User login
Concomitant depression in breast cancer survivors doubles health care costs
SAN ANTONIO – Annual health care costs and utilization jump several-fold in nonelderly breast cancer survivors with concomitant depression, according to an analysis from the U.S. military health system.
Analysis of the records of 2,851 breast cancer survivors whose care is provided by the Department of Defense military health system indicated that 15.9% were diagnosed with depression in the time interval within 1 year prior to and 2 years after their cancer diagnosis. These dual-diagnosis patients averaged $15,471 annually in health care costs covering inpatient and outpatient services and outpatient prescriptions in the first years after being diagnosed with breast cancer, compared with $8,297 per year in those without a diagnosis of depression, Diana D. Jeffery, Ph.D., reported at the San Antonio Breast Cancer Symposium.

The mean annual number of hospital admissions was tripled: 0.33 in breast cancer survivors with depression and 0.11 in survivors without depression. The dual-diagosis group averaged 1.94 hospital bed days annually, compared with 0.58 in breast cancer survivors without depression. Breast cancer survivors diagnosed with depression averaged 28 outpatient visits annually, while those without depression averaged 16.5, according to Dr. Jeffery, a senior researcher at the Defense Health Agency in Falls Church, Va.
Fifty percent of the breast cancer survivors were diagnosed with hypertension, making this the most common chronic comorbid condition. A diagnosis of depression, anxiety, adjustment, or stress disorder was present in 37.5% of the breast cancer survivors, making this group of psychiatric diagnoses the second most prevalent comorbidity. Twenty-three percent of the breast cancer survivors had received a diagnosis of heart disease, 20% had diabetes, 16% had asthma or chronic obstructive pulmonary disease, and 17% were obese. No demographic characteristics proved predictive of an increased likelihood of being diagnosed with depression, she said.
Of note, nearly one-half of the patients with depression had been diagnosed with the affective disorder during the year prior to receiving their breast cancer diagnosis.
Dr. Jeffery said that, while these data on health care costs and utilization in breast cancer survivors with concomitant depression are likely to be of particular interest to health plans, they also show what is likely to happen following adoption of the American Society of Clinical Oncology 2014 guidelines on screening and care of depression and anxiety in adults with cancer.
The guidelines recommend that all cancer patients and cancer survivors periodically be evaluated for symptoms of depression and anxiety using validated measures across the trajectory of care to “reduce the human cost of cancer” (J. Clin. Oncol. 2014;32:1605-19).
Adoption of the depression screening guidelines will likely increase the number of breast cancer survivors with a mental health diagnosis, which, as Dr. Jeffery’s study demonstrates, will boost health care costs and utilization. On the other hand, identifying and intervening effectively in patients with mild symptoms that haven’t yet risen to the level that meets diagnostic criteria for clinical depression should yield cost savings as well as quality-of-life benefits, she added.
The Department of Defense military health system, under a health plan known as Tricare, serves 9.5 million beneficiaries in 360 military treatment clinics worldwide. It’s a system with very few restrictions upon medical-ordered cancer follow-up care, according to Dr. Jeffery.
She reported having no financial conflicts regarding this study.
SAN ANTONIO – Annual health care costs and utilization jump several-fold in nonelderly breast cancer survivors with concomitant depression, according to an analysis from the U.S. military health system.
Analysis of the records of 2,851 breast cancer survivors whose care is provided by the Department of Defense military health system indicated that 15.9% were diagnosed with depression in the time interval within 1 year prior to and 2 years after their cancer diagnosis. These dual-diagnosis patients averaged $15,471 annually in health care costs covering inpatient and outpatient services and outpatient prescriptions in the first years after being diagnosed with breast cancer, compared with $8,297 per year in those without a diagnosis of depression, Diana D. Jeffery, Ph.D., reported at the San Antonio Breast Cancer Symposium.
The mean annual number of hospital admissions was tripled: 0.33 in breast cancer survivors with depression and 0.11 in survivors without depression. The dual-diagosis group averaged 1.94 hospital bed days annually, compared with 0.58 in breast cancer survivors without depression. Breast cancer survivors diagnosed with depression averaged 28 outpatient visits annually, while those without depression averaged 16.5, according to Dr. Jeffery, a senior researcher at the Defense Health Agency in Falls Church, Va.
Fifty percent of the breast cancer survivors were diagnosed with hypertension, making this the most common chronic comorbid condition. A diagnosis of depression, anxiety, adjustment, or stress disorder was present in 37.5% of the breast cancer survivors, making this group of psychiatric diagnoses the second most prevalent comorbidity. Twenty-three percent of the breast cancer survivors had received a diagnosis of heart disease, 20% had diabetes, 16% had asthma or chronic obstructive pulmonary disease, and 17% were obese. No demographic characteristics proved predictive of an increased likelihood of being diagnosed with depression, she said.
Of note, nearly one-half of the patients with depression had been diagnosed with the affective disorder during the year prior to receiving their breast cancer diagnosis.
Dr. Jeffery said that, while these data on health care costs and utilization in breast cancer survivors with concomitant depression are likely to be of particular interest to health plans, they also show what is likely to happen following adoption of the American Society of Clinical Oncology 2014 guidelines on screening and care of depression and anxiety in adults with cancer.
The guidelines recommend that all cancer patients and cancer survivors periodically be evaluated for symptoms of depression and anxiety using validated measures across the trajectory of care to “reduce the human cost of cancer” (J. Clin. Oncol. 2014;32:1605-19).
Adoption of the depression screening guidelines will likely increase the number of breast cancer survivors with a mental health diagnosis, which, as Dr. Jeffery’s study demonstrates, will boost health care costs and utilization. On the other hand, identifying and intervening effectively in patients with mild symptoms that haven’t yet risen to the level that meets diagnostic criteria for clinical depression should yield cost savings as well as quality-of-life benefits, she added.
The Department of Defense military health system, under a health plan known as Tricare, serves 9.5 million beneficiaries in 360 military treatment clinics worldwide. It’s a system with very few restrictions upon medical-ordered cancer follow-up care, according to Dr. Jeffery.
She reported having no financial conflicts regarding this study.
SAN ANTONIO – Annual health care costs and utilization jump several-fold in nonelderly breast cancer survivors with concomitant depression, according to an analysis from the U.S. military health system.
Analysis of the records of 2,851 breast cancer survivors whose care is provided by the Department of Defense military health system indicated that 15.9% were diagnosed with depression in the time interval within 1 year prior to and 2 years after their cancer diagnosis. These dual-diagnosis patients averaged $15,471 annually in health care costs covering inpatient and outpatient services and outpatient prescriptions in the first years after being diagnosed with breast cancer, compared with $8,297 per year in those without a diagnosis of depression, Diana D. Jeffery, Ph.D., reported at the San Antonio Breast Cancer Symposium.
The mean annual number of hospital admissions was tripled: 0.33 in breast cancer survivors with depression and 0.11 in survivors without depression. The dual-diagosis group averaged 1.94 hospital bed days annually, compared with 0.58 in breast cancer survivors without depression. Breast cancer survivors diagnosed with depression averaged 28 outpatient visits annually, while those without depression averaged 16.5, according to Dr. Jeffery, a senior researcher at the Defense Health Agency in Falls Church, Va.
Fifty percent of the breast cancer survivors were diagnosed with hypertension, making this the most common chronic comorbid condition. A diagnosis of depression, anxiety, adjustment, or stress disorder was present in 37.5% of the breast cancer survivors, making this group of psychiatric diagnoses the second most prevalent comorbidity. Twenty-three percent of the breast cancer survivors had received a diagnosis of heart disease, 20% had diabetes, 16% had asthma or chronic obstructive pulmonary disease, and 17% were obese. No demographic characteristics proved predictive of an increased likelihood of being diagnosed with depression, she said.
Of note, nearly one-half of the patients with depression had been diagnosed with the affective disorder during the year prior to receiving their breast cancer diagnosis.
Dr. Jeffery said that, while these data on health care costs and utilization in breast cancer survivors with concomitant depression are likely to be of particular interest to health plans, they also show what is likely to happen following adoption of the American Society of Clinical Oncology 2014 guidelines on screening and care of depression and anxiety in adults with cancer.
The guidelines recommend that all cancer patients and cancer survivors periodically be evaluated for symptoms of depression and anxiety using validated measures across the trajectory of care to “reduce the human cost of cancer” (J. Clin. Oncol. 2014;32:1605-19).
Adoption of the depression screening guidelines will likely increase the number of breast cancer survivors with a mental health diagnosis, which, as Dr. Jeffery’s study demonstrates, will boost health care costs and utilization. On the other hand, identifying and intervening effectively in patients with mild symptoms that haven’t yet risen to the level that meets diagnostic criteria for clinical depression should yield cost savings as well as quality-of-life benefits, she added.
The Department of Defense military health system, under a health plan known as Tricare, serves 9.5 million beneficiaries in 360 military treatment clinics worldwide. It’s a system with very few restrictions upon medical-ordered cancer follow-up care, according to Dr. Jeffery.
She reported having no financial conflicts regarding this study.
AT SABCS 2014
Key clinical point: Depression was diagnosed in 15.9% of breast cancer survivors within 1 year prior to, at the time of, or up to 2 years following their cancer diagnosis.
Major finding: Health care costs averaged $15,471 per year in breast cancer survivors with concomitant depression and $8,297 in those without depression.
Data source: This was a retrospective study of health care costs and utilization based upon administrative claims data for 2,851 breast cancer survivors in the military heath care system.
Disclosures: The study was funded by the Department of Defense. The presenter reported having no financial conflicts.

BOLERO-1: Everolimus shows strong signal in HER2+ advanced breast cancer
SAN ANTONIO – Adding daily everolimus to weekly trastuzumab and paclitaxel as first-line therapy resulted in a median 7.2-month gain in progression-free survival in women with hormone receptor-negative, HER2+ advanced breast cancer in the Phase III BOLERO-1 trial.
Median progression-free survival was 20.27 months with the addition of everolimus (Afinitor) compared with 13.08 months with placebo in the 309 patients with hormone receptor-negative disease who participated in the randomized, double-blind study conducted at 141 centers in 28 countries, Dr. Sara A. Hurvitz reported at the San Antonio Breast Cancer Symposium. This translated to a 34% relative risk reduction for disease progression in patients randomized to everolimus, an oral mTOR inhibitor (P = .0049). However, this seemingly robust outcome did not actually achieve statistical significance. Since this was a subgroup analysis -- the other 410 participants in BOLERO-1 had hormone receptor-positive, HER2+ advanced breast cancer -- the prespecified threshold for significance set by the study statisticians for the analysis in hormone receptor-negative patients was P = .0044.
An Australian statistician rose from the audience to take issue with the BOLERO-1 statisticians in setting the bar for statistical significance so high.
“This was a statistical decision that was made. We’re all thinking about that,” admitted Dr. Hurvitz, director of the breast oncology program in the division of hematology-oncology at the University of California, Los Angeles.

Everolimus showed no benefit in the full study population, where median progression-free survival was virtually identical in the two treatment arms: 14.95 months with everolimus at 10 mg daily, 14.49 months with placebo.
Trastuzumab (Herceptin) has dramatically improved outcomes in patients diagnosed with HER2+ breast cancer, both in the early-stage and advanced settings. But not everyone benefits.
“Resistance to treatment remains a major clinical unmet challenge,” she observed.
The rationale for BOLERO-1 was that hyperactivation of the P13 kinase/mTOR pathway is one likely mechanism for HER2 resistance, and therefore an mTOR inhibitor such as everolimus might close off this resistance.
The most common adverse events associated with everolimus in BOLERO-1 were stomatitis, diarrhea, neutropenia, and anemia.
Of greater concern was the 3.6% mortality due to adverse events in the everolimus group compared with none in placebo-treated controls. Most of the deaths were due to pulmonary causes. Study leaders noticed that these deaths were occurring in centers with little experience in using everolimus. A letter was sent to all investigators underscoring the need for proactive aggressive management of adverse events in patients taking everolimus with chemotherapy; after that there was only a single additional death.
Dr. C. Kent Osborne commented that he thought it was a mistake for the BOLERO-1 investigators not to allow endocrine therapy in the patients with hormone receptor-positive disease.
“I think it’s important to add endocrine therapy because the estrogen receptor provides an immediate escape mechanism. If you don’t block it in a HER2+ tumor, the estrogen receptor can start activating and signaling the tumor cell to survive. It’s a very important issue,” said Dr. Osborne, professor of medicine and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston.
Dr. Hurvitz concurred.
“Now, with our retrospectoscope on, I think ongoing and future studies are going to be utilizing endocrine therapy with HER2-targeted therapy and P13 kinase inhibitors in this setting,” the oncologist said.
The BOLERO-1 trial was sponsored by Novartis. Dr. Hurvitz reported receiving research support from Genentech, Roche, and Novartis.
SAN ANTONIO – Adding daily everolimus to weekly trastuzumab and paclitaxel as first-line therapy resulted in a median 7.2-month gain in progression-free survival in women with hormone receptor-negative, HER2+ advanced breast cancer in the Phase III BOLERO-1 trial.
Median progression-free survival was 20.27 months with the addition of everolimus (Afinitor) compared with 13.08 months with placebo in the 309 patients with hormone receptor-negative disease who participated in the randomized, double-blind study conducted at 141 centers in 28 countries, Dr. Sara A. Hurvitz reported at the San Antonio Breast Cancer Symposium. This translated to a 34% relative risk reduction for disease progression in patients randomized to everolimus, an oral mTOR inhibitor (P = .0049). However, this seemingly robust outcome did not actually achieve statistical significance. Since this was a subgroup analysis -- the other 410 participants in BOLERO-1 had hormone receptor-positive, HER2+ advanced breast cancer -- the prespecified threshold for significance set by the study statisticians for the analysis in hormone receptor-negative patients was P = .0044.
An Australian statistician rose from the audience to take issue with the BOLERO-1 statisticians in setting the bar for statistical significance so high.
“This was a statistical decision that was made. We’re all thinking about that,” admitted Dr. Hurvitz, director of the breast oncology program in the division of hematology-oncology at the University of California, Los Angeles.
Everolimus showed no benefit in the full study population, where median progression-free survival was virtually identical in the two treatment arms: 14.95 months with everolimus at 10 mg daily, 14.49 months with placebo.
Trastuzumab (Herceptin) has dramatically improved outcomes in patients diagnosed with HER2+ breast cancer, both in the early-stage and advanced settings. But not everyone benefits.
“Resistance to treatment remains a major clinical unmet challenge,” she observed.
The rationale for BOLERO-1 was that hyperactivation of the P13 kinase/mTOR pathway is one likely mechanism for HER2 resistance, and therefore an mTOR inhibitor such as everolimus might close off this resistance.
The most common adverse events associated with everolimus in BOLERO-1 were stomatitis, diarrhea, neutropenia, and anemia.
Of greater concern was the 3.6% mortality due to adverse events in the everolimus group compared with none in placebo-treated controls. Most of the deaths were due to pulmonary causes. Study leaders noticed that these deaths were occurring in centers with little experience in using everolimus. A letter was sent to all investigators underscoring the need for proactive aggressive management of adverse events in patients taking everolimus with chemotherapy; after that there was only a single additional death.
Dr. C. Kent Osborne commented that he thought it was a mistake for the BOLERO-1 investigators not to allow endocrine therapy in the patients with hormone receptor-positive disease.
“I think it’s important to add endocrine therapy because the estrogen receptor provides an immediate escape mechanism. If you don’t block it in a HER2+ tumor, the estrogen receptor can start activating and signaling the tumor cell to survive. It’s a very important issue,” said Dr. Osborne, professor of medicine and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston.
Dr. Hurvitz concurred.
“Now, with our retrospectoscope on, I think ongoing and future studies are going to be utilizing endocrine therapy with HER2-targeted therapy and P13 kinase inhibitors in this setting,” the oncologist said.
The BOLERO-1 trial was sponsored by Novartis. Dr. Hurvitz reported receiving research support from Genentech, Roche, and Novartis.
SAN ANTONIO – Adding daily everolimus to weekly trastuzumab and paclitaxel as first-line therapy resulted in a median 7.2-month gain in progression-free survival in women with hormone receptor-negative, HER2+ advanced breast cancer in the Phase III BOLERO-1 trial.
Median progression-free survival was 20.27 months with the addition of everolimus (Afinitor) compared with 13.08 months with placebo in the 309 patients with hormone receptor-negative disease who participated in the randomized, double-blind study conducted at 141 centers in 28 countries, Dr. Sara A. Hurvitz reported at the San Antonio Breast Cancer Symposium. This translated to a 34% relative risk reduction for disease progression in patients randomized to everolimus, an oral mTOR inhibitor (P = .0049). However, this seemingly robust outcome did not actually achieve statistical significance. Since this was a subgroup analysis -- the other 410 participants in BOLERO-1 had hormone receptor-positive, HER2+ advanced breast cancer -- the prespecified threshold for significance set by the study statisticians for the analysis in hormone receptor-negative patients was P = .0044.
An Australian statistician rose from the audience to take issue with the BOLERO-1 statisticians in setting the bar for statistical significance so high.
“This was a statistical decision that was made. We’re all thinking about that,” admitted Dr. Hurvitz, director of the breast oncology program in the division of hematology-oncology at the University of California, Los Angeles.
Everolimus showed no benefit in the full study population, where median progression-free survival was virtually identical in the two treatment arms: 14.95 months with everolimus at 10 mg daily, 14.49 months with placebo.
Trastuzumab (Herceptin) has dramatically improved outcomes in patients diagnosed with HER2+ breast cancer, both in the early-stage and advanced settings. But not everyone benefits.
“Resistance to treatment remains a major clinical unmet challenge,” she observed.
The rationale for BOLERO-1 was that hyperactivation of the P13 kinase/mTOR pathway is one likely mechanism for HER2 resistance, and therefore an mTOR inhibitor such as everolimus might close off this resistance.
The most common adverse events associated with everolimus in BOLERO-1 were stomatitis, diarrhea, neutropenia, and anemia.
Of greater concern was the 3.6% mortality due to adverse events in the everolimus group compared with none in placebo-treated controls. Most of the deaths were due to pulmonary causes. Study leaders noticed that these deaths were occurring in centers with little experience in using everolimus. A letter was sent to all investigators underscoring the need for proactive aggressive management of adverse events in patients taking everolimus with chemotherapy; after that there was only a single additional death.
Dr. C. Kent Osborne commented that he thought it was a mistake for the BOLERO-1 investigators not to allow endocrine therapy in the patients with hormone receptor-positive disease.
“I think it’s important to add endocrine therapy because the estrogen receptor provides an immediate escape mechanism. If you don’t block it in a HER2+ tumor, the estrogen receptor can start activating and signaling the tumor cell to survive. It’s a very important issue,” said Dr. Osborne, professor of medicine and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston.
Dr. Hurvitz concurred.
“Now, with our retrospectoscope on, I think ongoing and future studies are going to be utilizing endocrine therapy with HER2-targeted therapy and P13 kinase inhibitors in this setting,” the oncologist said.
The BOLERO-1 trial was sponsored by Novartis. Dr. Hurvitz reported receiving research support from Genentech, Roche, and Novartis.
AT SABCS 2014
Key clinical point: The risk of disease progression in women with hormone receptor-negative, HER2+ advanced breast cancer was reduced by 34% with everolimus rather than placebo in combination with weekly trastuzumab and paclitaxel.
Major finding: Median progression-free survival in hormone receptor-negative patients on everolimus was 20.27 months compared with 13.08 months with placebo.
Data source: The Phase III, double-blind BOLERO study randomized 309 patients with hormone receptor-negative and 410 with hormone receptor-positive, HER2+ advanced breast cancer to first-line therapy with trastuzumab, paclitaxel, and either everolimus or placebo.
Disclosures: The BOLERO-1 trial was sponsored by Novartis. The presenter reported receiving research support from Genentech, Roche, and Novartis.

New insights into relationship between alcohol, depression, and suicide
BERLIN– Alcohol dependence and major depressive disorder are similarly potent yet independent risk factors for suicidal behavior, according to Dr. Philip Gorwood.
Although alcohol use disorder and major depression are extremely common and often comorbid, the mechanisms by which they boost the risk for suicidal behavior are very different, he said at the annual congress of the European College of Neuropsychopharmacology.
“The ideation about suicidal behavior comes from the mood disorder, but the organization of the behavior – the suicidal attempt, especially when it is unplanned and impulsive – is driven by the alcohol consumption,” said Dr. Gorwood, professor of psychiatry at Rene Descartes University, Paris.

“The real take-home message is the difference between suicidal ideas and impulsive acts. Probably that was not well understood before. Alcohol dependence has no relationship with suicidal ideas. But once you have those ideas, alcohol consumption becomes very important in the risk of suicidal behavior,” he said.
A recent retrospective analysis of nearly 451,000 French patients hospitalized for suicide attempts during 2004-2011 showed their most common psychiatric diagnosis was major depressive disorder, present in 52% of the men and 65% of the women. Second most common – and far ahead of the rest of the pack – was alcohol use disorder, diagnosed in 36% of the hospitalized men and 49% of the women.
Alcohol probably facilitates suicidal behaviors in a variety of ways – by generating stressful life events, weakening social supports, worsening mood, restricting cognition and thereby inhibiting coping strategies, boosting impulsivity, and promoting inaccurate assessment of harm and pain.
A recent review of epidemiologic studies on the risk factors for suicide attempts and suicide among individuals with alcohol use disorder identified a clutch of risk factors that could be useful in clinical practice as a means of targeting problem drinkers at increased risk for suicidality: major depressive disorder, greater severity of alcohol use disorder, limited social support, stressful life events, aggression, medical illness, and economic adversity (Am. J. Prev. Med. 2014;47:S204-S208).
Other studies have identified additional risk factors that distinguish individuals with alcohol dependence who do attempt suicide from those who don’t: early onset of alcohol dependence, childhood trauma, a family history of suicidal behavior, and tobacco dependence. But if a clinician is going to rely on the two strongest risk factors in order to identify increased suicidal risk among alcohol-dependent patients, those would be major depression and the greater severity of alcohol dependence, according to Dr. Gorwood.
A study from the National Comorbidity Survey Replication based on a representative sample comprised of 9,282 U.S. adults concluded that alcohol abuse or dependence was associated with a 2.1-fold increased risk of a history of a suicide attempt, while major depressive disorder was independently associated with a 2.0-fold increased risk. In a multivariate analysis, major depressive disorder was associated with a statistically significant 2.3-fold increased risk of suicidal ideation but no significant increase in planned or unplanned suicide attempts. In contrast, alcohol abuse or dependence wasn’t associated with a significant increase in suicidal ideation but did carry a 2.9-fold increased risk of unplanned, impulsive suicide attempts (Mol. Psychiatry 2010;15:868-76).
A first-of-its-kind U.S. national study of postmortem blood alcohol levels as a means of assessing alcohol use prior to suicide concluded that men and women who committed suicide were 1.8- and 2.4-fold more likely, respectively, to have consumed alcohol within 48 hours prior to their death, compared with matched living controls. More importantly, in a multivariate analysis adjusted for potential confounders, men and women who committed suicide were 6.2-fold and 10-fold more likely to have been intoxicated. The investigators concluded that it’s essential for suicide prevention programs to include components that discourage intoxication (Ann. Epidemiol. 2014;24:588-92).
Dr. Gorwood said a popular misconception among clinicians is that focusing solely on antidepressant therapy in patients with major depressive disorder and comorbid alcohol dependence will reduce their risk of suicidal behavior. A large Finnish national study scrutinizing the use of antidepressants and cause-specific mortality over the course of a decade showed this is not the case (J. Affect. Disord. 2013;148:278-85).
“The Finnish data means that probably if you are not also taking care of the alcohol dependence, then independently treating the associated mood disorder will not be an efficient way of reducing the suicide risk,” Dr. Gorwood noted.
He added, however, that getting patients with alcohol use disorder to stop drinking is hardly a panacea.
“We shouldn’t be naive. Stopping drinking alcohol will not resolve a lot of the difficulties that affect these patients. They have to build a new life and new types of functioning, and it’s difficult. There’s a lot of work to do. But it’s a very important step in reducing suicidal risk.”
Dr. Gorwood reported receiving research grants from Eli Lilly and Servier, and serving on scientific advisory boards or speakers panels for those pharmaceutical companies and eight others.
BERLIN– Alcohol dependence and major depressive disorder are similarly potent yet independent risk factors for suicidal behavior, according to Dr. Philip Gorwood.
Although alcohol use disorder and major depression are extremely common and often comorbid, the mechanisms by which they boost the risk for suicidal behavior are very different, he said at the annual congress of the European College of Neuropsychopharmacology.
“The ideation about suicidal behavior comes from the mood disorder, but the organization of the behavior – the suicidal attempt, especially when it is unplanned and impulsive – is driven by the alcohol consumption,” said Dr. Gorwood, professor of psychiatry at Rene Descartes University, Paris.
“The real take-home message is the difference between suicidal ideas and impulsive acts. Probably that was not well understood before. Alcohol dependence has no relationship with suicidal ideas. But once you have those ideas, alcohol consumption becomes very important in the risk of suicidal behavior,” he said.
A recent retrospective analysis of nearly 451,000 French patients hospitalized for suicide attempts during 2004-2011 showed their most common psychiatric diagnosis was major depressive disorder, present in 52% of the men and 65% of the women. Second most common – and far ahead of the rest of the pack – was alcohol use disorder, diagnosed in 36% of the hospitalized men and 49% of the women.
Alcohol probably facilitates suicidal behaviors in a variety of ways – by generating stressful life events, weakening social supports, worsening mood, restricting cognition and thereby inhibiting coping strategies, boosting impulsivity, and promoting inaccurate assessment of harm and pain.
A recent review of epidemiologic studies on the risk factors for suicide attempts and suicide among individuals with alcohol use disorder identified a clutch of risk factors that could be useful in clinical practice as a means of targeting problem drinkers at increased risk for suicidality: major depressive disorder, greater severity of alcohol use disorder, limited social support, stressful life events, aggression, medical illness, and economic adversity (Am. J. Prev. Med. 2014;47:S204-S208).
Other studies have identified additional risk factors that distinguish individuals with alcohol dependence who do attempt suicide from those who don’t: early onset of alcohol dependence, childhood trauma, a family history of suicidal behavior, and tobacco dependence. But if a clinician is going to rely on the two strongest risk factors in order to identify increased suicidal risk among alcohol-dependent patients, those would be major depression and the greater severity of alcohol dependence, according to Dr. Gorwood.
A study from the National Comorbidity Survey Replication based on a representative sample comprised of 9,282 U.S. adults concluded that alcohol abuse or dependence was associated with a 2.1-fold increased risk of a history of a suicide attempt, while major depressive disorder was independently associated with a 2.0-fold increased risk. In a multivariate analysis, major depressive disorder was associated with a statistically significant 2.3-fold increased risk of suicidal ideation but no significant increase in planned or unplanned suicide attempts. In contrast, alcohol abuse or dependence wasn’t associated with a significant increase in suicidal ideation but did carry a 2.9-fold increased risk of unplanned, impulsive suicide attempts (Mol. Psychiatry 2010;15:868-76).
A first-of-its-kind U.S. national study of postmortem blood alcohol levels as a means of assessing alcohol use prior to suicide concluded that men and women who committed suicide were 1.8- and 2.4-fold more likely, respectively, to have consumed alcohol within 48 hours prior to their death, compared with matched living controls. More importantly, in a multivariate analysis adjusted for potential confounders, men and women who committed suicide were 6.2-fold and 10-fold more likely to have been intoxicated. The investigators concluded that it’s essential for suicide prevention programs to include components that discourage intoxication (Ann. Epidemiol. 2014;24:588-92).
Dr. Gorwood said a popular misconception among clinicians is that focusing solely on antidepressant therapy in patients with major depressive disorder and comorbid alcohol dependence will reduce their risk of suicidal behavior. A large Finnish national study scrutinizing the use of antidepressants and cause-specific mortality over the course of a decade showed this is not the case (J. Affect. Disord. 2013;148:278-85).
“The Finnish data means that probably if you are not also taking care of the alcohol dependence, then independently treating the associated mood disorder will not be an efficient way of reducing the suicide risk,” Dr. Gorwood noted.
He added, however, that getting patients with alcohol use disorder to stop drinking is hardly a panacea.
“We shouldn’t be naive. Stopping drinking alcohol will not resolve a lot of the difficulties that affect these patients. They have to build a new life and new types of functioning, and it’s difficult. There’s a lot of work to do. But it’s a very important step in reducing suicidal risk.”
Dr. Gorwood reported receiving research grants from Eli Lilly and Servier, and serving on scientific advisory boards or speakers panels for those pharmaceutical companies and eight others.
BERLIN– Alcohol dependence and major depressive disorder are similarly potent yet independent risk factors for suicidal behavior, according to Dr. Philip Gorwood.
Although alcohol use disorder and major depression are extremely common and often comorbid, the mechanisms by which they boost the risk for suicidal behavior are very different, he said at the annual congress of the European College of Neuropsychopharmacology.
“The ideation about suicidal behavior comes from the mood disorder, but the organization of the behavior – the suicidal attempt, especially when it is unplanned and impulsive – is driven by the alcohol consumption,” said Dr. Gorwood, professor of psychiatry at Rene Descartes University, Paris.
“The real take-home message is the difference between suicidal ideas and impulsive acts. Probably that was not well understood before. Alcohol dependence has no relationship with suicidal ideas. But once you have those ideas, alcohol consumption becomes very important in the risk of suicidal behavior,” he said.
A recent retrospective analysis of nearly 451,000 French patients hospitalized for suicide attempts during 2004-2011 showed their most common psychiatric diagnosis was major depressive disorder, present in 52% of the men and 65% of the women. Second most common – and far ahead of the rest of the pack – was alcohol use disorder, diagnosed in 36% of the hospitalized men and 49% of the women.
Alcohol probably facilitates suicidal behaviors in a variety of ways – by generating stressful life events, weakening social supports, worsening mood, restricting cognition and thereby inhibiting coping strategies, boosting impulsivity, and promoting inaccurate assessment of harm and pain.
A recent review of epidemiologic studies on the risk factors for suicide attempts and suicide among individuals with alcohol use disorder identified a clutch of risk factors that could be useful in clinical practice as a means of targeting problem drinkers at increased risk for suicidality: major depressive disorder, greater severity of alcohol use disorder, limited social support, stressful life events, aggression, medical illness, and economic adversity (Am. J. Prev. Med. 2014;47:S204-S208).
Other studies have identified additional risk factors that distinguish individuals with alcohol dependence who do attempt suicide from those who don’t: early onset of alcohol dependence, childhood trauma, a family history of suicidal behavior, and tobacco dependence. But if a clinician is going to rely on the two strongest risk factors in order to identify increased suicidal risk among alcohol-dependent patients, those would be major depression and the greater severity of alcohol dependence, according to Dr. Gorwood.
A study from the National Comorbidity Survey Replication based on a representative sample comprised of 9,282 U.S. adults concluded that alcohol abuse or dependence was associated with a 2.1-fold increased risk of a history of a suicide attempt, while major depressive disorder was independently associated with a 2.0-fold increased risk. In a multivariate analysis, major depressive disorder was associated with a statistically significant 2.3-fold increased risk of suicidal ideation but no significant increase in planned or unplanned suicide attempts. In contrast, alcohol abuse or dependence wasn’t associated with a significant increase in suicidal ideation but did carry a 2.9-fold increased risk of unplanned, impulsive suicide attempts (Mol. Psychiatry 2010;15:868-76).
A first-of-its-kind U.S. national study of postmortem blood alcohol levels as a means of assessing alcohol use prior to suicide concluded that men and women who committed suicide were 1.8- and 2.4-fold more likely, respectively, to have consumed alcohol within 48 hours prior to their death, compared with matched living controls. More importantly, in a multivariate analysis adjusted for potential confounders, men and women who committed suicide were 6.2-fold and 10-fold more likely to have been intoxicated. The investigators concluded that it’s essential for suicide prevention programs to include components that discourage intoxication (Ann. Epidemiol. 2014;24:588-92).
Dr. Gorwood said a popular misconception among clinicians is that focusing solely on antidepressant therapy in patients with major depressive disorder and comorbid alcohol dependence will reduce their risk of suicidal behavior. A large Finnish national study scrutinizing the use of antidepressants and cause-specific mortality over the course of a decade showed this is not the case (J. Affect. Disord. 2013;148:278-85).
“The Finnish data means that probably if you are not also taking care of the alcohol dependence, then independently treating the associated mood disorder will not be an efficient way of reducing the suicide risk,” Dr. Gorwood noted.
He added, however, that getting patients with alcohol use disorder to stop drinking is hardly a panacea.
“We shouldn’t be naive. Stopping drinking alcohol will not resolve a lot of the difficulties that affect these patients. They have to build a new life and new types of functioning, and it’s difficult. There’s a lot of work to do. But it’s a very important step in reducing suicidal risk.”
Dr. Gorwood reported receiving research grants from Eli Lilly and Servier, and serving on scientific advisory boards or speakers panels for those pharmaceutical companies and eight others.
EXPERT ANALYSIS FROM THE ECNP CONGRESS

Fulvestrant bests anastrozole in advanced breast cancer
SAN ANTONIO – Fulvestrant resulted in a 30% improvement in overall survival, compared with anastrozole as first-line therapy for postmenopausal women with hormone receptor–positive advanced or metastatic breast cancer in the randomized FIRST trial.
This new finding follows upon a previously reported 34% reduction in the risk of disease progression in an earlier FIRST analysis. Plus, significant improvements in both disease progression and overall survival were seen with fulvestrant at 500 mg as second-line endocrine therapy in the Phase III CONFIRM (Comparison of Faslodex in Recurrent or Metastatic Breast Cancer) trial (J. Natl. Cancer Inst. Jan 2014;106:djt337 [doi:10.1093/jnci/djt337]). The clinical performance of fulvestrant in these two studies outpaces that of any other endocrine therapy for advanced breast cancer, Dr. John Robertson observed in presenting the new FIRST overall survival results at the San Antonio Breast Cancer Symposium.
“I don’t know of any other endocrine therapy where you can see both a time-to-progression and overall survival benefit in both the second- and first-line settings. So I think this is a new and exciting development in endocrine therapy for women with advanced breast cancer,” declared Dr. John Robertson, professor of surgery at the University of Nottingham, England.

FIRST (Fulvestrant First-line Study Comparing Endocrine Treatments) was a phase II, open-label study involving 205 women randomized to intramuscular fulvestrant (Faslodex) at 500 mg once monthly or the aromatase inhibitor anastrozole (Arimidex) at 1 mg/day orally. Aromatase inhibitors have been considered the standard therapy in this setting.
At a median follow-up of 48.8 months, the median overall survival was 54.1 months in the fulvestrant arm, compared with 48.4 months with anastrozole, for a 5.7-month advantage in favor of fulvestrant. This translated to a 30% reduction in the risk of death in the fulvestrant group (P = .041), which Dr. Robertson believes patients and their families will consider highly clinically meaningful.
“When I first started taking care of breast cancer patients like these 30 years ago, the average survival was 24 months. In this study, with fulvestrant it’s 54 months. We’re seeing step-by-step improvements,” he commented.
The advantage in overall survival seen with fulvestrant was consistent across all predefined subgroups based upon age, prior chemotherapy or endocrine therapy, visceral involvement status, and progesterone receptor status.
Both treatments were generally well tolerated, with no new safety concerns observed.
“Fulvestrant is a drug that’s really well tolerated. I can’t think of another medication in oncology where you can double the dose – from 250 to 500 mg – with no increase in side effects,” Dr. Robertson observed.
Now underway is the phase III FALCON (Fulvestrant and Anastrozole Compared in Hormonal Therapy–Naive Advanced Breast Cancer) trial, in which 450 hormone therapy–naive women with advanced breast cancer are being randomized to fulvestrant at 500 mg or anastrozole.
Dr. C. Kent Osborne commented, “Many people, including myself, have thought since the time fulvestrant was developed in the lab that it was the best endocrine therapy that we have.” But the drug “has had a checkered past,” he noted, citing the inconvenience of the required once-monthly intramuscular injections, plus the fact that early studies of fulvestrant as adjuvant therapy in early breast cancer yielded unimpressive results because they used fulvestrant at 250 mg, which turned out to be the wrong dose.
“In view of the data from CONFIRM and FIRST, are there plans to bring fulvestrant back into the adjuvant setting?” asked Dr. Osborne, professor of medicine and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston.
Dr. Robertson replied that it’s now quite apparent that fulvestrant would likely outperform aromatase inhibitors or tamoxifen as adjuvant therapy in early breast cancer, but he doubts that AstraZeneca, which markets the selective estrogen receptor down-regulator, will sponsor the requisite clinical trials. It wouldn’t be commercially viable. Adjuvant breast cancer therapy trials take a long time to produce results, and the drug will be close to going off patent by then.
“It’s a study that’s crying out to be done given what we’ve seen here in the FIRST study, but I think it is unlikely to happen unless somebody like the NIH takes on the funding,” Dr. Robertson said.
Pharmaceutical companies are now developing next-generation selective estrogen receptor down-regulators that can be given orally. They’re so new that it’s not yet known whether they’re actually effective, but if they are, they’ll be the ones studied as adjuvant therapy in clinical trials, not fulvestrant, he predicted.
“I’m skeptical,” said Dr. Osborne. “Trying to develop a better fulvestrant might work, but remember that after tamoxifen came out many, many companies tried to develop a better tamoxifen – and here we are with tamoxifen 40 years later.”
The FIRST trial was funded by AstraZeneca. Dr. Robertson reported serving as a consultant to that company as well as Bayer HealthCare and receiving research funding from both companies along with Amgen and Novartis.
SAN ANTONIO – Fulvestrant resulted in a 30% improvement in overall survival, compared with anastrozole as first-line therapy for postmenopausal women with hormone receptor–positive advanced or metastatic breast cancer in the randomized FIRST trial.
This new finding follows upon a previously reported 34% reduction in the risk of disease progression in an earlier FIRST analysis. Plus, significant improvements in both disease progression and overall survival were seen with fulvestrant at 500 mg as second-line endocrine therapy in the Phase III CONFIRM (Comparison of Faslodex in Recurrent or Metastatic Breast Cancer) trial (J. Natl. Cancer Inst. Jan 2014;106:djt337 [doi:10.1093/jnci/djt337]). The clinical performance of fulvestrant in these two studies outpaces that of any other endocrine therapy for advanced breast cancer, Dr. John Robertson observed in presenting the new FIRST overall survival results at the San Antonio Breast Cancer Symposium.
“I don’t know of any other endocrine therapy where you can see both a time-to-progression and overall survival benefit in both the second- and first-line settings. So I think this is a new and exciting development in endocrine therapy for women with advanced breast cancer,” declared Dr. John Robertson, professor of surgery at the University of Nottingham, England.
FIRST (Fulvestrant First-line Study Comparing Endocrine Treatments) was a phase II, open-label study involving 205 women randomized to intramuscular fulvestrant (Faslodex) at 500 mg once monthly or the aromatase inhibitor anastrozole (Arimidex) at 1 mg/day orally. Aromatase inhibitors have been considered the standard therapy in this setting.
At a median follow-up of 48.8 months, the median overall survival was 54.1 months in the fulvestrant arm, compared with 48.4 months with anastrozole, for a 5.7-month advantage in favor of fulvestrant. This translated to a 30% reduction in the risk of death in the fulvestrant group (P = .041), which Dr. Robertson believes patients and their families will consider highly clinically meaningful.
“When I first started taking care of breast cancer patients like these 30 years ago, the average survival was 24 months. In this study, with fulvestrant it’s 54 months. We’re seeing step-by-step improvements,” he commented.
The advantage in overall survival seen with fulvestrant was consistent across all predefined subgroups based upon age, prior chemotherapy or endocrine therapy, visceral involvement status, and progesterone receptor status.
Both treatments were generally well tolerated, with no new safety concerns observed.
“Fulvestrant is a drug that’s really well tolerated. I can’t think of another medication in oncology where you can double the dose – from 250 to 500 mg – with no increase in side effects,” Dr. Robertson observed.
Now underway is the phase III FALCON (Fulvestrant and Anastrozole Compared in Hormonal Therapy–Naive Advanced Breast Cancer) trial, in which 450 hormone therapy–naive women with advanced breast cancer are being randomized to fulvestrant at 500 mg or anastrozole.
Dr. C. Kent Osborne commented, “Many people, including myself, have thought since the time fulvestrant was developed in the lab that it was the best endocrine therapy that we have.” But the drug “has had a checkered past,” he noted, citing the inconvenience of the required once-monthly intramuscular injections, plus the fact that early studies of fulvestrant as adjuvant therapy in early breast cancer yielded unimpressive results because they used fulvestrant at 250 mg, which turned out to be the wrong dose.
“In view of the data from CONFIRM and FIRST, are there plans to bring fulvestrant back into the adjuvant setting?” asked Dr. Osborne, professor of medicine and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston.
Dr. Robertson replied that it’s now quite apparent that fulvestrant would likely outperform aromatase inhibitors or tamoxifen as adjuvant therapy in early breast cancer, but he doubts that AstraZeneca, which markets the selective estrogen receptor down-regulator, will sponsor the requisite clinical trials. It wouldn’t be commercially viable. Adjuvant breast cancer therapy trials take a long time to produce results, and the drug will be close to going off patent by then.
“It’s a study that’s crying out to be done given what we’ve seen here in the FIRST study, but I think it is unlikely to happen unless somebody like the NIH takes on the funding,” Dr. Robertson said.
Pharmaceutical companies are now developing next-generation selective estrogen receptor down-regulators that can be given orally. They’re so new that it’s not yet known whether they’re actually effective, but if they are, they’ll be the ones studied as adjuvant therapy in clinical trials, not fulvestrant, he predicted.
“I’m skeptical,” said Dr. Osborne. “Trying to develop a better fulvestrant might work, but remember that after tamoxifen came out many, many companies tried to develop a better tamoxifen – and here we are with tamoxifen 40 years later.”
The FIRST trial was funded by AstraZeneca. Dr. Robertson reported serving as a consultant to that company as well as Bayer HealthCare and receiving research funding from both companies along with Amgen and Novartis.
SAN ANTONIO – Fulvestrant resulted in a 30% improvement in overall survival, compared with anastrozole as first-line therapy for postmenopausal women with hormone receptor–positive advanced or metastatic breast cancer in the randomized FIRST trial.
This new finding follows upon a previously reported 34% reduction in the risk of disease progression in an earlier FIRST analysis. Plus, significant improvements in both disease progression and overall survival were seen with fulvestrant at 500 mg as second-line endocrine therapy in the Phase III CONFIRM (Comparison of Faslodex in Recurrent or Metastatic Breast Cancer) trial (J. Natl. Cancer Inst. Jan 2014;106:djt337 [doi:10.1093/jnci/djt337]). The clinical performance of fulvestrant in these two studies outpaces that of any other endocrine therapy for advanced breast cancer, Dr. John Robertson observed in presenting the new FIRST overall survival results at the San Antonio Breast Cancer Symposium.
“I don’t know of any other endocrine therapy where you can see both a time-to-progression and overall survival benefit in both the second- and first-line settings. So I think this is a new and exciting development in endocrine therapy for women with advanced breast cancer,” declared Dr. John Robertson, professor of surgery at the University of Nottingham, England.
FIRST (Fulvestrant First-line Study Comparing Endocrine Treatments) was a phase II, open-label study involving 205 women randomized to intramuscular fulvestrant (Faslodex) at 500 mg once monthly or the aromatase inhibitor anastrozole (Arimidex) at 1 mg/day orally. Aromatase inhibitors have been considered the standard therapy in this setting.
At a median follow-up of 48.8 months, the median overall survival was 54.1 months in the fulvestrant arm, compared with 48.4 months with anastrozole, for a 5.7-month advantage in favor of fulvestrant. This translated to a 30% reduction in the risk of death in the fulvestrant group (P = .041), which Dr. Robertson believes patients and their families will consider highly clinically meaningful.
“When I first started taking care of breast cancer patients like these 30 years ago, the average survival was 24 months. In this study, with fulvestrant it’s 54 months. We’re seeing step-by-step improvements,” he commented.
The advantage in overall survival seen with fulvestrant was consistent across all predefined subgroups based upon age, prior chemotherapy or endocrine therapy, visceral involvement status, and progesterone receptor status.
Both treatments were generally well tolerated, with no new safety concerns observed.
“Fulvestrant is a drug that’s really well tolerated. I can’t think of another medication in oncology where you can double the dose – from 250 to 500 mg – with no increase in side effects,” Dr. Robertson observed.
Now underway is the phase III FALCON (Fulvestrant and Anastrozole Compared in Hormonal Therapy–Naive Advanced Breast Cancer) trial, in which 450 hormone therapy–naive women with advanced breast cancer are being randomized to fulvestrant at 500 mg or anastrozole.
Dr. C. Kent Osborne commented, “Many people, including myself, have thought since the time fulvestrant was developed in the lab that it was the best endocrine therapy that we have.” But the drug “has had a checkered past,” he noted, citing the inconvenience of the required once-monthly intramuscular injections, plus the fact that early studies of fulvestrant as adjuvant therapy in early breast cancer yielded unimpressive results because they used fulvestrant at 250 mg, which turned out to be the wrong dose.
“In view of the data from CONFIRM and FIRST, are there plans to bring fulvestrant back into the adjuvant setting?” asked Dr. Osborne, professor of medicine and director of the Dan L. Duncan Cancer Center at Baylor College of Medicine, Houston.
Dr. Robertson replied that it’s now quite apparent that fulvestrant would likely outperform aromatase inhibitors or tamoxifen as adjuvant therapy in early breast cancer, but he doubts that AstraZeneca, which markets the selective estrogen receptor down-regulator, will sponsor the requisite clinical trials. It wouldn’t be commercially viable. Adjuvant breast cancer therapy trials take a long time to produce results, and the drug will be close to going off patent by then.
“It’s a study that’s crying out to be done given what we’ve seen here in the FIRST study, but I think it is unlikely to happen unless somebody like the NIH takes on the funding,” Dr. Robertson said.
Pharmaceutical companies are now developing next-generation selective estrogen receptor down-regulators that can be given orally. They’re so new that it’s not yet known whether they’re actually effective, but if they are, they’ll be the ones studied as adjuvant therapy in clinical trials, not fulvestrant, he predicted.
“I’m skeptical,” said Dr. Osborne. “Trying to develop a better fulvestrant might work, but remember that after tamoxifen came out many, many companies tried to develop a better tamoxifen – and here we are with tamoxifen 40 years later.”
The FIRST trial was funded by AstraZeneca. Dr. Robertson reported serving as a consultant to that company as well as Bayer HealthCare and receiving research funding from both companies along with Amgen and Novartis.
AT SABCS 2014
Key clinical point: The selective estrogen receptor down-regulator fulvestrant proved superior to anastrozole in disease progression and overall survival in women with hormone receptor–positive advanced breast cancer.
Major finding: At a median follow-up of 48.8 months, overall survival was 54.1 months in patients on fulvestrant, fully 5.7 months more than the 48.4 months with anastrozole.
Data source: The FIRST trial was a phase II, open-label study of 205 women randomized to fulvestrant or anastrozole.
Disclosures: The FIRST trial was sponsored by AstraZeneca. The presenter has received research funds from and served as a consultant to the company.

Takotsubo cardiomyopathy: predicting in-hospital mortality
CHICAGO – A novel risk score has been developed for predicting the risk of in-hospital mortality in patients with takotsubo cardiomyopathy.
The new risk score’s unique strength is that it was developed using hospital data on a huge patient population with this rare and incompletely understood cardiac condition: 10,582 patients hospitalized for takotsubo cardiomyopathy in seven U.S. states, Dr. David P. Kao reported at the American Heart Association scientific sessions.
He used multivariate logistic regression analysis to identify seven independent characteristics predictive of mortality in the study population. Their collective area under the curve as predictors was 0.70, which is considered good. And while the overall in-hospital mortality rate was low at 4.4%, it varied enormously depending upon how many of the seven risk factors were present, according to Dr. Kao of the University of Colorado, Denver.
In-hospital mortality ranged from 1.6% in the 2,585 patients with none of the risk factors to 19.6% in those with three or more. The 616 patients with at least three risk factors accounted for 22% of all in-hospital deaths in patients with takotsubo cardiomyopathy in California, New York, New Jersey, Colorado, West Virginia, New Hampshire, and Vermont during 2006-2012.
Intracranial hemorrhage, which was present in 2% of hospitalized takotsubo cardiomyopathy patients, was the most potent predictor both of in-hospital mortality and major adverse events. In multivariate analysis, intracranial hemorrhage was independently associated with a 6.8-fold increased risk of in-hospital mortality. The other mortality risk factors and their associated odds ratios were age 60 years or older, with a 1.8-fold risk; Asian race, 1.8-fold; male sex, 1.9-fold; acute renal failure, 4.1-fold; atrial fibrillation or flutter, 1.7-fold; and stroke, 2.9-fold.
The simple, user-friendly risk score is derived by totaling the number of risk factors present in a given hospitalized patient. The presence of each additional risk factor increased the odds of in-hospital death by 2.2-fold, according to Dr. Kao.

Takotsubo cardiomyopathy is marked by acute, typically rapidly reversible left ventricular dysfunction without evidence of epicardial coronary artery occlusion. It occurs most often in postmenopausal women in response to emotional or physical stress. Indeed, 89% of the more than 10,000 affected patients in this series were women.
Most adverse events in patients with takotsubo cardiomyopathy occur during their first hospitalization for the disorder. In this large series, 22% of patients experienced major adverse events, including ventricular arrhythmias, acute heart failure, cardiogenic shock, pulmonary edema, or ventricular rupture.
In a separate multiple logistic regression analysis, Dr. Kao and coinvestigator Dr. JoAnn Lindenfeld, also of the University of Colorado, identified eight characteristics independently predictive of in-hospital major adverse events. Five of them were also predictors of in-hospital mortality: intracranial hemorrhage, male gender, stroke, atrial fibrillation/flutter, and acute renal failure. The other three were age less than 60, substance abuse, and anemia. The major adverse event rate ranged from 10% in patients with none of the risk factors to 56% in the 242 patients having four or more. The 1,057 patients with three or more risk factors had a 47% major adverse event rate and accounted for 20% of all such events.
Dr. Kao reported having no financial conflicts related to this study.
CHICAGO – A novel risk score has been developed for predicting the risk of in-hospital mortality in patients with takotsubo cardiomyopathy.
The new risk score’s unique strength is that it was developed using hospital data on a huge patient population with this rare and incompletely understood cardiac condition: 10,582 patients hospitalized for takotsubo cardiomyopathy in seven U.S. states, Dr. David P. Kao reported at the American Heart Association scientific sessions.
He used multivariate logistic regression analysis to identify seven independent characteristics predictive of mortality in the study population. Their collective area under the curve as predictors was 0.70, which is considered good. And while the overall in-hospital mortality rate was low at 4.4%, it varied enormously depending upon how many of the seven risk factors were present, according to Dr. Kao of the University of Colorado, Denver.
In-hospital mortality ranged from 1.6% in the 2,585 patients with none of the risk factors to 19.6% in those with three or more. The 616 patients with at least three risk factors accounted for 22% of all in-hospital deaths in patients with takotsubo cardiomyopathy in California, New York, New Jersey, Colorado, West Virginia, New Hampshire, and Vermont during 2006-2012.
Intracranial hemorrhage, which was present in 2% of hospitalized takotsubo cardiomyopathy patients, was the most potent predictor both of in-hospital mortality and major adverse events. In multivariate analysis, intracranial hemorrhage was independently associated with a 6.8-fold increased risk of in-hospital mortality. The other mortality risk factors and their associated odds ratios were age 60 years or older, with a 1.8-fold risk; Asian race, 1.8-fold; male sex, 1.9-fold; acute renal failure, 4.1-fold; atrial fibrillation or flutter, 1.7-fold; and stroke, 2.9-fold.
The simple, user-friendly risk score is derived by totaling the number of risk factors present in a given hospitalized patient. The presence of each additional risk factor increased the odds of in-hospital death by 2.2-fold, according to Dr. Kao.
Takotsubo cardiomyopathy is marked by acute, typically rapidly reversible left ventricular dysfunction without evidence of epicardial coronary artery occlusion. It occurs most often in postmenopausal women in response to emotional or physical stress. Indeed, 89% of the more than 10,000 affected patients in this series were women.
Most adverse events in patients with takotsubo cardiomyopathy occur during their first hospitalization for the disorder. In this large series, 22% of patients experienced major adverse events, including ventricular arrhythmias, acute heart failure, cardiogenic shock, pulmonary edema, or ventricular rupture.
In a separate multiple logistic regression analysis, Dr. Kao and coinvestigator Dr. JoAnn Lindenfeld, also of the University of Colorado, identified eight characteristics independently predictive of in-hospital major adverse events. Five of them were also predictors of in-hospital mortality: intracranial hemorrhage, male gender, stroke, atrial fibrillation/flutter, and acute renal failure. The other three were age less than 60, substance abuse, and anemia. The major adverse event rate ranged from 10% in patients with none of the risk factors to 56% in the 242 patients having four or more. The 1,057 patients with three or more risk factors had a 47% major adverse event rate and accounted for 20% of all such events.
Dr. Kao reported having no financial conflicts related to this study.
CHICAGO – A novel risk score has been developed for predicting the risk of in-hospital mortality in patients with takotsubo cardiomyopathy.
The new risk score’s unique strength is that it was developed using hospital data on a huge patient population with this rare and incompletely understood cardiac condition: 10,582 patients hospitalized for takotsubo cardiomyopathy in seven U.S. states, Dr. David P. Kao reported at the American Heart Association scientific sessions.
He used multivariate logistic regression analysis to identify seven independent characteristics predictive of mortality in the study population. Their collective area under the curve as predictors was 0.70, which is considered good. And while the overall in-hospital mortality rate was low at 4.4%, it varied enormously depending upon how many of the seven risk factors were present, according to Dr. Kao of the University of Colorado, Denver.
In-hospital mortality ranged from 1.6% in the 2,585 patients with none of the risk factors to 19.6% in those with three or more. The 616 patients with at least three risk factors accounted for 22% of all in-hospital deaths in patients with takotsubo cardiomyopathy in California, New York, New Jersey, Colorado, West Virginia, New Hampshire, and Vermont during 2006-2012.
Intracranial hemorrhage, which was present in 2% of hospitalized takotsubo cardiomyopathy patients, was the most potent predictor both of in-hospital mortality and major adverse events. In multivariate analysis, intracranial hemorrhage was independently associated with a 6.8-fold increased risk of in-hospital mortality. The other mortality risk factors and their associated odds ratios were age 60 years or older, with a 1.8-fold risk; Asian race, 1.8-fold; male sex, 1.9-fold; acute renal failure, 4.1-fold; atrial fibrillation or flutter, 1.7-fold; and stroke, 2.9-fold.
The simple, user-friendly risk score is derived by totaling the number of risk factors present in a given hospitalized patient. The presence of each additional risk factor increased the odds of in-hospital death by 2.2-fold, according to Dr. Kao.
Takotsubo cardiomyopathy is marked by acute, typically rapidly reversible left ventricular dysfunction without evidence of epicardial coronary artery occlusion. It occurs most often in postmenopausal women in response to emotional or physical stress. Indeed, 89% of the more than 10,000 affected patients in this series were women.
Most adverse events in patients with takotsubo cardiomyopathy occur during their first hospitalization for the disorder. In this large series, 22% of patients experienced major adverse events, including ventricular arrhythmias, acute heart failure, cardiogenic shock, pulmonary edema, or ventricular rupture.
In a separate multiple logistic regression analysis, Dr. Kao and coinvestigator Dr. JoAnn Lindenfeld, also of the University of Colorado, identified eight characteristics independently predictive of in-hospital major adverse events. Five of them were also predictors of in-hospital mortality: intracranial hemorrhage, male gender, stroke, atrial fibrillation/flutter, and acute renal failure. The other three were age less than 60, substance abuse, and anemia. The major adverse event rate ranged from 10% in patients with none of the risk factors to 56% in the 242 patients having four or more. The 1,057 patients with three or more risk factors had a 47% major adverse event rate and accounted for 20% of all such events.
Dr. Kao reported having no financial conflicts related to this study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: The risk of in-hospital mortality in patients with takotsubo cardiomyopathy can be predicted using a simple risk score based upon information readily available at the bedside.
Major finding: In-hospital mortality ranged from just 1.6% in patients with no risk factors to 19.6% in those with any three or more.
Data source: The seven independent characteristics associated with in-hospital mortality were identified through multivariate logistic regression analysis applied to the hospital records of 10,582 patients with takotsubo cardiomyopathy in seven states.
Disclosures: The presenter reported having no financial conflicts in connection with this study, conducted free of commercial interests.

Acupuncture beats gabapentin for hot flashes in RCT
SAN ANTONIO – Electroacupuncture proved significantly more effective than gabapentin for treatment of hot flashes in breast cancer survivors in a randomized, placebo-controlled clinical trial.
Acupuncture was far better tolerated as well. The rate of treatment-related adverse events was higher in patients randomized to gabapentin than to women assigned to electroacupuncture, sham acupuncture, or placebo, Dr. Jun J. Mao reported at the San Antonio Breast Cancer Symposium.
The study included 120 women who had completed their primary treatment for breast cancer and were experiencing troublesome hot flashes at least twice daily. Participants were randomized to 8 weeks of treatment with electroacupuncture, sham acupuncture, gabapentin at 300 mg t.i.d., or placebo. The primary endpoint was change from baseline to week 8 in patients’ hot flash composite score as gleaned from their daily hot flash diary. The secondary endpoint was durability of response based upon the hot flash composite score at week 24, fully 4 months after patients went off treatment, explained Dr. Mao, a family physician and licensed acupuncturist at the University of Pennsylvania, Philadelphia.

From a baseline mean hot flash score of 14.3, scores dropped by a mean of 7.4 points by week 8 in the electroacupuncture recipients. This represented a significantly greater treatment effect, compared with the reductions of 5.9 points with sham acupuncture, 5.2 points with gabapentin, and 3.4 points with placebo.
Only acupuncture showed a durable treatment benefit at 24 weeks. Indeed, the magnitude of the reduction in hot flash scores 4 months after the final acupuncture session was, intriguingly, even greater than at 8 weeks, both for electroacupuncture and sham acupuncture. The mean reduction in hot flash score at 24 weeks was 8.5 points in the electroacupuncture group, as compared with 7.4 points at week 8. Sham acupuncture showed a mean 6.1-point decrease in the hot flash score at week 24, gabapentin a 4.6-point reduction, and placebo a 2.8-point drop.
No serious adverse events were noted during the study. However, 48% of gabapentin-treated patients reported treatment-related adverse events, compared with 29% on placebo, 19% who got electroacupuncture, and 3% with sham acupuncture, Dr. Mao continued.
The adherence rate to acupuncture was 90%, versus 75% with gabapentin.
Electroacupuncture entailed using a TENS unit to pass a 2-Hz current through acupuncture needles placed at traditional points. There were two sessions per week for the first 2 weeks, then once-weekly sessions for the remaining 6 weeks.
“The needle insertion is generally brief, 5-10 minutes. Then the patient rests for about 20 minutes,” according to the family physician.
Sham acupuncture utilized nonpenetrating Streitberger needles at nontraditional acupuncture points.
Discussant Dr. Michelle E. Melisko noted that this is one of the largest randomized trials of acupuncture for hot flashes ever done, and it included women of widely varied ages and a substantial African American population. It’s also the first study she’s aware of to compare acupuncture to a nonhormonal medication.
She observed that hot flashes tend to be particularly frequent, severe, and often more debilitating in breast cancer survivors than in the general population. Gabapentin (Neurontin) and venlafaxine (Effexor) are probably the two most widely prescribed centrally acting drugs for treatment of hot flashes in breast cancer survivors.
“Gabapentin is often an appealing choice. In my practice it’s a drug often used to kill two birds with one stone. It can make people sleepy, so if patients are having hot flashes and night sweats it’s nice to give them an agent they can take at bedtime that might have the dual effects of reducing hot flashes as well as improving their sleep,” said Dr. Melisko, an oncologist at the University of California, San Francisco.
She noted that a systematic review of gabapentin for hot flashes in 901 patients in seven clinical trials, including four studies in breast cancer survivors, concluded the drug resulted in 20%-30% reductions in hot flash frequency and severity, but with a dropout rate twice that for placebo (Clin. Therapeutics 2009;31:221-35).But lots of breast cancer survivors say they don’t want to take an additional side effect–laden medication to treat a different set of treatment-induced side effects, Dr. Melisko continued. They’re interested in trying complementary and alternative medicine. And while a Cochrane review has concluded that acupuncture resulted in a significant reduction in hot flash severity but not frequency (Cochrane Database Syst. Rev. 2013 July 30;7:CD007410), Dr. Melisko noted that many of the trials included in that analysis may have been too brief to give acupuncture a fair shake.
Dr. Mao agreed.
“By 4 weeks in our trial you see only about one-half of the eventual effect of electroacupuncture. So if you design a short trial you may not get to the full therapeutic dose,” he said. “With acupuncture, it’s a slow start but eventual substantial effect. I tell patients you need to give acupuncture a therapeutic trial of at least six treatments. If at that point you don’t have any benefit, it may not work for you, but if you don’t try that amount it’s suboptimal.”
In acupuncture trials across the board, whether in the setting of cancer, chronic pain, or various other conditions, roughly one-third of patients are nonresponders, according to Dr. Mao.
His study was funded by the NIH’s National Center for Complementary and Alternative Medicine. He reported having no financial conflicts.
SAN ANTONIO – Electroacupuncture proved significantly more effective than gabapentin for treatment of hot flashes in breast cancer survivors in a randomized, placebo-controlled clinical trial.
Acupuncture was far better tolerated as well. The rate of treatment-related adverse events was higher in patients randomized to gabapentin than to women assigned to electroacupuncture, sham acupuncture, or placebo, Dr. Jun J. Mao reported at the San Antonio Breast Cancer Symposium.
The study included 120 women who had completed their primary treatment for breast cancer and were experiencing troublesome hot flashes at least twice daily. Participants were randomized to 8 weeks of treatment with electroacupuncture, sham acupuncture, gabapentin at 300 mg t.i.d., or placebo. The primary endpoint was change from baseline to week 8 in patients’ hot flash composite score as gleaned from their daily hot flash diary. The secondary endpoint was durability of response based upon the hot flash composite score at week 24, fully 4 months after patients went off treatment, explained Dr. Mao, a family physician and licensed acupuncturist at the University of Pennsylvania, Philadelphia.
From a baseline mean hot flash score of 14.3, scores dropped by a mean of 7.4 points by week 8 in the electroacupuncture recipients. This represented a significantly greater treatment effect, compared with the reductions of 5.9 points with sham acupuncture, 5.2 points with gabapentin, and 3.4 points with placebo.
Only acupuncture showed a durable treatment benefit at 24 weeks. Indeed, the magnitude of the reduction in hot flash scores 4 months after the final acupuncture session was, intriguingly, even greater than at 8 weeks, both for electroacupuncture and sham acupuncture. The mean reduction in hot flash score at 24 weeks was 8.5 points in the electroacupuncture group, as compared with 7.4 points at week 8. Sham acupuncture showed a mean 6.1-point decrease in the hot flash score at week 24, gabapentin a 4.6-point reduction, and placebo a 2.8-point drop.
No serious adverse events were noted during the study. However, 48% of gabapentin-treated patients reported treatment-related adverse events, compared with 29% on placebo, 19% who got electroacupuncture, and 3% with sham acupuncture, Dr. Mao continued.
The adherence rate to acupuncture was 90%, versus 75% with gabapentin.
Electroacupuncture entailed using a TENS unit to pass a 2-Hz current through acupuncture needles placed at traditional points. There were two sessions per week for the first 2 weeks, then once-weekly sessions for the remaining 6 weeks.
“The needle insertion is generally brief, 5-10 minutes. Then the patient rests for about 20 minutes,” according to the family physician.
Sham acupuncture utilized nonpenetrating Streitberger needles at nontraditional acupuncture points.
Discussant Dr. Michelle E. Melisko noted that this is one of the largest randomized trials of acupuncture for hot flashes ever done, and it included women of widely varied ages and a substantial African American population. It’s also the first study she’s aware of to compare acupuncture to a nonhormonal medication.
She observed that hot flashes tend to be particularly frequent, severe, and often more debilitating in breast cancer survivors than in the general population. Gabapentin (Neurontin) and venlafaxine (Effexor) are probably the two most widely prescribed centrally acting drugs for treatment of hot flashes in breast cancer survivors.
“Gabapentin is often an appealing choice. In my practice it’s a drug often used to kill two birds with one stone. It can make people sleepy, so if patients are having hot flashes and night sweats it’s nice to give them an agent they can take at bedtime that might have the dual effects of reducing hot flashes as well as improving their sleep,” said Dr. Melisko, an oncologist at the University of California, San Francisco.
She noted that a systematic review of gabapentin for hot flashes in 901 patients in seven clinical trials, including four studies in breast cancer survivors, concluded the drug resulted in 20%-30% reductions in hot flash frequency and severity, but with a dropout rate twice that for placebo (Clin. Therapeutics 2009;31:221-35).But lots of breast cancer survivors say they don’t want to take an additional side effect–laden medication to treat a different set of treatment-induced side effects, Dr. Melisko continued. They’re interested in trying complementary and alternative medicine. And while a Cochrane review has concluded that acupuncture resulted in a significant reduction in hot flash severity but not frequency (Cochrane Database Syst. Rev. 2013 July 30;7:CD007410), Dr. Melisko noted that many of the trials included in that analysis may have been too brief to give acupuncture a fair shake.
Dr. Mao agreed.
“By 4 weeks in our trial you see only about one-half of the eventual effect of electroacupuncture. So if you design a short trial you may not get to the full therapeutic dose,” he said. “With acupuncture, it’s a slow start but eventual substantial effect. I tell patients you need to give acupuncture a therapeutic trial of at least six treatments. If at that point you don’t have any benefit, it may not work for you, but if you don’t try that amount it’s suboptimal.”
In acupuncture trials across the board, whether in the setting of cancer, chronic pain, or various other conditions, roughly one-third of patients are nonresponders, according to Dr. Mao.
His study was funded by the NIH’s National Center for Complementary and Alternative Medicine. He reported having no financial conflicts.
SAN ANTONIO – Electroacupuncture proved significantly more effective than gabapentin for treatment of hot flashes in breast cancer survivors in a randomized, placebo-controlled clinical trial.
Acupuncture was far better tolerated as well. The rate of treatment-related adverse events was higher in patients randomized to gabapentin than to women assigned to electroacupuncture, sham acupuncture, or placebo, Dr. Jun J. Mao reported at the San Antonio Breast Cancer Symposium.
The study included 120 women who had completed their primary treatment for breast cancer and were experiencing troublesome hot flashes at least twice daily. Participants were randomized to 8 weeks of treatment with electroacupuncture, sham acupuncture, gabapentin at 300 mg t.i.d., or placebo. The primary endpoint was change from baseline to week 8 in patients’ hot flash composite score as gleaned from their daily hot flash diary. The secondary endpoint was durability of response based upon the hot flash composite score at week 24, fully 4 months after patients went off treatment, explained Dr. Mao, a family physician and licensed acupuncturist at the University of Pennsylvania, Philadelphia.
From a baseline mean hot flash score of 14.3, scores dropped by a mean of 7.4 points by week 8 in the electroacupuncture recipients. This represented a significantly greater treatment effect, compared with the reductions of 5.9 points with sham acupuncture, 5.2 points with gabapentin, and 3.4 points with placebo.
Only acupuncture showed a durable treatment benefit at 24 weeks. Indeed, the magnitude of the reduction in hot flash scores 4 months after the final acupuncture session was, intriguingly, even greater than at 8 weeks, both for electroacupuncture and sham acupuncture. The mean reduction in hot flash score at 24 weeks was 8.5 points in the electroacupuncture group, as compared with 7.4 points at week 8. Sham acupuncture showed a mean 6.1-point decrease in the hot flash score at week 24, gabapentin a 4.6-point reduction, and placebo a 2.8-point drop.
No serious adverse events were noted during the study. However, 48% of gabapentin-treated patients reported treatment-related adverse events, compared with 29% on placebo, 19% who got electroacupuncture, and 3% with sham acupuncture, Dr. Mao continued.
The adherence rate to acupuncture was 90%, versus 75% with gabapentin.
Electroacupuncture entailed using a TENS unit to pass a 2-Hz current through acupuncture needles placed at traditional points. There were two sessions per week for the first 2 weeks, then once-weekly sessions for the remaining 6 weeks.
“The needle insertion is generally brief, 5-10 minutes. Then the patient rests for about 20 minutes,” according to the family physician.
Sham acupuncture utilized nonpenetrating Streitberger needles at nontraditional acupuncture points.
Discussant Dr. Michelle E. Melisko noted that this is one of the largest randomized trials of acupuncture for hot flashes ever done, and it included women of widely varied ages and a substantial African American population. It’s also the first study she’s aware of to compare acupuncture to a nonhormonal medication.
She observed that hot flashes tend to be particularly frequent, severe, and often more debilitating in breast cancer survivors than in the general population. Gabapentin (Neurontin) and venlafaxine (Effexor) are probably the two most widely prescribed centrally acting drugs for treatment of hot flashes in breast cancer survivors.
“Gabapentin is often an appealing choice. In my practice it’s a drug often used to kill two birds with one stone. It can make people sleepy, so if patients are having hot flashes and night sweats it’s nice to give them an agent they can take at bedtime that might have the dual effects of reducing hot flashes as well as improving their sleep,” said Dr. Melisko, an oncologist at the University of California, San Francisco.
She noted that a systematic review of gabapentin for hot flashes in 901 patients in seven clinical trials, including four studies in breast cancer survivors, concluded the drug resulted in 20%-30% reductions in hot flash frequency and severity, but with a dropout rate twice that for placebo (Clin. Therapeutics 2009;31:221-35).But lots of breast cancer survivors say they don’t want to take an additional side effect–laden medication to treat a different set of treatment-induced side effects, Dr. Melisko continued. They’re interested in trying complementary and alternative medicine. And while a Cochrane review has concluded that acupuncture resulted in a significant reduction in hot flash severity but not frequency (Cochrane Database Syst. Rev. 2013 July 30;7:CD007410), Dr. Melisko noted that many of the trials included in that analysis may have been too brief to give acupuncture a fair shake.
Dr. Mao agreed.
“By 4 weeks in our trial you see only about one-half of the eventual effect of electroacupuncture. So if you design a short trial you may not get to the full therapeutic dose,” he said. “With acupuncture, it’s a slow start but eventual substantial effect. I tell patients you need to give acupuncture a therapeutic trial of at least six treatments. If at that point you don’t have any benefit, it may not work for you, but if you don’t try that amount it’s suboptimal.”
In acupuncture trials across the board, whether in the setting of cancer, chronic pain, or various other conditions, roughly one-third of patients are nonresponders, according to Dr. Mao.
His study was funded by the NIH’s National Center for Complementary and Alternative Medicine. He reported having no financial conflicts.
AT SABCS 2014
Key clinical point: Breast cancer survivors with frequent hot flashes obtained more benefit from 8 weeks of electroacupuncture than gabapentin.
Major finding: Mean hot flash composite scores after 8 weeks of electroacupuncture fell by 7.4 points from baseline, compared with a 5.2-point drop with gabapentin at 900 mg/day.
Data source: This was a randomized, prospective trial including 120 breast cancer survivors with troublesome hot flashes at least twice daily.
Disclosures: The study was funded by the National Center for Complementary and Alternative Medicine. The presenter reported having no financial conflicts.

Maintenance Tacrolimus for Eczema Boosts Quality of Life
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
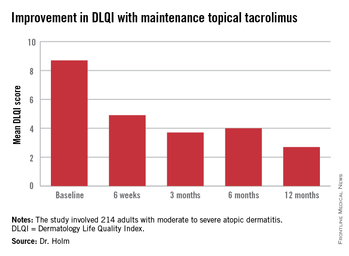
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
Continue for other outcomes >>
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
Continue for other outcomes >>
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
Continue for other outcomes >>
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AT THE EADV CONGRESS
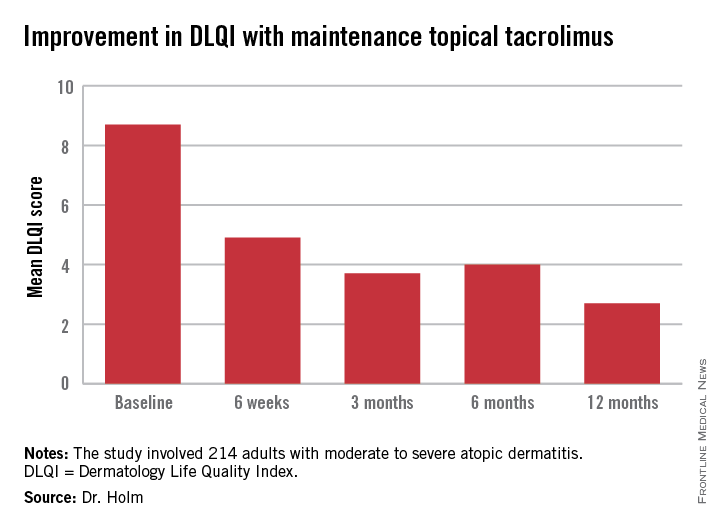
Maintenance tacrolimus for eczema boosts quality of life
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
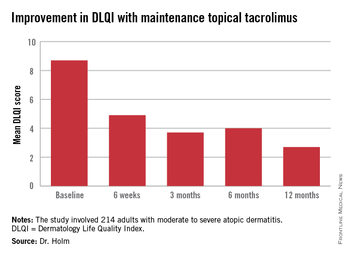
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AT THE EADV CONGRESS
Key clinical point: Twice-weekly proactive application of topical tacrolimus in adults with moderate to severe atopic dermatitis not only reduces flares, it dramatically improves patients’ self-rated quality of life.
Major finding: Mean scores on the Dermatology Life Quality Index in patients on maintenance therapy improved from 8.7 at baseline to 2.7 at 12 months, indicative of minimal disease impact upon daily life.
Data source: This was a 41-site, two-nation study involving 214 adults with moderate to severe atopic dermatitis.
Disclosures: The study was sponsored by Astellas. The presenter is a consultant to the company.
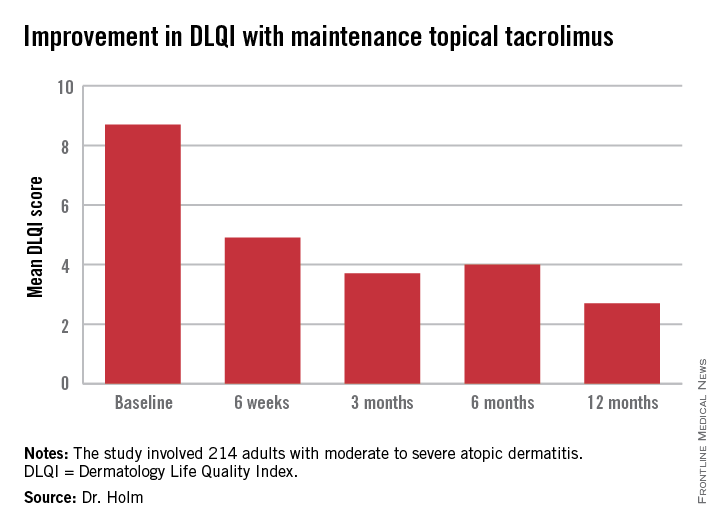
Introducing a better bleeding risk score in atrial fib
CHICAGO – The ORBIT-AF bleeding risk score is a simple, user-friendly new tool for assessing the risk of major bleeding in patients with atrial fibrillation on oral anticoagulation, Emily C. O’Brien, Ph.D., announced at the American Heart Association scientific sessions.
This novel score offers significant advantages over existing bleeding risk scores, including HAS-BLED and ATRIA. Those scores were developed on the basis of small numbers of bleeding events, they show inconsistent performance, and their calculation requires data that’s often not readily accessible in busy daily practice, according to Dr. O’Brien of the Duke Clinical Research Institute in Durham, N.C.

The new score was derived from the ORBIT-AF registry, the largest prospective U.S. registry of patients with atrial fibrillation (AF).
The score was constructed using data on 7,411 AF patients in community practice settings at 173 U.S. sites. All subjects were on oral anticoagulant therapy at baseline. During 2 years of prospective follow-up, 581 patients (7.8%) experienced a major bleeding event as defined by International Society on Thrombosis and Haemostasis criteria.
After sifting through numerous potential candidate variables, Dr. O’Brien and coinvestigators settled upon five they identified as the most potent and practical baseline predictors of major bleeding risk while on oral anticoagulation. Then they packaged them in a convenient acronym: ORBIT, for Older than 74, Renal insufficiency with an estimated glomerular filtration rate below 60 mL/minute per/1.73 m2, Bleeding history, Insufficient hemoglobin/hematocrit or anemia, and Treatment with an antiplatelet agent. The two strongest predictors – renal insufficiency and bleeding history– were awarded two points each; the others are worth one point each.
The observed major bleeding rate among patients enrolled in the ORBIT-AF registry rose with an increasing risk score. The same was true upon application of the ORBIT bleeding score to an independent study sample comprised of participants in the ROCKET-AF randomized clinical trial.
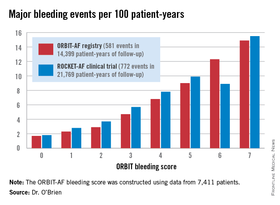
Dr. O’Brien also compared the performance of the ORBIT bleeding score to that of two existing bleeding risk scores – HAS-BLED and ATRIA – in the ORBIT-AF and ROCKET-AF cohorts. The simpler, more user friendly ORBIT bleeding score had a C-statistic of 0.67, similar to the 0.64 for HAS-BLED and 0.66 for ATRIA.
Thus, the ORBIT bleeding score is a practical new tool for use alongside the CHA2DS2-VASc stroke risk score to support clinical decision making regarding whether or not to place an individual AF patient on oral anticoagulation, Dr. O’Brien concluded.
She reported having no financial conflicts regarding this study. The ORBIT-AF registry is sponsored by Janssen.
CHICAGO – The ORBIT-AF bleeding risk score is a simple, user-friendly new tool for assessing the risk of major bleeding in patients with atrial fibrillation on oral anticoagulation, Emily C. O’Brien, Ph.D., announced at the American Heart Association scientific sessions.
This novel score offers significant advantages over existing bleeding risk scores, including HAS-BLED and ATRIA. Those scores were developed on the basis of small numbers of bleeding events, they show inconsistent performance, and their calculation requires data that’s often not readily accessible in busy daily practice, according to Dr. O’Brien of the Duke Clinical Research Institute in Durham, N.C.
The new score was derived from the ORBIT-AF registry, the largest prospective U.S. registry of patients with atrial fibrillation (AF).
The score was constructed using data on 7,411 AF patients in community practice settings at 173 U.S. sites. All subjects were on oral anticoagulant therapy at baseline. During 2 years of prospective follow-up, 581 patients (7.8%) experienced a major bleeding event as defined by International Society on Thrombosis and Haemostasis criteria.
After sifting through numerous potential candidate variables, Dr. O’Brien and coinvestigators settled upon five they identified as the most potent and practical baseline predictors of major bleeding risk while on oral anticoagulation. Then they packaged them in a convenient acronym: ORBIT, for Older than 74, Renal insufficiency with an estimated glomerular filtration rate below 60 mL/minute per/1.73 m2, Bleeding history, Insufficient hemoglobin/hematocrit or anemia, and Treatment with an antiplatelet agent. The two strongest predictors – renal insufficiency and bleeding history– were awarded two points each; the others are worth one point each.
The observed major bleeding rate among patients enrolled in the ORBIT-AF registry rose with an increasing risk score. The same was true upon application of the ORBIT bleeding score to an independent study sample comprised of participants in the ROCKET-AF randomized clinical trial.
Dr. O’Brien also compared the performance of the ORBIT bleeding score to that of two existing bleeding risk scores – HAS-BLED and ATRIA – in the ORBIT-AF and ROCKET-AF cohorts. The simpler, more user friendly ORBIT bleeding score had a C-statistic of 0.67, similar to the 0.64 for HAS-BLED and 0.66 for ATRIA.
Thus, the ORBIT bleeding score is a practical new tool for use alongside the CHA2DS2-VASc stroke risk score to support clinical decision making regarding whether or not to place an individual AF patient on oral anticoagulation, Dr. O’Brien concluded.
She reported having no financial conflicts regarding this study. The ORBIT-AF registry is sponsored by Janssen.
CHICAGO – The ORBIT-AF bleeding risk score is a simple, user-friendly new tool for assessing the risk of major bleeding in patients with atrial fibrillation on oral anticoagulation, Emily C. O’Brien, Ph.D., announced at the American Heart Association scientific sessions.
This novel score offers significant advantages over existing bleeding risk scores, including HAS-BLED and ATRIA. Those scores were developed on the basis of small numbers of bleeding events, they show inconsistent performance, and their calculation requires data that’s often not readily accessible in busy daily practice, according to Dr. O’Brien of the Duke Clinical Research Institute in Durham, N.C.
The new score was derived from the ORBIT-AF registry, the largest prospective U.S. registry of patients with atrial fibrillation (AF).
The score was constructed using data on 7,411 AF patients in community practice settings at 173 U.S. sites. All subjects were on oral anticoagulant therapy at baseline. During 2 years of prospective follow-up, 581 patients (7.8%) experienced a major bleeding event as defined by International Society on Thrombosis and Haemostasis criteria.
After sifting through numerous potential candidate variables, Dr. O’Brien and coinvestigators settled upon five they identified as the most potent and practical baseline predictors of major bleeding risk while on oral anticoagulation. Then they packaged them in a convenient acronym: ORBIT, for Older than 74, Renal insufficiency with an estimated glomerular filtration rate below 60 mL/minute per/1.73 m2, Bleeding history, Insufficient hemoglobin/hematocrit or anemia, and Treatment with an antiplatelet agent. The two strongest predictors – renal insufficiency and bleeding history– were awarded two points each; the others are worth one point each.
The observed major bleeding rate among patients enrolled in the ORBIT-AF registry rose with an increasing risk score. The same was true upon application of the ORBIT bleeding score to an independent study sample comprised of participants in the ROCKET-AF randomized clinical trial.
Dr. O’Brien also compared the performance of the ORBIT bleeding score to that of two existing bleeding risk scores – HAS-BLED and ATRIA – in the ORBIT-AF and ROCKET-AF cohorts. The simpler, more user friendly ORBIT bleeding score had a C-statistic of 0.67, similar to the 0.64 for HAS-BLED and 0.66 for ATRIA.
Thus, the ORBIT bleeding score is a practical new tool for use alongside the CHA2DS2-VASc stroke risk score to support clinical decision making regarding whether or not to place an individual AF patient on oral anticoagulation, Dr. O’Brien concluded.
She reported having no financial conflicts regarding this study. The ORBIT-AF registry is sponsored by Janssen.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: A simple new score is available to assess major bleeding risk in patients with atrial fibrillation on oral anticoagulation.
Major finding: The major bleeding risk in patients with atrial fibrillation on oral anticoagulation ranged from 1.7 per 100 patient-years in those with an ORBIT risk score of 0% to 14.9% in those with a maximum score of 7.
Data source: The risk score was derived by analyzing prospective 2-year follow-up data on 7,411 U.S. patients with atrial fibrillation in a large registry.
Disclosures: The ORBIT-AF registry is sponsored by Janssen. The presenter reported having no financial conflicts.

Ixekizumab linked to decrease in psoriasis-related sexual difficulties
AMSTERDAM – Patient complaints of psoriasis-related sexual difficulties decreased significantly in response to treatment with the investigational biologic agent ixekizumab in a phase 2 dose-ranging study.
Sexual problems attributed by psoriasis patients to their skin condition are a common, underappreciated, and understudied problem. Most physicians simply don’t ask. But when they do, as was done formally in this study, it turned out that at baseline roughly one-third of the 142 participating subjects with moderate to severe chronic plaque psoriasis reported some degree of sexual problems they believed due specifically to their skin disease, Dr. Lyn Guenther reported at the annual congress of the European Academy of Dermatology and Venereology.
That rate dropped precipitously and in dose-dependent fashion in response to subcutaneous therapy with ixekizumab, a super-potent psoriasis medication directed against interleukin 17A, according to Dr. Guenther, professor of dermatology at the University of Western Ontario, London.
The study entailed double-blind randomization of the 142 participants to subcutaneous injections of ixekizumab at 10, 25, 75, or 150 mg or placebo at 0, 2, 4, 8, 12, and 16 weeks. The standard primary outcome -- the proportion of patients with a PASI 75 improvement at 12 weeks -- has previously been reported as highly positive (N. Engl. J. Med. 2012;366:1190-9).
For her secondary analysis of psoriasis-related sexual difficulties and their response to treatment, Dr. Guenther used as her metric the patients’ response to item 9 on the Dermatology Life Quality Index, which all subjects completed at weeks 0, 8, and 16. Item 9 asks the extent to which the responder’s skin “caused any sexual difficulties” during the past week. The options range from 0 (none at all) to 3 (very much). She categorized a response of 1 or more as evidence of sexual difficulties. And because of the relatively small sample size in this study, she lumped together as the low-dose therapy group those patients assigned to ixekizumab at 10 or 25 mg, with the high-dose group being comprised of patients on 75 or
After 8 weeks on low-dose ixekizumab, the proportion of patients reporting any skin disease-related sexual difficulties within the past week fell from a baseline of 30% to 16%. After 8 weeks of high-dose ixekizumab, the figure was just 7%. Those rates remained unchanged at 16 weeks. In contrast, the placebo group remained unchanged over time, with 32% of patients still reporting sexual difficulties caused by their skin disease at week 8.
The degree to which a patient’s psoriasis improved in response to therapy with the humanized monoclonal antibody was closely related to the reduction in skin-related sexual problems. Among the 76 ixekizumab-treated patients who achieved a PASI 75 response at week 16, the rate of self-reported sexual difficulties within the previous week was 7%. For those with less than a PASI 75 response, the rate was 24%.
An impressively high 38% percent of patients on high-dose ixekizumab achieved a PASI 100 response. Only 5% of them reported any skin-related sexual difficulties at week 8, as did 9% at week 16.
Dr. Guenther also looked at the data restricting the analysis to patients with more severe baseline sexual impairment as defined by a response of 2 or 3 on item 9 of the DLQI. Among patients on high-dose izekizumab, the rate dropped from 10.5% at baseline to 1.8% at week 8 to zero at week 16. For patients on low-dose izekizumab, the progression was 13.8% to 8.8% to 3.5% at week 16. Rates remained unchanged over time in the control group.
Although this phase 2 study was limited in size, Dr. Guenther found much the same thing earlier in the much larger phase 3 PHOENIX 1 and 2 trials of ustekinumab (Stelara), which together featured 1,334 psoriasis patients randomized to the human anti-interkelukin-12/23 monoclonal antibody. In that analysis, the proportion of ustekinumab-treated patients with impaired sexual function as assessed by DLQI item 9 plunged from 22.4% at baseline to 2.7% at week 12, compared with no change in placebo-treated controls. The bigger the PASI improvement, the greater the reduction in psoriasis-related sexual dysfunction (J. Eur. Acad. Dermatol. Venereol. 2011;25:851-7).
The phase 2 ixekizumab study was funded by Eli Lilly. Dr. Guenther is a consultant to the company. Positive primary outcomes in three pivotal phase 3 clinical trials of ixekizumab totalling nearly 3,900 randomized psoriasis patients have since been reported. The company plans to apply for marketing approval of the biologic in the first half of 2015.
AMSTERDAM – Patient complaints of psoriasis-related sexual difficulties decreased significantly in response to treatment with the investigational biologic agent ixekizumab in a phase 2 dose-ranging study.
Sexual problems attributed by psoriasis patients to their skin condition are a common, underappreciated, and understudied problem. Most physicians simply don’t ask. But when they do, as was done formally in this study, it turned out that at baseline roughly one-third of the 142 participating subjects with moderate to severe chronic plaque psoriasis reported some degree of sexual problems they believed due specifically to their skin disease, Dr. Lyn Guenther reported at the annual congress of the European Academy of Dermatology and Venereology.
That rate dropped precipitously and in dose-dependent fashion in response to subcutaneous therapy with ixekizumab, a super-potent psoriasis medication directed against interleukin 17A, according to Dr. Guenther, professor of dermatology at the University of Western Ontario, London.
The study entailed double-blind randomization of the 142 participants to subcutaneous injections of ixekizumab at 10, 25, 75, or 150 mg or placebo at 0, 2, 4, 8, 12, and 16 weeks. The standard primary outcome -- the proportion of patients with a PASI 75 improvement at 12 weeks -- has previously been reported as highly positive (N. Engl. J. Med. 2012;366:1190-9).
For her secondary analysis of psoriasis-related sexual difficulties and their response to treatment, Dr. Guenther used as her metric the patients’ response to item 9 on the Dermatology Life Quality Index, which all subjects completed at weeks 0, 8, and 16. Item 9 asks the extent to which the responder’s skin “caused any sexual difficulties” during the past week. The options range from 0 (none at all) to 3 (very much). She categorized a response of 1 or more as evidence of sexual difficulties. And because of the relatively small sample size in this study, she lumped together as the low-dose therapy group those patients assigned to ixekizumab at 10 or 25 mg, with the high-dose group being comprised of patients on 75 or
After 8 weeks on low-dose ixekizumab, the proportion of patients reporting any skin disease-related sexual difficulties within the past week fell from a baseline of 30% to 16%. After 8 weeks of high-dose ixekizumab, the figure was just 7%. Those rates remained unchanged at 16 weeks. In contrast, the placebo group remained unchanged over time, with 32% of patients still reporting sexual difficulties caused by their skin disease at week 8.
The degree to which a patient’s psoriasis improved in response to therapy with the humanized monoclonal antibody was closely related to the reduction in skin-related sexual problems. Among the 76 ixekizumab-treated patients who achieved a PASI 75 response at week 16, the rate of self-reported sexual difficulties within the previous week was 7%. For those with less than a PASI 75 response, the rate was 24%.
An impressively high 38% percent of patients on high-dose ixekizumab achieved a PASI 100 response. Only 5% of them reported any skin-related sexual difficulties at week 8, as did 9% at week 16.
Dr. Guenther also looked at the data restricting the analysis to patients with more severe baseline sexual impairment as defined by a response of 2 or 3 on item 9 of the DLQI. Among patients on high-dose izekizumab, the rate dropped from 10.5% at baseline to 1.8% at week 8 to zero at week 16. For patients on low-dose izekizumab, the progression was 13.8% to 8.8% to 3.5% at week 16. Rates remained unchanged over time in the control group.
Although this phase 2 study was limited in size, Dr. Guenther found much the same thing earlier in the much larger phase 3 PHOENIX 1 and 2 trials of ustekinumab (Stelara), which together featured 1,334 psoriasis patients randomized to the human anti-interkelukin-12/23 monoclonal antibody. In that analysis, the proportion of ustekinumab-treated patients with impaired sexual function as assessed by DLQI item 9 plunged from 22.4% at baseline to 2.7% at week 12, compared with no change in placebo-treated controls. The bigger the PASI improvement, the greater the reduction in psoriasis-related sexual dysfunction (J. Eur. Acad. Dermatol. Venereol. 2011;25:851-7).
The phase 2 ixekizumab study was funded by Eli Lilly. Dr. Guenther is a consultant to the company. Positive primary outcomes in three pivotal phase 3 clinical trials of ixekizumab totalling nearly 3,900 randomized psoriasis patients have since been reported. The company plans to apply for marketing approval of the biologic in the first half of 2015.
AMSTERDAM – Patient complaints of psoriasis-related sexual difficulties decreased significantly in response to treatment with the investigational biologic agent ixekizumab in a phase 2 dose-ranging study.
Sexual problems attributed by psoriasis patients to their skin condition are a common, underappreciated, and understudied problem. Most physicians simply don’t ask. But when they do, as was done formally in this study, it turned out that at baseline roughly one-third of the 142 participating subjects with moderate to severe chronic plaque psoriasis reported some degree of sexual problems they believed due specifically to their skin disease, Dr. Lyn Guenther reported at the annual congress of the European Academy of Dermatology and Venereology.
That rate dropped precipitously and in dose-dependent fashion in response to subcutaneous therapy with ixekizumab, a super-potent psoriasis medication directed against interleukin 17A, according to Dr. Guenther, professor of dermatology at the University of Western Ontario, London.
The study entailed double-blind randomization of the 142 participants to subcutaneous injections of ixekizumab at 10, 25, 75, or 150 mg or placebo at 0, 2, 4, 8, 12, and 16 weeks. The standard primary outcome -- the proportion of patients with a PASI 75 improvement at 12 weeks -- has previously been reported as highly positive (N. Engl. J. Med. 2012;366:1190-9).
For her secondary analysis of psoriasis-related sexual difficulties and their response to treatment, Dr. Guenther used as her metric the patients’ response to item 9 on the Dermatology Life Quality Index, which all subjects completed at weeks 0, 8, and 16. Item 9 asks the extent to which the responder’s skin “caused any sexual difficulties” during the past week. The options range from 0 (none at all) to 3 (very much). She categorized a response of 1 or more as evidence of sexual difficulties. And because of the relatively small sample size in this study, she lumped together as the low-dose therapy group those patients assigned to ixekizumab at 10 or 25 mg, with the high-dose group being comprised of patients on 75 or
After 8 weeks on low-dose ixekizumab, the proportion of patients reporting any skin disease-related sexual difficulties within the past week fell from a baseline of 30% to 16%. After 8 weeks of high-dose ixekizumab, the figure was just 7%. Those rates remained unchanged at 16 weeks. In contrast, the placebo group remained unchanged over time, with 32% of patients still reporting sexual difficulties caused by their skin disease at week 8.
The degree to which a patient’s psoriasis improved in response to therapy with the humanized monoclonal antibody was closely related to the reduction in skin-related sexual problems. Among the 76 ixekizumab-treated patients who achieved a PASI 75 response at week 16, the rate of self-reported sexual difficulties within the previous week was 7%. For those with less than a PASI 75 response, the rate was 24%.
An impressively high 38% percent of patients on high-dose ixekizumab achieved a PASI 100 response. Only 5% of them reported any skin-related sexual difficulties at week 8, as did 9% at week 16.
Dr. Guenther also looked at the data restricting the analysis to patients with more severe baseline sexual impairment as defined by a response of 2 or 3 on item 9 of the DLQI. Among patients on high-dose izekizumab, the rate dropped from 10.5% at baseline to 1.8% at week 8 to zero at week 16. For patients on low-dose izekizumab, the progression was 13.8% to 8.8% to 3.5% at week 16. Rates remained unchanged over time in the control group.
Although this phase 2 study was limited in size, Dr. Guenther found much the same thing earlier in the much larger phase 3 PHOENIX 1 and 2 trials of ustekinumab (Stelara), which together featured 1,334 psoriasis patients randomized to the human anti-interkelukin-12/23 monoclonal antibody. In that analysis, the proportion of ustekinumab-treated patients with impaired sexual function as assessed by DLQI item 9 plunged from 22.4% at baseline to 2.7% at week 12, compared with no change in placebo-treated controls. The bigger the PASI improvement, the greater the reduction in psoriasis-related sexual dysfunction (J. Eur. Acad. Dermatol. Venereol. 2011;25:851-7).
The phase 2 ixekizumab study was funded by Eli Lilly. Dr. Guenther is a consultant to the company. Positive primary outcomes in three pivotal phase 3 clinical trials of ixekizumab totalling nearly 3,900 randomized psoriasis patients have since been reported. The company plans to apply for marketing approval of the biologic in the first half of 2015.
AT THE EADV CONGRESS
Key clinical point: Psoriasis patients have a high rate of sexual problems they attribute to their skin disease, and which decrease with effective psoriasis therapy.
Major finding: The prevalence of self-reported psoriasis-related sexual difficulties within the previous week fell from 32% at baseline to 7% among patients with a PASI 75 response to ixekizumab at week 16.
Data source: This was a double-blind, phase 2, dose-ranging study involving 142 patients with moderate to severe chronic plaque psoriasis randomized to 16 weeks of ixekizumab or placebo.
Disclosures: The study was funded by Eli Lilly. The presenter is a consultant to the company.