User login
‘You’re not going to tell my parents about this are you?’
You are on the front lines of the prevention, screening, and treatment decisions for adolescent substance use disorders. You often must choose whether to disclose information about substance use to parents and other concerned adults.
The risk of developing a substance use disorder increases dramatically the earlier an individual begins using a given substance.1 The neurobiology behind this risk is becoming increasingly clear. Young brains are undergoing crucial developmental processes, including synaptic pruning and myelination. The brain increasingly becomes more efficient in a staggered pattern, with limbic regions preceding frontal and executive regions, so we see adolescents with “more gas than brakes.” This has wisely been identified as developmentally appropriate, and even beneficial, rather than evidence that adolescents are somehow broken.2
Age-appropriate screening for substance use should occur as early as the preteen years and continue throughout adolescence. The most widely studied screening tools include the CRAFFT screening instrument and the Screening, Brief Intervention, and Referral to Treatment (SBIRT) approach.3,4 During formal and informal screening, you should lead with genuine concern for the well-being of the adolescent. Beginning a discussion with open-ended questions about substance use in the school and home is a way to build understanding of an adolescent’s environment prior to asking about personal use. While screening, consider well known risk factors including family history of substance use disorders, poor parental supervision, childhood maltreatment or abuse, low academic achievement, and untreated psychiatric disorders such as ADHD, depression, or anxiety, which may contribute to a higher likelihood or more rapid progression of a substance use disorder. Adolescents are more likely to disclose substance use when screening is done in private, rather than in the presence of a parent.5
Discussing the limits of confidentiality (generally when there is substantial risk of harm to self or others) with an adolescent shows respect and can be an expression of genuine care and concern. Once substance use or other risk-associated behaviors and choices are disclosed, you often may be asked not to share the information with parents. In some instances, privacy cannot be broken without consent. Be aware of your state laws governing parental and adolescent rights related to confidentiality.
You should strongly consider discussing substance use with the concerned adults when there are these red flags: daily use of any substance, any intravenous substance use, a score of 2 or higher on the CRAFFT, prescription medication misuse, or any change in medical status resulting from substance use, such as alcohol-related blackouts.
In most cases, adolescents should be informed of a decision to disclose substance use to their parents. Inviting adolescents to discuss how this will be done, including if the adolescent will be present, and whether you or the adolescent will disclose the use can be an opportunity to discuss their concerns. You should seek to understand if an adolescent has specific fears related to such a disclosure including careful consideration of any history of domestic violence or abuse.
Although adolescents increasingly identify with the opinions and values of their peers, it is a mistake to assume that they therefore do not value the opinions of their parents and the concerned adults in their lives. Parents play an integral role in preventing and treating adolescent substance use disorders. Except in rare instances of severe parent-child relationship problems or abuse, parents can and should be engaged as invaluable participants
Being aware of the legal and ethical obligations in treatment of adolescents presenting with any level of substance use, you can improve outcomes by thoughtfully inviting the participation of parents and other concerned adults into the prevention, screening, and treatment of adolescent substance use disorders.
Dr. Jackson is a child and adolescent psychiatrist at the University of Vermont, Burlington.
References
1. “Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings.” NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. (Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013).
2. “The Amazing Teen Brain,” Jay N. Geidd, Scientific American, May 2016.
3. Pediatrics 2011 Oct. doi: 10.1542/peds.2011-1754.
4. Alcohol Screening and Brief Intervention for Youth: A Practitioner’s Guide.
5. Pediatrics. 2016 Jul 1. doi: 10.1542/peds.2016-1211.
6. J Fam Commun. 2014 Jan 1:14(4):328-51.
7. J Clin Child Adolesc. Psychol. 2008;37(1):236-59.
8. J Child Adolesc Subst Abuse. 2015 May 4;24(3):155-65.
9. Arch Pediatr Adolesc Med. 2012;166(12):1132-9.
You are on the front lines of the prevention, screening, and treatment decisions for adolescent substance use disorders. You often must choose whether to disclose information about substance use to parents and other concerned adults.
The risk of developing a substance use disorder increases dramatically the earlier an individual begins using a given substance.1 The neurobiology behind this risk is becoming increasingly clear. Young brains are undergoing crucial developmental processes, including synaptic pruning and myelination. The brain increasingly becomes more efficient in a staggered pattern, with limbic regions preceding frontal and executive regions, so we see adolescents with “more gas than brakes.” This has wisely been identified as developmentally appropriate, and even beneficial, rather than evidence that adolescents are somehow broken.2
Age-appropriate screening for substance use should occur as early as the preteen years and continue throughout adolescence. The most widely studied screening tools include the CRAFFT screening instrument and the Screening, Brief Intervention, and Referral to Treatment (SBIRT) approach.3,4 During formal and informal screening, you should lead with genuine concern for the well-being of the adolescent. Beginning a discussion with open-ended questions about substance use in the school and home is a way to build understanding of an adolescent’s environment prior to asking about personal use. While screening, consider well known risk factors including family history of substance use disorders, poor parental supervision, childhood maltreatment or abuse, low academic achievement, and untreated psychiatric disorders such as ADHD, depression, or anxiety, which may contribute to a higher likelihood or more rapid progression of a substance use disorder. Adolescents are more likely to disclose substance use when screening is done in private, rather than in the presence of a parent.5
Discussing the limits of confidentiality (generally when there is substantial risk of harm to self or others) with an adolescent shows respect and can be an expression of genuine care and concern. Once substance use or other risk-associated behaviors and choices are disclosed, you often may be asked not to share the information with parents. In some instances, privacy cannot be broken without consent. Be aware of your state laws governing parental and adolescent rights related to confidentiality.
You should strongly consider discussing substance use with the concerned adults when there are these red flags: daily use of any substance, any intravenous substance use, a score of 2 or higher on the CRAFFT, prescription medication misuse, or any change in medical status resulting from substance use, such as alcohol-related blackouts.
In most cases, adolescents should be informed of a decision to disclose substance use to their parents. Inviting adolescents to discuss how this will be done, including if the adolescent will be present, and whether you or the adolescent will disclose the use can be an opportunity to discuss their concerns. You should seek to understand if an adolescent has specific fears related to such a disclosure including careful consideration of any history of domestic violence or abuse.
Although adolescents increasingly identify with the opinions and values of their peers, it is a mistake to assume that they therefore do not value the opinions of their parents and the concerned adults in their lives. Parents play an integral role in preventing and treating adolescent substance use disorders. Except in rare instances of severe parent-child relationship problems or abuse, parents can and should be engaged as invaluable participants
Being aware of the legal and ethical obligations in treatment of adolescents presenting with any level of substance use, you can improve outcomes by thoughtfully inviting the participation of parents and other concerned adults into the prevention, screening, and treatment of adolescent substance use disorders.
Dr. Jackson is a child and adolescent psychiatrist at the University of Vermont, Burlington.
References
1. “Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings.” NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. (Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013).
2. “The Amazing Teen Brain,” Jay N. Geidd, Scientific American, May 2016.
3. Pediatrics 2011 Oct. doi: 10.1542/peds.2011-1754.
4. Alcohol Screening and Brief Intervention for Youth: A Practitioner’s Guide.
5. Pediatrics. 2016 Jul 1. doi: 10.1542/peds.2016-1211.
6. J Fam Commun. 2014 Jan 1:14(4):328-51.
7. J Clin Child Adolesc. Psychol. 2008;37(1):236-59.
8. J Child Adolesc Subst Abuse. 2015 May 4;24(3):155-65.
9. Arch Pediatr Adolesc Med. 2012;166(12):1132-9.
You are on the front lines of the prevention, screening, and treatment decisions for adolescent substance use disorders. You often must choose whether to disclose information about substance use to parents and other concerned adults.
The risk of developing a substance use disorder increases dramatically the earlier an individual begins using a given substance.1 The neurobiology behind this risk is becoming increasingly clear. Young brains are undergoing crucial developmental processes, including synaptic pruning and myelination. The brain increasingly becomes more efficient in a staggered pattern, with limbic regions preceding frontal and executive regions, so we see adolescents with “more gas than brakes.” This has wisely been identified as developmentally appropriate, and even beneficial, rather than evidence that adolescents are somehow broken.2
Age-appropriate screening for substance use should occur as early as the preteen years and continue throughout adolescence. The most widely studied screening tools include the CRAFFT screening instrument and the Screening, Brief Intervention, and Referral to Treatment (SBIRT) approach.3,4 During formal and informal screening, you should lead with genuine concern for the well-being of the adolescent. Beginning a discussion with open-ended questions about substance use in the school and home is a way to build understanding of an adolescent’s environment prior to asking about personal use. While screening, consider well known risk factors including family history of substance use disorders, poor parental supervision, childhood maltreatment or abuse, low academic achievement, and untreated psychiatric disorders such as ADHD, depression, or anxiety, which may contribute to a higher likelihood or more rapid progression of a substance use disorder. Adolescents are more likely to disclose substance use when screening is done in private, rather than in the presence of a parent.5
Discussing the limits of confidentiality (generally when there is substantial risk of harm to self or others) with an adolescent shows respect and can be an expression of genuine care and concern. Once substance use or other risk-associated behaviors and choices are disclosed, you often may be asked not to share the information with parents. In some instances, privacy cannot be broken without consent. Be aware of your state laws governing parental and adolescent rights related to confidentiality.
You should strongly consider discussing substance use with the concerned adults when there are these red flags: daily use of any substance, any intravenous substance use, a score of 2 or higher on the CRAFFT, prescription medication misuse, or any change in medical status resulting from substance use, such as alcohol-related blackouts.
In most cases, adolescents should be informed of a decision to disclose substance use to their parents. Inviting adolescents to discuss how this will be done, including if the adolescent will be present, and whether you or the adolescent will disclose the use can be an opportunity to discuss their concerns. You should seek to understand if an adolescent has specific fears related to such a disclosure including careful consideration of any history of domestic violence or abuse.
Although adolescents increasingly identify with the opinions and values of their peers, it is a mistake to assume that they therefore do not value the opinions of their parents and the concerned adults in their lives. Parents play an integral role in preventing and treating adolescent substance use disorders. Except in rare instances of severe parent-child relationship problems or abuse, parents can and should be engaged as invaluable participants
Being aware of the legal and ethical obligations in treatment of adolescents presenting with any level of substance use, you can improve outcomes by thoughtfully inviting the participation of parents and other concerned adults into the prevention, screening, and treatment of adolescent substance use disorders.
Dr. Jackson is a child and adolescent psychiatrist at the University of Vermont, Burlington.
References
1. “Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings.” NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. (Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013).
2. “The Amazing Teen Brain,” Jay N. Geidd, Scientific American, May 2016.
3. Pediatrics 2011 Oct. doi: 10.1542/peds.2011-1754.
4. Alcohol Screening and Brief Intervention for Youth: A Practitioner’s Guide.
5. Pediatrics. 2016 Jul 1. doi: 10.1542/peds.2016-1211.
6. J Fam Commun. 2014 Jan 1:14(4):328-51.
7. J Clin Child Adolesc. Psychol. 2008;37(1):236-59.
8. J Child Adolesc Subst Abuse. 2015 May 4;24(3):155-65.
9. Arch Pediatr Adolesc Med. 2012;166(12):1132-9.
Update on AGA-Medtronic Research and Development Pilot Award in Technology
BOSTON – It’s been just a year since Bani Chander Roland, MD, FACG, was awarded the 2017 AGA-Medtronic Research and Development Pilot Award in Technology, and her team already has recruited 30 patients with irritable bowel syndrome (IBS) and small intestinal bacterial overgrowth (SIBO) for a study of the gut microbiome and functioning. Interim data from her grant will be presented at Digestive Disease Week® 2018 in June in Washington, D.C., as a poster of distinction.
Dr. Roland and her team are testing the hypothesis that IBS and SIBO result from several distinct pathophysiologic mechanisms, each of which are associated with their own distinct microbial and inflammatory profile. For the study, they are using the Wireless Motility Capsule (WMC, SmartPill) to assess alterations in gastrointestinal pathophysiology in patients with suspected IBS and SIBO – just the sort of innovative technology that the AGA Center for GI Innovation and Technology (CGIT) has fostered. They also are obtaining microflora from oropharyngeal, gastric, small bowel, and fecal samples for DNA sequencing. In addition, the team is beginning to study serum samples to test the hypothesis that patients with IBS and SIBO have increased expression of pro-inflammatory markers compared to those with only IBS; they are attempting to correlate the inflammatory markers to specific bacteria.
“IBS is a very common gastrointestinal disorder, and we’re continuing to see an increase in prevalence in Western countries, without understanding the etiology for this syndrome,” said Dr. Roland, director of gastrointestinal motility at Lenox Hill Hospital and Northwell Health System in New York. “Unfortunately, we don’t have any specific or targeted therapies for this patient population because the underlying physiological mechanisms that cause IBS are not very well understood. When we treat these patients with antibiotics, often their symptoms come right back. If we can target the causes of disease in subsets of these patients, we may be able to successfully treat them.”
“We’re very excited to see what changes in the microbiome exist in this patient population, to determine if the microbiome may be another potential area that we can target for treatment,” she added.
In data to be presented in the DDW poster, Dr. Roland’s team used the SmartPill to measure the gastrointestinal transit times, pH, and ileocecal junction pressures of patients with IBS and SIBO as compared to patients with IBS without evidence of SIBO. “Interestingly, patients who had IBS and SIBO had significantly higher contraction frequency in the stomach and small bowel compared to patients with IBS alone,” Dr. Roland said. Those with both conditions also had lower ileocecal junction pressures. “These are physiological mechanisms that have not been well understood before,” Dr. Roland said. “We have been able to begin delineating some of the underlying physiological mechanisms in this challenging patient population for the first time, using a noninvasive, wireless motility capsule.”
Dr. Roland’s team is now partnering with the hospital’s endocrinology division to compare the circulating inflammatory markers in patients with IBS and SIBO, such as TNF (tumor necrosis factor)-alpha and IL (interleukin)-6, to patients with IBS alone. They will use their data to apply for future funding.
BOSTON – It’s been just a year since Bani Chander Roland, MD, FACG, was awarded the 2017 AGA-Medtronic Research and Development Pilot Award in Technology, and her team already has recruited 30 patients with irritable bowel syndrome (IBS) and small intestinal bacterial overgrowth (SIBO) for a study of the gut microbiome and functioning. Interim data from her grant will be presented at Digestive Disease Week® 2018 in June in Washington, D.C., as a poster of distinction.
Dr. Roland and her team are testing the hypothesis that IBS and SIBO result from several distinct pathophysiologic mechanisms, each of which are associated with their own distinct microbial and inflammatory profile. For the study, they are using the Wireless Motility Capsule (WMC, SmartPill) to assess alterations in gastrointestinal pathophysiology in patients with suspected IBS and SIBO – just the sort of innovative technology that the AGA Center for GI Innovation and Technology (CGIT) has fostered. They also are obtaining microflora from oropharyngeal, gastric, small bowel, and fecal samples for DNA sequencing. In addition, the team is beginning to study serum samples to test the hypothesis that patients with IBS and SIBO have increased expression of pro-inflammatory markers compared to those with only IBS; they are attempting to correlate the inflammatory markers to specific bacteria.
“IBS is a very common gastrointestinal disorder, and we’re continuing to see an increase in prevalence in Western countries, without understanding the etiology for this syndrome,” said Dr. Roland, director of gastrointestinal motility at Lenox Hill Hospital and Northwell Health System in New York. “Unfortunately, we don’t have any specific or targeted therapies for this patient population because the underlying physiological mechanisms that cause IBS are not very well understood. When we treat these patients with antibiotics, often their symptoms come right back. If we can target the causes of disease in subsets of these patients, we may be able to successfully treat them.”
“We’re very excited to see what changes in the microbiome exist in this patient population, to determine if the microbiome may be another potential area that we can target for treatment,” she added.
In data to be presented in the DDW poster, Dr. Roland’s team used the SmartPill to measure the gastrointestinal transit times, pH, and ileocecal junction pressures of patients with IBS and SIBO as compared to patients with IBS without evidence of SIBO. “Interestingly, patients who had IBS and SIBO had significantly higher contraction frequency in the stomach and small bowel compared to patients with IBS alone,” Dr. Roland said. Those with both conditions also had lower ileocecal junction pressures. “These are physiological mechanisms that have not been well understood before,” Dr. Roland said. “We have been able to begin delineating some of the underlying physiological mechanisms in this challenging patient population for the first time, using a noninvasive, wireless motility capsule.”
Dr. Roland’s team is now partnering with the hospital’s endocrinology division to compare the circulating inflammatory markers in patients with IBS and SIBO, such as TNF (tumor necrosis factor)-alpha and IL (interleukin)-6, to patients with IBS alone. They will use their data to apply for future funding.
BOSTON – It’s been just a year since Bani Chander Roland, MD, FACG, was awarded the 2017 AGA-Medtronic Research and Development Pilot Award in Technology, and her team already has recruited 30 patients with irritable bowel syndrome (IBS) and small intestinal bacterial overgrowth (SIBO) for a study of the gut microbiome and functioning. Interim data from her grant will be presented at Digestive Disease Week® 2018 in June in Washington, D.C., as a poster of distinction.
Dr. Roland and her team are testing the hypothesis that IBS and SIBO result from several distinct pathophysiologic mechanisms, each of which are associated with their own distinct microbial and inflammatory profile. For the study, they are using the Wireless Motility Capsule (WMC, SmartPill) to assess alterations in gastrointestinal pathophysiology in patients with suspected IBS and SIBO – just the sort of innovative technology that the AGA Center for GI Innovation and Technology (CGIT) has fostered. They also are obtaining microflora from oropharyngeal, gastric, small bowel, and fecal samples for DNA sequencing. In addition, the team is beginning to study serum samples to test the hypothesis that patients with IBS and SIBO have increased expression of pro-inflammatory markers compared to those with only IBS; they are attempting to correlate the inflammatory markers to specific bacteria.
“IBS is a very common gastrointestinal disorder, and we’re continuing to see an increase in prevalence in Western countries, without understanding the etiology for this syndrome,” said Dr. Roland, director of gastrointestinal motility at Lenox Hill Hospital and Northwell Health System in New York. “Unfortunately, we don’t have any specific or targeted therapies for this patient population because the underlying physiological mechanisms that cause IBS are not very well understood. When we treat these patients with antibiotics, often their symptoms come right back. If we can target the causes of disease in subsets of these patients, we may be able to successfully treat them.”
“We’re very excited to see what changes in the microbiome exist in this patient population, to determine if the microbiome may be another potential area that we can target for treatment,” she added.
In data to be presented in the DDW poster, Dr. Roland’s team used the SmartPill to measure the gastrointestinal transit times, pH, and ileocecal junction pressures of patients with IBS and SIBO as compared to patients with IBS without evidence of SIBO. “Interestingly, patients who had IBS and SIBO had significantly higher contraction frequency in the stomach and small bowel compared to patients with IBS alone,” Dr. Roland said. Those with both conditions also had lower ileocecal junction pressures. “These are physiological mechanisms that have not been well understood before,” Dr. Roland said. “We have been able to begin delineating some of the underlying physiological mechanisms in this challenging patient population for the first time, using a noninvasive, wireless motility capsule.”
Dr. Roland’s team is now partnering with the hospital’s endocrinology division to compare the circulating inflammatory markers in patients with IBS and SIBO, such as TNF (tumor necrosis factor)-alpha and IL (interleukin)-6, to patients with IBS alone. They will use their data to apply for future funding.
2018 AGA TECH SUMMIT
Variants in One Gene May Account for 7% of Juvenile Myoclonic Epilepsy Cases
Rare genetic variants that affect the maturation, migration, and death of neurons appear to be responsible for about 7% of cases of juvenile myoclonic epilepsy. 
Variants of the intestinal-cell kinase gene (ICK) occurred in 12 members of a family affected by the disorder and were confirmed in 22 of 310 additional patients, Julia N. Bailey, PhD, of the University of California, Los Angeles (UCLA), and her colleagues reported in the March 15 issue of the New England Journal of Medicine.
But among these 34 patients, the variants manifested as different epileptic phenotypes, suggesting genetic pleiotropism, the investigators said.
Clinical Heterogeneity
“We report striking variation with respect to epilepsy phenotypes both within and among families,” the researchers said. “Of 34 affected nonproband family members, five (15%) had juvenile myoclonic epilepsy, 10 (29%) had myoclonic-tonic-clonic seizures, four (12%) had pyknoleptic petit mal seizures alone or with myoclonic-tonic-clonic seizures, four (12%) had febrile seizures alone or with absence seizures or myoclonias, and 11 (32%) were clinically asymptomatic but had polyspikes or focal spikes on EEG. These results strongly suggest that ICK is pleiotropic ... and that epistatic loci with different genes are present in affected family members and interact with ICK and contribute to pleiotropism and clinical heterogeneity.”
ICK “is expressed in all tissues,” said senior study author Antonio Delgado-Escueta, MD, Professor of Neurology at UCLA. The subtle brain dysplasia, or microdysgenesis, that occurs in patients with juvenile myoclonic epilepsy is “diagnosed mainly microscopically, and has neuronal cells that migrated from periventricular zones to the wrong places in wrong layers of the cortical gray matter and even the white matter of the brain,” he said. “The cells can also be abnormally large and bunch up as a thicker gray matter. On voxel-based brain MRI ... focal thickenings of these abnormally migrated cells can also be partly explained by decreased pruning of cells and circuits (apoptosis).”
The gene encoding for ICK is located close to EFHC1 on chromosome 6p12. EFHC1, which encodes for a calcium-binding protein, has been implicated in juvenile myoclonic epilepsy. Dr. Bailey and her colleagues examined whether several genes in close proximity to EFHC1 also influenced that risk.
An Epilepsy Database
The investigators drew data from the GENESS (Genetic Epilepsies Studies) consortium, which has study sites in the United States, Mexico, Honduras, Brazil, and Japan. The current study analyzed information from 334 families with genetic generalized epilepsies. Among these families, 310 patients had adolescent-onset myoclonic seizures and polyspike waves or had a diagnosis of juvenile myoclonic epilepsy.
The investigators first performed an exome-wide analysis of four affected members of a large family with genetic juvenile myoclonic epilepsy. They observed the same variants in all four patients, then ran the screen in all 37 family members. Next, they screened these candidate genes in all 334 of the GENESS families and calculated risk scores for juvenile myoclonic epilepsy.
A linkage analysis confirmed two candidate genes on chromosome 6p12.2. Further analyses pinpointed a single variant: K305T on the ICK gene. This trait was present in each of the 12 affected members and three unaffected members of the initial family examined. Of those affected, three had juvenile myoclonic epilepsy, two had myoclonic-tonic-clonic convulsions only, two had febrile convulsions plus childhood absence seizures or neonatal myoclonus, one had febrile convulsions only, and four had polyspikes on EEG and were clinically asymptomatic.
“These results genetically implicated K305T as an autosomal dominant, possibly disease-causing trait,” the authors noted.
ICK variants were also present in 24 of the 310 database patients who had juvenile myoclonic epilepsy (8%). Of these, nine belonged to families with other affected members. The researchers tested 24 ICK variants for pathogenicity and determined that 13 exerted significant juvenile myoclonic epilepsy risk, with odds ratios exceeding 5.0.
When the researchers looked for these variants in the Genome Aggregation Database (gnomAD), they found that 12 of the variants were present but extremely rare, and eight were absent. They also found an additional ICK variant in a Mexican patient who was in gnomAD. That variant was a benign polymorphism in Africans.
Dr. Bailey and her colleagues thus concluded that 21 ICK variants in 22 patients with juvenile myoclonic epilepsy accounted for 7% of the juvenile myoclonic epilepsy among the 310 cases examined.
Experiments in Mice
The team also conducted a series of in vitro and in vivo mouse experiments. They determined that ICK variants impaired the migration of neuronal progenitor cells and lowered their mitotic index. ICK transgenic mice during light sleep displayed muscle movements similar to human myoclonic seizures. These mice also displayed diffuse polyspike brain waves on EEG recordings.
“The data we obtained through the use of electroporated slices of mouse brain support the conclusion that pathogenic variants in ICK cause 7% of cases of juvenile myoclonic epilepsy by disrupting mitosis, neuroblast migration, and apoptosis,” they concluded.
The study was funded by private and public grants. Several authors are coholders of patents on EFHC1-based diagnostics and therapeutics that have been licensed to Athena Diagnostics.
—Michele G. Sullivan
Suggested Reading
Bailey JN, de Nijs L, Bai D, et al. Variant intestinal-cell kinase in juvenile myoclonic epilepsy. N Engl J Med. 2018; 378(11): 1018-1028.
Rare genetic variants that affect the maturation, migration, and death of neurons appear to be responsible for about 7% of cases of juvenile myoclonic epilepsy.
Variants of the intestinal-cell kinase gene (ICK) occurred in 12 members of a family affected by the disorder and were confirmed in 22 of 310 additional patients, Julia N. Bailey, PhD, of the University of California, Los Angeles (UCLA), and her colleagues reported in the March 15 issue of the New England Journal of Medicine.
But among these 34 patients, the variants manifested as different epileptic phenotypes, suggesting genetic pleiotropism, the investigators said.
Clinical Heterogeneity
“We report striking variation with respect to epilepsy phenotypes both within and among families,” the researchers said. “Of 34 affected nonproband family members, five (15%) had juvenile myoclonic epilepsy, 10 (29%) had myoclonic-tonic-clonic seizures, four (12%) had pyknoleptic petit mal seizures alone or with myoclonic-tonic-clonic seizures, four (12%) had febrile seizures alone or with absence seizures or myoclonias, and 11 (32%) were clinically asymptomatic but had polyspikes or focal spikes on EEG. These results strongly suggest that ICK is pleiotropic ... and that epistatic loci with different genes are present in affected family members and interact with ICK and contribute to pleiotropism and clinical heterogeneity.”
ICK “is expressed in all tissues,” said senior study author Antonio Delgado-Escueta, MD, Professor of Neurology at UCLA. The subtle brain dysplasia, or microdysgenesis, that occurs in patients with juvenile myoclonic epilepsy is “diagnosed mainly microscopically, and has neuronal cells that migrated from periventricular zones to the wrong places in wrong layers of the cortical gray matter and even the white matter of the brain,” he said. “The cells can also be abnormally large and bunch up as a thicker gray matter. On voxel-based brain MRI ... focal thickenings of these abnormally migrated cells can also be partly explained by decreased pruning of cells and circuits (apoptosis).”
The gene encoding for ICK is located close to EFHC1 on chromosome 6p12. EFHC1, which encodes for a calcium-binding protein, has been implicated in juvenile myoclonic epilepsy. Dr. Bailey and her colleagues examined whether several genes in close proximity to EFHC1 also influenced that risk.
An Epilepsy Database
The investigators drew data from the GENESS (Genetic Epilepsies Studies) consortium, which has study sites in the United States, Mexico, Honduras, Brazil, and Japan. The current study analyzed information from 334 families with genetic generalized epilepsies. Among these families, 310 patients had adolescent-onset myoclonic seizures and polyspike waves or had a diagnosis of juvenile myoclonic epilepsy.
The investigators first performed an exome-wide analysis of four affected members of a large family with genetic juvenile myoclonic epilepsy. They observed the same variants in all four patients, then ran the screen in all 37 family members. Next, they screened these candidate genes in all 334 of the GENESS families and calculated risk scores for juvenile myoclonic epilepsy.
A linkage analysis confirmed two candidate genes on chromosome 6p12.2. Further analyses pinpointed a single variant: K305T on the ICK gene. This trait was present in each of the 12 affected members and three unaffected members of the initial family examined. Of those affected, three had juvenile myoclonic epilepsy, two had myoclonic-tonic-clonic convulsions only, two had febrile convulsions plus childhood absence seizures or neonatal myoclonus, one had febrile convulsions only, and four had polyspikes on EEG and were clinically asymptomatic.
“These results genetically implicated K305T as an autosomal dominant, possibly disease-causing trait,” the authors noted.
ICK variants were also present in 24 of the 310 database patients who had juvenile myoclonic epilepsy (8%). Of these, nine belonged to families with other affected members. The researchers tested 24 ICK variants for pathogenicity and determined that 13 exerted significant juvenile myoclonic epilepsy risk, with odds ratios exceeding 5.0.
When the researchers looked for these variants in the Genome Aggregation Database (gnomAD), they found that 12 of the variants were present but extremely rare, and eight were absent. They also found an additional ICK variant in a Mexican patient who was in gnomAD. That variant was a benign polymorphism in Africans.
Dr. Bailey and her colleagues thus concluded that 21 ICK variants in 22 patients with juvenile myoclonic epilepsy accounted for 7% of the juvenile myoclonic epilepsy among the 310 cases examined.
Experiments in Mice
The team also conducted a series of in vitro and in vivo mouse experiments. They determined that ICK variants impaired the migration of neuronal progenitor cells and lowered their mitotic index. ICK transgenic mice during light sleep displayed muscle movements similar to human myoclonic seizures. These mice also displayed diffuse polyspike brain waves on EEG recordings.
“The data we obtained through the use of electroporated slices of mouse brain support the conclusion that pathogenic variants in ICK cause 7% of cases of juvenile myoclonic epilepsy by disrupting mitosis, neuroblast migration, and apoptosis,” they concluded.
The study was funded by private and public grants. Several authors are coholders of patents on EFHC1-based diagnostics and therapeutics that have been licensed to Athena Diagnostics.
—Michele G. Sullivan
Suggested Reading
Bailey JN, de Nijs L, Bai D, et al. Variant intestinal-cell kinase in juvenile myoclonic epilepsy. N Engl J Med. 2018; 378(11): 1018-1028.
Rare genetic variants that affect the maturation, migration, and death of neurons appear to be responsible for about 7% of cases of juvenile myoclonic epilepsy.
Variants of the intestinal-cell kinase gene (ICK) occurred in 12 members of a family affected by the disorder and were confirmed in 22 of 310 additional patients, Julia N. Bailey, PhD, of the University of California, Los Angeles (UCLA), and her colleagues reported in the March 15 issue of the New England Journal of Medicine.
But among these 34 patients, the variants manifested as different epileptic phenotypes, suggesting genetic pleiotropism, the investigators said.
Clinical Heterogeneity
“We report striking variation with respect to epilepsy phenotypes both within and among families,” the researchers said. “Of 34 affected nonproband family members, five (15%) had juvenile myoclonic epilepsy, 10 (29%) had myoclonic-tonic-clonic seizures, four (12%) had pyknoleptic petit mal seizures alone or with myoclonic-tonic-clonic seizures, four (12%) had febrile seizures alone or with absence seizures or myoclonias, and 11 (32%) were clinically asymptomatic but had polyspikes or focal spikes on EEG. These results strongly suggest that ICK is pleiotropic ... and that epistatic loci with different genes are present in affected family members and interact with ICK and contribute to pleiotropism and clinical heterogeneity.”
ICK “is expressed in all tissues,” said senior study author Antonio Delgado-Escueta, MD, Professor of Neurology at UCLA. The subtle brain dysplasia, or microdysgenesis, that occurs in patients with juvenile myoclonic epilepsy is “diagnosed mainly microscopically, and has neuronal cells that migrated from periventricular zones to the wrong places in wrong layers of the cortical gray matter and even the white matter of the brain,” he said. “The cells can also be abnormally large and bunch up as a thicker gray matter. On voxel-based brain MRI ... focal thickenings of these abnormally migrated cells can also be partly explained by decreased pruning of cells and circuits (apoptosis).”
The gene encoding for ICK is located close to EFHC1 on chromosome 6p12. EFHC1, which encodes for a calcium-binding protein, has been implicated in juvenile myoclonic epilepsy. Dr. Bailey and her colleagues examined whether several genes in close proximity to EFHC1 also influenced that risk.
An Epilepsy Database
The investigators drew data from the GENESS (Genetic Epilepsies Studies) consortium, which has study sites in the United States, Mexico, Honduras, Brazil, and Japan. The current study analyzed information from 334 families with genetic generalized epilepsies. Among these families, 310 patients had adolescent-onset myoclonic seizures and polyspike waves or had a diagnosis of juvenile myoclonic epilepsy.
The investigators first performed an exome-wide analysis of four affected members of a large family with genetic juvenile myoclonic epilepsy. They observed the same variants in all four patients, then ran the screen in all 37 family members. Next, they screened these candidate genes in all 334 of the GENESS families and calculated risk scores for juvenile myoclonic epilepsy.
A linkage analysis confirmed two candidate genes on chromosome 6p12.2. Further analyses pinpointed a single variant: K305T on the ICK gene. This trait was present in each of the 12 affected members and three unaffected members of the initial family examined. Of those affected, three had juvenile myoclonic epilepsy, two had myoclonic-tonic-clonic convulsions only, two had febrile convulsions plus childhood absence seizures or neonatal myoclonus, one had febrile convulsions only, and four had polyspikes on EEG and were clinically asymptomatic.
“These results genetically implicated K305T as an autosomal dominant, possibly disease-causing trait,” the authors noted.
ICK variants were also present in 24 of the 310 database patients who had juvenile myoclonic epilepsy (8%). Of these, nine belonged to families with other affected members. The researchers tested 24 ICK variants for pathogenicity and determined that 13 exerted significant juvenile myoclonic epilepsy risk, with odds ratios exceeding 5.0.
When the researchers looked for these variants in the Genome Aggregation Database (gnomAD), they found that 12 of the variants were present but extremely rare, and eight were absent. They also found an additional ICK variant in a Mexican patient who was in gnomAD. That variant was a benign polymorphism in Africans.
Dr. Bailey and her colleagues thus concluded that 21 ICK variants in 22 patients with juvenile myoclonic epilepsy accounted for 7% of the juvenile myoclonic epilepsy among the 310 cases examined.
Experiments in Mice
The team also conducted a series of in vitro and in vivo mouse experiments. They determined that ICK variants impaired the migration of neuronal progenitor cells and lowered their mitotic index. ICK transgenic mice during light sleep displayed muscle movements similar to human myoclonic seizures. These mice also displayed diffuse polyspike brain waves on EEG recordings.
“The data we obtained through the use of electroporated slices of mouse brain support the conclusion that pathogenic variants in ICK cause 7% of cases of juvenile myoclonic epilepsy by disrupting mitosis, neuroblast migration, and apoptosis,” they concluded.
The study was funded by private and public grants. Several authors are coholders of patents on EFHC1-based diagnostics and therapeutics that have been licensed to Athena Diagnostics.
—Michele G. Sullivan
Suggested Reading
Bailey JN, de Nijs L, Bai D, et al. Variant intestinal-cell kinase in juvenile myoclonic epilepsy. N Engl J Med. 2018; 378(11): 1018-1028.
Constipation on opioids? Follow these three steps to ID the true cause
LAS VEGAS – To appropriately manage patients on opioids who develop constipation, one of the most important distinctions to make is whether the condition was caused by the pain treatment or was just exacerbated by it, according to Darren M. Brenner, MD.
Because of the rampant use of opioids, the answer to that question is increasingly relevant to clinical practice, said Dr. Brenner, associate professor of medicine (gastroenterology and hepatology) and surgery at Northwestern University, Chicago.
Dr. Brenner described a concise algorithm (Curr Gastroenterol Rep. 2017 Mar;19[3]:12) for discerning these patient groups; he codeveloped the algorithm with meeting cochair Brooks D. Cash, MD, chief of the division of gastroenterology, hepatology, and nutrition at the University of Texas, Houston.
Step 1 in the algorithm is simply to ask patients whether they are constipated. “You should ask all of your patients who are on opioids if they have this problem,” Dr. Brenner said. “A significant percentage of individuals using opioids will develop constipation.”
According to the results of studies that Dr. Brenner summarized, up to 80% of patients taking opioids for chronic, noncancer pain will develop opioid-induced constipation, and more than 90% of opioid-taking patients with advanced illness will need laxatives.
Given this prevalence, clinicians might want to be skeptical when patients on opioids reply “no” when asked whether they are constipated.
“From my own clinical experience, you will miss a third of your population that has constipation,” Dr. Brenner said, noting that some patients will instead think of their condition in terms of incomplete evacuation or decreased stool frequency.
Step 2 of the algorithm, therefore, is to assess for signs and symptoms of functional constipation in all patients, regardless of whether they report the condition.
The recently published Rome IV diagnostic criteria included a new category for opioid-induced constipation. According to the new definition, opioid-induced constipation must include new or worsening symptoms, such as fewer than three solid bowel movements per week, and straining, blockage sensation, or manual maneuvers on at least 25% of bowel movements, among other symptoms listed in the report.
If patients do have constipation meeting these criteria, then step 3 of the algorithm is to determine whether the symptoms were present prior to taking opioids.
If onset of constipation is related to the start of opioid treatment, options may include prescribing peripherally acting mu-opioid receptor antagonists (PAMORAs). By contrast, onset unrelated to the start of opioids, also known as opioid-exacerbated constipation, may require treatment according to the underlying cause. For example, slow-transit constipation may respond to laxatives, while evacuation disorders may be treated with surgery, biofeedback, or physical therapy.
The hardest group to identify, according to Dr. Brenner, is individuals whose symptoms were so minor that they didn’t even realize they had constipation symptoms prior to opioids.
Because treatment protocols for opioid-induced and opioid-exacerbated constipation are so different, “we must tease these people out,” Dr. Brenner said.
Global Academy and this news organization are owned by the same parent company.
Dr. Brenner reported disclosures related to Allergan, Daiichi Sankyo, Ironwood Pharmaceuticals, Prius Medical, Salix Pharmaceuticals, Synergy Pharmaceuticals, Shionogi, and others.
LAS VEGAS – To appropriately manage patients on opioids who develop constipation, one of the most important distinctions to make is whether the condition was caused by the pain treatment or was just exacerbated by it, according to Darren M. Brenner, MD.
Because of the rampant use of opioids, the answer to that question is increasingly relevant to clinical practice, said Dr. Brenner, associate professor of medicine (gastroenterology and hepatology) and surgery at Northwestern University, Chicago.
Dr. Brenner described a concise algorithm (Curr Gastroenterol Rep. 2017 Mar;19[3]:12) for discerning these patient groups; he codeveloped the algorithm with meeting cochair Brooks D. Cash, MD, chief of the division of gastroenterology, hepatology, and nutrition at the University of Texas, Houston.
Step 1 in the algorithm is simply to ask patients whether they are constipated. “You should ask all of your patients who are on opioids if they have this problem,” Dr. Brenner said. “A significant percentage of individuals using opioids will develop constipation.”
According to the results of studies that Dr. Brenner summarized, up to 80% of patients taking opioids for chronic, noncancer pain will develop opioid-induced constipation, and more than 90% of opioid-taking patients with advanced illness will need laxatives.
Given this prevalence, clinicians might want to be skeptical when patients on opioids reply “no” when asked whether they are constipated.
“From my own clinical experience, you will miss a third of your population that has constipation,” Dr. Brenner said, noting that some patients will instead think of their condition in terms of incomplete evacuation or decreased stool frequency.
Step 2 of the algorithm, therefore, is to assess for signs and symptoms of functional constipation in all patients, regardless of whether they report the condition.
The recently published Rome IV diagnostic criteria included a new category for opioid-induced constipation. According to the new definition, opioid-induced constipation must include new or worsening symptoms, such as fewer than three solid bowel movements per week, and straining, blockage sensation, or manual maneuvers on at least 25% of bowel movements, among other symptoms listed in the report.
If patients do have constipation meeting these criteria, then step 3 of the algorithm is to determine whether the symptoms were present prior to taking opioids.
If onset of constipation is related to the start of opioid treatment, options may include prescribing peripherally acting mu-opioid receptor antagonists (PAMORAs). By contrast, onset unrelated to the start of opioids, also known as opioid-exacerbated constipation, may require treatment according to the underlying cause. For example, slow-transit constipation may respond to laxatives, while evacuation disorders may be treated with surgery, biofeedback, or physical therapy.
The hardest group to identify, according to Dr. Brenner, is individuals whose symptoms were so minor that they didn’t even realize they had constipation symptoms prior to opioids.
Because treatment protocols for opioid-induced and opioid-exacerbated constipation are so different, “we must tease these people out,” Dr. Brenner said.
Global Academy and this news organization are owned by the same parent company.
Dr. Brenner reported disclosures related to Allergan, Daiichi Sankyo, Ironwood Pharmaceuticals, Prius Medical, Salix Pharmaceuticals, Synergy Pharmaceuticals, Shionogi, and others.
LAS VEGAS – To appropriately manage patients on opioids who develop constipation, one of the most important distinctions to make is whether the condition was caused by the pain treatment or was just exacerbated by it, according to Darren M. Brenner, MD.
Because of the rampant use of opioids, the answer to that question is increasingly relevant to clinical practice, said Dr. Brenner, associate professor of medicine (gastroenterology and hepatology) and surgery at Northwestern University, Chicago.
Dr. Brenner described a concise algorithm (Curr Gastroenterol Rep. 2017 Mar;19[3]:12) for discerning these patient groups; he codeveloped the algorithm with meeting cochair Brooks D. Cash, MD, chief of the division of gastroenterology, hepatology, and nutrition at the University of Texas, Houston.
Step 1 in the algorithm is simply to ask patients whether they are constipated. “You should ask all of your patients who are on opioids if they have this problem,” Dr. Brenner said. “A significant percentage of individuals using opioids will develop constipation.”
According to the results of studies that Dr. Brenner summarized, up to 80% of patients taking opioids for chronic, noncancer pain will develop opioid-induced constipation, and more than 90% of opioid-taking patients with advanced illness will need laxatives.
Given this prevalence, clinicians might want to be skeptical when patients on opioids reply “no” when asked whether they are constipated.
“From my own clinical experience, you will miss a third of your population that has constipation,” Dr. Brenner said, noting that some patients will instead think of their condition in terms of incomplete evacuation or decreased stool frequency.
Step 2 of the algorithm, therefore, is to assess for signs and symptoms of functional constipation in all patients, regardless of whether they report the condition.
The recently published Rome IV diagnostic criteria included a new category for opioid-induced constipation. According to the new definition, opioid-induced constipation must include new or worsening symptoms, such as fewer than three solid bowel movements per week, and straining, blockage sensation, or manual maneuvers on at least 25% of bowel movements, among other symptoms listed in the report.
If patients do have constipation meeting these criteria, then step 3 of the algorithm is to determine whether the symptoms were present prior to taking opioids.
If onset of constipation is related to the start of opioid treatment, options may include prescribing peripherally acting mu-opioid receptor antagonists (PAMORAs). By contrast, onset unrelated to the start of opioids, also known as opioid-exacerbated constipation, may require treatment according to the underlying cause. For example, slow-transit constipation may respond to laxatives, while evacuation disorders may be treated with surgery, biofeedback, or physical therapy.
The hardest group to identify, according to Dr. Brenner, is individuals whose symptoms were so minor that they didn’t even realize they had constipation symptoms prior to opioids.
Because treatment protocols for opioid-induced and opioid-exacerbated constipation are so different, “we must tease these people out,” Dr. Brenner said.
Global Academy and this news organization are owned by the same parent company.
Dr. Brenner reported disclosures related to Allergan, Daiichi Sankyo, Ironwood Pharmaceuticals, Prius Medical, Salix Pharmaceuticals, Synergy Pharmaceuticals, Shionogi, and others.
EXPERT ANALYSIS FROM PERSPECTIVES IN DIGESTIVE DISEASES
Simplified HCT-CI better predicts outcomes in young patients
NEWPORT BEACH, CALIF. – A revised hematopoietic stem cell transplantation comorbidity index developed for adolescents and young adults is useful for predicting nonrelapse mortality in this specific population, according to Brian Friend, MD.
In a retrospective study of 241 patients aged 15-39 years who underwent a first allogeneic hematopoietic stem cell transplant (HCT) between 2005 and 2015 at the University of California, Los Angeles, nonrelapse mortality incidence was particularly high, with rates of 26%, 28%, and 30% at 1, 2, and 3 years, respectively, Dr. Friend, a clinical research fellow at the David Geffen School of Medicine, Los Angeles, reported in a poster at the Acute Leukemia Forum of Hemedicus.

Rather, a history of pulmonary disease – found in 44% of the patients – was the most common comorbidity, and although this was based on pulmonary function tests alone and not necessarily on patient symptoms, it was a surprising finding, he said. It was associated with lower overall survival and with nonrelapse mortality, he added.
A psychosocial component, which took into account factors such as stressors, social support, financial issues, and substance abuse, was also fairly frequent in the patients, but was not necessarily associated with worse outcomes, he noted.
“In multivariable analysis, only a history of prior malignancy (hazard ratio, 2.04) and moderate and severe pulmonary disease (hazard ratios, 1.39 and 1.84, respectively) were associated with a higher incidence of nonrelapse mortality,” he reported.
The existing HCT-CI was developed in adults to help risk-stratify patients undergoing transplant, but adolescents and young adults undergoing HCT tend to have fewer comorbidities compared with older adults, though they still having a significant nonrelapse mortality rate, Dr. Friend said.
“We sought to develop a modified HCT-CI that would be more practical and efficient in predicting outcomes of adolescent and young adult patients,” he wrote.
Data were collected on 15 comorbidities included in the original HCT-CI study, as well as the psychosocial risk factors. The relationship between multiple variables and the incidence of nonrelapse mortality was investigated via the Fine and Gray competing risk model with adjustments for patient- and transplant-specific factors.
A few things were “looked at differently,” he said, explaining, for example, that multiple cardiovascular risk factors were combined into one since they are rare in younger patients.
The study demonstrated that an index including only a few comorbidities important in adolescents and young adults is more predictive in these younger patients vs. adults, suggesting that a simpler model is more practical and useful, Dr. Friend said.
A larger study is planned in conjunction with the Center for International Blood and Marrow Transplant Research (CIBMTR). The researchers for that study will take an in-depth look at this younger population in an effort to develop a novel risk score for them. Other future efforts will focus on developing interventions to target high risk patients – and in particular, modifiable risk factors – with a focus on preventive measures, he said.
Dr. Friend reported having no financial disclosures.
NEWPORT BEACH, CALIF. – A revised hematopoietic stem cell transplantation comorbidity index developed for adolescents and young adults is useful for predicting nonrelapse mortality in this specific population, according to Brian Friend, MD.
In a retrospective study of 241 patients aged 15-39 years who underwent a first allogeneic hematopoietic stem cell transplant (HCT) between 2005 and 2015 at the University of California, Los Angeles, nonrelapse mortality incidence was particularly high, with rates of 26%, 28%, and 30% at 1, 2, and 3 years, respectively, Dr. Friend, a clinical research fellow at the David Geffen School of Medicine, Los Angeles, reported in a poster at the Acute Leukemia Forum of Hemedicus.
Rather, a history of pulmonary disease – found in 44% of the patients – was the most common comorbidity, and although this was based on pulmonary function tests alone and not necessarily on patient symptoms, it was a surprising finding, he said. It was associated with lower overall survival and with nonrelapse mortality, he added.
A psychosocial component, which took into account factors such as stressors, social support, financial issues, and substance abuse, was also fairly frequent in the patients, but was not necessarily associated with worse outcomes, he noted.
“In multivariable analysis, only a history of prior malignancy (hazard ratio, 2.04) and moderate and severe pulmonary disease (hazard ratios, 1.39 and 1.84, respectively) were associated with a higher incidence of nonrelapse mortality,” he reported.
The existing HCT-CI was developed in adults to help risk-stratify patients undergoing transplant, but adolescents and young adults undergoing HCT tend to have fewer comorbidities compared with older adults, though they still having a significant nonrelapse mortality rate, Dr. Friend said.
“We sought to develop a modified HCT-CI that would be more practical and efficient in predicting outcomes of adolescent and young adult patients,” he wrote.
Data were collected on 15 comorbidities included in the original HCT-CI study, as well as the psychosocial risk factors. The relationship between multiple variables and the incidence of nonrelapse mortality was investigated via the Fine and Gray competing risk model with adjustments for patient- and transplant-specific factors.
A few things were “looked at differently,” he said, explaining, for example, that multiple cardiovascular risk factors were combined into one since they are rare in younger patients.
The study demonstrated that an index including only a few comorbidities important in adolescents and young adults is more predictive in these younger patients vs. adults, suggesting that a simpler model is more practical and useful, Dr. Friend said.
A larger study is planned in conjunction with the Center for International Blood and Marrow Transplant Research (CIBMTR). The researchers for that study will take an in-depth look at this younger population in an effort to develop a novel risk score for them. Other future efforts will focus on developing interventions to target high risk patients – and in particular, modifiable risk factors – with a focus on preventive measures, he said.
Dr. Friend reported having no financial disclosures.
NEWPORT BEACH, CALIF. – A revised hematopoietic stem cell transplantation comorbidity index developed for adolescents and young adults is useful for predicting nonrelapse mortality in this specific population, according to Brian Friend, MD.
In a retrospective study of 241 patients aged 15-39 years who underwent a first allogeneic hematopoietic stem cell transplant (HCT) between 2005 and 2015 at the University of California, Los Angeles, nonrelapse mortality incidence was particularly high, with rates of 26%, 28%, and 30% at 1, 2, and 3 years, respectively, Dr. Friend, a clinical research fellow at the David Geffen School of Medicine, Los Angeles, reported in a poster at the Acute Leukemia Forum of Hemedicus.
Rather, a history of pulmonary disease – found in 44% of the patients – was the most common comorbidity, and although this was based on pulmonary function tests alone and not necessarily on patient symptoms, it was a surprising finding, he said. It was associated with lower overall survival and with nonrelapse mortality, he added.
A psychosocial component, which took into account factors such as stressors, social support, financial issues, and substance abuse, was also fairly frequent in the patients, but was not necessarily associated with worse outcomes, he noted.
“In multivariable analysis, only a history of prior malignancy (hazard ratio, 2.04) and moderate and severe pulmonary disease (hazard ratios, 1.39 and 1.84, respectively) were associated with a higher incidence of nonrelapse mortality,” he reported.
The existing HCT-CI was developed in adults to help risk-stratify patients undergoing transplant, but adolescents and young adults undergoing HCT tend to have fewer comorbidities compared with older adults, though they still having a significant nonrelapse mortality rate, Dr. Friend said.
“We sought to develop a modified HCT-CI that would be more practical and efficient in predicting outcomes of adolescent and young adult patients,” he wrote.
Data were collected on 15 comorbidities included in the original HCT-CI study, as well as the psychosocial risk factors. The relationship between multiple variables and the incidence of nonrelapse mortality was investigated via the Fine and Gray competing risk model with adjustments for patient- and transplant-specific factors.
A few things were “looked at differently,” he said, explaining, for example, that multiple cardiovascular risk factors were combined into one since they are rare in younger patients.
The study demonstrated that an index including only a few comorbidities important in adolescents and young adults is more predictive in these younger patients vs. adults, suggesting that a simpler model is more practical and useful, Dr. Friend said.
A larger study is planned in conjunction with the Center for International Blood and Marrow Transplant Research (CIBMTR). The researchers for that study will take an in-depth look at this younger population in an effort to develop a novel risk score for them. Other future efforts will focus on developing interventions to target high risk patients – and in particular, modifiable risk factors – with a focus on preventive measures, he said.
Dr. Friend reported having no financial disclosures.
REPORTING FROM ALF 2018
Key clinical point:
Major finding: As many as 60% of the comorbidities included in the HCT-CI had no significant prevalence in young patients.
Study details: A retrospective study of 241 adolescents and young adults.
Disclosures: Dr. Friend reported having no financial disclosures.
Source: Friend B et al. ALF 2018, Poster Session.
What Are the Top Missed Imaging Diagnoses in Epilepsy?
WASHINGTON, DC—Neuroimaging is a core competency for epileptologists, according to an overview presented at the 71st Annual Meeting of the American Epilepsy Society. Neurologists trained in this subspecialty must bring “value-added” skills to the routine reports that radiologists provide—ensuring that both a proper diagnostic protocol and a quality-assurance mindset are in place so that when images are used, they are of sufficient quality to exclude wrong diagnoses.
Ultimately, it is the role of the epileptologist to review these images in the context of other localizing data and to work with radiologists in an integrative way, said Graeme Jackson, MD, Senior Deputy Director of the Florey Institute of Neuroscience and Mental Health in Melbourne.

“Finding a focal abnormality can truly change the path that patients move forward on, and it can change whether we have implantations, whether we have regional resections or focal resections…. It is critically important for good imaging to be a part of the path these patients travel on,” he said. Hippocampal sclerosis and bottom-of-sulcus dysplasia (BOSD) are entities that epileptologists “can’t miss,” he added.
What Is the Protocol?
In a presentation comprised largely of imaging studies in cases across the lifespan—infant, young child, teenager, adult, and senior citizen—Dr. Jackson discussed the diagnostic information essential for all patients with epilepsy: a clinical history for context, an EEG for function, and structural MRI with an epilepsy protocol for structure.
To map out the proper protocol, clinicians have to contend with many choices for MRI studies. Eventually, the process results in images. One pathway leads to a report from the radiologist, and another pathway leads to the epileptologist’s review.
Epileptologists are responsible for obtaining images that are adequate—not just taking what they get, said Dr. Jackson. “The radiologist is sitting there—[with] probably 2,000 images … a couple of minutes and a lot of cases.” As the “epileptologist, you have the advantage of having other information. You have the focus [and] the hypotheses.… It is critical that they be
Four “Can’t Miss” Imaging Diagnoses
The top four missed imaging diagnoses in epilepsy are obvious abnormalities, hippocampal sclerosis, malformations of cortical development, and a diagnosis of nothing, in which the clinician must be confident because the implicit observation is that the brain is completely structurally normal. Clinicians sometimes miss subtle things that can only be identified by looking correctly in the proper location, said Dr. Jackson.
In contrast to the four “can’t miss” diagnoses, focal cortical dysplasia, bilateral hippocampal sclerosis, temporal encephalocele, and parahippocampal dysplasia are among the many subtle lesions that clinicians can easily miss.
Examining a Case Study
Dr. Jackson assessed the case of Rachel, age 17, who has BOSD. This form of dysplasia encompasses localized seizures and can present at any time from infancy to adulthood. Although these entities are often intractable, 90% of patients who undergo resection of the cortical BOSD remain seizure-free.
Rachel had her first seizure at age 15. It lasted a few seconds and caused her to drop her ice cream. Her facial appearance was blank and she was pointing her right index finger, said Dr. Jackson. Her condition evolved into intractable tonic-clonic seizures at night, resulting in multiple medication use and side effects. After imaging revealed that Rachel—a left-dominant-language individual with aspirations to be a teacher—had a tiny abnormality at the base of the sulci, she underwent surgery.
“Before surgery, we could never convince our radiologist that this was abnormal,” said Dr. Jackson. “But because we believe these small BOSDs could cause this sort of epilepsy, we convinced our surgeon to take a tiny resection … that just took out [an] area of abnormal connectivity.”
The surgery was so precise that Rachel has been seizure-free for nearly three years, reported Dr. Jackson. “We did quite a remarkable job of taking out exactly that bit and only that bit within the middle of her language area,” he said. “When [Rachel] came out of the anesthetic, she was much more interactive, and [we] noticed the personality change.… She did not have that delay we often see in patients, even though she was on the same medications.”
“Really tiny bits of the brain can drive pretty nasty epilepsy,” said Dr. Jackson. Since Rachel’s procedure, she has graduated college and earned her first degree. “I published this [research] just to make the point that not all epilepsy [cases] are like this, but there are some, and we should try to find them.”
—Fred Balzac
Suggested Reading
Abou-Hamden A, Lau M, Fabinyi G, et al. Small temporal pole encephaloceles: a treatable cause of “lesion negative” temporal lobe epilepsy. Epilepsia. 2010;51(10):2199-2202.
Hofman PA, Fitt GJ, Harvey AS, et al. Bottom-of-sulcus dysplasia: imaging features. AJR Am J Roentgenol. 2011;196(4):881-885.
Jackson GD, Pedersen M, Harvey AS. How small can the epileptogenic region be?: a case in point. Neurology. 2017;88(21):2017-2019.
Jackson GD, Berkovic SF, Duncan JS, et al. Optimizing the diagnosis of hippocampal sclerosis using MR imaging. AJNR Am J Neuroradiol. 1993;14(3):753-762.
Jackson GD, Berkovic SF, Tress BM, et al. Hippocampal sclerosis can be reliably detected by magnetic resonance imaging. Neurology. 1990;40(12):1869-1875.
Pillay N, Fabinyi GC, Myles TS, et al. Parahippocampal epilepsy with subtle dysplasia: A cause of “imaging negative” partial epilepsy. Epilepsia. 2009;50(12):2611-2618.
WASHINGTON, DC—Neuroimaging is a core competency for epileptologists, according to an overview presented at the 71st Annual Meeting of the American Epilepsy Society. Neurologists trained in this subspecialty must bring “value-added” skills to the routine reports that radiologists provide—ensuring that both a proper diagnostic protocol and a quality-assurance mindset are in place so that when images are used, they are of sufficient quality to exclude wrong diagnoses.
Ultimately, it is the role of the epileptologist to review these images in the context of other localizing data and to work with radiologists in an integrative way, said Graeme Jackson, MD, Senior Deputy Director of the Florey Institute of Neuroscience and Mental Health in Melbourne.
“Finding a focal abnormality can truly change the path that patients move forward on, and it can change whether we have implantations, whether we have regional resections or focal resections…. It is critically important for good imaging to be a part of the path these patients travel on,” he said. Hippocampal sclerosis and bottom-of-sulcus dysplasia (BOSD) are entities that epileptologists “can’t miss,” he added.
What Is the Protocol?
In a presentation comprised largely of imaging studies in cases across the lifespan—infant, young child, teenager, adult, and senior citizen—Dr. Jackson discussed the diagnostic information essential for all patients with epilepsy: a clinical history for context, an EEG for function, and structural MRI with an epilepsy protocol for structure.
To map out the proper protocol, clinicians have to contend with many choices for MRI studies. Eventually, the process results in images. One pathway leads to a report from the radiologist, and another pathway leads to the epileptologist’s review.
Epileptologists are responsible for obtaining images that are adequate—not just taking what they get, said Dr. Jackson. “The radiologist is sitting there—[with] probably 2,000 images … a couple of minutes and a lot of cases.” As the “epileptologist, you have the advantage of having other information. You have the focus [and] the hypotheses.… It is critical that they be
Four “Can’t Miss” Imaging Diagnoses
The top four missed imaging diagnoses in epilepsy are obvious abnormalities, hippocampal sclerosis, malformations of cortical development, and a diagnosis of nothing, in which the clinician must be confident because the implicit observation is that the brain is completely structurally normal. Clinicians sometimes miss subtle things that can only be identified by looking correctly in the proper location, said Dr. Jackson.
In contrast to the four “can’t miss” diagnoses, focal cortical dysplasia, bilateral hippocampal sclerosis, temporal encephalocele, and parahippocampal dysplasia are among the many subtle lesions that clinicians can easily miss.
Examining a Case Study
Dr. Jackson assessed the case of Rachel, age 17, who has BOSD. This form of dysplasia encompasses localized seizures and can present at any time from infancy to adulthood. Although these entities are often intractable, 90% of patients who undergo resection of the cortical BOSD remain seizure-free.
Rachel had her first seizure at age 15. It lasted a few seconds and caused her to drop her ice cream. Her facial appearance was blank and she was pointing her right index finger, said Dr. Jackson. Her condition evolved into intractable tonic-clonic seizures at night, resulting in multiple medication use and side effects. After imaging revealed that Rachel—a left-dominant-language individual with aspirations to be a teacher—had a tiny abnormality at the base of the sulci, she underwent surgery.
“Before surgery, we could never convince our radiologist that this was abnormal,” said Dr. Jackson. “But because we believe these small BOSDs could cause this sort of epilepsy, we convinced our surgeon to take a tiny resection … that just took out [an] area of abnormal connectivity.”
The surgery was so precise that Rachel has been seizure-free for nearly three years, reported Dr. Jackson. “We did quite a remarkable job of taking out exactly that bit and only that bit within the middle of her language area,” he said. “When [Rachel] came out of the anesthetic, she was much more interactive, and [we] noticed the personality change.… She did not have that delay we often see in patients, even though she was on the same medications.”
“Really tiny bits of the brain can drive pretty nasty epilepsy,” said Dr. Jackson. Since Rachel’s procedure, she has graduated college and earned her first degree. “I published this [research] just to make the point that not all epilepsy [cases] are like this, but there are some, and we should try to find them.”
—Fred Balzac
Suggested Reading
Abou-Hamden A, Lau M, Fabinyi G, et al. Small temporal pole encephaloceles: a treatable cause of “lesion negative” temporal lobe epilepsy. Epilepsia. 2010;51(10):2199-2202.
Hofman PA, Fitt GJ, Harvey AS, et al. Bottom-of-sulcus dysplasia: imaging features. AJR Am J Roentgenol. 2011;196(4):881-885.
Jackson GD, Pedersen M, Harvey AS. How small can the epileptogenic region be?: a case in point. Neurology. 2017;88(21):2017-2019.
Jackson GD, Berkovic SF, Duncan JS, et al. Optimizing the diagnosis of hippocampal sclerosis using MR imaging. AJNR Am J Neuroradiol. 1993;14(3):753-762.
Jackson GD, Berkovic SF, Tress BM, et al. Hippocampal sclerosis can be reliably detected by magnetic resonance imaging. Neurology. 1990;40(12):1869-1875.
Pillay N, Fabinyi GC, Myles TS, et al. Parahippocampal epilepsy with subtle dysplasia: A cause of “imaging negative” partial epilepsy. Epilepsia. 2009;50(12):2611-2618.
WASHINGTON, DC—Neuroimaging is a core competency for epileptologists, according to an overview presented at the 71st Annual Meeting of the American Epilepsy Society. Neurologists trained in this subspecialty must bring “value-added” skills to the routine reports that radiologists provide—ensuring that both a proper diagnostic protocol and a quality-assurance mindset are in place so that when images are used, they are of sufficient quality to exclude wrong diagnoses.
Ultimately, it is the role of the epileptologist to review these images in the context of other localizing data and to work with radiologists in an integrative way, said Graeme Jackson, MD, Senior Deputy Director of the Florey Institute of Neuroscience and Mental Health in Melbourne.
“Finding a focal abnormality can truly change the path that patients move forward on, and it can change whether we have implantations, whether we have regional resections or focal resections…. It is critically important for good imaging to be a part of the path these patients travel on,” he said. Hippocampal sclerosis and bottom-of-sulcus dysplasia (BOSD) are entities that epileptologists “can’t miss,” he added.
What Is the Protocol?
In a presentation comprised largely of imaging studies in cases across the lifespan—infant, young child, teenager, adult, and senior citizen—Dr. Jackson discussed the diagnostic information essential for all patients with epilepsy: a clinical history for context, an EEG for function, and structural MRI with an epilepsy protocol for structure.
To map out the proper protocol, clinicians have to contend with many choices for MRI studies. Eventually, the process results in images. One pathway leads to a report from the radiologist, and another pathway leads to the epileptologist’s review.
Epileptologists are responsible for obtaining images that are adequate—not just taking what they get, said Dr. Jackson. “The radiologist is sitting there—[with] probably 2,000 images … a couple of minutes and a lot of cases.” As the “epileptologist, you have the advantage of having other information. You have the focus [and] the hypotheses.… It is critical that they be
Four “Can’t Miss” Imaging Diagnoses
The top four missed imaging diagnoses in epilepsy are obvious abnormalities, hippocampal sclerosis, malformations of cortical development, and a diagnosis of nothing, in which the clinician must be confident because the implicit observation is that the brain is completely structurally normal. Clinicians sometimes miss subtle things that can only be identified by looking correctly in the proper location, said Dr. Jackson.
In contrast to the four “can’t miss” diagnoses, focal cortical dysplasia, bilateral hippocampal sclerosis, temporal encephalocele, and parahippocampal dysplasia are among the many subtle lesions that clinicians can easily miss.
Examining a Case Study
Dr. Jackson assessed the case of Rachel, age 17, who has BOSD. This form of dysplasia encompasses localized seizures and can present at any time from infancy to adulthood. Although these entities are often intractable, 90% of patients who undergo resection of the cortical BOSD remain seizure-free.
Rachel had her first seizure at age 15. It lasted a few seconds and caused her to drop her ice cream. Her facial appearance was blank and she was pointing her right index finger, said Dr. Jackson. Her condition evolved into intractable tonic-clonic seizures at night, resulting in multiple medication use and side effects. After imaging revealed that Rachel—a left-dominant-language individual with aspirations to be a teacher—had a tiny abnormality at the base of the sulci, she underwent surgery.
“Before surgery, we could never convince our radiologist that this was abnormal,” said Dr. Jackson. “But because we believe these small BOSDs could cause this sort of epilepsy, we convinced our surgeon to take a tiny resection … that just took out [an] area of abnormal connectivity.”
The surgery was so precise that Rachel has been seizure-free for nearly three years, reported Dr. Jackson. “We did quite a remarkable job of taking out exactly that bit and only that bit within the middle of her language area,” he said. “When [Rachel] came out of the anesthetic, she was much more interactive, and [we] noticed the personality change.… She did not have that delay we often see in patients, even though she was on the same medications.”
“Really tiny bits of the brain can drive pretty nasty epilepsy,” said Dr. Jackson. Since Rachel’s procedure, she has graduated college and earned her first degree. “I published this [research] just to make the point that not all epilepsy [cases] are like this, but there are some, and we should try to find them.”
—Fred Balzac
Suggested Reading
Abou-Hamden A, Lau M, Fabinyi G, et al. Small temporal pole encephaloceles: a treatable cause of “lesion negative” temporal lobe epilepsy. Epilepsia. 2010;51(10):2199-2202.
Hofman PA, Fitt GJ, Harvey AS, et al. Bottom-of-sulcus dysplasia: imaging features. AJR Am J Roentgenol. 2011;196(4):881-885.
Jackson GD, Pedersen M, Harvey AS. How small can the epileptogenic region be?: a case in point. Neurology. 2017;88(21):2017-2019.
Jackson GD, Berkovic SF, Duncan JS, et al. Optimizing the diagnosis of hippocampal sclerosis using MR imaging. AJNR Am J Neuroradiol. 1993;14(3):753-762.
Jackson GD, Berkovic SF, Tress BM, et al. Hippocampal sclerosis can be reliably detected by magnetic resonance imaging. Neurology. 1990;40(12):1869-1875.
Pillay N, Fabinyi GC, Myles TS, et al. Parahippocampal epilepsy with subtle dysplasia: A cause of “imaging negative” partial epilepsy. Epilepsia. 2009;50(12):2611-2618.
MRI May Reveal PML in Patients With Undetectable JCV
Patients with multiple sclerosis (MS) who are treated with natalizumab can have small progressive multifocal leukoencephalopathy (PML) lesions on MRI, yet have undetectable JC virus (JCV) DNA in their CSF, according to a cross-sectional, retrospective study published online ahead of print March 12 in JAMA Neurology.
The findings show that for some people with MS, PML diagnosis could be delayed if CSF sampling is negative and patients are asymptomatic, potentially resulting in worse functional outcomes and survival rates, according to Martijn T. Wijburg, MD, a neurologist at the MS Center at VU University Medical Center in Amsterdam, and colleagues.
The study also described a potential correlation between PML lesion volume and JCV copy numbers. “To our knowledge, this is the first study that shows an association between total PML lesion volume measured by brain MRI and CSF JCV polymerase chain reaction [PCR] results in patients with [natalizumab-associated PML]. This finding may have considerable implications for patient care,” said the authors.
A Retrospective Study
PML, a lytic infection of glial and neuronal cells by the JCV, can be diagnosed when a patient exhibits clinical symptoms, when JCV DNA is detected in CSF by PCR, and when specific brain lesions are seen on MRI, according to a consensus statement from the Neuroinfectious Disease section of the American Academy of Neurology.
Dr. Wijburg and his coinvestigators reviewed data from Dutch and Belgian patients considered to have natalizumab-associated PML between January 2007 and December 2014. Patients were required to meet one of the following criteria:
- Definite or probable PML, based on positive PCR and MRI findings suggestive of PML, with or without PML symptoms.
- In the absence of a positive PCR, the presence of all four of the following features: high risk of PML development, such as positive anti-JCV serostatus and natalizumab treatment duration greater than 12 months; no MS disease activity prior to PML suspicion; MRI lesions highly suggestive of PML, with lesion characteristics as previously reported and absence of lesion characteristics suggestive of other diseases, as judged by an experienced neuroradiologist; and a lesion evolution on follow-up MRI scans suggestive of PML, including development of immune reconstitution inflammatory syndrome.
In the study of 56 patients (37 women), nine patients (16.1%) had undetectable JCV DNA in CSF, and 14 (25%) were asymptomatic for PML. At the time of PML diagnosis, the median age was 45, and the median natalizumab treatment duration was 43 months. Patients with a positive PCR had larger total PML lesion volumes than did those with undetectable JCV DNA (median volume, 22.9 mL vs 6.7 mL). Logistic regression showed that a smaller PML lesion volume significantly increased the probability for undetectable JCV DNA.
The research team also observed a positive correlation between PML lesion volume and JCV copy numbers. PML lesion volume was greater in patients with PML symptoms and in patients with more widespread lesion dissemination. But no association was found between PCR results and PML lesion dissemination, signs of inflammation, or PML symptoms.
Results Suggest Need for Pharmacovigilance
The findings suggest that patients with a smaller PML lesion volume were more likely to have a negative test result for JCV, which may lead to a delayed diagnosis of PML. Patients with smaller lesion volume were also more likely to be asymptomatic, which may further delay diagnosis.
“This [finding] can result in a therapeutic dilemma. Unjustly excluding PML may have serious consequences (eg, when switching from [natalizumab] to even more potent immunosuppressive treatments, such as alemtuzumab),” said the authors.
“In patients with [natalizumab-associated PML], both the probability for a positive CSF JCV PCR result and the JCV viral load are associated with the total PML lesion volume.... As a consequence, patients with smaller PML lesion volumes are more likely to have undetectable JCV DNA, and PML can thus not reliably be excluded based on a negative PCR.”
Strict pharmacovigilance by MRI “will lead to identification of smaller [PML] lesions that associate with a higher likelihood of negative PCR results, which hampers a formal diagnosis of [PML] and may complicate patient treatment,” said the authors.
Meticulous clinical and MRI follow-up, in combination with repeated CSF JCV PCR testing, was warranted in these patients, they added. Complementary PML diagnostic approaches, such as assessing intrathecal antibody synthesis to JCV by determining the CSF JCV antibody index, may also be of additional value.
“Furthermore, undetectable JCV DNA does not completely preclude the presence of JCV DNA. Further development and improvement of ultrasensitive PCR assays may improve the diagnostic accuracy in the future.”
MRI Alone Cannot Yet Support Diagnosis
“Dr. Wijburg and colleagues raise an important point in our understanding of the development of PML by showing that small brain lesions may be present at what may be the start of JCV infection when the virus is still undetectable in CSF,” said Eugene O. Major, PhD, a consultant in the Division of Neuroimmunology and Neurovirology at NINDS in Bethesda, Maryland, in an accompanying editorial. “However, it is not yet clear how well the relationship between viral load in CSF and MRI brain lesions approximates the stages of the disease and the processes with which it affects its target brain cells.”
Repeat testing may be worthwhile when CSF testing is negative, because some patients test positive weeks after testing negative, he added. “Suspicion for PML may be increased when MRI shows signs of PML despite negative CSF testing, but it is too early to rely on MRI alone for diagnosis.”
Dr. Major has received consulting fees while serving on independent adjudication committees for Takeda/Millennium, Roche/Genentech, and GlaxoSmithKline.He has patent rights at the NIH as coinventor of the Ultrasensitive Quantitative PCR Multiplex assay for the detection of JCV DNA–distinguishing viral variants.
—Nicola Garrett
Suggested Reading
Major EO. Progressive multifocal leukoencephalopathy lesions and JC virus: the limits and value of imaging. JAMA Neurol. 2018 Mar 12 [Epub ahead of print].
Wijburg MT, Kleerekooper I, Lissenberg-Witte BI, et al. Association of progressive multifocal leukoencephalopathy lesion volume with JC virus polymerase chain reaction results in cerebrospinal fluid of natalizumab-treated patients with multiple sclerosis. JAMA Neurol. 2018 Mar 12 [Epub ahead of print].
Patients with multiple sclerosis (MS) who are treated with natalizumab can have small progressive multifocal leukoencephalopathy (PML) lesions on MRI, yet have undetectable JC virus (JCV) DNA in their CSF, according to a cross-sectional, retrospective study published online ahead of print March 12 in JAMA Neurology.
The findings show that for some people with MS, PML diagnosis could be delayed if CSF sampling is negative and patients are asymptomatic, potentially resulting in worse functional outcomes and survival rates, according to Martijn T. Wijburg, MD, a neurologist at the MS Center at VU University Medical Center in Amsterdam, and colleagues.
The study also described a potential correlation between PML lesion volume and JCV copy numbers. “To our knowledge, this is the first study that shows an association between total PML lesion volume measured by brain MRI and CSF JCV polymerase chain reaction [PCR] results in patients with [natalizumab-associated PML]. This finding may have considerable implications for patient care,” said the authors.
A Retrospective Study
PML, a lytic infection of glial and neuronal cells by the JCV, can be diagnosed when a patient exhibits clinical symptoms, when JCV DNA is detected in CSF by PCR, and when specific brain lesions are seen on MRI, according to a consensus statement from the Neuroinfectious Disease section of the American Academy of Neurology.
Dr. Wijburg and his coinvestigators reviewed data from Dutch and Belgian patients considered to have natalizumab-associated PML between January 2007 and December 2014. Patients were required to meet one of the following criteria:
- Definite or probable PML, based on positive PCR and MRI findings suggestive of PML, with or without PML symptoms.
- In the absence of a positive PCR, the presence of all four of the following features: high risk of PML development, such as positive anti-JCV serostatus and natalizumab treatment duration greater than 12 months; no MS disease activity prior to PML suspicion; MRI lesions highly suggestive of PML, with lesion characteristics as previously reported and absence of lesion characteristics suggestive of other diseases, as judged by an experienced neuroradiologist; and a lesion evolution on follow-up MRI scans suggestive of PML, including development of immune reconstitution inflammatory syndrome.
In the study of 56 patients (37 women), nine patients (16.1%) had undetectable JCV DNA in CSF, and 14 (25%) were asymptomatic for PML. At the time of PML diagnosis, the median age was 45, and the median natalizumab treatment duration was 43 months. Patients with a positive PCR had larger total PML lesion volumes than did those with undetectable JCV DNA (median volume, 22.9 mL vs 6.7 mL). Logistic regression showed that a smaller PML lesion volume significantly increased the probability for undetectable JCV DNA.
The research team also observed a positive correlation between PML lesion volume and JCV copy numbers. PML lesion volume was greater in patients with PML symptoms and in patients with more widespread lesion dissemination. But no association was found between PCR results and PML lesion dissemination, signs of inflammation, or PML symptoms.
Results Suggest Need for Pharmacovigilance
The findings suggest that patients with a smaller PML lesion volume were more likely to have a negative test result for JCV, which may lead to a delayed diagnosis of PML. Patients with smaller lesion volume were also more likely to be asymptomatic, which may further delay diagnosis.
“This [finding] can result in a therapeutic dilemma. Unjustly excluding PML may have serious consequences (eg, when switching from [natalizumab] to even more potent immunosuppressive treatments, such as alemtuzumab),” said the authors.
“In patients with [natalizumab-associated PML], both the probability for a positive CSF JCV PCR result and the JCV viral load are associated with the total PML lesion volume.... As a consequence, patients with smaller PML lesion volumes are more likely to have undetectable JCV DNA, and PML can thus not reliably be excluded based on a negative PCR.”
Strict pharmacovigilance by MRI “will lead to identification of smaller [PML] lesions that associate with a higher likelihood of negative PCR results, which hampers a formal diagnosis of [PML] and may complicate patient treatment,” said the authors.
Meticulous clinical and MRI follow-up, in combination with repeated CSF JCV PCR testing, was warranted in these patients, they added. Complementary PML diagnostic approaches, such as assessing intrathecal antibody synthesis to JCV by determining the CSF JCV antibody index, may also be of additional value.
“Furthermore, undetectable JCV DNA does not completely preclude the presence of JCV DNA. Further development and improvement of ultrasensitive PCR assays may improve the diagnostic accuracy in the future.”
MRI Alone Cannot Yet Support Diagnosis
“Dr. Wijburg and colleagues raise an important point in our understanding of the development of PML by showing that small brain lesions may be present at what may be the start of JCV infection when the virus is still undetectable in CSF,” said Eugene O. Major, PhD, a consultant in the Division of Neuroimmunology and Neurovirology at NINDS in Bethesda, Maryland, in an accompanying editorial. “However, it is not yet clear how well the relationship between viral load in CSF and MRI brain lesions approximates the stages of the disease and the processes with which it affects its target brain cells.”
Repeat testing may be worthwhile when CSF testing is negative, because some patients test positive weeks after testing negative, he added. “Suspicion for PML may be increased when MRI shows signs of PML despite negative CSF testing, but it is too early to rely on MRI alone for diagnosis.”
Dr. Major has received consulting fees while serving on independent adjudication committees for Takeda/Millennium, Roche/Genentech, and GlaxoSmithKline.He has patent rights at the NIH as coinventor of the Ultrasensitive Quantitative PCR Multiplex assay for the detection of JCV DNA–distinguishing viral variants.
—Nicola Garrett
Suggested Reading
Major EO. Progressive multifocal leukoencephalopathy lesions and JC virus: the limits and value of imaging. JAMA Neurol. 2018 Mar 12 [Epub ahead of print].
Wijburg MT, Kleerekooper I, Lissenberg-Witte BI, et al. Association of progressive multifocal leukoencephalopathy lesion volume with JC virus polymerase chain reaction results in cerebrospinal fluid of natalizumab-treated patients with multiple sclerosis. JAMA Neurol. 2018 Mar 12 [Epub ahead of print].
Patients with multiple sclerosis (MS) who are treated with natalizumab can have small progressive multifocal leukoencephalopathy (PML) lesions on MRI, yet have undetectable JC virus (JCV) DNA in their CSF, according to a cross-sectional, retrospective study published online ahead of print March 12 in JAMA Neurology.
The findings show that for some people with MS, PML diagnosis could be delayed if CSF sampling is negative and patients are asymptomatic, potentially resulting in worse functional outcomes and survival rates, according to Martijn T. Wijburg, MD, a neurologist at the MS Center at VU University Medical Center in Amsterdam, and colleagues.
The study also described a potential correlation between PML lesion volume and JCV copy numbers. “To our knowledge, this is the first study that shows an association between total PML lesion volume measured by brain MRI and CSF JCV polymerase chain reaction [PCR] results in patients with [natalizumab-associated PML]. This finding may have considerable implications for patient care,” said the authors.
A Retrospective Study
PML, a lytic infection of glial and neuronal cells by the JCV, can be diagnosed when a patient exhibits clinical symptoms, when JCV DNA is detected in CSF by PCR, and when specific brain lesions are seen on MRI, according to a consensus statement from the Neuroinfectious Disease section of the American Academy of Neurology.
Dr. Wijburg and his coinvestigators reviewed data from Dutch and Belgian patients considered to have natalizumab-associated PML between January 2007 and December 2014. Patients were required to meet one of the following criteria:
- Definite or probable PML, based on positive PCR and MRI findings suggestive of PML, with or without PML symptoms.
- In the absence of a positive PCR, the presence of all four of the following features: high risk of PML development, such as positive anti-JCV serostatus and natalizumab treatment duration greater than 12 months; no MS disease activity prior to PML suspicion; MRI lesions highly suggestive of PML, with lesion characteristics as previously reported and absence of lesion characteristics suggestive of other diseases, as judged by an experienced neuroradiologist; and a lesion evolution on follow-up MRI scans suggestive of PML, including development of immune reconstitution inflammatory syndrome.
In the study of 56 patients (37 women), nine patients (16.1%) had undetectable JCV DNA in CSF, and 14 (25%) were asymptomatic for PML. At the time of PML diagnosis, the median age was 45, and the median natalizumab treatment duration was 43 months. Patients with a positive PCR had larger total PML lesion volumes than did those with undetectable JCV DNA (median volume, 22.9 mL vs 6.7 mL). Logistic regression showed that a smaller PML lesion volume significantly increased the probability for undetectable JCV DNA.
The research team also observed a positive correlation between PML lesion volume and JCV copy numbers. PML lesion volume was greater in patients with PML symptoms and in patients with more widespread lesion dissemination. But no association was found between PCR results and PML lesion dissemination, signs of inflammation, or PML symptoms.
Results Suggest Need for Pharmacovigilance
The findings suggest that patients with a smaller PML lesion volume were more likely to have a negative test result for JCV, which may lead to a delayed diagnosis of PML. Patients with smaller lesion volume were also more likely to be asymptomatic, which may further delay diagnosis.
“This [finding] can result in a therapeutic dilemma. Unjustly excluding PML may have serious consequences (eg, when switching from [natalizumab] to even more potent immunosuppressive treatments, such as alemtuzumab),” said the authors.
“In patients with [natalizumab-associated PML], both the probability for a positive CSF JCV PCR result and the JCV viral load are associated with the total PML lesion volume.... As a consequence, patients with smaller PML lesion volumes are more likely to have undetectable JCV DNA, and PML can thus not reliably be excluded based on a negative PCR.”
Strict pharmacovigilance by MRI “will lead to identification of smaller [PML] lesions that associate with a higher likelihood of negative PCR results, which hampers a formal diagnosis of [PML] and may complicate patient treatment,” said the authors.
Meticulous clinical and MRI follow-up, in combination with repeated CSF JCV PCR testing, was warranted in these patients, they added. Complementary PML diagnostic approaches, such as assessing intrathecal antibody synthesis to JCV by determining the CSF JCV antibody index, may also be of additional value.
“Furthermore, undetectable JCV DNA does not completely preclude the presence of JCV DNA. Further development and improvement of ultrasensitive PCR assays may improve the diagnostic accuracy in the future.”
MRI Alone Cannot Yet Support Diagnosis
“Dr. Wijburg and colleagues raise an important point in our understanding of the development of PML by showing that small brain lesions may be present at what may be the start of JCV infection when the virus is still undetectable in CSF,” said Eugene O. Major, PhD, a consultant in the Division of Neuroimmunology and Neurovirology at NINDS in Bethesda, Maryland, in an accompanying editorial. “However, it is not yet clear how well the relationship between viral load in CSF and MRI brain lesions approximates the stages of the disease and the processes with which it affects its target brain cells.”
Repeat testing may be worthwhile when CSF testing is negative, because some patients test positive weeks after testing negative, he added. “Suspicion for PML may be increased when MRI shows signs of PML despite negative CSF testing, but it is too early to rely on MRI alone for diagnosis.”
Dr. Major has received consulting fees while serving on independent adjudication committees for Takeda/Millennium, Roche/Genentech, and GlaxoSmithKline.He has patent rights at the NIH as coinventor of the Ultrasensitive Quantitative PCR Multiplex assay for the detection of JCV DNA–distinguishing viral variants.
—Nicola Garrett
Suggested Reading
Major EO. Progressive multifocal leukoencephalopathy lesions and JC virus: the limits and value of imaging. JAMA Neurol. 2018 Mar 12 [Epub ahead of print].
Wijburg MT, Kleerekooper I, Lissenberg-Witte BI, et al. Association of progressive multifocal leukoencephalopathy lesion volume with JC virus polymerase chain reaction results in cerebrospinal fluid of natalizumab-treated patients with multiple sclerosis. JAMA Neurol. 2018 Mar 12 [Epub ahead of print].
Sonified EEG Could Be Useful Triage Tool
Medical students and nurses who listen to 15 seconds of single-channel sonified EEGs may detect seizures with 95% to 98% sensitivity, thus outperforming neurologists who review traditional visual EEG displays, according to the results of a single-center study published in the April issue of Epilepsia.
“Individuals without EEG training can detect ongoing seizures or seizurelike rhythmic and periodic patterns by merely listening to short clips of sonified EEG,” said Josef Parvizi, MD, PhD, Professor of Neurology at Stanford University Medical Center in California, and his associates. “Ours is also the first study to test the capability of a sonification method to detect a range of significant abnormalities when it is used by clinical staff (eg, physicians, nurses, and students).” 
The sonification technique is based on an algorithm that translates low-frequency EEG signals into “speechlike declamations,” the investigators said. Vocal pitch, loudness, and resonance vary depending on input. Unlike prior sonification methods, the new method conserves brain rhythms, rate, and seizure severity.
To test the method, 34 medical students and 30 nurses watched a four-minute training video before listening to 84 sonified EEGs, including seven seizures, 52 slowing or normal patterns, and 25 seizurelike abnormalities (ie, generalized periodic discharges, lateralized periodic discharges, triphasic waves, or burst suppression). For each patient, listeners heard two sonified EEG clips, one from each hemisphere, and designated them as “seizure,” “nonseizure,” or “don’t know.” For comparison, 12 EEG-trained neurologists and 29 EEG-trained medical students reviewed traditional visual displays of the same EEGs.
Using sonified EEGs, nurses identified seizures with a sensitivity of 95%, and medical students identified seizures with a sensitivity of 98%. In contrast, the sensitivity of visual displays was 88% when reviewed by neurologists and 76% when reviewed by EEG-trained medical students. Specificity of sonified EEGs was 85% when heard by the medical students and 82% when heard by the nurses. Specificity of traditional review was 90% for neurologists and 65% for medical students.
The study was based on a representative sample, not a prospectively and consecutively recruited cohort, which limits conclusions about how this technique might perform at the bedside, said the researchers. In addition, the sonification method would not identify focal seizures occurring outside the individual channels selected.
The study was funded by a Stanford University BioX Seed Grant. Dr. Parvizi and one coinvestigator invented the sonification method and cofounded a startup that has licensed the technology from Stanford University. The other two investigators had no conflicts of interest.
—Amy Karon
Suggested Reading
Parvizi J, Gururangan
Medical students and nurses who listen to 15 seconds of single-channel sonified EEGs may detect seizures with 95% to 98% sensitivity, thus outperforming neurologists who review traditional visual EEG displays, according to the results of a single-center study published in the April issue of Epilepsia.
“Individuals without EEG training can detect ongoing seizures or seizurelike rhythmic and periodic patterns by merely listening to short clips of sonified EEG,” said Josef Parvizi, MD, PhD, Professor of Neurology at Stanford University Medical Center in California, and his associates. “Ours is also the first study to test the capability of a sonification method to detect a range of significant abnormalities when it is used by clinical staff (eg, physicians, nurses, and students).”
The sonification technique is based on an algorithm that translates low-frequency EEG signals into “speechlike declamations,” the investigators said. Vocal pitch, loudness, and resonance vary depending on input. Unlike prior sonification methods, the new method conserves brain rhythms, rate, and seizure severity.
To test the method, 34 medical students and 30 nurses watched a four-minute training video before listening to 84 sonified EEGs, including seven seizures, 52 slowing or normal patterns, and 25 seizurelike abnormalities (ie, generalized periodic discharges, lateralized periodic discharges, triphasic waves, or burst suppression). For each patient, listeners heard two sonified EEG clips, one from each hemisphere, and designated them as “seizure,” “nonseizure,” or “don’t know.” For comparison, 12 EEG-trained neurologists and 29 EEG-trained medical students reviewed traditional visual displays of the same EEGs.
Using sonified EEGs, nurses identified seizures with a sensitivity of 95%, and medical students identified seizures with a sensitivity of 98%. In contrast, the sensitivity of visual displays was 88% when reviewed by neurologists and 76% when reviewed by EEG-trained medical students. Specificity of sonified EEGs was 85% when heard by the medical students and 82% when heard by the nurses. Specificity of traditional review was 90% for neurologists and 65% for medical students.
The study was based on a representative sample, not a prospectively and consecutively recruited cohort, which limits conclusions about how this technique might perform at the bedside, said the researchers. In addition, the sonification method would not identify focal seizures occurring outside the individual channels selected.
The study was funded by a Stanford University BioX Seed Grant. Dr. Parvizi and one coinvestigator invented the sonification method and cofounded a startup that has licensed the technology from Stanford University. The other two investigators had no conflicts of interest.
—Amy Karon
Suggested Reading
Parvizi J, Gururangan
Medical students and nurses who listen to 15 seconds of single-channel sonified EEGs may detect seizures with 95% to 98% sensitivity, thus outperforming neurologists who review traditional visual EEG displays, according to the results of a single-center study published in the April issue of Epilepsia.
“Individuals without EEG training can detect ongoing seizures or seizurelike rhythmic and periodic patterns by merely listening to short clips of sonified EEG,” said Josef Parvizi, MD, PhD, Professor of Neurology at Stanford University Medical Center in California, and his associates. “Ours is also the first study to test the capability of a sonification method to detect a range of significant abnormalities when it is used by clinical staff (eg, physicians, nurses, and students).”
The sonification technique is based on an algorithm that translates low-frequency EEG signals into “speechlike declamations,” the investigators said. Vocal pitch, loudness, and resonance vary depending on input. Unlike prior sonification methods, the new method conserves brain rhythms, rate, and seizure severity.
To test the method, 34 medical students and 30 nurses watched a four-minute training video before listening to 84 sonified EEGs, including seven seizures, 52 slowing or normal patterns, and 25 seizurelike abnormalities (ie, generalized periodic discharges, lateralized periodic discharges, triphasic waves, or burst suppression). For each patient, listeners heard two sonified EEG clips, one from each hemisphere, and designated them as “seizure,” “nonseizure,” or “don’t know.” For comparison, 12 EEG-trained neurologists and 29 EEG-trained medical students reviewed traditional visual displays of the same EEGs.
Using sonified EEGs, nurses identified seizures with a sensitivity of 95%, and medical students identified seizures with a sensitivity of 98%. In contrast, the sensitivity of visual displays was 88% when reviewed by neurologists and 76% when reviewed by EEG-trained medical students. Specificity of sonified EEGs was 85% when heard by the medical students and 82% when heard by the nurses. Specificity of traditional review was 90% for neurologists and 65% for medical students.
The study was based on a representative sample, not a prospectively and consecutively recruited cohort, which limits conclusions about how this technique might perform at the bedside, said the researchers. In addition, the sonification method would not identify focal seizures occurring outside the individual channels selected.
The study was funded by a Stanford University BioX Seed Grant. Dr. Parvizi and one coinvestigator invented the sonification method and cofounded a startup that has licensed the technology from Stanford University. The other two investigators had no conflicts of interest.
—Amy Karon
Suggested Reading
Parvizi J, Gururangan
Highlights from the 2018 Society of Gynecologic Surgeons Scientific Meeting
PART 1

- Leading best gynecologic surgical care into the next decade
- Optimal surgical management of stage 3 and 4 pelvic organ prolapse
- Patient experience: It’s not about satisfaction
Andrew P. Cassidenti, MD
Chief, Female Pelvic Medicine and Reconstructive Surgery
Kern Medical,
Bakersfield, California
Amanda White, MD
Assistant Professor, Department of Women’s Health
Female Pelvic Medicine and Reconstructive Surgery
Dell Medical School, University of Texas
Austin, Texas
Vivian Aguilar, MD
Assistant Professor, Obstetrics and Gynecology
Female Pelvic Medicine and Reconstructive Surgery
Dell Medical School, University of Texas
Austin, Texas
Rebecca G. Rogers, MD
Professor, Department of Women’s Health
Female Pelvic Medicine and Reconstructive Surgery
Associate Chair, Clinical Integration and Operations
Dell Medical School, University of Texas
Austin, Texas
Patrick Culligan, MD
Director, Urogynecology and The Center for Female Pelvic Health
Department of Urology
Weill Cornell Medical College, New York Presbyterian/Weill Cornell Medical Center
New York, New York
Sarah Huber, MD
Fellow, Female Pelvic Medicine and Reconstructive Surgery
Department of Urology
Weill Cornell Medical College, New York Presbyterian/Weill Cornell Medical Center
New York, New York
Vincent R. Lucente, MD, MBA
Chief, Gynecology, St. Luke’s University Health Network
Medical Director, The Institute for Female Pelvic Medicine and Reconstructive Surgery
Allentown, Pennsylvania
Jessica B. Ton, MD
AAGL Fellow, Minimally Invasive Gynecologic Surgery
St. Luke’s University Health Network
Bethlehem, Pennsylvania
James I. Merlino, MD
President and Chief Medical Officer of Advisory and Strategic Consulting
Press Ganey Associates
Cleveland, Ohio
Amy A. Merlino, MD
Maternal Fetal Medicine Specialist
Department of Obstetrics and Gynecology
Enterprise Chief Informatics Officer
Cleveland Clinic, Cleveland, Ohio
PART 2

- Deep infiltrating endometriosis: Evaluation and management
- What’s new in simulation training for hysterectomy
Rosanne M. Kho, MD
Head, Section of Benign Gynecology
Women’s Health Institute
Department of Obstetrics and Gynecology
Cleveland Clinic
Cleveland, Ohio
Mauricio S. Abrão, MD
Associate Professor and
Director, Endometriosis Division
Department of Obstetrics and Gynecology
São Paulo University Medical School
São Paulo, Brazil
Alicia Scribner, MD, MPH
Director, Ob/Gyn Simulation Curriculum
Madigan Army Medical Center
Tacoma, Washington
Clinical Instructor
Department of Obstetrics and Gynecology
University of Washington, Seattle
Christine Vaccaro, DO
Medical Director, Andersen Simulation Center
Madigan Army Medical Center
Tacoma, Washington
Clinical Assistant Professor
Department of Obstetrics and Gynecology
University of Washington, Seattle
Uniformed Services University of Health Sciences
Bethesda, Maryland
PART 1
- Leading best gynecologic surgical care into the next decade
- Optimal surgical management of stage 3 and 4 pelvic organ prolapse
- Patient experience: It’s not about satisfaction
Andrew P. Cassidenti, MD
Chief, Female Pelvic Medicine and Reconstructive Surgery
Kern Medical,
Bakersfield, California
Amanda White, MD
Assistant Professor, Department of Women’s Health
Female Pelvic Medicine and Reconstructive Surgery
Dell Medical School, University of Texas
Austin, Texas
Vivian Aguilar, MD
Assistant Professor, Obstetrics and Gynecology
Female Pelvic Medicine and Reconstructive Surgery
Dell Medical School, University of Texas
Austin, Texas
Rebecca G. Rogers, MD
Professor, Department of Women’s Health
Female Pelvic Medicine and Reconstructive Surgery
Associate Chair, Clinical Integration and Operations
Dell Medical School, University of Texas
Austin, Texas
Patrick Culligan, MD
Director, Urogynecology and The Center for Female Pelvic Health
Department of Urology
Weill Cornell Medical College, New York Presbyterian/Weill Cornell Medical Center
New York, New York
Sarah Huber, MD
Fellow, Female Pelvic Medicine and Reconstructive Surgery
Department of Urology
Weill Cornell Medical College, New York Presbyterian/Weill Cornell Medical Center
New York, New York
Vincent R. Lucente, MD, MBA
Chief, Gynecology, St. Luke’s University Health Network
Medical Director, The Institute for Female Pelvic Medicine and Reconstructive Surgery
Allentown, Pennsylvania
Jessica B. Ton, MD
AAGL Fellow, Minimally Invasive Gynecologic Surgery
St. Luke’s University Health Network
Bethlehem, Pennsylvania
James I. Merlino, MD
President and Chief Medical Officer of Advisory and Strategic Consulting
Press Ganey Associates
Cleveland, Ohio
Amy A. Merlino, MD
Maternal Fetal Medicine Specialist
Department of Obstetrics and Gynecology
Enterprise Chief Informatics Officer
Cleveland Clinic, Cleveland, Ohio
PART 2
- Deep infiltrating endometriosis: Evaluation and management
- What’s new in simulation training for hysterectomy
Rosanne M. Kho, MD
Head, Section of Benign Gynecology
Women’s Health Institute
Department of Obstetrics and Gynecology
Cleveland Clinic
Cleveland, Ohio
Mauricio S. Abrão, MD
Associate Professor and
Director, Endometriosis Division
Department of Obstetrics and Gynecology
São Paulo University Medical School
São Paulo, Brazil
Alicia Scribner, MD, MPH
Director, Ob/Gyn Simulation Curriculum
Madigan Army Medical Center
Tacoma, Washington
Clinical Instructor
Department of Obstetrics and Gynecology
University of Washington, Seattle
Christine Vaccaro, DO
Medical Director, Andersen Simulation Center
Madigan Army Medical Center
Tacoma, Washington
Clinical Assistant Professor
Department of Obstetrics and Gynecology
University of Washington, Seattle
Uniformed Services University of Health Sciences
Bethesda, Maryland
PART 1
- Leading best gynecologic surgical care into the next decade
- Optimal surgical management of stage 3 and 4 pelvic organ prolapse
- Patient experience: It’s not about satisfaction
Andrew P. Cassidenti, MD
Chief, Female Pelvic Medicine and Reconstructive Surgery
Kern Medical,
Bakersfield, California
Amanda White, MD
Assistant Professor, Department of Women’s Health
Female Pelvic Medicine and Reconstructive Surgery
Dell Medical School, University of Texas
Austin, Texas
Vivian Aguilar, MD
Assistant Professor, Obstetrics and Gynecology
Female Pelvic Medicine and Reconstructive Surgery
Dell Medical School, University of Texas
Austin, Texas
Rebecca G. Rogers, MD
Professor, Department of Women’s Health
Female Pelvic Medicine and Reconstructive Surgery
Associate Chair, Clinical Integration and Operations
Dell Medical School, University of Texas
Austin, Texas
Patrick Culligan, MD
Director, Urogynecology and The Center for Female Pelvic Health
Department of Urology
Weill Cornell Medical College, New York Presbyterian/Weill Cornell Medical Center
New York, New York
Sarah Huber, MD
Fellow, Female Pelvic Medicine and Reconstructive Surgery
Department of Urology
Weill Cornell Medical College, New York Presbyterian/Weill Cornell Medical Center
New York, New York
Vincent R. Lucente, MD, MBA
Chief, Gynecology, St. Luke’s University Health Network
Medical Director, The Institute for Female Pelvic Medicine and Reconstructive Surgery
Allentown, Pennsylvania
Jessica B. Ton, MD
AAGL Fellow, Minimally Invasive Gynecologic Surgery
St. Luke’s University Health Network
Bethlehem, Pennsylvania
James I. Merlino, MD
President and Chief Medical Officer of Advisory and Strategic Consulting
Press Ganey Associates
Cleveland, Ohio
Amy A. Merlino, MD
Maternal Fetal Medicine Specialist
Department of Obstetrics and Gynecology
Enterprise Chief Informatics Officer
Cleveland Clinic, Cleveland, Ohio
PART 2
- Deep infiltrating endometriosis: Evaluation and management
- What’s new in simulation training for hysterectomy
Rosanne M. Kho, MD
Head, Section of Benign Gynecology
Women’s Health Institute
Department of Obstetrics and Gynecology
Cleveland Clinic
Cleveland, Ohio
Mauricio S. Abrão, MD
Associate Professor and
Director, Endometriosis Division
Department of Obstetrics and Gynecology
São Paulo University Medical School
São Paulo, Brazil
Alicia Scribner, MD, MPH
Director, Ob/Gyn Simulation Curriculum
Madigan Army Medical Center
Tacoma, Washington
Clinical Instructor
Department of Obstetrics and Gynecology
University of Washington, Seattle
Christine Vaccaro, DO
Medical Director, Andersen Simulation Center
Madigan Army Medical Center
Tacoma, Washington
Clinical Assistant Professor
Department of Obstetrics and Gynecology
University of Washington, Seattle
Uniformed Services University of Health Sciences
Bethesda, Maryland

What’s new in simulation training for hysterectomy
Due to an increase in minimally invasive approaches to hysterectomy, including vaginal and laparoscopic approaches, gynecologic surgeons may need to turn to simulation training to augment practice and hone skills. Simulation is useful for all surgeons, especially for low-volume surgeons, as a warm-up to sharpen technical skills prior to starting the day’s cases. Additionally, educators are uniquely poised to use simulation to teach residents and to evaluate their procedural competency.
In this article, we provide an overview of the 3 approaches to hysterectomy—vaginal, laparoscopic, abdominal—through medical modeling and simulation techniques. We focus on practical issues, including current resources available online, cost, setup time, fidelity, and limitations of some commonly available vaginal, laparoscopic, and open hysterectomy models.
Simulation directly influences patient safety. Thus, the value of simulation cannot be overstated, as it can increase the quality of health care by improving patient outcomes and lowering overall costs. In 2008, the American College of Obstetricians and Gynecologists (ACOG) founded the Simulations Working Group to establish simulation as a pillar in education for women’s health through collaboration, advocacy, research, and the development and implementation of multidisciplinary simulations-based educational resources and opportunities.
Refer to the ACOG Simulations Working Group Toolkit online to see the objectives, simulation, and videos related to each module. Under the “Hysterectomy” section, you will find how to construct the “flower pot” model for abdominal and vaginal hysterectomy, as well as the AAGL vaginal and laparoscopic hysterectomy webinars. All content is reaffirmed frequently to keep it up to date. You can access the toolkit, with your ACOG login and passcode, at https://www.acog.org/About-ACOG/ACOG-Departments/Simulations-Consortium/Simulations-Consortium-Tool-Kit.
For a comprehensive gynecology curriculum to include vaginal, laparoscopic, and abdominal approaches to hysterectomy, refer to ACOG’s Surgical Curriculum in Obstetrics and Gynecology page at https://cfweb.acog.org/scog/. This page lists the standardized surgical skills curriculum for use in training residents in obstetrics and gynecology by procedure. It includes:
- the objective, description, and assessment of the module
- a description of the simulation
- a description of the surgical procedure
- a quiz that must be passed to proceed to evaluation by a faculty member
- an evaluation form to be downloaded and printed by the learner.
Takeaway. Value of Simulation = Quality (Improved Patient Outcomes) ÷ Direct and Indirect Costs.
Simulation models for training in vaginal hysterectomy
According to the Accreditation Council for Graduate Medical Education (ACGME), the minimum number of vaginal hysterectomies is 15; this number represents the minimum accepted exposure, however, and does not imply competency. Exposure to vaginal hysterectomy in residency training has significantly declined over the years, with a mean of only 19 vaginal hysterectomies performed by the time of graduation in 2014.1
A wide range of simulation models are available that you either can construct or purchase, based on your budget. We discuss 3 such models below.
The Miya model
The Miya Model Pelvic Surgery Training Model (Miyazaki Enterprises) consists of a bony pelvic frame and multiple replaceable and realistic anatomic structures, including the uterus, cervix, and adnexa (1 structure), vagina, bladder, and a few selected muscles and ligaments for pelvic floor disorders (FIGURE 1). The model incorporates features to simulate actual surgical experiences, such as realistic cutting and puncturing tensions, palpable surgical landmarks, a pressurized vascular system with bleeding for inadequate technique, and an inflatable bladder that can leak water if damaged.

Mounted on a rotating stand with the top of the pelvis open, the Miya model is designed to provide access and visibility, enabling supervising physicians the ability to give immediate guidance and feedback. The interchangeable parts allow the learner to be challenged at the appropriate skill level with the use of a large uterus versus a smaller uterus.
New in 2018 is an “intern” uterus and vagina that have no vascular supply and a single-layer vagina; this model is one-third of the cost of the larger, high-fidelity uterus (which has a vascular supply and additional tissue layers).
The Miya model reusable bony pelvic frame has a one-time cost of a few thousand dollars. Advantages include its high fidelity, low technology, light weight, portability, and quick setup. To view a video of the Miya model, go to https://www.youtube.com/watch?time_continue=49&v=A2RjOgVRclo. To see a simulated vaginal hysterectomy, visit https://www.youtube.com/watch?time_continue=13&v=dwiQz4DTyy8.
The gynecologic surgeon and inventor, Dr. Douglas Miyazaki, has improved the vesicouterine peritoneal fold (usually the most challenging for the surgeon) to have a more realistic, slippery feel when palpated.
This model’s weaknesses are its cost (relative to low-fidelity models) and the inability to use energy devices.
Takeaway. The Miya model is a high-fidelity, portable vaginal hysterectomy model with a reusable base and consumable replacement parts
The Gynesim model
The Gynesim Vaginal Hysterectomy Model, developed by Dr. Malcolm “Kip” Mackenzie (Gynesim), is a high-fidelity surgical simulation model constructed from animal tissue to provide realistic training in pelvic surgery (FIGURE 2).

These “real tissue models” are hand-constructed from animal tissue harvested from US Department of Agriculture inspected meat processing centers. The models mimic normal and abnormal abdominal and pelvic anatomy, providing realistic feel (haptics) and response to all surgical energy modalities. The “cassette” tissues are placed within a vaginal approach platform, which is portable.
Each model (including a 120- to 240-g uterus, bladder, ureter, uterine artery, cardinal and uterosacral ligaments, and rectum) supports critical gaps in surgical techniques such as peritoneal entry and cuff closure. Gynesim staff set up the entire laboratory, including the simulation models, instruments, and/or cameras; however, surgical energy systems are secured from the host institution.
The advantages of this model are its excellent tissue haptics and the minimal preparation time required from the busy gynecologic teaching faculty, as the company performs the setup and breakdown. Disadvantages include the model’s cost (relative to low-fidelity models), that it does not bleed, its one-time use, and the need for technical assistance from the company for setup.
This model can be used for laparoscopic and open hysterectomy approaches, as well as for vaginal hysterectomy. For more information, visit the Gynesim website at https://www.gynesim.com/vaginal-hysterectomy/.
Takeaway. The high-fidelity Gynesim model can be used to practice vaginal, laparoscopic, or open hysterectomy approaches. It offers excellent tissue haptics, one-time use “cassettes” made from animal tissue, and compatibility with energy devices.
The milk jug model
The milk jug and fabric uterus model, developed by Dr. Dee Fenner, is a low-cost simulation model and an alternative to the flower pot model (described later in this article). The bony pelvis is simulated by a 1-gallon milk carton that is taped to a foam ring. Other materials used to make the uterus are fabric, stuffing, and a needle and thread (or a sewing machine). Each model costs approximately $5 and takes approximately 15 minutes to create. For instructions on how to construct this model, see the Society for Gynecologic Surgeons (SGS) award-winning video from 2012 at https://vimeo.com/123804677.
The advantages of this model are that it is inexpensive and is a good tool with which novice gynecologic surgeons can learn the basic steps of the procedure. The disadvantages are that it does not bleed, is not compatible with energy devices, and must be constructed by hand (adding considerable time) or with a sewing machine.
Takeaway. The milk jug model is a low-cost, low-fidelity model for the novice surgeon that can be quickly constructed with the use of a sewing machine.
Read about simulation models for training in laparoscopic hysterectomy.
Simulation models for training in laparoscopic hysterectomy
While overall hysterectomy numbers have remained relatively stable during the last 10 years, the proportion of laparoscopic hysterectomy procedures is increasing in residency training.1 Many toolkits and models are available for practicing skills, from low-fidelity models on which to rehearse laparoscopic techniques (suturing, instrument handling) to high-fidelity models that provide augmented reality views of the abdominal cavity as well as the operating room itself. We offer a sampling of 4 such models below.
The FLS trainer system
The Fundamentals of Laparoscopic Surgery (FLS) Trainer Box (Limbs & Things Ltd) provides hands-on manual skills practice and training for laparoscopic surgery (FIGURE 3). The FLS trainer box uses 5 skills to challenge a surgeon’s dexterity and psychomotor skills. The set includes the trainer box with a camera and light source as well as the equipment needed to perform the 5 FLS tasks (peg transfer, pattern cutting, ligating loop, and intracorporeal and extracorporeal knot tying). The kit does not include laparoscopic instruments or a monitor.

The FLS trainer box with camera costs $1,164. The advantages are that it is portable and can be used to warm-up prior to surgery or for practice to improve technical skills. It is a great tool for junior residents who are learning the basics of laparoscopic surgery. This trainer’s disadvantages are that it is a low-fidelity unit that is procedure agnostic. For more information, visit the Limbs & Things website at https://www.fls-products.com.
Notably, ObGyn residents who graduate after May 31, 2020, will be required to successfully complete the FLS program as a prerequisite for specialty board certification.2 The FLS program is endorsed by the American College of Surgeons and is run through the Society of American Gastrointestinal and Endoscopic Surgeons. The FLS test is proctored and must be taken at a testing center.
Takeaway. The FLS trainer box is readily available, portable, relatively inexpensive, low-tech, and has valid benchmarks for proficiency. The FLS test will be required for ObGyn residents by 2020.
The SimPraxis software trainer
The SimPraxis Laparoscopic Hysterectomy Trainer (Red Llama, Inc) is an interactive simulation software platform that is available in DVD or USB format (FIGURE 4). The software is designed to review anatomy, surgical instrumentation, and specific steps of the procedure. It provides formative assessments and offers summative feedback for users.

The SimPraxis training software would make a useful tool to familiarize medical students and interns with the basics of the procedure before advancing to other simulation trainers. The software costs $100. For more information, visit https://www.3-dmed.com/product/simpraxis%C3%82%C2%AE-laparoscopic-hysterectomy-trainer.
Takeaway. The SimPraxis software is ideal for novice learners and can be used on a home or office computer.
The LapSim virtual reality trainer
The LapSim Haptic System (Surgical Science) is a virtual reality skills trainer. The hysterectomy module includes right and left uterine artery dissection, vaginal cuff opening, and cuff closure (FIGURE 5). One advantage of this simulator is its haptic feedback system, which enhances the fidelity of the training.
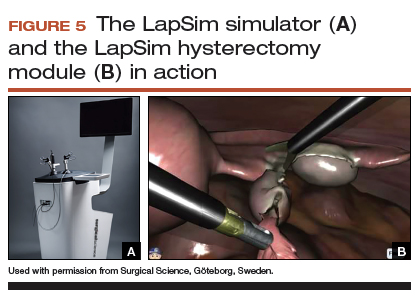
The LapSim simulator includes a training module for students and early learners and modules to improve camera handling. The virtual reality base system costs $70,720, and the hysterectomy software module is an additional $15,600.
For more information, visit the company’s website at https://surgicalscience.com/systems/lapsim/. For an informational video, go to https://surgicalscience.com/systems/lapsim/video/.
Takeaway. The LapSim is an expensive, high-fidelity, virtual reality simulator with enhanced haptics and software for practicing laparoscopic hysterectomy.
The LAP Mentor virtual reality simulator
The LAP Mentor VR (3D Systems) is another virtual reality simulator that has modules for laparoscopic hysterectomy and cuff closure (FIGURE 6). The trainee uses a virtual reality headset and becomes fully immersed in the operating room environment with audio and visual cues that mimic a real surgical experience.
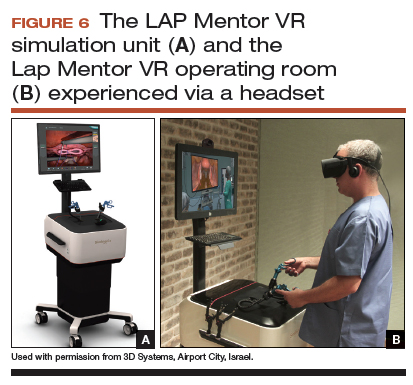
The hysterectomy module allows the user to manipulate the uterus, identify the ureters, divide the superior pedicles, mobilize the bladder, expose and divide the uterine artery, and perform the colpotomy. The cuff closure module allows the user to suture the vaginal cuff using barbed suture. The module also can expose the learner to complications, such as bladder, ureteral, colon, or vascular injury.
The LAP Mentor VR base system costs $84,000 and the modules cost about $15,000. For additional information, visit the company’s website at http://simbionix.com/simulators/lap-mentor/lap-mentor-vr-or/.
Takeaway. The LAP Mentor is an expensive, high-fidelity simulation platform with a virtual reality headset that simulates a laparoscopic hysterectomy (with complications) in the operating room.
Read about simulations models for robot-assisted lap hysterectomy and abdominal hysterectomy.
Simulation models for training in robot-assisted laparoscopic hysterectomy
All robot-assisted simulation platforms have highly realistic graphics, and they are expensive (TABLE). However, the da Vinci Skills Simulator (backpack) platform is included with the da Vinci Si and Xi Systems. Note, though, that it can be challenging to access the surgeon console and backpack at institutions with high volumes of robot-assisted surgery.
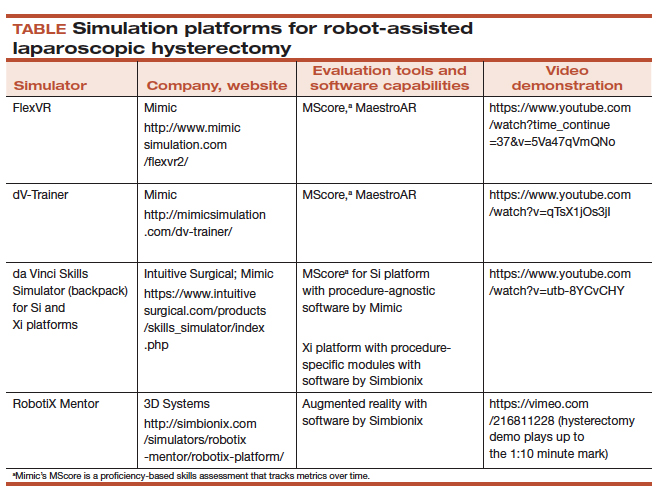
Other options that generally reside outside of the operating room include Mimic’s FlexVR and dV-Trainer and the Robotix Mentor by 3D Systems (FIGURES 7–11). Mimic’s new technology, called MaestroAR (augmented reality), allows trainees to manipulate virtual robotic instruments to interact with anatomic regions within augmented 3D surgical video footage, with narration and instruction by Dr. Arnold Advincula.
Newer software by Simbionix allows augmented reality to assist the simulation of robot-assisted hysterectomy with the da Vinci Xi backpack and RobotiX platforms.
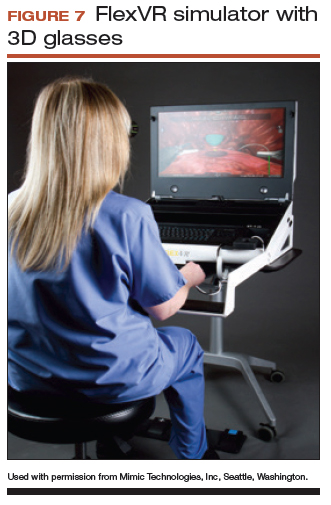

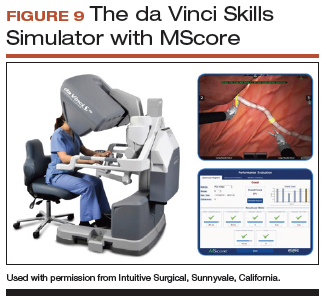
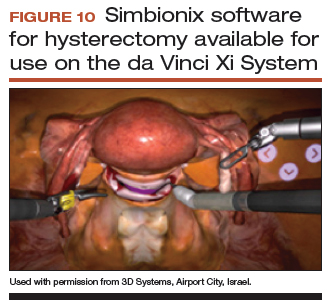
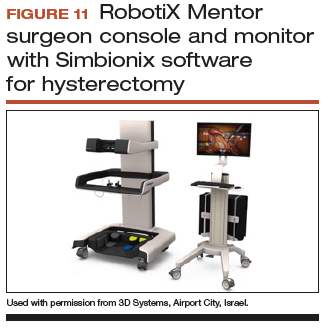
Models for training in abdominal hysterectomy
In the last 10 years, there has been a 30% decrease in the number of abdominal hysterectomies performed by residents.1 Because of this decline in operating room experience, simulation training can be an important tool to bolster residency experience.
There are not many simulation models available for teaching abdominal hysterectomy, but here we discuss 2 that we utilize in our residency program.
Adaptable task trainer
The Surgical Female Pelvic Trainer (SFPT) (Limbs & Things Ltd), a pelvic task trainer primarily used for simulation of laparoscopic hysterectomy, can be adapted for abdominal hysterectomy by removing the abdominal cover (FIGURE 12). This trainer can be used with simulated blood to increase the realism of training. The SFPT trainer costs $2,190. For more information, go to https://www.limbsandthings.com/us/our-products/details/surgical-female-pelvic-trainer-sfpt-mk-2.
Takeaway. The SFPT is a medium-fidelity task trainer with a reusable base and consumable replacement parts.
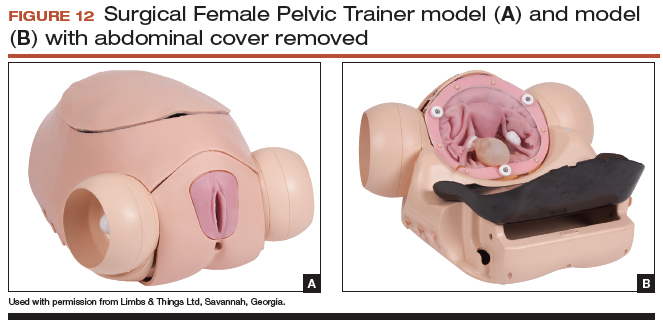
ACOG’s do-it-yourself flower pot model
The flower pot model (developed by the ACOG Simulation Working Group, Washington, DC) is a comprehensive educational package that includes learning objectives, simulation construction instructions, content review of the abdominal hysterectomy, quiz, and evaluation form.3 ACOG has endorsed this low-cost model for residency education. Each model costs approximately $20, and the base (flower pot) is reusable (FIGURE 13).Construction time for each model is 30 to 60 minutes, and learners can participate in the construction. This can aid in anatomy review and familiarization with the model prior to training in the surgical procedure.
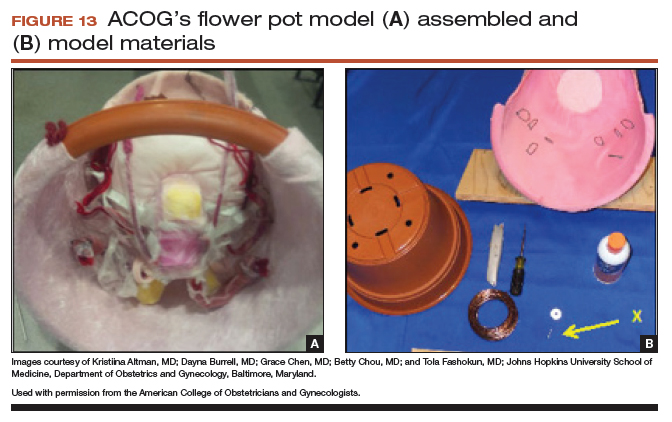
The learning objectives, content review, quiz, and evaluation form can be used for the flower pot model or for high-fidelity models.
The advantages of this model are the low cost and that it provides enough fidelity to teach each of the critical steps of the procedure. The disadvantages include that it is a lower-fidelity model, requires a considerable amount of time for construction, does not bleed, and is not compatible with energy devices. This model also can be used for training in laparoscopic and vaginal hysterectomy. For more information, visit ACOG’s Surgical Curriculum website at https://cfweb.acog.org/scog/.
Takeaway. ACOG’s flower pot model for hysterectomy training is a comprehensive, low-cost, low-fidelity simulation model that requires significant setup time.
Simulation’s offerings
Simulation training is the present and future of medicine that bridges the gap between textbook learning and technical proficiency. Although in this article we describe only a handful of the simulation resources available, we hope that you will incorporate such tools into your practice for continuing education and skill development. Utilize peer-reviewed resources, such as the ACOG curriculum module and evaluation tools for abdominal, laparoscopic, and vaginal hysterectomy, which can be used with any simulation model to provide a comprehensive and complimentary learning experience.
The future of health care depends on the commitment and ingenuity of educators who embrace medical simulation’s purpose: improved patient safety, effectiveness, and efficiency. Join the movement!
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Washburn EE, Cohen SL, Manoucheri E, Zurawin RK, Einarsson JI. Trends in reported resident surgical experience in hysterectomy. J Minim Invasive Gynecol. 2014;21(6):1067–1070.
- American Board of Obstetrics and Gynecology. ABOG announces new eligibility requirement for board certification. https://www.abog.org/new/ABOG_FLS.aspx. Published January 22, 2018. Accessed April 10, 2018.
- Altman K, Burrell D, Chen G, Chou B, Fashokun T. Surgical curriculum in obstetrics and gynecology: vaginal hysterectomy simulation. https://cfweb.acog.org/scog/scog008/Simulation.cfm. Published December 2014. Accessed April 10, 2018.
Due to an increase in minimally invasive approaches to hysterectomy, including vaginal and laparoscopic approaches, gynecologic surgeons may need to turn to simulation training to augment practice and hone skills. Simulation is useful for all surgeons, especially for low-volume surgeons, as a warm-up to sharpen technical skills prior to starting the day’s cases. Additionally, educators are uniquely poised to use simulation to teach residents and to evaluate their procedural competency.
In this article, we provide an overview of the 3 approaches to hysterectomy—vaginal, laparoscopic, abdominal—through medical modeling and simulation techniques. We focus on practical issues, including current resources available online, cost, setup time, fidelity, and limitations of some commonly available vaginal, laparoscopic, and open hysterectomy models.
Simulation directly influences patient safety. Thus, the value of simulation cannot be overstated, as it can increase the quality of health care by improving patient outcomes and lowering overall costs. In 2008, the American College of Obstetricians and Gynecologists (ACOG) founded the Simulations Working Group to establish simulation as a pillar in education for women’s health through collaboration, advocacy, research, and the development and implementation of multidisciplinary simulations-based educational resources and opportunities.
Refer to the ACOG Simulations Working Group Toolkit online to see the objectives, simulation, and videos related to each module. Under the “Hysterectomy” section, you will find how to construct the “flower pot” model for abdominal and vaginal hysterectomy, as well as the AAGL vaginal and laparoscopic hysterectomy webinars. All content is reaffirmed frequently to keep it up to date. You can access the toolkit, with your ACOG login and passcode, at https://www.acog.org/About-ACOG/ACOG-Departments/Simulations-Consortium/Simulations-Consortium-Tool-Kit.
For a comprehensive gynecology curriculum to include vaginal, laparoscopic, and abdominal approaches to hysterectomy, refer to ACOG’s Surgical Curriculum in Obstetrics and Gynecology page at https://cfweb.acog.org/scog/. This page lists the standardized surgical skills curriculum for use in training residents in obstetrics and gynecology by procedure. It includes:
- the objective, description, and assessment of the module
- a description of the simulation
- a description of the surgical procedure
- a quiz that must be passed to proceed to evaluation by a faculty member
- an evaluation form to be downloaded and printed by the learner.
Takeaway. Value of Simulation = Quality (Improved Patient Outcomes) ÷ Direct and Indirect Costs.
Simulation models for training in vaginal hysterectomy
According to the Accreditation Council for Graduate Medical Education (ACGME), the minimum number of vaginal hysterectomies is 15; this number represents the minimum accepted exposure, however, and does not imply competency. Exposure to vaginal hysterectomy in residency training has significantly declined over the years, with a mean of only 19 vaginal hysterectomies performed by the time of graduation in 2014.1
A wide range of simulation models are available that you either can construct or purchase, based on your budget. We discuss 3 such models below.
The Miya model
The Miya Model Pelvic Surgery Training Model (Miyazaki Enterprises) consists of a bony pelvic frame and multiple replaceable and realistic anatomic structures, including the uterus, cervix, and adnexa (1 structure), vagina, bladder, and a few selected muscles and ligaments for pelvic floor disorders (FIGURE 1). The model incorporates features to simulate actual surgical experiences, such as realistic cutting and puncturing tensions, palpable surgical landmarks, a pressurized vascular system with bleeding for inadequate technique, and an inflatable bladder that can leak water if damaged.
Mounted on a rotating stand with the top of the pelvis open, the Miya model is designed to provide access and visibility, enabling supervising physicians the ability to give immediate guidance and feedback. The interchangeable parts allow the learner to be challenged at the appropriate skill level with the use of a large uterus versus a smaller uterus.
New in 2018 is an “intern” uterus and vagina that have no vascular supply and a single-layer vagina; this model is one-third of the cost of the larger, high-fidelity uterus (which has a vascular supply and additional tissue layers).
The Miya model reusable bony pelvic frame has a one-time cost of a few thousand dollars. Advantages include its high fidelity, low technology, light weight, portability, and quick setup. To view a video of the Miya model, go to https://www.youtube.com/watch?time_continue=49&v=A2RjOgVRclo. To see a simulated vaginal hysterectomy, visit https://www.youtube.com/watch?time_continue=13&v=dwiQz4DTyy8.
The gynecologic surgeon and inventor, Dr. Douglas Miyazaki, has improved the vesicouterine peritoneal fold (usually the most challenging for the surgeon) to have a more realistic, slippery feel when palpated.
This model’s weaknesses are its cost (relative to low-fidelity models) and the inability to use energy devices.
Takeaway. The Miya model is a high-fidelity, portable vaginal hysterectomy model with a reusable base and consumable replacement parts
The Gynesim model
The Gynesim Vaginal Hysterectomy Model, developed by Dr. Malcolm “Kip” Mackenzie (Gynesim), is a high-fidelity surgical simulation model constructed from animal tissue to provide realistic training in pelvic surgery (FIGURE 2).
These “real tissue models” are hand-constructed from animal tissue harvested from US Department of Agriculture inspected meat processing centers. The models mimic normal and abnormal abdominal and pelvic anatomy, providing realistic feel (haptics) and response to all surgical energy modalities. The “cassette” tissues are placed within a vaginal approach platform, which is portable.
Each model (including a 120- to 240-g uterus, bladder, ureter, uterine artery, cardinal and uterosacral ligaments, and rectum) supports critical gaps in surgical techniques such as peritoneal entry and cuff closure. Gynesim staff set up the entire laboratory, including the simulation models, instruments, and/or cameras; however, surgical energy systems are secured from the host institution.
The advantages of this model are its excellent tissue haptics and the minimal preparation time required from the busy gynecologic teaching faculty, as the company performs the setup and breakdown. Disadvantages include the model’s cost (relative to low-fidelity models), that it does not bleed, its one-time use, and the need for technical assistance from the company for setup.
This model can be used for laparoscopic and open hysterectomy approaches, as well as for vaginal hysterectomy. For more information, visit the Gynesim website at https://www.gynesim.com/vaginal-hysterectomy/.
Takeaway. The high-fidelity Gynesim model can be used to practice vaginal, laparoscopic, or open hysterectomy approaches. It offers excellent tissue haptics, one-time use “cassettes” made from animal tissue, and compatibility with energy devices.
The milk jug model
The milk jug and fabric uterus model, developed by Dr. Dee Fenner, is a low-cost simulation model and an alternative to the flower pot model (described later in this article). The bony pelvis is simulated by a 1-gallon milk carton that is taped to a foam ring. Other materials used to make the uterus are fabric, stuffing, and a needle and thread (or a sewing machine). Each model costs approximately $5 and takes approximately 15 minutes to create. For instructions on how to construct this model, see the Society for Gynecologic Surgeons (SGS) award-winning video from 2012 at https://vimeo.com/123804677.
The advantages of this model are that it is inexpensive and is a good tool with which novice gynecologic surgeons can learn the basic steps of the procedure. The disadvantages are that it does not bleed, is not compatible with energy devices, and must be constructed by hand (adding considerable time) or with a sewing machine.
Takeaway. The milk jug model is a low-cost, low-fidelity model for the novice surgeon that can be quickly constructed with the use of a sewing machine.
Read about simulation models for training in laparoscopic hysterectomy.
Simulation models for training in laparoscopic hysterectomy
While overall hysterectomy numbers have remained relatively stable during the last 10 years, the proportion of laparoscopic hysterectomy procedures is increasing in residency training.1 Many toolkits and models are available for practicing skills, from low-fidelity models on which to rehearse laparoscopic techniques (suturing, instrument handling) to high-fidelity models that provide augmented reality views of the abdominal cavity as well as the operating room itself. We offer a sampling of 4 such models below.
The FLS trainer system
The Fundamentals of Laparoscopic Surgery (FLS) Trainer Box (Limbs & Things Ltd) provides hands-on manual skills practice and training for laparoscopic surgery (FIGURE 3). The FLS trainer box uses 5 skills to challenge a surgeon’s dexterity and psychomotor skills. The set includes the trainer box with a camera and light source as well as the equipment needed to perform the 5 FLS tasks (peg transfer, pattern cutting, ligating loop, and intracorporeal and extracorporeal knot tying). The kit does not include laparoscopic instruments or a monitor.
The FLS trainer box with camera costs $1,164. The advantages are that it is portable and can be used to warm-up prior to surgery or for practice to improve technical skills. It is a great tool for junior residents who are learning the basics of laparoscopic surgery. This trainer’s disadvantages are that it is a low-fidelity unit that is procedure agnostic. For more information, visit the Limbs & Things website at https://www.fls-products.com.
Notably, ObGyn residents who graduate after May 31, 2020, will be required to successfully complete the FLS program as a prerequisite for specialty board certification.2 The FLS program is endorsed by the American College of Surgeons and is run through the Society of American Gastrointestinal and Endoscopic Surgeons. The FLS test is proctored and must be taken at a testing center.
Takeaway. The FLS trainer box is readily available, portable, relatively inexpensive, low-tech, and has valid benchmarks for proficiency. The FLS test will be required for ObGyn residents by 2020.
The SimPraxis software trainer
The SimPraxis Laparoscopic Hysterectomy Trainer (Red Llama, Inc) is an interactive simulation software platform that is available in DVD or USB format (FIGURE 4). The software is designed to review anatomy, surgical instrumentation, and specific steps of the procedure. It provides formative assessments and offers summative feedback for users.
The SimPraxis training software would make a useful tool to familiarize medical students and interns with the basics of the procedure before advancing to other simulation trainers. The software costs $100. For more information, visit https://www.3-dmed.com/product/simpraxis%C3%82%C2%AE-laparoscopic-hysterectomy-trainer.
Takeaway. The SimPraxis software is ideal for novice learners and can be used on a home or office computer.
The LapSim virtual reality trainer
The LapSim Haptic System (Surgical Science) is a virtual reality skills trainer. The hysterectomy module includes right and left uterine artery dissection, vaginal cuff opening, and cuff closure (FIGURE 5). One advantage of this simulator is its haptic feedback system, which enhances the fidelity of the training.
The LapSim simulator includes a training module for students and early learners and modules to improve camera handling. The virtual reality base system costs $70,720, and the hysterectomy software module is an additional $15,600.
For more information, visit the company’s website at https://surgicalscience.com/systems/lapsim/. For an informational video, go to https://surgicalscience.com/systems/lapsim/video/.
Takeaway. The LapSim is an expensive, high-fidelity, virtual reality simulator with enhanced haptics and software for practicing laparoscopic hysterectomy.
The LAP Mentor virtual reality simulator
The LAP Mentor VR (3D Systems) is another virtual reality simulator that has modules for laparoscopic hysterectomy and cuff closure (FIGURE 6). The trainee uses a virtual reality headset and becomes fully immersed in the operating room environment with audio and visual cues that mimic a real surgical experience.
The hysterectomy module allows the user to manipulate the uterus, identify the ureters, divide the superior pedicles, mobilize the bladder, expose and divide the uterine artery, and perform the colpotomy. The cuff closure module allows the user to suture the vaginal cuff using barbed suture. The module also can expose the learner to complications, such as bladder, ureteral, colon, or vascular injury.
The LAP Mentor VR base system costs $84,000 and the modules cost about $15,000. For additional information, visit the company’s website at http://simbionix.com/simulators/lap-mentor/lap-mentor-vr-or/.
Takeaway. The LAP Mentor is an expensive, high-fidelity simulation platform with a virtual reality headset that simulates a laparoscopic hysterectomy (with complications) in the operating room.
Read about simulations models for robot-assisted lap hysterectomy and abdominal hysterectomy.
Simulation models for training in robot-assisted laparoscopic hysterectomy
All robot-assisted simulation platforms have highly realistic graphics, and they are expensive (TABLE). However, the da Vinci Skills Simulator (backpack) platform is included with the da Vinci Si and Xi Systems. Note, though, that it can be challenging to access the surgeon console and backpack at institutions with high volumes of robot-assisted surgery.
Other options that generally reside outside of the operating room include Mimic’s FlexVR and dV-Trainer and the Robotix Mentor by 3D Systems (FIGURES 7–11). Mimic’s new technology, called MaestroAR (augmented reality), allows trainees to manipulate virtual robotic instruments to interact with anatomic regions within augmented 3D surgical video footage, with narration and instruction by Dr. Arnold Advincula.
Newer software by Simbionix allows augmented reality to assist the simulation of robot-assisted hysterectomy with the da Vinci Xi backpack and RobotiX platforms.
Models for training in abdominal hysterectomy
In the last 10 years, there has been a 30% decrease in the number of abdominal hysterectomies performed by residents.1 Because of this decline in operating room experience, simulation training can be an important tool to bolster residency experience.
There are not many simulation models available for teaching abdominal hysterectomy, but here we discuss 2 that we utilize in our residency program.
Adaptable task trainer
The Surgical Female Pelvic Trainer (SFPT) (Limbs & Things Ltd), a pelvic task trainer primarily used for simulation of laparoscopic hysterectomy, can be adapted for abdominal hysterectomy by removing the abdominal cover (FIGURE 12). This trainer can be used with simulated blood to increase the realism of training. The SFPT trainer costs $2,190. For more information, go to https://www.limbsandthings.com/us/our-products/details/surgical-female-pelvic-trainer-sfpt-mk-2.
Takeaway. The SFPT is a medium-fidelity task trainer with a reusable base and consumable replacement parts.
ACOG’s do-it-yourself flower pot model
The flower pot model (developed by the ACOG Simulation Working Group, Washington, DC) is a comprehensive educational package that includes learning objectives, simulation construction instructions, content review of the abdominal hysterectomy, quiz, and evaluation form.3 ACOG has endorsed this low-cost model for residency education. Each model costs approximately $20, and the base (flower pot) is reusable (FIGURE 13).Construction time for each model is 30 to 60 minutes, and learners can participate in the construction. This can aid in anatomy review and familiarization with the model prior to training in the surgical procedure.
The learning objectives, content review, quiz, and evaluation form can be used for the flower pot model or for high-fidelity models.
The advantages of this model are the low cost and that it provides enough fidelity to teach each of the critical steps of the procedure. The disadvantages include that it is a lower-fidelity model, requires a considerable amount of time for construction, does not bleed, and is not compatible with energy devices. This model also can be used for training in laparoscopic and vaginal hysterectomy. For more information, visit ACOG’s Surgical Curriculum website at https://cfweb.acog.org/scog/.
Takeaway. ACOG’s flower pot model for hysterectomy training is a comprehensive, low-cost, low-fidelity simulation model that requires significant setup time.
Simulation’s offerings
Simulation training is the present and future of medicine that bridges the gap between textbook learning and technical proficiency. Although in this article we describe only a handful of the simulation resources available, we hope that you will incorporate such tools into your practice for continuing education and skill development. Utilize peer-reviewed resources, such as the ACOG curriculum module and evaluation tools for abdominal, laparoscopic, and vaginal hysterectomy, which can be used with any simulation model to provide a comprehensive and complimentary learning experience.
The future of health care depends on the commitment and ingenuity of educators who embrace medical simulation’s purpose: improved patient safety, effectiveness, and efficiency. Join the movement!
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
Due to an increase in minimally invasive approaches to hysterectomy, including vaginal and laparoscopic approaches, gynecologic surgeons may need to turn to simulation training to augment practice and hone skills. Simulation is useful for all surgeons, especially for low-volume surgeons, as a warm-up to sharpen technical skills prior to starting the day’s cases. Additionally, educators are uniquely poised to use simulation to teach residents and to evaluate their procedural competency.
In this article, we provide an overview of the 3 approaches to hysterectomy—vaginal, laparoscopic, abdominal—through medical modeling and simulation techniques. We focus on practical issues, including current resources available online, cost, setup time, fidelity, and limitations of some commonly available vaginal, laparoscopic, and open hysterectomy models.
Simulation directly influences patient safety. Thus, the value of simulation cannot be overstated, as it can increase the quality of health care by improving patient outcomes and lowering overall costs. In 2008, the American College of Obstetricians and Gynecologists (ACOG) founded the Simulations Working Group to establish simulation as a pillar in education for women’s health through collaboration, advocacy, research, and the development and implementation of multidisciplinary simulations-based educational resources and opportunities.
Refer to the ACOG Simulations Working Group Toolkit online to see the objectives, simulation, and videos related to each module. Under the “Hysterectomy” section, you will find how to construct the “flower pot” model for abdominal and vaginal hysterectomy, as well as the AAGL vaginal and laparoscopic hysterectomy webinars. All content is reaffirmed frequently to keep it up to date. You can access the toolkit, with your ACOG login and passcode, at https://www.acog.org/About-ACOG/ACOG-Departments/Simulations-Consortium/Simulations-Consortium-Tool-Kit.
For a comprehensive gynecology curriculum to include vaginal, laparoscopic, and abdominal approaches to hysterectomy, refer to ACOG’s Surgical Curriculum in Obstetrics and Gynecology page at https://cfweb.acog.org/scog/. This page lists the standardized surgical skills curriculum for use in training residents in obstetrics and gynecology by procedure. It includes:
- the objective, description, and assessment of the module
- a description of the simulation
- a description of the surgical procedure
- a quiz that must be passed to proceed to evaluation by a faculty member
- an evaluation form to be downloaded and printed by the learner.
Takeaway. Value of Simulation = Quality (Improved Patient Outcomes) ÷ Direct and Indirect Costs.
Simulation models for training in vaginal hysterectomy
According to the Accreditation Council for Graduate Medical Education (ACGME), the minimum number of vaginal hysterectomies is 15; this number represents the minimum accepted exposure, however, and does not imply competency. Exposure to vaginal hysterectomy in residency training has significantly declined over the years, with a mean of only 19 vaginal hysterectomies performed by the time of graduation in 2014.1
A wide range of simulation models are available that you either can construct or purchase, based on your budget. We discuss 3 such models below.
The Miya model
The Miya Model Pelvic Surgery Training Model (Miyazaki Enterprises) consists of a bony pelvic frame and multiple replaceable and realistic anatomic structures, including the uterus, cervix, and adnexa (1 structure), vagina, bladder, and a few selected muscles and ligaments for pelvic floor disorders (FIGURE 1). The model incorporates features to simulate actual surgical experiences, such as realistic cutting and puncturing tensions, palpable surgical landmarks, a pressurized vascular system with bleeding for inadequate technique, and an inflatable bladder that can leak water if damaged.
Mounted on a rotating stand with the top of the pelvis open, the Miya model is designed to provide access and visibility, enabling supervising physicians the ability to give immediate guidance and feedback. The interchangeable parts allow the learner to be challenged at the appropriate skill level with the use of a large uterus versus a smaller uterus.
New in 2018 is an “intern” uterus and vagina that have no vascular supply and a single-layer vagina; this model is one-third of the cost of the larger, high-fidelity uterus (which has a vascular supply and additional tissue layers).
The Miya model reusable bony pelvic frame has a one-time cost of a few thousand dollars. Advantages include its high fidelity, low technology, light weight, portability, and quick setup. To view a video of the Miya model, go to https://www.youtube.com/watch?time_continue=49&v=A2RjOgVRclo. To see a simulated vaginal hysterectomy, visit https://www.youtube.com/watch?time_continue=13&v=dwiQz4DTyy8.
The gynecologic surgeon and inventor, Dr. Douglas Miyazaki, has improved the vesicouterine peritoneal fold (usually the most challenging for the surgeon) to have a more realistic, slippery feel when palpated.
This model’s weaknesses are its cost (relative to low-fidelity models) and the inability to use energy devices.
Takeaway. The Miya model is a high-fidelity, portable vaginal hysterectomy model with a reusable base and consumable replacement parts
The Gynesim model
The Gynesim Vaginal Hysterectomy Model, developed by Dr. Malcolm “Kip” Mackenzie (Gynesim), is a high-fidelity surgical simulation model constructed from animal tissue to provide realistic training in pelvic surgery (FIGURE 2).
These “real tissue models” are hand-constructed from animal tissue harvested from US Department of Agriculture inspected meat processing centers. The models mimic normal and abnormal abdominal and pelvic anatomy, providing realistic feel (haptics) and response to all surgical energy modalities. The “cassette” tissues are placed within a vaginal approach platform, which is portable.
Each model (including a 120- to 240-g uterus, bladder, ureter, uterine artery, cardinal and uterosacral ligaments, and rectum) supports critical gaps in surgical techniques such as peritoneal entry and cuff closure. Gynesim staff set up the entire laboratory, including the simulation models, instruments, and/or cameras; however, surgical energy systems are secured from the host institution.
The advantages of this model are its excellent tissue haptics and the minimal preparation time required from the busy gynecologic teaching faculty, as the company performs the setup and breakdown. Disadvantages include the model’s cost (relative to low-fidelity models), that it does not bleed, its one-time use, and the need for technical assistance from the company for setup.
This model can be used for laparoscopic and open hysterectomy approaches, as well as for vaginal hysterectomy. For more information, visit the Gynesim website at https://www.gynesim.com/vaginal-hysterectomy/.
Takeaway. The high-fidelity Gynesim model can be used to practice vaginal, laparoscopic, or open hysterectomy approaches. It offers excellent tissue haptics, one-time use “cassettes” made from animal tissue, and compatibility with energy devices.
The milk jug model
The milk jug and fabric uterus model, developed by Dr. Dee Fenner, is a low-cost simulation model and an alternative to the flower pot model (described later in this article). The bony pelvis is simulated by a 1-gallon milk carton that is taped to a foam ring. Other materials used to make the uterus are fabric, stuffing, and a needle and thread (or a sewing machine). Each model costs approximately $5 and takes approximately 15 minutes to create. For instructions on how to construct this model, see the Society for Gynecologic Surgeons (SGS) award-winning video from 2012 at https://vimeo.com/123804677.
The advantages of this model are that it is inexpensive and is a good tool with which novice gynecologic surgeons can learn the basic steps of the procedure. The disadvantages are that it does not bleed, is not compatible with energy devices, and must be constructed by hand (adding considerable time) or with a sewing machine.
Takeaway. The milk jug model is a low-cost, low-fidelity model for the novice surgeon that can be quickly constructed with the use of a sewing machine.
Read about simulation models for training in laparoscopic hysterectomy.
Simulation models for training in laparoscopic hysterectomy
While overall hysterectomy numbers have remained relatively stable during the last 10 years, the proportion of laparoscopic hysterectomy procedures is increasing in residency training.1 Many toolkits and models are available for practicing skills, from low-fidelity models on which to rehearse laparoscopic techniques (suturing, instrument handling) to high-fidelity models that provide augmented reality views of the abdominal cavity as well as the operating room itself. We offer a sampling of 4 such models below.
The FLS trainer system
The Fundamentals of Laparoscopic Surgery (FLS) Trainer Box (Limbs & Things Ltd) provides hands-on manual skills practice and training for laparoscopic surgery (FIGURE 3). The FLS trainer box uses 5 skills to challenge a surgeon’s dexterity and psychomotor skills. The set includes the trainer box with a camera and light source as well as the equipment needed to perform the 5 FLS tasks (peg transfer, pattern cutting, ligating loop, and intracorporeal and extracorporeal knot tying). The kit does not include laparoscopic instruments or a monitor.
The FLS trainer box with camera costs $1,164. The advantages are that it is portable and can be used to warm-up prior to surgery or for practice to improve technical skills. It is a great tool for junior residents who are learning the basics of laparoscopic surgery. This trainer’s disadvantages are that it is a low-fidelity unit that is procedure agnostic. For more information, visit the Limbs & Things website at https://www.fls-products.com.
Notably, ObGyn residents who graduate after May 31, 2020, will be required to successfully complete the FLS program as a prerequisite for specialty board certification.2 The FLS program is endorsed by the American College of Surgeons and is run through the Society of American Gastrointestinal and Endoscopic Surgeons. The FLS test is proctored and must be taken at a testing center.
Takeaway. The FLS trainer box is readily available, portable, relatively inexpensive, low-tech, and has valid benchmarks for proficiency. The FLS test will be required for ObGyn residents by 2020.
The SimPraxis software trainer
The SimPraxis Laparoscopic Hysterectomy Trainer (Red Llama, Inc) is an interactive simulation software platform that is available in DVD or USB format (FIGURE 4). The software is designed to review anatomy, surgical instrumentation, and specific steps of the procedure. It provides formative assessments and offers summative feedback for users.
The SimPraxis training software would make a useful tool to familiarize medical students and interns with the basics of the procedure before advancing to other simulation trainers. The software costs $100. For more information, visit https://www.3-dmed.com/product/simpraxis%C3%82%C2%AE-laparoscopic-hysterectomy-trainer.
Takeaway. The SimPraxis software is ideal for novice learners and can be used on a home or office computer.
The LapSim virtual reality trainer
The LapSim Haptic System (Surgical Science) is a virtual reality skills trainer. The hysterectomy module includes right and left uterine artery dissection, vaginal cuff opening, and cuff closure (FIGURE 5). One advantage of this simulator is its haptic feedback system, which enhances the fidelity of the training.
The LapSim simulator includes a training module for students and early learners and modules to improve camera handling. The virtual reality base system costs $70,720, and the hysterectomy software module is an additional $15,600.
For more information, visit the company’s website at https://surgicalscience.com/systems/lapsim/. For an informational video, go to https://surgicalscience.com/systems/lapsim/video/.
Takeaway. The LapSim is an expensive, high-fidelity, virtual reality simulator with enhanced haptics and software for practicing laparoscopic hysterectomy.
The LAP Mentor virtual reality simulator
The LAP Mentor VR (3D Systems) is another virtual reality simulator that has modules for laparoscopic hysterectomy and cuff closure (FIGURE 6). The trainee uses a virtual reality headset and becomes fully immersed in the operating room environment with audio and visual cues that mimic a real surgical experience.
The hysterectomy module allows the user to manipulate the uterus, identify the ureters, divide the superior pedicles, mobilize the bladder, expose and divide the uterine artery, and perform the colpotomy. The cuff closure module allows the user to suture the vaginal cuff using barbed suture. The module also can expose the learner to complications, such as bladder, ureteral, colon, or vascular injury.
The LAP Mentor VR base system costs $84,000 and the modules cost about $15,000. For additional information, visit the company’s website at http://simbionix.com/simulators/lap-mentor/lap-mentor-vr-or/.
Takeaway. The LAP Mentor is an expensive, high-fidelity simulation platform with a virtual reality headset that simulates a laparoscopic hysterectomy (with complications) in the operating room.
Read about simulations models for robot-assisted lap hysterectomy and abdominal hysterectomy.
Simulation models for training in robot-assisted laparoscopic hysterectomy
All robot-assisted simulation platforms have highly realistic graphics, and they are expensive (TABLE). However, the da Vinci Skills Simulator (backpack) platform is included with the da Vinci Si and Xi Systems. Note, though, that it can be challenging to access the surgeon console and backpack at institutions with high volumes of robot-assisted surgery.
Other options that generally reside outside of the operating room include Mimic’s FlexVR and dV-Trainer and the Robotix Mentor by 3D Systems (FIGURES 7–11). Mimic’s new technology, called MaestroAR (augmented reality), allows trainees to manipulate virtual robotic instruments to interact with anatomic regions within augmented 3D surgical video footage, with narration and instruction by Dr. Arnold Advincula.
Newer software by Simbionix allows augmented reality to assist the simulation of robot-assisted hysterectomy with the da Vinci Xi backpack and RobotiX platforms.
Models for training in abdominal hysterectomy
In the last 10 years, there has been a 30% decrease in the number of abdominal hysterectomies performed by residents.1 Because of this decline in operating room experience, simulation training can be an important tool to bolster residency experience.
There are not many simulation models available for teaching abdominal hysterectomy, but here we discuss 2 that we utilize in our residency program.
Adaptable task trainer
The Surgical Female Pelvic Trainer (SFPT) (Limbs & Things Ltd), a pelvic task trainer primarily used for simulation of laparoscopic hysterectomy, can be adapted for abdominal hysterectomy by removing the abdominal cover (FIGURE 12). This trainer can be used with simulated blood to increase the realism of training. The SFPT trainer costs $2,190. For more information, go to https://www.limbsandthings.com/us/our-products/details/surgical-female-pelvic-trainer-sfpt-mk-2.
Takeaway. The SFPT is a medium-fidelity task trainer with a reusable base and consumable replacement parts.
ACOG’s do-it-yourself flower pot model
The flower pot model (developed by the ACOG Simulation Working Group, Washington, DC) is a comprehensive educational package that includes learning objectives, simulation construction instructions, content review of the abdominal hysterectomy, quiz, and evaluation form.3 ACOG has endorsed this low-cost model for residency education. Each model costs approximately $20, and the base (flower pot) is reusable (FIGURE 13).Construction time for each model is 30 to 60 minutes, and learners can participate in the construction. This can aid in anatomy review and familiarization with the model prior to training in the surgical procedure.
The learning objectives, content review, quiz, and evaluation form can be used for the flower pot model or for high-fidelity models.
The advantages of this model are the low cost and that it provides enough fidelity to teach each of the critical steps of the procedure. The disadvantages include that it is a lower-fidelity model, requires a considerable amount of time for construction, does not bleed, and is not compatible with energy devices. This model also can be used for training in laparoscopic and vaginal hysterectomy. For more information, visit ACOG’s Surgical Curriculum website at https://cfweb.acog.org/scog/.
Takeaway. ACOG’s flower pot model for hysterectomy training is a comprehensive, low-cost, low-fidelity simulation model that requires significant setup time.
Simulation’s offerings
Simulation training is the present and future of medicine that bridges the gap between textbook learning and technical proficiency. Although in this article we describe only a handful of the simulation resources available, we hope that you will incorporate such tools into your practice for continuing education and skill development. Utilize peer-reviewed resources, such as the ACOG curriculum module and evaluation tools for abdominal, laparoscopic, and vaginal hysterectomy, which can be used with any simulation model to provide a comprehensive and complimentary learning experience.
The future of health care depends on the commitment and ingenuity of educators who embrace medical simulation’s purpose: improved patient safety, effectiveness, and efficiency. Join the movement!
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Washburn EE, Cohen SL, Manoucheri E, Zurawin RK, Einarsson JI. Trends in reported resident surgical experience in hysterectomy. J Minim Invasive Gynecol. 2014;21(6):1067–1070.
- American Board of Obstetrics and Gynecology. ABOG announces new eligibility requirement for board certification. https://www.abog.org/new/ABOG_FLS.aspx. Published January 22, 2018. Accessed April 10, 2018.
- Altman K, Burrell D, Chen G, Chou B, Fashokun T. Surgical curriculum in obstetrics and gynecology: vaginal hysterectomy simulation. https://cfweb.acog.org/scog/scog008/Simulation.cfm. Published December 2014. Accessed April 10, 2018.
- Washburn EE, Cohen SL, Manoucheri E, Zurawin RK, Einarsson JI. Trends in reported resident surgical experience in hysterectomy. J Minim Invasive Gynecol. 2014;21(6):1067–1070.
- American Board of Obstetrics and Gynecology. ABOG announces new eligibility requirement for board certification. https://www.abog.org/new/ABOG_FLS.aspx. Published January 22, 2018. Accessed April 10, 2018.
- Altman K, Burrell D, Chen G, Chou B, Fashokun T. Surgical curriculum in obstetrics and gynecology: vaginal hysterectomy simulation. https://cfweb.acog.org/scog/scog008/Simulation.cfm. Published December 2014. Accessed April 10, 2018.