome.”
“These traditional terms often connote a permanent syndrome or assumption that the concussion itself is solely responsible for 100% of symptoms, which can be harmful to a patient’s recovery,” the editorialists wrote. “Conversely, PSAC offers room for the clinician to discuss how other causes may be maintaining, magnifying, or mimicking concussion symptoms.”
Commenting on the findings, Richard Figler, MD, an orthopedic surgeon at the Cleveland Clinic, Cleveland, praised the researchers for addressing concussion in younger children, a field in which little research has been conducted. The research supports the current approaches to treatment. The approach has shifted toward easing children quickly and safely back into normal routines. “We don’t cocoon kids. We don’t send them to dark rooms,” Figler added.
He also commended the researchers’ decision to examine data about concussions linked to limited contact sports. In contact sports, participants may be more likely to anticipate and prepare for a hit. That’s not the case with injuries sustained in limited contact sports.
“Dodgeball is basically a sucker punch. That’s why these kids have so many concussions,” said Figler. “They typically don’t see the ball coming, or they can’t get out of the way, and they can’t tense themselves to take that blow.”
The Predicting and Preventing Postconcussive Problems in Pediatrics study was funded by the Canadian Institutes of Health Research and the Canadian Institutes of Health Research-Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team. Ledoux reported receiving grants from the Children’s Hospital of Eastern Ontario Foundation, Ontario Brain Institute, and University of Ottawa Brain and Mind Research Institute. She received nonfinancial support from Mobio Interactive outside the submitted work. Zuckerman reported receiving personal fees from the National Football League and Medtronic outside the submitted work. Figler had no relevant financial disclosures.
A version of this article appeared on Medscape.com.
“With that result, it means we don’t need to change management protocols” depending on the cause of the concussion, study author Andrée-Anne Ledoux, PhD, a scientist at Children’s Hospital of Eastern Ontario Research Institute in Ottawa, Ontario, Canada, said in an interview. “That’s kind of good news. We’re applying the right management protocols with them.”
The data were published on December 4 in JAMA Network Open.
Secondary Analysis
The results stem from a planned secondary analysis of the prospective Predicting and Preventing Postconcussive Problems in Pediatrics study. Conducted from August 2013 to June 2015 at nine pediatric emergency departments in Canada, it included children of different ages (5 to < 18 years), genders, demographic characteristics, and comorbidities. All participants had a concussion.
The secondary analysis focused on study participants who were aged 5-12 years and had presented within 48 hours of injury. The primary outcome was symptom change, which was defined as current ratings minus preinjury ratings, across time (1, 2, 4, 8, and 12 weeks), measured using the Post-Concussion Symptom Inventory.
No significant differences in postinjury recovery curves were found between participants with sport-related concussions (SRC) and those with non-SRC. The latter injuries resulted from causes such as falls and objects dropped on heads. SRC and non-SRC showed a nonlinear association with time, with symptoms decreasing over time.
Perhaps surprisingly, the researchers also reported a higher rate of persisting symptoms after concussion (PSAC) following limited contact sports than following contact sports such as hockey, soccer, rugby, lacrosse, and football. Limited contact sports include activities such as bicycling, horseback riding, tobogganing, gymnastics, and cheerleading.
This finding suggests that the management of SRC may not require distinct strategies based on sports classification, the researchers wrote. “Instead, it may be more appropriate for clinicians to consider the specific dynamics of the activity, such as velocity and risk of falls from heights. This nuanced perspective can aid in assessing the likelihood of persisting symptoms.” The researchers urged more investigation of this question. “A larger sample with more information on injury height and velocity would be required to confirm whether an association exists.”
In addition, the researchers cited guidelines that include a recommendation for a gradual return to low to moderate physical and cognitive activity starting 24-48 hours after a concussion at a level that does not result in recurrence or exacerbation of symptoms.
“Children do need to return to their lives. They need to return to school,” said Ledoux. “They can have accommodations while they return to school, but just returning to school has huge benefits because you’re reintegrating the child into their typical lifestyle and socialization as well.”
A potential limitation of the study was its reliance on participants who had been seen in emergency departments and thus may have been experiencing more intense symptoms than those seen elsewhere.
The researchers also excluded cases of concussion resulting from assaults and motor vehicle crashes. This decision may explain why they didn’t reproduce the previous observation that patients with SRC tended to recover faster than those with concussions from other causes.
Injuries resulting from assaults and motor vehicle crashes can involve damage beyond concussions, Ledoux said. Including these cases would not allow for an apples-to-apples comparison of SRC and non-SRC.
‘Don’t Cocoon Kids’
The authors of an accompanying editorial wrote that the researchers had done “a beautiful job highlighting this important nuance.” Noncontact sports with seemingly little risk “actually carry substantial risks when one imagines the high-impact forces that can occur with a fall from height, albeit rare,” Scott Zuckerman, MD, MPH, assistant professor of neurological surgery at Vanderbilt University Medical Center, Nashville, Tennessee, and colleagues wrote.
The new analysis suggests a need to rethink a “somewhat archaic way of classifying sport risk, which may oversimplify how we categorize risk of brain and spine injuries.”
The commentary also noted how the researchers used the term PSAC to describe lingering symptoms instead of more widely used terms like “persistent postconcussive symptoms” or “postconcussive syndrome.”
“These traditional terms often connote a permanent syndrome or assumption that the concussion itself is solely responsible for 100% of symptoms, which can be harmful to a patient’s recovery,” the editorialists wrote. “Conversely, PSAC offers room for the clinician to discuss how other causes may be maintaining, magnifying, or mimicking concussion symptoms.”
Commenting on the findings, Richard Figler, MD, an orthopedic surgeon at the Cleveland Clinic, Cleveland, praised the researchers for addressing concussion in younger children, a field in which little research has been conducted. The research supports the current approaches to treatment. The approach has shifted toward easing children quickly and safely back into normal routines. “We don’t cocoon kids. We don’t send them to dark rooms,” Figler added.
He also commended the researchers’ decision to examine data about concussions linked to limited contact sports. In contact sports, participants may be more likely to anticipate and prepare for a hit. That’s not the case with injuries sustained in limited contact sports.
“Dodgeball is basically a sucker punch. That’s why these kids have so many concussions,” said Figler. “They typically don’t see the ball coming, or they can’t get out of the way, and they can’t tense themselves to take that blow.”
The Predicting and Preventing Postconcussive Problems in Pediatrics study was funded by the Canadian Institutes of Health Research and the Canadian Institutes of Health Research-Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team. Ledoux reported receiving grants from the Children’s Hospital of Eastern Ontario Foundation, Ontario Brain Institute, and University of Ottawa Brain and Mind Research Institute. She received nonfinancial support from Mobio Interactive outside the submitted work. Zuckerman reported receiving personal fees from the National Football League and Medtronic outside the submitted work. Figler had no relevant financial disclosures.
A version of this article appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Clinicians More Likely to Flag Black Kids’ Injuries as Abuse
TOPLINE:
Among children with traumatic injury, those of Black ethnicity are more likely than those of White ethnicity to be suspected of experiencing child abuse. Young patients and those from low socioeconomic backgrounds also face an increased likelihood of suspicion for child abuse (SCA).
METHODOLOGY:
- Researchers analyzed data on pediatric patients admitted to hospitals after sustaining a traumatic injury between 2006 and 2016 using the Kids’ Inpatient Database (KID) to investigate racial and ethnic disparities in cases in which SCA codes from the 9th and 10th editions of the International Classification of Diseases were used.
- The analysis included a weighted total of 634,309 pediatric patients with complete data, comprising 13,579 patients in the SCA subgroup and 620,730 in the non-SCA subgroup.
- Patient demographics, injury severity, and hospitalization characteristics were classified by race and ethnicity.
- The primary outcome was differences in racial and ethnic composition between the SCA and non-SCA groups, as well as compared with the overall US population using 2010 US Census data.
TAKEAWAY:
- Black patients had 75% higher odds of having a SCA code, compared with White patients; the latter ethnicity was relatively underrepresented in the SCA subgroup, compared with the distribution reported by the US Census.
- Black patients had 10% higher odds of having a SCA code (odds ratio, 1.10; P =.004) than White patients, after socioeconomic factors such as insurance type, household income based on zip code, and injury severity were controlled for.
- Black patients in the SCA subgroup experienced a 26.5% (P < .001) longer hospital stay for mild to moderate injuries and a 40.1% (P < .001) longer stay for serious injuries compared with White patients.
- Patients in the SCA subgroup were significantly younger (mean, 1.70 years vs 9.70 years), were more likely to have Medicaid insurance (76.6% vs 42.0%), and had higher mortality rates (5.6% vs 1.0%) than those in the non-SCA subgroup; they were also more likely to come from lower socioeconomic backgrounds and present with more severe injuries.
IN PRACTICE:
“However, we can identify and appropriately respond to patients with potential child abuse in an equitable way by using clinical decision support tools, seeking clinical consultation of child abuse pediatricians, practicing cultural humility, and enhancing the education and training for health care professionals on child abuse recognition, response, and prevention,” Allison M. Jackson, MD, MPH, of the Child and Adolescent Protection Center at Children’s National Hospital, Washington, DC, wrote in an accompanying editorial.
SOURCE:
The study was led by Fereshteh Salimi-Jazi, MD, of Stanford University School of Medicine in California. It was published online on December 18, 2024, in JAMA Network Open.
LIMITATIONS:
The study relied on data from KID, which has limitations such as potential coding errors and the inability to follow patients over time. The database combines race and ethnicity in a single field as well. The study only included hospitalized patients, which may not represent all clinician suspicions of SCA cases.
DISCLOSURES:
This study was supported by a grant from the National Center for Advancing Translational Sciences of the National Institutes of Health. The authors reported no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Among children with traumatic injury, those of Black ethnicity are more likely than those of White ethnicity to be suspected of experiencing child abuse. Young patients and those from low socioeconomic backgrounds also face an increased likelihood of suspicion for child abuse (SCA).
METHODOLOGY:
- Researchers analyzed data on pediatric patients admitted to hospitals after sustaining a traumatic injury between 2006 and 2016 using the Kids’ Inpatient Database (KID) to investigate racial and ethnic disparities in cases in which SCA codes from the 9th and 10th editions of the International Classification of Diseases were used.
- The analysis included a weighted total of 634,309 pediatric patients with complete data, comprising 13,579 patients in the SCA subgroup and 620,730 in the non-SCA subgroup.
- Patient demographics, injury severity, and hospitalization characteristics were classified by race and ethnicity.
- The primary outcome was differences in racial and ethnic composition between the SCA and non-SCA groups, as well as compared with the overall US population using 2010 US Census data.
TAKEAWAY:
- Black patients had 75% higher odds of having a SCA code, compared with White patients; the latter ethnicity was relatively underrepresented in the SCA subgroup, compared with the distribution reported by the US Census.
- Black patients had 10% higher odds of having a SCA code (odds ratio, 1.10; P =.004) than White patients, after socioeconomic factors such as insurance type, household income based on zip code, and injury severity were controlled for.
- Black patients in the SCA subgroup experienced a 26.5% (P < .001) longer hospital stay for mild to moderate injuries and a 40.1% (P < .001) longer stay for serious injuries compared with White patients.
- Patients in the SCA subgroup were significantly younger (mean, 1.70 years vs 9.70 years), were more likely to have Medicaid insurance (76.6% vs 42.0%), and had higher mortality rates (5.6% vs 1.0%) than those in the non-SCA subgroup; they were also more likely to come from lower socioeconomic backgrounds and present with more severe injuries.
IN PRACTICE:
“However, we can identify and appropriately respond to patients with potential child abuse in an equitable way by using clinical decision support tools, seeking clinical consultation of child abuse pediatricians, practicing cultural humility, and enhancing the education and training for health care professionals on child abuse recognition, response, and prevention,” Allison M. Jackson, MD, MPH, of the Child and Adolescent Protection Center at Children’s National Hospital, Washington, DC, wrote in an accompanying editorial.
SOURCE:
The study was led by Fereshteh Salimi-Jazi, MD, of Stanford University School of Medicine in California. It was published online on December 18, 2024, in JAMA Network Open.
LIMITATIONS:
The study relied on data from KID, which has limitations such as potential coding errors and the inability to follow patients over time. The database combines race and ethnicity in a single field as well. The study only included hospitalized patients, which may not represent all clinician suspicions of SCA cases.
DISCLOSURES:
This study was supported by a grant from the National Center for Advancing Translational Sciences of the National Institutes of Health. The authors reported no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Among children with traumatic injury, those of Black ethnicity are more likely than those of White ethnicity to be suspected of experiencing child abuse. Young patients and those from low socioeconomic backgrounds also face an increased likelihood of suspicion for child abuse (SCA).
METHODOLOGY:
- Researchers analyzed data on pediatric patients admitted to hospitals after sustaining a traumatic injury between 2006 and 2016 using the Kids’ Inpatient Database (KID) to investigate racial and ethnic disparities in cases in which SCA codes from the 9th and 10th editions of the International Classification of Diseases were used.
- The analysis included a weighted total of 634,309 pediatric patients with complete data, comprising 13,579 patients in the SCA subgroup and 620,730 in the non-SCA subgroup.
- Patient demographics, injury severity, and hospitalization characteristics were classified by race and ethnicity.
- The primary outcome was differences in racial and ethnic composition between the SCA and non-SCA groups, as well as compared with the overall US population using 2010 US Census data.
TAKEAWAY:
- Black patients had 75% higher odds of having a SCA code, compared with White patients; the latter ethnicity was relatively underrepresented in the SCA subgroup, compared with the distribution reported by the US Census.
- Black patients had 10% higher odds of having a SCA code (odds ratio, 1.10; P =.004) than White patients, after socioeconomic factors such as insurance type, household income based on zip code, and injury severity were controlled for.
- Black patients in the SCA subgroup experienced a 26.5% (P < .001) longer hospital stay for mild to moderate injuries and a 40.1% (P < .001) longer stay for serious injuries compared with White patients.
- Patients in the SCA subgroup were significantly younger (mean, 1.70 years vs 9.70 years), were more likely to have Medicaid insurance (76.6% vs 42.0%), and had higher mortality rates (5.6% vs 1.0%) than those in the non-SCA subgroup; they were also more likely to come from lower socioeconomic backgrounds and present with more severe injuries.
IN PRACTICE:
“However, we can identify and appropriately respond to patients with potential child abuse in an equitable way by using clinical decision support tools, seeking clinical consultation of child abuse pediatricians, practicing cultural humility, and enhancing the education and training for health care professionals on child abuse recognition, response, and prevention,” Allison M. Jackson, MD, MPH, of the Child and Adolescent Protection Center at Children’s National Hospital, Washington, DC, wrote in an accompanying editorial.
SOURCE:
The study was led by Fereshteh Salimi-Jazi, MD, of Stanford University School of Medicine in California. It was published online on December 18, 2024, in JAMA Network Open.
LIMITATIONS:
The study relied on data from KID, which has limitations such as potential coding errors and the inability to follow patients over time. The database combines race and ethnicity in a single field as well. The study only included hospitalized patients, which may not represent all clinician suspicions of SCA cases.
DISCLOSURES:
This study was supported by a grant from the National Center for Advancing Translational Sciences of the National Institutes of Health. The authors reported no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Nodding Off While Feeding an Infant
In a recent survey of 1259 mothers published in the journal Pediatrics, 28% reported they had fallen asleep while feeding their babies, and 83% of those mothers reported that the sleep was unplanned. Although the study sample was small, the investigators found that sociodemographic factors did not increase the odds that a mother would fall asleep while feeding.
These numbers are not surprising, but nonetheless they are concerning because co-sleeping is a known risk factor for sudden unexplained infant death (SUID). Every parent will tell you during the first 6 months of their adventure in parenting they didn’t get enough sleep. In fact some will tell you that sleep deprivation was their chronic state for the child’s first year.
Falling asleep easily at times and places not intended for sleep is the primary symptom of sleep deprivation. SUID is the most tragic event associated with parental sleep deprivation, but it is certainly not the only one. Overtired parents are more likely to be involved in accidents and are more likely to make poor decisions, particularly those regarding how to respond to a crying or misbehaving child.
The investigators found that 24% of mothers who reported that their usual nighttime feeding location was a chair or sofa (14%). Not surprisingly, mothers who fed in chairs were less likely to fall asleep while feeding. Many of these mothers reported that they chose the chair because they thought they would be less likely to fall asleep and/or disturb other family members. One wonders how we should interpret these numbers in light of other research that has found it is “relatively less hazardous to fall asleep with an infant in the adult bed than on a chair or sofa.” Had these chair feeding mothers made the better choice under the circumstances? It would take a much larger and more granular study to answer that question.
Mothers who exclusively breastfed were more likely to fall asleep feeding than were those who partially breastfed or used formula. The investigators postulated that the infants of mothers who exclusively breastfed may have required more feedings because breast milk is more easily and quickly digested. I know this is a common explanation, but in my experience I have found that exclusively breastfed infants often use nursing as pacification and a sleep trigger and spend more time at the breast regardless of how quickly they emptied their stomachs.
This study also examined the effect of repeated educational interventions and support and found that mothers who received an intervention based on safe sleep practices were less likely to fall asleep while feeding than were the mothers who had received the intervention focused on exclusive breastfeeding value and barriers to its adoption.
Education is one avenue, particularly when it includes the mother’s partner who can play an important role as standby lifeguard to make sure the mother doesn’t fall asleep. Obviously, this is easier said than done because when there is a new baby in the house sleep deprivation is usually a shared experience.
Although I believe that my family is on the verge of gifting me a smartwatch to protect me from my own misadventures, I don’t have any personal experience with these wonders of modern technology. However, I suspect with very little tweaking a wearable sensor could be easily programmed to detect when a mother is beginning to fall asleep while she is feeding her infant. A smartwatch would be an expensive intervention and is unlikely to filter down to economically challenged families. On the other hand, this paper has reinforced our suspicions that sleep-deprived infant feeding is a significant problem. A subsidized loaner program for those families that can’t afford a smartwatch is an option that should be considered.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
In a recent survey of 1259 mothers published in the journal Pediatrics, 28% reported they had fallen asleep while feeding their babies, and 83% of those mothers reported that the sleep was unplanned. Although the study sample was small, the investigators found that sociodemographic factors did not increase the odds that a mother would fall asleep while feeding.
These numbers are not surprising, but nonetheless they are concerning because co-sleeping is a known risk factor for sudden unexplained infant death (SUID). Every parent will tell you during the first 6 months of their adventure in parenting they didn’t get enough sleep. In fact some will tell you that sleep deprivation was their chronic state for the child’s first year.
Falling asleep easily at times and places not intended for sleep is the primary symptom of sleep deprivation. SUID is the most tragic event associated with parental sleep deprivation, but it is certainly not the only one. Overtired parents are more likely to be involved in accidents and are more likely to make poor decisions, particularly those regarding how to respond to a crying or misbehaving child.
The investigators found that 24% of mothers who reported that their usual nighttime feeding location was a chair or sofa (14%). Not surprisingly, mothers who fed in chairs were less likely to fall asleep while feeding. Many of these mothers reported that they chose the chair because they thought they would be less likely to fall asleep and/or disturb other family members. One wonders how we should interpret these numbers in light of other research that has found it is “relatively less hazardous to fall asleep with an infant in the adult bed than on a chair or sofa.” Had these chair feeding mothers made the better choice under the circumstances? It would take a much larger and more granular study to answer that question.
Mothers who exclusively breastfed were more likely to fall asleep feeding than were those who partially breastfed or used formula. The investigators postulated that the infants of mothers who exclusively breastfed may have required more feedings because breast milk is more easily and quickly digested. I know this is a common explanation, but in my experience I have found that exclusively breastfed infants often use nursing as pacification and a sleep trigger and spend more time at the breast regardless of how quickly they emptied their stomachs.
This study also examined the effect of repeated educational interventions and support and found that mothers who received an intervention based on safe sleep practices were less likely to fall asleep while feeding than were the mothers who had received the intervention focused on exclusive breastfeeding value and barriers to its adoption.
Education is one avenue, particularly when it includes the mother’s partner who can play an important role as standby lifeguard to make sure the mother doesn’t fall asleep. Obviously, this is easier said than done because when there is a new baby in the house sleep deprivation is usually a shared experience.
Although I believe that my family is on the verge of gifting me a smartwatch to protect me from my own misadventures, I don’t have any personal experience with these wonders of modern technology. However, I suspect with very little tweaking a wearable sensor could be easily programmed to detect when a mother is beginning to fall asleep while she is feeding her infant. A smartwatch would be an expensive intervention and is unlikely to filter down to economically challenged families. On the other hand, this paper has reinforced our suspicions that sleep-deprived infant feeding is a significant problem. A subsidized loaner program for those families that can’t afford a smartwatch is an option that should be considered.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
In a recent survey of 1259 mothers published in the journal Pediatrics, 28% reported they had fallen asleep while feeding their babies, and 83% of those mothers reported that the sleep was unplanned. Although the study sample was small, the investigators found that sociodemographic factors did not increase the odds that a mother would fall asleep while feeding.
These numbers are not surprising, but nonetheless they are concerning because co-sleeping is a known risk factor for sudden unexplained infant death (SUID). Every parent will tell you during the first 6 months of their adventure in parenting they didn’t get enough sleep. In fact some will tell you that sleep deprivation was their chronic state for the child’s first year.
Falling asleep easily at times and places not intended for sleep is the primary symptom of sleep deprivation. SUID is the most tragic event associated with parental sleep deprivation, but it is certainly not the only one. Overtired parents are more likely to be involved in accidents and are more likely to make poor decisions, particularly those regarding how to respond to a crying or misbehaving child.
The investigators found that 24% of mothers who reported that their usual nighttime feeding location was a chair or sofa (14%). Not surprisingly, mothers who fed in chairs were less likely to fall asleep while feeding. Many of these mothers reported that they chose the chair because they thought they would be less likely to fall asleep and/or disturb other family members. One wonders how we should interpret these numbers in light of other research that has found it is “relatively less hazardous to fall asleep with an infant in the adult bed than on a chair or sofa.” Had these chair feeding mothers made the better choice under the circumstances? It would take a much larger and more granular study to answer that question.
Mothers who exclusively breastfed were more likely to fall asleep feeding than were those who partially breastfed or used formula. The investigators postulated that the infants of mothers who exclusively breastfed may have required more feedings because breast milk is more easily and quickly digested. I know this is a common explanation, but in my experience I have found that exclusively breastfed infants often use nursing as pacification and a sleep trigger and spend more time at the breast regardless of how quickly they emptied their stomachs.
This study also examined the effect of repeated educational interventions and support and found that mothers who received an intervention based on safe sleep practices were less likely to fall asleep while feeding than were the mothers who had received the intervention focused on exclusive breastfeeding value and barriers to its adoption.
Education is one avenue, particularly when it includes the mother’s partner who can play an important role as standby lifeguard to make sure the mother doesn’t fall asleep. Obviously, this is easier said than done because when there is a new baby in the house sleep deprivation is usually a shared experience.
Although I believe that my family is on the verge of gifting me a smartwatch to protect me from my own misadventures, I don’t have any personal experience with these wonders of modern technology. However, I suspect with very little tweaking a wearable sensor could be easily programmed to detect when a mother is beginning to fall asleep while she is feeding her infant. A smartwatch would be an expensive intervention and is unlikely to filter down to economically challenged families. On the other hand, this paper has reinforced our suspicions that sleep-deprived infant feeding is a significant problem. A subsidized loaner program for those families that can’t afford a smartwatch is an option that should be considered.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Fibrosis Risk High in Young Adults With Both Obesity and T2D
TOPLINE:
METHODOLOGY:
- Researchers aimed to assess the prevalence of hepatic steatosis and clinically significant fibrosis (stage ≥ 2) in young adults without a history of metabolic dysfunction–associated steatotic liver disease (MASLD), hypothesizing that the rates would be comparable with those in older adults, especially in the presence of cardiometabolic risk factors.
- Overall, 1420 participants aged 21-79 years with or without T2D (63% or 37%, respectively) were included from outpatient clinics at the University of Florida, Gainesville, Florida, and divided into two age groups: < 45 years (n = 243) and ≥ 45 years (n = 1177).
- All the participants underwent assessment of liver stiffness via transient elastography, with magnetic resonance elastography (MRE) or liver biopsy recommended when indicated.
- Participants also underwent a medical history review, physical examination, and fasting blood tests to rule out secondary causes of liver disease.
TAKEAWAY:
- Overall, 52% of participants had hepatic steatosis, and 9.5% had clinically significant fibrosis.
- There were no significant differences in the frequencies of hepatic steatosis (50.2% vs 52.7%; P = .6) or clinically significant hepatic fibrosis (7.5% vs 9.9%; P = .2) observed between young and older adults.
- The presence of either T2D or obesity was linked to an increased prevalence of both hepatic steatosis and fibrosis in both the age groups (P < .01).
- In young and older adults, the presence of both T2D and obesity led to the highest rates of both hepatic steatosis and clinically significant fibrosis, with the latter rate being statistically similar between the groups (15.7% vs 17.3%; P = .2).
- The presence of T2D and obesity was the strongest risk factors for hepatic fibrosis in young adults (odds ratios, 4.33 and 1.16, respectively; P < .05 for both).
IN PRACTICE:
“The clinical implication is that young adults with obesity and T2D carry a high risk of future cirrhosis, possibly as high as older adults, and must be aggressively screened at the first visit and carefully followed,” the authors wrote.
SOURCE:
This study, led by Anu Sharma, University of Florida College of Medicine, Gainesville, was published online in Obesity.
LIMITATIONS:
The diagnosis of clinically significant hepatic fibrosis was confirmed via MRE and/or liver biopsy in only 30% of all participants. The study population included a slightly higher proportion of young adults with obesity, T2D, and other cardiometabolic risk factors than that in national averages, which may have limited its generalizability. Genetic variants associated with MASLD were not included in this study.
DISCLOSURES:
This study was funded partly by grants from the National Institutes of Health and Echosens. One author disclosed receiving research support and serving as a consultant for various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers aimed to assess the prevalence of hepatic steatosis and clinically significant fibrosis (stage ≥ 2) in young adults without a history of metabolic dysfunction–associated steatotic liver disease (MASLD), hypothesizing that the rates would be comparable with those in older adults, especially in the presence of cardiometabolic risk factors.
- Overall, 1420 participants aged 21-79 years with or without T2D (63% or 37%, respectively) were included from outpatient clinics at the University of Florida, Gainesville, Florida, and divided into two age groups: < 45 years (n = 243) and ≥ 45 years (n = 1177).
- All the participants underwent assessment of liver stiffness via transient elastography, with magnetic resonance elastography (MRE) or liver biopsy recommended when indicated.
- Participants also underwent a medical history review, physical examination, and fasting blood tests to rule out secondary causes of liver disease.
TAKEAWAY:
- Overall, 52% of participants had hepatic steatosis, and 9.5% had clinically significant fibrosis.
- There were no significant differences in the frequencies of hepatic steatosis (50.2% vs 52.7%; P = .6) or clinically significant hepatic fibrosis (7.5% vs 9.9%; P = .2) observed between young and older adults.
- The presence of either T2D or obesity was linked to an increased prevalence of both hepatic steatosis and fibrosis in both the age groups (P < .01).
- In young and older adults, the presence of both T2D and obesity led to the highest rates of both hepatic steatosis and clinically significant fibrosis, with the latter rate being statistically similar between the groups (15.7% vs 17.3%; P = .2).
- The presence of T2D and obesity was the strongest risk factors for hepatic fibrosis in young adults (odds ratios, 4.33 and 1.16, respectively; P < .05 for both).
IN PRACTICE:
“The clinical implication is that young adults with obesity and T2D carry a high risk of future cirrhosis, possibly as high as older adults, and must be aggressively screened at the first visit and carefully followed,” the authors wrote.
SOURCE:
This study, led by Anu Sharma, University of Florida College of Medicine, Gainesville, was published online in Obesity.
LIMITATIONS:
The diagnosis of clinically significant hepatic fibrosis was confirmed via MRE and/or liver biopsy in only 30% of all participants. The study population included a slightly higher proportion of young adults with obesity, T2D, and other cardiometabolic risk factors than that in national averages, which may have limited its generalizability. Genetic variants associated with MASLD were not included in this study.
DISCLOSURES:
This study was funded partly by grants from the National Institutes of Health and Echosens. One author disclosed receiving research support and serving as a consultant for various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers aimed to assess the prevalence of hepatic steatosis and clinically significant fibrosis (stage ≥ 2) in young adults without a history of metabolic dysfunction–associated steatotic liver disease (MASLD), hypothesizing that the rates would be comparable with those in older adults, especially in the presence of cardiometabolic risk factors.
- Overall, 1420 participants aged 21-79 years with or without T2D (63% or 37%, respectively) were included from outpatient clinics at the University of Florida, Gainesville, Florida, and divided into two age groups: < 45 years (n = 243) and ≥ 45 years (n = 1177).
- All the participants underwent assessment of liver stiffness via transient elastography, with magnetic resonance elastography (MRE) or liver biopsy recommended when indicated.
- Participants also underwent a medical history review, physical examination, and fasting blood tests to rule out secondary causes of liver disease.
TAKEAWAY:
- Overall, 52% of participants had hepatic steatosis, and 9.5% had clinically significant fibrosis.
- There were no significant differences in the frequencies of hepatic steatosis (50.2% vs 52.7%; P = .6) or clinically significant hepatic fibrosis (7.5% vs 9.9%; P = .2) observed between young and older adults.
- The presence of either T2D or obesity was linked to an increased prevalence of both hepatic steatosis and fibrosis in both the age groups (P < .01).
- In young and older adults, the presence of both T2D and obesity led to the highest rates of both hepatic steatosis and clinically significant fibrosis, with the latter rate being statistically similar between the groups (15.7% vs 17.3%; P = .2).
- The presence of T2D and obesity was the strongest risk factors for hepatic fibrosis in young adults (odds ratios, 4.33 and 1.16, respectively; P < .05 for both).
IN PRACTICE:
“The clinical implication is that young adults with obesity and T2D carry a high risk of future cirrhosis, possibly as high as older adults, and must be aggressively screened at the first visit and carefully followed,” the authors wrote.
SOURCE:
This study, led by Anu Sharma, University of Florida College of Medicine, Gainesville, was published online in Obesity.
LIMITATIONS:
The diagnosis of clinically significant hepatic fibrosis was confirmed via MRE and/or liver biopsy in only 30% of all participants. The study population included a slightly higher proportion of young adults with obesity, T2D, and other cardiometabolic risk factors than that in national averages, which may have limited its generalizability. Genetic variants associated with MASLD were not included in this study.
DISCLOSURES:
This study was funded partly by grants from the National Institutes of Health and Echosens. One author disclosed receiving research support and serving as a consultant for various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Satisfaction With Department of Veterans Affairs Prosthetics and Support Services as Reported by Women and Men Veterans
Satisfaction With Department of Veterans Affairs Prosthetics and Support Services as Reported by Women and Men Veterans
Limb loss is a significant and growing concern in the United States. Nearly 2 million Americans are living with limb loss, and up to 185,000 people undergo amputations annually.1-4 Of these patients, about 35% are women.5 The Veterans Health Administration (VHA) provides about 10% of US amputations.6-8 Between 2015 and 2019, the number of prosthetic devices provided to female veterans increased from 3.3 million to 4.6 million.5,9,10
Previous research identified disparities in prosthetic care between men and women, both within and outside the VHA. These disparities include slower prosthesis prescription and receipt among women, in addition to differences in self-reported mobility, satisfaction, rates of prosthesis rejection, and challenges related to prosthesis appearance and fit.5,10,11 Recent studies suggest women tend to have worse outcomes following amputation, and are underrepresented in amputation research.12,13 However, these disparities are poorly described in a large, national sample. Because women represent a growing portion of patients with limb loss in the VHA, understanding their needs is critical.14
The Johnny Isakson and David P. Roe, MD Veterans Health Care and Benefits Improvement Act of 2020 was enacted, in part, to improve the care provided to women veterans.15 The law required the VHA to conduct a survey of ≥ 50,000 veterans to assess the satisfaction of women veterans with prostheses provided by the VHA. To comply with this legislation and understand how women veterans rate their prostheses and related care in the VHA, the US Department of Veterans Affairs (VA) Center for Collaborative Evaluation (VACE) conducted a large national survey of veterans with limb loss that oversampled women veterans. This article describes the survey results, including characteristics of female veterans with limb loss receiving care from the VHA, assesses their satisfaction with prostheses and prosthetic care, and highlights where their responses differ from those of male veterans.
Methods
We conducted a cross-sectional, mixedmode survey of eligible amputees in the VHA Support Service Capital Assets Amputee Data Cube. We identified a cohort of veterans with any major amputation (above the ankle or wrist) or partial hand or foot amputation who received VHA care between October 1, 2019, and September 30, 2020. The final cohort yielded 46,646 potentially eligible veterans. Thirty-three had invalid contact information, leaving 46,613 veterans who were asked to participate, including 1356 women.
Survey
We created a survey instrument de novo that included questions from validated instruments, including the Trinity Amputation Prosthesis and Experience Scales to assess prosthetic device satisfaction, the Prosthesis Evaluation Questionnaire to assess quality of life (QOL) satisfaction, and the Orthotics Prosthetics Users Survey to assess prosthesis-related care satisfaction. 16-18 Additional questions were incorporated from a survey of veterans with upper limb amputation to assess the importance of cosmetic considerations related to the prosthesis and comfort with prosthesis use in intimate relationships.19 Questions were also included to assess amputation type, year of amputation, if a prosthesis was currently used, reasons for ceasing use of a prosthesis, reasons for never using a prosthesis, the types of prostheses used, intensity of prosthesis use, satisfaction with time required to receive a prosthetic limb, and if the prosthesis reflected the veteran’s selfidentified gender. Veterans were asked to answer questions based on their most recent amputation.
We tested the survey using cognitive interviews with 6 veterans to refine the survey and better understand how veterans interpreted the questions. Pilot testers completed the survey and participated in individual interviews with experienced interviewers (CL and RRK) to describe how they selected their responses.20 This feedback was used to refine the survey. The online survey was programmed using Qualtrics Software and manually translated into Spanish.
Given the multimodal design, surveys were distributed by email, text message, and US Postal Service (USPS). Surveys were emailed to all veterans for whom a valid email address was available. If emails were undeliverable, veterans were contacted via text message or the USPS. Surveys were distributed by text message to all veterans without an email address but with a cellphone number. We were unable to consistently identify invalid numbers among all text message recipients. Invitations with a survey URL and QR code were sent via USPS to veterans who had no valid email address or cellphone number. Targeted efforts were made to increase the response rate for women. A random sample of 200 women who had not completed the survey 2 weeks prior to the closing date (15% of women in sample) was selected to receive personal phone calls. Another random sample of 400 women was selected to receive personalized outreach emails. The survey data were confidential, and responses could not be traced to identifying information.
Data Analyses
We conducted a descriptive analysis, including percentages and means for responses to variables focused on describing amputation characteristics, prosthesis characteristics, and QOL. All data, including missing values, were used to document the percentage of respondents for each question. Removing missing data from the denominator when calculating percentages could introduce bias to the analysis because we cannot be certain data are missing at random. Missing variables were removed to avoid underinflation of mean scores.
We compared responses across 2 groups: individuals who self-identified as men and individuals who self-identified as women. For each question, we assessed whether each of these groups differed significantly from the remaining sample. For example, we examined whether the percentage of men who answered affirmatively to a question was significantly higher or lower than that of individuals not identifying as male, and whether the percentage of women who answered affirmatively was significantly higher or lower than that of individuals not identifying as female. We utilized x2 tests to determine significant differences for percentage calculations and t tests to determine significant differences in means across gender.
Since conducting multiple comparisons within a dataset may result in inflating statistical significance (type 1 errors), we used a more conservative estimate of statistical significance (α = 0.01) and high significance (α = 0.001). This study was deemed quality improvement by the VHA Rehabilitation and Prosthetic Services (12RPS) and acknowledged by the VA Research Office at Eastern Colorado Health Care System and was not subject to institutional review board review.
Results
Surveys were distributed to 46,613 veterans and were completed by 4981 respondents for a 10.7% overall response rate. Survey respondents were generally similar to the eligible population invited to participate, but the proportion of women who completed the survey was higher than the proportion of women eligible to participate (2.0% of eligible population vs 16.7% of respondents), likely due to specific efforts to target women. Survey respondents were slightly younger than the general population (67.3 years vs 68.7 years), less likely to be male (97.1% vs 83.3%), showed similar representation of Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans (4.4% vs 4.1%), and were less likely to have diabetes (58.0% vs 52.7% had diabetes) (Table 1).
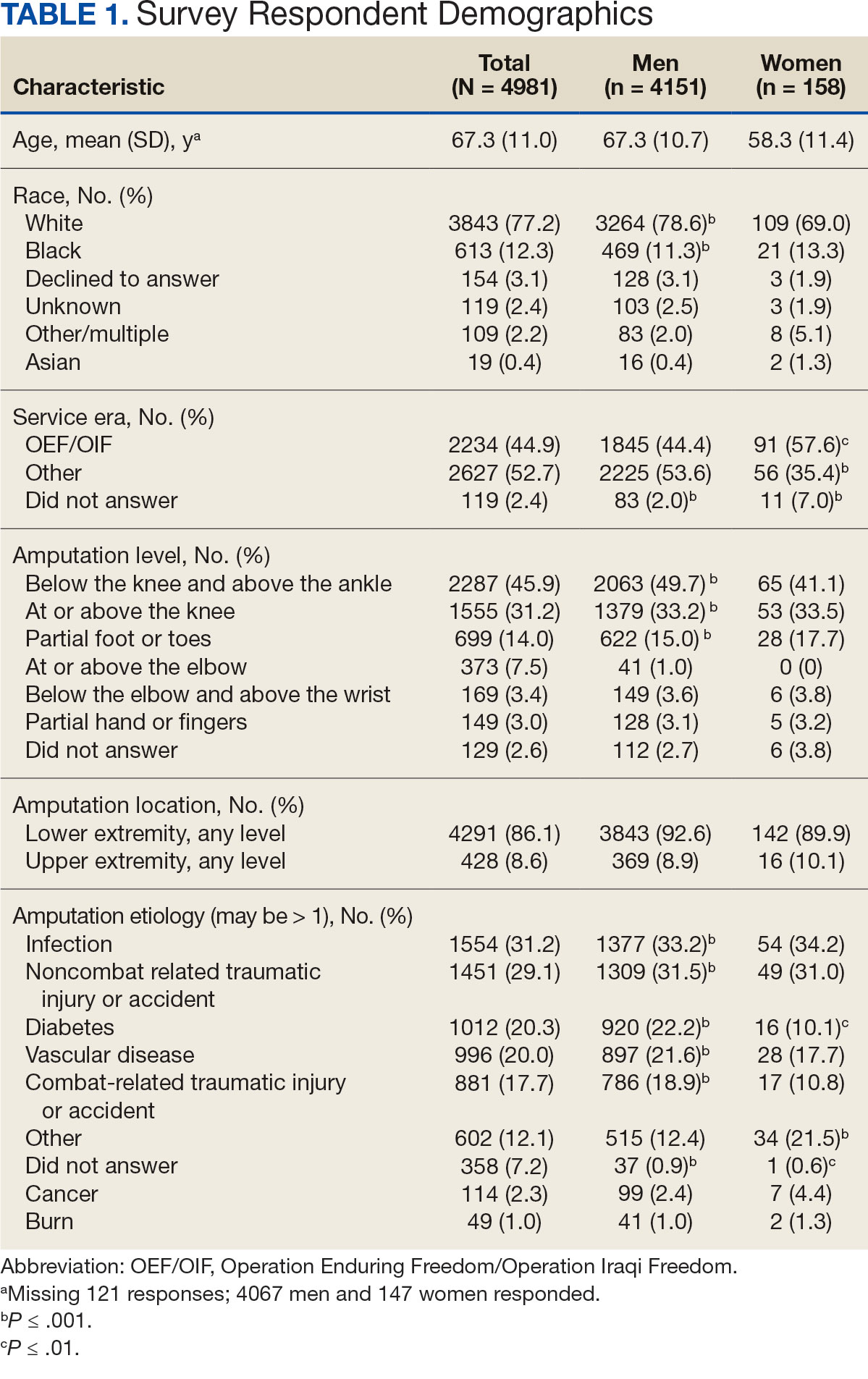
The mean age of male respondents was 67.3 years, while the mean age of female respondents was 58.3 years. The majority of respondents were male (83.3%) and White (77.2%). Female respondents were less likely to have diabetes (35.4% of women vs 53.5% of men) and less likely to report that their most recent amputation resulted from diabetes (10.1% of women vs 22.2% of men). Women respondents were more likely to report an amputation due to other causes, such as adverse results of surgery, neurologic disease, suicide attempt, blood clots, tumors, rheumatoid arthritis, and revisions of previous amputations. Most women respondents did not serve during the OEF or OIF eras. The most common amputation site for women respondents was lower limb, either below the knee and above the ankle or above the knee.
Most participants use an everyday prosthesis, but women were more likely to report using a sports-specific prosthesis (Table 2). Overall, most respondents report using a prosthesis (87.7%); however, women were more likely to report not using a prosthesis (19.4% of women vs 11.1% of men; P ≤ .01). Additionally, a lower proportion of women report using a prosthesis for < 12 hours per day (30.6% of women vs 46.4% of men; P ≤ .01) or using a prosthesis every day (54.8% of women vs 74.6% of men; P ≤ .001).
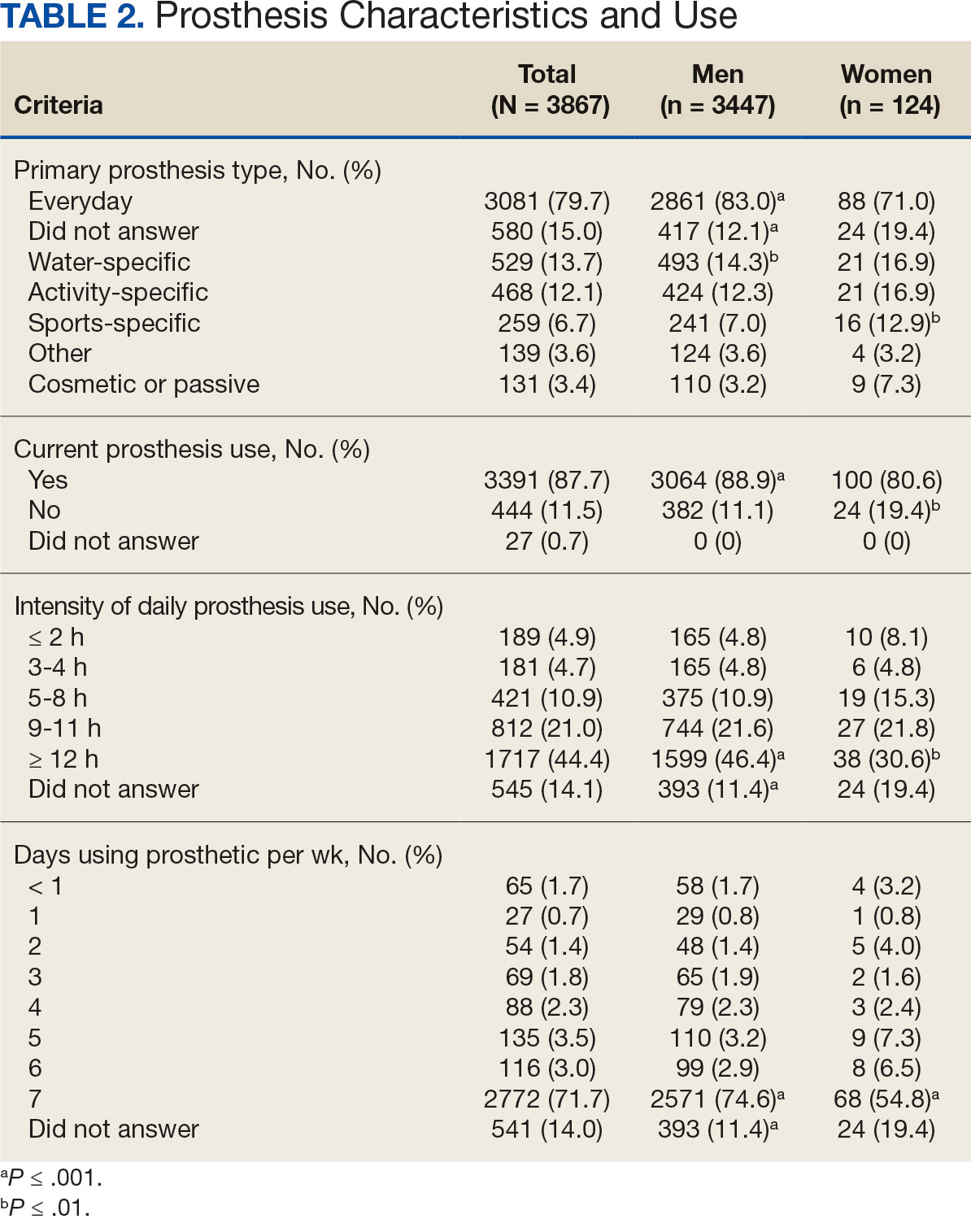
In the overall sample, the mean satisfaction score with a prosthesis was 2.7 on a 5-point scale, and women had slightly lower overall satisfaction scores (2.6 for women vs 2.7 for men; P ≤ .001) (Table 3). Women also had lower satisfaction scores related to appearance, usefulness, reliability, and comfort. Women were more likely to indicate that it was very important to be able to wear jewelry and accessories (20.2% of women vs 11.6% of men; P ≤ .01), while men were less likely to indicate that it was somewhat or very important that the prosthesis not restrict clothing or shoes (95.2% of women vs 82.9% of men; P ≤ .001). Men were more likely than women to report being comfortable or very comfortable using their prosthesis in intimate contact: 40.5% vs 29.0%, respectively (P ≤ .001).
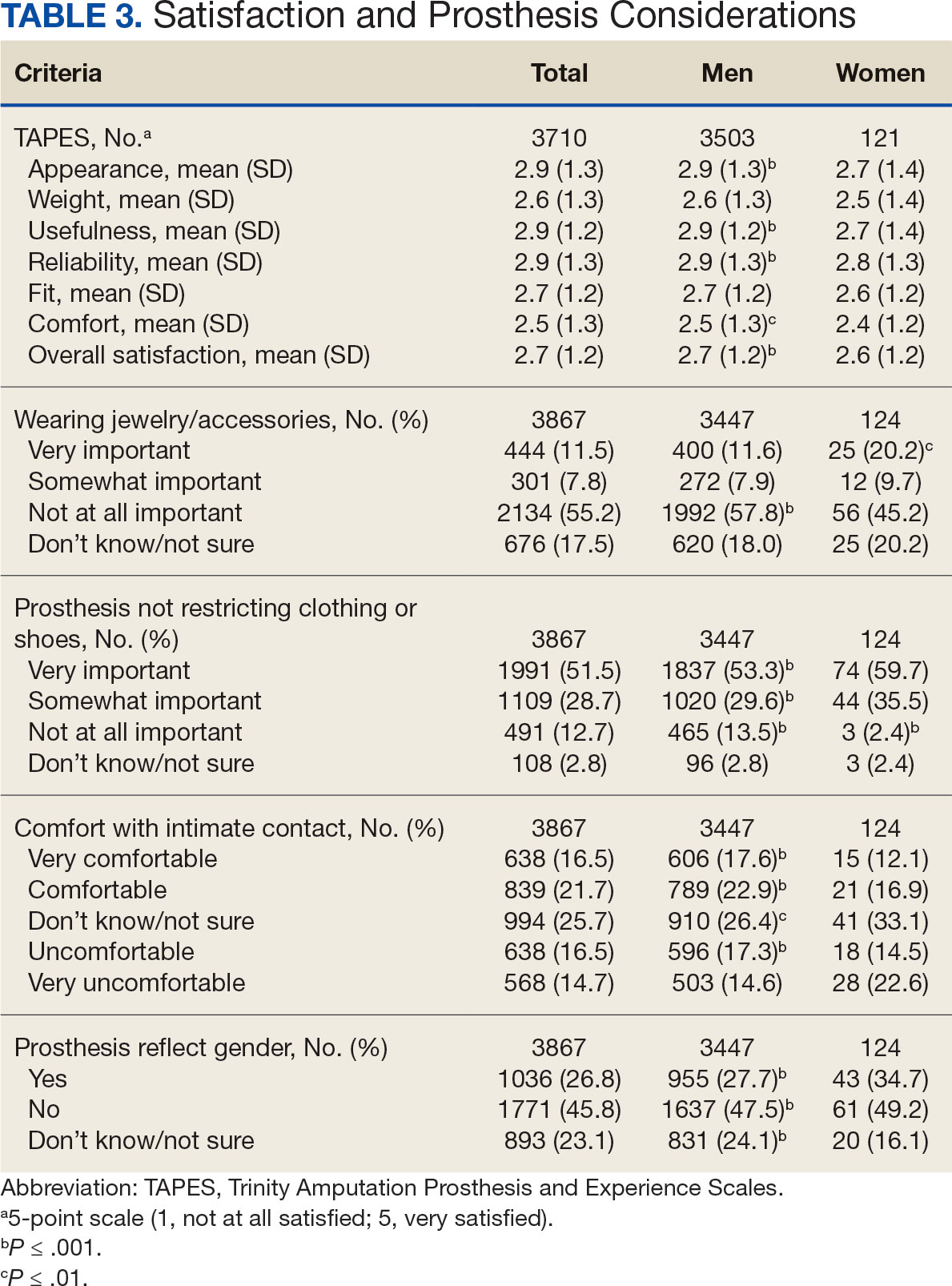
Overall, participants reported high satisfaction with appointment times, wait times, courteous treatment, opportunities to express concerns, and staff responsiveness. Men were slightly more likely than women to be satisfied with training (P ≤ 0.001) and problem discussion (P ≤ 0.01) (Table 4). There were no statistically significant differences in satisfaction or QOL ratings between women and men. The overall sample rated both QOL and satisfaction with QOL 6.7 on a 10-point scale.
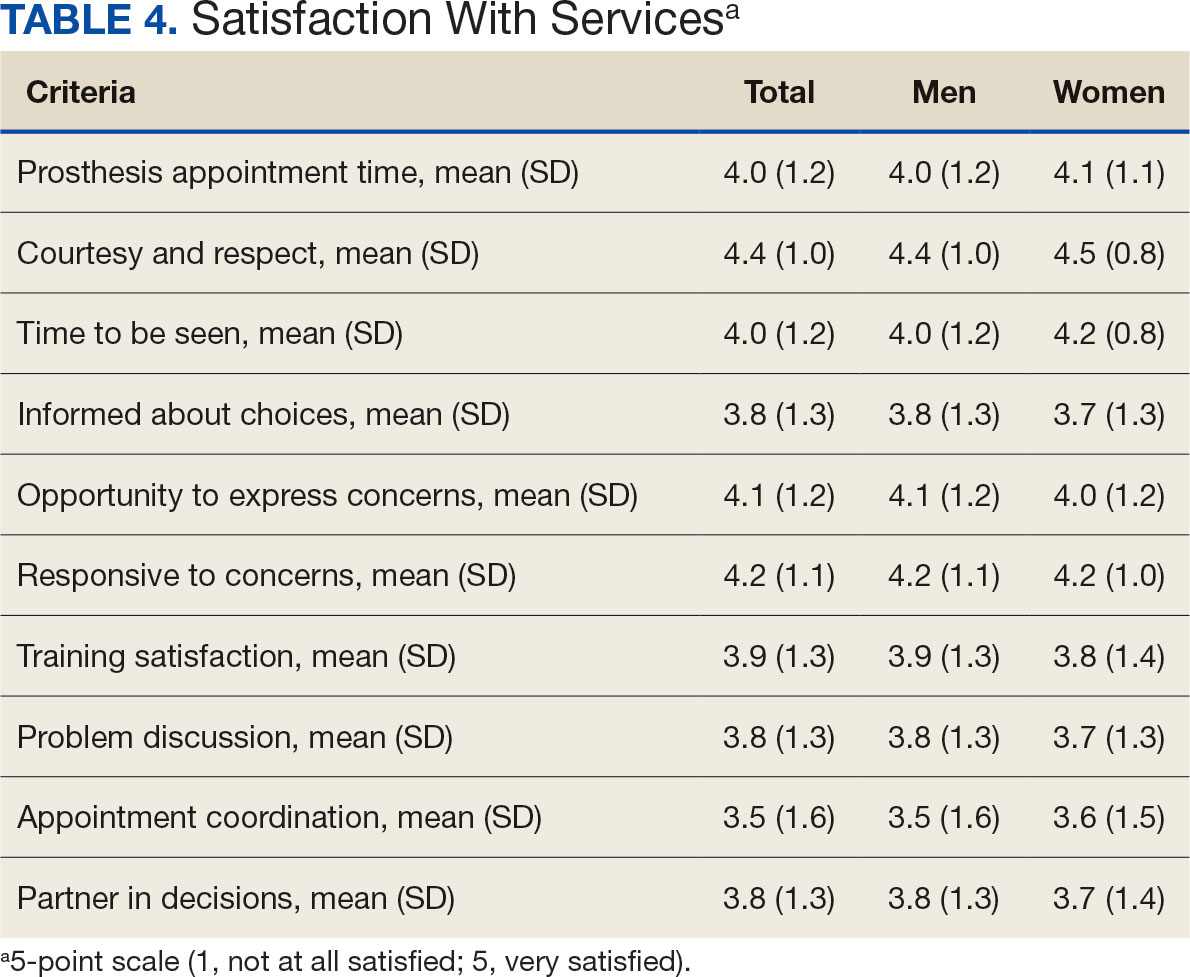
Discussion
The goal of this study was to characterize the experience of veterans with limb loss receiving care in the VHA and assess their satisfaction with prostheses and prosthetic care. We received responses from nearly 5000 veterans, 158 of whom were women. Women veteran respondents were slightly younger and less likely to have an amputation due to diabetes. We did not observe significant differences in amputation level between men and women but women were less likely to use a prosthesis, reported lower intensity of prosthesis use, and were less satisfied with certain aspects of their prostheses. Women may also be less satisfied with prosthesis training and problem discussion. However, we found no differences in QOL ratings between men and women.
Findings indicating women were more likely to report not using a prosthesis and that a lower proportion of women report using a prosthesis for > 12 hours a day or every day are consistent with previous research. 21,22 Interestingly, women were more likely to report using a sports-specific prosthesis. This is notable because prior research suggests that individuals with amputations may avoid participating in sports and exercise, and a lack of access to sports-specific prostheses may inhibit physical activity.23,24 Women in this sample were slightly less satisfied with their prostheses overall and reported lower satisfaction scores regarding appearance, usefulness, reliability, and comfort, consistent with previous findings.25
A lower percentage of women in this sample reported being comfortable or very comfortable using their prosthesis during intimate contact. Previous research on prosthesis satisfaction suggests individuals who rate prosthesis satisfaction lower also report lower body image across genders. 26 While women in this sample did not rate their prosthesis satisfaction lower than men, they did report lower intensity of prosthesis use, suggesting potential issues with their prostheses this survey did not evaluate. Women indicated the importance of prostheses not restricting jewelry, accessories, clothing, or shoes. These results have significant clinical and social implications. A recent qualitative study emphasizes that women veterans feel prostheses are primarily designed for men and may not work well with their physiological needs.9 Research focused on limbs better suited to women’s bodies could result in better fitting sockets, lightweight limbs, or less bulky designs. Additional research has also explored the difficulties in accommodating a range of footwear for patients with lower limb amputation. One study found that varying footwear heights affect the function of adjustable prosthetic feet in ways that may not be optimal.27
Ratings of satisfaction with prosthesisrelated services between men and women in this sample are consistent with a recent study showing that women veterans do not have significant differences in satisfaction with prosthesis-related services.28 However, this study focused specifically on lower limb amputations, while the respondents of this study include those with both upper and lower limb amputations. Importantly, our findings that women are less likely to be satisfied with prosthesis training and problem discussions support recent qualitative findings in which women expressed a desire to work with prosthetists who listen to them, take their concerns seriously, and seek solutions that fit their needs. We did not observe a difference in QOL ratings between men and women in the sample despite lower satisfaction among women with some elements of prosthesis-related services. Previous research suggests many factors impact QOL after amputation, most notably time since amputation.16,29
Limitations
This survey was deployed in a short timeline that did not allow for careful sample selection or implementing strategies to increase response rate. Additionally, the study was conducted among veterans receiving care in the VHA, and findings may not be generalizable to limb loss in other settings. Finally, the discrepancy in number of respondents who identified as men vs women made it difficult to compare differences between the 2 groups.
Conclusions
This is the largest sample of survey respondents of veterans with limb loss to date. While the findings suggest veterans are generally satisfied with prosthetic-related services overall, they also highlight several areas for improvement with services or prostheses. Given that most veterans with limb loss are men, there is a significant discrepancy between the number of women and men respondents. Additional studies with more comparable numbers of men and women have found similar ratings of satisfaction with prostheses and services.28 Further research specifically focused on improving the experiences of women should focus on better characterizing their experiences and identifying how they differ from those of male veterans. For example, understanding how to engage female veterans with limb loss in prosthesis training and problem discussions may improve their experience with their care teams and improve their use of prostheses. Understanding experiences and needs that are specific to women could lead to the development of processes, resources, or devices that are tailored to the unique requirements of women with limb loss.
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422-429. doi:10.1016/j.apmr.2007.11.005
- Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the united states. South Med J. 2002;95(8):875-883. doi:10.1097/00007611-200208000-00018
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005;86(3):480-486. doi:10.1016/j.apmr.2004.06.072
- Centers for Disease Control and Prevention. Ambulatory and inpatient procedures in the United States. Accessed September 30, 2024. https://www.cdc.gov/nchs/pressroom/98facts/ambulat.htm
- Ljung J, Iacangelo A. Identifying and acknowledging a sex gap in lower-limb prosthetics. JPO. 2024;36(1):e18-e24. doi:10.1097/JPO.0000000000000470
- Feinglass J, Brown JL, LoSasso A, et al. Rates of lower-extremity amputation and arterial reconstruction in the united states, 1979 to 1996. Am J Public Health. 1999;89(8):1222- 1227. doi:10.2105/ajph.89.8.1222
- Mayfield JA, Reiber GE, Maynard C, Czerniecki JM, Caps MT, Sangeorzan BJ. Trends in lower limb amputation in the Veterans Health Administration, 1989-1998. J Rehabil Res Dev. 2000;37(1):23-30.
- Feinglass J, Pearce WH, Martin GJ, et al. Postoperative and late survival outcomes after major amputation: findings from the department of veterans affairs national surgical quality improvement program. Surgery. 2001;130(1):21-29. doi:10.1067/msy.2001.115359
- Lehavot K, Young JP, Thomas RM, et al. Voices of women veterans with lower limb prostheses: a qualitative study. J Gen Intern Med. 2022;37(3):799-805. doi:10.1007/s11606-022-07572-8
- US Government Accountability Office. COVID-19: Opportunities to improve federal response. GAO-21-60. Published November 12, 2020. Accessed September 30, 2024. https://www.gao.gov/products/gao-21-60
- Littman AJ, Peterson AC, Korpak A, et al. Differences in prosthetic prescription between men and women veterans after transtibial or transfemoral lowerextremity amputation: a longitudinal cohort study. Arch Phys Med Rehabil. 2023;104(8)1274-1281. doi:10.1016/j.amjsurg.2023.02.011
- Cimino SR, Vijayakumar A, MacKay C, Mayo AL, Hitzig SL, Guilcher SJT. Sex and gender differences in quality of life and related domains for individuals with adult acquired lower-limb amputation: a scoping review. Disabil Rehabil. 2022 Oct 23;44(22):6899-6925. doi:10.1080/09638288.2021.1974106
- DadeMatthews OO, Roper JA, Vazquez A, Shannon DM, Sefton JM. Prosthetic device and service satisfaction, quality of life, and functional performance in lower limb prosthesis clients. Prosthet Orthot Int. 2024;48(4):422-430. doi:10.1097/PXR.0000000000000285
- Hamilton AB, Schwarz EB, Thomas HN, Goldstein KM. Moving women veterans’ health research forward: a special supplement. J Gen Intern Med. 2022;37(Suppl3):665– 667. doi:10.1007/s11606-022-07606-1
- US Congress. Public Law 116-315: An Act to Improve the Lives of Veterans, S 5108 (2) (F). 116th Congress; 2021. Accessed September 30, 2024. https://www.congress.gov/116/plaws/publ315/PLAW-116publ315.pdf
- Gallagher P, MacLachlan M. The Trinity amputation and prosthesis experience scales and quality of life in people with lower-limb amputation. Arch Phys Med Rehabil. 2004;85(5):730-736. doi:10.1016/j.apmr.2003.07.009
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Heinemann AW, Bode RK, O’Reilly C. Development and measurement properties of the orthotics and prosthetics users’ survey (OPUS): a comprehensive set of clinical outcome instruments. Prosthet Orthot Int. 2003;27(3):191-206. doi:10.1080/03093640308726682
- Resnik LJ, Borgia ML, Clark MA. A national survey of prosthesis use in veterans with major upper limb amputation: comparisons by gender. PM R. 2020;12(11):1086-1098. doi:10.1002/pmrj.12351
- Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229-238. doi:10.1023/a:1023254226592
- Østlie K, Lesjø IM, Franklin RJ, Garfelt B, Skjeldal OH, Magnus P. Prosthesis rejection in acquired major upper-limb amputees: a population-based survey. Disabil Rehabil Assist Technol. 2012;7(4):294-303. doi:10.3109/17483107.2011.635405
- Pezzin LE, Dillingham TR, MacKenzie EJ, Ephraim P, Rossbach P. Use and satisfaction with prosthetic limb devices and related services. Arch Phys Med Rehabil. 2004;85(5):723-729. doi:10.1016/j.apmr.2003.06.002
- Deans S, Burns D, McGarry A, Murray K, Mutrie N. Motivations and barriers to prosthesis users participation in physical activity, exercise and sport: a review of the literature. Prosthet Orthot Int. 2012;36(3):260-269. doi:10.1177/0309364612437905
- McDonald CL, Kahn A, Hafner BJ, Morgan SJ. Prevalence of secondary prosthesis use in lower limb prosthesis users. Disabil Rehabil. 2023;46(5):1016-1022. doi:10.1080/09638288.2023.2182919
- Baars EC, Schrier E, Dijkstra PU, Geertzen JHB. Prosthesis satisfaction in lower limb amputees: a systematic review of associated factors and questionnaires. Medicine (Baltimore). 2018;97(39):e12296. doi:10.1097/MD.0000000000012296
- Murray CD, Fox J. Body image and prosthesis satisfaction in the lower limb amputee. Disabil Rehabil. 2002;24(17):925–931. doi:10.1080/09638280210150014
- Major MJ, Quinlan J, Hansen AH, Esposito ER. Effects of women’s footwear on the mechanical function of heel-height accommodating prosthetic feet. PLoS One. 2022;17(1). doi:10.1371/journal.pone.0262910.
- Kuo PB, Lehavot K, Thomas RM, et al. Gender differences in prosthesis-related outcomes among veterans: results of a national survey of U.S. veterans. PM R. 2024;16(3):239- 249. doi:10.1002/pmrj.13028
- Asano M, Rushton P, Miller WC, Deathe BA. Predictors of quality of life among individuals who have a lower limb amputation. Prosthet Orthot Int. 2008;32(2):231-243. doi:10.1080/03093640802024955
Limb loss is a significant and growing concern in the United States. Nearly 2 million Americans are living with limb loss, and up to 185,000 people undergo amputations annually.1-4 Of these patients, about 35% are women.5 The Veterans Health Administration (VHA) provides about 10% of US amputations.6-8 Between 2015 and 2019, the number of prosthetic devices provided to female veterans increased from 3.3 million to 4.6 million.5,9,10
Previous research identified disparities in prosthetic care between men and women, both within and outside the VHA. These disparities include slower prosthesis prescription and receipt among women, in addition to differences in self-reported mobility, satisfaction, rates of prosthesis rejection, and challenges related to prosthesis appearance and fit.5,10,11 Recent studies suggest women tend to have worse outcomes following amputation, and are underrepresented in amputation research.12,13 However, these disparities are poorly described in a large, national sample. Because women represent a growing portion of patients with limb loss in the VHA, understanding their needs is critical.14
The Johnny Isakson and David P. Roe, MD Veterans Health Care and Benefits Improvement Act of 2020 was enacted, in part, to improve the care provided to women veterans.15 The law required the VHA to conduct a survey of ≥ 50,000 veterans to assess the satisfaction of women veterans with prostheses provided by the VHA. To comply with this legislation and understand how women veterans rate their prostheses and related care in the VHA, the US Department of Veterans Affairs (VA) Center for Collaborative Evaluation (VACE) conducted a large national survey of veterans with limb loss that oversampled women veterans. This article describes the survey results, including characteristics of female veterans with limb loss receiving care from the VHA, assesses their satisfaction with prostheses and prosthetic care, and highlights where their responses differ from those of male veterans.
Methods
We conducted a cross-sectional, mixedmode survey of eligible amputees in the VHA Support Service Capital Assets Amputee Data Cube. We identified a cohort of veterans with any major amputation (above the ankle or wrist) or partial hand or foot amputation who received VHA care between October 1, 2019, and September 30, 2020. The final cohort yielded 46,646 potentially eligible veterans. Thirty-three had invalid contact information, leaving 46,613 veterans who were asked to participate, including 1356 women.
Survey
We created a survey instrument de novo that included questions from validated instruments, including the Trinity Amputation Prosthesis and Experience Scales to assess prosthetic device satisfaction, the Prosthesis Evaluation Questionnaire to assess quality of life (QOL) satisfaction, and the Orthotics Prosthetics Users Survey to assess prosthesis-related care satisfaction. 16-18 Additional questions were incorporated from a survey of veterans with upper limb amputation to assess the importance of cosmetic considerations related to the prosthesis and comfort with prosthesis use in intimate relationships.19 Questions were also included to assess amputation type, year of amputation, if a prosthesis was currently used, reasons for ceasing use of a prosthesis, reasons for never using a prosthesis, the types of prostheses used, intensity of prosthesis use, satisfaction with time required to receive a prosthetic limb, and if the prosthesis reflected the veteran’s selfidentified gender. Veterans were asked to answer questions based on their most recent amputation.
We tested the survey using cognitive interviews with 6 veterans to refine the survey and better understand how veterans interpreted the questions. Pilot testers completed the survey and participated in individual interviews with experienced interviewers (CL and RRK) to describe how they selected their responses.20 This feedback was used to refine the survey. The online survey was programmed using Qualtrics Software and manually translated into Spanish.
Given the multimodal design, surveys were distributed by email, text message, and US Postal Service (USPS). Surveys were emailed to all veterans for whom a valid email address was available. If emails were undeliverable, veterans were contacted via text message or the USPS. Surveys were distributed by text message to all veterans without an email address but with a cellphone number. We were unable to consistently identify invalid numbers among all text message recipients. Invitations with a survey URL and QR code were sent via USPS to veterans who had no valid email address or cellphone number. Targeted efforts were made to increase the response rate for women. A random sample of 200 women who had not completed the survey 2 weeks prior to the closing date (15% of women in sample) was selected to receive personal phone calls. Another random sample of 400 women was selected to receive personalized outreach emails. The survey data were confidential, and responses could not be traced to identifying information.
Data Analyses
We conducted a descriptive analysis, including percentages and means for responses to variables focused on describing amputation characteristics, prosthesis characteristics, and QOL. All data, including missing values, were used to document the percentage of respondents for each question. Removing missing data from the denominator when calculating percentages could introduce bias to the analysis because we cannot be certain data are missing at random. Missing variables were removed to avoid underinflation of mean scores.
We compared responses across 2 groups: individuals who self-identified as men and individuals who self-identified as women. For each question, we assessed whether each of these groups differed significantly from the remaining sample. For example, we examined whether the percentage of men who answered affirmatively to a question was significantly higher or lower than that of individuals not identifying as male, and whether the percentage of women who answered affirmatively was significantly higher or lower than that of individuals not identifying as female. We utilized x2 tests to determine significant differences for percentage calculations and t tests to determine significant differences in means across gender.
Since conducting multiple comparisons within a dataset may result in inflating statistical significance (type 1 errors), we used a more conservative estimate of statistical significance (α = 0.01) and high significance (α = 0.001). This study was deemed quality improvement by the VHA Rehabilitation and Prosthetic Services (12RPS) and acknowledged by the VA Research Office at Eastern Colorado Health Care System and was not subject to institutional review board review.
Results
Surveys were distributed to 46,613 veterans and were completed by 4981 respondents for a 10.7% overall response rate. Survey respondents were generally similar to the eligible population invited to participate, but the proportion of women who completed the survey was higher than the proportion of women eligible to participate (2.0% of eligible population vs 16.7% of respondents), likely due to specific efforts to target women. Survey respondents were slightly younger than the general population (67.3 years vs 68.7 years), less likely to be male (97.1% vs 83.3%), showed similar representation of Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans (4.4% vs 4.1%), and were less likely to have diabetes (58.0% vs 52.7% had diabetes) (Table 1).
The mean age of male respondents was 67.3 years, while the mean age of female respondents was 58.3 years. The majority of respondents were male (83.3%) and White (77.2%). Female respondents were less likely to have diabetes (35.4% of women vs 53.5% of men) and less likely to report that their most recent amputation resulted from diabetes (10.1% of women vs 22.2% of men). Women respondents were more likely to report an amputation due to other causes, such as adverse results of surgery, neurologic disease, suicide attempt, blood clots, tumors, rheumatoid arthritis, and revisions of previous amputations. Most women respondents did not serve during the OEF or OIF eras. The most common amputation site for women respondents was lower limb, either below the knee and above the ankle or above the knee.
Most participants use an everyday prosthesis, but women were more likely to report using a sports-specific prosthesis (Table 2). Overall, most respondents report using a prosthesis (87.7%); however, women were more likely to report not using a prosthesis (19.4% of women vs 11.1% of men; P ≤ .01). Additionally, a lower proportion of women report using a prosthesis for < 12 hours per day (30.6% of women vs 46.4% of men; P ≤ .01) or using a prosthesis every day (54.8% of women vs 74.6% of men; P ≤ .001).
In the overall sample, the mean satisfaction score with a prosthesis was 2.7 on a 5-point scale, and women had slightly lower overall satisfaction scores (2.6 for women vs 2.7 for men; P ≤ .001) (Table 3). Women also had lower satisfaction scores related to appearance, usefulness, reliability, and comfort. Women were more likely to indicate that it was very important to be able to wear jewelry and accessories (20.2% of women vs 11.6% of men; P ≤ .01), while men were less likely to indicate that it was somewhat or very important that the prosthesis not restrict clothing or shoes (95.2% of women vs 82.9% of men; P ≤ .001). Men were more likely than women to report being comfortable or very comfortable using their prosthesis in intimate contact: 40.5% vs 29.0%, respectively (P ≤ .001).
Overall, participants reported high satisfaction with appointment times, wait times, courteous treatment, opportunities to express concerns, and staff responsiveness. Men were slightly more likely than women to be satisfied with training (P ≤ 0.001) and problem discussion (P ≤ 0.01) (Table 4). There were no statistically significant differences in satisfaction or QOL ratings between women and men. The overall sample rated both QOL and satisfaction with QOL 6.7 on a 10-point scale.
Discussion
The goal of this study was to characterize the experience of veterans with limb loss receiving care in the VHA and assess their satisfaction with prostheses and prosthetic care. We received responses from nearly 5000 veterans, 158 of whom were women. Women veteran respondents were slightly younger and less likely to have an amputation due to diabetes. We did not observe significant differences in amputation level between men and women but women were less likely to use a prosthesis, reported lower intensity of prosthesis use, and were less satisfied with certain aspects of their prostheses. Women may also be less satisfied with prosthesis training and problem discussion. However, we found no differences in QOL ratings between men and women.
Findings indicating women were more likely to report not using a prosthesis and that a lower proportion of women report using a prosthesis for > 12 hours a day or every day are consistent with previous research. 21,22 Interestingly, women were more likely to report using a sports-specific prosthesis. This is notable because prior research suggests that individuals with amputations may avoid participating in sports and exercise, and a lack of access to sports-specific prostheses may inhibit physical activity.23,24 Women in this sample were slightly less satisfied with their prostheses overall and reported lower satisfaction scores regarding appearance, usefulness, reliability, and comfort, consistent with previous findings.25
A lower percentage of women in this sample reported being comfortable or very comfortable using their prosthesis during intimate contact. Previous research on prosthesis satisfaction suggests individuals who rate prosthesis satisfaction lower also report lower body image across genders. 26 While women in this sample did not rate their prosthesis satisfaction lower than men, they did report lower intensity of prosthesis use, suggesting potential issues with their prostheses this survey did not evaluate. Women indicated the importance of prostheses not restricting jewelry, accessories, clothing, or shoes. These results have significant clinical and social implications. A recent qualitative study emphasizes that women veterans feel prostheses are primarily designed for men and may not work well with their physiological needs.9 Research focused on limbs better suited to women’s bodies could result in better fitting sockets, lightweight limbs, or less bulky designs. Additional research has also explored the difficulties in accommodating a range of footwear for patients with lower limb amputation. One study found that varying footwear heights affect the function of adjustable prosthetic feet in ways that may not be optimal.27
Ratings of satisfaction with prosthesisrelated services between men and women in this sample are consistent with a recent study showing that women veterans do not have significant differences in satisfaction with prosthesis-related services.28 However, this study focused specifically on lower limb amputations, while the respondents of this study include those with both upper and lower limb amputations. Importantly, our findings that women are less likely to be satisfied with prosthesis training and problem discussions support recent qualitative findings in which women expressed a desire to work with prosthetists who listen to them, take their concerns seriously, and seek solutions that fit their needs. We did not observe a difference in QOL ratings between men and women in the sample despite lower satisfaction among women with some elements of prosthesis-related services. Previous research suggests many factors impact QOL after amputation, most notably time since amputation.16,29
Limitations
This survey was deployed in a short timeline that did not allow for careful sample selection or implementing strategies to increase response rate. Additionally, the study was conducted among veterans receiving care in the VHA, and findings may not be generalizable to limb loss in other settings. Finally, the discrepancy in number of respondents who identified as men vs women made it difficult to compare differences between the 2 groups.
Conclusions
This is the largest sample of survey respondents of veterans with limb loss to date. While the findings suggest veterans are generally satisfied with prosthetic-related services overall, they also highlight several areas for improvement with services or prostheses. Given that most veterans with limb loss are men, there is a significant discrepancy between the number of women and men respondents. Additional studies with more comparable numbers of men and women have found similar ratings of satisfaction with prostheses and services.28 Further research specifically focused on improving the experiences of women should focus on better characterizing their experiences and identifying how they differ from those of male veterans. For example, understanding how to engage female veterans with limb loss in prosthesis training and problem discussions may improve their experience with their care teams and improve their use of prostheses. Understanding experiences and needs that are specific to women could lead to the development of processes, resources, or devices that are tailored to the unique requirements of women with limb loss.
Limb loss is a significant and growing concern in the United States. Nearly 2 million Americans are living with limb loss, and up to 185,000 people undergo amputations annually.1-4 Of these patients, about 35% are women.5 The Veterans Health Administration (VHA) provides about 10% of US amputations.6-8 Between 2015 and 2019, the number of prosthetic devices provided to female veterans increased from 3.3 million to 4.6 million.5,9,10
Previous research identified disparities in prosthetic care between men and women, both within and outside the VHA. These disparities include slower prosthesis prescription and receipt among women, in addition to differences in self-reported mobility, satisfaction, rates of prosthesis rejection, and challenges related to prosthesis appearance and fit.5,10,11 Recent studies suggest women tend to have worse outcomes following amputation, and are underrepresented in amputation research.12,13 However, these disparities are poorly described in a large, national sample. Because women represent a growing portion of patients with limb loss in the VHA, understanding their needs is critical.14
The Johnny Isakson and David P. Roe, MD Veterans Health Care and Benefits Improvement Act of 2020 was enacted, in part, to improve the care provided to women veterans.15 The law required the VHA to conduct a survey of ≥ 50,000 veterans to assess the satisfaction of women veterans with prostheses provided by the VHA. To comply with this legislation and understand how women veterans rate their prostheses and related care in the VHA, the US Department of Veterans Affairs (VA) Center for Collaborative Evaluation (VACE) conducted a large national survey of veterans with limb loss that oversampled women veterans. This article describes the survey results, including characteristics of female veterans with limb loss receiving care from the VHA, assesses their satisfaction with prostheses and prosthetic care, and highlights where their responses differ from those of male veterans.
Methods
We conducted a cross-sectional, mixedmode survey of eligible amputees in the VHA Support Service Capital Assets Amputee Data Cube. We identified a cohort of veterans with any major amputation (above the ankle or wrist) or partial hand or foot amputation who received VHA care between October 1, 2019, and September 30, 2020. The final cohort yielded 46,646 potentially eligible veterans. Thirty-three had invalid contact information, leaving 46,613 veterans who were asked to participate, including 1356 women.
Survey
We created a survey instrument de novo that included questions from validated instruments, including the Trinity Amputation Prosthesis and Experience Scales to assess prosthetic device satisfaction, the Prosthesis Evaluation Questionnaire to assess quality of life (QOL) satisfaction, and the Orthotics Prosthetics Users Survey to assess prosthesis-related care satisfaction. 16-18 Additional questions were incorporated from a survey of veterans with upper limb amputation to assess the importance of cosmetic considerations related to the prosthesis and comfort with prosthesis use in intimate relationships.19 Questions were also included to assess amputation type, year of amputation, if a prosthesis was currently used, reasons for ceasing use of a prosthesis, reasons for never using a prosthesis, the types of prostheses used, intensity of prosthesis use, satisfaction with time required to receive a prosthetic limb, and if the prosthesis reflected the veteran’s selfidentified gender. Veterans were asked to answer questions based on their most recent amputation.
We tested the survey using cognitive interviews with 6 veterans to refine the survey and better understand how veterans interpreted the questions. Pilot testers completed the survey and participated in individual interviews with experienced interviewers (CL and RRK) to describe how they selected their responses.20 This feedback was used to refine the survey. The online survey was programmed using Qualtrics Software and manually translated into Spanish.
Given the multimodal design, surveys were distributed by email, text message, and US Postal Service (USPS). Surveys were emailed to all veterans for whom a valid email address was available. If emails were undeliverable, veterans were contacted via text message or the USPS. Surveys were distributed by text message to all veterans without an email address but with a cellphone number. We were unable to consistently identify invalid numbers among all text message recipients. Invitations with a survey URL and QR code were sent via USPS to veterans who had no valid email address or cellphone number. Targeted efforts were made to increase the response rate for women. A random sample of 200 women who had not completed the survey 2 weeks prior to the closing date (15% of women in sample) was selected to receive personal phone calls. Another random sample of 400 women was selected to receive personalized outreach emails. The survey data were confidential, and responses could not be traced to identifying information.
Data Analyses
We conducted a descriptive analysis, including percentages and means for responses to variables focused on describing amputation characteristics, prosthesis characteristics, and QOL. All data, including missing values, were used to document the percentage of respondents for each question. Removing missing data from the denominator when calculating percentages could introduce bias to the analysis because we cannot be certain data are missing at random. Missing variables were removed to avoid underinflation of mean scores.
We compared responses across 2 groups: individuals who self-identified as men and individuals who self-identified as women. For each question, we assessed whether each of these groups differed significantly from the remaining sample. For example, we examined whether the percentage of men who answered affirmatively to a question was significantly higher or lower than that of individuals not identifying as male, and whether the percentage of women who answered affirmatively was significantly higher or lower than that of individuals not identifying as female. We utilized x2 tests to determine significant differences for percentage calculations and t tests to determine significant differences in means across gender.
Since conducting multiple comparisons within a dataset may result in inflating statistical significance (type 1 errors), we used a more conservative estimate of statistical significance (α = 0.01) and high significance (α = 0.001). This study was deemed quality improvement by the VHA Rehabilitation and Prosthetic Services (12RPS) and acknowledged by the VA Research Office at Eastern Colorado Health Care System and was not subject to institutional review board review.
Results
Surveys were distributed to 46,613 veterans and were completed by 4981 respondents for a 10.7% overall response rate. Survey respondents were generally similar to the eligible population invited to participate, but the proportion of women who completed the survey was higher than the proportion of women eligible to participate (2.0% of eligible population vs 16.7% of respondents), likely due to specific efforts to target women. Survey respondents were slightly younger than the general population (67.3 years vs 68.7 years), less likely to be male (97.1% vs 83.3%), showed similar representation of Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans (4.4% vs 4.1%), and were less likely to have diabetes (58.0% vs 52.7% had diabetes) (Table 1).
The mean age of male respondents was 67.3 years, while the mean age of female respondents was 58.3 years. The majority of respondents were male (83.3%) and White (77.2%). Female respondents were less likely to have diabetes (35.4% of women vs 53.5% of men) and less likely to report that their most recent amputation resulted from diabetes (10.1% of women vs 22.2% of men). Women respondents were more likely to report an amputation due to other causes, such as adverse results of surgery, neurologic disease, suicide attempt, blood clots, tumors, rheumatoid arthritis, and revisions of previous amputations. Most women respondents did not serve during the OEF or OIF eras. The most common amputation site for women respondents was lower limb, either below the knee and above the ankle or above the knee.
Most participants use an everyday prosthesis, but women were more likely to report using a sports-specific prosthesis (Table 2). Overall, most respondents report using a prosthesis (87.7%); however, women were more likely to report not using a prosthesis (19.4% of women vs 11.1% of men; P ≤ .01). Additionally, a lower proportion of women report using a prosthesis for < 12 hours per day (30.6% of women vs 46.4% of men; P ≤ .01) or using a prosthesis every day (54.8% of women vs 74.6% of men; P ≤ .001).
In the overall sample, the mean satisfaction score with a prosthesis was 2.7 on a 5-point scale, and women had slightly lower overall satisfaction scores (2.6 for women vs 2.7 for men; P ≤ .001) (Table 3). Women also had lower satisfaction scores related to appearance, usefulness, reliability, and comfort. Women were more likely to indicate that it was very important to be able to wear jewelry and accessories (20.2% of women vs 11.6% of men; P ≤ .01), while men were less likely to indicate that it was somewhat or very important that the prosthesis not restrict clothing or shoes (95.2% of women vs 82.9% of men; P ≤ .001). Men were more likely than women to report being comfortable or very comfortable using their prosthesis in intimate contact: 40.5% vs 29.0%, respectively (P ≤ .001).
Overall, participants reported high satisfaction with appointment times, wait times, courteous treatment, opportunities to express concerns, and staff responsiveness. Men were slightly more likely than women to be satisfied with training (P ≤ 0.001) and problem discussion (P ≤ 0.01) (Table 4). There were no statistically significant differences in satisfaction or QOL ratings between women and men. The overall sample rated both QOL and satisfaction with QOL 6.7 on a 10-point scale.
Discussion
The goal of this study was to characterize the experience of veterans with limb loss receiving care in the VHA and assess their satisfaction with prostheses and prosthetic care. We received responses from nearly 5000 veterans, 158 of whom were women. Women veteran respondents were slightly younger and less likely to have an amputation due to diabetes. We did not observe significant differences in amputation level between men and women but women were less likely to use a prosthesis, reported lower intensity of prosthesis use, and were less satisfied with certain aspects of their prostheses. Women may also be less satisfied with prosthesis training and problem discussion. However, we found no differences in QOL ratings between men and women.
Findings indicating women were more likely to report not using a prosthesis and that a lower proportion of women report using a prosthesis for > 12 hours a day or every day are consistent with previous research. 21,22 Interestingly, women were more likely to report using a sports-specific prosthesis. This is notable because prior research suggests that individuals with amputations may avoid participating in sports and exercise, and a lack of access to sports-specific prostheses may inhibit physical activity.23,24 Women in this sample were slightly less satisfied with their prostheses overall and reported lower satisfaction scores regarding appearance, usefulness, reliability, and comfort, consistent with previous findings.25
A lower percentage of women in this sample reported being comfortable or very comfortable using their prosthesis during intimate contact. Previous research on prosthesis satisfaction suggests individuals who rate prosthesis satisfaction lower also report lower body image across genders. 26 While women in this sample did not rate their prosthesis satisfaction lower than men, they did report lower intensity of prosthesis use, suggesting potential issues with their prostheses this survey did not evaluate. Women indicated the importance of prostheses not restricting jewelry, accessories, clothing, or shoes. These results have significant clinical and social implications. A recent qualitative study emphasizes that women veterans feel prostheses are primarily designed for men and may not work well with their physiological needs.9 Research focused on limbs better suited to women’s bodies could result in better fitting sockets, lightweight limbs, or less bulky designs. Additional research has also explored the difficulties in accommodating a range of footwear for patients with lower limb amputation. One study found that varying footwear heights affect the function of adjustable prosthetic feet in ways that may not be optimal.27
Ratings of satisfaction with prosthesisrelated services between men and women in this sample are consistent with a recent study showing that women veterans do not have significant differences in satisfaction with prosthesis-related services.28 However, this study focused specifically on lower limb amputations, while the respondents of this study include those with both upper and lower limb amputations. Importantly, our findings that women are less likely to be satisfied with prosthesis training and problem discussions support recent qualitative findings in which women expressed a desire to work with prosthetists who listen to them, take their concerns seriously, and seek solutions that fit their needs. We did not observe a difference in QOL ratings between men and women in the sample despite lower satisfaction among women with some elements of prosthesis-related services. Previous research suggests many factors impact QOL after amputation, most notably time since amputation.16,29
Limitations
This survey was deployed in a short timeline that did not allow for careful sample selection or implementing strategies to increase response rate. Additionally, the study was conducted among veterans receiving care in the VHA, and findings may not be generalizable to limb loss in other settings. Finally, the discrepancy in number of respondents who identified as men vs women made it difficult to compare differences between the 2 groups.
Conclusions
This is the largest sample of survey respondents of veterans with limb loss to date. While the findings suggest veterans are generally satisfied with prosthetic-related services overall, they also highlight several areas for improvement with services or prostheses. Given that most veterans with limb loss are men, there is a significant discrepancy between the number of women and men respondents. Additional studies with more comparable numbers of men and women have found similar ratings of satisfaction with prostheses and services.28 Further research specifically focused on improving the experiences of women should focus on better characterizing their experiences and identifying how they differ from those of male veterans. For example, understanding how to engage female veterans with limb loss in prosthesis training and problem discussions may improve their experience with their care teams and improve their use of prostheses. Understanding experiences and needs that are specific to women could lead to the development of processes, resources, or devices that are tailored to the unique requirements of women with limb loss.
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422-429. doi:10.1016/j.apmr.2007.11.005
- Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the united states. South Med J. 2002;95(8):875-883. doi:10.1097/00007611-200208000-00018
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005;86(3):480-486. doi:10.1016/j.apmr.2004.06.072
- Centers for Disease Control and Prevention. Ambulatory and inpatient procedures in the United States. Accessed September 30, 2024. https://www.cdc.gov/nchs/pressroom/98facts/ambulat.htm
- Ljung J, Iacangelo A. Identifying and acknowledging a sex gap in lower-limb prosthetics. JPO. 2024;36(1):e18-e24. doi:10.1097/JPO.0000000000000470
- Feinglass J, Brown JL, LoSasso A, et al. Rates of lower-extremity amputation and arterial reconstruction in the united states, 1979 to 1996. Am J Public Health. 1999;89(8):1222- 1227. doi:10.2105/ajph.89.8.1222
- Mayfield JA, Reiber GE, Maynard C, Czerniecki JM, Caps MT, Sangeorzan BJ. Trends in lower limb amputation in the Veterans Health Administration, 1989-1998. J Rehabil Res Dev. 2000;37(1):23-30.
- Feinglass J, Pearce WH, Martin GJ, et al. Postoperative and late survival outcomes after major amputation: findings from the department of veterans affairs national surgical quality improvement program. Surgery. 2001;130(1):21-29. doi:10.1067/msy.2001.115359
- Lehavot K, Young JP, Thomas RM, et al. Voices of women veterans with lower limb prostheses: a qualitative study. J Gen Intern Med. 2022;37(3):799-805. doi:10.1007/s11606-022-07572-8
- US Government Accountability Office. COVID-19: Opportunities to improve federal response. GAO-21-60. Published November 12, 2020. Accessed September 30, 2024. https://www.gao.gov/products/gao-21-60
- Littman AJ, Peterson AC, Korpak A, et al. Differences in prosthetic prescription between men and women veterans after transtibial or transfemoral lowerextremity amputation: a longitudinal cohort study. Arch Phys Med Rehabil. 2023;104(8)1274-1281. doi:10.1016/j.amjsurg.2023.02.011
- Cimino SR, Vijayakumar A, MacKay C, Mayo AL, Hitzig SL, Guilcher SJT. Sex and gender differences in quality of life and related domains for individuals with adult acquired lower-limb amputation: a scoping review. Disabil Rehabil. 2022 Oct 23;44(22):6899-6925. doi:10.1080/09638288.2021.1974106
- DadeMatthews OO, Roper JA, Vazquez A, Shannon DM, Sefton JM. Prosthetic device and service satisfaction, quality of life, and functional performance in lower limb prosthesis clients. Prosthet Orthot Int. 2024;48(4):422-430. doi:10.1097/PXR.0000000000000285
- Hamilton AB, Schwarz EB, Thomas HN, Goldstein KM. Moving women veterans’ health research forward: a special supplement. J Gen Intern Med. 2022;37(Suppl3):665– 667. doi:10.1007/s11606-022-07606-1
- US Congress. Public Law 116-315: An Act to Improve the Lives of Veterans, S 5108 (2) (F). 116th Congress; 2021. Accessed September 30, 2024. https://www.congress.gov/116/plaws/publ315/PLAW-116publ315.pdf
- Gallagher P, MacLachlan M. The Trinity amputation and prosthesis experience scales and quality of life in people with lower-limb amputation. Arch Phys Med Rehabil. 2004;85(5):730-736. doi:10.1016/j.apmr.2003.07.009
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Heinemann AW, Bode RK, O’Reilly C. Development and measurement properties of the orthotics and prosthetics users’ survey (OPUS): a comprehensive set of clinical outcome instruments. Prosthet Orthot Int. 2003;27(3):191-206. doi:10.1080/03093640308726682
- Resnik LJ, Borgia ML, Clark MA. A national survey of prosthesis use in veterans with major upper limb amputation: comparisons by gender. PM R. 2020;12(11):1086-1098. doi:10.1002/pmrj.12351
- Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229-238. doi:10.1023/a:1023254226592
- Østlie K, Lesjø IM, Franklin RJ, Garfelt B, Skjeldal OH, Magnus P. Prosthesis rejection in acquired major upper-limb amputees: a population-based survey. Disabil Rehabil Assist Technol. 2012;7(4):294-303. doi:10.3109/17483107.2011.635405
- Pezzin LE, Dillingham TR, MacKenzie EJ, Ephraim P, Rossbach P. Use and satisfaction with prosthetic limb devices and related services. Arch Phys Med Rehabil. 2004;85(5):723-729. doi:10.1016/j.apmr.2003.06.002
- Deans S, Burns D, McGarry A, Murray K, Mutrie N. Motivations and barriers to prosthesis users participation in physical activity, exercise and sport: a review of the literature. Prosthet Orthot Int. 2012;36(3):260-269. doi:10.1177/0309364612437905
- McDonald CL, Kahn A, Hafner BJ, Morgan SJ. Prevalence of secondary prosthesis use in lower limb prosthesis users. Disabil Rehabil. 2023;46(5):1016-1022. doi:10.1080/09638288.2023.2182919
- Baars EC, Schrier E, Dijkstra PU, Geertzen JHB. Prosthesis satisfaction in lower limb amputees: a systematic review of associated factors and questionnaires. Medicine (Baltimore). 2018;97(39):e12296. doi:10.1097/MD.0000000000012296
- Murray CD, Fox J. Body image and prosthesis satisfaction in the lower limb amputee. Disabil Rehabil. 2002;24(17):925–931. doi:10.1080/09638280210150014
- Major MJ, Quinlan J, Hansen AH, Esposito ER. Effects of women’s footwear on the mechanical function of heel-height accommodating prosthetic feet. PLoS One. 2022;17(1). doi:10.1371/journal.pone.0262910.
- Kuo PB, Lehavot K, Thomas RM, et al. Gender differences in prosthesis-related outcomes among veterans: results of a national survey of U.S. veterans. PM R. 2024;16(3):239- 249. doi:10.1002/pmrj.13028
- Asano M, Rushton P, Miller WC, Deathe BA. Predictors of quality of life among individuals who have a lower limb amputation. Prosthet Orthot Int. 2008;32(2):231-243. doi:10.1080/03093640802024955
- Ziegler-Graham K, MacKenzie EJ, Ephraim PL, Travison TG, Brookmeyer R. Estimating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422-429. doi:10.1016/j.apmr.2007.11.005
- Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputation and limb deficiency: epidemiology and recent trends in the united states. South Med J. 2002;95(8):875-883. doi:10.1097/00007611-200208000-00018
- Dillingham TR, Pezzin LE, Shore AD. Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil. 2005;86(3):480-486. doi:10.1016/j.apmr.2004.06.072
- Centers for Disease Control and Prevention. Ambulatory and inpatient procedures in the United States. Accessed September 30, 2024. https://www.cdc.gov/nchs/pressroom/98facts/ambulat.htm
- Ljung J, Iacangelo A. Identifying and acknowledging a sex gap in lower-limb prosthetics. JPO. 2024;36(1):e18-e24. doi:10.1097/JPO.0000000000000470
- Feinglass J, Brown JL, LoSasso A, et al. Rates of lower-extremity amputation and arterial reconstruction in the united states, 1979 to 1996. Am J Public Health. 1999;89(8):1222- 1227. doi:10.2105/ajph.89.8.1222
- Mayfield JA, Reiber GE, Maynard C, Czerniecki JM, Caps MT, Sangeorzan BJ. Trends in lower limb amputation in the Veterans Health Administration, 1989-1998. J Rehabil Res Dev. 2000;37(1):23-30.
- Feinglass J, Pearce WH, Martin GJ, et al. Postoperative and late survival outcomes after major amputation: findings from the department of veterans affairs national surgical quality improvement program. Surgery. 2001;130(1):21-29. doi:10.1067/msy.2001.115359
- Lehavot K, Young JP, Thomas RM, et al. Voices of women veterans with lower limb prostheses: a qualitative study. J Gen Intern Med. 2022;37(3):799-805. doi:10.1007/s11606-022-07572-8
- US Government Accountability Office. COVID-19: Opportunities to improve federal response. GAO-21-60. Published November 12, 2020. Accessed September 30, 2024. https://www.gao.gov/products/gao-21-60
- Littman AJ, Peterson AC, Korpak A, et al. Differences in prosthetic prescription between men and women veterans after transtibial or transfemoral lowerextremity amputation: a longitudinal cohort study. Arch Phys Med Rehabil. 2023;104(8)1274-1281. doi:10.1016/j.amjsurg.2023.02.011
- Cimino SR, Vijayakumar A, MacKay C, Mayo AL, Hitzig SL, Guilcher SJT. Sex and gender differences in quality of life and related domains for individuals with adult acquired lower-limb amputation: a scoping review. Disabil Rehabil. 2022 Oct 23;44(22):6899-6925. doi:10.1080/09638288.2021.1974106
- DadeMatthews OO, Roper JA, Vazquez A, Shannon DM, Sefton JM. Prosthetic device and service satisfaction, quality of life, and functional performance in lower limb prosthesis clients. Prosthet Orthot Int. 2024;48(4):422-430. doi:10.1097/PXR.0000000000000285
- Hamilton AB, Schwarz EB, Thomas HN, Goldstein KM. Moving women veterans’ health research forward: a special supplement. J Gen Intern Med. 2022;37(Suppl3):665– 667. doi:10.1007/s11606-022-07606-1
- US Congress. Public Law 116-315: An Act to Improve the Lives of Veterans, S 5108 (2) (F). 116th Congress; 2021. Accessed September 30, 2024. https://www.congress.gov/116/plaws/publ315/PLAW-116publ315.pdf
- Gallagher P, MacLachlan M. The Trinity amputation and prosthesis experience scales and quality of life in people with lower-limb amputation. Arch Phys Med Rehabil. 2004;85(5):730-736. doi:10.1016/j.apmr.2003.07.009
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for persons with lower limb amputations: assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931-938. doi:10.1016/s0003-9993(98)90090-9
- Heinemann AW, Bode RK, O’Reilly C. Development and measurement properties of the orthotics and prosthetics users’ survey (OPUS): a comprehensive set of clinical outcome instruments. Prosthet Orthot Int. 2003;27(3):191-206. doi:10.1080/03093640308726682
- Resnik LJ, Borgia ML, Clark MA. A national survey of prosthesis use in veterans with major upper limb amputation: comparisons by gender. PM R. 2020;12(11):1086-1098. doi:10.1002/pmrj.12351
- Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229-238. doi:10.1023/a:1023254226592
- Østlie K, Lesjø IM, Franklin RJ, Garfelt B, Skjeldal OH, Magnus P. Prosthesis rejection in acquired major upper-limb amputees: a population-based survey. Disabil Rehabil Assist Technol. 2012;7(4):294-303. doi:10.3109/17483107.2011.635405
- Pezzin LE, Dillingham TR, MacKenzie EJ, Ephraim P, Rossbach P. Use and satisfaction with prosthetic limb devices and related services. Arch Phys Med Rehabil. 2004;85(5):723-729. doi:10.1016/j.apmr.2003.06.002
- Deans S, Burns D, McGarry A, Murray K, Mutrie N. Motivations and barriers to prosthesis users participation in physical activity, exercise and sport: a review of the literature. Prosthet Orthot Int. 2012;36(3):260-269. doi:10.1177/0309364612437905
- McDonald CL, Kahn A, Hafner BJ, Morgan SJ. Prevalence of secondary prosthesis use in lower limb prosthesis users. Disabil Rehabil. 2023;46(5):1016-1022. doi:10.1080/09638288.2023.2182919
- Baars EC, Schrier E, Dijkstra PU, Geertzen JHB. Prosthesis satisfaction in lower limb amputees: a systematic review of associated factors and questionnaires. Medicine (Baltimore). 2018;97(39):e12296. doi:10.1097/MD.0000000000012296
- Murray CD, Fox J. Body image and prosthesis satisfaction in the lower limb amputee. Disabil Rehabil. 2002;24(17):925–931. doi:10.1080/09638280210150014
- Major MJ, Quinlan J, Hansen AH, Esposito ER. Effects of women’s footwear on the mechanical function of heel-height accommodating prosthetic feet. PLoS One. 2022;17(1). doi:10.1371/journal.pone.0262910.
- Kuo PB, Lehavot K, Thomas RM, et al. Gender differences in prosthesis-related outcomes among veterans: results of a national survey of U.S. veterans. PM R. 2024;16(3):239- 249. doi:10.1002/pmrj.13028
- Asano M, Rushton P, Miller WC, Deathe BA. Predictors of quality of life among individuals who have a lower limb amputation. Prosthet Orthot Int. 2008;32(2):231-243. doi:10.1080/03093640802024955
Satisfaction With Department of Veterans Affairs Prosthetics and Support Services as Reported by Women and Men Veterans
Satisfaction With Department of Veterans Affairs Prosthetics and Support Services as Reported by Women and Men Veterans
 visual information does not imply or constitute DoD endorsement.")
Key Updates in Resuscitation Procedure After Drowning
New recommendations on rescuing adults and children who have drowned include an important update for healthcare professionals, trained rescuers, and untrained lay rescuers.
The American Heart Association (AHA) and the American Academy of Pediatrics (AAP) have issued recommendations that highlight delivering rescue breaths as well as calling 911 and performing chest compressions in cardiopulmonary resuscitation (CPR) as first steps when a person pulled from the water is in cardiac arrest.
This is the first collaboration between the two organizations on resuscitation after drowning. The recommendations were published simultaneously in Circulation and Pediatrics.
Included in the recommendations are two key principles:
- Anyone pulled from the water who has no signs of normal breathing or consciousness should be presumed to be in cardiac arrest.
- Rescuers should immediately start CPR that includes rescue breathing in addition to chest compressions. Multiple large studies show more people with cardiac arrest from noncardiac causes such as drowning survive when CPR includes rescue breaths, compared with hands-only CPR (calling 911 and pushing hard and fast in the center of the chest).
If someone is untrained, unwilling, or unable to give breaths, they can perform chest compressions until help arrives, the recommendations advise.
Reasoning Behind the Update
The authors, led by writing group cochair Tracy E. McCallin, MD, associate professor in the division of pediatric emergency medicine at Rainbow Babies and Children’s Hospital in Cleveland , Ohio, explained that drowning generally advances from initial respiratory arrest from submersion-related hypoxia to cardiac arrest, and therefore it can be difficult to distinguish respiratory arrest from cardiac arrest because pulses are difficult to accurately palpate within the recommended 10-second window.
“Therefore, resuscitation from cardiac arrest due to this specific circumstance must focus on restoring breathing as much as it does circulation,” the authors wrote.
Resuscitation after drowning may begin in the water with rescue breathing when safely provided by trained rescuers and should continue with chest compressions, once the drowned person and the rescuer are on land or in a boat, the report authors wrote.
“The focused update on drowning contains the most up-to-date, evidence-based recommendations on how to resuscitate someone who has drowned,” McCallin states in a press release.
In addition to the new guidance on rescue breaths, the update includes new topics that the AHA has not previously addressed with treatment recommendations, such as oxygen administration after drowning; automated external defibrillator use in cardiac arrest after drowning and public-access defibrillation programs.
Pediatricians Can Help Spread the Word
Alexandra Stern, MD, assistant professor in the Department of Pediatrics at University of Florida, Gainesville, who was not part of the update, said pediatricians can help disseminate this new information.
“Water safety is a topic frequently discussed as a pediatrician, with focus often being on primary prevention of drowning,” she said. “We stress the importance of the multiple layers of protection against drowning, such as touch supervision (staying within arm’s length); secure fencing, access to appropriate life jackets, and teaching our children to swim. Learning CPR is a large part of these measures and continuing these discussions with our patients and families is important.”
She added that updating the recommended procedures will likely require changes to all forms of education and community outreach regarding drowning from basic life support classes to more advanced lifeguard training. She noted that the update provides practical guidance not just for trained rescuers and healthcare professionals, but also for family members.
The paper notes that drowning is the third leading cause of death from unintentional injury globally, accounting for 7% of all injury-related deaths. In the United States, drowning is the leading cause of death in children aged 1-4 years and the second leading cause of death from unintentional injury in children aged 5-14 years.
The update is based on systematic reviews from 2021 to 2023 performed by the International Liaison Committee on Resuscitation related to the resuscitation of drowning.
The authors and Stern reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
New recommendations on rescuing adults and children who have drowned include an important update for healthcare professionals, trained rescuers, and untrained lay rescuers.
The American Heart Association (AHA) and the American Academy of Pediatrics (AAP) have issued recommendations that highlight delivering rescue breaths as well as calling 911 and performing chest compressions in cardiopulmonary resuscitation (CPR) as first steps when a person pulled from the water is in cardiac arrest.
This is the first collaboration between the two organizations on resuscitation after drowning. The recommendations were published simultaneously in Circulation and Pediatrics.
Included in the recommendations are two key principles:
- Anyone pulled from the water who has no signs of normal breathing or consciousness should be presumed to be in cardiac arrest.
- Rescuers should immediately start CPR that includes rescue breathing in addition to chest compressions. Multiple large studies show more people with cardiac arrest from noncardiac causes such as drowning survive when CPR includes rescue breaths, compared with hands-only CPR (calling 911 and pushing hard and fast in the center of the chest).
If someone is untrained, unwilling, or unable to give breaths, they can perform chest compressions until help arrives, the recommendations advise.
Reasoning Behind the Update
The authors, led by writing group cochair Tracy E. McCallin, MD, associate professor in the division of pediatric emergency medicine at Rainbow Babies and Children’s Hospital in Cleveland , Ohio, explained that drowning generally advances from initial respiratory arrest from submersion-related hypoxia to cardiac arrest, and therefore it can be difficult to distinguish respiratory arrest from cardiac arrest because pulses are difficult to accurately palpate within the recommended 10-second window.
“Therefore, resuscitation from cardiac arrest due to this specific circumstance must focus on restoring breathing as much as it does circulation,” the authors wrote.
Resuscitation after drowning may begin in the water with rescue breathing when safely provided by trained rescuers and should continue with chest compressions, once the drowned person and the rescuer are on land or in a boat, the report authors wrote.
“The focused update on drowning contains the most up-to-date, evidence-based recommendations on how to resuscitate someone who has drowned,” McCallin states in a press release.
In addition to the new guidance on rescue breaths, the update includes new topics that the AHA has not previously addressed with treatment recommendations, such as oxygen administration after drowning; automated external defibrillator use in cardiac arrest after drowning and public-access defibrillation programs.
Pediatricians Can Help Spread the Word
Alexandra Stern, MD, assistant professor in the Department of Pediatrics at University of Florida, Gainesville, who was not part of the update, said pediatricians can help disseminate this new information.
“Water safety is a topic frequently discussed as a pediatrician, with focus often being on primary prevention of drowning,” she said. “We stress the importance of the multiple layers of protection against drowning, such as touch supervision (staying within arm’s length); secure fencing, access to appropriate life jackets, and teaching our children to swim. Learning CPR is a large part of these measures and continuing these discussions with our patients and families is important.”
She added that updating the recommended procedures will likely require changes to all forms of education and community outreach regarding drowning from basic life support classes to more advanced lifeguard training. She noted that the update provides practical guidance not just for trained rescuers and healthcare professionals, but also for family members.
The paper notes that drowning is the third leading cause of death from unintentional injury globally, accounting for 7% of all injury-related deaths. In the United States, drowning is the leading cause of death in children aged 1-4 years and the second leading cause of death from unintentional injury in children aged 5-14 years.
The update is based on systematic reviews from 2021 to 2023 performed by the International Liaison Committee on Resuscitation related to the resuscitation of drowning.
The authors and Stern reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
New recommendations on rescuing adults and children who have drowned include an important update for healthcare professionals, trained rescuers, and untrained lay rescuers.
The American Heart Association (AHA) and the American Academy of Pediatrics (AAP) have issued recommendations that highlight delivering rescue breaths as well as calling 911 and performing chest compressions in cardiopulmonary resuscitation (CPR) as first steps when a person pulled from the water is in cardiac arrest.
This is the first collaboration between the two organizations on resuscitation after drowning. The recommendations were published simultaneously in Circulation and Pediatrics.
Included in the recommendations are two key principles:
- Anyone pulled from the water who has no signs of normal breathing or consciousness should be presumed to be in cardiac arrest.
- Rescuers should immediately start CPR that includes rescue breathing in addition to chest compressions. Multiple large studies show more people with cardiac arrest from noncardiac causes such as drowning survive when CPR includes rescue breaths, compared with hands-only CPR (calling 911 and pushing hard and fast in the center of the chest).
If someone is untrained, unwilling, or unable to give breaths, they can perform chest compressions until help arrives, the recommendations advise.
Reasoning Behind the Update
The authors, led by writing group cochair Tracy E. McCallin, MD, associate professor in the division of pediatric emergency medicine at Rainbow Babies and Children’s Hospital in Cleveland , Ohio, explained that drowning generally advances from initial respiratory arrest from submersion-related hypoxia to cardiac arrest, and therefore it can be difficult to distinguish respiratory arrest from cardiac arrest because pulses are difficult to accurately palpate within the recommended 10-second window.
“Therefore, resuscitation from cardiac arrest due to this specific circumstance must focus on restoring breathing as much as it does circulation,” the authors wrote.
Resuscitation after drowning may begin in the water with rescue breathing when safely provided by trained rescuers and should continue with chest compressions, once the drowned person and the rescuer are on land or in a boat, the report authors wrote.
“The focused update on drowning contains the most up-to-date, evidence-based recommendations on how to resuscitate someone who has drowned,” McCallin states in a press release.
In addition to the new guidance on rescue breaths, the update includes new topics that the AHA has not previously addressed with treatment recommendations, such as oxygen administration after drowning; automated external defibrillator use in cardiac arrest after drowning and public-access defibrillation programs.
Pediatricians Can Help Spread the Word
Alexandra Stern, MD, assistant professor in the Department of Pediatrics at University of Florida, Gainesville, who was not part of the update, said pediatricians can help disseminate this new information.
“Water safety is a topic frequently discussed as a pediatrician, with focus often being on primary prevention of drowning,” she said. “We stress the importance of the multiple layers of protection against drowning, such as touch supervision (staying within arm’s length); secure fencing, access to appropriate life jackets, and teaching our children to swim. Learning CPR is a large part of these measures and continuing these discussions with our patients and families is important.”
She added that updating the recommended procedures will likely require changes to all forms of education and community outreach regarding drowning from basic life support classes to more advanced lifeguard training. She noted that the update provides practical guidance not just for trained rescuers and healthcare professionals, but also for family members.
The paper notes that drowning is the third leading cause of death from unintentional injury globally, accounting for 7% of all injury-related deaths. In the United States, drowning is the leading cause of death in children aged 1-4 years and the second leading cause of death from unintentional injury in children aged 5-14 years.
The update is based on systematic reviews from 2021 to 2023 performed by the International Liaison Committee on Resuscitation related to the resuscitation of drowning.
The authors and Stern reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
From Pediatrics
Caregiver Surveys on Firearms, Suicide Offer Pediatricians Prevention Opportunities
ORLANDO, FLORIDA — , according to researchers who presented their findings at the American Academy of Pediatrics (AAP) 2024 National Conference.
An estimated 4.6 million US homes with children have firearms that are loaded and unlocked, a risk factor for youth suicide, yet only about half of parents of suicidal children had been screened for gun ownership in the hospital even as most would be receptive to both firearm screening and counseling, found one study in Texas.
In another study in Colorado, nearly all firearm owners believed that securely storing guns reduces the risk for firearm injury or death, but owners were less likely than non-owners to believe suicide is preventable or that removing a gun from the home reduces the risk for injury or death.
“Previous studies have shown that when pediatricians discuss the importance of armed safe storage guidance with families, families are actually more likely to go home and store firearms safely — storing them locked, unloaded, and separate from the ammunition,” said study author Taylor Rosenbaum, MD, a former pediatric fellow at Baylor College of Medicine/Texas Children’s Hospital in Houston and now an assistant professor at Children’s Hospital University of Miami. “However, previous studies have also shown that pediatricians really are not discussing firearm safe storage with our patients and their families, and we see this both in the outpatient setting, but especially in the inpatient setting for youth suicides, which have risen since 2020 and now are the second leading cause of death for those who are 10-24 years old in the United States.”

Firearm Safety Is a Necessary Conversation
The leading cause of death among children and teens aged 1-19 years is actually firearms, which are also the most fatal method for suicide. While only 4% of all suicide attempts in youth are fatal, 90% of those attempted with a firearm are fatal, Dr. Rosenbaum said. In addition, she said, 80% of the guns used in attempted suicide by children and teens belonged to a family member, and an estimated 70% of firearm-related suicides in youth can be prevented with safe storage of guns.
“This really gives us, as pediatricians, something actionable to do during these hospitalizations” for suicidal ideation or attempts, Dr. Rosenbaum said. “We know that when pediatricians discuss the importance of firearm safe storage guidance with families, they’re more likely to store their firearm safely,” Dr. Rosenbaum said. “We also know that families are not being screened for firearm ownership, that caregivers of youth who are in the hospital for suicidal thoughts or actions want their healthcare team to be screening for firearms, to be giving them information on how to safely secure their firearms, and to be providing free firearm blocks.”
Nathan Boonstra, MD, a general pediatrician at Blank Children’s Hospital, Des Moines, Iowa, said these findings are encouraging in terms of the opportunity pediatricians have.
“There is so much politicization around even basic firearm safety that pediatricians might shy away from the topic, but this research is reassuring that parents are receptive to our advice on safe gun storage,” said Dr. Boonstra, who was not involved in any of this presented research. “It’s especially important for pediatricians to address home firearms when their patient has a history of suicidal ideation or an attempt.”
Reducing the Risk
The Colorado findings similarly reinforce the opportunity physicians have to help caregivers reduce suicide risk, according to Maya Haasz, MD, an associate professor of pediatrics and emergency medicine at the University of Colorado Anschutz Medical Campus, Aurora, Colorado.
“Only 60% of firearm owners believed that removing firearms from the home in times of mental health crisis can decrease the risk of suicide,” she said. “These findings are really concerning, but what we found on the flip side was that 93% of firearm owners actually believe that secure storage can overall decrease the risk for firearm injury and death. So overall, we are underestimating the risk for suicide in our community, and we’re also underestimating our ability to prevent it.”

That presents an opportunity, Dr. Haasz said, “to educate families both about the preventability of suicide but also to have specific strategies, like secure storage and temporary removable requirements from the home, that can prevent suicide.”
Dr. Boonstra found it “disheartening that so many children live in a house with an unlocked and even loaded firearm when the evidence is so clear that this is a significant risk factor for youth suicide,” he said. “It’s also disheartening, though not too surprising, that families with a firearm are less likely to think that youth suicide can be prevented.”
Survey Results
Dr. Rosenbaum’s team conducted the survey in Houston with caregivers whose children were 8-21 years old and hospitalized for suicidal ideation or attempts at a large children’s hospital and two nearby community hospitals between June 2023 and May 2024. The respondents were 46% White and 23% Black, and 47% of the population were Hispanic, all but three of whom were not gun owners.
Among 244 potential participants, only 150 were eligible and approached, and 100 of these completed the surveys, including 26% firearm owners and 68% non-owners. Most of the youth (74%) were aged 14-17 years, and about three in four respondents were their mothers. Only half of the respondents (51%) said the healthcare provider had asked them whether they owned a gun.
One of the key findings Dr. Rosenbaum highlighted was the receptiveness of firearm-owning caregivers to advice from healthcare providers about ownership. If the healthcare team advised parents not to have any guns in the home for the safety of their child with self-arm, 58% of the firearm owners would follow the advice and 27% would consider it, with none saying they would be offended by it.
Among the firearm owners, 81% said their guns were safely secured where they did not believe their child could access it, which meant one in five youth had unsecured access to firearms. Most of the gun owners (77%), like the non-owners (70%), were “not at all worried” about their child getting ahold of a gun in the home, though 11.5% of the firearm owners were “very worried” about it. Interestingly, more gun owners (19%) were very worried about their children accessing a gun outside their home, a concern shared by 37% of non-owners. Nearly twice as many gun owners (46%) as non-owners (25%) were not at all worried about their child getting a gun outside the home.
The vast majority of respondents — 88% of gun owners and 91% of non-owners — felt it was “very important for the healthcare team to ask parents of children with suicidal ideation/attempts about firearms in the home.” Similarly, high proportions believed it was important for the healthcare team to counsel those parents on safe gun storage. Although only 69% of firearm owners believed it was important to distribute firearm locks in the hospital, 81% would be interested in receiving a free one. Significantly more of the non-owners (80%; P = .02) believed free lock distribution was important, and 72% of non-owners would also be interested in one.
About half the respondents (55%) preferred to hear firearm counseling one-on-one from a provider, whereas 31% would like written information and 27% would be interested in a video. In terms of what information parents preferred to receive, a little over half of owners (54%) and non-owners (56%) were interested in how or when (50% and 40%, respectively) to discuss the topic with their child. Only about a third (35% owners and 37% non-owners) wanted information on how to discuss the topic with the parents of their child’s friends.
The survey’s biggest limitations after its small size were the selection bias of those willing to complete the survey and potential response bias from the self-reported data.
The study of Colorado caregivers, just published in Pediatrics, surveyed 512 Colorado caregivers in April-May 2023 to learn about their beliefs and perceptions regarding firearms, firearm storage and risk, and youth suicide (2024 Oct 1;154[4]:e2024066930. doi: 10.1542/peds.2024-066930). Just over half the respondents (52%) had grown up in a household with firearms, and 44% currently lived in a household with a gun. The sample was 43% men and 88% White, predominantly non-Hispanic (75%), with 11% living in rural areas and 19% who currently or previously served in the military. Most (79%) had a child age 12 or younger in the home.
Only about one in four caregivers (24%) correctly answered that suicide is the leading cause of firearm death in Colorado, with similar rates of correct responses among both firearm owners and non-firearm owners. Both groups were also similarly likely (64% overall) to be concerned about youth suicide in their community, though those from homes with firearms were less likely to be concerned about youth suicide in their own family (28%) than those from homes without firearms (39%; P = .013).
In addition, caregivers from homes with versus without firearms were considerably less likely to believe suicide can be prevented (48% vs 69%) and were less likely to believe that temporarily removing a firearm from the home reduces the risk for gun injury or death (60% vs 78%; P < .001 for both comparisons).
Firearm owners were also much less likely than non-owners to believe keeping a gun in the home makes it more dangerous (7% vs 29%) and over twice as likely to think keeping a firearm makes their home safer (52% vs 22%; P < .001). The vast majority of respondents (89%) believed secure storage of guns reduces the risk for injury or death, though the response was higher for firearm owners (93%) than for non-owners (86%; P < .001).
“Our finding that most firearm owners believe that secure firearm storage is protective against firearm injury is a promising messaging strategy,” the authors wrote. “It presents a preventive education opportunity for adults living with children who have mental health concerns, who may benefit most from secure in-home storage and/or temporary and voluntary storage of firearms away from home.”
Firearm Injuries
A separate study at the AAP conference underscored the devastating impact of firearm injuries even among those who survive, whether self-inflicted or not, and the potential for reducing healthcare treatment and costs from effective prevention efforts. A national analysis of pediatric inpatient data from 2017 to 2020 calculated how much greater the burden of healthcare treatment and costs is for firearm injuries of any kind compared with penetrating traumas and blunt traumas.
“As a surgical resident, I have seen these patients who make it into the trauma bed that we are then faced to care for,” said Colleen Nofi, DO, PhD, MBA, a general surgery resident at Cohen Children’s Medical Center at Northwell Health in New York. “Anecdotally, we understand that the devastation and injury caused by bullets far outweighs the injuries caused by other trauma mechanisms,” but the actual calculation of the burden hasn’t been studied.

Among 6615 firearm injuries, 9787 penetrating traumas and 66,003 blunt traumas examined from the National Inpatient Sample Healthcare Cost and Utilization Project Database, 11% of firearm traumas required a transfusion of red blood cells, compared with 1.4% of penetrating traumas and 3% of blunt traumas (P < .001). Patients with firearm injuries also had a longer length of stay — 10.8 days compared with 8.3 for patients with penetrating trauma and 9.8 for those with blunt trauma — and significantly higher rates of CPR, pericardiotomy, chest tube, exploratory laparotomy and/or thoracotomy, colorectal surgery, small bowel surgery, ostomy formation, splenectomy, hepatic resection, tracheostomy, and feeding tube placement.
Pulmonary complications were higher for firearm injuries (4.9%) than for penetrating trauma (0.6%) or blunt trauma (2.9%), and septicemia rates were also higher (1.7% vs 0.2% and 1%, respectively). Cardiac, neurologic, and urinary complications were also significantly and substantially higher for firearm injuries, 6.9% of which resulted in death compared with 0.2% of penetrating traumas and 1.2% of blunt traumas.
The costs from firearm injuries were also significantly higher than the costs from other traumas; “firearm injury remained independently predictive of greater hospital costs, even when controlling for injury severity as well as age, sex, race, insurance, region, hospital type, and household income.
“These findings underscore the urgent need for targeted prevention, supportive measures, and resource allocation to mitigate the devastating impact of firearm injuries on children and healthcare systems alike,” Dr. Nofi said.
The Colorado study was funded by the Colorado Department of Public Health and Environment and a National Institutes of Health grant to Dr. Haasz. The Texas study and the one from Northwell Health did not note any external funding. Dr. Haasz, Dr. Rosenbaum, Dr. Boonstra, and Dr. Nofi had no disclosures.
A version of this article appeared on Medscape.com.
ORLANDO, FLORIDA — , according to researchers who presented their findings at the American Academy of Pediatrics (AAP) 2024 National Conference.
An estimated 4.6 million US homes with children have firearms that are loaded and unlocked, a risk factor for youth suicide, yet only about half of parents of suicidal children had been screened for gun ownership in the hospital even as most would be receptive to both firearm screening and counseling, found one study in Texas.
In another study in Colorado, nearly all firearm owners believed that securely storing guns reduces the risk for firearm injury or death, but owners were less likely than non-owners to believe suicide is preventable or that removing a gun from the home reduces the risk for injury or death.
“Previous studies have shown that when pediatricians discuss the importance of armed safe storage guidance with families, families are actually more likely to go home and store firearms safely — storing them locked, unloaded, and separate from the ammunition,” said study author Taylor Rosenbaum, MD, a former pediatric fellow at Baylor College of Medicine/Texas Children’s Hospital in Houston and now an assistant professor at Children’s Hospital University of Miami. “However, previous studies have also shown that pediatricians really are not discussing firearm safe storage with our patients and their families, and we see this both in the outpatient setting, but especially in the inpatient setting for youth suicides, which have risen since 2020 and now are the second leading cause of death for those who are 10-24 years old in the United States.”
Firearm Safety Is a Necessary Conversation
The leading cause of death among children and teens aged 1-19 years is actually firearms, which are also the most fatal method for suicide. While only 4% of all suicide attempts in youth are fatal, 90% of those attempted with a firearm are fatal, Dr. Rosenbaum said. In addition, she said, 80% of the guns used in attempted suicide by children and teens belonged to a family member, and an estimated 70% of firearm-related suicides in youth can be prevented with safe storage of guns.
“This really gives us, as pediatricians, something actionable to do during these hospitalizations” for suicidal ideation or attempts, Dr. Rosenbaum said. “We know that when pediatricians discuss the importance of firearm safe storage guidance with families, they’re more likely to store their firearm safely,” Dr. Rosenbaum said. “We also know that families are not being screened for firearm ownership, that caregivers of youth who are in the hospital for suicidal thoughts or actions want their healthcare team to be screening for firearms, to be giving them information on how to safely secure their firearms, and to be providing free firearm blocks.”
Nathan Boonstra, MD, a general pediatrician at Blank Children’s Hospital, Des Moines, Iowa, said these findings are encouraging in terms of the opportunity pediatricians have.
“There is so much politicization around even basic firearm safety that pediatricians might shy away from the topic, but this research is reassuring that parents are receptive to our advice on safe gun storage,” said Dr. Boonstra, who was not involved in any of this presented research. “It’s especially important for pediatricians to address home firearms when their patient has a history of suicidal ideation or an attempt.”
Reducing the Risk
The Colorado findings similarly reinforce the opportunity physicians have to help caregivers reduce suicide risk, according to Maya Haasz, MD, an associate professor of pediatrics and emergency medicine at the University of Colorado Anschutz Medical Campus, Aurora, Colorado.
“Only 60% of firearm owners believed that removing firearms from the home in times of mental health crisis can decrease the risk of suicide,” she said. “These findings are really concerning, but what we found on the flip side was that 93% of firearm owners actually believe that secure storage can overall decrease the risk for firearm injury and death. So overall, we are underestimating the risk for suicide in our community, and we’re also underestimating our ability to prevent it.”
That presents an opportunity, Dr. Haasz said, “to educate families both about the preventability of suicide but also to have specific strategies, like secure storage and temporary removable requirements from the home, that can prevent suicide.”
Dr. Boonstra found it “disheartening that so many children live in a house with an unlocked and even loaded firearm when the evidence is so clear that this is a significant risk factor for youth suicide,” he said. “It’s also disheartening, though not too surprising, that families with a firearm are less likely to think that youth suicide can be prevented.”
Survey Results
Dr. Rosenbaum’s team conducted the survey in Houston with caregivers whose children were 8-21 years old and hospitalized for suicidal ideation or attempts at a large children’s hospital and two nearby community hospitals between June 2023 and May 2024. The respondents were 46% White and 23% Black, and 47% of the population were Hispanic, all but three of whom were not gun owners.
Among 244 potential participants, only 150 were eligible and approached, and 100 of these completed the surveys, including 26% firearm owners and 68% non-owners. Most of the youth (74%) were aged 14-17 years, and about three in four respondents were their mothers. Only half of the respondents (51%) said the healthcare provider had asked them whether they owned a gun.
One of the key findings Dr. Rosenbaum highlighted was the receptiveness of firearm-owning caregivers to advice from healthcare providers about ownership. If the healthcare team advised parents not to have any guns in the home for the safety of their child with self-arm, 58% of the firearm owners would follow the advice and 27% would consider it, with none saying they would be offended by it.
Among the firearm owners, 81% said their guns were safely secured where they did not believe their child could access it, which meant one in five youth had unsecured access to firearms. Most of the gun owners (77%), like the non-owners (70%), were “not at all worried” about their child getting ahold of a gun in the home, though 11.5% of the firearm owners were “very worried” about it. Interestingly, more gun owners (19%) were very worried about their children accessing a gun outside their home, a concern shared by 37% of non-owners. Nearly twice as many gun owners (46%) as non-owners (25%) were not at all worried about their child getting a gun outside the home.
The vast majority of respondents — 88% of gun owners and 91% of non-owners — felt it was “very important for the healthcare team to ask parents of children with suicidal ideation/attempts about firearms in the home.” Similarly, high proportions believed it was important for the healthcare team to counsel those parents on safe gun storage. Although only 69% of firearm owners believed it was important to distribute firearm locks in the hospital, 81% would be interested in receiving a free one. Significantly more of the non-owners (80%; P = .02) believed free lock distribution was important, and 72% of non-owners would also be interested in one.
About half the respondents (55%) preferred to hear firearm counseling one-on-one from a provider, whereas 31% would like written information and 27% would be interested in a video. In terms of what information parents preferred to receive, a little over half of owners (54%) and non-owners (56%) were interested in how or when (50% and 40%, respectively) to discuss the topic with their child. Only about a third (35% owners and 37% non-owners) wanted information on how to discuss the topic with the parents of their child’s friends.
The survey’s biggest limitations after its small size were the selection bias of those willing to complete the survey and potential response bias from the self-reported data.
The study of Colorado caregivers, just published in Pediatrics, surveyed 512 Colorado caregivers in April-May 2023 to learn about their beliefs and perceptions regarding firearms, firearm storage and risk, and youth suicide (2024 Oct 1;154[4]:e2024066930. doi: 10.1542/peds.2024-066930). Just over half the respondents (52%) had grown up in a household with firearms, and 44% currently lived in a household with a gun. The sample was 43% men and 88% White, predominantly non-Hispanic (75%), with 11% living in rural areas and 19% who currently or previously served in the military. Most (79%) had a child age 12 or younger in the home.
Only about one in four caregivers (24%) correctly answered that suicide is the leading cause of firearm death in Colorado, with similar rates of correct responses among both firearm owners and non-firearm owners. Both groups were also similarly likely (64% overall) to be concerned about youth suicide in their community, though those from homes with firearms were less likely to be concerned about youth suicide in their own family (28%) than those from homes without firearms (39%; P = .013).
In addition, caregivers from homes with versus without firearms were considerably less likely to believe suicide can be prevented (48% vs 69%) and were less likely to believe that temporarily removing a firearm from the home reduces the risk for gun injury or death (60% vs 78%; P < .001 for both comparisons).
Firearm owners were also much less likely than non-owners to believe keeping a gun in the home makes it more dangerous (7% vs 29%) and over twice as likely to think keeping a firearm makes their home safer (52% vs 22%; P < .001). The vast majority of respondents (89%) believed secure storage of guns reduces the risk for injury or death, though the response was higher for firearm owners (93%) than for non-owners (86%; P < .001).
“Our finding that most firearm owners believe that secure firearm storage is protective against firearm injury is a promising messaging strategy,” the authors wrote. “It presents a preventive education opportunity for adults living with children who have mental health concerns, who may benefit most from secure in-home storage and/or temporary and voluntary storage of firearms away from home.”
Firearm Injuries
A separate study at the AAP conference underscored the devastating impact of firearm injuries even among those who survive, whether self-inflicted or not, and the potential for reducing healthcare treatment and costs from effective prevention efforts. A national analysis of pediatric inpatient data from 2017 to 2020 calculated how much greater the burden of healthcare treatment and costs is for firearm injuries of any kind compared with penetrating traumas and blunt traumas.
“As a surgical resident, I have seen these patients who make it into the trauma bed that we are then faced to care for,” said Colleen Nofi, DO, PhD, MBA, a general surgery resident at Cohen Children’s Medical Center at Northwell Health in New York. “Anecdotally, we understand that the devastation and injury caused by bullets far outweighs the injuries caused by other trauma mechanisms,” but the actual calculation of the burden hasn’t been studied.
Among 6615 firearm injuries, 9787 penetrating traumas and 66,003 blunt traumas examined from the National Inpatient Sample Healthcare Cost and Utilization Project Database, 11% of firearm traumas required a transfusion of red blood cells, compared with 1.4% of penetrating traumas and 3% of blunt traumas (P < .001). Patients with firearm injuries also had a longer length of stay — 10.8 days compared with 8.3 for patients with penetrating trauma and 9.8 for those with blunt trauma — and significantly higher rates of CPR, pericardiotomy, chest tube, exploratory laparotomy and/or thoracotomy, colorectal surgery, small bowel surgery, ostomy formation, splenectomy, hepatic resection, tracheostomy, and feeding tube placement.
Pulmonary complications were higher for firearm injuries (4.9%) than for penetrating trauma (0.6%) or blunt trauma (2.9%), and septicemia rates were also higher (1.7% vs 0.2% and 1%, respectively). Cardiac, neurologic, and urinary complications were also significantly and substantially higher for firearm injuries, 6.9% of which resulted in death compared with 0.2% of penetrating traumas and 1.2% of blunt traumas.
The costs from firearm injuries were also significantly higher than the costs from other traumas; “firearm injury remained independently predictive of greater hospital costs, even when controlling for injury severity as well as age, sex, race, insurance, region, hospital type, and household income.
“These findings underscore the urgent need for targeted prevention, supportive measures, and resource allocation to mitigate the devastating impact of firearm injuries on children and healthcare systems alike,” Dr. Nofi said.
The Colorado study was funded by the Colorado Department of Public Health and Environment and a National Institutes of Health grant to Dr. Haasz. The Texas study and the one from Northwell Health did not note any external funding. Dr. Haasz, Dr. Rosenbaum, Dr. Boonstra, and Dr. Nofi had no disclosures.
A version of this article appeared on Medscape.com.
ORLANDO, FLORIDA — , according to researchers who presented their findings at the American Academy of Pediatrics (AAP) 2024 National Conference.
An estimated 4.6 million US homes with children have firearms that are loaded and unlocked, a risk factor for youth suicide, yet only about half of parents of suicidal children had been screened for gun ownership in the hospital even as most would be receptive to both firearm screening and counseling, found one study in Texas.
In another study in Colorado, nearly all firearm owners believed that securely storing guns reduces the risk for firearm injury or death, but owners were less likely than non-owners to believe suicide is preventable or that removing a gun from the home reduces the risk for injury or death.
“Previous studies have shown that when pediatricians discuss the importance of armed safe storage guidance with families, families are actually more likely to go home and store firearms safely — storing them locked, unloaded, and separate from the ammunition,” said study author Taylor Rosenbaum, MD, a former pediatric fellow at Baylor College of Medicine/Texas Children’s Hospital in Houston and now an assistant professor at Children’s Hospital University of Miami. “However, previous studies have also shown that pediatricians really are not discussing firearm safe storage with our patients and their families, and we see this both in the outpatient setting, but especially in the inpatient setting for youth suicides, which have risen since 2020 and now are the second leading cause of death for those who are 10-24 years old in the United States.”
Firearm Safety Is a Necessary Conversation
The leading cause of death among children and teens aged 1-19 years is actually firearms, which are also the most fatal method for suicide. While only 4% of all suicide attempts in youth are fatal, 90% of those attempted with a firearm are fatal, Dr. Rosenbaum said. In addition, she said, 80% of the guns used in attempted suicide by children and teens belonged to a family member, and an estimated 70% of firearm-related suicides in youth can be prevented with safe storage of guns.
“This really gives us, as pediatricians, something actionable to do during these hospitalizations” for suicidal ideation or attempts, Dr. Rosenbaum said. “We know that when pediatricians discuss the importance of firearm safe storage guidance with families, they’re more likely to store their firearm safely,” Dr. Rosenbaum said. “We also know that families are not being screened for firearm ownership, that caregivers of youth who are in the hospital for suicidal thoughts or actions want their healthcare team to be screening for firearms, to be giving them information on how to safely secure their firearms, and to be providing free firearm blocks.”
Nathan Boonstra, MD, a general pediatrician at Blank Children’s Hospital, Des Moines, Iowa, said these findings are encouraging in terms of the opportunity pediatricians have.
“There is so much politicization around even basic firearm safety that pediatricians might shy away from the topic, but this research is reassuring that parents are receptive to our advice on safe gun storage,” said Dr. Boonstra, who was not involved in any of this presented research. “It’s especially important for pediatricians to address home firearms when their patient has a history of suicidal ideation or an attempt.”
Reducing the Risk
The Colorado findings similarly reinforce the opportunity physicians have to help caregivers reduce suicide risk, according to Maya Haasz, MD, an associate professor of pediatrics and emergency medicine at the University of Colorado Anschutz Medical Campus, Aurora, Colorado.
“Only 60% of firearm owners believed that removing firearms from the home in times of mental health crisis can decrease the risk of suicide,” she said. “These findings are really concerning, but what we found on the flip side was that 93% of firearm owners actually believe that secure storage can overall decrease the risk for firearm injury and death. So overall, we are underestimating the risk for suicide in our community, and we’re also underestimating our ability to prevent it.”
That presents an opportunity, Dr. Haasz said, “to educate families both about the preventability of suicide but also to have specific strategies, like secure storage and temporary removable requirements from the home, that can prevent suicide.”
Dr. Boonstra found it “disheartening that so many children live in a house with an unlocked and even loaded firearm when the evidence is so clear that this is a significant risk factor for youth suicide,” he said. “It’s also disheartening, though not too surprising, that families with a firearm are less likely to think that youth suicide can be prevented.”
Survey Results
Dr. Rosenbaum’s team conducted the survey in Houston with caregivers whose children were 8-21 years old and hospitalized for suicidal ideation or attempts at a large children’s hospital and two nearby community hospitals between June 2023 and May 2024. The respondents were 46% White and 23% Black, and 47% of the population were Hispanic, all but three of whom were not gun owners.
Among 244 potential participants, only 150 were eligible and approached, and 100 of these completed the surveys, including 26% firearm owners and 68% non-owners. Most of the youth (74%) were aged 14-17 years, and about three in four respondents were their mothers. Only half of the respondents (51%) said the healthcare provider had asked them whether they owned a gun.
One of the key findings Dr. Rosenbaum highlighted was the receptiveness of firearm-owning caregivers to advice from healthcare providers about ownership. If the healthcare team advised parents not to have any guns in the home for the safety of their child with self-arm, 58% of the firearm owners would follow the advice and 27% would consider it, with none saying they would be offended by it.
Among the firearm owners, 81% said their guns were safely secured where they did not believe their child could access it, which meant one in five youth had unsecured access to firearms. Most of the gun owners (77%), like the non-owners (70%), were “not at all worried” about their child getting ahold of a gun in the home, though 11.5% of the firearm owners were “very worried” about it. Interestingly, more gun owners (19%) were very worried about their children accessing a gun outside their home, a concern shared by 37% of non-owners. Nearly twice as many gun owners (46%) as non-owners (25%) were not at all worried about their child getting a gun outside the home.
The vast majority of respondents — 88% of gun owners and 91% of non-owners — felt it was “very important for the healthcare team to ask parents of children with suicidal ideation/attempts about firearms in the home.” Similarly, high proportions believed it was important for the healthcare team to counsel those parents on safe gun storage. Although only 69% of firearm owners believed it was important to distribute firearm locks in the hospital, 81% would be interested in receiving a free one. Significantly more of the non-owners (80%; P = .02) believed free lock distribution was important, and 72% of non-owners would also be interested in one.
About half the respondents (55%) preferred to hear firearm counseling one-on-one from a provider, whereas 31% would like written information and 27% would be interested in a video. In terms of what information parents preferred to receive, a little over half of owners (54%) and non-owners (56%) were interested in how or when (50% and 40%, respectively) to discuss the topic with their child. Only about a third (35% owners and 37% non-owners) wanted information on how to discuss the topic with the parents of their child’s friends.
The survey’s biggest limitations after its small size were the selection bias of those willing to complete the survey and potential response bias from the self-reported data.
The study of Colorado caregivers, just published in Pediatrics, surveyed 512 Colorado caregivers in April-May 2023 to learn about their beliefs and perceptions regarding firearms, firearm storage and risk, and youth suicide (2024 Oct 1;154[4]:e2024066930. doi: 10.1542/peds.2024-066930). Just over half the respondents (52%) had grown up in a household with firearms, and 44% currently lived in a household with a gun. The sample was 43% men and 88% White, predominantly non-Hispanic (75%), with 11% living in rural areas and 19% who currently or previously served in the military. Most (79%) had a child age 12 or younger in the home.
Only about one in four caregivers (24%) correctly answered that suicide is the leading cause of firearm death in Colorado, with similar rates of correct responses among both firearm owners and non-firearm owners. Both groups were also similarly likely (64% overall) to be concerned about youth suicide in their community, though those from homes with firearms were less likely to be concerned about youth suicide in their own family (28%) than those from homes without firearms (39%; P = .013).
In addition, caregivers from homes with versus without firearms were considerably less likely to believe suicide can be prevented (48% vs 69%) and were less likely to believe that temporarily removing a firearm from the home reduces the risk for gun injury or death (60% vs 78%; P < .001 for both comparisons).
Firearm owners were also much less likely than non-owners to believe keeping a gun in the home makes it more dangerous (7% vs 29%) and over twice as likely to think keeping a firearm makes their home safer (52% vs 22%; P < .001). The vast majority of respondents (89%) believed secure storage of guns reduces the risk for injury or death, though the response was higher for firearm owners (93%) than for non-owners (86%; P < .001).
“Our finding that most firearm owners believe that secure firearm storage is protective against firearm injury is a promising messaging strategy,” the authors wrote. “It presents a preventive education opportunity for adults living with children who have mental health concerns, who may benefit most from secure in-home storage and/or temporary and voluntary storage of firearms away from home.”
Firearm Injuries
A separate study at the AAP conference underscored the devastating impact of firearm injuries even among those who survive, whether self-inflicted or not, and the potential for reducing healthcare treatment and costs from effective prevention efforts. A national analysis of pediatric inpatient data from 2017 to 2020 calculated how much greater the burden of healthcare treatment and costs is for firearm injuries of any kind compared with penetrating traumas and blunt traumas.
“As a surgical resident, I have seen these patients who make it into the trauma bed that we are then faced to care for,” said Colleen Nofi, DO, PhD, MBA, a general surgery resident at Cohen Children’s Medical Center at Northwell Health in New York. “Anecdotally, we understand that the devastation and injury caused by bullets far outweighs the injuries caused by other trauma mechanisms,” but the actual calculation of the burden hasn’t been studied.
Among 6615 firearm injuries, 9787 penetrating traumas and 66,003 blunt traumas examined from the National Inpatient Sample Healthcare Cost and Utilization Project Database, 11% of firearm traumas required a transfusion of red blood cells, compared with 1.4% of penetrating traumas and 3% of blunt traumas (P < .001). Patients with firearm injuries also had a longer length of stay — 10.8 days compared with 8.3 for patients with penetrating trauma and 9.8 for those with blunt trauma — and significantly higher rates of CPR, pericardiotomy, chest tube, exploratory laparotomy and/or thoracotomy, colorectal surgery, small bowel surgery, ostomy formation, splenectomy, hepatic resection, tracheostomy, and feeding tube placement.
Pulmonary complications were higher for firearm injuries (4.9%) than for penetrating trauma (0.6%) or blunt trauma (2.9%), and septicemia rates were also higher (1.7% vs 0.2% and 1%, respectively). Cardiac, neurologic, and urinary complications were also significantly and substantially higher for firearm injuries, 6.9% of which resulted in death compared with 0.2% of penetrating traumas and 1.2% of blunt traumas.
The costs from firearm injuries were also significantly higher than the costs from other traumas; “firearm injury remained independently predictive of greater hospital costs, even when controlling for injury severity as well as age, sex, race, insurance, region, hospital type, and household income.
“These findings underscore the urgent need for targeted prevention, supportive measures, and resource allocation to mitigate the devastating impact of firearm injuries on children and healthcare systems alike,” Dr. Nofi said.
The Colorado study was funded by the Colorado Department of Public Health and Environment and a National Institutes of Health grant to Dr. Haasz. The Texas study and the one from Northwell Health did not note any external funding. Dr. Haasz, Dr. Rosenbaum, Dr. Boonstra, and Dr. Nofi had no disclosures.
A version of this article appeared on Medscape.com.
From AAP 2024
Heat-Related Pediatric ED Visits More Than Double
ORLANDO – according to research presented at the annual meeting of the American Academy of Pediatrics (AAP).
“Our study really highlights the adverse effects that can come from extreme heat, and how increasing heat-related illness is affecting our children,” Taylor Merritt, MD, a pediatric resident at the University of Texas Southwestern Medical Center and Children’s Health in Dallas, said during a press briefing.

Underestimating the Problem?
Lori Byron, MD, a pediatrician from Red Lodge, Montana, who heads the AAP Chapter Climate Advocates program and was not involved in this research, was not surprised by the findings. “If anything, we’re vastly underestimating it because when people come in with heat exhaustion or heat smoke, that gets coded correctly, but when people come in with heart attacks, asthma attacks, strokes, and other exacerbations of chronic disease, it very rarely gets coded as a heat-related illness.”
Record-breaking summer temperatures from the changing climate have led to increased heat-related morbidity and mortality. Past research suggests that children and teens make up nearly half of all those affected by heat-related illnesses, she noted. 2023, for example, was the hottest year on record, and 2024 is predicted to be hotter, Dr. Merritt said.
A Sharp Increase in Cases
The retrospective study examined emergency department diagnoses during May-September from 2012-2023 at two large children’s hospitals within a north Texas pediatric health care system. The researchers compared heat-specific conditions with rhabdomyolysis encounters based on ICD-10 coding.
Heat-specific conditions include heatstroke/sunstroke, exertion heatstroke, heat syncope, heat crap, heat exhaustion, heat fatigue, heat edema, and exposure to excessive natural heat. Rhabdomyolysis encounters included both exertional and nonexertional rhabdomyolysis as well as non-traumatic rhabdomyolysis and elevated creatine kinase (CK) levels.
Among 542 heat-related encounters, 77% had heat-specific diagnoses and 24% had a rhabdomyolysis diagnosis. Combined, heat-related encounters increased 170% from 2012 to 2023, from 4.3 per 10,000 to 11.6 per 10,000 (P = .1). Summer months with higher peak temperatures were also associated with higher heat-related volume in the emergency department (P < .001).
Teenage boys were most likely to have rhabdomyolysis, with 82% of the cases occurring in boys and 70% in ages 12-18 (P < .001). “Compared to the rhabdomyolysis group, the heat-specific group was more likely to be younger, Hispanic, use government-based insurance, and live in an area with a lower Child Opportunity Index,” Dr. Merritt reported. “Most heat-specific encounters resulted in an ED discharge (96%), while most rhabdomyolysis encounters resulted in hospital admission (63%)” (P < .001).
”Thankfully, pediatric heat-related illness is still relatively rare,” Dr. Merritt said. “However, given the context of increasing temperatures, this is important for us all to know, anyone who cares for children, whether that be families or parents or pediatricians.”
Prevention Is Key
Dr. Byron noted that about half of AAP chapters now have climate committees, many of which have created educational materials on heat and wildfire smoke and on talking with athletes about risk of heat-related illnesses.
“A lot of the state high school sports associations are actually now adopting guidelines on when it’s safe to practice and when it’s safe to play for heat and for smoke, so that’s definitely something that we can talk to parents about and kids about,” Dr. Byron said. “Otherwise, you still have a lot of coaches and a lot of kids out there that think you’re just supposed to be tough and barrel through it.”
Rhabdomyolysis and heat stroke are both potentially deadly illnesses, so the biggest focus needs to be on prevention, Dr. Byron said. “Not just working with individuals in your office, but working within your school or within your state high school sports association is totally within the lane of a pediatrician to get involved.”
The research had no external funding. Dr. Merritt and Dr. Byron had no disclosures.
ORLANDO – according to research presented at the annual meeting of the American Academy of Pediatrics (AAP).
“Our study really highlights the adverse effects that can come from extreme heat, and how increasing heat-related illness is affecting our children,” Taylor Merritt, MD, a pediatric resident at the University of Texas Southwestern Medical Center and Children’s Health in Dallas, said during a press briefing.
Underestimating the Problem?
Lori Byron, MD, a pediatrician from Red Lodge, Montana, who heads the AAP Chapter Climate Advocates program and was not involved in this research, was not surprised by the findings. “If anything, we’re vastly underestimating it because when people come in with heat exhaustion or heat smoke, that gets coded correctly, but when people come in with heart attacks, asthma attacks, strokes, and other exacerbations of chronic disease, it very rarely gets coded as a heat-related illness.”
Record-breaking summer temperatures from the changing climate have led to increased heat-related morbidity and mortality. Past research suggests that children and teens make up nearly half of all those affected by heat-related illnesses, she noted. 2023, for example, was the hottest year on record, and 2024 is predicted to be hotter, Dr. Merritt said.
A Sharp Increase in Cases
The retrospective study examined emergency department diagnoses during May-September from 2012-2023 at two large children’s hospitals within a north Texas pediatric health care system. The researchers compared heat-specific conditions with rhabdomyolysis encounters based on ICD-10 coding.
Heat-specific conditions include heatstroke/sunstroke, exertion heatstroke, heat syncope, heat crap, heat exhaustion, heat fatigue, heat edema, and exposure to excessive natural heat. Rhabdomyolysis encounters included both exertional and nonexertional rhabdomyolysis as well as non-traumatic rhabdomyolysis and elevated creatine kinase (CK) levels.
Among 542 heat-related encounters, 77% had heat-specific diagnoses and 24% had a rhabdomyolysis diagnosis. Combined, heat-related encounters increased 170% from 2012 to 2023, from 4.3 per 10,000 to 11.6 per 10,000 (P = .1). Summer months with higher peak temperatures were also associated with higher heat-related volume in the emergency department (P < .001).
Teenage boys were most likely to have rhabdomyolysis, with 82% of the cases occurring in boys and 70% in ages 12-18 (P < .001). “Compared to the rhabdomyolysis group, the heat-specific group was more likely to be younger, Hispanic, use government-based insurance, and live in an area with a lower Child Opportunity Index,” Dr. Merritt reported. “Most heat-specific encounters resulted in an ED discharge (96%), while most rhabdomyolysis encounters resulted in hospital admission (63%)” (P < .001).
”Thankfully, pediatric heat-related illness is still relatively rare,” Dr. Merritt said. “However, given the context of increasing temperatures, this is important for us all to know, anyone who cares for children, whether that be families or parents or pediatricians.”
Prevention Is Key
Dr. Byron noted that about half of AAP chapters now have climate committees, many of which have created educational materials on heat and wildfire smoke and on talking with athletes about risk of heat-related illnesses.
“A lot of the state high school sports associations are actually now adopting guidelines on when it’s safe to practice and when it’s safe to play for heat and for smoke, so that’s definitely something that we can talk to parents about and kids about,” Dr. Byron said. “Otherwise, you still have a lot of coaches and a lot of kids out there that think you’re just supposed to be tough and barrel through it.”
Rhabdomyolysis and heat stroke are both potentially deadly illnesses, so the biggest focus needs to be on prevention, Dr. Byron said. “Not just working with individuals in your office, but working within your school or within your state high school sports association is totally within the lane of a pediatrician to get involved.”
The research had no external funding. Dr. Merritt and Dr. Byron had no disclosures.
ORLANDO – according to research presented at the annual meeting of the American Academy of Pediatrics (AAP).
“Our study really highlights the adverse effects that can come from extreme heat, and how increasing heat-related illness is affecting our children,” Taylor Merritt, MD, a pediatric resident at the University of Texas Southwestern Medical Center and Children’s Health in Dallas, said during a press briefing.
Underestimating the Problem?
Lori Byron, MD, a pediatrician from Red Lodge, Montana, who heads the AAP Chapter Climate Advocates program and was not involved in this research, was not surprised by the findings. “If anything, we’re vastly underestimating it because when people come in with heat exhaustion or heat smoke, that gets coded correctly, but when people come in with heart attacks, asthma attacks, strokes, and other exacerbations of chronic disease, it very rarely gets coded as a heat-related illness.”
Record-breaking summer temperatures from the changing climate have led to increased heat-related morbidity and mortality. Past research suggests that children and teens make up nearly half of all those affected by heat-related illnesses, she noted. 2023, for example, was the hottest year on record, and 2024 is predicted to be hotter, Dr. Merritt said.
A Sharp Increase in Cases
The retrospective study examined emergency department diagnoses during May-September from 2012-2023 at two large children’s hospitals within a north Texas pediatric health care system. The researchers compared heat-specific conditions with rhabdomyolysis encounters based on ICD-10 coding.
Heat-specific conditions include heatstroke/sunstroke, exertion heatstroke, heat syncope, heat crap, heat exhaustion, heat fatigue, heat edema, and exposure to excessive natural heat. Rhabdomyolysis encounters included both exertional and nonexertional rhabdomyolysis as well as non-traumatic rhabdomyolysis and elevated creatine kinase (CK) levels.
Among 542 heat-related encounters, 77% had heat-specific diagnoses and 24% had a rhabdomyolysis diagnosis. Combined, heat-related encounters increased 170% from 2012 to 2023, from 4.3 per 10,000 to 11.6 per 10,000 (P = .1). Summer months with higher peak temperatures were also associated with higher heat-related volume in the emergency department (P < .001).
Teenage boys were most likely to have rhabdomyolysis, with 82% of the cases occurring in boys and 70% in ages 12-18 (P < .001). “Compared to the rhabdomyolysis group, the heat-specific group was more likely to be younger, Hispanic, use government-based insurance, and live in an area with a lower Child Opportunity Index,” Dr. Merritt reported. “Most heat-specific encounters resulted in an ED discharge (96%), while most rhabdomyolysis encounters resulted in hospital admission (63%)” (P < .001).
”Thankfully, pediatric heat-related illness is still relatively rare,” Dr. Merritt said. “However, given the context of increasing temperatures, this is important for us all to know, anyone who cares for children, whether that be families or parents or pediatricians.”
Prevention Is Key
Dr. Byron noted that about half of AAP chapters now have climate committees, many of which have created educational materials on heat and wildfire smoke and on talking with athletes about risk of heat-related illnesses.
“A lot of the state high school sports associations are actually now adopting guidelines on when it’s safe to practice and when it’s safe to play for heat and for smoke, so that’s definitely something that we can talk to parents about and kids about,” Dr. Byron said. “Otherwise, you still have a lot of coaches and a lot of kids out there that think you’re just supposed to be tough and barrel through it.”
Rhabdomyolysis and heat stroke are both potentially deadly illnesses, so the biggest focus needs to be on prevention, Dr. Byron said. “Not just working with individuals in your office, but working within your school or within your state high school sports association is totally within the lane of a pediatrician to get involved.”
The research had no external funding. Dr. Merritt and Dr. Byron had no disclosures.
FROM AAP 2024