User login
Statins don’t cut fracture risk
Daily rosuvastatin did not decrease fracture risk in a large international clinical trial involving older men and women who had elevated CRP levels, according to a report published online Dec. 1 in JAMA Internal Medicine.
Statins are thought to stimulate bone formation and increase bone mineral density, suggesting that they may exert clinical benefits beyond cardiovascular disease (CVD) prevention. Several observational studies have reported that statin users show a decreased risk of osteoporotic fractures, compared with nonusers. To examine this possible benefit, the JUPITER (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) trial enrolled 17,802 men older than 50 years and women older than 60 years to receive either rosuvastatin or matching placebo and be followed for up to 5 years (median follow-up, 2 years) for both CVD and fracture events. The study was conducted at 1,315 medical centers in 26 countries, said Dr. Jessica M. Peña of the division of cardiology, Montefiore Medical Center, New York, and her associates.

A total of 431 participants sustained fractures: 221 in the rosuvastatin group and 210 in the placebo group, a nonsignificant difference. The corresponding rate of fracture was 1.20 per 100 person-years with the statin and 1.14 per 100 person-years with placebo, also a nonsignificant difference. The lack of protection associated with the active drug was consistent between men and women, across all fracture sites, and regardless of the participants’ fracture history. It also persisted through several sensitivity analyses, the investigators said (JAMA Intern. Med. 2014 Dec. 1 [doi:10.1001/jamainternmed.2014.6388]).
“Our study does not support the use of statins in doses used for cardiovascular disease prevention to reduce the risk of fracture,” the researchers noted.
Daily rosuvastatin did not decrease fracture risk in a large international clinical trial involving older men and women who had elevated CRP levels, according to a report published online Dec. 1 in JAMA Internal Medicine.
Statins are thought to stimulate bone formation and increase bone mineral density, suggesting that they may exert clinical benefits beyond cardiovascular disease (CVD) prevention. Several observational studies have reported that statin users show a decreased risk of osteoporotic fractures, compared with nonusers. To examine this possible benefit, the JUPITER (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) trial enrolled 17,802 men older than 50 years and women older than 60 years to receive either rosuvastatin or matching placebo and be followed for up to 5 years (median follow-up, 2 years) for both CVD and fracture events. The study was conducted at 1,315 medical centers in 26 countries, said Dr. Jessica M. Peña of the division of cardiology, Montefiore Medical Center, New York, and her associates.
A total of 431 participants sustained fractures: 221 in the rosuvastatin group and 210 in the placebo group, a nonsignificant difference. The corresponding rate of fracture was 1.20 per 100 person-years with the statin and 1.14 per 100 person-years with placebo, also a nonsignificant difference. The lack of protection associated with the active drug was consistent between men and women, across all fracture sites, and regardless of the participants’ fracture history. It also persisted through several sensitivity analyses, the investigators said (JAMA Intern. Med. 2014 Dec. 1 [doi:10.1001/jamainternmed.2014.6388]).
“Our study does not support the use of statins in doses used for cardiovascular disease prevention to reduce the risk of fracture,” the researchers noted.
Daily rosuvastatin did not decrease fracture risk in a large international clinical trial involving older men and women who had elevated CRP levels, according to a report published online Dec. 1 in JAMA Internal Medicine.
Statins are thought to stimulate bone formation and increase bone mineral density, suggesting that they may exert clinical benefits beyond cardiovascular disease (CVD) prevention. Several observational studies have reported that statin users show a decreased risk of osteoporotic fractures, compared with nonusers. To examine this possible benefit, the JUPITER (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) trial enrolled 17,802 men older than 50 years and women older than 60 years to receive either rosuvastatin or matching placebo and be followed for up to 5 years (median follow-up, 2 years) for both CVD and fracture events. The study was conducted at 1,315 medical centers in 26 countries, said Dr. Jessica M. Peña of the division of cardiology, Montefiore Medical Center, New York, and her associates.
A total of 431 participants sustained fractures: 221 in the rosuvastatin group and 210 in the placebo group, a nonsignificant difference. The corresponding rate of fracture was 1.20 per 100 person-years with the statin and 1.14 per 100 person-years with placebo, also a nonsignificant difference. The lack of protection associated with the active drug was consistent between men and women, across all fracture sites, and regardless of the participants’ fracture history. It also persisted through several sensitivity analyses, the investigators said (JAMA Intern. Med. 2014 Dec. 1 [doi:10.1001/jamainternmed.2014.6388]).
“Our study does not support the use of statins in doses used for cardiovascular disease prevention to reduce the risk of fracture,” the researchers noted.
Key clinical point: Rosuvastatin didn’t lower the risk of bone fracture, compared with placebo.
Major finding: 221 participants given rosuvastatin and 210 given placebo sustained fractures, a nonsignificant difference.
Data source: An international randomized double-blind trial in which 17,802 older adults with elevated CRP received either rosuvastatin or placebo and were followed for a median of 2 years.
Disclosures: The JUPITER trial was supported by AstraZeneca, and Dr. Pena was supported by the National Heart, Lung, and Blood Institute. She reported having no financial disclosures; her associates reported numerous ties to industry sources.

Prehospital epinephrine tied to lower neurologically intact survival
Using epinephrine during resuscitation for out-of-hospital cardiac arrest may lower neurologically intact survival, according to an observational study published online Dec. 1 in the Journal of the American College of Cardiology.
This negative effect was dose related and unaffected by postresuscitation interventions such as percutaneous coronary intervention or therapeutic hypothermia in a single-center observational cohort study, said Dr. Florence Dumas of the Parisian Cardiovascular Research Center, Paris Descartes University, and her associates.
In this study, as in some previous studies, epinephrine was associated with an improved rate of return of spontaneous circulation. But that benefit didn’t translate into higher long-term survival, possibly because of an as-yet unidentified harmful effect during the postresuscitation phase of treatment, the investigators noted.
International resuscitation guidelines recommend giving epinephrine every 3-5 minutes during cardiac arrest resuscitation efforts, regardless of the initial cardiac rhythm. This approach has been shown to enhance the return of spontaneous circulation. However it is unclear how the treatment affects long-term survival, with some studies reporting no effect or even deleterious effects on that outcome. To examine the issue, Dr. Dumas and her associates assessed outcomes for 1,556 patients who had nontraumatic out-of-hospital cardiac arrest, achieved return of spontaneous circulation, and were then admitted to a large specialized medical center during a 12-year period.
The average patient age was 60 years, and 71% were men. Nearly 75% of the participants received epinephrine during resuscitation. As expected, those who were given epinephrine had less favorable prognostic characteristics than patients who were not given the drug; they were older, less likely to have had a witnessed cardiac arrest, and less likely to have had a shockable rhythm when paramedics arrived, and they had longer durations of resuscitation.
A total of 449 patients (29%) survived to hospital discharge with a good neurologic status, defined as a Cerebral Performance Category of 1 or 2. Patients who received epinephrine during resuscitation were markedly less likely to do so (17%) than patients who didn’t receive epinephrine (60%).
To control for the baseline differences between the two study groups that may have contributed to this discrepancy in survival, the investigators performed several adjusted analyses of the data, including propensity scoring, cross matching, and numerous sensitivity analyses. The negative effect associated with epinephrine “was robust to a variety of different methodological approaches designed to limit confounding,” Dr. Dumas and her associates said (J. Am. Coll. Cardiol. 2014 Dec. 1 [doi:10.1016/j.jacc.2014.09.036]).
There was a stepwise association between increasing dose of epinephrine and decreasing odds of surviving neurologically intact, with an odds ratio of 0.48 for 1 mg epinephrine, 0.30 for 2-5 mg, and 0.23 for more than 5 mg. The timing of administration also showed a linear association with survival odds. Patients who received epinephrine within 9 minutes of cardiac arrest had an odds ratio of neurologically intact survival of 0.54, those who received it at 10-15 minutes had an OR of 0.33, those who received it at 16-22 minutes had an OR of 0.23, and those who received it after 22 minutes had an OR of 0.17.
“Before incriminating the drug itself, our findings probably should provoke further discussion on the most appropriate scheme of treatment and its interaction regarding the resuscitation phases,” the researchers said, referring to the “electrical phase” within the first few minutes after cardiac arrest, when epinephrine isn’t required; the subsequent “circulatory phase” when both epinephrine and chest compressions enhance reperfusion; and the later “metabolic phase” when epinephrine might be detrimental.
“It is highly probable that patients receiving late or repeated doses of epinephrine have little or no chance of survival. Altogether, the scheme and timing of administration may be crucial to provide the appropriate effect of epinephrine,” they said.
Dr. Dumas and her associates emphasized that an observational study such as theirs cannot determine causality, so it cannot be said that epinephrine caused the negative effect on intact survival. They also noted that findings from their single-center study may not be generalizable to all communities.
Dr. Dumas and her associates reported having no relevant financial disclosures.
The report by Dr. Dumas and her colleagues adds to the growing number of articles questioning the role of epinephrine in managing out-of-hospital cardiac arrest.
The key question now is whether epinephrine is the optimal vasopressor in this setting. Future research should assess whether using a pure alpha-adrenergic agent such as phenylephrine or methoxamine, or combining epinephrine with a beta-adrenergic blocker, might produce better outcomes.
Dr. Gordon A. Ewy of the Sarver Heart Center at the University of Arizona, Tucson, made these remarks in an editorial comment accompanying Dr. Dumas’s report (J. Am. Coll. Cardiol. 2014 Dec. 1 [doi:10.1016/j.jacc.2014.09.035]). He reported having no relevant conflicts of interest.
The report by Dr. Dumas and her colleagues adds to the growing number of articles questioning the role of epinephrine in managing out-of-hospital cardiac arrest.
The key question now is whether epinephrine is the optimal vasopressor in this setting. Future research should assess whether using a pure alpha-adrenergic agent such as phenylephrine or methoxamine, or combining epinephrine with a beta-adrenergic blocker, might produce better outcomes.
Dr. Gordon A. Ewy of the Sarver Heart Center at the University of Arizona, Tucson, made these remarks in an editorial comment accompanying Dr. Dumas’s report (J. Am. Coll. Cardiol. 2014 Dec. 1 [doi:10.1016/j.jacc.2014.09.035]). He reported having no relevant conflicts of interest.
The report by Dr. Dumas and her colleagues adds to the growing number of articles questioning the role of epinephrine in managing out-of-hospital cardiac arrest.
The key question now is whether epinephrine is the optimal vasopressor in this setting. Future research should assess whether using a pure alpha-adrenergic agent such as phenylephrine or methoxamine, or combining epinephrine with a beta-adrenergic blocker, might produce better outcomes.
Dr. Gordon A. Ewy of the Sarver Heart Center at the University of Arizona, Tucson, made these remarks in an editorial comment accompanying Dr. Dumas’s report (J. Am. Coll. Cardiol. 2014 Dec. 1 [doi:10.1016/j.jacc.2014.09.035]). He reported having no relevant conflicts of interest.
Using epinephrine during resuscitation for out-of-hospital cardiac arrest may lower neurologically intact survival, according to an observational study published online Dec. 1 in the Journal of the American College of Cardiology.
This negative effect was dose related and unaffected by postresuscitation interventions such as percutaneous coronary intervention or therapeutic hypothermia in a single-center observational cohort study, said Dr. Florence Dumas of the Parisian Cardiovascular Research Center, Paris Descartes University, and her associates.
In this study, as in some previous studies, epinephrine was associated with an improved rate of return of spontaneous circulation. But that benefit didn’t translate into higher long-term survival, possibly because of an as-yet unidentified harmful effect during the postresuscitation phase of treatment, the investigators noted.
International resuscitation guidelines recommend giving epinephrine every 3-5 minutes during cardiac arrest resuscitation efforts, regardless of the initial cardiac rhythm. This approach has been shown to enhance the return of spontaneous circulation. However it is unclear how the treatment affects long-term survival, with some studies reporting no effect or even deleterious effects on that outcome. To examine the issue, Dr. Dumas and her associates assessed outcomes for 1,556 patients who had nontraumatic out-of-hospital cardiac arrest, achieved return of spontaneous circulation, and were then admitted to a large specialized medical center during a 12-year period.
The average patient age was 60 years, and 71% were men. Nearly 75% of the participants received epinephrine during resuscitation. As expected, those who were given epinephrine had less favorable prognostic characteristics than patients who were not given the drug; they were older, less likely to have had a witnessed cardiac arrest, and less likely to have had a shockable rhythm when paramedics arrived, and they had longer durations of resuscitation.
A total of 449 patients (29%) survived to hospital discharge with a good neurologic status, defined as a Cerebral Performance Category of 1 or 2. Patients who received epinephrine during resuscitation were markedly less likely to do so (17%) than patients who didn’t receive epinephrine (60%).
To control for the baseline differences between the two study groups that may have contributed to this discrepancy in survival, the investigators performed several adjusted analyses of the data, including propensity scoring, cross matching, and numerous sensitivity analyses. The negative effect associated with epinephrine “was robust to a variety of different methodological approaches designed to limit confounding,” Dr. Dumas and her associates said (J. Am. Coll. Cardiol. 2014 Dec. 1 [doi:10.1016/j.jacc.2014.09.036]).
There was a stepwise association between increasing dose of epinephrine and decreasing odds of surviving neurologically intact, with an odds ratio of 0.48 for 1 mg epinephrine, 0.30 for 2-5 mg, and 0.23 for more than 5 mg. The timing of administration also showed a linear association with survival odds. Patients who received epinephrine within 9 minutes of cardiac arrest had an odds ratio of neurologically intact survival of 0.54, those who received it at 10-15 minutes had an OR of 0.33, those who received it at 16-22 minutes had an OR of 0.23, and those who received it after 22 minutes had an OR of 0.17.
“Before incriminating the drug itself, our findings probably should provoke further discussion on the most appropriate scheme of treatment and its interaction regarding the resuscitation phases,” the researchers said, referring to the “electrical phase” within the first few minutes after cardiac arrest, when epinephrine isn’t required; the subsequent “circulatory phase” when both epinephrine and chest compressions enhance reperfusion; and the later “metabolic phase” when epinephrine might be detrimental.
“It is highly probable that patients receiving late or repeated doses of epinephrine have little or no chance of survival. Altogether, the scheme and timing of administration may be crucial to provide the appropriate effect of epinephrine,” they said.
Dr. Dumas and her associates emphasized that an observational study such as theirs cannot determine causality, so it cannot be said that epinephrine caused the negative effect on intact survival. They also noted that findings from their single-center study may not be generalizable to all communities.
Dr. Dumas and her associates reported having no relevant financial disclosures.
Using epinephrine during resuscitation for out-of-hospital cardiac arrest may lower neurologically intact survival, according to an observational study published online Dec. 1 in the Journal of the American College of Cardiology.
This negative effect was dose related and unaffected by postresuscitation interventions such as percutaneous coronary intervention or therapeutic hypothermia in a single-center observational cohort study, said Dr. Florence Dumas of the Parisian Cardiovascular Research Center, Paris Descartes University, and her associates.
In this study, as in some previous studies, epinephrine was associated with an improved rate of return of spontaneous circulation. But that benefit didn’t translate into higher long-term survival, possibly because of an as-yet unidentified harmful effect during the postresuscitation phase of treatment, the investigators noted.
International resuscitation guidelines recommend giving epinephrine every 3-5 minutes during cardiac arrest resuscitation efforts, regardless of the initial cardiac rhythm. This approach has been shown to enhance the return of spontaneous circulation. However it is unclear how the treatment affects long-term survival, with some studies reporting no effect or even deleterious effects on that outcome. To examine the issue, Dr. Dumas and her associates assessed outcomes for 1,556 patients who had nontraumatic out-of-hospital cardiac arrest, achieved return of spontaneous circulation, and were then admitted to a large specialized medical center during a 12-year period.
The average patient age was 60 years, and 71% were men. Nearly 75% of the participants received epinephrine during resuscitation. As expected, those who were given epinephrine had less favorable prognostic characteristics than patients who were not given the drug; they were older, less likely to have had a witnessed cardiac arrest, and less likely to have had a shockable rhythm when paramedics arrived, and they had longer durations of resuscitation.
A total of 449 patients (29%) survived to hospital discharge with a good neurologic status, defined as a Cerebral Performance Category of 1 or 2. Patients who received epinephrine during resuscitation were markedly less likely to do so (17%) than patients who didn’t receive epinephrine (60%).
To control for the baseline differences between the two study groups that may have contributed to this discrepancy in survival, the investigators performed several adjusted analyses of the data, including propensity scoring, cross matching, and numerous sensitivity analyses. The negative effect associated with epinephrine “was robust to a variety of different methodological approaches designed to limit confounding,” Dr. Dumas and her associates said (J. Am. Coll. Cardiol. 2014 Dec. 1 [doi:10.1016/j.jacc.2014.09.036]).
There was a stepwise association between increasing dose of epinephrine and decreasing odds of surviving neurologically intact, with an odds ratio of 0.48 for 1 mg epinephrine, 0.30 for 2-5 mg, and 0.23 for more than 5 mg. The timing of administration also showed a linear association with survival odds. Patients who received epinephrine within 9 minutes of cardiac arrest had an odds ratio of neurologically intact survival of 0.54, those who received it at 10-15 minutes had an OR of 0.33, those who received it at 16-22 minutes had an OR of 0.23, and those who received it after 22 minutes had an OR of 0.17.
“Before incriminating the drug itself, our findings probably should provoke further discussion on the most appropriate scheme of treatment and its interaction regarding the resuscitation phases,” the researchers said, referring to the “electrical phase” within the first few minutes after cardiac arrest, when epinephrine isn’t required; the subsequent “circulatory phase” when both epinephrine and chest compressions enhance reperfusion; and the later “metabolic phase” when epinephrine might be detrimental.
“It is highly probable that patients receiving late or repeated doses of epinephrine have little or no chance of survival. Altogether, the scheme and timing of administration may be crucial to provide the appropriate effect of epinephrine,” they said.
Dr. Dumas and her associates emphasized that an observational study such as theirs cannot determine causality, so it cannot be said that epinephrine caused the negative effect on intact survival. They also noted that findings from their single-center study may not be generalizable to all communities.
Dr. Dumas and her associates reported having no relevant financial disclosures.
Key clinical point: Use of epinephrine during resuscitation after out-of-hospital cardiac arrest is associated with lower neurologically intact survival.
Major finding: Patients who received epinephrine during resuscitation were markedly less likely to survive to hospital discharge neurologically intact (17%) than those who didn’t receive epinephrine (60%).
Data source: A single-center cohort study involving 1,556 patients who had out-of-hospital cardiac arrest followed by successful return of spontaneous circulation and admission to a cardiac arrest center in Paris during a 12-year period.
Disclosures: Dr. Dumas and her associates reported having no relevant financial disclosures.
USPSTF: Not Enough Evidence for Vitamin D Screening
The U.S. Preventive Services Task Force made no recommendation for or against primary care clinicians screening asymptomatic adults for vitamin D deficiency, because the current evidence is insufficient to adequately assess the benefits and harms of doing so, according to a report published online Nov. 24 in Annals of Internal Medicine.
The USPSTF reviewed the evidence on screening and treatment for vitamin D deficiency, because the condition may contribute to fractures, falls, functional limitations, cancer, diabetes, cardiovascular disease, depression, and excess mortality.

In addition, testing of vitamin D levels has increased markedly in recent years. One national survey showed the annual rate of outpatient visits with a diagnosis code for vitamin D deficiency more than tripled between 2008 and 2010, and a 2009 survey of clinical laboratories reported that the testing increased by at least half in the space of just 1 year, said Dr. Michael L. LeFevre, chair of the task force and professor of family medicine at the University of Missouri, Columbia, and his associates.
The organization is a voluntary expert group tasked with making recommendations about specific preventive care services, devices, and medications for asymptomatic people, with a view to improving Americans’ general health.
The task force reviewed the evidence presented in 16 randomized trials, as well as nested case-control studies using data from the Women’s Health Initiative. They found that no study has directly examined the effects of vitamin D screening, compared with no screening, on clinical outcomes. There isn’t even any consensus about what constitutes vitamin D deficiency, or what the optimal circulating level of 25-hydroxyvitamin D is.
Many testing methods are available, including competitive protein binding, immunoassay, high-performance liquid chromatography, and mass spectrometry. But the sensitivity and specificity of these tests remains unknown, because there is no internationally recognized reference standard. Moreover, the USPSTF found that test results vary not just by which test is used, but even between laboratories using the same test.
Continued >>
Symptomatic vitamin D deficiency is known to affect health adversely, as is asymptomatic vitamin D deficiency in certain patient populations. But the evidence that deficiency contributes to adverse health outcomes in asymptomatic adults is inadequate. The evidence that screening for such deficiency and treating “low” vitamin D levels prevents adverse outcomes or simply improves general health also is inadequate, Dr. LeFevre and his associates said.
Similarly, no studies to date have directly examined possible harms of screening for and treating vitamin D deficiency. Although there are concerns that vitamin D supplements may lead to hypercalcemia, kidney stones, or gastrointestinal symptoms, there is no evidence of such effects in the asymptomatic patient population.
The USPSTF concluded that the harms of screening for and treating vitamin D deficiency are likely “small to none,” but it still is not possible to determine whether the benefits outweigh even that small amount of harm.
At present, no national primary care professional organization recommends screening of the general adult population for vitamin D deficiency. The American Academy of Family Physicians, the Endocrine Society, the American College of Obstetricians and Gynecologists, the American Geriatrics Society, and the National Osteoporosis Foundation all recommend screening for patients at risk for fractures or falls only. The Institute of Medicine has no formal guidelines regarding vitamin D screening, Dr. LeFevre and his associates noted.
The USPSTF summary report and the review of the evidence are available at www.uspreventiveservicestaskforce.org.
The USPSTF is focused on providing a firm evidential base for early detection and prevention of disease, noted Dr. Robert P. Heaney and Dr. Laura A. G. Armas in an accompanying editorial. But perhaps clinicians should have a different focus: full nutrient repletion in their patients, to optimize their health.
A strict disease-avoidance approach is too simplistic with regard to micronutrients, because they don’t directly cause the effects often attributed to them. Instead, when supplies of micronutrients are inadequate, cellular responses are blunted, Dr. Heaney and Dr. Armas noted. That is dysfunction, but not clinically manifest disease.
Such dysfunction may indeed lead ultimately to various diseases, they added, but disease prevention is a dull tool for discerning the defect. And a disease-prevention approach clearly doesn’t show whether there is enough of the nutrient present to enable appropriate physiological responses.
Dr. Heaney and Dr. Armas are at Creighton University in Omaha, Neb. Their remarks are drawn from an editorial accompanying the USPSTF reports.
The USPSTF is focused on providing a firm evidential base for early detection and prevention of disease, noted Dr. Robert P. Heaney and Dr. Laura A. G. Armas in an accompanying editorial. But perhaps clinicians should have a different focus: full nutrient repletion in their patients, to optimize their health.
A strict disease-avoidance approach is too simplistic with regard to micronutrients, because they don’t directly cause the effects often attributed to them. Instead, when supplies of micronutrients are inadequate, cellular responses are blunted, Dr. Heaney and Dr. Armas noted. That is dysfunction, but not clinically manifest disease.
Such dysfunction may indeed lead ultimately to various diseases, they added, but disease prevention is a dull tool for discerning the defect. And a disease-prevention approach clearly doesn’t show whether there is enough of the nutrient present to enable appropriate physiological responses.
Dr. Heaney and Dr. Armas are at Creighton University in Omaha, Neb. Their remarks are drawn from an editorial accompanying the USPSTF reports.
The USPSTF is focused on providing a firm evidential base for early detection and prevention of disease, noted Dr. Robert P. Heaney and Dr. Laura A. G. Armas in an accompanying editorial. But perhaps clinicians should have a different focus: full nutrient repletion in their patients, to optimize their health.
A strict disease-avoidance approach is too simplistic with regard to micronutrients, because they don’t directly cause the effects often attributed to them. Instead, when supplies of micronutrients are inadequate, cellular responses are blunted, Dr. Heaney and Dr. Armas noted. That is dysfunction, but not clinically manifest disease.
Such dysfunction may indeed lead ultimately to various diseases, they added, but disease prevention is a dull tool for discerning the defect. And a disease-prevention approach clearly doesn’t show whether there is enough of the nutrient present to enable appropriate physiological responses.
Dr. Heaney and Dr. Armas are at Creighton University in Omaha, Neb. Their remarks are drawn from an editorial accompanying the USPSTF reports.
The U.S. Preventive Services Task Force made no recommendation for or against primary care clinicians screening asymptomatic adults for vitamin D deficiency, because the current evidence is insufficient to adequately assess the benefits and harms of doing so, according to a report published online Nov. 24 in Annals of Internal Medicine.
The USPSTF reviewed the evidence on screening and treatment for vitamin D deficiency, because the condition may contribute to fractures, falls, functional limitations, cancer, diabetes, cardiovascular disease, depression, and excess mortality.
In addition, testing of vitamin D levels has increased markedly in recent years. One national survey showed the annual rate of outpatient visits with a diagnosis code for vitamin D deficiency more than tripled between 2008 and 2010, and a 2009 survey of clinical laboratories reported that the testing increased by at least half in the space of just 1 year, said Dr. Michael L. LeFevre, chair of the task force and professor of family medicine at the University of Missouri, Columbia, and his associates.
The organization is a voluntary expert group tasked with making recommendations about specific preventive care services, devices, and medications for asymptomatic people, with a view to improving Americans’ general health.
The task force reviewed the evidence presented in 16 randomized trials, as well as nested case-control studies using data from the Women’s Health Initiative. They found that no study has directly examined the effects of vitamin D screening, compared with no screening, on clinical outcomes. There isn’t even any consensus about what constitutes vitamin D deficiency, or what the optimal circulating level of 25-hydroxyvitamin D is.
Many testing methods are available, including competitive protein binding, immunoassay, high-performance liquid chromatography, and mass spectrometry. But the sensitivity and specificity of these tests remains unknown, because there is no internationally recognized reference standard. Moreover, the USPSTF found that test results vary not just by which test is used, but even between laboratories using the same test.
Continued >>
Symptomatic vitamin D deficiency is known to affect health adversely, as is asymptomatic vitamin D deficiency in certain patient populations. But the evidence that deficiency contributes to adverse health outcomes in asymptomatic adults is inadequate. The evidence that screening for such deficiency and treating “low” vitamin D levels prevents adverse outcomes or simply improves general health also is inadequate, Dr. LeFevre and his associates said.
Similarly, no studies to date have directly examined possible harms of screening for and treating vitamin D deficiency. Although there are concerns that vitamin D supplements may lead to hypercalcemia, kidney stones, or gastrointestinal symptoms, there is no evidence of such effects in the asymptomatic patient population.
The USPSTF concluded that the harms of screening for and treating vitamin D deficiency are likely “small to none,” but it still is not possible to determine whether the benefits outweigh even that small amount of harm.
At present, no national primary care professional organization recommends screening of the general adult population for vitamin D deficiency. The American Academy of Family Physicians, the Endocrine Society, the American College of Obstetricians and Gynecologists, the American Geriatrics Society, and the National Osteoporosis Foundation all recommend screening for patients at risk for fractures or falls only. The Institute of Medicine has no formal guidelines regarding vitamin D screening, Dr. LeFevre and his associates noted.
The USPSTF summary report and the review of the evidence are available at www.uspreventiveservicestaskforce.org.
The U.S. Preventive Services Task Force made no recommendation for or against primary care clinicians screening asymptomatic adults for vitamin D deficiency, because the current evidence is insufficient to adequately assess the benefits and harms of doing so, according to a report published online Nov. 24 in Annals of Internal Medicine.
The USPSTF reviewed the evidence on screening and treatment for vitamin D deficiency, because the condition may contribute to fractures, falls, functional limitations, cancer, diabetes, cardiovascular disease, depression, and excess mortality.
In addition, testing of vitamin D levels has increased markedly in recent years. One national survey showed the annual rate of outpatient visits with a diagnosis code for vitamin D deficiency more than tripled between 2008 and 2010, and a 2009 survey of clinical laboratories reported that the testing increased by at least half in the space of just 1 year, said Dr. Michael L. LeFevre, chair of the task force and professor of family medicine at the University of Missouri, Columbia, and his associates.
The organization is a voluntary expert group tasked with making recommendations about specific preventive care services, devices, and medications for asymptomatic people, with a view to improving Americans’ general health.
The task force reviewed the evidence presented in 16 randomized trials, as well as nested case-control studies using data from the Women’s Health Initiative. They found that no study has directly examined the effects of vitamin D screening, compared with no screening, on clinical outcomes. There isn’t even any consensus about what constitutes vitamin D deficiency, or what the optimal circulating level of 25-hydroxyvitamin D is.
Many testing methods are available, including competitive protein binding, immunoassay, high-performance liquid chromatography, and mass spectrometry. But the sensitivity and specificity of these tests remains unknown, because there is no internationally recognized reference standard. Moreover, the USPSTF found that test results vary not just by which test is used, but even between laboratories using the same test.
Continued >>
Symptomatic vitamin D deficiency is known to affect health adversely, as is asymptomatic vitamin D deficiency in certain patient populations. But the evidence that deficiency contributes to adverse health outcomes in asymptomatic adults is inadequate. The evidence that screening for such deficiency and treating “low” vitamin D levels prevents adverse outcomes or simply improves general health also is inadequate, Dr. LeFevre and his associates said.
Similarly, no studies to date have directly examined possible harms of screening for and treating vitamin D deficiency. Although there are concerns that vitamin D supplements may lead to hypercalcemia, kidney stones, or gastrointestinal symptoms, there is no evidence of such effects in the asymptomatic patient population.
The USPSTF concluded that the harms of screening for and treating vitamin D deficiency are likely “small to none,” but it still is not possible to determine whether the benefits outweigh even that small amount of harm.
At present, no national primary care professional organization recommends screening of the general adult population for vitamin D deficiency. The American Academy of Family Physicians, the Endocrine Society, the American College of Obstetricians and Gynecologists, the American Geriatrics Society, and the National Osteoporosis Foundation all recommend screening for patients at risk for fractures or falls only. The Institute of Medicine has no formal guidelines regarding vitamin D screening, Dr. LeFevre and his associates noted.
The USPSTF summary report and the review of the evidence are available at www.uspreventiveservicestaskforce.org.
FROM ANNALS OF INTERNAL MEDICINE

USPSTF: Not enough evidence for vitamin D screening
The U.S. Preventive Services Task Force made no recommendation for or against primary care physicians screening asymptomatic adults for vitamin D deficiency, because the current evidence is insufficient to adequately assess the benefits and harms of doing so, according to a report published online Nov. 24 in Annals of Internal Medicine.
The USPSTF reviewed the evidence on screening and treatment for vitamin D deficiency, because the condition may contribute to fractures, falls, functional limitations, cancer, diabetes, cardiovascular disease, depression, and excess mortality.
In addition, testing of vitamin D levels has increased markedly in recent years. One national survey showed the annual rate of outpatient visits with a diagnosis code for vitamin D deficiency more than tripled between 2008 and 2010, and a 2009 survey of clinical laboratories reported that the testing increased by at least half in the space of just 1 year, said Dr. Michael L. LeFevre, chair of the task force and professor of family medicine at the University of Missouri, Columbia, and his associates.

The organization is a voluntary expert group tasked with making recommendations about specific preventive care services, devices, and medications for asymptomatic people, with a view to improving Americans’ general health.
The task force reviewed the evidence presented in 16 randomized trials, as well as nested case-control studies using data from the Women’s Health Initiative. They found that no study has directly examined the effects of vitamin D screening, compared with no screening, on clinical outcomes. There isn’t even any consensus about what constitutes vitamin D deficiency, or what the optimal circulating level of 25-hydroxyvitamin D is.
Many testing methods are available, including competitive protein binding, immunoassay, high-performance liquid chromatography, and mass spectrometry. But the sensitivity and specificity of these tests remains unknown, because there is no internationally recognized reference standard. Moreover, the USPSTF found that test results vary not just by which test is used, but even between laboratories using the same test.
Symptomatic vitamin D deficiency is known to affect health adversely, as is asymptomatic vitamin D deficiency in certain patient populations. But the evidence that deficiency contributes to adverse health outcomes in asymptomatic adults is inadequate. The evidence that screening for such deficiency and treating “low” vitamin D levels prevents adverse outcomes or simply improves general health also is inadequate, Dr. LeFevre and his associates said.
Similarly, no studies to date have directly examined possible harms of screening for and treating vitamin D deficiency. Although there are concerns that vitamin D supplements may lead to hypercalcemia, kidney stones, or gastrointestinal symptoms, there is no evidence of such effects in the asymptomatic patient population.
The USPSTF concluded that the harms of screening for and treating vitamin D deficiency are likely “small to none,” but it still is not possible to determine whether the benefits outweigh even that small amount of harm.
At present, no national primary care professional organization recommends screening of the general adult population for vitamin D deficiency. The American Academy of Family Physicians, the Endocrine Society, the American College of Obstetricians and Gynecologists, the American Geriatrics Society, and the National Osteoporosis Foundation all recommend screening for patients at risk for fractures or falls only. The Institute of Medicine has no formal guidelines regarding vitamin D screening, Dr. LeFevre and his associates noted.
The USPSTF summary report and the review of the evidence are available at www.uspreventiveservicestaskforce.org.
The USPSTF is focused on providing a firm evidential base for early detection and prevention of disease, noted Dr. Robert P. Heaney and Dr. Laura A. G. Armas in an accompanying editorial. But perhaps clinicians should have a different focus: full nutrient repletion in their patients, to optimize their health.
A strict disease-avoidance approach is too simplistic with regard to micronutrients, because they don’t directly cause the effects often attributed to them. Instead, when supplies of micronutrients are inadequate, cellular responses are blunted, Dr. Heaney and Dr. Armas noted. That is dysfunction, but not clinically manifest disease.
Such dysfunction may indeed lead ultimately to various diseases, they added, but disease prevention is a dull tool for discerning the defect. And a disease-prevention approach clearly doesn’t show whether there is enough of the nutrient present to enable appropriate physiological responses.
Dr. Heaney and Dr. Armas are at Creighton University in Omaha, Neb. Their remarks are drawn from an editorial accompanying the USPSTF reports.
The USPSTF is focused on providing a firm evidential base for early detection and prevention of disease, noted Dr. Robert P. Heaney and Dr. Laura A. G. Armas in an accompanying editorial. But perhaps clinicians should have a different focus: full nutrient repletion in their patients, to optimize their health.
A strict disease-avoidance approach is too simplistic with regard to micronutrients, because they don’t directly cause the effects often attributed to them. Instead, when supplies of micronutrients are inadequate, cellular responses are blunted, Dr. Heaney and Dr. Armas noted. That is dysfunction, but not clinically manifest disease.
Such dysfunction may indeed lead ultimately to various diseases, they added, but disease prevention is a dull tool for discerning the defect. And a disease-prevention approach clearly doesn’t show whether there is enough of the nutrient present to enable appropriate physiological responses.
Dr. Heaney and Dr. Armas are at Creighton University in Omaha, Neb. Their remarks are drawn from an editorial accompanying the USPSTF reports.
The USPSTF is focused on providing a firm evidential base for early detection and prevention of disease, noted Dr. Robert P. Heaney and Dr. Laura A. G. Armas in an accompanying editorial. But perhaps clinicians should have a different focus: full nutrient repletion in their patients, to optimize their health.
A strict disease-avoidance approach is too simplistic with regard to micronutrients, because they don’t directly cause the effects often attributed to them. Instead, when supplies of micronutrients are inadequate, cellular responses are blunted, Dr. Heaney and Dr. Armas noted. That is dysfunction, but not clinically manifest disease.
Such dysfunction may indeed lead ultimately to various diseases, they added, but disease prevention is a dull tool for discerning the defect. And a disease-prevention approach clearly doesn’t show whether there is enough of the nutrient present to enable appropriate physiological responses.
Dr. Heaney and Dr. Armas are at Creighton University in Omaha, Neb. Their remarks are drawn from an editorial accompanying the USPSTF reports.
The U.S. Preventive Services Task Force made no recommendation for or against primary care physicians screening asymptomatic adults for vitamin D deficiency, because the current evidence is insufficient to adequately assess the benefits and harms of doing so, according to a report published online Nov. 24 in Annals of Internal Medicine.
The USPSTF reviewed the evidence on screening and treatment for vitamin D deficiency, because the condition may contribute to fractures, falls, functional limitations, cancer, diabetes, cardiovascular disease, depression, and excess mortality.
In addition, testing of vitamin D levels has increased markedly in recent years. One national survey showed the annual rate of outpatient visits with a diagnosis code for vitamin D deficiency more than tripled between 2008 and 2010, and a 2009 survey of clinical laboratories reported that the testing increased by at least half in the space of just 1 year, said Dr. Michael L. LeFevre, chair of the task force and professor of family medicine at the University of Missouri, Columbia, and his associates.
The organization is a voluntary expert group tasked with making recommendations about specific preventive care services, devices, and medications for asymptomatic people, with a view to improving Americans’ general health.
The task force reviewed the evidence presented in 16 randomized trials, as well as nested case-control studies using data from the Women’s Health Initiative. They found that no study has directly examined the effects of vitamin D screening, compared with no screening, on clinical outcomes. There isn’t even any consensus about what constitutes vitamin D deficiency, or what the optimal circulating level of 25-hydroxyvitamin D is.
Many testing methods are available, including competitive protein binding, immunoassay, high-performance liquid chromatography, and mass spectrometry. But the sensitivity and specificity of these tests remains unknown, because there is no internationally recognized reference standard. Moreover, the USPSTF found that test results vary not just by which test is used, but even between laboratories using the same test.
Symptomatic vitamin D deficiency is known to affect health adversely, as is asymptomatic vitamin D deficiency in certain patient populations. But the evidence that deficiency contributes to adverse health outcomes in asymptomatic adults is inadequate. The evidence that screening for such deficiency and treating “low” vitamin D levels prevents adverse outcomes or simply improves general health also is inadequate, Dr. LeFevre and his associates said.
Similarly, no studies to date have directly examined possible harms of screening for and treating vitamin D deficiency. Although there are concerns that vitamin D supplements may lead to hypercalcemia, kidney stones, or gastrointestinal symptoms, there is no evidence of such effects in the asymptomatic patient population.
The USPSTF concluded that the harms of screening for and treating vitamin D deficiency are likely “small to none,” but it still is not possible to determine whether the benefits outweigh even that small amount of harm.
At present, no national primary care professional organization recommends screening of the general adult population for vitamin D deficiency. The American Academy of Family Physicians, the Endocrine Society, the American College of Obstetricians and Gynecologists, the American Geriatrics Society, and the National Osteoporosis Foundation all recommend screening for patients at risk for fractures or falls only. The Institute of Medicine has no formal guidelines regarding vitamin D screening, Dr. LeFevre and his associates noted.
The USPSTF summary report and the review of the evidence are available at www.uspreventiveservicestaskforce.org.
The U.S. Preventive Services Task Force made no recommendation for or against primary care physicians screening asymptomatic adults for vitamin D deficiency, because the current evidence is insufficient to adequately assess the benefits and harms of doing so, according to a report published online Nov. 24 in Annals of Internal Medicine.
The USPSTF reviewed the evidence on screening and treatment for vitamin D deficiency, because the condition may contribute to fractures, falls, functional limitations, cancer, diabetes, cardiovascular disease, depression, and excess mortality.
In addition, testing of vitamin D levels has increased markedly in recent years. One national survey showed the annual rate of outpatient visits with a diagnosis code for vitamin D deficiency more than tripled between 2008 and 2010, and a 2009 survey of clinical laboratories reported that the testing increased by at least half in the space of just 1 year, said Dr. Michael L. LeFevre, chair of the task force and professor of family medicine at the University of Missouri, Columbia, and his associates.
The organization is a voluntary expert group tasked with making recommendations about specific preventive care services, devices, and medications for asymptomatic people, with a view to improving Americans’ general health.
The task force reviewed the evidence presented in 16 randomized trials, as well as nested case-control studies using data from the Women’s Health Initiative. They found that no study has directly examined the effects of vitamin D screening, compared with no screening, on clinical outcomes. There isn’t even any consensus about what constitutes vitamin D deficiency, or what the optimal circulating level of 25-hydroxyvitamin D is.
Many testing methods are available, including competitive protein binding, immunoassay, high-performance liquid chromatography, and mass spectrometry. But the sensitivity and specificity of these tests remains unknown, because there is no internationally recognized reference standard. Moreover, the USPSTF found that test results vary not just by which test is used, but even between laboratories using the same test.
Symptomatic vitamin D deficiency is known to affect health adversely, as is asymptomatic vitamin D deficiency in certain patient populations. But the evidence that deficiency contributes to adverse health outcomes in asymptomatic adults is inadequate. The evidence that screening for such deficiency and treating “low” vitamin D levels prevents adverse outcomes or simply improves general health also is inadequate, Dr. LeFevre and his associates said.
Similarly, no studies to date have directly examined possible harms of screening for and treating vitamin D deficiency. Although there are concerns that vitamin D supplements may lead to hypercalcemia, kidney stones, or gastrointestinal symptoms, there is no evidence of such effects in the asymptomatic patient population.
The USPSTF concluded that the harms of screening for and treating vitamin D deficiency are likely “small to none,” but it still is not possible to determine whether the benefits outweigh even that small amount of harm.
At present, no national primary care professional organization recommends screening of the general adult population for vitamin D deficiency. The American Academy of Family Physicians, the Endocrine Society, the American College of Obstetricians and Gynecologists, the American Geriatrics Society, and the National Osteoporosis Foundation all recommend screening for patients at risk for fractures or falls only. The Institute of Medicine has no formal guidelines regarding vitamin D screening, Dr. LeFevre and his associates noted.
The USPSTF summary report and the review of the evidence are available at www.uspreventiveservicestaskforce.org.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: The USPSTF makes no recommendation for or against screening and treating asymptomatic adults for vitamin D deficiency, because the evidence regarding the benefits and harms is insufficient.
Major finding: Testing of vitamin D levels has increased markedly, with one national survey showing the annual rate of outpatient visits with a diagnosis code for vitamin D deficiency more than tripled between 2008 and 2010, and a 2009 survey of clinical laboratories reporting that the testing increased by at least half in the space of just 1 year.
Data source: A detailed review of the evidence and an expert consensus regarding screening asymptomatic adults for vitamin D deficiency to prevent fractures, cancer, CVD, and other adverse outcomes.
Disclosures: The USPSTF is an independent, voluntary group supported by the U.S. Agency for Healthcare Research and Quality to improve Americans’ health by making recommendations concerning preventive services such as screenings and medications. Dr. LeFevre and his associates reported having no relevant financial disclosures.

Carboplatin, etoposide yield similar survival in NSCLC
Chemotherapy with carboplatin and paclitaxel yielded similar overall survival with fewer adverse effects than did etoposide-plus-cisplatin chemotherapy in the first large study to directly compare the two approaches for stage-3 non–small-cell lung cancer, according to a report published online Nov. 24 in the Journal of Clinical Oncology.
When given concurrently with radiotherapy, the etoposide-based chemotherapy has been considered the most effective for these patients, but the carboplatin combination has recently emerged as an alternative because it is less toxic. Yet, “there is considerable concern that carboplatin plus paclitaxel, although better tolerated than etoposide plus cisplatin, may be inferior in terms of disease control,” said Dr. Rafael Santana-Davila of the University of Washington, Seattle, and his associates.
To compare the two combination chemotherapies, the investigators reviewed the records of 1,842 Veterans Affairs patients (98% men) newly diagnosed as having stage-3 NSCLC during a 10-year period. A total of 27% were treated with the etoposide combination and 73% with the carboplatin combination. In the initial, unadjusted data analysis, etoposide was associated with a longer median survival (17.3 months vs 14.6 months), but further investigation showed that the difference was attributable to patients’ baseline characteristics rather than their chemotherapy regimen.
Since baseline traits differed between the two groups of patients, a subgroup of 381 patients who received etoposide was propensity matched with the same number who received carboplatin. This eliminated baseline differences between the two study groups in age, hemoglobin level, albumin level, percentage of weight loss, and comorbidities. This analysis also demonstrated no survival advantage for etoposide.
The researchers then discovered that some of the medical centers in the study showed definite preferences for or against etoposide, with 8 using the drug more than half the time (in 55%-81% of patients) and 11 using it in fewer than 10% of cases (in 0-9% of patients).
In two final analyses that corrected for this discrepancy, the etoposide combination again carried no survival advantage, compared with the carboplatin combination. Patients who received etoposide plus cisplatin, however, had a higher rate of adverse events during treatment, more oncology visits (mean, 17.6 visits vs. 12.6 for carboplatin), and more hospitalizations during treatment (mean, 2.4 vs 1.7), Dr. Santana-Davila and his associates said (J. Clin. Oncol. 2014 Nov. 24 [doi:10.1200/JCO.2014.56.2587]).
“We believe this study shows that there is considerable equipoise regarding which regimen should be preferred. Given the prevalence of unresectable stage-3 lung cancer, we believe a phase III randomized controlled trial should be considered to definitively answer this question,” they said.
Chemotherapy with carboplatin and paclitaxel yielded similar overall survival with fewer adverse effects than did etoposide-plus-cisplatin chemotherapy in the first large study to directly compare the two approaches for stage-3 non–small-cell lung cancer, according to a report published online Nov. 24 in the Journal of Clinical Oncology.
When given concurrently with radiotherapy, the etoposide-based chemotherapy has been considered the most effective for these patients, but the carboplatin combination has recently emerged as an alternative because it is less toxic. Yet, “there is considerable concern that carboplatin plus paclitaxel, although better tolerated than etoposide plus cisplatin, may be inferior in terms of disease control,” said Dr. Rafael Santana-Davila of the University of Washington, Seattle, and his associates.
To compare the two combination chemotherapies, the investigators reviewed the records of 1,842 Veterans Affairs patients (98% men) newly diagnosed as having stage-3 NSCLC during a 10-year period. A total of 27% were treated with the etoposide combination and 73% with the carboplatin combination. In the initial, unadjusted data analysis, etoposide was associated with a longer median survival (17.3 months vs 14.6 months), but further investigation showed that the difference was attributable to patients’ baseline characteristics rather than their chemotherapy regimen.
Since baseline traits differed between the two groups of patients, a subgroup of 381 patients who received etoposide was propensity matched with the same number who received carboplatin. This eliminated baseline differences between the two study groups in age, hemoglobin level, albumin level, percentage of weight loss, and comorbidities. This analysis also demonstrated no survival advantage for etoposide.
The researchers then discovered that some of the medical centers in the study showed definite preferences for or against etoposide, with 8 using the drug more than half the time (in 55%-81% of patients) and 11 using it in fewer than 10% of cases (in 0-9% of patients).
In two final analyses that corrected for this discrepancy, the etoposide combination again carried no survival advantage, compared with the carboplatin combination. Patients who received etoposide plus cisplatin, however, had a higher rate of adverse events during treatment, more oncology visits (mean, 17.6 visits vs. 12.6 for carboplatin), and more hospitalizations during treatment (mean, 2.4 vs 1.7), Dr. Santana-Davila and his associates said (J. Clin. Oncol. 2014 Nov. 24 [doi:10.1200/JCO.2014.56.2587]).
“We believe this study shows that there is considerable equipoise regarding which regimen should be preferred. Given the prevalence of unresectable stage-3 lung cancer, we believe a phase III randomized controlled trial should be considered to definitively answer this question,” they said.
Chemotherapy with carboplatin and paclitaxel yielded similar overall survival with fewer adverse effects than did etoposide-plus-cisplatin chemotherapy in the first large study to directly compare the two approaches for stage-3 non–small-cell lung cancer, according to a report published online Nov. 24 in the Journal of Clinical Oncology.
When given concurrently with radiotherapy, the etoposide-based chemotherapy has been considered the most effective for these patients, but the carboplatin combination has recently emerged as an alternative because it is less toxic. Yet, “there is considerable concern that carboplatin plus paclitaxel, although better tolerated than etoposide plus cisplatin, may be inferior in terms of disease control,” said Dr. Rafael Santana-Davila of the University of Washington, Seattle, and his associates.
To compare the two combination chemotherapies, the investigators reviewed the records of 1,842 Veterans Affairs patients (98% men) newly diagnosed as having stage-3 NSCLC during a 10-year period. A total of 27% were treated with the etoposide combination and 73% with the carboplatin combination. In the initial, unadjusted data analysis, etoposide was associated with a longer median survival (17.3 months vs 14.6 months), but further investigation showed that the difference was attributable to patients’ baseline characteristics rather than their chemotherapy regimen.
Since baseline traits differed between the two groups of patients, a subgroup of 381 patients who received etoposide was propensity matched with the same number who received carboplatin. This eliminated baseline differences between the two study groups in age, hemoglobin level, albumin level, percentage of weight loss, and comorbidities. This analysis also demonstrated no survival advantage for etoposide.
The researchers then discovered that some of the medical centers in the study showed definite preferences for or against etoposide, with 8 using the drug more than half the time (in 55%-81% of patients) and 11 using it in fewer than 10% of cases (in 0-9% of patients).
In two final analyses that corrected for this discrepancy, the etoposide combination again carried no survival advantage, compared with the carboplatin combination. Patients who received etoposide plus cisplatin, however, had a higher rate of adverse events during treatment, more oncology visits (mean, 17.6 visits vs. 12.6 for carboplatin), and more hospitalizations during treatment (mean, 2.4 vs 1.7), Dr. Santana-Davila and his associates said (J. Clin. Oncol. 2014 Nov. 24 [doi:10.1200/JCO.2014.56.2587]).
“We believe this study shows that there is considerable equipoise regarding which regimen should be preferred. Given the prevalence of unresectable stage-3 lung cancer, we believe a phase III randomized controlled trial should be considered to definitively answer this question,” they said.
Key clinical point: Carboplatin + paclitaxel yielded similar overall survival with fewer adverse effects than etoposide + cisplatin for stage-3 NSCLC.
Major finding: Four separate statistical analyses demonstrated that overall survival was similar between 499 patients given etoposide-based chemotherapy and 1,343 given carboplatin-based chemotherapy.
Data source: A retrospective database analysis involving 1,842 VA patients with newly diagnosed stage-3 NSCLC.
Disclosures: Dr. Santana-Davila reported having no financial disclosures; one of his associates reported owning stock in Abbott and AbbVie.
Palliative tumor removal extends survival
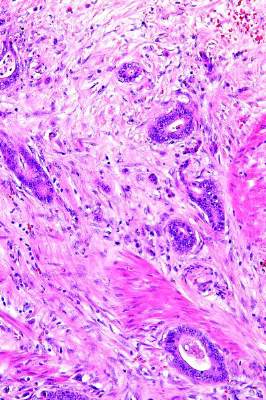
Palliative resection of the primary tumor actually extends survival in patients with metastatic colorectal adenocarcinoma, according to a report published online Nov. 4 in Annals of Surgery.
In what the investigators described as the first population-based study to assess trends in cancer-specific and overall survival among U.S. patients who did or did not undergo palliative removal of the primary tumor, the resection consistently conferred statistically significant and clinically meaningful survival benefits among 37,793 patients treated during a 12-year period.
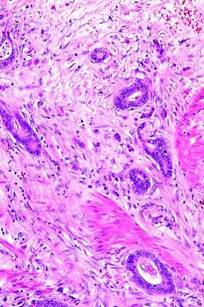
“There is a heated debate in the medical and surgical oncology community regarding whether or not an asymptomatic primary tumor should be removed in patients with unresectable, synchronous cancer metastases,” wrote Dr. Ignazio Tarantino of the department of surgery, Kantonsspital St. Gallen (Switzerland) and the department of general, abdominal, and transplant surgery, University of Heidelberg (Germany) and his associates.
Current National Comprehensive Cancer Network guidelines recommend against palliative surgery in this setting, primarily because of evidence that leaving the primary tumor in situ seldom leads to life-threatening complications such as bleeding or bowel obstruction, while resection can cause complications and is not strictly necessary in terminally ill patients. But given these new findings of a significant survival benefit, “the dogma that [such tumors] never should be resected ... must be questioned,” the investigators wrote.
Dr. Tarantino and his associates analyzed Surveillance, Epidemiology, and End Results (SEER) data for 23,004 patients (60.9% of the total study population) who underwent primary tumor resection and 14,789 (39.1%) who did not. The percentage of patients who had the surgery steadily declined throughout the study period.
Palliative removal of the primary tumor was a significant protective factor for overall survival (HR of death, 0.49) and for cancer-specific survival (HR of cancer death, 0.49) in both the primary data analysis and a proportional hazard regression analysis.
Patients undergoing resection tended to be younger and healthier than those who did not have the procedure, so the researchers performed a propensity-score matching analysis to account for baseline differences between the two study groups. After adjustment for numerous potential confounders, palliative primary tumor resection continued to exert a significant protective effect for overall and cancer-specific survival, with HRs of 0.40 and 0.39, respectively. The survival benefit also persisted, with identical hazard ratios, in two further sensitivity analyses of the data, Dr. Tarantino and his associates noted (Ann. Surg. 2014 Nov. 4 [doi: 10.1097/SLA.0000000000000860]).
The mechanism by which palliative resection imparts a survival benefit is not yet known, they added.
Major advances in systemic treatment of metastatic colorectal cancer were achieved during the study period, and survival improved accordingly across both groups of patients over time. “Because of the improvement in systemic treatment, we anticipated that the differences in survival between the subsets of patients who did and who did not undergo palliative primary tumor resection would decrease over time. However – against our a priori hypothesis – our analysis demonstrates the contrary,” the investigators noted.
No financial or material support was provided for this study. Dr. Tarantino and his associates reported having no financial disclosures.
Palliative resection of the primary tumor actually extends survival in patients with metastatic colorectal adenocarcinoma, according to a report published online Nov. 4 in Annals of Surgery.
In what the investigators described as the first population-based study to assess trends in cancer-specific and overall survival among U.S. patients who did or did not undergo palliative removal of the primary tumor, the resection consistently conferred statistically significant and clinically meaningful survival benefits among 37,793 patients treated during a 12-year period.
“There is a heated debate in the medical and surgical oncology community regarding whether or not an asymptomatic primary tumor should be removed in patients with unresectable, synchronous cancer metastases,” wrote Dr. Ignazio Tarantino of the department of surgery, Kantonsspital St. Gallen (Switzerland) and the department of general, abdominal, and transplant surgery, University of Heidelberg (Germany) and his associates.
Current National Comprehensive Cancer Network guidelines recommend against palliative surgery in this setting, primarily because of evidence that leaving the primary tumor in situ seldom leads to life-threatening complications such as bleeding or bowel obstruction, while resection can cause complications and is not strictly necessary in terminally ill patients. But given these new findings of a significant survival benefit, “the dogma that [such tumors] never should be resected ... must be questioned,” the investigators wrote.
Dr. Tarantino and his associates analyzed Surveillance, Epidemiology, and End Results (SEER) data for 23,004 patients (60.9% of the total study population) who underwent primary tumor resection and 14,789 (39.1%) who did not. The percentage of patients who had the surgery steadily declined throughout the study period.
Palliative removal of the primary tumor was a significant protective factor for overall survival (HR of death, 0.49) and for cancer-specific survival (HR of cancer death, 0.49) in both the primary data analysis and a proportional hazard regression analysis.
Patients undergoing resection tended to be younger and healthier than those who did not have the procedure, so the researchers performed a propensity-score matching analysis to account for baseline differences between the two study groups. After adjustment for numerous potential confounders, palliative primary tumor resection continued to exert a significant protective effect for overall and cancer-specific survival, with HRs of 0.40 and 0.39, respectively. The survival benefit also persisted, with identical hazard ratios, in two further sensitivity analyses of the data, Dr. Tarantino and his associates noted (Ann. Surg. 2014 Nov. 4 [doi: 10.1097/SLA.0000000000000860]).
The mechanism by which palliative resection imparts a survival benefit is not yet known, they added.
Major advances in systemic treatment of metastatic colorectal cancer were achieved during the study period, and survival improved accordingly across both groups of patients over time. “Because of the improvement in systemic treatment, we anticipated that the differences in survival between the subsets of patients who did and who did not undergo palliative primary tumor resection would decrease over time. However – against our a priori hypothesis – our analysis demonstrates the contrary,” the investigators noted.
No financial or material support was provided for this study. Dr. Tarantino and his associates reported having no financial disclosures.
Palliative resection of the primary tumor actually extends survival in patients with metastatic colorectal adenocarcinoma, according to a report published online Nov. 4 in Annals of Surgery.
In what the investigators described as the first population-based study to assess trends in cancer-specific and overall survival among U.S. patients who did or did not undergo palliative removal of the primary tumor, the resection consistently conferred statistically significant and clinically meaningful survival benefits among 37,793 patients treated during a 12-year period.
“There is a heated debate in the medical and surgical oncology community regarding whether or not an asymptomatic primary tumor should be removed in patients with unresectable, synchronous cancer metastases,” wrote Dr. Ignazio Tarantino of the department of surgery, Kantonsspital St. Gallen (Switzerland) and the department of general, abdominal, and transplant surgery, University of Heidelberg (Germany) and his associates.
Current National Comprehensive Cancer Network guidelines recommend against palliative surgery in this setting, primarily because of evidence that leaving the primary tumor in situ seldom leads to life-threatening complications such as bleeding or bowel obstruction, while resection can cause complications and is not strictly necessary in terminally ill patients. But given these new findings of a significant survival benefit, “the dogma that [such tumors] never should be resected ... must be questioned,” the investigators wrote.
Dr. Tarantino and his associates analyzed Surveillance, Epidemiology, and End Results (SEER) data for 23,004 patients (60.9% of the total study population) who underwent primary tumor resection and 14,789 (39.1%) who did not. The percentage of patients who had the surgery steadily declined throughout the study period.
Palliative removal of the primary tumor was a significant protective factor for overall survival (HR of death, 0.49) and for cancer-specific survival (HR of cancer death, 0.49) in both the primary data analysis and a proportional hazard regression analysis.
Patients undergoing resection tended to be younger and healthier than those who did not have the procedure, so the researchers performed a propensity-score matching analysis to account for baseline differences between the two study groups. After adjustment for numerous potential confounders, palliative primary tumor resection continued to exert a significant protective effect for overall and cancer-specific survival, with HRs of 0.40 and 0.39, respectively. The survival benefit also persisted, with identical hazard ratios, in two further sensitivity analyses of the data, Dr. Tarantino and his associates noted (Ann. Surg. 2014 Nov. 4 [doi: 10.1097/SLA.0000000000000860]).
The mechanism by which palliative resection imparts a survival benefit is not yet known, they added.
Major advances in systemic treatment of metastatic colorectal cancer were achieved during the study period, and survival improved accordingly across both groups of patients over time. “Because of the improvement in systemic treatment, we anticipated that the differences in survival between the subsets of patients who did and who did not undergo palliative primary tumor resection would decrease over time. However – against our a priori hypothesis – our analysis demonstrates the contrary,” the investigators noted.
No financial or material support was provided for this study. Dr. Tarantino and his associates reported having no financial disclosures.
Key clinical point: Palliative removal of the primary tumor extends survival in patients with metastatic colorectal cancer.
Major finding: Palliative resection of the primary tumor was a significant protective factor for overall survival (HR of death, 0.49) and for cancer-specific survival (HR of cancer death, 0.49) in both the primary data analysis and a proportional hazard regression analysis.
Data source: A population-based study of the duration of survival in 23,004 patients with metastatic colorectal cancer who had palliative removal of the primary tumor and 14,789 who did not during a 12-year period.
Disclosures: No financial or material support was provided for this study. Dr. Tarantino and his associates reported having no disclosures.
On-target glycemic control does not lessen excess mortality
Adults with type 1 diabetes who had on-target glycemic control still showed twice the risk of death from any cause and death from cardiovascular causes as did the general population, according to findings from a Swedish study involving virtually every affected patient in that country that was reported online Nov. 20.
The excess mortality despite good glycemic control was attributed almost entirely to diabetes itself (ketoacidosis or hypoglycemia) or to cardiovascular disease (CVD), which is particularly puzzling because adults with type 1 diabetes “generally do not have excess rates of obesity, hypertension, or hypercholesterolemia.” Moreover, the diabetes patients in this study were four to five times more likely than controls to be taking cardioprotective drugs such as statins or renin-angiotensin-aldosterone system inhibitors, said Dr. Marcus Lind of Uddevalla Hospital and the University of Gothenburg in Sweden, and his associates.
The investigators assessed mortality risks in patients who had varying degrees of glycemic control using data from the Swedish National Diabetes Register and national mortality databases during a 14-year period. They matched 33,915 patients for age, sex, and region of residence with 169,249 adults in the general population. The mean duration of diabetes was 20 years, and the mean glycosylated hemoglobin level at baseline was 8.2%.
Overall mortality for patients with type 1 diabetes was 8% (9.97 per 1,000 observation-years), compared with 2.9% (3.45 per 1,000 observation-years) for controls. After the data were adjusted to account for education level and other possible confounding factors, hazard ratios for patients vs. controls were still high at 3.52 for death from any cause and 4.60 for death from CVD causes, the investigators said (N. Engl. J. Med. 2014 November 20 [doi:10.1056/NEJMoa1408214]).
Even patients who had good glycemic control, with a mean glycosylated hemoglobin level of 6.9% or lower, had an hazard ratio for death from any cause of 2.36 and an HR for cardiovascular death of 2.92, in relation to controls. Mortality increased as mean glycosylated hemoglobin level increased, so that patients with a mean glycosylated hemoglobin level of 9.7% or higher were 8 times more likely to die from any cause and 10 times more likely to die from cardiovascular causes, in relation to controls.
Adults with type 1 diabetes who had on-target glycemic control still showed twice the risk of death from any cause and death from cardiovascular causes as did the general population, according to findings from a Swedish study involving virtually every affected patient in that country that was reported online Nov. 20.
The excess mortality despite good glycemic control was attributed almost entirely to diabetes itself (ketoacidosis or hypoglycemia) or to cardiovascular disease (CVD), which is particularly puzzling because adults with type 1 diabetes “generally do not have excess rates of obesity, hypertension, or hypercholesterolemia.” Moreover, the diabetes patients in this study were four to five times more likely than controls to be taking cardioprotective drugs such as statins or renin-angiotensin-aldosterone system inhibitors, said Dr. Marcus Lind of Uddevalla Hospital and the University of Gothenburg in Sweden, and his associates.
The investigators assessed mortality risks in patients who had varying degrees of glycemic control using data from the Swedish National Diabetes Register and national mortality databases during a 14-year period. They matched 33,915 patients for age, sex, and region of residence with 169,249 adults in the general population. The mean duration of diabetes was 20 years, and the mean glycosylated hemoglobin level at baseline was 8.2%.
Overall mortality for patients with type 1 diabetes was 8% (9.97 per 1,000 observation-years), compared with 2.9% (3.45 per 1,000 observation-years) for controls. After the data were adjusted to account for education level and other possible confounding factors, hazard ratios for patients vs. controls were still high at 3.52 for death from any cause and 4.60 for death from CVD causes, the investigators said (N. Engl. J. Med. 2014 November 20 [doi:10.1056/NEJMoa1408214]).
Even patients who had good glycemic control, with a mean glycosylated hemoglobin level of 6.9% or lower, had an hazard ratio for death from any cause of 2.36 and an HR for cardiovascular death of 2.92, in relation to controls. Mortality increased as mean glycosylated hemoglobin level increased, so that patients with a mean glycosylated hemoglobin level of 9.7% or higher were 8 times more likely to die from any cause and 10 times more likely to die from cardiovascular causes, in relation to controls.
Adults with type 1 diabetes who had on-target glycemic control still showed twice the risk of death from any cause and death from cardiovascular causes as did the general population, according to findings from a Swedish study involving virtually every affected patient in that country that was reported online Nov. 20.
The excess mortality despite good glycemic control was attributed almost entirely to diabetes itself (ketoacidosis or hypoglycemia) or to cardiovascular disease (CVD), which is particularly puzzling because adults with type 1 diabetes “generally do not have excess rates of obesity, hypertension, or hypercholesterolemia.” Moreover, the diabetes patients in this study were four to five times more likely than controls to be taking cardioprotective drugs such as statins or renin-angiotensin-aldosterone system inhibitors, said Dr. Marcus Lind of Uddevalla Hospital and the University of Gothenburg in Sweden, and his associates.
The investigators assessed mortality risks in patients who had varying degrees of glycemic control using data from the Swedish National Diabetes Register and national mortality databases during a 14-year period. They matched 33,915 patients for age, sex, and region of residence with 169,249 adults in the general population. The mean duration of diabetes was 20 years, and the mean glycosylated hemoglobin level at baseline was 8.2%.
Overall mortality for patients with type 1 diabetes was 8% (9.97 per 1,000 observation-years), compared with 2.9% (3.45 per 1,000 observation-years) for controls. After the data were adjusted to account for education level and other possible confounding factors, hazard ratios for patients vs. controls were still high at 3.52 for death from any cause and 4.60 for death from CVD causes, the investigators said (N. Engl. J. Med. 2014 November 20 [doi:10.1056/NEJMoa1408214]).
Even patients who had good glycemic control, with a mean glycosylated hemoglobin level of 6.9% or lower, had an hazard ratio for death from any cause of 2.36 and an HR for cardiovascular death of 2.92, in relation to controls. Mortality increased as mean glycosylated hemoglobin level increased, so that patients with a mean glycosylated hemoglobin level of 9.7% or higher were 8 times more likely to die from any cause and 10 times more likely to die from cardiovascular causes, in relation to controls.
Key clinical point: Adults with type 1 diabetes who have good glycemic control still have twice the all-cause and CVD mortality as the general population.
Major finding: Even patients who had good glycemic control, with a mean glycosylated hemoglobin level of 6.9% or lower, had an HR for death from any cause of 2.36 and an HR for cardiovascular death of 2.92, in relation to controls.
Data source: An observational analysis of glycemic control and mortality data involving 33,915 adults with type 1 diabetes and 169,249 controls in the general population matched for age, sex, and area of residence in Sweden.
Disclosures: This study was supported by the Swedish government, the Swedish Society of Medicine, the Regional Vastra Gotaland Executive Board’s Health and Medical Care Committee, the Swedish Heart and Lung Foundation, Diabetes Wellness, and the Swedish Research Council. Dr. Lind reported receiving honoraria and grant support from AstraZeneca, Novo Nordisk, Pfizer, Medtronic, Abbott, and Dexcom; his associates reported ties to numerous industry sources.
Early nasoenteric feeding not beneficial in acute pancreatitis
Early nasoenteric tube feeding was not superior to an oral diet introduced at 72 hours in decreasing infection or death among patients with acute pancreatitis who were at high risk for complications, according to a report published online Nov. 20 in the New England Journal of Medicine.
Most current American and European guidelines recommend routine early enteral feeding for such patients. But “the methodologic quality of the trials that form the basis for these recommendations has been criticized ... [and] large, high-quality, randomized controlled trials that show an improved outcome with early enteral feeding are lacking,” said Dr. Olaf J. Bakker of the department of surgery, University of Utrecht (the Netherlands) Medical Center, and his associates in the Dutch Pancreatitis Study Group.
The researchers compared the two feeding approaches in the Pancreatitis, Very Early Compared with Selective Delayed Start of Enteral Feeding (PYTHON) study, a randomized, controlled superiority trial involving 208 patients treated at six university medical centers and 13 large teaching hospitals in the Netherlands.
The participants were adults with a first episode of acute pancreatitis who were judged to be at high risk for complications when they presented to emergency departments. They were randomly assigned to receive either nasoenteric tube feeding initiated within 24 hours (102 patients in the early group), or oral feeding beginning at 72 hours (106 patients in the on-demand group) that was switched to nasoenteric tube feeding only if the oral intake was insufficient or not tolerated.
The primary endpoint of the study – a composite of major infection or death within 6 months – occurred in 30% of patients in the early group and 27% in the on-demand group, which did not demonstrate superiority.
“These findings do not support clinical guidelines recommending the early start of nasoenteric tube feeding in all patients with acute pancreatitis in order to reduce the risks of infection and death,” Dr. Bakker and his associates said (N. Engl. J. Med. 2014;371:1983-93).
The rationale for early enteral feeding is that its trophic effect would stabilize the integrity of the gut mucosa, reducing inflammation and susceptibility to infection. In the study, however, early enteral feeding did not reduce any of the variables indicating inflammation, the investigators noted.
“A feeding tube frequently causes discomfort, excessive gagging, or esophagitis and is often dislodged or becomes obstructed,” so avoiding tube feeding when possible would reduce both patient discomfort and costs, the investigators added.
The PYTHON study was supported by the Netherlands Organization for Health Research and Development, the ZonMw Health Care Efficiency Research Program, and Nutricia. Dr. Bakker reported having no financial disclosures; two of his associates had numerous ties to industry sources.
Early nasoenteric tube feeding was not superior to an oral diet introduced at 72 hours in decreasing infection or death among patients with acute pancreatitis who were at high risk for complications, according to a report published online Nov. 20 in the New England Journal of Medicine.
Most current American and European guidelines recommend routine early enteral feeding for such patients. But “the methodologic quality of the trials that form the basis for these recommendations has been criticized ... [and] large, high-quality, randomized controlled trials that show an improved outcome with early enteral feeding are lacking,” said Dr. Olaf J. Bakker of the department of surgery, University of Utrecht (the Netherlands) Medical Center, and his associates in the Dutch Pancreatitis Study Group.
The researchers compared the two feeding approaches in the Pancreatitis, Very Early Compared with Selective Delayed Start of Enteral Feeding (PYTHON) study, a randomized, controlled superiority trial involving 208 patients treated at six university medical centers and 13 large teaching hospitals in the Netherlands.
The participants were adults with a first episode of acute pancreatitis who were judged to be at high risk for complications when they presented to emergency departments. They were randomly assigned to receive either nasoenteric tube feeding initiated within 24 hours (102 patients in the early group), or oral feeding beginning at 72 hours (106 patients in the on-demand group) that was switched to nasoenteric tube feeding only if the oral intake was insufficient or not tolerated.
The primary endpoint of the study – a composite of major infection or death within 6 months – occurred in 30% of patients in the early group and 27% in the on-demand group, which did not demonstrate superiority.
“These findings do not support clinical guidelines recommending the early start of nasoenteric tube feeding in all patients with acute pancreatitis in order to reduce the risks of infection and death,” Dr. Bakker and his associates said (N. Engl. J. Med. 2014;371:1983-93).
The rationale for early enteral feeding is that its trophic effect would stabilize the integrity of the gut mucosa, reducing inflammation and susceptibility to infection. In the study, however, early enteral feeding did not reduce any of the variables indicating inflammation, the investigators noted.
“A feeding tube frequently causes discomfort, excessive gagging, or esophagitis and is often dislodged or becomes obstructed,” so avoiding tube feeding when possible would reduce both patient discomfort and costs, the investigators added.
The PYTHON study was supported by the Netherlands Organization for Health Research and Development, the ZonMw Health Care Efficiency Research Program, and Nutricia. Dr. Bakker reported having no financial disclosures; two of his associates had numerous ties to industry sources.
Early nasoenteric tube feeding was not superior to an oral diet introduced at 72 hours in decreasing infection or death among patients with acute pancreatitis who were at high risk for complications, according to a report published online Nov. 20 in the New England Journal of Medicine.
Most current American and European guidelines recommend routine early enteral feeding for such patients. But “the methodologic quality of the trials that form the basis for these recommendations has been criticized ... [and] large, high-quality, randomized controlled trials that show an improved outcome with early enteral feeding are lacking,” said Dr. Olaf J. Bakker of the department of surgery, University of Utrecht (the Netherlands) Medical Center, and his associates in the Dutch Pancreatitis Study Group.
The researchers compared the two feeding approaches in the Pancreatitis, Very Early Compared with Selective Delayed Start of Enteral Feeding (PYTHON) study, a randomized, controlled superiority trial involving 208 patients treated at six university medical centers and 13 large teaching hospitals in the Netherlands.
The participants were adults with a first episode of acute pancreatitis who were judged to be at high risk for complications when they presented to emergency departments. They were randomly assigned to receive either nasoenteric tube feeding initiated within 24 hours (102 patients in the early group), or oral feeding beginning at 72 hours (106 patients in the on-demand group) that was switched to nasoenteric tube feeding only if the oral intake was insufficient or not tolerated.
The primary endpoint of the study – a composite of major infection or death within 6 months – occurred in 30% of patients in the early group and 27% in the on-demand group, which did not demonstrate superiority.
“These findings do not support clinical guidelines recommending the early start of nasoenteric tube feeding in all patients with acute pancreatitis in order to reduce the risks of infection and death,” Dr. Bakker and his associates said (N. Engl. J. Med. 2014;371:1983-93).
The rationale for early enteral feeding is that its trophic effect would stabilize the integrity of the gut mucosa, reducing inflammation and susceptibility to infection. In the study, however, early enteral feeding did not reduce any of the variables indicating inflammation, the investigators noted.
“A feeding tube frequently causes discomfort, excessive gagging, or esophagitis and is often dislodged or becomes obstructed,” so avoiding tube feeding when possible would reduce both patient discomfort and costs, the investigators added.
The PYTHON study was supported by the Netherlands Organization for Health Research and Development, the ZonMw Health Care Efficiency Research Program, and Nutricia. Dr. Bakker reported having no financial disclosures; two of his associates had numerous ties to industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Early nasoenteric tube feeding was not superior to an oral diet at 72 hours in acute high-risk pancreatitis.
Major finding: The primary endpoint of the study – a composite of major infection or death within 6 months – occurred in 30% of patients who received early nasoenteric tube feeding and 27% who received an oral diet at 72 hours.
Data source: A multicenter, randomized, controlled superiority trial involving 208 adults with acute, high-risk pancreatitis who were followed for 6 months.
Disclosures: The PYTHON study was supported by the Netherlands Organization for Health Research and Development, the ZonMw Health Care Efficiency Research Program, and Nutricia. Dr. Bakker reported having no financial disclosures; two of his associates had numerous ties to industry sources.
'Lottery' incentive increases compliance with FOBT
A financial incentive – offering patients a 10% chance of winning a $50 lottery if they completed a fecal occult blood test – improved compliance with the colorectal cancer screen by approximately 20%, according to a report published online Nov. 17 in Annals of Internal Medicine.
In a randomized controlled trial assessing six different financial incentives for completing fecal occult blood tests (FOBTs), only this “lottery” incentive improved compliance. It is based on a central tenet of behavioral economics: people attach more value to near-term than long-term costs and benefits. In this specific case, patients may fail to complete FOBTs because the tests entail “a certain and immediate disutility” (i.e., a cost) in return for “an uncertain and distant benefit of early detection of colorectal cancer for a few patients and no tangible benefit for most patients, who screen negative,” said Dr. Jeffrey T. Kullgren of the Center for Clinical Management Research at the Veterans Affairs Ann Arbor (Mich.) Health System and his associates.
Their findings demonstrate that “a low-cost, scalable innovation ... can improve health care quality by promoting patient adherence to a high-value clinical preventive service” in a real-world primary care setting.
The investigators performed the two-stage trial during an 8-month period at a single primary care VA clinic. Most of the participants were white males in their 60s, and nearly half had a disease or injury related to military service. Approximately one-third had not completed a prescribed FOBT at their previous annual physical examination.
In the first stage of the study, 713 patients prescribed an FOBT were randomly assigned to usual care or to receive $5, $10, or $20 incentives for completing their FOBT within 30 days. The intent was to determine which of these dollar amounts was the smallest effective “dose” to enhance compliance, so that that amount could be further tested in the second stage of the study. However, none of these amounts proved effective. So in the second stage, 836 patients were assigned to usual care or to one of three incentives using the lowest amount ($5): a fixed payment of $5, a lottery with a 1 in 10 chance of winning $50, or a raffle in which one patient would win $500.
Only the lottery incentive for a 10% chance of winning $50 improved patient compliance with the FOBT. The rate of completing an FOBT within 30 days in this group was 19.6% higher than the rates in the other groups, Dr. Kullgren and his associates said (Ann. Intern. Med. 2014 Nov. 17 [doi:10.7326/M13-3015]).
A financial incentive – offering patients a 10% chance of winning a $50 lottery if they completed a fecal occult blood test – improved compliance with the colorectal cancer screen by approximately 20%, according to a report published online Nov. 17 in Annals of Internal Medicine.
In a randomized controlled trial assessing six different financial incentives for completing fecal occult blood tests (FOBTs), only this “lottery” incentive improved compliance. It is based on a central tenet of behavioral economics: people attach more value to near-term than long-term costs and benefits. In this specific case, patients may fail to complete FOBTs because the tests entail “a certain and immediate disutility” (i.e., a cost) in return for “an uncertain and distant benefit of early detection of colorectal cancer for a few patients and no tangible benefit for most patients, who screen negative,” said Dr. Jeffrey T. Kullgren of the Center for Clinical Management Research at the Veterans Affairs Ann Arbor (Mich.) Health System and his associates.
Their findings demonstrate that “a low-cost, scalable innovation ... can improve health care quality by promoting patient adherence to a high-value clinical preventive service” in a real-world primary care setting.
The investigators performed the two-stage trial during an 8-month period at a single primary care VA clinic. Most of the participants were white males in their 60s, and nearly half had a disease or injury related to military service. Approximately one-third had not completed a prescribed FOBT at their previous annual physical examination.
In the first stage of the study, 713 patients prescribed an FOBT were randomly assigned to usual care or to receive $5, $10, or $20 incentives for completing their FOBT within 30 days. The intent was to determine which of these dollar amounts was the smallest effective “dose” to enhance compliance, so that that amount could be further tested in the second stage of the study. However, none of these amounts proved effective. So in the second stage, 836 patients were assigned to usual care or to one of three incentives using the lowest amount ($5): a fixed payment of $5, a lottery with a 1 in 10 chance of winning $50, or a raffle in which one patient would win $500.
Only the lottery incentive for a 10% chance of winning $50 improved patient compliance with the FOBT. The rate of completing an FOBT within 30 days in this group was 19.6% higher than the rates in the other groups, Dr. Kullgren and his associates said (Ann. Intern. Med. 2014 Nov. 17 [doi:10.7326/M13-3015]).
A financial incentive – offering patients a 10% chance of winning a $50 lottery if they completed a fecal occult blood test – improved compliance with the colorectal cancer screen by approximately 20%, according to a report published online Nov. 17 in Annals of Internal Medicine.
In a randomized controlled trial assessing six different financial incentives for completing fecal occult blood tests (FOBTs), only this “lottery” incentive improved compliance. It is based on a central tenet of behavioral economics: people attach more value to near-term than long-term costs and benefits. In this specific case, patients may fail to complete FOBTs because the tests entail “a certain and immediate disutility” (i.e., a cost) in return for “an uncertain and distant benefit of early detection of colorectal cancer for a few patients and no tangible benefit for most patients, who screen negative,” said Dr. Jeffrey T. Kullgren of the Center for Clinical Management Research at the Veterans Affairs Ann Arbor (Mich.) Health System and his associates.
Their findings demonstrate that “a low-cost, scalable innovation ... can improve health care quality by promoting patient adherence to a high-value clinical preventive service” in a real-world primary care setting.
The investigators performed the two-stage trial during an 8-month period at a single primary care VA clinic. Most of the participants were white males in their 60s, and nearly half had a disease or injury related to military service. Approximately one-third had not completed a prescribed FOBT at their previous annual physical examination.
In the first stage of the study, 713 patients prescribed an FOBT were randomly assigned to usual care or to receive $5, $10, or $20 incentives for completing their FOBT within 30 days. The intent was to determine which of these dollar amounts was the smallest effective “dose” to enhance compliance, so that that amount could be further tested in the second stage of the study. However, none of these amounts proved effective. So in the second stage, 836 patients were assigned to usual care or to one of three incentives using the lowest amount ($5): a fixed payment of $5, a lottery with a 1 in 10 chance of winning $50, or a raffle in which one patient would win $500.
Only the lottery incentive for a 10% chance of winning $50 improved patient compliance with the FOBT. The rate of completing an FOBT within 30 days in this group was 19.6% higher than the rates in the other groups, Dr. Kullgren and his associates said (Ann. Intern. Med. 2014 Nov. 17 [doi:10.7326/M13-3015]).
Key clinical point: A financial incentive – earning a 10% chance of winning a $50 lottery – increased patient compliance with FOBT screening for colorectal cancer.
Major finding: Patients in the group with the lottery incentive had a 19.6% higher rate of compliance with the FOBT within 30 days than those in the other groups.
Data source: A two-stage randomized controlled clinical trial involving 1,549 Veterans Affairs patients, assessing six different financial incentives to improve compliance with FOBT screening.
Disclosures: This study was funded by the Veterans Affairs Center for Health Equity and Promotion and the Robert Wood Johnson Foundation.
Schools rarely comply with USDA nutritional standards
Less than 2% of middle school and less than 1% of high school students attend public schools that adhere to all five components of the U.S. Department of Agriculture nutritional standards for schools, according to a report published online Nov. 17 in JAMA Pediatrics.
Beginning with the current school year, schools participating in federally reimbursable meal programs must implement the USDA nutritional standards for foods and drinks sold in school stores, snack bars, vending machines, food carts, a la carte cafeteria lines, and at sporting and other events – not just in cafeterias.

The standards, developed in response to the obesity epidemic among American children and adolescents, include five components: eliminate all sugar-sweetened beverages, eliminate all whole and 2% milk (i.e., offer only skim milk), eliminate all candy and regular-fat (as opposed to low-fat) snacks, eliminate French fries, and make fruits or vegetables available in all food venues, said Yvonne M. Terry-McElrath of the Institute for Social Research, University of Michigan, Ann Arbor, and her associates.
To assess adherence to these standards before the requirement takes effect, the investigators analyzed questionnaire responses from nationally representative samples of 22,716 middle school students, 30,596 high school students, and school administrators during a 5-year period.
Only 1.8% of middle school and 0.3% of high school students attended schools that complied with all five components of the USDA nutritional standards. Conversely, 21% of middle and 30% of high school students attended schools that failed to comply with any of the five components. The mean number of components that were adhered to was 1.59 for middle schools and 1.27 for high schools. The components that most schools complied with were eliminating French fries and offering only skim milk, the investigators said (JAMA Pediatrics 2014 Nov. 17 [doi:10.1001/jamapediatrics.2014.2048]). High school students whose schools had fruits or vegetables available, offered only skim milk, or complied with three or more of the components had modestly but significantly lower odds of being overweight or obese. For example, the probability that students in somewhat compliant schools would be overweight or obese was estimated to be 25.4%, while that of students in noncompliant schools was 27.7%. Taken together, these findings suggest that fully implementing the USDA nutritional standards would make a measurable improvement in student body mass index across the country, Ms. Terry-McElrath and her associates noted. Ms. Terry-McElrath and her associates reported having no financial disclosures.
These findings offer a glimmer of hope that the new federal policy might make a dent in the nation’s childhood obesity epidemic. It appears that schools can and will remove unhealthy choices and increase access to healthy foods and that doing so is associated with lower rates of overweight and obesity.
But as Terry-McElrath et al. show, only 20% of middle and 17% of high schools prohibit the sale of candy and high-fat snacks, most likely because the proceeds may go toward the regular meal program, the hiring of teachers’ aides, and the funding of athletic and other noncurricular programs. If administrators assume that switching to more healthful options will cut into the schools’ incomes, they’ll be reluctant to comply with the USDA standards.
Leslie A. Lytle, Ph.D., is chair of the department of health behavior and professor of nutrition at Gillings School of Global Public Health at the University of North Carolina at Chapel Hill. She reported having no financial conflicts of interest. Dr. Lytle made these remarks in an editorial accompanying Ms. Terry-McElrath’s report (JAMA Ped. 2014 Nov. 17 [doi:10.1001/jamapediatrics.2014.2325]).
These findings offer a glimmer of hope that the new federal policy might make a dent in the nation’s childhood obesity epidemic. It appears that schools can and will remove unhealthy choices and increase access to healthy foods and that doing so is associated with lower rates of overweight and obesity.
But as Terry-McElrath et al. show, only 20% of middle and 17% of high schools prohibit the sale of candy and high-fat snacks, most likely because the proceeds may go toward the regular meal program, the hiring of teachers’ aides, and the funding of athletic and other noncurricular programs. If administrators assume that switching to more healthful options will cut into the schools’ incomes, they’ll be reluctant to comply with the USDA standards.
Leslie A. Lytle, Ph.D., is chair of the department of health behavior and professor of nutrition at Gillings School of Global Public Health at the University of North Carolina at Chapel Hill. She reported having no financial conflicts of interest. Dr. Lytle made these remarks in an editorial accompanying Ms. Terry-McElrath’s report (JAMA Ped. 2014 Nov. 17 [doi:10.1001/jamapediatrics.2014.2325]).
These findings offer a glimmer of hope that the new federal policy might make a dent in the nation’s childhood obesity epidemic. It appears that schools can and will remove unhealthy choices and increase access to healthy foods and that doing so is associated with lower rates of overweight and obesity.
But as Terry-McElrath et al. show, only 20% of middle and 17% of high schools prohibit the sale of candy and high-fat snacks, most likely because the proceeds may go toward the regular meal program, the hiring of teachers’ aides, and the funding of athletic and other noncurricular programs. If administrators assume that switching to more healthful options will cut into the schools’ incomes, they’ll be reluctant to comply with the USDA standards.
Leslie A. Lytle, Ph.D., is chair of the department of health behavior and professor of nutrition at Gillings School of Global Public Health at the University of North Carolina at Chapel Hill. She reported having no financial conflicts of interest. Dr. Lytle made these remarks in an editorial accompanying Ms. Terry-McElrath’s report (JAMA Ped. 2014 Nov. 17 [doi:10.1001/jamapediatrics.2014.2325]).
Less than 2% of middle school and less than 1% of high school students attend public schools that adhere to all five components of the U.S. Department of Agriculture nutritional standards for schools, according to a report published online Nov. 17 in JAMA Pediatrics.
Beginning with the current school year, schools participating in federally reimbursable meal programs must implement the USDA nutritional standards for foods and drinks sold in school stores, snack bars, vending machines, food carts, a la carte cafeteria lines, and at sporting and other events – not just in cafeterias.
The standards, developed in response to the obesity epidemic among American children and adolescents, include five components: eliminate all sugar-sweetened beverages, eliminate all whole and 2% milk (i.e., offer only skim milk), eliminate all candy and regular-fat (as opposed to low-fat) snacks, eliminate French fries, and make fruits or vegetables available in all food venues, said Yvonne M. Terry-McElrath of the Institute for Social Research, University of Michigan, Ann Arbor, and her associates.
To assess adherence to these standards before the requirement takes effect, the investigators analyzed questionnaire responses from nationally representative samples of 22,716 middle school students, 30,596 high school students, and school administrators during a 5-year period.
Only 1.8% of middle school and 0.3% of high school students attended schools that complied with all five components of the USDA nutritional standards. Conversely, 21% of middle and 30% of high school students attended schools that failed to comply with any of the five components. The mean number of components that were adhered to was 1.59 for middle schools and 1.27 for high schools. The components that most schools complied with were eliminating French fries and offering only skim milk, the investigators said (JAMA Pediatrics 2014 Nov. 17 [doi:10.1001/jamapediatrics.2014.2048]). High school students whose schools had fruits or vegetables available, offered only skim milk, or complied with three or more of the components had modestly but significantly lower odds of being overweight or obese. For example, the probability that students in somewhat compliant schools would be overweight or obese was estimated to be 25.4%, while that of students in noncompliant schools was 27.7%. Taken together, these findings suggest that fully implementing the USDA nutritional standards would make a measurable improvement in student body mass index across the country, Ms. Terry-McElrath and her associates noted. Ms. Terry-McElrath and her associates reported having no financial disclosures.
Less than 2% of middle school and less than 1% of high school students attend public schools that adhere to all five components of the U.S. Department of Agriculture nutritional standards for schools, according to a report published online Nov. 17 in JAMA Pediatrics.
Beginning with the current school year, schools participating in federally reimbursable meal programs must implement the USDA nutritional standards for foods and drinks sold in school stores, snack bars, vending machines, food carts, a la carte cafeteria lines, and at sporting and other events – not just in cafeterias.
The standards, developed in response to the obesity epidemic among American children and adolescents, include five components: eliminate all sugar-sweetened beverages, eliminate all whole and 2% milk (i.e., offer only skim milk), eliminate all candy and regular-fat (as opposed to low-fat) snacks, eliminate French fries, and make fruits or vegetables available in all food venues, said Yvonne M. Terry-McElrath of the Institute for Social Research, University of Michigan, Ann Arbor, and her associates.
To assess adherence to these standards before the requirement takes effect, the investigators analyzed questionnaire responses from nationally representative samples of 22,716 middle school students, 30,596 high school students, and school administrators during a 5-year period.
Only 1.8% of middle school and 0.3% of high school students attended schools that complied with all five components of the USDA nutritional standards. Conversely, 21% of middle and 30% of high school students attended schools that failed to comply with any of the five components. The mean number of components that were adhered to was 1.59 for middle schools and 1.27 for high schools. The components that most schools complied with were eliminating French fries and offering only skim milk, the investigators said (JAMA Pediatrics 2014 Nov. 17 [doi:10.1001/jamapediatrics.2014.2048]). High school students whose schools had fruits or vegetables available, offered only skim milk, or complied with three or more of the components had modestly but significantly lower odds of being overweight or obese. For example, the probability that students in somewhat compliant schools would be overweight or obese was estimated to be 25.4%, while that of students in noncompliant schools was 27.7%. Taken together, these findings suggest that fully implementing the USDA nutritional standards would make a measurable improvement in student body mass index across the country, Ms. Terry-McElrath and her associates noted. Ms. Terry-McElrath and her associates reported having no financial disclosures.
Key clinical point: Less than 2% of middle and high school students attend schools that comply with all five components of the USDA’s school nutritional standards.
Major finding: Only 1.8% of middle and 0.3% of high school students attended schools that complied with all five components of the USDA nutritional standards, while 21% of middle and 30% of high school students attended schools that failed to comply with any of the five components.
Data source: A cross-sectional analysis of data from nationally representative samples of 22,716 middle school and 30,596 high school students regarding foods and drinks available in their schools.
Disclosures: This study was supported by the National Institute on Drug Abuse and the Robert Wood Johnson Foundation. Ms. Terry-McElrath and her associates reported having no financial disclosures.
