User login
Novel BioFreedom coronary stent looks promising
PARIS – A unique polymer- and carrier-free drug-eluting stent demonstrated a highly desirable early healing profile and a mere 4% target vessel revascularization rate at 9 months of follow-up in a 100-patient study presented at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“This study is a proof of concept of the polymer-free approach. The stent retains neointimal suppression and antiproliferative efficacy like any other drug-eluting stent. If supported by long-term clinical results, this concept could have a major impact on future new stent platform development,” said Dr. Stephen Lee, professor of cardiology at the University of Hong Kong.

The BioFreedom stent was designed to avoid the chronic inflammation caused by the polymers and drug carriers utilized in other drug-eluting stents (DES), which necessitates long-term dual antiplatelet therapy (DAPT). The novel stent is a bare metal stent whose outer surface of stainless steel contains microstructural crevasses harboring a proprietary antirestenosis drug known as Biolimus A9. This is a highly lipophilic agent and hence has a strong affinity for the vessel wall. All of the drug elutes into the arterial tissue within 1 month, at which point the BioFreedom device becomes a bare metal stent – the type of stent that doesn’t require prolonged DAPT, with its attendant increased bleeding risks, Dr. Lee explained.
The 100-patient study, featuring a 100% follow-up rate at 12 months, utilized optical coherence tomography to assess the primary endpoint, which was stent strut coverage through 9 months as an indicator of early healing post intervention. At 1 month post-PCI, 85.8% of all struts were covered, as were 96.8% at 4 months, 97.1% at 5 months, and 99.6% at 9 months.
Neointimal thickness as assessed in a core laboratory increased minimally and slowly, confirming the drug’s antiproliferative effect. Neointimal thickness was 0.04 mm at 1 month, 0.06 mm at 5 months, and 1 mm at 9 months.
“This is the most important message of the study,” according to Dr. Lee. “It confirms the efficacy of the BioFreedom stent as a DES. If it didn’t curb neointimal thickness and just acted like a bare metal stent, there would be no point in using this mechanism.”
In-stent neointimal volume increased from 4.3% at 1 month to 13% at 9 months, which is “still very low” compared to other stent types, he added.
Four of 100 patients experienced asymptomatic in-stent restenosis requiring intervention within the first 9 months. With a mean follow-up duration of 468 days, there have been no additional cases of in-stent restenosis requiring treatment, no cases of late stent thrombosis, and indeed no other major adverse cardiovascular events.
Now well underway is a vastly larger clinical trial designed to confirm that the BioFreedom stent is as safe as a bare metal stent in patients at high risk of bleeding, while at the same time delivering the antirestenosis benefits of a DES. The LEADERS FREE trial is a 2,466-patient, prospective, randomized, double-blind clinical trial employing a 1-month course of DAPT following implantation of the BioFreedom stent or a bare metal stent. Results are anticipated late this year.
Dr. Lee received a research grant from Biosensors International, which sponsored the proof-of-concept study and is funding the LEADERS FREE trial.
PARIS – A unique polymer- and carrier-free drug-eluting stent demonstrated a highly desirable early healing profile and a mere 4% target vessel revascularization rate at 9 months of follow-up in a 100-patient study presented at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“This study is a proof of concept of the polymer-free approach. The stent retains neointimal suppression and antiproliferative efficacy like any other drug-eluting stent. If supported by long-term clinical results, this concept could have a major impact on future new stent platform development,” said Dr. Stephen Lee, professor of cardiology at the University of Hong Kong.
The BioFreedom stent was designed to avoid the chronic inflammation caused by the polymers and drug carriers utilized in other drug-eluting stents (DES), which necessitates long-term dual antiplatelet therapy (DAPT). The novel stent is a bare metal stent whose outer surface of stainless steel contains microstructural crevasses harboring a proprietary antirestenosis drug known as Biolimus A9. This is a highly lipophilic agent and hence has a strong affinity for the vessel wall. All of the drug elutes into the arterial tissue within 1 month, at which point the BioFreedom device becomes a bare metal stent – the type of stent that doesn’t require prolonged DAPT, with its attendant increased bleeding risks, Dr. Lee explained.
The 100-patient study, featuring a 100% follow-up rate at 12 months, utilized optical coherence tomography to assess the primary endpoint, which was stent strut coverage through 9 months as an indicator of early healing post intervention. At 1 month post-PCI, 85.8% of all struts were covered, as were 96.8% at 4 months, 97.1% at 5 months, and 99.6% at 9 months.
Neointimal thickness as assessed in a core laboratory increased minimally and slowly, confirming the drug’s antiproliferative effect. Neointimal thickness was 0.04 mm at 1 month, 0.06 mm at 5 months, and 1 mm at 9 months.
“This is the most important message of the study,” according to Dr. Lee. “It confirms the efficacy of the BioFreedom stent as a DES. If it didn’t curb neointimal thickness and just acted like a bare metal stent, there would be no point in using this mechanism.”
In-stent neointimal volume increased from 4.3% at 1 month to 13% at 9 months, which is “still very low” compared to other stent types, he added.
Four of 100 patients experienced asymptomatic in-stent restenosis requiring intervention within the first 9 months. With a mean follow-up duration of 468 days, there have been no additional cases of in-stent restenosis requiring treatment, no cases of late stent thrombosis, and indeed no other major adverse cardiovascular events.
Now well underway is a vastly larger clinical trial designed to confirm that the BioFreedom stent is as safe as a bare metal stent in patients at high risk of bleeding, while at the same time delivering the antirestenosis benefits of a DES. The LEADERS FREE trial is a 2,466-patient, prospective, randomized, double-blind clinical trial employing a 1-month course of DAPT following implantation of the BioFreedom stent or a bare metal stent. Results are anticipated late this year.
Dr. Lee received a research grant from Biosensors International, which sponsored the proof-of-concept study and is funding the LEADERS FREE trial.
PARIS – A unique polymer- and carrier-free drug-eluting stent demonstrated a highly desirable early healing profile and a mere 4% target vessel revascularization rate at 9 months of follow-up in a 100-patient study presented at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“This study is a proof of concept of the polymer-free approach. The stent retains neointimal suppression and antiproliferative efficacy like any other drug-eluting stent. If supported by long-term clinical results, this concept could have a major impact on future new stent platform development,” said Dr. Stephen Lee, professor of cardiology at the University of Hong Kong.
The BioFreedom stent was designed to avoid the chronic inflammation caused by the polymers and drug carriers utilized in other drug-eluting stents (DES), which necessitates long-term dual antiplatelet therapy (DAPT). The novel stent is a bare metal stent whose outer surface of stainless steel contains microstructural crevasses harboring a proprietary antirestenosis drug known as Biolimus A9. This is a highly lipophilic agent and hence has a strong affinity for the vessel wall. All of the drug elutes into the arterial tissue within 1 month, at which point the BioFreedom device becomes a bare metal stent – the type of stent that doesn’t require prolonged DAPT, with its attendant increased bleeding risks, Dr. Lee explained.
The 100-patient study, featuring a 100% follow-up rate at 12 months, utilized optical coherence tomography to assess the primary endpoint, which was stent strut coverage through 9 months as an indicator of early healing post intervention. At 1 month post-PCI, 85.8% of all struts were covered, as were 96.8% at 4 months, 97.1% at 5 months, and 99.6% at 9 months.
Neointimal thickness as assessed in a core laboratory increased minimally and slowly, confirming the drug’s antiproliferative effect. Neointimal thickness was 0.04 mm at 1 month, 0.06 mm at 5 months, and 1 mm at 9 months.
“This is the most important message of the study,” according to Dr. Lee. “It confirms the efficacy of the BioFreedom stent as a DES. If it didn’t curb neointimal thickness and just acted like a bare metal stent, there would be no point in using this mechanism.”
In-stent neointimal volume increased from 4.3% at 1 month to 13% at 9 months, which is “still very low” compared to other stent types, he added.
Four of 100 patients experienced asymptomatic in-stent restenosis requiring intervention within the first 9 months. With a mean follow-up duration of 468 days, there have been no additional cases of in-stent restenosis requiring treatment, no cases of late stent thrombosis, and indeed no other major adverse cardiovascular events.
Now well underway is a vastly larger clinical trial designed to confirm that the BioFreedom stent is as safe as a bare metal stent in patients at high risk of bleeding, while at the same time delivering the antirestenosis benefits of a DES. The LEADERS FREE trial is a 2,466-patient, prospective, randomized, double-blind clinical trial employing a 1-month course of DAPT following implantation of the BioFreedom stent or a bare metal stent. Results are anticipated late this year.
Dr. Lee received a research grant from Biosensors International, which sponsored the proof-of-concept study and is funding the LEADERS FREE trial.
AT EUROPCR 2015
Key clinical point: A novel coronary stent combines the antirestenotic benefits of a drug-eluting stent with the safety of a bare metal stent.
Major finding: One month after placement of the novel polymer- and carrier-free BioFreedom stainless steel DES, 85.8% of all struts were covered, as were 96.8% of struts at 4 months and 99.6% at 9 months.
Data source: This was a prospective proof-of-concept study in which 100 consecutive patients received the novel BioFreedom stent and underwent serial assessment of strut coverage by optical coherence tomography to document early healing.
Disclosures: The study was sponsored by Biosensors International, which provided the presenter with a research grant.

WCD: Touch Avoidance Is a New Dimension of Psoriatic Impairment
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.

“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.
“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.
“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
AT WCD 2015

WCD: Touch avoidance is a new dimension of psoriatic impairment
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.

“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.
“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
VANCOUVER – Touch impairment is an important but largely unappreciated aspect of quality-of-life impairment in psoriasis, Dr. April Armstrong said at the World Congress of Dermatology.
“Touch avoidance is a new concept in dermatology, and I think it’s great because it really brings home a humanistic aspect to research,” observed Dr. Armstrong, director of the psoriasis program at the University of Colorado, Denver.
“Touch is a fundamental human gesture that conveys understanding, connection, validation, as well as being cared for or caring for someone,” she added.
She presented an online study of 1,109 psoriasis patients, 70% of whom were female. When asked whether within the past 2 weeks they had avoided hugging, shaking hands, or other touching of others, or of being touched, because of how their skin looks or feels, 48% responded yes. On a 0-10 scale, 27% of the overall patient population rated themselves as having touch avoidance at the level of 4-10, corresponding to moderate to severe.
In a multivariate analysis, the prevalence or severity of touch avoidance didn’t vary by gender. However, touch avoidance was reported most often by patients under age 25 years. And touch avoidance was strongly associated with disease severity: Those with mild psoriasis as defined by body surface area of involvement were only about one-third as likely to report touch avoidance, compared with those with severe disease. Also, psoriatic itching was an important correlate of touch avoidance: Those with itch were roughly fivefold more likely to report recent touch avoidance.
In addition, patients with psoriasis on exposed areas such as the face and neck or in sensitive areas such as the genitalia were more likely to report touch avoidance.
Touch avoidance had a strong negative impact on quality of life. Scores on the Dermatology Life Quality Index averaged nearly threefold higher – indicating worse quality of life – in participants who reported touch avoidance. They were at similarly increased risk for mild or greater depressive symptoms based upon their scores on the Quick Inventory of Depressive Symptoms.
Thus, touch avoidance is an important new patient-reported outcome, and these study results open up a new area of psoriasis research, according to Dr. Armstrong.
“Future research may reveal that therapies offering clearance of psoriasis, particularly in sensitive areas, could lead to large improvements in the initiation and acceptance of interpersonal touch by patients with psoriasis,” she noted.
This study was supported by the National Psoriasis Foundation. Dr. Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.
AT WCD 2015
Key clinical point: Touch avoidance among psoriasis patients is an important new patient-reported outcome having a major negative quality-of-life impact.
Major finding: A total of 48 of a large group of psoriasis patients reported having avoided touching others, or having others touching them, within the prior 2 weeks because of how their skin looks or feels.
Data source: This was an online survey of 1,109 psoriasis patients.
Disclosures: The study was supported by the National Psoriasis Foundation. Dr. April Armstrong reported receiving research grants from and/or serving as a consultant to more than half a dozen pharmaceutical companies as well as the National Institutes of Health.

Double chin therapy scores high in patient satisfaction
VANCOUVER – Patients who underwent injections of ATX-101 (Kybella) for treatment of an unsightly double chin reported a high degree of satisfaction with the results, according to a pooled analysis of four large, double-blind, placebo-controlled, phase III trials.
Two of the trials were conducted in North America, two were conducted in Europe. The patient-reported outcomes were consistently favorable across this wide geographic and cultural range, Dr. Nowell Solish reported at the World Congress of Dermatology.
ATX-101 is a proprietary formulation of nonhuman, nonanimal deoxycholic acid. Injected directly into the excess submental fat also known as a double chin, it causes lysis of adipocytes. Earlier this year the product became the first Food and Drug Administration–approved nonsurgical treatment for double chins.
Although physician-scored ratings of improvement played a key role in obtaining regulatory approval, Dr. Solish, a dermatologist at the University of Toronto, focused on the patient-reported outcomes, which are particularly germane given that this is an aesthetic treatment.
The pooled analysis was restricted to 315 placebo-treated controls and 413 participants who received the FDA-approved dosing regimen, in which a single treatment consists of up to 50 injections of 0.2 mL each, placed 1 cm apart, which translates to 2 mg/cm2. The pooled analysis included patients who had up to four treatment sessions placed at least 1 month apart. All subjects had to have moderate to severe excess submental fat and dissatisfaction with the appearance of their face and chin.
A variety of outcome measures collectively painted a picture of improved patient satisfaction with face and chin appearance, significant psychological improvement, and satisfaction with the therapy itself.
For example, on the Subject Self-Rating Scale, which assesses satisfaction with face and chin appearance, 70% of North American and 72% of European ATX-101–treated patients were classified as satisfied as defined by a score of 4 or more on the 0-6 scale 12 weeks after the final treatment. This was the case for only 27% of North American and 32% of European placebo-treated controls.
On the 0-10 Patient-Response Submental Fat Impact Scale, which assesses the psychological impact of the visual appearance of the chin as well as emotional self-perception, average scores in the active treatment arms improved by 3-4 points from a baseline of 7, compared with 1- to 2-point improvements in the control groups.
Roughly 80% of patients who received the chin-fat buster in the double-blind studies declared themselves to be “a little,” “moderately,” or “extremely” satisfied with the posttreatment definition between their chin and neck as well as with the treatment itself, as did 25%-45% of controls.
Pain, burning, swelling, and/or numbness occurred in 60%-84% of ATX-101–treated patients. These adverse events were mostly mild in intensity and short lived.
The pooled analysis was sponsored by Kythera Biopharmaceuticals, which markets ATX-101 as Kybella. Dr. Solish reported serving as a consultant to Allergan, which in June announced a definitive agreement to acquire Kythera.
VANCOUVER – Patients who underwent injections of ATX-101 (Kybella) for treatment of an unsightly double chin reported a high degree of satisfaction with the results, according to a pooled analysis of four large, double-blind, placebo-controlled, phase III trials.
Two of the trials were conducted in North America, two were conducted in Europe. The patient-reported outcomes were consistently favorable across this wide geographic and cultural range, Dr. Nowell Solish reported at the World Congress of Dermatology.
ATX-101 is a proprietary formulation of nonhuman, nonanimal deoxycholic acid. Injected directly into the excess submental fat also known as a double chin, it causes lysis of adipocytes. Earlier this year the product became the first Food and Drug Administration–approved nonsurgical treatment for double chins.
Although physician-scored ratings of improvement played a key role in obtaining regulatory approval, Dr. Solish, a dermatologist at the University of Toronto, focused on the patient-reported outcomes, which are particularly germane given that this is an aesthetic treatment.
The pooled analysis was restricted to 315 placebo-treated controls and 413 participants who received the FDA-approved dosing regimen, in which a single treatment consists of up to 50 injections of 0.2 mL each, placed 1 cm apart, which translates to 2 mg/cm2. The pooled analysis included patients who had up to four treatment sessions placed at least 1 month apart. All subjects had to have moderate to severe excess submental fat and dissatisfaction with the appearance of their face and chin.
A variety of outcome measures collectively painted a picture of improved patient satisfaction with face and chin appearance, significant psychological improvement, and satisfaction with the therapy itself.
For example, on the Subject Self-Rating Scale, which assesses satisfaction with face and chin appearance, 70% of North American and 72% of European ATX-101–treated patients were classified as satisfied as defined by a score of 4 or more on the 0-6 scale 12 weeks after the final treatment. This was the case for only 27% of North American and 32% of European placebo-treated controls.
On the 0-10 Patient-Response Submental Fat Impact Scale, which assesses the psychological impact of the visual appearance of the chin as well as emotional self-perception, average scores in the active treatment arms improved by 3-4 points from a baseline of 7, compared with 1- to 2-point improvements in the control groups.
Roughly 80% of patients who received the chin-fat buster in the double-blind studies declared themselves to be “a little,” “moderately,” or “extremely” satisfied with the posttreatment definition between their chin and neck as well as with the treatment itself, as did 25%-45% of controls.
Pain, burning, swelling, and/or numbness occurred in 60%-84% of ATX-101–treated patients. These adverse events were mostly mild in intensity and short lived.
The pooled analysis was sponsored by Kythera Biopharmaceuticals, which markets ATX-101 as Kybella. Dr. Solish reported serving as a consultant to Allergan, which in June announced a definitive agreement to acquire Kythera.
VANCOUVER – Patients who underwent injections of ATX-101 (Kybella) for treatment of an unsightly double chin reported a high degree of satisfaction with the results, according to a pooled analysis of four large, double-blind, placebo-controlled, phase III trials.
Two of the trials were conducted in North America, two were conducted in Europe. The patient-reported outcomes were consistently favorable across this wide geographic and cultural range, Dr. Nowell Solish reported at the World Congress of Dermatology.
ATX-101 is a proprietary formulation of nonhuman, nonanimal deoxycholic acid. Injected directly into the excess submental fat also known as a double chin, it causes lysis of adipocytes. Earlier this year the product became the first Food and Drug Administration–approved nonsurgical treatment for double chins.
Although physician-scored ratings of improvement played a key role in obtaining regulatory approval, Dr. Solish, a dermatologist at the University of Toronto, focused on the patient-reported outcomes, which are particularly germane given that this is an aesthetic treatment.
The pooled analysis was restricted to 315 placebo-treated controls and 413 participants who received the FDA-approved dosing regimen, in which a single treatment consists of up to 50 injections of 0.2 mL each, placed 1 cm apart, which translates to 2 mg/cm2. The pooled analysis included patients who had up to four treatment sessions placed at least 1 month apart. All subjects had to have moderate to severe excess submental fat and dissatisfaction with the appearance of their face and chin.
A variety of outcome measures collectively painted a picture of improved patient satisfaction with face and chin appearance, significant psychological improvement, and satisfaction with the therapy itself.
For example, on the Subject Self-Rating Scale, which assesses satisfaction with face and chin appearance, 70% of North American and 72% of European ATX-101–treated patients were classified as satisfied as defined by a score of 4 or more on the 0-6 scale 12 weeks after the final treatment. This was the case for only 27% of North American and 32% of European placebo-treated controls.
On the 0-10 Patient-Response Submental Fat Impact Scale, which assesses the psychological impact of the visual appearance of the chin as well as emotional self-perception, average scores in the active treatment arms improved by 3-4 points from a baseline of 7, compared with 1- to 2-point improvements in the control groups.
Roughly 80% of patients who received the chin-fat buster in the double-blind studies declared themselves to be “a little,” “moderately,” or “extremely” satisfied with the posttreatment definition between their chin and neck as well as with the treatment itself, as did 25%-45% of controls.
Pain, burning, swelling, and/or numbness occurred in 60%-84% of ATX-101–treated patients. These adverse events were mostly mild in intensity and short lived.
The pooled analysis was sponsored by Kythera Biopharmaceuticals, which markets ATX-101 as Kybella. Dr. Solish reported serving as a consultant to Allergan, which in June announced a definitive agreement to acquire Kythera.
AT WCD 2015
Key clinical point: ATX-101, the first FDA-approved nonsurgical treatment for double chins, is a hit with patients who’ve undergone the injections in double-blind trials.
Major finding: A total of 70% of North American and 72% of European patients declared satisfaction with their face and chin appearance following a course of injections of the fat-busting agent ATX-101, compared with 30% of placebo-treated controls.
Data source: This was a pooled analysis of patient-reported outcomes in four large, double-blind, placebo-controlled randomized phase III trials conducted in North America and Europe.
Disclosures: The pooled analysis was funded by Kythera Biopharmaceuticals. Dr. Nowell Solish reported serving as a consultant to Allergan, which in June announced a definitive agreement to acquire Kythera.
In PCI, switching clopidogrel nonresponders to prasugrel halved 2-year cardiac mortality
PARIS – Clopidogrel nonresponsiveness is a modifiable cardiovascular risk factor in patients undergoing percutaneous coronary intervention, according to the results of the third Responsiveness to Clopidogrel and Stent-Related Events (RECLOSE-3) study.
High residual platelet activity following a loading dose of clopidogrel in patients undergoing PCI was shown in the earlier RECLOSE-2 study to be a potent predictor of an increased 2-year cardiovascular event rate (JAMA 2011;306:1215-23). This left open the question of whether switching to a different antiplatelet drug would reduce that elevated 2-year risk.

The new RECLOSE-3 study shows that this clopidogrel nonresponsiveness is indeed a modifiable risk factor. All that’s necessary is to identify affected patients via a commercially available in vitro assay, switch them to prasugrel, and their long-term cardiac outcomes become markedly better than if they stayed on clopidogrel, Dr. David Antoniucci reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The prospective RECLOSE-3 study included 302 consecutive patients undergoing PCI who were determined to be clopidogrel nonresponders based upon residual platelet activity of 70% or more as measured by light transmittance aggregometry. All were switched to prasugrel and underwent repeat platelet activity measurement. The control group consisted of 248 clopidogrel nonresponders who stayed on the antiplatelet agent in RECLOSE-2.
It was necessary to rely on historical controls for ethical reasons; based upon the RECLOSE-2 results, it’s no longer appropriate to randomize clopidogrel nonresponders to continued use of clopidogrel, according to Dr. Antoniucci, head of the division of cardiology at Careggi Hospital in Florence, Italy.
Mean residual platelet reactivity improved from 78% in RECLOSE-3 participants on clopidogrel to 47% on prasugrel. All but 6% of clopidogrel nonresponders demonstrated acceptable suppression of platelet activity on prasugrel.
The primary study endpoint was 2-year cardiac mortality. With a follow-up rate of 99%, the rate was 4% in clopidogrel nonresponders switched to prasugrel, significantly better than the 9.7% in controls. Moreover, the rate of definite stent thrombosis – a key secondary endpoint – was 0.7% in the group switched to prasugrel, fourfold lower than in controls. Probable stent thrombosis was diagnosed in 1.6% of controls and none of the prasugrel group.
All patients in the control group from RECLOSE-2 had been admitted with an acute coronary syndrome. Restricting the analysis to the 126 RECLOSE-3 participants switched to prasugrel who had an acute coronary syndrome upon hospitalization, the 2-year cardiac death rate was 3.2%, still significantly lower than the 9.7% in controls.
In a multivariate analysis that controlled for potential confounders – including the more frequent use of drug-eluting stents and lower prevalence of a left ventricular ejection fraction of 40% or less in the RECLOSE-3 patients – switching clopidogrel nonresponders to prasugrel was associated with a highly significant 50% reduction in the risk of cardiac death at 2 years’ follow-up. The only other significant predictors were a baseline serum creatinine greater than 1.5 mg/dL and advanced age, both of which were associated with increased risk.
The RECLOSE-3 study was sponsored by the Italian Department of Health. Dr. Antoniucci reported having no financial conflicts.
bjancin@frontlinemedcom.com
PARIS – Clopidogrel nonresponsiveness is a modifiable cardiovascular risk factor in patients undergoing percutaneous coronary intervention, according to the results of the third Responsiveness to Clopidogrel and Stent-Related Events (RECLOSE-3) study.
High residual platelet activity following a loading dose of clopidogrel in patients undergoing PCI was shown in the earlier RECLOSE-2 study to be a potent predictor of an increased 2-year cardiovascular event rate (JAMA 2011;306:1215-23). This left open the question of whether switching to a different antiplatelet drug would reduce that elevated 2-year risk.
The new RECLOSE-3 study shows that this clopidogrel nonresponsiveness is indeed a modifiable risk factor. All that’s necessary is to identify affected patients via a commercially available in vitro assay, switch them to prasugrel, and their long-term cardiac outcomes become markedly better than if they stayed on clopidogrel, Dr. David Antoniucci reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The prospective RECLOSE-3 study included 302 consecutive patients undergoing PCI who were determined to be clopidogrel nonresponders based upon residual platelet activity of 70% or more as measured by light transmittance aggregometry. All were switched to prasugrel and underwent repeat platelet activity measurement. The control group consisted of 248 clopidogrel nonresponders who stayed on the antiplatelet agent in RECLOSE-2.
It was necessary to rely on historical controls for ethical reasons; based upon the RECLOSE-2 results, it’s no longer appropriate to randomize clopidogrel nonresponders to continued use of clopidogrel, according to Dr. Antoniucci, head of the division of cardiology at Careggi Hospital in Florence, Italy.
Mean residual platelet reactivity improved from 78% in RECLOSE-3 participants on clopidogrel to 47% on prasugrel. All but 6% of clopidogrel nonresponders demonstrated acceptable suppression of platelet activity on prasugrel.
The primary study endpoint was 2-year cardiac mortality. With a follow-up rate of 99%, the rate was 4% in clopidogrel nonresponders switched to prasugrel, significantly better than the 9.7% in controls. Moreover, the rate of definite stent thrombosis – a key secondary endpoint – was 0.7% in the group switched to prasugrel, fourfold lower than in controls. Probable stent thrombosis was diagnosed in 1.6% of controls and none of the prasugrel group.
All patients in the control group from RECLOSE-2 had been admitted with an acute coronary syndrome. Restricting the analysis to the 126 RECLOSE-3 participants switched to prasugrel who had an acute coronary syndrome upon hospitalization, the 2-year cardiac death rate was 3.2%, still significantly lower than the 9.7% in controls.
In a multivariate analysis that controlled for potential confounders – including the more frequent use of drug-eluting stents and lower prevalence of a left ventricular ejection fraction of 40% or less in the RECLOSE-3 patients – switching clopidogrel nonresponders to prasugrel was associated with a highly significant 50% reduction in the risk of cardiac death at 2 years’ follow-up. The only other significant predictors were a baseline serum creatinine greater than 1.5 mg/dL and advanced age, both of which were associated with increased risk.
The RECLOSE-3 study was sponsored by the Italian Department of Health. Dr. Antoniucci reported having no financial conflicts.
bjancin@frontlinemedcom.com
PARIS – Clopidogrel nonresponsiveness is a modifiable cardiovascular risk factor in patients undergoing percutaneous coronary intervention, according to the results of the third Responsiveness to Clopidogrel and Stent-Related Events (RECLOSE-3) study.
High residual platelet activity following a loading dose of clopidogrel in patients undergoing PCI was shown in the earlier RECLOSE-2 study to be a potent predictor of an increased 2-year cardiovascular event rate (JAMA 2011;306:1215-23). This left open the question of whether switching to a different antiplatelet drug would reduce that elevated 2-year risk.
The new RECLOSE-3 study shows that this clopidogrel nonresponsiveness is indeed a modifiable risk factor. All that’s necessary is to identify affected patients via a commercially available in vitro assay, switch them to prasugrel, and their long-term cardiac outcomes become markedly better than if they stayed on clopidogrel, Dr. David Antoniucci reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The prospective RECLOSE-3 study included 302 consecutive patients undergoing PCI who were determined to be clopidogrel nonresponders based upon residual platelet activity of 70% or more as measured by light transmittance aggregometry. All were switched to prasugrel and underwent repeat platelet activity measurement. The control group consisted of 248 clopidogrel nonresponders who stayed on the antiplatelet agent in RECLOSE-2.
It was necessary to rely on historical controls for ethical reasons; based upon the RECLOSE-2 results, it’s no longer appropriate to randomize clopidogrel nonresponders to continued use of clopidogrel, according to Dr. Antoniucci, head of the division of cardiology at Careggi Hospital in Florence, Italy.
Mean residual platelet reactivity improved from 78% in RECLOSE-3 participants on clopidogrel to 47% on prasugrel. All but 6% of clopidogrel nonresponders demonstrated acceptable suppression of platelet activity on prasugrel.
The primary study endpoint was 2-year cardiac mortality. With a follow-up rate of 99%, the rate was 4% in clopidogrel nonresponders switched to prasugrel, significantly better than the 9.7% in controls. Moreover, the rate of definite stent thrombosis – a key secondary endpoint – was 0.7% in the group switched to prasugrel, fourfold lower than in controls. Probable stent thrombosis was diagnosed in 1.6% of controls and none of the prasugrel group.
All patients in the control group from RECLOSE-2 had been admitted with an acute coronary syndrome. Restricting the analysis to the 126 RECLOSE-3 participants switched to prasugrel who had an acute coronary syndrome upon hospitalization, the 2-year cardiac death rate was 3.2%, still significantly lower than the 9.7% in controls.
In a multivariate analysis that controlled for potential confounders – including the more frequent use of drug-eluting stents and lower prevalence of a left ventricular ejection fraction of 40% or less in the RECLOSE-3 patients – switching clopidogrel nonresponders to prasugrel was associated with a highly significant 50% reduction in the risk of cardiac death at 2 years’ follow-up. The only other significant predictors were a baseline serum creatinine greater than 1.5 mg/dL and advanced age, both of which were associated with increased risk.
The RECLOSE-3 study was sponsored by the Italian Department of Health. Dr. Antoniucci reported having no financial conflicts.
bjancin@frontlinemedcom.com
AT EuroPCR 2015
Key clinical point: Switch clopidogrel nonresponders undergoing PCI to prasugrel in order to cut their 2-year cardiac mortality risk in half.
Major finding: Patients undergoing PCI who switch to prasugrel because they show high residual platelet activity after a loading dose of clopidogrel have a 2-year cardiac mortality half that of clopidogrel nonresponders who remain on the drug.
Data source: RECLOSE-3, a prospective study of 302 patients undergoing PCI who were switched to prasugrel upon being identified as clopidogrel nonresponders and a historical control group of 248 clopidogrel nonresponders who remained on the antiplatelet agent.
Disclosures: RECLOSE-3 was funded by the Italian Department of Health. The presenter reported having no financial conflicts.

Intranasal evaporative cooling quickly quelled migraine
VALENCIA, SPAIN – The day may be coming when physicians simply advise their patients experiencing migraine onset to “just chill.”
Literally.
A few minutes of intranasal evaporative cooling brought rapid improvement in headache pain and other migraine-associated symptoms, sustained for 24 hours, in 87% of patients in a small proof-of-concept study, Dr. Jitka Vanderpol reported at the International Headache Congress.
The novel migraine therapy, which also shows potential for treatment of cluster headaches, utilizes the same proprietary therapeutic hypothermia technology approved by European regulators as a method to increase neurologically intact survival after cardiac arrest. The RhinoChill technology, marketed by BeneChill International, utilizes an intranasal cooling catheter to deliver cooling. And it’s portable: The system weighs less than 5 kg, making it suitable for prehospital therapeutic cooling by first responders in cases of cardiac arrest.
While the current device is being used in the ongoing migraine studies, it’s bulkier and more powerful than necessary for this purpose, which doesn’t necessitate lowering core temperature. The company is developing a much smaller, more portable version specifically for treatment of headaches, explained Dr. Vanderpol, a neurologist at Cumbria Partnership National Health Service Foundation Trust in Penrith, England.
The proof-of-concept study involved 20 cryotherapy sessions in 15 patients. Participants were hospitalized for treatment so Dr. Vanderpol and coinvestigators could monitor its safety. The two efficacy endpoints were change from admission through 24 hours in headache pain scores on a 0-10 scale, and change in migraine-associated symptom severity, also self-rated on a 0-10 scale.
* Headache pain: From a mean baseline score of 5.96 at admission, scores improved significantly at every evaluation point: 4.28 after 5 minutes of intranasal cooling; 3.79 after 15 minutes of cooling, at which point treatment stopped; 3.12 immediately after treatment halted; 2.42 at 2 hours post-treatment; and 1.97 at 24 hours post-treatment.
* Migraine-associated symptom severity: From a mean score of 4.25 at baseline, scores dropped to 1.9 immediately after treatment, 0.9 at 2 hours, and 0.7 at 24 hours post-treatment.
Two hours post-treatment, 9 of 20 treatments had resulted in dual zero scores – that is, complete freedom both from headache pain and other migraine-associated symptoms. Another 9 of the 20 treatment applications provided partial improvement on both measures.
When patients were asked how intranasal cooling compared with their current rescue medications, 9 of the 15 rated intranasal cooling as superior, and 4 deemed it equal. There were no side effects in the study.
The cooling of the nasal passages and their associated blood vessels is achieved using medicinal air at a temperature of 2 degrees Celsius. Tympanic temperature didn’t change.
“We were not cooling the head, brain, or patient’s body,” Dr. Vanderpol said at the meeting sponsored by the International Headache Society and the American Headache Society.
In an interview, she cited several possible mechanisms of benefit.
One draws upon the neurovascular theory of migraine: Because of the configuration of vascular anatomy, cooled venous blood from the nasal and paranasal mucous membranes can flow to the dura matter. There is also some preliminary evidence to suggest cooling can affect certain calcitonin gene-related peptide receptors. In addition, cooling tissue results in reduced demand for adenosine triphosphate and oxygen.
The sphenopalatine ganglion is another possible site of action, although this would be more relevant for the treatment of cluster headaches, the neurologist added.
In an ongoing clinical trial, patients received instruction in use of the RhinoChill cooling device and were sent home with a loaner for self treatment. A large, definitive, randomized, controlled trial to confirm the therapeutic benefits and safety will be conducted once the mini-cooling system is available.
The pilot study received partial support from Benechill International in the form of loaner equipment and funding for a research nurse. Dr. Vanderpol reported having no financial conflicts.
bjancin@frontlinemedcom
VALENCIA, SPAIN – The day may be coming when physicians simply advise their patients experiencing migraine onset to “just chill.”
Literally.
A few minutes of intranasal evaporative cooling brought rapid improvement in headache pain and other migraine-associated symptoms, sustained for 24 hours, in 87% of patients in a small proof-of-concept study, Dr. Jitka Vanderpol reported at the International Headache Congress.
The novel migraine therapy, which also shows potential for treatment of cluster headaches, utilizes the same proprietary therapeutic hypothermia technology approved by European regulators as a method to increase neurologically intact survival after cardiac arrest. The RhinoChill technology, marketed by BeneChill International, utilizes an intranasal cooling catheter to deliver cooling. And it’s portable: The system weighs less than 5 kg, making it suitable for prehospital therapeutic cooling by first responders in cases of cardiac arrest.
While the current device is being used in the ongoing migraine studies, it’s bulkier and more powerful than necessary for this purpose, which doesn’t necessitate lowering core temperature. The company is developing a much smaller, more portable version specifically for treatment of headaches, explained Dr. Vanderpol, a neurologist at Cumbria Partnership National Health Service Foundation Trust in Penrith, England.
The proof-of-concept study involved 20 cryotherapy sessions in 15 patients. Participants were hospitalized for treatment so Dr. Vanderpol and coinvestigators could monitor its safety. The two efficacy endpoints were change from admission through 24 hours in headache pain scores on a 0-10 scale, and change in migraine-associated symptom severity, also self-rated on a 0-10 scale.
* Headache pain: From a mean baseline score of 5.96 at admission, scores improved significantly at every evaluation point: 4.28 after 5 minutes of intranasal cooling; 3.79 after 15 minutes of cooling, at which point treatment stopped; 3.12 immediately after treatment halted; 2.42 at 2 hours post-treatment; and 1.97 at 24 hours post-treatment.
* Migraine-associated symptom severity: From a mean score of 4.25 at baseline, scores dropped to 1.9 immediately after treatment, 0.9 at 2 hours, and 0.7 at 24 hours post-treatment.
Two hours post-treatment, 9 of 20 treatments had resulted in dual zero scores – that is, complete freedom both from headache pain and other migraine-associated symptoms. Another 9 of the 20 treatment applications provided partial improvement on both measures.
When patients were asked how intranasal cooling compared with their current rescue medications, 9 of the 15 rated intranasal cooling as superior, and 4 deemed it equal. There were no side effects in the study.
The cooling of the nasal passages and their associated blood vessels is achieved using medicinal air at a temperature of 2 degrees Celsius. Tympanic temperature didn’t change.
“We were not cooling the head, brain, or patient’s body,” Dr. Vanderpol said at the meeting sponsored by the International Headache Society and the American Headache Society.
In an interview, she cited several possible mechanisms of benefit.
One draws upon the neurovascular theory of migraine: Because of the configuration of vascular anatomy, cooled venous blood from the nasal and paranasal mucous membranes can flow to the dura matter. There is also some preliminary evidence to suggest cooling can affect certain calcitonin gene-related peptide receptors. In addition, cooling tissue results in reduced demand for adenosine triphosphate and oxygen.
The sphenopalatine ganglion is another possible site of action, although this would be more relevant for the treatment of cluster headaches, the neurologist added.
In an ongoing clinical trial, patients received instruction in use of the RhinoChill cooling device and were sent home with a loaner for self treatment. A large, definitive, randomized, controlled trial to confirm the therapeutic benefits and safety will be conducted once the mini-cooling system is available.
The pilot study received partial support from Benechill International in the form of loaner equipment and funding for a research nurse. Dr. Vanderpol reported having no financial conflicts.
bjancin@frontlinemedcom
VALENCIA, SPAIN – The day may be coming when physicians simply advise their patients experiencing migraine onset to “just chill.”
Literally.
A few minutes of intranasal evaporative cooling brought rapid improvement in headache pain and other migraine-associated symptoms, sustained for 24 hours, in 87% of patients in a small proof-of-concept study, Dr. Jitka Vanderpol reported at the International Headache Congress.
The novel migraine therapy, which also shows potential for treatment of cluster headaches, utilizes the same proprietary therapeutic hypothermia technology approved by European regulators as a method to increase neurologically intact survival after cardiac arrest. The RhinoChill technology, marketed by BeneChill International, utilizes an intranasal cooling catheter to deliver cooling. And it’s portable: The system weighs less than 5 kg, making it suitable for prehospital therapeutic cooling by first responders in cases of cardiac arrest.
While the current device is being used in the ongoing migraine studies, it’s bulkier and more powerful than necessary for this purpose, which doesn’t necessitate lowering core temperature. The company is developing a much smaller, more portable version specifically for treatment of headaches, explained Dr. Vanderpol, a neurologist at Cumbria Partnership National Health Service Foundation Trust in Penrith, England.
The proof-of-concept study involved 20 cryotherapy sessions in 15 patients. Participants were hospitalized for treatment so Dr. Vanderpol and coinvestigators could monitor its safety. The two efficacy endpoints were change from admission through 24 hours in headache pain scores on a 0-10 scale, and change in migraine-associated symptom severity, also self-rated on a 0-10 scale.
* Headache pain: From a mean baseline score of 5.96 at admission, scores improved significantly at every evaluation point: 4.28 after 5 minutes of intranasal cooling; 3.79 after 15 minutes of cooling, at which point treatment stopped; 3.12 immediately after treatment halted; 2.42 at 2 hours post-treatment; and 1.97 at 24 hours post-treatment.
* Migraine-associated symptom severity: From a mean score of 4.25 at baseline, scores dropped to 1.9 immediately after treatment, 0.9 at 2 hours, and 0.7 at 24 hours post-treatment.
Two hours post-treatment, 9 of 20 treatments had resulted in dual zero scores – that is, complete freedom both from headache pain and other migraine-associated symptoms. Another 9 of the 20 treatment applications provided partial improvement on both measures.
When patients were asked how intranasal cooling compared with their current rescue medications, 9 of the 15 rated intranasal cooling as superior, and 4 deemed it equal. There were no side effects in the study.
The cooling of the nasal passages and their associated blood vessels is achieved using medicinal air at a temperature of 2 degrees Celsius. Tympanic temperature didn’t change.
“We were not cooling the head, brain, or patient’s body,” Dr. Vanderpol said at the meeting sponsored by the International Headache Society and the American Headache Society.
In an interview, she cited several possible mechanisms of benefit.
One draws upon the neurovascular theory of migraine: Because of the configuration of vascular anatomy, cooled venous blood from the nasal and paranasal mucous membranes can flow to the dura matter. There is also some preliminary evidence to suggest cooling can affect certain calcitonin gene-related peptide receptors. In addition, cooling tissue results in reduced demand for adenosine triphosphate and oxygen.
The sphenopalatine ganglion is another possible site of action, although this would be more relevant for the treatment of cluster headaches, the neurologist added.
In an ongoing clinical trial, patients received instruction in use of the RhinoChill cooling device and were sent home with a loaner for self treatment. A large, definitive, randomized, controlled trial to confirm the therapeutic benefits and safety will be conducted once the mini-cooling system is available.
The pilot study received partial support from Benechill International in the form of loaner equipment and funding for a research nurse. Dr. Vanderpol reported having no financial conflicts.
bjancin@frontlinemedcom
AT IHC 2015
Key clinical point: A few minutes of concentrated intranasal hypothermia shows promise as rescue therapy for migraine attacks.
Major finding: After 5 minutes of intranasal evaporative cooling, mean scores on measures of headache pain and migraine-associated symptoms decreased significantly, and they dropped further continuously through 24 hours.
Data source: This was a prospective, single-arm, proof-of-concept study involving 15 migraine patients who collectively received 20 intranasal cooling treatments.
Disclosures: The presenter reported having no financial conflicts regarding the study.
WCD: How to submit a proper nail specimen
VANCOUVER – Dr. Curtis T. Thompson is on a mission: to improve the often-shoddy quality of nail biopsy specimens submitted to pathologists.
No standardized protocols for nail specimens exist. The quality of pathologic diagnosis often suffers as a result, Dr. Thompson said at the World Congress of Dermatology.
“What often happens is the nail specimens get put into a bottle of formaldehyde, they float around and get torn up, and then when they come to the lab, we have no idea what’s proximal and dorsal. This is an issue. We’re all used to just putting a nail specimen in a bottle and sending it away, so all the grossing happens in the laboratory. What I submit to you is you need to be more involved in the grossing side so the specimen can be properly processed,” said Dr. Thompson, a dermatopathologist in group practice in Tigard, Ore.
He added that clear and concise guidelines for standardized specimen submission are needed, and he offered several specific suggestions regarding the orientation of the tissue and securing it for transport.
“Careful submission of tissue specimens is of great importance and allows for better diagnostics,” Dr. Thompson stressed. “There’s really nothing more terrifying than to be told you’re being sent a pigmented lesion and then not being able to find anything at all in the specimen. You really worry that it’s ended up in the trash can through leveling. This is why dermatopathologists don’t want to read nail biopsies very much.”
When a nail specimen is submitted properly, such mix-ups become “almost impossible,” according to the dermatopathologist.
Dr. Thompson borrowed one of his key ideas on efficient handling of nail specimens from opthalmologic pathology. Ophthalmologists routinely send delicate tissue segments and margins from the operating room, and they do so with consistent success because they place the segments on a cartoon of the eye so the pathologist can see exactly where the tissue was located on the patient.
Dermatologists and surgeons can do the same after printing out a sheaf of nail diagrams gratis at the Website for Dr. Thompson’s dermatopathology practice.
The rest of the necessary equipment is similarly simple and readily obtainable from any pathology laboratory, which routinely purchases small plastic cassettes by the tens of thousands for handling of tissue specimens.
“You don’t need to go out and buy them; just ask the lab you work with to send over 10 or so,” Dr. Thompson advised.
The cassette comes with a small fitted sponge to be placed over the tissue to keep it securely in place on the nail diagram rather than floating off. Ink one end of the specimen using the wooden end of a cotton-tip applicator so the lab knows which end is proximal and which is distal. The wooden tip provides more precise inking than the cotton-tip end. Then place the closed cassette in a larger bottle of formaldehyde for shipping.
One more thing: Separate the nail plate from the nail bed or matrix whenever possible, and place them in separate cassettes. Lab technicians typically devote a lot of attention to trying to get the nail plate to stick to a slide, but the diagnostic material is usually present in the nail bed or matrix, and keeping those soft tissues separate makes it less likely they’ll get lost in the shuffle.
“I recommend putting the nail plate cassette and the lesional tissue in the same bottle because then you don’t have two specimens with double the charge for the patient,” Dr. Thompson said.
He reported having no relevant financial conflicts.
VANCOUVER – Dr. Curtis T. Thompson is on a mission: to improve the often-shoddy quality of nail biopsy specimens submitted to pathologists.
No standardized protocols for nail specimens exist. The quality of pathologic diagnosis often suffers as a result, Dr. Thompson said at the World Congress of Dermatology.
“What often happens is the nail specimens get put into a bottle of formaldehyde, they float around and get torn up, and then when they come to the lab, we have no idea what’s proximal and dorsal. This is an issue. We’re all used to just putting a nail specimen in a bottle and sending it away, so all the grossing happens in the laboratory. What I submit to you is you need to be more involved in the grossing side so the specimen can be properly processed,” said Dr. Thompson, a dermatopathologist in group practice in Tigard, Ore.
He added that clear and concise guidelines for standardized specimen submission are needed, and he offered several specific suggestions regarding the orientation of the tissue and securing it for transport.
“Careful submission of tissue specimens is of great importance and allows for better diagnostics,” Dr. Thompson stressed. “There’s really nothing more terrifying than to be told you’re being sent a pigmented lesion and then not being able to find anything at all in the specimen. You really worry that it’s ended up in the trash can through leveling. This is why dermatopathologists don’t want to read nail biopsies very much.”
When a nail specimen is submitted properly, such mix-ups become “almost impossible,” according to the dermatopathologist.
Dr. Thompson borrowed one of his key ideas on efficient handling of nail specimens from opthalmologic pathology. Ophthalmologists routinely send delicate tissue segments and margins from the operating room, and they do so with consistent success because they place the segments on a cartoon of the eye so the pathologist can see exactly where the tissue was located on the patient.
Dermatologists and surgeons can do the same after printing out a sheaf of nail diagrams gratis at the Website for Dr. Thompson’s dermatopathology practice.
The rest of the necessary equipment is similarly simple and readily obtainable from any pathology laboratory, which routinely purchases small plastic cassettes by the tens of thousands for handling of tissue specimens.
“You don’t need to go out and buy them; just ask the lab you work with to send over 10 or so,” Dr. Thompson advised.
The cassette comes with a small fitted sponge to be placed over the tissue to keep it securely in place on the nail diagram rather than floating off. Ink one end of the specimen using the wooden end of a cotton-tip applicator so the lab knows which end is proximal and which is distal. The wooden tip provides more precise inking than the cotton-tip end. Then place the closed cassette in a larger bottle of formaldehyde for shipping.
One more thing: Separate the nail plate from the nail bed or matrix whenever possible, and place them in separate cassettes. Lab technicians typically devote a lot of attention to trying to get the nail plate to stick to a slide, but the diagnostic material is usually present in the nail bed or matrix, and keeping those soft tissues separate makes it less likely they’ll get lost in the shuffle.
“I recommend putting the nail plate cassette and the lesional tissue in the same bottle because then you don’t have two specimens with double the charge for the patient,” Dr. Thompson said.
He reported having no relevant financial conflicts.
VANCOUVER – Dr. Curtis T. Thompson is on a mission: to improve the often-shoddy quality of nail biopsy specimens submitted to pathologists.
No standardized protocols for nail specimens exist. The quality of pathologic diagnosis often suffers as a result, Dr. Thompson said at the World Congress of Dermatology.
“What often happens is the nail specimens get put into a bottle of formaldehyde, they float around and get torn up, and then when they come to the lab, we have no idea what’s proximal and dorsal. This is an issue. We’re all used to just putting a nail specimen in a bottle and sending it away, so all the grossing happens in the laboratory. What I submit to you is you need to be more involved in the grossing side so the specimen can be properly processed,” said Dr. Thompson, a dermatopathologist in group practice in Tigard, Ore.
He added that clear and concise guidelines for standardized specimen submission are needed, and he offered several specific suggestions regarding the orientation of the tissue and securing it for transport.
“Careful submission of tissue specimens is of great importance and allows for better diagnostics,” Dr. Thompson stressed. “There’s really nothing more terrifying than to be told you’re being sent a pigmented lesion and then not being able to find anything at all in the specimen. You really worry that it’s ended up in the trash can through leveling. This is why dermatopathologists don’t want to read nail biopsies very much.”
When a nail specimen is submitted properly, such mix-ups become “almost impossible,” according to the dermatopathologist.
Dr. Thompson borrowed one of his key ideas on efficient handling of nail specimens from opthalmologic pathology. Ophthalmologists routinely send delicate tissue segments and margins from the operating room, and they do so with consistent success because they place the segments on a cartoon of the eye so the pathologist can see exactly where the tissue was located on the patient.
Dermatologists and surgeons can do the same after printing out a sheaf of nail diagrams gratis at the Website for Dr. Thompson’s dermatopathology practice.
The rest of the necessary equipment is similarly simple and readily obtainable from any pathology laboratory, which routinely purchases small plastic cassettes by the tens of thousands for handling of tissue specimens.
“You don’t need to go out and buy them; just ask the lab you work with to send over 10 or so,” Dr. Thompson advised.
The cassette comes with a small fitted sponge to be placed over the tissue to keep it securely in place on the nail diagram rather than floating off. Ink one end of the specimen using the wooden end of a cotton-tip applicator so the lab knows which end is proximal and which is distal. The wooden tip provides more precise inking than the cotton-tip end. Then place the closed cassette in a larger bottle of formaldehyde for shipping.
One more thing: Separate the nail plate from the nail bed or matrix whenever possible, and place them in separate cassettes. Lab technicians typically devote a lot of attention to trying to get the nail plate to stick to a slide, but the diagnostic material is usually present in the nail bed or matrix, and keeping those soft tissues separate makes it less likely they’ll get lost in the shuffle.
“I recommend putting the nail plate cassette and the lesional tissue in the same bottle because then you don’t have two specimens with double the charge for the patient,” Dr. Thompson said.
He reported having no relevant financial conflicts.
EXPERT ANALYSIS FROM WCD 2015
WCD: Dapsone Gel Effective for Acne in Women of Color
VANCOUVER – Dapsone gel 5% proved effective and well tolerated for facial acne in women with skin of color in a multicenter pilot study.
The study was conducted because even though dapsone gel 5% (Aczone) is approved for the treatment of acne on the strength of two pivotal randomized, double-blind clinical trials totaling more than 3,000 patients, scant data exist on the topical agent’s performance in women with skin of color, Dr. Andrew F. Alexis explained at the World Congress of Dermatology.

He presented an open-label, seven-center, 12-week, single-arm study involving 68 women of color – three-quarters of whom were black – who treated their facial acne with dapsone gel 5% twice daily as monotherapy.
Participants averaged a mean baseline score of 2.6 on the 0-4 Global Acne Assessment Score (GAAS), with a mean total of 50 inflammatory and noninflammatory acne lesions on the face.
The primary endpoint was change in GAAS at 12 weeks, although patients also were formally assessed at 2 and 6 weeks. The average reduction in GAAS was 8.8% at 2 weeks, 20% at 6 weeks, and 39% at 12 weeks. At week 12, 43% of the women were categorized as responders, meaning they had a GAAS of 0 (meaning no acne lesions) or 1 (indicating mild disease), reported Dr. Alexis of Mt. Sinai Hospital in New York.
Total lesion counts dropped steadily throughout the 12-week trial: by 16% from baseline to week 2, 30% at week 6, and 52% at week 12. Inflammatory lesions responded best, with a 65% reduction in number at week 12.
Patient-reported outcomes on the validated, 17-item Acne Symptom and Impact Scale were favorable: Reductions of roughly 50% were documented over 12 weeks on the scale’s two domains, acne signs and quality of life impact.
No clinically meaningful treatment-related adverse events were reported in the study, although a handful of women reported trace levels of redness, burning, dryness, and/or oiliness.
Acne is more common among African American than white women. In a large epidemiologic study of adolescent and adult women, the prevalence of acne vulgaris was 37% in African Americans, compared with 24% in whites (J. Eur. Acad. Dermatol. Venereol. 2011;25:1054-60).
Dr. Alexis’ study was sponsored by Allergan. He reported serving as a consultant to and receiving research grants from the company.
VANCOUVER – Dapsone gel 5% proved effective and well tolerated for facial acne in women with skin of color in a multicenter pilot study.
The study was conducted because even though dapsone gel 5% (Aczone) is approved for the treatment of acne on the strength of two pivotal randomized, double-blind clinical trials totaling more than 3,000 patients, scant data exist on the topical agent’s performance in women with skin of color, Dr. Andrew F. Alexis explained at the World Congress of Dermatology.
He presented an open-label, seven-center, 12-week, single-arm study involving 68 women of color – three-quarters of whom were black – who treated their facial acne with dapsone gel 5% twice daily as monotherapy.
Participants averaged a mean baseline score of 2.6 on the 0-4 Global Acne Assessment Score (GAAS), with a mean total of 50 inflammatory and noninflammatory acne lesions on the face.
The primary endpoint was change in GAAS at 12 weeks, although patients also were formally assessed at 2 and 6 weeks. The average reduction in GAAS was 8.8% at 2 weeks, 20% at 6 weeks, and 39% at 12 weeks. At week 12, 43% of the women were categorized as responders, meaning they had a GAAS of 0 (meaning no acne lesions) or 1 (indicating mild disease), reported Dr. Alexis of Mt. Sinai Hospital in New York.
Total lesion counts dropped steadily throughout the 12-week trial: by 16% from baseline to week 2, 30% at week 6, and 52% at week 12. Inflammatory lesions responded best, with a 65% reduction in number at week 12.
Patient-reported outcomes on the validated, 17-item Acne Symptom and Impact Scale were favorable: Reductions of roughly 50% were documented over 12 weeks on the scale’s two domains, acne signs and quality of life impact.
No clinically meaningful treatment-related adverse events were reported in the study, although a handful of women reported trace levels of redness, burning, dryness, and/or oiliness.
Acne is more common among African American than white women. In a large epidemiologic study of adolescent and adult women, the prevalence of acne vulgaris was 37% in African Americans, compared with 24% in whites (J. Eur. Acad. Dermatol. Venereol. 2011;25:1054-60).
Dr. Alexis’ study was sponsored by Allergan. He reported serving as a consultant to and receiving research grants from the company.
VANCOUVER – Dapsone gel 5% proved effective and well tolerated for facial acne in women with skin of color in a multicenter pilot study.
The study was conducted because even though dapsone gel 5% (Aczone) is approved for the treatment of acne on the strength of two pivotal randomized, double-blind clinical trials totaling more than 3,000 patients, scant data exist on the topical agent’s performance in women with skin of color, Dr. Andrew F. Alexis explained at the World Congress of Dermatology.
He presented an open-label, seven-center, 12-week, single-arm study involving 68 women of color – three-quarters of whom were black – who treated their facial acne with dapsone gel 5% twice daily as monotherapy.
Participants averaged a mean baseline score of 2.6 on the 0-4 Global Acne Assessment Score (GAAS), with a mean total of 50 inflammatory and noninflammatory acne lesions on the face.
The primary endpoint was change in GAAS at 12 weeks, although patients also were formally assessed at 2 and 6 weeks. The average reduction in GAAS was 8.8% at 2 weeks, 20% at 6 weeks, and 39% at 12 weeks. At week 12, 43% of the women were categorized as responders, meaning they had a GAAS of 0 (meaning no acne lesions) or 1 (indicating mild disease), reported Dr. Alexis of Mt. Sinai Hospital in New York.
Total lesion counts dropped steadily throughout the 12-week trial: by 16% from baseline to week 2, 30% at week 6, and 52% at week 12. Inflammatory lesions responded best, with a 65% reduction in number at week 12.
Patient-reported outcomes on the validated, 17-item Acne Symptom and Impact Scale were favorable: Reductions of roughly 50% were documented over 12 weeks on the scale’s two domains, acne signs and quality of life impact.
No clinically meaningful treatment-related adverse events were reported in the study, although a handful of women reported trace levels of redness, burning, dryness, and/or oiliness.
Acne is more common among African American than white women. In a large epidemiologic study of adolescent and adult women, the prevalence of acne vulgaris was 37% in African Americans, compared with 24% in whites (J. Eur. Acad. Dermatol. Venereol. 2011;25:1054-60).
Dr. Alexis’ study was sponsored by Allergan. He reported serving as a consultant to and receiving research grants from the company.
AT WCD 2015

WCD: Dapsone gel effective for acne in women of color
VANCOUVER – Dapsone gel 5% proved effective and well tolerated for facial acne in women with skin of color in a multicenter pilot study.
The study was conducted because even though dapsone gel 5% (Aczone) is approved for the treatment of acne on the strength of two pivotal randomized, double-blind clinical trials totaling more than 3,000 patients, scant data exist on the topical agent’s performance in women with skin of color, Dr. Andrew F. Alexis explained at the World Congress of Dermatology.

He presented an open-label, seven-center, 12-week, single-arm study involving 68 women of color – three-quarters of whom were black – who treated their facial acne with dapsone gel 5% twice daily as monotherapy.
Participants averaged a mean baseline score of 2.6 on the 0-4 Global Acne Assessment Score (GAAS), with a mean total of 50 inflammatory and noninflammatory acne lesions on the face.
The primary endpoint was change in GAAS at 12 weeks, although patients also were formally assessed at 2 and 6 weeks. The average reduction in GAAS was 8.8% at 2 weeks, 20% at 6 weeks, and 39% at 12 weeks. At week 12, 43% of the women were categorized as responders, meaning they had a GAAS of 0 (meaning no acne lesions) or 1 (indicating mild disease), reported Dr. Alexis of Mt. Sinai Hospital in New York.
Total lesion counts dropped steadily throughout the 12-week trial: by 16% from baseline to week 2, 30% at week 6, and 52% at week 12. Inflammatory lesions responded best, with a 65% reduction in number at week 12.
Patient-reported outcomes on the validated, 17-item Acne Symptom and Impact Scale were favorable: Reductions of roughly 50% were documented over 12 weeks on the scale’s two domains, acne signs and quality of life impact.
No clinically meaningful treatment-related adverse events were reported in the study, although a handful of women reported trace levels of redness, burning, dryness, and/or oiliness.
Acne is more common among African American than white women. In a large epidemiologic study of adolescent and adult women, the prevalence of acne vulgaris was 37% in African Americans, compared with 24% in whites (J. Eur. Acad. Dermatol. Venereol. 2011;25:1054-60).
Dr. Alexis’ study was sponsored by Allergan. He reported serving as a consultant to and receiving research grants from the company.
VANCOUVER – Dapsone gel 5% proved effective and well tolerated for facial acne in women with skin of color in a multicenter pilot study.
The study was conducted because even though dapsone gel 5% (Aczone) is approved for the treatment of acne on the strength of two pivotal randomized, double-blind clinical trials totaling more than 3,000 patients, scant data exist on the topical agent’s performance in women with skin of color, Dr. Andrew F. Alexis explained at the World Congress of Dermatology.
He presented an open-label, seven-center, 12-week, single-arm study involving 68 women of color – three-quarters of whom were black – who treated their facial acne with dapsone gel 5% twice daily as monotherapy.
Participants averaged a mean baseline score of 2.6 on the 0-4 Global Acne Assessment Score (GAAS), with a mean total of 50 inflammatory and noninflammatory acne lesions on the face.
The primary endpoint was change in GAAS at 12 weeks, although patients also were formally assessed at 2 and 6 weeks. The average reduction in GAAS was 8.8% at 2 weeks, 20% at 6 weeks, and 39% at 12 weeks. At week 12, 43% of the women were categorized as responders, meaning they had a GAAS of 0 (meaning no acne lesions) or 1 (indicating mild disease), reported Dr. Alexis of Mt. Sinai Hospital in New York.
Total lesion counts dropped steadily throughout the 12-week trial: by 16% from baseline to week 2, 30% at week 6, and 52% at week 12. Inflammatory lesions responded best, with a 65% reduction in number at week 12.
Patient-reported outcomes on the validated, 17-item Acne Symptom and Impact Scale were favorable: Reductions of roughly 50% were documented over 12 weeks on the scale’s two domains, acne signs and quality of life impact.
No clinically meaningful treatment-related adverse events were reported in the study, although a handful of women reported trace levels of redness, burning, dryness, and/or oiliness.
Acne is more common among African American than white women. In a large epidemiologic study of adolescent and adult women, the prevalence of acne vulgaris was 37% in African Americans, compared with 24% in whites (J. Eur. Acad. Dermatol. Venereol. 2011;25:1054-60).
Dr. Alexis’ study was sponsored by Allergan. He reported serving as a consultant to and receiving research grants from the company.
VANCOUVER – Dapsone gel 5% proved effective and well tolerated for facial acne in women with skin of color in a multicenter pilot study.
The study was conducted because even though dapsone gel 5% (Aczone) is approved for the treatment of acne on the strength of two pivotal randomized, double-blind clinical trials totaling more than 3,000 patients, scant data exist on the topical agent’s performance in women with skin of color, Dr. Andrew F. Alexis explained at the World Congress of Dermatology.
He presented an open-label, seven-center, 12-week, single-arm study involving 68 women of color – three-quarters of whom were black – who treated their facial acne with dapsone gel 5% twice daily as monotherapy.
Participants averaged a mean baseline score of 2.6 on the 0-4 Global Acne Assessment Score (GAAS), with a mean total of 50 inflammatory and noninflammatory acne lesions on the face.
The primary endpoint was change in GAAS at 12 weeks, although patients also were formally assessed at 2 and 6 weeks. The average reduction in GAAS was 8.8% at 2 weeks, 20% at 6 weeks, and 39% at 12 weeks. At week 12, 43% of the women were categorized as responders, meaning they had a GAAS of 0 (meaning no acne lesions) or 1 (indicating mild disease), reported Dr. Alexis of Mt. Sinai Hospital in New York.
Total lesion counts dropped steadily throughout the 12-week trial: by 16% from baseline to week 2, 30% at week 6, and 52% at week 12. Inflammatory lesions responded best, with a 65% reduction in number at week 12.
Patient-reported outcomes on the validated, 17-item Acne Symptom and Impact Scale were favorable: Reductions of roughly 50% were documented over 12 weeks on the scale’s two domains, acne signs and quality of life impact.
No clinically meaningful treatment-related adverse events were reported in the study, although a handful of women reported trace levels of redness, burning, dryness, and/or oiliness.
Acne is more common among African American than white women. In a large epidemiologic study of adolescent and adult women, the prevalence of acne vulgaris was 37% in African Americans, compared with 24% in whites (J. Eur. Acad. Dermatol. Venereol. 2011;25:1054-60).
Dr. Alexis’ study was sponsored by Allergan. He reported serving as a consultant to and receiving research grants from the company.
AT WCD 2015
Key clinical point: Dapsone gel 5% is effective and well tolerated for treatment of facial acne in women with skin of color.
Major finding: Women of color experienced a mean 39% reduction in Global Acne Assessment Scores after 12 weeks of self-treatment of facial acne using dapsone gel 5% twice daily as monotherapy.
Data source: This was a 68-patient, open-label, seven-site, single-arm, 12-week study.
Disclosures: The study was sponsored by Allergan. Dr. Andrew F. Alexis reported serving as a consultant to and receiving research grants from the company.

WCD: Topical Tofacitinib Hits Marks in Atopic Dermatitis
VANCOUVER, B.C. – Topical tofacitinib shows promise as a novel treatment for atopic dermatitis on the basis of a highly positive phase II randomized clinical trial.
The topical Janus kinase inhibitor hit all of its efficacy endpoints and was well tolerated, with infrequent side effects, none of them serious, Dr. Robert Bissonnette reported at the World Congress of Dermatology.
An unmet need exists for additional topical therapies for atopic dermatitis, a condition whose prevalence has been estimated at up to 20%. Existing topical agents, including corticosteroids and calcineurin inhibitors, have limitations involving long-term safety concerns and application site reactions, noted Dr. Bissonnette, president of Innovaderm Research in Montreal.
The Janus kinases have been implicated in the pathogenesis of atopic dermatitis due to their effects upon the interleukin-4, IL-5, and IL-31 signaling pathways and the resultant dysregulation of the immune response.
Dr. Bissonnette presented a phase II, 4-week, double-blind, vehicle-controlled, multicenter Canadian study involving 65 adults with mild to moderate atopic dermatitis. They applied tofacitinib ointment 2% or its vehicle twice daily for 4 weeks. Participants averaged 31 years of age, with a median 21 years since receiving the diagnosis of atopic dermatitis. Roughly three-quarters of subjects had moderate disease based upon Physician Global Assessment.
The primary study endpoint was change in Eczema Area and Severity Index (EASI) total score after 4 weeks. From a baseline EASI score of 5.4, the topical tofacitinib group experienced a mean 82% reduction, significantly outperforming the control group, which showed a 30% reduction. The difference between the two study arms reached significance at the first assessment, at week 1.
Patients on the topical Janus kinase (JAK) inhibitor also showed significantly better outcomes than controls on all secondary endpoints, with the differences reaching statistical significance at week 1 with the exception of improvement in self-assessed Itch Severity Item, where topical tofacitinib’s advantage became significant on treatment day 2.
Two patients on topical tofacitinib and five controls developed treatment area adverse events, consisting of skin irritation and/or pain, which was mild in all cases. There were no cases of herpes simplex or zoster, no opportunistic infections, no laboratory abnormalities, and no one required a dose reduction or temporary discontinuation of the topical JAK inhibitor, according to the dermatologist.
Oral tofacitinib is Food and Drug Administration–approved as Xeljanz for the treatment of rheumatoid arthritis and is currently under FDA review as a potential treatment for moderate to severe chronic plaque psoriasis, with a regulatory decision anticipated in October 2015.
The atopic dermatitis study was funded by Pfizer. Dr. Bissonnette is a consultant to and recipient of research grants from more than a dozen pharmaceutical companies, including Pfizer.
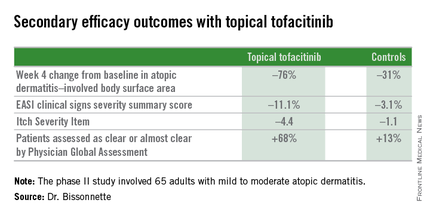
VANCOUVER, B.C. – Topical tofacitinib shows promise as a novel treatment for atopic dermatitis on the basis of a highly positive phase II randomized clinical trial.
The topical Janus kinase inhibitor hit all of its efficacy endpoints and was well tolerated, with infrequent side effects, none of them serious, Dr. Robert Bissonnette reported at the World Congress of Dermatology.
An unmet need exists for additional topical therapies for atopic dermatitis, a condition whose prevalence has been estimated at up to 20%. Existing topical agents, including corticosteroids and calcineurin inhibitors, have limitations involving long-term safety concerns and application site reactions, noted Dr. Bissonnette, president of Innovaderm Research in Montreal.
The Janus kinases have been implicated in the pathogenesis of atopic dermatitis due to their effects upon the interleukin-4, IL-5, and IL-31 signaling pathways and the resultant dysregulation of the immune response.
Dr. Bissonnette presented a phase II, 4-week, double-blind, vehicle-controlled, multicenter Canadian study involving 65 adults with mild to moderate atopic dermatitis. They applied tofacitinib ointment 2% or its vehicle twice daily for 4 weeks. Participants averaged 31 years of age, with a median 21 years since receiving the diagnosis of atopic dermatitis. Roughly three-quarters of subjects had moderate disease based upon Physician Global Assessment.
The primary study endpoint was change in Eczema Area and Severity Index (EASI) total score after 4 weeks. From a baseline EASI score of 5.4, the topical tofacitinib group experienced a mean 82% reduction, significantly outperforming the control group, which showed a 30% reduction. The difference between the two study arms reached significance at the first assessment, at week 1.
Patients on the topical Janus kinase (JAK) inhibitor also showed significantly better outcomes than controls on all secondary endpoints, with the differences reaching statistical significance at week 1 with the exception of improvement in self-assessed Itch Severity Item, where topical tofacitinib’s advantage became significant on treatment day 2.
Two patients on topical tofacitinib and five controls developed treatment area adverse events, consisting of skin irritation and/or pain, which was mild in all cases. There were no cases of herpes simplex or zoster, no opportunistic infections, no laboratory abnormalities, and no one required a dose reduction or temporary discontinuation of the topical JAK inhibitor, according to the dermatologist.
Oral tofacitinib is Food and Drug Administration–approved as Xeljanz for the treatment of rheumatoid arthritis and is currently under FDA review as a potential treatment for moderate to severe chronic plaque psoriasis, with a regulatory decision anticipated in October 2015.
The atopic dermatitis study was funded by Pfizer. Dr. Bissonnette is a consultant to and recipient of research grants from more than a dozen pharmaceutical companies, including Pfizer.
VANCOUVER, B.C. – Topical tofacitinib shows promise as a novel treatment for atopic dermatitis on the basis of a highly positive phase II randomized clinical trial.
The topical Janus kinase inhibitor hit all of its efficacy endpoints and was well tolerated, with infrequent side effects, none of them serious, Dr. Robert Bissonnette reported at the World Congress of Dermatology.
An unmet need exists for additional topical therapies for atopic dermatitis, a condition whose prevalence has been estimated at up to 20%. Existing topical agents, including corticosteroids and calcineurin inhibitors, have limitations involving long-term safety concerns and application site reactions, noted Dr. Bissonnette, president of Innovaderm Research in Montreal.
The Janus kinases have been implicated in the pathogenesis of atopic dermatitis due to their effects upon the interleukin-4, IL-5, and IL-31 signaling pathways and the resultant dysregulation of the immune response.
Dr. Bissonnette presented a phase II, 4-week, double-blind, vehicle-controlled, multicenter Canadian study involving 65 adults with mild to moderate atopic dermatitis. They applied tofacitinib ointment 2% or its vehicle twice daily for 4 weeks. Participants averaged 31 years of age, with a median 21 years since receiving the diagnosis of atopic dermatitis. Roughly three-quarters of subjects had moderate disease based upon Physician Global Assessment.
The primary study endpoint was change in Eczema Area and Severity Index (EASI) total score after 4 weeks. From a baseline EASI score of 5.4, the topical tofacitinib group experienced a mean 82% reduction, significantly outperforming the control group, which showed a 30% reduction. The difference between the two study arms reached significance at the first assessment, at week 1.
Patients on the topical Janus kinase (JAK) inhibitor also showed significantly better outcomes than controls on all secondary endpoints, with the differences reaching statistical significance at week 1 with the exception of improvement in self-assessed Itch Severity Item, where topical tofacitinib’s advantage became significant on treatment day 2.
Two patients on topical tofacitinib and five controls developed treatment area adverse events, consisting of skin irritation and/or pain, which was mild in all cases. There were no cases of herpes simplex or zoster, no opportunistic infections, no laboratory abnormalities, and no one required a dose reduction or temporary discontinuation of the topical JAK inhibitor, according to the dermatologist.
Oral tofacitinib is Food and Drug Administration–approved as Xeljanz for the treatment of rheumatoid arthritis and is currently under FDA review as a potential treatment for moderate to severe chronic plaque psoriasis, with a regulatory decision anticipated in October 2015.
The atopic dermatitis study was funded by Pfizer. Dr. Bissonnette is a consultant to and recipient of research grants from more than a dozen pharmaceutical companies, including Pfizer.
AT WCD 2015