User login
Using Telehealth Rehabilitation Therapy to Treat a Finger Flexor Tendon Repair During COVID-19
Telehealth-assisted finger rehabilitat ion therapy demonstrated good functional results following repair of a zone 2 flexor tendon laceration.
In 1948, Sterling Bunnell, MD, used the term no man’s land to describe the area between the A1 pulley at the volar aspect of the metacarpophalangeal joint and the insertion of the flexor digitorum superficialis tendons on the middle phalanx (zone 2).1 Bunnell’s description referenced the area of land in World War I between the trenches of opposing armies, and his goal was to emphasize the heightened risks of performing tendon repair in this area, as these repairs were notorious for poor outcomes. In lieu of tendon repair, Bunnell advocated treatment of tendon lacerations in this area with tendon excision and grafting.
It was not until the 1960s that researchers began to advocate for acute repair of tendons in this area.2,3 Since Verdan’s and Kleinart’s work, fastidious adherence to atraumatic technique and improvements in suture technique and rehabilitation protocols have allowed hand surgeons to repair tendons in this area with some level of success. Over the ensuing decades, acute repair of flexor tendon injuries within zone 2 has become the standard of care. The importance of meticulous technique during flexor tendon repair cannot be overemphasized; however, without appropriate hand therapy, even the most meticulous repair may fail.
COVID-19 has created significant barriers to patient care. Reducing travel and limiting face-to-face patient visits have been emphasized as methods that reduce spread of the virus, but these restrictions also prevent patients from easily accessing hand therapy. Recent adoption of telemedicine and videoconferencing technologies may help to reduce some of these barriers, but few previous studies have described the use of videoconferencing technology to supplant face-to-face hand therapy visits. This case describes the use of videoconferencing technology to provide hand therapy for a patient following repair of an acute flexor tendon laceration in zone 2.
Case Presentation
A patient aged < 50 years presented to a US Department of Veterans Affairs (VA) hand surgery clinic 2 days after sustaining a laceration to the flexor digitorum profundus (FDP) in zone 2 of the small finger while cleaning a knife. During the discussion of their treatment options and the recommended postoperative hand therapy protocol, the patient noted difficulty attending postoperative appointments due to COVID-19 as well as a lack of resources. Given these limitations and following discussion with our hand therapist, we discussed the potential for telehealth follow-up with videoconferencing. Four days following the injury, the patient underwent repair of the FDP. During surgery, the laceration was present at the level of the A3 pulley. The FDP was repaired using a 6-0 polypropylene synthetic suture for the epitendinous repair and 4-strand core suture repair using 3-0 Fiberwire suture in a modified cruciate fashion. The A2 and A4 pulleys were preserved, and venting of the pulleys was not required. At the time of surgery, the flexor digitorum superficialis and radial and ulnar digital neurovascular bundles were intact. Following surgical repair of the tendon, the patient was placed into a dorsal blocking splint with a plan for follow-up within 2 to 3 days.
The patient attended the first postoperative visit in person on postoperative day 2. During this visit, the postoperative splint and dressings were removed, and a forearm-based dorsal blocking orthosis was fabricated using thermoplastic. At this visit, the veteran relayed concerns regarding psychosocial and resource barriers in addition to concerns surrounding COVID-19 that would prevent travel to and from hand therapy appointments. Due to these concerns, a passive-motion protocol was initiated using the Indiana manual as a guide.4 The patient returned to the hand clinic at 2 weeks after surgery for evaluation by the operating surgeon and suture removal. All visits after the suture removal were conducted via either telehealth with videoconferencing or by telephone (Table 1).
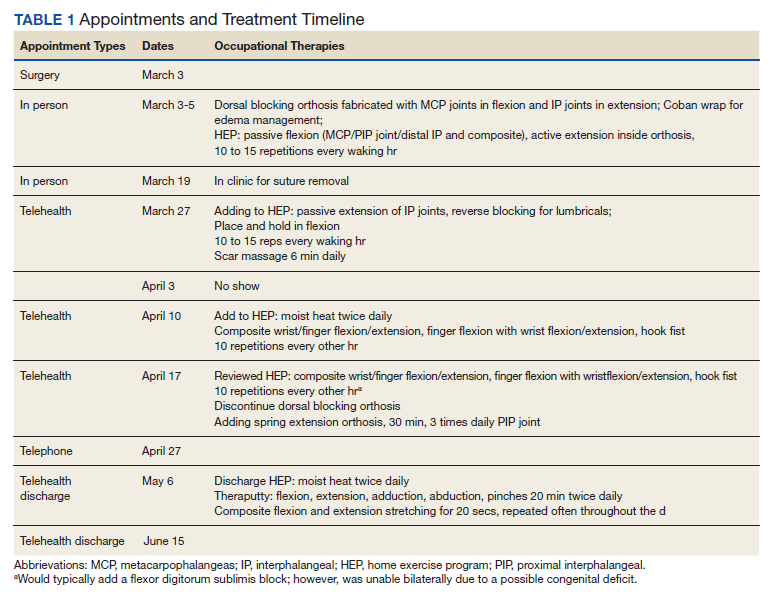
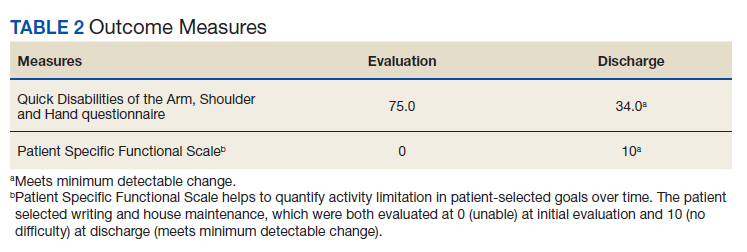
The operative team evaluated the patient 5 times following surgery. Only 2 of these visits were in-person. The patient attended 6 hand therapy sessions with 2 in-person visits to occupational therapy (Figure 1). The remaining 4 visits were conducted using videoconferencing. The patient received therapy supplies by mail as needed, and their use was reviewed in telerehabilitation sessions with videoconferencing as needed. During their postoperative course, the patient experienced little edema or scar tissue formation, and recovery was uncomplicated. The patient developed a mild extensor lag for which a proximal interphalangeal joint spring extension orthosis was provided via mail (Figure 2). The patient admitted only partial adherence with this orthosis, and at discharge, a 10-degree extensor lag remained. The patient was not concerned by this extension deficit and did not experience any associated functional deficits, demonstrated by scores on the Quick Disabilities of the Arm, Shoulder and Hand questionnaire and Patient Specific Functional Scale (Table 2).

Discussion
Few studies have been published that address the efficacy of telerehabilitation after surgical management of traumatic injuries involving the upper extremity. One Australian study performed by Worboys and colleagues concluded that utilization of telehealth services for hand therapy visits may provide accurate patient assessment with favorable patient satisfaction.5 Another study performed in the UK by Gilbert and colleagues demonstrated that videoconferencing is well received by patients, as it may offer shorter wait times, improved convenience, and reduced travel cost.
The authors noted that although videoconferencing may not completely replace in-person therapy, it could act as an adjunct.6 While these in-person visits may be necessary, particularly to establish care, at least one study has demonstrated that patients may prefer follow-up via telehealth if provided the option.7 In a randomized, controlled study performed in Norway, patients were randomized to either an in-person or video consultation with an orthopedic outpatient clinic. Of patients randomized to the in-person clinic visit, 86% preferred to have follow-up via videoconferencing.7
Previous studies have demonstrated that telehealth may produce accurate patient assessment, with relatively high patient satisfaction. Given the COVID-19 pandemic and the limitations that this crisis has placed on in-person outpatient visits, clinics that previously may have been resistant to telehealth are adapting and using the technology to meet the needs of their population.8 The present case demonstrates that videoconferencing is feasible and may lead to successful results, even for cases requiring significant hand therapy follow-up, such as flexor tendon repairs.
Conclusions
Although in-person hand therapy remains the standard of care following flexor tendon repair of the hand, situations may exist in which hand therapy conducted via telehealth is better than no hand therapy at all. The present case study highlights the use of telehealth as an acceptable supplement to in-person postoperative visits.
In our case, use of a standardized protocol with an emphasis on hand function and patient satisfaction as opposed to strict range of motion measurements produced good results. Although a specific telehealth satisfaction measure was not used in this case, commonly used questionnaires may be integrated into future visits to improve telehealth implementation and patient experience. In this specific case, the veteran felt that hand function was regained and expressed general satisfaction with the telemedicine process at the conclusion of care. While telehealth was a useful adjunct in the treatment of the present patient, further study of videoconferencing should be conducted to determine whether hand therapy conducted via telehealth could be implemented more broadly following upper extremity surgery.
1. Hege JJ. History off-hand: Bunnell’s no-man’s land. Hand (NY). 2019;14(4):570-574. doi:10.1177/1558944717744337
2. Verdan C. Primary repair of flexor tendons. J Bone Joint Surg Am. 1960;42-A:647-657.
3. Kleinert HE, Kutz JE, Ashbell TS, et al. Primary repair of lacerated flexor tendon in no man’s land (abstract). J Bone Joint Surg. 1967;49A:577.
4. Cannon NM. Diagnosis and Treatment Manual for Physicians and Therapists: Upper Extremity Rehabilitation. 4th ed. Hand Rehabilitation Center of Indiana; 2001.
5. Worboys T, Brassington M, Ward EC, Cornwell PL. Delivering occupational therapy hand assessment and treatment sessions via telehealth. J Telemed Telecare. 2018;24(3):185-192. doi:10.1177/1357633X17691861
6. Gilbert AW, Jaggi A, May CR. What is the patient acceptability of real time 1:1 videoconferencing in an orthopaedics setting? A systematic review. Physiotherapy. 2018;104(2):178-186. doi:10.1016/j.physio.2017.11.217
7. Buvik A, Bugge E, Knutsen G, Smatresk A, Wilsgaard T. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25(8):451-459. doi:10.1177/1357633X18783921
8. Loeb AE, Rao SS, Ficke JR, Morris CD, Riley LH 3rd, Levin AS. Departmental experience and lessons learned with accelerated introduction of telemedicine during the COVID-19 crisis. J Am Acad Orthop Surg. 2020;28(11):e469-e476. doi:10.5435/JAAOS-D-20-00380
Telehealth-assisted finger rehabilitat ion therapy demonstrated good functional results following repair of a zone 2 flexor tendon laceration.
Telehealth-assisted finger rehabilitat ion therapy demonstrated good functional results following repair of a zone 2 flexor tendon laceration.
In 1948, Sterling Bunnell, MD, used the term no man’s land to describe the area between the A1 pulley at the volar aspect of the metacarpophalangeal joint and the insertion of the flexor digitorum superficialis tendons on the middle phalanx (zone 2).1 Bunnell’s description referenced the area of land in World War I between the trenches of opposing armies, and his goal was to emphasize the heightened risks of performing tendon repair in this area, as these repairs were notorious for poor outcomes. In lieu of tendon repair, Bunnell advocated treatment of tendon lacerations in this area with tendon excision and grafting.
It was not until the 1960s that researchers began to advocate for acute repair of tendons in this area.2,3 Since Verdan’s and Kleinart’s work, fastidious adherence to atraumatic technique and improvements in suture technique and rehabilitation protocols have allowed hand surgeons to repair tendons in this area with some level of success. Over the ensuing decades, acute repair of flexor tendon injuries within zone 2 has become the standard of care. The importance of meticulous technique during flexor tendon repair cannot be overemphasized; however, without appropriate hand therapy, even the most meticulous repair may fail.
COVID-19 has created significant barriers to patient care. Reducing travel and limiting face-to-face patient visits have been emphasized as methods that reduce spread of the virus, but these restrictions also prevent patients from easily accessing hand therapy. Recent adoption of telemedicine and videoconferencing technologies may help to reduce some of these barriers, but few previous studies have described the use of videoconferencing technology to supplant face-to-face hand therapy visits. This case describes the use of videoconferencing technology to provide hand therapy for a patient following repair of an acute flexor tendon laceration in zone 2.
Case Presentation
A patient aged < 50 years presented to a US Department of Veterans Affairs (VA) hand surgery clinic 2 days after sustaining a laceration to the flexor digitorum profundus (FDP) in zone 2 of the small finger while cleaning a knife. During the discussion of their treatment options and the recommended postoperative hand therapy protocol, the patient noted difficulty attending postoperative appointments due to COVID-19 as well as a lack of resources. Given these limitations and following discussion with our hand therapist, we discussed the potential for telehealth follow-up with videoconferencing. Four days following the injury, the patient underwent repair of the FDP. During surgery, the laceration was present at the level of the A3 pulley. The FDP was repaired using a 6-0 polypropylene synthetic suture for the epitendinous repair and 4-strand core suture repair using 3-0 Fiberwire suture in a modified cruciate fashion. The A2 and A4 pulleys were preserved, and venting of the pulleys was not required. At the time of surgery, the flexor digitorum superficialis and radial and ulnar digital neurovascular bundles were intact. Following surgical repair of the tendon, the patient was placed into a dorsal blocking splint with a plan for follow-up within 2 to 3 days.
The patient attended the first postoperative visit in person on postoperative day 2. During this visit, the postoperative splint and dressings were removed, and a forearm-based dorsal blocking orthosis was fabricated using thermoplastic. At this visit, the veteran relayed concerns regarding psychosocial and resource barriers in addition to concerns surrounding COVID-19 that would prevent travel to and from hand therapy appointments. Due to these concerns, a passive-motion protocol was initiated using the Indiana manual as a guide.4 The patient returned to the hand clinic at 2 weeks after surgery for evaluation by the operating surgeon and suture removal. All visits after the suture removal were conducted via either telehealth with videoconferencing or by telephone (Table 1).
The operative team evaluated the patient 5 times following surgery. Only 2 of these visits were in-person. The patient attended 6 hand therapy sessions with 2 in-person visits to occupational therapy (Figure 1). The remaining 4 visits were conducted using videoconferencing. The patient received therapy supplies by mail as needed, and their use was reviewed in telerehabilitation sessions with videoconferencing as needed. During their postoperative course, the patient experienced little edema or scar tissue formation, and recovery was uncomplicated. The patient developed a mild extensor lag for which a proximal interphalangeal joint spring extension orthosis was provided via mail (Figure 2). The patient admitted only partial adherence with this orthosis, and at discharge, a 10-degree extensor lag remained. The patient was not concerned by this extension deficit and did not experience any associated functional deficits, demonstrated by scores on the Quick Disabilities of the Arm, Shoulder and Hand questionnaire and Patient Specific Functional Scale (Table 2).
Discussion
Few studies have been published that address the efficacy of telerehabilitation after surgical management of traumatic injuries involving the upper extremity. One Australian study performed by Worboys and colleagues concluded that utilization of telehealth services for hand therapy visits may provide accurate patient assessment with favorable patient satisfaction.5 Another study performed in the UK by Gilbert and colleagues demonstrated that videoconferencing is well received by patients, as it may offer shorter wait times, improved convenience, and reduced travel cost.
The authors noted that although videoconferencing may not completely replace in-person therapy, it could act as an adjunct.6 While these in-person visits may be necessary, particularly to establish care, at least one study has demonstrated that patients may prefer follow-up via telehealth if provided the option.7 In a randomized, controlled study performed in Norway, patients were randomized to either an in-person or video consultation with an orthopedic outpatient clinic. Of patients randomized to the in-person clinic visit, 86% preferred to have follow-up via videoconferencing.7
Previous studies have demonstrated that telehealth may produce accurate patient assessment, with relatively high patient satisfaction. Given the COVID-19 pandemic and the limitations that this crisis has placed on in-person outpatient visits, clinics that previously may have been resistant to telehealth are adapting and using the technology to meet the needs of their population.8 The present case demonstrates that videoconferencing is feasible and may lead to successful results, even for cases requiring significant hand therapy follow-up, such as flexor tendon repairs.
Conclusions
Although in-person hand therapy remains the standard of care following flexor tendon repair of the hand, situations may exist in which hand therapy conducted via telehealth is better than no hand therapy at all. The present case study highlights the use of telehealth as an acceptable supplement to in-person postoperative visits.
In our case, use of a standardized protocol with an emphasis on hand function and patient satisfaction as opposed to strict range of motion measurements produced good results. Although a specific telehealth satisfaction measure was not used in this case, commonly used questionnaires may be integrated into future visits to improve telehealth implementation and patient experience. In this specific case, the veteran felt that hand function was regained and expressed general satisfaction with the telemedicine process at the conclusion of care. While telehealth was a useful adjunct in the treatment of the present patient, further study of videoconferencing should be conducted to determine whether hand therapy conducted via telehealth could be implemented more broadly following upper extremity surgery.
In 1948, Sterling Bunnell, MD, used the term no man’s land to describe the area between the A1 pulley at the volar aspect of the metacarpophalangeal joint and the insertion of the flexor digitorum superficialis tendons on the middle phalanx (zone 2).1 Bunnell’s description referenced the area of land in World War I between the trenches of opposing armies, and his goal was to emphasize the heightened risks of performing tendon repair in this area, as these repairs were notorious for poor outcomes. In lieu of tendon repair, Bunnell advocated treatment of tendon lacerations in this area with tendon excision and grafting.
It was not until the 1960s that researchers began to advocate for acute repair of tendons in this area.2,3 Since Verdan’s and Kleinart’s work, fastidious adherence to atraumatic technique and improvements in suture technique and rehabilitation protocols have allowed hand surgeons to repair tendons in this area with some level of success. Over the ensuing decades, acute repair of flexor tendon injuries within zone 2 has become the standard of care. The importance of meticulous technique during flexor tendon repair cannot be overemphasized; however, without appropriate hand therapy, even the most meticulous repair may fail.
COVID-19 has created significant barriers to patient care. Reducing travel and limiting face-to-face patient visits have been emphasized as methods that reduce spread of the virus, but these restrictions also prevent patients from easily accessing hand therapy. Recent adoption of telemedicine and videoconferencing technologies may help to reduce some of these barriers, but few previous studies have described the use of videoconferencing technology to supplant face-to-face hand therapy visits. This case describes the use of videoconferencing technology to provide hand therapy for a patient following repair of an acute flexor tendon laceration in zone 2.
Case Presentation
A patient aged < 50 years presented to a US Department of Veterans Affairs (VA) hand surgery clinic 2 days after sustaining a laceration to the flexor digitorum profundus (FDP) in zone 2 of the small finger while cleaning a knife. During the discussion of their treatment options and the recommended postoperative hand therapy protocol, the patient noted difficulty attending postoperative appointments due to COVID-19 as well as a lack of resources. Given these limitations and following discussion with our hand therapist, we discussed the potential for telehealth follow-up with videoconferencing. Four days following the injury, the patient underwent repair of the FDP. During surgery, the laceration was present at the level of the A3 pulley. The FDP was repaired using a 6-0 polypropylene synthetic suture for the epitendinous repair and 4-strand core suture repair using 3-0 Fiberwire suture in a modified cruciate fashion. The A2 and A4 pulleys were preserved, and venting of the pulleys was not required. At the time of surgery, the flexor digitorum superficialis and radial and ulnar digital neurovascular bundles were intact. Following surgical repair of the tendon, the patient was placed into a dorsal blocking splint with a plan for follow-up within 2 to 3 days.
The patient attended the first postoperative visit in person on postoperative day 2. During this visit, the postoperative splint and dressings were removed, and a forearm-based dorsal blocking orthosis was fabricated using thermoplastic. At this visit, the veteran relayed concerns regarding psychosocial and resource barriers in addition to concerns surrounding COVID-19 that would prevent travel to and from hand therapy appointments. Due to these concerns, a passive-motion protocol was initiated using the Indiana manual as a guide.4 The patient returned to the hand clinic at 2 weeks after surgery for evaluation by the operating surgeon and suture removal. All visits after the suture removal were conducted via either telehealth with videoconferencing or by telephone (Table 1).
The operative team evaluated the patient 5 times following surgery. Only 2 of these visits were in-person. The patient attended 6 hand therapy sessions with 2 in-person visits to occupational therapy (Figure 1). The remaining 4 visits were conducted using videoconferencing. The patient received therapy supplies by mail as needed, and their use was reviewed in telerehabilitation sessions with videoconferencing as needed. During their postoperative course, the patient experienced little edema or scar tissue formation, and recovery was uncomplicated. The patient developed a mild extensor lag for which a proximal interphalangeal joint spring extension orthosis was provided via mail (Figure 2). The patient admitted only partial adherence with this orthosis, and at discharge, a 10-degree extensor lag remained. The patient was not concerned by this extension deficit and did not experience any associated functional deficits, demonstrated by scores on the Quick Disabilities of the Arm, Shoulder and Hand questionnaire and Patient Specific Functional Scale (Table 2).
Discussion
Few studies have been published that address the efficacy of telerehabilitation after surgical management of traumatic injuries involving the upper extremity. One Australian study performed by Worboys and colleagues concluded that utilization of telehealth services for hand therapy visits may provide accurate patient assessment with favorable patient satisfaction.5 Another study performed in the UK by Gilbert and colleagues demonstrated that videoconferencing is well received by patients, as it may offer shorter wait times, improved convenience, and reduced travel cost.
The authors noted that although videoconferencing may not completely replace in-person therapy, it could act as an adjunct.6 While these in-person visits may be necessary, particularly to establish care, at least one study has demonstrated that patients may prefer follow-up via telehealth if provided the option.7 In a randomized, controlled study performed in Norway, patients were randomized to either an in-person or video consultation with an orthopedic outpatient clinic. Of patients randomized to the in-person clinic visit, 86% preferred to have follow-up via videoconferencing.7
Previous studies have demonstrated that telehealth may produce accurate patient assessment, with relatively high patient satisfaction. Given the COVID-19 pandemic and the limitations that this crisis has placed on in-person outpatient visits, clinics that previously may have been resistant to telehealth are adapting and using the technology to meet the needs of their population.8 The present case demonstrates that videoconferencing is feasible and may lead to successful results, even for cases requiring significant hand therapy follow-up, such as flexor tendon repairs.
Conclusions
Although in-person hand therapy remains the standard of care following flexor tendon repair of the hand, situations may exist in which hand therapy conducted via telehealth is better than no hand therapy at all. The present case study highlights the use of telehealth as an acceptable supplement to in-person postoperative visits.
In our case, use of a standardized protocol with an emphasis on hand function and patient satisfaction as opposed to strict range of motion measurements produced good results. Although a specific telehealth satisfaction measure was not used in this case, commonly used questionnaires may be integrated into future visits to improve telehealth implementation and patient experience. In this specific case, the veteran felt that hand function was regained and expressed general satisfaction with the telemedicine process at the conclusion of care. While telehealth was a useful adjunct in the treatment of the present patient, further study of videoconferencing should be conducted to determine whether hand therapy conducted via telehealth could be implemented more broadly following upper extremity surgery.
1. Hege JJ. History off-hand: Bunnell’s no-man’s land. Hand (NY). 2019;14(4):570-574. doi:10.1177/1558944717744337
2. Verdan C. Primary repair of flexor tendons. J Bone Joint Surg Am. 1960;42-A:647-657.
3. Kleinert HE, Kutz JE, Ashbell TS, et al. Primary repair of lacerated flexor tendon in no man’s land (abstract). J Bone Joint Surg. 1967;49A:577.
4. Cannon NM. Diagnosis and Treatment Manual for Physicians and Therapists: Upper Extremity Rehabilitation. 4th ed. Hand Rehabilitation Center of Indiana; 2001.
5. Worboys T, Brassington M, Ward EC, Cornwell PL. Delivering occupational therapy hand assessment and treatment sessions via telehealth. J Telemed Telecare. 2018;24(3):185-192. doi:10.1177/1357633X17691861
6. Gilbert AW, Jaggi A, May CR. What is the patient acceptability of real time 1:1 videoconferencing in an orthopaedics setting? A systematic review. Physiotherapy. 2018;104(2):178-186. doi:10.1016/j.physio.2017.11.217
7. Buvik A, Bugge E, Knutsen G, Smatresk A, Wilsgaard T. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25(8):451-459. doi:10.1177/1357633X18783921
8. Loeb AE, Rao SS, Ficke JR, Morris CD, Riley LH 3rd, Levin AS. Departmental experience and lessons learned with accelerated introduction of telemedicine during the COVID-19 crisis. J Am Acad Orthop Surg. 2020;28(11):e469-e476. doi:10.5435/JAAOS-D-20-00380
1. Hege JJ. History off-hand: Bunnell’s no-man’s land. Hand (NY). 2019;14(4):570-574. doi:10.1177/1558944717744337
2. Verdan C. Primary repair of flexor tendons. J Bone Joint Surg Am. 1960;42-A:647-657.
3. Kleinert HE, Kutz JE, Ashbell TS, et al. Primary repair of lacerated flexor tendon in no man’s land (abstract). J Bone Joint Surg. 1967;49A:577.
4. Cannon NM. Diagnosis and Treatment Manual for Physicians and Therapists: Upper Extremity Rehabilitation. 4th ed. Hand Rehabilitation Center of Indiana; 2001.
5. Worboys T, Brassington M, Ward EC, Cornwell PL. Delivering occupational therapy hand assessment and treatment sessions via telehealth. J Telemed Telecare. 2018;24(3):185-192. doi:10.1177/1357633X17691861
6. Gilbert AW, Jaggi A, May CR. What is the patient acceptability of real time 1:1 videoconferencing in an orthopaedics setting? A systematic review. Physiotherapy. 2018;104(2):178-186. doi:10.1016/j.physio.2017.11.217
7. Buvik A, Bugge E, Knutsen G, Smatresk A, Wilsgaard T. Patient reported outcomes with remote orthopaedic consultations by telemedicine: A randomised controlled trial. J Telemed Telecare. 2019;25(8):451-459. doi:10.1177/1357633X18783921
8. Loeb AE, Rao SS, Ficke JR, Morris CD, Riley LH 3rd, Levin AS. Departmental experience and lessons learned with accelerated introduction of telemedicine during the COVID-19 crisis. J Am Acad Orthop Surg. 2020;28(11):e469-e476. doi:10.5435/JAAOS-D-20-00380
Midlife cardiovascular conditions tied to greater cognitive decline in women
Even though men in midlife have more cardiovascular (CV) conditions and risk factors than women of the same age, women are more affected by these conditions in terms of cognitive decline, new research suggests.
Analyses of almost 1,400 participants in the population-based Mayo Clinic Study of Aging showed that diabetes, dyslipidemia, and coronary heart disease (CHD) all had stronger associations with global cognitive decline in women than in men.
“All men and women should be treated for cardiovascular risk factors and conditions, but this study really highlights the importance of very early and perhaps more aggressive treatment in women with these conditions,” co-investigator Michelle M. Mielke, PhD, professor of epidemiology and neurology, Mayo Clinic, Rochester, Minn., told this news organization.
The findings were published online Jan. 5 in Neurology.
Assessing sex differences
Most previous studies in this area have focused on CV risk factors in midlife in relation to late-life dementia (after age 75) or on late-life vascular risk factors and late-life dementia, Dr. Mielke noted.
However, a few recent studies have suggested vascular risk factors can affect cognition even in midlife. The current investigators sought to determine whether there are sex differences in these associations.
They assessed 1,857 nondemented participants aged 50 to 69 years from the Mayo Clinic Study on Aging. The mean education level was 14.9 years, and the mean body mass index (BMI) was 29.7.
Among the participants, 78.9% had at least one CV condition or risk factor, and the proportion was higher in men than women (83.4% vs. 74.5%; P < .0001).
Frequency of each individual CV condition or risk factor was also higher in men than women, and they had more years of education and higher BMI but took fewer medications.
Every 15 months, participants had an in-person interview and physical examination that included a neurologic assessment and short test of memory.
The neuropsychological battery included nine tests across four domains: memory, language, executive function, and visuospatial skills. Researchers calculated z-scores for these domains and for global cognition.
Multiple cognitive domains
Whereas this study evaluated multiple cognitive domains, most previous research has focused on global cognitive decline and/or decline in only one or two cognitive domains, the investigators note.
They collected information from medical records on CV conditions such as CHD, arrhythmias, congestive heart failure, peripheral vascular disease (PVD), and stroke; and CV risk factors such as hypertension, diabetes, dyslipidemia, smoking status, and BMI.
Because of the small number of patients with stroke and PVD, these were classified as “other cardiovascular conditions” in the statistical analysis.
Researchers adjusted for sex, age, years of education, depressive symptoms, comorbidities, medications, and apolipoprotein E (APOE) genotyping. The mean follow-up was 3 years and did not differ by sex.
As some participants didn’t have a follow-up visit, the current analysis included 1,394 individuals. Those without follow-up visits were younger, had less education and more comorbidities, and took more medications compared with those with a follow-up.
Results showed most CV conditions were more strongly associated with cognitive function among women than men. For example, CHD was associated with global decline only in women (P < .05).
CHD, diabetes, and dyslipidemia were associated with language decline in women only (all, P < .05), but congestive heart failure was significantly associated with language decline in men only.
Dr. Mielke cautioned about reading too much into the language results for women.
“It’s an intriguing finding and definitely we need to follow up on it,” she said. However, “more studies are needed to examine sex differences before we start saying it only has an effect on language.”
‘Treat aggressively and right away’
The researchers were somewhat surprised by the study findings. Because there is a higher prevalence of CV conditions and risk factors in men, they presumed men would be more affected by these conditions, said Dr. Mielke.
“But that’s not what we saw; we saw the reverse. It was actually the women who were affected more by these cardiovascular risk factors and conditions,” she said.
As midlife is when women enter menopause, fluctuating estrogen levels may help explain the differential impact on cognition among women. But Dr. Mielke said she wants to “move beyond” just looking at hormones.
She pointed out there are a variety of psychosocial factors that may also contribute to an imbalance in the cognitive impact of CV conditions on women.
“Midlife is when many women are still taking care of their children at home, are also taking care of their adult parents, and may be undergoing more stress while continuing to do a job,” Dr. Miekle said.
Structural brain development and genetics may also contribute to the greater effect on cognition in women, the investigators note.
Dr. Mielke stressed that the current study only identifies associations. “The next steps are to understand what some of the underlying mechanisms for this are,” she said.
In the meantime, these new results suggest middle-aged women with high blood pressure, cholesterol, or glucose measures “should be treated aggressively and right away” said Dr. Mielke.
“For example, for women who are just starting to become hypertensive, clinicians should treat them right away and not watch and wait.”
Study limitations cited include that its sample was limited to Olmsted County, Minnesota – so results may not be generalized to other populations. Also, as researchers combined PVD and stroke into one group, larger sample sizes are needed, especially for stroke. Another limitation was the study did not have information on duration of all CV conditions or risk factors.
Helpful for tailoring interventions?
Commenting on the study, Glen R. Finney, MD, director, Memory and Cognition Program, Geisinger Health Clinic, Wilkes-Barre, Pennsylvania, said the results are important.
“The more we understand about risk factors for the development of Alzheimer’s disease and related dementias, the better we understand how we can reduce the risks,” said Dr. Finney, who was not involved with the research.
Awareness that CV conditions are major risk factors in midlife has been “definitely rising,” said Dr. Finney. “Many studies originally were looking at late life and are now looking more at earlier in the disease process, and I think that’s important.”
Understanding how sex, ethnicity, and other demographic variables affect risks can help to “tailor interventions” for individual patients, he said.
The study was supported by the National Institutes of Health, the GHR Foundation, and the Rochester Epidemiology Project. Dr. Mielke is a consultant for Biogen and Brain Protection Company and is on the editorial boards of Neurology and Alzheimer’s and Dementia. Dr. Finney has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Even though men in midlife have more cardiovascular (CV) conditions and risk factors than women of the same age, women are more affected by these conditions in terms of cognitive decline, new research suggests.
Analyses of almost 1,400 participants in the population-based Mayo Clinic Study of Aging showed that diabetes, dyslipidemia, and coronary heart disease (CHD) all had stronger associations with global cognitive decline in women than in men.
“All men and women should be treated for cardiovascular risk factors and conditions, but this study really highlights the importance of very early and perhaps more aggressive treatment in women with these conditions,” co-investigator Michelle M. Mielke, PhD, professor of epidemiology and neurology, Mayo Clinic, Rochester, Minn., told this news organization.
The findings were published online Jan. 5 in Neurology.
Assessing sex differences
Most previous studies in this area have focused on CV risk factors in midlife in relation to late-life dementia (after age 75) or on late-life vascular risk factors and late-life dementia, Dr. Mielke noted.
However, a few recent studies have suggested vascular risk factors can affect cognition even in midlife. The current investigators sought to determine whether there are sex differences in these associations.
They assessed 1,857 nondemented participants aged 50 to 69 years from the Mayo Clinic Study on Aging. The mean education level was 14.9 years, and the mean body mass index (BMI) was 29.7.
Among the participants, 78.9% had at least one CV condition or risk factor, and the proportion was higher in men than women (83.4% vs. 74.5%; P < .0001).
Frequency of each individual CV condition or risk factor was also higher in men than women, and they had more years of education and higher BMI but took fewer medications.
Every 15 months, participants had an in-person interview and physical examination that included a neurologic assessment and short test of memory.
The neuropsychological battery included nine tests across four domains: memory, language, executive function, and visuospatial skills. Researchers calculated z-scores for these domains and for global cognition.
Multiple cognitive domains
Whereas this study evaluated multiple cognitive domains, most previous research has focused on global cognitive decline and/or decline in only one or two cognitive domains, the investigators note.
They collected information from medical records on CV conditions such as CHD, arrhythmias, congestive heart failure, peripheral vascular disease (PVD), and stroke; and CV risk factors such as hypertension, diabetes, dyslipidemia, smoking status, and BMI.
Because of the small number of patients with stroke and PVD, these were classified as “other cardiovascular conditions” in the statistical analysis.
Researchers adjusted for sex, age, years of education, depressive symptoms, comorbidities, medications, and apolipoprotein E (APOE) genotyping. The mean follow-up was 3 years and did not differ by sex.
As some participants didn’t have a follow-up visit, the current analysis included 1,394 individuals. Those without follow-up visits were younger, had less education and more comorbidities, and took more medications compared with those with a follow-up.
Results showed most CV conditions were more strongly associated with cognitive function among women than men. For example, CHD was associated with global decline only in women (P < .05).
CHD, diabetes, and dyslipidemia were associated with language decline in women only (all, P < .05), but congestive heart failure was significantly associated with language decline in men only.
Dr. Mielke cautioned about reading too much into the language results for women.
“It’s an intriguing finding and definitely we need to follow up on it,” she said. However, “more studies are needed to examine sex differences before we start saying it only has an effect on language.”
‘Treat aggressively and right away’
The researchers were somewhat surprised by the study findings. Because there is a higher prevalence of CV conditions and risk factors in men, they presumed men would be more affected by these conditions, said Dr. Mielke.
“But that’s not what we saw; we saw the reverse. It was actually the women who were affected more by these cardiovascular risk factors and conditions,” she said.
As midlife is when women enter menopause, fluctuating estrogen levels may help explain the differential impact on cognition among women. But Dr. Mielke said she wants to “move beyond” just looking at hormones.
She pointed out there are a variety of psychosocial factors that may also contribute to an imbalance in the cognitive impact of CV conditions on women.
“Midlife is when many women are still taking care of their children at home, are also taking care of their adult parents, and may be undergoing more stress while continuing to do a job,” Dr. Miekle said.
Structural brain development and genetics may also contribute to the greater effect on cognition in women, the investigators note.
Dr. Mielke stressed that the current study only identifies associations. “The next steps are to understand what some of the underlying mechanisms for this are,” she said.
In the meantime, these new results suggest middle-aged women with high blood pressure, cholesterol, or glucose measures “should be treated aggressively and right away” said Dr. Mielke.
“For example, for women who are just starting to become hypertensive, clinicians should treat them right away and not watch and wait.”
Study limitations cited include that its sample was limited to Olmsted County, Minnesota – so results may not be generalized to other populations. Also, as researchers combined PVD and stroke into one group, larger sample sizes are needed, especially for stroke. Another limitation was the study did not have information on duration of all CV conditions or risk factors.
Helpful for tailoring interventions?
Commenting on the study, Glen R. Finney, MD, director, Memory and Cognition Program, Geisinger Health Clinic, Wilkes-Barre, Pennsylvania, said the results are important.
“The more we understand about risk factors for the development of Alzheimer’s disease and related dementias, the better we understand how we can reduce the risks,” said Dr. Finney, who was not involved with the research.
Awareness that CV conditions are major risk factors in midlife has been “definitely rising,” said Dr. Finney. “Many studies originally were looking at late life and are now looking more at earlier in the disease process, and I think that’s important.”
Understanding how sex, ethnicity, and other demographic variables affect risks can help to “tailor interventions” for individual patients, he said.
The study was supported by the National Institutes of Health, the GHR Foundation, and the Rochester Epidemiology Project. Dr. Mielke is a consultant for Biogen and Brain Protection Company and is on the editorial boards of Neurology and Alzheimer’s and Dementia. Dr. Finney has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Even though men in midlife have more cardiovascular (CV) conditions and risk factors than women of the same age, women are more affected by these conditions in terms of cognitive decline, new research suggests.
Analyses of almost 1,400 participants in the population-based Mayo Clinic Study of Aging showed that diabetes, dyslipidemia, and coronary heart disease (CHD) all had stronger associations with global cognitive decline in women than in men.
“All men and women should be treated for cardiovascular risk factors and conditions, but this study really highlights the importance of very early and perhaps more aggressive treatment in women with these conditions,” co-investigator Michelle M. Mielke, PhD, professor of epidemiology and neurology, Mayo Clinic, Rochester, Minn., told this news organization.
The findings were published online Jan. 5 in Neurology.
Assessing sex differences
Most previous studies in this area have focused on CV risk factors in midlife in relation to late-life dementia (after age 75) or on late-life vascular risk factors and late-life dementia, Dr. Mielke noted.
However, a few recent studies have suggested vascular risk factors can affect cognition even in midlife. The current investigators sought to determine whether there are sex differences in these associations.
They assessed 1,857 nondemented participants aged 50 to 69 years from the Mayo Clinic Study on Aging. The mean education level was 14.9 years, and the mean body mass index (BMI) was 29.7.
Among the participants, 78.9% had at least one CV condition or risk factor, and the proportion was higher in men than women (83.4% vs. 74.5%; P < .0001).
Frequency of each individual CV condition or risk factor was also higher in men than women, and they had more years of education and higher BMI but took fewer medications.
Every 15 months, participants had an in-person interview and physical examination that included a neurologic assessment and short test of memory.
The neuropsychological battery included nine tests across four domains: memory, language, executive function, and visuospatial skills. Researchers calculated z-scores for these domains and for global cognition.
Multiple cognitive domains
Whereas this study evaluated multiple cognitive domains, most previous research has focused on global cognitive decline and/or decline in only one or two cognitive domains, the investigators note.
They collected information from medical records on CV conditions such as CHD, arrhythmias, congestive heart failure, peripheral vascular disease (PVD), and stroke; and CV risk factors such as hypertension, diabetes, dyslipidemia, smoking status, and BMI.
Because of the small number of patients with stroke and PVD, these were classified as “other cardiovascular conditions” in the statistical analysis.
Researchers adjusted for sex, age, years of education, depressive symptoms, comorbidities, medications, and apolipoprotein E (APOE) genotyping. The mean follow-up was 3 years and did not differ by sex.
As some participants didn’t have a follow-up visit, the current analysis included 1,394 individuals. Those without follow-up visits were younger, had less education and more comorbidities, and took more medications compared with those with a follow-up.
Results showed most CV conditions were more strongly associated with cognitive function among women than men. For example, CHD was associated with global decline only in women (P < .05).
CHD, diabetes, and dyslipidemia were associated with language decline in women only (all, P < .05), but congestive heart failure was significantly associated with language decline in men only.
Dr. Mielke cautioned about reading too much into the language results for women.
“It’s an intriguing finding and definitely we need to follow up on it,” she said. However, “more studies are needed to examine sex differences before we start saying it only has an effect on language.”
‘Treat aggressively and right away’
The researchers were somewhat surprised by the study findings. Because there is a higher prevalence of CV conditions and risk factors in men, they presumed men would be more affected by these conditions, said Dr. Mielke.
“But that’s not what we saw; we saw the reverse. It was actually the women who were affected more by these cardiovascular risk factors and conditions,” she said.
As midlife is when women enter menopause, fluctuating estrogen levels may help explain the differential impact on cognition among women. But Dr. Mielke said she wants to “move beyond” just looking at hormones.
She pointed out there are a variety of psychosocial factors that may also contribute to an imbalance in the cognitive impact of CV conditions on women.
“Midlife is when many women are still taking care of their children at home, are also taking care of their adult parents, and may be undergoing more stress while continuing to do a job,” Dr. Miekle said.
Structural brain development and genetics may also contribute to the greater effect on cognition in women, the investigators note.
Dr. Mielke stressed that the current study only identifies associations. “The next steps are to understand what some of the underlying mechanisms for this are,” she said.
In the meantime, these new results suggest middle-aged women with high blood pressure, cholesterol, or glucose measures “should be treated aggressively and right away” said Dr. Mielke.
“For example, for women who are just starting to become hypertensive, clinicians should treat them right away and not watch and wait.”
Study limitations cited include that its sample was limited to Olmsted County, Minnesota – so results may not be generalized to other populations. Also, as researchers combined PVD and stroke into one group, larger sample sizes are needed, especially for stroke. Another limitation was the study did not have information on duration of all CV conditions or risk factors.
Helpful for tailoring interventions?
Commenting on the study, Glen R. Finney, MD, director, Memory and Cognition Program, Geisinger Health Clinic, Wilkes-Barre, Pennsylvania, said the results are important.
“The more we understand about risk factors for the development of Alzheimer’s disease and related dementias, the better we understand how we can reduce the risks,” said Dr. Finney, who was not involved with the research.
Awareness that CV conditions are major risk factors in midlife has been “definitely rising,” said Dr. Finney. “Many studies originally were looking at late life and are now looking more at earlier in the disease process, and I think that’s important.”
Understanding how sex, ethnicity, and other demographic variables affect risks can help to “tailor interventions” for individual patients, he said.
The study was supported by the National Institutes of Health, the GHR Foundation, and the Rochester Epidemiology Project. Dr. Mielke is a consultant for Biogen and Brain Protection Company and is on the editorial boards of Neurology and Alzheimer’s and Dementia. Dr. Finney has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
COVID-19 vaccination has little impact on menstrual cycle
Women may rest a bit easier thanks to results from a study showing that vaccination against the SARS-CoV-2 virus has almost no impact on a woman’s menstrual cycle. The issue is significant, as regular menstruation is a sign of health and fertility, and fears of disturbances might increase vaccination hesitancy as COVID-19 cases continue to surge.
Alison Edelman, MD, MPH, a professor of obstetrics and gynecology at Oregon Health & Science University, Portland, led a group studying prospective data on almost 24,000 menstrual cycles reported by almost 4,000 U.S. women.
The investigators found that COVID-19 vaccination was associated with a less than 1-day change in cycle length for the menstrual cycles after the first and second inoculations, compared with prevaccine cycles. Vaccination had no effect on the actual number of days menstrual bleeding lasted.
The study looked at the menstrual patterns of women aged 18-45 years with normal cycle lengths of 24-38 days for the three consecutive cycles before the first vaccine dose and for three consecutive postvaccine cycles. The final sample included 2,403 vaccinated and 1,556 unvaccinated individuals.
In vaccinated women, the study initially found a slight average increase in cycle length after dose one of 71% of a day and 91% of a day after dose two. Following adjustments, those increases dropped to 64% of a day after the first dose and 79% of a day after the second dose.
In unvaccinated women, the study looked at six cycles over a similar time period and found no significant changes from baseline.
“Coronavirus disease 2019 vaccination is associated with a small change in cycle length but not menses length,” Dr. Edelman’s group concluded in Obstetrics and Gynecology.
In the rare instance that a woman received two vaccine doses within the same menstrual cycle, the change in length could increase to 2 days. These variations appear to resolve quickly, possibly as soon as the next cycle after vaccination and do not indicate any cause for long-term physical or reproductive health concern, according to the authors.
Reports by women on social media, however, have suggested that postvaccine menstrual disruptions are more common with, for example, heavier and breakthrough bleeding. But it appears such changes are temporary and resolve quickly.
“These findings are reassuring and validating,” Dr. Edelman said in an interview. On a population level, the changes indicate no cause for concern for long-term physical or reproductive health and no reason to avoid vaccination. “On a personal level, people want this information so they know what to expect when they get vaccinated, and not worry about a pregnancy scare or be disappointed if they were trying for pregnancy.”
According to the International Federation of Gynecologists and Obstetricians, variations in cycle length of fewer than 8 days are considered normal, said Christine Metz, PhD, a research biologist and a professor of molecular medicine at the Feinstein Institutes for Medical Research in Manhasset, N.Y. “Thus, the extra 17 hours added to the menstrual cycle length in the vaccination group in this study is well within the ‘normal’ range.”
In a group of about 1,600 menstruating women being studied at Dr. Metz’s center, some have anecdotally reported transient cycle changes post vaccination for COVID-19, including delays in menstruation onset and changes in bleeding patterns.
Exactly how vaccination might alter menstrual cycle length is not known and has not been studied with vaccination against other infections such as influenza and meningococcal disease.
“Many factors are known to affect menstrual cycle length including changes in diet, sleep, and exercise, as well as sickness, travel, and stress,” Dr. Metz said. The COVID-19 vaccines have affected people in different ways, with side effects ranging from injection-site pain to nausea, aches, fever, and fatigue. “Vaccination side effects, particularly if severe, could lead to changes in diet, exercise, and sleep, and feelings of sickness and/or stress.”
These stressors can alter hormone production and stability, as well as the body’s response to hormones such as estrogen, progesterone, follicle-stimulating hormone, luteinizing hormone, and other hormones associated with female reproduction. “Because these hormones regulate the menstrual cycle, variations in these hormones can either shorten or lengthen the cycle,” Dr. Metz explained.
More research needs to be done at the global level, according to the authors. “Questions remain about other possible changes in menstrual cycles, such as menstrual symptoms, unscheduled bleeding, and changes in the quality and quantity of menstrual bleeding.”
This research was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health’s Office of Research on Women’s Health. Dr. Edelman reported support from the American College of Obstetrics and Gynecology, the World Health Organization, Gynuity, and the Karolinska Institute as well as royalties from UpToDate. Other study authors reported similar relationships with not-for-profit and private-sector companies. Three coauthors are employees of Natural Cycles, a fertility tracking device that was used in the study. Dr. Metz disclosed no conflicts of interest with regard to her comments.
Women may rest a bit easier thanks to results from a study showing that vaccination against the SARS-CoV-2 virus has almost no impact on a woman’s menstrual cycle. The issue is significant, as regular menstruation is a sign of health and fertility, and fears of disturbances might increase vaccination hesitancy as COVID-19 cases continue to surge.
Alison Edelman, MD, MPH, a professor of obstetrics and gynecology at Oregon Health & Science University, Portland, led a group studying prospective data on almost 24,000 menstrual cycles reported by almost 4,000 U.S. women.
The investigators found that COVID-19 vaccination was associated with a less than 1-day change in cycle length for the menstrual cycles after the first and second inoculations, compared with prevaccine cycles. Vaccination had no effect on the actual number of days menstrual bleeding lasted.
The study looked at the menstrual patterns of women aged 18-45 years with normal cycle lengths of 24-38 days for the three consecutive cycles before the first vaccine dose and for three consecutive postvaccine cycles. The final sample included 2,403 vaccinated and 1,556 unvaccinated individuals.
In vaccinated women, the study initially found a slight average increase in cycle length after dose one of 71% of a day and 91% of a day after dose two. Following adjustments, those increases dropped to 64% of a day after the first dose and 79% of a day after the second dose.
In unvaccinated women, the study looked at six cycles over a similar time period and found no significant changes from baseline.
“Coronavirus disease 2019 vaccination is associated with a small change in cycle length but not menses length,” Dr. Edelman’s group concluded in Obstetrics and Gynecology.
In the rare instance that a woman received two vaccine doses within the same menstrual cycle, the change in length could increase to 2 days. These variations appear to resolve quickly, possibly as soon as the next cycle after vaccination and do not indicate any cause for long-term physical or reproductive health concern, according to the authors.
Reports by women on social media, however, have suggested that postvaccine menstrual disruptions are more common with, for example, heavier and breakthrough bleeding. But it appears such changes are temporary and resolve quickly.
“These findings are reassuring and validating,” Dr. Edelman said in an interview. On a population level, the changes indicate no cause for concern for long-term physical or reproductive health and no reason to avoid vaccination. “On a personal level, people want this information so they know what to expect when they get vaccinated, and not worry about a pregnancy scare or be disappointed if they were trying for pregnancy.”
According to the International Federation of Gynecologists and Obstetricians, variations in cycle length of fewer than 8 days are considered normal, said Christine Metz, PhD, a research biologist and a professor of molecular medicine at the Feinstein Institutes for Medical Research in Manhasset, N.Y. “Thus, the extra 17 hours added to the menstrual cycle length in the vaccination group in this study is well within the ‘normal’ range.”
In a group of about 1,600 menstruating women being studied at Dr. Metz’s center, some have anecdotally reported transient cycle changes post vaccination for COVID-19, including delays in menstruation onset and changes in bleeding patterns.
Exactly how vaccination might alter menstrual cycle length is not known and has not been studied with vaccination against other infections such as influenza and meningococcal disease.
“Many factors are known to affect menstrual cycle length including changes in diet, sleep, and exercise, as well as sickness, travel, and stress,” Dr. Metz said. The COVID-19 vaccines have affected people in different ways, with side effects ranging from injection-site pain to nausea, aches, fever, and fatigue. “Vaccination side effects, particularly if severe, could lead to changes in diet, exercise, and sleep, and feelings of sickness and/or stress.”
These stressors can alter hormone production and stability, as well as the body’s response to hormones such as estrogen, progesterone, follicle-stimulating hormone, luteinizing hormone, and other hormones associated with female reproduction. “Because these hormones regulate the menstrual cycle, variations in these hormones can either shorten or lengthen the cycle,” Dr. Metz explained.
More research needs to be done at the global level, according to the authors. “Questions remain about other possible changes in menstrual cycles, such as menstrual symptoms, unscheduled bleeding, and changes in the quality and quantity of menstrual bleeding.”
This research was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health’s Office of Research on Women’s Health. Dr. Edelman reported support from the American College of Obstetrics and Gynecology, the World Health Organization, Gynuity, and the Karolinska Institute as well as royalties from UpToDate. Other study authors reported similar relationships with not-for-profit and private-sector companies. Three coauthors are employees of Natural Cycles, a fertility tracking device that was used in the study. Dr. Metz disclosed no conflicts of interest with regard to her comments.
Women may rest a bit easier thanks to results from a study showing that vaccination against the SARS-CoV-2 virus has almost no impact on a woman’s menstrual cycle. The issue is significant, as regular menstruation is a sign of health and fertility, and fears of disturbances might increase vaccination hesitancy as COVID-19 cases continue to surge.
Alison Edelman, MD, MPH, a professor of obstetrics and gynecology at Oregon Health & Science University, Portland, led a group studying prospective data on almost 24,000 menstrual cycles reported by almost 4,000 U.S. women.
The investigators found that COVID-19 vaccination was associated with a less than 1-day change in cycle length for the menstrual cycles after the first and second inoculations, compared with prevaccine cycles. Vaccination had no effect on the actual number of days menstrual bleeding lasted.
The study looked at the menstrual patterns of women aged 18-45 years with normal cycle lengths of 24-38 days for the three consecutive cycles before the first vaccine dose and for three consecutive postvaccine cycles. The final sample included 2,403 vaccinated and 1,556 unvaccinated individuals.
In vaccinated women, the study initially found a slight average increase in cycle length after dose one of 71% of a day and 91% of a day after dose two. Following adjustments, those increases dropped to 64% of a day after the first dose and 79% of a day after the second dose.
In unvaccinated women, the study looked at six cycles over a similar time period and found no significant changes from baseline.
“Coronavirus disease 2019 vaccination is associated with a small change in cycle length but not menses length,” Dr. Edelman’s group concluded in Obstetrics and Gynecology.
In the rare instance that a woman received two vaccine doses within the same menstrual cycle, the change in length could increase to 2 days. These variations appear to resolve quickly, possibly as soon as the next cycle after vaccination and do not indicate any cause for long-term physical or reproductive health concern, according to the authors.
Reports by women on social media, however, have suggested that postvaccine menstrual disruptions are more common with, for example, heavier and breakthrough bleeding. But it appears such changes are temporary and resolve quickly.
“These findings are reassuring and validating,” Dr. Edelman said in an interview. On a population level, the changes indicate no cause for concern for long-term physical or reproductive health and no reason to avoid vaccination. “On a personal level, people want this information so they know what to expect when they get vaccinated, and not worry about a pregnancy scare or be disappointed if they were trying for pregnancy.”
According to the International Federation of Gynecologists and Obstetricians, variations in cycle length of fewer than 8 days are considered normal, said Christine Metz, PhD, a research biologist and a professor of molecular medicine at the Feinstein Institutes for Medical Research in Manhasset, N.Y. “Thus, the extra 17 hours added to the menstrual cycle length in the vaccination group in this study is well within the ‘normal’ range.”
In a group of about 1,600 menstruating women being studied at Dr. Metz’s center, some have anecdotally reported transient cycle changes post vaccination for COVID-19, including delays in menstruation onset and changes in bleeding patterns.
Exactly how vaccination might alter menstrual cycle length is not known and has not been studied with vaccination against other infections such as influenza and meningococcal disease.
“Many factors are known to affect menstrual cycle length including changes in diet, sleep, and exercise, as well as sickness, travel, and stress,” Dr. Metz said. The COVID-19 vaccines have affected people in different ways, with side effects ranging from injection-site pain to nausea, aches, fever, and fatigue. “Vaccination side effects, particularly if severe, could lead to changes in diet, exercise, and sleep, and feelings of sickness and/or stress.”
These stressors can alter hormone production and stability, as well as the body’s response to hormones such as estrogen, progesterone, follicle-stimulating hormone, luteinizing hormone, and other hormones associated with female reproduction. “Because these hormones regulate the menstrual cycle, variations in these hormones can either shorten or lengthen the cycle,” Dr. Metz explained.
More research needs to be done at the global level, according to the authors. “Questions remain about other possible changes in menstrual cycles, such as menstrual symptoms, unscheduled bleeding, and changes in the quality and quantity of menstrual bleeding.”
This research was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institutes of Health’s Office of Research on Women’s Health. Dr. Edelman reported support from the American College of Obstetrics and Gynecology, the World Health Organization, Gynuity, and the Karolinska Institute as well as royalties from UpToDate. Other study authors reported similar relationships with not-for-profit and private-sector companies. Three coauthors are employees of Natural Cycles, a fertility tracking device that was used in the study. Dr. Metz disclosed no conflicts of interest with regard to her comments.
FROM OBSTETRICS & GYNECOLOGY
New blood test could identify pregnant women who are at risk of preeclampsia
Pregnant women who are at risk of preeclampsia can now be identified early before symptoms develop, finds new research from Kings College London and Guy’s and St Thomas’ NHS Foundation Trust, published in Nature.
The study, supported by the National Institute for Health Research and in partnership with the Mirvie RNA platform, analyzed the genetic material from over 2,500 blood samples of pregnant women from eight independent cohorts with multiple demographics, including socioeconomic background, geographic location, ethnicity, and nationality, collected 14.5 weeks before delivery.
“Because the study drew upon samples for a diverse group of women, including participants recruited across King’s Health Partners, the molecular signature is very reliable and has potential to outperform currently available tests,” said Rachel Tribe, PhD, department of women and children’s health, King’s College London.
Researchers used plasma cell-free RNA (cfRNA) transcripts to examine the standard molecular mechanism between the fetus, maternal, and placental tissues in order to determine fetal development and healthy pregnancy progression. Deviation from the standard cfRNA expression was also observed to establish the molecular pathway for those at risk of preeclampsia before clinical presentation.
A cfRNA signal from a single blood sample showed a 32.3% positive-predictive value and 75% sensitivity, which exceeds current positive-predictive values from recent clinical state-of-the-art models.
In addition, 73% of participants with a positive-predictive value were identified “as destined to have a medically indicated preterm birth over 3 months in advance of the preeclampsia symptoms,” said the authors.
With up to 1 in 12 pregnancies affected by preeclampsia, and the diagnosis most often only being made in the third trimester, these results provide a promising outlook for pregnant women “so that they can be more closely monitored and treated by the clinicians involved,” commented Dr. Tribe.
“We are now focused on ongoing clinical research to further validate these results and improve the understanding of other pregnancy complications,” she said. “As a scientist, it was also extremely interesting to see that the molecular signature tells us something about mechanisms associated with health in pregnancy and complications including preeclampsia; such knowledge will aid development of treatment strategies in the future.”
A version of this article first appeared on Medscape.com.
Pregnant women who are at risk of preeclampsia can now be identified early before symptoms develop, finds new research from Kings College London and Guy’s and St Thomas’ NHS Foundation Trust, published in Nature.
The study, supported by the National Institute for Health Research and in partnership with the Mirvie RNA platform, analyzed the genetic material from over 2,500 blood samples of pregnant women from eight independent cohorts with multiple demographics, including socioeconomic background, geographic location, ethnicity, and nationality, collected 14.5 weeks before delivery.
“Because the study drew upon samples for a diverse group of women, including participants recruited across King’s Health Partners, the molecular signature is very reliable and has potential to outperform currently available tests,” said Rachel Tribe, PhD, department of women and children’s health, King’s College London.
Researchers used plasma cell-free RNA (cfRNA) transcripts to examine the standard molecular mechanism between the fetus, maternal, and placental tissues in order to determine fetal development and healthy pregnancy progression. Deviation from the standard cfRNA expression was also observed to establish the molecular pathway for those at risk of preeclampsia before clinical presentation.
A cfRNA signal from a single blood sample showed a 32.3% positive-predictive value and 75% sensitivity, which exceeds current positive-predictive values from recent clinical state-of-the-art models.
In addition, 73% of participants with a positive-predictive value were identified “as destined to have a medically indicated preterm birth over 3 months in advance of the preeclampsia symptoms,” said the authors.
With up to 1 in 12 pregnancies affected by preeclampsia, and the diagnosis most often only being made in the third trimester, these results provide a promising outlook for pregnant women “so that they can be more closely monitored and treated by the clinicians involved,” commented Dr. Tribe.
“We are now focused on ongoing clinical research to further validate these results and improve the understanding of other pregnancy complications,” she said. “As a scientist, it was also extremely interesting to see that the molecular signature tells us something about mechanisms associated with health in pregnancy and complications including preeclampsia; such knowledge will aid development of treatment strategies in the future.”
A version of this article first appeared on Medscape.com.
Pregnant women who are at risk of preeclampsia can now be identified early before symptoms develop, finds new research from Kings College London and Guy’s and St Thomas’ NHS Foundation Trust, published in Nature.
The study, supported by the National Institute for Health Research and in partnership with the Mirvie RNA platform, analyzed the genetic material from over 2,500 blood samples of pregnant women from eight independent cohorts with multiple demographics, including socioeconomic background, geographic location, ethnicity, and nationality, collected 14.5 weeks before delivery.
“Because the study drew upon samples for a diverse group of women, including participants recruited across King’s Health Partners, the molecular signature is very reliable and has potential to outperform currently available tests,” said Rachel Tribe, PhD, department of women and children’s health, King’s College London.
Researchers used plasma cell-free RNA (cfRNA) transcripts to examine the standard molecular mechanism between the fetus, maternal, and placental tissues in order to determine fetal development and healthy pregnancy progression. Deviation from the standard cfRNA expression was also observed to establish the molecular pathway for those at risk of preeclampsia before clinical presentation.
A cfRNA signal from a single blood sample showed a 32.3% positive-predictive value and 75% sensitivity, which exceeds current positive-predictive values from recent clinical state-of-the-art models.
In addition, 73% of participants with a positive-predictive value were identified “as destined to have a medically indicated preterm birth over 3 months in advance of the preeclampsia symptoms,” said the authors.
With up to 1 in 12 pregnancies affected by preeclampsia, and the diagnosis most often only being made in the third trimester, these results provide a promising outlook for pregnant women “so that they can be more closely monitored and treated by the clinicians involved,” commented Dr. Tribe.
“We are now focused on ongoing clinical research to further validate these results and improve the understanding of other pregnancy complications,” she said. “As a scientist, it was also extremely interesting to see that the molecular signature tells us something about mechanisms associated with health in pregnancy and complications including preeclampsia; such knowledge will aid development of treatment strategies in the future.”
A version of this article first appeared on Medscape.com.
FROM NATURE
Pill not enough for ‘sexual problems’ female cancer patients face
The antidepressant bupropion failed to improve sexual dysfunction in female cancer survivors, according to new findings published online in the Journal of Clinical Oncology.
Using the Female Sexual Function Index (FSFI) as a measurement tool, investigators found that desire scores were not significantly different for participants who received bupropion versus a placebo over the 9-week study period.
“Sexual health is a complex phenomenon and [our results suggest that] no one intervention is going to solve the broader issue,” lead author Debra Barton, RN, PhD, FAAN, professor in the School of Nursing at the University of Michigan, Ann Arbor, told this news organization.
Sexual dysfunction is common among cancer survivors and experienced across multiple cancer types and stages of disease. Research shows that as many as 70% of female cancer survivors report loss of desire, compared with up to one-third of the general population.
Common sexual concerns among female cancer survivors include low desire, arousal issues, lack of appropriate lubrication, difficulty in achieving orgasm, and pain with penetrative sexual activity. Additionally, these women may experience significant overlap of symptoms, and often encounter multiple sexual issues that are exacerbated by a range of cancer treatments.
“It’s a huge problem,” Maryam B. Lustberg, MD, MPH, from Yale Cancer Center, New Haven, Conn., and colleagues wrote in an accompanying editorial.
Despite the prevalence of sexual dysfunction among cancer survivors, effective treatments remain elusive. Preliminary evidence suggests that bupropion, already approved for seasonal affective disorder, major depressive disorder, and smoking cessation, may also enhance libido.
Dr. Barton and colleagues conducted this phase 2 trial to determine whether bupropion can improve sexual desire in female cancer survivors without undesirable side effects.
In the study, Dr. Barton and colleagues compared two dose levels of extended-release bupropion in a cohort of 230 postmenopausal women diagnosed with breast or gynecologic cancer and low baseline FSFI desire scores (<3.3), who had completed definitive cancer therapy.
Participants were randomized to receive either 150 mg (79 patients) or 300 mg (74 patients) once daily of extended-release bupropion, or placebo (77 patients).
Barton and colleagues then evaluated whether sexual desire significantly improved over the 9-week study period comparing the bupropion arms and the placebo group.
Overall, the authors found no significant differences (mean between-arm change for 150 mg once daily and placebo of 0.02; P = .93; mean between-arm change for 300 mg once daily and placebo of –0.02; P = .92). Mean scores at 9 weeks on the desire subscale were 2.17, 2.27, and 2.30 for 150 mg, 300 mg, and the placebo group, respectively.
In addition, none of the subscales – which included arousal, lubrication, and orgasm – or the total score showed a significant difference between arms at either 5 or 9 weeks.
Bupropion did, however, appear to be well tolerated. No grade 4-5 treatment-related adverse events occurred. In the 150-mg bupropion arm, two patients (2.6%) experienced a grade 3 event (insomnia and headache) and one patient in the 300-mg bupropion arm (1.4%) and placebo arm (1.3%) experienced a grade 3 event related to treatment (hypertension and headache, respectively).
In the accompanying editorial, Dr. Lustberg and colleagues “applaud the authors for conducting a study in this population of cancer survivors,” noting that “evidenced-based approaches have not been extensively studied.”
Dr. Lustberg and colleagues also commented that other randomized controlled clinical trials evaluating sexual desire disorder assessed outcomes using additional metrics, such as the Female Sexual Distress Scale–Revised questionnaire, which measures distress related to sexual dysfunction and low desire, in particular.
“The use of specific validated instruments for libido in place of the FSFI might have helped determine the effect of the study intervention in this reported trial,” they wrote.
Overall, according to Dr. Lustberg and colleagues, the negative results of this study indicate that a multidisciplinary clinical approach may be needed.
“As much as we would like to have one intervention that addresses this prominent issue, the evidence strongly suggests that cancer-related sexual problems may need an integrative biopsychosocial model that intervenes on biologic, psychologic, interpersonal, and social-cultural factors, not just on one factor, such as libido,” they wrote. “Such work may require access to multidisciplinary care with specialists in women’s health, pelvic floor rehabilitation, and psychosocial oncology.”
Dr. Barton said she has been developing a multicomponent approach to addressing sexual health in female cancer survivors.
However, she noted, “there is still much we do not fully understand about the broader impact of the degree of hormone deprivation in the population of female cancer survivors. A better understanding would provide clearer targets for interventions.”
The study was supported by the National Cancer Institute and Breast Cancer Research Foundation. Dr. Barton has disclosed research funding from Merck. Dr. Lustberg reported receiving honoraria from Novartis and Biotheranostics; consulting or advising with PledPharma, Disarm Therapeutics, Pfizer; and other relationships with Cynosure/Hologic.
A version of this article first appeared on Medscape.com.
The antidepressant bupropion failed to improve sexual dysfunction in female cancer survivors, according to new findings published online in the Journal of Clinical Oncology.
Using the Female Sexual Function Index (FSFI) as a measurement tool, investigators found that desire scores were not significantly different for participants who received bupropion versus a placebo over the 9-week study period.
“Sexual health is a complex phenomenon and [our results suggest that] no one intervention is going to solve the broader issue,” lead author Debra Barton, RN, PhD, FAAN, professor in the School of Nursing at the University of Michigan, Ann Arbor, told this news organization.
Sexual dysfunction is common among cancer survivors and experienced across multiple cancer types and stages of disease. Research shows that as many as 70% of female cancer survivors report loss of desire, compared with up to one-third of the general population.
Common sexual concerns among female cancer survivors include low desire, arousal issues, lack of appropriate lubrication, difficulty in achieving orgasm, and pain with penetrative sexual activity. Additionally, these women may experience significant overlap of symptoms, and often encounter multiple sexual issues that are exacerbated by a range of cancer treatments.
“It’s a huge problem,” Maryam B. Lustberg, MD, MPH, from Yale Cancer Center, New Haven, Conn., and colleagues wrote in an accompanying editorial.
Despite the prevalence of sexual dysfunction among cancer survivors, effective treatments remain elusive. Preliminary evidence suggests that bupropion, already approved for seasonal affective disorder, major depressive disorder, and smoking cessation, may also enhance libido.
Dr. Barton and colleagues conducted this phase 2 trial to determine whether bupropion can improve sexual desire in female cancer survivors without undesirable side effects.
In the study, Dr. Barton and colleagues compared two dose levels of extended-release bupropion in a cohort of 230 postmenopausal women diagnosed with breast or gynecologic cancer and low baseline FSFI desire scores (<3.3), who had completed definitive cancer therapy.
Participants were randomized to receive either 150 mg (79 patients) or 300 mg (74 patients) once daily of extended-release bupropion, or placebo (77 patients).
Barton and colleagues then evaluated whether sexual desire significantly improved over the 9-week study period comparing the bupropion arms and the placebo group.
Overall, the authors found no significant differences (mean between-arm change for 150 mg once daily and placebo of 0.02; P = .93; mean between-arm change for 300 mg once daily and placebo of –0.02; P = .92). Mean scores at 9 weeks on the desire subscale were 2.17, 2.27, and 2.30 for 150 mg, 300 mg, and the placebo group, respectively.
In addition, none of the subscales – which included arousal, lubrication, and orgasm – or the total score showed a significant difference between arms at either 5 or 9 weeks.
Bupropion did, however, appear to be well tolerated. No grade 4-5 treatment-related adverse events occurred. In the 150-mg bupropion arm, two patients (2.6%) experienced a grade 3 event (insomnia and headache) and one patient in the 300-mg bupropion arm (1.4%) and placebo arm (1.3%) experienced a grade 3 event related to treatment (hypertension and headache, respectively).
In the accompanying editorial, Dr. Lustberg and colleagues “applaud the authors for conducting a study in this population of cancer survivors,” noting that “evidenced-based approaches have not been extensively studied.”
Dr. Lustberg and colleagues also commented that other randomized controlled clinical trials evaluating sexual desire disorder assessed outcomes using additional metrics, such as the Female Sexual Distress Scale–Revised questionnaire, which measures distress related to sexual dysfunction and low desire, in particular.
“The use of specific validated instruments for libido in place of the FSFI might have helped determine the effect of the study intervention in this reported trial,” they wrote.
Overall, according to Dr. Lustberg and colleagues, the negative results of this study indicate that a multidisciplinary clinical approach may be needed.
“As much as we would like to have one intervention that addresses this prominent issue, the evidence strongly suggests that cancer-related sexual problems may need an integrative biopsychosocial model that intervenes on biologic, psychologic, interpersonal, and social-cultural factors, not just on one factor, such as libido,” they wrote. “Such work may require access to multidisciplinary care with specialists in women’s health, pelvic floor rehabilitation, and psychosocial oncology.”
Dr. Barton said she has been developing a multicomponent approach to addressing sexual health in female cancer survivors.
However, she noted, “there is still much we do not fully understand about the broader impact of the degree of hormone deprivation in the population of female cancer survivors. A better understanding would provide clearer targets for interventions.”
The study was supported by the National Cancer Institute and Breast Cancer Research Foundation. Dr. Barton has disclosed research funding from Merck. Dr. Lustberg reported receiving honoraria from Novartis and Biotheranostics; consulting or advising with PledPharma, Disarm Therapeutics, Pfizer; and other relationships with Cynosure/Hologic.
A version of this article first appeared on Medscape.com.
The antidepressant bupropion failed to improve sexual dysfunction in female cancer survivors, according to new findings published online in the Journal of Clinical Oncology.
Using the Female Sexual Function Index (FSFI) as a measurement tool, investigators found that desire scores were not significantly different for participants who received bupropion versus a placebo over the 9-week study period.
“Sexual health is a complex phenomenon and [our results suggest that] no one intervention is going to solve the broader issue,” lead author Debra Barton, RN, PhD, FAAN, professor in the School of Nursing at the University of Michigan, Ann Arbor, told this news organization.
Sexual dysfunction is common among cancer survivors and experienced across multiple cancer types and stages of disease. Research shows that as many as 70% of female cancer survivors report loss of desire, compared with up to one-third of the general population.
Common sexual concerns among female cancer survivors include low desire, arousal issues, lack of appropriate lubrication, difficulty in achieving orgasm, and pain with penetrative sexual activity. Additionally, these women may experience significant overlap of symptoms, and often encounter multiple sexual issues that are exacerbated by a range of cancer treatments.
“It’s a huge problem,” Maryam B. Lustberg, MD, MPH, from Yale Cancer Center, New Haven, Conn., and colleagues wrote in an accompanying editorial.
Despite the prevalence of sexual dysfunction among cancer survivors, effective treatments remain elusive. Preliminary evidence suggests that bupropion, already approved for seasonal affective disorder, major depressive disorder, and smoking cessation, may also enhance libido.
Dr. Barton and colleagues conducted this phase 2 trial to determine whether bupropion can improve sexual desire in female cancer survivors without undesirable side effects.
In the study, Dr. Barton and colleagues compared two dose levels of extended-release bupropion in a cohort of 230 postmenopausal women diagnosed with breast or gynecologic cancer and low baseline FSFI desire scores (<3.3), who had completed definitive cancer therapy.
Participants were randomized to receive either 150 mg (79 patients) or 300 mg (74 patients) once daily of extended-release bupropion, or placebo (77 patients).
Barton and colleagues then evaluated whether sexual desire significantly improved over the 9-week study period comparing the bupropion arms and the placebo group.
Overall, the authors found no significant differences (mean between-arm change for 150 mg once daily and placebo of 0.02; P = .93; mean between-arm change for 300 mg once daily and placebo of –0.02; P = .92). Mean scores at 9 weeks on the desire subscale were 2.17, 2.27, and 2.30 for 150 mg, 300 mg, and the placebo group, respectively.
In addition, none of the subscales – which included arousal, lubrication, and orgasm – or the total score showed a significant difference between arms at either 5 or 9 weeks.
Bupropion did, however, appear to be well tolerated. No grade 4-5 treatment-related adverse events occurred. In the 150-mg bupropion arm, two patients (2.6%) experienced a grade 3 event (insomnia and headache) and one patient in the 300-mg bupropion arm (1.4%) and placebo arm (1.3%) experienced a grade 3 event related to treatment (hypertension and headache, respectively).
In the accompanying editorial, Dr. Lustberg and colleagues “applaud the authors for conducting a study in this population of cancer survivors,” noting that “evidenced-based approaches have not been extensively studied.”
Dr. Lustberg and colleagues also commented that other randomized controlled clinical trials evaluating sexual desire disorder assessed outcomes using additional metrics, such as the Female Sexual Distress Scale–Revised questionnaire, which measures distress related to sexual dysfunction and low desire, in particular.
“The use of specific validated instruments for libido in place of the FSFI might have helped determine the effect of the study intervention in this reported trial,” they wrote.
Overall, according to Dr. Lustberg and colleagues, the negative results of this study indicate that a multidisciplinary clinical approach may be needed.
“As much as we would like to have one intervention that addresses this prominent issue, the evidence strongly suggests that cancer-related sexual problems may need an integrative biopsychosocial model that intervenes on biologic, psychologic, interpersonal, and social-cultural factors, not just on one factor, such as libido,” they wrote. “Such work may require access to multidisciplinary care with specialists in women’s health, pelvic floor rehabilitation, and psychosocial oncology.”
Dr. Barton said she has been developing a multicomponent approach to addressing sexual health in female cancer survivors.
However, she noted, “there is still much we do not fully understand about the broader impact of the degree of hormone deprivation in the population of female cancer survivors. A better understanding would provide clearer targets for interventions.”
The study was supported by the National Cancer Institute and Breast Cancer Research Foundation. Dr. Barton has disclosed research funding from Merck. Dr. Lustberg reported receiving honoraria from Novartis and Biotheranostics; consulting or advising with PledPharma, Disarm Therapeutics, Pfizer; and other relationships with Cynosure/Hologic.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Statin therapy seems safe in pregnancy
Statins may be safe when used during pregnancy, with no increase in risk for fetal anomalies, although there may be a higher risk for low birth weight and preterm labor, results of a large study from Taiwan suggest.
The Food and Drug Administration relaxed its warning on statins in July 2021, removing the drug’s blanket contraindication in all pregnant women.
Removal of the broadly worded contraindication should “enable health care professionals and patients to make individual decisions about benefit and risk, especially for those at very high risk of heart attack or stroke,” the FDA said in their announcement.
“Our findings suggested that statins may be used during pregnancy with no increase in the rate of congenital anomalies,” wrote Jui-Chun Chang, MD, from Taichung Veterans General Hospital, Taiwan, and colleagues in the new study, published online Dec. 30, 2021, in JAMA Network Open.
“For pregnant women at low risk, statins should be used carefully after assessing the risks of low birth weight and preterm birth,” they said. “For women with dyslipidemia or high-risk cardiovascular disease, as well as those who use statins before conception, statins may be continuously used with no increased risks of neonatal adverse effects.”
The study included more than 1.4 million pregnant women aged 18 years and older who gave birth to their first child between 2004 and 2014.
A total of 469 women (mean age, 32.6 years; mean gestational age, 38.4 weeks) who used statins during pregnancy were compared with 4,690 matched controls who had no statin exposure during pregnancy.
After controlling for maternal comorbidities and age, women who used statins during pregnancy were more apt to have low-birth-weight babies weighing less than 2,500 g (risk ratio, 1.51; 95% confidence interval, 1.05-2.16) and to deliver preterm (RR, 1.99; 95% CI, 1.46-2.71).
The statin-exposed babies were also more likely to have a lower 1-minute Apgar score (RR, 1.83; 95% CI, 1.04-3.20). Importantly, however, there was no increase in risk for fetal anomalies in the statin-exposed infants, the researchers said.
In addition, for women who used statins for more than 3 months prior to pregnancy, maintaining statin use during pregnancy did not increase the risk for adverse neonatal outcomes, including congenital anomalies, low birth weight, preterm birth, very low birth weight, low Apgar scores, and fetal distress.
The researchers called for further studies to confirm their observations.
Funding for the study was provided by Taichung Veterans General Hospital. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Statins may be safe when used during pregnancy, with no increase in risk for fetal anomalies, although there may be a higher risk for low birth weight and preterm labor, results of a large study from Taiwan suggest.
The Food and Drug Administration relaxed its warning on statins in July 2021, removing the drug’s blanket contraindication in all pregnant women.
Removal of the broadly worded contraindication should “enable health care professionals and patients to make individual decisions about benefit and risk, especially for those at very high risk of heart attack or stroke,” the FDA said in their announcement.
“Our findings suggested that statins may be used during pregnancy with no increase in the rate of congenital anomalies,” wrote Jui-Chun Chang, MD, from Taichung Veterans General Hospital, Taiwan, and colleagues in the new study, published online Dec. 30, 2021, in JAMA Network Open.
“For pregnant women at low risk, statins should be used carefully after assessing the risks of low birth weight and preterm birth,” they said. “For women with dyslipidemia or high-risk cardiovascular disease, as well as those who use statins before conception, statins may be continuously used with no increased risks of neonatal adverse effects.”
The study included more than 1.4 million pregnant women aged 18 years and older who gave birth to their first child between 2004 and 2014.
A total of 469 women (mean age, 32.6 years; mean gestational age, 38.4 weeks) who used statins during pregnancy were compared with 4,690 matched controls who had no statin exposure during pregnancy.
After controlling for maternal comorbidities and age, women who used statins during pregnancy were more apt to have low-birth-weight babies weighing less than 2,500 g (risk ratio, 1.51; 95% confidence interval, 1.05-2.16) and to deliver preterm (RR, 1.99; 95% CI, 1.46-2.71).
The statin-exposed babies were also more likely to have a lower 1-minute Apgar score (RR, 1.83; 95% CI, 1.04-3.20). Importantly, however, there was no increase in risk for fetal anomalies in the statin-exposed infants, the researchers said.
In addition, for women who used statins for more than 3 months prior to pregnancy, maintaining statin use during pregnancy did not increase the risk for adverse neonatal outcomes, including congenital anomalies, low birth weight, preterm birth, very low birth weight, low Apgar scores, and fetal distress.
The researchers called for further studies to confirm their observations.
Funding for the study was provided by Taichung Veterans General Hospital. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Statins may be safe when used during pregnancy, with no increase in risk for fetal anomalies, although there may be a higher risk for low birth weight and preterm labor, results of a large study from Taiwan suggest.
The Food and Drug Administration relaxed its warning on statins in July 2021, removing the drug’s blanket contraindication in all pregnant women.
Removal of the broadly worded contraindication should “enable health care professionals and patients to make individual decisions about benefit and risk, especially for those at very high risk of heart attack or stroke,” the FDA said in their announcement.
“Our findings suggested that statins may be used during pregnancy with no increase in the rate of congenital anomalies,” wrote Jui-Chun Chang, MD, from Taichung Veterans General Hospital, Taiwan, and colleagues in the new study, published online Dec. 30, 2021, in JAMA Network Open.
“For pregnant women at low risk, statins should be used carefully after assessing the risks of low birth weight and preterm birth,” they said. “For women with dyslipidemia or high-risk cardiovascular disease, as well as those who use statins before conception, statins may be continuously used with no increased risks of neonatal adverse effects.”
The study included more than 1.4 million pregnant women aged 18 years and older who gave birth to their first child between 2004 and 2014.
A total of 469 women (mean age, 32.6 years; mean gestational age, 38.4 weeks) who used statins during pregnancy were compared with 4,690 matched controls who had no statin exposure during pregnancy.
After controlling for maternal comorbidities and age, women who used statins during pregnancy were more apt to have low-birth-weight babies weighing less than 2,500 g (risk ratio, 1.51; 95% confidence interval, 1.05-2.16) and to deliver preterm (RR, 1.99; 95% CI, 1.46-2.71).
The statin-exposed babies were also more likely to have a lower 1-minute Apgar score (RR, 1.83; 95% CI, 1.04-3.20). Importantly, however, there was no increase in risk for fetal anomalies in the statin-exposed infants, the researchers said.
In addition, for women who used statins for more than 3 months prior to pregnancy, maintaining statin use during pregnancy did not increase the risk for adverse neonatal outcomes, including congenital anomalies, low birth weight, preterm birth, very low birth weight, low Apgar scores, and fetal distress.
The researchers called for further studies to confirm their observations.
Funding for the study was provided by Taichung Veterans General Hospital. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Helping teens make the switch from pediatrics to gynecology
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Tech can help teens connect with docs about sexual health
Maria Trent, MD, MPH, was studying ways clinicians can leverage technology to care for adolescents years before COVID-19 exposed the challenges and advantages of telehealth.
Dr. Trent, a pediatrician and adolescent medicine specialist and professor of pediatrics at Johns Hopkins University, Baltimore, has long believed that the phones in her patients’ pockets have the potential to improve the sexual health of youth. The pandemic has only made that view stronger.
“They’re a generation that’s really wired and online,” Dr. Trent told this news organization. “I think that we can meet them in that space.”
Her research has incorporated texting, apps, and videos. Out of necessity, technology increasingly became part of patient care during the pandemic. “We had to stretch our ability to do some basic triage and assessments of patients online,” Dr. Trent said.
Even when clinics are closed, doctors might be able to provide initial care remotely, such as writing prescriptions to manage symptoms or directing patients to a lab for testing.
Telemedicine could allow a clinician to guide a teenager who thinks they might be pregnant to take a store-bought test and avoid possible exposure to COVID-19 in the ED, for instance.
But doctors have concerns about the legal and practical limits of privacy and confidentiality. Who else is at home listening to a phone conversation? Are parents accessing the patient’s online portal? Will parents receive an explanation of benefits that lists testing for a sexually transmitted infection, or see a testing kit that is delivered to their home?
When a young patient needs in-person care, transportation can be a barrier. And then there’s the matter of clinicians being able to bill for telehealth services.
Practices are learning how to navigate these issues, and relevant laws vary by state.
“I think this is going to become part of standard practice,” Dr. Trent said. “I think we have to do the hard work to make sure that it’s safe, that it’s accessible, and that it is actually improving care.”
Texts, apps, videos
In one early study, Dr. Trent and colleagues found that showing adolescents with pelvic inflammatory disease a 6-minute video may improve treatment rates for their sexual partners.
Another study provided preliminary evidence that text messaging support might improve clinic attendance for moderately long-acting reversible contraception.
A third trial showed that adolescents and young adults with pelvic inflammatory disease who were randomly assigned to receive text-message prompts to take their medications and provide information about the doses they consumed had greater decreases in Neisseria gonorrhoeae and Chlamydia trachomatis infections, compared with patients who received standard care.
Dr. Trent and coinvestigators are assessing a technology-based intervention for youth with HIV, in which patients can use an app to submit videos of themselves taking antiretroviral therapy and report any side effects. The technology provides a way to monitor patients remotely and support them between visits, she said.
Will pandemic-driven options remain?
In 2020, Laura D. Lindberg, PhD, principal research scientist at the Guttmacher Institute in New York, and coauthors discussed the possible ramifications of the pandemic on the sexual and reproductive health of adolescents and young adults.
If telemedicine options driven by COVID-19 are here to stay, adolescents and young adults could be “the age group most likely to continue that approach rather than returning to traditional in-person visits,” the researchers wrote. “Innovations in health care service provision, such as use of telemedicine and obtaining contraceptives and STI testing by mail, will help expand access to [sexual and reproductive health] care for young people.”
At the 2021 annual conference of the American Academy of Pediatrics, Dr. Trent described telehealth as a viable way to provide sexual and reproductive health care to adolescents and young adults, including anticipatory guidance, contraception counseling, coordination of follow-up care and testing, and connecting patients to resources.
Her presentation cited several websites that can help patients receive testing for STIs, including Yes Means Test, the Centers for Disease Control and Prevention’s GetTested page, and I Want the Kit. Planned Parenthood has telehealth options, and the Kaiser Family Foundation compiled information about 26 online platforms that were providing contraception or STI services.
Who else is in the room?
“There’s only so much time in the day and so many patients you can see, regardless of whether you have telehealth or not,” said David L. Bell, MD, MPH, president of the Society for Adolescent Health and Medicine and a coauthor of the Perspectives on Sexual and Reproductive Health paper. In addition, “you never know who else is in the room” with the patient on the other end, added Dr. Bell, a professor of population and family health and pediatrics at the Columbia University Medical Center and medical director of the Young Men’s Clinic, both in New York.
In some respects, young patients may not be able to participate in telehealth visits the same way they would in a medical office, Dr. Trent acknowledged. Encouraging the use of headphones is one way to help protect confidentiality when talking with patients who are at home and might not be alone.
But if patients are able to find a private space for remote visits, they might be more open than usual. In that way, telemedicine could provide additional opportunities to address issues like substance use disorders and mental health, as well, she said.
“Then, if they need something, we have to problem solve,” Dr. Trent said. Next steps may involve engaging a parent or getting the patient to a lab or the clinic.
Sex ed may be lacking
The Perspectives article also raised concerns that the pandemic might exacerbate shortcomings in sex education, which already may have been lacking.
“Before the pandemic, schools were a key source of formal sex education for young people,” the authors wrote. “Sex education, which was already limited in many areas of the country, has likely not been included in the national shift to online learning. Even when in-person schooling resumes, missed sex education instruction is unlikely to be made up, given the modest attention it received prior to the pandemic.”
A recently published study in the Journal of Adolescent Health indicates that American teenagers currently receive less formal sex education than they did 25 years ago, with “troubling” inequities by race.
Researchers surveyed adolescents about what they had learned about topics such as how to say no to sex, methods of birth control and where to get them, and STIs.
Dr. Lindberg and Leslie M. Kantor, PhD, MPH, professor and chair of the department of urban-global public health at Rutgers University, Newark, N.J., conducted the analysis.
“Pediatricians and other health care providers that work with children and adolescents have a critical role to play in providing information about sexuality to both the patients and to the parents,” said Dr. Kantor, who also coauthored the Perspectives article with Dr. Lindberg and Dr. Bell. The new research “shows that doctors play an even more critical role, because they can’t assume that their patients are going to get the information that they need in a timely way from schools.”
By age 15, 21% of girls and 20% of boys have had sexual intercourse at least once, according to data from the 2015-2017 National Survey of Family Growth. By age 17, the percentages were 53% of girls and 48% of boys. By age 20, the percentages were 79% of women and 77% of men. The CDC’s 2021 guidelines on treatment and screening for STIs note that prevalence rates of certain infections – such as chlamydia and gonorrhea in females – are highest among adolescents and young adults.
Those trends underscore the importance of counseling on sexual health that clinicians can provide, but time constraints may limit how much they can discuss in a single session with a patient. To cover all topics that are important to parents and patients, doctors may need to discuss sexual and reproductive health sooner and more frequently.
Young people are getting more and more explicit information from their phones and media, yet educators are giving them less information to navigate these topics and learn what’s real, Dr. Kantor said. That mismatch can be toxic. In a December 2021 interview with Howard Stern, the pop star Billie Eilish said she started watching pornography at about age 11 and frequently watched videos that were violent. “I think it really destroyed my brain and I feel incredibly devastated that I was exposed to so much porn,” Ms. Eilish told Mr. Stern.
Researchers and a psychologist told CNN that the singer’s story may be typical. It also highlights a need to be aware of kids’ online activities and to have conversations about how pornography may not depict healthy interactions, they said.
Beyond discussing a plan for preventing pregnancy and STIs, Dr. Kantor encouraged discussions about what constitutes healthy relationships, as well as check-ins about intimate partner violence and how romantic relationships are going.
“I think for pediatricians and for parents, it’s a muscle,” she said. “As you bring up these topics more, listen, and respond, you get more comfortable with it.”
Dr. Trent has served as an advisory board member on a sexual health council for Trojan (Church & Dwight Company) and has received research funding from Hologic and research supplies from SpeeDx. Dr. Bell has received funds from the Merck Foundation, Merck, and Gilead. Dr. Kantor had no disclosures.
A version of this article first appeared on Medscape.com.
Maria Trent, MD, MPH, was studying ways clinicians can leverage technology to care for adolescents years before COVID-19 exposed the challenges and advantages of telehealth.
Dr. Trent, a pediatrician and adolescent medicine specialist and professor of pediatrics at Johns Hopkins University, Baltimore, has long believed that the phones in her patients’ pockets have the potential to improve the sexual health of youth. The pandemic has only made that view stronger.
“They’re a generation that’s really wired and online,” Dr. Trent told this news organization. “I think that we can meet them in that space.”
Her research has incorporated texting, apps, and videos. Out of necessity, technology increasingly became part of patient care during the pandemic. “We had to stretch our ability to do some basic triage and assessments of patients online,” Dr. Trent said.
Even when clinics are closed, doctors might be able to provide initial care remotely, such as writing prescriptions to manage symptoms or directing patients to a lab for testing.
Telemedicine could allow a clinician to guide a teenager who thinks they might be pregnant to take a store-bought test and avoid possible exposure to COVID-19 in the ED, for instance.
But doctors have concerns about the legal and practical limits of privacy and confidentiality. Who else is at home listening to a phone conversation? Are parents accessing the patient’s online portal? Will parents receive an explanation of benefits that lists testing for a sexually transmitted infection, or see a testing kit that is delivered to their home?
When a young patient needs in-person care, transportation can be a barrier. And then there’s the matter of clinicians being able to bill for telehealth services.
Practices are learning how to navigate these issues, and relevant laws vary by state.
“I think this is going to become part of standard practice,” Dr. Trent said. “I think we have to do the hard work to make sure that it’s safe, that it’s accessible, and that it is actually improving care.”
Texts, apps, videos
In one early study, Dr. Trent and colleagues found that showing adolescents with pelvic inflammatory disease a 6-minute video may improve treatment rates for their sexual partners.
Another study provided preliminary evidence that text messaging support might improve clinic attendance for moderately long-acting reversible contraception.
A third trial showed that adolescents and young adults with pelvic inflammatory disease who were randomly assigned to receive text-message prompts to take their medications and provide information about the doses they consumed had greater decreases in Neisseria gonorrhoeae and Chlamydia trachomatis infections, compared with patients who received standard care.
Dr. Trent and coinvestigators are assessing a technology-based intervention for youth with HIV, in which patients can use an app to submit videos of themselves taking antiretroviral therapy and report any side effects. The technology provides a way to monitor patients remotely and support them between visits, she said.
Will pandemic-driven options remain?
In 2020, Laura D. Lindberg, PhD, principal research scientist at the Guttmacher Institute in New York, and coauthors discussed the possible ramifications of the pandemic on the sexual and reproductive health of adolescents and young adults.
If telemedicine options driven by COVID-19 are here to stay, adolescents and young adults could be “the age group most likely to continue that approach rather than returning to traditional in-person visits,” the researchers wrote. “Innovations in health care service provision, such as use of telemedicine and obtaining contraceptives and STI testing by mail, will help expand access to [sexual and reproductive health] care for young people.”
At the 2021 annual conference of the American Academy of Pediatrics, Dr. Trent described telehealth as a viable way to provide sexual and reproductive health care to adolescents and young adults, including anticipatory guidance, contraception counseling, coordination of follow-up care and testing, and connecting patients to resources.
Her presentation cited several websites that can help patients receive testing for STIs, including Yes Means Test, the Centers for Disease Control and Prevention’s GetTested page, and I Want the Kit. Planned Parenthood has telehealth options, and the Kaiser Family Foundation compiled information about 26 online platforms that were providing contraception or STI services.
Who else is in the room?
“There’s only so much time in the day and so many patients you can see, regardless of whether you have telehealth or not,” said David L. Bell, MD, MPH, president of the Society for Adolescent Health and Medicine and a coauthor of the Perspectives on Sexual and Reproductive Health paper. In addition, “you never know who else is in the room” with the patient on the other end, added Dr. Bell, a professor of population and family health and pediatrics at the Columbia University Medical Center and medical director of the Young Men’s Clinic, both in New York.
In some respects, young patients may not be able to participate in telehealth visits the same way they would in a medical office, Dr. Trent acknowledged. Encouraging the use of headphones is one way to help protect confidentiality when talking with patients who are at home and might not be alone.
But if patients are able to find a private space for remote visits, they might be more open than usual. In that way, telemedicine could provide additional opportunities to address issues like substance use disorders and mental health, as well, she said.
“Then, if they need something, we have to problem solve,” Dr. Trent said. Next steps may involve engaging a parent or getting the patient to a lab or the clinic.
Sex ed may be lacking
The Perspectives article also raised concerns that the pandemic might exacerbate shortcomings in sex education, which already may have been lacking.
“Before the pandemic, schools were a key source of formal sex education for young people,” the authors wrote. “Sex education, which was already limited in many areas of the country, has likely not been included in the national shift to online learning. Even when in-person schooling resumes, missed sex education instruction is unlikely to be made up, given the modest attention it received prior to the pandemic.”
A recently published study in the Journal of Adolescent Health indicates that American teenagers currently receive less formal sex education than they did 25 years ago, with “troubling” inequities by race.
Researchers surveyed adolescents about what they had learned about topics such as how to say no to sex, methods of birth control and where to get them, and STIs.
Dr. Lindberg and Leslie M. Kantor, PhD, MPH, professor and chair of the department of urban-global public health at Rutgers University, Newark, N.J., conducted the analysis.
“Pediatricians and other health care providers that work with children and adolescents have a critical role to play in providing information about sexuality to both the patients and to the parents,” said Dr. Kantor, who also coauthored the Perspectives article with Dr. Lindberg and Dr. Bell. The new research “shows that doctors play an even more critical role, because they can’t assume that their patients are going to get the information that they need in a timely way from schools.”
By age 15, 21% of girls and 20% of boys have had sexual intercourse at least once, according to data from the 2015-2017 National Survey of Family Growth. By age 17, the percentages were 53% of girls and 48% of boys. By age 20, the percentages were 79% of women and 77% of men. The CDC’s 2021 guidelines on treatment and screening for STIs note that prevalence rates of certain infections – such as chlamydia and gonorrhea in females – are highest among adolescents and young adults.
Those trends underscore the importance of counseling on sexual health that clinicians can provide, but time constraints may limit how much they can discuss in a single session with a patient. To cover all topics that are important to parents and patients, doctors may need to discuss sexual and reproductive health sooner and more frequently.
Young people are getting more and more explicit information from their phones and media, yet educators are giving them less information to navigate these topics and learn what’s real, Dr. Kantor said. That mismatch can be toxic. In a December 2021 interview with Howard Stern, the pop star Billie Eilish said she started watching pornography at about age 11 and frequently watched videos that were violent. “I think it really destroyed my brain and I feel incredibly devastated that I was exposed to so much porn,” Ms. Eilish told Mr. Stern.
Researchers and a psychologist told CNN that the singer’s story may be typical. It also highlights a need to be aware of kids’ online activities and to have conversations about how pornography may not depict healthy interactions, they said.
Beyond discussing a plan for preventing pregnancy and STIs, Dr. Kantor encouraged discussions about what constitutes healthy relationships, as well as check-ins about intimate partner violence and how romantic relationships are going.
“I think for pediatricians and for parents, it’s a muscle,” she said. “As you bring up these topics more, listen, and respond, you get more comfortable with it.”
Dr. Trent has served as an advisory board member on a sexual health council for Trojan (Church & Dwight Company) and has received research funding from Hologic and research supplies from SpeeDx. Dr. Bell has received funds from the Merck Foundation, Merck, and Gilead. Dr. Kantor had no disclosures.
A version of this article first appeared on Medscape.com.
Maria Trent, MD, MPH, was studying ways clinicians can leverage technology to care for adolescents years before COVID-19 exposed the challenges and advantages of telehealth.
Dr. Trent, a pediatrician and adolescent medicine specialist and professor of pediatrics at Johns Hopkins University, Baltimore, has long believed that the phones in her patients’ pockets have the potential to improve the sexual health of youth. The pandemic has only made that view stronger.
“They’re a generation that’s really wired and online,” Dr. Trent told this news organization. “I think that we can meet them in that space.”
Her research has incorporated texting, apps, and videos. Out of necessity, technology increasingly became part of patient care during the pandemic. “We had to stretch our ability to do some basic triage and assessments of patients online,” Dr. Trent said.
Even when clinics are closed, doctors might be able to provide initial care remotely, such as writing prescriptions to manage symptoms or directing patients to a lab for testing.
Telemedicine could allow a clinician to guide a teenager who thinks they might be pregnant to take a store-bought test and avoid possible exposure to COVID-19 in the ED, for instance.
But doctors have concerns about the legal and practical limits of privacy and confidentiality. Who else is at home listening to a phone conversation? Are parents accessing the patient’s online portal? Will parents receive an explanation of benefits that lists testing for a sexually transmitted infection, or see a testing kit that is delivered to their home?
When a young patient needs in-person care, transportation can be a barrier. And then there’s the matter of clinicians being able to bill for telehealth services.
Practices are learning how to navigate these issues, and relevant laws vary by state.
“I think this is going to become part of standard practice,” Dr. Trent said. “I think we have to do the hard work to make sure that it’s safe, that it’s accessible, and that it is actually improving care.”
Texts, apps, videos
In one early study, Dr. Trent and colleagues found that showing adolescents with pelvic inflammatory disease a 6-minute video may improve treatment rates for their sexual partners.
Another study provided preliminary evidence that text messaging support might improve clinic attendance for moderately long-acting reversible contraception.
A third trial showed that adolescents and young adults with pelvic inflammatory disease who were randomly assigned to receive text-message prompts to take their medications and provide information about the doses they consumed had greater decreases in Neisseria gonorrhoeae and Chlamydia trachomatis infections, compared with patients who received standard care.
Dr. Trent and coinvestigators are assessing a technology-based intervention for youth with HIV, in which patients can use an app to submit videos of themselves taking antiretroviral therapy and report any side effects. The technology provides a way to monitor patients remotely and support them between visits, she said.
Will pandemic-driven options remain?
In 2020, Laura D. Lindberg, PhD, principal research scientist at the Guttmacher Institute in New York, and coauthors discussed the possible ramifications of the pandemic on the sexual and reproductive health of adolescents and young adults.
If telemedicine options driven by COVID-19 are here to stay, adolescents and young adults could be “the age group most likely to continue that approach rather than returning to traditional in-person visits,” the researchers wrote. “Innovations in health care service provision, such as use of telemedicine and obtaining contraceptives and STI testing by mail, will help expand access to [sexual and reproductive health] care for young people.”
At the 2021 annual conference of the American Academy of Pediatrics, Dr. Trent described telehealth as a viable way to provide sexual and reproductive health care to adolescents and young adults, including anticipatory guidance, contraception counseling, coordination of follow-up care and testing, and connecting patients to resources.
Her presentation cited several websites that can help patients receive testing for STIs, including Yes Means Test, the Centers for Disease Control and Prevention’s GetTested page, and I Want the Kit. Planned Parenthood has telehealth options, and the Kaiser Family Foundation compiled information about 26 online platforms that were providing contraception or STI services.
Who else is in the room?
“There’s only so much time in the day and so many patients you can see, regardless of whether you have telehealth or not,” said David L. Bell, MD, MPH, president of the Society for Adolescent Health and Medicine and a coauthor of the Perspectives on Sexual and Reproductive Health paper. In addition, “you never know who else is in the room” with the patient on the other end, added Dr. Bell, a professor of population and family health and pediatrics at the Columbia University Medical Center and medical director of the Young Men’s Clinic, both in New York.
In some respects, young patients may not be able to participate in telehealth visits the same way they would in a medical office, Dr. Trent acknowledged. Encouraging the use of headphones is one way to help protect confidentiality when talking with patients who are at home and might not be alone.
But if patients are able to find a private space for remote visits, they might be more open than usual. In that way, telemedicine could provide additional opportunities to address issues like substance use disorders and mental health, as well, she said.
“Then, if they need something, we have to problem solve,” Dr. Trent said. Next steps may involve engaging a parent or getting the patient to a lab or the clinic.
Sex ed may be lacking
The Perspectives article also raised concerns that the pandemic might exacerbate shortcomings in sex education, which already may have been lacking.
“Before the pandemic, schools were a key source of formal sex education for young people,” the authors wrote. “Sex education, which was already limited in many areas of the country, has likely not been included in the national shift to online learning. Even when in-person schooling resumes, missed sex education instruction is unlikely to be made up, given the modest attention it received prior to the pandemic.”
A recently published study in the Journal of Adolescent Health indicates that American teenagers currently receive less formal sex education than they did 25 years ago, with “troubling” inequities by race.
Researchers surveyed adolescents about what they had learned about topics such as how to say no to sex, methods of birth control and where to get them, and STIs.
Dr. Lindberg and Leslie M. Kantor, PhD, MPH, professor and chair of the department of urban-global public health at Rutgers University, Newark, N.J., conducted the analysis.
“Pediatricians and other health care providers that work with children and adolescents have a critical role to play in providing information about sexuality to both the patients and to the parents,” said Dr. Kantor, who also coauthored the Perspectives article with Dr. Lindberg and Dr. Bell. The new research “shows that doctors play an even more critical role, because they can’t assume that their patients are going to get the information that they need in a timely way from schools.”
By age 15, 21% of girls and 20% of boys have had sexual intercourse at least once, according to data from the 2015-2017 National Survey of Family Growth. By age 17, the percentages were 53% of girls and 48% of boys. By age 20, the percentages were 79% of women and 77% of men. The CDC’s 2021 guidelines on treatment and screening for STIs note that prevalence rates of certain infections – such as chlamydia and gonorrhea in females – are highest among adolescents and young adults.
Those trends underscore the importance of counseling on sexual health that clinicians can provide, but time constraints may limit how much they can discuss in a single session with a patient. To cover all topics that are important to parents and patients, doctors may need to discuss sexual and reproductive health sooner and more frequently.
Young people are getting more and more explicit information from their phones and media, yet educators are giving them less information to navigate these topics and learn what’s real, Dr. Kantor said. That mismatch can be toxic. In a December 2021 interview with Howard Stern, the pop star Billie Eilish said she started watching pornography at about age 11 and frequently watched videos that were violent. “I think it really destroyed my brain and I feel incredibly devastated that I was exposed to so much porn,” Ms. Eilish told Mr. Stern.
Researchers and a psychologist told CNN that the singer’s story may be typical. It also highlights a need to be aware of kids’ online activities and to have conversations about how pornography may not depict healthy interactions, they said.
Beyond discussing a plan for preventing pregnancy and STIs, Dr. Kantor encouraged discussions about what constitutes healthy relationships, as well as check-ins about intimate partner violence and how romantic relationships are going.
“I think for pediatricians and for parents, it’s a muscle,” she said. “As you bring up these topics more, listen, and respond, you get more comfortable with it.”
Dr. Trent has served as an advisory board member on a sexual health council for Trojan (Church & Dwight Company) and has received research funding from Hologic and research supplies from SpeeDx. Dr. Bell has received funds from the Merck Foundation, Merck, and Gilead. Dr. Kantor had no disclosures.
A version of this article first appeared on Medscape.com.
Even healthy Black and Hispanic women have more cesareans than White women
New research offers more insight into potentially dangerous racial disparities in cesarean deliveries: In first-time live births, healthy African-American and Hispanic mothers were 21% and 26% more likely than White mothers, respectively, to deliver by cesarean section despite being low risk. The higher number of cesareans appeared to boost their risk of morbidity.
“A 20% increased odds of cesarean among otherwise healthy, low-risk, nulliparous individuals at term – with limited medical or obstetric explanation – is a significant concern, especially when considering that cesarean is the most common surgical procedure in the U.S.,” said study author Michelle P. Debbink, MD, PhD, an assistant professor with the department of obstetrics and gynecology at the University of Utah, in an interview.
Dr. Debbink and colleagues launched the study, published in the Jan. 2022 issue of Obstetrics & Gynecology, to better understand the racial gap in cesarean sections, which are considered riskier than vaginal deliveries. “Several studies have shown that Black women undergo cesarean more frequently than non-Hispanic White women. Numerous studies also show that Hispanic/Latina women undergo cesarean more frequently than White women, although these data are a bit more mixed,” she said. “What we don’t know, however, is why these differences occur and whether there are clues in the data which can point us toward interventions to close the gap.”
One theory, she said, is that Black and Hispanic women have more comorbidities and therefore more cesareans. To test that idea, the researchers found a cohort of healthy women in a randomized trial that studied the induction of labor.
For the study, they focused on 5,759 women (24.3% Black, 30% Hispanic, 46.6% White). Major differences between the groups included maternal age (average = 21 for Black, 22 for Hispanic, and 26 for White, P < .001), private insurance (17% for Black and Hispanic, 75% for White; P < .001), and full or part-time employment (37% for Black, 31% for Hispanic, and 71% for White; P < .001).
A total of 1,158 of the women (20.1%) underwent cesarean deliveries, accounting for 23% of deliveries by Black women, 22.8% of those by Hispanic women, and 17.6% of those by White women (P < .001). Black women were 21% more likely than White women to give birth via cesarean (adjusted relative risk = 1.21, 95% CI: 1.03-1.42) and Hispanic women were 26% more likely (aRR = 1.26, 95% CI: 1.08-1.46).
The study doesn’t explore why Black and Hispanic women have more cesarean deliveries. However, Dr. Debbink said, “we hypothesize that the difference likely stems more from differing treatment of Black or Hispanic individuals during labor.” It’s unlikely, she said, that these women are more likely to prefer cesarean sections. For one thing, she said, other research hasn’t shown a difference in preferences by race.
The researchers also analyzed maternal morbidity, defined as “transfusion of 4 or more units of red blood cells, any transfusion of other products, postpartum infection, intensive care unit admission, hysterectomy, venous thromboembolism, or maternal death.”
The study found that while few women (2.3%) suffered from morbidity, Black (aRR = 2.05, 95% CI: 1.21-3.47) and Hispanic (aRR = 1.92, 95% CI: 1.17-3.14) women were more likely to suffer from it than White women.
The researchers report that “cesarean birth accounted for an estimated 15.8% (95% CI: 2.1%-48.7%) and 16.5% (95% CI: 4.0%-44.0%) of excess maternal morbidity among non-Hispanic Black and Hispanic people, respectively.”
“Both endometritis and wound complications are much more common among individuals with cesarean, and blood clots, hysterectomy, and ICU admission are also more common after cesarean compared with vaginal delivery,” Dr. Debbink said.
The message of the study, she said, is that the health care system “perpetuates gaps in cesarean delivery for Black and Hispanic individuals compared to White individuals” even in low-risk, first-time live births. “We do not yet know exactly what the right levers are to address this gap, but it is important that we ob-gyns examine our practice patterns and our hospitals’ practice patterns to ensure equity for all our patients.”
Rebecca Delafield, PhD, an assistant professor of Native Hawaiian Health at the University of Hawaii, praised the study as “well-conducted” in an interview. “I agree with the assessment that while the cesarean delivery accounts for a modest proportion of excess morbidity in this study, the impact at the population level is significant,” said Dr. Delafield, who studies health disparities and didn’t take part in the study. “Delivery is complex and the causes of disparities observed are likely multifactorial, therefore research such as this is necessary and compelling.”
She added: “It is becoming increasingly evident that studies investigating racial/ethnic disparities in cesarean delivery and other maternal health outcomes must look beyond maternal behavioral or medical risk factors – e.g., obesity or hypertension – and consider the contribution of a broader set of factors, including societal prejudices.”
The study is funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Center for Advancing Translational Sciences. One study author reports funding from GlaxoSmithKline, Pfizer, Moderna, and UpToDate (contributor) and from the Centers for Disease Control and Prevention (via her institution). Dr. Debbink, the other authors, and Dr. Delafield report no disclosures.
New research offers more insight into potentially dangerous racial disparities in cesarean deliveries: In first-time live births, healthy African-American and Hispanic mothers were 21% and 26% more likely than White mothers, respectively, to deliver by cesarean section despite being low risk. The higher number of cesareans appeared to boost their risk of morbidity.
“A 20% increased odds of cesarean among otherwise healthy, low-risk, nulliparous individuals at term – with limited medical or obstetric explanation – is a significant concern, especially when considering that cesarean is the most common surgical procedure in the U.S.,” said study author Michelle P. Debbink, MD, PhD, an assistant professor with the department of obstetrics and gynecology at the University of Utah, in an interview.
Dr. Debbink and colleagues launched the study, published in the Jan. 2022 issue of Obstetrics & Gynecology, to better understand the racial gap in cesarean sections, which are considered riskier than vaginal deliveries. “Several studies have shown that Black women undergo cesarean more frequently than non-Hispanic White women. Numerous studies also show that Hispanic/Latina women undergo cesarean more frequently than White women, although these data are a bit more mixed,” she said. “What we don’t know, however, is why these differences occur and whether there are clues in the data which can point us toward interventions to close the gap.”
One theory, she said, is that Black and Hispanic women have more comorbidities and therefore more cesareans. To test that idea, the researchers found a cohort of healthy women in a randomized trial that studied the induction of labor.
For the study, they focused on 5,759 women (24.3% Black, 30% Hispanic, 46.6% White). Major differences between the groups included maternal age (average = 21 for Black, 22 for Hispanic, and 26 for White, P < .001), private insurance (17% for Black and Hispanic, 75% for White; P < .001), and full or part-time employment (37% for Black, 31% for Hispanic, and 71% for White; P < .001).
A total of 1,158 of the women (20.1%) underwent cesarean deliveries, accounting for 23% of deliveries by Black women, 22.8% of those by Hispanic women, and 17.6% of those by White women (P < .001). Black women were 21% more likely than White women to give birth via cesarean (adjusted relative risk = 1.21, 95% CI: 1.03-1.42) and Hispanic women were 26% more likely (aRR = 1.26, 95% CI: 1.08-1.46).
The study doesn’t explore why Black and Hispanic women have more cesarean deliveries. However, Dr. Debbink said, “we hypothesize that the difference likely stems more from differing treatment of Black or Hispanic individuals during labor.” It’s unlikely, she said, that these women are more likely to prefer cesarean sections. For one thing, she said, other research hasn’t shown a difference in preferences by race.
The researchers also analyzed maternal morbidity, defined as “transfusion of 4 or more units of red blood cells, any transfusion of other products, postpartum infection, intensive care unit admission, hysterectomy, venous thromboembolism, or maternal death.”
The study found that while few women (2.3%) suffered from morbidity, Black (aRR = 2.05, 95% CI: 1.21-3.47) and Hispanic (aRR = 1.92, 95% CI: 1.17-3.14) women were more likely to suffer from it than White women.
The researchers report that “cesarean birth accounted for an estimated 15.8% (95% CI: 2.1%-48.7%) and 16.5% (95% CI: 4.0%-44.0%) of excess maternal morbidity among non-Hispanic Black and Hispanic people, respectively.”
“Both endometritis and wound complications are much more common among individuals with cesarean, and blood clots, hysterectomy, and ICU admission are also more common after cesarean compared with vaginal delivery,” Dr. Debbink said.
The message of the study, she said, is that the health care system “perpetuates gaps in cesarean delivery for Black and Hispanic individuals compared to White individuals” even in low-risk, first-time live births. “We do not yet know exactly what the right levers are to address this gap, but it is important that we ob-gyns examine our practice patterns and our hospitals’ practice patterns to ensure equity for all our patients.”
Rebecca Delafield, PhD, an assistant professor of Native Hawaiian Health at the University of Hawaii, praised the study as “well-conducted” in an interview. “I agree with the assessment that while the cesarean delivery accounts for a modest proportion of excess morbidity in this study, the impact at the population level is significant,” said Dr. Delafield, who studies health disparities and didn’t take part in the study. “Delivery is complex and the causes of disparities observed are likely multifactorial, therefore research such as this is necessary and compelling.”
She added: “It is becoming increasingly evident that studies investigating racial/ethnic disparities in cesarean delivery and other maternal health outcomes must look beyond maternal behavioral or medical risk factors – e.g., obesity or hypertension – and consider the contribution of a broader set of factors, including societal prejudices.”
The study is funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Center for Advancing Translational Sciences. One study author reports funding from GlaxoSmithKline, Pfizer, Moderna, and UpToDate (contributor) and from the Centers for Disease Control and Prevention (via her institution). Dr. Debbink, the other authors, and Dr. Delafield report no disclosures.
New research offers more insight into potentially dangerous racial disparities in cesarean deliveries: In first-time live births, healthy African-American and Hispanic mothers were 21% and 26% more likely than White mothers, respectively, to deliver by cesarean section despite being low risk. The higher number of cesareans appeared to boost their risk of morbidity.
“A 20% increased odds of cesarean among otherwise healthy, low-risk, nulliparous individuals at term – with limited medical or obstetric explanation – is a significant concern, especially when considering that cesarean is the most common surgical procedure in the U.S.,” said study author Michelle P. Debbink, MD, PhD, an assistant professor with the department of obstetrics and gynecology at the University of Utah, in an interview.
Dr. Debbink and colleagues launched the study, published in the Jan. 2022 issue of Obstetrics & Gynecology, to better understand the racial gap in cesarean sections, which are considered riskier than vaginal deliveries. “Several studies have shown that Black women undergo cesarean more frequently than non-Hispanic White women. Numerous studies also show that Hispanic/Latina women undergo cesarean more frequently than White women, although these data are a bit more mixed,” she said. “What we don’t know, however, is why these differences occur and whether there are clues in the data which can point us toward interventions to close the gap.”
One theory, she said, is that Black and Hispanic women have more comorbidities and therefore more cesareans. To test that idea, the researchers found a cohort of healthy women in a randomized trial that studied the induction of labor.
For the study, they focused on 5,759 women (24.3% Black, 30% Hispanic, 46.6% White). Major differences between the groups included maternal age (average = 21 for Black, 22 for Hispanic, and 26 for White, P < .001), private insurance (17% for Black and Hispanic, 75% for White; P < .001), and full or part-time employment (37% for Black, 31% for Hispanic, and 71% for White; P < .001).
A total of 1,158 of the women (20.1%) underwent cesarean deliveries, accounting for 23% of deliveries by Black women, 22.8% of those by Hispanic women, and 17.6% of those by White women (P < .001). Black women were 21% more likely than White women to give birth via cesarean (adjusted relative risk = 1.21, 95% CI: 1.03-1.42) and Hispanic women were 26% more likely (aRR = 1.26, 95% CI: 1.08-1.46).
The study doesn’t explore why Black and Hispanic women have more cesarean deliveries. However, Dr. Debbink said, “we hypothesize that the difference likely stems more from differing treatment of Black or Hispanic individuals during labor.” It’s unlikely, she said, that these women are more likely to prefer cesarean sections. For one thing, she said, other research hasn’t shown a difference in preferences by race.
The researchers also analyzed maternal morbidity, defined as “transfusion of 4 or more units of red blood cells, any transfusion of other products, postpartum infection, intensive care unit admission, hysterectomy, venous thromboembolism, or maternal death.”
The study found that while few women (2.3%) suffered from morbidity, Black (aRR = 2.05, 95% CI: 1.21-3.47) and Hispanic (aRR = 1.92, 95% CI: 1.17-3.14) women were more likely to suffer from it than White women.
The researchers report that “cesarean birth accounted for an estimated 15.8% (95% CI: 2.1%-48.7%) and 16.5% (95% CI: 4.0%-44.0%) of excess maternal morbidity among non-Hispanic Black and Hispanic people, respectively.”
“Both endometritis and wound complications are much more common among individuals with cesarean, and blood clots, hysterectomy, and ICU admission are also more common after cesarean compared with vaginal delivery,” Dr. Debbink said.
The message of the study, she said, is that the health care system “perpetuates gaps in cesarean delivery for Black and Hispanic individuals compared to White individuals” even in low-risk, first-time live births. “We do not yet know exactly what the right levers are to address this gap, but it is important that we ob-gyns examine our practice patterns and our hospitals’ practice patterns to ensure equity for all our patients.”
Rebecca Delafield, PhD, an assistant professor of Native Hawaiian Health at the University of Hawaii, praised the study as “well-conducted” in an interview. “I agree with the assessment that while the cesarean delivery accounts for a modest proportion of excess morbidity in this study, the impact at the population level is significant,” said Dr. Delafield, who studies health disparities and didn’t take part in the study. “Delivery is complex and the causes of disparities observed are likely multifactorial, therefore research such as this is necessary and compelling.”
She added: “It is becoming increasingly evident that studies investigating racial/ethnic disparities in cesarean delivery and other maternal health outcomes must look beyond maternal behavioral or medical risk factors – e.g., obesity or hypertension – and consider the contribution of a broader set of factors, including societal prejudices.”
The study is funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Center for Advancing Translational Sciences. One study author reports funding from GlaxoSmithKline, Pfizer, Moderna, and UpToDate (contributor) and from the Centers for Disease Control and Prevention (via her institution). Dr. Debbink, the other authors, and Dr. Delafield report no disclosures.
FROM OBSTETRICS & GYNECOLOGY
EMA panel backs linzagolix for uterine fibroid symptoms
The European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) on December 17 recommended approval of linzagolix (Yselty, ObsEva), an oral gonadotropin-releasing hormone (GnRH) antagonist, for the management of moderate to severe symptoms of uterine fibroids (UF) in adult women of reproductive age.
If approved, linzagolix – which is taken once per day – would become the first GnRH receptor antagonist with a nonhormonal option to reach the market. The U.S. Food and Drug Administration in November accepted ObsEva’s new drug application for the medication, with a decision expected by September 2022.
“The positive CHMP opinion is an important milestone for millions of women in the EU living with UF to address the diverse medical needs of the women who suffer from this condition,” said Brian O’Callaghan, CEO of ObsEva, in a statement. “We will continue our productive, ongoing dialogue with [the] EMA toward potential marketing authorization in the EU and, in parallel, continue to work with the FDA to advance linzagolix through the U.S. regulatory process.”
The committee’s positive opinion was based on 52-week results from PRIMROSE 1 and PRIMROSE 2 phase 3 trials, involving more than 1,000 patients in the United States and Europe, as well as results from 76-week follow-up studies of patients in those trials. The two phase 3 trials assessed a 200-mg and 100-mg dose of linzagolix, with and without hormone add-back therapy (ABT; 1 mg estradiol and 0.5 mg norethisterone acetate).
According to ObsEVA, both trials met their primary endpoints, with all doses showing statistically significant and clinically relevant reductions in heavy menstrual bleeding (HMB) compared to placebo. The trials also achieved several secondary endpoints, including reduction in pain, rates of amenorrhea, time to reduced HMB, and amenorrhea and for the high dose without ABT, reductions in uterine and fibroid volume, the company said.
A version of this article first appeared on Medscape.com.
The European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) on December 17 recommended approval of linzagolix (Yselty, ObsEva), an oral gonadotropin-releasing hormone (GnRH) antagonist, for the management of moderate to severe symptoms of uterine fibroids (UF) in adult women of reproductive age.
If approved, linzagolix – which is taken once per day – would become the first GnRH receptor antagonist with a nonhormonal option to reach the market. The U.S. Food and Drug Administration in November accepted ObsEva’s new drug application for the medication, with a decision expected by September 2022.
“The positive CHMP opinion is an important milestone for millions of women in the EU living with UF to address the diverse medical needs of the women who suffer from this condition,” said Brian O’Callaghan, CEO of ObsEva, in a statement. “We will continue our productive, ongoing dialogue with [the] EMA toward potential marketing authorization in the EU and, in parallel, continue to work with the FDA to advance linzagolix through the U.S. regulatory process.”
The committee’s positive opinion was based on 52-week results from PRIMROSE 1 and PRIMROSE 2 phase 3 trials, involving more than 1,000 patients in the United States and Europe, as well as results from 76-week follow-up studies of patients in those trials. The two phase 3 trials assessed a 200-mg and 100-mg dose of linzagolix, with and without hormone add-back therapy (ABT; 1 mg estradiol and 0.5 mg norethisterone acetate).
According to ObsEVA, both trials met their primary endpoints, with all doses showing statistically significant and clinically relevant reductions in heavy menstrual bleeding (HMB) compared to placebo. The trials also achieved several secondary endpoints, including reduction in pain, rates of amenorrhea, time to reduced HMB, and amenorrhea and for the high dose without ABT, reductions in uterine and fibroid volume, the company said.
A version of this article first appeared on Medscape.com.
The European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) on December 17 recommended approval of linzagolix (Yselty, ObsEva), an oral gonadotropin-releasing hormone (GnRH) antagonist, for the management of moderate to severe symptoms of uterine fibroids (UF) in adult women of reproductive age.
If approved, linzagolix – which is taken once per day – would become the first GnRH receptor antagonist with a nonhormonal option to reach the market. The U.S. Food and Drug Administration in November accepted ObsEva’s new drug application for the medication, with a decision expected by September 2022.
“The positive CHMP opinion is an important milestone for millions of women in the EU living with UF to address the diverse medical needs of the women who suffer from this condition,” said Brian O’Callaghan, CEO of ObsEva, in a statement. “We will continue our productive, ongoing dialogue with [the] EMA toward potential marketing authorization in the EU and, in parallel, continue to work with the FDA to advance linzagolix through the U.S. regulatory process.”
The committee’s positive opinion was based on 52-week results from PRIMROSE 1 and PRIMROSE 2 phase 3 trials, involving more than 1,000 patients in the United States and Europe, as well as results from 76-week follow-up studies of patients in those trials. The two phase 3 trials assessed a 200-mg and 100-mg dose of linzagolix, with and without hormone add-back therapy (ABT; 1 mg estradiol and 0.5 mg norethisterone acetate).
According to ObsEVA, both trials met their primary endpoints, with all doses showing statistically significant and clinically relevant reductions in heavy menstrual bleeding (HMB) compared to placebo. The trials also achieved several secondary endpoints, including reduction in pain, rates of amenorrhea, time to reduced HMB, and amenorrhea and for the high dose without ABT, reductions in uterine and fibroid volume, the company said.
A version of this article first appeared on Medscape.com.