User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Higher Doses of Vitamin D3 Do Not Reduce Cardiac Biomarkers in Older Adults
TOPLINE:
Higher doses of vitamin D3 supplementation did not significantly reduce cardiac biomarkers in older adults with low serum vitamin D levels. The STURDY trial found no significant differences in high-sensitivity cardiac troponin I (hs-cTnI) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) between low- and high-dose groups.
METHODOLOGY:
- A total of 688 participants aged 70 years or older with low serum 25-hydroxy vitamin D levels (10-29 ng/mL) were included in the STURDY trial.
- Participants were randomized to receive one of four doses of vitamin D3 supplementation: 200, 1000, 2000, or 4000 IU/d, with 200 IU/d as the reference dose.
- Cardiac biomarkers, including hs-cTnI and NT-proBNP, were measured at baseline, 3 months, 12 months, and 24 months.
- The trial was conducted at two community-based research institutions in the United States between July 2015 and March 2019.
- The effects of vitamin D3 dose on biomarkers were assessed via mixed-effects tobit models, with participants followed up to 24 months or until study termination.
TAKEAWAY:
- Higher doses of vitamin D3 supplementation did not significantly affect hs-cTnI levels compared with the low-dose group (1.6% difference; 95% CI, −5.3 to 8.9).
- No significant differences were observed in NT-proBNP levels between the high-dose and low-dose groups (−1.8% difference; 95% CI, −9.3 to 6.3).
- Both hs-cTnI and NT-proBNP levels increased in both low- and high-dose groups over time, with hs-cTnI increasing by 5.2% and 7.0%, respectively, and NT-proBNP increasing by 11.3% and 9.3%, respectively.
- The findings suggest that higher doses of vitamin D3 supplementation do not reduce markers of subclinical cardiovascular disease in older adults with low serum vitamin D levels.
IN PRACTICE:
“We can speculate that the systemic effects of vitamin D deficiency are more profound among the very old, and there may be an inverse relationship between supplementation and inflammation. It is also possible that serum vitamin D level is a risk marker but not a risk factor for CVD risk and related underlying mechanisms,” wrote the authors of the study.
SOURCE:
The study was led by Katharine W. Rainer, MD, Beth Israel Deaconess Medical Center in Boston. It was published online in the Journal of the American College of Cardiology.
LIMITATIONS:
The study’s community-based population may limit the generalizability of the findings to populations at higher risk for cardiovascular disease. Additionally, the baseline cardiac biomarkers were lower than those in some high-risk populations, which may affect the precision of the assay performance. The study may not have had adequate power for cross-sectional and subgroup analyses. Both groups received some vitamin D3 supplementation, making it difficult to determine the impact of lower-dose supplementation vs no supplementation.
DISCLOSURES:
The study was supported by grants from the National Institute on Aging, the Office of Dietary Supplements, the Mid-Atlantic Nutrition Obesity Research Center, and the Johns Hopkins Institute for Clinical and Translational Research. Rainer disclosed receiving grants from these organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Higher doses of vitamin D3 supplementation did not significantly reduce cardiac biomarkers in older adults with low serum vitamin D levels. The STURDY trial found no significant differences in high-sensitivity cardiac troponin I (hs-cTnI) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) between low- and high-dose groups.
METHODOLOGY:
- A total of 688 participants aged 70 years or older with low serum 25-hydroxy vitamin D levels (10-29 ng/mL) were included in the STURDY trial.
- Participants were randomized to receive one of four doses of vitamin D3 supplementation: 200, 1000, 2000, or 4000 IU/d, with 200 IU/d as the reference dose.
- Cardiac biomarkers, including hs-cTnI and NT-proBNP, were measured at baseline, 3 months, 12 months, and 24 months.
- The trial was conducted at two community-based research institutions in the United States between July 2015 and March 2019.
- The effects of vitamin D3 dose on biomarkers were assessed via mixed-effects tobit models, with participants followed up to 24 months or until study termination.
TAKEAWAY:
- Higher doses of vitamin D3 supplementation did not significantly affect hs-cTnI levels compared with the low-dose group (1.6% difference; 95% CI, −5.3 to 8.9).
- No significant differences were observed in NT-proBNP levels between the high-dose and low-dose groups (−1.8% difference; 95% CI, −9.3 to 6.3).
- Both hs-cTnI and NT-proBNP levels increased in both low- and high-dose groups over time, with hs-cTnI increasing by 5.2% and 7.0%, respectively, and NT-proBNP increasing by 11.3% and 9.3%, respectively.
- The findings suggest that higher doses of vitamin D3 supplementation do not reduce markers of subclinical cardiovascular disease in older adults with low serum vitamin D levels.
IN PRACTICE:
“We can speculate that the systemic effects of vitamin D deficiency are more profound among the very old, and there may be an inverse relationship between supplementation and inflammation. It is also possible that serum vitamin D level is a risk marker but not a risk factor for CVD risk and related underlying mechanisms,” wrote the authors of the study.
SOURCE:
The study was led by Katharine W. Rainer, MD, Beth Israel Deaconess Medical Center in Boston. It was published online in the Journal of the American College of Cardiology.
LIMITATIONS:
The study’s community-based population may limit the generalizability of the findings to populations at higher risk for cardiovascular disease. Additionally, the baseline cardiac biomarkers were lower than those in some high-risk populations, which may affect the precision of the assay performance. The study may not have had adequate power for cross-sectional and subgroup analyses. Both groups received some vitamin D3 supplementation, making it difficult to determine the impact of lower-dose supplementation vs no supplementation.
DISCLOSURES:
The study was supported by grants from the National Institute on Aging, the Office of Dietary Supplements, the Mid-Atlantic Nutrition Obesity Research Center, and the Johns Hopkins Institute for Clinical and Translational Research. Rainer disclosed receiving grants from these organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Higher doses of vitamin D3 supplementation did not significantly reduce cardiac biomarkers in older adults with low serum vitamin D levels. The STURDY trial found no significant differences in high-sensitivity cardiac troponin I (hs-cTnI) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) between low- and high-dose groups.
METHODOLOGY:
- A total of 688 participants aged 70 years or older with low serum 25-hydroxy vitamin D levels (10-29 ng/mL) were included in the STURDY trial.
- Participants were randomized to receive one of four doses of vitamin D3 supplementation: 200, 1000, 2000, or 4000 IU/d, with 200 IU/d as the reference dose.
- Cardiac biomarkers, including hs-cTnI and NT-proBNP, were measured at baseline, 3 months, 12 months, and 24 months.
- The trial was conducted at two community-based research institutions in the United States between July 2015 and March 2019.
- The effects of vitamin D3 dose on biomarkers were assessed via mixed-effects tobit models, with participants followed up to 24 months or until study termination.
TAKEAWAY:
- Higher doses of vitamin D3 supplementation did not significantly affect hs-cTnI levels compared with the low-dose group (1.6% difference; 95% CI, −5.3 to 8.9).
- No significant differences were observed in NT-proBNP levels between the high-dose and low-dose groups (−1.8% difference; 95% CI, −9.3 to 6.3).
- Both hs-cTnI and NT-proBNP levels increased in both low- and high-dose groups over time, with hs-cTnI increasing by 5.2% and 7.0%, respectively, and NT-proBNP increasing by 11.3% and 9.3%, respectively.
- The findings suggest that higher doses of vitamin D3 supplementation do not reduce markers of subclinical cardiovascular disease in older adults with low serum vitamin D levels.
IN PRACTICE:
“We can speculate that the systemic effects of vitamin D deficiency are more profound among the very old, and there may be an inverse relationship between supplementation and inflammation. It is also possible that serum vitamin D level is a risk marker but not a risk factor for CVD risk and related underlying mechanisms,” wrote the authors of the study.
SOURCE:
The study was led by Katharine W. Rainer, MD, Beth Israel Deaconess Medical Center in Boston. It was published online in the Journal of the American College of Cardiology.
LIMITATIONS:
The study’s community-based population may limit the generalizability of the findings to populations at higher risk for cardiovascular disease. Additionally, the baseline cardiac biomarkers were lower than those in some high-risk populations, which may affect the precision of the assay performance. The study may not have had adequate power for cross-sectional and subgroup analyses. Both groups received some vitamin D3 supplementation, making it difficult to determine the impact of lower-dose supplementation vs no supplementation.
DISCLOSURES:
The study was supported by grants from the National Institute on Aging, the Office of Dietary Supplements, the Mid-Atlantic Nutrition Obesity Research Center, and the Johns Hopkins Institute for Clinical and Translational Research. Rainer disclosed receiving grants from these organizations.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Is It Possible To Treat Patients You Dislike?
This transcript has been edited for clarity.
What do we do if we don’t like patients? We take the Hippocratic Oath as young students in Glasgow. We do that just before our graduation ceremony; we hold our hands up and repeat the Hippocratic Oath: “First, do no harm,” and so on.
I was thinking back over a long career. I’ve been a cancer doctor for 40 years and I quite like saying that.
I can only think genuinely over a couple of times in which I’ve acted reflexively when a patient has done something awful. The couple of times it happened, it was just terrible racist comments to junior doctors who were with me. Extraordinarily dreadful things such as, “I don’t want to be touched by ...” or something of that sort.
Without really thinking about it, you react as a normal citizen and say, “That’s absolutely awful. Apologize immediately or leave the consultation room, and never ever come back again.”
I remember that it happened once in Glasgow and once when I was a young professor in Birmingham, and it’s just an automatic gut reaction. The patient got a fright, and I immediately apologized and groveled around. In that relationship, we hold all the power, don’t we? Rather than being gentle about it, I was genuinely angry because of these ridiculous comments.
Otherwise, I think most of the doctor-patient relationships are predicated on nonromantic love. I think patients want us to love them as one would a son, mother, father, or daughter, because if we do, then we will do better for them and we’ll pull out all the stops. “Placebo” means “I will please.” I think in the vast majority of cases, at least in our National Health Service (NHS), patients come with trust and a sense of wanting to build that relationship. That may be changing, but not for me.
What about putting the boot on the other foot? What if the patients don’t like us rather than vice versa? As part of our accreditation appraisal process, from time to time we have to take patient surveys as to whether the patients felt that, after they had been seen in a consultation, they were treated with dignity, the quality of information given was appropriate, and they were treated with kindness.
It’s an excellent exercise. Without bragging about it, patients objectively, according to these measures, appreciate the service that I give. It’s like getting five-star reviews on Trustpilot, or whatever these things are, that allow you to review car salesmen and so on. I have always had five-star reviews across the board.
That, again, I thought was just a feature of that relationship, of patients wanting to please. These are patients who had been treated, who were in the outpatient department, who were in the midst of battle. Still, the scores are very high. I speak to my colleagues and that’s not uniformly the case. Patients actually do use these feedback forms, I think in a positive rather than negative way, reflecting back on the way that they were treated.
It has caused some of my colleagues to think quite hard about their personal style and approach to patients. That sense of feedback is important.
What about losing trust? If that’s at the heart of everything that we do, then what would be an objective measure of losing trust? Again, in our healthcare system, it has been exceedingly unusual for a patient to request a second opinion. Now, that’s changing. The government is trying to change it. Leaders of the NHS are trying to change it so that patients feel assured that they can seek second opinions.
Again, in all the years I’ve been a cancer doctor, it has been incredibly infrequent that somebody has sought a second opinion after I’ve said something. That may be a measure of trust. Again, I’ve lived through an NHS in which seeking second opinions was something of a rarity.
I’d be really interested to see what you think. In your own sphere of healthcare practice, is it possible for us to look after patients that we don’t like, or should we be honest and say, “I don’t like you. Our relationship has broken down. I want you to be seen by a colleague,” or “I want you to be nursed by somebody else”?
Has that happened? Is that something that you think is common or may become more common? What about when trust breaks down the other way? Can you think of instances in which the relationship, for whatever reason, just didn’t work and the patient had to move on because of that loss of trust and what underpinned it? I’d be really interested to know.
I seek to be informed rather than the other way around. Can we truly look after patients that we don’t like or can we rise above it as Hippocrates might have done?
Thanks for listening, as always. For the time being, over and out.
Dr. Kerr, Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford; Professor of Cancer Medicine, Oxford Cancer Centre, Oxford, United Kingdom, disclosed ties with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Bayer HealthCare Pharmaceuticals, Genomic Health, Merck Serono, and Roche.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
What do we do if we don’t like patients? We take the Hippocratic Oath as young students in Glasgow. We do that just before our graduation ceremony; we hold our hands up and repeat the Hippocratic Oath: “First, do no harm,” and so on.
I was thinking back over a long career. I’ve been a cancer doctor for 40 years and I quite like saying that.
I can only think genuinely over a couple of times in which I’ve acted reflexively when a patient has done something awful. The couple of times it happened, it was just terrible racist comments to junior doctors who were with me. Extraordinarily dreadful things such as, “I don’t want to be touched by ...” or something of that sort.
Without really thinking about it, you react as a normal citizen and say, “That’s absolutely awful. Apologize immediately or leave the consultation room, and never ever come back again.”
I remember that it happened once in Glasgow and once when I was a young professor in Birmingham, and it’s just an automatic gut reaction. The patient got a fright, and I immediately apologized and groveled around. In that relationship, we hold all the power, don’t we? Rather than being gentle about it, I was genuinely angry because of these ridiculous comments.
Otherwise, I think most of the doctor-patient relationships are predicated on nonromantic love. I think patients want us to love them as one would a son, mother, father, or daughter, because if we do, then we will do better for them and we’ll pull out all the stops. “Placebo” means “I will please.” I think in the vast majority of cases, at least in our National Health Service (NHS), patients come with trust and a sense of wanting to build that relationship. That may be changing, but not for me.
What about putting the boot on the other foot? What if the patients don’t like us rather than vice versa? As part of our accreditation appraisal process, from time to time we have to take patient surveys as to whether the patients felt that, after they had been seen in a consultation, they were treated with dignity, the quality of information given was appropriate, and they were treated with kindness.
It’s an excellent exercise. Without bragging about it, patients objectively, according to these measures, appreciate the service that I give. It’s like getting five-star reviews on Trustpilot, or whatever these things are, that allow you to review car salesmen and so on. I have always had five-star reviews across the board.
That, again, I thought was just a feature of that relationship, of patients wanting to please. These are patients who had been treated, who were in the outpatient department, who were in the midst of battle. Still, the scores are very high. I speak to my colleagues and that’s not uniformly the case. Patients actually do use these feedback forms, I think in a positive rather than negative way, reflecting back on the way that they were treated.
It has caused some of my colleagues to think quite hard about their personal style and approach to patients. That sense of feedback is important.
What about losing trust? If that’s at the heart of everything that we do, then what would be an objective measure of losing trust? Again, in our healthcare system, it has been exceedingly unusual for a patient to request a second opinion. Now, that’s changing. The government is trying to change it. Leaders of the NHS are trying to change it so that patients feel assured that they can seek second opinions.
Again, in all the years I’ve been a cancer doctor, it has been incredibly infrequent that somebody has sought a second opinion after I’ve said something. That may be a measure of trust. Again, I’ve lived through an NHS in which seeking second opinions was something of a rarity.
I’d be really interested to see what you think. In your own sphere of healthcare practice, is it possible for us to look after patients that we don’t like, or should we be honest and say, “I don’t like you. Our relationship has broken down. I want you to be seen by a colleague,” or “I want you to be nursed by somebody else”?
Has that happened? Is that something that you think is common or may become more common? What about when trust breaks down the other way? Can you think of instances in which the relationship, for whatever reason, just didn’t work and the patient had to move on because of that loss of trust and what underpinned it? I’d be really interested to know.
I seek to be informed rather than the other way around. Can we truly look after patients that we don’t like or can we rise above it as Hippocrates might have done?
Thanks for listening, as always. For the time being, over and out.
Dr. Kerr, Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford; Professor of Cancer Medicine, Oxford Cancer Centre, Oxford, United Kingdom, disclosed ties with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Bayer HealthCare Pharmaceuticals, Genomic Health, Merck Serono, and Roche.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
What do we do if we don’t like patients? We take the Hippocratic Oath as young students in Glasgow. We do that just before our graduation ceremony; we hold our hands up and repeat the Hippocratic Oath: “First, do no harm,” and so on.
I was thinking back over a long career. I’ve been a cancer doctor for 40 years and I quite like saying that.
I can only think genuinely over a couple of times in which I’ve acted reflexively when a patient has done something awful. The couple of times it happened, it was just terrible racist comments to junior doctors who were with me. Extraordinarily dreadful things such as, “I don’t want to be touched by ...” or something of that sort.
Without really thinking about it, you react as a normal citizen and say, “That’s absolutely awful. Apologize immediately or leave the consultation room, and never ever come back again.”
I remember that it happened once in Glasgow and once when I was a young professor in Birmingham, and it’s just an automatic gut reaction. The patient got a fright, and I immediately apologized and groveled around. In that relationship, we hold all the power, don’t we? Rather than being gentle about it, I was genuinely angry because of these ridiculous comments.
Otherwise, I think most of the doctor-patient relationships are predicated on nonromantic love. I think patients want us to love them as one would a son, mother, father, or daughter, because if we do, then we will do better for them and we’ll pull out all the stops. “Placebo” means “I will please.” I think in the vast majority of cases, at least in our National Health Service (NHS), patients come with trust and a sense of wanting to build that relationship. That may be changing, but not for me.
What about putting the boot on the other foot? What if the patients don’t like us rather than vice versa? As part of our accreditation appraisal process, from time to time we have to take patient surveys as to whether the patients felt that, after they had been seen in a consultation, they were treated with dignity, the quality of information given was appropriate, and they were treated with kindness.
It’s an excellent exercise. Without bragging about it, patients objectively, according to these measures, appreciate the service that I give. It’s like getting five-star reviews on Trustpilot, or whatever these things are, that allow you to review car salesmen and so on. I have always had five-star reviews across the board.
That, again, I thought was just a feature of that relationship, of patients wanting to please. These are patients who had been treated, who were in the outpatient department, who were in the midst of battle. Still, the scores are very high. I speak to my colleagues and that’s not uniformly the case. Patients actually do use these feedback forms, I think in a positive rather than negative way, reflecting back on the way that they were treated.
It has caused some of my colleagues to think quite hard about their personal style and approach to patients. That sense of feedback is important.
What about losing trust? If that’s at the heart of everything that we do, then what would be an objective measure of losing trust? Again, in our healthcare system, it has been exceedingly unusual for a patient to request a second opinion. Now, that’s changing. The government is trying to change it. Leaders of the NHS are trying to change it so that patients feel assured that they can seek second opinions.
Again, in all the years I’ve been a cancer doctor, it has been incredibly infrequent that somebody has sought a second opinion after I’ve said something. That may be a measure of trust. Again, I’ve lived through an NHS in which seeking second opinions was something of a rarity.
I’d be really interested to see what you think. In your own sphere of healthcare practice, is it possible for us to look after patients that we don’t like, or should we be honest and say, “I don’t like you. Our relationship has broken down. I want you to be seen by a colleague,” or “I want you to be nursed by somebody else”?
Has that happened? Is that something that you think is common or may become more common? What about when trust breaks down the other way? Can you think of instances in which the relationship, for whatever reason, just didn’t work and the patient had to move on because of that loss of trust and what underpinned it? I’d be really interested to know.
I seek to be informed rather than the other way around. Can we truly look after patients that we don’t like or can we rise above it as Hippocrates might have done?
Thanks for listening, as always. For the time being, over and out.
Dr. Kerr, Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford; Professor of Cancer Medicine, Oxford Cancer Centre, Oxford, United Kingdom, disclosed ties with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Bayer HealthCare Pharmaceuticals, Genomic Health, Merck Serono, and Roche.
A version of this article appeared on Medscape.com.
ASA Releases New Primary Stroke Prevention Guideline
The first update in a decade, the 2024 Guideline for the Primary Prevention of Stroke, replaces the 2014 version and is intended to be a resource for clinicians to help them implement a variety of prevention strategies in patients with no previous history of stroke. It aligns with the American Heart Association’s Life’s Essential 8.
“This guideline is an important and timely update from 2014 for multiple reasons. First, there have been groundbreaking clinical trials that have been published with new medications to not only treat the target disease [including] diabetes/obesity and high cholesterol], but also lower the risk of stroke and heart disease,” said chair of the guideline writing group, Cheryl D. Bushnell, MD, MHS, FAHA, and vice chair of the research, Department of Neurology, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
It was published online on October 21 in Stroke.
Up to 80% of Strokes Preventable
Estimates show that every year in the United States, more than 500,000 individuals have a first stroke. However, the guideline authors noted that up to 80% of strokes may be preventable. As a result, they called for better primary stroke prevention that includes improved screening and lifestyle changes.
This includes adoption of the Mediterranean diet, which has been shown to significantly reduce stroke risk, especially when supplemented with consumption of nuts and olive oil.
The guideline recommendations also emphasize the need for physical activity, which is “essential” for cardiovascular health and stroke reduction. The authors underscored this point and provided a new recommendation to screen for sedentary behavior and advise patients to avoid inactivity and engage in regular moderate to vigorous physical activity.
Another new recommendation is based on “robust” data that glucagon-like peptide 1 receptor agonists (GLP-1s) significantly improve the management of type 2 diabetes, weight loss, and lower the risk for cardiovascular disease. As a result, guideline authors called for the use of GLP-1s in patients with diabetes and high cardiovascular risk or established cardiovascular disease.
“The glucagon-like peptide receptor agonists have been shown to not only drastically reduce blood sugars in patients with diabetes, but they also lead to significant weight loss in these patients, which has many downstream benefits. Together, this reduces the risk of stroke and other complications of diabetes,” said Bushnell.
She also noted that another drug class introduced since the 2014 guidelines were published, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, have proven to be highly effective in lowering low-density lipoprotein cholesterol. These medications have also been shown to reduce the risk for stroke.
At Least Two Meds Needed to Reduce BP
Effective blood pressure (BP) management is crucial for stroke prevention. Randomized controlled trials show that a single antihypertensive medication helps only about 30% of participants reach their BP target.
Most patients only achieve the desired BP target with two to three medications. In line with these data, the committee recommends using at least two antihypertensives for primary stroke prevention in most patients who require BP-lowering medications for hypertension.
In patients with antiphospholipid syndrome or systemic lupus erythematosus and no history of stroke or unprovoked venous thromboembolism, the authors recommended antiplatelet therapy to prevent stroke. They added that patients with antiphospholipid syndrome who have had a prior unprovoked venous thrombosis will likely benefit from vitamin K antagonist therapy (target international normalized ratio, 2-3) over direct oral anticoagulants.
Emphasis on Women’s Health
Preventing pregnancy-related stroke is achieved primarily by managing hypertension, the guideline authors noted. They recommended treating verified systolic BP over 160 mm Hg or diastolic BP over 110 mm Hg during pregnancy and up to 6 weeks postpartum to lower the risk for fatal maternal intracerebral hemorrhage.
They noted that adverse pregnancy outcomes are also common and linked to chronic hypertension, which increases stroke risk later in life. Therefore, they recommended screening for these outcomes to assess and manage vascular risk factors. The guideline includes a screening tool to help with this in clinical practice.
Endometriosis, premature ovarian failure (before age 40 years), and early-onset menopause (before age 45 years) are all associated with increased stroke risk. As a result, the guideline authors said screening for all three of these conditions is a “reasonable step in the evaluation and management of vascular risk factors in these individuals to reduce stroke risk.”
Finally, the guideline authors addressed primary stroke prevention in transgender individuals, noting that transgender women undergoing estrogen therapy for gender affirmation are at increased risk. They emphasized that evaluating and modifying risk factors could be beneficial for reducing stroke risk in this patient population.
Challenges Lie Ahead
Now that the guideline has been published, the challenge lies in determining how best to implement “its screening recommendations in primary care and other practices when these clinicians are already pushed to see as many patients as possible,” Bushnell said.
Development of screening tools that can be easily incorporated into the clinic visit or the electronic health record, as well as additional personnel to provide counseling, are probably needed to disseminate them, she added.
Bushnell also emphasized that the guideline includes a strong focus on social determinants of health and related social needs.
“We worked hard to use inclusive language and to consider populations historically excluded from research. In acknowledging that social determinants of health including access to healthcare, access to education, economic stability, neighborhood and geographic location, and social and community context have a tremendous influence on stroke risk, we describe how these factors are closely tied to the prevalence and management of many medical risks like obesity, hypertension, and diabetes.
“Our recommendations offer practical steps for screening and addressing essential health-related social needs, including access to nutritious food, stable housing, and reliable transportation, within clinical practice. By considering these factors more comprehensively, we believe we can make meaningful strides toward reducing the disparities in stroke risk,” said Bushnell.
A version of this article appeared on Medscape.com.
The first update in a decade, the 2024 Guideline for the Primary Prevention of Stroke, replaces the 2014 version and is intended to be a resource for clinicians to help them implement a variety of prevention strategies in patients with no previous history of stroke. It aligns with the American Heart Association’s Life’s Essential 8.
“This guideline is an important and timely update from 2014 for multiple reasons. First, there have been groundbreaking clinical trials that have been published with new medications to not only treat the target disease [including] diabetes/obesity and high cholesterol], but also lower the risk of stroke and heart disease,” said chair of the guideline writing group, Cheryl D. Bushnell, MD, MHS, FAHA, and vice chair of the research, Department of Neurology, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
It was published online on October 21 in Stroke.
Up to 80% of Strokes Preventable
Estimates show that every year in the United States, more than 500,000 individuals have a first stroke. However, the guideline authors noted that up to 80% of strokes may be preventable. As a result, they called for better primary stroke prevention that includes improved screening and lifestyle changes.
This includes adoption of the Mediterranean diet, which has been shown to significantly reduce stroke risk, especially when supplemented with consumption of nuts and olive oil.
The guideline recommendations also emphasize the need for physical activity, which is “essential” for cardiovascular health and stroke reduction. The authors underscored this point and provided a new recommendation to screen for sedentary behavior and advise patients to avoid inactivity and engage in regular moderate to vigorous physical activity.
Another new recommendation is based on “robust” data that glucagon-like peptide 1 receptor agonists (GLP-1s) significantly improve the management of type 2 diabetes, weight loss, and lower the risk for cardiovascular disease. As a result, guideline authors called for the use of GLP-1s in patients with diabetes and high cardiovascular risk or established cardiovascular disease.
“The glucagon-like peptide receptor agonists have been shown to not only drastically reduce blood sugars in patients with diabetes, but they also lead to significant weight loss in these patients, which has many downstream benefits. Together, this reduces the risk of stroke and other complications of diabetes,” said Bushnell.
She also noted that another drug class introduced since the 2014 guidelines were published, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, have proven to be highly effective in lowering low-density lipoprotein cholesterol. These medications have also been shown to reduce the risk for stroke.
At Least Two Meds Needed to Reduce BP
Effective blood pressure (BP) management is crucial for stroke prevention. Randomized controlled trials show that a single antihypertensive medication helps only about 30% of participants reach their BP target.
Most patients only achieve the desired BP target with two to three medications. In line with these data, the committee recommends using at least two antihypertensives for primary stroke prevention in most patients who require BP-lowering medications for hypertension.
In patients with antiphospholipid syndrome or systemic lupus erythematosus and no history of stroke or unprovoked venous thromboembolism, the authors recommended antiplatelet therapy to prevent stroke. They added that patients with antiphospholipid syndrome who have had a prior unprovoked venous thrombosis will likely benefit from vitamin K antagonist therapy (target international normalized ratio, 2-3) over direct oral anticoagulants.
Emphasis on Women’s Health
Preventing pregnancy-related stroke is achieved primarily by managing hypertension, the guideline authors noted. They recommended treating verified systolic BP over 160 mm Hg or diastolic BP over 110 mm Hg during pregnancy and up to 6 weeks postpartum to lower the risk for fatal maternal intracerebral hemorrhage.
They noted that adverse pregnancy outcomes are also common and linked to chronic hypertension, which increases stroke risk later in life. Therefore, they recommended screening for these outcomes to assess and manage vascular risk factors. The guideline includes a screening tool to help with this in clinical practice.
Endometriosis, premature ovarian failure (before age 40 years), and early-onset menopause (before age 45 years) are all associated with increased stroke risk. As a result, the guideline authors said screening for all three of these conditions is a “reasonable step in the evaluation and management of vascular risk factors in these individuals to reduce stroke risk.”
Finally, the guideline authors addressed primary stroke prevention in transgender individuals, noting that transgender women undergoing estrogen therapy for gender affirmation are at increased risk. They emphasized that evaluating and modifying risk factors could be beneficial for reducing stroke risk in this patient population.
Challenges Lie Ahead
Now that the guideline has been published, the challenge lies in determining how best to implement “its screening recommendations in primary care and other practices when these clinicians are already pushed to see as many patients as possible,” Bushnell said.
Development of screening tools that can be easily incorporated into the clinic visit or the electronic health record, as well as additional personnel to provide counseling, are probably needed to disseminate them, she added.
Bushnell also emphasized that the guideline includes a strong focus on social determinants of health and related social needs.
“We worked hard to use inclusive language and to consider populations historically excluded from research. In acknowledging that social determinants of health including access to healthcare, access to education, economic stability, neighborhood and geographic location, and social and community context have a tremendous influence on stroke risk, we describe how these factors are closely tied to the prevalence and management of many medical risks like obesity, hypertension, and diabetes.
“Our recommendations offer practical steps for screening and addressing essential health-related social needs, including access to nutritious food, stable housing, and reliable transportation, within clinical practice. By considering these factors more comprehensively, we believe we can make meaningful strides toward reducing the disparities in stroke risk,” said Bushnell.
A version of this article appeared on Medscape.com.
The first update in a decade, the 2024 Guideline for the Primary Prevention of Stroke, replaces the 2014 version and is intended to be a resource for clinicians to help them implement a variety of prevention strategies in patients with no previous history of stroke. It aligns with the American Heart Association’s Life’s Essential 8.
“This guideline is an important and timely update from 2014 for multiple reasons. First, there have been groundbreaking clinical trials that have been published with new medications to not only treat the target disease [including] diabetes/obesity and high cholesterol], but also lower the risk of stroke and heart disease,” said chair of the guideline writing group, Cheryl D. Bushnell, MD, MHS, FAHA, and vice chair of the research, Department of Neurology, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
It was published online on October 21 in Stroke.
Up to 80% of Strokes Preventable
Estimates show that every year in the United States, more than 500,000 individuals have a first stroke. However, the guideline authors noted that up to 80% of strokes may be preventable. As a result, they called for better primary stroke prevention that includes improved screening and lifestyle changes.
This includes adoption of the Mediterranean diet, which has been shown to significantly reduce stroke risk, especially when supplemented with consumption of nuts and olive oil.
The guideline recommendations also emphasize the need for physical activity, which is “essential” for cardiovascular health and stroke reduction. The authors underscored this point and provided a new recommendation to screen for sedentary behavior and advise patients to avoid inactivity and engage in regular moderate to vigorous physical activity.
Another new recommendation is based on “robust” data that glucagon-like peptide 1 receptor agonists (GLP-1s) significantly improve the management of type 2 diabetes, weight loss, and lower the risk for cardiovascular disease. As a result, guideline authors called for the use of GLP-1s in patients with diabetes and high cardiovascular risk or established cardiovascular disease.
“The glucagon-like peptide receptor agonists have been shown to not only drastically reduce blood sugars in patients with diabetes, but they also lead to significant weight loss in these patients, which has many downstream benefits. Together, this reduces the risk of stroke and other complications of diabetes,” said Bushnell.
She also noted that another drug class introduced since the 2014 guidelines were published, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, have proven to be highly effective in lowering low-density lipoprotein cholesterol. These medications have also been shown to reduce the risk for stroke.
At Least Two Meds Needed to Reduce BP
Effective blood pressure (BP) management is crucial for stroke prevention. Randomized controlled trials show that a single antihypertensive medication helps only about 30% of participants reach their BP target.
Most patients only achieve the desired BP target with two to three medications. In line with these data, the committee recommends using at least two antihypertensives for primary stroke prevention in most patients who require BP-lowering medications for hypertension.
In patients with antiphospholipid syndrome or systemic lupus erythematosus and no history of stroke or unprovoked venous thromboembolism, the authors recommended antiplatelet therapy to prevent stroke. They added that patients with antiphospholipid syndrome who have had a prior unprovoked venous thrombosis will likely benefit from vitamin K antagonist therapy (target international normalized ratio, 2-3) over direct oral anticoagulants.
Emphasis on Women’s Health
Preventing pregnancy-related stroke is achieved primarily by managing hypertension, the guideline authors noted. They recommended treating verified systolic BP over 160 mm Hg or diastolic BP over 110 mm Hg during pregnancy and up to 6 weeks postpartum to lower the risk for fatal maternal intracerebral hemorrhage.
They noted that adverse pregnancy outcomes are also common and linked to chronic hypertension, which increases stroke risk later in life. Therefore, they recommended screening for these outcomes to assess and manage vascular risk factors. The guideline includes a screening tool to help with this in clinical practice.
Endometriosis, premature ovarian failure (before age 40 years), and early-onset menopause (before age 45 years) are all associated with increased stroke risk. As a result, the guideline authors said screening for all three of these conditions is a “reasonable step in the evaluation and management of vascular risk factors in these individuals to reduce stroke risk.”
Finally, the guideline authors addressed primary stroke prevention in transgender individuals, noting that transgender women undergoing estrogen therapy for gender affirmation are at increased risk. They emphasized that evaluating and modifying risk factors could be beneficial for reducing stroke risk in this patient population.
Challenges Lie Ahead
Now that the guideline has been published, the challenge lies in determining how best to implement “its screening recommendations in primary care and other practices when these clinicians are already pushed to see as many patients as possible,” Bushnell said.
Development of screening tools that can be easily incorporated into the clinic visit or the electronic health record, as well as additional personnel to provide counseling, are probably needed to disseminate them, she added.
Bushnell also emphasized that the guideline includes a strong focus on social determinants of health and related social needs.
“We worked hard to use inclusive language and to consider populations historically excluded from research. In acknowledging that social determinants of health including access to healthcare, access to education, economic stability, neighborhood and geographic location, and social and community context have a tremendous influence on stroke risk, we describe how these factors are closely tied to the prevalence and management of many medical risks like obesity, hypertension, and diabetes.
“Our recommendations offer practical steps for screening and addressing essential health-related social needs, including access to nutritious food, stable housing, and reliable transportation, within clinical practice. By considering these factors more comprehensively, we believe we can make meaningful strides toward reducing the disparities in stroke risk,” said Bushnell.
A version of this article appeared on Medscape.com.
A Single Jog Can Improve Glucose Metabolism in Young Adults
TOPLINE:
In healthy young adults, a single 30-minute bout of outdoor aerobic exercise significantly reduces fasting and 1-hour glucose levels during an oral glucose tolerance test (OGTT) the next day and improves insulin sensitivity.
METHODOLOGY:
- Recent studies have identified 1-hour post-load glucose concentration during an OGTT as a specific and early predictor of diabetes, and exercise has long been known for its metabolic benefits in people with and without diabetes.
- The researchers investigated the effect of a single bout of aerobic exercise on 1-hour post-load glucose levels during an OGTT in 32 young, healthy, normal-weight or marginally overweight individuals (mean age, 35 years; 14 women and 18 men) with a sedentary or moderately active lifestyle.
- The participants underwent an initial OGTT after at least 4 days of physical inactivity, followed by a second OGTT the day after a single 30-minute bout of aerobic exercise.
- The exercise session consisted of a light jog for 30 minutes, monitored using a metabolic holter to quantify energy expenditure and exercise intensity. The participants did not undertake any exercise outside the lab sessions.
- Blood glucose levels were measured, and insulin sensitivity and secretion were estimated using surrogate indices derived from OGTT glucose and insulin assays, including the Matsuda index, oral glucose insulin sensitivity (OGIS) index, and quantitative insulin sensitivity check index, as well as the homeostasis model assessment (HOMA) of insulin resistance and of beta-cell function (HOMA-B).
TAKEAWAY:
- Postexercise insulin levels also were significantly lower 1 hour after glucose load, decreasing from 57.4 IU/mL at baseline to 43.5 IU/mL the day after exercise (P = .01).
- Insulin sensitivity improved significantly after exercise, as indicated by increases in the Matsuda index (P = .02) and OGIS index (P = .04), along with a reduction in insulin resistance (P = .04).
- The study found a trend toward increased beta-cell function the day after an exercise bout, as indicated by a nonsignificant increase in HOMA-B from 144.7 at baseline to 167.1 after exercise.
IN PRACTICE:
“Improvement in 1-hour post-load plasma glucose following a single session of aerobic physical activity suggests that exercise could have a direct effect on T2D [type 2 diabetes] risk and cardiovascular risk,” the authors wrote.
SOURCE:
The study was led by Simona Moffa, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, and Gian Pio Sorice, Università Degli Studi di Bari “Aldo Moro,” Bari, Italy. It was published online in the Journal of Endocrinological Investigation.
LIMITATIONS:
The study had a limited sample size, which may affect the generalizability of the findings. C-peptide levels, which could have provided additional insights into insulin secretion, were not assessed in the study.
DISCLOSURES:
The study was supported by grants from Università Cattolica del Sacro Cuore. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
In healthy young adults, a single 30-minute bout of outdoor aerobic exercise significantly reduces fasting and 1-hour glucose levels during an oral glucose tolerance test (OGTT) the next day and improves insulin sensitivity.
METHODOLOGY:
- Recent studies have identified 1-hour post-load glucose concentration during an OGTT as a specific and early predictor of diabetes, and exercise has long been known for its metabolic benefits in people with and without diabetes.
- The researchers investigated the effect of a single bout of aerobic exercise on 1-hour post-load glucose levels during an OGTT in 32 young, healthy, normal-weight or marginally overweight individuals (mean age, 35 years; 14 women and 18 men) with a sedentary or moderately active lifestyle.
- The participants underwent an initial OGTT after at least 4 days of physical inactivity, followed by a second OGTT the day after a single 30-minute bout of aerobic exercise.
- The exercise session consisted of a light jog for 30 minutes, monitored using a metabolic holter to quantify energy expenditure and exercise intensity. The participants did not undertake any exercise outside the lab sessions.
- Blood glucose levels were measured, and insulin sensitivity and secretion were estimated using surrogate indices derived from OGTT glucose and insulin assays, including the Matsuda index, oral glucose insulin sensitivity (OGIS) index, and quantitative insulin sensitivity check index, as well as the homeostasis model assessment (HOMA) of insulin resistance and of beta-cell function (HOMA-B).
TAKEAWAY:
- Postexercise insulin levels also were significantly lower 1 hour after glucose load, decreasing from 57.4 IU/mL at baseline to 43.5 IU/mL the day after exercise (P = .01).
- Insulin sensitivity improved significantly after exercise, as indicated by increases in the Matsuda index (P = .02) and OGIS index (P = .04), along with a reduction in insulin resistance (P = .04).
- The study found a trend toward increased beta-cell function the day after an exercise bout, as indicated by a nonsignificant increase in HOMA-B from 144.7 at baseline to 167.1 after exercise.
IN PRACTICE:
“Improvement in 1-hour post-load plasma glucose following a single session of aerobic physical activity suggests that exercise could have a direct effect on T2D [type 2 diabetes] risk and cardiovascular risk,” the authors wrote.
SOURCE:
The study was led by Simona Moffa, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, and Gian Pio Sorice, Università Degli Studi di Bari “Aldo Moro,” Bari, Italy. It was published online in the Journal of Endocrinological Investigation.
LIMITATIONS:
The study had a limited sample size, which may affect the generalizability of the findings. C-peptide levels, which could have provided additional insights into insulin secretion, were not assessed in the study.
DISCLOSURES:
The study was supported by grants from Università Cattolica del Sacro Cuore. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
In healthy young adults, a single 30-minute bout of outdoor aerobic exercise significantly reduces fasting and 1-hour glucose levels during an oral glucose tolerance test (OGTT) the next day and improves insulin sensitivity.
METHODOLOGY:
- Recent studies have identified 1-hour post-load glucose concentration during an OGTT as a specific and early predictor of diabetes, and exercise has long been known for its metabolic benefits in people with and without diabetes.
- The researchers investigated the effect of a single bout of aerobic exercise on 1-hour post-load glucose levels during an OGTT in 32 young, healthy, normal-weight or marginally overweight individuals (mean age, 35 years; 14 women and 18 men) with a sedentary or moderately active lifestyle.
- The participants underwent an initial OGTT after at least 4 days of physical inactivity, followed by a second OGTT the day after a single 30-minute bout of aerobic exercise.
- The exercise session consisted of a light jog for 30 minutes, monitored using a metabolic holter to quantify energy expenditure and exercise intensity. The participants did not undertake any exercise outside the lab sessions.
- Blood glucose levels were measured, and insulin sensitivity and secretion were estimated using surrogate indices derived from OGTT glucose and insulin assays, including the Matsuda index, oral glucose insulin sensitivity (OGIS) index, and quantitative insulin sensitivity check index, as well as the homeostasis model assessment (HOMA) of insulin resistance and of beta-cell function (HOMA-B).
TAKEAWAY:
- Postexercise insulin levels also were significantly lower 1 hour after glucose load, decreasing from 57.4 IU/mL at baseline to 43.5 IU/mL the day after exercise (P = .01).
- Insulin sensitivity improved significantly after exercise, as indicated by increases in the Matsuda index (P = .02) and OGIS index (P = .04), along with a reduction in insulin resistance (P = .04).
- The study found a trend toward increased beta-cell function the day after an exercise bout, as indicated by a nonsignificant increase in HOMA-B from 144.7 at baseline to 167.1 after exercise.
IN PRACTICE:
“Improvement in 1-hour post-load plasma glucose following a single session of aerobic physical activity suggests that exercise could have a direct effect on T2D [type 2 diabetes] risk and cardiovascular risk,” the authors wrote.
SOURCE:
The study was led by Simona Moffa, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, and Gian Pio Sorice, Università Degli Studi di Bari “Aldo Moro,” Bari, Italy. It was published online in the Journal of Endocrinological Investigation.
LIMITATIONS:
The study had a limited sample size, which may affect the generalizability of the findings. C-peptide levels, which could have provided additional insights into insulin secretion, were not assessed in the study.
DISCLOSURES:
The study was supported by grants from Università Cattolica del Sacro Cuore. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
State of Confusion: Should All Children Get Lipid Labs for High Cholesterol?
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
AHA Scientific Statement Links Three Common Cardiovascular Diseases to Cognitive Decline, Dementia
The statement includes an extensive research review and offers compelling evidence of the inextricable link between heart health and brain health, which investigators said underscores the benefit of early intervention.
The cumulative evidence “confirms that the trajectories of cardiac health and brain health are inextricably intertwined through modifiable and nonmodifiable factors,” the authors wrote.
Investigators say the findings reinforce the message that addressing cardiovascular health early in life may deter the onset or progression of cognitive impairment later on.
And the earlier this is done, the better, said lead author Fernando D. Testai, MD, PhD, a professor of neurology and the vascular neurology section head, Department of Neurology and Rehabilitation, University of Illinois, Chicago.
The statement was published online in Stroke.
Bridging the Research Gap
It’s well known that there’s a bidirectional relationship between heart and brain function. For example, heart failure can lead to decreased blood flow that can damage the brain, and stroke in some areas of the brain can affect the heart.
However, that’s only part of the puzzle and doesn’t address all the gaps in the understanding of how cardiovascular disease contributes to cognition, said Testai.
“What we’re trying to do here is to go one step further and describe other connections between the heart and the brain,” he said.
Investigators carried out an extensive PubMed search for heart failure, atrial fibrillation, and coronary heart disease. Researchers detailed the frequency of each condition, mechanisms by which they might cause cognitive impairment, and prospects for prevention and treatment to maintain brain health.
A recurring theme in the paper is the role of inflammation. Evidence shows there are “remarkable similarities in the inflammatory response that takes place,” with both cardiac disease and cognitive decline, said Testai.
Another potential shared mechanism relates to biomarkers, particularly amyloid, which is strongly linked to Alzheimer’s disease.
“But some studies show amyloid can also be present in the heart, especially in patients who have decreased ejection fraction,” said Testai.
Robust Heart-Brain Connection
The statement’s authors collected a substantial amount of evidence showing vascular risk factors such as hypertension and diabetes “can change how the brain processes and clears up amyloid,” Testai added.
The paper also provides a compilation of evidence of shared genetic predispositions when it comes to heart and brain disorders.
“We noticed that some genetic signatures that have historically been associated with heart disease seem to also correlate with structural changes in the brain. That means that at the end of the day, some patients may be born with a genetic predisposition to developing both conditions,” said Testai.
This indicates that the link between the two organs “begins as early as conception” and underscores the importance of adopting healthy lifestyle habits as early as possible, he added.
“That means you can avoid bad habits that eventually lead to hypertension, diabetes, and cholesterol, that eventually will lead to cardiac disease, which eventually will lead to stroke, which eventually will lead to cognitive decline,” Testai noted.
However, cardiovascular health is more complicated than having good genes and adhering to a healthy lifestyle. It’s not clear, for example, why some people who should be predisposed to developing heart disease do not develop it, something Testai refers to as enhanced “resilience.”
For example, Hispanic or Latino patients, who have relatively poor cardiovascular risk factor profiles, seem to be less susceptible to developing cardiac disease.
More Research Needed
While genetics may partly explain the paradox, Testai believes other protective factors are at play, including strong social support networks.
Testai referred to the AHA’s “Life’s Essential 8” — the eight components of cardiovascular health. These include a healthy diet, participation in physical activity, nicotine avoidance, healthy sleep, healthy weight, and healthy levels of blood lipids, blood glucose, and blood pressure.
More evidence is needed to show that effective management of cardiac disease positively affects cognition. Currently, cognitive measures are rarely included in studies examining various heart disease treatments, said Testai.
“There should probably be an effort to include brain health outcomes in some of the cardiac literature to make sure we can also measure whether the intervention in the heart leads to an advantage for the brain,” he said.
More research is also needed to determine whether immunomodulation has a beneficial effect on the cognitive trajectory, the statement’s authors noted.
They point out that the interpretation and generalizability of the studies described in the statement are confounded by disparate methodologies, including small sample sizes, cross-sectional designs, and underrepresentation of Black and Hispanic individuals.
‘An Important Step’
Reached for a comment, Natalia S. Rost, MD, Chief of the Stroke Division at Massachusetts General Hospital and professor of neurology at Harvard Medical School, both in Boston, said this paper “is an important step” in terms of pulling together pertinent information on the topic of heart-brain health.
She praised the authors for gathering evidence on risk factors related to atrial fibrillation, heart failure, and coronary heart disease, which is “the part of the puzzle that is controllable.”
This helps reinforce the message that controlling vascular risk factors helps with brain health, said Rost.
But brain health is “much more complex than just vascular health,” she said. It includes other elements such as freedom from epilepsy, migraine, traumatic brain injury, and adult learning disabilities.
No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
The statement includes an extensive research review and offers compelling evidence of the inextricable link between heart health and brain health, which investigators said underscores the benefit of early intervention.
The cumulative evidence “confirms that the trajectories of cardiac health and brain health are inextricably intertwined through modifiable and nonmodifiable factors,” the authors wrote.
Investigators say the findings reinforce the message that addressing cardiovascular health early in life may deter the onset or progression of cognitive impairment later on.
And the earlier this is done, the better, said lead author Fernando D. Testai, MD, PhD, a professor of neurology and the vascular neurology section head, Department of Neurology and Rehabilitation, University of Illinois, Chicago.
The statement was published online in Stroke.
Bridging the Research Gap
It’s well known that there’s a bidirectional relationship between heart and brain function. For example, heart failure can lead to decreased blood flow that can damage the brain, and stroke in some areas of the brain can affect the heart.
However, that’s only part of the puzzle and doesn’t address all the gaps in the understanding of how cardiovascular disease contributes to cognition, said Testai.
“What we’re trying to do here is to go one step further and describe other connections between the heart and the brain,” he said.
Investigators carried out an extensive PubMed search for heart failure, atrial fibrillation, and coronary heart disease. Researchers detailed the frequency of each condition, mechanisms by which they might cause cognitive impairment, and prospects for prevention and treatment to maintain brain health.
A recurring theme in the paper is the role of inflammation. Evidence shows there are “remarkable similarities in the inflammatory response that takes place,” with both cardiac disease and cognitive decline, said Testai.
Another potential shared mechanism relates to biomarkers, particularly amyloid, which is strongly linked to Alzheimer’s disease.
“But some studies show amyloid can also be present in the heart, especially in patients who have decreased ejection fraction,” said Testai.
Robust Heart-Brain Connection
The statement’s authors collected a substantial amount of evidence showing vascular risk factors such as hypertension and diabetes “can change how the brain processes and clears up amyloid,” Testai added.
The paper also provides a compilation of evidence of shared genetic predispositions when it comes to heart and brain disorders.
“We noticed that some genetic signatures that have historically been associated with heart disease seem to also correlate with structural changes in the brain. That means that at the end of the day, some patients may be born with a genetic predisposition to developing both conditions,” said Testai.
This indicates that the link between the two organs “begins as early as conception” and underscores the importance of adopting healthy lifestyle habits as early as possible, he added.
“That means you can avoid bad habits that eventually lead to hypertension, diabetes, and cholesterol, that eventually will lead to cardiac disease, which eventually will lead to stroke, which eventually will lead to cognitive decline,” Testai noted.
However, cardiovascular health is more complicated than having good genes and adhering to a healthy lifestyle. It’s not clear, for example, why some people who should be predisposed to developing heart disease do not develop it, something Testai refers to as enhanced “resilience.”
For example, Hispanic or Latino patients, who have relatively poor cardiovascular risk factor profiles, seem to be less susceptible to developing cardiac disease.
More Research Needed
While genetics may partly explain the paradox, Testai believes other protective factors are at play, including strong social support networks.
Testai referred to the AHA’s “Life’s Essential 8” — the eight components of cardiovascular health. These include a healthy diet, participation in physical activity, nicotine avoidance, healthy sleep, healthy weight, and healthy levels of blood lipids, blood glucose, and blood pressure.
More evidence is needed to show that effective management of cardiac disease positively affects cognition. Currently, cognitive measures are rarely included in studies examining various heart disease treatments, said Testai.
“There should probably be an effort to include brain health outcomes in some of the cardiac literature to make sure we can also measure whether the intervention in the heart leads to an advantage for the brain,” he said.
More research is also needed to determine whether immunomodulation has a beneficial effect on the cognitive trajectory, the statement’s authors noted.
They point out that the interpretation and generalizability of the studies described in the statement are confounded by disparate methodologies, including small sample sizes, cross-sectional designs, and underrepresentation of Black and Hispanic individuals.
‘An Important Step’
Reached for a comment, Natalia S. Rost, MD, Chief of the Stroke Division at Massachusetts General Hospital and professor of neurology at Harvard Medical School, both in Boston, said this paper “is an important step” in terms of pulling together pertinent information on the topic of heart-brain health.
She praised the authors for gathering evidence on risk factors related to atrial fibrillation, heart failure, and coronary heart disease, which is “the part of the puzzle that is controllable.”
This helps reinforce the message that controlling vascular risk factors helps with brain health, said Rost.
But brain health is “much more complex than just vascular health,” she said. It includes other elements such as freedom from epilepsy, migraine, traumatic brain injury, and adult learning disabilities.
No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
The statement includes an extensive research review and offers compelling evidence of the inextricable link between heart health and brain health, which investigators said underscores the benefit of early intervention.
The cumulative evidence “confirms that the trajectories of cardiac health and brain health are inextricably intertwined through modifiable and nonmodifiable factors,” the authors wrote.
Investigators say the findings reinforce the message that addressing cardiovascular health early in life may deter the onset or progression of cognitive impairment later on.
And the earlier this is done, the better, said lead author Fernando D. Testai, MD, PhD, a professor of neurology and the vascular neurology section head, Department of Neurology and Rehabilitation, University of Illinois, Chicago.
The statement was published online in Stroke.
Bridging the Research Gap
It’s well known that there’s a bidirectional relationship between heart and brain function. For example, heart failure can lead to decreased blood flow that can damage the brain, and stroke in some areas of the brain can affect the heart.
However, that’s only part of the puzzle and doesn’t address all the gaps in the understanding of how cardiovascular disease contributes to cognition, said Testai.
“What we’re trying to do here is to go one step further and describe other connections between the heart and the brain,” he said.
Investigators carried out an extensive PubMed search for heart failure, atrial fibrillation, and coronary heart disease. Researchers detailed the frequency of each condition, mechanisms by which they might cause cognitive impairment, and prospects for prevention and treatment to maintain brain health.
A recurring theme in the paper is the role of inflammation. Evidence shows there are “remarkable similarities in the inflammatory response that takes place,” with both cardiac disease and cognitive decline, said Testai.
Another potential shared mechanism relates to biomarkers, particularly amyloid, which is strongly linked to Alzheimer’s disease.
“But some studies show amyloid can also be present in the heart, especially in patients who have decreased ejection fraction,” said Testai.
Robust Heart-Brain Connection
The statement’s authors collected a substantial amount of evidence showing vascular risk factors such as hypertension and diabetes “can change how the brain processes and clears up amyloid,” Testai added.
The paper also provides a compilation of evidence of shared genetic predispositions when it comes to heart and brain disorders.
“We noticed that some genetic signatures that have historically been associated with heart disease seem to also correlate with structural changes in the brain. That means that at the end of the day, some patients may be born with a genetic predisposition to developing both conditions,” said Testai.
This indicates that the link between the two organs “begins as early as conception” and underscores the importance of adopting healthy lifestyle habits as early as possible, he added.
“That means you can avoid bad habits that eventually lead to hypertension, diabetes, and cholesterol, that eventually will lead to cardiac disease, which eventually will lead to stroke, which eventually will lead to cognitive decline,” Testai noted.
However, cardiovascular health is more complicated than having good genes and adhering to a healthy lifestyle. It’s not clear, for example, why some people who should be predisposed to developing heart disease do not develop it, something Testai refers to as enhanced “resilience.”
For example, Hispanic or Latino patients, who have relatively poor cardiovascular risk factor profiles, seem to be less susceptible to developing cardiac disease.
More Research Needed
While genetics may partly explain the paradox, Testai believes other protective factors are at play, including strong social support networks.
Testai referred to the AHA’s “Life’s Essential 8” — the eight components of cardiovascular health. These include a healthy diet, participation in physical activity, nicotine avoidance, healthy sleep, healthy weight, and healthy levels of blood lipids, blood glucose, and blood pressure.
More evidence is needed to show that effective management of cardiac disease positively affects cognition. Currently, cognitive measures are rarely included in studies examining various heart disease treatments, said Testai.
“There should probably be an effort to include brain health outcomes in some of the cardiac literature to make sure we can also measure whether the intervention in the heart leads to an advantage for the brain,” he said.
More research is also needed to determine whether immunomodulation has a beneficial effect on the cognitive trajectory, the statement’s authors noted.
They point out that the interpretation and generalizability of the studies described in the statement are confounded by disparate methodologies, including small sample sizes, cross-sectional designs, and underrepresentation of Black and Hispanic individuals.
‘An Important Step’
Reached for a comment, Natalia S. Rost, MD, Chief of the Stroke Division at Massachusetts General Hospital and professor of neurology at Harvard Medical School, both in Boston, said this paper “is an important step” in terms of pulling together pertinent information on the topic of heart-brain health.
She praised the authors for gathering evidence on risk factors related to atrial fibrillation, heart failure, and coronary heart disease, which is “the part of the puzzle that is controllable.”
This helps reinforce the message that controlling vascular risk factors helps with brain health, said Rost.
But brain health is “much more complex than just vascular health,” she said. It includes other elements such as freedom from epilepsy, migraine, traumatic brain injury, and adult learning disabilities.
No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
FROM STROKE
Ultraprocessed Foods and CVD: Myths vs Facts
I’d like to talk with you about ultraprocessed foods (UPFs) and risk for cardiovascular disease (CVD) and try to separate some of the facts from the myths. I’d like to discuss a recent report in The Lancet Regional Health that looks at this topic comprehensively and in detail.
This report includes three large-scale prospective cohort studies of US female and male health professionals, more than 200,000 participants in total. It also includes a meta-analysis of 22 international cohorts with about 1.2 million participants. I’d like to acknowledge that I’m a co-author of this study.
What are UPFs, and why are they important? Why do we care, and what are the knowledge gaps? UPFs are generally packaged foods that contain ingredients to extend shelf life and improve taste and palatability. It’s important because 60%-70% of the US diet, if not more, is made up of UPFs. So, the relationship between UPFs and CVD and other health outcomes is actually very important.
And the research to date on this subject has been quite limited.
In other studies, these UPFs have been linked to weight gain and dyslipidemia; some tissue glycation has been found, and some changes in the microbiome. Some studies have linked higher UPF intake with type 2 diabetes. A few have looked at certain selected UPF foods and found a higher risk for CVD, but a really comprehensive look at this question hasn’t been done.
So, that’s what we did in this paper and in the meta-analysis with the 22 cohorts, and we saw a very clear and distinct significant increase in coronary heart disease by 23%, total CVD by 17%, and stroke by 9% when comparing the highest vs the lowest category [of UPF intake]. When we drilled down deeply into the types of UPFs in the US health professional cohorts, we saw that there were some major differences in the relationship with CVD depending on the type of UPF.
In comparing the highest quintile vs the lowest quintile [of total UPF intake], we saw that some of the UPFs were associated with significant elevations in risk for CVD. These included sugar-sweetened beverages and processed meats. But some UPFs were linked with a lower risk for CVD. These included breakfast cereals, yogurt, some dairy desserts, and whole grains.
Overall, it seemed that UPFs are actually quite diverse in their association with health. It’s not one size fits all. They’re not all created equal, and some of these differences matter. Although overall we would recommend that our diets be focused on whole foods, primarily plant based, lots of fruits and vegetables, whole grains, fish, and other whole foods, it seems from this report and the meta-analysis that certain types of UPFs can be incorporated into a healthy diet and don’t need to be avoided entirely.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and Chief of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston, Massachusetts. She reported receiving donations and infrastructure support from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
I’d like to talk with you about ultraprocessed foods (UPFs) and risk for cardiovascular disease (CVD) and try to separate some of the facts from the myths. I’d like to discuss a recent report in The Lancet Regional Health that looks at this topic comprehensively and in detail.
This report includes three large-scale prospective cohort studies of US female and male health professionals, more than 200,000 participants in total. It also includes a meta-analysis of 22 international cohorts with about 1.2 million participants. I’d like to acknowledge that I’m a co-author of this study.
What are UPFs, and why are they important? Why do we care, and what are the knowledge gaps? UPFs are generally packaged foods that contain ingredients to extend shelf life and improve taste and palatability. It’s important because 60%-70% of the US diet, if not more, is made up of UPFs. So, the relationship between UPFs and CVD and other health outcomes is actually very important.
And the research to date on this subject has been quite limited.
In other studies, these UPFs have been linked to weight gain and dyslipidemia; some tissue glycation has been found, and some changes in the microbiome. Some studies have linked higher UPF intake with type 2 diabetes. A few have looked at certain selected UPF foods and found a higher risk for CVD, but a really comprehensive look at this question hasn’t been done.
So, that’s what we did in this paper and in the meta-analysis with the 22 cohorts, and we saw a very clear and distinct significant increase in coronary heart disease by 23%, total CVD by 17%, and stroke by 9% when comparing the highest vs the lowest category [of UPF intake]. When we drilled down deeply into the types of UPFs in the US health professional cohorts, we saw that there were some major differences in the relationship with CVD depending on the type of UPF.
In comparing the highest quintile vs the lowest quintile [of total UPF intake], we saw that some of the UPFs were associated with significant elevations in risk for CVD. These included sugar-sweetened beverages and processed meats. But some UPFs were linked with a lower risk for CVD. These included breakfast cereals, yogurt, some dairy desserts, and whole grains.
Overall, it seemed that UPFs are actually quite diverse in their association with health. It’s not one size fits all. They’re not all created equal, and some of these differences matter. Although overall we would recommend that our diets be focused on whole foods, primarily plant based, lots of fruits and vegetables, whole grains, fish, and other whole foods, it seems from this report and the meta-analysis that certain types of UPFs can be incorporated into a healthy diet and don’t need to be avoided entirely.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and Chief of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston, Massachusetts. She reported receiving donations and infrastructure support from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
I’d like to talk with you about ultraprocessed foods (UPFs) and risk for cardiovascular disease (CVD) and try to separate some of the facts from the myths. I’d like to discuss a recent report in The Lancet Regional Health that looks at this topic comprehensively and in detail.
This report includes three large-scale prospective cohort studies of US female and male health professionals, more than 200,000 participants in total. It also includes a meta-analysis of 22 international cohorts with about 1.2 million participants. I’d like to acknowledge that I’m a co-author of this study.
What are UPFs, and why are they important? Why do we care, and what are the knowledge gaps? UPFs are generally packaged foods that contain ingredients to extend shelf life and improve taste and palatability. It’s important because 60%-70% of the US diet, if not more, is made up of UPFs. So, the relationship between UPFs and CVD and other health outcomes is actually very important.
And the research to date on this subject has been quite limited.
In other studies, these UPFs have been linked to weight gain and dyslipidemia; some tissue glycation has been found, and some changes in the microbiome. Some studies have linked higher UPF intake with type 2 diabetes. A few have looked at certain selected UPF foods and found a higher risk for CVD, but a really comprehensive look at this question hasn’t been done.
So, that’s what we did in this paper and in the meta-analysis with the 22 cohorts, and we saw a very clear and distinct significant increase in coronary heart disease by 23%, total CVD by 17%, and stroke by 9% when comparing the highest vs the lowest category [of UPF intake]. When we drilled down deeply into the types of UPFs in the US health professional cohorts, we saw that there were some major differences in the relationship with CVD depending on the type of UPF.
In comparing the highest quintile vs the lowest quintile [of total UPF intake], we saw that some of the UPFs were associated with significant elevations in risk for CVD. These included sugar-sweetened beverages and processed meats. But some UPFs were linked with a lower risk for CVD. These included breakfast cereals, yogurt, some dairy desserts, and whole grains.
Overall, it seemed that UPFs are actually quite diverse in their association with health. It’s not one size fits all. They’re not all created equal, and some of these differences matter. Although overall we would recommend that our diets be focused on whole foods, primarily plant based, lots of fruits and vegetables, whole grains, fish, and other whole foods, it seems from this report and the meta-analysis that certain types of UPFs can be incorporated into a healthy diet and don’t need to be avoided entirely.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, and Chief of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston, Massachusetts. She reported receiving donations and infrastructure support from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
How Doctors Use Music to Learn Faster and Perform Better
“Because you know I’m all about that base, ‘bout that base, no acid.”
Do those words sound familiar? That’s because they’re the lyrics to Meghan Trainor’s “All About That Bass,” slightly tweaked to function as a medical study tool.
Early in med school, J.C. Sue, DO, now a family medicine physician, refashioned the song’s words to help him prepare for a test on acid extruders and loaders. Sue’s version, “All About That Base,” contained his lecture notes. During the exam, he found himself mentally singing his parody and easily recalling the information. Plus, the approach made cramming a lot more palatable.
Sound silly? It’s not. Sue’s approach is backed up by science. Recently, a 2024 study from Canada suggested that musical memory doesn’t decrease with age. And a 2023 study revealed music was a better cue than food for helping both young and older adults recall autobiographical memories.
Inspired by his success, Sue gave popular songs a medical spin throughout his medical training. “There’s no rule that says studying must be boring, tedious, or torturous,” Sue said. “If you can make it fun, why not?”
Sue isn’t alone. Many physicians say that writing songs, listening to music, or playing instruments improves their focus, energy, and work performance, along with their confidence and well-being.
Why does music work so well?
Tune Your Brain to Work With Tunes
Remember learning your ABCs to the tune of “Twinkle, Twinkle, Little Star?” (Or ask any Gen X person about Schoolhouse Rock.)
In the classroom, music is an established tool for teaching kids, said Ruth Gotian, EdD, MS, chief learning officer and associate professor of education in anesthesiology at Weill Cornell Medicine, New York City. But she said musical strategies make studying easier for adults, too, no matter how complex the material.
Christopher Emdin, PhD, Maxine Greene chair and professor of science education at Teachers College, Columbia University, New York City, shares Gotian’s view. When teaching science, engineering, technology, and mathematics (STEM) subjects to high school kids, he challenged them to write raps about the new concepts.
That’s when he saw visible results: As his students took exams, Emdin noticed them nodding and moving their mouths and heads.
“They were literally performing the songs they’d written for themselves,” Emdin said. “When you write a song to a beat, it’s almost like your heartbeat. You know it so well; you can conjure up your memories by reciting the lyrics.”
If songwriting isn’t in your repertoire, you’ll be glad to hear that just listening to music while studying can help with retention. “Music keeps both sides of the brain stimulated, which has been shown to increase focus and motivation,” explained Anita A. Paschall, MD, PhD, Medical School and Healthcare Admissions expert/director of Medical School and Healthcare Admissions at The Princeton Review.
‘Mind on a Permanent Vacation’
Paschall’s enthusiasm comes from personal experience. While preparing for her board exams, Jimmy Buffet’s catalog was her study soundtrack. “His songs stayed in my mind. I could hum along without having to think about it, so my brain was free to focus,” she recalled.
Because Paschall grew up listening to Buffet’s tunes, they also evoked relaxing moments from her earlier life, which she found comforting and uplifting. The combination helped make long, intense study sessions more pleasant. After all, when you’re “wasting away again in Margaritaville,” how can you feel stressed and despondent?
Alexander Remy Bonnel, MD, clinical assistant professor of medicine at the University of Pennsylvania and a physician at Pennsylvania Hospital, both in Philadelphia, found ways to incorporate both auditory and visual stimuli in his med school study routine. He listened to music while color-coding his notes to link both cues to the information. As with Paschall, these tactics helped reduce the monotony of learning reams of material.
That gave Bonnel an easy way to establish an important element for memory: Novelty.
“When you need to memorize so many things in a short amount of time, you’re trying to vary ways of internalizing information,” he observed. “You have a higher chance of retaining information if there’s something unique about it.”
Building Team Harmony
“Almost every single OR I rotated through in med school had music playing,” Bonnel also recalled. Furthermore, he noticed a pattern to the chosen songs: Regardless of their age, surgeons selected playlists of tunes that had been popular when they were in their 20s. Those golden oldies, from any era, could turn the OR team into a focused, cohesive unit.
Kyle McCormick, MD, a fifth-year resident in orthopedic surgery at New York–Presbyterian Hospital, Columbia University Irving Medical Center, New York City, has also noticed the ubiquity of background music in ORs. Her observation: Surgeons tend to choose universally popular, inoffensive songs, like tracks from Hall & Oates and Fleetwood Mac.
This meshes with the results of a joint survey of nearly 700 surgeons and other healthcare professionals conducted by Spotify and Figure 1 in 2021; 90% of the surgeons and surgical residents who responded said they listened to music in the OR. Rock and pop were the most popular genres, followed by classical, jazz, and then R&B.
Regardless of genre, music helped the surgical teams focus and feel less tense, the surgeons reported. But when training younger doctors, managing complications, or performing during critical points in surgery, many said they’d lower the volume.
Outside the OR, music can also help foster connection between colleagues. For Lawrence C. Loh, MD, MPH, adjunct professor at Dalla Lana School of Public Health at the University of Toronto in Ontario, Canada, playing guitar and piano has helped him connect with his staff. “I’ve played tunes at staff gatherings and recorded videos as encouragement during the emergency response for COVID-19,” he shared.
In his free time, Loh has also organized outings to his local pub’s weekly karaoke show for more than a decade. His goal: “Promote social cohesion and combat loneliness among my friend and social networks.”
Get Your Own Musical Boost
If all this sounds like music to your ears, here are some ways to try it yourself.
Find a study soundtrack. When choosing study music, follow Paschall’s lead and pick songs you know well so they’ll remain in the background. Also, compile a soundtrack you find pleasant and mood-boosting to help relieve the tedium of study and decrease stress.
Keep in mind that we all take in and process information differently, said Gotian. So background music during study sessions might not work for you. According to a 2017 study published in Frontiers in Psychology, it can be a distraction and impair learning for some. Do what works.
Get pumped with a “walkup song.” What songs make you feel like you could conquer the world? asked Emdin. Or what soundtrack would be playing if you were ascending a stage to accept an award or walking out to take the mound in the ninth inning? Those songs should be on what he calls your “superhero” or “walkup” playlist. His prescription: Tune in before you begin your workday or start a challenging procedure.
Paschall agrees and recommends her students and clients listen to music before sitting down for an exam. Forget reviewing flashcards for the nth time, she counseled. Putting on headphones (or earbuds) will put you in a “better headspace.”
Choose work and play playlists. As well as incorporating tunes in your clinic or hospital, music can help relieve stress at the end of the workday. “Medical culture can often be detrimental to doctors’ health,” said Sue, who credits music with helping him maintain equanimity.
Bonnel can relate. Practicing and performing with the Penn Medicine Symphony Orchestra offers him a sense of community and relief from the stress of modern life. “For 2 hours every Tuesday, I put my phone away and just play,” he said. “It’s nice to have those moments when I’m temporarily disconnected and can just focus on one thing: Playing.”
Scale Up Your Career
Years after med school graduation, Sue still recalls many of the tunes he wrote to help him remember information. When he sings a song in his head, he’ll get a refresher on pediatric developmental milestones, medication side effects, anatomical details, and more, which informs the treatment plans he devises for patients. To help other doctors reap these benefits, Sue created the website Tune Rx, a medical music study resource that includes many of the roughly 100 songs he’s written.
Emdin often discusses his musical strategies during talks on STEM education. Initially, people are skeptical, he said. But the idea quickly rings a bell for audience members. “They come up to me afterward to share anecdotes,” Emdin said. “If you have enough anecdotes, there’s a pattern. So let’s create a process. Let’s be intentional about using music as a learning strategy,” he urged.
A version of this article first appeared on Medscape.com.
“Because you know I’m all about that base, ‘bout that base, no acid.”
Do those words sound familiar? That’s because they’re the lyrics to Meghan Trainor’s “All About That Bass,” slightly tweaked to function as a medical study tool.
Early in med school, J.C. Sue, DO, now a family medicine physician, refashioned the song’s words to help him prepare for a test on acid extruders and loaders. Sue’s version, “All About That Base,” contained his lecture notes. During the exam, he found himself mentally singing his parody and easily recalling the information. Plus, the approach made cramming a lot more palatable.
Sound silly? It’s not. Sue’s approach is backed up by science. Recently, a 2024 study from Canada suggested that musical memory doesn’t decrease with age. And a 2023 study revealed music was a better cue than food for helping both young and older adults recall autobiographical memories.
Inspired by his success, Sue gave popular songs a medical spin throughout his medical training. “There’s no rule that says studying must be boring, tedious, or torturous,” Sue said. “If you can make it fun, why not?”
Sue isn’t alone. Many physicians say that writing songs, listening to music, or playing instruments improves their focus, energy, and work performance, along with their confidence and well-being.
Why does music work so well?
Tune Your Brain to Work With Tunes
Remember learning your ABCs to the tune of “Twinkle, Twinkle, Little Star?” (Or ask any Gen X person about Schoolhouse Rock.)
In the classroom, music is an established tool for teaching kids, said Ruth Gotian, EdD, MS, chief learning officer and associate professor of education in anesthesiology at Weill Cornell Medicine, New York City. But she said musical strategies make studying easier for adults, too, no matter how complex the material.
Christopher Emdin, PhD, Maxine Greene chair and professor of science education at Teachers College, Columbia University, New York City, shares Gotian’s view. When teaching science, engineering, technology, and mathematics (STEM) subjects to high school kids, he challenged them to write raps about the new concepts.
That’s when he saw visible results: As his students took exams, Emdin noticed them nodding and moving their mouths and heads.
“They were literally performing the songs they’d written for themselves,” Emdin said. “When you write a song to a beat, it’s almost like your heartbeat. You know it so well; you can conjure up your memories by reciting the lyrics.”
If songwriting isn’t in your repertoire, you’ll be glad to hear that just listening to music while studying can help with retention. “Music keeps both sides of the brain stimulated, which has been shown to increase focus and motivation,” explained Anita A. Paschall, MD, PhD, Medical School and Healthcare Admissions expert/director of Medical School and Healthcare Admissions at The Princeton Review.
‘Mind on a Permanent Vacation’
Paschall’s enthusiasm comes from personal experience. While preparing for her board exams, Jimmy Buffet’s catalog was her study soundtrack. “His songs stayed in my mind. I could hum along without having to think about it, so my brain was free to focus,” she recalled.
Because Paschall grew up listening to Buffet’s tunes, they also evoked relaxing moments from her earlier life, which she found comforting and uplifting. The combination helped make long, intense study sessions more pleasant. After all, when you’re “wasting away again in Margaritaville,” how can you feel stressed and despondent?
Alexander Remy Bonnel, MD, clinical assistant professor of medicine at the University of Pennsylvania and a physician at Pennsylvania Hospital, both in Philadelphia, found ways to incorporate both auditory and visual stimuli in his med school study routine. He listened to music while color-coding his notes to link both cues to the information. As with Paschall, these tactics helped reduce the monotony of learning reams of material.
That gave Bonnel an easy way to establish an important element for memory: Novelty.
“When you need to memorize so many things in a short amount of time, you’re trying to vary ways of internalizing information,” he observed. “You have a higher chance of retaining information if there’s something unique about it.”
Building Team Harmony
“Almost every single OR I rotated through in med school had music playing,” Bonnel also recalled. Furthermore, he noticed a pattern to the chosen songs: Regardless of their age, surgeons selected playlists of tunes that had been popular when they were in their 20s. Those golden oldies, from any era, could turn the OR team into a focused, cohesive unit.
Kyle McCormick, MD, a fifth-year resident in orthopedic surgery at New York–Presbyterian Hospital, Columbia University Irving Medical Center, New York City, has also noticed the ubiquity of background music in ORs. Her observation: Surgeons tend to choose universally popular, inoffensive songs, like tracks from Hall & Oates and Fleetwood Mac.
This meshes with the results of a joint survey of nearly 700 surgeons and other healthcare professionals conducted by Spotify and Figure 1 in 2021; 90% of the surgeons and surgical residents who responded said they listened to music in the OR. Rock and pop were the most popular genres, followed by classical, jazz, and then R&B.
Regardless of genre, music helped the surgical teams focus and feel less tense, the surgeons reported. But when training younger doctors, managing complications, or performing during critical points in surgery, many said they’d lower the volume.
Outside the OR, music can also help foster connection between colleagues. For Lawrence C. Loh, MD, MPH, adjunct professor at Dalla Lana School of Public Health at the University of Toronto in Ontario, Canada, playing guitar and piano has helped him connect with his staff. “I’ve played tunes at staff gatherings and recorded videos as encouragement during the emergency response for COVID-19,” he shared.
In his free time, Loh has also organized outings to his local pub’s weekly karaoke show for more than a decade. His goal: “Promote social cohesion and combat loneliness among my friend and social networks.”
Get Your Own Musical Boost
If all this sounds like music to your ears, here are some ways to try it yourself.
Find a study soundtrack. When choosing study music, follow Paschall’s lead and pick songs you know well so they’ll remain in the background. Also, compile a soundtrack you find pleasant and mood-boosting to help relieve the tedium of study and decrease stress.
Keep in mind that we all take in and process information differently, said Gotian. So background music during study sessions might not work for you. According to a 2017 study published in Frontiers in Psychology, it can be a distraction and impair learning for some. Do what works.
Get pumped with a “walkup song.” What songs make you feel like you could conquer the world? asked Emdin. Or what soundtrack would be playing if you were ascending a stage to accept an award or walking out to take the mound in the ninth inning? Those songs should be on what he calls your “superhero” or “walkup” playlist. His prescription: Tune in before you begin your workday or start a challenging procedure.
Paschall agrees and recommends her students and clients listen to music before sitting down for an exam. Forget reviewing flashcards for the nth time, she counseled. Putting on headphones (or earbuds) will put you in a “better headspace.”
Choose work and play playlists. As well as incorporating tunes in your clinic or hospital, music can help relieve stress at the end of the workday. “Medical culture can often be detrimental to doctors’ health,” said Sue, who credits music with helping him maintain equanimity.
Bonnel can relate. Practicing and performing with the Penn Medicine Symphony Orchestra offers him a sense of community and relief from the stress of modern life. “For 2 hours every Tuesday, I put my phone away and just play,” he said. “It’s nice to have those moments when I’m temporarily disconnected and can just focus on one thing: Playing.”
Scale Up Your Career
Years after med school graduation, Sue still recalls many of the tunes he wrote to help him remember information. When he sings a song in his head, he’ll get a refresher on pediatric developmental milestones, medication side effects, anatomical details, and more, which informs the treatment plans he devises for patients. To help other doctors reap these benefits, Sue created the website Tune Rx, a medical music study resource that includes many of the roughly 100 songs he’s written.
Emdin often discusses his musical strategies during talks on STEM education. Initially, people are skeptical, he said. But the idea quickly rings a bell for audience members. “They come up to me afterward to share anecdotes,” Emdin said. “If you have enough anecdotes, there’s a pattern. So let’s create a process. Let’s be intentional about using music as a learning strategy,” he urged.
A version of this article first appeared on Medscape.com.
“Because you know I’m all about that base, ‘bout that base, no acid.”
Do those words sound familiar? That’s because they’re the lyrics to Meghan Trainor’s “All About That Bass,” slightly tweaked to function as a medical study tool.
Early in med school, J.C. Sue, DO, now a family medicine physician, refashioned the song’s words to help him prepare for a test on acid extruders and loaders. Sue’s version, “All About That Base,” contained his lecture notes. During the exam, he found himself mentally singing his parody and easily recalling the information. Plus, the approach made cramming a lot more palatable.
Sound silly? It’s not. Sue’s approach is backed up by science. Recently, a 2024 study from Canada suggested that musical memory doesn’t decrease with age. And a 2023 study revealed music was a better cue than food for helping both young and older adults recall autobiographical memories.
Inspired by his success, Sue gave popular songs a medical spin throughout his medical training. “There’s no rule that says studying must be boring, tedious, or torturous,” Sue said. “If you can make it fun, why not?”
Sue isn’t alone. Many physicians say that writing songs, listening to music, or playing instruments improves their focus, energy, and work performance, along with their confidence and well-being.
Why does music work so well?
Tune Your Brain to Work With Tunes
Remember learning your ABCs to the tune of “Twinkle, Twinkle, Little Star?” (Or ask any Gen X person about Schoolhouse Rock.)
In the classroom, music is an established tool for teaching kids, said Ruth Gotian, EdD, MS, chief learning officer and associate professor of education in anesthesiology at Weill Cornell Medicine, New York City. But she said musical strategies make studying easier for adults, too, no matter how complex the material.
Christopher Emdin, PhD, Maxine Greene chair and professor of science education at Teachers College, Columbia University, New York City, shares Gotian’s view. When teaching science, engineering, technology, and mathematics (STEM) subjects to high school kids, he challenged them to write raps about the new concepts.
That’s when he saw visible results: As his students took exams, Emdin noticed them nodding and moving their mouths and heads.
“They were literally performing the songs they’d written for themselves,” Emdin said. “When you write a song to a beat, it’s almost like your heartbeat. You know it so well; you can conjure up your memories by reciting the lyrics.”
If songwriting isn’t in your repertoire, you’ll be glad to hear that just listening to music while studying can help with retention. “Music keeps both sides of the brain stimulated, which has been shown to increase focus and motivation,” explained Anita A. Paschall, MD, PhD, Medical School and Healthcare Admissions expert/director of Medical School and Healthcare Admissions at The Princeton Review.
‘Mind on a Permanent Vacation’
Paschall’s enthusiasm comes from personal experience. While preparing for her board exams, Jimmy Buffet’s catalog was her study soundtrack. “His songs stayed in my mind. I could hum along without having to think about it, so my brain was free to focus,” she recalled.
Because Paschall grew up listening to Buffet’s tunes, they also evoked relaxing moments from her earlier life, which she found comforting and uplifting. The combination helped make long, intense study sessions more pleasant. After all, when you’re “wasting away again in Margaritaville,” how can you feel stressed and despondent?
Alexander Remy Bonnel, MD, clinical assistant professor of medicine at the University of Pennsylvania and a physician at Pennsylvania Hospital, both in Philadelphia, found ways to incorporate both auditory and visual stimuli in his med school study routine. He listened to music while color-coding his notes to link both cues to the information. As with Paschall, these tactics helped reduce the monotony of learning reams of material.
That gave Bonnel an easy way to establish an important element for memory: Novelty.
“When you need to memorize so many things in a short amount of time, you’re trying to vary ways of internalizing information,” he observed. “You have a higher chance of retaining information if there’s something unique about it.”
Building Team Harmony
“Almost every single OR I rotated through in med school had music playing,” Bonnel also recalled. Furthermore, he noticed a pattern to the chosen songs: Regardless of their age, surgeons selected playlists of tunes that had been popular when they were in their 20s. Those golden oldies, from any era, could turn the OR team into a focused, cohesive unit.
Kyle McCormick, MD, a fifth-year resident in orthopedic surgery at New York–Presbyterian Hospital, Columbia University Irving Medical Center, New York City, has also noticed the ubiquity of background music in ORs. Her observation: Surgeons tend to choose universally popular, inoffensive songs, like tracks from Hall & Oates and Fleetwood Mac.
This meshes with the results of a joint survey of nearly 700 surgeons and other healthcare professionals conducted by Spotify and Figure 1 in 2021; 90% of the surgeons and surgical residents who responded said they listened to music in the OR. Rock and pop were the most popular genres, followed by classical, jazz, and then R&B.
Regardless of genre, music helped the surgical teams focus and feel less tense, the surgeons reported. But when training younger doctors, managing complications, or performing during critical points in surgery, many said they’d lower the volume.
Outside the OR, music can also help foster connection between colleagues. For Lawrence C. Loh, MD, MPH, adjunct professor at Dalla Lana School of Public Health at the University of Toronto in Ontario, Canada, playing guitar and piano has helped him connect with his staff. “I’ve played tunes at staff gatherings and recorded videos as encouragement during the emergency response for COVID-19,” he shared.
In his free time, Loh has also organized outings to his local pub’s weekly karaoke show for more than a decade. His goal: “Promote social cohesion and combat loneliness among my friend and social networks.”
Get Your Own Musical Boost
If all this sounds like music to your ears, here are some ways to try it yourself.
Find a study soundtrack. When choosing study music, follow Paschall’s lead and pick songs you know well so they’ll remain in the background. Also, compile a soundtrack you find pleasant and mood-boosting to help relieve the tedium of study and decrease stress.
Keep in mind that we all take in and process information differently, said Gotian. So background music during study sessions might not work for you. According to a 2017 study published in Frontiers in Psychology, it can be a distraction and impair learning for some. Do what works.
Get pumped with a “walkup song.” What songs make you feel like you could conquer the world? asked Emdin. Or what soundtrack would be playing if you were ascending a stage to accept an award or walking out to take the mound in the ninth inning? Those songs should be on what he calls your “superhero” or “walkup” playlist. His prescription: Tune in before you begin your workday or start a challenging procedure.
Paschall agrees and recommends her students and clients listen to music before sitting down for an exam. Forget reviewing flashcards for the nth time, she counseled. Putting on headphones (or earbuds) will put you in a “better headspace.”
Choose work and play playlists. As well as incorporating tunes in your clinic or hospital, music can help relieve stress at the end of the workday. “Medical culture can often be detrimental to doctors’ health,” said Sue, who credits music with helping him maintain equanimity.
Bonnel can relate. Practicing and performing with the Penn Medicine Symphony Orchestra offers him a sense of community and relief from the stress of modern life. “For 2 hours every Tuesday, I put my phone away and just play,” he said. “It’s nice to have those moments when I’m temporarily disconnected and can just focus on one thing: Playing.”
Scale Up Your Career
Years after med school graduation, Sue still recalls many of the tunes he wrote to help him remember information. When he sings a song in his head, he’ll get a refresher on pediatric developmental milestones, medication side effects, anatomical details, and more, which informs the treatment plans he devises for patients. To help other doctors reap these benefits, Sue created the website Tune Rx, a medical music study resource that includes many of the roughly 100 songs he’s written.
Emdin often discusses his musical strategies during talks on STEM education. Initially, people are skeptical, he said. But the idea quickly rings a bell for audience members. “They come up to me afterward to share anecdotes,” Emdin said. “If you have enough anecdotes, there’s a pattern. So let’s create a process. Let’s be intentional about using music as a learning strategy,” he urged.
A version of this article first appeared on Medscape.com.
Heard of ApoB Testing? New Guidelines
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
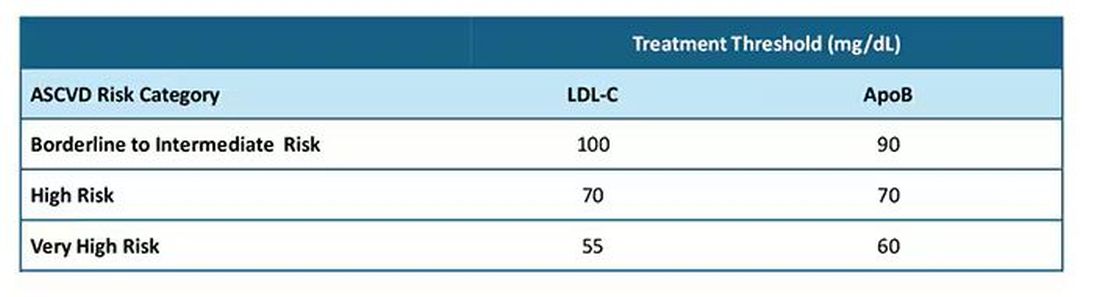
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I've been hearing a lot about apolipoprotein B (apoB) lately. It keeps popping up, but I've not been sure where it fits in or what I should do about it. The new Expert Clinical Consensus from the National Lipid Association now finally gives us clear guidance.
ApoB is the main protein that is found on all atherogenic lipoproteins. It is found on low-density lipoprotein (LDL) but also on other atherogenic lipoprotein particles. Because it is a part of all atherogenic particles, it predicts cardiovascular (CV) risk more accurately than does LDL cholesterol (LDL-C).
ApoB and LDL-C tend to run together, but not always. While they are correlated fairly well on a population level, for a given individual they can diverge; and when they do, apoB is the better predictor of future CV outcomes. This divergence occurs frequently, and it can occur even more frequently after treatment with statins. When LDL decreases to reach the LDL threshold for treatment, but apoB remains elevated, there is the potential for misclassification of CV risk and essentially the risk for undertreatment of someone whose CV risk is actually higher than it appears to be if we only look at their LDL-C. The consensus statement says, "Where there is discordance between apoB and LDL-C, risk follows apoB."
This understanding leads to the places where measurement of apoB may be helpful:
In patients with borderline atherosclerotic cardiovascular disease risk in whom a shared decision about statin therapy is being determined and the patient prefers not to start a statin, apoB can be useful for further risk stratification. If apoB suggests low risk, then statin therapy could be withheld, and if apoB is high, that would favor starting statin therapy. Certain common conditions, such as obesity and insulin resistance, can lead to smaller cholesterol-depleted LDL particles that result in lower LDL-C, but elevated apoB levels in this circumstance may drive the decision to treat with a statin.
In patients already treated with statins, but a decision must be made about whether treatment intensification is warranted. If the LDL-C is to goal and apoB is above threshold, treatment intensification may be considered. In patients who are not yet to goal, based on an elevated apoB, the first step is intensification of statin therapy. After that, intensification would be the same as has already been addressed in my review of the 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering.
After clarifying the importance of apoB in providing additional discrimination of CV risk, the consensus statement clarifies the treatment thresholds, or goals for treatment, for apoB that correlate with established LDL-C thresholds, as shown in this table:
Let me be really clear: The consensus statement does not say that we need to measure apoB in all patients or that such measurement is the standard of care. It is not. It says, and I'll quote, "At present, the use of apoB to assess the effectiveness of lipid-lowering therapies remains a matter of clinical judgment." This guideline is helpful in pointing out the patients most likely to benefit from this additional measurement, including those with hypertriglyceridemia, diabetes, visceral adiposity, insulin resistance/metabolic syndrome, low HDL-C, or very low LDL-C levels.
In summary, measurement of apoB can be helpful for further risk stratification in patients with borderline or intermediate LDL-C levels, and for deciding whether further intensification of lipid-lowering therapy may be warranted when the LDL threshold has been reached.
Lipid management is something that we do every day in the office. This is new information, or at least clarifying information, for most of us. Hopefully it is helpful. I'm interested in your thoughts on this topic, including whether and how you plan to use apoB measurements.
Dr. Skolnik, Professor, Department of Family Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia; Associate Director, Department of Family Medicine, Abington Jefferson Health, Abington, Pennsylvania, disclosed ties with AstraZeneca, Teva, Eli Lilly, Boehringer Ingelheim, Sanofi, Sanofi Pasteur, GlaxoSmithKline, Merck, and Bayer.
A version of this article first appeared on Medscape.com.
Fewer Recurrent Cardiovascular Events Seen With TNF Inhibitor Use in Axial Spondyloarthritis
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Tumor necrosis factor (TNF) inhibitors are associated with a reduced risk for recurrent cardiovascular events in patients with radiographic axial spondyloarthritis (axSpA) and a history of cardiovascular events.
METHODOLOGY:
- The researchers conducted a nationwide cohort study using data from the Korean National Claims Database, including 413 patients diagnosed with cardiovascular events following a radiographic axSpA diagnosis.
- Of all patients, 75 received TNF inhibitors (mean age, 51.9 years; 92% men) and 338 did not receive TNF inhibitors (mean age, 60.7 years; 74.9% men).
- Patients were followed from the date of the first cardiovascular event to the date of recurrence, the last date with claims data, or up to December 2021.
- The study outcome was recurrent cardiovascular events that occurred within 28 days of the first incidence and included myocardial infarction and stroke.
- The effect of TNF inhibitor exposure on the risk for recurrent cardiovascular events was assessed using an inverse probability weighted Cox regression analysis.
TAKEAWAY:
- The incidence of recurrent cardiovascular events in patients with radiographic axSpA was 32 per 1000 person-years.
- The incidence was 19 per 1000 person-years in the patients exposed to TNF inhibitors, whereas it was 36 per 1000 person-years in those not exposed to TNF inhibitors.
- Exposure to TNF inhibitors was associated with a 67% lower risk for recurrent cardiovascular events than non-exposure (P = .038).
IN PRACTICE:
“Our data add to previous knowledge by providing more direct evidence that TNFi [tumor necrosis factor inhibitors] could reduce the risk of recurrent cardiovascular events,” the authors wrote.
SOURCE:
The study was led by Oh Chan Kwon, MD, PhD, and Hye Sun Lee, PhD, Yonsei University College of Medicine, Seoul, South Korea. It was published online on October 4, 2024, in Arthritis Research & Therapy.
LIMITATIONS:
The lack of data on certain cardiovascular risk factors such as obesity, smoking, and lifestyle may have led to residual confounding. The patient count in the TNF inhibitor exposure group was not adequate to analyze each TNF inhibitor medication separately. The study included only Korean patients, limiting the generalizability to other ethnic populations. The number of recurrent stroke events was relatively small, making it infeasible to analyze myocardial infarction and stroke separately.
DISCLOSURES:
The study was funded by Yuhan Corporation as part of its “2023 Investigator Initiated Translation Research Program.” The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.