User login
Contraceptive Care Clinic Focuses on Military Readiness
SAN DIEGO — Not surprisingly, the contraception clinic at Madigan Army Medical Center near Tacoma, Wash., is popular among female soldiers seeking to avoid pregnancy. However, about half of the patients drop by for other reasons, the military pharmacist who runs the program told colleagues here at the Joint Federal Pharmacy Seminar.
“They come to suppress menstruation, to get help with pain, to get help with PCOS [polycystic ovary syndrome] symptoms. They're coming for a wide range of indications that we use contraception to treat,” said Sarah Abel, PharmD, a clinical pharmacist.
Regardless of the reason, Abel emphasized that contraceptives can significantly impact the ability of female soldiers to do their jobs. “If you have heavy periods and can't make it in work, or you have endometriosis and requiring a lot of doctor's appointments, or you're deployed and you get pregnant, these are all situations where contraceptive care matters,” she said. Rates of unintended pregnancy are higher in servicewomen than in the general population.
Abel, who opened the medical center’s contraceptive clinic about 10 years ago, stressed that it’s crucial to military readiness considering that the percentage of women in the American military is approaching 20%.
Thanks to a 2022 edict, military hospitals and clinics are required to offer walk-in contraceptive services with same-day access, no requirements for appointments or referrals. An announcement about the mandate noted that these contraceptive services, such as preventing unplanned pregnancy and decreasing menstrual periods, “support the overall well-being of the force and optimize personal warrior readiness.”
As Abel noted, 29 states and Washington D.C. allow pharmacists to prescribe contraception to outpatients, although the requirements vary. “Can we start practicing at the top of our license and start prescribing in the outpatient setting? Absolutely we should,” she said. “Pharmacists have a very unique opportunity to be a part of this.”
Abel also shared that setting up a contraceptive program requires patience and education. “I cannot tell you how many women have come to me who don't know the different names of their body parts, women who've had two babies that don't understand how their body works. So, I constantly find myself taking extra time to do general sexual education,” she said.
There are many lessons to impart to patients about sexual health. For example, birth control drugs and devices do not prevent transmission of sexually transmitted infections (STIs). “So I have bowls of condoms literally everywhere because condoms are the only thing that protects against STIs,” Abel said.
In terms of devices, “we have diaphragms available and cervical caps,” she said. “The Caya diaphragm is a TRICARE-covered benefit. It’s a small purple diaphragm, one size fits most. We can prescribe it, and it is good for 2 years. Unfortunately, spermicide, which you have to use with these things, is not a TRICARE-covered benefit.”
Hormonal contraceptives are also available, with Abel recommending the continuous monophasic type for most women. “Please don't tell women they have to have their periods. They don't,” she said. “What I'm trying to do is give a woman some stability in her hormones. She can know and expect what she's going to feel like. She's not going to wake up and say, ‘Oh God, today's the day. I'm going to be like this for a week.’”
Patches are another option, and a flurry of patients have been asking about them because of recent TikTok videos promoting their use. “We have the Xulane patch, our bread and butter. They wear it on their shoulder, their hip, their butt, or their back. They leave it in place for a week at a time. And every week, they will change that patch. I usually have to walk patients through a whole month to help them understand how that works.”
Another option, the NuvaRing, is notable because it’s linked to low amounts of breakthrough bleeding Abel noted. An extended form is now available that doesn’t need to be removed during menstrual periods.
Medroxyprogesterone injections, which are linked to bone loss, and subdermal implants, which may be less effective in women over 130% of their ideal weight are also available, she said.
Finally, IUDs are an option, although when they fail, they’re linked to ectopic pregnancies.
Abel has no disclosures.
SAN DIEGO — Not surprisingly, the contraception clinic at Madigan Army Medical Center near Tacoma, Wash., is popular among female soldiers seeking to avoid pregnancy. However, about half of the patients drop by for other reasons, the military pharmacist who runs the program told colleagues here at the Joint Federal Pharmacy Seminar.
“They come to suppress menstruation, to get help with pain, to get help with PCOS [polycystic ovary syndrome] symptoms. They're coming for a wide range of indications that we use contraception to treat,” said Sarah Abel, PharmD, a clinical pharmacist.
Regardless of the reason, Abel emphasized that contraceptives can significantly impact the ability of female soldiers to do their jobs. “If you have heavy periods and can't make it in work, or you have endometriosis and requiring a lot of doctor's appointments, or you're deployed and you get pregnant, these are all situations where contraceptive care matters,” she said. Rates of unintended pregnancy are higher in servicewomen than in the general population.
Abel, who opened the medical center’s contraceptive clinic about 10 years ago, stressed that it’s crucial to military readiness considering that the percentage of women in the American military is approaching 20%.
Thanks to a 2022 edict, military hospitals and clinics are required to offer walk-in contraceptive services with same-day access, no requirements for appointments or referrals. An announcement about the mandate noted that these contraceptive services, such as preventing unplanned pregnancy and decreasing menstrual periods, “support the overall well-being of the force and optimize personal warrior readiness.”
As Abel noted, 29 states and Washington D.C. allow pharmacists to prescribe contraception to outpatients, although the requirements vary. “Can we start practicing at the top of our license and start prescribing in the outpatient setting? Absolutely we should,” she said. “Pharmacists have a very unique opportunity to be a part of this.”
Abel also shared that setting up a contraceptive program requires patience and education. “I cannot tell you how many women have come to me who don't know the different names of their body parts, women who've had two babies that don't understand how their body works. So, I constantly find myself taking extra time to do general sexual education,” she said.
There are many lessons to impart to patients about sexual health. For example, birth control drugs and devices do not prevent transmission of sexually transmitted infections (STIs). “So I have bowls of condoms literally everywhere because condoms are the only thing that protects against STIs,” Abel said.
In terms of devices, “we have diaphragms available and cervical caps,” she said. “The Caya diaphragm is a TRICARE-covered benefit. It’s a small purple diaphragm, one size fits most. We can prescribe it, and it is good for 2 years. Unfortunately, spermicide, which you have to use with these things, is not a TRICARE-covered benefit.”
Hormonal contraceptives are also available, with Abel recommending the continuous monophasic type for most women. “Please don't tell women they have to have their periods. They don't,” she said. “What I'm trying to do is give a woman some stability in her hormones. She can know and expect what she's going to feel like. She's not going to wake up and say, ‘Oh God, today's the day. I'm going to be like this for a week.’”
Patches are another option, and a flurry of patients have been asking about them because of recent TikTok videos promoting their use. “We have the Xulane patch, our bread and butter. They wear it on their shoulder, their hip, their butt, or their back. They leave it in place for a week at a time. And every week, they will change that patch. I usually have to walk patients through a whole month to help them understand how that works.”
Another option, the NuvaRing, is notable because it’s linked to low amounts of breakthrough bleeding Abel noted. An extended form is now available that doesn’t need to be removed during menstrual periods.
Medroxyprogesterone injections, which are linked to bone loss, and subdermal implants, which may be less effective in women over 130% of their ideal weight are also available, she said.
Finally, IUDs are an option, although when they fail, they’re linked to ectopic pregnancies.
Abel has no disclosures.
SAN DIEGO — Not surprisingly, the contraception clinic at Madigan Army Medical Center near Tacoma, Wash., is popular among female soldiers seeking to avoid pregnancy. However, about half of the patients drop by for other reasons, the military pharmacist who runs the program told colleagues here at the Joint Federal Pharmacy Seminar.
“They come to suppress menstruation, to get help with pain, to get help with PCOS [polycystic ovary syndrome] symptoms. They're coming for a wide range of indications that we use contraception to treat,” said Sarah Abel, PharmD, a clinical pharmacist.
Regardless of the reason, Abel emphasized that contraceptives can significantly impact the ability of female soldiers to do their jobs. “If you have heavy periods and can't make it in work, or you have endometriosis and requiring a lot of doctor's appointments, or you're deployed and you get pregnant, these are all situations where contraceptive care matters,” she said. Rates of unintended pregnancy are higher in servicewomen than in the general population.
Abel, who opened the medical center’s contraceptive clinic about 10 years ago, stressed that it’s crucial to military readiness considering that the percentage of women in the American military is approaching 20%.
Thanks to a 2022 edict, military hospitals and clinics are required to offer walk-in contraceptive services with same-day access, no requirements for appointments or referrals. An announcement about the mandate noted that these contraceptive services, such as preventing unplanned pregnancy and decreasing menstrual periods, “support the overall well-being of the force and optimize personal warrior readiness.”
As Abel noted, 29 states and Washington D.C. allow pharmacists to prescribe contraception to outpatients, although the requirements vary. “Can we start practicing at the top of our license and start prescribing in the outpatient setting? Absolutely we should,” she said. “Pharmacists have a very unique opportunity to be a part of this.”
Abel also shared that setting up a contraceptive program requires patience and education. “I cannot tell you how many women have come to me who don't know the different names of their body parts, women who've had two babies that don't understand how their body works. So, I constantly find myself taking extra time to do general sexual education,” she said.
There are many lessons to impart to patients about sexual health. For example, birth control drugs and devices do not prevent transmission of sexually transmitted infections (STIs). “So I have bowls of condoms literally everywhere because condoms are the only thing that protects against STIs,” Abel said.
In terms of devices, “we have diaphragms available and cervical caps,” she said. “The Caya diaphragm is a TRICARE-covered benefit. It’s a small purple diaphragm, one size fits most. We can prescribe it, and it is good for 2 years. Unfortunately, spermicide, which you have to use with these things, is not a TRICARE-covered benefit.”
Hormonal contraceptives are also available, with Abel recommending the continuous monophasic type for most women. “Please don't tell women they have to have their periods. They don't,” she said. “What I'm trying to do is give a woman some stability in her hormones. She can know and expect what she's going to feel like. She's not going to wake up and say, ‘Oh God, today's the day. I'm going to be like this for a week.’”
Patches are another option, and a flurry of patients have been asking about them because of recent TikTok videos promoting their use. “We have the Xulane patch, our bread and butter. They wear it on their shoulder, their hip, their butt, or their back. They leave it in place for a week at a time. And every week, they will change that patch. I usually have to walk patients through a whole month to help them understand how that works.”
Another option, the NuvaRing, is notable because it’s linked to low amounts of breakthrough bleeding Abel noted. An extended form is now available that doesn’t need to be removed during menstrual periods.
Medroxyprogesterone injections, which are linked to bone loss, and subdermal implants, which may be less effective in women over 130% of their ideal weight are also available, she said.
Finally, IUDs are an option, although when they fail, they’re linked to ectopic pregnancies.
Abel has no disclosures.

Rising Cancer Rates Among Young People Spur New Fertility Preservation Options
Rising Cancer Rates Among Young People Spur New Fertility Preservation Options
ATLANTA —Jacqueline Lee, MD, a reproductive endocrinologist at Emory School of Medicine, frequently treats patients with cancer. Recently, she treated 4 women in their 30s with histories of colon cancer, acute lymphoblastic leukemia, lymphoma, and breast cancer. A young man in his 20s sought her care, to discuss his case of lymphoma.
All these patients sought guidance from Lee because they want to protect their ability to have children. At the annual meeting of the Association of VA Hematology/Oncology, Lee explained that plenty of patients are finding themselves in similar straits due in part to recent trends.
Cancer rates in the US have been rising among people aged 15 to 39 years, who now account for 4.2% of all cancer cases. An estimated 84,100 people in this age group are expected to be diagnosed with cancer this year. Meanwhile, women are having children later in life-birth rates are up among those aged 25 to 49 years-making it more likely that they have histories of cancer.
Although it's difficult to predict how cancer will affect fertility, Lee emphasized that many chemotherapy medications, including cisplatin and carboplatin, are cytotoxic. "It's hard to always predict what someone's arc of care is going to be," she said, "so I really have a low threshold for recommending fertility preservation in patients who have a strong desire to have future childbearing."
For women with cancer, egg preservation isn't the only strategy. Clinicians can also try to protect ovarian tissue from pelvic radiation through surgical reposition of the ovaries, Lee noted. In addition goserelin, a hormone-suppressing therapy, may protect the ovaries from chemotherapy, though its effectiveness in boosting pregnancy rates is still unclear.
"When I mentioned this option, it's usually for patients who can't preserve fertility via egg or embryo preservation, or we don't have the luxury of that kind of time," Lee said. "I say that if helps at all, it might help you resume menses after treatment. But infertility is still very common."
For some patients, freezing eggs is an easy decision. "They don't have a reproductive partner they're ready to make embryos with, so we proceed with egg preservation. It's no longer considered experimental and comes with lower upfront costs since the costs of actually making embryos are deferred until the future."
In addition, she said, freezing eggs also avoids the touchy topic of disposing of embryos. Lee cautions patients that retrieving eggs is a 2-week process that requires any initiation of cancer care to be delayed. However, the retrieval process can be adjusted in patients with special needs due to the type of cancer they have.
For prepubertal girls with cancer, ovarian tissue can be removed and frozen as a fertility preservation option. However, this is not considered standard of care. "We don't do it," she said. "We refer out if needed. Hopefully we'll develop a program in the future."
As for the 5 patients that Lee mentioned, with details changed to protect their privacy, their outcomes were as follows:
- The woman with colon cancer, who had undergone a hemicolectomy, chose to defer fertility preservation.
- The woman with acute lymphoblastic leukemia, who was taking depo-Lupron, had undetectable anti-Müllerian hormone (AMH) levels. Lee discussed the possibility of IVF with a donor egg.
- The woman with breast cancer, who was newly diagnosed, deferred fertility preservation.
- The man with lymphoma (Hodgkin's), who was awaiting chemotherapy, had his sperm frozen.
- The woman with lymphoma (new diagnosis) had 27 eggs frozen.
Lee had no disclosures to report.
ATLANTA —Jacqueline Lee, MD, a reproductive endocrinologist at Emory School of Medicine, frequently treats patients with cancer. Recently, she treated 4 women in their 30s with histories of colon cancer, acute lymphoblastic leukemia, lymphoma, and breast cancer. A young man in his 20s sought her care, to discuss his case of lymphoma.
All these patients sought guidance from Lee because they want to protect their ability to have children. At the annual meeting of the Association of VA Hematology/Oncology, Lee explained that plenty of patients are finding themselves in similar straits due in part to recent trends.
Cancer rates in the US have been rising among people aged 15 to 39 years, who now account for 4.2% of all cancer cases. An estimated 84,100 people in this age group are expected to be diagnosed with cancer this year. Meanwhile, women are having children later in life-birth rates are up among those aged 25 to 49 years-making it more likely that they have histories of cancer.
Although it's difficult to predict how cancer will affect fertility, Lee emphasized that many chemotherapy medications, including cisplatin and carboplatin, are cytotoxic. "It's hard to always predict what someone's arc of care is going to be," she said, "so I really have a low threshold for recommending fertility preservation in patients who have a strong desire to have future childbearing."
For women with cancer, egg preservation isn't the only strategy. Clinicians can also try to protect ovarian tissue from pelvic radiation through surgical reposition of the ovaries, Lee noted. In addition goserelin, a hormone-suppressing therapy, may protect the ovaries from chemotherapy, though its effectiveness in boosting pregnancy rates is still unclear.
"When I mentioned this option, it's usually for patients who can't preserve fertility via egg or embryo preservation, or we don't have the luxury of that kind of time," Lee said. "I say that if helps at all, it might help you resume menses after treatment. But infertility is still very common."
For some patients, freezing eggs is an easy decision. "They don't have a reproductive partner they're ready to make embryos with, so we proceed with egg preservation. It's no longer considered experimental and comes with lower upfront costs since the costs of actually making embryos are deferred until the future."
In addition, she said, freezing eggs also avoids the touchy topic of disposing of embryos. Lee cautions patients that retrieving eggs is a 2-week process that requires any initiation of cancer care to be delayed. However, the retrieval process can be adjusted in patients with special needs due to the type of cancer they have.
For prepubertal girls with cancer, ovarian tissue can be removed and frozen as a fertility preservation option. However, this is not considered standard of care. "We don't do it," she said. "We refer out if needed. Hopefully we'll develop a program in the future."
As for the 5 patients that Lee mentioned, with details changed to protect their privacy, their outcomes were as follows:
- The woman with colon cancer, who had undergone a hemicolectomy, chose to defer fertility preservation.
- The woman with acute lymphoblastic leukemia, who was taking depo-Lupron, had undetectable anti-Müllerian hormone (AMH) levels. Lee discussed the possibility of IVF with a donor egg.
- The woman with breast cancer, who was newly diagnosed, deferred fertility preservation.
- The man with lymphoma (Hodgkin's), who was awaiting chemotherapy, had his sperm frozen.
- The woman with lymphoma (new diagnosis) had 27 eggs frozen.
Lee had no disclosures to report.
ATLANTA —Jacqueline Lee, MD, a reproductive endocrinologist at Emory School of Medicine, frequently treats patients with cancer. Recently, she treated 4 women in their 30s with histories of colon cancer, acute lymphoblastic leukemia, lymphoma, and breast cancer. A young man in his 20s sought her care, to discuss his case of lymphoma.
All these patients sought guidance from Lee because they want to protect their ability to have children. At the annual meeting of the Association of VA Hematology/Oncology, Lee explained that plenty of patients are finding themselves in similar straits due in part to recent trends.
Cancer rates in the US have been rising among people aged 15 to 39 years, who now account for 4.2% of all cancer cases. An estimated 84,100 people in this age group are expected to be diagnosed with cancer this year. Meanwhile, women are having children later in life-birth rates are up among those aged 25 to 49 years-making it more likely that they have histories of cancer.
Although it's difficult to predict how cancer will affect fertility, Lee emphasized that many chemotherapy medications, including cisplatin and carboplatin, are cytotoxic. "It's hard to always predict what someone's arc of care is going to be," she said, "so I really have a low threshold for recommending fertility preservation in patients who have a strong desire to have future childbearing."
For women with cancer, egg preservation isn't the only strategy. Clinicians can also try to protect ovarian tissue from pelvic radiation through surgical reposition of the ovaries, Lee noted. In addition goserelin, a hormone-suppressing therapy, may protect the ovaries from chemotherapy, though its effectiveness in boosting pregnancy rates is still unclear.
"When I mentioned this option, it's usually for patients who can't preserve fertility via egg or embryo preservation, or we don't have the luxury of that kind of time," Lee said. "I say that if helps at all, it might help you resume menses after treatment. But infertility is still very common."
For some patients, freezing eggs is an easy decision. "They don't have a reproductive partner they're ready to make embryos with, so we proceed with egg preservation. It's no longer considered experimental and comes with lower upfront costs since the costs of actually making embryos are deferred until the future."
In addition, she said, freezing eggs also avoids the touchy topic of disposing of embryos. Lee cautions patients that retrieving eggs is a 2-week process that requires any initiation of cancer care to be delayed. However, the retrieval process can be adjusted in patients with special needs due to the type of cancer they have.
For prepubertal girls with cancer, ovarian tissue can be removed and frozen as a fertility preservation option. However, this is not considered standard of care. "We don't do it," she said. "We refer out if needed. Hopefully we'll develop a program in the future."
As for the 5 patients that Lee mentioned, with details changed to protect their privacy, their outcomes were as follows:
- The woman with colon cancer, who had undergone a hemicolectomy, chose to defer fertility preservation.
- The woman with acute lymphoblastic leukemia, who was taking depo-Lupron, had undetectable anti-Müllerian hormone (AMH) levels. Lee discussed the possibility of IVF with a donor egg.
- The woman with breast cancer, who was newly diagnosed, deferred fertility preservation.
- The man with lymphoma (Hodgkin's), who was awaiting chemotherapy, had his sperm frozen.
- The woman with lymphoma (new diagnosis) had 27 eggs frozen.
Lee had no disclosures to report.
Rising Cancer Rates Among Young People Spur New Fertility Preservation Options
Rising Cancer Rates Among Young People Spur New Fertility Preservation Options

Can Fasting Around Chemo Improve Ovarian Cancer Outcomes?
Can Fasting Around Chemo Improve Ovarian Cancer Outcomes?
A few days of fasting around chemotherapy sessions may improve treatment response and outcomes for some patients with advanced ovarian cancer, a small phase 2 trial suggests.
The study, of 36 patients with stage III or IV high-grade ovarian cancer, found that those randomly assigned to fast for 36 hours before chemotherapy and 24 hours afterward had stronger pathologic responses to chemotherapy and longer progression-free survival than patients who ate normally during treatment.
The findings, reported at a press briefing ahead the American Society of Clinical Oncology (ASCO) 2026, hint at a straightforward measure to potentially improve patients’ outcomes.
The working theory is that short-term fasting boosts chemotherapy response by lowering insulin and IGF-1 levels, both of which are implicated in tumor growth and chemotherapy resistance, said study presenter Claudia Marchetti, MD, of Agostino Gemelli University in Rome, Italy.
Speaking at the briefing, ASCO President Eric Small, MD, of the University of California San Francisco, called the study “a great example of a very simple intervention that has benefit and can be undertaken and implemented anywhere in the world.”
“It’s not an expensive new drug,” he said, “and yet it has the potential to really have an impact on this cancer.”
Ovarian cancer affects more than 324,000 women worldwide each year and causes more than 206,000 deaths annually. Around 80% of patients are diagnosed at an advanced stage, and up to 60% receive neoadjuvant chemotherapy to reduce tumor size and facilitate surgery.
Despite advances in surgery and chemotherapy, patients with advanced disease still face poor outcomes. There is, Marchetti said, “an urgent need for safe, low-cost, and easily implementable strategies that can enhance treatment efficacy and improve patient prognosis.”
Given evidence on the role of insulin in tumor growth and chemotherapy response, her team hypothesized that short bouts of fasting around the time of treatment might have benefits.
To test that idea, the researchers recruited 36 patients with newly diagnosed stage III or IV high-grade serous ovarian carcinoma who were not candidates for primary cytoreduction. All were in good general health, with a mean age of 62 years.
All patients received 3 rounds of carboplatin and paclitaxel before surgery. Prior to starting chemotherapy, half were randomly assigned to fast for 36 hours before and 24 hours after chemotherapy, whereas the other half ate normally throughout treatment.
Patients in the fasting group consumed no more than 350 calories per day during the fasting window. They were allowed to have unrestricted water, herbal tea, limited vegetable juice, and small amounts of light vegetable broth. (A ketogenic diet group had initially been planned but was closed early because of poor patient compliance.)
The study met its primary endpoint of change in insulin levels during chemotherapy, Marchetti reported. Baseline insulin levels were comparable between the 2 groups, but after 3 rounds of chemotherapy, they’d dipped by an average of 1.12 µIU/mL in the fasting group and increased by 9.76 µIU/mL in the control group (P = .01).
Fasting also improved clinical outcomes. Specifically, Marchetti said, 59% of fasting patients achieved a chemotherapy response score of 3 — indicating complete or near-complete tumor response before surgery — compared with 17% of patients in the control group.
Median progression-free survival was significantly longer in the fasting group, at 38 vs 24 months.
Importantly, Marchetti said, the fasting protocol was feasible, well tolerated, and safe: All patients assigned to the fasting group completed treatment, and rates of chemotherapy-related toxicities were similar between the 2 groups.
Additional analyses shed more light on the possible mechanisms underlying the fasting group’s improved outcomes: The researchers found that those patients tended to have lower levels of circulating suppressor granulocyte and monocyte populations that have been linked to tumor immune escape, which suggests, Marchetti said, fasting may have set the stage for a “more favorable immune environment” during chemotherapy.
However, she cautioned that much more research is needed. Her team is planning a larger multicenter trial to validate the current findings, and longer-term follow-up is necessary to see whether fasting ultimately impacts patients’ survival, Marchetti said.
In a statement, Eleonora Teplinsky, MD, an ASCO expert in gynecologic cancers, said these early findings are “encouraging, support earlier data, and highlight a promising area of cancer research.”
But she, too, emphasized the need for larger clinical trials to build on the results.
The study had no commercial funding. Marchetti disclosed having relationships with Arquer Diagnostics, AstraZeneca, Clovis Oncology, and other companies. Small disclosed having relationships with Janssen, Johnson & Johnson, and others. Teplinsky had no disclosures.
A version of this article first appeared on Medscape.com.
A few days of fasting around chemotherapy sessions may improve treatment response and outcomes for some patients with advanced ovarian cancer, a small phase 2 trial suggests.
The study, of 36 patients with stage III or IV high-grade ovarian cancer, found that those randomly assigned to fast for 36 hours before chemotherapy and 24 hours afterward had stronger pathologic responses to chemotherapy and longer progression-free survival than patients who ate normally during treatment.
The findings, reported at a press briefing ahead the American Society of Clinical Oncology (ASCO) 2026, hint at a straightforward measure to potentially improve patients’ outcomes.
The working theory is that short-term fasting boosts chemotherapy response by lowering insulin and IGF-1 levels, both of which are implicated in tumor growth and chemotherapy resistance, said study presenter Claudia Marchetti, MD, of Agostino Gemelli University in Rome, Italy.
Speaking at the briefing, ASCO President Eric Small, MD, of the University of California San Francisco, called the study “a great example of a very simple intervention that has benefit and can be undertaken and implemented anywhere in the world.”
“It’s not an expensive new drug,” he said, “and yet it has the potential to really have an impact on this cancer.”
Ovarian cancer affects more than 324,000 women worldwide each year and causes more than 206,000 deaths annually. Around 80% of patients are diagnosed at an advanced stage, and up to 60% receive neoadjuvant chemotherapy to reduce tumor size and facilitate surgery.
Despite advances in surgery and chemotherapy, patients with advanced disease still face poor outcomes. There is, Marchetti said, “an urgent need for safe, low-cost, and easily implementable strategies that can enhance treatment efficacy and improve patient prognosis.”
Given evidence on the role of insulin in tumor growth and chemotherapy response, her team hypothesized that short bouts of fasting around the time of treatment might have benefits.
To test that idea, the researchers recruited 36 patients with newly diagnosed stage III or IV high-grade serous ovarian carcinoma who were not candidates for primary cytoreduction. All were in good general health, with a mean age of 62 years.
All patients received 3 rounds of carboplatin and paclitaxel before surgery. Prior to starting chemotherapy, half were randomly assigned to fast for 36 hours before and 24 hours after chemotherapy, whereas the other half ate normally throughout treatment.
Patients in the fasting group consumed no more than 350 calories per day during the fasting window. They were allowed to have unrestricted water, herbal tea, limited vegetable juice, and small amounts of light vegetable broth. (A ketogenic diet group had initially been planned but was closed early because of poor patient compliance.)
The study met its primary endpoint of change in insulin levels during chemotherapy, Marchetti reported. Baseline insulin levels were comparable between the 2 groups, but after 3 rounds of chemotherapy, they’d dipped by an average of 1.12 µIU/mL in the fasting group and increased by 9.76 µIU/mL in the control group (P = .01).
Fasting also improved clinical outcomes. Specifically, Marchetti said, 59% of fasting patients achieved a chemotherapy response score of 3 — indicating complete or near-complete tumor response before surgery — compared with 17% of patients in the control group.
Median progression-free survival was significantly longer in the fasting group, at 38 vs 24 months.
Importantly, Marchetti said, the fasting protocol was feasible, well tolerated, and safe: All patients assigned to the fasting group completed treatment, and rates of chemotherapy-related toxicities were similar between the 2 groups.
Additional analyses shed more light on the possible mechanisms underlying the fasting group’s improved outcomes: The researchers found that those patients tended to have lower levels of circulating suppressor granulocyte and monocyte populations that have been linked to tumor immune escape, which suggests, Marchetti said, fasting may have set the stage for a “more favorable immune environment” during chemotherapy.
However, she cautioned that much more research is needed. Her team is planning a larger multicenter trial to validate the current findings, and longer-term follow-up is necessary to see whether fasting ultimately impacts patients’ survival, Marchetti said.
In a statement, Eleonora Teplinsky, MD, an ASCO expert in gynecologic cancers, said these early findings are “encouraging, support earlier data, and highlight a promising area of cancer research.”
But she, too, emphasized the need for larger clinical trials to build on the results.
The study had no commercial funding. Marchetti disclosed having relationships with Arquer Diagnostics, AstraZeneca, Clovis Oncology, and other companies. Small disclosed having relationships with Janssen, Johnson & Johnson, and others. Teplinsky had no disclosures.
A version of this article first appeared on Medscape.com.
A few days of fasting around chemotherapy sessions may improve treatment response and outcomes for some patients with advanced ovarian cancer, a small phase 2 trial suggests.
The study, of 36 patients with stage III or IV high-grade ovarian cancer, found that those randomly assigned to fast for 36 hours before chemotherapy and 24 hours afterward had stronger pathologic responses to chemotherapy and longer progression-free survival than patients who ate normally during treatment.
The findings, reported at a press briefing ahead the American Society of Clinical Oncology (ASCO) 2026, hint at a straightforward measure to potentially improve patients’ outcomes.
The working theory is that short-term fasting boosts chemotherapy response by lowering insulin and IGF-1 levels, both of which are implicated in tumor growth and chemotherapy resistance, said study presenter Claudia Marchetti, MD, of Agostino Gemelli University in Rome, Italy.
Speaking at the briefing, ASCO President Eric Small, MD, of the University of California San Francisco, called the study “a great example of a very simple intervention that has benefit and can be undertaken and implemented anywhere in the world.”
“It’s not an expensive new drug,” he said, “and yet it has the potential to really have an impact on this cancer.”
Ovarian cancer affects more than 324,000 women worldwide each year and causes more than 206,000 deaths annually. Around 80% of patients are diagnosed at an advanced stage, and up to 60% receive neoadjuvant chemotherapy to reduce tumor size and facilitate surgery.
Despite advances in surgery and chemotherapy, patients with advanced disease still face poor outcomes. There is, Marchetti said, “an urgent need for safe, low-cost, and easily implementable strategies that can enhance treatment efficacy and improve patient prognosis.”
Given evidence on the role of insulin in tumor growth and chemotherapy response, her team hypothesized that short bouts of fasting around the time of treatment might have benefits.
To test that idea, the researchers recruited 36 patients with newly diagnosed stage III or IV high-grade serous ovarian carcinoma who were not candidates for primary cytoreduction. All were in good general health, with a mean age of 62 years.
All patients received 3 rounds of carboplatin and paclitaxel before surgery. Prior to starting chemotherapy, half were randomly assigned to fast for 36 hours before and 24 hours after chemotherapy, whereas the other half ate normally throughout treatment.
Patients in the fasting group consumed no more than 350 calories per day during the fasting window. They were allowed to have unrestricted water, herbal tea, limited vegetable juice, and small amounts of light vegetable broth. (A ketogenic diet group had initially been planned but was closed early because of poor patient compliance.)
The study met its primary endpoint of change in insulin levels during chemotherapy, Marchetti reported. Baseline insulin levels were comparable between the 2 groups, but after 3 rounds of chemotherapy, they’d dipped by an average of 1.12 µIU/mL in the fasting group and increased by 9.76 µIU/mL in the control group (P = .01).
Fasting also improved clinical outcomes. Specifically, Marchetti said, 59% of fasting patients achieved a chemotherapy response score of 3 — indicating complete or near-complete tumor response before surgery — compared with 17% of patients in the control group.
Median progression-free survival was significantly longer in the fasting group, at 38 vs 24 months.
Importantly, Marchetti said, the fasting protocol was feasible, well tolerated, and safe: All patients assigned to the fasting group completed treatment, and rates of chemotherapy-related toxicities were similar between the 2 groups.
Additional analyses shed more light on the possible mechanisms underlying the fasting group’s improved outcomes: The researchers found that those patients tended to have lower levels of circulating suppressor granulocyte and monocyte populations that have been linked to tumor immune escape, which suggests, Marchetti said, fasting may have set the stage for a “more favorable immune environment” during chemotherapy.
However, she cautioned that much more research is needed. Her team is planning a larger multicenter trial to validate the current findings, and longer-term follow-up is necessary to see whether fasting ultimately impacts patients’ survival, Marchetti said.
In a statement, Eleonora Teplinsky, MD, an ASCO expert in gynecologic cancers, said these early findings are “encouraging, support earlier data, and highlight a promising area of cancer research.”
But she, too, emphasized the need for larger clinical trials to build on the results.
The study had no commercial funding. Marchetti disclosed having relationships with Arquer Diagnostics, AstraZeneca, Clovis Oncology, and other companies. Small disclosed having relationships with Janssen, Johnson & Johnson, and others. Teplinsky had no disclosures.
A version of this article first appeared on Medscape.com.
Can Fasting Around Chemo Improve Ovarian Cancer Outcomes?
Can Fasting Around Chemo Improve Ovarian Cancer Outcomes?
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Telephone outreach by a nurse practitioner (NP) providing counseling and care coordination reduced the gaps in breast and cervical cancer screenings among women veterans in rural areas, according to a retrospective study.
METHODOLOGY:
- Researchers conducted a retrospective chart review of 55 women veterans who received interventions related to breast or cervical cancer screening at a rural Veterans Health Administration health care system.
- A Boost team, including an NP, a medical director, a program coordinator, and a program evaluation team, was established to provide care coordination and counseling for these participants.
- The NP conducted outreach by telephone to these participants receiving care at five community-based outpatient clinics located in rural counties and helped coordinate access to screening appointments through the Office of Community Care.
- Outcomes included the number of veterans due for breast or cervical cancer screening at the time of outreach and the number of mammograms and Pap smears completed in the 12-month period following the intervention.
TAKEAWAY:
- Of the 55 veterans who received Boost interventions related to cancer screening, 35 (64%) were due for breast cancer screening and 27 (49%) were due for cervical cancer screening before the intervention.
- Following the Boost intervention, the number of veterans due for breast cancer and cervical cancer screenings decreased to 18 (32%) and 16 (29%), respectively.
- Among veterans due for breast cancer screening, 29 (83%) received counseling regarding screening and 17 (59%) of counseled participants completed mammography; however, among those due for cervical cancer screening, 22 (81%) received counseling and 11 (50%) completed screening.
- None of the veterans who were due for screening but did not receive counseling completed their screening, demonstrating the critical role of clinician-provided education and counseling.
IN PRACTICE:
“We hope to expand Boost outreach from one NP working part-time across two health systems to a national partnership of licensed independent providers conducting clinician-initiated outreach to a broader and geographically more diverse group of veterans,” the authors wrote.
SOURCE:
This study was led by Lina Vadlamani, MD, MBA, San Francisco Internal Medicine Residency Program, University of California, San Francisco. It was published online on April 24, 2026, in Military Medicine.
LIMITATIONS:
This study was a secondary analysis in which participants were not randomly assigned, limiting causal inferences. Veterans who answered the phone and engaged with the NP were likely easier to reach and potentially more proactive about their health than those who did not engage, and this selection bias may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded by the Department of Veterans Affairs, Veterans Health Administration, and Office of Rural Health. The authors reported having no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Nurse Practitioner-Led Outreach Boosts Cancer Screening Rates Among Women Veterans in Rural Settings
Rising Lung Cancer Burden Among Women
Rising Lung Cancer Burden Among Women
While the incidence of lung cancer is decreasing in men, it continues to rise in women. With more than 19,000 new cases in France each year, lung cancer is now the third most commonly diagnosed cancer among women. This trend is also seen in other European countries but appears to be region-specific because other continents report a decline in incidence among women. Moreover, although overall prognosis remains better in the female population, the trend is worrying: Mortality associated with the disease is increasing in women, unlike in men with lung cancer. A session at the French-Language Pneumology Congress held from January 30 to February 1, 2026, in Lille, France, provided an opportunity to review the situation.
Efficacy and Toxicity
Lung tumors in women have a distinct tumor profile: Women have a higher proportion of adenocarcinomas than men and a higher frequency of somatic mutations (EGFR, BRAF, or HER2), including in nonsmokers. In addition, 65% of lung cancers in women are associated with smoking compared with 87% of those in men.
The role of estrogens is central because they interact directly with tumor growth signaling pathways. Moreover, “sex is the second leading factor of variability in drug pharmacokinetics after weight and accounts for 28% of anticancer drug kinetics,” emphasized Julien Mazières, pulmonologist, Toulouse University Hospital, Toulouse, France. Also involved in this equation are a higher body fat percentage, lower gastric acidity, and, above all, reduced renal and hepatic clearance.
As a result, exposure to drugs — represented by the area under the curve — is often greater in women and translates into not only improved progression-free survival with targeted therapies and chemotherapy but also increased toxicity. Carboplatin and paclitaxel are among the drugs whose kinetics are most affected by clearance. There are differences in clearance of more than 20% for these drugs in women vs men, though dosages are not systematically adjusted except for weight-based dosing. This vulnerability to adverse effects is particularly pronounced with targeted therapies, with more neuropsychiatric and gastrointestinal disorders. Data on the efficacy of immunotherapy in lung cancer by sex are contradictory. However, endocrine-related adverse effects and pneumonitis are more frequent in women, especially before menopause.
Women remain underrepresented in clinical trials, and sex-specific analyses of results are too rarely performed, which limits understanding of mechanisms and prevents tailoring management recommendations according to sex.
Impaired Quality of Life
Lung cancer most severely impairs physical functioning in women. “In the absence of sex-stratified studies, psycho-oncologists’ experience suggests that women have more cognitive disorders, anxiety, and depression associated with this disease. Its impact on quality of life is major, with deterioration of social relationships and reduced treatment adherence,” summarized Céline Mascaux, MD, PhD, pulmonologist, Strasbourg University Hospital, Strasbourg, France. Women also face social and family pressure — a mental burden that pushes them to “hold on” for their loved ones. Regarding sexual health, women with lung cancer who are sexually active often report dissatisfaction with the quality of their sexual relations because of fatigue, lack of energy, sadness, and shortness of breath, not to mention treatment-related sexual dysfunction. These problems are often not given sufficient attention by physicians.
Finally, fertility requires greater attention from the medical community: According to the VICAN study conducted by France’s National Health Insurance Fund, a discussion about fertility preservation did not take place at the time of cancer diagnosis for 60% of men and 67% of women of childbearing age. “In lung cancer specifically, the desire for children nevertheless exists in nearly 40% of patients of childbearing age,” regretted Jacques Cadranel, pulmonologist, Tenon Hospital, Paris, France. This desire does not appear to have influenced therapeutic strategy, and fertility preservation was ultimately proposed in only a third of cases and was carried out in only 3% of women compared with21% of men.
This story has been translated from Univadis France, part of the Medscape Professional Network.
A version of this story first appeared on Medscape.com
While the incidence of lung cancer is decreasing in men, it continues to rise in women. With more than 19,000 new cases in France each year, lung cancer is now the third most commonly diagnosed cancer among women. This trend is also seen in other European countries but appears to be region-specific because other continents report a decline in incidence among women. Moreover, although overall prognosis remains better in the female population, the trend is worrying: Mortality associated with the disease is increasing in women, unlike in men with lung cancer. A session at the French-Language Pneumology Congress held from January 30 to February 1, 2026, in Lille, France, provided an opportunity to review the situation.
Efficacy and Toxicity
Lung tumors in women have a distinct tumor profile: Women have a higher proportion of adenocarcinomas than men and a higher frequency of somatic mutations (EGFR, BRAF, or HER2), including in nonsmokers. In addition, 65% of lung cancers in women are associated with smoking compared with 87% of those in men.
The role of estrogens is central because they interact directly with tumor growth signaling pathways. Moreover, “sex is the second leading factor of variability in drug pharmacokinetics after weight and accounts for 28% of anticancer drug kinetics,” emphasized Julien Mazières, pulmonologist, Toulouse University Hospital, Toulouse, France. Also involved in this equation are a higher body fat percentage, lower gastric acidity, and, above all, reduced renal and hepatic clearance.
As a result, exposure to drugs — represented by the area under the curve — is often greater in women and translates into not only improved progression-free survival with targeted therapies and chemotherapy but also increased toxicity. Carboplatin and paclitaxel are among the drugs whose kinetics are most affected by clearance. There are differences in clearance of more than 20% for these drugs in women vs men, though dosages are not systematically adjusted except for weight-based dosing. This vulnerability to adverse effects is particularly pronounced with targeted therapies, with more neuropsychiatric and gastrointestinal disorders. Data on the efficacy of immunotherapy in lung cancer by sex are contradictory. However, endocrine-related adverse effects and pneumonitis are more frequent in women, especially before menopause.
Women remain underrepresented in clinical trials, and sex-specific analyses of results are too rarely performed, which limits understanding of mechanisms and prevents tailoring management recommendations according to sex.
Impaired Quality of Life
Lung cancer most severely impairs physical functioning in women. “In the absence of sex-stratified studies, psycho-oncologists’ experience suggests that women have more cognitive disorders, anxiety, and depression associated with this disease. Its impact on quality of life is major, with deterioration of social relationships and reduced treatment adherence,” summarized Céline Mascaux, MD, PhD, pulmonologist, Strasbourg University Hospital, Strasbourg, France. Women also face social and family pressure — a mental burden that pushes them to “hold on” for their loved ones. Regarding sexual health, women with lung cancer who are sexually active often report dissatisfaction with the quality of their sexual relations because of fatigue, lack of energy, sadness, and shortness of breath, not to mention treatment-related sexual dysfunction. These problems are often not given sufficient attention by physicians.
Finally, fertility requires greater attention from the medical community: According to the VICAN study conducted by France’s National Health Insurance Fund, a discussion about fertility preservation did not take place at the time of cancer diagnosis for 60% of men and 67% of women of childbearing age. “In lung cancer specifically, the desire for children nevertheless exists in nearly 40% of patients of childbearing age,” regretted Jacques Cadranel, pulmonologist, Tenon Hospital, Paris, France. This desire does not appear to have influenced therapeutic strategy, and fertility preservation was ultimately proposed in only a third of cases and was carried out in only 3% of women compared with21% of men.
This story has been translated from Univadis France, part of the Medscape Professional Network.
A version of this story first appeared on Medscape.com
While the incidence of lung cancer is decreasing in men, it continues to rise in women. With more than 19,000 new cases in France each year, lung cancer is now the third most commonly diagnosed cancer among women. This trend is also seen in other European countries but appears to be region-specific because other continents report a decline in incidence among women. Moreover, although overall prognosis remains better in the female population, the trend is worrying: Mortality associated with the disease is increasing in women, unlike in men with lung cancer. A session at the French-Language Pneumology Congress held from January 30 to February 1, 2026, in Lille, France, provided an opportunity to review the situation.
Efficacy and Toxicity
Lung tumors in women have a distinct tumor profile: Women have a higher proportion of adenocarcinomas than men and a higher frequency of somatic mutations (EGFR, BRAF, or HER2), including in nonsmokers. In addition, 65% of lung cancers in women are associated with smoking compared with 87% of those in men.
The role of estrogens is central because they interact directly with tumor growth signaling pathways. Moreover, “sex is the second leading factor of variability in drug pharmacokinetics after weight and accounts for 28% of anticancer drug kinetics,” emphasized Julien Mazières, pulmonologist, Toulouse University Hospital, Toulouse, France. Also involved in this equation are a higher body fat percentage, lower gastric acidity, and, above all, reduced renal and hepatic clearance.
As a result, exposure to drugs — represented by the area under the curve — is often greater in women and translates into not only improved progression-free survival with targeted therapies and chemotherapy but also increased toxicity. Carboplatin and paclitaxel are among the drugs whose kinetics are most affected by clearance. There are differences in clearance of more than 20% for these drugs in women vs men, though dosages are not systematically adjusted except for weight-based dosing. This vulnerability to adverse effects is particularly pronounced with targeted therapies, with more neuropsychiatric and gastrointestinal disorders. Data on the efficacy of immunotherapy in lung cancer by sex are contradictory. However, endocrine-related adverse effects and pneumonitis are more frequent in women, especially before menopause.
Women remain underrepresented in clinical trials, and sex-specific analyses of results are too rarely performed, which limits understanding of mechanisms and prevents tailoring management recommendations according to sex.
Impaired Quality of Life
Lung cancer most severely impairs physical functioning in women. “In the absence of sex-stratified studies, psycho-oncologists’ experience suggests that women have more cognitive disorders, anxiety, and depression associated with this disease. Its impact on quality of life is major, with deterioration of social relationships and reduced treatment adherence,” summarized Céline Mascaux, MD, PhD, pulmonologist, Strasbourg University Hospital, Strasbourg, France. Women also face social and family pressure — a mental burden that pushes them to “hold on” for their loved ones. Regarding sexual health, women with lung cancer who are sexually active often report dissatisfaction with the quality of their sexual relations because of fatigue, lack of energy, sadness, and shortness of breath, not to mention treatment-related sexual dysfunction. These problems are often not given sufficient attention by physicians.
Finally, fertility requires greater attention from the medical community: According to the VICAN study conducted by France’s National Health Insurance Fund, a discussion about fertility preservation did not take place at the time of cancer diagnosis for 60% of men and 67% of women of childbearing age. “In lung cancer specifically, the desire for children nevertheless exists in nearly 40% of patients of childbearing age,” regretted Jacques Cadranel, pulmonologist, Tenon Hospital, Paris, France. This desire does not appear to have influenced therapeutic strategy, and fertility preservation was ultimately proposed in only a third of cases and was carried out in only 3% of women compared with21% of men.
This story has been translated from Univadis France, part of the Medscape Professional Network.
A version of this story first appeared on Medscape.com
Rising Lung Cancer Burden Among Women
Rising Lung Cancer Burden Among Women
Building Trust: Enhancing Rural Women Veterans’ Healthcare Experiences Through Need-Supportive Patient-Centered Communication
Background
Rural women veterans often confront unique healthcare barriers—geographic isolation, gender-related stigma, and limited provider cultural sensitivity that undermine trust and engagement. In response, we co-designed an interprofessional communication curriculum to promote relational, patient-centered care grounded in psychological need support.
Innovation
Anchored in Self Determination Theory (SDT), this curriculum equips nurses and social workers with need-supportive communication strategies that nurture autonomy, competence, and relatedness, integrating two transformative learning methods for enhancing respectful and inclusive listening:
- Cultural humility reflections for veteran-centered care—personal narratives, storytelling, and power-awareness discussions to build lifelong reflective practices.
- Medical improv simulations—adaptive improvisational role plays for healthcare environments fostering presence, adaptability, empathy, trust-building, and real-time responsiveness.
Delivered via a multiday health professions learning lab, the training combines asynchronous workshops with in-person facilitated interactions. Core modules cover SDT foundations, need supportive dialogue, veteran-centered cultural humility, and shared decision-making practices that uplift rural women veterans’ voices. Using Kirkpatrick’s Four Level Model, we assess impact at multiple tiers:
- Reaction: Participant satisfaction and perceived training relevance.
- Learning: Pre/post assessments track SDT knowledge and communication skills gains.
- Behavior: Observe simulations and self-reported changes in communication practices.
- Results: Qualitative satisfaction metrics and care engagement trends among rural women veterans.
Results
A pilot cohort (N = 20) across two rural sites is pending implementation. pre/post surveys will assess any improved confidence in applying need supportive communication and the most effective component in building empathetic presence. Feedback measures will also indicate the significance of combined uses of medical improv and cultural humility on deepened relational capacity and trust.
Discussion
This program operationalizes SDT within healthcare communications, integrating cultural humility and improvisation learning modalities to enhance care quality for rural women veterans, ultimately strengthening provider-patient connections. Using health professions learning lab environments can foster sustained behavioral impacts. Future iterations will expand to additional rural VA sites, co-designing with the voices of women veterans through focus groups.
Background
Rural women veterans often confront unique healthcare barriers—geographic isolation, gender-related stigma, and limited provider cultural sensitivity that undermine trust and engagement. In response, we co-designed an interprofessional communication curriculum to promote relational, patient-centered care grounded in psychological need support.
Innovation
Anchored in Self Determination Theory (SDT), this curriculum equips nurses and social workers with need-supportive communication strategies that nurture autonomy, competence, and relatedness, integrating two transformative learning methods for enhancing respectful and inclusive listening:
- Cultural humility reflections for veteran-centered care—personal narratives, storytelling, and power-awareness discussions to build lifelong reflective practices.
- Medical improv simulations—adaptive improvisational role plays for healthcare environments fostering presence, adaptability, empathy, trust-building, and real-time responsiveness.
Delivered via a multiday health professions learning lab, the training combines asynchronous workshops with in-person facilitated interactions. Core modules cover SDT foundations, need supportive dialogue, veteran-centered cultural humility, and shared decision-making practices that uplift rural women veterans’ voices. Using Kirkpatrick’s Four Level Model, we assess impact at multiple tiers:
- Reaction: Participant satisfaction and perceived training relevance.
- Learning: Pre/post assessments track SDT knowledge and communication skills gains.
- Behavior: Observe simulations and self-reported changes in communication practices.
- Results: Qualitative satisfaction metrics and care engagement trends among rural women veterans.
Results
A pilot cohort (N = 20) across two rural sites is pending implementation. pre/post surveys will assess any improved confidence in applying need supportive communication and the most effective component in building empathetic presence. Feedback measures will also indicate the significance of combined uses of medical improv and cultural humility on deepened relational capacity and trust.
Discussion
This program operationalizes SDT within healthcare communications, integrating cultural humility and improvisation learning modalities to enhance care quality for rural women veterans, ultimately strengthening provider-patient connections. Using health professions learning lab environments can foster sustained behavioral impacts. Future iterations will expand to additional rural VA sites, co-designing with the voices of women veterans through focus groups.
Background
Rural women veterans often confront unique healthcare barriers—geographic isolation, gender-related stigma, and limited provider cultural sensitivity that undermine trust and engagement. In response, we co-designed an interprofessional communication curriculum to promote relational, patient-centered care grounded in psychological need support.
Innovation
Anchored in Self Determination Theory (SDT), this curriculum equips nurses and social workers with need-supportive communication strategies that nurture autonomy, competence, and relatedness, integrating two transformative learning methods for enhancing respectful and inclusive listening:
- Cultural humility reflections for veteran-centered care—personal narratives, storytelling, and power-awareness discussions to build lifelong reflective practices.
- Medical improv simulations—adaptive improvisational role plays for healthcare environments fostering presence, adaptability, empathy, trust-building, and real-time responsiveness.
Delivered via a multiday health professions learning lab, the training combines asynchronous workshops with in-person facilitated interactions. Core modules cover SDT foundations, need supportive dialogue, veteran-centered cultural humility, and shared decision-making practices that uplift rural women veterans’ voices. Using Kirkpatrick’s Four Level Model, we assess impact at multiple tiers:
- Reaction: Participant satisfaction and perceived training relevance.
- Learning: Pre/post assessments track SDT knowledge and communication skills gains.
- Behavior: Observe simulations and self-reported changes in communication practices.
- Results: Qualitative satisfaction metrics and care engagement trends among rural women veterans.
Results
A pilot cohort (N = 20) across two rural sites is pending implementation. pre/post surveys will assess any improved confidence in applying need supportive communication and the most effective component in building empathetic presence. Feedback measures will also indicate the significance of combined uses of medical improv and cultural humility on deepened relational capacity and trust.
Discussion
This program operationalizes SDT within healthcare communications, integrating cultural humility and improvisation learning modalities to enhance care quality for rural women veterans, ultimately strengthening provider-patient connections. Using health professions learning lab environments can foster sustained behavioral impacts. Future iterations will expand to additional rural VA sites, co-designing with the voices of women veterans through focus groups.
UK Approves Targeted Therapy for Cervical Cancer
UK Approves Targeted Therapy for Cervical Cancer
The Medicines and Healthcare products Regulatory Agency (MHRA) has approved tisotumab vedotin (Genmab AS) for adults with recurrent or metastatic cervical cancer.
The decision, made via the International Recognition Procedure, applies to patients whose disease has progressed after prior systemic therapy. It provides a new treatment option for a high-risk group with limited alternatives.
How the Treatment Works
Tisotumab vedotin is an antibody-drug conjugate that combines a tissue factor-directed human monoclonal antibody with monomethyl auristatin E, a microtubule-disrupting agent. The therapy targets tissue factor, which is overexpressed in a several solid tumours, including recurrent cervical cancer.
It is administered as a 30-minute intravenous infusion once every 3 weeks.
What Trials Showed
The approval is based on evidence from multiple clinical studies demonstrating tisotumab vedotin's efficacy in previously treated patients.
In the phase 2 innovaTV 204 study, 102 patients were enrolled and 101 received at least 1 dose of tisotumab vedotin. The confirmed objective response rate was 24%, including seven complete responses and 17 partial responses, demonstrating clinically meaningful activity in a heavily pretreated population.
Further evidence came from the phase 3 innovaTV-301 trial, which randomly assigned 502 patients to receive either tisotumab vedotin or investigator's-choice chemotherapy.
Median overall survival was 11.5 months with the new therapy compared with 9.5 months in the chemotherapy arm, translating to roughly a 30% reduction in the risk for death. The confirmed objective response rate was also significantly higher with tisotumab vedotin—17.8% vs 5.2%—underscoring its advantage over standard treatment options.
Safety and Tolerability
Ocular toxicity and peripheral neuropathy were the most notable adverse reactions.
Common treatment-related events in the phase 2 study included alopecia (38%), epistaxis (30%), nausea, conjunctivitis (26%), and fatigue (26%).
Grade 3 or higher treatment-related adverse events occurred in about 28% of patients. Clinicians should be alert to conjunctivitis and keratitis as well as sensory neuropathic symptoms (numbness, tingling, or a burning sensation in the hands and feet).
Julian Beach, interim executive director of healthcare quality and access at the MHRA, said that patient safety is the agency's "top priority." "We will continue to monitor its safety closely as it becomes more widely used," he added.
The Summary of Product Characteristics and Patient Information Leaflets will be published on the MHRA website within 7 days of approval.
A version of this article first appeared on Medscape.com.
The Medicines and Healthcare products Regulatory Agency (MHRA) has approved tisotumab vedotin (Genmab AS) for adults with recurrent or metastatic cervical cancer.
The decision, made via the International Recognition Procedure, applies to patients whose disease has progressed after prior systemic therapy. It provides a new treatment option for a high-risk group with limited alternatives.
How the Treatment Works
Tisotumab vedotin is an antibody-drug conjugate that combines a tissue factor-directed human monoclonal antibody with monomethyl auristatin E, a microtubule-disrupting agent. The therapy targets tissue factor, which is overexpressed in a several solid tumours, including recurrent cervical cancer.
It is administered as a 30-minute intravenous infusion once every 3 weeks.
What Trials Showed
The approval is based on evidence from multiple clinical studies demonstrating tisotumab vedotin's efficacy in previously treated patients.
In the phase 2 innovaTV 204 study, 102 patients were enrolled and 101 received at least 1 dose of tisotumab vedotin. The confirmed objective response rate was 24%, including seven complete responses and 17 partial responses, demonstrating clinically meaningful activity in a heavily pretreated population.
Further evidence came from the phase 3 innovaTV-301 trial, which randomly assigned 502 patients to receive either tisotumab vedotin or investigator's-choice chemotherapy.
Median overall survival was 11.5 months with the new therapy compared with 9.5 months in the chemotherapy arm, translating to roughly a 30% reduction in the risk for death. The confirmed objective response rate was also significantly higher with tisotumab vedotin—17.8% vs 5.2%—underscoring its advantage over standard treatment options.
Safety and Tolerability
Ocular toxicity and peripheral neuropathy were the most notable adverse reactions.
Common treatment-related events in the phase 2 study included alopecia (38%), epistaxis (30%), nausea, conjunctivitis (26%), and fatigue (26%).
Grade 3 or higher treatment-related adverse events occurred in about 28% of patients. Clinicians should be alert to conjunctivitis and keratitis as well as sensory neuropathic symptoms (numbness, tingling, or a burning sensation in the hands and feet).
Julian Beach, interim executive director of healthcare quality and access at the MHRA, said that patient safety is the agency's "top priority." "We will continue to monitor its safety closely as it becomes more widely used," he added.
The Summary of Product Characteristics and Patient Information Leaflets will be published on the MHRA website within 7 days of approval.
A version of this article first appeared on Medscape.com.
The Medicines and Healthcare products Regulatory Agency (MHRA) has approved tisotumab vedotin (Genmab AS) for adults with recurrent or metastatic cervical cancer.
The decision, made via the International Recognition Procedure, applies to patients whose disease has progressed after prior systemic therapy. It provides a new treatment option for a high-risk group with limited alternatives.
How the Treatment Works
Tisotumab vedotin is an antibody-drug conjugate that combines a tissue factor-directed human monoclonal antibody with monomethyl auristatin E, a microtubule-disrupting agent. The therapy targets tissue factor, which is overexpressed in a several solid tumours, including recurrent cervical cancer.
It is administered as a 30-minute intravenous infusion once every 3 weeks.
What Trials Showed
The approval is based on evidence from multiple clinical studies demonstrating tisotumab vedotin's efficacy in previously treated patients.
In the phase 2 innovaTV 204 study, 102 patients were enrolled and 101 received at least 1 dose of tisotumab vedotin. The confirmed objective response rate was 24%, including seven complete responses and 17 partial responses, demonstrating clinically meaningful activity in a heavily pretreated population.
Further evidence came from the phase 3 innovaTV-301 trial, which randomly assigned 502 patients to receive either tisotumab vedotin or investigator's-choice chemotherapy.
Median overall survival was 11.5 months with the new therapy compared with 9.5 months in the chemotherapy arm, translating to roughly a 30% reduction in the risk for death. The confirmed objective response rate was also significantly higher with tisotumab vedotin—17.8% vs 5.2%—underscoring its advantage over standard treatment options.
Safety and Tolerability
Ocular toxicity and peripheral neuropathy were the most notable adverse reactions.
Common treatment-related events in the phase 2 study included alopecia (38%), epistaxis (30%), nausea, conjunctivitis (26%), and fatigue (26%).
Grade 3 or higher treatment-related adverse events occurred in about 28% of patients. Clinicians should be alert to conjunctivitis and keratitis as well as sensory neuropathic symptoms (numbness, tingling, or a burning sensation in the hands and feet).
Julian Beach, interim executive director of healthcare quality and access at the MHRA, said that patient safety is the agency's "top priority." "We will continue to monitor its safety closely as it becomes more widely used," he added.
The Summary of Product Characteristics and Patient Information Leaflets will be published on the MHRA website within 7 days of approval.
A version of this article first appeared on Medscape.com.
UK Approves Targeted Therapy for Cervical Cancer
UK Approves Targeted Therapy for Cervical Cancer
Research Focuses on Mental Health Needs of Women Veterans
The more than 2 million women US veterans are the fastest-growing military population. While research into women veterans has traditionally lagged, more recently studies have begun to focus on their needs impacts of combat and service on women. These studies have found that women veterans preferred tailored solutions focused on women veterans.
A November 2025 study is one of the first to examine the impact of combat on women veterans. It found that those in combat roles had higher levels of depression, posttraumatic stress disorder (PTSD), dissociation, and overall poorer health compared with civilians and noncombat women military personnel. Previous research had found that women veterans had higher rates of lifetime and past-year PTSD (13.4%) compared with female civilians (8.0%), male veterans (7.7%), and male civilians (3.4%). A 2020 US Department of Veterans (VA) study of 4,928,638 men and 448,455 women similarly found that women had nearly twice the rates of depression and anxiety compared with men.
For many veterans, mental health issues may develop or be exacerbated in their return to civilian life. That transition can be especially confusing and isolating for women veterans, according to a 2024 study: “They neither fit in the military due to gendered relations centered on masculinity, or civilian life where they are largely misunderstood as ‘veterans.’ This ‘no woman’s land’ is poorly understood.” Few programs for transitioning veterans have been found effective for women veterans because they’ve been developed for a largely male veteran population. That includes mental health support programs.
Some women may prefer women-only groups, and even that choice may be dependent on their background, service history, socioeconomic level, and other factors. They may feel more comfortable in women-only groups if they’ve experienced MST. Others who have served in combat may choose mixed-gender programs. One study found that some women benefited from being in a mixed-gender group because it enabled them to work on difficulties with men in a safe environment. Other research has found that women veterans with substance use disorders are reluctant to seek help alongside men in the same facilities.
Accessing care may be especially challenging for rural women veterans. However, separate facilities and women-only groups are not always available, particularly in rural areas where there may be very few women veterans. And even if they are available, rural women are often up against barriers that urban women do not face, such as having to travel long distances to get care. Clinicians also may be hard to find in rural areas. Some participants in a 2025 study were hampered not only by a lack of female practitioners, but practitioners who were well trained to understand and treat the unique needs of female veterans: “[It’s] incredibly difficult to find a mental health practitioner that understands a veteran’s unique experience as a woman,” a participant said.
The more than 2 million women US veterans are the fastest-growing military population. While research into women veterans has traditionally lagged, more recently studies have begun to focus on their needs impacts of combat and service on women. These studies have found that women veterans preferred tailored solutions focused on women veterans.
A November 2025 study is one of the first to examine the impact of combat on women veterans. It found that those in combat roles had higher levels of depression, posttraumatic stress disorder (PTSD), dissociation, and overall poorer health compared with civilians and noncombat women military personnel. Previous research had found that women veterans had higher rates of lifetime and past-year PTSD (13.4%) compared with female civilians (8.0%), male veterans (7.7%), and male civilians (3.4%). A 2020 US Department of Veterans (VA) study of 4,928,638 men and 448,455 women similarly found that women had nearly twice the rates of depression and anxiety compared with men.
For many veterans, mental health issues may develop or be exacerbated in their return to civilian life. That transition can be especially confusing and isolating for women veterans, according to a 2024 study: “They neither fit in the military due to gendered relations centered on masculinity, or civilian life where they are largely misunderstood as ‘veterans.’ This ‘no woman’s land’ is poorly understood.” Few programs for transitioning veterans have been found effective for women veterans because they’ve been developed for a largely male veteran population. That includes mental health support programs.
Some women may prefer women-only groups, and even that choice may be dependent on their background, service history, socioeconomic level, and other factors. They may feel more comfortable in women-only groups if they’ve experienced MST. Others who have served in combat may choose mixed-gender programs. One study found that some women benefited from being in a mixed-gender group because it enabled them to work on difficulties with men in a safe environment. Other research has found that women veterans with substance use disorders are reluctant to seek help alongside men in the same facilities.
Accessing care may be especially challenging for rural women veterans. However, separate facilities and women-only groups are not always available, particularly in rural areas where there may be very few women veterans. And even if they are available, rural women are often up against barriers that urban women do not face, such as having to travel long distances to get care. Clinicians also may be hard to find in rural areas. Some participants in a 2025 study were hampered not only by a lack of female practitioners, but practitioners who were well trained to understand and treat the unique needs of female veterans: “[It’s] incredibly difficult to find a mental health practitioner that understands a veteran’s unique experience as a woman,” a participant said.
The more than 2 million women US veterans are the fastest-growing military population. While research into women veterans has traditionally lagged, more recently studies have begun to focus on their needs impacts of combat and service on women. These studies have found that women veterans preferred tailored solutions focused on women veterans.
A November 2025 study is one of the first to examine the impact of combat on women veterans. It found that those in combat roles had higher levels of depression, posttraumatic stress disorder (PTSD), dissociation, and overall poorer health compared with civilians and noncombat women military personnel. Previous research had found that women veterans had higher rates of lifetime and past-year PTSD (13.4%) compared with female civilians (8.0%), male veterans (7.7%), and male civilians (3.4%). A 2020 US Department of Veterans (VA) study of 4,928,638 men and 448,455 women similarly found that women had nearly twice the rates of depression and anxiety compared with men.
For many veterans, mental health issues may develop or be exacerbated in their return to civilian life. That transition can be especially confusing and isolating for women veterans, according to a 2024 study: “They neither fit in the military due to gendered relations centered on masculinity, or civilian life where they are largely misunderstood as ‘veterans.’ This ‘no woman’s land’ is poorly understood.” Few programs for transitioning veterans have been found effective for women veterans because they’ve been developed for a largely male veteran population. That includes mental health support programs.
Some women may prefer women-only groups, and even that choice may be dependent on their background, service history, socioeconomic level, and other factors. They may feel more comfortable in women-only groups if they’ve experienced MST. Others who have served in combat may choose mixed-gender programs. One study found that some women benefited from being in a mixed-gender group because it enabled them to work on difficulties with men in a safe environment. Other research has found that women veterans with substance use disorders are reluctant to seek help alongside men in the same facilities.
Accessing care may be especially challenging for rural women veterans. However, separate facilities and women-only groups are not always available, particularly in rural areas where there may be very few women veterans. And even if they are available, rural women are often up against barriers that urban women do not face, such as having to travel long distances to get care. Clinicians also may be hard to find in rural areas. Some participants in a 2025 study were hampered not only by a lack of female practitioners, but practitioners who were well trained to understand and treat the unique needs of female veterans: “[It’s] incredibly difficult to find a mental health practitioner that understands a veteran’s unique experience as a woman,” a participant said.
Socioeconomic Status Linked to Psychiatric Disorders in Older Women Veterans
TOPLINE: Psychiatric disorders affect 37.8% of veteran vs 37.3% of nonveteran in a study of > 42,000 women aged ≥ 65 years. Most differences between veterans and nonveterans were statistically insignificant after removing confounders.
METHODOLOGY:
Researchers analyzed 42,031 Women's Health Initiative (WHI) participants aged > 65 years at enrollment (1993-1998), including 1,512 veterans and 40,519 non-veterans, through linked WHI-Medicare databases with approximately 15 years of follow-up.
Analysis included multivariable logistic and Cox regression models to evaluate characteristics associated with prevalent and incident psychiatric disorders, respectively.
Participants were followed from WHI enrollment until first psychiatric diagnosis, with censoring at death, end of follow-up, or December 31, 2013.
Investigators examined relationships between individual-level and neighborhood-level socioeconomic status indicators with psychiatric disorders before and after stratification by veteran status.
TAKEAWAY:
The overall prevalence of psychiatric disorders was 37.3%, with an incidence rate of 25.5 per 1,000 person-years, showing no significant differences between veterans and non-veterans (odds ratio [OR], 0.95; 95% confidence interval [CI], 0.85-0.06).
There was a higher prevalence of psychiatric disorders for women veterans with technical, sales, or administrative occupations (adjusted OR [aOR], 1.72; 95 % CI, 1.02, 2.89) and those with “other” occupations (aOR, 2.09; 95 % CI, 1.13, 3.88) when compared with women veterans with managerial or professional occupations.
Mood and anxiety disorders emerged as the leading types of psychiatric conditions among both veteran and nonveteran women.
IN PRACTICE: "Although interaction effects by veteran status were nonsignificant,” the authors of the study explained, “lower education, household income, and neighborhood socioeconomic status were associated with higher frequencies of psychiatric disorders only among women non-veterans.”
SOURCE: The study was led by Jack Tsai and the US Department of Veterans Affairs National Center on Homelessness Among Veterans in Washington, DC. It was published online in Journal of Affective Disorders.
LIMITATIONS: The study faced several limitations including potential selection and survival biases, as findings correspond only to Women's Health Initiative participants who survived until age 65 or later. Information bias likely occurred due to self-reported measures and sole reliance on International Classification of Disease, 9th revision, Clinical Modification diagnostic codes from Medicare claims. Additionally, socioeconomic status indicators assessed at enrollment may not reflect early life or midlife exposures that could influence psychiatric diagnoses.
DISCLOSURES: The Women’s Health Initiative program received funding from the National Heart, Lung, and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services through grants 75N92021D00001, 75N92021D00002, 75N92021D00003, 75N92021D00004, and 75N92021D00005.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Psychiatric disorders affect 37.8% of veteran vs 37.3% of nonveteran in a study of > 42,000 women aged ≥ 65 years. Most differences between veterans and nonveterans were statistically insignificant after removing confounders.
METHODOLOGY:
Researchers analyzed 42,031 Women's Health Initiative (WHI) participants aged > 65 years at enrollment (1993-1998), including 1,512 veterans and 40,519 non-veterans, through linked WHI-Medicare databases with approximately 15 years of follow-up.
Analysis included multivariable logistic and Cox regression models to evaluate characteristics associated with prevalent and incident psychiatric disorders, respectively.
Participants were followed from WHI enrollment until first psychiatric diagnosis, with censoring at death, end of follow-up, or December 31, 2013.
Investigators examined relationships between individual-level and neighborhood-level socioeconomic status indicators with psychiatric disorders before and after stratification by veteran status.
TAKEAWAY:
The overall prevalence of psychiatric disorders was 37.3%, with an incidence rate of 25.5 per 1,000 person-years, showing no significant differences between veterans and non-veterans (odds ratio [OR], 0.95; 95% confidence interval [CI], 0.85-0.06).
There was a higher prevalence of psychiatric disorders for women veterans with technical, sales, or administrative occupations (adjusted OR [aOR], 1.72; 95 % CI, 1.02, 2.89) and those with “other” occupations (aOR, 2.09; 95 % CI, 1.13, 3.88) when compared with women veterans with managerial or professional occupations.
Mood and anxiety disorders emerged as the leading types of psychiatric conditions among both veteran and nonveteran women.
IN PRACTICE: "Although interaction effects by veteran status were nonsignificant,” the authors of the study explained, “lower education, household income, and neighborhood socioeconomic status were associated with higher frequencies of psychiatric disorders only among women non-veterans.”
SOURCE: The study was led by Jack Tsai and the US Department of Veterans Affairs National Center on Homelessness Among Veterans in Washington, DC. It was published online in Journal of Affective Disorders.
LIMITATIONS: The study faced several limitations including potential selection and survival biases, as findings correspond only to Women's Health Initiative participants who survived until age 65 or later. Information bias likely occurred due to self-reported measures and sole reliance on International Classification of Disease, 9th revision, Clinical Modification diagnostic codes from Medicare claims. Additionally, socioeconomic status indicators assessed at enrollment may not reflect early life or midlife exposures that could influence psychiatric diagnoses.
DISCLOSURES: The Women’s Health Initiative program received funding from the National Heart, Lung, and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services through grants 75N92021D00001, 75N92021D00002, 75N92021D00003, 75N92021D00004, and 75N92021D00005.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Psychiatric disorders affect 37.8% of veteran vs 37.3% of nonveteran in a study of > 42,000 women aged ≥ 65 years. Most differences between veterans and nonveterans were statistically insignificant after removing confounders.
METHODOLOGY:
Researchers analyzed 42,031 Women's Health Initiative (WHI) participants aged > 65 years at enrollment (1993-1998), including 1,512 veterans and 40,519 non-veterans, through linked WHI-Medicare databases with approximately 15 years of follow-up.
Analysis included multivariable logistic and Cox regression models to evaluate characteristics associated with prevalent and incident psychiatric disorders, respectively.
Participants were followed from WHI enrollment until first psychiatric diagnosis, with censoring at death, end of follow-up, or December 31, 2013.
Investigators examined relationships between individual-level and neighborhood-level socioeconomic status indicators with psychiatric disorders before and after stratification by veteran status.
TAKEAWAY:
The overall prevalence of psychiatric disorders was 37.3%, with an incidence rate of 25.5 per 1,000 person-years, showing no significant differences between veterans and non-veterans (odds ratio [OR], 0.95; 95% confidence interval [CI], 0.85-0.06).
There was a higher prevalence of psychiatric disorders for women veterans with technical, sales, or administrative occupations (adjusted OR [aOR], 1.72; 95 % CI, 1.02, 2.89) and those with “other” occupations (aOR, 2.09; 95 % CI, 1.13, 3.88) when compared with women veterans with managerial or professional occupations.
Mood and anxiety disorders emerged as the leading types of psychiatric conditions among both veteran and nonveteran women.
IN PRACTICE: "Although interaction effects by veteran status were nonsignificant,” the authors of the study explained, “lower education, household income, and neighborhood socioeconomic status were associated with higher frequencies of psychiatric disorders only among women non-veterans.”
SOURCE: The study was led by Jack Tsai and the US Department of Veterans Affairs National Center on Homelessness Among Veterans in Washington, DC. It was published online in Journal of Affective Disorders.
LIMITATIONS: The study faced several limitations including potential selection and survival biases, as findings correspond only to Women's Health Initiative participants who survived until age 65 or later. Information bias likely occurred due to self-reported measures and sole reliance on International Classification of Disease, 9th revision, Clinical Modification diagnostic codes from Medicare claims. Additionally, socioeconomic status indicators assessed at enrollment may not reflect early life or midlife exposures that could influence psychiatric diagnoses.
DISCLOSURES: The Women’s Health Initiative program received funding from the National Heart, Lung, and Blood Institute, National Institutes of Health, U.S. Department of Health and Human Services through grants 75N92021D00001, 75N92021D00002, 75N92021D00003, 75N92021D00004, and 75N92021D00005.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
Reducing Sex Disparities in Statin Therapy Among Female Veterans With Type 2 Diabetes and/or Cardiovascular Disease
Reducing Sex Disparities in Statin Therapy Among Female Veterans With Type 2 Diabetes and/or Cardiovascular Disease
Cardiovascular disease (CVD) is the leading cause of death among women in the United States.1 Most CVD is due to the buildup of plaque (ie, cholesterol, proteins, calcium, and inflammatory cells) in artery walls.2 The plaque may lead to atherosclerotic cardiovascular disease (ASCVD), which includes coronary heart disease, cerebrovascular disease, peripheral artery disease, and aortic atherosclerotic disease.2,3 Control and reduction of ASCVD risk factors, including high cholesterol levels, elevated blood pressure, insulin resistance, smoking, and a sedentary lifestyle, can contribute to a reduction in ASCVD morbidity and mortality.2 People with type 2 diabetes mellitus (T2DM) have an increased prevalence of lipid abnormalities, contributing to their high risk of ASCVD.4,5
The prescribing of statins (3-hydroxy-3-methyl-glutaryl-coenzmye A reductase inhibitors) is the cornerstone of lipid-lowering therapy and cardiovascular risk reduction for primary and secondary prevention of ASCVD.6 The American Diabetes Association (ADA) and American College of Cardiology/American Heart Association (ACC/AHA) recommend moderate- to high-intensity statins for primary prevention in patients with T2DM and high-intensity statins for secondary prevention in those with or without diabetes when not contraindicated.4,5,7 Despite eligibility according to guideline recommendations, research predominantly shows that women are less likely to receive statin therapy; however, this trend is improving. [6,8-11] To explain the sex differences in statin use, Nanna et al found that there is a combination of women being offered statin therapy less frequently, declining therapy more frequently, and discontinuing treatment more frequently.11 One possibility for discontinuing treatment could be statin-associated muscle symptoms (SAMS), which occur in about 10% of patients.12 The incidence of adverse effects (AEs) may be related to the way statins are metabolized.
Pharmacogenomic testing is free for veterans through the US Department of Veterans Affairs (VA) PHASER program, which offers information and recommendations for a panel of 11 gene variants. The panel includes genes related to common medication classes such as anticoagulants, antiplatelets, proton pump inhibitors, nonsteroidal anti-inflammatory drugs, opioids, antidepressants, and statins. The VA PHASER panel includes the solute carrier organic anion transporter family member 1B1 (SLCO1B1) gene, which is predominantly expressed in the liver and facilitates the hepatic uptake of most statins.13,14 A reduced function of SLCO1B1 can lead to higher statin levels, resulting in increased concentrations that may potentially cause SAMS.13,14 Some alleles associated with reduced function include SLCO1B1*5, *15, *23, *31, and *46 to *49, whereas others are associated with increased function, such as SLCO1B1 *14 and *20 (Appendix).15 Supporting evidence shows the SLCO1B1*5 nucleotide polymorphism increases plasma levels of simvastatin and atorvastatin, affecting effectiveness or toxicity. 13 Females tend to have a lower body weight and higher percentage of body fat compared with males, which might lead to higher concentrations of lipophilic drugs, including atorvastatin and simvastatin, which may be exacerbated by decreased function of SLCO1B1*5.15 With pharmacogenomic testing, therapeutic recommendations can be made to improve the overall safety and efficacy of statins, thus improving adherence using a patient-specific approach.14,15
Methods
Carl Vinson VA Medical Center (CVVAMC) serves about 42,000 veterans in Central and South Georgia, of which about 15% are female. Of the female veterans enrolled in care, 63% identify as Black, 27% White, and 1.5% as Asian, American Indian/Alaska Native, or Native Hawaiian/Other Pacific Islander. The 2020 Veterans Chartbook report showed that female veterans and minority racial and ethnic groups had worse access to health care and higher mortality rates than their male and non-Hispanic White counterparts.16
The Primary Care Equity Dashboard (PCED) was developed to engage the VA health care workforce in the process of identifying and addressing inequities in local patient populations.17 Using electronic quality measure data, the PCED provides Veterans Integrated Service Network-level and facility-level performance on several metrics.18 The PCED had not been previously used at the CVVAMC, and few publications or quality improvement projects regarding its use have been reported by the VA Office of Health Equity. PCED helped identify disparities when comparing female to male patients in the prescribing of statin therapy for patients with CVD and statin therapy for patients with T2DM.
VA PHASER pharmacogenomic analyses provided an opportunity to expand this quality improvement project. Sanford Health and the VA collaborated on the PHASER program to offer free genetic testing for veterans. The program launched in 2019 and expanded to various VA sites, including CVVAMC in March 2023. This program has been extended to December 31, 2025.
The primary objective of this quality improvement project was to increase statin prescribing among female veterans with T2DM and/or CVD to reduce cardiovascular risk. Secondary outcomes included increased pharmacogenomic testing and the assessment of pharmacogenomic results related to statin therapy. This project was approved by the CVVAMC Pharmacy and Therapeutics Committee. The PCED was used to identify female veterans with T2DM and/or CVD without an active prescription for a statin between July and October 2023. A review of Computerized Patient Record System patient charts was completed to screen for prespecified inclusion and exclusion criteria. Veterans were included if they were assigned female at birth, were enrolled in care at CVVAMC, and had a diagnosis of T2DM or CVD (history of myocardial infarction, coronary bypass graft, percutaneous coronary intervention, or other revascularization in any setting).
Veterans were excluded if they were currently pregnant, trying to conceive, breastfeeding, had a T1DM diagnosis, had previously documented hypersensitivity to a statin, active liver failure or decompensated cirrhosis, previously documented statin-associated rhabdomyolysis or autoimmune myopathy, an active prescription for a proprotein convertase subtilisin/kexin type 9 inhibitor, or previously documented statin intolerance (defined as the inability to tolerate ≥ 3 statins, with ≥ 1 prescribed at low intensity or alternate-day dosing). The female veterans were compared to 2 comparators: the facility's male veterans and the VA national average, identified via the PCED.
Once a veteran was screened, they were telephoned between October 2023 and February 2024 and provided education on statin use and pharmacogenomic testing using a standardized note template. An order was placed for participants who provided verbal consent for pharmacogenomic testing. Those who agreed to statin initiation were referred to a clinical pharmacist practitioner (CPP) who contacted them at a later date to prescribe a statin following the recommendations of the 2019 ACC/AHA and 2023 ADA guidelines and pharmacogenomic testing, if applicable.4,5,7 Appropriate monitoring and follow-up occurred at the discretion of each CPP. Data collection included: age, race, diagnoses (T2DM, CVD, or both), baseline lipid panel (total cholesterol, triglycerides, high-density lipoprotein, low-density lipoprotein), hepatic function, name and dose of statin, reasons for declining statin therapy, and pharmacogenomic testing results related to SLCO1B1.
Results
At baseline in July 2023, 77.8% of female veterans with T2DM were prescribed a statin, which exceeded the national VA average (77.0%), but was below the rate for male veterans (78.7%) in the facility comparator group.17 Additionally, 82.2% of females with CVD were prescribed a statin, which was below the national VA average of 86.0% and the 84.9% of male veterans in the facility comparator group.17 The PCED identified 189 female veterans from July 2023 to October 2023 who may benefit from statin therapy. Thirty-three females met the exclusion criteria. Of the 156 included veterans, 129 (82.7%) were successfully contacted and 27 (17.3%) could not be reached by telephone after 3 attempts (Figure 1). The 129 female veterans contacted had a mean age of 59 years and the majority were Black (82.9%) (Table 1).
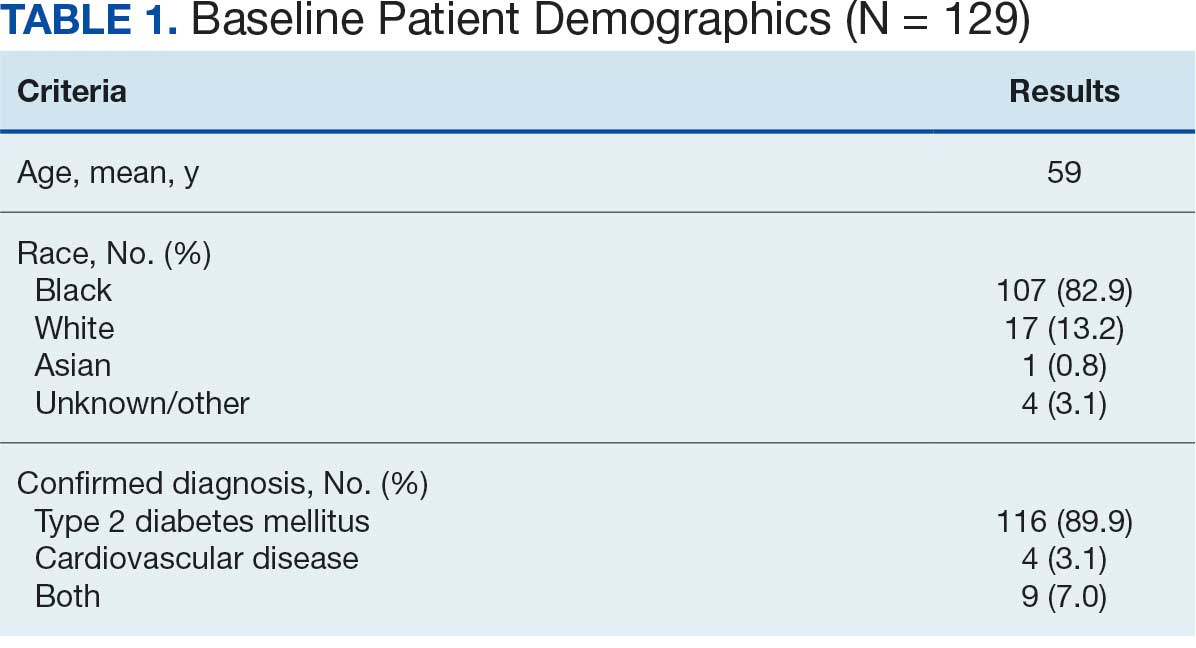
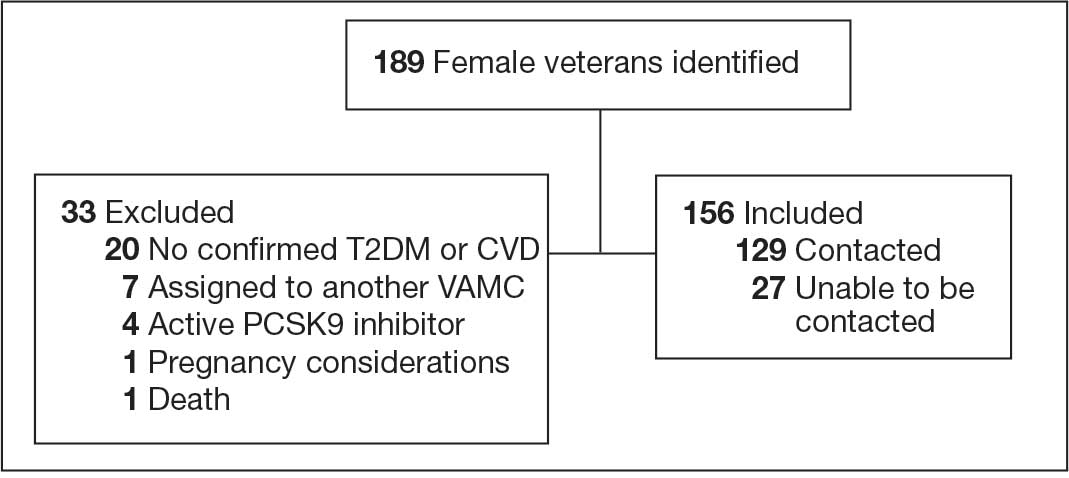
Abbreviations: CVD, cardiovascular disease; PCSK9, proprotein convertase subtilisin/
kexin type 9; T2DM, type 2 diabetes mellitus; VAMC, Veterans Affairs medical center.
Primary Outcomes
Of the 129 contacted veterans, 31 (24.0%) had a non-VA statin prescription, 13 (10.1%) had an active VA statin prescription, and 85 (65.9%) did not have a statin prescription, despite being eligible. Statin adherence was confirmed with participants, and the medication list was updated accordingly.
Of the 85 veterans with no active statin therapy, 37 (43.5%) accepted a new statin prescription and 48 (56.5%) declined. There were various reasons provided for declining statin therapy: 17 participants (35.4%) declined due to concern for AEs (Table 2).
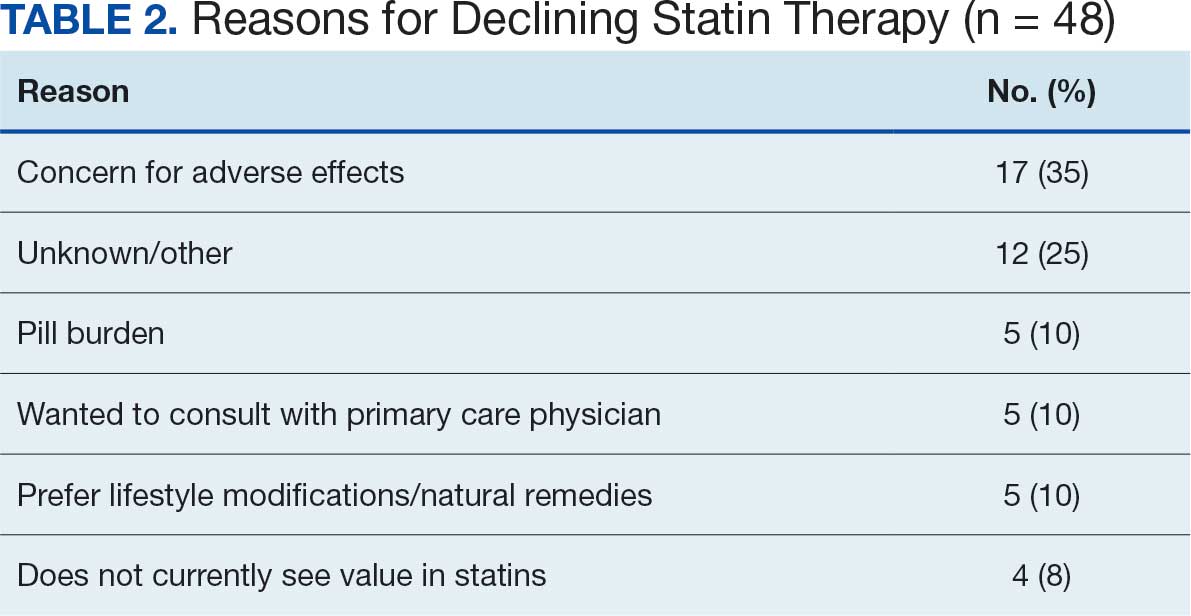
From July 2023 to March 2024, the percentage of female veterans with active statin therapy with T2DM increased from 77.8% to 79.0%. For those with active statin therapy with CVD, usage increased from 82.2% to 90.2%, which exceeded the national VA average and facility male comparator group (Figures 2 and 3).17
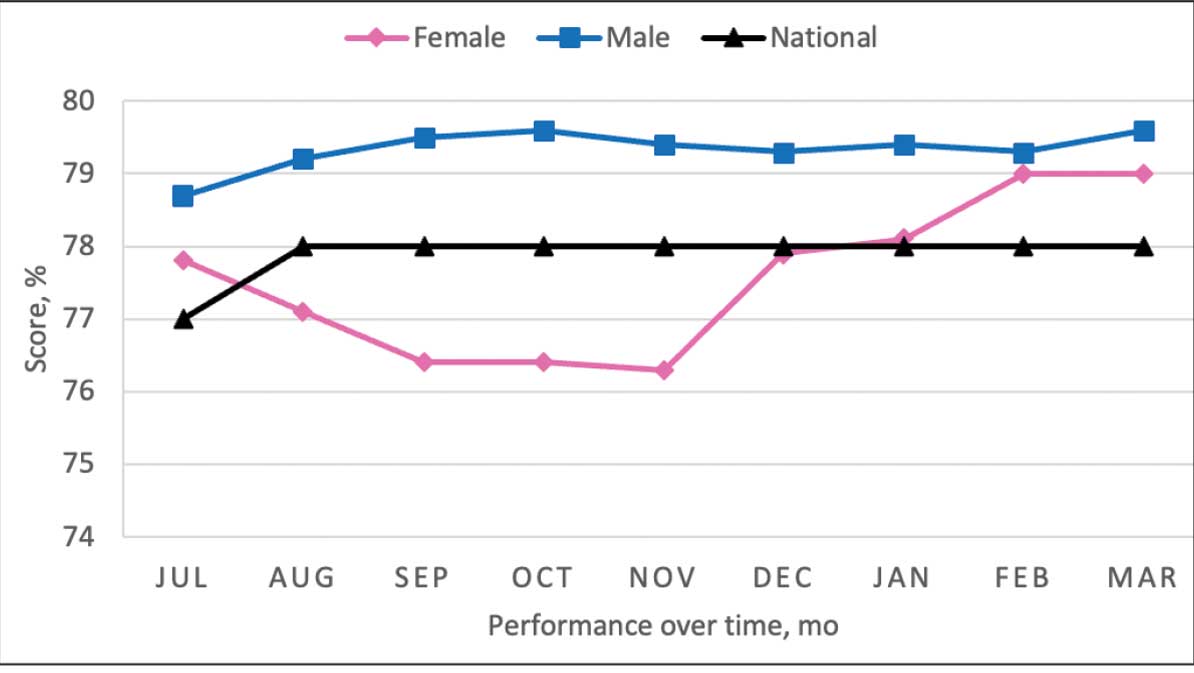
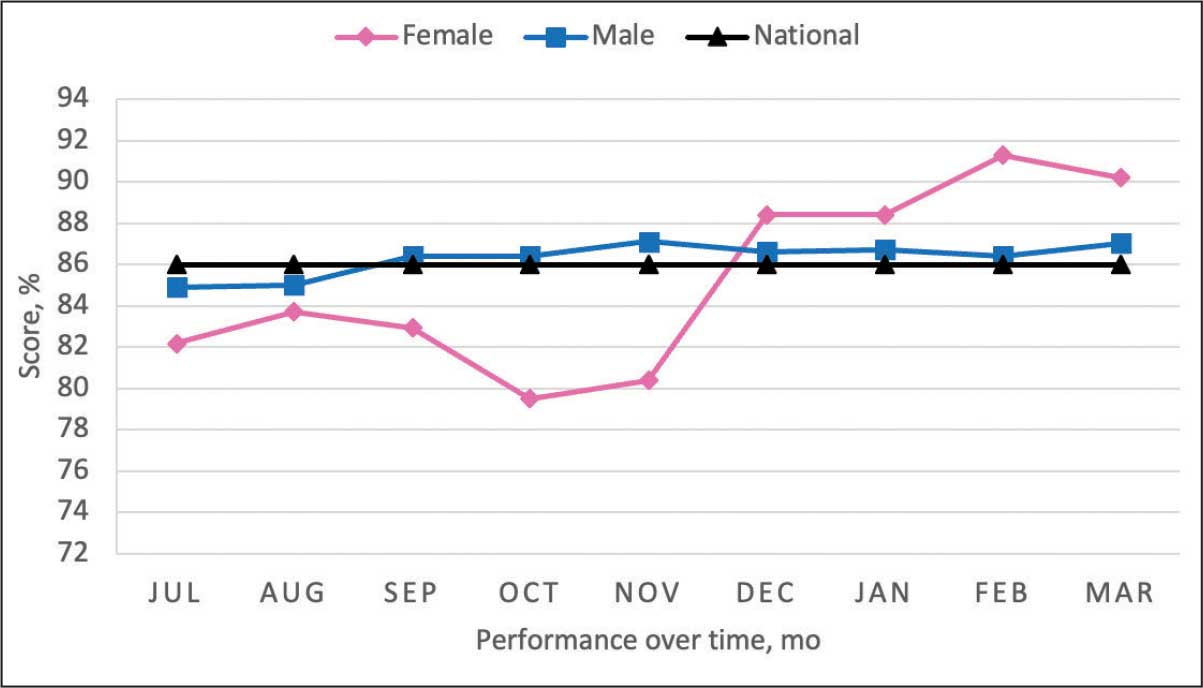
Secondary Outcomes
Seventy-one of 129 veterans (55.0%) gave verbal consent, and 47 (66.2%) completed the pharmacogenomic testing; 58 (45.0%) declined. Five veterans (10.6%) had a known SLCO1B1 allele variant present. One veteran required a change in statin therapy based on the results (eAppendix).
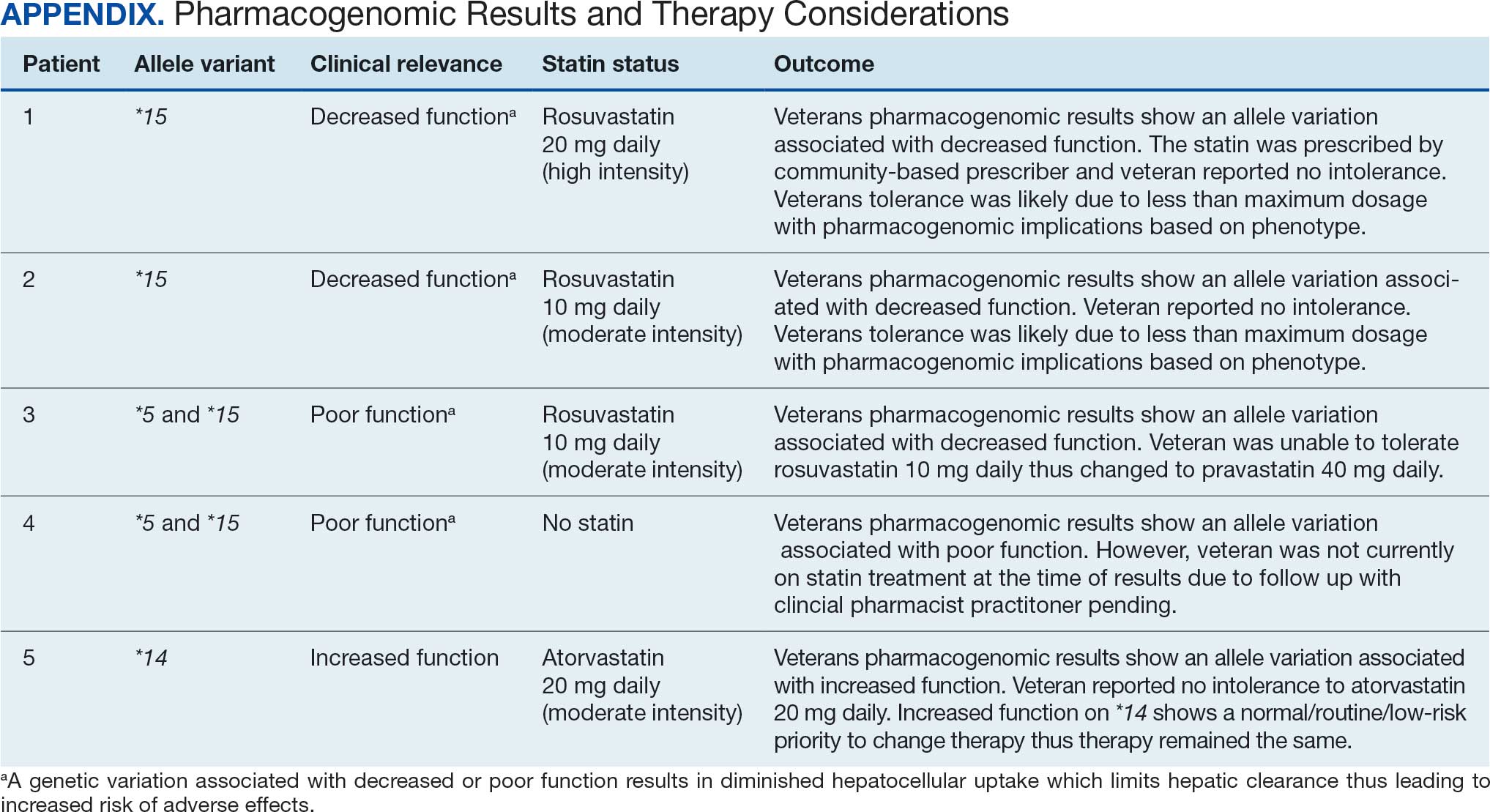
Discussion
This project aimed to increase statin prescribing among female veterans with T2DM and/or CVD to reduce cardiovascular risk and increase pharmacogenomic testing using the PCED and care managed by CPPs. The results of this quality improvement project illustrated that both metrics have improved at CVVAMC as a result of the intervention. The results in both metrics now exceed the PCED national VA average, and the CVD metric also exceeds that of the facility male comparator group. While there was only a 1.2% increase from July 2023 to March 2024 for patients with T2DM, there was an 8.0% increase for patients with CVD. Despite standardized education on statin use, more veterans declined therapy than accepted it, mostly due to concern for AEs. Recording the reasons for declining statin therapy offered valuable insight that can be used in additional discussions with veterans and clinicians.
Pharmacogenomics gives clinicians the unique opportunity to take a proactive approach to better predict drug responses, potentially allowing for less trial and error with medications, fewer AEs, greater trust in the clinician, and improved medication adherence. The CPPs incorporated pharmacogenomic testing into their practice, which led to identifying 5 SLCO1B1 gene abnormalities. The PCED served as a powerful tool for advancing equity-focused quality improvement initiatives on a local level and was crucial in prioritizing the detection of veterans potentially receiving suboptimal care.
Limitations
The nature of “cold calls” made it challenging to establish contact for inclusion in this study. An alternative to increase engagement could have been scheduled phone or face-to-face visits. While the use of the PCED was crucial, data did not account for statins listed in the non-VA medication list. All 31 patients with statins prescribed outside the VA had a start date added to provide the most accurate representation of the data moving forward.
Another limitation in this project was its small sample size and population. CVVAMC serves about 6200 female veterans, with roughly 63% identifying as Black. The preponderance of Black individuals (83%) in this project is typical for the female patient population at CVVAMC but may not reflect the demographics of other populations. Other limitations to this project consisted of scheduling conflicts. Appointments for laboratory draws at community-based outpatient clinics were subject to availability, which resulted in some delay in completion of pharmacogenomic testing.
Conclusions
CPPs can help reduce inequity in health care delivery. Increased incorporation of the PCED into regular practice within the VA is recommended to continue addressing sex disparities in statin use, diabetes control, blood pressure management, cancer screenings, and vaccination needs. CVVAMC plans to expand its use through another quality improvement project focused on reducing sex disparities in blood pressure management. Improving educational resources made available to veterans on the importance of statin therapy and potential to mitigate AEs through use of the VA PHASER program also would be helpful. This project successfully improved CVVAMC metrics for female veterans appropriately prescribed statin therapy and increased access to pharmacogenomic testing. Most importantly, it helped close the sex-based gap in CVD risk reduction care.
- Heron M. Deaths: leading causes for 2018. Nat Vital Stat Rep. 2021;70:1-114.
- US Department of Veterans Affairs, US Department of Defense. VA/DoD Clinical practice guideline for the management of dyslipidemia for cardiovascular risk reduction. Published June 2020. Accessed August 25, 2025. https://www.healthquality.va.gov/guidelines/CD/lipids/VADODDyslipidemiaCPG5087212020.pdf
- Atherosclerotic Cardiovascular Disease (ASCVD). American Heart Association. Accessed August 26, 2025. https:// www.heart.org/en/professional/quality-improvement/ascvd
- American Diabetes Association Professional Practice Committee. 10. Cardiovascular disease and risk management: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S144-S174. doi:10.2337/dc22-S010
- American Diabetes Association. Standards of Care in Diabetes— 2023 abridged for primary care providers. Clinical Diabetes. 2022;41(1):4-31. doi:10.2337/cd23-as01
- Virani SS, Woodard LD, Ramsey DJ, et al. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am J Cardiol. 2015;115:21-26. doi:10.1016/j.amjcard.2014.09.041
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/ AHA Guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/ American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596-e646. doi:10.1161/CIR.0000000000000678
- Buchanan CH, Brown EA, Bishu KG, et al. The magnitude and potential causes of gender disparities in statin therapy in veterans with type 2 diabetes: a 10-year nationwide longitudinal cohort study. Womens Health Issues. 2022;32:274-283. doi:10.1016/j.whi.2021.10.003
- Ahmed F, Lin J, Ahmed T, et al. Health disparities: statin prescribing patterns among patients with diabetes in a family medicine clinic. Health Equity. 2022;6:291-297. doi:10.1089/heq.2021.0144
- Metser G, Bradley C, Moise N, Liyanage-Don N, Kronish I, Ye S. Gaps and disparities in primary prevention statin prescription during outpatient care. Am J Cardiol. 2021;161:36-41. doi:10.1016/j.amjcard.2021.08.070
- Nanna MG, Wang TY, Xiang Q, et al. Sex differences in the use of statins in community practice. Circ Cardiovasc Qual Outcomes. 2019;12(8):e005562. doi:10.1161/CIRCOUTCOMES.118.005562
- Kitzmiller JP, Mikulik EB, Dauki AM, Murkherjee C, Luzum JA. Pharmacogenomics of statins: understanding susceptibility to adverse effects. Pharmgenomics Pers Med. 2016;9:97-106. doi:10.2147/PGPM.S86013
- Türkmen D, Masoli JAH, Kuo CL, Bowden J, Melzer D, Pilling LC. Statin treatment effectiveness and the SLCO1B1*5 reduced function genotype: long-term outcomes in women and men. Br J Clin Pharmacol. 2022;88:3230-3240. doi:10.1111/bcp.15245
- Cooper-DeHoff RM, Niemi M, Ramsey LB, et al. The Clinical Pharmacogenetics Implementation Consortium guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and statin-associated musculoskeletal symptoms. Clin Pharmacol Ther. 2022;111:1007-1021. doi:10.1002/cpt.2557
- Ramsey LB, Gong L, Lee SB, et al. PharmVar GeneFocus: SLCO1B1. Clin Pharmacol Ther. 2023;113:782-793. doi:10.1002/cpt.2705
- National Healthcare Quality and Disparities Report: Chartbook on Healthcare for Veterans. Rockville (MD): Agency for Healthcare Research and Quality (US); November 2020.
- Procario G. Primary Care Equity Dashboard [database online]. Power Bi. 2023. Accessed August 26, 2025. https://app.powerbigov.us
- Hausmann LRM, Lamorte C, Estock JL. Understanding the context for incorporating equity into quality improvement throughout a national health care system. Health Equity. 2023;7(1):312-320. doi:10.1089/heq.2023.0009
Cardiovascular disease (CVD) is the leading cause of death among women in the United States.1 Most CVD is due to the buildup of plaque (ie, cholesterol, proteins, calcium, and inflammatory cells) in artery walls.2 The plaque may lead to atherosclerotic cardiovascular disease (ASCVD), which includes coronary heart disease, cerebrovascular disease, peripheral artery disease, and aortic atherosclerotic disease.2,3 Control and reduction of ASCVD risk factors, including high cholesterol levels, elevated blood pressure, insulin resistance, smoking, and a sedentary lifestyle, can contribute to a reduction in ASCVD morbidity and mortality.2 People with type 2 diabetes mellitus (T2DM) have an increased prevalence of lipid abnormalities, contributing to their high risk of ASCVD.4,5
The prescribing of statins (3-hydroxy-3-methyl-glutaryl-coenzmye A reductase inhibitors) is the cornerstone of lipid-lowering therapy and cardiovascular risk reduction for primary and secondary prevention of ASCVD.6 The American Diabetes Association (ADA) and American College of Cardiology/American Heart Association (ACC/AHA) recommend moderate- to high-intensity statins for primary prevention in patients with T2DM and high-intensity statins for secondary prevention in those with or without diabetes when not contraindicated.4,5,7 Despite eligibility according to guideline recommendations, research predominantly shows that women are less likely to receive statin therapy; however, this trend is improving. [6,8-11] To explain the sex differences in statin use, Nanna et al found that there is a combination of women being offered statin therapy less frequently, declining therapy more frequently, and discontinuing treatment more frequently.11 One possibility for discontinuing treatment could be statin-associated muscle symptoms (SAMS), which occur in about 10% of patients.12 The incidence of adverse effects (AEs) may be related to the way statins are metabolized.
Pharmacogenomic testing is free for veterans through the US Department of Veterans Affairs (VA) PHASER program, which offers information and recommendations for a panel of 11 gene variants. The panel includes genes related to common medication classes such as anticoagulants, antiplatelets, proton pump inhibitors, nonsteroidal anti-inflammatory drugs, opioids, antidepressants, and statins. The VA PHASER panel includes the solute carrier organic anion transporter family member 1B1 (SLCO1B1) gene, which is predominantly expressed in the liver and facilitates the hepatic uptake of most statins.13,14 A reduced function of SLCO1B1 can lead to higher statin levels, resulting in increased concentrations that may potentially cause SAMS.13,14 Some alleles associated with reduced function include SLCO1B1*5, *15, *23, *31, and *46 to *49, whereas others are associated with increased function, such as SLCO1B1 *14 and *20 (Appendix).15 Supporting evidence shows the SLCO1B1*5 nucleotide polymorphism increases plasma levels of simvastatin and atorvastatin, affecting effectiveness or toxicity. 13 Females tend to have a lower body weight and higher percentage of body fat compared with males, which might lead to higher concentrations of lipophilic drugs, including atorvastatin and simvastatin, which may be exacerbated by decreased function of SLCO1B1*5.15 With pharmacogenomic testing, therapeutic recommendations can be made to improve the overall safety and efficacy of statins, thus improving adherence using a patient-specific approach.14,15
Methods
Carl Vinson VA Medical Center (CVVAMC) serves about 42,000 veterans in Central and South Georgia, of which about 15% are female. Of the female veterans enrolled in care, 63% identify as Black, 27% White, and 1.5% as Asian, American Indian/Alaska Native, or Native Hawaiian/Other Pacific Islander. The 2020 Veterans Chartbook report showed that female veterans and minority racial and ethnic groups had worse access to health care and higher mortality rates than their male and non-Hispanic White counterparts.16
The Primary Care Equity Dashboard (PCED) was developed to engage the VA health care workforce in the process of identifying and addressing inequities in local patient populations.17 Using electronic quality measure data, the PCED provides Veterans Integrated Service Network-level and facility-level performance on several metrics.18 The PCED had not been previously used at the CVVAMC, and few publications or quality improvement projects regarding its use have been reported by the VA Office of Health Equity. PCED helped identify disparities when comparing female to male patients in the prescribing of statin therapy for patients with CVD and statin therapy for patients with T2DM.
VA PHASER pharmacogenomic analyses provided an opportunity to expand this quality improvement project. Sanford Health and the VA collaborated on the PHASER program to offer free genetic testing for veterans. The program launched in 2019 and expanded to various VA sites, including CVVAMC in March 2023. This program has been extended to December 31, 2025.
The primary objective of this quality improvement project was to increase statin prescribing among female veterans with T2DM and/or CVD to reduce cardiovascular risk. Secondary outcomes included increased pharmacogenomic testing and the assessment of pharmacogenomic results related to statin therapy. This project was approved by the CVVAMC Pharmacy and Therapeutics Committee. The PCED was used to identify female veterans with T2DM and/or CVD without an active prescription for a statin between July and October 2023. A review of Computerized Patient Record System patient charts was completed to screen for prespecified inclusion and exclusion criteria. Veterans were included if they were assigned female at birth, were enrolled in care at CVVAMC, and had a diagnosis of T2DM or CVD (history of myocardial infarction, coronary bypass graft, percutaneous coronary intervention, or other revascularization in any setting).
Veterans were excluded if they were currently pregnant, trying to conceive, breastfeeding, had a T1DM diagnosis, had previously documented hypersensitivity to a statin, active liver failure or decompensated cirrhosis, previously documented statin-associated rhabdomyolysis or autoimmune myopathy, an active prescription for a proprotein convertase subtilisin/kexin type 9 inhibitor, or previously documented statin intolerance (defined as the inability to tolerate ≥ 3 statins, with ≥ 1 prescribed at low intensity or alternate-day dosing). The female veterans were compared to 2 comparators: the facility's male veterans and the VA national average, identified via the PCED.
Once a veteran was screened, they were telephoned between October 2023 and February 2024 and provided education on statin use and pharmacogenomic testing using a standardized note template. An order was placed for participants who provided verbal consent for pharmacogenomic testing. Those who agreed to statin initiation were referred to a clinical pharmacist practitioner (CPP) who contacted them at a later date to prescribe a statin following the recommendations of the 2019 ACC/AHA and 2023 ADA guidelines and pharmacogenomic testing, if applicable.4,5,7 Appropriate monitoring and follow-up occurred at the discretion of each CPP. Data collection included: age, race, diagnoses (T2DM, CVD, or both), baseline lipid panel (total cholesterol, triglycerides, high-density lipoprotein, low-density lipoprotein), hepatic function, name and dose of statin, reasons for declining statin therapy, and pharmacogenomic testing results related to SLCO1B1.
Results
At baseline in July 2023, 77.8% of female veterans with T2DM were prescribed a statin, which exceeded the national VA average (77.0%), but was below the rate for male veterans (78.7%) in the facility comparator group.17 Additionally, 82.2% of females with CVD were prescribed a statin, which was below the national VA average of 86.0% and the 84.9% of male veterans in the facility comparator group.17 The PCED identified 189 female veterans from July 2023 to October 2023 who may benefit from statin therapy. Thirty-three females met the exclusion criteria. Of the 156 included veterans, 129 (82.7%) were successfully contacted and 27 (17.3%) could not be reached by telephone after 3 attempts (Figure 1). The 129 female veterans contacted had a mean age of 59 years and the majority were Black (82.9%) (Table 1).
Abbreviations: CVD, cardiovascular disease; PCSK9, proprotein convertase subtilisin/
kexin type 9; T2DM, type 2 diabetes mellitus; VAMC, Veterans Affairs medical center.
Primary Outcomes
Of the 129 contacted veterans, 31 (24.0%) had a non-VA statin prescription, 13 (10.1%) had an active VA statin prescription, and 85 (65.9%) did not have a statin prescription, despite being eligible. Statin adherence was confirmed with participants, and the medication list was updated accordingly.
Of the 85 veterans with no active statin therapy, 37 (43.5%) accepted a new statin prescription and 48 (56.5%) declined. There were various reasons provided for declining statin therapy: 17 participants (35.4%) declined due to concern for AEs (Table 2).
From July 2023 to March 2024, the percentage of female veterans with active statin therapy with T2DM increased from 77.8% to 79.0%. For those with active statin therapy with CVD, usage increased from 82.2% to 90.2%, which exceeded the national VA average and facility male comparator group (Figures 2 and 3).17
Secondary Outcomes
Seventy-one of 129 veterans (55.0%) gave verbal consent, and 47 (66.2%) completed the pharmacogenomic testing; 58 (45.0%) declined. Five veterans (10.6%) had a known SLCO1B1 allele variant present. One veteran required a change in statin therapy based on the results (eAppendix).
Discussion
This project aimed to increase statin prescribing among female veterans with T2DM and/or CVD to reduce cardiovascular risk and increase pharmacogenomic testing using the PCED and care managed by CPPs. The results of this quality improvement project illustrated that both metrics have improved at CVVAMC as a result of the intervention. The results in both metrics now exceed the PCED national VA average, and the CVD metric also exceeds that of the facility male comparator group. While there was only a 1.2% increase from July 2023 to March 2024 for patients with T2DM, there was an 8.0% increase for patients with CVD. Despite standardized education on statin use, more veterans declined therapy than accepted it, mostly due to concern for AEs. Recording the reasons for declining statin therapy offered valuable insight that can be used in additional discussions with veterans and clinicians.
Pharmacogenomics gives clinicians the unique opportunity to take a proactive approach to better predict drug responses, potentially allowing for less trial and error with medications, fewer AEs, greater trust in the clinician, and improved medication adherence. The CPPs incorporated pharmacogenomic testing into their practice, which led to identifying 5 SLCO1B1 gene abnormalities. The PCED served as a powerful tool for advancing equity-focused quality improvement initiatives on a local level and was crucial in prioritizing the detection of veterans potentially receiving suboptimal care.
Limitations
The nature of “cold calls” made it challenging to establish contact for inclusion in this study. An alternative to increase engagement could have been scheduled phone or face-to-face visits. While the use of the PCED was crucial, data did not account for statins listed in the non-VA medication list. All 31 patients with statins prescribed outside the VA had a start date added to provide the most accurate representation of the data moving forward.
Another limitation in this project was its small sample size and population. CVVAMC serves about 6200 female veterans, with roughly 63% identifying as Black. The preponderance of Black individuals (83%) in this project is typical for the female patient population at CVVAMC but may not reflect the demographics of other populations. Other limitations to this project consisted of scheduling conflicts. Appointments for laboratory draws at community-based outpatient clinics were subject to availability, which resulted in some delay in completion of pharmacogenomic testing.
Conclusions
CPPs can help reduce inequity in health care delivery. Increased incorporation of the PCED into regular practice within the VA is recommended to continue addressing sex disparities in statin use, diabetes control, blood pressure management, cancer screenings, and vaccination needs. CVVAMC plans to expand its use through another quality improvement project focused on reducing sex disparities in blood pressure management. Improving educational resources made available to veterans on the importance of statin therapy and potential to mitigate AEs through use of the VA PHASER program also would be helpful. This project successfully improved CVVAMC metrics for female veterans appropriately prescribed statin therapy and increased access to pharmacogenomic testing. Most importantly, it helped close the sex-based gap in CVD risk reduction care.
Cardiovascular disease (CVD) is the leading cause of death among women in the United States.1 Most CVD is due to the buildup of plaque (ie, cholesterol, proteins, calcium, and inflammatory cells) in artery walls.2 The plaque may lead to atherosclerotic cardiovascular disease (ASCVD), which includes coronary heart disease, cerebrovascular disease, peripheral artery disease, and aortic atherosclerotic disease.2,3 Control and reduction of ASCVD risk factors, including high cholesterol levels, elevated blood pressure, insulin resistance, smoking, and a sedentary lifestyle, can contribute to a reduction in ASCVD morbidity and mortality.2 People with type 2 diabetes mellitus (T2DM) have an increased prevalence of lipid abnormalities, contributing to their high risk of ASCVD.4,5
The prescribing of statins (3-hydroxy-3-methyl-glutaryl-coenzmye A reductase inhibitors) is the cornerstone of lipid-lowering therapy and cardiovascular risk reduction for primary and secondary prevention of ASCVD.6 The American Diabetes Association (ADA) and American College of Cardiology/American Heart Association (ACC/AHA) recommend moderate- to high-intensity statins for primary prevention in patients with T2DM and high-intensity statins for secondary prevention in those with or without diabetes when not contraindicated.4,5,7 Despite eligibility according to guideline recommendations, research predominantly shows that women are less likely to receive statin therapy; however, this trend is improving. [6,8-11] To explain the sex differences in statin use, Nanna et al found that there is a combination of women being offered statin therapy less frequently, declining therapy more frequently, and discontinuing treatment more frequently.11 One possibility for discontinuing treatment could be statin-associated muscle symptoms (SAMS), which occur in about 10% of patients.12 The incidence of adverse effects (AEs) may be related to the way statins are metabolized.
Pharmacogenomic testing is free for veterans through the US Department of Veterans Affairs (VA) PHASER program, which offers information and recommendations for a panel of 11 gene variants. The panel includes genes related to common medication classes such as anticoagulants, antiplatelets, proton pump inhibitors, nonsteroidal anti-inflammatory drugs, opioids, antidepressants, and statins. The VA PHASER panel includes the solute carrier organic anion transporter family member 1B1 (SLCO1B1) gene, which is predominantly expressed in the liver and facilitates the hepatic uptake of most statins.13,14 A reduced function of SLCO1B1 can lead to higher statin levels, resulting in increased concentrations that may potentially cause SAMS.13,14 Some alleles associated with reduced function include SLCO1B1*5, *15, *23, *31, and *46 to *49, whereas others are associated with increased function, such as SLCO1B1 *14 and *20 (Appendix).15 Supporting evidence shows the SLCO1B1*5 nucleotide polymorphism increases plasma levels of simvastatin and atorvastatin, affecting effectiveness or toxicity. 13 Females tend to have a lower body weight and higher percentage of body fat compared with males, which might lead to higher concentrations of lipophilic drugs, including atorvastatin and simvastatin, which may be exacerbated by decreased function of SLCO1B1*5.15 With pharmacogenomic testing, therapeutic recommendations can be made to improve the overall safety and efficacy of statins, thus improving adherence using a patient-specific approach.14,15
Methods
Carl Vinson VA Medical Center (CVVAMC) serves about 42,000 veterans in Central and South Georgia, of which about 15% are female. Of the female veterans enrolled in care, 63% identify as Black, 27% White, and 1.5% as Asian, American Indian/Alaska Native, or Native Hawaiian/Other Pacific Islander. The 2020 Veterans Chartbook report showed that female veterans and minority racial and ethnic groups had worse access to health care and higher mortality rates than their male and non-Hispanic White counterparts.16
The Primary Care Equity Dashboard (PCED) was developed to engage the VA health care workforce in the process of identifying and addressing inequities in local patient populations.17 Using electronic quality measure data, the PCED provides Veterans Integrated Service Network-level and facility-level performance on several metrics.18 The PCED had not been previously used at the CVVAMC, and few publications or quality improvement projects regarding its use have been reported by the VA Office of Health Equity. PCED helped identify disparities when comparing female to male patients in the prescribing of statin therapy for patients with CVD and statin therapy for patients with T2DM.
VA PHASER pharmacogenomic analyses provided an opportunity to expand this quality improvement project. Sanford Health and the VA collaborated on the PHASER program to offer free genetic testing for veterans. The program launched in 2019 and expanded to various VA sites, including CVVAMC in March 2023. This program has been extended to December 31, 2025.
The primary objective of this quality improvement project was to increase statin prescribing among female veterans with T2DM and/or CVD to reduce cardiovascular risk. Secondary outcomes included increased pharmacogenomic testing and the assessment of pharmacogenomic results related to statin therapy. This project was approved by the CVVAMC Pharmacy and Therapeutics Committee. The PCED was used to identify female veterans with T2DM and/or CVD without an active prescription for a statin between July and October 2023. A review of Computerized Patient Record System patient charts was completed to screen for prespecified inclusion and exclusion criteria. Veterans were included if they were assigned female at birth, were enrolled in care at CVVAMC, and had a diagnosis of T2DM or CVD (history of myocardial infarction, coronary bypass graft, percutaneous coronary intervention, or other revascularization in any setting).
Veterans were excluded if they were currently pregnant, trying to conceive, breastfeeding, had a T1DM diagnosis, had previously documented hypersensitivity to a statin, active liver failure or decompensated cirrhosis, previously documented statin-associated rhabdomyolysis or autoimmune myopathy, an active prescription for a proprotein convertase subtilisin/kexin type 9 inhibitor, or previously documented statin intolerance (defined as the inability to tolerate ≥ 3 statins, with ≥ 1 prescribed at low intensity or alternate-day dosing). The female veterans were compared to 2 comparators: the facility's male veterans and the VA national average, identified via the PCED.
Once a veteran was screened, they were telephoned between October 2023 and February 2024 and provided education on statin use and pharmacogenomic testing using a standardized note template. An order was placed for participants who provided verbal consent for pharmacogenomic testing. Those who agreed to statin initiation were referred to a clinical pharmacist practitioner (CPP) who contacted them at a later date to prescribe a statin following the recommendations of the 2019 ACC/AHA and 2023 ADA guidelines and pharmacogenomic testing, if applicable.4,5,7 Appropriate monitoring and follow-up occurred at the discretion of each CPP. Data collection included: age, race, diagnoses (T2DM, CVD, or both), baseline lipid panel (total cholesterol, triglycerides, high-density lipoprotein, low-density lipoprotein), hepatic function, name and dose of statin, reasons for declining statin therapy, and pharmacogenomic testing results related to SLCO1B1.
Results
At baseline in July 2023, 77.8% of female veterans with T2DM were prescribed a statin, which exceeded the national VA average (77.0%), but was below the rate for male veterans (78.7%) in the facility comparator group.17 Additionally, 82.2% of females with CVD were prescribed a statin, which was below the national VA average of 86.0% and the 84.9% of male veterans in the facility comparator group.17 The PCED identified 189 female veterans from July 2023 to October 2023 who may benefit from statin therapy. Thirty-three females met the exclusion criteria. Of the 156 included veterans, 129 (82.7%) were successfully contacted and 27 (17.3%) could not be reached by telephone after 3 attempts (Figure 1). The 129 female veterans contacted had a mean age of 59 years and the majority were Black (82.9%) (Table 1).
Abbreviations: CVD, cardiovascular disease; PCSK9, proprotein convertase subtilisin/
kexin type 9; T2DM, type 2 diabetes mellitus; VAMC, Veterans Affairs medical center.
Primary Outcomes
Of the 129 contacted veterans, 31 (24.0%) had a non-VA statin prescription, 13 (10.1%) had an active VA statin prescription, and 85 (65.9%) did not have a statin prescription, despite being eligible. Statin adherence was confirmed with participants, and the medication list was updated accordingly.
Of the 85 veterans with no active statin therapy, 37 (43.5%) accepted a new statin prescription and 48 (56.5%) declined. There were various reasons provided for declining statin therapy: 17 participants (35.4%) declined due to concern for AEs (Table 2).
From July 2023 to March 2024, the percentage of female veterans with active statin therapy with T2DM increased from 77.8% to 79.0%. For those with active statin therapy with CVD, usage increased from 82.2% to 90.2%, which exceeded the national VA average and facility male comparator group (Figures 2 and 3).17
Secondary Outcomes
Seventy-one of 129 veterans (55.0%) gave verbal consent, and 47 (66.2%) completed the pharmacogenomic testing; 58 (45.0%) declined. Five veterans (10.6%) had a known SLCO1B1 allele variant present. One veteran required a change in statin therapy based on the results (eAppendix).
Discussion
This project aimed to increase statin prescribing among female veterans with T2DM and/or CVD to reduce cardiovascular risk and increase pharmacogenomic testing using the PCED and care managed by CPPs. The results of this quality improvement project illustrated that both metrics have improved at CVVAMC as a result of the intervention. The results in both metrics now exceed the PCED national VA average, and the CVD metric also exceeds that of the facility male comparator group. While there was only a 1.2% increase from July 2023 to March 2024 for patients with T2DM, there was an 8.0% increase for patients with CVD. Despite standardized education on statin use, more veterans declined therapy than accepted it, mostly due to concern for AEs. Recording the reasons for declining statin therapy offered valuable insight that can be used in additional discussions with veterans and clinicians.
Pharmacogenomics gives clinicians the unique opportunity to take a proactive approach to better predict drug responses, potentially allowing for less trial and error with medications, fewer AEs, greater trust in the clinician, and improved medication adherence. The CPPs incorporated pharmacogenomic testing into their practice, which led to identifying 5 SLCO1B1 gene abnormalities. The PCED served as a powerful tool for advancing equity-focused quality improvement initiatives on a local level and was crucial in prioritizing the detection of veterans potentially receiving suboptimal care.
Limitations
The nature of “cold calls” made it challenging to establish contact for inclusion in this study. An alternative to increase engagement could have been scheduled phone or face-to-face visits. While the use of the PCED was crucial, data did not account for statins listed in the non-VA medication list. All 31 patients with statins prescribed outside the VA had a start date added to provide the most accurate representation of the data moving forward.
Another limitation in this project was its small sample size and population. CVVAMC serves about 6200 female veterans, with roughly 63% identifying as Black. The preponderance of Black individuals (83%) in this project is typical for the female patient population at CVVAMC but may not reflect the demographics of other populations. Other limitations to this project consisted of scheduling conflicts. Appointments for laboratory draws at community-based outpatient clinics were subject to availability, which resulted in some delay in completion of pharmacogenomic testing.
Conclusions
CPPs can help reduce inequity in health care delivery. Increased incorporation of the PCED into regular practice within the VA is recommended to continue addressing sex disparities in statin use, diabetes control, blood pressure management, cancer screenings, and vaccination needs. CVVAMC plans to expand its use through another quality improvement project focused on reducing sex disparities in blood pressure management. Improving educational resources made available to veterans on the importance of statin therapy and potential to mitigate AEs through use of the VA PHASER program also would be helpful. This project successfully improved CVVAMC metrics for female veterans appropriately prescribed statin therapy and increased access to pharmacogenomic testing. Most importantly, it helped close the sex-based gap in CVD risk reduction care.
- Heron M. Deaths: leading causes for 2018. Nat Vital Stat Rep. 2021;70:1-114.
- US Department of Veterans Affairs, US Department of Defense. VA/DoD Clinical practice guideline for the management of dyslipidemia for cardiovascular risk reduction. Published June 2020. Accessed August 25, 2025. https://www.healthquality.va.gov/guidelines/CD/lipids/VADODDyslipidemiaCPG5087212020.pdf
- Atherosclerotic Cardiovascular Disease (ASCVD). American Heart Association. Accessed August 26, 2025. https:// www.heart.org/en/professional/quality-improvement/ascvd
- American Diabetes Association Professional Practice Committee. 10. Cardiovascular disease and risk management: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S144-S174. doi:10.2337/dc22-S010
- American Diabetes Association. Standards of Care in Diabetes— 2023 abridged for primary care providers. Clinical Diabetes. 2022;41(1):4-31. doi:10.2337/cd23-as01
- Virani SS, Woodard LD, Ramsey DJ, et al. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am J Cardiol. 2015;115:21-26. doi:10.1016/j.amjcard.2014.09.041
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/ AHA Guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/ American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596-e646. doi:10.1161/CIR.0000000000000678
- Buchanan CH, Brown EA, Bishu KG, et al. The magnitude and potential causes of gender disparities in statin therapy in veterans with type 2 diabetes: a 10-year nationwide longitudinal cohort study. Womens Health Issues. 2022;32:274-283. doi:10.1016/j.whi.2021.10.003
- Ahmed F, Lin J, Ahmed T, et al. Health disparities: statin prescribing patterns among patients with diabetes in a family medicine clinic. Health Equity. 2022;6:291-297. doi:10.1089/heq.2021.0144
- Metser G, Bradley C, Moise N, Liyanage-Don N, Kronish I, Ye S. Gaps and disparities in primary prevention statin prescription during outpatient care. Am J Cardiol. 2021;161:36-41. doi:10.1016/j.amjcard.2021.08.070
- Nanna MG, Wang TY, Xiang Q, et al. Sex differences in the use of statins in community practice. Circ Cardiovasc Qual Outcomes. 2019;12(8):e005562. doi:10.1161/CIRCOUTCOMES.118.005562
- Kitzmiller JP, Mikulik EB, Dauki AM, Murkherjee C, Luzum JA. Pharmacogenomics of statins: understanding susceptibility to adverse effects. Pharmgenomics Pers Med. 2016;9:97-106. doi:10.2147/PGPM.S86013
- Türkmen D, Masoli JAH, Kuo CL, Bowden J, Melzer D, Pilling LC. Statin treatment effectiveness and the SLCO1B1*5 reduced function genotype: long-term outcomes in women and men. Br J Clin Pharmacol. 2022;88:3230-3240. doi:10.1111/bcp.15245
- Cooper-DeHoff RM, Niemi M, Ramsey LB, et al. The Clinical Pharmacogenetics Implementation Consortium guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and statin-associated musculoskeletal symptoms. Clin Pharmacol Ther. 2022;111:1007-1021. doi:10.1002/cpt.2557
- Ramsey LB, Gong L, Lee SB, et al. PharmVar GeneFocus: SLCO1B1. Clin Pharmacol Ther. 2023;113:782-793. doi:10.1002/cpt.2705
- National Healthcare Quality and Disparities Report: Chartbook on Healthcare for Veterans. Rockville (MD): Agency for Healthcare Research and Quality (US); November 2020.
- Procario G. Primary Care Equity Dashboard [database online]. Power Bi. 2023. Accessed August 26, 2025. https://app.powerbigov.us
- Hausmann LRM, Lamorte C, Estock JL. Understanding the context for incorporating equity into quality improvement throughout a national health care system. Health Equity. 2023;7(1):312-320. doi:10.1089/heq.2023.0009
- Heron M. Deaths: leading causes for 2018. Nat Vital Stat Rep. 2021;70:1-114.
- US Department of Veterans Affairs, US Department of Defense. VA/DoD Clinical practice guideline for the management of dyslipidemia for cardiovascular risk reduction. Published June 2020. Accessed August 25, 2025. https://www.healthquality.va.gov/guidelines/CD/lipids/VADODDyslipidemiaCPG5087212020.pdf
- Atherosclerotic Cardiovascular Disease (ASCVD). American Heart Association. Accessed August 26, 2025. https:// www.heart.org/en/professional/quality-improvement/ascvd
- American Diabetes Association Professional Practice Committee. 10. Cardiovascular disease and risk management: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S144-S174. doi:10.2337/dc22-S010
- American Diabetes Association. Standards of Care in Diabetes— 2023 abridged for primary care providers. Clinical Diabetes. 2022;41(1):4-31. doi:10.2337/cd23-as01
- Virani SS, Woodard LD, Ramsey DJ, et al. Gender disparities in evidence-based statin therapy in patients with cardiovascular disease. Am J Cardiol. 2015;115:21-26. doi:10.1016/j.amjcard.2014.09.041
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/ AHA Guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/ American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596-e646. doi:10.1161/CIR.0000000000000678
- Buchanan CH, Brown EA, Bishu KG, et al. The magnitude and potential causes of gender disparities in statin therapy in veterans with type 2 diabetes: a 10-year nationwide longitudinal cohort study. Womens Health Issues. 2022;32:274-283. doi:10.1016/j.whi.2021.10.003
- Ahmed F, Lin J, Ahmed T, et al. Health disparities: statin prescribing patterns among patients with diabetes in a family medicine clinic. Health Equity. 2022;6:291-297. doi:10.1089/heq.2021.0144
- Metser G, Bradley C, Moise N, Liyanage-Don N, Kronish I, Ye S. Gaps and disparities in primary prevention statin prescription during outpatient care. Am J Cardiol. 2021;161:36-41. doi:10.1016/j.amjcard.2021.08.070
- Nanna MG, Wang TY, Xiang Q, et al. Sex differences in the use of statins in community practice. Circ Cardiovasc Qual Outcomes. 2019;12(8):e005562. doi:10.1161/CIRCOUTCOMES.118.005562
- Kitzmiller JP, Mikulik EB, Dauki AM, Murkherjee C, Luzum JA. Pharmacogenomics of statins: understanding susceptibility to adverse effects. Pharmgenomics Pers Med. 2016;9:97-106. doi:10.2147/PGPM.S86013
- Türkmen D, Masoli JAH, Kuo CL, Bowden J, Melzer D, Pilling LC. Statin treatment effectiveness and the SLCO1B1*5 reduced function genotype: long-term outcomes in women and men. Br J Clin Pharmacol. 2022;88:3230-3240. doi:10.1111/bcp.15245
- Cooper-DeHoff RM, Niemi M, Ramsey LB, et al. The Clinical Pharmacogenetics Implementation Consortium guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and statin-associated musculoskeletal symptoms. Clin Pharmacol Ther. 2022;111:1007-1021. doi:10.1002/cpt.2557
- Ramsey LB, Gong L, Lee SB, et al. PharmVar GeneFocus: SLCO1B1. Clin Pharmacol Ther. 2023;113:782-793. doi:10.1002/cpt.2705
- National Healthcare Quality and Disparities Report: Chartbook on Healthcare for Veterans. Rockville (MD): Agency for Healthcare Research and Quality (US); November 2020.
- Procario G. Primary Care Equity Dashboard [database online]. Power Bi. 2023. Accessed August 26, 2025. https://app.powerbigov.us
- Hausmann LRM, Lamorte C, Estock JL. Understanding the context for incorporating equity into quality improvement throughout a national health care system. Health Equity. 2023;7(1):312-320. doi:10.1089/heq.2023.0009
Reducing Sex Disparities in Statin Therapy Among Female Veterans With Type 2 Diabetes and/or Cardiovascular Disease
Reducing Sex Disparities in Statin Therapy Among Female Veterans With Type 2 Diabetes and/or Cardiovascular Disease